effect of the anticonvulsant medications pregabalin and lamotrigine on urodynamic parameters in an...
TRANSCRIPT

Neurourology and Urodynamics 31:1197–1202 (2012)
Effect of the Anticonvulsant Medications Pregabalin andLamotrigine on Urodynamic Parameters in an Animal
Model of Neurogenic Detrusor Overactivity
Oleg Loutochin, Tala Al Afraa, Lysanne Campeau, Wally Mahfouz, Ehab Elzayat, and Jacques Corcos*Department of Urology, McGill University, Montreal, Quebec, Canada
Aims: To assess the effects of different doses and treatment durations of Pregabalin and Lamotrigine on the urody-namic parameters of an animal model of neurogenic detrusor overactivity (NDO). Materials and Methods: Ninetyrats were used; six as normal controls and the remaining 84 were divided as follows: Six ‘‘paraplegic controls,’’ 6 ‘‘para-plegic-vehicle controls,’’ and the remaining 72 divided into two equal groups. Group 1 was divided into six subgroups;Pregabalin was given in doses of 10 mg/kg, 20 mg/kg, or 30 mg/kg for 1 or 2 weeks. Group 2 was similarly subdivided;Lamotrigine was given in doses of 1.5 mg/kg, 3 mg/kg, or 6 mg/kg for 1 or 2 weeks. Results: All paraplegic controlsdeveloped NDO within 3 weeks from spinalization. Their baseline bladder pressure (BBP) 19 � 4.4 cmH2O, detrusorpressure at maximum capacity (DPMaxC) 47.6 � 4.3 cmH2O, bladder capacity (BC) 0.45 � 0.1 ml, and frequencyof detrusor overactivity (FDO) 3.7 � 0.9/min. Both Pregabalin and Lamotrigine produced significant improvement.Urodynamic values in those treated with 20 mg Pregabalin for 1 or 2 weeks were: BBP 11.7 � 1.3 and9 � 0.2 cmH2O, BC 0.6 � 0.1 and 0.7 � 0.01 ml, DPMaxC 17.3 � 4.0 and 23 � 2.6 cmH2O, FDO 2.1 � 0.2/min and1.7 � 0.1/min. Urodynamic values in those treated with 3 mg/kg Lamotrigine for 1 or 2 weeks were: BBP 9.7 � 2.2and 8.6 � 1.9 cmH2O, DPMaxC 17.2 � 1.8 and 29 � 1.2 cmH2O, BC 0.7 � 0.1 and 0.8 � 0.1 ml, FDO 1.9 � 0.2/minand 1.9 � 0.2/min (P < 0.001). Conclusions: Pregabalin and Lamotrigine may represent novel alternative treat-ments of NDO. Clinical trials remain to be performed. Neurourol. Urodynam. 31:1197–1202, 2012.� 2012 Wiley Periodicals, Inc.
Key words: antiepileptics; Lamotrigine; neurogenic bladder; Pregabalin; spinal cord injury
INTRODUCTION
The International Continence Society defines neurogenicdetrusor overactivity (NDO) as a voiding dysfunction inpatients with relevant neurological conditions.1 Characteristicsymptoms are urinary frequency, urgency, and urge inconti-nence.2,3 NDO can significantly impact quality of life and sleepas well as mental health. Without proper treatment, thesepatients are at risk of upper tract deterioration and renal fail-ure, a leading cause of mortality among them.4
The pathophysiology of NDO involves bladder (detrusor)receptors, afferent pathway spinal cord interneurons,5 andthe central nervous system. After spinal cord injury (SCI), thebladder is initially areflexic, but then most frequentlybecomes overactive because of increased afferent input tosacral spinal cord centers.6 Several approaches are takennowadays to treat NDO, including intravesical instillation ofanticholinergics and intradetrusor injections of botulinumtoxin A.78 New therapeutic avenues need to be explored tocounteract the limitations of existing treatments.
Antiepileptic agents may have a role in the management ofNDO. In a previous work, we reported that Levetiracetam(LEV) was effective in a neurogenic rat model by increasingbladder capacity (BC) and reducing the frequency of detrusoroveractivity (FDO) as well as micturition pressure (MP). Weconcluded that LEV could be a novel alternative therapeuticoption in NDO.9
Several new antiepileptic medications (AEM) have becomeavailable recently to treat neuropathic pain and seizures. Themechanism of action is multiple for each AEM. Lamotrigen(Lamictal) belongs to broad-spectrum AEM and works byblocking release of Glutamate, the brain’s main escitatory neu-rotransmitter. Pregabalin (Lyrica) belongs to narrow-spectrum
AEM and it is similar to the structure of GABA (gamma amino-butyric acid). GABA is inhibitory neurotransmitter; it preventsnerve cells firing to quickly.Pregabalin (LyricaTM, 3-isobutyl g-aminobutyric acid [GABA])
is an analog of the inhibitory neurotransmitter GABA, but isfunctionally unrelated to it. Pregabalin binds the presynapticalpha-2-delta subunit of voltage-sensitive calcium channelsand reduces depolarization-induced calcium influx at nerveterminals, which decreases the release of several excitatoryneurotransmitters.10 It has been approved in North Americafor neuropathic pain and epilepsy.Lamotrigine (Lamictal 3,5-diamino-6-(2,3-dichlorophenyl)-as-
triazine), a second-generation anticonvulsant,11 acts on volt-age-sensitive sodium channels, inhibiting the release of theexcitatory neurotransmitter glutamate and increasing that ofGABA.12 Lamotrigine too has been approved in North Americafor the treatment of epilepsy.The aim of the study was to investigate the efficacy of
Pregabalin and Lamotrigine at different dose levels and treat-ment durations in an animal model of NDO, by performingcystometry (CM) before and after treatment in spinal cordtransected (SCT) rats, and comparing the evolution of urody-namic parameters.
Conflict of interest: none.Lori Birder led the peer-review process as the Associate Editor responsible for thepaper.*Correspondence to: Jacques Corcos, Urology Department, Jewish GeneralHospital, McGill University, 3755 Cote Sainte-Catherine, Montreal, Quebec,Canada H3T 1E2. E-mail: [email protected] 15 April 2011; Accepted 1 August 2011Published online 30 March 2012 in Wiley Online Library
(wileyonlinelibrary.com).
DOI 10.1002/nau.21214
� 2012 Wiley Periodicals, Inc.

MATERIALS AND METHODS
The protocol of the present experiment complied with Cana-dian Council on Animal Care guidelines and was approved bythe McGill University Animal Care Committee.
Animals and SCT
Ninety female Sprague-Dawley rats weighing 250–300 gwere obtained from Charles River Laboratories (Montreal, QC,Canada). Six of them served as normal controls (without SCT).Eighty-four underwent SCT at the level of the 10th thoracicvertebra (T10). Each rat was anesthetized with isoflurane andplaced in a prone position for skin sterilization. The skin wasthen opened at T10 and the paravertebral muscles were split.Laminectomy with curved scissors exposed the spinal cord,which was cut completely under magnification and a piece ofGelfoam placed between the two cut ends. Then, the muscleswere approximated with absorbable 3/0 cat gut sutures andthe skin was closed with 3/0 cat gut sutures. Buprenorphine0.01–0.05 mg/kg was given before spinalization and every12 hr for up to 2 days after surgery. The rats were injectedsubcutaneously with 3 ml of lactated Ringer solution duringthe procedure and with 5 ml of lactated Ringer solution intra-peritoneally after the procedure. They were warmed through-out the procedure and in the post-operative period until fullrecovery (2–4 hr). Trimethoprim 2.2 mg/kg was given pre-operatively and post-operatively, and each rat was housed ina separate cage containing wood shaving bedding to preventthe formation of decubitus ulcers. The animals’ bladderswere evacuated three times daily by the Crede maneuver(finger pressure on the lower abdomen) for the first two post-operative weeks until recovery of the voiding reflex.
Animal Grouping and Drug Administration
Of the 90 female Sprague-Dawley rats studied, 6 were usedas normal controls (without SCT) and 84 were spinalized(T10-SCT). Of the latter, 6 served as ‘‘paraplegic controls,’’ 6 as‘‘paraplegic-vehicle controls’’ (SCT plus placebo), and theremaining 72 were divided into two equal groups (n ¼ 36).Group 1 was divided into six subgroups, each containing sixrats that received Pregabalin at dose levels of 10 mg/kg,20 mg/kg, or 30 mg/kg for 1 or 2 weeks. Group 2 was similarlysubdivided to receive Lamotrigine in doses of 1.5 mg/kg,3 mg/kg, or 6 mg/kg for 1 or 2 weeks (Fig. 1).
CM was undertaken 4 weeks after SCT (1 week of treatment)in the first dose sub-groups and 5 weeks after SCT (2 weeks oftreatment) in the second dose sub-groups.Pregabalin was synthesized and supplied by Pfizer Inc.
(Groton, CT), dissolved in normal saline.Lamotrigine was synthesized by GlaxoSmithKline (Oakville,
ON) and supplied by Sigma–Aldrich (Oakville, ON, Canada),dissolved in 50% dimethyl sulfoxide and 50% sterile water.Pregabalin and Lamotrigine compounds were delivered viaModel 2ML1 and 2ML2 ALZET osmotic pumps (DURECT Corp.,Cupertino, CA) inserted into a subcutaneous pouch in the 1-and 2-week treatment groups, respectively.
Cystometry
CM was performed on awake rats 24 hr after insertion of apolyethylene catheter into the bladder dome. Employing thesame methods of anesthesia described above for SCT, the blad-der was exposed through a midline incision for placement of aPE-90 polyethylene catheter (Clay-Adams, Parsippany, NJ)through the bladder dome. It was secured with a 4/0 silkpurse-string suture, and its other end was delivered subcuta-neously through the back of the animal’s neck. Twenty-fourhours after catheter insertion, CM was undertaken with ahigh-sensitivity pressure transducer (AD Instruments, Inc.,Colorado Springs, CO) connected via a three-way stop-cock tothe catheter and a KDS 100 Series infusion pump (Fisher Scien-tific, Montreal, QC). After the bladder was emptied, room tem-perature saline was infused at a rate of 0.1 ml/min.Intravesical pressure was monitored continuously with aPowerLab 4/30 Chart Pro (AD Instruments Inc., ColoradoSprings, CO). At least three voiding cycles per rat wererecorded. The following variables were studied during CM: thepresence, frequency and amplitude of spontaneous bladdercontractions, resting bladder pressure, MP, and BC. CM wascontinued until the animals urinated, which was consideredas BC.
Statistical Analysis
All CM data are presented as means � SD, and P < 0.001was considered significant. The various groups were com-pared overall by Stats Direct software. Statistics were ana-lyzed by non-parametric two-way ANOVA with Bonferroniinequality analysis to compare parameters between the SCTgroups and different treatment groups.
RESULTS
Normal Controls
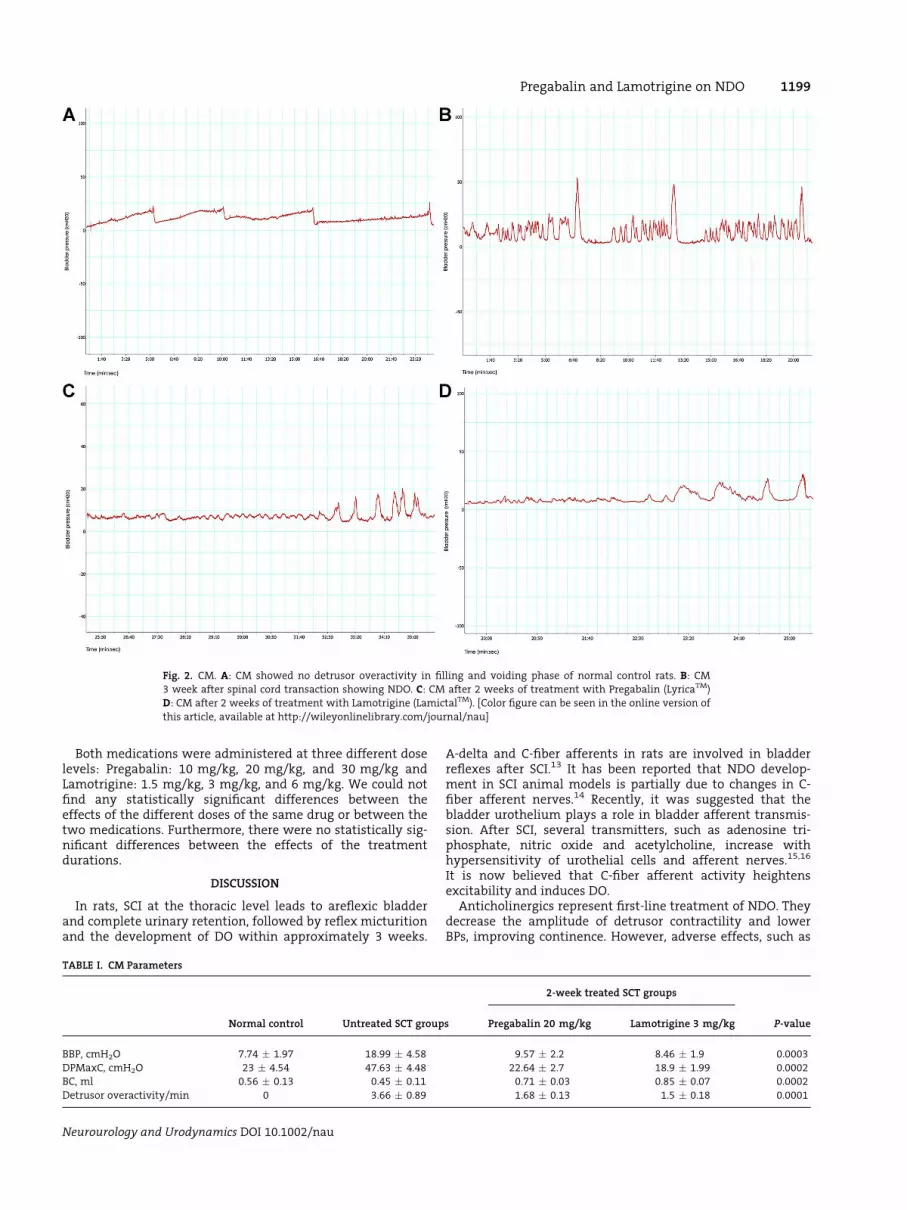
Mean � SD baseline bladder pressure (BBP) was 7.74 �1.97 cmH2O, mean � SD BC was 0.56 � 0.13 ml, and mean �SD MP was 23 � 4.54 cmH2O. None of the normal controlshad detrusor overactivity (DO) (Fig. 2A).
Paraplegic Controls
All paraplegic rats developed NDO 3 weeks after SCT(Fig. 2B). Mean � SD FDO was 3.66 � 0.89/min. Mean � SDBBP was 18.99 � 4.58 cmH2O, mean � SD BC was 0.45 �0.11 ml, and mean � SD detrusor pressure at maximumcapacity (DPMaxC) was 47.63 � 4.48 cmH2O.
Treated Paraplegic Rats
CM values after 2-week treatment of paraplegic rats showedstatistically significant improvement of all parameters com-pared to the untreated group (Table I, Fig. 2C, D and Figs. 3–6).
Fig. 1. Animal grouping and study design. [Color figure can be seen in the
online version of this article, available at http://wileyonlinelibrary.com/
journal/nau]
1198 Loutochin et al.
Neurourology and Urodynamics DOI 10.1002/nau
Both medications were administered at three different doselevels: Pregabalin: 10 mg/kg, 20 mg/kg, and 30 mg/kg andLamotrigine: 1.5 mg/kg, 3 mg/kg, and 6 mg/kg. We could notfind any statistically significant differences between theeffects of the different doses of the same drug or between thetwo medications. Furthermore, there were no statistically sig-nificant differences between the effects of the treatmentdurations.
DISCUSSION
In rats, SCI at the thoracic level leads to areflexic bladderand complete urinary retention, followed by reflex micturitionand the development of DO within approximately 3 weeks.
A-delta and C-fiber afferents in rats are involved in bladderreflexes after SCI.13 It has been reported that NDO develop-ment in SCI animal models is partially due to changes in C-fiber afferent nerves.14 Recently, it was suggested that thebladder urothelium plays a role in bladder afferent transmis-sion. After SCI, several transmitters, such as adenosine tri-phosphate, nitric oxide and acetylcholine, increase withhypersensitivity of urothelial cells and afferent nerves.15,16
It is now believed that C-fiber afferent activity heightensexcitability and induces DO.Anticholinergics represent first-line treatment of NDO. They
decrease the amplitude of detrusor contractility and lowerBPs, improving continence. However, adverse effects, such as
TABLE I. CM Parameters
Normal control Untreated SCT groups
2-week treated SCT groups
P-valuePregabalin 20 mg/kg Lamotrigine 3 mg/kg
BBP, cmH2O 7.74 � 1.97 18.99 � 4.58 9.57 � 2.2 8.46 � 1.9 0.0003
DPMaxC, cmH2O 23 � 4.54 47.63 � 4.48 22.64 � 2.7 18.9 � 1.99 0.0002
BC, ml 0.56 � 0.13 0.45 � 0.11 0.71 � 0.03 0.85 � 0.07 0.0002
Detrusor overactivity/min 0 3.66 � 0.89 1.68 � 0.13 1.5 � 0.18 0.0001
Fig. 2. CM. A: CM showed no detrusor overactivity in filling and voiding phase of normal control rats. B: CM3 week after spinal cord transaction showing NDO. C: CM after 2 weeks of treatment with Pregabalin (LyricaTM)
D: CM after 2 weeks of treatment with Lamotrigine (LamictalTM). [Color figure can be seen in the online version of
this article, available at http://wileyonlinelibrary.com/journal/nau]
Pregabalin and Lamotrigine on NDO 1199
Neurourology and Urodynamics DOI 10.1002/nau
dry mouth, blurred vision, and constipation, limit theiruse.17,18 Previous studies have demonstrated the effectivenessof Botox A administration in the management of NDO.19
Recently, antiepileptics were introduced for the treatment ofoveractive bladder.20 These drugs appear to act through inhi-bition of C-fiber afferent nerves.9
Pregabalin is an analog of the inhibitory neurotransmitterGABA, but does not interact with GABA receptors or mimicGABA’s action.10 Its exact mechanism of action remainsunknown. Pregabalin interacts with an auxiliary subunit(alpha2-delta subunit) of voltage-gated calcium channels.Potent binding at this site attenuates depolarization-inducedcalcium influx at nerve terminals, with subsequent reductionin the central release of excitatory neurotransmitters,
including glutamate, noradrenaline, and substance P.21 Pe-ripheral release may lead to subsequent inhibition of bladdersmooth muscle contraction and to decreased amplitude ofdetrusor contractions. Pregabalin’s capacity to suppress the re-lease of excitatory neurotransmitters is probably responsiblefor its analgesic properties. This analgesic effect may increasethe intervals between urgency episodes, helping to augmentBC. Pregabalin was assessed the efficacy and safety in alone orcombination with tolterodine ER in subjects with idiopathicOAB.22
Lamotrigine, a second-generation anticonvulsant, inhibitsvoltage-sensitive sodium channels, stabilizing neuronal mem-branes and modulating the presynaptic transmitter release ofexcitatory amino acids, such as glutamate and aspartate. This
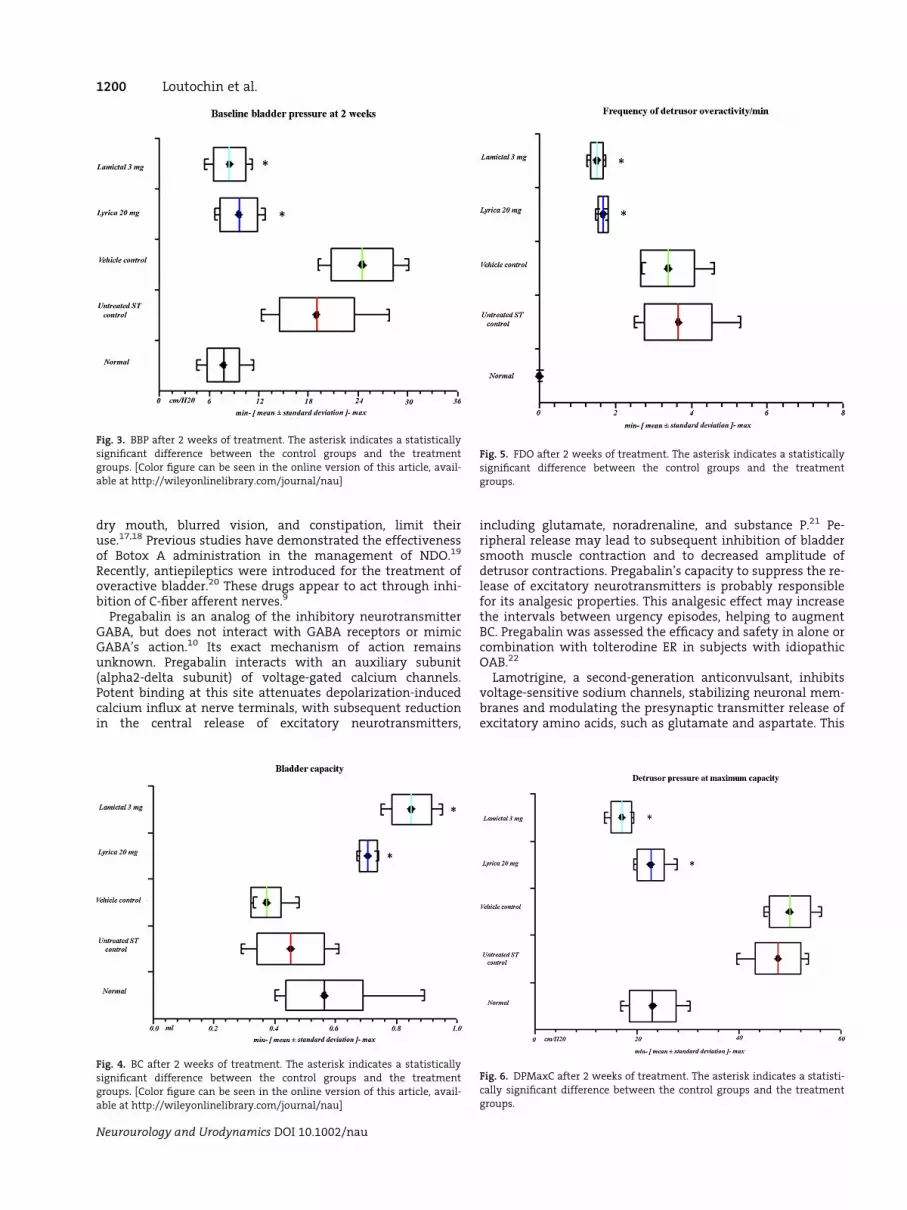
Fig. 3. BBP after 2 weeks of treatment. The asterisk indicates a statistically
significant difference between the control groups and the treatment
groups. [Color figure can be seen in the online version of this article, avail-
able at http://wileyonlinelibrary.com/journal/nau]
Fig. 4. BC after 2 weeks of treatment. The asterisk indicates a statistically
significant difference between the control groups and the treatment
groups. [Color figure can be seen in the online version of this article, avail-
able at http://wileyonlinelibrary.com/journal/nau]
Fig. 5. FDO after 2 weeks of treatment. The asterisk indicates a statistically
significant difference between the control groups and the treatment
groups.
Fig. 6. DPMaxC after 2 weeks of treatment. The asterisk indicates a statisti-
cally significant difference between the control groups and the treatment
groups.
1200 Loutochin et al.
Neurourology and Urodynamics DOI 10.1002/nau

is unlikely to be its sole mechanism. Action through calciumchannels has also been proposed.23 Inhibition of sodium chan-nels will lead to decreased sodium influx, with possible resul-tant reduction of muscle action potentials and suppression ofdetrusor muscle contractility.
In our study, we measured the following urodynamicparameters: FDO, BBP, DPMaxC, and BC. Urodynamic changeswere evaluated with different doses and durations of twoAEMs, Pregabalin, and Lamotrigine.
Urodynamic measurements were performed in awake ratsvia a catheter inserted into the bladder.24 After 3 weeks of SCI,the rats developed FDO of 3.66 � 0.89/min. Comparison ofnormal controls and the SCI groups showed that BBP increasedfrom 7.74 to 18.99 cmH20 and DPMaxC from 23.0 to47.63 cmH2O. BC of 0.56 ml in normal controls decreased to0.45 ml in SCI rats. Elhilali et al. reported that BC improved1 week after injury to 0.7 ml and declined after 2 weeks to0.5 ml.
A previous study noted significantly decreased pain inpatients with diabetic polyneuropathy after 300 mg of Prega-balin daily.25 In chronically spinalized rats, hyperexcitabilityof C-fiber bladder afferents contributes to bladder hyperre-flexia during the filling phase.26 Pregabalin, at a dose level of30 mg/kg, is effective against different stages of convulsion.27
We assume that the mechanism of action in the SCI animalmodel is reduced FDO due to decreased release of excitatoryneurotransmitters.
Our study, with 20 mg/kg of Pregabalin, disclosed signifi-cant improvement of FDO from 3.66/min to 1.5/min, BC from0.45 to 0.71 ml, DPMaxC from 47.63 to 22.64 cmH20, and BBPfrom 18.99 to 9.57 cmH20.
We also demonstrated that the urodynamic parameterswere significantly improved by 2 weeks of treatment with3 mg/kg of Lamotrigine. BBP fell from 18.99 to 8.46 cmH20,DPMaxC decreased from 47.63 to 22.64 cmH20, BC increasedfrom 0.45 to 0.85 ml, and FDO diminished from 3.66/min to1.5/min.
Information on the safety and tolerability of Pregabalincan be garnered from studies on chronic pain and seizuredisorder. These data indicate that Pregabalin is very safe,with mostly mild to moderate side-effects and minimaldrug interactions.28 Its commonly reported adverse effectsare dizziness, somnolence, and peripheral edema, whichoccur more frequently with higher doses. Other trouble-some side effects include visual disturbances, ataxia, confu-sion, and weight gain. The most serious adverse reactionsreported include angioedema with respiratory compromiseand hypersensitivity reactions. An additional concern is anincrease in suicidal ideation or behavior, although this isconsidered a class effect seen in antiepileptic drugs in gen-eral. Pregabalin does not bind to plasma proteins andundergoes minimal metabolism; therefore, it does notappear to have significant pharmacokinetic effects on co-administered medications.21 Additive actions on gross mo-tor function and cognition are observed when Pregabalin isco-administered with ethanol, benzodiazepines, andopioids. Pregabalin is listed as class C in pregnancy and, assuch, should be given only if the benefits significantlyoutweigh the risks. Elderly patients may exhibit a higherfrequency of previously mentioned side effects. Pregabalincan be considered as safe in the setting of renal insufficien-cy or failure, albeit at reduced doses. The appropriate dosageshould be based on creatinine clearance in patients.21
Lamotrigine has common side effects, such as blurred ordouble vision, clumsiness or unsteadiness, nausea, insomnia,sleepiness, back pain, fatigue, runny or stuffy nose, abdominal
pain, and dry mouth. Less common side effects are anxiety,confusion, depression, continuous, uncontrolled back andforth movements, and/or rolling eyes.Analysis of a German registry revealed Stevens-Johnson
syndrome and toxic epidermal necrolysis in 1 per 10,000 newusers of Lamotrigine.29 There have been isolated reports ofother potentially serious adverse effects, including interstitialnephritis and hemophagocytic syndrome.30
CONCLUSIONS
To our knowledge, our findings on the treatment of NDO ina SCI animal model with new generation antiepileptics arethe first to be published. We clearly demonstrated thatPregabalin and Lamotrigine significantly improved all CMparameters in our rat model of NDO. Considering our resultsand the relative safety of these drugs, we propose their studyin clinical practice as a novel treatment of NDO.
ACKNOWLEDGMENTS
This research was supported by Pfizer, Inc.
REFERENCES
1. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminologyin lower urinary tract function: Report from the standardisationsub-committee of the International Continence Society. Urology 2003;61:37–49.
2. Fowler CJ. Neurological disorders of micturition and their treatment. Brain1999;122:1213–31.
3. Rantell A. Lower urinary tract symptoms in women with multiple sclerosis:Part 1. Br J Nurs 2009;18:S16–8.
4. Samson G, Cardenas DD. Neurogenic bladder in spinal cord injury. Phys MedRehabil Clin N Am 2007;18:255–74, vi.
5. Steers WD. Pathophysiology of overactive bladder and urge urinary inconti-nence. Rev Urol 2002;4:S7–18.
6. de Groat WC, Yoshimura N. Mechanisms underlying the recovery of lowerurinary tract function following spinal cord injury. Prog Brain Res 2006;152:59–84.
7. Chancellor MB, Anderson RU, Boone TB. Pharmacotherapy for neurogenicdetrusor overactivity. Am J Phys Med Rehabil 2006;85:536–45.
8. Karsenty G, Denys P, Amarenco G, et al. Botulinum toxin A (Botox)intradetrusor injections in adults with neurogenic detrusor overactivity/neurogenic overactive bladder: A systematic literature review. Eur Urol2008;53:275–87.
9. Elzayat EA, Campeau L, Karsenty G, et al. Effect of antiepileptic agent, leve-tiracetam, on urodynamic parameters and neurogenic bladder overactivityin chronically paraplegic rats. Urology 2009;73:922–7.
10. Joshi I, Taylor CP. Pregabalin action at a model synapse: Binding to presyn-aptic calcium channel alpha2-delta subunit reduces neurotransmission inmice. Eur J Pharmacol 2006;553:82–8.
11. Sridhar B, Ravikumar K. Lamotrigine, an antiepileptic drug, and its chlorideand nitrate salts. Acta Crystallogr C 2009;65:460–4.
12. Tsenov G, Redkozubova O, Kubova H, et al. Effects of lamotrigine on cortical-ly-elicited phenomena in adult rats: Differences between acute applicationand late consequences of early postnatal administration. Brain Res 2009;1258:65–70.
13. de Groat WC, Yoshimura N. Changes in afferent activity after spinal cordinjury. Neurourol Urodyn 29:63–76.
14. Fowler CJ, Griffiths D, de Groat WC. The neural control of micturition. NatRev Neurosci 2008;9:453–66.
15. Birder LA. Role of the urothelium in urinary bladder dysfunction followingspinal cord injury. Prog Brain Res 2006;152:135–46.
16. Birder LA. More than just a barrier: Urothelium as a drug target for urinarybladder pain. Am J Physiol Renal Physiol 2005;289:F489–95.
17. Chapple CR, Yamanishi T, Chess-Williams R. Muscarinic receptor subtypesand management of the overactive bladder. Urology 2002;60:82–8 (discus-sion 88–9).
18. Yamaguchi O. Antimuscarinics and overactive bladder: Other mechanism ofaction. Neurourol Urodyn 29:112–5.
19. Smith CP, Nishiguchi J, O’Leary M, et al. Single-institution experience in 110patients with botulinum toxin A injection into bladder or urethra. Urology2005;65:37–41.
20. Andersson KE. New pharmacologic targets for the treatment of the overac-tive bladder: An update. Urology 2004;63:32–41.
Pregabalin and Lamotrigine on NDO 1201
Neurourology and Urodynamics DOI 10.1002/nau

21. Durkin B, Page C, Glass P. Pregabalin for the treatment of postsurgical pain.Expert Opin Pharmacother 11:2751–8.
22. Marencak J, Cossons NH, Darekar A, et al. Investigation of the clinical effica-cy and safety of pregabalin alone or combined with tolterodine in femalesubjects with idiopathic overactive bladder. Neurourol Urodyn 30:75–82.
23. Stefani A, Spadoni F, Siniscalchi A, et al. Lamotrigine inhibits Ca2þ currentsin cortical neurons: Functional implications. Eur J Pharmacol 1996;307:113–16.
24. Abdel-Karim AM, Bialecki RA, Elhilali MM. Effects of ZD6169 and ZD0947, 2potassium adenosine triphosphate channel openers, on bladder function ofspinalized rats. J Urol 2002;168:837–42.
25. Zaremba PD, Bialek M, Blaszczyk B, et al. Non-epilepsy uses of antiepilepsydrugs. Pharmacol Rep 2006;58:1–12.
26. Miyazato M, Sasatomi K, Hiragata S, et al. Suppression of detrusor-sphincterdysynergia by GABA-receptor activation in the lumbosacral spinal cord in
spinal cord-injured rats. Am J Physiol Regul Integr Comp Physiol 2008;295:R336–42.
27. Akula KK, Dhir A, Kulkarni SK. Effect of various antiepileptic drugs in apentylenetetrazol-induced seizure model in mice. Methods Find Exp ClinPharmacol 2009;31:423–32.
28. Straube S, Derry S, Moore RA, et al. Pregabalin in fibromyalgia: Meta-analysis of efficacy and safety from company clinical trial reports. Rheuma-tology (Oxford) 49:706–15.
29. Mockenhaupt M, Messenheimer J, Tennis P, et al. Risk of Stevens-Johnsonsyndrome and toxic epidermal necrolysis in new users of antiepileptics.Neurology 2005;64:1134–8.
30. Bialer M, Johannessen SI, Kupferberg HJ, et al. Progress report on newantiepileptic drugs: A summary of the Eigth Eilat Conference (EILAT VIII).Epilepsy Res 2007;73:1–52.
1202 Loutochin et al.
Neurourology and Urodynamics DOI 10.1002/nau