gp5+/6+ sybr green methodology for simultaneous screening and quantification of human papillomavirus
TRANSCRIPT

J
Go
MGa
b
c
a
ARRA
KHSVSR
1
figcHvaudhp
1d
ARTICLE IN PRESSG ModelCV-1677; No. of Pages 6
Journal of Clinical Virology xxx (2009) xxx–xxx
Contents lists available at ScienceDirect
Journal of Clinical Virology
journa l homepage: www.e lsev ier .com/ locate / j cv
P5+/6+ SYBR Green methodology for simultaneous screening and quantificationf human papillomavirus
elissa Rodrigues de Araujoa,b, Laura De Marcob, Carlos F. Santosa, Izabel Regina Fisher Rubira-Bullena,uglielmo Roncoc, Ilenia Penninib, Loredana Vizzinib, Franco Merlettib,c, Anna Gillio-Tosb,∗
Bauru School of Dentistry, University of São Paulo, Al. Octávio Pinheiro Brisola, 9-75, Bauru, São Paulo 17012-901, BrazilUnit of Cancer Epidemiology, C.E.R.M.S., University of Turin, Via Santena 7, 10126 Turin, ItalyCenter for Oncologic Prevention, Via San Francesco da Paola 31, 10123 Turin, Italy
r t i c l e i n f o
rticle history:eceived 17 November 2008eceived in revised form 9 March 2009ccepted 19 March 2009
eywords:uman papillomaviruscreeningiral loadYBR Greeneal-time PCR
a b s t r a c t
Background: Detection and quantification of human papillomavirus (HPV) may help in predicting theevolution of HPV infection and progression of associated lesions.Objectives: We propose a novel protocol using consensus primers GP5+/6+ in a SYBR Green quantitativereal-time (Q-RT) polymerase chain reaction (PCR). The strategy permits screening for HPV infection andviral load quantification simultaneously.Study design: DNA from 153 archived cervical samples, previously tested for HPV detection by GP5+/6+ PCRand typed by EIA-RLB (enzyme immunoassay-reverse line blot) or sequence analysis, was analysed usingSYBR Green Q-RT PCR. Melting temperature assay (Tm) and cycle threshold (Ct) were used to evaluate HPVpositivity and viral load. The Tm in the range of 77–82 ◦C was considered to be positive for HPV-DNA. HPVresults generated through GP5+/6+ conventional PCR were considered the gold standard against whichsensitivity and specificity of our assay were measured.
Results: Out of 104 HPV positive samples, 100 (96.2%) were also determined as positive by SYBR GreenQ-RT PCR; of the 49 HPV-negative samples, all were determined as negative. There was an excellentpositivity agreement (� = 0.94) between the SYBR Green Q-RT and the previous methods employed. Thespecificity and sensitivity were 100% and 96.2%, respectively. Comparison of SYBR Green Q-RT and TaqManoligo-probe technologies gave an excellent concordance (�c = 0.95) which validated the proposed strategy.Conclusions: We propose a sensitive and easy-to-perform technique for HPV screening and viral loadquantification simultaneously.. Background
Human papillomaviruses (HPVs) are recognised as risk factorsor development of skin and mucous membrane neoplasias.1–5 Thedentification of HPV infection alone may not represent a sufficientuideline to identify patients at increased risk for developing can-er. Several viral factors may play a role in carcinogenesis, includingPV genotype, multiple infections, viral load, HPV variants andiral integration.3,6 A conclusive agreement has thus far not beenchieved regarding the value of these parameters, which are still
Please cite this article in press as: de Araujo MR, et al. GP5+/6+ SYBR Gof human papillomavirus. J Clin Virol (2009), doi:10.1016/j.jcv.2009.03
nder investigation to evaluate their predictive power.7 In the lastecade, attention to viral load relevance has increased becauseigh viral load has been associated with persistent infection androgression to high-grade lesions.8–10 Although the utility of viral
∗ Corresponding author. Tel.: +39 011 6336863; fax: +39 011 6334664.E-mail address: gilliotos [email protected] (A. Gillio-Tos).
386-6532/$ – see front matter © 2009 Elsevier B.V. All rights reserved.oi:10.1016/j.jcv.2009.03.020
© 2009 Elsevier B.V. All rights reserved.
load varies with HPV type and a clinical application should beapproached with caution,10 some authors claim that viral load per-mits identification of high-risk populations regardless of the levelof lesion severity, thereby allowing selection of more appropriatemanagement protocols.9,11,12
Determination of the HPV titre may help when assessing thepossible evolution of an infection towards clearance or lesion pro-gression. Reduction of viral load may predict the regression ofcervical intra-epithelial neoplasia to normality.13
Several methods for HPV quantification have been described;however, most of them use TaqMan oligo-probes technology andare mainly focused on HPV16, 18, 31 and 33.14 These methodsare expensive, time consuming and are not available for all HPV
reen methodology for simultaneous screening and quantification.020
types. Indeed, few studies described the quantification for othergenotypes.13,15 The diversity of HPV genotypes and high incidenceof multiple infections require to establish reliable methods for HPVidentification and quantification for epidemiological studies andpotentially for patient management.16

IN PRESSJ
2 Clinical Virology xxx (2009) xxx–xxx
2
ebmagsar
3
3
H
wvbacsigba
aat
(4
3
Hfb
3
oH
(
io
9fi5
bs5HDl
Table 1HPV positivity using GP5+/6+ EIA-RLB or direct sequence analysis genotypes andGP5+/6+ SYBR Green analysis.
Number of samples GP5+/6+ EIA-RLB ordirect sequence analysis
GP5+/6+ SYBR Green
Single infections Positive Negative
HPV low-risk type2 6 2 01 11 1 01 42 1 03 70 3 04 81 4 02 90 2 07 Others (32,43,54, 72, 74,
87, 89)7 0
HPV high-risk type24 16 24 0
4 18 4 04 31 4 01 33 1 03 39 2 14 45 4 03 51 3 04 56 4 04 58 4 03 59 3 03 66 3 03 67 3 02 68 1 14 Others (52, 73, 82, 91) 4 0
Number of samples GP5+/6+ EIA-RLB ordirect sequence analysis
GP5+/6+ SYBR Green
Multiple infections Positive Negative
14 Double infectiona 12 22 Triple infectionb 2 0
ARTICLEG ModelCV-1677; No. of Pages 6
M.R. de Araujo et al. / Journal of
. Objectives
The objective of this study was to perform a novel protocolmploying the quantitative ability and dynamic range providedy real-time polymerase chain reaction (PCR) in an SYBR Greenethodology using the consensus primers GP5+/6+. These primers
re known for their efficient detection of a broad spectrum of HPVenotypes associated with neoplastic evolution.17 We propose atrategy that permits to combine the screening for HPV infectionnd the quantification of HPV viral load by using a low-cost fluo-ophore and quick microplate setting.
. Study design
.1. Study population
A total of 153 archived DNA samples positive and negative forPV detection from the previous studies18,19 were used.
DNA had been extracted from cervical samples obtained fromomen aged 25–70 years attending a screening programme for cer-
ical cancer in Turin, Italy. As described previously,18,19 DNA hadeen purified from 100 �l of cervical cell samples which presentedmean of 5.25 × 108 cells per 100 �l (range: 3.3 × 102 to 4.97 × 1010
ells per 100 �l) by silica-gel columns (Qiagen, Milan, Italy). All DNAamples had been tested for HPV positivity by PCR analysis employ-ng GP5+/6+ primers. The positive samples had subsequently beenenotyped by GP5+/6+ EIA-RLB (enzyme immunoassay-reverse linelot) or, when not identified by this method, by direct sequencenalysis. Residual material had been stored at −80 ◦C.
All DNA samples before inclusion in this study were evaluated bymplification of the �-globin gene as an internal control for DNAdequacy, to avoid false-negative results in the quantitative real-ime (Q-RT) PCR assays.
The sample distribution is as follows: 104 were positive for HPV84 high and 20 low risk) according to the IARC classification,1 and9 were negative (Table 1).
.2. Cell lines
SiHa20 and CaSki21 cervical carcinoma cell lines harbouringPV16 genomes (ATCC, Manassas, VA, USA), were used as controls
or cellular HPV-DNA. DNA isolation from cell lines was performedy silica gel columns (Qiagen, Milan, Italy).
.3. SYBR Green quantitative real-time (Q-RT) PCR
Quantification of the �-globin gene and HPV-DNA were carriedut in an iCycler iQTM Real-Time PCR Detection System (BioRad®,ercules, CA, USA).
Samples and controls were analysed in duplicate.22 NegativeDNA-free) and positive controls were included in each run.
All reactions were performed in a final volume of 25 �l, contain-ng 2× SYBR Green Supermix (BioRad®), either 0.3 �M of �-globin23
r 50 pmol of each GP5+/6+16 primers, and 1 �l of DNA sample.The amplification protocol for �-globin analysis was: 90 s at
5 ◦C, 50 repeats at 95 ◦C for 15 s and 50 ◦C for 1 min. After ampli-cation, a melting curve was performed at temperatures between5 ◦C and 95 ◦C, with temperature increasing at a rate of 0.5 ◦C s−1.
For HPV-DNA analysis the amplification protocol was optimisedefore testing the study samples. The annealing temperature was
Please cite this article in press as: de Araujo MR, et al. GP5+/6+ SYBR Gof human papillomavirus. J Clin Virol (2009), doi:10.1016/j.jcv.2009.03
elected by automatic gradient analysis in the range between0.0 ◦C24 and 38.0 ◦C25,26 by testing six HPV-DNA negative, fourPV-DNA positive (types 18, 54, 66, 82), one CaSki DNA, one SiHaNA and one DNA-free samples. HPV-DNA positive samples (cell
ine included) chosen for the optimisation of the protocol had a phy-
a Double infections genotypes: 16/18, 16/31, 16/56, 16/59, 16/66, 18/51, 18/58,31/39, 31/56, 35/53, 39/66, 56/58, 56/68, 66/68;
b Triple infection genotypes: 16/33/56, 16/56/82.
logenetic heterogeneity, since they belong to five different speciesclades (7, 13, 6, 5 and 9).
To verify the correct discrimination between GP5+/6+ ampliconsand non-specific or primer dimer products as well as PCR efficacy,gel electrophoresis was performed onto a 2% agarose gel.27 A 48.0 ◦Cannealing temperature produced the best yield and discrimina-tion of the target. Lower temperatures showed lack of specificity.Higher temperatures decreased the sensitivity. Therefore, we usedthe following amplification protocol for HPV-DNA analysis: 90 s at95 ◦C, followed by 50 repeats at 94 ◦C for 15 s and 48 ◦C for 30 s.After amplification, a melting curve was performed at tempera-tures between 65 ◦C and 95 ◦C, with temperature increasing at arate of 0.5 ◦C s−1. We identified the melting temperature (Tm) rangeto discriminate GP5+/6+ amplicons between 77 ◦C and 82 ◦C.
External standard calibration curves were generated using10-fold dilutions (2 × 102 ng �l−1 to 2 × 10−1 ng �l−1) of humanplacental DNA (Sigma–Aldrich, St. Louis, MO, USA) or 10-fold dilu-tions (106, 105, 104, 103 and 102 viral copies) of a plasmid carryingthe complete HPV16 genome (Clonit, Milan, Italy). The Ct (cyclethreshold) values were calculated with a software program fordata analysis using an automatic setting of the baseline (BioRad).The �-globin amounts were given as nanogram of �-globin in 1 �lof input DNA. Viral load results were reported as HPV copies/cellequivalent.28 The sensitivity of the method was 102 viral copies.
reen methodology for simultaneous screening and quantification.020
3.4. TaqMan Q-RT
TaqMan Q-RT assays were performed using primers and TaqManoligo-probes previously described that target the �-globin gene23
and HPV16 E6 region,29,30 respectively. Amplification conditions
Please cite this article in press as: de Araujo MR, et al. GP5+/6+ SYBR Green methodology for simultaneous screening and quantificationof human papillomavirus. J Clin Virol (2009), doi:10.1016/j.jcv.2009.03.020
ARTICLE IN PRESSG ModelJCV-1677; No. of Pages 6
M.R. de Araujo et al. / Journal of Clinical Virology xxx (2009) xxx–xxx 3
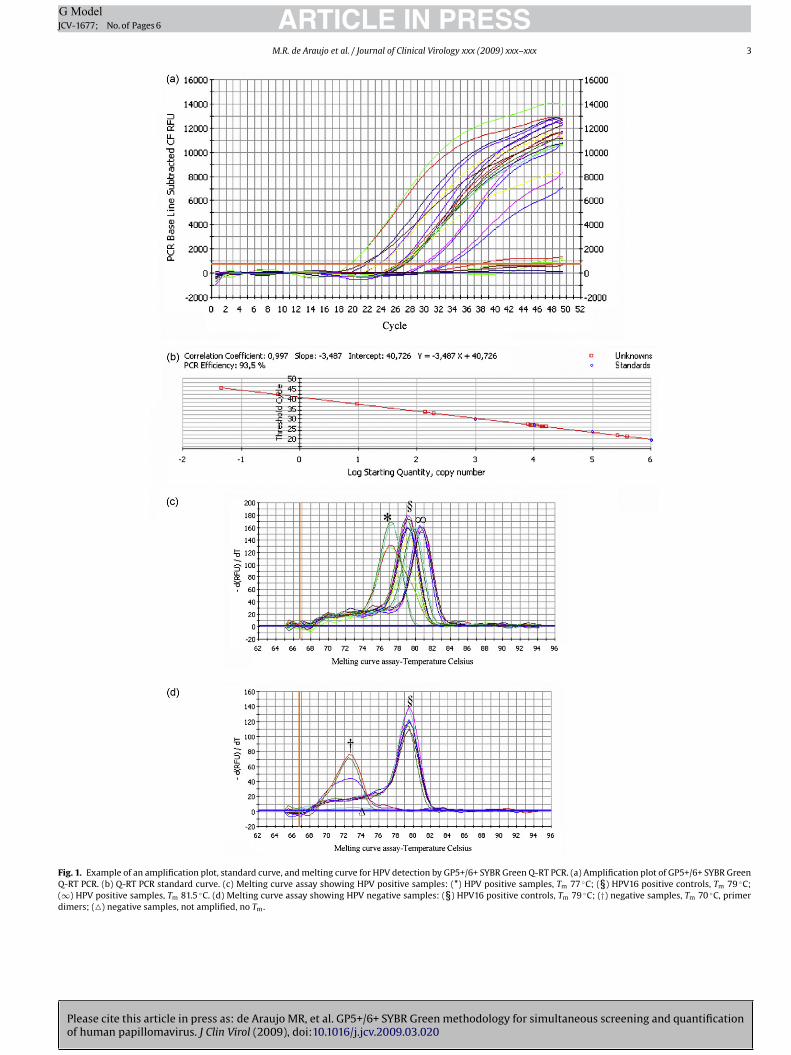
Fig. 1. Example of an amplification plot, standard curve, and melting curve for HPV detection by GP5+/6+ SYBR Green Q-RT PCR. (a) Amplification plot of GP5+/6+ SYBR GreenQ-RT PCR. (b) Q-RT PCR standard curve. (c) Melting curve assay showing HPV positive samples: (*) HPV positive samples, Tm 77 ◦C; (§) HPV16 positive controls, Tm 79 ◦C;(∞) HPV positive samples, Tm 81.5 ◦C. (d) Melting curve assay showing HPV negative samples: (§) HPV16 positive controls, Tm 79 ◦C; (†) negative samples, Tm 70 ◦C, primerdimers; (�) negative samples, not amplified, no Tm.
IN PRESSJ
4 Clinical Virology xxx (2009) xxx–xxx
wo
am
e
3
wSrb
ic
sat
4
od
4
btAHw1tmwiwepfifa
HmpdnT(
t(
4
Qt
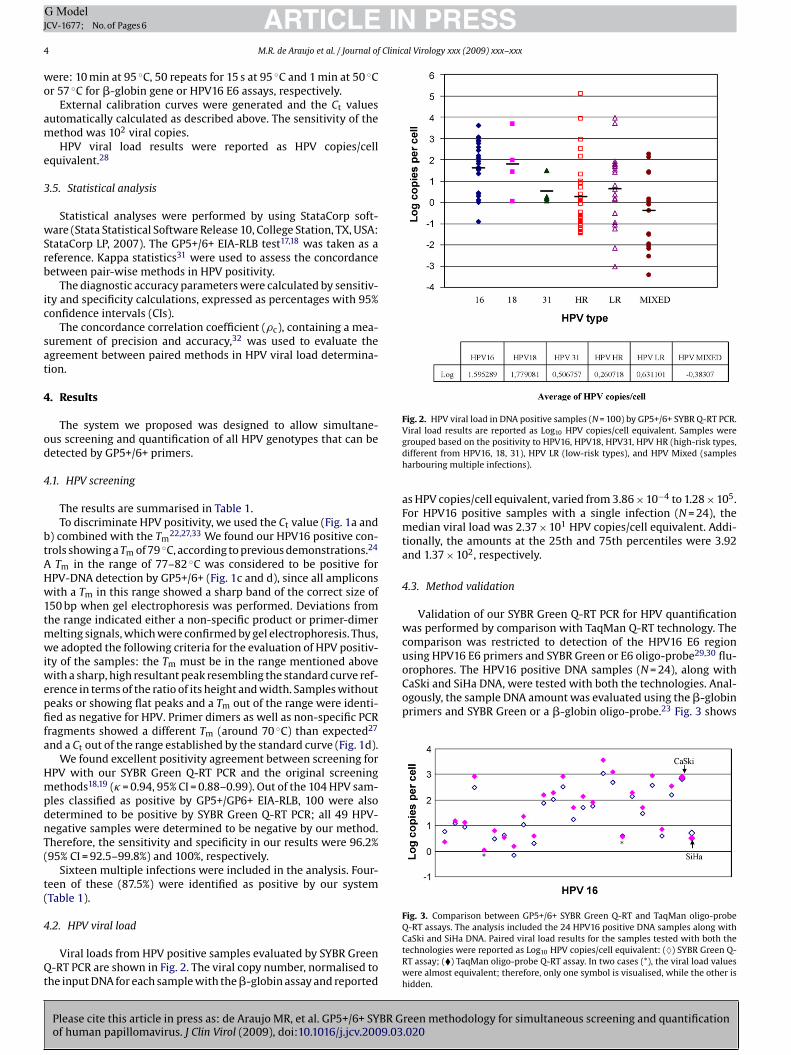
Fig. 2. HPV viral load in DNA positive samples (N = 100) by GP5+/6+ SYBR Q-RT PCR.
orophores. The HPV16 positive DNA samples (N = 24), along withCaSki and SiHa DNA, were tested with both the technologies. Anal-ogously, the sample DNA amount was evaluated using the �-globinprimers and SYBR Green or a �-globin oligo-probe.23 Fig. 3 shows
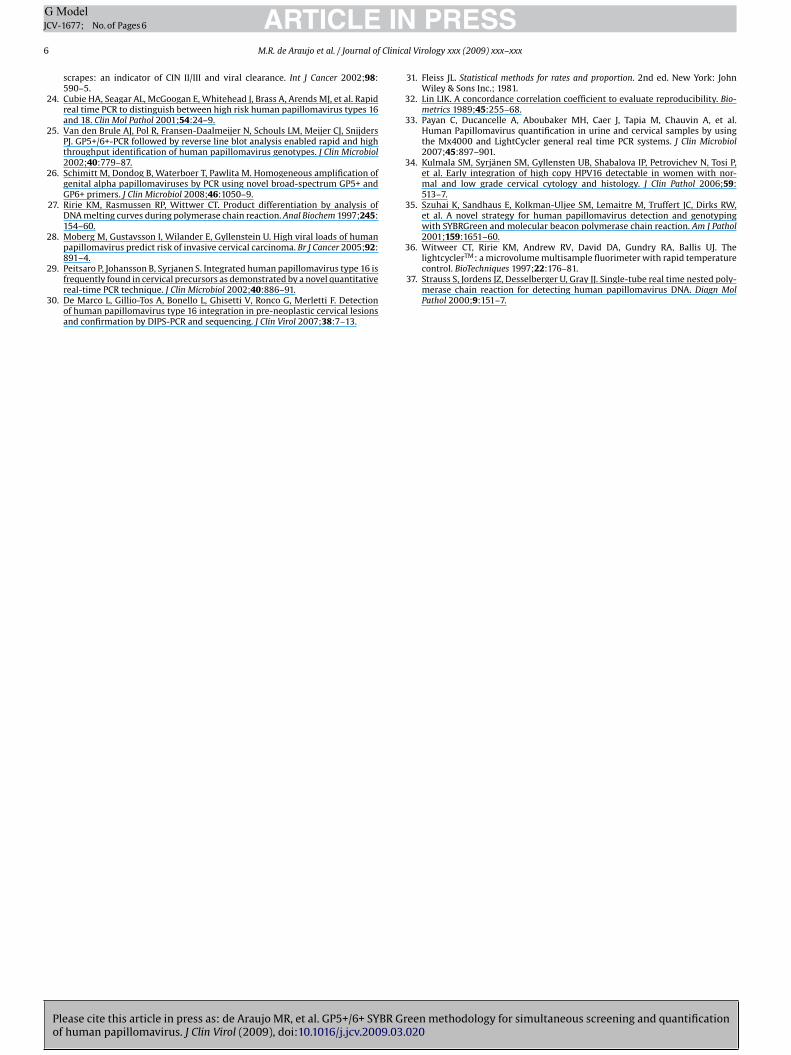
Fig. 3. Comparison between GP5+/6+ SYBR Green Q-RT and TaqMan oligo-probe
ARTICLEG ModelCV-1677; No. of Pages 6
M.R. de Araujo et al. / Journal of
ere: 10 min at 95 ◦C, 50 repeats for 15 s at 95 ◦C and 1 min at 50 ◦Cr 57 ◦C for �-globin gene or HPV16 E6 assays, respectively.
External calibration curves were generated and the Ct valuesutomatically calculated as described above. The sensitivity of theethod was 102 viral copies.HPV viral load results were reported as HPV copies/cell
quivalent.28
.5. Statistical analysis
Statistical analyses were performed by using StataCorp soft-are (Stata Statistical Software Release 10, College Station, TX, USA:
tataCorp LP, 2007). The GP5+/6+ EIA-RLB test17,18 was taken as aeference. Kappa statistics31 were used to assess the concordanceetween pair-wise methods in HPV positivity.
The diagnostic accuracy parameters were calculated by sensitiv-ty and specificity calculations, expressed as percentages with 95%onfidence intervals (CIs).
The concordance correlation coefficient (�c), containing a mea-urement of precision and accuracy,32 was used to evaluate thegreement between paired methods in HPV viral load determina-ion.
. Results
The system we proposed was designed to allow simultane-us screening and quantification of all HPV genotypes that can beetected by GP5+/6+ primers.
.1. HPV screening
The results are summarised in Table 1.To discriminate HPV positivity, we used the Ct value (Fig. 1a and
) combined with the Tm22,27,33 We found our HPV16 positive con-
rols showing a Tm of 79 ◦C, according to previous demonstrations.24
Tm in the range of 77–82 ◦C was considered to be positive forPV-DNA detection by GP5+/6+ (Fig. 1c and d), since all ampliconsith a Tm in this range showed a sharp band of the correct size of
50 bp when gel electrophoresis was performed. Deviations fromhe range indicated either a non-specific product or primer-dimer
elting signals, which were confirmed by gel electrophoresis. Thus,e adopted the following criteria for the evaluation of HPV positiv-
ty of the samples: the Tm must be in the range mentioned aboveith a sharp, high resultant peak resembling the standard curve ref-
rence in terms of the ratio of its height and width. Samples withouteaks or showing flat peaks and a Tm out of the range were identi-ed as negative for HPV. Primer dimers as well as non-specific PCR
ragments showed a different Tm (around 70 ◦C) than expected27
nd a Ct out of the range established by the standard curve (Fig. 1d).We found excellent positivity agreement between screening for
PV with our SYBR Green Q-RT PCR and the original screeningethods18,19 (� = 0.94, 95% CI = 0.88–0.99). Out of the 104 HPV sam-
les classified as positive by GP5+/GP6+ EIA-RLB, 100 were alsoetermined to be positive by SYBR Green Q-RT PCR; all 49 HPV-egative samples were determined to be negative by our method.herefore, the sensitivity and specificity in our results were 96.2%95% CI = 92.5–99.8%) and 100%, respectively.
Sixteen multiple infections were included in the analysis. Four-een of these (87.5%) were identified as positive by our systemTable 1).
Please cite this article in press as: de Araujo MR, et al. GP5+/6+ SYBR Gof human papillomavirus. J Clin Virol (2009), doi:10.1016/j.jcv.2009.03
.2. HPV viral load
Viral loads from HPV positive samples evaluated by SYBR Green-RT PCR are shown in Fig. 2. The viral copy number, normalised to
he input DNA for each sample with the �-globin assay and reported
Viral load results are reported as Log10 HPV copies/cell equivalent. Samples weregrouped based on the positivity to HPV16, HPV18, HPV31, HPV HR (high-risk types,different from HPV16, 18, 31), HPV LR (low-risk types), and HPV Mixed (samplesharbouring multiple infections).
as HPV copies/cell equivalent, varied from 3.86 × 10−4 to 1.28 × 105.For HPV16 positive samples with a single infection (N = 24), themedian viral load was 2.37 × 101 HPV copies/cell equivalent. Addi-tionally, the amounts at the 25th and 75th percentiles were 3.92and 1.37 × 102, respectively.
4.3. Method validation
Validation of our SYBR Green Q-RT PCR for HPV quantificationwas performed by comparison with TaqMan Q-RT technology. Thecomparison was restricted to detection of the HPV16 E6 regionusing HPV16 E6 primers and SYBR Green or E6 oligo-probe29,30 flu-
reen methodology for simultaneous screening and quantification.020
Q-RT assays. The analysis included the 24 HPV16 positive DNA samples along withCaSki and SiHa DNA. Paired viral load results for the samples tested with both thetechnologies were reported as Log10 HPV copies/cell equivalent: (♦) SYBR Green Q-RT assay; (�) TaqMan oligo-probe Q-RT assay. In two cases (*), the viral load valueswere almost equivalent; therefore, only one symbol is visualised, while the other ishidden.

INJ
Clinic
tg0
5
tcuai
fmovtofsat
pavs
afGE
wacvtaGoSctm3
gbmm
ssp
C
A
G
ARTICLEG ModelCV-1677; No. of Pages 6
M.R. de Araujo et al. / Journal of
he HPV16 copies/cell equivalent obtained with the two technolo-ies, demonstrating an excellent concordance (�c = 0.982, 95% CI:.921–0.983) between the two methods.
. Conclusions
There is increasing interest in the use of quantification methodso better predict the evolution of HPV infection. Although a ‘clini-al significance’ of HPV viral load and its prognostic value are stillnder investigation,10 viral load of HPV-DNA has been proposeds a biomarker of persistent infection,15 which might lead to anncreased occurrence of cervical lesions.34
The present study describes a suitable real-time PCR for per-orming HPV screening and quantification simultaneously, thereby
inimising the number of parallel analyses for each sample. The usef the widely described GP5+/6+ primers permits the evaluation ofiral load of different HPV types (including multiple infections) inhe same set of analyses for HPV screening, although identificationf high- and low-risk subtypes will be necessary in the follow-upor clinical management of HPV infection. SYBR Green was cho-en as a fluorophore that intercalates with double-stranded DNAnd may determine the total HPV viral load without suffering fromemplate-sequence variation among types.
Small sample sizes and use of archived samples with incompleteathological information can be listed as limitations of the study. Toscribe clinical sensitivity/specificity of the assay, we plan furtheralidation on a greater number of samples, by testing longitudinaleries and measuring disease outcomes.
Despite limitations of the study, our methodology showed highnalytical sensitivity, as demonstrated by the good agreementound in the samples tested between the detection of HPV byP5+/6+ SYBR Green Q-RT and the original analysis by GP5+/6+IA-RLB or direct sequencing analysis.
Only four (3.85%) discrepant results between these methodsere observed, and all were false negative (Table 1). These discrep-
ncies may be due to a low HPV viral load in the sample, whichould cause deviations in Tm towards non-specific peaks as pre-iously reported.35 No false-positive results were obtained usinghe SYBR Green methodology, which demonstrates the specificitychieved. The reliability of the viral load estimated by GP5+/6+ SYBRreen Q-RT was also supported by comparable viral load valuesbtained when HPV16 positive samples were analysed with bothYBR Green Q-RT and TaqMan oligo-probe technologies. Indeed, theomparison resulted in an excellent concordance between theseests, showing the detection of amplified product with approxi-
ately the same sensitivity as that described by other authors.6
HPV-DNA quantification is currently established for a few HPVenotypes.14 Measuring viral loads in other HPV genotypes maye relevant for managing high-risk subsets of populations,15 and aethodology using the easy-to-handle22 and low-cost SYBR Greenay be convenient.In conclusion, this study described a sensitive technique for the
creening and quantification of a wide range of HPV-DNA that isuitable for large-scale studies37 of high-risk patients, and is inex-ensive and easy to perform.
onflict of interest
None of the authors has competing interests.
Please cite this article in press as: de Araujo MR, et al. GP5+/6+ SYBR Gof human papillomavirus. J Clin Virol (2009), doi:10.1016/j.jcv.2009.03
cknowledgments
M.R. Araujo, received a PhD scholarship from CAPES, Brazilianovernment (2184-07-9).
PRESSal Virology xxx (2009) xxx–xxx 5
This work was partially supported by the Special Project ‘Oncol-ogy’, Compagnia di San Paolo/FIRMS, the Italian Association forCancer Research and by Piedmont Region.
Ethical approval was not required for this study.
References
1. IARC monographs on the evaluation of carcinogenic risks to humans, vol. 90. Humanpapillomaviruses. Lyon, France: International Agency for Research on Cancer(IARC); 2007. pp. 55–9.
2. Porro AM, Alchorne MM, Mota GR, Michalany N, Pignatari AC, Souza IE.Detection and typing of human papillomavirus in cutaneous warts ofpatients infected with human immunodeficiency virus type I. Br J Dermatol2003;149:1192–9.
3. Munoz N, Bosch FX, Castellsangué X, Diaz M, de Sanjose S, Hammouda D, et al.Against which human papillomavirus types shall we vaccinate and screen? Theinternational perspective. Int J Cancer 2004;111:278–85.
4. Chan SY, Delius H, Halpern AL, Bernard HU. Analysis of genomic sequencesof 95 papillomavirus types: uniting typing, phylogeny, and taxonomy. J Virol1995;69:3074–83.
5. Zur Hausen H. Papillomavirus infections—a major cause of human cancers.Biochim Biophys Acta 1996;1288:F55–78.
6. Steben M, Duarte-Franco E. Human papillomavirus infection: epidemiology andpathophysiology. Gynecol Oncol 2007;107:S2–5.
7. Lillo FB, Lodini S, Ferrari D, Stayton C, Taccagni G, Galli L, et al. Determinationof human papillomavirus (HPV) load and type in high grade cervical lesionssurgically resected from HIV-infected women during follow up of HPV infection.Clin Infect Dis 2005;40:451–7.
8. Dalstein V, Riethmuller D, Pretet JL, Le Bail CK, Sautiere JL, Carbillet JP, etal. Persistence and load of high risk HPV are predictors for development ofhigh-grade cervical lesions: a longitudinal French cohort study. Int J Cancer2003;106:396–403.
9. Hernandez-Hernandez DM, Ornelas-Bernal L, Guido-Jimenez M, Apresa-GarciaT, Alvarado-Cabrero I, Salcedo-Vargas M, et al. Association between high-riskhuman papillomavirus DNA load and precursor lesions of cervical cancer inMexican women. Gynecol Oncol 2003;90:310–7.
10. Gravitt PE, Kovacic MB, Herrero R, Schiffman M, Bratti C, Hildesheim A, et al.High load for most high risk human papillomavirus genotypes is associatedwith prevalent cervical cancer precursors but only HPV16 load predicts thedevelopment of incident disease. Int J Cancer 2007;121:2787–93.
11. Weissenborn SJ, Funke AM, Hellmich M, Mallmann P, Fuchs PG, Pfister HJ, etal. Oncogenic human papillomavirus DNA loads in human immunodeficiencyvirus–positive women with high-grade cervical lesions are strongly elevated. JClin Microbiol 2003;41:2763–7.
12. Sun CA, Liu JF, Wu DM, Nieh S, Yu CP, Chu TY. Viral load of high risk humanpapillomavirus in cervical squamous intraepithelial lesions. Int J Gynaecol Obstet2002;76:41–7.
13. Josefsson AM, Magnusson PK, Ylitalo N, Sorensen P, Qwarforth-Tubbin P, Ander-sen PK, et al. Viral load of human papillomavirus 16 as a determinant fordevelopment of cervical carcinoma in situ: a nested case–control study. Lancet2000;355:2189–93.
14. Snijders PJ, Hogewoning CJ, Hesselink AT, Berkhof J, Voorhorst FJ, Bleeker MC,et al. Determination of viral load thresholds in cervical scarpings to rule out CIN3 in HPV16, 18, 31, and 33-positive women with normal cytology. Int J Cancer2006;119:1102–7.
15. Broccolo F, Cocuzza CE. Automated extraction and quantification of oncogenicHPV genotypes from cervical samples by a real-time PCR-based system. J VirolMethods 2008;148:48–57.
16. Sotlar K, Diemer D, Dethleffs A, Hack Y, Stubner A, Vollmer N, et al. Detection andtyping of HPV by E6 nested multiplex PCR. J Clin Microbiol 2004;42:3176–84.
17. Jacobs MV, De Roda Husman AM, Van Den Brule AJC, Snijders PJF, Meijer CJLM,Walboomers JMM. Group-specific differentiation between high and low-riskhuman papillomavirus genotypes by general primer-mediated PCR and twococktails of oligonucleotide probes. J Clin Microbiol 1995;33:901–5.
18. Gillio-Tos A, De Marco L, Ghisetti V, Snijders PJF, Segnan N, Ronco G, et al.Human papillomavirus typing with GP5+/6+ polymerase chain reaction reverseline blotting and with commercial type-specific PCR kits. J Clin Virol 2006;36:126–32.
19. Ronco G, Ghisetti V, Segnan N, Snijders PJ, Gillio-Tos A, Meijer CJ, et al. Preva-lence of papillomavirus infection in women in Turin, Italy. Eur J Cancer 2005;41:297–305.
20. Durst M, Croce CM, Gissmann L, Schwarz E, Huebner K. Papillomavirussequences integrate near cellular oncogenes in some cervical carcinomas. ProcNatl Acad Sci USA 1987;84:1070–4.
21. Corstjens P, Zuiderwijk M, Brink A, Li S, Feindt H, Niedbala RS, et al. Use of up-converting phosphor reporters in lateral-flow assays to detect specific nucleicacid sequences: a rapid, sensitive DNA test to identify human papillomavirustype 16 infection. Clin Chem 2001;47:1885–93.
reen methodology for simultaneous screening and quantification.020
22. Biedermann K, Dandachi N, Trattner M, Vogl G, Doppelmayr H, Moré E, et al.Comparison of real-time PCR signal-amplified in situ hybridization and conven-tional PCR for detection and quantification of human papillomavirus in archivalcervical cancer tissue. J Clin Microbiol 2004;42:3758–65.
23. Van Duin M, Snijders PJ, Schrijnemakers HFJ, Voorhorst FJ, Rozendaal L, Nobbe-huis AE, et al. Human papillomavirus 16 load in normal and abnormal cervical
INJ
6 Clinic
36. Witweer CT, Ririe KM, Andrew RV, David DA, Gundry RA, Ballis UJ. ThelightcyclerTM: a microvolume multisample fluorimeter with rapid temperature
ARTICLEG ModelCV-1677; No. of Pages 6
M.R. de Araujo et al. / Journal of
scrapes: an indicator of CIN II/III and viral clearance. Int J Cancer 2002;98:590–5.
24. Cubie HA, Seagar AL, McGoogan E, Whitehead J, Brass A, Arends MJ, et al. Rapidreal time PCR to distinguish between high risk human papillomavirus types 16and 18. Clin Mol Pathol 2001;54:24–9.
25. Van den Brule AJ, Pol R, Fransen-Daalmeijer N, Schouls LM, Meijer CJ, SnijdersPJ. GP5+/6+-PCR followed by reverse line blot analysis enabled rapid and highthroughput identification of human papillomavirus genotypes. J Clin Microbiol2002;40:779–87.
26. Schimitt M, Dondog B, Waterboer T, Pawlita M. Homogeneous amplification ofgenital alpha papillomaviruses by PCR using novel broad-spectrum GP5+ andGP6+ primers. J Clin Microbiol 2008;46:1050–9.
27. Ririe KM, Rasmussen RP, Wittwer CT. Product differentiation by analysis ofDNA melting curves during polymerase chain reaction. Anal Biochem 1997;245:154–60.
28. Moberg M, Gustavsson I, Wilander E, Gyllenstein U. High viral loads of humanpapillomavirus predict risk of invasive cervical carcinoma. Br J Cancer 2005;92:891–4.
Please cite this article in press as: de Araujo MR, et al. GP5+/6+ SYBR Gof human papillomavirus. J Clin Virol (2009), doi:10.1016/j.jcv.2009.03
29. Peitsaro P, Johansson B, Syrjanen S. Integrated human papillomavirus type 16 isfrequently found in cervical precursors as demonstrated by a novel quantitativereal-time PCR technique. J Clin Microbiol 2002;40:886–91.
30. De Marco L, Gillio-Tos A, Bonello L, Ghisetti V, Ronco G, Merletti F. Detectionof human papillomavirus type 16 integration in pre-neoplastic cervical lesionsand confirmation by DIPS-PCR and sequencing. J Clin Virol 2007;38:7–13.
PRESSal Virology xxx (2009) xxx–xxx
31. Fleiss JL. Statistical methods for rates and proportion. 2nd ed. New York: JohnWiley & Sons Inc.; 1981.
32. Lin LIK. A concordance correlation coefficient to evaluate reproducibility. Bio-metrics 1989;45:255–68.
33. Payan C, Ducancelle A, Aboubaker MH, Caer J, Tapia M, Chauvin A, et al.Human Papillomavirus quantification in urine and cervical samples by usingthe Mx4000 and LightCycler general real time PCR systems. J Clin Microbiol2007;45:897–901.
34. Kulmala SM, Syrjänen SM, Gyllensten UB, Shabalova IP, Petrovichev N, Tosi P,et al. Early integration of high copy HPV16 detectable in women with nor-mal and low grade cervical cytology and histology. J Clin Pathol 2006;59:513–7.
35. Szuhai K, Sandhaus E, Kolkman-Uljee SM, Lemaitre M, Truffert JC, Dirks RW,et al. A novel strategy for human papillomavirus detection and genotypingwith SYBRGreen and molecular beacon polymerase chain reaction. Am J Pathol2001;159:1651–60.
reen methodology for simultaneous screening and quantification.020
control. BioTechniques 1997;22:176–81.37. Strauss S, Jordens JZ, Desselberger U, Gray JJ. Single-tube real time nested poly-
merase chain reaction for detecting human papillomavirus DNA. Diagn MolPathol 2000;9:151–7.