electrophysiologic basis for the suppression by amiodarone of orthodromic supraventricular...
TRANSCRIPT

1298 lACC Vol. 3. NO.5May 1984:1298-307
Electrophysiologic Basis for the Suppression by Amiodarone ofOrthodromic Supraventricular Tachycardias ComplicatingPre-excitation Syndromes
GREGORY K. FELD, MD, KOONLAWEE NADEMANEE, MD, FACC, JAMES WEISS, MD,
WILLIAM STEVENSON, MD, BRAMAH N. SINGH, MD, DPhil, FACC
Los Angeles, California
Ten patients with refractory recurrent supraventriculartachycardia were found by electrophysiologic study tohave bypass tracts and orthodromic atrioventricularreentrant tachycardia. All had failed to respond to conventional antiarrhythmic therapy and were thereforetreated with oral amiodarone (l,600 to 2,000 mg/day for2 weeks, then 800 to 1,200 mg/day for another 2 weekswith subsequent 200 to 600 mg/day maintenance doses).During or after the fourth week of therapy, electrophysiologic study was repeated. In 9 of 10 patients,supraventricular tachycardia could not be reinduced byprogrammed stimulation. In the remaining patient, nonsustained supraventricular tachycardia (>10 beats, lasting <30 seconds) with a slower basic cycle length thanthat during the control period was provoked. Significantincreases in the effective refractory period of the acces-
Numerous studies (1-9) recently provided convincing evidence for the marked effectiveness of the long-term administration of amiodarone in the prophylactic control of ventricular and supraventricular tachyarrhythmias resistant toconventional antiarrhythmic therapy. Rosenbaum et al. (I)
first observed that the drug might also be remarkably effective in controlling the supraventricular tachyarrhythmiasthat complicate the Wolff-Parkinson-White syndrome.However, subsequent studies (10-15) using varying doseregimens reported variable effects on orthodromic paroxysmal supraventricular tachycardia. No study has utilized
From the Departments of Cardiology and Medicine. Wadsworth Veterans Administration Medical Center and Center for Health Sciences. LosAngeles, California. This study was supported by grants from the MedicalResearch Service for the Veterans Administration and the American HeartAssociation. Greater Los Angeles Affiliate. Los Angeles. California.Manuscript received May 9. 1983; revised manuscript received October31. 1983. accepted December 15, 1983.
Address for reprints: Koonlawee Nadernanee, MD. Cardiology Section(691/111 E). Wadsworth Veterans Administration Medical Center. Wilshireand Sawtelle Boulevards. Los Angeles. California 90073.
© 1984 by the American College of Cardiology
sory pathway in both the anterograde (+26%, P < 0.05)and retrograde (+40%, p < 0.02) directions were noted,the magnitude of change being independent of the con.trol effective refractory period. There were also significant increases in the effective refractory period of theright atrium (+ 24%, P < 0.01) and the right ventricle(+ 15%, P < 0.01) during long-term therapy withamiodarone.
Over a mean follow-up period of 20 months, symptomatic control of the arrhythmia occurred in all patients; in only one patient treatment with amiodaronecould not be continued because of side effects. Thesedata establish the electrophysiologic basis for the effectiveness of amiodarone in the prophylactic control ofrefractory paroxysmal supraventricular tachycardiacomplicating the bypass tract syndromes.
initial high dose treatment to attain optimal "arniodaronization" (16) before evaluating the electrophysiologic correlates of long-term maintenance treatment with amiodaroneto prevent recurrences of paroxysmal supraventriculartachycardia in previously resistant cases.
The main objectives of the present study, therefore, wereto determine the electrophysiologic effects correlating withsuppression by amiodarone of inducible supraventriculartachycardia in previously resistant cases and to define therole of the drug in the long-term prophylactic control ofrefractory orthodromic paroxysmal supraventricular tachycardia complicating accessory pathway syndromes.
MethodsPatients. Ten male patients with paroxysmal supraven
tricular tachycardia developing in association with an accessory pathway were studied. Their ages ranged from 22to 74 years (mean 43). The accessory pathway was leftsided in six patients and right-sided in four, having a para-
0735-1097/84/$3()()

lACC Vol. 3, No.5May 1984: 1298-307
FELD ET AL.AMIODARONE IN ORTHODROMIC BYPASS TRACT TACHYCARDIA
1299
septal location in six and a free wall location in four (Table1). In all cases, recurrent sustained episodes of paroxysmalsupraventricular tachycardia had been documented electrocardiographically; all had been refractory to one or moreantiarrhythmic drugs previously administered (Table 1). Before the electrophysiologic studies were done and amiodarone was administered, a complete history and physicalexamination, complete blood count; serum biochemistryprofile, liver function, pulmonary and thyroid function tests,two-dimensional echocardiogram and 12 lead electrocardiogram were obtained. Informed written consent was obtained from all patients; the protocol for use of amiodaronewas approved by the Committee for the Use of HumanSubjects for Research in 1979.
Electrophysiologic study. After discontinuation of anyprevious medication for at least 5 half-lives, the patientsunderwent electrophysiologic study in the postabsorptivenonsedated state. Endocardial electrode catheters (USCI)were placed in the high lateral right atrium, coronary sinus,right ventricular apex and His bundle region of the interventricular septum (17,18). Pacing was performed using aMedtronic 5325 programmable stimulator. Recordings fromsurface electrodes I, aVF, VI and endocardial electrodes inthe right atrium, coronary sinus, His bundle and the rightventricle were obtained on an Electronics for Medicine recorder (VR-12). Refractory periods of the right atrium,atrioventricular (AV) node, right ventricle and accessory
pathway were determined using single premature stimuli(S IS2) with scanning during diastole with stimuli of increasing prematurity, each delivered after an eight beat pacingsequence (Medtronic 5325) with a cycle length (SISI) 10to 20% above the normal sinus rate during the control period. The same basic cycle length was then used in eachpatient during amiodarone treatment. Refractory periods weredefined as previously described (18,19), and tachycardiainduction is summarized herein:
Tachycardia induction. Ventricularpacing at two or morebasic cycle lengths (S,SI), 10 to 25% above sinus cyclelength, was followed by single premature stimuli (S,S2) withscanning during diastole until the refractory period of theright ventricle was reached. If supraventricular tachycardiawas not produced, double premature stimuli (SIS2S3) weredelivered after two or more basic cycle lengths (SISI)' Thediastole was scarined with the double stimuli, with the shortening of the interval between S2 and S3 initially and thenwith that between SI and S2 until both S2 and S3 approachedthe right ventricular effective refractory period. If supraventricular tachycardia was not induced by these measures,rapid ventricular pacing at increasing rates was used untilretrograde ventriculoatrial (VA) block occurred or untilsupraventricular tachycardia was induced.
Atrial pacing from the right atrium and coronary sinuswas then performed using the S,S2 and S,S2S3 technique ina manner identical to that described for ventricular pacing.
Table 1. Clinical Characteristics and Location of Accessory Pathways in 10 Patients WithOrthodromic Paroxysmal Supraventricular Tachycardia
Previously
Location of Duration of Used
Age (yr) Accessory Tachycardia Antiarrhythmic
Case &Sex Pathways* (yr) Agents
26M Left-sided 15 0, PAparaseptal
2 27M Right-sided 5 P,PAparaseptal
3 74M Left-sided 5 D, P, °parasepta1
4 54M Right-sided 28 PA. P, Dparaseptal
5 38M Left lateral 5 PA, P, Dwall
6 34M Right-sided 7 O,D, Pparaseptal
7 63M Left lateral 25 Qwall
8 66M Left lateral 42 D.Q,Pwall
9 22M Right-sided 4P, °
paraseptal10 43M Left lateral 3 v: 0, PA
wallMean 43 14
*Demonstrated by electrophysiologic studies (see Table 2). D = digoxin: F = female: M = male; P =
propranolol: PA = procainamide; Q = quinidine; V = verapamil.

1300 FEW ET AL.AMIODARONE IN ORTHODROMIC BYPASS TRACT TACHYCARDIA
lACC Vol. 3. No.5May 1984:1298~307
If supraventricular tachycardia was not induced, rapid atrialpacing was then undertaken at increasing rates until anterograde block or supraventricular tachycardia was produced.Atrial fibrillation was not routinely induced in our patients.
Tachycardia induction was performed during long-termtreatment with amiodarone in a manner identical to thatperformed during the control study in each patient.
Location of bypass tracts. The tachycardia cycle lengthand the activation sequence of the reentrant tachycardia weredetermined from endocardial and surface lead recordingsobtained during pacing and supraventricular tachycardia (20).The location of the bypass tracts was defined on the basisof the endocardial retrograde (VA) activation sequence during ventricular pacing and supraventricular tachycardia asfollows:
A) Left ventricular lateral wall-activation of the leftatrium first (distal coronary sinus electrode), then low rightatrium (His bundle electrode) and high right atrium.
B) Left ventricular paraseptal-low right atrium, leftatrium and high right atrium.
C) Right ventricular paraseptal-low right atrium, highright atrium and left atrium.
Drug treatment protocol. Only patients with sustained,inducible supraventricular tachycardia refractory to otherantiarrhythmic drugs were treated. After electrophysiologicstudy, treatment was started with oral amiodarone, initiallyat 1,600 to 2,000 mg (in two divided doses)/day for 2 weeks.The dose was then decreased to 800 to 1,200 mg for another2 weeks, at or after which time electrophysiologic studywas repeated. The dose was then decreased to 200 to 400mg/day in all patients. In one patient, amiodarone was discontinued after 2 months because of fever and pulmonaryinfiltrates, which resolved spontaneously on cessation ofamiodarone. During the treatment period, patients' laboratory determinations were repeated at regular intervals toassess evidence of impending toxicity, the development ofwhich was also monitored clinically.
Statistical analysis. Data are presented for individualpatients as well as for the study group as a whole as meanvalues ± 1 standard deviation. Statistical significance ofthe difference of means before and during treatment wasdetermined by the Student's two-tailed t test for paired datawith probability (p) < 0.05 as the limit of significance.
ResultsThe overall data with respect to the effects of amiodarone
on the inducibility of paroxysmal supraventricular tachycardia and on the electrophysiologic variables of the heartare summarized in Table 2 and illustrated in Figures I through5.
Effects on inducible supraventricular tachycardia.Before amiodarone was given, sustained supraventriculartachycardia was inducible in all 10 patients by programmed
electrical stimulation of the heart (Table 2). During therapywith amiodarone, supraventricular tachycardia became noninducible in 9 of 10 patients. In the remaining patient, oneepisode of supraventricular tachycardia occurred spontaneously during electrophysiologic study but was not reproducibly inducible; it was nonsustained (> 10 beats, lasting <30 seconds) and had a cycle length that was 130 ms(300 versus 430 ms) longer than it was before amiodaronewas started (Fig. 1).
Effect on the refractoriness of the accessory path.way. In all seven patients in whom the anterograde conduction over the accessory pathway could be demonstratedduring the control electrophysiologic study, the effectiverefractory period (anterograde) was lengthened (Table 2).
In patients in whom the exact value for the effective refractory period could be determined, the mean ± standarddeviation of the effective refractory period (anterograde) ofthe accessory pathway was 293 ± 30 ms before amiodaroneand 368 ± 26 ms (+ 26%, P < 0.05) during amiodaronetreatment. The corresponding values for the retrograde effective refractory period of the accessory pathway beforeand during amiodarone therapy were 277 ± 29 ms and 388± 72 ms, respectively (+40%, P < 0.02).
Figure 2 illustrates the increase in the anterograde refractory period of the accessory pathway plus prolongationof conduction in the AV node and prevention of supraventricular tachycardia by amiodarone. During control electrophysiologic study anterograde block of the accessory pathway occurs at SIS2 coupling intervals of 290 ms duration.Anterograde conduction through the AV node then occurswith retrograde conduction through the accessory pathwayand induction of supraventricular tachycardia. Amiodaroneincreased the anterograde effective refractory period of theaccessory pathway to 390 ms (not shown) and markedlyprolonged the atrio-His conduction time (450 ms) at similarSIS2 coupling intervals (300 ms). Retrograde conductionthrough the accessory pathway is then followed by anterograde AV node block, thus preventing induction of supraventricular tachycardia.
Figure 3 illustrates the increase in retrograde refractoryperiod of the accessory pathway produced by amiodarone.During control electrophysiologic study, retrograde blockoccurs at S I S2 intervals of 310 ms. The retrograde effectiverefractory period of the accessory pathway is increased to400 ms after administration of amiodarone.
Effect of amiodarone on effective refractory periodof atrium, right ventricle and AV node (Table 2).Amiodarone increased the effective refractory period in allthe tissues. The increase in the mean effective refractoryperiods was 24% (p < 0.01) in the atrium and 15% (p <0.01) in the right ventricle. Although the anterograde effective refractory period of the AV node was increased byamiodarone, it could not be measured in most cases becauseof anterograde conduction through the accessory pathway.

lACC Vol. 3. No.5May 1984:1298-307
FELD ETAL.AMIODARONE IN ORTHODROMIC BYPASS TRACT TACHYCARDIA
1301
Table 2. Effects of Long-Term Amiodarone Therapy on the Electrophysiologic Variables and Inducibility of SupraventricularTachycardia in Patients With Accessory Pathways
Effective Refractory Period (ms) InducibilityofSVT at
AP Ante AP Retro RV Atria AV Node EPS
Case C A C A C A C A C A C A
I <300 340 <320 410 220 280 240 330 NA NA Yes No2 320 380 <350 410 250 285 210 270 NA NA Yes No3 < 240 360 <240 550 240 270 240 280 NA NA Yes No4 NA NA 250 320 220 260 300 310 < 315 340 Yes No5 250 370 240 500 220 240 210 280 220 300 Yes No6 310 330 < 280 <310 210 240 210 250 240 > 330 Yes No7 NA NA 31 0 440 250 290 250 360 NA NA Yes Yes*8 290 390 310 400 260 280 NA NA NA NA Yes No9 NA NA 280 350 250 270 260 300 NA NA Yes No
10 <260 <340 270 320 210 250 215 260 NA NA Yes NoTotals 293 368 277 388 233 267 237 293
± 30 ± 26 ± 29 ± 72 ± 19 ± 18 ± 30 ± 35 10(n = 4) (n = 4) (n = 6) (n = 6) (n = 10) (n = 10) (n = 9) (n = 9)
*Nonsustained. A = during amiodarone therapy; Ante = anterograde; AP = accessory pathway; AV = atrioventricular; C = control; EPS =electrophysiologic study; NA = not applicable or could not be done; Retro = retrograde; RV = right ventricle; SVT = supraventricular tachycardia.
An example of AV node anterograde conduction block aftertreatment with amiodarone is shown in Figure 2.
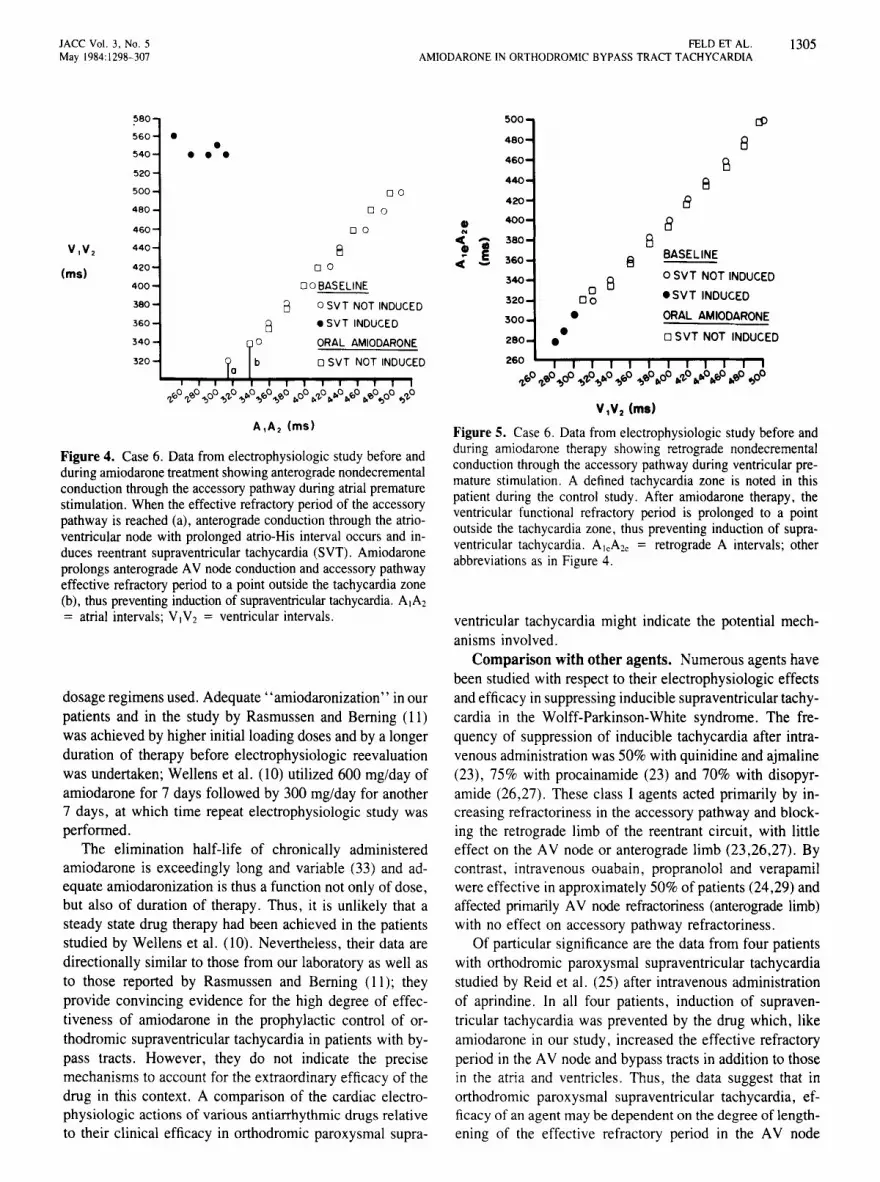
Figures 4 and 5 further demonstrate the effects of amiodarone on AV node and ventricular refractoriness and induction of supraventricular tachycardia. In Figure 4, atrialpacing with progressively premature stimuli (A\A2) producesnondecremental conduction through the accessory pathway(VIV2) until the effective refractoryperiod is reached. Whenthe effective refractory period of the accessory pathway isreached, anterograde conduction through the AV node witha prolonged atrio-His interval occurs. Retrograde conduction through the accessory pathway results in induction ofsupraventricular tachycardia. Amiodarone prolongs the anterograde AV node refractory period to an extent where AVnode block occurs before the anterograde effective refractory period of the accessory pathway is reached, thus preventing the induction of supraventricular tachycardia. Theanterograde effective refractory period of the accessorypathway is also increased. During ventricular pacing (Fig.5), amiodarone prolongs the functional refractory period ofthe right ventricle to a point outside the tachycardia zonenoted during controlelectrophysiologicstudy in this patient,thus preventing the induction of supraventricular tachycardia.
Long-term clinical outcome and drug side effects. In9 of 10 patients, the recurrence of spontaneous supraventricular tachycardia was suppressed 100% after the first monthof amiodarone therapy over a mean duration of therapy of20 months (range 10 to 29). In one patient, amiodarone hadto be discontinued after 2 months of therapy because of theonset of fever, pulmonary infiltrates and elevated serumlevels of hepatic enzymes. The nine patients remaining on
long-term therapy (200 to 400 mg/day) have been free ofclinically significant side effects.
DiscussionThe reentrant nature of orthodromic paroxysmal supra
ventricular tachycardia in patients with accessory pathwaysis now well defined (20-22) . The reentrant circuit incorporates the atrioventricular (AV) node and His bundle (andbranches) as the anterograde limb and the anomalous tractas the retrograde limb, while atrial and ventricular tissuesprovide the final proximal and distal common pathways forthe initiation and perpetuation of the tachycardia. Thus, therational approach for its control is to prolong refractorinessor conduction, or both, in one or more components of theentire reentrant circuit or to eliminate the trigger mechanism(for example, ventricular or supraventricular extrasystoles)initiating the arrhythmia. Different antiarrhythmic compounds have been shown to exhibit variable potencies inthis regard (23- 29).
Inconsistency in amiodarone's effects on supraventricular tachycardia. In the case of amiodarone, the success rate varying between 33 and 100% (1,3 , 10- 15) is noteworthy because the electrophysiologic properties of thedrugduring long-term administration are reasonably uniform (5,7).It lengthens repolarization and effective refractoryperiod inall cardiac tissue (5,7,30,31). One might, therefore, expecta greater consistency in the overall therapeutic effects ofamiodarone in orthodromic paroxysmal supraventriculartachycardia than has been reported (10,12, 13- 15).
Present study . Our results show that when the drug isgiven orally for at least 4 weeks (in our patients at a high

1302 FEW ET AL.AMIODARONE IN ORTHODROMIC BYPASS TRACTTACHYCARDIA
JACC Vol. 3. No.5May 1984: 1298-307
AVF
Figure 1. Case 7. Effect of long-termamiodarone administration on the inducibility of supraventricular tachycardia in a patient with a bypass tractsubject to recurrent orthodromic paroxysmal supraventricular tachycardia.Upper panel, Induction of supraventricular tachycardia by atrial pacingbefore amiodarone was started. Lowerpanel, Spontaneous supraventriculartachycardia occurs during electrophysiologic study after two prematureventricular complexes. With amiodarone, the supraventricular tachycardiawas nonsustained with a tachycardiacycle length longer than that undercontrol conditions. The tachycardiacould not be reinduced by pacing. I,AYF, Y I = surface electrocardiographic leads; A = atrial deflection;Ae = retrograde deflection; DCS =distal coronary sinus electrogram; Hor HBE = His deflection or His bundle electrogram, respectively;HRA =high right atrial electrogram; PCS =proximal coronary sinus electrogram;S = stimulus; Y = ventriculardeflection.
'.-c • .. - ... =' =
loading dosage), it leads to a significant increase in theeffective refractory period of the atria, AV node, ventricleand accessory pathways (anterograde and retrograde). Inour 10 patients, this was associated with the near completesuppression of the tendency for electrically inducible supraventricular tachycardia. Furthermore, over a mean followup period of 20 months on maintenance doses (200 to 400m/day), the drug was uniformly effective in eliminatingrecurrences of paroxysmal supraventricular tachycardia, withside effects occurring in only one patient.
Previous studies. Such a response is in line with the lessstandardized approach to dosage regimen used by Rosenbaum et al. (I) and others (3,32). Of particular significanceis the preliminary report by Rasmussen and Berning (II),who found amiodarone-induced increases in the refractoryperiod in the atrium, AV node and accessory pathway as afunction of duration of treatment in six patients with inducible supraventricular tachycardia. Their initial dose ofamiodarone was 600 mg/day for 10 to 14 days, followedby 400 mg/day until the appropriate response had been obtained, after which the dose was reduced to 250 to 400
mg/day. They repeated electrophysiologic study in four suchpatients after 26 to 85 days of treatment; induction of supraventricular tachycardia was prevented in all four patients.
These data, which are comparable with our own, are incontrast to those of Wellens et al. (10), who found thatamiodarone prevented inducible supraventricular tachycardia in only 5 of 15 patients. Nevertheless, the drug invariably prolonged the tachycardia cycle length in those inwhom it was reinducible. As in our study, Wellens et al.(10) noted a marked increase in the effective refractoryperiod of the accessory pathway in the anterograde direction;however, they found a less striking effect on this variablein the retrograde direction. By contrast, we found a greaterincrease in the effective refractory period in the retrograde(40%) than in the anterograde (26%) direction, in additionto the somewhat larger increase in the right ventricular effective refractory period (about 34 ms) than that (23 ms)reported by Wellens et al. (10).
Dosage regimen and duration of therapy. The differences between our data and those of Rasmussen and Berning(II) and Wellens et ai. (10) may be due to the differing

JACC Vol. 3, No.5May 1984:1298-307
FELD ET AL.AMIODARONE IN ORTHODROMIC BYPASS TRACT TACHYCARDIA
1303
Figure 2. Case 8. Changes in atrioventricular (AV) conduction and tachycardiainduction before and after long-termarniodarone therapy in another patient witha bypass tract. Upper panel, Control recordings during atrial stimulation demonstrating ventricular pre-excitation.Middle panel, Control recordings showing the anterograde effective refractoryperiod of the accessory pathway duringatrial premature stimulation, anterogradeconduction through the AV node and induction of supraventricular tachycardia.Lower panel, Note that amiodaronelengthened the anterograde effective refractory period of the accessory pathwayand AV conduction, thus preventing induction of supraventricular tachycardia byanterograde AV node block. RV = rightventricular electrogram; other abbreviations as in Figure I.
;-~_-4-4-....!L..::::::=:::::==::::::::r=--__A,--_-!....-__--===:=!:::A:
---~----::DeS
.t:, • L&
v
~,-

1304 FEW ET AL.AMIODARONE IN ORTHODROMIC BYPASS TRACT TACHYCARDIA
lACC Vol 3. No.5May 1984 1298-307
DCS
_-------'lalw,h j "'-"-
I I I I
~--.....-x,-+-
------~I
Figure 3. Case 8. An example of theprolongation of the retrograde effective refractory period of the accessorypathway induced by long-term administration of oral amiodarone. Upperand middle panels, Control recordings during right ventricular pacingdemonstrating accessory pathwayconduction and the effective refractoryperiod (310 ms). Lower panel, Recordings during amiodarone treatment. The drug markedly lengthenedthe effective refractory period (400 ms)of the accessory pathway. Abbreviations as in Figure I.
I--'--+---.,----....-----.~--------.-
,,!.~.d.r I
2
RV ~'.if .. 600 ~~- ~..... :.."..,.. .~ __- ,. f-- I!;j;~~_.._. --_.- - =£
lACC Vol. 3. No.5May 1984:1298-307
FELD ET AL.AMIODARONE IN ORTHODROMIC BYPASS TRACTTACHYCARDIA
1305
~80
~60 • •~40 • • •~20
~OO D O
480 D O
460 D O
V,V, 440 8(ms)
420 D O
400 DOBASELINE
380 B o SVT NOT INDUCED
360 B • SVT INDUCED
340 0 ORAL AMIODARONE
320 b o SVT NOT INDUCEDa
A,A, (rns)
Figure 4. Case6. Datafrom electrophysiologic study before andduring amiodarone treatment showing anterograde nondecrementaIconduction through theaccessory pathway during atrial prematurestimulation. When the effective refractory period of the accessorypathway is reached (a), anterograde conduction through the atrioventricular node with prolonged atrio-His interval occurs and induces reentrant supraventricular tachycardia (SVT). Amiodaroneprolongs anterograde AV nodeconduction and accessory pathwayeffective refractory period to a point outside the tachycardia zone(b), thus preventing induction of supraventricular tachycardia. A)A2
= atrial intervals; VIV2 = ventricular intervals.
dosage regimens used. Adequate' 'amiodaronization' in ourpatients and in the study by Rasmussen and Berning (11)was achieved by higher initial loading doses and by a longerduration of therapy before electrophysiologic reevaluationwas undertaken; Wellens et al. (10) utilized 600 mg/day ofamiodarone for 7 days followed by 300 mg/day for another7 days, at which time repeat electrophysiologic study wasperformed .
The elimination half-life of chronically administeredamiodarone is exceedingly long and variable (33) and adequate amiodaronization is thus a function not only of dose,but also of duration of therapy. Thus, it is unlikely that asteady state drug therapy had been achieved in the patientsstudied by Wellens et al. (10). Nevertheless, their data aredirectionally similar to those from our laboratory as well asto those reported by Rasmussen and Berning (II ); theyprovide convincing evidence for the high degree of effectiveness of amiodarone in the prophylactic control of orthodromic supraventricular tachycardia in patients with bypass tracts. However, they do not indicate the precisemechanisms to account for the extraordinary efficacy of thedrug in this context. A comparison of the cardiac electrophysiologic actions of various antiarrhythmic drugs relativeto their clinical efficacy in orthodromic paroxysmal supra-
~oo (j)
480 8460 B440 B4 20 B
tl 400 aN
-e - 380 8! •! 360 8
BASELINEC
340 B o SVT NOT INDUCED0 • SVT INDUCED320 d o
30 0 • ORAL AMIODARONE
• o 5VT NOT INDUCED280 •260
",f>0 ",,,,0..,00 ..,iJ..,r;.o ..,f>0 ..,,,,0..0° r;."'o r;.r;.or;.f>0 r;.'lP -flO
VlV2 (ms)
Figure 5. Case 6. Datafrom electrophysiologic study before andduring amiodarone therapy showing retrograde nondecrementalconduction through the accessory pathway during ventricular premature stimulation. A defined tachycardia zone is noted in thispatient during the control study. After amiodarone therapy, theventricular functional refractory period is prolonged to a pointoutside the tachycardia zone, thus preventing induction of supraventricular tachycardia. A1cA2c = retrograde A intervals; otherabbreviations as in Figure 4.
ventricular tachycardia might indicate the potential mechanisms involved.
Comparison with other agents. Numerous agents havebeen studied with respect to their electrophysiologic effectsand efficacy in suppressing inducible supraventricular tachycardia in the Wolff-Parkinson-White syndrome. The frequency of suppression of inducible tachycardia after intravenous administration was 50% with quinidine and ajmaline(23), 75% with procainamide (23) and 70% with disopyramide (26,27). These class I agents acted primarily by increasing refractoriness in the accessory pathway and blocking the retrograde limb of the reentrant circuit, with littleeffect on the AV node or anterograde limb (23,26,27). Bycontrast, intravenous ouabain , propranolol and verapamilwere effective in approximately 50% of patients (24,29) andaffected primarily AV node refractoriness (anterograde limb)with no effect on accessory pathway refractoriness .
Of particular significance are the data from four patientswith orthodromic paroxysmal supraventricular tachycardiastudied by Reid et al. (25) after intravenous administrationof aprindine . In all four patients, induction of supraventricular tachycardia was prevented by the drug which, likeamiodarone in our study, increased the effective refractoryperiod in the AV node and bypass tracts in addition to thosein the atria and ventricles. Thus, the data suggest that inorthodromic paroxysmal supraventricular tachycardia, efficacy of an agent may be dependent on the degree of lengthening of the effective refractory period in the AV node

1306 FELD ET AL.AMIODARONE IN ORTHODROMIC BYPASS TRACT TACHYCARDIA
lACC Vol. 3, No.5May 1984: 1298-307
(anterograde) as well as in the bypass tracts (retrograde).For this reason, compared with that of amiodarone or aprindine, a lower rate of efficacy in orthodromic paroxysmalsupraventricular tachycardia might be expected for agentswith a narrower spectrum of electrophysiologic effects (forexample, class I agents, digoxin, propranolol and verapamil).
Mechanisms of action. In our study, amiodarone wasshown to prevent induction of supraventricular tachycardiaby several potential mechanisms. These included prolongation of refractory periods and block of anterograde conduction in the AV node and retrograde conduction in theaccessory pathway and, in one case, prolongation of therefractory period of the right ventricle to a point outside thetachycardia zone. The possibility must also be consideredthat in paroxysmal supraventricular tachycardia, the drugadditionally might act by the reduction of premature atrialand ventricular complexes that provide the trigger mechanism for the initiation of the tachycardia (34). At least forpremature ventricular complexes, amiodarone has been shownto be a powerful suppressant (4,5,16).
Implications. Orally administered amiodarone appearsto be extremely effective in suppressing inducible sustainedsupraventricular tachycardia in the Wolff-Parkinson-Whitesyndrome. The incidence of side effects with the patientreceiving the minimal dose required to suppress spontaneously recurring paroxysmal supraventricular tachycardia(generally 200 to 400 mg/day) over a 20 month follow-upperiod was found to be low. The data suggest that the highrate of prophylactic efficacy of amiodarone in orthodromicparoxysmal supraventricular tachycardia may relate to thesignificant increases in the effective refractory period of thevarious components of the reentrant circuit, especially theAV node and the bypass tracts.
We are much indebted to Alma Gump and Lacy Goede for typing thismanuscript. We are also grateful to 10Ann Hendrickson and the technicalstaff of Electrophysiologic Laboratories at the Veterans AdministrationMedical Center, West Los Angeles and the Center for Health Sciences atthe University of California at Los Angeles, California for their assistancein the studies.
ReferencesI. Rosenbaum MB, Chiale PA, Ryka D, Elizari MV. Control of tachy
arrhythmias associated with the Wolff-Parkinson-White syndrome byamiodarone hydrochloride. Am 1 Cardiol 1974;34:215-23.
2. Rosenbaum MB, Chiale PA, Halpern MS. Clinical efficacy of amiodarone as an antiarrhythmic agent. Am 1 Cardiol 1976;38:934-44.
3. Leak D, Eydt IN. Control of refractory cardiac arrhythmias withamiodarone. Arch Intern Med 1979;139:425-8.
4. Nademanee K, Hendrickson lA, Cannom DS, Goldreyer BN, SinghBN. Control of refractory life-threatening ventricular arrhythmias byamiodarone. Am Heart 1 1981;101:759-65.
5. Nademanee K, Hendrickson lA, Kannan R, Singh BN. Electrophysiological effects of amiodarone in patients with life-threatening ventricular arrhythmias: modifications of induced ventricular tachycardia
versus suppression of spontaneously occurring tachyarrhythmias. AmHeart 1 1982;103:950-9.
6. Nademanee K, Singh BN; Hendrickson lA, Reed AW, Melmed S,Hershman 1M. Pharmacokinetic significance of serum reverse T3 levelsduring amiodarone treatment: a potential method for monitoring chronicdrug therapy. Circulation 1982;66:202-11.
7. Heger 11, Prystowsky E, lackman WM, et al. Amiodarone: clinicalefficacy and electrophysiology during long-term therapy for recurrentventricular tachycardia or ventricular fibrillation. N Engl 1 Med1981;305:539-45.
8. Kaski lC, Girotti LA, Messuti H, Rubitzky B, Rosenbaum MB. Longterm management of sustained recurrent symptomatic ventriculartachycardia with amiodarone. Circulation 1981;64:273-80.
9. Podrid Pl , Lown B. Amiodarone therapy in symptomatic sustainedrefractory atrial and ventricular tachyarrhythmias. Am Heart J1981;101:374-9.
10. Wellens H11, Lie KI, Bar FW, et al. Effect of amiodarone in theWolff-Parkinson-White syndrome. Am 1 Cardiol 1976;38:189-94.
II. Rasmussen V, Berning 1. Effect of amiodarone in the Wolff-Parkinson-White syndrome. Acta Med Scand 1979;205:31-7.
12. Wellens H11, Bar FW, Dassen WR, Brugada P, Vanagt sr, Farre 1.Effects of drugs in the Wolff-Parkinson- White syndrome. Importanceof initial length of effective refractory period of the accessory pathway.Am 1 Cardiol 1980;46:665-9.
13. Ward DE, Camm AJ, Spurrell RAJ. Clinical antiarrhythmic effectsof amiodarone in patients with resistant paroxysmal tachycardias. BrHeart 1 1980;44:91-5.
14. Rowland E, Krikler D. Electrophysiological assessment of amiodaronein treatment of resistant supraventricular arrhythmias. Br Heart 11980;44:82-90.
15. Wellens H11, Brugada P, Abdullah H. Effect of amiodarone in paroxsymal supraventricular tachycardia with or without Wolff-Parkinson-White syndrome. Am Heart 1 1983;106:876-9.
16. Nadamanee K, Singh BN, Hendrickson lA, et al. Amiodarone inrefractory life-threatening ventricular arrhythmias. Ann Intern Med1983;98:577-84.
17. Scherlag Bl, Lau SH, Helfant RH, et al. Catheter technique for recording His bundle activity in man. Circulation 1969;39:13-8.
18. losephson ME, Seides SF. Clinical Electrophysiology. Philadelphia:Lea & Febiger, 1976:41.
19. Narula OS. Electrophysiology of normal impulse propagation. In:Narula OS, ed. Cardiac Arrhythmias: Electrophysiology, Diagnosisand Management. Baltimore: Williams & Wilkins, 1979:57-65.
20. Wellens HJJ, Durrer D. The role of an accessory atrioventricularpathway in reciprocal tachycardia. Observations in patients with andwithout the Wolff-Parkinson-White syndrome. Circulation1975;52:58-72.
21. Gallagher JJ, Pritchett ELC, Sealy WC, Kasell J, Wallace AG. Thepre-excitation syndromes. Cardiovasc Dis 1978;20:285-327.
22. Josephson ME, Kastor lA. Supraventricular tachycardia: mechanismsand management. Ann Intern Med 1977;87:346-58.
23. Wellens HJJ, Durrer D. Effect of procainamide, quinidine and ajmaline in the Wolff-Parkinson-White syndrome. Circulation1974;50:114-20.
24. Wu D, Fernando AL, Simpson Rl, et al. Electrophysiologic studywith multiple drugs in patients with atrioventricular re-entry tachycardias utilizing an extranodal pathway. Circulation 1979;56:727-36.
25. Reid PR, Greene HL, Varghese Pl. Suppression of refractory arrhythmias by aprindine in patients with Wolff-Parkinson-White syndrome. Br Heart 1 1977;39:1353-60.
26. Kou HC, Hung is. Lee YS, Wu D. Effects of oral disopyramidephosphate on induction and sustenance of atrioventricular re-entranttachycardia incorporating retrograde accessory pathway conduction.Circulation 1982;66:454-62.

JACC Vo;. J, No.5May 1984:1298-307
FEW ETAL.AMIODARONE INORTHODROMIC BYPASS TRACT TACHYCARDIA
1307
27. Swirya S, Bauernfeind RA, Wyndham CRC, et al. Effect of oraldisopyramide phosphate on induction of paroxysmal supraventriculartachycardia. Circulation 1981;64:169-75.
28. RosenKM, BarwolfC, EhsaniA, Rahimtoola SH. Effectsof lidocaineand propranolol on the normal and anomalous pathways in patientswith pre-excitation. Am J Cardiol 1976;38:934-40.
29. Klein GJ, Gulamhussein S, Prystowsky EN. Comparison of the electrophysiological effects of intravenous and oral verapamil in patientswith supraventricular tachycardia. Am J Cardiol 1981 :49:117-24.
30. Singh BN, Vaughn Williams EM. The effect of amiodarone, a newantianginal drug, on cardiacmuscle. Br J Pharmacol 1970:39:657-67.
31. Singh BN, Collett JT. Chew CYC. New perspectives in the pharmacologic therapy of cardiac arrhythmias. Prog Cardiovasc Dis1980;22:243-30 I.
32. SwanJH, ChisholmAW. Controlof recurrent supraventricular tachycardia withamiodarone hydrochloride. CanMedAssoc 1 1976;114:43-6.
33. Kannan R, Nademanee K, Hendrickson lA, Rostami Hl, Singh BN.Amiodarone kinetics after oral doses. Clin Pharmacol Ther1982:31 :438-44.
34. Durrer D. Schoo L, Schuilenburg RM, Wellens HJJ. The role ofpremature beats in the initiation and termination of supraventriculartachycardia in the Wolff-Parkinson-White syndrome. Circulation1967;36:644-52.