effectiveness of cognitive-behavioural, person-centred, and psychodynamic therapies in uk...
TRANSCRIPT

Effectiveness of cognitive-behavioural, person-centredand psychodynamic therapies as practised in UK
National Health Service settings
WILLIAM B. STILES1*, MICHAEL BARKHAM2, ELSPETH TWIGG2,JOHN MELLOR-CLARK3
AND MICK COOPER4
1 Miami University, Oxford, USA ; 2 University of Leeds, UK ; 3 CORE Information Management Systems,Rugby, UK ; 4 University of Strathclyde, UK
ABSTRACT
Background. Psychotherapy’s equivalence paradox is that treatments have equivalently positiveoutcomes despite non-equivalent theories and techniques. We compared the outcomes of con-trasting approaches practised in routine care.
Method. Patients (n=1309) who received cognitive-behavioural therapy (CBT), person-centredtherapy (PCT) and psychodynamic therapy (PDT) at one of 58 National Health Service (NHS)primary and secondary care sites in the UK during a 3-year period completed the Clinical Outcomesin Routine Evaluation-OutcomeMeasure (CORE-OM) at the beginning and end of their treatment.Therapists indicated which treatment approaches were used on an End of Therapy form. Wecompared outcomes of six groups: three treated with CBT, PCT or PDT only, and three treatedwith one of these plus one additional approach (e.g. integrative, supportive, art), designatedCBT+1, PCT+1 or PDT+1 respectively.
Results. All six groups averaged marked improvement (pre–post effect size=1.36). Treatmentapproach and degree of purity (‘only’ vs. ‘+1’) each accounted for statistically significant butcomparatively tiny proportions of the variance in CORE-OM scores (respectively 1% and 0.5% asmuch as pre–post change). Distributions of change scores were largely overlapping.
Conclusions. Results for these three treatment approaches as practised routinely across a rangeof NHS settings were generally consistent with previous findings that theoretically differentapproaches tend to have equivalent outcomes. Caution is warranted because of limited treatmentspecification, non-random assignment, lack of a control group, missing data and other issues.
INTRODUCTION
Three widely influential approaches to coun-selling and psychotherapy are cognitive-behavioural therapy (CBT), person-centredtherapy (PCT) and psychodynamic or psycho-analytic therapy (PDT). Each encompasses arange of techniques and should be considereda family of treatments rather than a specifictreatment protocol. Nevertheless, they are
distinct from each other in terms of their usualrepertoires of interventions and their assump-tions about the nature and sources of psycho-pathology, and each is considered by itspractitioners as widely applicable to the prob-lems presented for psychotherapeutic treatment(Gabbard et al. 2005; Feltham &Horton, 2006).We studied the outcomes of treatments usingvaried versions of these three approaches asdelivered to 1309 patients in 58 National HealthService (NHS) mental health service settings inthe UK during a 3-year period from January1999 to November 2001.
* Address for correspondence: William B. Stiles, Department ofPsychology, Miami University, Oxford, OH 45056, USA.(Email : [email protected])
Psychological Medicine, 2006, 36, 555–566. f 2006 Cambridge University Pressdoi:10.1017/S0033291706007136 First published online 14 February 2006. Printed in the United Kingdom
555

There is strong evidence for the efficacy andeffectiveness of CBT for a wide variety of dis-orders (e.g. Dobson, 1989; Hollon et al. 2002;Hollon & Beck, 2004;Westbrook &Kirk, 2005).Fewer studies have systematically examined out-comes of the other two approaches, but avail-able evidence similarly supports the efficacy andeffectiveness of at least some varieties of PCT(Greenberg & Watson, 1998; Ward et al. 2000;Elliott et al. 2004; Goldman et al. in press) andPDT (Leichsenring, 2001; Leichsenring &Leibing, 2003; Leichsenring et al. 2004). Clinicaltrials comparing alternative approaches (e.g.Elkin et al. 1989; Shapiro et al. 1994; Barkhamet al. 1996) and broadly based reviews (e.g.Wampold, 2001; Roth & Fonagy, 2004) haveconcluded that bonafide therapies that have beenactively researched tend to be similarly effective.This is the equivalence paradox: many psycho-therapies appear to have equivalently positiveoutcomes despite manifestly non-equivalenttheoriesandtechniques.Theparadoxisexpressedby the Dodo verdict, ‘Everybody has won, andall must have prizes ’ (Carroll, 1865/1946, p. 28;italics in original), which has been quoted bypsychotherapy researchers for sevendecades (e.g.Rosenzweig, 1936; Stiles et al. 1986; Luborskyet al. 1975; Beutler, 1991; Seligman, 1995).
Despite these indications of equivalent out-comes across many treatments, the over-whelming quantity of published research onCBT (Wampold, 2001; Roth & Fonagy, 2004)has given CBT a greater credibility than theother approaches. For example, the greatmajority of approaches on the list of empiricallysupported treatments (formerly, empiricallyvalidated treatments) produced by the AmericanPsychological Association’s Division 12 Taskforce (Chambless et al. 1998) were in the CBTfamily, having been included because of thequantity and quality of research about them(Chambless & Hollon, 1998) rather than theirdemonstrated superiority over alternative bonafide treatments.
Holmes (2002) argued that CBT has beenoversold within the British NHS. AlthoughCBT is clearly effective, its dominance is more afunction of differential research attention thanevidence of differential effectiveness (but seealso Tarrier, 2002). Thus, the question arises,are there differences in effectiveness betweenalternative approaches in routine practice?
Ward et al. (2000) randomly assigned de-pressed patients to PCT (which they called non-directive counselling) or CBT, each delivered indoses of up to 12 sessions, at 24 NHS practicesin London and Manchester. Both psycho-therapies outperformed general practitioner(GP) care over a 4-month interval, although at a12-month follow-up, the GP care group hadcaught up, and patients in all three conditionsshowed similar and substantial improvement.Barkham et al. (1996) randomly assignedpatients to PDT (which they called psycho-dynamic-interpersonal therapy) with CBT fordepression, each delivered in eight- or 16-sessiondoses at three NHS sites. Again, results showedboth approaches were similarly efficacious,although there was no untreated comparisongroup. Our study complements these efficacystudies by addressing the effectiveness of differ-ent treatments as they are applied in routinepractice. The logic of effectiveness research isthat the risks of selection biases associated withlack of randomization and the lack of assurancethat the treatments were delivered in a standardway are balanced by the greater realism, orexternal validity (cf. Seligman, 1995). Resultsaddress the effects of treatments as routinelydelivered, using practitioners’ versions of thetreatments and the patients who typically receivethem.
Our study answers calls for clinically rep-resentative research (e.g. Shadish et al. 2000;Street et al. 2000; Stirman et al. 2003), drawingon routine treatments and using data collectedprimarily for clinical and administrative use,rather than for research. Our null hypothesiswas that there would be no difference in out-comes between CBT, PCT and PDT as deliveredin routine practice. We assessed effectivenessby comparing pretreatment to post-treatmentscores on the Clinical Outcomes in RoutineEvaluation-Outcome Measure (CORE-OM;Barkham et al. 1998, 2001, 2005; Evans et al.2000, 2002; Cahill et al. in press ; Connell et al.unpublished observations).
METHOD
Participants
We studied data from 1309 patients whoreceived CBT, PCT or PDT and completed the
556 W. B. Stiles et al.

CORE-OM at the beginning and end of theirtreatment. The data were collected during a3-year period (January 1999 to November 2001)at 58 NHS sites delivering counselling andpsychotherapy services where the CORE-OMwas routinely administered. The 58 NHS siteseach contributed from 1 to 111 of the patients(median=16.5; 24 of the sites each contributed20 or more of the patients). Most of the patients(n=844; 64.5%) were seen in primary carecounselling services ; the others were seen inpsychology and counselling services (n=286;21.8%), secondary care psychology services(n=136; 10.4%) or tertiary care/specialistservices (n=43; 3.3%). Therapist character-istics were not recorded. Based on the 878patients for whom therapist ID numbers wererecorded, however, 251 therapists each sawfrom one to 29 of the patients (median=2; 15 ofthe therapists each saw 10 or more of thepatients). These patients were a subsample ofthe patients described by Barkham et al. (2005) ;selection procedures are described later.
Of the 1309 patients, 29.3% (n=383) weremale ; 2.8% (n=36) were aged under 20 years,19.6% (n=257) aged 20–29, 29.7% (n=389)aged 30–39, 24.7% (n=323) aged 40–49, 15.2%(n=199) aged 50–59, and 8.0% (n=105) agedover 60. Patients presented a variety of psycho-logical problems, as described later. Nearly halfof the patients (n=638; 48.7%) were taking pre-scribed psychotropic medication at the start oftherapy, including 79 (6.1%) who were pre-scribed more than one type of medication(data missing for n=44; 3.4%). Of thoseprescribed medications, 88.7% were takingantidepressants, 14.7% anxiolytics/hypnotics,4.7% antipsychotics, and 2.7% other psycho-tropic medications.
Measures
Self-report outcome measure
The CORE-OM comprises 34 items addressingdomains of subjective well-being, symptoms(anxiety, depression, physical problems, trau-ma), functioning (general functioning, closerelationships, social relationships) and risk (riskto self, risk to others). Half the items focus onlow-intensity problems (e.g. ‘I feel anxious/nervous’) and half focus on high-intensityproblems (e.g. ‘I feel panic/terror ’). Items are
scored on a five-point, 0–4 scale, anchored Notat all, Only occasionally, Sometimes, Often, andAll or most of the time. CORE clinical scores arecomputed as the mean of all completed items,which is then multiplied by 10, so that clinicallymeaningful differences are represented by wholenumbers. Thus, CORE clinical scores canrange from 0 to 40. Forms are considered validif up to three items are omitted (Evans et al.2002). Internal consistency reliability for the34-item scale in clinical (n=713) and non-clinical (n=1009) samples was 0.94 and 0.94respectively (Barkham et al. 2001). The 1-weektest–retest correlation was Spearman’s rho=0.90 (n=43) in a student sample (Evans et al.2002).
Therapist assessments
The CORE Assessment (Mellor-Clark et al.1999; Mellor-Clark & Barkham, 2000) com-prises the Therapist Assessment form, completedat intake, and the End of Therapy form. On theTherapist Assessment form, therapists gavereferral information, patient demographics anddata on the nature, severity and duration ofpresenting problems using the following 14 cat-egories: depression, anxiety, psychosis, person-ality problems, cognitive/learning difficulties,eating disorder, physical problems, addictions,trauma/abuse, bereavement, self-esteem, inter-personal problems, living/welfare and work/academic.
On the End of Therapy form, therapists indi-cate which type(s) of therapy was(were) under-taken with the patient – as many as appropri-ate. Categories were psychodynamic, psycho-analytic, cognitive, behavioural, cognitive/behavioural, structured/brief, person-centred,integrative, systemic, supportive, art, and other.Therapists also report the number of sessionsattended and other aspects of the treatments.
Procedure
Data collection
All patients attending for psychological assess-ment or therapy at participating services wereasked to complete a CORE-OM before treat-ment began. Forms were completed duringscreening or assessment by 77.1% of the patientsand immediately before the first therapy sessionby the remaining 22.9%. Patients were allocated
Treatment therapies in UK NHS settings 557

to treatments and therapists following normalprocedures at these sites. Sites were instructed togive the post-treatment CORE-OM at the lastsession; the timing and specific procedures weredetermined by what worked best for eachservice administratively and were not recorded.Therapists completed the Therapist Assessmentform after the intake session and the End ofTherapy form when the patient was dischargedor stopped attending for therapy. Data collec-tion complied with data protection proceduresfor the use of routinely collected clinical data.Completed measures were compiled by a datamanagement service and sent to the Universityof Leeds for processing with no patient identi-fiers. Each patient was allocated a unique codenumber by the site.
Selection of patients
We selected our sample from the 10 351 patientsseen at these sites who returned at least oneCORE-OM or CORE Assessment form duringthe 3-year data collection period. Of these, 1345were excluded because they did not return apretreatment CORE-OM form, and 138 wereexcluded because their pretreatment form hadmore than three items missing (most of theseapparently failed to turn over the page on theform). A further 5444 failed to return a post-treatment CORE-OM form, including thosewho did not attend any sessions and those whohad not ended their treatment by the closingdate; 14 more returned a post-treatment CORE-OM that was incomplete ; and the therapists of359 more failed to complete an End of Therapyform. Barkham et al. (2005) reported descriptivedetails of this sample, which (based on a largesubsample of n=7651) was demographicallysimilar to our subsample, with 29.9% male; and4.3% aged under 20 years, 23.0% aged 20–29,32.6% aged 30–39, 21.5% aged 40–49, 13.0%aged 50–59, and 5.5% aged over 60.
From the remaining 3051 patients who com-pleted reliable pre- and post-treatment CORE-OM forms and whose therapists completed Endof Therapy forms, we selected six treatmentgroups based on therapists’ reports on the Endof Therapy form regarding the type(s) oftherapy undertaken. Most therapists indicatedmore than one of the 12 categories provided(mean=2.06, range=1–10). For the purposes
of this study, we classified the three targetedapproaches as follows:
CBT=cognitive, behavioural and/or cognitive/behavioural ;PCT=person-centred;PDT=psychodynamic and/or psychoanalytic.
Using these targeted approaches, we defined sixgroups of patients. Three groups were thosewhose therapists specified therapies belongingto one and only one of the targeted ap-proaches – CBT, PCT or PDT. The otherthree groups were those whose therapistsspecified one of the targeted approaches plusone treatment not included in the targeted ap-proaches (i.e. one of the following: structured/brief, integrative, systemic, supportive, artor other), abbreviated CBT+1, PCT+1 andPDT+1 respectively. We reasoned that thelatter three groups offered comparisons amongthe targeted approaches that were parallel to,but, depending on one’s perspective, somewhatdiluted or somewhat enhanced.
Of the 3051 patients who completed pre- andpost-treatment CORE-OM forms, 1309 metspecifications for one of the six groups.Numbers in each group are shown in Table 1.Patients who received either none of thetargeted approaches (n=685) or more than oneof the targeted approaches (n=305), or whoreceived more than one treatment in addition toone of the targeted approaches (n=752), werenot considered further in this study. Each ofthese residual categories comprised a large var-iety of different combinations of the approacheslisted on the CORE End of Therapy form.
RESULTS
Outcomes of treatment in NHS settings
Patients in these treatments showed verysubstantial gains, with patients improving, onaverage, from 17.41 (S.D.=6.52; internal con-sistency a=0.93) to 8.50 (S.D.=6.27) on theCORE-OM, a difference of 8.9 (S.D.=6.81).The overall treatment effect size, calculatedas the mean pre–post difference divided by thepre-therapy S.D., was 1.36.
Table 1 shows the mean pre- and post-treatment CORE-OM clinical scores for eachof the six groups, mean differences acrosstreatment, and effect sizes. A one-way analysis
558 W. B. Stiles et al.
of variance (ANOVA) comparing the pre-therapy means across the six groups was notsignificant, F(5, 1303)=0.66, p=0.654, partialg2=0.003 (g2, calculated as effect variancedivided by effect plus error variance), indicatingthat all groups began treatment with roughlyequivalent levels of disturbance.
To assess treatment outcomes, we conducteda repeated-measures (pretreatment versus post-treatment) ANOVA, with treatment approach(CBT vs. PCT vs. PDT) and degree of purity(pure vs. ‘+1’) as fixed factors. Results showeda very large overall within-patients main effectof treatment [F(1, 1303)=1905.70, p<0.001,partial g2=0.594], indicating that improvementacross treatment accounted for a large pro-portion of the variation in the CORE-OMscores obtained. In this analysis, a differentialtreatment effect appears as a treatment byoccasion of assessment (pre–post) interaction.The results showed that this effect was signifi-cant but very small [F(2, 1303)=3.94, p=0.020,partial g2=0.006] ; none of the post-hoc com-parisons among group means were significant.The comparative effectiveness of the pure versus‘+1’ forms of treatments (the purity by occasionof assessment interaction) was also significantbut very small [F(1, 1303)=4.02, p=0.045,partial g2=0.003]. The three-way treatment bypurity by occasion interaction, which wouldhave indicated that purity was differentiallyimportant for the therapies, was not significant[F(2, 1303)=1.40, p=0.248, partial g2<0.001].
Fig. 1 depicts the distributions of the pre–postdifferences in CORE-OM clinical scores foreach group in the form of notched box plots,which indicate the median, middle 50%, and
range. Although these change scores rangedwidely (from x21 to 32 out of the possibleCORE-OM range of x40 to 40), the medianswere similar, and the distributions of all sixgroups were largely overlapping.
As an additional approach to the same ques-tion, following Jacobson & Truax (1991), wedistinguished patients who had achieved reliableand clinically significant improvement (RCSI)as those who met two criteria : (a) reliableimprovement, defined as a pre–post differencethat, when divided by the standard error of thedifference, is equal to 1.96, which was a decreaseof 4.8 points on the CORE-OM, based onthis sample, and (b) clinically significant im-provement – entering treatment scoring withinthe clinical population and leaving treatment innormal population – defined as moving fromabove to below the recommended CORE-OMclinical cut-off score of 10 (Connell et al.unpublished observations).
Table 2 shows the number and percentage ofpatients in each treatment group who (a)achieved RCSI, (b) achieved reliable improve-ment only, (c) showed no reliable change, and(d ) showed reliable deterioration, defined as anincrease of 4.8 or more points on the CORE-OM. We restricted this analysis to the 1129patients whose pre-therapy CORE-OM scoreswere 10 or higher, insofar as patients whoseinitial scores were below the clinical cut-offcould not, by definition, achieve clinically sig-nificant improvement (Barkham et al. in press).The results showed substantial rates of improve-ment in all groups. A 2r3 x2 test comparing therates of RCSI versus non-RCSI (combining theother three cells in each row of Table 2) across
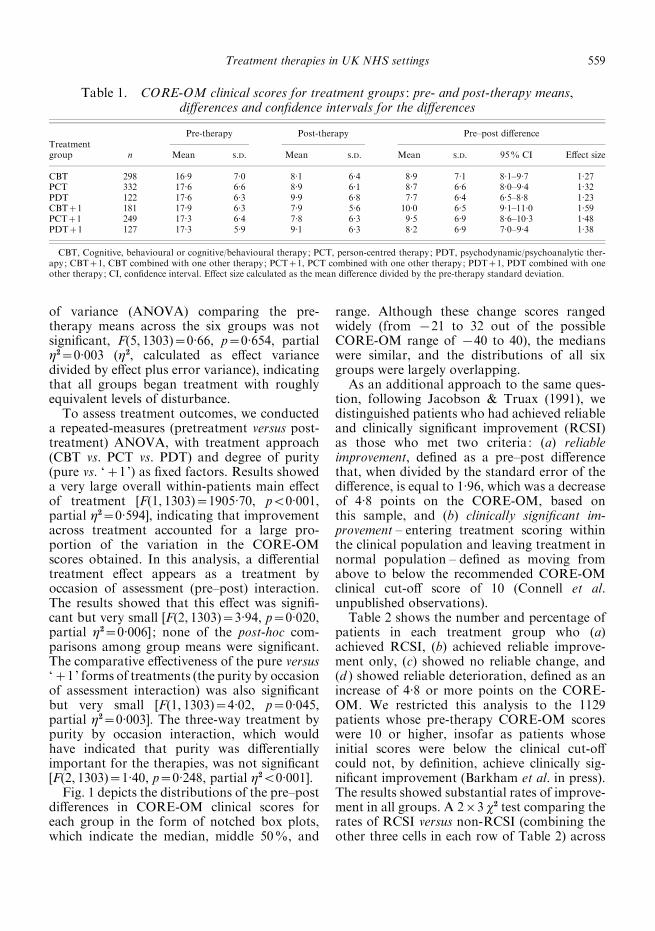
Table 1. CORE-OM clinical scores for treatment groups : pre- and post-therapy means,differences and confidence intervals for the differences
Treatmentgroup n
Pre-therapy Post-therapy Pre–post difference
Mean S.D. Mean S.D. Mean S.D. 95% CI Effect size
CBT 298 16.9 7.0 8.1 6.4 8.9 7.1 8.1–9.7 1.27PCT 332 17.6 6.6 8.9 6.1 8.7 6.6 8.0–9.4 1.32PDT 122 17.6 6.3 9.9 6.8 7.7 6.4 6.5–8.8 1.23CBT+1 181 17.9 6.3 7.9 5.6 10.0 6.5 9.1–11.0 1.59PCT+1 249 17.3 6.4 7.8 6.3 9.5 6.9 8.6–10.3 1.48PDT+1 127 17.3 5.9 9.1 6.3 8.2 6.9 7.0–9.4 1.38
CBT, Cognitive, behavioural or cognitive/behavioural therapy; PCT, person-centred therapy; PDT, psychodynamic/psychoanalytic ther-apy; CBT+1, CBT combined with one other therapy; PCT+1, PCT combined with one other therapy; PDT+1, PDT combined with oneother therapy; CI, confidence interval. Effect size calculated as the mean difference divided by the pre-therapy standard deviation.
Treatment therapies in UK NHS settings 559

the three pure treatment groups (CBT, PCT,PDT) was nearly significant [x2(2)=5.89,p=0.053, n=641], reflecting the 13.9% spreadin RCSI rates across groups (CBT highest, PDTlowest). The parallel test across the three ‘+1’groups (CBT+1, PCT+1, PDT+1) was notsignificant [x2(2)=1.92, p=0.382, n=488].
The 2r2 x2 test comparing RCSI rates acrossthe combined pure versus ‘+1’ groups wassignificant [x2(1)=8.38, p=0.004, n=1129],reflecting a somewhat higher RCSI rate in thegroups given ‘+1’ versions of the therapiesthan in the groups given pure versions (66.2%vs. 57.7%).
40
20
0
–20
Pre–
post
dif
fere
nce
in C
OR
E-O
M c
linic
al s
core
–40
CBT PCT PDT CBT+1
Treatment group
PCT+1 PDT+1
FIG. 1. Notched box plots showing pre–post differences in CORE-OM clinical scores. The notch shows the 95% confidenceinterval around the median. The boxes show the middle 50% of the distribution. The whiskers show the range, except thatobservations falling 1.5 times the interquartile range or more away from the top or bottom of the box are considered outliersand are shown separately. CBT, cognitive, behavioural or cognitive/behavioural therapy; PCT, person-centred therapy; PDT,psychodynamic/psychoanalytic therapy; CBT+1, CBT combined with one other therapy; PCT+1, PCT combined with one othertherapy; PDT+1, PDT combined with one other therapy.
Table 2. Reliable and clinically significant improvement in treatment groups
Treatmentgroup
RCSI Reliable improvement No reliable change Deterioration
Count Row % Count Row % Count Row % Count Row %
CBT 152 62.0 46 18.8 44 18.0 3 1.2PCT 167 57.6 63 21.7 55 19.0 5 1.7PDT 51 48.1 23 21.7 31 29.2 1 0.9CBT+1 116 70.3 28 17.0 18 10.9 3 1.8PCT+1 136 64.5 35 16.6 39 18.5 1 0.5PDT+1 71 63.4 17 15.2 23 20.5 1 0.9
n=1129 patients whose pre-therapy CORE-OM scores were at or above the recommended cut-off of 10 (Connell et al. unpublishedobservations).RCSI, Reliable and clinically significant improvement; CBT, cognitive, behavioural or cognitive/behavioural therapy; PCT, person-centred
therapy; PDT, psychodynamic/psychoanalytic therapy; CBT+1, CBT combined with one other therapy; PCT+1, PCT combined with oneother therapy; PDT+1, PDT combined with one other therapy.
560 W. B. Stiles et al.

Characteristics of patients allocated totreatment groups
Table 3 shows distribution of treatment groupsacross types of NHS settings in this sample.Most notably, CBT was delivered at a varietyof settings, whereas the other treatments weredelivered mainly in primary care counsellingservices.
Table 3 also shows the distribution of pre-senting problems across treatment groups, asreported by the therapists just following theirfirst contact with the patients. Note that thera-pists could indicate multiple problems, so thecolumns sum to more than the number ofpatients in each group. Broadly similar dis-tributions of problems were treated withineach group, but there appeared to be a few
Table 3. Distribution of treatments across types of services and presenting problems
Characteristic
Treatment group
CBT(n=298)
PCT(n=332)
PDT(n=122)
CBT+1(n=181)
PCT+1(n=249)
PDT+1(n=127)
Type of servicePrimary care counselling 83 298 91 120 149 103Psychology and counselling 102 34 5 27 99 19Secondary care/psychology 102 0 13 17 0 4Tertiary care/specialist 11 0 13 17 1 1
Presenting problemsAnxiety 252 236 95 144 194 109Depression 200 220 91 126 190 107Interpersonal problems 99 169 75 90 147 86Self-esteem 120 132 54 89 129 74Bereavement/loss 34 119 50 49 81 51Work/academic 51 66 30 45 54 31Trauma/abuse 42 51 33 33 45 25Physical problems 32 65 15 35 47 24Living/welfare 27 40 10 32 29 14Addictions 12 11 10 6 15 2Personality problems 10 2 5 8 6 2Eating disorder 7 9 5 3 7 2Cognitive/learning 2 8 2 2 4 1Psychosis 4 3 3 0 1 1Other 9 10 1 6 4 8
Based on n=1309 patients.CBT, Cognitive, behavioural or cognitive/behavioural therapy; PCT, person-centred therapy; PDT, psychodynamic/psychoanalytic ther-
apy; CBT+1, CBT combined with one other therapy; PCT+1, PCT combined with one other therapy; PDT+1, PDT combined with oneother therapy.Columns in the presenting problems section add to more than the number of patients in each treatment because therapists indicated multiple
problems for many patients.
Table 4. Demographics and mean numbers of presenting problems and sessions attended bytreatment groups
Treatment group % maleMean age(years)
Mean of number ofpresenting problems
Mean number ofsessions attended
CBT (n=298) 40.9 41.1 3.13 6.52PCT (n=332) 22.9 40.4 3.52 6.11PDT (n=122) 25.4 40.9 4.20 8.53CBT+1 (n=181) 28.4 39.1 3.80 6.03PCT+1 (n=249) 29.3 39.7 3.86 5.62PDT+1 (n=127) 23.6 40.6 4.23 6.11
Based on n=1309 patients.CBT, Cognitive, behavioural or cognitive/behavioural therapy; PCT, person-centred therapy; PDT, psychodynamic/psychoanalytic ther-
apy; CBT+1, CBT combined with one other therapy; PCT+1, PCT combined with one other therapy; PDT+1, PDT combined with oneother therapy.
Treatment therapies in UK NHS settings 561

differences. For example, patients presentingwith interpersonal problems seemed differen-tially likely to be seen in PCT.
Table 4 shows the gender, age, mean numberof problems indicated, and mean number ofsessions attended for patients in each treatmentgroup. Gender was somewhat unevenly distrib-uted across groups [x2(5)=29.07, p<0.001, n=1309], with a relatively higher percentage of malepatients in the CBT group.Mean age was similarin the three groups; a one-way ANOVAwas notsignificant [F(5, 1303)=0.72, p=0.607, partialg2=0.003]. The numbers of presenting problemsacross treatment groups varied significantlyacross the six groups [F(5, 1270)=13.76, p<0.001, partial g2=0.051], reflecting somewhatlarger numbers of problems being attributed topatients in the PDT and PDT+1 groups. Therewas also a modest but significant variation innumbers of sessions attended [F(5, 1266)=8.90,p<0.001, partial g2=0.034], as patients in PDTaveraged a somewhat higher number of sessionsthan patients in other groups.
DISCUSSION
These therapies appeared effective, on average,with effect sizes on the CORE-OM comparableto effect sizes observed on similar measuresin previous efficacy and effectiveness trials(Dobson, 1989; Lipsey &Wilson, 1993; Shapiroet al. 1994; Barkham et al. 1996; Ward et al.2000; Wampold, 2001; Roth & Fonagy, 2004;Westbrook & Kirk, 2005). The mean differencesamong the three targeted approaches, CBT,PCT and PDT, although statistically significant,were small in relation to this substantial changeacross treatment. Mean improvement acrosstreatment accounted for approximately 100times as much of the variance in CORE-OMscores as did the differential effects of the threeapproaches (partial g2 of 0.594 vs. 0.006). AsFig. 1 shows, the distributions of change scoreswere largely overlapping, with little differenceamong the groups’ median scores. All of thetreatment groups had substantial RCSI rates,although there was a nearly significant trendtowards a lower rate in the PDT group (Table2). In summary, our results tended to supportthe Dodo verdict for these three treatmentapproaches as practised routinely across a rangeof NHS settings.
The diluted/enhanced (‘+1’) treatmentgroups averaged slightly better outcomes thandid the pure treatment groups in this sample (seeTables 1 and 2), although the size of this effectwas also very small (partial g2=0.003). At leastacross the range of purity represented by thecomparisons in this study, dilution of CBT,PCT or PDT did not appear to yield worseoutcomes. By the same token, the benefit ofenhancement, although nominally significant,was too small to yield clinical recommendations.There was a great deal of variation in outcomeswithin each group (see Fig. 1), contrasting withthe minor differences between groups.
Our results extend the findings of Ward et al.(2000) and Barkham et al. (1996) by showingthat the equivalence of these treatments withinthe NHS may be observed in routine practice aswell as in randomized trials. Our results may beof particular interest to practitioners of PCTand PDT, insofar as the comparable effective-ness of these approaches to CBT in routinepractice may not have been appreciated (cf.Holmes, 2002).
Limitations
The limitations of our design, althoughcommon in research on routine treatments(Shadish et al. 2000; Westbrook & Kirk, 2005),place restrictions on how data can be inter-preted.
Limited specification of treatments
We had no independent check on whether orhow the therapists delivered the treatments theyindicated and, indeed, no precise definitions ofwhat these treatments comprised or details ofthe therapists’ qualifications. The observedapproximately equivalent outcomes could, inprinciple, reflect a lack of differences in howthe treatments were conducted. Alternatively,systematic failure to implement a treatmentcorrectly could account for its having failed toprove superior.
Nevertheless, we know of no reason why thetherapists would have misrepresented thetheoretical approach from which they worked.The most plausible assumption, we suggest, isthat they sincerely sought to implement theapproach they specified. To put it another way,for better or worse, these treatments represented
562 W. B. Stiles et al.

the way CBT, PCT and PDT are currentlypractised in these settings.
Of course, even protocol-driven psycho-therapies are far from standardized. More thanmost medical treatments, psychotherapies mustbe adapted to the emerging needs of variedpatients in ways that are not specified in a pro-tocol but depend on the skill and interpersonalresponsiveness of the therapist (Hardy et al.1998; Stiles et al. 1998).
Non-random assignment of patients totreatment groups
We did not randomly assign patients to treat-ments, so we cannot rule out selective referral asan explanation for our results. In principle, theobserved approximate equivalence could reflectnon-random assignment that placed the mostdifficult patients in the most effective therapiesand vice versa, compensating for outcome dif-ferences that would have otherwise emerged.For example, a relatively larger number of CBTpatients were treated in secondary care settings(Table 3). If secondary care treatment weresystematically more effective than primary caretreatment (cf. Raine et al. 2005), then thisselective assignment could have masked rela-tively better CBT outcomes.
However, there was no statistically significantdifference among groups on the pretreatmentCORE-OM, indicating that the groups beganwith similar overall levels of disturbance(Table 1). There were significant differences inthe patient mix across groups, including arelatively larger proportion of males in the CBTgroup (Table 4), a relatively larger number ofinterpersonal problems in the PCT group (Table3), and a relatively larger total number ofproblems in the PDT group (Table 3). Ifpatients with more problems tended to be as-signed to PDT, this might help to explain theirtrend towards a lower RCSI rate and theirtendency to receive more sessions than patientsin the other groups (Table 4). Of course, data onthe number and nature of problems were drawnfrom therapists’ reports and thus could reflectdifferences in case conceptualization acrossapproaches.
Absence of a control group
Although the pre–post change scores indicatedsubstantial improvement (see Table 1 and
Fig. 1), there was no comparison group ofuntreated patients. Consequently, we cannotattribute the improvement to the treatmentswith certainty (cf. Corney & Simpson, 2005).
Control groups are often not feasible in rou-tine settings. Ethically, it would be difficult tojustify withholding treatment from comparablepatients seeking care within the NHS, andrestricting consideration to patients who agreedto be randomized would undermine the clinicalrepresentativeness. In this respect, it is reassur-ing that the pre–post effect sizes in these thera-pies were comparable to those observed inefficacy studies where superiority to comparisongroups was observed (e.g. Ward et al. 2000).Our results may be considered as complemen-tary to such studies.
Missing data
As is typical in routine practice settings (e.g.Stiles et al. 2003; Greasley & Small, 2005;Gilbert et al. in press), many patients whocompleted a pre-therapy CORE-OM sub-sequently failed to appear for treatment orfailed to complete a form after treatment. Thereis evidence that, even among patients who doreceive treatment, those who complete post-treatment measures are (a) more likely to haveagreed with their therapist about when treat-ment should end (Barkham et al. in press) and(b) likely to have improved more during treat-ment (Stiles et al. 2003) than are patients whofail to complete them. Our results may not gen-eralize to patients who leave treatment withoutcompleting post-treatment measures.
Restriction to a single self-report measure
As a self-report instrument, the CORE-OMdoes not provide a clinician-rated or externalassessment. In principle, self-report instrumentsare vulnerable to distortions. Patients may haveexaggerated their distress before treatment orexaggerated their improvement following treat-ment. The CORE-OM is a broad spectrummeasure and does not focus on the specificproblems. Qualitatively different results of thedifferent treatments might have shown up onmore targeted measures.
Arguably, however, subjective symptoms anddistress define the need for psychotherapeutictreatment in most cases ; in this sense, self-report
Treatment therapies in UK NHS settings 563

could be considered as a criterion. We note thatthe CORE-OM is highly correlated with otherself-report and clinician-rated measures thathave been widely used to assess psychotherapyoutcome (Evans et al. 2002; Cahill et al. inpress ; Leach et al. 2005, in press). It would, ofcourse, be useful and informative to addition-ally examine external measures of functioning infuture research.
Investigator allegiance
In a review of psychotherapy outcome studies,Luborsky et al. (1999) reported that the in-vestigator’s allegiance, assessed by ratings ofprevious publications, ratings by colleagues andself-ratings, was strongly correlated with theoutcomes of the treatments in published reports(r=0.85, p<0.001, n=29 studies). The presentstudy’s first author has published papers dealingwith the equivalence paradox, so in a sensethis report fits the pattern. He, along withthe fifth author, has a particular interest inthe PCT approach. The second author is anaccredited CBT therapist and has deliveredmanualized versions of both CBT and PDT inrandomized efficacy studies. The third andfourth authors are not qualified therapists, al-though one of them belongs to an organizationwhose members have predominantly PCTorientations.
The Dodo verdict and responsiveness
Equivalent outcomes, such as we observed, areoften ascribed to common factors in therelationship, such as the alliance, empathy andcollaborative involvement (Norcross, 2002).Self-regulatory processes may cut across treat-ment approaches, yielding equivalent results, astherapists and patients responsively optimizegains, given limited time and resources (Stileset al. 1998). For example, participants appear toregulate the dose of therapy – in terms of num-ber of sessions, if that choice is available(Barkham et al. in press), or in terms of accel-eration of processes, if the number of sessions isfixed (Reynolds et al. 1996) – to achieve a com-mon, good enough level of outcome (Barkhamet al. in press). This logic of appropriateresponsiveness does not argue against thetheoretical accounts. Instead, it suggests that allprovide appropriate concepts and techniques,
which the participants use to achieve what theyseek – or what they will settle for – given avail-able resources and constraints.
ACKNOWLEDGEMENTS
Authors affiliated to the Psychological Thera-pies Research Centre, University of Leeds, weresupported by the Priorities and Needs Researchand Development Levy from Leeds CommunityMental Health and Teaching Trust. We thankJanice Connell for comments and assistancewith the analysis.
DECLARATION OF INTEREST
Michael Barkham and John Mellor-Clarkreceived funding from the UK Mental HealthFoundation to develop the CORE-OM, ameasure used in this study. John Mellor-Clarkruns a company that supplies training, softwaresupport and data analysis and benchmarkingservices to users of the CORE System.
REFERENCES
Barkham, M., Connell, J., Stiles, W. B., Miles, J. N. V., Margison,
F., Evans, C. & Mellor-Clark, J. (in press). Dose–effect relationsand responsive regulation of treatment duration: the good enoughlevel. Journal of Consulting and Clinical Psychology.
Barkham, M., Evans, C., Margison, F., McGrath, G., Mellor-Clark,
J., Milne, D. & Connell, J. (1998). The rationale for developingand implementing core outcome batteries for routine use in servicesettings and psychotherapy outcome research. Journal of MentalHealth 7, 35–47.
Barkham, M., Gilbert, N., Connell, J., Marshall, C. & Twigg, E.
(2005). Suitability and utility of the CORE-OM and CORE-A forassessing severity of presenting problems in psychological therapyservices based in primary and secondary care settings. BritishJournal of Psychiatry 186, 239–246.
Barkham, M., Margison, F., Leach, C., Lucock, M., Mellor-Clark, J.,
Evans, C., Benson, L., Connell, J., Audin, K. &McGrath, G. (2001).Service profiling and outcomes benchmarking using the CORE-OM: towards practice-based evidence in the psychological thera-pies. Journal of Consulting and Clinical Psychology 69, 184–196.
Barkham, M., Rees, A., Shapiro, D. A., Stiles, W. B., Agnew, R. M.,
Halstead, J., Culverwell, A. & Harrington, V. M. G. (1996).Outcomes of time-limited psychotherapy in applied settings : re-plicating the Second Sheffield Psychotherapy Project. Journal ofConsulting and Clinical Psychology 64, 1079–1085.
Beutler, L. E. (1991). Have all won and must all have prizes?Revisiting Luborsky et al.’s verdict. Journal of Consulting andClinical Psychology 59, 226–232.
Cahill, J., Barkham, M., Stiles, W. B., Twigg, E., Hardy, G. E., Rees,
A. & Evans, C. (in press). Convergent validity of the COREMeasures with measures of depression for clients in cognitivetherapy for depression. Journal of Counseling Psychology.
Carroll, L. (1946). Alice’s Adventures in Wonderland. RandomHouse: New York. (Original work published 1865.)
Chambless, D. L., Baker, M. J., Baucom, D. H., Beutler, L. E.,
Calhoun, K. S., Crits-Christoph, P., Daiuto, A., DeRubeis, R.,
Detweiler, J., Haaga, D. A. F., Johnson, S. B., McCurry, S.,
564 W. B. Stiles et al.

Mueser, K. T., Pope, K. S., Sanderson, W. C., Shoham, V.,
Stickle, T., Williams, D. A. & Woody, S. R. (1998). Update onempirically validated therapies, II. The Clinical Psychologist 51,3–16.
Chambless, D. L. & Hollon, S. D. (1998). Defining empiricallysupported therapies. Journal of Consulting and Clinical Psychology66, 7–18.
Corney, R. & Simpson, S. (2005). Thirty-six month outcome datafrom a trial of counselling with chronically depressed patients in ageneral practice setting. Psychology and Psychotherapy: Theory,Research and Practice 78, 127–138.
Dobson K. (1989). A meta-analysis of the efficacy of cognitive therapyfor depression. Journal of Consulting and Clinical Psychology 57,414–420.
Elkin, I., Shea, M. T., Watkins, J. T., Imber, S. D., Sotsky, S. M.,
Collins, J. F., Glass, D. R., Pilkonis, P. A., Leber, W. R., Docherty,
J. P., Fiester, S. J. & Parloff, M. B. (1989). National Institute ofMental Health Treatment of Depression Collaborative ResearchProgram: General effectiveness of treatments. Archives of GeneralPsychiatry 46, 971–982.
Elliott, R., Greenberg, L. S. & Lietaer, G. (2004). Research onexperiential psychotherapies. In Bergin and Garfield’s Handbook ofPsychotherapy and Behavior Change (5th edn) (ed. M. J. Lambert),pp. 493–539. Wiley: New York.
Evans, C., Connell, J., Barkham, M., Margison, F., Mellor-Clark, J.,
McGrath, G. & Audin, K. (2002). Towards a standardised briefoutcome measure : psychometric properties and utility of theCORE-OM. British Journal of Psychiatry 180, 51–60.
Evans, C., Mellor-Clark, J., Margison, F., Barkham, M., Audin, K.,
Connell, J. & McGrath, G. (2000). CORE: clinical outcomes inroutine evaluation. Journal of Mental Health 9, 247–255.
Feltham, C. & Horton, I. E. (eds) (2006). Handbook of Counsellingand Psychotherapy (2nd edn). Sage: London.
Gabbard, G. O., Beck, J. S. & Holmes, J. (eds) (2005). OxfordTextbook of Psychotherapy. Oxford University Press: Oxford,UK.
Gilbert, N., Barkham, M., Richards, A. & Cameron, I. (in press). Theeffectiveness of a primary care mental health service deliveringbrief psychological interventions: a benchmarking study using theCORE System. Primary Care Mental Health.
Goldman, R. N., Greenberg, L. S. &Angus, L. (in press). The effects ofadding emotion-focused interventions to the therapeutic relation-ship in the treatment of depression. Psychotherapy Research.
Greasley, P. & Small, N. (2005). Evaluating a primary care counsel-ing service : outcomes and issues. Primary Care Research andDevelopment 6, 124–136.
Greenberg, L. S. & Watson, J. C. (1998). Experiential therapyof depression: differential effects of client-centered relationshipconditions and process experiential interventions. PsychotherapyResearch 8, 210–224.
Hardy, G. E., Stiles, W. B., Barkham, M. & Startup, M. (1998).Therapist responsiveness to client interpersonal styles during time-limited treatments for depression. Journal of Consulting andClinical Psychology 66, 304–312.
Hollon, S. D. & Beck, A. T. (2004). Cognitive and cognitivebehavioral therapies. In Bergin and Garfield’s Handbook ofPsychotherapy and Behavior Change (5th edn) (ed. M. J. Lambert),pp. 447–492. Wiley: New York.
Hollon, S. D., Thase, M. E. & Markowitz, J. C. (2002). Treatmentand prevention of depression. Psychological Science in the PublicInterest 3, 39–77.
Holmes, J. (2002). All you need is cognitive-behaviour therapy?British Medical Journal 324, 288–290.
Jacobson, N. S. & Truax, P. (1991). Clinical significance: astatistical approach to defining meaningful change in psycho-therapy research. Journal of Consulting and Clinical Psychology59, 12–19.
Leach, C., Lucock, M., Barkham, M., Noble, R., Clarke, L. & Iveson,
S. (2005). Assessing risk and emotional disturbance using theCORE-OM & HoNOS outcome measures. Psychiatric Bulletin29, 419–422.
Leach, C., Lucock, M., Barkham, M., Stiles, W. B., Noble, R. &
Iveson, S. (in press). Transforming between Beck DepressionInventory and CORE-OM scores in routine clinical practice.British Journal of Clinical Psychology.
Leichsenring, F. (2001). Comparative effects of short-term psycho-dynamic psychotherapy and cognitive-behavioral therapy indepression: a meta-analytic approach. Clinical Psychology Review21, 401–419.
Leichsenring, F. & Leibing, E. (2003). The effectiveness of psycho-dynamic therapy and cognitive behavior therapy in the treatmentof personality disorders : a meta-analysis. American Journal ofPsychiatry 160, 1223–1232.
Leichsenring, F., Rabung, S. & Leibing, E. (2004). The efficacy ofshort-term psychodynamic psychotherapy in specific psychiatricdisorders : a meta-analysis. Archives of General Psychiatry 6,1208–1216.
Lipsey, M. W. & Wilson, D. B. (1993). The efficacy of psychological,educational, and behavioral treatment: confirmation from meta-analysis. American Psychologist 48, 1181–1209.
Luborsky, L., Diguer, L., Seligman, D. A., Rosenthal, R., Krause,
E. D., Johnson, S., Halperin, G., Bishop, M., Berman, J. S. &
Schweizer, E. (1999). The researcher’s own therapy allegiances: a‘wild card’ in comparisons of treatment efficacy. ClinicalPsychology: Science and Practice 6, 95–106.
Luborsky, L., Singer, B. & Luborsky, L. (1975). Comparative studiesof psychotherapies : is it true that ‘Everyone has won and all musthave prizes ’? Archives of General Psychiatry 32, 995–1008.
Mellor-Clark, J. & Barkham, M. (2000) Quality evaluation:methods, measures and meaning. In Handbook of Counselling andPsychotherapy (ed. C. Feltham and I. Horton), pp. 225–270. SagePublications : London.
Mellor-Clark, J., Barkham, M., Connell, J. & Evans, C.
(1999). Practice-based evidence and standardized evaluation:informing the design of the CORE system. European Journal ofPsychotherapy, Counselling and Health 2, 357–374.
Norcross, J. C. (ed.) (2002). Psychotherapy Relationships that Work:Therapist Contributions and Responsiveness to Patient Needs.Oxford University Press : New York.
Raine, R., Haines, A., Sensky, T., Hutchings, A., Larkin, K. & Black,
N. (2005). Systematic review of mental health interventions forpatients with common somatic symptoms: can research evidencefrom secondary care be extrapolated to primary care? BritishMedical Journal 325, 1082–1092.
Reynolds, S., Stiles, W. B., Barkham, M., Shapiro, D. A., Hardy,
G. E. & Rees, A. (1996). Acceleration of changes in session impactduring contrasting time-limited psychotherapies. Journal ofConsulting and Clinical Psychology 64, 577–586.
Roth, A. & Fonagy, P. (2004). What Works for Whom? A CriticalReview of Psychotherapy Research (2nd edn). Guilford: New York.
Rosenzweig, S. (1936). Some implicit common factors in diversemethods of psychotherapy.American Journal of Orthopsychiatry 6,412–415.
Seligman, M. (1995). The effectiveness of psychotherapy. AmericanPsychologist 50, 965–974.
Shadish, W. R., Navarro, A. M., Matt, G. E. & Phillips, G.
(2000). The effects of psychological therapies under clinicallyrepresentative conditions: a meta-analysis. Psychological Bulletin126, 512–529.
Shapiro, D. A., Barkham, M., Rees, A., Hardy, G. E., Reynolds, S. &
Startup, M. (1994). Effects of treatment duration and severity ofdepression on the effectiveness of cognitive-behavioural and psy-chodynamic-interpersonal psychotherapy. Journal of Consultingand Clinical Psychology 62, 522–534.
Stiles, W. B., Honos-Webb, L. & Surko, M. (1998). Responsivenessin psychotherapy. Clinical Psychology: Science and Practice 5,439–458.
Stiles, W. B., Leach, C., Barkham, M., Lucock, M., Iveson, S.,
Shapiro, D. A., Iveson, M. & Hardy, G. (2003). Early suddengains in psychotherapy under routine clinic conditions: practice-based evidence. Journal of Consulting and Clinical Psychology 71,14–21.
Treatment therapies in UK NHS settings 565

Stiles, W. B., Shapiro, D. A. & Elliott, R. (1986). ‘Are allpsychotherapies equivalent? ’ American Psychologist 41, 165–180.
Stirman, S. W., DeRubeis, R. J., Crits-Christoph, P. & Brody, P. E.
(2003). Are samples in randomized controlled trials ofpsychotherapy representative of community outpatients? A newmethodology and initial findings. Journal of Consulting andClinical Psychology 71, 963–972.
Street, L., Niederehe, G. & Lebowitz, B. (2000). Toward greaterpublic health relevance for psychotherapeutic interventionresearch: an NIMH workshop report. Clinical Psychology:Science and Practice 7, 127–137.
Tarrier, N. (2002). Yes, cognitive behavioural therapy may wellbe all you need. British Medical Journal 324, 291–292.
Wampold, B. E. (2001). The Great Psychotherapy Debate:Models, Methods, and Findings. Lawrence Erlbaum Associates :Mahwah, NJ.
Ward, E., King, M., Lloyd, M., Bower, P., Sibbald, B., Farrelly, S.,
Gabbay, M., Tarrier, N. & Addington-Hall, J. (2000). Randomisedcontrolled trial of non-directive counselling, cognitive-behaviourtherapy, and usual general practitioner care for patients withdepression. I: Clinical effectiveness. British Medical Journal 321,1383–1388.
Westbrook, D. & Kirk, J. (2005). The clinical effectiveness ofcognitive behaviour therapy: outcome for a large sample of adultstreated in routine practice. Behaviour Research and Therapy 43,1243–1261.
566 W. B. Stiles et al.