empowerment interventions for older adults
TRANSCRIPT
http://wjn.sagepub.com/
ResearchWestern Journal of Nursing
http://wjn.sagepub.com/content/early/2010/07/27/0193945910377887The online version of this article can be found at:
DOI: 10.1177/0193945910377887
published online 30 July 2010West J Nurs ResNelma B. C. Shearer, Julie Fleury, Kathy A. Ward and Anne-Marie O'Brien
Empowerment Interventions for Older Adults
Published by:
http://www.sagepublications.com
On behalf of:
Midwest Nursing Research Society
at: can be foundWestern Journal of Nursing ResearchAdditional services and information for
http://wjn.sagepub.com/cgi/alertsEmail Alerts:
http://wjn.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from

Western Journal of Nursing ResearchXX(X) 1 –28
© The Author(s) 2010Reprints and permission: http://www.sagepub.com/journalsPermissions.nav
DOI: 10.1177/0193945910377887http://wjn.sagepub.com
377887WJNXXX10.1177/0193945910377887Shearer et al.Western Journal of Nursing Research© The Author(s) 2010Reprints and permission: http://www.sagepub.com/journalsPermissions.nav
1Arizona State University, Phoenix
Corresponding Author:Nelma B. C. Shearer, 500 N. 3rd Street, Phoenix, AZ 85004 Email: [email protected]
Empowerment Interventions for Older Adults
Nelma B.C. Shearer1, Julie Fleury1,Kathy A. Ward1, and Anne-Marie O’Brien1
Abstract
There has been much discussion regarding the need to empower older adults to make informed health decisions and to test interventions targeting empowerment to promote health among older adults. It has been suggested that an empowerment approach may nurture an older adult’s participation in health care decisions and promote positive health outcomes. The purpose of this article is to report the findings of a critical review of published empowerment intervention studies with community-dwelling older adults. A descriptive literature review was conducted to examine how empowerment is conceptualized across interventions, the guiding theoretical frameworks, the outcomes measured, as well as the health outcomes of these interventions. Based on the findings from this review, recommendations for future empowerment intervention research with older adults as well as implications for practice are proposed.
Keywords
empowerment, interventions, older adults
Never before in our nation’s history have we experienced such a rapid and unprecedented growth in the number of older adults, defined by the American
West J Nurs Res OnlineFirst, published on July 30, 2010 as doi:10.1177/0193945910377887
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
2 Western Journal of Nursing Research XX(X)
Association of Retired Persons (http://www.aarp.org/) as someone aged 50 years and older. By the year 2030, approximately 20% of the U.S. popula-tion will be compromised older adults, many of whom will seek health care (Administration on Aging [AOA], United States Department of Health and Human Services, 2007; Centers for Disease Control and Prevention & The Merck Company Foundation, 2007). The aging of the U.S. population and the concomitant rise in health care needs underscore the importance of facili-tating meaningful and innovative ways to foster positive health outcomes among older adults.
There has been much discussion regarding the need to empower older adults to make informed health decisions (AOA, 2007) and to test interven-tions targeting empowerment to promote health among older adults (e.g., DeCoster & George, 2005; Keller & Fleury, 2000). It has been suggested that an empowerment approach may nurture an older adult’s participation in health care decisions and promote positive health outcomes (AOA, 2007; Toofany, 2006, 2007). The purpose of this article, therefore, is to report the findings of a critical review of published empowerment intervention studies with community-dwelling older adults. Specifically, a descriptive literature review was conducted to examine how empowerment is conceptualized across inter-ventions, the guiding theoretical frameworks, the outcomes measured, as well as the health outcomes of these interventions. Based on the findings from this review, recommendations for future empowerment intervention research with older adults as well as implications for practice are proposed.
Conceptualization of EmpowermentIn the health education and health promotion literature, empowerment has been conceptualized as a framework for understanding the process and conse-quences of efforts to exert control and influence over the decisions that affect one’s life, including perceptions of personal control as well as behaviors to realize control (Perkins & Zimmerman, 1995; Rappaport, 1984). Empowerment as a process focuses on relationships with others and the transfer of power with the outcome of “liberation, emancipation, energy and sharing power” (Leyshon, 2002, p. 467), and can be understood from several perspectives, including social and developmental (Shearer, 2004; Shearer & Reed, 2004). Such perspectives provide a basis for identifying and evaluat-ing empowerment interventions among older adults.
As a social process, empowerment is associated with external social forces that act on the person and affect his or her sense of control and feelings of power (Shearer, 2004; Shearer & Reed, 2004). Social support as an external feedback
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
Shearer et al. 3
mechanism has been studied as a process that can provide needed reinforce-ment, resources, assistance, and motivation (Ellis-Stoll & Popkess-Vawter, 1998; Shearer & Fleury 2006) and enable the individual to make decisions (Hawks, 1992). Other external social forces have been studied from the per-spective of emancipation from oppression. Several authors have suggested that empowerment could be promoted by addressing political constraints (Gutierrez, 1995; Labonte, 1994), environmental constraints (Ryles, 1999), and social constraints (Fulton, 1997).
Empowerment may also be understood in reference to the life span devel-opmental perspective (Lerner, 1997). Life span development is an orientation to the study of human beings who are viewed as continuously innovative, embedded in a dynamic environment, and equipped with inherent potential. Change derives from mutual influences in the personal and environmental contexts. Person–environment interactions, particularly human relationships, are central to developmental progress and well-being (Shearer & Reed, 2004). Health cannot be narrowly defined by illness or chronic conditions; rather, health must be viewed within a network of relationships and respon-sibilities. From a life span development perspective, the person is viewed as an active participant and resource in health care (Shearer & Reed, 2004). Empowerment from this approach considers the strengths and health goals of the individual rather than those of the health care provider (Baltes, Lindenberger, & Staudinger, 1998).
Theoretical frameworks underlying health empowerment interventions often address constraints in order to facilitate power. Three theories that offer a perspective on power related to empowerment include critical social theory, feminist theory, and Bandura’s theory of self-efficacy. Critical social theory emerged from Marxism and from Freire’s perspective that human beings’ “ontological vocation is to be a subject who actions upon and transforms one’s world” (Richard Shaull, as cited in Freire, 1968/1981, p. 12). Critical social theory focuses on making people aware of the social constraints under which they live, freeing their thinking, establishing unconstrained communi-cation, and facilitating empowerment through increased participation, includ-ing movement toward creating change (Shearer & Reed, 2004). Feminist theory acknowledges basic human potential and includes life experiences that may contribute to a transformation of oppressive situations, facilitating empowerment (Kane & Thomas, 2000). Empowerment from a feminist per-spective emphasizes choice and freedom (Shearer & Reed, 2004). Based on social behavior and social learning theory, Bandura’s concept of self- efficacy is often linked with empowerment. Self-efficacy refers to a per-son’s belief that they have the ability to succeed in a given situation.
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
4 Western Journal of Nursing Research XX(X)
Empowerment from a self-efficacy perspective focuses on enhancing per-ceived self-efficacy and movement toward positive health behaviors, sense of control and choice, and power through mastery experiences, social modeling, social persuasion, and psychological responses (Bandura, 1992, 1994).
MethodSearch Process
Computerized and manual searches were conducted of articles in the English-language literature from 1995 to 2008. Computerized searches of Academic Search Premier, Medline, and CINAHL databases were conducted using the following search terms: empowerment and elder*, empowerment approach, empowerment model, empowerment program, and empowerment + adults + intervention. Primary inclusion criteria for articles targeted (a) English lan-guage, peer-reviewed articles; (b) adults 50 years and older; (c) intervention study designed to foster older adult empowerment as stated by authors; (d) ran-domized controlled trials or quasi-experimental designs; and (e) conducted in community settings. Exclusion criteria included (a) case study, qualitative, and/or retrospective study; (b) study did not use empowerment either as an approach or an outcome; (c) study population was inpatient and/or living in group setting such as a long-term-care facility; and (d) mean age of study population was less than 50 years of age. Studies referenced by articles found in those databases were also considered. As a result of the search, 558 cita-tions were reviewed, and 11 studies were found to meet the inclusion and exclusion criteria.
Classification and Review ProcessA coding frame as described by Blue and Black (2005) was developed to record the following critical elements of the studies reviewed: (a) author’s last name(s), year published, and title of the intervention; (b) how empower-ment was defined; (c) theoretical framework guiding the intervention; (d) study methods (design/participants/outcome measures); and (e) results/conclusions. Specific coded study participant characteristics included the targeted patient population and the participants’ gender, race, age, and socioeconomic status. Specific coded design elements included randomized controlled trial versus quasi-experimental, sample size, mode of intervention delivery (i.e., in a group vs. individual setting), number of dose-weeks over which the interven-tion was delivered, coded theory elements, and intervention components.
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
Shearer et al. 5
Finally, coded outcomes included the targeted participant outcome vari-ables and instruments used to measure any change in the target variables over time
ResultsStudy Characteristics
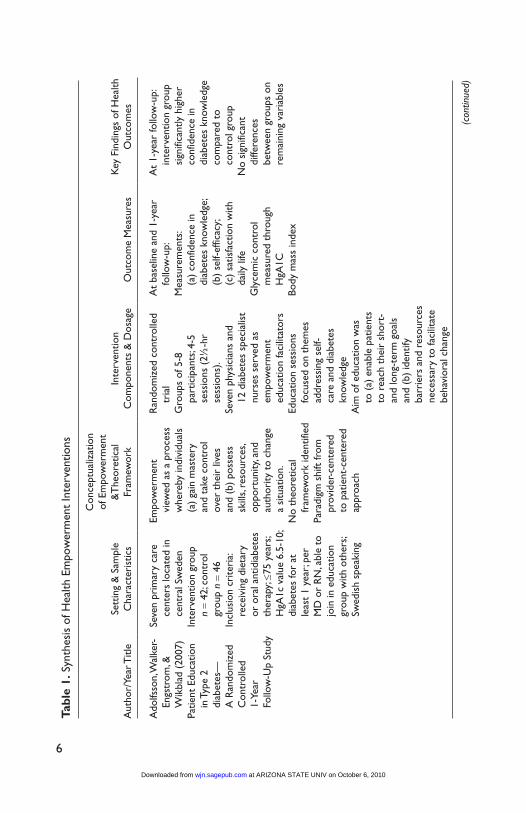
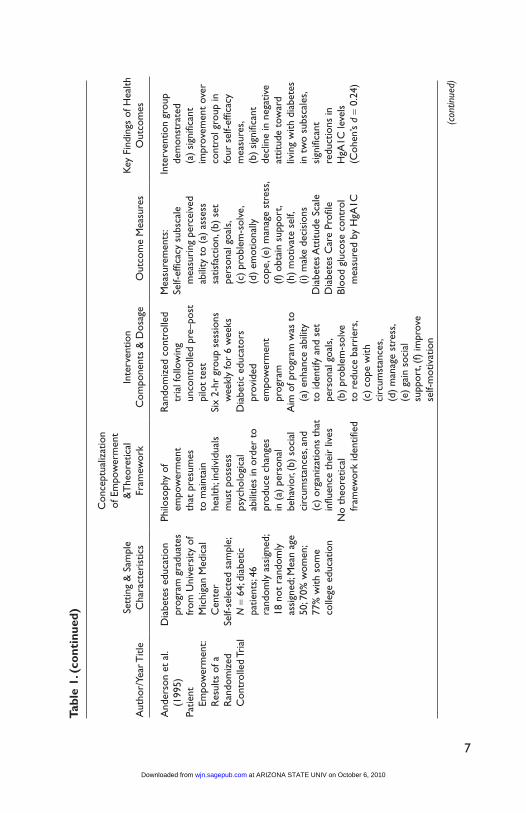
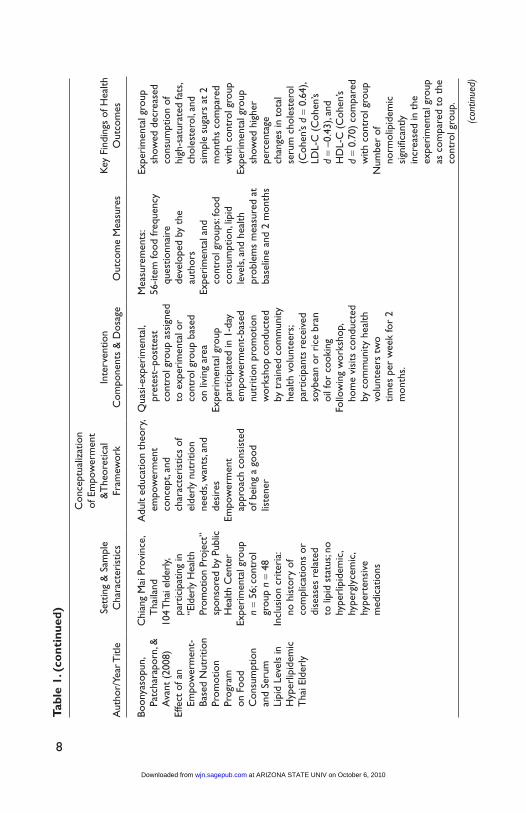
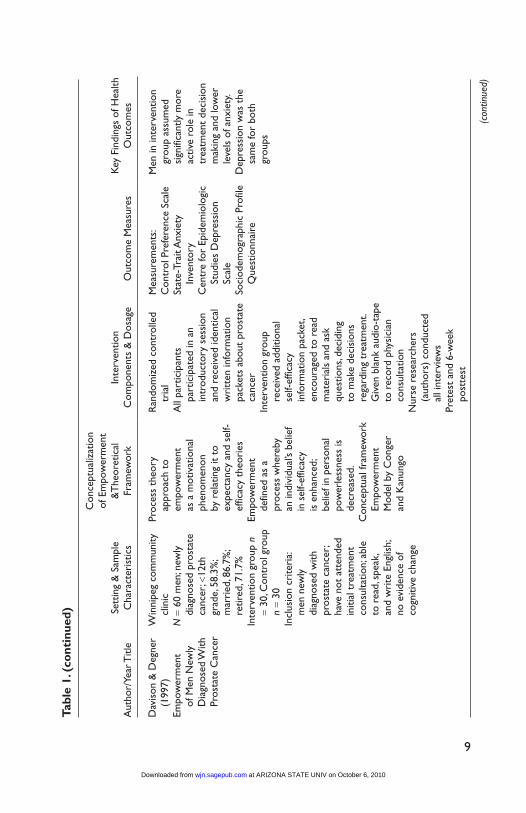
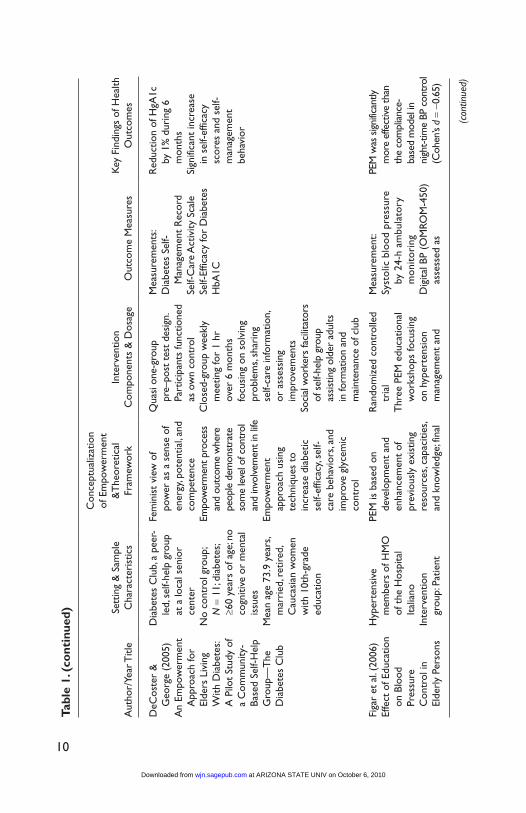
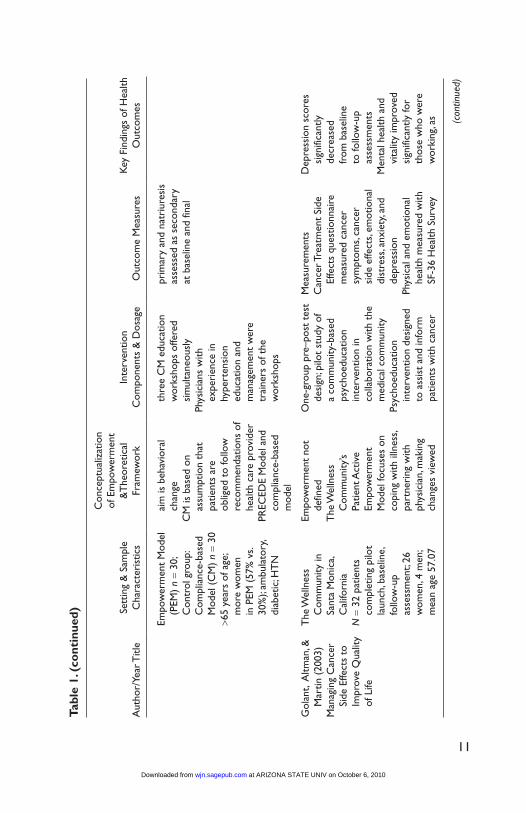
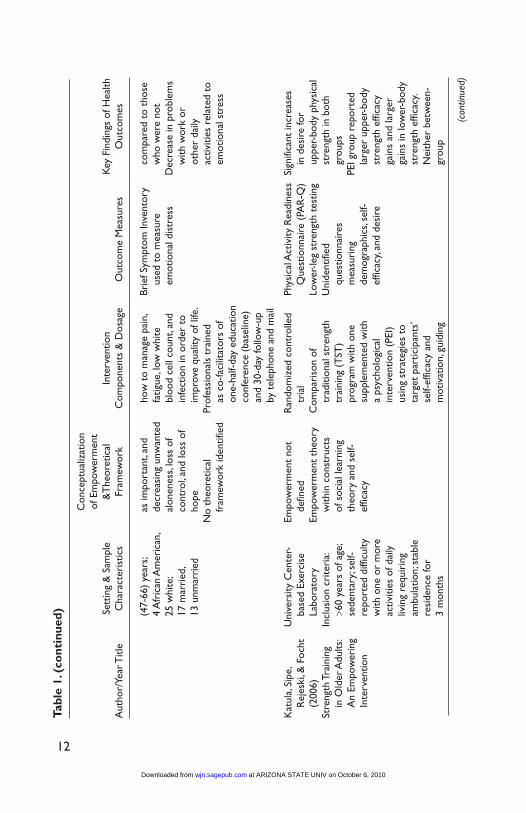
Eleven empowerment intervention studies focusing on older adults were found that met eligibility criteria. Six of the reviewed studies were random-ized controlled trials (Adolfsson, Walker-Engstrom, Smide, & Wikblad, 2007; Anderson et al., 1995; Davison & Degner, 1997; Figar et al., 2006; Katula, Sipe, Rejeski, & Focht, 2006; Tsay & Hung, 2004), and five used a quasi-experimental design (Boonyasopun, Aree, & Avant, 2008; DeCoster & George, 2005; Golant, Altman, & Martin, 2003; Pibernik-Okanovic, Prasek, Poljicanin-Filipovic, Pavlic-Renar, & Metelko, 2004; Wong, Harker, Lau, Shatzel, & Port, 2004) to address the needs of older adults related to the prevention and management of chronic illness and cancer. Table 1 presents a detailed description of the studies reviewed.
Sample and SettingParticipants included community-dwelling men and women with a mean age ranging from 50 years to 74 years. Two of the 11 studies reviewed targeted adults aged 60 years and older (DeCoster & George, 2005; Katula et al., 2006); one study targeted adults aged 65 years and older (Figar et al., 2006). One study did not report the age of participants but did indicate that the sample population was “elderly” (Boonyasopun et al., 2008). In 8 of the 11 studies women comprised the majority of the study participants, two were majority men (Adolfsson et al., 2007; Pibernik-Okanovic et al., 2004), and one study comprised only men (Davison & Degner, 1997). Of note, nearly half the study samples were international (Argentina, Canada, Croatia, Sweden, Taiwan, and Thailand), and one U.S. study comprised only foreign-born Hispanics (Wong et al., 2004). The remaining studies were conducted in the United States and included either predominately Caucasian (DeCoster & George, 2005; Golant et al., 2003; Katula et al., 2006) or did not report par-ticipant race (Anderson et al., 1995). Only one study reviewed included income level of the sample (DeCoster & George, 2005) and two studies did not report either education or income level of the sample (Adolfsson et al., 2007; Golant et al., 2003). Of the nine studies that did report years of education,
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
6
Tabl
e 1.
Syn
thes
is o
f Hea
lth E
mpo
wer
men
t In
terv
entio
ns
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
Ado
lfsso
n, W
alke
r-En
gstr
om, &
W
ikbl
ad (
2007
)Pa
tient
Edu
catio
n in
Typ
e 2
diab
etes
—
A R
ando
miz
ed
Con
trol
led
1-Ye
ar
Follo
w-U
p St
udy
Seve
n pr
imar
y ca
re
cent
ers
loca
ted
in
cent
ral S
wed
enIn
terv
entio
n gr
oup
n =
42; c
ontr
ol
grou
p n =
46In
clus
ion
crite
ria:
rece
ivin
g di
etar
y or
ora
l ant
idia
bete
s th
erap
y; ≤7
5 ye
ars;
HgA
1c v
alue
6.5
-10;
di
abet
es fo
r at
le
ast
1 ye
ar; p
er
MD
or
RN
, abl
e to
jo
in in
edu
catio
n gr
oup
with
oth
ers;
Swed
ish
spea
king
Empo
wer
men
t vi
ewed
as
a pr
oces
s w
here
by in
divi
dual
s (a
) ga
in m
aste
ry
and
take
con
trol
ov
er t
heir
live
s an
d (b
) po
sses
s sk
ills,
reso
urce
s, op
port
unity
, and
au
thor
ity t
o ch
ange
a
situ
atio
n.N
o th
eore
tical
fr
amew
ork
iden
tifie
dPa
radi
gm s
hift
from
pr
ovid
er-c
ente
red
to p
atie
nt-c
ente
red
appr
oach
Ran
dom
ized
con
trol
led
tria
lG
roup
s of
5-8
pa
rtic
ipan
ts; 4
-5
sess
ions
(2½
-hr
sess
ions
).Se
ven
phys
icia
ns a
nd
12 d
iabe
tes
spec
ialis
t nu
rses
ser
ved
as
empo
wer
men
t ed
ucat
ion
faci
litat
ors
Educ
atio
n se
ssio
ns
focu
sed
on t
hem
es
addr
essi
ng s
elf-
care
and
dia
bete
s kn
owle
dge
Aim
of e
duca
tion
was
to
(a)
ena
ble
patie
nts
to r
each
the
ir s
hort
- an
d lo
ng-t
erm
goa
ls
and
(b)
iden
tify
barr
iers
and
res
ourc
es
nece
ssar
y to
faci
litat
e be
havi
oral
cha
nge
At
base
line
and
1-ye
ar
follo
w-u
p:M
easu
rem
ents
: (a
) co
nfid
ence
in
diab
etes
kno
wle
dge;
(b
) se
lf-ef
ficac
y; (c
) sa
tisfa
ctio
n w
ith
daily
life
Gly
cem
ic c
ontr
ol
mea
sure
d th
roug
h H
gA1C
Body
mas
s in
dex
At
1-ye
ar fo
llow
-up:
in
terv
entio
n gr
oup
sign
ifica
ntly
hig
her
conf
iden
ce in
di
abet
es k
now
ledg
e co
mpa
red
to
cont
rol g
roup
No
sign
ifica
nt
diffe
renc
es
betw
een
grou
ps o
n re
mai
ning
var
iabl
es
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
7
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
And
erso
n et
al.
(199
5)Pa
tient
Em
pow
erm
ent:
Res
ults
of a
R
ando
miz
ed
Con
trol
led
Tria
l
Dia
bete
s ed
ucat
ion
prog
ram
gra
duat
es
from
Uni
vers
ity o
f M
ichi
gan
Med
ical
C
ente
rSe
lf-se
lect
ed s
ampl
e;
N =
64;
dia
betic
pa
tient
s; 46
ra
ndom
ly a
ssig
ned;
18
not
ran
dom
ly
assi
gned
; Mea
n ag
e 50
; 70%
wom
en;
77%
with
som
e co
llege
edu
catio
n
Philo
soph
y of
em
pow
erm
ent
that
pre
sum
es
to m
aint
ain
heal
th; i
ndiv
idua
ls
mus
t po
sses
s ps
ycho
logi
cal
abili
ties
in o
rder
to
prod
uce
chan
ges
in (
a) p
erso
nal
beha
vior
, (b)
soc
ial
circ
umst
ance
s, an
d (c
) or
gani
zatio
ns t
hat
influ
ence
the
ir li
ves
No
theo
retic
al
fram
ewor
k id
entif
ied
Ran
dom
ized
con
trol
led
tria
l fol
low
ing
unco
ntro
lled
pre–
post
pi
lot
test
Six
2-hr
gro
up s
essi
ons
wee
kly
for
6 w
eeks
Dia
betic
edu
cato
rs
prov
ided
em
pow
erm
ent
prog
ram
Aim
of p
rogr
am w
as t
o (a
) en
hanc
e ab
ility
to
iden
tify
and
set
pers
onal
goa
ls,
(b)
prob
lem
-sol
ve
to r
educ
e ba
rrie
rs,
(c)
cope
with
ci
rcum
stan
ces,
(d)
man
age
stre
ss,
(e)
gain
soc
ial
supp
ort,
(f) im
prov
e se
lf-m
otiv
atio
n
Mea
sure
men
ts:
Self-
effic
acy
subs
cale
m
easu
ring
per
ceiv
ed
abili
ty t
o (a
) as
sess
sa
tisfa
ctio
n, (
b) s
et
pers
onal
goa
ls,
(c)
prob
lem
-sol
ve,
(d)
emot
iona
lly
cope
, (e)
man
age
stre
ss,
(f) o
btai
n su
ppor
t, (h
) m
otiv
ate
self,
(i)
mak
e de
cisi
ons
Dia
bete
s Att
itude
Sca
leD
iabe
tes
Car
e Pr
ofile
Bloo
d gl
ucos
e co
ntro
l m
easu
red
by H
gA1C
Inte
rven
tion
grou
p de
mon
stra
ted
(a)
sign
ifica
nt
impr
ovem
ent
over
co
ntro
l gro
up in
fo
ur s
elf-e
ffica
cy
mea
sure
s, (b
) si
gnifi
cant
de
clin
e in
neg
ativ
e at
titud
e to
war
d liv
ing
with
dia
bete
s in
tw
o su
bsca
les,
sign
ifica
nt
redu
ctio
ns in
H
gA1C
leve
ls
(Coh
en’s
d =
0.24
)
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
8
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
Boon
yaso
pun,
Pa
tcha
rapo
rn, &
A
vant
(20
08)
Effe
ct o
f an
Empo
wer
men
t-Ba
sed
Nut
ritio
n Pr
omot
ion
Prog
ram
on
Foo
d C
onsu
mpt
ion
and
Seru
m
Lipi
d Le
vels
in
Hyp
erlip
idem
ic
Tha
i Eld
erly
Chi
ang
Mai
Pro
vinc
e,
Tha
iland
104
Tha
i eld
erly,
pa
rtic
ipat
ing
in
“Eld
erly
Hea
lth
Prom
otio
n Pr
ojec
t”
spon
sore
d by
Pub
lic
Hea
lth C
ente
rEx
peri
men
tal g
roup
n =
56; c
ontr
ol
grou
p n =
48In
clus
ion
crite
ria:
no h
isto
ry o
f co
mpl
icat
ions
or
dise
ases
rel
ated
to
lipi
d st
atus
; no
hype
rlip
idem
ic,
hype
rgly
cem
ic,
hype
rten
sive
m
edic
atio
ns
Adu
lt ed
ucat
ion
theo
ry,
empo
wer
men
t co
ncep
t, an
d ch
arac
teri
stic
s of
el
derl
y nu
triti
on
need
s, w
ants
, and
de
sire
sEm
pow
erm
ent
appr
oach
con
sist
ed
of b
eing
a g
ood
liste
ner
Qua
si-e
xper
imen
tal,
pret
est–
post
test
co
ntro
l gro
up a
ssig
ned
to e
xper
imen
tal o
r co
ntro
l gro
up b
ased
on
livi
ng a
rea
Expe
rim
enta
l gro
up
part
icip
ated
in 1
-day
em
pow
erm
ent-
base
d nu
triti
on p
rom
otio
n w
orks
hop
cond
ucte
d by
tra
ined
com
mun
ity
heal
th v
olun
teer
s; pa
rtic
ipan
ts r
ecei
ved
soyb
ean
or r
ice
bran
oi
l for
coo
king
Follo
win
g w
orks
hop,
ho
me
visi
ts c
ondu
cted
by
com
mun
ity h
ealth
vo
lunt
eers
tw
o tim
es p
er w
eek
for
2 m
onth
s.
Mea
sure
men
ts:
56-it
em fo
od fr
eque
ncy
ques
tionn
aire
de
velo
ped
by t
he
auth
ors
Expe
rim
enta
l and
co
ntro
l gro
ups:
food
co
nsum
ptio
n, li
pid
leve
ls, a
nd h
ealth
pr
oble
ms
mea
sure
d at
ba
selin
e an
d 2
mon
ths
Expe
rim
enta
l gro
up
show
ed d
ecre
ased
co
nsum
ptio
n of
hi
gh-s
atur
ated
fats
, ch
oles
tero
l, an
d si
mpl
e su
gars
at
2 m
onth
s co
mpa
red
with
con
trol
gro
upEx
peri
men
tal g
roup
sh
owed
hig
her
perc
enta
ge
chan
ges
in t
otal
se
rum
cho
lest
erol
(C
ohen
’s d =
0.64
), LD
L-C
(C
ohen
’s d =
–0.4
3), a
nd
HD
L-C
(C
ohen
’s d =
0.70
) co
mpa
red
with
con
trol
gro
upN
umbe
r of
no
rmol
ipid
emic
si
gnifi
cant
ly
incr
ease
d in
the
ex
peri
men
tal g
roup
as
com
pare
d to
the
co
ntro
l gro
up.
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
9
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
Dav
ison
& D
egne
r (1
997)
Empo
wer
men
t of
Men
New
ly
Dia
gnos
ed W
ith
Pros
tate
Can
cer
Win
nipe
g co
mm
unity
cl
inic
N =
60
men
; new
ly
diag
nose
d pr
osta
te
canc
er; <
12th
gr
ade,
58.
3%;
mar
ried
, 86.
7%;
retir
ed, 7
1.7%
Inte
rven
tion
grou
p n
= 30
, Con
trol
gro
up
n =
30In
clus
ion
crite
ria:
men
new
ly
diag
nose
d w
ith
pros
tate
can
cer;
have
not
att
ende
d in
itial
tre
atm
ent
cons
ulta
tion;
abl
e to
rea
d, s
peak
, an
d w
rite
Eng
lish;
no
evi
denc
e of
co
gniti
ve c
hang
e
Proc
ess
theo
ry
appr
oach
to
empo
wer
men
t as
a m
otiv
atio
nal
phen
omen
on
by r
elat
ing
it to
ex
pect
ancy
and
sel
f-ef
ficac
y th
eori
esEm
pow
erm
ent
defin
ed a
s a
proc
ess
whe
reby
an
indi
vidu
al’s
belie
f in
sel
f-effi
cacy
is
enh
ance
d;
belie
f in
pers
onal
po
wer
less
ness
is
decr
ease
d.C
once
ptua
l fra
mew
ork
Empo
wer
men
t M
odel
by
Con
ger
and
Kan
ungo
Ran
dom
ized
con
trol
led
tria
lA
ll pa
rtic
ipan
ts
part
icip
ated
in a
n in
trod
ucto
ry s
essi
on
and
rece
ived
iden
tical
w
ritt
en in
form
atio
n pa
cket
s ab
out
pros
tate
ca
ncer
Inte
rven
tion
grou
p re
ceiv
ed a
dditi
onal
se
lf-ef
ficac
y in
form
atio
n pa
cket
, en
cour
aged
to
read
m
ater
ials
and
ask
qu
estio
ns, d
ecid
ing
to m
ake
deci
sion
s re
gard
ing
trea
tmen
t. G
iven
bla
nk a
udio
-tap
e to
rec
ord
phys
icia
n co
nsul
tatio
nN
urse
res
earc
hers
(a
utho
rs)
cond
ucte
d al
l int
ervi
ews
Pret
est
and
6-w
eek
post
test
Mea
sure
men
ts:
Con
trol
Pre
fere
nce
Scal
eSt
ate-
Trai
t Anx
iety
In
vent
ory
Cen
tre
for
Epid
emio
logi
c St
udie
s D
epre
ssio
n Sc
ale
Soci
odem
ogra
phic
Pro
file
Que
stio
nnai
re
Men
in in
terv
entio
n gr
oup
assu
med
si
gnifi
cant
ly m
ore
activ
e ro
le in
tr
eatm
ent
deci
sion
m
akin
g an
d lo
wer
le
vels
of a
nxie
ty.
Dep
ress
ion
was
the
sa
me
for
both
gr
oups
(con
tinue
d)
Tabl
e 1.
(co
ntin
ued)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
10
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
DeC
oste
r &
G
eorg
e (2
005)
An
Empo
wer
men
t A
ppro
ach
for
Elde
rs L
ivin
g W
ith D
iabe
tes:
A P
ilot
Stud
y of
a
Com
mun
ity-
Base
d Se
lf-H
elp
Gro
up—
The
D
iabe
tes
Clu
b
Dia
bete
s C
lub,
a p
eer-
led,
sel
f-hel
p gr
oup
at a
loca
l sen
ior
cent
erN
o co
ntro
l gro
up;
N =
11;
dia
bete
s; ≥6
0 ye
ars
of a
ge; n
o co
gniti
ve o
r m
enta
l is
sues
Mea
n ag
e 73
.9 y
ears
, m
arri
ed, r
etir
ed,
Cau
casi
an w
omen
w
ith 1
0th-
grad
e ed
ucat
ion
Fem
inis
t vi
ew o
f po
wer
as
a se
nse
of
ener
gy, p
oten
tial,
and
com
pete
nce
Empo
wer
men
t pro
cess
an
d ou
tcom
e w
here
pe
ople
dem
onst
rate
so
me
leve
l of c
ontr
ol
and
invo
lvem
ent i
n lif
eEm
pow
erm
ent
appr
oach
usi
ng
tech
niqu
es t
o in
crea
se d
iabe
tic
self-
effic
acy,
self-
care
beh
avio
rs, a
nd
impr
ove
glyc
emic
co
ntro
l
Qua
si o
ne-g
roup
pr
e–po
st t
est
desi
gn.
Part
icip
ants
func
tione
d as
ow
n co
ntro
lC
lose
d-gr
oup
wee
kly
mee
ting
for
1 hr
ov
er 6
mon
ths
focu
sing
on
solv
ing
prob
lem
s, sh
arin
g se
lf-ca
re in
form
atio
n,
or a
sses
sing
im
prov
emen
tsSo
cial
wor
kers
faci
litat
ors
of s
elf-h
elp
grou
p as
sist
ing
olde
r ad
ults
in
form
atio
n an
d m
aint
enan
ce o
f clu
b
Mea
sure
men
ts:
Dia
bete
s Se
lf-M
anag
emen
t R
ecor
dSe
lf-C
are
Act
ivity
Sca
leSe
lf-Ef
ficac
y fo
r D
iabe
tes
HbA
1C
Red
uctio
n of
HgA
1c
by 1
% d
urin
g 6
mon
ths
Sign
ifica
nt in
crea
se
in s
elf-e
ffica
cy
scor
es a
nd s
elf-
man
agem
ent
beha
vior
Figa
r et
al.
(200
6)Ef
fect
of E
duca
tion
on B
lood
Pr
essu
re
Con
trol
in
Elde
rly
Pers
ons
Hyp
erte
nsiv
e m
embe
rs o
f HM
O
of t
he H
ospi
tal
Ital
iano
Inte
rven
tion
grou
p: P
atie
nt
PEM
is b
ased
on
deve
lopm
ent
and
enha
ncem
ent
of
prev
ious
ly e
xist
ing
reso
urce
s, ca
paci
ties,
and
know
ledg
e; fi
nal
Ran
dom
ized
con
trol
led
tria
lT
hree
PEM
edu
catio
nal
wor
ksho
ps fo
cusi
ng
on h
yper
tens
ion
man
agem
ent
and
Mea
sure
men
t:Sy
stol
ic b
lood
pre
ssur
e by
24-
h am
bula
tory
m
onit
orin
gD
igita
l BP
(OM
ROM
-450
) as
sess
ed a
s
PEM
was
sig
nific
antly
m
ore
effe
ctiv
e th
an
the
com
plia
nce-
base
d m
odel
in
nigh
t-tim
e BP
con
trol
(C
ohen
’s d = -0
.65)
(con
tinue
d)
Tabl
e 1.
(co
ntin
ued)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
11
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
Empo
wer
men
t M
odel
(P
EM)
n =
30;
Con
trol
gro
up:
Com
plia
nce-
base
d M
odel
(C
M)
n =
30>6
5 ye
ars
of a
ge;
mor
e w
omen
in
PEM
(57
% v
s. 30
%);
ambu
lato
ry,
diab
etic
; HT
N
aim
is b
ehav
iora
l ch
ange
CM
is b
ased
on
assu
mpt
ion
that
pa
tient
s ar
e ob
liged
to
follo
w
reco
mm
enda
tions
of
heal
th c
are
prov
ider
PREC
EDE
Mod
el a
nd
com
plia
nce-
base
d m
odel
thre
e C
M e
duca
tion
wor
ksho
ps o
ffere
d si
mul
tane
ousl
yPh
ysic
ians
with
ex
peri
ence
in
hype
rten
sion
ed
ucat
ion
and
man
agem
ent
wer
e tr
aine
rs o
f the
w
orks
hops
prim
ary
and
natr
iure
sis
asse
ssed
as
seco
ndar
y at
bas
elin
e an
d fin
al
Gol
ant,
Altm
an, &
M
artin
(20
03)
Man
agin
g C
ance
r Si
de E
ffect
s to
Im
prov
e Q
ualit
y of
Life
The
Wel
lnes
s C
omm
unity
in
Sant
a M
onic
a, C
alifo
rnia
N =
32
patie
nts
com
plet
ing
pilo
t la
unch
, bas
elin
e,
follo
w-u
p as
sess
men
t; 26
w
omen
, 4 m
en;
mea
n ag
e 57
.07
Empo
wer
men
t no
t de
fined
The
Wel
lnes
s C
omm
unity
’s Pa
tient
Act
ive
Empo
wer
men
t M
odel
focu
ses
on
copi
ng w
ith il
lnes
s, pa
rtne
ring
with
ph
ysic
ian,
mak
ing
chan
ges
view
ed
One
-gro
up p
re–p
ost
test
de
sign
; pilo
t st
udy
of
a co
mm
unity
-bas
ed
psyc
hoed
ucat
ion
inte
rven
tion
in
colla
bora
tion
with
the
m
edic
al c
omm
unity
Psyc
hoed
ucat
ion
inte
rven
tion
desi
gned
to
ass
ist
and
info
rm
patie
nts
with
can
cer
Mea
sure
men
tsC
ance
r Tre
atm
ent
Side
Ef
fect
s qu
estio
nnai
re
mea
sure
d ca
ncer
sy
mpt
oms,
canc
er
side
effe
cts,
emot
iona
l di
stre
ss, a
nxie
ty, a
nd
depr
essi
onPh
ysic
al a
nd e
mot
iona
l he
alth
mea
sure
d w
ith
SF-3
6 H
ealth
Sur
vey
Dep
ress
ion
scor
es
sign
ifica
ntly
de
crea
sed
from
bas
elin
e to
follo
w-u
p as
sess
men
tsM
enta
l hea
lth a
nd
vita
lity
impr
oved
si
gnifi
cant
ly fo
r th
ose
who
wer
e w
orki
ng, a
s
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
12
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
(47-
66)
year
s; 4
Afr
ican
Am
eric
an,
25 w
hite
; 17
mar
ried
, 13
unm
arri
ed
as im
port
ant,
and
decr
easi
ng u
nwan
ted
alon
enes
s, lo
ss o
f co
ntro
l, an
d lo
ss o
f ho
peN
o th
eore
tical
fr
amew
ork
iden
tifie
d
how
to
man
age
pain
, fa
tigue
, low
whi
te
bloo
d ce
ll co
unt,
and
infe
ctio
n in
ord
er t
o im
prov
e qu
ality
of l
ife.
Prof
essi
onal
s tr
aine
d as
co-
faci
litat
ors
of
one-
half-
day
educ
atio
n co
nfer
ence
(ba
selin
e)
and
30-d
ay fo
llow
-up
by t
elep
hone
and
mai
l
Brie
f Sym
ptom
Inve
ntor
y us
ed t
o m
easu
re
emot
iona
l dis
tres
s
com
pare
d to
tho
se
who
wer
e no
tD
ecre
ase
in p
robl
ems
with
wor
k or
ot
her
daily
ac
tiviti
es r
elat
ed t
o em
otio
nal s
tres
s
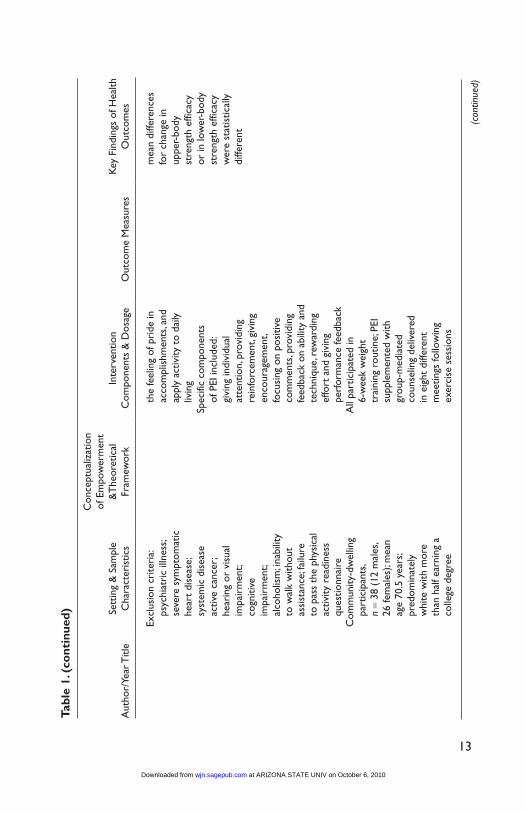
Kat
ula,
Sipe
, R
ejes
ki, &
Foc
ht
(200
6)St
reng
th T
rain
ing
in O
lder
Adu
lts:
An
Empo
wer
ing
Inte
rven
tion
Uni
vers
ity C
ente
r-ba
sed
Exer
cise
La
bora
tory
Incl
usio
n cr
iteri
a: >6
0 ye
ars
of a
ge;
sede
ntar
y; se
lf-re
port
ed d
iffic
ulty
w
ith o
ne o
r m
ore
activ
ities
of d
aily
liv
ing
requ
irin
g am
bula
tion;
sta
ble
resi
denc
e fo
r 3
mon
ths
Empo
wer
men
t no
t de
fined
Empo
wer
men
t th
eory
w
ithin
con
stru
cts
of s
ocia
l lea
rnin
g th
eory
and
sel
f-ef
ficac
y
Ran
dom
ized
con
trol
led
tria
lC
ompa
riso
n of
tr
aditi
onal
str
engt
h tr
aini
ng (
TST
) pr
ogra
m w
ith o
ne
supp
lem
ente
d w
ith
a ps
ycho
logi
cal
inte
rven
tion
(PEI
) us
ing
stra
tegi
es t
o ta
rget
par
ticip
ants
’ se
lf-ef
ficac
y an
d m
otiv
atio
n, g
uidi
ng
Phys
ical
Act
ivity
Rea
dine
ss
Que
stio
nnai
re (
PAR
-Q)
Low
er-le
g st
reng
th t
estin
gU
nide
ntifi
ed
ques
tionn
aire
s m
easu
ring
de
mog
raph
ics,
self-
effic
acy,
and
desi
re
Sign
ifica
nt in
crea
ses
in d
esir
e fo
r up
per-
body
phy
sica
l st
reng
th in
bot
h gr
oups
PEI g
roup
rep
orte
d la
rger
upp
er-b
ody
stre
ngth
effi
cacy
ga
ins
and
larg
er
gain
s in
low
er-b
ody
stre
ngth
effi
cacy
. N
eith
er b
etw
een-
grou
p
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
13
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
Excl
usio
n cr
iteri
a: ps
ychi
atri
c ill
ness
; se
vere
sym
ptom
atic
he
art
dise
ase;
sy
stem
ic d
isea
se
activ
e ca
ncer
; he
arin
g or
vis
ual
impa
irm
ent;
cogn
itive
im
pair
men
t; al
coho
lism
; ina
bilit
y
the
feel
ing
of p
ride
in
acco
mpl
ishm
ents
, and
ap
ply
activ
ity t
o da
ily
livin
gSp
ecifi
c co
mpo
nent
s of
PEI
incl
uded
: gi
ving
indi
vidu
al
atte
ntio
n, p
rovi
ding
re
info
rcem
ent,
givi
ng
enco
urag
emen
t, fo
cusi
ng o
n po
sitiv
e
mea
n di
ffere
nces
fo
r ch
ange
in
uppe
r-bo
dy
stre
ngth
effi
cacy
or
in lo
wer
-bod
y st
reng
th e
ffica
cy
wer
e st
atis
tical
ly
diffe
rent
to w
alk
with
out
assi
stan
ce; f
ailu
re
to p
ass
the
phys
ical
ac
tivity
rea
dine
ss
ques
tionn
aire
Com
mun
ity-d
wel
ling
part
icip
ants
, n =
38 (
12 m
ales
, 26
fem
ales
); m
ean
age
70.5
yea
rs;
pred
omin
atel
y w
hite
with
mor
e th
an h
alf e
arni
ng a
co
llege
deg
ree
com
men
ts, p
rovi
ding
fe
edba
ck o
n ab
ility
and
te
chni
que,
rew
ardi
ng
effo
rt a
nd g
ivin
g pe
rfor
man
ce fe
edba
ckA
ll pa
rtic
ipat
ed in
6-
wee
k w
eigh
t tr
aini
ng r
outin
e; P
EI
supp
lem
ente
d w
ith
grou
p-m
edia
ted
coun
selin
g de
liver
ed
in e
ight
diff
eren
t m
eetin
gs fo
llow
ing
exer
cise
ses
sion
s
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
14
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
Both
gro
ups
met
2 d
ays/
wee
k fo
r ce
nter
-bas
ed
trai
ning
and
1 d
ay/
wee
k ho
me-
base
d tr
aini
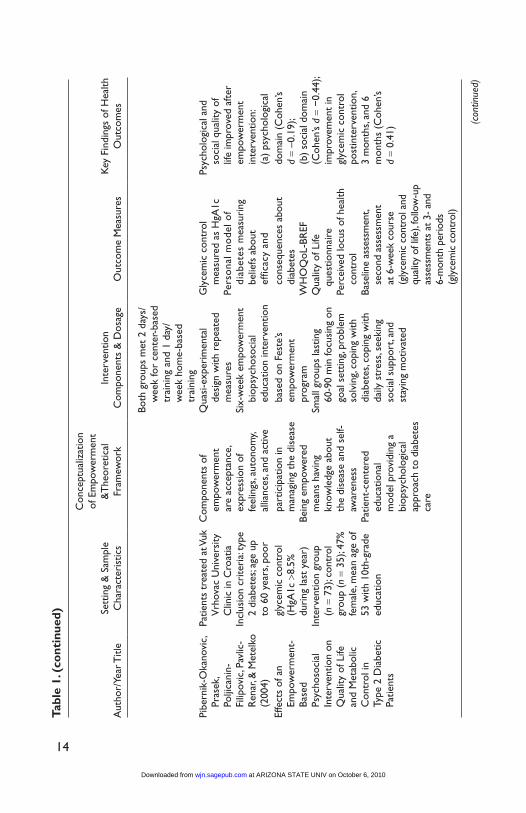
ngPi
bern
ik-O
kano
vic,
Pras
ek,
Polji
cani
n-Fi
lipov
ic, P
avlic
-R
enar
, & M
etel
ko
(200
4)
Patie
nts
trea
ted
at V
uk
Vrh
ovac
Uni
vers
ity
Clin
ic in
Cro
atia
Incl
usio
n cr
iteri
a: ty
pe
2 di
abet
es; a
ge u
p to
60
year
s, po
or
Com
pone
nts
of
empo
wer
men
t ar
e ac
cept
ance
, ex
pres
sion
of
feel
ings
, aut
onom
y, al
lianc
es, a
nd a
ctiv
e
Qua
si-e
xper
imen
tal
desi
gn w
ith r
epea
ted
mea
sure
sSi
x-w
eek
empo
wer
men
t bi
opsy
chos
ocia
l ed
ucat
ion
inte
rven
tion
Gly
cem
ic c
ontr
ol
mea
sure
d as
HgA
1cPe
rso
nal m
ode
l of
diab
etes
mea
suri
ng
belie
fs a
bout
ef
ficac
y an
d
Psyc
holo
gica
l and
so
cial
qua
lity
of
life
impr
oved
aft
er
empo
wer
men
t in
terv
entio
n:
(a)
psyc
holo
gica
lEf
fect
s of
an
Empo
wer
men
t-Ba
sed
Psyc
hoso
cial
In
terv
entio
n on
Q
ualit
y of
Life
an
d M
etab
olic
C
ontr
ol in
Ty
pe 2
Dia
betic
Pa
tient
s
glyc
emic
con
trol
(H
gA1c
>8.
5%
duri
ng la
st y
ear)
Inte
rven
tion
grou
p (n
= 7
3); c
ontr
ol
grou
p (n
= 3
5); 4
7%
fem
ale,
mea
n ag
e of
53
with
10t
h-gr
ade
educ
atio
n
part
icip
atio
n in
m
anag
ing
the
dise
ase
Bein
g em
pow
ered
m
eans
hav
ing
know
ledg
e ab
out
the
dise
ase
and
self-
awar
enes
sPa
tient
-cen
tere
d ed
ucat
iona
l m
odel
pro
vidi
ng a
bi
opsy
chol
ogic
al
appr
oach
to
diab
etes
ca
re
base
d on
Fes
te’s
empo
wer
men
t pr
ogra
mSm
all g
roup
s la
stin
g 60
-90
min
focu
sing
on
goal
set
ting,
prob
lem
so
lvin
g, co
ping
with
di
abet
es, c
opin
g w
ith
daily
str
ess,
seek
ing
soci
al s
uppo
rt, a
nd
stay
ing
mot
ivat
ed
cons
eque
nces
abo
ut
diab
etes
WH
OQ
oL-B
REF
Q
ualit
y of
Life
ques
tionn
aire
Perc
eive
d lo
cus
of h
ealth
co
ntro
lBa
selin
e as
sess
men
t, se
cond
ass
essm
ent
at 6
-wee
k co
urse
(g
lyce
mic
con
trol
and
qu
ality
of l
ife),
follo
w-u
p as
sess
men
ts a
t 3-
and
6-
mon
th p
erio
ds
(gly
cem
ic c
ontr
ol)
dom
ain
(Coh
en’s
d =
–0.1
9);
(b)
soci
al d
omai
n (C
ohen
’s d =
−0.
44);
impr
ovem
ent
in
glyc
emic
con
trol
po
stin
terv
entio
n,
3 m
onth
s, an
d 6
mon
ths
(Coh
en’s
d =
0.41
)
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
15
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
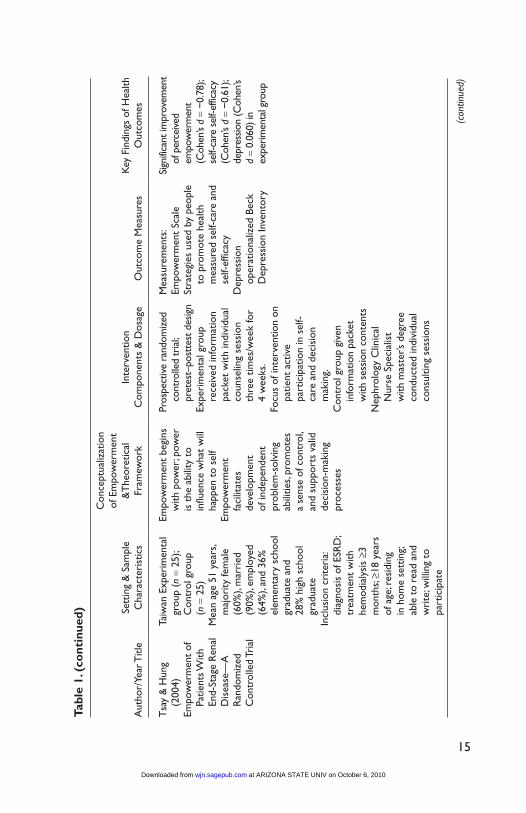
Tsa
y &
Hun
g (2
004)
Empo
wer
men
t of
Pa
tient
s With
En
d-St
age
Ren
al
Dis
ease
—A
R
ando
miz
ed
Con
trol
led
Tria
l
Taiw
an E
xper
imen
tal
grou
p (n
= 2
5);
Con
trol
gro
up
(n =
25)
Mea
n ag
e 51
yea
rs,
maj
ority
fem
ale
(60%
), m
arri
ed
(90%
), em
ploy
ed
(64%
), an
d 36
%
elem
enta
ry s
choo
l gr
adua
te a
nd28
% h
igh
scho
ol
grad
uate
Incl
usio
n cr
iteri
a: di
agno
sis
of E
SRD
; tr
eatm
ent
with
he
mod
ialy
sis
≥3
mon
ths;
≥18
year
s of
age
; res
idin
g in
hom
e se
ttin
g; ab
le t
o re
ad a
nd
wri
te; w
illin
g to
pa
rtic
ipat
e
Empo
wer
men
t be
gins
w
ith p
ower
; pow
er
is t
he a
bilit
y to
in
fluen
ce w
hat
will
ha
ppen
to
self
Empo
wer
men
t fa
cilit
ates
de
velo
pmen
t of
inde
pend
ent
prob
lem
-sol
ving
ab
ilitie
s, pr
omot
esa
sens
e of
con
trol
, an
d su
ppor
ts v
alid
de
cisi
on-m
akin
g pr
oces
ses
Pros
pect
ive
rand
omiz
ed
cont
rolle
d tr
ial;
pret
est–
post
test
des
ign
Expe
rim
enta
l gro
up
rece
ived
info
rmat
ion
pack
et w
ith in
divi
dual
co
unse
ling
sess
ion
thre
e tim
es/w
eek
for
4 w
eeks
.Fo
cus
of in
terv
entio
n on
pa
tient
act
ive
part
icip
atio
n in
sel
f-ca
re a
nd d
ecis
ion
mak
ing.
Con
trol
gro
up g
iven
in
form
atio
n pa
cket
w
ith s
essi
on c
onte
nts
Nep
hrol
ogy
Clin
ical
N
urse
Spe
cial
ist
with
mas
ter’s
deg
ree
cond
ucte
d in
divi
dual
co
nsul
ting
sess
ions
Mea
sure
men
ts:
Empo
wer
men
t Sc
ale
Stra
tegi
es u
sed
by p
eopl
e to
pro
mot
e he
alth
m
easu
red
self-
care
and
se
lf-ef
ficac
yD
epre
ssio
n op
erat
iona
lized
Bec
k D
epre
ssio
n In
vent
ory
Sign
ifica
nt im
prov
emen
t of
per
ceiv
ed
empo
wer
men
t (C
ohen
’s d =
−0.7
8);
self-
care
sel
f-effi
cacy
(C
ohen
’s d =
−0.6
1);
depr
essio
n (C
ohen
’s d =
0.06
0) in
ex
perim
enta
l gro
up
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
16
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
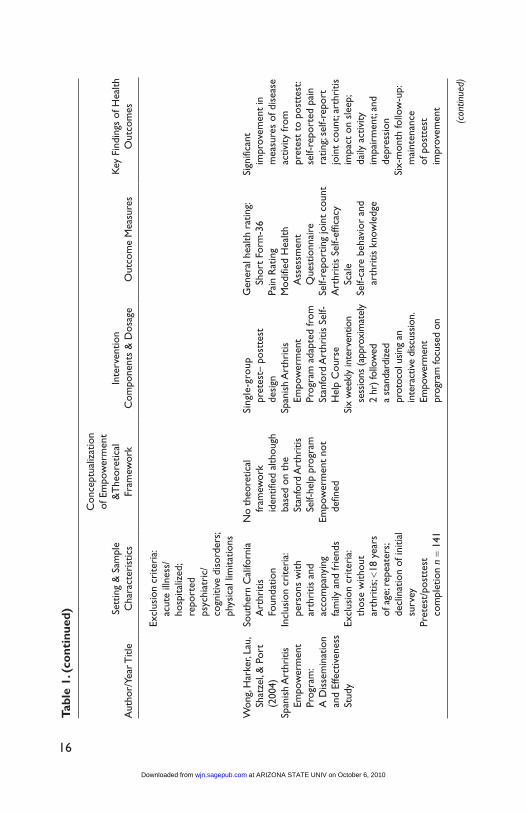
Excl
usio
n cr
iteri
a: ac
ute
illne
ss/
hosp
italiz
ed;
repo
rted
ps
ychi
atri
c/co
gniti
ve d
isor
ders
; ph
ysic
al li
mita
tions
Won
g, H
arke
r, La
u,
Shat
zel,
& P
ort
(200
4)Sp
anis
h A
rthr
itis
Empo
wer
men
t Pr
ogra
m:
A D
isse
min
atio
n an
d Ef
fect
iven
ess
Stud
y
Sout
hern
Cal
iforn
ia
Art
hriti
s Fo
unda
tion
Incl
usio
n cr
iteri
a: pe
rson
s w
ith
arth
ritis
and
acco
mpa
nyin
g fa
mily
and
frie
nds
Excl
usio
n cr
iteri
a: th
ose
with
out
arth
ritis
; <18
yea
rs
of a
ge; r
epea
ters
; de
clin
atio
n of
initi
al
surv
eyPr
etes
t/po
stte
st
com
plet
ion
n =
141
No
theo
retic
al
fram
ewor
k id
entif
ied
alth
ough
ba
sed
on t
he
Stan
ford
Art
hriti
s Se
lf-he
lp p
rogr
amEm
pow
erm
ent
not
defin
ed
Sing
le-g
roup
pr
etes
t– p
ostt
est
desi
gnSp
anis
h A
rthr
itis
Empo
wer
men
t Pr
ogra
m a
dapt
ed fr
omSt
anfo
rd A
rthr
itis
Self-
Hel
p C
ours
eSi
x w
eekl
y in
terv
entio
n se
ssio
ns (a
ppro
xim
atel
y 2
hr) f
ollo
wed
a
stan
dard
ized
pr
otoc
ol u
sing
an
inte
ract
ive
disc
ussio
n.
Empo
wer
men
t pr
ogra
m fo
cuse
d on
Gen
eral
hea
lth r
atin
g: Sh
ort
Form
-36
Pain
Rat
ing
Mod
ified
Hea
lth
Ass
essm
ent
Que
stio
nnai
reSe
lf-re
port
ing
join
t co
unt
Art
hriti
s Se
lf-ef
ficac
y Sc
ale
Self-
care
beh
avio
r an
d ar
thri
tis k
now
ledg
e
Sign
ifica
nt
impr
ovem
ent
in
mea
sure
s of
dis
ease
ac
tivity
from
pr
etes
t to
pos
ttes
t: se
lf-re
port
ed p
ain
ratin
g; se
lf-re
port
jo
int
coun
t; ar
thri
tis
impa
ct o
n sl
eep;
da
ily a
ctiv
ity
impa
irm
ent;
and
depr
essi
onSi
x-m
onth
follo
w-u
p:
mai
nten
ance
of
pos
ttes
t im
prov
emen
t
Tabl
e 1.
(co
ntin
ued)
(con
tinue
d)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
17
Aut
hor/
Year
Titl
eSe
ttin
g &
Sam
ple
Cha
ract
eris
tics
Con
cept
ualiz
atio
n of
Em
pow
erm
ent
&T
heor
etic
al
Fram
ewor
kIn
terv
entio
n C
ompo
nent
s &
Dos
age
Out
com
e M
easu
res
Key
Fin
ding
s of
Hea
lth
Out
com
es
6-m
onth
follo
w-u
p ev
alua
tion
n =
118
Mea
n ag
e 50
.7 y
ears
; 92
.2%
wom
en,
60%
spo
ke o
nly
Span
ish,
60%
re
port
ed h
avin
g no
m
edic
al in
sura
nce,
m
ajor
ity e
duca
ted
at e
lem
enta
ry le
vel
or le
ssN
atio
n of
ori
gin:
M
exic
o, 8
4%;
Cen
tral
Am
eric
a, 10
%; S
outh
Am
eric
a, 5%
; Car
ibbe
an/
Cub
a 0.
7%
enha
ncin
g se
lf-ef
ficac
y an
d ac
cess
ing
heal
th
care
.To
pics
incl
uded
:(a
) se
lf-m
anag
emen
t sk
ills,
(b)
lear
ning
to
acce
ss
heal
th c
are,
(c)
find
ing
appr
opri
ate
phys
icia
n ca
re, a
nd (
d) e
ffect
ive
com
mun
icat
ion
with
ph
ysic
ian
Faci
litat
or (
prom
otor
a)
cert
ified
by
arth
ritis
fo
unda
tion
led
inte
ract
ive
disc
ussi
on
form
atM
ater
ials
: boo
k,
audi
otap
es, i
llust
rate
d ex
erci
se b
ook
Tran
slat
ions
of m
ater
ials
in
dire
ct (
refle
cted
cu
ltura
l var
iatio
ns o
f co
ncep
ts, c
onte
nt, a
nd
proc
ess)
scor
es: g
ener
al
heal
th m
ean
ratin
g im
prov
ed fr
om
pret
est
to 6
-mon
th
follo
w-u
pPr
etes
t to
6-m
onth
fo
llow
-up
show
ed
sign
ifica
nt
impr
ovem
ent:
phys
ical
func
tion
Not
e: L
DL-
C =
low
-den
sity
lipo
prot
ein
chol
este
rol;
HD
L-C
= h
igh-
dens
ity li
popr
otei
n ch
oles
tero
l; ES
RD
= e
nd-s
tage
ren
al d
isea
se.
Tabl
e 1.
(co
ntin
ued)
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
18 Western Journal of Nursing Research XX(X)
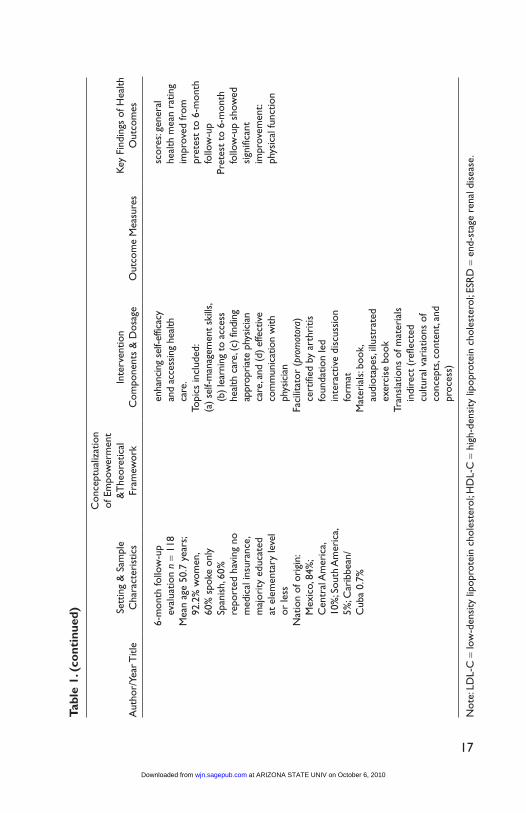
the levels varied, with some study populations comprising predominately elementary school–educated adults (Boonyasopun et al., 2008; Wong et al., 2004) to those with greater than 75% of the adults having some postsecond-ary education (Anderson et al., 1995; Katula et al., 2006). Sample sizes ranged from 13 to 108 participants.
The interventions were community based and ranged in approach from individually focused (Davison & Degner, 1997; Tsay & Hung, 2004) to group focused (Adolfsson et al., 2007; Anderson et al., 1995; DeCoster & George, 2005; Figar et al., 2006; Golant et al., 2003; Pibernik-Okanovic et al., 2004; Wong et al., 2004). Only Boonyasopun et al. (2008) and Katula et al. (2006) used a combination of both. The interventions were carried out in homes (Tsay & Hung, 2004), community-based organizations, schools and churches (Wong et al.), senior centers (DeCoster & George, 2005), clinics (Adolfsson et al., 2007; Anderson et al., 1995; Davison & Degner, 2005; Figar et al., 2006; Golant et al., 2003; Pibernik-Okanovic et al., 2004), and a combination of centers and homes (Boonyasopun et al., 2008; Katula et al., 2006).
Theoretical PerspectiveOf the articles reviewed, all conceptualized empowerment from a social process perspective involving relationships and social forces that act on the individual and promote a sense of control and feelings of power, including the transfer of power from one group to another. Nearly half of the studies reviewed (Adolfsson et al., 2007; Anderson et al., 1995; Boonyasopun et al., 2008; Pibernik-Okanovic et al., 2004; Tsay & Hung, 2004) were informed by Feste’s (1991) patient empowerment program (PEP), which argues that patient acquisition of knowledge and psychosocial skills empowers them to develop and implement a successful self-care plan that not only enhances their health, but also their quality of life (Anderson et al., 1995). The authors define empowerment “as one’s inherent capacity to be responsible for one’s own life” (Funnell et al., 1992, p. 55). This definition is guided by Rappaport’s (1987) perspective of empowerment as autonomous self-regulation. Empowerment is thus viewed as an outcome rather than an intervention or strategy to encourage behavior change (Anderson et al., 1995; Tsay & Hung, 2004). Although Figar and colleagues (2006) emphasized the importance of using multiple theories to develop and tailor their self-management program for blood pressure control, they also cited the PEP to explain their approach to patient empowerment. Additional theoretical frameworks included a feminist empowerment perspective to guide a peer-led, self-help Diabetes Club (DeCoster & George, 2005) and a psychological empowerment perspective
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from

Shearer et al. 19
(based on social cognitive theory and empowerment theory) to guide a strength training intervention (Katula et al., 2006). Finally, Davison and Degner (1997) used Conger and Kanungo’s (1988) Empowerment Model for their theoreti-cal framework, which is based on management and psychology theories as well as the concept of self-efficacy. With this approach, empowerment is viewed from a motivational perspective where belief in one’s own ability to successfully execute a desired goal leads to increased sense of personal mas-tery (Davison & Degner, 1997).
Intervention Strategies and DoseAll interventions reviewed included a health education component to foster empowerment by increasing knowledge to make informed choices and facilitating disease management specific to diabetes (Adolfsson et al., 2007; Anderson et al., 1995; DeCoster & George, 2005; Pibernik-Okanovic et al., 2004), hyperlipidemia (Boonyasopun et al., 2008), hypertension (Figar et al., 2006), cancer (Davison & Degner, 1997; Golant et al., 2003), end-stage renal disease (ESRD; Tsay & Hung, 2004), or disability including sarcopenia (Katula et al., 2006) and arthritis (Wong et al., 2004). In addition to health education, intervention content targeting type 2 diabetes self-management focused on optimal diabetes management by providing psychosocial edu-cation incorporating diet, exercise, medication compliance, and self-care behavior. Anderson and colleagues (1995), Adolfsson and colleagues (2007), and Pibernik-Okanovic and colleagues (2004) used a patient-centered, empowerment-based diabetes psychosocial educational program designed by Feste (1991). Key components that guided the six program sessions in these studies included enhancing the patient’s ability to identify and set real-istic goals, applying a problem-solving process to eliminate barriers to reach goals, coping with diabetes, managing stress related to living with diabetes, identifying and obtaining social support, and improving self-motivation (Anderson et al., 1995).
These studies (Adolfsson et al., 2007; Anderson et al., 1995; Boonyasopun et al., 2008; Katula et al., 2006; Tsay & Hung, 2004) also included a social support component to foster participant empowerment, but varied in both the degree of emphasis and the rationale. For example, Katula and colleagues (2006) coupled social interaction during supervised strength training exer-cises with a group counseling psychological empowerment process targeting strength efficacy and desire for physical strength. The group counseling com-ponents of the empowerment intervention were based on previous work in the promotion of a physically active lifestyle and included topics related to
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from

20 Western Journal of Nursing Research XX(X)
self-awareness and self-monitoring of progress, accomplishments, motiva-tion, and changes in daily life. Boonyasopun and colleagues (2008) used social support as the primary strategy for effecting change in the participants’ health behaviors. According to the authors, the community health volunteers’ biweekly home visits over the course of 2 months facilitated participant adherence through monitoring, teaching, and reinforcement. Tsay and Hung (2004) encouraged participants to identify sources of social support as a way to foster the participants’ ability to manage stress and to assume a more active role in the management of their ESRD.
Across the studies reviewed, the dosage of the interventions varied. Golant and colleagues (2003) held one half-day education program in the commu-nity, and Boonyasopun and colleagues (2008) held a full-day education program; other authors reported programs ranging from 4 to 10 sessions. Reported group attendance rates varied from 82.5% to greater than 85%. Among the 11 studies, 9 used either lay and/or health care professionals to deliver the intervention in a group format, and two used individual consulting provided by clinical nurse specialists (Davison & Degner, 1997; Tsay & Hung, 2004).
Outcome MeasuresAlthough all of the studies reviewed focused on enhancing patient empower-ment, empowerment was operationalized differently across studies. Outcome measures included self-efficacy (Adolfsson et al., 2007; Anderson et al., 1995; DeCoster & George, 2005; Katula et al., 2006; Wong et al., 2004); disease self-management (DeCoster & George, 2005; Figar et al., 2006; Golant et al., 2003; Pibernik-Okanovic et al., 2004; Wong et al., 2004); knowl-edge, attitude, behavioral, and health outcomes (Adolfsson et al., 1995; Boonyasopun et al., 2008); and taking a more active role in treatment deci-sion making (Davison & Degner, 1997). Even among those studies that conceptualized empowerment in the same way, the empirical referents var-ied. For example, self-efficacy was measured using SEDS (DeCoster & George, 2005), whereas others developed measures including confidence in lifting weights (Katula et al., 2006) and self-efficacy related to personal self-care (Adolfsson et al., 2007; Anderson et al., 1995; Wong et al., 2004).
Of note, only Tsay and Hung (2004) differentiated empowerment from self-efficacy as an outcome measure. The authors used a modified Empowerment Scale developed by Anderson, Fitzgerald, Funnell, and Marrero (2000) to evaluate the intervention’s effect on empowerment in patients with end-stage renal disease. The authors then measured self-care
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from

Shearer et al. 21
self-efficacy using Lev and Owen’s (1996) Strategies Used by People to Promote Health (SUPPH) scale.
Targeted health outcomes also varied across the studies reviewed and included blood pressure control (Figar et al., 2006), physical and emotional health (Davison & Degner, 1997; Golant et al., 2003; Tsay & Hung, 2004), pain scores (Wong et al., 2004), physical functioning (Katula et al., 2006; Wong et al., 2004), and reduced glycated hemoglobin (Adolfsson et al., 2007; Anderson et al., 1995; Boonyasopun et al., 2008; DeCoster & George, 2005; Pibernik-Okanovic et al., 2004).
Measurement time points also varied and ranged from 30 days to 9 months. Limited rationale, however, was provided for measurement time points.
Study OutcomesAcross reviewed studies, significant effects on outcomes were varied. Interventions based on Feste’s PEP had a significant impact on outcomes, including diabetes knowledge and self-care management skills (Adolfsson et al., 2007), self-efficacy (Anderson et al., 1995; Tsay & Hung, 2004), quality of life and glycemic control (Pibernik-Okanovic et al., 2004), hyper-lipidemia and food consumption (Boonyasopun et al., 2008), and levels of depression (Tsay & Hung, 2004). Studies incorporating other empowerment models to guide the intervention also had significant effects, including increased self-efficacy (DeCoster & George, 2005; Katula et al., 2006), improved glycemic control (DeCoster & George, 2005), decreased depres-sion (Golant et al., 2003), improved blood pressure control (Figar et al., 2006), and a more active role in decision making, and lowered state anxiety levels (Davison & Degner, 1997). It is important to note that the sample size in a number of studies was small; thus this review likely included studies without adequate statistical power. Among studies that provided adequate data, effect size ranged from .19 to .78, with most studies showing small to moderate effects.
DiscussionGiven the growing numbers of older adults, a greater understanding of rele-vant and effective empowerment interventions for this population is essen-tial. The findings from this review support the efficacy of empowerment interventions to enhance management of chronic illness among older adults and improve health outcomes. However, limitations in attention to theory, specification of intervention strategies used, and outcomes measured make it
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from

22 Western Journal of Nursing Research XX(X)
difficult to draw conclusions about the overall effectiveness of empowerment interventions in older adults.
Although a number of the studies reviewed used a theoretical perspective to guide program implementation and evaluation, often insufficient detail was provided to permit understanding of the operationalization of the major concepts in the intervention, particularly from a culturally relevant perspec-tive. Among studies that have achieved intervention effects, the mechanisms underlying treatment are not always clear, limiting the applicability of exist-ing intervention findings to practice. Ongoing research efforts are needed to better operationalize and test theoretical frameworks for empowerment inter-ventions and to evaluate the effectiveness of multilevel interventions that address cultural, contextual, and sustainability issues. Theory-based pro-grams that incorporate formative mechanisms and relevance to older adults in the community may show more promising results than those that lack a theoretical basis. A stronger theoretical approach may include specification of and program tailoring to select theoretical mediators.
Across the studies reviewed, consistency between the empowerment conceptualization and the clinical problem addressed was inferred. Few of the studies reviewed conceptualized the problem guiding the intervention from a theoretical perspective. Specification of the problem should detail defining experiences consistent with intervention theory, such as lack of self-efficacy, or low levels of perceived power, mastery, skills, or resources as part of inclusion criteria. The assumption that chronic illness or risk among older adults is associated with low levels of empowerment may result in interventions being delivered to those who do not need them, and will not benefit from them, limiting intervention effects. Continued efforts are needed to clearly specify the factors that put older adults at risk for low levels of perceived empowerment, thus more clearly targeting the causes for lack of empowerment and the design and evaluation of relevant and effective interventions.
Overall, intervention strategies were not well defined and were not clearly linked to theoretical referents. Although the majority of strategies focused on knowledge, social support, motivational factors, self-efficacy, self-management, goal setting, and education, it is not clear how these strategies comprise core empowerment components in an intervention. Without understanding the core empowerment components underpinning the interventions, includ-ing such factors as how and why the interventions worked or the conditions under which the treatment was thought to work, application to practice is limited. A greater level of specificity in construct definition as well as clear links between intervention theory and intervention strategies are needed to
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
Shearer et al. 23
evaluate specific predictions from theory and provide meaningful guidelines for intervention development targeting these constructs (Baranowski, 2006), strengthening the contribution of studies to the empirical literature. General statements about intervention content and delivery methods limit evaluation of the relationship between empowerment outcomes and intervention deliv-ery, including which component of multiple interventions may be responsible for an effect. Thus, greater attention is needed to intervention specification and related quantification of intervention fidelity to the planned protocol.
The conceptualization of empowerment and operationalization of empow-erment in the intervention were not consistent. Adolfsson and colleagues (2007) conceptualized empowerment as including mastery and control, oper-ationalizing empowerment in the intervention as education. Similarly, Figar and colleagues (2006) conceptualized empowerment as enhancement of capac-ities, operationalizing empowerment in the intervention as education and digital blood pressure monitoring. Davidson and Degner (1997) conceptual-ized empowerment as enhancing self-efficacy, operationalizing empowerment as information. DeCoster and George (2005) conceptualized empowerment as including control, self-efficacy, energy, potential, and competence, opera-tionalizing empowerment as a self-help group focusing on diabetes manage-ment. In some studies reviewed, empowerment was not defined, but relied on education to address problems such as quality of life among cancer patients (Golant et al., 2003). In other studies, the conceptualization of empowerment was outlined, with little information regarding operationalization in the inter-vention (Boonyasopun et al., 2008; Pibernik-Okanovic et al., 2004; Tsay & Hung, 2004; Wong et al., 2004). With any health promotion intervention or program, one of the greatest challenges is the maintenance of relevant effects over time. Many interventions within this review implemented comprehen-sive programs, but did not necessarily plan for, facilitate, or evaluate mainte-nance of program activities.
The majority of the studies reviewed conceptualized empowerment from a social perspective that involves relationships and social forces that act on the individual and promote a sense of control and feelings of power (Shearer & Reed, 2004), including the transfer of power from one group to another (Leyshon, 2002). However, a focus on individual strengths, skills, and access to needed resources may be a more sustainable approach. Empowerment may be viewed from a life span developmental perspective (Lerner, 1997) in which human beings are viewed as continuously innovative, embedded in a dynamic environment, and possessing inherent potential (Shearer & Reed, 2004). Successful intervention design from this perspective requires an inte-grative understanding of cultural and contextual perspectives, characteristics,
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from

24 Western Journal of Nursing Research XX(X)
and resources of the target population, as well as the theoretically relevant determinants of empowerment that can be transformed into culturally sensi-tive behavior change strategies (Fleury & Lee, 2006). Interventions from a life span perspective focus on maximizing strengths and minimizing weak-nesses (Baltes et al., 1998) rather than changing behavior. The participant is a resource and active partner, and the intervention, directed less toward changing the participant and more toward optimizing human potential (Shearer & Reed, 2004). Similarly, studies reviewed tested standardized empowerment interventions primarily focused on the management of chronic illness using a one-size-fits-all approach. Further research is needed designed to facilitate the engagement of the older adult in the process of recognizing personal resources, social contextual resources including social network, and accessing social services and the identification of desired health goals and the means to attain these goals (Shearer, 2009). Indeed, researchers have called for an empowerment approach from a paradigm focused on the inherent poten-tial, skills, and resources of older adults rather than their deficits (Shearer, 2007; Shearer & Reed, 2004).
In a number of studies outcome measures were clearly linked to the con-ceptualization of empowerment (Anderson et al., 1995; Boonyasopun et al., 2008; Pibernik-Okanovic et al., 2004; Tsay & Hung, 2004; Wong et al., 2004), whereas in others the link was less clear. Adolfsson and colleagues (2007) conceptualized empowerment as including mastery and control, with outcome measures targeting knowledge, self-efficacy, HgA1C, and body mass index. Davidson and Degner (1997) conceptualized empowerment as self-efficacy, with outcome measures targeting treatment control preferences, anxiety, and depression. Figar and colleagues (2006) conceptualized empow-erment as enhancement of resources, capacity, and knowledge, with outcome as systolic blood pressure. Katula and colleagues (2006) based their interven-tion on Empowerment Theory and self-efficacy, with outcomes of physical activity readiness and lower leg strength. Outcomes evaluation was typically not comprehensive in addressing all theoretically relevant outcomes. Among outcomes addressed, effects were stronger overall for physiologic outcome variables and for outcomes measured immediately following the interven-tion. Tsay and Hung (2004) used an empowerment-specific scale to measure intervention outcomes, with an effect size of .78.
One area of concern within the studies reviewed is the lack of significant follow-up to determine the long-term impact of interventions. Although mod-est changes in health behaviors and outcomes can be achieved with empow-erment interventions, the extent to which such outcomes are lasting is less clear. With some interventions implemented for only several weeks, and an
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from

Shearer et al. 25
overall limited time to follow up, the lasting impact of health empowerment interventions on relevant outcomes is difficult to evaluate.
In summary, a limited amount of intervention research has been conducted focusing on empowerment in older adults. This review raises many important questions regarding the definition and measurement of the concept of empow-erment, the strategies used to guide interventions, and the theory guiding the intervention. The clinical relevance and utility of empowerment-based inter-vention research is limited given the lack of clarity regarding the concept of empowerment, its measurement, and the specific interventions addressed.
Declaration of Conflicting Interests
The authors declared no conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The authors disclosed that they received the following support for their research and/or authorship of this article: The authors received funding from National Institutes of Health–National Institute of Nursing Research: 1R15 NR009225-01A2.
References
Administration on Aging, United States Department of Health and Human Services. (2007). A profile of older Americans: 2007. Washington, DC: Author.
Adolfsson, E. T., Walker-Engstrom, M. L., Smide, B., & Wikblad, K. (2007). Patient education in type 2 diabetes—A randomized controlled 1 year follow-up study. Diabetes Research and Clinical Practice, 76, 341-350.
Anderson, R. M., Fitzgerald, J. T., Funnell, M. M., & Marrero, D. G. (2000). The diabetes empowerment scale: A measure of psychosocial self-efficacy. Diabetes Care, 23, 739-743.
Anderson, R. M., Funnell, M. M., Butler, P. M., Arnold, M. S., Fitzgerald, J. T., & Feste, C. C. (1995). Patient empowerment: Results of a randomized controlled trial. Diabetes Care, 18, 943-949.
Baltes, P. B., Lindenberger, U., & Staudinger, U. M. (1998). Life-span theory in devel-opmental psychology. In R. Lerner (Ed.), Theoretical models of human develop-ment (pp. 1029-1143). New York, NY: John Wiley.
Bandura, A. (1992). Exercise of personal agency through the self-efficacy mecha-nisms. In R. Schwarzer (Ed.), Self-efficacy: Thought control of action (pp. 3-38). Washington, DC: Hemisphere.
Bandura, A. (1994). Self-efficacy. In V. S. Ramachandran (Ed.), Encyclopedia of human behavior (pp. 71-81). New York, NY: Academic Press.
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from

26 Western Journal of Nursing Research XX(X)
Baranowski, T. (2006). Advances in basic behavioral research will make the most important contributions to effective dietary change programs at this time. Journal of the American Dietetic Association, 106, 808-811.
Blue, C. L., & Black, D. R. (2005). Synthesis of intervention research to modify physical activity and dietary behaviors. Research and Theory for Nursing Prac-tice: An International Journal, 19, 25-61.
Boonyasopun, U., Aree, P., & Avant, K. C. (2008). Effect of an empowerment-based nutrition promotion program on food consumption and serum lipid levels in hyperlipidemic Thai elderly. Nursing and Health Sciences, 10, 93-100.
Centers for Disease Control and Prevention & The Merck Company Foundation. (2007). The state of aging and health in America 2007. Whitehouse Station, NJ: The Merck Company Foundation. Retrieved from http://www.cdc.gov/aging/pdf/saha_2007.pdf
Conger, J. A., & Kanungo, R. N. (1988). The empowering process: Integrating theory and practice. Academy of Management Review, 13, 471-482.
Davison, B. J., & Degner, L. F. (1997). Empowerment of men newly diagnosed with prostate cancer. Cancer Nursing, 20, 187-196.
DeCoster, V. A., & George, L. (2005). An empowerment approach for elders living with diabetes: A pilot study of a community-based self-help group—The diabetes club. Educational Gerontology, 31, 699-713.
Ellis-Stoll, C., & Popkess-Vawter, S. (1998). A concept analysis on the process of empowerment. Advances in Nursing Science, 21, 62-68.
Feste, C. C. (1991). Empowerment: Facilitating a path to personal self-care. Elkhart, IN: Miles Diagnostic Division.
Figar, S., Glarza, C., Petrlik, E., Hornstein, L., Loria, G. R., Waisman, G., . . . de Quirós, F. G. B. (2006). Effect of education on blood pressure control in elderly persons. American Journal of Hypertension, 19, 737-743.
Fleury, J., & Lee, S. (2006). The social ecological model and physical activity in African American women. American Journal of Community Psychology, 37, 129-140.
Fulton, Y. (1997). Nurses’ views on empowerment: A critical social theory perspec-tive. Journal of Advanced Nursing, 26, 529-536.
Funnell, M. M., Anderson, R. M., Arnold, M. S., Barr, P. A., Donnelly, M., Johnson, P. D., … White, N. H. (1992). Empowerment: An idea whose time has come in diabetes education. Beta Release, 16, 54-58.
Freire, P. (1981). Pedagogy of the oppressed (M. B. Ramos, Trans.). New York: Con-tinuum Publishing. (Original work published 1968.)
Golant, M., Altman, T., & Martin, C. (2003). Managing cancer side effects to improve quality of life. Cancer Nursing, 26, 37-44.
Gutierrez, L. (1995). Understanding the empowerment process: Does consciousness make a difference? Social Work Research, 19, 229-237.
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
Shearer et al. 27
Hawks, J. (1992). Empowerment in nursing education: Concept analysis and applica-tion to philosophy, learning and instruction. Journal of Advanced Nursing, 17, 609-618.
Kane, D., & Thomas, B. (2000). Nursing and the “F” word. Nursing Forum, 35, 17-24.Katula, J. A., Sipe, M., Rejeski, W. J., & Focht, B. C. (2006). Strength training in older
adults: An empowering intervention. Medicine & Science in Sports & Exercise, 38, 106-111.
Keller, C., & Fleury, J. (2000). Health promotion for the elderly. Thousand Oaks, CA: Sage.
Labonte, R. (1994). Health promotion and empowerment: Reflections on professional practice. Health Education Quarterly, 21, 253-268.
Lerner, R. (1997). Concepts and theories of human development (2nd ed.). Mahwah, NJ: Lawrence Erlbaum.
Lev, E. L., & Owen, S. V. (1996). A measurement of self-care self-efficacy. Research in Nursing & Health, 19, 421-429.
Leyshon, S. (2002). Empowering practitioners: An unrealistic expectation of nurse education? Journal of Advanced Nursing, 40, 466-474.
Perkins, D. D., & Zimmerman, M. A. (1995). Empowerment, theory, research, and application. American Journal of Community Psychology, 23, 569-579.
Pibernik-Okanovic, M., Prasek, M., Poljicanin-Filipovic, T., Pavlic-Renar, I., & Metelko, Z. (2004). Effects of an empowerment-based psychosocial intervention on quality of life and metabolic control in type 2 diabetic patients. Patient Educa-tion and Counseling, 52, 193-199.
Rappaport, J. (1984). Studies in empowerment: Introduction to the issue. Prevention in Human Services, 3, 1-7.
Rappaport, J. (1987). Terms of empowerment/exemplars of prevention: Toward a theory for community psychology. American Journal of Community Psychology, 15, 121-147.
Ryles, S. (1999). A concept analysis of empowerment: Its relationship to mental health nursing. Journal of Advanced Nursing, 29, 600-607.
Shearer, N. B. C. (2004). Relationships of contextual and relational factors to health empowerment in women. Research and Theory for Nursing Practice, 18, 357-370.
Shearer, N. B. C. (2007). Toward a nursing theory of health empowerment in home-bound older women. Journal of Gerontological Nursing, 33, 38-45.
Shearer, N. B. C. (2009). Health empowerment theory as a guide for practice. Geriat-ric Nursing, 30(2 Suppl. 1), 4-10.
Shearer, N. B. C., & Fleury, J. (2006). Social support promoting health in older women. Journal of Women & Aging, 18(4), 3-17.
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from
28 Western Journal of Nursing Research XX(X)
Shearer, N. B. C., & Reed, P. G. (2004). Empowerment: Reformulation of a non-Rogerian concept. Nursing Science Quarterly, 17, 253-259.
Toofany, S. (2006). Patient empowerment. Nursing Management, 13, 18-22.Toofany, S. (2007). Empowering older people. Nursing Older People, 19(2), 12-14.Tsay, S. L., & Hung, L. O (2004). Empowerment of patients with end-stage renal
disease—A randomized controlled trial. International Journal of Nursing Studies, 41, 59-65.
Wong, A. L., Harker, J. O., Lau, V. P., Shatzel, S., & Port, L. H. (2004). Spanish Arthri-tis Empowerment Program: A dissemination and effectiveness study. Arthritis & Rheumatism, 51, 332-336.
at ARIZONA STATE UNIV on October 6, 2010wjn.sagepub.comDownloaded from