curcumin and liver cancer: a review
TRANSCRIPT

218 Current Pharmaceutical Biotechnology, 2012, 13, 218-228
1389-2010/12 $58.00+.00 © 2012 Bentham Science Publishers
Curcumin and Liver Cancer: A Review
Altaf S. Darvesha, Bharat B. Aggarwal
b and Anupam Bishayee
a,c,*
aCancer Therapeutics and Chemoprevention Group, Department of Pharmaceutical Sciences, College of Pharmacy,
Northeast Ohio Medical University, Rootstown, OH 44272, USA; bCytokine Research Laboratory, Department of Ex-
perimental Therapeutics, The University of Texas M.D. Anderson Cancer Center, Houston, TX 77030, USA; cDepart-
ment of Internal Medicine, College of Medicine, Northeast Ohio Medical University, Rootstown, OH 44272, USA
Abstract: Primary liver cancer, also known as hepatocellular carcinoma (HCC), is one of the most lethal cancers having
worldwide prevalence. Although most HCC cases are reported in the developing countries of Asia and Africa, there has
been an alarming increase in HCC cases in Western Europe as well as United States. Chronic liver diseases, viral hepati-
tis, alcoholism as well as dietary carcinogens, such as aflatoxins and nitrosoamines, contribute to HCC. Liver transplanta-
tion as well as surgical resection at best offer limited treatment options. Thus, there exists a critical need to investigate and
evaluate possible alternative chemopreventive and therapeutic strategies which may be effective in the control of liver
cancer. HCC, most often, develops and progresses in a milieu of oxidative stress and inflammation. Phytochemicals, such
as dietary polyphenols endowed with potent antioxidant as well as anti-inflammatory properties, provide a suitable alter-
native in affording alleviation of HCC. Curcumin, the principal polyphenolic curcuminoid, obtained from the turmeric
rhizome Curcuma longa has long been used to cure several chronic ailments, such as neoplastic and neurodegenerative
diseases. Studies suggest that curcumin may have antitumor, antioxidant, and anti-inflammatory properties. This article
reviews the effects of curcumin in preclinical in vitro and in vivo models of HCC with particular emphasis to its antioxi-
dant, apoptotic and anti-inflammatory effects as well as involvement in various molecular signaling mechanisms. This re-
view also discusses potential challenges involved in the use of curcumin in HCC, such as bioavailability, pharmacokinet-
ics, drug delivery as well as paucity of clinical studies.
Keywords: Chemoprevention, curcumin, inflammation, liver cancer, oxidative stress, therapy.
INTRODUCTION
Primary liver cancer, essentially hepatocellular carci-
noma (HCC), remains the fifth largest cause of cancer in
men and the eighth largest in women [1-3]. HCC remains the
third leading cause of cancer-related deaths worldwide with
about 700,000 deaths reported annually [4, 5]. HCC is a ma-
lignancy with extremely grim prospects and a five-year sur-
vival rate reported below 9% [6]. HCC incidence has shown
a precipitous increase worldwide especially in the develop-
ing countries of Asia, such as China, as well as sub-Saharan
Africa. An alarming increase in HCC cases has also been
reported in parts of Central and Southern Europe as well as
the North American continent [7, 8]. The past three decades
has witnessed a dramatic increase in the occurrence of hu-
man HCC in the United States. Current statistics predict ap-
proximately 25,000 new cases and 19,000 deaths due to liver
cancer in 2010 in this country [9]. Although, the majority of
HCC cases are a result of infections due to the hepatitis B
and C viruses, risk factors such as obesity, iron overload,
both alcoholic and non-alcoholic cirrhosis, as well as dietary
hepatocarcinogenes, such as aflatoxins and nitrosoamines,
have also been implicated as important key causes of HCC
[5, 10-13]. Both surgery and liver transplant offer limited
*Address correspondence to this author at the Department of Pharmaceuti-
cal and Administrative Sciences, School of Pharmacy, 1600 East Hill Street,
Signal Hill, CA 90755, USA; Tel: +562 988 2278, Ext. 2038; Fax: +562 988
1791; E-mail: [email protected]
treatment options for HCC. Several factors, such as tumor
size, multifocality along with vascular invasion limit the
option of surgical resection in only about 20% of HCC pa-
tients. The recurrence rates of post-surgery HCC are also as
high as 50% [14]. Although, liver transplantation is useful in
treatment of early-stage HCC, it is available only to a small
number of HCC patients primarily due to scarcity of donor
organs. The effectiveness of the transplant option is also se-
verely limited due to the swift and frequent reappearance of
HCC in the transplanted liver [11, 15]. Several alternative
treatment approaches, such as Yttrium-90 intra-arterial de-
livery as microspheres, arterial chemoembolization, micro-
wave coagulation, intra-tumor ethanol injection as well as
radiofrequency ablation, have limited usefulness, being ap-
plicable only to patients with localized liver tumors [11, 16-
20]. Sorafenib, a vascular endothelial growth factor receptor
and tyrosine kinase inhibitor, is currently approved in the
United States for the treatment of unresectable HCC.
Although sorafenib has been shown to prolong the medial
survival time by almost three months in patients with ad-
vanced HCC, its therapeutic usefulness is limited due to se-
vere adverse effects including a considerable risk of hemor-
rhage [21, 22] as well as unprecedented high cost [23]. In
view of the aforementioned limitations of the current treat-
ment options available for HCC, novel approaches, espe-
cially chemoprevention, has been suggested as the para-
mount approach in lowering the occurrence and mortality
associated with HCC [24, 25].
Curcumin and Liver Cancer Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 219
Primary liver cancer occurs in the milieu of oxidative
stress and inflammation (reviewed in ref. [26]). Hepatic in-
flammation, resulting from hepatropic viral infections,
chronic hepatitis, cirrhosis, as well as exposure to toxic hepa-
tocarcinogens, represents an early malignant step with the
consequent epigenetic events occurring as a consequence of
a protracted inflammatory response. Considerable evidence,
accumulated over the past several years, implicates inflam-
mation-driven processes such as production of cytokines,
chemokines, as well as both reactive oxygen and nitrogen
species which contribute to the process of hepatocarcino-
genesis [27-31]. Oxidative stress, due to environmental in-
sults including hepatotoxicants, generates reactive oxygen
species such as superoxide anion and the hydroxyl radical
and is a predisposing factor to hepatocarcinogenesis [32-34].
Besides the involvement of the oxidative stress and the in-
flammatory cascade, various molecular and signaling
mechanisms have been proposed in the pathogenesis of HCC
[35, 36].
Phytochemicals, obtained from both dietary and non-
dietary sources, have shown potential usefulness as therapeu-
tic as well as chemopreventive agents for several chronic
maladies such as cardiovascular, metabolic, neoplastic and
neurodegenerative diseases [37-44]. Dietary components,
present in fruits, vegetables, nuts and spices, have demon-
strated significant potential in their ability to suppress car-
cinogenesis in pre-clinical models and prevent and delay the
occurrence of cancer in high-risk populations [45-48]. Of
particular interest are a multitude of polyphenolic com-
pounds found in the aforementioned dietary resources. Die-
tary polyphenols, such as anthocyanidins obtained from ber-
ries, catechins present in green tea, curcumin in turmeric,
ellagic acid present in pomegranates, lycopene found in to-
matoes, resveratrol in peanuts, grapes and red wine, quer-
cetin present in apples and red onions and many others, have
shown considerable promise as both preventive and thera-
peutic agents in cancer affecting several organ systems such
as breast, liver, lung, prostate and skin [40, 47, 49-51]. Poly-
phenolic compounds exert anticarcinogenic effects primarily
due to their antioxidant and anti-inflammatory properties as
well as their ability to modulate diverse molecular signaling
mechanisms implicated in carcinogenesis [45, 52-55]. Glau-
ert et al. [56] have recently reviewed the preventive potential
of dietary antioxidants such as vitamin C, vitamin E, sele-
nium as well as several phytochemicals in preclinical animal
models of HCC as well as human studies. Mann and col-
leagues [57] have also documented the promising chemopre-
ventive and therapeutic properties of several phytochemicals,
including dietary polyphenols in hepatocarcinogenesis. In
this article, we review the potential role of curcumin as a
chemopreventive and therapeutic agent for HCC.
CURCUMIN
Turmeric (Curcuma longa), also known as Indian saffron
is a rhizomatous herbaceous plant of the ginger family,
Zingiberaceae, native to the Indian sub-continent, Southeast
Asia as well as several other tropical countries. The dried
rhizome is ground to yield a yellow powder, also known as
yellow ginger, yellow root or natural yellow, and is widely
used as a spice in ethnic South and Southeast Asian cuisine
[58]. India, the major producer of turmeric, consumes about
90% of it with the remainder exported to be utilized by the
food industry as additive, preservative, flavoring and color-
ing agent [59]. Turmeric has customarily been used in tradi-
tional Ayurvedic medicine, primarily in South Asia, for
thousands of years as an antiseptic, antibacterial, antiin-
flammatory agent in the treatment of infections, respiratory
ailments, swelling and rheumatism [60-64]. Turmeric has
also been attributed with antiarthritic, anticarcinogenic, an-
tilipidogenic, cardioprotective, hepatoprotective, hypogly-
cemic and thrombosuppressive properties [65-70]. Polyphe-
nolic, yellow-colored curcuminoids are the primary chemical
constituents present in turmeric. Along with curcumin (cur-
cumin I), the principal curcuminoid, three other curcumi-
noids, namely demethoxycurcumin (curcumin II), bisde-
methoxycurcumin (curcumin III) and the recently identified
cyclocurcumin are present in turmeric. Commercial curcu-
min is a mixture of curcuminoids containing approximately
77% curcumin, 18% demethoxycurcumin and 5% bisde-
methoxycurcumin [58, 68, 69, 71].
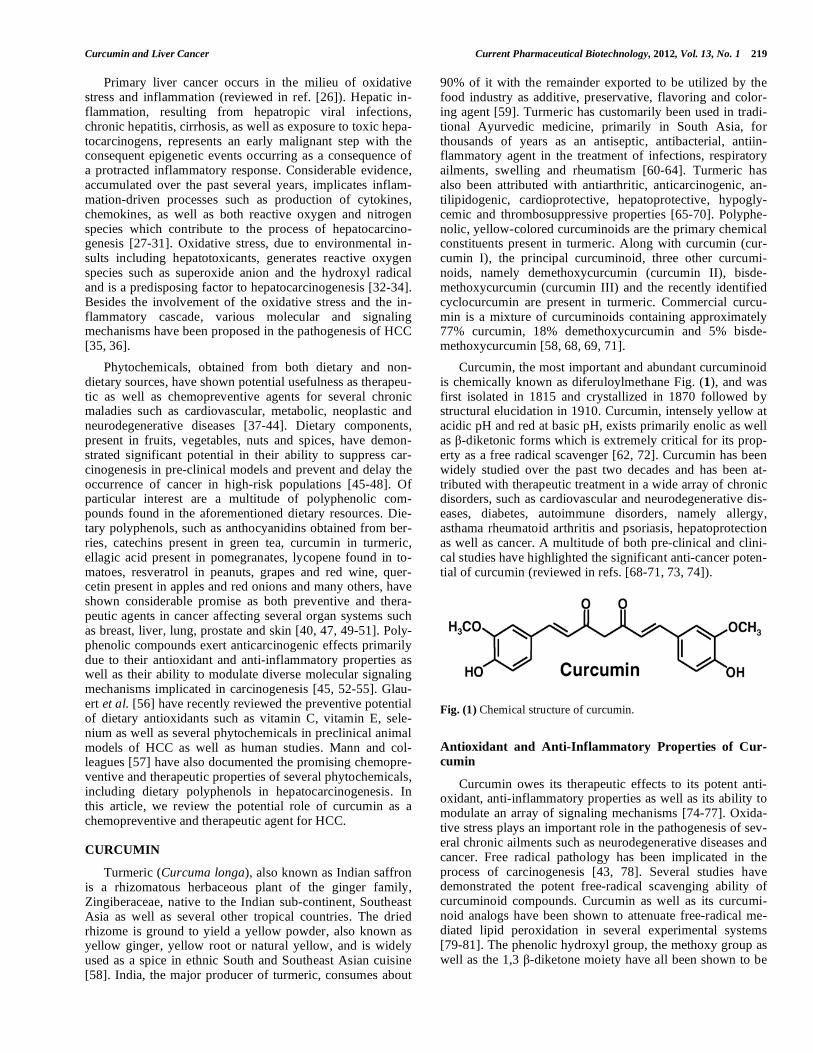
Curcumin, the most important and abundant curcuminoid
is chemically known as diferuloylmethane Fig. (1), and was
first isolated in 1815 and crystallized in 1870 followed by
structural elucidation in 1910. Curcumin, intensely yellow at
acidic pH and red at basic pH, exists primarily enolic as well
as -diketonic forms which is extremely critical for its prop-
erty as a free radical scavenger [62, 72]. Curcumin has been
widely studied over the past two decades and has been at-
tributed with therapeutic treatment in a wide array of chronic
disorders, such as cardiovascular and neurodegenerative dis-
eases, diabetes, autoimmune disorders, namely allergy,
asthama rheumatoid arthritis and psoriasis, hepatoprotection
as well as cancer. A multitude of both pre-clinical and clini-
cal studies have highlighted the significant anti-cancer poten-
tial of curcumin (reviewed in refs. [68-71, 73, 74]).
Fig. (1) Chemical structure of curcumin.
Antioxidant and Anti-Inflammatory Properties of Cur-
cumin
Curcumin owes its therapeutic effects to its potent anti-
oxidant, anti-inflammatory properties as well as its ability to
modulate an array of signaling mechanisms [74-77]. Oxida-
tive stress plays an important role in the pathogenesis of sev-
eral chronic ailments such as neurodegenerative diseases and
cancer. Free radical pathology has been implicated in the
process of carcinogenesis [43, 78]. Several studies have
demonstrated the potent free-radical scavenging ability of
curcuminoid compounds. Curcumin as well as its curcumi-
noid analogs have been shown to attenuate free-radical me-
diated lipid peroxidation in several experimental systems
[79-81]. The phenolic hydroxyl group, the methoxy group as
well as the 1,3 -diketone moiety have all been shown to be

220 Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 Darvesh et al.
important structural features in the antioxidant properties of
curcuminoids [82].
The inflammatory cascade has been held as a key media-
tor of the pathogenesis of several chronic illnesses such as
autoimmune, cardiovascular, neurodegenerative as well as
neoplastic diseases [83-86]. Kundu and Surh [30] in their
elegant review discuss the critical and multifaceted role of
inflammation in carcinogenesis. Curcumin has been shown
to possess potent antiinflammatory properties which contrib-
ute to its therapeutic effects in the aforementioned illnesses
[73, 87, 88]. Pioneering research by the Aggarwal laboratory
has highlighted the powerful anti-inflammatory properties of
curcumin [73, 89, 90]. One of the key findings to emerge
almost a decade ago is the curcumin-mediated suppression of
nuclear factor- B (NF- B), the master switch in the inflam-
matory cascade [91]. NF- B activation is known to regulate
several key inflammatory mediators such as cytokines,
chemokines and kinases, which have been shown to play a
critical role in the pathogenesis of most chronic illnesses [85,
92, 93]. The curcumin-mediated attenuation of the NF- B
activated inflammatory cascade is an extremely critical
mechanism of its widespread therapeutic profile [94]. Sev-
eral investigators have delineated the mechanisms involved
in curcumin-mediated attenuation of NF- B expression and
the NF- B gene products which suppress apoptosis and me-
diate cell proliferation, invasion and angiogenesis [95-99].
Curcumin treatment also leads to suppression of several in-
flammatory cytokines such as interleukin (IL)-1, IL-1 , IL-6,
IL-8, chemokines as well as tumor necrosis factor- and cy-
clooxygenases [95, 100-102]. Curcumin also affects a pleth-
ora of signaling mechanisms implicated in process of car-
cinogenesis. Curcumin interacts with multiple cell signaling
proteins such as transcriptional factors, protein kinases, cy-
tokine signaling receptors, growth factors, adhesion mole-
cules as well as anti-apoptotic proteins. The aforementioned
molecular effects of curcumin lead to inhibition of cell pro-
liferation, cell invasion and apoptosis causing suppression of
metastasis (reviewed in ref. [75]).
Pharmacokinetics and Bioavailability of Curcumin
The pharmacokinetic profile of curcumin has been a sub-
ject of detailed investigation over the past few decades [103-
107]. Studies reveal poor absorption and rapid metabolism to
form glucoronoid conjugates which result in limited
bioavailability of curcumin. The Aggarwal laboratory has
contributed several excellent articles which review the phar-
macokinetics and bioavailability of curcumin [68, 69, 73, 76,
108]. Several strategies have been utilized to enhance the
poor bioavailability of curcumin. Shoba and colleagues [109]
demonstrated that co-administration of piperine, a hepatic
and intestinal inhibitor of glucoronidation, significantly en-
hanced curcumin bioavailability. Use of nanoparticle tech-
nology, liposomal formulations, phosphotidylcholine and
cyclodextrin complexes, as well as synthetic analogs of cur-
cumin resulted in superior bioavailability [110-116]. Several
recent studies have investigated the potential anti-cancer
properties of synthetic curcumin derivatives. John and co-
workers [117] demonstrated the enhanced cytotoxic and anti-
tumor activity of four synthetic curcuminoids as well as their
copper complexes. In a recent study, Padhye et al. [118]
showed that novel difluoro Knoevenagel curcumin conden-
sates, their Schiff bases as well as copper complexes causes
both growth inhibition and induction of apoptosis in colon
and pancreatic cancer cell lines. Salicyl curcumin inhibited
tumor specific angiogenesis in C57BL/6 mice injected with
B16F-10 melanoma cells [119].
Several clinical trials conducted over the past several
years, as well as currently ongoing, have studied the chemo-
preventive and therapeutic effects of curcumin in cancer of
various organ systems such as colon, gall bladder, liver, pan-
creas, as well as the gastrointestinal tract. Although trial re-
sults remain encouraging, there exists a critical need to criti-
cally evaluate the clinical effects of curcumin. Several inves-
tigators are of the opinion that encouraging in vitro as well as
in vivo pre-clinical data has not been reflected in the clinical
results in curcumin studies essentially due to poor bioavail-
ability. Hence, it is important to utilize the various aforemen-
tioned novel drug delivery systems to enhance curcumin’s
bioavailability, which may result in improved clinical thera-
peutic effects [68, 76, 120].
Toxicity Studies
Curcumin is an extremely well tolerated, bioactive and
nontoxic evident from it being an integral component of the
South Asian diet for thousands of years [68, 121, 122].
However, it has been opined that the high doses administered
in clinical trials remain a cause for potential concern since
the genotoxic and long-term effects of curcumin administra-
tion have not been systematically investigated [123]. Also,
there exist rare anecdotal reports of curcumin-induced ad-
verse effects. Curcumin-induced allergic contact dermatitis
and urticaria has also been reported in humans [124-126].
Role of Synergy
The role of synergy in the chemopreventive and thera-
peutic effects of dietary polyphenols has been a subject of
recent investigation [127-130]. Besides curcumin, turmeric
also contains three known curcuminoids. Sandur and co-
workers [131] have systematically evaluated the antioxidant,
antiinflammatory and antiproliferative effects of curcumin as
well as other curcuminoids. Although, curcumin displayed
higher activity than the other curcuminoids, the combination
of all the curcuminoids was more potent than any individual
curcuminoid, including curcumin, indicating a role of syn-
ergy in the pharmacological effects of curcuminoids.
CURCUMIN AND LIVER CANCER: IN VITRO STUD-
IES
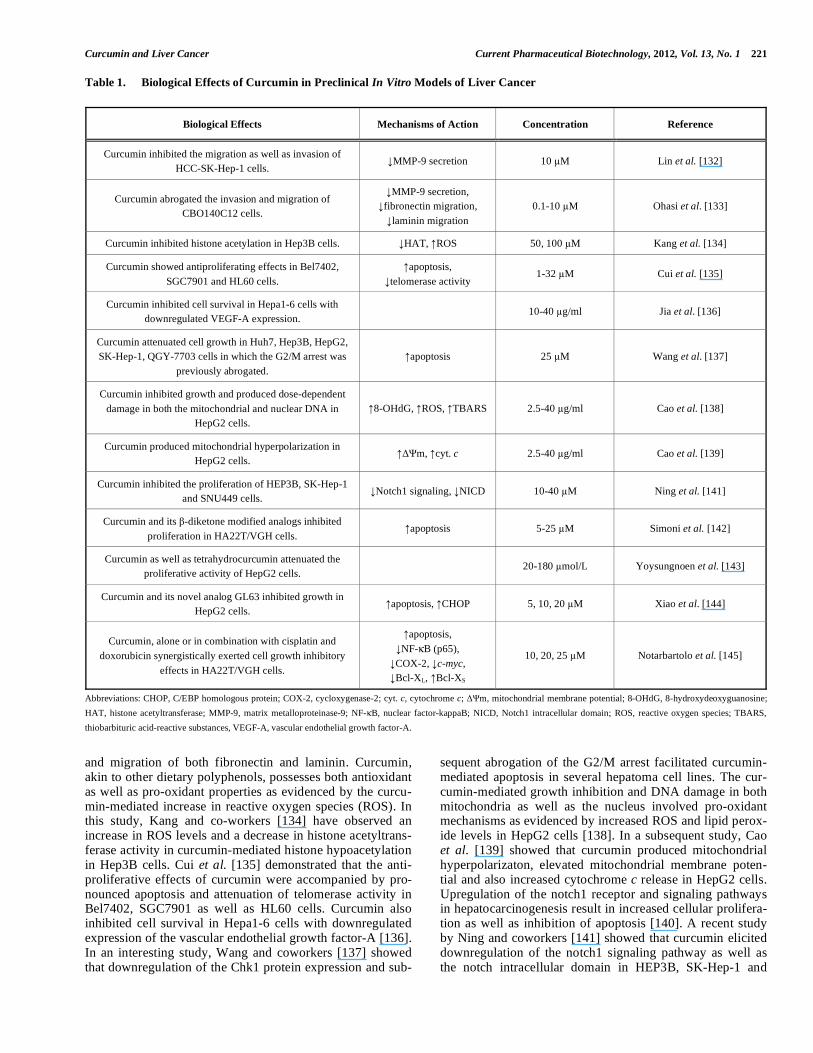
Numerous studies, over the past several years, have
evaluated the effects of curcumin and its analogs in several
rodent as well as human hepatoma cells. In one of the initial
studies, Lin et al. [132] showed that curcumin decreased the
secretion of matrix metalloproteinase-9 (MMP-9) and conse-
quently inhibited both the migration as well as invasion of
SK-Hep-1 cells (Table 1). The anti-invasive and anti-
migratory effects of curcumin have also been shown in
CBO140C12 cells. In this study, Ohasi and colleagues [133]
showed that curcumin-mediated decrease in MMP-9 secretion
was accompanied by a significant inhibition of the adhesion
Curcumin and Liver Cancer Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 221
Table 1. Biological Effects of Curcumin in Preclinical In Vitro Models of Liver Cancer
Biological Effects Mechanisms of Action Concentration Reference
Curcumin inhibited the migration as well as invasion of
HCC-SK-Hep-1 cells. MMP-9 secretion 10 M Lin et al. [132]
Curcumin abrogated the invasion and migration of
CBO140C12 cells.
MMP-9 secretion,
fibronectin migration,
laminin migration
0.1-10 M Ohasi et al. [133]
Curcumin inhibited histone acetylation in Hep3B cells. HAT, ROS 50, 100 M Kang et al. [134]
Curcumin showed antiproliferating effects in Bel7402,
SGC7901 and HL60 cells.
apoptosis,
telomerase activity 1-32 M Cui et al. [135]
Curcumin inhibited cell survival in Hepa1-6 cells with
downregulated VEGF-A expression. 10-40 g/ml Jia et al. [136]
Curcumin attenuated cell growth in Huh7, Hep3B, HepG2,
SK-Hep-1, QGY-7703 cells in which the G2/M arrest was
previously abrogated.
apoptosis 25 M Wang et al. [137]
Curcumin inhibited growth and produced dose-dependent
damage in both the mitochondrial and nuclear DNA in
HepG2 cells.
8-OHdG, ROS, TBARS 2.5-40 g/ml Cao et al. [138]
Curcumin produced mitochondrial hyperpolarization in
HepG2 cells. m, cyt. c 2.5-40 g/ml Cao et al. [139]
Curcumin inhibited the proliferation of HEP3B, SK-Hep-1
and SNU449 cells. Notch1 signaling, NICD 10-40 M Ning et al. [141]
Curcumin and its -diketone modified analogs inhibited
proliferation in HA22T/VGH cells. apoptosis 5-25 M Simoni et al. [142]
Curcumin as well as tetrahydrocurcumin attenuated the
proliferative activity of HepG2 cells. 20-180 mol/L Yoysungnoen et al. [143]
Curcumin and its novel analog GL63 inhibited growth in
HepG2 cells. apoptosis, CHOP 5, 10, 20 M Xiao et al. [144]
Curcumin, alone or in combination with cisplatin and
doxorubicin synergistically exerted cell growth inhibitory
effects in HA22T/VGH cells.
apoptosis,
NF- B (p65),
COX-2, c-myc,
Bcl-XL, Bcl-XS
10, 20, 25 M Notarbartolo et al. [145]
Abbreviations: CHOP, C/EBP homologous protein; COX-2, cycloxygenase-2; cyt. c, cytochrome c; m, mitochondrial membrane potential; 8-OHdG, 8-hydroxydeoxyguanosine;
HAT, histone acetyltransferase; MMP-9, matrix metalloproteinase-9; NF- B, nuclear factor-kappaB; NICD, Notch1 intracellular domain; ROS, reactive oxygen species; TBARS,
thiobarbituric acid-reactive substances, VEGF-A, vascular endothelial growth factor-A.
and migration of both fibronectin and laminin. Curcumin,
akin to other dietary polyphenols, possesses both antioxidant
as well as pro-oxidant properties as evidenced by the curcu-
min-mediated increase in reactive oxygen species (ROS). In
this study, Kang and co-workers [134] have observed an
increase in ROS levels and a decrease in histone acetyltrans-
ferase activity in curcumin-mediated histone hypoacetylation
in Hep3B cells. Cui et al. [135] demonstrated that the anti-
proliferative effects of curcumin were accompanied by pro-
nounced apoptosis and attenuation of telomerase activity in
Bel7402, SGC7901 as well as HL60 cells. Curcumin also
inhibited cell survival in Hepa1-6 cells with downregulated
expression of the vascular endothelial growth factor-A [136].
In an interesting study, Wang and coworkers [137] showed
that downregulation of the Chk1 protein expression and sub-
sequent abrogation of the G2/M arrest facilitated curcumin-
mediated apoptosis in several hepatoma cell lines. The cur-
cumin-mediated growth inhibition and DNA damage in both
mitochondria as well as the nucleus involved pro-oxidant
mechanisms as evidenced by increased ROS and lipid perox-
ide levels in HepG2 cells [138]. In a subsequent study, Cao
et al. [139] showed that curcumin produced mitochondrial
hyperpolarizaton, elevated mitochondrial membrane poten-
tial and also increased cytochrome c release in HepG2 cells.
Upregulation of the notch1 receptor and signaling pathways
in hepatocarcinogenesis result in increased cellular prolifera-
tion as well as inhibition of apoptosis [140]. A recent study
by Ning and coworkers [141] showed that curcumin elicited
downregulation of the notch1 signaling pathway as well as
the notch intracellular domain in HEP3B, SK-Hep-1 and

222 Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 Darvesh et al.
SNU449 cells. Curcumin as well as its analogs have shown
anti-proliferative effects in various hepatoma cells [142-
144]. Simoni and colleagues [142] showed that curcumin and
its -diketone modified analogs stimulated apoptosis and
produced antiproliferative activity in HA22T/ VGH cells.
Tetrahydrocurcumin showed comparable results to curcumin
with regards to the attenuation of the proliferative activity of
HepG2 cells [143]. In an equivalent study, curcumin as well
as its novel analog GL63 produced an inhibitory effect on
HepG2 cells. The inhibitory effect was accompanied by in-
creased apoptosis and enhanced expression of C/EBP ho-
mologous protein, a pro-apoptotic activating protein [144].
The effects of curcumin in combination with standard che-
motherapeutic agents have also been investigated. In an in-
teresting study, Notarbartalo and colleagues [145] showed
that curcumin when combined with cisplatin and doxorubicin
caused a synergistic cell growth inhibition in HA22T/VGH
cells. The aforementioned effect was accompanied by an
increase in apoptosis and a decrease in NF- B activation as
well as a lowering of COX-2 levels.
CURCUMIN AND LIVER CANCER: IN VIVO STUD-
IES
The effects of curcumin and its analogous compounds
have been a subject of considerable investigation over more
than the past decade in several chemically-induced as well as
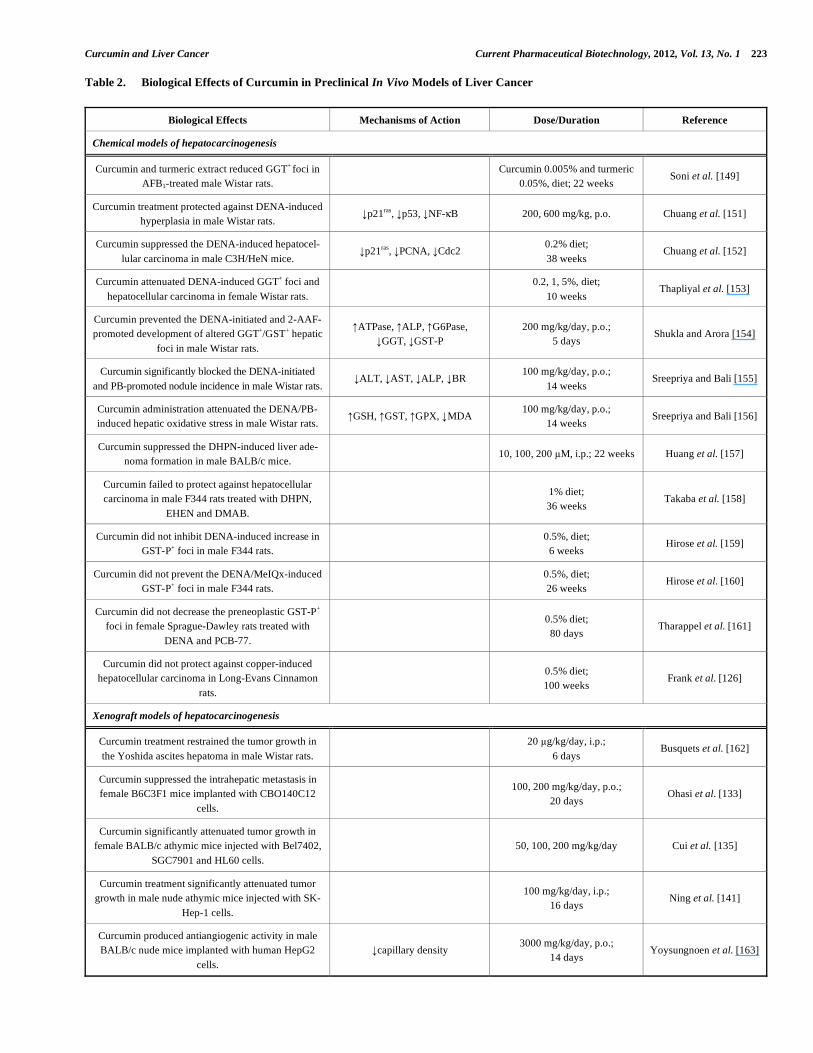
xenograft preclinical rodent models of HCC. These studies
document the potential role of curcumin as well as its ana-
logs in the prevention and treatment of HCC (Table 2).
Chemical Models of Hepatocarcinogenesis
Chemically-induced HCC remains one of the most exten-
sively used methods both of the study of the biological
mechanisms of HCC as well as the elucidation of the che-
mopreventive and therapeutic effects of potential anti-cancer
agents [146-148]. In one of the earliest studies, Soni and
colleagues [149] demonstrated that curcumin as well as tur-
meric extract reduced the number of gamma glutamyl
transpeptidase-positive foci in rats challenged with aflatoxin
B1. Nitrosoamines in general and diethylnitrosoamine
(DENA) in particular, either used alone or in presence of a
promoter such as phenobarbital (PB) have been a corner-
stone of pre-clinical liver cancer research [146, 147, 150].
Several studies have investigated the pharmacological effects
of curcumin and its analogs in DENA-induced HCC. Chuang
et al. [152, 153] have shown that curcumin protected against
DENA-induced hyperplasia and HCC in rodents. The
authors of the aforementioned studies also investigated the
underlying biochemical mechanisms of curcumin in DENA-
treated rodents. Curcumin strongly inhibited the DENA-
induced increase in the expression of the oncogenic p21ras
and tumor suppressor p53 protein as well as the elevated
levels of proliferating cell nuclear antigen as well as NF- B.
Thapliyal and coworkers [153] have also documented the
attenuation of DENA-induced hepatocarcinogenesis in rats
by dietary curcumin. The suppressive effects of curcumin in
the DENA-initiated and 2-acetylaminofluorene-promoted
alteration of hepatic foci in rats was accompanied by the
restoration of the normal levels of several hepatic metabolic
enzymes [154]. Sreepriya and Bali [155, 156] utilized the
well-characterized DENA-initiated and PB-promoted two-
stage model to investigate the potential anti-hepatocarcino-
genic properties of curcumin. In these studies, curcumin ad-
ministration prevented hepatocellular carcinogenesis in rats.
The investigators also reported that curcumin normalized the
elevated levels of several enzymes of liver function and bili-
rubin, increased glutathione content, elevated antioxidant
enzymes and attenuated lipid peroxidation. Curcumin has
also been shown to suppress the formation of hepatic ade-
nomas in mice treated with, 2,2'-dihydroxy-di-n-propylnitro-
samine (DHPN) [157].
In addition to aforementioned positive reports, several
studies have documented the failure of curcumin in protect-
ing against chemical hepatocarcinogenesis in rodents. Using
a multi-organ hepatocarcinogenesis rat model Takaba and
colleagues [158] reported the inability of curcumin to pre-
vent HCC in rats treated with DNPN, N-ethyl-N-hydroxy-
ethylnitrosamine and 3, 2'-methyl-4-aminobiphenyl. Curcu-
min also failed to attenuate both the DENA-induced increase
in formation of glutathione S-transferase (GST)-positive foci
as well as the DENA/2-amino-3,8-dimethylimidazo[4,5-f] quinoxaline-induced hepatocarcinogenesis in rats [159, 160].
Curcumin treatment did not prevent the GST-positive foci
formation in rats treated with DENA and 3,3',4,4'-tetrachlo-
robiphenyl [161]. In an interesting study, chronic curcumin
administration did not prevent the copper-induced HCC in
rats [126]. A common feature of the aforementioned studies
which document the inability of curcumin to protect against
chemically-induced hepatocarcinogenesis is the administra-
tion of a relatively low dose of dietary curcumin which may
lead to its pro-oxidant effects. A low dietary dose may also
offer limited bioavailability of curcumin.
Xenograft Models of Hepatocarcinogenesis
A few investigators have studied the therapeutic effects
of curcumin in xenograft models of hepatocarcinogenesis.
Busquets et al. [162], demonstrated that curcumin treatment
blocked tumor growth in the Yoshida ascites hepatoma in
rats. Curcumin also suppressed the intrahepatic metastasis in
female mice implanted with CBO140C12 cells [132]. Subse-
quent studies have also demonstrated the curcumin-mediated
tumor inhibition in mice xenografted with several hepatoma
cells [135, 141]. Although the aforementioned xenograft
studies highlight the protective role of curcumin, the investi-
gators do not provide any mechanistic explanation to curcu-
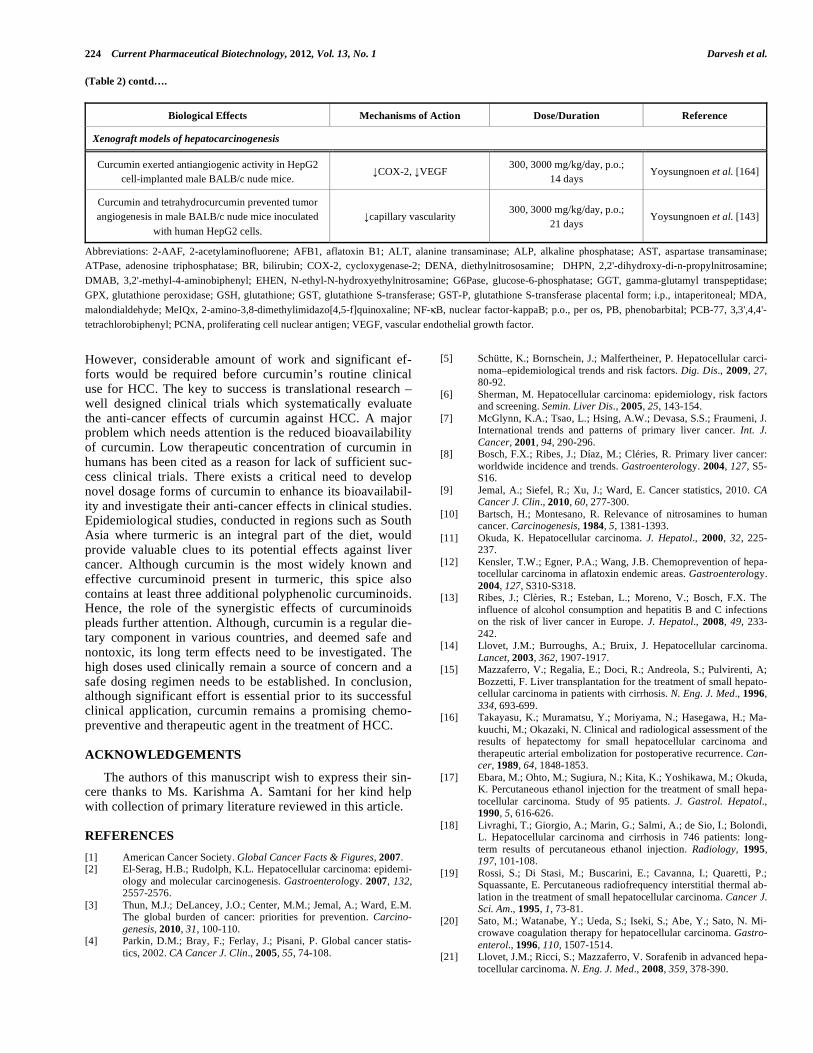
min’s anti-tumor properties. Yoysungnoen and colleagues
[143, 163, 164] in a series of studies document the signifi-
cant antiangiogenic property of curcumin and its analog in
nude mice implanted with human HepG2 cells. Curcumin
treatment decreased both capillary density and vascularity
and also decreased expression of the pro-angiogenic vascular
endothelial growth factor.
CONCLUSION
The essential premise for the potential use of curcumin as
a chemopreventive and therapeutic agent in HCC rests on its
potent antioxidant and anti-inflammatory properties as well
as its ability to modulate a multitude of signaling mecha-
nisms. It is clearly evident from the in vitro as well as in vivo
pre-clinical models that curcumin, along with other curcumi-
noids, hold great promise as curative agents for HCC.
Curcumin and Liver Cancer Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 223
Table 2. Biological Effects of Curcumin in Preclinical In Vivo Models of Liver Cancer
Biological Effects Mechanisms of Action Dose/Duration Reference
Chemical models of hepatocarcinogenesis
Curcumin and turmeric extract reduced GGT+ foci in
AFB1-treated male Wistar rats.
Curcumin 0.005% and turmeric
0.05%, diet; 22 weeks Soni et al. [149]
Curcumin treatment protected against DENA-induced
hyperplasia in male Wistar rats. p21
ras, p53, NF- B 200, 600 mg/kg, p.o. Chuang et al. [151]
Curcumin suppressed the DENA-induced hepatocel-
lular carcinoma in male C3H/HeN mice. p21
ras, PCNA, Cdc2
0.2% diet;
38 weeks Chuang et al. [152]
Curcumin attenuated DENA-induced GGT+ foci and
hepatocellular carcinoma in female Wistar rats.
0.2, 1, 5%, diet;
10 weeks Thapliyal et al. [153]
Curcumin prevented the DENA-initiated and 2-AAF-
promoted development of altered GGT+/GST
+ hepatic
foci in male Wistar rats.
ATPase, ALP, G6Pase,
GGT, GST-P
200 mg/kg/day, p.o.;
5 days Shukla and Arora [154]
Curcumin significantly blocked the DENA-initiated
and PB-promoted nodule incidence in male Wistar rats. ALT, AST, ALP, BR
100 mg/kg/day, p.o.;
14 weeks Sreepriya and Bali [155]
Curcumin administration attenuated the DENA/PB-
induced hepatic oxidative stress in male Wistar rats. GSH, GST, GPX, MDA
100 mg/kg/day, p.o.;
14 weeks Sreepriya and Bali [156]
Curcumin suppressed the DHPN-induced liver ade-
noma formation in male BALB/c mice. 10, 100, 200 M, i.p.; 22 weeks Huang et al. [157]
Curcumin failed to protect against hepatocellular
carcinoma in male F344 rats treated with DHPN,
EHEN and DMAB.
1% diet;
36 weeks Takaba et al. [158]
Curcumin did not inhibit DENA-induced increase in
GST-P+ foci in male F344 rats.
0.5%, diet;
6 weeks Hirose et al. [159]
Curcumin did not prevent the DENA/MeIQx-induced
GST-P+ foci in male F344 rats.
0.5%, diet;
26 weeks Hirose et al. [160]
Curcumin did not decrease the preneoplastic GST-P+
foci in female Sprague-Dawley rats treated with
DENA and PCB-77.
0.5% diet;
80 days Tharappel et al. [161]
Curcumin did not protect against copper-induced
hepatocellular carcinoma in Long-Evans Cinnamon
rats.
0.5% diet;
100 weeks Frank et al. [126]
Xenograft models of hepatocarcinogenesis
Curcumin treatment restrained the tumor growth in
the Yoshida ascites hepatoma in male Wistar rats.
20 g/kg/day, i.p.;
6 days Busquets et al. [162]
Curcumin suppressed the intrahepatic metastasis in
female B6C3F1 mice implanted with CBO140C12
cells.
100, 200 mg/kg/day, p.o.;
20 days Ohasi et al. [133]
Curcumin significantly attenuated tumor growth in
female BALB/c athymic mice injected with Bel7402,
SGC7901 and HL60 cells.
50, 100, 200 mg/kg/day Cui et al. [135]
Curcumin treatment significantly attenuated tumor
growth in male nude athymic mice injected with SK-
Hep-1 cells.
100 mg/kg/day, i.p.;
16 days Ning et al. [141]
Curcumin produced antiangiogenic activity in male
BALB/c nude mice implanted with human HepG2
cells.
capillary density 3000 mg/kg/day, p.o.;
14 days Yoysungnoen et al. [163]
224 Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 Darvesh et al.
(Table 2) contd….
Biological Effects Mechanisms of Action Dose/Duration Reference
Xenograft models of hepatocarcinogenesis
Curcumin exerted antiangiogenic activity in HepG2
cell-implanted male BALB/c nude mice. COX-2, VEGF
300, 3000 mg/kg/day, p.o.;
14 days Yoysungnoen et al. [164]
Curcumin and tetrahydrocurcumin prevented tumor
angiogenesis in male BALB/c nude mice inoculated
with human HepG2 cells.
capillary vascularity 300, 3000 mg/kg/day, p.o.;
21 days Yoysungnoen et al. [143]
Abbreviations: 2-AAF, 2-acetylaminofluorene; AFB1, aflatoxin B1; ALT, alanine transaminase; ALP, alkaline phosphatase; AST, aspartase transaminase;
ATPase, adenosine triphosphatase; BR, bilirubin; COX-2, cycloxygenase-2; DENA, diethylnitrososamine; DHPN, 2,2'-dihydroxy-di-n-propylnitrosamine;
DMAB, 3,2'-methyl-4-aminobiphenyl; EHEN, N-ethyl-N-hydroxyethylnitrosamine; G6Pase, glucose-6-phosphatase; GGT, gamma-glutamyl transpeptidase;
GPX, glutathione peroxidase; GSH, glutathione; GST, glutathione S-transferase; GST-P, glutathione S-transferase placental form; i.p., intaperitoneal; MDA,
malondialdehyde; MeIQx, 2-amino-3,8-dimethylimidazo[4,5-f]quinoxaline; NF- B, nuclear factor-kappaB; p.o., per os, PB, phenobarbital; PCB-77, 3,3',4,4'-
tetrachlorobiphenyl; PCNA, proliferating cell nuclear antigen; VEGF, vascular endothelial growth factor.
However, considerable amount of work and significant ef-
forts would be required before curcumin’s routine clinical
use for HCC. The key to success is translational research –
well designed clinical trials which systematically evaluate
the anti-cancer effects of curcumin against HCC. A major
problem which needs attention is the reduced bioavailability
of curcumin. Low therapeutic concentration of curcumin in
humans has been cited as a reason for lack of sufficient suc-
cess clinical trials. There exists a critical need to develop
novel dosage forms of curcumin to enhance its bioavailabil-
ity and investigate their anti-cancer effects in clinical studies.
Epidemiological studies, conducted in regions such as South
Asia where turmeric is an integral part of the diet, would
provide valuable clues to its potential effects against liver
cancer. Although curcumin is the most widely known and
effective curcuminoid present in turmeric, this spice also
contains at least three additional polyphenolic curcuminoids.
Hence, the role of the synergistic effects of curcuminoids
pleads further attention. Although, curcumin is a regular die-
tary component in various countries, and deemed safe and
nontoxic, its long term effects need to be investigated. The
high doses used clinically remain a source of concern and a
safe dosing regimen needs to be established. In conclusion,
although significant effort is essential prior to its successful
clinical application, curcumin remains a promising chemo-
preventive and therapeutic agent in the treatment of HCC.
ACKNOWLEDGEMENTS
The authors of this manuscript wish to express their sin-
cere thanks to Ms. Karishma A. Samtani for her kind help
with collection of primary literature reviewed in this article.
REFERENCES
[1] American Cancer Society. Global Cancer Facts & Figures, 2007.
[2] El-Serag, H.B.; Rudolph, K.L. Hepatocellular carcinoma: epidemi-
ology and molecular carcinogenesis. Gastroenterology. 2007, 132,
2557-2576.
[3] Thun, M.J.; DeLancey, J.O.; Center, M.M.; Jemal, A.; Ward, E.M.
The global burden of cancer: priorities for prevention. Carcino-
genesis, 2010, 31, 100-110.
[4] Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statis-
tics, 2002. CA Cancer J. Clin., 2005, 55, 74-108.
[5] Schütte, K.; Bornschein, J.; Malfertheiner, P. Hepatocellular carci-
noma–epidemiological trends and risk factors. Dig. Dis., 2009, 27,
80-92.
[6] Sherman, M. Hepatocellular carcinoma: epidemiology, risk factors
and screening. Semin. Liver Dis., 2005, 25, 143-154.
[7] McGlynn, K.A.; Tsao, L.; Hsing, A.W.; Devasa, S.S.; Fraumeni, J.
International trends and patterns of primary liver cancer. Int. J.
Cancer, 2001, 94, 290-296.
[8] Bosch, F.X.; Ribes, J.; Díaz, M.; Cléries, R. Primary liver cancer:
worldwide incidence and trends. Gastroenterology. 2004, 127, S5-
S16.
[9] Jemal, A.; Siefel, R.; Xu, J.; Ward, E. Cancer statistics, 2010. CA Cancer J. Clin., 2010, 60, 277-300.
[10] Bartsch, H.; Montesano, R. Relevance of nitrosamines to human
cancer. Carcinogenesis, 1984, 5, 1381-1393.
[11] Okuda, K. Hepatocellular carcinoma. J. Hepatol., 2000, 32, 225-
237.
[12] Kensler, T.W.; Egner, P.A.; Wang, J.B. Chemoprevention of hepa-
tocellular carcinoma in aflatoxin endemic areas. Gastroenterology.
2004, 127, S310-S318.
[13] Ribes, J.; Clèries, R.; Esteban, L.; Moreno, V.; Bosch, F.X. The
influence of alcohol consumption and hepatitis B and C infections
on the risk of liver cancer in Europe. J. Hepatol., 2008, 49, 233-
242.
[14] Llovet, J.M.; Burroughs, A.; Bruix, J. Hepatocellular carcinoma.
Lancet, 2003, 362, 1907-1917.
[15] Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A;
Bozzetti, F. Liver transplantation for the treatment of small hepato-
cellular carcinoma in patients with cirrhosis. N. Eng. J. Med., 1996,
334, 693-699.
[16] Takayasu, K.; Muramatsu, Y.; Moriyama, N.; Hasegawa, H.; Ma-
kuuchi, M.; Okazaki, N. Clinical and radiological assessment of the
results of hepatectomy for small hepatocellular carcinoma and
therapeutic arterial embolization for postoperative recurrence. Can-cer, 1989, 64, 1848-1853.
[17] Ebara, M.; Ohto, M.; Sugiura, N.; Kita, K.; Yoshikawa, M.; Okuda,
K. Percutaneous ethanol injection for the treatment of small hepa-
tocellular carcinoma. Study of 95 patients. J. Gastrol. Hepatol., 1990, 5, 616-626.
[18] Livraghi, T.; Giorgio, A.; Marin, G.; Salmi, A.; de Sio, I.; Bolondi,
L. Hepatocellular carcinoma and cirrhosis in 746 patients: long-
term results of percutaneous ethanol injection. Radiology, 1995,
197, 101-108.
[19] Rossi, S.; Di Stasi, M.; Buscarini, E.; Cavanna, I.; Quaretti, P.;
Squassante, E. Percutaneous radiofrequency interstitial thermal ab-
lation in the treatment of small hepatocellular carcinoma. Cancer J. Sci. Am., 1995, 1, 73-81.
[20] Sato, M.; Watanabe, Y.; Ueda, S.; Iseki, S.; Abe, Y.; Sato, N. Mi-
crowave coagulation therapy for hepatocellular carcinoma. Gastro-
enterol., 1996, 110, 1507-1514.
[21] Llovet, J.M.; Ricci, S.; Mazzaferro, V. Sorafenib in advanced hepa-
tocellular carcinoma. N. Eng. J. Med., 2008, 359, 378-390.
Curcumin and Liver Cancer Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 225
[22] Je, Y.; Schutz, F.A.B.; Choueiri, T.K. Risk of bleeding with vascu-
lar endothelial growth factor receptor tyrosine-kinase inhibitors
sunitinib and sorafenib: a systematic review and meta-analysis of
clinical trials. Lancet Oncol., 2009, 10, 967-974.
[23] Lu, S.C. Where are we in the chemoprevention of hepatocellular
carcinoma? Hepatol., 2010, 51, 734-736.
[24] Okuno, M.; Kojima, S.; Moriwaki, H. Chemoprevention of hepato-
cellular carcinoma: concept, progress and perspectives. J. Gastro-enterol. Hepatol., 2001, 16, 1329-1335.
[25] Kensler, T.W.; Quain, G.S.; Chen, J.G.; Groopman, J.D. Transla-
tional strategies for cancer prevention in liver. J. Natl. Cancer Inst.,
2003, 3, 321-329.
[26] Bishayee, A.; Politis, T.; Darvesh, A.S. Resveratrol in the chemo-
prevenion and treatment of hepatocellular carcinoma. Cancer Treat. Rev., 2010, 36, 43-53.
[27] Laurent-Puig, P.; Zucman-Rossi, J. Genetics of hepatocellular
tumors. Oncogene, 2006, 25, 3778-3786.
[28] Prieto, J. Inflammation, HCC and sex: IL-6 in the centre of the
triangle. J. Hepatol., 2008, 48, 380-381.
[29] Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related
inflammation. Nature, 2008, 454, 436-444.
[30] Kundu, J.K.; Surh, Y.-J. Inflammation: gearing the journey to
cancer. Mut. Res., 2008, 659, 15-30.
[31] Berasain, C.; Casillo, J.; Perugorria, M.J.; Latasa, M.U.; Prieto, J.;
Avila, M.A. Inflammation and liver cancer: new molecular links.
Ann. N.Y. Acad. Sci., 2009, 1155, 206-221.
[32] Klaunig, J.E.; Kamendulis, L.M. The oxidative stress in carcino-
genesis. Annu. Rev. Pharmacol. Toxicol., 2004, 44, 239-267.
[33] Kawanishi, S.; Hiraku, Y.; Pinlaor, S.; Ma, N. Oxidative stress and
nitrative DNA damage in animals and patients with inflammatory
diseases in relation to inflammation-related carcinogenesis. Biol.
Chem., 2006, 387, 365-372.
[34] Gius, D.; Spitz, D.R. Redox signaling in cancer biology. Antioxid.
Redox Signal, 2006, 8, 1249-1252.
[35] Pang, R.; Tse, E.; Poon, R.T.P. Molecular pathways in hepatocellu-
lar carcinoma. Cancer Lett., 2006, 240, 157-169.
[36] Wong, C.-M.; Ng, I.O.L. Molecular pathogenesis of hepatocellular
carcinoma. Liver Int., 2007, 160-174.
[37] Lee, K.W.; Lee, H.J.; Lee, C.Y. Vitamins, phytochemicals, diets,
and their implementation in cancer chemoprevention. Crit. Rev. Food Sci. Nutr., 2004, 44, 437-452.
[38] Aggarwal, B.B.; Shishodia, S. Molecular targets of dietary agents
for prevention and therapy of cancer. Biochem. Pharmacol., 2006,
71, 1397-1421.
[39] Aggarwal, B.B.; Ichikawa, H.; Garodia, P.; Weersinghe, P.; Sethi,
G.; Bhatt, I.D.; Pandey, M.K.; Shishodia, S.; Nair, M.G. From tra-
ditional ayurvedic medicine to modern medicine: identification to
therapeutic targets for suppression of inflammation and cancer.
Exp. Opin. Ther. Targets, 2006, 10, 87-118.
[40] Ullah, M.F.; Khan, M.W. Food as Medicine: Potential therapeutic
tendencies of plant derived polyphenolic compounds. Asian Pacific
J. Cancer Prev., 2008, 9, 187-196.
[41] Moiseeva, E.P.; Manson, M.M. Dietary chemopreventive phyto-
chemicals: Too little or too much. Cancer Prev. Res., 2009, 2, 611-
616.
[42] Manach, C.; Hubert, J.; Llorach, R.; Scalbert, A. The complex links
between dietary phytochemicals and human health deciphered by
metabolomics. Mol. Nutr. Food Res., 2009, 53, 1303-1315.
[43] Bishayee, A.; Darvesh, A.S. Oxidative stress in cancer and neu-
rodegenerative diseases: prevention and treatment by dietary anti-
oxidants. In: Free Radicals: Formation, Types and Effects, Eds:
Kozyrev, D., Slutsky, V., Nova Science Publishers, Inc, Haup-
pauge, NY, 2010, 1-55.
[44] Darvesh, A.S.; Carroll, R.T.; Bishayee, A.; Geldenhuys, W.J.; Van
der Schyf, C.J. Oxidative stress and Alzheimer’s disease: dietary
polyphenols as potential therapeutic agents. Exp. Rev. Neurother.,
2010, 10, 729-745.
[45] Johnson, I.T. Phytochemicals and cancer. Proc. Nutr. Soc.; 2007, 6,
207-215.
[46] Russo, G.L. Ins and outs of dietary phytochemicals in cancer che-
moprevention. Biochem. Pharmacol.; 2007, 74, 533-544.
[47] Khan, N.; Afaq, F.; Mukhtar, H. Cancer chemoprevention through
dietary antioxidants: progress and promise. Antioxid. Redox. Sig-
nal., 2008, 10, 475-510.
[48] Stan, S.D.; Kar, S.; Stoner, G.D.; Singh, S.V. Bioactive food com-
ponents and cancer risk reduction. J. Cell. Biochem., 2008, 104,
339-356.
[49] Manach, C.; Scalbert, A.; Morand, C.; Remesy, C.; Jimenes, L.
Polyphenols: food sources and bioavailability. Am. J. Clin, Nutr.,
2004, 79, 727-747.
[50] Manach, C.; Williamson, G.; Morand, C.; Scalbert, A.; Remesy, C.
Bioavailability and bioefficacy of polyphenols in humans. I. Re-
view of 97 bioavailability studies. Am. J. Clin. Nutr., 2005, 81,
230S-242S.
[51] Lee, K.W.; Lee, H.J. The roles of polyphenols in cancer chemopre-
vention. Biofactors, 2006, 26, 105-121.
[52] Surh, Y.J. Cancer chemoprevention with dietary phytochemicals.
Nat. Rev. Cancer, 2003, 3, 768-780.
[53] Milner, J.A. Molecular targets for bioactive food components. J.
Nutr., 2004, 134, 2492S-2498S.
[54] Rahman, I.; Biswas, S.K.; Kirkham, P.A. Regulation of inflamma-
tion and redox signaling by dietary polyphenols. Biochem. Phar-macol., 2005, 72, 1439-1452.
[55] Kim, Y.S.; Young, M.R.; Bobe, G.; Colbum, N.H.; Milner, J.A.
Bioactive food components, inflammatory targets, and cancer pre-
vention. Cancer Prev. Res., 2009, 2, 200-208.
[56] Glauert, H.P.; Mason-Calfee, K.; Stemm, D.V.; Tharappel, J.C.
Dietary antioxidants in the prevention of hepatocarcinogenesis: A
review. Mol. Nutr. Food Res., 2010, 54, 875-896.
[57] Mann, C.D.; Neal, C.P.; Garcea, G.; Manson, M.M.; Dennison,
A.R.; Berry, D.P. Phytochemicals as potential chemopreventive
and chemotherapeutic agents in hepatocarcinogenesis. Eur. J. Can-cer Prev., 2009, 18, 13-25.
[58] Ravindran, P.N. Turmeric-the golden spice of life. In: Turmeric: The genus Curcuma. Taylor and Francis Group: London, 2006, pp.
1-14.
[59] Ploto, A. Post-production management for improved market access
for herbs and spices – turmeric. Food and Agriculture Organization of the United Nations (FAO), 2003.
[60] Ammon, H.P.; Wahl, M.A. Pharmacology of Curcuma longa.
Planta Med., 1991, 57, 1-7.
[61] Araujo, C.C.; Leon, L.L. Biological activities of Curcuma longa L. Mem. Inst. Oswaldo Cruz., 2001, 96, 723-728.
[62] Aggarwal, B.B.; Kumar, A.; Bharti, A.C. Anticancer potential of
curcumin: preclinical and clinical studies. Anticancer Res., 2003,
23, 363-398.
[63] Aggarwal, B.B.; Bhatt, I.D.; Ichikawa, H.; Ahn, K.S.; Sethi, G.;
Sandur, S.K. Curcumin-biological and medicinal properties. In:
Turmeric: The genus Curcuma. Taylor and Francis Group: London,
2006, pp. 297-368.
[64] Aggarwal, B.B.; Sundaram, C.; Malani, N.; Ichikawa, H. Curcu-
min: the Indian solid gold. Adv. Exp. Med. Biol., 2007, 595, 1-75.
[65] Kiso, Y.; Suzuki, Y.; Watanabe, N.; Oshima, Y.; Hikino, H. Anti-
hepatotoxic principles of Curcuma longa rhizomes. Planta Med.,
1983, 49, 185-187.
[66] Srivastava, R.; Dikshit, M.; Srimal, R.C.; Dhawan, B.N. Anti-
thrombotic effect of curcumin. Thromb. Res., 1985, 40, 413-417.
[67] Babu, P.S.; Srinivasa, K. Infulence of dietary curcumin and choles-
terol on the progression of experimentally induced diabetes in al-
bino rats. Mol. Cell Biochem., 1995, 152, 13-21.
[68] Goel, A.; Kunnumakkara, A.B.; Aggarwal, B.B. Curcumin as
‘Curecumin”: from kitchen to clinic. Biochem. Pharmacol., 2008,
75, 787-809.
[69] Goel, A.; Jhurani, S.; Aggarwal, B.B. Multi-targeted therapy by
curcumin: how spicy is it? Mol. Nutr. Food Res., 2008, 52, 1010-
1030.
[70] Rivera-Espinoza, Y.; Muriel, P. Pharmacological actions of curcu-
min in liver diseases or damage. Liver Int., 2009, 1457-1466.
[71] Anand, P.; Sundaram, C.; Jhurani, S.; Kunnumakkara, A.B.; Ag-
garwal, B.B. Curcumin and cancer: an “old-age” disease with an
“age-old” solution. Cancer Lett., 2008, 267, 133-164.
[72] Shen, L.; Ji, H.F. Theoretical study on physiochemical properties of
curcumin. Spectrochim. Acta A. Mol. Biomol. Spectrom., 2007, 67,
619-623.
[73] Aggarwal, B.B.; Harikumar, K.B. Potential therapeutic effects of
curcumin, the anti-inflammatory agent, against neurodegenerative,
cardiovascular, pulmonary, metabolic, autoimmune and neoplastic
diseases. Int. J. Biochem. Cell Biol., 2009, 41, 40-59.
[74] Sethi, G.; Sung, B.; Aggarwal, B.B. The role of curcumin in mod-
ern medicine. In: Herbal Drugs: Ethnomedicine to Modern Medi-
226 Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 Darvesh et al.
cine, Ramawat, K.G., Ed., Springler-Verlag Berlin, Heidelberg,
2009, 97-113.
[75] Calabrese, V.; Bates, T.E.; Mancuso, C.; Cornelius, C.; Ven-
timiglia, B.; Cambria, M.T.; Di Renzo, L.; De Lorenzo, A.;
Dinkova-Kostova, A.T. Curcumin and the cellular stress response
in free radical-related diseases. Mol. Nutr. Food Res., 2008, 52,
1062-1073.
[76] Kunnumakkara, A.B.; Anand, P.; Aggarwal, B.B. Curcumin inhib-
its proliferation, invasion, angiogenesis and metastasis of different
cancers through interaction with multiple cell signaling proteins.
Cancer Lett., 2008, 269, 199-225.
[77] Sarkar, F.H.; Li, Y.; Wang, Z.; Padhye, S. Lesson learned from
nature for the development of novel anti-cancer agents: implication
of isoflavone, curcumin, and their synthetic analogs. Curr. Pharm. Des., 2010, 16, 1801-1812.
[78] Valko, M.; Rhodes, C.J.; Moncol, J.; Izaokovic, M.; Mazur, M.
Free radicals, metals and antioxidants in oxidative stress-induced
cancer. Chem. Biol. Interact., 2006, 160, 1-40.
[79] Sharma, O.P. Antioxidant activity curcumin and related com-
pounds. Biochem. Pharmacol., 1976, 25, 1811-1812.
[80] Osawa, T.; Sugiyama, Y.; Inayoshi, M.; Kawakishi, S. Antioxida-
tive activity of tetrahydrocurcuminoids. Biosci. Biotechnol. Bio-chem., 1995, 59, 1609-1612.
[81] Ak, T.; Gulcin, I. Antioxidant and radical scavenging properties of
curcumin. Chem. Biol. Interact., 2008, 174, 27-37.
[82] Sugiyama, Y.; Kawakishi, S.; Osawa, T. Involvement of the beta-
diketone moiety in the antioxidative mechanism of tetrahydrocur-
cumin. Biochem. Pharmacol., 1996, 52, 519-525.
[83] Aggarwal, B.B.; Shishodia, S.; Sandur, S.K.; Pandey, M.K.; Sethi,
G. Inflammation and cancer: how hot is the link? Biochem. Phar-macol., 2006, 72, 1605-1621.
[84] Hansson, G.K.; Robertson, A.K.; Soderberg-Naucler, C. Inflamma-
tion and atherosclerosis. Annu. Rev. Pathol., 2006, 1, 297-329.
[85] Libby, P. Inflammatory mechanisms: the molecular basis of in-
flammation and disease. Nutr. Rev., 2007, 65, S140-S146.
[86] Packard, R.R.; Libby, P. Inflammation in atherosclerosis: from
vascular biology to biomarker discovery and risk prediction. Clin.
Chem., 2008, 54, 24-38.
[87] Murakami, Y.; Ishii, H.; Takeda, N.; Tanaka, S.; Machino, M.; Ito,
S.; Fujisawa, S. Comparative anti-inflammatory activities of cur-
cumin and tetrahydrocurcumin based on the phenolic O-H bond
dissociation enthalpy, ionization potential and quantum chemical
descriptor. Anticancer Res., 2008, 28, 699-707.
[88] Jurenka, J.S. Anti-inflammatory properties of curcumin, a major
constituent of Curcuma longa: a review of preclinical and clinical
research. Altern. Med. Rev., 2009, 14, 141-153.
[89] Aggarwal, B.B.; Sung, B. Pharmacological basis for the role of
curcumin in chronic diseases: an age old spice with modern targets.
Trends Pharmacol. Sci., 2009, 30, 85-94.
[90] Gupta, S.C.; Kim, J.H.; Prasad, H.; Aggarwal, B.B. Regulation of
survival, proliferation, invasion, angiogenesis, and metastasis, of
tumor cells through modulation of inflammatory pathways by nu-
traceuticals. Cancer Metas. Rev., 2010, 29, 405-434.
[91] Singh, S.; Aggarwal, B.B. Activation of transcription factor NF-
kappa B is suppressed by curcumin (diferuloylmethane). J. Biol.
Chem., 1995, 270, 24995-25000.
[92] Sethi, G.; Sung, B.; Aggarwal, B.B. Nucelar factor-kappaB activa-
tion: from bench to bedside. Exp. Biol. Med., 2008, 233, 21-31.
[93] Ralhan, R.; Pandey, M.K.; Aggarwal, B.B. Nuclear factor-kappa B
links carcinogenic and chemopreventive agents. Front. Biosci., 2009, 1, 45-60.
[94] Aggarwal, B.B.; Kunnumakkara, A.B.; Harikumar, K.B.; Tharakan,
S.T.; Sung, B.; Anand, P. Potential of spice derived phytochemicals
for cancer prevention. Planta Med., 2008, 74, 1560-1569.
[95] Shishodia, S.; Amin, H.M.; Lai, R.; Aggarwal, B.B. Curcumin
(diferuloylmethane) inhibits constitutive NF-kappaB activation, in-
duced G1/S arrest, suppresses proliferation, and induces apoptosis
in mantle cell lymphoma. Biochem. Pharmacol., 2005, 70, 700-
713.
[96] Aggarwal, B.B.; Shishodia, S.; Takeda, Y.; Banerjee, S.; Newman,
R.A.; Bueso-Ramos, C.E.; Price, J.E. Curcumin suppresses the
paclitaxel-induced nuclear factor-kappaB pathway in breast cancer
cells and inhibits lung metastasis of human breast cancer in nude
mice. Clin. Cancer Res., 2005, 11, 7490-7498.
[97] Aggarwal S.; Ichikawa, H.; Takada, Y.; Sandur, S.K.; Shishodia,
S.; Aggarwal, B.B. Curcumin (diferuloylmethane) down-regulates
expression of cell proliferation and anti-apoptotic and metastatis
gene products through suppression of IkappaBalpha kinase and Akt
activation. Mol. Pharmacol., 2006, 69, 195-206.
[98] Kamat, A.M.; Sethi, S.; Aggarwal, B.B. Curcumin potentiates the
apoptotic effects of chemotherapeutic agents and cytokines through
down-regulation of nuclear factor-kappaB and nuclear factor-
kappaB-regulated gene products in IFN-alpha-sensitive and IFN-
alpha-resistant human bladder cancer cells. Mol. Cancer Ther.,
2007, 6, 1022-1030.
[99] Deeb, D.; Jiang, H.; Gao, X.; Al-Holou, S.; Danyluk, A.L.; Dul-
chavsky, S.A. Curcumin sensitizes human prostate cancer cells to
tumor necrosis factor-related apoptosis-inducing ligand/Apo2L-
induced apoptosis by suppressing nuclear factor-kappab via inhibi-
tion of the prosurvival Akt signaling pathway. J. Pharmacol. Exp. Ther., 2007, 321, 616-625.
[100] Li, L.; Aggarwal, B.B.; Shishodia, S.; Abbruzzese, J.; Kurzrock, R.
Nuclear factor-kappaB and Ikappa-B kinase are constitutively ac-
tive in human pancreatic cells, and their down-regulation by cur-
cumin (diferuloylmethane) is associated with the suppression of
proliferation and the induction of apoptosis. Cancer, 2004, 101,
2351-2362.
[101] Shakibaei, M.; Schulze-Tanzil, G.; John, T.; Mobasheri, A. Curcu-
min protects human chodrocytes from IL-1beta-induced inhibition
of collagen type II and beta1-integrin expression and activatin of
caspase-3: an immunomorphological study. Ann. Anat., 2005, 187,
487-497.
[102] Skommer, J.; Wlodkowic, D.; Pelkonen, J. Gene-expression profil-
ing during curcumin-induced apoptosis reveals downregulation of
CXCR4. Exp. Hematol., 2007, 35, 85-95.
[103] Wahlstrom, B.; Blennow, G. A study on the fate of curcumin in the
rat. Acta Pharmacol. Toxicol. (Copenh.), 1978, 43, 86-92.
[104] Holder, G.M.; Plummer, J.L.; Ryan, A.J. The metabolism and
excretion of curcumin in the rat. Xenobiotica, 1978, 8, 761-768.
[105] Ravindranath, V.; Chandrasekhara, N. Absorption and tissue distri-
bution of curcumin in rats. Toxicol., 1980, 16, 259-265.
[106] Ireson, C.; Orr, S.; Jones, D.J.; Verschoyle, R.; Lim, C.K.; Luo,
J.L. Characterization of metabolites of f the chemopreventive agent
curcumin in human and rat hepatocytes and in the rat in vivo, and
evaluation of their ability to inhibit phorbol ester-induced prosta-
glandin E2 production. Cancer Res., 2001, 61, 1058-1064.
[107] Garcea, G.; Jones, D.J.; Singh, R.; Dennison, A.R.; Farmer, P.B.;
Sharma, R.A. Detection of curcumin and its metabolites in hepatic
tissue and portal blood of patients following oral administration.
Br. J. Cancer, 2004, 90, 1011-1015.
[108] Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B.
Bioavailability of curcumin: problems and promises. Mol. Pharm.,
2007, 4, 807-818.
[109] Shoba, G.; Joy, D.; Joseph, T.; Majeed, M.; Rajendran, R.; Srini-
vas, P.S. Influence of piperine on the pharmacokinetics of curcu-
min in animals and human volunteers. Planta Med., 1998, 64, 353-
356.
[110] Li, L.; braiteh, F.S.; Kurzrock, R. Liposome-encapsulated curcu-
min: in vitro and in vivo effects on proliferation, apoptosis, signal-
ing, and angiogenesis. Cancer, 2005, 104, 1322-1331.
[111] Sun, A.; Shoji, M.: Lu, Y.J.; Liotta, D.C.; Snyder, J.P. Synthesis of
EF24-tripeptide chloromethyl ketone: a novel curcumin-related
anticancer drug delivery system. J. Med. Chem., 2006, 49, 3153-
3158.
[112] Bisht, S.; Feldmann, G.; Soni, S.; Ravi, R.; Karikar, C.; Maitra, A.
Polymeric nanoparticle-encapsulated curcumin (“nanocurcumin”):
a novel strategy for human cancer therapy. J. Nanobiotechnol.,
2007, 5, 3.
[113] Marczylo, T.H.; Verschoyle, R.D.; Cooke, D.N.; Morazzoni, P.;
Steward, W.P.; Gescher, A.J. Comparison of systematic availability
of curcumin with that of curcumin formulated with phosphatadiyl-
choline. Cancer Chemother. Pharmacol., 2007, 60, 171-177.
[114] Anand, P.; Nair, H.B.; Sung, B.; Kunnumakkara, A.B.; Yadav,
V.R.; Tekmal, R.R.; Aggarwal, B.B. Design of curcumin-loaded
PLGA nanoparticles formulation with enhanced cellular uptake,
and increased bioactivity in vitro and superior bioavailability in vivo. Biochem. Pharmacol., 2010, 79, 330-338.
[115] Nair, H.B.; Sung, B.; Yadav, V.R.; Kannappan, R.; Chaturvedi,
M.M.; Aggarwal, B.B. Delivery of anti-inflammatory nutraceuti-
cals by nanoparticles for the prevention and treatment of cancer.
Biochem. Pharmacol., 2010, 80, 1833-1843.
Curcumin and Liver Cancer Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 227
[116] Yadav, V.R.; Prasad, S.; Kannappan, R.; Ravindran, J.; Chaturvedi,
M.M.; Vaahtera, L.; Parkkinen, J.; Aggarwal, B.B. Cyclo-dextrin-
complexed curcumin exhibits anti-inflammatory and antiprolifera-
tive activities superior to those of curcumin through higher cellular
uptake. Biochem. Pharmacol., 2010, 80, 1021-1032.
[117] John, V.D.; Kuttan, G.; Krishnankutty, K. Anti-tumour studies of
metal chelates of synthetic curcuminoids. J. Exp. Clin. Cancer
Res., 2002, 21, 219-224.
[118] Padhye, S.; Yang, H.; Jamadar, A.; Cui, Q.C.; Chavan, D.;
Dominiak, K.; McKinney, J.; Banerjee, S.; Dou, Q.P.; Sarkar, F.H.
New difluoro Knoevenagel condensates of curcumin, their Schiff
bases and copper complexes as proteasome inhibitors and apoptosis
inducers in cancer cells. Pharm. Res., 2009, 26, 1874-1880.
[119] Leyon, P.V.; Kuttan, G. Studies on the role of some synthetic cur-
cuminoid derivatives in the inhibition of tumour specific angio-
genesis. J. Exp. Clin. Cancer Res., 2003, 22, 77-83.
[120] Bar-Sela, G.; Epelbaum, R.; Schaffer, M. Curcumin as an anti-
cancer agent: review of the gap between basic and clinical applica-
tions. Curr. Med. Chem., 2010, 17, 190-197.
[121] Aggarwal, B.B.; Takada, Y.; Oommen, O.V. From chemopreven-
tion to chemotherapy: common targets and common goals. Exp.
Opin. Invest. Drugs, 2004, 13, 1327-1338.
[122] Shishodia, S.; Sethi, G.; Aggarwal, B.B. Curcumin: getting back to
the roots. Ann. N.Y. Acad. Sci., 2005, 1056, 206-217.
[123] Burgos-Morón, E.; Calderón-Montano, J.M.; Salvador, J.; Robles,
A.; López-Lázaro, M. The dark side of curcumin. Int. J. Cancer,
2010, 126, 1771-1775.
[124] Hata, M; Sasaki, E.; ota, M.; Fujimoto, K.; Yajima, J.; Shichida, T.
Allergic contact dermatitis from curcumin (turmeric). Contact
Dermat., 1997, 36, 107-108.
[125] Swierczynska, M.K.; Krecisz, B. occupational skin changes in
persons working in contact with food spices. Med. Pr., 1998, 49,
187-190.
[126] Frank, N.; Knauft, J.; Amelung, F.; Nair, J.; Wesch, H.; Bartsch, H.
No prevention of liver and kidney tumors in Long-Evans Cinna-
mon rats by dietary curcumin, but inhibition at other sites and of
metastases. Mutat. Res., 2003, 523, 127-135.
[127] Liu, R.H. Potential synergy of phytochemicals in cancer preven-
tion: mechanism of action. J. Nutr., 2004, 3479S-3485S.
[128] de Kok, T.M.; van Breda, S.G.; Manson, M.M. Mechanisms of
combined action of different chemopreventive dietary compounds.
Eur. J. Nutr., 2008, 47, 51-59.
[129] Korkina, L.G.; de Luca, C.; Kostyuk, V.A.; Pastore, S. Plant poly-
phenols and tumors: from mechanisms to therapies, prevention and
protection against toxicity of anti-cancer treatments. Curr. Med.
Chem., 2009, 16, 3943-3965.
[130] Sheepens, A., Tan, K., Paxton, J.W. Improving the oral bioavail-
ability of beneficial polyphenols through designed synergies. Genes Nutr., 2010, 5, 75-87.
[131] Sandur, S.K.; Pandey, M.K.; Sung, B.; Ahn, K.S.; Murakami, A.;
Sethi, G.; Limtrakul, V.; Badmaev, V., Aggarwal, B.B. Curcumin,
demethoxycurcumin, bisdemethoxycurcumin, tetrahydrocurcumin,
and tumerones differentially regulate anti-inflammatory and anti-
proliferative responses through a ROS-independent mechanism.
Carcinogenesis, 2007, 8, 1765-1773.
[132] Lin, L.-I.; Ke, Y.-F.; Ko, Y.-C.; Lin, J.-K. Curcumin inhibits SK-
Hep-1 hepatocellular carcinoma cell invasion in vitro and sup-
presses matric metalloproteinase-9 secretion. Oncology, 1998, 55,
349-353.
[133] Ohashi, Y.; Tsuchiya, Y.; Koizumi, K.; Sakurai, H.; Saiki, Y. Pre-
vention of intrahepatic metastasis by curcumin in an orthotopic im-
plantation model. Oncology, 2003, 65, 250-258.
[134] Kang, J.; Chen, J.; Shi, Y.; Jia, J.; Zhang, Y. Curcumin-induced
histone hypoacetylation: the role of reactive oxygen species. Bio-chem. Pharmacol., 2005, 69, 1205-1213.
[135] Cui, S.-X.; Qu, X.-J.; Xie, Y.-Y.; Zhou, L.; Nakata, M.; Makuuchi,
M.; Tang, W. Curcumin inhibits telomerase activity in human can-
cer cell lines. Int. J. Mol. Med., 2006, 18, 227-231.
[136] Jia, L.; Wang, H.; Qu, S.; Miao, X.; Zhang, J. CD147 regulates
vascular endothelial growth factor–A expression, tumorigenicity,
and chemosensitivity to curcumin in hepatocellular carcinoma.
Life, 2008, 60, 57-63.
[137] Wang, W.-Z.; Cheng, J.; Luo, J.; Zhuang, S.-M. Abrogation of
G2/M arrest sensitizes curcumin-resistant hepatoma cells to apop-
tosis. F.E.B.S. Lett., 2008, 582, 2689-2695.
[138] Cao, J., Jia, L.; Zhou, H.-M.; Liu, Y.; Zhong, L.-F. Mitochondrial
and nuclear DNA damage induced by curcumin in human hepa-
toma G2 cells. Toxicol. Sci., 2006, 91, 476-483.
[139] Cao, J.; Liu, Y.; Jia, L.; Zhou, H.-M.; Kong, Y.; Yang, G.; Jiang,
L.P.; Li, Q.J.; Zhong, L.-F. Curcumin induces apoptosis through
mitochondrial hyperpolarization and mtDNA damage in human he-
patoma G2 cells. Free Rad. Biol. Med., 2007, 43, 968-975.
[140] Roy, M.; Pear, W.S.; Aster, J.C. The multifaceted role of Notch in
cancer. Curr. Opin. Genet. Dev., 2007, 17, 52-59.
[141] Ning, L.; Wentworth, L.; Chen, H.; Weber, S.M. Down-regulation
of notch1 signaling inhibits tumor growth in human hepatocellular
carcinoma. Am. J. Transl. Res., 2009, 1, 358-366.
[142] Simoni, D.; Rizzi, M.; Rondanin, R.; Baruchello, R.; Marchetti, P.;
Invidiata, F.P.; Labbozzetta, M.; Poma, P.; Carina, V.; Notarbar-
tolo, M.; Alaimo, A.; D’Alessandro, N. Antitumor effects of cur-
cumin and structurally -diketone modified analogs on multidrug
resistant cancer cells. Bioorg. Med. Chem. Lett., 2008, 18, 845-849.
[143] Yoysungneon, P.; Wirachwong, P.; Changtam, C.; Suksamrarn, A.;
Patumraj, S. Anti-cancer and anti-angiogenic effects of curcumin
and tetrahydrocurcumin on implanted hepatocellular carcinoma in
nude mice. World J. Gastroenterol., 2008, 14, 2003-2009.
[144] Xiao, J.; Chu, Y.; Hu, K.; Wan, J.; Huang, Y.; Jiang, C.; Liang, G.;
Li, X. Synthesis and biological analysis of a new curcumin ana-
logue for enhanced anti-tumor activity in HepG2 cells. Oncol. Rep.,
2010, 23, 1435-1441.
[145] Notarbartolo, M.; Poma, P.; Perri, D.; Dusonchet, L.; Cervello, M.;
D’Alessandro, N. Antitumor effects of curcumin, alone or in com-
bination with cisplatin or doxorubicin, on human hepatic cancer
cells. Analysis of their possible relationship to changes in NF-kB
activation levels and in IAP gene expression. Cancer Lett., 2005,
224, 53-65.
[146] Bishayee, A.; Chatterjee, M. Inhibitory effect of vanadium on rat
liver carcinogenesis initiated with diethylnotisoamine and pro-
moted with phenobarbital. Br. J. Cancer, 1995, 71, 1214-1220.
[147] Bishayee, A; Dhir, N. Resveratrol-mediated chemoprevention of
diethylnitrosoamine-initiated hepatocarcinogenesis: inhibition of
cell proliferation and induction of apoptosis. Chem.-Biol. Interact.,
2009, 10, 131-144.
[148] Darvesh, A.S.; Bishayee, A. Selenium in the prevention and treat-
ment of hepatocellular carcinoma. Anti-Cancer Agents Med. Chem., 2010, 10, 338-345.
[149] Soni, K.B.; Lahiri, M.; Chackradeo, P.; Bhide, S.V.; Kuttan, R.
Protective effect of food additives on aflatoxin-induced mutagenic-
ity and hepatocarcinogenicity. Cancer Lett., 1997, 115, 129-133.
[150] Bishayee, A.; Sarkar, A.; Chatterjee, M. Further evidence for che-
mopreventive potential of beta-carotene against experimental car-
cinogenesis: diethylnitrosamine-initiated and Phenobarbital-
promoted hepatocarcinogenesis prevented more effected by beta-
carotene than by retinoic acid. Nutr. Cancer, 2000, 37, 89-98.
[151] Chuang, S.E.; Cheng, A.-L.; Lin, J.-K.; Kuo, M.-L. Inhibition by
curcumin of diethylnitrosamine-induced hepatic hyperplasia, in-
flammation, cellular gene products and cell-cycle-related proteins
in rats. Food Chem. Toxicol., 2000, 38, 991-995.
[152] Chuang, S.E.; Kuo, M.L.; Hsu, C.H.; Chen, C.R.; Lin, J.K.; Lai,
G.M.; Hsieh, C.Y.; Cheng, A.L. Curcumin-containing diet inhibits
diethylnitrosamine-induced murine hepatocarcinogenesis. Carcino-genesis, 2000, 21, 331-335.
[153] Thapliyal, R.; Naresh, K.N.; Rao, K.V.K.; Maru, G.B. Inhibition of
nitrosoamine-induced hepatocarcinogenesis by dietary turmeric in
rats. Toxicol. Lett., 2003, 139, 45-54.
[154] Shukla, Y.; Arora, A. Suppression of altered hepatic foci develop-
ment by curcumin in Wistar rats. Nutr. Cancer, 2003, 45, 53-59.
[155] Sreepriya, M; Bali, G. Chemopreventive effects of embelin and
curcumin against N-nitrosodiethylamine/phenobarbital-induced he-
patocarcinogenesis in Wistar rats. Fitoterapia, 2005, 76, 549-555.
[156] Sreepriya, M.; Bali, G. Effects of administration of embelin and
curcumin on lipid peroxidation, hepatic glutathione antioxidant de-
fense and hematopoietic system during N-nitrosodiethylamine/
phenobarbital-induced hepatocarcinogenesis in Wistar rats. Mol.
Cell. Biochem., 2006, 284, 49-55.
[157] Huang, A.-C.; Lin, S.-Y.; Su, C.-C.; Lin, S.-S.; Ho, C.-C.; Hsia, T.-
C.; Chiu, T.-H.; Yu, C.-S.; Ip, S.W.; Lin, T.-P.; Chung, J.-G. Ef-
fects of curcumin on N-bis(2-hydroxypropyl) nitrosamine (DHPN)-
induced lung and liver tumorigenesis in BALB/c mice in vivo. In Vivo, 2008, 22, 781-786.
228 Current Pharmaceutical Biotechnology, 2012, Vol. 13, No. 1 Darvesh et al.
[158] Takaba, K.; Hirose, M.; Yoshida, Y.; Kimura, J.; Ito, N.; Shirai, T.
Effects of n-trtricontane-16,18-dione, curcumin, chlorophyllin,
dihydroguaiaretic acid, tannic acid and phytic acid on the initiation
stage in a rat multi-organ carcinogenesis model. Cancer Lett., 1997, 113, 39-46.
[159] Hirose, M.; Takahashi, S.; Ogawa, K.; Futakuchi, M.; Shirai, T.;
Shibutani, M.; Uneyama, C.; Toyoda, K.; Iwata, H. Chemopreven-
tion of heterocyclic amine-induced carcinogenesis by phenolic
compounds in rats. Cancer Lett., 1999, 143, 173-178.
[160] Hirose, M.; Takahashi, S.; Ogawa, K.; Futakuchi, M.; Shirai. Phe-
nolics: Blocking agents for heterocyclic amine-induced carcino-
genesis. Food Chem. Toxicol., 1999, 37, 985-992.
[161] Tharappel, J.C.; Lehmler, H.-J.; Srinivasan, C.; Robertson, L.W.;
Spear, B.T.; Glauert, H.P. Effect of antioxidant phytochemicals on
the hepatic tumor promoting activity of 3,3', 4,4'-
tetrachlorobiphenyl (PCB-77). Food Chem. Toxicol., 2008, 46,
3467-3474.
[162] Busquets, S.; Carb , N.; Almendro, V.; Quiles, M.T.; L pez-
Soriano, F.J.; Argilés, J.M. Curcumin, a natural product present in
turmeric, decreases tumor growth but does not behave as an anti-
cachectic compound in a rat model. Cancer Lett., 2001, 167, 33-38.
[163] Yoysungnoen, P.; Wirachwong, P.; Bhattarakosol, P.; Niimi, H.;
Patumraj, S. Antiangiogenic activity of curcumin in hepatocellular
carcinoma cells implanted nude mice. Clin. Hemor. Microcirc.,
2005, 33, 127-135.
[164] Yoysungnoen, P.; Wirachwong, P.; Bhattarakosol, P.; Niimi, H.;
Patumraj, S. Effects of curcumin on tumor angiogenesis and bio-
markers, COX-2 and VEGF, in hepatocellular carcinoma cell-
implanted carcinoma cell-implanted nude mice. Clin. Hemor. Mi-crocirc., 2006, 34, 109-115.
Received: September 03, 2010 Revised: September 29, 2010 Accepted: October 01, 2010