distribution and correlates of total impaired fasting glucose in oman
TRANSCRIPT

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
Eastern Mediterranean Health Journal, Vol. 9, No. 3, 2003 377
Distribution and correlates of totalimpaired fasting glucose in OmanA.A. Al-Riyami1 and M. Afifi1
1Department of Research and Studies, Ministry of Health, Muscat, Oman.Received: 10/02/02; accepted: 06/08/02
ABSTRACT To determine the distribution and correlates of total impaired fasting glucose in Oman, weconducted a cross-sectional survey of 1968 households with 7011 eligible residents in 2000. During face-to-face interviews, demographic data, blood pressure, fasting blood glucose, serum cholesterol, weight, heightand waist and hip measurements were obtained. Of 5788 subjects tested for total impaired fasting glucose(response rate: 83%), crude prevalence was 17.3% and age-adjusted prevalence was 20.3%. Associatedfactors in bivariate analysis were older age, male gender, lower education, hypercholesterolaemia, beingmarried, obesity, abnormal waist to hip ratio and hypertension. Total impaired fasting glucose is a significantpublic health problem in Oman. Increasing the awareness of health care providers and community throughhealth education is crucial.
Distribution et corrélats de l’intolérance au glucose et de la glycémie à jeun anormale à OmanRESUME Pour déterminer la distribution et les corrélats de l’intolérance au glucose et de la glycémie à jeunanormale à Oman, nous avons réalisé une enquête transversale auprès de 1968 ménages composés de7011 résidents éligibles en 2000. Au cours d’entretiens face à face, on a recueilli des donnéesdémographiques, effectué des mesures de la pression artérielle, de la glycémie à jeun, du cholestérolsérique, du poids, de la taille, du tour de taille et du tour de hanches. Chez les 5788 sujets testés pourl’intolérance au glucose et la glycémie à jeun anormale (taux de réponse : 83 %), la prévalence brute s’élevaità 17,3 % et la prévalence ajustée selon l’âge était de 20,3 %. Les facteurs associés dans l’analyse bivariéeétait l’âge plus élevé, le sexe masculin, le niveau d’instruction plus bas, l’hypercholestérolémie, le fait d’êtremarié, l’obésité, le rapport tour de taille/tour de hanches anormal et l’hypertension. L’intolérance au glucoseet la glycémie à jeun anormale représentent un problème important de santé publique à Oman. Lasensibilisation des prestataires de soins de santé et de la communauté par l’éducation sanitaire est cruciale.
ȷǠȶłȝ Ž ȨɅȀȱǟ ɂȲȝ ȳǼȱǟ ȀȮȅ ȰȲǹ ǧɍǠǵ Ȱȶƭ ȔǣǟȀǩȿ țȁɀǩɄȵǠɅȀȱǟ ǦɆȅǓÛɄȦɆȦȝ ɂȦȖȎȵ
ƪǟǦøȍɎ:ȷǠȶłȝ Ž ȨɅȀȱǟ ɂȲȝ ȀȮȆȱǟ ȰȲǹ ǧɍǠǵ Ȱȶƭ țŊȁɀǩ ȀɅǼȪǪȱÛȰƽ DŽǠȑȀȞǪȆȵ DŽǠǶȆȵ ǠȺɅȀDZǕ1968ȷǠȮȆȱǟ ȸȵȿ7011ȳǠȝ ȷǠȶłȝ Ž ƙȶɆȪƫǟ ȸȵ2000ÛȶȒǩȿȃǠɆȩȿ ǦɆȥǟȀȢƹǻ ǧǠɆȖȞȵ ɂȲȝ ȯɀȎƩǟȿ ǦɆȎǺȉ ǧɎǣǠȪȵ ǒǟȀDZǙ ǴȆƫǟ ȸ
ȏɀƩǟȿ ȀȎƪǟ ȔɆƮȿ ȯɀȖȱǟȿ ȷȁɀȱǟȿ ȰȎƫǟ ȯȿȀǪȆɆȱɀȭȿ ȨɅȀȱǟ ɂȲȝ ȳǼȱǟ ȀȮȅȿ ȳǼȱǟ ȔȢȑ.ǧǟǿǠǤǪǹɍǟ ǻǼȝ ȠȲǣ ǼȩȿȨɅȀȱǟ ɂȲȝ ȳǼȱǟ ȀȮȅ ȃǠɆȪȱ ǥǟȀŎǟ5788)ǦǣǠDzǪȅǟ ǦǤȆȹ ȰƍǮƢȿ83(%ǟ ȀȮȅ ȰȲǹ ǿǠȊǪȹǟ ȯǼȞȵ ȷǠȭǠȾɆȥ ȳǼȱ17.3%Û
ȀȶȞȲȱ DŽǠȪȥȿ ǴʼnǶȎƫǟ ǿǠȊǪȹɍǟ ȯǼȞȵ ȷǠȭ ƙǵ Ž20.3.%ȳŊǼȪǪȱǟ ɄȽ ȰȵǟɀȞȱǟ ɄǝǠȺǮȱǟ ȰɆȲǶǪȱǟ Ž ǦǤǵǠȎǪƫǟ ȰȵǟɀȞȱǟ ǨȹǠȭȿȀȶȞȱǟ ŽÛǥǿɀȭǾȱǟÛȴɆȲȞǪȱǟ ɁɀǪȆȵ ȏǠȦƳǟÛȳǼȱǟ ȯȿȀǪȆȱɀȭ ȓȀȥÛǯǟȿȂȱǟÛǦȹǟǼǤȱǟÛȏɀƩǟ ƂǙ ȀȎƪǟ ǦǤȆȹ ȯɎǪǹǟÛ
ȳǼȱǟ ȔȢȑ țǠȦǩǿǟȿ.Ž ǦɆȵɀȶȞȱǟ ǦǶȎȱǟ Ž ǦȵǠƬǟ ǧɎȮȊƫǟ ǼǵǕ ŊǼŁȞłɅ ȨɅȀȱǟ ɂȲȝ ȳǼȱǟ ȀȮȅ ȰȲǹ ȷǕ ǦȅǟǿǼȱǟ ȸȵ ȸʼnɆǤǪɅȿȳǠȽ ȀȵǕ ɄǶȎȱǟ ȤɆȪǮǪȱǠǣ ǦɆǶȎȱǟ ǦɅǠȝȀȱǟ ǒǠǪɅǙ ɂȲȝ ƙȶǝǠȪȱǟ ɁǼȱȿ ȜȶǪŎǟ ɁǼȱ Ʉȝɀȱǟ ɁɀǪȆȵ Ȝȥǿ ȷǕȿ ÜȷǠȶłȝ.
18 Distribution and correlates.p65 20/09/25, 09:23 ã377

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
378 La Revue de Santé de la Méditerranée orientale, Vol. 9, NO 3, 2003
Introduction
Social advances in Oman since 1970 havebeen accompanied by cultural changes, areduced incidence of communicable disea-ses, increased life expectancy, changes innutritional habits and habitual physicalactivity, and an increased incidence ofnoncommunicable diseases such as hyper-tension and diabetes [1]. Development ofdiabetes mellitus, in particular, is associatedwith increased mortality and a high risk ofdeveloping vascular, renal, retinal and neu-ropathic complications leading to pre-mature disability and death.
In a study from 1 January 1991 to 31July 1991, adult diabetes in the generalpopulation of Oman was surveyed to esti-mate the prevalence of and associationsbetween diabetes, impaired glucose tole-rance, hyperlipidaemia, obesity and hyper-tension. Using the American DiabeticAssociation 1997 criteria, the prevalence ofdiabetes and impaired glucose tolerance for4682 persons aged 20 years or older was8.3% and 5.7% respectively, or a totalprevalence of 14.0% [2].
McCarty and Zimmet [3] projected anincrease of 189% in diabetes prevalence inOman between 1994 and 2010. King et al.[4] projected a 30% increase in diabetesprevalence in the Middle East crescent andan approximate 14% increase in Omanbetween 1995 and 2025.
The aim of our study was to estimatethe distribution and study the correlates oftotal impaired fasting glucose, i.e. diabetesmellitus and impaired fasting glycaemia, ina community-based survey as a part of theOman National Health Survey, 2000.
Methods
SampleThe survey sample was selected to reflectas closely as possible the national situation.The survey adopted a multi-stage, stratifiedprobability-sampling design. All 10 regionsof the Sultanate were sampled propor-tionally, with one or more wilayat, ordistricts, depending on population chosenrandomly from each region and resulting inthe selection of 16 of 59 wilayat nationally.Each wilayat was classified as either urban(major population centres) or rural (villagesor remote areas). The urban to rural ratio of2:1 was similar to that of the 1993 nationalcensus.
In the second stage of study design,enumeration areas within each stratumwere randomly selected. Enumerationareas were defined during the 1993 popu-lation census and each contains approxi-mately 80 households. In the third stage,households were selected within eachenumeration area. Maps of the selectedenumeration areas were updated and acomplete list of Omani households in eachwas made to obtain the sampling frame.Households were then randomly selected.All subjects aged 20 years or older in theselected households were invited to par-ticipate in the survey.
The total number of households selec-ted was 1968 in which 7011 subjects metselection criteria. The response rate variedfrom 83% to 91% according to the type ofmeasurement or laboratory investigationcompleted. Of 7011 eligible subjects, 5788(83%) completed the questionnaire, hadblood drawn for fasting blood glucose,
18 Distribution and correlates.p65 20/09/25, 09:23 ã378

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
Eastern Mediterranean Health Journal, Vol. 9, No. 3, 2003 379
completed most measurements and labo-ratory investigations and had their dataanalysed for total impaired fasting glucose.
Questionnaire and measurementsOur household health status questionnairecovered demographic data such as age,sex, marital, educational and employmentstatus and self-reporting of diabetes mel-litus, hypertension and smoking habits.World Health Organization (WHO) pro-cedures [5] were used to measure bloodpressure, weight, height and waist and hipcircumference. The questionnaire alsocovered the results of laboratory inves-tigations for fasting blood glucose andserum cholesterol levels.
Specimen collection and analysisFor specimen collection and analysis, 25teams were assembled and trained in themethodology of the survey for 2 weeks.Each team consisted of a nurse to takemeasurements, a laboratory technician todraw samples, a health educator to inter-view subjects, a health inspector to trans-port laboratory samples and a fieldsupervisor (statistician) to supervise andreview the questionnaires in the field.
Eligible members in selected householdswere requested to commence fasting 1–2hours before midnight the night before theywere to be visited by the survey team. At07:00 the following morning, householdmembers were interviewed and measuredand venous fasting blood glucose sampleswere collected. Fasting blood samples forglucose were collected in sodium fluoridepotassium oxalate tubes, labelled and trans-ferred immediately with laboratory formsto the laboratory at the wilayat hospital incold boxes. Samples were immediatelycentrifuged, the plasma was separated andfasting plasma glucose was determined by
a glucose oxidase method on the same dayusing a Hitachi 911 automated clinicalchemistry analyser (Hitachi 911 analyserand reagents supplied by Boehringer Man-nheim, Roche Diagnostics, Dubai, UnitedArab Emirates). Samples for estimation ofcholesterol were collected in tubes con-taining lithium heparin anticoagulants andtransferred to the laboratory. At the labora-tory, investigations were performed withthe enzymatic colorimetric method usingthe same Hitachi 911 automated clinicalchemistry analyser.
Diagnostic criteriaWHO criteria were used for the diagnosisof hypertension, hypercholesterolaemia,anthropometric measurements and glucoseintolerance [6].
Patients who self-reported hypertensionwere categorized as having diastolic hyper-tension even if their blood pressure readingat the time of screening was normal only ifthe interviewer either sighted their medi-cation or verified that the subject had beendiagnosed by a medical practitioner. Pa-tients were also categorized as havingdiastolic hypertension if the mean of twoblood pressure (BP) readings was≥ 90 mmHg diastolic phase 5, regardless ofsystolic BP. Hypertensive subjects werefurther classified in the logistic regressionmodels as having mild hypertension (dias-tolic BP 90-104 mmHg) or moderate/severe hypertension (diastolic BP ≥ 105mmHg).
Patients were categorized as havinghypercholesterolaemia if their totalcholesterol reading was ≥ 5.2 mmol/L or≥ 200 mg/dL.
Body mass index (BMI = weight (kg)/height2 (m2)) was classified according toaccepted norms: underweight (BMI < 18.5kg/m2), normal (18.5–24.9 kg/m2), over-
18 Distribution and correlates.p65 20/09/25, 09:23 ã379

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
380 La Revue de Santé de la Méditerranée orientale, Vol. 9, NO 3, 2003
weight (25.0–29.9 kg/m2), obese (30.0–39.9 kg/m2) and morbidly obese (≥ 40.0kg/m2).
Abnormal waist to hip ratio (WHR)measurements, or central obesity, were≥ 0.85 for females and ≥ 0.95 for males.
Subjects were classified as having im-paired fasting glycaemia with fasting bloodglucose ≥ 6.1–6.9 mmol/L and diabetesmellitus if they self-reported diabetesmellitus or had fasting blood glucose ≥ 7.0mmol/L. Total impaired fasting glucosewas calculated by adding the two groups.
Data processing and analysisData were entered using Epi-Info version6.04. The process of preparing the data filewas completed by July 2000. Data wereanalysed using SPSS version 9.0. Datawere given as counts, means and per-centages. Variance among the group meanswere analysed (ANOVA) and the dist-ribution of data using the likelihood ratiowas examined with the chi-squared test.Step-wise logistic regression tested forfactors most strongly associated with thestudied dependent variables and to obtainthe adjusted odds ratios (OR) for thesefactors. All independent variables used inthe logistic models were dichotomous(after recoding some). P-value < 0.05 wassignificant.
Results
A crude prevalence of total impaired fastingglucose of 17.3% in the total sample ofsubjects aged 20-120 years was obtainedby summing the percentage of diabetesmellitus cases (crude prevalence = 11.2%)and the impaired fasting glucose cases(crude prevalence = 6.1%). Using the Segistandard world population [7], the totalimpaired fasting glucose age-adjusted pre-
Table 1 Demographic and socialcharacteristics of subjects
Characteristic No. %
Age group (years)
20–39 4353 62.1
40–59 1753 25.0
≥ 60 905 12.9
Total 7011 100.0
Sex
Male 3506 50.0
Female 3505 50.0
Total 7011 100.0
Residence
Urban 5143 73.4
Rural 1868 26.4
Total 7011 100.0
Education
Illiterate 2333 33.8
< Secondary 2824 40.9
≥ Secondary 1753 25.3
Total 6910 100.0
Employment status
Working 2778 39.9
Not working 4191 60.1
Total 6969 100.0
Marital status
Married 4668 66.7
Not married 2327 33.3
Total 6995 100.0
Family size
≤ 10 members 3696 52.7
> 10 members 3315 47.3
Total 7011 100.0
Current smoking
Yes 488 7.0
No 6515 93.0
Total 7003 100.0
18 Distribution and correlates.p65 20/09/25, 09:23 ã380
ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
Eastern Mediterranean Health Journal, Vol. 9, No. 3, 2003 381
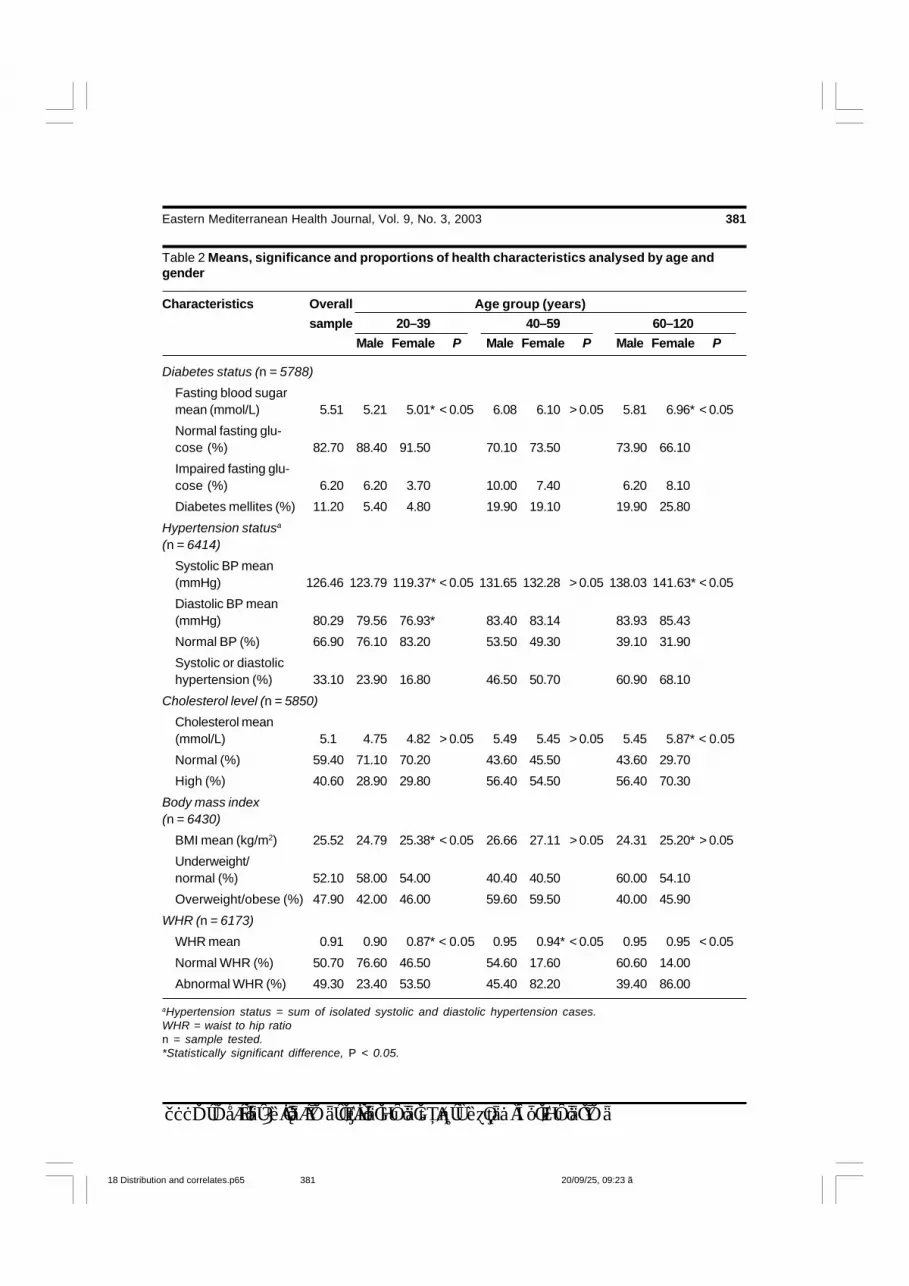
Table 2 Means, significance and proportions of health characteristics analysed by age andgender
Characteristics Overall Age group (years)
sample 20–39 40–59 60–120
Male Female P Male Female P Male Female P
Diabetes status (n = 5788)
Fasting blood sugarmean (mmol/L) 5.51 5.21 5.01* < 0.05 6.08 6.10 > 0.05 5.81 6.96* < 0.05
Normal fasting glu-cose (%) 82.70 88.40 91.50 70.10 73.50 73.90 66.10
Impaired fasting glu-cose (%) 6.20 6.20 3.70 10.00 7.40 6.20 8.10
Diabetes mellites (%) 11.20 5.40 4.80 19.90 19.10 19.90 25.80
Hypertension statusa
(n = 6414)
Systolic BP mean(mmHg) 126.46 123.79 119.37* < 0.05 131.65 132.28 > 0.05 138.03 141.63* < 0.05
Diastolic BP mean(mmHg) 80.29 79.56 76.93* 83.40 83.14 83.93 85.43
Normal BP (%) 66.90 76.10 83.20 53.50 49.30 39.10 31.90
Systolic or diastolichypertension (%) 33.10 23.90 16.80 46.50 50.70 60.90 68.10
Cholesterol level (n = 5850)
Cholesterol mean(mmol/L) 5.1 4.75 4.82 > 0.05 5.49 5.45 > 0.05 5.45 5.87* < 0.05
Normal (%) 59.40 71.10 70.20 43.60 45.50 43.60 29.70
High (%) 40.60 28.90 29.80 56.40 54.50 56.40 70.30
Body mass index(n = 6430)
BMI mean (kg/m2) 25.52 24.79 25.38* < 0.05 26.66 27.11 > 0.05 24.31 25.20* > 0.05
Underweight/normal (%) 52.10 58.00 54.00 40.40 40.50 60.00 54.10
Overweight/obese (%) 47.90 42.00 46.00 59.60 59.50 40.00 45.90
WHR (n = 6173)
WHR mean 0.91 0.90 0.87* < 0.05 0.95 0.94* < 0.05 0.95 0.95 < 0.05
Normal WHR (%) 50.70 76.60 46.50 54.60 17.60 60.60 14.00
Abnormal WHR (%) 49.30 23.40 53.50 45.40 82.20 39.40 86.00
aHypertension status = sum of isolated systolic and diastolic hypertension cases.WHR = waist to hip ration = sample tested.*Statistically significant difference, P < 0.05.
18 Distribution and correlates.p65 20/09/25, 09:23 ã381
ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
382 La Revue de Santé de la Méditerranée orientale, Vol. 9, NO 3, 2003
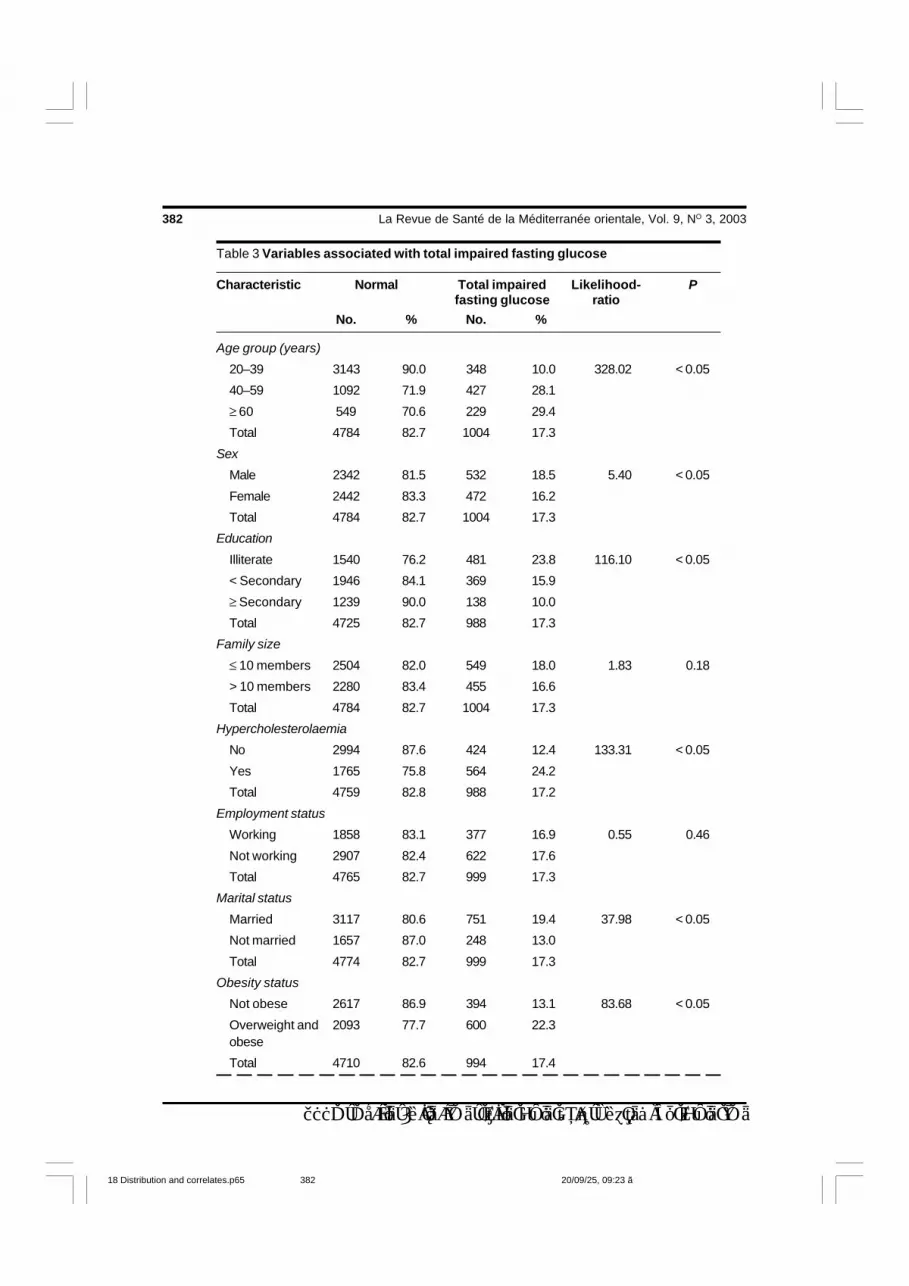
Table 3 Variables associated with total impaired fasting glucose
Characteristic Normal Total impaired Likelihood- Pfasting glucose ratio
No. % No. %
Age group (years)
20–39 3143 90.0 348 10.0 328.02 < 0.05
40–59 1092 71.9 427 28.1
≥ 60 549 70.6 229 29.4
Total 4784 82.7 1004 17.3
Sex
Male 2342 81.5 532 18.5 5.40 < 0.05
Female 2442 83.3 472 16.2
Total 4784 82.7 1004 17.3
Education
Illiterate 1540 76.2 481 23.8 116.10 < 0.05
< Secondary 1946 84.1 369 15.9
≥ Secondary 1239 90.0 138 10.0
Total 4725 82.7 988 17.3
Family size
≤ 10 members 2504 82.0 549 18.0 1.83 0.18
> 10 members 2280 83.4 455 16.6
Total 4784 82.7 1004 17.3
Hypercholesterolaemia
No 2994 87.6 424 12.4 133.31 < 0.05
Yes 1765 75.8 564 24.2
Total 4759 82.8 988 17.2
Employment status
Working 1858 83.1 377 16.9 0.55 0.46
Not working 2907 82.4 622 17.6
Total 4765 82.7 999 17.3
Marital status
Married 3117 80.6 751 19.4 37.98 < 0.05
Not married 1657 87.0 248 13.0
Total 4774 82.7 999 17.3
Obesity status
Not obese 2617 86.9 394 13.1 83.68 < 0.05
Overweight and 2093 77.7 600 22.3obese
Total 4710 82.6 994 17.4
18 Distribution and correlates.p65 20/09/25, 09:23 ã382

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
Eastern Mediterranean Health Journal, Vol. 9, No. 3, 2003 383
valence for the overall sample within 5-yearbands in the truncated age range of 20-89years was 20.3% (21.3% for males and19.3% for females).
Table 1 shows subjects’ demographicand social characteristics. Males and fe-males were equally represented, the majo-rity (62.1%) were between 20 and 39 yearsof age, 73% lived in rural areas, approxi-mately 34% were illiterate and 7% weresmokers.
Table 2 shows the mean and proportionof selected characteristics of the sampleaccording to age group and gender. Chi-squared test and ANOVA for comparison ofmeans were used to determine the signi-ficance of the results. The significantgender difference in most of the para-
meters in the youngest group was mar-kedly less apparent in the middle-agedgroup and re-emerged to a lesser extent inthe age group 60–120 years.
Table 3 shows selected characteristicsof subjects with total impaired fastingglucose. In bivariate analysis, older age,male gender, high cholesterol level, over-weight or obesity, abnormal WHR andsystolic or diastolic hypertension weresignificantly associated with higher rates oftotal impaired fasting glucose (P < 0.05).Being married (possibly because in Omanbeing unmarried is usually associated withbeing young, i.e. age is a confounder withmarital status) and illiteracy (in Oman oldersubjects are more likely to be illiterate)were also significantly associated with
Table 3 Variables associated with total impaired fasting glucose (concluded)
Characteristic Normal Total impaired Likelihood- Pfasting glucose ratio
No. % No. %
Waist to hip ratio
Normal 2427 87.1 358 12.9 76.60 < 0.05
Abnormal 2099 78.2 584 21.8
Total 4526 82.8 942 17.2
Hypertension
No 3329 87.6 472 12.4 189.40 < 0.05
Yes 1387 72.6 524 27.4
Total 4716 82.6 996 17.4
Current smoking
Yes 330 80.1 82 19.9 1.99 0.16
No 4451 82.9 920 17.1
Total 4781 82.7 1002 17.3
Residence
Urban 3531 82.8 735 17.2 0.15 0.69
Rural 1253 82.3 269 17.7
Total 4784 82.7 1004 17.3
Significant at P < 0.05.
18 Distribution and correlates.p65 20/09/25, 09:23 ã383

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
384 La Revue de Santé de la Méditerranée orientale, Vol. 9, NO 3, 2003
higher rates of total impaired fasting glu-cose (P < 0.05). There was no significantassociation between family size, workingstatus, current smoking, or urban or ruralresidence and total impaired fasting glucoserates (P > 0.05).
Table 4 shows the variables significant-ly associated with total impaired fastingglucose and with diabetes mellitus in themultiple logistic regression and OR in termsof the overall sample. (Marital status andeducation level were not included becauseof the age-related nature of these characte-ristics in Oman.) The OR for each variablewas adjusted for the other variables in themodel to account for confounding betweenthem. Some of the significantly associatedvariables, such as gender, cholesterol leveland abnormal WHR were binary. Agegroup, obesity and hypertension werecategorical. For example, relative to thereference age group of 20–39 years, theodds of having total impaired fasting glu-cose increased significantly for the agegroup aged = 60 years (OR = 2.53)compared to the age group 40–59 years(OR = 2.39). In terms of total impairedfasting glucose, for the hypertension varia-ble relative to the reference category(normotensive subjects), the significantincrease in OR was more apparent betweenthe moderately/severely hypertensivegroup (OR = 2.7) and the mildlyhypertensive group (OR = 1.64). Femalesex appeared to be a protective variableagainst total impaired fasting glucose afteradjustment for age and other variables(OR = 0.76). All variables significantlyassociated with total impaired fasting glu-cose were also significant for diabetesmellitus, except for sex.
Discussion
Despite the efforts of the Ministry of Healthto control the problem of increasing preva-lence of noncommunicable diseases, dia-betes and impaired fasting glucose ratescontinue to rise. Since 1991, a formaldiabetes control programme has been inplace. Specialist services for diabetics arenow available at the regional level, althoughpreviously they had been available only inthe major referral hospital in the capital,Muscat. In 1997, the Ministry initiated apilot primary prevention project in Nizwa,the old capital, in the hope of curbing therise in diabetes-associated mortality andmorbidity.
Between 1991 and 2000, the crudeprevalence of total impaired fasting glucoseincreased from 14.0% to 17.4%. Thismight be partially explained by the Neel‘thrifty genotype’ hypothesis or by a failureto adapt to relatively rapid environmentalchanges. In 2000 (the year of our study),the percentage of new and old cases ofdiabetics registered and treated in Ministryof Health institutions was 3.04% amongthose aged = 20 years [8]. Thus, projec-tions of the magnitude of the problem willbe underestimated if planners rely solely onhospital-based statistics.
Identifying the distribution and cor-relates of total impaired fasting glucose in acommunity-based study provides moreaccurate data about the magnitude of theproblem and its associated factors in re-gional settings. Primary health care doctorsand their patients can benefit greatly fromthe dissemination of data about factorssignificantly associated with total impairedfasting glucose. Doctors would be able to
18 Distribution and correlates.p65 20/09/25, 09:23 ã384

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
Eastern Mediterranean Health Journal, Vol. 9, No. 3, 2003 385
more accurately predict which patients areat greatest risk, thereby resulting in moreprompt investigations of at-risk patientsand improved management of patients withdiabetes. Widely disseminated, such infor-mation has the potential to prevent andreduce morbidity and mortality of diabetesat the primary health care level.
In our study, obesity, central obesity,high cholesterol, older age and presence ofhypertension were the common correlatesof total impaired fasting glucose and dia-betes mellitus in multivariate analysis in thelogistic regression models. Female genderwas significantly protective against totalimpaired fasting glucose, although not
Table 4 Variables significantly associated with total impaired fastingglucose according to multiple logistic regression for the overall sample
Variable Total impaired Diabetesfasting glucose mellitus
Adjusted ORa P Adjusted OR P
Age group (years)
20–39*
40–59 2.39 2.99
60–120 2.53 < 0.05 3.72 < 0.05
Hypercholesterolaemia
No = 0
Yes = 1 1.47 < 0.05 1.43 < 0.05
Obesity
Underweight or normal*
Overweight 1.48 1.63
Obese or morbidly obese 1.67 < 0.05 1.77 < 0.05
Gender
Male = 0
Female = 1 0.76 < 0.05 NS
Hypertension
Normotensive*
Mildly hypertensive 1.64 1.7
Moderately/severelyhypertensive 2.71 < 0.05 2.25 < 0.05
Waist to height ratio
Normal = 0
Abnormal = 1 1.36 < 0.05 1.39 < 0.05
aOR, or odds ratio, of each variable is adjusted for the other variables in the model.*Reference category.NS = not significant.
18 Distribution and correlates.p65 20/09/25, 09:23 ã385

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
386 La Revue de Santé de la Méditerranée orientale, Vol. 9, NO 3, 2003
against diabetes mellitus. Romero et al.found that age was strongly associatedwith diabetes prevalence with a chi-squared risk of 39.1 (P < 0.0001) [9]. Asignificant proportion (5.9%) of youngerindividuals (35–44 years of age) wasaffected by the disease. Diabetes wasassociated with advanced age, was morecommon among the low-income group andhad increased OR for hypertension,dyslipidaemia and myocardial infarction inboth men and women and for obesity inwomen only.
In Jamaica, 12.6% of 669 females haddiabetes compared with 7.8% of 649 males[10]. The same pattern was observed in theLibyan Arab Jamahiriya despite the lowprevalence of diabetes among adults aged20 years or older (3.8% for the overallsample, 4.7% in females and 2.9% inmales, P < 0.01) [11]. In our study, femalesex was protective for total impairedfasting glucose and was not significantlyassociated with diabetes mellitus.
These results differed from SouthAfrican data in which prevalence ofdiabetes in male and female workers (P =0.31) was similar and the highest incidencewas observed in the age group 40–59years. No subject under 40 years of agewas diabetic and the prevalence of thedisease increased with age. Impairedglucose tolerance was observed in 3.4% ofmale and 1.5% of female workersrespectively (P = 0.13) with the peakprevalence occurring among the age group30–49 years [12].
In South Africa, diabetes mellitus wasmore common in women (5.2% versus2.3% for males), although the reverse wastrue of impaired glucose tolerance (5.5%vs. 11.5% for males). The mean age-adjusted BMIs of diabetic (31.3 ± 1.9 kg/m2) and impaired glucose tolerant subjects
(29.7 ± 1.9 kg/m2) were significantlyhigher than those with normal glucosetolerance (28 ± 0.5 kg/m2). Femalesubjects with all types of glucose tolerancehad a significantly higher mean BMI thanmen. For women, there was a significantcorrelation between BMI and both fastingglucose (r = 0.16, P = 0.0039) and 2-hour plasma levels (r = 0.15, P =0.0065), although for men only the fastinglevels were similarly related (r = 0.21, P =0.01719) [13].
In another study, subjects with diabetesmellitus were significantly older (mean age50.7 years) than those with a normal glu-cose tolerance test result (mean age 30.9years), but of similar age distribution com-pared with the impaired glucose tolerancegroup (mean age 46 years). Subjects with anormal glucose tolerance test had asignificantly lower mean BMI (22.1 ± 2.8kg/m2) compared with diabetic subjects(26.1 ± 5.2 kg/m2) or the impaired glucosetolerance group (25.8 ± 6.6 kg/m2). Obesi-ty was commonly associated with bothdiabetes mellitus and impaired glucosetolerance, particularly among women [14].
In Finland, the prevalence of impairedglucose tolerance and diabetes increasedwith age more steeply among women thanmen [15]. In the Sudan, family history ofdiabetes, obesity and advanced age wereassociated with higher rates of diabetes[16].
In Tanzania, the overall age-adjustedprevalence of impaired glucose tolerancewas 21.5%, a little higher than the pre-valence of total impaired fasting glucose inour study (20.3%), but with almost thesame associated factors. Swai et al. re-ported a mean BMI of 24.3 kg/m2 and 26.4kg/m2 for males and females respectively,but with similar age-adjusted diabetes rates(7.0% and 7.6% respectively). Diabetes
18 Distribution and correlates.p65 20/09/25, 09:23 ã386

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
Eastern Mediterranean Health Journal, Vol. 9, No. 3, 2003 387
and impaired glucose tolerance were morecommon in those with BMI > 25 kg/m2
only in the older age groups. Diabetes andimpaired glucose tolerance were morecommon in those with a family history ofdiabetes. Increasing parity was also as-sociated with higher diabetes prevalence.Diabetes and impaired glucose tolerancewere thus higher among Asians in Tanzaniathan among the indigenous community.Rates were higher than among most otherimmigrant Asian communities [17].
In India, the prevalence of known dia-betes and abnormal glucose tolerancetesting steadily increased with age with thehighest prevalence in the age group = 70years (P < 0.001). Obese subjects hadsignificantly higher base and 2-hour bloodglucose readings for males and females.Subjects with diabetes on glucose tolerancetesting had higher waist to hip ratios.
We found no significant associationbetween total impaired fasting glucose andplace of residence (urban or rural). Zargaret al. reported similar results, although theydid find that in bivariate analysis theprevalence of both diabetes and impairedglucose testing were significantly higher inurban populations. However, when theresults were analysed by gender, the dif-ference between urban and rural popula-tions was statistically significant onlyamong females. When the data were fur-ther analysed using multiple logistic reg-ression even this difference was notsignificant [18]. Al-Nuaim found that theage-adjusted prevalence of diabetes mel-litus but not impaired glucose tolerancewas higher among urban populations [19].
The absence of any significant dif-ference in the prevalence of either totalimpaired fasting glucose or diabetes mel-litus between rural and urban populations inour study may be because the majority ofour subjects who lived in urban areas were
relatively recent arrivals from the country-side, having lived in an urban environmentfor only a few years, or were only tem-porary urban residents. Additionally, thedifference in conditions in urban and ruralenvironments in the Sultanate, with theexception of Muscat, is less distinct. Thus,the full impact of a sedentary lifestyle andstressful working conditions resulting fromthe increasing modernization of Oman haveperhaps not had time to show up in the datacollected among the urban dwellers in oursurvey.
Conclusions
Both diabetes mellitus and impaired fastingglucose are important public health prob-lems in Oman. The crude and age-adjustedprevalence of total impaired fasting glucoseare quite high. The participation rate in oursurvey was high and it is therefore unlikelythat we missed many cases of diabetesmellitus or impaired fasting glucose as non-responders. The crude prevalence of totalimpaired fasting glucose has increased byapproximately 24% since the 1991 survey.
At the national government level there isan existing 5-year programme for controlof chronic noncommunicable diseases.Controlling diabetes mellitus and its comp-lication is an important component of theprogramme. To prevent or minimize morbi-dity and mortality arising from these disea-ses, heightening the level of surveillanceamong primary health care doctors and thelevel of community awareness are perhapsthe best strategies to aid early diagnosis andmanagement of total impaired fasting glu-cose. Primary health care and other medi-cal professionals need to be vigilantbecause the onset of type 2 diabetes canoccur up to 4 years before clinical diag-nosis as evidenced by the presence of
18 Distribution and correlates.p65 20/09/25, 09:23 ã387

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
388 La Revue de Santé de la Méditerranée orientale, Vol. 9, NO 3, 2003
diabetic retinopathy or micro-angiopathy atthe time of clinical diagnosis. Primary caredoctors should always suspect total im-paired fasting glucose or diabetes mellitusamong males who are aged 40 years orolder and who are obese, those with abnor-mal waist to hip ratios and hypertensive
subjects with or without high cholesterollevels. Maintaining diabetes registration andimproving community awareness for self-reporting of diabetes are also highly recom-mended. Improving awareness of theproblem can be achieved through healtheducation campaigns.
References
1. Asfour AG et al. Diabetes mellitus in theSultanate of Oman. Diabetic medicine,1991, 8:76–80.
2. Al-Lawati JA, Mohammed AJ. Diabetesin Oman: Comparison of 1997 AmericanDiabetes Association classification ofdiabetes mellitus with 1985 WHO clas-sification. Annals of Saudi medicine,2000, 1:12–4.
3. McCarty D, Zimmet P. Diabetes 1994 to2010: Global estimates and projections.Melbourne, International Diabetes Ins-titute, 1994.
4. King H, Aubert RE, Herman WH. Globalburden of diabetes, 1995–2025: Preva-lence, numerical estimates, and projec-tions. Diabetes care, 1998, 21:1414–31.
5. King H, Minjoot-Pereira G, eds. Diabetesand noncommunicable disease risk fac-tor surveys. Geneva, World Health Orga-nization, 1999:64–86.
6. Definition, diagnosis and classificationof diabetes mellitus and its complica-tions. Report of a WHO consultation. Part1: Diagnosis and classification of dia-betes mellitus. Geneva, World HealthOrganization, Department of Noncom-municable Disease Surveillance, 1999.
7. Segi M. Cancer mortality for selectedsites in 24 countries (1950–1957). Sen-dai, Japan, Tohuku University of Medi-cine, 1960.
8. Annual health report, 2000. Muscat,Oman, Ministry of Health, 2001:9.61.
9. Posadas-Romero C et al. The preva-lence of NIDDM and associated coro-nary risk factors in Mexico City. Diabetescare, 1994, 17:1441–8.
10. Eldemire D, Hagley K. Diabetes mellitusin the Jamaican elderly. West Indianmedical journal, 1996, 45:82–4.
11. Kadiki OA, Roaed RB. Epidemiologicaland clinical patterns of diabetes mellitusin Benghazi, Libyan Arab Jamahiriya.Eastern Mediterranean health journal,1999, 5:6–13.
12. Erasmus RT et al. Prevalence of dia-betes mellitus and impaired glucose to-lerance in factory workers from Transkei,South Africa. South African medical jour-nal. Suid-Afrikaanse tydskrif vir gene-eskunde, 2001, 91:157–60.
13. Omar MA et al. The prevalence of dia-betes mellitus and impaired glucose to-lerance in a group of urban SouthAfrican blacks. South African medicaljournal. Suid-Afrikaanse tydskrif vir ge-neeskunde, 1993, 83:641–3.
14. Omar MA et al. The prevalence of dia-betes mellitus in a large group of SouthAfrican Indians. South African medicaljournal. Suid-Afrikaanse tydskrif vir ge-neeskunde, 1985, 67:924–6.
18 Distribution and correlates.p65 20/09/25, 09:23 ã388

ǼȲŎǟ ÛǦɆƫǠȞȱǟ ǦǶȎȱǟ ǦȶȚȺȵ ÛȔȅɀǪƫǟ ȧȀȊȱ ǦɆǶȎȱǟ ǦȲŎǟȜȅǠǪȱǟǻǼȞȱǟ ÛĎÛčċċĎ
Eastern Mediterranean Health Journal, Vol. 9, No. 3, 2003 389
munity in Tanzania. Diabetes researchand clinical practice, 1990, 8:227–34.
18. Zargar AH et al. Prevalence of type 2diabetes mellitus and impaired glucosetolerance in the Kashmir Valley of theIndian subcontinent. Diabetes researchand clinical practice, 2000, 47:135–46.
19. Al-Nuaim AR. Prevalence of glucoseintolerance in urban and rural com-munities in Saudi Arabia. Diabetic me-dicine, 1997, 14:595–602.
15. Tuomilehto J et al. Prevalence of dia-betes mellitus and impaired glucose to-lerance in the middle-aged population ofthree areas in Finland. Internationaljournal of epidemiology, 1991, 20:1010–7.
16. Elbagir MN et al. A high prevalence ofdiabetes mellitus and impaired glucosetolerance in the Danagla community innorthern Sudan. Diabetic medicine,1998, 15:164–9.
17. Swai AB et al. Diabetes and impairedglucose tolerance in an Asian com-
Regional Consultation on Early Diabetes Prevention and ControlThe World Health Organization (WHO) organized a Regional Consulta-tion on Diabetes Prevention and Control in Teheran, Islamic Republicof Iran from 2 to 5 February 2003. The objectives of the Consultationwere: to review the activities of diabetes control programmes in theRegion; to develop strategies to integrate diabetes control pro-grammes into primary health care services; and to prepare regionalguidelines for prevention and control of diabetes. Experts fromEgypt, Islamic Republic of Iran, Jordan, Lebanon, Libyan ArabJamarhiriya, Oman, Pakistan, Saudi Arabia, Sudan, Syrian Arab Re-public, Tunisia, United Kingdom, United States of America as well asWHO concerned staff participated in the consultation.
18 Distribution and correlates.p65 20/09/25, 09:23 ã389