combined histologic grading of prostatic carcinoma
TRANSCRIPT

Combined Histologic Grading of Prostatic Carcinoma
ALFRED BWKING, MD, JOACHIM KIEHN, MD, AND MONIKA HEINZEL-WACH
A new histologic grading system for prostatic adenocarcinomas is presented, and its clinical significance tested. Histologic growth patterns and nuclear anaplasia found therein are evaluated independently of each other. The diagnostic categories are in accordance with the histologic classification recently published by the WHO." The tumor is denominated according to the least differentiated fraction. Three grades of malignancy, which correspond to significantly different survival probabilities, are distinguished. The prognosis of grade I patients is not reduced in comparison to that of healthy males of the same age. Grade 1 patients did not reveal metastases. The rate of tumor-specific deaths increases with the malignancy grade of the tumor. Interobserver reproducibility of this grading is found to be 91%. With 5% undergradings, the representativity is found to be satisfactory. Prostatic carcinomas tend to change their malignancy grades in time. The question of whether grade I prostatic carcinoma patients with early clinical stages benefit from therapy is discussed.
Cancer 50:288-294, 1982.
ISTOLOGIC CLASSIFICATIONS of tumors discrimi- H nate neoplasms primarily according to their dif- ferent histogenetic derivations and allow predictions about the biological behavior of the tumors, (e.g., hor- monal sensitivity). Histologic grading systems subdivide tumors of the same histogenetic origin into groups with different degrees of malignancy and different prognoses. The prognostic significance of a grading system should be accepted only if good correlations of tumor grades with the survival probabilities of the different groups of patients can be demonstrated. Thus, the clinical rel- evance of a grading system is established by correlating individual tumor grades with the clinical course of the disease. No more grades should be distinguished than allow the corresponding survival probabilities to reveal significant differences. Basic conditions of achieving this goal are: ( 1 ) that each applied diagnostic criterion should correlate with tumor malignancy and prognosis; (2) that the subjective grading results should be suffi- ciently reproducible; and (3) that the grading results
From the Department of Pathology, Ludwig-Aschoff-Haus. Uni- versity of Freiburg i.Br., West Germany.
Supported by the Deutsche Forschungsgemeinschaft. Grant Bo 58912.
The calculations of survival probabilities were performed by M. Heinzel-Wach at the Institute for Medical Statistics and Documen- tation (Director: Prof. Dr. E. Walter), University of Freiburg i.Br.
Address for reprints: Priv. Doz. Dr. A. Bijcking, Pathologisches Institut der Universitlt, AlberstraBe 19, D-7800 Freiburg, West Ger- many.
The authors thank Miss S. Vucikuja and Mrs. U. Wiehle for ex- cellent technical assistance.
Accepted for publication May 23, 1981.
obtained from random biopsies should be sufficiently representative of the tumor as a whole.
At least 40 different histologic classifications for pros- tatic carcinomas have been published, but only 19 have been examined closely for their prognostic significance. Only six of them may be accepted as grading systems since these were demonstrated to be sufficiently corre- lated with the clinical courses: ( 1 ) the systems of Kah- ler'V2 and Pool and T h ~ m p s o n , ~ which are based on the very first grading system published by Br~ders;~. ' (2) the system of Evans et aL6 ( 3 ) the system of Shelley et ~ l . , ~ examined by Wiederanders et a1.;' (4) the system of G l e a ~ o n , ~ examined by Gleason et al.;" ( 5 ) the sys- tem of Bijcking and Sinagowitz;" and ( 6 ) the system of Gaeta et al." Currently, no published clinical data establishes the clinical significance of the grading sys- tem proposed by Mo~tofi , ' '* '~ although he demonstrated the prognostic significance of the individual diagnostic criteria applied.'* In six other publications, the mor- phologic criteria applied were defined insufficiently for reproducible application.16-2' Five other grading systems revealed no sufficient correlation with progno-
In the current investigation the prognostic signifi- cance, interobserver variation and representativity, of a new grading system for prostatic adeno~arc inoma~~ are examined.
sis.22-26
Materials and Methods
Tissue specimens from prostatic carcinomas of 758 patients at 23 different hospitals and in the care of eight
0008-543)</82/07 I5/0288 $0.85 0 American Cancer Society
288
No. 2 PROSTATIC CANCER GRADING - Bocking et al. 289
urologists in private practice were reviewed microscop- ically ( 5 17 punch biopsies, 3 I5 transurethral resections, and 44 enucleated prostates). Punch biopsies and re- sected material were available from 11 8 patients. The tissue cylinders from punch biopsies were cut into serial sections, and five slides of histologic sections were cut from the resectated material. Information concerning the therapy performed on 430 patients was available. Of the patients, 56% had received contrasexual hor- monal therapy, orchiectomy and/or Honvan (= fosfes- trole) or Estradurin (Ayerst) (= polyestradiolphosphate + mepivacaine + nicotinamide), 7% surgical therapy (transurethral resection or enucleation of the prostate), and 37% had received combined surgical and hormonal therapy after histologic confirmation of the diagnosis. No term of therapy was used in preference to any par- ticular histologic diagnosis. The mean age of all patients at the time of diagnosis was 71 years; that of patients with combined malignancy grade I was 70 years.
The four following histologic growth patterns were distinguished for histologic
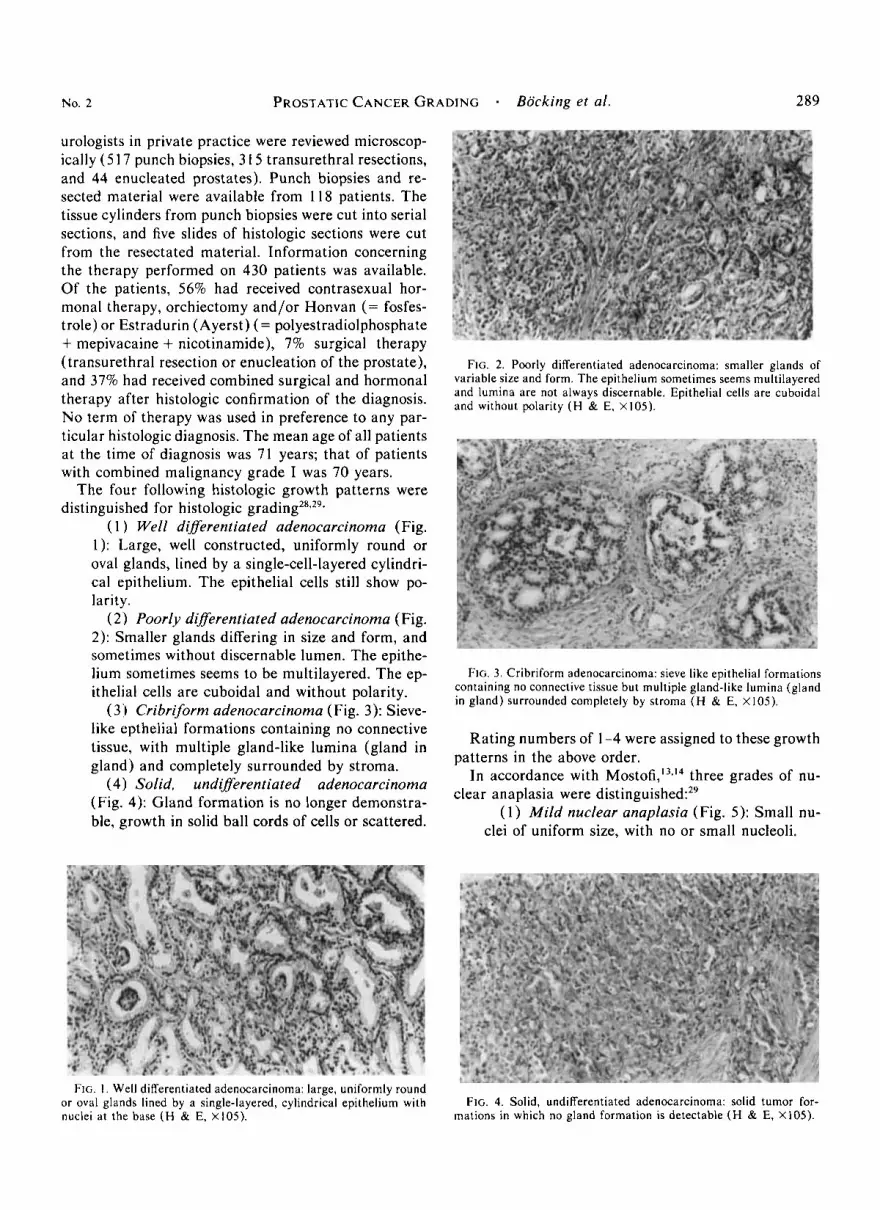
( 1 ) Well diflerentiated adenocarcinoma (Fig. 1): Large, well constructed, uniformly round or oval glands, lined by a single-cell-layered cylindri- cal epithelium. The epithelial cells still show po- larity.
( 2 1 Poorly diflerentiated adenocarcinoma (Fig. 2): Smaller glands differing in size and form, and sometimes without discernable lumen. The epithe- lium sometimes seems to be multilayered. The ep- ithelial cells are cuboidal and without polarity.
(3') Cribriform adenocarcinoma (Fig. 3): Sieve- like epthelial formations containing no connective tissue, with multiple gland-like lumina (gland in gland) and completely surrounded by stroma.
(4) Solid, undiflerentiated adenocarcinoma (Fig. 4): Gland formation is no longer demonstra- ble, growth in solid ball cords of cells or scattered.
FIG. 2. Poorly differentiated adenocarcinoma: smaller glands of variable size and form. The epithelium sometimes seems multilayered and lurnina are not always discernable. Epithelial cells are cuboidal and without polarity ( H & E. X105).
FIG. 3. Cribriform adenocarcinoma: sieve like epithelial formations containing no connective tissue but multiple gland-like lumina (gland in gland) surrounded completely by stroma ( H & E, Xl05).
Rating numbers of 1-4 were assigned to these growth
In accordance with M o ~ t o f i , ' ~ . ~ ~ three grades of nu-
( 1 ) Mild nuclear anaplasia (Fig. 5 ) : Small nu-
patterns in the above order.
clear anaplasia were d is t ingui~hed:~~
clei of uniform size, with no or small nucleoli.
FIG. I . Well differentiated adenocarcinoma: large, uniformly round or oval glands lined by a single-layered, cylindrical epithelium with nuclei at the base (H & E, X 105).
FIG. 4. Solid, undifferentiated adenocarcinoma: solid tumor for- mations in which no gland formation is detectable (H & E, X105).

290 CANCER July 15 1982 Vol. 50
FIG. 5. Mild nuclear anaplasia: small nuclei of uniform size with no or small nucleoli (H & E X430).
FIG. 6. Moderate nuclear anaplasia: medium sized nuclei and nu- cleoli with moderate variation of nuclear and nucleolar size ( H & E, X430).
(2) Moderate nuclear anaplasia (Fig. 6): Me- dium sized nuclei and nucleoli with moderate vari- ation of nuclear and nucleolar size.
(3) Marked nuclear anaplasia (Fig. 7): Large nuclei and nucleoli with marked variation of nu- clear and nucleolar size.
Rating numbers 1-3 were assigned to these grades of nuclear anaplasia in the above order.
The combined grade of prostatic carcinoma results from adding the rating number of the histologic growth pattern to the rating number of nuclear anaplasia which is found therein. The sum of rating numbers 2-3 cor- responds to grade I, 4-5 to grade 11, and 6-7 to grade 111 prostatic carcinoma. The tumors, mostly growing simultaneously in a plurality of forms, are designated according to the growth pattern revealing the highest grade of malignancy. Unlike Hobach and DhomZ8 and D h ~ m , ~ ' who consider the present histologic variants in tumors with several structural patterns, and unlike Gleason,' who considers the two quantitatively predom- inating patterns, we employ rather the qualitatively poorest grade of differentiation.
Evaluation of survival probabilities were carried out according to a life table ana ly~is .~ ' A survival proba- bility (Po,) of 1,0 corresponds to a survival rate of 100%. Significancies were proved by the Kolmogoroff-Smir- noff test and calculated for the total survival curves not for a certain moment.31 Survival probabilities for age- matched control groups were taken from the Statistical Yearbook for the Federal Republic of Germany.32 Clin- ical information about the supposed cause of death was available in 108 cases. Death as a consequence of me- tastases or tumor cachexia was considered tumor-spe- cific. Clinical stages were determined according to
To evaluate interobserver variation of the proposed grading system, the same slides of 100 prostatic car- cinomas (from 50 punch biopsies and 50 transurethral resections) were graded by three pathologists and one semiskilled young physician. For instructions, the pa- thologists received only the grading direction given above in writing and no verbal feed back. The person untrained in histologic diagnostic procedures was, in addition, trained by the author in this grading. No one knew the grading results of his colleagues. To evaluate intraobserver variation, the author of this grading
in 21 3 cases.
TABLE I . Levels of Significance of the Differences in Survival Probability Between Groups of Patients According to Different
Histologic Growth Patterns (KolmogoroK-Smirnoff Test) -~
Well Poorly differentiated differentiated Cribriform Solid
carcinoma carcinoma carcinoma carcinoma
Control 0 ++ +++ +++ Well differentiated
carcinoma 0 0 +++ Poorly differentiated
carcinoma + +++ Cribriform
carcinoma +++ FIG. 7 . Marked nuclear anaplasia: Large nuclei and nucleoli with
marked variation of nuclear and nucleolar size (H & E, X430). 0: no significant difference (P > 0.05); +: weakly significant ( P < 0.05);
++: significant (P < 0.01); +++: highly significant (P < 0 .OOI) .

KO. 2 PROSTATIC CAKCEK GRADING * Bocking et al. 29 1
(A.B.) graded the histologic sections of 100 patients for a second time after an interval of three months. To determine whether the grading results obtained from punch biopsy material were representative of the tumor as a whole, the malignancy grades of 57 biopsies were compared to those obtained from transurethral resec- tates performed during the next half a year. To evaluate a progression of tumor-malignancy, a comparison was made of the grades of 78 prostatic carcinomas as re- vealed by double biopsies taken at intervals of 1-8 years.
Results
At the date of diagnosis, 4% of the patients were found to be in Stage A according to Flocks,33 23% were in Stage B, 45% in Stage C, and 18% in Stage D with distant metastases. Ten per cent of the carcinomas of the prostate were found incidentally. None of the pa- tients with combined grade I-prostatic carcinoma re- vealed metastases during the time of observation, but 53% of the patients with grade I11 carcinoma had me- tastases at the time of diagnosis. Combined histologic malignancy grade I was encountered in 8%, grade I1 i n 57%, and grade 111 in 35% of the cases.
The survival probabilities of prostatic carcinoma pa- tients were found to differ according to the actual least differentiated histologic growth pattern, as shown in Figure 8. Survival time decreases with decreasing his- tological differentiation of the prostatic adenocarcino- mas in the rank order of the rating numbers. The ma- lignancy of the cribriform adenocarcinoma lies between those of poorly differentiated and undifferentiated solid adenocarcinoma. The survival probability of patients with well-differentiated adenocarcinoma is not signifi- cantly different from that of healthy age-matched con- trol males, whereas all other histologic variants revealed a significantly decreased probability of survival (Fig. 8, Table 2). The survival probabilities of patients with three different grades of nuclear anaplasia are signifi- cantly different from each other (Fig. 9, Table 3), but the survival time for patients with slight nuclear ana- plasia is not significantly reduced in comparison to that of healthy males of the same age. The survival proba- bilities of patients with three different combined his- tologic malignancy grades differ from each other sig- nificantly also (Fig. 10, Table 4). Survival time is significantly reduced in patients with grade I1 and I11 carcinomas, but there is no significant difference be- tween the prognoses for grade I carcinoma patients and healthy males of the same age. These statements are also valid when the survival probabilities are calculated for patients who have received essentially the same ther- apy, either hormonal therapy only (Fig. 1 1 ) or surgical combined with hormonal therapy. Survival probabilities
TABLE 2. Levels of Significance of the Differences in Survival Probability between Groups of Patients According to Different
Nuclear Anaplasia Grades of 758 Patients with Prostatic Carcinoma ( Kolmogoroff-Smirnoff Test)
Mild Moderate Market anaplasia anaplasia anaplasia
Control 0 ++ ++ Mild anaplasia ++ ++ Moderate anaplasia + 0: no significant difference ( P > 0.05); +: weakly significant ( P
< 0.05); ++: significant ( P < 0.01); +++: highly significant ( P < 0.00 I ),
TABLE 3. Levels of Significance of the Differences in Survival Probability Between Groups of Patients According to Different Combined Histologic Malignancy Grades of 758 Patients with
Prostatic Carcinoma ( Kolmogoroff-Smirnoff Test)
Grade I Grade I I Grade 1 1 1 carcinoma carcinoma carcinoma
Control 0 ++ ++ Grade I carcinoma + + Grade I1 carcinoma ++*
0: no significant difference ( P > 0.05); +: weakly significant ( P < 0.05); ++: significant ( P < 0.01); +++: highly significant ( P < 0.001 ).
for patients with different clinical stages of prostatic carcinoma revealed the best prognosis for Stage A pa- tients. Prognosis for Stage C patients was significantly better than for Stage D patients (Fig. 12). Patients with distant metastases and grade 111 prostatic adenocarci- noma died four years after the diagnosis was made, whereas those with grade I11 prostatic carcinoma lived an average of one year longer.
When one of the authors (A.B.) graded the same 100 tumors for a second time three months later, he found the same grade of malignancy in 87.5% of the cases. This intraobserver reproducibility was lower for the histologic (85.5%) or the cytologic results (73.5%) alone. In 95% of the cases, he agreed with the tumor grade that was most often assigned by all of the inves- tigators. The other investigators agreed with this grad-
TABLE 4. Percentage of Tumor-Specific Deaths (cachexia, metastases) in Relation to the Malignancy Grades
of Prostatic Carcinoma -.
Sum of Malignancy rating numbers ?h grade %
I 25 2 0 3 33
38 56
78 83
11
1 1 1
47
80

292 CANCER July 15 1982 Vol. 50
PO.
FIG. 8-12. Decrease in survival probabilities (pox) among patients with treated prostatic carcinoma in the years after diagnosis in relation to different morphologic and clinical parameters. The dashed lines represent the survival curves of 71-year-old men in the Federal Re- public of Germany.
I 1 I
2 3 4 5 6 7years8 1
FIG. 8. Survival probabilities of 758 patients, receiving different treatments in relation to different histologic growth patterns of pros- tatic carcinomas.
PO.
1 2 3 4 5 6 7yearsf3
FIG. 9. Survival probabilities of 758 patients receiving different treatments in relation to different degrees of nuclear anaplasia of prostatic carcinomas.
PO.
n c
grade II
1 2 3 4 5 6 7years0
FIG. I I. Survival probabilities of 241 prostatic carcinoma patients receiving hormonal treatment in relation to histologic grades of ma- lignancy.
ing results in 86% of the cases on an average. When the different grading results were compared against the diagnosis with the highest degree of accordance, the
P O "
1 - 1 5 5 1 4 6 7yearse
FIG. 10. Survival probabilities of 758 patients receiving different treatments i n relation to three combined histologic grades of malig- nancy of prostatic carcinomas.
PO,
1 '.stage D
1 2 3 4 5years6
FIG. 12. Survival probabilities of 21 3 prostatic carcinoma patients, in relation to the clinical staging.
mean interobserver reproducibility was found to be 91%. The person specially trained for this grading, al- though unexperienced in histologic diagnosis, achieved

No. 2 PROSTATIC C A N C E R G R A D I N G Bocking el a/. 29 3
a higher degree of agreement with the grades most often assigned (94%) than the graduated pathologists not spe- cially trained (87%).
The malignancy grades found in transurethral resec- tions within six months after the initial punch biopsy, were seen to be one grade lower in 19% of the cases and i n 5%, one grade higher than at the time of the first biopsy ( representativity). Differences of more than one grade did not occur. In 54% of the biopsies per- formed from 1-8 years after the initial biopsy, the tu- mor grade had risen by one histologic grade.
Discussion
The grading system for prostatic adenocarcinomas described above allows us to discriminate three groups of patients with significantly different survival proba- bilities. The prognosis of grade I prostatic carcinoma patients receiving different forms of therapy is not re- duced significantly in comparison to healthy males of the same mean age. However, survival time is signifi- cantly reduced among grade 11 and grade 111 patients (Figs. 10 and 1 1 and Table 4). This grading is based upon the separate and independent evaluation of two different diagnostic criteria, i .e., the histologic growth pattern (Fig. 8) and the nuclear anaplasia (Fig. 9), each of which shows good correlation with prognosis. Dif- fering with our earlier publication^,^^." we no longer regard nuclear polymorphism, nuclear hyperchromasia, or nuclear anisochromasia as diagnostic criteria of any prognostic ~ignif icance.~~ As grading has all the char- acteristics of a subjective test, the separate rating of more than one criterion of prognostic significance re- duces the possibility of misjudgment and improves di- agnostic accuracy. Thus, the reproducibility of the com- bined grading results increases over that of its separate components (84.5% for the histologic and 84% for the cytologic result) and is found to be 91% among various persons according to our grading system. Interobserver reproducibility has otherwise been tested only on the grading system of Gleason9 by Harada et af.,” and has been found to be 64%. The degree of agreement between the authors’ application of a grading instruction and the application by others depends on the willingness to understand and apply an unfamiliar instruction. Di- agnostic experience of the graduated pathologists seems to have interfered with this goal, seeing that an unex- perienced person accepted and applied the new diag- nostic criteria more easily. The consequence is that even the application of new grading systems must be taught, since they may interfer with traditional criteria and are still subjective procedures. Our grading system differs from that of M~s to f i ” , ’~ and Gaeta et a/.” in the respect that we assume that the various appearances of pros-
tatic carcinomas do, within certain limits, represent variable combinations of the four histologic growth pat- terns with different grades of nuclear anaplasia. Both criteria have to be rated within the same growth pattern.
the cribriform pattern is in fact associated mostly (61.9%) with moderate nuclear an- aplasia, but still in 13% with mild and in 25.1% with marked anaplasia. Well differentiated adenoacrinoma is in 52.6% associated with mild but in 47.4% with moderate anaplasia. In solid, undifferentiated carcino- mas mostly marked (72%), but sometimes moderate anaplasia (27%) is found. A fixed combination of an histologic growth pattern with any degree of nuclear anaplasia is therefore unreal and makes no use of the possibility of gaining additional prognostic information by another diagnostic criterion that is in itself prog- nostically significant. and may therefore serve to find a prognostic index of greater accuracy.
The current grading system is so far in accordance with the proposals of the World Health Organization2’ and the International Union Against C a n c e P as it dif- ferentiates three grades of malignancy and uses the same histologic and cytologic categories as the WHO classification does. Unlike other grading systems (such as Gleason’) ours assigns the qualitatively highest ma- lignancy grade found in the diagnostic material under examination to the tumor as a whole. Considering the quantitatively predominating growth patterns (as in Gleason’) attaches in our opinion too much weight to sample size and introduce another subjective criterion, wiz. the quantification of areas of different growth pat- terns. In our opinion that fraction of a tumor will decide the fate of the patient which has the highest growth rate” and malignancy. As the pattern with the highest mitotic rate will sooner or later occupy most of the tumor volume it seems unjustified to neglect the least differentiated tumor fraction when only a small area of it is found in a random biopsy. If the tumor is graded according to the least differentiated fraction found even in small biopsies, these have to be searched thoroughly to detect it. This seems to be the reason why in only 5% of the transrectal resections performed within six months after the initial punch biopsy the diagnosis had to be changed to a grade higher. We feel that the above mentioned characteristics of the proposed new grading system are responsible for its good interobserver repro- ducibility and repesentativity.
The prognostic significance of our grading is further demonstrated by the facts that none of the grade I pa- tients had metastases, but 53% of the grade 111 patients did, and that the rate of tumor specific deaths increased with the grade of malignancy (Table 1). That prostatic carcinomas may increase their grade of malignancy in time is demonstrated by the fact that in 57% of the
As we found

CANCER July 15 1982 Vol. 50
patients who underwent a second biopsy from 1-8 years later, a higher grade was found. We do not believe that these higher tumor grades are a result of therapy, for therapy-induced regressive changes tend rather to sim- ulate lower grades of nuclear anaplasia and hardly af- fect the histologic growth pattern. The result of a lower malignancy grade found in 19% of a second biopsy per- formed within six months after the initial biopsy, com- pared to only 5% higher grades, may in fact be related to a therapy induced reduction in nuclear anaplasia. The implication of these findings is that the clinician has to check regularly the grade of malignancy if his choice of therapy depends on the grading results.
As the grade of malignancy greatly influences sur- vival time, no studies of different therapeutic effects should be published unless it is certain that the groups compared have the same spectrum of malignancy grades. As it is the grade of malignancy which deter- mines how quickly tumors spread, we feel that grading gives reliable information on the prognosis even without staging. As low-grade, low-stage prostatic carcinoma patients most likely do not benefit from conventional
we question whether grade I prostatic car- cinoma patients should be treated in early tumor stages. They should rather be supervised regularly to detect tumor progression, which is revealed by a progressing tumor grade or stage.
REFERENCES
1. Kahler JE. Carcinoma of the prostate gland. Muyo Clin Proc 1938; I3:589- 592.
2. Kahler JE. Carcinoma of prostate gland: Pathologic study. J Urol 1939; 41:557-574.
3. Pool TL. Thompson GJ. Conservative treatment of carcinoma of the prostate. J Anr Med Assoc 1956; 160:833-837.
4. Broders AC. The grading of carcinoma. Minn Med 1925; 8:726 730.
5. Broders AC. Grading and practical application. Arch Parhol 1926; 2:376-38 1
6. Evans N. Barnes RW, Brown AF. Carcinoma of the prostate; correlation between the histological observations and the clinical course. Arch Pathol 1942; 34:473-483.
7. Shelley HS, Auerbach StH, Classen KL, Marks C H , Wieran- ders RE. Carcinoma of the prostate: A new system of classification. Arch Surg 1958; 77:751-756.
8. Wiederanders RE, Stuber RV, Mota C, OConnell D, Haslam GJ. Prognostic value of grading prostatic carcinoma. J Urol 1963;
9. Gleason DF. Classification of prostatic carcinomas. Cancer Chemorher Rep 1966; 50: I25 - 128.
10. Gleason DF. Mellinger GT. The Veterans Administration Co- operative Urological Research Group. Prediction of prognosis for pros- tatic adenocarcinoma by combined histological grading and clinical staging. J Urol 1974; I I I:%-63.
I I . Baking A. Sinagowitz E. Histologic grading of prostatic car- cinoma. Puthol Res Pracr 1980; 168: 1 15- 125.
12. Gaeta JF , Asirwatham JE. Miller G, Murphy GP. llistologic grading of primary prostatic cancer: A new approach to an old prob- lem. J Urol 1980; 123:689-693.
13. Mostofi FK. Grading of prostatic carcinoma. Cuncer Chem- olher Rep 1975; 59:111-117.
14. Mostofi FK. Problems of grading carcinoma of prostate. I n
891881-888.
Jarbo J W , ed. Seminars in Oncology, Vol. 3. Washington. Grune & Stratton, 1976.
15. Harada M, Mostofi FK, C o r k DK, Byar DP, Trump BF. Pre- liminary studies of histological prognosis in cancer of the prostate. Cancer Treat Rep 1977; 61:223 225.
16. Bauer WC, McGavran MH, Carlin MR. Unsuspected carci- noma of the prostate in suprapubic prostatectomy specimens: A clin- ico-pathological study of 55 consecutive cases. Cancer 1960 I3:370- 378.
17. Vickery AL, Kerr WS. Carcinoma of the prostate treated by radical prostatectomy: A.clinicopathologicaI survey of I87 cases fol- lowed for 5 years and 148 cases followed for 10 years. Cuncer 1963; 16: I 598- 1608.
18. Jewett HJ. Bridges RW, Gray GF, el at. The palpable nodule of prostatic cancer: Results 15 years after radical excision. J A M A
19. Mobley TL. Frank J N . Influence of tumor grade on survival and on serum acid phosphatase levels in metastatic carcinoma of the prostate. J Urol 1968; 99:321 323.
20. Denis LJ. Clinical cancer of prostate: Influence of tumor stage and grade on five-year survival. Acro Urol Belg 1972; 40: 126- 132.
21. Belt E, Schroeder 1-H. Total perineal prostatectomy for car- cinoma of the prostate. J Urol 1972; 107:91-96.
22. Foot NC, Humphreys GA, Coats EC. Carcinoma of the pros- tate: A review of 162 cases with pathological classification. NY Siure J Med 1950 50:84-88.
23. Mobius G, Schneider HJ. flesse P. Zum biologischen Verhalten des Prostatacarcinoms i n Abhangigkeit vom histologischen Typ. Z Krebsforsch 1961; 64:267-277.
24. McNeal JE. Morphogenesis of prostatic carcinoma. Cuncer 1965; 18:1659 1666.
25. UIZ DC, Farrow GM. Pathologic differentiation and prognosis of prostatic carcinoma J A M A 1969; 209: I701 - 1705.
26. Esch W, Latal D. Das Prostatakarzinom als Zufallsbefund bei Prostatektomie. Z Urol 1972; 65:389-395.
27. Bllcking A, Sommerkamp H. Histologisches Malignitats-Grad- ing des Prostatakarainoms. Proknostische Validitit, Reproduzierbar- keit und Reprlsentativitlt. 32. Kongress Dtsch. Ges. f. Urologie. Ber- lin, Sept. 1980 (Abstract).
28. Hohbach M, Dhom G. Aktuelle Probleme des Prostatakarzi- noms. Munch Med Wschr 1972; 114;45-54.
29. Mostofi FK, Sesterhenn I, Sobin LH. Histological typing of prostate tumours. International Histological Classification of Tu- mours Nr. 22. Geneva, World Health Organization, 1980.
30. Dhom G. Differentialdiagnostische Probleme des Prostatacar- cinoms (Erfahrungen mit dem Prostatacarcinom-Register). Beilr Pu- rho1 1974; 153:203 220.
31. Walter E. Biomathematik filr Mediziner. Stuttgart: B. G. Teubner, 1975.
32. Statistisches Jahrbuch 1975 fur die Bundesrepublik Deutsch- land. Herausgeber: Statistisches Bundesamt Wiesbaden. Stuttgart und Mainz, Verlag W. Kohlhammer, 1975.
33. Flocks RH. Carcinoma of the prostate. J Urol 1969; 101:741- 749.
34. Btkking A, Sinagowitz E, Thon W, Nattenmiiller E, Wagner J , Sandritter W. Histologisches Grading des Prostatakarzinoms. Med Welt 1979; 30:275-279.
35. Baking A. Grading des Prostatakarzinoms. Habilitationssch- rift 1980. Med. Fak. Univ. Freiburg.
36. Harmer MH. T N M Classification of Malignant Tumors, ed 3. Geneva, International Union Against Cancer, 1978.
37. Helpap B, Stiens R, BrUhl P. Autoradiographische Untersu- chungen an inkubierten Prostatapunktaten nach Doppelmarkierung mit C- 14-und H-3-Thymidin. Beilr Pathol 1974; I5 I :65 74.
38. Helpap B. Stiens R, Brilhl P. The proliferative pattern of the prostatic carcinoma before and under hormonal treatment. Z Krebs- forsch 1976; 87:31 1-320.
39. Kirchheim D. Das Prostatakarzinom. Dlsch Arzreblart 1980; 77:807 814.
40. Mellinger GT. Prognosis of prostatic carcinoma. I n Grund- mann E, Vahlsieck W, eds. Tumors of the Male Genital System: Recent Results in Cancer Research. Vol 60. Berlin, Springer-Verlag, 1977; 61 72.
1968: 203:403-406.