comparative effect of power training and high-speed yoga on motor function in older patients with...
TRANSCRIPT

edicine and Rehabilitation
Archives of Physical M journal homepage: www.archives-pmr.orgArchives of Physical Medicine and Rehabilitation 2016;97:345-54
ORIGINAL RESEARCH
Comparative Effect of Power Training andHigh-Speed Yoga on Motor Function in Older PatientsWith Parkinson Disease
Meng Ni, PhD,a Joseph F. Signorile, PhD,a,b Kiersten Mooney, MS,c
Anoop Balachandran, MS,a Melanie Potiaumpai, MS,a Corneliu Luca, MD, PhD,d
James G. Moore, PT, PhD,e Christopher M. Kuenze, PhD,a Moataz Eltoukhy, PhD,a
Arlette C. Perry, PhDa
From the aLaboratory of Neuromuscular Research and Active Aging, University of Miami, Coral Gables, FL; bCenter on Aging, University of MiamiSchool of Medicine, Miami, FL; cGreen Monkey Yoga, Miami, FL; and Departments of dNeurology and ePhysical Therapy, University of Miami,Coral Gables, FL.
Abstract
Objectives: To compare the effects of power training (PWT) and a high-speed yoga program on physical performances in older patients with
Parkinson disease (PD), and to test the hypothesis that both training interventions would attenuate PD symptoms and improve physical
performance.
Design: Randomized controlled trial.
Setting: A laboratory of neuromuscular research and active aging.
Participants: Patients with PD (NZ41; mean age � SD, 72.2�6.5y).
Interventions: Two high-speed exercise interventions (specifically designed yoga program and PWT) were given for 12 weeks (twice a week),
and 1 nonexercise control group.
Main Outcome Measures: Unified Parkinson Disease Rating Scale motor score (UPDRSMS), Berg Balance Scale (BBS), Mini-Balance Evalu-
ation Systems Test (Mini-BESTest), Timed Up and Go, functional reach, single leg stance (SLS), postural sway test, 10-m usual and maximal
walking speed tests, 1 repetition maximum (RM), and peak power (PPW) for leg press.
Results: For the posttests, both training groups showed significant improvements (P<.05) in all physical measurements except functional reach
on the more affected side, SLS, and postural sway compared with the pretests, and significantly better scores for UPDRSMS, BBS, Mini-BESTest,
Timed Up and Go, functional reach on the less affected side, 10-m usual and maximal walking speed tests, 1RM, and PPW than controls, with no
differences detected between the yoga program and PWT.
Conclusions: Both the specially designed yoga programandPWTprograms can significantly improve physical performance in older personswithPD.
Archives of Physical Medicine and Rehabilitation 2016;97:345-54
ª 2016 by the American Congress of Rehabilitation Medicine
Reduced motor function in Parkinson disease (PD), especiallybalance and mobility, typically results in loss of independence,increased fall incidence and related injuries, and reduced activitylevels.1,2 Bradykinesia, 1 of the cardinal symptoms of PD, hasbeen attributed to rigidity, tremor, and muscle weakness.3 Musclepower (force � velocity), especially leg power, has a greater effect
Disclosures: none.
0003-9993/15/$36 - see front matter ª 2016 by the American Congress of Re
http://dx.doi.org/10.1016/j.apmr.2015.10.095
on independence,4,5 mobility,3 and fall reduction6,7 than strengthin healthy older and PD populations, while decreased movementspeed and muscle weakness significantly contribute to loss ofmuscle power in PD, especially when moving light to moderateloads.3 These factors are especially important since most dailyactivities,4 such as housekeeping, walking, and recovering from astumble, require rapid movements under light to moderateexternal loading conditions.
habilitation Medicine

346 M. Ni et al
Movement speed is an essential consideration in any exerciseintervention designed to address bradykinesia and physicalfunction in PD.3,8 Power-based resistance training (high speed,low resistance) has been shown to improve muscle strength andpower, and physical functions, including gait speed, balance, andwhole-body functional level, in older adults.9 The only existingstudy9 examining the efficacy of power training (PWT) showsthat 12 weeks of PWT has a beneficial effect on leg musclestrength, power, and movement speed, but not on balance and gaitspeed. Therefore, whether PWT could attenuate PD symptomsand improve balance and mobility in PD needs furtherinvestigation.
Power Vinyasa yoga, characterized by fast transitions from 1posture to another,10 may be another effective exercise strategyto target bradykinesia, rigidity, and muscle function in PD. Thisis supported by our recent study11 demonstrating that partici-pation in a 3-month Power Vinyasa yoga intervention producedsignificant improvements in balance in healthy older fallers.Additionally, the benefits of classic yogic training in healthypopulations include improvements in muscle strength,12,13
power,14 flexibility,12,13 balance, and coordination.11 Finally,yoga-based treatments have the potential to reduce fall risks11,15
and improve quality of life16 in individuals with musculoskeletaldisorders. For patients with PD, 1 pilot study17 indicated that a12-week Iyengar yoga intervention improved motor function,balance, flexibility, and locomotion over a control groupreceiving no intervention.
To our knowledge, no previous study has compared the effectsof high-speed resistance training and yoga in a controlled design.Therefore, the purpose of this study was to compare the effec-tiveness of high-speed yoga and PWT as interventions foraddressing motor symptoms, balance, mobility, and muscle per-formance in older patients with mild to moderate PD. We hy-pothesized that both training interventions would attenuate PDsymptoms and improve physical performance, but that the PWTprogram would produce a greater improvement.
Methods
Design
This study used a randomized controlled trial design. Participantswere recruited from support groups and clinics in the area byadvertising and physician referrals. After baseline assessments,the study coordinator allocated participants to PWT, the yogagroup, or a control group using block randomization based onthe Hoehn and Yahr Classification of Disability for PD (Hoehnand Yahr Scale), by using Excel software.a All testing was
List of abbreviations:
APDavg anterior-posterior average displacement
BBS Berg Balance Scale
Mini-BESTest Mini-Balance Evaluation Systems Test
MLDavg medial-lateral average displacement
PD Parkinson disease
PPW peak power
PWT power training
RM repetition maximum
SLS single leg stance
UPDRSMS Unified Parkinson Disease Rating Scale motor score
conducted at the Laboratory of Neuromuscular Research andActive Aging 1 hour after participants took their usual PDmedications (“on” state), to minimize motor fluctuation andvariability of motor symptoms among participants. The testingorder was standardized among subjects and testing sessions.Pretests and posttests were performed within 2 weeks of theintervention.
Participants
Older patients (60e90y) with idiopathic PD, mildly to moderatelyimpaired (Hoehn and Yahr Scale IeIII), capable of ambulating forat least 50ft with or without an assistive device and rising fromthe floor with minimal assistance, with a score of �24 on theFolstein Mini-Mental State Examination, participated in thisstudy. Exclusion criteria included the following: above stage IIIsymptoms; progressive degenerative disease besides PD; spinalfusion or other orthopedic surgery in the previous 6 months; se-vere visual deficits; major depression or dementia; greater thanminimal assistance required for gait and transfers; and regularpractice (1e2 times/wk) of yoga or resistance training within thepast year. All participants signed an informed written consentapproved by the university’s Human Subjects’ Subcommittee.Participants were allowed to pursue their routine exercise duringthe study, but were instructed to discontinue participation in anyresistance training or yoga program in which they hadalready enrolled.
Outcome measures
Unified Parkinson Disease Rating Scale motor scoreThe Unified Parkinson Disease Rating Scale motor score(UPDRSMS) was the primary outcome measure used to evaluatethe effectiveness of the 2 interventions in addressing motordysfunction. The more and less affected sides were determinedbased on a sum of bradykinesia subscores (items 23e26).18 Twotesters evaluated subjects’ performance separately, and interraterreliability (.904) was high for this test.
BalanceTwo scales, the Berg Balance Scale (BBS)19 and Mini-BalanceEvaluation Systems Test (Mini-BESTest)20; 2 static balancetests, the single leg stance (SLS)21 and postural sway tests22; and 2dynamic balance tests, the Timed Up and Go19 and functionalreach,19 were used. The SLS and functional reach were measuredon both sides (less and more affected side). For the postural swaytest, a portable force platformb recorded the sway area of the 95%confidence ellipse, the medial-lateral and anterior-posterioraverage displacement (MLDavg, APDavg) and SD (MLDSD,APDSD) with the patient during quiet standing with the feet a hip-width apart for 10 seconds with the eyes open and closed.23 Threetrials occurred under each condition, and the average value wasrecorded for each variable.
Leg press strength and peak powerMuscle strength (1 repetition maximum [RM]) and peak power(PPW) (the highest power achieved among 7 loading conditions:30%, 40%, 50%, 60%, 70%, 80%, and 90% 1RM) were assessedusing computerized pneumatic resistance machinesc to evaluateneuromuscular capacity related to fall risk.24 The 1RM protocolwas used previously with older individuals.25 After a warm-up,
www.archives-pmr.org

Effect of exercise on Parkinson disease 347
participants performed 10 repetitions of the exercise at a lowperceived resistance. The test began using a weight agreed on bythe tester and subject to be close to the expected maximum. Theweight was then increased or reduced depending on the subject’ssuccess or failure. A 1- to 2-minute recovery was provided be-tween attempts, and 1RM was reached by all subjects within 4 or5 attempts.
Optimal loads for power were assessed as described previ-ously.26 Power outputs for intensities between 30% and 90% of1RM were assessed on all machines on 3 separate days separatedby 1 or 2 days. A 45- to 60-second recovery was provided betweenattempts. Loads were randomized to reduce any order effect. Theload that generated the highest power across the 7 intensities wasconsidered the optimal load for power for each exercise and usedduring PWT. The testing order was randomized to reduce anyfatigue or learning effects.
Gait speedThe 10-m usual (self-selected) and perceived maximal (fastest)walking speeds (10-m walk test) were measured using a stopwatchand used to evaluate mobility.
Interventions
Power trainingPWT used evolving optimal loads on 11 pneumatic machines,including biceps curl, triceps push-down, chest press, seated row,latissimus pull-down, shoulder press, leg press, leg curl, hipabduction, hip adduction, and seated calf. Each session included 3circuits of 10 to 12 repetitions, twice per week, for 12 weeks (24sessions). Upper and lower body exercises were alternated duringthe circuits.
Training loads were determined using the PPW established oneach machine. After a 1-week adaptation period at loads of 50%and 75% of the optimal loads for PWT, training loads for eachexercise were increased weekly based on participants reachingpower plateaus. Briefly, when the power seen for any exerciseshowed no sustentative increase (defined as value within 5%)across 2 consecutive sessions, loads were increased by 5% andtraining continued until the next similar occurrence.26 For eachexercise, participants were instructed to exert force as fast aspossible during the concentric phase and move slowly through theeccentric phase. Additionally, two 2-week (weeks 5 and 6, weeks11 and 12) translational training cycles were incorporated into thePWT program. These cycles used balance and agility activities,including line, cone, ladder, chair, step, and ball drills. The drillswere designed to improve movement speed and coordination,thereby translating improvements in strength and power intoimproved functional performances through motor skill practice.11
Resistance and translational sessions averaged between 45 mi-nutes and 1 hour. Training occurred according to subject avail-ability between 10 AM and 2 PM daily. For each participant, atrainer provided individualized training.
YogaThe yoga program was designed to improve movement speed,muscle strength and power, and balance specific to PD-relateddecrements. This program was based on our earlier studies27,28
showing variations in muscle utilization patterns among Vinyasayoga poses, and the positive effect of a specially designed yogaprogram on balance in older fallers.11 The yoga training program
www.archives-pmr.org
was provided as a group class, 1 hour per class, twice per week, for12 weeks (24 classes). During class, participants were instructed tohold a pose statically for 1 breath and quickly transition to the nextpose. Also, static poses were included to strengthen and stabilizemuscles, and stretching was included to increase flexibility. Theprogram incorporated 3 difficulty levels: easy, moderate, and hard(supplemental appendix S1, available online only at http://www.archives-pmr.org/). All participants started at the same difficultylevel of yoga practice, and they all went through all difficulty levels.Althoughmodificationswere applied to accommodate an individualsubject’s progress, the same sequencing was applied to all subjects.Three certified yoga instructors taught the program. The class wasoffered at 11 AM. All training occurred within 3 hours of the subjectstaking their medication.
ControlFor CON, a 1-hour nonexercise, health education class, concen-trating on lifestyle modification, medication, therapy and exercise,nutrition, and long-term care, was provided once per month over12 weeks.
Data analyses
Power analysis indicated that a sample size of 14 participants pergroup was required to detect an effect size of Cohen’s dZ.5629 forreduction in the UPDRSMS in the exercise groups compared withCON (power, 0.8; aZ.05; correlation with covariate, .05). Thesample size calculation allowed a 10% dropout rate.
All statistical analyses were performed using SPSS (version22d). A repeated-measures analysis of covariance was used toexamine time (pretest vs posttest) and group (PWT vs yoga trainingprogram vs CON) differences while using the prescore as the co-variate. Post hoc tests using Bonferroni adjustments were used todetect statistical significance for time or group. For skewed data(from the PS test), a Friedman test was used to determine groupdifferences, and Wilcoxon signed-rank tests were used to examinetime differences within groups. Pearson correlation coefficientswere calculated to evaluate the relationship between the changes inbalance measures and leg muscle function (1RM and PPW). The1RM and PPW were normalized to subjects’ body weight. Effectsizes (Hedge’s g) and 95% confidence intervals were calculated forthe UPDRSMS and balance measurements (except PS). Hedge’s gwas calculated using the pretest and posttest means and SDs, andstandardized using posttest score SDs.30 The interpretation of g issimilar to the interpretation of Cohen’s d (.80, large; .50, medium;.20, small). A P value of .05 was required to establish significance.
Results
Flow of participants
Forty-eight participants were randomized into PWT, yoga trainingprogram, or control group. Figure 1 shows the study design andflow of participants through the study. Both interventions werewell tolerated by participants and resulted in an exceptional levelof exercise adherence, with no adverse effects or injuries. Theaverage � SD number of sessions attended by each group was22.79�1.2 for PWTand 22.08�1.2 for yoga intervention (table 1).
Participants’ characteristics are presented in table 1. No sig-nificant group difference was observed in the Hoehn and Yahr

Fig 1 Flowchart of study design and flow of participants through the study.
348 M. Ni et al
stage, age, sex, height, weight, disease duration, and exerciselevel. At the beginning of the study, 25 participants in PWT andyoga training were taking carbidopa/levodopa (Sinemet). Duringthe study period, 1 PWT participant had her Sinemet doseincreased because of increased tremor. No modifications inSinemet dosing were reported for participants in yoga training orcontrol group. Exercise levels refer to the number of hoursparticipating in any type of exercise, including physical therapyand participants’ recreational exercise.
Effect of intervention
Motor performance and balance results are presented in table 2.PWT and yoga training showed significant improvements inUPDRSMS and balance measurements, except for functional reachand SLS on the more affected side for yoga training, and SLS onthe less affected side for PWT. Both training groups producedsignificantly better scores than controls for the UPDRSMS, BBS,Mini-BESTest, Timed Up and Go, and FR on the less affected side,with no group differences detected between PWT and yoga trainingfor any measurement. Walking speed and leg press results are
shown in tables 3 and 4, respectively. The PWT and yoga traininggroups showed significant improvements in all measures andsignificantly differed from the control group. No differences weredetected between training groups. As can be seen in table 5,postural sway results differed by variable, with significant differ-ences from the control group and improvements for the sway areaof the 95% confidence ellipse, APDSD, and the average velocity ofthe center of pressure, for the yoga training group during eyes openand eyes closed. PWT produced significantly greater improvementsthan controls for eyes open APDSD and eyes closed MLDavg,APDavg, and average velocity of the center of pressure, andsignificantly greater improvements than yoga training for MLDavg
and APDavg, as well as a significant improvement in MLDavg.A significant correlation was only found between changes in
the Mini-BESTest and leg PPW (rZ.49, P<.05) for the yogatraining program.
Discussion
This is the first randomized trial to investigate the effect of a high-speed yoga intervention on physical function in patients with PD
www.archives-pmr.org

Table 1 Participant characteristics
Characteristics
PWT
(nZ14)
YOGA
(nZ13)
CON
(nZ10)
H&Y stage 2.2�0.6 2.2�0.7 2.1�0.7
Sex (M/F) 9/5 11/2 4/6
Age (y) 71.6�6.6 71.2�6.5 74.9�8.3
Weight (kg) 78.0�18.9 75.1�11.9 71.5�13.4
Height (m) 1.73�0.1 1.73�0.8 1.64�1.0
Duration of disease (y) 6.6�4.4 6.9�6.3 5.9�6.2
Exercise level at
pretest (h$wk�1)*
3.8�3.3 3.6�2.8 3.3�3.2
Sessions attended 22.79�1.2 22.08�1.2 2.5�2.3
Sinemet as single
medication
4 5 4
Sinemet combined
with other PD
medications
9 7 6
No PD medication 1 1 0
NOTE. Values are mean � SD or n.
Abbreviations: CON, control group; F, female; H&Y, Hoehn and Yahr;
M, male; YOGA, yoga training group.
* As reported through a standard health status questionnaire
approved by the University Subcommittee for the Use and Protection of
Human Subjects.
Effect of exercise on Parkinson disease 349
and the relationship between the improvements in the leg strength/power and balance measurements. The principal finding of thisstudy was that 3 months of PWT and our specially designed yogatraining program was effective at improving physical function andbalance in older adults with PD; however, levels of improvementfor specific variables varied between the 2 exercise interventions.
Both PWT and yoga training produced statistically significantimprovements in the primary outcome measure, the UPDRSMS,suggesting that both interventions can attenuate PD symptoms andimprove movement function. The minimal clinically importantdifference for the UPDRSMS is 5 of 108 points, while 11points in-dicates “much improved” and 12.3 points indicates “very muchimproved.”31 The change scores in this study suggest that our in-terventions (PWT, 10; yoga training, 11) produced a substantialtraining effect. The effect sizes in the current study, compared withthose from a previous meta-analysis,32 indicate the effectiveness ofboth interventions relative to physical therapy, gait-specific training,Tai Chi, dance, and other selected modalities (fig 2A). Additionally,the lack of significant differences between our 2 training groupsindicates that, when targeting improvements in motor function,patients have the opportunity to choose either program or a com-bination of both depending on their exercise preference.
Balance measurement results suggest that participants fromboth training programs had some degrees of improvement in mostmeasures. Both groups produced approximately a 5-point increasein BBS score, which represents a clinically meaningful improve-ment.19 However, as the pretest scores of both training groups(PWTZ48.1; yoga trainingZ49.2) indicated a low fall risk (46e58,low risk; 21e40, medium risk; 0e20, high risk), improvementswere likely limited by a ceiling effect since the sensitivity of theBBS is modest for patients with a low fall risk (fig 2B). Incontrast, the Mini-BESTest is more sensitive than the BBS indetecting abnormal postural responses in PD.20 A suggestedminimal clinically important difference is 4 points for people withbalance disorders.33 In response to training, increases of 3.4 and
www.archives-pmr.org
4.0 points were seen for PWT and yoga training, respectively, andboth groups reached the threshold of 21 recommended fordetecting balance deficits. Our PWT intervention showed a similareffect size to a previously tested balance-training program,34 but aslightly smaller effect size than yoga training and interventionsinvolving dance training (fig 2C).35,36 For the Timed Up and Go,yoga training generated a large effect size (gZ�1.2), and thetraining effect was comparative to previous studies incorporatingother types of training (fig 2D).32 The differences that were seenmay be attributable to the more functional characteristics of ouryoga training program, which allowed a greater transfer ofmuscular power into daily activity patterns because of the incor-poration of high-speed, multidirectional transitions using bodyweight and kinetic movement chains.
Body asymmetry was reflected in some balance tests. For thefunctional reach test, the significant improvement on the moreaffected side only occurred in PWT. This may be explained by thefact that training was bilateral, allowing the less affected side tocompensate, thereby providing less overload and reduced trainingresponses in the more affected limbs. By comparison, many yogaposes were unilateral and may have required greater levels ofexertion, thereby reducing the participants’ willingness or capacityto produce sufficient overload for meaningful adaptation on theirmore affected side (fig 2E). Based on this finding, caution should betaken during yoga training to ensure symmetrical movement, andinstructors should motivate patients to exert maximal effort on theirmore affected side. Finally, the lack of significant differences in theSLS test for both intervention groups comparedwith controls,whichstill compared favorably to results of previous studies (fig 2F), mayhave been due to the large variability between subjects.
Weattempted to investigate the relationshipbetween improvementsinbalance and legmuscle function.Although significant improvementswere found in both measurements, few significant correlations weredetected. The significant correlation between leg power and the Mini-BESTest for yoga training group may be an indication that improve-ment in balance results from increased leg power, as some itemsincluded in this test require fast postural adjustments. Furthermore,addingmore functional power tests, such as chair stands, stair climbing,or object transfers in future studies, to assess the effectiveness of in-terventions under more practical conditions using kinetic chains ratherthan isolated movements may be advisable.
For postural sway, the significant reductions for eyes open andeyes closed sway area of the 95% confidence ellipse across thetraining period observed for our yoga training group indicate thisintervention’s potential to improve postural stability37 and reduceassociated fall risks.38 The ellipse area of patients with PD is largerthan that of the general population, predominantly because ofincreased anterior-posterior sway. The decreased area as a result ofthe yoga training program suggests improved postural control.39
The task-specific training effect of static poses during our yogaprogram may have induced improvement in static balance. ForPWT, decreased EC MLDavg seen after training is likely due to theinclusion of hip abduction and adduction exercises in the trainingprogram. These high-speedmovements likely increased the speed atwhich patients could adjust their body positions laterally during thetest.40 Additionally, the translational cycles included in the PWTinterventionmay have improved proprioceptive feedback just as theposes and pose transitions did during our yoga training program.This suggestion is supported by our previous study11 using yoga andstandard balance training with older fallers.
Both training programs were effective at increasing gait speed,as evidenced by the increases in the 10-m usual walking speed for

Table 2 Results for outcome measures related to motor function and balance for PWT group, YOGA, and CON
EXE (PWT: nZ14/YOGA: nZ13), CON (nZ10)
Outcome Measures Baseline Changes at 3-mo Time Point Treatment Effect Effect Size, g (95% CI) Adjusted P
UPDRSMS*
PWT
YOGA
CON
32.9�12.0
28.15�11
27.6�7.8
�10.7 (�13.1 to �8.4)y
�10.9 (�14.0 to �7.8)y
0.4 (�1.4 to 2.2)
�11.1 (�14.1 to �8.1)
�11.3 (�14.7 to �7.9)
�1.07 (�1.91 to �.23)
�1.20 (�2.07 to �.33)
.000z
.000z
Balance
BBS
PWT
YOGA
CON
48.8 �5.8
49.22�3.9
50.9�6.1
4.4 (2.9 to 6.0)y
4.2 (2.4 to 5.9)y
0.4 (�0.1 to 0.9)
4.0 (2.4 to 5.6)
3.8 (2.0 to 5.5)
.75 (�.07 to 1.57)
.84 (.01 to 1.67)
.000z
.000z
Mini-BESTest
PWT
YOGA
CON
17.6�4.6
18.92�3.9
16.9�5.1
3.4 (2.3 to 4.4)y
4.0 (3.1 to 4.9)y
0.7 (�0.1 to 1.5)
2.7 (1.3 to 4.0)
3.3 (2.2 to 4.4)
.57 (�.23 to 1.37)
.73 (�.09 to 1.55)
.000z
.000z
TUG (s)*
PWT
YOGA
CON
10.8�5.5
10.27�3.9
10.2�2.4
�1.3 (�2.4 to �0.3)y
�2.3 (�4.1 to �0.6)y
0.3 (�0.3 to .9)
�1.6 (�2.9 to �0.4)
�2.6 (�4.6 to �0.6)
�.35 (�1.14 to .44)
�1.20 (�2.07 to �.33)
.014z
.013*
FR more affected (cm)
PWT
YOGA
CON
26.4�5.3
27.94�3.8
26.2�4.6
4.3 (1.5 to 7.2)y
1.0 (�2.0 to 4.0)
0.1 (�1.4 to 1.7)
4.2 (1.1 to 4.8)
0.8 (�2.4 to 4.1)
.65 (�.19 to 1.45)
.13 (�.67 to .93)
.026z
.568
FR less affected (cm)
PWT
YOGA
CON
29.4�5.8
29.36�4.8
28.5�5.3
4.8 (2.5 to 7.3)y
3.3 (1.4 to 5.2)y
0.6 (�2.1 to 0.8)
5.5 (2.6 to 8.5)
3.9 (1.6 to 6.3)
.92 (.09 to 1.75)
.65 (�.19 to 1.45)
.000z
.002z
SLS more affected (s)
PWT
YOGA
CON
4.2�4.1
6.11�2.6
10.5�8.2
8.4 (�2.8 to 19.6)y
5.9 (1.7 to 10.2)
4.1 (�4.0 to 12.2)
4.3 (�4.2 to 20.9)
1.9 (�6.9 to 10.6)
.22 (�.57 to 1.01)
.13 (�.67 to .93)
.536
.657
SLS less affected (s)
PWT
YOGA
CON
4.8�3.6
9.24�7.4
15.1�25.6
11.8 (2.5 to 21.0)
17.7 (�0.3 to 35.8)y
3.4 (�5.4 to 12.2)
8.4 (�9.9 to 18.6)
14.3 (�5.0 to 33.6)
.37 (�.42 to 1.16)
.45 (�.36 to 1.26)
.180
.136
NOTE. Values are mean � SD, mean (95% CI), or as otherwise indicated.
Abbreviations: CI, confidence interval; CON, control group; EXE, exercise; FR, functional reach; SLS, single leg stance; TUG, Timed Up and Go; YOGA,
yoga training group.
* High score reflects poor performance.y Significant difference from pretest.z Significant difference from CON, is adjusted for pretest score based on analysis of covariance.
350 M. Ni et al
PWT (.14m$s�1) and yoga training (.16m$s�1) after training,which were greater than the minimal clinically important differ-ence of .05m$s�1 and “substantial meaningful change” of.13m$s�1 reported in the literature.41 Our interventions yieldedmoderate effect sizes, similar to the training effect for treadmill orgait-specific training (fig 2G).32 Furthermore, the significantimprovement in the 10-m maximal walking speed seen after PWTand our modified yoga program may be attributed to the increasedleg muscle power, which has been shown to be positively corre-lated to the maximal walking speed.42 The moderate effect size(gZ.56) produced by the yoga program may have been the resultof the intervention providing a greater volume of work at highercontractile speeds than classic yoga training because of the use ofthe lower body musculature during most high-speed transitions(fig 2H).
Study limitations
This study had a number of limitations. First, testers were notblinded to the interventions assigned to participants, which mayhave affected evaluations. Second, the sample was small, and thislikely affected our power to detect differences in some measures,such as the SLS. Third, because of the variability in disease statesof the participants, the magnitude of improvement for some spe-cific tests may vary, and this may have affected the precision ofeffect sizes and their confidence intervals. Thus, further studies areneeded to evaluate the interaction between disease stages andtreatment effects. Finally, all assessments were conducted in the“on-medication” state, and it is uncertain whether the trainingeffects resulting from PWT or our yoga program would be repli-cated during the “off-medication” states.
www.archives-pmr.org

Table 3 Results for outcome measures related to gait for PWT group, YOGA, and CON
EXE (PWT: nZ14/YOGA: nZ13), CON (nZ10)
Outcome Measures Baseline Changes at 3-mo Time Point Treatment Effect Effect Size, g (95% CI) Adjusted P
Gait (10-MWS)
Uwalk speed (m$s�1)
PWT
YOGA
CON
1.03�.27
1.06�.20
1.04�.28
.12 (.06 to .18)*
.14 (.02 to .26)*
�.03 (�.06 to .01)
.15 (.08 to 21)
.17 (.05 to .29)
.52 (�.28 to 1.32)
.55 (�.26 to 1.36)
.000y
.011y
Mwalk speed (m$s�1)
PWT
YOGA
CON
1.52�.42
1.49�.25
1.41�.43
.16 (.08 to .24)*
.22 (.08 to .36)*
.002 (�.06 to .06)
.16 (.04 to .26)
.22 (.07 to .37)
.35 (�.44 to 1.14)
.56 (�.26 to 1.38)
.005y
.008y
NOTE. Values are mean � SD, mean (95% CI), or as otherwise indicated.
Abbreviations: CI, confidence interval; CON, control group; EXE, exercise; Mwalk, 10-m maximal walking speed; 10-MWS, 10-m walking speed; Uw , 10-m usual walking speed; YOGA, yoga training group.
* Significant difference from pretest.y Significant difference from CON, is adjusted for pretest score based on analysis of covariance.
Table 4 Results for outcome measures related to neuromuscular performance for PWT group, YOGA, and CON
EXE (PWT: nZ14/YOGA: nZ13), CON (nZ10)
Outcome Measures Baseline Changes at 3-mo Time Point Treatment Effect Effect Size, g (95% CI) Adjusted P
Leg press
Strength (kg)/BW (kg)
PWT
YOGA
CON
1.4�0.5
1.6�0.6
1.4�0.9
0.2 (0.1 to 0.3)*
0.3 (0.2 to 0.5)*
.008 (�.06 to .07)
.21 (�.01 to .43)
.31 (.09 to .53)
.29 (�.51 to 1.07)
.42 (�.40 to 1.21)
.003y
.004y
Peak power (W)/BW (kg)
PWT
YOGA
CON
7.1�2.3
7.8�4.8
5.9�3.0
2.6 (1.8 to 3.4)*
1.8 (0.8 to 2.7)*
�.09 (�0.3 to 0.1)
2.7 (1.3 to 4.1)
1.9 (0.4 to 3.3)
.88 (.03 to 1.67)
.52 (�.31 to 1.31)
.000y
.008y
NOTE. Values are mean � SD, mean (95% CI), or as otherwise indicated.
Abbreviations: BW, body weight; CI, confidence interval; CON, control group; EXE, exercise; YOGA, yoga training group.
* Significant difference from pretest.y Significant difference from CON, is adjusted for pretest score based on analysis of covariance.
Effectofexercise
onParkin
sondisease
351
www.arch
ives-pmr.o
rg
alk

Table 5 Results for outcome variables in postural sway test
Outcome Measures
PWT (nZ14) YOGA (nZ13) CON (nZ10)
Pre Post Pre Post Pre Post
Eyes Open
COParea (cm2) .71�.58 .64�.38 .56�.53 .41�.30*,y .46�.43 .64�.71
MLDavg (cm) .66�2.08 .58�1.73 .48�1.24 .51�1.40 .25�1.09 1.09�1.52
APDavg (cm) �2.54�1.30 �2.13�1.55 �2.90�1.75 �2.87�1.52 �1.42�1.12 �2.41�1.78
MLDSD (cm) .20�.08 .20�.08 .15�.08 .13�.05 .15�.14 .18�.10
APDSD (cm) .48�.15 .43�.10*,y .43�.20 .41�.20*,y .33�.15 .41�.20
Vavg (cm/s) 2.16�.99 2.21�.76 1.55�.66 1.50�.61* 1.45�.71 2.03�1.32
Eyes Closed
COParea (cm2) .94�.84 .99�.64 .97�1.63 .43�.30*,y .61�.76 .89�1.12
MLDavg (cm) .79�2.11 .18�2.01*,y,z .38�1.55 .79�1.17 .25�1.12 1.09�1.57
APDavg (cm) �2.87�1.30 �2.18�1.37*,z �2.59�1.70 �3.07�1.63 �1.42�1.30 �2.57�1.75
MLDSD (cm) .23�.13 .25�.10 .18�.15 .15�.08 .15�.13 .20�.18
APDSD (cm) .56�.20 .51�.13 .53�.36 .38�.15y .43�.23 .43�.25
Vavg (cm/s) 2.72�1.40 2.67�.86* 1.91�.86 1.78�.86* 1.75�.94 2.64�1.93
NOTE. Values are mean � SD. For all measures, higher scores indicate poorer performances (cm).
Abbreviations: CON, control group; COParea, sway area of the 95% confidence ellipse; MLDSD, medial-lateral displacement SD; APDSD, anterior-posterior
displacement SD; Vavg, average velocity of the center of pressure; YOGA, yoga training group.
* Significant difference from CON, adjusted for pretest score based on Friedman test.y Significant difference from pretest based on Wilcoxon signed-rank test.z Significant difference from YOGA, adjusted for pretest score based on Friedman test.
Fig 2 Comparison of effect sizes seen in the current study with those reported in a previous meta-analysis.32 (A) UPDRSMS. (B) BBS. (C) Mini-
BESTest. (D) Timed Up and Go. (E) FR. (F) SLS. (G) Usual walking speed. (H) Maximal walking speed. Abbreviations: C.I., confidence interval; prev,
prevention; PT, physical therapy; SEN, sensory attention focused exercise; WT, weight training; YOGA, yoga training group.
352 M. Ni et al
www.archives-pmr.org

Effect of exercise on Parkinson disease 353
Conclusions
Our 3-month, twice-weekly PWT and our modified yoga trainingprograms were able to alleviate motor symptoms, improve balancefunction and gait, and increase leg muscle strength and power inpatients with mild to moderate PD. These 2 training systemsshould be considered viable interventions in rehabilitation pro-grams designed to translate improvements in physical functioninto improvements in functionality and reductions in fallprobability.
Suppliers
a. Excel software; Microsoft Corp.b. Portable force platform; AMTI.c. Computerized pneumatic resistance machines (Keiser A420);
Keiser.d. SPSS (version 22); IBM Corp.
Keywords
Aging; Exercise therapy; Muscle strength; Postural balance;Rehabilitation; Resistance training
Corresponding author
Joseph F. Signorile, PhD, 1507 Levante Ave, Rm 114, CoralGables, FL 33146. E-mail address: [email protected].
Acknowledgments
We thank Michelle Potiaumpai, BS, Elizabeth Foley, MS, RikaPark, BS, and Green Monkey Yoga Studio (previous Bala VinyasaYoga Studio) for their contributions to the exercise interventions.
References
1. Speelman AD, van de Warrenburg BP, van Nimwegen M,
Petzinger GM, Munneke M, Bloem BR. How might physical ac-
tivity benefit patients with Parkinson disease? Nat Rev Neurol 2011;
7:528-34.
2. Wood BH, Bilclough JA, Bowron A, Walker RW. Incidence and
prediction of falls in Parkinson’s disease: a prospective multidisci-
plinary study. J Neurol Neurosurg Psychiatry 2002;72:721-5.
3. Allen NE, Canning CG, Sherrington C, Fung VS. Bradykinesia,
muscle weakness and reduced muscle power in Parkinson’s disease.
Mov Disord 2009;24:1344-51.
4. Foldvari M, Clark M, Laviolette LC, et al. Association of muscle
power with functional status in community-dwelling elderly women. J
Gerontol A Biol Sci Med Sci 2000;55:M192-9.
5. Skelton DA, Kennedy J, Rutherford OM. Explosive power and
asymmetry in leg muscle function in frequent fallers and non-fallers
aged over 65. Age Ageing 2002;31:119-25.
6. Whipple R, Wolfson L, Amerman P. The relationship of knee and
ankle weakness to falls in nursing home residents: an isokinetic study.
J Am Geriatr Soc 1987;35:13-20.
7. Lamb S, Morse R, Evans JG. Mobility after proximal femoral fracture:
the relevance of leg extensor power, postural sway and other factors.
Age Ageing 1995;24:308-14.
www.archives-pmr.org
8. King LA, Horak FB. Delaying mobility disability in people with
Parkinson disease using a sensorimotor agility exercise program. Phys
Ther 2009;89:384-93.
9. Paul SS, Canning CG, Song J, Fung VS, Sherrington C. Leg muscle
power is enhanced by training in people with Parkinson’s disease: a
randomized controlled trial. Clin Rehabil 2014;28:275-88.
10. Srivasta R. The complete book of Vinyasa yoga. New York: Marlowe
& Co.; 2005.
11. Ni M, Mooney K, Richards L, et al. Comparative impacts of tai chi,
balance training, and a specially-designed yoga program on balance in
older fallers. Arch Phys Med Rehabil 2014;95:1620-8.
12. Tran MD. Effects of hatha yoga practice on the health-related aspects
of physical fitness. Prev Cardiol 2001;4:165-70.
13. Gharote ML, Ganguly SK. Effects of a nine-week yogic training
programme on some aspects of physical fitness of physically condi-
tioned young males. Indian J Med Sci 1979;33:258-63.
14. Bera TK, Rajapurkar MV. Body composition, cardiovascular endur-
ance and anaerobic power of yogic practitioner. Indian J Physiol
Pharmacol 1993;37:225-8.
15. DiBenedetto M, Innes KE, Taylor AG, et al. Effect of a gentle
Iyengar yoga program on gait in the elderly: an exploratory study.
Arch Phys Med Rehabil 2005;86:1830.
16. Kolasinski SL, Garfinkel M, Tsai AG, Matz W, Van Dyke A,
Schumacher HR. Iyengar yoga for treating symptoms of osteoarthritis
of the knees: a pilot study. J Altern Complement Med 2005;11:689-93.
17. Colgrove Y, Sharma N, Kluding P, Potter D, Imming K, VandeHoef J.
Effect of yoga on motor function in people with Parkinson’s disease: a
randomized, controlled pilot study. J Yoga Phys Ther 2012;2:112.
18. Zampieri C, Salarian A, Carlson-Kuhta P, Aminian K, Nutt JG,
Horak FB. The instrumented Timed Up and Go test: potential outcome
measure for disease modifying therapies in Parkinson’s disease. J
Neurol Neurosurg Psychiatry 2010;81:171-6.
19. Steffen T, Seney M. Test-retest reliability and minimal detectable
change on balance and ambulation tests, the 36-Item Short-Form
Health Survey, and the Unified Parkinson Disease Rating Scale in
people with parkinsonism. Phys Ther 2008;88:733-46.
20. King LA, Priest KC, Salarian A, Pierce D, Horak FB. Comparing the
mini-BESTest with the Berg Balance Scale to evaluate balance dis-
orders in Parkinson’s disease. Parkinsons Dis 2012;2012:375419.
21. Adkin AL, Frank JS, Jog MS. Fear of falling and postural control in
Parkinson’s disease. Mov Disord 2003;18:496-502.
22. Rocchi L, Chiari L, Cappello A, Horak FB. Identification of distinct
characteristics of postural sway in Parkinson’s disease: a feature se-
lection procedure based on principal component analysis. Neurosci
Lett 2006;394:140-5.
23. D’Andrea Greve JM, Luna NM, de Siqueira JP, Prota C, Alonso AC.
Assessment of postural balance among individuals with Parkinson
disease with and without effects from dopaminergic medications. Am
J Phys Med Rehabil 2014;93:365-71.
24. Latt MD, Lord SR, Morris JG, Fung VS. Clinical and physiological
assessments for elucidating falls risk in Parkinson’s disease. Mov
Disord 2009;24:1280-9.
25. Henwood TR, Riek S, Taaffe DR. Strength versus muscle power-
specific resistance training in community-dwelling older adults. J
Gerontol A Biol Sci Med Sci 2008;63:83-91.
26. Balachandran A, Krawczyk SN, Potiaumpai M, Signorile JF. High-
speed circuit training vs hypertrophy training to improve physical
function in sarcopenic obese adults: a randomized controlled trial. Exp
Gerontol 2014;60:64-71.
27. Ni M, Mooney K, Harriell K, Balachandran A, Signorile J. Core
muscle function during specific yoga poses. Complement Ther Med
2014;22:235-43.
28. Ni M, Mooney K, Balachandran A, Richards L, Harriell K,
Signorile JF. Muscle utilization patterns vary by skill levels of the
practitioners across specific yoga poses (asanas). Complement Ther
Med 2014;22:662-9.
29. Ellis T, de Goede CJ, Feldman RG, Wolters EC, Kwakkel G,
Wagenaar RC. Efficacy of a physical therapy program in patients with

354 M. Ni et al
Parkinson’s disease: a randomized controlled trial. Arch Phys Med
Rehabil 2005;86:626-32.
30. Allen NE, Sherrington C, Paul SS, Canning CG. Balance and falls in
Parkinson’s disease: a meta-analysis of the effect of exercise and
motor training. Mov Disord 2011;26:1605-15.
31. Korczyn AD, Brooks DJ, Brunt ER, Poewe WH, Rascol O, Stocchi F.
Ropinirole versus bromocriptine in the treatment of early Parkinson’s dis-
ease: a6-month interimreportof a3-year study.MovDisord1998;13:46-51.
32. Tomlinson CL, Patel S, Meek C, et al. Physiotherapy intervention in
Parkinson’s disease: systematic review and meta-analysis. BMJ 2012;
345:e5004.
33. Godi M, Franchignoni F, Caligari M, Giordano A, Turcato AM,
Nardone A. Comparison of reliability, validity, and responsiveness of
the mini-BESTest and Berg Balance Scale in patients with balance
disorders. Phys Ther 2013;93:158-67.
34. Conradsson D, Lofgren N, Nero H, et al. The effects of highly chal-
lenging balance training in elderly with Parkinson’s disease: a ran-
domized controlled trial. Neurorehabil Neural Repair 2015;29:827-36.
35. Duncan RP, Earhart GM. Are the effects of community-based dance
on Parkinson disease severity, balance, and functional mobility
reduced with time? A 2-year prospective pilot study. J Altern Com-
plement Med 2014;20:757-63.
36. Romenets SR, Anang J, Fereshtehnejad S, Pelletier A, Postuma R.
Tango for treatment of motor and non-motor manifestations in Par-
kinson’s disease: a randomized control study. Complement Ther Med
2015;23:175-84.
37. Horak FB, Shupert CL, Mirka A. Components of postural dyscontrol
in the elderly: a review. Neurobiol Aging 1989;10:727-38.
38. Maki BE, Holliday PJ, Topper AK. A prospective study of postural
balance and risk of falling in an ambulatory and independent elderly
population. J Gerontol 1994;49:M72-84.
39. Rocchi L, Chiari L, Horak FB. Effects of deep brain stimulation and
levodopa on postural sway in Parkinson’s disease. J Neurol Neurosurg
Psychiatry 2002;73:267-74.
40. Izquierdo M, Aguado X, Gonzalez R, Lopez J, Hakkinen K.
Maximal and explosive force production capacity and balance
performance in men of different ages. Eur J Appl Physiol Occup
Physiol 1999;79:260-7.
41. Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change
and responsiveness in common physical performance measures in
older adults. J Am Geriatr Soc 2006;54:743-9.
42. Rantanen T, Avela J. Leg extension power and walking speed in very
old people living independently. J Gerontol A Biol Sci Med Sci 1997;
52:M225-31.
www.archives-pmr.org

Supplemental Appendix S1 Power Yoga Program for Parkinson Disease
Stage 1
Warmup
B Tadasana- Teach e Ujjayi breath.- Walk with feet in place and maintaining feet directly forward.- Lift 1 heel. Lift the other heel. Progress to lifting both heels (toe stand).- Alternate reaching arms toward the ceiling 5 times, hold the last stretch for each arm for 3 breaths. Reach arms across the body 6
times keeping the hip bones facing forward during reaches, then twist the trunk with the arm swings 10 times, and finally rotatearms in the sleepwalker position 5 times.
- Alternate full range of motion (ROM) circles forward and backward with strap 5 times. For the final position with the strap behindthe back, slide the hands along the strap to a close grip position and perform a standing backbend like “rocket man” (1 time).
- Head and neck movements. Alternate neck stretches chin to chest, back of skull to spine 3 times, ear to shoulder alternating sides 4times, head rolls in both directions 5 times each.
- Halfway lift hands on thighs, alternating cat and cow 3 times each. Alternate arms forward 3 times on each side, then both armsforward 2 times, holding for 3 breaths.
Effect of exercise on Parkinson disease 354.e1
www.archives-pmr.org

Strengthening
B To the floor- Half lift to forward fold, hands on blocks 4 times.
- Table top push up 5 times and crock hop 5 times.
354.e2 M. Ni et al
www.archives-pmr.org

- Bird Dog opposite arm and leg extensions with lifts 4 times on each side.
- Lateral opposite leg and arm reach to the side 1 on each side.
- Dynamic “thread the needle” twist 5 times on each side.
- Knee lifts: Lift knees 3 inches off the ground and return to the ground 5 times.- Down Dog walking feet and hands together, to standing.
Effect of exercise on Parkinson disease 354.e3
www.archives-pmr.org

Standing
- Chair with toes up and dynamic chair twist.
- Chair step back into crescent step alternating sides 4 times.
- Stepping back alternating diagonal lunge hands in “T” 5 times on each side.
354.e4 M. Ni et al
www.archives-pmr.org

Balancing
- Wall dynamic single knee raise up, then rotate out to the side, then airplane (straight leg extended arm), then foot down, pivot and stepforward to the other side.
Effect of exercise on Parkinson disease 354.e5
www.archives-pmr.org

- Wall Eagle
- Wall Tree: Foot placed below or above the opposite knee.
- From the middle of the yoga mat, from Warrior 1 or Warrior 2 move into triangle (bend to straighten) 2 times with hand to shin.
354.e6 M. Ni et al
www.archives-pmr.org
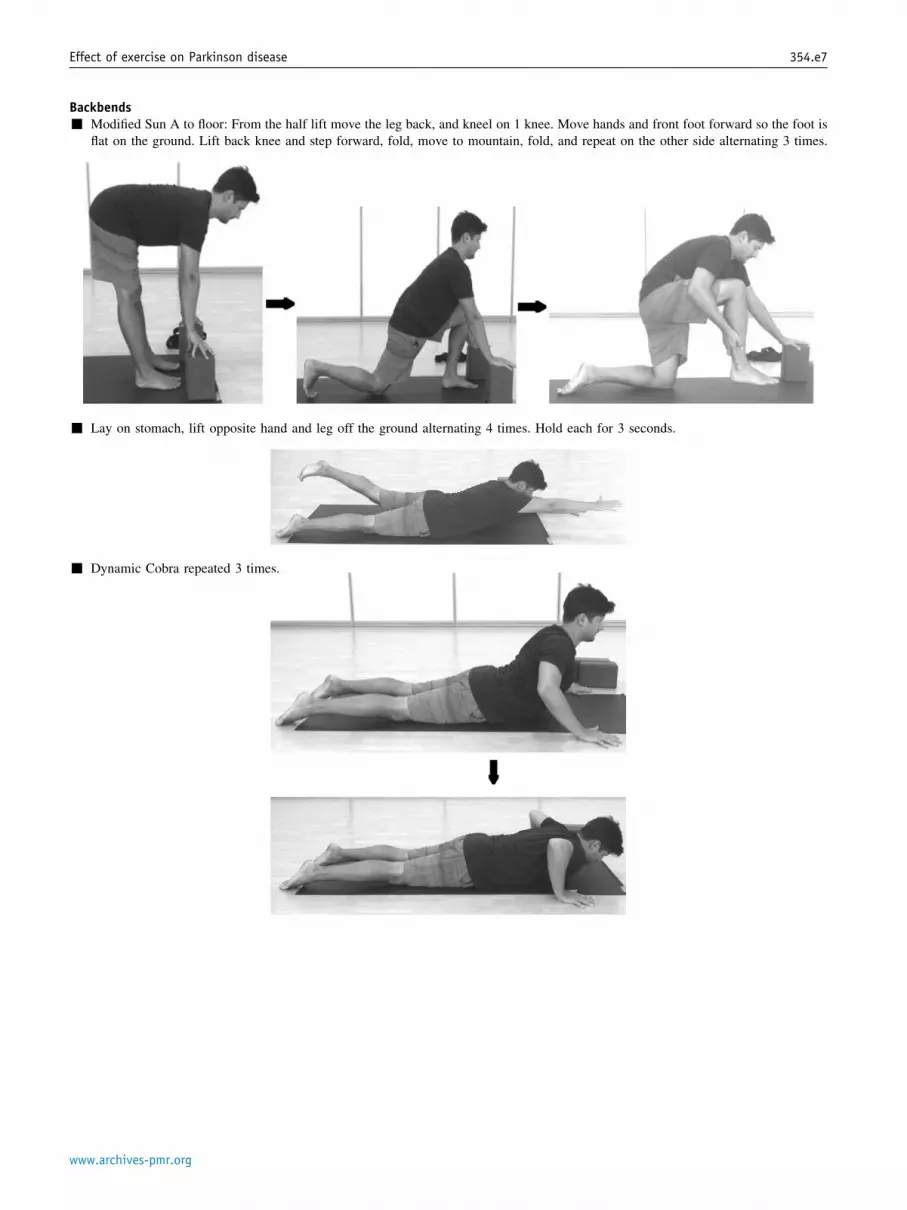
Backbends- Modified Sun A to floor: From the half lift move the leg back, and kneel on 1 knee. Move hands and front foot forward so the foot is
flat on the ground. Lift back knee and step forward, fold, move to mountain, fold, and repeat on the other side alternating 3 times.
- Lay on stomach, lift opposite hand and leg off the ground alternating 4 times. Hold each for 3 seconds.
- Dynamic Cobra repeated 3 times.
Effect of exercise on Parkinson disease 354.e7
www.archives-pmr.org

- Move from child’s pose to camel 3 times.
Stretching- Bridge with block under sacrum holding 1 to 3 minutes.
354.e8 M. Ni et al
www.archives-pmr.org

- Hamstring stretch: Place strap across the ball of the foot, then hold vertical straight leg position for 5 to 10 breaths, leg across the bodyposition for 5 breaths, and the figure 4 position for 5 breaths.
- Knees into chest rock and roll performed 3 to 5 times.
- Supta baddha konasana: With blocks under the scapula and shoulder opening with breaths perform “square breaths,” breathing in for 4seconds and out for 4 seconds.
Effect of exercise on Parkinson disease 354.e9
www.archives-pmr.org

- Perform dynamic twists both knee 6 times, then hold with 1 knee in and 1 leg straight.
Cooldown- Savasana
- Bring knees into chest, roll to 1 side, then hands to knees and walk to the front of the mat to standing position.
- Meditate for 3 breaths with hands at prayer.
354.e10 M. Ni et al
www.archives-pmr.org

Stage 2
Warmup
B Tadasana- Build from the foundation up, walk with feet in place keeping feet pointed directly forward.- Shift the weight from 1 foot to the other, lifting the unsupported foot.- Lift toes, then perform a calf raise, pausing at the top before lowering. Repeat this 5 times.- Bring 1 hand to sacrum and 1 hand to lower belly, press sacrum bone toward the ground and lift the lower belly, tilting the sacrum
5 times.
- Roll the shoulders toward the back of the body.- Perform 5 deep Ujjayi breaths with eyes closed.- Alternate reaching arms toward the ceiling 5 times, holding the last stretch for each arm. Reach arms across body 6 times (square
hip bones forward during reaches), the twist with “floppy” arms 10 times.- Perform sleepwalker arm rotations 4 times.- Alternate full ROM circles forward and backward with strap 5 times. For the final position with the strap behind the back, slide the
hands along the strap to a close grip position and perform a standing backbend like “rocket man” 1 time.- Perform neck stretches chin to chest and back of skull to spine 3 times, ear to shoulder on both sides 4 times, and head rolls both
directions 5 times.- Halfway lift with hands on thighs, alternating the cat and cow positions 3 times each, then alternate arms forward 1 time on each
side, and finally hold both arms forward a single time for 3 breaths.
StrengtheningB To the floor
- Half lift to forward fold, hands on blocks performed 4 times.- Table top push-ups 10 times.- Crock hops 10 times.- Hands and knees cat and cow alternating 4 times, wag tail 3 times on each side, stretch nose toward hip on the ipsilateral side.- Bird Dog with opposite arm and leg both extended, then lift 4 times each.- Lateral opposite leg and arm reach out to each side 1 time each.- Elbow to knee 5 times on each side.- Dynamic “thread the needle” twist 5 times on each side.- Knee lifts 10 times, lifting knees 3 inches off the ground and lowering without touching the ground.- Hold Down Dog for 3 to 5 breaths, then walk feet and hands together moving to a standing position.
Effect of exercise on Parkinson disease 354.e11
www.archives-pmr.org

B Standing- Chair pose with toes up and arms extended forward (sleep walker).- Dynamic chair twists 3 times each side.- Hold a chair pose, clasping hands at the low back and fold forward, hooking thumbs or holding a strap 1 time.- From chair pose, step 1 knee up and then step back into crescent step, then forward to a chair pose. Alternate sides 3 times,
increasing speed with each transition.- Step back alternating diagonal lunges with hands in “T,” repeating 5 times on each side.- Pivot lunge 2 times on each side. Step backward as far as possible to the back edge of the mat, then turn and step to the back.
Observe the distance from the toe tips to end of mat and repeat the movement on the other side, each time shortening the spacebetween the foot and the mat edge.
- Four directional lunges starting by lunging forward and pivoting 3 times each side. Then forward and backward lunges on thesame leg 3 times each with opposite arm movements during the pivot. Begin in the middle of the mat with the right foot forward,pivot to the right and then to the back of the mat. Next with the right foot pivot back to front of the mat. Step to the middle of themat. Then repeat the sequence with the left foot forward.
354.e12 M. Ni et al
www.archives-pmr.org

Balancing (without using a wall)- Perform a dynamic knee raise, rotate the knee out to the side, transition to an airplane pose, then place the foot down and pivot. Step
forward on the other side. Perform the movements 5 times at moderate speed and 2 times at fast speed.- Transfer from an eagle pose to an airplane pose, then back to the eagle 3 times on each side.- Assume a tree pose, move the foot to calf with the hands in a “T” once on each side.- From the middle of the mat perform a Warrior 1 and Warrior 2, moving into a triangle with hand to shin.Backbends- Modified Sun A to floor: From the half lift move the leg back and kneel on 1 knee. Move hands and front foot forward so the foot is
flat on the ground. Lift back knee and step forward, fold, move to mountain, fold, and repeat on the other side, alternating 3 times.- Modified Sun A to floor: From the half lift move the leg back and kneel on 1 knee. With hands, move front foot forward and flat to the
ground. Move hands to the front knee, point arms up toward the ceiling, and twist over the forward thigh. Now untwist the torso witharms up, then hands to blocks, lift the back knee and step forward, then fold. Finally, take the mountain position, then fold again.Repeat the sequence on the other side. Performing each of the sequences 1 time on each side.
- Perform 5 croc hops.- Perform 5 cobra lifts.- Perform the Locus. Lying prone, alternate raising and reaching with opposing hand and leg, holding each for 5 breaths. Next raise the
arms and legs, extending them upward and outward 3 times, holding each for 3 breaths. Finally, clasp the hands at the lower back withpalms facing upward, rest with elbows open.
- Perform the 1-leg floor bow 3 times.- Perform the dynamic cobra 3 times.- Perform the Cobra followed by the child pose, camel, and backbend 4 times.- Perform the Cobra with the right arm locking around the right leg 3 times, then change sides.- Bridge with a block, then hip raise 3 times, pause briefly and remove the block.
Stretching- Hamstring stretch: Place strap across the ball of the foot, then hold vertical straight leg position for 5 to 10 breaths, leg across the body
position for 5 breaths, and the figure 4 position for 5 breaths.- Knees into chest rock and roll with hold 3 to 5 times.- Dynamic twists on both sides, 3 times per side.- Supta baddha konasana: With blocks under the scapula and shoulder opening with breaths perform “square breaths,” breathe in for 6
seconds, hold for 6 seconds, breathe out for 6 seconds, then hold for 6 seconds.
Effect of exercise on Parkinson disease 354.e13
www.archives-pmr.org

Cooldown- Savasana- Bring knees into chest, roll to 1 side, then hands to knees and walk to the front of the mat to standing position.- Meditate for 3 breaths with hands at prayer.
Stage 3
Warmup
B Tadasana- Build from the foundation up, walk with feet in place keeping feet pointed directly forward.- Shift the weight from 1 foot to the other, lifting the unsupported foot.- Lift toes, then perform a calf raise, pausing at the top before lowering. Repeat this 5 times.- Bring 1 hand to sacrum and 1 hand to lower belly, press sacrum bone toward the ground and lift the lower belly, tilting the sacrum
5 times.- Roll the shoulders toward the back of the body.- Perform 5 deep Ujjayi breaths with eyes closed.- Alternate reaching arms toward the ceiling 5 times, holding the last stretch for each arm. Reach arms across body 6 times (square
hip bones forward during reaches), the twist with “floppy” arms 10 times.- Perform sleepwalker arm rotations 4 times.- Alternate full ROM circles forward and backward with strap 5 times. For the final position with the strap behind the back, slide the
hands along the strap to a close grip position and perform a standing backbend like “rocket man” 1 time.- Perform neck stretches chin to chest and back of skull to spine 3 times, ear to shoulder on both sides 4 times, and head rolls both
directions 5 times.- Halfway lift with hands on thighs, alternating the cat and cow positions 3 times each, then alternate arms forward 1 time on each
side, and finally hold both arms forward a single time for 3 breaths.
StrengtheningB To the floor
- Half lift to forward fold, hands on blocks performed 4 times. Bring shoulder blades together while consciously moving forwardand stabilizing the spine.
- Hands and knees cat and cow alternating 4 times, wag tail 3 times on each side, stretch nose toward hip on the ipsilateral side.- Bird Dog with opposite arm and leg both extended, then lift 4 times each, then perform the movement laterally.- Perform a plank, straighten 1 leg then the other. Then hold with both legs extended for 5 breaths.- Perform 10 modified push-ups.- Perform 10 crock hops with knees down.- Hold a plank with both legs extended for 5 breaths.- Dynamic “thread the needle” twist 5 times on each side.- Hold Down Dog for 3 to 5 breaths, then walk feet and hands together moving to a standing position.
B Standing- Maintain the sleepwalker arm stance while holding a block, shift to the chair pose with a block between the upper thighs and lift
toes for a greater challenge. Sit low and stand 5 times, holding each position for 3 breaths.- Perform a dynamic chair twist with a block between the thighs once on each side.- Hold a chair pose, clasping hands at the low back and fold forward, hooking thumbs or holding a strap 1 time.- Standing hold the knee into chest with your hands, pause and step back into crescent lunge. Step forward then to other side. Do
this 1 time slowly and 4 times at high speed on each side.- Stepping back alternate diagonal lunges with arms in a “T” position 5 times per side.- Pivot lunge 2 times on each side. Step backward as far as possible to the back edge of the mat, then turn and step to the back.
Observe the distance from the toe tips to end of mat and repeat the movement on the other side, each time shortening the spacebetween the foot and the mat edge.
- Four directional lunges starting by lunging forward and pivoting 3 times each side. Then forward and backward lunges on thesame leg 3 times each with opposite arm movements during the pivot. Begin in the middle of the mat with the right foot forward,pivot to the right and then to the back of the mat. Next with the right foot, pivot back to front of the mat. Step to the middle of themat. Then repeat the sequence with the left foot forward.
Balancing (without using a wall)- Perform the eagle pose, transition to the airplane, then back to the eagle 3 times.- Assume a tree pose, move the foot to calf with the hands at prayer once on each side.- Modified Sun A to floor: From half lift move the leg back and go down to 1 knee. With hands, move front foot forward and flat to the
ground. Move hands to the front knee, point arms up toward the ceiling, and twist over the forward thigh. Now untwist the torso with
354.e14 M. Ni et al
www.archives-pmr.org

arms up, then hands to blocks, lift the back knee and step forward, then fold. Finally, take the mountain position, then fold again. Repeatthe sequence on the other side. Performing each of the sequences 1 time on each side.
- Modified Sun A with half-lift to the floor, stepping back with 1 leg, bringing the contralateral knee up while keeping the back healdown, raising the arms up into a Warrior 2, transitioning into a triangle with hand to shin. Then put your hands on blocks, lift yourback heal, lunge forward, fold, and perform a halfway lift. Repeat the sequence on the other side.
Backbends- Perform the Locus. Lying prone, alternate raising and reaching with opposing hand and leg, holding each for 5 breaths. Next raise the
arms and legs, extending them upward and outward 3 times, holding each for 3 breaths. Finally, clasp the hands at the lower back withpalms facing upward, rest with elbows open.
- Perform the Sphinx- including a 1 leg floor bow on each side as illustrated in the picture below.
- Perform the dynamic cobra pose 3 times.- Transition from cobra to child pose to camel and fall forward 4 times.- Bridge with block, “square breaths” at 4/6/8 inhale, hold and exhale, then remove block.Stretching- Hamstring stretch: Place strap across the ball of the foot, then hold vertical straight leg position for 5 to 10 breaths, leg across the body
position for 5 breaths, and the figure 4 position for 5 breaths.- Knees into chest, rock and roll with hold 3 to 5 times.- Dynamic twists on both sides 3 times per side.- Supta baddha konasana: With blocks under the scapula and shoulder opening with breaths perform “square breaths,” breathe in for 6
seconds, hold for 6 seconds, breathe out for 6 seconds, then hold for 6 seconds.Cooldown� Savasana.� Bring knees into chest, roll to 1 side, then hands to knees and walk to the front of the mat to standing position.� Meditate for 3 breaths with hands at prayer.
(Several photos were from our previous yoga program for fall prevention: Ni M, Mooney K, Richards L, et al. Comparative impacts of TaiChi, balance training, and a specially-designed yoga program on balance in older fallers. Arch Phys Med Rehabil 2014;95:1620-8.)
Effect of exercise on Parkinson disease 354.e15
www.archives-pmr.org