college/school of pharmacy affiliation and community pharmacies' involvement in public health...
TRANSCRIPT

RESEARCH ARTICLES
College/School of Pharmacy Affiliation and Community Pharmacies’Involvement in Public Health Activities
Salisa C. Westrick, PhD,a* Jeanine Mount, PhD,b and Suntaree Watcharadamrongkun, MSb,c
aHarrison School of Pharmacy, Auburn UniversitybSchool of Pharmacy, University of Wisconsin-MadisoncChulalongkorn University, Bangkok, Thailand
Submitted January 3, 2009; accepted April 5, 2009; published November 12, 2009.
Objectives. To examine the relationship between pharmacy college/school affiliation and communitypharmacies’ involvement in immunization and emergency preparedness activities.Methods. Telephone interviews were completed with 1,704 community pharmacies randomly sampledfrom 17 states to determine the pharmacies’ involvement in immunization promotion, vaccine distri-bution, in-house immunization delivery, and health emergency preparedness and response, affiliationwith college/school of pharmacy, and selected pharmacy and public health-related characteristics.Results. Pharmacy college/school-affiliated community pharmacies were more likely than non-affiliated pharmacies to participate in immunization and emergency preparedness when controllingfor pharmacy characteristics. College/school affiliation generally became nonsignificant, however,when public health-related characteristics were included in the analysis.Conclusions. Affiliation with a college/school of pharmacy was related to community pharmacies’involvement in immunization and emergency preparedness.
Keywords: experiential learning, public health, school of pharmacy, college of pharmacy, communitypharmacy, immunization
INTRODUCTIONPharmacists have a responsibility to engage in disease
prevention and health promotion activities such as smok-ing cessation, immunization delivery, and prevention ofheart disease, stroke, and diabetes.1,2 The 2004 educa-tional outcomes released by the Center for the Advance-ment of Pharmaceutical Education (CAPE) include publichealth as a major competency in pharmaceutical educa-tion.3 The Accreditation Council for Pharmacy Education(ACPE) also incorporated these outcomes into Standards2007.4 Hence, colleges and schools of pharmacy must pre-pare future pharmacists for expanding public health rolesby incorporating public health content in their curricula.
While teaching public health can be accomplishedthrough didactic coursework,5 colleges and schools ofpharmacy should go beyond this to integrate public healthinto experiential education.6-8 Experiential education haslong been recognized as an effective way to facilitate
student learning.9 During experiential education, stu-dents should have opportunities to actively participate inpharmacy-based public health activities, acquire in-depthexperiences, and master public health skills.
The need for exceptional experiential education sitesto guide the development of pharmacy students is great.10
Sending students to experiential education sites that donot provide public health services may cause student frus-tration due to the perceived dissonance between what theyare being taught as the ideal practice and what they see inactual practice.11 Students assigned to sites who do notengage in public health activities may not gain sufficientexperiences to master the skills necessary to provide pub-lic health activities and achieve the outcomes specified byCAPE.
Community pharmacies’ participation as experientialeducation sites is an essential mechanism for pharmaciesto be affiliated with colleges/schools of pharmacy. In ad-dition, community pharmacies’ affiliations with collegesand schools of pharmacy may be based on the pharmacy’sparticipation in practice-based research networks, resi-dency programs, and/or classroom teaching or researchactivities. Little information is available regarding theextent to which pharmacies affiliated with colleges andschools of pharmacy offer public health services and how
Corresponding Author: Salisa C. Westrick, 207 DunstanHall, Pharmacy Care Systems, Auburn University,AL 36849. Tel: 334-844-5152. Fax: 334-844-8307.E-mail: [email protected]*All authors contributed equally to this work and their namesappear in random order.
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
1

these pharmacies compare to non-affiliated pharmacies interms of involvement in public health activities.
The goal of this study was to better understand therelationship between a pharmacy’s affiliation with a phar-macy college/school and its involvement in public healthactivities. In this study, public health activities were con-ceptualized as innovations to be studied. Social networktheory was used to provide an explanation for why college/school-affiliated pharmacies were more involved in publichealth activities than their non-affiliated counterparts.According to this theory, knowledge transfer and resourcesharing occur among organizations that are connected toone another in the same social context.12,13 Informationand resource exchange enhance organizations’ capabil-ities to discover new opportunities, obtain new knowl-edge, and explore new innovations.14-16 In the case ofcommunity pharmacies, through affiliation with collegesand schools of pharmacy, community pharmacies learnnew knowledge, are exposed to new opportunities, andgain critical competencies that contribute to advancementin their practices. We then posited that community phar-macies affiliated with a pharmacy college/school weremore likely to be involved in public health activities thancommunity pharmacies not affiliated with a pharmacycollege/school. We explored 4 selected public health ac-tivities: immunization promotion, vaccine distribution,in-house immunization delivery, and emergency pre-paredness and response. Our objectives were to: (1) com-pare community pharmacies with and without pharmacycollege/school affiliation in terms of general pharmacycharacteristics and public health-related characteristics,(2) compare community pharmacies with and withoutpharmacy college/school affiliation in terms of extentand type of public health involvement, and (3) examinethe relationship between pharmacy college/school affilia-tion and pharmacy involvement in public health activitieswhen controlling for general pharmacy characteristics andpublic health-related characteristics.
METHODSThis study was part of a larger national study (17 states)
describing community pharmacies’ participation in immu-nization and emergency preparedness and response activ-ities. Seventeen states were purposely selected to maximizevariability along 3 dimensions: the flexibility of state im-munization-related laws, the overall level of pharmacist/pharmacy participation in public health activities at thestate-level, and geographical location (Figure 1).17 Thisstudy received exempt status by the University of Wiscon-sin-Madison’s Institutional Review Board.
A systematic random sample of 150 community phar-macies (158 in one state due to error) was selected from
each state. Prenotification letters and study descriptionswere sent to 2,558 pharmacies prior to contacting them bytelephone. A computer-assisted telephone interview wasthen conducted with key informants (pharmacy managersor on-duty pharmacists) at each of the pharmacies be-tween July 2005 and February 2006. When making tele-phone contact, the interviewer requested to speak with thepharmacy manager or a pharmacist on duty. If an appro-priate individual was not available, the interviewerattempted to call back; calling was limited to 35 attemptsper sampled pharmacy. Details of interview proceduresappear in a previously published study.18
VariablesWe determined each pharmacy’s affiliation status by
asking key informants whether their practice site was af-filiated with a college or school of pharmacy (responserecorded as yes or no). To measure pharmacy involvementin public health activities, the key informants were asked toidentify whether their pharmacy was involved in immuni-zation promotion, vaccine distribution, in-house immuni-zation delivery, or emergency preparedness and response.For example, for immunization promotion, key informantswere asked whether their practice site participated in anycampaign to promote the importance of immunizations.Similarly, 3 additional questions were asked about theirinvolvement in vaccine distribution, immunization deliv-ery, and emergency preparedness and response. These 4questions yielded 4 dichotomous variables (yes/no). A fifthdichotomous dependent variable was created based on keyinformants’ responses related to the 4 public health activ-ities; if the key informant responded yes to at least 1 of thetargeted public health activities, the pharmacy was coded1; pharmacies offering none of these services were coded 0.
Control variables were categorized into 2 groups:general pharmacy characteristics and characteristics re-lated to public health. General pharmacy characteristics
Figure 1. States with a lighter shade were included in thisstudy.
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
2

included type of pharmacy (independent/chain/mass mer-chant/supermarket), pharmacy location (rural/suburban/urban), number of full-time equivalent pharmacists(count), and pharmacist workload (prescriptions filledper full-time pharmacist per week). For the publichealth-related characteristics, key informants were askedto report whether their practice site had at least 1 pharma-cist trained in in-house immunization delivery (yes/no) andin emergency preparedness and response (yes/no). Theyalso were asked the extent of perceived support from var-ious groups for in-house immunization delivery and foremergency preparedness and response. These groups were:pharmacy profession (state board, state/local pharmacy as-sociations, and national pharmacy associations), publichealth (health department and physicians/clinics), andpharmacy practice (employing organization, supervisor,and other pharmacists). To measure perceived supportvariables, key informants were asked to rate how stronglyeach group opposed or supported pharmacist participa-tion in these activities on a scale ranging from -5 (stronglyoppose) to 5 (strongly support). A zero was assigned whenthe key informants saw a particular group as neither sup-portive nor opposed or had no opinions.
Data AnalysisData were analyzed using SPSS, version 16.0 (SPSS,
Chicago). To assess the potential for nonresponse bias,characteristics of hard-to-contact pharmacies (those re-quiring more than 9 calls) and easy-to-contact pharmacies(those requiring less than 2 calls) were compared.18
Descriptive statistics, including general pharmacycharacteristics and characteristics related to public health,were used to describe participating pharmacies. Bivariateanalyses were conducted to assess relationships betweenpharmacy college/school affiliation and (1) pharmacycharacteristics, (2) public health-related characteristics(characteristics specific to immunization delivery andemergency preparedness and response), and (3) pharmacyinvolvement in public health activities. A series of logisticregression analyses were conducted to assess the relation-ship between pharmacy college/school affiliation andpublic health involvement when controlling for pharmacycharacteristics and characteristics specific to immuniza-tion delivery and emergency preparedness and response.
RESULTSOf the 2,558 randomly selected community pharma-
cies, 92 were excluded because they did not provide directpharmacy services to the public, were nonpharmacy tele-phone numbers, or were non-working telephone numbers.Results showed no significant differences between easy-and hard-to-contact pharmacies with respect to general
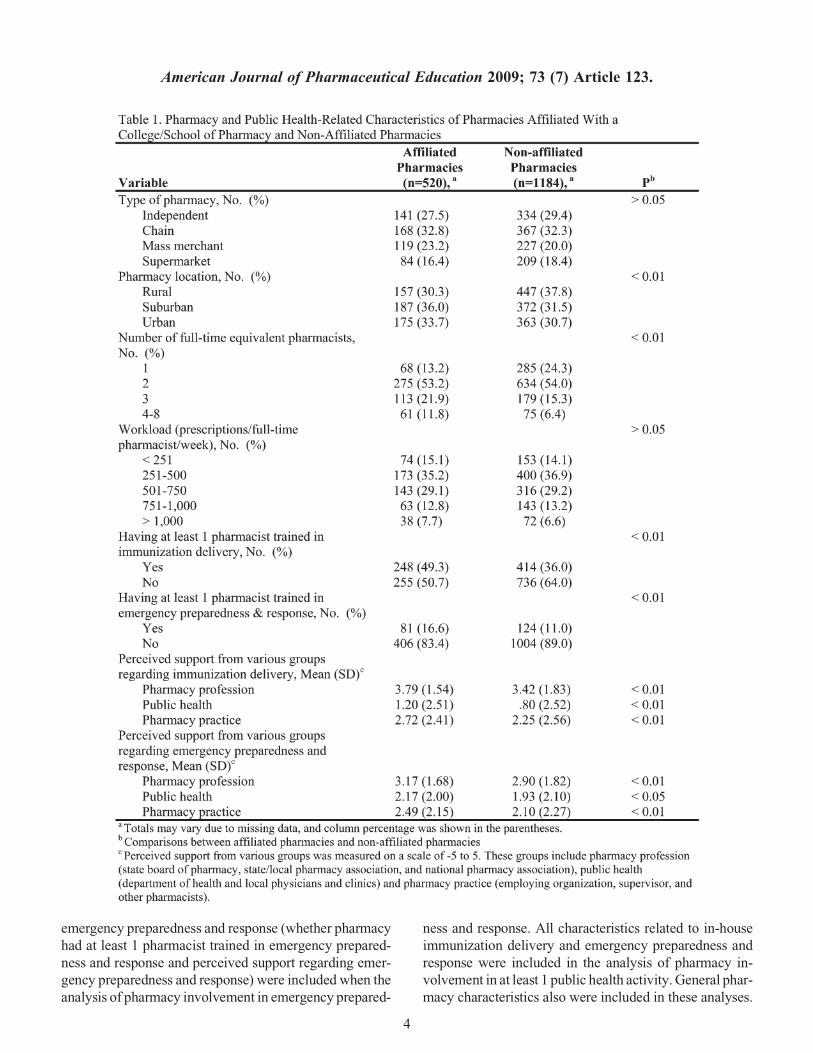
pharmacy characteristics and involvement in emergencypreparedness and response. However, easy-to-contactcases differed from hard-to-contact cases in that thosewho provided immunization services were more promptin responding to the telephone survey request. Of the 1,704(69% response rate) participating pharmacies, 520 wereaffiliated with a college or school of pharmacy and 1,184were not (Table 1). Pharmacies affiliated with pharmacycollege or school differed from non-affiliated pharmaciesin terms of their location (x2 5 9.1; p , 0.01) and numberof full-time equivalent pharmacists (x2 5 43.4; p , 0.01).Pharmacies affiliated with a college/school were morelikely to be located in suburban and urban locations andto employ a greater number of full-time equivalent phar-macists compared to non-affiliated pharmacies. As for thepublic health-related characteristics, pharmacies affiliatedwith a college/school were more likely to have at least 1pharmacist trained in immunization delivery (x2 5 25.8;p , 0.01) and in emergency preparedness and response(x2 5 9.8; p , 0.01). Further, pharmacies affiliated witha college/school perceived a greater level of support fromthe pharmacy profession, public health, and pharmacypractice groups compared to pharmacies that were notaffiliated with a college or school of pharmacy.
Compared to non-affiliated pharmacies, pharmaciesaffiliated with a college/school were more likely to be in-volved in each of the 4 targeted public health activities(Table 2). For example, 28.1% of pharmacies affiliated witha college/school were involved in vaccine distribution,compared to 19.9% of non-affiliated pharmacies (x2 5
13.8; p , 0.01). Pharmacies affiliated with a college/schoolof pharmacy were involved in a greater number of publichealth activities than non-affiliated pharmacies (x2 5 31.1;p , 0.01; Table 2). An independent t test was also employedto examine the difference in the total number of publichealth activities in which affiliated and non-affiliated phar-macies were involved. On average, pharmacies affiliatedwith a college/school engaged in 1.14 activities, which wassignificantly higher than the average of 0.88 activities en-gaged in by non-affiliated pharmacies (t 5 4.99; p , 0.01;data not shown in Table 2).
Even when controlling for the effect of general phar-macy characteristics, pharmacy college/school affiliationremained a significant predictor (Table 3). We next in-cluded public health-related characteristics in logistic re-gression analyses (Table 4). Characteristics related toimmunization delivery (whether pharmacy had at least 1pharmacist trained in immunization delivery and perceivedsupport regarding immunization delivery) were included inthe analyses of pharmacy involvement in immuniza-tion promotion, vaccine distribution, and in-house immu-nization delivery. Similarly, characteristics related to
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
3
emergency preparedness and response (whether pharmacyhad at least 1 pharmacist trained in emergency prepared-ness and response and perceived support regarding emer-gency preparedness and response) were included when theanalysis of pharmacy involvement in emergency prepared-
ness and response. All characteristics related to in-houseimmunization delivery and emergency preparedness andresponse were included in the analysis of pharmacy in-volvement in at least 1 public health activity. General phar-macy characteristics also were included in these analyses.
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
4
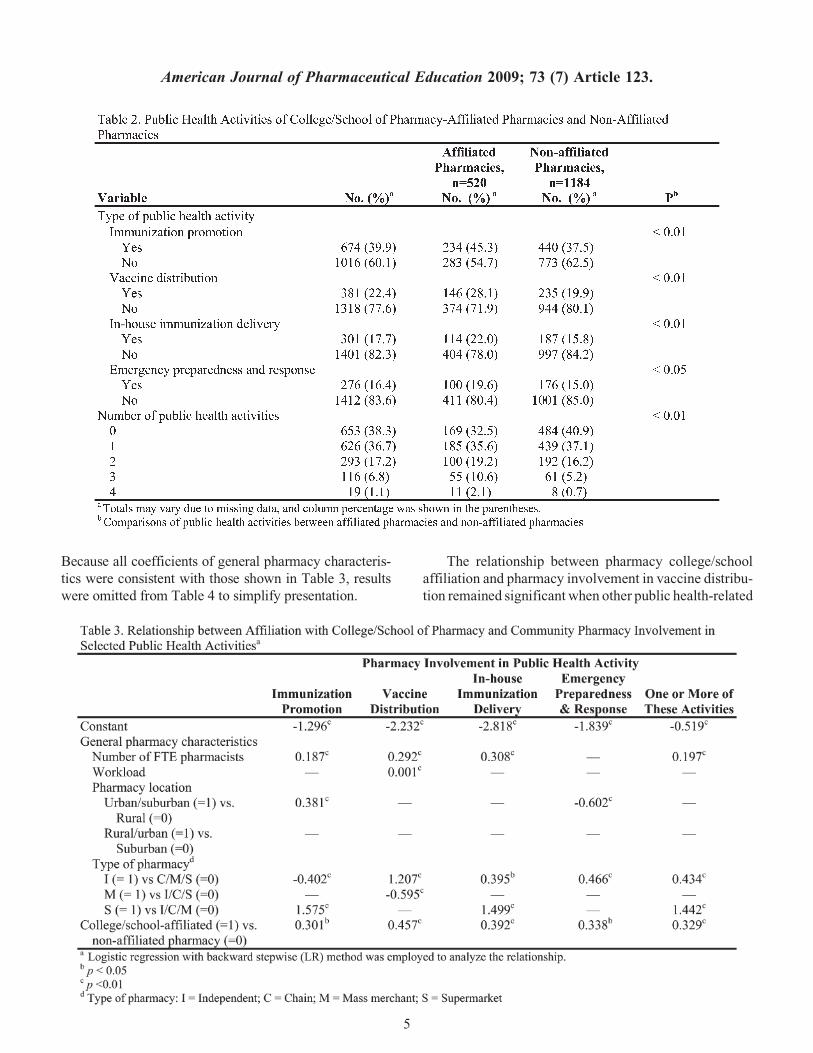
Because all coefficients of general pharmacy characteris-tics were consistent with those shown in Table 3, resultswere omitted from Table 4 to simplify presentation.
The relationship between pharmacy college/schoolaffiliation and pharmacy involvement in vaccine distribu-tion remained significant when other public health-related
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
5
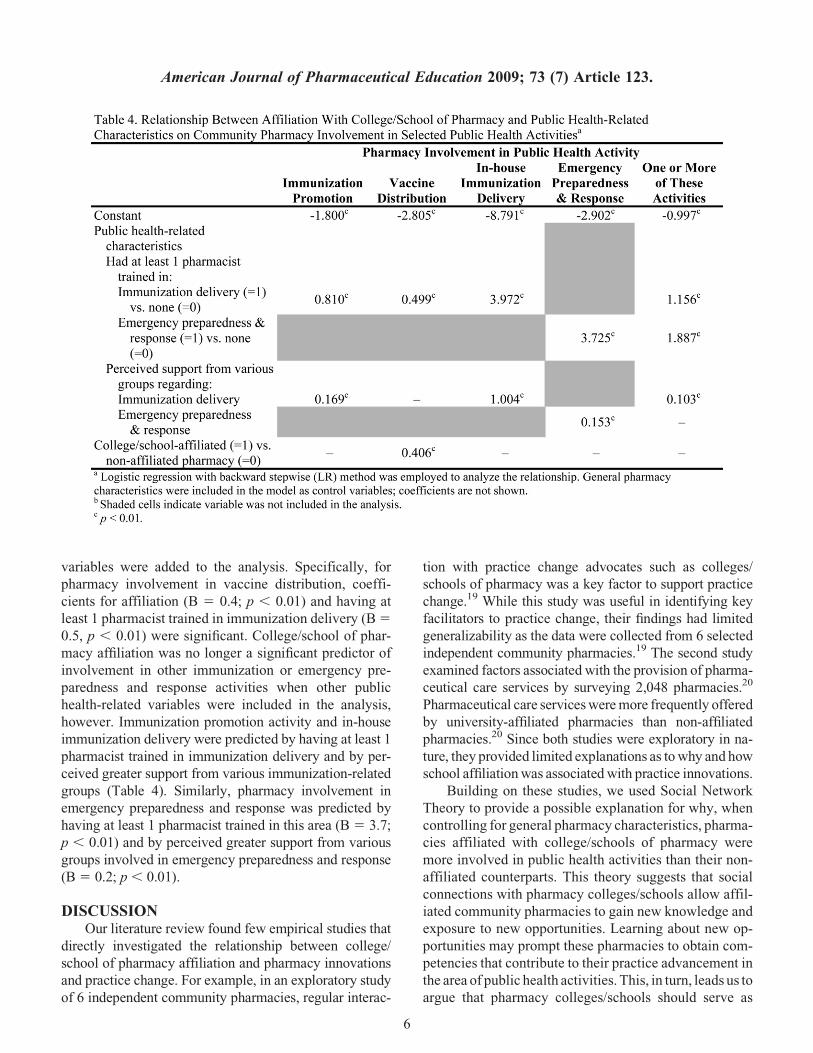
variables were added to the analysis. Specifically, forpharmacy involvement in vaccine distribution, coeffi-cients for affiliation (B 5 0.4; p , 0.01) and having atleast 1 pharmacist trained in immunization delivery (B 5
0.5, p , 0.01) were significant. College/school of phar-macy affiliation was no longer a significant predictor ofinvolvement in other immunization or emergency pre-paredness and response activities when other publichealth-related variables were included in the analysis,however. Immunization promotion activity and in-houseimmunization delivery were predicted by having at least 1pharmacist trained in immunization delivery and by per-ceived greater support from various immunization-relatedgroups (Table 4). Similarly, pharmacy involvement inemergency preparedness and response was predicted byhaving at least 1 pharmacist trained in this area (B 5 3.7;p , 0.01) and by perceived greater support from variousgroups involved in emergency preparedness and response(B 5 0.2; p , 0.01).
DISCUSSIONOur literature review found few empirical studies that
directly investigated the relationship between college/school of pharmacy affiliation and pharmacy innovationsand practice change. For example, in an exploratory studyof 6 independent community pharmacies, regular interac-
tion with practice change advocates such as colleges/schools of pharmacy was a key factor to support practicechange.19 While this study was useful in identifying keyfacilitators to practice change, their findings had limitedgeneralizability as the data were collected from 6 selectedindependent community pharmacies.19 The second studyexamined factors associated with the provision of pharma-ceutical care services by surveying 2,048 pharmacies.20
Pharmaceutical care services were more frequently offeredby university-affiliated pharmacies than non-affiliatedpharmacies.20 Since both studies were exploratory in na-ture, they provided limited explanations as to why and howschool affiliation was associated with practice innovations.
Building on these studies, we used Social NetworkTheory to provide a possible explanation for why, whencontrolling for general pharmacy characteristics, pharma-cies affiliated with college/schools of pharmacy weremore involved in public health activities than their non-affiliated counterparts. This theory suggests that socialconnections with pharmacy colleges/schools allow affil-iated community pharmacies to gain new knowledge andexposure to new opportunities. Learning about new op-portunities may prompt these pharmacies to obtain com-petencies that contribute to their practice advancement inthe area of public health activities. This, in turn, leads us toargue that pharmacy colleges/schools should serve as
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
6

change agents by facilitating the diffusion of public healthactivities among community pharmacies.21 To accom-plish this, colleges and schools should introduce innova-tive ideas in community pharmacies, assist practitionersin developing a need for change, help practitionerstranslate intent to change into action, and stabilize theadoption of new practices.21 Relationships developedthrough network connections between community phar-macies and pharmacy colleges/schools are mutuallybeneficial. For example, community pharmacies thatserve as experiential education sites may learn new ideasfrom preceptor training programs offered by colleges/schools and subsequently develop their competenciesto build competitive advantage. Benefits for the college/school of pharmacy result when students gain experi-ences during their experiential education and ultimatelyare able to achieve the outcomes at the level specified byCAPE.3
Public health-related variables were added to themodel; The effects of college/school affiliation dimin-ished. This was true for all selected public health activitiesexcept vaccine distribution. These findings do not contra-dict our previous explanations of the relationship betweencollege/school and pharmacy involvement in publichealth activities; instead, they provide additional insightsinto the importance of social networks. First, the findingsemphasized the importance of having at least 1 staff phar-macist who was trained in immunization delivery oremergency preparedness and response. Through connec-tions with a college/school of pharmacy, staff pharmacistsmay have been exposed to new opportunities and thussought formal training to advance their practice sites.We recommend that to facilitate pharmacy involvementin public health activities colleges/school of pharmacyoffer training programs in immunization delivery andemergency preparedness and response for communitypharmacies on a regular basis. Second, another significantfactor included in the analysis was the degree of perceivedsupport for public health activities; community pharma-cies were more likely to participate in public health ac-tivities if they perceived a greater degree of support fromvarious groups, including physicians and clinics, healthdepartments, employing organizations, and the stateboard of pharmacy. Similar to the explanation givenabove for affiliation with a college/school of pharmacy,network connections between community pharmacies andthese groups may help facilitate the implementation ofpublic health activities. For example, for pharmacies toprovide in-house immunization services, state boards ofpharmacy need to grant or recognize authority for pharma-cists in their states to administer vaccines, employing or-ganizations and supervisors need to provide support for
immunization activities, and physicians need to providesupport by referring patients to and/or entering into col-laborative practice agreements with community pharma-cies. Without such supports, community pharmaciescannot engage in successful public health activities. Forthis reason, we also recommend that colleges/schools ofpharmacy communicate with these groups regarding howpharmacists and pharmacies can help to promote publichealth.
Our study uses Social Network Theory to offer oneexplanation for the relationships between affiliation witha college/school of pharmacy and pharmacies involve-ment in public health activities. Since a key limitationof this study is its use of cross-sectional data, causal ef-fects cannot be established and at least 2 alternative ex-planations for these findings should be noted. First,pharmacy involvement in public health could facilitateaffiliation with a college/school of pharmacy. That is,pharmacies that are involved in public health may beattractive to colleges/schools of pharmacy, promptingthe colleges/schools to seek out these pharmacies andask to collaborate with them, for example, by serving asexperiential education sites or participating in a practice-based research network. A second alternative explanationfor our results is that the significant relationship betweenaffiliation with a pharmacy college/school and pharmacyinvolvement in public health activities was a result ofa spurious effect. That is, affiliation may have had nocausal connection with public health involvement; in-stead both variables could have been caused by a thirdfactor, such as being an innovative practitioner. For ex-ample, an innovative practitioner might both affiliatewith a pharmacy college/school and provide publichealth-related services. Since our study could not estab-lish causal effect, future research should examine pro-cesses that could further explain the relationship betweencollege/school of pharmacy affiliation and pharmacyinvolvement in public health or other innovations. Astudy of the processes in which pharmacy schools attractand collaborate with experiential education sites couldprovide important insights into research questions suchas: How did connection between the pharmacy and thecollege/school originate? What characteristics attractedthe college/school to the pharmacy and/or the pharmacyto the college/school? What types of assistance do expe-riential education sites receive from colleges/schools ofpharmacy and what effects do these have? And what aremechanisms used by the college/school of pharmacy toadvance experiential education sites?
Our study shows that affiliation with colleges/schoolswas positively associated with community pharmacies’involvement in public health activities. We recognize that
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
7

the nature of college/school affiliation may differ acrossparticipating pharmacies; for example, some affiliatedpharmacies serve as experiential education sites whileothers serve as practice-based research sites. Therefore,future research should address the following questions:What is the nature and strength of college/school affilia-tion(s) in relation to pharmacy involvement in publichealth activities or other innovative practices? How dodifferent types of college/school affiliation influencepharmacy involvement in public health activities or in-novative practices? How might the influence of affiliationbe enhanced?
Experiential education sites that engage in publichealth activities are needed to provide adequate opportuni-ties for students to actively participate in pharmacy-basedpublic health activities and acquire in-depth experiencesin public health activities. College/school of pharmacygoals are to ensure that student learning achieves theCAPE outcomes and prepare them for expanded publichealth roles. Because little is known about how best toimprove student learning outcomes related to public health,colleges and schools of pharmacy should reexamine theircurricula to ensure that competencies in public health areadequately achieved to prepare future pharmacists.22 Fu-ture research should explore the following possible re-search questions: To what extent do students engage inpublic health activities during pharmacy practice experi-ences? What mechanisms used in experiential educationsites improve student learning outcomes? And whatmethods can best prepare students to carry out key publichealth activities?
LimitationsBeyond reliance on cross-sectional data, certain
limitations need to be considered when interpreting andgeneralizing the results presented here. First, key infor-mants may have been subject to recall errors. We did notbelieve this was a problem, as key informants were ableto access pharmacy records while being interviewed. Sec-ond, this study investigated the effects of only particularfactors; it did not evaluate all factors that may be associ-ated with pharmacy involvement in public health activi-ties. Lastly, the study may have limited generalizabilityto nonrespondents, other states beyond the 17 study states,other public health activities, and pharmacy practiceinnovations.
CONCLUSIONPharmacy college/school-affiliated community phar-
macies were more likely than non-affiliated pharmaciesto participate in public health activities. However, affili-ation generally became nonsignificant when other
public health-related characteristics were included inthe analysis. Research further examining how best to de-velop experiential education sites and improve student-learning outcomes related to public health activities isneeded.
ACKNOWLEDGEMENTSThis research was supported by grant R06-CCR
523387 from the Public Health Law Program of the USCenters for Disease Control and Prevention (CDC). Theideas expressed in this manuscript are those of the authorsand in no way are intended to represent the position ofUniversity of Wisconsin-Madison School of Pharmacyand Harrison School of Pharmacy Auburn University.
REFERENCES1. Babb VJ, Babb J. Pharmacist involvement in healthy people2010. J Am Pharm Assoc. 2003;43(1):56-60.2. Hurd PD, Levin BL, Hanson A. Introduction and overview ofpharmacy and public health. In Levin BL, Hurd PD, Hanson A, eds.Introduction to Public Health in Pharmacy. Sadbury, MA: Jones andBartlett Publishers; 2007: 1-15.3. American Association of Colleges of Pharmacy, Center for theAdvancement of Pharmaceutical Education (CAPE). Educationaloutcomes, revised version 2004. http://www.aacp.org/resources/education/Documents/CAPE2004.pdf Accessed October 20, 2009.4. Accreditation Council for Pharmacy Education. AccreditationStandards and Guidelines for the Professional Program in PharmacyLeading to the Doctor of Pharmacy Degree (ACPE Standards2007). http://www.acpe-accredit.org/pdf/ACPE_Revised_PharmD_Standards_Adopted_Jan152006.pdf Accessed October 20, 2009.5. Crawford SY. Pharmacists’ roles in health promotion anddisease prevention. Am J Pharm Educ. 2005;69(4):534-540.6. Globe DR, Johnson K, Conant L, Frausto S. Implementinga community-based health promotion program into the pharmacycurriculum: the USC FUENTE initiative. Am J Pharm Educ.2004;68(2):Article 32.7. Doty RE, Latham KM, Stewart RB. Public health screenings asa component of introductory practice experiences. Am J Pharm Educ.2000;64(4):425-430.8. Anderson AS, Goode J-VR. Engaging students in wellness anddisease prevention services. Am J Pharm Educ. 2006;70(2):Article 40.9. Beck DE, Thomas SG, Janer AL. Introductory practiceexperiences: a conceptual framework. Am J Pharm Educ.1996;60(2):122-131.10. Cerulli J. Experiential education in community pharmacy. Am JPharm Educ. 2006;70(1):Article 19.11. Speedie M. Introductory experiential education: a means forintroducing concepts of healthcare improvement. Am J Pharm Educ.2006;70(6):Article 145.12. Blau PM, Scott WR. Formal Organizations: A ComparativeApproach. Stanford: CA: Stanford University Press; 2003.13. Gresov C, Stephens C. The context of interunit influenceattempts. Adm Sci Q. 1993;38(2):252-276.14. Venkataraman S, ed. The distinctive domain of entrepreneurshipresearch. In: Katz, JA, ed. Advances in Entrepreneurship, FirmEmergence and Growth; No. 3. Greenwich, CT: JAI Press; 1997.
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
8

15. Tsai W. Knowledge transfer in intraorganizational networks:effects of network position and absorptive capacity on business unitinnovation and performance. Acad Manage J. 2001(5);44:996-1004.16. Ahuja G. Collaboration networks, structural holes, andinnovation: a longitudinal study. Adm Sci Q. 2000;45(3):425-455.17. Westrick SC, Mount JK, Watcharadamrongkun S, Breland ML.Pharmacy stages of involvement in pharmacy-based immunizationservices: results from a 17-state survey. J Am Pharm Assoc.2008;48(6):764-773.18. Westrick SC, Mount JK. Effects of repeated callbacks onresponse rate and nonresponse bias: results from a 17-state pharmacysurvey. Res Social Adm Pharm. 2008;4(1):46-58.
19. Doucette WR, Koch YD. An exploratory study of communitypharmacy practice change. J Am Pharm Assoc. 2000;40(3):384-391.20. McDermott JH, Christensen DB. Provision of pharmaceuticalcare services in North Carolina: a 1999 survey. J Am Pharm Assoc.2002(1);42:26-35.21. Rogers EM. Diffusion of Innovations. 5th ed. New York: FreePress; 2003.22. O’Neil CK, Levin BL, Hanson A. Education and training. In:Levin BL, Hurd PD, Hanson A, eds. Introduction to public health inpharmacy. Sudbury, MA: Jones and Bartlett Publishers; 2008:337-350.
American Journal of Pharmaceutical Education 2009; 73 (7) Article 123.
9