discussing side effects of over-the-counter medicines: impact of adding percentage data
TRANSCRIPT
JOBNAME: No Job Name PAGE: 1 SESS: 18 OUTPUT: Wed Jul 28 20:07:44 2010 SUM: A5B5D9B4/v2451/blackwell/journals/ijpp_v0_i0/ijpp_57
Discussing side effects of over-the-counter medicines:impact of adding percentage dataijpp_57 1..8
Mahsa Seyed-Hosseinia, Jeff Taylora and Dale Questb
a College of Pharmacy and Nutrition, University of Saskatchewan, Saskatoon, Saskatchewan, Canada andb Medical Education, Paul L. Foster School of Medicine, Texas Tech University Health Science Center, ElPaso, TX, USA
Abstract
Objective Discussing side effects with patients continues to be a difficult area of practice.Questions arise as to how many should be mentioned and which ones. The way suchinformation is presented can affect drug-taking decisions. This study examined how over-the-counter (OTC) medicine users are influenced by numerical risk estimates of side effects.Methods As part of a larger study on patient decision-making, 30 participants over 50years were asked to consider three OTC headache medicines. They responded to one of twoheadache scenarios, one with symptoms described as mild but common and the other severebut rare. Participants made their selection based on drug efficacy and side effects, at first notlinked to occurrence rates and then when this information provided.Key findings Average age was 66.6 years and the majority were female. Most werecurrently using some form of drug therapy. Drug choices differed in relation to mild versussevere headache scenarios. A stronger preference for drug X (50% effective and two sideeffects) was evident when the headaches were mild, shifting to a more effective agent (butwith more side effects) when more severe. Addition of occurrence rates to the side effectshad the greatest effect within the severe headache scenario, where more participants optedfor the most effective agent (drug Z at 100% effective but six side effects) upon seeing thenumbers. Overall, however, most kept the same drug in spite of the numerical information.Conclusions Inclusion of numerical data for side effects did not negatively influencepotential OTC medicine users. For most, effectiveness and side effects were the concernbefore receiving the percentages, while effectiveness became more important when thefrequency data seemed to instil a sense of reassurance.Keywords decision-making; OTC medicines; over-the-counter medicines; patient educa-tion; side effects
Introduction
During discussions with patients about medicines, an area of trepidation for healthcarepractitioners is the provision of side-effect information. While all are likely to acknowledgethe importance of such material, for some there may be concern that their simple mentionwill cause occurrence in a patient. For others, there may be uncertainty as to how many sideeffects to actually mention or which ones to include. Researchers in the field of riskcommunication have shown that risk (such as side effects) is a complex matter and the wayinformation is presented will affect decisions.[1–3] For example, how information is framed –in the context of a potential gain or loss – can play a role in how decisions are made.[4]
When pharmacists provide advice on a medicine it is customary to verbally mention theones deemed to be the most relevant. The patient may also be directed to a computer-generated leaflet in support of this process. At some point, the pharmacist may note thechances a person might have of experiencing the ones identified. On determining howpharmacists might do this, Deschamps et al. found they often described the rate of occur-rence by using terms and phrases such as ‘might happen’, ‘rarely’ and ‘not that common’.[5]
Elsewhere, side-effect information has been disclosed using similar semantic descriptions,such as ‘some people may experience . . .’, ‘side effects may include . . .’ and ‘commonlyreported side effects are . . .’.[1,2,6]
Unfortunately, the use of verbal descriptors to convey such information may lead toan over-estimation of the level of harm, possibly leading patients to make inappropriate
1
2
3
4
567
8
9
1011121314151617181920212223242526272829303132
33
34
35363738394041424344454647484950515253
Research Paper
IJPP 2010, ••: ••–••© 2010 The AuthorsJournal compilation © 2010Royal Pharmaceutical Society ofGreat BritainReceived January 29, 2010Accepted July 1, 2010DOI10.1111/j.2042-7174.2010.00057.xISSN 0961-7671
Correspondence: Professor JeffTaylor, College of Pharmacy andNutrition, University ofSaskatchewan, 110 SciencePlace, Saskatoon, Saskatchewan,Canada, S7N 5C9E-mail: [email protected]
1

JOBNAME: No Job Name PAGE: 2 SESS: 18 OUTPUT: Wed Jul 28 20:07:44 2010 SUM: AC1CF2AA/v2451/blackwell/journals/ijpp_v0_i0/ijpp_57
decisions.[1] That said, there has been little evidence-basedguidance on how best to communicate the information.[7,8]
There is always the possibility of misunderstanding evenwhen patients and doctors use identical words. As an example,a group of researchers investigated how readers interpretedthe level of likelihood intended by a ‘low risk’. They foundthat some individuals concluded it to mean odds as high as 1in 5, while others said they would expect the term to be usedfor odds of 1 in 10 000; it depended on people’s knowledge orexpectations of the context.[9] For a review, Edwards andElwyn found that terms such as ‘probable’, ‘unlikely’ and‘rare’ conveyed elastic concepts, that one person’s under-standing of each can vary.[6] Individuals may also interpretsuch terms differently in different contexts. For example, a‘rare’ outcome is a different prospect in the context of genetictests than in the context of antibiotic treatment for tonsillitis.
One answer to this problem might be to utilize more deci-sive rates of occurrence (if known): the use of numericalinformation. In fact, it appears that patients may prefer anumerical format (e.g. 2 chances in 100 or 2%) rather thanverbal descriptors (rare, infrequent, common, etc.) and areable to use that format to make more accurate predictions oftheir chances of experiencing a particular reaction.[7,10,11]
Studies show that patients who were informed in terms offrequencies were less anxious about taking their drugs.[3,12,13]
Young and Oppenheimer proposed that informing people ofthe actual percentage risk of side effects might reduce fear andincrease intentions for adherence.[2]
Information leaflets in their current form may not be idealfor patients.[14–17] Current medication packaging and insertsusually provide lists of adverse effects but may not providefrequency of occurrence.[1,15,18] Adverse effects listed withoutfrequency or percentage data may make it harder to under-stand individual risk.[1,16] There appears to be a need forfurther understanding of how to discuss medicine risks. Thisshould include those agents available without prescription.Many over-the-counter (OTC) purchase decisions in pharma-cies take place without pharmacist involvement. In these situ-ations, it is the written information on the box or insert thatmust convey such detail. This study examined aspects of howOTC medicine users process side-effect information whencontemplating product use. The objective was to determinehow potential users are influenced when given numerical riskestimates of side effects.
Methods
Only a small segment of the methods are described here, inwhat was otherwise a complex protocol to examine a host ofissues (including attitudes to medicines, perceptions of effi-cacy balanced against risk and preferences for side-effectframing). Regardless of whether for the broader study or justthe aspects described here, an overview of the methods meantthat subjects individually arrived at the study site, respondedto questions and scenarios involving drug therapy, and thenwere interviewed.
Participants were residents of Saskatoon over 50 years ofage and were required to have English as their first language.Each was to have reached a minimum score of 19 on the RapidEstimate of Adult Literacy in Medicine (REALM) test in
order to be able to read the study materials.[19] Subjects wererecruited using posters placed in 30 randomly chosen phar-macies. Recruitment was complete when 30 people meetingthe entrance requirements had volunteered. Demanding studyrequirements (including interviews) and past research involv-ing a previous report guided the decision to enlist this numberof subjects.[20] To gauge existing health status, the Short-Formhealth survey (SF-8) was used.[21]
An OTC medicine for a headache was considered so par-ticipants would have a reasonable chance for familiarity withthe symptom under consideration. An actual brand name (orrecognizable generic name) was not used. Rather, the termsdrug X, drug Y and drug Z were the options presented toparticipants. It was thought this might prevent direct associa-tion with agents they may have used in real life. Precedencefor this approach exists.[2,17,22]
As symptom severity is likely to influence patientdecision-making, the sample was asked to respond to one oftwo headache scenarios. Half were given a scenario where theheadache was described as mild but common, as follows.
Whether true or not, consider for a moment that you getheadaches. They tend to be mild and occur six times ayear. You need a pain killer for these headaches in orderto focus better on your daily activities. You have thechoice of three headache medicines for relief.
The other half responded to a scenario where the headachewas severe but rare, as follows.
Whether true or not, please consider for a moment thatyou get headaches. They tend to be severe and occurtwice a year. You need a pain killer in order to get out ofbed. You have a choice of three headache medicines forrelief.
Regardless of which scenario given, participants were askedto perform the product-selection task twice: once where theside effects did not have frequency data and a second timewhere frequency data were added (see Tables 1 and 2). Thisdesign would allow a comparison of drug preference bothwith percentages and without percentages for side effects.Subjects were asked to choose one of these drugs as thepreferred agent for their headache scenario at each juncture(or they could opt for none). Upon seeing both side-effectformats, the outcome could be either a participant stayingwith his/her first choice or changing a decision based on thenew information. They were also asked for their preference inhow they are given information on side effects.
Side effects were chosen from product monographs ofAdvil, Motrin, Tylenol and acetylsalicylic acid, and thus were
Table 1 First version of side-effect information given to participants
Trait Drug X Drug Y Drug Z
Headache relief 50% 75% 100%Side effects Nausea Nausea Nausea
Rash Rash RashDizziness DizzinessHeartburn Heartburn
DiarrhoeaDry eyes
123456789
1011121314151617181920212223242526272829303132333435363738394041424344
45
46
47484950515253545556575859
60
61
6263646566676869
7071727374757677787980818283848586878889
9091929394
9596
979899
100101
102103104105106107108109110111112113114115116
2 International Journal of Pharmacy Practice 2010; ••: ••–••

JOBNAME: No Job Name PAGE: 3 SESS: 18 OUTPUT: Wed Jul 28 20:07:44 2010 SUM: ABAE5C0D/v2451/blackwell/journals/ijpp_v0_i0/ijpp_57
similar and relevant to existing medication. Further justifica-tion was provided by common drug advertisements, where themost commonly occurring side effects were diarrhoea(reported in 18 of 20 advertisements), nausea (17 of 20) anddizziness (10 of 11).[2]
The agents outlined in the figures were configured to varyin effectiveness and side-effect profile, characterized fromlower efficacy (with few potential side effects) up to highefficacy (but more potential side effects). This was a require-ment of the larger study, where efficacy versus risk was a keycomponent of inquiry. In essence, then, subject choicesinvolved a balancing between levels of efficacy in relation toassociated side effects. Subjects were provided their scenarioand were asked to choose between one of three OTC drugs forthe headache, first with just side-effect information, thenwhen provided information for how often the side effectsmight occur. Data-collection forms were created by theresearchers, simply encompassing the scenario and check-offboxes for the drug option of their choosing.
Once the participants had made all the decisions asked ofthem, they were interviewed by one researcher (using a semi-structured interview format) to garner greater insight into theirthought process during decision-making.
Data were analysed descriptively and via chi-square tests(for choices of drugs).
Approval from the University of Saskatchewan AdvisoryCommittee on Ethics in Behavioural Research was obtained.
Results
The age of the 30 respondents ranged from 51 to 89 years,with an average of 66.6 � 10.6 years. The majority (n = 19)were female. Five had less than grade 12 (the final year ofsecondary school), whereas the remainder had a high schooldiploma or higher. Twenty-three participants were currentlyusing OTCs and 23 were taking prescription medications. AShort-Form health survey (SF-8) revealed that all participantshad some health issues. Scores could range from eight to 42,with eight meaning no physical or mental health concerns,whereas scores approaching 42 would be indicative of physi-cal and emotional problems. The mean for the 30 participantswas 32.4 (�5.7) and ranged from 22 to 42. Based on theREALM data, all participants had the ability to read mostpatient education materials.
In response to the question ‘Have you had any experiencewith side effects of medication in the last 6 months?’, 11reported yes, whereas 19 felt they had not had any such
experience. Seven of the 11 mentioned that they experiencedsome of the side effects listed for our OTC agents (nausea,rash, dizziness, heartburn, diarrhoea and dry eyes), whereasthe other four had experienced different ones (shortness ofbreath and muscle pain, among others).
Drug choices differed in relation to mild versus severeheadache scenarios. Pearson chi-square showed a significantdifference between the hypothetical OTC drug and headacheseverity for both methods of presenting side effects (withoutand with percentages) (c2(3) = 11.083, P < 0.05 andc2(3) = 10.597, P < 0.05 respectively; see Table 3). This indi-cates a stronger preference for drug X when the headacheswere mild, but shifting to a more effective agent when theheadaches were more severe. The addition of percentages tothe side-effect information had the greatest effect within thesevere headache scenario, where more participants opted forthe most effective agent (drug Z) upon seeing how often theside effects might occur. While decisions were indeedchanged, most kept the same drug (see Table 4) in spite of thenew information presented to them.
To determine whether exposure to our study materialsmight influence future reaction to side-effect information, acomparison of pre- and post-study preferences was made.Before the main aspects of the study were conducted, partici-pants responded to this question.
Side effects can be communicated to patients by listingthem, with the option of adding numbers that representthe percentage of people who experience a particular
Table 2 Second version of side-effect information given to participants
Trait Drug X Drug Y Drug Z
Headache relief 50% 75% 100%Side effects Nausea 3% (3 in 100) Nausea 3% (3 in 100) Nausea 3% (3 in 100)
Rash 4% (4 in 100) Rash 4% (4 in 100) Rash 4% (4 in 100)Dizziness 7% (7 in 100) Dizziness 7% (7 in 100)Heartburn 5% (5 in 100) Heartburn 5% (5 in 100)
Diarrhoea 2% (2 in 100)Dry eyes <1% (<1 in 100)
Table 3 Preferred drug for mild and severe headache scenarios
Preferred drug Headache severity Total
Mild Severe
Without side effectpercentagesNone 1 3 4Drug X 9 1 10Drug Y 1 6 7Drug Z 4 5 9Total 15 15 30
With side effect percentagesNone 1 0 1Drug X 9 2 11Drug Y 0 4 4Drug Z 5 9 14Total 15 15 30
1
2
3456789
10
11
121314151617181920212223242526272829303132333435363738
39
40
4142434445464748495051525354555657
58
59
60
61626364656667
68697071727374
75
767778798081828384858687888990919293949596979899
100
101102103
Side effects of OTC medicines Seyed-Hosseini et al. 3
JOBNAME: No Job Name PAGE: 4 SESS: 18 OUTPUT: Wed Jul 28 20:07:44 2010 SUM: AACFE568/v2451/blackwell/journals/ijpp_v0_i0/ijpp_57
side effect. For example, a pharmacist or doctor couldsay: ‘The most common side effects are stomach ache,back ache, and drowsiness.’ Or they could say: ‘Themost common side effects are stomach ache (12%),back ache (6%), and drowsiness (2%).’ Whichapproach, if any, do you prefer?
They were presented with three options: (1) just the sideeffects, (2) the side effects and the percentages or (3) nopreference. Most were interested in seeing the percentages forside effects before starting the study (see Table 5). Upon com-pleting the study, participants were again asked to respond tothose same preferences for presentation of side effects.
From what you read (side effects with and withoutpercentages), which explanation would YOU prefer tobe given on medication side effects? Check ONE of thefollowing options: The first version (a list of possibleside effects), the second version (a list of possible sideeffects plus the percentages that they may occur), or Nopreference.
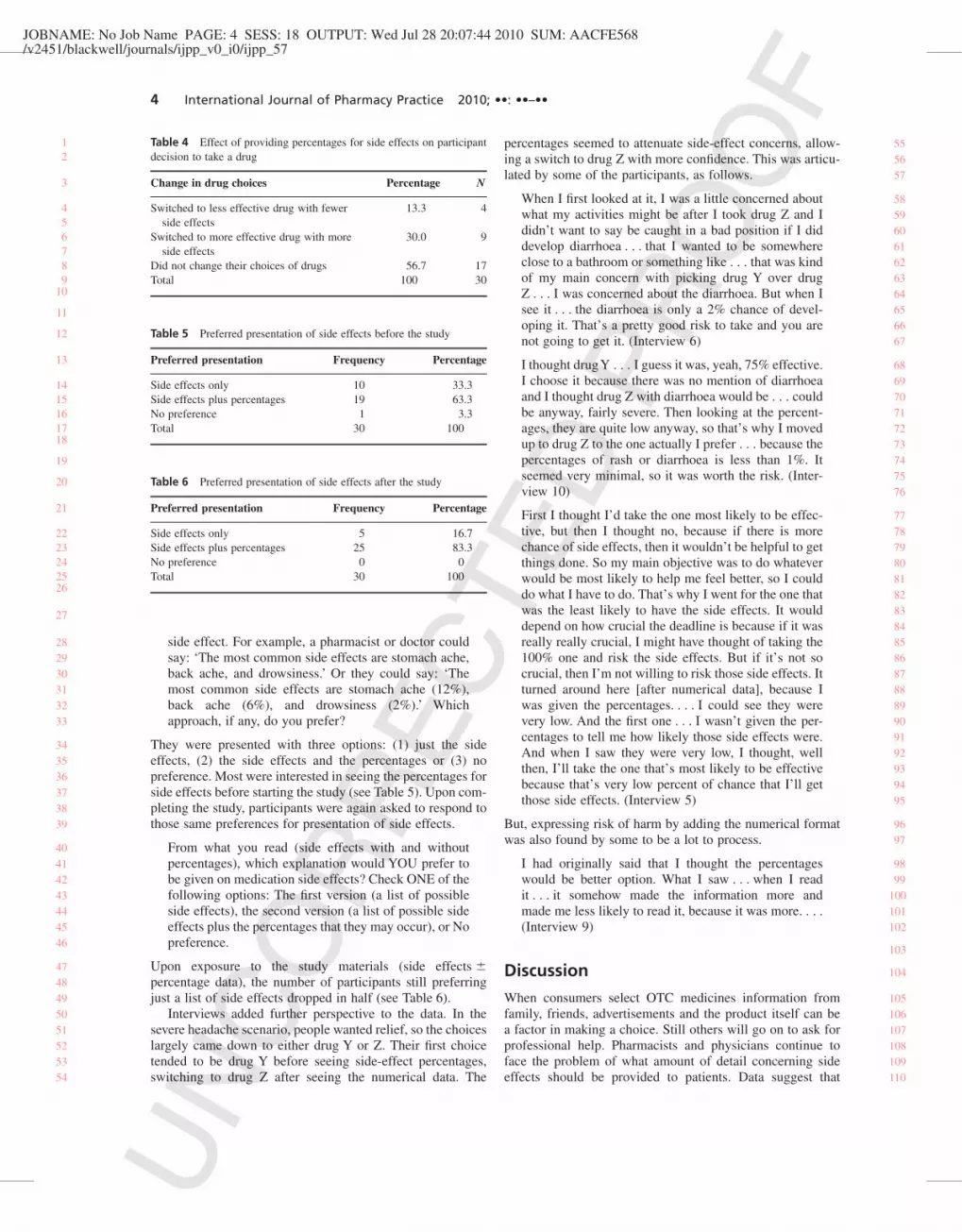
Upon exposure to the study materials (side effects �percentage data), the number of participants still preferringjust a list of side effects dropped in half (see Table 6).
Interviews added further perspective to the data. In thesevere headache scenario, people wanted relief, so the choiceslargely came down to either drug Y or Z. Their first choicetended to be drug Y before seeing side-effect percentages,switching to drug Z after seeing the numerical data. The
percentages seemed to attenuate side-effect concerns, allow-ing a switch to drug Z with more confidence. This was articu-lated by some of the participants, as follows.
When I first looked at it, I was a little concerned aboutwhat my activities might be after I took drug Z and Ididn’t want to say be caught in a bad position if I diddevelop diarrhoea . . . that I wanted to be somewhereclose to a bathroom or something like . . . that was kindof my main concern with picking drug Y over drugZ . . . I was concerned about the diarrhoea. But when Isee it . . . the diarrhoea is only a 2% chance of devel-oping it. That’s a pretty good risk to take and you arenot going to get it. (Interview 6)
I thought drugY . . . I guess it was, yeah, 75% effective.I choose it because there was no mention of diarrhoeaand I thought drug Z with diarrhoea would be . . . couldbe anyway, fairly severe. Then looking at the percent-ages, they are quite low anyway, so that’s why I movedup to drug Z to the one actually I prefer . . . because thepercentages of rash or diarrhoea is less than 1%. Itseemed very minimal, so it was worth the risk. (Inter-view 10)
First I thought I’d take the one most likely to be effec-tive, but then I thought no, because if there is morechance of side effects, then it wouldn’t be helpful to getthings done. So my main objective was to do whateverwould be most likely to help me feel better, so I coulddo what I have to do. That’s why I went for the one thatwas the least likely to have the side effects. It woulddepend on how crucial the deadline is because if it wasreally really crucial, I might have thought of taking the100% one and risk the side effects. But if it’s not socrucial, then I’m not willing to risk those side effects. Itturned around here [after numerical data], because Iwas given the percentages. . . . I could see they werevery low. And the first one . . . I wasn’t given the per-centages to tell me how likely those side effects were.And when I saw they were very low, I thought, wellthen, I’ll take the one that’s most likely to be effectivebecause that’s very low percent of chance that I’ll getthose side effects. (Interview 5)
But, expressing risk of harm by adding the numerical formatwas also found by some to be a lot to process.
I had originally said that I thought the percentageswould be better option. What I saw . . . when I readit . . . it somehow made the information more andmade me less likely to read it, because it was more. . . .(Interview 9)
Discussion
When consumers select OTC medicines information fromfamily, friends, advertisements and the product itself can bea factor in making a choice. Still others will go on to ask forprofessional help. Pharmacists and physicians continue toface the problem of what amount of detail concerning sideeffects should be provided to patients. Data suggest that
Table 4 Effect of providing percentages for side effects on participantdecision to take a drug
Change in drug choices Percentage N
Switched to less effective drug with fewerside effects
13.3 4
Switched to more effective drug with moreside effects
30.0 9
Did not change their choices of drugs 56.7 17Total 100 30
Table 5 Preferred presentation of side effects before the study
Preferred presentation Frequency Percentage
Side effects only 10 33.3Side effects plus percentages 19 63.3No preference 1 3.3Total 30 100
Table 6 Preferred presentation of side effects after the study
Preferred presentation Frequency Percentage
Side effects only 5 16.7Side effects plus percentages 25 83.3No preference 0 0Total 30 100
12
3
456789
10
11
12
13
1415161718
19
20
21
2223242526
27
282930313233
343536373839
40414243444546
4748495051525354
555657
58596061626364656667
686970717273747576
77787980818283848586878889909192939495
9697
9899
100101102
103
104
105106107108109110
4 International Journal of Pharmacy Practice 2010; ••: ••–••

JOBNAME: No Job Name PAGE: 5 SESS: 18 OUTPUT: Wed Jul 28 20:07:44 2010 SUM: A06B7F81/v2451/blackwell/journals/ijpp_v0_i0/ijpp_57
side-effect information is a high priority for patients[15,23–25]
and the perception of them is influential in many decisionsabout medicines.[17] Some people appear to want to know allpotential adverse reactions, even if they are relativelyrare.[8,26,27] Healthcare workers, on the other hand, contendthat explaining to patients (for each medication prescribed)every possible adverse effect would take an unacceptableamount of time and be of questionable advisability.[8] Howthen should pharmacists choose the level and extent of infor-mation to give? Our study assessed the impact of addingpercentages to verbal descriptors for OTC drug choices forheadaches. Thirty participants were given the option of threehypothetical OTC medicines, described as 50, 75 and 100%effective, while exhibiting two, four and six side effects,respectively. While side effects are the focus of this report, ameasure of effectiveness was needed for our larger studydesign. This set in motion a situation requiring subjects tobalance risk/benefit information during decision-making.One question we had is would the propensity to take drug X(for example) change with the provision of numerical side-effect data?
In the severe headache scenario it appeared respondentswere not interested in drug X because, at only 50% effective-ness, it would not be strong enough for more troublesomeheadaches. People wanted relief, so the choices largely camedown to either drug Y or Z. Their first choice was drug Ybefore seeing side-effect percentages. After seeing thenumerical data, most changed their selection to drug Z. Whatmay have been the issue between drug Y and Z was that thenew side effects (diarrhoea and dry eyes) seemed to drivepeople away from drug Z. After seeing the percentages, thevalues attached to those ‘problematic’ side effects seemed toattenuate the concern, allowing a switch to drug Z with moreconfidence.
In the mild headache scenario, drug Y was rarely consid-ered; drug X was largely perceived as the better option. Peoplewere very pragmatic: it was still considered somewhat effec-tive, but if it did not work for them (in real life), they couldeasily move on to a stronger agent in a day or so. For that levelof headache, though, there seemed to be low tolerance for sideeffects; thus people chose the agent with the least risk.Numerical frequency data for side effects at this juncture hadthe effect of further justifying their choice in selecting drug X.
The percentages chosen were undoubtedly importantduring deliberations and decisions might have been differentif higher values were attached to the given side effects. Forexample, if the possibility of experiencing dizziness was 17%instead of 7%, participants may not have considered the lattertwo agents.
The choice of side effects was also likely a factor in anydecisions. If a participant actually suffered from dry eyes(drug Z for example), even a small chance of getting it mightbe considered an unacceptable risk. By extension, selection ofside effects considered more severe (e.g. kidney problems,troubled breathing) would also create stronger hesitationtowards use. The effect of either situation might be reduced ifthe side effects were applicable to all three agents.
Volunteering for the study may potentially bias the sample.Volunteers can have certain characteristics that differentiatethem from the population of patients as a whole. The high
education level of our participants – a third had an educationlevel higher than a bachelor’s degree – may be another limi-tation in generalizing our sample to the population of people50 years and older.
Our study design encompassed both frequency and per-centage formats. Since a clear picture was not evident a priorifor the best approach, the decision to use both formats wasmade. Including both the percentages and frequency data wasa limitation in some respects in that it did not allow for anassessment of which of the two formats was most influentialto any person. For some, the two could have been helpful. Forothers, it could have been perceived as an extra piece ofmaterial to process. Schommer et al. suggested there is abalance between the need for information at a level sufficientfor individuals to make decisions and the need not to overloadindividuals as they cognitively process it.[28] Future researchmay be able to assess the effect of each separately on people’sdecision to use a medicine. More sophisticated techniquescould be utilized to assess the importance of attributes as wellas the levels of each attribute.[29,30]
Our results show that respondents expressed a strongerintention to use OTC medicines upon receiving numericaldata compared to just the side effects. Of particular interest isthat 19 of 30 wanted numerical information upon arrival intothis study. Some contrast to this has been evident elsewhere,albeit from the perspective of information providers. A studyof family physicians showed that 189 of 300 agreed thatcommunicating risk both qualitatively and numerically wasequally important.[31] Of the remaining 111 physicians,however, 94% endorsed the importance of communicatingqualitatively more strongly than numerically.
In choosing numerical data in addition to verbal descrip-tors, healthcare professionals have another decision to make:describing the numerical probabilities as either percentages(e.g. this side effect will happen in 2% of users), as frequen-cies (e.g. this side effect will be seen in 5 out of every 100users), or perhaps both. The competency of the public withnumeracy soon comes to play in this discussion, in that theinterpretation of numerical information can also be problem-atic. The International Adult Literacy and Skills Survey testedmore than 23 000 adult Canadians (c.2003) on their profi-ciency in four domains, including numeracy.[32] Skills wererated on the basis of levels one to five (lowest to highest).About 50% scored below level three on the numeracy scale.Levels below three are considered to indicate limited profi-ciency and such individuals are likely to have difficultiescoping with increasing numeracy-related demands in every-day life. As another example of numeracy assessment,Yamagishi found that a death rate of 1286 out of 10 000 wasrated as more risky than a rate of 24.14 out of 100.[33]
Providing numerical data (in percentage or frequencyformat) for side effects has been suggested by several stud-ies.,[2,24,34,35] Some have reported advantages in using frequen-cies rather than percentages,[35–38] but Berry et al. found nodifference between people’s interpretations using the two dif-ferent response formats.[16] Another study by Schapira et al.noted the advantages of each format: frequency formatsprovide ease of interpretation and simplicity, whereas percent-age formats provide an association with personal risk estima-tion and a mathematical quality.[39] Evans et al. found that
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
616263646566676869707172737475767778798081828384858687888990919293949596979899
100101102103104105106107108109110111112113114115116117118119120
Side effects of OTC medicines Seyed-Hosseini et al. 5
JOBNAME: No Job Name PAGE: 6 SESS: 18 OUTPUT: Wed Jul 28 20:07:44 2010 SUM: 9019C3BB/v2451/blackwell/journals/ijpp_v0_i0/ijpp_57
frequency formats were not generally associated with betterperformance than probability formats.[40]
Still, the optimal format to assist human judgement is notclear yet. Nor does the one-dimensional approach takenduring this study completely reflect how consumers go aboutchoosing an OTC drug.[41,42] Hypothetical scenarios do notallow an opportunity to fully incorporate the impact ofrespondents’ concerns on medicine-taking behaviour. So, inspite of a trend favouring the inclusion of numerical frequencydata from our small study, one should be cautious about con-cluding that pharmacists should include it with side-effectdata in practice. The same precaution would apply to productlabelling and advertisements. Far more needs to be done fordifferent illnesses and for different drugs, and with moresevere types of side effects.
ConclusionCommunicating medication information effectively shouldhelp patients make personal decisions about treatments andhopefully to find ways to integrate medication-taking intodaily activities. Drug information on labels and inserts is amajor source of knowledge for patients as they attempt tobalance risks and benefits of drugs and administer themsafely. It is not easy to present a single best approach forconveying a medication’s adverse effects to individuals.
Results here suggest that the inclusion of numerical datadid not negatively influence potential OTC medicine users, atleast with the percentages used. For most participants, effec-tiveness and side effects were the concern before receiving thepercentages, while effectiveness became more importantwhen the frequency data appeared to instil a sense of relief.
Declarations
Conflict of interestThe Author(s) declare(s) that they have no conflicts of interestto disclose.
FundingThis research received no specific grant from any fundingagency in the public, commercial or not-for-profit sectors.
References1. Knapp P et al. Comparison of two methods of presenting
risk information to patients about the side effects of medicines.Qual Saf Health Care 2004; 13: 176–180.
2. Young SD, Oppenheimer DM. Different methods of presentingrisk information and their influence on medication complianceintentions: results of three studies. Clin Ther 2006; 28: 129–139.
3. Edwards A et al. Presenting risk information a review of theeffects of framing and other manipulations on patient outcomes.J Health Commun 2001; 6: 61–82.
4. Tversky A, Kahneman D. The framing of decisions and thepsychology of choice. Science 1981; 211: 453–458.
5. Deschamps M et al. What are we saying? Content and organi-zation of patient counselling by community pharmacists. CanPharm J 2003; 136: 42–47.
6. Edwards A, Elwyn GJ. Explaining risks: turning numerical datainto meaningful pictures. BMJ 2002; 324: 827–830.
7. Berry DC. Informing people about the risks and benefits ofmedicines: implications for the safe and effective use of medici-nal products. Curr Drug Saf 2006; 1: 121–126.
8. Ziegler DK et al. How much information about adverse effects ofmedication do patients want from physicians? Arch Intern Med2001; 161: 706–713.
9. Paling J. Bad points about current practices. In: Paling J, editor.Helping Patients Understand Risks: Seven Simple Strategies forSuccessful Communication. Gainesville, FL: The Risk Commu-nication Institute, 2006.
10. Dyck A et al. Pharmacists’ discussions of medication sideeffects: a descriptive study. Patient Educ Counsel 2005; 56:21–27.
11. Franic DM, Pathak DS. Communicating the frequency ofadverse drug reactions to female patients. Drug Inf J 2000; 34:251–272.
12. Berry DC et al. Expressing medicine side effects: assessing theeffectiveness of absolute risk, relative risk, and number needed toharm, and the provision of baseline risk information. PatientEduc Counsel 2006; 63: 89–96.
13. Berry DC et al. Patients understanding of risk associated withmedication use: impact of European Commission guidelines andother risk scales. Drug Saf 2003; 26: 1–11.
14. Raynor DK et al. A systematic review of quantitative and quali-tative research on the role and effectiveness of written informa-tion available to patients about individual medicines. HealthTechnol Assess 2007; 11: iii.
15. Berry DC et al. Provision of information about drug side effectsto patients. Lancet 2002; 359: 853–854.
16. Berry DC et al. Is 15 percent very common? Informing peopleabout the risks of medication side effect. Int J Pharm Pract 2002;10: 144–151.
17. Berry DC et al. Communicating information about medicationside effects: effects on satisfaction, perceived risk to health andintention to comply. Psychol Health 2002; 17: 247–267.
18. Clark C. Improvements needed in risk communication. HospPharm 2004; 11: 426.
19. Davis TC et al. Rapid estimate of adult literacy in medicine: ashortened screening instrument. Fam Med 1993; 25: 391–395.
20. Bissell P et al. The dependent consumer: reflection on accountsof the risks of non-prescription medicines. Health 2001; 5: 5–30.
21. Turner-Bowker DM et al. Usefulness of the SF-8 health surveyfor comparing the impact of migraine and conditions. Qual LifeRes 2003; 12: 1003–1012.
22. Schwartz LM et al. Can patients interpret health information? Anassessment of the medical data interpretation test. Med DecisMaking 2005; 25: 290–300.
23. Raynor DK et al. How do patients use medicine informationleaflets in the UK? Int J Pharm 2007; 15: 209–218.
24. Knapp P et al. Do patient information leaflets meet patients’needs for describing the likelihood of side effects? Int J PharmPract 2007; 15 (suppl. 1): A26–A27.
25. Berry DC et al. What do patients want to know: an empiricalapproach to explanation generation and validation? Expert SystAppl 1995; 8: 419–429.
26. Howard J et al. The importance of drug information from apatient perspective. J Soc Admin Pharm 1999; 16: 115–126.
27. Nair K et al. What patients want to know about their medica-tions? Can Fam Phys 2002; 48: 104–110.
28. Schommer JC et al. Processing prescription drug informationunder different conditions of presentation. Patient Educ Counsel2001; 43: 49–59.
29. Johnson FR et al. Multiple sclerosis patients’ benefit-risk pre-ferences: serious adverse event risks versus treatment efficacy.J Neurol 2009; 256: 554–562.
123456789
1011121314151617
1819202122232425262728293031
32
33
34
35363738
3940
41
42
43444546474849505152535455565758
5960616263646566676869707172737475767778798081828384858687888990919293949596979899
100101102103104105106107108109110111112113114115116117118119120121122123
6 International Journal of Pharmacy Practice 2010; ••: ••–••

JOBNAME: No Job Name PAGE: 7 SESS: 18 OUTPUT: Wed Jul 28 20:07:44 2010 SUM: AF10207E/v2451/blackwell/journals/ijpp_v0_i0/ijpp_57
30. Seston EM et al. Balancing the benefits and risks of drug treat-ment: a stated-preference, discrete choice experiment withpatients with psoriasis. Arch Dermatol 2007; 143: 1175–1179.
31. Gramling R et al. Numeracy and medicine: key family physicianattitudes about communicating probability with patients. J AmBoard Fam Pract 2004; 17: 473.
32. Statistics Canada and the Organisation for EconomicCo-operation and Development. Learning a Living: First Resultsof the Adult Literacy and Life Skills Survey. Statistics CanadaCatalogue number 89-603-XWE.Ottawa: Statistics Canadaand the Organisation for Economic Co-operation and Develop-ment, 2005. http://www.oecd.org/dataoecd/44/7/34867438.pdf(accessed 21 July 2010).
33. Yamagishi K. When a 12.86 percent mortality is more dangerousthan 24.14 percent: implications for risk communication. ApplCogn Psychol 1997; 11: 495–506.
34. Berry DC et al. Evaluating explanations about drug prescrip-tions: effects of varying the nature of information about sideeffects and its relative position in explanations. Psychol Health1998; 13: 767–784.
35. Gigerenzer G, Edwards A. Simple tools for understanding risks:from innumeracy to insight. BMJ 2003; 327: 741–744.
36. Butterworth B. Statistics: what seems natural? Science 2001;292: 853–855.
37. Eddy DM. Probabilistic reasoning in clinical medicine: problemsand opportunities. In: Kahneman D et al., editors. Judg-ment Under Uncertainty: Heuristic and Biases. Cambridge:Cambridge University Press, 1982: 249–267.
38. Hoffrage U et al. Communicating statistical information.Science 2000; 290: 2261–2262.
39. Schapira MM et al. Frequency or probability? A qualitative studyof risk communication formats used in health care. Med DecisMaking 2001; 21: 459–467.
40. Evans JB et al. Frequency versus probability formats in statisti-cal word problems. Cognition 2000; 77: 197–213.
41. Bissell P et al. Mapping the contours of risk: consumer percep-tions of non-prescription medicines. J Soc Admin Pharm 2000;17: 136–142.
42. Johnson MMS, Drungle SC. Purchasing over-the-counter medi-cations: the influence of age and familiarity. Exp Aging Res2000; 26: 245–261.
123456789
101112131415161718192021
222324252627282930313233343536373839404142
Side effects of OTC medicines Seyed-Hosseini et al. 7

JOBNAME: No Job Name PAGE: 8 SESS: 18 OUTPUT: Wed Jul 28 20:07:44 2010 SUM: 03C1A06C/v2451/blackwell/journals/ijpp_v0_i0/ijpp_57
SNP Best-set Typesetter Ltd.Journal Code: IJPP Proofreader: ElsieArticle No: 57 Page Extent: 7

MARKED PROOF
Please correct and return this set
Instruction to printer
Leave unchanged under matter to remain
through single character, rule or underline
New matter followed byor
or
or
or
or
or
or
or
or
and/or
and/or
e.g.
e.g.
under character
over character
new character new characters
through all characters to be deleted
through letter orthrough characters
under matter to be changedunder matter to be changedunder matter to be changedunder matter to be changedunder matter to be changed
Encircle matter to be changed
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
linking characters
through character orwhere required
between characters orwords affected
through character orwhere required
or
indicated in the marginDelete
Substitute character orsubstitute part of one ormore word(s)
Change to italicsChange to capitalsChange to small capitalsChange to bold typeChange to bold italicChange to lower case
Change italic to upright type
Change bold to non-bold type
Insert ‘superior’ character
Insert ‘inferior’ character
Insert full stop
Insert comma
Insert single quotation marks
Insert double quotation marks
Insert hyphenStart new paragraph
No new paragraph
Transpose
Close up
Insert or substitute spacebetween characters or words
Reduce space betweencharacters or words
Insert in text the matter
Textual mark Marginal mark
Please use the proof correction marks shown below for all alterations and corrections. If you
in dark ink and are made well within the page margins.wish to return your proof by fax you should ensure that all amendments are written clearly