emergence, persistence, and resolution of suicidal ideation during treatment of depression in old...
TRANSCRIPT
Seediscussionsstatsandauthorprofilesforthispublicationathttpswwwresearchgatenetpublication6854829
Emergencepersistenceandresolutionofsuicidalideationduringtreatmentofdepressioninoldage
ArticleinJournalofAffectiveDisordersmiddotMarch2007
DOI101016jjad200607015middotSourcePubMed
CITATIONS
43
READS
30
7authorsincluding
KatalinSzanto
UniversityofPittsburgh
74PUBLICATIONS2265CITATIONS
SEEPROFILE
PatriciaRHouck
UniversityofPittsburgh
340PUBLICATIONS18961CITATIONS
SEEPROFILE
AlexandreYDombrovski
UniversityofPittsburgh
52PUBLICATIONS1105CITATIONS
SEEPROFILE
BruceGPollock
CentreforAddictionandMentalHealth
492PUBLICATIONS16490CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyKatalinSzantoon19June2015
TheuserhasrequestedenhancementofthedownloadedfileAllin-textreferencesunderlinedinblueareaddedtotheoriginaldocumentandarelinkedtopublicationsonResearchGatelettingyouaccessandreadthemimmediately
Journal of Affective Disorders 98 (2007) 153ndash161wwwelseviercomlocatejad
Research report
Emergence persistence and resolution of suicidal ideationduring treatment of depression in old age
Katalin Szanto a Benoit H Mulsant ac Patricia R Houck a Mary Amanda Dew abAlexandre Dombrovski a Bruce G Pollock ad Charles F Reynolds III aefg
a University of Pittsburgh School of Medicine Department of Psychiatry Pittsburgh Pennsylvania United Statesb University of Pittsburgh School of Medicine Departments of Psychology and Epidemiology Pittsburgh Pennsylvania United States
c University of Pittsburgh School of Medicine Department of Psychiatry and Center for Addiction and Mental HealthDepartment of Psychiatry University of Toronto Canada
d The Rotman Research Institute Baycrest Centre for Geriatric Care University of Toronto Canadae Advanced Center for Interventions and Services Research for Late-Life Mood Disorders
University of Pittsburgh School of Medicine Pittsburgh Pennsylvania United Statesf The John A Hartford Center of Excellence in Geriatric Psychiatry University of Pittsburgh School of Medicine
Pittsburgh Pennsylvania United Statesg Project EXPORT at the Center for Minority Health Graduate School of Public Health University of Pittsburgh School of Medicine
Pittsburgh Pennsylvania United States
Received 16 February 2006 received in revised form 20 July 2006 accepted 25 July 2006Available online 24 August 2006
Abstract
Introduction To determine the rate and clinical correlates of emergent persistent and resolved suicidal ideation during treatment ofmajor depression in the elderlyMethods Based on the course of suicidal ideation before and during 12 weeks of antidepressant treatment we classified 437 elderlypatients (234 treated with paroxetine 203 with nortriptyline) as either non-suicidal or as having ldquoemergentrdquo ldquopersistentrdquo orldquoresolvedrdquo suicidality We compared the four groups on pretreatment demographic and clinical measures and with respect todepression anxiety and akathisia during treatment Results Rates of emergent persistent and resolved suicidality were 78 126and 156 respectively Patients with persistent suicidal ideation were more likely to have recurrent depression than non-suicidalpatients or patients whose suicidality resolved with treatment At the start of treatment patients in all three suicidal groups had lowerself-esteem than non-suicidal patients During the course of treatment emergent suicidality was not associated with akathisia nor didrates of emergent suicidality differ between paroxetine- and nortriptyline-treated patients While at baseline the levels of depressionand anxiety and agitation were similar in the four groups patients with resolved suicidality had a favorable treatment response whilepatients with emergent and persistent suicidality were more likely to maintain higher depression scores and had higher levels ofanxiety and agitation during treatmentDiscussion Emergence of suicidal ideation is not common but is clinically significant during treatment of late-life depression andmay signal more difficult-to-treat-depressioncopy 2006 Elsevier BV All rights reserved
Keywords Elderly Major depression Suicidal ideation Treatment
Corresponding author University of Pittsburgh School of Medicine 315 S Bellefield Street Bellefield Towers 537 Pittsburgh PA 15213 USATel +1 412 586 9601 fax +1 412 246 6030
E-mail address szantokupmcedu (K Szanto)
0165-0327$ - see front matter copy 2006 Elsevier BV All rights reserveddoi101016jjad200607015
154 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
1 Background
Older adults (age 60 and above) have the highestsuicide rate among all age groups in most countries of theworld (World Health Organization 2005) Althoughdepression is the most common diagnosis in elderlysuicide attempters and completers (Conwell et al 2000Beautrais 2002) to our knowledge no study has syste-matically examined emergence persistence and resolu-tion of suicidality during treatment of late-life depressionRecent concerns about emergent suicidality during de-pression treatment in children and adolescent (US Foodand Drug Administration 2004) and its apparentassociation with akathisia or agitation induced byselective serotonin reuptake inhibitors (SSRIs) highlightthe clinical importance of this issue In late-life theliterature is inconclusive with respect to these issues andto the implication of prior course (eg single versusrecurrent depression) for suicide risk
Patients whose mood remains low when they regainenergy may be at increased risk for suicide (Detre andJarecki 1971) Alternatively increased anxiety and agi-tation in the face of non- or partially remitting depressionmay increase suicide risk (Akiskal et al 2005) A fewcase series (Power and Cowen 1992) and case reports(Rothschild and Locke 1991) have suggested anassociation between suicidality and akathisia Howeverother investigators did not find a relationship betweentreatment-emergent adverse events and suicidality (Tol-lefson et al 1994) A review of the literature (Hansen2001 pp 495) concluded that ldquoakathisia cannot be un-equivocally linked to suicidal behavior however it iscertain that the condition of akathisia does cause con-siderable distress in an already vulnerable group of pa-tientsrdquo To our knowledge no study other than casereports(Hansen andWilkinson 2001) has investigated apossible relationship between medication-induced anx-ietyagitation and suicidality in the elderly
According to psychological autopsy studies anxietydisorders without comorbid mood disorders only mo-destly increase suicide risk in the elderly (Waern et al2002b) However in one study insomnia and severepsychic anxiety predicted suicide in mid-life patientswith major depressive disorder (Fawcett et al 1990) andtwo recent reports found an association between mixeddepression often marked by psychomotor agitation andsuicidal ideation and attempts (Akiskal et al 2005Balazs et al 2006) The authors note that psychomotoragitation maybe related to an activation syndromecaused by antidepressants In our previous study in el-derly patients decline in suicidal ideation was associatedwith remission of depression (Szanto et al 2003) Thus
based on literature review our previous findings andclinical experience we hypothesized that
1) Emergence and persistence of suicidality during treat-ment would be associated with chronicrecurrentdepression and higher baseline anxiety or agitation
2) Patientswith emergent or persistent suicidalitywould bemore likely to have persisting low mood and higherlevels of anxietyagitationakathisia compared to non-suicidal patients and to thosewhose suicidality resolved
3) Patients treated with a SSRI would be more likely tobecome suicidal than patients receiving a tricylicThis association if present could be due to the onsetof akathisia in the SSRI-treated group
2 Methods
21 Study group
Data for this analysis were available for 473 par-ticipants in three federally-supported clinical trials ofgeriatric depressionWe pooled data from the three studiesbecause all dealt with the treatment of non-psychotic non-bipolar major depressive episodes in old age and utilizedsimilar assessment and treatment approaches administeredin the same research setting Patients were required to be60 years or older to have nonpsychotic unipolar majordepression determined by administration of either theSchedule for Affective Disorders and Schizophrenia(SADS) (Spitzer 1978) or the SCID for DSM-IV (Firstet al 1995) to score 15 or higher on the 17-itemHamiltonRating Scale for Depression (HRSD-17) (Hamilton1967) and 15 or higher on the Folstein Mini-MentalState Exam (MMSE) (Folstein et al 1975) Patients withunstable medical conditions or medications that couldcause depressionwere excludedWritten informed consentwas obtained from each patient following proceduresapproved by our Institutional Review Board (see Fig 1)
Because the course of suicidality during treatmentcannot be reliably established if patients are not closelymonitored and suicidal ideation is not formally assessedlongitudinally we excluded 36 patients who did notcomplete at least four assessments (baseline and threeweekly assessments during treatment) Of these 36patients 10 withdrew consent and 26 were terminatedReasons for termination were severe side effects (n=13)need for electroconvulsive therapy (n=2) psychosis(n=1) non-compliance with protocol (n=2) medicalillness precluding further treatment (n=5) and otherreasons (n=3) We compared the clinical characteristicsand the presence of suicidality in those 36 patients withthe 437 who remained in treatment for more than three
Fig 1
155K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
weeks Subjects with fewer than four assessments hadhigher levels of co-existing medical burden (scores on theCumulative Illness Rating Scale for Geriatrics [CIRS-G](Miller et al 1992) 111 vs 87 t=371 df=463pb00002) Baseline severity of depression was similar inthe two groups while patients who left the study had lowerMMSE scores (271 vs 280 t=202 df=464 pb005)and were more likely to endorse ideation suicidal (21 outof 36 vs 161 out of 437 χ2=649 df=1 pb002)
3 Treatment
Patients were treated as in- andor outpatients in threestudiesMaintenance Therapies in Late-Life Depression-1 and-2 (Reynolds et al 2006) (MTLD-1 andMTLD-2)or Nortriptyline versus Paroxetine (NTPX) (Mulsantet al 2001) Participants in MTLD-1 and MTLD-2received open (non-blinded) acute treatment beforebeing randomized to maintenance treatments MTLD-1patients received combined nortriptyline and Interper-sonal Psychotherapy Treatment (IPT) MTLD-2 patientsreceived combined paroxetine and IPT NTPX patientsreceived randomized acute treatment with either parox-etine or nortriptyline under double-blind conditionsMTLD-1 and-2 patients had weekly medication visitchecks and 45-minute IPT sessions NTPX patients hadweekly medication visits In all three studies patientscould receive lorazepam as an adjunctive medication foranxiety or insomnia In MTLD-1 and MTLD-2 if pa-tients did not respond or only partially responded to
treatment a second antidepressant or lithium was ad-ministered as combined treatment The data reportedhere are derived from the first 12 weeks of the opentreatment in MTLD-1 and MTLD-2 and from the12 weeks of randomized double-blind treatment of NTPX In all 203 patients were treated with nortriptylineand 234 with paroxetine
4 Assessments
Assessments before the start of treatment includedthe 17-item Hamilton Rating Scale for Depression(HRSD) (Hamilton 1967) Interpersonal SupportEvaluation List (Cohen et al 1985) (ISEL) Cumula-tive Illness Rating Scale-Geriatric (Miller et al 1992)(CIRS-G) and Folstein Mini-Mental State Exam(Folstein et al 1975) The ISEL measures perceivedemotional and practical support as well as self-esteemAll subjects were also rated weekly with the HRSD InMTLD-2 and NTPX medication side effects weremeasured weekly using the UKU scale (Lingjaerde etal 1987) Raters supervision measurements of inter-rater reliability for the HRSD and the UKU andreviews of diagnoses were carried out regularly Duringthe most recent assessment of interrater reliabilityintraclass correlation coefficients were 093 for theHRSD total score 097 for the HRSD suicide item and075 for the total UKU score Interrater reliability ofthe HRSD suicide item was greater than 085 for thelast 6 years
156 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
The HRSD suicide item assesses suicidal behaviorsuicidal thoughts thoughts of death and desire to livewithin the past 7 days Suicidality was defined as ascore of 2 or higher on this item (ldquopatient reports orwishes heshe were dead recurrent thought of death orsuicidal ideation or had a recent suicide attemptrdquo)Wechose this particular cut-point for the following reasonsfirst based on data from 6891 psychiatric outpatientswhowere evaluated at the Center for Cognitive Therapyof the University of Pennsylvania those who scored 2or higher on the Hamilton Depression Rating Scalesuicide item were 49 times (95 CI 27ndash90) morelikely to commit suicide than those who scored less than2 during a 20-year prospective study (httpwwwnimhnihgovsuicideresearch adultsuicidepdf) Second wehave shown in an earlier study (Szanto et al 1996) thatolder depressed patients with either active or passivesuicidal ideation had similar rates of life-time suicideattempts and similarly high levels of hopelessnessdiffering significantly from patients who deniedsuicidal ideation or thoughts of death
We further classified patients as having persistentsuicidality if they reported suicidality during the first twoassessments and continued to endorse it at any point after4 weeks of treatment Patients who did not endorsesuicidality at any of the first 2 assessments but reported itlater at any point during treatment were classified ashaving emergent suicidality Patients who endorsedsuicidality during the first two assessments but did notreport it after 4 weeks of treatment were considered tohave resolved suicidality Patients were judged to benon-suicidal if they never reported suicidality and neverreported the feeling that life is empty or not worth living(ie they had a score of 0 on the HRSD suicide item atthe inception of treatment and during each of the 12weekly assessments) To ensure that we did not mis-classify patients as non-suicidal we used this criterionfor non-suicidality (score of 0 on HRSD suicide item) forall 12-weeks of data Thus we excluded from furtheranalysis 176 patients who were neither clearly suicidalnor non-suicidal that is patients who had an HRSDsuicide item score of 1 at any time (ldquolife is empty notworth livingrdquo) but who never had a score of 2 or higher(recurrent thoughts of death wishes heshe were dead orsuicidal ideation) We compared the demographic andbaseline clinical characteristics of the 176 ambiguouscases with the 261 cases who were used for furtheranalyses There was no significant difference betweenthese two groups regarding age gender educationallevel baseline severity of depression lifetime age ofonset of first depressive episode or levels of self-esteem(results are not shown but available upon request)
As an additional check of the validity of our suicidegroup classification we examined the Scale for SuicideIdeation (SSI) (Beck et al 1979) scores in a subgroup(N=307) for whom SSI scores were available for the firsttwo assessments (SSI scale was introduced later in thestudy) We used the highest summarized scores from thefirst two assessments for the first 5 (screening) items ofthe SSI (possible scores 0ndash10) Three SSI screeningitems assess the wish to live or the wish to die and twoitems assess the desire to attempt suicide There is noclear cut-off point for the SSI some studies have used anSSI score of 1 or higher to define suicidality (eg Bruceet al 2004) while others used a score of 2 or higher(eg Brown et al 2000) The classification by theHRSD suicide item was confirmed by the SSI Of 69non-suicidal patients where SSI data were available 67had a total score of 0 on the SSI first 5 items only 2 had ascore of 1 (97 agreement across scales) Within thepersistent and resolved groups 65 of the 72 (86) had atotal SSI score of 1 or higher and 28 of those had a scoreof 2 or higher showing a significant level of suicidalityOf the 28 patients classified as emergent suicidality 20subjects had a baseline score of 0 six had a score of 1and 2 had a score of 2 (thus using a cut-off score of two79 was misclassified based on the SSI) Of the 138ambiguous cases with concurrent SSI ratings 119 (86)had a score of 0 and 7 had a score of 2 or higher
5 Assessment of combined symptoms of agitationanxiety
We assessed agitationanxiety using three items of theHRSD item 9 (agitation) item 10 (psychologicalanxiety) and item 11 (somatic anxiety) and noting ateach assessment whether subjects scorege2 on any singleitem We used this categorical approach to investigatewhether patients with emergent suicidal ideation weremore likely than other patients to have these symptoms
6 Assessment of akathisia
UKU data were available for a subgroup of MTLD-2and NTPX patients (n=161) Using the UKU akathisiaitem (item 16 score 0ndash4) we investigated whetherpatients with emergent suicidal ideationweremore likelyto experience akathisia than other groups A score of 1 onthis item indicates ldquoSlight akathisia however thepatient can keep still without effortrdquo a score of 2ldquoModerate akathisia however the patient can with aneffort remain sitting during the interviewrdquo and a scoreof 3 ldquothe patient has to rise to his feet several timesduring the interview because of akathisiardquo Although the
157K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
UKU is intended to assess medication side effects wealso administered the UKU before treatment to insurethat symptoms present before the inception of antide-pressant pharmacotherapy (such as agitation) were notmisattributed to treatment
7 Statistical analysis
In comparing the demographic and clinical character-istics of the four groups we used a one-way analysis ofvariance for continuous variables followed by Tukeypost-hoc contrasts for significant results For categoricalvariables (eg presence of akathisia) we used chi-squaretests Mixed-effect models were used to examinedepression (HRSD minus item 3 suicide item) overthe 12 weeks of treatment The mixed-effect includedgroup as a fixed effect while subject and time wereincluded as random effects The fixed-effect parameter(group and group by time) of each suicidal group wasexamined and compared in models that demonstrated anoverall significant effect Satterthwaite degrees offreedom was used in the mixed effect model A ge-neralized logit model with repeated measures over timetested for differences in anxietyagitation as indicated bya score of ge2 on any of items 9 10 or 11 of the HRSD
8 Results
Of the 437 patients (the sample with at least fourassessments) 123 patients (28) reported suicidality dur-ing the first two assessments of these 55(126) reported
Table 1Sociodemographic and clinical characteristics of patients based on the prese
(N) Non-suicidalN=104
(R) ResolvedsuicidalityN=68
(P) PsuicidN=55
Age (years) 731 (68) 733 (79) 703 Men 28 25 31 White 84 93 96Education (years) 123 (27) 126 (33) 123CIRS-G1 89 (37) 84 (39) 86 Recurrent depression 65 54 82Age of onset (lifetime) 604 (162) 604 (200) 511 Age of onset before age 60 378 353 630Hamilton-162 at week 0 189 (39) 200 (45) 196MMSE3 278 (27) 274 (27) 288ISEL-Self-esteem4 63 (29) 47 (28) 45Agitationanxiety5 45(16) 44(17) 45(1CIRS-G Cumulative Illness Rating Scale-Geriatric2HRSD Hamilton Rating Scale for Depression3MMSE Folstein Mini-Mental State Exam4ISEL Interpersonal Support Evaluation List ISEL-Self-esteem positive co5Agitationanxiety Hamilton Rating Scale of Depression aggregate score of11 (somatic anxiety)
suicidality longer than the first 4 weeks (ldquopersistentrdquo) while68 (156) did not report suicidality after 4 weeks intreatment (ldquoresolvedrdquo) Thirty-four patients (78) did notreport suicidality during the first 2 assessments but did solater during acute treatment (ldquoemergentrdquo) Of these 34 53showed emergent suicidal ideation in the first month oftreatment 21 in the second month and 26 in the thirdmonth of treatment There were 104 patients who werenon-suicidal throughout the 12-week treatment (ieconsistently scored 0 on the HRSD suicide item) Thusthe rates of emergent suicidality in the sample of 437 were78 (34437) persistent suicidality 126 (55437) andresolved suicidality 156 (68437)
There were 4 patients who had attempted suicide theweek before entering the study No patient attempted orcompleted suicide during the 12 weeks of acute treat-ment However one patient attempted suicide duringmaintenance treatment and one patient completed sui-cide after leaving the study and discontinuing treatmentagainst medical advice
Hypothesis 1 Association of suicidality with the pre-sence of chronicrecurrent depressive illness anxietyand agitation before treatment (Table 1)
Patients with persistent suicidality had their first epi-sode of depression on average 9 years earlier than non-suicidal patients or patients whose suicidality resolvedand were more likely to have recurrent episodes than theresolved and non-suicidal groups Patients in all threesuicidal groups reported lower self-esteem (ISEL self-esteem score) than the non-suicidal patients while
nceabsence of suicidality (meanplusmnSD)
ersistentality
(E) EmergentsuicidalityN=34
F or χ2 Df p Post-hoc
(89) 734 (74) 205 257 1124 080 3 8594 833 3 04 NP
(26) 125 (25) 019 256 90(48) 88 (37) 022 254 88
74 1112 3 02 NP RP(192) 534 (191) 415 249 007 NP RP
636 1621 3 001 NE NP PR RE(41) 197 (44) 103 257 38(18) 288 (15) 537 253 002 PR RE(32) 46 (32) 568 216 001 NP NR NE15) 45(19) 006 257 98
mparison when comparing oneself to othersitems item 9 (agitation) item 10 (psychological anxiety) and item
Table 2Adjunctive medication use during the 12-week treatment of late-life depression in non-suicidal patients and in patients with resolved persistent andemergent suicidality
Non-suicidal (N) N=104 Resolved (R) N=68 Persistent (P) N=55 Emergent (E) N=34 χ2 p Post-hoc
Lithium 4 (4) 1 (1) 9 (16) 3 (9) 1312 004 NP RPSecond antidepressant 7 (7) 1 (1) 6 (11) 6 (18) 942 03 RP RELorazepam 43(41) 27(40) 22(40) 15(44) 021 098
158 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
perceived availability of material aid perceived avail-ability of someone to talk to and to do things with did notdiffer among the four groups Pretreatment levels ofanxiety and agitation co-existing medical burden andseverity of the current depressive episode did not differamong the groups The UKU akathisia item scores alsodid not differ among the four groups at baseline
Hypothesis 2 Association of emergent and persistentsuicidality with persisting low mood and high levels ofanxietyagitation or akathisia during treatment
9 Association of suicidal status with remission ofdepression
A mixed-effect model indicated a significant groupand group by time interaction (16-item HRSD groupF=1076 df=3296 pb00001 interaction F=794df=3241 pb00001) The fixed-effect parameters fromthe model showed that all 3 suicidal groups had higherlevels of depressive symptoms over the 12 weeks oftreatment than the reference (non-suicidal) group(resolved t=245 df=299 pb002 persistent t=556df= 294 pb00001 emergent t= 276 df= 298pb0007) There was a significant group by time inter-action for the emergent group compared to the non-suicidal group (t=385 df=245 pb00002) Patientswith emergent suicidality had levels of depressionsimilar to those with persistent suicidality while patientswith resolved suicidality had lower levels of depressionthan those with persistent suicidality (t=minus300 df=294pb0003) The results for the mixed effects were thesame when we included only patients who receivedcombined pharmacotherapy and IPT
10 Association of suicidal status with agitationanxiety
The repeated-measures logit model indicated a sign-ificant group difference between the non-suicidal andthose with persistent suicidality (Z=326 pb 002) aswell as between those with resolved and persistentsuicidality (Z=241 pb 02) Non-suicidal patients andthose whose suicidality resolved were less likely to score
ge2 on items measuring anxiety or agitation than patientswith persistent suicidality A significant group-by-timeinteraction was found between patients with persistentand emergent ideation (Z=205 pb 05) the latterdemonstrated an increase in the percentage of patientsscoring ge2 on anxiety or agitation by week 12
101 Akathisia
Of the 161 patients with UKU data 97 had noakathisia (score=0) and 64 patients had akathisia scoresof ge1 at any time during treatment Only seven patientshad moderate akathisia (score=2) and only one hadsevere akathisia (score=3) There was no significantdifference among the groups 40 of the non-suicidal26 of the emergent 43 of the persistent and 44 ofthe resolved suicidality patients had a score of 1 or higherat any time on the UKU akathisia item (χ23=184p=061)
11 Adjunctive medication use during the 12-weektreatment (Table 2)
Patients who had persistent suicidal ideation weresignificantly more likely to receive lithium augmentationthan non-suicidal patients or those whose suicidalityresolved Patients with emergent or persistent suicidalideation were significantly more likely to receive anti-depressant augmentation than those whose suicidalityresolved The use of lorazepam as anxiolytichypnoticwas similar across the groups
Hypothesis 3 Potential effect of nortriptyline versusparoxetine on emergence of ideation
We limited our comparison of the effects of nortri-ptyline vs paroxetine to the patients who were treatedunder randomized double-blind conditions (NTPXstudy) because important clinical characteristics thatmay have influenced suicidality (eg rate of recurrenceof illness) differed in the two open-treatment studies(MTLD-1 and MTLD-2) and because the NTPX studydid not allow augmentation with a second antidepres-sant In 61 patients treated under double-blind random-ized conditions the proportions of patients with
159K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
emergent suicidal ideation and thoughts of death did notdiffer between treatments (1 subject [3] receivedparoxetine and none [0] received nortriptyline) (Fisherexact p=027)
12 Discussion
In 437 elderly patients with major depression during12 weeks of acute treatment 78 showed emergence ofsuicidality 126 persistence and 156 resolutionWhile at the inception of treatment the suicidal and non-suicidal groups had similar severity of symptoms duringtreatment patients with emergent and persistent suicid-ality had higher levels of depression and anxiety thannon-suicidal patients or those whose suicidality re-solved Emergent suicidality was associated with lowself-esteem earlier lifetime onset and non- or partialresponse to treatment (as indicated by high levels ofdepression and anxiety) but not with akathisia Patientsrandomized to nortriptyline or paroxetine were equallylikely to have emergent suicidality however this lastresult should be interpreted cautiously because of thesmall sample size
To our knowledge no study has examined emergentpersistent and resolved suicidality in older adults duringtreatment of depression The current study extends ourprevious finding that depressed elderly who endorsesuicidal ideation or recurrent thoughts of death experi-ence slower and less robust treatment response(Szantoet al 2003) This study also expands the previous find-ings by providing a potentially useful classification ofsuicidality during treatment by examining emergentpersistent and resolved suicidality We also showed thatthere are two distinct subgroups among depressedelderly patients who originally present with suicidalitythose whose suicidality resolves quickly after initiationof treatment and those who remain suicidal for a longerperiod of time (ie in our study often for up to 3 months)
Half of patients with emergent suicidality reportedsuicidal ideation or recurrent thoughts of death for thefirst time during the third and fourth week of treatmentone quarter in the second month and one quarter in thethird month Further studies could clarify whether thismight indicate different mediators For example in thosewhose suicidality emerged at the beginning of treatmentsuicide risk may be more likely due to medicationeffects In those who reported suicidality only afterseveral weeks of treatment non-response and giving uphope of ever getting better may be a causal factor
The strengths of this study include a large study groupof elderly depressed patients referred from both mentalhealth specialty clinics and primary care offices who
were well characterized at baseline received protoco-lized treatment over 12 weeks and were assessed weeklyusing well-defined reliable methods The studies in-cluded frail and old subjects those who were 70 andolder and patients with ldquodoublerdquo depression (ie majordepression superimposed on dysthymia)
Although the classification of suicidality based on thesingle suicide item of the HRSD administered weeklyover 12 weeks was confirmed by the SSI scores it is alimitation of the study that we did not have SSI scores inthewhole sample for each time point Based on theHRSDsuicide item 176 patients who were neither clearlysuicidal nor clearly non-suicidal were excluded Usingscales more specific to the assessment of suicidal ideationmay have increased our ability to identify suicidal ideatorsand to reduce the number of ldquoambiguousrdquo cases Visualinspection of the HRSD scores over time showed that theldquoambiguousrdquo group fell in between the two groups withbest treatment response (non-suicidal and resolved) andthe two groups with worse response (persistent and emer-gent suicidality)
We reported previously in a subsample of the currentstudy group that 155 of our study participants had alife-time history of suicide attempt Because we did nothave data in the whole study group on previous episodesof suicidality we could not investigate the relation oflife-time ideation and attempts to the course of currentsuicidality Nonetheless despite the limited informationavailable the use of repeated assessments and the asso-ciation observed with distinct patterns of treatment out-comes provide evidence of the clinical utility andvalidity of our classification of suicidality
The relatively low rates of suicidality in part could bedue to the exclusion of psychotic and bipolar patientsEven though the burden of co-existing medical illness instudy participants was moderately high patients whodropped out from the study (N=36) were medicallymore burdened than those who remained in the studyHence results may not be generalizable to the most frailelderly who may be at the highest risk for completedsuicide (Waern et al 2002a)
We noted that African Americans were more likely tobe in the non-suicidal group than Caucasians It isunclear whether this reflects a real difference in rates ofsuicidal ideation corresponding to lower elderlyAfrican American suicide rates or whether themeasures used are not sensitive to assess suicidality inAfrican Americans
The rate of emergent suicidality (78) was lowerthan the rate of emergent suicidality reported in a sampleof medication-free depressed adolescent outpatients whoreceived psychotherapy over a 12ndash16 week period
160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention

Journal of Affective Disorders 98 (2007) 153ndash161wwwelseviercomlocatejad
Research report
Emergence persistence and resolution of suicidal ideationduring treatment of depression in old age
Katalin Szanto a Benoit H Mulsant ac Patricia R Houck a Mary Amanda Dew abAlexandre Dombrovski a Bruce G Pollock ad Charles F Reynolds III aefg
a University of Pittsburgh School of Medicine Department of Psychiatry Pittsburgh Pennsylvania United Statesb University of Pittsburgh School of Medicine Departments of Psychology and Epidemiology Pittsburgh Pennsylvania United States
c University of Pittsburgh School of Medicine Department of Psychiatry and Center for Addiction and Mental HealthDepartment of Psychiatry University of Toronto Canada
d The Rotman Research Institute Baycrest Centre for Geriatric Care University of Toronto Canadae Advanced Center for Interventions and Services Research for Late-Life Mood Disorders
University of Pittsburgh School of Medicine Pittsburgh Pennsylvania United Statesf The John A Hartford Center of Excellence in Geriatric Psychiatry University of Pittsburgh School of Medicine
Pittsburgh Pennsylvania United Statesg Project EXPORT at the Center for Minority Health Graduate School of Public Health University of Pittsburgh School of Medicine
Pittsburgh Pennsylvania United States
Received 16 February 2006 received in revised form 20 July 2006 accepted 25 July 2006Available online 24 August 2006
Abstract
Introduction To determine the rate and clinical correlates of emergent persistent and resolved suicidal ideation during treatment ofmajor depression in the elderlyMethods Based on the course of suicidal ideation before and during 12 weeks of antidepressant treatment we classified 437 elderlypatients (234 treated with paroxetine 203 with nortriptyline) as either non-suicidal or as having ldquoemergentrdquo ldquopersistentrdquo orldquoresolvedrdquo suicidality We compared the four groups on pretreatment demographic and clinical measures and with respect todepression anxiety and akathisia during treatment Results Rates of emergent persistent and resolved suicidality were 78 126and 156 respectively Patients with persistent suicidal ideation were more likely to have recurrent depression than non-suicidalpatients or patients whose suicidality resolved with treatment At the start of treatment patients in all three suicidal groups had lowerself-esteem than non-suicidal patients During the course of treatment emergent suicidality was not associated with akathisia nor didrates of emergent suicidality differ between paroxetine- and nortriptyline-treated patients While at baseline the levels of depressionand anxiety and agitation were similar in the four groups patients with resolved suicidality had a favorable treatment response whilepatients with emergent and persistent suicidality were more likely to maintain higher depression scores and had higher levels ofanxiety and agitation during treatmentDiscussion Emergence of suicidal ideation is not common but is clinically significant during treatment of late-life depression andmay signal more difficult-to-treat-depressioncopy 2006 Elsevier BV All rights reserved
Keywords Elderly Major depression Suicidal ideation Treatment
Corresponding author University of Pittsburgh School of Medicine 315 S Bellefield Street Bellefield Towers 537 Pittsburgh PA 15213 USATel +1 412 586 9601 fax +1 412 246 6030
E-mail address szantokupmcedu (K Szanto)
0165-0327$ - see front matter copy 2006 Elsevier BV All rights reserveddoi101016jjad200607015
154 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
1 Background
Older adults (age 60 and above) have the highestsuicide rate among all age groups in most countries of theworld (World Health Organization 2005) Althoughdepression is the most common diagnosis in elderlysuicide attempters and completers (Conwell et al 2000Beautrais 2002) to our knowledge no study has syste-matically examined emergence persistence and resolu-tion of suicidality during treatment of late-life depressionRecent concerns about emergent suicidality during de-pression treatment in children and adolescent (US Foodand Drug Administration 2004) and its apparentassociation with akathisia or agitation induced byselective serotonin reuptake inhibitors (SSRIs) highlightthe clinical importance of this issue In late-life theliterature is inconclusive with respect to these issues andto the implication of prior course (eg single versusrecurrent depression) for suicide risk
Patients whose mood remains low when they regainenergy may be at increased risk for suicide (Detre andJarecki 1971) Alternatively increased anxiety and agi-tation in the face of non- or partially remitting depressionmay increase suicide risk (Akiskal et al 2005) A fewcase series (Power and Cowen 1992) and case reports(Rothschild and Locke 1991) have suggested anassociation between suicidality and akathisia Howeverother investigators did not find a relationship betweentreatment-emergent adverse events and suicidality (Tol-lefson et al 1994) A review of the literature (Hansen2001 pp 495) concluded that ldquoakathisia cannot be un-equivocally linked to suicidal behavior however it iscertain that the condition of akathisia does cause con-siderable distress in an already vulnerable group of pa-tientsrdquo To our knowledge no study other than casereports(Hansen andWilkinson 2001) has investigated apossible relationship between medication-induced anx-ietyagitation and suicidality in the elderly
According to psychological autopsy studies anxietydisorders without comorbid mood disorders only mo-destly increase suicide risk in the elderly (Waern et al2002b) However in one study insomnia and severepsychic anxiety predicted suicide in mid-life patientswith major depressive disorder (Fawcett et al 1990) andtwo recent reports found an association between mixeddepression often marked by psychomotor agitation andsuicidal ideation and attempts (Akiskal et al 2005Balazs et al 2006) The authors note that psychomotoragitation maybe related to an activation syndromecaused by antidepressants In our previous study in el-derly patients decline in suicidal ideation was associatedwith remission of depression (Szanto et al 2003) Thus
based on literature review our previous findings andclinical experience we hypothesized that
1) Emergence and persistence of suicidality during treat-ment would be associated with chronicrecurrentdepression and higher baseline anxiety or agitation
2) Patientswith emergent or persistent suicidalitywould bemore likely to have persisting low mood and higherlevels of anxietyagitationakathisia compared to non-suicidal patients and to thosewhose suicidality resolved
3) Patients treated with a SSRI would be more likely tobecome suicidal than patients receiving a tricylicThis association if present could be due to the onsetof akathisia in the SSRI-treated group
2 Methods
21 Study group
Data for this analysis were available for 473 par-ticipants in three federally-supported clinical trials ofgeriatric depressionWe pooled data from the three studiesbecause all dealt with the treatment of non-psychotic non-bipolar major depressive episodes in old age and utilizedsimilar assessment and treatment approaches administeredin the same research setting Patients were required to be60 years or older to have nonpsychotic unipolar majordepression determined by administration of either theSchedule for Affective Disorders and Schizophrenia(SADS) (Spitzer 1978) or the SCID for DSM-IV (Firstet al 1995) to score 15 or higher on the 17-itemHamiltonRating Scale for Depression (HRSD-17) (Hamilton1967) and 15 or higher on the Folstein Mini-MentalState Exam (MMSE) (Folstein et al 1975) Patients withunstable medical conditions or medications that couldcause depressionwere excludedWritten informed consentwas obtained from each patient following proceduresapproved by our Institutional Review Board (see Fig 1)
Because the course of suicidality during treatmentcannot be reliably established if patients are not closelymonitored and suicidal ideation is not formally assessedlongitudinally we excluded 36 patients who did notcomplete at least four assessments (baseline and threeweekly assessments during treatment) Of these 36patients 10 withdrew consent and 26 were terminatedReasons for termination were severe side effects (n=13)need for electroconvulsive therapy (n=2) psychosis(n=1) non-compliance with protocol (n=2) medicalillness precluding further treatment (n=5) and otherreasons (n=3) We compared the clinical characteristicsand the presence of suicidality in those 36 patients withthe 437 who remained in treatment for more than three
Fig 1
155K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
weeks Subjects with fewer than four assessments hadhigher levels of co-existing medical burden (scores on theCumulative Illness Rating Scale for Geriatrics [CIRS-G](Miller et al 1992) 111 vs 87 t=371 df=463pb00002) Baseline severity of depression was similar inthe two groups while patients who left the study had lowerMMSE scores (271 vs 280 t=202 df=464 pb005)and were more likely to endorse ideation suicidal (21 outof 36 vs 161 out of 437 χ2=649 df=1 pb002)
3 Treatment
Patients were treated as in- andor outpatients in threestudiesMaintenance Therapies in Late-Life Depression-1 and-2 (Reynolds et al 2006) (MTLD-1 andMTLD-2)or Nortriptyline versus Paroxetine (NTPX) (Mulsantet al 2001) Participants in MTLD-1 and MTLD-2received open (non-blinded) acute treatment beforebeing randomized to maintenance treatments MTLD-1patients received combined nortriptyline and Interper-sonal Psychotherapy Treatment (IPT) MTLD-2 patientsreceived combined paroxetine and IPT NTPX patientsreceived randomized acute treatment with either parox-etine or nortriptyline under double-blind conditionsMTLD-1 and-2 patients had weekly medication visitchecks and 45-minute IPT sessions NTPX patients hadweekly medication visits In all three studies patientscould receive lorazepam as an adjunctive medication foranxiety or insomnia In MTLD-1 and MTLD-2 if pa-tients did not respond or only partially responded to
treatment a second antidepressant or lithium was ad-ministered as combined treatment The data reportedhere are derived from the first 12 weeks of the opentreatment in MTLD-1 and MTLD-2 and from the12 weeks of randomized double-blind treatment of NTPX In all 203 patients were treated with nortriptylineand 234 with paroxetine
4 Assessments
Assessments before the start of treatment includedthe 17-item Hamilton Rating Scale for Depression(HRSD) (Hamilton 1967) Interpersonal SupportEvaluation List (Cohen et al 1985) (ISEL) Cumula-tive Illness Rating Scale-Geriatric (Miller et al 1992)(CIRS-G) and Folstein Mini-Mental State Exam(Folstein et al 1975) The ISEL measures perceivedemotional and practical support as well as self-esteemAll subjects were also rated weekly with the HRSD InMTLD-2 and NTPX medication side effects weremeasured weekly using the UKU scale (Lingjaerde etal 1987) Raters supervision measurements of inter-rater reliability for the HRSD and the UKU andreviews of diagnoses were carried out regularly Duringthe most recent assessment of interrater reliabilityintraclass correlation coefficients were 093 for theHRSD total score 097 for the HRSD suicide item and075 for the total UKU score Interrater reliability ofthe HRSD suicide item was greater than 085 for thelast 6 years
156 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
The HRSD suicide item assesses suicidal behaviorsuicidal thoughts thoughts of death and desire to livewithin the past 7 days Suicidality was defined as ascore of 2 or higher on this item (ldquopatient reports orwishes heshe were dead recurrent thought of death orsuicidal ideation or had a recent suicide attemptrdquo)Wechose this particular cut-point for the following reasonsfirst based on data from 6891 psychiatric outpatientswhowere evaluated at the Center for Cognitive Therapyof the University of Pennsylvania those who scored 2or higher on the Hamilton Depression Rating Scalesuicide item were 49 times (95 CI 27ndash90) morelikely to commit suicide than those who scored less than2 during a 20-year prospective study (httpwwwnimhnihgovsuicideresearch adultsuicidepdf) Second wehave shown in an earlier study (Szanto et al 1996) thatolder depressed patients with either active or passivesuicidal ideation had similar rates of life-time suicideattempts and similarly high levels of hopelessnessdiffering significantly from patients who deniedsuicidal ideation or thoughts of death
We further classified patients as having persistentsuicidality if they reported suicidality during the first twoassessments and continued to endorse it at any point after4 weeks of treatment Patients who did not endorsesuicidality at any of the first 2 assessments but reported itlater at any point during treatment were classified ashaving emergent suicidality Patients who endorsedsuicidality during the first two assessments but did notreport it after 4 weeks of treatment were considered tohave resolved suicidality Patients were judged to benon-suicidal if they never reported suicidality and neverreported the feeling that life is empty or not worth living(ie they had a score of 0 on the HRSD suicide item atthe inception of treatment and during each of the 12weekly assessments) To ensure that we did not mis-classify patients as non-suicidal we used this criterionfor non-suicidality (score of 0 on HRSD suicide item) forall 12-weeks of data Thus we excluded from furtheranalysis 176 patients who were neither clearly suicidalnor non-suicidal that is patients who had an HRSDsuicide item score of 1 at any time (ldquolife is empty notworth livingrdquo) but who never had a score of 2 or higher(recurrent thoughts of death wishes heshe were dead orsuicidal ideation) We compared the demographic andbaseline clinical characteristics of the 176 ambiguouscases with the 261 cases who were used for furtheranalyses There was no significant difference betweenthese two groups regarding age gender educationallevel baseline severity of depression lifetime age ofonset of first depressive episode or levels of self-esteem(results are not shown but available upon request)
As an additional check of the validity of our suicidegroup classification we examined the Scale for SuicideIdeation (SSI) (Beck et al 1979) scores in a subgroup(N=307) for whom SSI scores were available for the firsttwo assessments (SSI scale was introduced later in thestudy) We used the highest summarized scores from thefirst two assessments for the first 5 (screening) items ofthe SSI (possible scores 0ndash10) Three SSI screeningitems assess the wish to live or the wish to die and twoitems assess the desire to attempt suicide There is noclear cut-off point for the SSI some studies have used anSSI score of 1 or higher to define suicidality (eg Bruceet al 2004) while others used a score of 2 or higher(eg Brown et al 2000) The classification by theHRSD suicide item was confirmed by the SSI Of 69non-suicidal patients where SSI data were available 67had a total score of 0 on the SSI first 5 items only 2 had ascore of 1 (97 agreement across scales) Within thepersistent and resolved groups 65 of the 72 (86) had atotal SSI score of 1 or higher and 28 of those had a scoreof 2 or higher showing a significant level of suicidalityOf the 28 patients classified as emergent suicidality 20subjects had a baseline score of 0 six had a score of 1and 2 had a score of 2 (thus using a cut-off score of two79 was misclassified based on the SSI) Of the 138ambiguous cases with concurrent SSI ratings 119 (86)had a score of 0 and 7 had a score of 2 or higher
5 Assessment of combined symptoms of agitationanxiety
We assessed agitationanxiety using three items of theHRSD item 9 (agitation) item 10 (psychologicalanxiety) and item 11 (somatic anxiety) and noting ateach assessment whether subjects scorege2 on any singleitem We used this categorical approach to investigatewhether patients with emergent suicidal ideation weremore likely than other patients to have these symptoms
6 Assessment of akathisia
UKU data were available for a subgroup of MTLD-2and NTPX patients (n=161) Using the UKU akathisiaitem (item 16 score 0ndash4) we investigated whetherpatients with emergent suicidal ideationweremore likelyto experience akathisia than other groups A score of 1 onthis item indicates ldquoSlight akathisia however thepatient can keep still without effortrdquo a score of 2ldquoModerate akathisia however the patient can with aneffort remain sitting during the interviewrdquo and a scoreof 3 ldquothe patient has to rise to his feet several timesduring the interview because of akathisiardquo Although the
157K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
UKU is intended to assess medication side effects wealso administered the UKU before treatment to insurethat symptoms present before the inception of antide-pressant pharmacotherapy (such as agitation) were notmisattributed to treatment
7 Statistical analysis
In comparing the demographic and clinical character-istics of the four groups we used a one-way analysis ofvariance for continuous variables followed by Tukeypost-hoc contrasts for significant results For categoricalvariables (eg presence of akathisia) we used chi-squaretests Mixed-effect models were used to examinedepression (HRSD minus item 3 suicide item) overthe 12 weeks of treatment The mixed-effect includedgroup as a fixed effect while subject and time wereincluded as random effects The fixed-effect parameter(group and group by time) of each suicidal group wasexamined and compared in models that demonstrated anoverall significant effect Satterthwaite degrees offreedom was used in the mixed effect model A ge-neralized logit model with repeated measures over timetested for differences in anxietyagitation as indicated bya score of ge2 on any of items 9 10 or 11 of the HRSD
8 Results
Of the 437 patients (the sample with at least fourassessments) 123 patients (28) reported suicidality dur-ing the first two assessments of these 55(126) reported
Table 1Sociodemographic and clinical characteristics of patients based on the prese
(N) Non-suicidalN=104
(R) ResolvedsuicidalityN=68
(P) PsuicidN=55
Age (years) 731 (68) 733 (79) 703 Men 28 25 31 White 84 93 96Education (years) 123 (27) 126 (33) 123CIRS-G1 89 (37) 84 (39) 86 Recurrent depression 65 54 82Age of onset (lifetime) 604 (162) 604 (200) 511 Age of onset before age 60 378 353 630Hamilton-162 at week 0 189 (39) 200 (45) 196MMSE3 278 (27) 274 (27) 288ISEL-Self-esteem4 63 (29) 47 (28) 45Agitationanxiety5 45(16) 44(17) 45(1CIRS-G Cumulative Illness Rating Scale-Geriatric2HRSD Hamilton Rating Scale for Depression3MMSE Folstein Mini-Mental State Exam4ISEL Interpersonal Support Evaluation List ISEL-Self-esteem positive co5Agitationanxiety Hamilton Rating Scale of Depression aggregate score of11 (somatic anxiety)
suicidality longer than the first 4 weeks (ldquopersistentrdquo) while68 (156) did not report suicidality after 4 weeks intreatment (ldquoresolvedrdquo) Thirty-four patients (78) did notreport suicidality during the first 2 assessments but did solater during acute treatment (ldquoemergentrdquo) Of these 34 53showed emergent suicidal ideation in the first month oftreatment 21 in the second month and 26 in the thirdmonth of treatment There were 104 patients who werenon-suicidal throughout the 12-week treatment (ieconsistently scored 0 on the HRSD suicide item) Thusthe rates of emergent suicidality in the sample of 437 were78 (34437) persistent suicidality 126 (55437) andresolved suicidality 156 (68437)
There were 4 patients who had attempted suicide theweek before entering the study No patient attempted orcompleted suicide during the 12 weeks of acute treat-ment However one patient attempted suicide duringmaintenance treatment and one patient completed sui-cide after leaving the study and discontinuing treatmentagainst medical advice
Hypothesis 1 Association of suicidality with the pre-sence of chronicrecurrent depressive illness anxietyand agitation before treatment (Table 1)
Patients with persistent suicidality had their first epi-sode of depression on average 9 years earlier than non-suicidal patients or patients whose suicidality resolvedand were more likely to have recurrent episodes than theresolved and non-suicidal groups Patients in all threesuicidal groups reported lower self-esteem (ISEL self-esteem score) than the non-suicidal patients while
nceabsence of suicidality (meanplusmnSD)
ersistentality
(E) EmergentsuicidalityN=34
F or χ2 Df p Post-hoc
(89) 734 (74) 205 257 1124 080 3 8594 833 3 04 NP
(26) 125 (25) 019 256 90(48) 88 (37) 022 254 88
74 1112 3 02 NP RP(192) 534 (191) 415 249 007 NP RP
636 1621 3 001 NE NP PR RE(41) 197 (44) 103 257 38(18) 288 (15) 537 253 002 PR RE(32) 46 (32) 568 216 001 NP NR NE15) 45(19) 006 257 98
mparison when comparing oneself to othersitems item 9 (agitation) item 10 (psychological anxiety) and item
Table 2Adjunctive medication use during the 12-week treatment of late-life depression in non-suicidal patients and in patients with resolved persistent andemergent suicidality
Non-suicidal (N) N=104 Resolved (R) N=68 Persistent (P) N=55 Emergent (E) N=34 χ2 p Post-hoc
Lithium 4 (4) 1 (1) 9 (16) 3 (9) 1312 004 NP RPSecond antidepressant 7 (7) 1 (1) 6 (11) 6 (18) 942 03 RP RELorazepam 43(41) 27(40) 22(40) 15(44) 021 098
158 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
perceived availability of material aid perceived avail-ability of someone to talk to and to do things with did notdiffer among the four groups Pretreatment levels ofanxiety and agitation co-existing medical burden andseverity of the current depressive episode did not differamong the groups The UKU akathisia item scores alsodid not differ among the four groups at baseline
Hypothesis 2 Association of emergent and persistentsuicidality with persisting low mood and high levels ofanxietyagitation or akathisia during treatment
9 Association of suicidal status with remission ofdepression
A mixed-effect model indicated a significant groupand group by time interaction (16-item HRSD groupF=1076 df=3296 pb00001 interaction F=794df=3241 pb00001) The fixed-effect parameters fromthe model showed that all 3 suicidal groups had higherlevels of depressive symptoms over the 12 weeks oftreatment than the reference (non-suicidal) group(resolved t=245 df=299 pb002 persistent t=556df= 294 pb00001 emergent t= 276 df= 298pb0007) There was a significant group by time inter-action for the emergent group compared to the non-suicidal group (t=385 df=245 pb00002) Patientswith emergent suicidality had levels of depressionsimilar to those with persistent suicidality while patientswith resolved suicidality had lower levels of depressionthan those with persistent suicidality (t=minus300 df=294pb0003) The results for the mixed effects were thesame when we included only patients who receivedcombined pharmacotherapy and IPT
10 Association of suicidal status with agitationanxiety
The repeated-measures logit model indicated a sign-ificant group difference between the non-suicidal andthose with persistent suicidality (Z=326 pb 002) aswell as between those with resolved and persistentsuicidality (Z=241 pb 02) Non-suicidal patients andthose whose suicidality resolved were less likely to score
ge2 on items measuring anxiety or agitation than patientswith persistent suicidality A significant group-by-timeinteraction was found between patients with persistentand emergent ideation (Z=205 pb 05) the latterdemonstrated an increase in the percentage of patientsscoring ge2 on anxiety or agitation by week 12
101 Akathisia
Of the 161 patients with UKU data 97 had noakathisia (score=0) and 64 patients had akathisia scoresof ge1 at any time during treatment Only seven patientshad moderate akathisia (score=2) and only one hadsevere akathisia (score=3) There was no significantdifference among the groups 40 of the non-suicidal26 of the emergent 43 of the persistent and 44 ofthe resolved suicidality patients had a score of 1 or higherat any time on the UKU akathisia item (χ23=184p=061)
11 Adjunctive medication use during the 12-weektreatment (Table 2)
Patients who had persistent suicidal ideation weresignificantly more likely to receive lithium augmentationthan non-suicidal patients or those whose suicidalityresolved Patients with emergent or persistent suicidalideation were significantly more likely to receive anti-depressant augmentation than those whose suicidalityresolved The use of lorazepam as anxiolytichypnoticwas similar across the groups
Hypothesis 3 Potential effect of nortriptyline versusparoxetine on emergence of ideation
We limited our comparison of the effects of nortri-ptyline vs paroxetine to the patients who were treatedunder randomized double-blind conditions (NTPXstudy) because important clinical characteristics thatmay have influenced suicidality (eg rate of recurrenceof illness) differed in the two open-treatment studies(MTLD-1 and MTLD-2) and because the NTPX studydid not allow augmentation with a second antidepres-sant In 61 patients treated under double-blind random-ized conditions the proportions of patients with
159K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
emergent suicidal ideation and thoughts of death did notdiffer between treatments (1 subject [3] receivedparoxetine and none [0] received nortriptyline) (Fisherexact p=027)
12 Discussion
In 437 elderly patients with major depression during12 weeks of acute treatment 78 showed emergence ofsuicidality 126 persistence and 156 resolutionWhile at the inception of treatment the suicidal and non-suicidal groups had similar severity of symptoms duringtreatment patients with emergent and persistent suicid-ality had higher levels of depression and anxiety thannon-suicidal patients or those whose suicidality re-solved Emergent suicidality was associated with lowself-esteem earlier lifetime onset and non- or partialresponse to treatment (as indicated by high levels ofdepression and anxiety) but not with akathisia Patientsrandomized to nortriptyline or paroxetine were equallylikely to have emergent suicidality however this lastresult should be interpreted cautiously because of thesmall sample size
To our knowledge no study has examined emergentpersistent and resolved suicidality in older adults duringtreatment of depression The current study extends ourprevious finding that depressed elderly who endorsesuicidal ideation or recurrent thoughts of death experi-ence slower and less robust treatment response(Szantoet al 2003) This study also expands the previous find-ings by providing a potentially useful classification ofsuicidality during treatment by examining emergentpersistent and resolved suicidality We also showed thatthere are two distinct subgroups among depressedelderly patients who originally present with suicidalitythose whose suicidality resolves quickly after initiationof treatment and those who remain suicidal for a longerperiod of time (ie in our study often for up to 3 months)
Half of patients with emergent suicidality reportedsuicidal ideation or recurrent thoughts of death for thefirst time during the third and fourth week of treatmentone quarter in the second month and one quarter in thethird month Further studies could clarify whether thismight indicate different mediators For example in thosewhose suicidality emerged at the beginning of treatmentsuicide risk may be more likely due to medicationeffects In those who reported suicidality only afterseveral weeks of treatment non-response and giving uphope of ever getting better may be a causal factor
The strengths of this study include a large study groupof elderly depressed patients referred from both mentalhealth specialty clinics and primary care offices who
were well characterized at baseline received protoco-lized treatment over 12 weeks and were assessed weeklyusing well-defined reliable methods The studies in-cluded frail and old subjects those who were 70 andolder and patients with ldquodoublerdquo depression (ie majordepression superimposed on dysthymia)
Although the classification of suicidality based on thesingle suicide item of the HRSD administered weeklyover 12 weeks was confirmed by the SSI scores it is alimitation of the study that we did not have SSI scores inthewhole sample for each time point Based on theHRSDsuicide item 176 patients who were neither clearlysuicidal nor clearly non-suicidal were excluded Usingscales more specific to the assessment of suicidal ideationmay have increased our ability to identify suicidal ideatorsand to reduce the number of ldquoambiguousrdquo cases Visualinspection of the HRSD scores over time showed that theldquoambiguousrdquo group fell in between the two groups withbest treatment response (non-suicidal and resolved) andthe two groups with worse response (persistent and emer-gent suicidality)
We reported previously in a subsample of the currentstudy group that 155 of our study participants had alife-time history of suicide attempt Because we did nothave data in the whole study group on previous episodesof suicidality we could not investigate the relation oflife-time ideation and attempts to the course of currentsuicidality Nonetheless despite the limited informationavailable the use of repeated assessments and the asso-ciation observed with distinct patterns of treatment out-comes provide evidence of the clinical utility andvalidity of our classification of suicidality
The relatively low rates of suicidality in part could bedue to the exclusion of psychotic and bipolar patientsEven though the burden of co-existing medical illness instudy participants was moderately high patients whodropped out from the study (N=36) were medicallymore burdened than those who remained in the studyHence results may not be generalizable to the most frailelderly who may be at the highest risk for completedsuicide (Waern et al 2002a)
We noted that African Americans were more likely tobe in the non-suicidal group than Caucasians It isunclear whether this reflects a real difference in rates ofsuicidal ideation corresponding to lower elderlyAfrican American suicide rates or whether themeasures used are not sensitive to assess suicidality inAfrican Americans
The rate of emergent suicidality (78) was lowerthan the rate of emergent suicidality reported in a sampleof medication-free depressed adolescent outpatients whoreceived psychotherapy over a 12ndash16 week period
160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention
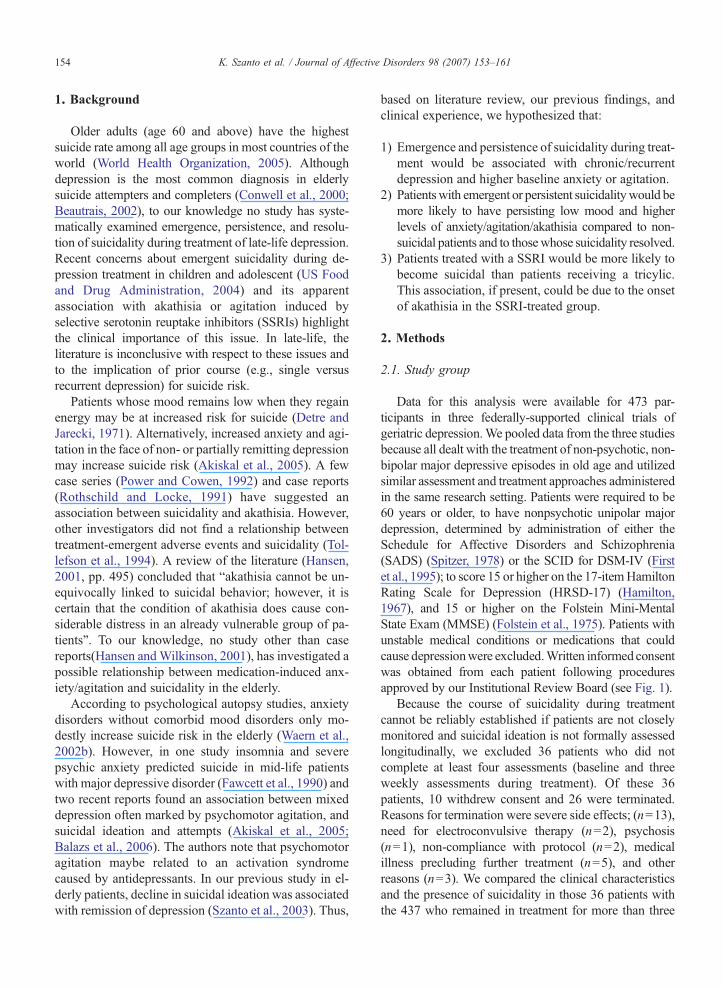
154 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
1 Background
Older adults (age 60 and above) have the highestsuicide rate among all age groups in most countries of theworld (World Health Organization 2005) Althoughdepression is the most common diagnosis in elderlysuicide attempters and completers (Conwell et al 2000Beautrais 2002) to our knowledge no study has syste-matically examined emergence persistence and resolu-tion of suicidality during treatment of late-life depressionRecent concerns about emergent suicidality during de-pression treatment in children and adolescent (US Foodand Drug Administration 2004) and its apparentassociation with akathisia or agitation induced byselective serotonin reuptake inhibitors (SSRIs) highlightthe clinical importance of this issue In late-life theliterature is inconclusive with respect to these issues andto the implication of prior course (eg single versusrecurrent depression) for suicide risk
Patients whose mood remains low when they regainenergy may be at increased risk for suicide (Detre andJarecki 1971) Alternatively increased anxiety and agi-tation in the face of non- or partially remitting depressionmay increase suicide risk (Akiskal et al 2005) A fewcase series (Power and Cowen 1992) and case reports(Rothschild and Locke 1991) have suggested anassociation between suicidality and akathisia Howeverother investigators did not find a relationship betweentreatment-emergent adverse events and suicidality (Tol-lefson et al 1994) A review of the literature (Hansen2001 pp 495) concluded that ldquoakathisia cannot be un-equivocally linked to suicidal behavior however it iscertain that the condition of akathisia does cause con-siderable distress in an already vulnerable group of pa-tientsrdquo To our knowledge no study other than casereports(Hansen andWilkinson 2001) has investigated apossible relationship between medication-induced anx-ietyagitation and suicidality in the elderly
According to psychological autopsy studies anxietydisorders without comorbid mood disorders only mo-destly increase suicide risk in the elderly (Waern et al2002b) However in one study insomnia and severepsychic anxiety predicted suicide in mid-life patientswith major depressive disorder (Fawcett et al 1990) andtwo recent reports found an association between mixeddepression often marked by psychomotor agitation andsuicidal ideation and attempts (Akiskal et al 2005Balazs et al 2006) The authors note that psychomotoragitation maybe related to an activation syndromecaused by antidepressants In our previous study in el-derly patients decline in suicidal ideation was associatedwith remission of depression (Szanto et al 2003) Thus
based on literature review our previous findings andclinical experience we hypothesized that
1) Emergence and persistence of suicidality during treat-ment would be associated with chronicrecurrentdepression and higher baseline anxiety or agitation
2) Patientswith emergent or persistent suicidalitywould bemore likely to have persisting low mood and higherlevels of anxietyagitationakathisia compared to non-suicidal patients and to thosewhose suicidality resolved
3) Patients treated with a SSRI would be more likely tobecome suicidal than patients receiving a tricylicThis association if present could be due to the onsetof akathisia in the SSRI-treated group
2 Methods
21 Study group
Data for this analysis were available for 473 par-ticipants in three federally-supported clinical trials ofgeriatric depressionWe pooled data from the three studiesbecause all dealt with the treatment of non-psychotic non-bipolar major depressive episodes in old age and utilizedsimilar assessment and treatment approaches administeredin the same research setting Patients were required to be60 years or older to have nonpsychotic unipolar majordepression determined by administration of either theSchedule for Affective Disorders and Schizophrenia(SADS) (Spitzer 1978) or the SCID for DSM-IV (Firstet al 1995) to score 15 or higher on the 17-itemHamiltonRating Scale for Depression (HRSD-17) (Hamilton1967) and 15 or higher on the Folstein Mini-MentalState Exam (MMSE) (Folstein et al 1975) Patients withunstable medical conditions or medications that couldcause depressionwere excludedWritten informed consentwas obtained from each patient following proceduresapproved by our Institutional Review Board (see Fig 1)
Because the course of suicidality during treatmentcannot be reliably established if patients are not closelymonitored and suicidal ideation is not formally assessedlongitudinally we excluded 36 patients who did notcomplete at least four assessments (baseline and threeweekly assessments during treatment) Of these 36patients 10 withdrew consent and 26 were terminatedReasons for termination were severe side effects (n=13)need for electroconvulsive therapy (n=2) psychosis(n=1) non-compliance with protocol (n=2) medicalillness precluding further treatment (n=5) and otherreasons (n=3) We compared the clinical characteristicsand the presence of suicidality in those 36 patients withthe 437 who remained in treatment for more than three
Fig 1
155K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
weeks Subjects with fewer than four assessments hadhigher levels of co-existing medical burden (scores on theCumulative Illness Rating Scale for Geriatrics [CIRS-G](Miller et al 1992) 111 vs 87 t=371 df=463pb00002) Baseline severity of depression was similar inthe two groups while patients who left the study had lowerMMSE scores (271 vs 280 t=202 df=464 pb005)and were more likely to endorse ideation suicidal (21 outof 36 vs 161 out of 437 χ2=649 df=1 pb002)
3 Treatment
Patients were treated as in- andor outpatients in threestudiesMaintenance Therapies in Late-Life Depression-1 and-2 (Reynolds et al 2006) (MTLD-1 andMTLD-2)or Nortriptyline versus Paroxetine (NTPX) (Mulsantet al 2001) Participants in MTLD-1 and MTLD-2received open (non-blinded) acute treatment beforebeing randomized to maintenance treatments MTLD-1patients received combined nortriptyline and Interper-sonal Psychotherapy Treatment (IPT) MTLD-2 patientsreceived combined paroxetine and IPT NTPX patientsreceived randomized acute treatment with either parox-etine or nortriptyline under double-blind conditionsMTLD-1 and-2 patients had weekly medication visitchecks and 45-minute IPT sessions NTPX patients hadweekly medication visits In all three studies patientscould receive lorazepam as an adjunctive medication foranxiety or insomnia In MTLD-1 and MTLD-2 if pa-tients did not respond or only partially responded to
treatment a second antidepressant or lithium was ad-ministered as combined treatment The data reportedhere are derived from the first 12 weeks of the opentreatment in MTLD-1 and MTLD-2 and from the12 weeks of randomized double-blind treatment of NTPX In all 203 patients were treated with nortriptylineand 234 with paroxetine
4 Assessments
Assessments before the start of treatment includedthe 17-item Hamilton Rating Scale for Depression(HRSD) (Hamilton 1967) Interpersonal SupportEvaluation List (Cohen et al 1985) (ISEL) Cumula-tive Illness Rating Scale-Geriatric (Miller et al 1992)(CIRS-G) and Folstein Mini-Mental State Exam(Folstein et al 1975) The ISEL measures perceivedemotional and practical support as well as self-esteemAll subjects were also rated weekly with the HRSD InMTLD-2 and NTPX medication side effects weremeasured weekly using the UKU scale (Lingjaerde etal 1987) Raters supervision measurements of inter-rater reliability for the HRSD and the UKU andreviews of diagnoses were carried out regularly Duringthe most recent assessment of interrater reliabilityintraclass correlation coefficients were 093 for theHRSD total score 097 for the HRSD suicide item and075 for the total UKU score Interrater reliability ofthe HRSD suicide item was greater than 085 for thelast 6 years
156 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
The HRSD suicide item assesses suicidal behaviorsuicidal thoughts thoughts of death and desire to livewithin the past 7 days Suicidality was defined as ascore of 2 or higher on this item (ldquopatient reports orwishes heshe were dead recurrent thought of death orsuicidal ideation or had a recent suicide attemptrdquo)Wechose this particular cut-point for the following reasonsfirst based on data from 6891 psychiatric outpatientswhowere evaluated at the Center for Cognitive Therapyof the University of Pennsylvania those who scored 2or higher on the Hamilton Depression Rating Scalesuicide item were 49 times (95 CI 27ndash90) morelikely to commit suicide than those who scored less than2 during a 20-year prospective study (httpwwwnimhnihgovsuicideresearch adultsuicidepdf) Second wehave shown in an earlier study (Szanto et al 1996) thatolder depressed patients with either active or passivesuicidal ideation had similar rates of life-time suicideattempts and similarly high levels of hopelessnessdiffering significantly from patients who deniedsuicidal ideation or thoughts of death
We further classified patients as having persistentsuicidality if they reported suicidality during the first twoassessments and continued to endorse it at any point after4 weeks of treatment Patients who did not endorsesuicidality at any of the first 2 assessments but reported itlater at any point during treatment were classified ashaving emergent suicidality Patients who endorsedsuicidality during the first two assessments but did notreport it after 4 weeks of treatment were considered tohave resolved suicidality Patients were judged to benon-suicidal if they never reported suicidality and neverreported the feeling that life is empty or not worth living(ie they had a score of 0 on the HRSD suicide item atthe inception of treatment and during each of the 12weekly assessments) To ensure that we did not mis-classify patients as non-suicidal we used this criterionfor non-suicidality (score of 0 on HRSD suicide item) forall 12-weeks of data Thus we excluded from furtheranalysis 176 patients who were neither clearly suicidalnor non-suicidal that is patients who had an HRSDsuicide item score of 1 at any time (ldquolife is empty notworth livingrdquo) but who never had a score of 2 or higher(recurrent thoughts of death wishes heshe were dead orsuicidal ideation) We compared the demographic andbaseline clinical characteristics of the 176 ambiguouscases with the 261 cases who were used for furtheranalyses There was no significant difference betweenthese two groups regarding age gender educationallevel baseline severity of depression lifetime age ofonset of first depressive episode or levels of self-esteem(results are not shown but available upon request)
As an additional check of the validity of our suicidegroup classification we examined the Scale for SuicideIdeation (SSI) (Beck et al 1979) scores in a subgroup(N=307) for whom SSI scores were available for the firsttwo assessments (SSI scale was introduced later in thestudy) We used the highest summarized scores from thefirst two assessments for the first 5 (screening) items ofthe SSI (possible scores 0ndash10) Three SSI screeningitems assess the wish to live or the wish to die and twoitems assess the desire to attempt suicide There is noclear cut-off point for the SSI some studies have used anSSI score of 1 or higher to define suicidality (eg Bruceet al 2004) while others used a score of 2 or higher(eg Brown et al 2000) The classification by theHRSD suicide item was confirmed by the SSI Of 69non-suicidal patients where SSI data were available 67had a total score of 0 on the SSI first 5 items only 2 had ascore of 1 (97 agreement across scales) Within thepersistent and resolved groups 65 of the 72 (86) had atotal SSI score of 1 or higher and 28 of those had a scoreof 2 or higher showing a significant level of suicidalityOf the 28 patients classified as emergent suicidality 20subjects had a baseline score of 0 six had a score of 1and 2 had a score of 2 (thus using a cut-off score of two79 was misclassified based on the SSI) Of the 138ambiguous cases with concurrent SSI ratings 119 (86)had a score of 0 and 7 had a score of 2 or higher
5 Assessment of combined symptoms of agitationanxiety
We assessed agitationanxiety using three items of theHRSD item 9 (agitation) item 10 (psychologicalanxiety) and item 11 (somatic anxiety) and noting ateach assessment whether subjects scorege2 on any singleitem We used this categorical approach to investigatewhether patients with emergent suicidal ideation weremore likely than other patients to have these symptoms
6 Assessment of akathisia
UKU data were available for a subgroup of MTLD-2and NTPX patients (n=161) Using the UKU akathisiaitem (item 16 score 0ndash4) we investigated whetherpatients with emergent suicidal ideationweremore likelyto experience akathisia than other groups A score of 1 onthis item indicates ldquoSlight akathisia however thepatient can keep still without effortrdquo a score of 2ldquoModerate akathisia however the patient can with aneffort remain sitting during the interviewrdquo and a scoreof 3 ldquothe patient has to rise to his feet several timesduring the interview because of akathisiardquo Although the
157K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
UKU is intended to assess medication side effects wealso administered the UKU before treatment to insurethat symptoms present before the inception of antide-pressant pharmacotherapy (such as agitation) were notmisattributed to treatment
7 Statistical analysis
In comparing the demographic and clinical character-istics of the four groups we used a one-way analysis ofvariance for continuous variables followed by Tukeypost-hoc contrasts for significant results For categoricalvariables (eg presence of akathisia) we used chi-squaretests Mixed-effect models were used to examinedepression (HRSD minus item 3 suicide item) overthe 12 weeks of treatment The mixed-effect includedgroup as a fixed effect while subject and time wereincluded as random effects The fixed-effect parameter(group and group by time) of each suicidal group wasexamined and compared in models that demonstrated anoverall significant effect Satterthwaite degrees offreedom was used in the mixed effect model A ge-neralized logit model with repeated measures over timetested for differences in anxietyagitation as indicated bya score of ge2 on any of items 9 10 or 11 of the HRSD
8 Results
Of the 437 patients (the sample with at least fourassessments) 123 patients (28) reported suicidality dur-ing the first two assessments of these 55(126) reported
Table 1Sociodemographic and clinical characteristics of patients based on the prese
(N) Non-suicidalN=104
(R) ResolvedsuicidalityN=68
(P) PsuicidN=55
Age (years) 731 (68) 733 (79) 703 Men 28 25 31 White 84 93 96Education (years) 123 (27) 126 (33) 123CIRS-G1 89 (37) 84 (39) 86 Recurrent depression 65 54 82Age of onset (lifetime) 604 (162) 604 (200) 511 Age of onset before age 60 378 353 630Hamilton-162 at week 0 189 (39) 200 (45) 196MMSE3 278 (27) 274 (27) 288ISEL-Self-esteem4 63 (29) 47 (28) 45Agitationanxiety5 45(16) 44(17) 45(1CIRS-G Cumulative Illness Rating Scale-Geriatric2HRSD Hamilton Rating Scale for Depression3MMSE Folstein Mini-Mental State Exam4ISEL Interpersonal Support Evaluation List ISEL-Self-esteem positive co5Agitationanxiety Hamilton Rating Scale of Depression aggregate score of11 (somatic anxiety)
suicidality longer than the first 4 weeks (ldquopersistentrdquo) while68 (156) did not report suicidality after 4 weeks intreatment (ldquoresolvedrdquo) Thirty-four patients (78) did notreport suicidality during the first 2 assessments but did solater during acute treatment (ldquoemergentrdquo) Of these 34 53showed emergent suicidal ideation in the first month oftreatment 21 in the second month and 26 in the thirdmonth of treatment There were 104 patients who werenon-suicidal throughout the 12-week treatment (ieconsistently scored 0 on the HRSD suicide item) Thusthe rates of emergent suicidality in the sample of 437 were78 (34437) persistent suicidality 126 (55437) andresolved suicidality 156 (68437)
There were 4 patients who had attempted suicide theweek before entering the study No patient attempted orcompleted suicide during the 12 weeks of acute treat-ment However one patient attempted suicide duringmaintenance treatment and one patient completed sui-cide after leaving the study and discontinuing treatmentagainst medical advice
Hypothesis 1 Association of suicidality with the pre-sence of chronicrecurrent depressive illness anxietyand agitation before treatment (Table 1)
Patients with persistent suicidality had their first epi-sode of depression on average 9 years earlier than non-suicidal patients or patients whose suicidality resolvedand were more likely to have recurrent episodes than theresolved and non-suicidal groups Patients in all threesuicidal groups reported lower self-esteem (ISEL self-esteem score) than the non-suicidal patients while
nceabsence of suicidality (meanplusmnSD)
ersistentality
(E) EmergentsuicidalityN=34
F or χ2 Df p Post-hoc
(89) 734 (74) 205 257 1124 080 3 8594 833 3 04 NP
(26) 125 (25) 019 256 90(48) 88 (37) 022 254 88
74 1112 3 02 NP RP(192) 534 (191) 415 249 007 NP RP
636 1621 3 001 NE NP PR RE(41) 197 (44) 103 257 38(18) 288 (15) 537 253 002 PR RE(32) 46 (32) 568 216 001 NP NR NE15) 45(19) 006 257 98
mparison when comparing oneself to othersitems item 9 (agitation) item 10 (psychological anxiety) and item
Table 2Adjunctive medication use during the 12-week treatment of late-life depression in non-suicidal patients and in patients with resolved persistent andemergent suicidality
Non-suicidal (N) N=104 Resolved (R) N=68 Persistent (P) N=55 Emergent (E) N=34 χ2 p Post-hoc
Lithium 4 (4) 1 (1) 9 (16) 3 (9) 1312 004 NP RPSecond antidepressant 7 (7) 1 (1) 6 (11) 6 (18) 942 03 RP RELorazepam 43(41) 27(40) 22(40) 15(44) 021 098
158 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
perceived availability of material aid perceived avail-ability of someone to talk to and to do things with did notdiffer among the four groups Pretreatment levels ofanxiety and agitation co-existing medical burden andseverity of the current depressive episode did not differamong the groups The UKU akathisia item scores alsodid not differ among the four groups at baseline
Hypothesis 2 Association of emergent and persistentsuicidality with persisting low mood and high levels ofanxietyagitation or akathisia during treatment
9 Association of suicidal status with remission ofdepression
A mixed-effect model indicated a significant groupand group by time interaction (16-item HRSD groupF=1076 df=3296 pb00001 interaction F=794df=3241 pb00001) The fixed-effect parameters fromthe model showed that all 3 suicidal groups had higherlevels of depressive symptoms over the 12 weeks oftreatment than the reference (non-suicidal) group(resolved t=245 df=299 pb002 persistent t=556df= 294 pb00001 emergent t= 276 df= 298pb0007) There was a significant group by time inter-action for the emergent group compared to the non-suicidal group (t=385 df=245 pb00002) Patientswith emergent suicidality had levels of depressionsimilar to those with persistent suicidality while patientswith resolved suicidality had lower levels of depressionthan those with persistent suicidality (t=minus300 df=294pb0003) The results for the mixed effects were thesame when we included only patients who receivedcombined pharmacotherapy and IPT
10 Association of suicidal status with agitationanxiety
The repeated-measures logit model indicated a sign-ificant group difference between the non-suicidal andthose with persistent suicidality (Z=326 pb 002) aswell as between those with resolved and persistentsuicidality (Z=241 pb 02) Non-suicidal patients andthose whose suicidality resolved were less likely to score
ge2 on items measuring anxiety or agitation than patientswith persistent suicidality A significant group-by-timeinteraction was found between patients with persistentand emergent ideation (Z=205 pb 05) the latterdemonstrated an increase in the percentage of patientsscoring ge2 on anxiety or agitation by week 12
101 Akathisia
Of the 161 patients with UKU data 97 had noakathisia (score=0) and 64 patients had akathisia scoresof ge1 at any time during treatment Only seven patientshad moderate akathisia (score=2) and only one hadsevere akathisia (score=3) There was no significantdifference among the groups 40 of the non-suicidal26 of the emergent 43 of the persistent and 44 ofthe resolved suicidality patients had a score of 1 or higherat any time on the UKU akathisia item (χ23=184p=061)
11 Adjunctive medication use during the 12-weektreatment (Table 2)
Patients who had persistent suicidal ideation weresignificantly more likely to receive lithium augmentationthan non-suicidal patients or those whose suicidalityresolved Patients with emergent or persistent suicidalideation were significantly more likely to receive anti-depressant augmentation than those whose suicidalityresolved The use of lorazepam as anxiolytichypnoticwas similar across the groups
Hypothesis 3 Potential effect of nortriptyline versusparoxetine on emergence of ideation
We limited our comparison of the effects of nortri-ptyline vs paroxetine to the patients who were treatedunder randomized double-blind conditions (NTPXstudy) because important clinical characteristics thatmay have influenced suicidality (eg rate of recurrenceof illness) differed in the two open-treatment studies(MTLD-1 and MTLD-2) and because the NTPX studydid not allow augmentation with a second antidepres-sant In 61 patients treated under double-blind random-ized conditions the proportions of patients with
159K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
emergent suicidal ideation and thoughts of death did notdiffer between treatments (1 subject [3] receivedparoxetine and none [0] received nortriptyline) (Fisherexact p=027)
12 Discussion
In 437 elderly patients with major depression during12 weeks of acute treatment 78 showed emergence ofsuicidality 126 persistence and 156 resolutionWhile at the inception of treatment the suicidal and non-suicidal groups had similar severity of symptoms duringtreatment patients with emergent and persistent suicid-ality had higher levels of depression and anxiety thannon-suicidal patients or those whose suicidality re-solved Emergent suicidality was associated with lowself-esteem earlier lifetime onset and non- or partialresponse to treatment (as indicated by high levels ofdepression and anxiety) but not with akathisia Patientsrandomized to nortriptyline or paroxetine were equallylikely to have emergent suicidality however this lastresult should be interpreted cautiously because of thesmall sample size
To our knowledge no study has examined emergentpersistent and resolved suicidality in older adults duringtreatment of depression The current study extends ourprevious finding that depressed elderly who endorsesuicidal ideation or recurrent thoughts of death experi-ence slower and less robust treatment response(Szantoet al 2003) This study also expands the previous find-ings by providing a potentially useful classification ofsuicidality during treatment by examining emergentpersistent and resolved suicidality We also showed thatthere are two distinct subgroups among depressedelderly patients who originally present with suicidalitythose whose suicidality resolves quickly after initiationof treatment and those who remain suicidal for a longerperiod of time (ie in our study often for up to 3 months)
Half of patients with emergent suicidality reportedsuicidal ideation or recurrent thoughts of death for thefirst time during the third and fourth week of treatmentone quarter in the second month and one quarter in thethird month Further studies could clarify whether thismight indicate different mediators For example in thosewhose suicidality emerged at the beginning of treatmentsuicide risk may be more likely due to medicationeffects In those who reported suicidality only afterseveral weeks of treatment non-response and giving uphope of ever getting better may be a causal factor
The strengths of this study include a large study groupof elderly depressed patients referred from both mentalhealth specialty clinics and primary care offices who
were well characterized at baseline received protoco-lized treatment over 12 weeks and were assessed weeklyusing well-defined reliable methods The studies in-cluded frail and old subjects those who were 70 andolder and patients with ldquodoublerdquo depression (ie majordepression superimposed on dysthymia)
Although the classification of suicidality based on thesingle suicide item of the HRSD administered weeklyover 12 weeks was confirmed by the SSI scores it is alimitation of the study that we did not have SSI scores inthewhole sample for each time point Based on theHRSDsuicide item 176 patients who were neither clearlysuicidal nor clearly non-suicidal were excluded Usingscales more specific to the assessment of suicidal ideationmay have increased our ability to identify suicidal ideatorsand to reduce the number of ldquoambiguousrdquo cases Visualinspection of the HRSD scores over time showed that theldquoambiguousrdquo group fell in between the two groups withbest treatment response (non-suicidal and resolved) andthe two groups with worse response (persistent and emer-gent suicidality)
We reported previously in a subsample of the currentstudy group that 155 of our study participants had alife-time history of suicide attempt Because we did nothave data in the whole study group on previous episodesof suicidality we could not investigate the relation oflife-time ideation and attempts to the course of currentsuicidality Nonetheless despite the limited informationavailable the use of repeated assessments and the asso-ciation observed with distinct patterns of treatment out-comes provide evidence of the clinical utility andvalidity of our classification of suicidality
The relatively low rates of suicidality in part could bedue to the exclusion of psychotic and bipolar patientsEven though the burden of co-existing medical illness instudy participants was moderately high patients whodropped out from the study (N=36) were medicallymore burdened than those who remained in the studyHence results may not be generalizable to the most frailelderly who may be at the highest risk for completedsuicide (Waern et al 2002a)
We noted that African Americans were more likely tobe in the non-suicidal group than Caucasians It isunclear whether this reflects a real difference in rates ofsuicidal ideation corresponding to lower elderlyAfrican American suicide rates or whether themeasures used are not sensitive to assess suicidality inAfrican Americans
The rate of emergent suicidality (78) was lowerthan the rate of emergent suicidality reported in a sampleof medication-free depressed adolescent outpatients whoreceived psychotherapy over a 12ndash16 week period
160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention
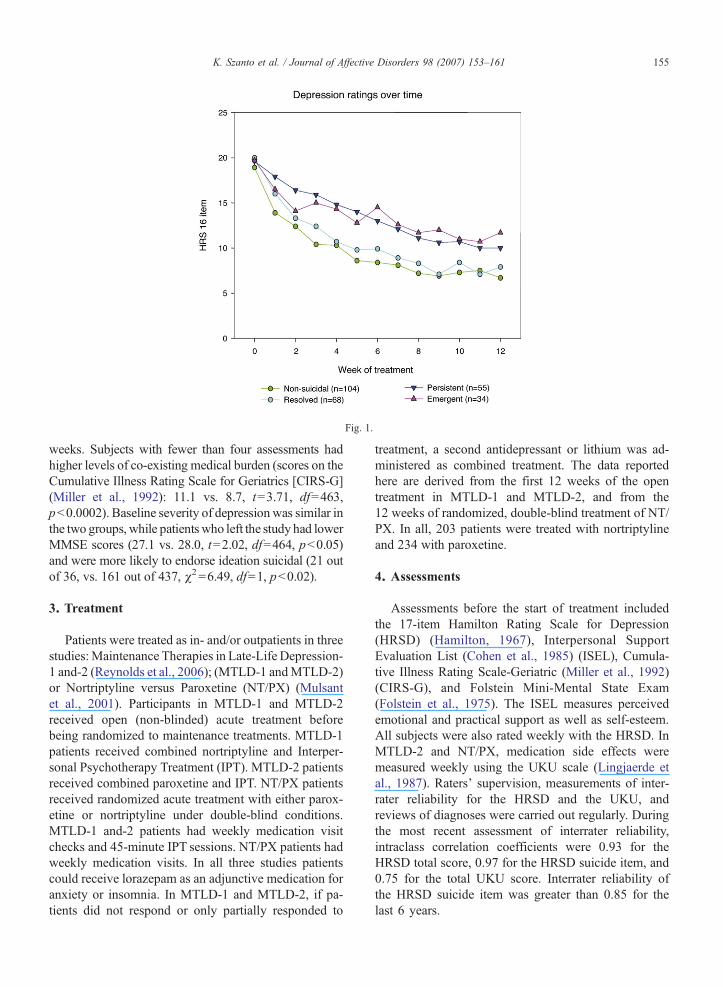
Fig 1
155K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
weeks Subjects with fewer than four assessments hadhigher levels of co-existing medical burden (scores on theCumulative Illness Rating Scale for Geriatrics [CIRS-G](Miller et al 1992) 111 vs 87 t=371 df=463pb00002) Baseline severity of depression was similar inthe two groups while patients who left the study had lowerMMSE scores (271 vs 280 t=202 df=464 pb005)and were more likely to endorse ideation suicidal (21 outof 36 vs 161 out of 437 χ2=649 df=1 pb002)
3 Treatment
Patients were treated as in- andor outpatients in threestudiesMaintenance Therapies in Late-Life Depression-1 and-2 (Reynolds et al 2006) (MTLD-1 andMTLD-2)or Nortriptyline versus Paroxetine (NTPX) (Mulsantet al 2001) Participants in MTLD-1 and MTLD-2received open (non-blinded) acute treatment beforebeing randomized to maintenance treatments MTLD-1patients received combined nortriptyline and Interper-sonal Psychotherapy Treatment (IPT) MTLD-2 patientsreceived combined paroxetine and IPT NTPX patientsreceived randomized acute treatment with either parox-etine or nortriptyline under double-blind conditionsMTLD-1 and-2 patients had weekly medication visitchecks and 45-minute IPT sessions NTPX patients hadweekly medication visits In all three studies patientscould receive lorazepam as an adjunctive medication foranxiety or insomnia In MTLD-1 and MTLD-2 if pa-tients did not respond or only partially responded to
treatment a second antidepressant or lithium was ad-ministered as combined treatment The data reportedhere are derived from the first 12 weeks of the opentreatment in MTLD-1 and MTLD-2 and from the12 weeks of randomized double-blind treatment of NTPX In all 203 patients were treated with nortriptylineand 234 with paroxetine
4 Assessments
Assessments before the start of treatment includedthe 17-item Hamilton Rating Scale for Depression(HRSD) (Hamilton 1967) Interpersonal SupportEvaluation List (Cohen et al 1985) (ISEL) Cumula-tive Illness Rating Scale-Geriatric (Miller et al 1992)(CIRS-G) and Folstein Mini-Mental State Exam(Folstein et al 1975) The ISEL measures perceivedemotional and practical support as well as self-esteemAll subjects were also rated weekly with the HRSD InMTLD-2 and NTPX medication side effects weremeasured weekly using the UKU scale (Lingjaerde etal 1987) Raters supervision measurements of inter-rater reliability for the HRSD and the UKU andreviews of diagnoses were carried out regularly Duringthe most recent assessment of interrater reliabilityintraclass correlation coefficients were 093 for theHRSD total score 097 for the HRSD suicide item and075 for the total UKU score Interrater reliability ofthe HRSD suicide item was greater than 085 for thelast 6 years
156 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
The HRSD suicide item assesses suicidal behaviorsuicidal thoughts thoughts of death and desire to livewithin the past 7 days Suicidality was defined as ascore of 2 or higher on this item (ldquopatient reports orwishes heshe were dead recurrent thought of death orsuicidal ideation or had a recent suicide attemptrdquo)Wechose this particular cut-point for the following reasonsfirst based on data from 6891 psychiatric outpatientswhowere evaluated at the Center for Cognitive Therapyof the University of Pennsylvania those who scored 2or higher on the Hamilton Depression Rating Scalesuicide item were 49 times (95 CI 27ndash90) morelikely to commit suicide than those who scored less than2 during a 20-year prospective study (httpwwwnimhnihgovsuicideresearch adultsuicidepdf) Second wehave shown in an earlier study (Szanto et al 1996) thatolder depressed patients with either active or passivesuicidal ideation had similar rates of life-time suicideattempts and similarly high levels of hopelessnessdiffering significantly from patients who deniedsuicidal ideation or thoughts of death
We further classified patients as having persistentsuicidality if they reported suicidality during the first twoassessments and continued to endorse it at any point after4 weeks of treatment Patients who did not endorsesuicidality at any of the first 2 assessments but reported itlater at any point during treatment were classified ashaving emergent suicidality Patients who endorsedsuicidality during the first two assessments but did notreport it after 4 weeks of treatment were considered tohave resolved suicidality Patients were judged to benon-suicidal if they never reported suicidality and neverreported the feeling that life is empty or not worth living(ie they had a score of 0 on the HRSD suicide item atthe inception of treatment and during each of the 12weekly assessments) To ensure that we did not mis-classify patients as non-suicidal we used this criterionfor non-suicidality (score of 0 on HRSD suicide item) forall 12-weeks of data Thus we excluded from furtheranalysis 176 patients who were neither clearly suicidalnor non-suicidal that is patients who had an HRSDsuicide item score of 1 at any time (ldquolife is empty notworth livingrdquo) but who never had a score of 2 or higher(recurrent thoughts of death wishes heshe were dead orsuicidal ideation) We compared the demographic andbaseline clinical characteristics of the 176 ambiguouscases with the 261 cases who were used for furtheranalyses There was no significant difference betweenthese two groups regarding age gender educationallevel baseline severity of depression lifetime age ofonset of first depressive episode or levels of self-esteem(results are not shown but available upon request)
As an additional check of the validity of our suicidegroup classification we examined the Scale for SuicideIdeation (SSI) (Beck et al 1979) scores in a subgroup(N=307) for whom SSI scores were available for the firsttwo assessments (SSI scale was introduced later in thestudy) We used the highest summarized scores from thefirst two assessments for the first 5 (screening) items ofthe SSI (possible scores 0ndash10) Three SSI screeningitems assess the wish to live or the wish to die and twoitems assess the desire to attempt suicide There is noclear cut-off point for the SSI some studies have used anSSI score of 1 or higher to define suicidality (eg Bruceet al 2004) while others used a score of 2 or higher(eg Brown et al 2000) The classification by theHRSD suicide item was confirmed by the SSI Of 69non-suicidal patients where SSI data were available 67had a total score of 0 on the SSI first 5 items only 2 had ascore of 1 (97 agreement across scales) Within thepersistent and resolved groups 65 of the 72 (86) had atotal SSI score of 1 or higher and 28 of those had a scoreof 2 or higher showing a significant level of suicidalityOf the 28 patients classified as emergent suicidality 20subjects had a baseline score of 0 six had a score of 1and 2 had a score of 2 (thus using a cut-off score of two79 was misclassified based on the SSI) Of the 138ambiguous cases with concurrent SSI ratings 119 (86)had a score of 0 and 7 had a score of 2 or higher
5 Assessment of combined symptoms of agitationanxiety
We assessed agitationanxiety using three items of theHRSD item 9 (agitation) item 10 (psychologicalanxiety) and item 11 (somatic anxiety) and noting ateach assessment whether subjects scorege2 on any singleitem We used this categorical approach to investigatewhether patients with emergent suicidal ideation weremore likely than other patients to have these symptoms
6 Assessment of akathisia
UKU data were available for a subgroup of MTLD-2and NTPX patients (n=161) Using the UKU akathisiaitem (item 16 score 0ndash4) we investigated whetherpatients with emergent suicidal ideationweremore likelyto experience akathisia than other groups A score of 1 onthis item indicates ldquoSlight akathisia however thepatient can keep still without effortrdquo a score of 2ldquoModerate akathisia however the patient can with aneffort remain sitting during the interviewrdquo and a scoreof 3 ldquothe patient has to rise to his feet several timesduring the interview because of akathisiardquo Although the
157K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
UKU is intended to assess medication side effects wealso administered the UKU before treatment to insurethat symptoms present before the inception of antide-pressant pharmacotherapy (such as agitation) were notmisattributed to treatment
7 Statistical analysis
In comparing the demographic and clinical character-istics of the four groups we used a one-way analysis ofvariance for continuous variables followed by Tukeypost-hoc contrasts for significant results For categoricalvariables (eg presence of akathisia) we used chi-squaretests Mixed-effect models were used to examinedepression (HRSD minus item 3 suicide item) overthe 12 weeks of treatment The mixed-effect includedgroup as a fixed effect while subject and time wereincluded as random effects The fixed-effect parameter(group and group by time) of each suicidal group wasexamined and compared in models that demonstrated anoverall significant effect Satterthwaite degrees offreedom was used in the mixed effect model A ge-neralized logit model with repeated measures over timetested for differences in anxietyagitation as indicated bya score of ge2 on any of items 9 10 or 11 of the HRSD
8 Results
Of the 437 patients (the sample with at least fourassessments) 123 patients (28) reported suicidality dur-ing the first two assessments of these 55(126) reported
Table 1Sociodemographic and clinical characteristics of patients based on the prese
(N) Non-suicidalN=104
(R) ResolvedsuicidalityN=68
(P) PsuicidN=55
Age (years) 731 (68) 733 (79) 703 Men 28 25 31 White 84 93 96Education (years) 123 (27) 126 (33) 123CIRS-G1 89 (37) 84 (39) 86 Recurrent depression 65 54 82Age of onset (lifetime) 604 (162) 604 (200) 511 Age of onset before age 60 378 353 630Hamilton-162 at week 0 189 (39) 200 (45) 196MMSE3 278 (27) 274 (27) 288ISEL-Self-esteem4 63 (29) 47 (28) 45Agitationanxiety5 45(16) 44(17) 45(1CIRS-G Cumulative Illness Rating Scale-Geriatric2HRSD Hamilton Rating Scale for Depression3MMSE Folstein Mini-Mental State Exam4ISEL Interpersonal Support Evaluation List ISEL-Self-esteem positive co5Agitationanxiety Hamilton Rating Scale of Depression aggregate score of11 (somatic anxiety)
suicidality longer than the first 4 weeks (ldquopersistentrdquo) while68 (156) did not report suicidality after 4 weeks intreatment (ldquoresolvedrdquo) Thirty-four patients (78) did notreport suicidality during the first 2 assessments but did solater during acute treatment (ldquoemergentrdquo) Of these 34 53showed emergent suicidal ideation in the first month oftreatment 21 in the second month and 26 in the thirdmonth of treatment There were 104 patients who werenon-suicidal throughout the 12-week treatment (ieconsistently scored 0 on the HRSD suicide item) Thusthe rates of emergent suicidality in the sample of 437 were78 (34437) persistent suicidality 126 (55437) andresolved suicidality 156 (68437)
There were 4 patients who had attempted suicide theweek before entering the study No patient attempted orcompleted suicide during the 12 weeks of acute treat-ment However one patient attempted suicide duringmaintenance treatment and one patient completed sui-cide after leaving the study and discontinuing treatmentagainst medical advice
Hypothesis 1 Association of suicidality with the pre-sence of chronicrecurrent depressive illness anxietyand agitation before treatment (Table 1)
Patients with persistent suicidality had their first epi-sode of depression on average 9 years earlier than non-suicidal patients or patients whose suicidality resolvedand were more likely to have recurrent episodes than theresolved and non-suicidal groups Patients in all threesuicidal groups reported lower self-esteem (ISEL self-esteem score) than the non-suicidal patients while
nceabsence of suicidality (meanplusmnSD)
ersistentality
(E) EmergentsuicidalityN=34
F or χ2 Df p Post-hoc
(89) 734 (74) 205 257 1124 080 3 8594 833 3 04 NP
(26) 125 (25) 019 256 90(48) 88 (37) 022 254 88
74 1112 3 02 NP RP(192) 534 (191) 415 249 007 NP RP
636 1621 3 001 NE NP PR RE(41) 197 (44) 103 257 38(18) 288 (15) 537 253 002 PR RE(32) 46 (32) 568 216 001 NP NR NE15) 45(19) 006 257 98
mparison when comparing oneself to othersitems item 9 (agitation) item 10 (psychological anxiety) and item
Table 2Adjunctive medication use during the 12-week treatment of late-life depression in non-suicidal patients and in patients with resolved persistent andemergent suicidality
Non-suicidal (N) N=104 Resolved (R) N=68 Persistent (P) N=55 Emergent (E) N=34 χ2 p Post-hoc
Lithium 4 (4) 1 (1) 9 (16) 3 (9) 1312 004 NP RPSecond antidepressant 7 (7) 1 (1) 6 (11) 6 (18) 942 03 RP RELorazepam 43(41) 27(40) 22(40) 15(44) 021 098
158 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
perceived availability of material aid perceived avail-ability of someone to talk to and to do things with did notdiffer among the four groups Pretreatment levels ofanxiety and agitation co-existing medical burden andseverity of the current depressive episode did not differamong the groups The UKU akathisia item scores alsodid not differ among the four groups at baseline
Hypothesis 2 Association of emergent and persistentsuicidality with persisting low mood and high levels ofanxietyagitation or akathisia during treatment
9 Association of suicidal status with remission ofdepression
A mixed-effect model indicated a significant groupand group by time interaction (16-item HRSD groupF=1076 df=3296 pb00001 interaction F=794df=3241 pb00001) The fixed-effect parameters fromthe model showed that all 3 suicidal groups had higherlevels of depressive symptoms over the 12 weeks oftreatment than the reference (non-suicidal) group(resolved t=245 df=299 pb002 persistent t=556df= 294 pb00001 emergent t= 276 df= 298pb0007) There was a significant group by time inter-action for the emergent group compared to the non-suicidal group (t=385 df=245 pb00002) Patientswith emergent suicidality had levels of depressionsimilar to those with persistent suicidality while patientswith resolved suicidality had lower levels of depressionthan those with persistent suicidality (t=minus300 df=294pb0003) The results for the mixed effects were thesame when we included only patients who receivedcombined pharmacotherapy and IPT
10 Association of suicidal status with agitationanxiety
The repeated-measures logit model indicated a sign-ificant group difference between the non-suicidal andthose with persistent suicidality (Z=326 pb 002) aswell as between those with resolved and persistentsuicidality (Z=241 pb 02) Non-suicidal patients andthose whose suicidality resolved were less likely to score
ge2 on items measuring anxiety or agitation than patientswith persistent suicidality A significant group-by-timeinteraction was found between patients with persistentand emergent ideation (Z=205 pb 05) the latterdemonstrated an increase in the percentage of patientsscoring ge2 on anxiety or agitation by week 12
101 Akathisia
Of the 161 patients with UKU data 97 had noakathisia (score=0) and 64 patients had akathisia scoresof ge1 at any time during treatment Only seven patientshad moderate akathisia (score=2) and only one hadsevere akathisia (score=3) There was no significantdifference among the groups 40 of the non-suicidal26 of the emergent 43 of the persistent and 44 ofthe resolved suicidality patients had a score of 1 or higherat any time on the UKU akathisia item (χ23=184p=061)
11 Adjunctive medication use during the 12-weektreatment (Table 2)
Patients who had persistent suicidal ideation weresignificantly more likely to receive lithium augmentationthan non-suicidal patients or those whose suicidalityresolved Patients with emergent or persistent suicidalideation were significantly more likely to receive anti-depressant augmentation than those whose suicidalityresolved The use of lorazepam as anxiolytichypnoticwas similar across the groups
Hypothesis 3 Potential effect of nortriptyline versusparoxetine on emergence of ideation
We limited our comparison of the effects of nortri-ptyline vs paroxetine to the patients who were treatedunder randomized double-blind conditions (NTPXstudy) because important clinical characteristics thatmay have influenced suicidality (eg rate of recurrenceof illness) differed in the two open-treatment studies(MTLD-1 and MTLD-2) and because the NTPX studydid not allow augmentation with a second antidepres-sant In 61 patients treated under double-blind random-ized conditions the proportions of patients with
159K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
emergent suicidal ideation and thoughts of death did notdiffer between treatments (1 subject [3] receivedparoxetine and none [0] received nortriptyline) (Fisherexact p=027)
12 Discussion
In 437 elderly patients with major depression during12 weeks of acute treatment 78 showed emergence ofsuicidality 126 persistence and 156 resolutionWhile at the inception of treatment the suicidal and non-suicidal groups had similar severity of symptoms duringtreatment patients with emergent and persistent suicid-ality had higher levels of depression and anxiety thannon-suicidal patients or those whose suicidality re-solved Emergent suicidality was associated with lowself-esteem earlier lifetime onset and non- or partialresponse to treatment (as indicated by high levels ofdepression and anxiety) but not with akathisia Patientsrandomized to nortriptyline or paroxetine were equallylikely to have emergent suicidality however this lastresult should be interpreted cautiously because of thesmall sample size
To our knowledge no study has examined emergentpersistent and resolved suicidality in older adults duringtreatment of depression The current study extends ourprevious finding that depressed elderly who endorsesuicidal ideation or recurrent thoughts of death experi-ence slower and less robust treatment response(Szantoet al 2003) This study also expands the previous find-ings by providing a potentially useful classification ofsuicidality during treatment by examining emergentpersistent and resolved suicidality We also showed thatthere are two distinct subgroups among depressedelderly patients who originally present with suicidalitythose whose suicidality resolves quickly after initiationof treatment and those who remain suicidal for a longerperiod of time (ie in our study often for up to 3 months)
Half of patients with emergent suicidality reportedsuicidal ideation or recurrent thoughts of death for thefirst time during the third and fourth week of treatmentone quarter in the second month and one quarter in thethird month Further studies could clarify whether thismight indicate different mediators For example in thosewhose suicidality emerged at the beginning of treatmentsuicide risk may be more likely due to medicationeffects In those who reported suicidality only afterseveral weeks of treatment non-response and giving uphope of ever getting better may be a causal factor
The strengths of this study include a large study groupof elderly depressed patients referred from both mentalhealth specialty clinics and primary care offices who
were well characterized at baseline received protoco-lized treatment over 12 weeks and were assessed weeklyusing well-defined reliable methods The studies in-cluded frail and old subjects those who were 70 andolder and patients with ldquodoublerdquo depression (ie majordepression superimposed on dysthymia)
Although the classification of suicidality based on thesingle suicide item of the HRSD administered weeklyover 12 weeks was confirmed by the SSI scores it is alimitation of the study that we did not have SSI scores inthewhole sample for each time point Based on theHRSDsuicide item 176 patients who were neither clearlysuicidal nor clearly non-suicidal were excluded Usingscales more specific to the assessment of suicidal ideationmay have increased our ability to identify suicidal ideatorsand to reduce the number of ldquoambiguousrdquo cases Visualinspection of the HRSD scores over time showed that theldquoambiguousrdquo group fell in between the two groups withbest treatment response (non-suicidal and resolved) andthe two groups with worse response (persistent and emer-gent suicidality)
We reported previously in a subsample of the currentstudy group that 155 of our study participants had alife-time history of suicide attempt Because we did nothave data in the whole study group on previous episodesof suicidality we could not investigate the relation oflife-time ideation and attempts to the course of currentsuicidality Nonetheless despite the limited informationavailable the use of repeated assessments and the asso-ciation observed with distinct patterns of treatment out-comes provide evidence of the clinical utility andvalidity of our classification of suicidality
The relatively low rates of suicidality in part could bedue to the exclusion of psychotic and bipolar patientsEven though the burden of co-existing medical illness instudy participants was moderately high patients whodropped out from the study (N=36) were medicallymore burdened than those who remained in the studyHence results may not be generalizable to the most frailelderly who may be at the highest risk for completedsuicide (Waern et al 2002a)
We noted that African Americans were more likely tobe in the non-suicidal group than Caucasians It isunclear whether this reflects a real difference in rates ofsuicidal ideation corresponding to lower elderlyAfrican American suicide rates or whether themeasures used are not sensitive to assess suicidality inAfrican Americans
The rate of emergent suicidality (78) was lowerthan the rate of emergent suicidality reported in a sampleof medication-free depressed adolescent outpatients whoreceived psychotherapy over a 12ndash16 week period
160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention

156 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
The HRSD suicide item assesses suicidal behaviorsuicidal thoughts thoughts of death and desire to livewithin the past 7 days Suicidality was defined as ascore of 2 or higher on this item (ldquopatient reports orwishes heshe were dead recurrent thought of death orsuicidal ideation or had a recent suicide attemptrdquo)Wechose this particular cut-point for the following reasonsfirst based on data from 6891 psychiatric outpatientswhowere evaluated at the Center for Cognitive Therapyof the University of Pennsylvania those who scored 2or higher on the Hamilton Depression Rating Scalesuicide item were 49 times (95 CI 27ndash90) morelikely to commit suicide than those who scored less than2 during a 20-year prospective study (httpwwwnimhnihgovsuicideresearch adultsuicidepdf) Second wehave shown in an earlier study (Szanto et al 1996) thatolder depressed patients with either active or passivesuicidal ideation had similar rates of life-time suicideattempts and similarly high levels of hopelessnessdiffering significantly from patients who deniedsuicidal ideation or thoughts of death
We further classified patients as having persistentsuicidality if they reported suicidality during the first twoassessments and continued to endorse it at any point after4 weeks of treatment Patients who did not endorsesuicidality at any of the first 2 assessments but reported itlater at any point during treatment were classified ashaving emergent suicidality Patients who endorsedsuicidality during the first two assessments but did notreport it after 4 weeks of treatment were considered tohave resolved suicidality Patients were judged to benon-suicidal if they never reported suicidality and neverreported the feeling that life is empty or not worth living(ie they had a score of 0 on the HRSD suicide item atthe inception of treatment and during each of the 12weekly assessments) To ensure that we did not mis-classify patients as non-suicidal we used this criterionfor non-suicidality (score of 0 on HRSD suicide item) forall 12-weeks of data Thus we excluded from furtheranalysis 176 patients who were neither clearly suicidalnor non-suicidal that is patients who had an HRSDsuicide item score of 1 at any time (ldquolife is empty notworth livingrdquo) but who never had a score of 2 or higher(recurrent thoughts of death wishes heshe were dead orsuicidal ideation) We compared the demographic andbaseline clinical characteristics of the 176 ambiguouscases with the 261 cases who were used for furtheranalyses There was no significant difference betweenthese two groups regarding age gender educationallevel baseline severity of depression lifetime age ofonset of first depressive episode or levels of self-esteem(results are not shown but available upon request)
As an additional check of the validity of our suicidegroup classification we examined the Scale for SuicideIdeation (SSI) (Beck et al 1979) scores in a subgroup(N=307) for whom SSI scores were available for the firsttwo assessments (SSI scale was introduced later in thestudy) We used the highest summarized scores from thefirst two assessments for the first 5 (screening) items ofthe SSI (possible scores 0ndash10) Three SSI screeningitems assess the wish to live or the wish to die and twoitems assess the desire to attempt suicide There is noclear cut-off point for the SSI some studies have used anSSI score of 1 or higher to define suicidality (eg Bruceet al 2004) while others used a score of 2 or higher(eg Brown et al 2000) The classification by theHRSD suicide item was confirmed by the SSI Of 69non-suicidal patients where SSI data were available 67had a total score of 0 on the SSI first 5 items only 2 had ascore of 1 (97 agreement across scales) Within thepersistent and resolved groups 65 of the 72 (86) had atotal SSI score of 1 or higher and 28 of those had a scoreof 2 or higher showing a significant level of suicidalityOf the 28 patients classified as emergent suicidality 20subjects had a baseline score of 0 six had a score of 1and 2 had a score of 2 (thus using a cut-off score of two79 was misclassified based on the SSI) Of the 138ambiguous cases with concurrent SSI ratings 119 (86)had a score of 0 and 7 had a score of 2 or higher
5 Assessment of combined symptoms of agitationanxiety
We assessed agitationanxiety using three items of theHRSD item 9 (agitation) item 10 (psychologicalanxiety) and item 11 (somatic anxiety) and noting ateach assessment whether subjects scorege2 on any singleitem We used this categorical approach to investigatewhether patients with emergent suicidal ideation weremore likely than other patients to have these symptoms
6 Assessment of akathisia
UKU data were available for a subgroup of MTLD-2and NTPX patients (n=161) Using the UKU akathisiaitem (item 16 score 0ndash4) we investigated whetherpatients with emergent suicidal ideationweremore likelyto experience akathisia than other groups A score of 1 onthis item indicates ldquoSlight akathisia however thepatient can keep still without effortrdquo a score of 2ldquoModerate akathisia however the patient can with aneffort remain sitting during the interviewrdquo and a scoreof 3 ldquothe patient has to rise to his feet several timesduring the interview because of akathisiardquo Although the
157K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
UKU is intended to assess medication side effects wealso administered the UKU before treatment to insurethat symptoms present before the inception of antide-pressant pharmacotherapy (such as agitation) were notmisattributed to treatment
7 Statistical analysis
In comparing the demographic and clinical character-istics of the four groups we used a one-way analysis ofvariance for continuous variables followed by Tukeypost-hoc contrasts for significant results For categoricalvariables (eg presence of akathisia) we used chi-squaretests Mixed-effect models were used to examinedepression (HRSD minus item 3 suicide item) overthe 12 weeks of treatment The mixed-effect includedgroup as a fixed effect while subject and time wereincluded as random effects The fixed-effect parameter(group and group by time) of each suicidal group wasexamined and compared in models that demonstrated anoverall significant effect Satterthwaite degrees offreedom was used in the mixed effect model A ge-neralized logit model with repeated measures over timetested for differences in anxietyagitation as indicated bya score of ge2 on any of items 9 10 or 11 of the HRSD
8 Results
Of the 437 patients (the sample with at least fourassessments) 123 patients (28) reported suicidality dur-ing the first two assessments of these 55(126) reported
Table 1Sociodemographic and clinical characteristics of patients based on the prese
(N) Non-suicidalN=104
(R) ResolvedsuicidalityN=68
(P) PsuicidN=55
Age (years) 731 (68) 733 (79) 703 Men 28 25 31 White 84 93 96Education (years) 123 (27) 126 (33) 123CIRS-G1 89 (37) 84 (39) 86 Recurrent depression 65 54 82Age of onset (lifetime) 604 (162) 604 (200) 511 Age of onset before age 60 378 353 630Hamilton-162 at week 0 189 (39) 200 (45) 196MMSE3 278 (27) 274 (27) 288ISEL-Self-esteem4 63 (29) 47 (28) 45Agitationanxiety5 45(16) 44(17) 45(1CIRS-G Cumulative Illness Rating Scale-Geriatric2HRSD Hamilton Rating Scale for Depression3MMSE Folstein Mini-Mental State Exam4ISEL Interpersonal Support Evaluation List ISEL-Self-esteem positive co5Agitationanxiety Hamilton Rating Scale of Depression aggregate score of11 (somatic anxiety)
suicidality longer than the first 4 weeks (ldquopersistentrdquo) while68 (156) did not report suicidality after 4 weeks intreatment (ldquoresolvedrdquo) Thirty-four patients (78) did notreport suicidality during the first 2 assessments but did solater during acute treatment (ldquoemergentrdquo) Of these 34 53showed emergent suicidal ideation in the first month oftreatment 21 in the second month and 26 in the thirdmonth of treatment There were 104 patients who werenon-suicidal throughout the 12-week treatment (ieconsistently scored 0 on the HRSD suicide item) Thusthe rates of emergent suicidality in the sample of 437 were78 (34437) persistent suicidality 126 (55437) andresolved suicidality 156 (68437)
There were 4 patients who had attempted suicide theweek before entering the study No patient attempted orcompleted suicide during the 12 weeks of acute treat-ment However one patient attempted suicide duringmaintenance treatment and one patient completed sui-cide after leaving the study and discontinuing treatmentagainst medical advice
Hypothesis 1 Association of suicidality with the pre-sence of chronicrecurrent depressive illness anxietyand agitation before treatment (Table 1)
Patients with persistent suicidality had their first epi-sode of depression on average 9 years earlier than non-suicidal patients or patients whose suicidality resolvedand were more likely to have recurrent episodes than theresolved and non-suicidal groups Patients in all threesuicidal groups reported lower self-esteem (ISEL self-esteem score) than the non-suicidal patients while
nceabsence of suicidality (meanplusmnSD)
ersistentality
(E) EmergentsuicidalityN=34
F or χ2 Df p Post-hoc
(89) 734 (74) 205 257 1124 080 3 8594 833 3 04 NP
(26) 125 (25) 019 256 90(48) 88 (37) 022 254 88
74 1112 3 02 NP RP(192) 534 (191) 415 249 007 NP RP
636 1621 3 001 NE NP PR RE(41) 197 (44) 103 257 38(18) 288 (15) 537 253 002 PR RE(32) 46 (32) 568 216 001 NP NR NE15) 45(19) 006 257 98
mparison when comparing oneself to othersitems item 9 (agitation) item 10 (psychological anxiety) and item
Table 2Adjunctive medication use during the 12-week treatment of late-life depression in non-suicidal patients and in patients with resolved persistent andemergent suicidality
Non-suicidal (N) N=104 Resolved (R) N=68 Persistent (P) N=55 Emergent (E) N=34 χ2 p Post-hoc
Lithium 4 (4) 1 (1) 9 (16) 3 (9) 1312 004 NP RPSecond antidepressant 7 (7) 1 (1) 6 (11) 6 (18) 942 03 RP RELorazepam 43(41) 27(40) 22(40) 15(44) 021 098
158 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
perceived availability of material aid perceived avail-ability of someone to talk to and to do things with did notdiffer among the four groups Pretreatment levels ofanxiety and agitation co-existing medical burden andseverity of the current depressive episode did not differamong the groups The UKU akathisia item scores alsodid not differ among the four groups at baseline
Hypothesis 2 Association of emergent and persistentsuicidality with persisting low mood and high levels ofanxietyagitation or akathisia during treatment
9 Association of suicidal status with remission ofdepression
A mixed-effect model indicated a significant groupand group by time interaction (16-item HRSD groupF=1076 df=3296 pb00001 interaction F=794df=3241 pb00001) The fixed-effect parameters fromthe model showed that all 3 suicidal groups had higherlevels of depressive symptoms over the 12 weeks oftreatment than the reference (non-suicidal) group(resolved t=245 df=299 pb002 persistent t=556df= 294 pb00001 emergent t= 276 df= 298pb0007) There was a significant group by time inter-action for the emergent group compared to the non-suicidal group (t=385 df=245 pb00002) Patientswith emergent suicidality had levels of depressionsimilar to those with persistent suicidality while patientswith resolved suicidality had lower levels of depressionthan those with persistent suicidality (t=minus300 df=294pb0003) The results for the mixed effects were thesame when we included only patients who receivedcombined pharmacotherapy and IPT
10 Association of suicidal status with agitationanxiety
The repeated-measures logit model indicated a sign-ificant group difference between the non-suicidal andthose with persistent suicidality (Z=326 pb 002) aswell as between those with resolved and persistentsuicidality (Z=241 pb 02) Non-suicidal patients andthose whose suicidality resolved were less likely to score
ge2 on items measuring anxiety or agitation than patientswith persistent suicidality A significant group-by-timeinteraction was found between patients with persistentand emergent ideation (Z=205 pb 05) the latterdemonstrated an increase in the percentage of patientsscoring ge2 on anxiety or agitation by week 12
101 Akathisia
Of the 161 patients with UKU data 97 had noakathisia (score=0) and 64 patients had akathisia scoresof ge1 at any time during treatment Only seven patientshad moderate akathisia (score=2) and only one hadsevere akathisia (score=3) There was no significantdifference among the groups 40 of the non-suicidal26 of the emergent 43 of the persistent and 44 ofthe resolved suicidality patients had a score of 1 or higherat any time on the UKU akathisia item (χ23=184p=061)
11 Adjunctive medication use during the 12-weektreatment (Table 2)
Patients who had persistent suicidal ideation weresignificantly more likely to receive lithium augmentationthan non-suicidal patients or those whose suicidalityresolved Patients with emergent or persistent suicidalideation were significantly more likely to receive anti-depressant augmentation than those whose suicidalityresolved The use of lorazepam as anxiolytichypnoticwas similar across the groups
Hypothesis 3 Potential effect of nortriptyline versusparoxetine on emergence of ideation
We limited our comparison of the effects of nortri-ptyline vs paroxetine to the patients who were treatedunder randomized double-blind conditions (NTPXstudy) because important clinical characteristics thatmay have influenced suicidality (eg rate of recurrenceof illness) differed in the two open-treatment studies(MTLD-1 and MTLD-2) and because the NTPX studydid not allow augmentation with a second antidepres-sant In 61 patients treated under double-blind random-ized conditions the proportions of patients with
159K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
emergent suicidal ideation and thoughts of death did notdiffer between treatments (1 subject [3] receivedparoxetine and none [0] received nortriptyline) (Fisherexact p=027)
12 Discussion
In 437 elderly patients with major depression during12 weeks of acute treatment 78 showed emergence ofsuicidality 126 persistence and 156 resolutionWhile at the inception of treatment the suicidal and non-suicidal groups had similar severity of symptoms duringtreatment patients with emergent and persistent suicid-ality had higher levels of depression and anxiety thannon-suicidal patients or those whose suicidality re-solved Emergent suicidality was associated with lowself-esteem earlier lifetime onset and non- or partialresponse to treatment (as indicated by high levels ofdepression and anxiety) but not with akathisia Patientsrandomized to nortriptyline or paroxetine were equallylikely to have emergent suicidality however this lastresult should be interpreted cautiously because of thesmall sample size
To our knowledge no study has examined emergentpersistent and resolved suicidality in older adults duringtreatment of depression The current study extends ourprevious finding that depressed elderly who endorsesuicidal ideation or recurrent thoughts of death experi-ence slower and less robust treatment response(Szantoet al 2003) This study also expands the previous find-ings by providing a potentially useful classification ofsuicidality during treatment by examining emergentpersistent and resolved suicidality We also showed thatthere are two distinct subgroups among depressedelderly patients who originally present with suicidalitythose whose suicidality resolves quickly after initiationof treatment and those who remain suicidal for a longerperiod of time (ie in our study often for up to 3 months)
Half of patients with emergent suicidality reportedsuicidal ideation or recurrent thoughts of death for thefirst time during the third and fourth week of treatmentone quarter in the second month and one quarter in thethird month Further studies could clarify whether thismight indicate different mediators For example in thosewhose suicidality emerged at the beginning of treatmentsuicide risk may be more likely due to medicationeffects In those who reported suicidality only afterseveral weeks of treatment non-response and giving uphope of ever getting better may be a causal factor
The strengths of this study include a large study groupof elderly depressed patients referred from both mentalhealth specialty clinics and primary care offices who
were well characterized at baseline received protoco-lized treatment over 12 weeks and were assessed weeklyusing well-defined reliable methods The studies in-cluded frail and old subjects those who were 70 andolder and patients with ldquodoublerdquo depression (ie majordepression superimposed on dysthymia)
Although the classification of suicidality based on thesingle suicide item of the HRSD administered weeklyover 12 weeks was confirmed by the SSI scores it is alimitation of the study that we did not have SSI scores inthewhole sample for each time point Based on theHRSDsuicide item 176 patients who were neither clearlysuicidal nor clearly non-suicidal were excluded Usingscales more specific to the assessment of suicidal ideationmay have increased our ability to identify suicidal ideatorsand to reduce the number of ldquoambiguousrdquo cases Visualinspection of the HRSD scores over time showed that theldquoambiguousrdquo group fell in between the two groups withbest treatment response (non-suicidal and resolved) andthe two groups with worse response (persistent and emer-gent suicidality)
We reported previously in a subsample of the currentstudy group that 155 of our study participants had alife-time history of suicide attempt Because we did nothave data in the whole study group on previous episodesof suicidality we could not investigate the relation oflife-time ideation and attempts to the course of currentsuicidality Nonetheless despite the limited informationavailable the use of repeated assessments and the asso-ciation observed with distinct patterns of treatment out-comes provide evidence of the clinical utility andvalidity of our classification of suicidality
The relatively low rates of suicidality in part could bedue to the exclusion of psychotic and bipolar patientsEven though the burden of co-existing medical illness instudy participants was moderately high patients whodropped out from the study (N=36) were medicallymore burdened than those who remained in the studyHence results may not be generalizable to the most frailelderly who may be at the highest risk for completedsuicide (Waern et al 2002a)
We noted that African Americans were more likely tobe in the non-suicidal group than Caucasians It isunclear whether this reflects a real difference in rates ofsuicidal ideation corresponding to lower elderlyAfrican American suicide rates or whether themeasures used are not sensitive to assess suicidality inAfrican Americans
The rate of emergent suicidality (78) was lowerthan the rate of emergent suicidality reported in a sampleof medication-free depressed adolescent outpatients whoreceived psychotherapy over a 12ndash16 week period
160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention
157K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
UKU is intended to assess medication side effects wealso administered the UKU before treatment to insurethat symptoms present before the inception of antide-pressant pharmacotherapy (such as agitation) were notmisattributed to treatment
7 Statistical analysis
In comparing the demographic and clinical character-istics of the four groups we used a one-way analysis ofvariance for continuous variables followed by Tukeypost-hoc contrasts for significant results For categoricalvariables (eg presence of akathisia) we used chi-squaretests Mixed-effect models were used to examinedepression (HRSD minus item 3 suicide item) overthe 12 weeks of treatment The mixed-effect includedgroup as a fixed effect while subject and time wereincluded as random effects The fixed-effect parameter(group and group by time) of each suicidal group wasexamined and compared in models that demonstrated anoverall significant effect Satterthwaite degrees offreedom was used in the mixed effect model A ge-neralized logit model with repeated measures over timetested for differences in anxietyagitation as indicated bya score of ge2 on any of items 9 10 or 11 of the HRSD
8 Results
Of the 437 patients (the sample with at least fourassessments) 123 patients (28) reported suicidality dur-ing the first two assessments of these 55(126) reported
Table 1Sociodemographic and clinical characteristics of patients based on the prese
(N) Non-suicidalN=104
(R) ResolvedsuicidalityN=68
(P) PsuicidN=55
Age (years) 731 (68) 733 (79) 703 Men 28 25 31 White 84 93 96Education (years) 123 (27) 126 (33) 123CIRS-G1 89 (37) 84 (39) 86 Recurrent depression 65 54 82Age of onset (lifetime) 604 (162) 604 (200) 511 Age of onset before age 60 378 353 630Hamilton-162 at week 0 189 (39) 200 (45) 196MMSE3 278 (27) 274 (27) 288ISEL-Self-esteem4 63 (29) 47 (28) 45Agitationanxiety5 45(16) 44(17) 45(1CIRS-G Cumulative Illness Rating Scale-Geriatric2HRSD Hamilton Rating Scale for Depression3MMSE Folstein Mini-Mental State Exam4ISEL Interpersonal Support Evaluation List ISEL-Self-esteem positive co5Agitationanxiety Hamilton Rating Scale of Depression aggregate score of11 (somatic anxiety)
suicidality longer than the first 4 weeks (ldquopersistentrdquo) while68 (156) did not report suicidality after 4 weeks intreatment (ldquoresolvedrdquo) Thirty-four patients (78) did notreport suicidality during the first 2 assessments but did solater during acute treatment (ldquoemergentrdquo) Of these 34 53showed emergent suicidal ideation in the first month oftreatment 21 in the second month and 26 in the thirdmonth of treatment There were 104 patients who werenon-suicidal throughout the 12-week treatment (ieconsistently scored 0 on the HRSD suicide item) Thusthe rates of emergent suicidality in the sample of 437 were78 (34437) persistent suicidality 126 (55437) andresolved suicidality 156 (68437)
There were 4 patients who had attempted suicide theweek before entering the study No patient attempted orcompleted suicide during the 12 weeks of acute treat-ment However one patient attempted suicide duringmaintenance treatment and one patient completed sui-cide after leaving the study and discontinuing treatmentagainst medical advice
Hypothesis 1 Association of suicidality with the pre-sence of chronicrecurrent depressive illness anxietyand agitation before treatment (Table 1)
Patients with persistent suicidality had their first epi-sode of depression on average 9 years earlier than non-suicidal patients or patients whose suicidality resolvedand were more likely to have recurrent episodes than theresolved and non-suicidal groups Patients in all threesuicidal groups reported lower self-esteem (ISEL self-esteem score) than the non-suicidal patients while
nceabsence of suicidality (meanplusmnSD)
ersistentality
(E) EmergentsuicidalityN=34
F or χ2 Df p Post-hoc
(89) 734 (74) 205 257 1124 080 3 8594 833 3 04 NP
(26) 125 (25) 019 256 90(48) 88 (37) 022 254 88
74 1112 3 02 NP RP(192) 534 (191) 415 249 007 NP RP
636 1621 3 001 NE NP PR RE(41) 197 (44) 103 257 38(18) 288 (15) 537 253 002 PR RE(32) 46 (32) 568 216 001 NP NR NE15) 45(19) 006 257 98
mparison when comparing oneself to othersitems item 9 (agitation) item 10 (psychological anxiety) and item
Table 2Adjunctive medication use during the 12-week treatment of late-life depression in non-suicidal patients and in patients with resolved persistent andemergent suicidality
Non-suicidal (N) N=104 Resolved (R) N=68 Persistent (P) N=55 Emergent (E) N=34 χ2 p Post-hoc
Lithium 4 (4) 1 (1) 9 (16) 3 (9) 1312 004 NP RPSecond antidepressant 7 (7) 1 (1) 6 (11) 6 (18) 942 03 RP RELorazepam 43(41) 27(40) 22(40) 15(44) 021 098
158 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
perceived availability of material aid perceived avail-ability of someone to talk to and to do things with did notdiffer among the four groups Pretreatment levels ofanxiety and agitation co-existing medical burden andseverity of the current depressive episode did not differamong the groups The UKU akathisia item scores alsodid not differ among the four groups at baseline
Hypothesis 2 Association of emergent and persistentsuicidality with persisting low mood and high levels ofanxietyagitation or akathisia during treatment
9 Association of suicidal status with remission ofdepression
A mixed-effect model indicated a significant groupand group by time interaction (16-item HRSD groupF=1076 df=3296 pb00001 interaction F=794df=3241 pb00001) The fixed-effect parameters fromthe model showed that all 3 suicidal groups had higherlevels of depressive symptoms over the 12 weeks oftreatment than the reference (non-suicidal) group(resolved t=245 df=299 pb002 persistent t=556df= 294 pb00001 emergent t= 276 df= 298pb0007) There was a significant group by time inter-action for the emergent group compared to the non-suicidal group (t=385 df=245 pb00002) Patientswith emergent suicidality had levels of depressionsimilar to those with persistent suicidality while patientswith resolved suicidality had lower levels of depressionthan those with persistent suicidality (t=minus300 df=294pb0003) The results for the mixed effects were thesame when we included only patients who receivedcombined pharmacotherapy and IPT
10 Association of suicidal status with agitationanxiety
The repeated-measures logit model indicated a sign-ificant group difference between the non-suicidal andthose with persistent suicidality (Z=326 pb 002) aswell as between those with resolved and persistentsuicidality (Z=241 pb 02) Non-suicidal patients andthose whose suicidality resolved were less likely to score
ge2 on items measuring anxiety or agitation than patientswith persistent suicidality A significant group-by-timeinteraction was found between patients with persistentand emergent ideation (Z=205 pb 05) the latterdemonstrated an increase in the percentage of patientsscoring ge2 on anxiety or agitation by week 12
101 Akathisia
Of the 161 patients with UKU data 97 had noakathisia (score=0) and 64 patients had akathisia scoresof ge1 at any time during treatment Only seven patientshad moderate akathisia (score=2) and only one hadsevere akathisia (score=3) There was no significantdifference among the groups 40 of the non-suicidal26 of the emergent 43 of the persistent and 44 ofthe resolved suicidality patients had a score of 1 or higherat any time on the UKU akathisia item (χ23=184p=061)
11 Adjunctive medication use during the 12-weektreatment (Table 2)
Patients who had persistent suicidal ideation weresignificantly more likely to receive lithium augmentationthan non-suicidal patients or those whose suicidalityresolved Patients with emergent or persistent suicidalideation were significantly more likely to receive anti-depressant augmentation than those whose suicidalityresolved The use of lorazepam as anxiolytichypnoticwas similar across the groups
Hypothesis 3 Potential effect of nortriptyline versusparoxetine on emergence of ideation
We limited our comparison of the effects of nortri-ptyline vs paroxetine to the patients who were treatedunder randomized double-blind conditions (NTPXstudy) because important clinical characteristics thatmay have influenced suicidality (eg rate of recurrenceof illness) differed in the two open-treatment studies(MTLD-1 and MTLD-2) and because the NTPX studydid not allow augmentation with a second antidepres-sant In 61 patients treated under double-blind random-ized conditions the proportions of patients with
159K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
emergent suicidal ideation and thoughts of death did notdiffer between treatments (1 subject [3] receivedparoxetine and none [0] received nortriptyline) (Fisherexact p=027)
12 Discussion
In 437 elderly patients with major depression during12 weeks of acute treatment 78 showed emergence ofsuicidality 126 persistence and 156 resolutionWhile at the inception of treatment the suicidal and non-suicidal groups had similar severity of symptoms duringtreatment patients with emergent and persistent suicid-ality had higher levels of depression and anxiety thannon-suicidal patients or those whose suicidality re-solved Emergent suicidality was associated with lowself-esteem earlier lifetime onset and non- or partialresponse to treatment (as indicated by high levels ofdepression and anxiety) but not with akathisia Patientsrandomized to nortriptyline or paroxetine were equallylikely to have emergent suicidality however this lastresult should be interpreted cautiously because of thesmall sample size
To our knowledge no study has examined emergentpersistent and resolved suicidality in older adults duringtreatment of depression The current study extends ourprevious finding that depressed elderly who endorsesuicidal ideation or recurrent thoughts of death experi-ence slower and less robust treatment response(Szantoet al 2003) This study also expands the previous find-ings by providing a potentially useful classification ofsuicidality during treatment by examining emergentpersistent and resolved suicidality We also showed thatthere are two distinct subgroups among depressedelderly patients who originally present with suicidalitythose whose suicidality resolves quickly after initiationof treatment and those who remain suicidal for a longerperiod of time (ie in our study often for up to 3 months)
Half of patients with emergent suicidality reportedsuicidal ideation or recurrent thoughts of death for thefirst time during the third and fourth week of treatmentone quarter in the second month and one quarter in thethird month Further studies could clarify whether thismight indicate different mediators For example in thosewhose suicidality emerged at the beginning of treatmentsuicide risk may be more likely due to medicationeffects In those who reported suicidality only afterseveral weeks of treatment non-response and giving uphope of ever getting better may be a causal factor
The strengths of this study include a large study groupof elderly depressed patients referred from both mentalhealth specialty clinics and primary care offices who
were well characterized at baseline received protoco-lized treatment over 12 weeks and were assessed weeklyusing well-defined reliable methods The studies in-cluded frail and old subjects those who were 70 andolder and patients with ldquodoublerdquo depression (ie majordepression superimposed on dysthymia)
Although the classification of suicidality based on thesingle suicide item of the HRSD administered weeklyover 12 weeks was confirmed by the SSI scores it is alimitation of the study that we did not have SSI scores inthewhole sample for each time point Based on theHRSDsuicide item 176 patients who were neither clearlysuicidal nor clearly non-suicidal were excluded Usingscales more specific to the assessment of suicidal ideationmay have increased our ability to identify suicidal ideatorsand to reduce the number of ldquoambiguousrdquo cases Visualinspection of the HRSD scores over time showed that theldquoambiguousrdquo group fell in between the two groups withbest treatment response (non-suicidal and resolved) andthe two groups with worse response (persistent and emer-gent suicidality)
We reported previously in a subsample of the currentstudy group that 155 of our study participants had alife-time history of suicide attempt Because we did nothave data in the whole study group on previous episodesof suicidality we could not investigate the relation oflife-time ideation and attempts to the course of currentsuicidality Nonetheless despite the limited informationavailable the use of repeated assessments and the asso-ciation observed with distinct patterns of treatment out-comes provide evidence of the clinical utility andvalidity of our classification of suicidality
The relatively low rates of suicidality in part could bedue to the exclusion of psychotic and bipolar patientsEven though the burden of co-existing medical illness instudy participants was moderately high patients whodropped out from the study (N=36) were medicallymore burdened than those who remained in the studyHence results may not be generalizable to the most frailelderly who may be at the highest risk for completedsuicide (Waern et al 2002a)
We noted that African Americans were more likely tobe in the non-suicidal group than Caucasians It isunclear whether this reflects a real difference in rates ofsuicidal ideation corresponding to lower elderlyAfrican American suicide rates or whether themeasures used are not sensitive to assess suicidality inAfrican Americans
The rate of emergent suicidality (78) was lowerthan the rate of emergent suicidality reported in a sampleof medication-free depressed adolescent outpatients whoreceived psychotherapy over a 12ndash16 week period
160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention

Table 2Adjunctive medication use during the 12-week treatment of late-life depression in non-suicidal patients and in patients with resolved persistent andemergent suicidality
Non-suicidal (N) N=104 Resolved (R) N=68 Persistent (P) N=55 Emergent (E) N=34 χ2 p Post-hoc
Lithium 4 (4) 1 (1) 9 (16) 3 (9) 1312 004 NP RPSecond antidepressant 7 (7) 1 (1) 6 (11) 6 (18) 942 03 RP RELorazepam 43(41) 27(40) 22(40) 15(44) 021 098
158 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
perceived availability of material aid perceived avail-ability of someone to talk to and to do things with did notdiffer among the four groups Pretreatment levels ofanxiety and agitation co-existing medical burden andseverity of the current depressive episode did not differamong the groups The UKU akathisia item scores alsodid not differ among the four groups at baseline
Hypothesis 2 Association of emergent and persistentsuicidality with persisting low mood and high levels ofanxietyagitation or akathisia during treatment
9 Association of suicidal status with remission ofdepression
A mixed-effect model indicated a significant groupand group by time interaction (16-item HRSD groupF=1076 df=3296 pb00001 interaction F=794df=3241 pb00001) The fixed-effect parameters fromthe model showed that all 3 suicidal groups had higherlevels of depressive symptoms over the 12 weeks oftreatment than the reference (non-suicidal) group(resolved t=245 df=299 pb002 persistent t=556df= 294 pb00001 emergent t= 276 df= 298pb0007) There was a significant group by time inter-action for the emergent group compared to the non-suicidal group (t=385 df=245 pb00002) Patientswith emergent suicidality had levels of depressionsimilar to those with persistent suicidality while patientswith resolved suicidality had lower levels of depressionthan those with persistent suicidality (t=minus300 df=294pb0003) The results for the mixed effects were thesame when we included only patients who receivedcombined pharmacotherapy and IPT
10 Association of suicidal status with agitationanxiety
The repeated-measures logit model indicated a sign-ificant group difference between the non-suicidal andthose with persistent suicidality (Z=326 pb 002) aswell as between those with resolved and persistentsuicidality (Z=241 pb 02) Non-suicidal patients andthose whose suicidality resolved were less likely to score
ge2 on items measuring anxiety or agitation than patientswith persistent suicidality A significant group-by-timeinteraction was found between patients with persistentand emergent ideation (Z=205 pb 05) the latterdemonstrated an increase in the percentage of patientsscoring ge2 on anxiety or agitation by week 12
101 Akathisia
Of the 161 patients with UKU data 97 had noakathisia (score=0) and 64 patients had akathisia scoresof ge1 at any time during treatment Only seven patientshad moderate akathisia (score=2) and only one hadsevere akathisia (score=3) There was no significantdifference among the groups 40 of the non-suicidal26 of the emergent 43 of the persistent and 44 ofthe resolved suicidality patients had a score of 1 or higherat any time on the UKU akathisia item (χ23=184p=061)
11 Adjunctive medication use during the 12-weektreatment (Table 2)
Patients who had persistent suicidal ideation weresignificantly more likely to receive lithium augmentationthan non-suicidal patients or those whose suicidalityresolved Patients with emergent or persistent suicidalideation were significantly more likely to receive anti-depressant augmentation than those whose suicidalityresolved The use of lorazepam as anxiolytichypnoticwas similar across the groups
Hypothesis 3 Potential effect of nortriptyline versusparoxetine on emergence of ideation
We limited our comparison of the effects of nortri-ptyline vs paroxetine to the patients who were treatedunder randomized double-blind conditions (NTPXstudy) because important clinical characteristics thatmay have influenced suicidality (eg rate of recurrenceof illness) differed in the two open-treatment studies(MTLD-1 and MTLD-2) and because the NTPX studydid not allow augmentation with a second antidepres-sant In 61 patients treated under double-blind random-ized conditions the proportions of patients with
159K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
emergent suicidal ideation and thoughts of death did notdiffer between treatments (1 subject [3] receivedparoxetine and none [0] received nortriptyline) (Fisherexact p=027)
12 Discussion
In 437 elderly patients with major depression during12 weeks of acute treatment 78 showed emergence ofsuicidality 126 persistence and 156 resolutionWhile at the inception of treatment the suicidal and non-suicidal groups had similar severity of symptoms duringtreatment patients with emergent and persistent suicid-ality had higher levels of depression and anxiety thannon-suicidal patients or those whose suicidality re-solved Emergent suicidality was associated with lowself-esteem earlier lifetime onset and non- or partialresponse to treatment (as indicated by high levels ofdepression and anxiety) but not with akathisia Patientsrandomized to nortriptyline or paroxetine were equallylikely to have emergent suicidality however this lastresult should be interpreted cautiously because of thesmall sample size
To our knowledge no study has examined emergentpersistent and resolved suicidality in older adults duringtreatment of depression The current study extends ourprevious finding that depressed elderly who endorsesuicidal ideation or recurrent thoughts of death experi-ence slower and less robust treatment response(Szantoet al 2003) This study also expands the previous find-ings by providing a potentially useful classification ofsuicidality during treatment by examining emergentpersistent and resolved suicidality We also showed thatthere are two distinct subgroups among depressedelderly patients who originally present with suicidalitythose whose suicidality resolves quickly after initiationof treatment and those who remain suicidal for a longerperiod of time (ie in our study often for up to 3 months)
Half of patients with emergent suicidality reportedsuicidal ideation or recurrent thoughts of death for thefirst time during the third and fourth week of treatmentone quarter in the second month and one quarter in thethird month Further studies could clarify whether thismight indicate different mediators For example in thosewhose suicidality emerged at the beginning of treatmentsuicide risk may be more likely due to medicationeffects In those who reported suicidality only afterseveral weeks of treatment non-response and giving uphope of ever getting better may be a causal factor
The strengths of this study include a large study groupof elderly depressed patients referred from both mentalhealth specialty clinics and primary care offices who
were well characterized at baseline received protoco-lized treatment over 12 weeks and were assessed weeklyusing well-defined reliable methods The studies in-cluded frail and old subjects those who were 70 andolder and patients with ldquodoublerdquo depression (ie majordepression superimposed on dysthymia)
Although the classification of suicidality based on thesingle suicide item of the HRSD administered weeklyover 12 weeks was confirmed by the SSI scores it is alimitation of the study that we did not have SSI scores inthewhole sample for each time point Based on theHRSDsuicide item 176 patients who were neither clearlysuicidal nor clearly non-suicidal were excluded Usingscales more specific to the assessment of suicidal ideationmay have increased our ability to identify suicidal ideatorsand to reduce the number of ldquoambiguousrdquo cases Visualinspection of the HRSD scores over time showed that theldquoambiguousrdquo group fell in between the two groups withbest treatment response (non-suicidal and resolved) andthe two groups with worse response (persistent and emer-gent suicidality)
We reported previously in a subsample of the currentstudy group that 155 of our study participants had alife-time history of suicide attempt Because we did nothave data in the whole study group on previous episodesof suicidality we could not investigate the relation oflife-time ideation and attempts to the course of currentsuicidality Nonetheless despite the limited informationavailable the use of repeated assessments and the asso-ciation observed with distinct patterns of treatment out-comes provide evidence of the clinical utility andvalidity of our classification of suicidality
The relatively low rates of suicidality in part could bedue to the exclusion of psychotic and bipolar patientsEven though the burden of co-existing medical illness instudy participants was moderately high patients whodropped out from the study (N=36) were medicallymore burdened than those who remained in the studyHence results may not be generalizable to the most frailelderly who may be at the highest risk for completedsuicide (Waern et al 2002a)
We noted that African Americans were more likely tobe in the non-suicidal group than Caucasians It isunclear whether this reflects a real difference in rates ofsuicidal ideation corresponding to lower elderlyAfrican American suicide rates or whether themeasures used are not sensitive to assess suicidality inAfrican Americans
The rate of emergent suicidality (78) was lowerthan the rate of emergent suicidality reported in a sampleof medication-free depressed adolescent outpatients whoreceived psychotherapy over a 12ndash16 week period
160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention

159K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
emergent suicidal ideation and thoughts of death did notdiffer between treatments (1 subject [3] receivedparoxetine and none [0] received nortriptyline) (Fisherexact p=027)
12 Discussion
In 437 elderly patients with major depression during12 weeks of acute treatment 78 showed emergence ofsuicidality 126 persistence and 156 resolutionWhile at the inception of treatment the suicidal and non-suicidal groups had similar severity of symptoms duringtreatment patients with emergent and persistent suicid-ality had higher levels of depression and anxiety thannon-suicidal patients or those whose suicidality re-solved Emergent suicidality was associated with lowself-esteem earlier lifetime onset and non- or partialresponse to treatment (as indicated by high levels ofdepression and anxiety) but not with akathisia Patientsrandomized to nortriptyline or paroxetine were equallylikely to have emergent suicidality however this lastresult should be interpreted cautiously because of thesmall sample size
To our knowledge no study has examined emergentpersistent and resolved suicidality in older adults duringtreatment of depression The current study extends ourprevious finding that depressed elderly who endorsesuicidal ideation or recurrent thoughts of death experi-ence slower and less robust treatment response(Szantoet al 2003) This study also expands the previous find-ings by providing a potentially useful classification ofsuicidality during treatment by examining emergentpersistent and resolved suicidality We also showed thatthere are two distinct subgroups among depressedelderly patients who originally present with suicidalitythose whose suicidality resolves quickly after initiationof treatment and those who remain suicidal for a longerperiod of time (ie in our study often for up to 3 months)
Half of patients with emergent suicidality reportedsuicidal ideation or recurrent thoughts of death for thefirst time during the third and fourth week of treatmentone quarter in the second month and one quarter in thethird month Further studies could clarify whether thismight indicate different mediators For example in thosewhose suicidality emerged at the beginning of treatmentsuicide risk may be more likely due to medicationeffects In those who reported suicidality only afterseveral weeks of treatment non-response and giving uphope of ever getting better may be a causal factor
The strengths of this study include a large study groupof elderly depressed patients referred from both mentalhealth specialty clinics and primary care offices who
were well characterized at baseline received protoco-lized treatment over 12 weeks and were assessed weeklyusing well-defined reliable methods The studies in-cluded frail and old subjects those who were 70 andolder and patients with ldquodoublerdquo depression (ie majordepression superimposed on dysthymia)
Although the classification of suicidality based on thesingle suicide item of the HRSD administered weeklyover 12 weeks was confirmed by the SSI scores it is alimitation of the study that we did not have SSI scores inthewhole sample for each time point Based on theHRSDsuicide item 176 patients who were neither clearlysuicidal nor clearly non-suicidal were excluded Usingscales more specific to the assessment of suicidal ideationmay have increased our ability to identify suicidal ideatorsand to reduce the number of ldquoambiguousrdquo cases Visualinspection of the HRSD scores over time showed that theldquoambiguousrdquo group fell in between the two groups withbest treatment response (non-suicidal and resolved) andthe two groups with worse response (persistent and emer-gent suicidality)
We reported previously in a subsample of the currentstudy group that 155 of our study participants had alife-time history of suicide attempt Because we did nothave data in the whole study group on previous episodesof suicidality we could not investigate the relation oflife-time ideation and attempts to the course of currentsuicidality Nonetheless despite the limited informationavailable the use of repeated assessments and the asso-ciation observed with distinct patterns of treatment out-comes provide evidence of the clinical utility andvalidity of our classification of suicidality
The relatively low rates of suicidality in part could bedue to the exclusion of psychotic and bipolar patientsEven though the burden of co-existing medical illness instudy participants was moderately high patients whodropped out from the study (N=36) were medicallymore burdened than those who remained in the studyHence results may not be generalizable to the most frailelderly who may be at the highest risk for completedsuicide (Waern et al 2002a)
We noted that African Americans were more likely tobe in the non-suicidal group than Caucasians It isunclear whether this reflects a real difference in rates ofsuicidal ideation corresponding to lower elderlyAfrican American suicide rates or whether themeasures used are not sensitive to assess suicidality inAfrican Americans
The rate of emergent suicidality (78) was lowerthan the rate of emergent suicidality reported in a sampleof medication-free depressed adolescent outpatients whoreceived psychotherapy over a 12ndash16 week period
160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention

160 K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
(125) (1188) (Bridge et al 2005) In this study a self-report measure (Beck Depression Inventory) was moresensitive in identifying suicidal adolescents than clinicalinterviews Thus the majority of patients who haddenied significant suicidal ideation during the clinicalinterview and were classified as emergent ideators by theresearch staff also had endorsed suicidal ideation on theBDI at the start of treatment To ensure that we were notmistakenly classifying patients as non-suicidal atbaseline and then as having emergent suicidality werequired patients with emergent suicidality to have ascore 0 on the HRSD suicide item for two consecutiveweeks (at baseline and after 1 week of treatment) Stilldespite using repeated assessments and a structuredinterview (the HRSD) we cannot eliminate the possi-bility that some patients in the ldquoemergentrdquo group in factwere not free of suicidality at the time of the first twoassessments but were not willing to disclose it to theunfamiliar treatment team eg because of fear of beinghospitalized
The fundamental question is whether the course ofsuicidal ideation in late-life reflects illness character-istics and relates to treatment response variability or isan adverse consequence of treatment Because of theabsence of a placebo group we cannot make any causalinference linking treatment to emergence of suicidalityClinicians followed a treatment protocol that took intoconsideration the results of the weekly structured as-sessments and the global clinical picture The fact thatpatients with emergent and persistent suicidality weremore likely to be prescribed a second antidepressantsuggests that these patients were not responding to thefirst-line treatment Further as their persistently higherlevels of depression and anxiety indicate they were lesslikely to respond to second-line treatment as well We didnot find an association between akathisia and suicidalstatus We should emphasize that akathisia was assessedonly in a limited part of the sample Further we cannotrefute the possibility that the low rate of akathisia in thesample was due to the successful psychopharmacologicalmanagement of the patients or the exclusion of psychoticpatients probably those with the most severe agitationOur observation that patients with emergent suicidalityhad persistently high levels of depression and anxietydespite augmentation pharmacotherapy supports theimportance of partial or non-response to the emergenceof suicidality rather than akathisia
It is also clinically important that patientswith emergentsuicidality had lower level of self-esteem at baseline thannon-suicidal patients similarly to thosewho presentedwithsuicidality at the start of treatment Patients with persistentsuicidality had an age of onset of depression on average
9 years earlier than the non-suicidal and the resolvedgroups and the greatest percentage with depression onsetbelow age 60 mdash suggesting that this may be a morepersistently depresseddysthymic group in general
While patients whose suicidal ideation resolvesrapidly have a favorable illness course similar to non-suicidal patients those with persistent ideation present asignificant challenge to clinicians A small group ofolder patients with emerging suicidality share thecharacteristics and treatment course of these challengingpatients Our data indicate that patients with emergentand persistent suicidality have had a more chronicillness course compared to non-suicidal patients andthose whose suicidality resolved marked by an earlierage of onset and by the higher percentage of patientshaving recurrent depressive episodes Thus emergenceof suicidal ideation or thoughts of death thoughrelatively infrequent is clinically important and oftena signal of difficult-to-treat-depression
Acknowledgements
Supported by P30 MH52247 P30 MH071944 R37MH43832 R01 MH37869 R25 MH60473 K24MH65416 K24 MH069430 K23 MH070471
Dr Mulsant has received honoraria andor researchsupport from antidepressant manufacturers BristolndashMyers Squibb Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Reynolds has received researchsupport from Eli Lilly Forest Laboratories GlaxoS-mithKline and Pfizer Dr Pollock has received honorariaandor research support from antidepressant manufac-turers Forest Laboratories GlaxoSmithKline and Solvay
References
Akiskal HS Benazzi F Perugi G Rihmer Z 2005 Agitatedldquounipolarrdquo depression re-conceptualized as a depressive mixedstate implications for the antidepressant-suicide controversyJ Affect Disord 85 245ndash258
Balazs J Benazzi F Rihmer Z Rihmer A Akiskal KK AkiskalHS 2006 The close link between suicide attempts and mixed(bipolar) depression implications for suicide prevention J AffectDisord 91 133ndash138
Beautrais AL 2002 A case control study of suicide and attemptedsuicide in older adults Suicide Life-Threat Behav 32 1ndash9
Beck AT Kovacs M Weissman A 1979 Assessment of suicidalintention the scale for suicide ideation J Consult Clin Psychol47 343ndash352
Bridge JA Barbe RP Birmaher B Kolko DJ Brent DA2005 Emergent suicidality in a clinical psychotherapy trial foradolescent depression Am J Psychiatry 162 2173ndash2175
Brown GK Beck AT Steer RA Grisham JR 2000 Riskfactors for suicide in psychiatric outpatients a 20-year prospectivestudy J Consult Clin Psychol 68 371ndash377
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention
161K Szanto et al Journal of Affective Disorders 98 (2007) 153ndash161
BruceML TenHave TR Reynolds CF Katz IR Schulberg HCMulsant BH Brown GK McAvay GJ Pearson JLAlexopoulos GS 2004 Reducing suicidal ideation and depressivesymptoms in depressed older primary care patients a randomizedcontrolled trial JAMA 291 1081ndash1090
Cohen S Mermelstein R Kamarck T Hoberman HM 1985Measuring the functional components of social support In SarasonIG Sarason B (Eds) Social Support Theory Research andApplications Martinus Nijhoff The Hague Netherlands pp 73ndash94
Conwell Y Lyness JM Duberstein P Cox C Seidlitz LDiGiorgio A Caine ED 2000 Completed suicide among olderpatients in primary care practices a controlled study J Am GeriatrSoc 48 23ndash29
Detre TP Jarecki HG 1971 Modern Psychiatric TreatmentLippincott Philadelphia
Fawcett J Scheftner WA Fogg L Clark DC Young MAHedeker D Gibbons R 1990 Time-related predictors of suicidein major affective disorder Am J Psychiatry 147 1189ndash1194
First M Spitzer RL GibbonMWilliams JBW 1995 StructuredClinical Interview for DSM-IV Axis I Disorders-Patient Edition(SCID-IP) New York State Psychiatric Institute New York
Folstein MF Folstein SW McHugh PR 1975 Mini-mental statea practical method for grading the cognitive state of patients for theclinician J Psychiatr Res 12 189ndash198
Hamilton M 1967 Development of a rating scale for primarydepressive illness Br J Soc Clin Psychol 6 278ndash296
Hansen L 2001A critical reviewof akathisia and its possible associationwith suicidal behaviour Hum Psychopharmacol 16 495ndash505
Hansen L Wilkinson DG 2001 Drug induced akathisia suicidalideation and its treatment in the elderly Int J Geriatr Psychiatry16 231ndash233
Lingjaerde O Ahlfors UG Bech P Dencker SJ Elgen K 1987The UKU side effect rating scale A new comprehensive ratingscale for psychotropic drugs and a cross-sectional study of sideeffects in neuroleptic-treated patients Acta Psychiatr ScandSuppl 334 1ndash100
Miller MD Paradis CF Houck PR Mazumdar S Stack JARifai AH Mulsant B Reynolds CF 1992 Rating chronicmedical illness burden in geropsychiatric practice and researchapplication of the Cumulative Illness Rating Scale Psychiatry Res41 237ndash248
Mulsant BH Pollock BG Nebes R Miller MD Sweet RAStack J Houck PR Bensasi S Mazumdar S Reynolds CF
2001 A twelve-week double-blind randomized comparison ofnortriptyline and paroxetine in older depressed inpatients andoutpatients Am J Geriatr Psychiatry 9 406ndash414
Power AC Cowen PJ 1992 Fluoxetine and suicidal behaviourSome clinical and theoretical aspects of a controversy BrJ Psychiatry 161 735ndash741
Reynolds CF Dew MA Pollock BG Mulsant BH Frank EMiller MD Houck PR Mazumdar S Butters M Stack JASchlernitzauer MA Whyte E Gildengers A Karp J Lenze ESzanto K Bensasi S Kupfer DJ 2006Maintenance treatment ofmajor depression in old age N Engl J Med 354 1130ndash1138
Rothschild AJ Locke CA 1991 Reexposure to fluoxetine afterserious suicide attempts by three patients the role of akathisiaJ Clin Psychiatry 52 491ndash493
Spitzer RL 1978 Schedule for Affective Disorders and Schizo-phrenia-Lifetime Version (SADS-L) New York State PsychiatricInstitute New York
Szanto K Reynolds CF Frank E Stack J Fasiczka AL MillerMD Mulsant BH Mazumdar S 1996 Suicide in elderlydepressed patients is ldquoactiverdquo vs ldquopassiverdquo suicidal ideation aclinically valid distinction Am J Geriatr Psychiatry 4 197ndash207
Szanto K Mulsant BH Houck P Dew MA Reynolds CF 2003Occurrence and course of suicidality during short-term treatment oflate-life depression Arch Gen Psychiatry 60 610ndash617
Tollefson GD Rampey AH Beasley CM Enas GG Potvin JH1994 Absence of a relationship between adverse events and sui-cidality during pharmacotherapy for depression J Clin Psycho-pharmacol 14 163ndash169
US Food and Drug Administration 2004 Labeling change requestletter for antidepressant medications httpwwwfdagovcderdrugantidepressantsSSRIlabelChangehtm
Waern M Rubenowitz E Runeson B Skoog I Wilhelmsson KAllebeck P 2002a Burden of illness and suicide in elderlypeople case-control study Br Med J 324 1355
Waern M Runeson BS Allebeck P Beskow J Rubenowitz ESkoog I Wilhelmsson K 2002b Mental disorder in elderlysuicides a case-control study Am J Psychiatry 159 450ndash455
World Health Organization Suicide prevention Available at httpwwwwhointmental-healthpreventionsuicidesuicidepreventen2005 Suicide prevention