general principles of orthopaedic clinical examination - net
TRANSCRIPT
Chapter
1General principles of orthopaedicclinical examinationStanley Jones and Fazal Ali
Clinical examination is an art and has to be learnt, asit does not come naturally. All patients must berespected, made to feel at ease and assured of theirconfidentiality and dignity.
A detailed history should always be taken followedby clinical examination.
It is often assumed that clinical examinationbegins on the couch. This should not be the case, assignificant information can be gained by observingthe patient as they enter the room and walk towardsyou or as you approach them.
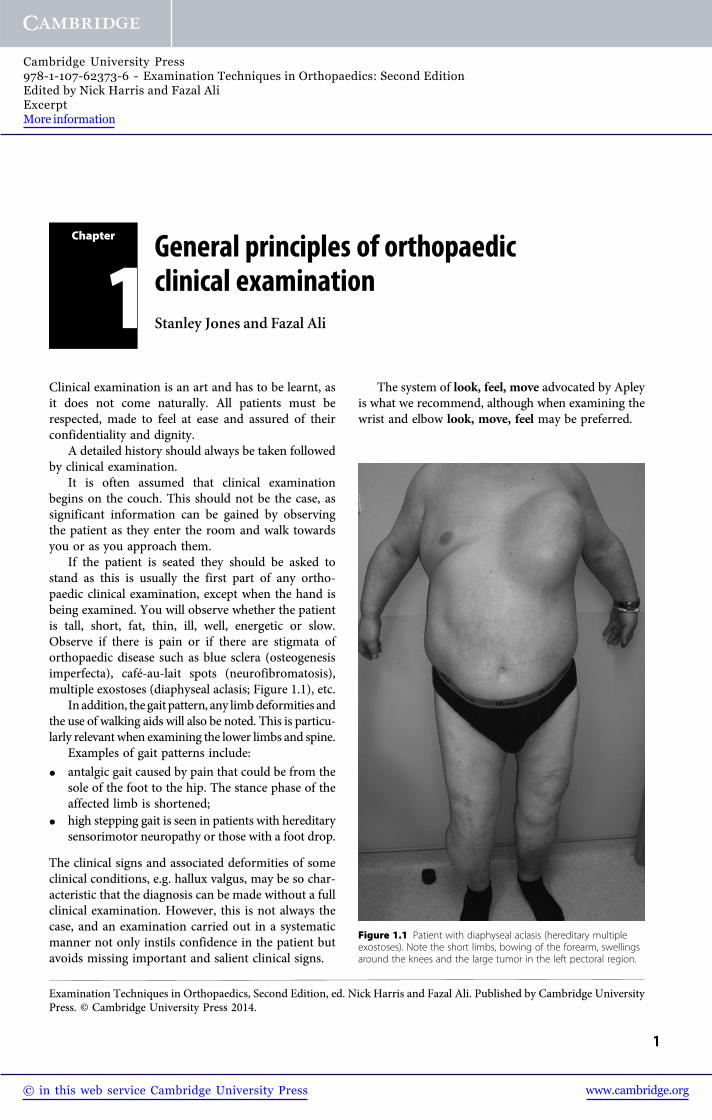
If the patient is seated they should be asked tostand as this is usually the first part of any ortho-paedic clinical examination, except when the hand isbeing examined. You will observe whether the patientis tall, short, fat, thin, ill, well, energetic or slow.Observe if there is pain or if there are stigmata oforthopaedic disease such as blue sclera (osteogenesisimperfecta), café-au-lait spots (neurofibromatosis),multiple exostoses (diaphyseal aclasis; Figure 1.1), etc.
In addition, the gait pattern, any limbdeformities andthe use of walking aids will also be noted. This is particu-larly relevant when examining the lower limbs and spine.
Examples of gait patterns include:
� antalgic gait caused by pain that could be from thesole of the foot to the hip. The stance phase of theaffected limb is shortened;
� high stepping gait is seen in patients with hereditarysensorimotor neuropathy or those with a foot drop.
The clinical signs and associated deformities of someclinical conditions, e.g. hallux valgus, may be so char-acteristic that the diagnosis can be made without a fullclinical examination. However, this is not always thecase, and an examination carried out in a systematicmanner not only instils confidence in the patient butavoids missing important and salient clinical signs.
The system of look, feel, move advocated by Apleyis what we recommend, although when examining thewrist and elbow look, move, feel may be preferred.
Figure 1.1 Patient with diaphyseal aclasis (hereditary multipleexostoses). Note the short limbs, bowing of the forearm, swellingsaround the knees and the large tumor in the left pectoral region.
Examination Techniques in Orthopaedics, Second Edition, ed. Nick Harris and Fazal Ali. Published by Cambridge UniversityPress. © Cambridge University Press 2014.
1
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information
The part of the musculoskeletal system beingexamined must be suitably exposed; for example,when examining the shoulder the patient should beundressed to the waist. Modesty in females shouldbe preserved by using a strapless garment to coverthe breasts. The patient must be given clear instruc-tions on which clothes to take off. The ease or difficultyof undressing and any associated pain experiencedwhilst doing so is useful information that helps inthe assessment. In addition, it is advisable to exposeboth limbs for comparison even though only one limbmay be affected.
Examination of paediatric patients requiresskill and flexibility. Remember to look at the parentsas the patient may be presenting with an inheritedclinical condition. More information can be acquiredby adopting methods of play than using a rigid systemof examination as previously suggested. Any testsfor tenderness must be carried out at the end.
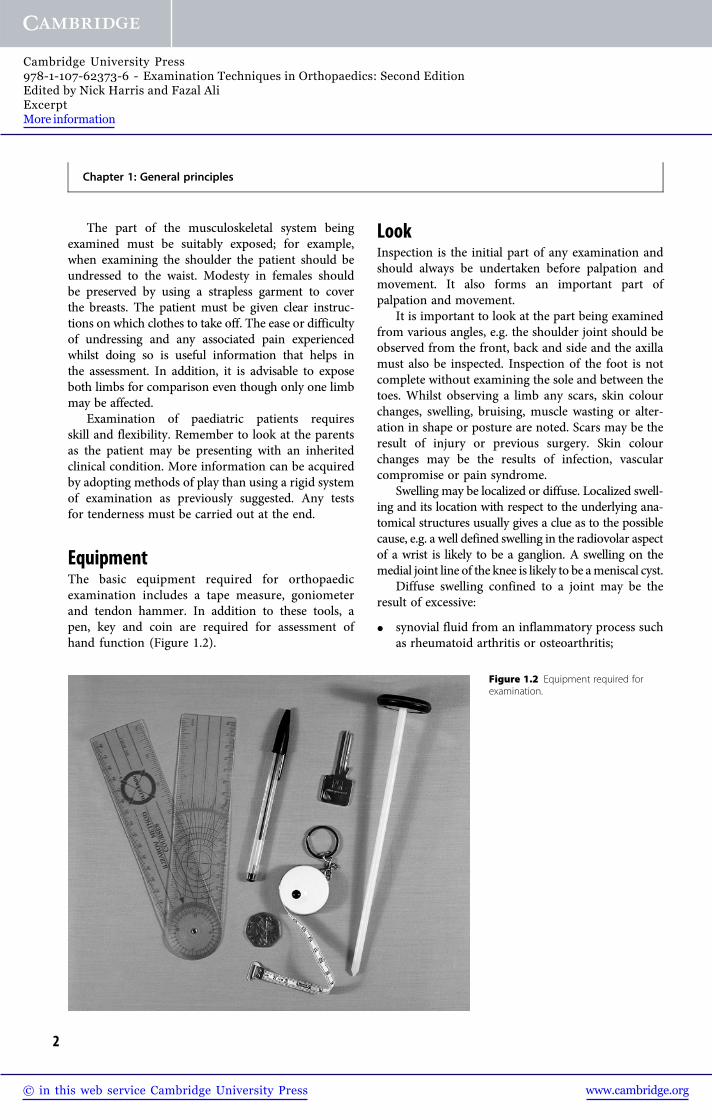
EquipmentThe basic equipment required for orthopaedicexamination includes a tape measure, goniometerand tendon hammer. In addition to these tools, apen, key and coin are required for assessment ofhand function (Figure 1.2).
LookInspection is the initial part of any examination andshould always be undertaken before palpation andmovement. It also forms an important part ofpalpation and movement.
It is important to look at the part being examinedfrom various angles, e.g. the shoulder joint should beobserved from the front, back and side and the axillamust also be inspected. Inspection of the foot is notcomplete without examining the sole and between thetoes. Whilst observing a limb any scars, skin colourchanges, swelling, bruising, muscle wasting or alter-ation in shape or posture are noted. Scars may be theresult of injury or previous surgery. Skin colourchanges may be the results of infection, vascularcompromise or pain syndrome.
Swelling may be localized or diffuse. Localized swell-ing and its location with respect to the underlying ana-tomical structures usually gives a clue as to the possiblecause, e.g. a well defined swelling in the radiovolar aspectof a wrist is likely to be a ganglion. A swelling on themedial joint line of the knee is likely to be ameniscal cyst.
Diffuse swelling confined to a joint may be theresult of excessive:
� synovial fluid from an inflammatory process suchas rheumatoid arthritis or osteoarthritis;
Figure 1.2 Equipment required forexamination.
Chapter 1: General principles
2
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information
� blood (haemarthrosis) from a recent injury, bloodcoagulation defect or medication such as warfarin;
� pus from an infection.
Bruising is usually the result of trauma to tissuesowing to a recent injury or surgery. Muscle wastingmay arise from disuse because of pain, other abnor-mality or muscle denervation. Muscle wasting isquantified by comparing the affected limb with thenormal limb or by measuring the circumference ofthe limb at a fixed point from a bony landmark.
Alteration in shape or posture may be causedby a congenital anomaly, skeletal dysplasia, jointdegeneration or the sequelae of a previous injury.
Finally, inspection should involve looking for anddescribing any orthosis or walking aid.
Inspection should always be thorough. In clinicalexaminations at a junior level it is desirable todescribe both positive and negative findings. In moresenior examinations inspection should still be
complete, but is performed much more rapidly withonly positive and important negative findingsexpressed. Examiners may become agitated if seniorcandidates spend too much time on inspection.
FeelIrrespective of the joint being examined palpationshould always be carried out in a systematic mannerwith reference to the anatomic landmarks. The detailsof how to carry out a satisfactory palpation of thevarious joints are discussed in the relevant chapters,but an essential aspect of palpation is that the exam-iner must not only look at the joint being examinedbut also look at the patient’s face to appreciate anyareas of tenderness (Figure 1.3).
Ensure that hands are washed or antiseptic gel isused. Rubbing your hands together to warm themmakes palpation more comfortable.
Some joints, such as the hip and shoulder, aredeeper and therefore significant information maynot be gained by palpation compared to the moresuperficial joints such as the hand, elbow, spine, knee,foot and ankle. By knowing the surface anatomy ofthese joints, tenderness over the relevant areas maylead to the diagnosis, e.g. tenderness over the lateralepicondyle of the elbow indicates tennis elbow andtenderness over the medial joint line of the knee mayindicate a medial meniscus tear.
MoveBoth active and passive range of movement of thejoint being examined should be assessed. It is advis-able to carry out active range of movement beforepassive as this gives the examiner an idea of thefunctional range of movement and any associatedpain. The patient must be given clear instruction ora demonstration of the range of movement to becarried out. Demonstration is sometimes the bestmethod of communicating to the patient.
� It is always advisable to compare the range ofmovement of the symptomatic with theasymptomatic or normal joint, and the rangeachieved should be recorded in degrees asmeasured by a goniometer.
� Sometimes it may not be possible to assess activerange of movement in certain situations (such aswith a very young child or a patient with cerebralpalsy or other neurological disorder).Figure 1.3 Observe the patient closely whilst examining.
Chapter 1: General principles
3
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information
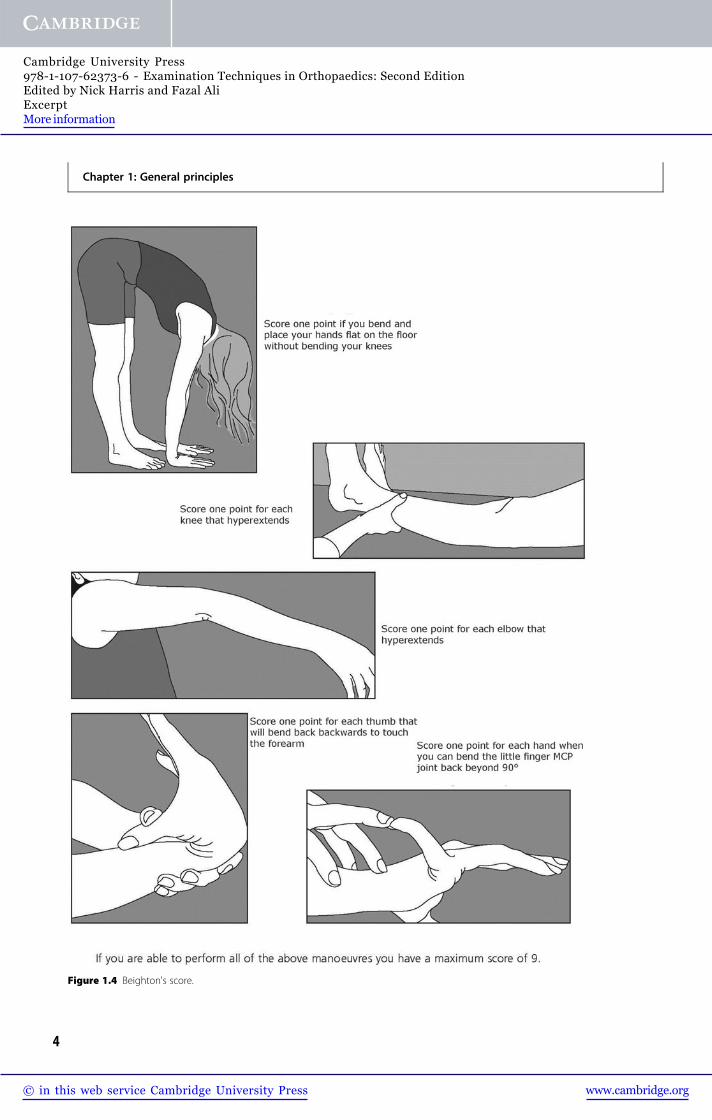
Figure 1.4 Beighton's score.
Chapter 1: General principles
4
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information

� Complete loss of (active and passive) movementmay be the result of previous surgery, e.g. in apatient who has had a previous arthrodesis.
� A joint that is grossly degenerate may have limitedactive or passive range of movement.
� Tendon, muscle or nerve injury may precludeactive movement and in these situations onlypassive movement can be assessed. However, beaware that the patient may use gravity or a trickmovement to move the affected joint, thusmisleading the examiner.
� Excessive passive joint movement or movement inabnormal planes may be the result of generalizedligamentous laxity or ligament/bony abnormality.
� Generalized ligamentous laxity can be assessedfully using Beighton’s scoring system (Figure 1.4).A total score greater than or equal to 4 indicateshypermobility.
Further examinationIn addition to the triad of look, feel, move, other testsspecific to the part being examined may be requiredto enable the examiner to reach a diagnosis, e.g. theanterior draw or Lachman test for anterior cruciateligament insufficiency. The various tests will be dis-cussed later in this book in the respective chapters.
The examiner must be prepared to examine thejoint above or below the one being examined as thepatient may be presenting with referred pain. Forexample, a patient with a slipped upper femoral
epiphysis may present with knee pain, and failure toexamine the hip joint will cause the examiner to missthe diagnosis. In addition, pathology in one joint maydirectly affect adjacent joints.
A neurovascular assessment is also an importantaspect of any examination. It is important to ascertainif there is a true neurological deficit or if neurologicalsymptoms are mimicking musculoskeletal symptoms.In some instances (e.g. in patients with nerve palsy) itmay be necessary to undertake this assessment earlyon in the examination after inspection.
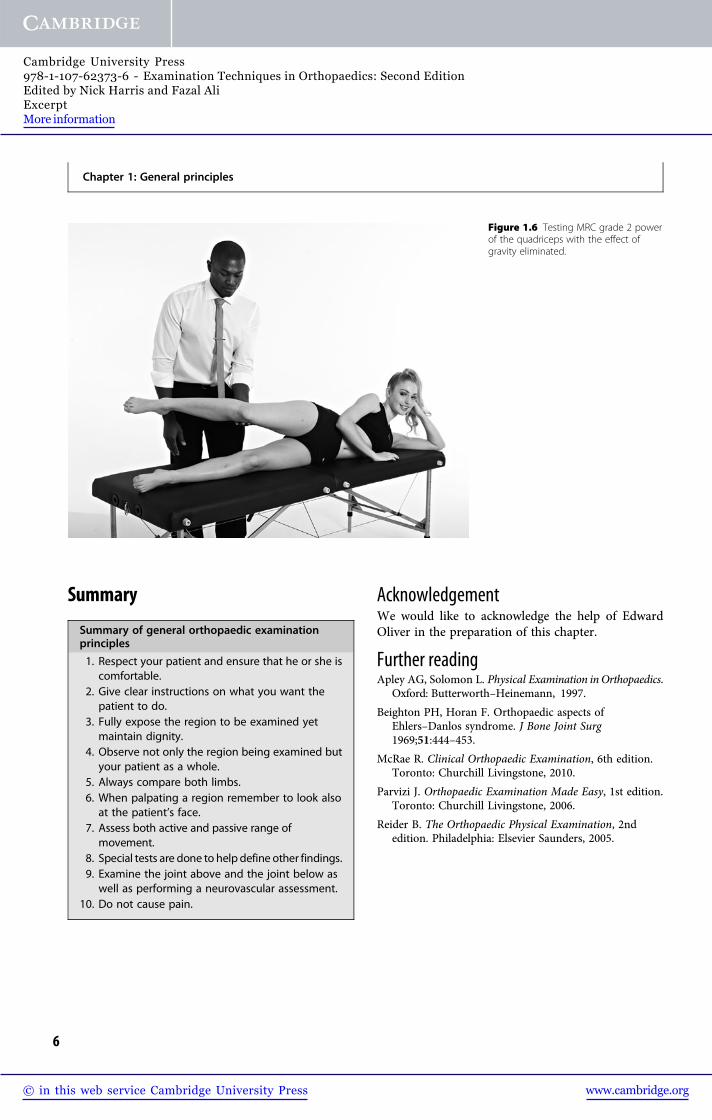
Muscle strength is an integral part of theneurological assessment and is best carried out ina systematic manner from proximal to distal andrecorded using the MRC scale (Table 1.1). It isimportant to understand how to differentiate betweengrade 2 and grade 3 by eliminating gravity (Figures1.5 and 1.6).
Figure 1.5 Testing MRC grade 3 musclepower of the quadriceps.
Table 1.1 MRC scale for muscle strength
Grade
0 No muscle contraction
1 Flicker of contraction
2 Movement with gravity eliminated
3 Movement against gravity
4 Movement against gravity and some resistance
5 Full power
Chapter 1: General principles
5
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information
Summary
Summary of general orthopaedic examinationprinciples
1. Respect your patient and ensure that he or she iscomfortable.
2. Give clear instructions on what you want thepatient to do.
3. Fully expose the region to be examined yetmaintain dignity.
4. Observe not only the region being examined butyour patient as a whole.
5. Always compare both limbs.6. When palpating a region remember to look also
at the patient’s face.7. Assess both active and passive range of
movement.8. Special tests are done to help define other findings.9. Examine the joint above and the joint below as
well as performing a neurovascular assessment.10. Do not cause pain.
AcknowledgementWe would like to acknowledge the help of EdwardOliver in the preparation of this chapter.
Further readingApley AG, Solomon L. Physical Examination inOrthopaedics.
Oxford: Butterworth–Heinemann, 1997.
Beighton PH, Horan F. Orthopaedic aspects ofEhlers–Danlos syndrome. J Bone Joint Surg1969;51:444–453.
McRae R. Clinical Orthopaedic Examination, 6th edition.Toronto: Churchill Livingstone, 2010.
Parvizi J. Orthopaedic Examination Made Easy, 1st edition.Toronto: Churchill Livingstone, 2006.
Reider B. The Orthopaedic Physical Examination, 2ndedition. Philadelphia: Elsevier Saunders, 2005.
Figure 1.6 Testing MRC grade 2 powerof the quadriceps with the effect ofgravity eliminated.
Chapter 1: General principles
6
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information
Chapter
2Examination of the shoulder
David Limb
IntroductionThere is rarely a need to carry out a comprehensiveexamination of the shoulder including all of the testsdescribed in this chapter. Described below are theelements that can be used to differentiate betweenpossible diagnoses suggested by the clinical presenta-tion. To be successful clinically and to demonstratecompetence in professional examinations, interpret-ation of the available history is combined with anappropriately directed examination of the shoulder.Each test answers a specific question about the stateand function of the components of the shoulder or thestructures that enable it to work effectively. Piecedtogether, the clinical examination narrows down thedifferential diagnosis and may direct one to supple-mentary investigations that prove a diagnosis. Alter-natively, the clinical examination may reassure thattreatment can proceed without further expensive tests,pending review to confirm the expected progress. Nodescription of clinical examination of the shoulder cantherefore be complete without mention of the historythat should be elicited, as this is primarily responsiblefor focusing the examination to those components thatmove one efficiently towards the correct diagnosis.
HistoryPatients often present with shoulders that are painful,unstable and/or stiff. Even basic demographic detailsare helpful, and it is important to document these formedicolegal reasons. Age, handedness and occupationshould be noted. Although an open mind should bekept at all times, instability tends to dominate in theyounger age group, impingement symptoms inmiddle age and rotator cuff tears and arthritis in theolder group.
Initially an account is gathered on how the prob-lem began and developed and whether any treatmentshave been undertaken already, with a note of theiroutcome. The past medical history and family historymay point to conditions or associations relevant tothe presenting complaint, whilst the social historymay be vital in formulating a treatment plan withthe patient – a frail elderly patient with a moderaterotator cuff tear who is complaining of overheadweakness but no pain is very unlikely to want a cuffrepair. However, the 50–year-old with the same tearand pseudoparalysis may take quite a different view.
Elements of the history are particularly useful indirecting the subsequent clinical examination andthese merit further attention. In particular, the sur-geon should consider the history of pain, weakness,stiffness and instability.
PainWhy do patients with shoulder problems suffer somuch night pain? It is a frequent complaint, oftenthe main presenting symptom, but elsewhere wouldsuggest tumour or infection. Whilst tumours andinfections of the shoulder do cause night pain, it isnot a red flag symptom in this context as it is socommon in patients with shoulder pathology.
The patient may describe pain that is accuratelylocalized or diffuse. Neck pain radiating to the scapulaor tip of the shoulder should trigger an assessment ofthe cervical spine, whilst radiation into the forearmand hand, particularly with parasthesiae, suggestscervical root entrapment. Pain at the tip of the scapulamay suggest abdominal pathology, though posteriorpain in the upper, outer part of the shoulder blade isusually glenohumeral in origin.
Examination Techniques in Orthopaedics, Second Edition, ed. Nick Harris and Fazal Ali. Published by Cambridge UniversityPress. © Cambridge University Press 2014.
7
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information

Acromioclavicular joint (ACJ) pain is classicallylocalized to the joint itself, the patient pointing with asingle finger to the source of their problem. However,it is not uncommon for ACJ pain to radiate towardsthe root of the neck and, furthermore, ACJ pathologymay coexist with impingement syndrome, giving awider distribution of perceived pain. The painassociated with impingement and rotator cuff diseaseis often diffusely felt over the deltoid region. How-ever, the patient may report painful clicks that theylocalize to the anterior and lateral subacromialregions. Just as hip arthritis can present with thighpain, shoulder arthritis commonly gives pain in theregion of the deltoid insertion, at the midpoint of thehumeral shaft.
There are some conditions that can be associatedwith excruciating pain so severe that it limits furtherclinical tests. Acute calcific tendonitis falls into thiscategory, and may be confirmed by ultrasound orradiographs. The early phases of frozen shouldercan also be extremely painful and the above testswill be negative – this is particularly common indiabetic patients, and the condition also tends tobe more severe and longer-lasting in this group.Also normal on radiography and ultrasound isParsonage–Turner syndrome or brachial neuritis,with neuralgic pain that is associated with weaknessand wasting in the distribution of affected peripheralnerves, unlike the nerve root distribution of cervicaldisc disease.
Finally, the relationship between pain and move-ment should be explored, not least to prevent theexaminer hurting the patient subsequently. Pain thatoccurs only through a particular range of movement isa painful arc: rotator cuff disease, including subacro-mial impingement, often causes a midrange painfularc between about 60° and 120° of abduction andelevation. A high painful arc (for example, the last30° of elevation) is typical of ACJ disorders.A painful arc with pain felt posteriorly is less common,but can occur with subscapular disorders such asenchondromata, which typically produce ratchet-likecrepitus as the lesion moves over the ribs. Morecommonly (but less understood), abnormal musclepatterning of the scapular muscles causes tilting andthe development of subscapular bursitis, causingsimilar subscapular crepitus. Often the patient withthis problem can voluntarily exacerbate their crepitus(and pain if bursitis has developed) by tensing theirshoulder girdle as they move the scapula.
WeaknessThe commonest cause of perceived weakness of theshoulder is pain inhibition – if a movement hurts, thepatient’s brain will not let the muscles contract toproduce the movement. Thus subacromial impinge-ment may present with weakness, but this may bereversed by an injection of local anaesthetic into thesubacromial space. Such diagnostic test injections areless commonly used now that diagnostic ultrasound ismore freely available and can even be integrated intothe clinical examination, observing deformation orbunching of the cuff as it moves under the acromion.Furthermore, weakness can be a manifestation ofstiffness – if the range is not available the patientmay interpret this as them not having the strengthto move the arm. A history of inherited disorders orof generalized problems may alert the surgeon to rareneurological or myopathic conditions such as fascio-scapulohumeral dystrophy.
However, the majority of patients presenting toshoulder clinic (or to examinations) have a disordereither of the rotator cuff or of the nerves supplyingthe shoulder girdle muscles. The latter can includeentrapment in the neck (cervical nerve rootentrapment) or more peripherally. This includesbrachial plexus injury, the assessment of whichrequires a detailed neurological assessment of theupper limb with mapping of all deficits to pinpointthe exact location of the lesion.
Other peripheral nerve problems that canmanifest as shoulder pain and weakness includesuprascapular nerve entrapment. This can occur inthe suprascapular notch, in which case it is known as‘rucksack palsy’ because prolonged downward trac-tion on the shoulder has been implicated. Wastingand weakness of the supraspinatus and infraspinatusoccurs and may be improved by nerve release. Inter-estingly, retraction of supraspinatus because of cufftears has been suggested to cause nerve kinking in thenotch, exacerbating cuff weakness with large tears.Entrapment of the suprascapular nerve can also occuras it winds round the spinoglenoid notch, often aresult of pressure from cysts or ganglia related to adegenerative posterior labrum. In this case only infra-spinatus is involved and the treatment relies on deal-ing with the cyst causing compression. Axillary nerveweakness, with deltoid wasting, may follow axillarynerve injury. Both this, and musculocutaneous nerveinjury, may follow anterior shoulder dislocation.
Chapter 2: Examination of the shoulder
8
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information

Common things being common, however, the mostfrequent cause of weakness in the shoulder clinic isrotator cuff disease and, in particular, rotator cuff tears.
StiffnessIs the shoulder really stiff, or is the patient referring topain, which limits them to moving the shoulderslowly or with assistance? If active movements arelimited check passive movements, being careful notto hurt the patient. Frozen shoulder causes restrictionof both active and passive movement in all planes(global restriction). Arthritic disorders can do thesame, but the latter are often associated with crepitusand radiographs demonstrate the pathology, whilstradiographs are normal in cases of frozen shoulder.
Frozen shoulder has been a loosely used term andshould best be reserved for the specific condition thatcauses inflammation, myofibroblastic transformationand contracture associated with severe pain which, forreasons that we do not understand, eventually ‘thawsout’, even without treatment. So-called secondaryfrozen shoulder refers to stiffness associated withother pathology that is associated with fibrous scar-ring or contracture of the glenohumeral capsule andsubacromial space and is often more resistant tocomplete reversal. This includes stiffness after evenminimally displaced fractures or rotator cuff tears. Inthe latter case it is important to treat the stiffness aswell as the tear – sequentially if necessary – as therehabilitation programme will be doomed to failure ifthe shoulder is already stiff before a repair is carriedout that typically requires a period of further relativeimmobility afterwards.
InstabilityLaxity may be found on examination of the asymp-tomatic shoulder. Indeed, an assessment of general-ized joint laxity is important in any patient in whominstability is suspected, and can be documented usingthe Beighton score (Chapter 1). Instability refers tothe symptomatic inability to maintain the humeralhead centred in the glenoid. Its most extreme manifest-ation is dislocation, though patients presenting to theshoulder clinic will not usually have a dislocated shoul-der (except in the case of chronic dislocation). Rather,they will complain that they can feel the shoulder slip-ping out of the joint and back in, with or without a pasthistory of dislocation. Silliman and Hawkins1 describeda simple classification that broadly categorizes patients
into those likely to need surgical treatment and thosewho may not. TUBS (traumatic, unidirectional,Bankart, surgery) and AMBRI (atraumatic,multidirec-tional, bilateral, rehabilitation, inferior capsular shift)are useful aide-memoires in this respect. However, thisis an oversimplification and the Stanmore classificationconsiders three axes – traumatic structural, atraumaticstructural and habitual non-structural (musclepatterning) – allowing any given patient to be plottedat a point recognizing the contribution of all factorsand allowing a more holistic treatment plan, andappreciating that more than one pathology can bepresent.2 Thus it is important to ask about previousdislocations and their treatment (including anyprevious surgery), but also about the evolution ofsymptoms and whether the patient can voluntarilyproduce subluxation or dislocation.
It should be noted that instability can present aspain in provocative positions of the arm. With fatiguein sports, in particular, anterosuperior instability canmanifest as typical impingement symptoms, but theseare not best addressed by subacromial decompression.
ExaminationLookInspection of the shoulder girdle should be systematicand this requires the patient to be undressed to thewaist. Garments worn for modesty should leave thescapulae visible and enquiry should be made as to anyconcealed scars. Observing preparation for examin-ation may be an adjunct to the history, revealingfunctional difficulties in arm positioning.
The general appearance of the patient may help toidentify underlying disease. The shoulder is inspectedfrom the front, back and side. Inspection of the axilla(Figure 2.1) is also required but may more conveni-ently be carried out during ‘move’.
Inspection of the bony contours may reveal prom-inence of the ACJ or sternoclavicular joint (SCJ) thatcould be degenerative or traumatic in origin. Deform-ity of the clavicle is most likely to be a consequence ofpast trauma. Prominence of the shoulder blade couldbe a result of structural problems, such as malunionor osteochondroma, but is more often positional(static winging) and will be investigated further whenmovements are checked.
Evidence of muscle wasting is important, thoughcan be difficult if there is a substantial layer of sub-cutaneous fat. However, deltoid wasting can give a
Chapter 2: Examination of the shoulder
9
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information
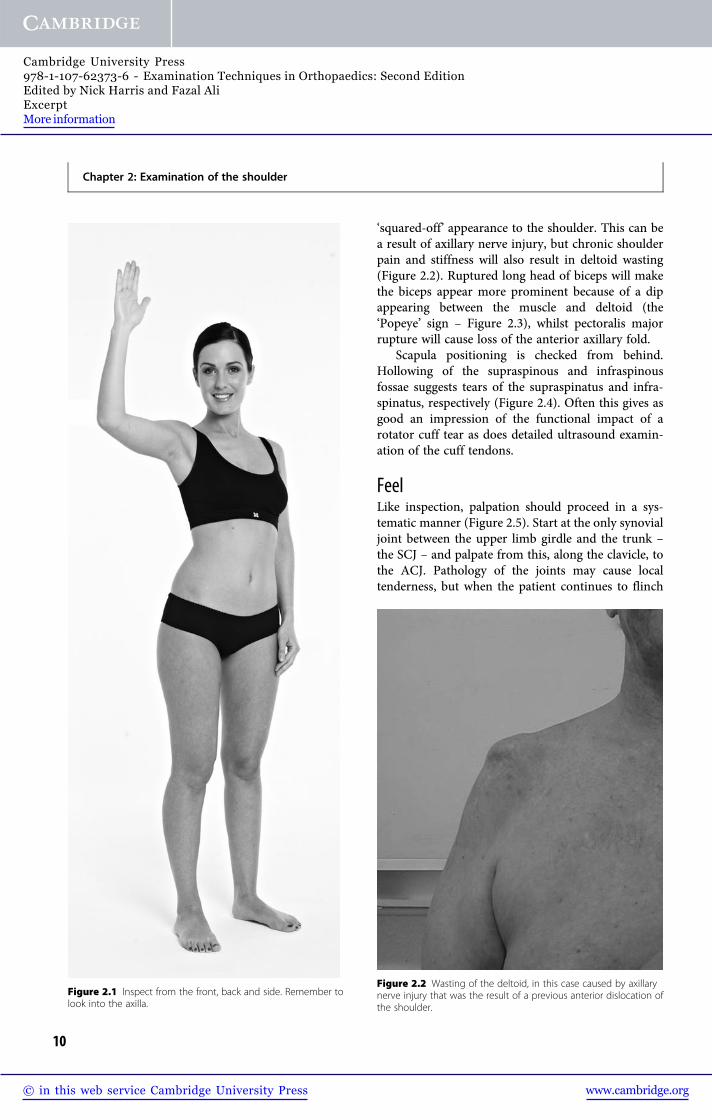
‘squared-off’ appearance to the shoulder. This can bea result of axillary nerve injury, but chronic shoulderpain and stiffness will also result in deltoid wasting(Figure 2.2). Ruptured long head of biceps will makethe biceps appear more prominent because of a dipappearing between the muscle and deltoid (the‘Popeye’ sign – Figure 2.3), whilst pectoralis majorrupture will cause loss of the anterior axillary fold.
Scapula positioning is checked from behind.Hollowing of the supraspinous and infraspinousfossae suggests tears of the supraspinatus and infra-spinatus, respectively (Figure 2.4). Often this gives asgood an impression of the functional impact of arotator cuff tear as does detailed ultrasound examin-ation of the cuff tendons.
FeelLike inspection, palpation should proceed in a sys-tematic manner (Figure 2.5). Start at the only synovialjoint between the upper limb girdle and the trunk –the SCJ – and palpate from this, along the clavicle, tothe ACJ. Pathology of the joints may cause localtenderness, but when the patient continues to flinch
Figure 2.1 Inspect from the front, back and side. Remember tolook into the axilla.
Figure 2.2 Wasting of the deltoid, in this case caused by axillarynerve injury that was the result of a previous anterior dislocation ofthe shoulder.
Chapter 2: Examination of the shoulder
10
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-62373-6 - Examination Techniques in Orthopaedics: Second EditionEdited by Nick Harris and Fazal AliExcerptMore information