decrease in acute myocardial ischemia by hyaluronidase in isolated, perfused, rabbit hearts
TRANSCRIPT

JOURNAL OF SURGICAL RESEARCH 30, 489-4% (1981)
Decrease in Acute Myocardial lschemia by Hyaluronidase in Isolated, Perfused, Rabbit Hearts’
LEWIS WETSTEIN, M.D.,2 MICHAEL S.NUSSBAUM, M.D., CLYDE H. BARLOW, PH.D., WESLEY R. HARDEN, M.D., MICHAEL B. SIMSON, M.D., BRUCE SLAGLE, B.S.,
AND ALDEN H. HARKEN, M.D.3
Divisions of Cardiothoracic Surgery and Cardiology, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania 19104
Presented at the Annual Meeting of the Association for Academic Surgery, Birmingham, Alabama, November 5-8, 1980
Hyaluronidase has been reported to reduce infarct size and cellular damage after coronary artery occlusion. The influence of hyaluronidase (H) on experimental myocardial ischemia was studied in isolated perfused rabbit hearts. Changes in ischemic area were assessed by epicardial NADH fluorescence photography, an intrinsic, high-resolution display of myocardial ischemia. Computerized determination of ischemic area was made from standardized photographs. H was begun 5 min after coronary artery ligation at 4 units/ml perfusate. NADH fluorophotographs were taken at IO-min intervals up to 40 min of ischemia. Coronary sinus oxygen tension (P,,O,), myo- cardial oxygen consumption (MvOz) and coronary flow were determined. After 40 mitt, the hearts were perfused with a rhodamine solution to indicate areas of myocardial perfusion. In 18 H- treated hearts 55 ? 6% (mean ? SE) of the nonperfused area was ischemic (NADH fluorescent) and the ischemic areas had a patchy distribution. In 26 untreated hearts 86 f 2% of the nonper- fused area was ischemic and the ischemic areas were uniform, (P < 0.001). The distance between perfused and ischemic tissue was 861 f 76 pm in the H-treated and 359 ? 19 pm in the untreated hearts, (P < 0.001). In the H-treated hearts P,,O, increased to 154% of the postligation control while it decresed to 77% in the untreated hearts (P < 0.001). M$‘O, decreased to 87% of control after ligation in both groups. The H-treated hearts had a further decline of 37% while the untreated hearts had no further change. In the H-treated hearts, coronary flow increased to 150% of the post- ligation control while it fell to 80% in the untreated group (P < 0.001). We conclude that hyaluroni- dase increases P,,O, and coronary flow while it decreases MVO, during acute ischemia. In hyaluronidase-treated hearts, significant amounts of myocardium remain normoxic within the nonperfused areas.
INTRODUCTION
An imbalance of oxygen supply and de- mand leads to myocardial ischemia and cell death. Classically, the zone between the ischemic and well-perfused areas is defined as a reversibly damaged “border zone.” Numerous studies have investigated the ex-
r Supported in part by USPHS Grants HL-223 15 and 1 F32 HL-06275-01.
* Measey Fellow in Investigative Surgery. 3 To whom requests for reprints should be sent at:
Department of Cardiothoracic Surgery, Hospital of the University of Pennsylvania, 3400 Spruce St., Phila- delphia, Pa. 19104.
tent and reversibility of myocardial ische- mic injury, however, the nature of the transition from reversible to irreversible damage remains obscure. Many techniques, including histochemical [ 11, metabolic [2, 31, and radioisotopic [4] have been em- ployed to measure this zone. Reported “border-zone” widths have appeared to be highly technique dependent and have varied from 2 to 15 mm [5].
A high-resolution (k 50 pm), autofluores- cent signal has previously been utilized in this laboratory to delineate myocardial oxy- gen supply/demand 16, 73. Reduced nico-
489 OO22-4804/81/05O489-08$01.00/O Copyright 0 1981 by Academic Press. Inc. AU rights of reproduction in any form reserved.

490 JOURNAL OF SURGICAL RESEARCH: VOL. 30, NO. 5, MAY 1981
tinamide adenine dinucleotide (NADH), a normal component of the intracellular mito- chondrial electron transport system in- creases in concentration during cellular hypoxia. The ratio between the reduced (NADH) and oxidized (NAD+) form reflects oxygen supply/demand. Reduced NADH in anoxic myocardium fluoresces when ex- cited with ultraviolet light while oxidized NAD in normoxic tissue does not. Employ- ing fluorescence angiography , a sharp de- marcation has been demonstrated between the normoxic-anoxic interface or border zone. This technique displays high temporal (kO.5 set) and spatial (-+50 pm) resolution in the assessment of myocardial redox state [g-lo] and correlates well with other methods of assessing myocardial ischemia [ll, 121.
Hyaluronidase has been reported to re- duce infarct size and cellular damage after coronary artery occlusion [ 13 - 161. The purpose of this report is to examine the influence and mechanism of hyaluronidase action on experimentally produced myo- cardial ischemia in the isolated, perfused rabbit heart.
Fourty-four 2- to 3-kg New Zealand rab- bits were anesthetized with sodium pento- barbitol (30 mg/kg). Hearts were rapidly excised and perfused with a blood-free crystalloid solution at 37°C. The perfusate consisted of Krebs-Ringer’s bicarbonate solution containing 5 n&I glucose and 2.5 n&I calcium and saturated with 95% oxygen and 5% carbon dioxide. The perfusion cir- cuit included an overflow reservoir placed 104 cm above the level of the aortic cannula to maintain perfusion pressure to 80 mm Hg.
The vena cavae and pulmonary veins were ligated, and a soft, plastic, cannula was secured in the pulmonary artery. Pulmonary artery flow was directed through a Clark- type oxygen electrode. Coronary venous PO, was recorded and temperature cor- rected on an oxygen electrode amplifier.4
4 Johnson Research Foundation.
Hearts were paced at 240 beats/min with bipolar leads placed on the right atria1 appendage. Pacing stimulus was provided by a Grass SD-9 stimulator. The left atrium was opened and the left ventricle decom- pressed by excising a portion of the mitral valve.
After establishment of stable atria1 pacing, epicardial NADH fluorescence photographs and myocardial oxygen consumption were recorded. Flows were measured by collect- ing the coronary venous and thebesian ef- fluent flow that dripped from the heart. Epicardial NADH fluorescence photographs were taken utilizing a Bronica S2A camera fitted with a 75-mm focal lens reversed to provide an image on film 1.5 times the actual size. Flash illumination was pro- vided by two xenon flash tubes (E. G. & G. Corp. FX-47C2), 400 joules each, covered with Corning 5840 filters yielding excitatory light in the 330- to 380-nm region. The camera lens was filtered with Wratten Nos. 2E and 4 filters which allowed transmission of fluorescence in the 430- to 510-nm region. The xenon flash tubes were triggered from the pacemaker 10 msec prior to the onset of the electrical stimulus. By this tech- nique, all photographs were taken at end diastole.
At 10 min a coronary artery supplying the anteroapical portion of the left ventricle was ligated, and coronary sinus P02, MvOp, and coronary flow were recorded. After 5 min of ischemic time, an epicardial NADH fluorophotograph was taken. The rabbits were then divided into two groups: eighteen were treated with hyaluronidase (40 pg/ ml), while 26 received no treatment. Coro- nary sinus P02, MVO,, and coronary flow were recroded and photographs taken at lo- min intervals. At 40 min, each heart was perfused with rhodamine. As soon as the dye was noted to emerge from the pulmo- nary artery catheter (2-3 set) the heart was quick-frozen between large metal tongs and plunged into liquid nitrogen [ 171.
After the heart was completely frozen,

WETSTEIN ET AL: HYALURONIDASE DECREASES MYOCARDIAL ISCHEMIA 491
the epicardium was filled to a depth of 0.5 mm in order to remove the epicardial vessels and surface ice. NADH fluoro- photographs were taken at this depth. Sub- sequently, the heart was removed from the aluminum block and weighed.
Photographs were enlarged (x 15) and areas computer digitized. Both the area not perfused with rhodamine and the anoxic zone of NADH fluorescence were digitized. In addition, the distance between rhoda- mine and NADH fluorescence was meas- ured at 20 points around the ischemic border.
Myocardial oxygen consumption was cal- culated and expressed as microliters of oxygen per minute per grams wet weight of heart. Calculations were based on the standard formula: MVO, = (P,OZ - PyO,) x 0.000029 ml O2 perfusate x flow/g wet wt of heart, where 0.000029 ml O,/Torr is the solubility of oxygen in milliliters of perfusate at 37°C.
The influence of hyaluronidase on myo- cardial oxygen consumption, myocardial perfusate flow, and the ischemic zone area and borderzone width were evaluated. Dif- ferences were assessed using a t test for paired and nonpaired data where appropriate.
RESULTS
There was no difference in coronary sinus oxygen tension (PoO,) between the two groups before and 5 min after ligation (Fig. 1). P,,O, increased in the hyaluroni- dase-treated group to 154% of the post- ligation control (278 + 18-426 t 18 Torr, mean f SE). The untreated hearts declined to 77% of control over the course of the experiment (247 2 13-191 * 26 Tot-r). The increase in coronary sinus PO, in the treated group was different from that of untreated hearts (P < 0.0001).
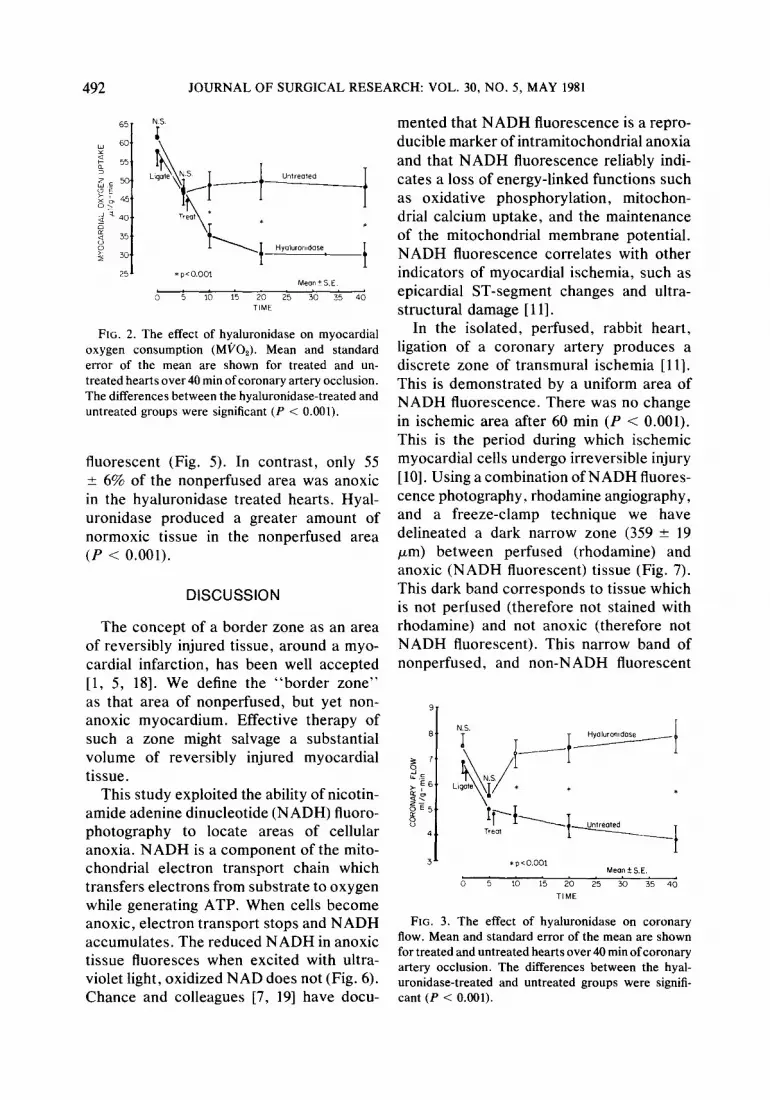
After ligation, myocardial oxygen con- sumption (MPO,) decreased to 87% of con- trol in both groups (Fig. 2). There was no difference between the two groups before
500-
450
0” a 400,’
2 350 m;
&E 300
2 P 250,
8 200
*
150 1 ‘p’oooo1
blean+s E
Control 5 10 15 20 25 30 35 ‘lo
TlME
FIG. 1. The effects of hyaluronidase on coronary sinus oxygen tension (P,,O,). Mean and standard error of the mean are shown for treated and untreated hearts over 40 min of coronary occlusion. The dif- ferences between the H-treated and untreated groups were significant (P < 0.0001).
and 5 min after ligation. The hyaluronidase- treated hearts had a further decline in MVO, of 36% (58 +- 4-37 +- 3 pi/g-min). The untreated hearts had no further change in MVO, (55 + 4-52 2 4 pi/g-min) (P < 0.001).
Coronary flow was reduced in both the treated and untreated hearts 5 min after coronary ligation (Fig. 3). There was no dif- ference between the groups before and after ligation. After hyaluronidase treatment, coronary flow increased to 150% of the post- ligation control (48 2 3-72 + 4 ml/min). With time the untreated hearts had a further drop in coronary flow to 80% of the post- ligation control (50 * 3-40 * 2 ml/min). The increase in flow in hyaluronidase treated hearts was different from that of untreated hearts (P < 0.001).
In all cases the transition from minimal to full NADH fluoresence was abrupt and less than 50 pm. In the untreated hearts, the distance between perfused and anoxic tissue was 359 t 19 ,um (Fig. 4). In the hyaluronidase-treated hearts, the distance was 861 ? 76 pm. The distance between perfused and anoxic tissue was larger in the hyaluronidase-treated hearts (P < 0.000 1).
In the untreated hearts, 86 + 2% of the nonperfused area was anoxic and NADH
492 JOURNAL OF SURGICAL RESEARCH: VOL. 30, NO. 5, MAY 1981
251 * p~o.001 Me0ntS.E
0 5 10 15 20 25 30 35 40 TIME
FIG. 2. The effect of hyaluronidase on myocardial oxygen consumption (MPO,). Mean and standard error of the mean are shown for treated and un- treated hearts over 40 min of coronary artery occlusion. The differences between the hyaluronidase-treated and untreated groups were significant (P < 0.001).
fluorescent (Fig. 5). In contrast, only 55 ? 6% of the nonperfused area was anoxic in the hyaluronidase treated hearts. Hyal- uronidase produced a greater amount of normoxic tissue in the nonperfused area (P < 0.001).
DISCUSSION
The concept of a border zone as an area of reversibly injured tissue, around a myo- cardial infarction, has been well accepted [l, 5, 181. We define the “border zone” as that area of nonperfused, but yet non- anoxic myocardium. Effective therapy of such a zone might salvage a substantial volume of reversibly injured myocardial tissue.
This study exploited the ability of nicotin- amide adenine dinucleotide (NADH) fluoro- photography to locate areas of cellular anoxia. NADH is a component of the mito- chondrial electron transport chain which transfers electrons from substrate to oxygen while generating ATP. When cells become anoxic, electron transport stops and NADH accumulates. The reduced NADH in anoxic tissue fluoresces when excited with ultra- violet light, oxidized NAD does not (Fig. 6). Chance and colleagues [7, 191 have docu-
mented that NADH fluorescence is a repro- ducible marker of intramitochondrial anoxia and that NADH fluorescence reliably indi- cates a loss of energy-linked functions such as oxidative phosphorylation, mitochon- drial calcium uptake, and the maintenance of the mitochondrial membrane potential. NADH fluorescence correlates with other indicators of myocardial ischemia, such as epicardial ST-segment changes and ultra- structural damage [ 1 I].
In the isolated, perfused, rabbit heart, ligation of a coronary artery produces a discrete zone of transmural ischemia [ 111. This is demonstrated by a uniform area of NADH fluorescence. There was no change in ischemic area after 60 min (P < 0.001). This is the period during which ischemic myocardial cells undergo irreversible injury [lo]. Using a combination of NADH fluores- cence photography. rhodamine angiography, and a freeze-clamp technique we have delineated a dark narrow zone (359 2 19 pm) between perfused (rhodamine) and anoxic (NADH fluorescent) tissue (Fig. 7). This dark band corresponds to tissue which is not perfused (therefore not stained with rhodamine) and not anoxic (therefore not NADH fluorescent). This narrow band of nonperfused, and non-NADH fluorescent
31 *p<o.oo, Meon f. SE.
0 5 10 15 20 25 30 35 40
TIME
FIG. 3. The effect of hyaluronidase on coronary flow. Mean and standard error of the mean are shown for treated and untreated hearts over 40 min of coronary artery occlusion. The differences between the hyal- uronidase-treated and untreated groups were signifi- cant (P < 0.001).

WETSTEIN ET AL: HYALURONIDASE DECREASES MYOCARDIAL ISCHEMIA 493
FIG. 4. The effect of hyaluronidase on border-zone width (distance between perfused and anoxic tissue). Mean and standard error of the mean are shown for the hyaluronidase-treated (H) and the untreated (U) hearts 40 min after coronary artery occlusion. The differences between the hyahrronidase-treated and un- treated groups were significant (P < 0.0001).
tissue was defined as peri-ischemic border zone and was observed in all hearts.
Hyaluronidase is a mucolytic enzyme that lyses hyaluronic acid, the primary muco- polysaccharide component of the intra- cellular ground substance. The function of hyaluronic acid relates to the binding of cells in a viscous matrix. Hyaluronidase has been employed in many clinical situations since it was first described as a “spread- ing factor” by Duran-Reynals [21]. No toxic effects have been reported [22]. The ratio of toxicity to therapeutic dose is 200,000/l [23].
Our results demonstrated an increase in coronary flow and a decrease in myocardial oxygen consumption during acute ischemia treated with hyaluronidase. Furthermore, we were able to delineate an increase in the distance between perfused and anoxic tissue at the ischemic border. Hyaluronidase therefore increases the amount of non- NADH fluorescent tissue within nonper- fused areas.
The mechanism by which hyaluronidase
exerts its salutary effect on ischemic myo- cardium remains unclear. It has been sug- gested that it might reduce tissue edema [24], improve collateral flow [25], increase nutrient delivery, and enhance washout of metabolic waste products [ 14). We were able to document an increase (P < 0.001) in coronary blood flow.
We interpret these results as support that hyaluronidase increases the distance that oxygen diffuses at the border of an ischemic area. There are several factors that may produce this result. Hyaluronidase decreased myocardial oxygen consumption and increased capillary perfusion. There- fore, tissue oxygen supply/demand was improved: increasing capillary oxygen ten- sion together with the increase in coronary flow may increase oxygen diffusion into the nonperfused zone. Previous work in our laboratory demonstrated that when MVO, is dramatically reduced with potassium car- dioplegia, the border zone width increased to 500 pm. Our present results delineate a distance of approximately 869 pm; by de- polymerizing mucopolysaccharides hyal- uronidase may promote bulk transport of
100
E 0" 60 6 a
60
40
20 1 U
FIG. 5. The ratio of anoxic area and nonperfused area in the treated (H) and untreated (U) hearts. Mean and standard error of the mean are shown. Hyaluroni- dase significantly decreased the ratio of anoxic area to nonperfused area, (P < 0.001).

494 JOURNAL OF SURGICAL RESEARCH: VOL. 30, NO. 5, MAY 1981
OXJ /gen into the ischemic area. We feel that We caution that these results were obl :ained hyz duronidase may have a role in the ther- in isolated hearts with high coronary o: wen am r of myocardial &hernia and infarction. tension and low myocardial oxygen con-
FIG. 6. Epicardial NADH fluorophotograph of isolated perfused rabbit heart after IO-min coronal artery occlusion. Fat and connective tissue fluoresce brightly (*). The epicardial tissue distal to tl ligation is anoxic (A) and NADH fluorescent. The normoxic (N) epicardium does not fluoresce.
‘Y ke

WETSTEIN ET AL: HYALURONIDASE DECREASES MYOCARDIAL ISCHEMIA 495
FIG. 7. NADH fluorescence photograph of frozen-treated (H) and untreated (U) hearts 40 min after ligation. There are three zones: (1) the area well perfused(P) and marked with rhodamine fluorescence, (2) the anoxic area (A) which is NADH fluorescent, (3) the borderzone (B) between perfused and anoxic tissue.
sumption. The response of ischemia to hyal- 3. Opie, L. H., Bruyneel, L., and Owen, P. Beneficial
uronidase must be further examined in the effects of glucose, potassium and insulin on
blood perfused working heart in viva. tissue metabolic changes within first hour of myocardial infarction in the baboon. Circulation
ACKNOWLEDGMENTS
We would like to acknowledge the superb technical assistance of Peter H. Feldman and the secretarial assistance of Linda Gauthier and Nancy Wells.
REFERENCES
1. Cox, J. L., McLaughlin, V. W., Flowers, N. C., et al. The ischemic zone surrounding acute
myocardial infarction. Its morphology as detected by dehydrogenase staining. Amer. Heart. J. 76: 650, 1968.
2. Opie, L. H., and Owen, P. Effect of glucose- insulin-potassium infusions on arteriovenous dif- ferences of glucose and of free fatty acids and on tissue metabolic changes in dogs with developing myocardial infarction. Amer. J. Cardiol. 38: 310, 1976.
52: 49, 1975. 4. Lubbe, W. F., Peisach, M., Pretorious, R.,
et a/. Distribution of myocardial blood flow be- fore and after coronary artery ligation in the baboon. Relation to early ventricular fibrillation. Cardiovasc. Res. 8: 478, 1974.
5. Hearse, D. J., Opie, L. H., Katzeff, I. E., Lubbe, W. F., VanderWerff, T., Peisach, M., and Boulle, G. Characterization of the “borderzone” in acute regional ischemia in the dog. Amer. J. Cardiol. 40: 716-726, 1977.
6. Simson, M. B., Harden, W. R., III, Barlow, C. H., and Harken, A. H. Visualization of the distance between perfusion and anoxia along an ischemic border. Circulation 60: 1151, 1979.
7. Barlow, C. H., Harken, A. H., and Chance, B. Evaluation of cardiac ischemia by NADH fluores- cence photography. Ann. Sup. 186: 737, 1977.
8. Harken, A. H., Barlow, C. H., Harden, W. R., and Chance, B. Two and three dimensional display

496 JOURNAL OF SURGICAL RESEARCH: VOL. 30, NO. 5, MAY 1981
9
10.
11.
12.
13.
14.
15.
of the myocardial ischemic “borderzone” in dogs. 16. Maroko, P. R., Davidson, D. M., Libby, P., Amer. .I. Cardiol. 42: 954, 1978. Hagan, A. D., and Braunwald, E. Effects of hyal- Harden, W. R., Barlow, C. H., and Harken, A. H. uronidase administration on myocardial ischemic Epicardial NADH fluorescence in altered mito- injury in acute infarction: A preliminary study in chondrial redox states. J. Surg. Res. 27: 156, 24 patients. Ann. Intern. Med. 82: 516, 1975. 1979. 17. Wollenberger, A., Ristua, O., and Schoffa, G. Harden, W. R., Barlow, C. H., Simson, M. B., and Harken, A. H. Myocardial ischemia and left ventricular failure in the isolated, perfused rabbit heart. Amer. J. Cardiol. 1979. Harden, W. R., Simson, M. B., Barlow, C. H., Soriano, R., and Harken, A. H. Display of epi- cardial ischemia by reduced nicotinamide adenine dinucleotide fluorescence photography, electron microscopy and ST segment mapping. Surgery 83: 723, 1978. Simson, M. B., Harden, W. R., Barlow, C. H., and Harken, A. H. Epicardial ischemia as de- lineated with epicardial ST segment mapping and nicotinamide adenine dinucleotide (NADH) flu- orescence photography. Amer. J. Cardiol. 44: 263, 1979. Martins de Olivera, J., Carballo, R., and Zimmer- man, H. A. Intravenous injection of hyaluroni- dase in acute myocardial infarction; preliminary report of clinical and experimental observations. Amer. Heart J. 57: 712, 1959. Maroko, P. R., Libby, P., Bloor, C. M., Sobel, B. E., and Braunwald, E. Reduction by hyaluroni- dase of myocardial necrosis following coronary artery occlusion. Circulation 46: 430, 1972. Hillis, L. D., Askenazi, J., Braunwald, E., Rad- vany, P., Muller, .I. E., Fishbein, M. C., and Maroko, P. R. Use of changes in the epicardial QRS complex to assess interventions which modify the extent of myocardial necrosis following coronary artery occlusion. Circulation 54: 591, 1976.
18.
19.
20.
21.
22.
23.
24.
25.
Eine Einfache Technik Der Extrem Schnellen Abkunlung Grosserer Gewehestucke. PJuger’s Arch. 270: 399, 1960. Sobel, B. E., and Shell, W. E. Jeopardized, blighted and necrotic myocardium. Circulation 47: 215, 1973. Barlow, C. H., and Chance, B. Ischemic areas in perfused rat hearts: Measurement by NADH fluorescence photography. Science 193: 909, 1976. Britton, R. C., and Habif, D. V. Clinical uses of hyaluronidase. A current review. Surgery 33: 917, 1953. Duran-Reynals, F. Tissue permeability and spread- ing factors in infections: Contribution to host parasite problem. Bacterio[. Rev. 6(Dec.): 197, 1942. Tislow, R., and Chase, J. F. Subacute and chronic toxicity experiments with hyaluronidase. Ann. N. Y. Acad. Sci. 52: 1156, 1950. Seifter, J., and Christian, J. J. Studies on the pharmacology and toxicology of hyaluronidase. In Proceedings N. Y. Academy of Science Con- ference, December 1948. P. 16. Martins de Oliveira, J., and Levy, M. N. Effect of hyaluronidase upon the water content of ische- mic myocardium. Amer. Heart J. 60: 106, 1960. Askenazi, J., Hillis, D., Diaz, P. E., Davis, M. A., Braunwald, E., and Maroko, P. R. The effects of hyaluronidase on coronary blood flow following coronary artery occlusion in the dog. Circulation 40: 55, 1977.