disturbances in acute phase plasma proteins during melancholia: additional evidence for the presence...
TRANSCRIPT
0278 -S&%6/92 816.00
8 1992 Rqanm Press Ud
DISTURBANCES IN ACUTE PHASE PLASMA PROTEINS DURING MEIANCHOLIA: ADDITIONAL
EVIDENCE FOR THE PRESENCE OF AN INFLAMMATORY PROCESS DURING THAT ILLNESS
MICHAEL MAES’, SIMON SCHARPE’, EUGENE BOSMANS’, MAURITS VANDEWOUDE4, EDUARD SW’. WIM UMTENBROECK~ WALTER COOREMAN? CARINE VANDERVORST? and JEF RAUS?
I Psychiatric Centre, Munslerbilzen, Belgium, ‘Department of Cllnlcal Biochemistry, University of Antwerp. Belgium, ‘Eurogenetics. Tessanderlo. Belgium, ‘Department of Internal Medicine,
Anhverp. Belgium ‘Dr. Willems Institute, Unlverslty of Diepenbeek, Belgium.
(Final form, September 1991)
BBsTRACT
MAES. MICHAEL, SIMON SCHARPE. EUGENE BOSMANS. MAURITS VANDEWOUDE, EDUARD SUY. WlM UYTIXNBROECK, WALTER COOREMAN. CARINE VANDERVORST and JEF RAUS: Disturbances in Acute Phase Plasma Proteins during Melancholia: Additional Evidence for an Inflammatory Process during that Illness. Prog. Neuro-Psychopharmacol. & Biol. Psychiat. 1992. 16(4):501-515.
t Leukocyte enumeration through flow cytometry has revealed that severe depression may be accompanied by a systemic immune activation, indicative of an Inflammatory response. The latter condition allegedly involves an important modification of acute phase plasma protein (APP) equilibrium.
2. In order to elucidate whether the state of severe depression Is represented by alterations in APPs, the authors measured: a, antltrypsln (a,AT). a, macroglobulln (GM), haptoglobin (HP), a, acid glycoprotein (a,S). transfer& (Tf), complement component 4 (C.) and C-reactive protein (CRP). Interleukin-f-6 (11-16) 8nd lnlerleukind (11-6) clrculatlng levels were determined.
3 Hyperhaptoglobinemia and hypotransferrinemia are hallmarks for major depression and depression per se, respectively. The disorders in Hp and Tf circulating levels are highly sensitive to (83%) and specific for (100%) melancholia as opposed to the healthy state.
4. Disorders in both APPs are significantly related to the absolute number of blood monocytes. 5. The authors observed a trend towards lower u,M and higher o,S values in severely depressed
subjects. Severity of depression was significantly related to Hp and a,S (both positively) and lo Q,M and Tf (both negatively) values.
6. No significant intercategory diierences in C, could be established, whilst only a few subjects exhibited measurable CRP, II-if3 and II-6 circulating levels.
7. Our findings may support the hypothesis that depression Is accompanied by an inflammatory response.
Kev word : a, acid glycoprotein. acute ph8Se proteins, a, antitrypsin. complement component 4. flow cytometry, depression, haploglobin, lnflammatlon, Interleukin-l-6, interieukin-6, at macroglobulin. monocytosis, plasma proteins, C-reactive protein, transferrin.
. Abbrevlatlons: a, acid glycoprotein (a, S), acute phase (AP), acute phase proteins (APPs), a, antitrypsin (a, AT), complement component 4 (C4). Hamllton Depression Rating Scale (HDRS). dipeptidylpeptidase IV (DPP IV), Haptoglobln (HP), hypolhalamlc-pituitary-adrenal (HPA). interleukin-l-6 (II-IQ interleukin-6 (II-6), C-reactive protein (CRP). Structured Cllnical interview DSM-IIIR (SCID). transferrin (Tf).
Some recent studies have documented that severe depression may bs accompanied by alterali-
ons in immune functions. The most consistent findings comprise a blunted mitogen-induced blastoge-
501
502 M. Maes et cd
nesis (Schlelfer et al.. 1984; 1985; Kronfol and House, 1985; Kronfol et al., 1986; Maes et al., 1989a;
1SSla) and a reduced natural killer ceil activity (Irwin, 1988; Irwin et al., 1930). Some authors have
reported on the presence of antfnuclear and antlphospholipid autoantlbodles In severe depression
(Deberdt et al.. 1976; Maes et al.. 1991c).
Recently. we were able to estabfish that severe depression may be characterized by: monocytosis.
increased numbers of T cells expressing both prfmary activation receptors and receptors that function
as accessory molecules, the appearance of previously unexpressed cell surface molecules, and
increased B cell numbers (Maes et al., 1SSte). In addltfon we have observed hfgher serum soluble-
interleukin-2~~~t~ levels together with lower di~p~~lpep~da~ fV (OPP IV) actfvlty in plasma of
severely depressed patients (t&es et al., 1991~; lQ91d). These phenomena may indicate ttte
existence of an inflammatory process with systemic immune activation via monocytosls (Fujta et al.,
1978: Stone et al., 1989: Maes et al.. lSQlc, 1991e).
Acute and chronic inflammatory processes are characterized by an alleged coordinated alteration
in the expression of several functionally essential plasma proteins. The best documented changes
during the acute phase of inflammation constitute those in circulating levels of a large number of
plasma proteins of hepatic origin (i.e. the acute phase proteins; APPs). e.g. increased levels of
positive APPs such as a, antitrypsin (a,AT), haptoglobfn (HP). a, acid glycoproteln (a$). and C-
reactive-protein (CRP), and a fall in negatlve APPs such as transferrin (Tf) and or macrogfobulln (o&4)
(Schmid. 1975; Laurel1 and Jeppsson, 1975; Putnam, 1975a; 1975b; 1975c; 19754; Kushner, 1982;
Keyser, 1979; Bernin~r, 1986; Robsrts, 1986: Fay~nvfl~ et al., 1987; Kremer et al., lQ88:
Mackiewfcz et al.. 1988; de Jong et al., 1990).
inflammatory processes are directly mediated by various actlons of the complement system,
whereby the classic complement pathway is activated by antigen-antibody complexes and by
substances such as CRP (Muller-Eberhard, 1975; Cooper, 1987). The complement cascade, in turn,
leads to immune cell activation (Roitt et al., 1989). Classic pathway activation affects especlaiiy the
fourth component of complement (C,) (Cooper, 1987). Congenital deflciencles of classical pathway
components (e.g. C,) are associated with chronic inflammatory disorders (Cooper, 1987; Ross and
Densen, 1984: Fries and Frank, 1988).
lnterleukin-1 (k-1) and interleukin-6 (k-6) - both of which are produced by the mon~~/macr~h-
age lineage - are potent modufators of APP synthesis in adult human hepatocytes (Caste11 et al.,
1988; Klasing, 1988; Helnrlch et al., 1990). Glucocorticofds act In concert wfth both lnterfeuklns to
mediate this protein synthesis (Kfaslng, 1988; Marlnkovfc et al., 1989; Prowse and Baumann, 1989).
Increased hypothalamic-pituitary-adrenal (liPA)-axis activity (Carroll, 1980; Maes et al., 1990~) and
higher Ii-10 accumulation in culture supernatant of mitogen-stimulated perlpheral blood leukocytes
(Maes et al., 1991 b) have been observed during melancholia.
The aim of this study was to determine whether higher positive and lower negative APP
circulating levels - indicative of acute or chronic inflammatory diseases - represent the state of severe
Acute phase plasma proteins during melancholia 503
depression. Hence, the authors examined (1) C.. a,AT. a,M. Hp. CAP, a$, and Tf In various depressl-
on categories and in normal volunteers, and (2) the relationship between these APP levels and some
of their regulatory mechanisms such as monocyte function, II-16 and II-6 clrculatlng levels, and
glucocorticoid activity.
In this study 82 subjects participated: 11 healthy controls - staff members - and 71 depressed
inpatients consecutively admitted to the Psychiatric Centre. The study period extended from January
1989 until 1 June 1990. The healthy volunteers were free of any medication during at least one
month previous to blood sampling. None were regular drinkers or had been taking psychotropic
drugs. They were free of any medical or psychiatric illness. All normal volunteers had scores c 9 on
the Beck Depression Inventory. and c 40 on the Zung Depresslon and Anxiety sccres. The depressed
patients were classified according to the DSM-III (APA, 1980) Into (a) dysthymlc dlsorder (300.40) and
adjustment disorder with depressed mood (309.00) (i.e. labeled as miner depression), (b) major
depression without melancholia or simple major depression (296.X2), and (c) major depression with
melancholia (296.X3). Diagnoses were made wlth the Structured Cllnlcal Interview for DSM-III-R (SCID)
Patient Version (Spitzer et al.. 1985). The melancholic depression criteria of the SCID-Inventory.
edition 1985. are based upon the DSM-III (and not DSM-III-R) depression diagnoses. Hamilton
Depression Rating Scale (HDRS) scores were determined 5-8 days after hospital admission (Hamilton.
1960). SCID and HDRS were scored by the same rater (MM). Anorexia and welght loss were assessed
by means of the HDRS items (scores: 0. 1 or 2). In addition, we have used a second measure of
overall severity of illness, i.e. a score ranging for 0 to 3; 0 is not depressed, 1: minor depressed , 2:
simple major depressed, and 3: melancholic depressed. This &ore may be used as an overall severity
index since DSM-III diagnosis for unipolar depression largely reflects severity of Illness (Maes et al.,
1990a: 1990b).
All subjects were free of any drugs known to interfere with the immune apparatus. In addition, all
subjects were free of acute (e.g. inflammatory, infectious or allergic diseases at least 2 weeks before
the study) and chronic medical illnesses known to affect the immune system.
The authors have omitted patients with bipolar disorders, and other axis I diagnoses beside
depression, including alcohol and drug abuse. In addition, we excluded patlents who were on lithium,
monoamlne oxidase lnhlbltors and neuroleptlcs (antl-psychotic dosages) or patlents who underwent
ECT the year prevlous to hospital admission.
Thirty-four depressed patients were drug free for at least 1 month prior to hospital admlsslon
(thus, 5 weeks prior to blood sampling; Table 1 shows number of patients In each category). The
others had been taking bsnzodlazeplnes, antidepressants or low-dosage neuroleptlcs. These drugs
were discontinued upon hospital admission. Consequently, these patlents underwent a wash-out
period of 7 days before blood samplings. We have administered a low dosage schedule for
504 M. Maes et crL
benzodtazeplnes (c 6 mg lorazepam/day) to 22 depressives In the case of sleep disorders and
severe agitation (see Table 1 for number of patients in each category).
Seven days after hospital admission, 6 a.m. fasting blood samples were collected for the assay of
APPs. k-18. 11-6, baseline ccrtisol and leukocyte enumeration (number of monocytes). The same day,
patients ingested 1 mg of dexamethasone (as a Ilquld) at 11 p.m. The next day, blood was sampled
at 8 a.m. after an overnight fast for the assay of postdexamethasone cortlsol. APPs were determined
in the department of clinical Mochemistry. Universitalre lnstelllng Antwerpen (UIA); II-18 and II-6 were
determined by Eurogenetics. Tessenderlo: leukocytes were enumerated at the Dr.Wlllems Institute.
University of Dfepenbeek; cortlsol was determlned In the Psychlatrlc Cenfre, Munsterbllzen. Belgium.
Assays of APPs. II-16 and II-6 were carrled out In all subjects (n = 82). Baseline and poetdexametha-
sone corttsol were determlned in all depressed patlents. Leukocyte enumeration was carrted out in 10
healthy controls and In 32 depressed subjects. Methods and results of leukocyte enumeration are
presented elsewhere (Maes et al.. 199le).
Transferrin. haptoglobfn. CRP. o, acid glycofxotetn. a,-antltrypsln. C. and a, mscroglobulln were
determlned by laser nephelometry (Behrlngwerke AG Marburg. FRG). Antisera. controls and standards
were obtained from Behrlngwerke. For each parameter we used one single batch of antiserum. All
calibrations were done with the same standard batch. For most parameters a single polnt callbratlon
was avakabfe. Only for transferrln and CRP a multlpolnt callbratlon was necessary. Appropriate
controls were included in each run. The lntra and interassay coefficients of variation for all APPs were
< 2% and < 5%. respectively.
The determlnation of II-16 was performed according to the instructions of the supplier of the II-1 8
ELISA kit, (Cistron, Eurogenetics). Mlcrotiterplates coated with a II-16 specific monoclonal antlbody
are incubated with 100 )JI of sample or calibrator. after washing a second lncubatfon step with 100 MI
rabbit anti II-18 antibody is performed, followed by a third incubation with a goat antirabbtt immuno-
globulin horse rash peroxidase conjugate. After a final substrate (H,OJ and chromogen (tetramethyl-
benzidlne. TMB) reaction, optical densities are recorded at 450 nm and II-18 concentrations are
calculated from the standard curve.
The determination of II-6 was performed wlth a sandwich ELISA method (Eurogenetics). In thls
procedure 100 FI of serum or calibrator are incubated for 2 hours wlth a mlcrotlterplate coated with
an II-6 specific monoclonal antibody, followed by a second incubation of 30 mlnutes with 100 )JI of
an II-6 specific polyclonal blotinylated antlbody. After washing, 100 ).rl of a streptavidlne horse radish
peroxidase conjugate is added for 30 minutes. Subsequently, the substrate reaction (H,O,/TMB) is
carried out for 30 minutes at room temperature, optical densities are recorded at 450 nm and
concentrations calculated from the standard curve wlth a dynamic range of 5 pg/mL to 500 pg/mL.
Acute phase plasma proteins durtng melatwholta 505
The independence of classfficatlon systems has been ascertained by means of contfngence
analysis (chi-square test with Yates’ correction). Relatfonships between variabfes were assessed by
means of Pearson’s product moment (r). point Mserial, and Spearman’s rank order (r,) correlation
coefficients, and by means of multiple regression analysis. Intergroup differences were tested with the
analysis of variance (ANOVA), analysis of covariance (ANCOVA), muitivariate ANOVA (MANOVA). and
linear dlscrlminant analysis &DA). Multiple a prior1 comparisons between group means were
ascertained with the Dunn test (with Bonferroni’s p conaction). The Koimogorov-Smirnov test has
been used In order to test normality of distribution. Transformationa (natural i~ithm) were used in
order to reach normality of dfstrfbutfon. The dfaQMstic performance of a test was computed by
means of ROC freceiver operatfnQ ~~act~fs~) analysfs (Mossman and Ckrnoaa, 1SSS), ser&fvIty,
specfftcfty, predict&e value for a poshive test rest& (PV+), K (with t-statistic and exact p value) and
Y-statistics (Maes et al.. WfM}. ROC analysis offers 3 criteria _ i.e. delta m, s. and AUC - that are
helpful In evaluating the discriminatory power of a given test. Delta m is the difference between the
disordered (i.e. melancholia) and non-disordered (i.e. healthy state) populations’ means when
measured in units of SDS. The ratio of the SDS in both catego&@ is ~iied 8. The overall accuracy of
the test may bs reflected by the area under the ROC curva (AUC). The RCKZ curve is obtained when
one plots true positive versus false positive rates for dffferent cut off points. The AUC of the WC
curve has been approximated by connecting the dlfferent pdnts in the plot of true positive versus
false positive resufts. and by summing up the areas of the resufting trapezoids. The AUC may range
from 50% (no better than chance) to fM)% (perfect performance). The greater 6s defta m and AUC,
the higher the overall accuracy of a dfagnostfc test.
1. Demoaraohic
Table 1 lists the demographic data of the 82 subjects in this study. There were no differences in
sex ratio between the 4 study samples. Patients with melancholia were significantly older than minor
depressives and healthy ct)ntrols. The HDRS-score was signfficantly different between the 3 depressive
subgroups and increased from minor depression --> simple major depression--> melancholia. We
found no slgnlffcant difterences in drug state between the DSM-III categories (use of benzodlazeplnes
and length of drug free period before hospital admission).
The authors found no significant dffferences In any of the APPs between men and women. Conse-
quent&, both groups were analyzed together. C., ~$8, Hp, a,AT, and Yf vafues showed a normal
distrfbution; a$ values were lognormally distributed. As a result, a$ values were processed in
logarithmic (natural logarfthm) transformation.
All posltlve APPs showed significant positive intercorrelations: C, was positively related to Hp (r, 5
0.32, p = 0.003), a,S (I, = 0.52. p < lo”) and a,AT (r, = 0.2% p = 0.008). Hp was significantly
correlated with a,AT (r, = 0.27. p = 0.01) and a,S (r, = 0.59, p < 10’). Finally, there was a
significant relationship between a,S and a.AT (r, = 0.23, p = 0.03).
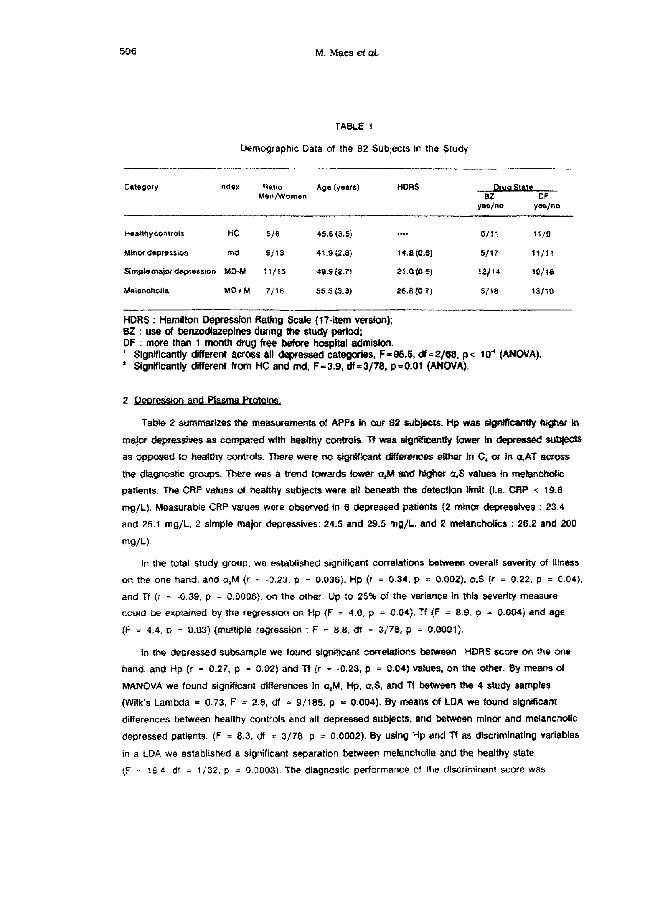
TABLE 1
Demographic Data of Ihe 82 Subjects in th% Study
Category mler Ratio Age lyerrs) HORS Masn/Womsn -e-@-F
yes/no yas/no _..
HC
Mrtancholia
516
S/l3
26.8 fG.7)
r*jtr
s/r8 r3/1o
HORS : Hamilton Depresa~on Rdng Scale (17-item ve&oi?); BZ : use of benzodfazeplne8 during the study period; DF : more than 1 month drug f@e before hospital admlslon. ’ SignWcantly different acro$$ alI depressed categories, F =95.5, df * Z/%9. p < 1 Cl’ (ANOVA). * Significantly different from HC and md. F-3.9. df=3/78. p=O.O1 (AN&N).
In the total study group, wg e$t#blished significant correlations betwecmn overall severity of Hlness
on the one hand, and a,M (P = -0.23, p T 0.036). Hp (I = 0.34. p = a.o02), a,$ (r = 0.22, p = 0.04),
and Tf {r = -0.39, p = 0,0006). on the other. #p :o 25% of the variance In tl~ls severity measure
could be expiairted by the re$resdon on Hp fF = 4.0, p = O.M], Tf IF = 8.9, p = 0X%34) and age
f-F = 4.4, p = 0.#3] &-nuiSpie regression : F = 8.8, bf = 3$‘78, fi = tUWl1).
In the dewem& sutrsampie we touffd signif#cant c#rektior% between WRS score 08-r %e oile
hand, and Hp fr = 0.27, p = 0,02) and Tf (r = -0.23, p = 0.04) values, on WA? other, 3~ ~MSWS of
MANOVA we found significant differences In a&l, Hp, sr,S, and Tf betvwean the 4 study sampfes
(Wilk’s Lambda = 0.73. F * 2.8, df = Q/185, p = 0.004). By meaw of LOA we found slgnlficant
differences between healthy c~r~trnls $nd all depressed subjects. and between minor and melancholic
depressed patients. (F = 8.3. d = 3/f& p = 0.0002). By using Hp and Tf a~ dlscrlminatlng variables
in a LDA we established a sigrrlficanr separation between melancholia and the healthy state
(F = 18.4, df = tj32, p = O.NNX%). She diagnostic performance of the discriminant score was
Acute phase plasma proteins during melancholia 507
SsnSitiVity = 83%. SpeCifiCity = 100%. PVt = 100% (K = 0.75. t = 3.5. p = 0.001. Y = 1); results of
ROC analysis: delta m = 1.92. s = 1.31. AUC = 90%.
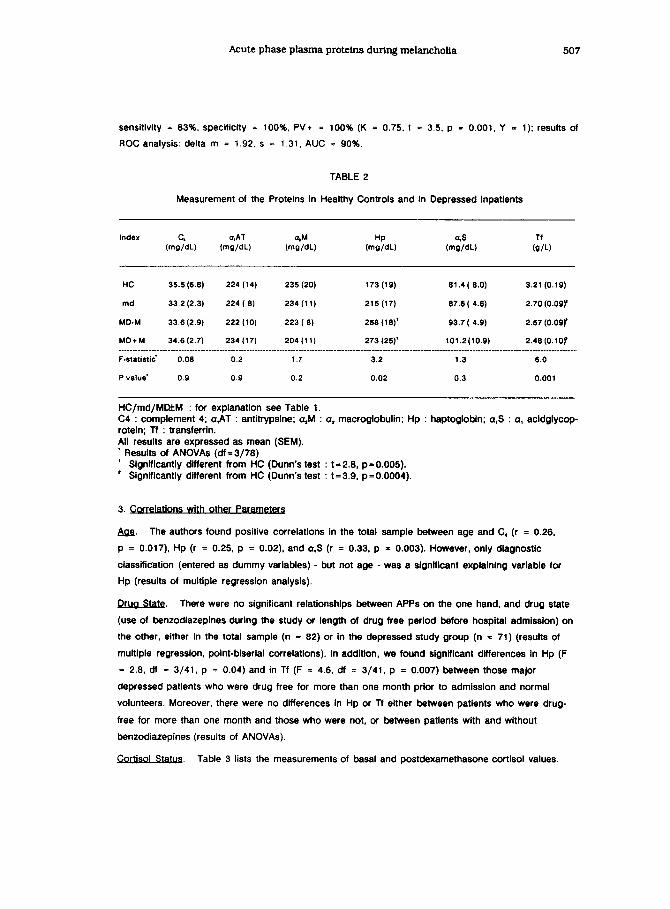
TABLE 2
Measurement of the Proteins in Healthy Controls and in Depressed Inpatients
Index
(me?dL)
a,AT Tf
(W/dL) (m%) (mi:dL) (m?dL) (Q/L)
HC 35.5 (6.6) 224 (14) 235 (20) 173(16) 61.4( 8.0) 3.21(0.(g)
md 33.2(2.3) 224( 8) 234 (11) 215(17) 67.6( 4.6) 2.70(0.09r
MD-M 33.6(2.9) 222 (10) 223(6) 256 (16)' 93.7( 4.9) 2.67(O.OSy
MD+M 34.6t2.7) 234(17) 204(11) 273(25)' 101.2(10.e) 2.46(O.lOy
F-statistic' 0.06 0.2 1.7 3.2 1.3 6.0
P value' 0.9 0.9 0.2 0.02 0.3 0.001
HC/md/MDtM : for explanation see Table 1. C4 : complement 4; a,AT : antitrypsine; a&f : a2 macroglobulin; Hp : haptoglobin; a,S : a, acidglycop- rotein; Tf : transferrin. All results are expressed as mean (SEM).
Results of ANOVAs (df=3/78) ’ Significantly different from HC (Dunn’s test : t=2.8, p=O.O05). ’ Signiffcantly dkferent from HC (Dunn’s test : t=3.9, p=O.OOOS).
3. Cotrelations with other Pa
&a. The authors found positive correlations in the total sample between age and C, (r = 0.26,
p = 0.017) Hp (r = 0.25, p = 0.02) and a,S (r = 0.33, p = 0.003). However, only diagnostic
classification (entered as dummy variables) - but not age - was a signlflcant explalnlng variable for
Hp (results of multiple regression analysis).
Qcgg_&k There were no significant relatlonshlps between APPs on the one hand, and drug state
(use of benzodlazepines during the study or length of drug free period before hospital admisslon) on
the other, either in the total sample (n = 82) or in the depressed study group (n = 71) (results of
multiple regression, point-biserial correlations). In addition, we found signlflcant differences In Hp (F
= 2.8, df = 3/41, p = 0.04) and in Tf (F = 4.6, df = 3/41, p = 0.007) between those major
depressed patients who were drug free for more than one month prior to admission and normal
volunteers. Moreover, there were no differences in Hp or Tf either between patients who were drug
free for more than one month and those who were not, or between patients with and without
benzodiazepines (results of ANOVAs).
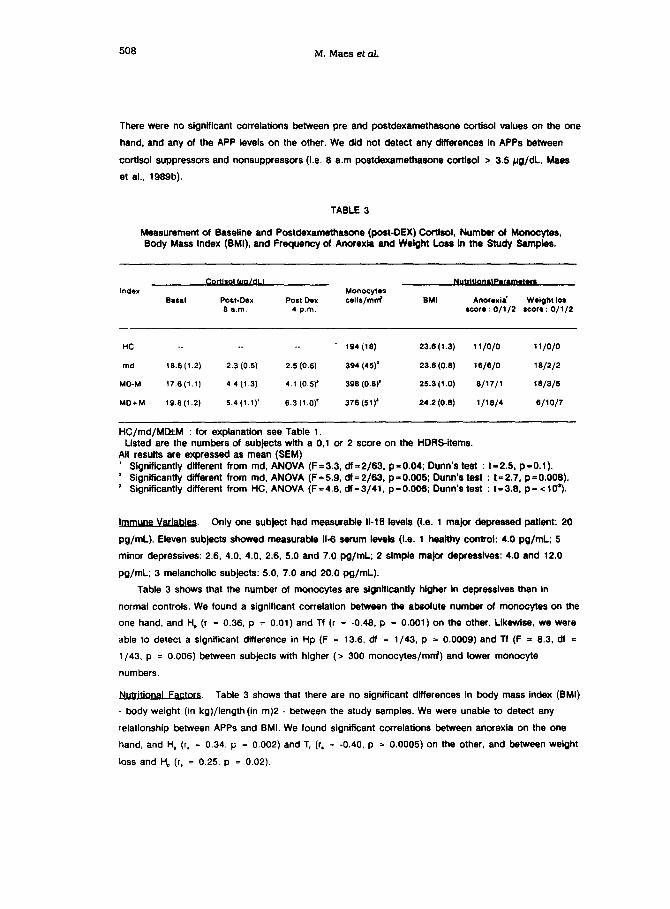
Cprtisol SW. Table 3 lists the measurements of basal and postdexamethasone cortisol values
508 M. Maes et al.
There were no signtficant correiatlons between pre and postdexamethasone cortisol values on the one
hand, and any of the APP levels on the other. We did not detect any dtfferences In APPs between
cortisol suppressors and nonsuppressors (i.e. 8 a.m postdexamethasone corttsol > 3.5 pg/dL. Maes
et al., 1989b).
TABLE 3
Measurement of Baseline and Postdexamethasone (post-DEX) Cortisol. Number of Monocytes. Body Mass Index (BMI). and Frequency of Anorexla and Weight Loss In the Study Sempfes.
Index Basal
Ccx&Q(&tldLI
POW-00X 8 a.m.
Posl Dex 4 p.m.
HC
md
MD-M
MD+M
. . . . . . 194 (IS) 23.6 (I .3) 11 /o/o 11/o/o
l&6(1.2) 2.3 (0.5) 2.5 (0.6) 394 (45)’ 23.6 (0.6) 16/6/O Is/z/n
17.6(1.1) 4.4 (1.3) 4.1 (0.5.y 39s (0.W 25.3(1.0) s/17/1 lS/3/5
19.S(l.2) 5.4 (1.1)’ 6.3 (1 .O)’ 37s (51)’ 24.2 (0.8) l/IS/4 6/lOf7
HC/md/MatM : for explanatlon see Table 1. Ltsted are the numbers of subjects with a 0,l or 2 score on the HORS-items.
All results are expressed as mean (SEM) ’ Signtftcantly different from md, ANOVA (F=3.3, df=2/63, p=O.O4; Dunn’s test : ts2.5, p=O.l). ’ Significantly different from md. ANOVA (F = 5.9, df = 2/63, p = 0.005; Dunn’s test : t = 2.7, p = 0.006). ’ Significantly different from HC. ANOVA (F=4.8, df=3/41. p=O.O06; Dunn’s test : t=3.8. p= <I@).
wVariables. Only one subject had measurable II-16 levels (Le. 1 major depressed patlent: 20
pg/mL). Eleven subjects showed measurable II-6 serum levels (I.e. 1 heafthy control: 4.0 pg/mL; 5
minor depressives: 2.6, 4.0. 4.0, 2.6, 5.0 and 7.0 pg/mL; 2 simple major depressives: 4.0 and 12.0
pg/mL; 3 melancholic subjects: 5.0, 7.0 and 20.0 pg/mL).
Table 3 shows that the number of monocytes are .slgntficantly hlgher In depressives than In
normal controls. We found a significant correlation between the absolute number of monocytes on the
one hand, and H, (r = 0.36, p = 0.01) and Tf (r = -0.46, p = 0.001) on the other. LIkewIse. we were
able to detect a significant difference in Hp (F = 13.6, df = l/43, p = 0.0009) and Tf (F = 6.3, dl =
l/43. p = 0.006) between subjects wlth higher (a 300 monocytes/mrrf) and lower monocyte
numbers.
F&QG. Table 3 shows that there are no significant difference6 In body mass index (BMI)
- body weight (in kg)/length(in m)2 - between the study samples. We were unable to detect any
relationship between APPs and 8MI. We found signtficant correlations between anorexia on the one
hand, and H, (r, = 0.34, p = 0.002) and T, (r, = -0.40. p = 0.0005) on the other, and between welght
loss and H, (r, = 0.25, p = 0.02).

Acute phase plasma protelns during melancholia 5OQ
1. p. To our knowledge, this is the first study reporting on
major depression-r&ted disturbances in haptogiobln plasma conoentrations. Like in one of our
previous reports we have found lower transferrin levels In depressed subjects than In normal contrals.
In addition. severity of illness was significantly related to higher Hp and a$. and to lower Tf and a&f
circulating levels. Moreover, the combined use of Hp and Tf ylelded a high degree of marker
positivhy for mefanchoiia which coufd not be improved by lncludlng a,S or u&i. By cumufatfve
evaluation of tip and Tf, the positfvity of these markers for meianchofff fncreased to 83% (sensitivity),
v&fist the specfffcky equalied 100%. This may prove that h~r~pt~o~~~ and h~an~~i~-
mfa are rather specific for severe depression versus the normal staie.
increased levels of positive APPs (e.g. Hp. a$) and a drop in negative APPs (eg. Tf, o,M) are
important indicators of inflammatory states (Romette et al., 1986; Kleesiek and Greiling, 1984;
Mackiewicz et al., lQ86). APPs probabfy play a role durfng inflammation: the site of inflammation is
provided by APPs via blood pool and tissue fluid: APPs may Interact with the Inflammatory agents,
neutralize toxic molecules, inhibit proteoiytic enzymes, and clear ceil memixanes (Gauidie et al.,
1985; Engler. 1988).
We observed that meianchoifa is characterized by dfsharmonk alteratfons of some APPs (I.e. Tf
and Hp, wfthout changes in C,, a&T, and CBP). Tftla dfssodatfon may be expiafned by the fact that each AP reactant has e oertafn specfficity depending on the kind of aggres&n suffered (Sanchaz et
ai., t968). Moreover, APPs exhfbft d&rent sensitMtfes fh dsteoting the ~~~ state, whilst the
latency times of the APPs’ response to the challenge may vary substantiaiiy (Lapaduia and Numo,
1987).
2. p. Another major finding of this study is the slgnifkant
relationship between hyperhaptoglobfnemla and hypotransferrinrmla, on the one hand, and the
estabflshed monocytoals durlng depression (Maes et al., 199le), on the other. These relationships
agree with the well-estabilshed findlngs that products of activated monocytes (e.g. k-1, 11-6. and tumor
necrosis factor) alter hepatk APP synthesis by acting locally as well as at d&ant &es (Baumann et
al., 1987; Beuscher et al.. 1987; Gddman and Lfu. 1987; Kfasfng, 5988; Gastell et al., $969; Pulficino
et al.. 1990; Baumann and Gauldie, 1QQQ).
Our negative fnterleukfn results do not rufe out the putative invofvement of these substances in
the observed AP response. Firstly, in a previous study we were abfe to establish a higher k-18
accumulation in culture supernatant of mitogen-induced peripheral leukocytes during melancholia
(Maes et al.. 1991 b). Secondly, it appears that monocyte membrane II-1 regulates the expression of
APPs in human hepatocytea, whereas this form of II-1 on the outer cell membrane may be dissociated
from II-1 release (Beuscher et al., 1987).
510 M. Maes et al
3. LiPA-axis and Acute Phase Prc&&& Glucocorticosteroids are needed to achieve a maximal II-1
and II-6 induced stimulation of hepatic APPs (Marinkovic et al., 1989; Prowse and Baumann, 1989;
van Vugt et al., 1988). Accordingly, increased circulating cortisol levels were found to precede the
elevation of various APPs (e.g. Hp and a,S) (Togart et al., 1986). Since melancholia is characterized
by increased HPA-axis activity (Carroll, 1980; Maes et al., 1986; 1989b), we must consider the role of
glucocorticoids in AP responses. However, we were unable to establish a significant correlation
between HPA-axis activity and the APPs, As a result, we have no evidence for a pivotal role of
giucocorticoid state of our patients in APP synthesis.
4. Qther Sources of f&s. Several other factors, such as age, malnu~ition, circadian rhythms in
APPs, and smoking behaviour, may interfere with the production rate of APPs.
Milman et al. (1988) found higher a-AT, lip and a,S production rates in elderly subjects as
opposed to younger persons. In our study we observed significant correlations between age on the
one hand, and circulating levels of C.. Hp and a,S, on the other. However, we established that only
the depressive state (diagnostic classification: severity of illness) _ but not age - exhibited a
significant relationship with hyperhaptoglobinemia.
Reduction in protein intake may lead to a downturn in Tf and a,AT concentrations, whereas Hp.
a& a,S remain unaffected (Voitko and latsyshina. 1985). Domtnioni and Dlonigi (1987) have
established that malnu~ltlon may suppress the AP response of some APPs. Anorexia and weight toss
~ons~tute core symptoms of severe depression (~~nch~ia) (f&es et al., 199Oa. t99Ob) and could,
therefore, endanger the patient’s nutritional state and, subsequently, Tf and a,AT synthesis. Hence,
one could hypothesize that anorexia with subsequent weight loss induces a state of malnutrition
(protetn deprivation) In melancholic patients explaining perhaps hypotransferrinemia but not hyperhap-
toglobinemia. The Importance of this sequence is underscored by our finding of a signtficant
relationship between anorexia and hypotransferrinemia. In this respect, Fleck (1989) has suggested
that a decrement in visceral proteins such as Tf cannot be assumed to reflect primary malnutrition
when there is evidence for an AP response. On the contrary, it Is tempting to speculate that anorexia
and weight loss are part of the AP response, via, for Instance, anorectic actions of II-1 or Ii-64nked
inflammatory responses (Gershenwaid et al., 1990; Klasing, 1988).
Bruguer~te et al., (1986) found sign~icant circadian rhythms in some (Le. a,AT, Tf, a,S) but not
all APPs. Putative effects of circadian rhythms were controlted for since all bfood samples were
collected at 8 a.m.
It is known that tobacco smoking may induce an AP response as indicated by increased CRP
levels, whilst other APPs (Le. a,AT. a,.% Tf. Hp) are not affected by smoking (Das, 1985). As our
study shows negative CRP, but positive a$. Tf and Hp results, we may conclude that any effects of
tobacco smoking on our results may be disregarded.
Finally, we have no evidence that the drug state of our subjects might have influenced our
Acute phase plasma protefns durfng melancholfa 511
results. We have established hypotransferrlnemia and hyperhaptoglobinemfa In those patients who
were drug-free for more than 1 month before hospital admission. In addition, no significant differen-
ces in any of the APP levels were detected between subjects with and without benzodiazepine
therapy during the study period.
The results of the present study and those from our previous reports (q.v. Introduction) fit in weft
with the existence of an inflammation in some severefy depressed subjects. The classic sequence of
t~am~tion involves the foilawing phases (Kieesiek and veiling, 1984).
Flrst phase : formation of inflammatory humcxal factors and systemic Immune actfvation. Evidence
for this step is provided by our findlngs of the following changes in the immune system during
depression: monocytosis, increased if-18 production in cufture supernatant of mltogen-stimulated
peripheral blood leukocytes, presence of activated T cells, and Increased serum II-2-Rs (Maes et al.,
1991b. 1991c. 199le).
The second phase involves alteratfons in APP biosynthesis and degradation In hepatocytes, a
phenomenon which is reportedly linked to monocyte function. Indirect confirmation is offered by our
observation that monocytosis and hyperhaptoglobfnemia or hypotransferrinemia are Interrelated
phenomena.
The end result can become apparent in our severely depressed patfents: a higher express&n of
positive APPs (i.e. Hp, a,S), and a fall in plasma concentratfons of negative APPs (I.e. a$&, Tf).
Interestfngly. ex vivo immunosuppressfon as revealed by lymphocyte hyporesponsitivlty to mitogens is
a common hallmark of severe depression (Schleifer et al., 1984; 1985; Mae8 et al., 1989a) and an AP
response in inflammatory illnesses (Kushner. 1982).
However, the APP response indicates a reactionary process towards an injury without being
specffic to a particular aetiology. Consequently, the key questlon remains whether a local inflammato-
ry reaction exists during severe depression?
Another consideration is that both the AP response (Kushner. 1982) and severe depresslon are
characterfzed by similar endocrinologlcal (i.e. HPA and HPT-axis disorders, noradrenergic spllfover),
bfochemical (changes In L-Utahan rne~~isrn~, and imrnun~~~al (lower mit~n-induced
~ast~esfs) markers. As a result, future research should conskfer the possibilfty that estabfished
enckxzrinofoglcal, biochemical, and immune markers of depressfon may constitute eplphenomena of
AP responses during that illness.
AMERICAN PSYCHIATRIC ASSOCIATION (1980) Diagnostic and Statistfcal Manual of Mental Disorders, 3rd ed. American Psychiatric Association, Washington. D.C.
BAUMANN, H., RICHARDS. C. and GAULDIE. J. (t987) Interaction among hepatocyte-stimulating
512 M. Maes et at.
factors, interleukin 1, and glucocorticoids for regulation of acute phase plasma protelns in human hepatoma (HepG2) cells. J. Immunol. j.5: 4122-4128.
BAUMANN, H. and GAULDIE. J. (1990) Regulation of hepatlc acute phase plasma protein genes by hepatocyte stimulating factors and other mediators of lnflammatlon. Mol. Blot Med. 1: 147-l 59.
BERNINGER. R.W. (1986) Alpha-1-antitrypsin. In: Reviews of Hematology, Volume II, 0. Murano (Ed.), pp 22-100. PJD Publications, Westbury.
BEUSCHER. H.U.. FALLON, R.J. and COLTEN, H.R. (1987) Macrophage membrane Interleukln-1 regulates the expression of acute phase proteins In human hepatoma Hep 38 cells. J. lmmunol QS: 1896-1901.
BRUGUEROLLE. B.. BOUVENOT. G.. ARNAUD, C., LEW, F., MECHKOURI. M., BARTOLIN, R. and PERONNE. R. (1986) Circadian rhythms of the so-called inflammatlon proteins in healthy subjects. Revue du Rhumatisme et des Maladles Osteo-Articulaires m: 313-316.
CARROLL, B.J. (1980) Clinical application of neuroendocrine research in depression. In: Handbook of Biological Psychiatry, Part Ill. M.H. van Praag. M.H. Lader, O.J. Rafaelsen and E.J. Sachar (Eds.), pp 179-193. Marcel Dekker. New York.
CASTELL. J.V., GOMEZ-LECHON. M.J.. DAVID, M., HIRANO. T., KISHIMOTO. T. and HEINRICH. PC. (1988) Recombinant human interleukln-6 (II-G/BSF-2/HSF)regulates the synthesis of acute phase proteins in human hepatocytes. FEBS Letters a: 347-350.
CASTELL, J.V.. GOMEZ-LECHON, M.J.. DAVID, M.. ANDUS, T.. GEIGER, T., TRUUENQUE. R.. FABRA, R. and HEINRICH. P.C. (1989) Interleukln-6 Is the major regulator of acute phase proteln synthesis in adult human hepatocytes. FEBS Letters 242: 237-239.
COOPER, N.R. (1987) The complement system. In: Basic and Clinical Immunology. D.P. Stites, J.D. Stobo and J.V. Wells (Eds.),pp 114-l 27. Prentice-Hall, New York.
DAS. I. (1965) Raised C-reactive protein levels in serum from smokers. Clin. Chlm. Acta m: 9-13.
DEBERDT. R., VAN HOOREN, J.. BIESBROUK, M. and AMERY, W. (1976) Antinuclear factor positivity In mental depression: a single disease entity? Biol. Psychiatry 11: 69-74.
DE JONG. G., VAN DIJK. J.P. and VAN EIJK. H.G. (1990) Critical review: the biology of transferrin. Clin. Chim. Acta 19p: l-46.
DOMINIONI. L. and DIONIGI. R. (1987) Immunological function and nutritional assessment. Japanese J. Parent. Ent. Nutr. 11: 709-72s.
ENGLER. R. (1988) Proteins of the inflammatory reactlon. Regulatory functions. Ann. Blot Clin. Pads 46: 336-342.
FAYMONVILLE, M.E., MICHEELS. J., BODSON, L., JACQUEMIN. D., LAMY, M.. ADAM, J. and DUCHATEAU. J. (1987) Biochemical investlgatlons after burnlng injury : complement system, protease-antiprotease balance and acute-phase reactants. Burns Incl. Therm. Inj. l;i: 26-33.
FLECK, A. (1989) Clinfcal and nutritional aspects of changes In acute-phase proteins durlng inflammation. Proc. NUV. Sot. 46: 347-354.
FRIES, L.F. and FRANK, M.M. (1966) Complement and related protelns. In: lrtflammatlon : Basic Prlnclples and Cllnlcal Correlates, J.I. Gallln, I.M. Goldsteln and R. Snyderman (Eds.), pp 89-100. Raven, New York.
FUJITA, K., HIRANO, M., OCHIAI, J., FUNABASHI, M.. NAGATSU, I., NAGATSU, T. and SAKAKIBARA, S. (1978) Serum glycylproline p-nltroanllldase actlvlty In rheumatold arthritfs and systemic lupus erythematosus. Clln. Chem. @: 15-20.
GAULDIE. J., LAMONTAGNE, L. and STADNYK. N. (1985) Acute phase response in infectious disease. Survey Synth. Pathol. Res. 4: 126-151.
GERSHENWALD, J.E.. FONG, Y.M., FAHEY, T.J., CALVANO, S.E., CHIZZONITE, R., KILIAN, P.L., LOWRY, S.F. and MOLDAWER, L.L. (1990) lnterleukln 1 receptor blockade attenuates the host inflammatory response. Proc. Nat. Acad. Sciences USA m: 4966-4970.
GOLDMAN, N.D. and LIU. T.Y. (1967) Biosynthesis of human C-reactive protein In cultured hepatoma
Acute phase plasma proteins during meisncholla 513
cells is induced by a monocyte factor(s) other than Interleukln-1. J. Blot Chem. fi: 2363-2368.
HAMILTON, ht. (1980) A rating scale for depression. J. Neurol. Neurosurg. Psychiatry B: 58-82.
HEINRICH, P.C.. CASTE& J.V. and ANDUS. T. (19wf) Review article: interleuklnd and the acute phase response. B&hem. J. 265: 621836.
IRWIN, M. (1988) Depression and Immune function. Stress Med. 4: 95-103.
IRWIN, M.. PATTERSON. T.. SMITH, T.L., CALDWELL, C.. BROWN, S.A.. GILLIN, J.C. and GRANT, I. (1990) Reduction of immune function in life stress and depresalon. B1d. Psychiatry a: 22-30.
KEYSER, J.W. (1979) Human Plasma Proteins: Thefr ln~d~~ In Pamological Condldons. In: J.W. Keyser (Ed.), John Wiley and Sons, New York.
KtASING, KC. (1988) Nutrltional aspects of leukocytfc cytokines. J. Nub. m: 14381448.
KLEESIEK, K. and GREILING, H. (1984) Pathoblochemlcal mechankms during the acute phase response. Int. J. Mlcroclrc. Clln. Exp. 9: 131-145.
KREMER, J.M.H., WILTING, J. and JANSSEN. L.H.M. (1988) Drug Mnding to human alpha-l-acid glycoprotein In frealth and disease. Pharm. Rev. 4p: l-47.
KRONFOL. t. and HOUSE, D.J. (1985) Depreaskx~ ~alarnk~~~~~ actlvtty and lymphocyte functton. Psychopharmacol. Bull. 22: 478.479.
KRONFOL, 2.. HOUSE, D.J.. SILVA, J.Jr., GREDEN, J. and CARROLL, B.J. (1988) Depression, urlnary free cortlsol excretion and lymphocyte function. Brlt. J. Psychiatry 148: 70-73.
KUSHNER, I. (1982) The phenomenon of the acute phase response. In: C-Reactive Proteln and the Plasma Protein Response to Tissue Injury. I. Kushner, J.E. Volanakls and H. Gewurz (Eds.), pp 39 48. The New York Academy of Sctences, New York.
LAPADULA, G. and NUMO, R. (1987) The acute phase protein profile In inflammatory arthropathies. Stand. J. Rheumatol. Suppl. @j: 90-93.
LAURELL. C-B. and JEPPSSON, J.-O. (1975) Protease Inhibitors in plasma. In: The Plasma Proteins: Structure, Function,.and Genetic Control (Volume I) F.W. Putnam (Ed.), pp 229-285. Academic Press, New York.
MACKIEWICZ. A., GANAPATHI, M.K., SCHULTZ, D., SAMOLS, D., REESE, J. and KUSHNER, I. (1988) Regulation of rabbft acute phase protein Wosynsthesis by monoklnes. Blochem. J. m: 851-857.
MAES. M., De RUYTER, M., HOBIN. P. and SUY. E. (1988) The dexamethasone suppression test, the Hamilton Depression Ratlng Scale and the DSM-III categories. J. Affect. Dlsord. 1p: 207-214.
MAW M., BOSMANS, E., SUY. E.. MINNER. B. and RAUS. J. (lQ89a) Impaired lymphocyte stimulation by mitogens in severely depressed patlents. A complex interface with HPA-axis hyperfunction, noradrenerglc actfvfty and the agelng process. Brlt. J. Psychiatry m: 793-798.
MAES, M., VANDEWOUDE. M., SCHOTTE, C, and COSYNS, P. (1989b) Results of the 8 a.m. dexamethasone suppression test constttute a s&able tool for conftrming the diagnosk of melancholia: a test unaffected by the vartatfons in the MoavaltaMlity of dexamethasone. Neuropsy- chobiol. 2: 2832.
MAES. M., COSYNS. P., MAES, L. D’HONDT, P. and SCHOTTE. C. (r9QOa) Clinical subtypes of unlpolar depression, part I : a validation of the vltal and non-vltal clusters. Psychlatr. Res. &t : 29-41.
MAES, M., SCHOTTE, C., MAES, L. and COSYNS, P. (199Ob) Cftnkal subtypes of unlpotar depression, part II : D~n~8~ and qualftabve cllnlcal differences between the v&al and non-v&al defxession soups Psychlatr. Res. ;F4, 43-57.
MAES, M., MAES, L.. SCHOTTE, C., VANDEWOUDE, M., MARTIN, M., D’HONDT, P., BLDCKX, P., SCHARPE, S. and COSYNS, P. (1990~) Clinical subtypes of unlpolar dapresslon. part Ill : Quantltative dtfferences In varlous M~ical markers between the cluster analysis-generated non- vital and vital depresslon classes. Psychiatr. Res. ;i?l: 59-75.
MAES, M., BOSMANS, E., SUY, E., MINNER, 8. and RAUS, J. (199la) A further exploration of the
514 M. Maes et at.
relationships between immune parameters and the HPA-axis activity in depressed inpatients. Psychol. Med. 21: 313-320.
MAES. M., BOBMANS. E.. SUY, E.. VANDERVORST, C.. DEJONCKHEERE, C., MINNER, B. and RAUS, J. (1991 b) Depression-related disturbances in mitogen-Induced lymphocyte responses, interleukin-l-6, and soluble interleukin-2-receptor production. Acta Psychiatr. Stand. (in press).
MAES. M., BOSMANS. E.. SUY, E., VANDERVORST, C., DEJ0NCKHEERE.C. and RAUS, J. (1991c) Antlphosphoilpid, anti-nuclear. Epsteln-Barr and cytomegalovirus antibodies, and solubie Interleukln- 2 receptors in depressive patients. J. Affect. Disord. 21: 133-140.
MAES. M.. DE MEESTER. I., VANHOOF, G., SCHARPE. S., BOSMANS, E., VANDERVORST, C.. VERKERK. R., MINNER, B., SUY. E. and RAUS, J. (199ld) Decreased serum dipeptidyl peptldase IV activity in major depression. Bloi. Psychiatry. (in press).
MAES, M.. LAMBRECHTS. J.. BOSMANS. E.. JACOBS, J., SUY. E., VANDERVORST. C., DEJONCKHEERE,C., MINNER, 8. and RAUS. J. (1991e) Evidence for a systemic immune acttvation during depression: results of leukocyte‘enu&ation by flow cytometry in conjuction with monocional antibody staining. Psychd. Med. (in press).
MARINKOVIC. S.. JAHREIS. G.P.. WONG. G.G. and BAUMANN, H.(1989) Ii-6 modulates the synthesis of a specific set of acute phase plasma proteins In vivo. J. Immunoi. j&?: 808-812.
MILMAN, N.. GRAUDAL. N. and ANDERSEN, H.C. (1988) Acute phase reactants in the elderly. Ciin Chim. Acta. m: 59-62.
MOSSMAN. D. and SOMOZA. E. (1989) Assessing improvements in the dexamethasone suppression test using receiver operating characteristic analysis. 8101. Psychiatry. 25: 159-173.
MULLER-EBERHARD. H.J. (1975) The complement system. In: The Plasma Proteins: Structure, Function and Genetic Control. F.W. Putnam (Ed.), pp 394432. Academic Press, New York.
PROWSE. K.R. and BAUMANN, H. (1989) Interleukin-1 and interleukln-6 stimulate acute-phase protein production in primary mouse hepatocytes. J. Leukocyte Biol. s: 55-61.
PULLICINO, E:A.. CARLI. F., POOLE, S.. RAFFERTY, B., MALIK, S.T. and ELIA, M. (1990) The relationship between the circulating concentrations of interleukin-6 (k-6), tumor necrosis factor (TNF) and the acute phase response to elective surgery and accidental Injury. Lymphoklne Res. 9: 231-238.
PUTNAM, F.W. (1975a) Perspectives-Past, Present en Future. in: The Plasma Proteins: Structure, Function, and Genetic Control (Volume I). F.W. Pumam (Ed.), pp 2-67. Academic Press, New York.
PUTNAM, F.W. (1975b) Alpha, beta, gamma, omega-the roster of the plasma protelns. In: The Plasma Proteins: Structure, Function, and Genetic Control (Volume I), F.W. Putnam (Ed.), pp 58-125. Academic Press, New York.
PUTNAM, F.W. (1975~) Haptoglobtn. In: The Plasma Protelns: Structure, Function and Genetic Control (Volume II). F.W. Putnam (Ed.), pp 2-51. Academic Press, New York.
PUTNAM, F.W. (1975d) Transferrin. in: The Plasma Proteins: Structure, Function, and Genetic Control (Volume I). F.W. Putnam (Ed.). pp 266-317. Academic Press, New York.
ROBERTS, R.C. (1986) Alpha-2-macroglobulin. In: Reviews of Hematology, Volume II, G. Murano. (Ed.), pp 129-244. PJD Publications, Westbury.
ROITT. I.. BROSTOFF, J. and MALE, D.K. (1989) Immunology. Gower Medical Pubilshing, New-York.
ROMETTE. J.. DI-COSTANZO-DUFETEL,J. and CHARREL. M. (1986) Inflammatory syndrome and changes in plasma proteins. Pathol. Biol. (Pads), a: 1006-1012.
ROSS, S.C. and DENSEN. P. (1984) Complement deficiency states and Infection: Epidemiology. pathogenesis and consequences of netsserial and other Infections In an immune deficiency. Med. 6.S: 243.
SANCHEZ, L., SOLARES, M.C.. ZOZAYA, J.M., MUNOZ. M. and LISO, P. (1988) Acute phase reaction after inflammatory Injury. Experimental study. Rev. Med. Unlversidad Navarra. a: 47-50.
SCHLEIFER. S.J.. KELLER, S.E.. MEYERSON. A.T., RASKIN, M.J.. DAVIS, K.L. and STEIN, M. (1984)
Acute phase plasma proteins during melancholta 515
Lymphocyte function in major depressive disorder. Arch. Gen. Psychiatry 41: 484-486.
SCHLEIFER, S.J., KELLER, S.E., SIRIS, S.G., DAVIS, K.L. and STEIN, M. (1985) Depresslon and Immunity : lymphocyte function in-ambulatory depressed pattents, hospitalized schizophrenic patients, and patients hospltallzed for hernlorrhaphy. Arch. Gen. Psychiatry 92: 124133.
SCHMID, K. (1975) a,-Acid glycoprotein. In: The Plasma Protelns: Structure, Function, and Genetic Control (Volume 1). F.W. Putnam (Ed.), pp 184-228. Academic Press, New York.
SPITZER. R.L.. WILLIAMS, J.B.W. and GIBBON, M. (1985) Structured Cllnlcal Interview for DSM-III Patient Version. Biometrics Research Department, New York State Psychiatric Institute, New York, NY.
STONE, B.A., KOOPERSMITH.T.B., QUINN, K., QUINN, P. and MARRS, R.P. (lB89) Levels of tnterleukin-2 receptor In serum of patients during the menstrual cycle and following embryo/gam- ete transfer. Am. J. Repr. Immunol. Microbial. 2p: 114-l 16.
TOGARI. H.. SUGIYAMA. S.. OGINO. T.. SUZUKI, S.. ITO. T., ICHIKI. T.. KAMIYA. K.. WATANABE, I.. OGAWA. Y. and WADA. Y. (1986) Interactions of endotoxln with cortlsol and acute phase proteins in septic shock neonates. Acta Paed. Stand. B: 69-74.
VAN VUGT, H.. VAN GOOL. J. and DEUTZ. N.E. (1988) Fever and acute phase reactants In the rat. Brit. J. Exp. Pathol. 69: 577588.
VOITKO. NE. and IATSYSHINA. T.A. (1985) Determination of acute-Inflammatory-phase proteins in the blood serum of volunteers consuming diets with various protein levels consisting of optlmum protein constituents. Voprosy Pltanlia. 1: 34-38.
Inquiries and reprint requests should be addressed to :
Dr. Michael Maes Dept. of Biological Psychiatry Case Western Reserve University 2040, Abington Road OHIO USA