fiber-reinforced dermis graft for ventral hernia repair
TRANSCRIPT

Available online at www.sciencedirect.com
www.elsevier.com/locate/jmbbm
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9
http://dx.doi.org/10.1751-6161/& 2014 El
nCorresponding aE-mail addresses:
Research Paper
Fiber-reinforced dermis graft for ventral hernia repair
Sambit Sahooa,n, Katherine R. DeLoziera,b, Rochelle A. Dumma,c,Michael J. Rosend, Kathleen A. Derwina
aDepartment of Biomedical Engineering, ND2-20, Lerner Research Institute, Cleveland Clinic, 9500 Euclid Avenue,Cleveland, OH 44195, USAbDepartment of Biomedical Engineering, University of Akron, Akron, OH 44325, USAcDepartment of Biomedical Engineering, Johns Hopkins University, Baltimore, MD 21218, USAdCase Comprehensive Hernia Center, University Hospitals Case Medical Center, 11100 Euclid Avenue, Cleveland, OH44106, USA
a r t i c l e i n f o
Article history:
Received 21 January 2014
Received in revised form
5 March 2014
Accepted 9 March 2014
Available online 15 March 2014
Keywords:
Abdominal wall repair
Biologic grafts
Enzymatic degradation
Mechanical properties
Biaxial tests
Ball burst tests
1016/j.jmbbm.2014.03.001sevier Ltd. All rights rese
uthor: Tel.: þ1 216 445 [email protected], sambit.
a b s t r a c t
Ventral hernia repair (VHR) continues to be a challenge for surgeons. Poor long-term
durability of the commonly-used human acellular dermal matrix (HADM) grafts often
results in VHR failure and reherniation. We hypothesized that fiber-reinforcement will
improve the mechanical properties of HADM grafts and maintain these properties after
enzymatic degradation. We designed a reinforced HADM (r-HADM) graft comprised of
HADM and a small amount (�10 wt% or 56 g/m2) of 2-0 monofilament polypropylene.
We evaluated the failure and fatigue biomechanics of r-HADM grafts and HADM controls,
before and after 8 h of in vitro enzymatic degradation, in ball-burst and planar biaxial
testing modes (n¼6–11/group/test). Fiber-reinforcement improved time-zero failure prop-
erties of HADM. While enzymatic degradation resulted in a significant reduction in nearly
all mechanical properties and frequent premature failure of HADM, key sub-failure
parameters and cyclic dilatational strain were maintained in r-HADM, with no sample
having premature failure. These data show that fiber-reinforcement improves biomecha-
nical properties and imparts mechanical durability to r-HADM during enzymatic degrada-
tion. Our findings suggest that fiber-reinforcement may be a strategy to mitigate the loss of
HADM graft mechanical properties after in vivo implantation, and thereby limit VHR
bulging and improve outcomes.
& 2014 Elsevier Ltd. All rights reserved.
rved.
39; fax: þ1 216 444 [email protected] (S. Sahoo).
1. Introduction
Incisional hernias occur in nearly one-third of the patientsover two million patients undergoing laparotomies in theUnited States each year (Poulose et al., 2012). These hernias
affect patient quality of life through pain and discomfort andcan also cause life-threatening visceral incarceration andstrangulation. The treatment of incisional hernias is surgicalrepair. An estimated 350,000 ventral hernia repairs (VHR) areperformed annually, involving total healthcare costs of US $3.2
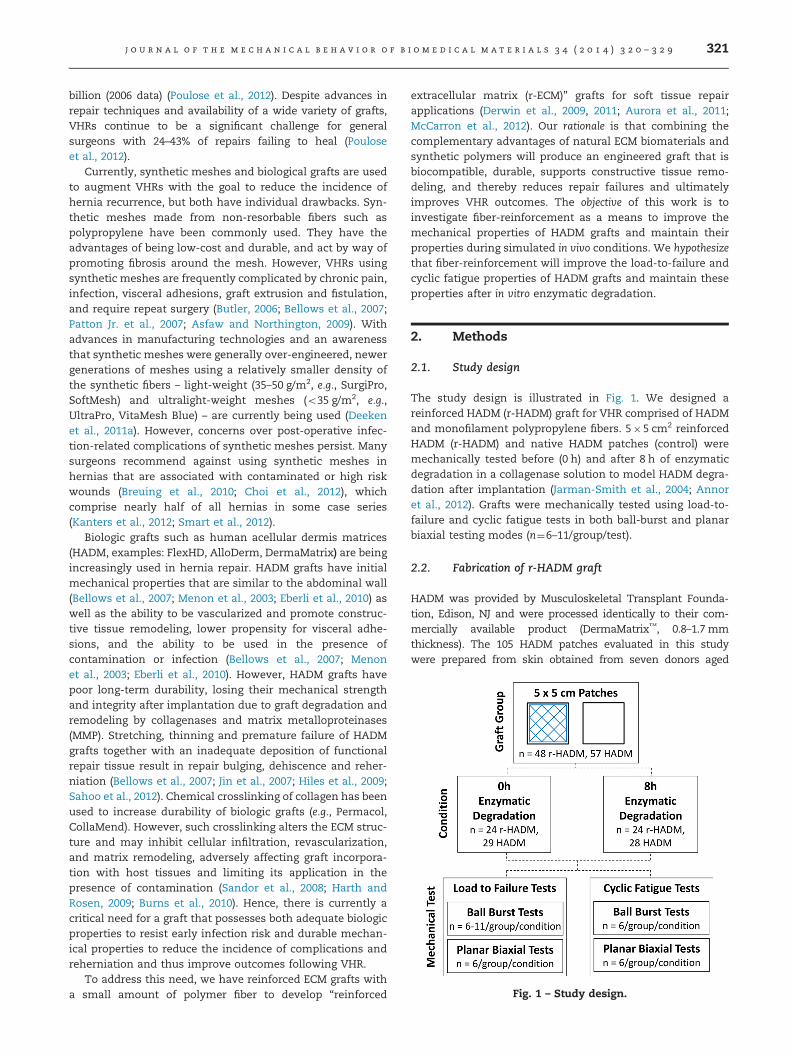
Fig. 1 – Study design.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9 321
billion (2006 data) (Poulose et al., 2012). Despite advances inrepair techniques and availability of a wide variety of grafts,VHRs continue to be a significant challenge for generalsurgeons with 24–43% of repairs failing to heal (Pouloseet al., 2012).
Currently, synthetic meshes and biological grafts are usedto augment VHRs with the goal to reduce the incidence ofhernia recurrence, but both have individual drawbacks. Syn-thetic meshes made from non-resorbable fibers such aspolypropylene have been commonly used. They have theadvantages of being low-cost and durable, and act by way ofpromoting fibrosis around the mesh. However, VHRs usingsynthetic meshes are frequently complicated by chronic pain,infection, visceral adhesions, graft extrusion and fistulation,and require repeat surgery (Butler, 2006; Bellows et al., 2007;Patton Jr. et al., 2007; Asfaw and Northington, 2009). Withadvances in manufacturing technologies and an awarenessthat synthetic meshes were generally over-engineered, newergenerations of meshes using a relatively smaller density ofthe synthetic fibers – light-weight (35–50 g/m2, e.g., SurgiPro,SoftMesh) and ultralight-weight meshes (o35 g/m2, e.g.,UltraPro, VitaMesh Blue) – are currently being used (Deekenet al., 2011a). However, concerns over post-operative infec-tion-related complications of synthetic meshes persist. Manysurgeons recommend against using synthetic meshes inhernias that are associated with contaminated or high riskwounds (Breuing et al., 2010; Choi et al., 2012), whichcomprise nearly half of all hernias in some case series(Kanters et al., 2012; Smart et al., 2012).
Biologic grafts such as human acellular dermis matrices(HADM, examples: FlexHD, AlloDerm, DermaMatrix) are beingincreasingly used in hernia repair. HADM grafts have initialmechanical properties that are similar to the abdominal wall(Bellows et al., 2007; Menon et al., 2003; Eberli et al., 2010) aswell as the ability to be vascularized and promote construc-tive tissue remodeling, lower propensity for visceral adhe-sions, and the ability to be used in the presence ofcontamination or infection (Bellows et al., 2007; Menonet al., 2003; Eberli et al., 2010). However, HADM grafts havepoor long-term durability, losing their mechanical strengthand integrity after implantation due to graft degradation andremodeling by collagenases and matrix metalloproteinases(MMP). Stretching, thinning and premature failure of HADMgrafts together with an inadequate deposition of functionalrepair tissue result in repair bulging, dehiscence and reher-niation (Bellows et al., 2007; Jin et al., 2007; Hiles et al., 2009;Sahoo et al., 2012). Chemical crosslinking of collagen has beenused to increase durability of biologic grafts (e.g., Permacol,CollaMend). However, such crosslinking alters the ECM struc-ture and may inhibit cellular infiltration, revascularization,and matrix remodeling, adversely affecting graft incorpora-tion with host tissues and limiting its application in thepresence of contamination (Sandor et al., 2008; Harth andRosen, 2009; Burns et al., 2010). Hence, there is currently acritical need for a graft that possesses both adequate biologicproperties to resist early infection risk and durable mechan-ical properties to reduce the incidence of complications andreherniation and thus improve outcomes following VHR.
To address this need, we have reinforced ECM grafts witha small amount of polymer fiber to develop “reinforced
extracellular matrix (r-ECM)” grafts for soft tissue repairapplications (Derwin et al., 2009, 2011; Aurora et al., 2011;McCarron et al., 2012). Our rationale is that combining thecomplementary advantages of natural ECM biomaterials andsynthetic polymers will produce an engineered graft that isbiocompatible, durable, supports constructive tissue remo-deling, and thereby reduces repair failures and ultimatelyimproves VHR outcomes. The objective of this work is toinvestigate fiber-reinforcement as a means to improve themechanical properties of HADM grafts and maintain theirproperties during simulated in vivo conditions. We hypothesizethat fiber-reinforcement will improve the load-to-failure andcyclic fatigue properties of HADM grafts and maintain theseproperties after in vitro enzymatic degradation.
2. Methods
2.1. Study design
The study design is illustrated in Fig. 1. We designed areinforced HADM (r-HADM) graft for VHR comprised of HADMand monofilament polypropylene fibers. 5�5 cm2 reinforcedHADM (r-HADM) and native HADM patches (control) weremechanically tested before (0 h) and after 8 h of enzymaticdegradation in a collagenase solution to model HADM degra-dation after implantation (Jarman-Smith et al., 2004; Annoret al., 2012). Grafts were mechanically tested using load-to-failure and cyclic fatigue tests in both ball-burst and planarbiaxial testing modes (n¼6–11/group/test).
2.2. Fabrication of r-HADM graft
HADM was provided by Musculoskeletal Transplant Founda-tion, Edison, NJ and were processed identically to their com-mercially available product (DermaMatrix™, 0.8–1.7 mmthickness). The 105 HADM patches evaluated in this studywere prepared from skin obtained from seven donors aged
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9322
18–55 years, processed as previously described (Eberli et al.,2010), freeze-dried, and packed under aseptic conditions. Sam-ples from at least four unique donors were represented in eachtest group (r-HADM: n¼48; HADM: n¼57). Dry HADM patcheswere trimmed to 5�5 cm2 and their thicknesses were mea-sured at eight locations using a standard caliper. Forty-eightHADM patches were reinforced with USP 2-0 monofilamentpolypropylene fibers (Proxy Biomedical, Cleveland, OH) in across-hatch stitch pattern using a computer-controlled indus-trial sewing machine (Juki AMS 221EN 2516). The pattern wasstitched in a continuous manner with minimal overlap ofstitches to minimize the amount of fiber used in the reinforce-ment. The average polypropylene content in the r-HADM graftswas estimated to be 56 g/cm2 and �10 wt%.
2.3. Graft preparation for mechanical testing
r-HADM and HADM patches were rehydrated in 1� PBS for10 min. Eight peripheral mattress sutures (#2 Fiberwire, Arthrex,Naples, FL) were applied to each patch using a curved reverse-cutting needle, �5–10mm from the edges. The peripheralsutures were tied around a custom frame to create eightuniform suture loops for mechanical testing (15 mm loops forball-burst tests and 45mm loops for planar biaxial tests) (Fig. 2).Interrupted mattress sutures were used to fix the grafts formechanical testing, instead of perfect clamping in grips, tosimulate the in vivo fixation method used for ventral herniagrafts (Bellows et al., 2007; Jin et al., 2007; Lee et al., 2009).
2.4. In vitro enzyme degradation
Twenty-four r-HADM and 28 HADM patches with pre-attached peripheral sutures were digested in a collagenasesolution to simulate in vivo degradation of the collagenousgrafts. Each graft was digested in 100 ml of 21 U/ml collage-nase solution (Collagenase Type 2, Worthington Biochemical,Lakewood, NJ) at 37 1C for 8 h under constant agitation.
2.5. Load-to-failure properties of r-HADM and HADMpatches
r-HADM and native HADM patches, with and without enzy-matic degradation, were mechanically tested by load-to-failure tests in both ball-burst and planar biaxial testingmodes. Since both ball-burst and planar biaxial tests are used
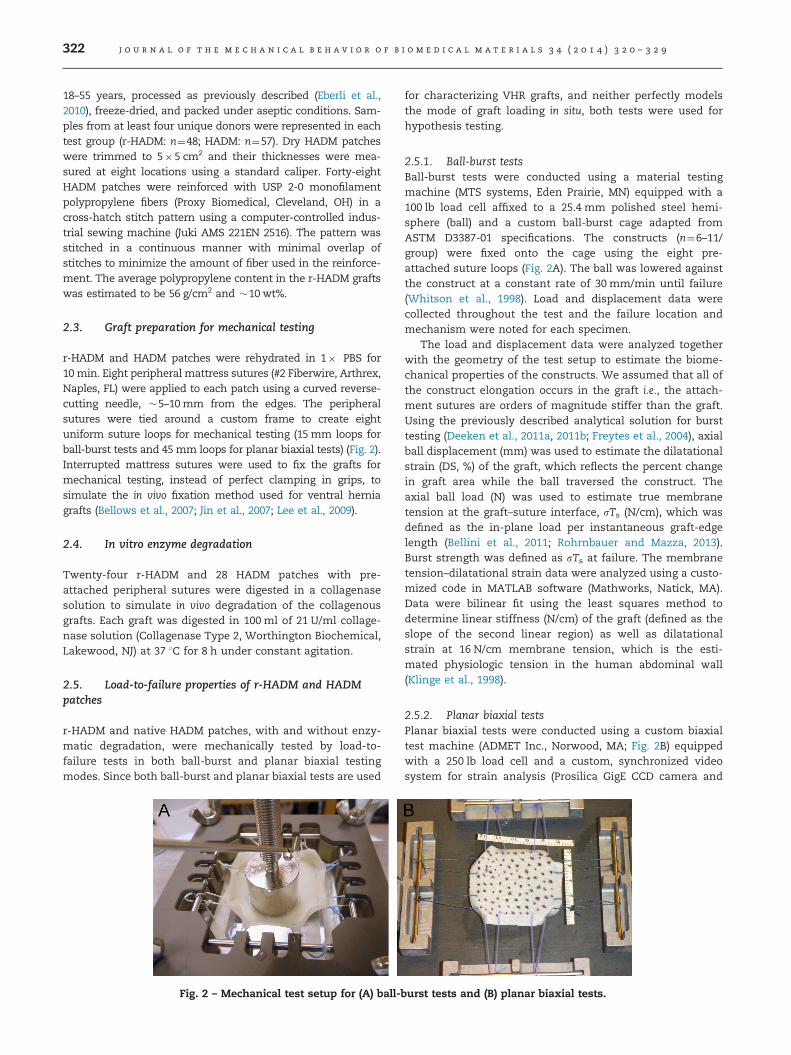
Fig. 2 – Mechanical test setup for (A) ball-
for characterizing VHR grafts, and neither perfectly modelsthe mode of graft loading in situ, both tests were used forhypothesis testing.
2.5.1. Ball-burst testsBall-burst tests were conducted using a material testingmachine (MTS systems, Eden Prairie, MN) equipped with a100 lb load cell affixed to a 25.4 mm polished steel hemi-sphere (ball) and a custom ball-burst cage adapted fromASTM D3387-01 specifications. The constructs (n¼6–11/group) were fixed onto the cage using the eight pre-attached suture loops (Fig. 2A). The ball was lowered againstthe construct at a constant rate of 30 mm/min until failure(Whitson et al., 1998). Load and displacement data werecollected throughout the test and the failure location andmechanism were noted for each specimen.
The load and displacement data were analyzed togetherwith the geometry of the test setup to estimate the biome-chanical properties of the constructs. We assumed that all ofthe construct elongation occurs in the graft i.e., the attach-ment sutures are orders of magnitude stiffer than the graft.Using the previously described analytical solution for bursttesting (Deeken et al., 2011a, 2011b; Freytes et al., 2004), axialball displacement (mm) was used to estimate the dilatationalstrain (DS, %) of the graft, which reflects the percent changein graft area while the ball traversed the construct. Theaxial ball load (N) was used to estimate true membranetension at the graft–suture interface, sTs (N/cm), which wasdefined as the in-plane load per instantaneous graft-edgelength (Bellini et al., 2011; Rohrnbauer and Mazza, 2013).Burst strength was defined as sTs at failure. The membranetension–dilatational strain data were analyzed using a custo-mized code in MATLAB software (Mathworks, Natick, MA).Data were bilinear fit using the least squares method todetermine linear stiffness (N/cm) of the graft (defined as theslope of the second linear region) as well as dilatationalstrain at 16 N/cm membrane tension, which is the esti-mated physiologic tension in the human abdominal wall(Klinge et al., 1998).
2.5.2. Planar biaxial testsPlanar biaxial tests were conducted using a custom biaxialtest machine (ADMET Inc., Norwood, MA; Fig. 2B) equippedwith a 250 lb load cell and a custom, synchronized videosystem for strain analysis (Prosilica GigE CCD camera and
burst tests and (B) planar biaxial tests.

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9 323
StreamPix videometric tracking system). The constructs(n¼6/group) were fixed onto the test fixtures using the eightpre-attached suture loops. The graft surface was sprayedwith black enamel paint to create a speckled pattern neededfor optical surface strain analysis. The constructs wereequibiaxially preloaded to 1 N, followed by equibiaxial load-ing at 150 N/min to failure. Load and image data werecollected throughout the test, and the failure location andmechanism were noted for each specimen.
Load and image data were analyzed together to determinethe biaxial biomechanical properties of the graft. For strainanalysis, all test images were analyzed using an incrementaldigital image correlation technique (DIC, Vic-2D software,Correlated Solutions, Inc., Columbia, SC) to determine localLagrangian strains (Exx and Eyy; Fig. 3), which were averagedover the graft portion of the construct (defined by the suturefixation points) to calculate the graft biaxial strains. The graftbiaxial strains were then converted to graft principal strains(E11 and E22). Finally, the dilatational strain (DS, %) of thegraft, reflecting the percent change in graft area, was calcu-lated from the sum of the graft principal strains (E11þE22)(Willems et al., 2008). The true membrane tension at thegraft–suture interface (N/cm) was estimated from the ratio ofthe biaxial load per the instantaneous graft-edge length(Bellini et al., 2011; Rohrnbauer and Mazza, 2013). While thegraft portion of the construct was initially square-shaped,concentrated loading of the constructs at suture fixationpoints caused the graft to deform into complex shapes (asshown in Fig. 3), such that edge lengths could not be mean-ingfully defined or measured. Therefore, we made the sim-plifying assumption of a square shape of the deformed graftand approximated the effective instantaneous graft-edgelength as the square root of the area of the deformed graft.The linear stiffness of the graft and the dilatational strain at16 N/cm membrane tension were calculated from a bilinearfit of the membrane tension and dilatational strain data asdescribed in ball-burst test analysis (Section 2.5.1). Themembrane tension and dilatational strain at failure werereported. The degree of mechanical anisotropy of the graft(Anisotropy Index) was calculated from the ratio of the
Fig. 3 – Representative local strain maps during planar biaxial lincrease in local Lagrangian strains (Exx and Eyy) with biaxial lo
difference in principal strains to the mean principal strainat failure [(E11�E22)/0.5(E11þE22)] (Langdon et al., 1999).
2.6. Cyclic fatigue properties of HADM and r-HADMpatches
r-HADM and native HADM patches, with and without enzy-matic degradation, were mechanically tested through 1000cycles of estimated physiologic load (Eliason et al., 2011), inboth ball-burst and planar biaxial testing modes. The graftswere kept moistened during the test using PBS for the 0 hgrafts or collagenase solution for the 8 h grafts.
2.6.1. Ball-burst testsCyclic ball-burst tests were conducted using the custom ball-burst test fixture described in Section 2.5.1. Constructs (n¼6/group) were preloaded to 10 N and cyclically loaded between10 and 80 N for 1000 cycles at 0.25 Hz. Eighty Newtons is theestimated physiologic load on a 5�5 cm2 graft, based on16 N/cm physiologic membrane tension in the abdominalwall (Klinge et al., 1998). The location and mechanism offailure, if any, were noted for each specimen. Dilatationalstrain (DS, %) of the graft after cyclic fatigue tests wascalculated from the axial ball displacement as in load-to-failure test analysis. The cumulative dilatational strain of thegraft was determined at the 10 N preload (DS0) and at the 10 Nvalley following each cycle (DSn). Dilatational strain data fromcycles 0, 1, 10, 100 and 1000 were compared across groups.
2.6.2. Planar biaxial testsCyclic planar biaxial tests were conducted using the ADMETbiaxial test machine described in Section 2.5.2. Constructs(n¼6/group) were equibiaxially preloaded to 5 N and cycli-cally and equibiaxially loaded between 5 and 40 N for 1000cycles at 120 mm/min. This loading regimen was chosenbecause it resulted in similar graft dilatational strain and testduration in the control group (0 h HADM) as the cyclic ball-burst tests. The location and mechanism of failure, if any,were noted for each specimen. Image data were analyzed asin load-to-failure biaxial tests to determine the dilatational
oad-to-failure testing of an HADM patch show the expectedading at: (A) 1 N preload and (B and C) at failure.
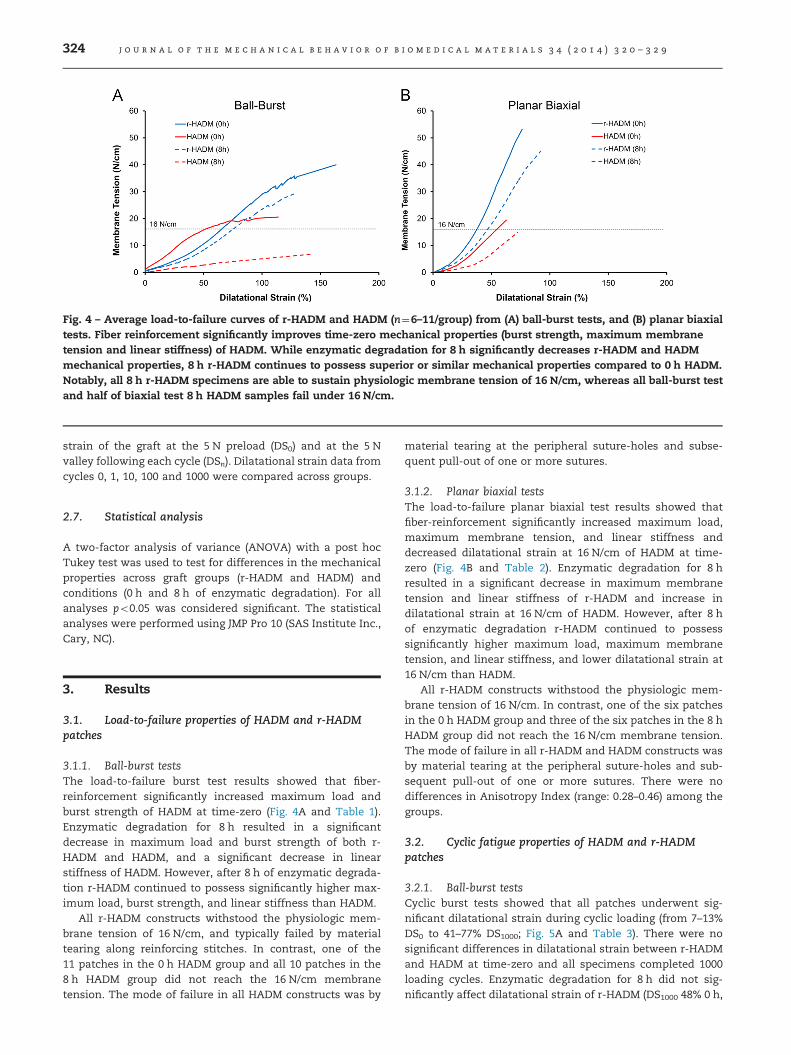
Fig. 4 – Average load-to-failure curves of r-HADM and HADM (n¼6–11/group) from (A) ball-burst tests, and (B) planar biaxialtests. Fiber reinforcement significantly improves time-zero mechanical properties (burst strength, maximum membranetension and linear stiffness) of HADM. While enzymatic degradation for 8 h significantly decreases r-HADM and HADMmechanical properties, 8 h r-HADM continues to possess superior or similar mechanical properties compared to 0 h HADM.Notably, all 8 h r-HADM specimens are able to sustain physiologic membrane tension of 16 N/cm, whereas all ball-burst testand half of biaxial test 8 h HADM samples fail under 16 N/cm.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9324
strain of the graft at the 5 N preload (DS0) and at the 5 Nvalley following each cycle (DSn). Dilatational strain data fromcycles 0, 1, 10, 100 and 1000 were compared across groups.
2.7. Statistical analysis
A two-factor analysis of variance (ANOVA) with a post hocTukey test was used to test for differences in the mechanicalproperties across graft groups (r-HADM and HADM) andconditions (0 h and 8 h of enzymatic degradation). For allanalyses po0.05 was considered significant. The statisticalanalyses were performed using JMP Pro 10 (SAS Institute Inc.,Cary, NC).
3. Results
3.1. Load-to-failure properties of HADM and r-HADMpatches
3.1.1. Ball-burst testsThe load-to-failure burst test results showed that fiber-reinforcement significantly increased maximum load andburst strength of HADM at time-zero (Fig. 4A and Table 1).Enzymatic degradation for 8 h resulted in a significantdecrease in maximum load and burst strength of both r-HADM and HADM, and a significant decrease in linearstiffness of HADM. However, after 8 h of enzymatic degrada-tion r-HADM continued to possess significantly higher max-imum load, burst strength, and linear stiffness than HADM.
All r-HADM constructs withstood the physiologic mem-brane tension of 16 N/cm, and typically failed by materialtearing along reinforcing stitches. In contrast, one of the11 patches in the 0 h HADM group and all 10 patches in the8 h HADM group did not reach the 16 N/cm membranetension. The mode of failure in all HADM constructs was by
material tearing at the peripheral suture-holes and subse-quent pull-out of one or more sutures.
3.1.2. Planar biaxial testsThe load-to-failure planar biaxial test results showed thatfiber-reinforcement significantly increased maximum load,maximum membrane tension, and linear stiffness anddecreased dilatational strain at 16 N/cm of HADM at time-zero (Fig. 4B and Table 2). Enzymatic degradation for 8 hresulted in a significant decrease in maximum membranetension and linear stiffness of r-HADM and increase indilatational strain at 16 N/cm of HADM. However, after 8 hof enzymatic degradation r-HADM continued to possesssignificantly higher maximum load, maximum membranetension, and linear stiffness, and lower dilatational strain at16 N/cm than HADM.
All r-HADM constructs withstood the physiologic mem-brane tension of 16 N/cm. In contrast, one of the six patchesin the 0 h HADM group and three of the six patches in the 8 hHADM group did not reach the 16 N/cm membrane tension.The mode of failure in all r-HADM and HADM constructs wasby material tearing at the peripheral suture-holes and sub-sequent pull-out of one or more sutures. There were nodifferences in Anisotropy Index (range: 0.28–0.46) among thegroups.
3.2. Cyclic fatigue properties of HADM and r-HADMpatches
3.2.1. Ball-burst testsCyclic burst tests showed that all patches underwent sig-nificant dilatational strain during cyclic loading (from 7–13%DS0 to 41–77% DS1000; Fig. 5A and Table 3). There were nosignificant differences in dilatational strain between r-HADMand HADM at time-zero and all specimens completed 1000loading cycles. Enzymatic degradation for 8 h did not sig-nificantly affect dilatational strain of r-HADM (DS1000 48% 0 h,

Table 1 – Load-to-failure results from ball-burst tests showing the effect of enzymatic degradation on r-HADM and HADM.
Time zero (0 h) Collagenase (8 h)
r-HADM (n¼6) HADM (n¼11) r-HADM (n¼6) HADM (n¼10)
Max load (N) 723782a 311766a 4707129a 115751a
Burst strength (N/cm) 40.073.5b 20.674.3b 29.277.5b 6.873.0b
Dilatational strain (%) at burst 163.3724.5c,d 114.0713.3c,e 127.5710.6d 142.5723.2e
Linear stiffness (N/cm) 43.677.3 37.977.9f 34.377.4g 9.575.1f,g
Dilatational strain (%) at 16 N/cm 66.5710.0 52.3715.6h,n 80.2717.2h n
a–hSimilar superscript letters indicate a significant difference between groups (po0.05).*One of 11 patches in the 0 h HADM group and 10 of 10 patches in the 8 h HADM group did not reach the physiologic membrane tension of16 N/cm.
Table 2 – Load-to-failure results from planar biaxial tests showing the effect of enzymatic degradation on r-HADMand HADM.
Time zero (0 h) Collagenase (8 h)
r-HADM (n¼6) HADM (n¼6) r-HADM (n¼6) HADM (n¼6)
Max load (N) 270723a 106738a,b 236731b,c 85742c
Max membrane tension (N/cm) 53.273.2d,e 19.475.4d 45.074.5d,e 14.876.3e
Dilatational strain (%) at failure 76.3717.0 62.7720.9 92.1716.7 72.4725.5Linear stiffness (N/cm) 112.8721.2f,g 50.7714.3f 76.476.7f,g 35.4713.6g
Dilatational strain (%) at 16 N/cm 37.675.5h 53.7710.4h,i,n 46.875.2j 76.478.8i,j,n
Anisotropy Index 0.3770.29 0.4670.33 0.2870.14 0.4570.20
a–jSimilar superscript letters indicate a significant difference between groups (po0.05).*One of six patches in the 0 h HADM group and three of six patches in the 8 h HADM group did not reach the physiologic membrane tension of16 N/cm.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9 325
63% 8 h), and all six 8 h r-HADM specimens completed 1000cycles. In contrast, there was a significant increase in dilata-tional strain of HADM (DS1000 41% 0 h, 77% 8 h), and one of six8 h HADM specimens failed before 1000 cycles. After 8 h ofenzymatic degradation, differences in dilatational strainbetween r-HADM and HADM did not reach the level ofstatistical significance.
3.2.2. Planar biaxial testsPlanar biaxial cyclic tests showed that all patches underwentsignificant dilatational strain during cyclic loading (from 6–13% DS0 to 27–67% DS1000; Fig. 5B and Table 4). There were nosignificant differences in dilatational strain between r-HADMand HADM at time-zero and all specimens completed 1000loading cycles. Enzymatic degradation for 8 h did not sig-nificantly affect dilatational strain of r-HADM (DS1000 27% 0 h,42% 8 h), and all six 8 h r-HADM specimens completed 1000cycles. In contrast, there was a significant increase in dilata-tional strain of HADM (DS1000 36% 0 h, 67% 8 h), with five ofsix specimens failing before 1000 cycles. After 8 h of enzy-matic degradation, r-HADM had significantly lower cyclicdilatational strain than HADM.
4. Discussion
The objective of this work was to investigate fiber-reinforcement as a means to improve and maintain themechanical properties of HADM during simulated in vivoconditions. To that end, we reinforced HADM with small
amounts (�10 wt% or 56 g/m2) of monofilament polypropy-lene fiber, and evaluated the failure and fatigue biomechanicsof r-HADM and HADM grafts before and after in vitro enzy-matic degradation. As hypothesized, load-to-failure resultsfrom both ball-burst and planar biaxial tests showed thatfiber-reinforcement improved time-zero mechanical proper-
ties of HADM. The load-to-failure properties of r-HADM were
mostly though not fully maintained after enzymatic degrada-
tion for 8 h. Importantly, r-HADM continued to possess
significantly superior mechanical properties (in terms of
maximum load, burst strength, maximum membrane ten-
sion, linear stiffness, and dilatational strain at 16 N/cm)
compared to HADM after 8 h of enzymatic degradation.
Furthermore, 8 h r-HADM possessed significantly higher
maximum load, burst strength, and maximum membrane
tension compared to 0 h HADM. Notably, while a portion of
the 0 h and 8 h HADM constructs failed before reaching the
physiologic membrane tension of 16 N/cm, all 0 h and 8 h
r-HADM constructs withstood the tension.In contrast to load-to-failure properties, fiber-reinforcement
showed no significant effect on cyclic fatigue properties ofHADM at time-zero (contrary to our hypothesis). Yet after8 h of enzymatic digestion, the cyclic fatigue properties ofr-HADM were maintained (supporting our hypothesis)whereas the properties of HADM were significantly reduced.A portion of the 8 h HADM constructs failed before reach-ing 1000 cycles whereas all 8 h r-HADM specimens com-pleted 1000 cycles. Under cyclic biaxial loading, thedilatational strain of 8 h r-HADM was significantly lowerthan 8 h HADM. Furthermore, the dilatational strain of 8 h
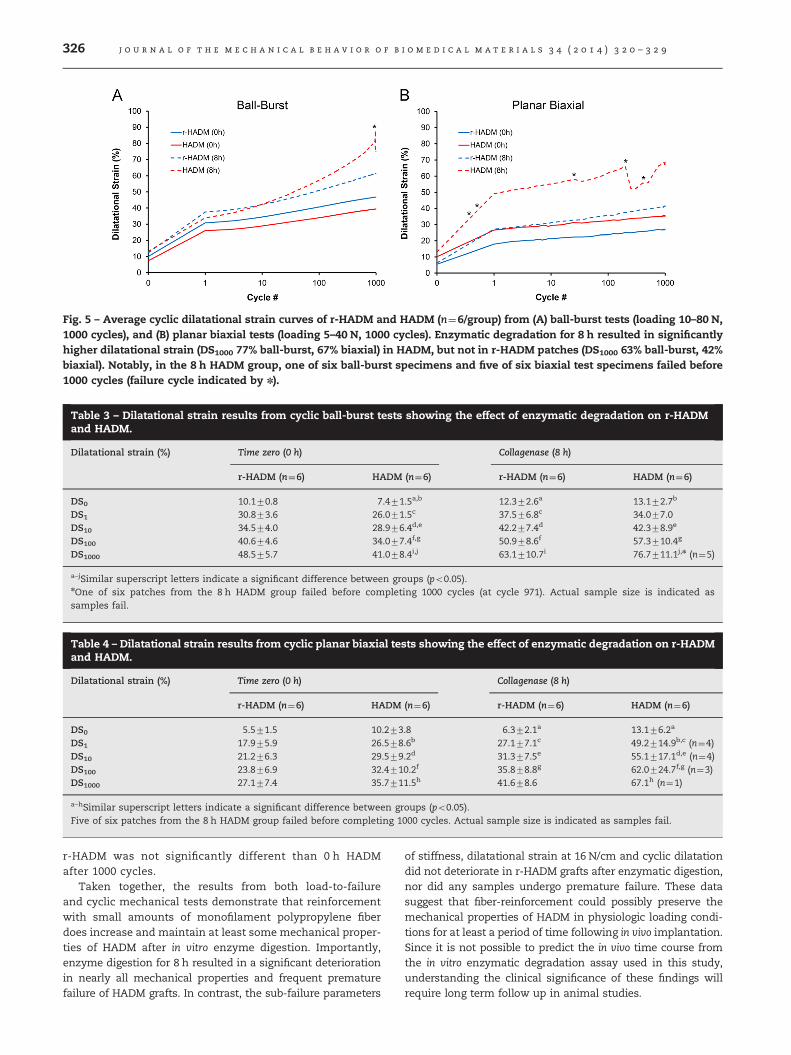
Fig. 5 – Average cyclic dilatational strain curves of r-HADM and HADM (n¼6/group) from (A) ball-burst tests (loading 10–80 N,1000 cycles), and (B) planar biaxial tests (loading 5–40 N, 1000 cycles). Enzymatic degradation for 8 h resulted in significantlyhigher dilatational strain (DS1000 77% ball-burst, 67% biaxial) in HADM, but not in r-HADM patches (DS1000 63% ball-burst, 42%biaxial). Notably, in the 8 h HADM group, one of six ball-burst specimens and five of six biaxial test specimens failed before1000 cycles (failure cycle indicated by n).
Table 3 – Dilatational strain results from cyclic ball-burst tests showing the effect of enzymatic degradation on r-HADMand HADM.
Dilatational strain (%) Time zero (0 h) Collagenase (8 h)
r-HADM (n¼6) HADM (n¼6) r-HADM (n¼6) HADM (n¼6)
DS0 10.170.8 7.471.5a,b 12.372.6a 13.172.7b
DS1 30.873.6 26.071.5c 37.576.8c 34.077.0DS10 34.574.0 28.976.4d,e 42.277.4d 42.378.9e
DS100 40.674.6 34.077.4f,g 50.978.6f 57.3710.4g
DS1000 48.575.7 41.078.4i,j 63.1710.7i 76.7711.1j,n (n¼5)
a–jSimilar superscript letters indicate a significant difference between groups (po0.05).nOne of six patches from the 8 h HADM group failed before completing 1000 cycles (at cycle 971). Actual sample size is indicated assamples fail.
Table 4 – Dilatational strain results from cyclic planar biaxial tests showing the effect of enzymatic degradation on r-HADMand HADM.
Dilatational strain (%) Time zero (0 h) Collagenase (8 h)
r-HADM (n¼6) HADM (n¼6) r-HADM (n¼6) HADM (n¼6)
DS0 5.571.5 10.273.8 6.372.1a 13.176.2a
DS1 17.975.9 26.578.6b 27.177.1c 49.2714.9b,c (n¼4)DS10 21.276.3 29.579.2d 31.377.5e 55.1717.1d,e (n¼4)DS100 23.876.9 32.4710.2f 35.878.8g 62.0724.7f,g (n¼3)DS1000 27.177.4 35.7711.5h 41.678.6 67.1h (n¼1)
a–hSimilar superscript letters indicate a significant difference between groups (po0.05).Five of six patches from the 8 h HADM group failed before completing 1000 cycles. Actual sample size is indicated as samples fail.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9326
r-HADM was not significantly different than 0 h HADMafter 1000 cycles.
Taken together, the results from both load-to-failureand cyclic mechanical tests demonstrate that reinforcementwith small amounts of monofilament polypropylene fiberdoes increase and maintain at least some mechanical proper-ties of HADM after in vitro enzyme digestion. Importantly,enzyme digestion for 8 h resulted in a significant deteriorationin nearly all mechanical properties and frequent prematurefailure of HADM grafts. In contrast, the sub-failure parameters
of stiffness, dilatational strain at 16 N/cm and cyclic dilatationdid not deteriorate in r-HADM grafts after enzymatic digestion,nor did any samples undergo premature failure. These datasuggest that fiber-reinforcement could possibly preserve themechanical properties of HADM in physiologic loading condi-tions for at least a period of time following in vivo implantation.Since it is not possible to predict the in vivo time course fromthe in vitro enzymatic degradation assay used in this study,understanding the clinical significance of these findings willrequire long term follow up in animal studies.

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9 327
We tested the r-HADM and HADM grafts in a patchgeometry by way of sutures to model the manner in whichthe grafts are applied and loaded clinically for ventral herniarepair. While clinically relevant, testing by way of suturesconcentrates the load at distinct points rather than evenlydistributing it along the graft-edge. Therefore, the membranetension is in fact highly non-uniform, and the estimatedmembrane tension which we report is more of an effective oraveraged parameter that is useful for making comparisonsamong groups or test modalities. Likewise, since failureoccurs at the points of suture loading, failure load has aclinical interpretation but no real meaning in relation tomaterial properties of the graft itself. Furthermore, we per-formed both load-to-failure and cyclic fatigue tests, extract-ing both failure and sub-failure mechanical properties suchas graft dilatation at low physiologic loads (16 N/cm) andlinear stiffness. Sub-failure mechanical properties are morerelevant to define the functional and clinical efficacy of graftsthan their failure properties (Sahoo et al., 2012; Yoder andElliott, 2010). We believe that the results using these testmethods and outcomes are likely to be more readily extra-polated to the clinical scenario than biomechanical data fromthe more common uniaxial strip tests of perfectly clampedspecimens.
We also tested the r-HADM and HADM grafts using ball-burst and planar biaxial tests, again, to model the manner inwhich the grafts are applied and loaded clinically for ventralhernia repair. Ball-burst tests constrain the graft edges whileapplying an orthogonal load to the central portion of thegraft, whereas the planar biaxial test applies in-plane loadingto the graft edges. Burst tests require membrane tension anddilatational strain in the graft to be estimated analyticallyfrom axial ball load and displacements, whereas these out-comes are estimated directly from biaxial load and opticalstrains in planar biaxial tests. Planar biaxial tests also havethe advantage of investigating anisotropic behavior of thegraft which could be relevant in VHR (Anurov et al., 2012). Forexample, our planar biaxial test results showed that HADMpossesses a low degree of mechanical anisotropy that wasnot significantly altered by fiber-reinforcement. While eachtest mode offers unique advantages and disadvantages, andneither is entirely physiologic, both tests provided the sameconclusion regarding hypothesis testing.
Since poor mechanical durability of HADM is the predo-minant cause of VHR failure with HADM grafts, our findingssuggest that fiber-reinforcement may be a strategy to miti-gate the loss of graft mechanical properties after in vivoimplantation, and thereby limit repair bulging and improveoutcomes. Prevention of premature failure and reduced cyclicdilatation after enzymatic degradation of r-HADM graftscould translate to reduced failure (true recurrence) or bulging(functional recurrence) of the ventral hernia repair. Severalseries have reported unacceptably high failure rates of brid-ging repairs of VHR with biologic grafts (Smart et al., 2012; Jinet al., 2007; Blatnik et al., 2008; Alaedeen et al., 2007; Candageet al., 2008; Shankaran et al., 2011), suggesting that biologicgrafts should not be used routinely as a bridge. However, incertain clinical scenarios as in large hernia defects, the fasciacannot be re-approximated and a bridged repair is necessary.While repairs with fascial closure experience physiologic
loads of 16 N/cm, a bridged repair is estimated to experiencea two-fold higher load of 32 N/cm (Klosterhalfen et al., 2005;Bringman et al., 2010). The load-to-failure results from thisstudy show that r-HADM continues to possess biomechanicalproperties adequate for such repairs even after enzymaticdigestion. Therefore in situations when a bridged repair isnecessary and a synthetic mesh is felt to be contraindicated,an r-HADM graft may provide a viable solution.
Fiber-reinforcement improved time-zero mechanical prop-erties of HADM and changed the failure mode from suturepull-out at relatively low loads (HADM) to tearing along innerreinforcing stitches or suture pull-out at high loads (r-HADM).These results suggest that fiber-reinforcement improvesr-HADM biomechanics by (i) load-sharing between ECMand stitched fiber in the composite graft, (ii) load-transferalong the reinforcement pattern resulting in a more uniformload distribution across the graft, and (iii) mitigatingstress-concentration in ECM at sutures and improving sutureretention strength. That fiber-reinforcement improvessuture-retention properties of HADM was confirmed in asupplementary study. 1.5�4.5 cm2 r-HADM strips reinforcedwith 2-0 polypropylene fiber possessed significantly highersuture-retention load compared to HADM at time-zero(154719.8 N versus 64.379.7 N, po0.05), and continued topossess significantly higher suture-retention load comparedto HADM after 8 h of enzymatic degradation (111712.4 Nversus 52.377.1 N, po0.05). We specifically investigatedmonofilament polypropylene and HADM in this studybecause these are commonly-used materials for ventralhernia repair devices. However, we expect that the reinfor-cing concept could provide the same advantages to otherallograft and xenograft ECMs, with select fibers and/or rein-forcing patterns, to design reinforced ECM scaffolds forvarious soft tissue repair applications (Derwin et al., 2009;Aurora et al., 2011). Furthermore, fiber-reinforcement reducedthe wide variability in dermis mechanical properties, aninherent feature of biologic materials (Smart et al., 2012).For example, the coefficient of variation of maximum mem-brane tension in biaxial tests dropped from 28% and 43% (0 hand 8 h HADM) to 6% and 10% respectively. Reduced varia-bility in mechanical properties could translate to morepredictable and consistent repair outcomes with biologicgrafts.
The study is not without limitations. First, the 5�5 cm2
graft size used in the study is on the lower range of sizescommonly used hernia repair. While we chose this size forproof-of-concept and its appropriateness for standard bursttest fixtures, the reinforcing technology could be easilyscaled-up to create larger grafts. Second, we used a singleECM graft material (HADM) to manufacture the r-HADM graft,and results from this study should be extrapolated to otherECM scaffolds with caution. Furthermore, caution should beexercised when comparing our data with results from otherstudies that used different test methods, e.g., uniaxial striptests or ball-burst tests with perfectly-clamped specimens.Third, the in vitro degradation assay with an arbitrary col-lagenase concentration and a single time-point simulates butdoes not accurately represent in vivo conditions follow-ing implantation, or allow for the effects of graft remodelingto be measured. Hence, the results reported herein should be

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9328
interpreted as proof-of-concept and would need to be con-firmed using an in vivo animal model. Finally, the implicationthat a reinforced HADM graft would perform well in abridging and/or contaminated clinical situation will have tobe confirmed in animal studies.
In conclusion, this study shows that reinforcement ofdermis with small amounts (�10 wt% or 56 g/m2) of mono-filament polypropylene fiber improves biomechanical proper-ties and imparts mechanical durability to r-HADM duringenzymatic degradation. In an ongoing work using a ventralhernia repair model in the minipig, we are investigating theextent to which repair with r-HADM improves VHR outcomescompared to repair with HADM. We expect the r-HADM graftto largely maintain its mechanical properties after in vivoimplantation, and thereby limit repair bulging and supportconstructive tissue remodeling at the repair site. By reducingthe incidence of complications and reherniation after VHR,r-HADM would significantly improve morbidity and quality oflife for the many patients with this debilitating condition.
Acknowledgments
We thank Ahmet Erdemir, Ph.D., for consultation on thebiomechanical data analysis and interpretation. HADM wasdonated by Musculoskeletal Transplant Foundation. Fundingwas provided by the Armed Forces Institute of RegenerativeMedicine (W81XWH-08-2-0034). The U.S. Army MedicalResearch Acquisition Activity, 820 Chandler Street, FortDetrick, MD 21702-5014 is the awarding and administeringacquisition office for the last source of funding listed. Thecontent of the manuscript does not necessarily reflect theposition or the policy of the Government, and no officialendorsement should be inferred.
r e f e r e n c e s
Alaedeen, D.I., Lipman, J., Medalie, D., Rosen, M.J., 2007. Thesingle-staged approach to the surgical management ofabdominal wall hernias in contaminated fields. Hernia 11 (1),41–45.
Annor, A.H., Tang, M.E., Pui, C.L., Ebersole, G.C., Frisella, M.M.,Matthews, B.D., Deeken, C.R., 2012. Effect of enzymaticdegradation on the mechanical properties of biological scaffoldmaterials. Surg. Endosc. 26 (10), 2767–2778.
Anurov, M.V., Titkova, S.M., Oettinger, A.P., 2012. Biomechanicalcompatibility of surgical mesh and fascia being reinforced:dependence of experimental hernia defect repair results onanisotropic surgical mesh positioning. Hernia 16 (2), 199–210.
Asfaw, T.S., Northington, G., 2009. Synthetic and biological graftmaterials: biological concepts. Semin. Colon Rectal Surg. 20(3), 112–117.
Aurora, A., Mesiha, M., Tan, C.D., Walker, E., Sahoo, S., Iannotti, J.P., McCarron, J.A., Derwin, K.A., 2011. Mechanicalcharacterization and biocompatibility of a novel reinforcedfascia patch for rotator cuff repair. J. Biomed. Mater. Res. A 99(2), 221–230.
Bellows, C.F., Albo, D., Berger, D.H., Awad, S.S., 2007. Abdominalwall repair using human acellular dermis. Am. J. Surg. 194 (2),192–198.
Bellini, C., Glass, P., Sitti, M., Di Martino, E.S., 2011. Biaxialmechanical modeling of the small intestine. J. Mech. Behav.Biomed. Mater. 4 (8), 1727–1740.
Blatnik, J., Jin, J., Rosen, M., 2008. Abdominal hernia repair withbridging acellular dermal matrix – an expensive hernia sac.Am. J. Surg. 196 (1), 47–50.
Breuing, K., Butler, C.E., Ferzoco, S., Franz, M., Hultman, C.S.,Kilbridge, J.F., Rosen, M., Silverman, R.P., Vargo, D., 2010.Incisional ventral hernias: review of the literature andrecommendations regarding the grading and technique ofrepair. Surgery 148 (3), 544–558.
Bringman, S., Conze, J., Cuccurullo, D., Deprest, J., Junge, K.,Klosterhalfen, B., Parra-Davila, E., Ramshaw, B., Schumpelick,V., 2010. Hernia repair: the search for ideal meshes. Hernia 14(1), 81–87.
Burns, N.K., Jaffari, M.V., Rios, C.N., Mathur, A.B., Butler, C.E.,2010. Non-cross-linked porcine acellular dermal matrices forabdominal wall reconstruction. Plast. Reconstr. Surg. 125 (1),167–176.
Butler, C.E., 2006. The role of bioprosthetics in abdominal wallreconstruction. Clin. Plast. Surg. 33 (2), 199–211 (v–vi).
Candage, R., Jones, K., Luchette, F.A., Sinacore, J.M., Vandevender,D., Reed II, R.L., 2008. Use of human acellular dermal matrixfor hernia repair: friend or foe?. Surgery 144 (4), 703–709(discussion 709–11).
Choi, J.J., Palaniappa, N.C., Dallas, K.B., Rudich, T.B., Colon, M.J.,Divino, C.M., 2012. Use of mesh during ventral hernia repair inclean-contaminated and contaminated cases: outcomes of33,832 cases. Ann. Surg. 255 (1), 176–180.
Deeken, C.R., Abdo, M.S., Frisella, M.M., Matthews, B.D., 2011a.Physicomechanical evaluation of polypropylene, polyester,and polytetrafluoroethylene meshes for inguinal herniarepair. J. Am. Coll. Surg. 212 (1), 68–79.
Deeken, C.R., Melman, L., Jenkins, E.D., Greco, S.C., Frisella, M.M.,Matthews, B.D., 2011b. Histologic and biomechanicalevaluation of crosslinked and non-crosslinked biologicmeshes in a porcine model of ventral incisional hernia repair.J. Am. Coll. Surg. 212 (5), 880–888.
Derwin, K.A., Aurora, A., Iannotti, J.P., McCarron, J.A., 2009.Cleveland Clinic Foundation, assignee. Reinforced TissueGraft. PCT/US2009/038570; US 2011/0014153 A1; US 12/934791.
Derwin, K.A., Iannotti, J.P., Sahoo, S., 2011. Cleveland ClinicFoundation, assignee. Reinforced Tissue Graft. US 2013/0053961 A1; US 13/663938.
Eberli, D., Rodriguez, S., Atala, A., Yoo, J.J., 2010. In vivo evaluationof acellular human dermis for abdominal wall repair. J.Biomed. Mater. Res. A 93 (4), 1527–1538.
Eliason, B.J., Frisella, M.M., Matthews, B.D., Deeken, C.R., 2011. Effectof repetitive loading on the mechanical properties of synthetichernia repair materials. J. Am. Coll. Surg. 213 (3), 430–435.
Freytes, D.O., Badylak, S.F., Webster, T.J., Geddes, L.A., Rundell, A.E., 2004. Biaxial strength of multilaminated extracellularmatrix scaffolds. Biomaterials 25 (12), 2353–2361.
Harth, K.C., Rosen, M.J., 2009. Major complications associatedwith xenograft biologic mesh implantation in abdominal wallreconstruction. Surg. Innov. 16 (4), 324–329.
Hiles, M., Record Ritchie, R.D., Altizer, A.M., 2009. Are biologicgrafts effective for hernia repair? A systematic review of theliterature. Surg. Innov. 16 (1), 26–37.
Jarman-Smith, M.L., Bodamyali, T., Stevens, C., Howell, J.A.,Horrocks, M., Chaudhuri, J.B., 2004. Porcine collagencrosslinking, degradation and its capability for fibroblastadhesion and proliferation. J. Mater. Sci. Mater. Med. 15 (8),925–932.
Jin, J., Rosen, M.J., Blatnik, J., McGee, M.F., Williams, C.P., Marks, J.,Ponsky, J., 2007. Use of acellular dermal matrix forcomplicated ventral hernia repair: does technique affectoutcomes?. J. Am. Coll. Surg. 205 (5), 654–660.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 4 ( 2 0 1 4 ) 3 2 0 – 3 2 9 329
Kanters, A.E., Krpata, D.M., Blatnik, J.A., Novitsky, Y.M.,Rosen, M.J., 2012. Modified hernia grading scale to stratifysurgical site occurrence after open ventral hernia repairs. J.Am. Coll. Surg. 215 (6), 787–793.
Klinge, U., Klosterhalfen, B., Conze, J., Limberg, W., Obolenski, B.,Ottinger, A.P., Schumpelick, V., 1998. Modified mesh for herniarepair that is adapted to the physiology of the abdominal wall.Eur. J. Surg. 164 (12), 951–960.
Klosterhalfen, B., Junge, K., Klinge, U., 2005. The lightweight andlarge porous mesh concept for hernia repair. Expert Rev. Med.Devices 2 (1), 103–117.
Langdon, S.E., Chernecky, R., Pereira, C.A., Abdulla, D., Lee, J.M.,1999. Biaxial mechanical/structural effects of equibiaxialstrain during crosslinking of bovine pericardial xenograftmaterials. Biomaterials 20 (2), 137–153.
Lee, E.I., Chike-Obi, C.J., Gonzalez, P., Garza, R., Leong, M.,Subramanian, A., Bullocks, J., 2009. Awad SS. Abdominal wallrepair using human acellular dermal matrix: a follow-upstudy. Am. J. Surg. 198 (5), 650–657.
McCarron, J.A., Milks, R.A., Mesiha, M., Aurora, A., Walker, E.,Iannotti, J.P., Derwin, K.A., 2012. Reinforced fascia patch limitscyclic gapping of rotator cuff repairs in a human cadavericmodel. J. Shoulder Elb. Surg. 21 (12), 1680–1686.
Menon, N.G., Rodriguez, E.D., Byrnes, C.K., Girotto, J.A., Goldberg,N.H., Silverman, R.P., 2003. Revascularization of humanacellular dermis in full-thickness abdominal wallreconstruction in the rabbit model. Ann. Plast. Surg. 50 (5),523–527.
Patton Jr., J.H., Berry, S., Kralovich, K.A., 2007. Use of humanacellular dermal matrix in complex and contaminatedabdominal wall reconstructions. Am. J. Surg. 193 (3), 360–363.
Poulose, B.K., Shelton, J., Phillips, S., Moore, D., Nealon, W.,Penson, D., Beck, W., Holzman, M.D., 2012. Epidemiology andcost of ventral hernia repair: making the case for herniaresearch. Hernia 16 (2), 179–183.
Rohrnbauer, B., Mazza, E., 2013. A non-biological model system tosimulate the in vivo mechanical behavior of prostheticmeshes. J. Mech. Behav. Biomed. Mater. 20, 305–315.
Sahoo, S., Greeson, C.B., McCarron, J.A., Milks, R.A., Aurora, A.,Walker, E., Iannotti, J.P., Derwin, K.A., 2012. Effect ofpretension and suture needle type on mechanical propertiesof acellular human dermis patches for rotator cuff repair.J. Shoulder Elb. Surg. 21 (10), 1413–1421.
Sandor, M., Xu, H., Connor, J., Lombardi, J., Harper, J.R., Silverman,R.P., McQuillan, D.J., 2008. Host response to implantedporcine-derived biologic materials in a primate model ofabdominal wall repair. Tissue Eng. Part A 14 (12), 2021–2031.
Shankaran, V., Weber, D.J., Reed 2nd, R.L., Luchette, F.A., 2011.A review of available prosthetics for ventral hernia repair.Ann. Surg. 253 (1), 16–26.
Smart, N.J., Marshall, M., Daniels, I.R., 2012. Biological meshes: areview of their use in abdominal wall hernia repairs. Surgeon10 (3), 159–171.
Whitson, B.A., Cheng, B.C., Kokini, K., Badylak, S.F., Patel, U., Morff, R.,O’Keefe, C.R., 1998. Multilaminate resorbable biomedical deviceunder biaxial loading. J. Biomed. Mater. Res. 43 (3), 277–281.
Willems, A, Lomov, SV, Verpoest, I, Vandepitte, D., 2008. Opticalstrain fields in shear and tensile testing of textilereinforcements. Compos. Sci. Technol. 68 (3–4), 807–819.
Yoder, J.H., Elliott, D.M., 2010. Nonlinear and anisotropic tensileproperties of graft materials used in soft tissue applications.Clin. Biomech. (Bristol, Avon) 25 (4), 378–382.