decentralization and social service delivery
TRANSCRIPT
DECENTRALIZATION AND SOCIAL SERVICE DELIVERY: A COMPARATIVE
CASE STUDY OF THE HEALTH AND SOCIAL WELFARE DEPARTMENTS IN
BUDADIRI COUNTY SIRONKO DISTRICT UGANDA
BY
BPA/40524/151JDU
WAMUNGA JOHN
A RESEARCH DISSERTATION SUBMITTED TO THE COLLEGE HUMANITIES
AND SOCIAL SCIENCES OF IN PARTIAL FULFILLMENT OF THE
REQUIREMENTS FOR THE AWA1Th OF BACHELOR’S DEGREE
IN PUBLIC ADMINISTRATION OF KAMPALA
INTERNATIONAL UNIVERSITY
MAY, 2017
DECLARATION
I Wamunga John declare that this research dissertation is a result of my own efforts. To the
best of my knowledge it has never been submitted to any university or institution or any
academic award.
al
16 /otjZcYJ7
APPROVAL
This is to confirm that this research dissertation by Wamunga John entitled decentralization and
social service delivery: A comparative case study of the health and social welfare departments in
Budadiri County Sironko District Uganda is under my supervision and is now ready for
submission to the College of Humanities and Social Sciences with my approval.
1~ •°5i~ia)]~
DEDICATION
I wish to dedicate this research proposal to my dear parents my dady Mr. Nabubolo J.
Wamunga, mum Negesa Firista. My sisters Carl Robinah Wasagali, Ester Masagali and my
beloved brothers John, Muzenze Rogers, Charles, for all their support and encouragement.
More so I dedicate this report to my supervisor Mrs. Turnwejukye Ruth for the tireless effort
which has enabled me to accomplish this research.
I would like to also take this opportunity to thank all my friends at Kampala International
University and outside particularly Justine Munuulo and Ronald for their guidance rendered to
me when preparing this research proposal.
Lastly, I dedicate this research proposal to all members of the College of Humanities for their
prayers which have enabled me overcome all the challenges faced during my studies.
I pray that God blesses them.
III
ACKNOWLEDGEMENT
First I would like to acknowledge the divine presence of my Almighty God to whom this
research study would not have been successful without his guidance, love, care and protection.
All the Glory belongs to Him.
Special thanks and gratitude go to my parent’s dad Mr. Nabubolo J. Wamunga, mum Negesa
Firista for approving me with all the support towards my studies. I also thank to my brothers and
sisters for their support. This has opened more chances especially the fact that I am now in
position to make a reasonable contribution to nation building.
I acknowledge all the efforts and support of the entire madam Rose Bisikwa, Carol and staff of
the College of 1-lumanities and Social Sciences for their contributions towards the success of my
studies in the University.
My special thanks go to my supervisor Mrs. Tumwejukye Ruth for the insight and answering a
number of inquiries I put to her without forgetting the very valuable suggestions and comments.
Indeed, her procurement perspectives were very constructive. I thank you all and God bless you.
Finally I thank all those who contributed to the outcome of this piece of work whose names
would not appear here because of space and am grateful and appreciative to you all, and may the
almighty God bless you abundantly.
iv
TABLE OF CONTENTS
DECLARATION
APPROVAL ii
DEDICATION
ACKNOWLEDGEMENT iv
TABLE OF CONTENTS V
LIST OF TABLES ix
LIST OF FIGURES X
LIST OF ABBREVIATIONS xi
ABSTRACT xiii
CHAPTER ONE xiii
1.0 Introduction 1
1.1 Background of the Study 1
I .2 Statement ofiheProblern 4
1.3 Objectives ofthe Study 4
1 .4 ResearchQuestions 5
1.5 Scope of the study 5
1.6 Significanceofihe Study 5
1.7 Definition of terms 6
CHAPTER TWO 8
LITERATURE REVIEW 8
2.0 Introduction 8V
2.1 Conceptualizing Decentralization. 8
2.2 Types of Decentralization 9
2,3 Objective of Decentralization 11
2.3.1 To describe how decentralization can promote service delivery at the local level 11
2.3.2 To identify there a sons for state institutions to be decentralized earlier than others
strategies 1 3
2.3.3 ToidentifyareasofcollaborationandcOordinatiOnbetWeentheDepartmentsofHealth and
Social Welfare in the provision of services 16
2.4 Decentralization and Service Delivery 17
2.5 Decentralization, Health Care and Social Welfare Service Delivery in Uganda 18
2.5.1 Social Welfare Service Delivery in Uganda 19
2.5.2 Health Care Service Delivery in Uganda 21
2.6 Conclusion 23
CHAPTER THREE 25
METHODOLOGY 25
3.0 Introduction 25
3.1 Research Design 25
3.2 Study population 25
3.3 Sample size 25
3.4 Sampling procedure 26
3.5 Instruments of data collection 27
3.6 Sources of data 27
vi
Primary Data. 27
Secondary Data 27
3.7 Data Analysis 28
3.8 Ethical issues 28
CHAPTER FOUR 29
STUDY FINDINGS, INTERPRETATION AND DISCUSSION 29
4.2 Personnel respondents’ distribution by Health Sub-district (HSD), unit ownership and unit
level 34
4.3 Effect of decentralization on job expectation 36
4.4 Performance facilitation: the constraints to effectiveness and the quality, quantity and
accessibility of personnel 37
4.4.1 Effect of decentralisation on improving personnel job knowledge and skills 37
4.4.2 Performance Feedback: re-focusing personnel for better quality 39
4.4.2.1 Nature ofjob performance feedback 40
4.4.2.2 Perceived effect of decentralization on performance feedback 40
4.4.5 Working space 42
4.5.1 State of working space 42
4.5.2 Effect of decentralization on improving workspace at health facilities 42
4.5.3 Organisational support 43
4.5.4 Relationship between politicians and health personnel 44
4.5.5 Effect of decentralization in improving job incentives 44
vU
4.6 Quality of service: expressing satisfaction or dissatisfaction with performance of
personnel
4.6.1 Treatment satisfaction 45
4.6.2 People’s perception of personnel performance 46
4.6.3 Effect of decentralisation to personnel output 47
CHAPTER FIVE 49
DISCUSSION OF THE FINDINGS, CONCLUSIONS AND RECOMMENDATIONS.... 49
5.0 Introduction 49
5.1 Discussions of the findings 49
5.2 Conclusions 53
5.3 Recommendations 56
REFERENCES 58
APPENDICES 60
APPENDIX I: QUESTIONNAIRES 60
APPENDIX II: TIME FRAMEWORK 63
APPENDIX III: BUDGET 64
VIII
LIST OF TABLES
Table 1: Showing age of the respondents. 30
Table 2: Showing Sex of the repondents 30
Table 3: Showing level of education 31
Table 4: Showing the duration in service 3 1
Table 5: Showing the positions held by personnel respondents 33
Table 6: Showing the unit ownership of the respondents 34
Table 7: Showing the health unit level 35
Table 8: Showing respondents’ perception of how decentralisation has improved their job
expectation knowledge 36
Table 9: Showing the effect of decentralisation on improving job knowledge and skills 38
Table 10: Showing the reported effect of decentralisation on personnel performance feedback. 41
Table 11: Showing the effect of decentralisation on improving workspace at health facilities. .43
Table 12: Showing the effect of decentralisation in improving job incentives 45
Table 13: Showing the exit clients’ prescribed drugs received from health unit 46
Table 14 : Showing the personnel views on the effect of decentralization to their job output 47
ix

LIST OF FIGURES
Figure I: Showing level of education 31
Figure 2: Showing the duration in Service 33
Figure 3: Showing the unit ownership of the respondents 35
Figure 4: Showing the effect of decentralisation on improving job knowledge and skills 39
LIST OF ABBREVIATIONS
AIDS Acquired Immune Deficiency Syndrome
CHSWT County Health and Social Welfare Team
CHVs Community Health Volunteers
CM Community Member
DSW Department of Social Welfare
EPI-IS Essential Package of I-Iealth Services
EPI Expanded Program on Immunization
EPR Emergency Response Program
EPSS Essential Package of Social Services
Fl-ID Family 1-Iealth Division
GoL Government of Uganda
HE I-Iealth Education
I-IHPs Household Health Promoters
HIV Human Immunodeficiency Virus
HO Health Officer
HP Health Promotion
JFKMC John F. Kennedy Medical Center
LAC Ugandan Agricultural Company
LAMCO Ugandan American Mining Company
LIBINC Ugandan oil palm plantation Incorporated
LIMINCO Ugandan Mining Company
xi
LISGIS Uganda Institute of Statistics and Geo-Information Services
MOHSW Ministry of Health and Social Welfare
MoLG Ministry of Local Government
NACP National AIDS and STI Control Program
NDPC National Development Planning Commission
NDU National Diagnostic Unit
NGO Non-Governmental Organisation
NHU National Health Promotion Unit
NLTCP National Leprosy and Tuberculosis Control Program
NMCP National Malaria Control Program
NTDs Neglected Tropical Diseases
OPDOut Patient Department
PBC Performance-Based Contracting
PCU Program Coordination Unit
PHC Primary Health Care
SWO Social Welfare Officer
TB Tuberculosis
TTMs Trained Traditional Midwives
UNDP United Nations Development Programme
xi
ABSTRACT
Decentralization has been viewed widely by many in Uganda as the panacea to the challenges
of development in Uganda. With close to five years of the decentralization of the Ministry
of Health, the study sought to examine the services delivery of the Departments of Health and
Social Welfare; comparing the progress challced by both Departments and the challenges that
are experienced in the process of decentralization in the Departments. Employing a qualitative
research method, in-depth interviews wcre held with selected participants who included
Ministry officials and Community Leaders. The study found that even though the Ministry had
started the implementation of the decentralization program, the Department of Health had
advanced far greatly than the Department of Social Welfare. There were great disparities in
the implementation of the decentralization program between the two Departments. The Health
Sector was better funded, had more logistics and staff than the Social Welfare Sector. The study
also found that Health officials tended to lead in every sphere of the Ministry’s operations,
relegating the welfare staff to the background. There was very minimal collaboration between
the Departments of I-Iealth and Social Welfare. Overall, even though the decentralization
program has had some positive impact on the service delivery in the Ministry of Health and
Social welfare, there is much to be done in order for the people at the local level to have the
real benefits of the program. It is therefore recommended that the government takes steps to
stem the fragmentations in social services delivery in the country, provide the needed funding
for Social Welfare service delivery and in the medium to long term, detach the Department of
Social Welfare from the Ministry of Health and create an all new Ministry to encompass Social
V~1elfare and allied agencies in the country.
XIII
CHAPTER ONE
1.0 Introduction
This chapter explains how the research was to be carried out, It covered background to the
study, statement of the problem, research objectives, research questions, scope, and significance
of the study and definition of terms.
1.1 Background of the Study
Decentralization was one of the essential institutional reform efforts pursued in developing
countries and was intended to bring numerous improvements.
It was also considered that decentralization can contribute to further democratization, more
efficient public administration, to more effective development, and to good governance, (Saito,
2001).
Decentralization therefore, allows for the reconsideration of local government as more than just
a technical or administrative extension of the central government and br a bureaucratic structure
with new autonomous powers and functions, (McCarney, 1996 as cited Hope, 2000).
“Decentralization was the process whereby management support systems are dc-concentrated
so that national government was relief of a variety of repetitive tasks and functions which can be
more effectively accomplished at the local levels where those task and functions are
occurring”, (Ministry of Health and Social Welfare [MOHSWJ, 2008:1). When Decentralization
took place, it gave the central government or institution time to concentrate more on policy
formulations. carryout strategic planning, mobilize resources that will facilitate
implementations, conduct effective monitoring and evaluations of policy implementations and
ensure coordination between the county government and its citizens, (MOHSW, 2012).
The United Nations Habitat Agenda (1996) recognizes the fact that in order for any country to
obtain successful human settlements development, it should be done through an effective
decentralization of management, policy, responsibilities, decision making authority and
allocation of sufficient resources inclusive of revenue collection authorities to the local
authorities who are believed to be closest to the people and also representatives of
constituencies.1
The trend towards the development of elected forms of local government that do not just have
vertical accountability, butalsowhosepublicservicedeliveryroleanddirectaceountabilitytoits
citizens are effective has become a global issue. Alcpan, (2007) presumes that lower levels of
government, for example, a local government, is better placed at perceiving the desires and
demands of its constituents for public services than a distant centralized government.
Uganda being a developing country has had the administration and governance of the country
controlledbyinstitutionsandstructuresthroughacentralizedprocess, as far as its history is
concerned.Thiskindofsystemhinderedtheparticipationoflhelocalgovermnentinhelping in the
formulation and implementation of policies that will meet the needs of the vulnerable
population. It also led to the gaps in equal access in the provision of public goods and services
throughout the country, (Governance Commission, 2010).
According to the Uganda National Policy on Decentralization and Local Governance (201 0),the
absence of decentralization has slowed the overall economic growth and development and
democratization processes. His has effectively led to under investment in human resources and
human wellbeing throughout the country. The Government of Uganda, thus, realized that there
was a need for the Ugandan people themselves to participate in any process of development that
will yield equal distribution of public goods and services. This can be achieving through the
promotion of the use of the country resources and international contributions. This realization by
the Government of Uganda through the administration of President Ellen Johnson-Sirleaf,
deemed it necessary to formulate the National Policy of Decentralization and Local Governance,
with the intent to share political, administrative and fiscal powers with the county authorities in
the fifteen counties. Five governmental institutions were named as the first agencies to initiate
the decentralization processes, amongst which was the Ministry of Health and Social Welfare.
The Ministry of Health and Social Welfare is divided into two main service delivery
departments namely:
The Department of I-Iealth Services and the Department of Social Welfare. They both benefit
from the functions of the Department of Administration and the Department of Planning,
Research and Development. While it is true that the Ministry emphasizes decentralization, the
Department of Social Welfare is yet to decentralize its services as compared to the Department
2
of Health. Through observation, it is seen that the Department of Health has advanced in terms
of human resources, finding and logistics as compared to the Department of Social Welfare.
The Department of Health is found to be functioning in all fifteen counties through its County
Health and Social Welfare Teams, which is the decentralized administrative branch. On these
Teams, there is ones lot allocated for the Department of Social Welfare occupied by the Social
Welfare Supervisor. The Social Welfare Supervisor presently is responsible to carry out all
functions of the Department. The Department of Health on the other hand has over twenty — one
staff on each of the fifteen County Health and Social Welfare Teams excluding staff assigned to
facilities and communities, with specific functions.
Looking at the situation in Uganda, the Department of Health has attracted much attention as
compared to the Department of Social Welfare. Interestingly, the Ministry is called, The
Ministry of Health and Social Welfare, but both have separate policies and plans. The
Department of Health has decentralized its services unlike the Department of Social Welfare
which is yet to decentralize its services.
In the case of human resources, the Department of Health has many staff ranging from medical
doctors to community health volunteers and the Department of Social Welfare has staff with
limited qualifications and also insufficient staff Logistically, the Department of I-lealth has
many vehicles to help in its service delivery unlike the Department of Social Welfare that barely
has three.
Decentralization of services and sustainability of development are important in addressing the
issues of rebuilding and governing in a country like Uganda which has gone through devastating
conditions. According to the Uganda National Policy on Decentralization and Local
Governance, (201 0),centralization limits the functions of the local authorities, thus creating an
environment where in they have to depend wholly and solely on central government for both
policy formation and the implementations,
3
1.2 Statement of the Problem
Uganda in implementing its structural adjustment program [SAP] it resulted into
decentralization of services and health inclusive which was extended to the district level, July
1994. This was aimed at improving on the quality of health services and pharmaceutical supplies
in the hospitals and health IV [units], with resultant increase in the level of utilization of health
services in Budadiri County Sironlco District Uganda. In the health sector, this has not been
successful due to inadequacy of funds to extend health services supervision. This was coupled
up with poor supervision and improper monitoring of health centres, corruption, inefficient
utilization of the resources available and worse of it inappropriate delivery of health services in
the town council.
According to the Uganda Bureau of statistics, in the town council health programmes on the
effectiveness of health service delivery of community information system 2009, statistics show
that the percentage distribution of health services is still low and vulnerability risks are high and
sanitation and clean water accessibility is still not well addressed, the working population is low
showing a risk of poverty in the community. Therefore the problem statement is focused to find
to find out why there is still poor performance in the delivery of health services through
“decentralization policy” in place which gives and attributed with community participation.
There is a need to understand the decentralization strategies used by the Department of Health to
meet its service delivery. It is also necessary to identi& the gaps and constraints within the
Social Welfare Department that is causing delays in its decentralization policy implementations.
It is also important to identify a point of collaboration and coordination between the Health and
Social Welfare Departments along with other implementing partners to improve service delivery
in Uganda.
1.3 Objectives of the Study
The research specifically aimed at addressing the following objectives:
I. To describe how decentralization can promote social service delivery at the local level In
Budadiri County Sironko District Uganda.
2. To identify the reasons for institutions being decentralized in Budadiri County Sironko District
Uganda.
4
ToidentifyareasofcollaborationandcoordinationbetweentheDepartrnefltsOf Health and Social
Welfare in the provision of services in Budadiri County Sironko District Uganda.
1.4 Research Questions
The above problem was examined with the hope of addressing the following research questions:
1. How does decentralization promote service delivery in Budadiri County Sironko District
Uganda?
2. Why do state institutions decentralize in Budadiri County Sironko District Uganda?
3. How can the Departments of Health and Social Welfare collaborate and coordinate to
improve service delivery in Budadiri County Sironko District Uganda?
1.5 Scope of the study
1.5.1 Geographic scope
The study was carried out in Budadiri which is located approximately 13 kilometres (8.1 mi), by
road, southeast of Sironko, the district headquarters. It is located within Mount Elgon National
Park.
1.5.2 Content scope
The research study is to study on decentralization and service delivery in Budadiri County
Sironko District Uganda, and also finding out the possible solutions to the problem statement
and finally the conclusion and recommendations.
1.5.3 Time scope
This research will be carried out in a period of four months that is from January to May 2017.
1.6 Significance of the Study
This research looked at how the Republic of Uganda can have an effective decentralized health
and social welfare system that will help in alleviating some of its social problems.
5
It was also intended to identify the point at which the Departments of Health and Social Welfare
can collaborate their services for the best interest of its population. The inability of the Social
Welfare for each the vulnerable population in the fifteen counties had the tendency to increase
the rates of social problems within the country, thus having an unhealthy country.
The findings from this research will add to the stock of knowledge on decentralization and
social service delivery specifically taking in to account the importance of the level of
collaboration and coordination between the Departments of Health and Social Welfare.
This study also gave strength to the definition of health by the Constitution of World Health
Organization (2006) emphasizing that health was not only the absence of diseases but also the
state where one has physical, mental and social well-being. In most cases the Social Welfare
Department was ignored by politicians not taking in to consideration that when the social
issues are handled, it has the tendency to improve economic growth and sustainable
development.
This study intended to inform and influence policy makers of the importance of social welfare
service provision to the nation.
It was also to help non-governmental organizations and community-based organizations focus
on the total wellbeing of the vulnerable population.
This study was also providing knowledge too there countries in helping to strengthen their health
and social welfare services to meet the wellbeing of the population for a sustainable
development.
1.7 Definition of terms
Decentralization: “Decentralization is the process whereby management support systems are
dc-concentrated so that national government is relief of a variety of repetitive tasks and
functions which can be more effectively accomplished at the local levels where those task and
functions are occurring
Social welfare services: are as the cornerstone of the new Ugandan National Social Welfare
case delivery strategy.
6
Service Delivery; can be usefully conceptualized as the relationship between policy makers,
service providers, and consumers of those services and encompasses both services and their
supporting systems.
Social Service Delivery System:
The social service delivery system refers to the transfer of goods and services from one source to
the other; from producers to consumers. It also refers to the organizational arrangements among
distributors and between distributors and consumers of social welfare benefits in the context of
the local community (Gilbert and Terrell, 1998).
7

CHAPTER TWO
LITERATURE REVIEW
2.0 Introduction
This chapter of the study focuses on their views of relevant literature. Their view is conducted
underthemeswhichhavebeenformulatedinlinewiththeobjectivesofthestudy and in a bid to seek
answers to questions that have been raised by the study. Their view begins by loolcing at the
concept of decentralization, its challenges and solutions. This is followed by a consideration of
decentralization as implemented in various countries across the world with special emphasis on
developing countries. There is then are view of literature on decentralization on health care and
social welfare service delivery in Uganda. The chapter ends with a conclusion by the researcher.
2.1 Conceptualizing Decentralization
Even though decentralization is not a new concept, having been used since the 1950s (European
Commission, 2007); According to Crawford (2004),it has become an increasingly widespread
and significant dimension of political and administrative form in many developing countries.
The coming in to prominence of the concept according to Crawford (2004) began in the late
1980s and has been strongly supported by a variety of actors ranging from international
development agencies through national governments to non-governmental and grass roots
organizations.
Decentralization is invariably defined by various authorities. Though the definitions vary, at the
core of the concept is devolution of power from the center to the local levels. The World Banlc
(2001) characterized decentralization as a complex multifaceted concept embracing a variety of
perceptions which must be carefully analyzed in any particular country before determining if
projects or programs should support reorganization of financial, administrative or service
delivery systems. The World Bank (2001) defines the concept as “the transfer of authority and
responsibility for public functions from central government to intermediate and local
government or quasi-independent government organizations and/or the private sector”. On the
other hand, the UNDP (2004) defines the concept of decentralization as a restructuring of
authority so that there is a system of co-responsibility between institutions of governance at the
central, regional and local levels according to the principle of subsidiarity. This definition by
8
UNDP connotes a sharing of power between the central government and the local authority
which otherwise was a preserve of the central government. This diverts slightly from the World
Bank’s definition which seems to suggest an outright transfer of power from the central to the
local government. The UNDP (2004) espouses that based on the principle of decentralization
functions or tasks are transferred to the lowest institutional or social level that has the potential
of completing them. The French Corporation (2009) characterizes decentralization as being part
of democratic governance which is intended to give local authorities their own resources and
responsibilities separate from those of central government.
The above definitions of the concept of decentralization can be summarized as any act in which
a central government formally relinquishes powers to actors and institutions at lower levels in a
political-administrative and territorial hierarchy (Mawhood 1983; Smith 1985, as cited by Ribot
2001)
2.2 Types of Decentralization
Generally, there are three types of decentralization, which are fiscal, political and administrative
decentralization (Falleti, 2004; Scott, 2009; World Bank, 2001).Fiscal decentralization entails
the transfer off financial resources in the form of grants and tax-raising powers to the sub-
national units or local governments (Scott, 2009; World Bank, 2001).This kind of
decentralization gives the local level authorities autonomy to appropriate the resources in
manners deemed necessary.
On the other hand, administrative decentralization, which may be sometimes be referred to as
de- concentration, connotes a situation where the functions performed by the central government
are transferred to geographically distinct administrative units (European Commission, 2007;
French Corporation, 2009; Scott, 2009; World Bank, 2001).
The European Commission (2007) indicates that this type of decentralization seeks to transfer
decision-making authority, resources and responsibilities for the delivery of a select number of
public services or functions from the central government to other levels of government, agencies
or field offices of central government line agencies.
Shah and Thompson (2004) concords with the definition of administrative decentralization but
also simplifies it by stating that an effective administrative decentralization requires lack of any
9
exante controls over the decision to hire, fire and set terms of employment of local staff. To
improve tax collection or the delivery of local public services, local government should have the
freedom to contract own taxing and spending responsibilities. Furthermore, local governments
should have the authority to pass by laws in their spheres of responsibility without having to
obtain prior clearance from the higher level government. The European Commission explains
that administrative decentralization has three possible variants which come with different
characteristics. These variants include de-concentration, delegation and divestment.
Decentralization refers to “a process in public administration in which a field office or official or
a central department or ministry acquires some degree of delegated authority to make decisions
or otherwise regulate operations” (European Commission, 2007, p.1 7).
Delegation on the other hand is said to refer to a more extensive form of administrative
decentralization and involves a redistribution of authority and responsibility to local units of
government or agencies that are not always necessarily branches or local offices of the
delegating authority (European Commission, 2007). The final variant of administrative
decentralization is divestment which the European Commission posits is a finance term but has
been co-opted into the field of public administration. According to the European Commission
(2007), divestment “occurs when planning and administrative responsibility or other public
functions are transferred from government to voluntary, private or non-governmental
institutions” (p. 17).
Political decentralization is the third type of decentralization and refers to the situation where
powers and responsibilities are devolved to elected local governments (Scott, 2009; World Bank,
2001).
The European Commission (2007) corroborates the definition of political decentralization by
Scottand World Bank and further explains that political decentralization normally involves a
partial transfer of power and authority with the central government reserving greater amount of
power and control.
Although, it is widely accepted that there are three types of decentralization, there are a few
instances of divergence.
10
The French Corporation (2009) in its clarification of decentralization presents the original three,
fiscal, administrative and political decentralization, but goes to add a fourth, divestment.
This is in sharp contrast to the views of the European Commission (2007)
Who indicates divestment as a variant of administrative decentralization?
Therefore, according to the French Corporation, there are four types of decentralization: fiscal,
administrative, political and divestment which involves the devolution of public functions to
voluntary, private or non- governmental institutions.
2.3 Objective of Decentralization
2.3.1 To describe how decentralization can promote service delivery at the local level
According to Francis [1996] in his suggestion, he found out that decentralization is untimely
called for the service delivery survey [SDS] which has enabled effective delivery of social
services to the local people for example in pursuit of this goal, the service delivery mostly social
services to the local level.
Despite, the service delivery survey had produced information to be used as baseline on the
delivery of health services for example, provision of drugs in the health center, giving of
mosquito nets to people, water and sanitation to the local people i.e. Malcara S [1 998],in his
book political and administrative relations in decentralization, he said that decentralization
policy has compelled the local council governments to be concerned with the questions of
efficiency outcomes and outputs while they have the responsibility for their delivery of health
services to areas under their jurisdictions. Though this was done, but the outcomes of
decentralization policy in its attempt to foster effective delivery of health and social services at
the local level is still questionable.
Francis L [1996] further reported and revealed that decentralization has worlced effectively on
the delivery of health services of people, this was then the government of Uganda through
institutional capacity building programme borrowed funds to establish the system and training to
implement the results oriented management.
11
However, even if it was true that the government of Uganda borrowed funds with the purpose of
enabling decentralization policy to work effectively on its attempt to deliver health services to
the local centers but there is still little improvement on the delivery of social services such as
road network mostly on the local level hence leading to absence of delivery of social services at
the local level.
1-lowever, the management structures at the health service delivery level remain unclear and are
at present supported by no central guidelines; the town clerk council has been established and is
operational in all centers. The planning capacity of the town council in different districts and
even within one district varies greatly.
That still there are also regional variations in the status of health infrastructure and staffing
pattern. The more affluent regions are found in and the capital of Kanipala, whereas the north
eastern part of the country was least developed. On average 45% of all households live with 5
kilometers walking distance of health care, but this number ranges from 8% in Kitgum to almost
100% in Kampala. Most town councils had at least one health care unit but only 40% of parishes
in the town council have a health facility within their boundaries. The infrastructure at most
peripheral health facilities are in deplorable state.
In practice, the health facility staffing does not meet the established standards. A study in 1999
indicated that only 34% of the existing positions were filled by qualified staff. In general, health
centers from II to IV have no access to electricity, but also depend primarily on firewood, gas
and charcoal, so as to meet their energy requirements for sterilization, lighting, and refrigeration
of vaccines.
District and referral hospital on the other hand were usually connected to the country’s main
electrical grid or had generators to supply their needs, consequences of decentralization for the
health sector with the shift of managerial responsibility, disciplining the recruitment and
dismissal of staff was a task of body within the respective districts and the district commission
service.
Recently, the central ministry of health [MOHJ is responsible for deployment of health sector
staff to the district despite the fact that ministry processed an overview of needs the country’s
distribution of staff is very uneven and peripheral districts went largely understaffed.
12
But with the decentralization the other hand, posts are now advertised and districts seek out
officers by recruitment process. However, the inquiry between peripheral and central districts
remains a major problem.
2.3.2 To identify the reasons for institutions to be decentralized with strategies
According to Apollo Nsibambi, the NGOs have played significant roles in the implementing of
health programmes. Such NGOs include: UNICEF, Plan International, Action Aid Uganda,
TASO, Marie Stopes among others have improved the PHC in the areas of immunization, latrine
coverage sensitization, informing people on prevention of STDs, AIDS and many more, for
example Plan International has donated health facilities and equipment’s such as beds,
mattresses, drugs, vaccine, sponsored health personnel training. All the above mentioned
activities have been done to improve on the performance of the health sector in delivery of
services.
According to Pierre land eli mill 1987, giving them a voice to demand more accountable in it is
beneficial for development especially in terms of efficiency resource mobilization and
sustainability participation in consultation, identification, selection, implementation,
management utilities are some of the aspects highlighted. However, there is for example
community participation in the health sectors the degree of community participation varies from
one NGO to another in some cases, for example priority activities are selected by the NGOs
while in other cases the task is left to the community or their leaders.
According to Betty Kwagalana, the failure of official administrative instruments to deliver
health services to the population in Uganda demonstrated among other issues the absence of
good governance. NOOs and the local authorities however, have been instrumental in filling up
the gaps.
The NOOs community and the central government are closely interlinked and constitute some of
the indispensible services for human survival. More emphasis is laid on the rural areas since in
comparison to urban areas, they are poorly served.
Samuel Paul [1989) has noted that it is difficult to incorporate community participation in
service delivery when the setting does not have a supportive social tradition. NOOs are known
13
as a key catalyst to community participation and are expected to eventually strengthen civil
society and the populace.
According to Francis L, democratic decentralization in Uganda revealed that the local
government has a challenge of incompetence among the staff that existed in the town council for
example the commonest qualifications among many staff had been ordinary level school
certificate hence affecting health services in most local levels thus affecting the delivery of
health services due to the result of the policy.
1-lowever, Francis L stated that ‘decentralization policy had contributed a lot towards the decline
on the delivery of social services still in most town councils, the delivery of health services and
social services are still very low. It was due to these that most council had lagged behind due to
poor supervision, recruitment and corruption thus the challenges faced by the local government.
Francis L further asserted that “for the public services standing orders for the purpose of
uniformity, issues by the central government, still given the conditions service country wide at
the district level. The central government continues to provide block grants to districts for
services planned for and delivered by the district to the council. These block grants have
replaced a system of earmarked votes determined by the ministry of finance. These were
introduced in a phased manner and since the fiscal 1996-1997, and all districts received them.
Therefore, several conditional! stringed grants have been instituted for specific purposes like
primary health care [P1-IC].
In practice, the allocation of funds to the districts does not correspond to the actual commitment
made by the central government on behalf of the district. Out of the recurring national budget for
fiscal 1997-1998, only 34.9% was allocated to the districts. In addition to that, the relative size
of the conditional grants declined from 25.6% of the local budgets in 1996-1997 to 22.8% in
1998-1999 ULLA [1998].
According to Apollo Nsibambi in his book “Decentralization and Civil society”, he pointed out
that local government is faced with a challenge in the recruitment of unqualified staff and
unstable staff In many schools for example Apollo Nsibambi cited Masaka district where
graduated nurses were employed without the knowledge of mixing drugs for patients.
14
However, to a bigger extent, it was true that the government had failed to extend health and
social services that were of quality standards due to the challenges of its activities to recruit
unqualified and unstable staff as told by Apollo Nsibambi in his book. It was because of this that
many hospitals and health centers failed to improve on the performance. He went further and
stipulated that decentralization had a challenge on the delivery of health services to the local
centers therefore; the local government faced a problem of receiving similar financial transfers
from the central government thus made the policy to fail to catch up on the delivery of social
services like health to the local centers.
However to a larger extent, this was true because many health centers at the local levels had
failed to buy the required equipment’s so as to increase on their performance due to small
percentage of the finance extended to them. This was associated with a lot of corruption among
the officials who used the money for meeting their personal gain and interest than using the
money for the interest focused on delivering services to the people in the local level [parameter].
However, central decentralization still has fiscal power that affects the districts, leaving a
considerable discrepancy between the formal powers given to the districts by the local
government Act” and the financial means to exercise them. The local revenue base is also very
small as the lion’s share of the income from the local revenue is also very small as the lion’s
share of the income from the central government.
There has been a very significant reduction in infant and material mortality 1990’s. Data from
the indicators of health status and health service delivery compared to the situation of 5 years
earlier.
Infant mortality and malaria morbidity are on the increase, and maternal maternity remains
constant at high level estimated at 506 details per 100,000 live births. The proportion of fully
immunized children has declined from 47% to 37% and a tetanus oxide TT immunization
pregnant woman shows a decline from 54% to 42%.
In 1995 to 1996 a burden of diseases study was carried out in 13 of the districts of Uganda the
unit selected for measuring disease burden was discounted life years lost due to the discounted
life years reduced to 10 preventable diseases with five of them according for approximately 60%
of the total burden.
15
According to Onyach — 099 [2003] said that the capacity to implement decentralized system is
several limits the politicians hence perpetuating the problem of coordination between the initial
stages of decentralization has caused perpetuated in the level of development especially at the
district.
Furthermore, the capacity problem had been increased due to the lack of essential data that could
be used for monitoring, planning and evaluating at the local levels.
The magnate of the capacity outcome is generally muffed by the general tendency to over eat the
ability of the local goverm~ent council leaders to the priorities, plan and implement local
development programs in some cases poorly implemented. Decentralization has also led to the
delegation of natural resources thus leading to over exploitation of forest resources and this can
be proved with the early stages of Uganda’s decentralization process where a reality prompted a
recentralization of the country’s forest management.
I-Ic also went ahead and analyzed the challenges of decentralization into the structural
constraints and capacity constraints where he said that donor’s assistance to Uganda has taken
the form on general budget support and project Aid.
The general budget support is often times earmarked by donors to finance as project Aid; it has
been channeled directly to local government by passing the local government. This has
fragmented local development structures resulting in the exacerbation of the problem of
coordinating and monitoring local development activities, more so it has undermined the
institutional growth of local government system weakened community linkages.
Also pointed that in the system of decentralization and devolution conflicts emerge. A clash
between resident district commissioners and the district chairman is case in point. These
Authorities often belong to opposing political groups resulting in division and inefficiency in
public sector management and development.
2.3.3 To identify areas of collaboration and coordination between the Departments of
Ficaith and Social Welfare in the provision of services
According to the local government act of 1997, decentralization refers to the shifting of power
planning, decision making and administrative authority from the center [central government] to
the local government.16
This term can also be used to refer to the system of government in which power is provided to
the local authorities of financial management, decision making, planning and so forth.
Local governments are sub — national bodies and body cooperates that can sue and be sued
under their cooperates names “local government” and they perform functions on behalf of the
state [national government].
And their system of governance is categorized into four types that are devolution,
decentralization, delegation and privatization.
According to Apollo Nsibambi, the NRM government before it attained power in 1986, one of
its manifestations was to empowering local governments through decentralization with an aim to
enable the locals to participate in decision, administration, planning and control of financial
management in their local units.
Service delivery, it is the process where the required non tangible demands are made recently
available for the clients (consumers) to receive and check upon their cun~ent situation & desires.
And health services are delivered by those working (employed) in the department of health.
Uganda in implementing its structural adjustment program (SAP) it resulted into
decentralization of services and health inclusive which was extended to the district level, July
1994. This was aimed at improving on the quality of health services and pharmaceutical supplies
in the hospitals and health center units.
According to the Uganda Bureau of Statistics, in the town council health programmes on the
effectiveness of health service delivery of community information system 2009, statistics show
that the percentage distribution of health services is still not well addressed; the working
population is low showing a risk of poverty in the community.
2.4 Decentralization and Service Delivery
Akpan (2007) opinesth at decentralization may result in better service delivery. Heal so stressed
that the decentralization of the provision of social services such as education, health, water and
sanitation may improve service delivery. Ahmed, Devarajan, Khemani and Shah (2005)also
corroborates with Akpan that a country can have a successful and sustainable service delivery if
thegovernmentintervenesandprovidethenecessaryresourcesandtechnicalassistanCetolower-tier
17
governments.(Republic of Rwanda, 2006) emphasizes that a sound intergovernmental system is
grounded on a clear definition of spending and revenue responsibilities between each level of
government. Failing to clarify assigned responsibilities will surely result in in efficiency and
instability of service delivery.
Darmawan (2008) Opinesal so that decentralization and service delivery can be achieved if
financial resource autonomy is given to local authorities and later inter-governmental transfers
and grants are established to address some specific problems such as fiscal gap or vertical
imbalance between expenditure and revenue at sub-national government level. Furthermore, the
transfers are important to correct fiscal inequality among the sub-national governments, improve
the fiscal efficiency across jurisdictions, overcome spillovers and establish fiscal harmonization.
2.5 Decentralization, Health Care and Social Welfare Service Delivery in Uganda
The Ugandan governance and public administration has since the country’s independence in
1847 remained highly centralized in the country’s capital, Monrovia (Governance Commission,
2010).
Thus, the governance and public administration of Uganda had been controlled largely by
institutions and structures of the central state. This situation according to the Governance
Commission indicates that it did not allow adequate legal opportunities for the establishment of
a system of participatory local governance.
Further, the Governance Commission espouses that the centralized nature of the governance and
public administrative structures of the country had impeded popular participation and local
initiatives, especially in regards to the provision of public goods and services. The consequent
effects of this system as hinted by the Governance Commission include potential gaps in
economic growth and development, equal access to social and economic opportunities and
human wellbeing between the center, Monrovia, and the rest of the country.
Ultimately, the Governance Commission laments that the situation had contributed greatly to a
slowdown in the country’s overall economic growth and development, as well as the
democratization processes and under investment in human resources and human wellbeing
throughout the Republic. Such challenges with a centralized system of governance and
18
administration as gaps in development and service delivery are factors that informed the
formulation and implementation of the decentralization program in Uganda.
The new National Health and Social Welfare Policy and Plan which covers a ten year span,
starting 2011 and folding 2021 entrusts the responsibility of the execution of the Ministry’s
decentralization program in the hands of the County Health and Social Welfare Teams
(CHSWT)-a combined team of health and social welfare personnel.
This Team is responsible for the delivery of services to the people of Uganda at the grassroots
level. According to the Ugandan National Health Policy and Plan (2008-2011), the County
Health and Social Welfare Teams was responsible to manage all Ministry-owned facilities,
Ministry-employed human resources and Ministry-provided material resources. The National
Health Policy and Plan,(2008-201 1, p. 10) intended that the center will gradually allocate and
transfer resources to the county It is expected that the County Health and Social Welfare Teams
were to strategize and respond to the local health and social welfare issues within their
communities.
2.5.1 Social Welfare Service Delivery in Uganda
The Government of Uganda’s Social Welfare Policy (2009) describes social welfare services as
the cornerstone of the new Ugandan National Social Welfare case delivery strategy. The
Department of Social Welfare, under the Ministry of Health and Social Welfare has the mandate
to deliver social welfare services in the Republic of Uganda (Ministry of Health and Social
Welfare,EssentialPackageofSocialServices,2O 11-2021 ).TheEssentialPackageof Social Services
indicates that the Department of Social Welfare is charged with the responsibility to provide
“equitable and high quality services targeting persons, families and communities, and strengthen
the modalities to enhance the voice of the vulnerable in defining priority needs and influencing
the character and content of service delivery” (p.7). However, the National Health Policy and
Plan (2007) portrays the Social Welfare Department as fragmented and under resourced, and
thus, unable to address the enormous needs of the Ugandan population.
According to the Essential Package of Social Services, (2011-2021), in order to ensure the
effective social welfare service delivery in Uganda, the Department of Social Welfare introduced
the Social Welfare Policy in 2011 to provided direction for reforming the Social Welfare
Department in line with the principles of the National Decentralization Policy.19
The objectives of their forms in the Social Welfare Department focus on improve deficiency and
effectiveness among the various actors in the Department, increased accountability and probity,
and an enhanced ability to support vulnerable persons.
The main aim of their forms in the Social Welfare Department in particular was to redirect the
operations of the Social Welfare Department “towards a developmental social welfare approach”
which would focus specifically on the establishment of a demand-driven, community-focus
social welfare response with strengthened institutions capable of delivering quality services
(Social Welfare Policy, 2009).
Three key achievements are targeted by the Social Welfare Department with regards to their
form efforts and these include the ability of the Department of Social Welfare to enable a better
coordination of social welfare service delivery; the ability of the Department to strengthen the
influence of vulnerable groups in decision-making in society; and finally, the ability of the
Department to enhance the socio-economic conditions of vulnerable groups in the country
(Social Welfare Policy, 2009). Thus, at the heart of the Social Welfare Policy that was
formulated in 2009, is a two —point aim of strengthening the Social Welfare Department as well
as protecting vulnerable groups. In the long-term, however, the Social Welfare Policy aimed at
three things: the first being the decentralization of social welfare services and there enforcement
of partnerships to effect the decentralization process; the second, the strengthening of
community social capital and family and extended family networks; and finally, the enabling
systems and Structures that allow the effective and equitable access to social services among the
populace who are most vulnerable and in need (Social Welfare Policy, 2009).
The delivery of social welfare services in Uganda should be organized into four divisions
according to the Essential Package of Social Services (2011-2021).The first of the divisions is
the Community Welfare Division which entails basic community services, psychosocial support
and services for the elderly. The second is the Family Welfare Division which involves the
promotion of family-base care, family reunification, and services for separated or orphaned
children, and children in contact with the law.(MOHSW’5EP55201 1 -2021, p.8).
There are fourtiers of care delivery in the Ugandan social service delivery system (EPSS,20l 1-
2021).
20
These follow the political structure of the country. The first tier is the community level which is
the lowest level. This is the level that involves community case workers, community outreach
volunteers and trained social service providers. Staffs at this level are supposed to work directly
with the people and thus, the direct link between the people and the chain of authorities. These
condtier is the district level workers who at this level serve as facilitators for case workers at the
community level. The social welfare supervisors at this level are responsible for the supervision
and monitoring of the community level. County level officers form the third tier officers of the
Department of Social Welfare. Officers at this level are supervisors and case managers. They
provide supervision for all county social welfare activities and are responsible for the training
andre training of staff of the Department of Social Welfare in their respective counties.
The final tier in the social welfare service delivery in the Republic of Uganda is the national
level. This refers to the central administration of the Department of Social Welfare and officers
here are senior members of the Department who have the responsibility to ensure that social
welfare services are render in gat the community level and it should be done through the county
social workers. Officers at this level are responsible for policy formulation and implementation.
2.5.2 Health Care Service Delivery in Uganda
The Essential Package of Health Services [EPHSI of the Ministry of Health and Social Welfare,
2011, indicates that the responsibility of ensuring that the Ugandan people are healthy and enjoy
good quality health care is entrusted to the Department of Health Services. Uganda’s health
services like many other sectors of the economy have been severely disrupted by years of
conflict and looting (MOHSW, 2007).Jhpiego (nd). Jhpiegoreite rates that the key among the
challenges included weak logistics, transportation and communications systems, as well as in
sufficient access to care and poor referral networks, particularly in remote rural areas.
The EPHS (2011) indicates maternal health care as one of the priority areas for the MOHSW
and Jhpiego (nd) indicates that maternal mortality in Uganda is among the highest in the world
and only 40% of the population has access to health services. This calls for frantic and pragmatic
efforts after building the Department through the building of infrastructure, workforce and the
utilization of all available services. In this regard, Jhpiego (nd) acknowledges that the efforts so
far taken by the Government of Uganda as it opines that within a short period, the MOHSW has
taken bold steps to transition from an emergency relief model of health care to a functioning,
21
decentralized health care system. Jhpiego (nd) acknowledges that there is still a long way to go
even though all fifteen counties of the country have begun operational management of health
services. It is important to note however that the countries are still operating under the direction
and support of the central Ministry of Health and Social Welfare (Jhpiego, nd).
The Government of Uganda’s National Health and Social Welfare Policy which was first
introduced in 2007, revised in 201 land billed to span up to 2021, spells out the modalities for
the delivery of health care services in Uganda. However, in order to ensure that services reach
the lowest level of the Ugandan population, and in line with the principles of the National
Decentralization program, the EPHS (2011) indicates that the Ugandan health care sector like the
social welfare sector is organized into three levels. The first level is primary is primary level
which includes community healthcare systems. This level is made up off our types of service
providers. The first of them is Community Level Services such as set standards for outreach,
health promotion and referral services for communities that are more than one hour walk (5km)
from the nearest health facility. This activity is the responsibility of the Community Health
Volunteers including Household I-lealth Promoters, Trained Traditional Midwives, and general
Community Health Volunteers. These categories of personnel are responsible for primary health
care education at the grass roots level. These condtier within the primary care system is the
Primary I-Iealth Care Clinic Level 1. This refers to community clinics that operate Out Patient
Department services. These clinics are opened eight hours a day from Monday to Friday. These
level covers cluster communities that are isolated from major settlement. Such communities
usually have a population of up to 3,500. The penultimate tier within the Primary Level health
care system is the Primary I-IealthCare Clinic Level 2 which covers catchments that are made up
of populations between 3,500 and 12,000. In addition to providing OPD services eight hours a
day from Monday to Friday, PHC Level 2 clinics also provide outreach services oportions of
their catchment population outside of a 5 km radius. The outreach program constitutes the last
but
Not leas to f the primary level care an dischristened the Integrated Outreach Program (EPHS,
2011).
The next level of health care in Uganda after primary health care is Secondary Care which is
referring to as District Level HealthCare System. It is the first provider of secondary health care
22
and focuses on maternal and child health care. Secondary health care is the referral point for the
community systenL
This system provides health care services for catchments with populations ranging between
25,000 and 40,000. A facility that provides services at this level includes Health Centers and
District Hospitals. County Health System is an advanced healthcare system in the secondary
healthcare system which provides expanded services within the secondary level of care. It
consists of county hospitals which are responsible for receiving referrals from the community
and district health systems. Such county hospitals provide general surgeries, pediatrics, general
medicine, obstetrics and gynecological services and are open twenty-four hours every day.
Tertiary Care, that is, the National Health System is the final level. This level consist of two
types of hospitals: Regional Hospitals and one National Hospital, John F. Kennedy Medical
Center (JFKMC).Regional Hospitals serve a catchment area of three to five counties and receive
referrals from County Hospitals. The National Hospital is the final referral point for cases in the
country.
Despite such a comprehensive structure of the health care system in the country, the
Decentralization Guidelines (2008) empowers county health authorities to manage county health
facilities, including county hospitals.
The Decentralization Guidelines indicates that proper administrative structures and
management tools would be introduced at county level, to make health authorities truly
autonomous. It further iterates that county health authorities would be given responsibility for
financial and asset management and personnel, and would be fully accountable to local
constituencies, as well as to overseeing public bodies. The Decentralization Guidelines (2008)
establishes a County Health Team which is entrusted with the responsibility of management of
county health service delivery. The Team is made up of senior staff and general members.
Senior staff on the Team includes the county health officer, the county health department
director, the county hospital medical director, the county health services administrator, the
county pharmacist, and the county laboratory supervisor.
2.6 Conclusion
According to Apollo Nsibambi, the NRM government before it attained power in 1986, one of
its manifestations was to empowering local governments through decentralization with an aim to23
enable the locals to participate in decision, administration, planning and control of financial
management in their local units.
Note: Service delivery, it is the process where the required non tangible demands are made
recently available for the clients (consumers) to receive and check upon their current situation &
desires. And health services are delivered by those working (employed) in the department of
health.
Uganda in implementing its structural adjustment program (SAP) it resulted into
decentralization of services and health inclusive which was extended to the district level, July
1994. This was aimed at improving on the quality of health services and pharmaceutical supplies
in the hospitals and health center (IV) units.
24
CHAPTER THREE
METHODOLOGY
3.0 Introduction
This chapter explains the methods that were being used in this research including the research
design, the study population and area of study sampling techniques, sources of primary and
secondary data, data collection instruments, data processing of presentation of research findings
and limitations of this research.
3.1 Research Design
The study employed a descriptive design because of the qualitative nature of the study. Both
quantitative and qualitative approaches were being used in data collection and analysis and
general information on the subject matter was collected from the different departments of the
Sironko district among employees. Qualitative design was being involved in-depth interviewing
of the departmental managers. On the other hand, the quantitative design was to involve use of
close-ended questionnaires which was to be issued to the employees in the different departments
as the method was convenient for them to fill during thier free time.
3.2 Study population
The population of the study was to be 100 got from all departments, these include the
Administrators, the I-Iuman Resource, Supervisors, because they knew what decentralization was
and how it affects social service delivery.
3.3 Sample size
The researcher was to use the Solven’s formula to determine the sample size out of study
population of 100 members, 80 respondents were being selected from the study population.
25

Solvens Formula is applied as follows,
N= 1 + N(e)2
Where n simple size
N= population of the study
1 constant
e = marginal error (0.05)
100— 1 + 100(0.05)2
100— 1 + 100(0.0025)
100
— 1 + 0.25
1001.25
= 80 respondents.
3.4 Sampling procedure
The respondents for the study were being selected using Simple random and purposive
sampling. The researcher was to sample the participants using the judgment that the participants
had the knowledge, experience and information that will require for the study.
Purposive sampling
Purposive sampling was to be used as respondents were to be grouped according to departments.
50 workers were interviewed while 20 supervisors and 10 Administrators were chosen in the
sample population. This procedure was less costly and time saving.
Sampling random sampling
The simple random sampling refers to a technique that selects a sample without bias from the
target/accessible population. The researcher was to ensure that each member of the target
population has an equal and independence chance of being included in the sample. Each
respondent was to have an equal chance of being selected.
26
3.5 Instruments of data collection
These are the tools that were being used in collecting data from the respondents and these were
to include the following;
Questionnaire
The researcher used questionnaires as one of the tools for data collection. This method was to
help the researcher to attain information from different respondents. The respondents were being
given questionnaires to fill in. The reason for opting for this instrument is because, it is simple
to administer and it gave respondents time to think about what they should answer. The
questionnaires were to be answered by the Employees and Administrators themselves and later
collected by the researcher;
A pre-test was to be conducted to ensure the clarity of questions, their effectiveness the time was
being required to complete the questionnaire and to make sure that the questionnaire measures
what it intended to measure, the researcher assessed its content validity and reliability. In depth
interviews were also to be used especially for top managers that will be human resource for
accurate information.
Interviews
This method was to be used to obtain primary information from respondents, mainly the key
informants. The tools were to help the researcher to asic questions about the decentralization and
social service delivery in Sironko district in Uganda. The reason for the use of interviews was
that the respondents were to be few, meaning that it would be easy to interview them; and
interviewing them would result into the collection of in-depth
3.6 Sources of data
There are two general sources of data, which include primary and secondary (Hair et al 2003).
Primary Data
This was data that provided first-hand information in research (Hair, et al 2003) primary data
which included questionnaires and interviews.
Secondary Data
Secondary data was to be collected and assembled for some research problems or opportunity
situation other than the current situation (Hair et al 2003) secondary data was useful for it
27
formed the baseline and starting point for the research study. It included document analysis
observation and focus group discussions.
3.7 Data Analysis
Data was to be continuously analyzed during data collection. The data categories was being
identified and edited with a view of checking for completeness and accuracy. Qualitative data
was being attributed to numerical codes so that it could be analyzed statistically.
3.8 Ethical issues
The researcher kept her word on the confidentiality of the respondents and none of their details
and opinions was shared with a third party.
The researcher was honest to the respondents by telling them the truth about the research.
The researcher kept her integrity by always presentable and professional in conducting of this
research.
28
CHAPTER FOUR
STUDY FINDINGS, INTERPRETATION AND DISCUSSION
4.0 Introduction
Chapter four presents and discusses the results of the study. Information was handled in the
order of respondents’ background characteristics, job expectations/performance definition,
performance facilitation, performance encouragement and quality of service. This arrangement
was picked because it presents the systematic flow of performance as earlier supported by
Cascio (1986, p.423) and outlined in chapters 1 and 2 above.
4.1 Background characteristics of respondents
A total of 150 Budadiri County Sironko District Uganda I-Iealth personnel and 60 exiting
patients/caretakers were interviewed by questionnaire from four of the Health Sub-districts of
Budadiri County Sironko District Uganda. Additionally, 10 focus group discussions were held in
Wakiso Health Sub-districts (the furthest and nearest to the district headquarters) targeting
female and male adolescents (10-19 years), female and male adults (20 years and above) and
community leaders. Key informant interviews were administered to 10 respondents who were
associated with the Budadiri County Sironko District Uganda Health Directorate 31 work,
including politicians and bureaucrats from the government and non-government health sector of
the district.
4.1.1 Background characteristics of personnel respondents
Table 3 below shows the summary of background characteristics of personnel respondents.
Starting with the age and sex of personnel respondents
29
Table 1: Showing age of the respondents
Age No of respondents Percentage
20-29 27 34
30-39 17 21
40-49 23 29
50-59 09 11
60- and above 4 5
Total 80 100Source: Primary Data 2017
The table: 1 show that age range of 20 to 29 years (31%) had the largest number of respondents
and age range 60 to 69 (3%) had the smallest number.
Table 2: Showing Sex of the repondents
The female constituted the largest number with 52% while the male were at 48%. This is
because it is the female who are most affected.
Source: Primary Data 2017
30
Table 3: Showing level of education
Level of education No of respondents Percentage
Primary 12 15
Secondary 41 51
Post-secondary 21 26
University 4 5
Others 2 3
Total 80 100Sourcc: Primary Data 2017
The majority of health personnel interviewed had attained
postsecondary (26%) and University (5%). Primary leavers were
they had never gone to school. This implies that most people had
Secondary education (62%),
(15%). Only (2%) reported that
less education.
The majority of health personnel interviewed had attained
postsecondary (26%) and University (5%). Primary leavers were
they had never gone to school. This implies that most people had
Secondary education (62%),
(15%). Only (2%) reported that
less education.
Figure 1: Showing level of education
31
Table 4: Showing the duration in Service
Duration of Service No of Respondents Percentage
itolO 37 46
llto2O 22 28
21to30 16 20
31to40 4 5
41to50 1 1
Total 80 100
Source: Primary Data 2017
As for duration in service, over half of the respondents had worlced for a duration of 1 to 10
years (46%) a possible indication of new staff recruited during years of decentralisation, they
were followed by (28%) for 11 to 20 years’ service range, (20%) for 21 to 30 years, (5%) for 31
to 40 years and lastly (1%) for 41 to 50 years of service.
32
Figure 2: Showing the duration in Service
37
rn~Tr
~ -~ Irt Ir --
~_~
S 16-
- --
L~~ I_____
1- -~ —__
Source: Primary Data 2017
According to figure above as per duration in service, over half of the respondents had worked
for a duration of 1 to 10 years (46%) a possible indication of new staff recruited during years of
decentralisation, they were followed by (28%) for 11 to 20 years’ service range, (20%) for 21 to
30 years, (5%) for 31 to 40 years and lastly (1%) for 41 to 50 years of service.
Table 5: Showing the positions held by personnel respondents
Position held No of respondents PercentageNursing assistant 18 23Nurse/midwife 17 21Support staff 13 16in-charge 12 15Others officers 08 09Vaccinator 4 5Clinical officer 3 4Laboratory 3 4Medical officer 2 3Total 80 100Source: Primary Data 2017
33
Positions held by personnel respondents constituted nursing assistants forming the biggest
proportion of the respondents interviewed (23%), followed by nurses/midwives (2 1%), support
staff (16%) and unit in-charges (15%) who included nursing assistants, nurses, midwives and
clinical officers. Other officers (9%) (Comprising of dispensers, dental, radiography and
orthopaedic officers), vaccinators (5%), clinical officers (4%), laboratory (4%) and medical
officers (3%).
4.2 Personnel respondents’ distribution by Health Sub-district (HSD), unit ownership and
unit level
Table 2 below shows the distribution of personnel respondents by HSD, health units’ ownership
and health unit levels. Budadiri County Sironko District Uganda HSD,
Table 6: Showing the unit ownership of the respondents.
Unit ownership No of respondents Percentage
Government 17 21
Non-government organization 43 54
Private 20 25
Total 80 100
Source: Primary Data 2017
In the above table 21% of personnel interviewed were from Government units, 54% personnel
came from NGO health units, while 25% were interviewed from private units. This is because
non-government organizations are the ones which were so much involved in the study as
compared to other units.
34
Figure 3: Showing the unit ownership of the respondents.
— —43 ~——— —————— —
r__-~~--—
~ >~r~
---- -j~ir--~-
1 20
~ I r—-~ F
——.—~ 1__~_.__________~ I
1 1-- ~- —- - —~
- -
Source: Primary Data 2017
In the above figure 21% of personnel interviewed were from Government units, 54% personnel
came from NGO health units, while 25% were interviewed from private units.
Table 7: Showing the health unit level.
Unit ownership No of respondents Percentage
Hospital 10 13
HCII 25 31
I-IC III 29 36
I-ICIV 16 20
Total 80 100Source: Primary Data 2017
Personnel interviewed as by health unit level were 13% at hospital level, 31% at HCII, at HCIII
were 36% and 20% from HCIV.
35
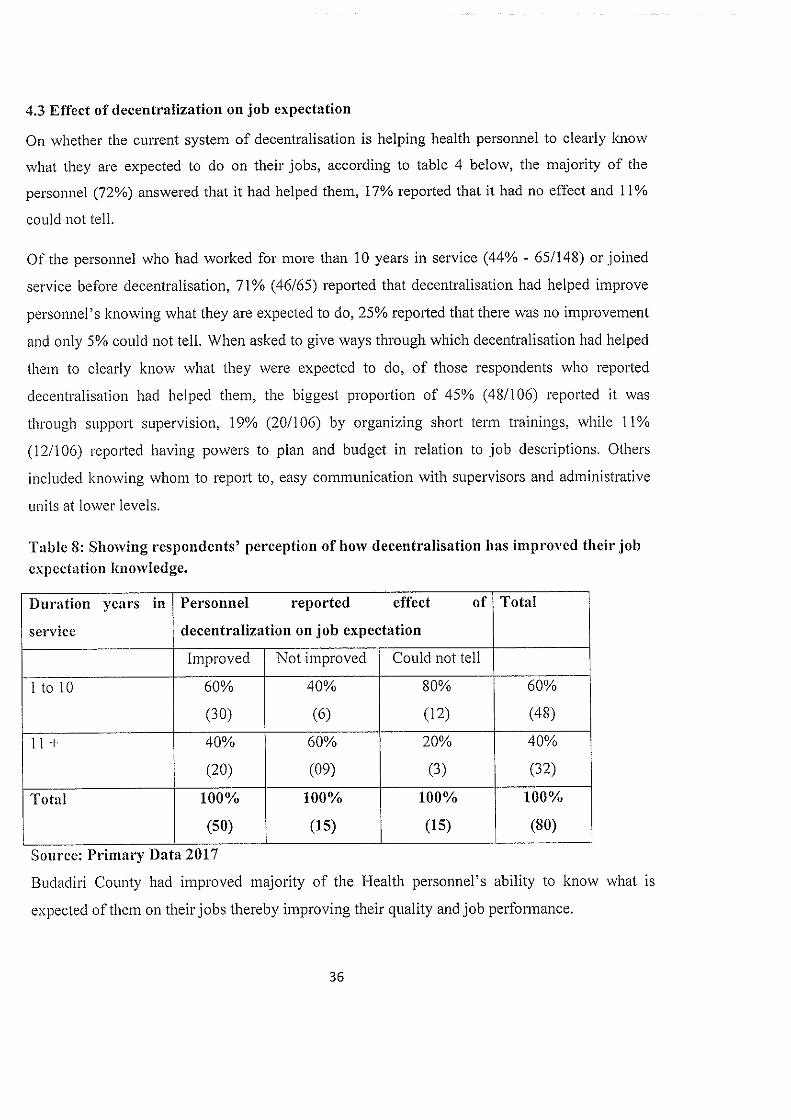
4.3 Effect of decentralization on job expectation
On whether the current system of decentralisation is helping health personnel to clearly know
what they are expected to do on their jobs, according to table 4 below, the majority of the
personnel (72%) answered that it had helped them, 17% reported that it had no effect and 11%
could not tell.
Of the personnel who had worlced for more than 10 years in service (44% - 65/148) or joined
service before decentralisation, 71% (46/65) reported that decentralisation had helped improve
personnel’s Ic owing what they are expected to do, 25% reported that there was no improvement
and only 5% could not tell. When asked to give ways through which decentralisation had helped
them to clearly know what they were expected to do, of those respondents who reported
decentralisation had helped them, the biggest proportion of 45% (48/106) reported it was
through support supervision, 19% (20/106) by organizing short term trainings, while 11%
(12/106) reported having powers to plan and budget in relation to job descriptions. Others
included knowing whom to report to, easy communication with supervisors and administrative
units at lower levels.
Table 8: Showing respondents’ perception of how decentralisation has improved their jobexpectation knowledge.
Duration years in Personnel reported effect of Total
service decentralization on job expectation
Improved Not improved Could not tell
1 to 10 60% 40% 80% 60%
(30) (6) (12) (48)
11 + 40% 60% 20% 40%
(20) (09) (3) (32)
Total 100% 100% 100% 100%
~___________________ (50) (15) (15) (80)
Source: Primary Data 2017
Budadiri County had improved majority of the Health personnel’s ability to know what is
expected of them on their jobs thereby improving their quality and job performance.
36
4.4 Performance facilitation: the constraints to effectiveness and the quality, quantity and
accessibility of personnel
Performance facilitation section presents results on the staffing status, action on elimination of
roadblocks to performance and provision of adequate resources for making easy personnel tasks.
It includes subsections on staffing, knowledge and skills, performance feedback, equipment,
supplies and workspace and organisational support.
4.4.1 Effect of decentralisation on improving personnel job knowledge and skills
Personnel explanation of how the system of decentralization had helped to improve their job
knowledge and skills were summarized in table below. The table illustrates the views of
personnel respondents on the effect of decentralisation on job knowledge and skills. In general,
the majority (74%) of all personnel interviewed reported that decentralisation had helped to
improve their job knowledge and skills while the rest (26%) reported that they had not improved
their job knowledge and skills under the decentralisation system. Of the personnel who had
worked for more than 10 years in service (65/140) or joined service before decentralisation, 75%
(49/65) reported that decentralisation had improved their job knowledge and skills and 25% said
they had not had their job knowledge and skills improved under decentralisation. On how
decentralisation had improved personnel job knowledge and skills, of those respondents who
reported improvement (104/140), 40% answered that it was through attending seminars and
workshops organized by the DDHS office, 26% was for training received, 14% through support
supervision and others included sharing knowledge with personnel from other units and
information passed on through grand rounds and radio. From the staff that gave reasons for why
they had had no improvement, the majority, 72% (15/28) argued that they had not gone for any
other training, seminar or workshop during decentralisation.
37
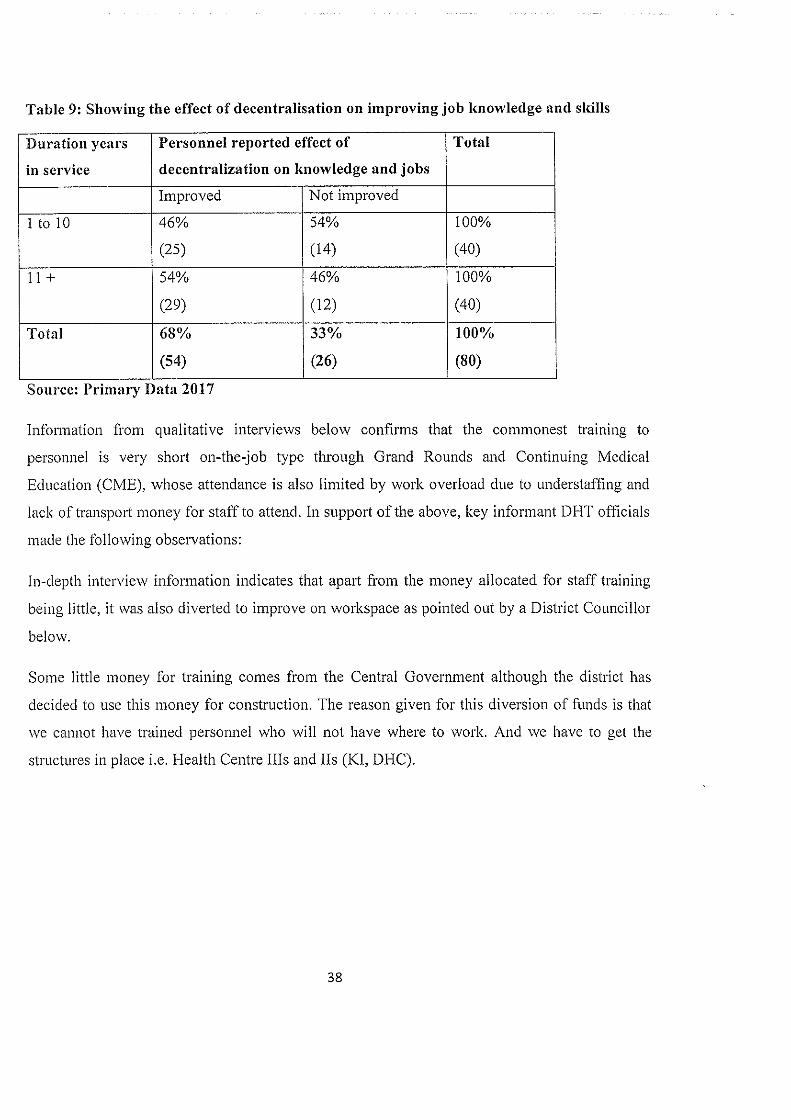
Table 9: Showing the effect of decentralisation on improving job knowledge and skills
Duration years Personnel reported effect of I Total
in service decentralization on knowledge and jobs
Improved Not improved
1 to 10 46% 54% 100%
(25) (14) (40)
11+ 54% 46% 100%
(29) (12) (40)
Total 68% 33% 100%
(54) (26) (80)
Source: Primary Data 2017
Information from qualitative interviews below confirms that the commonest training to
personnel is very short on-the-job type through Grand Rounds and Continuing Medical
Education (CME), whose attendance is also limited by work overload due to understaffing and
lack of transport money for staff to attend. In support of the above, key informant DI-IT officials
made the following observations:
In-depth interview information indicates that apart from the money allocated for staff training
being little, it was also diverted to improve on workspace as pointed out by a District Councillor
below.
Some little money for training comes from the Central Government although the district has
decided to use this money for construction. The reason given for this diversion of finds is that
we cannot have trained personnel who will not have where to work. And we have to get the
structures in place i.e. I-Iealth Centre Ills and us (Ku, DHC).
38
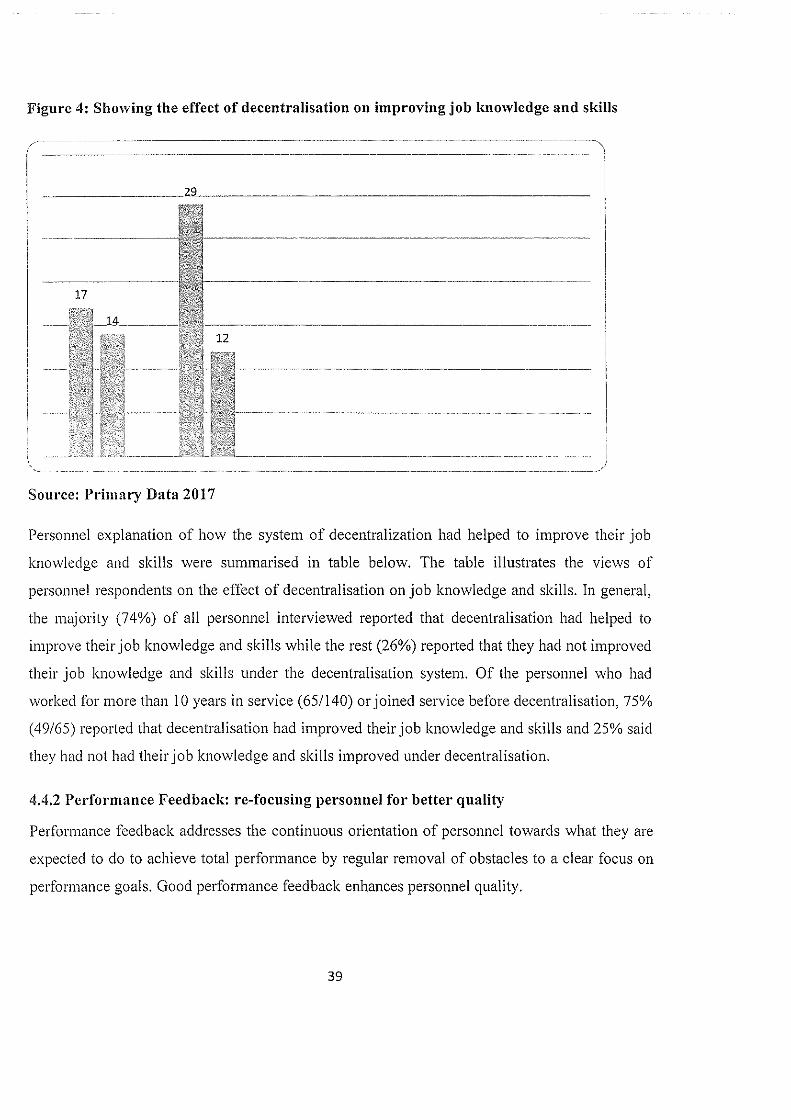
Figure 4: Showing the effect of decentralisation on improving job knowledge and skills
4______ ~—--- ---~-~--- —----------------------~ -----
--~
--— —-
44~;
17
-_-‘
- -
~:‘ -~
i;
U IE ~
I
Source: Primary Data 2017
Personnel explanation of how the system of decentralization had helped to improve their job
knowledge and skills were summarised in table below, The table illustrates the views of
personnel respondents on the effect of decentralisation on job knowledge and skills. In general,
the majority (74%) of all personnel interviewed reported that decentralisation had helped to
improve their job knowledge and skills while the rest (26%) reported that they had not improved
their job knowledge and skills under the decentralisation system. Of the personnel who had
worked for more than 10 years in service (65/140) or joined service before decentralisation. 75%
(49/65) reported that decentralisation had improved their job knowledge and skills and 25% said
they had not had their job knowledge and skills improved under decentralisation.
4.4.2 Performance Feedback; re-focusing personnel for better quality
Performance feedback addresses the continuous orientation of personnel towards what they are
expected to do to achieve total performance by regular removal of obstacles to a clear focus on
performance goals. Good performance feedback enhances personnel quality.
39
4.4.2.1 Nature of job performance feedback
The study revealed that the majority of the interviewed health personnel were getting some form
of job performance feedback. 45% of the respondents reported that they were getting job
performance feedback (reorientation to knowing they are doing what they are expected to do)
through verbal means, 37% reported that it was both verbal and written and 11% said it was by
written means only. 7% reported that they were not getting any feedback; these included a dental
officer, nurse, laboratory officer, an in-charge and a radiographer.
As regards the frequency of performance feedback, 49% indicated receiving feedback on
monthly basis, 17% quarterly, and 16% daily. However, only 8% reported receiving it annually.
Respondents under the category of “others” (11%) said that they either received feedback
weekly, rarely or did not get any feedback. When cross-tabulated with unit ownership, it was
noted that the majority of the personnel in government, NGO and private health units, reported
receiving feedback on monthly basis. From the above presentation, clearly, a big proportion of
personnel received feedback on a monthly basis, which is good for enhancing good
performance.
On the question of who assesses the personnel performance, 37% reported that they were
normally assessed by unit in-charges, 32% by Heads of Department, 18% said they were
assessed by health sub-district (HCIV) and 11% by the DDHS officials and 2% said by the
Parish Development Committee (PDC).
4,4.2.2 Perceived effect of dccentrallzation on performance feedback
Personnel were asked to explain how the system of decentralization had helped to improve their
performance feedback, their responses were summarized in table 6 below. According to the
table, the majority (23%) of the personnel respondents reported that decentralisation had helped
to improve on performance feedback, 17% said it had not improved on feedback and 9% could
not tell, these included a clinical officer, a dispenser, with the biggest proportion of 36% (9/2 5)
being nursing assistants. Of the personnel who had worked for more than 10 years in service
(65/150) or joined service before decentralisation, 27% (45/65) reported that decentralisation
had improved on performance feedback, 20% reported that there was no improvement while
40% could not tell whether there was improvement or not. On ways in which decentralisation
40
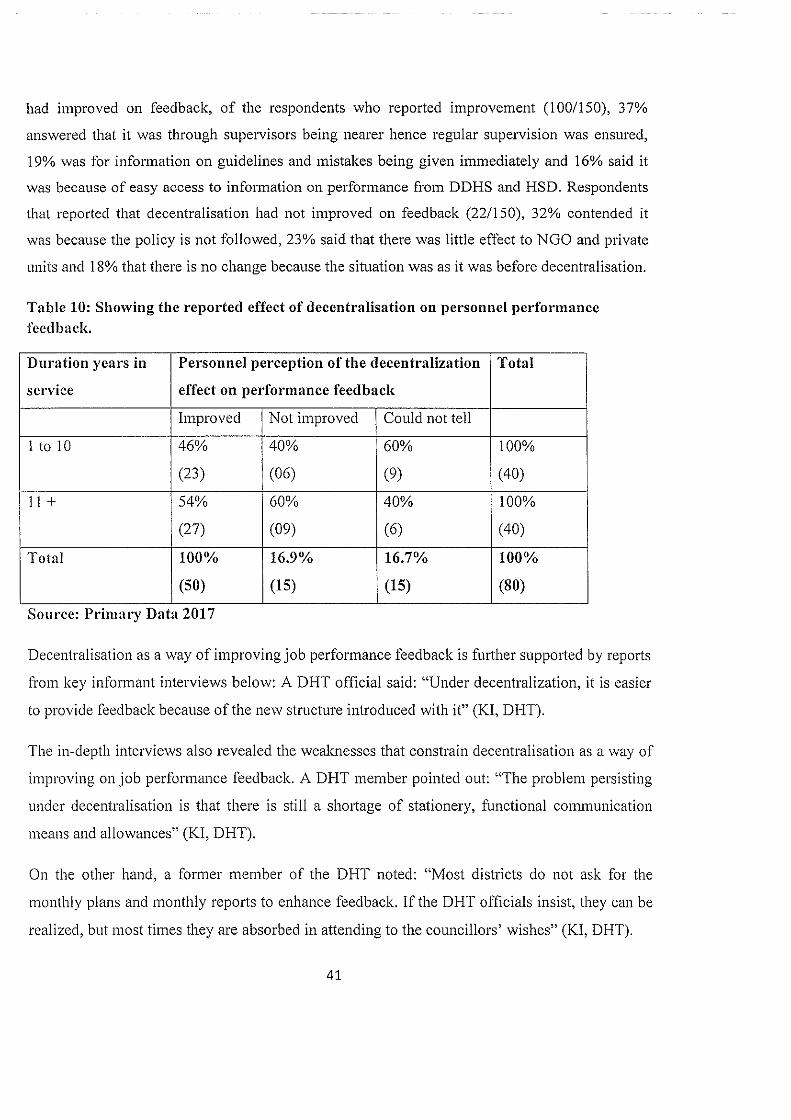
had improved on feedback, of the respondents who reported improvement (100/150), 37%
answered that it was through supervisors being nearer hence regular supervision was ensured,
19% was for information on guidelines and mistakes being given immediately and 16% said it
was because of easy access to information on performance from DDHS and HSD. Respondents
that reported that decentralisation had not improved on feedback (22/150), 32% contended it
was because the policy is not followed, 23% said that there was little effect to NGO and private
units and 18% that there is no change because the situation was as it was before decentralisation.
Table 10: Showing the reported effect of decentralisation on personnel performancefeedback.
Duration years in Personnel perception of the decentralization Total
service effect on performance feedback
Improved Not improved Could not tell
1 to 10 46% 40% 60% 100%
(23) (06) (9) (40)
11+ 54% 60% 40% 100%
(27) (09) (6) (40)
Total 100% 16.9% 16.7% 100%
(50) (15) (15) (80)
Source: Primary Data 2017
Decentralisation as a way of improving job performance feedback is further supported by reports
from key informant interviews below: A DHT official said: “Under decentralization, it is easier
to provide feedback because of the new structure introduced with it” (KI, DHT).
The in-depth interviews also revealed the weaknesses that constrain decentralisation as a way of
improving on job performance feedback. A DHT member pointed out: “The problem persisting
under decentralisation is that there is still a shortage of stationery, functional communication
means and allowances” (KI, DI-IT).
On the other hand, a former member of the DHT noted: “Most districts do not ask for the
monthly plans and monthly reports to enhance feedback. If the DHT officials insist, they can be
realized, but most times they are absorbed in attending to the councillors’ wishes” (KI, DHT).
41
Based on results presented above, performance feedbaclc in Tororo Health Directorate had been
largely improved upon as a result of decentralisation thereby farther improving on the
competence and performance of health personnel. However, meagre funds were still a hindrance
to better results.
4.4.5 Working space
4.5.1 State of working space
48% of the respondents reported that they did not have enough working space. Of those who
reported that they did not have enough space, 11/72 lacked enough room for delivery/maternity
wards, 10/72 for examination rooms, 9/72 needed injectionltreatment room and 9/72
immunisation rooms, 6 were for out-patient waiting room and 5 lacked counseling /family
planning space. The other space needed was for offices, storage, dispensary, antenatal,
laboratory, cold chain and monitoring of very sick patients.
In-depth interviews with health officials at the district further confirmed the problem of lack of
enough working space. A DHT official said: “There is lack of working space in most health
centres. Plans for construction of health centres are on paper and a few are completed. Space is
provided for as and when money is received from the Centre” (IU, DHT).
4.5.2 Effect of decentralization on improving workspace at health facilities
Personnel explanations on how the system of decentralization had helped to improve workspace
were summarised in table 7 below.
42
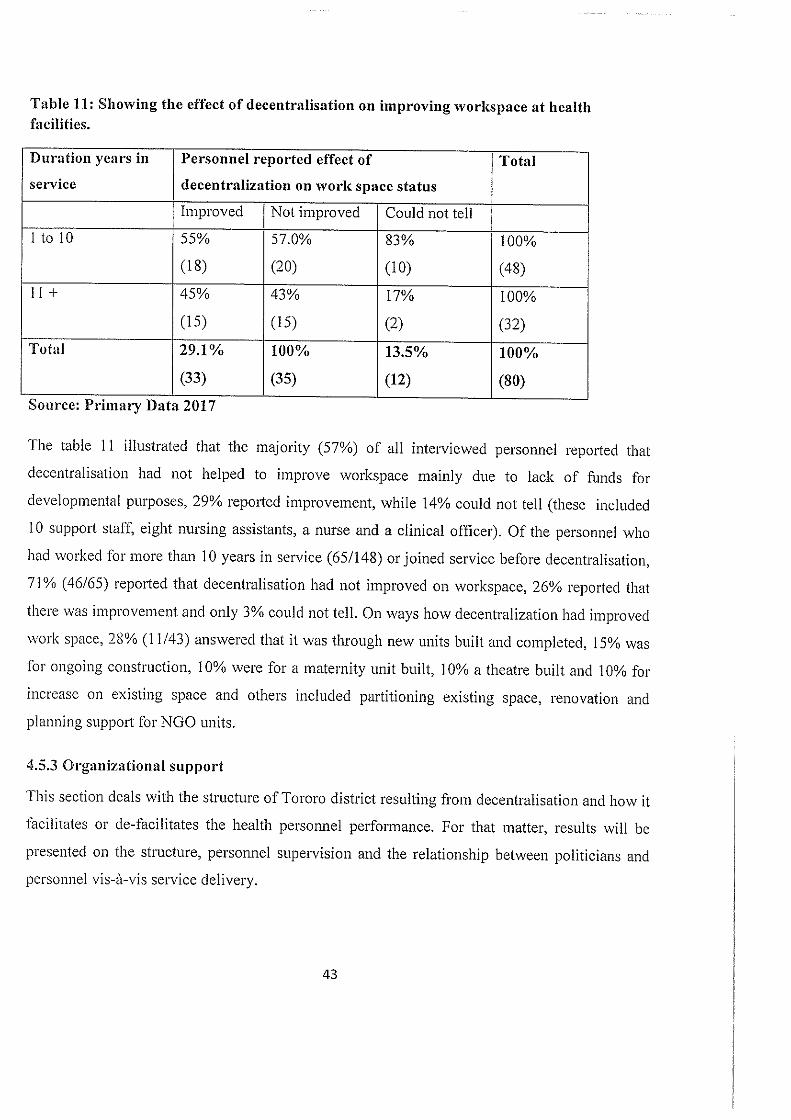
Table 11: Showing the effect of decentralisation on improving workspace at healthfacilities.
Duration years in Personnel reported effect of Total
service decentralization on work space status
Improved Not improved Could not tell
1 to 10 55% 57.0% 83% 100%
(18) (20) (10) (48)11+ 45% 43% 17% 100%
(15) (15) (2) (32)
Total 29.1% 100% 13.5% 100%
(33) (35) (12) (80)
Source: Primary Data 2017
The table 11 illustrated that the majority (57%) of all interviewed personnel reported that
decentralisation had not helped to improve workspace mainly due to lack of funds for
developmental purposes, 29% reported improvement, while 14% could not tell (these included
10 support staff, eight nursing assistants, a nurse and a clinical officer). Of the personnel who
had worked for more than 10 years in service (65/148) or joined service before decentralisation,
71% (46/65) reported that decentralisation had not improved on workspace, 26% reported that
there was improvement and only 3% could not tell. On ways how decentralization had improved
work space, 28% (11/43) answered that it was through new units built and completed, 15% was
for ongoing construction, 10% were for a maternity unit built, 10% a theatre built and 10% for
increase on existing space and others included partitioning existing space, renovation and
planning support for NOO units.
4.5.3 Organizational support
This section deals with the structure of Tororo district resulting from decentralisation and how it
facilitates or de-facilitates the health personnel performance. For that matter, results will be
presented on the structure, personnel supervision and the relationship between politicians and
personnel vis-à-vis service delivery.
43
4.5.4 Relationship between politicians and health personnel
The study revealed that 40% of the respondents observed that the relationship between health
personnel and politicians was not supportive to the delivery of services. However, 45% of the
respondents said that their relationship with politicians was good and that it helped to speed up
service delivery, while 14% (21/1 50) could not tell, with 13/21 working in NGO health units of
whom one was a medical officer and four were nurses. Of the 67 who praised the relationship,
57% said the politicians help in mobilising people, 15% reported that they increased supervision,
9% said that they participate in meetings for collective agreements and 8% said politicians
mobilise for drugs and equipment. From the 59 personnel that did not praise the politician-
personnel relationship for service delivery, 45 gave different reasons, of whom 29% observed
that politicians do not care about improving their relationship, 27% said that politicians did not
understand the personnel’s work but just harass them, 13% said that they take health workers as
being corrupt yet they are not, 9% said that they take long to make decisions and another 9%
said politicians only mind about their allowances.
4.5.5 Effect of decentralization in improving job incentives
Personnel were asked to explain how the system of decentralization had helped to improve their
job incentives, their responses were summarised in table 8 below, The table shows that 48% of
all personnel reported that decentralisation had not helped to improve job incentives, 35%
reported improvement while 17% could not tell, and they included mainly nursing assistants,
nurses and support staff. Of the personnel who had worked for more than 10 years in service
(65/147) or joined service before decentralisation, 54% (35/65) reported that decentralisation
had not improved job incentives, 41% said there was improvement and only 5% could not tell.
On ways through which decentralisation has improved job incentives, of the respondents who
reported improvement, 42% answered that it was through provision of incentives in form of
physical and monetary allowances, 38% was for assured rewards every month and others
included contribution to NGO staff allowances.
44
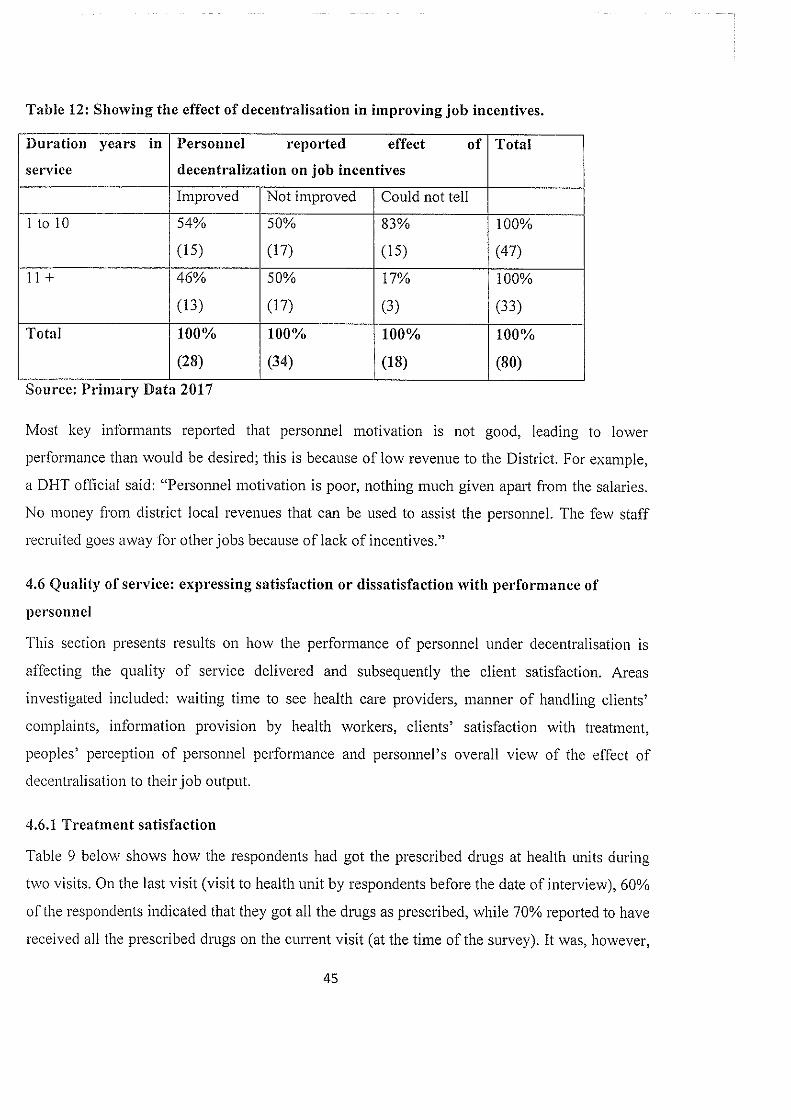
Table 12: Showing the effect of decentralisation in improving job incentives.
Duration years in Personnel reported effect of Total
service decentralization on job incentives
Improved Not improved Could not tell
1 to 10 54% 50% 83% 100%
(15) (17) (15) (47)
11+ 46% 50% 17% 100%
(13) (17) (3) (33)
Total 100% 100% 100% 100%
(28) (34) (18) (80)
Source: Primary Data 2017
Most key informants reported that personnel motivation is not good, leading to lower
performance than would be desired; this is because of low revenue to the District. For example,
a DHT official said: “Personnel motivation is poor, nothing much given apart from the salaries.
No money from district local revenues that can be used to assist the personnel. The few staff
recruited goes away for other jobs because of lacic of incentives.”
4.6 Quality of service: expressing satisfaction or dissatisfaction with performance of
personnel
This section presents results on how the performance of personnel under decentralisation is
affecting the quality of service delivered and subsequently the client satisfaction. Areas
investigated included: waiting time to see health care providers, manner of handling clients’
complaints, information provision by health workers, clients’ satisfaction with treatment,
peoples’ perception of personnel performance and personnel’s overall view of the effect of
decentralisation to their job output.
4.6.1 Treatment satisfaction
Table 9 below shows how the respondents had got the prescribed drugs at health units during
two visits. On the last visit (visit to health unit by respondents before the date of interview), 60%
of the respondents indicated that they got all the drugs as prescribed, while 70% reported to have
received all the prescribed drugs on the current visit (at the time of the survey). It was, however,
45
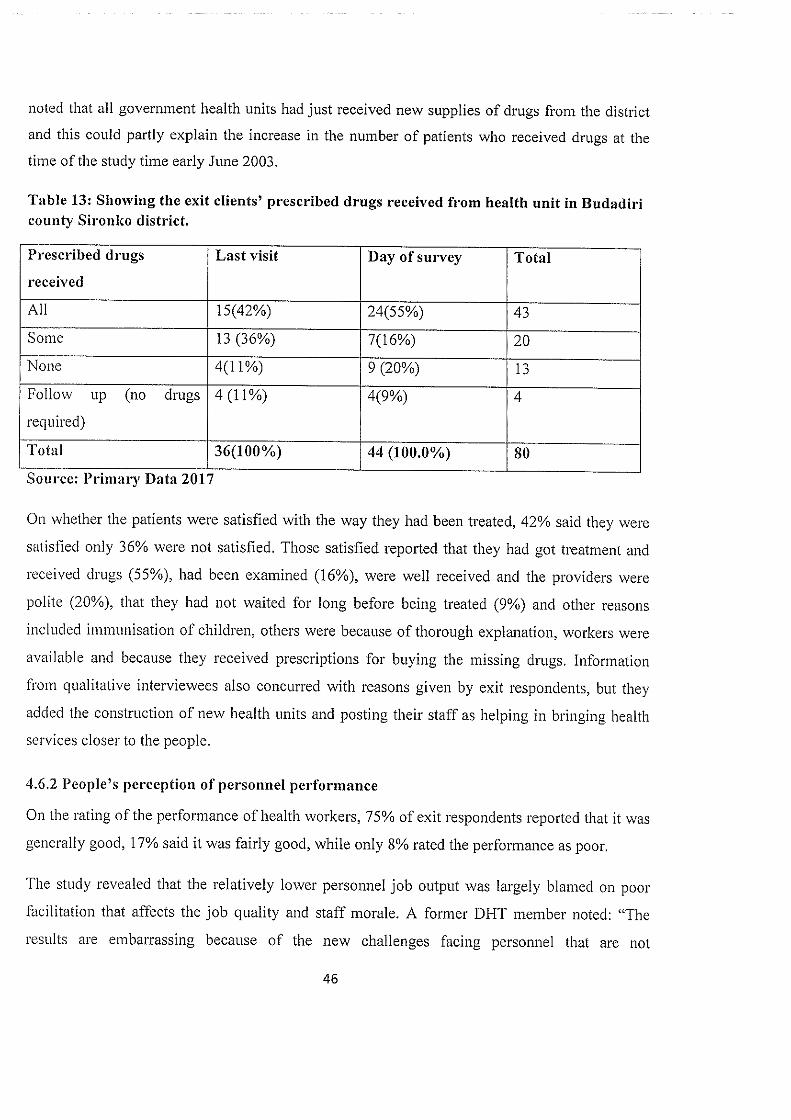
noted that all government health units had just received new supplies of drugs from the district
and this could partly explain the increase in the number of patients who received drugs at the
time of the study time early June 2003.
Table 13: Showing the exit clients’ prescribed drugs received from health unit in Budadiricounty Sironko district.
Prescribed drugs Last visit Day of survey Total
received
All 15(42%) 24(55%) 43
Some 13 (36%) 706%) 20
None 401%) 9(20%) 13
Follow up (no drugs 4 (11%) 4(9%) 4
required)
Total 36(100%) 44 (100.0%) 80
Source: Primary Data 2017
On whether the patients were satisfied with the way they had been treated, 42% said they were
satisfied only 36% were not satisfied. Those satisfied reported that they had got treatment and
received drugs (55%), had been examined (16%), were well received and the providers were
polite (20%), that they had not waited for long before being treated (9%) and other reasons
included immunisation of children, others were because of thorough explanation, workers were
available and because they received prescriptions for buying the missing drugs. Information
from qualitative interviewees also concurred with reasons given by exit respondents, but they
added the construction of new health units and posting their staff as helping in bringing health
services closer to the people.
4.6.2 People’s perception of personnel performance
On the rating of the performance of health workers, 75% of exit respondents reported that it was
generally good, 17% said it was fairly good, while only 8% rated the performance as poor.
The study revealed that the relatively lower personnel job output was largely blamed on poor
facilitation that affects the job quality and staff morale. A former DHT member noted: “The
results are embarrassing because of the new challenges facing personnel that are not
46
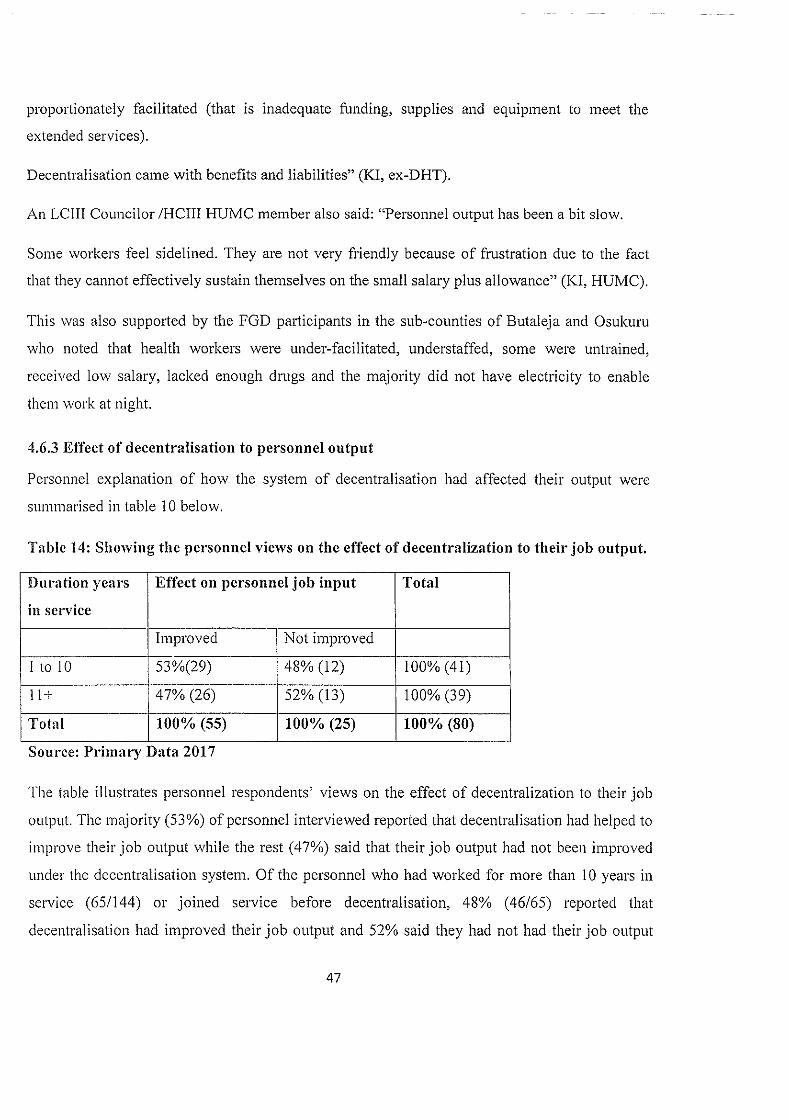
proportionately facilitated (that is inadequate Ending, supplies and equipment to meet the
extended services).
Decentralisation came with benefits and liabilities” (KI, ex-DHT).
An LCIII Councilor /HCIII HUMC member also said: “Personnel output has been a bit slow.
Some workers feel sidelined. They are not very friendly because of frustration due to the fact
that they cannot effectively sustain themselves on the small salary plus allowance” (1(1, HUMC).
This was also supported by the FGD participants in the sub-counties of Butaleja and Osukuru
who noted that health workers were under-facilitated, understaffed, some were untrained,
received low salary, lacked enough drugs and the majority did not have electricity to enable
them work at night.
4.6.3 Effect of decentralisation to personnel output
Personnel explanation of how the system of decentralisation had affected their output were
summarised in table 10 below.
Table 14: Showing the personnel views on the effect of decentralization to their job output.
I)uration years Effect on personnel job input Total
in service
Improved Not improved
I to 10 53%(29) 48% (12) 100% (41)
11+ 47% (26) 52% (13) 100% (39)
Total 100% (55) 100% (25) 100% (80)
Source: Primary Data 2017
The table illustrates personnel respondents’ views on the effect of decentralization to their job
output. The majority (53%) of personnel interviewed reported that decentralisation had helped to
improve their job output while the rest (47%) said that their job output had not been improved
under the decentralisation system. Of the personnel who had worked for more than 10 years in
service (65/144) or joined service before decentralisation, 48% (46/65) reported that
decentralisation had improved their job output and 52% said they had not had their job output
47

improved upon under decentralisation. This means that though decentralisation had helped the
majority improve performance, the other lot still needed to be uplifted for better results.
48
CHAPTER FIVE
DISCUSSION OF THE FINDINGS, CONCLUSIONS AND RECOMMENDATIONS
5.0 Introduction
This chapter presents the conclusions and recommendations drawn from the findings. This study
examined the effect of decentralisation on the performance of local government in Budadiri
County Sironico District Uganda Health Directorate personnel; it assessed the personnel
performance in terms of their quantity and quality, personnel accessibility to local people, the
clients’ satisfaction of personnel services and constraints to personnel performance under
decentralisation. In the process, it followed up the personnel performance factor; that is
performance definition or job expectation, performance facilitation and encouragement, and the
quality of service. Conclusions are therefore, presented on the personnel performance factors of
job expectations, staffing, lcnowledge and skills of personnel, equipment, supplies and
workspace, organizational support, job rewards and quality of service. Through these,
conclusions based on the study objectives are drawn.
5.1 Discussions of the findings
Decentralisation was found to have improved upon the ability of health personnel in Budadiri
County Sironlco District Uganda to lcnow their job expectations and consequently improve on
their quality. Performance goals were set within preset national standards. Reminders of
performance goals were clear (written and oral), and were both regular and timely. Personnel
were able to describe their performance goals in measurable terms, and the majority of them said
they had been given job descriptions. Both staff recruited before and after decentralisation
reported improvement on knowing their job expectations as a result of decentralisation, they
reported that this improvement was mainly through support supervision, short term trainings,
having more powers to plan and budget in relation to their job descriptions. Other improvements
were knowing whom to report to, easy communication with supervisors and administrative units
at lower levels.
In an effort to take health services closer to the Budadiri County communities, decentralisation
created more health units in categories of HCII, HCIII and HCIV; however, this was not
followed by proportionate increase in the numbers of relevant manpower, subsequently
49
overloading the available personnel. This led to many health units especially those falling under
HCII and HCIII category to be headed by under-qualified staff who did not measure up to the
required performance demands of planning, implementing and evaluation of activities as
managers of Health in the district. Even at hospitals, various categories of staff were
understaffed among these were the nurses while nursing assistants were overstaffed to cope with
the shortage of nurses. The staff resisted posting to rural areas where new units were being
created, this challenges the decentralisation powers to improve on service delivery. The I-lealth
Directorate had little influence on numbers of staff in NGO and private health units, while it has
direct influence on their staff qualifications. But results showed that many personnel in NGO
and private units were under qualified for the posts they occupied. Lack of funds was found to
be the biggest roadblock to eliminating staffing gaps; the DSC that was sometimes nonexistent
probably due to political reasons made the staffing problems worse.
The majority of staff interviewed felt that their pre-service training was adequate for their jobs.
However, most clients expressed dissatisfaction with the recruitment of personnel they deemed
to be unqualified. The majority (94%) of personnel expressed the need for on-the-job-training to
improve on their performance, but almost one-third (29%) had never attended any on-the-job
training while 54% had attended within the last one year. The majority of interviewed staff
(about ¼) that had worked before and after the introduction of decentralisation in the district
reported improvement on their job knowledge and skills; this was mainly through training
received, support supervision, sharing knowledge with personnel from other units and
information passed on through Grand Rounds and radio.
The type of staff training mainly given was of a very short-term nature, but this was also
hampered by inadequacy of funds for organizing the trainings and transporting participants and
facilitators.
Worse still, the training funds were diverted to construction of new health units. The
understaffing that leaves some staff unable to attend because they do not have partners to
delegate their duties to during their absence, also blocks personnel from attending training.
Regular verbal and written performance feedback on monthly, quarterly and daily basis received
by the majority of personnel, helped to remind them to properly focus their perfonnance to the
50
right services. In-charges, Heads of Department, HSD and DDHS, in that order, were reported to
be playing a big role in performance feedback. This is an indication that managers under
decentralisation are active in guiding personnel to stick to the right performance goals.
The majority of the personnel recruited both before decentralisation (69%) and afler (65%),
reported improvement on performance feedback during the decentralisation era. Reasons given
for the improvement included supervisors being nearer hence regular supervision was ensured,
information on guidelines and mistakes being given immediately and easy access to information
on performance from DDHS and HSD. However, meagre funds were still a hindrance to
achieving better results.
Availability of equipment to personnel was very poor with almost three quarters of interviewed
personnel reporting not having the equipment needed for their work. The majority of the
requests for equipment’s were not honoured. Equipment maintenance, on the other hand, was
very good with over three quarters of personnel saying that all their equipment’s were well
maintained. The relatively low amount of revenue collected by the district and that remitted by
the Central Government was largely blamed for the unavailability of equipment’s and its poor
maintenance in some cases.
The study revealed that the majority of the personnel did not have all supplies needed for their
work, neither were all their supplies’ requests honoured. Supplies most requested but not
received were drugs and protective wears. This led to demoralisation of patients and personnel.
The low funding situation in the district was mainly blamed on lack of supplies especially the
scarcity and irregularity of drugs in health units.
About half of the personnel interviewed did not have enough working space like rooms for
maternity services, patients’ examination, injection and counselling. A large proportion of both
staff recruited before and after decentralisation introduction in Budadiri County, reported that
decentralisation had not improved on their workspace status. Construction of new buildings for
workspace improvement was very slow due to inadequate funding which was given as a major
reason for diverting money meant for staff training to workspace construction. The inadequate
workspace makes staff inaccessible to all clients due to lack of rooms to conduct their duties in
confidence leading to client dissatisfaction of personnel services.
51
There was general agreement that the structure for decentralisation of health services in Budadiri
County had extended better health management to the lower communities especially through
creation of lower administrative centres. This had helped personnel to improve on their
performance through taking supervisors closer to them, by opening up health centers at different
levels it had brought their services closer to the community, and a little more quantity of drugs
than before. On the other hand, the structure was also making it difficult for health staff to
perform effectively because of delays in responding to requisitions like for drugs, delays in
release of funds and attending to problems, delay in appointing and confirming staff leading to
personnel getting overworked and collectively become less effective. The structure had not been
fully utilized to bolster personnel performance due to poor facilitation mainly because of
inadequate staff and funds to support supervisory work and provide logistics.
The relationship between politicians and health personnel was found to be both supportive and
unsupportive to service delivery. It was supportive because politicians helped in mobilising the
people, supplies and equipment for health service, supplementing supervision and participation
in meetings. While on the other hand, it was not supportive because some politicians did not
care about improving the relationship, politicians did not understand the personnel’s work but
just harassed them, politicians took all health workers to be corrupt yet this did not apply to all
of them, politicians were taking long to make decisions and only cared about securing future
votes and getting allowances. It was noted that the gap between politicians and personnel under
decentralisation was narrowing, leading to better service delivery, whereby the two increasingly
work as a team as time goes by.
The biggest proportion of personnel respondents indicated that they were receiving salary and
allowances as job rewards. The majority were not happy with the value and amount of their job
rewards, because the rewards could not meet all their basic needs. Just over half of the
interviewed personnel were happy with the timing of their job rewards while about a-half were
not happy as they received them late. Similarly, just over half of the personnel were getting job
rewards as promised by employers, while the rest were not happy because they had not received
accumulated salary arrears, no allowances paid, lacked salary increment and promotion.
Personnel promotions were generally inhibited by scarcity of funds, limited positions for
promotion in the district and further compounded by nepotism and tribalism. Generally, just
over a half of the personnel interviewed reported improvement of job incentives during52
decentralisation. The majority of the personnel were not encouraged by their job rewards to
sustain good performance.
Most patients were taking long to see health workers; the waiting time was at an average of lhr
15 mm. Some clients were also not able to see health staff in the afternoons as the staff was
leaving early before end of working hours. This made staff unavailable and the clients
dissatisfied.
Generally, most health workers were reported to be handling patients well despite the lack of
drugs at times, and for that the clients were satisfied. But some health workers were at times
rude, careless and money minded thereby not satisfying the patients with their service. Most
health workers gave clients the information that answered their needs for which the clients were
satisfied. On the other hand, some staff were reported to be overloaded by large numbers of
patients, not free with the local languages and some were rude hence not giving the needed
information and making the patients dissatisfied. Most patients were receiving all prescribed
drugs from the health units at which they were prescribed. However, about two fifths of patients
were either receiving some or no drugs at all which made them dissatisfied with the treatment
they were receiving from health workers.
Other common reasons given by citizens dissatisfied with treatment included unavailability of
staff, rudeness of staff, lack of comprehensive explanation from staff, poor or partial
examination and staff coming to health units late and leaving before end of working day. The
people perceived the health personnel performance as generally good. They further noted that
the relatively lower personnel job output was mainly due to under-facilitation of staff, which
negatively affects the quality of output and staff morale. The majority of the personnel reported
that decentralisation had helped to increase their job output.
5.2 Conclusions
In conclusion, the study achieved its general objective of assessing the effect of decentralisation
on the performance of district personnel in Uganda and Budadiri County Sironko District
Uganda Health Directorate in particular. It further attempted to answer the specific objectives of
assessing the nature of personnel performance in terms of their quantity and quality; the extent
to which personnel were accessible to their clients; the consumers’ satisfaction of personnel
services. The study also identified key constraints affecting effectiveness of the personnel53
performance under decentralisation in Budadiri County Sironko District Uganda as specifically
laid out below:
The improvement of personnel’s ability to know what they are expected to do on their jobs
under decentralisation led to improvement in personnel quality as being focused in their
performance.
The quantity of the Health Directorate personnel in Budadiri County Sironko District Uganda
was found to be lacking leading to overloading of personnel to serve the increasing numbers of
clients and increasing numbers of health units, it also led to understaffing hence constraining
service delivery. The personnel performance was also constrained by absence of the DSC that is
the top legal body in the district that oversees the smooth functioning of personnel. Personnel
quality was also found wanting especially in lower cadres of Government, NGOs and private
units where personnel were serving in positions for which they were under-qualified. The above
coupled with the lack of funds to recruit personnel were constraints to Budadiri County
personnel performance under decentralisation.
Personnel quality was partially enhanced under decentralisation by improvement of job
knowledge and skills through mainly very short-term training. Long-term courses were limited
and nonparticipation to available training of some personnel were caused by lack of funding and
understaffing that left no time for training to improve staff quality and subsequently their
performance.
The quality of personnel was in part improved by the regular verbal and written performance
feedback from the Health Directorate managers at lower levels created under decentralisation.
But meagre funds were again a constraint to the smooth flow of feedback in terms of transport
and stationery.
Personnel quality and accessibility were negatively affected by the general lack of equipment.
Staff without the essential equipment is viewed by the local people as inferior; and staffs are
also forced not to attend to clients when they lack the necessary equipment. The lack of
equipment and the funds that would purchase equipment were therefore major constraints to
personnel performance and contributed to some of the clients’ dissatisfaction.
54
Necessary supplies, especially drugs were scarce and irregular as a result of the poor financial
capacity of Budadiri County Sironlco District Uganda. Little amounts of drugs were purchased
as and when funds became available; this was a constraint to personnel performance leading to
the dissatisfaction of the local people who sometimes blamed staff for the situation based on
mere allegations. Lack of drugs is a major source of dissatisfaction among service users.
Workspace as venue for confidential personnel-client interaction was lacking to many personnel
thereby constraining health workers and making them not easy to access ending into
dissatisfaction of clients. On the other hand it is worth noting that an almost equal number of
personnel had their workspace made better under decentralisation. The lack of enough finds was
blamed for the inadequate and slow pace of workspace improvement.
Accessibility of health workers was improved upon through the creation of the health services
decentralisation structure that brought nearer more qualified cadre of personnel form hospitals to
lower health units, the same also partly improved health management at lower levels thus
enhancing personnel quality. But the structure was also found to be unhelpful when it came to its
inability to do away with the personnel constraints of poor staff appointment and confirmation,
and delayed in responding to calls for staff facilitation. The politicians were, on the one hand,
helpful to health workers in improving performance where they mobilised people and resources,
while on the other hand they constrained personnel performance especially the selfish ones, but
they were found to be progressing for better as time went by.
Personnel performance was constrained by poor job rewards, this made personnel less accessible
whenever they sought supplementary income activities (like gardening in the mornings) as an
alternative survival strategy and consequently dissatisfied the citizens. Personnel were not happy
with the value and amounts ofjob rewards that were not meeting their basic needs; the rewards
were sometimes received late, while promotions were inhibited by scarcity of funds, limited
positions in the district, nepotism and tribalism.
The clients expressed dissatisfaction with the way some personnel delivered services; clients
took long to see health workers, the personnel were sometimes unavailable, staff were
overloaded and could not avail enough time with patients, some were rude and others were not
conversant with the local languages. Sometimes, dissatisfaction was also directed to personnel
whenever patients did not receive the prescribed drugs. However, clients were satisfied with
55
some personnel labouring to handle patients carefully and giving thorough explanations
concerning patients’ ailments despite poor facilitation in terms supplies (drugs) and equipment.
All in all, the study revealed that decentralisation has helped to improve on personnel
perfonnance and is still beneficial to service delivery, but there is urgent need for proportionate
facilitation of the system to appropriately deliver the decentralised services.
5.3 Recommendations
In order to improve the quality of personnel, there is need to strengthen the lower administrative
units at the HCIV, HCIII and HCII to increase the reminders to personnel of performance goals
in written and oral form at timely and regular intervals. This will enhance the personnel’s ability
to know their job expectations or performance definitions thereby improving their service
delivery.
To enhance the personnel quantity, quality and accessibility, urgent action is required to
proportionately recruit personnel to fill the current 70% health personnel gap in Budadiri
County. Similarly, there is urgent need to allocate personnel to perform duties for which they are
qualified to give citizens the quality of service for which they pay taxes. In particular, urgent
action should be directed towards recruitment of enrolled comprehensive nurses and clinical
officers Grade I who are needed across all health facilities to head HCII and HCIII respectively
and to provide lead and supportive treatment elsewhere. Enrolled comprehensive nurses gap was
100%. while that of clinical officers Grade I was 85%.
Personnel quantity, quality and accessibility improvement requires to have a functional DSC,
which is operational at all times. This will allow it to perform its duties of ensuring adequate and
satisfied personnel for the district to fulfill its service delivery to the citizens. The Budadiri
County Sironko District Uganda Council should be made to realise the importance of the
existence of the DSC in personnel performance and go out to ensure its existence.
The need to regularly update the quality of personnel requires that the personnel office should
ensure that all personnel get equal chances of attending timely and regular on-the-job-training to
keep up with changes for better performance. In addition, more funds should be mobilised to
enable staff to attend longer-term training sessions. Health workers should also be encouraged to
56
expeditiously learn local languages of their areas of operation to communicate fully with their
clients.
Performance feedback should target all personnel to help them focus their performance to the
right goals. There is need to invest more in performance feedback activities like regular
meetings with stafi, supervisory visits and confidential discussion of individual appraisal forms.
To supplement personnel quality, availability and raise client satisfaction, more funds should be
mobilised for procurement of equipment and its maintenance, for regular and adequate purchase
of supplies of drugs, protective wears and others like stationery. Under the current
decentralization system, the Central Government takes biggest responsibility of securing Thnding
to districts as it retained the most lucrative revenue generation sources.
For better accessibility of personnel, extra funds should be mobilised to expedite construction of
new rooms and maintenance of existing workspace. The workspace status should always ensure
upholding of the principle of confidentiality for areas like the examination of patients, injection,
counselling and maternity services.
To reduce constraints resulting from poor relationships between politicians and personnel,
continuous team building between the two factions should be organised and most especially with
every new batch of politicians to cement the working relationship towards better performance
for service delivery. Roles for politicians and bureaucrats need to be clearly understood during
these team-building sessions for them to avoid confusion in the process of working alongside
each other as is required under decentralisation.
To minimize constraints to performance of personnel due to poor job rewards, there should be a
deliberate effort to significantly improve the job rewards given to personnel so as to encourage
them to continuously aim at better performance. The improvement should address the value and
amount of job rewards, timely release of all promised rewards, salary increment and promotion
of personnel.
Putting in place and implementing a system that ensures availability of personnel at the work
place for all the time they are supposed to be there should complement the improved rewards.
57
REFERENCES
Abramson, W. B. (2012).Uganda rebuilding basic health services (RBHS,): Evaluation of BornE
County Petforrnance-based Contracting-In Pilot. Monrovia: GoL/USAID
Ahmad, J., Devarajan, S., Khemani, S. &Shah, S.(2005).Decentralization and service delivery.
World Bank Policy Research Working Paper 3603. World Bank
Akpan, H. E. (2008). Decentralization and service delivery: A frame work prepared for the
African Economic Research Consortium. Nairobi: AERC
Crawford, G.(2004). Democratic decentralisation in Ghana: issues and prospects. POLlS
Working Paper No. 9. School of Politics and International Studies, University of Leeds
Crook R. 2003. Decentralisation and poverty reduction in Africa: thepolitics of central-local
relations. Public Administration and Development 23 (1): 77-88
Darmawan, R. E. D. (2008).The practices ofdecentralization in Indonesia and its implication on
local competitiveness. Twente: School of Management and Government, University of Twente.
Dethier, J. J. (ed.) (2000).Governance, decentralization and reform in China, India and Russia.
Dordrecht: Kluwer Academic Publishers.
Devas, N. (2005).The challenges of decentralization. Brasilia: Global Forum on Fighting
Corruption
European Commission. (2007). Supporting Decentralisation and Local Governance in Third
Countries. Tools and Methods Series. Italy: EC.
Falleti, T. G. (2004).A sequential theory of decentralization: Latin American Cases in
comparative perspective. American Political Science Review 99(3,)
Ministry of Health and Social Welfare. (201 3).Health sector drajibudget, 2013/2014 fiscal year.
Monrovia: MOHSW
Ministry of Health and Social Welfare.(2008).Guidelines for national decentralisation.
Monrovia: MOHSW
58
Nkrumah, S.A. (2000). Decentralisation for good governance and development: The Ghanaian
experience. Regional Development Dialogue Vol.21 No.1, pp.53-67
Olcojie, C. (2009). Decentralization and public service delivery in Nigeria. Abuja: International
Food Policy Research Institute
Republic of Rwanda. (2006). Making decentralized service delivery work: Putting the people at
the center ofservice provision. A policy Note. Kigali:
Ruiz—Casares,M.(20 11) .Childprotectionknowledge, attitudeandpracticesinC’entraland Western
Uganda. Monrovia: Save the Children and USAID
Saito, F (2001 ).Decentralization the o r i e s revisited: lessons from Uganda. Ryukoku RISS
Bulletin, No. 31.
Sandfort, J. & Milward, H. B. (2007). Collaborative service provision in the public sector. In
Cropper,S . ,Huxham,C.,Ebers, M .& Ring, P.S .(Eds j(2008). The Oxford Handbook of Inter-
Organizational Relations. Oxford University Press. Pp 147-174
Scott, Z. (2009).Decentralisation, local development and social cohesion: An analytical review.
AGSDRC Research Paper. GSDRC
Shah, A. & Thompson, T. (2004) Implementing decentralized local governance: A treacherous
road with potholes, detoursand road closures. World Bank Policy Research Working Paper
3353. Washington, D.C: World Bank issues. Canada: International Development Research
Center.
Steiner, S. (2006).Decentralisation in Uganda. Exploring the constraints for poverty reduction.
GIG Working Paper 31. Germanlnstitute of Global and Area Studies
1-larper Collins United Nations Development Programme (2004). Decentralised governance for
development: A combined practice note on decentralisation, local governance and urban/rural
development. UNDP
59
APPENDICES
APPENDIX I: QUESTIONNAIRES
Part 1 Background Information
Dear Respondents,
I am Wamunga John Reg No, BPA/40524/151/DU a final year student of the above named
institution, conducting a research on the topic ‘decentralisation and social service delivery; A
study of students of Kampala international University Uganda.
I humbly request your assistance in filling the questionnaire. All information gathered shall be
used purely for research purpose and shall be treated with confidentiality.
Yours faithfully
Researcher
Section A: Blo data
I. What is your sex?
Male DFemale D2. What is your age bracket?
18-24 D25-31 D32-38 D39-40 D
60
SECTION B
Please tell me your name and present position in the Ministry of I-Iealth and Social Welfare
Tell me about your roles and responsibilities within the Ministry
How long have you worked with the Ministry?
Part 2 Decentralization and Service Delivery
What informed the Ugandan Government’s decision to decentralize its ministries and agencies?
In the cases of the departments of Health and Social Welfare, How has the process been
successful in bringing about improvement in the areas of health and social welfare in the country
especially at the local level?
With the introduction of the decentralization process, what challenges do you still face as a
department?
Has the decentralization of the Ministry of Health and Social Welfare contributed in any way to
the resource fullness or other wise of the staff of the department at the local levels? Please throw
more light on this.
How many Social Welfare/Health officials are in atypical CHSWT at the local level?
On the average, how many health worker and DSW workers is one expected to find at the county
and district levels in Uganda?
How do the departments of health and social welfare fund their operations?
Part 3 Reasons for Disparity between the Departments of Health and Social Welfare
Kindly describe how services are delivered in the Department of Health / Social Welfare
There is an apparent disparity in the decentralization process between the Department of Health
and that of Social Welfare. What might have accounted for this disparity in your view?
What do you suggests makes it possible for the health department to have advanced in the
decentralization process compared to the DSW?
61
Do you think the slow pace of decentralization in the DSW has something to do with their
internal operational mechanisms?
Part 4 Promotion of Wellbeing by Collaboration through Decentralization Process
What is the level of collaboration between the Health and Social Welfare Departments in
delivery of services to meet the well-being of the population?
What do you think account for the low/high levels of collaboration?
What would be some of the areas of collaboration between our department and that of DSW in
your quest to fully decentralize?
Community leaders
F In time of sickness, how do you get to the nearest health facility?
Can you explain the kind of services that are provided?
When there are social problems like child abuse, domestic violence, old age people, etc. how do
you deal with them?
Who are those that provide you with social welfare services in your community?
I-low was service delivery in terms of health and social services some five years ago?
Decentralization is expected to bring services closer to you. What do you think about the health
and social welfare services?
What are some social problems in the community that you think can be handled by social welfare
and health?
62
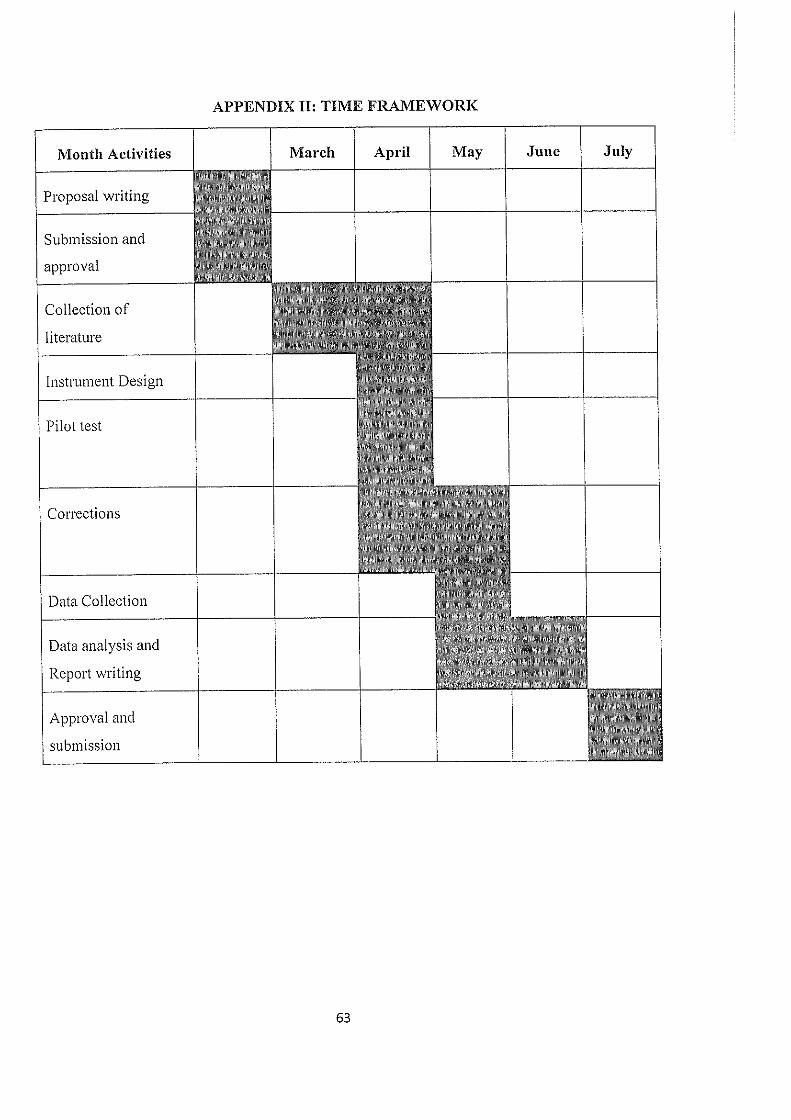
APPENDIX II: TIME FRAMEWORK
Proposal writing
Submission and
approval
Collection of
literature
Instrument Design
Month Activities March April May June July
Pilot test
Corrections
Data Collection
Data analysis and
Report writing
Approval and
submission
63
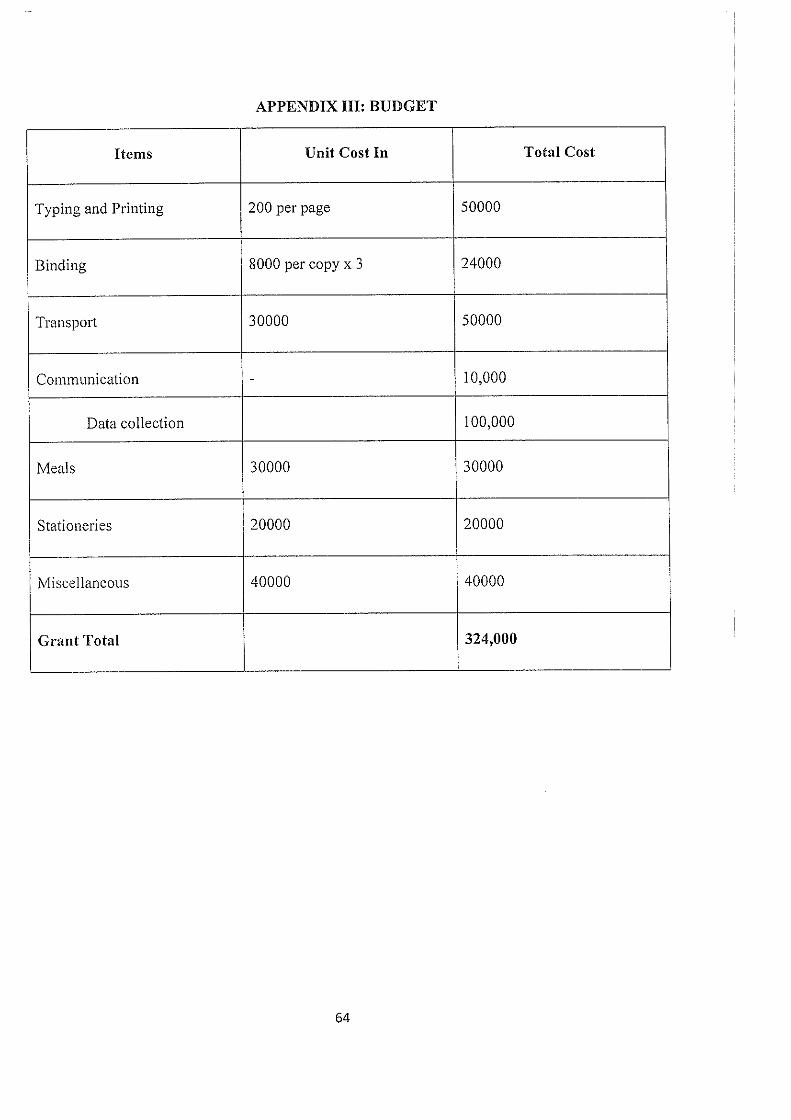
APPENDIX III: BUDGET
Items Unit Cost In Total Cost
Typing and Printing 200 per page 50000
Binding 8000 per copy x 3 24000
Transport 30000 50000
Communication — 10,000
Data collection 100,000
Meals 30000 30000
Stationeries 20000 20000
Miscellaneous 40000 40000
Grant Total 324,000
64