conversation analysis in psychotherapy
TRANSCRIPT

1 Introduction
Josef Breuer ’ s patient, known as “ Anna O. ” , coined the phrase “ talking cure ” to describe the treatment for hysteria she received from Breuer, who was, at the time, a close collaborator of Sigmund Freud. The treatment involved the patient narrat-ing her worries and fantasies. The expression the “ talking cure ” was adopted by Freud as a shorthand description of what takes place in psychoanalysis; ever since, this expression has been used as an apt gloss of psychotherapy.
Talking is indeed the key activity in all psychotherapies. It is often the only activity taking place in therapy sessions; and even in psychotherapies where other activities such as painting, playing or drama are involved, talking remains impor-tant. Conversation Analysis, as the study of talk - in - interaction, should therefore have much to say about psychotherapy.
In what follows, I summarize what a CA informed understanding of psycho-therapy might involve. I then discuss the background, present state, and future prospects of CA research on psychotherapy.
2 Working Sequentially with Understandings
In the introduction to a recent collection on CA and psychotherapy, Per ä kyl ä , et al. suggest that through its core theoretical idea, the notion of sequential organiza-tion of human action, CA can make a specifi c contribution to understanding psychotherapy (Per ä kyl ä , et al., 2008a : 16). Sequentiality involves relations of nextness between utterances (turns - at - talk): “ Next turns are understood by co - participants to display their speaker ’ s understanding of the just - prior turn and to
The Handbook of Conversation Analysis, First Edition. Edited by Jack Sidnell and Tanya Stivers.© 2013 Blackwell Publishing Ltd. Published 2013 by Blackwell Publishing Ltd.
27 Conversation Analysis in Psychotherapy
ANSSI PER Ä KYL Ä University of Helsinki

552 Key Contexts of Study in CA: Populations and Settings
embody an action responsive to the just - prior turn so understood ” (Schegloff, 2007b : 15). This kind of relation between turns is “ endemic to the organization of conversation ” (Schegloff, 2007b ) and as such, it is the backbone of the possibility of intersubjective understanding between humans (Heritage, 1984b ; Schegloff, 1992d ).
In the context of psychotherapy, this organization entails that anything a thera-pist or a patient does, is done and understood in the context of the other partici-pant ’ s previous turn. Because turns are tied together by nextness, “ the participants inevitably have to orient to and work with the understandings that they each bring about through their actions ” (Per ä kyl ä , et al., 2008a : 16). Thus, through their adja-cent utterances, therapist and patient inevitably create an intersubjective fi eld — an emergent fi eld of shared understandings regarding each other ’ s actions and the worlds of momentary experience that these actions embody. As in any interaction (and in psychotherapy, perhaps in specifi c and specifi able ways), this intersubjec-tive fi eld involves gaps, discontinuities and tensions, as well as moments where the participants ’ understandings converge. Therapists ’ and patients ’ actions, as specifi ed in CA research in psychotherapy and reviewed in what follows, involve movement in this intersubjective fi eld.
In their infl uential discussion of institutional interaction, Drew and Heritage (1992a: 21 – 5) single out particular inferential frameworks as one key feature charac-teristic to institutional encounters. In different institutions, participants hear each other ’ s conversational contributions in institutionally specifi c ways — for example, in medical, juridical and journalistic contexts, the client ’ s talk is usually not treated as a source of surprise or sympathy in the professional recipient (Drew & Heritage, 1992a : 24). What makes psychotherapy a specifi c form of institutional interaction is perhaps most distinctively linked to its inferential frameworks. While ordinarily in interaction, language and other signs are understood as means for displaying and recognizing the speaker ’ s communicative intentions (Grice, 1975 ; see also Enfi eld, 2009 : 2), in psychotherapy, there is an endemic orientation in the therapist, and usually also in the patient, to examine the patient ’ s talk beyond its intended meaning . The professional and lay understandings of ‘ beyond ’ vary across thera-pies. For example, in classical psychoanalysis it would be thoughts and feelings repressed due to confl icts between different aspects of the mind (e.g. Vehvil ä inen, 2003 ); in cognitive therapy, dysfunctional beliefs and ways of thinking (e.g. Voutilainen, Per ä kyl ä & Ruusuvuori, 2010b ); and in solution - oriented therapy, it would be the patient ’ s (unrecognized) coping resources (e.g. MacMartin, 2008 ). Many interactional practices of psychotherapy, investigated by CA and discussed below, involve therapists ’ and patients ’ methods of recognizing, examining, and dealing with this ‘ beyond ’ .
There are probably other ways in which psychotherapies are distinct as interac-tion, but in them, the variation across different therapies may be even bigger. Take, for example, constraints on participant contributions (see Drew & Heritage, 1992a : 23 – 4). While some psychotherapies are largely driven by turn - type pre - allocation, which assigns therapists the role of questioner and patients the role of the answerer (e.g. Gale, 1991 ; Halonen, 2008 ; MacMartin, 2008 ; Per ä kyl ä , 1995 ), other psycho-

Conversation Analysis in Psychotherapy 553
therapies, especially psychoanalysis, allocate patients the opportunity and obliga-tion for initiatory, multiunit turns often taking the form of extensive narration. Likewise, participant orientations to the goals of their interactions (Drew & Heritage, 1992a : 22 – 3) may vary across therapies, for example from fi nding means for reducing the patient ’ s acute anxiety, to enhancing the patient ’ s ability to observe states of mind in him - or herself and others.
3 History
Before the birth of the line of research that later on was to be labeled Conversation Analysis, a number of pioneering scholars started to investigate psychotherapy by methods that partially anticipated CA. Qualitative interactional analysis of audio - or video - recorded psychotherapy sessions was initiated by Pittenger, Hockett and Danehy (1960) , who described in detail an audio recording of the fi rst fi ve minutes of an initial psychiatric interview, paying particular attention to the implicit meanings conveyed by the lexical and prosodic choices of the partici-pants. A decade later, Schefl en (1973) presented an equally impressive microanaly-sis of a fi lmed segment of family therapy, focusing especially on the coordination of participants ’ language, posture and gesture. Labov and Fanshel (1977) analyzed a segment of psychotherapy interaction using speech act theory, and the line of their work was recently extended by Ferrara (1994) , who examined various dis-course strategies (such as repetition of the other ’ s talk, construction of metaphors, and joint production of utterances) in a large corpus of tape - recorded data. All these studies on interaction in psychotherapy have much in common with CA, but do not explicitly employ CA methods.
In his early work on naturally occurring conversations, Harvey Sacks used, among other types of recordings, a set of audio - taped recordings from a group therapy session (see especially Sacks, 1992 : 268 – 80). In investigating these record-ings, Sacks and his colleagues made a number of observations that generated further conversation analytic research, for example on storytelling (Jefferson, 1978 ; Sacks, 1974a ) and categorization (Sacks, 1974a ). These studies are useful for the study of psychotherapy. However, in focusing on generic properties of interaction, they do not involve an extensive effort to understand what is specifi c in psycho-therapy as interaction. An illuminating discussion of the “ omnirelevance ” of the categories therapist and patient in such interactions (Sacks, 1992 : e.g. 315 and 462) is perhaps the closest that Sacks came to the investigation of institutionally specifi c properties of psychotherapy interaction.
Conversation analytic work on practices pertaining especially to psychother-apy began with a now widely cited paper by Kathy Davis on problem reformulation in psychotherapy (Davis, 1986 ). As data, she used an initial inter-view between a patient and a psychotherapist — that is, the data were not from psychotherapy proper, but from a clinical interview preparatory to psychotherapy. Using the concept of formulation as defi ned by Heritage and Watson (1979) , Davis showed a process where the patient ’ s initial description of her trouble (involving

554 Key Contexts of Study in CA: Populations and Settings
dilemmas of being a housewife, her relationship with her husband, and possible complications of her current pregnancy) was redefi ned as a problem of not being able to express her emotions openly and honestly. Formulations were the vehicle for this redefi nition: by “ explaining, characterizing, translating, summarizing or furnishing gists for the talk - thus - far ” (Davis, 1986 : 47), the therapist in this par-ticular interview defi ned the patient ’ s problem, provided evidence for it, and fi nally persuaded the patient to undergo psychotherapeutic treatment for the (redefi ned) problem.
In hindsight, Davis ’ study appears to be rather inexact in many ways: in what she calls formulations, a wide variety of actions are included (such as candidate understandings, statements and assessments). In many cases, she does not expli-cate the local sequential context of these utterances, but rather maps these utter-ances onto the overall development of the narrative and negotiation of problem defi nition during the interview. But the study was nonetheless innovative. It introduced, as a topic of analysis, ways in which the therapist ’ s responses and interventions recast the troubles that the patient describes. In other words, it elaborated one aspect of the process through which the participants created an intersubjective fi eld through their adjacent turns - at - talk — seeking to show espe-cially the discontinuities and tensions in this process.
After Davis ’ seminal study, not much happened in the fi eld of conversation analytic research on psychotherapy for about ten years. In the later 1990s, however, there were new developments which eventually led to the busy scene of research of the past decade. I have organized the summary of current research under two umbrellas: some studies deal with sequentially organized practices through which psychotherapy gets done, while others focus more on aspects of the relation between the therapist and the patient, as realized through their interaction. It should be noted that the classifi cation into ‘ practices ’ and ‘ relation ’ is not at all mutually exclusive: any sequentially organized practice is a vehicle for the relation, and a relation emerges from sequentially organized practices.
4 Key Practices
4.1 Formulations in p sychotherapy Since Davis ’ (1986) initial paper, formulations have been perhaps the most exten-sively researched facet of psychotherapeutic interaction (e.g. Antaki, 2008 ; Antaki, Barnes & Leudar, 2005 ; Bercelli, Rossano & Viaro, 2008 ; Buttny, 1996 ; Hutchby, 2005 ; Madill, Widdicombe & Barkham, 2001 ; Per ä kyl ä , 2004 ; Vehvil ä inen, 2003 ). As Antaki (2008) points out, the term formulation lends itself to various usages, and therefore it is important to be quite precise in defi ning it. A core defi nition arises from Heritage and Watson ’ s (1979) study, according to which formulations are utterances in which the current speaker suggests a meaning of what another participant has said in the prior turn or turns (see also Garfi nkel & Sacks, 1970 ).

Conversation Analysis in Psychotherapy 555
A formulation is inevitably selective: it foregrounds something in the prior talk, and leaves something else in the background. It thereby, involves what Antaki (2008) calls local editing of the interlocutor ’ s talk. It makes relevant confi rmation or disconfi rmation by the recipient (the party whose talk is being edited).
Therapists ’ formulations of patients ’ talk have been shown to be multipurpose devices in psychotherapy. Formulations can serve, for example, to establish the events or experiences that the patient has spoken about as therapeutically relevant or therapeutically irrelevant, to intensify and underline emotional or confl ictual issues, to prepare the ground for interpretation, and to manage the agenda of the therapeutic session (cf. Antaki, 2008 ; Antaki, Barnes & Leudar, 2005 ; Hutchby, 2005 ; Per ä kyl ä , 2004 ; Vehvil ä inen, 2003 ).
In the Finnish Extract (1) below, the therapist formulates the patient ’ s talk. In the fi rst part of the extract, the patient talks about the career choices that he has made (working at some point in time with small children, and later on with ado-lescents). This topic emerged from a prior discussion of the patient ’ s ideas and experiences of associating and identifying himself with men or with women, in his childhood as well as in his adult working life.
(1) Vehvil ä inen ( 2003 : 585)
3 Pa: . . . sen takia mä oon nimeomaa hakeutunu tänneit’s for I am exactly sought my way to-here
. . . it is because of that that I have chosen °this area of
4 vaikeitten nuorten °hoito:< hoito° (0.4) °alalle°.difficult youth care care to-fieldthe care:< care° of difficult adolescents.
5 (3.0)
6 Pa: mähän oon ollu työssä lastenkodissaI have been in-work in-children’s-home
I have worked in a children’s home you know
7 ja (.) ollu pienten lasten °kanssa°.and been small children withand (.) I’ve been with small °children°.
8 (2.2)
9 Th: joka on jotenkin selvästi naisellista.which is somehow clearly femininewhich is somehow clearly feminine.
10 Pa: =nii:hPRT=yea:h.
11 (1.0)
12 Pa: mut et tässä< (.hhhhhhhhh) tässä kohtaa nin: #e::# (1.0)but that here here point PRTbut at this< (.hhhhhhhhh) this point erm:: (1.0)

556 Key Contexts of Study in CA: Populations and Settings
13 (mut jos<) (.) työskennellään näitten hankali#en (0.2)but if work these burdensome(but if<) (.) one works with these laborious (0.2)
14 epäsosiaalisten (0.6) va:ikeitte agressiiviisten (0.4)not-social difficult aggressiveantisocial (0.6) difficult aggressive (0.4)
15 >nuorten kanssa ni< ^sillon< miehen .hhhhhhhh paikka onyouth with PRT then man’s place is>adolescents< ^then< then there is .hhhhhhhh clearly
16 ihan selkeä.very cleara place for a man there.
17 (0.6)
18 Pa: #ja ja# sillä on niinku (tehtävänsä)/(tehtävä °siinä°).and and it is PRT his_task task thereand and he has his task (°there°).(2.0)
20 Th: et se on kohta mistä isä ei voi lähteä.=that it is point from-where father not can leaveso it is a point from which the father cannot leave.=
21 Pa: =nii:.PRT=yeah:.
22 (6.0)
23 Th: .nfff vähä niinku sinä sanoisit että .hhhh sairaanlittle PRT you would-say that sick
.nfff it’s a bit like you were saying that .hhhh the
24 lapsen jah (0.4) kuolevan lapsen ja (0.8) pienenchild and dying child and smallfather can abandon (0.4) a sick child and (0.8) a
25 lapsen< #i:# (1.0) isä voi hylätä.child father can abandondying child and a (1.0) small child.
26 (1.5)
27 Th: mutt tämmöstä >asosiaalista< lasta niin se on mahdotonta.but this-kind-of not-social child PRT it is impossiblebut this kind of >antisocial< child it is impossible.
28 (2.0)
29 Th: hänelle isä on aivan välttämätön.for-him father is quite unavoidablefor him the father is absolutely necessary.
30 (22.0)
31 Pa: nii:.PRTyeah:.
32 (10.0)
33 Pa: ((clears throat))
34 (34.0)
Conversation Analysis in Psychotherapy 557
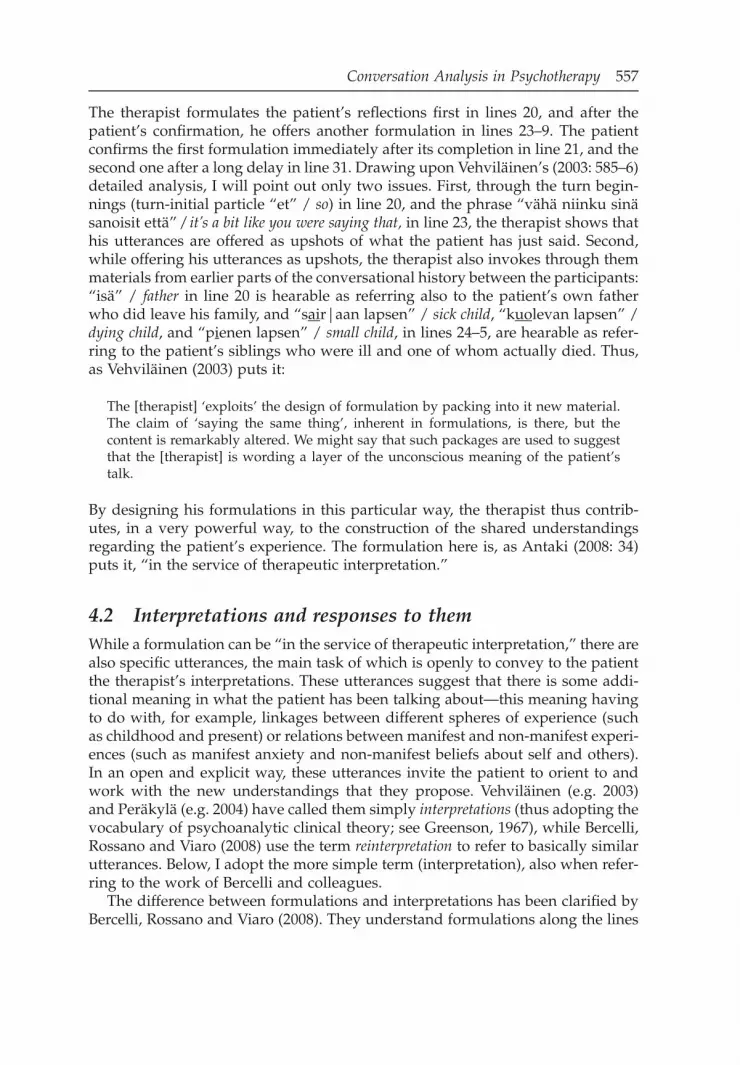
The therapist formulates the patient ’ s refl ections fi rst in lines 20, and after the patient ’ s confi rmation, he offers another formulation in lines 23 – 9. The patient confi rms the fi rst formulation immediately after its completion in line 21, and the second one after a long delay in line 31. Drawing upon Vehvil ä inen ’ s ( 2003 : 585 – 6) detailed analysis, I will point out only two issues. First, through the turn begin-nings (turn - initial particle “ et ” / so ) in line 20, and the phrase “ v ä h ä niinku sin ä sanoisit ett ä ” / it ’ s a bit like you were saying that, in line 23, the therapist shows that his utterances are offered as upshots of what the patient has just said. Second, while offering his utterances as upshots, the therapist also invokes through them materials from earlier parts of the conversational history between the participants: “ is ä ” / father in line 20 is hearable as referring also to the patient ’ s own father who did leave his family, and “ s ai r|aan lapsen ” / sick child , “ k uo levan lapsen ” / dying child , and “ p i enen lapsen ” / small child , in lines 24 – 5, are hearable as refer-ring to the patient ’ s siblings who were ill and one of whom actually died. Thus, as Vehvil ä inen (2003) puts it:
The [therapist] ‘ exploits ’ the design of formulation by packing into it new material. The claim of ‘ saying the same thing ’ , inherent in formulations, is there, but the content is remarkably altered. We might say that such packages are used to suggest that the [therapist] is wording a layer of the unconscious meaning of the patient ’ s talk.
By designing his formulations in this particular way, the therapist thus contrib-utes, in a very powerful way, to the construction of the shared understandings regarding the patient ’ s experience. The formulation here is, as Antaki ( 2008 : 34) puts it, “ in the service of therapeutic interpretation. ”
4.2 Interpretations and r esponses to t hem While a formulation can be “ in the service of therapeutic interpretation, ” there are also specifi c utterances, the main task of which is openly to convey to the patient the therapist ’ s interpretations. These utterances suggest that there is some addi-tional meaning in what the patient has been talking about — this meaning having to do with, for example, linkages between different spheres of experience (such as childhood and present) or relations between manifest and non - manifest experi-ences (such as manifest anxiety and non - manifest beliefs about self and others). In an open and explicit way, these utterances invite the patient to orient to and work with the new understandings that they propose. Vehvil ä inen (e.g. 2003 ) and Per ä kyl ä (e.g. 2004 ) have called them simply interpretations (thus adopting the vocabulary of psychoanalytic clinical theory; see Greenson, 1967 ), while Bercelli, Rossano and Viaro (2008) use the term reinterpretation to refer to basically similar utterances. Below, I adopt the more simple term (interpretation), also when refer-ring to the work of Bercelli and colleagues.
The difference between formulations and interpretations has been clarifi ed by Bercelli, Rossano and Viaro (2008) . They understand formulations along the lines

558 Key Contexts of Study in CA: Populations and Settings
suggested above, as utterances which, while proposing further signifi cance of what the patient has said, frame what they propose “ as something that was implic-itly meant by the client ” (46). An interpretation, on the other hand, presents the analysis “ as something that, though grounded in what the client has said, is caught and expressed from the therapist ’ s own perspective — therefore something possibly different, and ostensibly so, from what the client meant ” (47). Thus, the distinction made brings to the foreground the basic difference in the production format of the two therapeutic interventions: in formulation, the principal — ” the party whose position the words attest ” (Goffman, 1981b : 226) — of the therapist ’ s utterance is, at least nominally, the patient, and in interpretation, it is the therapist. Thus, in delivering an interpretation while speaking about the patient ’ s mind and circumstance, the therapist still uses his or her own ‘ voice ’ in full strength. Bercelli, Rossano and Viaro ( 2008 : 49) point out that the linkage of interpretations to the therapist ’ s own reasoning is often achieved by the use of epistemic markers and perspective markers, such as I think , in a sense or perhaps .
In Extract (2), the therapist delivers an interpretation from line 16 onwards. Prior to the interpretation, the patient talks about his disappointment in his mother for not having encouraged him as cross - country skier. In the interpretation, the therapist proposes that the patient has displaced his disappointment from father to mother, and that the target of the ‘ original ’ disappointment is the father who was not available for him in his childhood.
(2) Tul 6:3; 1A
1 Pa: Ja varsinkin se hiihto oli se mun,and especially it skiing was it myAnd especially skiing was my,
2 (2.2)
3 Pa: mun laji.my sportmy kind of sports.
4 (7.8)
5 Pa: .mthh >Mut et siin (>oli<) niinko äidillä olibut that there was PRT mother had
.mthh >But there (>was<) mother sort of had
6 jotenkin< nihkee |suhtautuminen siihen kokosomehow sticky relation to-it wholesomehow< negative |attitude to that whole
7 hommaan että se suorastaan vähän niinku esteli.to-job that it even a-little PRT hinderedbusiness so that she even tried to stop me.
8 (7.2)
9 Pa: >Jotenki mulla on niinku semmonen< (0.6) tunnesomehow I have PRT such feeling>Somehow I have the< (0.6) feeling that
Conversation Analysis in Psychotherapy 559
10 (.) oli sillon ja nyt (.) nyt vieläkin ettähad then and now now still that
(.) had it then and still (.) still have it
11 .hhh (0.2) että lasta pitäs päinvastointhat child should on-the-contrary
.hhh (0.2) °that instead of what she did a child
12 kannustaa niinkun tommoseen °(hommaan)°.encourage PRT to-such to-jobshould be encouraged to such °(activity)°.
13 (8.5)
14 Th: Joo:o,PRTYeah:.
15 (4.2)
16 Th: .hh Syvemmällä tasollahan se merkitsee sitäon-deeper level it means it
.hh On a deeper level it means you know
17 että (0.6) mt että äiti ei,that that mother notthat (0.6) tch that the mother ^wasn’t
18 (2.0)
19 Th: ^ollu isä.were fatherthe father.
20 (2.2)((13 lines omitted))
33 .hhh >ja koska se tämmönen<=#y::# >Mä luulenand because it such I think
.hhh >and because this kind<=#er::# >I think
34 et sun on< v:aikea oikeestaan (1.2)that you have difficult reallythat it’s actually< diff:icult for you (1.2)
35 myöntää sitä että että y’ (.)admit it that thatto admit that that eh (.)
36 is#ä:# isä puuttu sinul°ta°.father father was-missing from-youyou didn’t didn’t have a fa°ther°.
37 (1.2)
38 Th: Sillä tavalla et se oli vähän niinku äidin vika,on-it on-way that it was little PRT mother’s faultSo that it was as it were mother’s fault,
39 (1.3)
40 Th: mt |että isä puuttu.that father was-missing
tch |that the father wasn’t there.
41 (0.7)

560 Key Contexts of Study in CA: Populations and Settings
42 Th: .hh Ja se ilmenee tällä tavalla ettäand it emerges this way that
.hh And it shows in this way that
43 .hhh (0.2) #ä:# sie kaipaat niitä ominaisuuksiayou miss those properties
.hhh (0.2) #er:# you miss the characteristics
44 (0.8) joita <isässä olisi ollut>.which in-father would-have been
(0.8) that <the father would have had>.
45 (2.2)
46 Th: Ja (.) oot tyytymätön äitiin nytand are dissatisfied into-mother nowAnd (.) you are dissatisfied now with mother
47 siitä (0.7) mt että >äidillä eifrom-it that mother notfor the fact (0.7) tch that the >mother didn’t
48 |ollu< niitä ominai°suuksia°.had those properties
|have< those character°istics°.
49 (1.6)
50 Th: Että äiti ei ollu isä.that mother not was fatherThat the mother wasn’t the father.
51 (3.5)
52 Th: #Isän::# (1.0) tehtävänäh’n (.) tavallisestifather’s task usually#It’s the fa:ther’s (1.0) duty (.) normally
53 on: (1.0) #(juu:r) i::#nnostaa (0.5) poikaa u-is exactly inspire boy(1.0) #( ) to e#ncourage (0.5) the son to o-
54 ulkoiluun ja urhei°luun°.to-be-outdoors and to-sportoutdoor activities and °sports°.
55 (6.0)
56 Th: mt Metsälle ja,to-forest and
tch To hunting expeditions and,
57 (1.5)
58 Th: urheilukentille ja niin edel°leen°.to-sport-fields and so furtherto athletic fields and so °on°.
59 (18.5)
60 Pa: .mthhhhff hhhmthh (1.0) mt hhhh.mthhhhff hhhmthh (1.0) tch hhhh
61 (6.2)
62 Pa: .mthh Nii::, (.) Tottahan se on (.) on tietysti,PRT true it is is of-course
.mthh Yeah::, (.) It is true (.) true of course,

Conversation Analysis in Psychotherapy 561
63 =Isänhän siellä ladun varrellafather there track by=It is father who >should have been< there
64 >ois pitäny< olla.had should beby the skiing track.
65 (0.8)
66 Pa: Hihkumassa.=>Eikö niin<.whooping no soWhooping.=>shouldn’t he<.
67 Th: Niin.PRTYeah.
68 (10.0)
69 Th: .hh Ja urheiluseuran#::# johtokunnassaand sport-society’s in-board
.hh And in the steering committee of the sports club
70 (1.0) tukemassa nuorten työtä.supporting youth’s work
(1.0) supporting the youngsters’ work.
71 (5.2)
72 Pa: °Nii:°,PRT°Yeah:°,
73 (35.0)
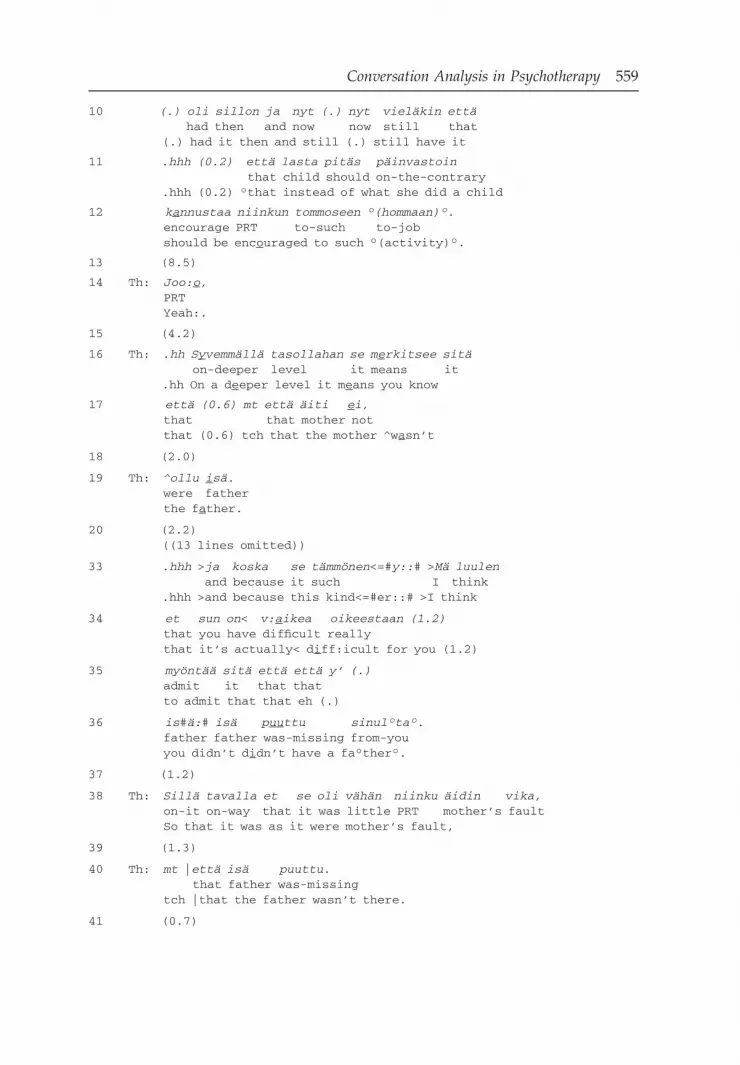
In lines 16, 34, and 42, the therapist produces the kind of epistemic and perspec-tive marking that Bercelli, Rossano and Viaro (2008) suggest is distinctive of psychotherapeutic interpretations: “ S y vemm ä ll ä tasollahan ” / On a deeper level(line 16) frames what the therapist says as involving a new perspective vis - à - vis the earlier talk; “ M ä luulen ” / I think (line 33) marks the proposal as arising from the therapist ’ s own reasoning, and “ Ja se ilmenee t ä ll ä tavalla ett ä ” / It shows in this way that (line 42) indicates the therapist ’ s reasoning from which the proposal arises.
According to Bercelli and colleagues, the projected response is another feature that makes interpretations different from formulations. While formulations make relevant confi rmations or disconfi rmations, which often take a minimal form (e.g. lines 21 and 31 of Extract (1)), interpretations are geared to project more extensive agreements or disagreements. Per ä kyl ä (2005) and Bercelli, Rossano and Viaro (2008) have made converging observations regarding the ways in which therapists design interpretative utterances so as elicit more than minimal response from the patient. A key technique involves, in the face of minimal or no response from the patient, the therapist adding increments to his/her own interpretations, thus pursuing a more elaborate response. In Extract (2), the interpretation is hearably complete, for example, in lines 36, 40, 44, 48, 50 and 54. In the absence of any

562 Key Contexts of Study in CA: Populations and Settings
response from the patient, the therapist continues, thus creating new opportuni-ties for the patient to respond.
Recurrently, patients respond to interpretations with what Per ä kyl ä (2005) calls elaboration and Bercelli, Rossano and Viaro (2008) call extended agreement : an utter-ance through which the patient shows his or her agreement and understanding of the interpretation by offering evidence for the interpretation (Bercelli, Rossano & Viaro, 2008 : 56 – 7), or illustrating or explaining what was proposed in the inter-pretation (Per ä kyl ä , 2005 : 165). There is a dramatic difference between this default response to psychotherapeutic interpretation, and the default response to diag-noses in medical interaction, as the latter are minimal or non - existent (Heath, 1992 ; Per ä kyl ä , 2002 ). The difference in responses embodies the difference in the task of the professional ’ s talk in these two types of encounters: while in medical consulta-tion it is to inform the patient about the professional ’ s view and to clear the way to the next phase of the encounter (discussion on treatment), in psychotherapy, it is to invite the patient to reconsider his or her understandings along the lines suggested by the clinician (i.e. the talk is the cure).
In Extract (2), the patient ’ s response to interpretation occurs in lines 62 – 4 (sim-plifi ed): the patient fi rst displays his agreement in compact form ( “ Nii, Tottahan se on tietysti ” / Yeah it is true of course ) and thereafter moves on to illustrate what was said in the interpretation ( “ I s ä nh ä n siell ä ladun varrella ois pit ä ny olla ” / Itis father who should have been there by the skiing track ). Through this extended agree-ment (elaboration), the patient documents his understanding of the interpretation. Below, we return to the design and placement of this response.
4.3 Questions Asking questions is the third recurrently addressed practice in contemporary conversation analytical research on psychotherapy. An overall impression of empirical materials presented in conversation analytic and other empirical studies on psychotherapy is that questions are used in some therapies more than others. While in all kinds of psychotherapies there is a place for therapist ’ s questions, some therapies can be characterized as question driven (for example solution - oriented therapies and systemic family therapies), while others (such as psychoanalysis) appear as response driven (Per ä kyl ä & Vehvil ä inen, 2007 ). In response - driven therapies, the therapist ’ s understandings of the patient ’ s experi-ences are conveyed through formulations, interpretations and other interventions, which are made in response to the patient ’ s narratives. These responses drive the topic and manage the agenda. In question - driven therapies (e.g. Gale, 1991 ; Halonen, 2008 ; MacMartin, 2008 ; Per ä kyl ä , 1995 ) therapists ’ work is done largely through questions.
Solution - oriented therapies are an impressive example of the question - driven framework (see Gale, 1991 ; MacMartin, 2008 ). The therapist ’ s understandings of the patient ’ s experiences are largely conveyed through optimistic questions, char-acterized by MacMartin as presuppositional questions that are “ built so as to prefer answers from [patients] that affi rm . . . their agency, competence, resilience,

Conversation Analysis in Psychotherapy 563
(3a) MacMartin, 2008 : 83 – 4
1 Th: So they might have (0.2) what-what would’ve (0.4)2 the >kind=of-< (0.6) average person might=of3 (0.8) done in that situ^a|tion4 (1.1)5 Pa: UH:: well honestly try an’ (0.3) find somebody6 else to live with?7 (0.2)8 Th: Mm hm9 (0.9)10 Pa: Run away:.
((17 lines omitted))
28 Pa: That’s about #it.# (.) #Get out er stay:.#29 (0.2)30 Th: Yeah31 (.)32 Pa: An’ deal with it.33 (0.4)34 Th: .Hg (.) hgh=what do you think it says about you35 that you’ve-you were able to:, (0.2) to:,36 ^not |leave to stay there (0.5) to make the choice37 to stay: an’ kind of deal with (0.2) things that38 were going on.
abilities, achievements, or some combination thereof ” (MacMartin, 2008 : 82). Extract (3a) illustrates this. Prior to the extract, the patient, a man in his twenties, has been explaining diffi culties in living with his parents.
As MacMartin (2008) points out, the therapist ’ s question in lines 34 – 8 is designed to invite “ the client to describe himself in relation to a number of optimistic pre-suppositions about his ablility to cope. ” By reorganizing some of the materials presented by the patient in his answer to the prior question, the therapist ’ s query in lines 34 – 8 foregrounds the patient as “ able to not leave ” and to “ make the choiceto stay and to deal with things ” (simplifi ed).
Questions can be used to convey different understandings, not only optimistic ones as in MacMartin ’ s materials. In a recent study on the use of questions in group therapy for alcohol addicts, Halonen ( 2006 ; see also Halonen, 2008 ) shows the ways in which the design and placement of therapists ’ follow - up questions after patient narratives highlight elements in the narrative that can be heard by patients as symptoms of their addiction. The question “ puts this symptom to the patient to accept or reject ” (Halonen, 2006 : 286). In a certain sense, these ques-tions work in the opposite direction as compared to those in solution - oriented therapy: whereas in the latter, the patient ’ s experience is recast as involving agency and competence, in the former, it is recast as involving powerlessness in relation to alcohol.

564 Key Contexts of Study in CA: Populations and Settings
5 Relational Aspects of Practices
Above, we examined some key practices of psychotherapists as they have been described in CA research. These practices pertain to particularly designed utter-ances that occupy specifi c positions in specifi c sequences of psychotherapeutic interaction: formulations, interpretations and questions. All convey specifi c, therapeutically relevant understandings of patients ’ prior talk and patients ’ expe-riences embodied in this talk, and all invite patients to orient to and to work with these understandings. In the next part of the chapter, we continue the exposition of the results of CA research on psychotherapy, but from a slightly different angle. We take up aspects of practice that pertain to the relation between therapist and patient, as realized through their interaction.
The relationship between therapist and patient is widely recognized among psychotherapy practitioners and researchers as of the utmost importance. The therapist - patient relation is understood to be a key aspect of the ‘ common factors ’ (features of therapy that do not pertain to any particular therapeutic approach such as psychoanalysis or CBT) that arguably explain a great deal of the outcome of psychotherapy (cf. Wampold, 2001 ). Early in his career, Freud thought that the emotional relation (discussed in terms of transference and counter- transference ) between the patient and the therapist was a potential risk for the therapy; but later on, he (e.g. Freud, 1914 ) and especially many of his contempo-rary followers (e.g. Mitchell, 2000 ), rather saw that the healing in psychotherapy takes place through this therapeutic relationship. As a curative factor, the relation-ship may thus be more important than, for example, the insight brought about through interpretations.
The relational aspects of psychotherapy practice discussed below include resist-ance , affi liation and emotion. The relation between therapist and patient is embodied in the recurrent patterns of interaction that we discussed above (i.e. formulations, interpretations and questions), as well as in other sequences.
5.1 Resistance As Vehvil ä inen ( 2008 : 120) points out, some mismatch between the professionals ’ and the clients ’ actions is common in institutional settings: “ professionals encoun-ter moments where patients resist their actions and institutional agendas. ” Numerous CA studies have focused on these moments. For psychotherapies, patient resistance is a pertinent feature: resistance is not only an obstacle for psy-chotherapy (i.e. something that needs to be sorted out in order for the therapy to take place), but rather, resistance and the therapist ’ s ways of dealing with it are part and parcel of the very activity of doing therapy.
Let us return to optimistic questioning, introduced in the preceding section. Such questions typically meet with patient resistance — in spite of the presupposi-tions embodied in the questions, patients do not , in their answers, view themselves as competent, resilient and able.
Conversation Analysis in Psychotherapy 565
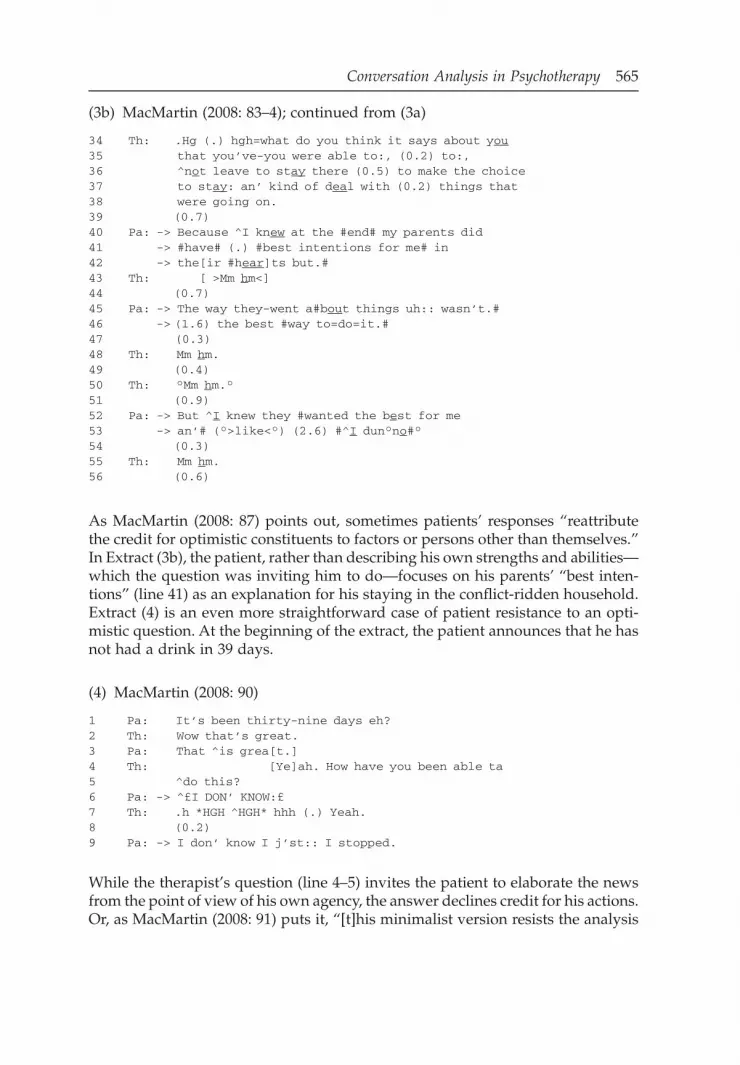
As MacMartin ( 2008 : 87) points out, sometimes patients ’ responses “ reattribute the credit for optimistic constituents to factors or persons other than themselves. ” In Extract (3b), the patient, rather than describing his own strengths and abilities — which the question was inviting him to do — focuses on his parents ’ “ best inten-tions ” (line 41) as an explanation for his staying in the confl ict - ridden household. Extract (4) is an even more straightforward case of patient resistance to an opti-mistic question. At the beginning of the extract, the patient announces that he has not had a drink in 39 days.
(4) MacMartin ( 2008 : 90)
1 Pa: It’s been thirty-nine days eh?2 Th: Wow that’s great.3 Pa: That ^is grea[t.]4 Th: [Ye]ah. How have you been able ta5 ^do this?6 Pa: -> ^£I DON’ KNOW:£7 Th: .h *HGH ^HGH* hhh (.) Yeah.8 (0.2)9 Pa: -> I don’ know I j’st:: I stopped.
(3b) MacMartin ( 2008 : 83 – 4); continued from (3a)
34 Th: .Hg (.) hgh=what do you think it says about you35 that you’ve-you were able to:, (0.2) to:,36 ^not leave to stay there (0.5) to make the choice37 to stay: an’ kind of deal with (0.2) things that38 were going on.39 (0.7)40 Pa: -> Because ^I knew at the #end# my parents did41 -> #have# (.) #best intentions for me# in42 -> the[ir #hear]ts but.#43 Th: [ >Mm hm<]44 (0.7)45 Pa: -> The way they-went a#bout things uh:: wasn’t.#46 -> (1.6) the best #way to=do=it.#47 (0.3)48 Th: Mm hm.49 (0.4)50 Th: °Mm hm.°51 (0.9)52 Pa: -> But ^I knew they #wanted the best for me53 -> an’# (°>like<°) (2.6) #^I dun°no#°54 (0.3)55 Th: Mm hm.56 (0.6)
While the therapist ’ s question (line 4 – 5) invites the patient to elaborate the news from the point of view of his own agency, the answer declines credit for his actions. Or, as MacMartin ( 2008 : 91) puts it, “ [t]his minimalist version resists the analysis

566 Key Contexts of Study in CA: Populations and Settings
and the refl ective self - statements called for by the therapist ’ s optimistic question, even though the earlier contributions (lines 1/3) clearly display the client ’ s orien-tation to his news as jubilantly positive. ”
In dealing with patients ’ resistance toward optimistic questions, the therapists in MacMartin ’ s data resort to a number of techniques, including replacing one form of optimistic question with another form, moving on to more neutral ques-tions, or by reframing patients ’ misaligned contributions with more optimistic alternatives. Most often, however, the therapists recycle their optimistic questions, frequently “ incorporat[ing] material from patients ’ prior disaffi liative turns in a way that acknowledge[s] (while simultaneously transforming) this resistant mate-rial in the reissued question ” (MacMartin, 2008 : 93). Extract (5) below shows the optimistic question from Extract (3b), now reissued after the patient ’ s resistance.
As MacMartin ( 2008 : 93) points out, alongside the materials that the question in Extract (5) reuses from the question in Extract (3b), the therapist adds material taken from the patient ’ s initial response (see lines 68 – 71, cf. lines 40 – 1, 45 – 6 in Extract (3b)). Thus the reissued question underlies “ additional competencies of the patient in terms of his capacity to see his parents in a respectful, positive light despite the diffi culties of the situation ” (MacMartin, 2008 : 94). But as we see from lines 79 and 81, the reissued question is not more successful than the initial one.
Patient resistance is not restricted to question - answer sequences: it can occur in any second - position action that patients are involved in (for resistance in response to formulations, see Madill, Widdicombe & Barkham, 2001 ). 1 Consider Extract (2) again, and the patient ’ s receipt of the therapist ’ s interpretation. He remains silent through a number of transition - relevance places (lines 20, 37, 41, 45, 49, 51, 55), 2 thereby not affi liating with the reconsideration of his experience
(5) MacMartin, 2008 ; follow - up from (3b)
64 Th: ^>What would ^it (was) ^it< (0.2) about you:65 that makes: (0.2) °#i-y-#° (0.6) makes it possible66 for you to be able to stay and deal with those67 things. tuh (0.2) recognize ^you know ^that, (.)68 yer parents wer:e, (0.3) in fact having yer best69 intentions in mind even though they may not have70 been, (0.3) um going about it in a way that (0.6)71 kind of (.) fit with (0.5) how you would have72 preferred,73 (2.3)74 Pa: .pt U::M: (1.2) °what does that #say about me?#°75 (0.3)76 Th: Yeah. (0.4) that- (0.2) .h >you know I’m I’m77 getting the sense too that78 (.)79 Pa: -> Y’a[sk that ques]tion °y’ask that question°=80 Th: [somebody else]81 Pa: -> =°a lot eh?°

Conversation Analysis in Psychotherapy 567
from the perspective suggested by the therapist. Above, we suggested that the therapist deals with the lack of patient response by adding new increments to the interpretation. If we now consider the topical development of the interpreta-tion that ensues, we see that the therapist eventually offers an account of a father ’ s conventional duties as evidence for his statement regarding the displacement of disappointment from father to mother. By focusing his elaboration on this fi nal, incremental part of the interpretation, the patient avoids elaborating the material offered in the earlier parts of the interpretation (the displacement of the disap-pointment from mother to father). As Per ä kyl ä (2005) has suggested, this involves what might be called indirect resistance to the interpretation.
5.2 Affi liation In spite of the fact that resistance may be an ever - present feature of therapeutic interaction, there are also moments in which the therapist ’ s and the patient ’ s actions and understandings do meet (on affi liation more generally, see Lindstr ö m & Sorjonen, this volume). These may be therapeutically signifi cant moments in which the therapist and the patient collaborate in constructing new understand-ings regarding the patient ’ s experience. In clinical theory, Stern ’ s (2004) well - known phrase moments of meeting refers to such occasions. Patients ’ extended agreements to interpretations are one locus where such a convergence can take place. Consider Extract (6), in Italian, which is taken from the analysis of cognitive and systemic therapies by Bercelli, Rossano and Viaro (2008) :
(6) Bercelli, Rossano & Viaro ( 2008 : 57 – 8)
1 Th: (allora) è venuto fuori anche (0.5) questa- h cosa quiso is come out also this thing here(so) what’s come up as well (0.5) is this- h (.) interesting
2 (.) interessante.=quindi allora (0.3) il fatto di essere a tavola,interesting so then the fact of being at table
thing.=so then (0.3) the fact of being at the ta:ble,
3 (1.0) e di essere un po’ (.) ingabbiato (.) a tavola::and of being a bit caged at table
(1.0) and being a bit (.) caged (.) at the ta::ble
4 Pa: a questo punto, ripensandoci potrebbe essere.at this point rethinking-to-it could beat this point, thinking back it might be.
5 Th: potrebbe essere che lei si senta- poi lei lo risolvecould be that you self feel then you it resolveit might be that you feel- then you resolve it
6 Pa: alzandomi=raising-myselfby getting up=
7 Th: =alzandosi e togliendosi (.)raising-yourself and taking-out-yourself=by getting up and getting out (.)

568 Key Contexts of Study in CA: Populations and Settings
8 Pa: da[lof-theo[f
9 Th: [dalla gabbietta.of-the little-cage[of the cage.
10 (3.0)
11 Pa: °sì.°yes°yes.°
12 (5.0)
13 Pa: a questo punto no? (0.5) penso che la nascita° delat this point no I-think that the birth of-theh °at this point right? (0.5) I think that the birth° of my
14 secondo figlio no? perché poi (.) non- (cr[esce)second son no because then not growssecond son right? because then (.) not- he’ll gr[ow
15 Th: [heh hehheh heh[heh heh
16 Pa: mi: mi faccia:: provare questa aggressività perché::to-me to-me makes to-feel this aggressiveness becauseit: it: makes me:: feel this aggressiveness because::
17 mi ingabbia °secondo me, ancora di più.°me cages according to-me even of moreit cages me °in my opinion, even more.°
18 (1.5)
19 Pa: °non so.°not I-know°I don’t know.°
20 (1.0)
In the initial part of the interpretation, taking place before this segment, the thera-pist has suggested that the violent fantasies disturbing the patient during family mealtimes, of attacking his wife with a knife, might arise from a feeling of being caged at the table (see Bercelli, Rossano & Viaro, 2008 : 52). In lines 1 – 9, the thera-pist produces an expansion on this interpretation, suggesting that getting up from the table might be the patient ’ s way of “ resolving ” this problem ( “ risolve ” in line 5). The patient receives the interpretative utterance with agreement (see lines 4 and 11), in addition to collaboratively fi nishing the therapist ’ s turns (cf. sequence from lines 5 – 7 and 7 – 9). In line 13, he produces an extended agreement (elabora-tion) in which he links his wife ’ s pregnancy and the coming birth of his second son to the feeling of being caged. In an illuminating way, Bercelli and colleagues ( 2008 : 58) show how the patient displays that the interpretation has changed his perspective here and now:

Conversation Analysis in Psychotherapy 569
[T]he evidence in support of the therapist ’ s interpretation is presented by the client as something that he has considered from this perspective right at this moment, just after the therapist ’ s last increment to his interpretation (line 13, “ at this point right? I think . . . ” uttered in a low voice). This makes the previous rather long silences (lines 10, 12), before and after the low - uttered agreement token, retroactively hearable as silences during which the client ’ s idea has emerged. And the client ’ s hesitations and low voice utterances throughout his response (lines 10 – 20) convey the same sense of an idea under construction. Such design features . . . characterize the client ’ s response as displaying a change of perspective about the talked - about matters, and moreover a change triggered by the therapist ’ s previous reinterpretation.
Thus, the patient ’ s extended agreement involves a moment where his and the therapist ’ s understandings meet (cf. Stern, 2004 ). Now, from this perspective, reconsider Extract (2), shown above. The patient ’ s elaboration of interpretation is preceded by a long silence (lines 59 – 61), and the elaboration is (through the preface “ Tottahan se o n (.) on tietysti ” / It i s true (.) true of course, through the marked word order in the Finnish original, and through the emphasis on “ I s ä nh ä n ” / f a ther ) designed as one that conveys a sense of ‘ Now I realized this, as you said it to me ’ . Here, as well as in Extract (6), the patient displays a change in perspec-tive, and the understandings of the participants momentarily converge. The display of meeting of understandings is there in spite of the fact that the patient ’ s elaboration may, as was pointed out above, also embody selectiveness and thereby implicit resistance to some aspect(s) of the interpretation.
The meetings of therapists ’ and patients ’ understandings that take place in and through patients ’ extended agreements/elaborations after therapists ’ interpreta-tions also have a further sequential component to them. As Bercelli, Rossano and Viaro ( 2008 : 57) point out, therapists regularly expand the sequence after patients ’ extended agreements by producing comments, follow - up questions and/or further reinterpretations, through which they show that patients ’ responses are “ valuable contributions to the therapeutic work. ” Per ä kyl ä (2010, 2011) has pointed out similar characteristics in the therapists ’ third - position utterances that follow the patients ’ responses to interpretation. According to him, third - position utter-ances that are designed as formulations or extensions of the patient ’ s responses convey the therapist ’ s acceptance and ratifi cation of the understandings that the patient conveys in his/her responses (elaborations). Thus, in lines 68 – 9 of Extract (2), the therapist takes up the patient ’ s elaboration (which was in line 63 – 5). The third - position utterance is designed as a grammatical continuation (extension; see Vehvil ä inen, 2003 ) of the patient ’ s preceding turn, and it is hearable as being in line with that turn, ratifying the patient ’ s understandings. However, the third - position utterances also seem to involve (usually implicit) shifts of perspective: alongside appreciating and ratifying patient elaborations, they also indirectly suggest that there is something else or something more in what the patient describes in his or her elaboration. In Extract (2), the therapist ’ s characterization of the patient ’ s missing father (he should have been on the steering committee of the skiing club supporting the youngsters ’ work; see lines 69 – 70) is, in a particular sense, different from the patient ’ s initial characterization of him (he should have

570 Key Contexts of Study in CA: Populations and Settings
been there by the skiing track, cheering, or literally, “ hihkumassa ” / whooping it up ; see lines 63 – 6): while the patient presents the father ’ s attention as dependent on his son ’ s achievement, and the father as a somewhat childish fi gure who is “ whooping ” to cheer for his son, the therapist portrays the father as an independ-ent and powerful fi gure. Per ä kyl ä (2010, 2011) argues that through perspective shifts like this, the therapists do further interpretative work, in this case enriching and intensifying the joint characterization of what the patient missed.
5.3 Emotion Although emotion is arguably ubiquitous in any interaction because there is always some background feeling (Damasio, 1999 ) associated with what is being said, there are specifi c junctures in interaction where emotion is attended to and worked with in particular ways (see Sacks, 1992 : ff. 570; Sorjonen & Per ä kyl ä , 2012). Much of the work in any psychotherapy revolves around the patient ’ s emo-tions: emotions that are painful, emotions that are diffi cult to deal with, emotions that are perceived as inappropriate, or emotions that should be there but are not (see Voutilainen, 2012). Recently, emotions have emerged as a topic for CA research, and likewise, CA researchers working with psychotherapy data have started to focus on emotions in psychotherapy (see Per ä kyl ä 2008 ). (On emotion more gener-ally, see Ruusuvuori, this volume).
In a recent case study on one psychotherapeutic session, Rae (2008) identifi ed a practice that can serve as a vehicle for work with emotions. This practice involves the use of a particular technique for repair — other - initiated other correction, accomplished through what Rae calls lexical substitution — in response to utter-ances that have emotional valence in them.
(7) Rae ( 2008 : 64)
1 Pa: I am surviving and I am2 Th: But it feels (.) doesn’t feel right3 Pa: It feels a little uncomfortable4 Th: Or a lot uncomfortable.5 Pa: It feels a l(hoh)ot unc(huh)omfortable actually
(8) Rae, 2008
1 Pa: tis the season to be jolly and y’know2 I can play I can do jo- I can do jolly3 Th: Pretend jolly4 Pa: I can pretend jolly I can just be out there
In both extracts, the patients are involved in a description of their current circum-stances, and these descriptions have an emotional valence in them: in (7), “ It feels a little uncomfortable ” , and in (8), “ I can play I can do jo - I can do jolly ” . In response to these descriptions, the therapists propose modifi ed expressions (in (7), “ or a lot uncomfortable ” , and in (8), “ pretend jolly ” ). In the subsequent lines (line

Conversation Analysis in Psychotherapy 571
5 of (7); line 4 of (8)) the patients adopt the proposals. As Rae points out, these lexical substitutions show the patient that the therapist is closely monitoring and making sense of his/her talk, and they propose the patient should express his/her feelings more explicitly. Put another way, lexical substitutions in the context of patient utterances that have emotional stance in them show that the therapist has recognized the patient ’ s emotion, and perhaps perceives it as more intense than the patient described.
A recent article by Voutilainen, Per ä kyl ä and Ruusuvuori (2010) suggests that there may be two broad frames through which psychotherapists respond to patients ’ narratives with emotional stance. One frame involves interpretation , namely therapist ’ s suggestions that there is something more or something else in what the patient says. Interpretative utterances and responses to them were described above. The other frame has to do with a recognition of emotion, and it might be called empathy . In responses within this frame, the therapist does not suggest new meanings, but instead, indicates that s/he recognizes, and considers valid, the emotions that patient descriptions are implicating or explicating. In the data from cognitive - constructivist psychotherapy examined by Voutilainen and colleagues, these two frames were both present, combined in different ways, in therapists ’ ways of responding to patients ’ narratives with emotional stance. In Extract (9), the therapist, in one utterance, recognizes the patient ’ s emotion, and in a subsequent one, offers an interpretation. At the beginning of the extract (lines 1 – 5), the patient is answering the therapist ’ s question about her capability to defend herself against her mother ’ s criticism, describing her anxiety in a situation where the mother would criticize her face - to - face.
(9) Voutilainen, Per ä kyl ä & Ruusuvuori (2010: 89 – 90)
1 (0.7)
2 Pa: .hh >Ehkä PU<HELIMES ET jos semaybe in-phone so if it
.hh >Maybe on the PH<ONE I MEAN if it
3 KASVOKKAIN se on jotenki nii ÄLYTTÖMÄN voimakasface-to-face it is somehow so insanely strongFACE TO FACE it is somehow so INSANELY strong
4 (.) tai sillä lailla että jos se on kasvokkainor such way that if it is face-to-face
(.) or like that so that if it is face to face
5 .hh nii sitten (.) sit kyllä niinku: (.) saattasso then then really PRT could
.hh so then (.) then I guess I could li:ke(.)
6 mennä #lukkoo että#.go into-lock that#seize up so that#.
7 (0.7)
8 Th: <Ts sä et vois °katsookkaa° äitiä> (.)you not could look at-mother
<Ts you wouldn’t even be able to °look at° mother> (.)

572 Key Contexts of Study in CA: Populations and Settings
9 ^mm[mm.mm[mm.
10 Pa: [N- NII:.PRT
[Y- YEA:H.
11 (0.9)
12 Pa: .hff Et se: (.) se niinku jotenki (.)so it it PRT somehow
.hff So that she: (.) she like somehow (.)
13 katseen voimalla £SHAIS .hh sais mutof-gaze strength could could mejust by looking at me £WOULD .hh floor me
14 maan tasalle et^tä:£.ground’s to-level thatso ^that£
15 (0.5)
16 Th: Nii (.) sit se olis se taas se: ä:itiPRT then it would-be again it mother(that’s) Right (.) then she would be again tha:t mo:ther
17 jota sä oot pienenä pe[län^ny.which you have as-small fearedthat you as a child were af[^raid of.
18 Pa: [Yea:h (.) yea-h.PRT PRT
[Nii: (.) nii-i.
19 (.)
20 Th: Enemmän °^vie[lä.°more stillEven °^mo[re°
21 Pa: [Nii::.PRT[Yea::h.
In lines 7 – 8, the therapist rephrases what would happen in the hypothetical situ-ation. She upgrades the emotion involved in the patient ’ s description by adopting an extreme case formulation (Pomerantz, 1986 ), reusing the patient ’ s own words from an earlier point in the session (data not shown), and by using a soft and comforting voice. Through this turn design, the therapist “ concreti[z]es the patient ’ s fi gurative, idiomatic expression of seizing up, and thus preserves the patient ’ s emotion in the focus of description and views it from a similar perspec-tive as the patient did ” (Voutilainen, Per ä kyl ä & Ruusuvuori 2010b : 90). In doing this, she recognizes the patient ’ s emotional experience.
After the therapist ’ s recognizing utterance, the patient goes on to describe her emotional reaction in the hypothetical situation (lines 12 – 14). In lines 16 – 17, the therapist produces another kind of response to the patient ’ s (expanded) descrip-tion: she interprets the patient ’ s problematic experience by linking it to the fear she felt as a child. Voutilainen and colleagues point out that this way of combining

Conversation Analysis in Psychotherapy 573
recognition and interpretation — recognition comes fi rst, and interpretation thereafter — recurs in their data, and they suggest that the recognition, coming before interpretation and inviting further elaboration of the experience by the patient (see lines 12 – 14 above), contributes to “ a stronger ‘ shared ground ’ for the interpretation ” (Voutilainen, Per ä kyl ä & Ruusuvuori 2010b : 98).
6 Future Directions
CA research on psychotherapy has expanded signifi cantly since the year 2000. In comparison to CA research on medical interaction, however, this fi eld remains in its infancy. Even though some convergence between studies on psychotherapy has occurred (e.g. in studies showing complementary facets of formulations (Antaki, 2008 ), and studies on responses to interpretations, described above), research results have, by and large, not had the cumulative character that studies on primary care encounters have had (see Heritage & Maynard, 2006a ). This is the result of there being fewer studies of psychotherapy and the fact that the psychotherapeutic interactions studied are themselves quite variable. Whereas the medical consultation has a fairly standard form, psychotherapy is done in a mul-titude of different ways, not only in terms of participation (individual, group and family therapies) but also in terms of guiding clinical theories (psychodynamic, cognitive, solution - oriented, interpersonal, etc.). It is likely that ‘ psychotherapy ’ as a practice is far less uniform than the medical consultation is. But we do not know for sure, or in detail, and therefore, comparative studies across different forms of psychotherapy are needed.
Studies that address clinically relevant issues are also needed. From the clinical point of view, change in the patient that comes about in psychotherapy is of the utmost interest because change of some sort is the motivation for all psychothera-pies. Psychotherapy research using methods other than CA largely focuses on processes of change (e.g. Angus, Levitt & Hardtke, 1999 ; Leiman & Stiles, 2001 ; Stiles, et al., 1990 ). Traditionally, CA has been used to investigate rather stable patterns of interaction: ones that remain consistent over time and across situations. The practices of formulating, interpreting and questioning are such stable pat-terns. However, recently in the study of classrooms (Mondada & Doehler, 2004 ; Young & Miller, 2004 ; see also Gardner, this volume) and of physiotherapy (Martin, 2004 ), as well as of speech therapy (Sellman, 2008 ), CA scholars have started to unravel processes of change in learners ’ ways of participating in interactions — showing that conversation analytic description of practices can be adopted in the study of change in these practices. A similar kind of approach can be taken up in the study of psychotherapy, with the aim of showing how patients ’ contributions to psychotherapeutic interaction evolve over time (see Voutilainen, Per ä kyl ä & Ruusuvuori, 2011 ).
Another clinically relevant issue that could and should be taken up by conver-sation analysts involves what is common to psychotherapy relations that work well. It is widely agreed that the effectiveness of psychotherapy rests not only

574 Key Contexts of Study in CA: Populations and Settings
upon the techniques that are specifi c to one or another approach, but on nonspecifi c factors such as the therapist ’ s person and especially the alliance (positive emo-tional relation, trust and collaboration) between the patient and the therapist (e.g. Oei & Shuttlewood, 1996 ; Wampold, 2001 ). In the research literature, these char-acteristics of the therapeutic relation are described on a general level. It would be a key challenge for conversation analytical psychotherapy research to explore the makings of an effective therapeutic alliance (for general CA informed discussion on therapeutic relation, see Pain, 2009 : 51 – 69; and for case studies on therapeutic relation employing CA methodology alongside a quantitative approach, see Lepper & Mergenthaler, 2007, 2008 ). It is obvious that building or maintaining an alliance is not a distinct practice such as formulating, interpreting, questioning, or even the use of recognizing responses to emotional description. Rather, what makes up what is experienced as an alliance must be scattered through various practices and small - scale interactional events between the participants (see Streeck, 2008 ). Through its descriptive apparatus, CA should be able to pin down these practices and events.
NOTES
I wish to thank Charles Antaki, Sanna Vehvil ä inen and Ivan Leudar for joint work on CA and psycho-therapy. Many ideas presented in this chapter have their origins in the chapters that we recently co - authored (Per ä kyl ä , et al., 2008a ; Vehvil ä inen, et al., 2008 ). I also thank Tanya Stivers and Jack Sidnell for many helpful comments on earlier drafts of this chapter. 1 Obviously, fi rst - position actions can also be vehicles of resistance: for example topic initial questions
could be a way to evade the therapist ’ s agenda. However, this has not been investigated in CA studies on psychotherapy.
2 Even though the idiomatic English translation fails to show it, line 39 is not a transition - relevance place: through its syntactic and prosodic features, line 38 projects continuation. Pronoun “ se ” / itin line 38 (see the morphemic gloss) serves here as a projective indexical.