contract grant and disclosure form equal opportunity pol
TRANSCRIPT
Proposal Signature Page
All Agreement and
Compliance Pages
E.O. 98-04 - Contract Grant
and Disclosure Form
Equal Opportunity Policy
Proposed Subcontractors Form
Other Documents and/or Information
Technical Proposal Response to the Information for Evaluation section of
the Technical Proposal Packet
Proposal
Signature
Page
RFP Response Packet Bid No. 710-21-0003
SIGNATURE PAGE
ype or rt t e o owing m ormat on. T Ph th fi II . . t
PROSPECTIVE CONTRACTOR'S INFORMATION ,,
Company: Northeast Arkansas Community Mental Health Center d/b/a Midsoulb Heallh Systems, Inc. affiliate of Arisa Real th, Inc.
Address: 12707 Browns Lane
City: Jonesboro I State: 1 AR 1 Zip Code: j 72401
Business 0 Individual D Sole Proprietorship □ Public Service Corp Designation: □ Partnership □ Corporation ~onprofil
Minority and \!!Not Applicable D American Indian □ Asian American D Service Disabled Veteran Women-Owned D African American □ Hispanic American □ Pacific Islander American □ Women-Owned Designation*:
AR Certification#: • See Minority and Women-Owned Business Policy
PROSPECTIVE CONTRACTOR eONTAC.f INFORMATION Provide contact information to be used for bid solicitation related matters.
Contact Person: Christie Ring Title: Director of Substance Abuse Services
Phone: 870-886-7924 Alternate Phone: 870-878-1128
Email:
- - -CONFIRMATION OF REDACT.ED COPY r, - "
D YES, a redacted copy of submission documents is enclosed. ~O, a redacted copy of submission documents Is not enclosed. I understand a full copy of non-redacted submission documents will be released if requested.
Note: If a redacted copy of the submission documents is not provided with Prospective Contractor's response packet, and neither box is checked. a copy of the non-redacted documents, with the exception of financial data (other than pricing}, will be released in response to any request made under the Arkansas Freedom of Information Act (FOIA). See Bid Solicitation for additional Information.
U.LEGAL IMMl~RANT CONFIRMATION .,.
By signing and submitting a response to this Bid Solicitation, a Prospective Contractor agrees and certifies that they do not employ or contract with Illegal immigrants. If selected, the Prospective Contractor certtfies that they will not employ or contract with illegal immigrants during the aggregate term of a contract.
ISRAEL B0:YCOTT RESTRICTION GONFIBMAflON
By checking the box below, a Prospective Contractor agrees and certifies that they do not boycott Israel, and if selected, will not boycott Israel during the aggregate term of the contract.
i'Prospective Contractor does not and will not boycott Israel.
An official authorized to bind the Prospective Contractor to a resultant contract must sign below.
The signature below signifies agreement that any exception that conflicts with a Requirement of this Bid Solicitation will cause the Prospective Contractor's bid to be disqualified:
V) / \ ,r---_ l
Authorized Signature: I< ·:t-t""I .) G(;t/v Use Ink Only.
Title: Executive Director
Printed/Typed Name: Ruth Allison Dover Date: 9-30-20
I
Agreement
and
Compliance
Pages
RFP Response Packet Bid No. 710-21-0003
SECTION 1 - VENDOR AGREEMENT AND COMPLIANCE
• Any requested exceptions to items in this section which are NON-mandatory must be declared below or as an attachment to this page. Vendor mus t clearly explain the requested exception, and should label the request to reference the specific solicitation item number to which the exception applies.
• Exceptions to Requirements shall cause the vendors proposal lo be disqualified,
By signature below, vendor agrees to and shall fully comply with all Requirements as shown In this section of the bid solicitation. Use Ink Only
Vendor Name: Northeast Arkansas Community Mental Health Center Date: 9-30-20 d/b/a Midsoulh Health Systems, Inc. affiliate of Arisa Health Inc.
Authorized Signature: l6~~-,()1')1Vt/ ·1 / Title: Executive Director
Print{fype Name: Ruth Allison Dover
RFP Response Packet Bid No. 710-21-0003
SECTION 2 - VENDOR AGREEMENT AND COMPLIANCE
• Any requested exceptions to items in this section which are NON-mandatorv must be declared below or as an attachment to this page. Vendor must clearly explain the requested exception, and should label the request to reference the specific solicitation item number to which the exception applies.
• Exceptions to Requirements shall cause the vendor's proposal to be disqualified.
By s ignature below, vendor agrees to and shall fully comply with all Requirements as shown in this section of the bid solicitation. Use Ink Only
Vendor Name: !Northeast Arkansas Community Mental Health Center Date: 9~30 .. 20 d/b/a Midsouth Health Systems, Inc. affiliate of Arisa Health, foe_
Authorized Signature: \? J,l\/{dl){)Vt/ Title: Executive Director
Print/Type Name: Ruth Allison Dover
Pane 4 nfB
RFP Response Packet Bid No. 710-21-0003
SECTION 3,4,5 - VENDOR AGREEMENT AND COMPLIANCE
• Exceptions to Requirements shall cause the vendor's proposal lo be disqualified.
By signature below, vendor agrees to and shall fully comply with al l Requirements as shown in this section of the bid solicitation. Use Ink Only
Vendor Name: Northeast Arkansas Community Mental Health Center kl/b/a Midsouth Health Systems, Inc. affiliate of Arisa
Date: 9-30-20
Health, Inc.
Authorized Signature: VJJ~{)f ~. f'- ~ .. ' ) •UL./)..,..,.✓ Title: Executive Director
Print(Type Name: Ruth Allison Dover
p,,,.,,, t; nf R
E.O. 98-04
Contract
Grant and
Disclosure
Form
CO
NT
RA
CT
AN
D G
RA
NT
DIS
CL
OS
UR
E A
ND
CE
RT
IFIC
AT
ION
FO
RM
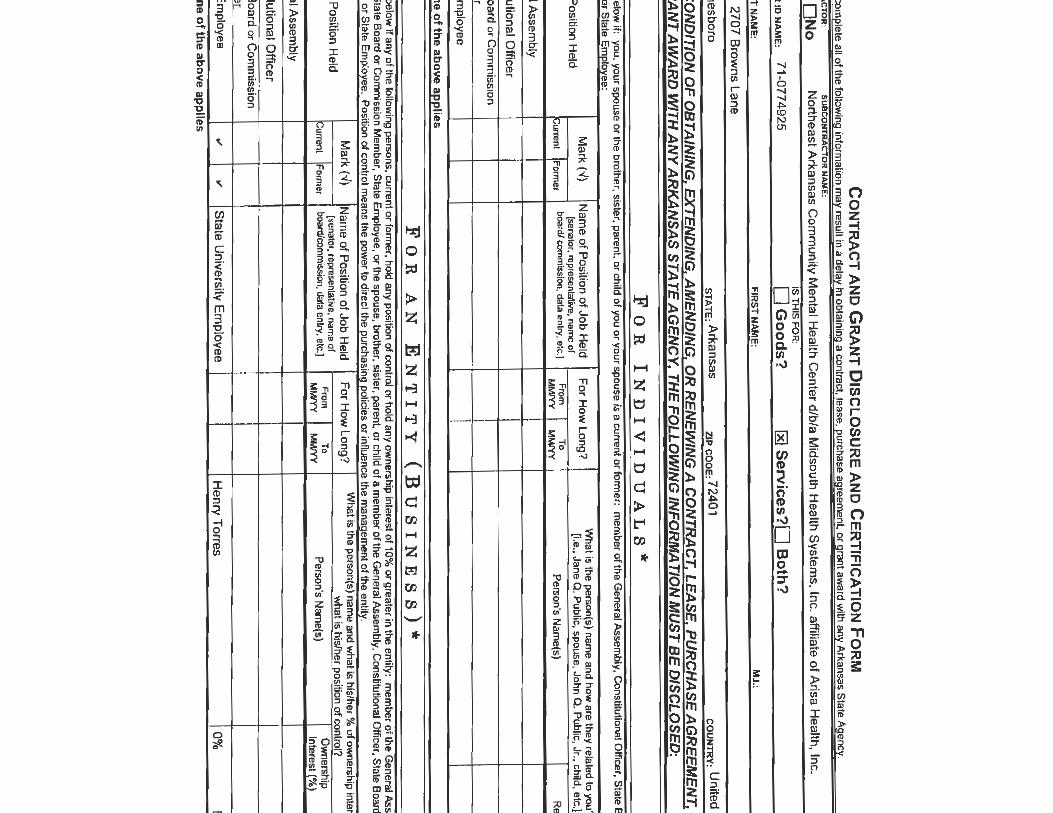
F
ailure to complete all o
f the following in
formatio
n m
ay result in
a delay in o
btaining a contract, lease
, purchase agreement, o
r grant award w
ith any Arkansas S
tate Agency.
SU
BC
OH
TR
AC
TO
R:
SU
BC
OIT
TR
AC
TO
R H
AM
E:
OY
es
ON
o
No
rthe
ast A
rka
nsa
s C
om
mu
nity
Me
nta
l He
alth
Ce
nte
r d/b
/a M
idso
uth
He
alth
Syste
ms
, Inc
. affilia
te o
f Aris
a H
ea
lth, In
c.
ISTH
IS FOR
: T
AX
PA
YE
R ID
NA
ME
: 7
1-0
77
49
25
D
Go
od
s?
~ Services?
□ B
oth
?
YO
U£!_ LA
ST_ NA
ME
: F
I_RS
LNA
M~:
M.I.:
AD
DR
ES
S: 2
70
7 B
rown
s L
an
e
CIT
Y: J
on
esb
oro
S
TATE
: Ark
an
sa
s
ZJP co
oe
: 72
40
1
couNT
RY
: Un
ited
Sta
les
AS
A C
ON
DIT
ION
OF
OB
TA
ININ
G, E
XT
EN
DIN
G, A
ME
ND
ING
, OR
RE
NE
WIN
G A
CO
NT
RA
CT
, LE
AS
E, P
UR
CH
AS
E A
GR
EE
ME
NT
, O
R G
RA
NT
AW
AR
D W
ITH
AN
Y A
RK
AN
SA
S S
TA
TE
AG
EN
CY
, TH
E F
OL
LO
WIN
G IN
FO
RM
AT
ION
MU
ST
BE
DIS
CL
OS
ED
:
11 F
OR
IN
DIV
ID
UA
LS
*
Indicate below
if: you. your spouse or the brother, sister. parent, or child o
f you or yo
ur spouse Is a current or form
er: m
ember o
f the General A
ssembly, C
onstitutional Officer. S
tate Board o
r Com
mission
Mem
ber, ors
-. . ···-·-
--··
Po
sition
He
ld
Mark(✓)
Na
me
of P
ositio
n o
f Jo
b H
eld
F
or H
ow
lon
g?
Wh
al is the person(s) nam
e and ho
w are the
y related to you?
(senator, representative, name of
p, e., Jane Q. P
ublic, spouse, John a. P
ublic, Jr .• child, etc.}
Current
FOfm
llr board/ com
mission, d
ata
enlry, efc.J F
rom
To
Person's N
ame(s)
MM
/YY
M
MN
Y
Relation
Ge
ne
ral A
ssem
bly
Co
nstitu
tion
al O
ffice
r
Sta
le B
oa
rd o
r Co
mm
ission
I
Me
mb
er I
Sta
te Em
plo
yee
I
D
No
ne
of th
e a
bo
ve
ap
plie
s
FO
R
AN
E
NT
IT
Y
(B
US
IN
ES
S)*
Indicate below
if any of the follow
ing persons, current or form
er, hold any position o
f control or hold any ow
nership interest of 1
0% o
r greater in the
entity: m
ember of the G
eneral Assem
bly, Co
nstitutional
Officer, S
tate
Board o
r Com
mission M
ember, S
tate Em
ployee, o
r lhe
spouse, brother, sister, parent. or child of a m
ember o
f the General A
ssembly, C
onstitutional Officer, S
tate Board o
r Com
missio
n
Mem
ber, or Sla
te E
mploye
e. P
ositio
n o
l control
--
--
-· .
. • .•
r-
.• -
. .
. ---
..::11 •••••
•
Mark(✓
) N
am
e o
f Po
sition
of J
ob
He
ld
Fo
r Ho
w L
on
g?
W
hat is the person(s) name and w
ha
t is his/her% o
f ownership Interest and/or
what is his/her position o
f control? P
ositio
n H
eld
[seriator, representative. nam
e of F
rom
To
Ow
nership
P
osition of !C
urrent Form
er boartl/com
misslon, data entry, etc.)
MM
/YY
M
M/YY
Person's N
ame(s)
Interest (%
) C
ontrol
Ge
ne
ral A
sse
mb
ly
Co
nstitu
tion
al O
ffice
r
Sta
te B
oa
rd o
r Co
mm
ission
M
em
be
r
Sta
te E
mp
loye
e
.,, .,,
Sta
te U
niv
ersity
Em
plo
ye
e
He
nry
To
rres
0%
B
oa
rd M
em
D
No
ne o
f the ab
ove ap
plie
s
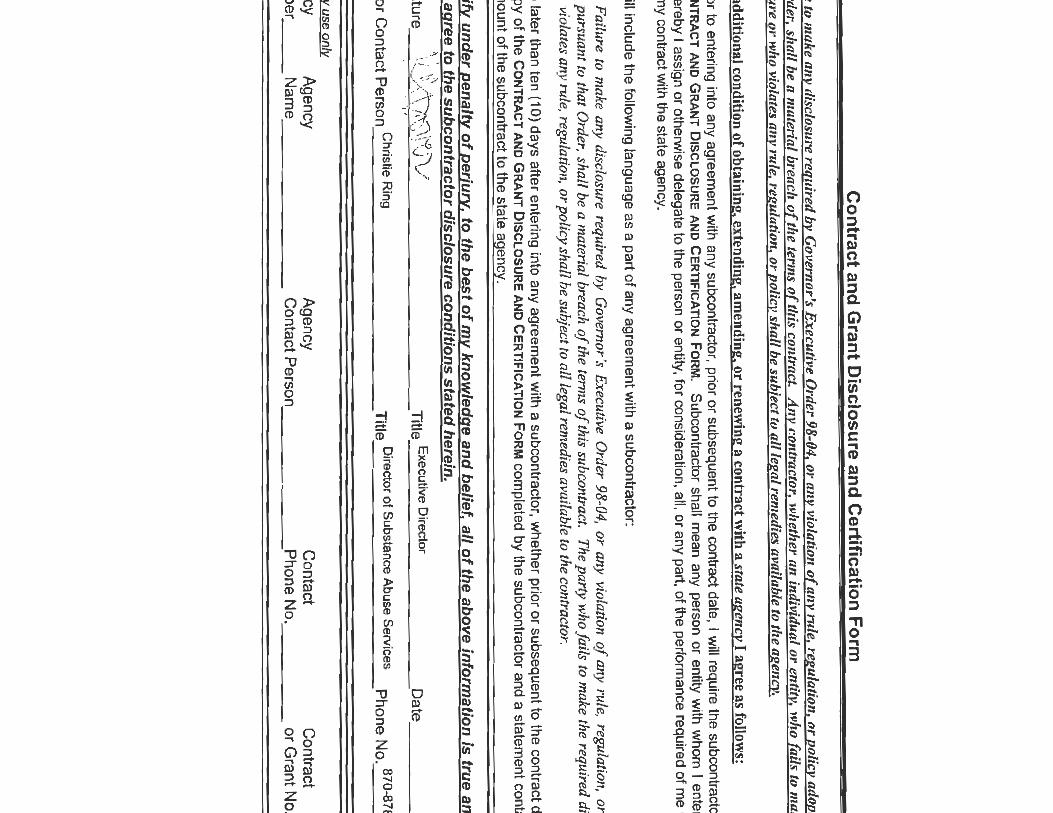
Co
ntra
ct an
d G
ran
t Disclo
sure
an
d C
ertifica
tion
Fo
rm
Failu
re to make a
ny disclosu
re requ
ired by G
overnor's E
xecutive O
rder 98-04, or a
m, violatioll o
f an
y rule, regulation
, or po/icy at/opted p
ursu
ant to
that O
rder, sha
ll be <t material b
l'each oft/re term
s of th
is contract.
An
y contractor, wh
ether llll individual o
r entity, w
ho fails to m
ake th
e required
disclosu
re or w
ho violates an
y mle, regulation, o
r policy shall be sub;ect to all legal rem
edies available to the agen
cy.
As an ad~
itiom1l condition o
f obtaining, extending, am
ending, or renewing a contract w
ith a stale agen
cy 1 agree as follows:
1. P
rior to
entering into any agreement w
ith any subcontractor, prior or subsequent to the contract date
, l will require the subcontractor to com
plete a C
ON
TR
AC
T A
ND
GR
AN
T D
ISC
LOS
UR
E A
ND
CE
RT
IFICA
TIO
N F
OR
M.
Subcontractor shall m
ean any person or entity w
ith wh
om
I enter an
agreement
wh
ere
by I assign o
r otherwise delegate to the person o
r entity, for consideration
, all, or a
ny part, o
f the performance required o
f me under the term
s o
f my contract w
ith the state agency.
2. I w
ill include the following la
ng
ua
ge
as a pa
rt of a
ny a
gre
em
en
t with a subcontracto
r:
Failure to m
ake any disclosure required b
y Governor's E
xecutive Order 98-04, o
r any violation o
f an
y rule, regulation, o
r policy adopted pursuant to that O
rder, shall be a m
aterial breach of the term
s of this subcontract.
The p
arty w
ho fails to ma
ke the required disclosure or w
ho violates any rule, regulation, o
r po
licy shall be subject to all legal rem
edies available to the contractor.
3.
No la
ter than ten (1
0) days a
fter entering into any ag
ree
me
nt w
ith a sub
con
tractor, w
hether p
rior or su
bseq
ue
nt to th
e contract date, I w
ill mail a
cop
y of th
e C
ON
TR
AC
T A
ND
GR
AN
T D
ISC
LO
SU
RE
AN
D C
ER
TIF
ICA
TIO
N F
OR
M com
pleted by the subco
ntractor and a statement containing th
e d
olla
r a
mo
un
t of the subcontract to th
e state agency.
I ce
rtify u
nd
er p
en
alty
of p
erju
ry. to th
e b
est o
f my kn
ow
led
ge
an
d b
elie
f. all o
f the
ab
ove
info
rma
tion
is tru
e a
nd
co
rrect a
nd
th
at I a
gre
e to
the
su
bco
ntra
cto
r dis
clo
su
re c
on
ditio
ns s
tate
d h
ere
in.
II ' ·,\
~ •
\i • ~\,--:>
\"\ / E
t·
o· ct
Sig
na
ture
i~!..~
}\ \ /\\~ ~ \J v
Title
xecu ive ire
or
-·,'
Da
te -------
Ve
nd
or C
on
tact P
erso
n C
hristie Ring
Title D
irector of Substance A
buse Servi~es
Ph
on
e No
. 87
0-87
8-11
28
Ag
en
cy use
on
ly
Agency
Agency
Ag
en
cy C
on
tact C
ontract N
um
be
r __
_ N
am
e __
__
__
__
_ C
on
tact P
erso
n __
__
__
__
Ph
on
e No
. __
__
_ o
r Gra
nt N
o. _
_
Equal
Opportunity
Policy
Mid-South Health Systems, Inc. PERSONNEL POLICIES AND PROCEDURES
SUBJECT I POLICY NUMBER Equal Employment Opportunity 1.10
EFFECTIVE DATE: July 1, 1999 PAGE NO. I OF I FILE UNDER SECTION: Employment Practices
REVISION DATE: November 12, 2008; August l, APPROVED BY: Bonnie White, ChiefExecutive Officer 2013
POLICY:
It is the official policy of this organization that no one will be denied service or be subjected to any form of discrimination on the basis of race, color, national origin, age, gender, sexual orientation, veteran's status, disability, ancestry or religion. The organization will not discriminate against individuals in the admission or access to, or treatment, or employment in, its programs and activities. This policy is adopted pursuant to Section 601 , Title VI and Title VII of the Civil Rights Act of 1964, Public Law 88-352, section 504 of the Rehabilitation Act of 1973 and Title VI and XVI of the Public Health Service Act and Americans with Disabilities Act of 1992.
We will endeavor to ensure that qualified applicants are employed, and that employees are treated equally during employment without regard to their race, color, religion, gender, sexual orientation, national origin, disability, veteran's status, ancestry, age or other legally protected status. Such action shall include, but not be limited to, the following: employment, upgrading, demotion, transfer recruitment or recruitment advertising, lay-off or termination, rates of pay, other fom1s of compensation and selection of training. We will post in conspicuous places, available to employees and applicants for employment, notices setting forth the provisions of this nondiscrimination clause.
The Human Resources Department will promote principles of equity in its efforts to staff available positions. The department will monitor labor market information and maintain contact with staffing sources to further these principles.
We will comply with all provisions of applicable laws prohibiting discrimination.
Any employee may request a reasonable accommodation under the Americans with Disabilities Act of 1992. Such requests should be made to the Human Resources Director. The HR Director shall review the request and respond in writing to the employee within a reasonable amount of time. The written response shall be retained in the employee's personnel file.
.,, ....................... ' .. , " , ........ ,~--~.~-.. " .. , ........ , .... ,.,., ....... ,. '" .. , ..... , .. ,.,. ,., ... , .... , ................. , .. ' ' ' ...... " ..... ---··----- ----~"·~··"·'·'·' ...... ,.,., ........ , .. ,.,
EQUAL EMPLOYMENT OPPORTUNITY
Arisa is an Equal Opportunity Employer. Employment at Arisa is based upon personal capabilities and qualifications without regard to race, color, rel igion, sex, gender (including pregnancy, childbirth, or related medical conditions), sexual orientation, gender identity or expression, national origin, age, disability, genetic information, marital status, citizenship status, veteran s tatus or any other protected characteristic as established by law.
This policy applies to all terms and conditions of employment, including, but not limited to, recruitment, hiring, placement, promotion1 termination, layoff, compensation, benefits, and all other terms and conditions of employment. It is Arisa's intent to comply with all federal and state laws regarding employment practices.
The Human Resources Department has overall responsibility for this policy and maintains reporting and rnonitorlng procedures. Staff members' questions or concerns should be referred to the Human Resources Department. Any staff member or applicant who believes he or she has been subjected to unlawful discrimination should report the incident immediately. Staff members, or applicants for employment, who seek assistance pursuant to this policy will not have their employment opportunities adversely affected because of such a complaint or be subject to any other type of retaliation.
Appropriate corrective action, up to and including termination, may be taken when any staff member violates this policy.
NON-DISCRIMINATION AND ANTI-HARASSMENT POLICY
Arisa is committed to a work environment in which all individuals are treated with respect and dignity. Everyone has t11e right to work in a professional atmosphere that promotes equal employment opportunities and prohibits discriminatory practices, including harassment. Therefore, Arisa expects that all relationships among persons in the workplace wil l be respectful, business-like and free of bias, prejudice and harassment.
Arisa prohibits discrimination and l1arassment based on race, color, religion, sex, gender (including pregnancy, childbirth, or related medical conditions), sexual orientation, gender identity or expression, national origin, disability, genetic information, n1arital status, citizenship status, veteran status, association with a person of a protected status, or any other characteristic protected by law. Arisa prohibits and will not tolerate any such discrimination or harassment.
9
Proposed
Subcontractors'
Form
RFP Response Packet Bid No. 710-21-0003
PROPOSED SUBCONTRACTORS FORM
• Do not include additional information relating to subcontractors on this form or as an attachment to this form.
PROSPECTIVE CONTRACTOR PROPOSES TO USE THE FOLLOWING SUBCONTRACTOR(S) TO PROVIDE SERVICES.
T voe or rm e o owm.a m orma wn P . t th fi II . . ~ t'
Subcontractor's Company Name Street Address City, State, ZIP
Northeast Arkansas Regional 6009 C.W. Post Road Jonesboro, AR, 72401 Recovery Center
Arkansas Cares-Methodist Family 1600 Aldersgate Road Little Rock, AR 72205 Health
□ PROSPECTIVE CONTRACTOR DOES NOT PROPOSE TO USE SUBCONTRACTORSTO
PERFORM SERVICES.
By signature below, vendor agrees to and shall fully comply with all Requirements related to subcontractors as shown In the bfd solicitation.
Vendor Name: Northeast Arkansas Community Mental Health Center Date: 9-30-20 d/b/a Midsouth Health Systems, Inc. affiliate of Arisa Health, Inc.
Authorized Signature: )~J ~ /1)nu,el} Title: Executive Director
Print(fype Name: Ru h Allison Dover
Paqe 6of8
Contents of other Documents
First Solid Blue
Solid Orange
Solid Red
Solid Green
Solid Yellow
Second Solid Blue
1.23 Prohibition of Employment of Illegal Immigrants
2.2 Minimum Qualifications, A.
2.2 Minimum Qualifications, B.
2.2 Minimum Qualifications, C.
2.2 Minimum Qualifications, D.
2.2 Minimum Qualifications, E.
M ( l\t:JlltftH:S Ut,~bl ll llCUJ ~ V I rllldlllt..:t, a1 1u l"'\Ul l l lllldUtlllUII
Home Wolcomo Agency - LQgl~ - ----------------------- ----------- --- .. ·--
Submission Confirmation
1 Thank you for your submission. This submission Is valid for one year.
We havo rocordod your submission. Please cllck here to return to the home page.
Print Disclosure Submission
Dlsclosure forms aro valid for one year.
Vendor:
Tax ID:
Disclosure Statement:
Contact E-mail :
Submitted on:
Yalld through:
hftnc ·//u11A11., :ark nrn/rlr:o/lmmlnrRnfllnrl"'v nhn/rl l-.r.ln-.1 ,r,./rnmnlRIAl~AQAR
NEACMHC dba Mid-South Health Systems, Inc.
4925
I certify that I DO NOT employ or contract with an illegal Immigrant.
01-27-20
01-26-21
1 /1
Contractor
and
Subcontractors'
Division of
Provider Services
and Quality
Assurance
Licenses
A R K A N 5 DEPARTMENT
A S OF
HUMAN SERVICES
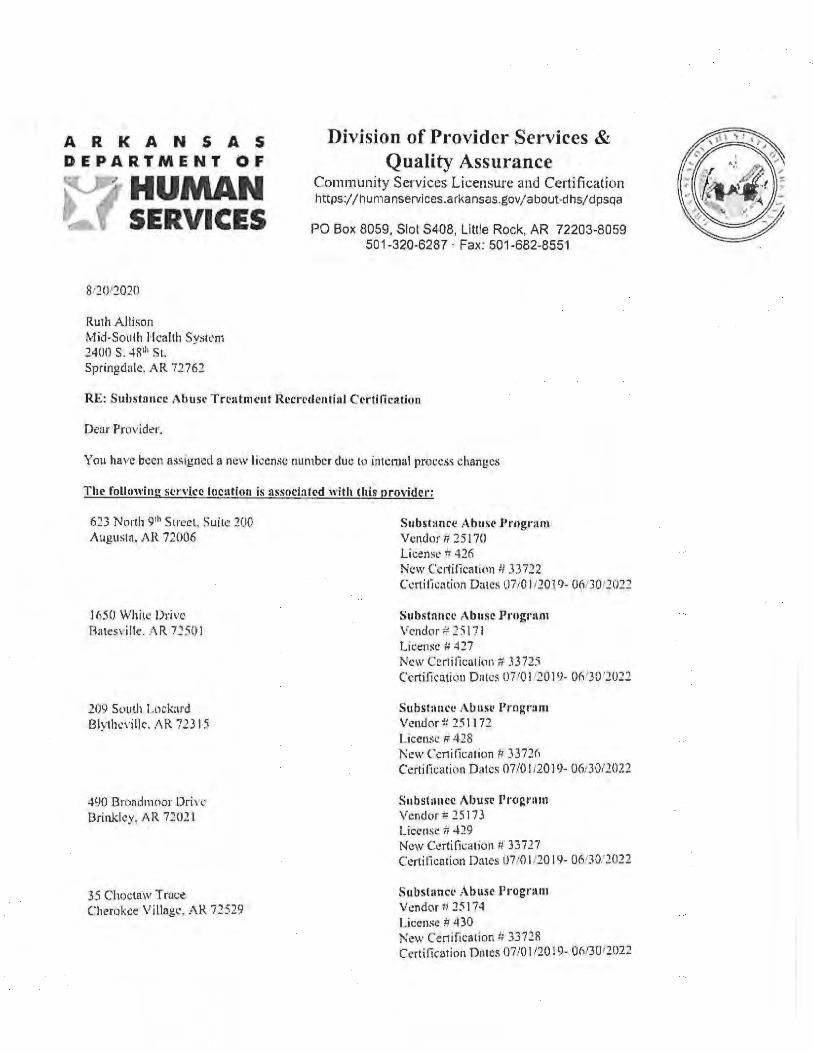
812()12020
Ruth All ison Mid-South Health Syskm 2400 S. -1 8tll Sl. Springdale. AR 72762
Division of Provider Services & Quality Assurance
Community Services Licensure and Ce11ification https://humanservices.arl<ansas.gov/about-dhs/ dpsqa
PO Box 8059, Slot S408, Little Rock, AR 72203-8059 501-320-6287 · Fax: 501-682-8551
RE: S uhstirncc Ah U S(' Trt•11lmc11t Rccrcdential Certification
Dear Provider.
You l1avc been assign~Ll a new licen.~e number due lo intt:nrnl process changes
T he following service location is associnled with this proYider;
623 NNth 9111 Street. Suite :wo Augusta. AH 72006
1650 White Dri ve Hatesdlle. ,\ R 7250 l
209 Sl,uth Lnckard Bly thl.'\'i llc. AR 723 1 S
490 Bro11d111oor Ori, ~· Brinklt'y, AR 72021
35 Cho<.:taw Trr1ce Cherokee Village, AR 72529
Substance Abuse l'rogrHm Vcndor#25 170 Licensr I= 426 New Certification !/ 33722 Cl'.nifkacion Dates U7/0 l /2019- 0l\130120:!2
Substance Abuse Prngr:im Vcndor # 2S l7 I Licen~c If 417 New Ccr1 ifica1io11 t:/ 3372:i Ccrtificati<m Dales 0710 I '2019- 01\ '30 '2022
Substance Ab11sl' l'rngram Vendnr -P. 2511 72 Licem;I.! # 428 New Ccnilica1ion ;; 3372(, Cerrilicati tln Dales 07/01/2019- 06:30/2022
S11bst:111cc i\busc Progl'am Vcndor ;;:!5173 License Tr 429 New Certilication I/ 33 727 Certifica tion Dates 07/0 l /20 19- 06130.'2022
Subslancr Abuse Program Vendor t, 25 174 License # 4 30 N~w Certification !: 33 728 Certification Dotes 07/0 I /20 19- 06/30/202.2
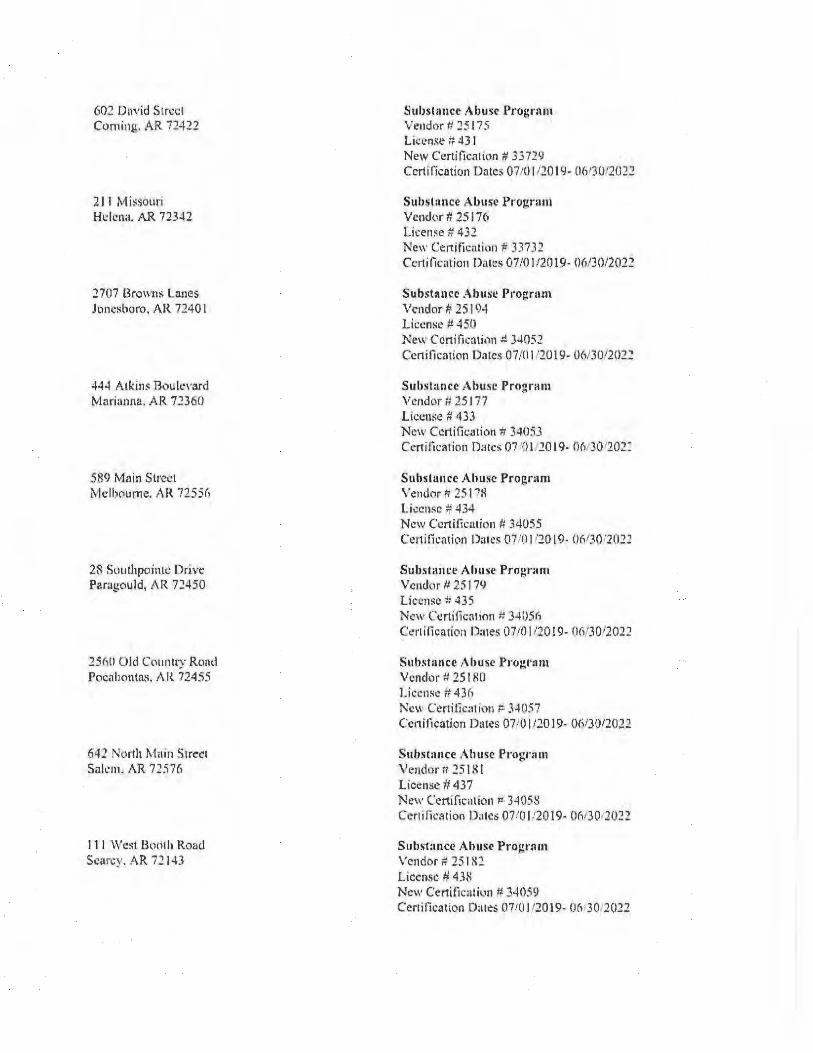
602 OaYid Stn:cl Corning. AR 72-122
211 Miss.ouri 1-h: lcna. AR 72342
2707 Browns Lanes Jonesboro, AR 7240 I
44-1 Atkin:: Bou levard Marianna. AR 71360
589 Main Stred Melbourne. AR 72556
28 Southpointi: Drive Par:igould, AR 72450
25MI Old Country Rt\ild Pocaliontai;, AR 724 55
642 1orth J\foin Street Sak'm. AR 72576
111 West Bocllh Roacl Scnr~y. AR 72 143
Su1>s1irnce Al>use Pr ogrnm Vendor t: ::15 175 Lic,;-nsc # 43 1 New Certilic,llion # 33729 Certilicotion Dates 07/0 I /?.O l 9- 0613012022
Substance Abuse Program Ve11dC1r # 25 176 License# 43?. Ne\\' Certificatinn f: 33732 Ccrtilicati011 Dates 07/01/20 19- 0(1/30/2012
Substance Ab use Program Vendor# 25 194 License fl. 45() New Ccnilicatinn :i 34052 Ccnilkation 0 :11es 07 /0 1 120 19- 06130/2()22
Suhstance Ahusc Program Vendor ft 25177 license # 433 New Certification ir 34();)3 Certification Dates 07 ·'0I 20 l9- Or1.'J01202J
Suhsluncc Ah use Program Vendor # 25 l"'X License ¢f 434 New Ccrtificnt ion # 34055 Certification Dates 0710 I ,·20 I 9- 06130 '2011
Subslance Alrnse l?rogr:im Vc11d<1r IJ 25 I 7CJ Lic..:nsc-# 435 New Ccrti!icnt ion # 34()511 Ct!rl ilicnrion Dates 07/0 I /2019- (l(,/30/2022
Suhstance Ahuse Program Vendor# 25 t RO Licct\SC ;; 43n New Cer1ilic:Hi('l11 p 34057 Ccn ihcntion Dmes 07/0I 120 19- ()6/30/2022
Substance Ah use Progrnm Vendorr/ 151 ~ I license# 437 New Certificn1io11 ;:. 34058 Ccr1ific:Hion Dates 07f01/2019- OMJ0,202'.!
S ubs tance Ah use P rogr:-.111 Vendor # 25 182 License # 43~ Nc·w Certi ticaliun # 34059 Cer1ification Dates 07101/2019- 06130 2022
807 West Main T runtann. A.R 72472
905 North 7'11 Street West Memphis. AR 7230 I
102 South Larkspur Walnllt Ridge. AR 72476
66 1 Addison Drive Wynne. J\R 72342
445'1 North Wnshington Forrest City. AR 72335
1507 rcc:in Newport. AR 72 1 12
10 11 MorganS1rec1 Pan1gould. A R 7.2450
$37 Wi]lell Road Jonesboro. AR 72.-JO I
~ubstancc Abuse Prngrnrn Vendor # 25 183 License# 439 New Ccrtilic:uion Ii 3-W60 Certifo:ation Dates 07/0 I /20 I 9- 06/30/2022
Stibsrnncc l\.l>usc Program Vt:ndor!/25 184 License # 440 New Certification # 34063 Certification Dates 071() I '2019- U(V301202'.!
S11bsh111cc Abu~e Progrn111 Vcnd~1r If 25 185 License # 4-1 l New Ccrtifo.:aticrn # 34064 ('4.-:rtitication Dates 07/0 112019- 06/30/2022
Suhstaucc Abusc Pro~r:1111 Vendor 1; 2518() License# 442 New Certification ;, 34065 Ccrti(kntion Dntt:~ 07101120 19- 06/30/2022
Subsllmcc Abuse Progralll Vendor ff- 25 187 License It 443 Nl!w Ccrtifirntion ti 34066 Ccrtifir.:ation Datl·s 07101 120 19- 06.'J(I, ~022
S11bsti111ce Abusr Program Vendor f. 25 188 Li cen~e ii 4-1-1 N~·,,· Certification Ii 34067 Ccntlicalion Dales 07/t) 1/20 I 9- 06/30,2022
S11bst1111cC' i\hus,• Progn1111 Vendor ;.; 2~ I !i9 Liccnst: /: 445 Ne\\' Ccnific:uion # 34069 Certitiea1ion Datt!i- (1710J /2019- 06/30 12022
Subst:111ce Al>USl' Progrflm Ven clot ff 25190 Lici.>ns~ A 425 N~w Ccrtificutiun 1134·103 Certi lkution Dates 07, l) l/20 l9- U(l'JU,20~2
On an ongoing basis. if ci ,cumstanct;S change regan.ling your SNYicc del ivery. site address(cs). M orga11i;m11011al structure, you mus( lH)tify DPSQA/Substnncc Abusl! Liet:nsuri: antl Ccniticntion oflice with applicnblc updates, Addilionully, please remember that nil 11lc~1hol and L,thcr drng abu~l' trcaunent programs in Arkansas arc requir~d to report olicm-rd :Hcd data in accordance with the requirements of lhe current .i\ lcohol and Drug M1111agcmenl lnfon11a1io11 System {ADtvUS l. Tascha J\:t.::r~cn is our stnff dedicated 10 ADMIS training and data. She can be reached il t (50 l) 686-9953.
Should you have any qtJllstiom:. pkase do not ht:$itnte i.;ontac t Darm Briscoe by email nl
1,•,-11• I',, l 1'.J,-11,_ :1•n· II ,11 .1, '-~ •· nra1 (501)320-6 1l 0.
Sincerdy.
( J-,-lli:)v<:_ Johnathan Jones Assistant Director Oi \'ision of Provider Servin!S and Qua I ity Assurance Community Services Lil:cnsun: and Certification h 1h1111 lm11 l,111, 'i:..1Jft,,,.,, ~ 111-,,1- -~•·
C: Liccn~un· File Daphne r~urk111~. DXC Tamera Bdin, OMIG Tn~lia Petersen C-tin1c;sa Cla•·k Taoya Gilts Cltri~lin:1 Wcstmi11s1.:r 0 1is l logan l' ;11m.:1a Cia1111 Shnntn [)t,nv:m Vivi:111 Ja,·kson Meli~.,n Wn1\l
~ · ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 33722
~bis Js to <!Cettifp ~bat
Northeast Arkansas CMHC; Mid-South Health Systems, Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at __ _ 623 North 9th Street, Suite 200
Augusta , County of Woodruff 'Arkansas.
License Effective: O? / Oi/ 2019 I License Expires: 06/30/2022
I~ (tt,
l~I 1■1·· ~< .l ~;-~ ,; ~7 ARKANSAS DEPARTMENT OF
. HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 33725
'Qf;bf~ 3l~ to <!Certtfp ~bat
Northeast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 1650 White Drive
Batesville , County of Independence , Arkansas.
License Effective: o7 / 01/2019 I License Expires: 06/30/2022
~ ARKANSAS DEPARTMENT OF
r -- .V HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 33726
m;bts Js to Qtertifp 1Ebat
Northeast Arkansas CMHC; Mid-South Health Systems, Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 209 South lockard
Blytheville , County of Mississippi , Arkansas.
License Effective: 07/ 01/2019 I License Expires: 06/30/2022
a-=:::-..
a /4 .. .. ~
~
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 33727
~bis 3Js to ([erttfp 1Ebat
Northeast Arkansas CMHC; Mid-South Health Systems, Inc.
is hereby granted a l icense by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 490 Broadmoore Drive
Brinkley 'County of Monroe ' Arkansas.
License Effective: 07/ 01/2019 I License Expires: 06/30/2022
~~
~ ARKANSAS DEPARTMENT OF
.f HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 33728
1!Cbts 3Js to <!Certtfp 'Qr;bat
Northeast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 35 Choctaw Trace
Cherokee Village County of Sharp A k _______________ , _______________ , r ansas.
'H .A~ • License Effective: 07/ 01/2019 I License Expires: 06/30/2022
~
~\ ,)

ARKANSAS DEPARTMENT OF HUMAN SERVICES
Division of Provider Services & Quatity Assurance
License Number: 33729
'<Ebts J~ to ~erttfp '<Ebat
Northeast Arkansas CMHC; Mid-South Heafth Systems, Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 602 David Street
..,,. . Corning , County of Clay , Arkansas .
License Effective: 07/ 01/ 2019 I License Expires: 06/30/2022
(IIN -~

ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number. 33732
~bts J~ to ~ertifp 1l[;bat
No·theast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 801 Newman Drive
Helena , County of Phillips , Arkansas.
License Effective: 07/ 01/ 2019 I License Expires: 06/30/2022
. :-.
I 'I
111 [11 ~ ARKANSAS DEPARTMENT OF
r -- .f HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number. 34052
m;bfs 3Js to ~erttfp m;bat
Northeast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 2707 Browns Lane
______ J_o_ne_s_b_o_ro ______ ' County of ______ c_ra_i_g_he_a_d _____ _, Arkansas.
License Effective: 07/ 01/2019 I License Expires: 06/30/2022
"· ·,
:( ~
1~ -~~
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34053
1[bfs Js to ~erttfp 1[bat
Northeast Arkansas CMHC; Mid-South Health Systems, Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 444 Atkins Boulevard
______ M_a_ria_n_n_a ______ , County of _______ L_e_e _______ , Arkansas.
License Effective: 07 / 01/ 201.9 I License Expires: 06/30/2022
~ -I I
~ ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number. 34055
~bi!i ll!i to ~erttfp 'UCbat
Norttieast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 589 Main Street
Melbourne , County of Izard , Arkansas. ' ~
License Effective: 07/ 01/ 2019 I License Expires: 06/30/2022
~ -
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34056
1Ebi~ 3ls tJ.l ~ertifp ~bat
Northeast Arkansas CMHC: Mid-South Health Systems, Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 28 Southpointe Drive
~:--____ P_a_ra_g_o_u_ld ______ , County of _______ G_r_ee_n_e _______ ,, Arkansas.
License Effective: 07/ 01/2019 I License Expires: 06/30/2022
.~s· _\ I •
~ / -\~·

ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34057
1[bf~ JJ~ to <!Certtf!' 1lCbat
Northeast Arkansas CMHC; Mid-South Health Systems1 Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 2560 Old Country Road
Pocahontas , County of Randolph , Arkansas.
License Effective: 0? / 01/ 2019 I License Expires: 06/30/2022
:--~ ·,
~ ~~
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34058
'Qf;bi~ 11' to ~erttf!' 'Qf;bat
Northeast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 642 North Main Street
Salem , County of Fulton , Arkansas.
License Effective: 07 / Oi/ 2019 I license Expires: 06/30/2022
~
~., ARKANSAS DEPARTMENT OF . HUMAN SERVICES
Division of Provider Services & Quality Assurance
License Number: 34059
~bfs Js to ClCettff!' 'atbat
Northeast Arkansas CMHC: Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 111 West Booth Road
_ Searcy , County of White , Arkansas.
License Effective: 07/ 01/ 2019 I License Expires: 06/30/2022
e
~. '7 ARKANSAS DEPARTMENT OF
~\f HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34060
1Ebfs Js to qterttfp ~bat
Northeast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 807 West Main
Trumann County of Poinsett , Arkansas. ~~ '
License Effective: o7 / 01/2019 t License Expires: 06/30/2022
a -~/
~1 ARKANSAS DEPARTMENT OF
"_.. HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34063
m;bt~ 3Js to QCertffp m;bat
Northeast Arkansas CMHC; Mid-South Health Systems, Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 905 North 7th Street
west Memphis , County of Crittenden , Arkansas.
:t_ License Effective: 07 / Ol/ 2019 I License Expires: 06/30/2022
Ill y• · .f[I
~ ARKANSAS DEPARTMENT OF
'!..f HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34064
'tEbis 3Js to QCertifp ~bat
Northeast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 102 South Lark.spur
Walnut Ridge , County of Lawrence , Arkansas.
License Effective: o7 / 01/2019 I license Expires: 06/30/2022
"1.IL,~-~
~\ ,1 \VI
l ;
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34065
m;bts Js to ~ertifp ~bat
Northeast Arkansas CMHC: Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 611 Addison Drive
Wynne C f C _______________ , ounty o ross , Arkansas.
License Effective: o7 / 01./ 201.9 I License Expires: 06/30/2022
~'~
~ ARKANSAS DEPARTMENT OF
r __ .f HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34066
~bfs Jti to C!Certtfp UCbat
Northeast Arkansas CMHC; Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 4451 North Washington
Forrest City , County of Saint Francis , Arkansas.
License Effective: o7 / Oi/2019 I License Expires: 06/30/2022
~ -1)
7 ARKANSAS DEPARTMENT OF
...._ HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34067
t[bfs Js to <teertffp 11tbat
Northeast Arkansas CMHC: Mid-South Health Systems, Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 1507 Pecan
Newport , County of Craighead Arkansas.
License Effective: 07/ 01/ 2019 I License Expires: 06/30/2022
'~) !
~7 ARKANSAS DEPARTMENT OF ..._ HUMAN SERVICES
Division of Provider Services · & Quality Assurance
License Number: 34069
~bis Js to <!Certffp ~bat
Northeast Arkansas CMHC: Mid-Sout~ Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 1011 Morgan Street
Paragould County of Greene A k --------------- , ______________ _, r ansas.
license Effective: 07/ 01/ 2019 I License Expires: 06/30/2022
/~ 1~' ,, ,1 ·~,
~ ARKANSAS DEPARTMENT OF
"-- ~ HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34103
mbis Jls to QCertff!' 11Cbat
Northeast Arkansas CMHC: Mid-South Health Systems. Inc.
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Program
on the premises located at 837 Willett Road
Jonesboro , County of Craighead Arkansas.
License Effective: 07/ 01/2019 l License Expires: 06/30/2022
. j
I
~ ARKANSAS DEPARTMENT OF
J ,HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 33730
tlebt11 J11 to QCertif!' ~at Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
602 David Street: Corning. AR; 72422
Therapeutic Communities - Level 1
has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01 /2019 to NIA (unless sooner revoked). .
~ -,~,\
A R K A N S A S DEPARTMENT OF
HUMAN SERVICES
08/05/2020
Ruth Allison Dover, CEO Jared Spnrks, VPC Mid South 1-kal th System:-. Inc 2707 Brnwn~ Lane Jonesboro, AR 72401
Division of Provider Services & Quality Assurance
Community Services Licensurc and Certi fication https:j / t1umanseNlces.arkansas.gov/ about·cihs/ dpsqa
PO Box 8059, Slo t S408, Little Rock, AR 72203-8059 501-320-6287 · Fax: 501-682-8551
R E: Licen se to Provide Substance Abuse Trcntmcnf
Dear Provider.
t---1id South Health Syi;tcrn:-. lnc."s license has been apprt)\'ed from July 23, 2020 through July 22. 2023, as long as iherc hus not b1:c11 a lapse in Licensurc Standards for /\ lcohol and Other On1g Abuse Treatment Programs.
The DJ>SQA Program License is included \\'ith this mailing. The DPSQA Program License shnuld be displayed al ft
prominent public location within the licensed site(s).
The follo\\'ing s~n ·icc loc:ation is associat~d with this provider:
3204 G. Moore Ave Searcy, AR 72 143
3202 C. Mot1re Ave Searcy. AR 72 143
Ccrtificntiun # 34059 Crrtifica tion Dates: 07/23/2020-07/22/2023
On an 011going bnsis. ir c in:umswnccs chnngc regarding your service delivery. ~i tc addrcss(cs), N organinHionnl ~tructurc, you 111us1 ntltify DPSQ.'\/Sub~tanee Abuse l. icensure aud Ceniliculion office with applicahlc updates. Additio1,ally, please remember tha t all alcolrnl and olhcr drug abuse h·catmcnt programs in Arkansas arc rcquin:J to report client-related dnt11 ir\ accordunce wilh the regu i1·1: 111cnts of the curren1 Alcohol and Dntg Managc111cnl lnfornrntion Sy:-lizm (AD1VJIS). Tasdrn Petersen is our staff dedicated to /\IJMIS trnining and data. She can be reached a l (50 I) 686-9953.
Should you have .1ny quc:ctions. pica.st do nnt he~itatc contact Dana Briscoi.: by email at l?.f>">V,.~.11·11\ f1k1 , 1,plil .II ll llJSI.(! u1i~.a 1'~ 1111, I . !,!l I'\ or lit (50 I) 320-(i 11 0.
Sincerely,
q,1£;~ Johnath.in Jone-~ Assistant Dir;:ctur Di\'ii;iqn of Pro\'ider Services and Qual ity Assurance Com1mmity Services I.iccnsure and Ccnification f': '.'I l i .J2(),1,5•J<l I .'i<J I A'-~ s: - ~ I ~,,,,, \ l.1111~[ ,f.,t\-4 ! ~
humanservices.arkansas.gov Protecting the vulnerable, fostering independe nce a nd promoting better health
I 1lll. R,11.'.k. \ H • ''11\
l11h11,,ll1,111.J~1 1,~~ d !JI' II k,11i~:t!--;;•I\
C· Liccn,ur.; File
r-it.:
J ltwh
Daphne Burkins, DXC Tamera 13din. OMIG Tnschu Pcrcfs,·n Conti.:s~o Clark Tan.yo Gile~ Ch ri stina \\11:.•aminsr<::r Patricia Gnnn Sharon D (11wn11
Vi1·iun Jack s1111 rvkli~_.;11 Ward
~7 ARKANSAS DEPARTMENT OF
'!.. · HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34059
'atbis 3Js to <!Certif!' 'at:bat
Mid South Hea Ith Systems. Inc
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Programs
on the premises located at 3202 E. Moore Ave
Searc}', AR 72143 , County of White , Arkansas.
License Effective: 07/ 23/ 2020 I License Expires: 07/ 22/2023
:(9
~., ARKANSAS DEPARTMENT OF
~ HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 34059
m;btS' 3J 1' to <lCerttfp «bat
Mid South Health Systems. Inc
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Programs
on the premises located at 3204 E. Moore Ave
, Searcy, AR 72143 , County of White , Arkansas.
~~ License Effective: 07/ 23/ 2020 f License Expires: 07/22/2023
A \ill
A R K A N S A S DEPARTMENT OF
HUMAN SERVICES
08/20/2020
Ruth All ison Mid-South I tea Ith System 2400 s. 48 11, S t. Springda le. AR 71762
Division of Provider Services & Quality Assurance
Community Services Liccnsurc and Certification https;//11 u manservices.a rkansas.gov/ a bout-d hs/ d psqa
PO Box 8059, Slot S408, Lit tle Rock, AR 72203-8059 501-320-6287 · Fax: 501-682-8551
1rn: lkha\1ior11l Ilcalth Agency (BHA) Rccrcdcntial Ccrrilication
IJcnr Provider,
Y <1u hnvc b.::cn assigned a ne\\' license number due lo in icntal prncc:-s changes. Your pre\"ious license number arc 31 1.67 .68,716,7 17,4 I 3.4 11,54) 75.69.56.63.64.57.5S.59.60.6 l.65.34lU86.3 I 2.66.307. and 313. Your prC\'tOll ~ vcndor number is 11 053, I 1433.1 1068. 11 055,11062. 11063) 1056. 11 057. 11058. l I 059, I I 060. 11 064, 11 406. 11446, 113 I 2. l 1065.1 l 307. 11 127.1 13 11 .11066. I 1067,12015.12016, l 1473.and 1147 1.
Enclosed ccni[ication (s):
445 1 North Washington Forrc:-:1 City. AR 72335
623 '.'/1)rth 9111 Street, Suite 200 A11gusl.J, AR 7'.!006
11 I M issot1ri l lck·11r1, A R 72342
905 North 7111 • trccl Wt.:Sl Memphis, AR 7230 I
28 Sou1hpoi111c Drive Paragould. AR 72450
Bch:"1iornl Health Agency Vendor H I I 053 License f I 54 New Certil'icntion ti 32034 Cl'rl1 ricnlinn Dotes 07 /0l /20 19- 04/30/20?. I
lkhaviornl Jk:t lth Agency Vendor ;; 11 433 License ;; 375 New Ccnifica1ion fi 3:2 186 Ci:r1ilici1tion Dates 07/01 2019-04/30 2021
lkhavion1I llcalth Agency Vendor /1 I [()68 Liccn:;c N ()9 New Ccrtilical ion fl 32190 Ccrtificillion Dales 07/0 l /2019- 04/30/202 1
Bchaviornl llcalth Agency Vendor II I 1055 License II 56 New Ccrlification It 32362 Ccr1ificr11 io11 Dates 07/01 /20 19- 04/30/202 1
Behavioral Health Agency Vendor fl 11062
huma ns C!rvices.arkansas.gov Protecting the vulnerable, fostering independence and promoting better health
101 I Morgan Street Paragould, AR 72450
80 I Newman Dnvc Wynne, AR 72396
66 1 Addison Dri\'C Wynne. AR 72342
602 Da,ritl Street Coming. AR 72-1 22
490 Broadmoor DrivcBrinklcy, AR 7202 1
-144 Atkin,; Roulcv:ird Marianna, AR 72360
2707 Browns l.1111~s Jonesboro. AR 72-Hl I
35 Chocta\\' Trace Cherokee Village. AR 72529
Liceu~c 11 63 New Ccnilica1irn\ 11 32364 Certifo;alion Dates 07/0 I/2019- 04/30/2021 Behnviornl Jlcaltb Agency Vendor ff. 110(13 · L iccnse ft r,4 New Ccrtilicnlion Ii 32370 Cert ification Dilh:~ 07 01,20 I 9- 04/30 '2021
BchnYiornl llcnlth Agl•ncy Vendor# 11 056 License ti 57 New Certilicat io11 If 3255 1 Cer1ificatk111 D:\lc:; 07/0 I /20 J 9- 04/301202 I
Behavioral llcal lh Agency Vendorf: 11057 Licen~e r; SR New Ccn ificati,111 !: 32555 Certificntiun Dates 07/0 I /2019- 04/30/2021
Behavioral Clcalth Agency Vendor ~ 11058 Licen:;c ti 59 :--lew Ccr1ilic.ilil1n ;; 32557 Certification O.itcs 07/0112019- 0-Vi0 '202 1
Behavioral Jl calth Agency VendClr II 11 059 License ti (10
New Ccrtitil::ation II 32611 Certilica1in11 IJatc, OH ) I 120 I 9- 04 Jn 1102 I
Behavioral fil' alth Agency Vendor fl 11060 License IJ 61 New Ccrti fi..:,11i(111 /I 32614 Certilica1i n11 Dates 07/01/2019- 04130/202 1
Belul\'ioral Jll'allh Agency Vendor 1i 11064 License 1/ 65 New Ccnificuti<1n // 32643 Certilication l);i\es 07/0I /2019- 04/30/202 1
Bch:wioral llealth Agency Vendor I; 11 40() License # 348 New Ccrti fi i.:mion ;; 327 1 I Certification Dates 07/01 12019- 04/30 2021
807 West Main Trumann. AR 72472
111 We l Bou1h Rt111d Searcy, AR 72 143
I 02 South Larkspur Walnut Ridge. AR 724 76
589 Main Street Mclboumc, AR 7155'1
1650 While Drive Batesville, AR 72501
642 Nonh Main Street Salem. AR 72576
2560 Old Country Road Pocahontas. /\.R 72-155
209 South Lockard Blytheville, AR 72315
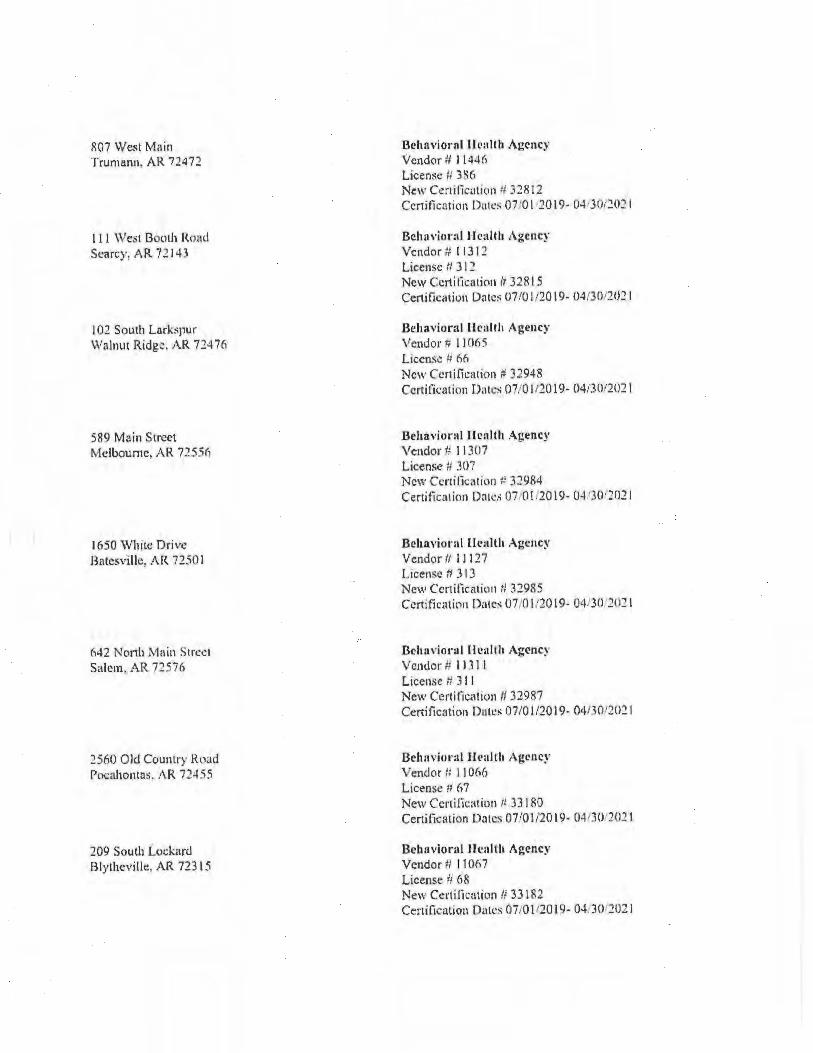
Oehnviornl IJeallh Agency Vendor # l 144(i License II 3~6 Ne\\' Certificatit111 :1 32812 Certilicution Dn1'.'!i 07 '01 20 19- O-J,J0.-2021
Beh:1"iornl Health Agency Vendor ti I 13 12 License II 312 New Ccrti ticatiCln /, 328 15 Certific,11iun Oates 0710 I120 19- 04/301202 1
Behavioral lkalth Agency Vendor;; 11065 License /; 66 New Cenifica1io11 P 32948 Ccrtifo:a tion Oaks 07/0112019- 04i30t202 I
Behavioral llcalth Agency Vendor # 11 307 License ii 307 'cw Ccnificatio11 :: 32984
Certiticnlion Dates 07 0I.2019- O-l: .30 '202 1
Bcha,1iornl 111:nllh Agency Vendor II 111 27 License fl 3 I 3 New Ccrtificatil111 II 32985 Ccrtificntion D:1tc, 07,01/20 19- 04130 202 1
Ochavioral ll callh Agcnc~ \/ cn<lor R 1131 I
Lice11se ti 3 I I New Certiticativn II 32987 Certification Date~ 07/0112019- 04130/20:! I
Behnviural ll<•al!h Agency Vendor /; 11066 License ;, fi 7 New Certification /i 33 180 Certilication Dates 07/01 /2019- 041301202 1
Behnviornl Health Agency Vendor # 11 067 License Ii 68 New C.:rtilkation /1 33182 Certilication Dates 07/01120 19- 0-UO 2021
211 Mis.sou ri Helena, AR n3"12
3700 Acces~ Road Jonesboro, A R 72450
1507 Pecan Newpo11, AR 72 112
83 7 Willett Rnad Jonesboro, A R 72401
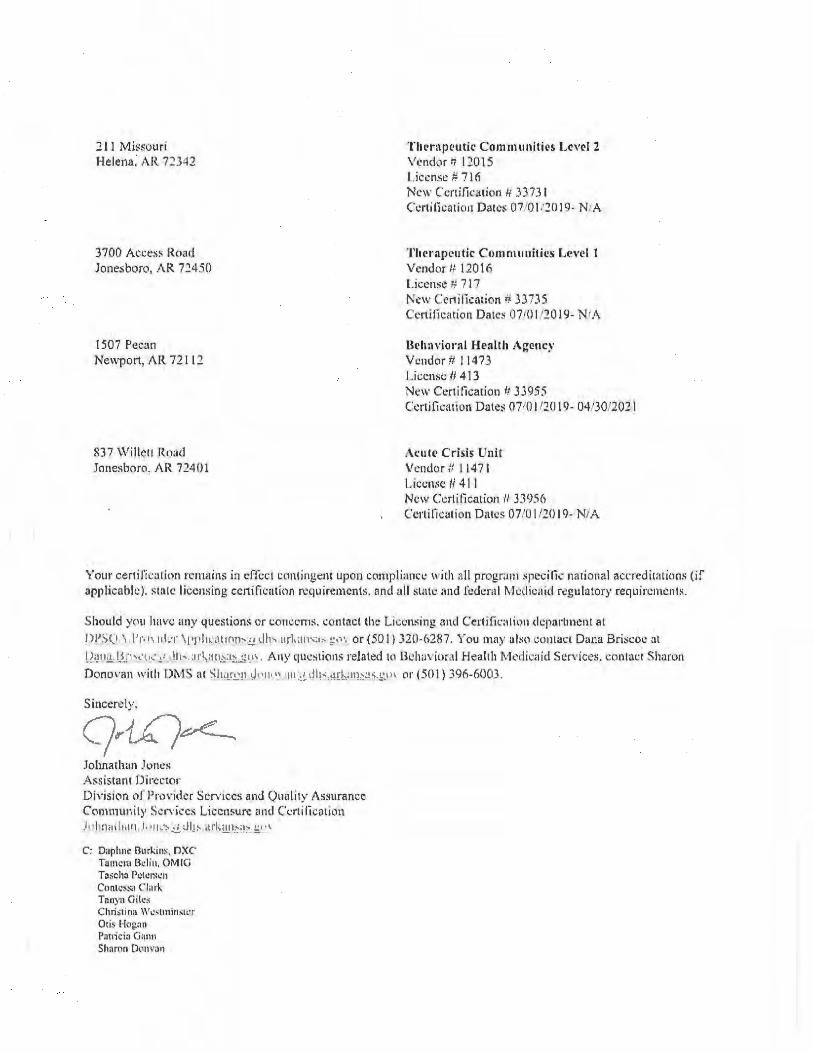
T hc·rnpcutil.' Com muniti"s Lcv"l 2 Vl'ndor I; 12015 l ,iccn.sc # 716 New C'cn ification Ii .3373 1 Ccr1ilica1io11 Dates 07 101: 20 19- NIA
'l'hcraprutk Comm1111ilics Level 1 Vendor/, 12016 License ;; 7 17 New Ccnificmion # 3J7JS Ccn itil:ation Date~ 0710 I 120 I(). NIA
l.k h:1vioral Health A~e11c~· Vendor tt l 1473 License ti 4 13 New Ceni!ication 11 33955 Certification Date:; 07(0 1110 19- 04 '30/202 I
A1:ut<' Crisis Unit Vcndur t/ I 147 1 License II 4 1 I New Certification /I 33956 Ccrlilicution Dates 07/01/20 19- NIA
Your oeni fic alinn remains in cffcc1 contingoimt upon C(lmpli,1r,cc with all prngr.1111 ~pccilic ,wional accreditaiiQn~ (if applicable). :-lalc licensing ce.rtification requirements. and all slate and fcdern l IVkllicil i cl rc:gulatory requircmi.'nls.
Should )'Cl\l lwvc any questions or co11ccm s, contacl lhl: Licensing and Certi fic: ,tit)n dcparlment al IW':>CJ , l'r, ,,, 111:r \t •1d1 •• ll 1on,-E,!. dh, arl.:111~·1,, .:!•· or (50 I J 320-6287. You 11rny alsl1 coi!litct Dana Briscoe at
I J,_11 1.i I~ ·1 ,._•u .. !1 Iii,. ·11!-.·111~.1~~<.1\ A11y question:; related tl, lkl1i1, iornl Health Medica id Services. conl.ict Sharon D ono1·an with 1)1\1] S at ~h.in,11 J, 111 •" 111 ., t1t,.tll'k'11b:3.!, ,1 or (50 l ) 396-6003.
Sincerely. q. -1,,(;ve.____ Johnatlwn Junes Assistant Director Dh·ision ot Pro,·idcr Scr;ices and Q11ali1y Assurance Com111u11i1y Scn·icc~ Liccnsurc c111d C1.:nilicntion .l 11luw«lin11 J, •11 - ~ .t1. Jlt, ,1l'k:1J1>i-. !:-• ,,
C': Daphne Ourkins, nxc Tamc1.1 lk lin, QMl(l Toscha l'c1c1~..:11 Conti:i~,1 C l:1rl,. Tnnyn Giles Christina W..:slminstL•r Otis Hognn Panicio Gann Shamn D01w:111
V1,·i,m Jutks11n Melissa Wnnl
JJ JR
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32034
1Ebts Js to ClCerttfp m;bat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
4451 North Washington: Forrest City. AR 72335
Behavioral Health Agency
has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021 (unless sooner revoked).
,,~
I[~
~1 ARKANSAS DEPARTMENT OF a,_ · HUMAN SERVICES
Division of Provider Services & Quality Assurance
Certificate Number: 32186
~~ts Js to Qeertff!' ~bat Northeast Arkansas CMHC: dba Mid-South Health Systems, Inc.
623 North 9th Street. Suite 200; Augusta. AR; 72006
Behavioral Health Agency
has met provider requirements to operate a(n)/as _____________________ _
\ Certificate effective from 07/01/2019 to 4/30/2021
~ Ll ~
!lffiD] r'-' '
(unless sooner revoked).
~7 ARKANSAS DEPARTMENT OF
~ HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32190
1!tbf1, J1, to ~erttfp 1ltbat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
211 Missouri: Helena. AR: 72342
Behavioral Health Agency
has met provider requirements to operate a(n}/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021 (unless sooner revoked).
~-
~7 ARKANSAS DEPARTMENT OF
I!... HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32362
m;bts 3Js to <!Certtfp t[bat Northeast Arkansas CMHC: dba Mid~South Health Systems. Inc.
905 North 7th Street; West Memphis. AR; 72301
Behavioral Health Agency has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021 (unless sooner revoked).
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32364
~bts Js to <tettifp ~bat Northeast Arkansas CMHC· dba Mid-South Health Systems. Inc.
28 Southpointe Drive: Paragould. AR: 72450
Behavioral Health Agency
has met provider requirements to operate a(n}/as ____________________ _
Certificate effective from 07/01/2019 to 4/30/2021
~"
i'
(unless sooner revoked).
ee,-s ·-f'F-!-4€-So,n•. 4-t§J-L:ZSj,tH:· 4·i·S ◄---•·= -:·-l:f '\. ·4:-_~½J
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32370
'QI;bts JJs to <!Certifp ~bat Northeast Arkansas CMHC: dba Mid-South Health Systems, Inc.
1011 Morgan Street: Paragould. AR· 72450
Behavioral Health Agency
has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021 (unless sooner rev(?ked).
--~-•
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assu ranee
Certificate Number: 32551
tEbts 3Js to ~ertffp ~bat Northeast Arkansas CMHC; dba Mid-South Health Systems. Inc.
801 Newman Drive: Helena, AR: 72342
Behavioral Health Agency has met provider requi rements to operate a(n)/as _____________________ _
fertificate effective from 07/01 /2019 to 4/30/2021 (unless sooner revoked).
~7 ARKANSAS DEPARTMENT OF
I!.. HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32555
m;bts Js to <!Certif!' ~bat Northeast J\rkansas CMHC: dba Mid-South Health Systems, Inc.
661 Addison Drive. Wynne. AR: 72396
Behavioral Health Agency has met provider requirements to operate a(n)/ as _____________________ _
:ertificate effective from 07/01/2019 to 4/30/2021
.~ a
(unless sooner revoked).
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32557
~bts lJs to ~erttfp ~at Northeast Arkansas CMHC: dba Mid►South Healtt, Systems. Inc.
602 David Street. Corning. AR; 72422
Behavioral Health Agency
has met provider requirements to operate a(n)/as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021
a '-8,
(unless sooner revoked).

ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32611
m;bts Js to QCertffp 1!Cbat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
490 Broadmoor Drive; Brinkley. AR: 72021
Behavioral Health Agency
has met provider requirements to operate a(n)/ as _____________________ _
~. Certificate effective from 07/01/2019 to 4/30/2021
..... ~ ..... ~~
. ~.,IAPJ) I~ ~ / \~~
(unless sooner revoked) .
~ l\RKANSAS DEPARTMENT OF
--.f HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32614
m;bis 3Ts to Qterttfp m;bat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
444 Atkins Boulevard: Marianna. AR; 72360
Behavioral Health Agency has met provider requirements to operate a(n)/as _____________________ _
Certificate effective from 07/01 /2019 to 4/30/2021 (unless sooner revoked).
V
~7 ARKANSAS DEPARTMENT OF I!.. HUMAN SERVICES
Division of Provider Services & Quality Assurance
Certificate Number: 32643
t!rbiti J~ to <!Certifp ~bat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
2707 Browns Lane: Jonesboro. AR: 72401
Behavioral Health Agency has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021 (unless sooner revoked).
/ ~ ,,,-~,\ _l~f ~
~. 7 ARKANSAS DEPARTMENT OF ~ HUMAN SERVICES
Division of Provider Services & Quality Assurance
Certificate Number: 32711
m;bts Jls to ~erttfp m;bat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
35 Choctaw Trace: Cherokee Village. AR: 72529
Behavioral Health Agency
has met provider requirements to operate a(n)/ as ____________________ _
Certificate effective from O 7/01/2019 to 4/30/2021
. ~ (v~ \,
~
(unless sooner revoked) .
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32812
m;bts ls to <lCerttfp ~at Northeast Arkansas CMHC: dba Mid~South Health Systems. Inc.
807 West Main; Trumann. AR: 724 72
Behavioral Health Agency has met provider requirements to operate a(n)/as _____________________ _
Certificate effective from 07/01 /2019 to 4/30/2021 (unless sooner revoked).
~B··~\ / f \w,
"'1f ARKANSAS DEPARTMENT OF
41..f HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32815
1lebis ls to C!Certif!' 1lebat Northeast Arkansas CMHC; dba Mid-South Health Systems, Inc.
111 West Booth Road: Searcy AR: 72143
Behavioral Health Agency
has met provider requirements to operate a(n)/ as _____________________ _
,Certificate effective from 07/01/2019 to 4/30/2021
I\ 11
·~·/ '~~
(unless sooner revoked).
•s=--;,s;; *'' aw:--* t&»:::••--t 1¥ ' · **'* t-· a a.__ > ... _-:,_.\
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider se,vices
& Quality Assurance
Certificate Number: 32948
m;bts Js to ~ertffp ~at Northeast Arkansas CMHC: dba Mid-South Health Systems. l11c.
102 South Larkspur. Walnut Ridge, AR; 724 76
Behavioral Health Agency
has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021 (unless sooner revoked).
~ ""~1·'',, '~ )
'~
,, ___ ,
ESivti=iHOca&,f1&2Z.r· ;- " · .. # Fl hr C.lf.• .-- ) , ~ _....;....:;;.. .
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32984
~bts ls to ~ettifp m;bat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
589 Mam Street: Melbourne. AR: 72556
Behavioral Health Agency
has met provider requirements to operate a(n)/as _____________________ _
07/01/2019 to4/30/2021 (unless sooner revoked).
-~
\ ~~w I
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32985
tlr;bts Jfs to QCerttfp ~bat Northeast Arkansas CMHC; dba Mid-South Health Systems. Inc.
1650 White Drive; Batesville. AR: 72501
Behavioral Health Agency
has met provider requirements to operate a(n)/as _____________________ _
Certificate effective from 07/01 /2019 to 4/30/2021 (unless sooner revoked).
G=--JI
i & 1
/
~
'' .. ~··~ f

~7 ARKANSAS DEPARTMENT OF
~ HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32987
'Qr;{Jts 3Js to ~ertif!' ~bat Northeast Arkansas CMHC: dba Mid-South Health Sys~ems! Inc.
642 North Main Street Salem. AR: 72576
Behavioral Health Agency
has met provider requirements to operate a(n)/as ___ __________________ _
ertificate effective from 07/01 /2019 to 4/30/2021 (unless sooner revoked).
4""--~
( ~
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 33180
~bis Js to <lCertffp ~bat Northeast Arkansas CMHC dba Mid-South Health Systems Inc.
2560 Old Country Road: Pocahontas. AR: 72455
Behavioral Health Agency
has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021 (unless sooner revoked}.
4 :j t ,,
,,. ,,.
~ ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 33182
m;bts Js to QCertifp ~bat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
209 South Lockard. Blytheville. AR: 72315
Behavioral Health Agency
has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021
,~
l~ I~ \ ,
~ , .;:
(unless sooner revoked).
- -- . .... , .. --~ I
ARKANSAS DEPARTMENT OF
HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 33735
~bis 3ls to <lCertffp ~bat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
3700 Access Road: Jonesboro. AR: 72450
Therapeutic Communities - Level 1
has met provider requirements to operate a(n)/as _____________________ _
Certificate effective from 07/01/2019 to NIA (unless sooner revoked).
~ .
a
'7 ARKANS. AS DEPARTMENT OF .-..f HUMAN SERVICES
Division of Provider Services & Quality Assurance
Certificate Number: 33956
tlrbi~ lf ~ to <!Certtfp tlrbat Northeast Arkansas CMHC; dba Mid-South Health Systems. Inc.
837 Willett Road: Jonesboro. AR; 72401
Acute Crisis Unit
has met provider requ irements to operate a(n)/as _____________________ _
Certificate effective from 07/01/2019 to N/A
a ~~
l ,1 ; ~
(unless sooner revoked).
ARKANSAS DEPARTMENT OF HUMAN SERVICES
Division of Provid_er Services & Quality Assurance
Certificate Number: 33955
~bis Js to QCerttfp ij[;bat Northeast Arkansas CMHC; dba Mid-South Health Systems. Inc.
1507 Pecan: Newport. AR· 72112
Behavioral Health Agency
has met provider requirements to operate a(n)/ as _____________________ _
Certificate effective from 07/01/2019 to 4/30/2021
=,
'
"·--=
(unless sooner revoked).
7 ARKANSAS DEPARTMENT OF
~ HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 33731
1[bis 3Js to <!Certtfp 1Ebat Northeast Arkansas CMHC: dba Mid-South Health Systems. Inc.
211 Missouri; Helena, AR: 72342
Therapeutic Communities - Level 2
has met provider requirements to operate a(n)/as _____________________ _
t~ ertificate effective from 07/01/2019 to N/A
I)"'~.~ 't:IY~JJ~ -~~ -~
I I
\
(unless sooner revoked).
3202 E. :,.toon: Ave Searcy. AR 72143
New Certification # 32815 Certificntio11 Dates: 07/23/2020- 04(30/202 t
Your ce11itica1ion remains in effect contingent upon compliance with all pl"(lgrnm specific national uccredil6tions (if applicable). slate licerlsing certification requm:ments, and all state and fedcrnl l\ ledicaid regulatory requirements. Plea!-c provide a copy of your current professional licensure ,md a copy o f any accreditation date changes (if applic.,blc) to DPSQA for our records prior to all expiration dates.
Should you have any questions or concerns. contact the Liccn:;ing and Ccnificauon department at
DP~~ Pr,•\ iJc~. \pplh-•lli 11 ..:.•Jh~...Jrkm•,:h.1'._,•\ or (50 I) 320-6287. You may also contact Dana Briscoe al
l),111.. lln,..:"'" ~ <lh, .u km, .. , ·--='l\ Any questions related to Bcha\'ioral Hc:ilth Medicaid SerYiccs. contac t Sharon OonO\";l!l \\•ith DMS at ~h,1r,,11.Jl•fh, \ <ltl ' . ,n .... 1d.·11i,;.1,.g ... or (50 I) 396-6003.
Sincerely .
. q.r1£)~ Jolmathan Jones Assistant Director Division of Provider Servrr.;cs and Q uality /\s.~urance Community Services Licensure and Cen ilication I' )I I L ,20.f• ~'-)\J
I 501 hS~ , ,5 1 °'1 Ill ', :'\ lam '-,t • ~ l1'! \-..:2-1111 k Rod , ,\R 722t1.:-J,1h11.11h.!11 1.,11,·,,,, dh,.ark.111,.1,~
humanservices.arkansas.gov Protecting the vulnerable, fostering independence and promoting better health
A R K A N S A S DEPARTMENT OF
HUMAN SERVICES
08/05/2020
Ruth Alli~on Dover. CEO Jared Sparks, VPC Mid South Health Sy:-tcms, Inc 2707 Browns Lane Jonesboro. AR 7240 l
Division of Provider Services & Quality Assurance
Community Services Licensure and Certification https://humanservices.arkansas.gov/ about-<lhs/dpsqa
PO Box 8059, Slot S408, Little Rock, AR 72203-8059 501 -320-6287 · Fax: 501-682-8551
RE: Behavioral Health Agency (BHA) Ccrlil1cation Approval
Dem:- Provider,
The Divi~ion of P rovider Scr\"iccs and Oualitv Assurance <DPSOA) has dctcm1ined 1ha1 all Arkansas Beha\'ioral
C: Daphne flurkins, DXC' Ta111cra l !cl in. OM IG T ascha Petersen Contessa Cl.irk Tanyu Giles Christina Westminster Patricia G,11111 Sharon Don, an Vivian .li!cbon Mclissu Ward
JJ/wh
~., ARKANSAS DEPARTMENT OF
~ HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 3281.5
1[bts Jrs to Qeertifp '<Ebat Mid South Health Systems. Inc
3202 E. Moore Ave Searcy. AR 72143
has met provider requirements to operate a(n}/ as Behavioral Health Agency.
ertificate effective from 07/23/2020 to 04/30/2021
a '.9,i
(unless sooner revoked).
M ARKANSAS DEPARTMENT OF
~f HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number: 32815
'Qrbts ls to ~erttfp 11tbat Mid South Health Systems. Inc
3204 E. Moore Ave Searcy, AR 72143
has met provider requirements to operate a(n)/ as Behavioral Health Agency.
Certificate effective from 07/23/2020 to 04/30/2021 (unless sooner revoked).
(.
A R K A N S A S DEPARTMENT OF
~ HUMAN ~f SERVICES
05/12/2020
WILLJAM A ALTON CEO
Division of Provider Services & Quality Assurance
Community Services Licensure and Certification https://h umanservlces.a rkansas .gov/ a bout-d hs/ d psqa
PO Box 8059, Slot S408, Little Rock, AR 72203-8059 501-320-6287 · Fax: 501-682-8651
UNITED METHODIST CHILDRENS HOME 1600 ALDERSGATE ROAD LITTLE ROCK AR 72205
RE: Behavioral Health Agency (BHA) Recredeolial Certification
Dear Provider,
You have been assigned a new license number due to internal process changes. Your previous license number is 070. Your previous vendornumber is 11069.
Enclosed certification (s):
2002 S. Fillmore St. Little Rock AR 72204
New Certification #32343 Certification Dates: 07/01/2019-12/30/2021
Your certification remains in effect contingent upon compliance with all program specific national accreditations (if applicable), state licensing certification requirements, and all state and federal Medicaid regulatory requirements.
Should you have any questions or concerns, contact the Licensing and Certification department at QI:S.QA.,P.roviderApplications(hcJhs.arkansas.gov or(501) 320-6287. You may also contact Dana Briscoe at Qana,Brisco~,a dhs.ark!l,D,;11::.g.ov. Any questions related to Behavioral Health Medicaid Services, contact Sheron Donovan with DMS at Sharon.donovnn(hdhs,arkansas.gov or (50 I) 396-6003.
Sincerely,
q~~ Johnathan Jones Assistant Director Division of Provider Services and Quality Assurance Community Services Liccnsure and Certification Johnathnn.Joncs(a,<lhs.erkansa~
C: Oapluie Burkins, DXC Tamera Belin, OMIG Tascha Pcte~cn Contessa Clark Tanya Giles Christina Wes1m111s1cr Otis Hoean Polrici~ Gann
humanservices.arkansas.gov Protecting the vulnerable, fostering independence and promoting better health
Sh:iron Oonvan V 1viftn Jackson Melissa Ward
JJ/wh
~7 ARKANSAS DEPARTMENT OF
... HUMAN SERVICES Division of Provider Services
& Quality Assurance
Certificate Number. 32343
~is Js to etertifp ~at United Methodist Children's Home / AR CARES
2002 S. Fillmore St. Little Rock AR 72204
has met provider requirements to operate a(n)/as Behavioral Health Agency.
Certificate effective from 07/01/2019 to 12/30/2021 (unless sooner revoked) •
•
A R K A N $ A S DEPARIMENT OF
HUMAN SERVICES
06/08/2020
A ndy Altom, CEO
Division of Provider Services & Quality Assurance
Communi ty Services Licensure and Certification https;//humanservices.arkansas.gov/about-dhs/dpsqa
PO Box 8059, Slo t S408, Little Rock, AR 72203-8059 501 -320-6287 · Fax: 501 -682-8551
United Methodist Chi ldren's Home l 600 Aldergatc Rond Little Rock, AR 72205
RE: Subslancl• Ah11s<.' Tl'eatn11mt R('Cr<.'cll•111ial Certification
Yoll hnve been a~signed a new license number due to internal process changes. Your new certiiic::nion number is 11069. Yt)Ur prcviou~ liccn~c number is 070. Your previons vendor number is 33776.
T hl' followi ng scrvic~ location is associated with this provider;
2002 South rillrnorc Street Little Rock, AR 72204
New C <.'rtific:i1io11 i,3377<, Ccrlifleation Oates: 07/01/2019 - 07/01/2022
0 11 un (rngoing bnsis. if cin.:u111~1unccs chongl! rcgru-ding your ~ervice deli\'ery. site addr.;:ss(C$). or org,ini1.01io111il slr'Ucture, you must 11i,1ily Dl'S(.).1\/S llbSltHH.!L' Abus~- Lic:cnsurc· and Certification oft.ice with applicable upd,1tc.s. Additionally, plc:ti;c r<'mcrn bcr thal all .ilcolwl illld olhcr drug abuse trea1menl programs in Arkansas an: required 1~, report clic111-rclatc:d tlal:1 i11 .iccord:inc.: wi1h th.: r.:quirements of lhe current .•'\lcohol and Drug Mnm1geme11I J11 fo r111arion Sys11:111 (/\ l)Ml S). Tasch a Petersen is our stnlT dcdicmcd to /\Dlvl!S trn ining and dato. She can be reached a l (50 I) 6R(1-9953.
Slwuld you hn, c any question~. plt"asc dn not lu:sitate contact Dana Briscoe by emai l at !)i•,r.,.\ 1'11 ,, 1d, 1 \i.'11!1 ,1 , .. ,. ,,_d .. , .nl...1,"., :.;•~ or al (501) 320-6 11 0.
S inccn:I)'.
Johnathan Jt,nc~ Assis1.in1 Director Division of Provider !jcrvicc~ n11d Qualtty Assuronce Comnnlnity Service~ l.it cnsurc and Ccrtif'ication I , lw tth.11, I ,11,•,,, dJ,, .. :d,;111,;, , ••1•\
Oaph11t llurki11.,, DXC Tnm,•m lklin. OMIG T:lscha l',·ttrscu Cumc,sa Clark l 'anyil Gil1..·~ Christina \Vc, unir1~11:r Oti, H1>g:111 Pa1rida Ci:11111 Sha11111 0 0 11\':111
Vivian Jarhun Meli~~:• Wurd
~7 ARKANSAS DEPARTMENT OF
~ HUMAN SERVICES Division of Provider Services
& Quality Assurance
License Number: 33776
1Ebts 3Js to ~ertif!' 1Ebat
United Methodist Children's Home / AR CARES
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Programs
on the premises located at 2002 South Fillmore Street
______ L_it_tl_e_R_o_c_k ______ ' County of Putaski Arkansas.
License Effective: O? / Oi/ 2019 I License Expires: 07/01 /2022
(.
,. l
)
j
A R K A N S A S DEP ARTMEN T OF
·HUMAN SERVICE
Tony ·1 homa..-;
Division of ProYidcr SrrYiccs & Quality Assu ranee
C\ i111munily Sc.:rviccs Li t:l.!llSllJ'l: and Cerll ltcalion 11 ttps:/ / 11 Li nic1 nserv/ces.mka nsus. gov/ a bou t-d hs/ d psqa
PO Bo.x 8059, Slot S408, Little Roell, AR 72203-8059 501·320-6287 - Fax: 501-682-8551
J\:c,n hcasl AR Rc!l,it1 11;il Rcc<,,·cry Center fi009 C W Po::t Rr•ad Jnncshoro, A R 7J-lt) I
RE: Su1Jst11 ucc .-\1111s1· Trcnlln en t Rc>r rccl l'tll ial Cc1·1ilica1io11
Dc.ir l'rn1 iLkt.
Ym1 ban : bc1:n ;1~.-.it! ncc.J a Ill'\\' lrccnsc m1111hl'I clue (p 111 1<.!rnal prm:c~~ cl11111:,:I.!~. Ynur lit::\\ cert rl1, 0111m m1111uc:r i,.
J:!549. Y11ur pri:,·i1•11~ licc11sc 11u111bcr 1:1 295. Yn11r pn:vious ,·end1,r 1111111lwr rs 250<10.
T he followiui.: s c·n ice· locat ion is assodalcll 11 ilh this pl'O\'ld ~i-:
(,(HJ9 C \\' Po~t R1,,1(1 fo11esbt1ro. . \ R 7 2 Ill I
;\cw Ccrtifira1io11 #: 315-1 9 Cc1·tific;1 I iun Da l l'!>: 03/2/!/20 I l) - IIJ /21:i.'21112
On nn IJl1J;?Ol11g b:i:.1s. ii' d 1cw11sta11cc~ change 1·cµ;1rding your sen ic,: dd i\\;ry. sitL· <1ddr~:;..~(,::; ). nr org,1111z11tiClnal slruct11re, you mu~l 11111 il~• IWSQA/Subsl,111cc /\ husc l..ici.:nsurc und l \:n ilii:.r tion t, t'fic:c 1,•j1h applic:ihlc updates. 1\dclitio11a lly. plca~c 1\:n1en,hcr 1hat :il l 11k1, lll'f ,11H.I Pth~r drug aim st' il'\'<1 1111l'lll prOl,ll'lllll~ i11 Ark,111s.,s ar,: rcq11 ired tn rl·port clic11t-rcl.ilcd d:11:1 in ai.:t'L•1·da11rc \\'ilh tho: 1·,:quiri:me111~ of1hi: , u,·l"\'111 /\klllml mid Drug ~la11:,gc111l'lll l,1 rorr11 ndc,11 sy~:tl·m (1\l)~ I IS). 'l'usdrn l'c \L'r,;L'II '" 11ur stnffd.::<l icMcd l1' ,\ i),\ 11'- 1r:1i11ing and tbta, ShL' i:im bi: r~:ich::d :u \5(1 I I f,s1,. o,J:•~
'ihnulrl yr)u h:I\ <.: ;rn~ qu,:,-1in11, . pica~,: Llv 11 111 h,·, iia1c Cl'llia.:1 D.111.1 Hri ,,:p,• 1,y l.:JJ1;11 I O\ JJ l'-.1,l , 1'1 ,., 1il1, \r _, ,. .,, " .,, di!, .t1 k.111-.,, . . ,1 nrn1 (50 I) 3211-/111 11.
Sinc~rcly,
J,,h11:11han J,,nc~ ,\ ,;:;i:;1r111t Direc t11r f1i vi~iC111 of J'rt11·i(k r .'ii:l" kc~ and Qu::d ily .\ ,~ur:111c,· C.'om n1l111 i1y Ser"\ i<:1•s I in :nsun.: and Ccr1i li1:atm11 1,,1 111.rh \l l 1,,1, • '"" 11·~ 111 •. , ... ,:,,1
(' I i, ,·n,11r~ f ik D:1111111: Our!.111, 1>:,:c (:1111~,·~ lk tin. \ l:,.tt(1
T11, ~hu l'~kr,m C,10l~>il1 (1:11 1.
ARKANSAS DEPARTMENT OF HUMAN SERVICES
Divisio:1 of ?roi ider Services & Quality Ass1m:mce;
license Number: 32549
'l!f;gtg J11 to ~erttfp m;gat
Northeast AR Regjonat Recovery 8enter
is hereby granted a license by the Arkansas Department of Human Services to maintain and operate a
N/ A capacity Alcohol and Other Drug Abuse Treatment Programs
on the premises located at 6009 cw Post Road
Jonesboro , County of Craighead , Arkansas.
License Effective: 0 3/ 28/ 2019 , License Expires: 03/28/2022
car~ ERNATIONAL
Survey Number:
Company Number:
Accreditation Decision:
Accreditation Expiration Date:
Company Submitting Application :
Program Summary:
Survey Accreditation D_etail As of 5/19/2020
98412
20323
Three-Year Accreditation
10/31/2020
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. 2707 Browns Lane Jonesboro, AR 72401
Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case ManagemenUServices Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOb/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents) Residential Treatment: Alcohol and Other Drugs/Addictions (Adults) Residential Treatment: Integrated: AOD/MH (Adults)
Companies with Programs:
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. (20323) 2707 Browns Lane Jonesboro, AR 72401
Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case ManagemenVServices Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Mid-South Health Systems (307610)
1650 White Drive Batesville, AR 72501 Case ManagemenVServices Coordination: r ntegrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOO/MH (Children and Adolescents)
,,-,c:, 1 ,-,f 7
Mid-South Health Systems (307611)
35 Choctaw Trace Cheroke Village, AR 72529
Survey Accreditation Detail
As of 5/19/2020
Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Mid-South Health Systems (307614)
642 North Main Street Salem, AR 72567 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Mid-South Health Systems (307618)
589 East Main Street Melbourne, AR 72556 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Mid-South Health Systems (307619)
1507 North Pecan Newport, AR 72112 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Mid-South Health Systems (307877)
111 West Booth Road Searcy, AR 72143 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
............ ., .... .i 7 98412
Mid-South Health Systems (311460}
623 North Ninth Street, Suite 200 Augusta, AR 72006
Survey Accreditation Detail As of 5/19/2020
Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination : Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated : AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Mid-South Health Systems Acute Crisis Unit (320822}
837 Willett Road Jonesboro, AR 72401 Outpatient Treatment: Integrated: AOD/MH (Adults)
MSHS Trumann Clinic (315221}
807 West Main Street Trumann, AR 72472 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems - Helena Clinic (75625} 801 Newman Drive Helena, AR 72342 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems - West Memphis (203514} 905 North Seventh Street West Memphis, AR 72301 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated : AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
98412
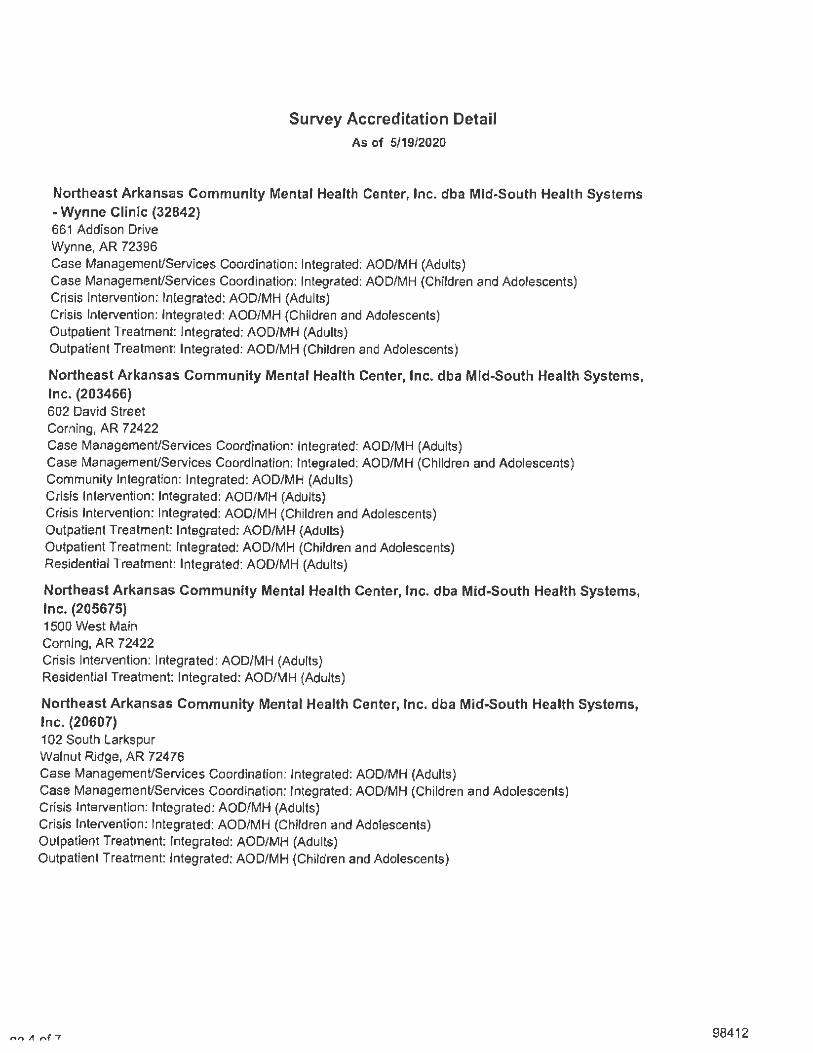
Survey Accreditation Detail As of 5/19/2020
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems - Wynne Clinic (32842) 661 Addison Drive Wynne, AR 72396 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. (203466) 602 David Street Corning, AR 72422 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adu lts) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment Integrated: AOD/MH (Children and Adolescents) Residential Treatment: Integrated; AOD/MH (Adults)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. (205675) 1500 West Main Corning, AR 72422 Crisis Intervention: Integrated: AOD/MH (Adults) Residential Treatment: Integrated: AOD/MH (Adults)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. (20607) 102 South Larkspur Walnut Ridge, AR 72476 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
no It nf 7 98412
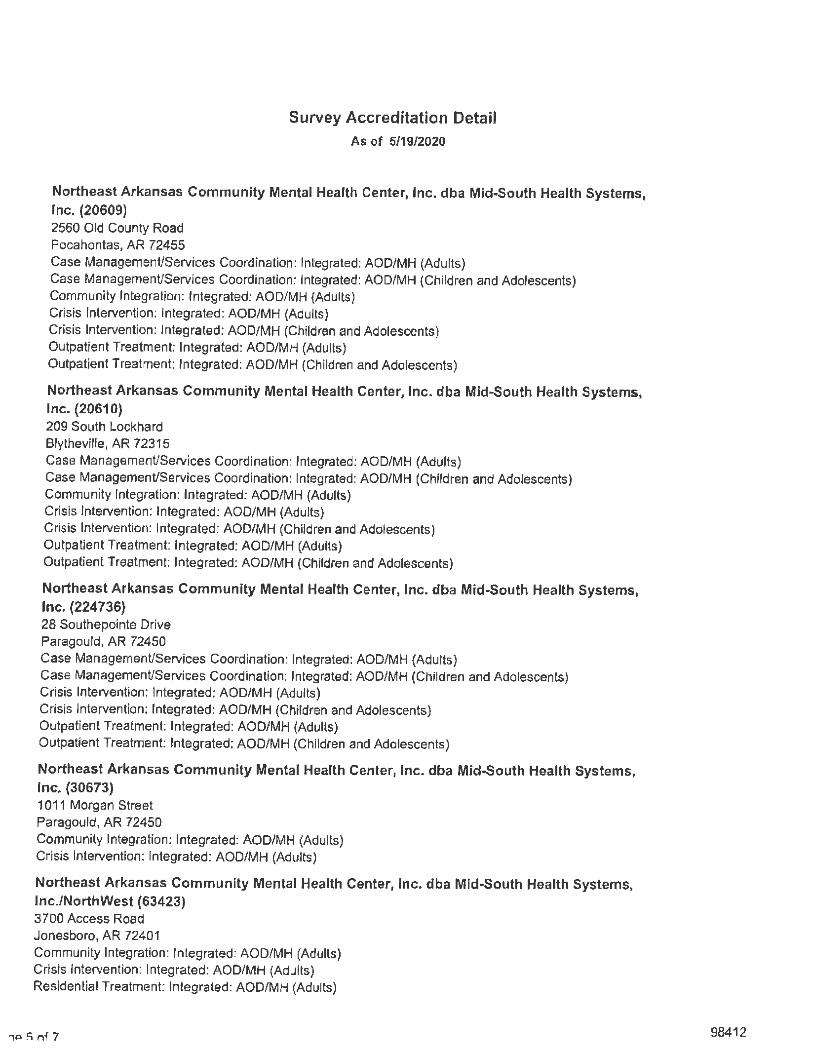
Survey Accreditation Detail As of 5/19/2020
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. (20609) 2560 Old County Road Pocahontas, AR 72455 Case Management/Services Coordination: Integrated; AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment Integrated: AOD/MH (Children and Adolescehts)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. (20610) 209 South Lockhard Blytheville, AR 72315 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. (224736) 28 Southepointe Drive Paragould, AR 72450 Case Management/Services Coordination: Integrated: AOD/MH (Adults) Case Management/Services Coordination: Integrated: AOD/MH (Children and Adolescents) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: lrUegrated: AOD/MH (Children and Adolescents)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems, Inc. (30673) 1011 Morgan Street Paragould, AR 72450 Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults)
Northeast Arkansas Community Mental Health Center, Inc. dba MidpSouth Health Systems, lnc./NorthWest (63423} 3700 Access Road Jonesboro, AR 72401 Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: lhtegrated: AOD/MH (Adults) Residential Treatment: Integrated; AOD/MH (Adults)
, ,:i !i nf 7 98412
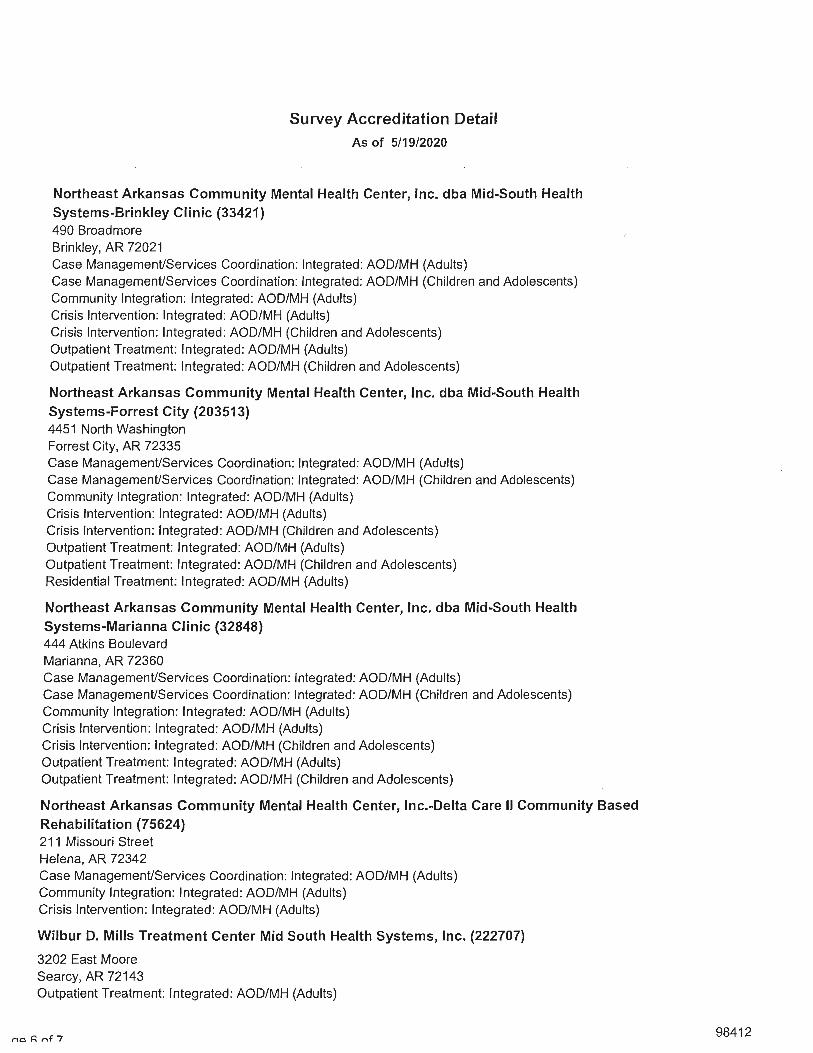
Survey Accreditation Detail As of 5/19/2020
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems-Brinkley Clinic (33421) 490 Broadmore Brinkley, AR 72021 Case ManagemenUServices Coordination: Integrated: AOD/MH (Adults) Case ManagemenUServices Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems-Forrest City (203513) 4451 North Washington Forrest City, AR 72335 Case ManagemenUServices Coordination: Integrated: AOD/MH (Adults) Case ManagemenUServices Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents) Residential Treatment: Integrated: AOD/MH (Adults)
Northeast Arkansas Community Mental Health Center, Inc. dba Mid-South Health Systems-Marianna Clinic (32848) 444 Atkins Boulevard Marianna, AR 72360 Case ManagemenUServices Coordination: Integrated: AOD/MH (Adults) Case ManagemenUServices Coordination: Integrated: AOD/MH (Children and Adolescents) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Children and Adolescents) Outpatient Treatment: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Children and Adolescents)
Northeast Arkansas Community Mental Health Center, lnc.-Delta Care II Community Based Rehabilitation (75624) 211 Missouri Street Helena, AR 72342 Case ManagemenUServices Coordination: Integrated: AOD/MH (Adults) Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults)
Wilbur D. Mills Treatment Center Mid South Health Systems, Inc. (222707)
3202 East Moore Searcy, AR 72143 Outpatient Treatment: Integrated: AOD/MH (Adults)
no P. nf 7 98412
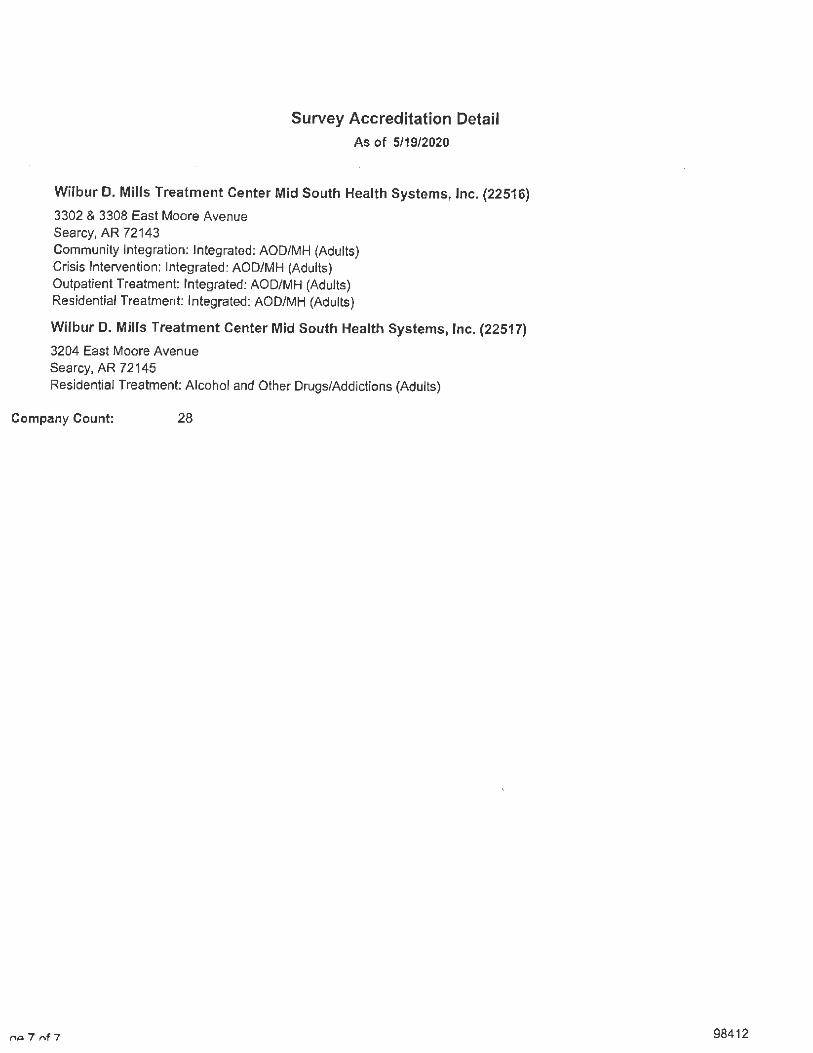
Survey Accreditation Detail
As of 5/19/2020
Wilbur D. Mills Treatment Center Mid South Health Systems, Inc. (22516)
3302 & 3308 East Moore Avenue Searcy, AR 72143 Community Integration: Integrated: AOD/MH (Adults) Crisis Intervention: Integrated: AOD/MH (Adults) Outpatient Treatment: Integrated: AOD/MH (Adults) Residential Treatment: Integrated: AOD/MH (Adults)
Wilbur D. Mills Treatment Center Mid South Health Systems, Inc. (22517)
3204 East Moore Avenue Searcy, AR 72145
Residential Treatment: A lcohol and Other Drugs/Addictions {Adults)
Company Count: 28
/"IQ 7 f'\f 7 98412
Contractor and
Subcontractors'
Staff
Li censure
and
Certification
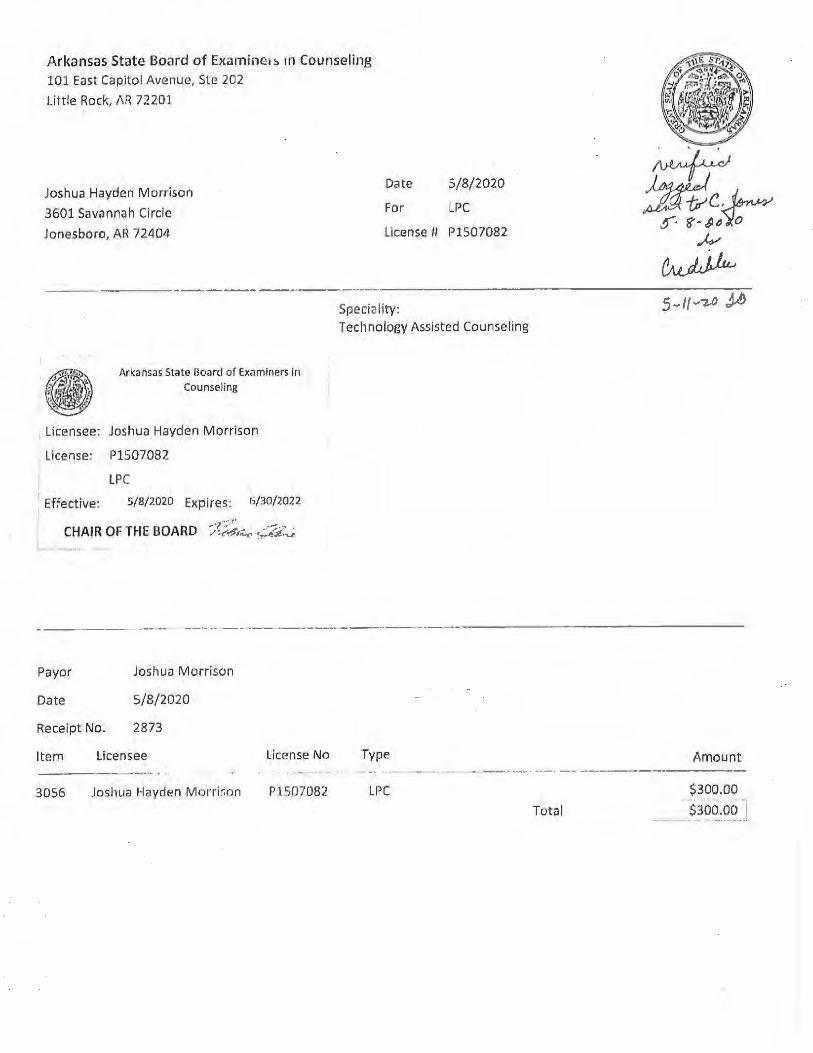
Arkansas State Board of Examine1:, rn Counseling
101 East Capitol Avenu e, Ste 202
Little Rock, /\R 72201
Joshua Hayden Morrison
3601 Savannah Circle
Jonesboro, A~ 72LI04
---------·------__________ _.
Date 5/8/2020
For LPC
License U P1507082
Speciality:
Arkansas State Board of Ex.imtners In Counseling
. Licensee: Joshua Hayden M orrison
License: P1507082
LPC
Effective: 5/8/2020 Expires: h/30/W22
Technology Assisted Counseling
--- ---·- - --------------------··---------·- ---------
Payor
Date
Receipt No.
Joshua Morrison
S/8/2020
2873
Item Licensee
3056 Joshua Hayden M orfr;on
License No
P1507082
Type
LPC
. -· ·-·- ---- -----
Total
Amount
$300.00
$30~.:~~J
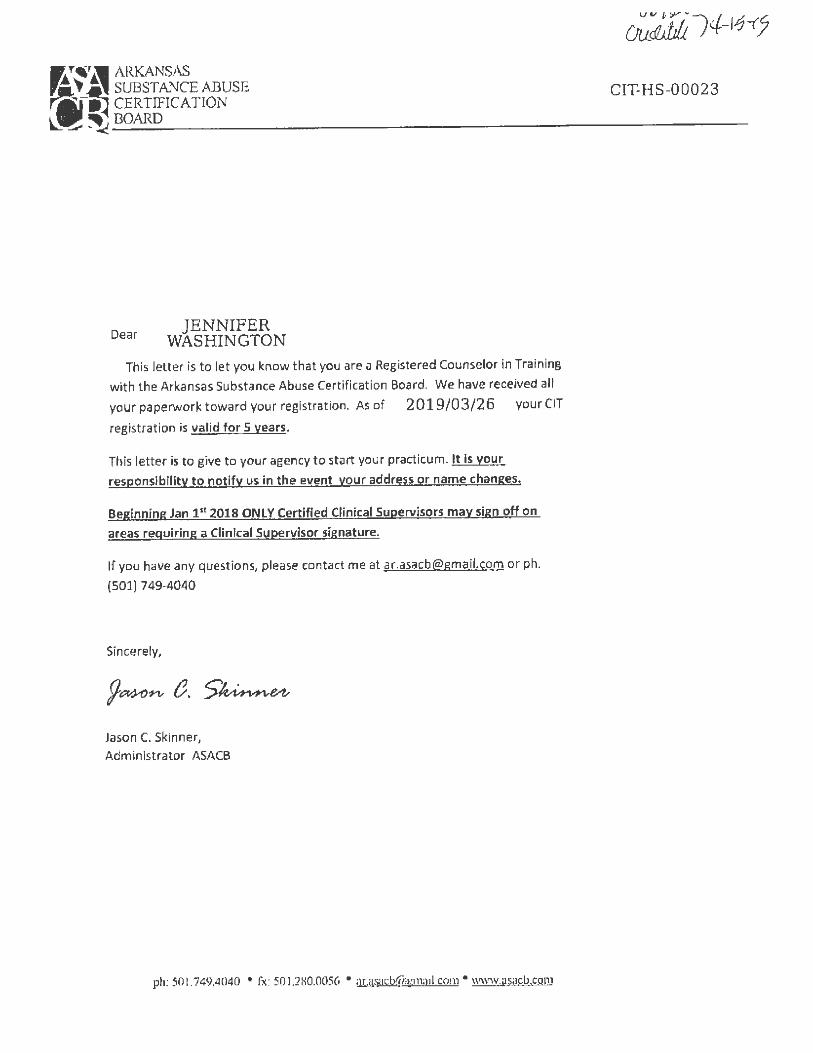
Dear JENNIFER
WASHINGTON This letter is to let you know that you are a Registered Counselor ill Training
with t he Arkansas Substance Abuse Certificat ion Board. We have received all
your paperwork toward your registration. As of 2019/03/26 your CIT
registration is valid for 5 years.
This letter is to give to your agency to start your practicum. It is your
responsibility to notify us in the event your address or name changes.
Beginning Jan 1st 2018 ONLY Certified Clinical Supervisors mav sign off on
areas requiring a Clinical Supervisor signature.
If you have any questions, please contact rne at [email protected] or ph.
(501) 749-4040
Sincerely,
Jason C. Skinner, Admin istrator ASACB
ph: 501.749.4040 • fx: 501.280.0056 • UL.\1sac:[email protected] • www.as;1cb.com
CIT•HS-00023
·----,
· ....
. .~
. --. :;; .
.. :. -~
.•
l~ ~
-? ..
.._:,,.
.~
.r
'•
.-''j
l'•.'1
;
.. .....
... . ,;
~-_-
J ....
.. •}
!-'· ~ .. _
., .:.
. •,
~
• ,..
·Y..-1
~-•"
t~~ --~
,..,
,.
.: .
·,)>,}!
,_ t. "
f-'·
.{f".~
.?(..-
; \·,.
.·, ,.
. " ,.,
.,
-=-
~:r
\ '.'~
~s=t
b±s:
"
----
----
•--·
•·•
~
.
(J!:rtiif
oa. .. W"
···· --··
~ ec
o-,g
n✓i•tton
· •
•t
ir.
~
• o
J_
;_
•
-,,,
\
_ .-; \.
• .
-..
. .. ,
• •
• .
.,
: ' ,
,
' . '/
"' <
:-;
:·:-:
\/::
;c
: ,,, ,
;:
-•
-
·•
..,,
. ·•
-~
•• _
--~
· .•
. ·.
-
,,i,
,
· ·
··,;-.•'
Jenn
jfer
Wa§
.hj'n
:g/p
p:, -.
.. ~ ·
·..
. .
IS .. C
ER
TIF
IED
. AS
A M
EN
TA
I.:.J
IBll
TH
it~~R
A.F
RC
)FE
SSIO
NA
L
-..:
., ,
II•
""
.-•
J. ,-
·-o,:.
.,.
, •
•
AND
1s Q
UA
I:JFI
BP.
To
wo1
¢: A
l;'. -~
;,
NO
RT
HE
AS
T A
RK
AN
SA
S _C
QM
MU
NIT
YM
EN
-TA
L.H
F;;
lLT
H C
EN
TE
R, I
NC
. lJN
DER
PRQF
ES:S
IONJ
\L .S
UP
ER
VIS
ION
. --~-
' .
TH
IS C
ER
TIF
ICA
TIO
N-I
S N
ON
-TR
AN
SF
ER
AB
.LE
.
Jun~
13,
201
8 D
ate
,·· ...
,.
.
~- .. , "··-
.:::
----
I , .
..
• ,
~
·.-. _
____ .
;on
Dov
er, E
xecu
tive
Dir
ecto
r
()
. ~
r
, 11
.._
~-·
-~
, , · ·
" •. '·'L
·:. .'.
,;;, :•
';,/
·. , ,,
,,
., ~-
: \.
_ ..
-;'.~/:.\'.
-).~·~:·
f ~J~ .
. . : .
...: .. ~ ,,..
~-: ,,, --~
.. : .... ~~at7:.:·
.-. •.!
. ·-
...
-·.
-
-...
...
·1
·· · ··•
· -
·-tr
::--
-·
-.
..,,,.
. ,,
"'' ~-
::.:
•-·-
·--
· --
----.
----~,.
,.;_.
·"'
~
\.,a\' ' 1 \' ,.\''\
'\~ 11 ' ,o ~r~r~ ARKANSAS f\,,._().QY' ,J ~',~ SUBSTANCE ABUSE t\-i, \J -\.l'h, ( CIT-A-00009 r~if!_~ CERTTFICATION y l_~ ~_B_O_AR_D ___________________ Y_1 __________ _
Dear SARIAH VALLEY
This letter is to let you know that you are a Registered Counselor in Training
with t he Arkansas Substance Abuse Certificat ion Board. We have received all
your paperwor k toward your registration. As of 2019/07/08 your CIT
registration is valid for 5 years.
This letter is to give to your agency to start your practicum. It is you r
responsibility to notify us in the event your address or name changes.
Beginning Jan 1•1 2018 ONLY Certified Clinical Supervisors may sign off on
areas requiring a Clinical Supervisor signature.
If you have any questions, please contact me at [email protected] or ph.
(501) 749-4040
Sincerely,
Jason C. Skinner,
Adm in istrator ASA CB
ph: 501.74~.4040 • fa: 50L280.0056 • :ir.:isacbw:w11i1 il.com • www.as:icb,com
-.. ?
_;~
;·•~
::_.·:
:;
_ ...
,\}-.l\
·· ·\::~:_
:;~~;/t~
\~}~\::
·· •;,
r'
-~:h
_~·
--·
••;-
t~,~
: !it
r:
<-••s
: -::
~,
,.,,
-1 :/
;·'.
·,<
.,. ~
4r-'5
,•,. ·
.,~
~ "
,·: ,
>,'r
:•,i
._
"~>"
't ', h
:
:;
. ~
l<:,-
. •'~
..... ·~
\... --~
" ~ ~~ l .
...... :,"•
~~ ..
,,, <
· ••
-.
• ~ ... ,
,
·.-·-·~-
·:. ·: ·.
/?_;_•~
~-.. :_;~
~ ~. ,
~J;,f:
:Ft· 1
\ ~~~::
.-i::~
-• .. 11
.)~·-= .
. , .
, ,,,.
._ __ ._
... " .
. ~
, ,,.
~ -,--
~--.-·
·,;....;..
..
.,~
. -.
,"'"
":'1
;\\
~:~f,'_
-;,,
~ ~
-,.-..
-.
-~:,"'~
:; -~:
_ ':.:
.... ';!
~~•;~
--,. ~
.r :~
\~
rJ·-·~
-_
---~· 5:~
~~::~;~·
;:,7:, .{
· ;'.-< -~
--___ -
"' _:, --
-l(
• r ~ -1
· lt~,~
~
----
-·
.. ·,.,
.. :·· ··
:::: ...
. :._·
·--·~::
.~-.-~
!::.:.::
~-·•!,· .
, . -~
-...
--
~\1
"
. ~
II!'
---
-~
---~
---, -
.-·-r
.--::--
.r:-=
-----.
: _;-
(}".
J::::
: .• -
... _
.:;1,
~ ..
.. .,
.
' .
·!:·
. ~
••
_ .-
J .
-...
,;"
, ,
-1 .
... .
-i
t . u
·-.
_-:-. ·?
:. '·:
. ?~f ··)
;~~: ;,.-,:_·'
~ --~·_:· :?, '
~ . ; '·
' ~
Certi
¾ct
itit >;
•();~.\
~-0
aniti
on
=
. ';F
f .
. ~i {?
\_::,~ ;-;~
>)~/ : :'
(/1;,
·, :-
., .-·;
-
·,.{
=-_ . .
.,. ,.'°
$.g,
r.fal
t..V.a
l(f!J
J.: ~-;
, -,: ...
-~--. _
. .
-•
t:,
·.
' <
J."
... -
;l #
,.,.J
......
. \.
·-·
··•·
~-.
..
. •
• .
IS_;C
~I.
tIJF
)'.J::T
IJ'~
~:-~
~Q:P
.~1
f:.~
;l~~
~~
~~-~
~-.,~
~T
;£}
_~R
QV
IDE
R
. -·
., ~ ·
.. ··~~A
~tIS
~QW
'#k.3
!'~~;
J.@-,W
@~
AJ
.-.
-. -
_ -N
OR
TH
EA
ST
A~
S,~
Sk(f
.()iJY
J~ff!
./f/f{
![{~..
~1
;~ftl
$~pT
!f C
EJVT
ER; I
NC.
UN
DB
R~P
.1tQ
FE£·S
[ON
ffi:)
:S!®
1P~~
Vl;&
ION
. .
· ,
~-·_ ··
~-:.
____ : 1
~::;
,•:, ..
_; ·_ ;
;.;;.: .<
Hf;_-~:r~
:------t~·:
\;~:~· ..
/:-.~ .... :
.. .
;: ___ ·_
TH
IS .O
ERT1
1JIC
;41:
,ia•'6
.fl~i
N:iJ
NiJJ
,,D.•'ll
NS!
JJER
A.B
LE .. ·
. •
. ,.
.
.. -~
, ,.,
. ••
ef.T
• •~
• .. ,•
r·
.. ,, •
. v~
~-.
. ,
. ~--,, :
. :, :>i
::; ,·,J~!
l:::I : :'.
--::<\: \
_ . .
Feb
ruar
~i.'6
i0
19
:
· .··
.. ··
· ~-
.. v1:
-":,1 •
.... -
:·
·-• .• -·
, ·.
:~
... -:
• -
•J
' '
.• • )
'-,\.
.-
,/ <
.;
.:'ii~
~·!,_
_ -• _
.., l
·~ #
•
••
..
.•
.,;.
Da
te·
: ·' ,
' ..
. '.
. \. l.i
\·t~~-j;t_
·:~·-✓-·/
J~-~~~~tlf
it~,
f~~~
~ Do_
je:1;
;:J/x
?.G
Utiv
e: D
irec
tor
::.·: ~, .•.· ~
~;::. ~-.. -:·;
~/~ -~~} <
.;:\:~~~~:-
-; ·., •
.·. ·';.-,
?;:;_
. ;
), f~
.,t
.·}"f.
: • . .,_
.
►--7(•
-~~
==
~~
~~
~=
=-~
~~
==
==
~=
.;;;;;;;~
~ttU
· ·
□:
Jll~
_ -.
. : _
_ -
. -
_ .. _
. .
. .
. .,
-
---
a.L]JJ
.v. .
~
•.
. ,.,_
~ ~
)~--
. -
-··
··
:· ·,:
.;
·;:.
~--
~ -
-·-·.
-·
·1
~-L
.. . -
-~ .. _ ~--=
-----
-.
-· -
. ~ --~
" _--
-.:.
. -
-=---
-·-·
-. -
. -~
-
. ,.
. ..
. ........
, ~.1
.
~/•.
:.',1.
• •. .'-~
! .;
:~:t~·-
~ T ~I~ ARKANSAS Yl" Ji SUBSTANCE ABUSE r~f ~1 CERTIFICATION ~ ~ _BO_:ARD __________________________ _
March 19, 2018
Demertic Johnson
120 S. 8th St.
West Helena, AR. 72390
Dear Demertic,
This letter is to let you know that you are a Registered Counselor in Training
with the Arkansas Substance Abuse Certification Board. We have received all
your paperwork toward your registration. As of March 19th, 2018 your CIT
registration is valid for 5 years.
This letter is to give to your agency to start your practicum. It Is your
responsibility to notify us In the event your address or name changes.
Beginning Jan 1 ' t 2018 ONLY Certified Clinical Supervisors may sign off on
areas requiring a Clinical Supervisor signature.
If you have any questions, please contact me at [email protected] or ph.
(501) 749-4040
Sincerely,
9~~e.~e,z, Jason C. Skinner, Adm in t<:tr::itnr A,ArR
~~ \' 0-(', --:::::. () c;) ,~ _,., Co'
\~ ~~
':"'
\"
. !
. .i:~;-:
_,
<
.. ,_
. .
•;-.
,),_
... _:
_;:~
:.
.. .. · , ..
C1 Iii .
. ,
'---
---
~
i_=·:
... :::
.-.:=
--'·_--· -
~:-.:::··
--·· -·_·
. -.
-. ~
IF
.. .. .
. .. ,
-.::. . -
---. ..
.,, ..
.. ~
-' ·-
..
""""'"
·"·
--~
--s ·
, --.,
..
--
. -~
.. :.:-
--,:
. . ;•
.,. '.
\='~
-.:~~ .
,.
;;;.
;:;;
,i; -
"'~
. ~~
, .!'
.-.;
....
~.:...~~-
.:-===
===-1
7&t"
..
·. =?
·· ~
]
.,.--
=--
:...
. ====
===-~
~~~~
Jrf
~----
-
/" rr
.4J4
f.;'n
f; ,,,
,tf:
~(P
O~i
j{J7
:1{ f
! <"n
~
I ~v
-~~ , ':)
.... _:~~~!{,~
~;, 1-
~1
,,~
-
Dem
.~rt
ic J
ohns
.on
. .
·;.-_
. ·'"
.
:.
IS C
ER
TIF
IED
AS
A M
EN
TA
L'H
EA
..r,~
H P
AR
A.P
RO
FE
SS
ION
AL
.
.. .....
A
ND
IS
QU
~IF
IED
TO
WO
RK
AT
N
OR
TH
EA
ST
AR
KA
NS
AS
CO
MM
UN
ITY
ME
NT
AL
HE
AL
TH
CE
NT
ER
, IN
C.
UN
DE
R P
RO
FE
SS
ION
AL
SU
PE
RV
ISIO
N.
TH
IS C
ER
TIF
ICA
TIO
N IS
NO
N-T
RA
NSF
ER
AB
LE
.
Mar
ch 2
1, 2
018
Da
te
a~
, ,.,.
Ru
ih:;
{,{so
nbov
er, E
xecu
tive
Dir
ecto
r
.. ,,
f!
►•
. . ...
' ._
'.!
=-f-4..
. .
. ~
Ci~
·--
-_, . .
. .;, --~.-
-.. -~
[]-·' -I--
-· e
-:-:
:..
•"~
~ ••
• ·'
-.
--~~-
~ --~
-, -
. J
---
, """
"' .
. . .
. •
,.
---1'
-···
:r
:~.; ..
... -
.,
~'f~~ ARKANSAS ,,:.-. I, SUBST/\NCF /\ l31 J~F ri~ CERTIFTCAT l()N ~ ~ -~_B_OAR_D __________________________ _
March 13, 2020
Jimmy Dixon
3204 E. Moore
Searcy, AR. 72143
Dear Jimmy,
This Jetter is to /e l you know that you are a Registered Counselor in Training
with the Arkansas Substance Abuse Certification Board. We have received all
your paperwork toward your registration. As of March 11, 2020 your CIT
registr.ition is valid for S years.
This letter is Lo give to your agency to start your practicum. It is your
responsibility to notify us in the even your address or name changes.
Beginning Jan 1st 2018 ONLY Clinical Supervisors may sign off on areas
requiring a Clinical Supervisor signature.
If you have any questions, please contact me at [email protected] or ph.
(501) 749-4040
Sincerely,
Jason Skipncr.
Admlnis1'r;)tnr /\S/\CI~
-Arkansas State Board of Exam11,..: rs in Counseling 101 East Capitol Avenue, Ste 202
Little Rock, AR 72201
Awanna Leigh Smilh
1314 W. Washington Ave.
Jonesboro, 72401 License II P2007041
Arkansas State Board of Examiners in Counseling
Licensee: Awanna Leigh Smith
License: P2007041
LPC
Effective: 7/28/2020 Expires: 6/'2.n/2022
CHAIR OF THE BOARD -i~~:~;,;: . . , ")°;.·?. ~
Arkansas State Board of Examine,:, in Counseling 101 East Capitol Avenue, Ste 202
Little Rock, AR 72201
Christie_ Dawn Ring
P.O. Box 372
Ravenden,AR72459
.:;~vi_:~.,_ ,~~-, °"/J~i~· ;-\: . :ff,.. ~-'••~ V '•• ~. Licensee:
License:
Arkansas State Board of Examiners in Counseling
Christie Dawn Ring
P1901013
LPC
Effect ive: 3/25/2020 Expires: 6/30/2022
CHAIR OF THE BOARD
License # P1901013
----------------------~-Speciality:
Rehabilitation
Arkansas State Board of EJrnminers in Counseling 101 East Capitol Avenue, Ste 202
Little Rock, AR 72201
Leighann Rattan Howr'lrd
101 Pickens Dr.
Newport, AR 72112
Arkansas State Board of £)('()miners in
CounselinB
Licensee: Leighann Ratton Howard
License: A1810146
Effective:
Payor
Date
Receipt No.
LAC
7/9/2020 Expires: 6/30/2022
Leighann Howarrl
7/9/2020
3727
Date 7/9/2020
For LAC
License I/ A1810146
Item Licensee License No Type Amount -----·--- .. ' -----------------~--- - ---- -3927 Leighann Rattan Howard A1810146 LAC
Total
$250.00
$250.00
Arkansas State Board of Examiners in Counseling
101 East Capitol Avenue, Ste 202
Little Rock, AR 72201
Date
For
5/29/2019
LPC Thomas Lee Norton
10518 County Road 9690
West Plains, MO 65775 License# Pl 712388
;-- - .-. ~ -- --Ark~nsas St~rd.of Exam~:~- --7] ,. • : Counsehng
• f. I •, . • I
1
1 Licensee: Thomas Lee Norton
License: P1712388
I LPC
' Effective: 5/2.9/2019 Expires: 6/30/2021
CHAIR OF THE BOARD 74,.; ~
Payor
Date
Receipt No.
Thomas Norton
5/29/2019
562
Item Licensee
589 Thomas Lee Norton
License No
P1712388
Type
LPC
Total
Amount
$312.36
$312.36
Arkansas State Board of Exam~. . sin Counseling
101 East Capito l Ave nue, Ste 202
Litt le Rock, AR 72201
Ralph Irvin Wray
P.O. Box 476
Swifton, AR 72471
Arkansas State Board 9f EXaf'!liiiers ln Counseling
Licensee: Ralph Irvin Wray
License: P1704280
LPC
Effective: 5/20/2019 Expires: 6/30/2021
.CHAIR OF THE BOARD ·J.:;.~f.;;-. ,4;::,,;
Payor
Date
Receipt No.
R.a lph Wray
5/20/2019
411
Date
For
5/20/2019
LPC
License# P1704280
Item Licensee License No Type Arnount ·--- . --- -- ·----------- --- ----------------- ---
422 Ralph Irvin Wray P1704280 LPC
Total
$312.36
$312.36
ST ATE OF ARKANSAS SOCIAL WORK LICENSING BOARD P. 0. Box 251965 Litile Rock, AR 72225
JW1e 10, 2019
Leslie Ann Tullos, LMSW 2106 Executive Loop Horseshoe Bend, AR 72064
Leslie Ann Tullos> LMSW;
Asa Hutchinson Governor
nuthic Bnin Executive Director
Phone: 501-372-5071 Fax: 501-372-6301
Email: swlb@arkaosas,iov Website: arkansas.gov/s,vlb
I, • • \ '
--This ·fs~torfO"tify"y"cro that')'O":l? !icet~tlr1hnrsm:1~~1firfbetm: approved"i'on.1lepC!J%ch:rt'"Ja1?172v19· -~ --through June 30, 2021. The attached wallet-size license card will serve as confirmation of I icense renewal.
Please remember to retain your continuing education documentation for a period of two-years in the event you are audited. If audited, you will be required to submit documented proof that you attended all of the continuing education you listed on your summary sheet. Tf you are unable to provide proof that you attended the workshops, an administrative hearing will be held to consider revocation of your license.
[n order to renew your license for your new expiration date, (June 30, 2021) you must obtain 48 hours of social work continuing education between the dates of July 1, 2019 through June 30, 2021. Only boors obtained between these dates will apply toward your next renewal period. Please see the Board's website for specific requirements for continuing education.
Future renewaJ notice rem inders will be mailed to the address on file in the Board office approximately two months prior to the expiration date of your license. It is your responsibility to notify the Board of any change in address and to renew your license in a timely manner even if you do not receive the reminder.
Congratulations on your license renewal, and please contact the Board office if you have questions or need additional information.
Please watch the Board's website on a regular basis for updates or changes that may affect your license.
Please remove card carefully! Bend back and forth along crease before separating. ·
Arkansas Social Work License Card
License No. ExpiHJlion Onie:
2604-M 6/30/2021 Leslie Ann Tullos, LMSW 2106 Execu1ive Loop Horseshoe Bend AR 72064
·d bearer is licensed nnd in good stnndi11g with U1e Arkansas :i~I Work Licensing Boai ~ ~-- -~
The card to the left is your ,oew social work license card, which reflects your new expiration date. This is the on ly card you will receive. Please punch it out carefully along the perforated line.
If lost or stolen, an additional card may be requested by writien request and a cashier's check or money order in the amount of nventy dollars ($20).
Please keep this letter for your records. You may wish to make a copy before you remove the card.
7/1/2020 1.icense Search
License Search
Arkansas Board of Examiners in Counseling and Marriage & Family Therapy
501-683-5800
Robbie Robinson LICENSE#: P0503012 I TYPE: LPC I STATUS: ACTIVE
Jonesboro, 72404
ADDITIONAL INFO Date of Issue: 3/2/2005
Date of Expiration: 6/30/2022 Standing: Good Standing
Email: [email protected]
hllps;//scarch.sla lesolulions.11s/l. lCP.1HlP.e/? 11.)=!i I :,,11·10 'I rm GG':111 f'CDl1?C /\ll97(1G06 I 95'1 2&L=P0503012&GUID=D07 A 1 E08272O4841AD588E794692... 111
Arkansas Social Work License Card
License No. Expiration Date:
17 49-M 2/28/202 l Gloria J. Shields-Rogers, LMSW 818 Canal Marion AR 72364
Card bearer is licensed and in good standing with the Arkansas Social Work Licensing Boru ~ ~ :,,..]b_...---. ~' c~ ,>
Chairman
I;)
)~~ ,J, ~~ -~
1---::i
t,"""I~ J
~~
~-::,...
~r1;attf5a.9 ~ubstante ~buse Q
terttttration ~oarb
JE,erebp (£ertifies
BA
RB
AR
A O
SB
OR
N
Wl10 ha~ (.om
pli rb lllitlJ tlJt rc(}ni remrn t~ rstiibli~hcb lJv tht ~
oarb mtb ht1~ ~11rrt~~fuH
1l obtai 111.·o tt,rst g,rnnlrn1·bg of ~t·ofcss1on<1l ,tBr1•fot·nm
ntr. anb in boinet so. 1mg Nn·nc-b ri\roaHttion n~ (1
<!tertifieb ~lcobol anb 7!lrug <!Coungelor
11
/05
/20
19
I <s m
' f>:ll~
'" . .
' \),_
..,. __ _
l'n-!->i1ko
t
, .. ' .. /
';,
'. \
\-
\ •
/.
I l
\ .. •. ·,
·,-.
--'
I. ~
I '· :.
I .
i ·.,
· ... , .
i "··
. .,,._
' .
4'
-, •
' I
I '-1
n·-l'n
'"•fr111 -.,
14
19
f't·rtifirn
lc "\um
ber
,d~f~f t~~i,,, .-.;~
~,~.,) ~(1f ~r, :,, .. -,.,.,,: ~>
,':
-ftJt;,lft';_?i{~
fj,~\. Sp.. t "'•····· Sr'AJ -·-·-{" ··-;; JiJ!i;¼v,Erill?JJ i: .. ,;\;~~~: .. -:,..{f:.·;l, i,-,·'t' ... _.\~
,;:,~ •. :. ~r-.---1.-
.• ,,. -
., '
y '".,...
·;.:, ,:; __ ~'.. ·-~,-':.J;:~, •. i ~t, .. ~;.~~-
1.~t·· /,_~:~,-r,==: ..,.,, /•~'· ~, .;,;-.. -
-~-.:"'I)..~•'-.,;,_"'•.,
,.,., .• H•,"ttJ•~
·t' . _. t~·1-'!fu~
i ,, .... .,~},..•· ,.l., ._ • ..
--~·F:f_~!,ii'.;:' .!>.~~-
_J_2/31/~02_1_
1 f
,11irn1i1m O
atr
' I
... (
'·,
: 1{
Y1 !, r1 l~
l; t-~-~
f} ', 'i['
, .. ·oc., ;•~
~ccn·c:11-~ 1.I
Arkansas · ·t ate Board of Examine, . in Counseling
101 East C ;:,ital Avenue, St e 202
Little Rock, AR 72201
Charles Jer :)me Jackson
P.O. Box 21::1
Paragould, .O.R 72451
Arkansas State Board of Exami· ::rs in Counseling
Licensee: '.':harles Jerome Jackson' '
License: :1/10806008 P0803027
LMFT LPC
Effective: 5/12/ 2020 Expires: 6/3f'/2022
CHAIR OF THE BOARD ~ er"" ?6Zv
Payor
Dat e
Receipt Ne
Charles Jackson
5/12/2020
2917
Date 5/12/2020
For LMFT LPC
License# M0806008 P0803027
Item I ·censee '.icense No Type Amount -------------------- ---------------------3102 Ci1arles Jerome Jackson M0806008 PO LMFT LPC
Total
$450.00
$450.00
Arkansas Social Work License Cf1rd
License No. 1462-C Kelli Leann Statler, LCSW 3304 Windover Garden CR Jonesboro AR 72401-5614
E~pir:1tion Dntc:
8/31/2021
Card licurcr is licensed and in good standing with the Arkansas Social Work Licensing Boa, -a~ ~~ • ~ :
Chaim1an
I.__, Arkansas Department of Health SOCIAL WORK LICENSTNG BOARD P. 0. Box 25 I 965 Little Rock, AR 72225
July 13, 2020
Kellie Lynn Letbetter, LCS W 5117 S Caraway Rd
Jonesboro, AR 72404
Kellie Lynn Letbetter, LCSW;
Nathaniel Smith, MD, MPII. Secretary of Meal th
Ruthie Baio Director
Phone: 501-372-507 1
Fax: 501 -372-6301 Email: [email protected]
Website: arkansas.gov/swlb
--•-•, . .,,,. ..... ---- .. "
This is to notify you that your licensure as a Sacral Worker has been approved for the period of August 1, 2020 through July 31, 2022. The attached wallet~size license card will serve as confirmation of license renewal.
Please remember to retain your continuing education documentation for a period of two-years in the event you are audited. If audited, you will be required to submit documented proof that you attended all of the continuing education you listed on your summnry sh~ct. Tfyou arc unable to provide proof that you attended the workshops, an adminis trative hearing v.ill be hekl to considc.:r revocation of your license.
In order to renew your license for you, new c~qifration date, (J.uly 31, 2022) you must obtain 30 hours of social work continuing education between the cl:-ites of August 1, 2020 throt1gh July 31, 2022. Only hours obtained betvvcen these dates will apply toward your next renewal period. Please see the Board's website for specific requirements for continuing education.
Future renewal noLice reminders will be mailed to the address on file in the Board office approximately two months prior to the expiration date of your I icense. It is your responsibility to notify the Board of any change in address and to renew your license in a timely manne.r ev~~ if you do not receive the reminder.
Congratulat ions on your license renewal, and please contact the Board office if you have questions or need additional information.
Please remove card carefully! Bend back and forth along crease before separating.
Arkansas Department of Health Social Work License Ca rd
License No. Expi rn (ion On (c:
4716-C 7/3 1/2022 Kellie Lynn Letbetter, LCSW 5117 ,S Caraway Rd Jonesboro AR 72404
~:Ht:I bMrer is licensed ,rnd in good slooding with 111c Arkansas
,<Jl:ial Work Licensing IJOard, ~ 4
~.w:l 'J>J-JJ. u,,)
Chair
The card to the left is your new social work I icense card, which . reflects your new exp iration date. This is the on ly card you will
receive. Please punch it out carefully along the perforated line.
If lost or stolen, an additional card may be requested by written requesf and a cashier's check or money order in the amount of twenty dollars ($20).
Please keep this letter for your records. You may wish to make a cor,y i:Jdore you remove the card.
i&lr~,"'1 ARKANSAS ~ v ~ SUBSTANCE ABUSE r .IJif!!_~ C:SRT1F1CAT10N ~ -~ _B_O_ARD ____________________________ _
June 24, 2016
Vicki Thomas
440 Lower Guntharp Rd.
Ravenden Springs, AR . 72460
Dear Vicki,
This letter is to let you know that you are a Registered Counselor in Training
with the Arkansas Substance Abuse Certificat ion Board. We have received all
your paperwork toward your registra t ion. As of June 241\ 2016 your CIT
registration is valid for 5 years,
This letter is to give to your agency to start your practicum. It is your
responsibility to notify us in t he even your address or name changes.
lf you have any questions, please contact me at [email protected] or ph.
(501) 749-4040
Sincerely,
Jason C. Skinner,
Administrator ASACB
r,h: 501.749.4040 • fie S01.280.0056 • ,11 .<[email protected].;om • www.nsacb.com
Arlrn nsas Social Work License Card
License No.
9742-C Lauren Ericka Pitman LCSW 9880 Pacific Heights Blvd. San Diego CA 92121
E~pirnti on D~ tc:
8/31/2021
Cart! bearer is licensed nnd in good standing with the Arkan~as Social Work Licensing Board.~~~ ,\..._C..o~
Chairman
Arkansas Social W orl< License Card
(..icc nsr No.
7843-M Debra Denise Hayes, LMSW PO Box 1924 Forrest City AR 72336
Expirn tion Date:
1/31/2021
••• I .. : 'i
Card bearer is liccns~d nnd in good stonding with the Arkansas Socinl Work Licensing Boni ~S" ~~ .. ~~
Chairmnn
7/1/2020 License Search
License Search
Arkansas Board of Examiners in Counseling and Marriage & Family Therapy
501-683-5800
---- ---
Cynthia Hampton LICENSE#: P1006045 I TYPE: LPC I STATUS: ACTIVE
Jonesboroj 72401
ADDITIONAL INFO Date of Issue: 6/30/2010
Date of Expiration: 6/30/2022 Standing: Good Standing
Email: [email protected]
l\llos://search.slatesolulions, ltS/1.ino11r.r1r,/'f'lrl" I)() 1 t)1r>rJ(P1"11: 11 Ftl rJAl1M40E(l52CC[:3'-8&L=P 1110604 5&GLJID=D07A1E0B?.72O'18'11 AD580E794692. .. l / 1
~ A ;"kansas St ate Board of Examine, ., m Counseling
101 East Capitol AVenue, Ste 202
Little Rock, AR 72201
Jcremey Leland Beasley
5289 Greene 628 Road
Paragou ld, AR 72450
Arkansas State Board of Examiners in
Counseling
I Licensee: Jeremey Leland Beasley
' License: P1707328
LPC
i Effective: 3/26/2019 Expires: 6/30/2021
CHAIR OF THE BOARD ~ ~._;
Payer
Dale
Receipt No.
Beasley, Jeremey
3/26/2019
28
Item Licensee
32 Jeremey Leland Beasley
License No
P1707328
Date 3/26/2019
For LPC
License # P1707328
Type
LPC
Amount
$300.00
Total . . I
$300.0D_ .I
~
\ -\ t===-
~
~.1~ \I°
~~
!-~~
'-'
Ark
ansas
Social W
ork L
icense C
ard
License N
o. E
xpiration
Date:
79
76
-C
7/31/2021 T
isha
Ra
nd
a M
axwell, L
CS
\N
4700 McP
hil Dr.
Paragould A
R 72450
Card bearer is licensed and in good stand
ing with the A
rkansas
Social W
ork Licensing B
oard. ~-
\6._~ ,L
L-b
LD
Chairm
an
..c.:'
~"."4''i9 ARKANSAS ~ l_~ SUBSTANCE ABUSE fAJ !~ CERTIFICATION l_~ ~_B_OARD ____________________________ _
May 25, 2016
Tisha Maxwell
4700 Mc Phil Dr.
Paragould, AR. 72450
Dear Tisha,
This letter is to let you know that you are a Registered Counselor in Training
with the Arkansas Substance Abuse Certificat ion Board. We have received all
your paperwork toward your registration. As of May 25 111, 2016 your CIT
registration is valid for 5 years.
This let ter is to give to your agency to start your practicum.
If you have any questions, please contact me at [email protected] or ph.
(501) 749-4040
Sincerely,
Jason Skinner,
Administrator ASACB
I \.,
'
!
. !
·.< .. t
State of A Board of E . rkans~s .
xaminers of Al and Drug Ab cohollsm use Couns I
cert·fl c ors ' es that
Ric Ke f ls currently I' e er icensed under
LICENSED A of Act 443 of 2009the authority 0 _ LCOHOLISM as a
ate of Issue & DRUG ABUS 09/14/20lS License No. E ~OUNSELOR . (". 423L Expiration Oat<?
~--6. 12/ 31/21
- ~L. Mob- ::b . Board Adm" 1- ic ,n strator
Social W Arkansas License No. ork License Card
n2~c . Richard Tho Expiration Date·
1212 Pleasa;ts Keefer, LCS~/31/202 I
Horsesh Valley Dr Card b oe Bend AR Social c_;cr is licensed and . 72512
ork Licensing Bo~n good standing with th ~¼ ~Ar~ansas
· ,.·:
Arkansas State Board of Exan:-,•i1, _, ~ in Counseling 'L01 Ease Capitol Avenue, Ste 202
Little Rock, AR 72201
MS Wenoka Lynne Young
186 Verkler Lane
Searcy, AR 72143
Arkansas State Board of Examiners In
Counseling
Licensee: MS Wenoka Lynne Young
License: Pl907090
LPC
Effective: 7/29/2019 Expires: 6/30/2021
CHAIR OF THE BOARD ·~";;;...1,. ,;::r-;r_:,_;
License # P1907090
~--::,
~ ~ ~-;-~;~ nJ '5- \
s ·-~
\
... - - - · .... . ~'•. ~-· - •· , . ... - - - - - .. ,.. - ·- - ••- ._. - ... . . . -- ,.. _ , - · - - - ... . t -
".--~ .~ r,.-:' .. .. -1;:· ,~,.... ~ ..,.:) .. _ ~ ... - . ~ ww·,: ~~-.. .,"' .... ~ ·. ~-:\ ::-,. . ··•' 'i}f \l=l'1
~~ > • i ,.' ~ .. ~ \\ /;,,;,.. .. ~....,,
~ /, '" -.::-.;.:...,.. ~
~- .•r ~ .
Arkansas Departme1rnt of Health. Social Work Licernse Card
Liceirnse Noc Expiration Date;
3085-C 1/31/2022 Bobby Davies Armstrong, LCSW 136 Western HiHs Drive Sear9y AR 72143
Card b~arer is lice11sed and in good standing with tl1e Ark:a11sas Social Work Licensing Boru ~ ~- ,.~: .
Chainnan \ ' <·
OS/16/201 7 Wlm 14: l1 FAX
f • I t>
lri"'"LW ARKANSAS ,t )~~, SUBSTANCE ABUSE - CERTJFICA TION
~~-- ~.::B..:::.OA:...:.RD:.=... __________________________ _
Apr/I 20, 2017 .
Darrel Levy
608 Campbell Dr.
Marlon, AR. 72364
Dear Darrel,
This letter is to let you know that vou are a Heg,stered Counselor in I raining
with the Arkansas Substance Abuse Certification Board. We have received all
your paperwork toward ·your registration. As of April 201~. 2017 your CIT
registration Is yalld fot 5 years.
This letter ls ~ogive to your agency to start your practicum. H rs your responslb[Jlty to notify us In the ev·en your address or name changes,
Beginning J;:m 1" 2018 ONl Y Clinical Supervisors may sign off on areas
requiring a Cllnlcal Supervisor signature,
If you have any questions, please contact me at [email protected] or ph. (501) 749-4040
Sincerely,
Jason Skinner, Administrator ASACB
'I
ph- .501.749.4040 • fx.; 501.280,0056 • t1r.H~ucb@11,nnll.cop1 • www 1mcb com
_,.
Arl,ansas State Board of E,caminers in Counseling J.01 East Capitol Avenue, Ste 202
Little Roel<, AR 72201
Stephanie Ann Hawkins
1116 Unio n Ave East
Wynne, AR 72396
Arkansas Slate Ooard of Examiners in Counseling
Licensee: Stephanie Ann Hawkins
License: Al808115
LAC
Effective: s/G/2020 Expires: G/30/2022
CHAIR OF Tt-lE BOARD
license It Al808115
Speciality: Technology Assisted Counseling
STATE OP ARKANSAS SOCIAL WORK LICENSING BOARD P. 0 . Box 251965 Little Rock, AR 72225
June J 0, 2019
Amanda Suzanne Myers, LMSW 5964 })arnela Ann Drive South Bartlett, TN 38135
Amanda Suzanne Myers, LMSW;
As:1 Hutchinson Governor
Ruthie Rnin Executive Dircclor
Phone: 501 -372-5071 Fa.-<: 501-372-6301
Email: [email protected] Website: arkansns.gov/swlb
This is to notify you tbat your licensure as a Social Worker has been approved for the period of J uly l, 2019 through June 30, 2021. The attached wallet-size license card will serve as confirmation oflicensc renewal.
Please remember to retain your continuing education documentation for a period of two-years in the event you arc audited. If audited, you will be required to submit documented proof that you attended all of the continujng education you listed on your summary sheet. If you are unable to provide proof that you attended the workshops, an administrative hearing will be held to consider revocation of your license.
ln order to renew your license for your new expiration date, (June 30, 2021) you must obtain 48 hours of social work continuing education between the dates of Joly 1, 2019 through June 30, 2021. Only hours obtained between these dates will apply toward your next renewal period. Please see the Board's website for specific requirements for continuing education.
Future renewal noLice reminders will be mailed to the address on file in the Board office approximately two months prior to the expiration date of your license. It is your responsibility to notify the Board of any change in address and to renew your license in a timely manner even if you do not receive the reminder.
Congratulations on your license renewal, and please cont.act the Board office if you have questions or need additional infonnation.
P lease watch the Board's website on a regular basis for updates or changes that may affect your license.
Please remove card carefully! Bend back and forth along crease before separating.
Arkansas Social Work License Card
License No. Expiration Dote:
8483-M 6/30/2021 Amanda Suzanne Myers, LMSW 5964 Pamela Ann Drive South Bartlett TN 38135
,rd bearer is licensed 1111d m good stMding \ \1th the Arkll11sa.s crnl Wo,k Licensing 00111 ~ ~~ ,--........-..,.
Clrnlmmn
The card to the le.ft is your 11cw social work license card, which reflects your new expiration date. This is the only card you will receive. Please punch it out carefully along the perforated line.
If lost or stolen, an additional card may be requested by written request and a cashier's check or money order in the amount of twenty dollars ($20).
Please keep this letter for your records. You may wish to make a copy before you remove the card.
~ Arkansas State Board or Examiners in Counc;l"ling
101 East Capitol /\venue, Sir 2m Little Rock, AR 72201
Eric Dane Busby
3719 Stadium Blvd Apl 820
Jonesboro, AR 72404
l\rkans.i~ ,_,.,.1,.. n,,.u·,J 111 rx:imlner~ in l ri, 11,~c-lillR
licensee: Eric Dane [hrsbv
license: P1901007
LPC
j Eff::I:~~ o/:~1;::AR:pl::;~,::;;:2
license fl P1901007
:ip!'r·irt lity:
7 f"C h /\s.'.;isted Counseling
6adl·na6eUJ1 07.0?.IA l/7.
'A TE OF ARKAN SAS iCIAL WORK LICENSING BOARD 0. Box 25 1965 t' ock, AR 72225
Jssue Date: J uly 23, 2019
Chelsea E Thielemier, LMSW 500 Marion St Paragou ld, AR 72450
Dear Chelsea;
Asa Hutchinson Governor
Ruthie 13:iin Executive Dirccior
l'honc: 501-372-.507 1 Fax ; 501-372-6301
Email: [email protected] Wcbsi1c; ark:insas.gov/swlb
The Social Work Licensing Board is ple!:ised to notify you of your licensure as a Licensed Masi er Social Worker since you have successfully completed the licensure examination. You are now entitled to all rights, privileges and responsibilities as prescribed in the Social Work Licensing Act (No. 79 1 of 198 1 ), including the use of the ini tials "LMSW" after your name on all professional correspondence.
Your license, No. 9534-M, is subject lo renewal July 3 I, 202 l and every two years 01ereafter. Your license may be renewed by submitting the renewal fee and verification tJ,at you completed 48 hours-of social work continuing education during the two-year licensure period (August [, 2019 - July 31, 2021). The specifics of the continuing education requirement can be found on line al www.arkansas.gov/swlb. Please bookmark and review the website often for any updates or changes.
renewal notice will be mailed to the most current address on file with the Board approximately two monlhs prior to your renewal date. lt is your responsibil ity to keep the Board infonned of any change of address.
A license certificate is being prepared and will be mailed to you at a later date. Your license number and your renewal date appear on the allached wallet-size license card. Please note your license number on all correspondence with the Board.
Congratulations on your liccnsure, and please contact the Board office for any additional information or assistance.
Sincerely,
Leigh Hudson, LCSW Chairman of the Board
------ 111 • .•. Arlc::i ru :.is
Social Work License Carc.J
cnsc No.
i34-M , 0 1sea E Thielemier, LMSW
larion St 3ragould AR 72450
Expir:11i nn l)a1c :
7/31/2021
bearer ,s liccnsccJ ~nd in good stMdrng 11·1111 1111: Arknnsns ,I Work Licensing Ooord ~~ ~~ -~!
' Chnlr111n11
I
The card to the left is your new social work license cord, which reflects your license number and expiration date. This is the only card you wi ll receive. Please punch it out carefully along the perforated line.
If lost or stolen, an additional card may be requested by written request and a cashier's check or money order in the amount of n..,enty dollars ($20). A request form is availAble on our website.
Please remove card carefully! Bend back and fort h along crease
before separating.
I l
7/1/2020 l .1Ct1n se bB:31t;l l
license Search
Arkansas Board of Examiners in Counseling and Marriage & Family Therapy
501 -683-5800
Sarah Elkins LICENSE#: P1403029 I TYPE: LPG I STATUS: ACTIVE
Searcy, 72143
ADDITIONAL INFO Date of Issue: 3/13/2014
Date of Expiration: 6/30/2022 Standing: Good Standing
F.mai l: [email protected] Speciality:
Tech Assisted Counseling
hl tm;:f/searcl1 .stotesolulions.us/l lc«IH""' '/? II J-.A!-lf,IH;l[l ·I 1 G(l()fi1M1J/\? All!i7f"J0f7.E3G60D&L=P11103029&GU 10-007 A 1 E0827204641AD588E794692 . . 1 /1
~-~\ ~,~l --~-::~-rJ
Arkansi;~
Social Wo r k License. C.ird
I kcn.,c :',o.
8576-C Debra Alberts. LCSV\I 307 Fanway De Horseshoe Beno AR 72:312
r.\:pi1 >tlHol\ D~lt:
1'L31 2!;21
C:11'(1 bc.~,cr 1s liccrw,<l and i11 ;;1.,vJ ;:~ndm~ ,, :tt: 11:c- -'d. ,,,,~, 'it1cral \vc,rk I ,ccns;ni; Boai ~-~ •-.>..,...,.____ -~
cri,:nn!ln
~ --L ';,!.
i§:,t-~ u· ~ -L ~
l ...__
-0
Arkansas State Board of-Examin(::rS in Counseling
101 East Capitol Avenue, Ste 202
Little flock, AR 72~01
Date
For
6/2/2019
LPC CASANDRA QUINN PATTERSON
5400 DEERFIELD DR.
JONESBORO, AR 72404 License # P9804008
;~~f,J~~ , i/J@.,itr:. )~l
1~!.J6 Arkansas State Board of Examiners in
Counseling
: Licensee: CASANDRA QUINN PATTERSON
License: P9804008
LPC
I Effect ive: 6/2/2019 Expi~~s~ 6/30/2021
CHAIR OF THE BOARD ·;;9.,""·;:r.,f: ?':?.J
Payor
Dat e
Receipt No.
CASANDRA PATTERSON
6/2/ 2019
657
Item Licensee License No
688 CASANDRA QUINN PATTER P9804008
Speciality:
Play Therapy
Type
LPC
Total
Amount
$312.36
$312.36 J
Arkansas State Boqrd of Examiners In CounsellHg
101 East Capitol Avenue, Ste 202
Little Hock, AR 72201
Date
For
6/5/2019
LPC AMANDA N. POLSTON
308 RUSSELL DR. APT. 20
JONESBORO, AR 72401 License# P1501001
tf,:n;;-;_ ·~1-·~ '1:t:~i'1 ,\)
Arkansas State Board of Examiners In Counseling
~ I
Licensee: AMANDA N. POLSTON
License: P1501001
LPC
Effective: 6/5/2019 Expires: 6/30/2021
CHAIR OF THE BOARD ?Z..a...: ~
Payor
Date
Receipt No,
AMANDA POLSTON
6/5/2019
745
Item Licensee
796 AMANDA N. POLSTON
License No
P1501001
Type
LPC
Total
Amount
$312.36
$312.36
Arkansas State Board of Examin;,.,-. . -.. in Counseling
101 East Capitol Avenue, Ste 207.
Litt le Rock, AR 72201
Haley L. Thomas
2105 Spring Hollow Drive
Jonesboro, AR 72404
Arkansas State tlo;ird of f:xamlners In Counselin,z
Licensee: Haley L. Thom;is
License: P1201011
LPC
Effective: s/1/2020 Expires: 6/30/2022
CHAIR OF THE BOARD ·: f(/ __ ;i..-,,; ,,,__:;j;-;.;.
Payor
Date
Receipt No.
Haley Thornt1s
5/1/2020
2778
Item Licensee
2958 Haley L. Thomas
License No
P120:J011
Date 5/1/2020
For LPC
License lt P1201011
Type
LPC
Total
Amount
$300.00
$300.00 I
Arkansas State Board of Exami11t,s in Counseling 101 East Capit ol Avenue, Ste 202
Little Rock, AR 72201
Date
For
6/2/2019
LPC MICHAEL CRAIG PATTERSON
2504 ALEXANDER DR #214
JONESBORO, AR 72401 License # P000902 7
Arkansas Stal e Board of bamlners in Counseline
Licensee: MICHAEL CRAIG PATTERSON
License: P0009027
LPC
Effective: r,/7/-;n,q Expires: 6/30/2021
CHAIR OF THE BOARD
Payor
Date
Receipt No.
MICHAEL PATTERSON
6/2/2019
646
Item Licensee License No
677 MICHAEL CRAIG PATTERSO P0009027
Type
LPC
Total
Amount
$312.36
$312.36
Arkansas State Board of Examiners In Counseling 101 East Capitol Avenue, Ste 202
Llttle Rock, AR 72201
MR VINCENT D. TOMPKINS
PO BOX431 LULA, MS 38644
Arkansas State Board of Ex~ml(lers In Counsellng
Licensee: MR VINCENT D. TOMPKINS
License; ?1312114
LPC
Effective: 6/25/201.!J Expires: 6/30/2021
CHAIR OF THE BOARD ·;:1,::.:·~.:_ .. , ·:;~'._;
Llceme # P1312114
Speciality: Technology Assisted Counseling
Arkansas Psycholop;y Board • 01 E. Capitol Avenue, Suite 415
_,ttle Rock
Del R. Thomas
2707 Browns Lane
Jonesboro, AR 72401
STATE OF ARKANSAS
ARKANSAS PSYCHOLOGY BOARD
6/20/1994 ----- -
Date Issued
Attests that
Del R. Thomas Is licensed as a
Psychologist - Active Status 6/30/2021
Expiration Date
ARKANSAS PSYCHOLOGY BOARD
License No. 94-lBP
Issued 6/20/l!J'.lll Expires G/30/(021
Signature
94-18P
License Number
\
, ... I
-~,.. l:°;~Z~~ (!~~~ ~K..~
Arkansas Soci.al v,:o .-k License C11rd
----.::_,,,· l.iccn, ~ ;',o.
8575-C Debra Alberts. LCSW 307 Fauway Or. Horseshoe Bend AR 72512
r,pir:Hion O:.rc:
s.·; I 2li2 t
C:u-d b~;:rtr is lie1:11s~d am.! ia g0<).I ;;aodo,!,! wn•1 :1·,<' ,,:1.~.,si~ <;n;:ml Work L1c~ns1r:g. Umir '..I ~ ... -,~.__-- '-~
Ch:1nn~ l
? ~ ~ ~~.½~ u-~ -L ~
l .._ .__(:'>
• • - "'" ·••L.:.l"i l Ut· llFAI TH SOCIAL WORK T fCENSING BO~IU> P. 0. Box 251%5 Little Rock, AR 72225
Issue Dato: December 30, 2019
Priscilla Leo Alc,'Candcr, LCSW 126 Harper Drive Brookland, AR 724 17
Nntbanlel Smith, MD, MPH Sccrelary of l\eolth
Ruthie Baio execu\\ve 0\1ce11,r
Phone: S0l-31'.2-507 \ P11><: S0 l -31Ml01
t!.mt.11: awlb@attanse,.gov Web,llc:: ~ .govhwlb
n,c Sodol Work Licensing Doardispleasc<l to notif:{you of y~ur licensure as a Licensed Certified Social Wofliersince you have successfully completed the licensure examination. You are now entitled to all rights, privileges and responsibilities as prescribed in the Social Work Licensing Act (No. 791 of 1981), including the use of the initials "LCSW'' after your name on all professional correspondence.
Your liccnso, No. 83 I 4-C, is subject to rcnewnl December 31, 2021 and every two years thereafter. Your license may be renewed by submitting the rcnew:il fee nnd verification that you completed 48 hours of social work continuing education during the two-year liccnsurc period (Janunry I, 2020 - December 31 , 2021). The specifics of the continuing education requirement can be found onlinc nt www.arJ.:nnsas.gov/swlb. Please bookmark and review the website often for any upda1es or changes.
A renewal notice will be mailed to the most current address on file wiU1 the Board approximately two months prior to your renewal date. ft is your responsibility to keep the Board informed of any change of address.
A license ccrtific!lle js being prepared and will be mailed to you at a later date. Your license number and yourreoewal dale appear on tho artached wallet-size liccnso card. Please note your license nwnber on an· correspondence with the Board.
iPtu/ations on your /icensure, and please contact t~e B_oard office for any additional information or assistance.
ly, ·---·- ----------- - . ----------------------
o-&~~\\..U,W .Ceigh Hudson, LCSW Cbairman ofthe Board
· (i · · · · ·· ~~~::; ~iiri~:~.: ;~~~ · · · ··, Expir11lioJ1 Date:
12/31/2021 B.31~ C ., . ~. PrlsclHa Lee:,,4Jexander, LCSW 126 Hiirpei,Drlv~ ; Bropkl~nd•AR' 724~ 7
Card beprcr ';s licenw!. 1111d i~ g~sfending,'wilh the /\r).:ansns
· S9cill1 Wor-",Llccn.~~f~~- ~ •~~\\UAW
. ~~~M ·
Your LMSW license is hereby retired and is not subject to renewal
The card to the left is your new social work license card, wh reflects your license number and expiration date. This is the 1
curd you will receive. Please punch it out carefully along the perforated line.
If lost or stolen, an additional card may be requested by wril request and a cashier's check or money order in the amount twenty dollars ($20). A request fonn is available-on our wel:
Please remove card carefully! Bend back and forth along crease
before separating.
A R K A N & A S D E P A R T M E NT OF
fXlM~~ $l~VID<;~S
Novem ber 21, 2019
Pricilla l ee Alexander, LMSW
Mid Sout h Health Syst em 2707 Brown Lane Jonesboro, AR 72401
Division of Aging, Adult, and Behavioral Health Services
Mental Health Services PO 0ox 1437, Slo t W241 · little Rock, AR 72203
Telephone · 501-686-9164
RE: APPROVAL AS AN INFANT MENTAL HEALTH THERAPIST
Dear Ms. Alexander,
This correspondence confirms that Prtcllla Lee Alexander, LMSW, has met the requirements of the Division of Aging, Adult, and Behavioral Health Services (DAABHS) as an Infant M ental Health (IMH) Therapist to prov ide outpatient behav toral health services for the Arkansas Medicaid population under the age of forty-seven (47) months. This approval wlll be effective November 21, 2019, ilnd wfll extend until Novernber 20,2021, <>S long as there is no lapse in professio nal licensure or compliance with any DepMtment of Humiln Services (DRS)
1
requirements related to Behavloral Health Agency (BHA}, lndependently licensed Practitioner (ILP) certtficatlon, or h1far1l M ental Heallh Tiit:r c1pi:;, t Sla11uc1rd!>, whid1t:wr is c1p1Jlit:c1blt!, Auuitiuno11fy1 t:uni1,1lictnc;it wilh c1II i!pp llcable sections of the Arkansas Medicaid Manual, including, but not limited to, the Outpatient Behavioral Health Services section, are mandatory. Furthermore, rehewal applications are due with all required supporting documentation at least fifteen (15) buslness days ptlor to DHS Infant Men ta I Health Therapist status expiration date.
The sites at which OHS approves you to provlde IMH Therapy services include the following:
Mic/South Health System 2707 Brown Lane, Jonesboro AR MCDlt 128707526
If circumstances change regarding your BHA employer, ILP business, address(es), phone number or any other contact Information, you wlll need to Immediately notify DAABHS In writing of all changes. An updated approval letter wlll be sent to you reflecting all changes of which DAABHS was notified. You will also be responsible for notifying Medicaid/HP Provider Enrollment and OHS Division of Provider Services and Quallty Assurance of any applicable changes.
Please cont act the DAABHS office at (S0l ) 68 2-0235 or emall at C>HS.BehaviorajH~alU:[email protected] for any updates, questions or clarification.
::in~iyr - ,/V<,....,_.... __
~r Program Coordinator Division of Aging, Adult & Behavio ral Health Services Office: S0I -682-023S Christ ina. W estml [email protected]
Cc: EQ Health; CW
huma nservJces.a rka nsas.gov Pro tecting the vulnera ble, foste ring Independence and promo ting better health
~~:.- ,\ ,·-:,.~-.~ ill• 11:'\H l ~ll:l\'J' (.H' BEAU I 1
-·.:( ; -~,: . \\ORK J ,,cr:NSJ :c; no A l{l)
'.\ ~i-.. :1Hc i A11(hoI1y Allen.c:.\',Orlh; !..CSW 5\16 !-"air Oaks C ircle :\.·fanon, r-\R 721611
~al'h :111 iel :)mirh, MD, .:Vl PH ~:1,;::rc1::1 ·.- <>:' t k,1r,:1
R11Lhil! [foi,; ! ''H;~11J1 ·1,1t, i)t1·:•. 1~,1
P hOill' , .501-372-S(l71 F;1~ ~0 1-37:. -6,CI
r.n~~il s1 •.•lb@urkun~,,:; .!('1'
\\ 'd:;;1tt . ;;rb11~3s.r,r1,!F,,d b
·n .... --,,,._,;.,. ;\\1rit L,j(;(;ilS:Jig uucird i~ ;1itils1:d (~I 11ut i1y yu.J 1)( >vu, iict\11..ilii \: .tli ii j ,IC0::/ 1:,Cd Ct:1 llih;u '.jo,;i;i i w'u1 i-.cr ~.:1 1.,l' y ,lll hav-: st..ct<tssfully coinpl<!ted th.: licensur~ cxrnnimit ion. Yut1 arc n,,w .~nritl..:J IIJ all rights, privileges 3tlcl
n',µ01)£;bi iiti~s as !Kescribtd in :he Social WtJrk Licensi11g ;\ct (No. 79 1 of I 98 1 ), rndJding i:,c use :)f the initi:ds "LCS\V" ~f.er vour n!lll1e en nl l l"ll'Ofessic11.1I corresooncten:::e. , r- '
Your li;;el!se, ~o. 7636..C, is suii_j ccL to reoewnl March 31, 2022 an<l every lWo ye;:i1~ •iJereaficr, Y0ur I it:ense inay bo renc1~ .;:a by submitting tile renewal fee and verificztior. that you cc-,:r.plctcd 4ll ho Lir5 1;f <;;>: ial work cnn1 inlling edut:at ion durin~ th~ two-year ]i:::c11sure pcr:od (April I. 2020 - Much 3 !, 2022). The :,;pl::;t,ic., 1:,1· 1hc continuing i.:ducaLion r~\qllirf~ntcnl ca;i be fuuctd onl ine at www.l!rk:lnsas.gn v/s.wlb Please bookr::::u k and r~v;i;:w the weh:ate ollcn for any •:.pclsles m clrnr1ges.
A r(;ncwal 11o l icc will be n1ailcd to the most cunc;it addre~s cin r:lc with rt:c Board app~Qxi1nntoly tW{l month~ r:r :tJr 10
your rt:icwal dl!.te. lt is your responsibility to kcc,c ti,:~ 8n.1rtl infonned of i :1y chang:: j f :idJr-.;ss.
A license cenifi.:ate i~ being prepared and" i!: !Jc inai}(:d 10 you a\ r: l;i.rcr dc1!\:. Y,:::r l'censc t1t1.nber 1:nrl your rcnc11 al date appc;;.I' on the anachcd I a I i<:t-si1.e : ite11~e cnr-:. Pknsc not:: ~·tiur i ic:~nsl' nu m'.' ~ ;· on :iii corrc.,pom.Jeocc 1,
1ith r!I~
Llu:\ r,1.
Co!1gra.ulations 011 y:i;,;r lil:ensure, c1nd plcusc comae( the Boord office fr,1 ~1:y addii.inn:i: 111lon~rntion or a;;~1str1 r.ce.
Sinc~rei~,
~ .~ \ \ Vt)"- \0~~,i!)•\ \\ __ LbW.
I ·tl •~I; ( liHhOli, i .r-~.\\·
(· :i!\li·1n J:1 o: th~ :3-J:t
ArKans11s S(lci;1 l \-V11r lt U ccusc <:arc!
E.xpirnliCtll U:m·:
3/31/2022 1,.':1c:·11~~1 A1111ony Al!erw.vo,111, LCSW ,•t'il:i F ;;:11 O;;~rn Chr;ti;
1.\ :11,1.111 .I\H 723EM wU ti:,11 • ,~ 1 ! ~\! ri11•.;.I !l,,.t 1n ;,,o-.H~ ·,~ ~":1~ 111~1 ,•tilil 1:1~ ~11:;J c1 ~~s
I r '1d::1.! ,)t·•.'J d :-_~._ \ ;,, :\. , _ .. -A!:;:-...,) '"'1~ '-1,,.'-&.,\ ..... ~ \.._ .. - -
- - --~0!11. I
The care to :he l~ft is )Ct.I' 1;c\\ s:;cial 1Ynrk l1c:e11s('. c1.1 rd1 which
rctlc-crs your license number· a11d cxi ira1ior1 <.late. This rs the 01ily
curd )'OI.! wi l1 receive::. P k:~ ~t: p1111ch ir out l'i\ rei'i il ly a Icing the pc r for a~cd I i 11.::.
Ir i o).L m- s tolen, ail acld1tifni,i! c,:rd 1nny be requested by writt(;n
req LI :!Sl and a r.11 ;;,hicr•s check or 11w ncy order in the ant0u111 of t,,~nt)' do!l,~rs ($20). A req1J(\:; t fc1r111 i.~ a v,iil:ible on 011 r ,i,eb~ili::.
l'k.1se rL'1,1ri,e '"'' LI cur:f1 11ly' R~ntl b,,cl, :1I1d t'0 n il ,ilo112 ,::-t:11~~
t,d~~a, ',L' p,,r,1 t i11f
05/21/20U 'l'Ul! 81 41 PAX 1870Z3f16ld Kid-S Hellth i•raooUld
Arkansas Social Work License Card
License No. Expiration Date:
1202 .. c s13112021 Brittany Rachelle Anders, LCSW 301 O Norman Rockwell St. Paragould AR 72450
Card bearer is licensed and in good standing with the Arkansas Social Work Licens,ng Boru ~~ ~bilte,,dWU,._ .,'-l!,11::, ,~
Chairman
Ol/lS/2019 PRI 10:36 PAX LS70S5736&7 MGHS CORNING --M ADMIN
J
STATE OF ARKANSAS SOCIAL WORK LICENSING BOARD P. 0. Box 251965 Little Rock, AR 72225
"1:)002/002
'Asu H11lchl11so11 Govt!rnor
January 14, 2019
Stacy Renee Amell, LCSW
1410 Sn1ith Stl·eel' Corning, AR 72422
. Stucy Re11ee Arnell, LCSW;
Rulhiu Boin E1".ecl1Livc. Director
?hone:: 501-372-50?1 . Fox: 501-J,2-GJOl
.8111all: [email protected] Website: 11r~ensas.gov/swlb
This is to notify you that your licensure as a Social Worker hos been approved for the period ofFebt•uary 1, 2019 throl1gh Juuua:ry 31, 2021. The nttached wallet-size license cal'd will servo as confirmalion of license 1•enewal.
Please remember to rotaln yollr continuing r:ducatio11 dooumentn.tion for a period of two-years in the event you are audited. lf audlt0d, you will be requirod to submit docume11ted proof that you alt1mdccl all of the continuing education you listed on your sucnmury sheer. If you nre unable to provide proof thal you attended the workshops, an administrative h0ar!ng will be held to consider n,vocn.tion of your license.
I11 ot·dcr to ronew your license for your new exp iration dntc, (,JanuAty 31, 2021) you must obte.in 48 hours of sooinl work continuing education between the datc..q of February 1, 2019 through Janmuy 311 202]. Only hours obtained betweon these do.tes wlll apply toward your next renewal period. Plca:se sec the Board's webs ite for specific (equirements for continuing ed ucalion,
Futuro renewal notice reminders will be mailed to the address OJI file in the Board office 0pproxim1-1tely two months prior to the expiration date ofyout liccni:;e. lt is your tespousibilily to notify the Board of any cha11ge in address and to renew you1· license in a tlmoly man11er,eve11 if you do not receive the reminder.
Congro.tulutions on your license renewfll, and please co11toct the Boru·d office if you have questions or need addltional informl'\tion.
[J leE\se watch tne Bourd· s website 011 fl regular bu sis for npdates or changes that may at'foct you1· licerxse.
Please 1·emove ca~d C!lrefullyl Bend back and forth along oi·cnse before scparnting.
Arlrnnsas Soclnl Work L1oen.!le CMcl
License No. E¥plrntlou Dote;
H55-0 I /31/2021 Stacy Renee Arnell, LCSW
410 Smith Street ..;ornlng AR 72422
j burcr is llce11scd R!ld in 11ovu Hundi11g with tho Al l<ans•s 1111 Werk l.iccnstn~ 0 0~1 ~ ~- ,~.....,
Chairm an
The card to tho left is your new social worlc license cnrd, which reflects your new expiration dnte. This is the only cord you will receive. Please punch it out carefl11ly aJ011g the pel'fomted line.
If los~ ur stolon, ar1 ndd ,ti on a.I co.rd may be requested by written request and a cai;h)e r'~ check or money order in the amount of twenty dollars ($20) .
Please keep this Jotter for yom recorcls. You 1n11y wish to mRke a copy beforo yQu remove the cat·d ,
Arkans,1!-l Dcpnrt111e11l of f-lcalth SOCIAL WORK LICJ,:NSING BOARD P. 0. Box 251965 Little Rock, AR 722?.)
June 8, 2020
Hcathcl' Hunlcr Bt1kcr, LC.SW
1209 Osage St. Wynne, /\.R 723')6
Heather 1-Iunlcr Baker, LCSW;
(1.J-R, vi , I t;/
J.,v}.t: <-·' . ,u.1,.:?';/t; (,, J0~u1.., -~~,
C ·':~•J[; :~~11 8 \{ct.fk_, y~;}/~i
' . ~- ~~<j,_& ,-11..~20 -~~~
.•;:i.c,..;..,v-.:....:. (
c, / 1,,. ~ u,U.J N:1th1lll i1~1 Smith, 1\-1 1>, M111I
.~ Sccrt:11111• ol'I lcallh
llu(liic 11:till (,)ircc11,r
Phone: 5fl 1-3 77.-5071 l~ux: .rn I -3 72-6]0 I
Email: ~wlb(~)111·ka11s1ts.g.ov Wcb~i(c; nrlrn11r.M,gov/.-;11 lh
Tl tis is to notify you th.it youl' liccnsurc n~ n ::3ocial Worker ha~ bec11 appl'ovcd f'or the pc.;riod or July l, 2020 through ,hmc 30, 2022. The ntlnel,ed wullct-sizc license c,mJ will serve: as co11 fi rnwlion or l iccl'1se renewal.
Plcnse rcme111 bcr lo retain your corttinuing cducntion docume11Cnt.ion for 11 period or lw{1-yc:1rs in ll rn uvl~nl you me a11dilcd. 1r :1ucfitcd, ytHr will be requ ired lo subtnil cloeumc11lctl proof 1h01 yu11 alt<.:11ded ull of the oontinuing cdw.:nl ion you listed on yum su111 11wry sheet. ff you arc 11nnblc In provide prnl)/' ili:rt yOL1 atlcnclcd the workshops, 1111 ad,nini:-trut ivc hearing will be held to consid<:r rcvoention or yo11r license.
ln order to rnm:w yo11r lil:c11~1~ for your new cxpirt1 t io11 dnll'. (June 30, 2022) yriu 111 11s1 olijn i11 118 hour:; or social work 1.a111fi1111 i11g cducntion between Che dales of ,July J, 2020 through June 301 2022. 0 11ly h(111r~ obtained between these dn(cs ,:vii i npply cowurd )'O\tr 11oxl renewal pcriof Plcnst: see the 13oarcf!; wcb~itc ror spocilic rcqllit·c.n1cnts fol' c.<111li1111i11g cd11cilt io11 .
Future rcncwnl rnilic:c re1111mlors wi ll he rnnilcd tt> the address 0 11 file in tho l3ocll'd ofli ce npproxi1nu1cly two 111onlhs prior lo tho L:l- pirnlion dntc of your license. fl is your responsibil ity to notify the Board of !luy chnngc in address 1t11d to rc11~1w y1>t1r l ic.:crrsc in u timely nrnnncr even ifym1 do not receive U1c rcm i11dcr.
Congrncula!ions on your license renewa l, and please conl'l\Cl tho Bonrd of'ficc i(" you have qLtcstions or need ndditionnl infonna(ion.
Please wiitch Che l3onrd'E: wcbsit_e o_n n regu lar bnsis for updates or ch~mges tlrnt inay.,nf(r::c't yo,ur li_9e11§q.
Please rcmcJvo card carefu lly! Dcncl bock 1111d 1<111'1 :dun[; ~:rc,r.sc before .scpnmli11g.
Arli:iusus l>cpnrt11,c11r of I !~;•Ith Suci:1 I Work I ,ii.:l:n ~c Cu nl
Llcrn5t Nu, l•'.,plr·r11 ir111 llulr :
6404-C (1/:l (lf).(l'.l)
Heather Hunter 0:ikor, I C:~:iW 1109 Osage SL Wynne AR 723!.lG
C~rtl l,cor~r is liccn,cd 1111d i,1 gt"•d ,:111111li1•1•. 11'•11• 11,~ l\ 1l1111r;11~
Snr.,~I Wl•rk L1~t11loi11tt 1J11111 -;,;~~~~- '-'-·'-"'---, _ ,,_-<.-..-.A'
The ca rd l(1 the lcll ii: )'Llllr 11uw sc-u..:in l work licc11su c.ird. which rcllccls your 11<.:w cxpirn1io11 date. This is llw lrnly card you will rccriv<:. l'lcusc punch ,1 out carelir lly .:i long (he pcrforn1cd l iru.:.
lf lost or stolon, nn addilio1wl cuf'CI mny be rcq11esi-ccl by wriltcn retp rcst and ;i cash ier's c.:ltcck or 111011cy ordc:r in llic a111ou11t o( lw~nly tlCJ llur!; ($20),
Please keep lltis h:Ucr lor your records. You 111ay wish lo 111aki..: a copy before you remove Lhc cord.
Arkansas State Board of Examiners in Counseling 101 Ea~l Cdµllul Avenu~, Ste 202
Li ttle Rock, AR 72201
Date
For
4/8/2019
LPC PHILLIP G. BEASLEY
1905 CLOVERDALE
PARAGOULD, AR 721150 llcense # P0S12070
Arkansas State Board of Examiners In Counseling
Ucensee: PHILLIP G. BEASLEY
License: P05 12070
LPC
Elfective: il/B/2019 Expires· 6/30/2.0'J.l ..
CHAIR OF THE BOARD . . ;;,.·,,: ._ ,~; :..,.
Date
Receipt No.
PHILLIP Bt:ASLEY
4/8/2019
60
/tern licensee
Gti j)HJLLIP G. BEASLEY
License No
P0512D70
Type
lPC
Total
$312.Jf,
$3 U ~ll
Arkansas State Board of Examir,~,:; in Counseling 101 Cast Capitol Avenue, Ste 202
Little Rock, AR 72201
MS. Carla Leann Blackburn
411 West Pyburn Street
Pocahontas, AR 72455
Arkc>nsas State Bonrd of Examiners in Co~nseling
License: P1608117
LPC
Effective: S/24/2019 Expires: 6/30/2021
CHAIR OF THE BOARD ·;[.~;;.,...., . • ,::1iJ.
License tt P1608117
Speciality: Technology-Assisted Counseling
A_rkansas State Board of Exami,~-· s in Counseling
101 East Capito I /\venue, Ste 202
Little Rock, AR 72201
Tae(or Fay Blankenship
2110 Munos l ane
Jonesboro, AR 72401
Arkansas State Board of Examiners In Counseling
licensee: Taelor Fay Blankenship
License: P1906078
LPC
Effective: 2/19/2020 Expires: 6/30/2022
CHAIR OF THE BOARD '??'~: 0 ... ;
Payor
Date
Receipt No.
Taelor Blankenship
2/19/2020
1875
Item Licensee
2028 Taelor Fay Blankenship
license No
P1906078
Date 2/19/2020
Fo r LPC
License ti P1906078
Speciality:
Technology Assisted Counseling
Type
LPC
Total
Amount
$300.00
$300.00
8/111/2020 IMG.jpg
- ·- - "''-'' ._...._.._._._ .,. __, ,""-'"' •- - - -, ... - - - ·-- - _._ . .,_. ... _ . ._,,,._ -·- __ .._ - · - - - - . ...,,.... - -- -·--·-·-- - ·- -
Lic:rasc No.
Ar!{ansas H)epairtment of llealth Social Worlk lJficense Card
Expiration Date:
2 5U'3-C 8/3 l /2022 Janice Kathryn Eonner, LCSW 4.99 Sue l ane Poc.:1t1ontr-ts A.R 72.455
·, ~':l_;d 'Jt~:-J.rcr i~ I icensr.d an ,J. in good st ,riding ,vith the Arkansas :~ )·_,i :i.l Work U Cl\ns in g B,,ard. • ft\ L , 1 n-. I .,,, .._:i
, _ Y.Ul.-ra_ ~_J t..'-1-f~wl .;-)J,t/J, u Chair
h llps://ma 11.gongle coni/m.illh1/0/l/lnl)Ox/Whcll<JVzcl1S FBLs T pOCTrtCMsHhlLwz Twdf skVl<rRBK nGdP MJQLNKjkGTwqcQdrVLzjOkq?proJoclor=1 &mess.. 1 / i
~\ ~
' ~
~
.. ~
~
I ~
'-b r,/~
·) ~~\-l~~
_'(~
-'=
-I'->, ~
rJ
-
~~
~\).,
-~...::::. ~
;.~-
\ ~
i!) .::,
t-.~., L
~
-c;,'-'-
'<")
..J
..._,
-~
., '
<:?
I I
AR
K.~.N
SA
S D
EP
AR
TM
'E~
T O
F H
EA
LT
H
SO
CIA
L W
OR
K L
lCE
NS
ll\'G B
OA
RD
Mailing A
ddra;ss; P
O B
ox 251965 Linlc R
ock, ~R
722~5-1965
Ph
ysi~
I Ad
dro?ss;
2020 W. T
hird, Suite 518 L
ittle Rock, A
R 72205
Phohe: 501-371-5071
ww
w.tirk:m
s~~s.oov,"wln
Fax:;501-372-6301 E
mail: sw
Ark
shsas
Social W
ork
license C
ard
Llc.cm
cNo.
7266-C
Ca(!1y Ilene B
oyd, LCS
W
21~H
ope St
Corping A
R
72422
~ira
tion
DaC(':
5/31/2022
Card bean:-r ;s licaiscd and in good standing 1vjU
1 the Aikansas
Social Worli L
icensing Board. ~ ~~ \\...c...bw
Chainn,m
-- -1,1.rkansas State Board of Examin~rs in Counseling
101 East Capitol Avenue, Ste 202
Little Rock, AR 72201
MS Kimberley Beth Boyett
1902 Sandbrook
Jonesboro, AR 72404
Ark,msa:; State Board of El<;:imlners In Counseling
Licensee: MS l<imberley Beth Boyett
license: P1206075
LPC
Effective: 4/6/2020 Expires: 6/30/2022
License I/ P1205075
Specia lity: Tech Assisted Counseling
ait!v.a d.{j ~ & t.lt ~ --:2.--2.020
ti
"ATE OF AR.KANSAS )CIAL WORK LICENSING BOARD 0 . Box 25 1965
,Ille.: Rock, AR 72225
August 12, 2019
Connie Lynn Bromky. I .MSW 465 Crcslmont Cir Blylheville, AR 723 15
Connie Lynn Bromley, LMSW;
Asa Hu(chinso11 Ciov::rnor
Ruthie Baio &xceut1vc Dirc,tPI'
l'hom:: 501-J72-SU71 PILX. 501-)72-(d0 I
Email: swlhr,,)nrka11~a~.J!C1'' Wchsi1c: u1•k1111sas.r,,,.•/~wlh
This is 10 notify you thnt your liccnsurc 11s :1 Social Worker has been approved for Lhc rcriod of August 1, 2019 through July 31, 202 J. 'fhc ut tacheJ wnllct-sizc license card will serve as confirmation of license rencwul.
Please remember 10 retain yolll" continuing education documuutation fol' a period of two-ycnrs in the event you urc uudi1cd. If audited, you will be required to submit documt'lntcd proof that you nuentlcd all of the continuing education you listed on your summary sheet. If you arc unable Lo provide proof that you uttcr1dccl the workshops, n11 admi11islr:.itivc hearing will be held lo consider revocation of your liocm;c.
ln order lo renew your license for your new cxpirnlion dole, (July 31, 2021) you must obtnin 46 hours of socinl work continuing education between the dales of August 1, 2019 through ,July 31, 2021. Only hours obtained between these dalt:S will apply toward your next rcncwnl period. Plc:nsc sec (he Board 's website for sp1:cific requirements for continuing cducntion.
f-'ullll'C rcncwul notice rcmi11dcrs will be moiled 10 the nddrcss on file in the Board office urproxi111nlcly two months prior to the expirntion d111c or your license. ll is your n:sponsibilily 10 notify the Ooard ofnny clwngc in address and lo renew your license in a timely n u1111H!r even if you do 1101 receive the rc111indcr.
Congra111lutio11s on your license renewal, and please contuct the Oo:ird of/ice if you hnvc questions lW 11ccd aclclitionnl inlornrnlion.
P lua:.w wutch the lfo,m.1' ~ website on u n.:gu lur bus is for updalt:S ur cl,angcs tr.at may n fft:c-1 )'Ollr I ict-n!i<!
--- ------- . -· -Plcnsc remove curd cnrc /i1lly! J Ocnd bilck a11d forth nluni; crease before scparatin~.
·- ----------
Arknnsas Social Work License Card
License No. F,~pi ra lion OM le:
2613-M 7/31/2021 Connie Lynn Bromley. LMSW 465 Crestmont Cir Blytheville AH 72315
l .'1111) bu:11cr 1s l1ctr,scd 111111 111 1i,1t1d , 1:int.11111• ~ llh the l\rk,m:rns -;,•:1:il Work 1.•~~nsinu I.S.,n1 ~~-~-.~
The cnrd lo the left is your new socia l work license card, which rcnccts your new expiration dale. This is the only cnrd you will receive. Plc.:asc punch it out cnrcfully ulcmg the pcrforntccl line.
If lost or stolen, nn additional card may be requested by wriHcn request and a cashier's check or money order in lhc ;imount of Lwcnty dollnrs ($20).
Please keep this lcLkr for your records. You may wish to make a copy before you remove the card.
• A, ~osas State Board of Exam in,;," in Counseling 101 East Capito l Avenue, St e 202
Little Rock, AR 72201
Kristen Nicole Bruc:e
27 Ashcraft Court
Paragould, AR 72450
Arkansas St;ite Uoard of (;)(,imlners in Counseling
Krist!:!n Nicole Bruce
l-'2005014
LPC
Effective: S/'V./7.07.0 Expires: G/30/2021
CHAIR OF THE BOARO ·.·,.~:;_-J,·,'-· ,;:; ~ .~
License U P2005014
A R. K A N S A S DEPARTMENT OF
Division of A-ging, Adu rt, and Behavioral Health Services
Mental Health Services PO Box 1437, Slot W24 l • little Rock, AR 72203
Telephone· 501-686-9164
July 1, 2019
Kristen Bruce, LAC 27 Ashcraft Court Paragould, AR 72450
RE: APPROVAL AS)!\!\! INFANT MENTAL HEALTH THFRAPIST ~~(
Dear Ms. Bruce,
This corresponc1ence confirms tha t Kristen Bruce, LAC, has met the rcquiremerits of the Division of Aging, Adult, and Behavioral Health Services (DAABHS) as an Infant Mental Health {IMH) Therapist to provide outpatient behav,oral health services for the Arkansas Medicaid population under the uge of forty-seven (47) months. This approval wlll be effective July 1, 2019, and wlll extend until June 30, 2021, as long as there ls no lapse in professional licensure or compliance with any Department of Human Services (OHS) requirements related to Beh;ivioral Health Agency (BHA), Independently Licensed Practitioner (ILP) cer t ification, or Infant Mental Health Therapist Standards. Whichever is applicable. Additionally, cornpllance with all appficable sections of the Arkansas M edlcai,j Manual, Including, but not limited to, the Outpatient Behavioral Health Services section, are mandatory. Furthermore, renewal appl ications are due with all required supporting documentat ion at least fifteen (15) business days prior to OHS Infant M ental Health Therapist status expiration date.
The sites at Which DHS approves you to provide IMH TheJ'l!~~ services include the following:
Mid-South Health Systems 2707 Browns Lane, Jonesboro Medicalq # 172106526
If clrcumstanc:es change regarding your BHA employ~r, ILP business, address(es), phone number or any other cohtact Information, you will need t o immediately notify DAABHS in writ ing of all change~. An UJ:,dat ed approval letter will be sent to yo,u reflecting alt changes of which DAABHS was notified. You Will also be resP,~n~iqle fqr n.otlfv lng MepipJld/HP Provl<ter Enrollment ,!n~ DHS Divis-ion pf ~rovict'!r ~11.rvloes an~ Quality Assurance of any applicable changes. ·
Please contact the DAABHS office at (501) 686-98S8 or emafl at lrn'll,l1'i.:[email protected]'1;.~ fo r any updates, questions or clarification.
Respectfully,
~~:-r'li.h®tu ... ~ Lindsay Colll~(MPA Program Coordinator Division of Aging, Adult & Behavioral Health Services Office: 5D1-686·9858 1'111rl~-u,.Collins(LD<lhs.ark<1nst1~.ug~
Cc: EQ Health; LC
humanservic:cs.arkansas.gov Pro tecting the vulner abl e, fostering independen ce and prom o ting better h ealth
Please remove card carefullyl
Bend back an
d forth along crease
before separating, Arkansas
~ln
l Wo
rk L
icense Card
Uttn
seNo.
E1plratton D
11tt:
66
97-M
7/31/2021
Am
anda Jo Caldw
ell, lMS
W
1770 Hannony R
d P
ocahontas AR
72455 C
ard beam is licensed end in good standing w
ilh the Arkansas
Social Work Li<:-.. ,nsing Boil!
~ ~
-.~
Chainnan
Th
e cru-d to thJ reflects your ne receive. P
lease\
If lost or stoleJ
request and a J
twenty dollars
Please k
eep thi
copy before y01
,,r ~
~5
:-,. ~
--~ _,.;-
..._~
·~,,,.~-;__
~,..-
~ -<
s
. -ii,.
t
,-:, ·-···
A R K A N $ A S DEPA RTMENT OF
March 9, 2020
Amanda caldwell, LMSW 1770 Harmony Rd. Pocahontas, AR 724S5
Division of Aging, Adult, and Behavioral Health Services
Mental Health services PO Box 1437, Slot W241 · little Rock, AR 72203
Telephone• 501-686-9164
RE: APPROVAL AS AN INFANT MENTAL HEALTH THERAPIST
oear Ms. Caldwell,
This correspondence confirms that Amanda Caldwell, LMSW, has met the requirements of the Division of Aging1
Adult, and Behavioral Health Services (DAABHS) as an Infant Mental Health ( IMH) Therapist to provide outpatient be,-,avloral t,ealth services for the Arkansas Medicaid population under the age of forty-seven (47) months. This approval will be effective March 9, 2020, and will extend until March 8, 2022, as long as there is no lapse in profession al ltcensure or compllance with any Department of Human Services (OHS) requirements related to Behavioral Health Agency (BHA), Independently Licensed Practitioner (ILP) certification, or Infant Mental Health Therapist Standards, Whichever is applicable. Additlonally, compllance with air applicable sections of the Arkansas Medicaid Manual, Including, but not limited to. the Outpatient Behavioral Health Services section, are mandatory. Furthermore, renewal appllcations are due with all required supporting documentation at least fifteen (1S) business days prior to OHS Infant Mental Health Therapist status expiration date.
The sites at which OHS approves you to provide IMH Therapy services include the following:
Mid-South Health Systems, 256.D Old County Rd, Pocahontas, AR MCD# 172105526
If circumstances change regarding your BHA emplo~er, llP business, address(es), phone number or any other contact Information, you wlll need to Immediately notify DAABHS in writing of all changes. An updated approval letter will be sent to you reflecting all changes of which DAABHS was notified. You will also be responsible for notifying Medicaid/HP Provider Enrollment ancl OHS OivisiQn of Provider Services and Quality Assurance of any appllcablfl changes.
Please contact the DAABHS office at (501) 682-0235 or emall at [email protected] for any updates, quest ions or clarification.
Program Coordinator Dlvlslon of Aging, Adult & Behavioral Health Services Office: 501-682-0235 Christina. [email protected]
Cc: EQ f-l ealth; CW
huntanservices.arl<ansas.gov Protecting the vul~erable, fostering independence and promoting better h ealth
---o Arkansas Stat e Board of Examiners in Counseling 101 East Capitol Avenue, Ste 202
Little Rock, AR 72201
Robbie Lee Cline
173CR369
Jonesboro, AR 72401
Arkansas State Board of Examiners in
Counseling
I
, Licensee: Robbie Lee Cline
, License: P0910069
LPC I Effective: 2/19/2020 Expires: 6/30/2022
..,.. • , .-;; I
CHAIR OF THE BOARD .,.~,;:,.,_. ~
·------ ---
Payor
Date
Receipt No.
Robbie Cline
2/19/2020
1876
Item Licensee
2029 Robbie Lee Cline
License No
P0910069
Date
For
2/19/2020
LPC
license# P0910069
Speciality:
Tech Assisted Counseling Drug & Alcohol
Pastoral Counseling
Type
LPC
Supervision:
Supervision Tech Assisted Supervision
Total
Amount
$300,00
$300.00
•~ . ..;.., .5
-,.•1 ~
rv1tj~ ~
StzteofArle.lB
SaiS B
oard of E)cam
!Mrs o
f Alcoholbm
a
nd
°""
fAb
c!MC
ou
~
certlfidth
a\
Robbie O
lne
Is currently Rcens.@
d under the authority
of A
ct 4
43
of 2
00
9 as a
LJC
D¥
D AI.CO¼iQUSM
il.DflU
G M
USE COONSElDR,
~e
of Issue
Lic:etlse No
. ~
tlon
~
rs/O!a/2013
358L
U/3
1/2
1
~o
.__
,,.J-,-¾~
B
oaid AdllllnlstratQ
r
·~ )
,~
, ........ ·11'--
fi
_11,-.:. 1.A.././4.(; / ,l.-1jji~(' ·Ji~;; _-ti,.- l:~LJ"I!.•:~) ~ , .....
t ✓ i , ,11, ~{)
_j,,,,;
C-uclJ..R~-~) -2--zo20
j6
Arkan~~s Still<.! Oo~rd of Ex.:in1l11crs iri Cour1s~lin13
Licensee: Ashley Morgan Counts
License: A1705214
LAC
Effective: 3/2/2020 Expires: 5/30/2022
CHAIR OF THE BOARD · ·: __ :; r. . --: , .. r rl .,,,.-, t , ( ;. 1 • .,_,.
)
STATE or, /\.RK/\.NSAS SOCIAL WORK LICENSING BOARD P. 0. Box 25 1965 Little Ro~k, AR 72225
January 14, 20 19
Ken Jarvis Allen Cross, LMSW 5930 Rees Rd. # 172
Jonesboro, AR 7240 I
Ken Jarvis Allen Cross, LMSW;
Asa llutchin~on Governor
Ruthie JJ:iin ~xccutivc Director
l'ho11c: :i0 1-3 72-5071 Fax. 501-372-6301
Email · [email protected] WchsiH:: 111 knnsas.gov/swlb
This is to noti fy you thac your l icensure as a Social Worker has been approved for the period of February l, 2019 through ,fanu:uy 31, 202 1. The atl'ached wallet-size license cnrd will serve as confirmation of license renewal.
Please remember to retain your continuing education documentation for a period of two-years in the event you are awdited. lf audited, you wi ll be required to submit documented proof that you attended all of the continuing education you listed on your summary sheet. I[ you are unable to provide proof that you attended the workshops, an administrative hearing will be held to consider revocation of your license.
fn order to renew your license fo r your new expiration date, (January 31, 2021) you must obtain 48 hours of social work continuing education between the dates of February 1, 2019 through Januai-y 31, 2021.. Only hours obtained between these dates will apply toward your next renewal period. Please see the Board 's website for specific requi rements for continuing education.
Future renewal notice reminders will be mailed to the address on file in the Board office approximately two months prior to the expiration date of your I icense. Jt is your responsibility to notify the Board of any change in address and to renew your license in a timely manne1· even if you do not receive the reminder.
Congratulations on your license renewal, and please contact the Board office if you have qLJestions or need additional information.
Please watch the l3oard 's websilc on a regutl:lr basis tor lipdares Of changes tl~~t nfay affect yotlr license.
Please remove cal'(f cc1refully! Bend back and forth along crease before sep.irating.
Arlrn ns::is Social Work Liccusc C:ird
Exr,irn1io11 DIile:
8109-M 1/J 1/202 1 Ken Jarvis Allen Cross, LMSW 5930 Rees Rd #172 Jonesboro AR 72401
·~rd bearer ,s lh;i;nsc(I 1111d 111 good sln11di1111, will\ 11\c /\r~nn.s:,s
oi:inl Work l.1ccnsi11g n11a1 ~½ ~.,,. •.•~-- .~
The card to the left is yot1r new social work license card, v,,hich reflects your new expiration date. This is the only card you will receive. Please punch it out carefully along the perforated line,
lf lost or stolen, an additiona l card may be requested by written request and a cashier's check or money order in the amount of
twenty dol lars ($20).
Please keep this letter for your records. You may wi!>h lo 111ake a copy before you remove the card.
Jul 17 20, 04:05p
-----Waller or Betty O~mell
\
Arkansas Department of Health SOCIAL \YORK LfCENSlNG BOARD P. 0. Box 251965 Little Rock. AR 72225
July 13, 2020
Walter A. Darnell, LCSW 91_0 College Helen.a, AR 72342-2812
Walter A. Darnell, LCSW;
8 70-.:-\38-3050
Nnthnni~f Smith, MD, MPH Secretary of Keallh
Ruthie B:'lin Director
Phone; 501 -372-5071 Fox: 501-372-6301
Emnil: swlb@arkaruas,sov Website: nrk~nsas.gov/swlb
__ _. .... _ - -· - - ··-·-----··. -·--- -- ·- ·-This is to notify you that your licensure RS a Soci,,i Worker has been approved for the period of A~g~ -1; 2020 through .July 31, 2022. The attached wallet-size li,cense card will serve as confirmation of license renewal.
Please remember to retain your continuing educatio11 documentation for a period of two-years in Ute event you nre audited. lf audited, you will b~ rcqllil'ccl to submit documented proof tl1at you attended all of the continuing education you listed oit your summaty :1heet. Jf you nrc unnblc to provide proof that you attended the workshops, an administrative hearing will lie he.Id to considcrrcvocntioo of your license.
fn order to renew you~ license for your Liew expit'a1lon date, (July 31, 202:Z) yon must obtain 30 hours of social work continuing education between the dates of August), 2,020 through July 3l, 2022. Only hours obtained between these dates will apply toward yollr next renewal period. PJe1rne see the Board's website for specific requirements for continuing education.
Future renewal notice retnindets will bo mailed to the address on file iu the Board office approximately two months prior to the expiration date of your license. lt is your responsibility to notify the Board of any change in address and to ren~w )'dt1r license in a ti1ncly cnanner evt>n if you do not receive the reminder.
Congratulations on your license renewal, a11d .,1i.:;;,:o contact the Board office if you have questions or need additional infonnation.
Please r<imove card corefully! Bend back ·and forth along crease before separatine;.
Arkansas Depnrtroent ofHealtli Social Worlt License Cnnt
062-C Walter A. Darnell, LCSW 930 College ~lefena. AR 72342·2812
7/31/2()22
('ll(d lx:.lrcr Is liccns,d and in good sll\Jldini wi1l1 the Arl:unsas Soel;\l Worl< Licensing Oo:ird. ;-.. 1 . J 1 . ,,.)
U.1211~ ;,,,g.~~ cr.i -·'- 1!',.n, Ls Chair
Thr. card to che left .is yolfr new social work license card, which rdlects yot1r new cxpiratioll date. This is the only card you will rccei\'~ . . Please punch il out carefully along the perforated line.
If. l~st o.r stolen, an additional card may be requested by written
n,,1ut'lst ,ind a ciishier's check or money order in the amount of 1"'·\'CI\L)' do! lo.rs ($20).
:',k• sJ, l:,·~,r l'his ktter for your records. You may wish to make a ,;~py !·1~.fo:c you remove li1e card.
____. Arkansas State Board of E><amin1::,;, in Counseling
101 East Capitol Avenue, Ste 202
Little Rock, AR 72201
Ashlee Nichole Davis
1001 Goldsmith Rd.
Paragould, AR 72450
Arkansas State Board of Examiners in Counseling
Licensee: Ashlee Nichole Davis
License: P1903029
LPC
Effective: 5/5/2020 Expires: 5/30/2022
License # Pl903029
. ~-~.,.__,,,._...._ .... ~J c,. , <,, . J C> .:l o
k
-~---=
::-~
-~'~.:t.:z \-l' ~
!,.,. .
L ~~
Ark
ansas D
epartm
ent o
f Healtlbl
Social W
ork L
icense Card
License N
o~
3757-M
Pam
ela Denice D
iaz, LMS
W
1600 Courtney C
ove Jonesboro A
R 72401
Expiration D
ate:
12/31/2021
Card bearer is licensed and in good standing w
ith the Arkansas
Social Work L
icensing Boat
~-~
-......... -
-,
" ~
J ';:)
·rr .s
~
~
-~
\
" -•l'c:o-\
---~ ........ _
,~' '
-=
<:) ::i-
. ~ ·~
~
,J -0
-d
? "Q
-~
-~~
<s
Chairm
an
--
-~
•n -~~
z:.2
.•~":..i._
~ ..... ._
_~
":r1
'~'..,.,..' ~--~
-~-·-'•"'~~C
T-,,;;;f~-,.._~~i
..fm
~~
~;l~
~~
~.· ?'.!~~ .
· ~
~.m
.....~
'llh
~,.s-«_ .. ~
~-
.._"\,;1 ~
"' ·
~
:'i: ...
· .
" ~~~~ E
h'Y
-~
~
'i:"1
~~~ ~
71 '6/20W . imageO.jpeg
httno ·ll= .. 11 r,nnnla rnm/m:,il/1 1/ni#inhox/lritXMmLnDWQfsBKdnwanwJxiCSM11TDARlkmhdLVPHNNRwDXcwXMRSqKhcMHlzvHSkKHrxvW?projeclor=1 1/1