cytofluorometric methods for assessing absolute numbers of cell subsets in blood
TRANSCRIPT

Review Article
Cytofluorometric Methods for Assessing AbsoluteNumbers of Cell Subsets in Blood
Bruno Brando,1* David Barnett,2 George Janossy,3 Francis Mandy,4 Brigitte Autran,5
Gregor Rothe,6 Barbara Scarpati,1 Giovanna D’Avanzo,1 Jean-Luc D’Hautcourt,7 Rodica Lenkei,8
Gerd Schmitz,6 Annalisa Kunkl,9 Rosa Chianese,10 Stefano Papa,11 and Jan Willem Gratama12
for the European Working Group on Clinical Cell Analysis (EWGCCA)1Transplant Immunology and Hematology Laboratory, Niguarda-Ca’ Granda Hospital, Milan, Italy2UK NEQAS, Department of Haematology, Royal Hallamshire Hospital Sheffield, United Kingdom
3HIV Immunology, Department of Immunology & Molecular Pathology, Royal Free and University College Medical School,London, United Kingdom
4Laboratory for Analytical Cytology, Health Canada, Ottawa, Canada5Laboratoire d’ Immunologie Cellulaire et Tissulaire, Hopital Pitie Salpetriere, Paris, France
6Institut fur Klinische Chimie und Laboratoriumsmedizin, Klinikum der Universitat, Regensburg, Germany7Hopital de Warquignies, Boussu, Belgium
8CALAB Medical Laboratories, Stockholm, Sweden9Department of Immunology, San Martino Hospital and University of Genova, Genova, Italy
10Hematology Laboratory and Blood Bank, Hospital of Legnano, Legnano, Italy11Istituto di Scienze Morfologiche, Universita di Urbino, Urbino, Italy
12Department of Clinical and Tumor Immunology, Daniel den Hoed Kliniek, Rotterdam, The Netherlands
The enumeration of absolute levels of cells and their subsets in clinical samples is of primary importance inhuman immunodeficiency virus (HIV)1 individuals (CD41 T- lymphocyte enumeration), in patients who arecandidates for autotransplantation (CD341 hematopoietic progenitor cells), and in evaluating leukoreducedblood products (residual white blood cells). These measurements share a number of technical options, namely,single- or multiple-color cell staining and logical gating strategies. These can be accomplished using single- ordual-platform counting technologies employing cytometric methods. Dual-platform counting technologies couplethe percentage of positive cell subsets obtained by cytometry and the absolute cell count obtained by automatedhematology analyzers to derive the absolute value of such subsets. Despite having many conceptual and technicallimitations, this approach is traditionally considered as the reference method for absolute cell count enumeration.As a result, the development of single-platform technologies has recently attracted attention with several differenttechnical approaches now being readily available. These single-platform approaches have less sources ofvariability. A number of reports clearly demonstrate that they provide better coefficients of variation (CVs) inmulticenter studies and a lower chance to generate aberrant results. These methods are therefore candidates forthe new gold standard for absolute cell assessments. The currently available technical options are discussed inthis review together with the results of some cross-comparative studies. Each analytical system has its ownspecific requirements as far as the dispensing precision steps are concerned. The importance of precision reversepipetting is emphasized. Issues still under development include the establishment of the critical error ranges, which aredifferent in each test setting, and the applicability of simplified low-cost techniques to be used in countrieswith limited resources. Cytometry (Comm. Clin. Cytometry) 42:327–346, 2000. © 2000 Wiley-Liss, Inc.
Key terms: flow cytometry (FCM); absolute cell count; single platform; counting beads; CD4; CD34;leukoreduced blood products; monoclonal antibodies; immunofluorescence (IF)
Grant sponsor: Concerted Action; Grant number: BMH4-97-2611.The EWGCCA, a collaborative initiative from 16 European laboratories,
is open to scientists active in this field. The goal of the group is theevaluation and standardization of analytical techniques for clinical cellanalysis. Currently, the core members are G. Schmitz and G. Rothe(Regensburg, Germany); B. Autran (Paris, France); B. Brando (Milan,Italy); J.L. D’ Hautcourt (Boussu, Belgium); J.W. Gratama (Rotterdam,The Netherlands); A. Huber (Aarau, Switzerland); G. Janossy (London,
UK); J. Kappelmayer (Debrecen, Hungary); R. Lenkei (Stockholm, Swe-den); A. Orfao (Salamanca, Spain); S. Papa (Urbino, Italy); M. Pa-pamichail (Athens, Greece); T. Tottermann (Uppsala, Sweden); G. Valet(Martinsried, Germany); and B. Zupanska (Warsaw, Poland).
*Correspondence to: Bruno Brando, Transplant Immunology and He-matology Laboratory, Niguarda-Ca’ Granda Hospital, 20162 Milan, Italy.
E-mail: [email protected] 29 December 1999; Accepted 27 September 2000
Cytometry (Communications in Clinical Cytometry) 42:327–346 (2000)
© 2000 Wiley-Liss, Inc.

Counting the absolute numbers of CD41 T cells,CD341 hematopoietic precursor cells (HPC), and residualwhite blood cells (rWBC) in whole blood by flow cytom-etry (FCM) represents different aspects of the same tech-nical problem: each setting requires single- or multiple-color surface or nuclear fluorescence analysis linked to anabsolute cell counting technology as well as to a logicalgating strategy to isolate the relevant cells. However, asthe percentages and absolute cell levels in these clinicalsettings are widely different, diverging technological re-quirements are set in terms of sensitivity, precision, andcounting accuracy for the tests performed. In this review,we critically assess the cytofluorometric and noncytoflu-orometric methods for absolute cell and cell subset count-ing in order to investigate how they can fulfill their clinicalrequirements. Most of the techniques we summarize hereare commercially available as cell counting systems and/orkit packages.
Clinical Utility of Absolute CD41 T-Cell Counting
Selective CD4 lymphopenia had been shown to be thehallmark of acquired immune deficiency syndrome(AIDS), even before the human immunodeficiency virus(HIV, LAV, HTLV-III) had been discovered (1). Ever since,absolute counting of CD41 T lymphocytes remains themajor laboratory tool for staging HIV-infected patients(2–11). It provides information about how far the patientshave progressed along the path of HIV disease, this pa-rameter being complementary to HIV plasma viral load(9–12). It is now universally accepted that the most suit-able CD4 value for the laboratory diagnosis occurs whenCD41 T-cell counts fall below 200/mL blood or 14% oftotal lymphocytes (13). CD4 counts are therefore impor-tant clinical tools to assess the likelihood of opportunisticcomplications, for the appropriate timing of preventivemedications, and to document the effects of intensiveantiretroviral (10,11,14,15), and possibly cytokine, ther-apy.
The absolute T CD4 level continues to be the bestvalidated predictor of the likelihood of an opportunisticinfection, whereas such risk has not yet been ade-quately related to plasma viral load (15). Moreover, thebest predictor of opportunistic infections is the mostrecently confirmed CD4 cell count, despite the occur-rence of substantially lower prior CD4 cell counts.The risk varies continuously over the spectrum of ab-solute CD4 cell counts (15). Additional surrogate indi-cators of disease progression include the assessment ofCD38 expression, as a measure of activation status ofCD81 T cells, of CD45RA/RO, and of CD28 on T cells(16 –21).
In diseases other than HIV infection, the percent andabsolute CD31CD41 T-cell count are also of clinicalrelevance. These areas include solid-organ transplanta-tion in patients in whom polyclonal antisera to humanlymphocytes and monoclonal antibodies to CD3 andT-cell receptor (TCR) are used posttransplant to avertorgan rejection (22–24). The T-cell depletion in bloodis observed by FCM and the dosage of antiserum or
CD3 antibody may accordingly be adjusted. In addition,the emergence of T cells (CD21,CD41 andCD21,CD81 lymphoid cells) that down-regulated theirCD3-TCR marker is monitored, pointing to one of theimmunosuppressive mechanisms that contributes tothe action of anti-CD3 antibody therapy (22). Using thisFCM approach, the relative immunosuppressive po-tency of the different antilymphocyte preparations andthe duration of their long-term effects can also be stud-ied (23,25). Sustained CD41 T depletion has beenshown to be associated with the emergence of oppor-tunistic infections and neoplasms including skin cancer(26).
During the periods of postchemotherapy and the recov-ery phase following bone marrow (stem cell) transplants(BMT), faster thymus-dependent T-cell regeneration isseen in juveniles. In adults, CD41 T-cell regeneration canremain slow due to impaired thymic function (27). Oneimportant aspect is that following BMT and the reinfusionof CD341 stem cells (HPC), the speed of CD41 T-cellrecovery may vary according to the technique used andthe purity of the preparation (28–30). This is becauseCD45R01 CD41 T cells of “memory” type in adults ap-pear to regenerate from peripheral T cells and not fromCD341 HPC (27). A prolonged reduction of CD4 counts isalso a known problem following therapy with purinenucleosides, e.g., 2-chlorodeoxy-adenosine (cladribine)for hairy cell leukemia (31,32).
In other diseases, infections are also frequently asso-ciated with a reduced CD41 T-cell level, both as apredisposing factor and as a consequence of an infectedstate (33,34). A reduced CD41 T-cell level has beenreported to be of prognostic value in cytomegalovirus(CMV) infection in immunocompromised patients (35).Conversely, in pediatric respiratory syncytial virus, theinfectious state seems to be associated with an increasein the CD41 T-cell count (36). T-cell count derange-ments have also been described in association withprotein-caloric malnutrition, anorexia nervosa, lactationand iron deficiency (37,38), smoking habit (39), auto-immune thyroiditis (40), bronchial asthma (41), multi-ple sclerosis (42), polymyalgia rheumatica (43), andamong synovial fluid cells taken from patients withrheumatoid arthritis (44). Finally, in some cancers, areduced CD41 T-cell count is often observed as anassociated, nonspecific finding (45).
Clinical Utility of Absolute CD341 ProgenitorCell (HPC) Counting
In normal blood, CD341 HPC circulate in very lownumbers, i.e., ,0.1% of leukocytes or ,5/mL (46). Fol-lowing high-dose chemotherapy and/or recombinant cellgrowth factor-induced stimulation, the cells are mobilized(0.05 to 6–8% of total leukocytes) and can be harvested.These cells can then be stored frozen for autotransplanta-tion and used to support further courses of chemotherapy(46–48) or to obtain the reset of the immune system insevere, life-threatening autoimmune diseases (49,50). Thecritical issue is that the wave of CD341 HPC that enters
328 BRANDO ET AL.

recirculation can be transient and variable. In order tomaximize economical HPC collection, an active monitor-ing of CD341 cells is needed for establishing the optimumtiming of leukapheresis (48,51). To be productive, leuka-pheresis is usually performed when total WBC are.1,000/mL and CD341 cells are at least 40–50/mL, or atleast 10–20/mL according to certain protocols (52,53).The CD341 HPC yield of a leukapheresis procedure canbe predicted rather accurately from the peripheral bloodstarting absolute CD341 cell level (54). Also, the compar-ison between the expected and obtained CD341 HPCyield is a useful consistency control of the entire proce-dure.
The final CD341 HPC content of the leukapheresis bagis then counted as the percent and absolute CD341 countper milliliter as well as the total CD341 cell number perbag. The exact determination of CD341 cells is importantbecause the autotransplantation engraftment rate is pro-portional to the number of viable and functional CD341per kilogram patient’s body weight (48,55). SimilarCD341 HPC counts are also useful for cord blood trans-plants (56) and during allogeneic mobilized peripheralblood transplants (57) and BMT (58).
The biological and technical aspects concerning thepercent and absolute CD341 cell assessment have beenextensively reviewed by another EWGCCA task force (47)and validated procedure and guidelines are now available(53,59–62). Robust and reliable percent and absoluteCD341 HPC counting methods and guidelines have beendeveloped that can be applied to the widest range ofspecimens (peripheral blood from mobilized cancer pa-tients and normal subjects, native and manipulatedapheresis products, bone marrow, and cord blood;47,51,53,59). An experimental stain-no-lyse procedure hasbeen recently described (63).
Clinical Utility of rWBC Counting in Blood Products
Leukocyte depletion of red cell, platelet, and freshplasma preparations for transfusion to critical patients hasbeen demonstrated to be a mandatory requirement toprevent a number of untoward events, such as febrilereactions, microorganism transfer (CMV, Epstein-Barr vi-rus [EBV], Creutzfeldt-Jacob disease variants), alloimmuni-zation, platelet refractoriness, and immunosuppression(64,65–73).
Leukoreduction is performed by separation and/or fil-tering techniques that may take place both in blood banksand at the patient’s bedside. Typically, a leukoreduced250–300 mL blood product bag must contain ,5 3 108
rWBC to prevent febrile reactions (i.e., about ,1,600rWBC per microliter), ,5 3 106–1 3 107 rWBC to mini-mize the transfer of organisms (i.e., about ,16 rWBC permicroliter), and ,1 3 106 rWBC (i.e., about ,3 rWBC permicroliter) to be considered virtually leukocyte free, as itcan be obtained by combined depletion techniques or bydouble filtering the product (64,65,69).
Especially in the United Kingdom, after the crazy cowdisease outbreak, the possibility to transmit prion diseasethrough blood products became of particular concern.
However, the real efficacy of current filtration proceduresin preventing the transmission of Creutzfeldt-Jacob dis-ease variants is still being debated (66,68).
Not every single leukoreduced blood product under-goes laboratory checking of rWBC. About 2–3% of pro-cessed products are sampled randomly in regular qualitycontrol programs aimed at the maintenance of establishedstandard performance levels of each depletion techniqueand filter batch.
The technical issue of rWBC counting implies the de-tection of WBC in a cell concentration range much lowerthan the sensitivity and linearity range of any hematologyanalyzer and other traditional counting techniques (74–77). The accurate detection of such rare numbers of WBCis particularly challenging. The development of robustFCM counting techniques is still in its infancy, as will bediscussed in the following sections.
CONCEPTS APPLIED DURING ABSOLUTE COUNTINGDual- and Single-Platform Techniques
Absolute cell subset counts by FCM can be performedusing dual- and single-platform techniques. The dual-plat-form technique utilizes FCM to provide the percentage ofa given cell subset among total blood leukocytes or lym-phocytes (i.e., a chosen reference denominator) alongwith a hematology analyzer. This second platform thenprovides absolute WBCC with a three- or five-part leuko-cyte differential count, when applicable, that must in-clude the reference denominator.
The single-platform technique directly provides the ab-solute cell counts by counting the identified cells of inter-est (i.e., the CD41 or CD341 populations, or the totalrWBC) in a precisely determined blood volume. The def-inition of a reference denominator is therefore notneeded. There are common features in the different tech-nologies that include procedures of cell identification andsubset counting by electronic selection of the cells. Thespecific steps that are most frequently referred to as thegating strategy (78) are, however, different for each pro-cedure.
On the dual platform, the reference populations (leuko-cytes or lymphocytes) need to be defined with the great-est precision. This can be accomplished by a gating strat-egy based on light scatter properties of the white cells or,even more precisely, by using a combination of lightscatter plus immunological characteristics such as theexpression of the pan-leukocyte CD45 marker used alongwith the monocyte marker CD14 (79), the monocyte/granulocyte marker CD13 (80), or without these markers(78). In this strategy, the aim of gating is to encompass allleukocytes (or lymphocytes) in the acquired file and max-imize their purity by excluding unwanted cells such asplatelets and red cells (and CD141 monocytes). The lightscatter (forward scatter [FSC] versus side scatter [SSC])lymphocyte gating alone is now considered as unaccept-able (78,81,82). The laboratories not using CD45 gatinghave been demonstrated to have two to three times morechances to provide inaccurate CD3141% results (82).
329ABSOLUTE CELL SUBSET COUNT

The reference lymphocyte population is used as thedenominator of the percent cell subset level measurementon the FCM. Clearly, the precision in terms of absolutecounting is restricted by the performance of the hematol-ogy counter and is based on a putative exact overlappingof the cell definition criteria between the two instru-ments.
A major source for potential error in this procedureoccurs when the FCM definition of the reference popula-tion (i.e., leukocytes or lymphocytes used in the particularprotocol) does not match exactly that of the hematologyanalyzer.
It is relevant here to summarize the role of hematologyanalyzers in absolute CD4, CD34, and rWBCC. Many stud-ies on dual-platform CD41 T and CD341 cell count haveemphasized that an intrinsic inaccuracy of the approachmay derive from the hematology analyzer (83–88). Thetotal WBCC and the three- or five-part leukocyte differen-tial count introduce variable factors into the calculation ofabsolute lymphocyte subsets. These are particularly appar-ent in interlaboratory studies that use different hematolog-ical analyzers in the collaborating centers, especially whenHIV1 patients are studied (84,89,90). The correct discrim-ination between lymphocytes and monocytes is still anunresolved issue and may account for inaccurate lympho-cyte identification (84,91,92). In many instances, the pa-tient samples contain cell numbers well outside the sen-sitivity and linearity response range of blood counters(i.e., severely leukopenic patients, leukapheresis bags,mobilized normal donors, rWBCC). Counting leukocyte-poor samples with hematology analyzers also introducesadditional variability. In such instruments, a fixed samplevolume is analyzed, not a predefined number of cellevents (93).
The basic principles and problems of hematology ana-lyzers have been reviewed (84,94) and the specific tech-nical features of the more widely diffused instrumentshave been described (95–102). In summary, the advent ofFCM has greatly improved the poor resolution of WBCsubpopulations obtained by electrical impedance mea-surement systems (84). Further improvements in cell def-inition criteria have been achieved by the implementationof flow cytochemistry and fluorescence techniques(99,101–104).
The existence of such a wide spectrum of hematologyanalyzers in multicenter FCM studies is, however, a signif-icant impediment to the interlaboratory standardizationprocess (90). Even the patients may notice these regularinterinstitutional discrepancies and use them to their ad-vantage. Nevertheless, the dual-platform technique can beperformed with any type of FCM using a single laser anddual-color immunofluorescence (IF). Thus, despite its lim-itations, this method is still frequently used and listed in anumber of institutional guidelines (13,78,82,105,106).
On the single platform, the aim of the gating strategy isto positively identify the cells of interest (e.g., by using arelevant lineage antibody or a cell dye) and exclude con-taminating cells, without the need for a reference popu-lation. The identified cell subset is then directly related to
the original blood volume. The blood volume can bedetermined with different methods: volumetric pumps,admixed microbeads, fixed volume capillaries, and flow-and-rate software-controlled systems. The precision of thesingle platforms depends on the FCM technology and thepipetting steps, which are a relatively recent issue in FCM.
The crucial role of the reverse pipetting technique, themost reliable dispensing method for absolute cell-count-ing assays, needs to be stressed here. Although an appar-ently trivial issue, pipetting precision is the major variabil-ity factor that may affect absolute counting by FCM(51,53,107). The pipette plunger is pressed to the secondstop, the fluid is aspirated in slight excess, and the aspi-rated sample is dispensed against the lower end of thewall of the tube until the first pipette stop, leaving someresidual sample in the pipette tip (51,53). A detailed list oftechnical aspects of sample pipetting and dispensing isincluded in the Appendix. During the performance ofboth dual- and single-platform methods, the so-called log-ical, boolean, or sequential gating has introduced preciseselection of cell subset hierarchy in order to greatly im-prove the ease and the statistical robustness of the analysis(53,78).
Red Cell Lysis and Washing Procedures
Another technical issue that determines the precision ofabsolute counting is the sample preparation. The twomajor approaches include the erythrocyte lyse-and-washand the lyse-no-wash techniques.
Lyse-and-wash techniques are now exclusively per-formed together with the dual-platform counting technol-ogies, particularly when the membrane markers of inter-est are expressed at a relatively low intensity. Theadvantage of such an approach resides in the lower fluo-rescence background, the better positive/negative cellresolution, the lower contamination of viable cells withcell debris, and its compatibility with indirect IF assays.However, when using such techniques, the initial relation-ship between blood cell number and blood volume islargely lost, and thus absolute values cannot be preciselycalculated. Moreover, the sample manipulation and cen-trifugation introduce cell losses that may drastically affectthe final cell count, especially when fixative-containinglysing agents are used and washed away in CD341 cellanalysis (53,62,108–110).
Lyse-no-wash techniques, initially described 20 yearsago (111), have only recently gained dominance in clinicalFCM with the emergence of single-platform assays, whenminimum sample manipulation is coupled with the avail-ability of directly conjugated reagents (108). During thelyse-no-wash techniques, the original relationship be-tween blood cell count and volume is fully retained byusing known dilution factors. Then, a known blood vol-ume is mixed with a fixed amount of reagents (i.e., anti-bodies, lysing, and microbeads). Both procedures havetheir own dispensing precision requirements. However,lyse-no-wash techniques have some disadvantages such asan increase in background fluorescence and the presenceof cell debris. Various red blood cell (RBC) lysing agents
330 BRANDO ET AL.

may also affect WBC populations differently in alteringtheir scatter and surface staining characteristics (112,113).A certain amount of cell loss is also demonstrable in anylysing procedure, which can affect different cell subsets indifferent ways. In addition, it may not be fully justified toassume 100% lymphocyte purity (114) during the lyse-no-wash techniques without appropriate additional studies.Many artifacts such as cell aggregates, platelet clusters,unlysed nucleated erythroid cells, immature cells, and theequivocal boundary between lymphocytes and monocytesmay interfere with lymphocyte purity even under well-controlled staining and lysing conditions (Fig. 1). Further-more, cell aggregation is variable between different pa-tients and also depends on the antibodies used (115).Immature nucleated red cells are frequently present butonly in abnormal subjects, so that disturbing occasionalartifacts are not always easily spotted. The use of CD45/CD14 gating (see below) plus CD3/CD4 and scatter pa-rameters in a quadruple color assay is theoretically thebest method to obtain a true 100% lymphocyte gate purityin single tubes simultaneously labeled with four antibod-ies (114). Nevertheless, the efficacy of this approach hasnot yet been extensively studied (see also below).
Stain-no-lyse procedures have been implemented so faron the FACSCount (Becton-Dickinson ImmunocytometrySystems [BDIS], Braintree, MA) for CD4 counting (116),and as an experimental analysis protocol for CD341 cells(63).
Precise Identification of Reference Populations
From the definitions above, it may appear that dual-platform methods are difficult to perform due to theirreliance on reference populations. Nevertheless, the iden-tification of lymphocytes as reference standards has beengreatly facilitated by the introduction of CD45 gating forthe following reasons. When lymphocytes are identifiedby scatter (or morphological) gating using FSC versusorthogonal SSC, nonlymphoid cells (i.e., basophils, nucle-ated unlysed erythrocytes, monocytes) may contaminatethe gates, whereas large lymphocytes and lymphoblastsmay be inadvertently excluded. In 1990, Loken et al. (79)described an IF gating method based on CD45-fluorescein
isothiocyante (FITC)/CD14-phycoerythrin (PE; 79). Usingthis method, also referred to as fluorescence backgating,the lymphocyte gate purity and the lymphoid cell recov-ery are easily calculated on the basis of the differentialCD45 antigen density expression. CD45 is a pan-leukocytemarker expressed on polymorphonuclear cells (CD451),monocytes (CD4511), and lymphocytes (CD45111) atdifferent intensities, respectively. Monocytes are identi-fied by their selective expression of the CD14 antigen.
Once CD45 gating is employed, scatter gates can also beredefined as follows (13): the highest possible fraction oflymphocytes (.95% CD45111, CD14-) is included inthe light scatter analysis gate and the purity of theseCD45111,CD14- lymphocytes in the light scatter analy-sis gate should be .90%. The percentage value of anylymphocyte subset obtained by a light scatter gate mustthen be corrected for this purity value.
The purity and recovery rates are inversely related vari-ables. When a gating policy is defined, a compromise mustbe sought between these two conflicting requirements.An acceptable FSC/SSC gate on lymphocytes using CD45/CD14 backgating is virtually impossible in samples thatcontain immature myeloid cells. In samples with very lowproportions of lymphocytes versus monocytes, basophilsmay also cause additional problems.
Some analysis software systems automatically use CD45gating for selecting relevant cells (e.g., Becton DickinsonMultiSET, Beckman-Coulter TetraONE System). However,the major limitation of the CD45/CD14 gating strategyused in the two-color IF system with replicate tubes isobvious: the analysis gate is set in Tube 1, which may notbe an exact replica of the other tubes (Tube 2 onward)that contain the lymphocyte markers. The tube-to-tubevariability is difficult to control; it has indeed been shownthat after lysing the cells, the characteristics were nolonger identical between the replicate tubes (13). As aconsequence, the two-color IF approach is no longerrecommended by the Centers for Disease Control (14; butsee other regulatory bodies, e.g., the NCCLS in ref. 105).Instead, recent modern recommendations (82,114) em-phasize the advantage of utilizing three to four-color IFtechniques including CD45 in single tubes (see below).
Thus, in three- and four-color immunophenotypingtechniques, CD45 staining has recently been included as aprimary (anchor) gating marker: lymphocytes are definedas CD45111 with low SSC enabling a putative 100%lymphocyte gate purity (114). The lymphocyte recoverycan be calculated as CD31 (T cells) 1 CD191 (B cells) 1CD16/561 (NK cells) and then compared with the totalCD45111 /low SSC events. The most compelling reasonfor CD45/SSC gating is that one can provide percentageT-cell subset values from the same tube simultaneously.The preferred use of CD45/SSC gating for CD41 T lym-phocytes has been given priority in recent UK guidelines(106). Finally, it is important to stress that the CD45 gatingapproach is not the only way to obtain a reliable absoluteCD41 count (see below; 81,90,116,117). Logical gatestrategies can also be used to avoid isotypic controls, bothin lymphocyte and CD341 HPC analysis (47,51,118).
FIG. 1. Lymphocyte selection by CD45 gating in lyse-no-wash (ammo-nium chloride) single-platform multicolor IF and TruCount beads. Left:Clearcut lymphocyte (L), monocyte (M), and polymorphonuclear (PMN)cell discrimination. Right: Presence of lymphocyte aggregates (arrow A)and immature erythroid cells or basophils (arrow B) that render thelymphocyte identification problematic.
331ABSOLUTE CELL SUBSET COUNT

In CD341 HPC dual-platform analysis, the referencecells are the total leukocytes and no morphologically orphenotypically defined cell subset can be identified as thereference population. CD45 gating is also highly recom-mended when counting CD341 HPC using the logicalgate strategy developed by the International Society ofHematotherapy and Graft Engineering (ISHAGE; 119), andsubsequently modified by others (47,51,53,120). TheISHAGE protocol and its modifications may be the bestcurrent examples of routinely applicable logical gating.They represent the most widely accepted procedure forCD341 HPC enumeration (51,53,59,61,121). The CD341cell events are filtered according to their CD451 and SSClow expression. The latter gating is further refined by theverification of a homogeneous FSC/SSC pattern. ISHAGEgating is particularly helpful in eliminating nonspecificallyCD34-stained platelets, especially when very low percentand absolute CD341 HPC are present (47,53).
The definition of the true reference leukocytes is, how-ever, further complicated by the particular features ofWBC occurring in the CD341 HPC analysis setting. Pe-ripheral blood may contain very low or very high totalWBC, cord blood is particularly rich in cell debris, themobilization protocols induce the release of a great deal ofimmature WBC and erythrocytes, and the leukapheresisprocedure facilitates platelet clumping. Therefore, addi-tional means to better define reference WBC may berequired. The use of nuclear dyes like LDS-751 or SYTO-type has been suggested (53,63) or included in commer-cial kits like ProCount (Becton Dickinson Biosciences, SanJose, CA; 53,122). Moreover, apheresis samples may re-quire dilution before staining, to obtain WBC within 10–20 3 109/L and ensure proper counting assay perfor-mance (51). Bovine serum albumin (BSA)-supplementedphosphate-buffered saline (PBS) should be used as a di-luent instead of plain PBS to avoid the occurrence of thevanishing bead phenomenon when using microbead-based counting techniques (123).
Specific Technical Issues of rWBCC
The accurate FCM detection of very rare rWBC eventsin blood products introduces a number of challengingtechnical issues. rWBC enumeration has been traditionallyperformed with visual microscopy and large-volume Na-geotte-type hemocytometers (74–77,104). The visualcounting method accounts for an intrinsic variance rang-ing from 25% to 91% (75,76), it is quite operator depen-dent, time-consuming, and may not be sensitive enough inthe lowest rWBC range, where some hemocytometers cangive zero rWBC counts in a number of cases (76).
An FCM counting technique using fluorescence signaldetection by propidium iodide (PI) incorporation into thenucleus of permeabilized rWBC was introduced in thisfield by Dzik 10 years ago (124,125). The subsequenttechnical development has been slow and difficult. Untilrecently, the FCM technical requirements for both rareevent detection and absolute cell counting were not en-tirely established (126–128). Several alternative FCM andhematological methods involving cell detection by pheno-
type and light scatter analysis have also been described(104,129–132), but also judged as overall inefficient (129)or inaccurate with platelet concentrates (104). The filtra-tion process was demonstrated to introduce cell activa-tion and undesired changes in WBC light scatter proper-ties (129).
More recently, significant improvements in FCM count-ing technology led to the development of more reliablerWBC detection and enumeration procedures. ModernFCM techniques are able to acquire and store a largenumber of events at higher speed. The need for adequatefluidic circuit cleaning and increased sample flow rate asprerequisites for rare rWBC analysis were stressed (126).Single-platform counting approaches with microbeads(131), marker chicken RBC (126), or volumetric tech-nique (107) were also introduced.
Although the WBC nuclear signal induced by PI isstrong and clearcut, the need for a prolonged run timeleads to the acquisition of many undesired backgroundevents. These events show a nonspecific diagonal fluores-cence pattern that differs from that of rWBC and countingparticles, as demonstrable in FL2 versus FL1 or FL3 dis-plays. They can be excluded by an appropriate instrumentsetup and gating (126).
The evaluation of virtually leukocyte-free blood prod-ucts represents a challenge for FCM operators. In conven-tional rare event analysis, it is generally accepted that atleast 100 positive events must be acquired to obtain ade-quate data representation. Following this assumption, therWBC enumeration in a virtually leukocyte-free productmay require the analysis of a very large sample volumeover an unacceptably long acquisition time. This is anexample where the concept of mathematical limits cannotbe applied to practical FCM. The monitoring of the ab-sence of a rare population may require a different algo-rithm compared with the conventional detection of a rarecell subset. When microsphere-based methods are used,the number of beads acquired is a good indicator of theapproximate blood volume analyzed, which is optimally10–20 mL. An appropriate acquisition gate counter can beset in most instruments to evaluate this parameter (107).When volumetric approaches are used, the sample prep-aration protocols must be adapted to acquire at least10–20 mL of the original blood sample (107).
In all currently available preparation methods, a deter-gent permeabilizes rWBC and lyses RBC and a nucleic aciddye (DAPI, PI, TO-PRO-3) stains the cell nuclei (107).
Two commercially available kits now exist that useTruCount microbeads (LeucoCount, Becton DickinsonBiosciences; 133) or volumetric capillary cytometry(CEQer PRP and RBC assays, Becton Dickinson Bio-sciences; 134). An appropriate analysis protocol has alsobeen developed for the volumetric FCM Dako Galaxy(107). Another simple counting protocol has been devel-oped for Partec PA and CCA particle analyzers using UV-lamp excitation and DAPI incorporation. Great care mustbe paid in pipetting and dispensing very viscous samplessuch as packed RBC and platelet concentrates. Plateletbags are definitely more difficult to check than RBC con-
332 BRANDO ET AL.

centrates, because cell clumping and a high nucleic acidbackground tend to generate more nonspecific staining.The addition of RNAse to the staining medium seems toimprove the detectability of rWBC in platelet concen-trates. The actual biological and clinical meaning of min-imal rWBC transfusions is still being debated, mostly be-cause the detection and counting methods available so farare not entirely satisfactory.
THE STATE OF THE ART: SINGLE PLATFORMFOR ABSOLUTE CELL COUNTING
To date, many different methods have been developedfor commercial use in order to count the absolute numberof CD41 T cells, CD341 HPC, and rWBC (Table 1). Mostof these methods have already been evaluated in multi-center studies (86,87,90,116,117,135). Some analysis sys-tems were marketed in the past and are briefly describedhere for historic purpose. All cytometric methods can beused to count both CD41 T cells and CD341 HPC. ForCD4 counts, a number of noncytometric options have alsobeen available but these are not suited for CD34 assays.Most of the methods also include cell fixation and virus-inactivating reagents, although this commendable feature(and its efficacy) is not always detailed in the samplepreparation protocols.
Volumetric Technologies
Conventional FCM analysis mostly ignores the require-ment of maintaining a stable relationship between theoriginal and final sample cell concentration. In contrast,volumetric methods strictly define this ratio for absolutecell counting and require stained and lysed blood samplesin a known final medium volume. The sample dilution
factor is therefore taken into account for the final calcu-lations. The volumetric techniques require dispensing pre-cision in all the pipetting steps and the final dilution factormust be strictly controlled. Volumetric techniques rely oninstrument and system calibration and normally do notrequire additional reagents for sample analysis. However,volumetric techniques may also require standard countingbeads for volume calibration. Some techniques may benegatively biased by a limited sample volume, which caninfluence the statistic robustness of rare event counts.
Ortho Cytoron Absolute plus Immunocount IIsoftware plus Trio reagents. The Ortho Cytoron Abso-lute (Ortho, Raritan, NJ) was manufactured between 1990and 1996 as the first benchtop FCM equipped with anabsolute counting option using a lyse-no-wash techniquewithout a need for CD45 gating (81,90). This system relieson a precise volumetric pump for sample aspiration anddelivery. The Immunocount II software automaticallyidentifies CD31, CD191, and CD161 cells by triple-colorIF and calculates their absolute values. Lymphocytes aredefined as the sum of T1B1NK cells (Immunosum orLymphosum). In the second tube, the absolute CD31,CD41 and CD31,CD81 counts are also given; internalconsistency controls are included from the CD3 replicatesand Lymphosum checks. The Immunocount II softwareitself requires manufacturer-defined staining and analysisprotocols using nine antibodies (including three isotypiccontrols) in three tubes. The assumptions regarding theLymphosum and the calculation giving CD31 5 CD41 Tplus CD81 T Cells might be challenged scientifically buthave proved to be robust in routine practice. Within-labquality assessment of the absolute count reproducibility isgood (coefficient of variation [CV] , 4%) and interlabo-ratory comparisons with lowest CV of 3.2–7.1% are facil-itated by the availability of stabilized samples (81,88). Alimitation of the the Ortho system is the maximumamount of cell sample acquired per run (i.e., 250 mL or65,520 cells), which may not be sufficient to analyze veryrare events such as CD341 HPC at the lower end of itsconcentration scale (,10–20/mL).
Partec PAS FCM. The Partec PAS (Partec GmbH,Muenster, Germany, marketed as Dako Galaxy by DakoA/S, Denmark) is a volumetric software-controlled abso-lute counting system with innovative electronics provid-ing a very short dead time. The excitation source includestwo lasers and a mercury arc lamp applicable for multiple-color phenotyping. In the currently available version, ab-solute counting occurs when the tips of two electrodesdip into the fluid at different levels. The counting is trig-gered when the higher electrode during the aspiration isno longer surrounded by fluid; when the sample level fallsbelow the second electrode, counting stops. From theaspirated volume (200 mL) and the dilution factor, theabsolute cell count is given. A more advanced version isalso being developed to perform continuous flow count-ing using integrated calculation of the cell rate per samplevolume flow (i.e., flow-and-rate counting). The PAS instru-ment, like the Cytoron, requires full dispensing precisionbut does not require daily calibration. The system func-
Table 1Currently Available Methods for Absolute Cell Subset Counting
a) Cytometric Methods1) FCM Immunophenotyping 1 Hematology (Dual-Platform
Approach)a1) Volumetric Technologies
2) ORTHO Cytoron Absolute 1 Immunocount II Software 1Trio Reagents
3) DAKO GALAXY 2 PARTEC PAS Instrument4) BIOMETRIC IMAGN 2000 1 Dedicated Cartridges
a2) Microbead-Based Technologies5) BECTON DICKINSON FACSCount 1 Dedicated Cartridges6) BECTON DICKINSON TRUCount Tubes 1 3 and 4 Color
Reagents7) BECKMAN 2 COULTER Flowcount Beads 1 3 and 4
Color Reagents8) BANGS 2 FCSC Count Standard
b) Hematologic Cytometric-Like Methods9) BAYER H2 1 Dedicated Module (Absorption
Immunocytochemistry)10) COULTER STKS 2 Gen’s 1 VCS Module11) ABBOTT Cell-Dyn 4000
c) Non-Cytometric Methods12) Beckman-Coulter Manual CD4 Count Kit13) T Cell Science TraX CD4 Kit14) Zynaxis Zymmune CD4/CD815) Pasteur-Sanofi Capcellia CD4/CD816) DuPont Medical CD4-CCS Kit
333ABSOLUTE CELL SUBSET COUNT

tions equally well with a CD45-independent and CD45-dependent approach because its software is not linked toa preset staining or analysis protocol. The system is alsosuitable for CD341 HPC counting. A specific protocol hasalso been described for rWBC counting (107). Because theelectronic dead time is very short (25 ms), virtually no cellevents are lost due to coincidence. Running a 200-mLsample may thus enable the acquisition of at least 100CD341 HPC even with levels as low as 10 CD341 HPCper microliter of blood (W. Goehde, personal communi-cation).
IMAGN 2000 system and dedicated cartridges.This automated instrument (previously developed by Bio-metric Imaging, Mountain View, CA; now marketed byBecton Dickinson Biosciences) is a small closed staticfluorescence cytometer that requires neither operator-dependent steps nor FCM training. Four different tech-niques are available including an automated stain/lyse/read option for CD4 and CD8 T-cell counting (4T8 assaykit), the absolute CD341 HPC count (STELLer kit), andthe rWBC count for leukoreduced blood bags (CEQer RBCkit) and platelet donations (CEQer PRP kit; 136).
For CD41 counting, blood is dispensed into dedicatedcartridges where sample staining and lysing are automat-ically performed. The cartridge tubing separates the sam-ple into two aliquots stained with CD3/CD4 and CD3/CD8mixtures labeled with Cy5 and Cy5.5, respectively. For thestained blood, the calibrated square-section glass capillarytubes act as the analysis chamber. Scanning stationarycells in the capillary tube is performed by a small, redHeNe laser: the emission of two different fluorescencechannels is recorded as an image analysis of the fluores-cence peaks generated by the positive cells (137). Theperformance data on CD4 counts show satisfactory results(intra-assay CV 6.7–14.3%; interassay CV 5.5–18.2%; 117)but larger multicenter trials are awaited.
The CD341 cell analysis is performed in dedicatedtubes with subsequent injection of the capillary withthe stained and lysed sample. The preliminary resultsare satisfactory (intra-assay CV 8 –17%). Some criticismcan be raised about the statistic robustness of this CD34method at very low cell counts (10 –50 CD341 cells permicroliter or WBC lower than 2,000/mL). Using theSTELLer kit, each reading capillary tube contains only2.2 mL of a 1:3 diluted sample (50 mL blood190 mLlysing) and the scanning laser operates on a fraction ofthe tube only. Consequently, the positive cell eventsrecorded may be below what is considered a safethreshold, around 100 CD341 cells. This may explainthe rather poor cross-comparison results obtained be-low 20 –30 CD341 cells per microliter (138 –140). Theparticular advantage of this method, however, is that itcan be performed at the bedside. By directly controllingthe strategy of HPC collection from granulocyte mac-rophage-colony stimulating factor (GM-CSF)-inducedperipheral blood at the bedside, the wasteful collectionof blood with low CD34 counts can be readily avoided.
Microbead-Based Technologies
This technology, conceived by Stewart and Steinkampas early as 1982 (141) and subsequently developed byValet (142), has recently undergone stability and consis-tency assessments in several commercial applications.Known amounts of fluorescent microbeads are admixedto a known volume of stained blood in a lyse-no-washtechnique and the beads are counted along with cells. Thenumber of cells (or cell subsets) per microliter is obtained:number of cells per microliter 5 number of cellscounted 3 concentration of beads/number of beadscounted. The prerequisite of microbead-based counts isthat both beads and the relevant cells must be acquiredsimultaneously and without any acquisition selection bias.Remarkably, this method is independent from lysing andantibody volumes and additional reagents can be addedwithout caring about dispensing precision. The number ofrelevant cell events should not exceed more than 10 timesthe number of bead events and at least 1,000 bead eventshave to be acquired to ensure adequate statistical robust-ness.
Several critical issues may influence the accuracy of themicrobead-based counts. Initial bead quantity or concen-tration must be strictly controlled by the manufacturerand kept consistent with time; dispensing proceduresmust be performed carefully; counting beads tend eitherto sediment or to float; a thorough mixing between mi-crobeads and sample cells must be ensured, but bubble orfoam formation from energic agitation must be avoided.Beads also tend to form aggregates, which may influencethe number of bead events to be used for counting (Fig. 2;107,143). A possible overlapping of fluorescence signalsfrom cells and beads may also be considered in somesettings, whereas high-intensity fluorescence signals maygenerate detector saturation and loss of bead events. Vir-tually any bead suspension can be used as a countingreference, provided stability and concentration consis-tency are well established. Other counting microbeadpreparations are commercially available, i.e., Bangs-FCSC
FIG. 2. Zoomed displays of Beckman-Coulter FlowCount and BectonDickinson TruCount counting beads in lyse-no-wash techniques withammonium chloride. Aggregation is evident with both bead types (re-gions R3 and R5, respectively). According to manufacturer recommen-dations, only FlowCount singlets must be considered, whereas all Tru-Count events must be included.
334 BRANDO ET AL.

Count Standard and Spherotech-Rainbow beads, but theyhave not yet been validated in the clinical setting. Someplasma protein or bovine albumin in resuspension mediaseems necessary with counting beads to prevent beadsticking to the tube walls. Quite recently, the drop of beadconcentration enhanced by vortexing (i.e., the vanishingbead phenomenon) was demonstrated to occur in pro-tein-poor leukapheresis samples (123). Detailed guidelineson counting bead dispensing and usage are included in theAppendix.
Becton Dickinson FACSCount plus dedicated re-agents. For this instrument (Becton Dickinson Bio-sciences), an exclusive stain-no-lyse technology has beendeveloped that relies on dedicated cartridges with anti-body mixtures (CD4PE/CD3Cy5 and CD8PE/CD3Cy5, re-spectively) plus reference microbeads in suspension. Be-cause the beads and antibodies are pipetted at the factory,the only source of technical error is blood aliquoting. Themanufacturer recommends reverse pipetting (see above)and the instrument comes with a calibrated electronicreverse pipette. Cell fluorescence is stimulated by a green,low-power HeNe laser and, as with the IMAGN 2000system, no compensation is required. First, CD31 cellsare detected using a closed Attractors software program.The calculation of absolute CD3, CD4, and CD8 levels isperformed automatically. This CD45-independent T-gatingapproach only provides percentage CD4 and CD8 valueswithin total CD31 T cells. Internal quality assurance in-cludes the acquisition of a defined number of CD41 Tcells, leading to a longer counting cycle in blood when thepatient shows severe CD4 lymphopenia. Although thesmall fluid tanks are inconvenient during prolonged use,the CVs in interlaboratory quality assessments are excel-lent (about 4%; 88,135). The equipment has been success-fully used in a rural setting in developing countries(116,144–146).
Becton Dickinson TruCount tubes plus multiple-color reagents. The TruCount system is preloaded witha lyophilized pellet of fluorescent 4.2 mm Ø microspheresretained at the bottom of 12 3 75-mm polystyrene tubesby a small metal grid. It is marketed only along withTriTest, MultiTest, ProCount, and LeucoCount kits but canbe used with other reagents on all FCM equipped with atleast two fluorescence channels (87,147,148). A lyse-no-wash technique by FACS lysing solution is recommendedbut ammonium chloride is also applicable. The fluores-cence emitted by the beads is detectable in all four-colorchannels and the beads can also be excited by a HeNe redlaser. Coupled with anti-CD45 to trigger the cell acquisi-tion, the analysis region is defined and the lymphocytesare identified. A disadvantage of the TruCount beads isthat they are too small to be included in a common scatterwindow together with cells. Thus, a common window forcells and beads must be set on a fluorescence channel andfluorescence must be used as the acquisition trigger. Con-sequently, the choice of a fluorescence threshold is re-stricted to a cell marker expressed on all the cells such asCD45 or a nuclear fluorescent dye (i.e., LDS-751) or atleast on the positively defined cell population (107). Tru-
Count beads tend to sediment with time. All microbeadevents, including singlets and the usual 6–10% of doublet/multiple bead aggregates, are to be taken into account asthis bead aggregation factor has also been compensatedwith each titrated bead preparation and lot number.When positive cells are at the bright end of the fluores-cence scale, some overlapping with the TruCount beadsignal may be observed (107). As with the FACSCcount,the precision requirement is limited to the reverse pipet-ting step of the sample only. However, this apparentsimplicity implies a high sensitivity of this system to pi-petting imprecision. Across-site reproducibility CVs forCD4 and CD341 counts range from 5.6% to 13%(87,88,149).
Beckman-Coulter-IL FlowCount microbead sus-pension. The same concepts as above are applicable tothis fluorescent 10-mm Ø microbead preparation obtainedin suspension with a certified particle concentration permicroliter from Coulter (Miami, FL; 86,120,143). Knownvolumes of bead and blood are added with precisely thesame 100 mL reverse pipetting and prepared using a lyse-no-wash technique (Coulter Q Prep or ammonium chlo-ride). FlowCount beads are larger than TruCount, and thuscan be used with reduced FSC thresholding without aneed for an associated fluorescent marker. However, anappropriate polygonal acquisition gate is necessary toeliminate the high amount of debris and electrical noise(53,120). The Beckman-Coulter method involves a four-color system using a single Argon-ion laser and the beadsemit on all four channels (86,148). FlowCount beads can-not be excited by the HeNe red laser in the BDIS instru-ments. FlowCount beads are also sold separately andtherefore can be used with any FCM equipped with atleast two-color fluorescence detectors. The Coulter Tetra-One software assists in relating the number of acquiredFlowCount beads to those of cells and to acquisition time,a useful internal consistency check (143). Replicate mea-surements within the same laboratory show CV rangingfrom 1.9% (143) to 4.9 (86). Nevertheless, great careneeds to be taken in storing, resuspending, aliquoting, anddispensing the beads (FlowCount float when the vial isstored); only bead singlets must be included in the count-ing strategy. Bead aggregation may tend to increase withvial usage, which should not exceed 30 days from the firstopening (see Appendix). An apparent disadvantage of theFlowCount beads is that the resuspension and the pipet-ting of the beads may introduce new variables, which canbe a contributing factor for a slightly increased interlabo-ratory variability (CV 9.4–12.1%; 86). However, the com-bined pipetting of beads and sample with exactly thesame dispenser is a factor that remarkably compensatesany pipetting imprecision.
Hematological Cytometric-Like Methods
The architecture of modern hematology analyzers ismuch like that of FCMs. Some hematology counters havebeen supplied with flow cytometric-like devices to obtainabsolute CD41 cell, reticulocyte, erythroblast, and rWBCcounts along with the routine hematological analysis. A
335ABSOLUTE CELL SUBSET COUNT

method claimed to perform direct HPC enumeration by ahematology analyzer based on cell phospholipid contenthas been also described (150).
The first hematology counter equipped with an immu-nocytochemical device to count CD41 cells, Bayer H2, isnot manufactured anymore. A new laser counter withfluorescence detectors, the Abbott Cell Dyn 4000 (102), isstill under development and no performance studies onabsolute cell subsets are available at the moment.
Coulter STKS-Gen’s plus VCS module. As an optionto the STKS and Gen’s Coulter hematology counters, aVacutainer tube used for the blood count is placed into anautomated aspiration device. To the blood sample, a mixof microbeads (anti-CD4- and anti-CD14-coated latex par-ticles of different diameters) is added and then transferredto another tube. The microbeads are the same as thoseemployed in the Coulter manual kit for microscopy count-ing (see below). The CD41 cells rosette with high num-bers of large microbeads, whereas monocytes rosette withsmall anti-CD14–coated spheres along with a few anti-CD4 beads. The CD41 T-cell count is then performedautomatically by combining the hematological counts andthose obtained by the scatter signals measured by the VCSmodule (96,145).
Noncytometric Methods
Alternative noncytometric methods have been pro-posed to determine CD4 and CD8 T-cell counts with aspectrum of different technologies. Most of them are notmarketed any more and are cited here for historic pur-pose. These include the Beckman-Coulter manual CD4count kit, currently the only available test that meetsWorld Health Organization (WHO) recommendations fora simple and inexpensive assay (151–153). In this rapidtest, CD41 T cells and monocytes are rosetted with anti-body-coated latex beads of different diameter (see above).The sample preparation does not require centrifugationand the absolute count is performed by the visual analysisof rosetted cells in a hemocytometer.
A second system, the T-Cell Science TraX CD4 assay,has been evaluated in extensive cross-comparison studiesin the past (145,146,154–157). It appears that this assaywas affected by soluble CD4 molecules in the serum andby a high background bias. Finally, the Zynaxis ZymmuneCD4/CD8 (145,154,158), the Pasteur-Sanofi CapcelliaCD4/CD8 (159,160), and the DuPont Medical CD4-CCS kitwere labor-intensive assays with a limited throughput,which suffered from design simplification by assumingthat CD4 expression by monocytes does not interfere.
COMPARATIVE STUDIES FOR ABSOLUTE CD41COUNTING METHODS
A Need for Appropriate Statistics
In clinical absolute cell or cell subset counting, the truevalues are unknown. Therefore, a comparison of differentanalysis methods can only measure the degree of agree-ment between the reference and the predicate method.Unfortunately, statistical methods traditionally utilized toanalyze such clinical comparisons have, in many studies,
been inappropriate because regression analyses are notvery informative when the task is to compare two meth-ods designed to provide similar results. When the line ofequality is compared and the level of agreement betweentwo analysis methods is sought, the Bland-Altman statisticsis more appropriate (161,162). Briefly, a correlation coef-ficient only gives information on the extent to which theresults defined by the two methods are correlated (i.e.,association). This is obviously quite high because the twomethods are designed to measure the same variable andthe range of observed data is usually wide (162). TheBland-Altman method examines, in a more discriminativefashion, if the methods agree sufficiently well to be usedinterchangeably and if a systematic bias exists. The cor-nerstone is the assumption that both methods do have anintrinsic error and therefore the difference between thetwo methods has to be analyzed. The Bland-Altman datadisplay includes a bias value (i.e., the systematic differ-ence from zero of the data differences), the bias error (i.e.,how much this difference varies), and the precision (i.e.,the upper and lower limits of agreement; 162). There areno established criteria to define acceptable agreement.Acceptable limits of agreement should be rather estab-lished before the planning of a comparison study andweighed according to the intrinsic variability of eachmethod and the magnitude of the variate range. Below,we give prominence to multicenter investigations thatused this advanced statistical approach (163,164) and tosingle-center studies that investigated large-scale clinicalsamples with the most recently developed methods (165–167).
Multicenter Comparisons for Dual- Versus Single-PlatformMethods for CD4 Counting
The most extensive study of dual- versus single-platformFCM is run every 2 months for a large number of labora-tories participating in the UK NEQAS for Leucocyte Im-munophenotyping Immune Monitoring Scheme. Stabi-lized whole blood samples are issued and participantsenumerate CD41 and CD31 T lymphocytes. The use ofstabilized material removes the variability seen in otherQA schemes due to the deterioration of fresh specimenswhile they reach the local laboratories through the mail.As a result, in the NEQAS study, the interlaboratory CVsare frequently ,5% (168). In a most recent trial, single-platform approaches (including both bead-based and volu-metric methods) were compared to the conventional dual-platform method. Although the interlaboratory variationfor dual-platform approaches was consistently 30% orgreater, the interlaboratory variation for the single-plat-form approaches was ,17%. Further analysis of this vari-ation revealed that the Ortho Cytoron Absolute gave thelowest interlaboratory variation (3.2%) for absolute CD41T-lymphocyte counting followed by the FACSCount(4.6%), TruCount (13.1%), and FlowCount (13.2%; 88).Other studies also involved extensive multicenter cooper-ations within the quality control schemes for additionalparameters in the United Kingdom and Spain (NEQAS andthe Iberian Society for Cytometry, respectively). Here, the
336 BRANDO ET AL.

interlaboratory reproducibility of the results was obtainedwith the FACSCount versus the conventional dualplatform (116,135) where a standardized staining and in-strument setup protocol was used (Simultest reagents,Autocomp, and Simulset software, Becton Dickinson Bio-sciences). A high degree of correlation between FAC-SCount and conventional dual-platform FCM plus hema-tology and a very low CV% on the FACSCount wereapparent, both for quadruplicate intralaboratory testingand for interlaboratory comparison. Interestingly, the in-terlaboratory CV of CD4/mL count ranged from 2.48% to3.76%, which is one of the lowest figures ever reported inthis type of investigation. Whereas the instrument, evenacross centers, was a stable factor, the sample preparationprotocol, i.e., the timing between sample drawing andprocessing, showed the highest factors of variability.
In a multicenter study sponsored by Becton Dickinson,percent and absolute values obtained in 126 subjects bythree- and four-color immunophenotyping and single-plat-form count by TruCount tubes were compared. The in-tralaboratory and multisite replicate reproducibility, thelinearity of percent and absolute subset counts, and theperformance of the MultiSET automated cell gating soft-ware were also evaluated (149). A single-tube, four-colorabsolute CD41 T-cell count gave a linearity slope of 0.997(90% CI 0.985–1.009) over a range of 0–5,000 cells permicroliter. The within-site reproducibility of duplicates bythe same technique gave a CV of 4.1–8.9%, the latterfigure in the range of 100–350 CD41 T cells per micro-liter. The multisite reproducibility CV ranged from 5.4% to8.1%. The cross-comparison of absolute CD4 count ob-tained by three-color versus four-color techniques gave aslope of 1.015 (90% CI 0.986–1.045) with r2 5 0.982.
Two multicenter studies were performed in the UnitedStates under the patronage of the Division of AIDS(DAIDS) of the National Institute of Allergy and InfectiousDiseases (NIAID; 86,87). In the first one (87), three-colorsingle-platform analysis using TruCount tubes was em-ployed in five laboratories receiving 60 external and 14internal HIV specimens. All samples were analyzed after 6and 24 h. Again, both the intralaboratory and interlabora-tory variability was significantly improved by the single-platform method. The bead-based technology also gave abetter reproducibility for aged samples, and enabled the“rescue” of samples that could not be analyzed because ofunacceptable gating criteria with predicate methods.
In the second study (86), the intralaboratory and inter-laboratory variability of absolute CD4 and CD8 counts bya single-platform method employing FlowCount micro-spheres plus two- or four-color staining, including theautomated TetraONE analysis system, was evaluated. Fivelaboratories received 103 specimens and analyzed further71 internal replicate samples. The intralaboratory CV wasoverall improved by either single-platform method com-pared with the predicate two-color, dual-platformmethod. The interlaboratory CV was some 40% lowerwith single-platform methods, and particularly when Te-traONE automated analysis was employed. Moreover, the
hematology counter was found to introduce counting biasin selected centers.
The NIAID/DAIDS is currently planning the release of adocument that approves the switch to single-platformmethods, provided an appropriate switch study is per-formed by each laboratory (document in preparation,169).
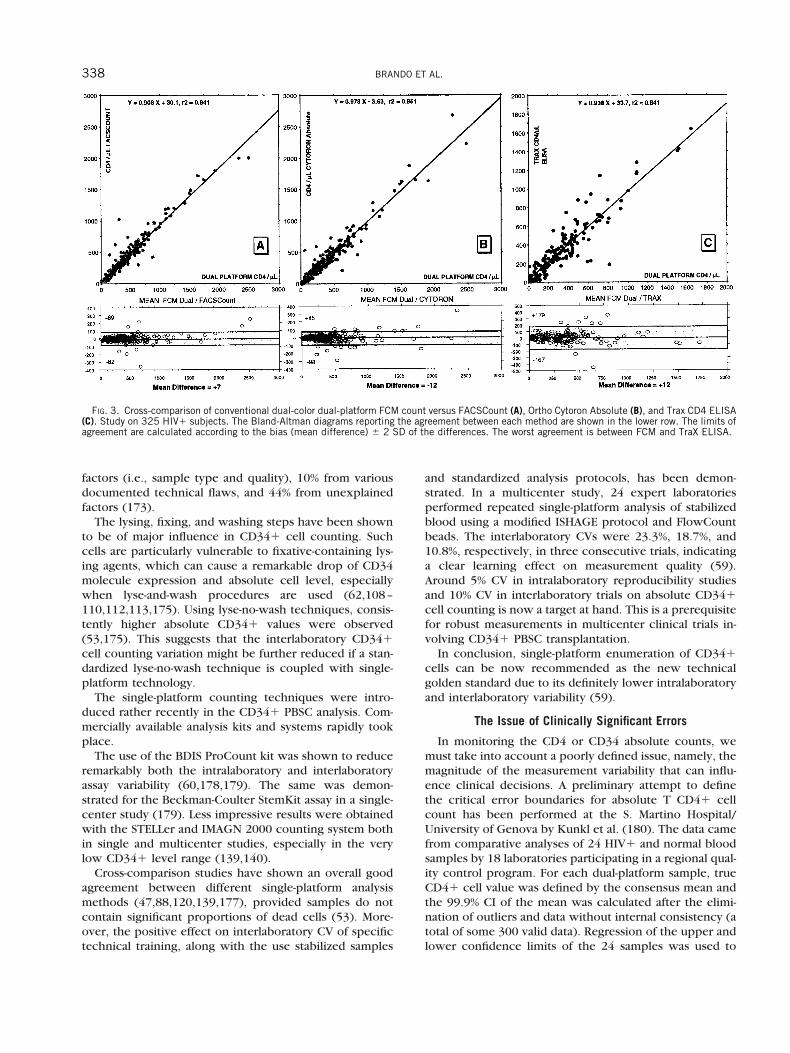
Finally, two large single-center studies in which Bland-Altman statistical analysis was used must be mentionedhere. In a study performed by Brando et al. (165), dual-platform FCM plus hematology was compared with single-platform Ortho Cytoron Absolute, FACSCount, and TraXenzyme-linked immunosorbent assays (ELISA) in a singleinstitution. Samples from 325 HIV1 subjects and 80 solid-organ transplant recipients at various disease states wereincluded (Fig. 3).. Importantly, the overall correlation andagreement among the four systems in HIV1 subjects wereexcellent but the highest degree of disagreement wasfound between TraX ELISA versus FCM. All three FCMtechniques performed in a perfectly overlapping fashiondespite remarkable technical and conceptual differences.Furthermore, the total lymphocyte count per microliterbtained by the Coulter STKS was well correlated with theimmunological lymphocyte sum obtained by Ortho Cy-toron (y 5 0.990 x - 25.8, r2 5 0.957, bias 5 12, limits ofagreement -108 and 1136, respectively, over a range of150–12,000 lymphocytes per microliter).
Two-hundred and ten normal and HIV1 subjects werestudied for absolute CD41 and CD81 T cells by dual-platform FCM and the IMAGN 2000 4T8 kit at the LegnanoHospital, Italy (166). The X slope and the correlationcoefficient of FCM versus IMAGN 2000 were 0.87 and r2 50.916 for CD4 and 0.84 and r2 5 0.948 for CD8. TheBland-Altman statistics for CD4 analysis gave -224 and1242, respectively, as the limits of agreement and a biasof 19 over a range of 5–2,250 CD41 T cells per microli-ter. For CD8, the limits of agreement were somewhatwider: -236 and 1358, respectively, and the bias was 161over a range of 165–3,230 CD81 T cells per microliter.
Multicenter Studies on CD341 Cell Counting: TheEmerging Consensus on Single-Platform Techniques
The first standardized dual-platform counting methodfor CD341 cells was developed in 1994 as the MilanProtocol (170). Despite its limitations (47), it is still usedin many centers. In the majority of early multicenter trialson CD341 HPC enumeration, an alarming interlaboratoryvariability was seen. Result variation was generated by theusage of local nonstandardized staining and gating proce-dures (171–174) and by sample instability (175). Usingnonstandardized staining and analysis methods, the inter-laboratory CVs of dual-platform CD341 cell values rangedfrom 50% to 284% (171–173,175), whereas the use of apredefined analysis protocol reduced the variability to amore acceptable 14–82% (140,173,176, 177).
Using the simple Milan Protocol, the interlaboratory CVwas limited to 20% in a large study in northern Europe(176). Even using a carefully standardized procedure,however, 46% of variation resulted from nontechnical
337ABSOLUTE CELL SUBSET COUNT
factors (i.e., sample type and quality), 10% from variousdocumented technical flaws, and 44% from unexplainedfactors (173).
The lysing, fixing, and washing steps have been shownto be of major influence in CD341 cell counting. Suchcells are particularly vulnerable to fixative-containing lys-ing agents, which can cause a remarkable drop of CD34molecule expression and absolute cell level, especiallywhen lyse-and-wash procedures are used (62,108–110,112,113,175). Using lyse-no-wash techniques, consis-tently higher absolute CD341 values were observed(53,175). This suggests that the interlaboratory CD341cell counting variation might be further reduced if a stan-dardized lyse-no-wash technique is coupled with single-platform technology.
The single-platform counting techniques were intro-duced rather recently in the CD341 PBSC analysis. Com-mercially available analysis kits and systems rapidly tookplace.
The use of the BDIS ProCount kit was shown to reduceremarkably both the intralaboratory and interlaboratoryassay variability (60,178,179). The same was demon-strated for the Beckman-Coulter StemKit assay in a single-center study (179). Less impressive results were obtainedwith the STELLer and IMAGN 2000 counting system bothin single and multicenter studies, especially in the verylow CD341 level range (139,140).
Cross-comparison studies have shown an overall goodagreement between different single-platform analysismethods (47,88,120,139,177), provided samples do notcontain significant proportions of dead cells (53). More-over, the positive effect on interlaboratory CV of specifictechnical training, along with the use stabilized samples
and standardized analysis protocols, has been demon-strated. In a multicenter study, 24 expert laboratoriesperformed repeated single-platform analysis of stabilizedblood using a modified ISHAGE protocol and FlowCountbeads. The interlaboratory CVs were 23.3%, 18.7%, and10.8%, respectively, in three consecutive trials, indicatinga clear learning effect on measurement quality (59).Around 5% CV in intralaboratory reproducibility studiesand 10% CV in interlaboratory trials on absolute CD341cell counting is now a target at hand. This is a prerequisitefor robust measurements in multicenter clinical trials in-volving CD341 PBSC transplantation.
In conclusion, single-platform enumeration of CD341cells can be now recommended as the new technicalgolden standard due to its definitely lower intralaboratoryand interlaboratory variability (59).
The Issue of Clinically Significant Errors
In monitoring the CD4 or CD34 absolute counts, wemust take into account a poorly defined issue, namely, themagnitude of the measurement variability that can influ-ence clinical decisions. A preliminary attempt to definethe critical error boundaries for absolute T CD41 cellcount has been performed at the S. Martino Hospital/University of Genova by Kunkl et al. (180). The data camefrom comparative analyses of 24 HIV1 and normal bloodsamples by 18 laboratories participating in a regional qual-ity control program. For each dual-platform sample, trueCD41 cell value was defined by the consensus mean andthe 99.9% CI of the mean was calculated after the elimi-nation of outliers and data without internal consistency (atotal of some 300 valid data). Regression of the upper andlower confidence limits of the 24 samples was used to
FIG. 3. Cross-comparison of conventional dual-color dual-platform FCM count versus FACSCount (A), Ortho Cytoron Absolute (B), and Trax CD4 ELISA(C). Study on 325 HIV1 subjects. The Bland-Altman diagrams reporting the agreement between each method are shown in the lower row. The limits ofagreement are calculated according to the bias (mean difference) 6 2 SD of the differences. The worst agreement is between FCM and TraX ELISA.
338 BRANDO ET AL.

extrapolate confidence ranges for any theoretical CD41value. CIs of true CD41 values have been taken as ameasure of the error due to the variation of CD41 counts.As an example, with this method, the 99.9% CI in the caseof measured CD41 of 100 and 300 CD41 T cells permicroliter were 80 and 120/mL and 254 and 346/mL,respectively. This matter must also be viewed in the lightof physiological, diurnal, and circannual variability ofCD41 T-cell counts (181–185).
CONCLUDING REMARKSReliability of FCM in Clinical Service
Until recently, the commercially available conjugatedantibodies were limited to FITC/PE/third-color combina-tions. These reagents could be employed on the majorityof FCM. In recent years, however, the development ofvarious four-color staining and analysis stategies has re-duced the wide reagent interchangeability that existed inthe past. This technical advance may partly impair the fullcross-comparison of methods.
Pipetting precision is an overall major issue in everyabsolute CD41 T-cell, CD341 cell, and rWBC countingprocedure. High precision pipetting requires appropriatecalibrated dispensers, manual or electronic reverse pipet-ting, periodic maintenance, volume calibration of dispens-ing devices, and the training of personnel (78).
When looking at external quality assurance programson CD41 and CD341 cell count with reverse pipetting,the interlaboratory CV could be greatly reduced with theuse of stabilized blood samples, unified staining and anal-ysis protocols (173,186), and the targeted training of theinvolved personnel (59,173,175). Even people from veryexperienced laboratories may experience difficulty whenapproaching single-platform absolute counting proce-dures for the first time.
The single-platform techniques can be now consideredas the new golden standard for CD41 and CD341 cellcounting. This is because many well-controlled studiesclearly indicate the definitely lower intrainstitutional andinterinstitutional variability of these methods. Each centermust perform adequate training on single-platform proce-dures, which may require more technical skill than theordinary dual-platform techniques.
The CD41 T-cell counting methods so far credited withthe lowest interlaboratory CV are the single-platform Or-tho Cytoron Absolute and the Becton Dickinson FAC-SCount with values both less than 4% CV, a considerabletechnical achievement in FCM (116,168). To date, severalalternative FCM techniques exist for absolute CD41 T-cellabsolute counting. Conceptually, every methodologicalaspect can be criticized (see above), but most of them canbe credited as valid for routine clinical use. It is interestingto note that the major single- and dual-platform FCMtechniques are based on entirely different concepts andbiological premises but perform equally well.
After adequate technical cross-comparison studies arecompleted, clearcut data on the superiority of FCM count-ing of rWBC over conventional techniques will also beavailable. A Dutch consortium between blood banks is
currently working intensively on that matter and they aregoing to publish a paper shortly.
Future Developments
Stain-no-lyse procedures for absolute cell subset count-ing can be considered as a remarkable step forward be-cause the flaws introduced by lysing agents have beenclearly demonstrated. The first applicable no-lyse technol-ogy was developed for CD4 counting on the FACSCountinstrument (116). Strangely, no further developments ofsuch a promising and effective technique have occurredsince that time. Quite recently, an experimental stain-no-lyse procedure for absolute CD341 cell counting usingSYTO-13 nuclear staining was described (63).
Besides the established absolute cell counting tech-niques, other experimental issues are on the verge of a fullclinical application. These include the absolute countingof blood CD341 cells in myelodysplastic syndromes (187)and of total cells in bone marrow aspirates (188), whichmay have relevance in BMT outcome and possibly also inleukemia diagnosis and staging. Interesting applicationsare emerging in quantitative and qualitative sperm analysis(189) and in the detection and counting of rare antigen-specific CD81 cell subsets by HLA-tetramer technology(190,191).
Single-tube, multiple-color systems are brilliantly simpleand precise, but expensive. Counting microbeads are del-icate, high-technology products, which introduce a re-markable extra cost to single-platform procedures. CD41T cell per microliter count, along with the minimuminternal consistency control, can be obtained now withthe use of four antibodies in a single tube using four-colorbead-based procedures provided by Becton Dickinson andBeckman-Coulter, which represent state-of-the-art tech-nology.
However, an issue of great concern is the cost of eachmethodology (151,163,164,167). Cost is a major limitingfactor for each laboratory testing, including CD41 T-celland CD341 cell count. It is still questionable whether theuse of alternative non-FCM technology may determine areal cost-saving; the answer is likely no.
Why is FCM, the golden standard technology for abso-lute cell counting, still such a high-cost procedure? Whatcan be done to enable countries with limited health careresources to satisfy the increasing demand of locally af-fordable testing to cope with the ever increasing AIDSepidemics?
We spent the last decade learning how to identify andcount cells properly. This process led to increasing preci-sion, but also to increasing complexity and costs. Nowthat all the assay variables have been identified in detail,some effort to simplify the technical burden and saveresources seems warranted. It is indeed a necessary pro-cess that took place similarly in many technical fields.
Reliable FCM CD41 cell counts may be generated withnewly designed low-cost minimalist procedures that aredemanded by countries with limited resources (Fig. 4)(163,164,167). The widespread clinical applicability ofgreatly simplified and cheaper assay systems (including
339ABSOLUTE CELL SUBSET COUNT

newly designed instruments) seems, however, in contrastwith the current recommendations of influential institu-tions like the CDC.
The procedure cost and assay complexity must also beweighed in comparison to another crucial issue, namely,the critical error we can afford with CD41 T-cell andCD341 cell count assays, which is much tighter in thelatter case. In other words, if the clinical decision-makingthreshold is narrow, every technical effort should be madeto ensure a very precise and accurate absolute cell levelmeasurement. This is typically the case of the delicateCD341 PBSC transplantation.
Looking back at the past few years, it is interesting tonote that a number of consensus threshold values forbiological testings have been established without any con-cern about the assay sensitivity, accuracy, and intrinsicvariability (i.e., ,200 CD41 cells per microliter as anAIDS-defining condition and the number of rWBC to beinfused). We are still unable to evaluate the exact clinicalimpact of many crucial biological variables, simply be-cause we have been unable to measure them properly.
LITERATURE CITED1. Fauci AS, Macher AM, Longo DL, Lane HC, Rook AH, Masur H,
Gelmann EP. NIH conference. Acquired immunodeficiency syn-drome: epidemiologic, clinical, immunologic, and therapeutic con-siderations. Ann Intern Med 1984;100:92–106.
2. Valentine ME, Jackson CR, Vavro C, Wilfert CM, McClernon D, StClair M, Katz SL, McKinney RE Jr. Evaluation of surrogate markersand clinical outcomes in two-year follow-up of 86 HIV-infectedpediatric patients. Pediatr Infect Dis J 1998;17:18–23.
3. Guarner J, Montoya P, del Rio C, Hernandez-Tepichin G. CD41T-lymphocyte variations in patients with advanced human immuno-deficiency virus infection and counts below 100 cells per microliter.Cytometry 1997;30:178–180.
4. Spino C, Kahn JO, Dolin R, Phair JP. Predictors of survival inHIV-infected persons with 50 or fewer CD4 cells/mm3. J AcquirImmune Defic Syndr Hum Retrovirol 1997;15:346–355.
5. Vanhems P, Allard R, Toma E, Cyr L, Beaulieu R. Prognostic value ofthe CD41 T cell count for HIV-1 infected patients with advancedimmunosuppression. Int J STD AIDS 1996;7:495–501.
6. Rabeneck L, Hartigan PM, Huang IW, Souchek J, Wray NP. Predict-ing outcomes in HIV-infected veterans: I. Progression to AIDS. II.Survival after AIDS. J Clin Epidemiol 1997;50:1231–1248.
7. Keet IP, Janssen M, Veugelers PJ, Miedema F, Klein MR, Goudsmit J,
Coutinho RA, de Wolf F. Longitudinal analysis of CD4 T cell counts,T cell reactivity, and human immunodeficiency virus type 1 RNAlevels in persons remaining AIDS-free despite CD4 cell counts ,200for .5 years. J Infect Dis 1997;176:665–671.
8. Sabin CA, Mocroft A, Bofill M, Janossy G, Johnson M, Lee CA, PhillipsAN. Survival after a very low (,5 3 10(6)/l) CD41 T-cell count inindividuals infected with HIV. AIDS 1997;11:1123–1127.
9. Phillips AN, Eron J, Bartlett J, Kuritzkes DR, Johnson VA, Gilbert C,Johnson J, Keller A, Hill AM. Correspondence between the effect ofzidovudine plus lamivudine on plasma HIV level/CD4 lymphocytecount and the incidence of clinical disease in infected individuals.North American Lamivudine HIV Working Group. AIDS 1997;11:169–175.
10. Furrer H, Egger M, Opravil M, Bernasconi E, Hirschel B, Battegay M,Telenti A, Vernazza PL, Rickenbach M, Flepp M, Malinverni R.Discontinuation of primary prophylaxis against Pneumocystis cari-nii pneumonia in HIV-1 infected adults treated with combinationantiretroviral therapy. N Engl J Med 1999;340:1301–1306.
11. Autran B, Carcelain G, Li TS, Blanc C, Mathez D, Tubiana R, KatlamaC, Debre P, Leibowitch J. Positive effects of combined antiretroviraltherapy on CD41 T cell homeostasis and function in advanced HIVdisease. Science 1997;277:112–116.
12. Mellors JW. Plasma viral load and CD41 lymphocytes as prognosticmarkers of HIV-1 infection. Ann Intern Med 1997;126:946–954.
13. CDC-Centers for Disease Control and Prevention 1997 Revisedguidelines for performing CD41 T-cell determinations in personsinfected with human immunodeficiency virus (HIV). MMWR 1997;46:1–29.
14. Department of Health and Human Services and Henry J. KaiserFamily Foundation. Guidelines for the use of antiretroviral agents inHIV-infected adults and adolescents. MMWR 1998;47:1–91 (updatedat http://www.hivatis.org).
15. Kovacs JA, Masur H. Prophylaxis against opportunistic infections inpatients with human immunodeficiency virus infection. N EnglJ Med 2000;342:1416–1429.
16. Roederer M, De Rosa SC, Watanabe N, Herzenberg LA. Dynamics offine T-cell subsets during HIV disease and after thymic ablation bymediastinal irradiation. Semin Immunol 1997;9:389–396.
17. Bofill M, Mocroft A, Lipman M, Medina E, Borthwick NJ, Sabin CA,Timms A, Winter M, Baptista L, Johnson MA, Lee CA, Phillips AN,Janossy G. Increased numbers of primed activated CD81CD381CD45RO1 T cells predict the decline of CD41 T cells in HIV-1-infected patients. AIDS 1996;10:827–834.
18. Ullum H, Lepri AC, Victor J, Skinhoj P, Phillips AN, Pedersen BK.Increased losses of CD41CD45RA1 cells in late stages of HIVinfection is related to increased risk of death: evidence from acohort of 347 HIV-infected individuals. AIDS 1997;11:1479–1485.
19. Caruso A, Licenziati S, Canaris AD, Cantalamessa A, Fiorentini S,Ausenda S, Ricotta D, Dima F, Malacarne F, Balsari A, Turano A.Contribution of CD41, CD81CD281, and CD81CD28- T cells toCD31 lymphocyte homeostasis during the natural course of HIV-1infection. J Clin Invest 1998;101:137–144.
20. Hultin LE, Matud JL, Giorgi JV. Quantitation of CD38 activationantigen expression on CD81 T cells in HIV-1 infection using CD4expression on CD41 T lymphocytes as a biological calibrator. Cy-tometry 1998;33:123–132.
21. Evans TG, Bonnez W, Soucier HR, Fitzgerald T, Gibbons DC, Reich-mann RC. Highly active antiretroviral therapy results in a decrease inCD81 T cell activation and preferential reconstitution of the periph-eral CD41 T cell population with memory rather than naive cells.Antiviral Res 1998;39:163–173.
22. Koene RAP. Immunosuppression by T cell antibodies in renal trans-plantation. Nephron 1992;61:383–392.
23. Civati G, Minetti E, Busnach G, Perego A, Brando B, Broggi ML,Sansalone V, Forti D. Low and very low incidence of acute rejectionin kidney grafts treated with initial quadruple therapy: a retrospec-tive analysis comparing two ATGs. Transplant Proc 1998;30:1343–1345.
24. Clark KR, Forsythe JL, Shenton BK, Lennard TW, Proud G, TaylorRM. Administration of ATG according to the absolute T lymphocytecount during therapy for steroid-resistant rejection. Transplant Int1993;1:18–21.
25. Bas J, Mestre M, Grinyo JM, Massip E, Alsina J, Castelao AM, Coromi-nas M, Buendia E. Peripheral blood lymphoid subsets and long-termclinical course of kidney recipients: a longitudinal study. Cytometry1998;34:103–112.
26. Ducloux D, Carron PL, Rebibou JM, Aubin F, Fournier V, Bresson-Vautrin C, Blanc D, Humbert P, Chalopin JM. CD4 lymphocytopeniaas a risk factor for skin cancers in renal transplant recipients. Trans-plantation 1998;65:1270–1272.
FIG. 4. Bland-Altman comparison of single-platform absolute CD4counting employing full technology (Ortho Cytoron plus Trio Immuno-count) versus reevaluation of single-color primary CD41 cell gating onthe same FCS files (minimal technology). The mean difference is -4, theCIs are -6 and 115, the lower and upper limits of agreement areindicated, along with linear regression. An isolated outlier (-650) hadT-cell lymphoma. Data modified from Janossy et al. (164).
340 BRANDO ET AL.
27. Mackall CL, Fleisher TA, Brown MR, Andrich MP, Chen CC, Feuer-stein IM, Horowitz ME, Magrath IT, Shad AT, Steinberg SM, WexlerLH, Gress RE. Age, thymopoiesis, and CD41 T-lymphocyte regener-ation after intensive chemotherapy. N Engl J Med 1995;332:143–149.
28. Bomberger C, Singh-Jairam M, Rodey G, Guerriero A, Yeager AM,Fleming WH, Holland HK, Waller EK. Lymphoid reconstitution afterautologous PBSC transplantation with FACS-sorted CD341 hemato-poietic progenitors. Blood 1998;91:2588–2600.
29. Pavletic ZS, Joshi SS, Pirruccello SJ, Tarantolo SR, Kollath J, Reed EC,Bierman PJ, Vose JM, Warkentin PI, Gross TG, Nasrati K, ArmitageJO, Kessinger A, Bishop MR. Lymphocyte reconstitution after allo-geneic blood stem cell transplantation for hematologic malignan-cies. Bone Marrow Transplant 1998;21:33–41.
30. Takeshima M, Takamatsu H, Iida M, Mochizuki Y, Okumura H,Yoshida T. Frequent viral infections and delayed CD41 cell recoveryfollowing CD341 cell-selected autologous peripheral blood stemcell transplantation. Int J Hematol 1999;70:193–199.
31. Schirmer M, Hilbe W, Geisen F, Thaler J, Konwalinka G. T cells andnatural killer cells after treatment of hairy cell leukemia with 2-chlo-rodeoxyadenosine. Acta Haematol 1997;97:180–183.
32. Raspadori D, Rondelli D, Birtolo S, Lenoci M, Nardi G, Scalia G,Sestigiani C, Tozzi M, Marotta G, Lauria F. Long-lasting decrease ofCD41/CD45RA1 T cells in HCL patients after 2-chlorodeoxyade-nosine (2-CdA) treatment. Leukemia 1999;13:1254–1257.
33. Hviid L, Kurtzhals JA, Goka BQ, Oliver-Commey JO, Nkrumah FK,Theander TG. Rapid reemergence of T cells into peripheral circula-tion following treatment of severe and uncomplicated Plasmodiumfalciparum malaria. Infect Immun 1997;65:4090–4093.
34. Sabatier F, Dignat-George F, Mege JL, Brunet C, Raoult D, Sampol J.CD41 T-cell lymphopenia in Q fever endocarditis. Clin Diagn LabImmunol 1997;4:89–92.
35. Mordacchini M, Vianello A, Calconi G. T-lymphocyte subsets in earlyand late phase of cytomegalovirus infection in renal transplantrecipients. Clin Transplant 1990;4:9–13.
36. Raes M, Peeters V, Alliet P, Gillis P, Kortleven J, Magerman K,Rummens JL. Peripheral blood T and B lymphocyte subpopulationsin infants with acute respiratory syncytial virus brochiolitis. PediatrAllergy Immunol 1997;8:97–102.
37. Zimmer JP, Garza C, Heller ME, Butte N, Goldman AS. Postpartummaternal blood helper T (CD31CD41) and cytotoxic T (CD31CD81) cells: correlations with iron status, parity, supplement use,and lactation status. Am J Clin Nutr 1998;67:897–904.
38. Mustafa A, Ward A, Treasure J, Peakman M. T lymphocyte subpopu-lations in anorexia nervosa and refeeding. Clin Immunol Immuno-pathol 1997;82:282–289.
39. Schaberg T, Theilacker C, Nitschke OT, Lode H. Lymphocyte sub-sets in peripheral blood and smoking habits. Lung 1997;175:387–394.
40. Gessl A, Waldhausl W. Elevated CD69 expression on naive periph-eral blood T-cells in hyperthyroid Graves’ disease and autoimmunethyroiditis: discordant effect of methimazole on HLA-DR and CD69.Clin Immunol Immunopathol 1998;87:168–175.
41. Krejsek J, Kral B, Vokurkova D, Derner V, Touskova M, Parakova Z,Kopecky O. Decreased peripheral blood gamma delta T cells inpatients with bronchial asthma. Allergy 1998;53:73–77.
42. Rohowsky-Kochan C, Molinaro D, Devereux C, Troiano R, Bansil S,Zito G, Wolansky L, Jotkowitz A, Denny T, Oleske J, Dowling P,Cook SD. The effect of total lymphoid irradiation and low-dosesteroids on T lymphocyte populations in multiple sclerosis: correla-tion with clinical and MRI status. J Neurol Sci 1997;152:182–192.
43. Boiardi L, Salvarani C, Macchioni P, Casadei Maldini M, Mancini R,Beltrandi E, Portioli I. CD8 lymphocyte subsets in active polymyalgiarheumatica: comparison with elderly-onset and adult rheumatoidarthritis and influence of prednisone therapy. Br J Rheumatol 1996;35:642–648.
44. Lacki JK, Mackiewicz SH. Relations between absolute number ofCD41 CD291 memory cells and levels of interleukin-6, rheumatoidfactors, and acute phase proteins in rheumatoid synovial fluid. RevRhum Engl Ed 1997;64:160–165.
45. Schroder W, Vering A, Stegmuller M, Strohmeier R. Lymphocytesubsets in patients with ovarian and breast cancer. Eur J GynaecolOncol 1997;18:474–477.
46. To LB, Haylock DN, Simmons PJ, Juttner CA. The biology andclinical uses of blood stem cells. Blood 1997;89:2233–2258.
47. Gratama JW, Orfao A, Barnett D, Brando B, Huber A, Janossy G,Johnsen HE, Keeney M, Marti GE, Preijers F, Rothe G, Serke S,Sutherland DR, Van der Schoot CE, Schmitz G, Papa S (EWGCCA).Flow cytometric enumeration of CD341 hematopoietic stem andprogenitor cells. Cytometry 1998;34:128–142.
48. Siena S, Schiavo R, Pedrazzoli P, Carlo-Stella C. The therapeuticrelevance of CD341 cell dose in blood cell transplantation forcancer therapy. J Clin Oncol 2000;18:1360–1377.
49. Traynor A, Burt RK. Haematopoietic stem cell transplantation foractive systemic lupus erythematosus. Rheumatology 1999;38:767–772.
50. Locatelli F, Perotti C, Torretta L, Maccario R, Montagna D, Ravelli A,Giorgiani G, De Benedetti F, Giraldi E, Magnani ML, De Stefano P,Martini A. Mobilization and selection of peripheral blood hemato-poietic progenitors in children with systemic sclerosis. Haemato-logica 1999;84:839–843.
51. Barnett D, Janossy G, Lubenko A, Matutes E, Newland AC, Reilly JT.Guideline for the flow cytometric enumeration of CD341 haemato-poietic cells. Clin Lab Haematol 1999;21:301–308.
52. Meldgaard Knudsen L, Gaarsdal E, Jensen L, Nikolaisen K, JohnsenHE. Evaluation of mobilized CD341 cell counts to guide timing andyield of large-scale collection by leukapheresis. J Hematother 1998;7:45–52.
53. Gratama JW, Keeney M, Sutherland DR. Enumeration of CD341hematopoietic stem and progenitor cells. In: Robinson JP, Darzynk-iewicz Z, Dean PN, Dressler LG, Rabinovitch PS, Stewart CC, TankeHJ, Wheeless LL, editors. Current protocols in cytometry. New York:John Wiley & Sons; 1999. p 6.4.1–6.4.22.
54. Chapple P, Prince HM, Quinn M, Bertoncello I, Juneja S, Wolf M,Januszewicz H, Brettell M, Gardyn J, Seymour C, Venter D. Periph-eral blood CD341 cell count reliably predicts autograft yield. BoneMarrow Transplant 1998;22:125–130.
55. Benedetti G, Patoia L, Giglietti A, Alessio M, Pelicci P, Grignani F.Very large amounts of peripheral blood progenitor cells eliminatesevere thrombocytopenia after high-dose melphalan in advancedbreast cancer patients. Bone Marrow Transplant 1999;24:971–979.
56. Ademokun JA, Chapman C, Dunn J, Lander D, Mair K, Proctor SJ,Dickinson AM. Umbilical cord blood collection and separation forhaematopoietic progenitor cell banking. Bone Marrow Transplant1997;19:1023–1028.
57. Aversa F, Tabilio A, Velardi A, Cunningham I, Terenzi A, Falzetti F,Ruggeri L, Barbabietola G, Aristei C, Latini P, Reisner Y, Martelli MF.Treatment of high-risk acute leukemia with T-cell-depleted stemcells from related donors with one fully mismatched HLA haplotype.N Engl J Med 1998;339:1186–1193.
58. Schmitz N, Bacigalupo A, Hasenclever D, Nagler A, Gluckman E,Clark P, Bourquelot P, Greinix H, Frickhofen N, Ringden O, ZanderA, Apperley JF, Gorin C, Borkett K, Schwab G, Goebel M, RussellNH, Gratwohl A. Allogeneic bone marrow transplantation vs filgras-tim-mobilised peripheral blood progenitor cell transplantation inpatients with early leukemia: first results of a randomised multicen-tre trial of the European Group for Blood and Marrow Transplanta-tion. Bone Marrow Transplant 1998;21:995–1003.
59. Barnett D, Granger V, Kraan J, Whitby L, Reilly JT, Papa S, GratamaJW. Reduction of intra- and inter-laboratory variation in CD341 stemcell enumeration by the use of stable test material, standard proto-cols and targeted training. Br J Haematol 2000;108:784–792.
60. Gratama JW, Braakman E, Kraan J, Lankheet P, Levering WH, VanDen Beemd MW, Van Der Schoot CE, Wijermans P, Preijers F.Comparison of single- and dual-platform assay formats for CD341haemopoietic progenitor cell enumeration. Clin Lab Haematol 1999;21:337–346.
61. Gratama JW, Keeney M, Sutherland DR, Papa S. The real CD341events: simplicity versus accuracy and flexibility. Exp Hematol 1999;27:975–977.
62. Keeney M, Chin-Yee I, Nayar R, Sutherland DR. Effect of fixatives onCD341 cell enumeration. J Hematother Stem Cell Res 1999;8:327–329.
63. Fornas O, Garcia J, Petriz J. Flow cytometry counting of CD341 cellsin whole blood. Nature Med 2000;6:833–836.
64. Lane TA. Leucocyte depletion of cellular blood components. CurrOpin Hematol 1994;1:443–451.
65. Standards for Blood Banks and Transfusion Services, 16th edition.Harvey G. Klein, chairman. Bethesda, MD: American Association ofBlood Banks; 1994. p 13.
66. Pamphilon DH, Rider JR, Barbara JA, Williamson LM. Prevention oftransfusion-transmitted cytomegalovirus infection. Transfus Med1999;9:115–123.
67. Wagner HJ, Kluter H, Kruse A, Bucsky P, Hornef M, Kirchner H.Determination of the number of Epstein-Barr virus genomes inwhole blood and red cell concentrates. Transfus Med 1995;5:297–302.
68. Prowse CV, Hornsey VS, Drummond O, MacGregor IR, Pepper DS,Barclay GR, Bethel H, Walker B, Barnard G, Kirby L, Hope J. Prelim-inary assessment of whole-blood, red-cell and platelet-leucodeplet-
341ABSOLUTE CELL SUBSET COUNT

ing filters for possible induction of prion release by leucocyte frag-mentation during room temperature processing. Br J Haematol1999;106:240–247.
69. Ten Haaft MA, Van den Berg-Loonen PM, Van Rhenen DJ. Preventionof primary HLA class I allo-immunization with leucocyte-poor bloodcomponents produced without the use of platelet filters. Vox Sang1992;63:257–261.
70. Heddle NM, Blajchman MA. The leukodepletion of cellular bloodproducts in the prevention of HLA-alloimmunization and refractori-ness to allogeneic platelet transfusions. Blood 1995;85:603–606.
71. Saarinen UM, Koskimies S, Myllyla G. Systematic use of leukocyte-free blood components to prevent alloimmunization and plateletrefractoriness in multitransfused children with cancer. Vox Sang1993;65:286–292.
72. van Prooijen HC, Aarts-Riemens MI, van Oostendorp WR, Hene RJ,Gmelig-Meyling FH, de Weger RA. Prevention of donor-specificT-cell unresponsiveness after buffy-coat-depleted blood transfusion.Br J Haematol 1995;91:219–223.
73. Willis JI, Lown JA, Simpson MC, Erber WN. White cells in fresh-frozen plasma: evaluation of a new white cell-reduction filter. Trans-fusion 1998;38:645–649.
74. Lutz P, Dzik WH. Large-volume hemocytometer chamber for accu-rate counting of white cells (wbcs) in wbc-reduced platelets: vali-dation and application for quality control of wbc-reduced plateletsprepared by apheresis and filtration. Transfusion 1993;33:409–412.
75. Masse M, Naegelen C, Pellegrini N, Segier JM, Marpaux N, BeaujeanF. Validation of a simple method to count very low white cellconcentrations in filtered red cells or platelets. Transfusion 1992;32:565–571.
76. Rebulla P, Porretti L, Bertolini F, Marangoni F, Prati D, Smacchia C,Pappalettera M, Parravicini A, Sirchia G. White cell-reduced red cellsprepared by filtration: a critical evaluation of current filters andmethods for counting residual white cells. Transfusion 1993;33:128–133.
77. Richter E, Matthes G, Tofote U, Rath E, Takahashi TA, Hosoda M,Sekiguchi S. 4-Log leukocyte depletion of erythrocyte concentrates.A comparison with 3 other filters. Beitr Infusionsther Transfu-sionsmed 1994;32:26–28.
78. Mandy FF, Bergeron M, Minkus T. Evolution of leukocyte immuno-phenotyping as influenced by the HIV/AIDS pandemic: a shorthistory of the development of gating strategies for CD41 T-cellenumeration. Cytometry 1997;30:157–165.
79. Loken MR, Brosnan JM, Bach BA, Ault KA. Establishing optimallymphocyte gates for immunophenotyping by flow cytometry. Cy-tometry 1990;11:453–459.
80. Gelman R, Cheng SC, Kidd P, Waxdal M, Kagan J. Assessment of theeffects of instrumentation, monoclonal antibody, and fluorochromeon flow cytometric immunophenotyping: a report based on 2 yearsof the NIAID DAIDS flow cytometry quality assessment program.Clin Immunol Immunopathol 1993;66:150–162.
81. Mercolino TJ, Connelly MC, Meyer EJ, Knight MD, Parker JW, StelzerGT, De Chirico G. Immunologic differentiation of absolute lympho-cyte count with an integrated flow cytometric system: a new con-cept for absolute T cell subset determinations. Cytometry 1995;22:48–59.
82. Gelman R, Wilkening C. Analyses of quality assessment studies usingCD45 for gating lymphocytes for CD3141%. Cytometry 2000;42:1–4.
83. Aboulker JP, Autran B, Beldjord K, Touraine F, Debre P. Consistencyof routine measurements of CD41, CD81 peripheral blood lympho-cytes. J Immunol Methods 1992;154:155–161.
84. Bentley SA, Johnson A, Bishop CA. A parallel evaluation of fourautomated hematology analyzers. Am J Clin Pathol 1993;100:626–632.
85. Robinson G, Morgan L, Evans M, McDermott S, Pereira S, Wans-brough-Jones M, Griffin G. Effect of type of haematology analyser onCD4 count [Letter]. Lancet 1992;340:485.
86. Reimann KA, O’Gorman MRG, Spritzler J, Wilkening C, Sabath DE,Helm K, Campbell DE. A multisite comparison of CD4 and CD8 Tlymphocyte counting by single vs multiple platform methodologies:evaluation of Beckman Coulter Flow-Count fluorospheres and tetra-ONE System. Clin Diagn Lab Immunol 2000;7:344–351.
87. Schnitzlein-Bick CT, Spritzler J, Wilkening C, Nicholson JKA,O’Gorman MRG. Evaluation of TruCount absolute count tubes fordetermining CD4 and CD8 cell numbers and their comparison toconventional immunophenotyping. Clin Diagn Lab Immunol 2000;7:336–343.
88. Barnett D, Granger V, Whitby L, Storie I, Reilly JT. Absolute CD41T-lymphocyte and CD341 stem cell counts by single-platform flowcytometry: the way forward. Br J Haematol 1999;106:1059–1062.
89. Cohen AJ, Peerschke EIB, Steigbigel RT. A comparison of the CoulterSTKS, Coulter S1IV, and manual analysis of white blood cell differ-ential counts in a human immunodeficiency virus-infected popula-tion. Am J Clin Pathol 1993;100:611–617.
90. Connelly MC, Knight M, Giorgi JV, Kagan J, Landay AL, Parker J,Page E, Spino C, Wilkening C, Mercolino TJ. Standardization ofabsolute CD41 lymphocyte counts across laboratories: an evalua-tion of the Ortho Cytoron Absolute flow cytometry system onnormal donors. Cytometry 1995;22:200–210.
91. Hubl W, Tlustos L, Erath A, Andert S, Bayer PM. Proposed referencemethod for peripheral-blood monocyte counting using fluores-cence-labelled monoclonal antibodies. Cytometry 1996;26:69–74.
92. Morillon M, Maslin J, De Pina JJ, Louis FJ, Martet G. Evaluation of themonocyte counting by the ABX Vega. Comparison with the manualmethod and fluoro-flow cytometry. Hematol Cell Ther 1999;41:47–50.
93. Hubl W, Tlustos L, Bayer PM. Use of precision profiles to evaluateprecision of the automated leukocyte differential. Clin Chem 1996;42:1068–1073.
94. Lombarts AJPF, Koevoet AL, Leijnse B. Basic principles and prob-lems of haemocytometry. Ann Clin Biochem 1986;23:390–404.
95. Warner BA, Reardon DM. A field evaluation of the Coulter STKS.Am J Clin Pathol 1991;95:207–217.
96. Hudson JC, Brunhouse RF, Garrison C, Rodriguez CM, Zwerner R,Russell TR. Lymphocyte subset determination using a hematologyanalyzer. Cytometry 1995;22:150–153.
97. Bollinger PB, Drewinko B, Brailas CD, Smeeton NA, Trujillo JM. TheTechnicon H1. An automated hematology analyzer for today andtomorrow. Am J Clin Pathol 1987;87:71–78.
98. Van Leeuwen L, Eggels PH, Bullen JA. A short evaluation of a newhaematological cell counter. The Cell-Dyn 3000, following a modi-fied tentative NCCLS-procedure. Eur J Clin Chem Clin Biochem1991;29:105–110.
99. Buttarello M, Bulian P, Temporin V, Rizzotti P. Sysmex SE-9000hematology analyzer: Performance evaluation on leukocyte differen-tial counts using an NCCLS H20-A protocol. National Committee forClinical Laboratory Standards. Am J Clin Pathol 1997;108:674–686.
100. Ferrero-Vacher C, Sudaka I, Jambou D, Vanhaeke D, Fischer F, BayleJ. Evaluation of the ABX Cobas Vega automated hematology analyzerand comparison with the Coulter STKS. Hematol Cell Ther 1997;39:149–158.
101. Fournier M, Gireau A, Chretien MC, Ghevaert C, Boniface B, Gou-demand J, Cosson A. Laboratory evaluation of the Abbott Cell DYN3500 5-part differential. Am J Clin Pathol 1996;105:286–292.
102. Kim YR, Yee M, Metha S, Chupp V, Kendall R, Scott CS. Simulta-neous differentiation and quantitation of erythroblasts and whiteblood cells on a high throughput clinical haematology analyser. ClinLab Haematol 1998;20:21–29.
103. Mentz F, Baudet S, Maloum K, Azgui Z, Sevin O, Vinsobre MF,Dujarric C, Brefort K, Chretien MC, Merle-Beral H. Quantification ofapoptosis by the Abbott CD4000 hematology analyzer. Hematol CellTher 1998;40:183–188.
104. Muller TH, Doscher A, Schunter F, Scott CS. Manual and automatedmethods for the determination of leukocyte counts at extreme lowlevels: comparative evaluation of the Nageotte chamber and theAbbott Cell Dyn 3500 analyser. Transfus Sci 1997;18:505–515.
105. No Authors Listed. Clinical applications of flow cytometry: qualityassurance and immunophenotyping of lymphocytes; approvedguideline. NCCLS document H42-A, December 1998.
106. Barnett D, Bird G, Hodges E, Linch DC, Matutes E, Newland AC,Reilly JT. Guidelines for the enumeration of CD41 T lymphocytes inimmunosuppressed individuals. Clin Lab Haematol 1997;19:231–241.
107. Mandy F, Brando B. Enumeration of absolute counts using immuno-phenotypic techniques. In: Robinson JP, Darzynkiewicz Z, Dean PN,et al., eds. Current protocols in cytometry. New York: John Wiley &Sons; 2000. p 6.8.1–6.8.26.
108. Menendez P, Redondo O, Rodriguez A, Lopez-Berges MC, Ercilla G,Lopez A, Duran A, Almeida J, Perez-Simon JA, San Miguel JF, GratamaJW, Orfao A. Comparison between a lyse-and-then-wash method anda lyse-non-wash technique for the enumeration of CD341 hemato-poietic progenitor cells. Cytometry 1998;34:264–271.
109. Cassens U, Gutensohn K, Garritsen H, Kelsch R, Kuehnl P, SibrowskiW. The influence of different erythrocyte lysing procedures on flowcytometric determination of CD341 cells in umbilical cord bloodtransplants. Transfus Med 1998;8:111–118.
110. Gratama JW, Menendez P, Kraan J, Orfao A. Loss of CD34(1)hematopoietic progenitor cells due to washing can be reduced bythe use of fixative-free erythrocyte lysing reagents. J Immunol Meth-ods 2000;239:13–23.
342 BRANDO ET AL.

111. Hoffman RA, Hansen WP. Simple and rapid measurement of humanT lymphocytes and their subclasses in peripheral blood. Proc NatlAcad Sci USA 1980;77:4914–4917.
112. Macey MG, McCarthy DA, Davies C, Newland AC. The Q-Prepsystem: effects on the apparent expression of leucocyte cell surfaceantigens. Cytometry 1997;30:67–71.
113. Bossuyt X, Marti GE, Fleisher TA. Comparative analysis of wholeblood lysis methods for flow cytometry. Cytometry 1997;30:124–133.
114. Nicholson J, Kidd P, Mandy F, Livnat D, Kagan J. Three-color sup-plement to the NIAID-DAIDS guideline for flow cytometric immu-nophenotyping. Cytometry 1996;26:227–230.
115. Gratama JW, van der Linden R, van der Holt B, Bolhuis RLH, van deWinkel JGJ. Analysis of factors contributing to the formation ofmononuclear cell aggregates (“escapees”) in flow cytometric immu-nophenotyping. Cytometry 1997;29:250–260.
116. Strauss K, Hannet I, Engels S, Shiba A, Ward DM, Ulley S, Jinguji G,Valinsky J, Barnett D, Orfao A, Kestens L. Performance evaluation ofthe FACSCount system: a dedicated system for clinical cellular anal-ysis. Cytometry 1996;26:52–59.
117. O’Gorman MR, Gelman R. Inter- and intrainstitutional evaluation ofautomated volumetric capillary cytometry for the quantitation ofCD4- and CD8-positive T lymphocytes in the peripheral blood ofpersons infected with human immunodeficiency virus. Site investi-gators and the NIAID New CD4 Technologies Focus Group. ClinDiagn Lab Immunol 1997;4:173–179.
118. Keeney M, Gratama JW, Chin-Yee IH, Sutherland DR. Isotype con-trols in the analysis of lymphocytes and CD341 stem/progenitorcells by flow cytometry: time to let go! Cytometry 1998;34:280–283.
119. Sutherland DR, Anderson L, Keeney M, Nayar R, Chin-Yee I. TheISHAGE guidelines for CD341 cell determination by flow cytom-etry. J Hematother 1996;5:213–226.
120. Keeney M, Yee IC, Weir K, Popma J, Nayar R, Sutherland DR. Singleplatform flow cytometric absolute CD341 cell counts based on theISHAGE guidelines. Cytometry 1998;34:61–70.
121. Basso G, Timeus F. Cytofluorimetric analysis of CD34 cells. BoneMarrow Transplant 1998;22 (Suppl 5):S17–20.
122. Chen CH, Lin W, Shye S, Kibler R, Grenier K, Recktenwald D,Terstappen LWMM. Automated enumeration of CD341 cells inperipheral blood and bone marrow. J Hematother 1994;3:3–13.
123. Brando B, Goehde W Jr, Scarpati B, D’Avanzo G. The “vanishingcounting bead phenomenon”: effect on absolute CD341 cell count-ing in PBS-diluted luekapheresis. Cytometry (submitted).
124. Dzik WH, Ragosta A, Cusack WF. Flow-cytometric method for count-ing very low numbers of leukocytes in platelet products. Vox Sang1990;59:153–159.
125. Dzik WH. White cell-reduced blood components: should we go withthe flow? Transfusion 1991;31:789–791.
126. Dumont LJ. Sampling errors and the precision associated withcounting very low numbers of white cells in blood components.Transfusion 1991;31: 428–432.
127. Scheckler VL, Loken MR. Routine quantitation of white cells as lowas 0.001 per mL in platelet components. Transfusion 1993;33:256–261.
128. Lombardo JF, Cusack NA, Rajagopalan C, Sangaline RJ, Ambruso DR.Flow cytometric analysis of residual white blood cell concentrationand platelet activation antigens in double filtered platelet concen-trates. J Lab Clin Med 1993;122:557–566.
129. Al EJ, Visser SC, Prins HK, Pietersz RN, Reesink HW, Huisman JG. Aflow cytometric method for determination of white cell subpopula-tions in filtered red cells. Transfusion 1991;31:835–842.
130. Wenz B, Burns ER. Phenotypic characterization of white cells inwhite cell-reduced red cell concentrate using flow cytometry. Trans-fusion 1991;31:829–834.
131. Neumuller J, Schwartz DW, Mayr WR. Demonstration by flow cy-tometry of the numbers of residual white blood cells and platelets infiltered red blood cell concentrates and plasma preparations. VoxSang 1997;73:220–229.
132. Sowemimo-Coker SO, Kim A, Tribble E, Brandwein HJ, Wenz B.White cell subsets in apheresis and filtered platelet concentrates.Transfusion 1998;38:650–657.
133. Barclay R, Walker B, Allan R, Reid C, Duffin E, Kane E, Turner M.Flow cytometric determination of residual leucocytes in filter-de-pleted blood products: an evaluation of Becton-Dickinson’s Leuco-COUNT system. Transfus Sci 1998;19:399–403.
134. Krailadsiri P, Seghatchian MJ. Evaluation of IMAGN 2000: a newsystem for absolute leucocyte count. Transfus Sci 1998;19:405–407.
135. Lopez A, Caragol I, Candeias J, Villamor N, Echaniz P, Ortuno F,Sempere A, Strauss K, Orfao A, for the Working Group on LymphoidSubset Analysis of the Iberian Society of Cytometry. Enumeration of
CD41 T-cells in the peripheral blood of HIV-infected patients: aninterlaboratory study of the FACSCount system. Cytometry 1999;38:231–237.
136. Adams MR, Johnson DK, Busch MP, Schembri CT, Hartz TP, HeatonWA. Automatic volumetric capillary cytometry for counting whitecells in white cell-reduced plateletpheresis components. Transfu-sion 1997;37:29–37.
137. Dietz LJ, Dubrow RS, Manian BS, Sizto NL. Volumetric capillarycytometry: a new method for absolute cell enumeration. Cytometry1996;23:177–186.
138. Sims LC, Brecher ME, Gertis K, Jenkins A, Nickischer D, Schmitz JL,Sparks S, Wright P, Bentley SA. Enumeration of CD34-positive stemcells: evaluation and comparison of three methods. J Hematother1997;6:213–226.
139. Cabezudo E, Querol S, Cancelas JA, Garcia J. Comparison of volu-metric capillary cytometry with standard flow cytometry for routineenumeration of CD341 cells. Transfusion 1999;39:864–872.
140. Dzik W, Sniecinski I, Fischer J. Toward standardization of CD341cell enumeration: an international study. Biomedical Excellence forSafer Transfusion Working Party. Transfusion 1999;39:856–863.
141. Stewart CC, Steinkamp JA. Quantitation of cell concentration usingthe flow cytometer. Cytomery 1982;2:238–243.
142. Valet G. A new method for fast blood cell counting and partialdifferentiation by flow cytometry. Blut 1984;49:83–90.
143. Schlenke P, Frohn C, Klueter H, Saballus M, Hammers HJ, Zajac SR,Kirchner H. Evaluation of a flow cytometric method for simulta-neous leukocyte phenotyping and quantification by fluorescent mi-crospheres. Cytometry 1998;33:310–317.
144. Levin A, Brubaker G, Shao JS, Kumby D, O’Brien TR, Goedert JJ,Strauss KW, Blattner WA, Hannet I. Determination of T-lymphocytesubsets on site in rural Tanzania: results in HIV-1 infected andnon-infected individuals. Int J STD AIDS 1996;7:288–291.
145. Johnson D, Hirschkorn D, Busch MP. Evaluation of four alternativemethodologies for determination of absolute CD41 lymphocytecounts. The National Heart, Lung, and Blood Institute RetrovirusEpidemiology Donor Study. J Acquir Immune Defic Syndr HumRetrovirol 1995;10:522–530.
146. Lyamuya EF, Kagoma C, Mbena EC, Urassa WK, Pallangyo K, MhaluFS, Biberfeld G. Evaluation of the FACScount, TRAx CD4 and Dyna-beads methods for CD4 lymphocyte determination. J ImmunolMethods 1996;195:103–112.
147. Nicholson JK, Stein D, Mui T, Mack R, Hubbard M, Denny T.Evaluation of a method for counting absolute numbers of cells witha flow cytometer. Clin Diagn Lab Immunol 1997;4:309–313.
148. Blanc C, Carcelain G, Peries L, Porcher I, Debre P, Autran B. Interetde la numeration absolue per citometrie en flux et du quadruplemarquage des sous-populations lymphocytaires lors de l’ infectionpar le VIH. Rev Fr Lab 1996;287:59–64.
149. Becton Dickinson Report. Part number 23-3670-00, June 1998.150. Takekawa K, Yamane T, Hino M, Tatsumi N. Determination of
hematopoietic stem cells in peripheral blood by an automated he-matology analyzer (SE-9000). Acta Haematol 1998;100:130–136.
151. WHO global programme on AIDS. 1991 Progress Report, ISBN92-4-156156-4, 1992.
152. Gernow A, Lisse IM, Bottiger B, Christensen L, Brattegaard K. De-termination of CD41 and CD81 lymphocytes with the cytosphereassay: a comparative study with flow cytometry and the immunoal-kaline phosphatase method. Clin Immunol Immunopathol 1995;76:135–141.
153. Carella AV, Moss MW, Provost V, Quinn TC. A manual bead assay forthe determination of absolute CD41 and CD81 lymphocyte countsin human immunodeficiency virus-infected individuals. Clin DiagnLab Immunol 1995;2:623–625.
154. Nicholson JK, Velleca WM, Jubert S, Green TA, Bryan L. Evaluationof alternative CD4 technologies for the enumeration of CD4 lym-phocytes. J Immunol Methods 1994;177:43–54.
155. Cordiali Fei P, Solmone M, Vanacore P, Giglio A, Bonifati C, CarducciM, Mussi A, Chiarotti F, Ameglio F. CD4 lymphocyte enumeration:comparison between flow cytometry and enzyme immunoassay.Cytometry 1995;22:70–74.
156. Paxton H, Pins M, Denton G, McGonigle AD, Meisner PS, Phair JP.Comparison of CD4 cell count by a simple enzyme-linked immu-nosorbent assay using the TRAx CD4 test kit and by flow cytometryand hematology. Clin Diagn Lab Immunol 1995;2:104–114.
157. Moss MW, Carella AV, Provost V, Quinn TC. Comparison of absoluteCD41 lymphocyte counts determined by enzyme immunoassay(TRAx CD4 test kit) and flow cytometry. Clin Diagn Lab Immunol1996;3:371–373.
158. Denny TN, Jensen BD, Gavin EI, Louzao AG, Vella FA, Oleske JM,Wong W. Determination of CD4 and CD8 lymphocyte subsets by a
343ABSOLUTE CELL SUBSET COUNT

new alternative fluorescence immunoassay. Clin Diagn Lab Immu-nol 1995;2:330–336.
159. Carriere D, Fontaine C, Berthier AM, Roquette AM, Carayon P,Laprode M, Juillard R, Jansen A, Paoli P, Paolucci F. Two-site enzymeimmunoassay of CD4 and CD8 molecules on the surface of T lym-phocytes from healthy subjects and HIV-1-infected patients. ClinChem 1994;40:30–37.
160. Carriere D, Vendrell JP, Fontaine C, Jansen A, Reynes J, Pages I,Holzmann C, Laprade M, Pau B. Whole blood Capcellia CD4/CD8immunoassay for enumeration of CD41 and CD81 peripheral Tlymphocytes. Clin Chem 1999;45:92–97.
161. Bland JM, Altman DG. Statistical methods for assessing agreementbetween two methods of clinical measurement. Lancet 1986;i:307–310.
162. Hollis S. Analysis of method comparison studies. J Int Fed Clin Chem1997;9:8–12.
163. Sherman GG, Galpin JS, Patel JM, Mendelow BV, Glencross DK.CD41 T cell enumeration in HIV infection with limited resources.J Immunol Methods 1999;222:209–217.
164. Janossy G, Jani I, Gohde W. Affordable CD41 T cell counts on“single-platform” flow cytometers. I. Primary CD4 gating. Br JHaematol 2000;111:720–729.
165. Brando B, Sommaruga E, Mazzola E, Sbressa C. CD41 T cell absolutecount. A crossed comparison among three flow cytometric methodsand plate ELISA test in 325 HIV1 patients. Cytometry 1996; Suppl8:77 (Abstract IH32).
166. Chianese R, Latella S. Use of the IMAGN2000 single-platformmethod for the quantitative evaluation of T CD41 peripheral bloodlymphocytes. Eur J Histochem 1999;43(Suppl 3):38 (Abstract).
167. Brando B. Development of a “minimal technology” procedure forabsolute counting of CD41 cells in HIV1 patients. Cytometry 2000;Suppl. 10:138 (Abstract 6390).
168. Barnett D, Granger V, Mayr P, Storie I, Wilson GA, Reilly JT. Evalu-ation of a novel stable whole blood quality control material forlymphocyte subset analysis: results from the UK NEQAS immunemonitoring scheme. Cytometry 1996;26:216–222.
169. NIAID Flow Cytometry Advisory Committee. Cynthia Wilkening.e-mail: [email protected].
170. Siena S, Bregni M, De Nicola M, Peccatori F, Magni M, Brando B,Ravagnan F, Gianni AM. Milan protocol for clinical CD341 cellestimations in peripheral blood for autografting in patients withcancer. In: Wunder E, Sovalat H, Henon PR, Serke S, editors. Hema-topoietic stem cells: the Mulhouse manual. Dayton, OH: Alpha MedPress; 1994. p 23–30.
171. Chang A, Ma DD. The influence of flow cytometric gating strategyon the standardization of CD341 cell quantitation: an Australianmulticenter study. Australasian BMT Scientists Study Group. J He-matother 1996;5:605–616.
172. Brecher ME, Sims L, Schmitz J, Shea T, Bentley SA. North Americanmulticenter study on flow cytometric enumeration of CD341 he-matopoietic stem cells. J Hematother 1996;5:227–236.
173. Gratama JW, Kraan J, Levering W, Van Bockstaele DR, Rijkers GT,Van der Schoot E. Analysis of variation in results of CD341 hema-topoietic progenitor cell enumeration in a multicenter study. Cy-tometry 1997;30:109–117.
174. Chin-Yee I, Anderson L, Keeney M, Sutherland DR, and the CanadianQASE Study Group. Quality assurance of stem cell enumeration byflow cytometry. Cytometry 1997;30:296–303.
175. Barnett D, Granger V, Storie I, Peel J, Pollitt R, Smart T, Reilly JT.Quality assessment of CD341 stem cell enumeration: experience ofthe United Kingdom National External Quality Assessment Scheme(UK NEQAS) using a unique stable whole blood preparation. Br JHaematol 1998;102:553–565.
176. Johnsen HE, Baech J, Nikolajsen K. Validation of the Nordic flowcytometry standard for CD341 cell enumeration in blood and au-tografts: report from the third workshop. Nordic Stem Cell Labora-tory Group. J Hematother 1999;8:15–28.
177. Leuner S, Arland M, Kahl C, Jentsch-Ullrich K, Franke A, Hoffkes HG.Enumeration of CD34-positive hematopoietic progenitor cells byflow cytometry: comparison of a volumetric assay and the ISHAGEgating strategy. Bone Marrow Transplant 1998;22:699–706.
178. McNiece I, Kern B, Zilm K, Brunaud C, Dziem G, Briddell R. Mini-mization of CD341 cell enumeration variability using the Pro-COUNT standardized methodology. J Hematother 1998;7:499–504.
179. Olivero S, Alario T, Ladaique P, Haccoun M, Viens P, Blaise D,Chabannon C. CD341 cell enumeration in peripheral blood andapheresis samples, using two laboratory diagnostic kits or an insti-tutional protocol. Bone Marrow Transplant 1999;23:387–394.
180. Kunkl A, Terranova MP, Mortara L, Bottone L. Measurement error ofabsolute CD41 T lymphocyte count double platform evaluations for
the assessment of laboratory performance in lymphocyte immuno-phenotyping quality control. Cytometry 2000; Suppl 10;45 (Abstract6415).
181. Hoover DR, Graham NMH, Chen B, Taylor JMG, Phair J, Zhou SYJ,Munoz A. Effect of CD41 cell count measurement variability onstaging HIV-1 infection. J Acquir Immune Defic Syndr Hum Retro-virol 1992;5:794–802.
182. Paglieroni TG, Holland PV. Circannual variation in lymphocyte sub-sets, revisited. Transfusion 1994;34:512–516.
183. Hughes MD, Stein DS, Gundacker HM, Valentine FT, Phair JP, Vol-berding PA. Within-subject variation in CD4 lymphocyte count inasymptomatic human immunodeficiency virus infection: implica-tions for patient monitoring. J Infect Dis 1994;169:28–36.
184. Raboud JM, Haley L, Montaner JS, Murphy C, Januszewska M,Schechter MT. Quantification of the variation due to laboratory andphysiologic sources in CD4 lymphocyte counts of clinically stableHIV-infected individuals. J Acquir Immune Defic Syndr Hum Retro-virol 1995;10 (Suppl 2):S67–S73.
185. Jones AR, Twedt D, Swaim W, Gottfried E. Diurnal change of bloodcount analytes in normal subjects. Am J Clin Pathol 1996;106:723–727.
186. Bergeron M, Faucher S, Minkus T, Lacroix F, Ding T, Phaneuf S,Somorjai R, Summers R, Mandy F. Impact of unified procedures asimplemented in the Canadian quality assurance program for T lym-phocyte subset enumeration. Cytometry 1998;33:146–155.
187. Fuchigami K, Mori H, Matsuo T, Iwanaga M, Nagai K, Kuriyama K,Tomonaga M. Absolute number of circulating CD341 cells is abnor-mally low in refractory anemias and extremely high in RAEB andRAEB-t. Novel pathologic features of myelodysplastic syndromesidentified by highly sensitive flow cytometry. Leuk Res 2000;24:163–174.
188. Singhal S, Powles R, Kulkarni S, Treleaven J, Sirohi B, Millar B,Shepherd V, Saso R, Rowland A, Long S, Cabral S, Horton C, MehtaJ. Comparison of marrow and blood cell yields from the samedonors in a double-blind, randomized study of allogeneic marrow vsblood stem cell transplantation. Bone Marrow Transplant 2000;25:501–505.
189. Ferrara F, Daverio R, Mazzini G, Bonini P, Banfi G. Automation ofhuman sperm cell analysis by flow cytometry. Clin Chem 1997;43:801–807.
190. Ogg GS, McMichael AJ. HLA-peptide tetrameric complexes. CurrOpin Immunol 1998;10:393–396.
191. Gray CM, Lawrence J, Schapiro JM, Altman JD, Winters MA, Cromp-ton M, Loi M, Kundu SK, Davis MM, MeriganTC. Frequency of classI HLA-restricted anti-HIV CD81 T cells in individuals receivinghighly active antiretroviral therapy (HAART). J Immunol 1999;162:1780–1788.
TECHNICAL APPENDIX: ADDITIONAL GUIDELINES FORABSOLUTE COUNTING TECHNIQUES: HOW TO
IMPROVE PRECISION AND ACCURACYA. Pipetting Technique
1. The primary sample pipetting step plays the majorrole in influencing measurement precision and accuracy.
2. Reverse pipetting is always mandatory. Press thepipette plunger at second stop, insert tip into the sample,draw sample (an excess sample is aspirated), then dis-pense at the first stop (the tip contains the excess sample,which must not be distributed).
3. Never use the first sample taken for dispensing (drytip dispensing). Draw sample at the second pipette stop,then do two to three gentle dispense/draw cycles at thefirst stop, keeping the pipette tip within the sample. Youare ready to dispense at the first stop (wet tip dispensing).
4. Before dispensing, wipe away the extra sample thatsticks to the outer wall of pipette tip using gauze or tissue.Avoid touching the terminal tip hole to prevent inadver-tent sample absorption due to capillarity.
5. Before dispensing, place the pipette tip at the dryround bottom of the test tube. Do not touch the tube wall
344 BRANDO ET AL.

with the tip side. This applies only with the primarysample dispensing (see point B.3).
6. DISPENSE at the first plunger stop.7. If repeated sample dispensing with the same tip is
made by manual pipetting, do not lift the thumb after eachdispensing. Keep the plunger pressed steadily at the firststop until another take/dispensing cycle is done (pointsA.3–A.6).
8. The same rules apply to the drawing and dispensingof FlowCount microbeads and for other small-aliquot re-agents in volumetric counting techniques.
B. Pipette Calibration
Always use the above described pipetting technique.
1. Blood is much more viscous than water, and itsspecific gravity is estimated around 1.08 g/mL.
2. The pipette (either manual or electronic) must becalibrated using a precision weighing scale. First, adjustthe volume using distilled water (1 mL water 5 1 mg) in arepeated series of reverse dispensings. Second, calibratefor blood dispensing keeping the 1.08 correction factorfor specific gravity (i.e., 100 mL blood 5 108 mg).
3. Pipette calibration must take into account the deci-sion about how to deal with residual droplets that mayremain at the pipette tip end. This mostly applies to thedispensing of secondary reagents such as counting beads.
4. Residual sample droplets are sensitive to thumb en-ergy: if the dispensing action is quick, droplets do nottend to form and vice versa.
5. Another calibration decision may also derive fromthe dispensing habit, namely, if the secondary reagent isinjected in air from above the existing sample or if thetube wall is touched just above the cell suspension sur-face. In either case, the residual droplet has a differentinfluence and must be taken into account accordingly.
6. The size of the pipette tip terminal bore influencesthe residual droplet formation. Narrow bores ensure lessdroplet formation. Recalibrate the dispensing procedurewhen new lots or different brands of pipette tips are used.
7. When FlowCount microbeads are added to lysedblood (i.e., when the sample is already present in thetube), the points from B.3 to B.5 are particularly critical.
C. General Rules for Counting With Microbeads
Whatever microbead type and brand are used, the fol-lowing rules must be applied to ensure best assay perfor-mance. The above-described pipetting technique and cal-ibration procedures must be applied.
1. Beads are mixed with samples so that the approx-imate final concentration of 1,000 beads per microliter oforiginal sample is usually obtained.
2. Sample cell concentration must be not higher than30,000 cells per microliter and the total cell/bead eventratio should not be .10. In case sample dilution is re-quired, always use PBS supplemented with 1% BSA toensure an adequate protein content.
3. At least 1,000 bead events must be included in thesample list mode file (best 2–3,000). The relevant cellevents must not exceed more than four to five times thebead events to ensure proper statistic robustness.
4. When the total analyzed sample amount is the mea-surement endpoint (e.g., in leukoreduced blood productsanalysis), the number of acquired microbeads is a roughindicator of how much sample has been processed.
5. Ensure proper instrument setup and sample injec-tion pressure to acquire at rates not higher than 3,000–4,000 events per second. This helps to minimize eventloss for coincidence and to reduce bead peak CV.
6. Ensure that highly intense microbead fluorescencesignals are as much as possible on scale. This helps toavoid prolonged photomultiplier tube (PMT) blinding andevent loss due to PMT oversaturation (increased PMT deadtime).
7. Ensure that sheath fluid tank is over 50% full. Thisseems to increase flow stability.
8. Avoid bubble formation in any instance. Bubblescapture beads by capillarity and remove them from thesuspension.
9. Vortexing can be applied with care, provided pro-teins are present in the resuspension medium. Vortexingstart must be gradual, and the mechanical mixing must notexceed 5 s at maximum 50% of tube height. Mixing sam-ples by inversion after tube capping is also applicable.
10. During very lengthy sample runs (i.e., more than8–10 min), beads tend either to sediment or to float, thuscausing a change in the proportion of cells and beadssimultaneously aspirated. An additional mixing is there-fore warranted if the run lasts more than 8–10 min.
D. Additional Usage Tips for Beckman-CoulterFlowCount Beads
The following guidelines may be in some contrast withofficial manufacturer’s instructions.
1. Always keep the bead bottle in upright position andtightly stopped.
2. FlowCount beads completely float at the suspen-sion medium surface if the bottle is kept unperturbed formore than 12 h.
3. The first bottle opening must be preceded by a verythorough mixing and the aluminum foil seal must becompletely removed after the first mixing.
4. Mark the date of the first opening and use the bottlepreferably within 1 month.
5. The bottle must be vortexed once a day, in themorning, then gently mixed by inversion just before anyusage during the same day.
6. The same pipetting precautions described abovemust be applied to the drawing and dispensing FlowCountbeads.
7. FlowCount beads must be dispensed using exactlythe same pipette and tip type used for the primary sample.
8. After adding FlowCount to lysed sample, mix bygentle vortexing (as described above) or by inversion aftertube capping.
345ABSOLUTE CELL SUBSET COUNT

9. Analyze immediately after mixing or keep the sam-ples in melting ice in the dark until analysis.
10. Instrument setup can include FSC as the primarythreshold and trigger, provided low-volume debris andelectrical noise are appropriately gated out during acqui-sition.
11. Take into account only bead singlets. Include timeas an additional parameter to better define bead singletsand to monitor possible fluidic perturbations in the acqui-sition process. Try to keep bead singlet CV for FSC andfluorescence within 3%.
12. FlowCount beads generate end-scale fluorescencesignals when used on Becton Dickinson instruments setup for routine IF analysis. Ensure that the bead events arefully on scale in at least one fluorescence channel.
13. FlowCount beads are not excited by He-Ne red lasersin instruments equipped with dual-laser configuration.
E. Additional Usage Tips for Becton DickinsonTruCount Beads
The following guidelines may be in some contrast withofficial manufacturer’s instructions.
1. Always keep the TruCount tube bag carefully air-tight (best with adhesive tape) and use an opened bagwithin 1 month.
2. Discard tubes where bead bolus is fragmented or ifbead dust is evident.
3. Discard the entire sample if the bead bolus does notdissolve quickly and completely.
4. Ensure maximum pipetting precision when usingTruCount beads. All the measurement precisions relyon this step and it is not compensated by the dual-steppipetting (i.e., sample and bead pipetting) as with Flow-Count.
5. TruCount beads must be used with primary thresh-old and trigger on a fluorescence channel, because theyare too small to be acquired when FSC is used as athreshold parameter.
6. A fluorescence marker must be used to define atleast the relevant cell population to be analyzed.
7. TruCount beads are some 10 times less brilliantthan FlowCount beads. This implies that end-scale beadevents are usually not generated, but that some interfer-ence between cell and bead signals can occur.
8. All bead events, including doublets and multipleaggregates, must be taken into account for absolute countcalculation. This is best accomplished with a dual-fluores-cence display and a upperright corner window includingend-scale events.
9. TruCount beads tend to sediment with time.10. TruCount beads are excited also by the He-Ne red
laser.
F. Additional Tips for Volumetric Counting Systems
1. Maximum dispensing precision and accuracy mustbe applied in any step. However, the primary sampledispensing still has the major influence on overall accu-racy.
2. If a limited amount of final sample is aspirated byvolumetric instruments, verify that the relative proportionbetween primary sample and lysing is set to ensure theacquisition of the minimum positive cell events or theminimum primary sample volume.
3. Avoid inadvertent final sample dilution by spillage ofsheath fluid drops from the sample injection port.
346 BRANDO ET AL.