cognitive and emotion regulation change processes in cognitive behavioural therapy for social...
TRANSCRIPT

Cognitive and Emotion Regulation ChangeProcesses in Cognitive BehaviouralTherapy for Social Anxiety Disorder
Mia S. O’Toole,1* Douglas S. Mennin,2 Esben Hougaard,1 Robert Zachariae1and Nicole K. Rosenberg31Department of Psychology and Behavioral Sciences, Aarhus University, Aarhus, Denmark2Department of Psychology, Hunter College, City University of New York, New York City, NY, USA3Clinic for Anxiety Disorders, Aarhus University Hospital, Risskov, Denmark
The objective of the study was to investigate variables, derived from both cognitive and emotion regu-lation conceptualizations of social anxiety disorder (SAD), as possible change processes in cognitive be-haviour therapy (CBT) for SAD. Several proposed change processes were investigated: estimatedprobability, estimated cost, safety behaviours, acceptance of emotions, cognitive reappraisal and expres-sive suppression. Participants were 50 patients with SAD, receiving a standard manualized CBTprogram, conducted in groups or individually. All variables were measured pre-therapy, mid-therapyand post-therapy. Lower level mediation models revealed that while a change in most process measuressignificantly predicted clinical improvement, only changes in estimated probability and cost and accep-tance of emotions showed significant indirect effects of CBT for SAD. The results are in accordancewith previous studies supporting the mediating role of changes in cognitive distortions in CBT forSAD. In addition, acceptance of emotions may also be a critical component to clinical improvementin SAD during CBT, although more research is needed on which elements of acceptance are mosthelpful for individuals with SAD. The study’s lack of a control condition limits any conclusion regard-ing the specificity of the findings to CBT. Copyright © 2013 John Wiley & Sons, Ltd.
Key Practitioner Message:• Change in estimated probability and cost, and acceptance of emotions showed an indirect effect of CBT
for SAD.• Cognitive distortions appear relevant to target with cognitive restructuring techniques.• Finding acceptance to have an indirect effect could be interpreted as support for contemporary CBT
approaches that include acceptance-based strategies.
Keywords: Social Phobia, CBT, Mediation, Emotion Regulation, Cognitive Distortion, Acceptance
INTRODUCTION
Social anxiety disorder (SAD) is one of the most commonpsychological conditions (Ramshaw, Chavira, & Stein,2010). SAD is defined by a marked and persistent fear ofone or more social situations, and if an individual fearsmost social situations, the condition may be specified asgeneralized SAD (in DSM-IV; APA, 2000). Untreated,SAD tends to run a chronic course and be associated withlower work productivity, impaired functioning in socialrelationships and poor quality of life (Hofmann & Bögels,2006; Wittchen et al., 2000). Although cognitive behav-ioural therapy (CBT) is a well-documented, effective
treatment for SAD (Pontoski, Heimberg, Turk, & Coles,2010), a large portion of patients (25–50%) does not oronly partially responds to therapy (Heimberg et al., 1998;Herbert et al., 2005; Hofmann & Bögels, 2006). Little isknown about how CBT works both for SAD and for othermental disorders (Kazdin, 2007). As argued Kazdin(2007), an understanding of why and how treatmentfacilitates change can aid in focusing more specificallyon crucial components of treatment packages, therebymaking it possible to develop effective augmentationstrategies. For this reason, studies of change processes orchange mechanisms may be one of the most critical areasof psychotherapy research.Cognitive behavioural theories of SAD propose that
distorted cognitions and safety behaviours are responsiblefor developing and maintaining SAD (Clark & Wells,1995; Rapee & Heimberg, 1997). Distorted cognitions
*Correspondence to: Mia Skytte O’Toole, Department of Psychologyand Behavioral Sciences, Aarhus University, Aarhus C, 8000, Denmark.E-mail: [email protected]
Clinical Psychology and PsychotherapyClin. Psychol. Psychother. (2014)Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/cpp.1926
Copyright © 2014 John Wiley & Sons, Ltd.

include overestimation of the probability and/or costs ofvarious negative social situations (e.g., the likelihood thatsomeone will reject you [i.e., probability] and theemotional consequences associated with it [i.e., cost];McManus, Clark, & Hackmann, 2000), whereas safety be-haviours refer to a range of strategies designed to reducethe likelihood of negative evaluation by others in thefeared social situations (Cuming et al., 2009). Correspond-ingly, CBT aims to change distorted cognitions anddysfunctional safety behaviour, and these changes areproposed to be central change processes in CBT for SAD.A complementary conceptualization of change in CBT is
based on emotion regulation theory (Gross & Thompson,2007), which has achieved growing influence within thearea of anxiety disorders in the last 10 years (Rodebaugh& Heimberg, 2008). Emotion regulation strategies suchas cognitive reappraisal and expressive suppression havereceived most attention. Cognitive reappraisal is definedas changing one’s thinking about a situation in a way thatalters its emotional impact (Gross & Thompson, 2007),and expressive suppression concerns the conscious effortto hide emotional expressions (Gross & Thompson,2007). Socially anxious individuals have been found tobe, and believe they are, less effective at employingcognitive reappraisal (Goldin, Manber, et al., 2009;Goldin, Manber-Ball, et al., 2009; Werner et al., 2011), whileothers have failed to find this association (Kashdan &Steger, 2006). Regarding expressive suppression, thisstrategy has been found to be highly characteristic ofindividuals with SAD (Turk et al., 2005; Werner et al.,2011). Although realistic reappraisal of emotional situa-tions is directly targeted in CBT, there has not been muchexplicit focus on changing expressive suppression(Hofmann & Asmundson, 2008). Expressive suppressionmay, however, be considered a type of safety behaviour(e.g., attempts at concealing anxiety symptoms, such ashiding one is shaking by keeping hands busy) (Vonken,Alden, & Bögels, 2006), which is directly targeted inCBT. Another emotion regulation strategy, namely accep-tance of emotions, is considered an important therapeuticgoal in newer, so called ‘third wave’ therapies, likeacceptance and commitment therapy (ACT; Hayes, 2004).Exposure in CBT involves confronting the anxiety provok-ing stimulus despite being anxious, which, besidescontributing to desensitization/habituation, may also leadto a reduction of emotion suppression and an increase inacceptance (Arch & Craske, 2008). Thus, an increase inacceptance could be considered an additional theory ofchange in CBT.The distinction between cognitive variables and emo-
tion regulation variables should not be considered a sharpdichotomy. Rather, the variables are derived from two dif-ferent models, embedded within two different traditions,each granting different weights to the specific roles ofcognition and emotion. We would like to think of the
variables as different ways of talking about targeting thearising emotions in SAD as described in the process modelof emotion regulation (Gross & Thompson, 2007). Thismodel differentiates between antecedent-focused andresponse-focused emotion regulation strategies, whereantecedent-focused strategies are employed before theemotion fully unfolds, and response-focused strategiesare aimed at changing the emotional responses after theyhave been generated.Studies on change processes in CBT for SAD are rather
few in number. Most studies have relied on a simple corre-lational pre-post design, measuring process and outcomevariables before and after therapy (e.g., Boden et al.,2012; Foa, Franklin, Perry, & Herbert, 1996; Goldin et al.,2012; Hofmann, 2004; McManus et al., 2000). Of these, onestudy found that a reduction in maladaptive beliefs, typi-cally found in SAD, was associated with clinical improve-ment (Boden et al., 2012). Some have found inflatedprobability estimates (McManus et al., 2000), others inflatedcost estimates (Foa et al., 1996; Hofmann, 2004) to be associ-atedwith symptom reduction. Goldin and colleagues (2012)found that CBT improved cognitive reappraisal self-efficacy(i.e., the belief that one can successfully employ cognitivereappraisal) and that cognitive reappraisal self-efficacymediated the effect of individual CBT on symptoms ofsocial anxiety.Some studies have attempted to handle the causality
question by experimentally manipulating the processvariable. Both Morgan and Raffle (1999) and Wells, Clark,Salkovskis, and Ludgate (1995) compared two exposureconditions, one without and one with the instruction toavoid the use of safety behaviours, with the latter condi-tion outperforming the former. Similarly, Rapee, Gaston,and Abbot (2009) compared CBT courses with and with-out specifically addressing cognitive biases and safetybehaviours. They found that estimated cost, but not safetybehaviours, was significantly more reduced in the CBTcondition in which the cognitive biases and safety behav-iours were directly targeted.A few studies have used repeated measures of both the
outcome and proposed mediators during the therapycourse. Smits, Rosenfield, McDonald, and Telch (2006) in-vestigated estimated probability and cost and found thatonly changes in estimated probability predicted subse-quent symptom changes in exposure treatment for SAD.Hoffart, Borge, Sexton, and Clark (2009) found thatchanges in cognitive biases, both probability and cost,safety behaviours and changes in acceptance by others,predicted subsequent symptom change in both cognitiveand interpersonal therapy. In both of these studies, how-ever, change in outcome variables also predicted subse-quent change in the proposed mediators, indicatingbidirectional associations between variables. Moscovitchand colleagues (2012) repeatedly measured both cognitiveand emotion regulation variables during CBT. They found
M. S. O’Toole et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

that an early acquisition of cognitive reappraisal skills pre-dicted a subsequent reduction in symptoms of social anx-iety, which was not the case for expressive suppression.Finally, Dalrymple and Herbert (2007), also in a studywith multiple measuring points, found that an initial in-crease in acceptance of emotions predicted later clinicalimprovement of SAD.Taken together, there is a relatively small number of
studies aimed at investigating mediators in CBT forSAD. Generally, the studies have generated only a fewpositive results that have been somewhat mixed, and onlya few studies have jointly investigated some of the abovepresented emotion regulation and cognitive behaviouralvariables.
Aims and Hypotheses
With the present study, we wanted to repeat and extendparts of the previous body of research in this field. Severalproposed processes of change derived from cognitive andemotion regulation theories were therefore simultaneouslyinvestigated at three measuring points: pre-therapy, mid-therapy and post-therapy. The aim was to investigatechange processes in CBT for SAD. Based on prior findings,it was hypothesized that a change in (1) cognitive distor-tions (estimated probability and cost), (2) safety behaviours,including expressive suppression, (3) cognitive reappraisaland (4) acceptance would show an indirect effect of CBTfor SAD.
METHODS
Participants
Participants were consecutively recruited from an outpa-tient anxiety clinic at Aarhus University Hospital,Denmark, which is a specialized facility for severe casesof anxiety disorders. The inclusion criterion was a primarydiagnosis of SAD. Exclusion criteria were a cluster A or Bpersonality disorder, psychotic disorders and bipolar dis-orders. Patients were also excluded if they had undergonea full therapeutic course at the clinic within 12monthsprior to the inclusion point, since such clients were notoffered the standard CBT program. All patients wereinterviewed with the Anxiety Disorders Interview Sched-ule for DSM-IV (ADIS-IV; Brown, DiNardo, & Barlow,1994). Diagnostic interviews were conducted by clinicianswho all had either a master’s or PhD degree in psychol-ogy, except for one occupational therapist that had under-gone clinical training. All clinicians were trained andexperienced in using the ADIS-IV and met on a weeklybasis to peer supervise diagnoses.
Fifty-seven participants were included in the study dur-ing the recruitment period (1.5 years), which was deter-mined by practical issues at the clinic. A total of sevenpatients dropped out of therapy before the last sessionwithout filling out the mid-therapy and post-therapyquestionnaires. Of these, five stopped without givingnotice, and twomentioned that they no longer needed ther-apy. Because the present study was not an outcome study,the seven individuals were excluded from the analyses.All participants had generalized SAD. Their mean age
was 31.7 years (SD=9.5), 64% were women, and all wereCaucasian. Thirty-two participants (64%) were employedor in school, and 26 (52%) claimed that their disorderprevented them from keeping a job or completing an edu-cation. Thirty-seven participants (74%) had a comorbidanxiety or depression diagnosis (5 had a comorbid anxietydisorder, 25 had a depressive disorder, including episodicdepression in remission, 7 had both a comorbid anxietyand depressive disorder). Twenty-seven participants(54%) received psychopharmacological treatment, primar-ily selective serotonin reuptake inhibitors and serotonin–norepinephrine reuptake inhibitors.
Treatment
All clinicians had completed or were enrolled in a national2-year psychotherapy training course specializing in CBT.The standard treatment of choice at the clinic was a groupCBT program led by two clinicians, but participants whoinsisted were offered individual therapy. Individual andgroup therapy followed the same manualized CBT pro-gram for SAD inspired by Clark and Wells (1995) andHeimberg and Becker (2002).1 The program includedpsychoeducation, cognitive restructuring, attentionaltraining, gradual exposure and behavioural experiments.Homework exercises consisted of symptom diaries,cognitive restructuring exercises and individualizedexposure/behavioural experiments. The first half of thetherapeutic course mostly concerned cognitive skills,whereas exposure exercises and behavioural experimentswere primarily stressed in the latter half. During the study,an unforeseen change in the treatment program occurred,due to the public health care system’s aim at reducingcosts of treatment, which resulted in a shortening of theduration of therapy from 13 to 10 sessions (however, afew individual treatments were extended up to 16 ses-sions; n=6 in the present study). Therapy was providedonce a week, although some individual sessions wererescheduled due to cancellations. Regardless of the dura-tion of therapy, participants received the full treatmentprogram including all main components.
1For a copy of the manual materials, please email the correspondingauthor.
Change Processes in CBT for SAD
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

Forty participants received group therapy (80%). Atbaseline, there were no differences regarding age,symptom severity (LSAS) or any of the proposed processmeasures between participants that had received groupor individual therapy; received or did not receive psycho-pharmacological treatment and had or did not have acomorbid anxiety or depressive disorder. There was nodifference in number of completed sessions in group(M=10.5, SD=2.0, range: 6–14) and individual therapy(M=10.6, SD=2.5, range: 7–16), t(48) =�0.2, p=0.866.Linear mixed models showed no interaction of group(group versus individual CBT: t(101.1) = 0.6, p=0.457; con-current psychopharmacological treatment: t(96.9) = 0.8,p=0.400; comorbidity: t(100.7) =�0.5, p=0.648) by timeon the outcome (LSAS). Subsequent analyses were there-fore conducted on the whole sample.
Measures
All measures were self-report measures. Cronbach’salphas were calculated before mean substitution (see pro-cedure below) and refer to internal reliability at the threetime points: pre-therapy, mid-therapy and post-therapy.
Outcome MeasureThe Liebowitz Social Anxiety Scale (LSAS; Liebowitz,
1987) is a 24-item measure of symptoms of social anxiety,here used in its self-report version. The scale can be sepa-rately scored for fear in and avoidance of various socialsituations. In this study, the full scale was used. Cronbach’sα in the present sample was found to be 0.94/0.95/0.97.
Process MeasuresThe Social Probability and Cost Questionnaire (SPCQ;
McManus et al., 2000, adapted from Foa et al., 1996) asksthe participants to rate the probability and cost on a scalefrom 0 to 100 of 33 negative social events. Half of theevents are concerned with the individual’s performance inthe situation (e.g., ”I will make a mistake in front of mycolleagues”), whereas the others are not (e.g., ”a friendwill cancel an agreement to meet me”). Cronbach’s α forthe probability scale was 0.94/0.93/0.97; for the cost scale,it was 0.94/0.96/0.97.
The Subtle Avoidance and Frequency Examination(SAFE; Cuming et al., 2009) was used as a measure of in-situation safety behaviours. The scale consists of 32 itemsthat can be scored from 1 to 7. The scale includes threefactor analytically derived subscales: active safety behav-iours (e.g., ‘remain silent’), subtle restriction behaviours(e.g., ‘rehearse sentences in your mind’) and behavioursaimed at avoiding or concealing physical symptoms(e.g., ‘wear clothes or makeup to hide blushing’).Cronbach’s α for the full scale was 0.85/0.86/0.87.
Reappraisal and expressive suppressionwere assessed bythe Emotion Regulation Questionnaire (ERQ; Gross & John,2003). The questionnaire consists of 10 items: 6 concerningcognitive reappraisal and 4 expressive suppression. The itemsare rated on a 7-point scale. Cronbach’s α for the six reap-praisal items was 0.89/0.80/0.79; Cronbach’s α for the fourexpressive suppression items was 0.63/0.65/0.79.
The Acceptance and Action Questionnaire (AAQ-I;Hayes et al., 2004) was used as a measure of acceptanceof emotions. The scale consists of 16 items that are ratedon a 7-point scale. Cronbach’s α was 0.68/0.71/0.73. TheAAQ-II was not published at the time of the study’s datacollection.
Procedure
Measures were administered three times: before therapy,after the fifth session of therapy (the mid-point in mosttherapeutic courses) and after therapy. Pre-therapy andpost-therapy questionnaires were mailed to participantsfor them to return by mail in a stamped addressed enve-lope (no more than a month prior to the beginning of ther-apy and immediately after therapy), while the mid-therapy questionnaires were handed out by the therapistand returned to him/her on the same day or at the nextsession. Informed consent was obtained from all partici-pants following the diagnostic assessment, and the studywas approved by the Danish data protection agency andthe local ethical committee.
Analytic Strategy
Process analyses followed the principles of lower levelmediation (Bauer, Preacher, & Gil, 2006; Kenny,Korchmaros, & Bolger, 2003), where lower level variablesin this case refer to variables measured multiple timesfor each individual.Determination of indirect effects were based on the prod-
uct-of-coefficients approach, which has been recommendedover the Baron and Kenny (1986) causal-steps strategy(MacKinnon, Lockwood, & Williams, 2004; MacKinnonet al., 2002), especially for analyzing multiple mediators(Preacher & Hayes, 2008). This approach calculates theproduct term between two paths (see Figure 1): (1) fromthe independent variable (time) to the process variables(numbered 1 to 6): path a and (2) from the processvariables to the outcome variable (LSAS): path b, in the
Figure 1. The basic mediation model
M. S. O’Toole et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

presence of the independent variable, path c′. Path c is thedirect path from the independent variable to outcomeindependent of the process variables.We tested the total effect of time (path c), that is, the
effectiveness of the treatment. In this model, the timevariable consisted of the number of sessions at the timeof observation (one for pre-therapy, five for mid-therapyand the number of completed session for post-therapy)and predicted the social anxiety symptom score (LSAS)at those time points.Indirect effects of the process variables were separately
investigated, according to the principles described byBauer and colleagues (2006). Following this strategy, allpaths necessary for determining indirect and direct effectsare estimated in one model. A new outcome variable isformed (Z) by stacking the dependent (Y) variable andthe process variable (P) for each time unit iwithin each in-dividual j. In order to distinguish the two variablesstacked in Z, two selection variables are created thatspecify when Z refers to the process variable (SPij) or thedependent variable (SYij) (see Eqn 1).
ZiJ ¼ SPij dPj þ aXij� �þ SYij dYj þ bMij þ c’Xij
� �þ eZij (1)
Finally, all process measures that individually showed astatistical significant indirect effect, see criterion below,were included together in one model. The same analyticprocedure was followed, only more selection variableswere created (cf. Bauer et al., 2006). All models were esti-mated using restricted maximum likelihood.Indirect effects were, as noted above, represented by the
product term for path a and b (ab). In order to assess statis-tical significance of mediation, we calculated the standarderror (SE) of ab following Eqn 10 (cf. Kenny et al., 2003):σ(ab)2 = b2σa
2 + a2σb2 + σa
2σb2, where σ refers to the variance
(SE) of the unstandardized regression coefficient. Thisequation may underestimate the variance of the indirecteffect as it does not take the covariance of path a and pathb (σab) into account as recommended when exploringlower level mediation in multilevel models (Bauer et al.,2006; Kenny et al., 2003). However, σab is calculated basedon the covariance of a and b per upper level unit (j), in this
case individuals. With only three observation points perparticipant and three predicting variables, the SE of bjwould be 0. Therefore, only the intercept was specifiedas random in the models. If the product term of path aand b divided by its standard error, ab/SE(ab), fell aboveor below the critical value of Z=1.96, the indirect effectwas considered statistically significant at p< 0.05.Effect sizes were calculated as the proportion reduction in
variance (PRV), comparing the variance explained in themodelwith orwithout the variables of interest (Raudenbush& Bryk, 2002; Singer & Willett, 2003) (see Eqn 2):
PRV ¼ varNoPredictor � varPredictorð Þ=varNoPredictor (2)
There were only few missing data. Across individualitems, the number of missing data at the item level rangedfrom 0 to 6%. To handle these missing numbers, mean sub-stitution, or ipsative mean imputation, was performed foreach (sub)scale separately, based on the individual’s meanat the specific time point.When scales have an acceptable in-ternal reliability and individuals have less than 50%missingin total on that scale, this method performs well (cf. Schafer& Graham, 2002). In total, the number of individuals withless than 50% missing items on a particular scale, and thusthe number of individuals for whom a mean wassubstituted, ranged from 0 to 10. The number of individualswith more than 50% missing items on a particular scale, andthus individuals for whom the total score was left missing,ranged from 0 and 2 across scales.We controlled for comorbidity and the use of medication
using categorical variables. In order not to compromisepower, these analyses were run separately for each of thecontrol variables.All statistical analyses were performedwith the Statistical
Package for the Social Sciences (SPSS) version 21.
RESULTS
Descriptives
Table 1 provides raw scores for the three observationpoints, and effect sizes for the magnitude of change from
Table 1. Raw scores at the three observation points and effect size of change
Pre-therapyM (SD) (n = 50)
Mid-therapyM (SD) (n= 50)
Post-therapyM (SD) (n= 50)
Effect size (Cohen’s d) for changescores pre-mid/mid-post
Social anxiety (LSAS) 85.5 (23.6) 80.4 (23.7) 60.4 (29.2) 0.53/2.30Probability (SPCQ) 17.3 (6.2) 16.2 (7.1) 13.0 (7.0) 0.55/1.77Cost (SPCQ) 20.2 (5.8) 18.0 (5.9) 14.1 (6.8) 1.16/1.99Safety behaviour (SAFE) 88.3 (14.8) 53.6 (14.1) 76.7 (15.3) 6.49/�4.36Reappraisal (ERQ) 23.2 (7.8) 26.8 (5.3) 28.4 (4.6) �1.15/�.07Expressive suppression (ERQ) 15.9 (4.8) 15.9 (4.4) 14.2 (4.9) �0.04/0.87Acceptance (AAQ) 57.2 (9.3) 61.0 (9.5) 63.5 (9.8) �0.97/�0.93
Change Processes in CBT for SAD
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)
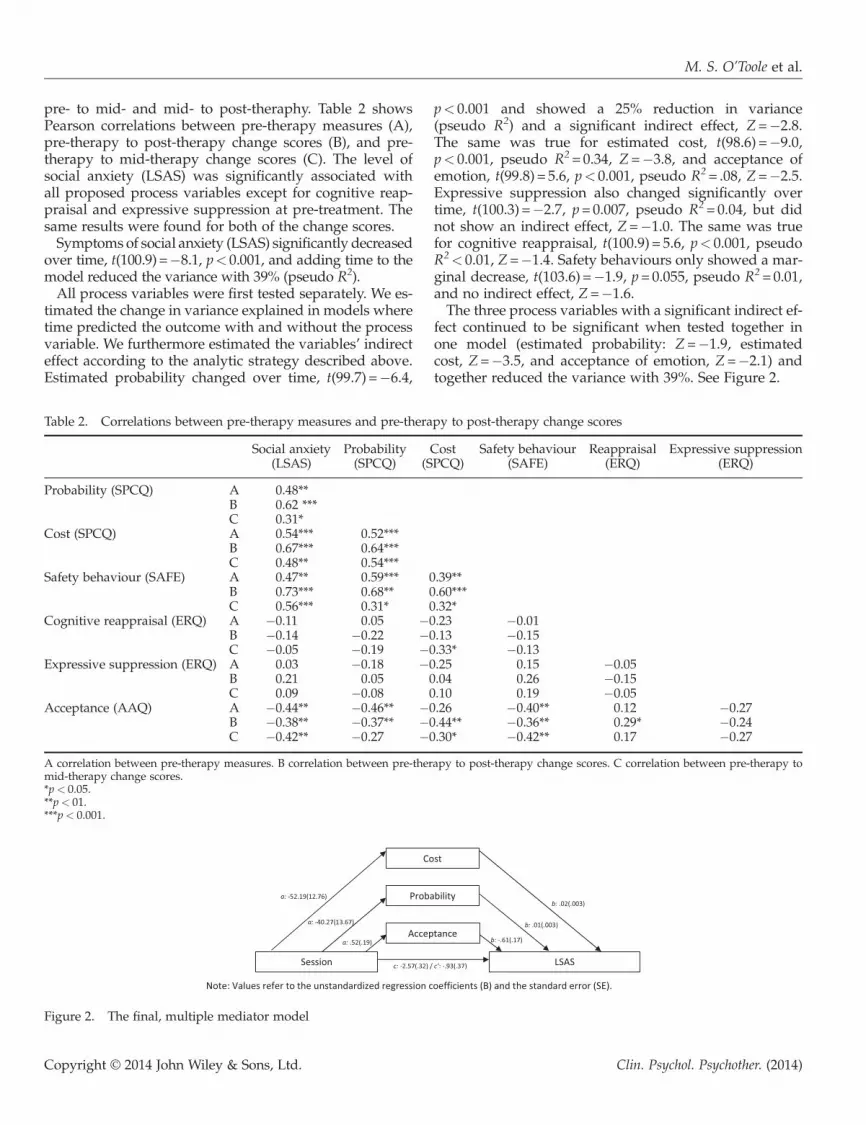
pre- to mid- and mid- to post-theraphy. Table 2 showsPearson correlations between pre-therapy measures (A),pre-therapy to post-therapy change scores (B), and pre-therapy to mid-therapy change scores (C). The level ofsocial anxiety (LSAS) was significantly associated withall proposed process variables except for cognitive reap-praisal and expressive suppression at pre-treatment. Thesame results were found for both of the change scores.Symptoms of social anxiety (LSAS) significantly decreased
over time, t(100.9) =�8.1, p< 0.001, and adding time to themodel reduced the variance with 39% (pseudo R2).All process variables were first tested separately. We es-
timated the change in variance explained in models wheretime predicted the outcome with and without the processvariable. We furthermore estimated the variables’ indirecteffect according to the analytic strategy described above.Estimated probability changed over time, t(99.7) =�6.4,
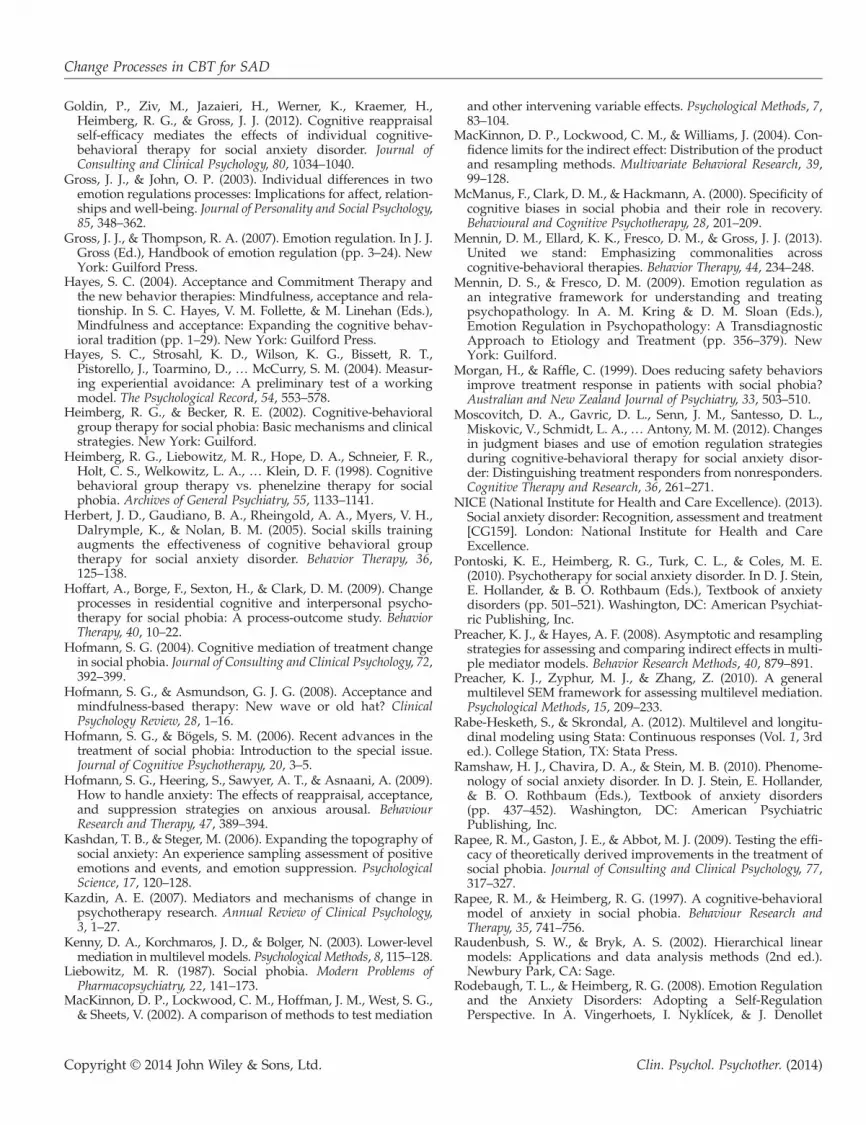
p< 0.001 and showed a 25% reduction in variance(pseudo R2) and a significant indirect effect, Z=�2.8.The same was true for estimated cost, t(98.6) =�9.0,p< 0.001, pseudo R2=0.34, Z=�3.8, and acceptance ofemotion, t(99.8) = 5.6, p< 0.001, pseudo R2= .08, Z=�2.5.Expressive suppression also changed significantly overtime, t(100.3) =�2.7, p=0.007, pseudo R2=0.04, but didnot show an indirect effect, Z=�1.0. The same was truefor cognitive reappraisal, t(100.9) = 5.6, p< 0.001, pseudoR2< 0.01, Z=�1.4. Safety behaviours only showed a mar-ginal decrease, t(103.6) =�1.9, p=0.055, pseudo R2=0.01,and no indirect effect, Z=�1.6.The three process variables with a significant indirect ef-
fect continued to be significant when tested together inone model (estimated probability: Z=�1.9, estimatedcost, Z=�3.5, and acceptance of emotion, Z=�2.1) andtogether reduced the variance with 39%. See Figure 2.
Table 2. Correlations between pre-therapy measures and pre-therapy to post-therapy change scores
Social anxiety(LSAS)
Probability(SPCQ)
Cost(SPCQ)
Safety behaviour(SAFE)
Reappraisal(ERQ)
Expressive suppression(ERQ)
Probability (SPCQ) A 0.48**B 0.62 ***C 0.31*
Cost (SPCQ) A 0.54*** 0.52***B 0.67*** 0.64***C 0.48** 0.54***
Safety behaviour (SAFE) A 0.47** 0.59*** 0.39**B 0.73*** 0.68** 0.60***C 0.56*** 0.31* 0.32*
Cognitive reappraisal (ERQ) A �0.11 0.05 �0.23 �0.01B �0.14 �0.22 �0.13 �0.15C �0.05 �0.19 �0.33* �0.13
Expressive suppression (ERQ) A 0.03 �0.18 �0.25 0.15 �0.05B 0.21 0.05 0.04 0.26 �0.15C 0.09 �0.08 0.10 0.19 �0.05
Acceptance (AAQ) A �0.44** �0.46** �0.26 �0.40** 0.12 �0.27B �0.38** �0.37** �0.44** �0.36** 0.29* �0.24C �0.42** �0.27 �0.30* �0.42** 0.17 �0.27
A correlation between pre-therapy measures. B correlation between pre-therapy to post-therapy change scores. C correlation between pre-therapy tomid-therapy change scores.*p< 0.05.**p< 01.***p< 0.001.
Figure 2. The final, multiple mediator model
M. S. O’Toole et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

None of the results above changed regarding signifi-cance, and they remained of similar magnitudes, whencontrolling for comorbidity and the use of medication.
DISCUSSION
Studies on mediation of clinical improvement in SADhave shown mixed results, and most studies have reliedon a simple pre-post correlation design without applyingformal tests of mediation. The present study used a threedata-point design and investigated change in what wasconceptualized as cognitive as well as emotion regulationvariables. Indirect effects of process variables were testedin lower level mediation analyses, where three variableshad a significant indirect effect both when investigatedseparately and together: estimated probability, estimatedcost and acceptance of emotions. Of these three variables,estimated cost showed the largest overall decrease (seeTable 1) and also yielded the largest effects in the media-tion model. Due to the chosen analytic strategy anddesign, causal inference cannot be made as temporal pre-cedence of change was not demonstrated.Regarding estimated probability and cost, the results are
in line with previous studies exploring the association be-tween distorted cognitions and symptoms of social anxi-ety. The results further align with studies indicating themediating role of threat reappraisal in CBT for anxiety dis-orders (Smits, Julian, Rosenfield, & Powers, 2012). Whileprevious studies on SAD sometimes have found one orthe other of the two cognitive variables to be associatedwith clinical improvement, the present study found thatchange in both types of distortions accounted for a reduc-tion in symptoms of SAD. This finding is in accordancewith classic cognitive models of SAD (Clark & Wells,1995; Rapee & Heimberg, 1997). Since change in the twotypes of cognitive distortions may be consideredantecedent-focused emotion regulation in the form ofstimulus (re)appraisal (cf. Gross & Thompson, 2007), thepresent results are in line with newer emotion regulationconceptualizations that also consider cognitive reap-praisal an adaptive and effective way to change negativeemotions (Gross & Thompson, 2007; Mennin, Ellard,Fresco, & Gross, 2013). When it comes to acceptance ofemotions, this strategy also turned out to be a significantmediator. Emotional acceptance has been argued to beboth an antecedent-focused (Hofmann, Heering, Sawyer,& Asnaani, 2009; Mennin et al., 2013) and a response-focused strategy (Hofmann & Asmundson, 2008), de-pending on when it is used in the unfolding of emotions.For an individual with SAD, acceptance may thereforebe proposed to facilitate both the accepting reappraisalof emotionally upsetting stimuli (antecedent focused) aswell as the acceptance of emotions after they unfold(response focused).
Two general points should be raised about the processvariables that did not show an indirect effect. First, a rela-tively small sample size precludes the conclusion that thevariables are not potentially important mediators as alarger sample would have been able to detect smaller ef-fect sizes. However, the present sample allowed for signif-icant indirect effect of a medium magnitude (r=0.3) to bedetected. Secondly, all measures were based on self-reportdata, and one may question if the measured constructscould be reliably reported by clients. Cognitive variables,reflecting information that is exclusively available to theparticipants, may be appropriately measured throughmeans of self-report, albeit subject to introspective bias.Furthermore, they may differ in the degree to which theyare reliably reported by clients. For instance, cognitive re-appraisal, as measured with the ERQ, did not show an in-direct effect, and one reason may be that the ERQmeasures the ability to reappraise situations in general.As such, it may have been easier for clients to evaluatethe specific probability and cost of social situations com-pared with evaluating their cross-contextual tendency toreappraise a situation. Behavioural variables, such assafety behaviours (although not exclusively behavioural),including expressive suppression, are per definition acces-sible, at least in part, to others, and may have been bettermeasured by observers. In addition, individuals with SADmay engage in safety behaviours in a habitual fashion andtherefore not be consciously aware that they are indeedusing safety behaviours. Albeit speculative, the rise insafety behaviours at mid-treatment could be indicativeof participants becoming aware of their safety behavioursas well as an actual rise in them.The present results point to a number of clinical implica-
tions and suggestions for future research. First, since achange in cognitive distortions may mediate clinical im-provement, it appears relevant to specifically target cogni-tive distortions with cognitive restructuring techniques,which is in accordance with the NICE (2013) guidelinesthat recommend CBT for treatment of SAD. Secondly,more work has to be carried out on the role of acceptancein CBT for SAD in order to target the appropriate elementsof the construct. Acceptance may not be fundamentallydifferent from cognitive restructuring; in fact, contrastingreappraisal and acceptance may be instilling a falsedichotomy. Acceptance-based approaches such as ACT,although not explicitly challenging the thought content,do emphasize the use of descriptive metaphors or analo-gies that encourage a change of perspectives. As such,acceptance may constitute an implicit reframing of cogni-tions about the averseness of emotional experience andthe need for it to be controlled (Mennin et al., 2013). Find-ing acceptance to be a mediator of change could beinterpreted as support for the more contemporaryCBT approaches that include acceptance-based strategies(e.g., Hayes, 2004; Mennin & Fresco, 2009). To further
Change Processes in CBT for SAD
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

investigate the identified processes of change in SAD,future treatment studies should include a control condi-tion in order to ensure the specificity to CBT. Further-more, in order to get at the causal relationship betweenthe variables, they should be investigated under rigorousexperimental conditions.The present study has several limitations. The correla-
tional design of the study and analytic strategy chosenare problematic since they preclude conclusions abouttemporal change. With more observation points, it wouldhave been possible to address the question of causality(e.g., Fentz et al., 2013). Furthermore, a larger samplewould have allowed for other statistical tests of indirecteffects such as multilevel structural equation modellingthat may be a superior analytic approach (Preacher,Zyphur, & Zhang, 2010). The study had no control condi-tion, which questions the specificity of the proposed ef-fects to CBT, and the lack of data on drop-outs limits theinterpretability of the findings to treatment completers.There was some potential unmodelled variance at a thirdlevel, represented by the different therapists and differenttreatment groups. However, six therapists and five treat-ment groups are below the recommended number of up-per level units (Rabe-Hesketh & Skrondal, 2012). Thestudy only included one outcome measure where otheroperationalizations of symptoms of SAD could haveyielded different results. Further regarding the measures,the Cronbach’s alphas for the ERQ expressive suppressionsubscale and the AAQ were rather low, calling intoquestion the reliability of the questionnaires. Treatmentduration varied between participants and constitutes apotential moderator that was not investigated in thisstudy due to the sample size. Moreover, many patientshad comorbid anxiety or depression, which questionsthe specificity of findings to SAD. However, controllingfor comorbidity did not change the results. Although di-agnoses were provided by experienced clinicians, no for-mal measure was obtained for diagnostic reliability, andadherence to the CBT methods was not evaluated. Finally,all clinicians were trained in CBT, but without adherenceratings, it cannot be ascertained that CBT was appropri-ately delivered.In conclusion, the present study yielded support for the
cognitive conceptualization of SAD. Specifically, thestudy found that reductions in inflated probability andcost estimates showed significant indirect effects in CBTfor SAD. In addition, acceptance also revealed a signifi-cant indirect effect, and its role in reducing symptomsof social anxiety should be further explored.
CONFLICT OF INTEREST
The authors report of no conflict of interest.
ACKNOWLEDGEMENTS
The authors would like to thank clinicians at the Clinic forAnxiety Disorders for their willingness to cooperateduring the data gathering process, as well as Dr. ThomasNielsen and Patrick O’Toole for invaluable commentsduring the preparation of the manuscript.
REFERENCESAmerican Psychiatric Association (APA). (2000). Diagnostic and
statistical manual of mental disorders (4th ed., text rev.).Washington, DC: American Psychiatric Association.
Arch, J. J., & Craske, M. G. (2008). Acceptance and commitmenttherapy and cognitive behavioral therapy for anxiety disor-ders: Different treatments, similar mechanisms? ClinicalPsychology: Science and Practice, 5, 263–279.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediatorvariable distinction in social psychological research: Concep-tual, strategic, and statistical considerations. Journal of Personal-ity and Social Psychology, 51, 1173–1182.
Bauer, D. J., Preacher, K. J., & Gil, K. M. (2006). Conceptualizingand testing random indirect effects and moderated mediationin multilevel models: New procedures and recommendations.Psychological Methods, 11, 142–163.
Boden, M. T., John, O. P., Goldin, P. R., Werner, K., Heimberg, R.G., & Gross, J. J. (2012). The role of maladaptive beliefs incognitive-behavioral therapy: Evidence from social anxietydisorder. Behaviour Research and Therapy, 50, 287–291.
Brown, T. A., DiNardo, P. A., & Barlow, D. A. (1994). Anxiety in-terview schedule for DSM-IV: Adult version. New York:Graywind Publication.
Clark, D. M., & Wells, A. (1995). A cognitive model of socialphobia. In R. Heimberg, M. Liebowitz, D. A. Hope, & F. R.Schneier (Eds.), Social phobia: Diagnosis, assessment andtreatment (pp. 69–93). New York: Guilford Press.
Cuming, S., Rapee, R. M., Kemp, N., Abbott, M. J., Peters, L., &Gaston, J. E. (2009). A self-report measure of subtle avoidanceand safety behaviors relevant to social anxiety: Developmentand psychometric properties. Journal of Anxiety Disorders, 23,879–883.
Dalrymple, K. L., & Herbert, J. D. (2007). Acceptance and Com-mitment Therapy for Generalized Social Anxiety Disorder: Apilot study. Behavior Modification, 31, 543–568.
Fentz, H. N., Hoffart, A., Jensen, M. B., Arendt, M., O’Toole, M.S., Rosenberg, N. K., & Hougaard, E. (2013). Mechanisms ofchange in cognitive behaviour therapy for panic disorder:The role of panic self-efficacy and catastrophic misinterpreta-tions. Behaviour Research and Therapy, 51, 579–587.
Foa, E. B., Franklin, M. E., Perry, K. J., & Herbert, J. D. (1996).Cognitive biases in generalized social phobia. Journal ofAbnormal Psychology, 105, 433–439.
Goldin, P. R., Manber, T., Hakimi, S., Canli, T., & Gross, J. J.(2009). Neural bases of social anxiety disorder: Emotional reac-tivity and cognitive regulation during social and physicalthreat. Archives of General Psychiatry, 66, 170–180.
Goldin, P. R., Manber-Ball, T., Werner, K., Heimberg, R., & Gross,J. J. (2009). Neural mechanisms of cognitive reappraisal of neg-ative self-beliefs in social anxiety disorder. Biological Psychiatry,66, 1091–1099.
M. S. O’Toole et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)
Goldin, P., Ziv, M., Jazaieri, H., Werner, K., Kraemer, H.,Heimberg, R. G., & Gross, J. J. (2012). Cognitive reappraisalself-efficacy mediates the effects of individual cognitive-behavioral therapy for social anxiety disorder. Journal ofConsulting and Clinical Psychology, 80, 1034–1040.
Gross, J. J., & John, O. P. (2003). Individual differences in twoemotion regulations processes: Implications for affect, relation-ships and well-being. Journal of Personality and Social Psychology,85, 348–362.
Gross, J. J., & Thompson, R. A. (2007). Emotion regulation. In J. J.Gross (Ed.), Handbook of emotion regulation (pp. 3–24). NewYork: Guilford Press.
Hayes, S. C. (2004). Acceptance and Commitment Therapy andthe new behavior therapies: Mindfulness, acceptance and rela-tionship. In S. C. Hayes, V. M. Follette, & M. Linehan (Eds.),Mindfulness and acceptance: Expanding the cognitive behav-ioral tradition (pp. 1–29). New York: Guilford Press.
Hayes, S. C., Strosahl, K. D., Wilson, K. G., Bissett, R. T.,Pistorello, J., Toarmino, D., … McCurry, S. M. (2004). Measur-ing experiential avoidance: A preliminary test of a workingmodel. The Psychological Record, 54, 553–578.
Heimberg, R. G., & Becker, R. E. (2002). Cognitive-behavioralgroup therapy for social phobia: Basic mechanisms and clinicalstrategies. New York: Guilford.
Heimberg, R. G., Liebowitz, M. R., Hope, D. A., Schneier, F. R.,Holt, C. S., Welkowitz, L. A., … Klein, D. F. (1998). Cognitivebehavioral group therapy vs. phenelzine therapy for socialphobia. Archives of General Psychiatry, 55, 1133–1141.
Herbert, J. D., Gaudiano, B. A., Rheingold, A. A., Myers, V. H.,Dalrymple, K., & Nolan, B. M. (2005). Social skills trainingaugments the effectiveness of cognitive behavioral grouptherapy for social anxiety disorder. Behavior Therapy, 36,125–138.
Hoffart, A., Borge, F., Sexton, H., & Clark, D. M. (2009). Changeprocesses in residential cognitive and interpersonal psycho-therapy for social phobia: A process-outcome study. BehaviorTherapy, 40, 10–22.
Hofmann, S. G. (2004). Cognitive mediation of treatment changein social phobia. Journal of Consulting and Clinical Psychology, 72,392–399.
Hofmann, S. G., & Asmundson, G. J. G. (2008). Acceptance andmindfulness-based therapy: New wave or old hat? ClinicalPsychology Review, 28, 1–16.
Hofmann, S. G., & Bögels, S. M. (2006). Recent advances in thetreatment of social phobia: Introduction to the special issue.Journal of Cognitive Psychotherapy, 20, 3–5.
Hofmann, S. G., Heering, S., Sawyer, A. T., & Asnaani, A. (2009).How to handle anxiety: The effects of reappraisal, acceptance,and suppression strategies on anxious arousal. BehaviourResearch and Therapy, 47, 389–394.
Kashdan, T. B., & Steger, M. (2006). Expanding the topography ofsocial anxiety: An experience sampling assessment of positiveemotions and events, and emotion suppression. PsychologicalScience, 17, 120–128.
Kazdin, A. E. (2007). Mediators and mechanisms of change inpsychotherapy research. Annual Review of Clinical Psychology,3, 1–27.
Kenny, D. A., Korchmaros, J. D., & Bolger, N. (2003). Lower-levelmediation in multilevel models. Psychological Methods, 8, 115–128.
Liebowitz, M. R. (1987). Social phobia. Modern Problems ofPharmacopsychiatry, 22, 141–173.
MacKinnon, D. P., Lockwood, C. M., Hoffman, J. M., West, S. G.,& Sheets, V. (2002). A comparison of methods to test mediation
and other intervening variable effects. Psychological Methods, 7,83–104.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Con-fidence limits for the indirect effect: Distribution of the productand resampling methods. Multivariate Behavioral Research, 39,99–128.
McManus, F., Clark, D. M., & Hackmann, A. (2000). Specificity ofcognitive biases in social phobia and their role in recovery.Behavioural and Cognitive Psychotherapy, 28, 201–209.
Mennin, D. M., Ellard, K. K., Fresco, D. M., & Gross, J. J. (2013).United we stand: Emphasizing commonalities acrosscognitive-behavioral therapies. Behavior Therapy, 44, 234–248.
Mennin, D. S., & Fresco, D. M. (2009). Emotion regulation asan integrative framework for understanding and treatingpsychopathology. In A. M. Kring & D. M. Sloan (Eds.),Emotion Regulation in Psychopathology: A TransdiagnosticApproach to Etiology and Treatment (pp. 356–379). NewYork: Guilford.
Morgan, H., & Raffle, C. (1999). Does reducing safety behaviorsimprove treatment response in patients with social phobia?Australian and New Zealand Journal of Psychiatry, 33, 503–510.
Moscovitch, D. A., Gavric, D. L., Senn, J. M., Santesso, D. L.,Miskovic, V., Schmidt, L. A., … Antony, M. M. (2012). Changesin judgment biases and use of emotion regulation strategiesduring cognitive-behavioral therapy for social anxiety disor-der: Distinguishing treatment responders from nonresponders.Cognitive Therapy and Research, 36, 261–271.
NICE (National Institute for Health and Care Excellence). (2013).Social anxiety disorder: Recognition, assessment and treatment[CG159]. London: National Institute for Health and CareExcellence.
Pontoski, K. E., Heimberg, R. G., Turk, C. L., & Coles, M. E.(2010). Psychotherapy for social anxiety disorder. In D. J. Stein,E. Hollander, & B. O. Rothbaum (Eds.), Textbook of anxietydisorders (pp. 501–521). Washington, DC: American Psychiat-ric Publishing, Inc.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resamplingstrategies for assessing and comparing indirect effects in multi-ple mediator models. Behavior Research Methods, 40, 879–891.
Preacher, K. J., Zyphur, M. J., & Zhang, Z. (2010). A generalmultilevel SEM framework for assessing multilevel mediation.Psychological Methods, 15, 209–233.
Rabe-Hesketh, S., & Skrondal, A. (2012). Multilevel and longitu-dinal modeling using Stata: Continuous responses (Vol. 1, 3rded.). College Station, TX: Stata Press.
Ramshaw, H. J., Chavira, D. A., & Stein, M. B. (2010). Phenome-nology of social anxiety disorder. In D. J. Stein, E. Hollander,& B. O. Rothbaum (Eds.), Textbook of anxiety disorders(pp. 437–452). Washington, DC: American PsychiatricPublishing, Inc.
Rapee, R. M., Gaston, J. E., & Abbot, M. J. (2009). Testing the effi-cacy of theoretically derived improvements in the treatment ofsocial phobia. Journal of Consulting and Clinical Psychology, 77,317–327.
Rapee, R. M., & Heimberg, R. G. (1997). A cognitive-behavioralmodel of anxiety in social phobia. Behaviour Research andTherapy, 35, 741–756.
Raudenbush, S. W., & Bryk, A. S. (2002). Hierarchical linearmodels: Applications and data analysis methods (2nd ed.).Newbury Park, CA: Sage.
Rodebaugh, T. L., & Heimberg, R. G. (2008). Emotion Regulationand the Anxiety Disorders: Adopting a Self-RegulationPerspective. In A. Vingerhoets, I. Nyklícek, & J. Denollet
Change Processes in CBT for SAD
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)

(Eds.), Emotion Regulation: Conceptual and clinical issues (pp.140–149). New York: Springer.
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view ofthe state of the art. Psychological Methods, 7, 147–177.
Singer, J. D., & Willett, J. B. (2003). Applied longitudinal dataanalysis: Modeling change and event occurrence. New York:Oxford University Press.
Smits, J. A., Julian, K., Rosenfield, D., & Powers,M. B. (2012). Threatreappraisal as a mediator of symptom change in cognitive-behavioral treatment of anxiety disorders: A systematic review.Journal of Consulting and Clinical Psychology, 80, 624–635.
Smits, J. A., Rosenfield, D., McDonald, R., & Telch, M. J. (2006).Cognitive mechanisms of social anxiety reduction: An exami-nation of specificity and temporality. Journal of Consulting andClinical Psychology, 74, 1203–1212.
Turk, C. L., Heimberg, R. G., Luterek, J. A., Mennin, D. S., &Fresco, D. M. (2005). Emotion dysregulation in generalized
anxiety disorder: A comparison with social anxiety disorder.Cognitive Therapy and Research, 29, 89–106.
Vonken, M., Alden, L. E., & Bögels, S. (2006). Predicted socialoutcomes of safety behaviours: A double standard. BehaviourResearch and Therapy, 44, 1663–1679.
Wells, A., Clark, D. M., Salkovskis, P., & Ludgate, J. (1995).Social phobia: The role of in-situation safety behaviors inmaintaining anxiety and negative beliefs. Behavior Therapy,26, 153–161.
Werner, K. H., Goldin, P. R., Ball, T. M., Heimberg, R. G., & Gross,J. J. (2011). Assessing emotion regulation in social anxiety dis-order: The Emotion Regulation Interview. Journal of Psychopa-thology and Behavioral Assessment, 33, 346–354.
Wittchen, H. U., Fuetsch, M., Sonntag, H., Müller, N., &Liebowitz, M. (2000). Disability and quality of life in pureand comorbid social phobia: Findings from a controlled study.European Psychiatry, 15, 46–58.
M. S. O’Toole et al.
Copyright © 2014 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. (2014)