cochrane review: selective serotonin reuptake inhibitors (ssris) for depressive disorders in...
TRANSCRIPT

Selective serotonin reuptake inhibitors (SSRIs) for autism
spectrum disorders (ASD) (Review)
Williams K Wheeler DM Silove N Hazell P
This is a reprint of a Cochrane review prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2010 Issue 9
httpwwwthecochranelibrarycom
Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
3OBJECTIVES
3METHODS
6RESULTS
Figure 1 8
15DISCUSSION
16AUTHORSrsquo CONCLUSIONS
16ACKNOWLEDGEMENTS
17REFERENCES
19CHARACTERISTICS OF STUDIES
26DATA AND ANALYSES
26APPENDICES
31WHATrsquoS NEW
31HISTORY
32CONTRIBUTIONS OF AUTHORS
32DECLARATIONS OF INTEREST
32SOURCES OF SUPPORT
32DIFFERENCES BETWEEN PROTOCOL AND REVIEW
iSelective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Selective serotonin reuptake inhibitors (SSRIs) for autismspectrum disorders (ASD)
Katrina Williams1 Danielle M Wheeler2 Natalie Silove3 Philip Hazell4
1School of Womenrsquos and Childrenrsquos Health University of New South Wales amp Sydney Childrenrsquos Hospital Sydney Australia 2co
Cochrane Developmental Psychosocial and Learning Problems Group Belfast UK 3Child Development Unit The Childrenrsquos Hospital
at Westmead Westmead Australia 4Department of Psychiatry Concord Clinical School Sydney Medical School Sydney Australia
Contact address Katrina Williams School of Womenrsquos and Childrenrsquos Health University of New South Wales amp Sydney Chil-
drenrsquos Hospital Sydney Childrenrsquos Community Health Centre Cnr Avoc amp Barker Street Randwick Sydney NSW 2031 Australia
KatrinaWilliamsSESIAHSHEALTHNSWGOVAU
Editorial group Cochrane Developmental Psychosocial and Learning Problems Group
Publication status and date Edited (no change to conclusions) published in Issue 9 2010
Review content assessed as up-to-date 30 May 2010
Citation Williams K Wheeler DM Silove N Hazell P Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders
(ASD) Cochrane Database of Systematic Reviews 2010 Issue 8 Art No CD004677 DOI 10100214651858CD004677pub2
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Autism spectrum disorders (ASD) are characterised by abnormalities in social interaction and communication skills as well as stereotypic
behaviours and restricted activities and interests Selective serotonin reuptake inhibitors (SSRIs) are prescribed for the treatment of co-
morbidity associated with ASD such as depression anxiety and obsessive-compulsive behaviours
Objectives
To determine if treatment with an SSRI
1 improves the core features of autism (social interaction communication and behavioural problems)
2 improves other non-core aspects of behaviour or function such as self-injurious behaviour
3 improves the quality of life of children and their carers
4 has short and long term effects on outcome
5 causes harms
Search strategy
We searched the Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4) MEDLINE ( December 2009)
EMBASE (December 2009) CINAHL (December 2009) PsycINFO (December 2009) and ERIC (December 2009) without language
restrictions
Selection criteria
Randomised controlled trials (RCTs) of any dose of oral SSRI compared with placebo in participants with autism spectrum disorders
Trials must have included at least one standardised outcome measure
1Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data collection and analysis
Two authors independently selected and appraised studies for inclusion and risk of bias All data were continuous Meta-analysis where
possible used a random-effects model
Main results
Seven RCTs with a total of 271 participants were included Four SSRIs were evaluated fluoxetine (two studies) fluvoxamine (two
studies) fenfluramine (two studies) and citalopram (one study) Five studies included only children and two studies included only adults
Varying inclusion criteria were used with regard to diagnostic criteria and intelligence of participants Seventeen different outcome
measures were reported Although more than one study reported data for Clinical Global Impression (CGI) and obsessive-compulsive
behaviour (OCB) different tool types or components of these outcomes were used in each study As such data were unsuitable for
meta-analysis One large high quality study in children showed no evidence of positive effect of citalopram Two small studies in adults
showed positive outcomes for CGI and OCB one study showed improvements in aggression and another in anxiety
Authorsrsquo conclusions
There is no evidence of effect of SSRIs in children and emerging evidence of harm There is limited evidence of the effectiveness of
SSRIs in adults from small studies in which risk of bias is unclear
P L A I N L A N G U A G E S U M M A R Y
Selective serotonin reuptake inhibitors for the treatment of autism spectrum disorders
Autism spectrum disorders (ASD) are characterised by problems with social interaction and communication as well as repetitive
behaviours and limited activities and interests Selective serotonin reuptake inhibitors (SSRIs) are a class of antidepressants which are
sometimes given to help anxiety or obsessive compulsive behaviours We found seven trials which evaluated four SSRIs fluoxetine
fluvoxamine fenfluramine and citalopram Five studies included only children and two studies included only adults One trial enrolled
149 children but all other trials were small We found no trials which evaluated sertraline paroxetine or escitalopram There is no
evidence to support the use of SSRIs to treat autism in children There is limited evidence which is not yet sufficiently robust to
suggest effectiveness of SSRIs in adults with autism Treatment with an SSRI may cause side effects Decisions about the use of SSRIs
for established clinical indications that may co-occur with autism such as obsessive compulsive disorder and depression in adults or
children and anxiety in adults should be made on a case by case basis
B A C K G R O U N D
Description of the condition
Autism spectrum disorders (ASD) are characterised by qualita-
tive impairment in social interaction and communication skills as
well as stereotypic behaviours and limited activities and interests
While ASD is a commonly used term in clinical practice it is not
recognised by current mainstream disease classification systems
such as the Diagnostic and Statistical Manual of Mental Disorders
fourth edition or fourth edition text revision (DSM-IV DSM-
IV-TR) (APA 1994 APA 2000) and International Classification
of Diseases (ICD-10) (WHO 1993) ASD is generally considered
to include autism defined in Diagnostic and Statistical Manual
of Mental Disorders third edition (DSM-III) (APA 1980) as In-
fantile Autism and the third edition revised (DSM-IIIR) (APA
1987) and DSM-IV (APA 1994) as Autistic Disorder and in ICD-
10 (WHO 1993) as Classical Autism Also included in the term
ASD are the diagnoses Pervasive Developmental Disorder - Not
Otherwise Specified (PDD-NOS) rsquoother pervasive developmen-
tal disordersrsquo rsquopervasive developmental disorder unspecifiedrsquo As-
perger syndrome or Asperger disorder and atypical autism
Estimates of the prevalence of autism using the DSM-III DSM-
IIIR DSM-IV or ICD-10 diagnostic classification systems from
published literature up to April 2004 vary between 1 and 40 per
10000 and for any ASD between 3 and 82 per 10000 (Williams
2006) Publications from 2006 have estimated the prevalence of
any ASD between 22 and 116 per 10000 (Baird 2006 Fombonne
2Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
2006 Gillberg 2006 Guillem 2006 Williams 2008) however
lower rates have also been reported (Atladottir 2007 Chen 2007)
Males are affected about four times more frequently than females
Problems usually present in early childhood and continue through-
out life Autism places a considerable burden of care on the family
and society Follow-up studies have found that only 3-10 of peo-
ple with autism are able to live independently as adults (Billstedt
2005 Howlin 2004)
Description of the intervention
Therapies for autism spectrum disorders (ASD)
The heterogeneous nature of problems seen within the autism
spectrum means that it is often difficult to be sure which indi-
viduals will benefit from the many available therapies It is also
likely that different timing of therapy in relation to age and onset
of problems will change outcomes Many therapies are invasive
time consuming andor expensive and little is known about their
potential to cause harm Pharmacological treatments have been
used most commonly as adjuncts to behavioural intervention to
target specific symptoms and behaviours These treatments have
been associated with reductions in sleep disturbance mood dis-
order poor attentionconcentration and self-harm or aggression
towards others (Gringras 2000)
Selective serotonin reuptake inhibitors (SSRIs)
Antidepressants (most of which are likely to be SSRIs) are the
most commonly prescribed psychotropic medications for ASD
and the class of medication for which there has been the greatest
increase in prescribing (Aman 2005) The prescribing of SSRI
drugs to children and adolescents for any indication has however
been curtailed since the Committee on Safety in Medicines (UK)
and the Food and Drugs Administration (USA) released safety
warnings in 2003 and 2004 respectively concerning an increased
risk of suicide-related behaviours associated with these medications
(Murray 2005 Nemeroff 2007)
How the intervention might work
Increased rates of platelet serotonin transport and levels of whole
blood and platelet serotonin (5-hydroxytryptamine 5-HT) have
been reported in people with ASD (Cook 1996) Serotonin is
linked to the mediation of several psychological processes many
of which are altered in ASD including mood social interaction
sleep obsessive compulsive behaviours and aggression (Saxena
1995) It is therefore plausible that inhibition of serotonin reup-
take will result in improvement of ASD symptoms
Why it is important to do this review
Several studies have reported improvements following adminis-
tration of SSRIs However the subject numbers are small espe-
cially for paediatric patients and serious side effects including in-
creases in maladaptive behaviours urinary retention and seizures
are reported (Branford 1998) A recent larger study of children has
shown no improvement (King 2009) To our knowledge no drug
authority has specifically approved the use of SSRIs for autism
The prescribing of SSRIs for autism is therefore either rsquooff-labelrsquo
or is directed to an associated indicated disorder such as obsessive
compulsive disorder (OCD) or depression
Regarding indications and prescribing for children there are be-
tween-country variations The FDA has approved (allowed the
marketing of ) sertraline in children six years and older fluoxetine
in children seven years and older and fluvoxamine in children
eight years and older for the treatment of OCD The FDA has
approved fluoxetine in children eight years and older and escitalo-
pram in adolescents 12 to 17 years for the treatment of depression
In the UK the Commission on Human Medicines (formerly the
Committee on Safety of Medicines) contraindicates all antidepres-
sants other than fluoxetine for the treatment of depression in chil-
dren and adolescents In Australia fluvoxamine has been given a
specific indication of OCD in children eight years and over while
prescribers are urged to exercise caution in prescribing other SSRIs
for children under the age of 18 years
A systematic review of SSRIs is required to assess the evidence of
efficacy and harms when used to treat ASD
O B J E C T I V E S
To determine if treatment with SSRIs
1 improves the core features of ASD (social interaction commu-
nication and behavioural problems)
2 improves other non-core aspects of behaviour or function such
as self-injurious behaviour
3 improves the quality of life of adults or children and their carers
4 has short and long term effects on outcome
5 causes harms
M E T H O D S
Criteria for considering studies for this review
Types of studies
3Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Trials were eligible for inclusion in the review if the assignment of
study participants to intervention or control group was random
Types of participants
Inclusion was limited to individuals with a diagnosis of an ASD de-
fined using DSM-IV or ICD-10 or equivalent as a Pervasive Devel-
opmental Disorder excluding Rett syndrome and Childhood Dis-
integrative Disorder Diagnosis must have been made using a stan-
dardised diagnostic instrument (Childhood Autism Rating Scale
(CARS) Autism Diagnostic Interview-Revised (ADI-R) Autism
Diagnostic Observation Schedule (ADOS) Diagnostic Interview
for Social and Communication Disorders (DISCO)) or by using
established diagnostic criteria (ICD-10 DSM-IV) No age limits
were applied
Types of interventions
Oral SSRIs regardless of dosage used or frequency of administra-
tion The control group must be a placebo group
Types of outcome measures
Types of outcomes
1 Core features of ASD ie social interaction
communication and behavioural problems including stereotypy
or restricted repetitive patterns of behaviour interests or
activities
2 Non-core aspects of behaviour and function such as sleep
disturbance self-mutilation aggression attention and
concentration problems and gastrointestinal function
3 Global assessment of health and function
4 Quality of life for the individual or their family
5 Adverse events
No outcome has been identified as primary because there is insuf-
ficient information at present to prioritise these outcomes We in-
tended to examine short (up to 3 months) medium (3-12 months)
and long term (greater than 12 months) outcomes if data were
available
Types of measures
1 Standardised diagnostic assessment instruments (CARS
ADI-R ADOS DISCO)
2 Standardised communication assessments
3 Quality of life questionnaires
4 Rating scales of emotions and behaviour including
depression anxiety aggression obsessive compulsive behaviour
5 Global impression rating scales
6 Other health outcome rating scales
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Tri-
als (CENTRAL) (The Cochrane Library issue 4 2009) and the
following biomedical science databases MEDLINE (December
2009) EMBASE (2009 Week 49) CINAHL (December 2009)
and PsycINFO (December 2009) We also searched the social sci-
ence and education databases Sociological Abstracts (December
2009) and ERIC (December 2009)
Search terms were modified to meet the requirements of indi-
vidual databases The optimally sensitive search strategy for ran-
domised controlled trials developed for the Cochrane Collabora-
tion (Clarke 2003) was combined with medical subject headings
and text words specific for autism and pervasive development dis-
orders as developed by the Cochrane Developmental Psychoso-
cial and Learning Problems Group Search terms were modified
to meet the requirements of individual databases regarding differ-
ences in fields and syntax The aim of the search strategy was for
high precision and recall There were no language restrictions
See Appendix 1 to Appendix 7 for details of search terms for each
database
Searching other resources
We also searched bibliographies of articles identified through the
search strategy and contacted known experts in the field
Data collection and analysis
Selection of studies
Titles and abstracts from the searches were screened by two au-
thors in 2004 2006 and 2008 (DW KW) and December 2009
(KW NS) Disagreement was resolved by consensus and articles
that did not fulfil the inclusion criteria were discarded Potentially
relevant articles were retrieved for full-text assessment and data
extraction
Data extraction and management
Data were organised using Review Manager Data extraction forms
were developed a priori and included information regarding meth-
ods participant details dose and frequency of SSRI administra-
tion and outcomes Data were extracted by two independent re-
viewers (KW and DW or NS) No disagreements arose
4Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Assessment of risk of bias in included studies
Two authors (KW and NS or DW) independently assessed each
included study using the risk of bias criteria outlined in chapter
8 of the Cochrane Handbook for Systematic Reviews of Interventions(Higgins 2008) without blinding to authorship or source The
assessments were compared for inconsistencies and differences in
interpretation were resolved by discussion and consensus Risk of
bias was assessed according to the following five domains with rat-
ings of rsquoYesrsquo (low risk of bias) rsquoNorsquo (high risk of bias) and rsquoUnclearrsquo
(uncertain risk of bias)
1 Sequence generation
Was the allocation sequence adequately generated
ldquoYesrdquo (computer generated random numbers table of random
numbers coin-tossing or similar) ldquoNordquo (day of week evenodd
clinic record number clinician judgment participant preference
laboratory test result such as haemoglobin value or similar) or
ldquoUnclearrdquo (insufficient information about the sequence generation
process to permit judgment)
2 Allocation concealment
Was allocation adequately concealed
ldquoYesrdquo (central independent unit sequentially numbered drug con-
tainers or sealed envelopes of identical appearance or similar)
ldquoNordquo (alternation or rotation date of birth non-opaque envelopes
open table of random numbers or similar) or ldquoUnclearrdquo (randomi-
sation stated but no information on method used is available)
3 Blinding
Was knowledge of the allocated intervention adequately prevented
during the study
ldquoYesrdquo (identical placebo medication or similar) ldquoNordquo (tablets ver-
sus liquid or similar) or ldquoUnclearrdquo (blinding stated but no infor-
mation on method used is available)
4 Incomplete outcome data
Were incomplete data dealt with adequately by the researchers
ldquoYesrdquo (no missing outcome data missing outcome data balanced
in numbers across intervention groups and reasons for dropouts
and withdrawals described or similar) ldquoNordquo (reason for missing
outcome data likely to be related to true outcome or similar) or
ldquoUnclearrdquo (number or reasons for dropouts and withdrawals not
described)
5 Selective outcome reporting
Are reports of the study free of suggestion of selective outcome
reporting
ldquoYesrdquo (study protocol is available published reports include all ex-
pected outcomes or similar) ldquoNordquo (not all of the studyrsquos pre-spec-
ified primary outcomes have been reported one or more reported
primary outcomes were not pre-specified or similar) or ldquoUnclearrdquo
(insufficient information to permit judgement of rsquoadequatersquo or rsquoin-
adequatersquo)
Any other potential sources of bias such as stopping the study
early or extreme baseline imbalance were also explored
Measures of treatment effect
Binary data
If two or more studies presented outcomes from either standard-
ised instruments or diagnostic evaluations as proportions the rela-
tive risk and risk difference with 95 confidence intervals would
have been calculated from meta-analysis Number needed to treat
would also have been calculated where appropriate However only
one study presented categorical outcomes
Continuous data
Where standardised assessment tools generated a score as the out-
come measure comparisons were made between the means of
these scores We calculated mean difference (MD) where possible
and calculated standard error (SE) using data available from the
same study or imputed it from another study in the same meta-
analysis as described in Chapters 7 9 and 16 of the CochraneHandbook for Systematic Reviews of Interventions (Higgins 2008)
Where studies did not use sufficiently similar instruments to mea-
sure an outcome we conducted meta-analysis using standardised
mean difference
Unit of analysis issues
No unit of analysis errors were identified In all included studies
randomisation reporting and analysis were per individual partic-
ipant
Dealing with missing data
Where possible missing data and dropouts were assessed for each
included study and reported Reasons for missing data were pro-
vided when reported in trials Where insufficient data were re-
ported we contacted the trial authors for further information No
replies were received Where data could not be included in meta-
analysis we have included a summary in the text of the review
Assessment of heterogeneity
Consistency of results was assessed visually and by examining I2 (Higgins 2002) a quantity which describes approximately the
proportion of variation in point estimates that is due to hetero-
geneity rather than sampling error
Assessment of reporting biases
Insufficient studies were found to allow for the use of funnel plots
to investigate any relationship between effect size and study pre-
cision (closely related to sample size)
5Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data synthesis
Where possible when two or more studies were found that were
suitable for inclusion we planned to perform a meta-analysis on
the results using a random-effects model
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was not possible because of a lack of data for
meta-analysis Anticipated clinical differences included
- age of participants adult versus paediatric preschool versus
school age
- diagnostic classification
- dose of medication
Sensitivity analysis
Sensitivity analysis was planned to assess the impact of risk of bias
on the results of meta-analyses However we could not conduct
this analysis because there were too few data available for meta-
analysis for the same drug therapy age group and clinical outcome
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
Seven studies are included in the review Five of the studies were
carried out in the USA 1 in France and 1 in Japan Participants
were children in five of the studies and adults in the other two
Results of the search
Electronic literature searches were conducted in December 2004
and yielded 46 titles Thirty-eight studies were excluded because
they were not randomised controlled trials (RCTs) or were not
about ASD Following full paper review four RCTs were identi-
fied The search was repeated in September 2006 and two further
trials were identified The search was repeated in December 2008
No new trials were found The search was repeated in December
2009 and one new trial was found Thus a total of seven RCTs
with 271 participants were included in this review
Of note fenfluramine was not searched for directly and is not
registered for use as an antidepressant but was identified as an
SSRI in electronic searches We debated its inclusion and chose
to retain the two trials to provide a complete clinical picture The
tricyclic antidepressant clomipramine was also identified using this
search method and is known to have serotonin uptake inhibitor
actions but was excluded because unlike fenfluramine it will be
included in a systematic review of tricyclic antidepressants and
ASD (currently in progress)
Different versions of assessment tools were used to measure sim-
ilar outcomes For example for CGI the Clinical Global Im-
pression - Severity scale (CGI-S) the Clinical Global Impression
- Improvement scale (CGI-I) and the Clinical Global Improve-
ment Scale Adapted to Global Autism (CGI-AD) were used and
sometimes the tool used was uncertain (CGI) (Guy 1976) Simi-
larly to measure Obsessive Compulsive Behaviour the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) (Scahill 2006) the
Childrenrsquos Yale-Brown Obsessive Compulsive scale (CY-BOCS)
(McKay 2003) and the Yale-Brown Obsessive-Compulsion Scale
(Goodman 1989Goodman 1989b) and a modified version of it
were used
Included studies
Five studies were conducted in children aged 3-17 years us-
ing fenfluramine (Barthelemy 1989 Leventhal 1993) fluoxe-
tine (Hollander 2005) fluvoxamine (Sugie 2005) and citalopram
(King 2009) Two studies were conducted in adults aged 18-
53 years using fluoxetine (Buchsbaum 2001) and fluvoxamine
(McDougle 1996)
Of the five trials in children two used DSM-IV-TR diagnoses of
Autistic Disorder Asperger Disorder or PDD-NOS (Hollander
2005 King 2009) One study (King 2009) also required at least
moderate severity on the CGI illness severity scale and a moderate
or greater score for compulsive behaviour items of the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) Both of these studies
included children with intelligence in the normal range with one
having an IQ range of 30-132 (Hollander 2005) and the other
reporting 61 of children with a non-verbal IQ over 70 (King
2009) One study included children ldquodiagnosed with autismrdquo using
DSM-IV but did not specify how criteria were applied or provide
information about intelligence (Sugie 2005) Two studies used
DSM-III criteria for a diagnosis of autism and included children
with intellectual impairment with IQ ranges of 16-63 (Leventhal
1993) and 30-75 (Barthelemy 1989)
Of the two adult studies one (Buchsbaum 2001) included adults
diagnosed using DSM-IV with autism or Asperger Disorders and
all patients were verbal with an IQ score range of 53 to 119
The other study included adults diagnosed with autism using the
DSM-III-R and ICD-10 criteria and individuals included were at
least ldquomoderaterdquo in severity using the CGI global severity of illness
rating Both intellectually able and disabled adults were included
(McDougle 1996)
One study (Leventhal 1993) included participants who had pre-
viously been treated with an SSRI Trial authors participated in a
multicentre non-randomised trial of 30 weeks duration and then
extended this trial with a 32 week cross-over RCT Thus there was
6Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
3OBJECTIVES
3METHODS
6RESULTS
Figure 1 8
15DISCUSSION
16AUTHORSrsquo CONCLUSIONS
16ACKNOWLEDGEMENTS
17REFERENCES
19CHARACTERISTICS OF STUDIES
26DATA AND ANALYSES
26APPENDICES
31WHATrsquoS NEW
31HISTORY
32CONTRIBUTIONS OF AUTHORS
32DECLARATIONS OF INTEREST
32SOURCES OF SUPPORT
32DIFFERENCES BETWEEN PROTOCOL AND REVIEW
iSelective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Selective serotonin reuptake inhibitors (SSRIs) for autismspectrum disorders (ASD)
Katrina Williams1 Danielle M Wheeler2 Natalie Silove3 Philip Hazell4
1School of Womenrsquos and Childrenrsquos Health University of New South Wales amp Sydney Childrenrsquos Hospital Sydney Australia 2co
Cochrane Developmental Psychosocial and Learning Problems Group Belfast UK 3Child Development Unit The Childrenrsquos Hospital
at Westmead Westmead Australia 4Department of Psychiatry Concord Clinical School Sydney Medical School Sydney Australia
Contact address Katrina Williams School of Womenrsquos and Childrenrsquos Health University of New South Wales amp Sydney Chil-
drenrsquos Hospital Sydney Childrenrsquos Community Health Centre Cnr Avoc amp Barker Street Randwick Sydney NSW 2031 Australia
KatrinaWilliamsSESIAHSHEALTHNSWGOVAU
Editorial group Cochrane Developmental Psychosocial and Learning Problems Group
Publication status and date Edited (no change to conclusions) published in Issue 9 2010
Review content assessed as up-to-date 30 May 2010
Citation Williams K Wheeler DM Silove N Hazell P Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders
(ASD) Cochrane Database of Systematic Reviews 2010 Issue 8 Art No CD004677 DOI 10100214651858CD004677pub2
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Autism spectrum disorders (ASD) are characterised by abnormalities in social interaction and communication skills as well as stereotypic
behaviours and restricted activities and interests Selective serotonin reuptake inhibitors (SSRIs) are prescribed for the treatment of co-
morbidity associated with ASD such as depression anxiety and obsessive-compulsive behaviours
Objectives
To determine if treatment with an SSRI
1 improves the core features of autism (social interaction communication and behavioural problems)
2 improves other non-core aspects of behaviour or function such as self-injurious behaviour
3 improves the quality of life of children and their carers
4 has short and long term effects on outcome
5 causes harms
Search strategy
We searched the Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4) MEDLINE ( December 2009)
EMBASE (December 2009) CINAHL (December 2009) PsycINFO (December 2009) and ERIC (December 2009) without language
restrictions
Selection criteria
Randomised controlled trials (RCTs) of any dose of oral SSRI compared with placebo in participants with autism spectrum disorders
Trials must have included at least one standardised outcome measure
1Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data collection and analysis
Two authors independently selected and appraised studies for inclusion and risk of bias All data were continuous Meta-analysis where
possible used a random-effects model
Main results
Seven RCTs with a total of 271 participants were included Four SSRIs were evaluated fluoxetine (two studies) fluvoxamine (two
studies) fenfluramine (two studies) and citalopram (one study) Five studies included only children and two studies included only adults
Varying inclusion criteria were used with regard to diagnostic criteria and intelligence of participants Seventeen different outcome
measures were reported Although more than one study reported data for Clinical Global Impression (CGI) and obsessive-compulsive
behaviour (OCB) different tool types or components of these outcomes were used in each study As such data were unsuitable for
meta-analysis One large high quality study in children showed no evidence of positive effect of citalopram Two small studies in adults
showed positive outcomes for CGI and OCB one study showed improvements in aggression and another in anxiety
Authorsrsquo conclusions
There is no evidence of effect of SSRIs in children and emerging evidence of harm There is limited evidence of the effectiveness of
SSRIs in adults from small studies in which risk of bias is unclear
P L A I N L A N G U A G E S U M M A R Y
Selective serotonin reuptake inhibitors for the treatment of autism spectrum disorders
Autism spectrum disorders (ASD) are characterised by problems with social interaction and communication as well as repetitive
behaviours and limited activities and interests Selective serotonin reuptake inhibitors (SSRIs) are a class of antidepressants which are
sometimes given to help anxiety or obsessive compulsive behaviours We found seven trials which evaluated four SSRIs fluoxetine
fluvoxamine fenfluramine and citalopram Five studies included only children and two studies included only adults One trial enrolled
149 children but all other trials were small We found no trials which evaluated sertraline paroxetine or escitalopram There is no
evidence to support the use of SSRIs to treat autism in children There is limited evidence which is not yet sufficiently robust to
suggest effectiveness of SSRIs in adults with autism Treatment with an SSRI may cause side effects Decisions about the use of SSRIs
for established clinical indications that may co-occur with autism such as obsessive compulsive disorder and depression in adults or
children and anxiety in adults should be made on a case by case basis
B A C K G R O U N D
Description of the condition
Autism spectrum disorders (ASD) are characterised by qualita-
tive impairment in social interaction and communication skills as
well as stereotypic behaviours and limited activities and interests
While ASD is a commonly used term in clinical practice it is not
recognised by current mainstream disease classification systems
such as the Diagnostic and Statistical Manual of Mental Disorders
fourth edition or fourth edition text revision (DSM-IV DSM-
IV-TR) (APA 1994 APA 2000) and International Classification
of Diseases (ICD-10) (WHO 1993) ASD is generally considered
to include autism defined in Diagnostic and Statistical Manual
of Mental Disorders third edition (DSM-III) (APA 1980) as In-
fantile Autism and the third edition revised (DSM-IIIR) (APA
1987) and DSM-IV (APA 1994) as Autistic Disorder and in ICD-
10 (WHO 1993) as Classical Autism Also included in the term
ASD are the diagnoses Pervasive Developmental Disorder - Not
Otherwise Specified (PDD-NOS) rsquoother pervasive developmen-
tal disordersrsquo rsquopervasive developmental disorder unspecifiedrsquo As-
perger syndrome or Asperger disorder and atypical autism
Estimates of the prevalence of autism using the DSM-III DSM-
IIIR DSM-IV or ICD-10 diagnostic classification systems from
published literature up to April 2004 vary between 1 and 40 per
10000 and for any ASD between 3 and 82 per 10000 (Williams
2006) Publications from 2006 have estimated the prevalence of
any ASD between 22 and 116 per 10000 (Baird 2006 Fombonne
2Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
2006 Gillberg 2006 Guillem 2006 Williams 2008) however
lower rates have also been reported (Atladottir 2007 Chen 2007)
Males are affected about four times more frequently than females
Problems usually present in early childhood and continue through-
out life Autism places a considerable burden of care on the family
and society Follow-up studies have found that only 3-10 of peo-
ple with autism are able to live independently as adults (Billstedt
2005 Howlin 2004)
Description of the intervention
Therapies for autism spectrum disorders (ASD)
The heterogeneous nature of problems seen within the autism
spectrum means that it is often difficult to be sure which indi-
viduals will benefit from the many available therapies It is also
likely that different timing of therapy in relation to age and onset
of problems will change outcomes Many therapies are invasive
time consuming andor expensive and little is known about their
potential to cause harm Pharmacological treatments have been
used most commonly as adjuncts to behavioural intervention to
target specific symptoms and behaviours These treatments have
been associated with reductions in sleep disturbance mood dis-
order poor attentionconcentration and self-harm or aggression
towards others (Gringras 2000)
Selective serotonin reuptake inhibitors (SSRIs)
Antidepressants (most of which are likely to be SSRIs) are the
most commonly prescribed psychotropic medications for ASD
and the class of medication for which there has been the greatest
increase in prescribing (Aman 2005) The prescribing of SSRI
drugs to children and adolescents for any indication has however
been curtailed since the Committee on Safety in Medicines (UK)
and the Food and Drugs Administration (USA) released safety
warnings in 2003 and 2004 respectively concerning an increased
risk of suicide-related behaviours associated with these medications
(Murray 2005 Nemeroff 2007)
How the intervention might work
Increased rates of platelet serotonin transport and levels of whole
blood and platelet serotonin (5-hydroxytryptamine 5-HT) have
been reported in people with ASD (Cook 1996) Serotonin is
linked to the mediation of several psychological processes many
of which are altered in ASD including mood social interaction
sleep obsessive compulsive behaviours and aggression (Saxena
1995) It is therefore plausible that inhibition of serotonin reup-
take will result in improvement of ASD symptoms
Why it is important to do this review
Several studies have reported improvements following adminis-
tration of SSRIs However the subject numbers are small espe-
cially for paediatric patients and serious side effects including in-
creases in maladaptive behaviours urinary retention and seizures
are reported (Branford 1998) A recent larger study of children has
shown no improvement (King 2009) To our knowledge no drug
authority has specifically approved the use of SSRIs for autism
The prescribing of SSRIs for autism is therefore either rsquooff-labelrsquo
or is directed to an associated indicated disorder such as obsessive
compulsive disorder (OCD) or depression
Regarding indications and prescribing for children there are be-
tween-country variations The FDA has approved (allowed the
marketing of ) sertraline in children six years and older fluoxetine
in children seven years and older and fluvoxamine in children
eight years and older for the treatment of OCD The FDA has
approved fluoxetine in children eight years and older and escitalo-
pram in adolescents 12 to 17 years for the treatment of depression
In the UK the Commission on Human Medicines (formerly the
Committee on Safety of Medicines) contraindicates all antidepres-
sants other than fluoxetine for the treatment of depression in chil-
dren and adolescents In Australia fluvoxamine has been given a
specific indication of OCD in children eight years and over while
prescribers are urged to exercise caution in prescribing other SSRIs
for children under the age of 18 years
A systematic review of SSRIs is required to assess the evidence of
efficacy and harms when used to treat ASD
O B J E C T I V E S
To determine if treatment with SSRIs
1 improves the core features of ASD (social interaction commu-
nication and behavioural problems)
2 improves other non-core aspects of behaviour or function such
as self-injurious behaviour
3 improves the quality of life of adults or children and their carers
4 has short and long term effects on outcome
5 causes harms
M E T H O D S
Criteria for considering studies for this review
Types of studies
3Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Trials were eligible for inclusion in the review if the assignment of
study participants to intervention or control group was random
Types of participants
Inclusion was limited to individuals with a diagnosis of an ASD de-
fined using DSM-IV or ICD-10 or equivalent as a Pervasive Devel-
opmental Disorder excluding Rett syndrome and Childhood Dis-
integrative Disorder Diagnosis must have been made using a stan-
dardised diagnostic instrument (Childhood Autism Rating Scale
(CARS) Autism Diagnostic Interview-Revised (ADI-R) Autism
Diagnostic Observation Schedule (ADOS) Diagnostic Interview
for Social and Communication Disorders (DISCO)) or by using
established diagnostic criteria (ICD-10 DSM-IV) No age limits
were applied
Types of interventions
Oral SSRIs regardless of dosage used or frequency of administra-
tion The control group must be a placebo group
Types of outcome measures
Types of outcomes
1 Core features of ASD ie social interaction
communication and behavioural problems including stereotypy
or restricted repetitive patterns of behaviour interests or
activities
2 Non-core aspects of behaviour and function such as sleep
disturbance self-mutilation aggression attention and
concentration problems and gastrointestinal function
3 Global assessment of health and function
4 Quality of life for the individual or their family
5 Adverse events
No outcome has been identified as primary because there is insuf-
ficient information at present to prioritise these outcomes We in-
tended to examine short (up to 3 months) medium (3-12 months)
and long term (greater than 12 months) outcomes if data were
available
Types of measures
1 Standardised diagnostic assessment instruments (CARS
ADI-R ADOS DISCO)
2 Standardised communication assessments
3 Quality of life questionnaires
4 Rating scales of emotions and behaviour including
depression anxiety aggression obsessive compulsive behaviour
5 Global impression rating scales
6 Other health outcome rating scales
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Tri-
als (CENTRAL) (The Cochrane Library issue 4 2009) and the
following biomedical science databases MEDLINE (December
2009) EMBASE (2009 Week 49) CINAHL (December 2009)
and PsycINFO (December 2009) We also searched the social sci-
ence and education databases Sociological Abstracts (December
2009) and ERIC (December 2009)
Search terms were modified to meet the requirements of indi-
vidual databases The optimally sensitive search strategy for ran-
domised controlled trials developed for the Cochrane Collabora-
tion (Clarke 2003) was combined with medical subject headings
and text words specific for autism and pervasive development dis-
orders as developed by the Cochrane Developmental Psychoso-
cial and Learning Problems Group Search terms were modified
to meet the requirements of individual databases regarding differ-
ences in fields and syntax The aim of the search strategy was for
high precision and recall There were no language restrictions
See Appendix 1 to Appendix 7 for details of search terms for each
database
Searching other resources
We also searched bibliographies of articles identified through the
search strategy and contacted known experts in the field
Data collection and analysis
Selection of studies
Titles and abstracts from the searches were screened by two au-
thors in 2004 2006 and 2008 (DW KW) and December 2009
(KW NS) Disagreement was resolved by consensus and articles
that did not fulfil the inclusion criteria were discarded Potentially
relevant articles were retrieved for full-text assessment and data
extraction
Data extraction and management
Data were organised using Review Manager Data extraction forms
were developed a priori and included information regarding meth-
ods participant details dose and frequency of SSRI administra-
tion and outcomes Data were extracted by two independent re-
viewers (KW and DW or NS) No disagreements arose
4Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Assessment of risk of bias in included studies
Two authors (KW and NS or DW) independently assessed each
included study using the risk of bias criteria outlined in chapter
8 of the Cochrane Handbook for Systematic Reviews of Interventions(Higgins 2008) without blinding to authorship or source The
assessments were compared for inconsistencies and differences in
interpretation were resolved by discussion and consensus Risk of
bias was assessed according to the following five domains with rat-
ings of rsquoYesrsquo (low risk of bias) rsquoNorsquo (high risk of bias) and rsquoUnclearrsquo
(uncertain risk of bias)
1 Sequence generation
Was the allocation sequence adequately generated
ldquoYesrdquo (computer generated random numbers table of random
numbers coin-tossing or similar) ldquoNordquo (day of week evenodd
clinic record number clinician judgment participant preference
laboratory test result such as haemoglobin value or similar) or
ldquoUnclearrdquo (insufficient information about the sequence generation
process to permit judgment)
2 Allocation concealment
Was allocation adequately concealed
ldquoYesrdquo (central independent unit sequentially numbered drug con-
tainers or sealed envelopes of identical appearance or similar)
ldquoNordquo (alternation or rotation date of birth non-opaque envelopes
open table of random numbers or similar) or ldquoUnclearrdquo (randomi-
sation stated but no information on method used is available)
3 Blinding
Was knowledge of the allocated intervention adequately prevented
during the study
ldquoYesrdquo (identical placebo medication or similar) ldquoNordquo (tablets ver-
sus liquid or similar) or ldquoUnclearrdquo (blinding stated but no infor-
mation on method used is available)
4 Incomplete outcome data
Were incomplete data dealt with adequately by the researchers
ldquoYesrdquo (no missing outcome data missing outcome data balanced
in numbers across intervention groups and reasons for dropouts
and withdrawals described or similar) ldquoNordquo (reason for missing
outcome data likely to be related to true outcome or similar) or
ldquoUnclearrdquo (number or reasons for dropouts and withdrawals not
described)
5 Selective outcome reporting
Are reports of the study free of suggestion of selective outcome
reporting
ldquoYesrdquo (study protocol is available published reports include all ex-
pected outcomes or similar) ldquoNordquo (not all of the studyrsquos pre-spec-
ified primary outcomes have been reported one or more reported
primary outcomes were not pre-specified or similar) or ldquoUnclearrdquo
(insufficient information to permit judgement of rsquoadequatersquo or rsquoin-
adequatersquo)
Any other potential sources of bias such as stopping the study
early or extreme baseline imbalance were also explored
Measures of treatment effect
Binary data
If two or more studies presented outcomes from either standard-
ised instruments or diagnostic evaluations as proportions the rela-
tive risk and risk difference with 95 confidence intervals would
have been calculated from meta-analysis Number needed to treat
would also have been calculated where appropriate However only
one study presented categorical outcomes
Continuous data
Where standardised assessment tools generated a score as the out-
come measure comparisons were made between the means of
these scores We calculated mean difference (MD) where possible
and calculated standard error (SE) using data available from the
same study or imputed it from another study in the same meta-
analysis as described in Chapters 7 9 and 16 of the CochraneHandbook for Systematic Reviews of Interventions (Higgins 2008)
Where studies did not use sufficiently similar instruments to mea-
sure an outcome we conducted meta-analysis using standardised
mean difference
Unit of analysis issues
No unit of analysis errors were identified In all included studies
randomisation reporting and analysis were per individual partic-
ipant
Dealing with missing data
Where possible missing data and dropouts were assessed for each
included study and reported Reasons for missing data were pro-
vided when reported in trials Where insufficient data were re-
ported we contacted the trial authors for further information No
replies were received Where data could not be included in meta-
analysis we have included a summary in the text of the review
Assessment of heterogeneity
Consistency of results was assessed visually and by examining I2 (Higgins 2002) a quantity which describes approximately the
proportion of variation in point estimates that is due to hetero-
geneity rather than sampling error
Assessment of reporting biases
Insufficient studies were found to allow for the use of funnel plots
to investigate any relationship between effect size and study pre-
cision (closely related to sample size)
5Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data synthesis
Where possible when two or more studies were found that were
suitable for inclusion we planned to perform a meta-analysis on
the results using a random-effects model
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was not possible because of a lack of data for
meta-analysis Anticipated clinical differences included
- age of participants adult versus paediatric preschool versus
school age
- diagnostic classification
- dose of medication
Sensitivity analysis
Sensitivity analysis was planned to assess the impact of risk of bias
on the results of meta-analyses However we could not conduct
this analysis because there were too few data available for meta-
analysis for the same drug therapy age group and clinical outcome
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
Seven studies are included in the review Five of the studies were
carried out in the USA 1 in France and 1 in Japan Participants
were children in five of the studies and adults in the other two
Results of the search
Electronic literature searches were conducted in December 2004
and yielded 46 titles Thirty-eight studies were excluded because
they were not randomised controlled trials (RCTs) or were not
about ASD Following full paper review four RCTs were identi-
fied The search was repeated in September 2006 and two further
trials were identified The search was repeated in December 2008
No new trials were found The search was repeated in December
2009 and one new trial was found Thus a total of seven RCTs
with 271 participants were included in this review
Of note fenfluramine was not searched for directly and is not
registered for use as an antidepressant but was identified as an
SSRI in electronic searches We debated its inclusion and chose
to retain the two trials to provide a complete clinical picture The
tricyclic antidepressant clomipramine was also identified using this
search method and is known to have serotonin uptake inhibitor
actions but was excluded because unlike fenfluramine it will be
included in a systematic review of tricyclic antidepressants and
ASD (currently in progress)
Different versions of assessment tools were used to measure sim-
ilar outcomes For example for CGI the Clinical Global Im-
pression - Severity scale (CGI-S) the Clinical Global Impression
- Improvement scale (CGI-I) and the Clinical Global Improve-
ment Scale Adapted to Global Autism (CGI-AD) were used and
sometimes the tool used was uncertain (CGI) (Guy 1976) Simi-
larly to measure Obsessive Compulsive Behaviour the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) (Scahill 2006) the
Childrenrsquos Yale-Brown Obsessive Compulsive scale (CY-BOCS)
(McKay 2003) and the Yale-Brown Obsessive-Compulsion Scale
(Goodman 1989Goodman 1989b) and a modified version of it
were used
Included studies
Five studies were conducted in children aged 3-17 years us-
ing fenfluramine (Barthelemy 1989 Leventhal 1993) fluoxe-
tine (Hollander 2005) fluvoxamine (Sugie 2005) and citalopram
(King 2009) Two studies were conducted in adults aged 18-
53 years using fluoxetine (Buchsbaum 2001) and fluvoxamine
(McDougle 1996)
Of the five trials in children two used DSM-IV-TR diagnoses of
Autistic Disorder Asperger Disorder or PDD-NOS (Hollander
2005 King 2009) One study (King 2009) also required at least
moderate severity on the CGI illness severity scale and a moderate
or greater score for compulsive behaviour items of the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) Both of these studies
included children with intelligence in the normal range with one
having an IQ range of 30-132 (Hollander 2005) and the other
reporting 61 of children with a non-verbal IQ over 70 (King
2009) One study included children ldquodiagnosed with autismrdquo using
DSM-IV but did not specify how criteria were applied or provide
information about intelligence (Sugie 2005) Two studies used
DSM-III criteria for a diagnosis of autism and included children
with intellectual impairment with IQ ranges of 16-63 (Leventhal
1993) and 30-75 (Barthelemy 1989)
Of the two adult studies one (Buchsbaum 2001) included adults
diagnosed using DSM-IV with autism or Asperger Disorders and
all patients were verbal with an IQ score range of 53 to 119
The other study included adults diagnosed with autism using the
DSM-III-R and ICD-10 criteria and individuals included were at
least ldquomoderaterdquo in severity using the CGI global severity of illness
rating Both intellectually able and disabled adults were included
(McDougle 1996)
One study (Leventhal 1993) included participants who had pre-
viously been treated with an SSRI Trial authors participated in a
multicentre non-randomised trial of 30 weeks duration and then
extended this trial with a 32 week cross-over RCT Thus there was
6Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Selective serotonin reuptake inhibitors (SSRIs) for autismspectrum disorders (ASD)
Katrina Williams1 Danielle M Wheeler2 Natalie Silove3 Philip Hazell4
1School of Womenrsquos and Childrenrsquos Health University of New South Wales amp Sydney Childrenrsquos Hospital Sydney Australia 2co
Cochrane Developmental Psychosocial and Learning Problems Group Belfast UK 3Child Development Unit The Childrenrsquos Hospital
at Westmead Westmead Australia 4Department of Psychiatry Concord Clinical School Sydney Medical School Sydney Australia
Contact address Katrina Williams School of Womenrsquos and Childrenrsquos Health University of New South Wales amp Sydney Chil-
drenrsquos Hospital Sydney Childrenrsquos Community Health Centre Cnr Avoc amp Barker Street Randwick Sydney NSW 2031 Australia
KatrinaWilliamsSESIAHSHEALTHNSWGOVAU
Editorial group Cochrane Developmental Psychosocial and Learning Problems Group
Publication status and date Edited (no change to conclusions) published in Issue 9 2010
Review content assessed as up-to-date 30 May 2010
Citation Williams K Wheeler DM Silove N Hazell P Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders
(ASD) Cochrane Database of Systematic Reviews 2010 Issue 8 Art No CD004677 DOI 10100214651858CD004677pub2
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Autism spectrum disorders (ASD) are characterised by abnormalities in social interaction and communication skills as well as stereotypic
behaviours and restricted activities and interests Selective serotonin reuptake inhibitors (SSRIs) are prescribed for the treatment of co-
morbidity associated with ASD such as depression anxiety and obsessive-compulsive behaviours
Objectives
To determine if treatment with an SSRI
1 improves the core features of autism (social interaction communication and behavioural problems)
2 improves other non-core aspects of behaviour or function such as self-injurious behaviour
3 improves the quality of life of children and their carers
4 has short and long term effects on outcome
5 causes harms
Search strategy
We searched the Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4) MEDLINE ( December 2009)
EMBASE (December 2009) CINAHL (December 2009) PsycINFO (December 2009) and ERIC (December 2009) without language
restrictions
Selection criteria
Randomised controlled trials (RCTs) of any dose of oral SSRI compared with placebo in participants with autism spectrum disorders
Trials must have included at least one standardised outcome measure
1Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data collection and analysis
Two authors independently selected and appraised studies for inclusion and risk of bias All data were continuous Meta-analysis where
possible used a random-effects model
Main results
Seven RCTs with a total of 271 participants were included Four SSRIs were evaluated fluoxetine (two studies) fluvoxamine (two
studies) fenfluramine (two studies) and citalopram (one study) Five studies included only children and two studies included only adults
Varying inclusion criteria were used with regard to diagnostic criteria and intelligence of participants Seventeen different outcome
measures were reported Although more than one study reported data for Clinical Global Impression (CGI) and obsessive-compulsive
behaviour (OCB) different tool types or components of these outcomes were used in each study As such data were unsuitable for
meta-analysis One large high quality study in children showed no evidence of positive effect of citalopram Two small studies in adults
showed positive outcomes for CGI and OCB one study showed improvements in aggression and another in anxiety
Authorsrsquo conclusions
There is no evidence of effect of SSRIs in children and emerging evidence of harm There is limited evidence of the effectiveness of
SSRIs in adults from small studies in which risk of bias is unclear
P L A I N L A N G U A G E S U M M A R Y
Selective serotonin reuptake inhibitors for the treatment of autism spectrum disorders
Autism spectrum disorders (ASD) are characterised by problems with social interaction and communication as well as repetitive
behaviours and limited activities and interests Selective serotonin reuptake inhibitors (SSRIs) are a class of antidepressants which are
sometimes given to help anxiety or obsessive compulsive behaviours We found seven trials which evaluated four SSRIs fluoxetine
fluvoxamine fenfluramine and citalopram Five studies included only children and two studies included only adults One trial enrolled
149 children but all other trials were small We found no trials which evaluated sertraline paroxetine or escitalopram There is no
evidence to support the use of SSRIs to treat autism in children There is limited evidence which is not yet sufficiently robust to
suggest effectiveness of SSRIs in adults with autism Treatment with an SSRI may cause side effects Decisions about the use of SSRIs
for established clinical indications that may co-occur with autism such as obsessive compulsive disorder and depression in adults or
children and anxiety in adults should be made on a case by case basis
B A C K G R O U N D
Description of the condition
Autism spectrum disorders (ASD) are characterised by qualita-
tive impairment in social interaction and communication skills as
well as stereotypic behaviours and limited activities and interests
While ASD is a commonly used term in clinical practice it is not
recognised by current mainstream disease classification systems
such as the Diagnostic and Statistical Manual of Mental Disorders
fourth edition or fourth edition text revision (DSM-IV DSM-
IV-TR) (APA 1994 APA 2000) and International Classification
of Diseases (ICD-10) (WHO 1993) ASD is generally considered
to include autism defined in Diagnostic and Statistical Manual
of Mental Disorders third edition (DSM-III) (APA 1980) as In-
fantile Autism and the third edition revised (DSM-IIIR) (APA
1987) and DSM-IV (APA 1994) as Autistic Disorder and in ICD-
10 (WHO 1993) as Classical Autism Also included in the term
ASD are the diagnoses Pervasive Developmental Disorder - Not
Otherwise Specified (PDD-NOS) rsquoother pervasive developmen-
tal disordersrsquo rsquopervasive developmental disorder unspecifiedrsquo As-
perger syndrome or Asperger disorder and atypical autism
Estimates of the prevalence of autism using the DSM-III DSM-
IIIR DSM-IV or ICD-10 diagnostic classification systems from
published literature up to April 2004 vary between 1 and 40 per
10000 and for any ASD between 3 and 82 per 10000 (Williams
2006) Publications from 2006 have estimated the prevalence of
any ASD between 22 and 116 per 10000 (Baird 2006 Fombonne
2Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
2006 Gillberg 2006 Guillem 2006 Williams 2008) however
lower rates have also been reported (Atladottir 2007 Chen 2007)
Males are affected about four times more frequently than females
Problems usually present in early childhood and continue through-
out life Autism places a considerable burden of care on the family
and society Follow-up studies have found that only 3-10 of peo-
ple with autism are able to live independently as adults (Billstedt
2005 Howlin 2004)
Description of the intervention
Therapies for autism spectrum disorders (ASD)
The heterogeneous nature of problems seen within the autism
spectrum means that it is often difficult to be sure which indi-
viduals will benefit from the many available therapies It is also
likely that different timing of therapy in relation to age and onset
of problems will change outcomes Many therapies are invasive
time consuming andor expensive and little is known about their
potential to cause harm Pharmacological treatments have been
used most commonly as adjuncts to behavioural intervention to
target specific symptoms and behaviours These treatments have
been associated with reductions in sleep disturbance mood dis-
order poor attentionconcentration and self-harm or aggression
towards others (Gringras 2000)
Selective serotonin reuptake inhibitors (SSRIs)
Antidepressants (most of which are likely to be SSRIs) are the
most commonly prescribed psychotropic medications for ASD
and the class of medication for which there has been the greatest
increase in prescribing (Aman 2005) The prescribing of SSRI
drugs to children and adolescents for any indication has however
been curtailed since the Committee on Safety in Medicines (UK)
and the Food and Drugs Administration (USA) released safety
warnings in 2003 and 2004 respectively concerning an increased
risk of suicide-related behaviours associated with these medications
(Murray 2005 Nemeroff 2007)
How the intervention might work
Increased rates of platelet serotonin transport and levels of whole
blood and platelet serotonin (5-hydroxytryptamine 5-HT) have
been reported in people with ASD (Cook 1996) Serotonin is
linked to the mediation of several psychological processes many
of which are altered in ASD including mood social interaction
sleep obsessive compulsive behaviours and aggression (Saxena
1995) It is therefore plausible that inhibition of serotonin reup-
take will result in improvement of ASD symptoms
Why it is important to do this review
Several studies have reported improvements following adminis-
tration of SSRIs However the subject numbers are small espe-
cially for paediatric patients and serious side effects including in-
creases in maladaptive behaviours urinary retention and seizures
are reported (Branford 1998) A recent larger study of children has
shown no improvement (King 2009) To our knowledge no drug
authority has specifically approved the use of SSRIs for autism
The prescribing of SSRIs for autism is therefore either rsquooff-labelrsquo
or is directed to an associated indicated disorder such as obsessive
compulsive disorder (OCD) or depression
Regarding indications and prescribing for children there are be-
tween-country variations The FDA has approved (allowed the
marketing of ) sertraline in children six years and older fluoxetine
in children seven years and older and fluvoxamine in children
eight years and older for the treatment of OCD The FDA has
approved fluoxetine in children eight years and older and escitalo-
pram in adolescents 12 to 17 years for the treatment of depression
In the UK the Commission on Human Medicines (formerly the
Committee on Safety of Medicines) contraindicates all antidepres-
sants other than fluoxetine for the treatment of depression in chil-
dren and adolescents In Australia fluvoxamine has been given a
specific indication of OCD in children eight years and over while
prescribers are urged to exercise caution in prescribing other SSRIs
for children under the age of 18 years
A systematic review of SSRIs is required to assess the evidence of
efficacy and harms when used to treat ASD
O B J E C T I V E S
To determine if treatment with SSRIs
1 improves the core features of ASD (social interaction commu-
nication and behavioural problems)
2 improves other non-core aspects of behaviour or function such
as self-injurious behaviour
3 improves the quality of life of adults or children and their carers
4 has short and long term effects on outcome
5 causes harms
M E T H O D S
Criteria for considering studies for this review
Types of studies
3Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Trials were eligible for inclusion in the review if the assignment of
study participants to intervention or control group was random
Types of participants
Inclusion was limited to individuals with a diagnosis of an ASD de-
fined using DSM-IV or ICD-10 or equivalent as a Pervasive Devel-
opmental Disorder excluding Rett syndrome and Childhood Dis-
integrative Disorder Diagnosis must have been made using a stan-
dardised diagnostic instrument (Childhood Autism Rating Scale
(CARS) Autism Diagnostic Interview-Revised (ADI-R) Autism
Diagnostic Observation Schedule (ADOS) Diagnostic Interview
for Social and Communication Disorders (DISCO)) or by using
established diagnostic criteria (ICD-10 DSM-IV) No age limits
were applied
Types of interventions
Oral SSRIs regardless of dosage used or frequency of administra-
tion The control group must be a placebo group
Types of outcome measures
Types of outcomes
1 Core features of ASD ie social interaction
communication and behavioural problems including stereotypy
or restricted repetitive patterns of behaviour interests or
activities
2 Non-core aspects of behaviour and function such as sleep
disturbance self-mutilation aggression attention and
concentration problems and gastrointestinal function
3 Global assessment of health and function
4 Quality of life for the individual or their family
5 Adverse events
No outcome has been identified as primary because there is insuf-
ficient information at present to prioritise these outcomes We in-
tended to examine short (up to 3 months) medium (3-12 months)
and long term (greater than 12 months) outcomes if data were
available
Types of measures
1 Standardised diagnostic assessment instruments (CARS
ADI-R ADOS DISCO)
2 Standardised communication assessments
3 Quality of life questionnaires
4 Rating scales of emotions and behaviour including
depression anxiety aggression obsessive compulsive behaviour
5 Global impression rating scales
6 Other health outcome rating scales
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Tri-
als (CENTRAL) (The Cochrane Library issue 4 2009) and the
following biomedical science databases MEDLINE (December
2009) EMBASE (2009 Week 49) CINAHL (December 2009)
and PsycINFO (December 2009) We also searched the social sci-
ence and education databases Sociological Abstracts (December
2009) and ERIC (December 2009)
Search terms were modified to meet the requirements of indi-
vidual databases The optimally sensitive search strategy for ran-
domised controlled trials developed for the Cochrane Collabora-
tion (Clarke 2003) was combined with medical subject headings
and text words specific for autism and pervasive development dis-
orders as developed by the Cochrane Developmental Psychoso-
cial and Learning Problems Group Search terms were modified
to meet the requirements of individual databases regarding differ-
ences in fields and syntax The aim of the search strategy was for
high precision and recall There were no language restrictions
See Appendix 1 to Appendix 7 for details of search terms for each
database
Searching other resources
We also searched bibliographies of articles identified through the
search strategy and contacted known experts in the field
Data collection and analysis
Selection of studies
Titles and abstracts from the searches were screened by two au-
thors in 2004 2006 and 2008 (DW KW) and December 2009
(KW NS) Disagreement was resolved by consensus and articles
that did not fulfil the inclusion criteria were discarded Potentially
relevant articles were retrieved for full-text assessment and data
extraction
Data extraction and management
Data were organised using Review Manager Data extraction forms
were developed a priori and included information regarding meth-
ods participant details dose and frequency of SSRI administra-
tion and outcomes Data were extracted by two independent re-
viewers (KW and DW or NS) No disagreements arose
4Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Assessment of risk of bias in included studies
Two authors (KW and NS or DW) independently assessed each
included study using the risk of bias criteria outlined in chapter
8 of the Cochrane Handbook for Systematic Reviews of Interventions(Higgins 2008) without blinding to authorship or source The
assessments were compared for inconsistencies and differences in
interpretation were resolved by discussion and consensus Risk of
bias was assessed according to the following five domains with rat-
ings of rsquoYesrsquo (low risk of bias) rsquoNorsquo (high risk of bias) and rsquoUnclearrsquo
(uncertain risk of bias)
1 Sequence generation
Was the allocation sequence adequately generated
ldquoYesrdquo (computer generated random numbers table of random
numbers coin-tossing or similar) ldquoNordquo (day of week evenodd
clinic record number clinician judgment participant preference
laboratory test result such as haemoglobin value or similar) or
ldquoUnclearrdquo (insufficient information about the sequence generation
process to permit judgment)
2 Allocation concealment
Was allocation adequately concealed
ldquoYesrdquo (central independent unit sequentially numbered drug con-
tainers or sealed envelopes of identical appearance or similar)
ldquoNordquo (alternation or rotation date of birth non-opaque envelopes
open table of random numbers or similar) or ldquoUnclearrdquo (randomi-
sation stated but no information on method used is available)
3 Blinding
Was knowledge of the allocated intervention adequately prevented
during the study
ldquoYesrdquo (identical placebo medication or similar) ldquoNordquo (tablets ver-
sus liquid or similar) or ldquoUnclearrdquo (blinding stated but no infor-
mation on method used is available)
4 Incomplete outcome data
Were incomplete data dealt with adequately by the researchers
ldquoYesrdquo (no missing outcome data missing outcome data balanced
in numbers across intervention groups and reasons for dropouts
and withdrawals described or similar) ldquoNordquo (reason for missing
outcome data likely to be related to true outcome or similar) or
ldquoUnclearrdquo (number or reasons for dropouts and withdrawals not
described)
5 Selective outcome reporting
Are reports of the study free of suggestion of selective outcome
reporting
ldquoYesrdquo (study protocol is available published reports include all ex-
pected outcomes or similar) ldquoNordquo (not all of the studyrsquos pre-spec-
ified primary outcomes have been reported one or more reported
primary outcomes were not pre-specified or similar) or ldquoUnclearrdquo
(insufficient information to permit judgement of rsquoadequatersquo or rsquoin-
adequatersquo)
Any other potential sources of bias such as stopping the study
early or extreme baseline imbalance were also explored
Measures of treatment effect
Binary data
If two or more studies presented outcomes from either standard-
ised instruments or diagnostic evaluations as proportions the rela-
tive risk and risk difference with 95 confidence intervals would
have been calculated from meta-analysis Number needed to treat
would also have been calculated where appropriate However only
one study presented categorical outcomes
Continuous data
Where standardised assessment tools generated a score as the out-
come measure comparisons were made between the means of
these scores We calculated mean difference (MD) where possible
and calculated standard error (SE) using data available from the
same study or imputed it from another study in the same meta-
analysis as described in Chapters 7 9 and 16 of the CochraneHandbook for Systematic Reviews of Interventions (Higgins 2008)
Where studies did not use sufficiently similar instruments to mea-
sure an outcome we conducted meta-analysis using standardised
mean difference
Unit of analysis issues
No unit of analysis errors were identified In all included studies
randomisation reporting and analysis were per individual partic-
ipant
Dealing with missing data
Where possible missing data and dropouts were assessed for each
included study and reported Reasons for missing data were pro-
vided when reported in trials Where insufficient data were re-
ported we contacted the trial authors for further information No
replies were received Where data could not be included in meta-
analysis we have included a summary in the text of the review
Assessment of heterogeneity
Consistency of results was assessed visually and by examining I2 (Higgins 2002) a quantity which describes approximately the
proportion of variation in point estimates that is due to hetero-
geneity rather than sampling error
Assessment of reporting biases
Insufficient studies were found to allow for the use of funnel plots
to investigate any relationship between effect size and study pre-
cision (closely related to sample size)
5Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data synthesis
Where possible when two or more studies were found that were
suitable for inclusion we planned to perform a meta-analysis on
the results using a random-effects model
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was not possible because of a lack of data for
meta-analysis Anticipated clinical differences included
- age of participants adult versus paediatric preschool versus
school age
- diagnostic classification
- dose of medication
Sensitivity analysis
Sensitivity analysis was planned to assess the impact of risk of bias
on the results of meta-analyses However we could not conduct
this analysis because there were too few data available for meta-
analysis for the same drug therapy age group and clinical outcome
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
Seven studies are included in the review Five of the studies were
carried out in the USA 1 in France and 1 in Japan Participants
were children in five of the studies and adults in the other two
Results of the search
Electronic literature searches were conducted in December 2004
and yielded 46 titles Thirty-eight studies were excluded because
they were not randomised controlled trials (RCTs) or were not
about ASD Following full paper review four RCTs were identi-
fied The search was repeated in September 2006 and two further
trials were identified The search was repeated in December 2008
No new trials were found The search was repeated in December
2009 and one new trial was found Thus a total of seven RCTs
with 271 participants were included in this review
Of note fenfluramine was not searched for directly and is not
registered for use as an antidepressant but was identified as an
SSRI in electronic searches We debated its inclusion and chose
to retain the two trials to provide a complete clinical picture The
tricyclic antidepressant clomipramine was also identified using this
search method and is known to have serotonin uptake inhibitor
actions but was excluded because unlike fenfluramine it will be
included in a systematic review of tricyclic antidepressants and
ASD (currently in progress)
Different versions of assessment tools were used to measure sim-
ilar outcomes For example for CGI the Clinical Global Im-
pression - Severity scale (CGI-S) the Clinical Global Impression
- Improvement scale (CGI-I) and the Clinical Global Improve-
ment Scale Adapted to Global Autism (CGI-AD) were used and
sometimes the tool used was uncertain (CGI) (Guy 1976) Simi-
larly to measure Obsessive Compulsive Behaviour the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) (Scahill 2006) the
Childrenrsquos Yale-Brown Obsessive Compulsive scale (CY-BOCS)
(McKay 2003) and the Yale-Brown Obsessive-Compulsion Scale
(Goodman 1989Goodman 1989b) and a modified version of it
were used
Included studies
Five studies were conducted in children aged 3-17 years us-
ing fenfluramine (Barthelemy 1989 Leventhal 1993) fluoxe-
tine (Hollander 2005) fluvoxamine (Sugie 2005) and citalopram
(King 2009) Two studies were conducted in adults aged 18-
53 years using fluoxetine (Buchsbaum 2001) and fluvoxamine
(McDougle 1996)
Of the five trials in children two used DSM-IV-TR diagnoses of
Autistic Disorder Asperger Disorder or PDD-NOS (Hollander
2005 King 2009) One study (King 2009) also required at least
moderate severity on the CGI illness severity scale and a moderate
or greater score for compulsive behaviour items of the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) Both of these studies
included children with intelligence in the normal range with one
having an IQ range of 30-132 (Hollander 2005) and the other
reporting 61 of children with a non-verbal IQ over 70 (King
2009) One study included children ldquodiagnosed with autismrdquo using
DSM-IV but did not specify how criteria were applied or provide
information about intelligence (Sugie 2005) Two studies used
DSM-III criteria for a diagnosis of autism and included children
with intellectual impairment with IQ ranges of 16-63 (Leventhal
1993) and 30-75 (Barthelemy 1989)
Of the two adult studies one (Buchsbaum 2001) included adults
diagnosed using DSM-IV with autism or Asperger Disorders and
all patients were verbal with an IQ score range of 53 to 119
The other study included adults diagnosed with autism using the
DSM-III-R and ICD-10 criteria and individuals included were at
least ldquomoderaterdquo in severity using the CGI global severity of illness
rating Both intellectually able and disabled adults were included
(McDougle 1996)
One study (Leventhal 1993) included participants who had pre-
viously been treated with an SSRI Trial authors participated in a
multicentre non-randomised trial of 30 weeks duration and then
extended this trial with a 32 week cross-over RCT Thus there was
6Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Data collection and analysis
Two authors independently selected and appraised studies for inclusion and risk of bias All data were continuous Meta-analysis where
possible used a random-effects model
Main results
Seven RCTs with a total of 271 participants were included Four SSRIs were evaluated fluoxetine (two studies) fluvoxamine (two
studies) fenfluramine (two studies) and citalopram (one study) Five studies included only children and two studies included only adults
Varying inclusion criteria were used with regard to diagnostic criteria and intelligence of participants Seventeen different outcome
measures were reported Although more than one study reported data for Clinical Global Impression (CGI) and obsessive-compulsive
behaviour (OCB) different tool types or components of these outcomes were used in each study As such data were unsuitable for
meta-analysis One large high quality study in children showed no evidence of positive effect of citalopram Two small studies in adults
showed positive outcomes for CGI and OCB one study showed improvements in aggression and another in anxiety
Authorsrsquo conclusions
There is no evidence of effect of SSRIs in children and emerging evidence of harm There is limited evidence of the effectiveness of
SSRIs in adults from small studies in which risk of bias is unclear
P L A I N L A N G U A G E S U M M A R Y
Selective serotonin reuptake inhibitors for the treatment of autism spectrum disorders
Autism spectrum disorders (ASD) are characterised by problems with social interaction and communication as well as repetitive
behaviours and limited activities and interests Selective serotonin reuptake inhibitors (SSRIs) are a class of antidepressants which are
sometimes given to help anxiety or obsessive compulsive behaviours We found seven trials which evaluated four SSRIs fluoxetine
fluvoxamine fenfluramine and citalopram Five studies included only children and two studies included only adults One trial enrolled
149 children but all other trials were small We found no trials which evaluated sertraline paroxetine or escitalopram There is no
evidence to support the use of SSRIs to treat autism in children There is limited evidence which is not yet sufficiently robust to
suggest effectiveness of SSRIs in adults with autism Treatment with an SSRI may cause side effects Decisions about the use of SSRIs
for established clinical indications that may co-occur with autism such as obsessive compulsive disorder and depression in adults or
children and anxiety in adults should be made on a case by case basis
B A C K G R O U N D
Description of the condition
Autism spectrum disorders (ASD) are characterised by qualita-
tive impairment in social interaction and communication skills as
well as stereotypic behaviours and limited activities and interests
While ASD is a commonly used term in clinical practice it is not
recognised by current mainstream disease classification systems
such as the Diagnostic and Statistical Manual of Mental Disorders
fourth edition or fourth edition text revision (DSM-IV DSM-
IV-TR) (APA 1994 APA 2000) and International Classification
of Diseases (ICD-10) (WHO 1993) ASD is generally considered
to include autism defined in Diagnostic and Statistical Manual
of Mental Disorders third edition (DSM-III) (APA 1980) as In-
fantile Autism and the third edition revised (DSM-IIIR) (APA
1987) and DSM-IV (APA 1994) as Autistic Disorder and in ICD-
10 (WHO 1993) as Classical Autism Also included in the term
ASD are the diagnoses Pervasive Developmental Disorder - Not
Otherwise Specified (PDD-NOS) rsquoother pervasive developmen-
tal disordersrsquo rsquopervasive developmental disorder unspecifiedrsquo As-
perger syndrome or Asperger disorder and atypical autism
Estimates of the prevalence of autism using the DSM-III DSM-
IIIR DSM-IV or ICD-10 diagnostic classification systems from
published literature up to April 2004 vary between 1 and 40 per
10000 and for any ASD between 3 and 82 per 10000 (Williams
2006) Publications from 2006 have estimated the prevalence of
any ASD between 22 and 116 per 10000 (Baird 2006 Fombonne
2Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
2006 Gillberg 2006 Guillem 2006 Williams 2008) however
lower rates have also been reported (Atladottir 2007 Chen 2007)
Males are affected about four times more frequently than females
Problems usually present in early childhood and continue through-
out life Autism places a considerable burden of care on the family
and society Follow-up studies have found that only 3-10 of peo-
ple with autism are able to live independently as adults (Billstedt
2005 Howlin 2004)
Description of the intervention
Therapies for autism spectrum disorders (ASD)
The heterogeneous nature of problems seen within the autism
spectrum means that it is often difficult to be sure which indi-
viduals will benefit from the many available therapies It is also
likely that different timing of therapy in relation to age and onset
of problems will change outcomes Many therapies are invasive
time consuming andor expensive and little is known about their
potential to cause harm Pharmacological treatments have been
used most commonly as adjuncts to behavioural intervention to
target specific symptoms and behaviours These treatments have
been associated with reductions in sleep disturbance mood dis-
order poor attentionconcentration and self-harm or aggression
towards others (Gringras 2000)
Selective serotonin reuptake inhibitors (SSRIs)
Antidepressants (most of which are likely to be SSRIs) are the
most commonly prescribed psychotropic medications for ASD
and the class of medication for which there has been the greatest
increase in prescribing (Aman 2005) The prescribing of SSRI
drugs to children and adolescents for any indication has however
been curtailed since the Committee on Safety in Medicines (UK)
and the Food and Drugs Administration (USA) released safety
warnings in 2003 and 2004 respectively concerning an increased
risk of suicide-related behaviours associated with these medications
(Murray 2005 Nemeroff 2007)
How the intervention might work
Increased rates of platelet serotonin transport and levels of whole
blood and platelet serotonin (5-hydroxytryptamine 5-HT) have
been reported in people with ASD (Cook 1996) Serotonin is
linked to the mediation of several psychological processes many
of which are altered in ASD including mood social interaction
sleep obsessive compulsive behaviours and aggression (Saxena
1995) It is therefore plausible that inhibition of serotonin reup-
take will result in improvement of ASD symptoms
Why it is important to do this review
Several studies have reported improvements following adminis-
tration of SSRIs However the subject numbers are small espe-
cially for paediatric patients and serious side effects including in-
creases in maladaptive behaviours urinary retention and seizures
are reported (Branford 1998) A recent larger study of children has
shown no improvement (King 2009) To our knowledge no drug
authority has specifically approved the use of SSRIs for autism
The prescribing of SSRIs for autism is therefore either rsquooff-labelrsquo
or is directed to an associated indicated disorder such as obsessive
compulsive disorder (OCD) or depression
Regarding indications and prescribing for children there are be-
tween-country variations The FDA has approved (allowed the
marketing of ) sertraline in children six years and older fluoxetine
in children seven years and older and fluvoxamine in children
eight years and older for the treatment of OCD The FDA has
approved fluoxetine in children eight years and older and escitalo-
pram in adolescents 12 to 17 years for the treatment of depression
In the UK the Commission on Human Medicines (formerly the
Committee on Safety of Medicines) contraindicates all antidepres-
sants other than fluoxetine for the treatment of depression in chil-
dren and adolescents In Australia fluvoxamine has been given a
specific indication of OCD in children eight years and over while
prescribers are urged to exercise caution in prescribing other SSRIs
for children under the age of 18 years
A systematic review of SSRIs is required to assess the evidence of
efficacy and harms when used to treat ASD
O B J E C T I V E S
To determine if treatment with SSRIs
1 improves the core features of ASD (social interaction commu-
nication and behavioural problems)
2 improves other non-core aspects of behaviour or function such
as self-injurious behaviour
3 improves the quality of life of adults or children and their carers
4 has short and long term effects on outcome
5 causes harms
M E T H O D S
Criteria for considering studies for this review
Types of studies
3Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Trials were eligible for inclusion in the review if the assignment of
study participants to intervention or control group was random
Types of participants
Inclusion was limited to individuals with a diagnosis of an ASD de-
fined using DSM-IV or ICD-10 or equivalent as a Pervasive Devel-
opmental Disorder excluding Rett syndrome and Childhood Dis-
integrative Disorder Diagnosis must have been made using a stan-
dardised diagnostic instrument (Childhood Autism Rating Scale
(CARS) Autism Diagnostic Interview-Revised (ADI-R) Autism
Diagnostic Observation Schedule (ADOS) Diagnostic Interview
for Social and Communication Disorders (DISCO)) or by using
established diagnostic criteria (ICD-10 DSM-IV) No age limits
were applied
Types of interventions
Oral SSRIs regardless of dosage used or frequency of administra-
tion The control group must be a placebo group
Types of outcome measures
Types of outcomes
1 Core features of ASD ie social interaction
communication and behavioural problems including stereotypy
or restricted repetitive patterns of behaviour interests or
activities
2 Non-core aspects of behaviour and function such as sleep
disturbance self-mutilation aggression attention and
concentration problems and gastrointestinal function
3 Global assessment of health and function
4 Quality of life for the individual or their family
5 Adverse events
No outcome has been identified as primary because there is insuf-
ficient information at present to prioritise these outcomes We in-
tended to examine short (up to 3 months) medium (3-12 months)
and long term (greater than 12 months) outcomes if data were
available
Types of measures
1 Standardised diagnostic assessment instruments (CARS
ADI-R ADOS DISCO)
2 Standardised communication assessments
3 Quality of life questionnaires
4 Rating scales of emotions and behaviour including
depression anxiety aggression obsessive compulsive behaviour
5 Global impression rating scales
6 Other health outcome rating scales
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Tri-
als (CENTRAL) (The Cochrane Library issue 4 2009) and the
following biomedical science databases MEDLINE (December
2009) EMBASE (2009 Week 49) CINAHL (December 2009)
and PsycINFO (December 2009) We also searched the social sci-
ence and education databases Sociological Abstracts (December
2009) and ERIC (December 2009)
Search terms were modified to meet the requirements of indi-
vidual databases The optimally sensitive search strategy for ran-
domised controlled trials developed for the Cochrane Collabora-
tion (Clarke 2003) was combined with medical subject headings
and text words specific for autism and pervasive development dis-
orders as developed by the Cochrane Developmental Psychoso-
cial and Learning Problems Group Search terms were modified
to meet the requirements of individual databases regarding differ-
ences in fields and syntax The aim of the search strategy was for
high precision and recall There were no language restrictions
See Appendix 1 to Appendix 7 for details of search terms for each
database
Searching other resources
We also searched bibliographies of articles identified through the
search strategy and contacted known experts in the field
Data collection and analysis
Selection of studies
Titles and abstracts from the searches were screened by two au-
thors in 2004 2006 and 2008 (DW KW) and December 2009
(KW NS) Disagreement was resolved by consensus and articles
that did not fulfil the inclusion criteria were discarded Potentially
relevant articles were retrieved for full-text assessment and data
extraction
Data extraction and management
Data were organised using Review Manager Data extraction forms
were developed a priori and included information regarding meth-
ods participant details dose and frequency of SSRI administra-
tion and outcomes Data were extracted by two independent re-
viewers (KW and DW or NS) No disagreements arose
4Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Assessment of risk of bias in included studies
Two authors (KW and NS or DW) independently assessed each
included study using the risk of bias criteria outlined in chapter
8 of the Cochrane Handbook for Systematic Reviews of Interventions(Higgins 2008) without blinding to authorship or source The
assessments were compared for inconsistencies and differences in
interpretation were resolved by discussion and consensus Risk of
bias was assessed according to the following five domains with rat-
ings of rsquoYesrsquo (low risk of bias) rsquoNorsquo (high risk of bias) and rsquoUnclearrsquo
(uncertain risk of bias)
1 Sequence generation
Was the allocation sequence adequately generated
ldquoYesrdquo (computer generated random numbers table of random
numbers coin-tossing or similar) ldquoNordquo (day of week evenodd
clinic record number clinician judgment participant preference
laboratory test result such as haemoglobin value or similar) or
ldquoUnclearrdquo (insufficient information about the sequence generation
process to permit judgment)
2 Allocation concealment
Was allocation adequately concealed
ldquoYesrdquo (central independent unit sequentially numbered drug con-
tainers or sealed envelopes of identical appearance or similar)
ldquoNordquo (alternation or rotation date of birth non-opaque envelopes
open table of random numbers or similar) or ldquoUnclearrdquo (randomi-
sation stated but no information on method used is available)
3 Blinding
Was knowledge of the allocated intervention adequately prevented
during the study
ldquoYesrdquo (identical placebo medication or similar) ldquoNordquo (tablets ver-
sus liquid or similar) or ldquoUnclearrdquo (blinding stated but no infor-
mation on method used is available)
4 Incomplete outcome data
Were incomplete data dealt with adequately by the researchers
ldquoYesrdquo (no missing outcome data missing outcome data balanced
in numbers across intervention groups and reasons for dropouts
and withdrawals described or similar) ldquoNordquo (reason for missing
outcome data likely to be related to true outcome or similar) or
ldquoUnclearrdquo (number or reasons for dropouts and withdrawals not
described)
5 Selective outcome reporting
Are reports of the study free of suggestion of selective outcome
reporting
ldquoYesrdquo (study protocol is available published reports include all ex-
pected outcomes or similar) ldquoNordquo (not all of the studyrsquos pre-spec-
ified primary outcomes have been reported one or more reported
primary outcomes were not pre-specified or similar) or ldquoUnclearrdquo
(insufficient information to permit judgement of rsquoadequatersquo or rsquoin-
adequatersquo)
Any other potential sources of bias such as stopping the study
early or extreme baseline imbalance were also explored
Measures of treatment effect
Binary data
If two or more studies presented outcomes from either standard-
ised instruments or diagnostic evaluations as proportions the rela-
tive risk and risk difference with 95 confidence intervals would
have been calculated from meta-analysis Number needed to treat
would also have been calculated where appropriate However only
one study presented categorical outcomes
Continuous data
Where standardised assessment tools generated a score as the out-
come measure comparisons were made between the means of
these scores We calculated mean difference (MD) where possible
and calculated standard error (SE) using data available from the
same study or imputed it from another study in the same meta-
analysis as described in Chapters 7 9 and 16 of the CochraneHandbook for Systematic Reviews of Interventions (Higgins 2008)
Where studies did not use sufficiently similar instruments to mea-
sure an outcome we conducted meta-analysis using standardised
mean difference
Unit of analysis issues
No unit of analysis errors were identified In all included studies
randomisation reporting and analysis were per individual partic-
ipant
Dealing with missing data
Where possible missing data and dropouts were assessed for each
included study and reported Reasons for missing data were pro-
vided when reported in trials Where insufficient data were re-
ported we contacted the trial authors for further information No
replies were received Where data could not be included in meta-
analysis we have included a summary in the text of the review
Assessment of heterogeneity
Consistency of results was assessed visually and by examining I2 (Higgins 2002) a quantity which describes approximately the
proportion of variation in point estimates that is due to hetero-
geneity rather than sampling error
Assessment of reporting biases
Insufficient studies were found to allow for the use of funnel plots
to investigate any relationship between effect size and study pre-
cision (closely related to sample size)
5Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data synthesis
Where possible when two or more studies were found that were
suitable for inclusion we planned to perform a meta-analysis on
the results using a random-effects model
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was not possible because of a lack of data for
meta-analysis Anticipated clinical differences included
- age of participants adult versus paediatric preschool versus
school age
- diagnostic classification
- dose of medication
Sensitivity analysis
Sensitivity analysis was planned to assess the impact of risk of bias
on the results of meta-analyses However we could not conduct
this analysis because there were too few data available for meta-
analysis for the same drug therapy age group and clinical outcome
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
Seven studies are included in the review Five of the studies were
carried out in the USA 1 in France and 1 in Japan Participants
were children in five of the studies and adults in the other two
Results of the search
Electronic literature searches were conducted in December 2004
and yielded 46 titles Thirty-eight studies were excluded because
they were not randomised controlled trials (RCTs) or were not
about ASD Following full paper review four RCTs were identi-
fied The search was repeated in September 2006 and two further
trials were identified The search was repeated in December 2008
No new trials were found The search was repeated in December
2009 and one new trial was found Thus a total of seven RCTs
with 271 participants were included in this review
Of note fenfluramine was not searched for directly and is not
registered for use as an antidepressant but was identified as an
SSRI in electronic searches We debated its inclusion and chose
to retain the two trials to provide a complete clinical picture The
tricyclic antidepressant clomipramine was also identified using this
search method and is known to have serotonin uptake inhibitor
actions but was excluded because unlike fenfluramine it will be
included in a systematic review of tricyclic antidepressants and
ASD (currently in progress)
Different versions of assessment tools were used to measure sim-
ilar outcomes For example for CGI the Clinical Global Im-
pression - Severity scale (CGI-S) the Clinical Global Impression
- Improvement scale (CGI-I) and the Clinical Global Improve-
ment Scale Adapted to Global Autism (CGI-AD) were used and
sometimes the tool used was uncertain (CGI) (Guy 1976) Simi-
larly to measure Obsessive Compulsive Behaviour the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) (Scahill 2006) the
Childrenrsquos Yale-Brown Obsessive Compulsive scale (CY-BOCS)
(McKay 2003) and the Yale-Brown Obsessive-Compulsion Scale
(Goodman 1989Goodman 1989b) and a modified version of it
were used
Included studies
Five studies were conducted in children aged 3-17 years us-
ing fenfluramine (Barthelemy 1989 Leventhal 1993) fluoxe-
tine (Hollander 2005) fluvoxamine (Sugie 2005) and citalopram
(King 2009) Two studies were conducted in adults aged 18-
53 years using fluoxetine (Buchsbaum 2001) and fluvoxamine
(McDougle 1996)
Of the five trials in children two used DSM-IV-TR diagnoses of
Autistic Disorder Asperger Disorder or PDD-NOS (Hollander
2005 King 2009) One study (King 2009) also required at least
moderate severity on the CGI illness severity scale and a moderate
or greater score for compulsive behaviour items of the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) Both of these studies
included children with intelligence in the normal range with one
having an IQ range of 30-132 (Hollander 2005) and the other
reporting 61 of children with a non-verbal IQ over 70 (King
2009) One study included children ldquodiagnosed with autismrdquo using
DSM-IV but did not specify how criteria were applied or provide
information about intelligence (Sugie 2005) Two studies used
DSM-III criteria for a diagnosis of autism and included children
with intellectual impairment with IQ ranges of 16-63 (Leventhal
1993) and 30-75 (Barthelemy 1989)
Of the two adult studies one (Buchsbaum 2001) included adults
diagnosed using DSM-IV with autism or Asperger Disorders and
all patients were verbal with an IQ score range of 53 to 119
The other study included adults diagnosed with autism using the
DSM-III-R and ICD-10 criteria and individuals included were at
least ldquomoderaterdquo in severity using the CGI global severity of illness
rating Both intellectually able and disabled adults were included
(McDougle 1996)
One study (Leventhal 1993) included participants who had pre-
viously been treated with an SSRI Trial authors participated in a
multicentre non-randomised trial of 30 weeks duration and then
extended this trial with a 32 week cross-over RCT Thus there was
6Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

2006 Gillberg 2006 Guillem 2006 Williams 2008) however
lower rates have also been reported (Atladottir 2007 Chen 2007)
Males are affected about four times more frequently than females
Problems usually present in early childhood and continue through-
out life Autism places a considerable burden of care on the family
and society Follow-up studies have found that only 3-10 of peo-
ple with autism are able to live independently as adults (Billstedt
2005 Howlin 2004)
Description of the intervention
Therapies for autism spectrum disorders (ASD)
The heterogeneous nature of problems seen within the autism
spectrum means that it is often difficult to be sure which indi-
viduals will benefit from the many available therapies It is also
likely that different timing of therapy in relation to age and onset
of problems will change outcomes Many therapies are invasive
time consuming andor expensive and little is known about their
potential to cause harm Pharmacological treatments have been
used most commonly as adjuncts to behavioural intervention to
target specific symptoms and behaviours These treatments have
been associated with reductions in sleep disturbance mood dis-
order poor attentionconcentration and self-harm or aggression
towards others (Gringras 2000)
Selective serotonin reuptake inhibitors (SSRIs)
Antidepressants (most of which are likely to be SSRIs) are the
most commonly prescribed psychotropic medications for ASD
and the class of medication for which there has been the greatest
increase in prescribing (Aman 2005) The prescribing of SSRI
drugs to children and adolescents for any indication has however
been curtailed since the Committee on Safety in Medicines (UK)
and the Food and Drugs Administration (USA) released safety
warnings in 2003 and 2004 respectively concerning an increased
risk of suicide-related behaviours associated with these medications
(Murray 2005 Nemeroff 2007)
How the intervention might work
Increased rates of platelet serotonin transport and levels of whole
blood and platelet serotonin (5-hydroxytryptamine 5-HT) have
been reported in people with ASD (Cook 1996) Serotonin is
linked to the mediation of several psychological processes many
of which are altered in ASD including mood social interaction
sleep obsessive compulsive behaviours and aggression (Saxena
1995) It is therefore plausible that inhibition of serotonin reup-
take will result in improvement of ASD symptoms
Why it is important to do this review
Several studies have reported improvements following adminis-
tration of SSRIs However the subject numbers are small espe-
cially for paediatric patients and serious side effects including in-
creases in maladaptive behaviours urinary retention and seizures
are reported (Branford 1998) A recent larger study of children has
shown no improvement (King 2009) To our knowledge no drug
authority has specifically approved the use of SSRIs for autism
The prescribing of SSRIs for autism is therefore either rsquooff-labelrsquo
or is directed to an associated indicated disorder such as obsessive
compulsive disorder (OCD) or depression
Regarding indications and prescribing for children there are be-
tween-country variations The FDA has approved (allowed the
marketing of ) sertraline in children six years and older fluoxetine
in children seven years and older and fluvoxamine in children
eight years and older for the treatment of OCD The FDA has
approved fluoxetine in children eight years and older and escitalo-
pram in adolescents 12 to 17 years for the treatment of depression
In the UK the Commission on Human Medicines (formerly the
Committee on Safety of Medicines) contraindicates all antidepres-
sants other than fluoxetine for the treatment of depression in chil-
dren and adolescents In Australia fluvoxamine has been given a
specific indication of OCD in children eight years and over while
prescribers are urged to exercise caution in prescribing other SSRIs
for children under the age of 18 years
A systematic review of SSRIs is required to assess the evidence of
efficacy and harms when used to treat ASD
O B J E C T I V E S
To determine if treatment with SSRIs
1 improves the core features of ASD (social interaction commu-
nication and behavioural problems)
2 improves other non-core aspects of behaviour or function such
as self-injurious behaviour
3 improves the quality of life of adults or children and their carers
4 has short and long term effects on outcome
5 causes harms
M E T H O D S
Criteria for considering studies for this review
Types of studies
3Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Trials were eligible for inclusion in the review if the assignment of
study participants to intervention or control group was random
Types of participants
Inclusion was limited to individuals with a diagnosis of an ASD de-
fined using DSM-IV or ICD-10 or equivalent as a Pervasive Devel-
opmental Disorder excluding Rett syndrome and Childhood Dis-
integrative Disorder Diagnosis must have been made using a stan-
dardised diagnostic instrument (Childhood Autism Rating Scale
(CARS) Autism Diagnostic Interview-Revised (ADI-R) Autism
Diagnostic Observation Schedule (ADOS) Diagnostic Interview
for Social and Communication Disorders (DISCO)) or by using
established diagnostic criteria (ICD-10 DSM-IV) No age limits
were applied
Types of interventions
Oral SSRIs regardless of dosage used or frequency of administra-
tion The control group must be a placebo group
Types of outcome measures
Types of outcomes
1 Core features of ASD ie social interaction
communication and behavioural problems including stereotypy
or restricted repetitive patterns of behaviour interests or
activities
2 Non-core aspects of behaviour and function such as sleep
disturbance self-mutilation aggression attention and
concentration problems and gastrointestinal function
3 Global assessment of health and function
4 Quality of life for the individual or their family
5 Adverse events
No outcome has been identified as primary because there is insuf-
ficient information at present to prioritise these outcomes We in-
tended to examine short (up to 3 months) medium (3-12 months)
and long term (greater than 12 months) outcomes if data were
available
Types of measures
1 Standardised diagnostic assessment instruments (CARS
ADI-R ADOS DISCO)
2 Standardised communication assessments
3 Quality of life questionnaires
4 Rating scales of emotions and behaviour including
depression anxiety aggression obsessive compulsive behaviour
5 Global impression rating scales
6 Other health outcome rating scales
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Tri-
als (CENTRAL) (The Cochrane Library issue 4 2009) and the
following biomedical science databases MEDLINE (December
2009) EMBASE (2009 Week 49) CINAHL (December 2009)
and PsycINFO (December 2009) We also searched the social sci-
ence and education databases Sociological Abstracts (December
2009) and ERIC (December 2009)
Search terms were modified to meet the requirements of indi-
vidual databases The optimally sensitive search strategy for ran-
domised controlled trials developed for the Cochrane Collabora-
tion (Clarke 2003) was combined with medical subject headings
and text words specific for autism and pervasive development dis-
orders as developed by the Cochrane Developmental Psychoso-
cial and Learning Problems Group Search terms were modified
to meet the requirements of individual databases regarding differ-
ences in fields and syntax The aim of the search strategy was for
high precision and recall There were no language restrictions
See Appendix 1 to Appendix 7 for details of search terms for each
database
Searching other resources
We also searched bibliographies of articles identified through the
search strategy and contacted known experts in the field
Data collection and analysis
Selection of studies
Titles and abstracts from the searches were screened by two au-
thors in 2004 2006 and 2008 (DW KW) and December 2009
(KW NS) Disagreement was resolved by consensus and articles
that did not fulfil the inclusion criteria were discarded Potentially
relevant articles were retrieved for full-text assessment and data
extraction
Data extraction and management
Data were organised using Review Manager Data extraction forms
were developed a priori and included information regarding meth-
ods participant details dose and frequency of SSRI administra-
tion and outcomes Data were extracted by two independent re-
viewers (KW and DW or NS) No disagreements arose
4Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Assessment of risk of bias in included studies
Two authors (KW and NS or DW) independently assessed each
included study using the risk of bias criteria outlined in chapter
8 of the Cochrane Handbook for Systematic Reviews of Interventions(Higgins 2008) without blinding to authorship or source The
assessments were compared for inconsistencies and differences in
interpretation were resolved by discussion and consensus Risk of
bias was assessed according to the following five domains with rat-
ings of rsquoYesrsquo (low risk of bias) rsquoNorsquo (high risk of bias) and rsquoUnclearrsquo
(uncertain risk of bias)
1 Sequence generation
Was the allocation sequence adequately generated
ldquoYesrdquo (computer generated random numbers table of random
numbers coin-tossing or similar) ldquoNordquo (day of week evenodd
clinic record number clinician judgment participant preference
laboratory test result such as haemoglobin value or similar) or
ldquoUnclearrdquo (insufficient information about the sequence generation
process to permit judgment)
2 Allocation concealment
Was allocation adequately concealed
ldquoYesrdquo (central independent unit sequentially numbered drug con-
tainers or sealed envelopes of identical appearance or similar)
ldquoNordquo (alternation or rotation date of birth non-opaque envelopes
open table of random numbers or similar) or ldquoUnclearrdquo (randomi-
sation stated but no information on method used is available)
3 Blinding
Was knowledge of the allocated intervention adequately prevented
during the study
ldquoYesrdquo (identical placebo medication or similar) ldquoNordquo (tablets ver-
sus liquid or similar) or ldquoUnclearrdquo (blinding stated but no infor-
mation on method used is available)
4 Incomplete outcome data
Were incomplete data dealt with adequately by the researchers
ldquoYesrdquo (no missing outcome data missing outcome data balanced
in numbers across intervention groups and reasons for dropouts
and withdrawals described or similar) ldquoNordquo (reason for missing
outcome data likely to be related to true outcome or similar) or
ldquoUnclearrdquo (number or reasons for dropouts and withdrawals not
described)
5 Selective outcome reporting
Are reports of the study free of suggestion of selective outcome
reporting
ldquoYesrdquo (study protocol is available published reports include all ex-
pected outcomes or similar) ldquoNordquo (not all of the studyrsquos pre-spec-
ified primary outcomes have been reported one or more reported
primary outcomes were not pre-specified or similar) or ldquoUnclearrdquo
(insufficient information to permit judgement of rsquoadequatersquo or rsquoin-
adequatersquo)
Any other potential sources of bias such as stopping the study
early or extreme baseline imbalance were also explored
Measures of treatment effect
Binary data
If two or more studies presented outcomes from either standard-
ised instruments or diagnostic evaluations as proportions the rela-
tive risk and risk difference with 95 confidence intervals would
have been calculated from meta-analysis Number needed to treat
would also have been calculated where appropriate However only
one study presented categorical outcomes
Continuous data
Where standardised assessment tools generated a score as the out-
come measure comparisons were made between the means of
these scores We calculated mean difference (MD) where possible
and calculated standard error (SE) using data available from the
same study or imputed it from another study in the same meta-
analysis as described in Chapters 7 9 and 16 of the CochraneHandbook for Systematic Reviews of Interventions (Higgins 2008)
Where studies did not use sufficiently similar instruments to mea-
sure an outcome we conducted meta-analysis using standardised
mean difference
Unit of analysis issues
No unit of analysis errors were identified In all included studies
randomisation reporting and analysis were per individual partic-
ipant
Dealing with missing data
Where possible missing data and dropouts were assessed for each
included study and reported Reasons for missing data were pro-
vided when reported in trials Where insufficient data were re-
ported we contacted the trial authors for further information No
replies were received Where data could not be included in meta-
analysis we have included a summary in the text of the review
Assessment of heterogeneity
Consistency of results was assessed visually and by examining I2 (Higgins 2002) a quantity which describes approximately the
proportion of variation in point estimates that is due to hetero-
geneity rather than sampling error
Assessment of reporting biases
Insufficient studies were found to allow for the use of funnel plots
to investigate any relationship between effect size and study pre-
cision (closely related to sample size)
5Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data synthesis
Where possible when two or more studies were found that were
suitable for inclusion we planned to perform a meta-analysis on
the results using a random-effects model
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was not possible because of a lack of data for
meta-analysis Anticipated clinical differences included
- age of participants adult versus paediatric preschool versus
school age
- diagnostic classification
- dose of medication
Sensitivity analysis
Sensitivity analysis was planned to assess the impact of risk of bias
on the results of meta-analyses However we could not conduct
this analysis because there were too few data available for meta-
analysis for the same drug therapy age group and clinical outcome
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
Seven studies are included in the review Five of the studies were
carried out in the USA 1 in France and 1 in Japan Participants
were children in five of the studies and adults in the other two
Results of the search
Electronic literature searches were conducted in December 2004
and yielded 46 titles Thirty-eight studies were excluded because
they were not randomised controlled trials (RCTs) or were not
about ASD Following full paper review four RCTs were identi-
fied The search was repeated in September 2006 and two further
trials were identified The search was repeated in December 2008
No new trials were found The search was repeated in December
2009 and one new trial was found Thus a total of seven RCTs
with 271 participants were included in this review
Of note fenfluramine was not searched for directly and is not
registered for use as an antidepressant but was identified as an
SSRI in electronic searches We debated its inclusion and chose
to retain the two trials to provide a complete clinical picture The
tricyclic antidepressant clomipramine was also identified using this
search method and is known to have serotonin uptake inhibitor
actions but was excluded because unlike fenfluramine it will be
included in a systematic review of tricyclic antidepressants and
ASD (currently in progress)
Different versions of assessment tools were used to measure sim-
ilar outcomes For example for CGI the Clinical Global Im-
pression - Severity scale (CGI-S) the Clinical Global Impression
- Improvement scale (CGI-I) and the Clinical Global Improve-
ment Scale Adapted to Global Autism (CGI-AD) were used and
sometimes the tool used was uncertain (CGI) (Guy 1976) Simi-
larly to measure Obsessive Compulsive Behaviour the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) (Scahill 2006) the
Childrenrsquos Yale-Brown Obsessive Compulsive scale (CY-BOCS)
(McKay 2003) and the Yale-Brown Obsessive-Compulsion Scale
(Goodman 1989Goodman 1989b) and a modified version of it
were used
Included studies
Five studies were conducted in children aged 3-17 years us-
ing fenfluramine (Barthelemy 1989 Leventhal 1993) fluoxe-
tine (Hollander 2005) fluvoxamine (Sugie 2005) and citalopram
(King 2009) Two studies were conducted in adults aged 18-
53 years using fluoxetine (Buchsbaum 2001) and fluvoxamine
(McDougle 1996)
Of the five trials in children two used DSM-IV-TR diagnoses of
Autistic Disorder Asperger Disorder or PDD-NOS (Hollander
2005 King 2009) One study (King 2009) also required at least
moderate severity on the CGI illness severity scale and a moderate
or greater score for compulsive behaviour items of the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) Both of these studies
included children with intelligence in the normal range with one
having an IQ range of 30-132 (Hollander 2005) and the other
reporting 61 of children with a non-verbal IQ over 70 (King
2009) One study included children ldquodiagnosed with autismrdquo using
DSM-IV but did not specify how criteria were applied or provide
information about intelligence (Sugie 2005) Two studies used
DSM-III criteria for a diagnosis of autism and included children
with intellectual impairment with IQ ranges of 16-63 (Leventhal
1993) and 30-75 (Barthelemy 1989)
Of the two adult studies one (Buchsbaum 2001) included adults
diagnosed using DSM-IV with autism or Asperger Disorders and
all patients were verbal with an IQ score range of 53 to 119
The other study included adults diagnosed with autism using the
DSM-III-R and ICD-10 criteria and individuals included were at
least ldquomoderaterdquo in severity using the CGI global severity of illness
rating Both intellectually able and disabled adults were included
(McDougle 1996)
One study (Leventhal 1993) included participants who had pre-
viously been treated with an SSRI Trial authors participated in a
multicentre non-randomised trial of 30 weeks duration and then
extended this trial with a 32 week cross-over RCT Thus there was
6Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Trials were eligible for inclusion in the review if the assignment of
study participants to intervention or control group was random
Types of participants
Inclusion was limited to individuals with a diagnosis of an ASD de-
fined using DSM-IV or ICD-10 or equivalent as a Pervasive Devel-
opmental Disorder excluding Rett syndrome and Childhood Dis-
integrative Disorder Diagnosis must have been made using a stan-
dardised diagnostic instrument (Childhood Autism Rating Scale
(CARS) Autism Diagnostic Interview-Revised (ADI-R) Autism
Diagnostic Observation Schedule (ADOS) Diagnostic Interview
for Social and Communication Disorders (DISCO)) or by using
established diagnostic criteria (ICD-10 DSM-IV) No age limits
were applied
Types of interventions
Oral SSRIs regardless of dosage used or frequency of administra-
tion The control group must be a placebo group
Types of outcome measures
Types of outcomes
1 Core features of ASD ie social interaction
communication and behavioural problems including stereotypy
or restricted repetitive patterns of behaviour interests or
activities
2 Non-core aspects of behaviour and function such as sleep
disturbance self-mutilation aggression attention and
concentration problems and gastrointestinal function
3 Global assessment of health and function
4 Quality of life for the individual or their family
5 Adverse events
No outcome has been identified as primary because there is insuf-
ficient information at present to prioritise these outcomes We in-
tended to examine short (up to 3 months) medium (3-12 months)
and long term (greater than 12 months) outcomes if data were
available
Types of measures
1 Standardised diagnostic assessment instruments (CARS
ADI-R ADOS DISCO)
2 Standardised communication assessments
3 Quality of life questionnaires
4 Rating scales of emotions and behaviour including
depression anxiety aggression obsessive compulsive behaviour
5 Global impression rating scales
6 Other health outcome rating scales
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Tri-
als (CENTRAL) (The Cochrane Library issue 4 2009) and the
following biomedical science databases MEDLINE (December
2009) EMBASE (2009 Week 49) CINAHL (December 2009)
and PsycINFO (December 2009) We also searched the social sci-
ence and education databases Sociological Abstracts (December
2009) and ERIC (December 2009)
Search terms were modified to meet the requirements of indi-
vidual databases The optimally sensitive search strategy for ran-
domised controlled trials developed for the Cochrane Collabora-
tion (Clarke 2003) was combined with medical subject headings
and text words specific for autism and pervasive development dis-
orders as developed by the Cochrane Developmental Psychoso-
cial and Learning Problems Group Search terms were modified
to meet the requirements of individual databases regarding differ-
ences in fields and syntax The aim of the search strategy was for
high precision and recall There were no language restrictions
See Appendix 1 to Appendix 7 for details of search terms for each
database
Searching other resources
We also searched bibliographies of articles identified through the
search strategy and contacted known experts in the field
Data collection and analysis
Selection of studies
Titles and abstracts from the searches were screened by two au-
thors in 2004 2006 and 2008 (DW KW) and December 2009
(KW NS) Disagreement was resolved by consensus and articles
that did not fulfil the inclusion criteria were discarded Potentially
relevant articles were retrieved for full-text assessment and data
extraction
Data extraction and management
Data were organised using Review Manager Data extraction forms
were developed a priori and included information regarding meth-
ods participant details dose and frequency of SSRI administra-
tion and outcomes Data were extracted by two independent re-
viewers (KW and DW or NS) No disagreements arose
4Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Assessment of risk of bias in included studies
Two authors (KW and NS or DW) independently assessed each
included study using the risk of bias criteria outlined in chapter
8 of the Cochrane Handbook for Systematic Reviews of Interventions(Higgins 2008) without blinding to authorship or source The
assessments were compared for inconsistencies and differences in
interpretation were resolved by discussion and consensus Risk of
bias was assessed according to the following five domains with rat-
ings of rsquoYesrsquo (low risk of bias) rsquoNorsquo (high risk of bias) and rsquoUnclearrsquo
(uncertain risk of bias)
1 Sequence generation
Was the allocation sequence adequately generated
ldquoYesrdquo (computer generated random numbers table of random
numbers coin-tossing or similar) ldquoNordquo (day of week evenodd
clinic record number clinician judgment participant preference
laboratory test result such as haemoglobin value or similar) or
ldquoUnclearrdquo (insufficient information about the sequence generation
process to permit judgment)
2 Allocation concealment
Was allocation adequately concealed
ldquoYesrdquo (central independent unit sequentially numbered drug con-
tainers or sealed envelopes of identical appearance or similar)
ldquoNordquo (alternation or rotation date of birth non-opaque envelopes
open table of random numbers or similar) or ldquoUnclearrdquo (randomi-
sation stated but no information on method used is available)
3 Blinding
Was knowledge of the allocated intervention adequately prevented
during the study
ldquoYesrdquo (identical placebo medication or similar) ldquoNordquo (tablets ver-
sus liquid or similar) or ldquoUnclearrdquo (blinding stated but no infor-
mation on method used is available)
4 Incomplete outcome data
Were incomplete data dealt with adequately by the researchers
ldquoYesrdquo (no missing outcome data missing outcome data balanced
in numbers across intervention groups and reasons for dropouts
and withdrawals described or similar) ldquoNordquo (reason for missing
outcome data likely to be related to true outcome or similar) or
ldquoUnclearrdquo (number or reasons for dropouts and withdrawals not
described)
5 Selective outcome reporting
Are reports of the study free of suggestion of selective outcome
reporting
ldquoYesrdquo (study protocol is available published reports include all ex-
pected outcomes or similar) ldquoNordquo (not all of the studyrsquos pre-spec-
ified primary outcomes have been reported one or more reported
primary outcomes were not pre-specified or similar) or ldquoUnclearrdquo
(insufficient information to permit judgement of rsquoadequatersquo or rsquoin-
adequatersquo)
Any other potential sources of bias such as stopping the study
early or extreme baseline imbalance were also explored
Measures of treatment effect
Binary data
If two or more studies presented outcomes from either standard-
ised instruments or diagnostic evaluations as proportions the rela-
tive risk and risk difference with 95 confidence intervals would
have been calculated from meta-analysis Number needed to treat
would also have been calculated where appropriate However only
one study presented categorical outcomes
Continuous data
Where standardised assessment tools generated a score as the out-
come measure comparisons were made between the means of
these scores We calculated mean difference (MD) where possible
and calculated standard error (SE) using data available from the
same study or imputed it from another study in the same meta-
analysis as described in Chapters 7 9 and 16 of the CochraneHandbook for Systematic Reviews of Interventions (Higgins 2008)
Where studies did not use sufficiently similar instruments to mea-
sure an outcome we conducted meta-analysis using standardised
mean difference
Unit of analysis issues
No unit of analysis errors were identified In all included studies
randomisation reporting and analysis were per individual partic-
ipant
Dealing with missing data
Where possible missing data and dropouts were assessed for each
included study and reported Reasons for missing data were pro-
vided when reported in trials Where insufficient data were re-
ported we contacted the trial authors for further information No
replies were received Where data could not be included in meta-
analysis we have included a summary in the text of the review
Assessment of heterogeneity
Consistency of results was assessed visually and by examining I2 (Higgins 2002) a quantity which describes approximately the
proportion of variation in point estimates that is due to hetero-
geneity rather than sampling error
Assessment of reporting biases
Insufficient studies were found to allow for the use of funnel plots
to investigate any relationship between effect size and study pre-
cision (closely related to sample size)
5Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data synthesis
Where possible when two or more studies were found that were
suitable for inclusion we planned to perform a meta-analysis on
the results using a random-effects model
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was not possible because of a lack of data for
meta-analysis Anticipated clinical differences included
- age of participants adult versus paediatric preschool versus
school age
- diagnostic classification
- dose of medication
Sensitivity analysis
Sensitivity analysis was planned to assess the impact of risk of bias
on the results of meta-analyses However we could not conduct
this analysis because there were too few data available for meta-
analysis for the same drug therapy age group and clinical outcome
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
Seven studies are included in the review Five of the studies were
carried out in the USA 1 in France and 1 in Japan Participants
were children in five of the studies and adults in the other two
Results of the search
Electronic literature searches were conducted in December 2004
and yielded 46 titles Thirty-eight studies were excluded because
they were not randomised controlled trials (RCTs) or were not
about ASD Following full paper review four RCTs were identi-
fied The search was repeated in September 2006 and two further
trials were identified The search was repeated in December 2008
No new trials were found The search was repeated in December
2009 and one new trial was found Thus a total of seven RCTs
with 271 participants were included in this review
Of note fenfluramine was not searched for directly and is not
registered for use as an antidepressant but was identified as an
SSRI in electronic searches We debated its inclusion and chose
to retain the two trials to provide a complete clinical picture The
tricyclic antidepressant clomipramine was also identified using this
search method and is known to have serotonin uptake inhibitor
actions but was excluded because unlike fenfluramine it will be
included in a systematic review of tricyclic antidepressants and
ASD (currently in progress)
Different versions of assessment tools were used to measure sim-
ilar outcomes For example for CGI the Clinical Global Im-
pression - Severity scale (CGI-S) the Clinical Global Impression
- Improvement scale (CGI-I) and the Clinical Global Improve-
ment Scale Adapted to Global Autism (CGI-AD) were used and
sometimes the tool used was uncertain (CGI) (Guy 1976) Simi-
larly to measure Obsessive Compulsive Behaviour the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) (Scahill 2006) the
Childrenrsquos Yale-Brown Obsessive Compulsive scale (CY-BOCS)
(McKay 2003) and the Yale-Brown Obsessive-Compulsion Scale
(Goodman 1989Goodman 1989b) and a modified version of it
were used
Included studies
Five studies were conducted in children aged 3-17 years us-
ing fenfluramine (Barthelemy 1989 Leventhal 1993) fluoxe-
tine (Hollander 2005) fluvoxamine (Sugie 2005) and citalopram
(King 2009) Two studies were conducted in adults aged 18-
53 years using fluoxetine (Buchsbaum 2001) and fluvoxamine
(McDougle 1996)
Of the five trials in children two used DSM-IV-TR diagnoses of
Autistic Disorder Asperger Disorder or PDD-NOS (Hollander
2005 King 2009) One study (King 2009) also required at least
moderate severity on the CGI illness severity scale and a moderate
or greater score for compulsive behaviour items of the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) Both of these studies
included children with intelligence in the normal range with one
having an IQ range of 30-132 (Hollander 2005) and the other
reporting 61 of children with a non-verbal IQ over 70 (King
2009) One study included children ldquodiagnosed with autismrdquo using
DSM-IV but did not specify how criteria were applied or provide
information about intelligence (Sugie 2005) Two studies used
DSM-III criteria for a diagnosis of autism and included children
with intellectual impairment with IQ ranges of 16-63 (Leventhal
1993) and 30-75 (Barthelemy 1989)
Of the two adult studies one (Buchsbaum 2001) included adults
diagnosed using DSM-IV with autism or Asperger Disorders and
all patients were verbal with an IQ score range of 53 to 119
The other study included adults diagnosed with autism using the
DSM-III-R and ICD-10 criteria and individuals included were at
least ldquomoderaterdquo in severity using the CGI global severity of illness
rating Both intellectually able and disabled adults were included
(McDougle 1996)
One study (Leventhal 1993) included participants who had pre-
viously been treated with an SSRI Trial authors participated in a
multicentre non-randomised trial of 30 weeks duration and then
extended this trial with a 32 week cross-over RCT Thus there was
6Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Assessment of risk of bias in included studies
Two authors (KW and NS or DW) independently assessed each
included study using the risk of bias criteria outlined in chapter
8 of the Cochrane Handbook for Systematic Reviews of Interventions(Higgins 2008) without blinding to authorship or source The
assessments were compared for inconsistencies and differences in
interpretation were resolved by discussion and consensus Risk of
bias was assessed according to the following five domains with rat-
ings of rsquoYesrsquo (low risk of bias) rsquoNorsquo (high risk of bias) and rsquoUnclearrsquo
(uncertain risk of bias)
1 Sequence generation
Was the allocation sequence adequately generated
ldquoYesrdquo (computer generated random numbers table of random
numbers coin-tossing or similar) ldquoNordquo (day of week evenodd
clinic record number clinician judgment participant preference
laboratory test result such as haemoglobin value or similar) or
ldquoUnclearrdquo (insufficient information about the sequence generation
process to permit judgment)
2 Allocation concealment
Was allocation adequately concealed
ldquoYesrdquo (central independent unit sequentially numbered drug con-
tainers or sealed envelopes of identical appearance or similar)
ldquoNordquo (alternation or rotation date of birth non-opaque envelopes
open table of random numbers or similar) or ldquoUnclearrdquo (randomi-
sation stated but no information on method used is available)
3 Blinding
Was knowledge of the allocated intervention adequately prevented
during the study
ldquoYesrdquo (identical placebo medication or similar) ldquoNordquo (tablets ver-
sus liquid or similar) or ldquoUnclearrdquo (blinding stated but no infor-
mation on method used is available)
4 Incomplete outcome data
Were incomplete data dealt with adequately by the researchers
ldquoYesrdquo (no missing outcome data missing outcome data balanced
in numbers across intervention groups and reasons for dropouts
and withdrawals described or similar) ldquoNordquo (reason for missing
outcome data likely to be related to true outcome or similar) or
ldquoUnclearrdquo (number or reasons for dropouts and withdrawals not
described)
5 Selective outcome reporting
Are reports of the study free of suggestion of selective outcome
reporting
ldquoYesrdquo (study protocol is available published reports include all ex-
pected outcomes or similar) ldquoNordquo (not all of the studyrsquos pre-spec-
ified primary outcomes have been reported one or more reported
primary outcomes were not pre-specified or similar) or ldquoUnclearrdquo
(insufficient information to permit judgement of rsquoadequatersquo or rsquoin-
adequatersquo)
Any other potential sources of bias such as stopping the study
early or extreme baseline imbalance were also explored
Measures of treatment effect
Binary data
If two or more studies presented outcomes from either standard-
ised instruments or diagnostic evaluations as proportions the rela-
tive risk and risk difference with 95 confidence intervals would
have been calculated from meta-analysis Number needed to treat
would also have been calculated where appropriate However only
one study presented categorical outcomes
Continuous data
Where standardised assessment tools generated a score as the out-
come measure comparisons were made between the means of
these scores We calculated mean difference (MD) where possible
and calculated standard error (SE) using data available from the
same study or imputed it from another study in the same meta-
analysis as described in Chapters 7 9 and 16 of the CochraneHandbook for Systematic Reviews of Interventions (Higgins 2008)
Where studies did not use sufficiently similar instruments to mea-
sure an outcome we conducted meta-analysis using standardised
mean difference
Unit of analysis issues
No unit of analysis errors were identified In all included studies
randomisation reporting and analysis were per individual partic-
ipant
Dealing with missing data
Where possible missing data and dropouts were assessed for each
included study and reported Reasons for missing data were pro-
vided when reported in trials Where insufficient data were re-
ported we contacted the trial authors for further information No
replies were received Where data could not be included in meta-
analysis we have included a summary in the text of the review
Assessment of heterogeneity
Consistency of results was assessed visually and by examining I2 (Higgins 2002) a quantity which describes approximately the
proportion of variation in point estimates that is due to hetero-
geneity rather than sampling error
Assessment of reporting biases
Insufficient studies were found to allow for the use of funnel plots
to investigate any relationship between effect size and study pre-
cision (closely related to sample size)
5Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data synthesis
Where possible when two or more studies were found that were
suitable for inclusion we planned to perform a meta-analysis on
the results using a random-effects model
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was not possible because of a lack of data for
meta-analysis Anticipated clinical differences included
- age of participants adult versus paediatric preschool versus
school age
- diagnostic classification
- dose of medication
Sensitivity analysis
Sensitivity analysis was planned to assess the impact of risk of bias
on the results of meta-analyses However we could not conduct
this analysis because there were too few data available for meta-
analysis for the same drug therapy age group and clinical outcome
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
Seven studies are included in the review Five of the studies were
carried out in the USA 1 in France and 1 in Japan Participants
were children in five of the studies and adults in the other two
Results of the search
Electronic literature searches were conducted in December 2004
and yielded 46 titles Thirty-eight studies were excluded because
they were not randomised controlled trials (RCTs) or were not
about ASD Following full paper review four RCTs were identi-
fied The search was repeated in September 2006 and two further
trials were identified The search was repeated in December 2008
No new trials were found The search was repeated in December
2009 and one new trial was found Thus a total of seven RCTs
with 271 participants were included in this review
Of note fenfluramine was not searched for directly and is not
registered for use as an antidepressant but was identified as an
SSRI in electronic searches We debated its inclusion and chose
to retain the two trials to provide a complete clinical picture The
tricyclic antidepressant clomipramine was also identified using this
search method and is known to have serotonin uptake inhibitor
actions but was excluded because unlike fenfluramine it will be
included in a systematic review of tricyclic antidepressants and
ASD (currently in progress)
Different versions of assessment tools were used to measure sim-
ilar outcomes For example for CGI the Clinical Global Im-
pression - Severity scale (CGI-S) the Clinical Global Impression
- Improvement scale (CGI-I) and the Clinical Global Improve-
ment Scale Adapted to Global Autism (CGI-AD) were used and
sometimes the tool used was uncertain (CGI) (Guy 1976) Simi-
larly to measure Obsessive Compulsive Behaviour the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) (Scahill 2006) the
Childrenrsquos Yale-Brown Obsessive Compulsive scale (CY-BOCS)
(McKay 2003) and the Yale-Brown Obsessive-Compulsion Scale
(Goodman 1989Goodman 1989b) and a modified version of it
were used
Included studies
Five studies were conducted in children aged 3-17 years us-
ing fenfluramine (Barthelemy 1989 Leventhal 1993) fluoxe-
tine (Hollander 2005) fluvoxamine (Sugie 2005) and citalopram
(King 2009) Two studies were conducted in adults aged 18-
53 years using fluoxetine (Buchsbaum 2001) and fluvoxamine
(McDougle 1996)
Of the five trials in children two used DSM-IV-TR diagnoses of
Autistic Disorder Asperger Disorder or PDD-NOS (Hollander
2005 King 2009) One study (King 2009) also required at least
moderate severity on the CGI illness severity scale and a moderate
or greater score for compulsive behaviour items of the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) Both of these studies
included children with intelligence in the normal range with one
having an IQ range of 30-132 (Hollander 2005) and the other
reporting 61 of children with a non-verbal IQ over 70 (King
2009) One study included children ldquodiagnosed with autismrdquo using
DSM-IV but did not specify how criteria were applied or provide
information about intelligence (Sugie 2005) Two studies used
DSM-III criteria for a diagnosis of autism and included children
with intellectual impairment with IQ ranges of 16-63 (Leventhal
1993) and 30-75 (Barthelemy 1989)
Of the two adult studies one (Buchsbaum 2001) included adults
diagnosed using DSM-IV with autism or Asperger Disorders and
all patients were verbal with an IQ score range of 53 to 119
The other study included adults diagnosed with autism using the
DSM-III-R and ICD-10 criteria and individuals included were at
least ldquomoderaterdquo in severity using the CGI global severity of illness
rating Both intellectually able and disabled adults were included
(McDougle 1996)
One study (Leventhal 1993) included participants who had pre-
viously been treated with an SSRI Trial authors participated in a
multicentre non-randomised trial of 30 weeks duration and then
extended this trial with a 32 week cross-over RCT Thus there was
6Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data synthesis
Where possible when two or more studies were found that were
suitable for inclusion we planned to perform a meta-analysis on
the results using a random-effects model
Subgroup analysis and investigation of heterogeneity
Subgroup analysis was not possible because of a lack of data for
meta-analysis Anticipated clinical differences included
- age of participants adult versus paediatric preschool versus
school age
- diagnostic classification
- dose of medication
Sensitivity analysis
Sensitivity analysis was planned to assess the impact of risk of bias
on the results of meta-analyses However we could not conduct
this analysis because there were too few data available for meta-
analysis for the same drug therapy age group and clinical outcome
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
Seven studies are included in the review Five of the studies were
carried out in the USA 1 in France and 1 in Japan Participants
were children in five of the studies and adults in the other two
Results of the search
Electronic literature searches were conducted in December 2004
and yielded 46 titles Thirty-eight studies were excluded because
they were not randomised controlled trials (RCTs) or were not
about ASD Following full paper review four RCTs were identi-
fied The search was repeated in September 2006 and two further
trials were identified The search was repeated in December 2008
No new trials were found The search was repeated in December
2009 and one new trial was found Thus a total of seven RCTs
with 271 participants were included in this review
Of note fenfluramine was not searched for directly and is not
registered for use as an antidepressant but was identified as an
SSRI in electronic searches We debated its inclusion and chose
to retain the two trials to provide a complete clinical picture The
tricyclic antidepressant clomipramine was also identified using this
search method and is known to have serotonin uptake inhibitor
actions but was excluded because unlike fenfluramine it will be
included in a systematic review of tricyclic antidepressants and
ASD (currently in progress)
Different versions of assessment tools were used to measure sim-
ilar outcomes For example for CGI the Clinical Global Im-
pression - Severity scale (CGI-S) the Clinical Global Impression
- Improvement scale (CGI-I) and the Clinical Global Improve-
ment Scale Adapted to Global Autism (CGI-AD) were used and
sometimes the tool used was uncertain (CGI) (Guy 1976) Simi-
larly to measure Obsessive Compulsive Behaviour the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) (Scahill 2006) the
Childrenrsquos Yale-Brown Obsessive Compulsive scale (CY-BOCS)
(McKay 2003) and the Yale-Brown Obsessive-Compulsion Scale
(Goodman 1989Goodman 1989b) and a modified version of it
were used
Included studies
Five studies were conducted in children aged 3-17 years us-
ing fenfluramine (Barthelemy 1989 Leventhal 1993) fluoxe-
tine (Hollander 2005) fluvoxamine (Sugie 2005) and citalopram
(King 2009) Two studies were conducted in adults aged 18-
53 years using fluoxetine (Buchsbaum 2001) and fluvoxamine
(McDougle 1996)
Of the five trials in children two used DSM-IV-TR diagnoses of
Autistic Disorder Asperger Disorder or PDD-NOS (Hollander
2005 King 2009) One study (King 2009) also required at least
moderate severity on the CGI illness severity scale and a moderate
or greater score for compulsive behaviour items of the Childrenrsquos
Yale-Brown Obsessive Compulsive Scales modified for pervasive
developmental disorders (CY-BOCS-PDD) Both of these studies
included children with intelligence in the normal range with one
having an IQ range of 30-132 (Hollander 2005) and the other
reporting 61 of children with a non-verbal IQ over 70 (King
2009) One study included children ldquodiagnosed with autismrdquo using
DSM-IV but did not specify how criteria were applied or provide
information about intelligence (Sugie 2005) Two studies used
DSM-III criteria for a diagnosis of autism and included children
with intellectual impairment with IQ ranges of 16-63 (Leventhal
1993) and 30-75 (Barthelemy 1989)
Of the two adult studies one (Buchsbaum 2001) included adults
diagnosed using DSM-IV with autism or Asperger Disorders and
all patients were verbal with an IQ score range of 53 to 119
The other study included adults diagnosed with autism using the
DSM-III-R and ICD-10 criteria and individuals included were at
least ldquomoderaterdquo in severity using the CGI global severity of illness
rating Both intellectually able and disabled adults were included
(McDougle 1996)
One study (Leventhal 1993) included participants who had pre-
viously been treated with an SSRI Trial authors participated in a
multicentre non-randomised trial of 30 weeks duration and then
extended this trial with a 32 week cross-over RCT Thus there was
6Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

potential for carry-over effects from initial treatment which could
result in an underestimate of treatment effect
Treatment duration ranged from five to twelve weeks (see
Characteristics of included studies table) One study (Barthelemy
1989) used a shortened placebo period where participants re-
ceived placebo for only one month and active treatment for three
months The trial authors adopted this method because of parent
concerns with a lengthy non-treatment phase In all studies fol-
low-up was short term (12 weeks or less)
Excluded studies
Seven studies were excluded after full paper review Two studies
(Gordon 1993 Remington 2001) were trials of clomipramine a
tricyclic antidepressant which has SSRI characteristics but is not
classed as such Four studies were not randomised controlled trials
(Doyle 2001 McDougle 1996 Peral 1999 Sanchez 1996) One
of these studies (Doyle 2001) was a cost analysis of a treatment
not classed as an SSRI A further study did not use participants
with ASD (Humble 2001)
Risk of bias in included studies
Study design
Two studies used a parallel design (King 2009 McDougle
1996) Four studies used a cross-over design (Barthelemy 1989
Buchsbaum 2001Hollander 2005Sugie 2005) No data were
available prior to the second phase One study had two treatment
phases four weeks placebo 16 weeks fenfluramine eight weeks
placebo followed by randomisation of 15 children to a cross-over
phase (Leventhal 1993) One study of fluoxetine observed a wash-
out period of four weeks (Hollander 2005) and another study of
fluvoxamine for two weeks (Sugie 2005) Different SSRIs have
different recommended wash-out periods ranging from 15 hours
(fluvoxamine) to 7-9 days (fluoxetine) Of the five studies that
reported using crossover methods for at least part of the study no
data was extracted from one (Sugie 2005) two studies used paired
t test analyses (Buchsbaum 2001 Leventhal 1993) and one also
used ANOVA analyses (Leventhal 1993) Two studies reported
comparative analyses using ANOVA (Hollander 2005 Barthelemy
1989) and one of these also used mixed regression models for com-
parative analyses (Barthelemy 1989) Figure 1 provides a summary
of the risk of bias of included studies
7Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
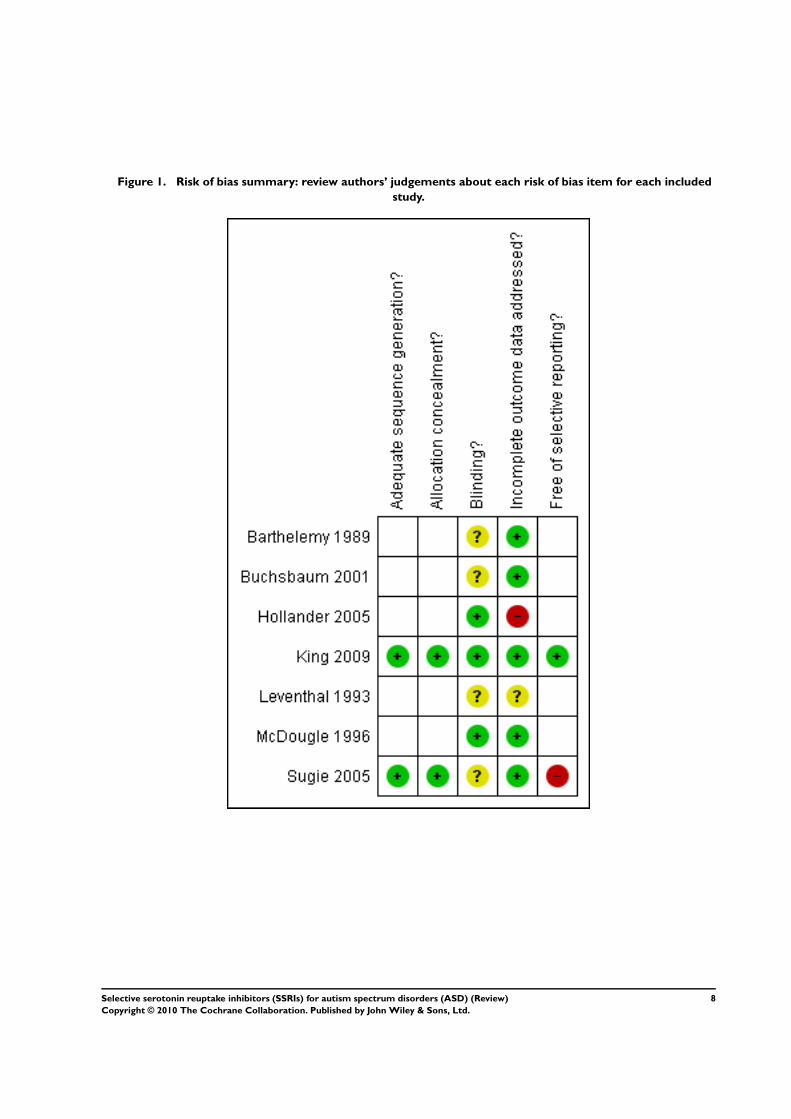
Figure 1 Risk of bias summary review authorsrsquo judgements about each risk of bias item for each included
study
8Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sequence generation
Sequence generation was adequate in two studies (King 2009
Sugie 2005 ) and unclear in the remaining five
Allocation
Allocation concealment was adequate in two studies (King 2009
Sugie 2005) Adequacy of allocation concealment was unclear in
five studies (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
Leventhal 1993 McDougle 1996) No further unpublished infor-
mation about allocation concealment was forthcoming from trial
authors
Blinding
Outcome assessors were reported as being blind to treatment al-
location in three studies (Hollander 2005 King 2009 McDougle
1996) In the remaining four studies it was not possible to ascertain
if outcome assessors were blinded Of these four studies two stud-
ies stated that participants and treating physicians were blinded but
did not report blinding of outcome assessors (Barthelemy 1989
Buchsbaum 2001) and two studies used the term ldquodouble blindrdquo
to refer to all blinding (Leventhal 1993 Sugie 2005) Given that
the outcome measures used rely on subjective observation and as-
sessment there is potential for bias where outcome assessors were
not adequately blinded to treatment allocation
Incomplete outcome data
Three studies reported no loss to follow-up (Barthelemy 1989
Buchsbaum 2001 McDougle 1996 ) One study (King 2009)
reported that 13 of 76 withdrew from the placebo arm and 13
of 73 withdrew from the treatment arm of the trial Reasons for
withdrawal included adverse events (one serious in the treatment
group) protocol violation and consent withdrawal One study
(Leventhal 1993) reported one withdrawal prior to the randomised
phase and reported no data from this participant One study (Sugie
2005) excluded one participant due to non-compliance One study
(Hollander 2005) reported that of 62 patients who consented
18 were excluded for non-eligibility or non-compliance and 44
were randomised Of these 39 participants were included and
completed outcome data were published three were excluded due
to non-compliance one due to lack of efficacy and one was lost
from analysis due to lost records The exclusion of a participant
due to lack of efficacy creates a risk of bias as does exclusion of
those who were not compliant with therapy
Three studies reported not using or were assessed as not using
an intention-to-treat analysis (Hollander 2005 Leventhal 1993
Sugie 2005) Four studies reported the use of intention-to-treat
analysis or did not require any statistical adjustments as they had no
losses to follow up or changes in treatment allocation (Barthelemy
1989 Buchsbaum 2001 King 2009 McDougle 1996)
Selective reporting
The likelihood of selective reporting that is reporting only those
outcomes which showed evidence of treatment effect was lowest
for the most recent publication (King 2009) which was registered
at the commencement of the trial No other trial reported being
registered prior to commencement Five trials reported negative
outcomes (Barthelemy 1989 Buchsbaum 2001 Hollander 2005
King 2009 Leventhal 1993) one reported only positive outcomes
(McDougle 1996) and one study only reported effectiveness for
genetic subgroups (Sugie 2005) All studies reported at least one
relevant clinical outcome
Other potential sources of bias
We are unaware of any further potential sources of bias in the
included studies
Effects of interventions
Seventeen different standardised outcome measures were used in
the seven included trials (Table 1) Use of a single outcome mea-
sure by more than one study was uncommon but occurred for
the CGI and the Childrsquos Yale-Brown Obsessive Compulsive (CY-
BOCS) scales albeit using different scales and subsections of exist-
ing scales allowing meta-analysis for these two outcome measures
using standardised mean difference Results are presented below
by age (children or adults) and compound
Table 1 Outcome measures used in included trials
Outcome
measure
Barthelemy King Buchsbaum Hollander Leventhal McDougle Sugie
Core features
of autism
9Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
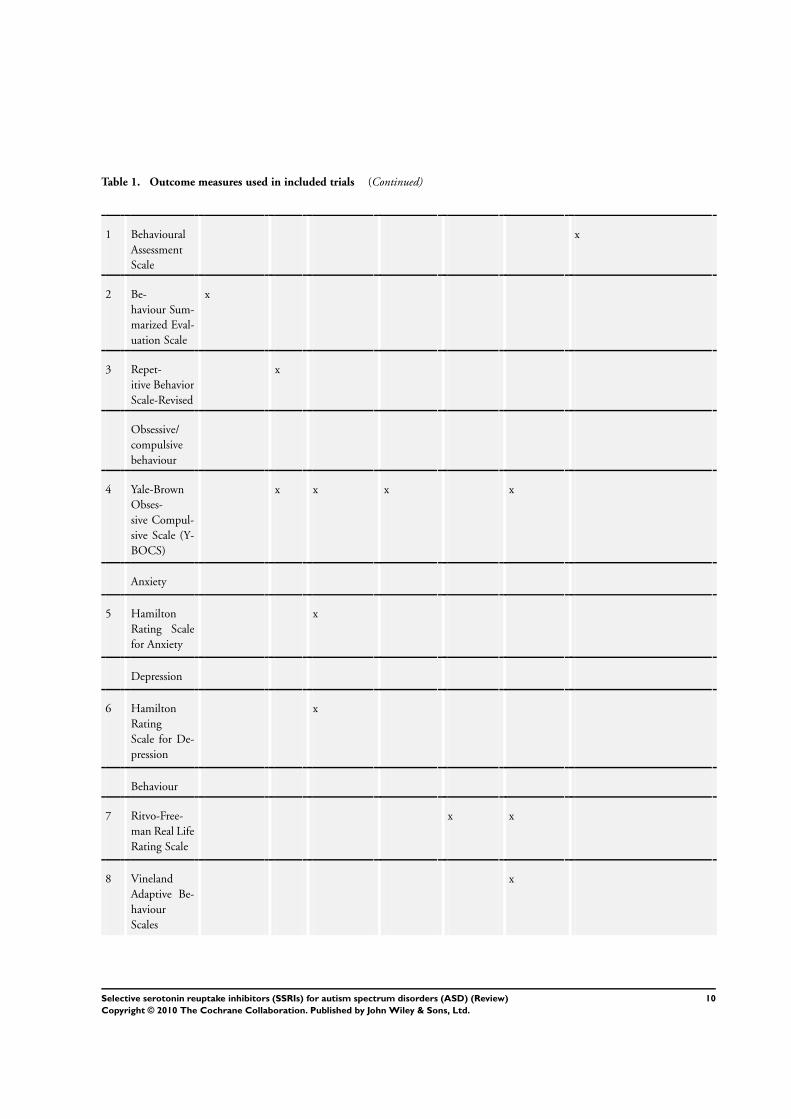
Table 1 Outcome measures used in included trials (Continued)
1 Behavioural
Assessment
Scale
x
2 Be-
haviour Sum-
marized Eval-
uation Scale
x
3 Repet-
itive Behavior
Scale-Revised
x
Obsessive
compulsive
behaviour
4 Yale-Brown
Obses-
sive Compul-
sive Scale (Y-
BOCS)
x x x x
Anxiety
5 Hamilton
Rating Scale
for Anxiety
x
Depression
6 Hamilton
Rating
Scale for De-
pression
x
Behaviour
7 Ritvo-Free-
man Real Life
Rating Scale
x x
8 Vineland
Adaptive Be-
haviour
Scales
x
10Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
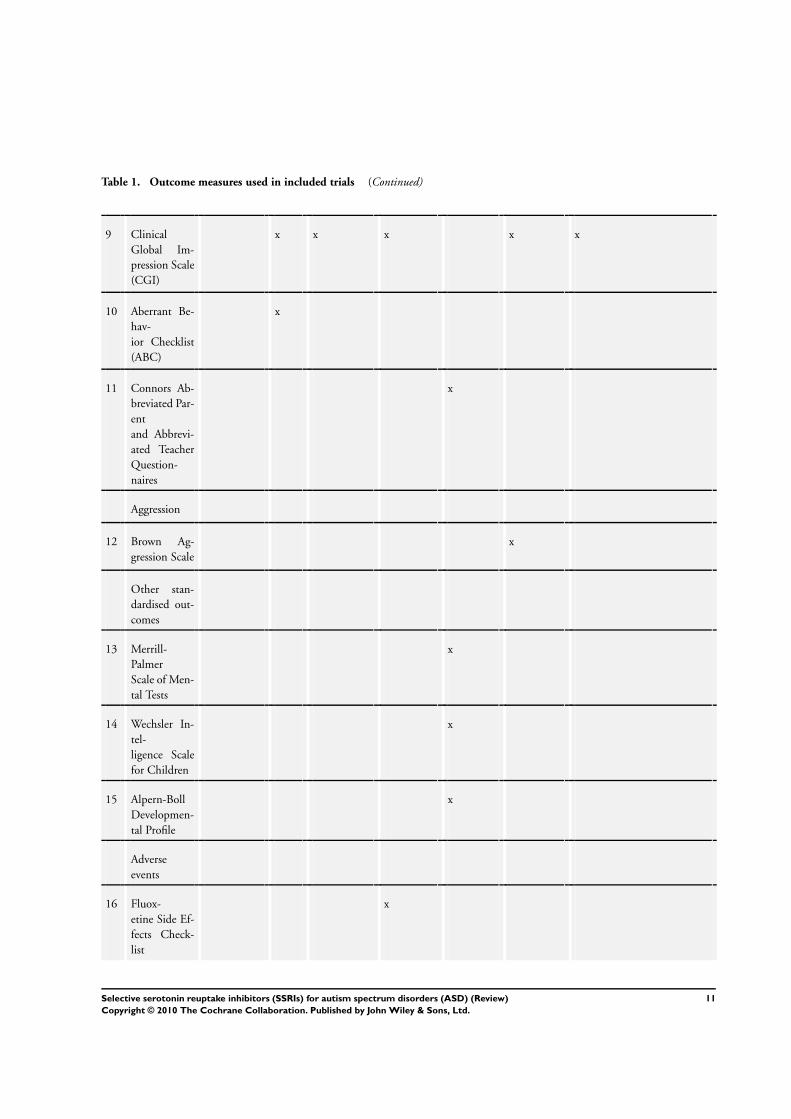
Table 1 Outcome measures used in included trials (Continued)
9 Clinical
Global Im-
pression Scale
(CGI)
x x x x x
10 Aberrant Be-
hav-
ior Checklist
(ABC)
x
11 Connors Ab-
breviated Par-
ent
and Abbrevi-
ated Teacher
Question-
naires
x
Aggression
12 Brown Ag-
gression Scale
x
Other stan-
dardised out-
comes
13 Merrill-
Palmer
Scale of Men-
tal Tests
x
14 Wechsler In-
tel-
ligence Scale
for Children
x
15 Alpern-Boll
Developmen-
tal Profile
x
Adverse
events
16 Fluox-
etine Side Ef-
fects Check-
list
x
11Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
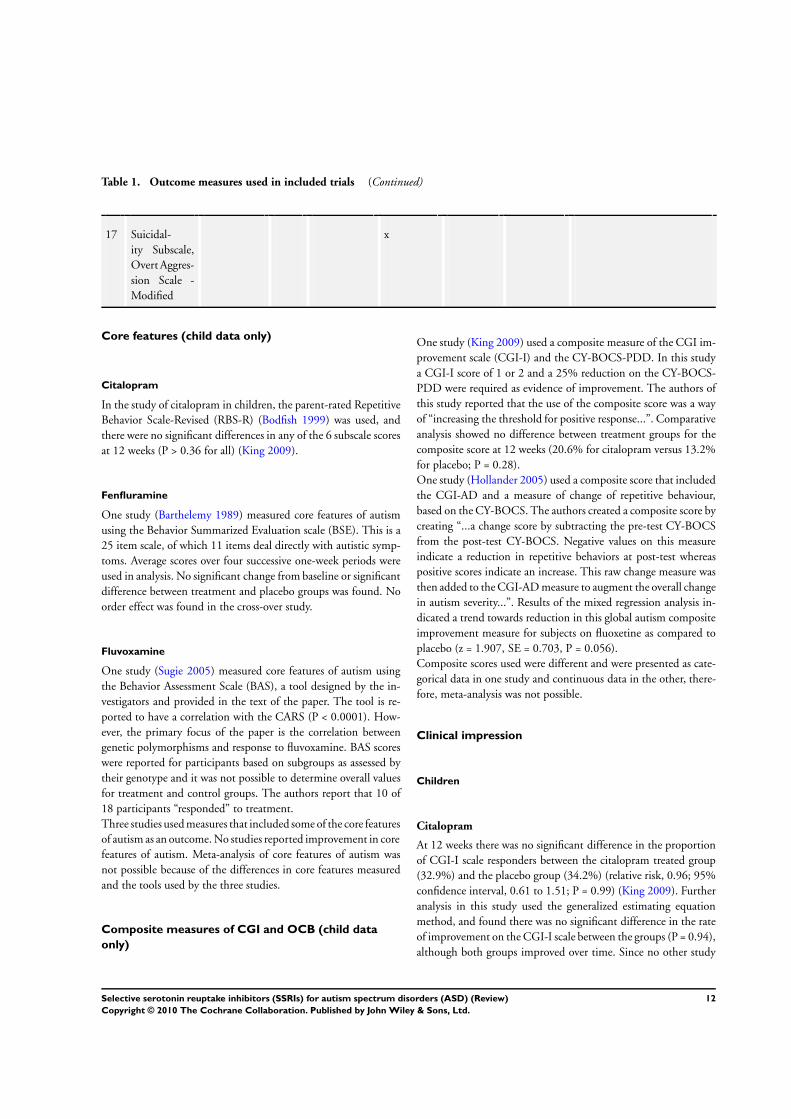
Table 1 Outcome measures used in included trials (Continued)
17 Suicidal-
ity Subscale
Overt Aggres-
sion Scale -
Modified
x
Core features (child data only)
Citalopram
In the study of citalopram in children the parent-rated Repetitive
Behavior Scale-Revised (RBS-R) (Bodfish 1999) was used and
there were no significant differences in any of the 6 subscale scores
at 12 weeks (P gt 036 for all) (King 2009)
Fenfluramine
One study (Barthelemy 1989) measured core features of autism
using the Behavior Summarized Evaluation scale (BSE) This is a
25 item scale of which 11 items deal directly with autistic symp-
toms Average scores over four successive one-week periods were
used in analysis No significant change from baseline or significant
difference between treatment and placebo groups was found No
order effect was found in the cross-over study
Fluvoxamine
One study (Sugie 2005) measured core features of autism using
the Behavior Assessment Scale (BAS) a tool designed by the in-
vestigators and provided in the text of the paper The tool is re-
ported to have a correlation with the CARS (P lt 00001) How-
ever the primary focus of the paper is the correlation between
genetic polymorphisms and response to fluvoxamine BAS scores
were reported for participants based on subgroups as assessed by
their genotype and it was not possible to determine overall values
for treatment and control groups The authors report that 10 of
18 participants ldquorespondedrdquo to treatment
Three studies used measures that included some of the core features
of autism as an outcome No studies reported improvement in core
features of autism Meta-analysis of core features of autism was
not possible because of the differences in core features measured
and the tools used by the three studies
Composite measures of CGI and OCB (child data
only)
One study (King 2009) used a composite measure of the CGI im-
provement scale (CGI-I) and the CY-BOCS-PDD In this study
a CGI-I score of 1 or 2 and a 25 reduction on the CY-BOCS-
PDD were required as evidence of improvement The authors of
this study reported that the use of the composite score was a way
of ldquoincreasing the threshold for positive responserdquo Comparative
analysis showed no difference between treatment groups for the
composite score at 12 weeks (206 for citalopram versus 132
for placebo P = 028)
One study (Hollander 2005) used a composite score that included
the CGI-AD and a measure of change of repetitive behaviour
based on the CY-BOCS The authors created a composite score by
creating ldquoa change score by subtracting the pre-test CY-BOCS
from the post-test CY-BOCS Negative values on this measure
indicate a reduction in repetitive behaviors at post-test whereas
positive scores indicate an increase This raw change measure was
then added to the CGI-AD measure to augment the overall change
in autism severityrdquo Results of the mixed regression analysis in-
dicated a trend towards reduction in this global autism composite
improvement measure for subjects on fluoxetine as compared to
placebo (z = 1907 SE = 0703 P = 0056)
Composite scores used were different and were presented as cate-
gorical data in one study and continuous data in the other there-
fore meta-analysis was not possible
Clinical impression
Children
Citalopram
At 12 weeks there was no significant difference in the proportion
of CGI-I scale responders between the citalopram treated group
(329) and the placebo group (342) (relative risk 096 95
confidence interval 061 to 151 P = 099) (King 2009) Further
analysis in this study used the generalized estimating equation
method and found there was no significant difference in the rate
of improvement on the CGI-I scale between the groups (P = 094)
although both groups improved over time Since no other study
12Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

reported percentage improvement for CGI-I scale these data could
not be included in a meta-analysis
Fluoxetine
One study (Hollander 2005) used the Clinical Global Impression
Scale Global Autism Score (CGIS-GAS) There was no significant
benefit from fluoxetine treatment for this score
Fluvoxamine
One study (Sugie 2005) of fluvoxamine used the CGI scale to assess
improvements in behaviour However the results were presented
for different genotypes and it was not possible to assess the overall
outcome score for treatment and control groups
Variation instruments analysis approach and availability of data
meant that meta-analysis was not possible for this outcome for
children
Adults
Fluoxetine
One study (Buchsbaum 2001) used the CGI-GAS to measure
changes in behaviour Three of six participants showed improve-
ment Continuous outcomes were compared using paired t-tests
and reported for rsquobaselinersquo and fluoxetine with no significant
change (mean difference -100 SD 126) However it is uncertain
whether rsquobaselinersquo represents the control phase so these data were
unsuitable for inclusion in a meta-analysis
Fluvoxamine
One study (McDougle 1996) reported statistically significant im-
provements in behaviour following treatment with fluvoxamine
as assessed using the CGI scale improvement item at 4 8 and 12
weeks When presented as a proportion who had shown improve-
ment 53 of participants in the treatment arm were reported to
have improved on the CGI improvement item while no partici-
pants in the placebo arm had improved
Non core features of behaviour
Obsessive compulsive behaviour
Although stereotypy or restricted repetitive patterns of behaviour
interests or activities are core features of autism and may mani-
fest in similar ways to obsessive-compulsive behaviour obsessive
compulsive behaviour per se is not a core feature of autism and is
therefore reported here under non-core features of behaviour
Children
Citalopram (combined obsession and compulsion score only)
Using CY-BOCS-PDD (Scahill 2006) there was no significant
difference between the groups in score reduction over time from
baseline (mean (SD) minus20 (34) points for the citalopram group
and minus19 (25) points for the placebo group P = 085) (King
2009) Results for obsessions and compulsions were not reported
separately
Fluoxetine (compulsion score only)
One study (Hollander 2005) used the compulsions questions of
the CY-BOCS as their participants were aged 5-16 years and re-
ported no statistically significant difference between groups (effect
size changes were mean of -13 for phase 1 and -06 for phase 2)
Although both studies in children report no statistically significant
change on the CY-BOCS presentation of different components of
the scales (obsession and compulsion as one score or compulsion
score only) meant that available data were not suitable for meta-
analyses
Adults
Fluoxetine
This study used the full adult version of the tool reporting a sta-
tistically significant improvement in obsessions (P = 003) but not
compulsions (P = 086) and a 4 point difference favouring treat-
ment groups that was not statically significant for the overall score
(P = 006) (Buchsbaum 2001) As reported for the CGI outcome
uncertainty about whether rsquobaselinersquo represents the control phase
meant that available data were unsuitable for inclusion in a meta-
analysis
Fluvoxamine
One study of fluvoxamine (McDougle 1996) used a modified ver-
sion of the Yale-Brown Obsessive-Compulsion Scale There was
no significant difference in baseline scores between treatment and
control groups Fluvoxamine was reported to show a treatment
benefit compared with placebo (mean difference -82 95 CI -
1392 to -248) Sample size was small (N = 30) Statistically signif-
icant improvements in both obsession (P lt 002) and compulsion
(P lt 002) scores were reported at 8 weeks and also at 12 weeks
(obsession P lt 002 compulsion P lt 0001)
Both studies reported improvement in obsessions as scored us-
ing the Yale-Brown Obsessive-Compulsion Scale One study
(McDougle 1996) also reported improvement in compulsions and
the combined obsession-compulsion score
13Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Behaviour (child data only)
Citalopram
Of the five subscales of the Aberrant Behavior Checklist-Com-
munity version only the irritability scale achieved statistical sig-
nificance (without any correction for multiple comparisons) from
baseline to week 12 and the difference in change scores was small
(227 points favouring the citalopram group)
Fenfluramine
One study (Leventhal 1993) used the Ritvo-Freeman Real Life
Rating Scale to assess possible improvements in behaviour The
complex arrangement of placebo and treatment phases including
two cross-overs made the data from this trial difficult to inter-
pret To ensure that there was no carry-over effect or learning of
responses from repeat administration of the outcome measures
outcome data from the first phase only were used Overall there
was no significant improvement in behaviour (mean fenfluramine
073 SD 011 mean placebo 080 SD 015) There was a signifi-
cant improvement reported in motor abnormalities and on parent
reports of hyperactivity (P values not reported)
Anxiety (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Anxiety and reported significant improvement in the treatment
group compared with the control group after eight weeks treat-
ment (mean difference 450 SD 351 P = 003) Sample size was
very small (N = 6)
Depression (adult data only)
Fluoxetine
One study (Buchsbaum 2001) used the Hamilton Rating Scale for
Depression There was no significant benefit seen in the treatment
group compared with the control group (mean difference 383
SD 387 P = 006)
Aggression (adult data only)
Fluvoxamine
One study (McDougle 1996) reported using the Brown Aggression
Scale as an outcome measure Fluvoxamine was significantly better
than placebo at reducing aggression (F = 457 P lt 003)
No other non-core behaviour outcomes such as sleep or self mu-
tilation were reported
Adverse effects
Children
Citalopram
Significantly more children in the citalopram-treated group had
one or more emergent adverse events compared to placebo (973
versus 868 P = 003) with adverse events recorded at each bi-
weekly visit using the Safety Monitoring Uniform Report Form
a semi-structured review of body systems (Greenhill 2004) One
child who had not previously suffered seizures experienced a pro-
longed seizure with loss of consciousness and required emergency
hospitalization Although citalopram treatment was ceased after
withdrawal from the trial the child continued to have frequent
seizures
Fenfluramine
One study (Barthelemy 1989) reported that one week after treat-
ment at 15 mgkg the dosage had to be reduced due to adverse ef-
fects in four children There were two cases of increased withdrawal
and sadness and two cases of increased stereotypies Dosage was
increased after one month in all but one child with no recurrence
of adverse symptoms Four children experienced poor appetite in
the first two weeks of treatment and four children displayed irri-
tability in the second month Mean weight significantly decreased
in the treatment group (P lt 002) in the first month of treatment
but stabilised by the second month and returned to normal one
month post-treatment
One study (Leventhal 1993) reported similar weight loss in the
first treatment phase with resolution by the second period of fen-
fluramine administration No further assessment of adverse effects
was reported
Fluoxetine
One study (Hollander 2005) used a side effects symptom check-
list There were no significant differences recorded in frequency
or severity of adverse effects between children in the treatment
or control groups There was no significant difference between
treatment and control groups on the suicide subscale of the Overt
Aggression Scale Six of 37 subjects had their dosage reduced due
to agitation and two of 36 had a ldquodosage reductionrdquo while on
placebo
14Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Fluvoxamine
One study (Sugie 2005) used only blood biochemistry to evaluate
adverse effects No significant differences were reported between
treatment and control groups
Three of the studies in children provided detailed reporting of ad-
verse events and one reported a serious adverse event and statisti-
cally significant differences between occurrence of adverse events
in treatment and placebo groups (King 2009)
Adults
Fluoxetine
One study (Buchsbaum 2001) did not report assessment of any
adverse effects This small study of six adults was primarily focused
on cerebral metabolism
Fluvoxamine
One study (McDougle 1996) of adult participants reported that
fluvoxamine was well tolerated Three participants in the treat-
ment group and one in the control group reported nausea Two
participants in the treatment group and one in the control group
reported moderate sedation All adverse effects were recorded in
the first two weeks of treatment There were no recorded anti-
cholinergic adverse effects no significant changes in pulse blood
pressure or electrocardiographic changes No seizures or dyskine-
sias were reported
Quality of life
No study used any standardised measure of quality of life
Long term outcomes
No study recorded outcome beyond the length of the trial du-
ration with the exception of Barthelemy 1989 who monitored
weight loss (see adverse effects)
D I S C U S S I O N
People with ASD are a heterogeneous group Studies included
in this review included children and adults covering a wide age
range diagnosed using different classification systems and assess-
ment procedures and with different severity of problems and in-
tellectual ability Despite these differences there is consistency of
findings for the studies conducted in children and for those con-
ducted in adults There is no evidence of benefit for children from
one large study of citalopram with low risk of bias and from four
smaller studies In adults only evidence from small studies with
unclear risk of bias is available to date which report significant
improvements in clinical global impression (fluvoxamine and flu-
oxetine) obsessive-compulsive behaviours (fluvoxamine) anxiety
(fluoxetine) and aggression (fluvoxamine)
This review again highlights problems with trial methods already
found in other systematic reviews of treatments for ASD (Jesner
2007 Sinha 2004 Williams 2005) Variations in the clinical pro-
file of ASD trial participants such as the age of participants their
IQ the severity of their problems and whether they have the prob-
lems that the treatment is suggested to ameliorate are likely to
lead to differences in treatment effectiveness It is not yet known
whether these factors influence the effectiveness of a treatment
under investigation independently or as inter-related factors It is
also possible that some measures are suitable for measuring change
in participants of some ages and not others or that they accurately
measure an outcome for individuals with one severity of ASD or
IQ but not for others This means that meaningful interpretation
of the variations in reported outcomes from the studies included
in this review is not straightforward
This review details the findings of seven randomised controlled
trials Two trials each evaluated the effectiveness of fluoxetine
fenfluramine and fluvoxamine and one trial looked at citalopram
In one multi-centre study the sample size was over 100 but the
next largest study recruited 39 participants Small sample sizes
increase the likelihood of type II error that is that no significant
change will be found where one exists Meta-analysis can address
this where sufficient studies use the same outcome measures but
only two meta-analyses were possible in this review
Exacerbating the above problem of small individual trial sample
size is the use of a variety of outcome measures Seventeen differ-
ent outcome measures were used in studies contributing to this
review and variations of measures generated for the same outcome
(different tool or different items from a given tool) also occurred
For this reason and because of important differences in the age of
the populations studied this review like others of treatments for
ASD (Sinha 2004 Williams 2005) found that meta-analyses were
not possible
A further concern with outcome measures is their sensitivity to
change and what magnitude of change individuals and families
would perceive as sufficient to warrant therapy Behavioural out-
comes such as sleep disturbance self-mutilation attention and
concentration problems and gastrointestinal function were not
assessed by any of the trials nor was quality of life Consumer
involvement in outcome measure selection is important to both
generate data that are meaningful to those who use them and to
facilitate practice change if clear evidence of effectiveness (or a lack
of effectiveness) is found
All studies reported outcomes until trial completion (maximum
duration 12 weeks) with the exception of weight loss which was
monitored for longer in one trial (Leventhal 1993) The lack of
15Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

medium and long-term follow-up remains a characteristic problem
of trials in ASD
Other SSRIs particularly sertraline are used in clinical practice
to treat problems associated with ASD Our review identified no
RCTs of sertraline nor RCTs of paroxetine and escitalopram
Treatment with SSRIs may cause various adverse effects One
study reported significantly more adverse events in children on
citalopram compared to placebo and one serious adverse event
a prolonged seizure (King 2009) Both studies of fenfluramine
reported adverse effects in children including withdrawal and
sadness which prompted dosage changes (Barthelemy 1989) and
weight loss (Barthelemy 1989 Leventhal 1993) With monitor-
ing dose adjustment and time all but one of these adverse effects
were resolved No significant differences were reported for side ef-
fects in children in the treatment or placebo group for fluoxetine
(Hollander 2005) and little information was available for side ef-
fects in children in the fluvoxamine study (Sugie 2005) The adult
studies (fluvoxamine and fluoxetine) both reported that treatment
was well tolerated
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
There is no evidence that SSRIs are effective as a treatment for
children with autism In fact there is emerging evidence that they
are not effective and can cause harm As such SSRIs cannot be
recommended as a treatment for children with autism at this time
For adults small positive effects have been seen with fewer side
effects reported but the possible risk of bias and small sample size
of the trials make clear recommendations impossible at this time
Decisions about the use of SSRIs for established clinical indica-
tions that may co-occur with autism such as obsessive-compulsive
disorder and depression and anxiety (in the case of adults) should
be made on a case by case basis
Not all the SSRIs currently in use have been subjected to con-
trolled trials for ASD As ASD causes substantial impairment par-
ents of children with the condition are motivated to try treatments
regardless of the evidence Nevertheless it is important that pre-
scribing clinicians are explicit to parents and patients about the
limited evidence discuss the risks of treatment and discuss other
pharmacological and non-pharmacological interventions
Implications for research
The present review has highlighted the significant challenges in
researching outcomes in the pharmacological treatment of autism
However quality studies are feasible if adequately resourced as
demonstrated by the trial of citalopram reported in this review
and the trial of the unrelated compound risperidone (McCracken
2002) presented in another review (Jesner 2007)
In our opinion knowledge about the effectiveness and safety of
SSRIs for childhood autism would be best served in the first in-
stance by a replication of the citalopram study which will either
confirm or refute the absence of effect on core symptoms For
completeness an adequately powered RCT should be conducted
on at least one other SSRI We would recommend fluoxetine ow-
ing to its favourable safety profile We are aware of one such study
that reached primary study completion in 2009 (ClinicalTrialsgov
identifier NCT 00515320) and another scheduled to commence
in 2010 (Virasinghe personal communication) Sufficiently large
trials would permit the examination of subgroup differences in
responsiveness to SSRIs Comparisons of interest include pre-pu-
berty versus puberty and low IQ versus normal IQ
Knowledge about the effectiveness and safety of SSRIs for adult
autism would be best served by the conduct of at least one ad-
equately powered RCT of a commonly prescribed drug such as
fluoxetine
Comparison between trials in all age groups would be aided by
the use of a core battery of standard outcome measures As a mini-
mum we recommend a measure of global functioning (eg CGI)
a measure of repetitive and stereotyped behaviours (eg Repetitive
Behavior Scale - Revised) a measure of disruptive behaviour (eg
Aberrant Behavior Checklist) and a measure of obsessive compul-
sive symptoms (eg Yale-Brown Obsessive Compulsive Scale)
If short term benefit is established in acute trials in the future for
one or more key clinical outcomes then sustained benefit could
be explored through the use of a relapse prevention trial con-
ducted over 12-18 months This is relevant as treatments directed
to autism tend to be long term A relapse prevention trial also af-
fords the opportunity to obtain systematic adverse event data over
a longer period
A C K N O W L E D G E M E N T S
The authors would like to thank the Cochrane Developmental
Psychosocial and Learning Problems Review Group for feedback
during the development of this review and Cochrane statisticians
for their advice
16Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Barthelemy 1989 published data onlylowast Barthelemy C Bruneau N Jouve J Martineau J Muh JP Lelord
G Urinary dopamine metabolites as indicators of the responsiveness
of fenfluramine treatment in children with autistic behavior
Journal of Autism and Developmental Disorders 198919(2)241ndash54
Buchsbaum 2001 published data onlylowast Buchsbaum M Hollander E Haznedar M Tong C Spiegal-
Cohen J Wei T et alEffect of fluoxetine on regional cerebral
metabolism in autistic spectrum disorders a pilot study
International Journal of Neuropsychopharmacology 20014119ndash25
Hollander 2005 published data onlylowast Hollander E Phillips A Chaplin W Zagursky K Novotny S A
placebo controlled crossover trial of liquid fluoxetine on repetitive
behaviours in childhood and adolescent autism
Neuropsychopharmacology 200530582ndash9
King 2009 published data only
King BH Hollander E Sikich L McCracken JT Scahill L
Bregman JD et alLack of efficacy of citalopram in children with
autism spectrum disorders and high levels of repetitive behavior
Archives of General Psychiatry 200966(6)583ndash90
Leventhal 1993 published data onlylowast Leventhal B Cook E Morford M Ravitz A Heller W Freedman
D Clinical and neurochemical effects of fenfluramine in children
with autism Journal of Neuropsychiatry 19935(3)307ndash15
McDougle 1996 published data onlylowast McDougle C Naylor S Cohen D Volkmar F Heninger G Price
L A double-blind placebo-controlled study of fluvoxamine in
adults with autistic disorder Archives of General Psychiatry 199653
(11)1001ndash8
Sugie 2005 published data onlylowast Sugie Y Sugie H Kukuda T Ito M Sasada Y Nakabayashi M et
alClinical efficacy of fluvoxamine and functional polymorphism in
a serotonin transporter gene on childhood autism Journal of
Autism and Developmental Disorders 200535(3)377ndash85
References to studies excluded from this review
Doyle 2001 published data only
Doyle J Casciano J Arikan S Tarride J-E Gonzales M Casciano
R A multinational pharmacoeconomic evaluation of acute major
depressive disorder (MDD) a comparison of cost-effectiveness
between venlafaxine SSRIs and TCAs Value in Health 20014(1)
16ndash31
Gordon 1993 published data onlylowast Gordon C State R Nelson J Hamburger S Rapoport J A
double-blind comparison of clomipramine desipramine and of
autistic disorder Archives of General Psychiatry 199350(6)441ndash7
Humble 2001 published data only
Humble M Bejerot S Bergqvist P Bengtsson F Reactivity of
serotonin in while blood relationship with drug response in
obsessive-compulsive disorder Biological Psychiatry 200149360ndash8
McDougle 1998 published data only
McDougle C Brodkin E Naylor S Carlson D Cohen D Price L
Sertraline in adults with pervasive developmental disorders a
prospective open-label investigation Journal of Clinical
Psychopharmacology 199818(1)62ndash6
Peral 1999 published data only
Peral M Alcami M Gilaberte I Fluoxetine in children with autism
Journal of the American Academy of Child and Adolescent Psychiatry
199938(12)1472ndash3
Remington 2001 published data onlylowast Remington G Sloman L Konstantareas M Parker K Gow R
Clomipramine versus haloperidol in the treatment of autistic
disorder a double-blind placebo-controlled cross-over study
Journal of Clinical Psychopharmacology 200121(4)440ndash4
Sanchez 1996 published data only
Sanchez L Campbell M Small A Cueva J Armenteros J Adams P
A pilot study of clomipramine in young autistic children Journal of
the American Academy of Child and Adolescent Psychiatry 199635
(4)537ndash44
Additional references
Aman 2005
Aman MG Lam KSL Van Bourgondien ME Medication patterns
in patients with autism temporal regional and demographic
influences Journal of Child amp Adolescent Psychopharmacology 2005
15(1)116ndash26
APA 1980
Diagnostic and Statistical Manual of Mental Disorders Third
Edition American Psychiatric Association 1980
APA 1987
Diagnostic and Statistical Manual of Mental Disorders Revised third
American Psychiatric Association 1987
APA 1994
Diagnostic and Statistical Manual of Mental Disorders Fourth
American Psychiatric Association 1994
APA 2000
Diagnostic and Statistical Manual of Mental Disorders Text revision
- fourth American Psychiatric Association 2000
Atladottir 2007
Atladottir HO Parner ET Schendel D Dalsgaard S Thomsen PH
Thorsen P Time trends in reported diagnoses of childhood
neuropsychiatric disorders A Danish cohort study Archives of
Pediatric amp Adolescent Medicine 2007161(2)193ndash8
Baird 2006
Baird G Simonoff E Pickles A Chandler S Loucas T Meldrum
D et alPrevalence of disorders of the autism spectrum in a
population cohort of children in South Thames the Special Needs
and Autism Project (SNAP) Lancet 2006368(9531)210ndash5
Billstedt 2005
Billstedt E Gillberg IC Gillberg C Autism after adolescence
population-based 13- to 22-year follow-up study of 120 individuals
with autism diagnosed in childhood Journal of Autism amp
Developmental Disorders 200535351ndash60
17Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Bodfish 1999
Bodfish JW Symons FW Lewis MH The Repetitive Behavior Scale
Morganton NC Western Carolina Center Research Reports 1999
Branford 1998
Branford D Bhaumik S Naik B Selective serotonin re-uptake
inhibitors for the treatment of perseverative and maladaptive
behaviours of people with intellectual disability Journal of
Intellectual Disability Research 199842(4)301ndash6
Chen 2007
Chen C-Y Liu C-Y Su W-C Huang S-L Lin K-M Factors
associated with the diagnosis of neurodevelopmental disorders A
population-based longitudinal study Pediatrics 2007119(7)
e435ndash43
Clarke 2003
Clarke M Oxman AD (editors) Cochrane Handbook for Systematic
Reviews of Interventions Oxford Update Software 2003
Cook 1996
Cook EH Leventhal BL The serotonin system in autism Current
Opinion in Pediatrics 19968348ndash54
Fombonne 2006
Fombonne E Zakarian R Bennett A Meng L McLean-Heywood
D Pervasive developmental disorders in Montreal Quebec
Canada Prevalence and links with immunizations Pediatrics 2006
118e139ndash50
Gillberg 2006
Gillberg C Cederlund M Lamberg K Zeijlon L Brief report The
ldquoAutism Epidemicrdquo The registered prevalence of autism in a
Swedish urban area Journal of Autism and Developmental Disorders
200626(3)429ndash35
Goodman 1989
Goodman WK Price LH Rasmussen SA Mazure C Delgado P
Heninger GR Charney DS The Yale-Brown Obsessive
Compulsive Scale II Validity Archives of General Psychiatry 1989
46(11)1012ndash16
Goodman 1989b
Goodman WK Price LH Rasmussen SA Mazure C Fleischman
RL Hill CL Heninger GR Charney DS The Yale-Brown
Obsessive Compuslive Scale I Development Use and Reliability
Archives of General Psychiatry 1989461006ndash11
Greenhill 2004
Greenhill LL Vitiello B Fisher P Levine J Davies M Abikoff H et
alComparison of increasingly detailed elicitation methods for the
assessment of adverse events in pediatric psychopharmacology
Journal of the American Academy of Child and Adolescent Psychiatry
200443(12)1488ndash96
Gringras 2000
Gringras P Practical paediatric psychopharmacological prescribing
in autism Autism 20004(3)229ndash47
Guillem 2006
Guillem P Cans C Guinchat V Ratel M Jouk P-S Trends
perinatal characteristics and medical conditions in pervasive
developmental disorders Developmental Medicine amp Child
Neurology 200648(11)896ndash900
Guy 1976
Guy W ECDEU Assessment Manual for Psychopharmacology Vol
NIMH Publication DHEW Publ No 76-388 Bethesda MD
National Institute of Mental Health 1976
Higgins 2002
Higgins JPT Thompson SG Quantifying heterogeneity in a meta-
analysis Statistics in Medicine 2002211539ndash58
Higgins 2008
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions Version 502 [updated
September 2009] The Cochrane Collaboration 2009 Available
from wwwcochrane-handbookorg
Howlin 2004
Howlin P Goode S Hutton J Rutter M Adult outcome for
children with autism Journal of Child Psychology amp Psychiatry amp
Allied Disciplines 200445212ndash29
Jesner 2007
Jesner OS Aref-Adib M Coren E Risperidone for autism spectrum
disorder Cochrane Database of Systematic Reviews 2007 Issue 1
McCracken 2002
McCracken JT McGough J Shah B Cronin P Hong D Aman
MG et alRisperidone in children with autism and serious
behavioral problems New England Journal of Medicine 2002347
(5)314ndash21
McKay 2003
McKay D Piacentinib J Greisberga S Graaec F Jafferc M Millerc
J Neziroglud F Yaryura-Tobiasd JA The Childrenrsquos Yale-Brown
Obsessive-Compulsive Scale Item Structure in an Outpatient
Setting Psychological Assessment 200315(4)578ndash81
Murray 2005
Murray ML Wong ICK Thompson M Do selective serotonin
reuptake inhibitors cause suicide Antidepressant prescribing to
children and adolescents by GPs has fallen since CSM advice
(Letter) BMJ 2005330(7500)1151
Nemeroff 2007
Nemeroff CB Kalali A Keller MB Charney DS Lenderts SE
Cascade EF et alImpact of publicity concerning pediatric
suicidality data on physician practice patterns in the United States
Archives of General Psychiatry 200764(4)466ndash72
Saxena 1995
Saxena PR Serotonin receptors subtypes functional responses and
therapeutic relevance Pharmacology and Therapeutics 199566(2)
339ndash68
Scahill 2006
Scahill L McDougle CJ Williams SK Dimitropoulos A Aman
MG McCracken JT et alThe Childrenrsquos Yale-Brown Obsessive
Compulsive Scales modified for pervasive developmental disorders
Journal of the American Academy of Child and Adolescent Psychiatry
200645(9)1114ndash23
Sinha 2004
Sinha Y Silove N Wheeler D Williams K Auditory integration
training and other sound therapies for autism spectrum disorders
Cochrane Database of Systematic Reviews 2004 Issue 1
18Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

WHO 1993
World Health Organisation International Classification of
Diseases International Classification of Diseases (ICD-10) World
Health Organisation 1993
Williams 2005
Williams KJ Wray JJ Wheeler DM Intravenous secretin for
autism spectrum disorder Cochrane Database of Systematic Reviews
2005 Issue 3
Williams 2006
Williams JG Higgins JPT Brayne CEG Systematic review of
prevalence studies of autism spectrum disorders Archives of Diseases
in Childhood 2006918ndash15 [DOI 101136adc2004062083]
Williams 2008
Williams K Macdermott S Ridley G Glasson EJ Wray JA The
prevalence of autism in Australia Can it be established from
existing data Journal of Paediatrics and Child Health 200844(9)
504ndash10lowast Indicates the major publication for the study
19Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Barthelemy 1989
Methods Cross-over
Participants blind
Treating physicians blind
Blinding of outcome assessors unclear
No loss to follow-up
Participants N = 13
8 males 5 females
Age range 3-10 yrs mean age 6 yrs 4 months Children only
Diagnosis DSM-III autism
IQ range 30-75 Obsessive-compulsive behaviours not required
Interventions Treatment Fenfluramine twice daily divided dose at total 15 mgkg
Reduced to 08 mgkg in 2 children due to adverse effects
Duration 3 months
Placebo identical placebo phase duration 1 month
Outcomes Weight
Behavior Summarised Evaluation
Urinary dopamine metabolites
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Buchsbaum 2001
Methods Cross-over
Participants blind
Blinding of treating physicians unclear
Blinding of outcome assessors unclear
No loss to follow-up
20Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Buchsbaum 2001 (Continued)
Participants N = 6
5 male 1 female
Mean age 305 plusmn 86 yrs Adults only
Diagnosis DSM-IV ADI
5 autism 1 Asperger disorder
IQ scores ranged from 53 to 119 and all participants were verbal Obsessive-compulsive
behaviours were not a requirement
Interventions Treatment fluoxetine starting dose 10 mgday up to maximum dose 40 mgday for 8
weeks
Placebo not described Duration of placebo phase = 8 weeks
Outcomes Yale-Brown Obsessive Compulsive Scale
Hamilton Rating Scale for Anxiety
Clinical Global Impression Scale
Positron Emission Tomography
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Unclear if there was blinding of outcome
assessors
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Hollander 2005
Methods Cross-over
Outcome assessors blind
Randomisation method not stated
44 children randomised of 62 consented 5 lost to follow-up
Participants N = 44 39 completed
30 males 9 females
mean age 818 plusmn 30 range 5-16 Children only
Diagnosis DSM-IV-TR of Autism PDD-NOS or Asperger Syndrome
IQ range 30-132 No required threshold for obsessive compulsive behaviours
Interventions Treatment fluoxetine 8 weeks treatment 4 weeks washout 8 weeks cross-over
25 mgday up to 08 mgkgday maximum
Outcomes Yale-Brown Obsessive-Compulsion Scale
Clinical Global Improvement Scale Adapted to Global Autism
Suicidality Subscale of Overt Aggression Scale
21Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
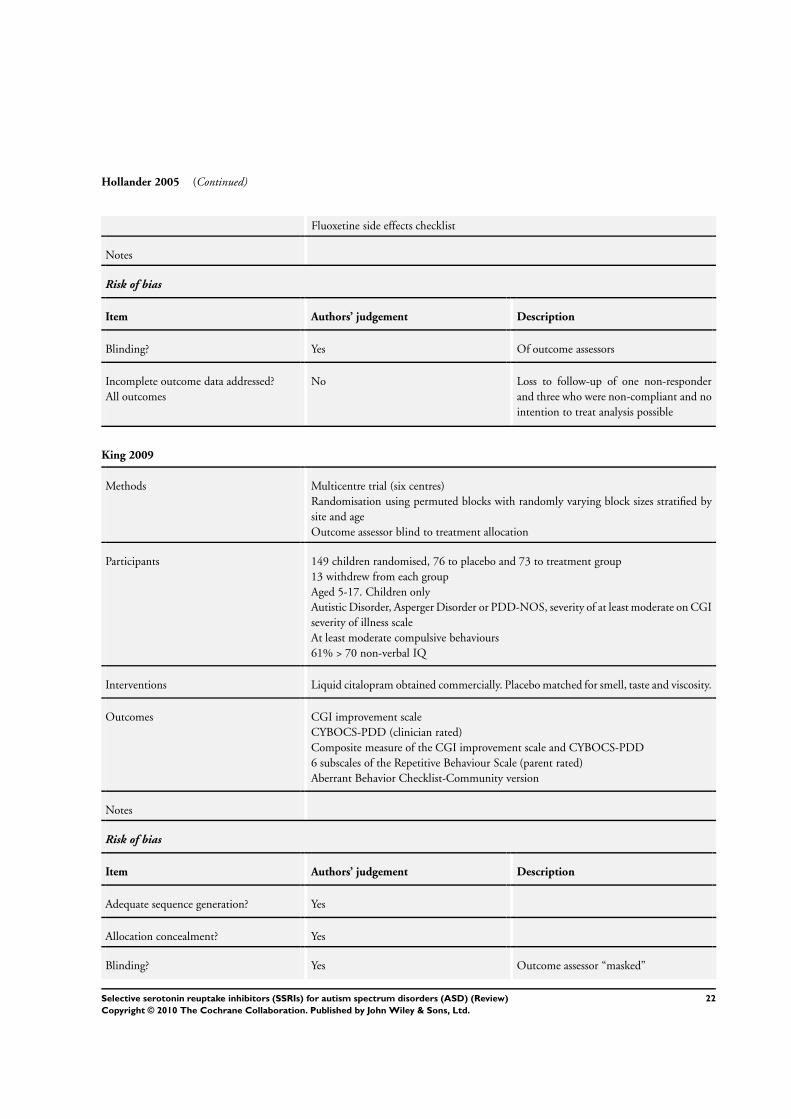
Hollander 2005 (Continued)
Fluoxetine side effects checklist
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Of outcome assessors
Incomplete outcome data addressed
All outcomes
No Loss to follow-up of one non-responder
and three who were non-compliant and no
intention to treat analysis possible
King 2009
Methods Multicentre trial (six centres)
Randomisation using permuted blocks with randomly varying block sizes stratified by
site and age
Outcome assessor blind to treatment allocation
Participants 149 children randomised 76 to placebo and 73 to treatment group
13 withdrew from each group
Aged 5-17 Children only
Autistic Disorder Asperger Disorder or PDD-NOS severity of at least moderate on CGI
severity of illness scale
At least moderate compulsive behaviours
61 gt 70 non-verbal IQ
Interventions Liquid citalopram obtained commercially Placebo matched for smell taste and viscosity
Outcomes CGI improvement scale
CYBOCS-PDD (clinician rated)
Composite measure of the CGI improvement scale and CYBOCS-PDD
6 subscales of the Repetitive Behaviour Scale (parent rated)
Aberrant Behavior Checklist-Community version
Notes
Risk of bias
Item Authorsrsquo judgement Description
Adequate sequence generation Yes
Allocation concealment Yes
Blinding Yes Outcome assessor ldquomaskedrdquo
22Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

King 2009 (Continued)
Incomplete outcome data addressed
All outcomes
Yes ITT analyses used
Free of selective reporting Yes Registered trial
Leventhal 1993
Methods Two phase placebo-treatment-placebo followed by randomised cross-over
ldquodouble blindrdquo no details
Participants N = 15
3-125 yrs (mean age 76 plusmn 26yrs) Children only
Diagnosis infantile autism DSM-III
No loss to follow-up Incomplete data for some outcomes
IQ range 16-63 Obsessive-compulsive behaviours not required
Interventions Fenfluramine
Outcomes Ritvo-Freeman Real Life Rating Scale
Connors Abbreviated Parent and Teacher Questionnaires
Notes Previous use of fenfluramine
Risk of bias
Item Authorsrsquo judgement Description
Blinding Unclear Uncertain if outcome assessors blind to
treatment group
Incomplete outcome data addressed
All outcomes
Unclear No loss to follow-up but incomplete data
for some outcomes
McDougle 1996
Methods Participants blind
Treating physicians blind
Outcome assessors blind
No loss to follow-up
Participants N = 30
27 males 3 females
Mean age 301 plusmn 77 yrs age range 18-53 yrs Adults only
Diagnosis of autism using DSM-III-R and ICD-10 at least ldquomoderaterdquo in severity using
the CGI global severity of illness rating
Obsessive-compulsive behaviours not required
23Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
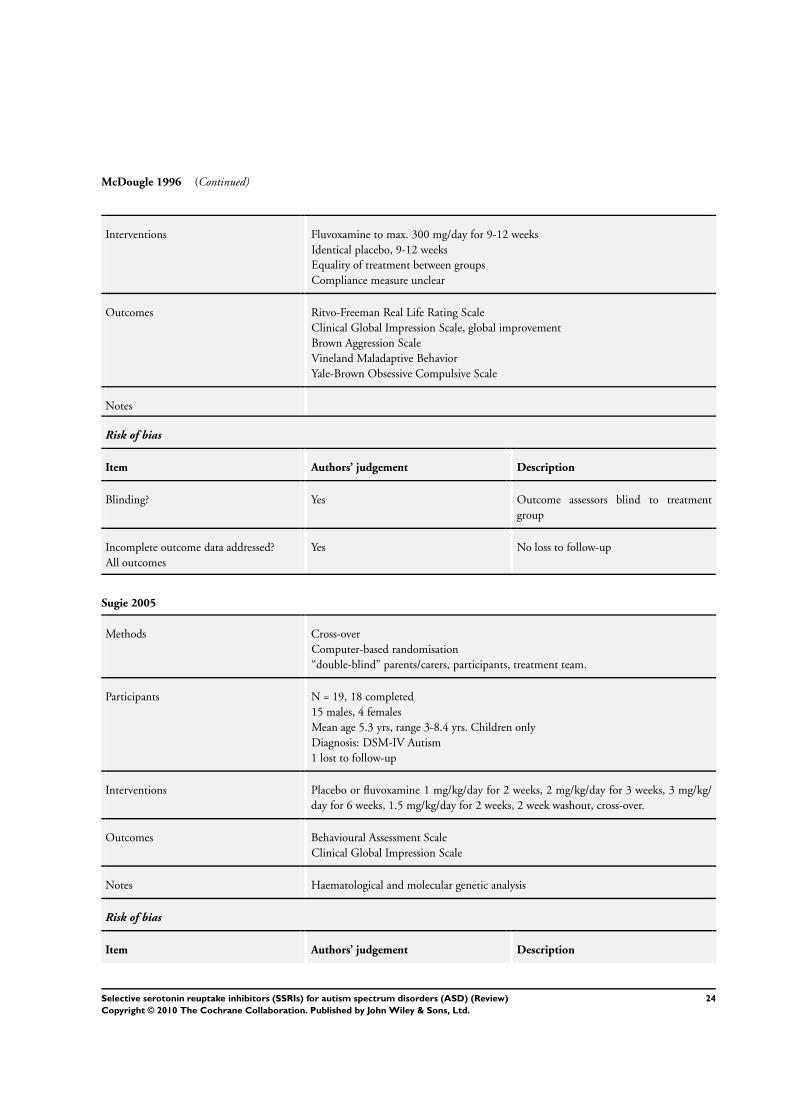
McDougle 1996 (Continued)
Interventions Fluvoxamine to max 300 mgday for 9-12 weeks
Identical placebo 9-12 weeks
Equality of treatment between groups
Compliance measure unclear
Outcomes Ritvo-Freeman Real Life Rating Scale
Clinical Global Impression Scale global improvement
Brown Aggression Scale
Vineland Maladaptive Behavior
Yale-Brown Obsessive Compulsive Scale
Notes
Risk of bias
Item Authorsrsquo judgement Description
Blinding Yes Outcome assessors blind to treatment
group
Incomplete outcome data addressed
All outcomes
Yes No loss to follow-up
Sugie 2005
Methods Cross-over
Computer-based randomisation
ldquodouble-blindrdquo parentscarers participants treatment team
Participants N = 19 18 completed
15 males 4 females
Mean age 53 yrs range 3-84 yrs Children only
Diagnosis DSM-IV Autism
1 lost to follow-up
Interventions Placebo or fluvoxamine 1 mgkgday for 2 weeks 2 mgkgday for 3 weeks 3 mgkg
day for 6 weeks 15 mgkgday for 2 weeks 2 week washout cross-over
Outcomes Behavioural Assessment Scale
Clinical Global Impression Scale
Notes Haematological and molecular genetic analysis
Risk of bias
Item Authorsrsquo judgement Description
24Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
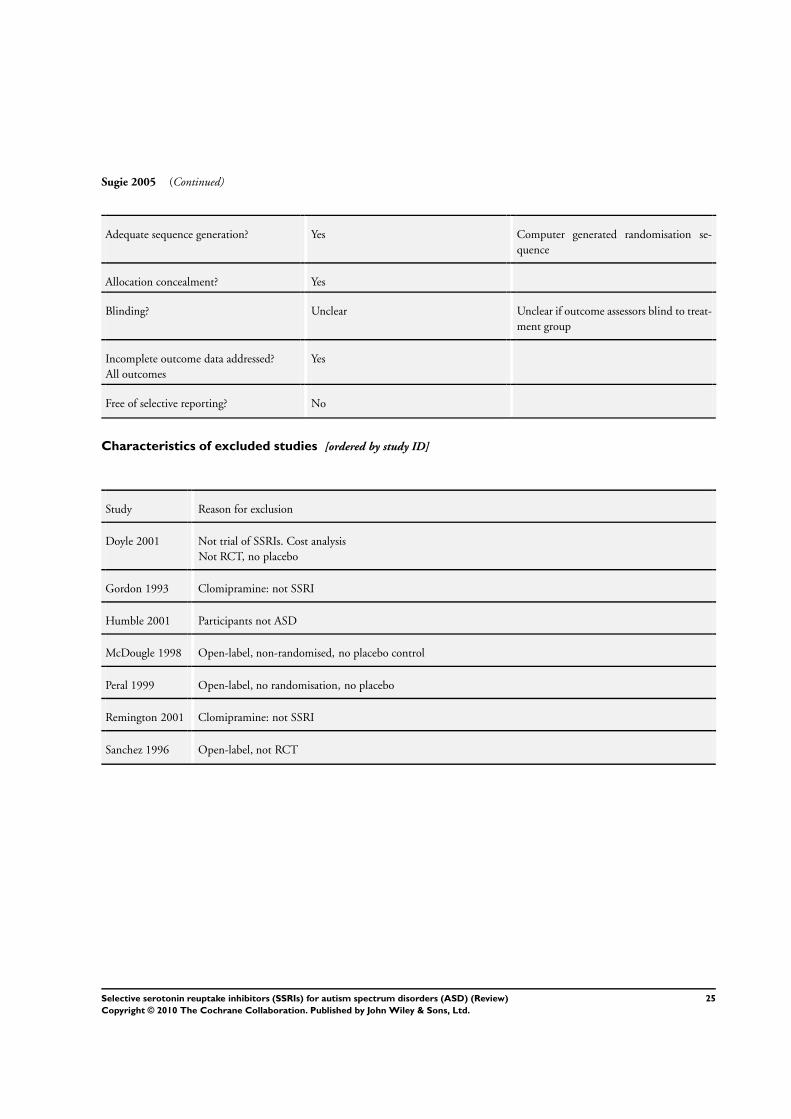
Sugie 2005 (Continued)
Adequate sequence generation Yes Computer generated randomisation se-
quence
Allocation concealment Yes
Blinding Unclear Unclear if outcome assessors blind to treat-
ment group
Incomplete outcome data addressed
All outcomes
Yes
Free of selective reporting No
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Doyle 2001 Not trial of SSRIs Cost analysis
Not RCT no placebo
Gordon 1993 Clomipramine not SSRI
Humble 2001 Participants not ASD
McDougle 1998 Open-label non-randomised no placebo control
Peral 1999 Open-label no randomisation no placebo
Remington 2001 Clomipramine not SSRI
Sanchez 1996 Open-label not RCT
25Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A P P E N D I C E S
Appendix 1 MEDLINE search strategy
MEDLINE (via OVID) searched December 4th 2009
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 randomized controlled trialpt
32 controlled clinical trialpt
33 randomizedab
34 placeboab
35 drug therapyfs
36 randomlyab
37 trialab
38 groupsab
39 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38
40 humanssh
26Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
41 39 and 40
42 30 and 41
Appendix 2 CENTRAL search strategy
Cochrane Central Register of Controlled Trials (The Cochrane Library 2009 Issue 4)
1 MeSH descriptor Child Development Disorders Pervasive explode all trees
2 (communicat)
3 (autis)
4 (PDD)
5 (pervasive next developmental disorder)
6 (language near3 delay)
7 speech near3 disorder
8 childhood next schizophrenia
9 kanner
10 asperg
11 (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10)
12 MeSH descriptor Serotonin Uptake Inhibitors this term only
13 (selective serotonin reuptake inhibitors)
14 (SSRI)
15 (5-hydroxytryptamine)
16 (5HT)
17 MeSH descriptor Fluvoxamine explode all trees
18 fluvoxamine
19 (fluvocamine)
20 (fluoxetine)
21 MeSH descriptor Fluoxetine explode all trees
22 MeSH descriptor Paroxetine explode all trees
23 paroxetine
24 MeSH descriptor Sertraline explode all trees
25 sertraline
26 MeSH descriptor Citalopram explode all trees
27 citalopram
28 venlafaxine
29 (12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 OR 25 OR 26
OR 27 OR 28)
30 (11 AND 29)
Appendix 3 EMBASE search strategy
EMBASE (via OVID) Searched 2009 Week 49
1 exp Child Development Disorders Pervasive
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
27Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$tw
11 or1-10
12 Serotonin Uptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
31 random$tw
32 factorial$tw
33 crossover$tw
34 cross over$tw
35 cross-over$tw
36 placebo$tw
37 (doubl$ adj blind$)tw
38 (singl$ adj blind$)tw
39 assign$tw
40 allocat$tw
41 volunteer$tw
42 Crossover Procedure
43 double-blind proceduretw
44 Randomized Controlled Trial
45 Single Blind Procedure
46 or31-45
47 30 and 46
Appendix 4 ERIC search strategy
ERIC (via Dialog Datastar) Searched December 2009
1 Pervasive-Developmental-DisordersDE
2 communicat$
3 autis$
4 PDD unrestricted
5 pervasive ADJ developmental ADJ disorder$
6 language NEAR delay$ unrestricted 690 show titles
7 speech NEAR disorder$
8 childhood ADJ schizophrenia
9 kanner$
28Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

10 asperg$
11 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12 selective ADJ serotonin ADJ reuptake ADJ inhibitor$
13 SSRI
14 5-hydroxytryptamine
15 5HT
16 fluvoxamine
17 fluvocamine
18 fluoxetine
19 paroxetine
20 sertraline
21 citalopram
22 venlafaxine
23 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24 11 AND 23
25 random$ OR control$ OR blind$ OR trial$ OR crossover
26 24 and 25
Appendix 5 PsycINFO search strategy
PsycINFO (via OVID) Searched December 2009 Week 2
1 exp Pervasive Developmental Disorders
2 communicat$tw
3 autis$tw
4 PDDtw
5 pervasive developmental disorder$tw
6 (language adj3 delay$)tw
7 (speech adj3 disorder$)tw
8 childhood schizophreniatw
9 kanner$tw
10 asperg$tw
11 or1-10
12 Serotonin Reuptake Inhibitors
13 selective serotonin reuptake inhibitor$tw
14 SSRItw
15 5-hydroxytryptaminetw
16 5HTtw
17 Fluvoxamine
18 fluvoxaminetw
19 fluvocaminetw
20 Fluoxetine
21 fluoxetinetw
22 Paroxetine
23 paroxetinetw
24 Sertraline
25 sertralinetw
26 Citalopram
27 citalopramtw
28 venlafaxinetw
29 or12-28
30 11 and 29
29Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
31 Treatment Effectiveness Evaluation
32 exp Treatment Outcomes
33 Psychotherapeutic Outcomes
34 PLACEBO
35 exp Followup Studies
36 placebo$tw
37 random$tw
38 comparative stud$tw
39 randomied controlled trial$tw
40 (clinical adj3 trial$)tw
41 (research adj3 design)tw
42 (evaluat$ adj3 stud$)tw
43 (prospectiv$ adj3 stud$)tw
44 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$))tw
45 control$tw
46 45 or 37 or 35 or 43 or 42 or 38 or 31 or 36 or 32 or 44 or 40 or 34 or 33 or 41 or 39
47 30 and 46
Appendix 6 CINAHL search strategy
CINAHL (via EBSCO) Searched December 2009
S46 S29 and S45
S45 S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40
or S41 or S42 or S43 or S44
S44 allocat random
S43 (MH ldquoQuantitative Studiesrdquo)
S42 (MH ldquoPlacebosrdquo)
S41 placebo
S40 random allocat
S39 (MH ldquoRandom Assignmentrdquo)
S38 (Randomied control trial)
S37 (singl mask )
S36 (doubl mask )
S35 (tripl mask )
S34 (trebl mask )
S33 (trebl blind )
S32 (tripl blind )
S31 (doubl blind )
S30 (singl blind )
S29 S11 and S28
S28 S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22
or S23 or S24 or S25 or S26 or S27
S27 Venlafaxine
S26 (MH ldquoVenlafaxinerdquo)
S25 Citalopram
S24 (MH ldquoCitalopramrdquo)
S23 Sertraline
S22 (MH ldquoSertraline Hydrochloriderdquo)
S21 Paroxetine
S20 (MH ldquoParoxetinerdquo)
S19 (MH ldquoFluoxetinerdquo)
30Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
S18 fluoxetine
S17 fluvoxamine or fluvocamine
S16 5HT
S14 SSRI
S13 selective serotonin reuptake inhibitor
S12 (MH ldquoSerotonin Uptake Inhibitorsrdquo)
S11 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10
S10 asperg
S9 kanner
S8 childhood schizophrenia
S7 speech N3 disorder
S6 language N3 delay
S5 pervasive developmental disorder
S4 PDD
S3 autis
S2 communicat
S1 (MH ldquoChild Development Disorders Pervasive+rdquo)
Appendix 7 Sociological Abstracts
Sociological Abstracts searched 10 December 2009
(((DE=ldquoautismrdquo) or(communicat) or (autis) or (PDD) or (pervasive developmental disorder) or(language within 3 delay)
or (speech within 3 disorder) or(childhood schizophrenia) or (kanner))
AND
((selective serotonin reuptake inhibitor) or(SSRI) or(5-hydroxytryptamine) or(5HT) or(fluvoxamine) or(fluvocamine)or(fluoxetine)
or(paroxetine) or(sertraline) or(citalopram)or(venlafaxine)))
AND
((random or trial or control) or (blind or crossover))
W H A T rsquo S N E W
Last assessed as up-to-date 30 May 2010
Date Event Description
4 August 2010 Amended Typographical error corrected
31Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
H I S T O R Y
Protocol first published Issue 1 2004
Review first published Issue 8 2010
Date Event Description
7 November 2008 Amended Converted to new review format
C O N T R I B U T I O N S O F A U T H O R S
Danielle Wheeler and Katrina Williams conducted literature searches extracted data and made decisions about data synthesis All
authors were involved in writing the protocol and review
D E C L A R A T I O N S O F I N T E R E S T
Professor Philip Hazell has worked as a consultant for Eli Lilly and Janssen He has had research contracts with Eli Lilly and Celltech
He is a member of the advisory board of Eli Lilly Australia Janssen Australia Novartis Australia and Shire International Professor
Hazell has given presentations for Eli Lilly Pfizer Janssen and Sanofi He is an investigator on a non-industry funded trial of fluoxetine
for autism spectrum disorders
Dr Natalie Silove is an investigator on a non-industry funded trial of fluoxetine for autism spectrum disorders
S O U R C E S O F S U P P O R T
Internal sources
bull Small Grants Scheme The Childrenrsquos Hospital at Westmead Sydney Australia
External sources
bull Financial Markets Foundation for Children Australia
bull Department of Health and Aging Australia
Cochrane Entities funding
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
No significant changes were made to the protocol
32Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD) (Review)
Copyright copy 2010 The Cochrane Collaboration Published by John Wiley amp Sons Ltd