contracting out of clinical services in zimbabwe
TRANSCRIPT

Pergamon 0277-9536(94)00303-3
Sot'. Sci. Med. Wol. 41, No. 1, pp. 13-24, 1995 Copyright ,~ 1995 Elsevier Science Ltd
Printed in Great Britain. All rights reserved 0277-9536/95 $9.50 + 0.00
CONTRACTING OUT OF CLINICAL SERVICES IN ZIMBABWE
B A R B A R A M C P A K E and C H A R L E S HONGORO- '
~Health Economics and Financing Programme, London School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, England and 2Blair Research Laboratory, Joseph Tongogara/Mazowe Street,
P.O. Box 8105, Causeway, Harare, Zimbabwe
Abstract--Contracting is increasingly recommended to developing countries as a way of improving the efficiency of the health sector. However, empirical evidence regarding its effectiveness in this respect is almost completely absent. In Zimbabwe, a long standing contract exists between the Ministry of Health and Wankie Colliery to provide clinical services in the Colliery's 400 bed hospital. This paper details a study of the Zimbabweans' experience with the contract. Its success is assessed using comparisons with a neighbouring government hospital of the price of services (vs the cost in the government hospital); the situation of hospital workers; and the quality of services delivered.The Colliery has established a monopoly position for hospital services in the district. However, it appears to oiler services of at least as good quality at prices which are lower than the unit costs of the government hospital when capital costs are included. Nevertheless, the contract cannot be considered a success due to the failure to contain its total cost. Approximately 70% of provincial non-salary recurrent expenditure is consumed by the contract while only a minority of the province's population have access to the Colliery hospital. Screening patients, both with respect to their ability to pay and to their need for secondary level services does not take place with the result that utilization levels are not controlled.The study highlights a number of important issues affecting contracting in developing country settings: First, contracted institutions attain powerful bargaining positions if there are no viable competitors and the government does not itself retain capacity to offer an alternative service. Second, specific skills are needed for the management of contracts at all levels. If the process of contract development responds to a crisis driven agenda resulting from civil service retrenchment and public expenditure cuts, it is unlikely that adequate consideration will be given to the development of such skills and the retention of key personnel. If such details are neglected, otherwise feasible efficiency gains will prove elusive.
INTRODUCTION
Global trends in favour of privatization of health services in developing countries in the 1980s [14] have undergone a process of modification in the 1990s whereby the stress has been placed on finding an appropriate mix of public and private actors in the health sector [5, 6]. The shift can be conceptualized in diagrammatic form (Fig. 1). Organizational arrange- ments for health systems can be separated into provision and financing components. Whereas the public-private debate has traditionally been con- ducted through comparison of sectors 1 and 4 of this figure [7, 8], it is sectors 2 and 3 which have attract,ed more recent attention. For example, the much debated policy of introducing user fees (private financing) for publicly provided services [9-12] would fall into section 2 of the figure.
In some industrialized countries, innovative strLtc- tures for health systems which use contracts between the public and private sectors are emerging [13]. The reforms of the National Health Service in
*The countries represented in the network are Ghana, India, Malawi, Mexico, Nepal, Pakistan, Papua New Guinea, South Africa, Tanzania, Thailand, Uganda and Zi:rn- babwe.
the United Kingdom represent an extended model based on the contracting principle. These policies can be categorized in section 3 of the figure. Increasingly, contracting on a small scale and other forms of 'managed competit ion' are being advo- cated in developing countries. For example, the 1993 World Development Report emphasized pub- lic finance of essential clinical services, but a greater role for private and N G O provision in this area [6]. The Collaborative Research Network on the Pub- lic-Private Mix for Health Care was established in 1991 in order to bring together researchers working in this area in 12 developing countries.* At a meeting in January 1993, experience of policy development in these countries was compared and the issue of contracting emerged as one increasingly important on policy agendas in countries with otherwise divergent characteristics.
FINANCING PROVISION PUBLIC PRIVATE
PUBLIC 1. 2. PRIVATE 3. 4.
Fig. 1. Framework for analysis ofthe public-privatemix in the health sector.
SSM 41/I--B 13
14 Barbara McPake and Charles Hongoro
While contracts may have many advantages as the basis for health service delivery in theory, in practice it is not clear that these advantages will be realised where infrastructural pre-conditions are absent. Two types of failure--those arising from the nature of the market (in particular entry requirements and economies of location), and those arising from public sector capacity to manage contracts--are predicted in a developing country context. Empirical evidence which would shed light on the success and failure of contracting arrange- ments in practice in the health sectors of developing countries is almost completely absent [14].
Contracting is defined here as a normal market exchange of services which is formalized in advance by the issuing of a contract binding the buyer and seller to the conditions of the exchange. It is assumed that the buyer is a government agent although that may be a health unit purchasing some of the services it needs, or a more centralized body such as the Ministry of Finance. The seller may be either a public or private sector institution.
In Zimbabwe, a long standing contract exists be- tween the Ministry of Health and the 400 bed hospital run by Wankie Colliery. The hospital is contracted to provide the services of a district hospital to the population of Hwange district. This appeared to be a particularly interesting test case since clinical contract- ing presents particular difficulties and complications and the long standing nature of the contract suggests a wealth of experience to be reviewed. The contract provides for the treatment of 'government responsibil- ity' patients by the Colliery hospital on a fee for service basis. A government almoner certifies patients who apply (at an office on the hospital site) as eligible for government responsibility status. They are then treated according to the recommendations of clinical staff and the bill sent to the Ministry of Health. No user fees are charged since in theory only those patients who would be exempted from user charges at government facilities are eligible to be 'government responsibility' patients. (In practice, as is discussed below, this is not the case.) The hospital is not ideally sited to serve as the district hospital and is probably only considered accessible by a minority of the population.
A study of this contract was carried out in March and April 1993 using a team consisting of two economists. This paper reports the results of the study. Section 1 describes the study questions and methods and Section 2 describes the results. Section 3 discusses the results and concludes regarding the implications for contract- ing out policy in developing countries.
DESCRIPTION OF METHODS USED TO APPRAISE THE CONTRACT
Introduction
The main objective of the research was to assess the success or otherwise of this case of contracting
between public and private institutions in the health sector. The approach used to judge this was to make a comparison of certain characteristics of service provision in the contracted hospital (the Colliery hospital) and a neighbouring hospital which is directly managed by the government (a 40 bed hospital at Victoria Falls). Both hospitals are located in Matabeleland North Province.
The choice of Victoria Falls hospital seemed appropriate given its proximity to the Colliery hospital, but the former differed in several import- ant respects which cause some difficulties for the comparison. Most importantly, Victoria Falls hos- pital is much smaller than the Colliery hospital (40 beds compared to 400 beds) and offers a much more limited range of facilities. However, the only government hospitals of comparable size are in Harare, Bulawayo and a few other provinces. Presumably, similar provision would not be planned for Matabeleland North Province in the absence of the contract. It is possible that a number of hospitals of the size of Victoria Falls might be planned in its absence. The full implications of such a scenario might therefore have been considered including the impact on access costs of a number of smaller hospitals rather than a single large referral hospital, and the increased use of referral facilities in Bulawayo and Harare.
The characteristics which were considered most relevant for comparison were:
(i) the costs of services at Victoria Falls hospital compared to the prices charged by the Colliery hospital;
(ii) the working conditions and remuneration levels of workers; and
(iii) the quality of services delivered. In addition, (iv) specific contextual issues such as the history
of the contract's development and its interaction with other policy issues in the Zimbabwean health sector, and the general level of satisfaction with the contract and the factors affecting i t - -as perceived by the Ministry of Health, the Provincial health office and the managers of the Colliery hospital--were reviewed.
The methods used to address each of these factors are reviewed in the corresponding sections below.
Price and cost
Arrangements between the government and the Colliery hospital specify departmental charges for outpatient attendances and inpatient days (separate charges for 'public' and 'private' patients and until September 1992, outpatients differentiated accord- ing to whether consultation was with nurse or doctor), and for X-ray and laboratory (per investi- gation), dental services (per consultation) and theatre (per minute). These charges form the basis
Contracting out of clinical services in Zimbabwe 15
of comparison with unit costs of alternative government provision. Separate charges were also levied for physiotherapy, primary care clinics and other miscellaneous services but since these were not provided at Victoria Falls hospital, they were ignored in both hospitals.
The total charges invoiced and paid for services were also collected by department. These data were all readily available from the assistant hospital secretary (the equivalent of the assistant hospital administrator in a government hospital).
In order to compare with the charge information from the Colliery hospital it was necessary to com- pute unit costs by hospital department: inpalient, outpatient, X-ray, laboratory, dental and theatre. Since expenditure information was only catego:rized by vote (see below), individual items of expenditure had to be reclassified according to department and some items (particularly larger items such as vehicle hire) had to be disaggregated to departmental level using apportionment methods. The methods used are described in detail below but are roughly equivalent to standard cost accounting methods adapted to account for the types of records available at government hospitals in Zimbab~e.
The expenditure votes used in government hospi- tals in Zimbabwe are as follows: hospital pro- visions; medical and surgical supplies; office and miscellaneous; domestic expenses; fuel, light and water; vehicle hire; printing and stationery; t]:avel and subsistence; fares; private vehicle allowa]aces; and bedding and linen.
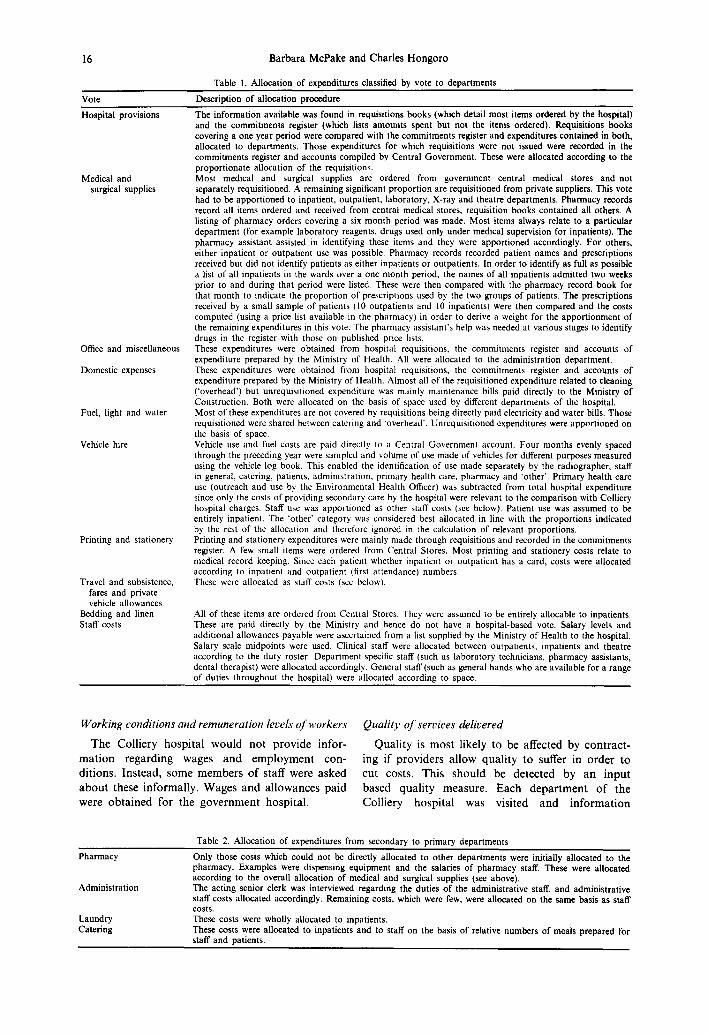
The methods of allocating each of these votes to the relevant departments are outlined in Tables 1 and 2. Expenditures were first allocated to the full range of departments in the hospital which are: inpatients; outpatients; theatre; dentist; laboratory; X-ray; pharmacy; administration; laundry; catering; and cleaning.
Allocation of expenditures by vote to these departments is described in Table 1. Some items were also allocated to an 'overhead' category which was later apportioned to departments on the basis of the space used by each department. For those departments which were not 'primary departments' (those at which charges were levied in the Colliery hospital), a further process of allocation was necess- ary. Table 2 describes the procedures used for this.
Capital costs were assessed using hospital build- ing costs associated with the Second Family Health Project: a hospital building and rehabilitation programme currently under way. These costs were supplied by the Ministry of Health. Since Victoria Falls hospital was not part of this project they are only estimates of the likely actual building costs. In addition, since none of the hospitals in this project were exactly the same size in bed terms as Victoria Falls, ward construction costs were estimated according to the relationship between bed numbers and ward construction cost observed within the
project. Simple linear regression was used to estimate this relationship since this produced an R 2 of 0.94 and more sophisticated approaches were therefore not deemed worth pursuing. Estimates for other items of hospital construction cost (such as theatre construction) might be inflated if they vary according to hospital size, but there was no evidence of such a relationship within the Second Family Health Project for any of these. Capital costs were annuitized using a discount rate of 5% and a building life of 20 years [15].
Unit costs require the division of total depart- mental costs by an appropriate denominator such as inpatient days, outpatient attendances or labora- tory investigations. Routinely reported statistics were obtained from the Provincial Health Office.
A number of difficulties were encountered in the costing exercise. It was not possible to separate out all primary health care costs from total hospital expendi- ture which would be necessary to compare hospital apportioned costs to charges for secondary level services. Since this was done for staff costs (using duty rosters) and for vehicle costs (using vehicle log costs), the overestimation of costs at the government hospitalis not likely to be large.
Most apportionment methods used required some sampling of records. Pragmatic approaches to sample size were adopted based on the availability of records and time available. For example, the six month period used for review of pharmacy records covered the one locatable register which was not currently in use and could therefore be taken away. However it included the January to March period of high malaria incidence and was probably not representative of the whole year. Estimates of relative inpatient and outpatient prescription costs were made towards the end of the costing exercise and the sample sizes feasible in the time available (10 of each) were probably too small for reliability.
The various alternative sources of expenditure information did agree with respect to most of the expenditure items but there were discrepancies, and judgement needed to be used regarding the most accurate source. Most commonly requisition books and commitment registers agreed while accounts from Central government differed. While the practice is to adjust the commitment register to the account, it is more likely that the account is in error.
Finally, some cost estimates relied on the pharmacy assistant's assessment of the use of particular items. While the best source available, there were probably some mistakes made at this stage of the exercise.
It would have been desirable to compare diagnostic mix in the two hospitals. Divergence between the two might help explain some of the findings presented below. Unfortunately, diagnostic information was inadequately compiled at Victoria Falls hospital. Full explanation of the results of the study was hampered by the lack of these measures.
16 Barbara McPake and Char les Hongoro
Table 1. Allocation of expenditures classified by vote to departments
Vote Description of allocation procedure
Hospital provisions
Medical and surgical supplies
Office and miscellaneous
Domestic expenses
Fuel, light and water
Vehicle hire
Printing and stationery
Travel and subsistence, fares and private vehicle allowances
Bedding and linen Staff costs
The information available was found in requisitions books (which detail most items ordered by the hospital) and the commitments register (which lists amounts spent but not the items ordered). Requisitions books covering a one year period were compared with the commitments register and expenditures contained in both, allocated to departments. Those expenditures for which requisitions were not issued were recorded in the commitments register and accounts compiled by Central Government. These were allocated according to the proportionate allocation of the requisitions. Most medical and surgical supplies are ordered from government central medical stores and not separately requisitioned. A remaining significant proportion are requisitioned from private suppliers. This vote had to be apportioned to inpatient, outpatient, laboratory, X-ray and theatre departments. Pharmacy records record all items ordered and received from central medical stores, requisition books contained all others. A listing of pharmacy orders covering a six month period was made. Most items always relate to a particular department (for example laboratory reagents, drugs used only under medical supervision for inpatients). The pharmacy assistant assisted in identifying these items and they were apportioned accordingly. For others, either inpatient or outpatient use was possible. Pharmacy records recorded patient names and prescriptions received but did not identify patients as either inpatients or outpatients. In order to identify as full as possible a list of all inpatients in the wards over a one month period, the names of all inpatients admitted two weeks prior to and during that period were listed. These were then compared with the pharmacy record book for that month to indicate the proportion of prescriptions used by the two groups of patients. The prescriptions received by a small sample of patients (10 outpatients and 10 inpatients) were then compared and the costs computed (using a price list available in the pharmacy) in order to derive a weight for the apportionment of the remaining expenditures in this vote. The pharmacy assistant's help was needed at various stages to identify drugs in the register with those on published price lists. These expenditures were obtained from hospital requisitions, the commitments register and accounts of expenditure prepared by the Ministry of Health. All were allocated to the administration department. These expenditures were obtained from hospital requisitions, the commitments register and accounts of expenditure prepared by the Ministry of Health. Almost all of the requisitioned expenditure related to cleaning ('overhead') but unrequisitioned expenditure was mainly maintenance bills paid directly to the Ministry of Construction. Both were allocated on the basis of space used by different departments of the hospital. Most of these expenditures are not covered by requisitions being directly paid electricity and water bills. Those requisitioned were shared between catering and 'overhead'. Unrequisitioned expenditures were apportioned on the basis of space. Vehicle use and fuel costs are paid directly to a Central Government account. Four months evenly spaced through the preceding year were sampled and volume of use made of vehicles for different purposes measured using the vehicle log book. This enabled the identification of use made separately by the radiographer, staff in general, catering, patients, administration, primary health care, pharmacy and 'other'. Primary health care use (outreach and use by the Environmental Health Officer) was subtracted from total hospital expenditure since only the costs of providing secondary care by the hospital were relevant to the comparison with Colliery hospital charges. Staff use was apportioned as other staff costs (see below). Patient use was assumed to be entirely inpatient. The 'other' category was considered best allocated in line with the proportions indicated by the rest of the allocation and therefore ignored in the calculation of relevant proportions. Printing and stationery expenditures were mainly made through requisitions and recorded in the commitments register. A few small items were ordered from Central Stores. Most printing and stationery costs relate to medical record keeping. Since each patient whether inpatient or outpatient has a card, costs were allocated according to inpatient and outpatient (first attendance) numbers. These were allocated as staff costs (see below).
All of these items are ordered from Central Stores. They were assumed to be entirely allocable to inpatients. These are paid directly by the Ministry and hence do not have a hospital-based vote. Salary levels and additional allowances payable were ascertained from a list supplied by the Ministry of Health to the hospital. Salary scale midpoints were used. Clinical staff were allocated between outpatients, inpatients and theatre according to the duty roster. Department-specific staff (such as laboratory technicians, pharmacy assistants, dental therapist) were allocated accordingly. General staff (such as general hands who are available for a range of duties throughout the hospital) were allocated according to space.
Working conditions and remuneration levels of workers
T h e C o l l i e r y h o s p i t a l w o u l d n o t p r o v i d e i n f o r -
m a t i o n r e g a r d i n g w a g e s a n d e m p l o y m e n t c o n -
d i t i o n s . I n s t e a d , s o m e m e m b e r s o f s t a f f w e r e a s k e d
a b o u t t h e s e i n f o r m a l l y . W a g e s a n d a l l o w a n c e s p a i d
w e r e o b t a i n e d fo r t h e g o v e r n m e n t h o s p i t a l .
Quality of services delivered
Q u a l i t y is m o s t l i k e l y t o be a f f e c t e d b y c o n t r a c t -
i n g i f p r o v i d e r s a l l o w q u a l i t y t o suf fe r in o r d e r t o
c u t cos t s . T h i s s h o u l d be d e t e c t e d b y a n i n p u t
b a s e d q u a l i t y m e a s u r e . E a c h d e p a r t m e n t o f t he
C o l l i e r y h o s p i t a l w a s v i s i t e d a n d i n f o r m a t i o n
Table 2. Allocation of expenditures from secondary to primary departments
Pharmacy
Administration
Laundry Catering
Only those costs which could not be directly allocated to other departments were initially allocated to the pharmacy. Examples were dispensing equipment and the salaries of pharmacy staff. These were allocated according to the overall allocation of medical and surgical supplies (see above). The acting senior clerk was interviewed regarding the duties of the administrative staff, and administrative staff costs allocated accordingly. Remaining costs, which were few, were allocated on the same basis as staff costs. These costs were wholly allocated to inpatients. These costs were allocated to inpatients and to staff on the basis of relative numbers of meals prepared for staff and patients.
Contracting out of clinical services in Zimbabwe
Table 3. Costs by primary department: Victoria Falls hospital (Zimbabwean dollars)
17
Supplies Staff Total recurrent Units Unit recurrent cost Capital Total Unit total cost
Inpatients 464,497 506,543 971,040 6887 (IP days) 141 720.737 1.691,777 246 Outpatients 137,632 94,466 232,098 12,176 (OP visits) 19 94,270 326.368 27 Laboratory 63,270 11,361 74,631 2507 (Lab tests) 30 11,141 85,772 34 X-Ray 77,740 11,985 89,725 1893 (films) 47 I 1,141 100.866 53 Dental 11,770 11,781 23,551 9427 32,978
Theatre 46,319 5387 51,706 10,284 61,990 Total 801,228 641,523 1,442,751 857,000 2,299,751
regarding staff numbers and qualifications and available beds and equipment was collected.
The equivalent exercise at the government hospi- tal was much simpler. The hospital was much smaller and had much less equipment and staff. In addition, it was clear that the comparison was not difficult and that it would not be necessary to try to identify subtle differences in level of available inputs.
While an input-based quality assessment method has several advantages: relative ease of use, objec- tivity and quantifiability, there are some aspects of quality which are ignored and might be expected to respond to the introduction of contracting. Process indicators of quality such as diagnostic, prescril:,tion and treatment practices might be affected by low staff morale (which might respond to such factors as security of employment rather than more obvious influences), by differences in ability to select quality staff or in the quality of supervision (rather than the amount which might be indicated by an input-based assessment). Outcome measures of quality might be affected in similar ways. However, an input-based assessment is likely to be most sensitive to deliberate cost cutting at the expense of quality and was sufficient to demonstrate major qualitative differences.
Other issues
Interviews were conducted with Ministry of Health officials, provincial health officials and the Colliery hospital administration regarding their perspectives on the appropriateness of the contract and the problems experienced with it. These were unstructured but focused interviews. Structured interviews (using short directly administered ques- tionnaires) with a small sample of both in and outpatients at the Colliery hospital were conducted to obtain information on the patients' level of satisfaction with the services provided and their suggestions for improvements.
The original contract was drawn up in the 1950s and much information regarding conditions at that time was unavailable. Specific contextual i:~sues were addressed in the unstructured, focused inter- views with Ministry of Health officials, provincial health officials and Colliery hospital administration and by reviewing minutes of meetings and corre- spondence between the contracting parties. In
addition, a recent attempt to redraft the contract by the Ministry of Health provided useful information.
RESULTS
Price and cost
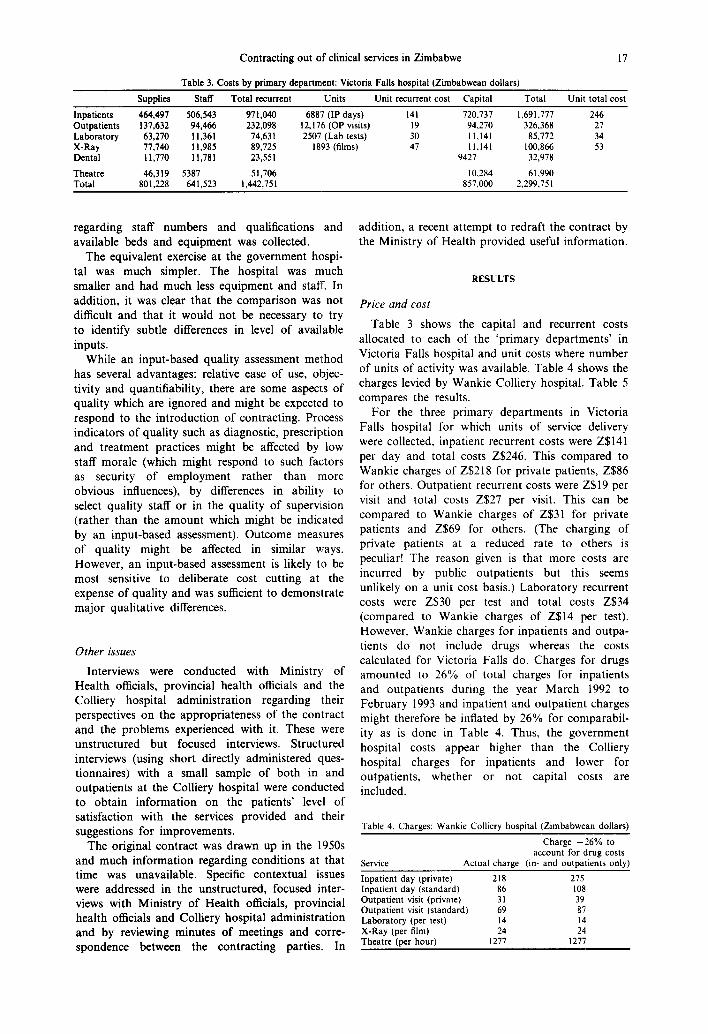
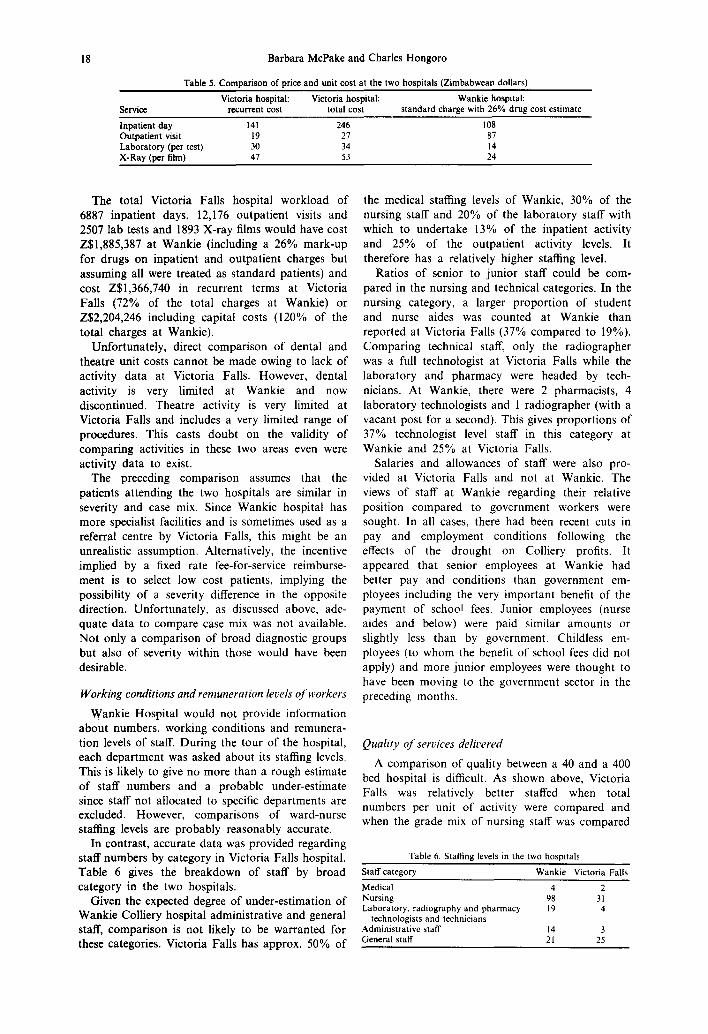
Table 3 shows the capital and recurrent costs allocated to each of the 'primary departments' in Victoria Falls hospital and unit costs where number of units of activity was available. Table 4 shows the charges levied by Wankie Colliery hospital. Table 5 compares the results.
For the three primary departments in Victoria Falls hospital for which units of service delivery were collected, inpatient recurrent costs were Z$141 per day and total costs Z$246. This compared to Wankie charges of Z$218 for private patients, Z$86 for others. Outpatient recurrent costs were Z$19 per visit and total costs Z$27 per visit. This can be compared to Wankie charges of Z$31 for private patients and Z$69 for others. (The charging of private patients at a reduced rate to others is peculiar! The reason given is that more costs are incurred by public outpatients but this seems unlikely on a unit cost basis.) Laboratory recurrent costs were Z$30 per test and total costs Z$34 (compared to Wankie charges of Z$14 per test). However, Wankie charges for inpatients and outpa- tients do not include drugs whereas the costs calculated for Victoria Falls do. Charges for drugs amounted to 26% of total charges for inpatients and outpatients during the year March 1992 to February 1993 and inpatient and outpatient charges might therefore be inflated by 26% for comparabil- ity as is done in Table 4. Thus, the government hospital costs appear higher than the Colliery hospital charges for inpatients and lower for outpatients, whether or not capital costs are included.
Table 4. Charges: Wankie Colliery hospital (Zimbabwean dollars)
Charge +26% to account for drug costs
Service Actual charge (in- and outpatients only)
Inpatient day (private) 218 275 Inpatient day (standard) 86 108 Outpatient visit (private) 31 39 Outpatient visit (standard) 69 87 Laboratory (per test) 14 14 X-Ray (per film) 24 24 Theatre (per hour) 1277 1277
18 Barbara McPake and Charles Hongoro
Table 5. Comparison of price and unit cost at the two hospitals (Zimbabwean dollars) Victoria hospital: Victoria hospital: Wankie hospital:
Service recurrent cost total cost standard charge with 26% drug cost estimate
Inpatient day 141 246 108 Outpatient visit 19 27 87 Laboratory (per test) 30 34 14 X-Ray (per film) 47 53 24
The total Victoria Falls hospital workload of 6887 inpatient days, 12,176 outpatient visits and 2507 lab tests and 1893 X-ray films would have cost Z$1,885,387 at Wankie (including a 26% mark-up for drugs on inpatient and outpatient charges but assuming all were treated as standard patients) and cost Z$1,366,740 in recurrent terms at Victoria Falls (72% of the total charges at Wankie) or Z$2,204,246 including capital costs (120% of the total charges at Wankie).
Unfortunately, direct comparison of dental and theatre unit costs cannot be made owing to lack of activity data at Victoria Falls. However, dental activity is very limited at Wankie and now discontinued. Theatre activity is very limited at Victoria Falls and includes a very limited range of procedures. This casts doubt on the validity of comparing activities in these two areas even were activity data to exist.
The preceding comparison assumes that the patients attending the two hospitals are similar in severity and case mix. Since Wankie hospital has more specialist facilities and is sometimes used as a referral centre by Victoria Falls, this might be an unrealistic assumption. Alternatively, the incentive implied by a fixed rate fee-for-service reimburse- ment is to select low cost patients, implying the possibility of a severity difference in the opposite direction. Unfortunately, as discussed above, ade- quate data to compare case mix was not available. Not only a comparison of broad diagnostic groups but also of severity within those would have been desirable.
Working conditions and remuneration levels of workers
Wankie Hospital would not provide information about numbers, working conditions and remunera- tion levels of staff. During the tour of the hospital, each department was asked about its staffing levels. This is likely to give no more than a rough estimate of staff numbers and a probable under-estimate since staff not allocated to specific departments are excluded. However, comparisons of ward-nurse staffing levels are probably reasonably accurate.
In contrast, accurate data was provided regarding staff numbers by category in Victoria Falls hospital. Table 6 gives the breakdown of staff by broad category in the two hospitals.
Given the expected degree of under-estimation of Wankie Colliery hospital administrative and general staff, comparison is not likely to be warranted for these categories. Victoria Falls has approx. 50% of
the medical staffing levels of Wankie, 30% of the nursing staff and 20% of the laboratory staff with which to undertake 13% of the inpatient activity and 25% of the outpatient activity levels. It therefore has a relatively higher staffing level.
Ratios of senior to junior staff could be com- pared in the nursing and technical categories. In the nursing category, a larger proportion of student and nurse aides was counted at Wankie than reported at Victoria Falls (37% compared to 19%). Comparing technical staff, only the radiographer was a full technologist at Victoria Falls while the laboratory and pharmacy were headed by tech- nicians. At Wankie, there were 2 pharmacists, 4 laboratory technologists and 1 radiographer (with a vacant post for a second). This gives proportions of 37% technologist level staff in this category at Wankie and 25% at Victoria Falls.
Salaries and allowances of staff were also pro- vided at Victoria Falls and not at Wankie. The views of staff at Wankie regarding their relative position compared to government workers were sought. In all cases, there had been recent cuts in pay and employment conditions following the effects of the drought on Colliery profits. It appeared that senior employees at Wankie had better pay and conditions than government em- ployees including the very important benefit of the payment of school fees. Junior employees (nurse aides and below) were paid similar amounts or slightly less than by government. Childless em- ployees (to whom the benefit of school fees did not apply) and more junior employees were thought to have been moving to the government sector in the preceding months.
Quality of services delivered
A comparison of quality between a 40 and a 400 bed hospital is difficult. As shown above, Victoria Falls was relatively better staffed when total numbers per unit of activity were compared and when the grade mix of nursing staff was compared
Table 6. Staffing levels in the two hospitals Staff category Wankie Victoria Falls Medical 4 2 Nursing 98 31 Laboratory, radiography and pharmacy 19 4
technologists and technicians Administrative staff 14 3 General staff 21 25

Contracting out of clinical services in Zimbabwe 19
but not when the grade mix of technical staff was compared.
A detailed inventory of facilities available taken at Wankie hospital revealed an extremely wide disparity between the hospitals which rendered a similarly detailed exercise unnecessary at Victoria Falls. For example, a comparison of laboratory facilities showed the following lists of equipment:
Wankie hospital
2 chemistry analyzers Sodium and potassium
analyzer Blood gas analyzer Glucose, urea and
creatinine analyzer 2 microscopes 1 cell washer 1 blood analyzer 1 coulter mixer 1 coulter counter Incubator Centrifuges
Victoria Falls hospital
2 microscopes Counting chamber Centrifuge Chemistry analyzer
(cast-off from Wankie hospital)
Spencer (very out-dated equipment for measuring haemoglobin levels)
Separate H I V room:
Washer Photometer Incubator Dynatec
Similarly, while the theatre at Victoria Falls was restricted to a very small range of simple operations, a very full range of surgical procedures was available at Wankie.
A small patient survey regarding levels of satisfac- tion was conducted at Wankie and suggested that patients were broadly satisfied with services there. However, this was conducted within the hospital grounds which is likely to have biased the finding [16, 17]. At Victoria Falls, the exercise was not carried out. At the time of study, the hospital was severely over-crowded and many patients were unconscious. This was attributed to the malaria outbreak and routine statistics did suggest that occupancy rates were far in excess of normal. The intrusiveness of questioning in the circumstances did not seem to be warranted by the probability of valuable results.
Other issues
The contract was originally signed before incLe- pendence and current knowledge within the Min- istry of Health regarding the rationale for it and the issues considered at the time is scant. It is thought that lack of government hospital facilities in the area prompted the contract and that little consider- ation was given to issues of cost and quality control. No charge rates were initially specified, although a fee for service system had operated since
the contract's inception. Currently, charges are revised only after agreement has been reached between the Ministry, the Provincial health office and the Colliery. The contract itself has never been reviewed since it was first developed but a new version is currently the subject of negotiation and the issues it raises are discussed further below.
More recently, the cost of the contract has come under scrutiny from both the provincial health office and the Ministry of Health. A World Bank health sector financing report for Zimbabwe [18] identified Matabeleland North Province as benefit- ting from the second highest expenditure per capita in the country. However, if payments under the contract were excluded, it would have been the worst financed in these terms. In addition, it is likely that population is underestimated in the Matabeleland North calculation. The contract cost the Ministry of Health Z$9.5 million in the financial year 1992-3. The recurrent budget for the whole province (excluding this payment and salaries which are not included in the provincial budget and would require a separate exercise to calculate) was only approx. Z$4 million.
There is no formal monitoring of the quality of services or the operation of the contract at present. The health services administrator at the Provincial office has recently been asked to prepare a document regarding a potential monitoring role. To date, the Provincial Medical Director has had the remit of monitoring on an informal basis without guidelines. While the quality of services has not been a serious cause for concern, the lack of filtering of pa t i en t~e i the r on grounds of ability to pay (in theory, only those earning below a given income level are entitled to free access) or whether their condition warrants secondary level services has caused concern. The Colliery hospital is included in the regular round of visits to govern- ment health facilities by the provincial health team.
A number of issues are apparent from review of a revised contract which is currently under nego- tiation, the minutes of a recent meeting in which the new contract was discussed, and correspondence between the Colliery and the Ministry of Health.
The proposed new contract lists a number of categories of patients for which the Ministry will take no responsibility. Important among these are:
(i) all persons on Medical Aid (insured persons);
(ii) persons earning more than Z$400 per month; and
(iii) persons without government health facility referral letters.
Medical Aid patients and those earning more than Z$400 per month, on whom charges are levied frequently default from payment. It has been the Ministry's responsibility to pursue bad debts but since many are very small, pursuit is not cost-effec-
20 Barbara McPake and Charles Hongoro
tive. As a result, a large total volume of unpaid debt has always been picked up by the government. Under the new contract, it would be the hospital's responsibility to ensure payment. This policy is contested by the Colliery who maintain that provision of health services to the whole district population is the government's responsibility. In their view, Medical Aid patients are treated on the government's behalf.
Furthermore, it is not clear who will certify the income of the patient or their insurance status. At present, there is a government clerical officer based at the hospital who has the responsibility of certifying patients as 'government responsibility'. No guidelines have been provided to her regarding the basis on which she should certify patients and consequently no screening takes place. All patients who request government responsibility status are certified.
The requirement to produce government health facility referral letters is an attempt to enforce the seeking of primary health care in government facilities. However, emergencies would be an excep- tion to this rule, and it is unclear how the existence or not of an emergency situation would be judged by the Chief Medical Officer. The Colliery takes the view that this judgement cannot be made prior to a medical consultation. With regard to access to Colliery owned primary care clinics, the Colliery argues that residents of Colliery compounds who are neither Colliery employees nor dependents will suffer hardship if they are unable to use primary health care centres which are located in the compounds.
The proposed new contract also provides that charges will in future be based on costs incurred by the hospital calculated using standard cost account- ing methods. At present, information regarding costs is absent and it is implied that auditors will be able to make the cost assessment.
The proposed new contract makes provision for the location of a Government medical officer (GMO) at the Colliery hospital. Although the role of this officer is not specified, it may be envisaged that medical judgement regarding emergency status for patients would be included. However, the government medical officer post has recently been allocated to Victoria Falls hospital as a more urgent priority and it is not clear that another position will be approved to fulfil this part of the contract.
Finally, further to the new contract under negotiation, the Ministry has refused to pay for HIV tests for government responsibility patients. The Colliery claims to subsidize these by 50%. In addition, the Colliery argues that its charges are in general subsidized--at least if capital cost allowance is made and if only 'junior' (public) patients who form the largest proportion of government respon- sibility patients are considered.
It is a condition of the original contract that the government will not develop 'competing' health facilities. This is seen in some parts of the Ministry as tying government hands and leaving a weak negotiating position as far as the new contract is concerned. Clearly, the Ministry cannot risk the loss of the services of the Colliery hospital before alternative services have been provided. While the existing contract gives a three month notice period for its termination by either party, this is not seen as a realistic option. It is thought that the Colliery will resist signing the new contract and strategies to deal with this scenario have not been agreed.
DISCUSSION
The general applicabilio, o/ the case stud)'
A number of features of the case study may not be typical of other contracting-out experiences either in Zimbabwe or in other countries.
First, the contract studied was originally negoti- ated in the mid 1950s. It was not therefore an example of a recent development responding to structural adjustment policy or recent privatization trends, and the process and effectiveness of its development and implementation are likely to be unrepresentative. No information was available regarding the conditions of negotiation, the issues which were evaluated at the time, or the objectives of the parties involved. Difficulties which might arise in trying to assess these, where at least some information was available, were therefore not evaluated.
Second, a clinical contract was selected whereas the most widespread experience of contracting out in network countries appears to be in non-clinical contracting [14]. Clinical contracting presents par- ticular difficulties of monitoring and may be more politically sensitive than the contracting of support services. However, the feasibility of clinical con- tracting is a stringent test of the policy, and central to the policy debate [6].
Third, the contract studied had not resulted from a competitive tendering process which is the most widely advocated form of contracting. Tendering procedures were developed by the Ministry of Finance in Zimbabwe in 1976, much later than the establishment of the Colliery contract. Therefore, none of the difficulties or opportunities associated with competitive tendering have been explored here. However, overview of current contracting experi- ence in Zimbabwe suggests that formalized com- petitive tendering is the exception rather than the rule, and this may be typical of other developing countries. A range of inter-institutional arrange- ments were common, many of which would be categorized as contracting only if a broad definition were adopted. For example, arrangements between public hospitals with only indirect payment (a
Contracting out of clinical services in Zimbabwe 21
rough estimate of the costs involved used te set hospital budgets) governed laundry organization in Harare and Bulawayo. Ad hoc recourse to the private sector was used when these arrangements repetitively failed. Boiler house and blood transfu- sion services were also shared around within the public sector and between the public and private sectors on bases resulting from historical accident rather than planned use of the potential of m~rket mechanisms. Planned and formalized competitive tendering may not be the most common forra of contract.
Despite these limitations in generalizability, it is likely that most of the conclusions reached below regrading the contract do have relevance to the policy debate on contracting out in developing countries. The environment of the health sector in Zimbabwe is typical of the region. Despite great strides having been made in health sector develop- ment in the early 1980s, from the mid-1980s, health expenditure has been under extreme pres~ure, reflecting economic stagnation. Structural adjust- ment policy has emphasized reduction in the :scale of the public sector and the civil service in particular. All this typifies the environment of health policy throughout sub-Saharan Africa and provides the context in which contracting policy is being developed [19].
Cost and charge differences between Wankie and Victoria Falls
The explanation for the relative cost and charge levels at the two hospitals is unclear. This results at least partly because the services of Wankie hospital were not costed. While the relevant comparison from the government's perspective is the difference between price and cost in the immediate term, understanding the reasons for divergence is also important. If future contracts are to be negotiated successfully the characteristics of companies likely to be able to maintain lower prices are of interest, and if the long term capacity of the contracted institution to offer the current price is important, the relationship between price and cost is relevant. The second consideration applies where there are insufficient competing companies to assume it will always be possible to switch to other providers in the face of price increases.
While there may be cross-subsidy explaining the differences in relative price and charge levels between Wankie and Victoria Falls for inpatients, outpatients and laboratory tests, it appears that Victoria Falls is considerably cheaper if capital costs are excluded and more expensive if they are included. It is surprising given the different levels of facilities offered that Victoria Falls is not unam- biguously and considerably cheaper from every perspective. The results may tally with the con- tention of the Colliery hospital management that charges cover recurrent but not capital costs.
Alternatively, the results could be viewed as supportive of the view of the Ministry of Health that patients who require only primary health care may be being treated at the Colliery hospital. If case mix severity is much lower than at Victoria Falls, unit costs are likely to be lower. Again, the lack of case mix information is regrettable.
The lack of a clear divergence may also reflect economies of scale. Laboratory, X-ray, dental and theatre costs account for 17% of recurrent and 12% of the total costs of Victoria Falls hospital and it is clearly more costly per unit of activity to provide these services in a 40 rather than 400 bed hospital. In addition, capital costs account for 37% of total costs, a relatively high proportion and likely to be higher in smaller hospitals (on simple engineering principles).
A further possible explanation is that the Colliery hospital is actually more efficient. Common expla- nations put forward for inefficiency in government units are over-staffing and under-utilization. The relatively high staffing levels in Victoria Falls clearly account for some of the extra cost. It is not clear whether these reflect economies of scale or pure efficiency differences between government and pri- vate sector providers. It is sometimes alleged that governments maintain excessive staffing levels in public service in order to pursue different political objectives [20]. Under-utilization seems an unlikely explanation in this case. Routine statistics suggest bed occupancy levels averaging 48% in Victoria Falls hospital and only 36% at Wankie. Observed occupancy levels at the time of the visit were higher (in excess of 100% at Victoria Falls and 69% at Wankie) but the relative levels were similar and the difference could be explained by the malaria outbreak.
Staff numbers, salaries and employment status
Concern over staff numbers arises both from concern for staff conditions and for the quality of service delivered. The extent to which staff numbers may indicate quality differences is discussed in the next section. It was difficult to assess the extent of normal workload differences between the two hospitals given the extraordinary conditions of the time of visit. However, staff at Victoria Falls hospital seemed to be under considerably greater pressure and the opinion of staff at both hospitals was that government staff workloads were higher. This contrasts with the findings. Economies of scale and divergence between severity of case mix again provide possible explanations of the findings which it would have been interesting to be able to explore further.
Relative working conditions between the two hospitals were found to vary according to the seniority of the staff concerned. This may reflect astute responses to market conditions on the part of the Colliery hospital management. Senior staff
22 Barbara McPake and Charles Hongoro
are relatively scarce and have to be attracted from alternative employment. Their better position suggests that the allegation that the Colliery hospital attracts staff away from the government sector where posts are then left vacant may have some justification. Victoria Falls hospital currently lacks a District Medical Officer and has 'borrowed' a laboratory technician from another hospital while they await a permanent appointment. Surplus labour supply for unskilled staff implies that the Colliery hospital does not have to attract such labour with competitive pay and conditions.
Recent cuts in pay and conditions at the Colliery hospital suggests a greater flexibility to respond to economic circumstances in the private sector. This aspect may appear less desirable in terms of staff conditions and morale than from an expenditure minimization perspective. However, inflationary conditions imply a similar ability to cut real pay in the public sector in response to recession and differences between the two may therefore be unimportant.
Quality
There are very great difficulties in comparing large and small hospitals in this respect. A wider range of facilities was evident at Wankie. At the time of study, the level of amenity was clearly also much higher at Wankie at least as far as inpatient services were concerned. This reflected over crowd- ing at Victoria Falls and probably was not the normal condition.
Staffing levels and ratios of senior to junior nursing staff appeared better at Victoria Falls. However, the extent to which this might reflect economies of scale rather than higher quality service was not clear. For example, one senior member of staff is probably required to supervise activities in all areas yet may be capable of supervising a much larger staff than required for a small hospital without quality losses. Similarly, the difference between the ratios in technical staff probably understates the quality implications of lacking fully qualified technologists in the pharmacy and laboratory.
This specific problem highlights a more general problem of input based quality indicators. It will never be clear whether input differences reflect efficiency rather than quality differences. This problem can equally apply to 'process' quality indicators, however, and true 'output' indicators (relating to the health status effects of health service provision) are hardly likely to be feasible to measure. It is probably more useful to give consideration to what efficiency factors may be confounding quality measures and the more likely explanation of findings. Here, economies of scale appear at least as likely to explain staff ratio differences (both senior to junior and staff to workload) as quality differences, particularly given
the perceived pressure levels expressed by staff at both hospitals.
Many of the above issues reflect the debate regarding the optimal size of hospitals which has been conducted in all countries for a considerable time. In this case, the Ministry of Health probably does face the choice between developing a number of smaller hospitals or continuing to pay for services offered by the Colliery. No assessment of the overall implications of this choice can be made without considering the accessibility advantages which the alternative strategy implies. Patient costs and their implications for access were not measured.
Other issues affecting the contract
The discussions which have been taking place between the Ministry of Health and the Colliery hospital suggest that many of the key questions surrounding the contract are managerial or concern the policy and contract negotiating process.
The magnitude of expenditure on the contract stands out as the key issue, particularly given the general inaccessibility of the Colliery hospital. Approximately 70% of provincial non-salary recur- rent expenditure is allocated to secondary care for a minority of the district population who have access. The fee for service nature of the contract and the failure to filter patients demanding the hospitals" services prevent adequate cost control. This appears to be more important than the level of the fees themselves. In other words, allocative rather than technical efficiency questions are paramount.
However, the Ministry is now in a weak position to control the situation. The decision to locate the GMO post at Victoria Falls may have been unwise with hindsight given the likely expenditure impli- cations of more effective screening at Wankie. Even without a GMO post at Wankie, training and guidelines supplied to the clerical officer currently responsible for screening could be effective. While the Ministry perceives its bargaining position over the new contract to be weak, the Colliery hospital is also highly dependent on government business which accounts for approx. 80% of inpatient and 55% of outpatient activity. The total revenue from government business (approx. Z$10 million in 1992 3) constitutes 5% of the Colliery's total turnover. In its weak financial position following the recent drought, it is unlikely to consider a stand off period in which government payments under the contract were not forthcoming to be acceptable.
The current administration has inherited many of the problems of the contract and has clearly identified a number of sensible strategies to coun- teract these. At the same time, the attempt to solve such an extreme problem as the potential mis-allo- cation of 70% of a whole province's recurrent budget appears to have been made late and
Contracting out of clinical services in Zimbabwe 23
probably in response only to the ex-Provincial Medical Director having moved to a Ministry position relevant to tackling the problem. Priority does not seem to have been given to managing the contract effectively. If authority to renegotiate the contract had been present at provincial level, the problem might have been tackled sooner but this would require contracting skills to be available at that level. Similarly, managerial capacity was lack- ing at the level of operation of contracts--in this case, the single clerical officer on site at the Colliery hospital lacking any specific training related to her expected duties.
Data shortages also appear to have affected the negotiation process. None of the data presented here have been compiled previously in any attempt to identify the priority negotiation points or to arbitrate between the conflicting positions of the two contracting parties. More serious still, data shortages at government facilities would appear to prevent future assessment of the contract on a comparative basis. The Ministry of Health believes that excessive provision of primary health care takes place at the Colliery hospital but has no basis on which to compare with primary health care provision at its own hospitals. In fact, excessive provision of PHC in government run district hospitals is a much debated problem throughout Africa [21].
In conclusion, this contract raises a number of important issues relevant to consideration of con- tracting out policy in developing countries more generally.
Many advantages have been claimed for con- tracting out of clinical and ancillary services. It is argued that services delivered by the private sector are typically perceived to be high in quality and that the creation of competition where the public sector is otherwise a monopoly is likely to increase efficiency and improve quality [6]. This case suggests that the private sector can provide good quality services at competitive prices. However, it also suggests that both types of failure predicted for contracting out in developing countries (thc se arising from market conditions and those frcm weak public sector capacity) apply, and may in practice be the most important considerations for a country contemplating the contracting of health services.
Specifically, the following issues arising from the case study should be considered by policy makers interested in contracting out as an option for the health sector: First, there is no competition for the contract. A monopoly supplier of clinical services exists in this district and has been entrenched rather than challenged by the terms of the contract. Lack of competitive arrangements is a frequent objection to the rationale for contracting and for the contract based models driving health sector reform in some industrialized countries. The combination of rno-
nopolist and monopsonist in health services mar- kets leads to unpredictable outcomes [22]. In this case, the outcome appears to arise from other factors affecting the balance of power between the two. Although the monopolist is perceived by the Ministry to have the upper bargaining hand, excessive provision rather than excessive pricing appears to have resulted. Limitations in competitive scope are likely to be even more severe in developing countries and in more remote areas of developing countries [14]. The power balance be- tween single buyers and sellers will determine the technical and allocative efficiency implications of this scenario.
Second, the Ministry's perception of political vulnerability in this context provides broader lessons. Where contracts are for clinical services, unless the Ministry maintains some capacity to provide an alternative to that contracted, or there is potential for a competitive provider to enter the market, such vulnerability appears inevitable. These must be seen as alternative pre-conditions to the introduction of successful clinical contracting.
Third, key skills shortages have contributed to some of the problems experienced under the contract. Under-staffing, lack of capacity and excessive pressure on Ministries is likely to be an issue affecting the administration of contracts in many countries. The most apparent example is the lack of a qualified government officer to effectively screen patients requesting government responsibility status. Skills shortages in the health sector are widespread in developing countries. If contracting is seen as a way of avoiding service cuts as a result of civil service retrenchment, these problems are likely to be compounded. Contracting may result in widespread resource wastage if careful consider- ation is not given to the skills needed within the public sector to manage the process, and priority given to ensuring prioritization of skilled staff in the roles identified. Decentralized responsibility for contracts may lead to earlier identification of problems but requires even greater investment in management capacity at lower levels of the health system.
Fourth, data shortages preventing adequate com- parison between government and contracting insti- tutions are likely to be a common problem facing government negotiators in identifying the most important issues to address, and even whether or not the contract represents an improvement when compared to direct public provision. These last two points emphasize a fifth: contracting is not free of administrative costs--any efficiency improvements resulting must more than compensate for these. This has been a key issue in the debate on contracting in developed countries [13] but appears over-looked in some contributions to the develop- ing country debate.
Both types of contracting failure thought most

24 Barbara McPake and Charles Hongoro
likely to arise in a developing country context are in evidence in this case study. The contract arose in an uncompetitive market environment characterized by extremely high entry costs. The Ministry of Health lacked the resources to allocate personnel with the requisite skills to manage key aspects of the contract. In addition, lack of data has pre- vented effective negotiat ion--part icularly concern- ing the probable excessive provision of primary health care at the hospital. An important criterion for the effective operation of contracts is that priority must be given to managing them effectively, and resources allocated for effective management and information system development. Only in this way can the monopol is t -monopsonis t balance be struck more evenly. As a tool of crisis management, the failure of contracts seems inevitable.
Contracting has potential to meet shortfalls in public sector capacity to provide services but the theoretical advantages of the contracting model will prove evasive in practice if the details of the process are neglected.
Acknowledgements--The Health Economics and Financing Programme is supported by ODA.
REFERENCES
1. World Bank. Financing Health Services in Developing Countries, an Agenda for Reform. World Bank, Washington DC, 1987.
2. Roth G. The Private Provision of Public SerL, ices in Developing Countries. EDI Series in Economic Develop- ment (World Bank), Oxford University Press, 1987.
3. Griffin C. C. Strengthening Health Services in Developing Countries Through the Private Sector. International Finance Corporation, Discussion Paper No. 4, World Bank, Washington DC, 1989.
4. World Bank. Developing the Private Sector: a Challenge for the Worm Bank Group. World Bank, Washington DC, 1989.
5. Bennett S. The Mystique of Markets: Public" and Private Health Care in Developing Countries. Department of Public Health and Policy publication No. 4, London School of Hygiene and Tropical Medicine, London, 1991.
6. World Bank. World Development Report: Investing in Health. World Bank, Washington DC, 1993.
7. Arrow K. J. Uncertainty and the welfare economics of medical care. Am. Econ. Rev. 53, 941, 1965.
8. Culyer A. J. The nature of the commodity 'health care' and its efficient allocation. Oxford Econ. Papers 23, 189, 1971.
9. Jimenez E. Pricing Policy in the Social Sectors. Johns Hopkins University Press, Baltimore, 1987.
10. Gilson L. Goz,ernment Health Care Charges: Is equity being abandoned? A Discussion Paper. EPC Publication No. 15. Spring, Evaluation and Planning Centre for Health Care, London School of Hygiene and Tropical Medicine, London, 1988.
11. Creese A. L. User Charges for Health Care: a Review of Recent Experience. Current Concerns, SHS Paper No. 1. Division of Health Service Strengthening, World Health Organisation, 1990.
12. McPakeB. User charges for health services in developing countries: a review of the economic literature. Soc. Sci. Med. 36, 1397, 1993.
13. Saltman R. B. and von Otter C. Planned Markets and Public Competition: Strategic Reform in Northern European Health Systems. Open University Press, Buckingham and Bristol, 1992.
14. McPake B. Contracting out of health services in developing countries. Hlth Pol. Planning 9, 25, 1994.
15. Creese A. and Parker D. (Eds) Cost Analysis in Primary Health Care: A Training Manual for Programme Managers. World Health Organisation, Aga Khan Foundation and UNICEF, (WHO/SHS/NHP/90.5) World Health Organisation, Geneva, 1990.
16. Kanji N., Kilima P. M. and Munishi G. M. Quality of Primary Curatiz~e Care in Dar-Es-Salaam. Health Policy Unit Report, London School of Hygiene and Tropical Medicine, 1992.
17. Atkinson S. Anthropology in research on quality of health services, Cadernos de Saude Publica (Rio de Janeiro), 1993.
18. World Bank. Zimbabwe: Health Sector Financing. World Bank, Washington DC, 1987.
19. Cornia G. A., van der Hoeven R. and Mkandawire T. Africa's Reco~,erv in the 1990s: from Stagnation and Adjustment to Human Development. St. Martin's Press, Basingstoke, 1992.
20. World Bank. Sub-Saharan Africa: from Crisis to Sustainable Growth. World Bank, Washington DC, 1989.
21. World Bank. Better Health in Africa. African Technical Department, Human Resources and Poverty Division, World Bank, Washington DC, 1994.
22. Bryan S. and Beech R. Cost information in a provider market for health care: a note. Financial Accountability Management 7, 99, 1991.