fungal infection of skin and nails by hendersonula toruloidea
TRANSCRIPT

British Journal of Dennatology (1973) 89, 45.
Fungal infection of skin and nails byHendersonula toruloidea
C.K.CAMPBELL, AZIZ KURWA, A-H.M.ABDEL-AZIZ*AND C.HODGSON
MRC Unit on the Experimental Pathology of the Skin, The Medical School,The University, Birmingham 15 and The Skin Hospital, Birmingham 15
Accepted for publication 5 January 1973
SUMMARY
Ten cases of skin and nail infection by Hendersonula toruloidea are described. All the patients werefrom tropical countries, though some had been in Britain for many years. Infections were confined tothe hands and feet, which showed scaling skin and dystrophic nails. Four of the patients presentedwith these symptoms, the remaining six having presented with other skin conditions. The presenceof brown-walled hyphae in nail tissue and the repeated isolation of//, toruloidea in pure culture aretaken as evidence that this species was infecting the tissues. In each of two patients there was evidenceof concurrent infection by a ringworm fungus in one of the sites examined.
Gentles & Evans (1970) were the first to present evidence of the possible pathogenicity to man of theplant parasite Hendersonula toruloidea. This species was first described in full by Natrass (1933) as acause of die-back of stone fruit trees in Egypt. It has since been recognized as a cause of branch wilt,canker and die-back diseases of a very wide range of trees, many of them of economic importance(Calavan & Wallace, 1954; Paxton & Wilson, 1965; Punithalingam & Waterston, 1970) and as a causeof fruit rot of bananas (Meredith, 1963). Its geographical range as a plant pathogen is pan-tropical,involving Central America, Africa and southern Asia.
Gentles & Evans (1970) described infection of nails and skin of feet of eight males, seven of whomwere immigrants to Britain from tropical countries. All showed a clinical picture resembling tineapedis, but H. toruloidea was repeatedly cultured. In only two cases were dermatophytes isolated.
The present paper reports ten further cases of hand and feet infection in which H. toruloidea wasimplicated, with particular emphasis on their clinical presentation. One of the cases (Case i) wasreported by Kurwa & Campbell (1972).
MATERIALS AND METHODS
The patients were referred to dermatological departments in the Birmingham area. Samples of skinand nail were examined by one of us (C.K.C.) as part of a general survey to ascertain the pattern ofarrival and spread of the non-indigenous mycoses in the West Midlands.
Laboratory methods involved the direct microscopical examination of KOH squash preparations of* Present address: Department of Dermatology and Vcnereology, Al-Azhar University, Cairo, Egypt.
45
46 C.K.Campbell et al.
samples, anci culture on two mecdia: (a) SAC mcdiuirij Sabouraud glucose agar (Oxoid), incorporating005 mg/ml chloramphenicol and 05 mg/ml cycloheximide; (b) MC medium, malt extract agar(Oxoid), with 05 mg/ml chloramphenicol. Incubation was at 27'C for at least 2 weeks.
The assays of sensitivity of H. toruloidea to griseofulvin (Glaxo Laboratories Ltd) were carriedout using a range of 3 ml aliquots of two-fold dilutions of the antibiotic in glucose peptone broth.The range covered was from 100 /(g/ml to 018 /ig/ml. These were each inoculated with o-1 ml of anaqueous suspension of arthospores, obtained by flooding a malt agar slope culture, and incubated at27 C for 4 weeks, after which the presence or absence of growth was recorded.
CASE HISTORIES
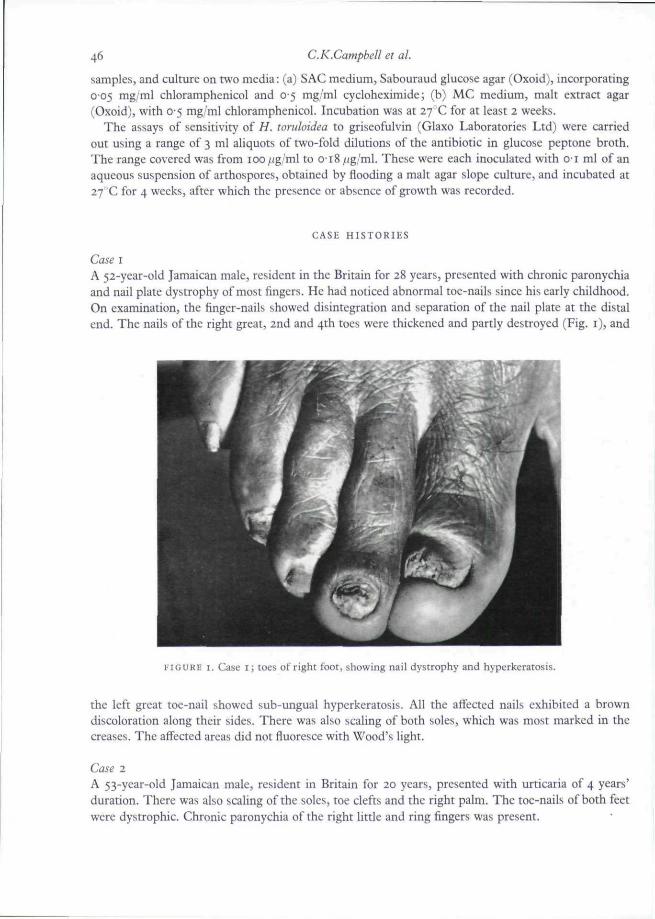
Case IA 52-year-old Jamaican male, resident in the Britain for 28 years, presented with chronic paronychiaand nail plate dystrophy of most fingers. He had noticed abnormal toe-nails since his early childhood.On examination, the finger-nails showed disintegration and separation of the nail plate at the distalend. The nails of the right great, 2nd and 4th toes were thickened and partly destroyed (Fig. i), and
FIGURE I. Case I] toes of right foot, showing nail dystrophy and hyperkeratosis.
the left great toe-nail showed sub-ungual hyperkeratosis. All the affeaed nails exhibited a browndiscoloration along their sides. There was also scaling of both soles, which was most marked in thecreases. The affected areas did not fiuoresce with Wood's light.
Case 2A 53-year-old Jamaican male, resident in Britain for 20 years, presented with urticaria of 4 years'duration. There was also scaling of the soles, toe clefts and the right palm. The toe-nails of both feetwere dystrophic. Chronic paronychia of the right little and ring fingers was present.
Skin and nail infection by H. toruloidea 47
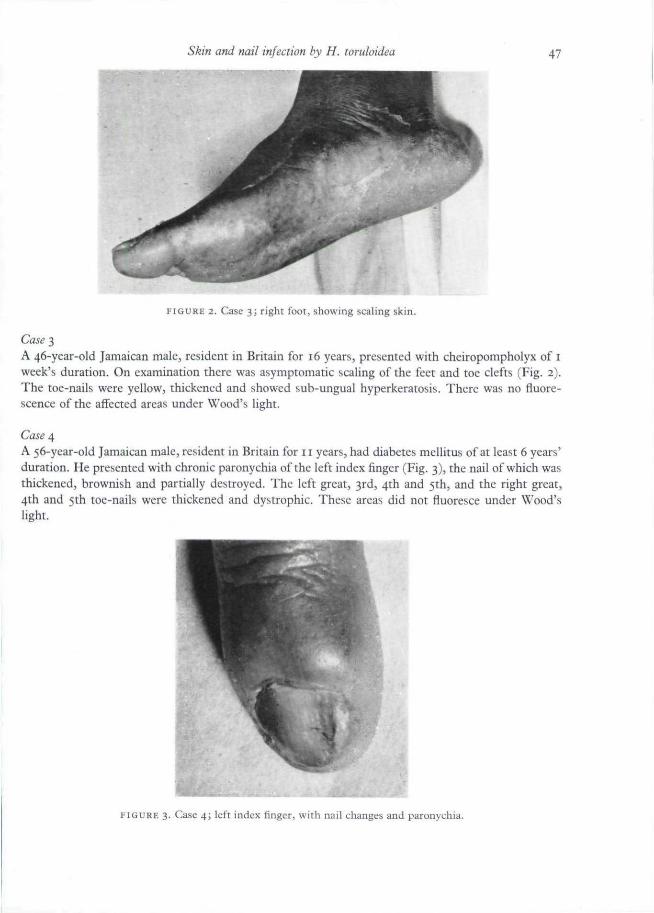
FIGURE 2. Case 3; right foot, showing scaling skin.
Case 3A 46-year-old Jamaican male, resident in Britain for 16 years, presented with cheiropompholyx of iweek's duration. On examination there was asymptomatic scahng of the feet and toe clefts (Fig. 2).The toe-nails were yellow, thickened and showed sub-ungual hyperkeratosis. There was no fluore-scence of the affected areas under Wood's light.
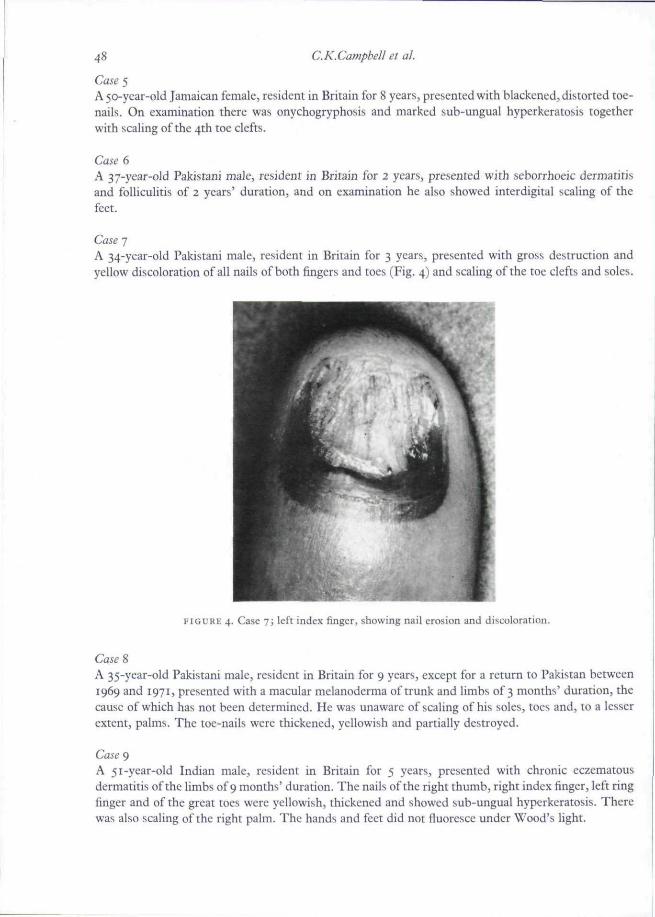
Case 4A 56-year-old Jamaican male, resident in Britain for 11 years, had diabetes mellitus of at least 6 years'duration. He presented with chronic paronychia of the left index finger (Fig. 3), the nail of which wasthickened, brownish and partially destroyed. The left great, 3rd, 4th and 5th, and the right great,4th and 5th toe-nails were thickened and dystrophic. These areas did not fluoresce under Wood'slight.
FIGURE 3. Case 4; left index finger, wiih nail changes and paronychia.
48 C.K.Campbell et al.
Case 5A 50-year-old Jamaican female, resident in Britain for 8 years, presented with blackened, distorted toe-nails. On examination there was onychogryphosis and marked sub-ungual hyperkcratosis togetherwith scaling of the 4th toe clefts.
Case 6A 37-year-old Pakistani male, resident in Britain for 2 years, presented with seborrhoeic dermatitisand foUiculitis of 2 years' duration, and on examination he also showed interdigital scaling of thefeet.
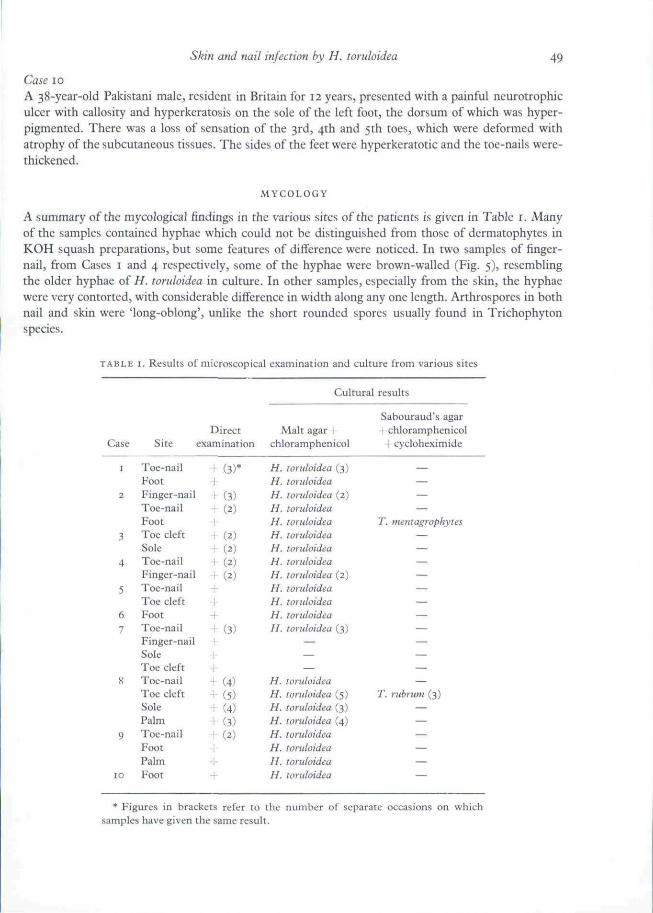
Case 7A 34-year-old Pakistani male, resident in Britain for 3 years, presented with gross destruction andyellow discoloration of all nails of both fingers and toes (Fig. 4) and scaling of the toe clefts and soles.
FIGURE 4. Case 7; left index finger, showing nail erosion and discoloration.
A 35-year-old Pakistani male, resident in Britain for 9 years, except for a return to Pakistan between1969 and 1971, presented with a macular melanoderma of trunk and limbs of 3 months' duration, thecause of which has not been determined. He was unaware of scaling of his soles, toes and, to a lesserextent, palms. The toe-nails were thickened, yellowish and partially destroyed.
Case 9A 51-year-old Indian male, resident in Britain for 5 years, presented with chronic eczematousdermatitis of the limbs of 9 months' duration. The nails of the right thumb, right index finger, left ringfinger and of the great toes were yellowish, thickened and showed sub-ungual hyperkeratosis. Therewas also scaling of the right palm. The hands and feet did not fluorcsce under Wood's light.
Skin and nail infection by H. toruloidea 49
Case 10
A 38-year-old Pakistani male, resident in Britain for 12 years, presented with a painful ncurotrophiculcer with callosity and hyperkeratosis on the sole of the left foot, the dorsum of which was hyper-pigmented. There was a loss of sensation of the 3rd, 4th and 5th toes, which were deformed withatrophy of the subcutaneous tissues. The sides of the feet were hyperkeratotic and the toe-nails were-thickened.
MYCOLOGY
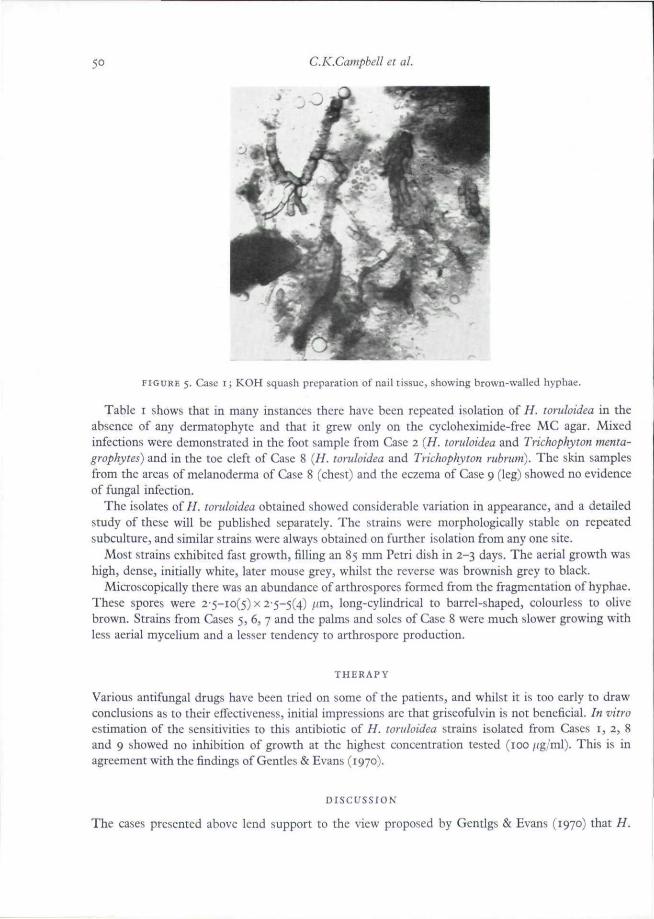
A summary of the mycological findings in the various sites of the patients is given in Table i. Manyof the samples contained hyphae which could not be distinguished from those of dermatophytes inKOH squash preparations, but some features of difference were noticed. In two samples of finger-nail, from Cases i and 4 respectively, some of the hyphae were brown-walled (Fig. 5), resemblingthe older hyphae of H. toruloidea in culture. In other samples, especially from the skin, the hyphaewere very contorted, with considerable difference in width along any one length. Arthrospores in bothnail and skin were 'long-oblong', unlike the short rounded spores usually found in Trichophytonspecies.
TABLE I. Results of micfoscopical examination and culture from various sites
Case
I
2
3
4
5
6
7
8
9
10
Site
Toe-nailFootFinger-nailToe-nailFootToe cleftSoleToe-nailFinger-nailToe-nailToe cleftFootToe-nailFinger-nailSoleToe cleftToe-nailToe cleftSolePalmToe-nailFootPalmFoot
Directexamination
1 (3)*
1 C3)• ( 2 )
•1-
• ( 2 )
•• ( 2 )
1 (2)+ (2)—
++\ (3)
a.
++•! ( 4 )
+ (5)+ (4)+ (3)+ (2)
+
+
Cultural results
Sabouraud's agarMalt agar I I chloramphenicol
chloramphenicol I cycloheximide
H. toruioidea (3) —H. loridoidea —H. toruloidea (2) —H. loridoidea —H. toruloidea T. mentagrophytesH. toruloidea —H. loruioidea —H. toruioidea —H. roruloidea (2) —H. toruloidea —H. toruloidea —/ / . toruloidea —H. toruloidea (3) —
— —— —— —
H. loruioidea —H. toruloidea (5) 7". rubrum (3)H. toruloidea (3) —H. loruioidea (4) —H. loruioidea —H. roruloidea —H. roruloidea —H. loruioidea —
* Figures in brackets refer to the number of separate occasions on whichsamples have given the same result.
50 C.K.Campbell et al.
FIGURE 5. Case i; KOH squash preparation of nail tissue, showing brown-wallcd hyphae.
Table i shows that in many instances there have been repeated isolation of H. toruloidea in theabsence of any dermatophyte and that it grew only on the cycloheximide-free MC agar. Mixedinfections were demonstrated in the foot sample from Case 2 (H. toruloidea and Trichophyton menta-grophytes) and in the toe cleft of Case 8 {//. toruloidea and Trichophyton rubrum). The skin samplesfrom the areas of melanoderma of Case 8 (chest) and the eczema of Case 9 (leg) showed no evidenceof fungal infection.
The isolates of//, toruloidea obtained showed considerable variation in appearance, and a detailedstudy of these will be published separately. The strains were morphologically stable on repeatedsubculture, and similar strains were always obtained on further isolation from any one site.
Most strains exhibited fast growth, filling an 85 mm Petri dish in 2-3 days. The aerial growth washigh, dense, initially white, later mouse grey, whilst the reverse was brownish grey to black.
Microscopically there was an abundance of arthrospores formed from the fragmentation of hyphae.These spores were 2'5-io(5) x 2-5-5(4) /'"i^ long-cylindrical to barrel-shaped, colourless to olivebrown. Strains from Cases 5, 6, 7 and the palms and soles of Case 8 were much slower growing withless aerial mycelium and a lesser tendency to arthrospore production.
THERAPY
Various antifungal drugs have been tried on some of the patients, and whilst it is too early to drawconclusions as to their effectiveness, initial impressions are that griseofulvin is not beneficial. In vitroestimation of the sensitivities to this antibiotic of H. toruloidea strains isolated from Cases t, 2, 8and 9 showed no inhibition of growth at the highest concentration tested (too /ig/ml). This is inagreement with the findings of Gentles & Evans (1970).
DISCUSSION
The cases presented above lend support to the view proposed by Gentlgs & Evans (1970) that H.
Skin and nail infection by H. toruloidea 51
toruloidea is capable of invading skin and nail tissue and giving a clinical appearance whichresembles dermatophytosis of the hands and feet. The most convincing evidence, apart from therepeated isolation of this species from the same site on several patients, is that brown-walled hyphaehave been found in some of the samples. Such hyphae could not have belonged to a true dermato-phyte. More knowledge is needed before the term pathogenic can be strictly applied to this fungus,however, since its part in producing the host response, and its status as a primary invader are not fullyestablished. The existence of multiple fungus infeaions is well recognized (Partridge, 1955) and itseems reasonable to postulate double infections in the two instances (Cases 2 and 8) in which dermato-phytes were isolated together with H. toruloidea.
The genus Hendersonula is a member of the Sphaeropsidales, a large group of asexual fungi whichproduce spores within flask-shaped structures known as pycnidia. Such pycnidia have so far beenobserved in strains from Cases i, 2, 3, 4 and 8. The identification of the remaining isolates has beenbased upon their production of brown arthrospores.
As this fungus is not a close relative of the ringworm fungi, it is not surprising that it differs fromthem in physiological respects, such as its susceptibility to cycloheximide and its tolerance of griseo-fulvin. Its inability to grow in the presence of cycloheximide probably accounts for its remainingunnoticed by medical mycologists until recently, since most laboratories use this compound for theisolation of ringworm ftingi.
Seven of the ten cases described here showed nail involvement, compared with only two of the eightreported by Gentles & Evans (1970). A single case found by Dr R.R.Davies (personal communication) in1964, and two others seen by Dr M.P.English (personal communication), all involved nails. It isdifficult to select any one clinical feature of the nails which may be pathognomonic for this infeaion.As in other types of onychomycosis some of the nails on the affected hand or foot remained normal,although other nails had apparently been infected for many years.
The nails in the present cases were generally dystrophic and exhibited yellowish to brownish-black discoloration. These changes appeared to begin at the nail edges, spreading to involve the wholenail-plate. The degree of dystrophy, separation of nail and subungual hyperkeratosis werevariable.
H. toruloidea is apparently unusual in its ability to invade the skin of hands and feet, since othernon-dermatophyte pathogens are typically restricted to infections of nail tissue (Walshe & English,1966; English, 1968; Zaias et al.., 1969). As in ringworm infections of feet and hands, the factorsrestricting the fungus to these sites are unknown.
The skin infection did not cause physical discomfort to the patients. In only four cases was the H.toruloidea infection the primary reason for attending the skin clinics, and some of the patients did notrealize their feet and hands were abnormal.
At present there is no reason to suppose that the Hendersonula infections were connected with thepresence of the other conditions (urticaria, pompholyx, eczematous dermatitis, melanoderma anddiabetes) found in the patients. Chronic paronychia was present in three patients (Cases i, 2 and 4)and in two it was the presenting symptom, although there is no proof that it was the direct resultof H. toruloidea infection.
The patients had been resident in Britain for between 3 and 28 years, and because of the geo-graphical distribution of the fungus it is assumed that the infections were contracted in the patients'countries of origin and had remained undetected for many years. The origins of the patients suggestthat there is a distinct probability that the infection occurs among the populations of Jamaica and theIndian sub-continent, and perhaps wherever the fungus is an indigenous plant pathogen.
The possibility that the infection is transmissible by means of infected skin and nail debris needsinvestigation. Work by one of us (C.K.C.) has shown that infected skin scales kept dry at roots
52 C.K.Campbell et al.
temperature for 6 months still contained viable fungus, so that the potential for the spread of infectionappears to exist.
ACKNOWLEDGMENTS
Our thanks are due to Dr E.A.Fairburn, Dr G.W.Senter and Mr K.E.Haynes, for allowing us toinclude details of patients under their care; to Mr R.P.Pfeiifer and other members of the MRC Uniton the Experimental Pathology of the Skin for technical assistance. We would also like to expressgratitude to Dr C.N.D.Cruickshank and Dr M.A.Cowan for encouragement and advice on themanuscript.
REFERENCES
CALAVAN, E.G. & WALLACE, J . M . (1954) Hendersonula wruloidea Natrass on citrus in California. Phytopathology,44. 635-
ENGLISH, M . P . (1968) Invasion of the skin by filamentous non-dermatophyte fungi, Briiishjouyna! of Dermatology.,80, 282.
GENTLES, J.G. & EVANS, E .G.V. (1970) Infection of the feet and nails with Hendersonula toruloidea. Sabouraudia,8,72.
KURWA, A.R. & GAMPBELL, G.K. (1972) Hendersonula wruloidea infection. British Journal of Dermatology, 86, 98.MEREDITH, I . D . S . (1963) Tip rot of banana fruits in Jamaica. I. Hendersonula wruloidea on dwarf Cavendish
bananas. Transactions of the British Mycological Society, 46, 473.NATRASS, R . M . (1933) A new species of Hendersonula (H. toruloidea) on deciduous trees in Egypt. Transactions
of the British Mycological Society, 18, 189.PARTRIDGE, B .M. (1955) Multiple fungus infections with special reference to their occurrence with the
Trichophyton rubrum syndrome. Transactions and Annual Report of the St John's Hospital DermatologicalSociety, 34, 41.
PAXTON, J . D . & WILSON E . E . (1965) Anatomical and physiological aspects of branch wilt disease of Persianwalnut. Phytopathology, 55, 21.
PUNITHALINGAM, E . & WATERSTON, J.M. (1970) CMl Descriptions of Pathogenic Fungi and Bacteria, No. 274.Commonwealth Mycological Institute, Kew, Surrey,
WALSHE, MARGARET M . & ENGLISH, MARY P. (1966) Fungi in nails, British Journal of Dermatology, 78, 198.ZAIAS, N . , OERTEL, I. & ELLIOTT, D . F . (1969) Fungi in toe adiW^. Journal of Investigative Dermatology, 53, 140.
