dementia services mini-screen: a simple method to identify patients and caregivers in need of...
TRANSCRIPT

Dementia Services Mini-Screen: A SimpleMethod to Identify Patients and
Caregivers in Need of Enhanced DementiaCare Services
Soo Borson, M.D., James M. Scanlan, Ph.D., Tatiana Sadak, A.R.N.P., Ph.D.,Mary Lessig, B.S., Peter Vitaliano, Ph.D.
Received OctobeSciences (SB, JMS(SB, TS), Univermeeting of the AConference, Bost
� 2013 Amehttp://dx.d
Am J Geriatr Ps
Objective: Improving dementia care in health systems requires estimates of need in
the population served. We explored whether dementia-specific service needs and gaps
for patients and caregivers could be predicted by simple information readily
captured in routine care settings. Method: Primary family caregivers (n ¼ 215)
rated their own current stress, challenging patient behaviors, and prior-year needs
and gaps in 16 medical and psychosocial services. These were evaluated with other
patient and caregiver characteristics in multivariate regressions to identify unique
predictors of service needs and gaps. Results: Caregiver stress and patient behavior
problems together accounted for an average of 24% of the whole-sample variance in
total needs and gaps. All other variables combined (comorbid chronic disease,
dementia severity, age, caregiver relationship, and residence) accounted for a mean
of 3%, with none yielding more than 4% in any equation. We combined stress and
behavior problem indicators into a simple screen. In early/mild dementia dyads
(n ¼ 111) typical in primary care settings, the screen identified gaps in total (84%)
and psychosocial (77%) care services for high stress/high behavior problem dyads
vs. 25% and 23%, respectively, of low stress/low behavior problem dyads. Medical
care gaps were dramatically higher in high stress/high behavior problem dyads
(66%) than all others (12%). Conclusion: The Dementia Services Mini-Screen is a
simple tool that could help clinicians and health systems rapidly identify dyads
needing enhanced dementia care, track key patient and caregiver outcomes of
interventions, and estimate population needs for new service development. (Am JGeriatr Psychiatry 2013; -:-e-)
Key Words: Dementia, health services, screening, chronic care
r 10, 2012; revised November 1, 2013; accepted November 6, 2013. From the Department of Psychiatry and Behavioral, ML, PV), University of Washington School of Medicine, Seattle, WA; Department of Psychosocial and Community Healthsity of Washington School of Nursing, Seattle, WA; and Screen Inc. (JMS), Seattle, WA. Presented in part at the annualmerican Association for Geriatric Psychiatry, Los Angeles CA, March 17, 2013, and the Alzheimer's Association Internationalon MA, July 13, 2013. Send correspondence to: [email protected] Association for Geriatric Psychiatryoi.org/10.1016/j.jagp.2013.11.001
ychiatry -:-, - 2013 1
Dementia Services Mini-Screen for Unmet Needs
INTRODUCTION
Nearly 5 million Americans have Alzheimer dis-ease, and prevalence will double by 2050.1 AnnualMedicare costs alone currently account for $11 billionin healthcare spending for patients with dementia,2
yet the quality of their medical care is suboptimal,3
and outcomes, measured in high cost acute care use,are cause for concern. In our recent study, personswith incident dementia had nearly 80% higher rates ofpotentially preventable hospitalizations than cogni-tively normal older adults.4 Moreover, the psychoso-cial aspects of dementia care, acknowledged byspecialists as integral to the delivery of high qualitycare,5 are not typically assessed in general medicalsettings; for example, family caregivers rarely spon-taneously disclose disruptive behavior and the asso-ciated stress to the patient’s primary care physician.6
These findings strongly suggest a need for strategicchanges in our overall approach to the ambulatorycare of dementia patients, including targeted im-provements in medical management and systematicintegration of psychosocial and behavioral assess-ments and interventions into routine outpatient care.7
Primary care clinicians find dementia more difficultto manage than other common chronic conditions oflate life,8 with its unpredictable time demands,9e11
clinical complexity,12 and need to actively engagethird parties—typically, family caregivers—over longperiods of time in both assessment and treatment ofcognitive, neuropsychiatric, and comorbid chronicmedical conditions.13 Many dementia-specific ser-vices are “nonmedical,” supportive in nature, andfocused on assisting the caregiver.14 As such, they areoutside the scope of usual primary care15,16 and areinconsistently if at all reimbursed. These services,together with informed, attentive general medicalcare, nevertheless are the backbone of successful long-range home care of persons with dementia,7 but thisprinciple is not yet widely operationalized: one studyfound that primary care clinicians are much less likelyto initiate referrals for psychosocial care than to pro-vide services generally accepted as part of the physi-cian’s role, such as writing orders for nursing homeadmission or home healthcare.9
The National Alzheimer’s Plan,17 created throughfederal legislation in 2011, calls for systemic upgradesin the quality and coordination of care for personswith
2
dementia and their family caregivers and recognizesthe need to focus care on the dyad. Healthcare modelsthat aim to unify medical and psychosocial care man-agement show promise,18e21 and, although the Centerfor Medicare & Medicaid Services has promotedPatient-Centered Medical Homes and organizationalaccountability for patient experience, healthcare qual-ity, and costs under Accountable Care Organizations,most health systems have yet to embrace the necessarysystem redesign or apply these concepts to healthcarefor dementia patients and caregivers. A simple, briefway to identify high needs dyads who are most likelyto show early benefit from integrated dementia caremanagement would be a useful step toward broaderimplementation.
Several informative studies have used extensivequestionnaires and surveys to describe health-relatedand psychosocial service needs of patients with de-mentia and their caregivers,22e26 but their findingsare too complex to translate well into front-linemedical settings where most patients receive theircare. We postulated that dyads with unmet needs fordementia-related services could be identified withoutrecourse to time-intensive, highly detailed question-naires that are impractical in primary care. Toaddress this, we tested candidate predictors from anexperimental protocol developed by the Consortiumto Establish a Registry for Alzheimer’s Disease(CERAD). CERAD investigators proposed a single-item stress index for caregivers and an inventory ofpatient and caregiver service needs.27 We combinedthese two elements with CERAD’s short list of highimpact behavioral problems and patient and care-giver variables that are easily captured in primarycare settings. Our goal was to create a useful tool thatwould enable primary care providers to quicklyidentify—preferably in 1e2 minutes—patient andcaregiver pairs in need of specialized dementia careinterventions. Such information could help bothproviders and health systems target the highest needsdyads first for care quality improvements.
METHODS
Overview and Study Sample
Participants were older adults identified in acommunity aging sample of over 600 persons as
Am J Geriatr Psychiatry -:-, - 2013

Borson et al.
having both clinically significant cognitive impairmentand a family caregiver. Subjects were identifiedthrough multimodal recruitment methods (commu-nity referrals, posted flyers, and “snowball” referralsfrom other enrollees) assessed at home as part of acommunity-based outreach program of the Universityof Washington’s Alzheimer’s Disease Research CenterSatellite. Of 231 cognitively impaired individuals, 215had complete data for all variables needed for thisanalysis and comprise the study sample. Most subjects(189, 88%) clearly met dementia criteria (ClinicalDementia Rating [CDR] 1þ),28 and 26 (12%) had mildcognitive impairment (MCI)/very mild dementia(CDR 0.5).
Written informed consent (assent, where appro-priate) was obtained as approved by the Universityof Washington Institutional Review Board. Althoughnot required for study participation, all carerecipients had some form of health insurance (usuallyMedicare A/B, with or without a supplemental plan)and an identified primary care physician, but fewhad a formal diagnosis of any cognitive impairmentdocumented in their medical records,29 and none wasreceiving care from a dementia specialist (geriatricpsychiatrist, geriatrician, or neurologist) at the timeof enrollment. Diagnoses were made as part of theoverall research program using uniform methodspreviously described in detail.29,30 Although all carerecipients were systematically diagnosed usingresearch criteria for dementia subtypes, etiology isnot included as a variable in the present studybecause primary care providers may not confidentlyclassify subtypes on their own.11
Variables
Patient variables included demographic descriptors,a defined set of five behavioral problems27 reported bycaregivers and/or observed during interview (anger/hostility, visual/auditory hallucinations, irritability,suspiciousness/paranoia, severe social withdrawal),dementia stage (CDR),28 and burden of chronic disease(Cumulative Illness Rating Scale, 13-itemmodificationfor medical conditions comorbid with cognitive dis-orders).31 Caregiver variables included relationship tothe care recipient (spouse or other relative), living sit-uation (together or apart), and the caregiver’s currentlevel of perceived stress using a single question:“Overall, how stressful is your caregiving situation at
Am J Geriatr Psychiatry -:-, - 2013
this time?” (scored 1 [not at all] to 5 [extremely]).Service needs and use were defined (yes/no) by aninterviewer-administered checklist of 16 specifieddementia- and care-related health and psychosocialservices27 with a free-response option for services notincluded in the inventory. Caregivers stated whetherthey had needed each service over the prior year and,if needed, whether they had or had not used it.
Service Variable Grouping
Two expert clinicians (S.B., T.S.) assigned each ofthe 16 services to either “medical” or “psychosocial”categories based on whether a physician or othermedical provider or an individual with knowledge ofcommunity resources and support services, usually asocial worker, would typically provide those ser-vices. The eight services designated as medicalincluded three aimed at caregivers (i.e., initial edu-cation and counseling about dementia, prescriptionof medication for caregiver stress or depression, andcaregiver hospitalization; these components mightrequire participation of two different primary careproviders, the patient’s and the caregiver’s) and fivefocused on the patient (i.e., prescription of medica-tion for mood or behavioral problems, patient hos-pitalization, enrollment in home healthcare,admission to hospice, and admission to a nursinghome). The eight psychosocial services were directcaregiver support and/or referral, companion care,overnight respite care, adult day health or activities,personal care for the care recipient at home, mealpreparation, chore help, and legal advice.
Scoring Service Needs, Use, and Gaps
For each provider type, total service need, use, andgap scores could each range from 0 to 8. For example,a caregiver might indicate a need for medication tohelp with stress but no other medical service needs,yielding a medical service need score of 1; if amedication was prescribed, the medical service usescore would be 1 and the gap score would be 0 (1need e 1 use ¼ 0 gap) and if not the gap score wouldbe 1 (1 need e 0 use ¼ 1 gap). The number of servicesfor which caregivers reported a need were summedfor each caregiverepatient dyad, and a mean scorewas derived for the whole sample and for subgroupsas described below and in Results. Total servicesneeded but not used are similarly reported as gaps.
3

TABLE 1. Characteristics of Cognitively Impaired Participants(N [ 215)
Characteristic Value
Demographic dataAge, mean (SD) 78 (8.4)Education, mean years (SD) 8.5 (5.7)Gender, % female 65%Caregiver relationship, n (%)Lives with spouse 69 (32)Lives with adult child or other relative 77 (36)Lives apart from caregiver 69 (32)
Cognitive impairment stage/type, n (%)CDR 0.5 (very mild) 26 (12)CDR 1þ (mild, moderate, severe dementia) 189 (88)Probable Alzheimer’s disease 124 (58)Vascular and mixed 46 (21)Othera 19 (9)Mean (SD) CDR 1.7 (0.8)
Behavioral problems, n (%) 183 (85)Anger, hostility 114 (53)Auditory and/or visual hallucinations 55 (26)Irritability 127 (59)Paranoia, suspiciousness 121 (56)Social withdrawal 102 (47)
Number of problems, mean (SD) 2.4 (1.6)0e1, n (%) 65 (34)2e5, n (%) 150 (66)
Chronic disease burden, modified CIRS-G, mean (SD) 11.1 (4.6)
Notes:modified CIRS-G: Cumulative Illness Rating Scale, 13-itemmodification for medical conditions comorbid with cognitivedisorders.31
aIncludes Parkinson dementia, other Lewy body dementia,progressive supranuclear palsy, alcoholic dementia, depressionwith dementia, dementia of etiology not yet specifiable.
Dementia Services Mini-Screen for Unmet Needs
Analytic Overview and Approach
All analyses were done (using SPSS 18 for Win-dows; IBM Corp., Somers, NY) to accomplish fivesequential goals: (1) to determine which caregiverand care recipient factors are most strongly relatedto total, medical careespecific, and psychosocialcareespecific service needs and gaps; (2) to simplifyscreening of patientecaregiver dyads by locatingcritical cut points on essential service predictorvariables; (3) to create a simple tool to screen fordyads with high service needs and gaps; (4) to testits utility in the total sample (with a broad range ofseverity of cognitive impairment); and (5) to retest itin the subset of dyads most typical of thoseencountered in primary care (MCI and very milddementia).
Goal 1 was evaluated using stepwise multipleregression. Dependent variables were total needs andgaps, medical care needs and gaps, and psychosocial
4
care needs and gaps. Independent (predictor) vari-ables for all equations were caregiver stress, numberof patient behavioral problems, CDR stage, relation-ship status (spouse versus other), residence (liveswith caregiver or apart), age, and comorbid chronicdisease. Data for service needs had symmetric dis-tributions; data for service gaps had minor negativeskews. However, skews were less than 1, and therelatively large number of participants relative topredictors minimizes deleterious effects on theregression analyses. Goal 2, to estimate the thresh-olds of caregiver and care-recipient variables usefulfor predicting service needs and gaps, was addressedby ANOVA with post-hoc least significant difference(LSD) comparisons, examining the strongest pre-dictors identified in Goal 1 analyses. Goal 3, to createa screening tool for unmet service needs, was done bycombining the variables found to be most predictive(Goal 1) in their simplest form (Goal 2) to form aDementia Services Mini-Screen. Goal 4 wasaddressed by applying the groupings created in Goal3 to the entire sample (ANOVA with LSD post-hoccomparisons). Goal 5 was accomplished by repli-cating analyses for Goal 4 using a subset of partici-pants with MCI and mild dementia (CDR ¼ 0.5 and1.0, respectively, N ¼ 111). Finally, we applied anadditional test of the mini-screen’s ability to detectgaps in medical and psychosocial services by calcu-lating its sensitivity and specificity in this early/mildstage group.
RESULTS
Demographic Data and Clinical Variables
Table 1 shows the characteristics of participants.About two-thirds of cognitively impaired partici-pants lived with their family caregivers, the restalone, and most had worked in business or serviceprofessions or as homemakers (data not shown).Overall burden of chronic disease was moderate, andabout two-thirds had two or more of the fivebehavior problems assessed.
Goal 1: Identifying Predictors of Service Needsand Gaps
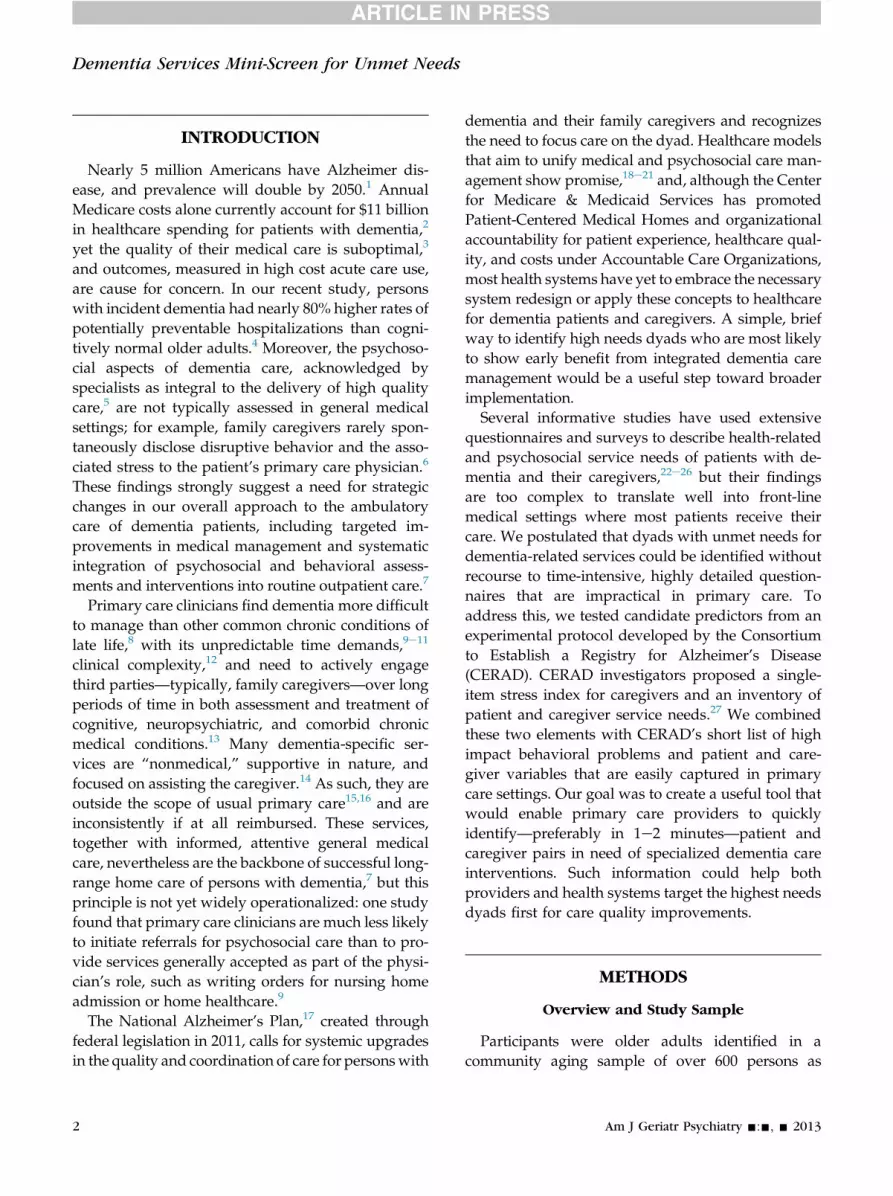
Table 2 shows the predictors of care needs andgaps. Caregiver stress and patient behavior problems
Am J Geriatr Psychiatry -:-, - 2013
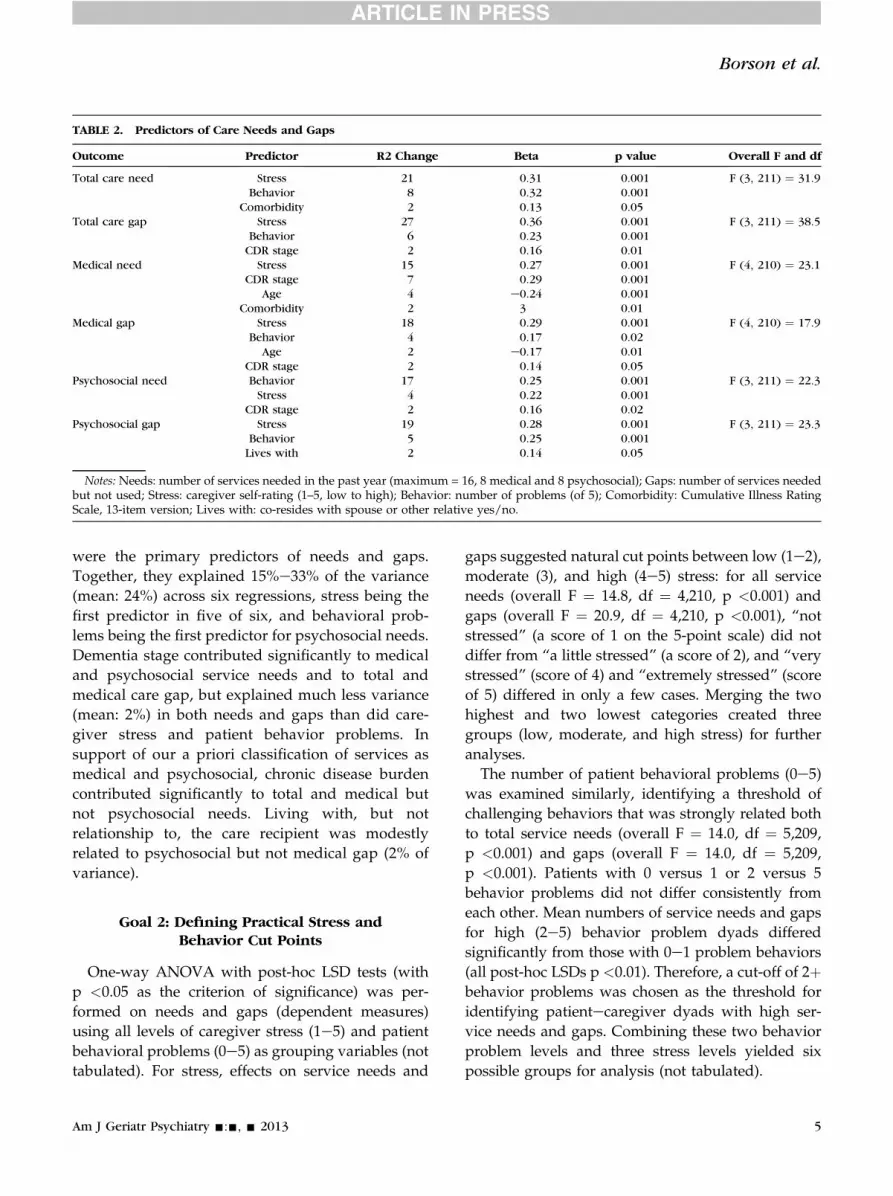
TABLE 2. Predictors of Care Needs and Gaps
Outcome Predictor R2 Change Beta p value Overall F and df
Total care need Stress 21 0.31 0.001 F (3, 211) ¼ 31.9Behavior 8 0.32 0.001
Comorbidity 2 0.13 0.05Total care gap Stress 27 0.36 0.001 F (3, 211) ¼ 38.5
Behavior 6 0.23 0.001CDR stage 2 0.16 0.01
Medical need Stress 15 0.27 0.001 F (4, 210) ¼ 23.1CDR stage 7 0.29 0.001
Age 4 e0.24 0.001Comorbidity 2 3 0.01
Medical gap Stress 18 0.29 0.001 F (4, 210) ¼ 17.9Behavior 4 0.17 0.02
Age 2 e0.17 0.01CDR stage 2 0.14 0.05
Psychosocial need Behavior 17 0.25 0.001 F (3, 211) ¼ 22.3Stress 4 0.22 0.001
CDR stage 2 0.16 0.02Psychosocial gap Stress 19 0.28 0.001 F (3, 211) ¼ 23.3
Behavior 5 0.25 0.001Lives with 2 0.14 0.05
Notes: Needs: number of services needed in the past year (maximum = 16, 8 medical and 8 psychosocial); Gaps: number of services neededbut not used; Stress: caregiver self-rating (1–5, low to high); Behavior: number of problems (of 5); Comorbidity: Cumulative Illness RatingScale, 13-item version; Lives with: co-resides with spouse or other relative yes/no.
Borson et al.
were the primary predictors of needs and gaps.Together, they explained 15%e33% of the variance(mean: 24%) across six regressions, stress being thefirst predictor in five of six, and behavioral prob-lems being the first predictor for psychosocial needs.Dementia stage contributed significantly to medicaland psychosocial service needs and to total andmedical care gap, but explained much less variance(mean: 2%) in both needs and gaps than did care-giver stress and patient behavior problems. Insupport of our a priori classification of services asmedical and psychosocial, chronic disease burdencontributed significantly to total and medical butnot psychosocial needs. Living with, but notrelationship to, the care recipient was modestlyrelated to psychosocial but not medical gap (2% ofvariance).
Goal 2: Defining Practical Stress andBehavior Cut Points
One-way ANOVA with post-hoc LSD tests (withp <0.05 as the criterion of significance) was per-formed on needs and gaps (dependent measures)using all levels of caregiver stress (1e5) and patientbehavioral problems (0e5) as grouping variables (nottabulated). For stress, effects on service needs and
Am J Geriatr Psychiatry -:-, - 2013
gaps suggested natural cut points between low (1e2),moderate (3), and high (4e5) stress: for all serviceneeds (overall F ¼ 14.8, df ¼ 4,210, p <0.001) andgaps (overall F ¼ 20.9, df ¼ 4,210, p <0.001), “notstressed” (a score of 1 on the 5-point scale) did notdiffer from “a little stressed” (a score of 2), and “verystressed” (score of 4) and “extremely stressed” (scoreof 5) differed in only a few cases. Merging the twohighest and two lowest categories created threegroups (low, moderate, and high stress) for furtheranalyses.
The number of patient behavioral problems (0e5)was examined similarly, identifying a threshold ofchallenging behaviors that was strongly related bothto total service needs (overall F ¼ 14.0, df ¼ 5,209,p <0.001) and gaps (overall F ¼ 14.0, df ¼ 5,209,p <0.001). Patients with 0 versus 1 or 2 versus 5behavior problems did not differ consistently fromeach other. Mean numbers of service needs and gapsfor high (2e5) behavior problem dyads differedsignificantly from those with 0e1 problem behaviors(all post-hoc LSDs p <0.01). Therefore, a cut-off of 2þbehavior problems was chosen as the threshold foridentifying patientecaregiver dyads with high ser-vice needs and gaps. Combining these two behaviorproblem levels and three stress levels yielded sixpossible groups for analysis (not tabulated).
5
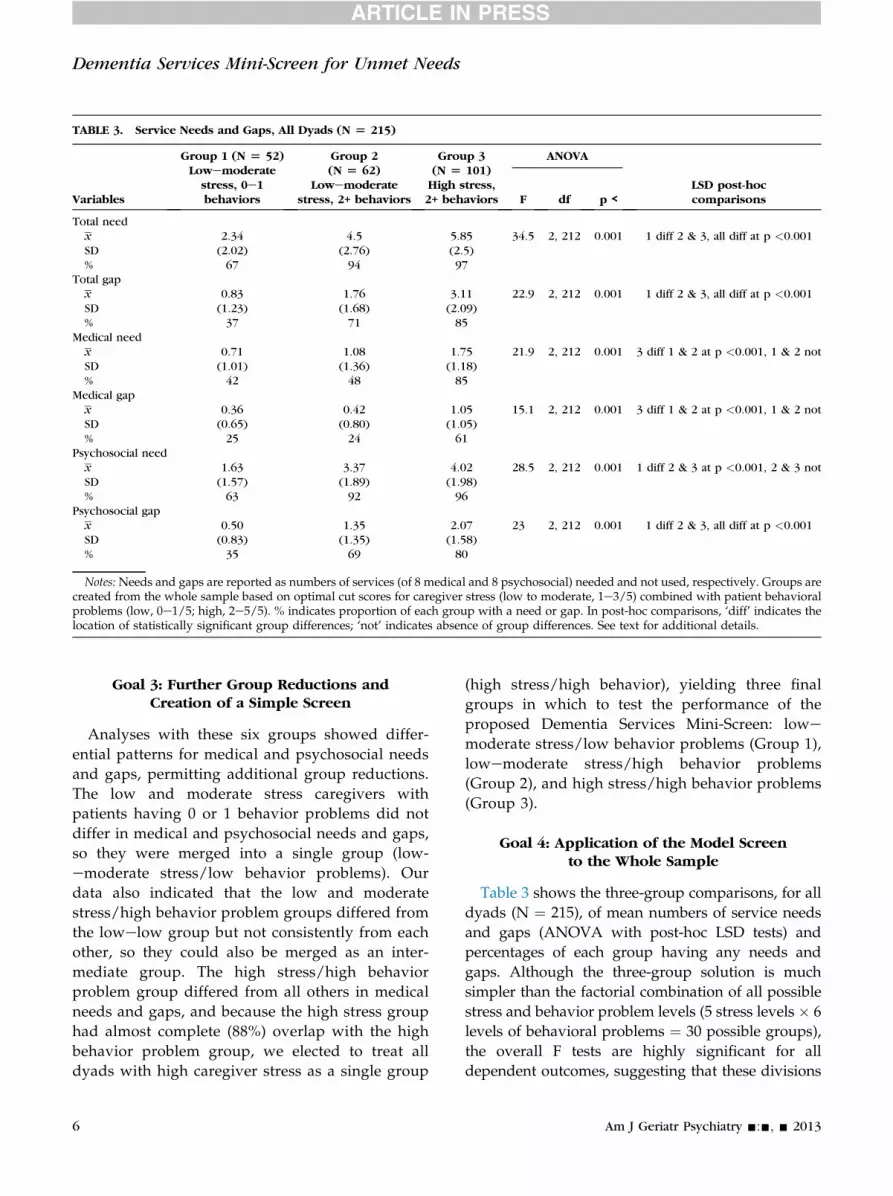
TABLE 3. Service Needs and Gaps, All Dyads (N [ 215)
Variables
Group 1 (N [ 52)Lowemoderatestress, 0e1behaviors
Group 2(N [ 62)
Lowemoderatestress, 2+ behaviors
Group 3(N [ 101)High stress,2+ behaviors
ANOVA
LSD post-hoccomparisonsF df p <
Total needx 2.34 4.5 5.85 34.5 2, 212 0.001 1 diff 2 & 3, all diff at p <0.001SD (2.02) (2.76) (2.5)% 67 94 97
Total gapx 0.83 1.76 3.11 22.9 2, 212 0.001 1 diff 2 & 3, all diff at p <0.001SD (1.23) (1.68) (2.09)% 37 71 85
Medical needx 0.71 1.08 1.75 21.9 2, 212 0.001 3 diff 1 & 2 at p <0.001, 1 & 2 notSD (1.01) (1.36) (1.18)% 42 48 85
Medical gapx 0.36 0.42 1.05 15.1 2, 212 0.001 3 diff 1 & 2 at p <0.001, 1 & 2 notSD (0.65) (0.80) (1.05)% 25 24 61
Psychosocial needx 1.63 3.37 4.02 28.5 2, 212 0.001 1 diff 2 & 3 at p <0.001, 2 & 3 notSD (1.57) (1.89) (1.98)% 63 92 96
Psychosocial gapx 0.50 1.35 2.07 23 2, 212 0.001 1 diff 2 & 3, all diff at p <0.001SD (0.83) (1.35) (1.58)% 35 69 80
Notes:Needs and gaps are reported as numbers of services (of 8 medical and 8 psychosocial) needed and not used, respectively. Groups arecreated from the whole sample based on optimal cut scores for caregiver stress (low to moderate, 1e3/5) combined with patient behavioralproblems (low, 0e1/5; high, 2e5/5). % indicates proportion of each group with a need or gap. In post-hoc comparisons, ‘diff’ indicates thelocation of statistically significant group differences; ‘not’ indicates absence of group differences. See text for additional details.
Dementia Services Mini-Screen for Unmet Needs
Goal 3: Further Group Reductions andCreation of a Simple Screen
Analyses with these six groups showed differ-ential patterns for medical and psychosocial needsand gaps, permitting additional group reductions.The low and moderate stress caregivers withpatients having 0 or 1 behavior problems did notdiffer in medical and psychosocial needs and gaps,so they were merged into a single group (low-emoderate stress/low behavior problems). Ourdata also indicated that the low and moderatestress/high behavior problem groups differed fromthe lowelow group but not consistently from eachother, so they could also be merged as an inter-mediate group. The high stress/high behaviorproblem group differed from all others in medicalneeds and gaps, and because the high stress grouphad almost complete (88%) overlap with the highbehavior problem group, we elected to treat alldyads with high caregiver stress as a single group
6
(high stress/high behavior), yielding three finalgroups in which to test the performance of theproposed Dementia Services Mini-Screen: lowe
moderate stress/low behavior problems (Group 1),lowemoderate stress/high behavior problems(Group 2), and high stress/high behavior problems(Group 3).
Goal 4: Application of the Model Screento the Whole Sample
Table 3 shows the three-group comparisons, for alldyads (N ¼ 215), of mean numbers of service needsand gaps (ANOVA with post-hoc LSD tests) andpercentages of each group having any needs andgaps. Although the three-group solution is muchsimpler than the factorial combination of all possiblestress and behavior problem levels (5 stress levels � 6levels of behavioral problems ¼ 30 possible groups),the overall F tests are highly significant for alldependent outcomes, suggesting that these divisions
Am J Geriatr Psychiatry -:-, - 2013

TABLE 4. Service Needs and Gaps, Mild Impairment Group (CDR 0.5e1, N [ 111)
Variables
Group 1 (N [ 52)Lowemoderatestress, 0e1behaviors
Group 2(N [ 62)
Lowemoderatestress, 2+ behaviors
Group 3(N [ 101)High stress,2+ behaviors
ANOVA
LSD post-hoc comparisonsF df p <
Total needx 1.68 3.81 5.3 30.5 2, 108 0.001 1, 2, & 3 all diff at p <0.01SD (1.59) (2.37) (2.38)% 60 93 98
Total gapx 0.48 1.18 2.81 26.8 2, 108 0.001 3 diff 1 & 2 at p <0.001,
1 & 2 diff at p <0.06SD (0.93) (1.44) (1.90)% 25 60 84
Medical needx 0.45 0.59 1.56 16.1 2, 108 0.001 3 diff 1 & 2 at p <0.001, 1 & 2 notSD (0.75) (1.01) (1.11)% 33 33 84
Medical gapx 0.20 0.15 0.98 16.7 2, 108 0.001 3 diff 1& 2 at p <0.001, 1 & 2 notSD (0.61) (0.46) (0.90)% 13 11 66
Psychosocial needx 1.25 3.22 3.61 19.6 2, 108 0.001 1 diff 2 & 3 at p <0.001, 2 & 3 notSD (1.50) (1.97) (1.97)% 53 89 95
Psychosocial gapx 0.30 1.07 1.82 15.8 2, 108 0.001 1 diff 2 & 3 at p <0.001, 2 & 3 notSD (0.61) (1.30) (1.57)% 23 59 77
Notes:Needs and gaps are reported as numbers of services (of 8 medical and 8 psychosocial) needed and not used, respectively. Groups arecreated from the very mildly/mildly impaired subsample based on optimal cut scores for caregiver stress (low to moderate, 1e3/5) combinedwith patient behavioral problems (low, 0e1/5; high, 2e5/5). See text for additional details.
Borson et al.
reasonably capture the relationships originally seenin multiple regressions (Table 2). Nonetheless,post-hoc group comparisons suggested further sim-plifications. For psychosocial needs, only Group 1(lowemoderate stress/low behavior problems)differed from Groups 2 and 3, which did not differsignificantly from each other. For medical needs andgaps, only the high stress group differed from theother two. By forming two groups (high stress versusall others for medical gap; lowemoderate stress/lowbehavior problems versus all others for psychosocialgap), we were able to calculate sensitivity and spec-ificity for the Dementia Services Mini-Screen. Acrossall dyads, sensitivity and specificity were 69% formedical gaps, and sensitivity was 88% and specificity47% for psychosocial gaps.
Relative to the patients typically seen in primarycare, our total sample over-represents the veryimpaired (CDR 2þ). The true test of an early needs/gaps-detection screen should be in the population forwhich it is primarily intended—dyads more typical
Am J Geriatr Psychiatry -:-, - 2013
of those seen in primary care, where MCI and milddementia (CDR ¼ 0.5 and 1.0, respectively) areprevalent.32
Goal 5: Retesting the Dementia Services Mini-Screen in MCI/Mild Dementia
Table 4 shows the service needs and gaps in the mildimpairment group. In analyses restricted to the less-impaired subset (N ¼ 111, CDR 0.5e1), we replicatedall ANOVAs shown in Table 3 with functionally iden-tical results. The contrasts for medical gaps and psy-chosocial gaps were particularly striking and areillustrated in Figure 1. Sensitivity/specificity analyses,classic benchmarks for screen performance, wereapplied to detection of medical and psychosocial gaps,using the empirical decision rules established in prioranalyses: “high stress” screens for gaps in dementia-specific medical care and “high behavior problems”screens for gaps in psychosocial care. Using thesecriteria, the mini-screen’s sensitivity was 88% and
7

FIGURE 1. Gaps in care for early/mild dementia dyads:Relationship to caregiver stress and dementia-related behavioral problems.
0%
10%
20%
30%
40%
50%
60%
70%
80%
Low/Moderate Stress High Stress+High Behavior Problems
Medical Care Gaps (CDR = 0.5 & 1)
Pe
rc
en
to
f S
am
ple
w
ith
G
ap
0%
10%
20%
30%
40%
50%
60%
70%
80%
Low Behavior Problems High Behavior Problems
Pe
rc
en
t o
f S
am
ple
w
ith
Ga
p
Psychosocial Care Gaps (CDR =0.5 & 1)
Dementia Services Mini-Screen for Unmet Needs
specificity78%formedical caregaps,whereas sensitivitywas 84% and specificity 60% for psychosocial care gaps.
DISCUSSION
In this study, we show that caregiver stress andpatient behavioral problems have powerful relation-ships with need for both medical and psychosocial careservices and with gaps in provision of those services.These factors are more important in predicting serviceneeds and gaps than dementia severity, relationshipbetween patient and caregiver, living situation, andpatients’ ages and chronic disease burden. Caregiverswere able to clearly identify needs and gaps in medicaland psychosocial services and, by the needs and gapsthey endorsed, to indicate that both types of cliniciansare important for both members of the dyad. The fullrange of dementia care services evaluated in this studyis not typically provided in the primary care settingand will require the collaborative expertise of special-ized dementia care clinicians and care managers wholink primary and psychosocial care services into acoherent framework for both patient and caregiver.
8
We found notable differences between perceivedneeds and gaps for medical care and psychosocialcare services. When the care recipient had two ormore behavior problems, nearly all caregiversreported need for psychosocial care, even when theyreported their stress as low, and most reported gapsin those services. In contrast, for medical care, majorgaps were found only when high caregiver stress wascoupled with high patient behavior problems, andthese gaps were specifically related to dementia careinterventions (counseling, medications to managepatient behavior problems and/or caregiver stress,data not shown). By using a new empirically derivedtool, the Dementia Services Mini-Screen, we suc-cessfully identified dyad characteristics associatedwith high medical and psychosocial needs and gaps.The Dementia Services Mini-Screen could be a viablefirst step in identifying high needs dyads in generalhealthcare settings. It offers a pragmatic approach toquantifying needs for developing dementia-specificmedical and psychosocial services at the health sys-tem level. It is simple enough to be used by clinicalsupport staff, easily incorporated into electronicmedical records, and readily tracked over time toassist clinicians in making appropriate care decisionsand help health systems develop a parsimonious butessential menu of services for delivering optimalhealthcare to dementia dyads, once dementia isrecognized and diagnosed.
Extensive prior research has shown that the causesof perceived stress in dementia caregivers are com-plex but are partly related to patient behavior prob-lems and that both are associated with caregivers’expressed needs for services.25 Asking caregiversabout services needs is well suited to the person-centered approach to care,33 which is receiving newemphasis in chronic disease management and whichis inherent in collaborative care models that linkspecialized medical and psychosocial dementia-related services to primary care.34 Guidance hasbeen lacking to help primary care providers andhealthcare systems quickly and systematically iden-tify patientecaregiver dyads who need enhanceddementia services embedded in a collaborative orintegrated service model. Based on data examined inthe present pilot study, we propose a pragmaticmethod that uses two very simple caregiver-reportedelements to achieve this goal. The Dementia ServicesMini-Screen may help to promote patient-centered
Am J Geriatr Psychiatry -:-, - 2013

Borson et al.
care by translating the large but highly specializedand complex literature on caregivers, patients, andservice needs into a practical algorithm for primarycare use.
We anticipate the time required to administer theDementia Services Mini-Screen to be brief (w1 min-ute), although this and administration by supportstaff remain to be empirically field tested. Knowledgeof the patient’s dementia history and stage and co-morbid illness history is important for comprehensivehealthcare but not required for validity or applicationof the screen, nor is its performance strongly influ-enced by patient age, residence, or caregiver relation-ship. It also shows very strong contrasts and goodsensitivity and specificity in dyads in the earlier stagesof dementia that are most often encountered in pri-mary care settings. It was in this group that the com-bination of caregiver stress and patient behaviorproblems most clearly separated dyads who haveservice gaps from those who do not. If combined witha very brief, well-established screen designed to detectclinically important cognitive impairment in primarycare, such as the Mini-Cog,29 a primary care providercould rapidly obtain useful indices of patient cognitivestatus and behavioral problems, a rough index ofcaregiver stress, and predictors of medical and psy-chosocial service gaps in 5 minutes or less. Withgrowing elderly populations, over-burdened physi-cians, and increasing healthcare costs, this would seema very efficient use of time and resources.
There are some limitations in the present work.Studyparticipantswere recruited through communityoutreach, so the sample cannot be considered repre-sentative of the older population in general or of olderadults in primary care. Sociodemographic factors thatcould have important influences on caregiver stress,patient behaviors, and service needs and gaps wereeither insufficiently variable for analysis (e.g., race,ethnicity) or not obtained (e.g., family support andinvolvement, income) in this study. The empirical cutpoints for stress and behavior indicators proposed fortargeting dyads with high service needs requireadditional validation in representative samples, andnot all patient behavior problems and neuropsychi-atric symptoms that affect needs for care wereincluded in the brief behavior scale. Also, the single-item CERAD caregiver stress question has not beenindependently validated. It was chosen for its promisefor use in healthcare settings, where longer, more
Am J Geriatr Psychiatry -:-, - 2013
detailed scales could not practically be used to screenlarge numbers of individuals. However, a single-itemmeasure of distress has been shown to perform wellwhen compared with longer standard distress scalesin cancer patients.35
There is broad agreement among dementiaspecialists that high quality care for patients withdementia requires both medical and psychosocialcomponents, attention to both patient and caregiver,and continuity of relationship between providers andpatientecaregiver dyads.36 However, there iscurrently no fully evidence-based consensus as tohow best to organize this care at the practice or healthsystem level. Although integrated or collaborativecare approaches that offer both medical and psy-chosocial services to dyads have inherent appeal,conform to geriatric care principles, and are sup-ported by results of early randomized trials18,19,37
and clinical demonstrations,20,21 comprehensive,intensive services are not needed by all patients andcaregivers or at all points along the course of de-mentia. Randomized trials of comprehensive de-mentia care tested thus far have provided the samepackage of services to all patientecaregiver dyadsand treated them as a uniform group. These studieshave found some positive but relatively modesteffects on target outcomes (including caregiver stressand patient behavioral problems). Such small effectscould discourage adoption of effective interventionsthat may be necessary for only a subset of patientecaregiver dyads. The Dementia Services Mini-Screenis designed to identify those dyads most likelyto benefit from comprehensive dementia careinterventions at a particular point in time. Use of thisscreen could be attractive to third-party payers andhealthcare organizations faced with rising demandsto provide high quality and cost-effective care fordementia, whether that need is for routine primarycare or specialized, intensive, team-based interven-tion for high-needs dyads seen in the same practices.
Acquisition of data and initial drafting of the manu-script was supported by the National Institute on Aging(P50 AG 5136, Alzheimer’s Disease Research Center [toSB, ML, and JMS]), the National Institute of MentalHealth (R01 MH 57663 to PV), and the Health Resourcesand Services Administration (to SB). TS receives supportfrom the JAHF Atlantic Philanthropies Claire FaginFellowship and the Robert Wood Johnson Foundation.
9

Dementia Services Mini-Screen for Unmet Needs
Ref
erences1. Hebert LE, Weuve J, Scherr PA, et al: Alzheimer disease in theUnited States (2010e2050) estimated using the 2010 census.Neurology 2013; 80:1778e1783
2. Hurd MD, Martorell P, Delavande A, et al: Monetary costs ofdementia in the United States. N Engl J Med 2013; 368:1326e1334
3. Chodosh J, Mittman BS, Connor KI, et al: Caring for patients withdementia: how good is the quality of care? Results from threehealth systems. J Am Geriatr Soc 2007; 55:1260e1268
4. Phelan EA, Borson S, Grothaus L, et al: Association of incidentdementia with hospitalizations. JAMA 2012; 307:165e172
5. Odenheimer G, Borson S, Sanders AE, et al: Quality improve-ment in neurology: Dementia Management Quality Measures.Neurology 2013; 81:1545e1549
6. Hunsaker AE, Schmidt K, Lingler JH: Discussing dementia-relatedbehaviors during medical visits for people with Alzheimer’s dis-ease. Am J Alz Dis Oth Dement 2010; 25:248e254
7. Borson S, Logsdon RG, Sadak T, et al: Redesigning health care fordementia: from wish through policy to practice. Am J GeriatrPsychiatry 2013; 21:30
8. Harris DP, Chodosh J, Vassar SD, et al: Primary care providers’views of challenges and rewards of dementia care relative toother conditions. J Am Geriatr Soc 2009; 57:2209e2216
9. Fortinsky RH, Zlateva I, Delaney C, et al: Primary care physicians’dementia care practices: evidence of geographic variation.Gerontologist 2010; 50:179e191
10. Pimlott NJ, Persaud M, Drummond N, et al: Family physicians anddementia in Canada: Part 1. Clinical practice guidelines: aware-ness, attitudes, and opinions. Can Fam Physician 2009; 55:506e507
11. Boise L, Camicioli R, Morgan DL, et al: Diagnosing dementia:perspectives of primary care physicians. Gerontologist 1999; 39:457e464
12. Brauner DJ, Muir JC, Sachs GA: Treating nondementia illnesses inpatients with dementia. JAMA 2000; 283:3230e3235
13. Fortinsky RH: Health care triads and dementia care: integrativeframework and future directions. Aging Ment Health 2001;5(Suppl 1):S35eS48
14. Robinson L, Iliffe S, Brayne C, et al: Primary care and dementia: 2.Long-term care at home: psychosocial interventions, informationprovision, carer support and case management. Int J GeriatrPsychiatry 2010; 25:657e664
15. Chodosh J, Pearson M, Connor K, et al: A dementia care man-agement intervention: which components improve quality? Am JManag Care 2012; 18:85e94
16. Connor K, McNeese-Smith D, van Servellen G, et al: Insight intodementia care management using social-behavioral theory andmixed methods. Nurs Res 2009; 58:348e358
17. National Plan to Address Alzheimer’s Disease. 2012. Washington,DC, US Department of Health and Human Services. Available at:http://aspe.hhs.gov/daltcp/napa/NatlPlan.pdf
18. Callahan CM, Boustani MA, Unverzagt FW, et al: Effectiveness ofcollaborative care for older adults with Alzheimer disease inprimary care: a randomized controlled trial. JAMA 2006; 295:2148e2157
19. Vickrey BG, Mittman BS, Connor KI, et al: The effect of a diseasemanagement intervention on quality and outcomes of dementia
10
care: a randomized, controlled trial. Ann Intern Med 2006; 145:713e726
20. Lessig M, Farrell J, Madhavan E, et al: Cooperative dementia careclinics: a new model for managing cognitively impaired patients.J Am Geriatr Soc 2006; 54:1937e1942
21. Murphy RHR, Borson S: Adaptation of a group visit dementia caremodel to a community setting. J Psychiatry Clin Neurosci 2013
22. van der Roest HG, Meiland FJ, Comijs HC, et al: What docommunity-dwelling people with dementia need? A survey ofthose who are known to care and welfare services. Int Psycho-geriatr 2009; 21:949e965
23. Toseland RW, McCallion P, Gerber T, et al: Use of health andhuman services by community-residing people with dementia.Soc Work 1999; 44:535e548
24. Toseland RW, McCallion P, Gerber T, et al: Predictors of healthand human services use by persons with dementia and theirfamily caregivers. Soc Sci Med 2002; 55:1255e1266
25. Stirling C, Andrews S, Croft T, et al: Measuring dementia carers’unmet need for services—an exploratory mixed method study.BMC Health Serv Res 2010; 10:122e132
26. Marziali E, McCleary L, Streiner DL: Evaluation of an assessmentbattery for estimating dementia caregiver needs for health andsocial care services. Am J Alzheim Dis Other Demen 2010; 25:446e454
27. Fillenbaum GG, van Belle G, Morris JC, et al: Consortium toEstablish a Registry for Alzheimer’s Disease (CERAD): the firsttwenty years. Alzheim Dement 2008; 4:96e109
28. Morris JC: Clinical dementia rating: a reliable and valid diagnosticand staging measure for dementia of the Alzheimer type. IntPsychogeriatr 1997; 9(Suppl 1):173e176; discussion 177e178
29. Borson S, Scanlan JM, Watanabe J, et al: Improving identificationof cognitive impairment in primary care. Int J Geriatr Soc 2006;21:349e355
30. Borson S, Brush M, Gil E, et al: The Clock Drawing Test: utility fordementia detection in multiethnic elders. J Gerontol Biol Sci MedSci 1999; 54A:M534eM540
31. Borson S, Scanlan JM, Lessig M, et al: Comorbidity in aging anddementia: scales differ, and the difference matters. Am J GeriatrPsychiatry 2010; 18:999e1006
32. Doraiswamy PM, Leon J, Cummings JL, et al: Prevalence andimpact of medical comorbidity in Alzheimer’s disease. J GerontolBiol Sci Med Sci 2002; 57A:M173eM177
33. Meaney AM, Croke M, Kirby M: Needs assessment in dementia.Int J Geriatr Psychiatry 2005; 20:322e329
34. Callahan CM, Boustani M, Sachs GA, et al: Integrating care forolder adults with cognitive impairment. Curr Alzheim Res 2009;6:368e374
35. Goebel S, Mehdorn HM: Measurement of psychological distress inpatients with intracranial tumours: the NCCN distress thermom-eter. J Neurooncol 2011; 104:357e364
36. Hogan DB, Bailey P, Carswell A, et al: Management of mild tomoderate Alzheimer’s disease and dementia. Alzheim Dement2007; 3:355e384
37. Reuben DB, Roth CP, Frank JC, et al: Assessing care of vulnerableelders—Alzheimer’s disease: a pilot study of a practice redesignintervention to improve the quality of dementia care. J Am Ger-iatr Soc 2010; 58:324e329
Am J Geriatr Psychiatry -:-, - 2013