evaluation of waist-mounted tri-axial accelerometer based fall-detection algorithms during scripted...
TRANSCRIPT

Journal of Biomechanics 43 (2010) 3051–3057
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jbiomech
Journal of Biomechanics
0021-92
doi:10.1
n Corr
Univers
fax: +3
E-m
(A.K. B
www.JBiomech.com
Short communication
Evaluation of waist-mounted tri-axial accelerometer based fall-detectionalgorithms during scripted and continuous unscripted activities
A.K. Bourke a,b,c,n, P. van de Ven b, M. Gamble d, R. O’Connor d, K. Murphy d,e, E. Bogan e,E. McQuade a,b, P. Finucane d, G. OLaighin c,f, J. Nelson b
a Biomedical Electronics Laboratory, Department of Electronic and Computer Engineering, Faculty of Science and Engineering, University of Limerick, Limerick, Irelandb Wireless Access Research Centre, Department of Electronic and Computer Engineering, Faculty of Science and Engineering, University of Limerick, Limerick, Irelandc National Centre for Biomedical Engineering Science, National University of Ireland, Galway, Irelandd Graduate-Entry Medical School, Faculty of Education and Health Science, University of Limerick, Limerick, Irelande Cois Abhann Primary Care Team, Mid-Western Health Board, Limerick, Irelandf Department of Electronic Engineering, National University of Ireland, Galway, Ireland
a r t i c l e i n f o
Article history:
Accepted 15 July 2010It is estimated that by 2050 more than one in five people will be aged 65 or over. In this age group, falls
are one of the most serious life-threatening events that can occur. Their automatic detection would help
Keywords:
Falls in the elderly
Fall-detection
Accelerometer
ADL
Sum-vector signal
Fall profile
Impact
Posture
Velocity
90/$ - see front matter & 2010 Elsevier Ltd. A
016/j.jbiomech.2010.07.005
esponding author at: Department of Electroni
ity of Limerick, Limerick, Ireland. Tel.: +353 8
53 61 338176.
ail addresses: [email protected], AlanKevinBo
ourke).
a b s t r a c t
reduce the time of arrival of medical attention, thus reducing the mortality rate and in turn promoting
independent living.
This study evaluated a variety of existing and novel fall-detection algorithms for a waist-mounted
accelerometer based system. In total, 21 algorithms of varying degrees of complexity were tested
against a comprehensive data-set recorded from 10 young healthy volunteers performing 240 falls and
120 activities of daily living (ADL) and 10 elderly healthy volunteers performing 240 scripted ADL and
52.4 waking hours of continuous unscripted normal ADL.
Results show that using an algorithm that employs thresholds in velocity, impact and posture
(velocity+impact+posture) achieves 100% specificity and sensitivity with a false-positive rate of less
than 1 false-positive (0.6 false-positives) per day of waking hours. This algorithm is the most suitable
method of fall-detection, when tested using continuous unscripted activities performed by elderly
healthy volunteers, which is the target environment for a fall-detection device.
& 2010 Elsevier Ltd. All rights reserved.
1. Introduction
By 2050, the proportion of the world’s population aged 65 orolder is set to double to more than 1 in 5, with those aged 80 orolder set to almost treble (UN, 2009). Falls and related injuries arenot only life threatening to older people (Noury et al., 2008b), butalso herald an inability to live independently (Gurley et al., 1996).Conversely, the automatic detection of falls facilitates theprovision of early medical attention, reduces the consequencesof prolonged lying following a fall (Lord et al., 2001) and promotesan independent lifestyle (Brownsell et al., 2000).
In recent years the number of proposed fall-detection systemsdeveloped has increased dramatically (Noury et al., 2008b). Thewaist is a popular location for fall-detection systems (Noury et al.,2008a), as it provides reliable indications of full-body movement,
ll rights reserved.
c and Computer Engineering,
6 6037831;
in addition to its ease of acceptance by allowing attachment to anexisting waist band (Mathie et al., 2004).
Recently, Kangas et al. (2009) evaluated a set of fall-detectionalgorithms (Kangas et al., 2008) on data recorded from 20 middle-aged volunteers (40–65 years old) performing 6 different falls(240 falls in total) and 4 scripted activities of daily living (ADL),these same ADL were also recorded from 21 adults (aged 58–98years) from a residential care unit (164 ADL in total). They showedthat thresholding of impact and posture can achieve 97.5%sensitivity and 100% specificity.
Chao et al. (2009) recorded 7 male subjects (2571.5 years)performing 8 different fall types and 17 functional ADL (total of 56falls and 119 ADL). Using a combination algorithm of accelerationcross-product and post-fall posture, a sensitivity of 100% and498% specificity were obtained.
The aim of this study is to evaluate the performance of 21,novel and existing, fall-detection algorithms of varying complex-ity on a comprehensive data-set containing simulated falls,normal ADL and including; continuous unscripted ADL performedby both urban and rural based elderly volunteers over extendedtime periods, which has not been previously performed. It isenvisaged, such an evaluation will uncover a more appropriate
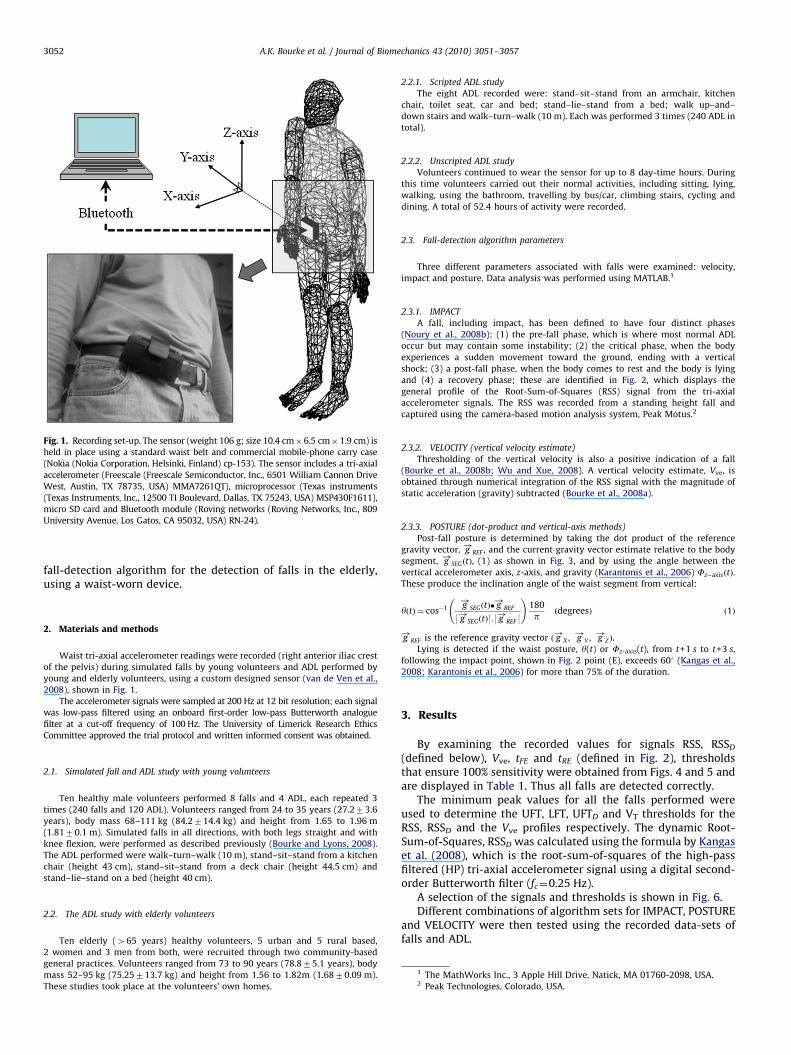
Fig. 1. Recording set-up. The sensor (weight 106 g; size 10.4 cm�6.5 cm�1.9 cm) is
held in place using a standard waist belt and commercial mobile-phone carry case
(Nokia (Nokia Corporation, Helsinki, Finland) cp-153). The sensor includes a tri-axial
accelerometer (Freescale (Freescale Semiconductor, Inc., 6501 William Cannon Drive
West, Austin, TX 78735, USA) MMA7261QT), microprocessor (Texas instruments
(Texas Instruments, Inc., 12500 TI Boulevard, Dallas, TX 75243, USA) MSP430F1611),
micro SD card and Bluetooth module (Roving networks (Roving Networks, Inc., 809
University Avenue, Los Gatos, CA 95032, USA) RN-24).
A.K. Bourke et al. / Journal of Biomechanics 43 (2010) 3051–30573052
fall-detection algorithm for the detection of falls in the elderly,using a waist-worn device.
2. Materials and methods
Waist tri-axial accelerometer readings were recorded (right anterior iliac crest
of the pelvis) during simulated falls by young volunteers and ADL performed by
young and elderly volunteers, using a custom designed sensor (van de Ven et al.,
2008), shown in Fig. 1.
The accelerometer signals were sampled at 200 Hz at 12 bit resolution; each signal
was low-pass filtered using an onboard first-order low-pass Butterworth analogue
filter at a cut-off frequency of 100 Hz. The University of Limerick Research Ethics
Committee approved the trial protocol and written informed consent was obtained.
2.1. Simulated fall and ADL study with young volunteers
Ten healthy male volunteers performed 8 falls and 4 ADL, each repeated 3
times (240 falls and 120 ADL). Volunteers ranged from 24 to 35 years (27.273.6
years), body mass 68–111 kg (84.2714.4 kg) and height from 1.65 to 1.96 m
(1.8170.1 m). Simulated falls in all directions, with both legs straight and with
knee flexion, were performed as described previously (Bourke and Lyons, 2008).
The ADL performed were walk–turn–walk (10 m), stand–sit–stand from a kitchen
chair (height 43 cm), stand–sit–stand from a deck chair (height 44.5 cm) and
stand–lie–stand on a bed (height 40 cm).
1 The MathWorks Inc., 3 Apple Hill Drive, Natick, MA 01760-2098, USA.2 Peak Technologies, Colorado, USA.
2.2. The ADL study with elderly volunteers
Ten elderly (465 years) healthy volunteers, 5 urban and 5 rural based,
2 women and 3 men from both, were recruited through two community-based
general practices. Volunteers ranged from 73 to 90 years (78.875.1 years), body
mass 52–95 kg (75.25713.7 kg) and height from 1.56 to 1.82m (1.6870.09 m).
These studies took place at the volunteers’ own homes.
2.2.1. Scripted ADL study
The eight ADL recorded were: stand–sit–stand from an armchair, kitchen
chair, toilet seat, car and bed; stand–lie–stand from a bed; walk up–and–
down stairs and walk–turn–walk (10 m). Each was performed 3 times (240 ADL in
total).
2.2.2. Unscripted ADL study
Volunteers continued to wear the sensor for up to 8 day-time hours. During
this time volunteers carried out their normal activities, including sitting, lying,
walking, using the bathroom, travelling by bus/car, climbing stairs, cycling and
dining. A total of 52.4 hours of activity were recorded.
2.3. Fall-detection algorithm parameters
Three different parameters associated with falls were examined: velocity,
impact and posture. Data analysis was performed using MATLAB.1
2.3.1. IMPACT
A fall, including impact, has been defined to have four distinct phases
(Noury et al., 2008b): (1) the pre-fall phase, which is where most normal ADL
occur but may contain some instability; (2) the critical phase, when the body
experiences a sudden movement toward the ground, ending with a vertical
shock; (3) a post-fall phase, when the body comes to rest and the body is lying
and (4) a recovery phase; these are identified in Fig. 2, which displays the
general profile of the Root-Sum-of-Squares (RSS) signal from the tri-axial
accelerometer signals. The RSS was recorded from a standing height fall and
captured using the camera-based motion analysis system, Peak Motus.2
2.3.2. VELOCITY (vertical velocity estimate)
Thresholding of the vertical velocity is also a positive indication of a fall
(Bourke et al., 2008b; Wu and Xue, 2008). A vertical velocity estimate, Vve, is
obtained through numerical integration of the RSS signal with the magnitude of
static acceleration (gravity) subtracted (Bourke et al., 2008a).
2.3.3. POSTURE (dot-product and vertical-axis methods)
Post-fall posture is determined by taking the dot product of the reference
gravity vector, g!
REF , and the current gravity vector estimate relative to the body
segment, g!
SEGðtÞ, (1) as shown in Fig. 3, and by using the angle between the
vertical accelerometer axis, z-axis, and gravity (Karantonis et al., 2006) Fz�axisðtÞ.
These produce the inclination angle of the waist segment from vertical:
yðtÞ ¼ cos�1 g!
SEGðtÞ� g!
REF
9 g!
SEGðtÞ9:9 g!
REF 9
!180
p ðdegreesÞ ð1Þ
g!
REF is the reference gravity vector ð g!
X , g!
Y , g!
Z Þ.
Lying is detected if the waist posture, y(t) or Fz-axis(t), from t+1 s to t+3 s,
following the impact point, shown in Fig. 2 point (E), exceeds 601 (Kangas et al.,
2008; Karantonis et al., 2006) for more than 75% of the duration.
3. Results
By examining the recorded values for signals RSS, RSSD
(defined below), Vve, tFE and tRE (defined in Fig. 2), thresholdsthat ensure 100% sensitivity were obtained from Figs. 4 and 5 andare displayed in Table 1. Thus all falls are detected correctly.
The minimum peak values for all the falls performed wereused to determine the UFT, LFT, UFTD and VT thresholds for theRSS, RSSD and the Vve profiles respectively. The dynamic Root-Sum-of-Squares, RSSD was calculated using the formula by Kangaset al. (2008), which is the root-sum-of-squares of the high-passfiltered (HP) tri-axial accelerometer signal using a digital second-order Butterworth filter (fc¼0.25 Hz).
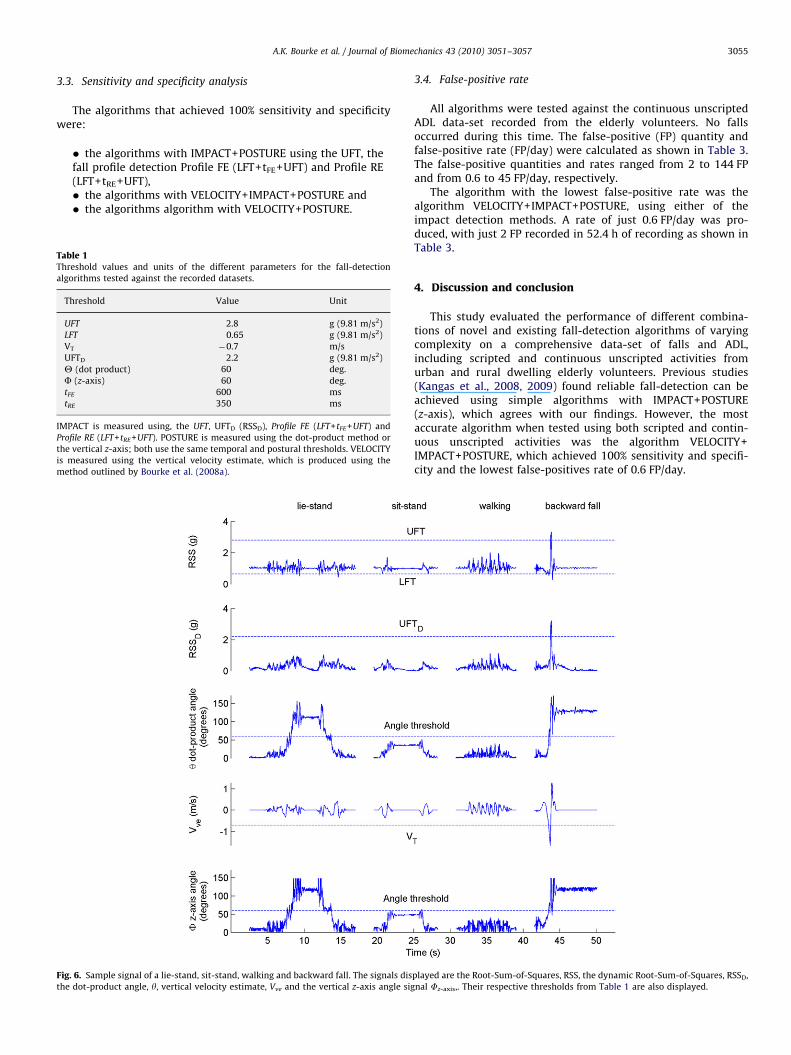
A selection of the signals and thresholds is shown in Fig. 6.Different combinations of algorithm sets for IMPACT, POSTURE
and VELOCITY were then tested using the recorded data-sets offalls and ADL.
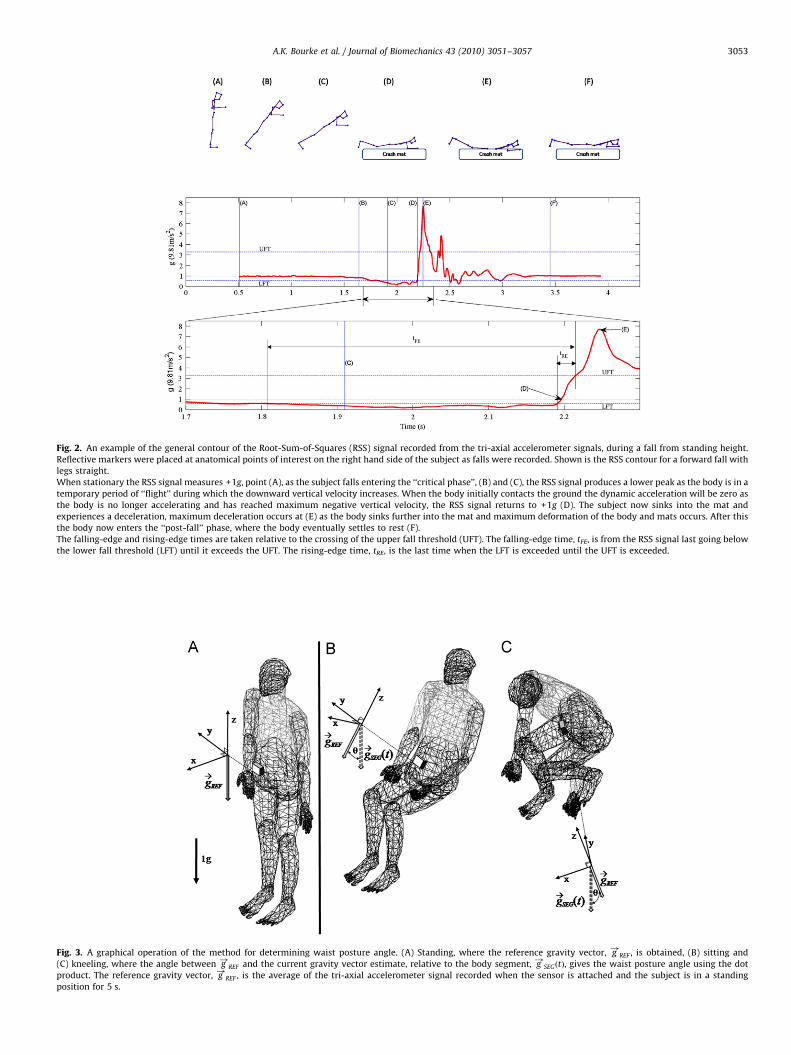
Fig. 3. A graphical operation of the method for determining waist posture angle. (A) Standing, where the reference gravity vector, g!
REF , is obtained, (B) sitting and
(C) kneeling, where the angle between g!
REF and the current gravity vector estimate, relative to the body segment, g!
SEGðtÞ, gives the waist posture angle using the dot
product. The reference gravity vector, g!
REF , is the average of the tri-axial accelerometer signal recorded when the sensor is attached and the subject is in a standing
position for 5 s.
Fig. 2. An example of the general contour of the Root-Sum-of-Squares (RSS) signal recorded from the tri-axial accelerometer signals, during a fall from standing height.
Reflective markers were placed at anatomical points of interest on the right hand side of the subject as falls were recorded. Shown is the RSS contour for a forward fall with
legs straight.
When stationary the RSS signal measures +1g, point (A), as the subject falls entering the ‘‘critical phase’’, (B) and (C), the RSS signal produces a lower peak as the body is in a
temporary period of ‘‘flight’’ during which the downward vertical velocity increases. When the body initially contacts the ground the dynamic acceleration will be zero as
the body is no longer accelerating and has reached maximum negative vertical velocity, the RSS signal returns to +1g (D). The subject now sinks into the mat and
experiences a deceleration, maximum deceleration occurs at (E) as the body sinks further into the mat and maximum deformation of the body and mats occurs. After this
the body now enters the ‘‘post-fall’’ phase, where the body eventually settles to rest (F).
The falling-edge and rising-edge times are taken relative to the crossing of the upper fall threshold (UFT). The falling-edge time, tFE, is from the RSS signal last going below
the lower fall threshold (LFT) until it exceeds the UFT. The rising-edge time, tRE, is the last time when the LFT is exceeded until the UFT is exceeded.
A.K. Bourke et al. / Journal of Biomechanics 43 (2010) 3051–3057 3053
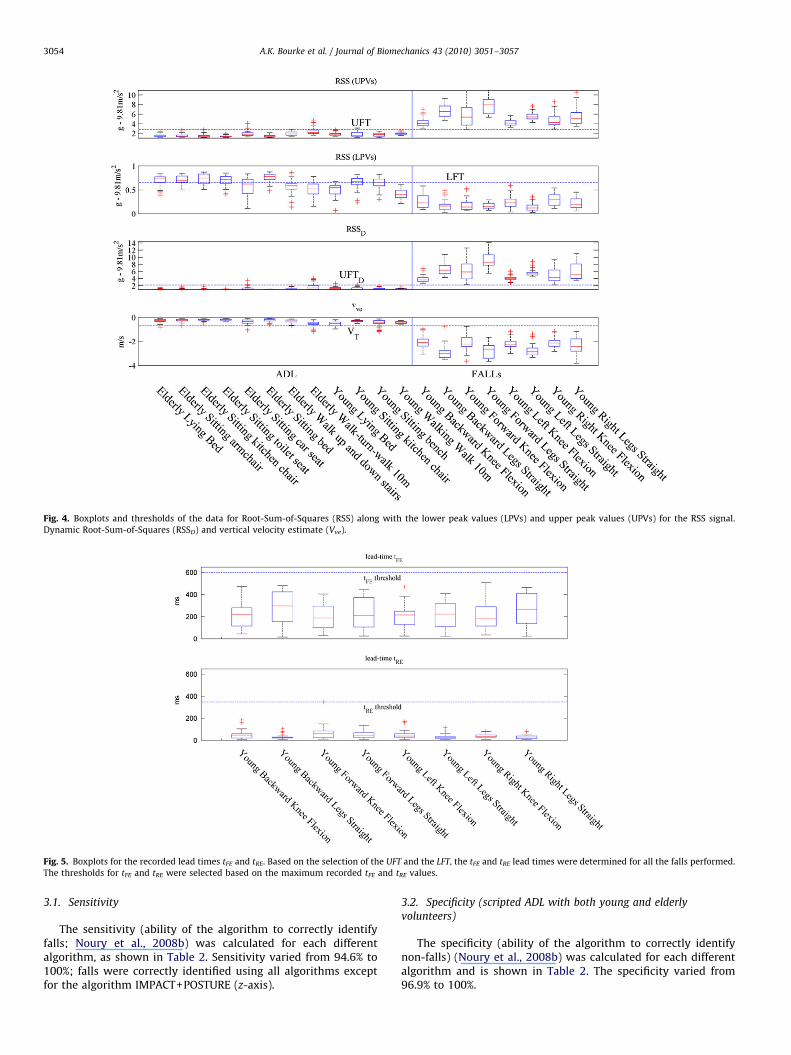
Fig. 4. Boxplots and thresholds of the data for Root-Sum-of-Squares (RSS) along with the lower peak values (LPVs) and upper peak values (UPVs) for the RSS signal.
Dynamic Root-Sum-of-Squares (RSSD) and vertical velocity estimate (Vve).
Fig. 5. Boxplots for the recorded lead times tFE and tRE. Based on the selection of the UFT and the LFT, the tFE and tRE lead times were determined for all the falls performed.
The thresholds for tFE and tRE were selected based on the maximum recorded tFE and tRE values.
A.K. Bourke et al. / Journal of Biomechanics 43 (2010) 3051–30573054
3.1. Sensitivity
The sensitivity (ability of the algorithm to correctly identifyfalls; Noury et al., 2008b) was calculated for each differentalgorithm, as shown in Table 2. Sensitivity varied from 94.6% to100%; falls were correctly identified using all algorithms exceptfor the algorithm IMPACT+POSTURE (z-axis).
3.2. Specificity (scripted ADL with both young and elderly
volunteers)
The specificity (ability of the algorithm to correctly identifynon-falls) (Noury et al., 2008b) was calculated for each differentalgorithm and is shown in Table 2. The specificity varied from96.9% to 100%.
A.K. Bourke et al. / Journal of Biomechanics 43 (2010) 3051–3057 3055
3.3. Sensitivity and specificity analysis
The algorithms that achieved 100% sensitivity and specificitywere:
� the algorithms with IMPACT+POSTURE using the UFT, thefall profile detection Profile FE (LFT+tFE+UFT) and Profile RE(LFT+tRE+UFT),� the algorithms with VELOCITY+IMPACT+POSTURE and� the algorithms algorithm with VELOCITY+POSTURE.
Fig. 6. Sample signal of a lie-stand, sit-stand, walking and backward fall. The signals dis
the dot-product angle, y, vertical velocity estimate, Vve and the vertical z-axis angle sig
Table 1Threshold values and units of the different parameters for the fall-detection
algorithms tested against the recorded datasets.
Threshold Value Unit
UFT 2.8 g (9.81 m/s2)
LFT 0.65 g (9.81 m/s2)
VT �0.7 m/s
UFTD 2.2 g (9.81 m/s2)
Y (dot product) 60 deg.
F (z-axis) 60 deg.
tFE 600 ms
tRE 350 ms
IMPACT is measured using, the UFT, UFTD (RSSD), Profile FE (LFT+tFE+UFT) and
Profile RE (LFT+tRE+UFT). POSTURE is measured using the dot-product method or
the vertical z-axis; both use the same temporal and postural thresholds. VELOCITY
is measured using the vertical velocity estimate, which is produced using the
method outlined by Bourke et al. (2008a).
3.4. False-positive rate
All algorithms were tested against the continuous unscriptedADL data-set recorded from the elderly volunteers. No fallsoccurred during this time. The false-positive (FP) quantity andfalse-positive rate (FP/day) were calculated as shown in Table 3.The false-positive quantities and rates ranged from 2 to 144 FPand from 0.6 to 45 FP/day, respectively.
The algorithm with the lowest false-positive rate was thealgorithm VELOCITY+IMPACT+POSTURE, using either of theimpact detection methods. A rate of just 0.6 FP/day was pro-duced, with just 2 FP recorded in 52.4 h of recording as shown inTable 3.
4. Discussion and conclusion
This study evaluated the performance of different combina-tions of novel and existing fall-detection algorithms of varyingcomplexity on a comprehensive data-set of falls and ADL,including scripted and continuous unscripted activities fromurban and rural dwelling elderly volunteers. Previous studies(Kangas et al., 2008, 2009) found reliable fall-detection can beachieved using simple algorithms with IMPACT+POSTURE(z-axis), which agrees with our findings. However, the mostaccurate algorithm when tested using both scripted and contin-uous unscripted activities was the algorithm VELOCITY+IMPACT+POSTURE, which achieved 100% sensitivity and specifi-city and the lowest false-positives rate of 0.6 FP/day.
played are the Root-Sum-of-Squares, RSS, the dynamic Root-Sum-of-Squares, RSSD,
nal Fz-axis,. Their respective thresholds from Table 1 are also displayed.
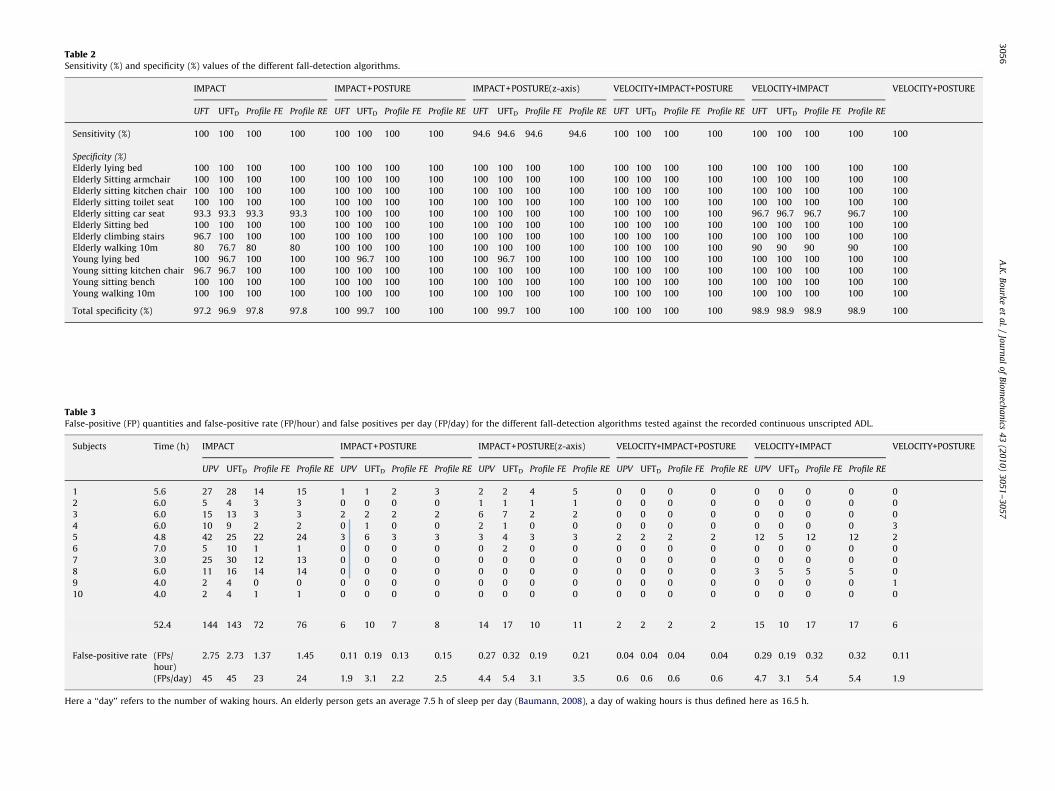
Table 2Sensitivity (%) and specificity (%) values of the different fall-detection algorithms.
IMPACT IMPACT+POSTURE IMPACT+POSTURE(z-axis) VELOCITY+IMPACT+POSTURE VELOCITY+IMPACT VELOCITY+POSTURE
UFT UFTD Profile FE Profile RE UFT UFTD Profile FE Profile RE UFT UFTD Profile FE Profile RE UFT UFTD Profile FE Profile RE UFT UFTD Profile FE Profile RE
Sensitivity (%) 100 100 100 100 100 100 100 100 94.6 94.6 94.6 94.6 100 100 100 100 100 100 100 100 100
Specificity (%)
Elderly lying bed 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Elderly Sitting armchair 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Elderly sitting kitchen chair 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Elderly sitting toilet seat 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Elderly sitting car seat 93.3 93.3 93.3 93.3 100 100 100 100 100 100 100 100 100 100 100 100 96.7 96.7 96.7 96.7 100
Elderly Sitting bed 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Elderly climbing stairs 96.7 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Elderly walking 10m 80 76.7 80 80 100 100 100 100 100 100 100 100 100 100 100 100 90 90 90 90 100
Young lying bed 100 96.7 100 100 100 96.7 100 100 100 96.7 100 100 100 100 100 100 100 100 100 100 100
Young sitting kitchen chair 96.7 96.7 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Young sitting bench 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Young walking 10m 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Total specificity (%) 97.2 96.9 97.8 97.8 100 99.7 100 100 100 99.7 100 100 100 100 100 100 98.9 98.9 98.9 98.9 100
Table 3False-positive (FP) quantities and false-positive rate (FP/hour) and false positives per day (FP/day) for the different fall-detection algorithms tested against the recorded continuous unscripted ADL.
Subjects Time (h) IMPACT IMPACT+POSTURE IMPACT+POSTURE(z-axis) VELOCITY+IMPACT+POSTURE VELOCITY+IMPACT VELOCITY+POSTURE
UPV UFTD Profile FE Profile RE UPV UFTD Profile FE Profile RE UPV UFTD Profile FE Profile RE UPV UFTD Profile FE Profile RE UPV UFTD Profile FE Profile RE
1 5.6 27 28 14 15 1 1 2 3 2 2 4 5 0 0 0 0 0 0 0 0 0
2 6.0 5 4 3 3 0 0 0 0 1 1 1 1 0 0 0 0 0 0 0 0 0
3 6.0 15 13 3 3 2 2 2 2 6 7 2 2 0 0 0 0 0 0 0 0 0
4 6.0 10 9 2 2 0 1 0 0 2 1 0 0 0 0 0 0 0 0 0 0 3
5 4.8 42 25 22 24 3 6 3 3 3 4 3 3 2 2 2 2 12 5 12 12 2
6 7.0 5 10 1 1 0 0 0 0 0 2 0 0 0 0 0 0 0 0 0 0 0
7 3.0 25 30 12 13 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
8 6.0 11 16 14 14 0 0 0 0 0 0 0 0 0 0 0 0 3 5 5 5 0
9 4.0 2 4 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1
10 4.0 2 4 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
52.4 144 143 72 76 6 10 7 8 14 17 10 11 2 2 2 2 15 10 17 17 6
False-positive rate (FPs/
hour)
2.75 2.73 1.37 1.45 0.11 0.19 0.13 0.15 0.27 0.32 0.19 0.21 0.04 0.04 0.04 0.04 0.29 0.19 0.32 0.32 0.11
(FPs/day) 45 45 23 24 1.9 3.1 2.2 2.5 4.4 5.4 3.1 3.5 0.6 0.6 0.6 0.6 4.7 3.1 5.4 5.4 1.9
Here a ‘‘day’’ refers to the number of waking hours. An elderly person gets an average 7.5 h of sleep per day (Baumann, 2008), a day of waking hours is thus defined here as 16.5 h.
A.K
.B
ou
rke
eta
l./
Jou
rna
lo
fB
iom
echa
nics
43
(20
10
)3
05
1–
30
57
30
56

A.K. Bourke et al. / Journal of Biomechanics 43 (2010) 3051–3057 3057
The dot-product posture detection method used here repre-sents an improvement over the vertical z-axis method, asthe sensor can initially be attached in any orientation, withoutthe need to nominate an individual axis as being incident to thegravity vector, thus making it a more practical method.
By performing fall-impact detection using the profile detectionwith tFE and tRE, these fall-detection algorithms will be lesssusceptible to acceleration spikes, not associated with falls, whichmay trigger an IMPACT if simply a single threshold is used.
This study uses simulated falls performed by young volunteersonto crash-mats, as opposed to real-life hard surfaces. Thus theimpact values recorded here are expected to be lower than wouldoccur in real conditions. Falls performed by middle-agedvolunteers, recorded previously (Kangas et al., 2009), representan advancement in this area; however fundamentally these arestill simulated falls. In addition, the difference between simulatedactivities and those recorded under real-world conditions isevident from results presented here, where 100% sensitivity andspecificity were achieved by algorithms tested using the completescripted data-sets. However, during real-world conditions, falsepositives did occur, indicating that some disparity exists betweensimulated and continuous unsupervised recorded activities.
In this study falls recorded from young subjects were used toassess the sensitivity of the fall-detection algorithms. In order todetermine a more significant sensitivity, further research isrequired to assess their performance in a long-term monitoringstudy, where elderly volunteers who inadvertently fall, are safelyrecorded wearing the proposed fall-detection system, in asupervised and controlled environment.
Previous studies have used ADL recorded from older adults(Kangas et al., 2008; Karantonis et al., 2006) and elderlyvolunteers (Kangas et al., 2009) to test their waist-mounted fall-detection algorithms. However, none to date have tested thesealgorithms against continuous unsupervised activities, performedby both urban and rural dwelling elderly. This is however theeventual target audience and operating environment for anautonomous fall-detection system.
In conclusion we have tested a variety of 21 fall-detectionalgorithms of varying degrees of complexity. The most successfulalgorithms, VELOCITY+IMPACT+POSTURE, achieved 100% specificityand sensitivity with less than 1 false positive (0.6 FP/day) foreach day of waking hours when tested in the most realisticoperating conditions to date.
Conflict of interest
The authors have no commercial stake in the outcomes of thisresearch and no patent has been filed in relation to this work.
Acknowledgments
We are grateful to all volunteers who gave their time tothe CAALYX project /www.caalyx.euS and the eCAALYX project/www.ecaalyx.orgS.
References
Baumann, C.R., 2008. Sleep: approaching the fundamental questions. CurrentBiology 18 (5), R665–R667.
Bourke, A.K., Lyons, G.M., 2008. A threshold-based fall-detection algorithm using abi-axial gyroscope sensor. Medical Engineering & Physics 30 (1), 84–90.
Bourke, A.K., O’Donovan, K.J., Nelson, J., OLaighin, G., 2008a. Fall-detection throughvertical velocity thresholding using a tri-axial accelerometer characterizedusing an optical motion-capture system. In: Conference Proceedings ofthe IEEE Engineering in Medicine and Biology Society, Vancouver, Canada,pp. 2832–2835.
Bourke, A.K., O’Donovan, K.J., OLaighin, G., 2008b. The identification of verticalvelocity profiles using an inertial sensor to investigate pre-impact detection offalls. Medical Engineering & Physics 30 (7), 937–946.
Brownsell, S.J., Bradley, D.A., Bragg, R., Catlin, P., Carlier, J., 2000. Do commu-nity alarm users want telecare? Journal of Telemedicine and Telecare 6199–204.
Chao, P.K., Chan, H.L., Tang, F.T., Chen, Y.C., Wong, M.K., 2009. A comparison ofautomatic fall detection by the cross-product and magnitude of tri-axialacceleration. Physiological Measurement 30 (10), 1027–1037.
Gurley, R.J., Lum, N., Sande, M., Lo, B., Katz, M.H., 1996. Persons found intheir homes helpless or dead. New England Journal of Medicine 334 (26),1710–1716.
Kangas, M., Konttila, A., Lindgren, P., Winblad, I., Jamsa, T., 2008. Comparison oflow-complexity fall detection algorithms for body attached accelerometers.Gait & Posture 28 (2), 285–291.
Kangas, M., Vikman, I., Wiklander, J., Lindgren, P., Nyberg, L., Jamsa, T., 2009.Sensitivity and specificity of fall detection in people aged 40 years and over.Gait & Posture 29 (4), 571–574.
Karantonis, D.M., Narayanan, M.R., Mathie, M., Lovell, N.H., Celler, B.G., 2006.Implementation of a real-time human movement classifier using a triaxialaccelerometer for ambulatory monitoring. IEEE Transactions on InformationTechnology in Biomedicine 10 (1), 156–167.
Lord, S.R., Sherrington, C., Menz, H.B., 2001. Falls in Older People: Risk Factors andStrategies for Prevention. Cambridge University Press, Cambridge.
Mathie, M.J., Celler, B.G., Lovell, N.H., Coster, A.C., 2004. Classification of basic dailymovements using a triaxial accelerometer. Medical Biological Engineering andComputing 42 (5), 679–687.
Noury, N., Galay, A., Pasquier, J., Ballussaud, M., 2008a. Preliminary investigationinto the use of Autonomous Fall Detectors. In: Conference Proceedings of theIEEE Engineering in Medical and Biology Society 2008, 2828–2831.
Noury, N., Rumeau, P., Bourke, A.K., OLaighin, G., Lundy, J.E., 2008b. A proposal forthe classification and evaluation of fall detectors. IRBM—Ingenierie etRecherche Biomedicale/Biomedical Engineering and Research 29 (6), 340–349.
UN, 2009. Population Ageing 2009. Population Division, Department of Economicand Social Affairs, United Nations.
van de Ven, P.W.J., Bourke, A.K., Nelson, J., OLaighin, G., 2008. A wearable wirelessplatform for fall and mobility monitoring. In: Proceedings of the firstInternational Conference on Pervasive Technologies Related to AssistiveEnvironments, Athens, Greece.
Wu, G., Xue, S., 2008. Portable preimpact fall detector with inertial sensors.IEEE Transactions on Neural Systems and Rehabilitation Engineering 16 (2),178–183.