clinical practice guideline for diabetes mellitus type 1
TRANSCRIPT
Clinical Practice Guidelinefor Diabetes Mellitus Type 1
CLINICAL PRACTICE GUIDELINTES IN THE NHS
MINISTRY OF HEALTH, SOCIAL SERVICES AND EQUALITY
MINISTERIODE ECONOMÍAY COMPETITIVIDAD
MINISTERIODE SANIDAD, SERVICIOS SOCIALESE IGUALDAD

OSASUN ETA KONTSUMO SAILA
DEPARTAMENTO DE SANIDAD Y CONSUMO
MINISTERIO
Y COMPETITIVIDADDE ECONOMÍA
MINISTERIODE SANIDAD, SERVICIOS SOCIALES E IGUALDAD
Vitoria-Gasteiz, 2012
Clinical Practice Guidelinefor Diabetes Mellitus Type 1
CLINICAL PRACTICE GUIDELINTES IN THE NHS
MINISTRY OF HEALTH, SOCIAL SERVICES AND EQUALITY
This CPG is an aid to decision making in health care. The compliance of this guide is not mandatory, nor does it replace the clinical judgement of the health care personnel.
A co bibliographic record of this work can be found in the catalogue of the Library of the Basque Government:http://www.bibliotekak.euskadi.net/WebOpac
Edition: 1st May 2012
Circulation: 4.000 CDs
Internet: http://publicaciones.administraciones.es
Edited by: Eusko Jaurlaritzaren Argitalpen Zerbitzu Nagusia Central Service of the Basque Government Publications c/Donostia-San Sebastián, 1 - 01010 Vitoria-Gasteiz
Photocomposition: Ipar, S. Coop. Zurbaran, 2-4 - 48007 Bilbao Zurbaran, 2-4 - 48007 Bilbao
Printing: Grafo, SA Graph, SA Cervantes etorb., 51 - 48970 Basauri (Bizkaia)
NIPO: 725-12-022-9 (Ministry of Economy and Competitiveness) NIPO: 680-12-018-5 (Ministry of Health, Social Services and Equality)
Legal Deposit: VI 130-201

This CPG has been funded by the agreement signed by the Instituto de Salud Carlos III, an autonomous body of the Ministry of Science and Innovation, and the Agency for Health Technology Assessment from the Basque Country - Osteba, in the framework of cooperation envisaged in the Quality Plan for the National Health Service of the Ministry of Health and Social Policy.
This guide should include:
Working Group of the Clinical Practice Guideline on Diabetes mellitus type 1. Clinical Practice Guidelines for Diabetes mellitus type 1. Quality Plan for the National Health Service of the Ministry of Health and Social Policy. Agency for Health Technology Assessment from the Basque Country -Osteba, 2012. Clinical Practice Guidelines in the NHS: OSTEBA n.º 2009/10.
OSASUN ETA KONTSUMO SAILA
DEPARTAMENTO DE SANIDAD Y CONSUMO
MINISTERIO
Y COMPETITIVIDADDE ECONOMÍA
MINISTERIODE SANIDAD, SERVICIOS SOCIALES E IGUALDAD

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 5
Index
Presentation 11
Authorship and collaborations 13
Questions to answer 17
Levels of evidence and grades of recommendations 21
Recommendations of the CPG 23
1. Introduction 55
2. Scope and aims 57
2.1. Scope 57
2.2. Aims of the CPG 57
2.3. Approach 58
2.4. People who should read this CPG 58
3. Methodology of the guide 59
3.1. Constitution of the guide development team 59
3.2. Systematic review 60
3.2.1. Formulation of clinical questions 60
3.2.2. Bibliographic Search 60
3.2.3. Assessment of the methodological quality 61
3.2.4. Data Extraction 61
3.2.5. Development of evidence tables 61
3.2.6. Classifi cation of studies and grades of recommendations 61
3.3. Edition of the Guide 62
4. Defi nition and diagnostic criteria of diabetes mellitus type 1 63
4.1. Defi nition of diabetes mellitus type1 63
4.2. Autoantibodies in the diagnosis of diabetes mellitus type 1 64
4.3. Predictors of ‘spontaneous remission’ 66
4.4. Genetic study to rule out MODY diabetes 68
4.5. Study of antibodies to rule out other autoimmune multiglandular diseases 72
4.5.1. Thyroid disease 73
4.5.2. Celiac disease (CD) 74
4.5.3. Addison’s disease 76
6 SNS CLINICAL PRACTICE GUIDELINES
5. Diabetes Education 79
5.1. Structured education aimed at families and / or patients withdiabetes mellitus 79
5.2. Education aimed at patients and family 84
5.3. Community Support arrangements 90
6. Feeding 95
6.1. Feeding specifi cations for people with diabetes mellitus type 1 95
6.1.1. Carbohydrates 95
6.1.2. Sucrose (table sugar) 96
6.1.3. Sweeteners 97
6.1.4. Glycaemic Index 98
6.1.5. Fibre 99
6.1.6. Proteins 99
6.1.6.1. Proteins in patients with nephropathy 99
6.1.7. Diet for the prevention and treatment of cardiovascular disease 101
6.2. Eating plan recommended for patients with diabetes mellitus type 1 104
6.2.1. Menus based method (Appendix 4) 104
6.2.2. Servings based method (Appendix 5) 104
6.2.3. Exchange and equivalents system (Appendix 6) 105
6.2.4. System based on counting carbohydrate servings 105
7. Exercising 107
7.1. Benefi ts of exercise in patients with DM1 108
7.1.1. Children and adolescents 108
7.1.2. Adults 109
7.1.3. All age groups 110
7.2. Type, intensity and duration of physical exercise in people with diabetes mellitus type 1 112
7.2.1. Children and adolescents 112
7.2.2. Adults 113
8. Glycaemic Control 115
8.1. Glycosylated haemoglobin 115
8.1.1. Glycosylated haemoglobin target fi gures 115
8.1.2. Criteria for the standardization and presentation of glycosylated haemoglobin analytical results 116
8.2. Systems of Continuous Glucose Monitoring 118
8.2.1. Retrospective monitoring 119
8.2.2. Real-time monitoring 119
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 7
8.3. Inpatient or outpatient clinical management of patients with diabetes mellitus type 1 at the time of diagnosis 121
8.4. Preparations of insulin in the treatment of patients with diabetes mellitus type 1 124
8.4.1. Fast acting analogues vs. human insulin 124
8.4.1.1. Adults. Fast acting analogues vs. human insulin 124
8.4.1.2. Children and adolescents. Fast acting analogues vs. human insulin 127
8.4.1.3. Pregnant. Fast acting analogues vs. human insulin 128
8.4.2. Slow-acting analogues vs. human insulin 129
8.4.2.1. Glargine vs. retarded human insulin (NPH) 129
8.4.2.1.1. Adults 129
8.4.2.1.2. Children and adolescents 132
8.4.2.1.3. Pregnant women 133
8.4.2.2. Detemir vs. human insulin 134
8.4.2.2.1. Adults 134
8.4.2.2.2. Children and adolescents 135
8.4.2.3. Glargine vs. detemir 136
8.5. Indications of the continuous subcutaneous insulin infusion pump (insulin pump or CSII) 137
8.5.1. Adults 137
8.5.2. Children and adolescents 141
8.5.3. Pregnant women 143
8.6. Methods of insulin administration in patients with diabetes mellitus type 1 144
8.6.1. Disposable syringe vs. prefi lled pen 144
8.6.1.1. Adults 144
8.6.1.2. Children and adolescents 145
8.6.2. Comparison of pre-fi lled pens 146
8.7. Insulin administration techniques 147
8.7.1. Administration site: injection site 147
8.7.2. Rotation of injection points 148
8.7.3. Injection technique (injection angle and skin fold) 149
8.7.4. Reusing needles 151
8.7.5. Injection through the clothes 151
8.7.6. Needle Size 152
8.8. Indications for the treatment with metformin added to insulin in adolescents with diabetes mellitus type 1 154
8.9. Pancreas and islet transplantation 156
8 SNS CLINICAL PRACTICE GUIDELINES
8.9.1. Pancreas Transplantation 156
8.9.2. Pancreatic islet transplantation 158
8.9.3. Islet transplantation vs. intensive insulin therapy 159
8.9.4. Pancreatic islet transplantation vs. pancreas transplantation 159
9. Management of diabetes mellitus type 1 in special situations 161
9.1. Insulin treatment guidelines during hospitalization of patients with diabetes mellitus type 1 161
9.1.1. Surgical Patient 162
9.1.2. Critical patient 164
9.1.3. Stable patient 166
9.2. Preventive and treatment measures in the case of outpatient acute intercurrent diseases in patients with diabetes mellitus type 1 168
9.3. Psychological disorders in patients with diabetes mellitus type 1 173
9.3.1. Affective disorders 173
9.3.2. Anxiety disorders 175
9.3.3. Eating disorders 176
9.4. Risk of decompensation of diabetes mellitus type 1 during adolescence 178
9.4.1. Risk of diabetic decompensation during adolescence 178
9.4.2. Psychological factors infl uencing metabolic control during adolescence 179
9.4.3. Adherence to the treatment 180
9.5. Pregnancy planning 182
9.6. Complications of diabetes mellitus type 1 during pregnancy 187
9.6.1. Evolution of retinopathy during pregnancy 187
9.6.2. Evolution of nephropathy during pregnancy 188
9.7. Metabolic control during pregnancy 189
9.8. Contraception and diabetes mellitus type 1 194
9.9 Clinical management of diabetes mellitus type 1 in patients with special needs 196
9.9.1. Immigrant Population 196
9.9.2. Patients with visual impairment 201
10. Acute complications 203
10.1. Hypoglycaemia 203
10.1.1. Symptoms of suspicion 204
10.1.2. Criteria for evaluating the severity 205
10.1.3. Performance measures in case of hypoglycaemia 206
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 9
10.1.3.1. Mild or moderate hypoglycaemia 206
10.1.3.2. Serious or severe hypoglycaemia 207
10.1.3.3. Pregnancy and breastfeeding 210
11. Chronic complications 213
11.1. Cardiovascular risk in patients with diabetes mellitus type 1 213
11.2. Diabetic retinopathy 217
11.2.1. Preventive medical treatment of diabetic retinopathy 217
11.2.2. Diabetic retinopathy screening techniques 222
11.2.3. Start time and frequency of screening for diabetic retinopathy 225
11.3. Diabetic nephropathy 227
11.3.1. Criteria for referral of patients with diabetic nephropathy to specialized care nephrology units 227
11.3.2. Treatment of patients with diabetes mellitus type 1 and microalbuminuria 231
11.3.3. Screening methods of diabetic nephropathy 232
11.3.4. Start time of screening for diabetic nephropathy 233
11.3.5. Frequency of screening for diabetic nephropathy 233
11.4. Diabetic foot 234
11.4.1. Effectiveness of screening for diabetic foot 234
11.4.2. Frequency of screening 235
11.4.3. Starting time of screening 235
11.4.4. Screening methods 235
11.5. Erectile dysfunction in people with diabetes mellitus type 1 238
11.5.1. Treatment of erectile dysfunction 238
11.6. Painful diabetic neuropathy 246
11.6.1. Treatment of painful diabetic neuropathy 246
12. Organizing the medical consultation 251
12.1. Transition of patients with diabetes mellitus type 1 from the paediatric services to the adult services 251
12.2. Initial study of the newly diagnosed patients with diabetes mellitus type 1 253
12.3. Follow-up and control consultations: tests and frequency 254
13. Dissemination and Implementation 257
13.1. Dissemination and implementation strategy 257
13.2. Implications for clinical practice 258
13.3. Proposed indicators 260
14. Future research 265
10 SNS CLINICAL PRACTICE GUIDELINES
Appendixes 269
Appendix 1. Reference centres which can carry out genetic studies to rule out MODY diabetes 269
Appendix 2. Sweeteners 272
Appendix 3. Caloric needs calculation 273
Appendix 4. Menu-based Method 274
Appendix 5. Servings based method and measuring cup 276
Appendix 6. Exchange and equivalence system 278
Appendix 7. Eligibility criteria for contraceptives in women with diabetes 282
Appendix 8. Treatment of hypoglycaemia 285
8.1. Mild hypoglycaemia 285
8.2. Severe Hypoglycaemia 286
Appendix 9. Use of the monofi lament (509) 287
Appendix 10. Drugs for neuropathic pain 288
Appendix 11. Information for patients: 289
11.1. International Charter of Rights and Responsibilities of people with diabetes 289
11.2. Support groups for people with diabetes 292
Appendix 12. Glossary 294
Appendix 13. Abbreviations 298
Appendix 14. Declaration of interest 300
Bibliography 302

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 11
Presentation
Documenting the variability of clinical practice, analyze its causes and adopt strategies to eliminate it have proven to be initiatives that promote effective and safe decision making by health profes-sionals focusing on the patient. Among these strategies, the most signifi cant is the preparation of clinical practice guidelines (CPG), a set of “systematically developed recommendations to help professionals and patients to make decisions about the most appropriate health care, and to select the diagnostic or therapeutic options best suited to addressing a health problem or a specifi c clini-cal condition”.
The 2010 Quality Plan for the Spanish National Health System (NHS) aims to address the challenges that it has to face, increasing the cohesion of the system, guaranteeing equity in health care to its citizens, regardless of where they reside and ensuring that this care is of the highest quality. Its objectives include the promotion of the development and use of GPC strategies related to health, consolidation and extension of the Guía-Salud Project. In this context, the CPG for Diabetes mellitus type 1 (DM1) can be framed.
Although DM1 usually represents only a minority of the total burden of diabetes on the popu-lation, it is the predominant disease in younger age groups in most developed countries and has a major impact on the patients’ lifestyle as well as their self-esteem.
The purpose of this guide is to improve the quality, effi ciency and equity of care for people with DM1 in the NHS. Thus, it addresses issues in the diagnosis of this disease and the detection of associated autoimmune diseases, diabetic education, glycaemic control, acute and chronic compli-cations and organizational aspects of care, paying special attention to the approach to patient care in special situations and with special needs.
This guide is the result of hard work carried out by a very large group of professionals, doctors and nurses and a group of patients who gave their vision of the whole process and how it could be improved.
From the Quality Agency we thank them for all the work they have done and we congratulate them for the elaboration of this CPG which will certainly allow healthcare professionals optimize their clinical practice and provide patients with DM1, their families and caregivers, with informa-tion and education to meet the needs and problems that may arise during the course of the disease, thus improving self-care and their quality of life.
Carmen Moya García
Director General of the Quality Agency of NHS


CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 13
Authorship and collaborations
Development Group of the CPG on Diabetes mellitus type 1 M.ª Ángeles Antón Miguel. Physician. Endocrinology and Nutrition Specialist. Araba
University Hospital. Txagorritxu, Vitoria-Gasteiz.
Beatriz Corcóstegui Santiago. Pharmacist. Specialist in Hospital Pharmacy. Galdakao-Usansolo Hospital, Bizkaia.
Alicia Cortazar Galarza. Physician. CIBERDEM. Endocrinology and Nutrition Specialist. Cruces University Hospital, Bizkaia.
Paz Gallego Saiz. Nurse. Diabetes Educator. Cruces University Hospital, Bizkaia.
Lorea García Cañibano. Patient.
Sonia Gaztambide Sáenz. Physician. Endocrinology and Nutrition Specialist. CIBERDEM. University of the Basque Country. Cruces University Hospital, Bizkaia
Virginia Guillén Cañas. Psychologist. Health Technology Assessment Service, Osteba, Vitoria-Gasteiz.
Paloma Jiménez Huertas. Nurse. Diabetes Educator. Cruces University Hospital, Vizcaya.
Marta López de Argumedo González de Durana. Physician. Specialist in Preventive Medicine and Public Health. Health Technology Assessment Service, Osteba, Vitoria-Gasteiz.
Oscar López de Briñas Ortega. Patient. Euskadi Diabetes Federation.
Itxaso Rica Echevarría. Physician. Specialist in Paediatric Endocrinology. Cruces University Hospital, Bizkaia
Federico Vázquez San Miguel. Physician. Endocrinology and Nutrition Specialist. CIBERDEM, University of the Basque Country. Cruces University Hospital, Bizkaia.
Alfredo Yoldi Arrieta. Physician. Endocrinology and Nutrition Specialist. University Hospital Donostia, Gipuzkoa Systematic review sub-working Group.
Systematic review sub-working GroupDavid Cantero González. Physician. Specialist in Preventive Medicine and Public Health.
Itziar Güemes Careaga. Psychologist.
M.ª Luisa Iruretagoiena Sánchez. Physician. Specialist in Preventive Medicine and Public Health.
Pedro Maria Latorre García. Physician. Specialist in Family and Community Medicine.
Eduardo Millán Ortuondo. Physician. Specialist in Preventive Medicine and Public Health.
M.ª Dolores Ramírez Ramírez. Documentalist
Jose Ramón Rueda Martínez de Santos. Physician. University of the Basque Country. Leioa, Bizkaia.
Jorge Taboada Gómez. Physician. Specialist in Preventive Medicine and Public Health
Gemma Villanueva Hernández. Psychologist. Specialist in Health Psychology

14 SNS CLINICAL PRACTICE GUIDELINES
Clinical Coordination Sonia Gaztambide Sáenz. Physician. Endocrinology and Nutrition Specialist.
CIBERDEM. University of the Basque Country. Cruces University Hospital Barakaldo, Bizkaia
Methodological coordination Marta López de Argumedo González de Durana. Physician. Specialist in Preventive
Medicine and Public Health. Service Health Technology Assessment, Osteba, Vitoria-Gasteiz
Virginia Guillén Cañas. Psychologist. Service Health Technology Assessment, Osteba, Vitoria-Gasteiz
Expert collaboration/External Review Manuel Aguilar Diosdado. Physician. Endocrinology and Nutrition Specialist. Puerta del
Mar Hospital, Cádiz
Ignacio Conget Donlo. Physician. Endocrinology and Nutrition Specialist. Hospital Clinic i Universitari, Barcelona
Ricardo V. García-Mayor. Physician. Endocrinology and Nutrition Specialist. Complexo Hospitalario Xeral-Cíes, Pontevedra
Juan Adrián Girbés Borrás. Physician. Endocrinology and Nutrition Specialist. Hospital “Arnau de Vilanova”, Valencia
Albert Goday Arnó. Physician. Endocrinology and Nutrition Specialist. Hospital del Mar, Barcelona.
Antonio Hernández Mijares. Physician. Endocrinology and Nutrition Specialist. University Hospital “Doctor Peset”, Valencia
Margarita Jansà Moretó. Nurse. Diabetes Educator. Hospital Clínic, Barcelona
Edelmiro Menéndez Torre. Physician. University Hospital “Central de Asturias”. Oviedo, Asturias
Mercedes Rodríguez Rigual. Physician. Specialist in Paediatric Endocrinology. Diabetes Unit. Hospital “Miguel Servet”. Zaragoza
Jose Antonio Vázquez García. Physician. Endocrinology and Nutrition Specialist. Professor, University of the Basque Country.
Clotilde Vázquez Martínez. Physician. Endocrinology and Nutrition Specialist. Hospital “Ramón y Cajal”. Madrid.
Luis Castaño González. Physician. Specialist in Paediatrics. CIBERDEM. University of the Basque Country. Cruces University Hospital, Barakaldo, Bizkaia
Gemma Peralta Pérez. Clinical psychologist. Fundació Rossend Carrasco I Formiguera. Universidad Autónoma de Barcelona.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 15
Other collaborations Arritxu Etxeberria Agirre. Primary Care Pharmacist. Teaching support
Idoia Fernández de Jáuregui Berrueta. Administrative support
Patrícia Fernández Ostolaza. Stlye proofreading.
Rosana Fuentes Gutiérrez. Managing bibliographical references, administrative support and editing.
Mar Gil Renedo. Patient.
Mª Asun M. Gutiérrez Iglesias. Economist. Support economic evaluation
Ana Larrabe González. Editing
Ana Maria Patiño Diez. Patient
Ana Maria Pedrueza. Patient
Rafael Rotaeche del Campo. Practitioner. Teaching support
Joseba Soloeta Eraso. Patient relative.
Marta Urban Echávarri. Administrative support
Acknowledgements Ángel Cabrera Hidalgo. Spanish Diabetes Federation
Itziar Etxeandia Ikobaltzeta. Service Health Technology Assessment of the Basque Government, Osteba
Tomás Lucas Morante. Spanish Society of Endocrinology and Nutrition (SEEN)
Rosa Rico Iturrioz. Health Technology Assessment Service of the Basque Government, Osteba
Flavia Salcedo Fernández. GuíaSalud. Aragon Institute of Health Sciences.
Cooperating Societies This CPG has the support of the following companies:
Diabetes Federation of the Basque Country belonging to the Spanish Diabetes Federation
Spanish Diabetes Society
Spanish Society for Paediatric Endocrinology
Spanish Society for Endocrinology and Nutrition
The members of these societies have participated in the creation, expert collaboration and exter-nal review of this CPG.
Declaration of interest: All members of the Working Group, as well as those who have partici-pated in the expert collaboration and external review, have made the declaration of interest as
appears in Appendix 14 of the full version.


CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 17
Questions to answer
Defi nition, diagnostic criteria for diabetes mellitus type 1
1. What is diabetes mellitus type 1?
2. What do the autoantibodies provide for the diagnosis of diabetes mellitus type 1?
3. What are the predictors of ‘spontaneous remission’?
4. When is it convenient to carry out a genetic study to rule out MODY diabetes?
5. What other autoimmune diseases are associated with diabetes mellitus type 1?
6. Is it necessary to rule out autoimmune diseases that are associated with diabetes mellitus type 1?
7. How should autoimmune diseases that are associated with diabetes mellitus type 1 in the initial study be considered?
8. How often should autoimmune diseases associated with diabetes mellitus type 1 be taken into account in the monitoring stage?
Diabetes Education
9. Are structured educational programs aimed at people with diabetes mellitus type 1 and their families effective?
10. Structured education aimed at families and people with diabetes mellitus type 1: When, how, by whom and what content is to be included?
11. Are the arrangements for community or extra sanitary support (schools, diabetic associa-tions, etc.) aimed at people with diabetes mellitus type 1 effective?
12. How to match the clinical management of diabetes mellitus type 1 in people with special needs?
Feeding
13. What is the most appropriate diet for people with diabetes mellitus type 1?
14. What meal plan is more advisable for people with diabetes mellitus type 1?
18 SNS CLINICAL PRACTICE GUIDELINES
Exercising
15. What are the benefi ts of exercise for people with diabetes mellitus type 1?
16. What kind of exercise is recommended for people with diabetes mellitus type 1?
Glycaemic Control
17. What are the target values of glycated haemoglobin?
18. What are the criteria for standardization and reporting of analytical results of glycated haemoglobin?
19. Do the continuous glucose monitoring systems provide better metabolic control?
20. What are the benefi ts and drawbacks of the management of patients with diabetes mellitus type 1 in the hospital at the time of diagnosis, compared with outpatient level management?
21. What is the effectiveness and safety of the different insulin preparations?
22. What are the indications for the continuous subcutaneous insulin infusion pump?
23. What are the safest and most effective methods of insulin administration?
24. What are the insulin administration techniques recommended for diabetes mellitus type 1?
25. Is it suitable to add metformin to insulin in adolescents?
26. What is the effectiveness of islet cells and pancreas transplantation?
Management of diabetes mellitus type 1 in special situations
27. What are the insulin therapy guidelines during hospitalization for patients whit diabetes mellitus type 1: surgical, critically ill and stable patients?
28. What are the preventive and treatment measures in case of ambulatory acute intercurrent diseases?
29. Are psychological disorders more common in people with diabetes mellitus type 1?
30. Does adolescence pose a risk for decompensation in diabetes mellitus type 1?
31. Is it important to plan pregnancy in women with diabetes mellitus type 1?
32. How does pregnancy affect the development of complications in diabetes mellitus type 1?
33. What should the before and during pregnancy metabolic control in women whit diabetes mellitus type 1 be?
34. What are the most recommended contraceptives in women with diabetes mellitus type 1?
35. How to adapt the clinical management of diabetes mellitus type 1 in patients whit special needs.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 19
Acute complications
36. When to suspect hypoglycaemia?
37. How to assess the severity of hypoglycaemia?
38. What should the performance measures against hypoglycaemic events be?
Chronic complications
39. How to evaluate the cardiovascular risk of patients with diabetes mellitus type 1?
40. Is there a medical (non-surgical, non-laser) treatment to prevent diabetic retinopathy?
41. What should the screening starting time for diabetic retinopathy be?
42. How often should screening for diabetic retinopathy be carried out?
43. What should the techniques for screening of diabetic retinopathy be?
44. What are the referral criteria to nephrology specialists for patients with diabetic nephrop-athy?
45. What is the pharmacological treatment for patients with diabetes mellitus type 1 and mi-croalbuminuria?
46. What should the screening frequency for diabetic nephropathy be?
47. At what age or years of evolution should diabetic nephropathy screening be performed?
48. What methods should be used for diabetic nephropathy screening?
49. It is necessary to carry out a diabetic foot screening?
50. What should the screening frequency for diabetic foot be?
51. At what age or years of evolution is diabetic foot screening to be carried out?
52. What method should be used for the diabetic foot screening?
53. What is the best treatment for erectile dysfunction in patients with diabetes mellitus type 1?
54. What is the best treatment for painful diabetic neuropathy?

20 SNS CLINICAL PRACTICE GUIDELINES
Organising the medical consultation
55. How should the transition of patients with diabetes mellitus type 1 from paediatric ser-vices to adult services be?
56. What is the initial study to be done to newly diagnosed patients of diabetes mellitus type 1?
57. What tests should be performed for people with diabetes mellitus type 1 in the monitoring and control consultations, and how often?
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 21
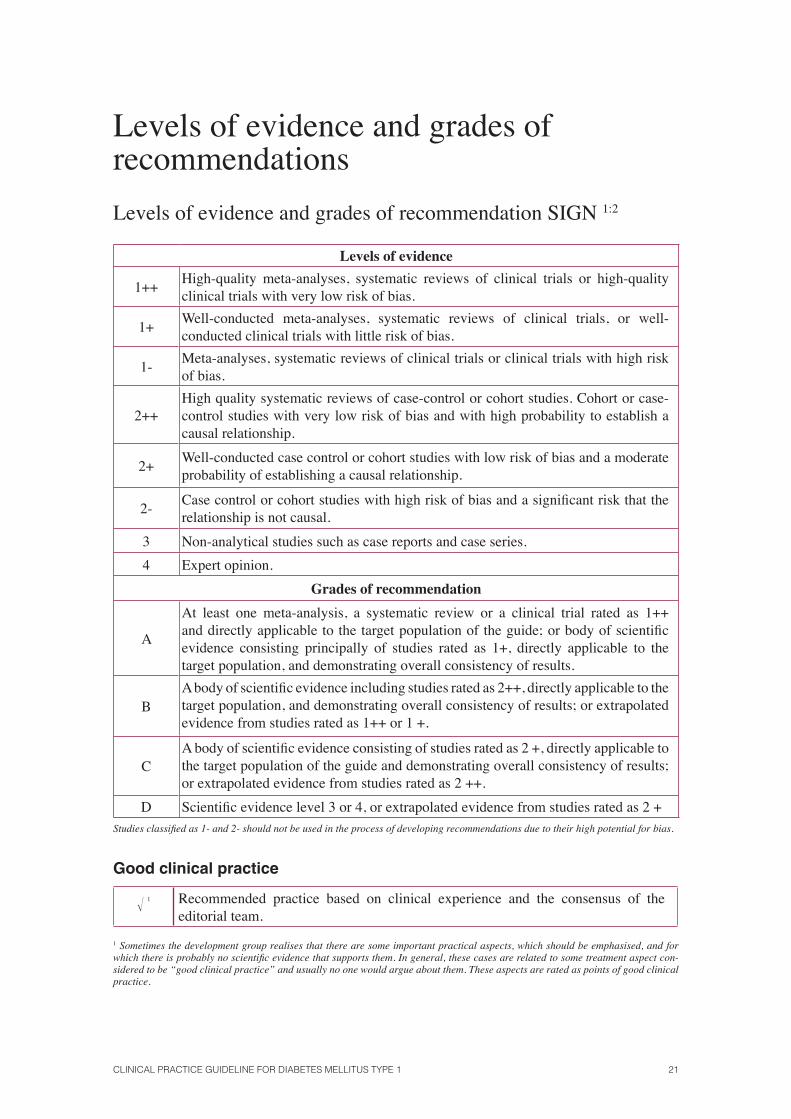
Levels of evidence and grades of recommendations
Levels of evidence and grades of recommendation SIGN 1:2
Levels of evidence
1++High-quality meta-analyses, systematic reviews of clinical trials or high-quality clinical trials with very low risk of bias.
1+Well-conducted meta-analyses, systematic reviews of clinical trials, or well-conducted clinical trials with little risk of bias.
1-Meta-analyses, systematic reviews of clinical trials or clinical trials with high risk of bias.
2++High quality systematic reviews of case-control or cohort studies. Cohort or case-control studies with very low risk of bias and with high probability to establish a causal relationship.
2+Well-conducted case control or cohort studies with low risk of bias and a moderate probability of establishing a causal relationship.
2-Case control or cohort studies with high risk of bias and a signifi cant risk that the relationship is not causal.
3 Non-analytical studies such as case reports and case series.
4 Expert opinion.
Grades of recommendation
A
At least one meta-analysis, a systematic review or a clinical trial rated as 1++ and directly applicable to the target population of the guide; or body of scientifi c evidence consisting principally of studies rated as 1+, directly applicable to the target population, and demonstrating overall consistency of results.
BA body of scientifi c evidence including studies rated as 2++, directly applicable to the target population, and demonstrating overall consistency of results; or extrapolated evidence from studies rated as 1++ or 1 +.
CA body of scientifi c evidence consisting of studies rated as 2 +, directly applicable to the target population of the guide and demonstrating overall consistency of results; or extrapolated evidence from studies rated as 2 ++.
D Scientifi c evidence level 3 or 4, or extrapolated evidence from studies rated as 2 + Studies classifi ed as 1- and 2- should not be used in the process of developing recommendations due to their high potential for bias.
Good clinical practice
� 1 Recommended practice based on clinical experience and the consensus of the editorial team.
1 Sometimes the development group realises that there are some important practical aspects, which should be emphasised, and for which there is probably no scientifi c evidence that supports them. In general, these cases are related to some treatment aspect con-sidered to be “good clinical practice” and usually no one would argue about them. These aspects are rated as points of good clinical practice.
22 SNS CLINICAL PRACTICE GUIDELINES
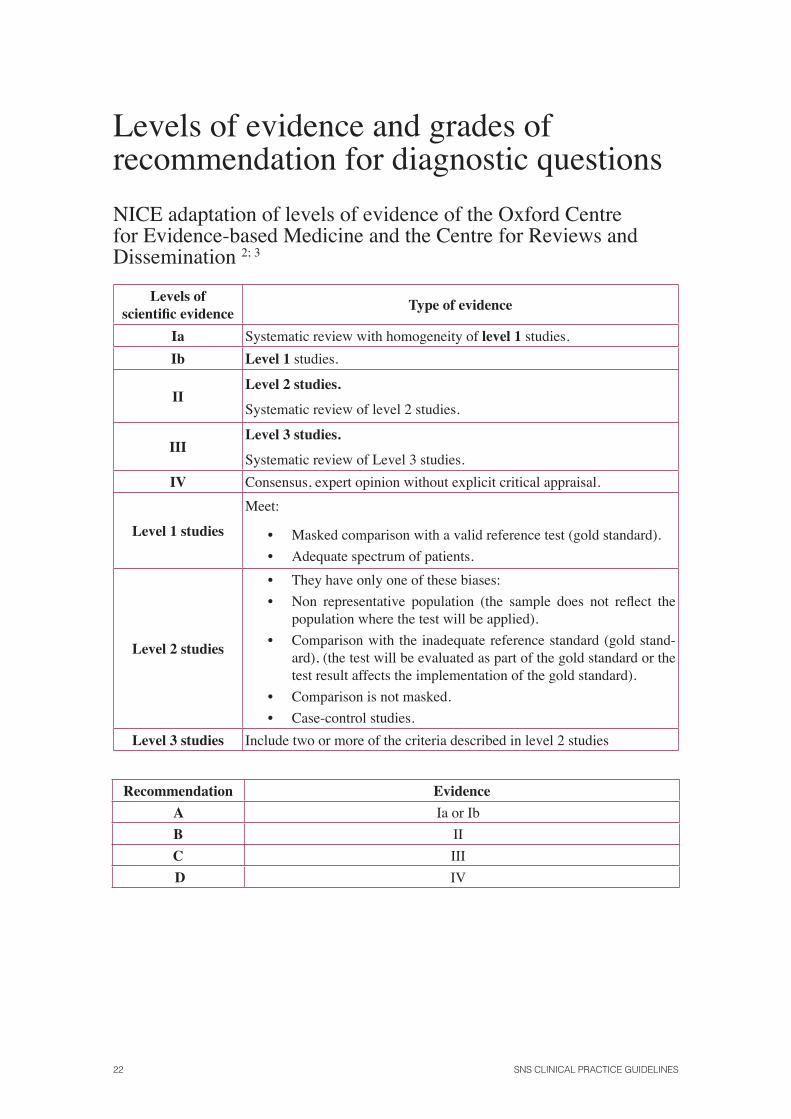
Levels of evidence and grades of recommendation for diagnostic questions
NICE adaptation of levels of evidence of the Oxford Centre for Evidence-based Medicine and the Centre for Reviews and Dissemination 2; 3
Levels of scientifi c evidence
Type of evidence
Ia Systematic review with homogeneity of level 1 studies.
Ib Level 1 studies.
IILevel 2 studies.
Systematic review of level 2 studies.
IIILevel 3 studies.
Systematic review of Level 3 studies.
IV Consensus, expert opinion without explicit critical appraisal.
Level 1 studies
Meet:
• Masked comparison with a valid reference test (gold standard).
• Adequate spectrum of patients.
Level 2 studies
• They have only one of these biases:
• Non representative population (the sample does not refl ect the population where the test will be applied).
• Comparison with the inadequate reference standard (gold stand-ard), (the test will be evaluated as part of the gold standard or the test result affects the implementation of the gold standard).
• Comparison is not masked.
• Case-control studies.
Level 3 studies Include two or more of the criteria described in level 2 studies
Recommendation Evidence
A Ia or Ib
B II
C III
D IV
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 23
Recommendations of the CPG
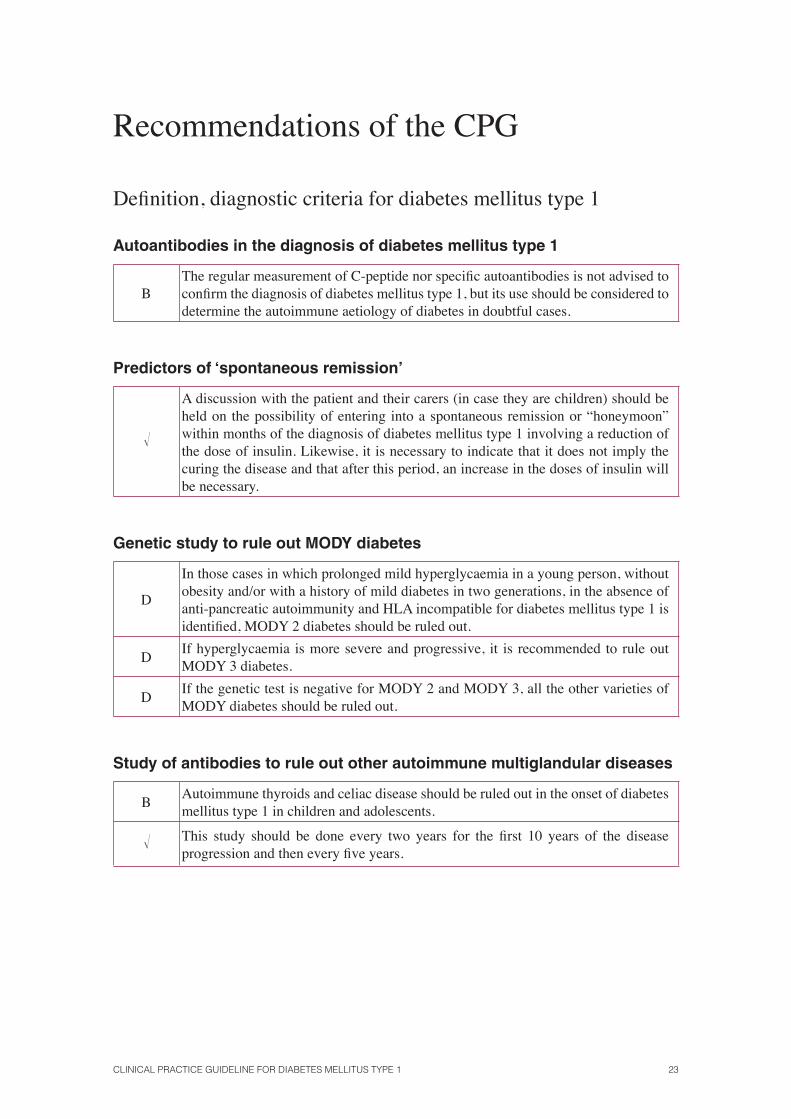
Defi nition, diagnostic criteria for diabetes mellitus type 1
Autoantibodies in the diagnosis of diabetes mellitus type 1
BThe regular measurement of C-peptide nor specifi c autoantibodies is not advised to confi rm the diagnosis of diabetes mellitus type 1, but its use should be considered to determine the autoimmune aetiology of diabetes in doubtful cases.
Predictors of ‘spontaneous remission’
�
A discussion with the patient and their carers (in case they are children) should be held on the possibility of entering into a spontaneous remission or “honeymoon” within months of the diagnosis of diabetes mellitus type 1 involving a reduction of the dose of insulin. Likewise, it is necessary to indicate that it does not imply the curing the disease and that after this period, an increase in the doses of insulin will be necessary.
Genetic study to rule out MODY diabetes
D
In those cases in which prolonged mild hyperglycaemia in a young person, without obesity and/or with a history of mild diabetes in two generations, in the absence of anti-pancreatic autoimmunity and HLA incompatible for diabetes mellitus type 1 is identifi ed, MODY 2 diabetes should be ruled out.
DIf hyperglycaemia is more severe and progressive, it is recommended to rule out MODY 3 diabetes.
DIf the genetic test is negative for MODY 2 and MODY 3, all the other varieties of MODY diabetes should be ruled out.
Study of antibodies to rule out other autoimmune multiglandular diseases
BAutoimmune thyroids and celiac disease should be ruled out in the onset of diabetes mellitus type 1 in children and adolescents.
� This study should be done every two years for the fi rst 10 years of the disease progression and then every fi ve years.
24 SNS CLINICAL PRACTICE GUIDELINES
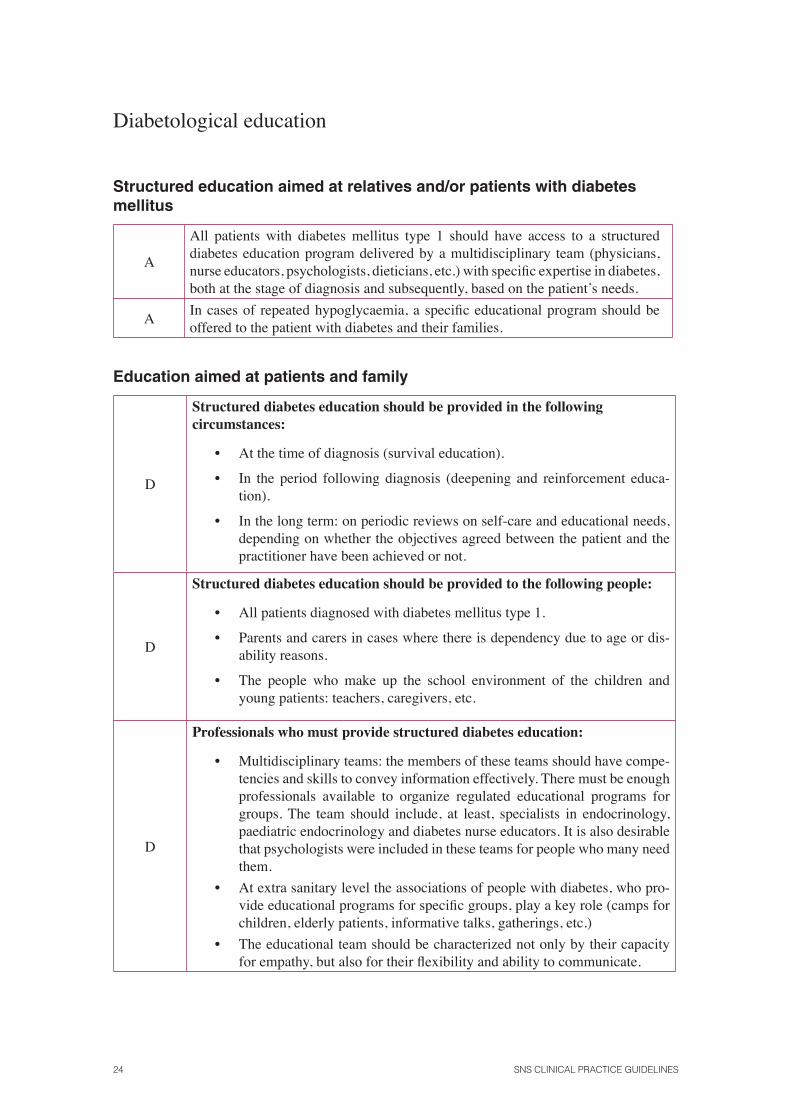
Diabetological education
Structured education aimed at relatives and/or patients with diabetes mellitus
A
All patients with diabetes mellitus type 1 should have access to a structured diabetes education program delivered by a multidisciplinary team (physicians, nurse educators, psychologists, dieticians, etc.) with specifi c expertise in diabetes, both at the stage of diagnosis and subsequently, based on the patient’s needs.
AIn cases of repeated hypoglycaemia, a specifi c educational program should be offered to the patient with diabetes and their families.
Education aimed at patients and family
D
Structured diabetes education should be provided in the following circumstances:
• At the time of diagnosis (survival education).
• In the period following diagnosis (deepening and reinforcement educa-tion).
• In the long term: on periodic reviews on self-care and educational needs, depending on whether the objectives agreed between the patient and the practitioner have been achieved or not.
D
Structured diabetes education should be provided to the following people:
• All patients diagnosed with diabetes mellitus type 1.
• Parents and carers in cases where there is dependency due to age or dis-ability reasons.
• The people who make up the school environment of the children and young patients: teachers, caregivers, etc.
D
Professionals who must provide structured diabetes education:
• Multidisciplinary teams: the members of these teams should have compe-tencies and skills to convey information effectively. There must be enough professionals available to organize regulated educational programs for groups. The team should include, at least, specialists in endocrinology, paediatric endocrinology and diabetes nurse educators. It is also desirable that psychologists were included in these teams for people who many need them.
• At extra sanitary level the associations of people with diabetes, who pro-vide educational programs for specifi c groups, play a key role (camps for children, elderly patients, informative talks, gatherings, etc.)
• The educational team should be characterized not only by their capacity for empathy, but also for their fl exibility and ability to communicate.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 25
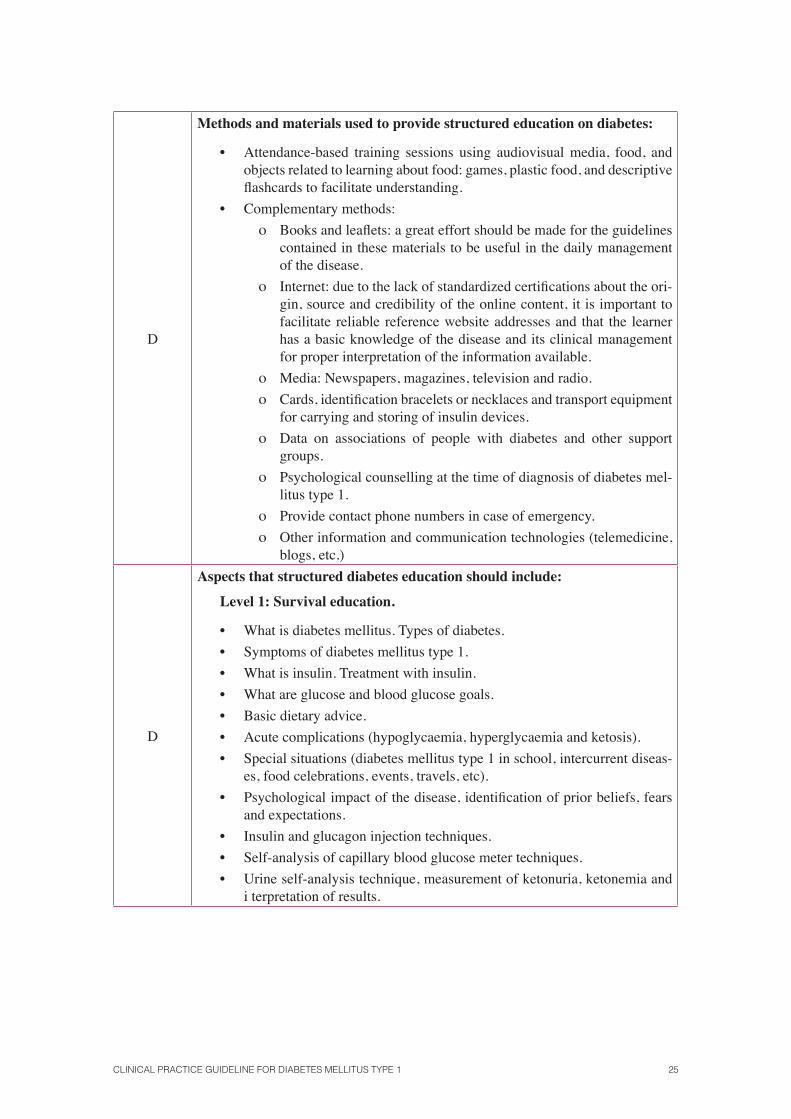
D
Methods and materials used to provide structured education on diabetes:
• Attendance-based training sessions using audiovisual media, food, and objects related to learning about food: games, plastic food, and descriptive fl ashcards to facilitate understanding.
• Complementary methods:
ο Books and leafl ets: a great effort should be made for the guidelines contained in these materials to be useful in the daily management of the disease.
ο Internet: due to the lack of standardized certifi cations about the ori-gin, source and credibility of the online content, it is important to facilitate reliable reference website addresses and that the learner has a basic knowledge of the disease and its clinical management for proper interpretation of the information available.
ο Media: Newspapers, magazines, television and radio.
ο Cards, identifi cation bracelets or necklaces and transport equipment for carrying and storing of insulin devices.
ο Data on associations of people with diabetes and other support groups.
ο Psychological counselling at the time of diagnosis of diabetes mel-litus type 1.
ο Provide contact phone numbers in case of emergency.
ο Other information and communication technologies (telemedicine, blogs, etc.)
D
Aspects that structured diabetes education should include:
Level 1: Survival education.
• What is diabetes mellitus. Types of diabetes.
• Symptoms of diabetes mellitus type 1.
• What is insulin. Treatment with insulin.
• What are glucose and blood glucose goals.
• Basic dietary advice.
• Acute complications (hypoglycaemia, hyperglycaemia and ketosis).
• Special situations (diabetes mellitus type 1 in school, intercurrent diseas-es, food celebrations, events, travels, etc).
• Psychological impact of the disease, identifi cation of prior beliefs, fears and expectations.
• Insulin and glucagon injection techniques.
• Self-analysis of capillary blood glucose meter techniques.
• Urine self-analysis technique, measurement of ketonuria, ketonemia and i terpretation of results.
26 SNS CLINICAL PRACTICE GUIDELINES
D
Level 2: Advanced Education.
• Physiopathology, epidemiology and classifi cation of diabetes.
• Types of insulin: absorption, action profi les, variability and adjustments.
• Food planning: qualitative and quantitative advice on immediate and fi -bre intakes, with special attention to carbohydrate intake.
• Control objectives, including the concept of glycated haemoglobin.
• Reinforcement of knowledge on acute complications.
• Problem solving and adjustment of treatment.
• Micro-and macrovascular complications: prevention and monitoring.
• Adjustment of insulin and feeding patterns in special situations, such as exercising, holidays and travelling.
• Tobacco, alcohol and other drugs.
• Adjustment to work and driving.
• Sexuality, contraception, teratogenic drugs, pregnancy and breast-feed-ing.
• Updated research on diabetes mellitus type 1.
• Continuous infusion pumps.
• Foot care.
D
Methods for teaching structured education about diabetes:
Several methods have been used successfully in diabetes education. The choice of one or another depends on the characteristics of the patient, the stage of the disease and the capacity of each team or health care centre.
Individualized education.
• An intensive individualized program should be provided to newly diag-nosed diabetes mellitus type 1 patients and in the case of pregnancy.
Education in groups.
• The groups should be organized according to age, socio-cultural back-ground, etc. It is desirable that family members and friends of patients also participate in the groups. Group education should include the fol-lowing aspects:
ο Structured training by explicative lectures.
ο Discussion groups, with analysis of the perceptions and experienc-es of all the group members.
ο Identifi cation of fears and anxieties.
ο Assessment of needs and expectations.
ο Manifestation of personal experiences regarding hypoglycaemia, physical activity, stress response, etc.
ο Audiovisual methods.
ο Support educational material, which the patient can read at home.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 27
D
Characteristics which structured education programs on diabetes must contain:
• Actively involve patients in all the stages of the educational program (de-sign, implementation, evaluation), providing them with the tools to make the best decisions about their own health.
• Set the benefi ts of learning new skills, including the daily monitoring of the treatment.
• Assess the educational needs of each patient.
• Assess patients’ personal perceptions.
• Be fl exible so that the programs are adapted to the specifi c educational, social and cultural needs.
• Have educational goals agreed with patients. The expectations of profes-sionals and patients may differ, so it is important to agree on common objectives, which may vary over time and require a continuous review. Any proposed therapeutic target should be achievable.
• Have a syllabus and a fi xed schedule.
• Do not create a very concentrated program and schedule frequent breaks.
• Schedule chats that do not exceed 25% of the total time, and include a time for asking and answering questions.
• Pay attention to the choice of words and expressions, avoiding an overly technical language.
• Provide standardized and consistent information between the different team members.
• Plan meetings between the professionals involved, to exchange ideas, discuss cases and review the program and methods.
• Facilitate that adults participate in their own health care by giving them the possibility to make judgments and choices about their own care.
• It is advisable to establish a dynamic contact process with the patient, ei-ther through visits, group discussions between patients, telephone contact or computer systems.
D
Other considerations:
• Discuss any changes that have taken place at biomedical level (new insu-lin requirements, glycaemia monitoring strategies, onset of ocular com-plications, etc).
• Evaluation: the educational program and the goals should be assessed by process and results indicators.
• Provision should be done of all the information needed to enable the de-velopment of the therapeutic education program: space required, enough qualifi ed personnel, necessary educational materials and work agendas and schedules.
28 SNS CLINICAL PRACTICE GUIDELINES
Community Support arrangements
B (Adults)/
A (Children)
Updated information should be provided to adults, children and adolescents with diabetes mellitus type 1 and to their families at the time of diagnosis, and periodically thereafter, about the existence of support groups for diabetics, both locally and nationally and the way to contact them (Appendix 11.2.).
BThe diabetes care teams should be aware that a poor psychosocial support has a negative impact on various outcomes of diabetes mellitus type 1 in children and young people, including glycaemic control and self-esteem.
A
A young person with diabetes mellitus type 1 should be offered specifi c support strategies such as self-analysis tutorials based on problem solving, to improve their self-esteem and glycaemic control, as well as provide them with gatherings to exchange experience and to reduce confl icts related to diabetes among family members.
�
There is no formal relationship between the health care services and the associations of diabetics. This relationship can be benefi cial if the actions are confl uent. It would be advisable that a physician and/or a diabetes nurse educator would participate in diabetics associations, as technical support for the activities to be developed.
Feeding
General recommendations
�
The nutrition recommendations for a healthy lifestyle which are valid among the general population, are also appropriate for people with diabetes mellitus type 1. Currently, several insulin options are available, allowing adapting the best-suited insulin regimen to the tastes and food choices of people with diabetes mellitus type 1 within the context of a healthy diet.
�The improvement in glycaemic control with insulin therapy is often associated to weight gain. As the potential weight gain can affect negatively to glycaemia, lipids, blood pressure and general health, it should be prevented.
�Although the carbohydrate content of the meal determines the pre-prandial insulin dose, the total intake of proteins and fats should also be taken into consideration.
Carbohydrates
A
The dose of insulin should be adjusted to the carbohydrate intake in people with diabetes mellitus type 1. This recommendation must be accompanied by the support of health professionals through comprehensive nutrition education.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 29
AIn patients with diabetes mellitus type 1, foods with table sugar can be replaced by other food containing other carbohydrate sources.
� If food with high sugar content is eaten, its absorption should be slowed by associating their food intake with fat or fi bre.
Artifi cial Sweeteners
BIn patients with diabetes mellitus type 1, it is preferable to use, artifi cial sweeteners, which do not interfere with glycaemic increase (see Appendix 2).
B
It is recommended to prevent the abuse of drinks and foods sweetened with fructose. This recommendation should not be extended to the fructose contained in fruits and vegetables, since these are healthy foods that provide small quantities of fructose in a normal diet.
Glycaemic Index
�For patients with diabetes mellitus type 1 who are evaluating the planning of their diet based exclusively on the glycaemic index of foods, health professionals should inform them about the lack of conclusive evidence regarding its benefi ts.
Fibre
A
The recommendations for fi bre intake in patients with diabetes mellitus type 1 are similar to those of the general population, that is, a diet containing 25 to 30 g fi bre/day, with special emphasis on soluble fi bre intake (7 to 13 g) is recommended.
Proteins in patients with nephropathy
AIn patients with diabetic nephropathy a protein intake of less than 0.8 g/kg/day is recommended.
AIn patients with advanced diabetic nephropathy (chronic renal failure in stages 3-5), a possible hypoalbuminemia should be monitored by modifying the protein and caloric intake to prevent malnutrition.
Diet for the prevention and treatment of cardiovascular disease
BNutritional interventions should be implemented to improve metabolic control and the lipid profi le in the prevention and treatment of cardiovascular disease in patients with diabetes mellitus type 1.
Advisable feeding plan for patients with diabetes mellitus type 1
�The feeding plan ought to be adjusted depending on the age, insulin dosage, physical activity, weight and personal situation (pregnancy, hypercholesterolemia, etc.) of the patient and his/her ability to understand.
30 SNS CLINICAL PRACTICE GUIDELINES
Exercising
Benefi ts of exercise in people with diabetes mellitus type 1
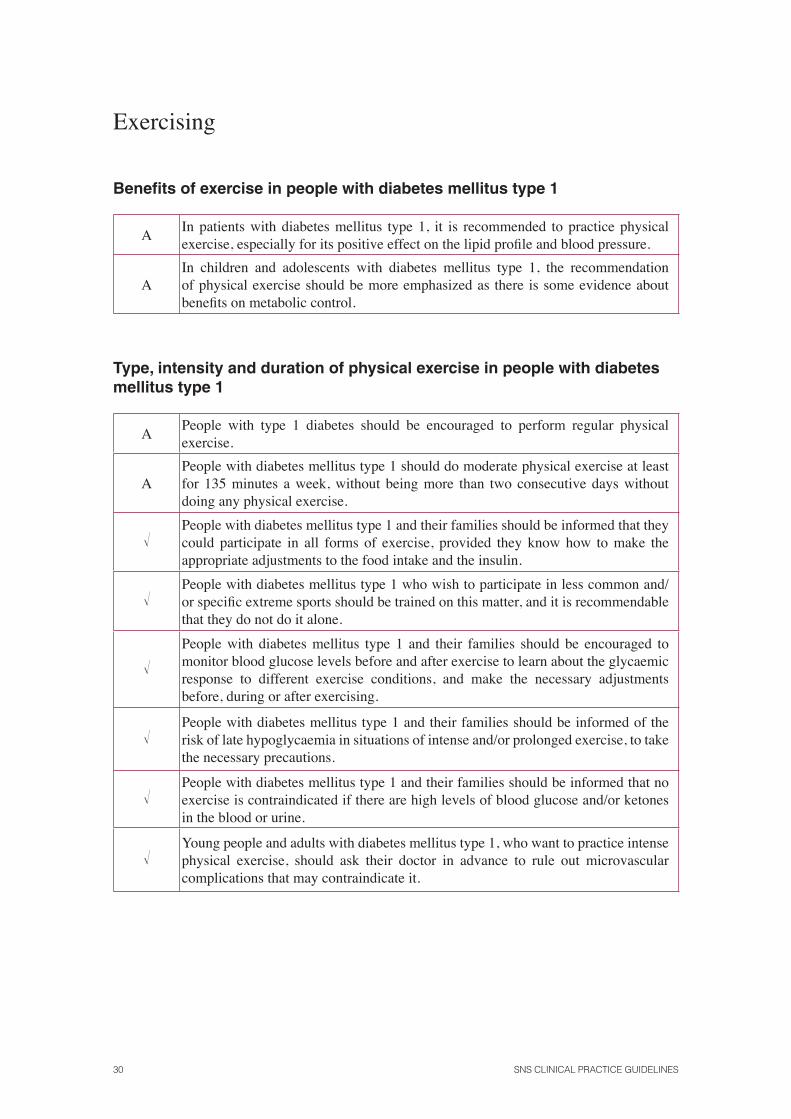
AIn patients with diabetes mellitus type 1, it is recommended to practice physical exercise, especially for its positive effect on the lipid profi le and blood pressure.
AIn children and adolescents with diabetes mellitus type 1, the recommendation of physical exercise should be more emphasized as there is some evidence about benefi ts on metabolic control.
Type, intensity and duration of physical exercise in people with diabetes mellitus type 1
APeople with type 1 diabetes should be encouraged to perform regular physical exercise.
APeople with diabetes mellitus type 1 should do moderate physical exercise at least for 135 minutes a week, without being more than two consecutive days without doing any physical exercise.
�People with diabetes mellitus type 1 and their families should be informed that they could participate in all forms of exercise, provided they know how to make the appropriate adjustments to the food intake and the insulin.
�People with diabetes mellitus type 1 who wish to participate in less common and/or specifi c extreme sports should be trained on this matter, and it is recommendable that they do not do it alone.
�People with diabetes mellitus type 1 and their families should be encouraged to monitor blood glucose levels before and after exercise to learn about the glycaemic response to different exercise conditions, and make the necessary adjustments before, during or after exercising.
�People with diabetes mellitus type 1 and their families should be informed of the risk of late hypoglycaemia in situations of intense and/or prolonged exercise, to take the necessary precautions.
�People with diabetes mellitus type 1 and their families should be informed that no exercise is contraindicated if there are high levels of blood glucose and/or ketones in the blood or urine.
�Young people and adults with diabetes mellitus type 1, who want to practice intense physical exercise, should ask their doctor in advance to rule out microvascular complications that may contraindicate it.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 31
Glycaemic Control
Glycosylated haemoglobin
Target fi gures of glycosylated haemoglobin
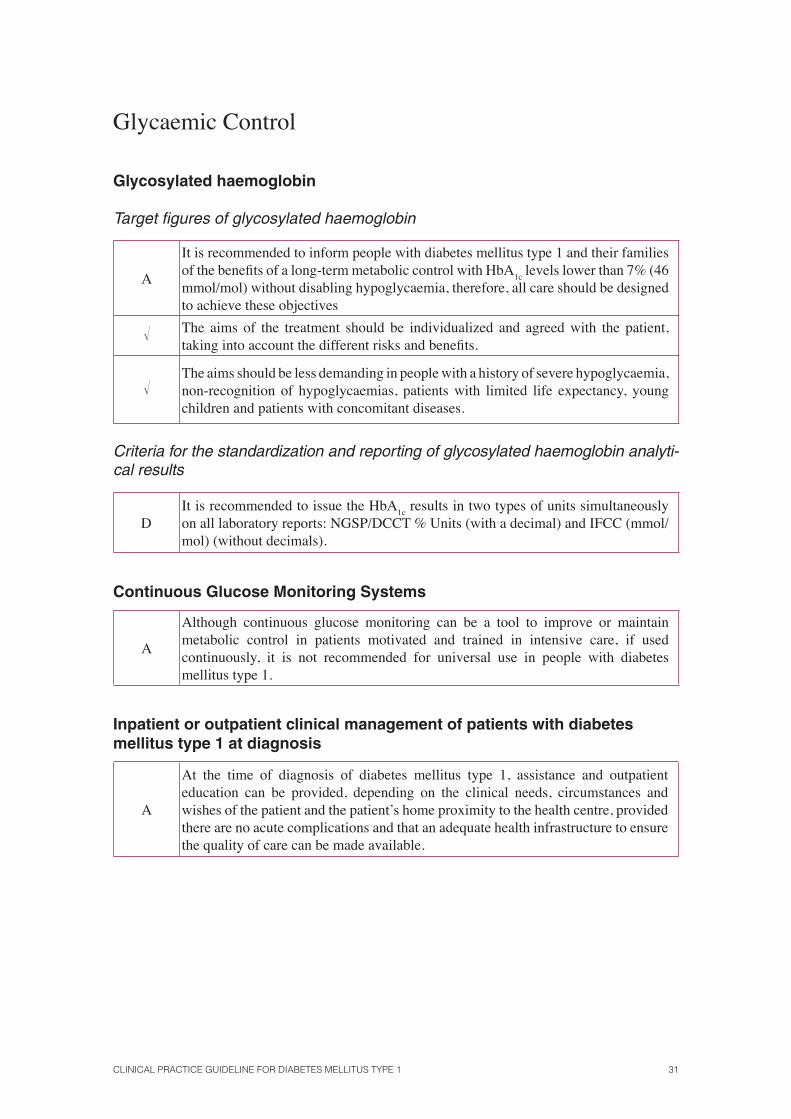
A
It is recommended to inform people with diabetes mellitus type 1 and their families of the benefi ts of a long-term metabolic control with HbA
1c levels lower than 7% (46
mmol/mol) without disabling hypoglycaemia, therefore, all care should be designed to achieve these objectives
� The aims of the treatment should be individualized and agreed with the patient, taking into account the different risks and benefi ts.
�The aims should be less demanding in people with a history of severe hypoglycaemia, non-recognition of hypoglycaemias, patients with limited life expectancy, young children and patients with concomitant diseases.
Criteria for the standardization and reporting of glycosylated haemoglobin analyti-cal results
DIt is recommended to issue the HbA
1c results in two types of units simultaneously
on all laboratory reports: NGSP/DCCT % Units (with a decimal) and IFCC (mmol/mol) (without decimals).
Continuous Glucose Monitoring Systems
A
Although continuous glucose monitoring can be a tool to improve or maintain metabolic control in patients motivated and trained in intensive care, if used continuously, it is not recommended for universal use in people with diabetes mellitus type 1.
Inpatient or outpatient clinical management of patients with diabetes mellitus type 1 at diagnosis
A
At the time of diagnosis of diabetes mellitus type 1, assistance and outpatient education can be provided, depending on the clinical needs, circumstances and wishes of the patient and the patient’s home proximity to the health centre, provided there are no acute complications and that an adequate health infrastructure to ensure the quality of care can be made available.
32 SNS CLINICAL PRACTICE GUIDELINES
Preparations of insulin in the treatment of patients with diabetes mellitus type 1
Fast acting analogues vs. human insulin. Adults, children and adolescents.
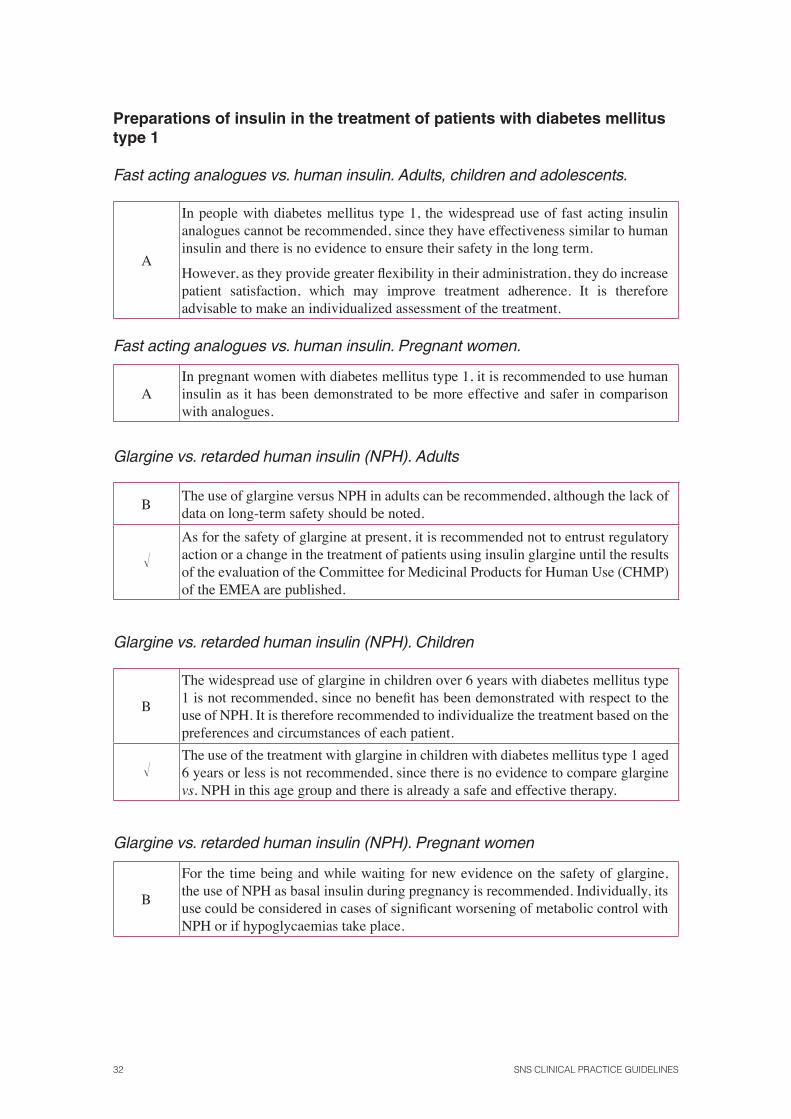
A
In people with diabetes mellitus type 1, the widespread use of fast acting insulin analogues cannot be recommended, since they have effectiveness similar to human insulin and there is no evidence to ensure their safety in the long term.
However, as they provide greater fl exibility in their administration, they do increase patient satisfaction, which may improve treatment adherence. It is therefore advisable to make an individualized assessment of the treatment.
Fast acting analogues vs. human insulin. Pregnant women.
AIn pregnant women with diabetes mellitus type 1, it is recommended to use human insulin as it has been demonstrated to be more effective and safer in comparison with analogues.
Glargine vs. retarded human insulin (NPH). Adults
BThe use of glargine versus NPH in adults can be recommended, although the lack of data on long-term safety should be noted.
�As for the safety of glargine at present, it is recommended not to entrust regulatory action or a change in the treatment of patients using insulin glargine until the results of the evaluation of the Committee for Medicinal Products for Human Use (CHMP) of the EMEA are published.
Glargine vs. retarded human insulin (NPH). Children
B
The widespread use of glargine in children over 6 years with diabetes mellitus type 1 is not recommended, since no benefi t has been demonstrated with respect to the use of NPH. It is therefore recommended to individualize the treatment based on the preferences and circumstances of each patient.
�The use of the treatment with glargine in children with diabetes mellitus type 1 aged 6 years or less is not recommended, since there is no evidence to compare glargine vs. NPH in this age group and there is already a safe and effective therapy.
Glargine vs. retarded human insulin (NPH). Pregnant women
B
For the time being and while waiting for new evidence on the safety of glargine, the use of NPH as basal insulin during pregnancy is recommended. Individually, its use could be considered in cases of signifi cant worsening of metabolic control with NPH or if hypoglycaemias take place.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 33
Detemir vs. retarded human insulin (NPH). Adults
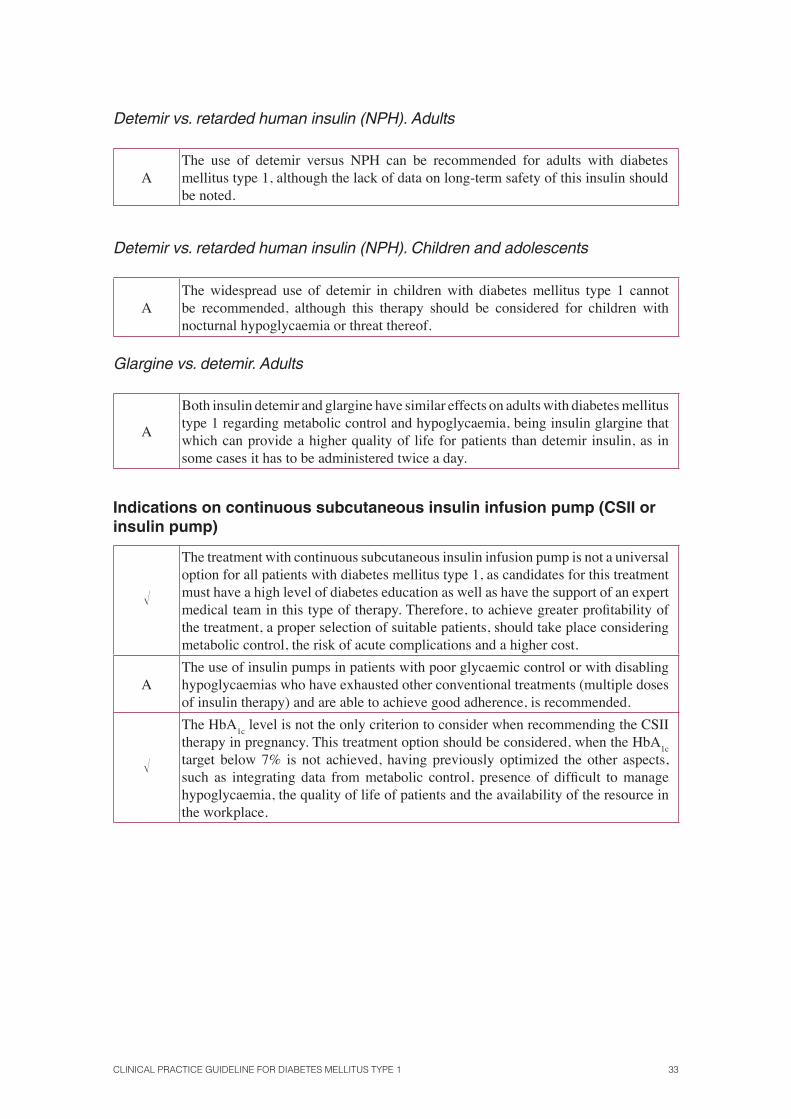
AThe use of detemir versus NPH can be recommended for adults with diabetes mellitus type 1, although the lack of data on long-term safety of this insulin should be noted.
Detemir vs. retarded human insulin (NPH). Children and adolescents
AThe widespread use of detemir in children with diabetes mellitus type 1 cannot be recommended, although this therapy should be considered for children with nocturnal hypoglycaemia or threat thereof.
Glargine vs. detemir. Adults
A
Both insulin detemir and glargine have similar effects on adults with diabetes mellitus type 1 regarding metabolic control and hypoglycaemia, being insulin glargine that which can provide a higher quality of life for patients than detemir insulin, as in some cases it has to be administered twice a day.
Indications on continuous subcutaneous insulin infusion pump (CSII or insulin pump)
�
The treatment with continuous subcutaneous insulin infusion pump is not a universal option for all patients with diabetes mellitus type 1, as candidates for this treatment must have a high level of diabetes education as well as have the support of an expert medical team in this type of therapy. Therefore, to achieve greater profi tability of the treatment, a proper selection of suitable patients, should take place considering metabolic control, the risk of acute complications and a higher cost.
AThe use of insulin pumps in patients with poor glycaemic control or with disabling hypoglycaemias who have exhausted other conventional treatments (multiple doses of insulin therapy) and are able to achieve good adherence, is recommended.
�
The HbA1c
level is not the only criterion to consider when recommending the CSII therapy in pregnancy. This treatment option should be considered, when the HbA
1c
target below 7% is not achieved, having previously optimized the other aspects, such as integrating data from metabolic control, presence of diffi cult to manage hypoglycaemia, the quality of life of patients and the availability of the resource in the workplace.
34 SNS CLINICAL PRACTICE GUIDELINES
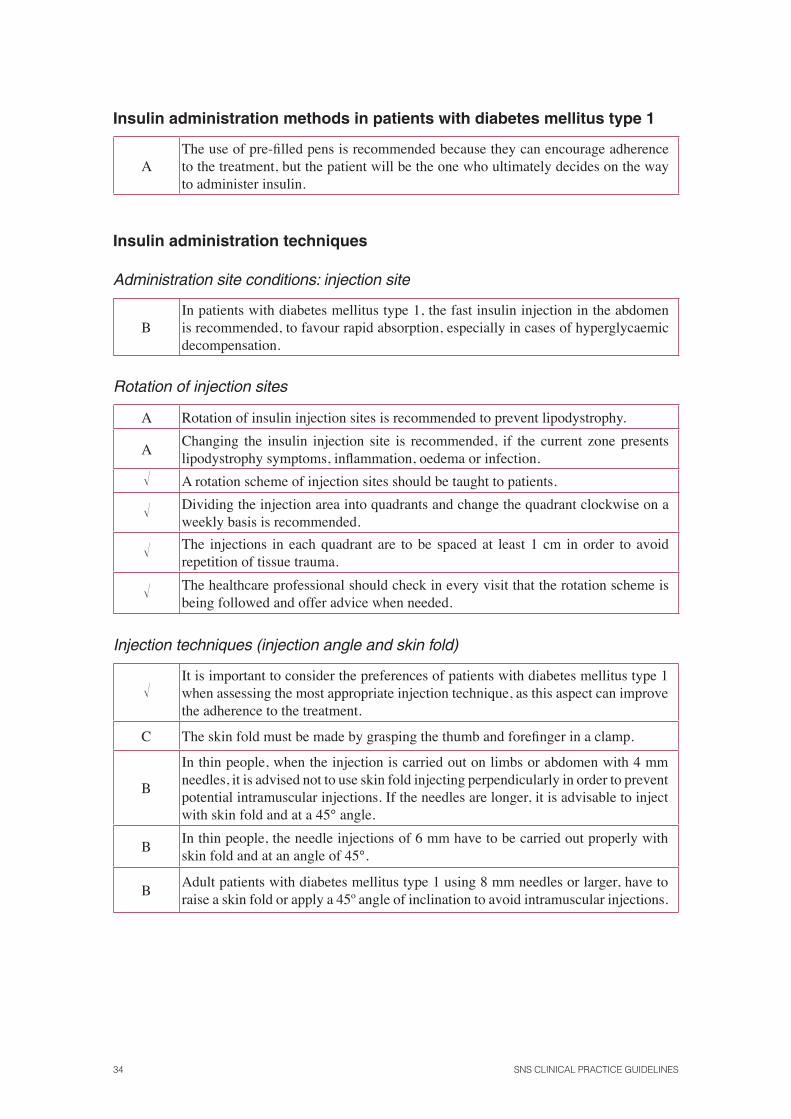
Insulin administration methods in patients with diabetes mellitus type 1
AThe use of pre-fi lled pens is recommended because they can encourage adherence to the treatment, but the patient will be the one who ultimately decides on the way to administer insulin.
Insulin administration techniques
Administration site conditions: injection site
BIn patients with diabetes mellitus type 1, the fast insulin injection in the abdomen is recommended, to favour rapid absorption, especially in cases of hyperglycaemic decompensation.
Rotation of injection sites
A Rotation of insulin injection sites is recommended to prevent lipodystrophy.
AChanging the insulin injection site is recommended, if the current zone presents lipodystrophy symptoms, infl ammation, oedema or infection.
� A rotation scheme of injection sites should be taught to patients.
� Dividing the injection area into quadrants and change the quadrant clockwise on a weekly basis is recommended.
� The injections in each quadrant are to be spaced at least 1 cm in order to avoid repetition of tissue trauma.
� The healthcare professional should check in every visit that the rotation scheme is being followed and offer advice when needed.
Injection techniques (injection angle and skin fold)
�It is important to consider the preferences of patients with diabetes mellitus type 1 when assessing the most appropriate injection technique, as this aspect can improve the adherence to the treatment.
C The skin fold must be made by grasping the thumb and forefi nger in a clamp.
B
In thin people, when the injection is carried out on limbs or abdomen with 4 mm needles, it is advised not to use skin fold injecting perpendicularly in order to prevent potential intramuscular injections. If the needles are longer, it is advisable to inject with skin fold and at a 45° angle.
BIn thin people, the needle injections of 6 mm have to be carried out properly with skin fold and at an angle of 45°.
BAdult patients with diabetes mellitus type 1 using 8 mm needles or larger, have to raise a skin fold or apply a 45º angle of inclination to avoid intramuscular injections.
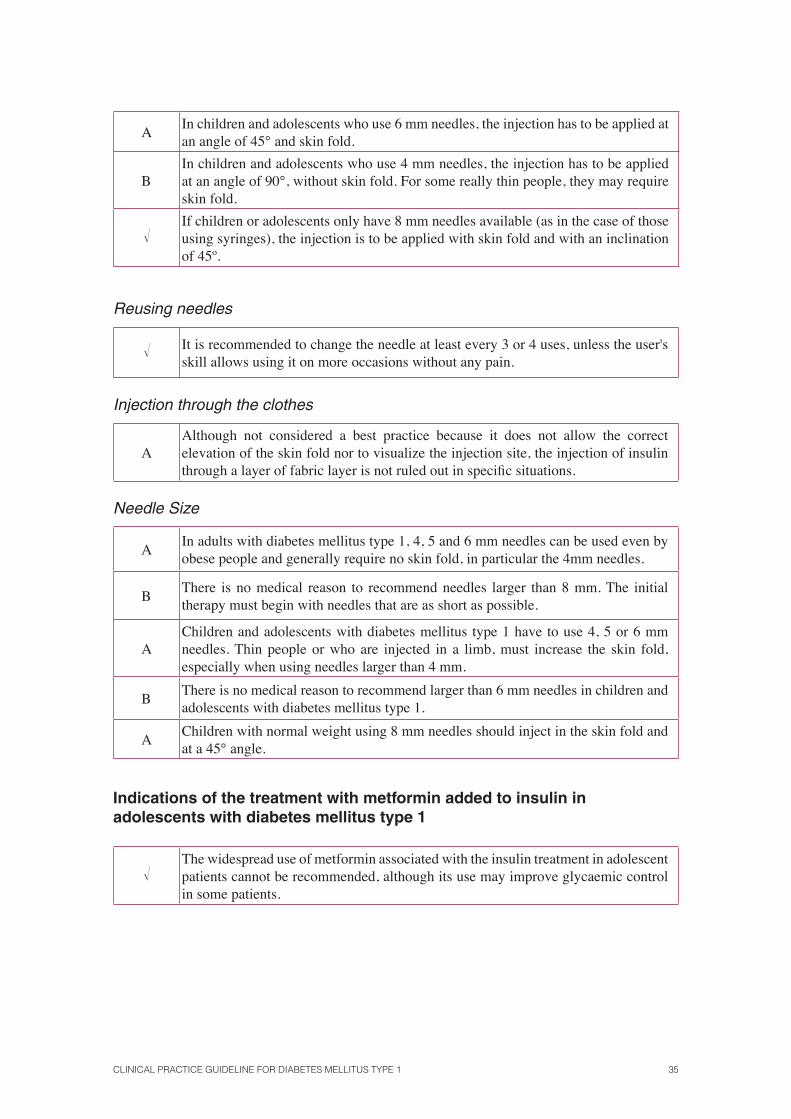
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 35
AIn children and adolescents who use 6 mm needles, the injection has to be applied at an angle of 45° and skin fold.
BIn children and adolescents who use 4 mm needles, the injection has to be applied at an angle of 90°, without skin fold. For some really thin people, they may require skin fold.
�If children or adolescents only have 8 mm needles available (as in the case of those using syringes), the injection is to be applied with skin fold and with an inclination of 45º.
Reusing needles
� It is recommended to change the needle at least every 3 or 4 uses, unless the user's skill allows using it on more occasions without any pain.
Injection through the clothes
AAlthough not considered a best practice because it does not allow the correct elevation of the skin fold nor to visualize the injection site, the injection of insulin through a layer of fabric layer is not ruled out in specifi c situations.
Needle Size
AIn adults with diabetes mellitus type 1, 4, 5 and 6 mm needles can be used even by obese people and generally require no skin fold, in particular the 4mm needles.
BThere is no medical reason to recommend needles larger than 8 mm. The initial therapy must begin with needles that are as short as possible.
AChildren and adolescents with diabetes mellitus type 1 have to use 4, 5 or 6 mm needles. Thin people or who are injected in a limb, must increase the skin fold, especially when using needles larger than 4 mm.
BThere is no medical reason to recommend larger than 6 mm needles in children and adolescents with diabetes mellitus type 1.
AChildren with normal weight using 8 mm needles should inject in the skin fold and at a 45° angle.
Indications of the treatment with metformin added to insulin in adolescents with diabetes mellitus type 1
�The widespread use of metformin associated with the insulin treatment in adolescent patients cannot be recommended, although its use may improve glycaemic control in some patients.
36 SNS CLINICAL PRACTICE GUIDELINES
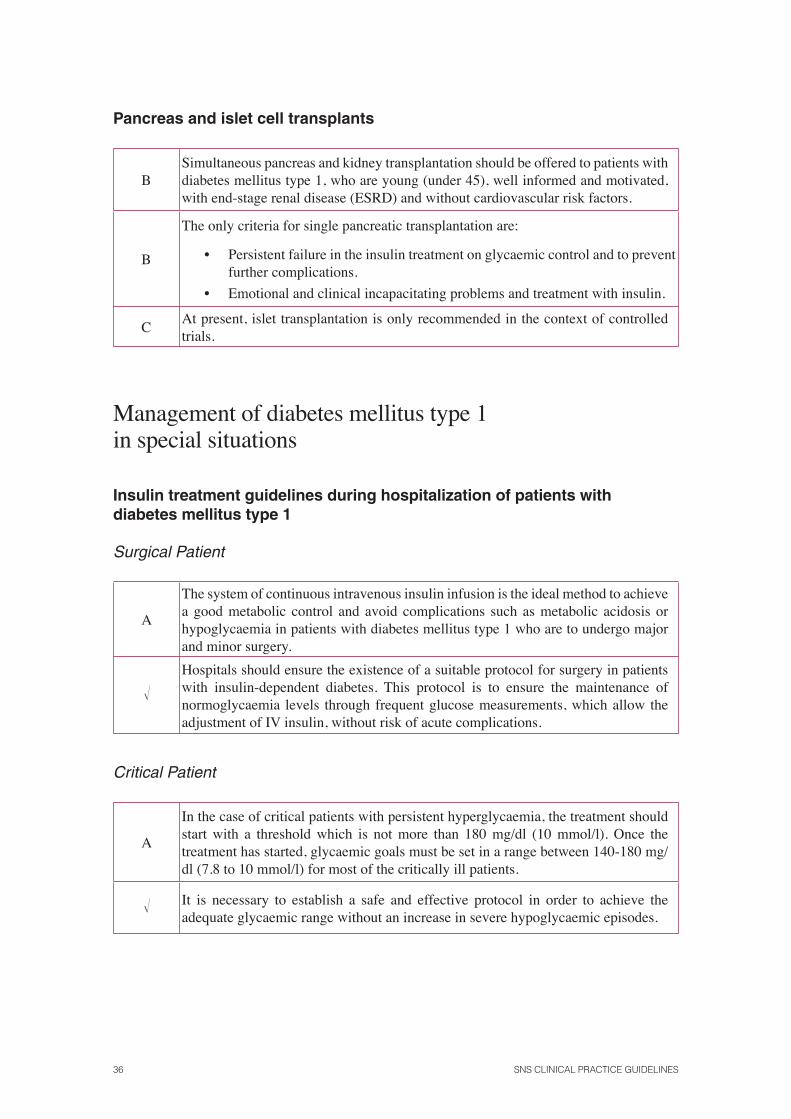
Pancreas and islet cell transplants
BSimultaneous pancreas and kidney transplantation should be offered to patients with diabetes mellitus type 1, who are young (under 45), well informed and motivated, with end-stage renal disease (ESRD) and without cardiovascular risk factors.
B
The only criteria for single pancreatic transplantation are:
• Persistent failure in the insulin treatment on glycaemic control and to prevent further complications.
• Emotional and clinical incapacitating problems and treatment with insulin.
CAt present, islet transplantation is only recommended in the context of controlled trials.
Management of diabetes mellitus type 1in special situations
Insulin treatment guidelines during hospitalization of patients with diabetes mellitus type 1
Surgical Patient
A
The system of continuous intravenous insulin infusion is the ideal method to achieve a good metabolic control and avoid complications such as metabolic acidosis or hypoglycaemia in patients with diabetes mellitus type 1 who are to undergo major and minor surgery.
�Hospitals should ensure the existence of a suitable protocol for surgery in patients with insulin-dependent diabetes. This protocol is to ensure the maintenance of normoglycaemia levels through frequent glucose measurements, which allow the adjustment of IV insulin, without risk of acute complications.
Critical Patient
A
In the case of critical patients with persistent hyperglycaemia, the treatment should start with a threshold which is not more than 180 mg/dl (10 mmol/l). Once the treatment has started, glycaemic goals must be set in a range between 140-180 mg/dl (7.8 to 10 mmol/l) for most of the critically ill patients.
� It is necessary to establish a safe and effective protocol in order to achieve the adequate glycaemic range without an increase in severe hypoglycaemic episodes.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 37
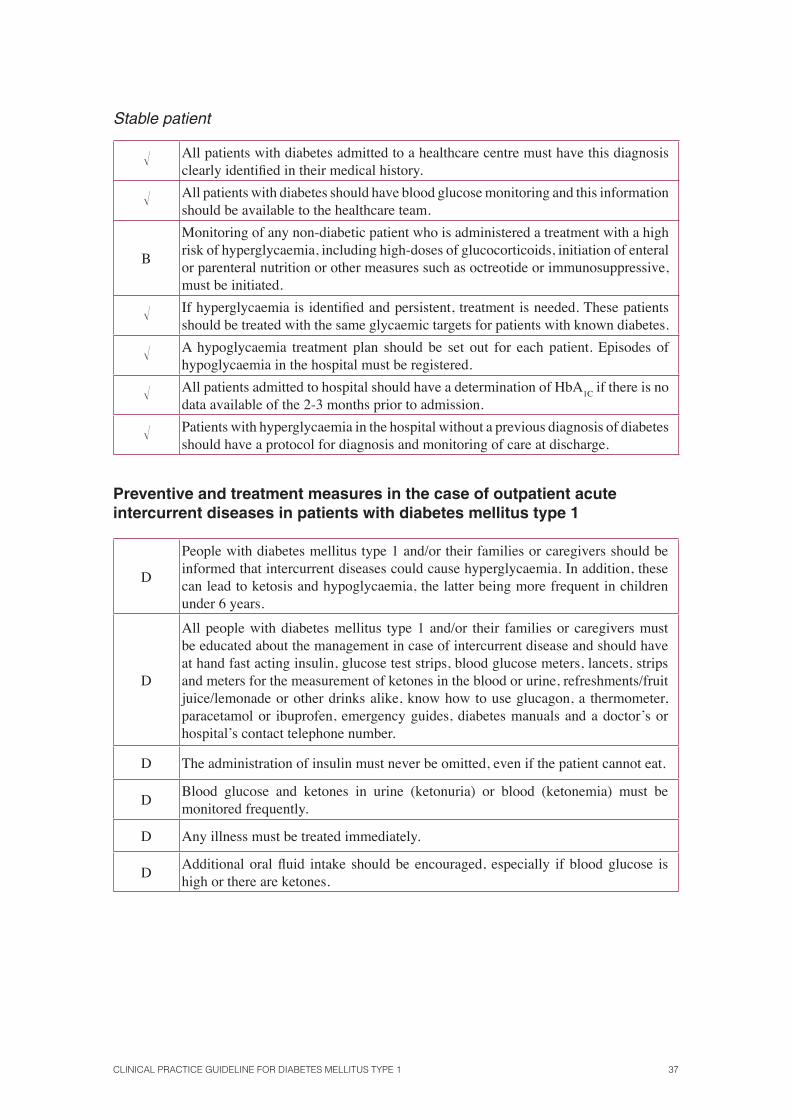
Stable patient
� All patients with diabetes admitted to a healthcare centre must have this diagnosis clearly identifi ed in their medical history.
� All patients with diabetes should have blood glucose monitoring and this information should be available to the healthcare team.
B
Monitoring of any non-diabetic patient who is administered a treatment with a high risk of hyperglycaemia, including high-doses of glucocorticoids, initiation of enteral or parenteral nutrition or other measures such as octreotide or immunosuppressive, must be initiated.
� If hyperglycaemia is identifi ed and persistent, treatment is needed. These patients should be treated with the same glycaemic targets for patients with known diabetes.
� A hypoglycaemia treatment plan should be set out for each patient. Episodes of hypoglycaemia in the hospital must be registered.
� All patients admitted to hospital should have a determination of HbA1C
if there is no data available of the 2-3 months prior to admission.
� Patients with hyperglycaemia in the hospital without a previous diagnosis of diabetes should have a protocol for diagnosis and monitoring of care at discharge.
Preventive and treatment measures in the case of outpatient acute intercurrent diseases in patients with diabetes mellitus type 1
D
People with diabetes mellitus type 1 and/or their families or caregivers should be informed that intercurrent diseases could cause hyperglycaemia. In addition, these can lead to ketosis and hypoglycaemia, the latter being more frequent in children under 6 years.
D
All people with diabetes mellitus type 1 and/or their families or caregivers must be educated about the management in case of intercurrent disease and should have at hand fast acting insulin, glucose test strips, blood glucose meters, lancets, strips and meters for the measurement of ketones in the blood or urine, refreshments/fruit juice/lemonade or other drinks alike, know how to use glucagon, a thermometer, paracetamol or ibuprofen, emergency guides, diabetes manuals and a doctor’s or hospital’s contact telephone number.
D The administration of insulin must never be omitted, even if the patient cannot eat.
DBlood glucose and ketones in urine (ketonuria) or blood (ketonemia) must be monitored frequently.
D Any illness must be treated immediately.
DAdditional oral fl uid intake should be encouraged, especially if blood glucose is high or there are ketones.
38 SNS CLINICAL PRACTICE GUIDELINES
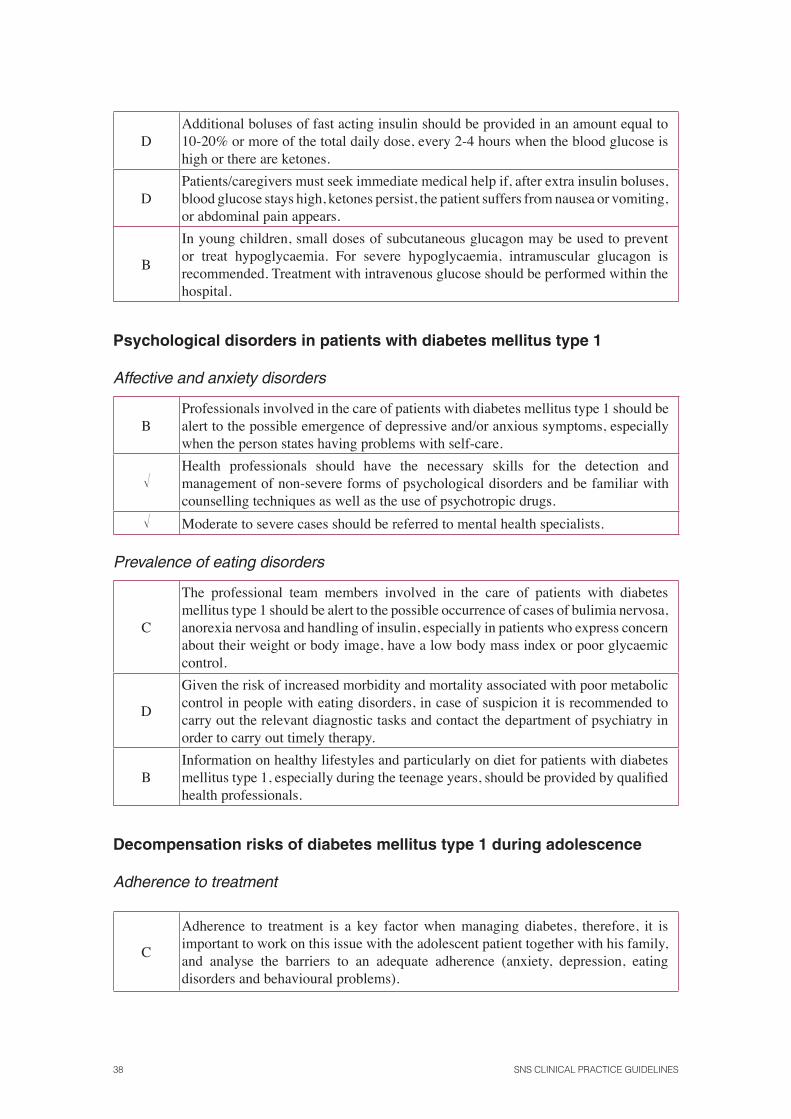
DAdditional boluses of fast acting insulin should be provided in an amount equal to 10-20% or more of the total daily dose, every 2-4 hours when the blood glucose is high or there are ketones.
DPatients/caregivers must seek immediate medical help if, after extra insulin boluses, blood glucose stays high, ketones persist, the patient suffers from nausea or vomiting, or abdominal pain appears.
B
In young children, small doses of subcutaneous glucagon may be used to prevent or treat hypoglycaemia. For severe hypoglycaemia, intramuscular glucagon is recommended. Treatment with intravenous glucose should be performed within the hospital.
Psychological disorders in patients with diabetes mellitus type 1
Affective and anxiety disorders
BProfessionals involved in the care of patients with diabetes mellitus type 1 should be alert to the possible emergence of depressive and/or anxious symptoms, especially when the person states having problems with self-care.
�Health professionals should have the necessary skills for the detection and management of non-severe forms of psychological disorders and be familiar with counselling techniques as well as the use of psychotropic drugs.
� Moderate to severe cases should be referred to mental health specialists.
Prevalence of eating disorders
C
The professional team members involved in the care of patients with diabetes mellitus type 1 should be alert to the possible occurrence of cases of bulimia nervosa, anorexia nervosa and handling of insulin, especially in patients who express concern about their weight or body image, have a low body mass index or poor glycaemic control.
D
Given the risk of increased morbidity and mortality associated with poor metabolic control in people with eating disorders, in case of suspicion it is recommended to carry out the relevant diagnostic tasks and contact the department of psychiatry in order to carry out timely therapy.
BInformation on healthy lifestyles and particularly on diet for patients with diabetes mellitus type 1, especially during the teenage years, should be provided by qualifi ed health professionals.
Decompensation risks of diabetes mellitus type 1 during adolescence
Adherence to treatment
C
Adherence to treatment is a key factor when managing diabetes, therefore, it is important to work on this issue with the adolescent patient together with his family, and analyse the barriers to an adequate adherence (anxiety, depression, eating disorders and behavioural problems).
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 39
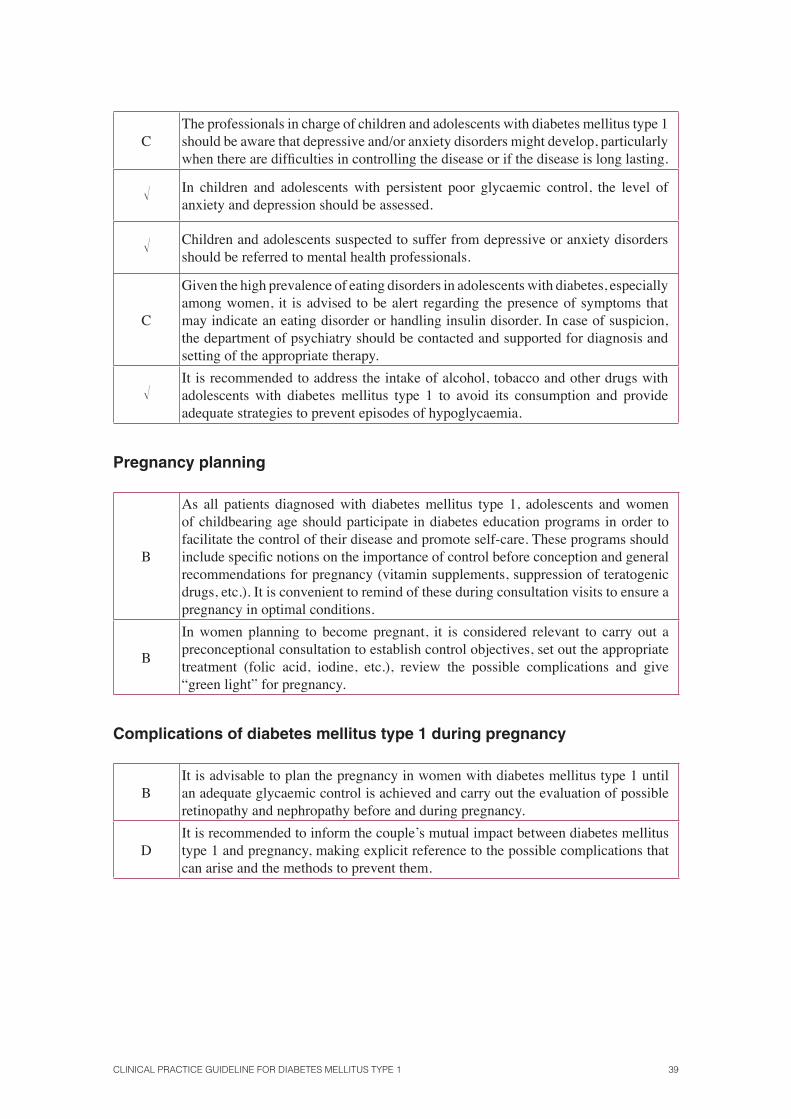
CThe professionals in charge of children and adolescents with diabetes mellitus type 1 should be aware that depressive and/or anxiety disorders might develop, particularly when there are diffi culties in controlling the disease or if the disease is long lasting.
� In children and adolescents with persistent poor glycaemic control, the level of anxiety and depression should be assessed.
� Children and adolescents suspected to suffer from depressive or anxiety disorders should be referred to mental health professionals.
C
Given the high prevalence of eating disorders in adolescents with diabetes, especially among women, it is advised to be alert regarding the presence of symptoms that may indicate an eating disorder or handling insulin disorder. In case of suspicion, the department of psychiatry should be contacted and supported for diagnosis and setting of the appropriate therapy.
�It is recommended to address the intake of alcohol, tobacco and other drugs with adolescents with diabetes mellitus type 1 to avoid its consumption and provide adequate strategies to prevent episodes of hypoglycaemia.
Pregnancy planning
B
As all patients diagnosed with diabetes mellitus type 1, adolescents and women of childbearing age should participate in diabetes education programs in order to facilitate the control of their disease and promote self-care. These programs should include specifi c notions on the importance of control before conception and general recommendations for pregnancy (vitamin supplements, suppression of teratogenic drugs, etc.). It is convenient to remind of these during consultation visits to ensure a pregnancy in optimal conditions.
B
In women planning to become pregnant, it is considered relevant to carry out a preconceptional consultation to establish control objectives, set out the appropriate treatment (folic acid, iodine, etc.), review the possible complications and give “green light” for pregnancy.
Complications of diabetes mellitus type 1 during pregnancy
BIt is advisable to plan the pregnancy in women with diabetes mellitus type 1 until an adequate glycaemic control is achieved and carry out the evaluation of possible retinopathy and nephropathy before and during pregnancy.
DIt is recommended to inform the couple’s mutual impact between diabetes mellitus type 1 and pregnancy, making explicit reference to the possible complications that can arise and the methods to prevent them.
40 SNS CLINICAL PRACTICE GUIDELINES
Metabolic control during pregnancy
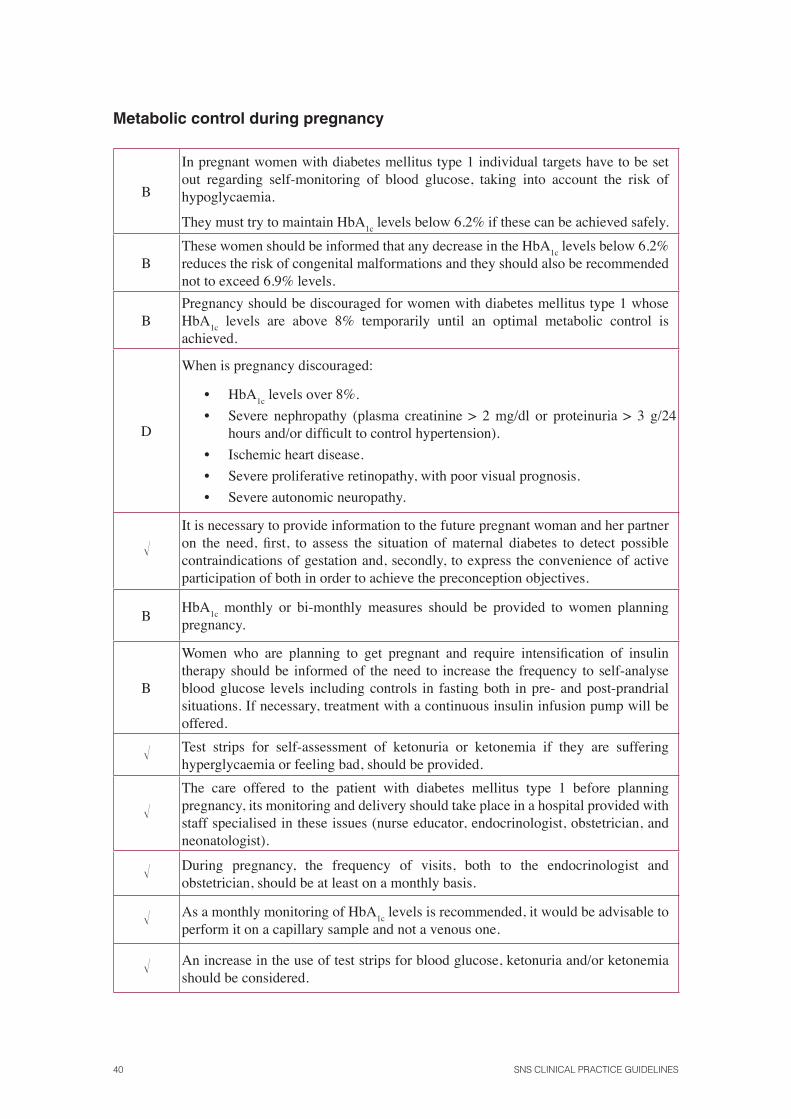
B
In pregnant women with diabetes mellitus type 1 individual targets have to be set out regarding self-monitoring of blood glucose, taking into account the risk of hypoglycaemia.
They must try to maintain HbA1c
levels below 6.2% if these can be achieved safely.
BThese women should be informed that any decrease in the HbA
1c levels below 6.2%
reduces the risk of congenital malformations and they should also be recommended not to exceed 6.9% levels.
BPregnancy should be discouraged for women with diabetes mellitus type 1 whose HbA
1c levels are above 8% temporarily until an optimal metabolic control is
achieved.
D
When is pregnancy discouraged:
• HbA1c
levels over 8%.
• Severe nephropathy (plasma creatinine > 2 mg/dl or proteinuria > 3 g/24 hours and/or diffi cult to control hypertension).
• Ischemic heart disease.
• Severe proliferative retinopathy, with poor visual prognosis.
• Severe autonomic neuropathy.
�It is necessary to provide information to the future pregnant woman and her partner on the need, fi rst, to assess the situation of maternal diabetes to detect possible contraindications of gestation and, secondly, to express the convenience of active participation of both in order to achieve the preconception objectives.
BHbA
1c monthly or bi-monthly measures should be provided to women planning
pregnancy.
B
Women who are planning to get pregnant and require intensifi cation of insulin therapy should be informed of the need to increase the frequency to self-analyse blood glucose levels including controls in fasting both in pre- and post-prandrial situations. If necessary, treatment with a continuous insulin infusion pump will be offered.
� Test strips for self-assessment of ketonuria or ketonemia if they are suffering hyperglycaemia or feeling bad, should be provided.
�The care offered to the patient with diabetes mellitus type 1 before planning pregnancy, its monitoring and delivery should take place in a hospital provided with staff specialised in these issues (nurse educator, endocrinologist, obstetrician, and neonatologist).
� During pregnancy, the frequency of visits, both to the endocrinologist and obstetrician, should be at least on a monthly basis.
� As a monthly monitoring of HbA1c
levels is recommended, it would be advisable to perform it on a capillary sample and not a venous one.
� An increase in the use of test strips for blood glucose, ketonuria and/or ketonemia should be considered.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 41
� Glycaemic control optimization protocols should exist.
�A treatment protocol in childbirth with general guidelines on the needs of carbohydrate and insulin intake, which must be known to the staff involved, as well as a protocol of newborn care is recommended.
Contraception and diabetes mellitus type 1
DIn women with diabetes mellitus type 1, it is recommended to use the copper IUD as the safest contraception method. The use of IUD that releases levonorgestrel should not be ruled out, since it has not been observed to affect the metabolism of glucose.
Clinical management of diabetes mellitus type 1 in patients with special needs
Immigrant population. General recommendations
�If the patient with diabetes mellitus type 1 has diffi culty understanding the language, the use of machine translation systems (telephone or audiovisual methods of open and closed questions) or direct translation during the consultation visit are recommended.
� It is also advisable to use simple graphics to facilitate understanding of the disease and the guidelines to be followed.
Recommendations for Muslim patients during Ramadan
Before Ramadan
� Inform the health care team about the concept of Ramadan and the risks posed by fasting.
� Plan the process in time for the celebration of Ramadan.
� Identify Muslim patients with diabetes mellitus type 1.
� Carry out a clinical interview with these patients to know their desire to fulfi l the precept of Ramadan.
� Inform patients about the possibility of not celebrating Ramadan due to having a chronic disease and the risks involved.
42 SNS CLINICAL PRACTICE GUIDELINES
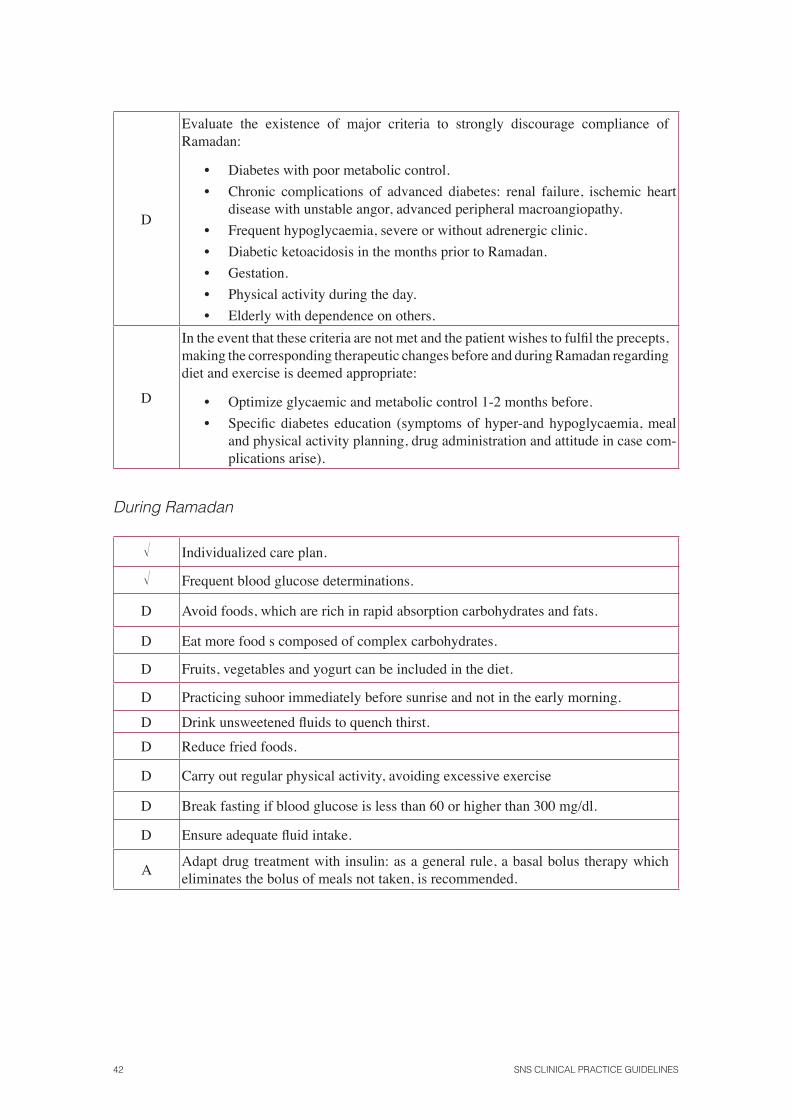
D
Evaluate the existence of major criteria to strongly discourage compliance of Ramadan:
• Diabetes with poor metabolic control.
• Chronic complications of advanced diabetes: renal failure, ischemic heart disease with unstable angor, advanced peripheral macroangiopathy.
• Frequent hypoglycaemia, severe or without adrenergic clinic.
• Diabetic ketoacidosis in the months prior to Ramadan.
• Gestation.
• Physical activity during the day.
• Elderly with dependence on others.
D
In the event that these criteria are not met and the patient wishes to fulfi l the precepts, making the corresponding therapeutic changes before and during Ramadan regarding diet and exercise is deemed appropriate:
• Optimize glycaemic and metabolic control 1-2 months before.
• Specifi c diabetes education (symptoms of hyper-and hypoglycaemia, meal and physical activity planning, drug administration and attitude in case com-plications arise).
During Ramadan
� Individualized care plan.
� Frequent blood glucose determinations.
D Avoid foods, which are rich in rapid absorption carbohydrates and fats.
D Eat more food s composed of complex carbohydrates.
D Fruits, vegetables and yogurt can be included in the diet.
D Practicing suhoor immediately before sunrise and not in the early morning.
D Drink unsweetened fl uids to quench thirst.
D Reduce fried foods.
D Carry out regular physical activity, avoiding excessive exercise
D Break fasting if blood glucose is less than 60 or higher than 300 mg/dl.
D Ensure adequate fl uid intake.
AAdapt drug treatment with insulin: as a general rule, a basal bolus therapy which eliminates the bolus of meals not taken, is recommended.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 43
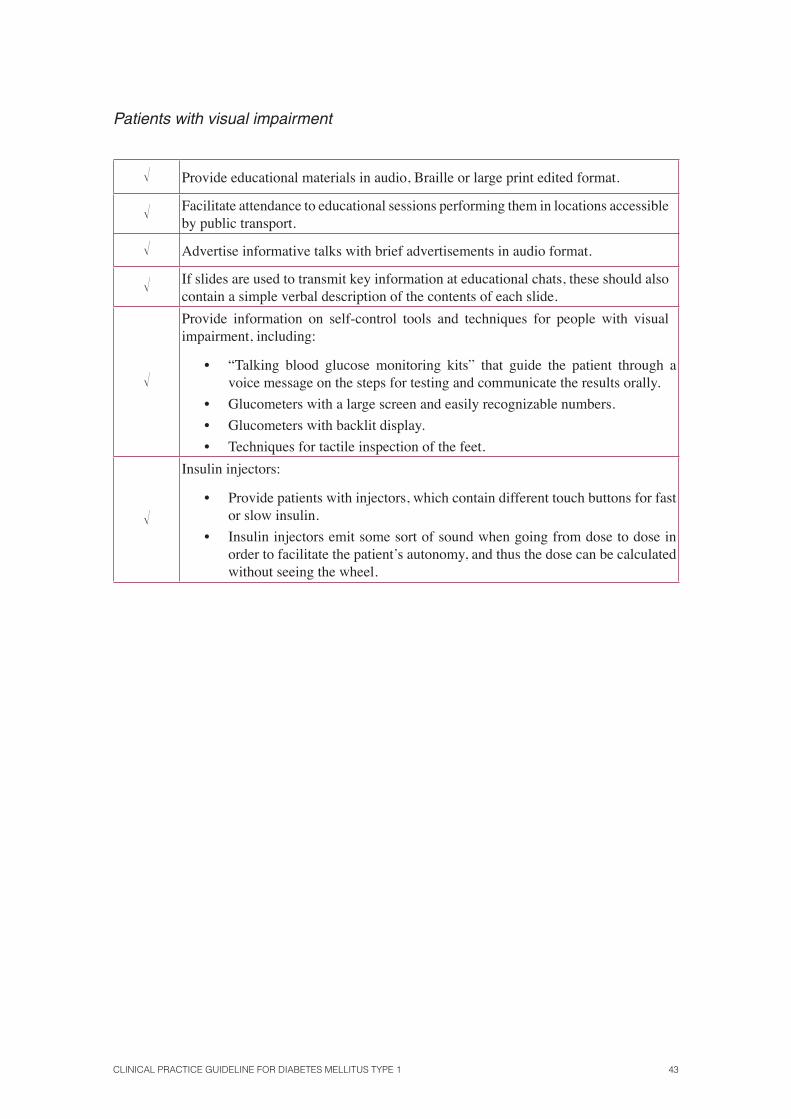
Patients with visual impairment
� Provide educational materials in audio, Braille or large print edited format.
� Facilitate attendance to educational sessions performing them in locations accessible by public transport.
� Advertise informative talks with brief advertisements in audio format.
� If slides are used to transmit key information at educational chats, these should also contain a simple verbal description of the contents of each slide.
�
Provide information on self-control tools and techniques for people with visual impairment, including:
• “Talking blood glucose monitoring kits” that guide the patient through a voice message on the steps for testing and communicate the results orally.
• Glucometers with a large screen and easily recognizable numbers.
• Glucometers with backlit display.
• Techniques for tactile inspection of the feet.
�
Insulin injectors:
• Provide patients with injectors, which contain different touch buttons for fast or slow insulin.
• Insulin injectors emit some sort of sound when going from dose to dose in order to facilitate the patient’s autonomy, and thus the dose can be calculated without seeing the wheel.
44 SNS CLINICAL PRACTICE GUIDELINES
Acute complications
Hypoglycaemia
Symptoms of suspicion
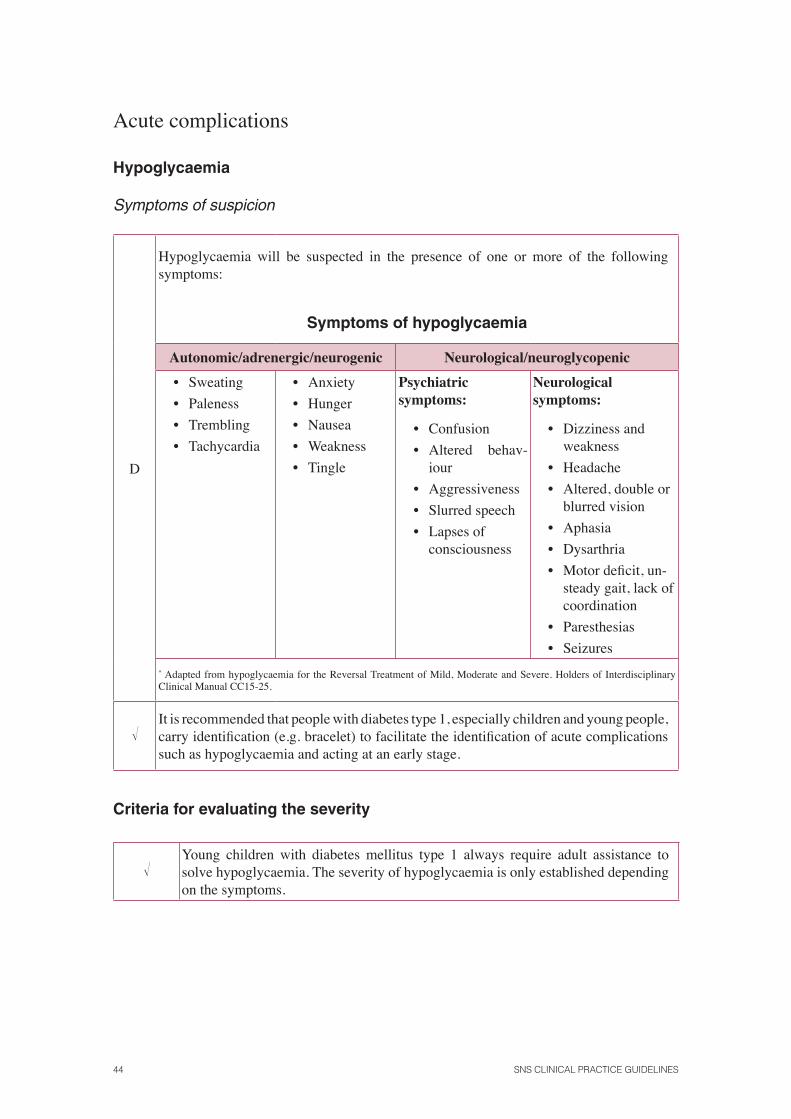
D
Hypoglycaemia will be suspected in the presence of one or more of the following symptoms:
Symptoms of hypoglycaemia
Autonomic/adrenergic/neurogenic Neurological/neuroglycopenic
• Sweating
• Paleness
• Trembling
• Tachycardia
• Anxiety
• Hunger
• Nausea
• Weakness
• Tingle
Psychiatric symptoms:
• Confusion
• Altered behav-iour
• Aggressiveness
• Slurred speech
• Lapses of consciousness
Neurological symptoms:
• Dizziness and weakness
• Headache
• Altered, double or blurred vision
• Aphasia
• Dysarthria
• Motor defi cit, un-steady gait, lack of coordination
• Paresthesias
• Seizures
* Adapted from hypoglycaemia for the Reversal Treatment of Mild, Moderate and Severe. Holders of Interdisciplinary Clinical Manual CC15-25.
�It is recommended that people with diabetes type 1, especially children and young people, carry identifi cation (e.g. bracelet) to facilitate the identifi cation of acute complications such as hypoglycaemia and acting at an early stage.
Criteria for evaluating the severity
�Young children with diabetes mellitus type 1 always require adult assistance to solve hypoglycaemia. The severity of hypoglycaemia is only established depending on the symptoms.
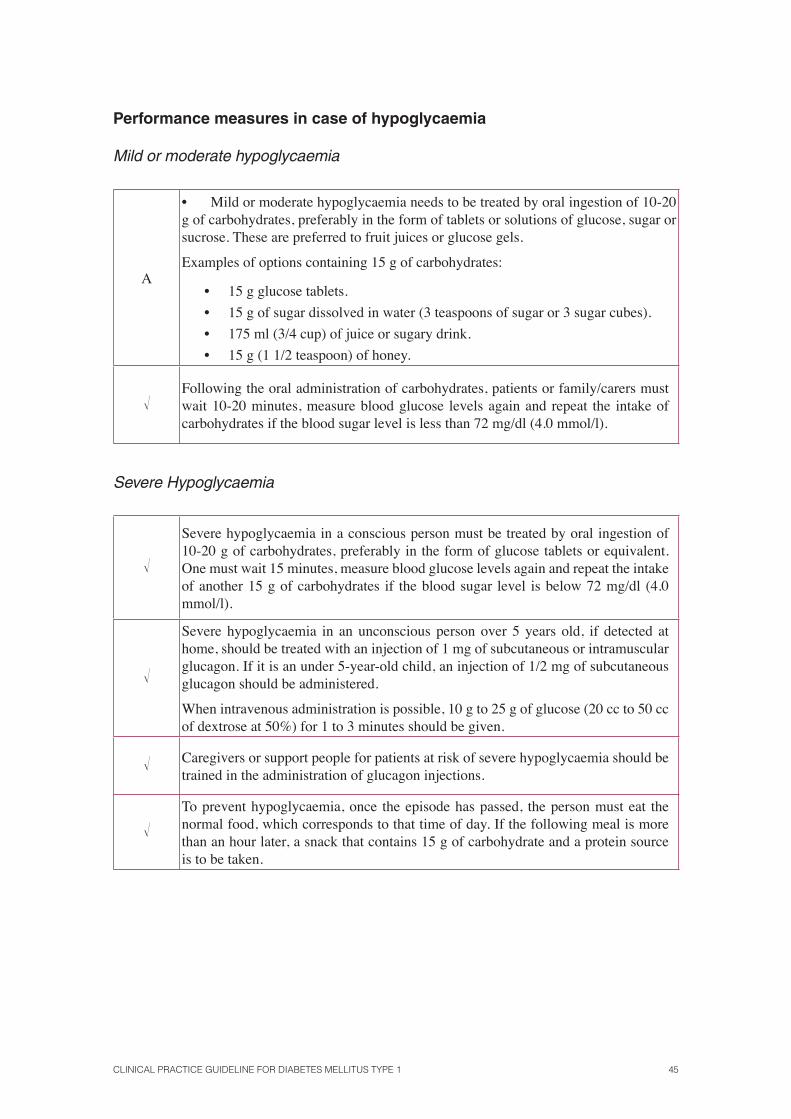
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 45
Performance measures in case of hypoglycaemia
Mild or moderate hypoglycaemia
A
• Mild or moderate hypoglycaemia needs to be treated by oral ingestion of 10-20 g of carbohydrates, preferably in the form of tablets or solutions of glucose, sugar or sucrose. These are preferred to fruit juices or glucose gels.
Examples of options containing 15 g of carbohydrates:
• 15 g glucose tablets.
• 15 g of sugar dissolved in water (3 teaspoons of sugar or 3 sugar cubes).
• 175 ml (3/4 cup) of juice or sugary drink.
• 15 g (1 1/2 teaspoon) of honey.
�Following the oral administration of carbohydrates, patients or family/carers must wait 10-20 minutes, measure blood glucose levels again and repeat the intake of carbohydrates if the blood sugar level is less than 72 mg/dl (4.0 mmol/l).
Severe Hypoglycaemia
�
Severe hypoglycaemia in a conscious person must be treated by oral ingestion of 10-20 g of carbohydrates, preferably in the form of glucose tablets or equivalent. One must wait 15 minutes, measure blood glucose levels again and repeat the intake of another 15 g of carbohydrates if the blood sugar level is below 72 mg/dl (4.0 mmol/l).
�
Severe hypoglycaemia in an unconscious person over 5 years old, if detected at home, should be treated with an injection of 1 mg of subcutaneous or intramuscular glucagon. If it is an under 5-year-old child, an injection of 1/2 mg of subcutaneous glucagon should be administered.
When intravenous administration is possible, 10 g to 25 g of glucose (20 cc to 50 cc of dextrose at 50%) for 1 to 3 minutes should be given.
� Caregivers or support people for patients at risk of severe hypoglycaemia should be trained in the administration of glucagon injections.
�To prevent hypoglycaemia, once the episode has passed, the person must eat the normal food, which corresponds to that time of day. If the following meal is more than an hour later, a snack that contains 15 g of carbohydrate and a protein source is to be taken.
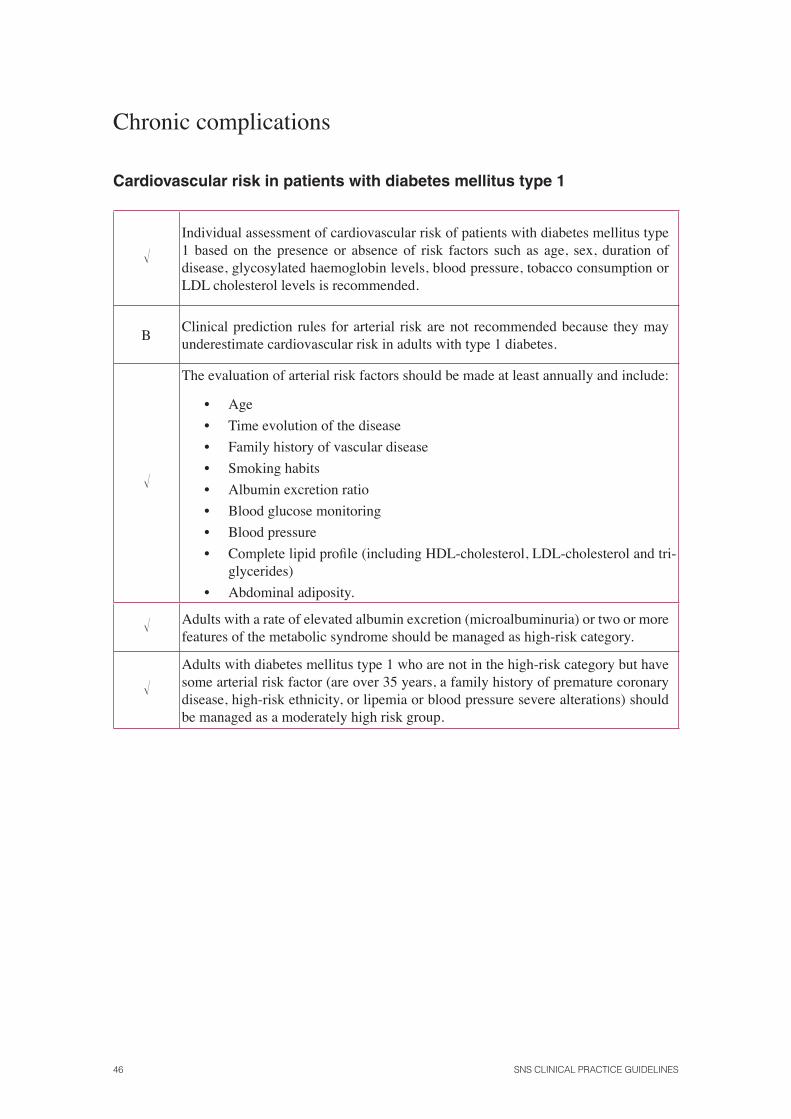
46 SNS CLINICAL PRACTICE GUIDELINES
Chronic complications
Cardiovascular risk in patients with diabetes mellitus type 1
�Individual assessment of cardiovascular risk of patients with diabetes mellitus type 1 based on the presence or absence of risk factors such as age, sex, duration of disease, glycosylated haemoglobin levels, blood pressure, tobacco consumption or LDL cholesterol levels is recommended.
BClinical prediction rules for arterial risk are not recommended because they may underestimate cardiovascular risk in adults with type 1 diabetes.
�
The evaluation of arterial risk factors should be made at least annually and include:
• Age
• Time evolution of the disease
• Family history of vascular disease
• Smoking habits
• Albumin excretion ratio
• Blood glucose monitoring
• Blood pressure
• Complete lipid profi le (including HDL-cholesterol, LDL-cholesterol and tri-glycerides)
• Abdominal adiposity.
� Adults with a rate of elevated albumin excretion (microalbuminuria) or two or more features of the metabolic syndrome should be managed as high-risk category.
�Adults with diabetes mellitus type 1 who are not in the high-risk category but have some arterial risk factor (are over 35 years, a family history of premature coronary disease, high-risk ethnicity, or lipemia or blood pressure severe alterations) should be managed as a moderately high risk group.
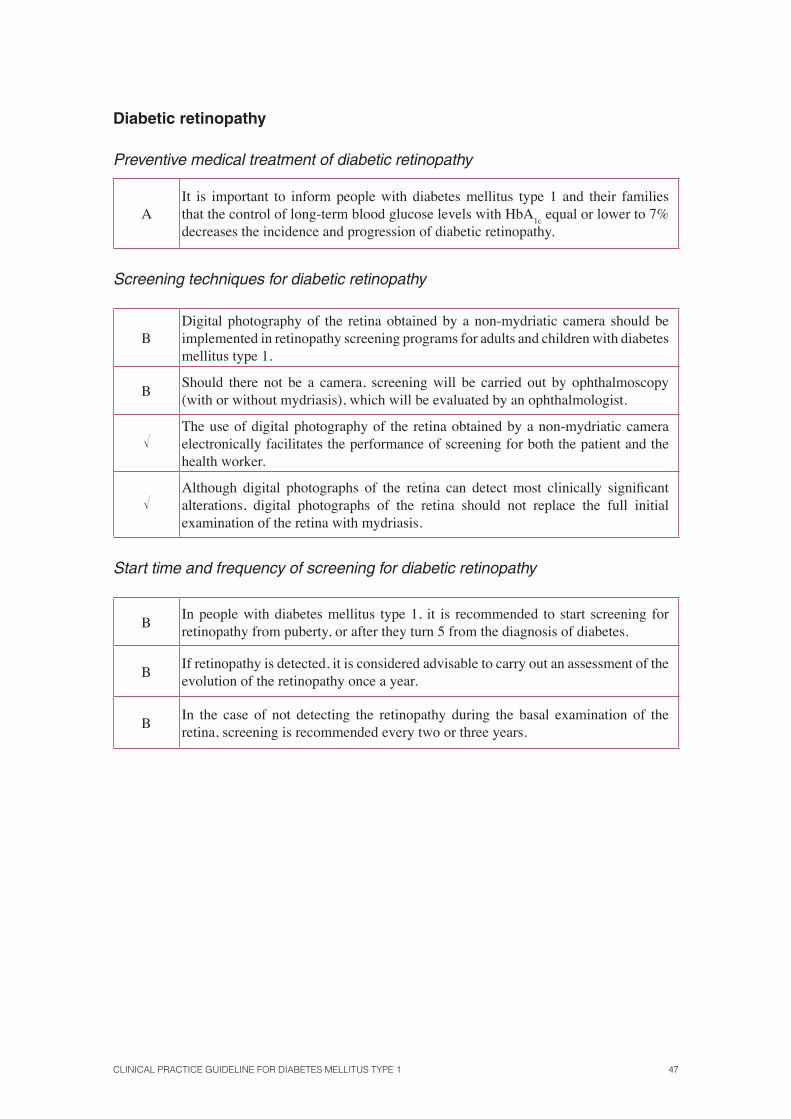
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 47
Diabetic retinopathy
Preventive medical treatment of diabetic retinopathy
AIt is important to inform people with diabetes mellitus type 1 and their families that the control of long-term blood glucose levels with HbA
1c equal or lower to 7%
decreases the incidence and progression of diabetic retinopathy.
Screening techniques for diabetic retinopathy
BDigital photography of the retina obtained by a non-mydriatic camera should be implemented in retinopathy screening programs for adults and children with diabetes mellitus type 1.
BShould there not be a camera, screening will be carried out by ophthalmoscopy (with or without mydriasis), which will be evaluated by an ophthalmologist.
�The use of digital photography of the retina obtained by a non-mydriatic camera electronically facilitates the performance of screening for both the patient and the health worker.
�Although digital photographs of the retina can detect most clinically signifi cant alterations, digital photographs of the retina should not replace the full initial examination of the retina with mydriasis.
Start time and frequency of screening for diabetic retinopathy
BIn people with diabetes mellitus type 1, it is recommended to start screening for retinopathy from puberty, or after they turn 5 from the diagnosis of diabetes.
BIf retinopathy is detected, it is considered advisable to carry out an assessment of the evolution of the retinopathy once a year.
BIn the case of not detecting the retinopathy during the basal examination of the retina, screening is recommended every two or three years.

48 SNS CLINICAL PRACTICE GUIDELINES
Diabetic nephropathy
Criteria for referral of patients with diabetic nephropathy to nephrology specialized care units
�
It is recommended to refer patients with diabetes mellitus type 1 with at least one of the following criteria to units specialized in nephrology:
1. With glomerular fi ltration rate (GFR)> 45 ml/min/1,73m2 of body surface area:
1.1. Albuminuria increased or albuminuria/creatinine ratio > 300 mg/g.
1.2. Uncorrected anaemia (Hb <11g/dl) despite iron treatment.
1.3. HTA refractory to treatment (3 drugs).
2. With 30-45ml/min/ GFR, 1,73 m2 body surface area:
2.1. Individual assessment, taking into account the age and rate of progression of renal failure, only if it meets the above criteria of proteinuria, anaemia and refractory hypertension.
3. With glomerular fi ltration rate <30 ml/min/1,73 m2 of body surface area:
3.1. In all cases.
Preferred referral criteria
4. Fast increase in serum creatinine: > 1 mg/dl in a month.
5. Hematuria associated to proteinuria once urologic diseases through renal ultrasound have been discarded.
6. Severe hyperkalaemia (> 7 mEq/l).
Treatment of patients with diabetes mellitus type 1 and microalbuminuria
A
The pharmacological treatment of choice in hypertensive and normotensive patients with microalbuminuria is an angiotensin converting enzyme (captopril, lisinopril, ramipril, enalapril and perindopril) inhibitor with a progressive increase in the therapeutic dose to achieve the desired response.
ADuring pregnancy and in the case of having bilateral stenosis of the renal artery an angiotensin converting enzyme inhibitor drug treatment is contraindicated.
� During the treatment with an angiotensin converting enzyme inhibitor, the levels of creatinine and potassium should be monitored.
� In case of contraindications or intolerance to angiotensin converting enzyme inhibitors, an angiotensin II receptor antagonist treatment is recommended.
� The aims of the treatment are to control blood pressure and reduce urinary albumin excretion. In normotensive patients, these will be given the maximum tolerated dose.
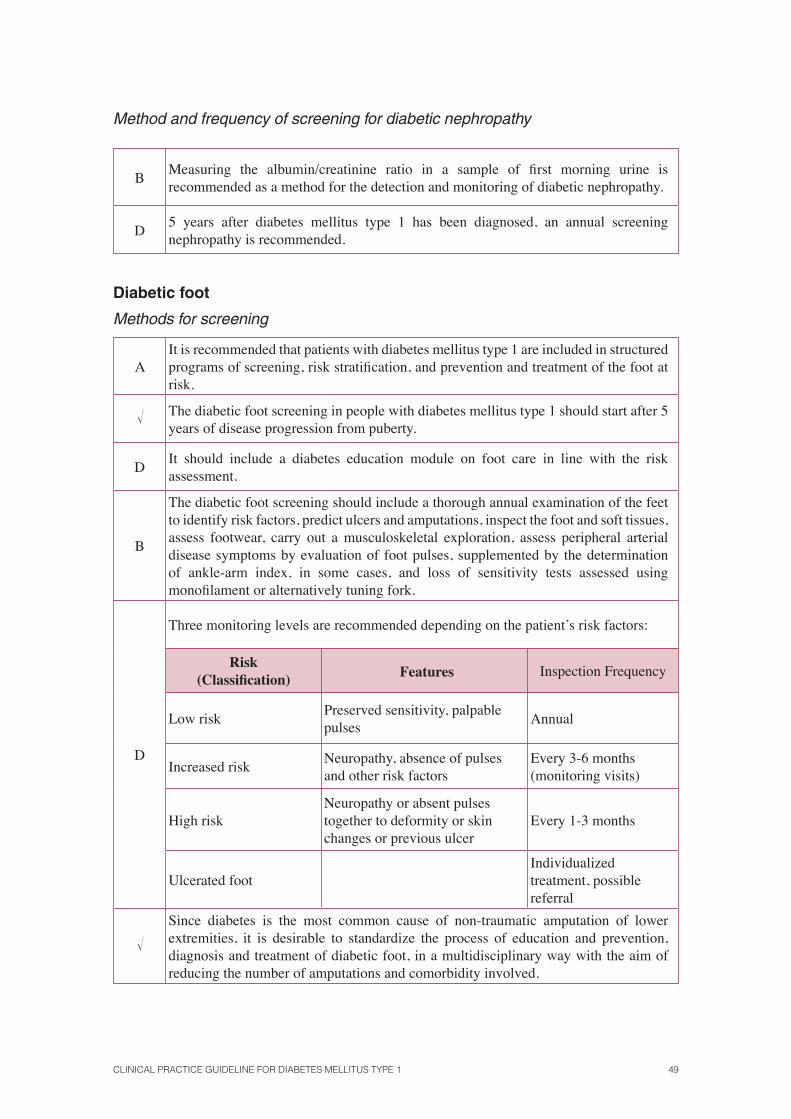
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 49
Method and frequency of screening for diabetic nephropathy
BMeasuring the albumin/creatinine ratio in a sample of fi rst morning urine is recommended as a method for the detection and monitoring of diabetic nephropathy.
D5 years after diabetes mellitus type 1 has been diagnosed, an annual screening nephropathy is recommended.
Diabetic foot
Methods for screening
AIt is recommended that patients with diabetes mellitus type 1 are included in structured programs of screening, risk stratifi cation, and prevention and treatment of the foot at risk.
� The diabetic foot screening in people with diabetes mellitus type 1 should start after 5 years of disease progression from puberty.
DIt should include a diabetes education module on foot care in line with the risk assessment.
B
The diabetic foot screening should include a thorough annual examination of the feet to identify risk factors, predict ulcers and amputations, inspect the foot and soft tissues, assess footwear, carry out a musculoskeletal exploration, assess peripheral arterial disease symptoms by evaluation of foot pulses, supplemented by the determination of ankle-arm index, in some cases, and loss of sensitivity tests assessed using monofi lament or alternatively tuning fork.
D
Three monitoring levels are recommended depending on the patient’s risk factors:
Risk (Classifi cation) Features Inspection Frequency
Low riskPreserved sensitivity, palpable pulses
Annual
Increased riskNeuropathy, absence of pulses and other risk factors
Every 3-6 months (monitoring visits)
High riskNeuropathy or absent pulses together to deformity or skin changes or previous ulcer
Every 1-3 months
Ulcerated footIndividualized treatment, possible referral
�Since diabetes is the most common cause of non-traumatic amputation of lower extremities, it is desirable to standardize the process of education and prevention, diagnosis and treatment of diabetic foot, in a multidisciplinary way with the aim of reducing the number of amputations and comorbidity involved.
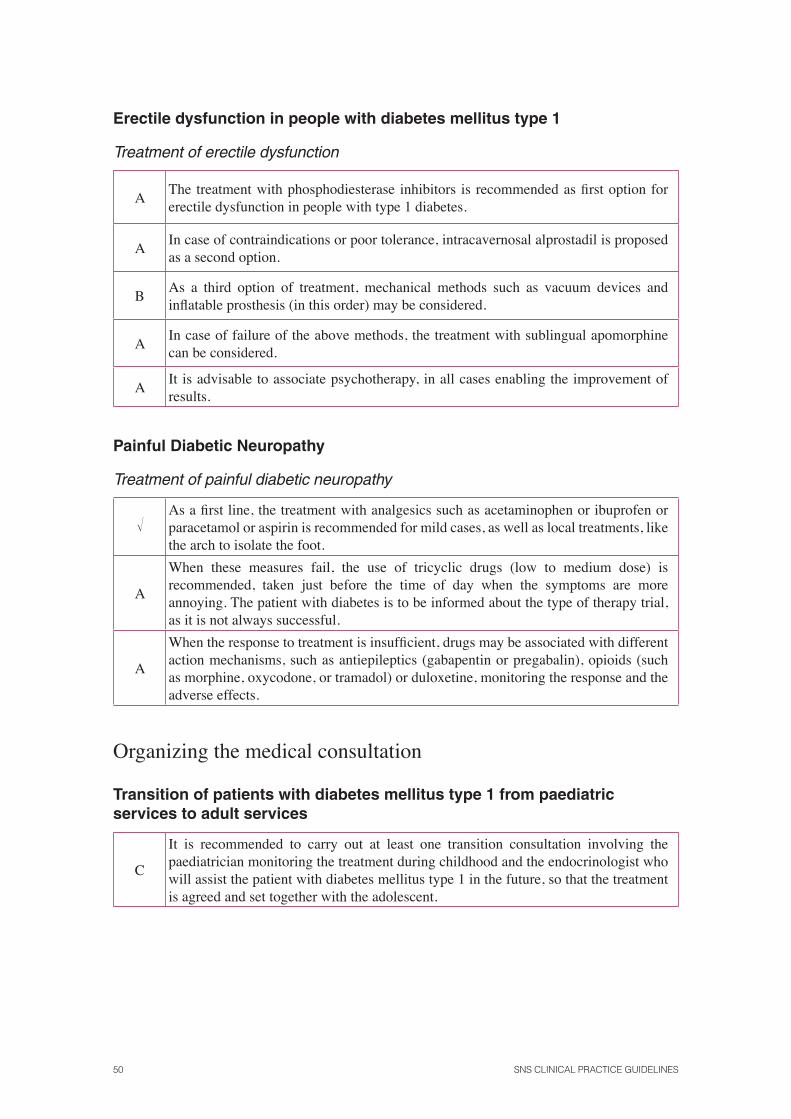
50 SNS CLINICAL PRACTICE GUIDELINES
Erectile dysfunction in people with diabetes mellitus type 1
Treatment of erectile dysfunction
AThe treatment with phosphodiesterase inhibitors is recommended as fi rst option for erectile dysfunction in people with type 1 diabetes.
AIn case of contraindications or poor tolerance, intracavernosal alprostadil is proposed as a second option.
BAs a third option of treatment, mechanical methods such as vacuum devices and infl atable prosthesis (in this order) may be considered.
A In case of failure of the above methods, the treatment with sublingual apomorphine can be considered.
AIt is advisable to associate psychotherapy, in all cases enabling the improvement of results.
Painful Diabetic Neuropathy
Treatment of painful diabetic neuropathy
�As a fi rst line, the treatment with analgesics such as acetaminophen or ibuprofen or paracetamol or aspirin is recommended for mild cases, as well as local treatments, like the arch to isolate the foot.
A
When these measures fail, the use of tricyclic drugs (low to medium dose) is recommended, taken just before the time of day when the symptoms are more annoying. The patient with diabetes is to be informed about the type of therapy trial, as it is not always successful.
A
When the response to treatment is insuffi cient, drugs may be associated with different action mechanisms, such as antiepileptics (gabapentin or pregabalin), opioids (such as morphine, oxycodone, or tramadol) or duloxetine, monitoring the response and the adverse effects.
Organizing the medical consultation
Transition of patients with diabetes mellitus type 1 from paediatric services to adult services
C
It is recommended to carry out at least one transition consultation involving the paediatrician monitoring the treatment during childhood and the endocrinologist who will assist the patient with diabetes mellitus type 1 in the future, so that the treatment is agreed and set together with the adolescent.
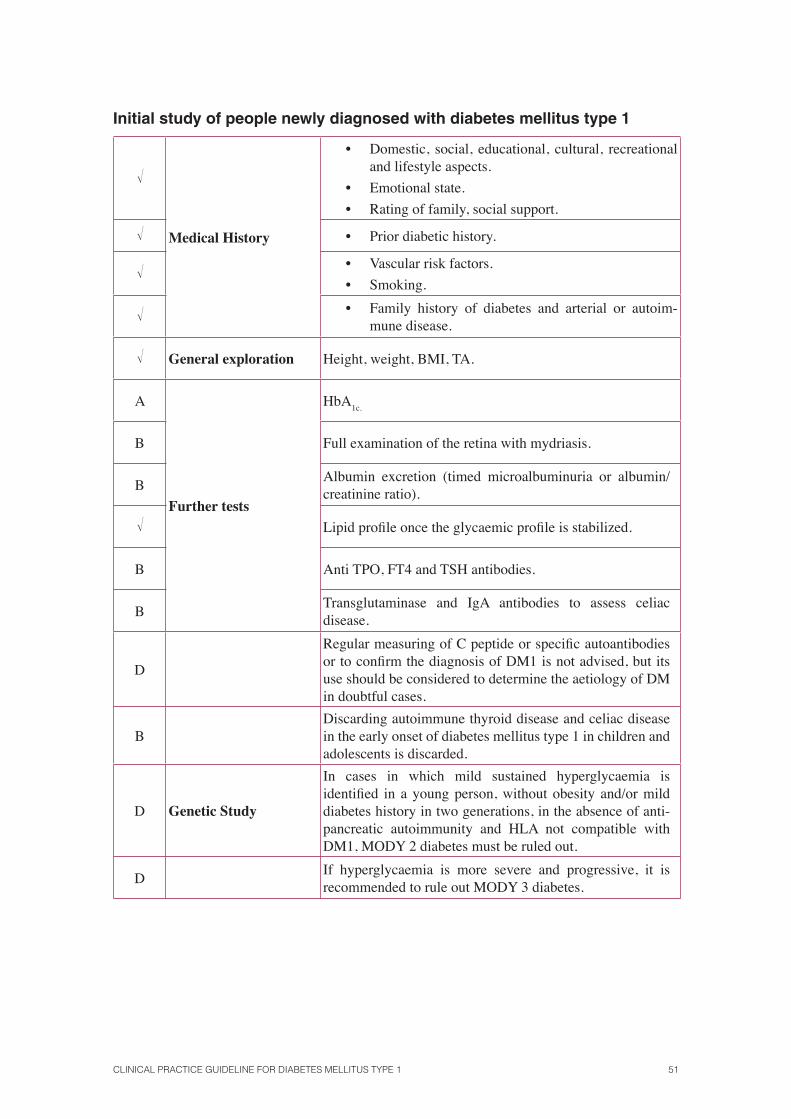
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 51
Initial study of people newly diagnosed with diabetes mellitus type 1
�
Medical History
• Domestic, social, educational, cultural, recreational and lifestyle aspects.
• Emotional state.
• Rating of family, social support.
� • Prior diabetic history.
� • Vascular risk factors.
• Smoking.
� • Family history of diabetes and arterial or autoim-mune disease.
� General exploration Height, weight, BMI, TA.
A
Further tests
HbA1c.
B Full examination of the retina with mydriasis.
BAlbumin excretion (timed microalbuminuria or albumin/creatinine ratio).
� Lipid profi le once the glycaemic profi le is stabilized.
B Anti TPO, FT4 and TSH antibodies.
BTransglutaminase and IgA antibodies to assess celiac disease.
D
Regular measuring of C peptide or specifi c autoantibodies or to confi rm the diagnosis of DM1 is not advised, but its use should be considered to determine the aetiology of DM in doubtful cases.
BDiscarding autoimmune thyroid disease and celiac disease in the early onset of diabetes mellitus type 1 in children and adolescents is discarded.
D Genetic Study
In cases in which mild sustained hyperglycaemia is identifi ed in a young person, without obesity and/or mild diabetes history in two generations, in the absence of anti-pancreatic autoimmunity and HLA not compatible with DM1, MODY 2 diabetes must be ruled out.
DIf hyperglycaemia is more severe and progressive, it is recommended to rule out MODY 3 diabetes.
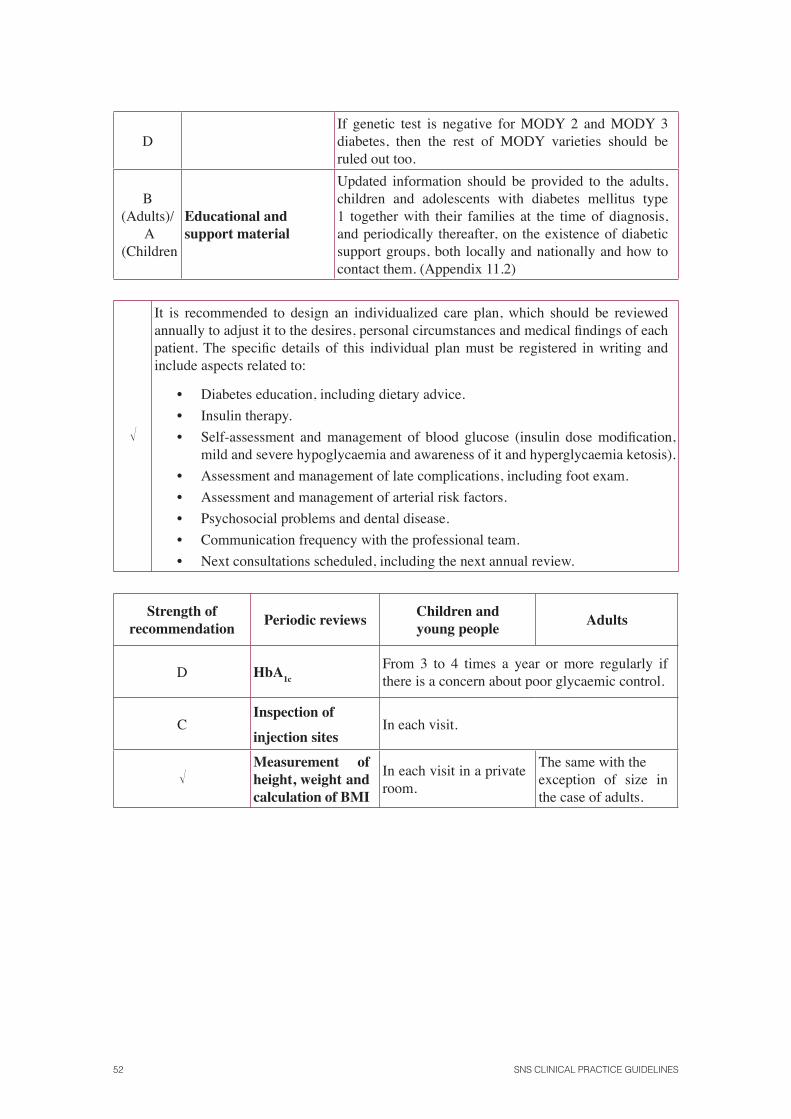
52 SNS CLINICAL PRACTICE GUIDELINES
DIf genetic test is negative for MODY 2 and MODY 3 diabetes, then the rest of MODY varieties should be ruled out too.
B(Adults)/
A (Children
Educational and support material
Updated information should be provided to the adults, children and adolescents with diabetes mellitus type 1 together with their families at the time of diagnosis, and periodically thereafter, on the existence of diabetic support groups, both locally and nationally and how to contact them. (Appendix 11.2)
�
It is recommended to design an individualized care plan, which should be reviewed annually to adjust it to the desires, personal circumstances and medical fi ndings of each patient. The specifi c details of this individual plan must be registered in writing and include aspects related to:
• Diabetes education, including dietary advice.
• Insulin therapy.
• Self-assessment and management of blood glucose (insulin dose modifi cation, mild and severe hypoglycaemia and awareness of it and hyperglycaemia ketosis).
• Assessment and management of late complications, including foot exam.
• Assessment and management of arterial risk factors.
• Psychosocial problems and dental disease.
• Communication frequency with the professional team.
• Next consultations scheduled, including the next annual review.
Strength of recommendation
Periodic reviewsChildren and young people
Adults
D HbA1c
From 3 to 4 times a year or more regularly if there is a concern about poor glycaemic control.
CInspection of
injection sitesIn each visit.
�Measurement of height, weight and calculation of BMI
In each visit in a private room.
The same with theexception of size in the case of adults.
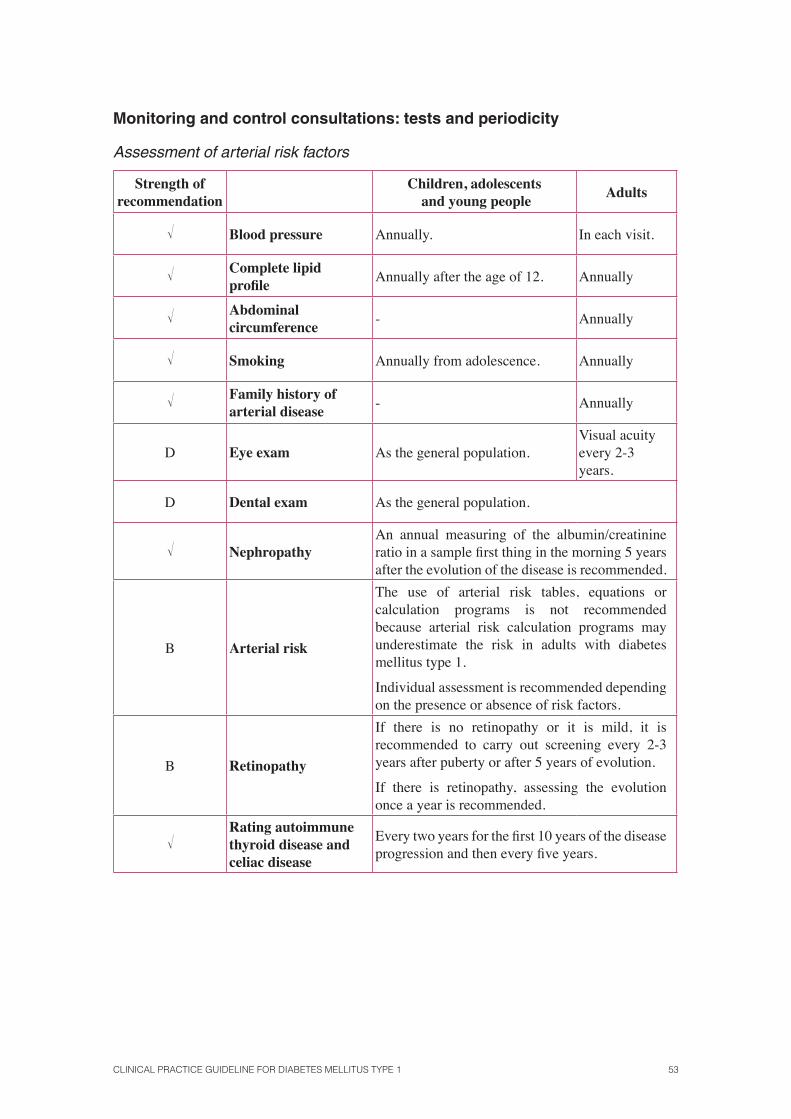
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 53
Monitoring and control consultations: tests and periodicity
Assessment of arterial risk factors
Strength ofrecommendation
Children, adolescents and young people
Adults
� Blood pressure Annually. In each visit.
� Complete lipid profi le
Annually after the age of 12. Annually
� Abdominal circumference
- Annually
� Smoking Annually from adolescence. Annually
� Family history of arterial disease
- Annually
D Eye exam As the general population.Visual acuity every 2-3 years.
D Dental exam As the general population.
� NephropathyAn annual measuring of the albumin/creatinine ratio in a sample fi rst thing in the morning 5 years after the evolution of the disease is recommended.
B Arterial risk
The use of arterial risk tables, equations or calculation programs is not recommended because arterial risk calculation programs may underestimate the risk in adults with diabetes mellitus type 1.
Individual assessment is recommended depending on the presence or absence of risk factors.
B Retinopathy
If there is no retinopathy or it is mild, it is recommended to carry out screening every 2-3 years after puberty or after 5 years of evolution.
If there is retinopathy, assessing the evolution once a year is recommended.
�Rating autoimmune thyroid disease and celiac disease
Every two years for the fi rst 10 years of the disease progression and then every fi ve years.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 55
1. Introduction
Diabetes mellitus (DM) comprises a group of metabolic diseases characterized by secondary hyperglycaemia to an absolute or relative defect in insulin secretion, which is accompanied, to a greater or lesser extent, by alterations in the metabolism of lipids and proteins. The chronic hyperglycaemia is associated with long-term alterations in various organs like eyes, kidneys, the nervous system and the circulatory system.
Diabetes mellitus type 1 (DM1) corresponds to the entity formerly termed insulin dependent or juvenile diabetes mellitus, in which the destruction of the pancreatic β cells leads to an absolute insulin defi ciency.
The prevalence of DM in Spain is around 13.8% in people over 18 years. (95% CI 12.8, 14.7%). For DM1 the prevalence is between 0.2 and 0.3%, representing between 10 to 15% of all people with diabetes. The annual incidence per 100,000 inhabitants ranges from 9.5 to 16 in people under 14 years, and 9.9 for those between 15 and 29 years. The incidence is low between 0 and 5 years, and the highest is in people aged 13-14 years. In the age group ranging from 0 to 14 years there is no difference in incidence regarding genre, while between 15 and 30 years there is a clear predominance of males4. Although DM1 normally represents only a minority of the total number of diabetes in the population, it is the predominant form of the disease in younger age groups in most developed countries5.
The Spanish Interregional Council of the National Health Service (NHS) decided on June 16, 2004 to address a joint strategy on Diabetes for the entire NHS, and thus created “Estrategia en Diabetes del Sistema Nacional de Salud” (Diabetes Strategy of the National Health System), submitted and approved by the Interregional Council of the NHS on 11 October 20065.
In addition, the Quality Plan 2010 for the Spanish National Health System (NHS) aims to address the challenges facing the NHS, increasing the coherence of the system, ensuring equity in health care to all citizens, regardless of where they live and ensuring that this care is of the high-est quality. Its aims include the promotion of the development and use of CPGs related to Health strategies, reinforcing and extending the “Guía-Salud” Project2.
The Department of Health of the Basque Government, an entity which belongs to the Agency for Health Technology Assessment of the Basque Country-Osteba, was commissioned to develop a CPG that would address the clinical management of diabetes mellitus type 1 in adults and chil-dren based on the latest evidence from scientifi c research. This document has been produced with-in a collaboration framework provided in the Quality Plan for the National Health System, under the collaboration agreement signed by the Instituto de Salud Carlos III, an autonomous body of the Ministry of Health and Social Policy and the Agency for Health Technology Assessment of the Basque Government-OSTEBA.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 57
2. Scope and Aims
The CPGs are a set of instructions, guidelines, statements or recommendations systematically developed which aims to help health professionals and patients make decisions about appropriate health care modality for specifi c clinical circumstances.
Although this term has spread to different products, good quality CPGs are documents that pose specifi c questions and organize the best available scientifi c evidence so as to be used in clini-cal decision making, in the form of fl exible recommendations.
This guide has been developed according to the following principles:
• Be useful and usable for all professionals.
• Take into account the perspectives of individuals with DM1 and their caregivers.
• Indicate areas of uncertainty or controversy needing further investigation.
2.1. Scope
This guide focuses on key issues affecting the care of people (adults, children and pregnant wom-en) with DM1 and addresses issues related to diagnosis, prognosis, screening, treatment, acute and chronic complications and the clinical monitoring of the disease.
2.2. Aims of the CPG
Main aim: to provide guidance on the various alternatives for the care provided to people with DM1, establishing the most relevant and up-to-date evidence-based recommendations. Under no circumstances does it replace the clinical judgment of professionals.
Specifi c aims:
• Develop standards that can maximize the quality, effi ciency and equity of care for people with DM1.
• Help patients make informed decisions to facilitate self-care.

58 SNS CLINICAL PRACTICE GUIDELINES
2.3. Approach
This CPG is focused on supporting health care in children, adolescents and adults with DM1, assisted in primary and specialty care, both in the intra-and outpatient means within the Spanish National Health System.
2.4. People who should read this CPG
This CPG is aimed at specialist care professionals within the Spanish National Health System in-volved in the treatment and care of patients with DM1, such as specialists in endocrinology, pae-diatric endocrinologists, specialized care staff and specialists treating the complications of DM1.
In addition, this guide is also aimed at patients, families and educational groups or scientifi c societies, as well as healthcare managers.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 59
3. Methodology of the guide
This CPG has been created following the Methodological Manual “Elaboración de Guías de Práctica Clínica en el Sistema Nacional de Salud” (Development of Clinical Practice Guidelines in the NHS)2 and the document “Descripción de la metodología de elaboración-adaptación-ac-tualización empleada en la Práctica Clínica sobre Asma en la CAPV” (Description of the devel-opment – adaptation – update methodology used in the Clinical Practice on Asthma within the Basque Autonomous Community)6 which can be consulted on the website of the Library of CPG of the NHS, GuíaSalud.
During the development process of this CPG, a mixed methodology has been applied, using a strategy of renovation and adaptation to the questions that are answered in the CPG “Type 1 diabetes: diagnosis and management of type 1 diabetes in children, young people and adults 2004 “ from the National Institute for Health and Clinical Excellence (NICE) published in 2004 (CPG NICE 2004)7 previously selected by the AGREE instrument for its highest quality. To address those questions that are not answered in the aforementioned guide the “de novo”6;8 development process has been followed.
For questions, regarding pregnant women with DM1, the upgrading and adaptation process has been made from the CPG ‘Diabetes in pregnancy management of diabetes and its complica-tions from preconception to the postnatal period. National Collaborating Centre for Women’s and Children’s Health Commissioned by the National Institute for Health and Clinical Excellence 2008” by NICE (NICE CPG 2008)9.
For questions 11.1 and 11.4, the upgrading process has been carried out from the diabetes CPG on diabetes type 2509 of the Spanish NHS.
The steps that taken during the preparation of the CPG were as follows:
3.1. Constitution of the guide development team
DM1 specialty care professionals (endocrinologists, paediatric endocrinologists and diabetes nurse educators) with proven expertise, experienced professionals in the development of CPG and evidence-based medicine, as well as experts on scientifi c literature and systematic revisions have collaborated in the development of this CPG. Likewise, people with DM1 and carers have partici-pated and contributed in various stages of the development process (defi ning the scope and focus of the CPG, formulating research questions, developing and reviewing the recommendations).
All the team members groups have provided a “declaration of interests” which is included in Appendix 14 of this guide.
60 SNS CLINICAL PRACTICE GUIDELINES
3.2. Systematic review Systematic reviews (SR) have been made for the development of this CPG in the following phases:
3.2.1. Formulation of clinical questions
It has been carried out using the PICO format: P (patients), I (interventions), C (comparisons) and O (outcomes or results). For proper formulation, a training workshop was provided previously for people involved in this process (doctors and nurses in DM1, experts in systematic reviews, people with DM1 and caregivers).
3.2.2. Bibliographic Search
There has been a search for CPG to identify the latest and of highest quality and clinical studies to identify the highest quality evidence available.
CPG Search:
Search period from 1998 to March 2011. Languages: Spanish, English, French and German. The following were consulted:
Agencies databases from collector bodies:
• Tripdatabase (European, American and English guides).
• NeLH (National Electronic Library of Health, United Kingdom).
• Canadian Medical Association.
• Guía Salud (Clinical Practice Guidelines in the NHS).
Databases from developing bodies:
• NICE (National Institute for Health and Clinical Excellence in the UK).
• SIGN (Scottish Intercollegiate Guidelines Network).
• FISTERRA Atención Primaria en la Red
• NGC (National Guideline Clearinghouse, U.S.).
A search of medicine databases based on evidence and general databases was also performed: MEDLINE (PubMed) and EMBASE (Elsevier).
Search for research studies. Search period: from 2003 to March 2011 (including warnings) for updated questions from the NICE CPG 2004. For the questions about pregnancy, which were based on the NICE CPG 2008, the search term was from 2007 to 2011 (including warnings).
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 61
After the identifi cation and selection of a CPG, a specifi c research was carried out on stud-ies for each clinical question in Cochrane Library Plus and the database of the National Health Service (NHS) Centre for Reviews and Dissemination, which in turn includes the HTA database (Health Technology Assessment) on assessment reports and the DARE base of reviews of effec-tiveness. General databases such as MEDLINE (PubMed) and EMBASE (Elsevier) were also used.
The whole process was completed using a general Internet search (scientifi c organizations and societies) and reverse lookup in articles from the most relevant studies to locate other relevant infor-mation.
The bibliographic search strategies are included in the document “Methodological material” available on the GuíaSalud website: http://www.guiasalud.es/ecpg/index.html.
3.2.3. Assessment of the methodological quality
The methodological quality of the CPGs found by the AGREE instrument10 was assessed, and the NICE CPG 20047 was selected for having the highest score. It was considered a reference CPG for its update/adaptation according to the methods proposed by the document “Descripción de la metodología de elaboración-adaptación-actualización empleada en la Práctica Clínica sobre Asma en la CAPV” (Description of the development – adaptation – update methodology used in the Clinical Practice on Asthma within the Basque Autonomous Community)6.
For those questions that were not addressed by this guide, a new search on research studies was carried out and the system proposed by SIGN11 for assessing the methodological quality of the studies was used.
3.2.4. Data Extraction
Performed by two independent reviewers.
3.2.5. Development of evidence tables
The evidence tables are included in the document «Methodological material» available in the website of GuíaSalud: http://www.guiasalud.es/ecpg/index.html.
3.2.6. Classifi cation of studies and grades of recommendations
For the classifi cation of levels of evidence and grades of recommendations, the SIGN11 scale was used for questions about effectiveness and safety of interventions or treatments and the Oxford12
classifi cation for the diagnostic questions.
62 SNS CLINICAL PRACTICE GUIDELINES
3.3. Edition of the Guide
Throughout this CPG there are recommendations based on publications of «consensus or expert opinion» qualifi ed with the letter «D».
The symbol «√» is used to defi ne «consensus of the development team». This last grade of recommendation is used in cases where there are no publications or when despite having studies, evidence must be adapted due to the context of application.
Along the document, the information provided by studies about the type and level of evi-dence refl ecting the possibility of bias in the literature reviewed is presented.
The text has undergone an external review by a multidisciplinary group of professionals. The fi nal version of the guide has been reviewed and approved by the development team.
The different scientifi c societies involved have been contacted:
• Federación de Asociaciones de Diabéticos de Euskadi (Federation of Diabetes Associations of the Basque Country) belonging to the Federación de Diabéticos Españoles (Spanish Diabetes Federation),
• Sociedad Española de Diabetes (Spanish Diabetes Society),
• Sociedad Española de Endocrinología y Nutrición (Spanish Society of Endocrinology and Nutrition), who participated through the development team and the external review.
This document is the «full» version of the Clinical Practice Guideline on Diabetes Mellitus type 1. The CPG is organized by chapters that provide answers to the questions at the beginning of it. A summary of the evidence and recommendations is presented at the end of each chapter. A “summarised” version of the CPG with the appendixes from the «complete» version and an educational guide aimed at young people and adults with DM1 is also available.
The link http://www.guiasalud.es/ecpg/index.html contains different versions of the CPG and the methodological material, which presents the information in detail with the preparation of the CPG, the search strategy for each clinical question and the evidence tables.
The update of this guide is scheduled every fi ve years without ruling out, if required, more frequent updating of the electronic version.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 63
4. Defi nition and diagnostic criteria ofdiabetes mellitus type 1
4.1. Defi nition of diabetes mellitus type1
Key question:
• What is diabetes mellitus type 1?
Diabetes mellitus (DM) comprises a group of metabolic diseases characterized by secondary hyperglycaemia to an absolute or relative defect in insulin secretion, which is accompanied, to a greater or lesser extent, by alterations in the metabolism of lipids and proteins, which leads to micro- and macro-vascular impairment affecting different organs such as eyes, kidneys, nerves, heart and vessels.
Diabetes mellitus type 1 (DM1) corresponds to the entity formerly termed insulin dependent or juvenile diabetes mellitus, in which the destruction of the pancreatic β cells leads to an absolute insulin defi ciency. In the current classifi cation, the DM1 is divided into two subtypes: DM1 A or autoimmune and DM1 B or idiopathic.
DM1 A or autoimmune: autoimmune disease in which there is a selective destruction of pancreatic β cells mediated by T lymphocytes activated in people with predisposing HLA haplo-types. After a preclinical period of variable duration, during which the patient is asymptomatic, when the mass of insulin-producing cells reaches a critical value the patient has classic symp-toms: polyuria, polydipsia, polyphagia, weight loss and a progressive ketosis that can lead to ketoacidosis, if not treated with exogenous insulin.
DM1 B or idiopathic: as opposed to DM1 A, DM1 B includes patients with the same or similar characteristics, without auto-immunity or predisposing HLA haplotypes data. As it has only been described recently as entity, little is known of its aetiology, development and prognosis.
64 SNS CLINICAL PRACTICE GUIDELINES
4.2. Autoantibodies in the diagnosis of diabetes mellitus type 1
Key question:
• What do the autoantibodies provide in the diagnosis of diabetes mellitus type 1?
DM type A or autoimmune is related to the destruction of β cells of the pancreatic Langerhans islet, usually because of an autoimmune response against specifi c molecules of the islet: insulin, glutamate decarboxylase, tyrosine phosphatase (IA-2), carboxypeptidase H; ICA69, etc.
The autoantibodies against these antigens can be detected in the serum of patients with DM1, and this has been used as an aid in the diagnosis, classifi cation, and prediction of the disease13. The autoantibodies can be detected even during the prodromal stage, as in the case of DM1 type A, during which although there are no clinical symptoms, there is a destruction of the β cells14. It is also possible to use these antibodies as markers of disease activity, and its measurement can help to defi ne the nature of the diabetes, providing autoimmune markers to classify as autoimmune or not, depending on the presence or absence of antibodies associated with the disease.
The NICE CPG 20047, based on a report carried out by consensus by the WHO15, does not recomm end regular measuring of the C-peptide nor specifi c autoantibodies to confi rm the diagnosis of DM1, but it does recommend its use if this will help to differentiate DM1 from DM2.
Expert consensus 4
This same CPG7, based on a consensus guide prepared by ISPAD16, recommends measuring specifi c immunological markers against β cells (ab-normal levels of anti-islet cell antibodies, anti-insulin and anti-glutamate decarboxylase antibodies) when there are doubts about the diagnosis of the type of DM.
Expert consensus 4
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 65
An SR of observational studies17 analyzed the clinical usefulness of the determination of some immunological markers, such as the antiglutamate decarboxylase 65 (GADA) antibodies, the islet cell antibodies (ICA), the insulin antibodies (IAA), the anti-tyrosine phosphatase antibodies (anti-IA2) and zinc antiporter (anti-ZnT8) in clinical practice, and described the utility of autoantibodies in the classifi cation of diabetes. The anti-islet antibodies (ICA) are associated with a different clinical course to that of patients who do not experience them: they are leaner, progress faster towards the need for insulin and have a lower secretion of the C-peptide. Moreover, the presence of GADA determines a slowly progressive autoimmune diabetes in adults. In the UKPDS study18 12% of patients with DM2 had ICA or GADA at the time of diagnosis, and 4% had both. The phenotype of patients with both antibod-ies was similar to that classically described for DM1 and at different ages, 59-94% required insulin within 6 years compared to 5-14% for those without either ICA or GADA. Both autoantibodies (isolated or combined) are associ-ated with an intermediate phenotype (lower body mass, greater HbA
1C and
lower β-cell function, compared with patients without antibodies). The posi-tive predictive value for insulin requirement was also intermediate.
In ketosis-prone diabetes: the isolated determination of autoantibodies has low sensitivity, but shows good results when combined with the func-tional determination of β cells. In people with maintained β function two weeks after an episode of ketoacidosis, the absence of autoantibodies was associated with greater functional preservation of β cells in the long term.
SR of observtional
studies 2++
Summary of evidence
SR ofobservational studies 2 + +
The determination of autoantibodies is valid for the differential diagnosis of DM1 with other types of diabetes 17.
Recommendations
B
Regular measurement of the C-peptide or specifi c antibodies to confi rm the diagnosis of diabetes mellitus type 1 is not advisable, but its use should be covnsidered to determine the aetiology of autoimmune diabetes in doubtful cases.
66 SNS CLINICAL PRACTICE GUIDELINES
4.3. Predictors of ‘spontaneous remission’
Key question:
• What are the predictors of ‘spontaneous remission’?
In newly diagnosed DM1 patients, a partial reset of the β function, shortly after diagnosis, is fre-quent leading to a reduction in the need for exogenous insulin and improved metabolic control. This phenomenon is known as “spontaneous remission” (SR) or ‘honeymoon’. The majority of patients still need a certain amount of insulin (even low doses) and very few can do completely without it.
The clinical defi nition of SR varies among the authors depending on the dose of insulin con-sidered necessary for the correct metabolic control (ranging between 0.3 and 0.5 IU/kg/day) and according to HbA
1c levels from which a metabolic control is considered adequate 19,20,21.
The Guide Development Group (GDG) has agreed that the defi nition of period of “spontane-ous remission” applicable in this CPG is that proposed by Bonfati22, according to which an SR period is considered that in which the need for exogenous insulin falls to doses lower than 0.3 IU/kg/day for a metabolic control in HbA
1c levels lower than 6% (36 mmol/mol) is reduced.
Different factors of individual, clinical, metabolic and immune character have been identi-fi ed as potential inducers of SR and determinants of its duration.
The NICE Guide 20047 evaluated the SR for diabetes in the section ‘Natural History of Diabetes “. In this text SR is defi ned as the period in which with insulin doses lower than 0.5 IU/kg/day, a patient has HbA
1c levels below 7% (46 mmol/mol) 23, or when with insulin doses lower
than 0.3 IU/kg/weight/day the patient has HbA1c
levels below 6% (36 mmol/mol)22. The preva-lence detected in different studies presents a very wide range (30-80%).
Factors that determine the occurrence of spontaneous remission
The NICE Guide 2004 includes in its review two observational studies23;24 that found no association between genre and the emergence of SR or its duration, while a third observational study25 found that men with DM1 are more likely to experience partial remission than women (73% vs. 53%) and during a longer period of time [mean (SD) 279 days22 vs. 210 days 25]
Observational studies
2 +
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 67
With respect to the infl uence of the age in the onset of SR, these same studies found that children with younger age at diagnosis were less likely to experience a phase of SR, which in turn showed that remissions were shorter.
A total of eight articles published after the NICE CPG 2004 have been found. Most are very heterogeneous observational studies regarding the defi ni-tions of SR and none of them matches the defi nition adopted by the develop-ment group of this CPG. Therefore, the results of two of these studies were not considered adequate to answer the question posed, according to the established criteria.
Summary of evidence
Observational studies 2 +
Currently there is not enough evidence on the predicting factors of spontaneous remission according to the criteria proposed by Bonfati et al.23, 24, 25, therefore the recommendations presented are based on the consensus of the Guide Development Group.
Recommendations
�
The patient and their caregivers (in case they are children) should be informed about the possibility of entering into a spontaneous remission or “honeymoon” stage within months of the diagnosis of diabetes mellitus type 1 that would imply a reduction of insulin doses. Likewise, it is necessary to point out that this entails no cure for the disease and that after this period insulin doses will have to be increased again.
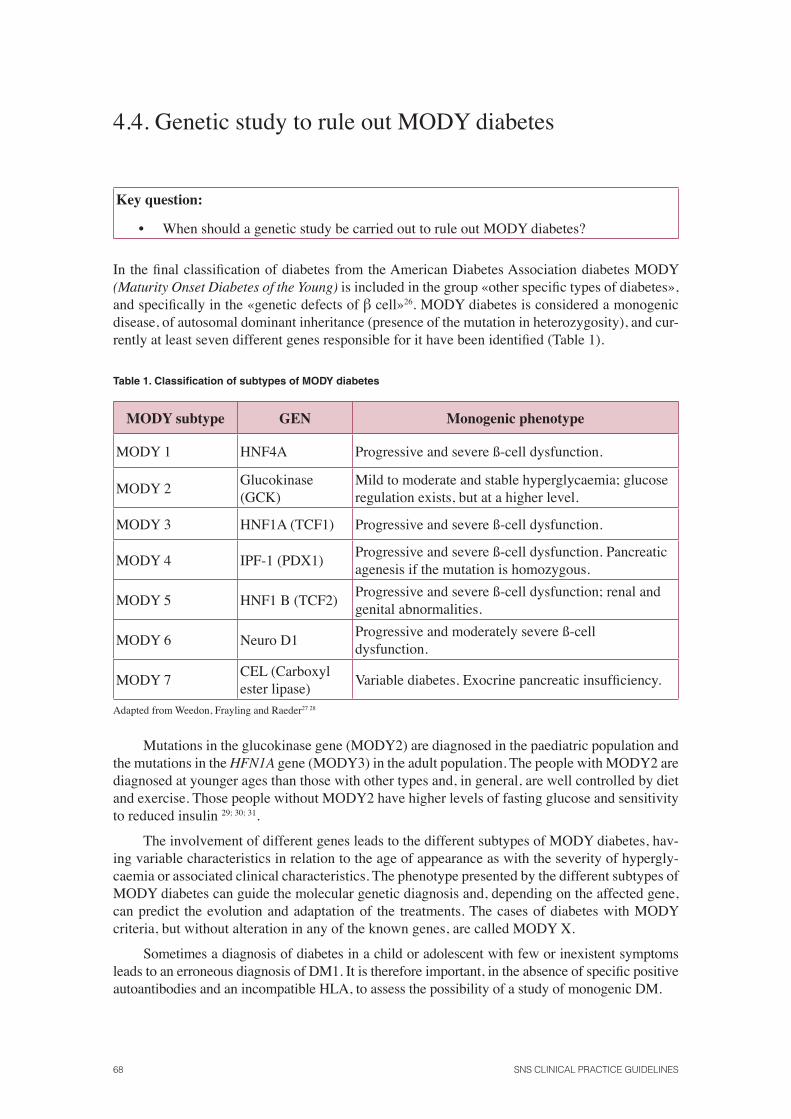
68 SNS CLINICAL PRACTICE GUIDELINES
4.4. Genetic study to rule out MODY diabetes
Key question:
• When should a genetic study be carried out to rule out MODY diabetes?
In the fi nal classifi cation of diabetes from the American Diabetes Association diabetes MODY (Maturity Onset Diabetes of the Young) is included in the group «other specifi c types of diabetes», and specifi cally in the «genetic defects of β cell»26. MODY diabetes is considered a monogenic disease, of autosomal dominant inheritance (presence of the mutation in heterozygosity), and cur-rently at least seven different genes responsible for it have been identifi ed (Table 1).
Table 1. Classifi cation of subtypes of MODY diabetes
MODY subtype GEN Monogenic phenotype
MODY 1 HNF4A Progressive and severe ß-cell dysfunction.
MODY 2Glucokinase (GCK)
Mild to moderate and stable hyperglycaemia; glucose regulation exists, but at a higher level.
MODY 3 HNF1A (TCF1) Progressive and severe ß-cell dysfunction.
MODY 4 IPF-1 (PDX1)Progressive and severe ß-cell dysfunction. Pancreatic agenesis if the mutation is homozygous.
MODY 5 HNF1 B (TCF2)Progressive and severe ß-cell dysfunction; renal and genital abnormalities.
MODY 6 Neuro D1Progressive and moderately severe ß-cell dysfunction.
MODY 7CEL (Carboxyl ester lipase)
Variable diabetes. Exocrine pancreatic insuffi ciency.
Adapted from Weedon, Frayling and Raeder27 28
Mutations in the glucokinase gene (MODY2) are diagnosed in the paediatric population and the mutations in the HFN1A gene (MODY3) in the adult population. The people with MODY2 are diagnosed at younger ages than those with other types and, in general, are well controlled by diet and exercise. Those people without MODY2 have higher levels of fasting glucose and sensitivity to reduced insulin 29; 30; 31.
The involvement of different genes leads to the different subtypes of MODY diabetes, hav-ing variable characteristics in relation to the age of appearance as with the severity of hypergly-caemia or associated clinical characteristics. The phenotype presented by the different subtypes of MODY diabetes can guide the molecular genetic diagnosis and, depending on the affected gene, can predict the evolution and adaptation of the treatments. The cases of diabetes with MODY criteria, but without alteration in any of the known genes, are called MODY X.
Sometimes a diagnosis of diabetes in a child or adolescent with few or inexistent symptoms leads to an erroneous diagnosis of DM1. It is therefore important, in the absence of specifi c positive autoantibodies and an incompatible HLA, to assess the possibility of a study of monogenic DM.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 69
The personal and family history, the severity and frequency can orientate towards the spe-cifi c type of study which to begin from. Performing a diagnosis of monogenic subtype DM can predict the most likely course of the disease and modify the treatment. Furthermore, the detection of gene alteration will allow early identifi cation of family and an earlier treatment.
The latest information regarding the indication of the genetic study to dis-card MODY diabetes comes from good practice guidelines for molecular genet-ic diagnosis of MODY diabetes developed by consensus by a group of European clinicians and scientists32. Consensual clinical criteria are as follows:
Mild fasting hyperglycaemia: evidence for mutations of the GCK gen
In a signifi cant proportion of young non-obese patients who presented mild and persistent fasting hyperglycaemia, a heterozygous mutation in the glucokinase gene will be found. The features that suggest a mutation of this gene are the fol-lowing:
• Fasting hyperglycaemia > 99 mg/dl (5.5 mmol/l) (in 98% of patients), persistent (at least on three separate occasions) and stable over a period of months or years.
• HbA1C
just above the upper limit of the normal range and rarely exceeds 7.5%.
• In the oral glucose tolerance test, the glucose increase is small (glucose after two hours - fasting glucose). In a major study conducted in Europe, 71% of patients had an increase <54 mg/dl (3 mmol/l). An increase of 83 mg/dl (4.6 mmol /) is used as a priority for testing and corresponds to the 90 percentile.
• Parents can be diagnosed with DM2 without complications or diabetes. In testing, one parent will usually undergo a slight increase in fasting glucose (99-144 mg/dl (5.5 to 8 mmol/l), unless the mutation has oc-curred de novo.
Gestational diabetes: evidence for mutations of the GCK gene
Patients with this disorder have slow and continuous fasting hyperglycaemia, and babies who do not inherit the mutation can be macrosomic. Its diagnosis is important, since the management is different in the case of this mutation to that of prediabetes type 2. The characteristics that suggest a mutation of this gene are the following:
• Persistent increase in fasting blood glucose in the range 99-144 mg/dl (5.5 to 8 mmol/l) before, during and after pregnancy.
• Increase of <83 mg/dl (4.6 mmol /) at least in an oral glucose tolerance test during or after pregnancy.
• A parent may have been diagnosed with mild DM2 but it often happens that it has not been detected; therefore, the absence of family history does not exclude the diagnosis.
Expert consensus
4
70 SNS CLINICAL PRACTICE GUIDELINES
Children and young adults with diabetes and family history of diabetes: evidence for HFN1A mutations
HFN1A mutation, along with that of GCK, is the most common cause of MODY diabetes. The characteristics that suggest a mutation of this gene are the follow-ing:
• Young-onset diabetes (often before the age of 25 in at least one family member).
• Appearance of “non-insulin dependent” (does not develop ketoacidosis in the absence of insulin, good glycaemic control with doses of insulin lower than usual, or measuring of detectable C-peptide when with in-sulin with glucose > 144 mg/dl (8 mmol/l) during the normal “honey-moon” period.
• Family history of diabetes (at least two generations). These can be treated with insulin and considered DM1 or DM2. At least two of the members have been diagnosed at the age of 20 or 30. There may be an affected grandparent, often diagnosed after the age of 45. The oral glu-cose tolerance test, in early stages, usually shows increases of > 90 mg/dl (5 mmol/l). Some people may have normal levels while fasting, but diabetes range levels after two hours.
• Absence of autoantibodies against pancreatic islets.
• Glycosuria with blood glucose levels at <180 mg/dl, because of the low renal threshold.
• Marked sensitivity to sulfonylureas, with hypoglycaemias despite a poor glycaemic control prior to treatment.
• Characteristics suggesting monogenic diabetes compared to young-on-set DM2: marked obesity is not seen nor evidence of insulin resistance in family members with diabetes, absence of acanthosis nigricans and ethnic background family with low prevalence of DM2.
Children and young adults with diabetes and family history of diabetes: evidence for HFN4A mutations
It is less frequent than the HFN1A mutation. It is associated with macrosomia (approximately 56% of mutation carriers) and transient neonatal hypoglycaemia (approximately 15% of the mutation carriers).
• It is similar to diabetes by HFN1A gene mutation, but there is no low renal threshold and the age of diagnosis may be later.
• This mutation should be considered when although molecular studies of the HNF1A gene are negative do not detect it, and the clinical character-istics are very suggestive.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 71
• Sensitivity to sulphonylureas.
• Family members with diabetes and marked macrosomia at birth (> 4.4 kg to conclusion).
• Diagnosis of neonatal hyperinsulinism sensitive to diazoxide in the context of family diabetes.
Babies with neonatal hyperinsulinemic hypoglycaemia sensitive to diazoxide and family history of diabetes: evidence for HFN4A mutations
• Macrosomic babies with hyperinsulinism sensitive to diazoxide and a family history of diabetes.
Summary of evidence
Expert consensus
4
In cases in which sustained hyperglycaemia is identifi ed in a young person with-out obesity and/or a history of diabetes in two generations, in the absence of antipancreatic autoimmunity and with HLA incompatible with diabetes melli-tus type 1, MODY diabetes should be ruled out. The most common types are MODY 2 and 3 diabetes.
In children, macrosomia and hyperinsulinism are signs of suspicion.
Diagnostic confi rmation must be made by genetic study 32.
Recommendations
DIn cases in which mild continuous hyperglycaemia is identifi ed in a young per-son, without obesity and/or diabetes history of mild to two generations, in the absence of antipancreatic autoimmunity and with HLA not compatible to diabe-tes mellitus type 1, MODY 2 diabetes should be ruled out.
DIf hyperglycaemia is more severe and progressive rule, it is recommended to rule out MODY 3 diabetes.
DIf genetic testing were negative for MODY 2 and MODY 3, the rest of MODY varieties would have to be ruled out.
Reference centres where these determinations can be made are detailed in Appendix 1
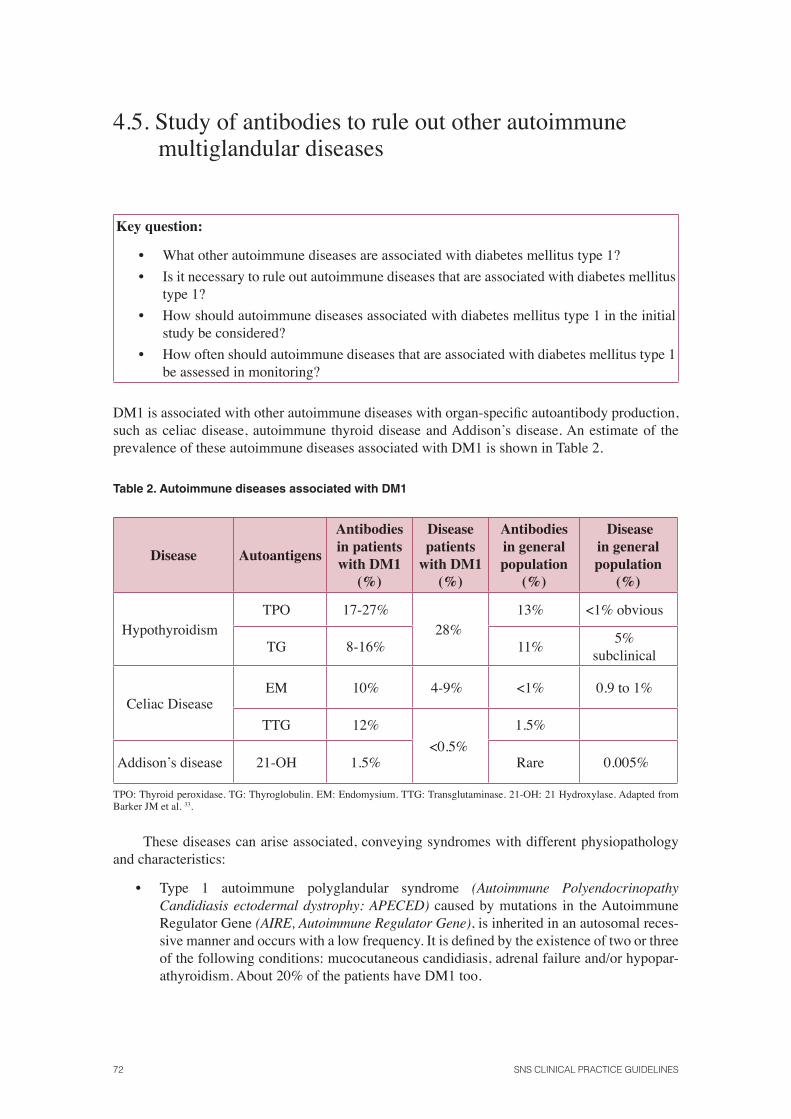
72 SNS CLINICAL PRACTICE GUIDELINES
4.5. Study of antibodies to rule out other autoimmune multiglandular diseases
Key question:
• What other autoimmune diseases are associated with diabetes mellitus type 1?
• Is it necessary to rule out autoimmune diseases that are associated with diabetes mellitus type 1?
• How should autoimmune diseases associated with diabetes mellitus type 1 in the initial study be considered?
• How often should autoimmune diseases that are associated with diabetes mellitus type 1 be assessed in monitoring?
DM1 is associated with other autoimmune diseases with organ-specifi c autoantibody production, such as celiac disease, autoimmune thyroid disease and Addison’s disease. An estimate of the prevalence of these autoimmune diseases associated with DM1 is shown in Table 2.
Table 2. Autoimmune diseases associated with DM1
Disease Autoantigens
Antibodies in patients with DM1
(%)
Disease patients
with DM1 (%)
Antibodies in general population
(%)
Disease in general population
(%)
HypothyroidismTPO 17-27%
28%13% <1% obvious
TG 8-16% 11%5%
subclinical
Celiac DiseaseEM 10% 4-9% <1% 0.9 to 1%
TTG 12%
<0.5%
1.5%
Addison’s disease 21-OH 1.5% Rare 0.005%
TPO: Thyroid peroxidase. TG: Thyroglobulin. EM: Endomysium. TTG: Transglutaminase. 21-OH: 21 Hydroxylase. Adapted from Barker JM et al. 33.
These diseases can arise associated, conveying syndromes with different physiopathology and characteristics:
• Type 1 autoimmune polyglandular syndrome (Autoimmune Polyendocrinopathy Candidiasis ectodermal dystrophy: APECED) caused by mutations in the Autoimmune Regulator Gene (AIRE, Autoimmune Regulator Gene), is inherited in an autosomal reces-sive manner and occurs with a low frequency. It is defi ned by the existence of two or three of the following conditions: mucocutaneous candidiasis, adrenal failure and/or hypopar-athyroidism. About 20% of the patients have DM1 too.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 73
• Type 2 polyglandular autoimmune syndrome: it is the combination of two major autoimmune endocrine disruptions (DM1, autoimmune thyroid disease and Addison’s disease). It is the most common and includes patients with DM1 and associated autoimmune diseases such as autoimmune thyroid disease, Addison’s disease, primary hypogonadism, myasthenia gravis, celiac disease, arthropathy and vitiligo. It has a genetic basis based on HLA just as DM1.
The screening of these autoantibodies in DM1 patients can detect organ-specifi c autoim-munity prior to the development of the disease and an early detection can prevent signifi cant morbidities and long-term complications of these diseases.
4.5.1. Thyroid disease
In connection with thyroid disease associated with DM1, the CPG by the International Society for Paediatric and Adolescent Diabetes (ISPAD) 2006-200734 indicates that 3-8% of children and adolescents with diabetes suffer pri-mary hypothyroidism due to autoimmune thyroiditis. Antithyroid antibodies ap-pear in the fi rst years in 25% of patients and are prone to develop, both clinical and subclinical, hypothyroidism. Hyperthyroidism, either by Graves disease or by the hyperthyroid phase of Hashimoto’s thyroiditis, is less common than hy-pothyroidism in patients with diabetes. However, hyperthyroidism is more com-mon in patients with diabetes than in the general population.
Based on these data, the ISPAD group recommends by consensus to carry out screening of the thyroid function based on the analysis of TSH and circu-lating antibodies at the time of diagnosis of diabetes and, thereafter, every two years in asymptomatic patients without goiter or absence of thyroid autoantibod-ies. These recommendations are consistent with those issued recently, also by consensus, by the American Diabetes Association 26.
Consensus document 4
In an SR35, the results show that antithyroid peroxinase antibodies (Ac. Anti-TPO) and thyroglobulin antibodies (Ac. Anti-Tg) are more frequent in pa-tients with DM1 than among the control population (Ac. Anti-TPO vs. 5.5 to 46.2%. 0 -27.0%, Ac. 2.1 to 40% Anti-Tg vs. 0-20%). Prevalence rates appear to be higher in women and increase with age and duration of DM1. The prevalence of clinical and subclinical hypothyroidism, depending on whether they have Ac. Anti-TPO, Ac. Anti-Tg or both, is between 6 and 72% in patients with DM1 compared with a prevalence reaching up to 25% in the control population.
In other standardized, prospective and multicenter observational study36 conducted in Germany and Austria from a database on children and adolescents with diabetes (Diabetes patiënten Verlaufsdokumentationsistem), the frequency of screening for celiac disease and Hashimoto’s thyroiditis was assessed in 31104 under 18 year-old patients with DM1 in 177 paediatric centres in Germany and Austria.
RS of observational
studies 2++
74 SNS CLINICAL PRACTICE GUIDELINES
15% of patients had thyroid antibodies and they were more frequent in women. The antibody-positive patients were older at the time of diagnosis of diabetes (8.4 vs. 8.1 years, P <0.001) and had a longer duration of diabetes (6.4 vs. 5.1 years, P <0.001). In the long term, there was a decrease in patients with positive antithyroid antibodies (1995: 21% vs. 2006: 12.4%, p <0.001), unlike in the case of celiac disease specifi c antibodies.
Observational study
2+
4.5.2. Celiac disease (CD)
According to data provided by the CPG ISPAD, the prevalence of CD is as-sociated with DM1 from 1 to 10% in children and adolescents with diabetes34. Often, the disease is asymptomatic and not necessarily associated with lower growth or poor glycaemic control.
Expertconsensus 4
The screening was based on the detection of anti-endomysial antibod-ies (EMA) and anti-transglutaminase antibodies (TG2), the fi rst more specifi c (100% vs. 96%) and the second more sensitive (91% vs. 86%). The authors of this CPG recommend carrying out an intestinal biopsy to confi rm the diagnosis when there is a rise in antibodies. The long-term benefi t of a gluten-free diet in asymptomatic children diagnosed with EC by routine screening has not been documented. The recommendations stated in this guide in relation to screening are:
• CD screening is recommended at the time of diagnosis of diabetes and, thereafter, every two years. Should the clinical condition suggest the existence of CD or in case the child has a fi rst degree relative with CD, assessment should be done more frequently.
• Children with DM1 to which CD has been detected in the screening should be referred to a paediatric gastroenterologist and, after confi r-mation of the diagnosis, support from a paediatric dietician with exper-tise in gluten-free diets should be provided.
The American Diabetes Association26 has issued the following recom-mendations:
• After the diagnosis of diabetes, children with DM1 should be assessed promptly by measuring antiendomysial antibodies or anti-tissue trans-glutaminase with data on normal IgA levels for the detection of CD.
• These determinations should be repeated if there were increasing defi -cits in growth, weight gain, weight loss or gastrointestinal symptoms.
• Regular assessment of asymptomatic individuals should be considered.
• Children with positive antibodies should be referred to a paediatric gastroenterologist for evaluation.
• Children where the diagnosis of celiac disease is confi rmed should consult a dietician and follow a gluten-free diet.
Expert consensus 4
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 75
In an SR35, the prevalence of EMA was higher in patients with DM1 (1.5 to 10%, IQR 5.1 to 8.7, P5-P953.4 to 9.8) than in the control population (0-2%, IQR 0 to 0.3, P5-P95 0 to 1.5) and showed no consensus regarding the age, sex and duration of diabetes. The biopsy confi rmed the diagnosis of CD between 44 and 100% of patients with DM1 and positive EMA.
SR ofobservational
studies 2++
A retrospective observational study37, conducted in Spain in 261 children and adolescents under 18 years with DM1, found an 8% prevalence of CD (21 of 261 patients studied). In 51% of cases, the diagnosis of CD took place after the diagnosis of DM1. Of these, 67% of cases were diagnosed after diagnosis of DM1in the fi rst 5 years; 2 cases after 8 years; 1 case after 10 years and 1 case after 13 years.
Observational study
2+
In a multicenter observational study36, the presence of CD if TG2 antibod-ies were greater than 10 U was assessed. Antigliadin antibodies were also ana-lysed and those values higher than 25 U/L were considered positive.
11% of patients with DM1 had EMA antibodies and/or positive TG2, and if antigliadin antibodies are also taken into account, the fi gure raises to 21%. The antibody-positive patients were younger at the time of diagnosis of diabetes (7.5 vs. 8.1 years, p <0.001) and had a longer duration of diabetes (5.5 vs. 4.9 years, p <0.001). In the long run, there was a slight increase in antibody-positive patients (1995: 11% vs. 2006: 12.4%, p <0.001).
Observational study
2+
A retrospective observational study38 conducted in a cohort of 950 children with DM1 in monitoring in the department of paediatric endocrinology of the University Hospital Robert Debré in Paris, assessed the prevalence of histologi-cally documented CD. The analysis of antigliadin, antirreticulin, EMA and TG2 antibodies was carried out between one and seven times in each patient and all patients with positive antibodies underwent an intestinal biopsy.
1.6% of patients (15/950) confi rmed the diagnosis of CD by biopsy. The suspected diagnosis was made based on the symptoms in 40% of patients [mean (SD): 7 years (4.6)] and by screening in 60% of patients [mean (SD): 6.1 years (3.6) in the time of diagnosis of diabetes]. CD was diagnosed after diagnosis of DM1 in 73% of cases, and the mean duration of DM1 at the time of diagnosis of CD was 4 years (0-13 years). The EMA antibodies were positive in 15 patients and antinuclear antibodies were positive in three patients. EMA seroconversion was observed in two patients after 2 and 6 years of diagnosis of diabetes, respec-tively.
The authors concluded that the prevalence of CD is higher in children with DM1 (16 ‰) than in the general paediatric population (0.41 ‰), while in the general population prevalence studies usually include only symptomatic forms of CD.
Observational study
2+
76 SNS CLINICAL PRACTICE GUIDELINES
A prospective cohort study39 investigated the prevalence of CD in a cohort of 300 children and adolescents with newly diagnosed DM1 and evaluated the screening procedure and the possible role of human leukocyte antigen (HLA-DQ) for a fi ve-year follow up. This analysis was performed at the time of di-agnosis and then a screening was carried out on an annual basis for EMA. In patients with positive EMA an intestinal biopsy was performed.
0.7% of children (2/300) had evident CD in the moment of diagnosis. 3.3% (10/300) had positive EMA and the intestinal biopsy confi rmed a silent CD at the time of diagnosis of DM1. During follow-up 6% (17/300) developed posi-tive EMA and confi rmed CD: 10 cases the fi rst year, 5 after 2 years; 1 after 3 years, and 1 case after 5 years. The cumulative frequency of confi rmed CD by intestinal biopsy was 10% (29/300).
The genotypes among patients with DM1 who developed CD were not dif-ferent from those with only DM1.
The results of this study confi rm the low prevalence of CD at the time of diagnosis of DM1. By screening, an increase in the prevalence of silent CD over fi ve years of follow up, with increased risk of development during the fi rst two years of diagnosis is observed.
Observational study
2+
4.5.3. Addison’s disease
In connection with Addison’s disease associated with DM1, ISPAD, as pub-lished in its CPG in 200734 indicates that up to 2% of patients with DM1 have detectable adrenal antibodies and that Addison’s disease is associated with DM1 in autoimmune syndromes. ISPAD does not establish specifi c recommendations for screening.
GPC Descriptive
studies 3
In the SR by Graaf et al.35, the results of the various studies show that adrenocortical antibodies (ACA) are more prevalent in patients with DM1 (0-4%) than in the control population (0-0.7%). There is no clear association of the presence of ACA with the age, sex and duration of diabetes. The data in this review suggest that between 3 and 40% of patients with positive ACA develop DM1 and Addison’s disease.
SR ofobservational studies 2++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 77
Summary of evidence
SR ofobservational
Studies 2++
Autoimmune thyroid diseases, celiac disease and Addison’s disease occur more frequently in people with diabetes mellitus type 1 than among the general population 34; 35; 36; 37.
SR of observational
Studies2++
The presence of antithyroid autoantibodies is more common in women and more frequent at an older age at the time of diagnosis of diabetes and when the duration of diabetes is longer 36.
Descriptivestudies
3
The presence of specifi c antibodies for celiac disease is more common at a younger age at the time of diagnosis of diabetes and when the duration of diabetes is longer 39.
Regarding Addison’s disease, there is currently not enough evidence available to make a recommendation on the systematic screening of autoimmune suprarenal disease.
Recommendations
BAutoimmune thyroid disease and celiac disease at the onset of diabetes mellitus type 1 in children and adolescents should be ruled out.
� This study should be done every two years for the fi rst 10 years of disease progression and then every fi ve years.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 79
5. Diabetes Education
5.1. Structured education aimed at families and/or patients with diabetes mellitus
Key question:
• Are structured educational programs aimed at people with diabetes mellitus type 1 and their families effective?
The education of a patient with DM1 is critical to have a proper control of the disease. The aim is to enable patients to take control of their disease in order to be autonomous, integrating the treat-ment in their daily lives.
According to ISPAD34, 40, the aspects that characterize a structured educational program are the following:
• It comprises a structured plan, which has been agreed and written.
• It is taught by trained educators.
• It is quality assured.
• There is a proper evaluation of the program.
80 SNS CLINICAL PRACTICE GUIDELINES
The CPG NICE 20047 partially addresses the issue of effectiveness of the structured educational programs in DM1: it assesses the effectiveness of edu-cational interventions in general, but not specifi cally that of the structured educational programs. However, this CPG includes some studies that pro-vide evidence of interest regarding this question.
GPC
Regarding the effectiveness of these interventions in children and ado-lescents, a report on health technology assessment41 that analyzed a large number of educational programs for children and adolescents with DM1 aged 9 to 21 years should be considered. The studies included in this review have a medium to high quality and most of them (68%) had been conducted in the United States. The meta-analysis on 14 studies that provided informa-tion on the psychological effects and on the 12 studies which analyzed HbA
1c
levels indicated a moderate positive effect of these educational interventions.
SR of RCT and observational
studies1++/2++
In terms of effectiveness in adults, an RCT42 that assessed the effects of a structured outpatient education program, taught over four weeks by nurses, dieticians and people affected by DM1, showed signifi cant benefi ts of these interventions on metabolic control and quality of life.
RCT1+
A medium sized RCT43 evaluated the effects of a monthly educational program with different educational aspects. After a year of education with this method, the HbA
1c levels were signifi cantly reduced in the intervention
group versus the control group in patients with DM1.
Following the NICE CPG 2004, two RS and two RCTs were published on this topic. In addition, the results of another RCT published in 2002 but which was not included in the NICE CPG 2004 have been incorporated.
RCT 1 +
The SR published by Couch et al 44 reviewed the effectiveness of educa-tional programs on diabetes that included at least one of the following: infor-mation about the disease process and treatment options, nutritional manage-ment, physical activity, monitoring blood glucose and ketone bodies in urine using the results to improve glycaemic control, use of treatments, preven-tion, detection and treatment of acute complications, control of risk factors, detection and treatment of chronic complications, setting targets for health improvement; solving daily life problems, and psychosocial adjustment.
Of the 12,756 items found, 80 studies, 53 randomized clinical trials or controlled clinical trials and 27 observational studies were included.
SR of RCT and observational
studies1++ /2++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 81
HbA1c: Most studies (35/52) that examined the effect of educational intervention on HbA
1c found no evidence of greater effectiveness of the in-
tervention regarding education than that provided with standard care. The in-terventions which achieved successful results were the cognitive behavioural therapy, family therapy, training in practical skills and training in diabetes in general.
Regarding children with poorly controlled diabetes, 13 studies exam-ined the effects on HbA
1C: two high quality RCTs that studied diabetes edu-
cation in general and family therapy concluded that the intervention had no impact on the level of HbA
1C. The results of the remaining studies were in-
consistent.
These studies indicate that it is not so much that programs are structured as that they are taught and that all their educational content is assimilated, albeit in an unstructured way.
Use of health services: 11 studies assessed the impact of diabetes edu-cation on the use of health care services (length of stay, emergency admission or hospitalization for complications related or not to diabetes). Most studies showed a lower use of health services, although the result was statistically signifi cant in less than half of them.
Acute complications: 15 studies examined the effects on acute compli-cations, most related to severe hypoglycaemia and 6 studies about diabetic ketoacidosis. Of these studies, 10 analyzed children with diabetes in general, three newly diagnosed children and one child with poor metabolic control. The results of these studies were not conclusive, since two studies in children with diabetes showed signifi cant improvements in terms of complications, but the rest found no signifi cant effects.
Practical skills: 9 studies measured the effects of diabetes education in the development of practical skills, including self-monitoring of blood glucose, nutrition and diet-related and urinary analysis practices. The results were inconclusive.
Adhesion: 14 of 21 studies showed signifi cant improvement in the re-sults and showed that interventions that improved adherence were general diabetes education, cognitive behavioural therapy and family therapy.
Psychosocial: 39 studies examined one or more connections (family and social relationships, family and social support, social skills, coping, self-perception, self-effi cacy, stress, depression and anxiety) and, in general, there was an improvement of various psychosocial outcomes; although it is not possible to draw fi rm conclusions because of the low quality and the heterogeneity of the studies.
82 SNS CLINICAL PRACTICE GUIDELINES
Another SR45 included 33 studies of educational interventions conduct-ed in adults with DM1. The results of this study indicated that these interven-tions improve signifi cantly the quality of life of patients (as measured by the SF-36 survey) in aspects of physical function, pain, social function, mental health, vitality and limitation due to physical problems, which leads to posi-tive changes in lifestyle, commitment with self-control and adherence to the treatment.
SR of RCT 1 + +
An RCT 46 with 78 children and adolescents with DM1 analyzed the effects of a structured program of education based on the family and showed that the effect depended on the number of sessions attended, as the families attending two or more sessions (up to four) had a signifi cant and benefi cial effect on metabolic control after 12 months. No signifi cant effects on quality of life or level of family responsibility were found.
RCT1+
Another RCT 47, conducted in 164 adult patients with DM1 with hypo-glycaemia problems, showed that a structured and specifi c program for this complication obtained signifi cant benefi ts in relation to awareness of hypo-glycaemia, a signifi cant increase in its detection threshold and a decrease in the number of undetected episodes.
RCT1+
A multicenter RCT published in 200248, but not included in the CPG NICE 2004, examined the effects of a structured educational program based on fi ve sessions aimed at improving skills in insulin management. This study showed a signifi cant improvement in metabolic control and quality of life after six months.
RCT1+
Summary of evidence
RCT1+
Structured educational programs targeted at adults with diabetes mellitus type 1 improve their quality of life42
RCT1+
Programs that include cognitive behavioural therapy and family therapy training in practical skills and diabetes improve metabolic control and reduce the risk of acute complications 44.
RCT1+
Studies carried out with children suggest that the structured nature of the program does not seem as important as how these are taught and that they include all the educational content 44.
RCT1+
There is evidence that specifi c education programs are effective in preventing hypoglycaemia complications and improve their management, and that specifi c education programs on insulin management improve metabolic control and quality of life 46, 47, 48.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 83
Recommendations
A
All patients with diabetes mellitus type 1 should have access to a diabetes education program delivered by a multidisciplinary team (doctors, nurse educators, psychologists, dieticians, etc.) with specifi c skills in diabetes, both in the diagnosis stage and subsequently, based on the patient’s needs..
AIn cases of repeated hypoglycaemia, the patient with diabetes and their families should be offered a specifi c educational program.

84 SNS CLINICAL PRACTICE GUIDELINES
5.2. Education aimed at patients and family
Key question:
• Structured education aimed at families and people with diabetes mellitus type 1: when, how, by whom and with what content is it taught?
There is great diversity in relation to the content and characteristics of educational programs. Knowledge about aspects that increase the effectiveness of these educational interventions will optimize their application and improve their results on health.
Given the heterogeneity of the interventions examined in the available scientifi c evidence, the recommendations that have been made on this issue are based on consensus documents published by the following international organizations:
• National Institute for Clinical Excellence (NICE CPG 2004) devotes sev-eral paragraphs of its CPG on DM1 to identify the effectiveness of the ele-ments of education and educational programs in diabetes, both in the case of adults and children and adolescents7.
• International Society for Paediatric and Adolescent Diabetes (ISPAD)49; 50.
• National Standards for Diabetes Self-Management Education. Diabetes Care (SRDS), issued by the working group of the American Diabetes Educators Association and the American Diabetes Association and rep-resentatives of the American Dietetic Association, the Veteran’s Health Administration, the Centres for Disease Control and Prevention, the Indian Health Service and the American Pharmaceutical Association 51, 52. These standards are reviewed approximately every fi ve years based on available evidence and with expert consensus.
• Teaching letters prepared by the Study Group on Diabetes Education from the European Association for the Study of Diabetes (EASD), aimed at doc-tors and other professionals involved in the daily care of patients with dia-betes, both type 1 and type 253; 54.
Expert consensus
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 85
Summary of evidence
Expert consensus
4
Given the heterogeneity of the interventions examined in the scientifi c evidence available the recommendations that have been made on this issue are based on the consensus of the GEG, which has taken into account the consensus documents published by the following international organizations: National Institute for Clinical Excellence (CPG NICE 2004)7. International Society for Paediatric and Adolescent Diabetes (ISPAD) 49, 50, National Standards for Diabetes Self-Management Education. Diabetes Care (EAMD), issued by the working group of the American Association of Diabetes Educators and the American Diabetes Association and representatives from the American Dietetic Association, the Veteran’s Health Administration, the Centres for Disease Control and Prevention, the Indian Health Service and the American Pharmaceutical Association 51, 52. Teaching letters prepared by the Study Group on Diabetes Education by the European Association for Study of Diabetes (EASD) 53, 54.
Recommendations
D
Structured diabetes education should be provided in the following circumstances:
• At the time of diagnosis (survival education).
• In the period following diagnosis (deepening and reinforcement education).
• In the long term: on periodic reviews on self-care and educational needs, depending on the achievement or not of the objectives agreed between the patient and the practitioner.
D
Structured diabetes education should be provided to the following people:
• All patients diagnosed with diabetes mellitus type 1.
• Parents and carers in cases where there is dependency because of age or disability.
• The people who make up the school environment of children or adolescents: teachers, caregivers, etc.
86 SNS CLINICAL PRACTICE GUIDELINES
D
Professionals who must provide structured diabetes education:
• Multidisciplinary teams: the members of these teams should have compe-tencies and skills to convey information effectively. There must be enough professionals available to organize regulated educational programs for groups. The team should include, at least, specialists in endocrinology, pae-diatric endocrinology and diabetes nurse educators. It is also desirable that psychologists were included in these teams for people who many need them.
• At extra sanitary level the associations of people with diabetes, who provide educational programs for specifi c groups, play a key role (camps for chil-dren, elderly patients, informative talks, gatherings, etc.)
The members of the educational team should be characterized not only by their capacity for empathy, but also for their fl exibility and ability to communicate.
D
Methods and materials used to provide structured education on diabetes:
• Attendance-based training sessions using audiovisual media, food, and ob-jects related to learning about food: games, plastic food, and descriptive fl ashcards to facilitate understanding.
• Complementary methods:
ο Books and leafl ets: a great effort should be made for the guidelines contained in these materials to be useful in the daily management of the disease.
ο Internet: due to the lack of standardized certifi cations about the origin, source and credibility of the online content, it is important to facilitate reliable reference website addresses and that the learner has a basic knowledge of the disease and its clinical management for proper in-terpretation of the information available.
ο Media: Newspapers, magazines, television and radio.
ο Cards, identifi cation bracelets or necklaces and transport equipment for carrying and storing of insulin devices.
ο Data on associations of people with diabetes and other support groups.
ο Psychological counselling at the time of diagnosis of diabetes mellitus type 1.
ο Provide contact phone numbers in case of emergency.
ο Other information and communication technologies (telemedicine, blogs, etc.)
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 87
D
Aspects that structured diabetes education should include:
Level 1: Survival education.
• What is diabetes mellitus. Types of diabetes.
• Symptoms of diabetes mellitus type 1.
• What is insulin. Treatment with insulin.
• What is glucose and blood glucose goals.
• Basic dietary advice.
• Acute complications (hypoglycaemia, hyperglycaemia and ketosis)
• Special situations (diabetes mellitus type 1 in school, intercurrent diseases, gastronomic celebrations, events, travels, etc.).
• Psychological impact of the disease, identifi cation of prior beliefs, fears and expectations.
• Techniques for the injection of insulin and glucagon.
• Self-analysis of capillary blood glucose meter techniques.
• Urine self-analysis technique, measurement of ketonuria, ketonemia and in-terpretation of results.
Level 2: Advanced Education.
• Physiopathology, epidemiology and classifi cation of diabetes.
• Types of insulin: absorption, action profi les, variability and adjustments.
• Food planning: qualitative and quantitative advice on immediate and fi bre intakes, with special attention to carbohydrate intake.
• Control objectives, including the concept of glycosylated haemoglobin.
• Reinforcement of knowledge of acute complications.
• Problem solving and adjustment of treatment.
• Micro-and macrovascular complications: prevention and monitoring.
• Adjustment of insulin patterns and feeding on special situations, such as exercising, holidays and travelling.
• Tobacco, alcohol and other drugs.
• Adjustment to work and driving.
• Sexuality, contraception, teratogenic drugs, pregnancy and breast-feeding.
• Updated research on diabetes mellitus type 1.
• Continuous infusion pumps.
• Foot care.
88 SNS CLINICAL PRACTICE GUIDELINES
D
Methods for teaching structured education about diabetes:
Several methods have been used successfully in diabetes education. The choice of one or the other depends on the characteristics of the patient, the disease stage and the capacity of each team or health care centre.
Individualized education.
• An intensive individualized program should be provided to newly diagnosed diabetes mellitus type 1 patients and in the case of pregnancy.
Education groups.
• The groups should be organized according to age, socio-cultural background, etc. It is desirable that family members and friends of patients also partici-pate in the groups. Group education should include the following aspects:
ο Structured training by explicative lectures.
ο Discussion groups, with analysis of the perceptions and experiences of all group members.
ο Identifi cation of fears and anxieties.
ο Assessment of needs and expectations.
ο Manifestation of personal experiences regarding hypoglycaemia, physical activity, stress response, etc.
ο Audiovisual methods.
ο Support educational material, which the patient can read at home.
D
Characteristics which structured education programs on diabetes must contain:
• Actively involve patients in all the stages of the educational program (de-sign, implementation, evaluation), providing them with the tools to make the best decisions about their own health.
• Set the benefi ts of learning new skills, including the daily monitoring of the treatment.
• Assess the educational needs of each patient.
• Assess patients’ personal perceptions.
• Be fl exible so that the programs are adapted to the specifi c educational, so-cial and cultural needs.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 89
D
• Have educational goals agreed with patients. The expectations of profes-sionals and patients may differ, so it is important to agree on common objec-tives, which may vary over time and require continuous review. Any pro-posed therapeutic target should be achievable.
• Have a syllabus and a fi xed schedule.
• Do not create a very concentrated program and schedule frequent breaks.
• Schedule lectures that do not exceed 25% of the total time, and include a time for asking and answering questions.
• Pay attention to the choice of words and expressions, avoiding an overly technical language.
• Provide standardized and consistent information between different team members.
• Plan meetings between the professionals involved, to exchange ideas, dis-cuss cases and review the program and methods.
• Facilitate that adults participate in their own health care by giving them the possibility to make judgments and choices about their own care.
• It is advisable to establish a dynamic contact process with the patient, ei-ther through visits, group discussions between patients, telephone contact or computer systems.
D
Other considerations:
• Discuss any changes that have taken place at biomedical level (new insulin requirements, glycaemia monitoring strategies, onset of ocular complica-tions, etc.).
• Evaluation: the educational program and the goals should be assessed by process and results indicators.
• Provision should be done of all the information needed to enable the de-velopment of the therapeutic education program: space required, enough qualifi ed personnel, necessary educational materials and work agendas and schedules.
90 SNS CLINICAL PRACTICE GUIDELINES
5.3. Community Support arrangements
Key question:
• How effective are the arrangements for community or extra sanitary support (schools, dia-betes associations, etc.) aimed at people with diabetes mellitus type 1?
DM1 has a major impact on the lifestyle of patients as well as their self-esteem. Both the psycho-logical characteristics of the individual and their social relationships affect the way to deal with this disease. DM1 patients and their families and caregivers, through contact and involvement with community support groups, can get information to address the needs and problems that can arise during the development of the disease.
The CPG NICE 20047 defi nes a support group as a group of people with DM1 that meets to provide support for themselves and others in their locality.” In our context, associations of people with diabetes usually carry out this role.
While these forms of community support are considered positive in the evolution of the dis-ease, it is important to know their effectiveness in terms of health.
In the CPG NICE 2004, the evidence comes from observational studies such as the DAWN study55, which states that emotional support, along with fam-ily support are key factors in the control of diabetes, and that social networks are considered at least as important as medication regarding management of the disease. Several studies have determined the following benefi ts of support groups for patients and caregivers:
• Psychological and emotional benefi ts, including improvements in the ability to deal with stress.
• Decreased burden and stress on caregivers.
• Improved quality of life.
• Improved self-care strategies through the promotion of health.
• Improved access to health services.
• Decreased isolation, overcoming depression and of the loss of self-esteem.
• Better knowledge of the conditions, symptoms and health care systems through education and information.
Observational studies
2 +
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 91
The CPG NICE 20047 affects the infl uence of psychosocial support in the acceptance of the disease, how to deal with it and the results in children and adolescents with DM1 and their families. However, the results found show a lack of good quality studies that assess the effectiveness of structured support in these patients.
RCT1+
There is evidence on the effectiveness of the systems of behavioural fam-ily therapy in reducing family confl ict related to diabetes and mentoring pro-grams with social and educational activities in young patients with DM1.
Cohort studies2+
One study56 has evaluated the interventions based on the support within the family context of peers with good results in the relationship between blood sugar levels and the support received.
Another study57 that examined the support of friends in an intervention program, found higher levels of knowledge of diabetes (p <0.0001) and a higher proportion of support from friends/family (p <0.05) compared to pre-intervention measures. The friends reported improvements in self-perception after intervention (p <0.0001), and the parents a decrease regarding the con-fl icts related to diabetes at home (p <0.05).
Cohort studies2+
An SR58 carried out by The Task Force on Community Preventive Services group studied the effectiveness of education for the self-management of diabe-tes developed outside the usual clinical settings (community assembly centres, home, workplace, recreational camps, school) reached the following conclu-sions:
• Recreational camps improve knowledge of the disease and its manage-ment in children and adolescents with DM1.
• The evidence was insuffi cient to assess both the effectiveness of edu-cational interventions in the workplace or in summer camps for DM1 patients, and to assess the effectiveness of education to co-workers and school personnel on diabetes.
SR of observa-tional studies
2++
Effectiveness of educational interventions in the workplace or in summer camps:
In a prospective study59 in 25 patients who participated in a 7-day summer camp, the effectiveness of the educational activity conducted therein was as-sessed. There was a signifi cant reduction of HbA
1C values after six and 12
months, with respect to the values before the camp, and an increase in knowl-edge about diabetes and self-control.
Descriptive study
3
92 SNS CLINICAL PRACTICE GUIDELINES
These results were confi rmed in another study60 during a fi ve-day camp in 60 patients who were taught knowledge of diabetes and self-management education (DSME) and were followed for six months to assess their level of knowledge and levels of HbA
1C, showing that children in diabetes camps
undergo a considerable blood glucose variability.
Descriptive study
3
A prospective cohort study61 compared two groups of children with DM1 (34 who received a specifi c educational program on knowledge, be-haviours, skills and psychological factors in a summer camp vs. 23 who re-ceived education and usual care). There were no signifi cant changes in mean annual HbA
1C, levels, BMI, knowledge of diabetes, anxiety, medical visits,
or in hospital admissions compared with those before the intervention. Only the adaptation to the school environment improved signifi cantly. The control group increased signifi cantly the BMI and HbA
1c levels.
Cohort studies 2+
A descriptive study was conducted on the basis of information con-tained in medical records62 of adolescents with DM1 aged 12-18 years, com-paring those who attended (n = 77) or not (n = 106) a camp for diabetes education. There was a decrease in HbA
1c levels in those attending the camp
during the follow-up compared with the baseline [mean (SD): 8.6% (1.8) vs. 8.3% (1.8)] while it increased in those who did not attend the camp [mean (DE): 8.4% (2.1) vs. 8.9% (2.3), P <0.005]. Seven months after the camp, there were still signifi cant differences in HbA
1c (p = 0.04) due to persistent
improvement in girls, but not in boys. Adherence to treatment (p <0.05) and the adjustment (p <0.05) was higher among the children who attended the camp.
Descriptivestudy
3
Another descriptive study63 examined the effects of an education pro-gram on self-management of diabetes taught to 60 patients in a 5-day camp. After training, the patients were divided into two groups based on the fre-quency of self-monitoring (<3 times/day vs.3-4 times/day) and were moni-tored for a period of 6 months. The HbA
1c was signifi cantly lower in the
group with the highest self-monitoring frequency after 3 months, but not after 6 months. Although the duration of the camp was short, there was an improvement in knowledge and a better attitude towards diabetes among the participants.
Descriptive study
3
Summary of evidence
Cohort studies
2+Social networks are key factors in controlling diabetes mellitus type 155
RCT 1+Methods of family therapy and tutoring programs with social and educational activi-ties for young patients with diabetes mellitus type 1 are effective in reducing family confl icts related to diabetes57.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 93
Cohort studies
2+
The support of friends and family in an intervention program aimed at children al-lows for higher levels of knowledge of diabetes and self-esteem56, 57.
Cohort studies
2+
Summer camps are effective in improving adherence to the treatment and metabolic control59, 60, 62, 63.
Recommendations
B (Adults)/
A(children)
Updated information should be provided to adults, children and adolescents with diabetes mellitus type 1 as well as to their families at the time of diagnosis, and periodically thereafter, on the existence of diabetes support groups, both locally and nationally and how to contact them. (Appendix 11.2.)
BThe diabetes care teams should be aware that a poor psychosocial support has a negative impact on various outcomes of diabetes mellitus type 1 in children and young patients, including glycaemic control and self-esteem.
A
Young patients with diabetes mellitus type 1 should be offered specifi c support strat-egies, such as tutoring on self-analysis supported by solution to problems, how to improve their self-esteem and glycaemic control, and retreats to exchange experi-ences, to reduce confl ict related to diabetes among family members.
√
There is no formal relationship between the health care services and diabetes associ-ations. This relationship can be benefi cial as long as the performances are confl uent. It would be advisable for a physician and/or diabetes nurse educator to participate in the diabetic associations in order to provide technical support for the activities to be developed.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 95
6. Feeding
6.1. Feeding specifi cations for people with diabetes mellitus type 1
It is important that the food intake of people with DM1 is balanced, varied and that it meets the ca-loric needs, and takes into account changes in glycaemic intakes and the relation with the insulin treatment. Young people and children with DM1 should acquire healthy eating habits to optimize their metabolic control. The food they eat should provide them enough energy and nutrients to ensure proper growth. In order to improve metabolic control and the prevention of complications, it is very important that people with this disease are aware and understand the close relationship between food and complications.
The evidence on nutrition in DM1 included in this CPG comes mainly from a high quality SR published in 201064, updated by subsequently published studies or studies not included in it.
6.1.1. Carbohydrates
Postprandial glucose levels mainly depend on the intake of carbohydrates (CH) and insulin avail-able. Adequate intake of CH is therefore a key strategy to achieve a good glycaemic control.
Three studies65, 66, 67 showed that even and regular distribution of carbo-hydrate intake during the day enhances metabolic control.
Observational studies 2 +
As for the strategy to adjust the insulin dose according to the planned intake of carbohydrates, 3 studies of patients with DM148, 68, 69 showed sig-nifi cant improvements in glycaemic control (p <0.0001), in quality of life (p <0.01) in the occurrence of severe hypoglycaemia, lipid profi le, as well as stability in the weight.
RCT 1+
The prospective observational study of Lowe et al.69, found benefi ts from the adjustment of the insulin dose and the planned intake of carbohy-drates during a one year follow up: HbA
1c decreased from 8.7% to 8.1% (p
= 0.0002), improved quality of life (p <0.05) and problem solving skills (p <0.00001).
Cohort studies2+
96 SNS CLINICAL PRACTICE GUIDELINES
Five trials examining diets with different percentages of carbohydrates did not obtain conclusive results. In two of these studies, monounsaturated fats were replaced by carbohydrates obtaining heterogeneous results regarding glycaemia and lipids70;
71. Other two studies66, 71 found benefi ts with diets low in carbohydrate percentage vs. diets high in carbohydrate percentages, while another study72, however, showed benefi ts of a diet with a high percentage of carbohydrates (80%) vs. a standard diet
RCT 1+
The Strong Health Study Study73 investigated the association between HbA1c
levels and macronutrient intake. The study included 1,284 American Indians with DM. This study found that a diet with less carbohydrate intake, along with higher consumption of total fat, saturated and monounsaturated fatty acids, was associated with poorer metabolic control.
Cohortstudies
2+
In DM1 patients who received intensive treatment in the Diabetes Control and Complication Trial 74, a diet low in carbohydrates and high in total fat and saturated fatty acids was associated with poorer metabolic control, regardless of the level of exercise and the Body Mass Index.
RCT1+
6.1.2. Sucrose (table sugar)
Fifteen studies examined the effect of sucrose intake on glycaemic control. Eleven of them lasted from 2 days to 4 months and used sucrose doses in the diet of between 19 and 42 g/day. There were no differences in metabolic control with the intake of carbohydrates in the form of sucrose or starch75, 76, 77, 78, 79, 80,
81, 82, 83, 84, 85.
RCT1+
In addition, three studies examined the effect of sucrose intake on plasma lipid levels. These studies found no signifi cant consequence75, 76, 84.
RCT1+
However, one 15-day long study comparing two diets containing 16% and 1% of sucrose respectively, concluded that the addition of sucrose in the diet increases blood glucose and lipid levels86.
RCT1+
A prospective study carried out in 19 young patients with DM187 found that, after 4 months of follow-up, HbA
1c levels decreased (p = 0.027) and cho-
lesterol and triglyceride levels were within normal ranges; thus it concluded that the sucrose consumption using the carbohydrates counting technique does not affect metabolic control in these patients with DM1.
Observational studies 2+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 97
6.1.3. Sweeteners
There are two types of substances that can sweeten foods according to their ability or inability to increase the glycaemia of the people taking it (Appendix 2):
• Non-caloric sweeteners (have no calories): saccharin, aspartame, cyclamate, acesulfame K, sucralose, etc.
• Caloric sweeteners (provide calories, raising blood sugar in a more or less abrupt way): glucose, sucrose (table sugar), fructose and polialcohols, such as sorbitol, maltitol, xy-litol, mannitol, etc.
Eight studies examined the effect of artifi cial sweeteners (AS) in people with DM1.
Three studies79, 88, 89 showed that the intake of artifi cial sweeteners has no effect on blood glucose and lipid levels.
RCT1+
A single study90 found a signifi cant decrease of blood glucose levels using sucralose.
Observational study 3
An American cross-sectional study91 found that adults and children with DM who consumed one or more light or diet drinks every day had higher HbA
1c levels than those who did not consume any drink.
Descriptivestudy
3+
Two studies examined the effect of stevioside and rebaudioside A92, 93 sweeteners and none of them found signifi cant effect on glycaemia, HbA
1c or
blood pressure in people with DM1
RCT1+
Regarding the role of fructose as a sweetener, an SR95 found that it produces a smaller increase in postprandial plasma glucose than other car-bohydrates and, therefore, could be a useful dietary sweetener for diabetics. However, fructose diets with percentages between 15% and 20% can raise levels of Low Density Lipoprotein (LDL) and triglyceride levels in men with and without diabetes96, 97 in the short-term. It was also considered that dietary fructose may foster weight gain and obesity, but there is no conclusive evi-dence on this matter.
SR of experimental
andobservational
studies1++ 2++
Within the Spanish health context, the Ministry of Health and the Diabetes Foundation published a consensus document on sweeteners and their effect on glycaemia, aimed at children with DM1. This information is available in the following web address: http://issuu.com/fundaciondiabetes/docs/alimenta-cion_ninos_diabetes0894.
Expertconsensus
4

98 SNS CLINICAL PRACTICE GUIDELINES
6.1.4. Glycaemic Index
In 1981, Jenkins et al. defi ned the concept of glycaemic index (GI) to order the food containing carbohydrates according to their ability to raise blood glucose levels compared with a reference food or food pattern, usually sugar or white bread.
There is also the concept of glycaemic load (GL), which is calculated by multiplying the glycaemic index of a food by the amount of carbohydrates it contains, expressed in grams, and dividing the total by 100. The glycaemic load serves to simultaneously describe both the quality (IG) and the amount of carbon hydrates of a particular food or dietary daily planning.
Although the balance between carbohydrate intake and insulin available is the main deter-minant of postprandial glycaemia, it has been shown that there are other factors infl uencing the glycaemic response to food intake, such as the content and type of food fi bre, fat content, the type of starch and the physical conditions of the food determined by the way it has been processed or cooked, temperature, etc.
12 studies that examined the relationship between the glycaemic index of foods and metabolic control in patients with DM167, 98 were found99, 100, 101, 102, 103,
104, 105, 106, 107, 108.
RCT1+
Of these 12 studies, an SR with meta-analysis104, an SR98 and 4 cohort studies67, 100, 103, 105 showed a benefi cial effect of a diet with low-glycaemic index food for HbA
1c.
SR ofexperimental
studies1++
Two studies, however, did not fi nd this benefi cial effect101, 102. Cohortstudies
2+RCT1+
A one day study107,108 in young people with DM1 undergoing continuous glucose monitoring showed lower mean levels of glycaemia, but no differences in the mean levels of nocturnal glycaemia with a diet rich in low glycaemic index foods.
RCT1+
In an attempt to clarify the effect of a low glycaemic index diet in people with DM1 and DM2, a review by Brand-Miller et al.104 analyzed this aspect. Considering those studies included in this SR which is at least 6 weeks long, it compared low and high glycaemic index diets, and an average decrease of 0.35% (range: 0 to 0.7%) in HbA
1c levels was found102.
SR ofobservational
studies2++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 99
6.1.5. Fibre
Five small RCTs compared a diet rich in fi bre (40-60 g) with diet low in fi bre (10-20 g) with a similar percentage of macronutrients and similar caloric con-tent. Two of them found no signifi cant difference between the two alternatives in relation to HbA
1c109, 110 and 3 demonstrated a benefi cial effect of a diet rich in
fi bre on metabolic control111, 112, 113.
RCT1+
Three studies examined the effect of fi bre intake on fasting glucose, two of which found no signifi cant effect114, 115, 116, while one study found improve-ment in fasting glucose with a diet rich in fi bre117.
RCT1+
A cross-sectional study found an inverse relationship between the amount of fi bre intake and HbA
1c levels118, while another119 did not fi nd this effect.
Descriptive study
3+
Studies carried out in the general population suggest that diets with high fi bre content (over 25 g/day) were associated with a lower risk of cardiovascu-lar diseases, due to the observed effect of a diet rich in total and soluble fi bre in reducing the total plasma cholesterol by 2-3% and LDL-cholesterol by 7%120.
SR of RCT/observational
studies 1++ 2++
6.1.6. Proteins
No direct evidence is available on the effect of protein intake in DM1 patients, as the 7 studies were performed with patients with DM2,121, 122, 123, 124, 125, 126, 127.
SR of RCT 1++ RCT1+
6.1.6.1. Proteins in patients with nephropathy
An SR Cochrane with meta-analysis on the low protein diet in diabetic nephrop-athy128, which included 12 studies, analyzed the effect of a low protein intake defi ned as “all types of dietary regimens with reduced or protein modifi cation (e.g., vegetable proteins rather than animal proteins) for a minimum period of four months” in patients with diabetic nephropathy. It showed a relative risk (RR) of end-stage renal disease (ESRD) or death of 0.23 (95% CI 0.07 to 0.72) for pa-tients assigned to a low-protein diet, after adjustment to initial values due to the existence of cardiovascular diseases (p = 0.01), and no signifi cant improvement in the glomerular fi ltration rate of 0.1 ml/min/month (95% CI: -0.1 to 0.3) within the same group. Regarding compliance, planned protein intake in the interven-tion groups ranged between 0.3 and 0.8 g/kg/day. The actual protein intake varied between 0.6 and 1.1 g/kg/day, what indicates a lack of compliance. As a recom-mendation, the authors proposed reducing protein intake to 1 g/kg/day or up to 0.8 g/kg/day in patients prepared to carry out this diet.
SR of RCT whit MA
1++
100 SNS CLINICAL PRACTICE GUIDELINES
Another SR129 analyzed 8 studies with 519 participants for a period between 6 months and 4 years, comparing a low protein diet (0.91 g/kg/day) vs. a control group (1.27 g/kg/day). No signifi cant differences were found between the two groups in the rate of glomerular fi ltration and creatinine clearance. The group with low protein diet showed a signifi cant reduction in the level of HbA
1c in 7 of the 8
trials that analyzed it [WMD 0.31% (95% CI -0.53% to -0.09%)].
RCT 1+
Nine studies investigated the effects of a low protein diet (less than 0.8 g of vegetable and animal proteins/kg/day) in the progression of nephropathy in patients with DM1. Three of these studies analyzed this effect in patients with incipient nephropathy130, 131, 132 and 5 with advanced nephropathy128, 129, 133, 134, 135, 136.
RCT1+
In patients with mild nephropathy (persistent microalbuminuria of 30-299 mg/24 hours or kidney failure in phases 1 and 2, defi ned as hyperfi ltration with glomerular fi ltration rates of 60 ml/min/1, 73 m2 of body surface), 2 studies com-pared dietary protein levels over 1 g/kg/day vs. 0.8 g/kg/day or less, proving that a poor protein intake decreases albuminuria, but has no effect on the glomerular fi ltration130, 131.
RCT1+
A study carried out in diabetic patients with incipient nephropathy showed no signifi cant effects on the glomerular fi ltration rate or excretion rate with a low protein diet vs. a normal diet132.
RCT1+
In patients with advanced nephropathy (macroalbuminuria defi ned as more than 300 mg/24 hours, chronic kidney disease (CKD) stages 3-5, defi ned as glo-merular fi ltration rate less than 60 ml/min/1, 73 m2 of body surface area), two studies found that intake of 0.7 to 0.9 g/kg/day of protein improved the excretion rate vs. the intake of 1.2 to 1.4 g/kg/day of protein, but not the glomerular fi ltration rate 133, 136.
RCT1+
Another study, however, showed no difference between the two diets134. RCT1+
Moreover, hypoalbuminemia, the malnutrition marker, was associated with a protein intake of 0.7 g/kg/day and not with a protein intake of 0.9 g/kg/day133, 136.
RCT1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 101
6.1.7. Diet for the prevention and treatment of cardiovascular disease
Five studies analyzed the effect of diet on augmented cardiovascular risk (CV) in patients with DM148, 137, 138, 139, 140, 141.
Studies examining the effects of the Mediterranean diet for at least one year141, as well as adequate control of HbA
1c levels137, 140, proved to reduce
cardiovascular risk in patients with DM1.
Observational studies
2 +
Likewise, in patients with DM1 in the DCCT study74 who received inten-sive treatment with a diet low in carbohydrates but rich in saturated and total fat showed a poorer glycaemic control (p = 0.01), a difference that remained signifi cant after adjusting for level of exercise, plasma triglycerides and body mass index (BMI) (p = 0.02).
Observational studies
2 +
Summary of evidence
RCT1+
The regular intake of carbohydrates has been shown to improve glycaemic control65, 66, 67.
RCT1+
Adjusting insulin doses based on the planned intake of carbohydrates improves metabolic control and the quality of life without producing side effects48, 68, 69.
RCT1+
The total intake of carbohydrates is the main determinant of the postprandial glucose levels, independently of the source being sucrose or starch75, 76, 77, 78, 79,
80, 81, 82, 83, 84, 85.
RCT1+
As to the effect of sucrose intake on plasma lipid levels, studies provide no conclusive data75, 76, 84, 86, 87.
Observationalstudies
2+
The intake of artifi cial non-caloric sweeteners has no signifi cant effects on short- term metabolic control in people with diabetes mellitus type 179, 88, 89, 92, 93.
SR ofobservational
studies2++
Fructose consumption in percentages between 15% and 20% of the caloric intake could produce a signifi cant increase in the levels of LDL-cholesterol and plasma triglycerides in men with and without diabetes95.
SR of RCT1++
SR of observational
2++
The use of the glycaemic index and glycaemic load may provide a modest additional benefi t to that provided by other interventions, such as carbohydrate counting. However, studies examining the effect of glycaemic index on metabolic control show great variability in the defi nition of glycaemic index and important confounding factors, so it is not possible to obtain conclusive information from them64, 67, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108.
102 SNS CLINICAL PRACTICE GUIDELINES
RCT1+
The available evidence on dietary fi bre intake in people with diabetes mellitus type 1 presents no conclusive results regarding its effect on metabolic control109,
110, 111, 112, 113, 114, 115, 116, 117, 118, 117.
SR of RCT/observational
studies1++/2++
A diet rich in total and soluble fi bre is associated with lower cardiovascular risk due to its lowering effect on total plasma cholesterol by 2-3%, and DL-cholesterol by 7%120.
SR of RCT 1 + + RCT 1 +
No direct evidence is available on the effect of protein intake in patients with diabetes mellitus type 1, as the studies found include only patients with DM2121,
122, 123, 124, 125, 126, 127.
SR of RCT 1 + + RCT 1 +
The dietary protein intake of less than 0.8 g/kg/day improves albuminuria in individuals with diabetic nephropathy, but has not shown any effect on glomerular fi ltration rates128, 129, 131, 132, 133, 134, 135, 136.
Observationalstudies
2+
Cardioprotective nutritional interventions, such as reducing saturated fatty acids, trans fatty acids and dietary cholesterol, reduce cardiovascular risk and improve the prognosis of cardiovascular disease in patients with diabetes mellitus type 148, 137, 138, 139, 140, 141, 137, 140, 74.
Recommendations
General recommendations
√
Nutrition recommendations for a healthy lifestyle valid among the general population are also appropriate for people with diabetes mellitus type 1. Currently, there are several insulin options available, allowing to adapt the best-suited insulin regimen to the taste preferences and food choices of people with diabetes mellitus type 1 in the context of a healthy diet.
√
The improvement in glycaemic control with insulin therapy is usually associated with increased body weight. As potential weight gain may adversely affect blood glucose, lipids, blood pressure and health in general, it is desirable to prevent it.
√Although the carbohydrate content of food determines the insulin dose, special attention should also be given to the total intake of proteins and fats.
Carbohydrates
AThe insulin dose should be adjusted to the carbohydrate intake in people with diabetes mellitus type 1. This recommendation should be accompanied by the support of health professionals through a comprehensive nutrition education.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 103
A In patients with diabetes mellitus type 1, foods with table sugar can be replaced with foods containing other sources of carbohydrates.
√If the patient eats food with high sugar content, its absorption should be slowed down by associating their food intake with fat or fi bre.
Artifi cial sweeteners
BIn patients with diabetes mellitus type 1 it is preferable to use artifi cial sweeteners which do not interfere with glycaemic increase (see Appendix 2).
B
It is recommended to prevent the abuse of drinks and foods sweetened with fructose. This recommendation should not be extended to the fructose contained in fruits and vegetables, as these are healthy foods that provide small amounts of fructose in a normal diet.
Glycaemic Index
AFor patients with diabetes mellitus type 1 who are assessing dietary planning based solely on the glycaemic index of foods, health professionals should inform them about the lack of conclusive evidence regarding its benefi ts.
Fibre
A
Recommendations for fi bre intake in patients with diabetes mellitus type 1 are similar to those of the general population: therefore, a diet containing 25 to 30 g fi bre/day, with special emphasis on the consumption of soluble fi bre (7 to 13 g) is advisable.
Proteins in patients with nephropathy
AIn people with diabetic nephropathy, a protein intake of less than 0.8 g/kg/day is recommended.
AIn people with advanced diabetic nephropathy (chronic renal failure in phases 3-5), a possible hypoalbuminemia should be monitored by modifying the protein and caloric intake to prevent malnutrition.
Diet for the prevention and treatment of cardiovascular disease
BNutritional interventions should be implemented to improve metabolic control and lipid profi le in the prevention and treatment of cardiovascular disease in patients with diabetes mellitus type 1.
104 SNS CLINICAL PRACTICE GUIDELINES
6.2. Eating plan recommended for patients with diabetes mellitus type 1
The recommendations regarding the diet of people with diabetes have undergone numerous fl uc-tuations over time, from the complete removal of carbohydrates and plenty of fat and protein, to the current situation, where the word “diet”, as synonym of bans and restrictions, has been ban-ished for people with diabetes. In these people it is of paramount importance to determine a meal plan according to each individual, not only taking into account circumstances such as weight, age and sex, but also the type of work, habits, schedules, physical activity, religious beliefs or economic resources. It is, in short, to adapt the meal plan to the characteristics and circumstances of each person, without forgetting that the most outstanding feature of this plan is the successful food distribution of carbohydrates throughout the day, along with the proportion of the other ma-cronutrients and observing its effect on weight.
There are many possibilities when planning food for people with DM1. The choice depends on the characteristics of each person and the availability of resources (material resources and ex-perienced professionals) to choose one plan or another.
6.2.1. Menus based method (Appendix 4)
It is based on the use of predefi ned and adapted meal plans tailored to daily menus, whilst main-taining adequate nutritional parameters.
They are very useful for those people who fi nd it diffi cult to organize themselves or are in the early stages of diabetes, a phase in which the patient or their family need simple and effective strategies.
6.2.2. Servings based method (Appendix 5)
It is based on a count of all the basic nutrients: the HC group, proteins group and lipids or fats group, thus contemplating their correct amount and distribution in the context of a healthy diet.
For an easier use there are 6 food groups based on the proportion of the most important nu-trients that contain:
1. Dairy products (HC).
2. Farinaceous (HC).
3. Vegetables and salads (HC).
4. Fruits (HC).
5. Proteins.
6. Fats.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 105
The concept serving, used as quantitative terminology, is defi ned as the amount of food con-taining 10 grams of each of the primary nutrients. For example:
20 grams of bread contain 10 grams of carbohydrates = 1 serving
50 grams of meat contain 10 grams of protein = 1 serving
10 g of oil contain 10 grams of fat = 1 serving
It should be noted that other countries use different contents of carbohydrates per serving, which is important for bibliographic queries or recipes, for example, in Germany one serving is equivalent to 12 grams of carbohydrates and in the United States, to 15 g.
Based on this servings’ method other systems have been developed to make meal plans easier.
6.2.3. Exchange and equivalents system (Appendix 6)
The system of exchange and equivalence is included as an extension of the method based on serv-ings to create a list of foods grouped by similar nutrient values. This allows, within the prescribed plan, to exchange equivalent food, offering more choice and more freedom for the design and adaptation of the menu.
Proper application requires that the person shows willingness to learn and receive proper training.
6.2.4. System based on counting carbohydrate servings
It is based on the concept that the amount and distribution of carbohydrates in the food provided is the most infl uential factor in postprandial glycaemia, although it is also important to pay atten-tion to proteins and fats.
Few studies attempt to assess the effectiveness of different types of diet in iso-lation. In fact, most studies assessed contain a specifi c method of diet included within complex and multidisciplinary education and intensive insulin therapy pro-grams. Therefore, it is diffi cult to extract the effectiveness of the diet in isolation in the overall intervention.
A poor quality methodological SR142 analyzed the dietary treatment in chil-dren and adolescents, based on studies published between 1990-2001 and found few consistent results among the 8 studies included, and concluded that the avail-able evidence cannot determine the differences between the carbohydrate count-ing method (carbohydrate counting) and the unrestricted diet.
SR1-
106 SNS CLINICAL PRACTICE GUIDELINES
The Goksen and Kalergis et al.143, 144 studies are the only studies that try to compare the HC counting method and the exchange system in isolation, outside the context of a structured program of education and intensive treatment. These studies showed no signifi cant differences between the two methods in terms of the effects on HbA
1c, BMI and quality of life.
RCT 1+
Summary of evidence
RCT 1 +
Evidence on the effectiveness of meal plans is limited and does not provide conclusive results regarding its effect on metabolic control and quality of life142,
143, 144.
Recommendations
√ A meal plan must be set adjusted to age, insulin dosage, physical activity, weight and personal situation (pregnancy, hypercholesterolemia, etc.) of the patient and his/her ability to understand.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 107
7. Exercising
Performing regular physical activity is, along with a balanced diet, one of the mainstays of the treatment of DM.
Metabolic and hormonal changes in response to exercise depend on several factors: intensity and duration of the exercise, metabolic control, type and dose of insulin administered before exer-cise, injection sites and time between the administration of insulin and the last meal.
Variations of glycaemia in connection with the exercise depend on several factors:
• Glycaemia tends to decrease during moderate-intensity aerobic exercise if a proper in-sulin level has been administered, it lasts longer than 30-60 minutes or in the absence of intake before or during the exercise.
• On the contrary, glycaemia cannot be changed if the period is short and low or moderate in intensity and adequate intakes are performed before or during the exercise.
• Finally, glycaemia tends to rise when a there is a situation of hypoinsulinemia, very intense exercise or carbohydrate intake before or during exercise is excessive.
• It is important to note that children have a smaller muscular and hepatic glycogen store and are more sensitive to the effect of exercise.
In normal people, insulin secretion decreases during moderate exercise, offsetting the in-creased insulin sensitivity in the muscle. This is not possible when the administration of insulin is exogenous, as is the case for patients with DM1. Insulin reduces the normal increase of hepatic glucose production and induces its uptake by the muscle, and also prevents the normal ascent non-esterifi ed fatty acids (NEFA) from the mobilization of fat stores. In cases of hypoinsulinemia, the production of hepatic glucose is increased and the muscle glucose uptake is reduced, and coun-terregulatory hormones (catecholamines, glucagon, cortisol and growth hormone) rise, and these changes are more prominent at higher exercise intensity. It also produces an increase in hepatic lipolysis and ketogenesis.
108 SNS CLINICAL PRACTICE GUIDELINES
7.1. Benefi ts of exercise in patients with DM1
Key question:
• What are the benefi ts of exercise for people with diabetes mellitus type 1?
The CPG NICE 20047 includes the following studies:
7.1.1. Children and adolescents
An RCT145 compared the effect on metabolic control of a program of intense regular physical activity (30 minutes three times a week for 12 weeks) in 9 children with DM1 vs. 10 children who did not participate in the program. The intervention group showed signifi cant improvement in HbA
1c levels [mean
(SD): 11.3% (0.5) vs. 13.3% (0.5), p <0.05].
RCT 1+
Another RCT146 with 32 children studied the effect of a program between workout once a week for three months and found no changes in HbA
1c levels,
urine glucose or maximal oxygen consumption.
RCT 1+
One before-after RCT evaluated the effect of three daily sessions of low intensity aerobic for two weeks (n = 20)147 obtaining an improvement in HbA
1c
levels [mean (SD): 8.28% (1.3) to 7.92% (1.42), P = 0.023] after the interven-tion.
RCT 1-
A cohort study148 with 19 143 children and adolescents with DM1 aged 3 to 20 years, evaluated the effect of regular physical activity on glycaemic control, insulin doses and frequency of hypoglycaemia.
Observational Studies
2 +
The HbA1c
levels were lower in the groups who practiced regular physi-cal activity more frequently (p <0.001), this difference remaining in all age groups and in both sexes. A higher frequency of physical activity was asso-ciated with a greater effect on HbA
1c: exercise 1-2 times per week reduced
HbA1c
levels by 30%, 3 or more times per week by 37%.
Children over 9 years who did not practice any physical activity required a higher daily dose of insulin than those who exercised 1-2 times per week (p <0.001).
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 109
7.1.2. Adults
The CPG NICE 20047 includes the following studies:
A small sample of RCT149 (n = 56) which studied the effect of a 16-week program of aerobic exercise in young men with DM1, identifi ed no signifi cant change in HbA
1c or glucose, although it did fi nd signifi cant differences regard-
ing the maximum oxygen consumption (higher) and the total cholesterol level in blood (less) in the intervention group.
RCT 1+
A prospective non-randomized study150 with a before-after design showed no signifi cant change on HbA
1c or microalbuminuria, but did fi nd signifi cant
decreases in total cholesterol and glucose compared to the starting point in the group that followed a supervised exercise program (at least 135 minutes/week) for three months compared with the group that did not perform any exercise.
Non-randomized
CT 1-
A before-after designed test151 found that an intervention consisting of a 10-hour educational module which included physical exercise three or four times a week, had no signifi cant changes in the blood glucose or fasting cho-lesterol levels.
Non-randomized
CT 1-
A small sample cross-sectional study152 found no signifi cant changes in blood pressure, lipid profi le, HbA
1c, fructosamine or glycaemia, relative to
baseline.
Descriptive study
3
The SR Conn et al.153 included 24 studies (n = 1435 adults with DM1) evaluating the effects of educational interventions that included physical ex-ercise. Despite the heterogeneity detected, it was found that interventions involving physical exercise improve metabolic control in adult patients with DM1 [Mean reduction of HbA
1c 0.33% (95% CI 0.26 to 1.28%)]. Besides
these compared the effect of interventions that included only physical exercise vs. those which also included dietary and pharmacological measures (9 stud-ies), proving that the latter had a greater effect on HbA
1c.
SR with MA of RCT
1++
110 SNS CLINICAL PRACTICE GUIDELINES
The Pedersen et al.154 SR reviewed the effect of exercise in patients with DM1 and identifi ed a protective effect on the development of cardiovascu-lar diseases, a positive effect on the lipid profi le (decreased LDL-cholesterol and triglycerides, increased HDL-cholesterol and the HDL-cholesterol/total cholesterol ratio). However, it did fi nd inconsistent results on the impact of exercise on the endothelial function. The authors of this SR concluded that although there are few studies analyzing specifi cally the effect of exercise in patients with DM1, the results indicate that there are minor differences in the metabolic control of active and inactive adults155, 156 or that there is no differ-ence149, 157, 158, 159. However, they felt that physical activity has possibly a benefi -cial effect on lipid profi le in people with DM1 by lowering LDL-cholesterol, triglycerides149 levels, increasing HDL-cholesterol and the HDL-cholesterol/total cholesterol ratio149, 158.
RT 1++/2++
An SR160 examined the effect of exercise on different result measures (glycaemic control, insulin requirement and lipid profi le) in people with DM1. No improvement was observed in terms of metabolic control through exercise, even if there was a reduction of insulin requirements, an improvement in lipid parameters, in blood pressure and on the endothelial function.
SR 1++
7.1.3. All age groups
An SR161 made in Spain analyzed the impact of exercise on metabolic control and the development of chronic complications in patients with DM1. Different results regarding the benefi ts of physical activity on glycaemic control, re-gardless of the level of evidence were observed: an SR showed no signifi -cant changes162 while another showed a signifi cant improvement of 0.33% in HbA
1c levels in the group who did take up some exercise153. From 16 RCTs,
10 showed no change and 6 found some minor improvements and from three observational studies, two showed some effects on those you had practiced exercise. The authors of the SR concluded that most of the studies show that the practice of regular physical activity affects positively (or at least does not worsen) the metabolic control of patients with DM1. Regarding the results on the development and progression of chronic complications, there is not enough information on this matter.
SR of RCT and
observational studies
1++/2++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 111
Summary of evidence
SR 1++/2++
RCT 1 +
Observational studies
2 +
In people with diabetes mellitus type 1, scientifi c evidence provides inconclusive results on the effect of regular exercise on metabolic control (HbA
1c) since some
studies fi nd benefi cial effects in patients who do practice exercise145, 147, 148, 153, while others149, 150, 152, 154, 160, 161 found no signifi cant differences with people who do not practice regular physical activity.
RCT 1 +
Observational studies
2 +
The analysis by age group has shown that the lack of studies in children and adolescents with diabetes mellitus type 1 show a benefi cial effect of physical exercise on metabolic control145, 147, 148, 163.
SR1++/2++
RCT 1 +
Most studies show that physical exercise has a positive effect on the lipid profi le, lowering LDL-cholesterol and the concentration of triglycerides, HDL cholesterol and increasing the HDL/total cholesterol ratio149, 150, 154, 160.
However, other studies have shown no signifi cant changes in lipid profi le151, 152.
SR1++
Descriptive study
3
As for the effects on blood pressure, a systematic review shows that physical exercise does decrease it160, nevertheless a descriptive study152 found no signifi cant change.
SR 1++/2++ SR 1++
Physical exercise leads to increased insulin sensitivity in patients with diabetes mellitus type 1, which is associated with a reduction in exogenous insulin intake160, of about 5%154.
Recommendations
A Patients with diabetes mellitus type 1 are recommended to do physical exercise, especially for its positive effect on the lipid profi le and on blood pressure.
AChildren and adolescents with diabetes mellitus type 1 should be highly recommended to do physical exercise as there is some evidence showing its benefi ts on metabolic control.
112 SNS CLINICAL PRACTICE GUIDELINES
7.2. Type, intensity and duration of physical exercise in people with diabetes mellitus type 1
Key question:
• What kind of physical exercise is recommended for people with diabetes mellitus type 1?
7.2.1. Children and adolescents
The CPG NICE7 includes the following studies:
An RCT145 that included 19 children with DM1 described the benefi cial effect on metabolic control of an intensive regular exercise program carried out for 30 minutes three times a week.
RCT 1 +
Another RCT146 with 32 children studied the effect of a once-a-week training program for three months, fi nding no changes in HbA
1c levels, urine
glucose or maximal oxygen consumption.
RCT 1 +
A cohort study148 with 19 143 children and adolescents with DM1 aged between 3 and 20 years found that the HbA
1c level was higher in the group
with no regular physical activity (8.4% in the group with less frequency vs. 8.1% in the group with greater frequency, P <0.001). This effect was found in both sexes and in all age groups (p <0.001). A multiple regression analysis revealed that regular physical activity was one of the most important factors that infl uence the HbA
1c level. There was no association observed between the
frequency of regular physical activity and the frequency of severe hypoglycae-mia or hypoglycaemia with loss of consciousness or convulsions. The study authors concluded that the regular practice of physical activity in children and adolescents with diabetes mellitus type 1 should be recommended, being the recommended frequency 3 or more times a week. This study defi ned “regular physical activity” as physical activity systematically practiced at least once a week for at least 30 minutes, excluding sport practiced at school.
Observational studies
2 +
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 113
7.2.2. Adults
The CPG NICE 20047 includes the following studies:
A prospective nonrandomized study150 with a before-after design con-cluded that conducting a supervised exercise program of at least 135 minutes per week for a period of three months, produces signifi cant benefi ts it decreas-es glucose levels and plasmatic cholesterol.
Non-randomized
CT 1-
A before-after study151 concluded that the practice of physical training three or four times a week, did not produce any signifi cant metabolic response.
Observational study
2+
In an SR154, it was recommended that people with DM1 should perform at least 30 minutes of moderate intensity physical activity every day or 3-4 hours a week in the form of light walk, cycling, swimming, rowing, golf, etc. In ad-dition, it was advised to include periods of mild exercise for 5 to 10 minutes before and after training with an adjustment of hydrocarbon intake and take into account the presence of autonomic neuropathy to adjust the intensity of exercise.
SR1++/2++
The Carral et al.161 SR noted that two clinical trials which examined the effects of exercise training programs with strength and muscle resistance exer-cises showed no signifi cant effects on the levels of HbA
1c164, 165.
SR1++/2++
Summary of evidence
2 + + Observational
study 2 +
In children and adolescents with diabetes mellitus type 1, the practice of moderate to intense exercise three to fi ve times a week for 20 to 60 minutes, produced a signifi cantv improvement on metabolic control145, 146, 148.
SR 2 + +
Moderate-intensity both aerobic and anaerobic exercise for 30 minutes a day or 3-4 hours a week, showed to have benefi cial effects in adult patients with diabetes mellitus type 1154.
Non-randomized
CT 1 -
Observational study 2 +
There is no clear relationship between the characteristics of physical exercise and the effects on metabolic control150, 151, 161, 164, 165.
114 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
A People with diabetes mellitus type 1 should be encouraged to perform regular physical exercise.
APeople with diabetes mellitus type 1 should be recommended moderate physical exercise for at least 135 minutes a week, without being more than two consecutive days without doing physical exercise.
√People with diabetes mellitus type 1 and their families should be informed that they can participate in all forms of exercise, providing they know how to perform the appropriate adjustments to the intake and insulin.
√The people with diabetes mellitus type 1 who wish to participate in less common/or specifi c risk sports should be educated on this matter, however it is not advisable to perform these alone.
√
People with diabetes mellitus type 1 and their families should be encouraged to monitor blood glucose levels before and after exercise to learn about the glycaemic response in different conditions of exercise, and make the necessary adjustments before, during or after it.
√People with diabetes mellitus type 1 and their families should be informed about late hypoglycaemia risk in situations of intense and/or prolonged exercise, to take the necessary precautions.
√People with diabetes mellitus type 1 and their families should be informed that exercise is contraindicated if there are high levels of blood glucose and/or ketones in the blood or urine.
√Young people and adults with diabetes mellitus type 1 who want to do intense physical exercise should consult a doctor to rule out microvascular complications that contraindicate it.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 115
8. Glycaemic Control
8.1. Glycosylated haemoglobin
Key question:
• What are the target values of glycosylated haemoglobin?
• What are the criteria for the standardization and presentation of glycosylated haemoglobin analytic results?
The risk of arterial disease and microvascular complications in people with diabetes is associated with inadequate metabolic control over time. Glycosylated haemoglobin (HbA
1c) has proved to
be a good indicator of metabolic control, but since very strict control is associated with more episodes of hypoglycaemia, it is important to identify the optimal value of this parameter to guide the treatment of people with diabetes.
8.1.1. Glycosylated haemoglobin target fi gures
The CPG NICE 20047 includes the results of a randomized trial published by the Diabetes Control and Complications Trial Research Group166 and the follow-up of that same cohort167, which assessed the occurrence of microvascular complications, comparing a group of 638 insulin dependent patients with intensive therapy (mean HbA
1c levels of 7%) vs. another group
of 638 diabetic patients treated with conventional therapy (mean HbA1c
levels of 8.8%). After 6.5 years of follow-up, it was observed that the group who underwent intensive therapy reduced the risk of retinopathy by 75%, and its progression by 54%, the risk of microalbuminuria decreased by 56%, the risk of neuropathy was reduced by 69% and its progression by 57%. However, there was three times the risk of hypoglycaemia and a higher rate of overweight in the intensive treatment group than in the conventional treatment group.
RCT 1
A medium-high quality SR from 8 RCTs (1,800 patients with DM1)168 evaluated the effect of long-term glycaemic control on macrovascular com-plications in patients with DM1 and DM2, comparing intensive treatment vs. non-intensive treatment, with an average difference of 1.25% (-11 mmol/mol) of HbA
1c levels between the two groups. It was found that patients with DM1
and intensive treatment had lower risk of macrovascular events [RR of macro-vascular events 0.38 (95% CI 0.26 to 0.56) and RR of cardiac events 0.41 (CI 95% CI 0.19 to 0.87), RR of peripheral vascular events 0.39 (95% CI: 0.25 to 0.62)].
SR of RCT 1 + +
116 SNS CLINICAL PRACTICE GUIDELINES
A high quality cohort study169 studied 879 patients with DM1 with no cardiovascular or kidney disease at baseline. These patients were divided into 4 groups according to their mean levels of HbA
1c at baseline: group 1, HbA
1c
= 5.6 - 9.4% (70 mmol/mol), group 2, HbA1c
= 9.5 - 10.5% (81 mmol/mol), group 3: HbA
1c = 10.6 - 12% (96 mmol/mol), group 4: HbA
1c = 12.1 to 19.5%
(171 mmol/mol). After a 20-year follow-up, the incidence of cardiovascular and overall mortality was compared between the groups. Analyzing the HbA
1c
as a continuous variable, it was observed that each HbA1c
unit increase was associated with a RR for death from all causes 1.16 (95% CI: 1.08 to 1.24) and RR for cardiovascular mortality 1.20. By analyzing the HbA
1c as a qualitative
variable, it was observed that people with greater than or equal to 7% HbA1c
showed an RR for mortality from all causes 2.66 (95% CI: 1.16 to 6.11) and RR for cardiovascular mortality 3.50 (95% CI 1.09 to 11.23).
Cohort studies 2+
A cross-sectional descriptive study170 reported a positive correlation (r = 0.427, p <0.001) between HbA
1c levels and severity of coronary disease, as
measured by the Gensini scale.
Descriptive study
3
8.1.2. Criteria for the standardization and presentation of glycosylated haemoglobin analytical results
Considering the variability of how analytical results are expressed in HbA1c
in Spain in 2002 (70% expressed in units JDS/JSCC and 30% in units NGSP/DCCT), a paper from expert consensus has been published in Spain to recommend a series of measures for the harmonization in stating the HbA
1c
results171.
The points agreed upon were as follows:
1. Laboratories shall use traceable methods to the IFCC reference method.
2. Following international recommendations172, it is agreed to issue HbA1c
results in two types of simultaneous units in all laboratory reports: NGSP/DCCT % units (with a decimal) and IFCC (mmol/mol) (no decimals).
3. The publications and clinical guidelines developed from the date of the agreement include the two units in their texts.
4. The transformation into units NGSP/DCCT (%) will be performed through different conversion equations, using the information technology systems of each laboratory:
• If working with calibration JDS/JSCC (Japan): NGSP (%) = 0.985 × JDS/JSCC % + 0.46.
• If working with Mono-Sweden calibration (Sweden): NGSP (%) = 0.923 × Mono – Sweden % + 1.34.
• If working with IFCC calibration (%): NGSP (%) = 0.915% + 2.15 × IFCC.
Expertconsensus 4
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 117
• To calculate the equivalent in IFCC units (mmol/mol) starting from NGSP/DCCT (%) units: IFCC (mmol/mol) = (NGSP % - 2.15/0.915) × 10.
5. The methods used should have an imprecision (coeffi cient of variation) of less than 4%, but the ultimate goal should be to achieve an accuracy of less than 2%.
6. In transient situations, such as the current use of JDS/JSCC (%), it is recommended to inform, if necessary, during a transitional period (12-14 months) in both units JDS/JSCC (%) and NGSP/DCCT (%) units.
7. The societies that underwrite this document will undertake to implement education and outreach programs for its members.
8. Including estimated mean glucose (eAG) with glucose and HbA1c
in glycaemic status reports is not based on enough scientifi c evidence to allow its use in the clinic. To determine the actual role it could play in the clinical practice, further research is required in all groups of diabetic patients, including paediatric patients, pregnant women and elderly, as well as the various ethnic groups.
Summary of evidence
RCT 1 +
Intensive therapy with medium HbA1c
levels of 7% reduces the microvascular complications risk but increases the risk of hypoglycaemia166, 167, 168, 169.
SR of RCT 1 + +
HbA1c
levels greater than 7% increase cardiovascular and death due to all causes risk168, 169, 170.
Recommendations
A
It is recommended to inform people with diabetes mellitus type 1 and their families of the benefi ts of a long-term metabolic control with HbA
1c levels
below 7% (46 mmol/mol) without disabling hypoglycaemia, therefore the care measures must be designed to achieve these aims.
√The aims of the treatment should be individualized and agreed with the patient, assessing the risks and benefi ts.
√The goals should be less demanding in people with a history of severe hypoglycaemia, no recognition of hypoglycaemia, patients with limited life expectancies, young children and patients with chronic concomitant diseases.
DThe HbA
1c results should be issued in two types of units simultaneously on all
laboratory reports: NGSP/DCCT % units (with a decimal) and IFCC (mmol/mol) (no decimals) units.

118 SNS CLINICAL PRACTICE GUIDELINES
8.2. Systems of Continuous Glucose Monitoring
Key question:
• Do the continuous glucose monitoring systems improve metabolic control?
In people with diabetes mellitus type 1 it is considered appropriate to assess blood glucose levels in different times during the day: before and after meals, before, during and after exercise, and occasionally overnight. However, intermittent measurements by capillary glucose do not always provide enough information about the time when the glucose changes, and, if it does, how fast it does so and in what direction. To overcome these limitations, systems have been developed that allow continuous glucose monitoring (CGM) in interstitial fl uid for more than 50 years.
On the one hand, non-invasive continuous monitoring systems have been searched for: en-zyme electrochemical sensors, spectroscopy, infrared or other, although currently most are under development173, 174, 175.
The MCG systems marketed today are invasive and measure the amount of glucose within the interstitial fl uid using a subcutaneous electrochemical enzyme sensor (Dexcom ®, Medtronic ®, Navigator ® systems), or by obtaining samples of interstitial fl uid by microdialysis techniques (Menarini ®)176, 177. These devices require capillary glucose measurements for calibration178.
Moreover, one must distinguish two types of MCGs according to the way the reading of the data is performed: with retrospective or real time reading.
In systems with retrospective reading, the information is downloaded after use, allowing adjustments in the therapy of patients with diabetes. Initially, the reading period was 72 hours, now it reaches up to a week.
In real-time systems a computer program, providing an interstitial glucose reading every few minutes, allowing adjustments of the real-time therapy, processes the information. In addition, these systems allow analyzing trends and set alarms for hypoglycaemia and hyperglycaemia and predictive alarms. The duration of the real-time sensor currently marketed is approximately one week. The technological evolution of the MCG is fast and constantly evolving, thus leading to the improvements of the monitoring systems.
The recommendations of the CPG NICE 20047 do not apply to this guide as technological developments in terms of comfort, applicability and capacity of monitoring devices in real time in recent years cannot compare the results of the current devices with those existing years ago. Therefore, only the evidence published in the last 7 years has been taken into account.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 119
8.2.1. Retrospective monitoring
Two meta-analysis179, 180 which included 7 and 5 randomized trials, respectively, including the one conducted by Chico et al.181 in Spain, concluded that using retrospective continuous monitoring systems is not associated with signifi cant reductions in HbA
1c compared to frequent capillary blood self-
analyses [HbA1c
reduction difference 0.22% (95% CI -0.439 to 0.004), P = 0.055].
Descriptive study
3
For continuous monitoring during pregnancy, a study of patients with DM1 and DM2 has demonstrated an improvement in HbA
1c levels and lower
macrosomia rates using retrospective MCG182. 71 pregnant women with dia-betes were studied, 46 of them with DM1, comparing the use of MCG (n = 38) versus standard 0glycaemic controls (n = 33), with treatment adjustments based on the results observed. The women with MCG had lower HbA
1c levels
during the last weeks of pregnancy [mean (SD): 5.8% (0.6)] than the group without MCG [mean (SD): 6.4% (0.7)]. The children of mothers with MCG had lower standard deviation values regarding birth weight [0.9 vs. 1.6, (95% CI: 0.0 to 1.3)]; smaller mean weight percentiles (69 vs. 93), and, above all, a reduced risk of macrosomia [OR 0.36 (95% CI 0.13 to 0.98)], compared to children of mothers with standard control.
RCT 1+
8.2.2. Real-time monitoring
The STAR1183 study performed a prospective trial with an integrated insulin pump and continuous glucose sensor system (Paradigm Real Time ®). 146 patients with DM1 and HbA
1c > 7.5% were randomized in 2 comparison
groups: continuous infusion pumps and real-time MCG vs. infusion pump and frequent self-analysis in capillary blood. After 6 months of follow-up, no signifi cant differences were found in HbA
1c levels between the two groups.
RCT 1+
The Juvenile Diabetes Research Foundation (JDRF) published a study in 2008184 that included 322 patients, randomly assigned to real time MCG (n = 165) or conventional monitoring via frequent capillary blood self-analysis (n = 156), and were evaluated for 6 months. Most patients used CSII (67-84%, depending on the groups) and measured their blood glucose levels more than 5 times a day with a capillary blood glucometer. 87% of the sample had an average HbA
1c level which was less than or equal to 8% (56 mmol/mol). In
patients older than 25 it was found that the average HbA1c
level was lower and statistically signifi cant in the MCG group [difference -0.53% (95% CI: -0.71 to -0.35), P <0.001].
RCT 1+
120 SNS CLINICAL PRACTICE GUIDELINES
Regarding side effects, the differences were not statistically signifi cant. The authors of this RCT concluded that the effect of MCG was strongly cor-related with age and that these devices can help motivated adults who are able to improve their glycaemic control.
This same group185 conducted a 26-week study with 126 patients with DM1 and good metabolic control (HbA
1c <7%). The group with MCG main-
tained its HbA1c
levels, while the group without MCG showed a 0.3% dete-rioration in HbA
1c levels (p <0.001). No differences were found in the number
of hypoglycaemias between the two groups, which was the study’s primary endpoint.
RCT 1+
Another study published by the JDRF185 evaluated the effectiveness of the continuous glucose monitoring system (CGM) used on a daily basis in patients with DM1. Patients who were assigned to the control group (n = 219), showed a decrease in the use of the monitoring system over time, although it was signifi cantly lower in those over 25 years (p <0.001). Regarding glycae-mic control, a signifi cant decrease in HbA
1c levels (p = 0.01) was observed.
RCT 1+
Summary of evidence
RCT 1 +
The continuous glucose monitoring systems (both retrospective and real time) developed in recent years have shown a slight improvement after a one year follow up of metabolic control in adult patients with diabetes mellitus type 1 179,
180, 181, 182, 183, 184, 185.
Recommendations
A
Although continuous glucose monitoring can be an instrument to improve or maintain metabolic control in patients motivated and trained in intensive care, if it is used continuously, its universal use is not recommended for people with diabetes mellitus type 1.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 121
8.3. Inpatient or outpatient clinical management of patients with diabetes mellitus type 1 at the time of diagnosis
Key question:
• What are the benefi ts and drawbacks of the management of patients with diabetes mellitus type 1 in the hospital at the time of diagnosis, compared with outpatient level management?
Traditionally in our health context, when a person is diagnosed with diabetes mellitus type 1, he/she was admitted into hospital in order to normalize blood sugar levels and control the symptoms and complications of the disease. During his/her stay in hospital, the patient and his/her family were educated about the disease. It is interesting to analyze the effectiveness of interventions per-formed in other health care settings, such as outpatient or home treatment, which, in the case of showing its usefulness, could arise as alternatives to hospitalization and therefore avoid the stress associated with hospitalization.
The CPG NICE 20047 analyzed the results of 13 trials and concluded that home care (home-based) carried out by a local clinical group specialised in diabetes management including permanent telephone contact, is as safe and ef-fective as hospital management, and therefore recommends that at the time of diagnosis of DM1 children and adolescents should be offered home or hospital care according to their clinical circumstances and the wishes of the family, and the proximity of the home to the hospital (strength of recommendation A).
The SR of Clar et al.186 includes seven studies that provide evidence for the following outcome measures:
CPG 1+
Metabolic Control
Four studies assessed HbA1c
levels relative to inpatient or outpatient management of patients with DM1 at the onset of the disease 187, 188, 189, 190. Two of the studies 187, 189 found no differences in HbA
1c levels (1, 2 and 5
years follow-up) between the two options, while in a third study188, HbA1c
values were lower in the group of ambulatory or home based patients than those treated in the hospital: 0.7% less after 2 years (p <0.05) and 3 years (p <0.02) of follow-up.
SR of RCT1+ +
122 SNS CLINICAL PRACTICE GUIDELINES
Psychosocial and behavioural measures
• Knowledge of diabetes The three studies that measured parental knowledge about diabetes188,
190, 191 found no signifi cant differences between the comparison groups in any of the points in time evaluated.
• Adherence to the treatment Dougherty et al. found no differences between the comparison groups regarding adherence to the treatment after one month, 12 months, or 24 months, according to what parents or adolescents reported. The reported adherence ranged from 66% to 86% 188.
On the contrary, Galatzer et al reported higher adherence rates in the out-patient/home based group than the hospital group (85% vs. 65.5%, P <0.001), but this effect is due to the behaviour of the group with a higher socioeconomic status192.
Siminerio et al. found no signifi cant differences in the adherence of the subscales regarding food and exercise regulation, while the group treated in the hospital scored signifi cantly higher on the subscale of glucose regulation (p <0.01)191.
• Family Impact In the study by Dougherty et al., no differences were observed be-tween the groups in the scores on the Family Assessment Scale after one month, 12 months and 24 months 188.
Galatzer et al. found higher rates of positive adaptation in the family relationship in the outpatient or home group (84% vs. 68%, p <0.02), but again, this result was observed in the socioeconomically higher group and was not evident in the lower socioeconomic group 192.
Siminerio et al, with the Family Assessment Device found no signifi -cant differences between groups in the subscales on general function-ing, problem solving, communication, affective involvement and af-fective response in any of the points in time evaluated. However, the outpatient group scored better in the behavioural control (p <0.005) and in the subscales roles (p <0.05) a month after the onset of the disease. No signifi cant differences were found between the groups of outpatients and inpatients in the share of responsibilities regarding diabetes care for children and their families 191.
Srinivasan et al. 190 found no signifi cant differences between the two groups with the scale Parent Emotional Adjustment to Diabetes Scale or the Diabetes Responsibility and Confl ict Scale after 6 or 12 months.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 123
• Coping and Stress The Dougherty and Siminerio et al studies 188, 191 showed no signifi cant differences between the two groups in the stress scales perceived when evaluating the parents after a month, 12 months or 24 months.
• Satisfaction with the treatment and quality of life The Dougherty and Siminerio et al studies 188, 191showed no signifi cant differences between the groups in the scales of satisfaction and quality of life in the assessments carried out after a month, 12 months or 24 months 188, 191.
• Truancy and performance at school or work Neither the Galatzer et al. nor the Dougherty et al. studies found any signifi cant differences between the groups in performance at school or work or school absences, respectively 188, 192.
Complications
• Need for hospital admissions or emergency unit visits The studies that analyzed this outcome187, 190, 191 found no signifi cant differences between the comparison groups in hospitalization, nor vis-its to the emergency units related to diabetes.
• Acute complications None of the four studies that analyzed severe hypoglycaemia, hyper-glycaemia and ketosis, diabetic ketoacidosis or chronic hyperglycae-mia 187, 188, 190, 193 showed signifi cant differences between the two com-parison groups for more than 5 years.
Summary of evidence
SR 1 + +
Ambulatory education at the onset of diabetes mellitus type 1 is as effective as hospitalization, provided that the patient is clinically well, his/her home is near the hospital and there is a hospital sanitary organization (12 hour day hospital and 24 hour telephone contact)7, 186, 187, 188, 189, 190, 191, 192, 193.
Recommendations
A
At the time of diagnosis of diabetes mellitus type 1 outpatient care and education can be offered versus hospital management, according to the clinical needs, circumstances and wishes of the patient and the patient’s home proximity to the health services, provided that there are no acute complications and that enough sanitary infrastructure can be guaranteed to ensure adequate health care quality.
124 SNS CLINICAL PRACTICE GUIDELINES
8.4. Preparations of insulin in the treatment of patients with diabetes mellitus type 1
Key question:
• What is the effectiveness and safety of the different insulin preparations?
Since the eighties new forms of insulin, called “insulin analogues” synthesized with genetic re-combination techniques are available. The fast acting analogues have fewer tendencies to be combined in hexamer complexes than human insulin and are absorbed more easily, so its onset of action is faster, its peak of action is higher and its duration is shorter. Currently, in the Spanish market there are three products with these features: lispro, aspart and glulisine.
Slow acting analogues (glargine) produce a more prolonged release of insulin and no peaks, with a lower risk of hypoglycaemia.
Insulin analogues have sought to imitate the physiological profi le of basal insulin secretion, improve the pharmacokinetic profi le of conventional insulins to overcome the limitations they had.
8.4.1. Fast acting analogues vs. human insulin
8.4.1.1. Adults. Fast acting analogues vs. human insulin
The CPG NICE 20047 analyzed a total of 20 good quality RCTs that compared fast-acting insulin analogues with soluble human insulin.
Eleven of these studies used a parallel design (2,425 patients were treated with an analogue treatment of fast acting insulin, 1821, with soluble insulin)194,
195, 196, 197, 198, 199, 200, 201, 202, 203, 204. In these studies, the levels of HbA1c
were lower [WMD -0.14% (95% CI -0.19 to 0.08%)] in patients using fast acting insulin analogues, compared with those treated with soluble human insulin.
RCT 1+
These results were confi rmed in the analysis for each insulin analogue. Thus the results of 8 RCTs comparing lispro insulin vs. soluble human insu-lin194, 195, 196, 197, 198, 199, 200, 201 showed a lower level of HbA
1c [WMD -0.13% (95%
CI -0.24 to -0.02%)] in the group that continued the treatment with fast acting insulin analogues.
RCT 1+
In addition, 3 RCTs comparing aspart insulin vs. soluble human insulin obtained a similar result [WMD -0.14% (95% CI: -0.20 to -0.07%)]202, 203, 204.
RCT1+
Twelve RCTs using a crossover design194, 205, 206, 207, 208, 209, 210, 211, 212 showed no signifi cant differences in HbA
1c levels in the treatment with fast acting insu-
lin analogues vs. soluble human insulin (WMD 0% (95% CI -0.09 to 0.08%)].
RCT1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 125
Seven systematic reviews that have examined the effectiveness and safe-ty of fast acting analogues vs. human insulin 213, 214, 215, 216, 217, 218, 219 have been located. In this guide, for the update of the CPG NICE 2004, the Cochrane review of Siebenhofer et al 214 will be used, due to its rigorous methodology regarding the defi nition of the disease, have a longer follow-up period (mini-mum 4 weeks) and include more recent studies. Although there is a review with a publication date later than that of Siebenhofer et al. 213, with a review period, which is very similar to the previous one and very similar results and conclusions, it applies less rigorous inclusion criteria, so the GEG has decided to disregard it.
SR of RCT1++
Metabolic Control
In the Cochrane review of Siebenhofer et al. 214 were 20 RCTs were analyzed, the WMD of HbA
1c was statistically signifi cant in favour of the insulin
analogue compared with human insulin [WMD -0.1% (95% CI: - 0.2% to -0.1%)]. However, in the sensitivity analysis carried out, the higher quality tests showed no better HbA
1c levels with insulin analogues, therefore the
above results should be considered with caution.
Sixteen RCTs compared lispro vs. human insulin and found no signifi cant differences HbA
1c [WMD -0.1% (95% CI: -0.2% to 0%)].
Six RCTs compared aspart with human insulin and found no signifi cant differences [WMD -0.1% (95% CI: -0.2% to 0%)].
No studies specifi cally designed to investigate the possible long-term ef-fects were found.
SR of RCT1++
In the study by Chen et al. 220 the HbA1c
levels measured after 12 weeks of treatment were better in the insulin aspart group than in the group with human insulin [geometric mean (range) 8.2 (6.7 to 9.7) vs. 8.7 (7.4 to 11.4), P <0.05].
RCT1+
An SR with meta-analysis221 that compared insulin analogues vs. human insulin included 68 RCTs and found a slightly greater reduction of HbA
1c with
lispro [WMD -0.09% (95% CI -0.16 to -0.02), P <0.05] and with aspart [DMP -0.13 (95% CI: -0.20 to -0.07) p <0.05] than with human insulin.
SR of RCT1++
Hypoglycaemia
In 10 of the studies included in the review of Siebenhofer et al.194, 195, 208, 212, 222,
223, 224, 225, 226, 227, with a total of 4266 patients, there were fewer hypoglycaemic episodes with insulin analogues than with human insulin [Weighted mean difference (WMD) of mean overall hypoglycaemic episodes per patient per month -0.2 (95% CI -1.1 to 0.7)].
SR of RCT1++
An SR 219 observed that in 13 of the 27 studies with fast acting insulin analogues a signifi cant reduction in the number of episodes of hypoglycaemia per patient per month [mean (SD) 14.0 (3.7) p <0.05] took place.
SR of RCT1++
126 SNS CLINICAL PRACTICE GUIDELINES
An RS with meta-analysis 221 compared insulin analogues vs. human in-sulin included 68 RCTs and found that use of insulin lispro led to a lower risk of severe hypoglycaemia [RR 0.80 (95% CI: 0.67 - 0.96)] and a lower rate of nocturnal hypoglycaemia [RR 0, 5 (95% CI 0.42 to 0.62)].
SR of RCT1+
Quality of Life
Twelve studies202, 205, 207, 208, 209, 226, 227, 228, 229, 230, 231, 232, 233, 234 analyzed aspects related to quality of life, but there was great heterogeneity in terms of the instruments and measurement scales used. Assessing quality of life with the most used instrument, the Diabetes Treatment Satisfaction Questionnaire, showed no signifi cant differences between the treatment used in 3 studies, while 4 studies found improvement in the group treated with insulin analogues in relation to the convenience, fl exibility and continuation of the treatment.
RCT1+
In an SR219 the quality of life in 13 of the 27 studies with insulin ana-logues vs. human insulin was assessed; 11 of which showed improvement and 2 showed no signifi cant changes.
SR of RCT1+
Summary of evidence
SR of RCT 1 + +
In adult patients with diabetes mellitus type 1, treatment with fast acting insulin analogues produces a slight improvement in glycaemic control, (overall less than 0.1% of HbA
1c)220, 221, 235 and less hypoglycaemic episodes, 194, 195, 208, 212, 222,
223, 224, 225, 226, 227 than the treatment with human insulin.
Some studies indicate that the treatment with analogues could improve the quality of life of patients, although the results are not consistent202, 205, 207, 208, 209,
226, 227, 228, 229, 230, 231, 232, 233, 234, 219.
It is not known how this treatment affects the development and evolution of microvascular complications, as there are no long-term data.
Recommendations for adults
A
In adults with diabetes, type 1 fast acting insulin analogues cannot be recommended in a generalised way, as they have similar effectiveness to human insulin and there is no evidence to ensure its long-term safety.
However, as these provide greater fl exibility in their administration, patients are more satisfi ed, which may improve adherence to the treatment. It is therefore advisable to make an individualized assessment of the treatment.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 127
8.4.1.2. Children and adolescents. Fast acting analogues vs. human insulin
The CPG NICE 20047 included 3 RCTs in children and adolescents that compared fast-acting analogues vs. human insulin207, 236, 237 and found no signifi cant differences in the metabolic control assessed based on the HbA
1c levels [WMD -0.03% (95% CI -0.21 to 0.14%)].
Metabolic Control
Two RCTs carried out in prepubertal children233, 238 assessed the difference between lispro and human insulin and found no signifi cant difference in the HbA
1c levels between the two drugs.
RCT1+
A subsequent study239 carried out with 26 children aged between 2 and 7 showed little difference between the treatment with aspart or human insulin.
RCT1+
Two studies carried out in adolescents, Holcombe et al.240, 241, found no signifi cant differences in metabolic control in this population group using fast acting analogues or human insulin.
An SR with meta-analysis221 that compared insulin analogues vs. human insulin and included 68 RCTs found no signifi cant difference in HbA
1c levels
between lispro and human insulin.
RCT1+
Hypoglycaemia
The trials that examined the incidence of hypoglycaemia in prepubertal patients236, 238 and adolescents240 found no signifi cant differences in the type of insulin used. Neither showed differences in the rate of severe hypoglycaemia in prepubertal children237.
The results of the studies were not consistent in the number of nocturnal hypoglycaemic episodes in children before puberty: of the three studies exam-ining the rate of overall nocturnal hypoglycaemic episodes, two found no sig-nifi cant differences237, 238 and one identifi ed differences statistically signifi cant in favour of the treatment with analogues240.
RCT1+
An SR with meta-analysis221 which compared insulin analogues vs. hu-man insulin included 68 RCTs and found only signifi cant differences in the risk of nocturnal hypoglycaemia in adolescents with lispro insulin versus hu-man insulin [RR 0.61 (95% CI 0.57 to 0.64)].
SR of RCT1++
Growth
The study by Mortensen et al.241 found lower increase in BMI in adolescents treated with aspart vs. those patients using human insulin; the difference was statistically signifi cant only in men [mean (SD) -0.13 kg/m2 (0.16) vs. 0.41 kg/m2 (0.18), P = 0.007].
RCT1+
128 SNS CLINICAL PRACTICE GUIDELINES
Summary of evidence
SR 1 + +
In children and adolescents with diabetes mellitus type 1, treatment with fast acting insulin analogues has not shown differences in glycaemic control or incidence of hypoglycaemic episodes compared with the results obtained with human insulin221; 236; 237; 233; 238; 240; 241, 221, 236, 237, 233, 238, 240, 241.
Recommendations for children and adolescents
A
In children and adolescents with type 1 diabetes, the widespread use of fast acting insulin analogues cannot be recommended, since they have similar effectiveness to human insulin and there is no evidence to ensure their long-term safety.
However, as they do provide greater fl exibility in their administration, patient’s satisfaction increases, thus it may improve adherence to the treatment. It is therefore advisable to make an individualized assessment of the treatment.
8.4.1.3. Pregnant. Fast acting analogues vs. human insulin
Metabolic control
Two trials carried out in pregnant women242, 243 found a similar HbA1c
re-duction in the group treated with lispro insulin analogue and the group treated with human insulin.
SR of RCT1++
An SR244 assessed the effectiveness of fast acting insulin analogues in pregnancy. The authors believe these drugs to be very helpful during preg-nancy, as they reduce postprandial hyperglycaemia better than human insulin.
SR of RCT1++
Hypoglycaemia
Regarding the risk of undergoing hypoglycaemic episodes, the Persson et al.242 study found that the rates of biochemical hypoglycaemias were signifi cantly higher in the gro up of analogues compared with the group of human insulin (5.5% vs. 3.9%, P <0.05), while the study by the Insulin Aspart Pregnancy Study Group243 found no signifi cant differences between the two treatments.
Regarding severe hypoglycaemic episodes, in the fi rst study, 2 women who were treated with human insulin had 4 severe hypoglycaemic episodes vs. no episode in any patient in the group with insulin analogues. Meanwhile, the study of Mathiesen et al. 243 showed no signifi cant differences.
RCT1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 129
In an SR244 the authors considered interesting the use of fast acting insulin analogues, since they can reduce episodes of pre-prandial hypoglycaemia.
SR of RCT1++
Adverse Effects
Two trials243, 245 found no signifi cant difference between the treatments in relation to the number of cases of live births, foetal loss or congenital malformations.
RCT1+
An SR246 examined the effectiveness and safety of analogues during preg-nancy and concluded that, although there are only studies on lispro and aspart during pregnancy available, studies show that teratogenicity, antigenicity and autoantibodies placental transport of these drugs is similar to human insulin.
SR of RCT1++
Summary of evidence
SR of RCT1++
In pregnant women with diabetes mellitus type 1, the results of the studies in terms of metabolic control, hypoglycaemia and adverse effects on the foetus of fast acting analogues vs. human insulin are not consistent242; 243; 244; 245; 246.242, 243,
244, 245, 246.
Recommendations in pregnant
AIn pregnant women with diabetes type 1, the use of human insulin is recommended by its demonstrated effi cacy and its greater safety against the use of analogues.
8.4.2. Slow-acting analogues vs. human insulin
8.4.2.1. Glargine vs. retarded human insulin (NPH)
8.4.2.1.1. Adults
The CPG NICE 20047 does not include studies that provide evidence on this matter.
Metabolic Control
In an SR247, 11 studies (n = 3279) examined the effects of glargine on metabolic control. The results were inconclusive, because only 5 studies demonstrated statistically signifi cant results in favour of glargine compared to human insulin (NPH) and the differences found were not clinically relevant (less than 1%).
SR of RCT1++
130 SNS CLINICAL PRACTICE GUIDELINES
Another SR248 compared NPH insulin preparations vs. slow acting ana-logues for basal insulin replacement in patients with DM1, administered sub-cutaneously once a day or more. 23 randomized controlled trials were iden-tifi ed. A total of 3,872 patients were analyzed in the intervention and 2915 in the control group. The weighted mean difference (WMD) for the level of HbA
1c was -0.08 (95% CI -0.12 to -0.04) in favour of slow-acting analogues.
The WMD between the groups in plasma glucose levels and fasting blood was -0.63 (95% CI: -0.86 to -0.40) and -0.86 (95% CI: -1.00 to -0.72) in favour of the analogues. The weight gain was more signifi cant in the control group. No differences were found in the number or acuteness of severe adverse events or deaths.
SR of RCT1++
A high quality SR with meta-analysis249 assessed differences in HbA1c
, the incidence of hypoglycaemias and weight gain between the treatment with human insulin and slow acting insulin analogues in adults with DM1. A total of 20 RCTs comparing NPH human insulin (2486 patients) with slow insulin analogues (detemir or glargine) (3693 patients) were selected. 7 of the 20 stud-ies showed a signifi cant improvement in HbA
1c levels in patients treated with
analogues (no differences in the remaining 13); in total there was a signifi cant reduction in HbA
1c levels with analogues [-0.07 % (95% CI -0.13 to -0.1), P
= 0.026]. In terms of weight, 9 studies found a signifi cantly lower gain with detemir vs. NPH, with differences in BMI [0.26 kg/m 2 (95% CI 0.06 to 0.47), P = 0.012]. However, no differences were found in the BMI when comparing insulin glargine with NPH insulin.
SR of RCT1++
An SR with meta-analysis221 which compared insulin analogues vs. hu-man insulin and included 49 RCTs with slow-acting insulin analogues, report-ed a small decrease in HbA
1c, but statistically signifi cant [WMD -0.11% (95%
CI -0.21 to -0.02)], with insulin glargine vs. NPH insulin.
SR of RCT1++
Hypoglycaemias
The review of Tran et al.247 showed no signifi cant differences in terms of overall, severe or nocturnal hypoglycaemias.
SR of RCT1++
Another SR248 found no signifi cant differences in the risk of hypoglycae-mias in patients treated with slow-acting analogues [OR 0.93 (95% CI 0.8 to 1.08)] vs. patients treated with NPH insulin. However, the differences were signifi cant for severe and nocturnal hypoglycaemic episodes: [OR 0.73 (95% CI 0.61 to 0.87) vs. 0.70 (95% CI: 0.63 to 0.79)] respectively. The WMD be-tween the NPH insulin groups and slow-acting analogues for hypoglycaemic events was not signifi cant [WMD -0.77 (95% CI: -0.89 to -0.65)].
SR of RCT1++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 131
An SR with meta-analysis249 of 16 studies compared the use of analogues (n = 264) vs. NPH (n = 225). With respect to hypoglycaemia and nocturnal hypoglycaemia, the risk was signifi cantly lower with slow acting insulin analogues [OR 0.73 (CI 95% 0.60 to 0.89), P = 0.002) and OR 0.69 (95% CI: 0.55 to 0.86), p = 0.001, respectively]. Comparing the analogues, detemir was associated with signifi cantly fewer episodes of hypoglycaemia and nocturnal hypoglycaemia than NPH.
SR of RCT1++
A meta-analysis SR221 that compared insulin analogues vs. human insulin, included 49 RCTs with slow-acting insulin analogues. No signifi cant differ-ences were found between the groups of insulin glargine and NPH insulin using equivalent doses in both groups.
SR of RCT1++
Quality of Life
The study by Kudva et al.250 found no statistically signifi cant differences regarding the score on the Fear of Hypoglycaemia Questionnaire scale among glargine users, but did fi nd statistically signifi cant differences in a lower score on the scale of concern among the glargine users.
RCT1+
Another study251 found a better score in glargine users for all areas of the Diabetes Treatment Satisfaction Questionnaire (DTSQ), which assesses satis-faction, usability, fl exibility and willingness to continue with the treatment. Meanwhile, with the Well-Being Questionnaire (WBQ) found no signifi cant differences between the treatments in relation to the presence of depression, anxiety, energy and wellbeing.
RCT1+
Safety
Four studies 252, 253, 254, 255 have suggested a relationship between the use of insulin glargine and cancer development, which has led the Committee for Medicinal Products for Human Use of the European Medicines Agency to conduct an assessment whose fi ndings are not yet available.
(http://www.ema.europa.eu/humandocs/PDFs/EPAR/Lantus/40847409en.pdf).
CohortStudies
2+
Summary of evidence
SR1++RCT1+
Cohortstudies
2+
In adults with diabetes mellitus type 1, glargine offers slight advantages versus NPH insulin in respect to metabolic control and occurrence of hypoglycaemia. As for the effects on the quality, the results are not conclusive221; 247; 248, 249, 250, 251, 252, 253, 254, 255.
132 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
BThe use of glargine versus NPH can be recommended in adults, although the lack of data on long-term safety should be noted.
√
Regarding the current safety of glargine, it is recommended not to take any regulatory action or instruct a change of treatment to the patients using insulin glargine until the results of the evaluation of the Committee for Medicinal Products for Human Use (CHMP) of the EMEA are published.
8.4.2.1.2. Children and adolescents
Metabolic Control
An RCT found statistically signifi cant differences in favour of glargine in HbA
1c256: in 14 children aged 6 to 12 years. On the contrary, another study257,
carried out with 42 young people aged between 6 to 21 years, found no signifi cant differences in HbA
1c levels.
SR of RCT1+
An SR with meta-analysis 221, which compared insulin analogues vs. hu-man insulin in 49 RCTs with slow acting insulin analogues, showed no signifi -cant differences in metabolic control in children or adolescents.
SR of RCT1++
Hypoglycaemia
Schober et al.258 found no signifi cant differences between the intervention group with glargine and the group treated with NPH insulin, either in severe hypoglycaemia (23% vs. 29%), or severe nocturnal hypoglycaemia (13% vs. 18%).
RCT1+
The SR by Singh et al.221 found no signifi cant differences between glar-gine vs. human insulin in severe hypoglycaemias and nocturnal hypoglycae-mias in children.
SR of RCT1++
Ketoacidosis
A prospective observational study259 analyzed 10,682 patients under 20 years with DM1 with at least 2 years of evolution of the disease, and a seven-year follow-up. The total rate of ketoacidosis episodes which required admittance to hospital /100 patients per year was on average (SD) 5.1 (0.2). While patients using insulin glargine or detemir (n = 5317) had a higher incidence of ketoacidosis episodes than those using NPH insulin. This difference remained signifi cant after the adjustment for age at diagnosis of DM1, HbA
1c, insulin
dose, sex, and history of emigration [OR 1.357; (95% CI: 1.062 to 1.734)].
Observa- tionalstudy
2+

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 133
Quality of Life
Regarding quality of life, the study by Hassan et al. 257 found no signifi cant differences between the two treatments.
RCT1+
Adverse Effects
The study by Schober et al. 258 found less severe adverse effects (reactions at the site of injection, antibody formation and ocular reactions) with glargine (p <0.02), while Hassan et al. 257 found no signifi cant differences between the treatments.
RCT1+
Summary of evidence
RCT 1 +
In children older than 6 years, no signifi cant differences have been found between the treatment with glargine vs. NPH human insulin in terms of metabolic control, hypoglycaemia and quality of life 221, 256, 257, 258.
A higher rate of episodes of ketoacidosis with insulin glargine than with NPH insulin was found 259.
Recommendations
B
The widespread use of glargine is not recommended in children with diabetes mellitus type 1 over 6 years, since no benefi t has been demonstrated for the use of NPH. It is therefore recommended to individualize treatment based on the preferences and circumstances of each patient.
√
The treatment with glargine is not recommended in children with diabetes mellitus type 1, aged 6 years or less, since there is no evidence to compare glargine vs. NPH in this age group and there is already an effective and safe therapeutic alternative.
8.4.2.1.3. Pregnant women
Summary of evidence
SR of observational
studies2 + +
An SR246 analyzed the safety of analogues during pregnancy. The results show a similar rate of congenital malformations with insulin glargine as with human insulin.
134 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
B
For the time being and waiting for new evidence on the safety of glargine, the use of NPH as basal insulin during pregnancy is recommended. Individually, its use could be considered in cases of signifi cant worsening of metabolic control with NPH or in the presence of hypoglycaemias.
8.4.2.2. Detemir vs. human insulin.
8.4.2.2.1 Adults
Metabolic Control
In the review by Tran et al.247, in which the levels of HbA1c
in 2937 patients with DM1 we analyzed, no statistically signifi cant differences were found between detemir and human insulin [WMD -0.05 (95% CI -0.12 to 0.03)].
SR of RCT1++
Another RS248 compared patients with NPH insulin vs. slow acting ana-logues basal for insulin replacement in DM1 patients administered subcutane-ously once a day or more. 23 were identifi ed in randomized controlled trials. A total of 3,872 and 2,915 participants in the intervention and control groups, respectively were analyzed. The WMD for HbA
1c was -0.08 (95% CI -0.12 to
-0.04) in favour of slow-acting analogues. The WMD between the 2 groups in fasting glycaemic levels was -0.63 (95% CI: -0.86 to -0.40) and -0.86 (95% CI: -1 to -0.72) in favour of the analogues. The weight gain was more signifi -cant in the control group. No differences in the number or characteristics of severe adverse events or deaths were found.
SR of RCT1++
Hypoglycaemias
In the review by Tran et al.247 no differences between treatments related to overall hypoglycaemia [RR 0.99 (95% CI 0.97 to 1.02)] were found, but there were in terms of nocturnal hypoglycaemia [RR 0.89 (95% CI 0.82 to 0.97)] and severe hypoglycaemia [RR 0.75 (95% CI 0.59 to 0.95)] in favour of detemir users. For severe hypoglycaemia signifi cant differences were found in studies that used bolus insulin analogue (aspart) [RR 0.70 (95% CI 0.52 to 0.95)], but not for those using human insulin bolus [RR 0.83, (95% CI 0.56 to 1.22)].
SR of RCT1++
In the SR by Vardi et al. 248, the number of patients experiencing at least one episode of severe or nocturnal hypoglycaemia was lower in the group us-ing detemir and glargine, but the number of total events did not differ. Detemir insulin had a greater infl uence on this parameter, with lower heterogeneity. The number of episodes was lower both with detemir and with glargine for total and nocturnal events, but not for serious episodes.
SR of RCT1++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 135
Summary of evidence
SR1 + +
In adult patients with diabetes mellitus type 1, detemir provides better metabolic control and lower rates of hypoglycaemia than NPH retarded human insulin247; 248.
Recommendations
AThe use of detemir vs. NPH in adults with diabetes mellitus type 1 can be recommended, although the lack of data on long-term safety of this insulin should be noted.
8.4.2.2.2. Children and adolescents
Only one unblinded 26-week long RCT of parallel design has been located260, comparing detemir vs. human insulin, both combined with aspart insulin in 140 prepubertal children (6 to 11 years) and 207 pubertal (12 to 17 years).
RCT1+
Metabolic Control
No signifi cant differences in HbA1c
levels were found between the treatment groups [WMD -0.1% (95% CI: -0.1 to 0.3)] 260.
RCT1+
Hypoglycaemias
No signifi cant differences were found in overall hypoglycaemia [RR 0.89 (95% CI 0.69 to 1.14)], or daytime hypoglycaemia [RR 0.92 (95% CI 0.71 to 1.18)]. Regarding the risk of nocturnal hypoglycaemia, the differences are statistically signifi cant in favour of detemir [RR 0.74 (95% CI 0.55 to 0.99), P = 0.041] 260.
RCT1+
Summary of evidence
RCT 1 +
The limited available evidence shows no benefi ts of detemir compared with NPH insulin in children with diabetes mellitus type 1, in terms of glycaemic control and daytime hypoglycaemia, although detemir could be used as an alternative in case of nocturnal hypoglycaemias260.
Recommendations
AThe widespread use of detemir cannot be recommended in children with diabetes mellitus type 1, although this therapy should be considered in children with nocturnal hypoglycaemia or threat thereof.
136 SNS CLINICAL PRACTICE GUIDELINES
8.4.2.3. Glargine vs. detemir
Pieber et al.261 in an unblinded RCT of parallel design, with 320 patients, compared detemir vs. glargine in people receiving aspart before meals. The decrease in HbA
1c levels was similar in both groups: 8.8 to 8.2% (64 to 58
mmol/mol) in the detemir group and from 8.7 to 8.2% (63 to 58 mmol/mol) in the glargine group.
The overall risk of hypoglycaemia was similar with both treatments, whereas the risk of severe and nocturnal hypoglycaemia was less among the detemir users.
RCT1+
An RCT262 compared the effi cacy of both drugs in 443 patients with DM1 adults and at least after one year from the time of diagnosis. After 52 weeks of follow-up these showed no signifi cant difference in the estimated HbA
1c
mean between the detemir and glargine groups (7.57% and 7.56%, respec-tively [Mean difference 0.01% (95% CI: -0, 13 to 0.16)] or in the proportion who achieved HbA
1c levels below 7% without severe hypoglycaemias (31.9%
and 28.9%, respectively).
RCT1+
Regarding the pharmacokinetics of these drugs, an RCT263 studied 24 patients with DM1: mean age (SD) 38 years (10), BMI 22.4 kg/m 2 (1.6), and HbA
1C 7.2% (0.7) to compare the pharmacokinetics and pharmacodynamics
of insulin analogues glargine and detemir. After two weeks of treatment with glargine or detemir insulin administered once a day (randomized, double blind, crossover), in patients treated with glargine, the plasma glucose remained as mean (SD) 103 mg/dl (3.6) up to 24 hours, and all the participants completed the study. Blood glucose levels increased progressively after 16 hours of treat-ment with detemir insulin, and only 8 participants (33%) completed the study with blood glucose less than 180 mg/dl. Detemir has effects similar to those of insulin glargine during the fi rst 12 hours after administration, but the effects are lower for 12 to 24 hours after administration.
RCT1+
Summary of evidence
RCT 1 +
Analogues glargine and detemir have not shown signifi cant differences between them in terms of metabolic control and the overall risk of hypoglycaemia, although detemir appears to have a lower risk of severe and nocturnal hypoglycaemia than glargine.
The most relevant clinical distinction between glargine and detemir, is the necessity of having 2 doses in the case of some patients using detemir, something that affects the quality of life 261, 262, 263.
Recommendations
A
Both detemir and insulin glargine have similar effects in adults with diabetes mellitus type 1 in terms of metabolic control and hypoglycaemia, being insulin glargine that which can provide a higher quality of life for patients as detemir insulin should be administered in some cases twice a day.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 137
8.5. Indications of the continuous subcutaneous insulin infusion pump (insulin pump or CSII)
In order to improve metabolic control, people with type 1 diabetes must inject different types of insulin several times a day (multiple dose insulin injection therapy or MDI) and determine their blood glucose levels at least 4 times a day. The aim of therapy with continuous subcutaneous in-sulin infusion pump (CSII or insulin pump) is to provide an accurate, continuous and controlled insulin input, and in pulses that can be regulated by the user to meet their objectives of glycaemic control. Different to the MDI therapy, the CSII offers patients the possibility of maintaining opti-mal metabolic control without insulin injections several times a day but, in return, require a lot of responsibility, discipline, training, education and dedication.
It is interesting to assess the aspects that infl uence the effectiveness and safety of the insulin pump therapy in order to establish the criteria for its indication.
8.5.1. Adults
The CPG NICE 20047 recommends the CSII as an option for people with DM1, provided that the treatment with MDI (including, where appropriate, the use of insulin glargine) has failed and provided that the people receiving treatment are responsible and competent.
CPG1++
The updated NICE guideline on insulin pumps 9 based on the systematic review by Cumminns et al.264 considered that, in comparison to the optimized MDI therapy, the CSII therapy achieved a slight improvement in HbA
1c, lev-
els, although its main value may be in reducing other problems such as hypo-glycaemia and the “dawn phenomenon” and on improving the quality of life by allowing greater fl exibility in the treatment.
CPG1++
Metabolic Control
The meta-analysis by Jeitler et al.235 included 12 RCTs that examined the level of HbA
1c at the end of the treatment, comparing the effi cacy and safety
of CSII vs. MDI on a daily basis.
The pooled analysis of 6 RCTs showed better metabolic control with the CSII therapy as measured by the level of HbA
1c [WMD -0.43% (95% CI: -0.65
to -0.20)], but in the studies measuring overall HbA1c
, the difference was not statistically signifi cant [WMD -0.60% (95% CI -1.34 to -0.14)].
The meta-analysis which combined data from studies that lasted less than 6 months found a WMD in the level of HbA
1c of -0.4% (95% CI: -0.82 to
-0.01). The studies which lasted 6 months or more, showed a difference of -0.7% (95% CI: -1.24 to -0.19).
SR of RCT 1 + +
138 SNS CLINICAL PRACTICE GUIDELINES
In studies of parallel design, the WMD in the level of HbA1c
was -0.9 [(95% CI: -1.64 to -0.10) I2 = 85%] in favour of CSII, with a reduction of 1.2%. In studies of crossover design, this difference was -0.4% units [WMD -0.4 (95% CI: -0.68 to -0.07) I2 = 52%].
On the other hand, the meta-analysis by Cummins et al.264 found no sig-nifi cant differences in the control of HbA
1c in users of the CSII therapy vs.
MDI users, being the WMD -0.64% (-1.28 to 0.01) after 4 months, -0.26% (-0.57 to 0.05) after 6 months, and -0.61% (-1.29 to 0.07) after 12 months.
SR of RCT1++
A more recent review265 presented a meta-analysis of studies in adults and identifi ed an HbA
1c level slightly lower in CSII users than with MDI [WMD
-0.18% (95% CI: -0.27 to -0.10)].
SR of RCT1++
In another SR266, in studies that included participants aged above 18 years267, 268, 269, 270, 271, 272, 273, 274, 275, 276, 277, 278, 279, 280 the mean difference of HbA
1c
was -0.3% (95% CI: -0.5 to -0.1) in favour of CSII compared with MDI.
SR of RCT1++
A before and after designed study carried out within our health environ-ment281, which included 20 patients with DM1 analyzed the effect after CSII therapy vs. the previous situation, where they received intensive therapy, found a better metabolic control (reduction in the incidence of symptomatic hypogly-caemia, improvements in HbA
1c levels [mean (SD) 7.99 (1.76) vs. 7.19 (0.51),
p = 0.001], and improved lipid profi le without changes in weight and with less insulin requirements. The patients’ satisfaction was higher with CSII.
Quasi-experi-mental study
1-
A multicentre, controlled and randomized study282 analyzed the effective-ness of the CSII therapy with sensors (n = 244) vs. MDI (n = 241) and found, after a one year follow-up, a signifi cant decrease from an 83% of HbA
1c at
basal level in both groups to 7.5% in the pump therapy group and 8.1% in the MDI group.
RCT1+
Total insulin requirements
The meta-analysis by Cummins et al.264, with data from 4 studies found a signifi cant reduction in mean insulin dose in CSII users compared to MDI [WMD UI -11.90 (-18.16 to -5, 63)]; a statistically signifi cant difference.
SR of RCT1++
In the meta-analysis by Jeitler et al.235 of the 14 studies that examined the effects of CSII on insulin requirements, 7 found that these were signifi cantly lower in patients treated with CSII than with MDI on a daily basis.
SR of RCT1++
An RCT283 found that the total insulin requirement at the end of the study was lower in the CSII group than in the MDI group [mean (SD) 36.2 (11.5) IU/day vs. 42.6 (15.5) IU/day].
RCT1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 139
Hypoglycaemias
In the meta-analysis by Jeitler et al.235 the number of overall hypoglycaemia events was similar: range from 0.9 to 3.1 episodes/patient/week in the group treated with CSII, and 1.1 to 3.3 in the group treated with MDI; the median weekly episodes was 1.9 and 1.7, respectively.
SR of RCT1++
Cummins et al.264 found 8 RCTs published between 2002 and 2007 that examined the number of episodes of hypoglycaemia. The RCT by Doyle et. al 284 found a statistically signifi cant difference in favour of the group treated with CSII vs. the group treated with MDI.
SR of RCT1++
A systematic review265 with meta-analysis found no signifi cant differenc-es in severe hypoglycaemia [OR 0.48 (95% CI: 0.23 to 1)], nocturnal hypo-glycaemia [OR 0.82 (95% CI 0.33 to 2.03)] or mild hypoglycaemia [OR -0.08 (95% CI -0.21 to 0.06)].
SR of RCT1++
In another SR266 23 studies that randomized 976 participants with DM1of all ages to treatment with CSII or MDI were included. No obvious differences were observed between the interventions in relation to non-severe hypoglycae-mia, but severe hypoglycaemia seemed to be reduced among patients assigned to the treatment with CSII.
SR of RCT1++
Other adverse effects
The available evidence on the adverse effects of CSII is generally scarce and of poor quality.
In reviewing Jeitler et al.235, only 4 of the 22 studies included information on serious adverse effects other than hypoglycaemia and not related to diabe-tes or its treatment. Incidence rates were generally low: in 2 studies279; 285 no serious adverse effects were observed and in another study286 only one severe adverse event (ketoacidosis) was reported in the intervention group with CSII. Another team287 reported 15 severe adverse events (ketoacidosis) in the group treated with MDI, as compared to 20 events in the CSII group.
Of 10 studies that provided information on episodes of ketoacidosis, only one274 found a signifi cant difference between the treatments, with the highest incidence of ketoacidosis in the group using MDI. The methodological quality of this study was low, so the results should be considered with caution.
Four studies278, 285, 287, 275 analyzed the problems at the site of injection, which were more frequent in patients treated with CSII.
SR of RCT1++
140 SNS CLINICAL PRACTICE GUIDELINES
Quality of Life
The systematic review by Barnard et al.288 analyzed the effect of the use of CSII in the quality of life of patients with DM1. Of the two RCTs involving adult patients, one study found moderate gains in quality of life268, although there was a high dropout rate and the other study found no signifi cant differences280.
SR of RCT1++
Cummins et al. found two studies published between 2002 and 2007284,
289; none of them showed signifi cant differences in quality of life between the treatments.
SR of RCT1++
In the SR by Misso et al.266, the measures of quality of life showed better results with CSII than with MDI.
SR of RCT1++
Costs
According to a study carried out in the Spanish context290, the average cost of the treatment with CSII was € 25,523 per treated patient, considering data from 2005. A cost-utility analysis indicates that although the CSII is a more expensive technology than MDI, it is a bit more effective than MDI (assuming a gain control base of HbA
1c of -0.51% in favour of the CSII therapies) with
a cost/utility incremental ratio of 29,947 €/QALY.
Economic evaluation
(cost-utility analysis)
Summary of evidence
Adults
SR of RCT 1 + + RCT 1 +
For adults with diabetes mellitus type 1, four systematic reviews235; 265; 266; 291, an RCT282 and a quasi-experimental study281 found a signifi cant improvement of metabolic control with the continuous subcutaneous insulin infusion pump therapy (CSII or insulin pump) vs. the multiple dose insulin injection therapy. However, a systematic review264 has not shown signifi cant differences between the treatments.
SR of RCT 1 + + RCT 1 +
The treatment with continuous subcutaneous insulin infusion pump (CSII or insulin pump) decreases the total requirements of insulin compared to the multiple dose insulin injection therapy in adults with diabetes mellitus type 1235,
264, 283.
SR of RCT 1 + +
The rate of hypoglycaemia is similar using the continuous subcutaneous insulin infusion pump therapy (CSII or insulin pump) or the multiple dose insulin injection therapy in adults with diabetes mellitus type 1235, 264, 265, 266, 267, 284.
SR of RCT 1 + +
The evidence comparing the quality of life of the treatment with continuous subcutaneous infusion insulin pump (CSII or insulin pump) vs. the multiple dose insulin injection therapy does not provide conclusive results in adults with diabetes mellitus type 1266, 284, 289.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 141
8.5.2. Children and adolescents
Metabolic Control
An RCT292 (n = 30), which compared the effi cacy of CSII vs. the therapy with MDI in children and adolescents with newly diagnosed DM1, found lower levels of HbA
1c with the CSII therapy after 2 years of follow up.
RCT1+
Another RCT293 compared the effectiveness CSII vs. MDI once a day, in 14 young people with newly diagnosed DM1 during the fi rst 28 to 62 days of treatment. During the intervention period, the treatment with CSII was as-sociated with lower levels of HbA
1c [mean (SD) 10.9 (0.6%) vs. 14.6 (0.7%),
P <0.005], lower fasting blood glucose levels and glycosuria, but at the end of the intervention period this difference persisted only statistically signifi cant in HbA
1c levels.
RCT1+
In an RCT with young people aged 13 to 19 years 294 no differences in HbA
1c levels were found 1 year after the onset of the treatment with CSII,
compared with the insulin injection therapy 1 or 2 times a day (n = 14).
RCT1+
The meta-analysis by Fatourechi et al.265 did not fi nd, in children, a sta-tistically signifi cant difference in the levels of HbA
1c [WMD -0.20% (95% CI:
-0.43 to 0.03)] between those using CSII or MDI.
SR of RCT1++
In the RCT by Doyle et al.284, no signifi cant differences were found in HbA
1c levels [8.1% vs. 7.2% (p <0.05)] between the group treated with CSII
vs. the group treated with MDI.
RCT1+
The Opipari-Arrigan et al.295 study in children aged around 4.5 years, found no signifi cant differences between the group treated with CSII vs. the group treated with MDI.
RCT1+
An RCT in young children with an average age of 4 years296 found that HbA
1c levels were not different in children treated with CSII vs. those children
receiving the MDI therapy (7.9 vs. 7.7%).
RCT1+
In an SR266, from studies that included participants under 18 years284, 297,
298, 299, 300, 301, 302, the mean difference in HbA1c
levels was -0.2% (95% CI: -0.4 to -0.03) in favour of the CSII therapy, compared with MDI.
SR of RCT1++
Insulin requirements
Three studies 284, 303, 296 found that insulin requirements were lower in patients treated with CSII; the result was statistically signifi cant in two of them, including adolescent patients.
RCT1+
Hypoglycaemia
The review by Fatourechi et al.265 performed a meta-analysis of parallel designed RCTs in children and found a signifi cantly higher rate in CSII users [WMD 0.68 (95% CI: 0.16 to 1.20), p = 0, 03)].
SR of RCT1++
142 SNS CLINICAL PRACTICE GUIDELINES
A meta-analysis of RCTs of crossover design, in adolescents and adults267, showed no signifi cant differences in episodes of mild hypoglycaemia per week among CSII and MDI users.
SR of RCT1++
Quality of Life
Three RCTs carried out in children found no signifi cant differences between the treatments296, 304, 305, while 2 RCTs271;301 did fi nd signifi cant differences in favour of the CSII therapy.
RCT1+
Summary of evidence
Children and adolescents
SR of RCT 1 + +
RCT 1 +
The results of studies in children and adolescents with diabetes mellitus type 1 do not provide conclusive information on the effects of the treatment with continuous subcutaneous insulin infusion pump in relation to metabolic control, hypoglycaemias and quality of life compared with the multiple daily insulin injections treatment265, 266, 284, 292, 293, 294, 295, 296, 297, 298, 299, 300, 301, 302.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 143
8.5.3. Pregnant women
Three systematic reviews examined the use of CSII vs. the conventional intensive therapy in pregnant women: a review by Farrar et al.306, the Nosari et al.307 study, which included 31 women with DM1 (32 pregnancies) and the Card et al.308 study, which included 15 women with DM1 and 14 with DM2.
SR of RCT1++
The SR by Farrar et al.306, which included two systematic reviews indi-cated that no signifi cant differences have been demonstrated in perinatal mor-tality [RR 2 (95% CI 0.20 to 19.91)], in foetal abnormalities [RR 1.07 (95% CI 0.07 to 15.54)], in maternal hypoglycaemia [RR 3 (95% CI 0.35 to 25.87)] or maternal hyperglycaemia [RR 7 (95% CI 0.39 to 125.44)].
Summary of evidence
SR of RCT 1 + +
In pregnant women with diabetes mellitus type 1, the available evidence shows no differences between the treatment with continuous subcutaneous insulin infusion pump (CSII or insulin pump) vs. multiple daily insulin injections regarding perinatal mortality [RR 2 (95% CI: 0.20 to 19.91)], foetal abnormalities [RR 1.07 (95% CI 0.07 to 15.54)], maternal hypoglycaemia [RR 3 (95% CI 0.35 to 25.87)], maternal hyperglycaemia [RR 7 (95% CI 0.39 to 125.44)], or macrosomia rate [RR 3.20 (95% CI 0.14 to 72.62)]306, 307, 308.
Recommendations
√
The treatment with continuous subcutaneous insulin infusion pump is not a universal option for all patients with diabetes mellitus type 1, as candidates for this treatment must have a high level of diabetes education and have the support of a health team expert in this type of therapy. Therefore, to achieve greater profi tability of the treatment, a proper selection of the candidate patients should be carried out, taking into account the metabolic control, the risk of acute complications acute and the higher cost.
A
The use of insulin pumps in patients with poor glycaemic control or disabling hypoglycaemias which have made invalid other conventional treatments (multiple dose insulin therapy) and which are able to achieve good adherence to the treatment, is recommended.
√
The HbA1c
level is not the only criterion to be considered when recommending the use of CSII treatment in pregnancy. This treatment option should be considered when a target less than 7% of HbA
1c level has not been achieved,
after previously having optimized other aspects, integrating data from metabolic control, presence of diffi cult to manage hypoglycaemia, the quality of life of patients and the availability of the resource in the workplace.
144 SNS CLINICAL PRACTICE GUIDELINES
8.6. Methods of insulin administration in patients with diabetes mellitus type 1
The usual route of administration is subcutaneous insulin (SC), except in the case of diabetic decompensation, when intravenous (IV) is generally used with fast acting insulin and with less frequency, intramuscularly (IM). Administration may be by disposable syringes or pre-fi lled pens.
It is of interest to know whether the use of these methods of administration may result in different health outcomes and to examine the patients’ preferences regarding these alternatives.
8.6.1. Disposable syringe vs. pre-fi lled pen
8.6.1.1. Adults
The CPG NICE 20047 provides the following evidence:
Metabolic Control
Five RCTs carried out with adult patients with DM1309, 310, 311, 312, 313 found no signifi cant differences between patients using disposable syringes or pre-fi lled pens, in relation to HbA
1c, glucose profi les (except in blood glucose
levels before dinner, which were signifi cantly lower in the group with the pen in the study by Murray et al.), or in relation to the episodes of hypoglycaemia.
RCT1+
Acceptability and patient preferences
The CPG NICE 20047 included 6 RCTs of crossover design310, 311, 312, 313, 314, which analyzed the patients’ preferences regarding injection techniques and found greater preference for prefi lled pens vs. disposable syringes (range of percentage of patients who preferred prefi lled pens: 96-74%).
RCT 1 +
Two RCTs315, 316 and an SR317 confi rmed the patients’ preference for pre-fi lled pens vs. disposable syringes, with values of 82%, 70% and 75% of pa-tients, respectively.
RCT 1 +
SR of RCT 1 + +
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 145
Another SR318, which included 5 studies analyzed patients’ adherence to insulin prefi lled pens vs. insulin disposable syringes; hypoglycaemic episodes, visits to the emergency unit due to hypoglycaemia, and the costs associated with diabetes and health care. The results stated that there was greater adher-ence to the treatment with insulin pre-fi lled pens than with syringes. In addi-tion, with the use of pen devices, the consumption of healthcare resources and costs decreased.
SR of RCT1++
A study carried out with 79 patients who had diffi culties to self-adminis-ter insulin315 found a higher percentage of patients who could self-administer insulin without help from caregivers or nurses with prefi lled pens than sy-ringes (53% vs. 20%).
RCT1+
Costs
An economic evaluation conducted in the Spanish context319 carried out an analysis on how to minimise costs by assuming that the 3 systems compared (syringe, prefi lled pen and prefi lled syringe) were equally effective in controlling the level of blood sugar. The estimated average cost for insulin injection was € 0.383 with syringe, € 0.341 with pre-fi lled pen, and € 0.329 with prefi lled syringe, resulting prefi lled pens and syringes more effi cient than syringes.
Economic analysis
A study in people with diffi culties to self-administer 315 found that use of prefi lled pens supposed savings because less insulin was wasted than with conventional syringes and assumed a lower cost associated with the time spent by nurses.
Economic analysis
8.6.1.2. Children and adolescents
The CPG NICE 20047 provides the following evidence:
Metabolic Control
The CPG NICE 20047 included an RCT320 comparing prefi lled pens vs. conventional syringes in 113 children and adolescents with DM1, aged between 8 and 18. This study showed no differences between the two systems in HbA
1c levels [mean (SD) 10.58 (2.4%) vs. 10.27 (2.6%)], in hypoglycaemic
episodes or unacceptably high levels of blood glucose.
RCT1+
Another study carried out with 20 children and adolescents with DM1, and aged between 8 and 19 years321, compared some specifi c prefi lled pens (Novopen II ®) vs. standard syringes, and found no differences between the treatments regarding the risk of nocturnal hypoglycaemia.
RCT1+
146 SNS CLINICAL PRACTICE GUIDELINES
Acceptability and patient preferences
The CPG NICE 20047 included an RCT320 that compared the preferences of children with DM1 between using the conventional syringe and the prefi lled pen, and found that 99.5% of the participants in the study preferred the prefi lled pens versus the conventional syringe.
RCT1+
In another study321 all participating children (n = 20) showed preference for the prefi lled pen against the conventional syringe.
RCT1+
8.6.2. Comparison of pre-fi lled pens
In the unblinded study of crossover design by Valk et al.322, prefi lled pens were compared for 6 months (Innovo ® and NovoPen 3 ®) and no signifi cant differences were found between the two options in terms of HbA
1c levels,
blood glucose levels, hypoglycaemia episodes or adverse effects.
RCT1+
Summary of evidence
RCT 1 +
The available evidence shows no differences in effectiveness or safety between the prefi lled pens and syringes in children and adults with diabetes mellitus type 1 309, 310, 311, 312, 313, 320, 321.
From the perspective of the patient preferences, evidence shows a greater predilection of patients for the pens rather than syringes187, 311, 312, 313, 314, 320, 321.
Recommendations
AThe use of pre-fi lled pens is recommended because they can encourage adherence to the treatment, but it will be the patient who decides on the administration system used.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 147
8.7. Insulin administration techniques
There is consensus regarding the best route of administration of insulin being the subcutaneous (SC). However, many factors can affect the subcutaneous absorption of insulin: type of insulin, patient gender, body mass index, morphology and abdominal fat distribution, site of injection, subcutaneous tissue thickness of the target area and the injection technique. Other factors to con-sider are the presence or absence of lipodystrophy, insulin injection volume, temperature of the site of injection, taking vasoconstrictor or vasodilator medication and the existence of muscle contraction underlying the injection area323.
8.7.1. Administration site: injection site
The systematic review conducted for the CPG NICE 20047 included several RCTs324, 325, 326, 327 that analyzed the relationship between the injection site of insulin and its effects. All these studies were carried out in adults; no study was found in children, adolescents and pregnant women.
SR of RCT1++
A working group composed of 127 experts from around the world328, 329 developed an SR that included 157 experimental and observational studies, with recommendations on injection in diabetic patients
SR of RCT1++/2++
Results on insulin absorption
A small observational study (n = 7)325 found a signifi cantly higher rate of insulin absorption and speed of insulin absorption in injections administered in the abdomen, intermediate in the arm, and lower in the thigh against arm or thigh, in this order.
Observational study
2+
Results on glycaemic control
Three studies examined blood glucose levels and found that levels were lower when the injection was made in the abdomen325, 326, 327.
RCT1+
An RCT with 35 adults who were followed up for 3 months324 observed that there were variations of glycaemia and episodes of nocturnal hypoglycae-mia signifi cantly more common in people who were administered insulin in the thigh vs. those who had been administered insulin in the abdomen.
RCT1+
A group of 40 experts330 proposed, based on the evidence from observa-tional studies, the following recommendations for the administration of insu-lin, depending on the type of insulin and the timing of administration:
Observational studies
2+
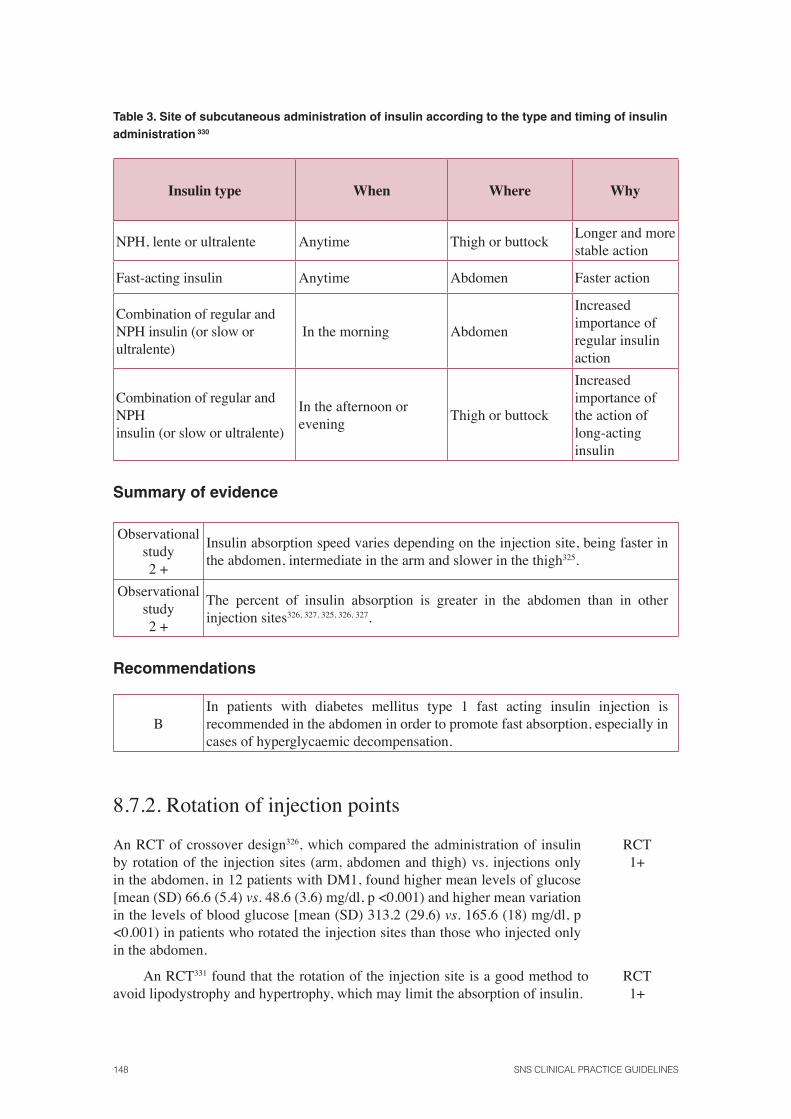
148 SNS CLINICAL PRACTICE GUIDELINES
Table 3. Site of subcutaneous administration of insulin according to the type and timing of insulin administration 330
Insulin type When Where Why
NPH, lente or ultralente Anytime Thigh or buttockLonger and more stable action
Fast-acting insulin Anytime Abdomen Faster action
Combination of regular and NPH insulin (or slow or ultralente)
In the morning Abdomen
Increased importance of regular insulin action
Combination of regular and NPH insulin (or slow or ultralente)
In the afternoon or evening
Thigh or buttock
Increased importance of the action of long-acting insulin
Summary of evidence
Observational study 2 +
Insulin absorption speed varies depending on the injection site, being faster in the abdomen, intermediate in the arm and slower in the thigh325.
Observational study 2 +
The percent of insulin absorption is greater in the abdomen than in other injection sites326, 327, 325, 326, 327.
Recommendations
BIn patients with diabetes mellitus type 1 fast acting insulin injection is recommended in the abdomen in order to promote fast absorption, especially in cases of hyperglycaemic decompensation.
8.7.2. Rotation of injection points
An RCT of crossover design326, which compared the administration of insulin by rotation of the injection sites (arm, abdomen and thigh) vs. injections only in the abdomen, in 12 patients with DM1, found higher mean levels of glucose [mean (SD) 66.6 (5.4) vs. 48.6 (3.6) mg/dl, p <0.001) and higher mean variation in the levels of blood glucose [mean (SD) 313.2 (29.6) vs. 165.6 (18) mg/dl, p <0.001) in patients who rotated the injection sites than those who injected only in the abdomen.
RCT1+
An RCT331 found that the rotation of the injection site is a good method to avoid lipodystrophy and hypertrophy, which may limit the absorption of insulin.
RCT1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 149
Summary of evidence
RCT 1 +
The rotation of the insulin injection sites results in increased plasma glucose levels and higher mean change in plasma glucose level than having the injection always in the abdomen326.
RCT 1 +
The rotation of the insulin injection site is a good way to keep the skin in good condition326, 328, 329, 331.
Recommendations
A Rotation in the insulin injection sites is recommended to prevent lipodystrophy.
AIt is recommended to change the insulin injections’ area if the current site is affected by lipodystrophy, infl ammation, oedema or infection.
√ Patients should be taught a rotation scheme of the different injection sites.
√It is recommended to divide the area into quadrants and change the quadrant clockwise weekly.
√The injections in each quadrant are to be spaced at least 1 cm in order to avoid repetition of tissue trauma.
√The clinician should verify in each visit that the rotation scheme is being followed and advice should be offered when needed.
8.7.3. Injection technique (injection angle and skin fold)
A descriptive study332 carried out in 14 patients with DM1 assessed the average thickness of subcutaneous fat and found great variability depending on the body areas and the people: in the abdomen the average thickness is 14 mm (range: 9.74 to 18, 26), in the lateral thigh the average thickness is 6 mm (range 2-19), in the upper thigh the average thickness is 8 mm (range 3-15 mm) and in the medial thigh the average thickness is 14 mm (range 4-25 mm).
Descriptivestudy
3
A descriptive study330 indicated a reduced risk of injection into the mus-cle, and therefore of hypoglycaemia, if skin fold was performed with the thumb and index fi nger vs. the fold being performed with all the fi ngers.
Descriptivestudy
3
An RCT 333, which included 28 adults who were injected with insulin pre-fi lled pens and skin fold injection, compared the injection with 45° vs. 90º injection angles. No signifi cant differences were found in levels of HbA
1c,
fructosamine, in fasting insulin doses administered or the number of episodes of moderate and severe hypoglycaemia.
RCT1+
150 SNS CLINICAL PRACTICE GUIDELINES
The Birkenbaek et al study334 analyzed in 21 children (16 males) and 32 adults (23 males) the risk of intramuscular injection with 4 mm and 6 mm needles in thin patients. It was determined that it to inject in the subcutaneous tissue was achieved more frequently using 4 mm needles than 6 mm needles in the abdomen (p = 0.032) and thigh (p = 0.001), without using skin fold. The authors suggest that in the cases using 6 mm needles, a skin fold is made and used at an angle of 45°.
RCT1+
Another study in thin men (BMI <25 kg/m2)335 determined that the injec-tion angle of 90° with an 8 mm needle into the thigh often reaches muscle tis-sue. The injection applied perpendicular to the skin and without folds, with a 4 mm needle favours the subcutaneous administration of insulin.
RCT1+
A trial in 72 children with DM1336 assessed the injection in the abdomen and thigh with a 6 mm needle and skin fold and compared the angle at 90° vs. an angle of 45° With perpendicular injection and skin fold, muscle tissue was reached in 32% of individuals and in 22% in muscular fascia; with an injection at 45º and skin fold, insulin administration was always subcutaneous.
RCT1+
Summary of evidence
RCT 1 +
In adult patients with diabetes mellitus type 1 metabolic control showed no differences if insulin injection is performed at 45º or 90º 333.
RCT 1 +
Thin people should use 4 mm needles, perpendicular to the skin and without skin fold to facilitate subcutaneous administration of insulin 334, 335. When using 6 mm needle, it is better to use skin fold and at an angle of 45° 334.
RCT 1 +
In children with diabetes mellitus type 1, if using a 6 mm needle, the injection at an angle of 45º and skin fold favours the subcutaneous administration of insulin336.
Recommendations
√It is important to consider the preferences of patients with diabetes mellitus type 1 when assessing the most appropriate injection technique as this aspect can improve adherence to the treatment.
C The skin fold must be made by grasping the thumb and forefi nger in a clamp.
B
In thin people, when the injection is performed on limbs or abdomen with 4mm needles, it is advised not to use skin fold injecting perpendicularly in order to prevent potential intramuscular injections. If the needles are longer, it is advisable to inject with skin fold and at an angle of 45°.
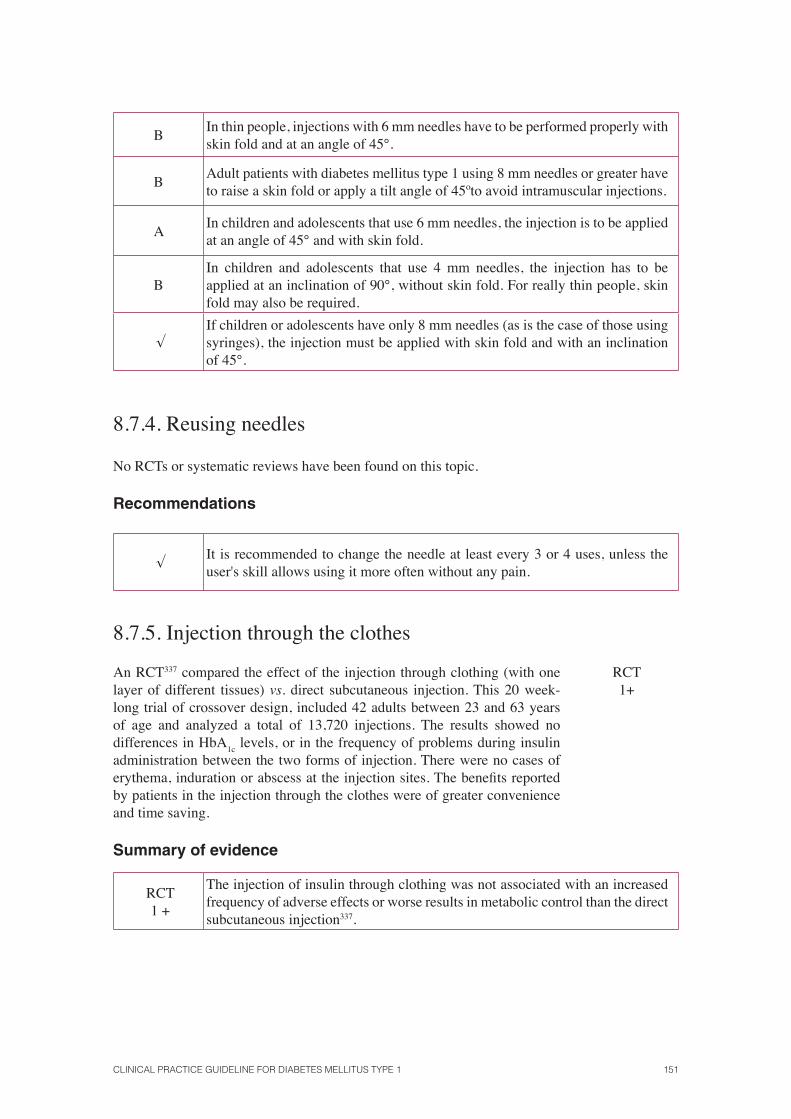
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 151
BIn thin people, injections with 6 mm needles have to be performed properly with skin fold and at an angle of 45°.
BAdult patients with diabetes mellitus type 1 using 8 mm needles or greater have to raise a skin fold or apply a tilt angle of 45ºto avoid intramuscular injections.
AIn children and adolescents that use 6 mm needles, the injection is to be applied at an angle of 45° and with skin fold.
BIn children and adolescents that use 4 mm needles, the injection has to be applied at an inclination of 90°, without skin fold. For really thin people, skin fold may also be required.
√If children or adolescents have only 8 mm needles (as is the case of those using syringes), the injection must be applied with skin fold and with an inclination of 45°.
8.7.4. Reusing needles
No RCTs or systematic reviews have been found on this topic.
Recommendations
√It is recommended to change the needle at least every 3 or 4 uses, unless the user's skill allows using it more often without any pain.
8.7.5. Injection through the clothes
An RCT337 compared the effect of the injection through clothing (with one layer of different tissues) vs. direct subcutaneous injection. This 20 week-long trial of crossover design, included 42 adults between 23 and 63 years of age and analyzed a total of 13,720 injections. The results showed no differences in HbA
1c levels, or in the frequency of problems during insulin
administration between the two forms of injection. There were no cases of erythema, induration or abscess at the injection sites. The benefi ts reported by patients in the injection through the clothes were of greater convenience and time saving.
RCT1+
Summary of evidence
RCT 1 +
The injection of insulin through clothing was not associated with an increased frequency of adverse effects or worse results in metabolic control than the direct subcutaneous injection337.

152 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
AAlthough not considered optimal practice since it does not allow the correct elevation of skin fold or to visualize the site of injection, injecting insulin through a layer of fabric is not ruled out in specifi c situations.
8.7.6. Needle Size
A study in obese adult patients (BMI ≥ 30 kg/m2) compared338 the abdominal injection with short needles (31 gauge × 6 mm) vs. long needles (29 gauge × 12.7 mm) and found no differences in metabolic control [HbA
1c fi nal mean
(SD) 7.6% (1.20) for the short needles vs. 7.9% (1.54) for the long needles]. Regarding patients’ preferences, short needles scored signifi cantly better than the long ones. No differences were found regarding adverse effects.
RCT1+
A trial published in 2010339 compared the use of 4mm needles vs.5 mm and 8 mm needles, in 168 adult patients with DM1 (37%) and DM2, and found no signifi cant differences between both groups in terms of changes in fructosa-mine levels (p = 0.878) and HbA
1c (p = 0.927), or the occurrence of adverse
effects. Patients with less pain reported to feel less pain with 4mm needles (p <0.005) and preferred the 4mm needles rather than the 5 mm or 8 mm ones.
RCT1+
Another study investigated the metabolic control340, safety and patient preferences depending on the length of the needles in 52 patients. The patients of a fi rst group used 5 mm needles during 13 weeks and then changed to longer needles (8 mm or 12 mm) during the same period. The second group followed the reverse order. The fi rst group underwent a slight increase in the HbA
1c
levels after changing from a short needle to a long one (baseline 7.67% 7.65% 13 weeks, 26 weeks 7.87%, p <0.05). The second group showed no signifi cant changes. No changes were found in the amounts of insulin administered, fre-quency or severity of hypoglycaemia, insulin or overfl ow between groups. 5 mm needles were signifi cantly associated with less bleeding, erosion and pain (p <0.05) and the patients reported a preference for them (p <0.05).
RCT1+
In order to assess the effects on glycaemic control when changing from a 12.7 mm needle to an 8 mm one in obese and non-obese patients, a prospective study was carried out in 106 patients341 and found that obese patients, when changing the needle size from 12.7 mm to 8 mm suffered less pain. No signifi -cant differences were found between obese and non-obese patients in terms of metabolic control or insulin overfl ow.
Observational study
2+
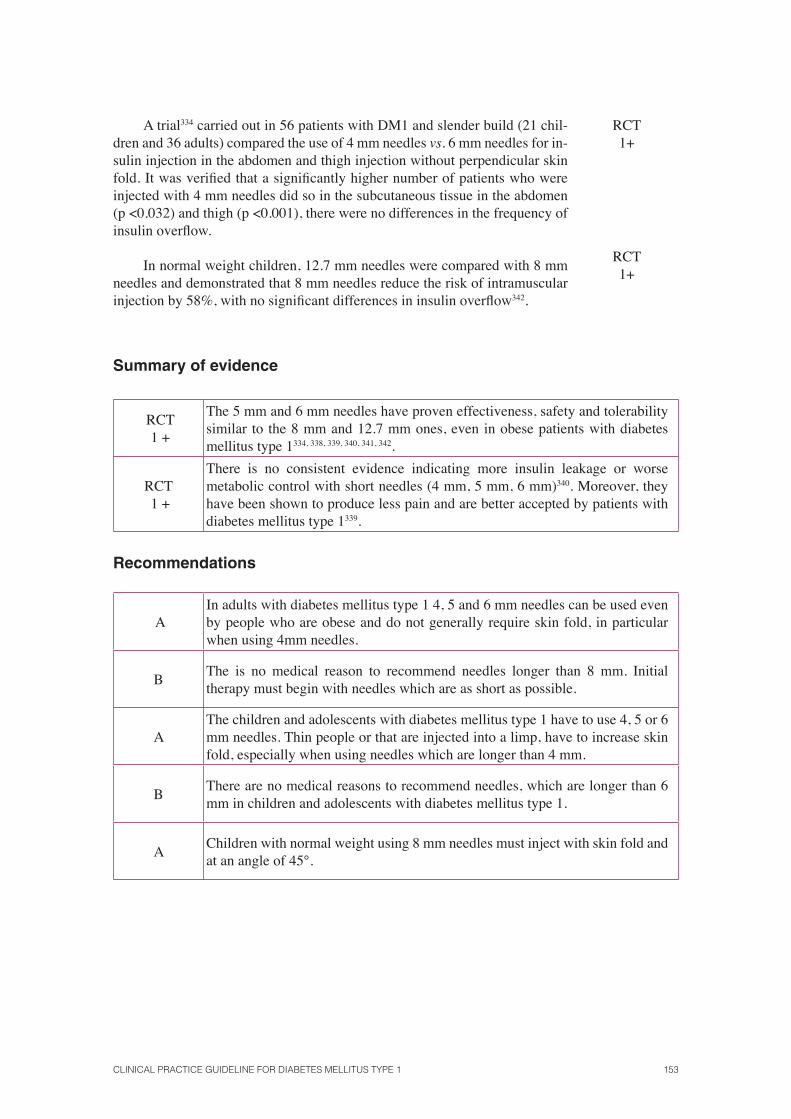
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 153
A trial334 carried out in 56 patients with DM1 and slender build (21 chil-dren and 36 adults) compared the use of 4 mm needles vs. 6 mm needles for in-sulin injection in the abdomen and thigh injection without perpendicular skin fold. It was verifi ed that a signifi cantly higher number of patients who were injected with 4 mm needles did so in the subcutaneous tissue in the abdomen (p <0.032) and thigh (p <0.001), there were no differences in the frequency of insulin overfl ow.
RCT1+
In normal weight children, 12.7 mm needles were compared with 8 mm needles and demonstrated that 8 mm needles reduce the risk of intramuscular injection by 58%, with no signifi cant differences in insulin overfl ow342.
RCT1+
Summary of evidence
RCT 1 +
The 5 mm and 6 mm needles have proven effectiveness, safety and tolerability similar to the 8 mm and 12.7 mm ones, even in obese patients with diabetes mellitus type 1334, 338, 339, 340, 341, 342.
RCT 1 +
There is no consistent evidence indicating more insulin leakage or worse metabolic control with short needles (4 mm, 5 mm, 6 mm)340. Moreover, they have been shown to produce less pain and are better accepted by patients with diabetes mellitus type 1339.
Recommendations
AIn adults with diabetes mellitus type 1 4, 5 and 6 mm needles can be used even by people who are obese and do not generally require skin fold, in particular when using 4mm needles.
BThe is no medical reason to recommend needles longer than 8 mm. Initial therapy must begin with needles which are as short as possible.
AThe children and adolescents with diabetes mellitus type 1 have to use 4, 5 or 6 mm needles. Thin people or that are injected into a limp, have to increase skin fold, especially when using needles which are longer than 4 mm.
BThere are no medical reasons to recommend needles, which are longer than 6 mm in children and adolescents with diabetes mellitus type 1.
AChildren with normal weight using 8 mm needles must inject with skin fold and at an angle of 45°.
154 SNS CLINICAL PRACTICE GUIDELINES
8.8. Indications for the treatment with metformin added to insulin in adolescents with diabetes mellitus type 1
Metformin, biguanide used for over 40 years in the treatment of diabetes, mainly acts to reduce hepatic glucose production as well as insulin resistance in peripheral tissues. In adolescents with DM1, metabolic control is diffi cult, due to insulin resistance, eating habits, exercising, lower ad-herence to measurement and to dose adjustments.
Metabolic Control
In two RCTs with 27343 and 26 patients respectively with DM1344, a 2,000 mg/day coadjutant to insulin dose of metformin was administered. After 3 months of intervention, the decrease in HbA
1c levels was 0.9% in absolute
terms in the Hamilton study and 0.6% in the Samblad study, versus placebo, in favour of the group treated with metformin.
RCT1+
An SR345 which included nine studies in which metformin was added to the insulin therapy compared with placebo or other treatment showed a reduction in insulin requirements (5.7 to 10.1 U/day in 6 of 7 studies) HbA
1c
(0.6-0.9% in 4 of 6 studies), weight (1.7 to 6.0 kg in 3 of 6 studies and total cholesterol (0.3 to 0.41 mmol/l in 3 of 7 studies). Metformin treatment was well tolerated, although it showed more episodes of hypoglycaemia in these patients.
SR ofRCT1+
A medium quality SR that included two RCTs (60 adolescents with DM1)346 indicated that metformin reduces HbA
1c in adolescents with DM1
with poor metabolic control.
SR of RCT 1++
Adverse Effects
In the study by Hamilton et al.343, no signifi cant differences were found in the occurrence of severe hypoglycaemia and gastrointestinal disturbances. Mild hypoglycaemia was more frequent in the metformin group than in the placebo group after 3 months of treatment [mean events per patient per week (DE) 1.75 (0.8) vs. 0.9 (0.4), P = 0.03].
RCT1+
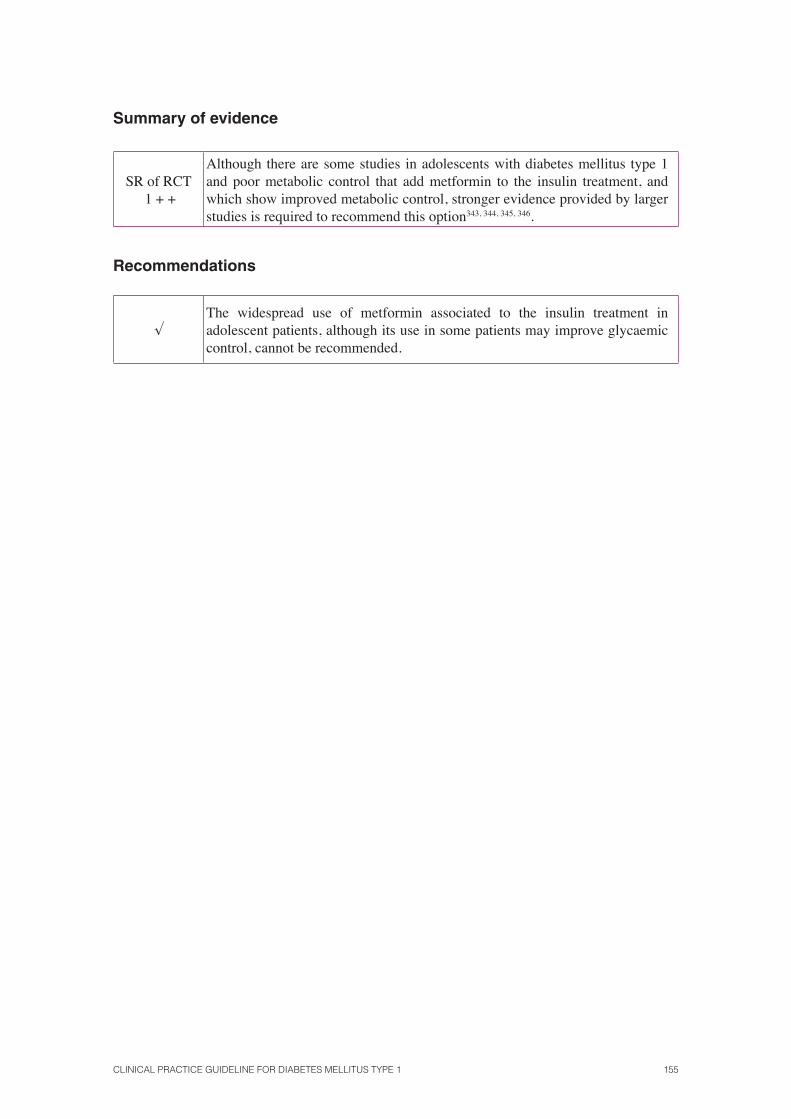
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 155
Summary of evidence
SR of RCT 1 + +
Although there are some studies in adolescents with diabetes mellitus type 1 and poor metabolic control that add metformin to the insulin treatment, and which show improved metabolic control, stronger evidence provided by larger studies is required to recommend this option343, 344, 345, 346.
Recommendations
√The widespread use of metformin associated to the insulin treatment in adolescent patients, although its use in some patients may improve glycaemic control, cannot be recommended.
156 SNS CLINICAL PRACTICE GUIDELINES
8.9. Pancreas and islet transplantation
The transplantation of pancreatic tissue, both the whole organ as well as isolated pancreatic islets, has become a therapeutic option to consider when treating patients with DM1.
8.9.1. Pancreas Transplantation
Mortality and graft survival
While mortality data vary depending on the surgical technique used and the patients’ characteristics, as published in 2006347, the survival rate after a pancreas transplant is between 95% and 97% per year, between 91 % and 92% after 3 years, and between 84% and 88% after 5 years. Most of the deaths are due to cardiovascular disease and usually occur within 3 years after discharge.
DescriptiveStudies
3
The graft survival rates (defi ned as complete independence from insu-lin therapy with normal fasting glucose and normal or slightly high levels of HbA
1c) for simultaneous kidney and pancreas transplant are of 86% per year
and 54% after 10 years. For isolated pancreatic transplantation, the rates are 80% per year and 27% after 10 years.
A retrospective cohort study348 that included 11,572 participants showed no difference in mortality rates between the two groups349, 350.
Cohort studies2+
Metabolic Control
According to data provided by several observational studies351, 352, 353, 354, 355,
356, 357, 358 pancreas transplants performed successfully restore the pancreatic function and lead to the independence of exogenous insulin therapy, normal blood sugar levels and normal or near-normal levels of HbA
1c. Patients with
normally functioning grafts have normal responses to oral glucose overload and stimulation with intravenous glucagon.
Cohort studies2+
The hormonal response to hypoglycaemia improves after a pancreas transplantation.353, 359, 360.
Cohort studies2+
Another observational study360 stated that the recognition of symptoms of hypoglycaemia also improves after transplantation.
Cohort studies2+
Studies as those carried out by Cottrell et al.361 have described hypogly-caemia as a complication of pancreatic transplantation, but these episodes are usually mild362.
Cohort studies2+
Prospective and crossover studies have shown that improved metabolic control is maintained over many years. Several centres reported a persistent improvement over 15 years356, 363, 364.
Descriptive studies
3
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 157
Microvascular complications
After a simultaneous pancreas and kidney transplant, renal structure is normalized as shown by the decrease in mesangial mass in patients receiving kidney and pancreas transplantation vs. patients with kidney transplant alone365, 366. One study367 described an improvement in non-transplant kidney structure after 10 years of follow up.
Cohort studies2+
Several studies have described an improvement of driving speed in mo-tor and sensory nerves and stabilization of the evolution of neuropathy358, 368,
369, 370, 371, 372, 373.
Cohort studies2+
Macrovascular
Combined pancreas and kidney transplant in patients with DM1 produced a greater reduction in cardiovascular risk than kidney transplant alone, which is associated with signifi cantly better changes in metabolic control in postprandial levels of homocysteine and lower levels of the von Willebrand factor374.
Descriptive study
3
158 SNS CLINICAL PRACTICE GUIDELINES
8.9.2 Pancreatic islet transplantation
Four SRs have analyzed the results of effectiveness and safety of pancreatic islet transplantation129, 375, 376, 377. This CPG will take into account the latest revision by Guo et al.129, as it includes the three latest versions. This review includes 11 series of cases378, 379, 380; 381, 382, 383, 384, 385, 386, 387, 388, with a total of 208 patients (mean age, 33-50 years), with follow-up periods ranging from 1 to 5 or 6 years.
SR of RCT 1++
Insulin independence: the percentage of people with good metabolic control without insulin in the 11 studies ranged from 30% above to 69% in the fi rst year, from 14% to 33% in the second year and up to 7.5 %, fi ve years after transplantation.
Case series 3
In the study by Edmonton with 7 patients with DM1389 who were treated with transplantation and immunosuppressive drugs, all patients had normal HbA
1c
levels without exogenous insulin after 1 year of follow-up.
In a 5-year follow-up of 65 patients with DM1381 from the Edmonton program, 47 patients (72%) achieved insulin independence. The median of this inde-pendence was 15 months and only 10% remained insulin independent after 5 years. However, 80% showed C-peptide secretion and required half the dose of insulin they took before transplantation and showed lower blood glucose liability.
Hypoglycaemia: nine studies analyzed results for hypoglycaemia. All insulin independent patients were fully free of hypoglycaemia episodes. The hypogly-caemic episodes of insulin dependent patients were mild episodes.
Quality of life: Only two studies388, 390 looked at the quality of life outcomes. Both studies showed reduced fear of hypoglycaemia after transplantation. However, the results were inconsistent in terms of total quality of life related to health.
Adverse effects: Islet transplantation is associated with complications related to the procedure and immunosuppression. None of these studies reported any preoperative or postoperative death as a direct result of the procedure.
However, there were 38 serious adverse events in 36 patients and 18 of them required hospitalization. Complications related to the procedure were mainly intraperitoneal bleeding (9% as mean, 23% in the study of Edmonton); the portal vein thrombosis, which in most cases was partial (described in 6 of the 11 studies percentages ranging between 6 and 17%) and liver abnormali-ties (described in 8 of the 11 studies, ranging from 10 to 100%).
Case series3
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 159
As for the adverse effects of immunosuppressive therapy, 7 of the 11 studies reported impairment of renal function from 17% to 50% of the pa-tients, forcing regime change in immunosuppression between 10% and 37 % of the cases.
Other complications observed in an international multicenter study227 were mouth sores (92%), anaemia (81%), leukopenia (75%), diarrhoea (64%), headache (56%), neutropenia (53%), nausea (50 %), vomiting (42%), and acne (39%).
8.9.3. Islet transplantation vs. intensive insulin therapy
A prospective observational study391 the metabolic control of 44 patients who received intensive insulin therapy vs. 21 patients who received islet transplantation compared for 29 months, fi nding HbA
1c levels being
signifi cantly lower in the transplant group.
Observational studies
2+
8.9.4. Pancreatic islet transplantation vs. pancreas transplantation
In a retrospective case series392 islet transplantation was compared with whole organ transplantation. In that study, 30 patients received pancreas transplantation and 13 patients islet transplantation; however, both groups were comparable in terms of poorly renal function (pancreas transplant group: 73% history of renal dialysis; islet transplantation group: 0%). There was no signifi cant difference in survival between the two groups. Pancreas transplantation performed better in terms of C-peptide levels, HbA
1c and
insulin requirement, but in this group negative results were also observed, such as longer hospital stays, higher readmission rates and increased postoperative morbidity.
Case series 3
Summary of evidence
Cohort study 2 +
The isolated pancreas transplantation and the simultaneous kidney and pancreas transplantation are effective for restoring endogenous insulin secretion, maintaining long-term glycaemic homeostasis and thereby prevent acute and chronic complications of diabetes, which improves the quality of life for people with diabetes mellitus type 1 relating to the fear of hypoglycaemia351, 352, 353, 354,
355, 356, 357, 358.
Case series
3
Although islet transplantation appears to reduce short-term insulin needs, long-term effectiveness and its effects on diabetic complications392 have not actually been proven.
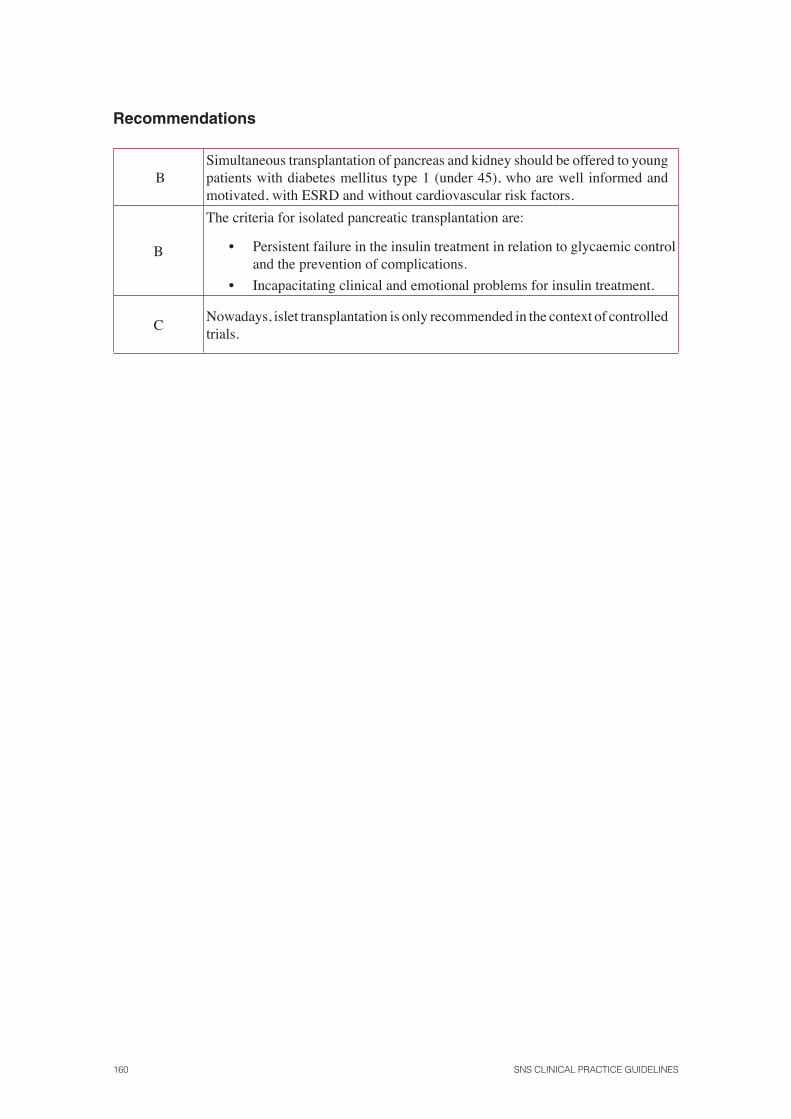
160 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
BSimultaneous transplantation of pancreas and kidney should be offered to young patients with diabetes mellitus type 1 (under 45), who are well informed and motivated, with ESRD and without cardiovascular risk factors.
B
The criteria for isolated pancreatic transplantation are:
• Persistent failure in the insulin treatment in relation to glycaemic control and the prevention of complications.
• Incapacitating clinical and emotional problems for insulin treatment.
CNowadays, islet transplantation is only recommended in the context of controlled trials.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 161
9. Management of diabetes mellitustype 1 in special situations
9.1. Insulin treatment guidelines during hospitalization of patients with diabetes mellitus type 1
Key question:
• What are the patterns of insulin therapy during hospitalization of patients with diabetes mellitus type 1: surgical patient, critically ill patient and stable patient?
Individuals with diabetes are a signifi cant percentage of hospitalized patients, as they make up 30-40% of patients seen in emergency units, 25% of inpatients in both medical and surgical areas, and about 30 % of patients undergoing aorto-coronary bypass. This follows the increase in the prevalence of DM and associated comorbidity and diagnostic and therapeutic procedures that require hospitalization. In addition, patients with diabetes stay in the hospital an average of 1-3 days more than non-diabetics, and patients with hyperglycaemia on admission are more likely to require the use of the ICU.
Insulin requirements to keep blood sugar within acceptable limits during hospitalization vary markedly according to the changes in nutrient inputs (fasting or nutrient reduction, glucose IV, enteral or parenteral nutrition), counterregulatory hormone release in response to stress, or the use of drugs with hyperglycaemic effect. In critically ill patients, there is a metabolic overload situation by releasing a number of counter-regulatory hormones in response to stress, hypergly-caemia generating and activate metabolic pathways releasing amino acids and fatty acids, increas-ing the resistance of peripheral tissues to the action of insulin. Furthermore, in intensive care units these effects are enhanced by the administration of exogenous glucocorticoid adrenergic drugs. Moreover, critically ill patients have impaired ability to detect the symptoms of hypoglycaemia, which is especially dangerous.
In DM1 patients requiring hospitalization glycaemic control can be altered among other causes by the underlying disease that has led to the hospitalization, dietary and schedule changes, forced periods of fasting, testing, the at least partial immobilization, drugs with hyperglycaemic potential, psychological stress and the absolute loss of control over the administration of insulin. The latter can be variable depending on the area of hospitalization and how often staff deal with patients with DM1 and their knowledge. Not infrequently, is the insulinization pattern on demand, depending on glucose levels before each meal or every 4-6-8 hours (always below their previ-ous requirements) and the inadequate supply of carbohydrates that cause large swings in blood glucose levels, prolonged stays and place patients at increased risk of infection. Therefore, it is essential to start up protocols for stable patients with treatment regimens depending on the most frequent variables, so that hospitalization for itself is not an added risk of diabetes control.
162 SNS CLINICAL PRACTICE GUIDELINES
9.1.1. Surgical Patient
The CPG NICE 20047 provides the following evidence in adult patients:
A cohort study393 on patients with diabetes showed that blood glucose levels the same day of the operation and three days after surgery, were signifi -cantly lower (p <0.0001) with the continuous intravenous infusion (IV) insulin compared with the subcutaneous insulin injection (SC).
Cohort Study
2+
Two trials compared IV insulin with the subcutaneous injection in mi-nor394 and major395 surgical procedures and found that the median glucose may be reduced during the fi rst day after surgery with the administration of IV insulin. Furthermore, the insulin/glucose ratio and the number of doses adjust-ments required were signifi cantly lower in those receiving IV insulin com-pared with the group that used the subcutaneous route of insulin.
RCT1+
Another study396 compared two regimens of intravenous insulin in 58 consecutive patients requiring preoperative insulin infusions. Patients were randomized to an infusion of glucose-insulin-potassium (GIK) or a more com-plex protocol that required two insulin infusion pumps. Both methods gave similar results in terms of glycaemic control. However, the dual pump system had a higher percentage of patients with glycaemia within target ranges, both preoperatively (47.4% vs. 60.1%) as well as postoperative (52.0% vs. 66.4%). The length of stay (15 vs. 16 days), duration of infusion (15 vs. 16 hours) were similar for both groups.
RCT1+
In a prospective cohort study397 3554 patients with hyperglycaemia who underwent cardiac surgery (coronary bypass graft) and who had been treated with either subcutaneous insulin or continuous infusion, were evaluated. The expected and observed mortality was compared using multivariate analysis models, showing a signifi cantly lower mortality in patients with continuous infusion (2.5%) than those receiving subcutaneous insulin (5.3%, P <0.0001). Glycaemic control was signifi cantly better in the group with continuous infu-sion [mean (SD) 177 mg/dL (30) vs. 213 mg/dL (41), P <0.0001].
CohortStudy
2+
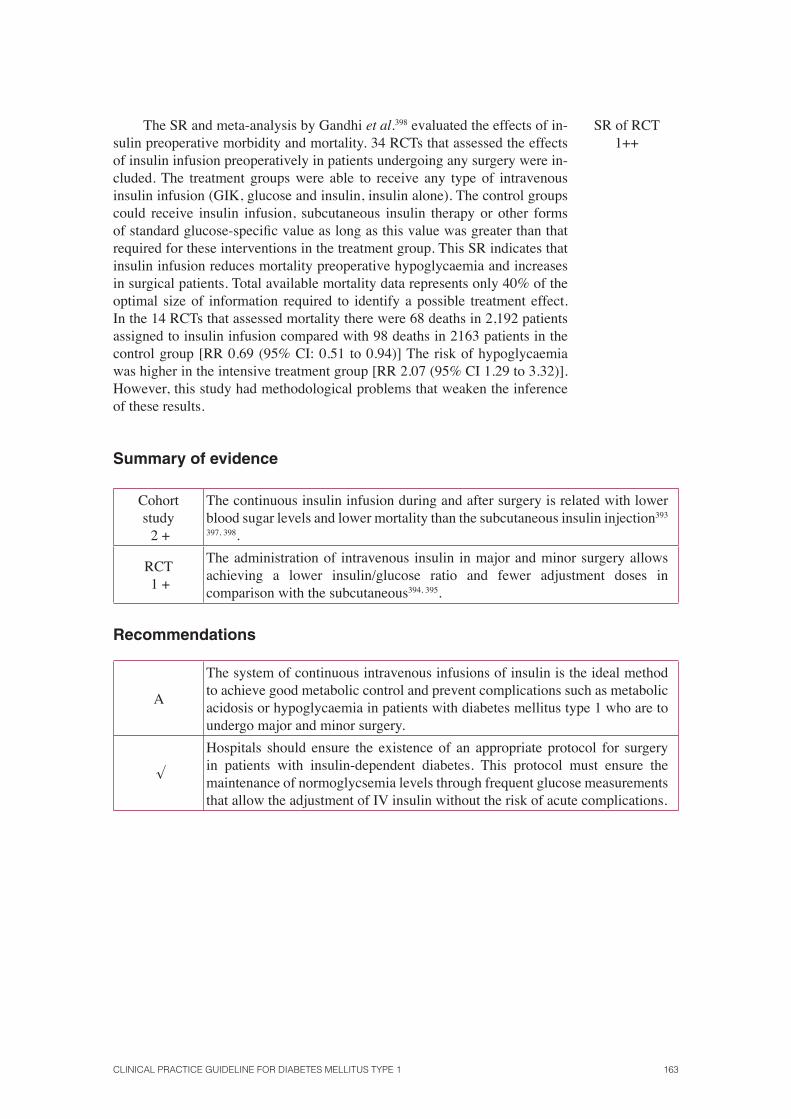
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 163
The SR and meta-analysis by Gandhi et al.398 evaluated the effects of in-sulin preoperative morbidity and mortality. 34 RCTs that assessed the effects of insulin infusion preoperatively in patients undergoing any surgery were in-cluded. The treatment groups were able to receive any type of intravenous insulin infusion (GIK, glucose and insulin, insulin alone). The control groups could receive insulin infusion, subcutaneous insulin therapy or other forms of standard glucose-specifi c value as long as this value was greater than that required for these interventions in the treatment group. This SR indicates that insulin infusion reduces mortality preoperative hypoglycaemia and increases in surgical patients. Total available mortality data represents only 40% of the optimal size of information required to identify a possible treatment effect. In the 14 RCTs that assessed mortality there were 68 deaths in 2,192 patients assigned to insulin infusion compared with 98 deaths in 2163 patients in the control group [RR 0.69 (95% CI: 0.51 to 0.94)] The risk of hypoglycaemia was higher in the intensive treatment group [RR 2.07 (95% CI 1.29 to 3.32)]. However, this study had methodological problems that weaken the inference of these results.
SR of RCT1++
Summary of evidence
Cohort study 2 +
The continuous insulin infusion during and after surgery is related with lower blood sugar levels and lower mortality than the subcutaneous insulin injection393
397, 398.
RCT 1 +
The administration of intravenous insulin in major and minor surgery allows achieving a lower insulin/glucose ratio and fewer adjustment doses in comparison with the subcutaneous394, 395.
Recommendations
A
The system of continuous intravenous infusions of insulin is the ideal method to achieve good metabolic control and prevent complications such as metabolic acidosis or hypoglycaemia in patients with diabetes mellitus type 1 who are to undergo major and minor surgery.
√
Hospitals should ensure the existence of an appropriate protocol for surgery in patients with insulin-dependent diabetes. This protocol must ensure the maintenance of normoglycsemia levels through frequent glucose measurements that allow the adjustment of IV insulin without the risk of acute complications.
164 SNS CLINICAL PRACTICE GUIDELINES
9.1.2. Critical patient
The CPG NICE 20047 includes the following evidence on the management of critically ill patients with DM1:
An RCT conducted in 620 patients who had suffered an acute myocar-dial infarction (AMI), of which 20% had DM1399, contrasted the effect of IV insulin and glucose infusion compared to a control group with conventional therapy. This study showed a lower incidence of cardiac death and reinfarction in patients receiving IV glucose-insulin infusion compared to controls after 3 months, one year and 3 and a half years of follow up. The HbA
1C levels de-
creased signifi cantly in both groups, but this decrease was more signifi cant in the group with IV insulin infusion after 3 months (p <0.0001) and even after 3 years (p <0.05).
RCT1+
A randomized controlled trial in an elderly population with diabetes (19% DM1) who had suffered an AMI400 compared IV insulin infusion during the fi rst 24 hours of admission with conventional treatment, which allowed to observe a signifi cant decrease in glucose levels in the IV infusion treat-ment group compared to the group with conventional treatment [mean (SD) 262.8 mg/dl (52.2) to 165.6 mg/dl (52.2) vs. 284.4 mg/dl (77.4) to 216 mg/dl (79.2) respectively, p <0.001). Regarding the adverse effects in the IV infusion group, 28 patients (17%) experienced an episode of hypoglycaemia (glucose <54 mg/dl), whereas no patients in the control group underwent any experi-ence (p <0.001).
RCT1+
Another RCT401 carried out in patients with DM1 and DM2, compared IV insulin infusion following predefi ned decision algorithms against an unde-fi ned logical method. The latter method allows obtaining a lowering of blood glucose (below 180 mg/dl) in less time [mean (SD) 7. 8 hours (0.7) vs. 13.2 hours (1.5) p < 0.02] than the IV infusion one, probably by a greater number of dose adjustments.
RCT1+
An RCT402 conducted in 763 critically ill patients (4% with DM1 in the conventional treatment group and 5% in the intensive treatment group) showed that tight control of glucose (between 80 and 110 mg/dl) was associated with lower mortality 4.6% vs. 8% (p <0.05) than in the group with conventional control. The morning blood glucose remained lower in the intensive treatment group than in the conventional treatment group [mean (SD) 103 (19) mg/dl vs. 153 (33) mg/dl, P <0.001]. The difference in hypoglycaemic episodes was not signifi cant.
RCT1+
An observational study403 found that the application of a protocol aimed to maintain blood glucose below 140 mg/dl in critically ill patients was associated with a reduction in mortality of 29.3% (p <0.02) and reduced ICU stay of 10.3% (p <0.01) without a signifi cant increase in the risk of hypoglycaemia.
Prospective observational
study2+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 165
An SR with meta-analysis404 analyzed 29 RCTs with a total of 8342 pa-tients admitted to the ICU with different pathologies, which varied widely be-tween the percentages of patients with diabetes. Hospital mortality remained unchanged in the control group with strict blood glucose vs. the group receiv-ing usual care [21.6% vs. 23.3% (RR 95% CI: 0.85 to 1.03)]. No signifi cant differences were observed when the glucose objectives were very strict (up to 110 mg/dl) or moderately strict (up to 150 mg/dl), or if the treatment was performed in a surgical, medical or surgical-medical ICU. Strict control was associated with a decreased risk of septicaemia [10.9% vs. 13.4% (RR 95% CI 0.59 to 0.97) and a signifi cantly increased risk of hypoglycaemia (RR 95% CI: 4. 09 to 6.43).
SR of RCT1+
In the NICE-SUGAR study405, 3015 patients (50 of them with DM1) were treated with intensive IV insulin therapy with a glycaemic control target between 81 and 108 mg/dl and 3014 (42 of them with DM1) with conven-tional treatment, with a blood glucose target less than or equal to 180 mg/dl. In the control group, insulin was administered only in the case of blood glucose above 180 mg/dl, and the infusion was stopped if the glycaemia fell below 144 mg/dl. Mortality was signifi cantly higher in the intensively treated group [OR 1.14 (95% CI: 1.02 to 1.28)], both in postsurgical patients as those with medi-cal pathology. However, patients with DM1 showed no difference in mortality after 90 days. Severe hypoglycaemia (<40 mg/dl) occurred in 6.8% of patients treated intensively compared with 0.5% of those treated conservatively.
RCT1+
Summary of evidence
SR of RCT 1 + +
RCT 1 +
Preliminary studies in critically ill patients with diabetes mellitus type 1 showed greater glycaemic control resulted in better health outcomes397, 402, 406. However, subsequent studies have failed to reproduce these results and found that intensive insulin therapy to achieve normoglycaemia increases the risk of hypoglycaemia, whose appearance is an independent predictor of mortality404, 407, 408. In a clinical trial with a before and after design403 found that the application of a protocol aimed at maintaining blood glucose between 80 and 110 mg/dl in critically ill patients was associated with a reduction in mortality, morbidity and ICU stay with no signifi cant increase in the risk of hypoglycaemia.
166 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
A
In the case of critical patients with persistent hyperglycaemia, the treatment must start with a threshold of no greater than 180 mg/dl (10 mmol/l). Once treatment has begun, glycaemic targets must be set in a range between 140-180 mg/dl (7.8 to 10 mmol/l) for the most critically ill patients.
√It is necessary to establish a safe and effective protocol to achieve an adequate blood glucose range without an increase in severe hypoglycaemic episodes.
9.1.3. Stable patient
The CPG NICE 20047 provides no evidence on this issue.
In the RABBIT 2 study409 the use of a basal-bolus regimen achieved better glycaemic control than the sliding scale or fast acting insulin scale administered every 6 hours in patients without previous insulin treatment. In this study, the mean blood glucose during hospitalization was lower [mean (SD): 166 (32) vs. 193 (54) mg/dl] and the percentage of patients achieving the blood glucose target less than 140 mg/dl was higher (66 vs. 38%) with the basal-bolus regimen than with the standard sliding scale, without increasing the incidence of hypoglycaemia (p <0.05). This study was conducted in patients with type 2 diabetes and has been taken into account in this CPG as a source of indirect evidence for patients with DM1.
RCT1+
During hospitalization of a stable patient, the American Diabetes Association410 considers reasonable basal glucose targets under 128 mg/dl and postprandial glucose less than 180-200 mg/dl if achieved safely.
CPG4
The consensus document of the SED411 recommends that, while waiting for further evidence, the blood glucose target during hospitalization should be that of normoglycaemia.
Expertconsensus
4
Summary of evidence
Expertconsensus
4
During hospitalization of stable patients with DM1, the targets for glycaemia should be similar to those of patients with diabetes who are not hospitalized409,
410, 411.
RCT 1 +
The use of a basal-bolus regimen achieved better glycaemic control than the sliding scale or fast acting insulin regimens administered every 6 hours in patients without previous insulin treatment409.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 167
Recommendations
√All patients with diabetes admitted to a health centre should have this diagnosis clearly identifi ed in their medical history.
√All patients with diabetes should have blood glucose levels monitored and this information should be available to the healthcare team.
B
Monitoring should be initiated in any known non-diabetic patient who is administered any treatment with a high risk of hyperglycaemia, including high doses of glucocorticoids, initiation of enteral or parenteral nutrition or other medications such as octreotide or immunosuppresives.
√If hyperglycaemia is identifi ed and persistent, treatment is needed. These patients should be treated with the same glycaemic targets as those applied for patients with known diabetes.
√A hypoglycaemia treatment plan should be set out for each patient. All episodes of hypoglycaemia in the hospital should be registered.
√All patients admitted to hospital have an HbA
1C level determination if data is
not available for the 2-3 months prior to admission.
√Patients with hyperglycaemia in the hospital with no prior accurate diagnosis of diabetes should have a protocol for diagnosis and monitoring of care at discharge.
168 SNS CLINICAL PRACTICE GUIDELINES
9.2. Preventive and treatment measures in the case of outpatient acute intercurrent diseases in patients with diabetes mellitus type 1
Key question:
• What are the preventive measures and treatment for outpatient acute intercurrent diseases?
Intercurrent diseases in DM1 patients can affect insulin requirements because they may be as-sociated with a lower caloric intake due to decreased appetite, loss of nutrients by vomiting and/or diarrhoea and a variable increase of the counterregulatory hormones caused by the stress of the disease.
The diseases associated with fever tend to increase glucose levels due to the hormones stress level, causing an increase to insulin resistance and an increase in glycogenolysis and gluconeo-genesis, which increases the risk of ketoacidosis. Associated diseases that present vomiting and diarrhoea may result in reducing blood glucose levels and thus in an increased risk of hypogly-caemia.
Decreasing calories by decreasing input (anorexia) or increased losses (vomiting) may cause hypoglycaemia. In older children, especially at puberty, a stressful disease is characterized by a relative insulin and hyperglycaemia defi ciency.
Adults
The CPG NICE 20047 provides no evidence on this issue but has published recommendations based on consensus, just as the document of the American Diabetes Association51 and the CPG of the Australian Government412.
Expertconsensus 4
While the most common problems in patients with diabetes mellitus type 1 associated with intercurrent diseases are hyperglycaemia and risk of ketoaci-dotic decompensation, found no relevant studies about adults. The evidence refers primarily to the management of hypoglycaemia and this is summarized in the corresponding section of this CPG.
Children and adolescents
The CPG NICE 20047 provides no evidence on this issue.
The ISPAD consensus guide from year 2009413 offers the following recommendations:
CPGconsensus
4
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 169
• The medical team responsible for the patient must provide patients and families clear recommendations on the management of the dis-ease when there are intercurrent diseases in order to avoid complica-tions such as:
ο Ketoacidosis.
ο Dehydration.
ο Uncontrolled or symptomatic hyperglycaemia.
ο Hypoglycaemia.
• Must never cease the administration of insulin.
• The dose of insulin is to be increased or decreased depending on the requirements.
• When a child with diabetes vomits, this must always be considered an insulin defi ciency until proven otherwise.
• A child with intercurrent disease must be requested with urgent health consultation in the following cases:
ο When the underlying condition is not clear.
ο When weight loss continuous, suggesting a worsening in dehy-dration.
ο When the vomiting persists for two hours (especially in small children).
ο When glucose continues to increase despite the extra adminis-tration of insulin.
ο When parents are unable to maintain blood glucose above 60 mg/dl (3.5 mmol/l).
ο When ketonuria increases or continues being high or when the ketonemia is> 1 to 1.5 mmol/l.
ο When the child is very tired, confused, hypervigilant, dehydrat-ed or has abdominal pain.
ο When the child is very young (under 2 or 3 years) or has an ill-ness other than diabetes.
ο When patients or relatives are exhausted, for example, by the night waking.
ο When language problems make it diffi cult to communicate with the family, the possibility of going to the hospital emergency unit should be considered if the situation does not improve quickly or if professional advice can be provided.
ο When the level of ketonemia is 3 mmol/l there is an immediate risk of ketoacidosis, being therefore insulin treatment urgently required and a consultation with the emergency services should be considered.
170 SNS CLINICAL PRACTICE GUIDELINES
An Australian CPG412 has proposed the following recommendations:
• Families must be informed that intercurrent diseases can cause very high or very low blood glucose levels [Strength of recommendation: D].
• All families are to receive education about managing diabetes in days of disease and must have at reach the kit including fast/ultra-fast acting insulin, glucose test capillary strips, lancets, glucose test strips or urine ketones or blood ketone test strips, telephone of the doctor or reference hospital, refreshments/juice fruit/lemonade or other similar beverages, glucagon, emergency guides or diabetes manuals, thermometer, and par-acetamol or ibuprofen [Strength of recommendation: D].
• Insulin is never to be omitted, even if the patient is not able to eat [Strength of recommendation: D].
• Blood glucose and ketones are to be monitored regularly [D].
• Any disease that is identifi ed, should be treated immediately to [Strength of recommendation: D].
• Taking additional oral fl uids should be encouraged, especially if the blood glucose is high or ketones are present [Strength of recommenda-tion: D].
• Additional boluses of rapid/ultra-fast acting insulin should be provided in an amount equal or greater than 10-20% of the total daily dose, every 2-4 hours if blood glucose level is high or ketones are present [Strength of recommendation: D].
• Parents/caregivers must offer assistance immediately if, after adminis-tering the extra insulin boluses, blood glucose stays high, ketones per-sist, nausea, vomiting or abdominal pain appear [Strength of recommen-dation: D].
• Severe hypoglycaemia is to be treated with intravenous dextrose (in the hospital setting)414, 415 [Strength of recommendation: A].
• If venous access is diffi cult or if the patient is outside the hospital set-ting, intramuscular glucagon is to be used to treat severe hypoglycaemia [Strength of recommendation: D].
• Under the supervision of a physician or a diabetes educator, small doses of subcutaneous glucagon can be administered to prevent or treat mean hypoglycaemia within outpatient settings416 [Strength of recommenda-tion: B].
CPG
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 171
Document from the American Diabetes Association417
• The goals of disease management are the prevention and early treatment of hypoglycaemia, signifi cant hyperglycaemia, ketosis and the preven-tion of acute ketoacidosis.
• The management of the days of disease requires frequent blood glucose and ketone levels in urine (or blood) monitoring, food and fl uids intake monitoring and supervision by an adult.
• A child can never be left in charge of the management of a day of dis-ease, thus being the implication of parents necessary and providing a contact telephone with the doctor.
• The child’s primary care physician must assess not only diabetes but also intercurrent diseases.
• The effects of the disease on insulin requirements are variable. The lack of appetite represents a decrease of calories intake, and in addition, the presence of vomits or diarrhoea may lead to a reduction of insulin needs. Furthermore, the stress of the disease can lead to increased counterregu-latory hormones, resulting in an increased need for insulin. In very small children (<6 years), in which the fast regulatory responses may not be well developed, the decrease in calories intake and the excess of the ac-tion of insulin may cause hypoglycaemia. However, in older children, particularly at puberty, a stressful disease is characterized by a relative insulin and hyperglycaemia defi ciency.
• Regular monitoring can help to determine the action to be preformed. Ketones have to be monitored regardless of the level of blood glucose, as acidosis can occur without elevated glucose levels, especially if oral intake is poor.
• Children with nauseas or vomits, may take sugary liquids and small dos-es of glucagon. If vomits persist, and if treatment at home fails to correct hypoglycaemia, hyperglycaemia or signifi cant ketoacidosis, it will be necessary to go to the emergency unit.
Consensus CPG
4
Summary of evidence
Expertconsensus
4
No scientifi c evidence has been found related to the management of diabetes mellitus type 1 with intercurrent diseases. The recommendations are based primarily on consensus of leading scientifi c institutions.
172 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
D
People with diabetes mellitus type 1 and/or their families or carers should be informed that intercurrent diseases could cause hyperglycaemia. They can also lead to ketosis and hypoglycaemia, the latter being more common in children under 6 years.
D
All people with diabetes mellitus type 1 and/or their families or carers have to be educated about disease management in case of intercurrent disease and should have at reach fast acting insulin, glucose test strips, blood glucose test strips, lancets, strips and meters for the measurement of ketones in the blood or urine, refreshments/fruit juice/lemonade or other drinks alike, know how to use glucagon, a thermometer, paracetamol or ibuprofen, emergency guides or diabetes manuals and a contact telephone of their doctor or the hospital.
D The administration of insulin should never be omitted, even if the patient is not able to eat.
DBlood glucose and ketone bodies in urine (ketonuria) or blood (ketonemia) must be monitored frequently.
D Any illness must be treated immediately.
DOral intake of extra liquids should be encouraged, especially if blood glucose is high or there are ketones.
DAdditional fast acting insulin boluses should be provided in an amount, which is the same or greater than 10-20% of the total daily dose, every 2-4 hours if the blood glucose is high or ketones are present.
DPatients/carers must immediately seek medical help if after the extra insulin boluses, blood glucose stays high, ketone bodies persist, nausea or vomiting or abdominal pain appear.
D
Small children may be administered small subcutaneous doses of glucagon to prevent or treat hypoglycaemia. For severe hypoglycaemia, intramuscular glucagon is recommended. Treatment with intravenous glucose should be performed within the hospital setting.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 173
9.3. Psychological disorders in patients with diabetes mellitus type 1
Key question:
• Are psychological disorders more common in people with diabetes mellitus type 1?
Diabetes is considered a possible trigger of psychological disorders. It is interesting to determine the prevalence of these problems in patients with DM1 in order to improve their health.
9.3.1. Affective disorders
The CPG NICE 2004 provides the following evidence7:
In a case-control study418, a signifi cantly higher number of patients with DM (12.8%) than those without DM (7.4%) were treated with antidepressants during the 12 months preceding the study [OR 1.59 (95% CI 1.43 to 1.76)].
Case control study
2+
In a prevalence study SR419 the presence of depression in patients with DM1 recorded was 21.7% compared to 8.6% in non-diabetic control patients [OR 2.9 (95% CI: 1.6 to 5, 5)].
SR ofdescriptive
studies3
Barnard et al. 420 conducted a prevalence study SR in adults that in-cluded 14 studies. The prevalence of depression found in the studies with the control group was 12% in people with DM1 and 3.2% in the people without diabetes.
SR ofdescriptive
studies3
The Kaneer et al. SR421 included four observational studies in children and adolescents, indicating that the prevalence of depressive symptom pathol-ogy is higher in people with DM1 compared with a control group with a preva-lence of 12% in children aged 8-12 years and 18% in adolescents that is 2-3 times higher than in people of the same age without DM.
SR ofdescriptive
studies3
Kessing et al.422 compared the risk of developing depression in a sample of individuals with DM1 and DM2 (n = 91,507) versus a group of patients with other chronic diseases such as osteoarthritis (n = 108,407). No signifi cant dif-ferences were demonstrated in the risk of developing severe forms of depres-sion between both chronic diseases (p = 0.07).
Descriptive study
3
174 SNS CLINICAL PRACTICE GUIDELINES
Other descriptive studies found signifi cant differences among people with diabetes compared to the general population, although there was vari-ability in the prevalence rates of depression found: 5.8% vs. 2.7% (p = 0.003) 423; moderate/severe depressive symptoms 6% vs. 3% (p = 0.04) 424; 12.6% vs. clinical depression 6.3% 425, in the Al-Ghamdi study426 34% vs. 13% (p = 0.04) and in the Khamseh study 427 64% vs. 36% (p = 0.0001).
Descriptive study
3
The retrospective study by Ali et al.428 aimed to examine the prevalence of depression in people with diabetes and the differences among ethnic groups in risk factors for depression diagnosis using multivariate logistic regression. The results showed that among people with DM1 (n = 1405) the prevalence of depression was 7.3 to 11.3%, and found no signifi cant differences between ethnic groups (10% of South-Asians vs. 7.9%, of Europeans, P = 0.355), which is consistent with previous literature showing similar prevalence rates. Furthermore, the prevalence rate was higher in women (females 11% vs. males 5.8%, P <0.001), also consistent with previous literature. Similarly, the preva-lence was signifi cantly higher in patients with other comorbidities (12% vs. 6.6% without them, P = 0.02) and in those patients who had complications associated with diabetes (9.4% vs. 6%; p = 0.021). There were no signifi cant differences in age (up to 59 years 7.8% vs. over 60 years 9%, P = 0.460); years of diabetes duration (between 0 and 5 years: 8.8%, between 6 and 14 years: 6.9% over 15 years: 8.1%, P = 0.663) or by HbA
1c levels (HbA
1c > 7%: 8.6%;
HbA1c
< 7%: 5.1 %, P = 0.101).
Descriptive study
3
Summary of evidence
Descriptive studies
3
DM1 is associated with higher rates of depressions than among the general population, regardless of age, race and the evolution of DM1, but not higher than other populations with chronic diseases420; 421, 423, 424, 425, 426, 427.
Descriptive study
3
The presence of depressions is associated with the presence of other diseases and the presence of diabetes-associated complications422.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 175
9.3.2. Anxiety disorders
A descriptive study423 showed no signifi cant differences in the prevalence of anxiety in newly diagnosed patients compared to a reference population (7.7% vs. 9.5%, P = 0.513).
Descriptive study
3
Hermanns et al.425 compared a group of DM1 or DM2 patients (n = 420) with a sample obtained from the general population. The prevalence of anxiety disorders observed were 5.9% versus 9% in people without DM.
Descriptive study
3
An observational study424 compared a group of patients with DM1 with another population without diabetes and found no difference in the prevalence rate of anxiety disorders among them (p = 0.31).
Case andcontrol studies
2+
A cross-sectional study429 with no control group noted that 35.5% of young adults with DM1 related stress, without any differences in gender, age or duration of diabetes being found. The use of CSII pumps is signifi cantly associated with higher scores on stress measured by the Achenbach scale (p = 0.01).
Descriptive study
3
Other descriptive studies indicated that the use of CSII is associated with higher levels of anxiety429. However, neither the duration of the disease, nor age seem to have a signifi cant effect on this disorder425, 429.
Descriptive study
3
Summary of evidence
Case control study
2 +
Descriptive studies
3
Anxiety is not related to the fact of suffering from diabetes mellitus type 1423,
424; 425, 429, but the use of continuous subcutaneous infusion pumps for insulin is associated with an increased level of anxiety in patients425, 429.
Recommendations
BProfessionals involved in the care of patients with diabetes mellitus type 1 should be alert to the possible emergence of depressive and/or anxious symptoms, especially when the person reports to have self-care problems.
√Health professionals should have the necessary skills for the detection and management of non-severe forms of psychological disorders and be familiar with counselling techniques and the administration of psychotropic drugs.
√ Moderate to severe cases should be referred to mental health specialists.
176 SNS CLINICAL PRACTICE GUIDELINES
9.3.3. Eating disorders
The CPG NICE 20047 includes the following studies related to this issue:
A prospective study430 compared possible eating disorders, weight changes or misuse of insulin in patients with and without diabetes, and found no increased incidence of eating disorders (ED), although higher BMI and greater concern on weight was observed among people with diabetes than among people without diabetes of the same age.
Descriptive study
3
A review of cross-sectional studies431 found a higher prevalence of bu-limia in women with DM1 than in the general population [OR 2.9 (95% CI 1.03 to 8.4)]. Misuse of insulin was increased when the ED coexisted with DM1 [OR 12.6 (95% CI: 7.8, 21.1)].
SR ofdescriptive
studies3
In a descriptive study, a rate of 5.3% ED was identifi ed in patients with DM1432.
Descriptive study
3
In a case-control study433 356 women with DM1 were compared to 1,098 controls, fi nding higher prevalence (10% vs. 4%) of ED in the group with dia-betes (p <0.001).
Case-control study 2+
According to the results of a study involving 91 young women with DM1434, those with eating disorders had worse metabolic control than those not suffering from these (p <0.001): baseline HbA
1C in the group with severe
ED: mean (SD) 11.1% (1.2) in the group with mild ED mean (SD) 8.9% (1.7), and without ED mean (SD) 8.7% (1.6). The ED at the beginning of the study were associated with the presence of retinopathy four years later (p = 0.004), occurring in 86% of women with severe eating disorders, 43% of those with mild disorders and 24% without ED.
Cohort studies2+
A cohort study435, which included 234 women, detected insulin con-straints in 30% of them. This was related to the presence of ED (p <0.05), higher mortality (p <0.05), early mortality (45 vs. 58 years, p <0.01) and in-creased risk of nephropathy and foot diabetes during a 28-year follow-up.
Cohort studies2+
Petrack et al.423 compared a gro up of newly diagnosed DM1 patients (n = 313) with a reference group of general population (n = 2046) and found no signifi cant differences in the prevalence of eating disorders at the time of diagnosis (1% vs. 0.3%).
Descriptive study
2
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 177
Grylli et al.436 conducted a study in 199 adolescents with DM1 (103 men/93 women) and found a higher prevalence of eating disorders in women than in men during this stage of life: 11.5% of women compared to 1% in males. The most common EDs were bulimia nervosa and non-specifi c eating disorders, with a very low incidence of cases of anorexia nervosa.
Descriptive study
3
Another comparative study437 indicated that the prevalence of eating dis-orders in patients with DM1 is four times higher than in the general population (p <0.001). The most commonly found weight control behaviour was dietary restriction (75%) and insulin management (40%).
Descriptive study
3
Summary of evidence
Descriptive studies
3
Eating disorders appear to be more frequent in patients with diabetes mellitus type 1 than in the general population423, 437, 436 especially in teenage girls.
Cohortstudies
2 +
People with diabetes mellitus type 1 who have eating disorders in adolescence have more medium-term microvascular complications434, 435 and increased long-term mortality435 than those who do not have these disorders.
Recommendations
C
The professional team members involved in the care of patients with diabetes mellitus type 1 should be alert about the possibility of occurrence of bulimia nervosa, anorexia nervosa and insulin management, especially in patients who express concern about their weight or body image, have a low body mass index or poor glycaemic control.
D
Given the risk of increased morbidity and mortality associated with poor metabolic control in people with eating disorders, it is recommended that in case of suspicion, the relevant diagnostic tasks are carried out and the department of psychiatry is contacted to apply the appropriate therapy.
BQualifi ed health professionals should provide information on healthy lifestyles and particularly on diet regularly to patients with diabetes mellitus type 1, especially in the teenage years.

178 SNS CLINICAL PRACTICE GUIDELINES
9.4. Risk of decompensation of diabetes mellitus type 1 during adolescence
Key question:
• Does adolescence pose a risk for decompensation in diabetes mellitus type 1?
Adolescence is a period involving signifi cant physical, psychological and social changes. These changes may have risks for adolescents with diabetes and provoke important metabolic decom-pensation, which may have long-term consequences on health, including kidney disease, cardio-vascular risk, retinopathy, etc.438.
In this chapter, the following aspects have been analyzed:
1. Risk of decompensation during adolescence.
2. Psychological factors that infl uence metabolic control during adolescence.
3. Adherence to the treatment during adolescence.
9.4.1. Risk of diabetic decompensation during adolescence
The CPG NICE 20047 includes the following studies:
A cohort study carried out in 42 children and adolescents with DM1 (mean age 12.9 years) examined whether pubertal development had an effect on metabolic control and adaptation to diabetes over four years439. Good control of the disease correlated with family cohesion (r = 0.38, p <0.01). In prepubertal young patients, family cohesion correlated well with the variable peer relationships (p = 0.008), the attitude towards diabetes (p = 0.03), and body image concerns (p = 0.05) in comparison with other adolescents.
Cohort studies2+
A study carried out in young patients with DM1 aged between 11 and 18 examined the effect of the psychological, behavioural and self-esteem on glycaemic control through an 8-year follow-up430. Behavioural problems in adolescence were signifi cantly associated with higher levels of HbA
1c. The
psychological state during the follow-up was a signifi cant predictor of recur-rent diabetic ketoacidosis admittance into hospital.
Descriptive study
3
In another descriptive study56 a positive association was found between the knowledge that the family has about DM1, the good family relationships and the younger age of the adolescent with good compliance with insulin regi-men.
Descriptive study
3
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 179
In a prospective observational study conducted on 15,967 young patients with DM1440 with a mean of 15.8 years, nine deaths related to diabetes dur-ing adolescence (6 due to acute complications and 3 due to neuropathy) were identifi ed. The risk of death was higher in adolescence than in childhood [RR 3.90 (95% CI 1.14 to 13.39)].
Observationalstudy
2+
9.4.2. Psychological factors infl uencing metabolic controlduring adolescence
The CPG NICE 20047 includes the following studies:
A cohort study441 showed that patients aged between 14 and 16 years with depressive symptoms had signifi cantly higher mean levels of HbA
1c than
patients without depressive symptoms [mean (SD): 9.0% (0.85) vs. 8.3% (1.4), P = 0.03].
Cohort studies
2+
In a small descriptive study442 (n = 16) of young patients with DM1 (age range: 15-18 years) depression was positively correlated with the deterioration of glycaemic control (r = 0.51, p <0.05).
Descriptivestudy
3
A cross-sectional study with no control group443 showed that depressive symptoms in adolescent girls and older, predicts poor adherence to the treat-ment (p <0.01).
Descriptivestudy
3
A multicenter cross-sectional study444 showed that depressive symptoms were associated with higher levels of HbA
1C and more visits to the emergency
unit, while no signifi cant relationship was stated regarding the number of hos-pitalizations, the number of episodes of hypoglycaemia, and/or ketoacidosis.
Descriptivestudy
3
A longitudinal observational study445 revealed that the presence of de-pressive symptoms at the beginning of the study predicted risk of hospitaliza-tion during the next 24 months [OR 2.58 (95% CI: 1.12 to 5.98)].
Longitudinalobservational
study2+
The study by Pinar et al.437 shows that the presence of ED predicts worse glycaemic control (p <0.001).
Descriptivestudy
3
180 SNS CLINICAL PRACTICE GUIDELINES
9.4.3. Adherence to the treatment
The CPG NICE 20047 includes the following studies:
A study in Scotland446 showed that people aged between 10 and 20 years old had signifi cantly higher levels of HbA
1c (p = 0.01) and lower adherence to
the insulin treatment (p <0.001) than the younger or older age group.
Descriptivestudy
3
A longitudinal study445 found that data reported by patients with DM1 regarding HbA
1c is the best predictor of HbA
1c, explaining the 30% of the
variance in the case of adolescents and the 19% in the case of parents. The cor-relation between the referred self-care and glycaemic control was signifi cant (p <0.01).
Descriptivestudy
3
Naar-King et al.447 examined the relationship between adherence and metabolic control, taking into account the role of the presence of psychologi-cal disorders. The presence of anxiety symptoms and behavioural problems were associated with poorer adherence, but ultimately only behaviour prob-lems predicted worse metabolic control (p <0.01).
Descriptivestudy
3
Summary of evidence
Descriptive study
3
Adolescence is associated with poorer metabolic control in patients with diabetes mellitus type 1446 especially if associated with behaviour problems430; 439.
Descriptive study
3
Good control of the disease correlates with family cohesion and its knowledge about diabetes mellitus type 156.
Descriptive study
3
Patients aged between 14 and 16 with depressive symptoms have signifi cantly higher HbA
1C levels than those patients without depressive symptoms441, 442, 443,
444, 445.
Descriptive study
3The presence of eating disorders predicts worse glycaemic control (p <0.001)437.
Descriptive study
3
People aged between 10 and 20 have signifi cantly higher HbA1C
levels (p = 0.01) and lower adherence to the insulin treatment (p <0.001) than the younger or older age group446.
Descriptive study
3
The presence of anxiety symptoms and behavioural problems are associated with poorer adherence, but ultimately only behaviour problems predicted worse metabolic control (p <0.01)447.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 181
Recommendations
C
Adherence to the treatment is a key factor in managing diabetes, so it is important to work on this aspect with the adolescent patient together with his family, and analyze barriers, which may impede an adequate adhesion (anxiety, depression, eating disorders and behavioural problems).
C
The professionals in charge of children and adolescents with diabetes mellitus type 1 should be aware they might develop depression and/or anxiety disorders, particularly when there are diffi culties in controlling the disease or if the disease is long lasting.
√In children and adolescents with persistent poor glycaemic control, the level of anxiety and depression should be assessed.
√Children and adolescents suspected to suffer anxiety or depression disorders should be referred to mental health professionals.
C
Given the high prevalence of eating disorders in adolescents with diabetes, especially among women, it is advised to be alert about the presence of symptoms that may indicate the presence of an eating disorder or insulin managing. In case of suspicion, the department of psychiatry for diagnosis and appropriate therapy should be contacted and worked with.
√It is recommended to address the issue of alcohol, smoking and other drugs with the teenager with diabetes mellitus type 1 to avoid its consumption and provide strategies to prevent episodes of hypoglycaemia.

182 SNS CLINICAL PRACTICE GUIDELINES
9.5. Pregnancy planning
Key question:
• Is it important to plan pregnancy in women with diabetes mellitus type 1?
Diabetes may favour the occurrence of certain events in pregnant women (urinary infections, vaginal candidiasis, polyhydramnios, hypertensive pregnancy and prematurity disorders) and in the foetus or newborn infant (malformations and/or abortions, retarded intrauterine growth, mac-rosomia, hypertrophic cardiomyopathy and foetal immaturity). In addition, pregnancy can affect glycaemic control in women with diabetes, increasing the frequency of hypoglycaemia and its inadvertence, or hyperglycaemia by increased placental lactogen especially after 20 weeks of gestation. The progression of certain complications of diabetes, especially diabetic retinopathy and nephropathy, may also be affected during this period.
It is considered of interest to analyze the benefi ts pregnancy planning can have in women with DM1, in terms of reduction of adverse perinatal outcomes (abortions, foetal malformations, eclampsia, perinatal death or other complications).
Planning pregnancy in pregnant women with DM1 is to use contraception to decide the most appropriate time for it to occur. This requires determining, based on maternal complications secondary to DM, the risk involved in a pregnancy, and reduce the maternal and foetal complica-tions with adequate metabolic control and medical monitoring before conception. This is done by informing the couple of the mutual impact between DM and pregnancy, as well as of the methods to prevent potential complications.
The CPG NICE on pregnancy 20089 includes the following studies:
A study449 conducted in 442 pregnant women with DM (73% with DM1) found an association between the lack of information about foetal risks before pregnancy and the risk of caesarean delivery [OR 2.9 (95% CI: 1, 1 to 8.2)] and increased neonatal mortality adjusted for maternal age and lower social status [OR 2.4 (95% CI: 1.0 to 5.8)].
Descriptivestudy
3
An SR with meta-analysis of 16 observational studies450 evaluated the infl uence of preconception care programs (PCP) in women with diabetes in reducing the risk of major congenital anomalies. The PCP consisted of glycae-mic control planning before pregnancy. The results obtained indicate that from the 2104 births, the weighted rate of major and minor anomalies was 2.4% for women included in the PCP compared with 7.7% for the group without PCP. The relatively low values of HbA
1c during the fi rst trimester in the group with
PCP suggest that glycaemic control during the fi rst weeks of pregnancy prob-ably plays an important role in preventing birth malformations.
SR of observa-tional studies
2++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 183
The cohort study by McElvy et al.451 evaluated the impact of a precon-ception care program made for 5 years in three stages (PPG I, II PPG, PPG III). During the period before the fi rst program (PPG I) (1973-1978) n = 79 revealed a perinatal mortality rate of 7% and a congenital malformation rate of 14%. The perinatal mortality rate dropped from 3% in the PPG I and 2% with the PPG II, to 0% in the PPG III. The rate of congenital malformations decreased to a minimum of 2.2% by PPG III.
Cohort study2+
In one trial452 84 women with DM (68% DM1) were trained for 17 weeks before and during pregnancy on concepts related to glucose monitoring, diet and exercise, insulin dose adjustments and complications of diabetes and they were compared with a group of 110 women (60% DM1) that was trained only during pregnancy. In the group that received the preconception education, a failure rate of 1.2% was found compared to the 10.9% found in the group that had only received education during the postconceptional period (p = 0.01).
RCT 1+
A prospective cohort study conducted in 160 women with DM1453 ana-lyzed the glycaemic control and the frequency of severe hypoglycaemia based on pregnancy planning. The results of the study were the following:
• 68.8% of pregnancies were planned vs. 33.8%, which were unplanned.
• 29.4% of women with DM1 had severe hypoglycaemia during preg-nancy, 21.9% in the fi rst trimester, 18.1% in the second trimester and 10.6% in the third trimester.
• The duration of diabetes was associated to an increased risk of severe hypoglycaemia during pregnancy (p = 0.012).
• The duration of diabetes was correlated with the total number of episodes of severe hypoglycaemia during pregnancy (r = 0.191, P = 0.017) and during the fi rst trimester (r = 0.16, p = 0.05). The duration of diabetes in women who had an episode of severe hypoglycaemia was on average (SD) 19.2 years (7.2).
• The total number of episodes of severe hypoglycaemia during preg-nancy is associated with the average HbA
1c level in the fi rst trimester
(r = 0.17, p = 0.043).
• 56% of U.S. women used 4 or more injections per day during periods before pregnancy, increasing to 77% and 83% in trimesters 1 and 3 respectively and this was not associated to an increase in hypoglycae-mia.
• Women who achieved HbA1c
levels less than 6.5% (n = 41) during the fi rst trimester were less likely to experience severe hypoglycaemia in the second trimester (7.3 vs. 25%; p = 0.019) and in the third trimester (0 vs. 16%, P = 0.003) than women with higher HbA
1c levels in the
fi rst trimester. These women had a lower mean duration of diabetes, although this difference is not signifi cant.
Cohort studies2+
184 SNS CLINICAL PRACTICE GUIDELINES
• The reduction in HbA1c
levels between the period before pregnancy and the fi rst trimester was not associated with severe hypoglycaemia in the fi rst trimester. However, a higher reduction of HbA
1c levels be-
tween the fi rst and second trimesters was correlated with the num-ber of episodes of severe hypoglycaemia in the second trimester (r = 0.194, P = 0.021).
• A signifi cant difference was found in HbA1c
levels between planned and unplanned pregnancies. In addition, among planned pregnancies there were more numbers of severe hypoglycaemia than in the un-planned ones (p = 0.047).
• No signifi cant differences were found in glycaemic control or the risk of severe hypoglycaemia among women using insulin analogues and those who did not take them during pregnancy, although there was a trend to signifi cance in the third trimester (HbA
1c6.4 vs. 6.7%, P =
0.06).
• The fall in the average HbA1c
levels between pre-pregnancy and the fi rst trimester was signifi cantly higher (1.0 vs. 0.5%) in women who used insulin analogues (n = 43, p = 0.005), but without noticing an increase in the number of severe hypoglycaemia.
Women smokers (n = 40) and those with retinopathy before pregnancy (n = 36) were 3 times more likely to suffer an episode of severe hypoglycaemia in the third trimester (p = 0.029, p = 0.03). Although those with retinopathy before pregnancy had a duration of diabetes (19.8 vs. 12.3 years, p = 0.001), the duration of diabetes was not associated with severe hypoglycaemia in the third trimester.
A cohort study454, which included 46 women with DM1 and nephropa-thy before pregnancy, analyzed the complications during pregnancy including abortion in the fi rst trimester, preeclampsia, premature delivery, baby weight and length, admission to the NICU and foetal loss. As results, these showed that 31 women (67%) had at least one complication during pregnancy. BMI was the only parameter with a signifi cant difference between the groups, be-ing higher in women with a complicated pregnancy compared to those who had no complications [mean (SD) 27 (9) vs. 24 (3), P = 0.027]. No differ-ences were found between the groups in relation to preconception counselling (60% vs. 67%), the pre-pregnancy glycaemic control (HbA
1c 7.5 vs. 7.1%), the
prevalence of patients who had an adequate glycaemic control (44% vs. 42%), weight gain during pregnancy (12.4 vs. 10.6 kg), duration of DM (18 vs. 19.7 years) and the proportion of patients treated with ACEi before pregnancy (26 vs. 33%). The authors concluded that overweight is associated with poor preg-nancy outcomes in patients with DM1 and different degrees of nephropathy.
Cohort studies 2+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 185
An SR with meta-analysis455 that included one RCT and 19 observational studies in patients with DM1 and DM2, analyzed the effects of glycaemic con-trol with fasting glucose levels ≤ 5.7 mmol/l or postprandial glucose levels ≤ 7.8 mmol/l and/or HbA
1c levels ≤ 7.0%, counselling or education about diabe-
tes, contraceptive use to optimize glycaemic control, multivitamin use and/or folic acid in the preconception period on complications during pregnancy. The results of the meta-analysis suggest that preconception care is effective in re-ducing birth defects, [RR 0.25 (95% CI: 0.15 to 0.42)], [NNT 17 (95% CI: 14-24)], preterm birth [RR 0.70 (95% CI 0.55 to 0.90)], [NNT 8 (95% CI 5-23)] and perinatal mortality [RR 0.35 (95% CI: 0.15 to 0.82)], [NNT 32 (95% CI 19-109)]. In these patients, the preconception care decreased HbA
1C levels in
the fi rst trimester of pregnancy by an average of 2.43% (95% CI: 2.27 to 2.58).
SR of RCT and Observa-tional studies
2++
Summary of evidence
Cohort studies 2 +
In women with diabetes mellitus type 1 planned pregnancies have a better metabolic control and an increased risk of hypoglycaemia453.
RCT 1 +
Cohort studies 2 +
SR of observational
studies 2++
Preconception care is effective in reducing congenital malformations450, 454, 455, 455 and in preterm delivery455 and perinatal mortality449, 451 452.
SR of observational
studies 2 + +
Preconception care decreases HbA1C
levels in the fi rst trimester of pregnancy455.
Cohort study 2 +
Being overweight is associated with poor pregnancy outcomes in patients with DM1 and different degrees of nephropathy454.
186 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
B
As all patients diagnosed with diabetes mellitus type 1, adolescents and women of childbearing age should participate in diabetes education programs in order to facilitate the control of their disease and promote self-care. These programs should include specifi c ideas about the importance of control before conception and general recommendations for pregnancy (vitamin supplements, suppression of teratogenic drugs, etc.). It is convenient to remind these patients about these points in all the visits to the health centre to ensure a pregnancy in optimal conditions.
B
In women planning to become pregnant, it is considered relevant performing a pre-conceptional visit to set out control targets, establishing the appropriate treatment (folic acid, iodine, etc.), review the possible complications and give “green light” to the pregnancy.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 187
9.6. Complications of diabetes mellitus type 1 during pregnancy
Key question:
• How does pregnancy affect the development of the complications of diabetes mellitus type 1?
9.6.1. Evolution of retinopathy during pregnancy
The CPG NICE on pregnancy 20089 provides evidence on this issue.
A prospective cohort study456 assessed the progression of retinopathy dur-ing pregnancy in 180 women (270 pregnancies) compared to 500 non-pregnant women during 6.5 years of follow up. It was observed that pregnant women had a 1.63 times greater risk of worsening retinopathy in the intensive treat-ment group compared with non-pregnant women (p <0.05). The OR peaked during the second trimester (OR 4.26, P = 0.001) and persisted until 12 months after pregnancy (OR 2.87, p = 0.005).
Cohort study 2+
An observational study457 evaluated the incidence, prevalence, and risk factors for progression of diabetic retinopathy during pregnancy. A total of 65 pregnant women with DM1 were evaluated before pregnancy, each trimester, and 12 months after delivery. Progression of retinopathy occurred in 77.5% of patients who had retinopathy before conception and 22.5% occurred in prolif-erative diabetic retinopathy. Only 26% of women who had no retinopathy in early pregnancy had a progression of it. Duration of diabetes (p = 0.007) and HbA
1c levels were higher in the progression group than in the group without
progression at all times when it was assessed, but only in the third trimester, was the difference statistically signifi cant (p = 0.04).
Longitudinal- observational
Study2+
A cohort study analyzed the progression of retinopathy in 154 women with DM1 during pregnancy and after 6 and 12 weeks after delivery458 and found that 51 women (33.11%) had progression of retinopathy during pregnancy and regression was observed in 13 postpartum women (8.44%). Progression of retinopathy was signifi cantly associated with changes in glycaemic control in early pregnancy, chronic hypertension and pregnancy-induced hypertension.
Cohort study
2+
188 SNS CLINICAL PRACTICE GUIDELINES
9.6.2. Evolution of nephropathy during pregnancy
No studies have been found to analyze this issue.
Summary of evidence
Cohort study 2 +
Retinopathy diagnosed before pregnancy tends to worsen during pregnancy456,
282, especially during the second trimester456.
Cohort study 2 +
The progression of retinopathy is associated with changes in glycaemic control in early pregnancy, chronic hypertension and pregnancy-induced hypertension458.
Recommendations
BIt is advisable to plan the pregnancy in women with diabetes mellitus type 1 to achieve adequate glycaemic control and conduct the evaluation of the possible retinopathy and nephropathy before and during pregnancy.
√It is recommended to inform the couple on the mutual repercussions between diabetes mellitus type 1 and pregnancy, making explicit reference to the possible complications that can arise and the methods to prevent them

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 189
9.7. Metabolic control during pregnancy
Key question:
• How does pregnancy affect the development of the complications of diabetes mellitus type 1?
Although there is agreement on the need to inform women with DM1 on the need for adequate glycaemic control before and during pregnancy, there is no agreement on what is meant by ad-equate glycaemic control during this time and what the goals to be set out are for these women in order to get better results for themselves and lower perinatal morbidity.
The CPG NICE 20089 included 23 cohort studies459, 460, 461, 462, 463, 464, 465, 466, 467,
468, 469, 470, 471, 472, 473, 474, 475, 476, 477, 478; 479, 480 and established an association between preconceptional control and the incidence of abortions and congenital malformations.
• Risk of congenital malformations:
A cohort study459 on 488 women with DM1 linked the HbA1C
levels in the fi rst trimester to the appearance of malformations (p = 0.02), demonstrating that the risk increases gradually to higher levels of HbA
1c in the fi rst trimester of
pregnancy
Cohortstudy
2+
Likewise, another cohort study474 found that the rate of major malforma-tions was signifi cantly higher in women whose HbA
1c level in the fi rst trimes-
ter exceeded values of 12.7%.
Cohortstudy
2+
A study460 that included 435 pregnant women (289 with DM1 and 146 with DM2) compared women with HbA
1C levels above 8% in the fi rst trimester
with women with HbA1C
levels lower than this value, noting higher rates of congenital malformations in the fi rst group [ (8.3% vs. 2.5%, OR 3.5 (95% CI: 1.3 to 8.9), P <0.01].
Cohortstudy
2+
Another cohort study that examined 142 pregnancies in women with DM1476 detected congenital malformations in 17 neonates (six minor and elev-en major). Baseline HbA
1c was signifi cantly higher in the group with minor
malformations [mean (SD): 9.3% (1.9), P <0.05)] and in the group with major malformations [mean (SD): 9, 6% (1.8), p <0.001)] than in the group without malformations [mean (SD): 8.0% (1.4)].
Congenital malformations were detected in 48% (3/63) of women with HbA
1C less than 8%, 12.9% (8/62) in those with HbA
1C from 8 to 8.9% and
35.3% (6/17) had average levels, which were equal, or greater than 10%.
Cohortstudy
2+
190 SNS CLINICAL PRACTICE GUIDELINES
A study by Miller et al. in 116 women with DM1470 showed that there were no malformations (0/19) in the offspring of women with HbA
1C levels of
6.9% or less. In women with HbA1C
levels in the range from 7.0 to 8.5%, the percentage who had malformations was 5.1% (2/39).
Cohort study
2+
A cohort study that followed up 83 pregnant women466, 63 with DM1 and 20 with DM2, examined the relationship between HbA
1c levels during the fi rst
trimester and congenital malformations. In 9 cases congenital malformations appeared, all with HbA
1C levels higher than 9.5% in the fi rst trimester (7 with
HbA1c above 11.5% and 6 with HbA1C higher than 13.5%).
Cohort study
2+
Another cohort study471 carried out in a sample of 229 pregnant women with DM1 found that the threshold for increased risk of abortion or malforma-tions is glycaemia in the fi rst trimester between 120 and 130 mg/dL or HbA
1c
levels of between 12 and 13%. Below these glycaemic levels, the risk is com-parable to that of non-diabetic women.
Cohort study
2+
• Risk of spontaneous abortions:
A cohort study with a sample of 105 women with DM1477 reported spontaneous abortions in 18 women. The HbA
1C levels during the fi rst
trimester were between [mean (SD) 9.4% (2.3)] which were not signifi cantly different from the mean HbA1C level of pregnancies that resulted in a baby with malformations [mean (SD) 10, 3 (1.9)] or no adverse outcome [mean (SD) 8.9% (2.3)].
Cohort study
2+
In a cohort study466 carried out in 83 women (63 women with DM1 and 20 DM2), the rate of spontaneous abortions was 26.5% (22 pregnancies). There were no spontaneous abortions in women with HbA
1C less than 7.5% in
the fi rst trimester. An abortion occurred in a woman with HbA1C
between 7.5 and 9.4%, 21 in women with HbA1C > 11.5% and two of them with HbA1C > 13.5%.
Cohort study
2+
A cohort study carried out in 303 women with DM1474 found that rates of spontaneous abortions were signifi cantly higher when the HbA
1c in the fi rst
trimester was higher than 11.0% compared to normal average in non-diabetic women [mean (SD) 5, 9% (0.57)].
Cohort study
2+
A cohort study that analyzed 84 pregnancies in women with DM1469 found that women who had a spontaneous abortion, had a signifi cantly higher HbA
1c [mean (SD) 12.0% (0.6)] than women whose pregnancy progressed
beyond 20 weeks [mean (SD) 10.7% (0.3), P <0.05]. The results suggest that poor glycaemic control around conception is a more important factor than in the weeks immediately preceding a spontaneous abortion.
Cohort study
2+
In another cohort study with 215 women with DM1471, 52 women (24%) had spontaneous abortions. The threshold value for increased risk of abortion or malformations is a glycaemia in the fi rst trimester between 120 to 130 mg/dL or HbA1c levels of between 12 and 13%.
Cohort study
2+
A cohort study of 116 pregnancies in 75 women with DM1468 found to be signifi cantly more likely for spontaneous abortions to occur when HbA
1C was
higher than 12% (p <0.05).
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 191
• Other neonatal outcomes:A cohort study examined the effect of glycaemic control at different times during pregnancy, in trimesters of adverse outcomes (perinatal death and/or congenital malformations in 990 pregnancies)465. The mean HbA1C in the 0 to 3 months prior to conception was 8.0% (interquartile range 7.3 to 9.1) in the adverse outcome group compared with 7.6% (interquartile range 6, 8 to 8.5) in the other group (p = 0.005). Women with adverse clinical outcomes received preconception counselling less frequently (42% vs. 59%, P = 0.002) and per-formed less measurements of glucose levels on a daily basis until conception (23% vs. 35%, p = 0.019).
Cohort study
2+
In an observational study481 211 pregnancies in 132 women were ana-lyzed, with 61 adverse outcomes (29%) including spontaneous abortions, ter-minations of pregnancy for medical reasons, neonatal deaths and congenital malformations. Mothers with poor glycaemic control before conception and at the time of conception (HbA1c ≥ 7.5%) had an adverse outcome rate almost three times higher than mothers with good glycaemic control [OR 2.59 (95% CI: 1.11 to 6.03) and OR 2.71, 95% CI 1.39 to 5.28, respectively)].
Observational study
3
In an SR482 RCTs that compared different targets of glycaemic control in pregnant women with DM1 and DM2 were included. Three trials in women with DM1 (223 women and children), and all with a high risk of bias were in-cluded. Two trials compared objectives of very strict glycaemic control (3.33 to 5.0 mmol/L fasting blood glucose) with strict-to-moderate glycaemic con-trol targets (4.45 to 6.38 mmol/L).
SR of poor quality RCT
1+/-
With a limited body of evidence, few differences in the outcomes be-tween strict glycaemic control measures and strict-to-moderate measures were found in pregnant women with pre-existing DM1. Adverse effects were noted (increased preeclampsia, caesarean deliveries and children with high birth weight percentile> 90) for fasting glucose levels above 7 mmol/L.
Summary of evidence
Cohort study 2 +
Several prospective studies have demonstrated an association between good metabolic control during the fi rst trimester of pregnancy and lower incidence of congenital malformations459, 460, 466, 469, 470, 471, 474, 476.
Cohort study 2 +
The level of HbA1C
that has proven to be related to the non-presence of malformations is 6.9% or less470.
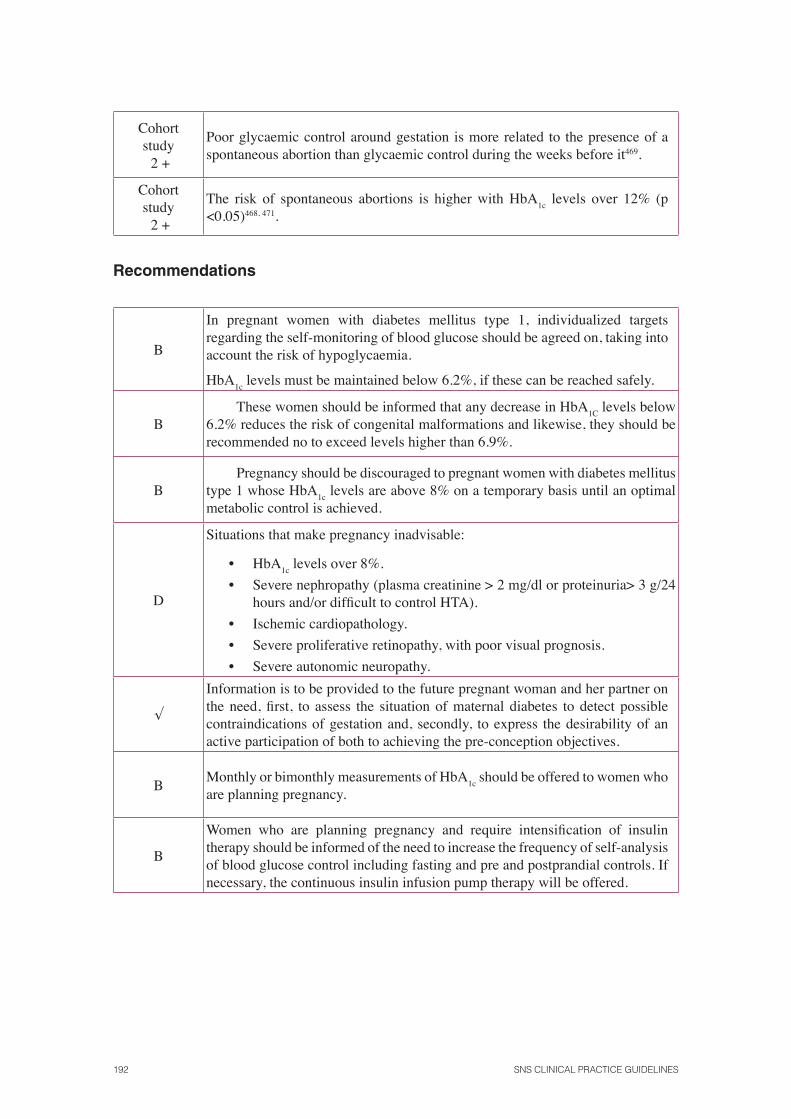
192 SNS CLINICAL PRACTICE GUIDELINES
Cohort study 2 +
Poor glycaemic control around gestation is more related to the presence of a spontaneous abortion than glycaemic control during the weeks before it469.
Cohort study 2 +
The risk of spontaneous abortions is higher with HbA1c
levels over 12% (p <0.05)468, 471.
Recommendations
B
In pregnant women with diabetes mellitus type 1, individualized targets regarding the self-monitoring of blood glucose should be agreed on, taking into account the risk of hypoglycaemia.
HbA1c
levels must be maintained below 6.2%, if these can be reached safely.
BThese women should be informed that any decrease in HbA
1C levels below
6.2% reduces the risk of congenital malformations and likewise, they should be recommended no to exceed levels higher than 6.9%.
BPregnancy should be discouraged to pregnant women with diabetes mellitus
type 1 whose HbA1c
levels are above 8% on a temporary basis until an optimal metabolic control is achieved.
D
Situations that make pregnancy inadvisable:
• HbA1c
levels over 8%.
• Severe nephropathy (plasma creatinine > 2 mg/dl or proteinuria> 3 g/24 hours and/or diffi cult to control HTA).
• Ischemic cardiopathology.
• Severe proliferative retinopathy, with poor visual prognosis.
• Severe autonomic neuropathy.
√
Information is to be provided to the future pregnant woman and her partner on the need, fi rst, to assess the situation of maternal diabetes to detect possible contraindications of gestation and, secondly, to express the desirability of an active participation of both to achieving the pre-conception objectives.
BMonthly or bimonthly measurements of HbA
1c should be offered to women who
are planning pregnancy.
B
Women who are planning pregnancy and require intensifi cation of insulin therapy should be informed of the need to increase the frequency of self-analysis of blood glucose control including fasting and pre and postprandial controls. If necessary, the continuous insulin infusion pump therapy will be offered.
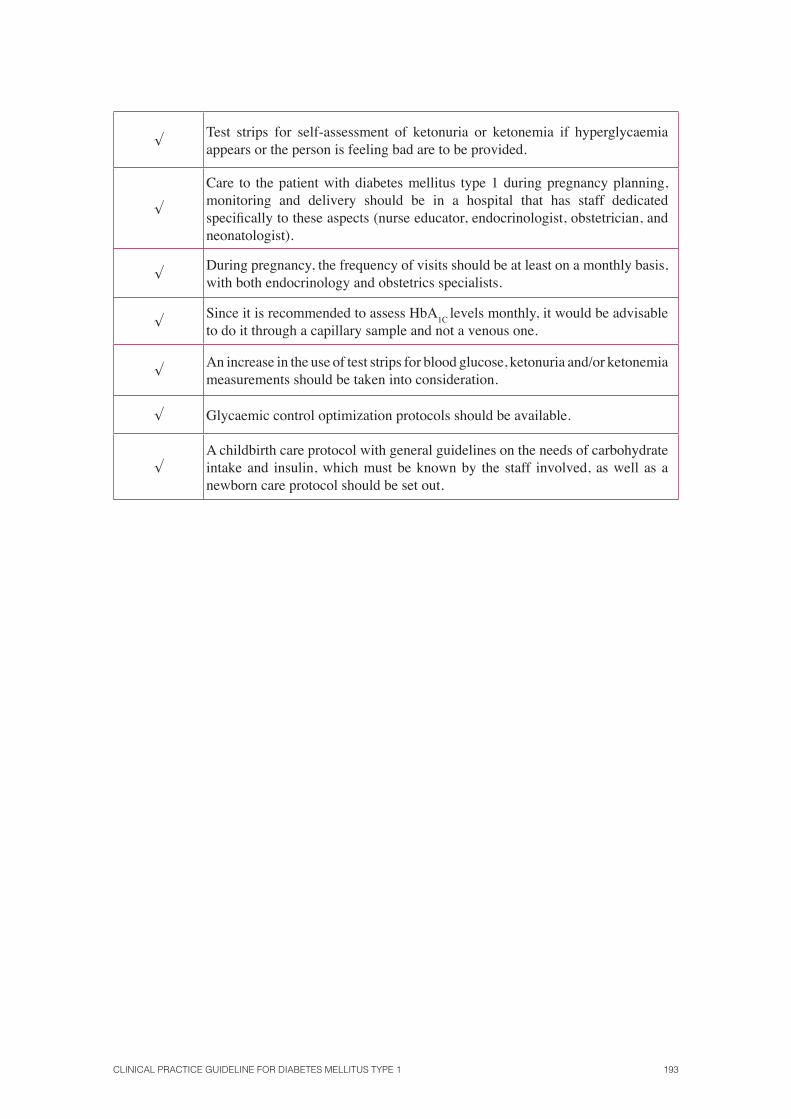
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 193
√Test strips for self-assessment of ketonuria or ketonemia if hyperglycaemia appears or the person is feeling bad are to be provided.
√
Care to the patient with diabetes mellitus type 1 during pregnancy planning, monitoring and delivery should be in a hospital that has staff dedicated specifi cally to these aspects (nurse educator, endocrinologist, obstetrician, and neonatologist).
√During pregnancy, the frequency of visits should be at least on a monthly basis, with both endocrinology and obstetrics specialists.
√Since it is recommended to assess HbA
1C levels monthly, it would be advisable
to do it through a capillary sample and not a venous one.
√An increase in the use of test strips for blood glucose, ketonuria and/or ketonemia measurements should be taken into consideration.
√ Glycaemic control optimization protocols should be available.
√A childbirth care protocol with general guidelines on the needs of carbohydrate intake and insulin, which must be known by the staff involved, as well as a newborn care protocol should be set out.

194 SNS CLINICAL PRACTICE GUIDELINES
9.8. Contraception and diabetes mellitus type 1
Key question:
• What are the most recommended contraceptives in women with diabetes mellitus type 1?
In previous questions the importance of pregnancy planning in women with DM1 has been deter-mined in order to intensify the treatment of DM1 until an adequate glycaemic control is achieved and collateral diseases are controlled (such as, retinopathy, nephropathy, etc.) prior to conception.
It is therefore important to identify the most effective and safest contraceptive methods for women with DM1.
The CPG NICE 20089 provides no evidence on this issue.
An SR conducted in women with diabetes (75% with DM1)483 included three RCTs to compare the effectiveness and safety of hormonal versus non-hormonal contraceptive methods. The authors concluded that there was insuffi cient evidence to decide whether to prescribe the convenience of hormonal or non-hormonal contraceptives for women with DM1. By consensus of the authors, the copper intrauterine device (IUD) was recommended as safest choice for patients with DM until the safety of hormonal contraceptives is proven. However, it was also considered probable that the IUD that releases levonorgestrel (LNG) would also be safe, as its use has not been associated with effects on the glucose metabolism.
SR of RCT 1++
A WHO report484 on medical eligibility criteria for different contraceptive methods evaluated both the medical condition of diabetes and all the compli-cations and circumstances that can occur, establishing different recommenda-tions based on the individual characteristics of each patient. These recommen-dations are summarised in Appendix 7.
Expertconsensus
4
Summary of evidence
SR of RCT 1 + +
Expertconsensus
4
There is insuffi cient evidence on the effectiveness and safety of all contraceptive methods in women with DM1. The consensus recommendations come from prestigious institutions and organizations.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 195
Recommendations
D
Women with type 1 diabetes are recommended to use the copper IUD as safest contraception method. The use of the IUD that releases levonorgestrel (LNG) cannot be ruled out, as it has not been observed to affect the metabolism of glucose.
196 SNS CLINICAL PRACTICE GUIDELINES
9.9. Clinical management of diabetes mellitus type 1 in patients with special needs
Key question:
• How can the clinical management of diabetes mellitus type 1 for patients with special needs be adapted?
9.9.1. Immigrant Population
In recent years, Spain has become one of the European Union countries that receives the high-est number of immigrants, being in 2009 the immigrant population 12% of the total number. It should be noted that 44.81% of all the immigrants registered in Spain are distributed among three provinces (Madrid, Barcelona and Alicante).
The clinical management of DM1 in immigrants can be diffi cult due to the existence of lin-guistic, cultural and religious barriers.
Clinical management of diabetes mellitus type 1 in Muslims patients during Ramadan
Ramadan is the holy month of Islam that takes place in the ninth month of the lunar calendar. During this period the Muslim believers practice fasting, both of solid and liquid foods including water, and medicine from sunrise to sunset. Generally, there are two intakes a day, one before dawn (suhoor) and one after sunset (iftar).
People under 12, the elderly, pregnant women and those with certain diseases are exempt from compliance. However, it is common for Muslim patients to insist on fasting during Ramadan, which signifi cantly increases the risk of acute complications in people with DM1. The risks asso-ciated with fasting in people with diabetes are hypoglycaemia, hyperglycaemia, diabetic ketoaci-dosis, dehydration and thrombosis485.
Al Arouj et al.486 have been categorized by consensus patients with DM according to risk of complications during fasting:
Very high risk if there is:
• Severe hypoglycaemia three months beforehand.
• History of recurrent hypoglycaemia.
• Poor diabetic control.
• Ketoacidosis three months beforehand.
• Diabetes Type 1.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 197
• Intercurrent disease.
• Hyperosmolar coma three months before.
• Intense physical work.
• Pregnancy.
• Haemodialysis.
High risk if there is:
• Moderate control of diabetes (glycaemia 150-300 mg/dl, HbA1c
7.5 to 9.0%).
• Renal insuffi ciency.
• Advanced macrovascular complications.
• Patients who live alone.
• Additional risk factors.
• Advanced age, health alterations.
• Drugs affecting the level of consciousness.
The categories identifi ed by the author as “moderate risk” and “low risk” are only applicable to patients with DM2.
The CPG NICE 20047 includes this issue, but does not provide specifi c evidence on the sub-ject and its recommendations were based on consensus.
The American Diabetes Association486 recommends the administration of two doses of a mixture of NPH insulin and fast acting insulin type 30/70 before the two main intakes. It also recommended inverting the doses, administering the usual morning dose before the evening meal (iftar), and halving the even-ing dose, to be administered prior to a meal before dawn (suhoor) thus reduc-ing the risk of hypoglycaemia during the day.
Expert opinion 4
In an RCT with crossover design at the University of Minnesota487 car-ried out in 15 patients with DM1 and HbA
1C levels less than 7.5%, a dose of
insulin glargine was administered at 10 pm and a dose of fast acting insulin before meals, comparing glucose levels every two hours during a day in which they received breakfast, lunch and dinner compared to another day in which they only received dinner (18 hour fast). No statistically signifi cant differences were found between the two groups, except for glucose at 9 am. Only two epi-sodes of mild hypoglycaemia were described during fasting.
RCT 1+
198 SNS CLINICAL PRACTICE GUIDELINES
In a randomized, crossover study in 64 patients with DM1 that was car-ried out in a health centre in Morocco, an insulin treatment based on two doses of mixed NPH and fast acting insulin versus two doses of mixed NPH insulin and ultra-fast insulin (lispro) analogue was compared. There was an improve-ment in postprandial glycaemia in the group treated with lispro (decrease of 45 vs. 61.2 mg/dl, p = 0.026). The number of hypoglycaemia was signifi cantly lower in the group treated with lispro insulin compared to the group treated with fast insulin (15 vs. 21, p = 0.004)488.
RCT 1+
In a study conducted in a medical centre in Lebanon that included 17 patients with DM1489, who were administered 85% of the usual dose of insulin into two equal parts between suhoor (pre-dawn) and iftar (after dark), 70% as ultraslow insulin and 30% as fast acting insulin. With this pattern, no changes were recorded in HbA
1C levels nor an increased risk of hypoglycaemia.
Before Ramadan, intermediate acting insulin was changed to ultra slow insulin in all patients. The total dose of insulin administered to the fasting patients at the end of Ramadan [mean (SD) 45.7 U/day (14.4)] was less than the total dose of insulin administered before fasting [mean (SD) 52.8 U/day (13.1), p <0.05]. No episodes of severe hypoglycaemia were observed during the day.
Observational study
2+
In a descriptive study490 conducted in Lebanon in 9 patients with DM1 who fasted during Ramadan a regimen based on a daily injection of insulin glargine and three doses of insulin lispro or aspart before each meal was ap-plied during the week before fasting. At the beginning of fasting, the dose prior to Ramadan was reduced to 20% and a dose of insulin glargine and two doses of lispro or aspart were administered before suhoor and iftar. No signifi cant differences were found in HbA
1c before and after fasting, although two pa-
tients discontinued fasting due to episodes of hypoglycaemia.
Descriptive study 3
Summary of evidence
1+The basal bolus therapy eliminating the bolus of meals, which do not take place, allows adequate metabolic control in people with diabetes mellitus type 1 who practice fasting during Ramadan486, 487, 488, 489.
Recommendations
Immigrant population. General recommendations
√
If the patient with diabetes mellitus type 1 presents diffi culties to understand the language, the use of automatic translation systems (via telephone or audiovisual methods of open and closed questions) or by direct translation during the visit is recommended.
√Likewise, the use of simple graphics that facilitate understanding of the disease and the guidelines to be followed, is recommendable.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 199
Recommendations for Muslim patients during Ramadan
Before Ramadan
√Inform the health care team about the concept of Ramadan and the risks posed by fasting.
√ Plan the process in time for the celebration of Ramadan.
√ Identify Muslim patients with diabetes mellitus type 1.
√Carry out a clinical interview with these patients to know their desire to fulfi l the precept of Ramadan.
√Inform patients about the possibility of not celebrating Ramadan due to having a chronic disease and the risks involved.
√
Evaluate the existence of major criteria to strongly discourage compliance of Ramadan:
• Diabetes with poor metabolic control.
• Chronic complications of advanced diabetes: renal failure, ischemic heart disease with unstable angor, advanced peripheral macroangiopathy.
• Frequent hypoglycaemia, severe or without adrenergic clinic.
• Diabetic ketoacidosis in the months prior to Ramadan.
• Gestation.
• Physical activity during the day.
• Aged with dependence on others.
√
In the event that these criteria are not met and the patient wishes to fulfi l the precepts, making the corresponding therapeutic changes before and during Ramadan regarding diet and exercise is deemed appropriate:
• Optimize glycaemic and metabolic control 1-2 months before.
• Specifi c diabetes education (symptoms of hyper-and hypoglycaemia, meal and physical activity planning, drug administration and attitude in case complications arise).
During Ramadan
√ Individualized care plan.
√ Frequent blood glucose determinations.
√ Avoid foods, which are rich in carbohydrates with rapid absorption and fats.
√ Eat more food s composed of complex carbohydrates.
√ Fruits, vegetables and yogurt can be included in the diet.
√ Practicing suhoor immediately before sunrise and not in the early morning.
200 SNS CLINICAL PRACTICE GUIDELINES
√ Drink unsweetened fl uids to quench thirst.
√ Reduce fried foods.
√ Carry out regular physical activity, avoiding excessive exercise.
√ Break fasting if blood glucose is less than 60 or higher than 300 mg/dl.
√ Ensure adequate fl uid intake.
AAdapt drug treatment with insulin: as a general rule, a basal bolus therapy, which eliminates the bolus of meals not taken, is recommended.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 201
9.9.2. Patients with visual impairment
No studies have been found in this regard.
Recommendations
√ Provide educational materials in audio, Braille, large print or edited format.
√Facilitate attendance to educational sessions performing them in locations accessible by public transport.
√ Advertise informative talks with brief advertisements in audio format.
√If slides are used to transmit key information at educational chats, these should also contain a simple verbal description of the contents of each slide.
√
Provide information on self-control tools and techniques for people with visual impairment, including:
• “Talking blood glucose monitoring kits” that guide the patient through a voice message on the steps for testing and communicate the results orally.
• Glucometers with a large screen and easily recognizable numbers.
• Glucometers with backlit display.
• Techniques for tactile inspection of the feet.
√
Insulin injectors:
• Provide patients with injectors, which contain different touch buttons for fast or slow insulin.
• Insulin injectors emit some sort of sound when going from dose to dose in order to facilitate the patient’s autonomy, and thus the dose can be calculated without seeing the wheel.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 203
10. Acute complications
10.1. Hypoglycaemia
Hypoglycaemia is the most common acute complication of diabetes. A Canadian CPG491 defi ned hypoglycaemia by Whipple’s triad:
1. Appearance of autonomic or neuroglycopenic symptoms;
2. A low level of glucose (<4.0 mmol/L or 72 mg/dl) for patients treated with insulin or products that cause insulin secretion;
3. Symptomatic improvement to the administration of carbohydrates.
However, there is no unanimity in defi ning the level of glucose to diagnose hypoglycaemia. The American Diabetes Association492 established the level of blood sugar to defi ne hypoglycaemia in adults at 70 mg/dl (3.9 mmol/l) and the Spanish Society of Diabetes493, at 60 mg/dl (3.3 mmol/l).
Hypoglycaemia can occur in different circumstances:
• Excessive insulin doses.
• Not enough carbohydrates in meals.
• Meals delayed in time.
• Extra exercise for the dose of insulin administered.
• Administration of intramuscular insulin instead of subcutaneous tissue.
• Errors in the administration of insulin (fast acting insulin instead of delayed insulin or mistake in the dose).
• Shower or bath with very hot water shortly after having injected insulin.
The effects and short-term risks of hypoglycaemia can range from mild discomfort and unpleas-ant situations due to associated symptoms to risk situations, which may occur mainly in cases of severe hypoglycaemia, such as during driving or while operating machinery.
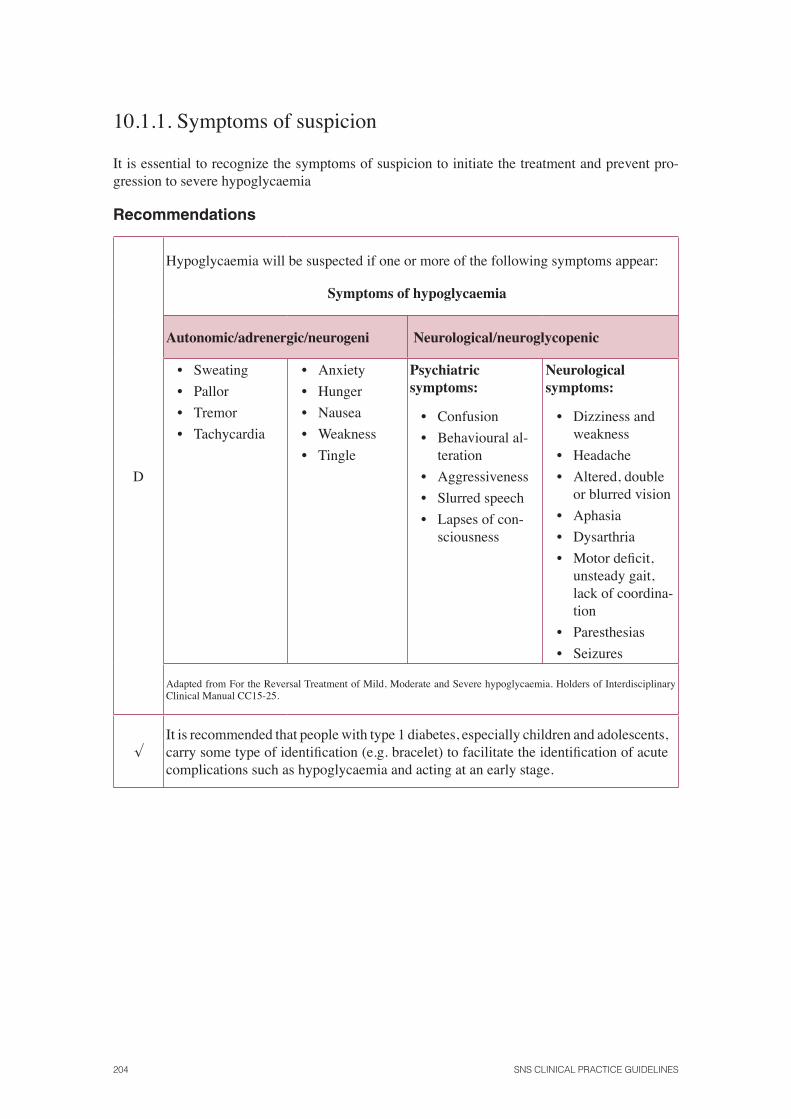
204 SNS CLINICAL PRACTICE GUIDELINES
10.1.1. Symptoms of suspicion
It is essential to recognize the symptoms of suspicion to initiate the treatment and prevent pro-gression to severe hypoglycaemia
Recommendations
D
Hypoglycaemia will be suspected if one or more of the following symptoms appear:
Symptoms of hypoglycaemia
Autonomic/adrenergic/neurogeni Neurological/neuroglycopenic
• Sweating
• Pallor
• Tremor
• Tachycardia
• Anxiety
• Hunger
• Nausea
• Weakness
• Tingle
Psychiatric symptoms:
• Confusion
• Behavioural al-teration
• Aggressiveness
• Slurred speech
• Lapses of con-sciousness
Neurological symptoms:
• Dizziness and weakness
• Headache
• Altered, double or blurred vision
• Aphasia
• Dysarthria
• Motor defi cit, unsteady gait, lack of coordina-tion
• Paresthesias
• Seizures
Adapted from For the Reversal Treatment of Mild, Moderate and Severe hypoglycaemia. Holders of Interdisciplinary Clinical Manual CC15-25.
√It is recommended that people with type 1 diabetes, especially children and adolescents, carry some type of identifi cation (e.g. bracelet) to facilitate the identifi cation of acute complications such as hypoglycaemia and acting at an early stage.
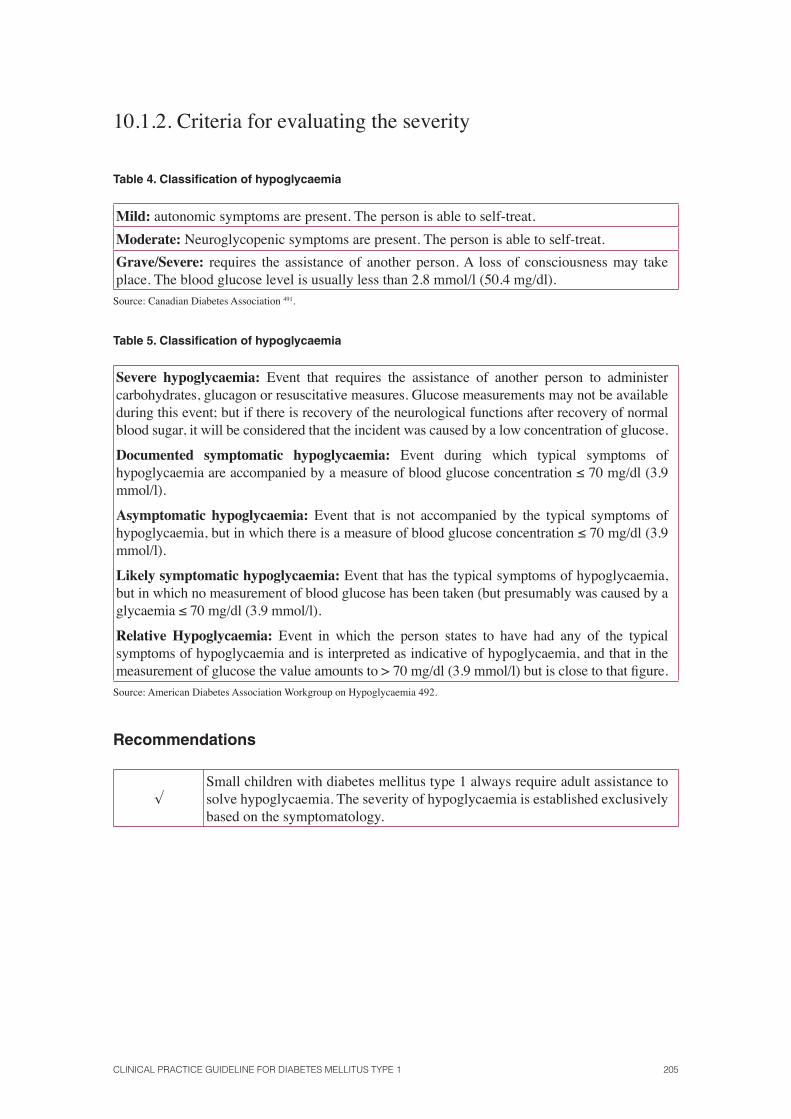
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 205
10.1.2. Criteria for evaluating the severity
Table 4. Classifi cation of hypoglycaemia
Mild: autonomic symptoms are present. The person is able to self-treat.
Moderate: Neuroglycopenic symptoms are present. The person is able to self-treat.
Grave/Severe: requires the assistance of another person. A loss of consciousness may take place. The blood glucose level is usually less than 2.8 mmol/l (50.4 mg/dl).
Source: Canadian Diabetes Association 491.
Table 5. Classifi cation of hypoglycaemia
Severe hypoglycaemia: Event that requires the assistance of another person to administer carbohydrates, glucagon or resuscitative measures. Glucose measurements may not be available during this event; but if there is recovery of the neurological functions after recovery of normal blood sugar, it will be considered that the incident was caused by a low concentration of glucose.
Documented symptomatic hypoglycaemia: Event during which typical symptoms of hypoglycaemia are accompanied by a measure of blood glucose concentration ≤ 70 mg/dl (3.9 mmol/l).
Asymptomatic hypoglycaemia: Event that is not accompanied by the typical symptoms of hypoglycaemia, but in which there is a measure of blood glucose concentration ≤ 70 mg/dl (3.9 mmol/l).
Likely symptomatic hypoglycaemia: Event that has the typical symptoms of hypoglycaemia, but in which no measurement of blood glucose has been taken (but presumably was caused by a glycaemia ≤ 70 mg/dl (3.9 mmol/l).
Relative Hypoglycaemia: Event in which the person states to have had any of the typical symptoms of hypoglycaemia and is interpreted as indicative of hypoglycaemia, and that in the measurement of glucose the value amounts to > 70 mg/dl (3.9 mmol/l) but is close to that fi gure.
Source: American Diabetes Association Workgroup on Hypoglycaemia 492.
Recommendations
√Small children with diabetes mellitus type 1 always require adult assistance to solve hypoglycaemia. The severity of hypoglycaemia is established exclusively based on the symptomatology.
206 SNS CLINICAL PRACTICE GUIDELINES
10.1.3. Performance measures in case of hypoglycaemia
The goal of the treatment for hypoglycaemia is to provide a rapid rise to a safe blood sugar level, eliminating the risk of accidents or damage to the patient, and relieving symptoms quickly. It is also important to avoid overtreatment, which can lead to rebound hyperglycaemia and weight gain.
10.1.3.1. Mild or moderate hypoglycaemia
The RCT by Wiethop et al.494 (n = 6) compared the administration of 10 g and 20 g of oral glucose, 1 mg of subcutaneous glucagon and placebo. Compared to placebo, the rest of the treatments signifi cantly increased plasma glucose levels, albeit transiently. Glucagon achieved signifi cantly higher glucose levels compared with other groups.
RCT 1+
Another RCT495, with 41 adults, compared seven methods of administer-ing oral glucose (glucose solution, glucose tablets, glucose gel, sucrose solu-tion, sucrose pellets, hydrolyzed polysaccharide solution and orange juice). The seven compounds were able to raise blood glucose levels after 20 minutes, although the glucose gel and orange juice did not increase, glucose levels as much as the others did.
RCT 1+
A Canadian guide491 proposes the administration of 15 g of oral glucose to produce an increase of approximately 37.8 mg/dl (2.1 mmol/l) in approxi-mately 20 minutes, which would achieve the improvement or disappearance of the symptoms in most patients. If the oral glucose dose is 20 g, an increase of around 64.8 mg/dl (3.6 mmol/l) occurs in 45 minutes. Other options, such as milk or orange juice, are slower in recovering glucose levels and improv-ing the symptoms. The use of glucose gel also produces a slow recovery (<1.0 mmol/l or 18 mg/dl increase in 20 minutes).
Subcutaneous or intramuscular administration of 1 mg of glucagon caus-es a signifi cant increase in blood glucose ranging from 54 mg/dl to 216 mg/dl (3.0 mmol/l to 12.0 mmol/l) in 60 minutes. This effect is prevented in people who have consumed more than two standard measures of alcohol in the hours before, or people with advanced liver disease. The guide states that there are no studies in patients with gastropathy.
No RCTs, which had been specifi cally carried out with children, adoles-cents and pregnant women, were found.
Expert opinion 4
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 207
10.1.3.2. Serious or severe hypoglycaemia
Intramuscular glucagon vs. intravenous glucose
An RCT414 compared the administration of 1 mg of IM glucagon with 50 ml of IV glucose at 50% in 29 adult patients who had been treated with insulin and had entered hypoglycaemic coma. There was a level of consciousness recovery signifi cantly slower in the group treated with glucagon. Two of the patients who had been treated with glucagon required an additional administration of IV glucose, as there were no signs of clinical improvement within 15 minutes of the treatment.
RCT 1+
Another RCT496 compared the administration of 1 mg of IM glucagon to 50 ml of glucose at 50% in 14 adults with severe hypoglycaemia. The recovery time ranged from 8 to 21 minutes in the group treated with glucagon and from 1 to 3 minutes in the group treated with IV glucose.
RCT 1+
Intravenous glucagon vs. intravenous glucose
An RCT415 compared the IV administration of 1 mg of glucagon vs. 50 ml of IV glucose at 50% in 49 adults treated with insulin and hypoglycaemic coma. There was a recovery of the normal level of consciousness signifi cantly slower in the group treated with glucagon.
RCT 1+
The authors of the NICE CPG 20047 consider that 10% is the maximum amount of IV glucose, which should be administered to children and youth.
CPG4
Intravenous glucagon (IV) vs. intramuscular glucagon (IM)
An RCT497 compared the effectiveness of glucagon depending on the route of administration (1 mg IM vs. 1 mg IV) in 99 patients (20 of them under 20 years old) following a treatment with insulin, with hypoglycaemia, treated in hospital emergency units. No signifi cant differences were found between the two groups in the number of patients who awoke or were able to take oral glucose after 15 minutes of treatment.
RCT 1+
A second RCT498 also compared 1 mg of IM glucagon vs. 1 mg of IV glucagon in 15 adults to whom hypoglycaemia was provoked. After 20 min-utes and 40 minutes of treatment, the treated group with IM glucagon showed glucose levels in plasma signifi cantly higher than the group treated with IV glucagon.
RCT 1+
208 SNS CLINICAL PRACTICE GUIDELINES
Intramuscular glucagon vs. subcutaneous glucagon
An RCT499 compared the IV and SC administration of 20 μg/kg of glucagon, in 30 children and young people who had been provoked hypoglycaemia. No differences were found between groups in the levels of glycaemia or glucagon in the blood.
RCT 1+
Intranasal glucagon vs. subcutaneous glucagon
An RCT500 compared the intranasal administration of glucagon vs. the SC administration, in 12 young people who had been provoked hypoglycaemia. No signifi cant differences were found in blood glucose levels after 15 minutes. However, after 45 minutes, the increase in glucose levels was signifi cantly higher in the group receiving the SC route. However, 90% of children and young people who received SC treatment had nausea, compared with the 10% in the group receiving intranasal insulin in which 4 children in this group had nasal irritation.
RCT 1+
Another RCT501, carried out with six adults who had been provoked hy-poglycaemia, showed no differences between the intranasal administration and the SC one, in the groups regarding an increase in plasma glucose levels.
RCT 1+
Intranasal glucagon vs. intramuscular glucagon
An RCT502 compared the administration of intranasal glucagon vs. the IM administration in 30 adults with hypoglycaemia. The average increase in the levels of blood glucose was higher in the group given IM glucagon.
RCT 1+
Combination therapy of intravenous glucose + intramuscular glucagon vs. intravenous glucose
An RCT503 comparing the combination therapy of IV glucose and IM glucagon vs. IV glucose in 18 adults with hypoglycaemia treated in emergency services found no signifi cant differences in plasma glucose levels between the groups.
RCT 1+
Intramuscular epinephrine vs. intramuscular glucagon
An RCT504 comparing the administration of IM epinephrine vs. IM glucagon in children and young people who had been provoked hypoglycaemia showed that epinephrine was signifi cantly less effective than glucagon to raise plasma glucose levels. Nine of the 10 children and young people complained of severe nausea after the administration of glucagon.
RCT 1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 209
Intravenous dextrose at 10% vs. intravenous dextrose at 50%
An RCT505 compared two dextrose solutions at different concentrations (10% vs. 50%), with increments of 5 g of dextrose to a maximum dose of 25 g in 51 adults, treated for hypoglycaemia by ambulance emergency paramedics. No differences were found between the two treatments in relation to mean recovery time (8 minutes), the mean score on the Glasgow Scale of Consciousness or recurrent episodes of hypoglycaemia in the next 24 hours. Those treated with dextrose at 10% received less total dose of dextrose and their glucose levels after the treatment were lower.
RCT 1+
Educational programs to improve the identifi cation of hypoglycaemia
Training to improve the identifi cation of hypoglycaemia aims to instruct patients on the interpretation of physical symptoms, diet, exercise, the dosage and insulin action, and the measurements of blood glucose to suspect.
An RCT compared an educational program to improve the identifi cation of hypoglycaemia and its impact on the number of hypoglycaemia vs. no edu-cation after starting more intensive management of diabetes506. No differences in the recognition of symptoms of hypoglycaemia between the groups were found, however, the educational program led to better detection of low glucose levels in patients who initiated intensive management of diabetes.
RCT 1+
An RCT in 111 adults with DM1507 analyzed an educational program vs. a control intervention and found a better recognition for both low and high glucose levels and a signifi cant reduction in the frequency of severe hypogly-caemia in the trained group.
RCT 1+
Another RCT508 examined the effect of a structured psycho-educational training program in anticipation, awareness and treatment of hypoglycaemia in 60 people with a history of recurrent severe hypoglycaemia evaluated for 18 months. This study found that the program signifi cantly decreased the number of mild, moderate and severe episodes of hypoglycaemia.
RCT 1+
An RCT47 examined the effect of an educational program (HyPOS) in 164 patients suffering from hypoglycaemia, and found that this intervention was more effective than the traditional program of clinical care with regard to increased recognition of hypoglycaemia awareness, signifi cantly increasing the threshold level of detection of hypoglycaemia and its treatment and signifi -cantly reducing the number of weekly episodes of hypoglycaemia undetected and the rate of mild hypoglycaemia. The rate of severe hypoglycaemia showed no statistically signifi cant differences.
RCT 1+
210 SNS CLINICAL PRACTICE GUIDELINES
10.1.3.3. Pregnancy and breastfeeding
Regarding pregnancy, the NICE CPG 20047 makes the following recommendations:
• Inform and advise pregnant women with diabetes on the risks of hy-poglycaemia and lack of recognition of hypoglycaemia during preg-nancy, particularly in the fi rst trimester.
• Give women a glucose concentrated solution and glucagon and edu-cate both themselves and their partners and acquaintances on their use.
CPG 4
Regarding the postpartum period, the NICE CPG 20089 made the following recommendations:
• Advise women to reduce the insulin dose immediately after delivery and to monitor their blood glucose levels carefully to establish the ap-propriate dose.
• Inform women of the increased risk of hypoglycaemia in the postna-tal period, especially during breastfeeding, and advise them to have a meal or snack available before or during breastfeeding.
CPG 4
Summary of evidence
Mild to moderate hypoglycaemia
RCT 1+
The administration of oral glucose causes a faster increase of glycaemia than orange juice and glucose gels491, 495.
RCT 1+
The administration of subcutaneous glucagon causes higher blood glucose levels than the oral administration of glucose494.
RCT 1+
The subcutaneous or intramuscular administration of 1 mg of glucagon causes a signifi cant increase of glucose from 54 to 216 mg/dl (3.0 mmol/l to 12.0 mmol/l) in 60 minutes491.
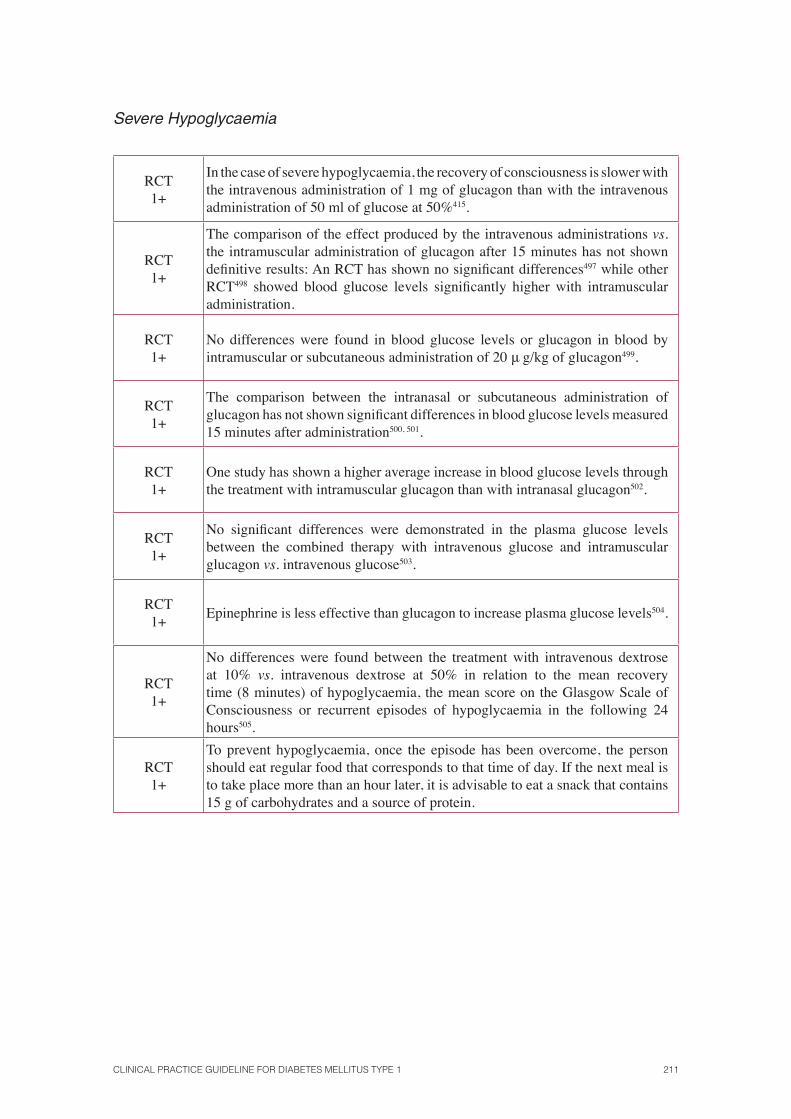
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 211
Severe Hypoglycaemia
RCT 1+
In the case of severe hypoglycaemia, the recovery of consciousness is slower with the intravenous administration of 1 mg of glucagon than with the intravenous administration of 50 ml of glucose at 50%415.
RCT 1+
The comparison of the effect produced by the intravenous administrations vs. the intramuscular administration of glucagon after 15 minutes has not shown defi nitive results: An RCT has shown no signifi cant differences497 while other RCT498 showed blood glucose levels signifi cantly higher with intramuscular administration.
RCT 1+
No differences were found in blood glucose levels or glucagon in blood by intramuscular or subcutaneous administration of 20 μ g/kg of glucagon499.
RCT 1+
The comparison between the intranasal or subcutaneous administration of glucagon has not shown signifi cant differences in blood glucose levels measured 15 minutes after administration500, 501.
RCT 1+
One study has shown a higher average increase in blood glucose levels through the treatment with intramuscular glucagon than with intranasal glucagon502.
RCT 1+
No signifi cant differences were demonstrated in the plasma glucose levels between the combined therapy with intravenous glucose and intramuscular glucagon vs. intravenous glucose503.
RCT 1+
Epinephrine is less effective than glucagon to increase plasma glucose levels504.
RCT 1+
No differences were found between the treatment with intravenous dextrose at 10% vs. intravenous dextrose at 50% in relation to the mean recovery time (8 minutes) of hypoglycaemia, the mean score on the Glasgow Scale of Consciousness or recurrent episodes of hypoglycaemia in the following 24 hours505.
RCT 1+
To prevent hypoglycaemia, once the episode has been overcome, the person should eat regular food that corresponds to that time of day. If the next meal is to take place more than an hour later, it is advisable to eat a snack that contains 15 g of carbohydrates and a source of protein.
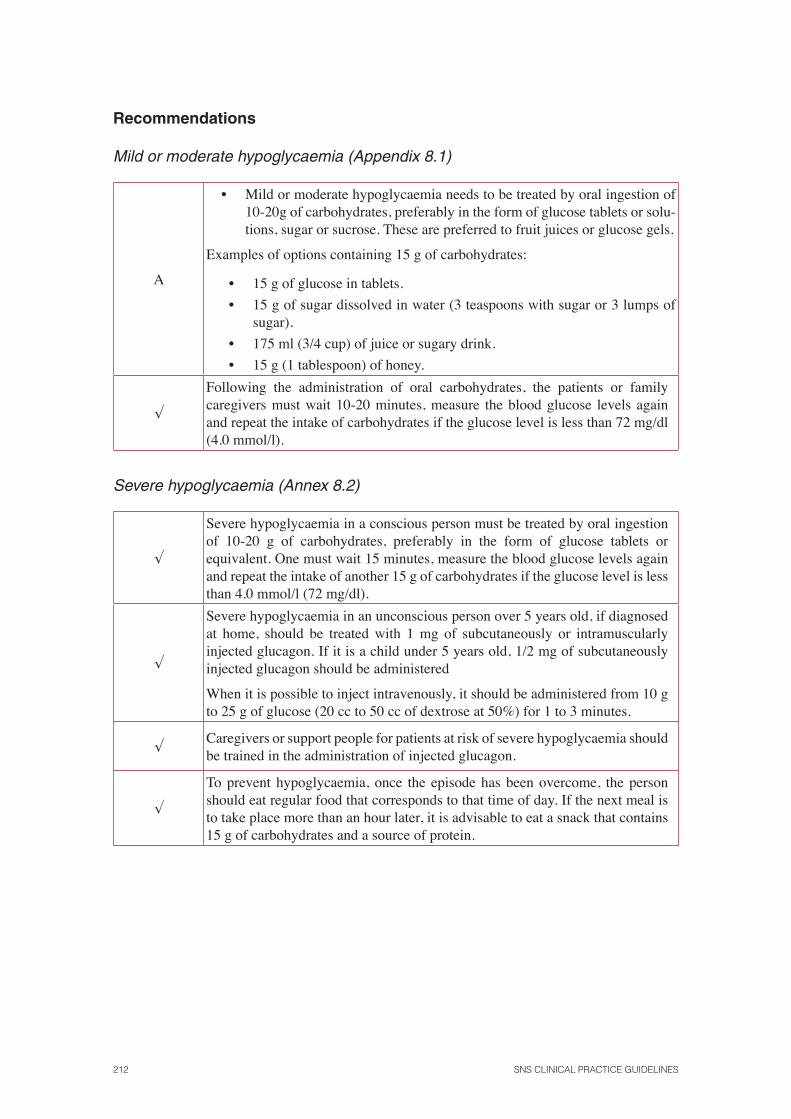
212 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
Mild or moderate hypoglycaemia (Appendix 8.1)
A
• Mild or moderate hypoglycaemia needs to be treated by oral ingestion of 10-20g of carbohydrates, preferably in the form of glucose tablets or solu-tions, sugar or sucrose. These are preferred to fruit juices or glucose gels.
Examples of options containing 15 g of carbohydrates:
• 15 g of glucose in tablets.
• 15 g of sugar dissolved in water (3 teaspoons with sugar or 3 lumps of sugar).
• 175 ml (3/4 cup) of juice or sugary drink.
• 15 g (1 tablespoon) of honey.
√
Following the administration of oral carbohydrates, the patients or family caregivers must wait 10-20 minutes, measure the blood glucose levels again and repeat the intake of carbohydrates if the glucose level is less than 72 mg/dl (4.0 mmol/l).
Severe hypoglycaemia (Annex 8.2)
√
Severe hypoglycaemia in a conscious person must be treated by oral ingestion of 10-20 g of carbohydrates, preferably in the form of glucose tablets or equivalent. One must wait 15 minutes, measure the blood glucose levels again and repeat the intake of another 15 g of carbohydrates if the glucose level is less than 4.0 mmol/l (72 mg/dl).
√
Severe hypoglycaemia in an unconscious person over 5 years old, if diagnosed at home, should be treated with 1 mg of subcutaneously or intramuscularly injected glucagon. If it is a child under 5 years old, 1/2 mg of subcutaneously injected glucagon should be administered
When it is possible to inject intravenously, it should be administered from 10 g to 25 g of glucose (20 cc to 50 cc of dextrose at 50%) for 1 to 3 minutes.
√Caregivers or support people for patients at risk of severe hypoglycaemia should be trained in the administration of injected glucagon.
√
To prevent hypoglycaemia, once the episode has been overcome, the person should eat regular food that corresponds to that time of day. If the next meal is to take place more than an hour later, it is advisable to eat a snack that contains 15 g of carbohydrates and a source of protein.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 213
11. Chronic complications
11.1. Cardiovascular risk in patients with diabetesmellitus type 1
Diabetes is associated with an increased risk of cardiovascular disease. There are different ap-proaches to calculate the level of cardiovascular risk in patients with diabetes. One school of thought suggests that the cardiovascular risk for diabetes is considered like a cardiovascular dis-ease. This assumption should be based on prognostic studies, which compare the risk of cardio-vascular events in patients with DM to patients who have suffered an acute myocardial infarction (AMI). Another option is to use cardiovascular or coronary risk equations or tables to select patients who can benefi t most from interventions in cardiovascular primary prevention. In order to make decisions on therapy or intensify therapy (glycaemic control, antiplatelet, lipid lowering, etc.) it is important to know which groups of patients are at increased cardiovascular (CV) risk and who would benefi t most of those treatments.
The CPG on DM2, published in our health context509, discussed this in its chapter on “Screening and treatment of macrovascular complications.” It has been upgraded for patients with DM1 from the evidence provided by this CPG, as no studies have been found on this matter.
To compare cardiovascular morbidity and mortality in patients with dia-betes and AMI 15 cohort studies were analyzed510, 511, 512, 513, 514 that assessed the risk of coronary events in diabetic patients compared to patients with a history of ischemic heart disease and compared to the general population. All studies show an increased coronary risk in diabetic patients compared to the general population. However, the comparative results of coronary mortality among diabetic people and people with a history of ischemic heart disease are contradictory. The differences in results could be explained by multiple fac-tors: differences in the inclusion criteria, lack of uniformity in the defi nition of diabetes and ischemic heart disease, the way to collect data, inclusion of in-cident or prevalent cases, patient characteristics (age groups, gender, years of evolution of diabetes), or methodological aspects (difference in the confound-ing factors considered, population-based cohort or not, different outcomes, follow-up losses, etc.).
Cohort studies2+
Studies analyzing the results by gender agree in pointing that DM in women involves a higher relative risk for coronary heart disease than in men with diabetes510, 511, 512, 514 and in some cases this risk is the same510, 512 or even higher510, 513 to that of women with a history of ischemic heart disease.

214 SNS CLINICAL PRACTICE GUIDELINES
Some studies have assessed the duration of DM and conclude that it is an independent risk factor515 and that, after 15 years of evolution of the disease, coronary risk is equated with a history of ischemic heart disease,514, 515, 516.
Based on this evidence it cannot be said that cardiovascular risk is the same in patients with diabetes and in patients with a history of CV disease, therefore other criteria are needed to identify patients at increased CV risk, being possibly the evolution for more than 15 years of diabetes one of them.
Another widely used tool to classify diabetic patients according to CV risk has been the implementation of cardiovascular or coronary risk tables. They estimate the probability of coronary or cardiovascular events in a given time depending on the presence or absence of other risk factors. The risks are constructed based on a special type of cohort study: the “clinical prediction rules” (CPR). The validity and applicability of a CPR to a given population fi rst requires its creation based on a cohort using a multivariate analysis and then a validation process, fi rst in the source population and then in different populations in which the rules want to be applied517.
There is a risk function exclusively for diabetic patients based on the re-sults of the UKPDS study. It has the advantage of using the years of duration of diabetes and HbA
1c levels as independent risk factors and providing, as well
as the coronary risk, the risk of stroke.
The Verifi ca study518, performed on 5732 patients, of whom 941 (16.4%) had diabetes, found no signifi cant differences between the expected event rate by the calibrated Framingham equation with those really observed in the follow-up cohort in the different risk categories. The study population was relatively young (mean 56.3 years) so it is assumable that the evolution of the disease was relatively short.
Currently, the REGICOR equation (also called calibrated Framingham), is the CPR that has a better validation among our population518, 519, 520.
The development group of this CPG (GEG) has considered that in case of using a clinical prediction rule, the most appropriate would be REGICOR. However, the population included in the Verifi ca study, who validated this prediction rule in Spain, includes general population over 35 years old with a very small proportion of patients with DM1. Therefore, none of the clinical prediction rules developed so far can be recommended, because they probably underestimate cardiovascular risk in patients with DM1.
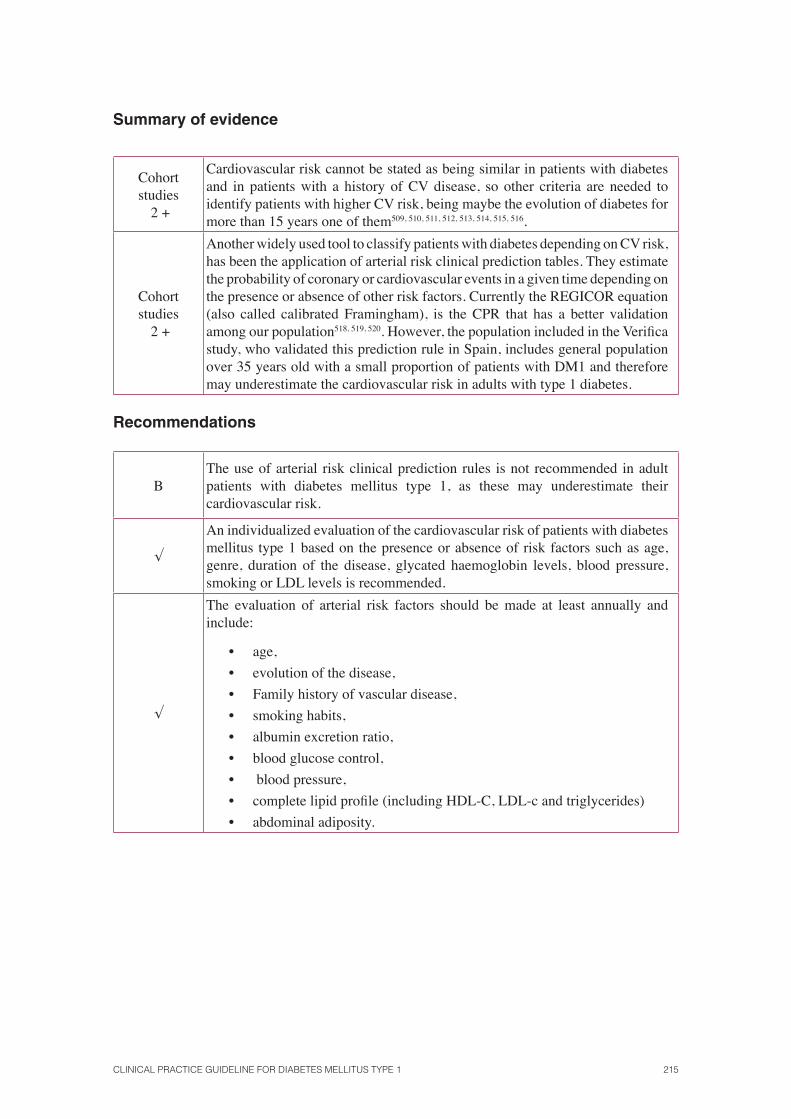
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 215
Summary of evidence
Cohortstudies
2 +
Cardiovascular risk cannot be stated as being similar in patients with diabetes and in patients with a history of CV disease, so other criteria are needed to identify patients with higher CV risk, being maybe the evolution of diabetes for more than 15 years one of them509, 510, 511, 512, 513, 514, 515, 516.
Cohortstudies
2 +
Another widely used tool to classify patients with diabetes depending on CV risk, has been the application of arterial risk clinical prediction tables. They estimate the probability of coronary or cardiovascular events in a given time depending on the presence or absence of other risk factors. Currently the REGICOR equation (also called calibrated Framingham), is the CPR that has a better validation among our population518, 519, 520. However, the population included in the Verifi ca study, who validated this prediction rule in Spain, includes general population over 35 years old with a small proportion of patients with DM1 and therefore may underestimate the cardiovascular risk in adults with type 1 diabetes.
Recommendations
BThe use of arterial risk clinical prediction rules is not recommended in adult patients with diabetes mellitus type 1, as these may underestimate their cardiovascular risk.
√
An individualized evaluation of the cardiovascular risk of patients with diabetes mellitus type 1 based on the presence or absence of risk factors such as age, genre, duration of the disease, glycated haemoglobin levels, blood pressure, smoking or LDL levels is recommended.
√
The evaluation of arterial risk factors should be made at least annually and include:
• age,
• evolution of the disease,
• Family history of vascular disease,
• smoking habits,
• albumin excretion ratio,
• blood glucose control,
• blood pressure,
• complete lipid profi le (including HDL-C, LDL-c and triglycerides)
• abdominal adiposity.
216 SNS CLINICAL PRACTICE GUIDELINES
√Adults with a high rate of albumin excretion (microalbumin) or two or more features of the metabolic syndrome should be managed as high-risk category.
√
Adults with diabetes mellitus type 1 who are not in the category of
higher risk but have some arterial risk factor (over 35 years old, family history of premature coronary disease, high-risk ethnicity or severe lipidemia alterations or blood pressure) should be managed as a moderately high risk group.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 217
11.2. Diabetic retinopathy
Key question:
• Is there any medical treatment (not surgical, not laser) to prevent diabetic retinopathy?
• When should the screening of diabetic retinopathy start?
• How often should diabetic retinopathy screening take place?
• What should be the techniques for the screening of diabetic retinopathy?
Diabetic retinopathy (DR) is a major complication of diabetes. The following information is known about its incidence:
• In developed countries, DR is the leading cause of blindness in people under 60.
• This disease is usually detected when more than 15 years have elapsed from the diagnose of diabetes.
• Most of the anomalies caused by DR are silent and do not cause any symptoms.
• Current treatments of DR are mainly based on laser photocoagulation and surgery. The laser photocoagulation treatment is an aggressive therapy, and requires an early diagnosis of the retinopathy to achieve good results.
Most patients who develop DR are asymptomatic until advanced stages (macular oedema and/or proliferative DR), and once they reach these phases treatment may be less effective. As progression can be fast and available therapies can be benefi cial to the improvement of symptoms and to slow the progression of the disease, it is important to perform regular screening for diabetic retinopathy.
11.2.1. Preventive medical treatment of diabetic retinopathy
Key question:
• Is there and medical treatment (not surgical, not laser) to prevent diabetic retinopathy?
The CPG NICE 20047 provides no evidence on this issue.
218 SNS CLINICAL PRACTICE GUIDELINES
The main source of evidence comes from a systematic review of good quality clinical trials521 that analyzes the effectiveness of interventions for pri-mary and secondary prevention of diabetic retinopathy and presents the fol-lowing results:
Primary prevention of retinopathy
Intensive diabetes treatment
The study Diabetes Control and Complications Trial (DCCT)522, carried out in 1441 DM1 patients randomly assigned to intensive treatment [(HbA
1c
<7.2% (48 mmol/mol)] vs. conventional treatment, found a 76% decrease in the incidence of DR (95% CI: 62% to 85%).
RCT 1+
Drugs that inhibit the renin-angiotensin-aldosterone
The DIRECT-Prevent 1 study523 included 1421 patients with DM1 without retinopathy, normotensice and with albuminuria, randomly assigned to a treatment with candesartan (16 mg/24 h during the fi rst month and 32 mg in the second month) vs. placebo, with a 4.7-year follow-up. According to this study, the treatment with candesartan did not reduce signifi cantly the incidence of DR, defi ned as two or more changes in the Early Treatment Diabetic Retinopathy Study scale levels [RR 0.82 (95% CI: 0.67 to 1)].
Instead, applying more restrictive criteria to defi ne the incidence (at least 3 levels in Early Treatment Diabetic Retinopathy Study scale), the protective effect was statistically signifi cant [RR 0.65 (95% CI 0.48 to 0, 87)] and per-sisted when adjusting for baseline characteristics such as duration of diabetes, HbA
1c and SBP [RR 0.71 (95% CI 0.53 to 0.95)].
RCT 1+
Vasodilator drugs
A Cochrane review524, which examined the effectiveness of pentoxifylline, concluded that while this drug can be effective in preventing retinal neovascularisation and its recovery, no studies have analyzed the methodological quality enough, thus, no conclusive results have been found.
SR pf RCT 1++
Angioprotector drugs
An RCT525 analyzed the effect of calcium dobesilate versus placebo in the permeability of the blood-retinal barrier in patients with type 2 diabetes and early diabetic retinopathy. This trial randomly assigned 194 patients to a treatment with 2 g of calcium dobesilate vs. placebo on a daily basis. A total of 137 patients completed the study, which lasted 24 months.
RCT1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 219
The primary outcome analyzed was the reason for further penetration into the vitreous (RPPV). The mean changes in the base levels after 24 months were signifi cantly lower in the treatment group [mean (SD) -3.87 (2.03), P = 0002] than in the placebo group [mean (SD) 2.03 (2.86)]. The difference remained regardless of the diabetes control levels. A subgroup analysis in pa-tients without antihypertensive and/or lipid-lowering drugs also showed a sig-nifi cant difference [mean (SD) -3.38 (13.44) vs. 3.50 (13.70), P = 0.002) after 24 months.
The fi ndings of the trial show a signifi cant activity of calcium dobesilate versus placebo in the prevention of the blood-retinal barrier breakdown re-gardless of diabetes control, being drugs well tolerated by patients.
Secondary prevention
Intensive treatment of diabetes
In a meta-analysis of 17 RCTs with a total of 529 patients526, 527, the conventional treatment was compared with the intensive treatment for 5 years. After 6 and 12 months of follow-up, the risk of retinopathy progression showed no statistically signifi cant differences between both groups but became signifi cantly lower in the intensive therapy group [OR 0.49 (95% CI 0.28 to 0.85), P = 0.011) after more than two years of follow up.
SR of RCT1+
The Diabetes Control and Complications Trial Study (DCCT) trial, which included 1055 adults and 156 adolescents, carried out eye examinations, as-sessment of visual acuity and eye fundus photographs. The study showed a reduction of 54% in the progression of DR (95% CI: 39% to 66%) in patients undergoing intensive treatment. The evaluation of the results after 10 years of follow up528 determined that the HbA
1c was similar between the original
group of intensive therapy and the group receiving conventional treatment. The adults from the intensive therapy group showed a slower progression of diabetic retinopathy than the conventional therapy group
RCT1+
Another trial529, involving 70 patients with DM1 with low C-peptide levels and nonproliferative mild to moderate DR, compared the intensive treatment (insulin pump) versus the conventional treatment. During the fi rst 2 years of follow-up, a greater progression of diabetic retinopathy was observed in the intensive treatment group. After 2 years, the trend equated, and even less deterioration was observed in the intensive treatment group.
RCT1+
In the Stockholm Diabetes Intervention Study trial530, the intensive treatment was compared to the conventional treatment in 96 patients with nonproliferative DR. Retinopathy increased in both groups, but after 5 years the outcome was worse for the conventional therapy group (OR 0.4, p = 0.04).
RCT1+
220 SNS CLINICAL PRACTICE GUIDELINES
The Oslo study275, 276, 277 compared 45 patients with DM1 who received intensive treatment with insulin pump vs. insulin treatment with multiple in-jections (5-6/per day) and vs. conventional treatment (2 injections per day). It was found that HbA
1c levels greater than 10% were associated with increased
risk of retinopathy progression (p = 0.014) and lower values of 7-8% with a lower risk of progression.
RCT1+
A more recent study531 included 65 patients randomized to a treatment group with infusion pump (n = 36) vs. a standard treatment group (n = 29). No signifi cant differences were found between the two groups in terms of baseline retinopathy, metabolic control or proteinuria, or of the progression of diabetic retinopathy.
RCT1+
Renin-angiotensin-aldosterone inhibitor drug
The DIRECT-Protect 1 study523 showed no signifi cant decrease in the risk of proliferation of DR in the treatment group with candesartan (16 mg/24 h during the fi rst month and 32 mg in the second month) vs. placebo [RR 1.02 (95% CI 0.80 to 1.31), P = 0.85].
RCT1+
The EUCLID (EURODIAB Controlled Trial of Lisinopril in Insulin-Dependent Diabetes Mellitus) study532 was carried out with 560 normoten-sive patients with DM1 and normal albumin, who were randomly assigned to a group treated with lisinopril (10 mg/day, increased to 20 mg/day after 3 months once having reached the DBP <75 mm Hg target) vs. placebo. After a 2-year follow-up, there was a 50% decrease in the progression of DR (95% CI: 28% to 89%) and the progression to proliferative DR was of 80%.
RCT1+
In the Renin Angiotensin System Study (RASS)533, a multicentre con-trolled trial with 285 normotensive patients with DM1 and normal albumin, the patients were randomized to a treatment with losartan (100 mg/per day), enalapril (20 mg/per day) or placebo. During the 5-year follow-up the progres-sion of diabetic retinopathy was assessed, this being defi ned as a progression of two or more steps in the retinopathy severity scale. The results showed a re-duction in the incidence of retinopathy progression in the groups treated with inhibitors of the renin-angiotensin-aldosterone system, which was reduced by 65% in the group treated with enalapril [OR 0.35, (95% CI 0.14 to 0.85)] and 70% in the group treated with losartan [OR = 0.30 (95% CI 0.12 to 0.73)], regardless of the changes in blood pressure.
RCT1+
Drugs with platelet antiaggregatory effect
An SR534 that evaluated the effectiveness of acetylsalicylic acid (ASA) alone or in combination with dipyridamole for the treatment of DR (ASA 650 mg/per day to 990 mg/per day, dipyridamole 225 mg/per day) in studies lasting from 8 weeks to 5 years, found a signifi cant increase of microaneurysms in the placebo group vs. the group that followed the treatment with ASA.
SR of RCT 1++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 221
The BTRS Belgian trial535 that evaluated the effectiveness and safety of a treatment with ticlopidine 250 mg/per day vs. placebo found no signifi cant differences between both groups.
RCT 1+
The TIMAD study536 evaluated the effectiveness and safety of ticlopidine (500 mg) for the treatment of diabetic retinopathy in patients with DM1 and DM2. Ticlopidine was effective in preventing the occurrence of microaneu-rysms (p = 0.03) versus placebo. However, the group receiving ticlopidine (n = 215) had higher rates of adverse effects and dropouts that the placebo group (n = 220).
RCT 1+
A study that evaluated the effects of the treatment with dipyridamole537 in 31 insulin-dependent patients, showed a lower retinopathy deterioration in patients treated with dipyridamole versus placebo after 30 months (p <0.05) and at the end of the study (36 months) (p <0.0025).
RCT 1+
A clinical trial carried out in the Spanish healthcare context538, in 17 pa-tients with insulin-dependent diabetes and retinopathy, found a signifi cantly better evolution (less leakage in the fl uorescein examination and fewer mi-croaneurysms) in the group treated with 300 g of trifl usal 3 times per day for 2 years. However, no signifi cant differences were found in terms of visual acuity and visual campimetry.
RCT 1+
Summary of evidence
Primary prevention
RCT1+
The intensive treatment of diabetes with HbA1c
levels below 7.2% reduces the risk of retinopathy522.
RCT1+
The treatment with candesartan (dose of 16 mg/24 hours to 32 mg/24 hours) may be protective to the occurrence of diabetic retinopathy (increase of at least 3 levels in the Early Treatment Diabetic Retinopathy Study scale)523.
RCT1+
The evidence available does not show conclusive results on the effectiveness of pentoxifylline in preventing retinal neovascularization524.
RCT1+
Calcium dobesilate (2 g/day) may be effective in preventing the blood-retinal barrier525 in patients with diabetes.
Secondary prevention
SR of RCT 1++
RCT1+
Intensive treatment of diabetes with HbA1c
levels below 7.2% could slow the progression of diabetic retinopathy after 2 years of evolution of the disease526, 527,
529 after 5 years and 10 years530 528, although no study has yet shown any signifi cant differences with the conventional treatment 531.
RCT 1 +
HbA1c
levels below 7% are associated with a better progression of diabetic retinopathy275, 276, 277.
RCT 1 +
Treatment with lisinopril (10 mg/per day, increased to 20 mg/per day after 3 months having reached the DBP <75 mm Hg target) may improve the progression of diabetic retinopathy compared to placebo (p <0.0025) 532.
222 SNS CLINICAL PRACTICE GUIDELINES
Recommendations
AIt is important to inform people with diabetes mellitus type 1 and their families that the control of long-term blood glucose with HbA
1c levels lower or equal to
7% decreases the incidence and progression of diabetic retinopathy.
11.2.2. Diabetic retinopathy screening techniques
The CPG NICE 20047 provides evidence that has been included in each of the subsections.
Direct ophthalmoscopy
According to the SR by Cummins et al.539, direct ophthalmoscopy does not comply with the necessary standards to constitute a screening tool because its sensitivity is low, regardless of the training received by the health professionals who use it:
• Direct ophthalmoscopy with mydriasis carried out by primary care phy-sicians:Sensitivity in detecting vision-threatening retinopathy 33-66%; detection of preproliferative retinopathy and proliferative retinopathy: 32-50%540.
• Direct ophthalmoscopy with mydriasis carried out by ophthalmologists:Sensitivity in detecting threatening retinopathy: 65% sensitivity for the detection of proliferative retinopathy: 70%540.
The CPG NICE 20047 places the sensitivity at 91% (76-97%), when performed by an ophthalmologist using a slit lamp in mydriatic eye.
• Direct ophthalmoscopy with mydriasis carried out by other profession-als: Sensitivity: 27% to 81% when performed by other professionals (endocrinologists, hospital doctors, technicians, etc.).
DS II
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 223
Indirect biomicroscopy with slit lamp
A study of diagnostic tests included in the systematic review Cummins et al.539 indicates that this technique, carried out by experienced staff, can achieve sensitivities similar to retinal photography.
DS II
A study541 carried out in 189 patients (32 patients with DM1) analyzed the diagnostic capability of slit lamp biomicroscopy for the detection of early vascular changes identifi ed by fl uorescein angiography, obtaining a sensitivity and specifi city of 91.2% and 97.9%, respectively. The concordance obtained between both tests was 87%.
DS Ia
The CPG SIGN DM 200111 states that:
The slit lamp biomicroscopy, used by properly trained staff, can achieve similar542 or higher543 sensitivities to those achieved by retinal photography, and with a less technical failure rate. However, the slit lamp biomicroscopy is of limited value as a screening tool 544.
DS II
Retinal Cameras
The CPG of DM SIGN 2001540 indicated that retinal photography often achieves a sensitivity of 80% and is more effective than direct ophthalmoscopy, reaching a sensitivity of 80% in rare cases, even when performed by trained specialists542.
DS II
A prospective study545 performed 108 ophthalmic scans on 55 people with DM to evaluate the diagnostic performance of the retinography at 45° non-mydriatic with a central image or three images compared to the technique used in the Early Treatment Diabetic Retinopathy Study (7 35 mm stereoscopic mydriatic colour photographs) as gold standard. The sensitivity and specifi c-ity of the non-mydriatic retinography system at 45 degrees with 3 images for DR were 82% and 92%, respectively, and for the system with a central image, the values were 71% and 96% respectively. This study concluded that the fun-dus images from 45º to 3-colour fi eld without mydriasis could be an effective screening tool to identify critical degrees of DR and diabetic macular oedema that need to be referred to a specialist. A central image at 45º is enough to de-termine the absence or presence of DR and diabetic macular oedema, but not enough to graduate its clinical signifi cance.
DS II
A study involving586 patients (103 with DM1)546 compared the use of the indirect ophthalmoscopy performed by an ophthalmologist (gold standard), conventional photography and digital photography, and found similar results to those reported in previous studies: lower sensitivities from the ophthalmos-copy than from the photography and similar sensitivities between the con-ventional and the digital photography (both above 90%) with 89% and 87% specifi cities, respectively. The rate of non-evaluable images or that required repetition was 50% lower in the digital photography.
DS II
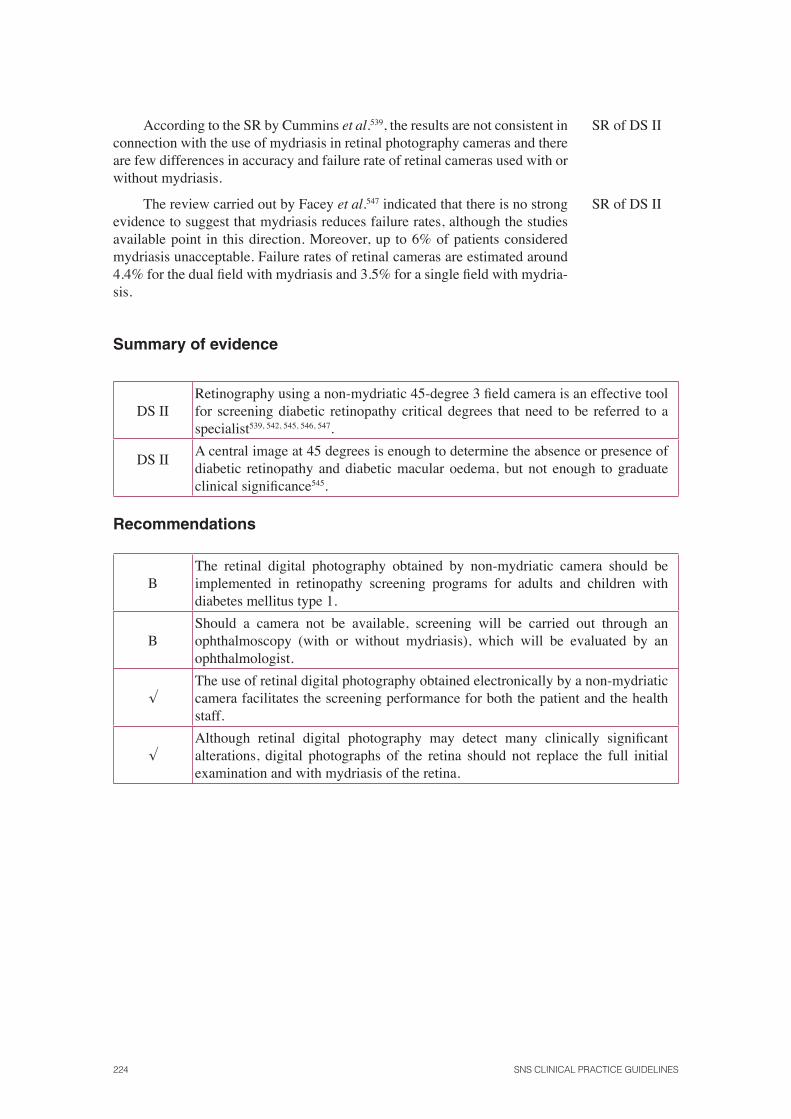
224 SNS CLINICAL PRACTICE GUIDELINES
According to the SR by Cummins et al.539, the results are not consistent in connection with the use of mydriasis in retinal photography cameras and there are few differences in accuracy and failure rate of retinal cameras used with or without mydriasis.
SR of DS II
The review carried out by Facey et al.547 indicated that there is no strong evidence to suggest that mydriasis reduces failure rates, although the studies available point in this direction. Moreover, up to 6% of patients considered mydriasis unacceptable. Failure rates of retinal cameras are estimated around 4.4% for the dual fi eld with mydriasis and 3.5% for a single fi eld with mydria-sis.
SR of DS II
Summary of evidence
DS IIRetinography using a non-mydriatic 45-degree 3 fi eld camera is an effective tool for screening diabetic retinopathy critical degrees that need to be referred to a specialist539, 542, 545, 546, 547.
DS II A central image at 45 degrees is enough to determine the absence or presence of diabetic retinopathy and diabetic macular oedema, but not enough to graduate clinical signifi cance545.
Recommendations
BThe retinal digital photography obtained by non-mydriatic camera should be implemented in retinopathy screening programs for adults and children with diabetes mellitus type 1.
BShould a camera not be available, screening will be carried out through an ophthalmoscopy (with or without mydriasis), which will be evaluated by an ophthalmologist.
√The use of retinal digital photography obtained electronically by a non-mydriatic camera facilitates the screening performance for both the patient and the health staff.
√Although retinal digital photography may detect many clinically signifi cant alterations, digital photographs of the retina should not replace the full initial examination and with mydriasis of the retina.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 225
11.2.3. Start time and frequency of screening for diabetic retinopathy
The CPG NICE 20047 includes the following evidence:
Age of onset for screening
A cohort study548 carried out in 937 patients aged 6 to 20 years old showed that 9% of children under 11 had retinopathy (n = 110, mean age 9.5 years), while in children over 11 years (n = 827, mean age 14 years) the percentage increased to 29%. The risk of developing retinopathy increased according to the duration of DM [OR 1.22 (95% CI: 1.16 to 1.29)], age [OR 1.13 (95% CI: 1.06 to 1, 21)], and higher levels of HbA
1c [OR 1.26 (95% CI: 1.11 to 1.43)].
Based on these data, the authors of this study recommend initiating screening of DR from the age of 12.
Cohort study
2+
Frequency of screening
The work by Younis et al.549 estimated optimum screening intervals by an actuarial survival analysis from the incidence rates found in the ‘Liverpool Screening Programme’ between 1991 and 1999.Thus, it determined a mean screening interval free of sight-threatening retinopathy of 5.7 years (95% CI: 3.5 to 7.6 years) for patients without retinopathy at baseline screening, 1.3 years (95% CI: 0.4 to 2.0 years) for incipient retinopathy, and 0.4 years (95% CI: 0 to 0.8 years) for mild preproliferative retinopathy.
Cohort study
2+
In the study by Olafdottir et al.550 296 diabetic patients were analyzed (96 with DM1) whose evolution of DR was assessed every two years for a period of 10 years. The study of these patients showed the following results:
• Of the total number of patients evaluated, 172 (46 with DM1) did not develop retinopathy within 10 years of follow-up [HbA
1c: Mean (SD)
7.8 (1.6), duration of diabetes: mean (SD) 18 years (7)].
• Of the total number of patients evaluated, 96 (38 with DM1) devel-oped mild nonproliferative DR [HbA
1c: Mean (SD) 8.1% (1.3), dura-
tion of diabetes mean (SD) 18 years (6)].
• Of the total number of patients evaluated, 6 (2 with DM1) developed clinically relevant macular oedema [HbA
1c: mean (SD) 9.6% (1.4);
duration of diabetes (SD) 20 years (4)].
• Of the total number of patients evaluated, 23 (11 with DM1) devel-oped preproliferative DR [HbA
1c: mean (SD) 8.4% (1.7), duration of
the diabetes mean (SD) 19 years (5)].
Cohort study
2+
226 SNS CLINICAL PRACTICE GUIDELINES
• Of the patients evaluated, 4 (2 with DM1) developed proliferative DR [HbA
1c: mean (SD) 9.5% (1.7), duration of diabetes 18, 15, 18 and 12
years].A retrospective observational study conducted in the Basque country551
that estimated the most adequate frequency of screening for diabetic retinopa-thy in 490 patients (70.8% with DM1), found that 86% of the patients free of retinopathy at the baseline examination remained free of retinopathy after 2 years. When considering the impact in relation to the development of high-risk retinopathy, it was found that among patients with DM1, over 95% of patients remained free of high-risk retinopathy at the end of the fourth year, regard-less of the time of evolution and the metabolic control of their diabetes. 94% of patients with non-proliferative mild retinopathy at baseline remained free of high-risk retinopathy at the end of the two years. The results of this study indicate that the frequency recommended to screen high-risk retinopathy in patients without retinopathy is 4 years and 2 years in people with diabetes mel-litus type 1 with nonproliferative mild diabetic retinopathy, although the data suggest that for people with good metabolic control of diabetes this interval could be even 3 years.
Observationalstudy
2+
Summary of evidence
Cohortstudy 2 +
The risk of developing retinopathy increases according to the duration of diabetes, age and higher HbA
1c levels548, 550.
Observational study 2 +
86% of patients free of retinopathy at the baseline examination remain free of retinopathy after 2 years of evolution549, 551.
Observational study 2 +
94% of patients with nonproliferative mild retinopathy at the baseline study remained free of high-risk retinopathy at the end of the 2-year follow-up549, 551.
Recommendations
BIn people with diabetes mellitus type 1, it is recommended to start screening for retinopathy after puberty, or after 5 years since the diagnosis of diabetes.
BIf retinopathy is detected, it is considered advisable to perform a screening for retinopathy once a year.
BShould retinopathy not be detected in the baseline examination of the retina, it is recommended to perform a retinopathy screening every 2 or 3 years.
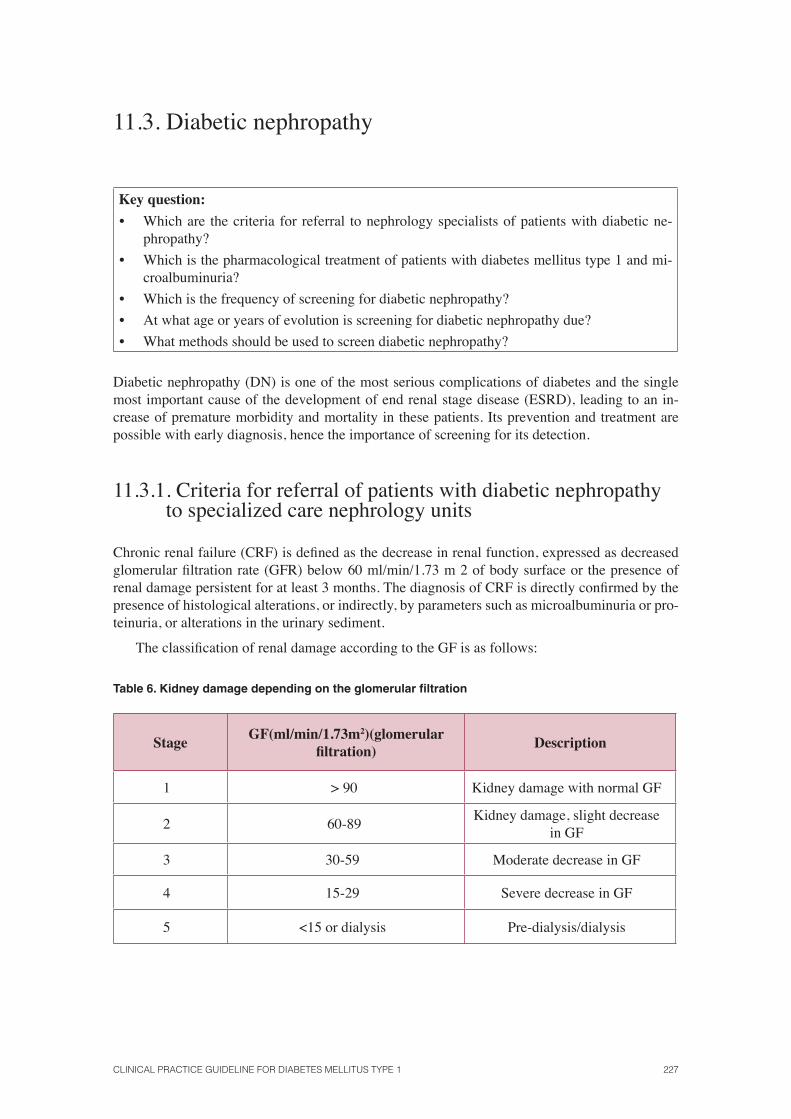
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 227
11.3. Diabetic nephropathy
Key question:
• Which are the criteria for referral to nephrology specialists of patients with diabetic ne-phropathy?
• Which is the pharmacological treatment of patients with diabetes mellitus type 1 and mi-croalbuminuria?
• Which is the frequency of screening for diabetic nephropathy?
• At what age or years of evolution is screening for diabetic nephropathy due?
• What methods should be used to screen diabetic nephropathy?
Diabetic nephropathy (DN) is one of the most serious complications of diabetes and the single most important cause of the development of end renal stage disease (ESRD), leading to an in-crease of premature morbidity and mortality in these patients. Its prevention and treatment are possible with early diagnosis, hence the importance of screening for its detection.
11.3.1. Criteria for referral of patients with diabetic nephropathy to specialized care nephrology units
Chronic renal failure (CRF) is defi ned as the decrease in renal function, expressed as decreased glomerular fi ltration rate (GFR) below 60 ml/min/1.73 m 2 of body surface or the presence of renal damage persistent for at least 3 months. The diagnosis of CRF is directly confi rmed by the presence of histological alterations, or indirectly, by parameters such as microalbuminuria or pro-teinuria, or alterations in the urinary sediment.
The classifi cation of renal damage according to the GF is as follows:
Table 6. Kidney damage depending on the glomerular fi ltration
Stage GF(ml/min/1.73m2)(glomerular
fi ltration)Description
1 > 90 Kidney damage with normal GF
2 60-89Kidney damage, slight decrease
in GF
3 30-59 Moderate decrease in GF
4 15-29 Severe decrease in GF
5 <15 or dialysis Pre-dialysis/dialysis

228 SNS CLINICAL PRACTICE GUIDELINES
From stage 3, it is considered that there is renal failure, although these alterations must be confi rmed for at least 3 months to confi rm the chronicity of the disorder.
In clinical practice, the assessment of the renal function must be performed by the following methods:
• Calculation of the GF through the MDRD or Cochcroft-Gault formulae. The determina-tion of serum creatinine cannot be used as single parameter for the assessment of the renal function.
• Microalbuminuria. Collecting a single morning urine sample by the determination of the albumin/creatinine ratio (normal <30 mg/g or mcg/mg) is advisable. This ratio represents a good estimation of proteinuria and prevents urine collection for 24 hours.
It is a known fact that late referral of CKD patients to specialized care units in nephrology is associated with negative consequences: initiation of renal replacement therapy in a worse clini-cal situation, in an unplanned way and with the need in many cases of urgent haemodialysis with vascular access through temporal catheters; preventable hospitalization; accelerated loss of renal function, etc. In addition, late referral of patients with CKD to specialized care units in nephrol-ogy has emerged as an independent factor of increased mortality risk after starting dialysis552, 553;
554, 555; 556; 557. Moreover, patients with diabetes start renal replacement therapy with a signifi cantly higher comorbidity than patients without diabetes558.
It is estimated that in Europe 35% of patients are referred late to a nephrologist559, 560. In Spain, the percentage is 23%, being the average creatinine clearance in these patients 30 ml/min552, 555. A study carried out in Canada that describes the characteristics of patients arriving for the fi rst time to the nephrology clinic561, indicated that the mean creatinine clearance (SD) in these patients was 64 ml/min 39, but two-thirds of the cases had a creatinine clearance less than 60 ml/min, and 20 patients (13%) had CKD at stage 4. Another study562, which retrospectively analyzed all patients seen for the fi rst time in the nephrology unit of the Hospital General Universitario Gregorio Marañón in Madrid between January and December 2003 (n = 612, 28.4% with dia-betes) observed renal insuffi ciency in 64% of cases, a high prevalence of arterial hypertension (HTN) (71%), and use of inhibitors of the renin-angiotensin system in only 42% of hypertensive patients. These studies show a delay in referral of patients to nephrology, which worsens the prognosis of the patient and the costs for the healthcare system. The ability to act promptly in the early stages of kidney damage and slow the evolution to progressive renal disease requires careful planning of renal damage detection and intensive treatment against two etiological factors of renal failure: hypertension and diabetes.
Therefore, it is important to determine the optimal time in the clinical course of the disease in relation to the degree of renal function in which a patient should be referred to the specialized care units in nephrology.
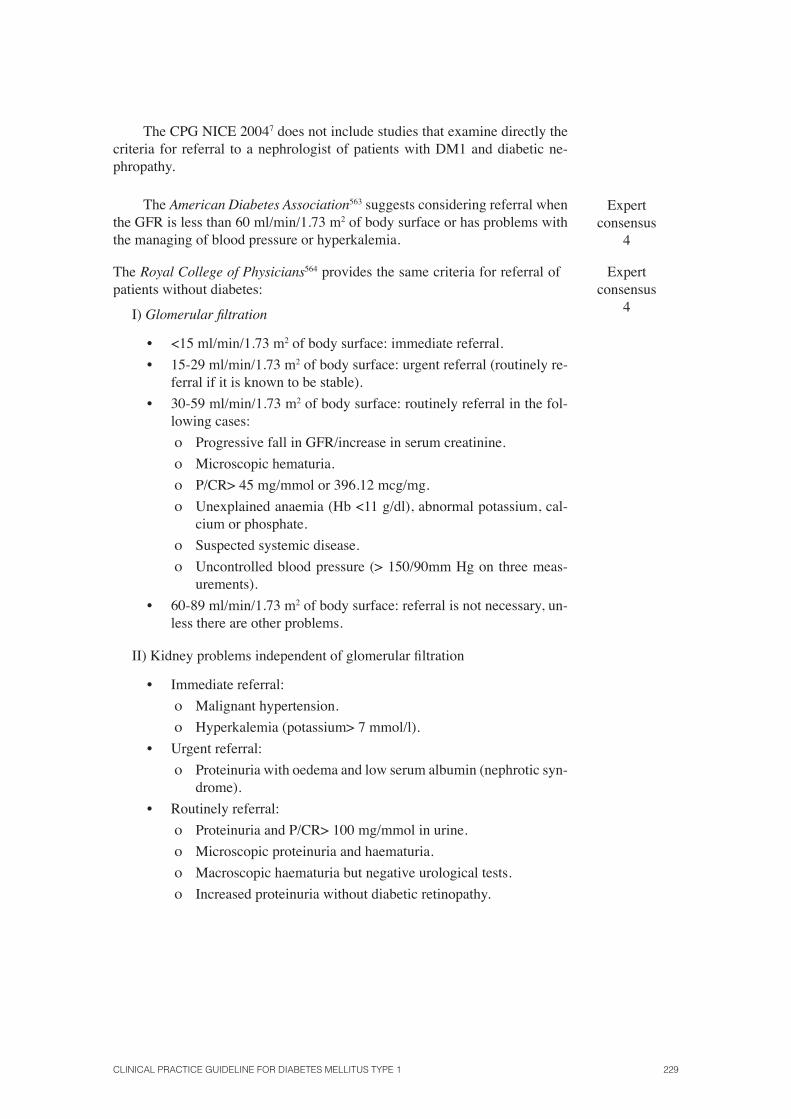
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 229
The CPG NICE 20047 does not include studies that examine directly the criteria for referral to a nephrologist of patients with DM1 and diabetic ne-phropathy.
The American Diabetes Association563 suggests considering referral when the GFR is less than 60 ml/min/1.73 m2 of body surface or has problems with the managing of blood pressure or hyperkalemia.
Expertconsensus
4
The Royal College of Physicians564 provides the same criteria for referral of patients without diabetes:
I) Glomerular fi ltration
• <15 ml/min/1.73 m2 of body surface: immediate referral.
• 15-29 ml/min/1.73 m2 of body surface: urgent referral (routinely re-ferral if it is known to be stable).
• 30-59 ml/min/1.73 m2 of body surface: routinely referral in the fol-lowing cases:
ο Progressive fall in GFR/increase in serum creatinine.
ο Microscopic hematuria.
ο P/CR> 45 mg/mmol or 396.12 mcg/mg.
ο Unexplained anaemia (Hb <11 g/dl), abnormal potassium, cal-cium or phosphate.
ο Suspected systemic disease.
ο Uncontrolled blood pressure (> 150/90mm Hg on three meas-urements).
• 60-89 ml/min/1.73 m2 of body surface: referral is not necessary, un-less there are other problems.
II) Kidney problems independent of glomerular fi ltration
• Immediate referral:
ο Malignant hypertension.
ο Hyperkalemia (potassium> 7 mmol/l).
• Urgent referral:
ο Proteinuria with oedema and low serum albumin (nephrotic syn-drome).
• Routinely referral:
ο Proteinuria and P/CR> 100 mg/mmol in urine.
ο Microscopic proteinuria and haematuria.
ο Macroscopic haematuria but negative urological tests.
ο Increased proteinuria without diabetic retinopathy.
Expertconsensus
4
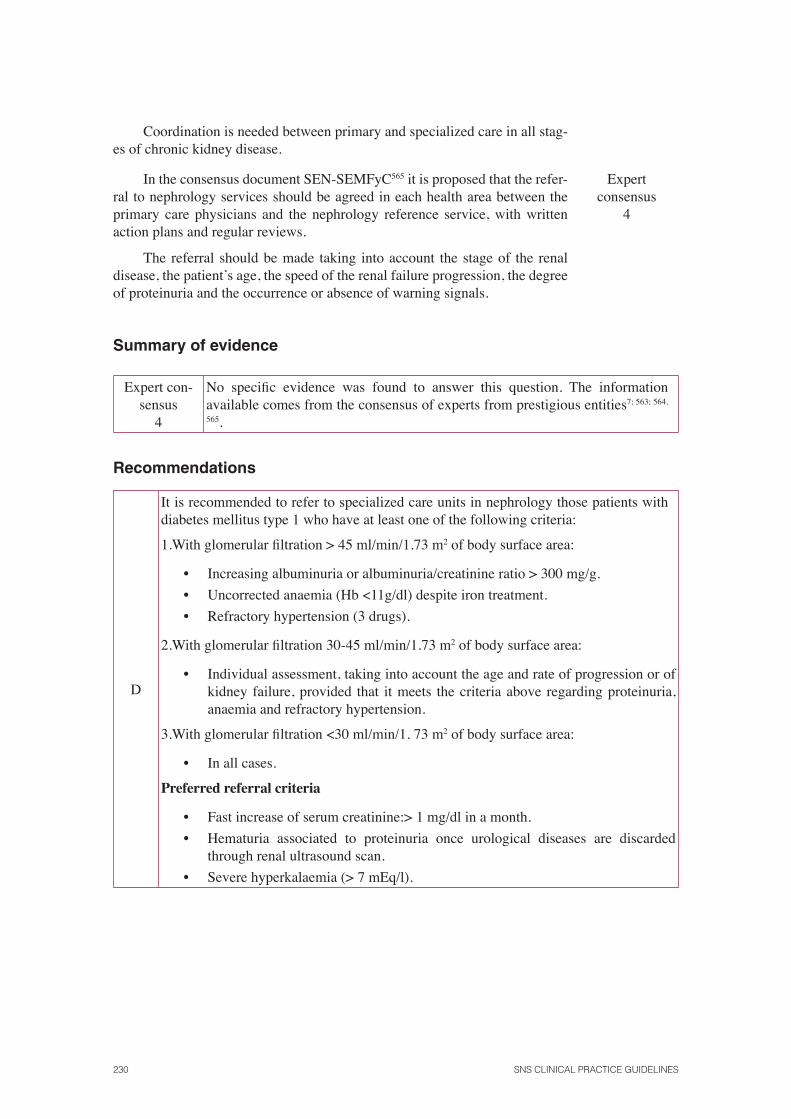
230 SNS CLINICAL PRACTICE GUIDELINES
Coordination is needed between primary and specialized care in all stag-es of chronic kidney disease.
In the consensus document SEN-SEMFyC565 it is proposed that the refer-ral to nephrology services should be agreed in each health area between the primary care physicians and the nephrology reference service, with written action plans and regular reviews.
Expertconsensus
4
The referral should be made taking into account the stage of the renal disease, the patient’s age, the speed of the renal failure progression, the degree of proteinuria and the occurrence or absence of warning signals.
Summary of evidence
Expert con-sensus
4
No specifi c evidence was found to answer this question. The information available comes from the consensus of experts from prestigious entities7; 563; 564,
565.
Recommendations
D
It is recommended to refer to specialized care units in nephrology those patients with diabetes mellitus type 1 who have at least one of the following criteria:
1.With glomerular fi ltration > 45 ml/min/1.73 m2 of body surface area:
• Increasing albuminuria or albuminuria/creatinine ratio > 300 mg/g.
• Uncorrected anaemia (Hb <11g/dl) despite iron treatment.
• Refractory hypertension (3 drugs).
2.With glomerular fi ltration 30-45 ml/min/1.73 m2 of body surface area:
• Individual assessment, taking into account the age and rate of progression or of kidney failure, provided that it meets the criteria above regarding proteinuria, anaemia and refractory hypertension.
3.With glomerular fi ltration <30 ml/min/1. 73 m2 of body surface area:
• In all cases.
Preferred referral criteria
• Fast increase of serum creatinine:> 1 mg/dl in a month.
• Hematuria associated to proteinuria once urological diseases are discarded through renal ultrasound scan.
• Severe hyperkalaemia (> 7 mEq/l).
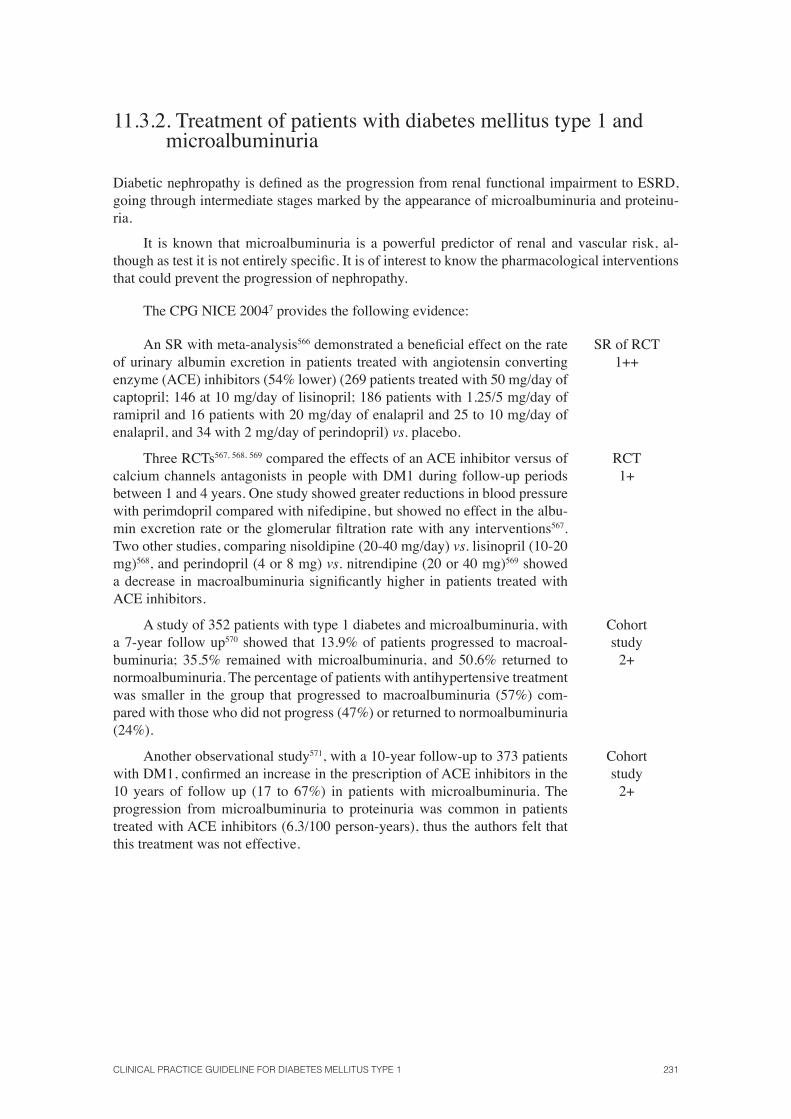
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 231
11.3.2. Treatment of patients with diabetes mellitus type 1 and microalbuminuria
Diabetic nephropathy is defi ned as the progression from renal functional impairment to ESRD, going through intermediate stages marked by the appearance of microalbuminuria and proteinu-ria.
It is known that microalbuminuria is a powerful predictor of renal and vascular risk, al-though as test it is not entirely specifi c. It is of interest to know the pharmacological interventions that could prevent the progression of nephropathy.
The CPG NICE 20047 provides the following evidence:
An SR with meta-analysis566 demonstrated a benefi cial effect on the rate of urinary albumin excretion in patients treated with angiotensin converting enzyme (ACE) inhibitors (54% lower) (269 patients treated with 50 mg/day of captopril; 146 at 10 mg/day of lisinopril; 186 patients with 1.25/5 mg/day of ramipril and 16 patients with 20 mg/day of enalapril and 25 to 10 mg/day of enalapril, and 34 with 2 mg/day of perindopril) vs. placebo.
SR of RCT1++
Three RCTs567, 568, 569 compared the effects of an ACE inhibitor versus of calcium channels antagonists in people with DM1 during follow-up periods between 1 and 4 years. One study showed greater reductions in blood pressure with perimdopril compared with nifedipine, but showed no effect in the albu-min excretion rate or the glomerular fi ltration rate with any interventions567. Two other studies, comparing nisoldipine (20-40 mg/day) vs. lisinopril (10-20 mg)568, and perindopril (4 or 8 mg) vs. nitrendipine (20 or 40 mg)569 showed a decrease in macroalbuminuria signifi cantly higher in patients treated with ACE inhibitors.
RCT1+
A study of 352 patients with type 1 diabetes and microalbuminuria, with a 7-year follow up570 showed that 13.9% of patients progressed to macroal-buminuria; 35.5% remained with microalbuminuria, and 50.6% returned to normoalbuminuria. The percentage of patients with antihypertensive treatment was smaller in the group that progressed to macroalbuminuria (57%) com-pared with those who did not progress (47%) or returned to normoalbuminuria (24%).
Cohort study
2+
Another observational study571, with a 10-year follow-up to 373 patients with DM1, confi rmed an increase in the prescription of ACE inhibitors in the 10 years of follow up (17 to 67%) in patients with microalbuminuria. The progression from microalbuminuria to proteinuria was common in patients treated with ACE inhibitors (6.3/100 person-years), thus the authors felt that this treatment was not effective.
Cohort study
2+
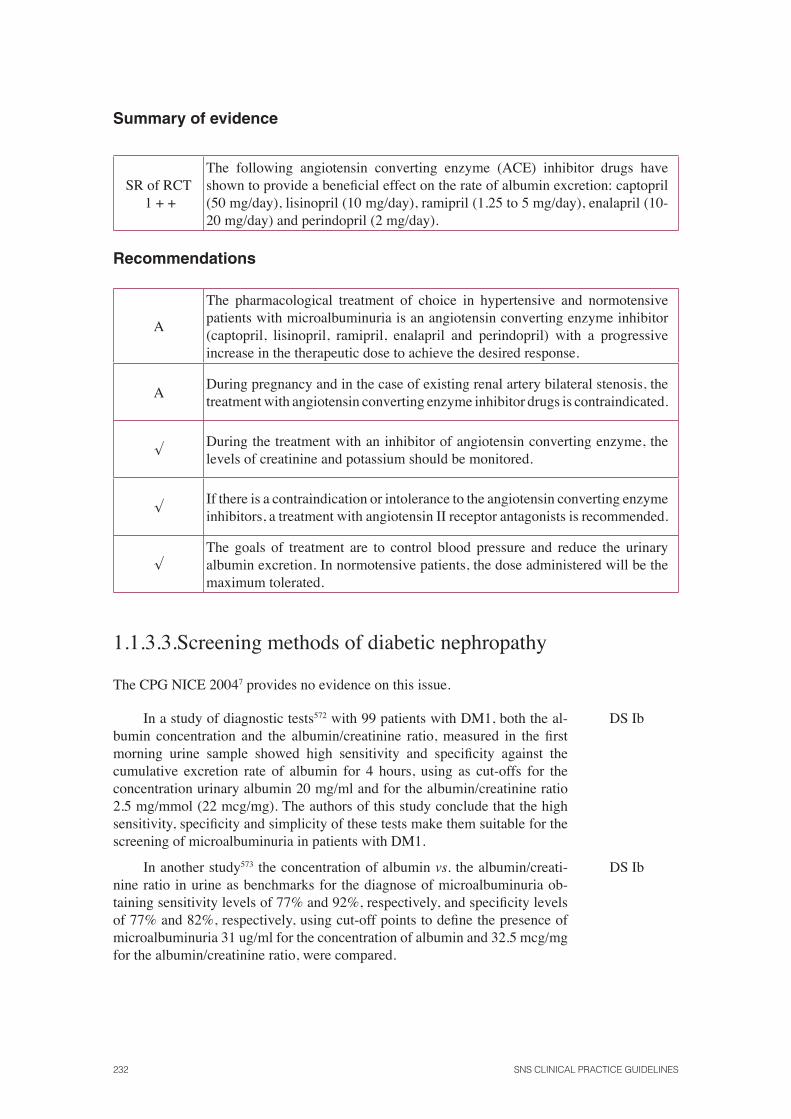
232 SNS CLINICAL PRACTICE GUIDELINES
Summary of evidence
SR of RCT 1 + +
The following angiotensin converting enzyme (ACE) inhibitor drugs have shown to provide a benefi cial effect on the rate of albumin excretion: captopril (50 mg/day), lisinopril (10 mg/day), ramipril (1.25 to 5 mg/day), enalapril (10-20 mg/day) and perindopril (2 mg/day).
Recommendations
A
The pharmacological treatment of choice in hypertensive and normotensive patients with microalbuminuria is an angiotensin converting enzyme inhibitor (captopril, lisinopril, ramipril, enalapril and perindopril) with a progressive increase in the therapeutic dose to achieve the desired response.
ADuring pregnancy and in the case of existing renal artery bilateral stenosis, the treatment with angiotensin converting enzyme inhibitor drugs is contraindicated.
√During the treatment with an inhibitor of angiotensin converting enzyme, the levels of creatinine and potassium should be monitored.
√If there is a contraindication or intolerance to the angiotensin converting enzyme inhibitors, a treatment with angiotensin II receptor antagonists is recommended.
√The goals of treatment are to control blood pressure and reduce the urinary albumin excretion. In normotensive patients, the dose administered will be the maximum tolerated.
1.1.3.3.Screening methods of diabetic nephropathy
The CPG NICE 20047 provides no evidence on this issue.
In a study of diagnostic tests572 with 99 patients with DM1, both the al-bumin concentration and the albumin/creatinine ratio, measured in the fi rst morning urine sample showed high sensitivity and specifi city against the cumulative excretion rate of albumin for 4 hours, using as cut-offs for the concentration urinary albumin 20 mg/ml and for the albumin/creatinine ratio 2.5 mg/mmol (22 mcg/mg). The authors of this study conclude that the high sensitivity, specifi city and simplicity of these tests make them suitable for the screening of microalbuminuria in patients with DM1.
DS Ib
In another study573 the concentration of albumin vs. the albumin/creati-nine ratio in urine as benchmarks for the diagnose of microalbuminuria ob-taining sensitivity levels of 77% and 92%, respectively, and specifi city levels of 77% and 82%, respectively, using cut-off points to defi ne the presence of microalbuminuria 31 ug/ml for the concentration of albumin and 32.5 mcg/mg for the albumin/creatinine ratio, were compared.
DS Ib
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 233
11.3.4. Start time of screening for diabetic nephropathy
The CPG NICE 20047 included a descriptive study that analyzed 3250 patients with DM574 and observed an albumin excretion greater than or equal to 20 g/min in 30.6% (95% CI: 29% to 32.2%) of patients and in 19.3% (95% CI: 15.6% to 23%) of the patients with a disease progression between 1 and 5 years.
Descriptive Study
3
11.3.5. Frequency of screening for diabetic nephropathy
No evidence has been found concerning this issue, so the recommendations are based on existing expert group consensus.
A CPG575 recommended carrying out an annual screening by determining microalbuminuria in urine.
Expert opinion 4
Another CPG published by the American Diabetes Association51 recom-mended by consensus as follows:
• Perform an annual evaluation of the urine albumin excretion in those patients with DM1 with a time of evolution of the disease equal to or longer than 5 years.
• Making a serum creatinine determination at least annually in adults with diabetes, with the aim of estimating the glomerular fi ltration rate (GFR) and study the degree of chronic renal disease.
Expert opinion 4
Summary of evidence
DS IbThe albumin/creatinine ratio in urine correlates well with albuminuria for 24 hours, and has high sensitivity (92%) and specifi city (82%) to detect microalbuminuria and macroalbuminuria572.
Descriptivestudy
3
Between 16% and 23% of people with an economic evolution of the disease between 1 to 5 years have a urinary albumin excretion higher than or equal to 20 g/min574.
Expertconsensus
4
An annual evaluation has been established as a criterion for screening diabetic nephropathy51; 575.
Recommendations
BThe measurement of the albumin/creatinine ratio in a sample of fi rst morning urine is recommended as a method for the detection and monitoring of diabetic nephropathy.
D5 after the diagnosis of diabetes mellitus type 1, an annual screening of the nephropathy is recommended.
234 SNS CLINICAL PRACTICE GUIDELINES
11.4. Diabetic foot
Key question:
• Should a diabetic foot screening take place?
• Which is the frequency of screening for diabetic foot?
• At what age or years of evolution should a diabetic foot screening take place?
• What method should be used to perform a diabetic foot screening?
Diabetic foot (DF) includes a group of syndromes in which the presence of neuropathy, ischemia and infection produces tissue damage or ulcers due to minor trauma, resulting in signifi cant mor-bidity that can even lead to amputation.
Diabetic foot complications can be prevented with a proper strategy, which includes early diagnosis, risk classifi cation and effective prevention and treatment measures.
11.4.1. Effectiveness of screening for diabetic foot
The CPG NICE 20047 does not provide evidence to answer this question.
An RCT576 that included 192 high-risk patients, in which they were ran-domly assigned to a detection and prevention program for diabetic foot (week-ly visits to the podiatrist and hygiene maintenance, protective footwear, every day care and footwear education) vs. usual care. In the intervention group a signifi cant reduction of amputations was observed compared to the group re-ceiving traditional care (p <0.01), but showed no signifi cant differences in the incidence of ulcers (2.4% in the experimental group vs. 3.5% in the control group)576.
RCT 1+
Prospective studies576, 577, 578 have shown signifi cant reductions in the in-cidence of amputations by careful inspection of the foot, artery evaluation, exploration by assessment of the skin colour, temperature, presence of pulses, determining the ankle-arm index and evaluation of sensory neuropathy using monofi lament.
Observational studies
2+
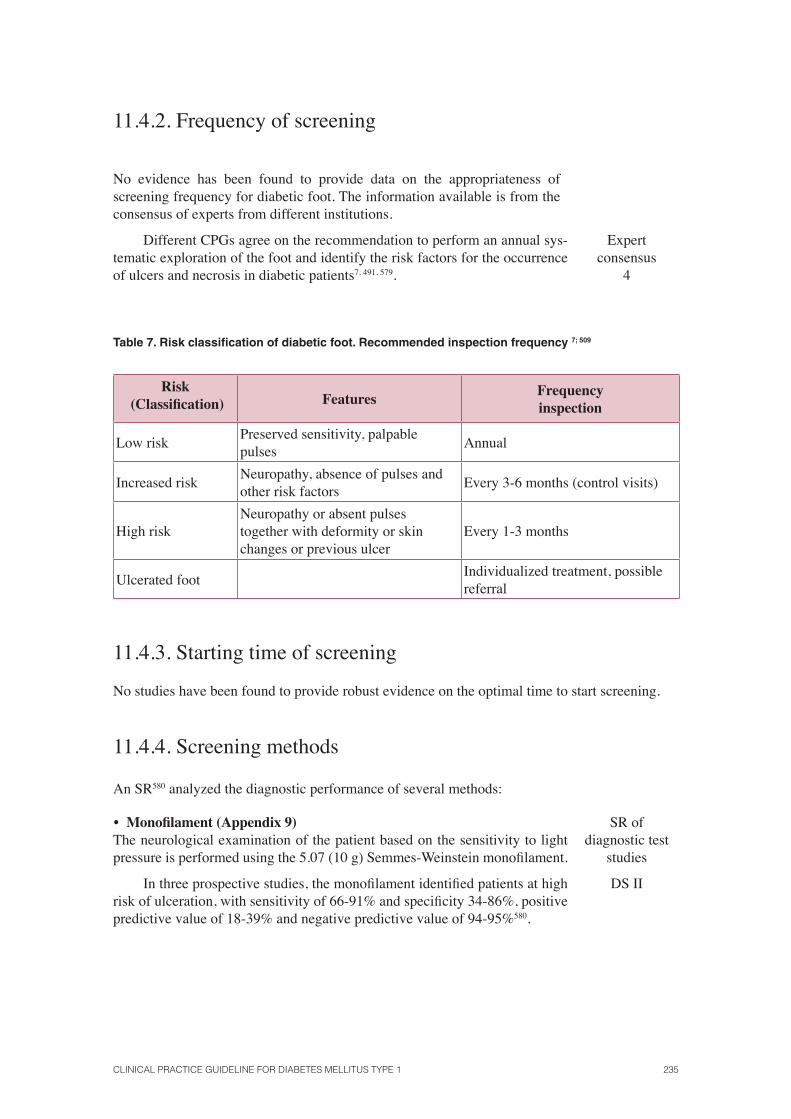
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 235
11.4.2. Frequency of screening
No evidence has been found to provide data on the appropriateness of screening frequency for diabetic foot. The information available is from the consensus of experts from different institutions.
Different CPGs agree on the recommendation to perform an annual sys-tematic exploration of the foot and identify the risk factors for the occurrence of ulcers and necrosis in diabetic patients7, 491, 579.
Expertconsensus
4
Table 7. Risk classifi cation of diabetic foot. Recommended inspection frequency 7; 509
Risk (Classifi cation) Features
Frequency inspection
Low riskPreserved sensitivity, palpable pulses
Annual
Increased riskNeuropathy, absence of pulses and other risk factors
Every 3-6 months (control visits)
High riskNeuropathy or absent pulses together with deformity or skin changes or previous ulcer
Every 1-3 months
Ulcerated footIndividualized treatment, possible referral
11.4.3. Starting time of screening
No studies have been found to provide robust evidence on the optimal time to start screening.
11.4.4. Screening methods
An SR580 analyzed the diagnostic performance of several methods:
• Monofi lament (Appendix 9)The neurological examination of the patient based on the sensitivity to light pressure is performed using the 5.07 (10 g) Semmes-Weinstein monofi lament.
SR ofdiagnostic test
studies
In three prospective studies, the monofi lament identifi ed patients at high risk of ulceration, with sensitivity of 66-91% and specifi city 34-86%, positive predictive value of 18-39% and negative predictive value of 94-95%580.
DS II
236 SNS CLINICAL PRACTICE GUIDELINES
• Turning forkIt is a simple and inexpensive method for measuring vibration sensa-
tion580, but has problems regarding reliability. According to a diagnostic tests study581 it is more inaccurate in predicting ulcers than the monofi lament, al-though it may be an alternative should there be no monofi lament available.
DS II
Oyer et al.582 analyzed diabetic peripheral neuropathy in 81 patients (11 with ulcers), through the 128 Hz turning fork, to assess its accuracy and repro-ducibility and compare it with the 10 g monofi lament. The RR of ulcer was 15.3 for patients whose perception of vibration of the tuning fork was equal to or less than 4 seconds. The authors of this study concluded that the turning fork method is effective and reproducible, provides a quantitative estimation of the degree of neuropathy in patients with diabetes and can demonstrate the presence of neuropathy in cases that are considered normal in the 10g mono-fi lament test.
• BiotensiometerAccording to the study results by Mayfi eld et al.581, the biotensiometer
exceeds the reliability limitations of the turning fork as it can regulate the different vibratory thresholds. A vibration threshold over 25V has 83% of sen-sitivity, 63% of specifi city, a positive probability quotient of 2.2 (95% CI 1.8 to 2.5), and a negative probability quotient of 0.27 (95% CI 0.14 to 0.48) to predict foot ulcer after 4 years.
DS II
Nather et al.583 studied the incidence of sensory peripheral neuropathy in patients with diabetes without previous diabetic foot problems at different times of the progression of the disease using 3 different tests (prick test, 5.07 Semmes-Weinstein 10 g monofi lament and the biotensiometer) to detect the threshold of perception.
No signifi cant differences were found in the ability to detect sensory neu-ropathy between the prick test and the neurometer, and the results of both tests were signifi cantly better than those performed with the 5.07 Semmes-Weinstein 10g monofi lament.
DS II
Summary of evidence
RCT 1 +
Diabetic foot screening decreases the incidence of amputation in patients with diabetes mellitus576, 577, 578.
Expertconsensus
4
Different clinical practice guidelines agree to carry out annual systematic explorations of the foot and identify the risk factors for the occurrence of ulcers and necrosis in patients with diabetes7, 491, 579.
SR of diagnostic test studies
2
Diabetic foot screening should include medical history, identifi cation of foot deformities and an assessment of the loss of sensitivity through monofi lament580.
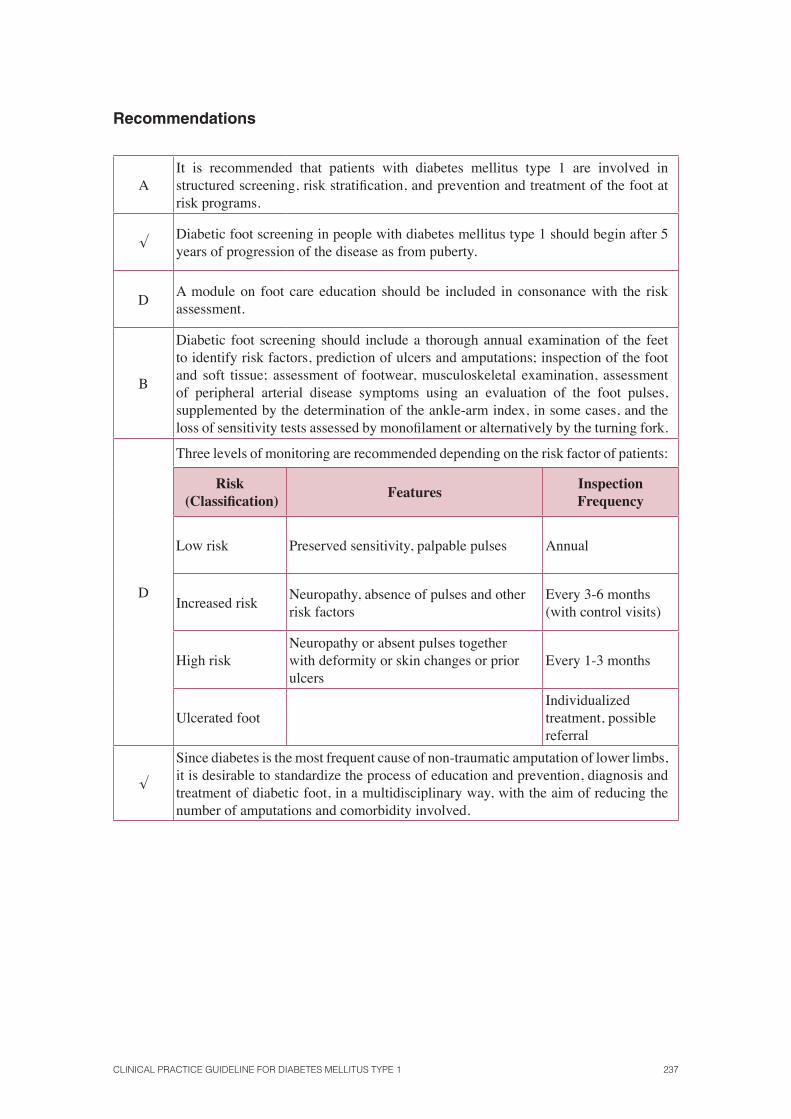
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 237
Recommendations
AIt is recommended that patients with diabetes mellitus type 1 are involved in structured screening, risk stratifi cation, and prevention and treatment of the foot at risk programs.
√Diabetic foot screening in people with diabetes mellitus type 1 should begin after 5 years of progression of the disease as from puberty.
DA module on foot care education should be included in consonance with the risk assessment.
B
Diabetic foot screening should include a thorough annual examination of the feet to identify risk factors, prediction of ulcers and amputations; inspection of the foot and soft tissue; assessment of footwear, musculoskeletal examination, assessment of peripheral arterial disease symptoms using an evaluation of the foot pulses, supplemented by the determination of the ankle-arm index, in some cases, and the loss of sensitivity tests assessed by monofi lament or alternatively by the turning fork.
D
Three levels of monitoring are recommended depending on the risk factor of patients:
Risk (Classifi cation)
FeaturesInspection Frequency
Low risk Preserved sensitivity, palpable pulses Annual
Increased riskNeuropathy, absence of pulses and other risk factors
Every 3-6 months (with control visits)
High riskNeuropathy or absent pulses together with deformity or skin changes or prior ulcers
Every 1-3 months
Ulcerated footIndividualized treatment, possible referral
√
Since diabetes is the most frequent cause of non-traumatic amputation of lower limbs, it is desirable to standardize the process of education and prevention, diagnosis and treatment of diabetic foot, in a multidisciplinary way, with the aim of reducing the number of amputations and comorbidity involved.

238 SNS CLINICAL PRACTICE GUIDELINES
11.5. Erectile dysfunction in people with diabetes mellitus type 1
Erectile dysfunction (ED) is known as the diffi culty to achieve and maintain an erection enough to be able to have a satisfying sexual relationship, microvascular or neuropathic complication that can occur in patients with diabetes 584.
The Study of Male Erectile Dysfunction (EDM), carried out in Spain585, determined that DE affects approximately 34-45% of men with diabetes, and 12% of men between 25 and 70 years of the general population. The risk factors include advanced age, longstanding diabetes, inadequate glycaemic control, smoking, hypertension, dyslipidemia, androgen defi ciency states and cardio-vascular disease.
11.5.1. Treatment of erectile dysfunction
• Phosphodiesterase inhibitors
Phosphodiesterase (PDE5) is an enzyme that hydrolyses the cyclic guanosine monophosphate
enzyme (GMPc) in the penile cavernous tissue, making it guanosine monophosphate. The inhibi-
tion of PDE5 increases the GMP
c level, which induces relaxation of the cavernous and vascular
musculature with vasodilatation and consequent penile erection586.
Sildenafi l, vardenafi l and tadalafi l are potent, reversible and competitive PDE5 inhibitors.
Their mechanism of action is to maintain the levels of nitric oxide, “universal vasodilator» previ-ously induced by the excitation.
The CPG NICE 20047 does not provide evidence to answer this question.
An RS587 identifi ed 8 RCTs (5 about sildenafi l) on the effi cacy of inhibi-tors of PDE
5 vs. placebo in patients with diabetes, of which 20% had DM1.
SR of RCT 1++
The meta-analysis on the effectiveness of PDE5 inhibitors indicated in a
consistent and signifi cant way that all three drugs (sildenafi l, vardenafi l and tadalafi l) were superior to placebo. Of the total, 976 men were assigned to receive a PDE
5 inhibitor and 741 to the control group. The results showed a
WMD 6.6 (95% CI 5.2 to 7.9) for the International Index of Erectile Function (IIEF) scale at the end of the study in favour of the PDE
5 inhibitors arm.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 239
Regarding the safety of the PDE5 inhibitors, the adverse event most fre-
quently reported was headache with a total of 141 episodes in the 1,012 pa-tients in the group of patients treated with PDE
5 inhibitors, compared with 28
of 755 in the control group [RR 3.66 (95% CI: 2.51 to 5.35)]. The second most frequent event was fl ushing, with 103 episodes in 970 patients in the group with PDE 5 inhibitors, [RR 13.21 (95% CI 6.01 to 29.03)]. Symptoms of the upper airway and fl u-like syndromes, dyspepsia, myalgia, back pain, and ab-normal vision, in descending order of frequency were also reported. The RR for developing any adverse reaction was 4.8 (95% CI 3.74 to 6.16) in the PDE
5
inhibitors arm, in comparison with the control group.
In the SR by Nehra et al.588 numerous studies evaluating the effi cacy and safety of PDE 5 in patients with DM1 and DM2 were included. Sildenafi l im-proved the erectile function compared to placebo (p = 0.0001) in DM1 patients regardless of the HbA
1c levels and the degree of progression of the disease.
Baseline HbA1c
levels did not appear to infl uence the response to tadalafi l in men with DM1 and DM2.
The response was similar to tadalafi l in men with DM and without DM, regardless of the levels of HbA
1c, the diabetes therapy, or the previous use of
other PDE 5 inhibitors (sildenafi l). Success rates were 60% with 10 mg of tadalafi l and 65% with 20 mg (p <0.001) vs. placebo, according to the scores on the SEP2, and 49% with 10 mg of tadalafi l and 53% with 20 mg (p <0.001) vs. placebo, according to the SEP3 scores.
These studies have shown similar effi cacy for the three agents (sildenafi l, tadalafi l, and vardenafi l), with a signifi cant improvement in the erectile func-tion of patients with DM.
SR of RCT 1++
Another SR589 included a total of 67 studies examining the PDE5 inhibi-
tors, intracavernous alprostadil and penile prostheses.
The PDE5 inhibitors were selected as a fi rst-line treatment for erectile
dysfunction, with an average effi ciency of 50% and a favourable safety pro-fi le. The alprostadil was the most commonly used drug, but the combination of papaverine, phentolamine and alprostadil represented the most effective medical treatment for patients whose erectile dysfunction was unresponsive to monotherapy.
The intracavernous administration of vasoactive drugs was the second line of treatment when PDE
5 inhibitors failed. Papaverine (20-80 mg) and alpros-
tadil were the main drugs used for the intracavernous treatment. Alprostadil represented the most effective and the only approved monotherapy treatment.
SR of RCT 1++
240 SNS CLINICAL PRACTICE GUIDELINES
Papaverine (7.5 to 45 mg) and phentolamine (0.25 to 1.5 mg), and com-binations of papaverine (8-16 mg), phentolamine (0.2-0.4 mg), and alprostadil (10-20 mg), showed the highest effi cacy rates (especially in the mixture of the three) in cases which were diffi cult to treat. Complications of intracav-ernous pharmacotherapy included penile pain (50% of patients, after 11% of injections), prolonged erections (5%), priapism (1%) and fi brosis (5-10%). However, no studies identifi ed the current incidence of complications by fi -brosis after intracavernous injections. The dropout rates were 41% to 68% on the desire for a permanent treatment modality, the lack of a suitable partner, due to the poor response (especially among older people), fear of needles, fear of complications and loss of spontaneity in sex.
Regarding penile prostheses, these showed excellent results at a func-tional and safety level in relation to the implantation of penile prostheses.
A placebo-controlled RCT in men with DM1 and DM2 (n = 425)352 showed signifi cant improvements in the erectile function scores of IIEF-EF and the Sexual Encounter Profi le 3 (SEP3), with satisfactory rates after 12 weeks with a 10 or 20 mg dose of vardenafi l, compared with placebo (p <0.0001). No association was found between vardenafi l and the level of gly-caemic control (defi ned as HbA
1c level). The responses to SEP3 were signifi -
cantly higher for those receiving 10 mg and 20 mg of vardenafi l regardless of the glycaemic control.
RCT 1+
• Apomorphine
The sublingual apomorphine (Uprima ®) or apomorphine hydrochloride is a non-selective ago-nist of dopamine receptors that acts on the paraventricular nucleus of the hypothalamus. This drug is marketed in Spain since 2001 with a sublingual formulation of 2 and 3 mg.
The CPG NICE 20047 does not provide evidence to answer this question.
An SR590 which included 4 RCTs studied sublingual apomorphine (2-6 mg) vs. placebo591, 592, 593, 594, with a total of 1594 men, stated that 45% of men had normal erections with apomorphine, compared to 29% in the placebo group [RR 1.4 (95% CI 1.3 to 1.7), NNT: 6.6 (95% CI: 5.0 to 9.6)].
SR of RCT1++
Another clinical trial carried out in 130 patients with diabetes594, ran-domly assigned to a treatment with sublingual apomorphine (14.74% patients with DM1) or placebo (15.25% patients with DM1) analyzed the improved erections after 4 weeks of treatment. The sexual response rate was 22% for apomorphine, compared with 17% for placebo, the difference not being rel-evant (p = 0.48).
RCT1+
The 2 RCTs included in this SR demonstrate that apomorphine is less effective than sildenafi l: the percentage of successful attempts was 75% in the group with sildenafi l vs. 35% in the group with apomorphine (p <0.001)595 and 73.1% in the group with sildenafi l vs. 62.7% with apomorphine (p <0.0004), with a 17.5% of the population with diabetes596.
RCT1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 241
Another RCT of crossover design597 evaluated the overall effectiveness of sublingual apomorphine versus sildenafi l (23.14% DM). Apomorphine was less effective than sildenafi l in the percentage of successful intercourses (40.3 vs. 83.3, p <0.001), in the sexual relationship satisfaction and overall satisfac-tion. Sildenafi l was preferred over apomorphine.
RCT 1+
An open, randomized crossover trial in 131 patients (9.3% DM1)598, previously untreated showed greater effi cacy of sildenafi l versus sublingual apomorphine (measured according to the IIEF questionnaire), in the percent-age of successful attempts (62.7 % vs. 28.3%) and in patient preference (95% preferred sildenafi l).
RCT 1++
A randomized crossover RCT599 studied 131 patients (7.6% DM), ran-domly divided into two groups: 66 with sildenafi l and 64 with sublingual apo-morphine without masking. A statistically signifi cant difference was found between the two interventions. The comparison between the before and after treatments showed differences in favour of sildenafi l (p <0.001).
RCT 1++
A descriptive study600, which conducted a survey to 11186 primary care physicians, concluded that the majority of patients treated with sublingual apo-morphine (28.5% with DM) considered it ineffective, and also that it had many adverse effects. The most reported adverse events were headache and nausea.
Descriptive Study
3
• Penile Prosthesis
The CPG NICE 20047 does not provide evidence to answer this question.
A systematic review included in an evaluation report601 with observation-al studies indicated that penile prostheses was highly effective, with rates of 80-90% of free persistent complication after 5 years, besides getting adequate erections for intercourse in 70-90% of patients. The surgical complications reported were: erosion or abrasion of the area, infection, mechanical failure of the prostheses or the cylinders or migration of any of its components. The het-erogeneity in the variables included in the follow-up and assessment criteria made it diffi cult to compare the results between the studies.
SR ofobservational studies 2++
Another study602 carried out a retrospective follow-up (1990-2004) of 200 patients with penile prostheses (40% with DM), analyzing three types of implants: AMS 700CX® (3- component infl atable), AMS Ambicor® (2-com-ponent infl atable) and 600-650 AMS® (semi-rigid prosthesis). Patient satis-faction and his partner was very high with the three types of prostheses, though it was less with the AMS 600-650®. Natural erections and higher stiffness than before the implantation in most cases were achieved. 20% of patients experienced serious complications after surgery: 9 (22.5%) had infections, 18 (45%) mechanical failure and 13 (32.5%) erosions.
SR ofobservational
studies 2+
242 SNS CLINICAL PRACTICE GUIDELINES
Another study603 analyzed the survival rate of the AMS 600® prosthesis, which was signifi cantly higher than that of the infl atable prosthesis AMS 700 CXM®. The overall failure rate of the AMS 600® prosthesis was 16.4%. The survival failure rate was 22.2% in the infl atable prosthesis and the most com-mon cause was some mechanical failure of the cylinder. Neurogenic erectile dysfunction is associated with increased failure of the AMS 700 CXM ® pros-thesis.
Observational study 3
• Psychotherapy
The CPG NICE 20047 does not provide evidence to answer this question.
In an SR604, nine randomized and two quasi-randomized trials were ana-lyzed, which included 398 men with ED (141 in the psychotherapy group, 109 in the medication group, 68 with psychotherapy along with medication, 20 with vacuum devices and 59 in the control group). The results of these studies indicated that group therapy focused on the symptoms showed greater effi cacy in comparison with the control group.
SR of RCT1+
In addition, group psychotherapy showed a greater reduction in the “per-sistence of erectile dysfunction” after the treatment than the control group (without treatment) [RR 0.40 (95% CI 0.17 to 0.98), n = 100, NNT 1.61 (95% CI: 0.97 to 4.76)].
Group psychotherapy with sildenafi l citrate, vs. sildenafi l alone, reduced more the “persistence of ED” [RR 0.46 (95% CI 0.24 to 0.88), NNT 3.57, (95% IC: 2 to 16.7), n = 71] and patients were less likely to drop out from the treatment [RR 0.29 (95% CI: 0.09, 0.93)].
• Vacuum devices
Vacuum devices (VD) essentially consist of a plastic cylinder connected to a pump, which can be operated by hand, or battery, and one or more tension rings. The penis is inserted into the cylinder and the activation of the pump removes the air from inside the cylinder causing the creation of a vacuum. This causes the blood to enter the penis, which immediately widens in a similar way to a natural erection. Once an adequate erection is produced, a tension band is fastened around the penis to maintain the erection impeding the outfl ow of blood. The vacuum inside the cylinder is then released and the cylinder removed from the penis. It is important that the tension ring be also removed within 30 minutes.
The CPG NICE 20047 does not provide evidence to answer this question.
Effectiveness
A retrospective study of cases among the Spanish population605 described that 63.3% of patients achieved satisfactory erections in over half of attempts with VDs.
DescriptiveStudy
3
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 243
Later another study606 compared the effectiveness of mono-therapy with VD vs. sildenafi l vs. both treatments in patients with various aetiologies of ED. It was observed that the mono-therapy and the combination therapy showed signifi cant differences in terms of erectile function compared to the pre-treat-ment. In all the other aspects analyzed (relationship satisfaction, orgasmic function, sexual desire and overall satisfaction) only the combined treatment was statistically signifi cant compared with the pre-treatment.
Observational study
2+
Another study607 included a sequence of interventions - sildenafi l citrate; vacuum devices (VD); intracavernosal injection (ICI) of alprostadil, sildenafi l citrate together with ICI of alprostadil; ICI of alprostadil together with VDs and penile prosthesis in patients with DM2 where the previous intervention had failed. The patients had a 2-year follow-up and the effectiveness was measured by the IIEF scale. The results showed that of 284 patients, 81 (28.5%) had a positive response to sildenafi l, 7 (2.5%), to DVC, 113 (39.8%) to ICI with alprostadil, 24 (8.5 %) to the combination of sildenafi l with ICI of alprostadil (0.7%), 2 to ICI together with VD, and 15 (5.3%) required a penile prosthesis implant. Fourteen patients (4.9%) had a negative response to all treatments. In conclusion, the progressive treatment program for ED seems very effective for patients with diabetes.
Observational study
2+
Adverse Effects
A study605 analyzed the side effects in 33 patients of which 27 had pain, 7 had penile ecchymosis, 5 had block in ejaculation and 5 had complaints with the rings. The only variables that were associated with lower use after 12 months were the lack of effectiveness of the device and the rejection of it by the couple (p <0.05). The presence of pain was associated with a higher rate of early dis-continuation in the medium term (p <0.05), but not to late dropout (p> 0.05).
DescriptiveStudy
3
A descriptive study608 that included 36 patients with ED who used VD stated that of the 36 patients studied, 3 (10%) had pain, 2 (5.5%), haematoma, 1 (2.7%), numbness; and 1 (2.7%), maceration.
DescriptiveStudy
3
Preferences of patients
A study608 assessed the preference of 36 patients with ED who had had suc-cessful results both with the vacuum devices and sildenafi l. Of all the patients, 12 (33.3%) chose to continue using a VD and 24 (66.6%) preferred sildenafi l. Those patients who preferred the vacuum device justifi ed their choice by the adverse side effects of sildenafi l. Those patients who chose sildenafi l justifi ed their preference for its greater effi ciency, convenience and ease of use.
DescriptiveStudy
3
244 SNS CLINICAL PRACTICE GUIDELINES
• Intracavernosal therapy: intracavernosal alprostadil
Alprostadil is the natural form of prostaglandin E1 (PGE1). It has a wide variety of pharmacologi-cal actions, including vasodilation and platelet aggregation inhibition. Erection occurs normally between 5 and 15 minutes after the intracavernous injection. Its duration depends on the dose administered.
The CPG NICE 20047 does not provide evidence to answer this question.
Alprostadil vs. placebo
An RCT609 compared the alprostadil injection with placebo in 296 men be-tween 21 and 74 years old. It compared injections of 2.5, 5, 10 and 20 mg of alprostadil vs. placebo. None of the men responded to placebo and all the doses of alprostadil increased the proportion of individuals with “full erection” under clinical evaluation (p <0.01) and achieved at least a 70% erection for 10 minutes or more (p < 0.001). It was also found that a higher proportion of men responded to higher doses, thus suggesting a dose-response relationship.
RCT 1+
The study published by Colli et al.610 compared alprostadil with placebo. Its results indicated a complete lack of response in the placebo group while the groups treated with different doses of alprostadil had a full erection in 38.6% at doses of 5 mg and 55.5% at doses of 10 mg. The latter considered the re-sponse good or excellent.
RCT 1+
Intracavernosal alprostadil vs. sildenafi l
The study by Wang et al.611 evaluated the results of the treatment in 54 rand-omized patients with ED to receive treatment with oral sildenafi l or intracav-ernosal injection of PGE1 for 4-9 months (mean 6 months). The effi cacy rates in the two groups were 80% for sildenafi l and 83.3% for PGE1, a difference that was not statistically signifi cant. Two of the six patients who did not re-spond to sildenafi l had enough erections when receiving the intracavernosal injection of PGE1. None of the 4 patients who did not respond to the intracav-ernosal injection of PGE1 achieved an erection enough for intercourse when they received sildenafi l. The authors concluded that both oral sildenafi l and the intracavernosal injection of PGE1 are effective for patients with different aetiologies of ED.
RCT 1+
A descriptive study in 31 patients with DM2612, found that 76.5% of the injections with alprostadil in trained patients were satisfactory to perform sexual intercourse, and 72.5% were satisfactory for the couples. Penile pain appeared in 61.3% of patients as adverse effect.
DescriptiveStudy
3
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 245
Heaton et al.613 evaluated the intracavernosal alprostadil therapy in 277 patients with diabetes, 31 of them with DM1. The response rates of total erec-tion were similar in DM1 (705/821, 86%) and DM2 (4869/5931, 82%).
DescriptiveStudy
3
Domínguez et al.614 evaluated 500 patients treated with intracavernosal alprostadil injection, and obtained a complete response in 405 cases (81%); incomplete in 70 (14%) negative in 25 (5%). Adverse effects were detected in 50 patients (10%).
DescriptiveStudy
3
Summary of evidence
RCT 1 +
As for the treatment of erectile dysfunction in patients with diabetes, the intervention that has better results in terms of effectiveness, safety and patient preference the treatment with phosphodiesterase inhibitors, especially if associated with group psychotherapy, followed by intracavernosal alprostadil and mechanical devices such as prosthesis and vacuum devices601, 602, 603, 604, 605,
607, 608, 609, 610, 611, 612, 613, 614.
Recommendations
AThe treatment with phosphodiesterase inhibitors is recommended as fi rst choice for the treatment of erectile dysfunction in people with type 1 diabetes.
AIn case of contraindication or poor tolerance, intracavernosal alprostadil is proposed as an alternative.
BAs a third option treatment, mechanical methods can be considered, such as vacuum devices and infl atable prosthesis (in this order).
AIn case all previous methods fail, sublingual apomorphine treatment can be considered.
246 SNS CLINICAL PRACTICE GUIDELINES
11.6. Painful diabetic neuropathy
The International Association for the Study of Pain defi nes neuropathic pain as pain triggered or caused by a primary lesion or dysfunction of the nervous system (central or peripheral)615. Diabetic peripheral neuropathy is a symmetric sensorimotor neuropathy predominantly affecting the lower limbs (foot and ankle) and, less frequently, to the top. The patient complains of continu-ous pain, burning, which can be accompanied by paroxysmal crises of lancinating or electric pain; this pain may be spontaneous or secondary to small stimuli. In this case, everyday environmental stimuli such as the touch of clothing, a light breeze and temperature variations can cause pain.
Appendix 10 shows the dosage and the most common side effects of the medications typi-cally used for neuropathic pain 616.
11.6.1. Treatment of painful diabetic neuropathy
The CPG NICE 20047 does not provide evidence to answer this question.
An SR617 evaluated the effi cacy of antidepressants, anticonvulsants, opi-oid antagonists of N-methyl-D-aspartic acid and capsaicin tramadol vs. pla-cebo in pain relief. The main result was expressed as “moderate pain relief or relief by 50%”.
Tricyclic antidepressants (amitriptyline, desipramine, imipramine) or classical anticonvulsants (carbamazepine, lamotrigine, valproate sodium) showed greater effi cacy against placebo than serotonine reuptake inhibitors antidepressants (SSRIs, citalopram or duloxetine) and that new anticonvul-sants (oxcarbazepine, gabapentin, pregabalin). The duration of the studies was less than six months, so it was not possible to draw conclusions about the long-term effectiveness.
SR of RCT1++
An SR on drugs for the treatment of diabetic neuropathic pain618 pub-lished 5 trials published up to 2004, comparing tricyclic antidepressants vs. gabapentin, carbamazepine or SSRIs antidepressants. No differences were found regarding a reduction in the intensity of pain, nor in the percentage of patients who discontinued the treatment due to adverse effects, except for a study comparing paroxetine vs. imipramine, which found more discontinua-tion in the treatment with imipramine. These studies included a small number of patients and a duration of between 2 and 6 weeks, which limits the validity of their results.
SR of RCT1++
Several systematic reviews have evaluated the effi cacy of gabapentin, car-bamazepine and opioids for neuropathic pain619, 620, 621, 622, in various indica-tions, which included the treatment of diabetic neuropathy. In the SR on opi-oids622, the intermediate term studies (from 8 days to 8 weeks) showed that oxycodone, morphine, methadone and levorphanol were effective in reducing neuropathic pain.
SR of RCT1++
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 247
A trial carried out in India623 compared amitriptyline vs. lamotrigine in a crossover study which lasted two weeks. No differences were found in effi -cacy. The adverse effects were more common with amitriptyline (drowsiness, anticholinergic effects) while lamotrigine resulted in increases in serum creati-nine that led to the discontinuation of the treatment in 4 patients with diabetes.
RCT1+
An RCT624 compared the intervention with duloxetine 60 mg vs. the usual treatment (mainly gabapentin, amitriptyline and venlafaxine) for neuropathic pain in DM1 (9.3%) and DM2 (90.7%), for 52 weeks, after a double-blind pe-riod of 13 weeks. No differences were found in effi cacy or quality of life and a good tolerance to duloxetine was observed.
RCT1+
An RCT625 compared the combination of morphine with gabapentin vs. the treatment with gabapentin or morphine alone. Pain relief was signifi cant with the association of these drugs, although adverse effects (constipation, se-dation and dry mouth) were more common with the drug combination.
RCT1+
An SR with meta-analysis626 analyzed 18 studies and compared the ef-fi cacy of gabapentin vs. tricyclic antidepressants to treat diabetic neuropathy and postherpetic neuralgia.
In the direct comparative studies no signifi cant differences were observed regarding pain control between gabapentin and tricyclic antidepressants in pa-tients with diabetic neuropathy [RR 0.98 (95% CI 0.69 to 1.38)]. Likewise, for both medical conditions, the abandonment of the therapy due to adverse events did not differ between patients treated with gabapentin and tricyclic antidepressants [RR 0.27 (95% CI: 0.03 to 2.34)]. In the studies with placebo (indirect comparisons), both gabapentin and tricyclic antidepressants were su-perior to placebo in pain control [RR 2.18 (95% CI 1.78 to 2.67) and [RR 5, 27 (95% CI 3.05 to 9.11)]. As regards adverse effects, gabapentin alone was sig-nifi cantly associated with an increased risk of discontinuation of the therapy due to the presence of adverse effects.
SR of RCT1++
An SR with meta-analysis627 carried out an indirect analysis to assess the effectiveness of duloxetine, pregabalin, gabapentin and amitriptyline, and their tolerance, using placebo as a common comparator. To this end, a total of 11 double-blind RCTs were selected with a placebo control group, with a parallel or crossover design, which lasted between 5 and 13 weeks, and pain reduction criterion of 50%. Of the 11 studies, 3 included duloxetine; 6 stud-ies, pregabalin, and 2 studies, gabapentin. The results indicated that all three drugs were more effective than placebo for the treatment of pain. Duloxetine was more effective than placebo (p <0.001), but caused a greater dropout due to the occurrence of side effects [NNT/NNH 11 (95% CI: 7-23), P <0.001] for duloxetine]. Pregabalin was also more effective than placebo and also showed higher percentage of dropout by the presence of adverse effects [NNT/NNH 19 (95% CI 10-48), P <0.001]. Gabapentin was also more effective than pla-cebo (p <0.001).
SR of RCT1++
248 SNS CLINICAL PRACTICE GUIDELINES
The authors concluded that duloxetine is a suitable option for the treat-ment of painful diabetic neuropathy, comparable to antiepileptic drugs such as gabapentin and pregabalin.
Another SR628 investigated the effi cacy of duloxetine for painful diabetic neuropathy and fi bromyalgia compared with other antidepressants. The review included six studies (three of them in patients with painful diabetic neuropa-thy), with a total of 2,216 patients (over 1,000 with painful diabetic neuropa-thy), 706 treated with placebo and 1,510 with duloxetine at doses of 20, 60 and 120 mg/day. 41% of patients treated with duloxetine achieved a pain reduc-tion of 50%, versus 24% in the placebo group [NNT 5.9 (95% CI: 4.8 to 7.7) to achieve a 50% reduction of pain]. No signifi cant differences were shown between the treatment with doses of 60 mg or 120 mg, or between patients with DM or fi bromyalgia. The dropout rates for treatment failure were 9% in placebo patients and 4% in patients with duloxetine. Dropout due to the oc-currence of side effects was higher in the group treated with duloxetine than among the patients treated with placebo (15% and 8%, respectively). The most common side effects (data from 3 trials) were nausea, drowsiness, constipation and loss of appetite.
SR of RCT1+
An SR629 with meta-analysis assessed the effi cacy of an adhesive dress-ing with lidocaine at 5% for pain management of diabetic neuropathy, com-pared with other treatments or placebo. This SR included an RCT that met the planned goals. The dressing showed signifi cantly better results in terms of quality of life (measured by EQ5D) than pregabalin. There was no differ-ence between the group treated with the dressing vs. other drugs (amitriptyline, capsaicin, gabapentin and pregabalin) in relieving pain, or patient satisfaction with the treatment. All treatments were rated more effective regarding pain relief than placebo.
SR of RCT1++
An RCT630 analyzed the effect of sodium valproate (A) and glyceril trinitrate (GTN) in spray (B) alone or in combination (C) for the treatment of neuropathic pain. The results showed a signifi cant pain reduction after 3 months (p <0.001/p <0.05) in the treatment groups A, B and C vs. placebo. Pain reduction was lower in the groups with a single drug than with the combination of both (p <0.05).
RCT1+
Another RCT631 compared the effi cacy, safety and tolerability of long-acting oxycodone (12 hours) in combination with gabapentin in comparison with placebo plus gabapentin in diabetic patients with moderate to severe neuropathic pain.
The results of the study indicate that those patients treated with oxyco-done in combination with gabapentin experienced a clinical reduction of pain of over 30% (p = 0.007) compared with the pretreatment (74% vs. 47%, p = 0.003). On the other hand, the treatment with oxycodone appears to reduce the need for additional analgesia (p = 0.029) and improves disrupted sleep (p = 0.05), although there are no differences in the quality of sleep (P = 0.209). With respect to the presence of side effects, there were differences between both groups (88% vs. 71%), being the most cited side effects constipation, fatigue, drowsiness, nausea, and dizziness. The reasons for leaving the clinical trial differed between the groups, being the main reason the presence of side effects (64%) for the experimental group versus the placebo group who did mostly for lack of therapeutic effect (54%, 3 times higher than in the experi-mental group).
RCT1+
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 249
An RCT632 evaluated the effi cacy of venlafaxine in the symptomatic treat-ment of painful neuropathy in patients with type 2 diabetes (n = 60). Analyzing the evolution of basal pain until the end of the study (8 weeks), signifi cant differences were observed from the second week through the questionnaire and the McGill Melzack numerical scale (p = 0.01). Given these results, the authors considered that the response to the treatment was good in 56% of cases (vs. 6.6% in the control group) and moderate in 36% (vs. 16.6% in the control group). 10% of patients in the treatment group and 76.6% in the control group did not respond to the treatment. The prospective evaluation showed that the decreasing intensity of pain was signifi cantly lower in the group treated with venlafaxine HC1 during the weeks 4 and 8 (p = 0.01) than in control group.
RCT1+
Summary of evidence
SR of RCT 1 + +
In the short term (treatments shorter than 6 months) classical antidepressants (amitriptyline, desipramine, imipramine) and classical anticonvulsants (carbamazepine, lamotrigine, valproate sodium) are more effective in the treatment of painful diabetic neuropathy than serotonin reuptake inhibitors antidepressants (citalopram, duloxetine) and new anticonvulsants (oxcarbazepine, gabapentin, pregabalin)617.
SR of RCT 1 + +
Opiates drugs (such as oxycodone, morphine, methadone, levorphanol) are more effective than placebo in treating painful diabetic neuropathy619, 620, 621, 622.
RCT 1 +
No signifi cant differences were demonstrated in the treatment of painful diabetic neuropathy with lamotrigine vs. amitriptyline623.
RCT 1 +
The treatment of diabetic neuropathy with duloxetine (60 mg) vs. gabapentin, amitriptyline or venlafaxine, showed no differences in pain relief624.
RCT 1 +
The combined treatment with gabapentin morphine is more effective than the treatment with one of the two drugs separately, but has more adverse effects625.
SR of RCT 1 + +
No direct comparative studies have shown signifi cant differences in terms of pain control between gabapentin and tricyclic antidepressants in patients with diabetic neuropathy [RR 0.98 (95% CI 0.69 to 1.38)]626.
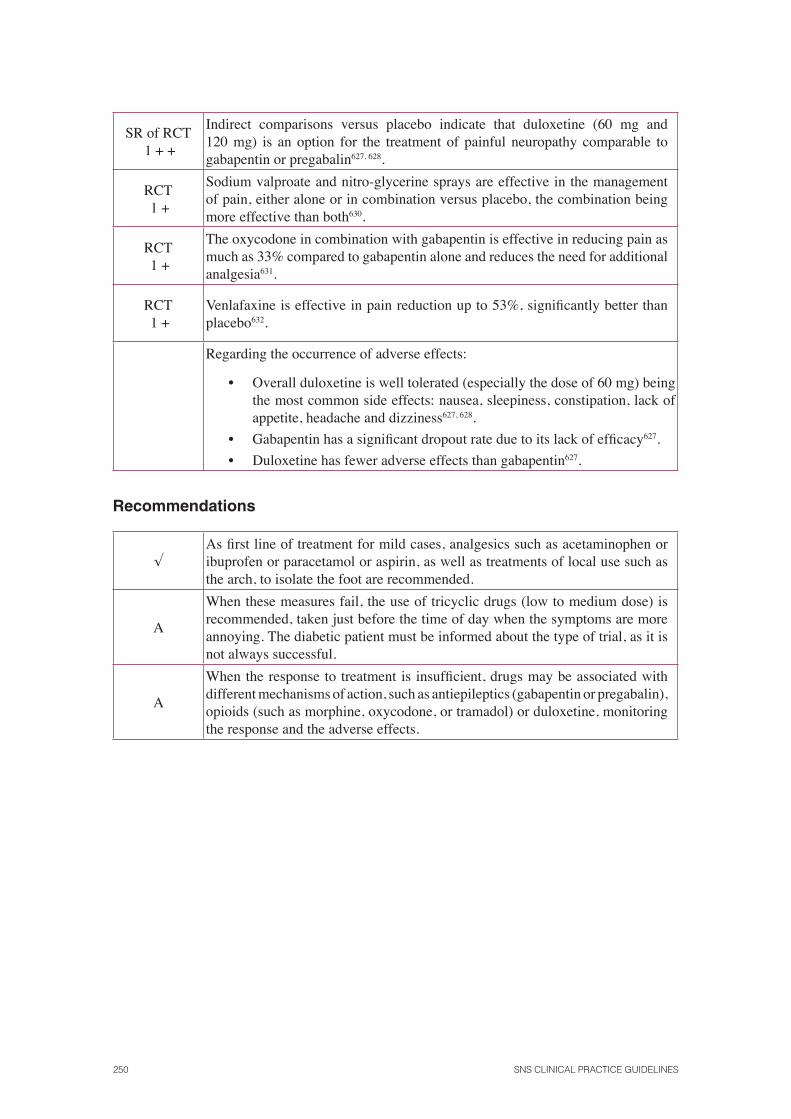
250 SNS CLINICAL PRACTICE GUIDELINES
SR of RCT 1 + +
Indirect comparisons versus placebo indicate that duloxetine (60 mg and 120 mg) is an option for the treatment of painful neuropathy comparable to gabapentin or pregabalin627, 628.
RCT 1 +
Sodium valproate and nitro-glycerine sprays are effective in the management of pain, either alone or in combination versus placebo, the combination being more effective than both630.
RCT 1 +
The oxycodone in combination with gabapentin is effective in reducing pain as much as 33% compared to gabapentin alone and reduces the need for additional analgesia631.
RCT 1 +
Venlafaxine is effective in pain reduction up to 53%, signifi cantly better than placebo632.
Regarding the occurrence of adverse effects:
• Overall duloxetine is well tolerated (especially the dose of 60 mg) being the most common side effects: nausea, sleepiness, constipation, lack of appetite, headache and dizziness627, 628.
• Gabapentin has a signifi cant dropout rate due to its lack of effi cacy627.
• Duloxetine has fewer adverse effects than gabapentin627.
Recommendations
√As fi rst line of treatment for mild cases, analgesics such as acetaminophen or ibuprofen or paracetamol or aspirin, as well as treatments of local use such as the arch, to isolate the foot are recommended.
A
When these measures fail, the use of tricyclic drugs (low to medium dose) is recommended, taken just before the time of day when the symptoms are more annoying. The diabetic patient must be informed about the type of trial, as it is not always successful.
A
When the response to treatment is insuffi cient, drugs may be associated with different mechanisms of action, such as antiepileptics (gabapentin or pregabalin), opioids (such as morphine, oxycodone, or tramadol) or duloxetine, monitoring the response and the adverse effects.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 251
12. Organizing the medical consultation
12.1.Transition of patients with diabetes mellitus type 1 from the paediatric services to the adult services
The transition of adolescents with DM1 from paediatric to adult care is a critical process that can generate a decline in self-care and affect glycaemic control.
No study has been found that examines the effectiveness of a structured inter-vention during the transition from paediatric services to adult services com-pared to the usual practice in people with DM1.
The NICE Guide 20047 summarized the information provided by studies that analyzed through surveys and which refl ected the perceptions of patients, their satisfaction with the care received, their opinion on the best age for the transition or the optimum time between the last paediatric visit and the fi rst on to adult care633, 634, 635, 636, 637, 638, 639.
Patient satisfaction
The study by Kipps et al.635 measured the satisfaction of some patients from Oxford (UK) that had recently been transferred was measured. 53% of patients considered important to know the endocrinologist before the transition, com-pared to 46% who did not consider it relevant.
Descriptive study
3
Age of transition
In the study by Salmi et al.639, the transition was performed at a mean age (SD) of 17.5 (0.5) years (range 16.5 to 18.8 years). The decision on the age at which the transition was to be made was taken by the doctor according to the level of maturity of each patient.
Descriptive study
3
In the study by Pacaud et al.636 the mean age of transition was 18.5 years, being the age proposed by patients less than this.
Descriptive study
3
In another study, in which a telephone survey was carried out in 101 pa-tients641, the optimal age for transfer was 18 years according to 58.4% of the participants.
Descriptive study
3
252 SNS CLINICAL PRACTICE GUIDELINES
Effects on glycaemic control
Another study642 involving 191 young people, analyzed the effect of an inter-vention based on a system of recall appointments (a coordinator contacted the young patients through telephone calls, messages to mobile phones or email reminders) with telephone support outside the usual hours of consultation, during the transition of adolescents to adult hospital care. Comparing the data with previous data obtained from other adolescents with diabetes, admissions due to diabetic ketoacidosis decreased 33% (p = 0.05), as well as the length of hospital stay for this cause in 3.6 days for 3.5 years (p = 0.02).
Observational study
2+
In the study by Busse et al.641 made by a telephone questionnaire to 101 patients [58 women, mean age (SD) 22.1 years (2.4)] after the transition, showed that after this phase, the attendance to medical consultation decreased [mean (SD) 8.5 years (2.3) vs. 6.7 years (3.2)]. However, the mean HbA
1c level
did not change signifi cantly before and after the transition [mean (SD) 8.5% (1.5) vs. 8.4% (1.7), P = 0.441].
Descriptive study
3
A retrospective study in 62 young patients with DM1640 which compared the transition with structured and unstructured programs identifi ed higher lev-els of HbA
1c, in the group that followed a structured transition program at the
fi rst visit in the adults service care (p < 0.01) and after a one-year follow-up (p <0.05).
Descriptive study
3
Summary of evidence
Descriptive study
3
For people with diabetes mellitus type 1 it is important to know the adult endocrinologist before the transition from paediatric endocrinology care640,
638, as well as the presence of the paediatrician at the fi rst visit with the endocrinologist640.
Descriptive study
3The transition is usually performed at around the age of 18639, 636, 641.
Descriptive study
3
Although during the transition, there can be lifestyle changes regarding attendance to checkups642, this does not appear to signifi cantly impact on glycaemic control641.
Recommendations
C
To set up at least one consultation visit involving both the paediatrician who has been responsible for the treatment during childhood and the endocrinology specialist who will attend the patient with diabetes mellitus type 1 in the future is recommended, so that they agree and fi x the treatment together with the adolescent.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 253
12.2. Initial study of the newly diagnosed patients with diabetes mellitus type 1
After the diagnosis of DM1, a full assessment of the patient is to be carried out to detect the exist-ence of possible complications and to set out the management plan, which will include aspects such as diabetes education, dietary advice and exercise and pharmacological treatment patterns. It is important to determine the elements that could enhance the effectiveness of this initial study.
No trials comparing the effi cacy and safety between the different options of initial study for people newly diagnosed with DM1 have been found.
Thus the recommendations have been developed by consensus of the GEG, from previous guidelines proposed in July,7; 51.
Recommendations
In the newly diagnosed DM1 patients, the following assessments are recommended:
√
Medical history
• Domestic, social, cultural-recreational as-pects, level of education.
• Emotional situation.
• Assessment of family and social support.
√ • Prior diabetic history.
å Vascular risk factors.
• Smoking.
å Family history of diabetes and artery or auto-
immune disease.
√ General exploration Height, weight, BMI, TA.
A
Further tests
HbA1c
.
B Full examination of the retina with mydriasis.
BAlbumin excretion (timed microalbuminuria or albumin/creatinine ratio).
√Lipid profi le once the glycaemic profi le is stabilized.
B Anti TPO, FT4 and TSH antibodies.
BTransglutaminase and IgA antibodies to assess celiac disease.
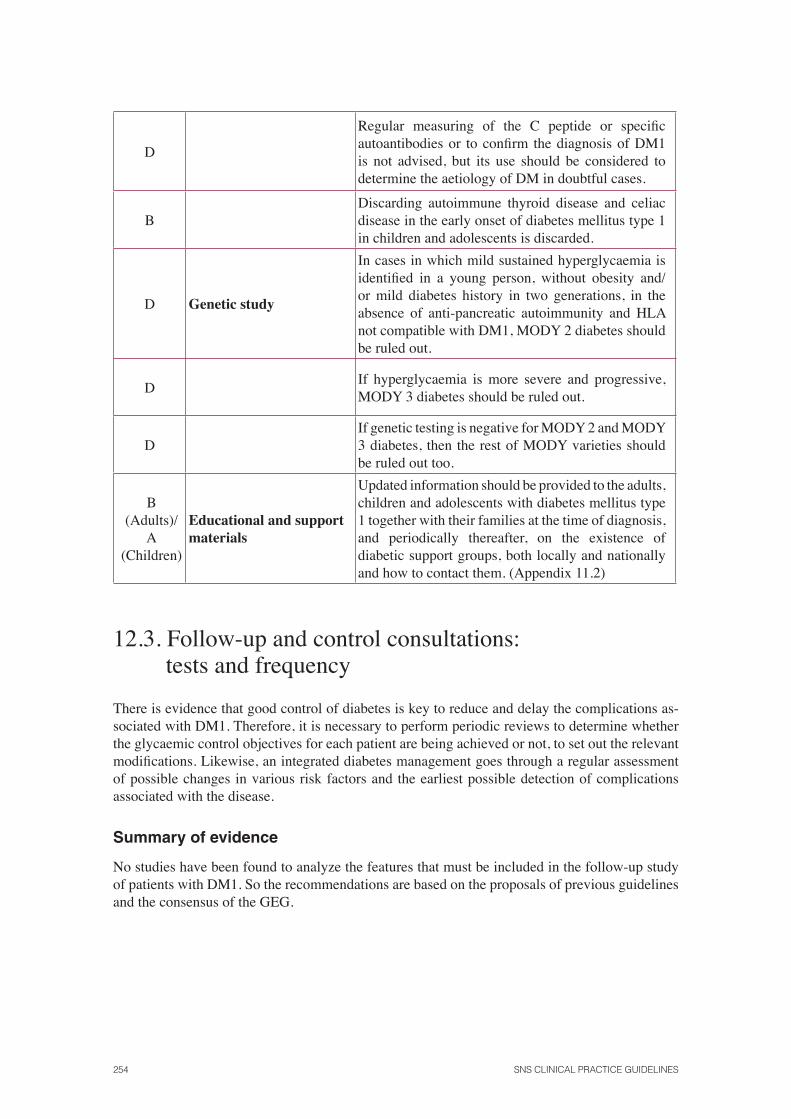
254 SNS CLINICAL PRACTICE GUIDELINES
D
Regular measuring of the C peptide or specifi c autoantibodies or to confi rm the diagnosis of DM1 is not advised, but its use should be considered to determine the aetiology of DM in doubtful cases.
BDiscarding autoimmune thyroid disease and celiac disease in the early onset of diabetes mellitus type 1 in children and adolescents is discarded.
D Genetic study
In cases in which mild sustained hyperglycaemia is identifi ed in a young person, without obesity and/or mild diabetes history in two generations, in the absence of anti-pancreatic autoimmunity and HLA not compatible with DM1, MODY 2 diabetes should be ruled out.
DIf hyperglycaemia is more severe and progressive, MODY 3 diabetes should be ruled out.
DIf genetic testing is negative for MODY 2 and MODY 3 diabetes, then the rest of MODY varieties should be ruled out too.
B (Adults)/
A (Children)
Educational and support materials
Updated information should be provided to the adults, children and adolescents with diabetes mellitus type 1 together with their families at the time of diagnosis, and periodically thereafter, on the existence of diabetic support groups, both locally and nationally and how to contact them. (Appendix 11.2)
12.3. Follow-up and control consultations: tests and frequency
There is evidence that good control of diabetes is key to reduce and delay the complications as-sociated with DM1. Therefore, it is necessary to perform periodic reviews to determine whether the glycaemic control objectives for each patient are being achieved or not, to set out the relevant modifi cations. Likewise, an integrated diabetes management goes through a regular assessment of possible changes in various risk factors and the earliest possible detection of complications associated with the disease.
Summary of evidence
No studies have been found to analyze the features that must be included in the follow-up study of patients with DM1. So the recommendations are based on the proposals of previous guidelines and the consensus of the GEG.
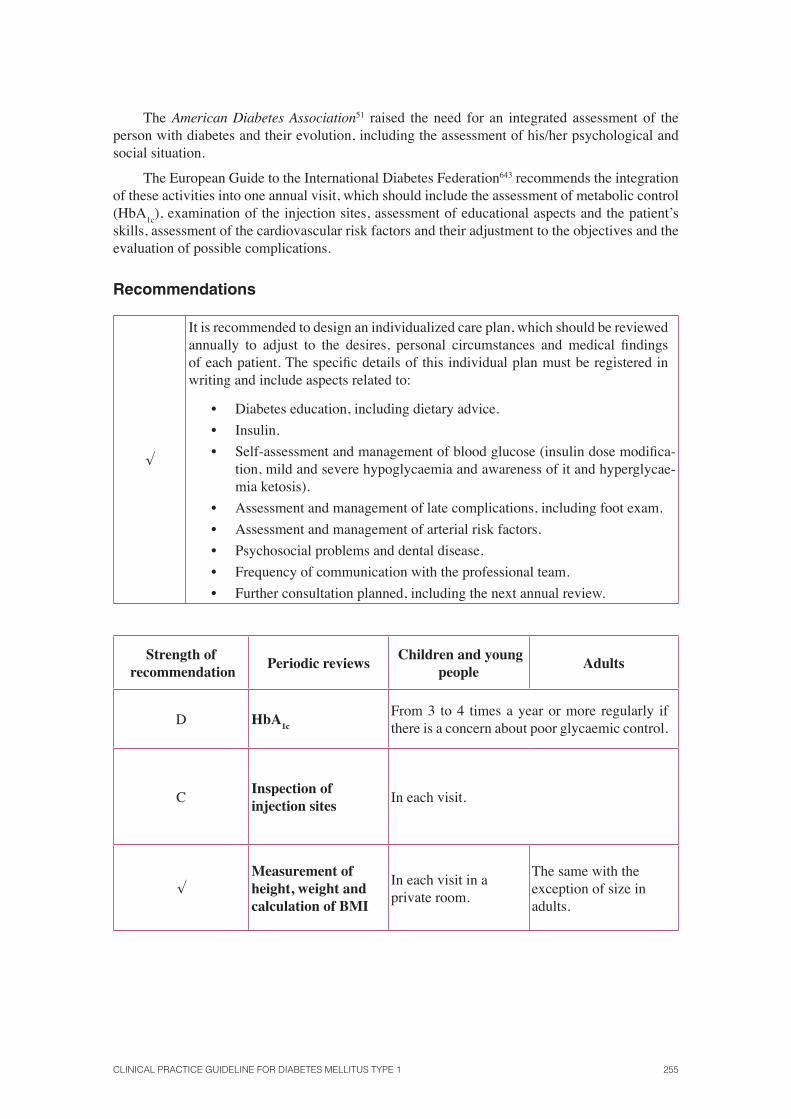
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 255
The American Diabetes Association51 raised the need for an integrated assessment of the person with diabetes and their evolution, including the assessment of his/her psychological and social situation.
The European Guide to the International Diabetes Federation643 recommends the integration of these activities into one annual visit, which should include the assessment of metabolic control (HbA
1c), examination of the injection sites, assessment of educational aspects and the patient’s
skills, assessment of the cardiovascular risk factors and their adjustment to the objectives and the evaluation of possible complications.
Recommendations
√
It is recommended to design an individualized care plan, which should be reviewed annually to adjust to the desires, personal circumstances and medical fi ndings of each patient. The specifi c details of this individual plan must be registered in writing and include aspects related to:
• Diabetes education, including dietary advice.
• Insulin.
• Self-assessment and management of blood glucose (insulin dose modifi ca-tion, mild and severe hypoglycaemia and awareness of it and hyperglycae-mia ketosis).
• Assessment and management of late complications, including foot exam.
• Assessment and management of arterial risk factors.
• Psychosocial problems and dental disease.
• Frequency of communication with the professional team.
• Further consultation planned, including the next annual review.
Strength of recommendation
Periodic reviews Children and young
peopleAdults
D HbA1c
From 3 to 4 times a year or more regularly if there is a concern about poor glycaemic control.
CInspection of injection sites
In each visit.
√Measurement of height, weight and calculation of BMI
In each visit in a private room.
The same with the exception of size in adults.
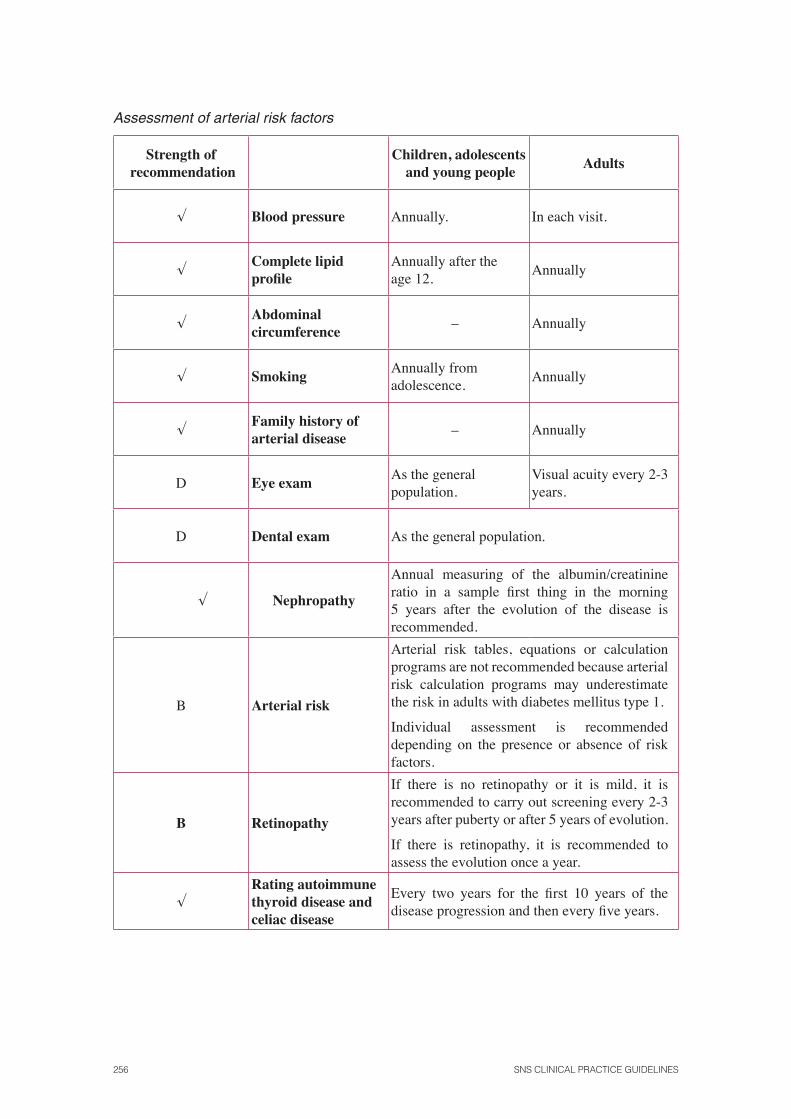
256 SNS CLINICAL PRACTICE GUIDELINES
Assessment of arterial risk factors
Strength of recommendation
Children, adolescents and young people
Adults
√ Blood pressure Annually. In each visit.
√Complete lipid profi le
Annually after the age 12.
Annually
√Abdominal circumference
– Annually
√ SmokingAnnually from adolescence.
Annually
√Family history of arterial disease
– Annually
D Eye examAs the general population.
Visual acuity every 2-3 years.
D Dental exam As the general population.
√ Nephropathy
Annual measuring of the albumin/creatinine ratio in a sample fi rst thing in the morning 5 years after the evolution of the disease is recommended.
B Arterial risk
Arterial risk tables, equations or calculation programs are not recommended because arterial risk calculation programs may underestimate the risk in adults with diabetes mellitus type 1.
Individual assessment is recommended depending on the presence or absence of risk factors.
B Retinopathy
If there is no retinopathy or it is mild, it is recommended to carry out screening every 2-3 years after puberty or after 5 years of evolution.
If there is retinopathy, it is recommended to assess the evolution once a year.
√Rating autoimmune thyroid disease and celiac disease
Every two years for the fi rst 10 years of the disease progression and then every fi ve years.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 257
13. Dissemination and Implementation
13.1. Dissemination and implementation strategy
Clinical practice guidelines are useful to improve the quality of care and outcomes for the patient. The big challenge now is to get the professional to adhere to the recommendations of these guide-lines. This calls for an implementation strategy aimed at overcoming the existing barriers in the environment in which it will be applied.
The plan to implement the DM1 guide includes the following interventions:
1. Presentation of the guide by the health authorities to the media.
2. Presentation of the guide to the Directorate and Sub-directorate of the Primary Health Care and Specialized Care Units of the different Health Services.
3. Institutional presentation of the guide in collaboration with the Quality Agency of the Ministry of Health, Social Policy and Equality, to the different scientifi c and profes-sional societies involved.
4. All presentations will highlight the educational material made for the patient in order to facilitate its distribution among all the health professionals as well as among the patients with this health problem.
5. Effective and addressed distribution to the professional groups involved (physicians specialized in Endocrinology and Nutrition, paediatric endocrinologists, diabetes nurse educators, nutritionists) to facilitate its distribution.
7. Dissemination of the guide in electronic format in the websites of the Ministry of Health, Social Policy and Equality, GuíaSalud, Osteba and the companies involved in the project.
8. Publishing of the guide in scientifi c magazines.
9. Setting up of criteria for good attention in contract programs and clinical management contracts, following the provisions of the guide.
10. Evaluation of the effectiveness of implantation, establishing systems to support the clin-ical decision, integrating the guide and the selected indicators in the computer program used in Specialized Care.
258 SNS CLINICAL PRACTICE GUIDELINES
13.2. Implications for clinical practice
Target fi gures of glycosylated haemoglobin
A strict metabolic control objective requires people with diabetes to involve highly and have a high level of knowledge about their disease and for the health staff to make an extra effort in dia-betes education and patient support. Therefore, the consultation time devoted to education, both initially and during the progression of the treatment should be programmed.
Proteins in patients with nephropathy
Formulating diets for people with type 1 diabetes and renal failure on dialysis poses diffi culties, since these patients should limit their intake of carbohydrates and proteins, together with the vol-ume of fl uid and ions (potassium). Therefore, this task requires the support of nutrition experts.
Continuous Glucose Monitoring Systems
Although the technology for continuous glucose monitoring is evolving towards greater simpli-fi cation of the systems and to a reduction of costs, there are diffi culties for its use in the clinical practice because of possible limitations in its availability, the diffi culties that new technologies can pose to patients, and the increase in the costs involved.
Hospital management vs. outpatient management, at the time of diagnosis of diabetes mellitus type 1
The outpatient management of newly diagnosed patients with diabetes mellitus type 1 can be infl uenced by the organization of healthcare services and the distance between the patient’s home and place of consultation, sometimes making hospitalization more appropriate.
Insulin preparations
The use of insulin analogues is widespread due to the preferences of patients and also partly due to the action policies of the pharmaceutical industry, which have been limiting the presentations available on human insulin.
Rotation of injection sites
The rotation of injection sites depends primarily on the patient’s preferences. However, the train-ing team teacher should stress the desirability of rotation to avoid lipodystrophy.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 259
Islet transplantation vs. pancreas transplantation
Pancreas transplantation should be performed, when indicated, in centres with a surgical team expert in transplants in general and pancreas in particular.
It is desirable that the monitoring of metabolic control is performed by a person specifi cally trained and knowledgeable in the management of immunosuppressive therapy, taking into ac-count its infl uence on metabolic control.
The performance of islet transplantation poses diffi culties in relation to the limitations on the number of donors, the technological limitations and the need for more than a pancreas for obtain-ing a suitable or suffi cient number of islets.
Start time and frequency of screening for diabetic retinopathy
The completion of the retinopathy screening with intervals of 2 or 3 years in the absence of retin-opathy at the baseline examination is a benefi t for the patient (reducing the number of trips to consultation, medical visits and loss of hours or work) without an increased risk of non-detection of retinopathy and also a benefi t for the health services, as it reduces the burden of care and the consequent release of medical and administrative time that can be spent on other tasks.
Criteria for referring the patient with diabetic nephropathy to a nephrologist
In some areas of the country, assistance to specialized care nephrology units will require patients to travel to health centres outside their treatment area.
Screening for diabetic foot
In Spain, the applicability of the recommended interventions for diabetic foot screening may be limited. While the activities of screening and risk stratifi cation are considered feasible, there are no uniform and structured benefi ts to derive and treat the foot at risk, with variations between the different autonomous communities.
Although the recommended measures are feasible and easy to implement, they require train-ing and especially consultation time, making them diffi cult to implement, given the lack of time to attend patients in an outpatient consultation.
Transition of patients from paediatric services to adult services
It is possible that the paediatrician and the adult endocrinology specialist do not see patients in the same centre, which would hamper the implementation of the minimum recommendations laid out in this CPG for the transfer of patients from paediatric services to adult health services.
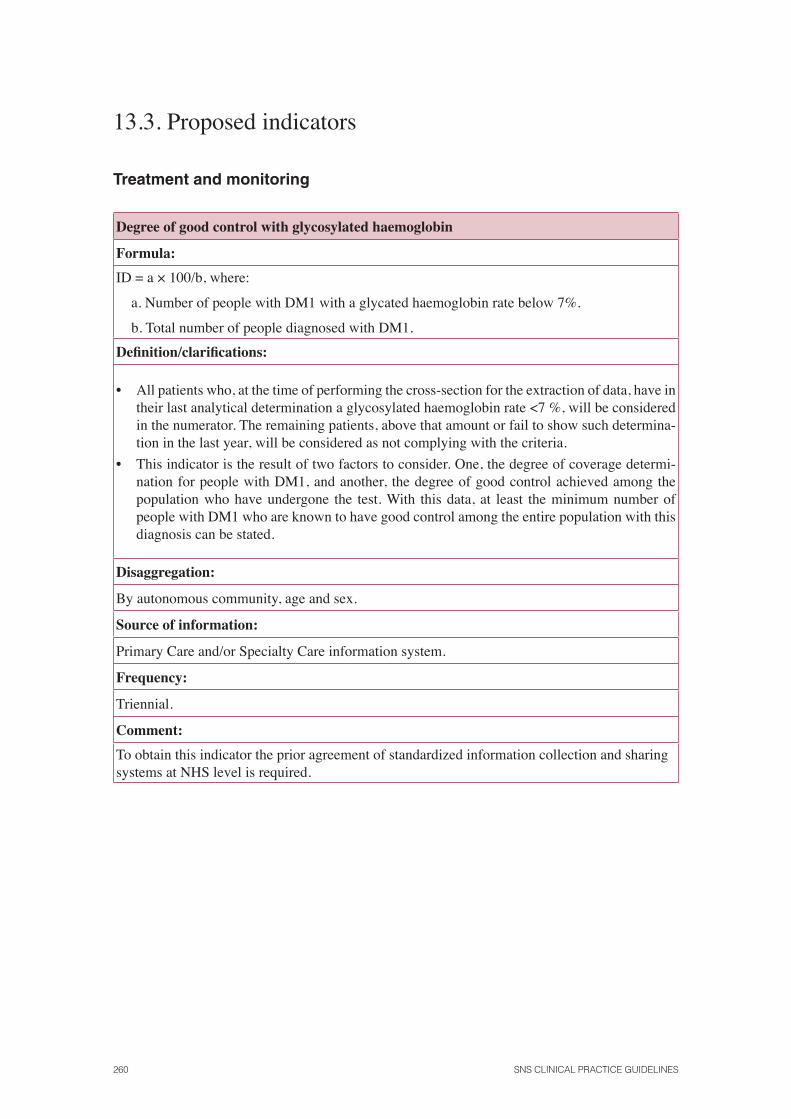
260 SNS CLINICAL PRACTICE GUIDELINES
13.3. Proposed indicators
Treatment and monitoring
Degree of good control with glycosylated haemoglobin
Formula:
ID = a × 100/b, where:
a. Number of people with DM1 with a glycated haemoglobin rate below 7%.
b. Total number of people diagnosed with DM1.
Defi nition/clarifi cations:
• All patients who, at the time of performing the cross-section for the extraction of data, have in their last analytical determination a glycosylated haemoglobin rate <7 %, will be considered in the numerator. The remaining patients, above that amount or fail to show such determina-tion in the last year, will be considered as not complying with the criteria.
• This indicator is the result of two factors to consider. One, the degree of coverage determi-nation for people with DM1, and another, the degree of good control achieved among the population who have undergone the test. With this data, at least the minimum number of people with DM1 who are known to have good control among the entire population with this diagnosis can be stated.
Disaggregation:
By autonomous community, age and sex.
Source of information:
Primary Care and/or Specialty Care information system.
Frequency:
Triennial.
Comment:
To obtain this indicator the prior agreement of standardized information collection and sharing systems at NHS level is required.
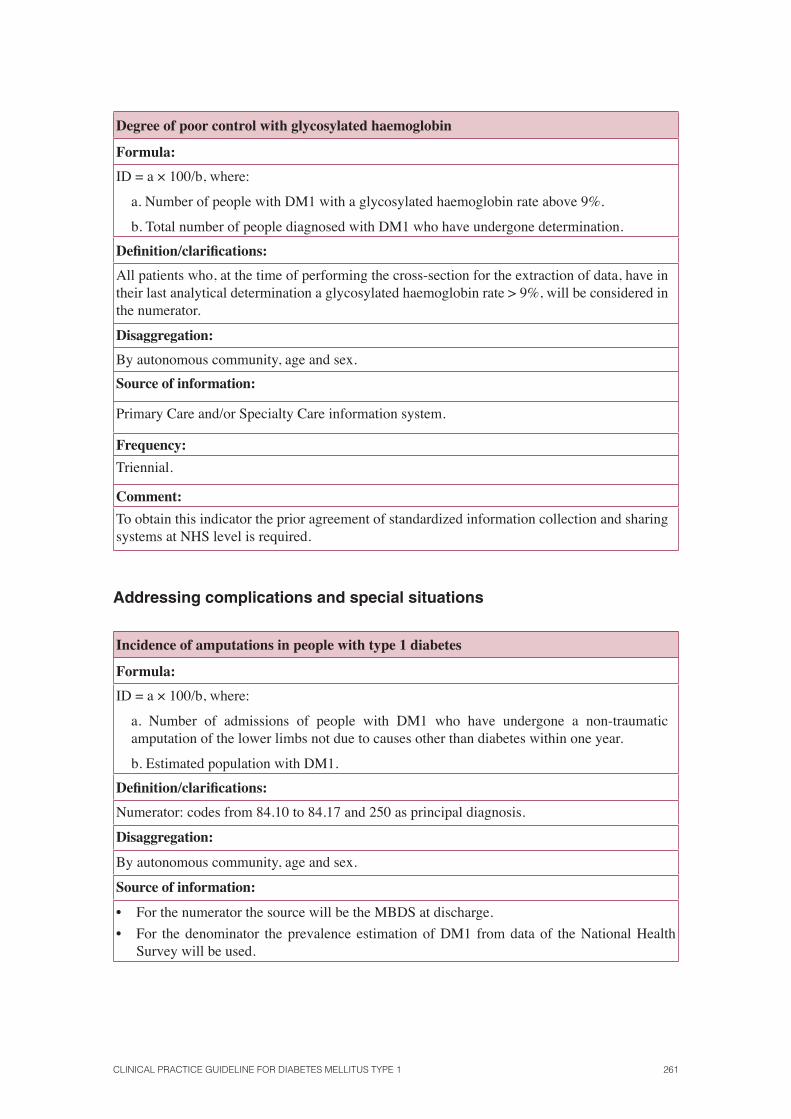
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 261
Degree of poor control with glycosylated haemoglobin
Formula:
ID = a × 100/b, where:
a. Number of people with DM1 with a glycosylated haemoglobin rate above 9%.
b. Total number of people diagnosed with DM1 who have undergone determination.
Defi nition/clarifi cations:
All patients who, at the time of performing the cross-section for the extraction of data, have in their last analytical determination a glycosylated haemoglobin rate > 9%, will be considered in the numerator.
Disaggregation:
By autonomous community, age and sex.
Source of information:
Primary Care and/or Specialty Care information system.
Frequency:
Triennial.
Comment:
To obtain this indicator the prior agreement of standardized information collection and sharing systems at NHS level is required.
Addressing complications and special situations
Incidence of amputations in people with type 1 diabetes
Formula:
ID = a × 100/b, where:
a. Number of admissions of people with DM1 who have undergone a non-traumatic amputation of the lower limbs not due to causes other than diabetes within one year.
b. Estimated population with DM1.
Defi nition/clarifi cations:
Numerator: codes from 84.10 to 84.17 and 250 as principal diagnosis.
Disaggregation:
By autonomous community, age and sex.
Source of information:
• For the numerator the source will be the MBDS at discharge.
• For the denominator the prevalence estimation of DM1 from data of the National Health Survey will be used.
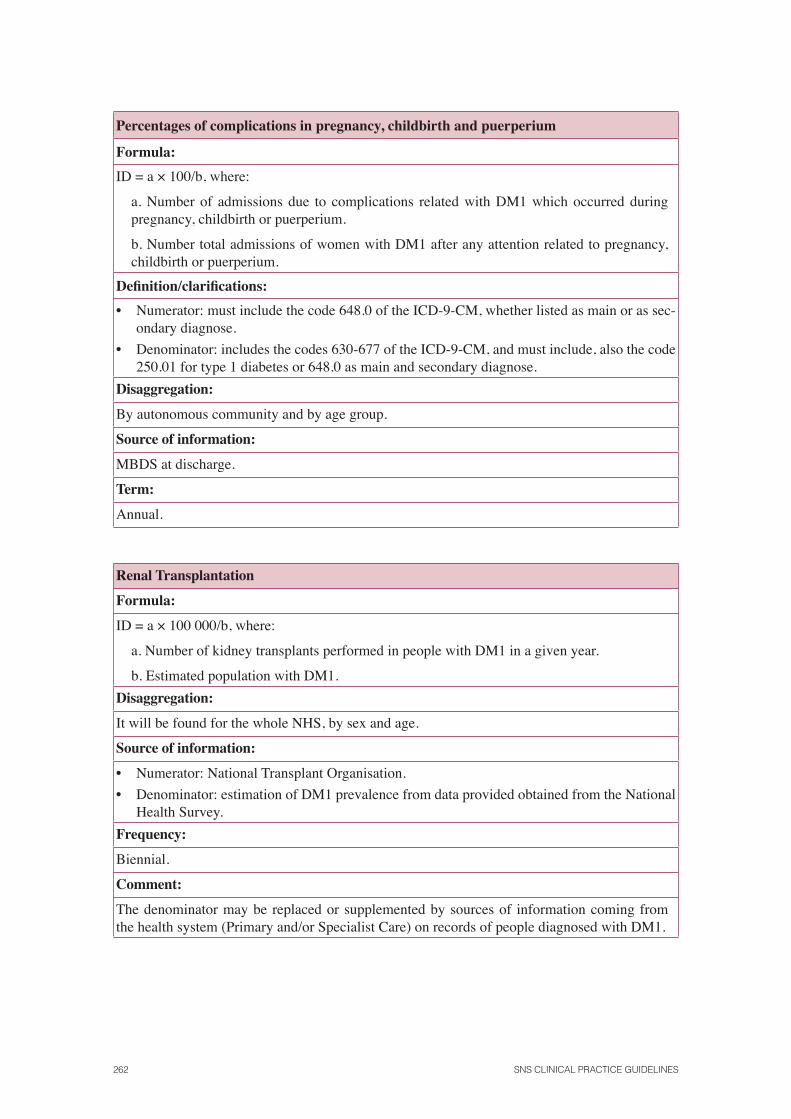
262 SNS CLINICAL PRACTICE GUIDELINES
Percentages of complications in pregnancy, childbirth and puerperium
Formula:
ID = a × 100/b, where:
a. Number of admissions due to complications related with DM1 which occurred during pregnancy, childbirth or puerperium.
b. Number total admissions of women with DM1 after any attention related to pregnancy, childbirth or puerperium.
Defi nition/clarifi cations:
• Numerator: must include the code 648.0 of the ICD-9-CM, whether listed as main or as sec-ondary diagnose.
• Denominator: includes the codes 630-677 of the ICD-9-CM, and must include, also the code 250.01 for type 1 diabetes or 648.0 as main and secondary diagnose.
Disaggregation:
By autonomous community and by age group.
Source of information:
MBDS at discharge.
Term:
Annual.
Renal Transplantation
Formula:
ID = a × 100 000/b, where:
a. Number of kidney transplants performed in people with DM1 in a given year.
b. Estimated population with DM1.
Disaggregation:
It will be found for the whole NHS, by sex and age.
Source of information:
• Numerator: National Transplant Organisation.
• Denominator: estimation of DM1 prevalence from data provided obtained from the National Health Survey.
Frequency:
Biennial.
Comment:
The denominator may be replaced or supplemented by sources of information coming from the health system (Primary and/or Specialist Care) on records of people diagnosed with DM1.
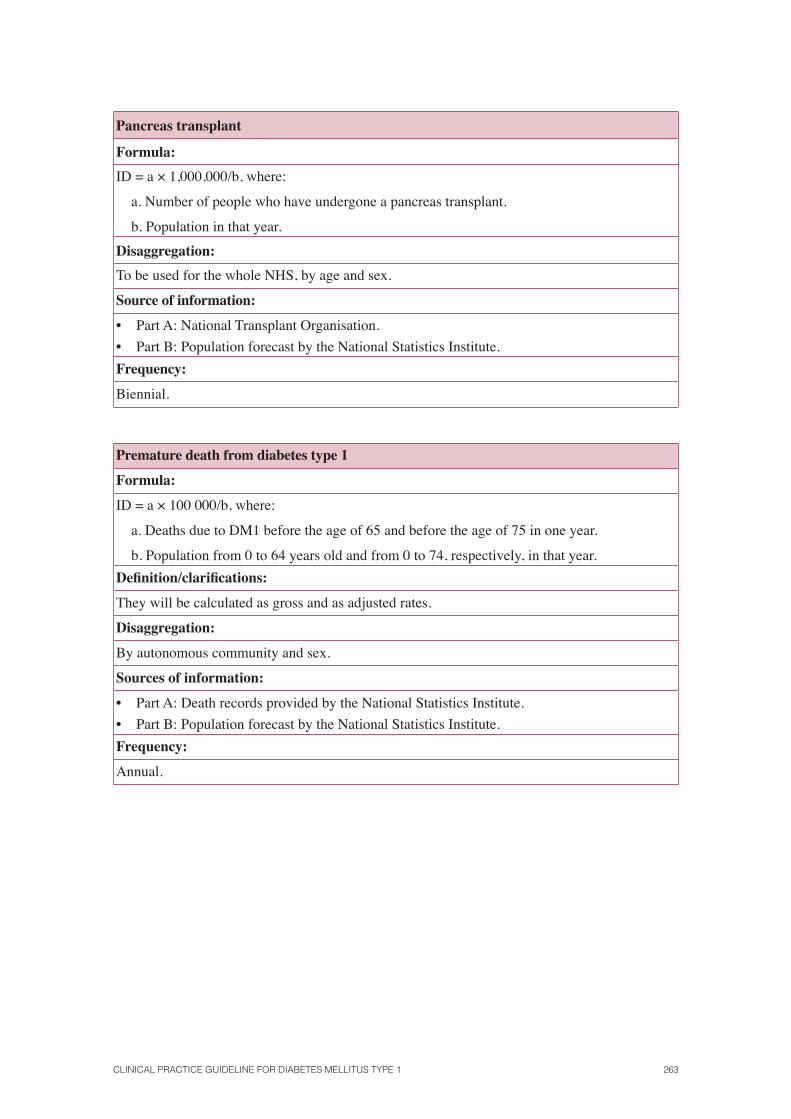
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 263
Pancreas transplant
Formula:
ID = a × 1,000,000/b, where:
a. Number of people who have undergone a pancreas transplant.
b. Population in that year.
Disaggregation:
To be used for the whole NHS, by age and sex.
Source of information:
• Part A: National Transplant Organisation.
• Part B: Population forecast by the National Statistics Institute.
Frequency:
Biennial.
Premature death from diabetes type 1
Formula:
ID = a × 100 000/b, where:
a. Deaths due to DM1 before the age of 65 and before the age of 75 in one year.
b. Population from 0 to 64 years old and from 0 to 74, respectively, in that year.
Defi nition/clarifi cations:
They will be calculated as gross and as adjusted rates.
Disaggregation:
By autonomous community and sex.
Sources of information:
• Part A: Death records provided by the National Statistics Institute.
• Part B: Population forecast by the National Statistics Institute.
Frequency:
Annual.
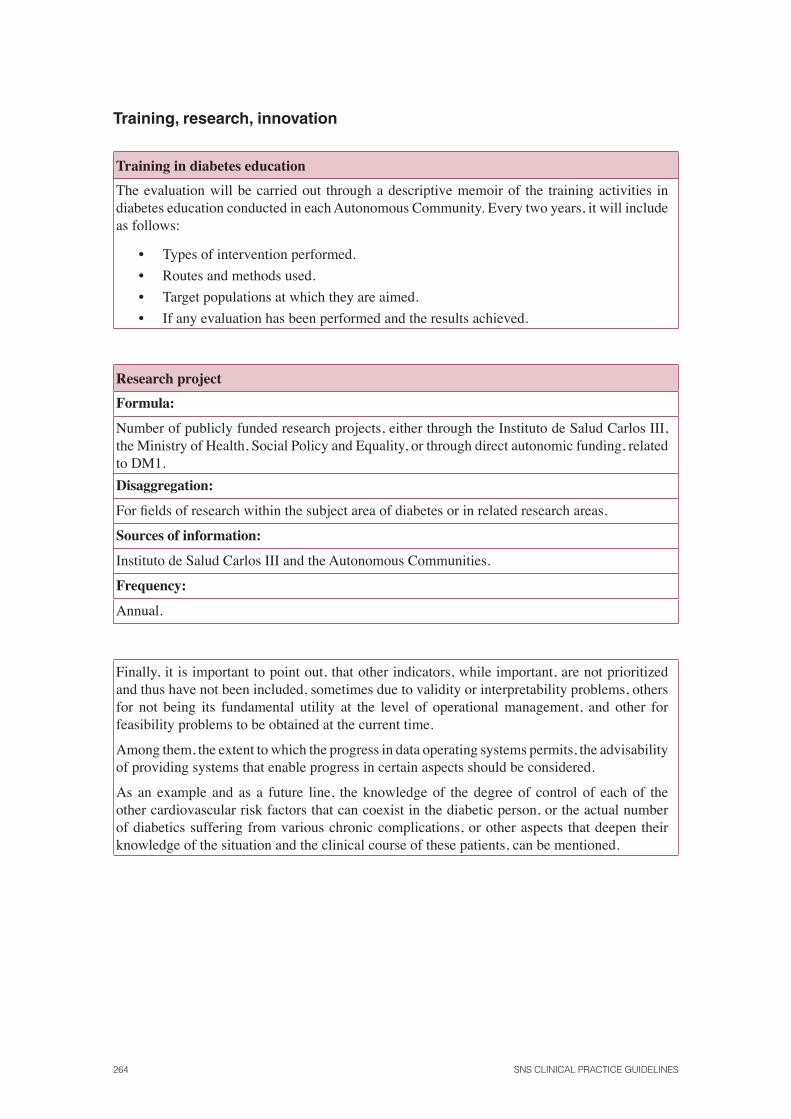
264 SNS CLINICAL PRACTICE GUIDELINES
Training, research, innovation
Training in diabetes education
The evaluation will be carried out through a descriptive memoir of the training activities in diabetes education conducted in each Autonomous Community. Every two years, it will include as follows:
• Types of intervention performed.
• Routes and methods used.
• Target populations at which they are aimed.
• If any evaluation has been performed and the results achieved.
Research project
Formula:
Number of publicly funded research projects, either through the Instituto de Salud Carlos III, the Ministry of Health, Social Policy and Equality, or through direct autonomic funding, related to DM1.
Disaggregation:
For fi elds of research within the subject area of diabetes or in related research areas.
Sources of information:
Instituto de Salud Carlos III and the Autonomous Communities.
Frequency:
Annual.
Finally, it is important to point out, that other indicators, while important, are not prioritized and thus have not been included, sometimes due to validity or interpretability problems, others for not being its fundamental utility at the level of operational management, and other for feasibility problems to be obtained at the current time.
Among them, the extent to which the progress in data operating systems permits, the advisability of providing systems that enable progress in certain aspects should be considered.
As an example and as a future line, the knowledge of the degree of control of each of the other cardiovascular risk factors that can coexist in the diabetic person, or the actual number of diabetics suffering from various chronic complications, or other aspects that deepen their knowledge of the situation and the clinical course of these patients, can be mentioned.
14. Future research
Usefulness of the diagnostic determination of autoantibodies
It would be desirable to conduct studies to evaluate the diagnostic technique of autoantibodies and use the one with better sensitivity and specifi city.
Further clinical trials are needed to analyze the inmunointervention in newly diagnosed pa-tients with diabetes mellitus type 1.
For the participation of people with diabetes mellitus type 1 in inmunointervention clinical trials, their characterization based on C-peptide, specifi c autoantibodies and HLA is essential.
Autoimmune diseases associated with diabetes mellitus type 1
New prospective studies are needed to determine the optimal screening interval for autoimmune diseases in patients with diabetes mellitus type 1.
Formal education for people with diabetes mellitus type 1 and/or their family
Investigating our health context about the possibility of education for patients with diabetes mel-litus type 1 in a more favourable environment than the health centres is proposed. In other coun-tries, it is possible to do it at home, both at the moment of diagnosis and during the follow-up. There is a professional called the “visiting nurse” who belongs to the patient’s referred endocri-nology service, who identifi es the problems at home and carries out a detailed analysis of the patient’s situation.
Studies are needed to analyze the effectiveness of educational programs, considering the potential confounders factors (time dedicated, changes in the treatment, frequency of visits, etc.).
Community support arrangements in diabetes mellitus type 1
Studies are needed regarding interventions conducted in the workplace and school to support people with diabetes mellitus type 1.
Fibre in the diet
Studies are needed to analyze the potential benefi ts of a diet high in fi bre for people with diabetes mellitus type 1.
266 SNS CLINICAL PRACTICE GUIDELINES
Continuous Glucose Monitoring Systems
More studies are needed on the various systems of continuous glucose monitoring, with more pa-tients and a longer follow-up and in specifi c patient groups such as pregnant women, children, etc.
Insulin preparations
There need to be long-term clinical trials carried out to verify the long-term safety and effective-ness of insulin analogues.
Continuous subcutaneous insulin infusion pump
Comparative studies should be carried out analysing pump infusion and multiple daily injections of insulin to properly assess the long-term effects on metabolic control and complications.
It would be desirable to perform prospective randomized studies that explore the use of con-tinuous subcutaneous insulin infusion pumps versus conventional treatment (especially multiple insulin injections) during pregnancy.
Rotation of injection sites
It would be interesting to conduct studies to rate the frequency of lipodystrophy, its relationship with the practice or not of rotating injection sites and their involvement in metabolic control.
Metformin added to insulin in adolescents with diabetes mellitus type 1
Studies are needed in adolescents with diabetes mellitus type 1 to analyze a larger sample and follow-up periods to evaluate the effi cacy and safety of long-term metformin.
Islet vs. pancreas transplantation
It would be advisable to carry out studies oriented at obtaining technical analysis of as many islets as possible, as well as to extend their viability.
Prevalence of mood disorders in people with diabetes mellitus type 1
It would be advisable to conduct studies that analyzed the prevalence of depression, anxiety or eating disorders in people with diabetes mellitus type 1 in our context.
Studies are needed to assess the effectiveness of possible strategies for early identifi cation of patients with eating disorders.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 267
Start time and frequency of screening for diabetic retinopathy
Considering the widespread non-mydriatic and digital retinal cameras at national level, carrying out a longitudinal study in patients with diabetes mellitus type 1 which allows setting out evolu-tion periods in the degree of involvement of retinopathy as a function of the different risk factors is proposed.
Criteria for referring the patient with diabetic nephropathy to a nephrologist
Further studies are necessary to determine the best time for referral of people with diabetes mel-litus type 1 to care units specializing in nephrology.

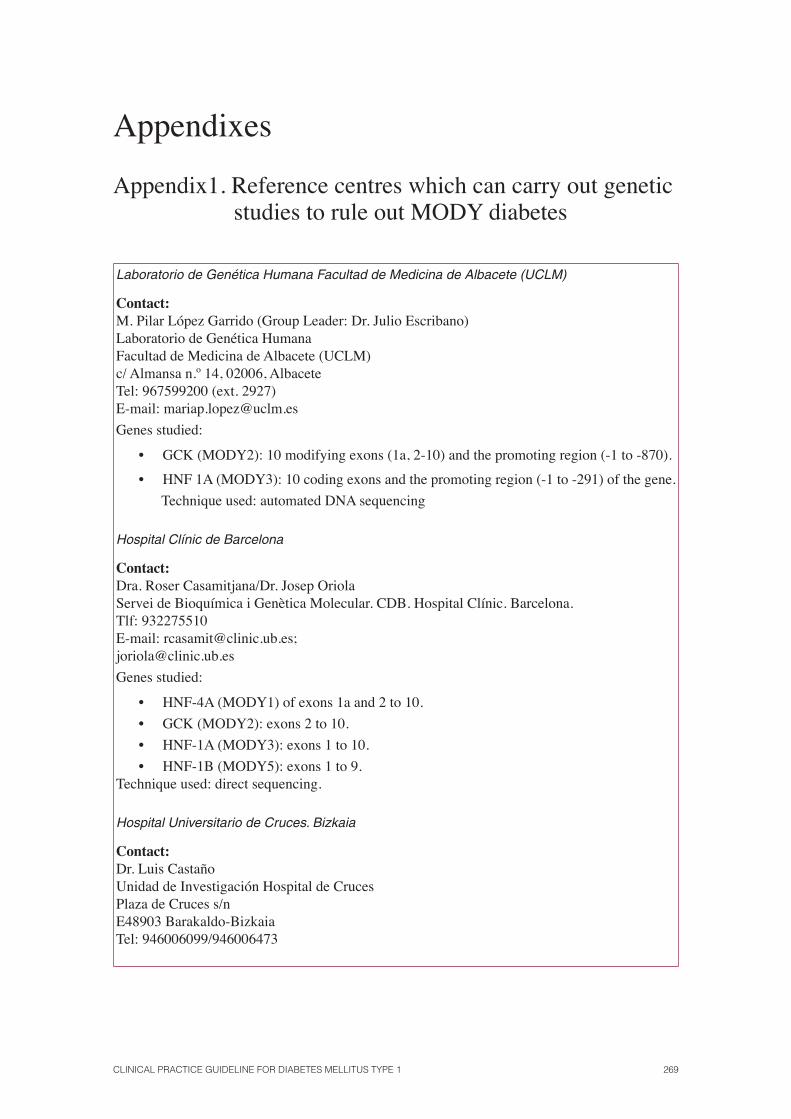
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 269
Appendixes
Appendix1. Reference centres which can carry out genetic studies to rule out MODY diabetes
Laboratorio de Genética Humana Facultad de Medicina de Albacete (UCLM)
Contact: M. Pilar López Garrido (Group Leader: Dr. Julio Escribano)Laboratorio de Genética HumanaFacultad de Medicina de Albacete (UCLM)c/ Almansa n.º 14, 02006, AlbaceteTel: 967599200 (ext. 2927)E-mail: [email protected]
Genes studied:
• GCK (MODY2): 10 modifying exons (1a, 2-10) and the promoting region (-1 to -870).
• HNF 1A (MODY3): 10 coding exons and the promoting region (-1 to -291) of the gene.
Technique used: automated DNA sequencing
Hospital Clínic de Barcelona
Contact: Dra. Roser Casamitjana/Dr. Josep OriolaServei de Bioquímica i Genètica Molecular. CDB. Hospital Clínic. Barcelona.Tlf: 932275510E-mail: [email protected];[email protected]
Genes studied:
• HNF-4A (MODY1) of exons 1a and 2 to 10.
• GCK (MODY2): exons 2 to 10.
• HNF-1A (MODY3): exons 1 to 10.
• HNF-1B (MODY5): exons 1 to 9. Technique used: direct sequencing.
Hospital Universitario de Cruces. Bizkaia
Contact: Dr. Luis CastañoUnidad de Investigación Hospital de CrucesPlaza de Cruces s/nE48903 Barakaldo-BizkaiaTel: 946006099/946006473
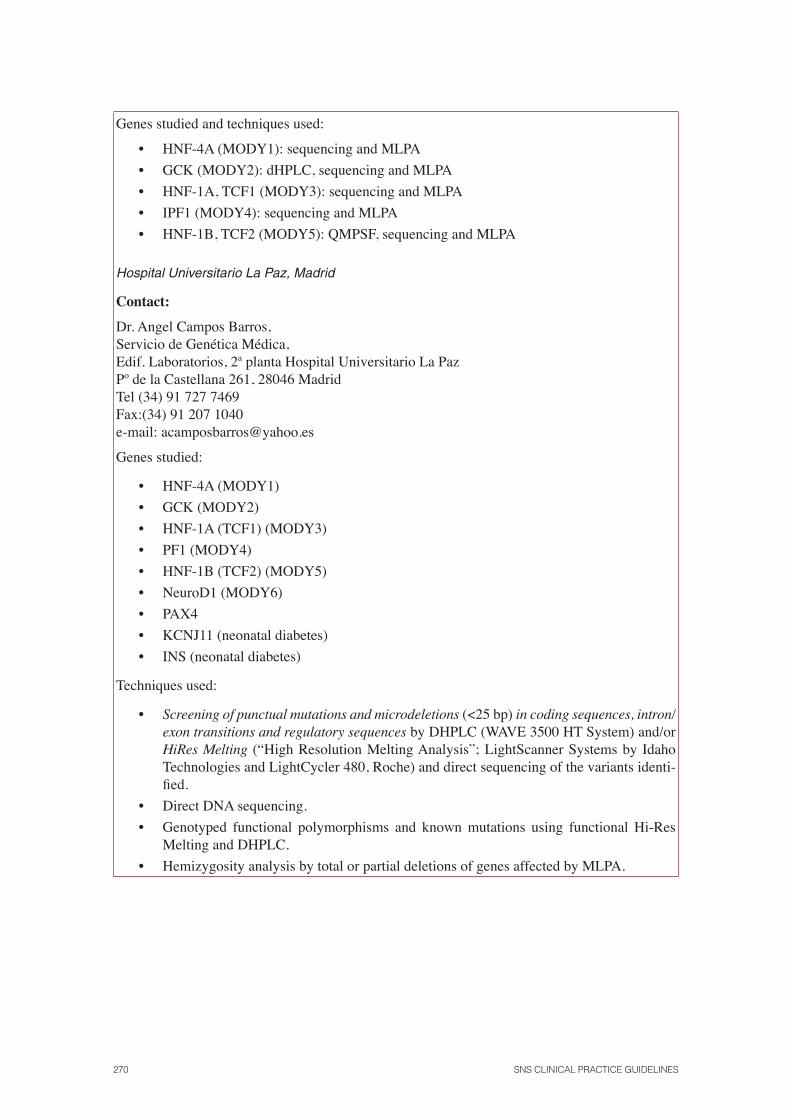
270 SNS CLINICAL PRACTICE GUIDELINES
Genes studied and techniques used:
• HNF-4A (MODY1): sequencing and MLPA
• GCK (MODY2): dHPLC, sequencing and MLPA
• HNF-1A, TCF1 (MODY3): sequencing and MLPA
• IPF1 (MODY4): sequencing and MLPA
• HNF-1B, TCF2 (MODY5): QMPSF, sequencing and MLPA
Hospital Universitario La Paz, Madrid
Contact:
Dr. Angel Campos Barros,Servicio de Genética Médica,Edif. Laboratorios, 2ª planta Hospital Universitario La PazPº de la Castellana 261, 28046 Madrid Tel (34) 91 727 7469Fax:(34) 91 207 1040e-mail: [email protected]
Genes studied:
• HNF-4A (MODY1)
• GCK (MODY2)
• HNF-1A (TCF1) (MODY3)
• PF1 (MODY4)
• HNF-1B (TCF2) (MODY5)
• NeuroD1 (MODY6)
• PAX4
• KCNJ11 (neonatal diabetes)
• INS (neonatal diabetes)
Techniques used:
• Screening of punctual mutations and microdeletions (<25 bp) in coding sequences, intron/exon transitions and regulatory sequences by DHPLC (WAVE 3500 HT System) and/or HiRes Melting (“High Resolution Melting Analysis”; LightScanner Systems by Idaho Technologies and LightCycler 480, Roche) and direct sequencing of the variants identi-fi ed.
• Direct DNA sequencing.
• Genotyped functional polymorphisms and known mutations using functional Hi-Res Melting and DHPLC.
• Hemizygosity analysis by total or partial deletions of genes affected by MLPA.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 271
Universidad Complutense de Madrid
Contact: Dra. M. Ángeles Navas/ Dr. E. Blázquez.Laboratorio de diagnóstico genético de alteraciones monogénicas de la homeostasis de glucosa.Departamento de Bioquímica y Biología Molecular III Facultad de Medicina. Universidad Complutense de Madrid Ciudad Universitaria 28040-MadridTel: 91 3941445 Fax: 91 3941691e-mail: [email protected]
Genes studied and techniques used:
• HNF-4A (MODY1) SSCP
• GCK (MODY2) SSCP
• HNF-1A (TCF1) (MODY3) Direct sequencing (DS)
• IPF1 (MODY4) DS
• HNF-1B (TCF2) (MODY5) DS
• NeuroD1 (MODY6) SSCP
• Kir 6.2 DS
Hospital Carlos Haya de Málaga
Contact: Dr. Federico Soriguer Escofet, Dr. Antonio Luis Cuesta Muñoz. Servicio Endocrinología y NutriciónHospital Regional Carlos HayaAvda Carlos Haya s/n. 29010 MálagaTel: 951 290 000.e-mail: [email protected];

272 SNS CLINICAL PRACTICE GUIDELINES
Appendix 2. Sweeteners
Non caloric
Do not alter glucose
Saccharin E 954 *
Aspartame E 951 *
Acesulfame K E 950 *
Cyclamate E 952 *
Sucralose E 955 *(can be used in cooking and baking)
Neohesperidine E 959 *
*Industrial terms for labelling
Caloric
Modify glycaemia
Sucrose: ordinary sugar
Fructose: fruit sugar and honey
Maltose: beer sugar
Lactose: milk sugar
Provide 4 calories per gram
Sugar alcohols or polyols:
Sorbitol E 420, E 967 Xylitol, Maltitol E 965,
Mannitol E 421, E 966 Lactitol inter alia
(Check the label so as to not exceed recommended intakes and avoid the laxative effect that may occur)
Provide about half the amount of calories of the fi rst
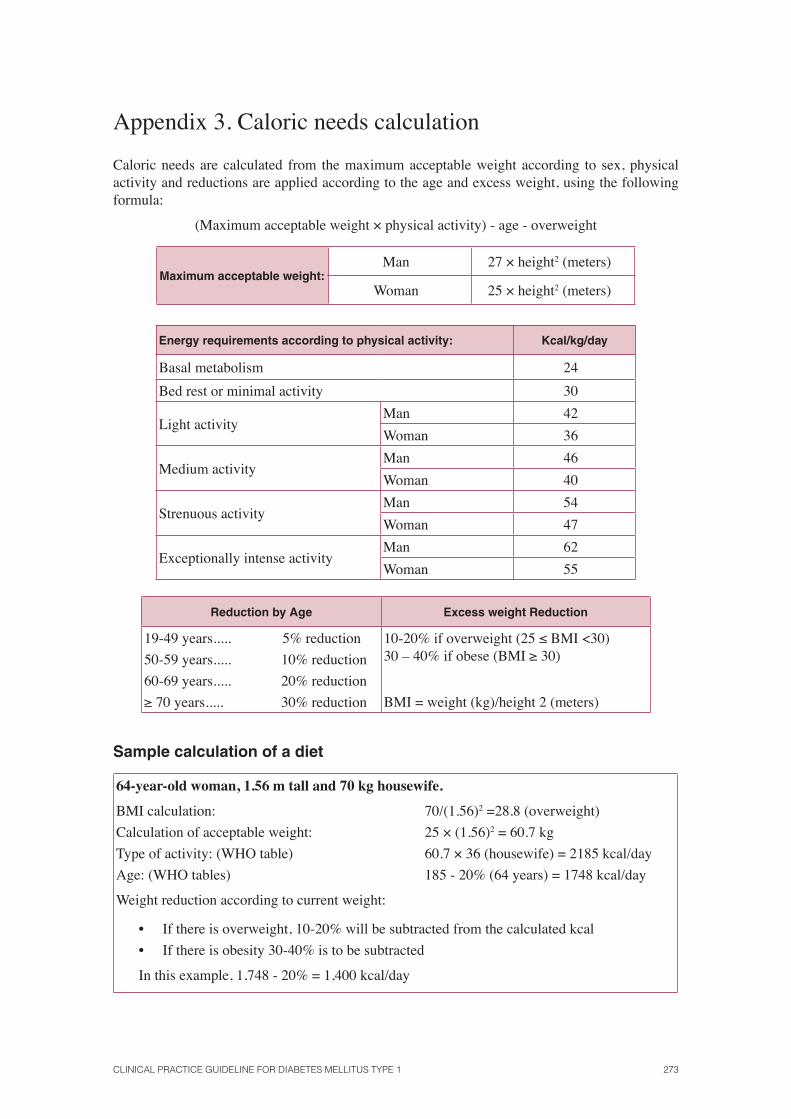
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 273
Appendix 3. Caloric needs calculation
Caloric needs are calculated from the maximum acceptable weight according to sex, physical activity and reductions are applied according to the age and excess weight, using the following formula:
(Maximum acceptable weight × physical activity) - age - overweight
Maximum acceptable weight:Man 27 × height2 (meters)
Woman 25 × height2 (meters)
Energy requirements according to physical activity: Kcal/kg/day
Basal metabolism 24
Bed rest or minimal activity 30
Light activityMan 42
Woman 36
Medium activityMan 46
Woman 40
Strenuous activityMan 54
Woman 47
Exceptionally intense activityMan 62
Woman 55
Reduction by Age Excess weight Reduction
19-49 years..... 5% reduction
50-59 years..... 10% reduction
60-69 years..... 20% reduction
≥ 70 years..... 30% reduction
10-20% if overweight (25 ≤ BMI <30)30 – 40% if obese (BMI ≥ 30)
BMI = weight (kg)/height 2 (meters)
Sample calculation of a diet
64-year-old woman, 1.56 m tall and 70 kg housewife.
BMI calculation: 70/(1.56)2 =28.8 (overweight)
Calculation of acceptable weight: 25 × (1.56)2 = 60.7 kg
Type of activity: (WHO table) 60.7 × 36 (housewife) = 2185 kcal/day
Age: (WHO tables) 185 - 20% (64 years) = 1748 kcal/day
Weight reduction according to current weight:
• If there is overweight, 10-20% will be subtracted from the calculated kcal
• If there is obesity 30-40% is to be subtracted
In this example, 1,748 - 20% = 1,400 kcal/day
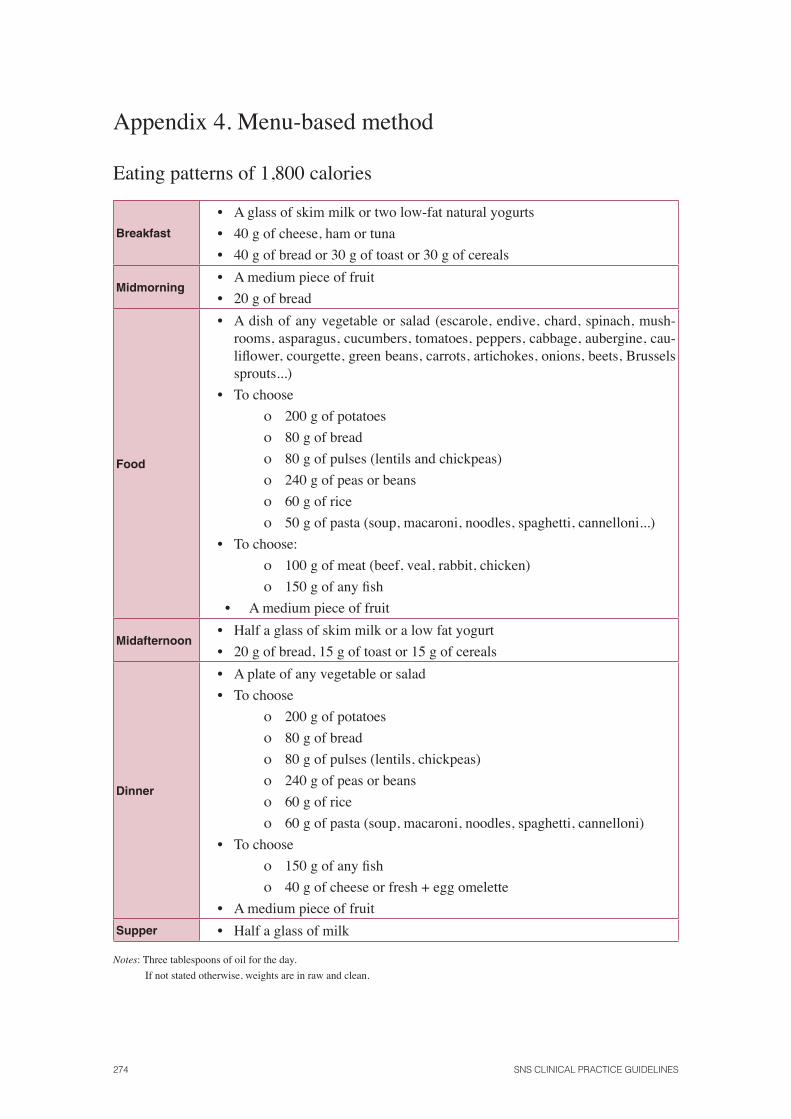
274 SNS CLINICAL PRACTICE GUIDELINES
Appendix 4. Menu-based method
Eating patterns of 1,800 calories
Breakfast
• A glass of skim milk or two low-fat natural yogurts
• 40 g of cheese, ham or tuna
• 40 g of bread or 30 g of toast or 30 g of cereals
Midmorning• A medium piece of fruit
• 20 g of bread
Food
• A dish of any vegetable or salad (escarole, endive, chard, spinach, mush-rooms, asparagus, cucumbers, tomatoes, peppers, cabbage, aubergine, cau-lifl ower, courgette, green beans, carrots, artichokes, onions, beets, Brussels sprouts...)
• To choose
ο 200 g of potatoes
ο 80 g of bread
ο 80 g of pulses (lentils and chickpeas)
ο 240 g of peas or beans
ο 60 g of rice
ο 50 g of pasta (soup, macaroni, noodles, spaghetti, cannelloni...)
• To choose:
ο 100 g of meat (beef, veal, rabbit, chicken)
ο 150 g of any fi sh
• A medium piece of fruit
Midafternoon• Half a glass of skim milk or a low fat yogurt
• 20 g of bread, 15 g of toast or 15 g of cereals
Dinner
• A plate of any vegetable or salad
• To choose
ο 200 g of potatoes
ο 80 g of bread
ο 80 g of pulses (lentils, chickpeas)
ο 240 g of peas or beans
ο 60 g of rice
ο 60 g of pasta (soup, macaroni, noodles, spaghetti, cannelloni)
• To choose
ο 150 g of any fi sh
ο 40 g of cheese or fresh + egg omelette
• A medium piece of fruit
Supper • Half a glass of milk
Notes: Three tablespoons of oil for the day.
If not stated otherwise, weights are in raw and clean.
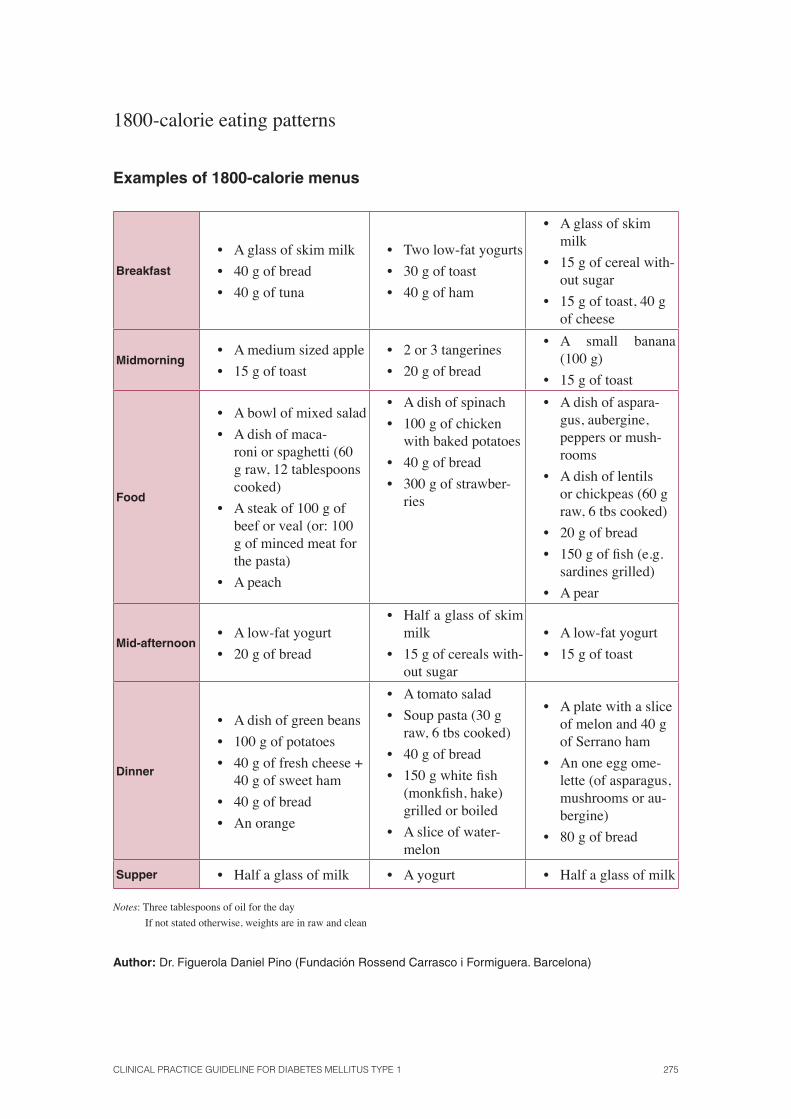
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 275
1800-calorie eating patterns
Examples of 1800-calorie menus
Breakfast
• A glass of skim milk
• 40 g of bread
• 40 g of tuna
• Two low-fat yogurts
• 30 g of toast
• 40 g of ham
• A glass of skim milk
• 15 g of cereal with-out sugar
• 15 g of toast, 40 g of cheese
Midmorning• A medium sized apple
• 15 g of toast
• 2 or 3 tangerines
• 20 g of bread
• A small banana (100 g)
• 15 g of toast
Food
• A bowl of mixed salad
• A dish of maca-roni or spaghetti (60 g raw, 12 tablespoons cooked)
• A steak of 100 g of beef or veal (or: 100 g of minced meat for the pasta)
• A peach
• A dish of spinach
• 100 g of chicken with baked potatoes
• 40 g of bread
• 300 g of strawber-ries
• A dish of aspara-gus, aubergine, peppers or mush-rooms
• A dish of lentils or chickpeas (60 g raw, 6 tbs cooked)
• 20 g of bread
• 150 g of fi sh (e.g. sardines grilled)
• A pear
Mid-afternoon • A low-fat yogurt
• 20 g of bread
• Half a glass of skim milk
• 15 g of cereals with-out sugar
• A low-fat yogurt
• 15 g of toast
Dinner
• A dish of green beans
• 100 g of potatoes
• 40 g of fresh cheese + 40 g of sweet ham
• 40 g of bread
• An orange
• A tomato salad
• Soup pasta (30 g raw, 6 tbs cooked)
• 40 g of bread
• 150 g white fi sh (monkfi sh, hake) grilled or boiled
• A slice of water-melon
• A plate with a slice of melon and 40 g of Serrano ham
• An one egg ome-lette (of asparagus, mushrooms or au-bergine)
• 80 g of bread
Supper • Half a glass of milk • A yogurt • Half a glass of milk
Notes: Three tablespoons of oil for the day
If not stated otherwise, weights are in raw and clean
Author: Dr. Figuerola Daniel Pino (Fundación Rossend Carrasco i Formiguera. Barcelona)
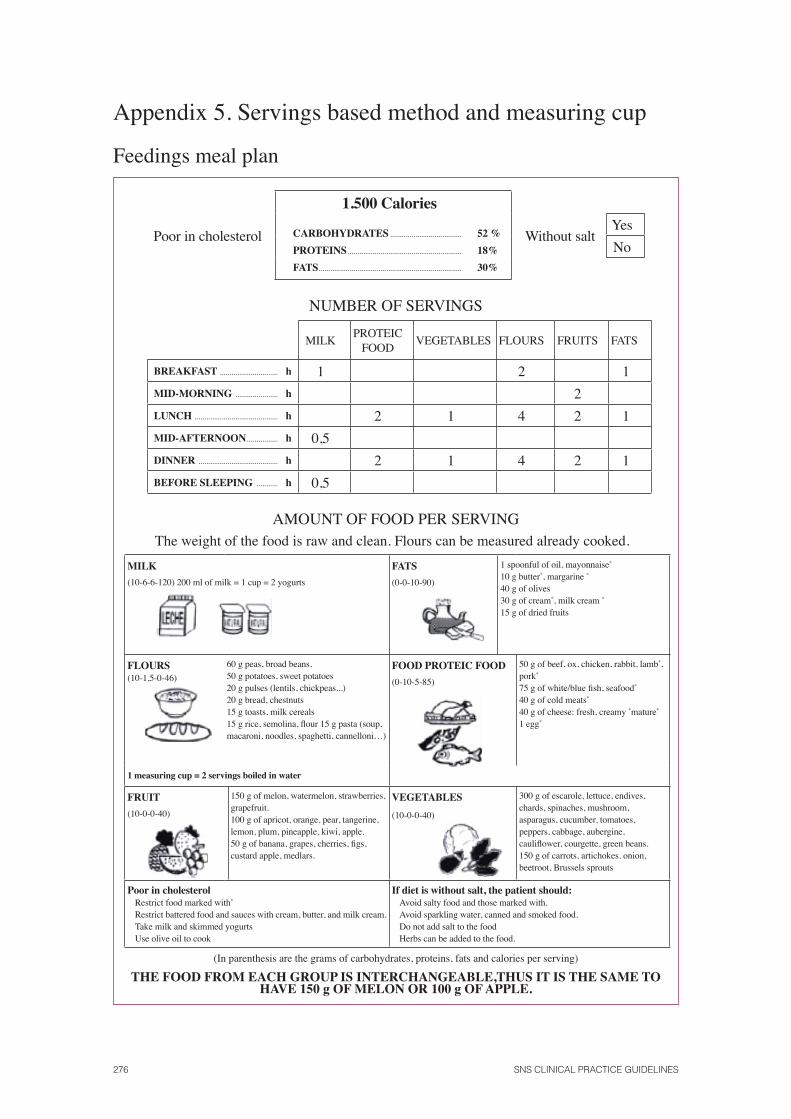
276 SNS CLINICAL PRACTICE GUIDELINES
Appendix 5. Servings based method and measuring cup
Feedings meal plan
Poor in cholesterol
1.500 Calories
CARBOHYDRATES ..................................... 52 %
PROTEINS ........................................................... 18%
FATS .......................................................................... 30%
Without saltYes
No
NUMBER OF SERVINGS
MILKPROTEIC
FOODVEGETABLES FLOURS FRUITS FATS
BREAKFAST .............................. h 1 2 1
MID-MORNING ...................... h 2
LUNCH ........................................... h 2 1 4 2 1
MID-AFTERNOON ................ h 0,5
DINNER ......................................... h 2 1 4 2 1
BEFORE SLEEPING ........... h 0,5
AMOUNT OF FOOD PER SERVINGThe weight of the food is raw and clean. Flours can be measured already cooked.
MILK
(10-6-6-120) 200 ml of milk = 1 cup = 2 yogurts
FATS (0-0-10-90)
1 spoonful of oil, mayonnaise*
10 g butter*, margarine *
40 g of olives 30 g of cream*, milk cream *
15 g of dried fruits
FLOURS(10-1,5-0-46)
60 g peas, broad beans, 50 g potatoes, sweet potatoes 20 g pulses (lentils, chickpeas...)20 g bread, chestnuts 15 g toasts, milk cereals15 g rice, semolina, fl our 15 g pasta (soup, macaroni, noodles, spaghetti, cannelloni…)
FOOD PROTEIC FOOD
(0-10-5-85)
50 g of beef, ox, chicken, rabbit, lamb*, pork*
75 g of white/blue fi sh, seafood*
40 g of cold meats*
40 g of cheese: fresh, creamy *mature*
1 egg*
1 measuring cup = 2 servings boiled in water
FRUIT
(10-0-0-40)
150 g of melon, watermelon, strawberries, grapefruit.100 g of apricot, orange, pear, tangerine, lemon, plum, pineapple, kiwi, apple.50 g of banana, grapes, cherries, fi gs, custard apple, medlars.
VEGETABLES
(10-0-0-40)
300 g of escarole, lettuce, endives, chards, spinaches, mushroom, asparagus, cucumber, tomatoes, peppers, cabbage, aubergine, caulifl ower, courgette, green beans.150 g of carrots, artichokes. onion, beetroot, Brussels sprouts
Poor in cholesterol Restrict food marked with*
Restrict battered food and sauces with cream, butter, and milk cream. Take milk and skimmed yogurts Use olive oil to cook
If diet is without salt, the patient should: Avoid salty food and those marked with.Avoid sparkling water, canned and smoked food. Do not add salt to the foodHerbs can be added to the food.
(In parenthesis are the grams of carbohydrates, proteins, fats and calories per serving)
THE FOOD FROM EACH GROUP IS INTERCHANGEABLE,THUS IT IS THE SAME TO HAVE 150 g OF MELON OR 100 g OF APPLE.
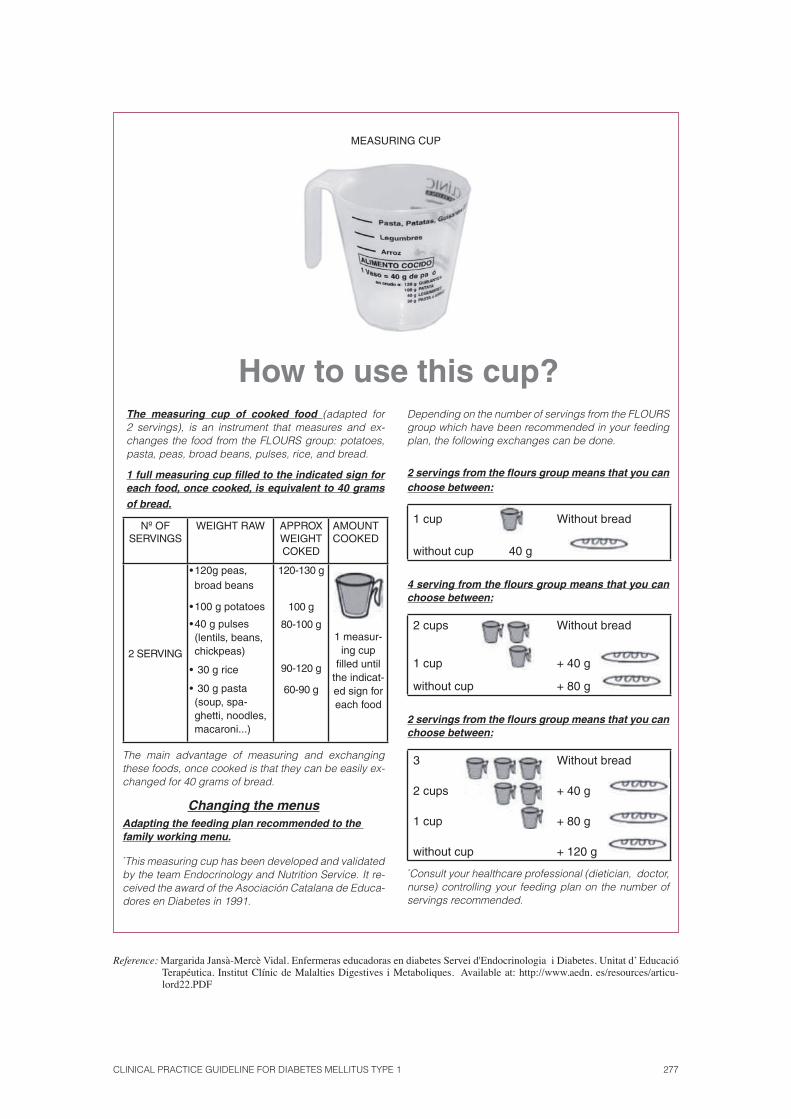
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 277
How to use this cup?The measuring cup of cooked food (adapted for 2 servings), is an instrument that measures and ex-changes the food from the FLOURS group: potatoes, pasta, peas, broad beans, pulses, rice, and bread.
1 full measuring cup fi lled to the indicated sign for each food, once cooked, is equivalent to 40 grams
of bread.
Nº OF SERVINGS
WEIGHT RAW APPROX WEIGHT COKED
AMOUNT COOKED
2 SERVING
• 120g peas, broad beans
• 100 g potatoes
• 40 g pulses (lentils, beans, chickpeas)
• 30 g rice
• 30 g pasta (soup, spa-ghetti, noodles, macaroni...)
120-130 g
100 g
80-100 g
90-120 g
60-90 g
1 measur-ing cup
fi lled until the indicat-ed sign for each food
The main advantage of measuring and exchanging these foods, once cooked is that they can be easily ex-changed for 40 grams of bread.
Changing the menusAdapting the feeding plan recommended to the family working menu.
*This measuring cup has been developed and validated by the team Endocrinology and Nutrition Service. It re-ceived the award of the Asociación Catalana de Educa-dores en Diabetes in 1991.
Depending on the number of servings from the FLOURS group which have been recommended in your feeding plan, the following exchanges can be done.
2 servings from the fl ours group means that you can choose between:
1 cup Without bread
without cup 40 g
4 serving from the fl ours group means that you can choose between:
2 cups Without bread
1 cup + 40 g
without cup + 80 g
2 servings from the fl ours group means that you can choose between:
3 Without bread
2 cups + 40 g
1 cup + 80 g
without cup + 120 g
*Consult your healthcare professional (dietician, doctor, nurse) controlling your feeding plan on the number of servings recommended.
Reference: Margarida Jansà-Mercè Vidal. Enfermeras educadoras en diabetes Servei d'Endocrinologia i Diabetes. Unitat d’ Educació Terapéutica. Institut Clínic de Malalties Digestives i Metaboliques. Available at: http://www.aedn. es/resources/articu-lord22.PDF
MEASURING CUP
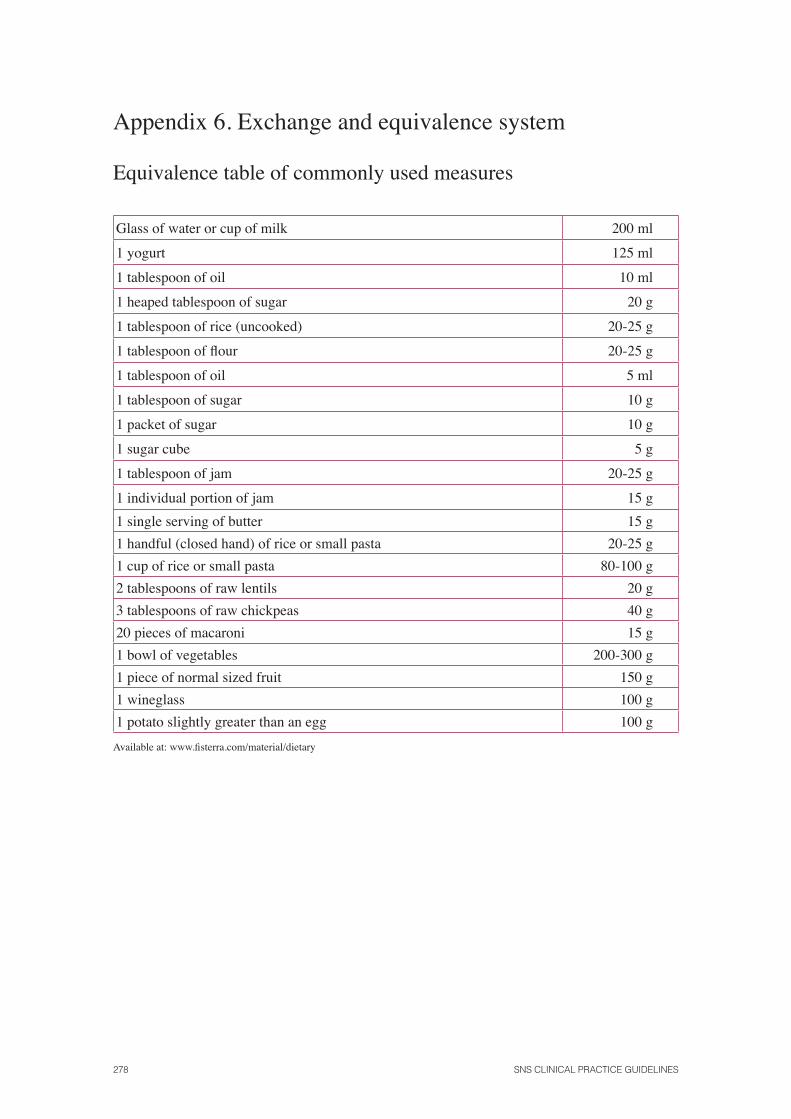
278 SNS CLINICAL PRACTICE GUIDELINES
Appendix 6. Exchange and equivalence system
Equivalence table of commonly used measures
Glass of water or cup of milk 200 ml
1 yogurt 125 ml
1 tablespoon of oil 10 ml
1 heaped tablespoon of sugar 20 g
1 tablespoon of rice (uncooked) 20-25 g
1 tablespoon of fl our 20-25 g
1 tablespoon of oil 5 ml
1 tablespoon of sugar 10 g
1 packet of sugar 10 g
1 sugar cube 5 g
1 tablespoon of jam 20-25 g
1 individual portion of jam 15 g
1 single serving of butter 15 g
1 handful (closed hand) of rice or small pasta 20-25 g
1 cup of rice or small pasta 80-100 g
2 tablespoons of raw lentils 20 g
3 tablespoons of raw chickpeas 40 g
20 pieces of macaroni 15 g
1 bowl of vegetables 200-300 g
1 piece of normal sized fruit 150 g
1 wineglass 100 g
1 potato slightly greater than an egg 100 g
Available at: www.fi sterra.com/material/dietary
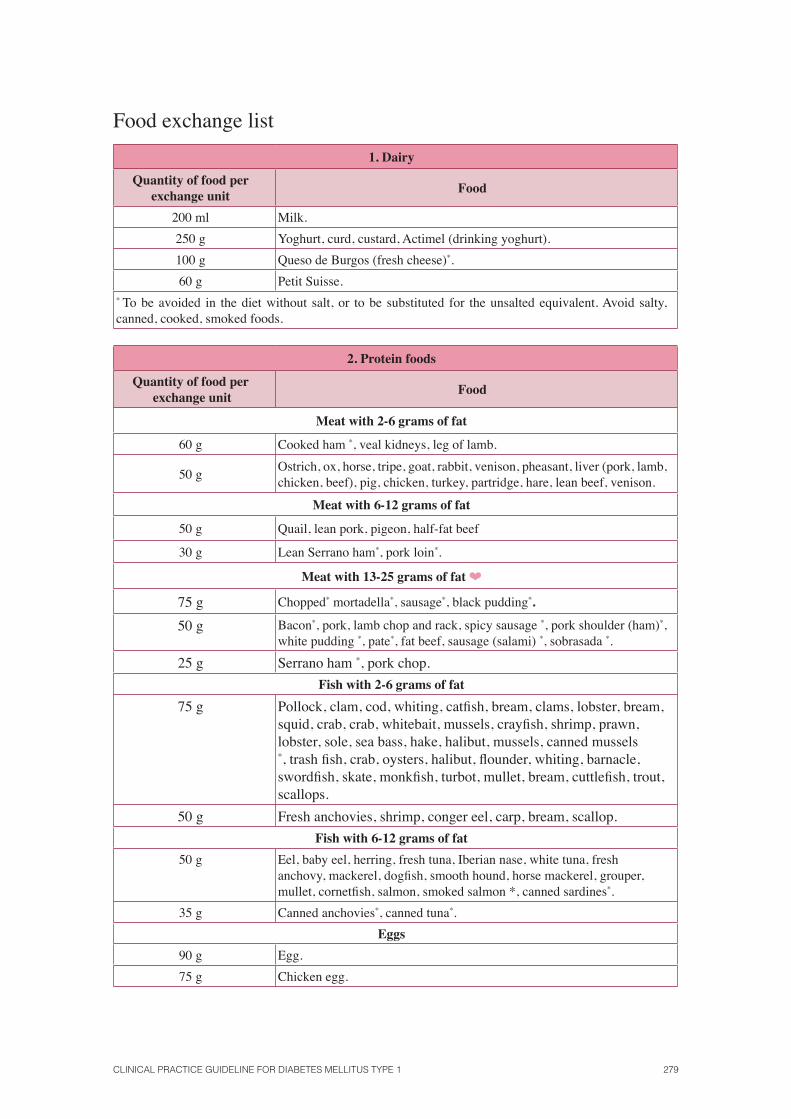
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 279
Food exchange list
1. Dairy
Quantity of food per exchange unit
Food
200 ml Milk.
250 g Yoghurt, curd, custard, Actimel (drinking yoghurt).
100 g Queso de Burgos (fresh cheese)*.
60 g Petit Suisse.* To be avoided in the diet without salt, or to be substituted for the unsalted equivalent. Avoid salty, canned, cooked, smoked foods.
2. Protein foods
Quantity of food per exchange unit
Food
Meat with 2-6 grams of fat
60 g Cooked ham *, veal kidneys, leg of lamb.
50 gOstrich, ox, horse, tripe, goat, rabbit, venison, pheasant, liver (pork, lamb, chicken, beef), pig, chicken, turkey, partridge, hare, lean beef, venison.
Meat with 6-12 grams of fat
50 g Quail, lean pork, pigeon, half-fat beef
30 g Lean Serrano ham*, pork loin*.
Meat with 13-25 grams of fat ❤
75 g Chopped* mortadella*, sausage*, black pudding*.
50 g Bacon*, pork, lamb chop and rack, spicy sausage *, pork shoulder (ham)*, white pudding *, pate*, fat beef, sausage (salami) *, sobrasada *.
25 g Serrano ham *, pork chop.
Fish with 2-6 grams of fat
75 g Pollock, clam, cod, whiting, catfi sh, bream, clams, lobster, bream, squid, crab, crab, whitebait, mussels, crayfi sh, shrimp, prawn, lobster, sole, sea bass, hake, halibut, mussels, canned mussels *, trash fi sh, crab, oysters, halibut, fl ounder, whiting, barnacle, swordfi sh, skate, monkfi sh, turbot, mullet, bream, cuttlefi sh, trout, scallops.
50 g Fresh anchovies, shrimp, conger eel, carp, bream, scallop.
Fish with 6-12 grams of fat
50 g Eel, baby eel, herring, fresh tuna, Iberian nase, white tuna, fresh anchovy, mackerel, dogfi sh, smooth hound, horse mackerel, grouper, mullet, cornetfi sh, salmon, smoked salmon *, canned sardines*.
35 g Canned anchovies*, canned tuna*.
Eggs
90 g Egg.
75 g Chicken egg.
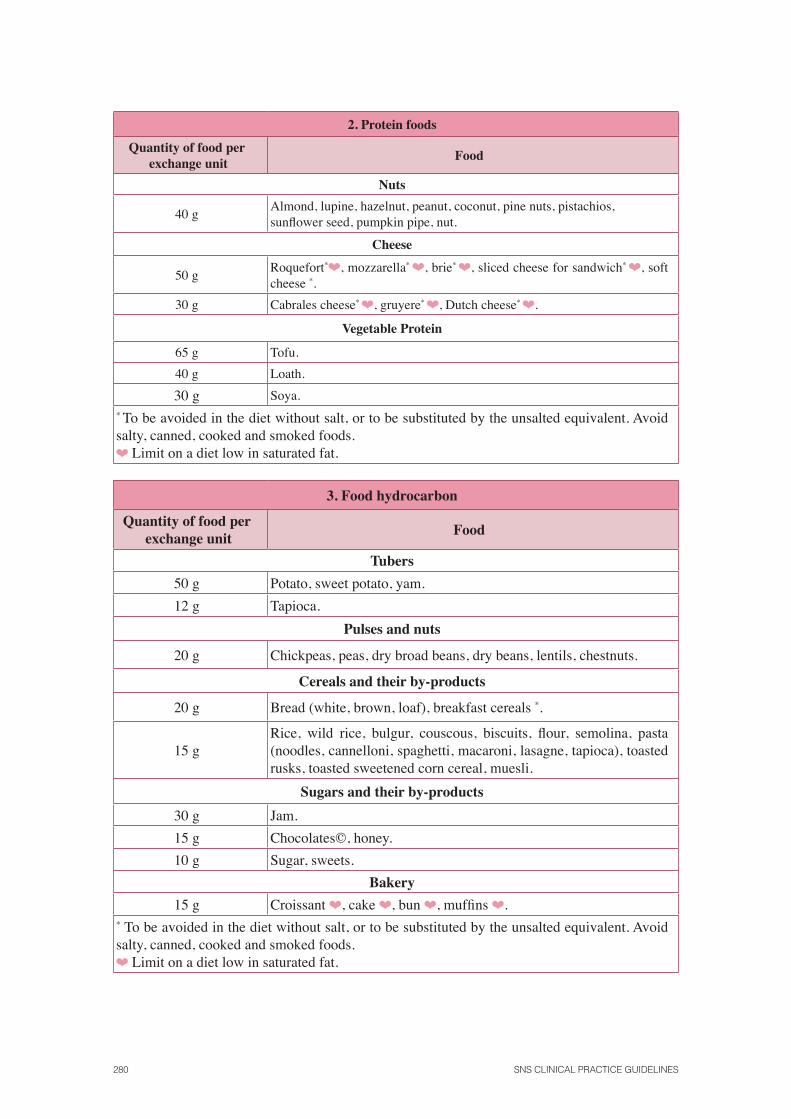
280 SNS CLINICAL PRACTICE GUIDELINES
2. Protein foods
Quantity of food per exchange unit
Food
Nuts
40 gAlmond, lupine, hazelnut, peanut, coconut, pine nuts, pistachios, sunfl ower seed, pumpkin pipe, nut.
Cheese
50 gRoquefort*❤, mozzarella* ❤, brie* ❤, sliced cheese for sandwich* ❤, soft cheese *.
30 g Cabrales cheese* ❤, gruyere* ❤, Dutch cheese* ❤.
Vegetable Protein
65 g Tofu.
40 g Loath.
30 g Soya.* To be avoided in the diet without salt, or to be substituted by the unsalted equivalent. Avoid salty, canned, cooked and smoked foods. ❤ Limit on a diet low in saturated fat.
3. Food hydrocarbon
Quantity of food per exchange unit
Food
Tubers
50 g Potato, sweet potato, yam.
12 g Tapioca.
Pulses and nuts
20 g Chickpeas, peas, dry broad beans, dry beans, lentils, chestnuts.
Cereals and their by-products
20 g Bread (white, brown, loaf), breakfast cereals *.
15 gRice, wild rice, bulgur, couscous, biscuits, fl our, semolina, pasta (noodles, cannelloni, spaghetti, macaroni, lasagne, tapioca), toasted rusks, toasted sweetened corn cereal, muesli.
Sugars and their by-products
30 g Jam.
15 g Chocolates©, honey.
10 g Sugar, sweets.
Bakery
15 g Croissant ❤, cake ❤, bun ❤, muffi ns ❤.* To be avoided in the diet without salt, or to be substituted by the unsalted equivalent. Avoid salty, canned, cooked and smoked foods.❤ Limit on a diet low in saturated fat.
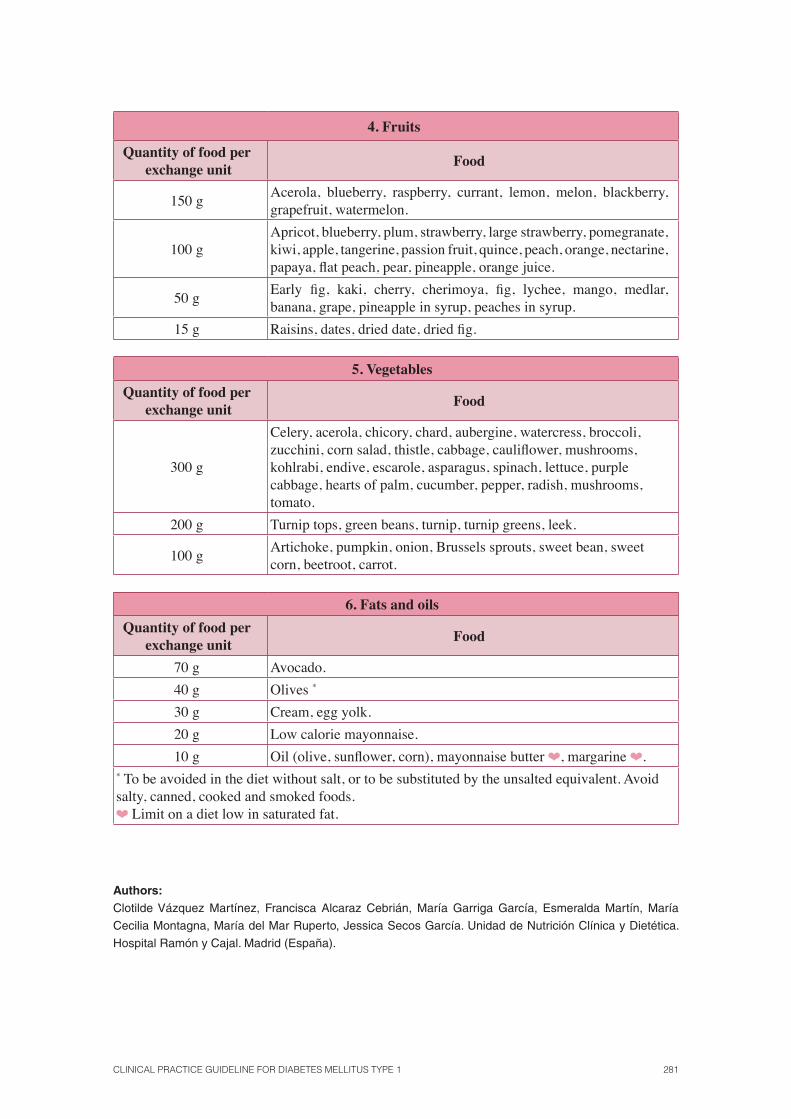
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 281
4. Fruits
Quantity of food per exchange unit
Food
150 gAcerola, blueberry, raspberry, currant, lemon, melon, blackberry, grapefruit, watermelon.
100 gApricot, blueberry, plum, strawberry, large strawberry, pomegranate, kiwi, apple, tangerine, passion fruit, quince, peach, orange, nectarine, papaya, fl at peach, pear, pineapple, orange juice.
50 gEarly fi g, kaki, cherry, cherimoya, fi g, lychee, mango, medlar, banana, grape, pineapple in syrup, peaches in syrup.
15 g Raisins, dates, dried date, dried fi g.
5. Vegetables
Quantity of food per exchange unit
Food
300 g
Celery, acerola, chicory, chard, aubergine, watercress, broccoli, zucchini, corn salad, thistle, cabbage, caulifl ower, mushrooms, kohlrabi, endive, escarole, asparagus, spinach, lettuce, purple cabbage, hearts of palm, cucumber, pepper, radish, mushrooms, tomato.
200 g Turnip tops, green beans, turnip, turnip greens, leek.
100 gArtichoke, pumpkin, onion, Brussels sprouts, sweet bean, sweet corn, beetroot, carrot.
6. Fats and oils
Quantity of food per exchange unit
Food
70 g Avocado.
40 g Olives *
30 g Cream, egg yolk.
20 g Low calorie mayonnaise.
10 g Oil (olive, sunfl ower, corn), mayonnaise butter ❤, margarine ❤.* To be avoided in the diet without salt, or to be substituted by the unsalted equivalent. Avoid salty, canned, cooked and smoked foods.❤ Limit on a diet low in saturated fat.
Authors: Clotilde Vázquez Martínez, Francisca Alcaraz Cebrián, María Garriga García, Esmeralda Martín, María
Cecilia Montagna, María del Mar Ruperto, Jessica Secos García. Unidad de Nutrición Clínica y Dietética.
Hospital Ramón y Cajal. Madrid (España).
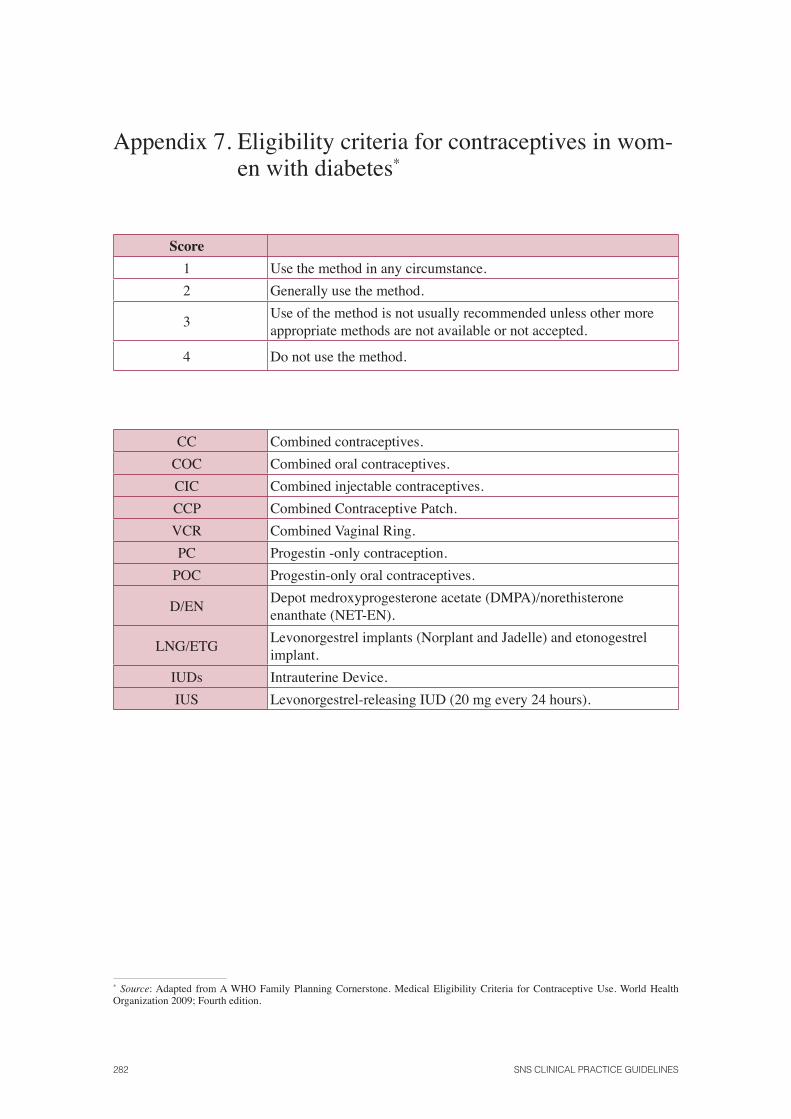
282 SNS CLINICAL PRACTICE GUIDELINES
Appendix 7. Eligibility criteria for contraceptives in wom-en with diabetes*
Score
1 Use the method in any circumstance.
2 Generally use the method.
3Use of the method is not usually recommended unless other more appropriate methods are not available or not accepted.
4 Do not use the method.
CC Combined contraceptives.
COC Combined oral contraceptives.
CIC Combined injectable contraceptives.
CCP Combined Contraceptive Patch.
VCR Combined Vaginal Ring.
PC Progestin -only contraception.
POC Progestin-only oral contraceptives.
D/ENDepot medroxyprogesterone acetate (DMPA)/norethisterone enanthate (NET-EN).
LNG/ETGLevonorgestrel implants (Norplant and Jadelle) and etonogestrel implant.
IUDs Intrauterine Device.
IUS Levonorgestrel-releasing IUD (20 mg every 24 hours).
* Source: Adapted from A WHO Family Planning Cornerstone. Medical Eligibility Criteria for Contraceptive Use. World Health Organization 2009; Fourth edition.
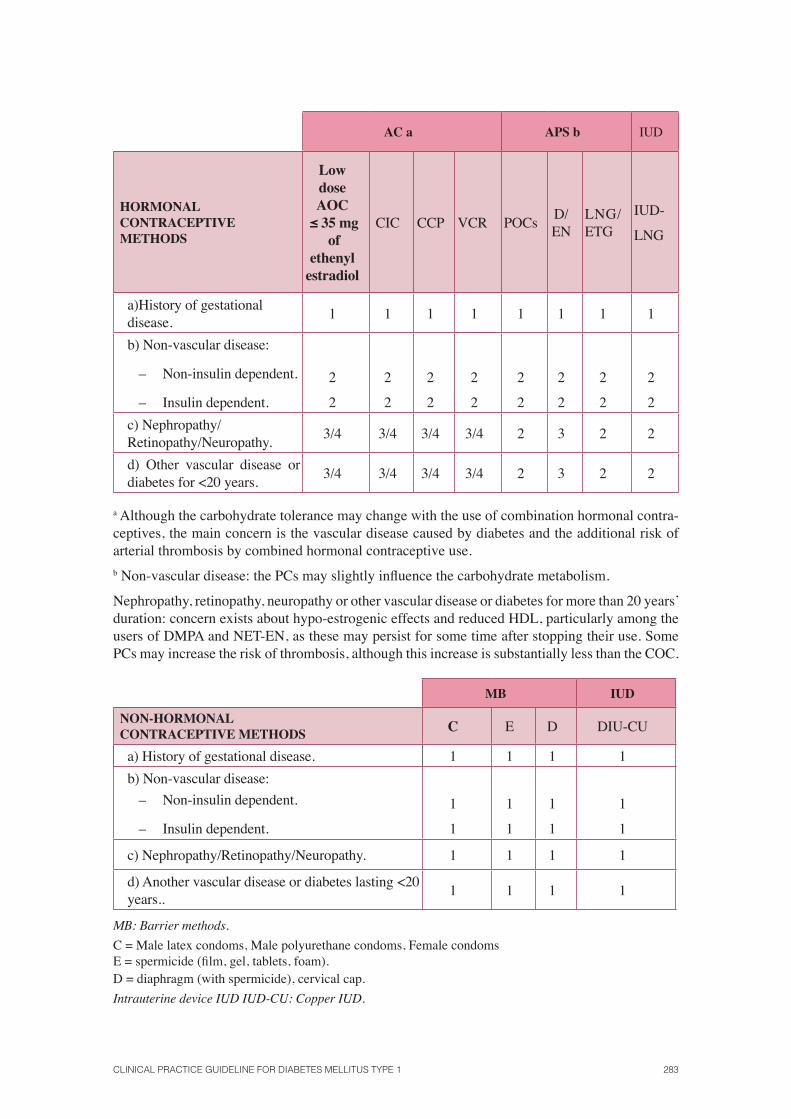
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 283
AC a APS b IUD
HORMONAL CONTRACEPTIVEMETHODS
Low dose AOC
≤ 35 mg of
ethenyl estradiol
CIC CCP VCR POCsD/EN
LNG/ETG
IUD-
LNG
a)History of gestational disease.
1 1 1 1 1 1 1 1
b) Non-vascular disease:
– Non-insulin dependent.
– Insulin dependent.
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
c) Nephropathy/Retinopathy/Neuropathy.
3/4 3/4 3/4 3/4 2 3 2 2
d) Other vascular disease or diabetes for <20 years.
3/4 3/4 3/4 3/4 2 3 2 2
a Although the carbohydrate tolerance may change with the use of combination hormonal contra-ceptives, the main concern is the vascular disease caused by diabetes and the additional risk of arterial thrombosis by combined hormonal contraceptive use. b Non-vascular disease: the PCs may slightly infl uence the carbohydrate metabolism.
Nephropathy, retinopathy, neuropathy or other vascular disease or diabetes for more than 20 years’ duration: concern exists about hypo-estrogenic effects and reduced HDL, particularly among the users of DMPA and NET-EN, as these may persist for some time after stopping their use. Some PCs may increase the risk of thrombosis, although this increase is substantially less than the COC.
MB IUD
NON-HORMONAL CONTRACEPTIVE METHODS C E D DIU-CU
a) History of gestational disease. 1 1 1 1
b) Non-vascular disease:
– Non-insulin dependent.
– Insulin dependent.
1
1
1
1
1
1
1
1
c) Nephropathy/Retinopathy/Neuropathy. 1 1 1 1
d) Another vascular disease or diabetes lasting <20 years..
1 1 1 1
MB: Barrier methods. C = Male latex condoms, Male polyurethane condoms, Female condoms E = spermicide (fi lm, gel, tablets, foam). D = diaphragm (with spermicide), cervical cap. Intrauterine device IUD IUD-CU: Copper IUD.
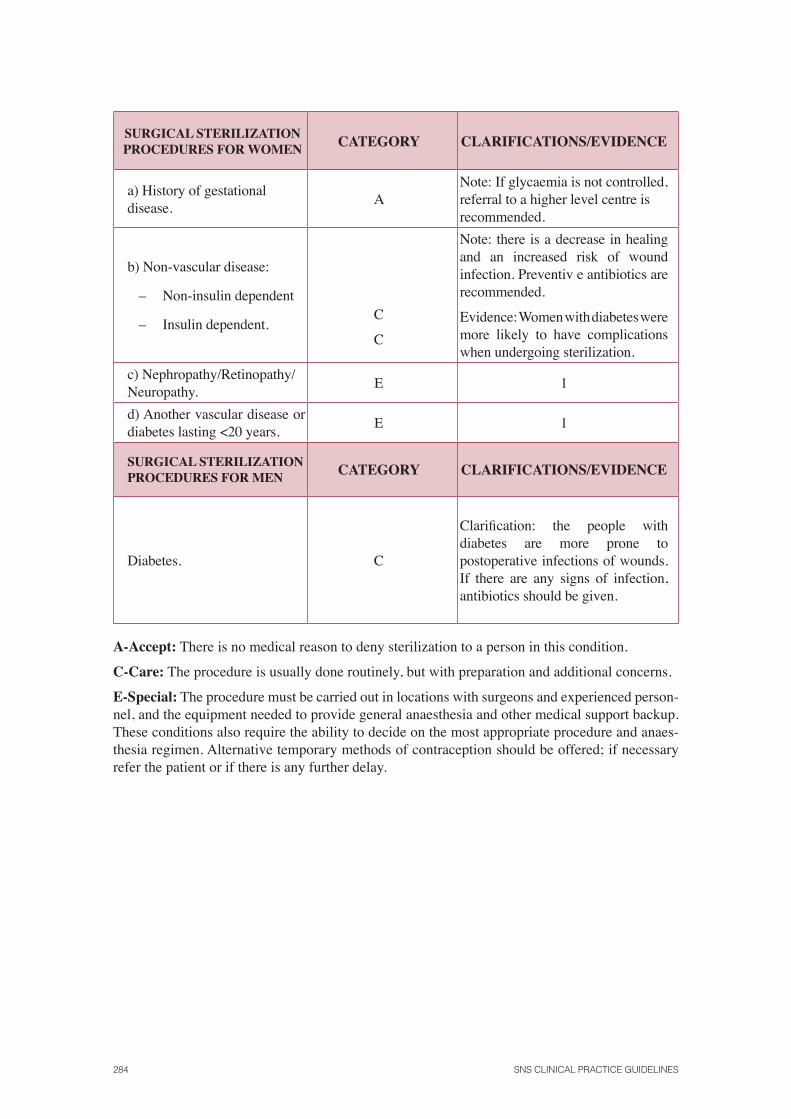
284 SNS CLINICAL PRACTICE GUIDELINES
SURGICAL STERILIZATION PROCEDURES FOR WOMEN CATEGORY CLARIFICATIONS/EVIDENCE
a) History of gestational disease.
ANote: If glycaemia is not controlled, referral to a higher level centre is recommended.
b) Non-vascular disease:
– Non-insulin dependent
– Insulin dependent. C
C
Note: there is a decrease in healing and an increased risk of wound infection. Preventiv e antibiotics are recommended.
Evidence: Women with diabetes were more likely to have complications when undergoing sterilization.
c) Nephropathy/Retinopathy/Neuropathy.
E 1
d) Another vascular disease or diabetes lasting <20 years.
E 1
SURGICAL STERILIZATION PROCEDURES FOR MEN CATEGORY CLARIFICATIONS/EVIDENCE
Diabetes. C
Clarifi cation: the people with diabetes are more prone to postoperative infections of wounds. If there are any signs of infection, antibiotics should be given.
A-Accept: There is no medical reason to deny sterilization to a person in this condition.
C-Care: The procedure is usually done routinely, but with preparation and additional concerns.
E-Special: The procedure must be carried out in locations with surgeons and experienced person-nel, and the equipment needed to provide general anaesthesia and other medical support backup. These conditions also require the ability to decide on the most appropriate procedure and anaes-thesia regimen. Alternative temporary methods of contraception should be offered; if necessary refer the patient or if there is any further delay.
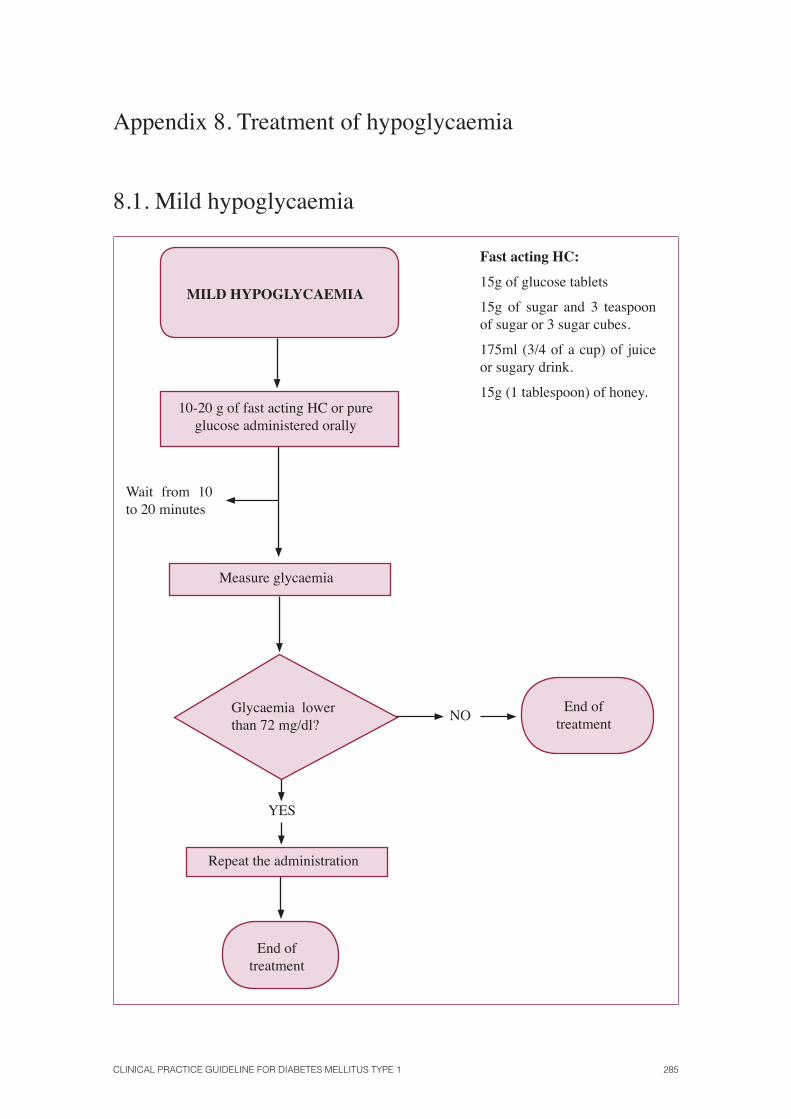
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 285
Appendix 8. Treatment of hypoglycaemia
8.1. Mild hypoglycaemia
MILD HYPOGLYCAEMIA
10-20 g of fast acting HC or pure glucose administered orally
Measure glycaemia
Glycaemia lower than 72 mg/dl?
NOEnd of
treatment
YES
Repeat the administration
End of treatment
Wait from 10 to 20 minutes
Fast acting HC:
15g of glucose tablets
15g of sugar and 3 teaspoon of sugar or 3 sugar cubes.
175ml (3/4 of a cup) of juice or sugary drink.
15g (1 tablespoon) of honey.
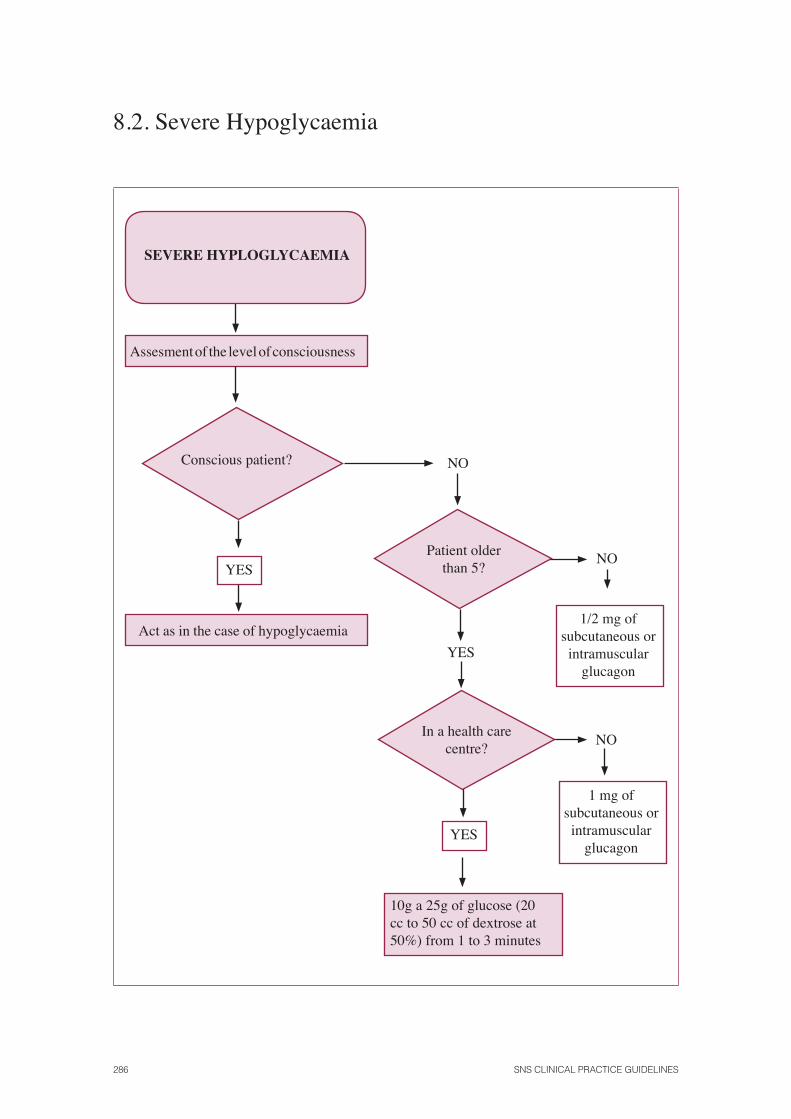
286 SNS CLINICAL PRACTICE GUIDELINES
8.2. Severe Hypoglycaemia
Assesment of the level of consciousness
Conscious patient?
YES
Act as in the case of hypoglycaemia
NO
Patient older than 5?
YES
In a health care centre?
YES
NO
NO
1 mg of subcutaneous or intramuscular
glucagon
10g a 25g of glucose (20 cc to 50 cc of dextrose at 50%) from 1 to 3 minutes
SEVERE HYPLOGLYCAEMIA
1/2 mg of subcutaneous or intramuscular
glucagon
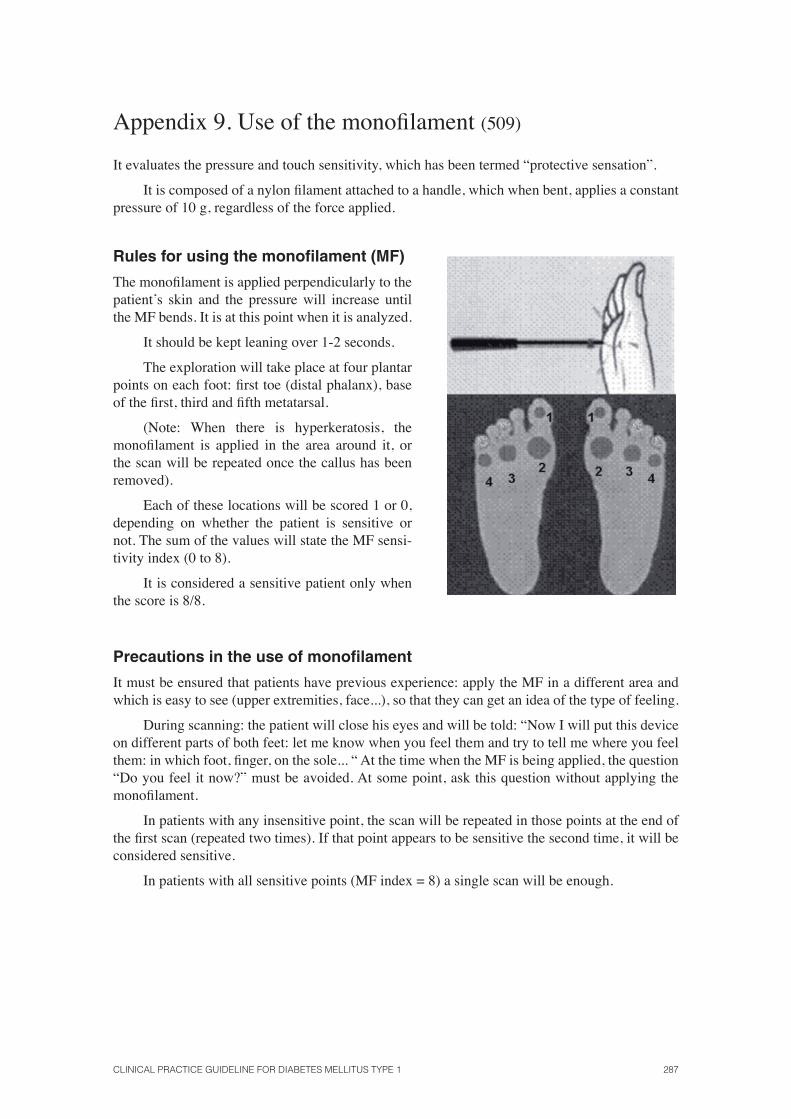
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 287
Appendix 9. Use of the monofi lament (509)
It evaluates the pressure and touch sensitivity, which has been termed “protective sensation”.
It is composed of a nylon fi lament attached to a handle, which when bent, applies a constant pressure of 10 g, regardless of the force applied.
Rules for using the monofi lament (MF)
The monofi lament is applied perpendicularly to the patient’s skin and the pressure will increase until the MF bends. It is at this point when it is analyzed.
It should be kept leaning over 1-2 seconds.
The exploration will take place at four plantar points on each foot: fi rst toe (distal phalanx), base of the fi rst, third and fi fth metatarsal.
(Note: When there is hyperkeratosis, the monofi lament is applied in the area around it, or the scan will be repeated once the callus has been removed).
Each of these locations will be scored 1 or 0, depending on whether the patient is sensitive or not. The sum of the values will state the MF sensi-tivity index (0 to 8).
It is considered a sensitive patient only when the score is 8/8.
Precautions in the use of monofi lament
It must be ensured that patients have previous experience: apply the MF in a different area and which is easy to see (upper extremities, face...), so that they can get an idea of the type of feeling.
During scanning: the patient will close his eyes and will be told: “Now I will put this device on different parts of both feet: let me know when you feel them and try to tell me where you feel them: in which foot, fi nger, on the sole... “ At the time when the MF is being applied, the question “Do you feel it now?” must be avoided. At some point, ask this question without applying the monofi lament.
In patients with any insensitive point, the scan will be repeated in those points at the end of the fi rst scan (repeated two times). If that point appears to be sensitive the second time, it will be considered sensitive.
In patients with all sensitive points (MF index = 8) a single scan will be enough.
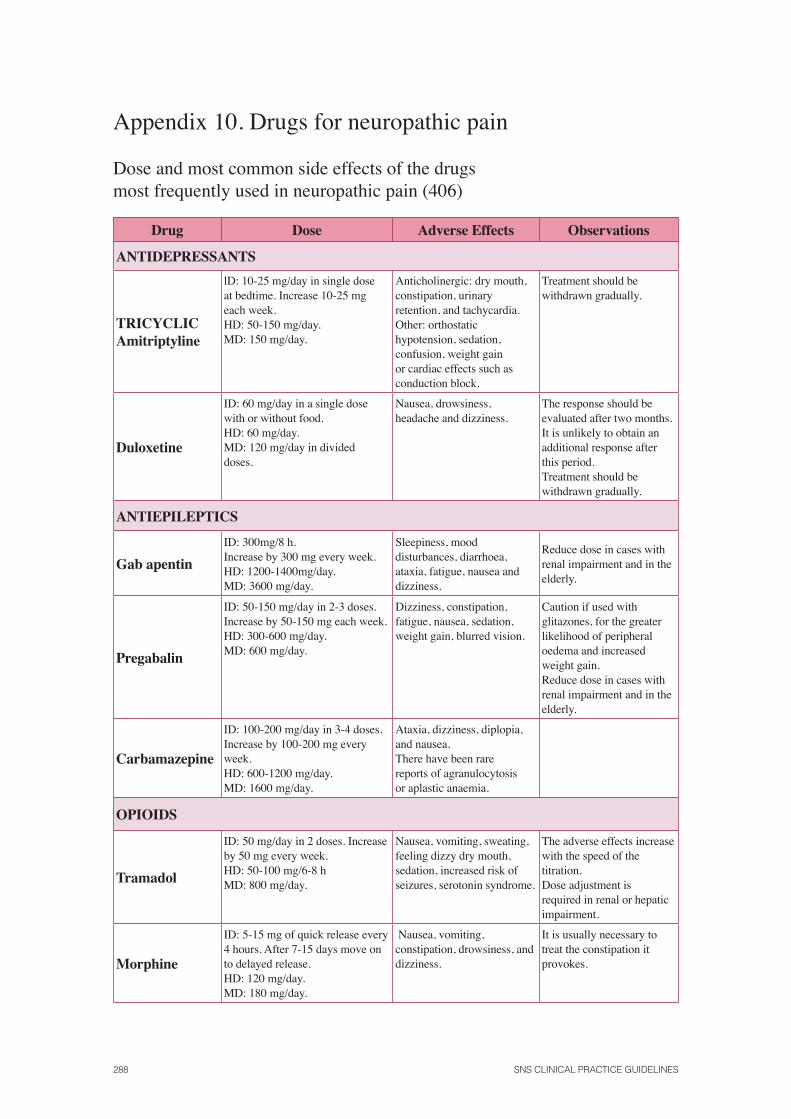
288 SNS CLINICAL PRACTICE GUIDELINES
Appendix 10. Drugs for neuropathic pain
Dose and most common side effects of the drugsmost frequently used in neuropathic pain (406)
Drug Dose Adverse Effects Observations
ANTIDEPRESSANTS
TRICYCLIC Amitriptyline
lD: 10-25 mg/day in single dose at bedtime. Increase 10-25 mg each week. HD: 50-150 mg/day. MD: 150 mg/day.
Anticholinergic: dry mouth, constipation, urinary retention, and tachycardia. Other: orthostatic hypotension, sedation, confusion, weight gain or cardiac effects such as conduction block.
Treatment should be withdrawn gradually.
Duloxetine
ID: 60 mg/day in a single dose with or without food. HD: 60 mg/day. MD: 120 mg/day in divided doses.
Nausea, drowsiness, headache and dizziness.
The response should be evaluated after two months. It is unlikely to obtain an additional response after this period. Treatment should be withdrawn gradually.
ANTIEPILEPTICS
Gab apentin
ID: 300mg/8 h.Increase by 300 mg every week. HD: 1200-1400mg/day. MD: 3600 mg/day.
Sleepiness, mood disturbances, diarrhoea, ataxia, fatigue, nausea and dizziness.
Reduce dose in cases with renal impairment and in the elderly.
Pregabalin
ID: 50-150 mg/day in 2-3 doses. Increase by 50-150 mg each week. HD: 300-600 mg/day. MD: 600 mg/day.
Dizziness, constipation, fatigue, nausea, sedation, weight gain, blurred vision.
Caution if used with glitazones, for the greater likelihood of peripheral oedema and increased weight gain. Reduce dose in cases with renal impairment and in the elderly.
Carbamazepine
ID: 100-200 mg/day in 3-4 doses. Increase by 100-200 mg every week. HD: 600-1200 mg/day. MD: 1600 mg/day.
Ataxia, dizziness, diplopia, and nausea. There have been rare reports of agranulocytosis or aplastic anaemia.
OPIOIDS
Tramadol
ID: 50 mg/day in 2 doses. Increase by 50 mg every week. HD: 50-100 mg/6-8 h MD: 800 mg/day.
Nausea, vomiting, sweating, feeling dizzy dry mouth, sedation, increased risk of seizures, serotonin syndrome.
The adverse effects increase with the speed of the titration. Dose adjustment is required in renal or hepatic impairment.
Morphine
ID: 5-15 mg of quick release every 4 hours. After 7-15 days move on to delayed release. HD: 120 mg/day. MD: 180 mg/day.
Nausea, vomiting, constipation, drowsiness, and dizziness.
It is usually necessary to treat the constipation it provokes.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 289
Appendix 11. Information for Patients
11.1. International Charter of rights and responsibilities of people with diabetes
Vision
The vision of the Charter is to:
• Optimise the health and quality of life of people with diabetes
• Enable people with diabetes to have as normal a life as possible
• Reduce or eliminate the barriers to people with diabetes realising their full potential as members of society.
The Charter
• Sets out the rights as well as the responsibilities of people with diabetes
• Acknowledges the wide global variety in the quality of healthcare as well as customs and practice that impact in different ways on people with diabetes
• Represents the ‘gold standard’ in care, treatment, prevention and education to which all countries and people can aspire.
1. The Right to care
People with diabetes have the right to:
• Early diagnosis and affordable and equitable access to care and treatment, regardless of race, ethnicity, gender and age, including access to psychosocial care and support.
• Receive regular, reliable advice, education and treatment in accordance with evidence-based practice that centres on their needs, irrespective of the setting in which they receive that care.
• Benefi t from proactive health sector community outreach, education and prevention campaigns in every healthcare setting.
• Access to high-quality services and care during and after pregnancy and childbirth.
• Access to high-quality services and care during childhood and adolescence, recognising the special needs of those not necessarily in a position to represent themselves.
290 SNS CLINICAL PRACTICE GUIDELINES
• Appropriate transitional care, addressing the progression of the disease and the changes that occur with age.
• Continuity of appropriate care in disaster and emergency situations.
• Be treated with dignity and respect - including respect for individual, religious or cul-tural beliefs and parental insights - by healthcare providers, and feel free to make com-plaints about any aspects of diabetes services without detriment to their care and treat-ment.
• Information relating to their diabetes being kept confi dential and not disclosed to third parties without their consent and the choice whether or not to take part in research pro-grammes, without detriment to care and treatment.
• Advocate, individually and collectively, to health providers and decision makers for improvements in diabetes care and services.
2. Right to Information and Education
People with diabetes and the parents or carers of people with diabetes have the right to:
• Information and education about diabetes, including how it can be prevented, how early detection in high-risk individuals is an advantage, how the disease can be managed ef-fectively and how to access education and clinical resources.
• High quality diabetes self-management education at diagnosis and whenever needed that integrates the clinical, behavioural and psychosocial aspects of diabetes in a group or individually.
• Be involved in assessing, planning and implementing as well as monitoring their own care and health goals.
• Reliable information about the names and dosage of any therapies and medication, their actions and potential side effects and interactions with other medical conditions and therapies, specifi c to the individual.
• Individual access to their medical records and other relevant information if requested and the right for that information to be shared.
3. Right to Social Justice
People with diabetes are entitled to:
• Be a fully engaged member of society, treated with respect and dignity by all, without feeling the need to conceal the fact they have diabetes.
• Affordable medicines and monitoring technologies.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 291
• Be treated fairly in employment and career progression while acknowledging that there are certain occupations where identifi able risks may limit the employment of people with diabetes.
• Be treated with respect and dignity by all sections of society.
• Not to be discriminated against in the provision of all forms of insurance cover and in applying for a driving licence.
• Be fully supported in pre-school activities, schools, during extra-curricular activities and social clubs as well as in workplaces and be given time to attend medical appoint-ments as well as the time and privacy to self-test and administer medicines in a clean and safe environment.
• Create or participate in a representative patient organisation and seek the support for that organisation from health and health-related bodies and civil society.
4. Responsibilities
People with diabetes have a responsibility to:
• Share information with their healthcare providers on their current state of health, all types of medicines they are using, allergies, social setting, lifestyle behaviour and any other information that would be relevant in a health provider determining the most suit-able treatment and advice.
• Manage their agreed care and treatment plan.
• Adopt, implement and monitor healthy lifestyle behaviours as part of their self-man-agement of diabetes.
• Share with their healthcare providers any problems they experience with their recom-mended treatment plan, including any barriers to its successful implementation.
• Inform family, school, work and social colleagues they have diabetes so that they can be supportive to people with diabetes, if and when needed.
• Show consideration and respect for the rights of other people with diabetes and their healthcare providers.
Source: International Diabetes Federation.
Available at: http://www.idf.org/webdata/docs/advocacy-kit/Charter-of-rights-ES.pdf
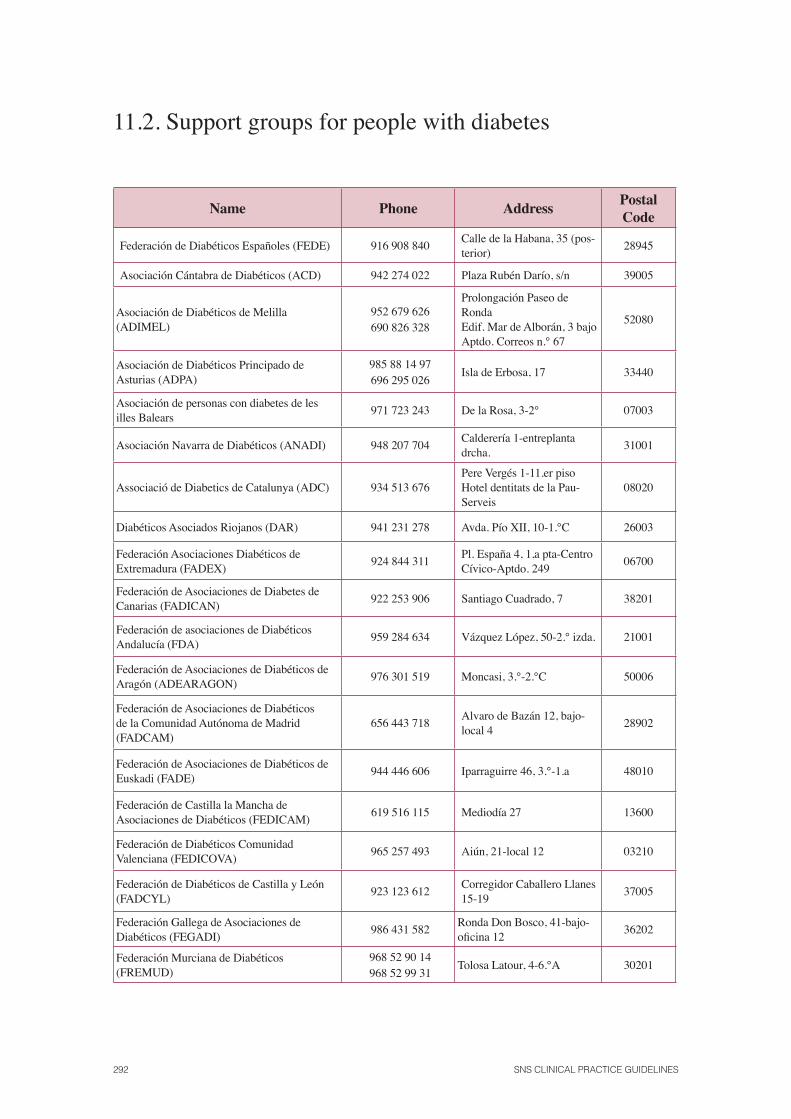
292 SNS CLINICAL PRACTICE GUIDELINES
11.2. Support groups for people with diabetes
Name Phone AddressPostalCode
Federación de Diabéticos Españoles (FEDE) 916 908 840Calle de la Habana, 35 (pos-terior)
28945
Asociación Cántabra de Diabéticos (ACD) 942 274 022 Plaza Rubén Darío, s/n 39005
Asociación de Diabéticos de Melilla (ADIMEL)
952 679 626 690 826 328
Prolongación Paseo de RondaEdif. Mar de Alborán, 3 bajo Aptdo. Correos n.° 67
52080
Asociación de Diabéticos Principado de Asturias (ADPA)
985 88 14 97696 295 026
Isla de Erbosa, 17 33440
Asociación de personas con diabetes de les illes Balears
971 723 243 De la Rosa, 3-2° 07003
Asociación Navarra de Diabéticos (ANADI) 948 207 704Calderería 1-entreplanta drcha.
31001
Associació de Diabetics de Catalunya (ADC) 934 513 676Pere Vergés 1-11.er pisoHotel dentitats de la Pau-Serveis
08020
Diabéticos Asociados Riojanos (DAR) 941 231 278 Avda. Pío XII, 10-1.°C 26003
Federación Asociaciones Diabéticos de Extremadura (FADEX)
924 844 311Pl. España 4, 1,a pta-Centro Cívico-Aptdo. 249
06700
Federación de Asociaciones de Diabetes de Canarias (FADICAN)
922 253 906 Santiago Cuadrado, 7 38201
Federación de asociaciones de Diabéticos Andalucía (FDA)
959 284 634 Vázquez López, 50-2.° izda. 21001
Federación de Asociaciones de Diabéticos de Aragón (ADEARAGON)
976 301 519 Moncasi, 3.°-2.°C 50006
Federación de Asociaciones de Diabéticos de la Comunidad Autónoma de Madrid (FADCAM)
656 443 718Alvaro de Bazán 12, bajo-local 4
28902
Federación de Asociaciones de Diabéticos de Euskadi (FADE)
944 446 606 Iparraguirre 46, 3.°-1.a 48010
Federación de Castilla la Mancha de Asociaciones de Diabéticos (FEDICAM)
619 516 115 Mediodía 27 13600
Federación de Diabéticos Comunidad Valenciana (FEDICOVA)
965 257 493 Aiún, 21-local 12 03210
Federación de Diabéticos de Castilla y León (FADCYL)
923 123 612Corregidor Caballero Llanes 15-19
37005
Federación Gallega de Asociaciones de Diabéticos (FEGADI)
986 431 582Ronda Don Bosco, 41-bajo-ofi cina 12
36202
Federación Murciana de Diabéticos (FREMUD)
968 52 90 14 968 52 99 31
Tolosa Latour, 4-6.°A 30201
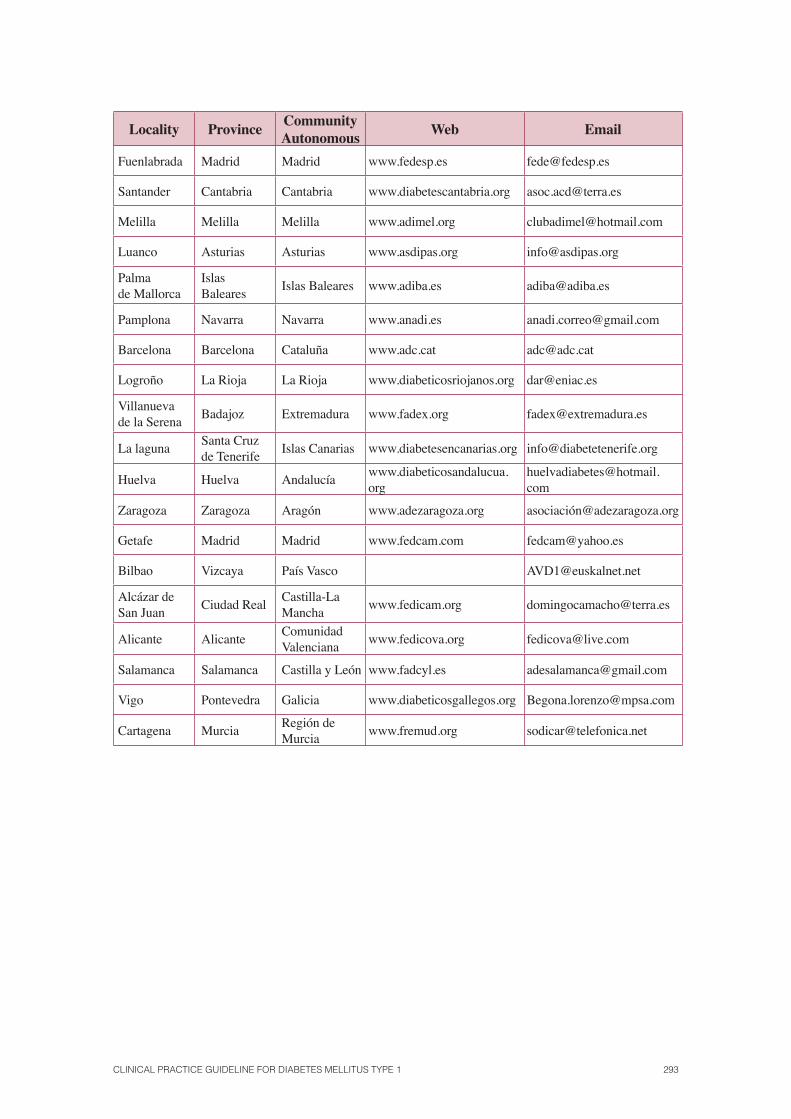
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 293
Locality ProvinceCommunity Autonomous
Web Email
Fuenlabrada Madrid Madrid www.fedesp.es [email protected]
Santander Cantabria Cantabria www.diabetescantabria.org [email protected]
Melilla Melilla Melilla www.adimel.org [email protected]
Luanco Asturias Asturias www.asdipas.org [email protected]
Palmade Mallorca
Islas Baleares
Islas Baleares www.adiba.es [email protected]
Pamplona Navarra Navarra www.anadi.es [email protected]
Barcelona Barcelona Cataluña www.adc.cat [email protected]
Logroño La Rioja La Rioja www.diabeticosriojanos.org [email protected]
Villanuevade la Serena
Badajoz Extremadura www.fadex.org [email protected]
La lagunaSanta Cruz de Tenerife
Islas Canarias www.diabetesencanarias.org [email protected]
Huelva Huelva Andalucíawww.diabeticosandalucua.org
Zaragoza Zaragoza Aragón www.adezaragoza.org asociació[email protected]
Getafe Madrid Madrid www.fedcam.com [email protected]
Bilbao Vizcaya País Vasco [email protected]
Alcázar deSan Juan
Ciudad RealCastilla-La Mancha
www.fedicam.org [email protected]
Alicante AlicanteComunidadValenciana
www.fedicova.org [email protected]
Salamanca Salamanca Castilla y León www.fadcyl.es [email protected]
Vigo Pontevedra Galicia www.diabeticosgallegos.org [email protected]
Cartagena MurciaRegión de Murcia
www.fremud.org [email protected]
294 SNS CLINICAL PRACTICE GUIDELINES
Appendix 12. Glossary
Angiotensin converting enzyme inhibitors (ACE): drugs, which exert their main action by inhibiting the transformation of the angiotensin I enzyme to the angiotensin II enzyme, thus obtaining a limitation of the vasoconstrictor effect of this enzyme at peripheral level.
Ankle-arm index: systolic pressure ratio in the ankle and the arm.
Antagonists of angiotensin II receptors (ARBs), exert their vasodilatory action by blocking the enzyme angiotensin II at its receptors AT1 levels.
Anti-21-hydroxylase antibodies: autoantibodies recognizing the 21-hydroxylase enzyme, which are associated with Addison’s disease.
Anti-GAD antibodies (GAD =glutamic acid decarboxylase): autoantibodies associated with the autoimmune response of DM1, which recognize the glutamic acid decarboxylase enzyme.
Anti-IA2 antibodies: autoantibodies associated with the autoimmune response of DM1, which recognize the tyrosine phosphatase.
Anti-Insulin antibodies (AIA =insulin autoantibodies): autoantibodies associated with the autoimmune response of DM1, which recognise insulin.
Anti-Islet cell antibodies (ICA =islet cell antibodies): autoantibodies associated with the autoimmune response of DM1, detected by immunofl uorescence that recognize antigens of pancreatic islets.
Anti-TPO antibodies: circulating autoantibodies that recognize the thyroid peroxidase enzyme, which is associated with the autoimmune thyroid disease.
Anti-transglutaminase antibodies (ATA): autoantibodies that recognise human transglutaminase, and are associated with celiac disease.
Anti-zinc transporter antibodies (ZnT8): autoantibodies associated with the autoimmune response of DM1, which recognizes a Zn transporter protein in the beta cells and plays a crucial role in its maturation and thus also in the secretion of insulin.
ASR Scale (Achenbach-scale): instrument to assess the skills and behavioural problems in children.
Biomicroscopy: Examination of living tissues under a microscope. In ophthalmology, eye examination with a microscope (anterior chamber, lens, vitreous), using special lighting focused with the slit lamp.
Case-control study: a study that identifi es people with a disease (cases), i.e. lung cancer, and is compared with a group without the disease (control). The relationship between one or more factors (i.e. smoking) related to the disease is examined by comparing the frequency of exposure to this or other factors between the cases and the controls.
Clinical Prediction Rule: is a clinical tool that quantifi es the individual contribution of various components of the clinical history, physical examination, and laboratory results and other variables on the diagnosis, prognosis or likely response to a treatment in a particular patient.
Cochrane Library: database on effectiveness created by the Cochrane Collaboration, composed among others by original systematic reviews of this organization.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 295
Cognitive behavioural therapy or cognitive therapy: a psychotherapeutic intervention, which highlights prominently cognitive restructuring, the promotion of a collaborative therapeutic alliance and associated behavioural and emotional methods using a structured framework. Its working hypothesis is that thought patterns, called cognitive distortions, have adverse effects on the emotions and behaviour and therefore its restructuring, through psycho-educational interventions and continuous practice, can improve the state of the patient.
Cohort study: consists of monitoring one or more cohorts of individuals who have different degrees of exposure to a risk factor, and in whom the onset of the disease or the condition being studied is measured.
Confi dence interval is the range, which lies within the true magnitude of the effect (never known with absolute exactitude) with a predetermined degree of security or confi dence. The most common phrase used is the “confi dence interval at 95%” (or “confi dence limits at 95%”). This means that within that range, the true value would be found in 95% of the cases.
Conventional insulin syringe: 1 ml syringe, graduated to be able to administer insulin in units.
Copper IUD: intrauterine device used as a non-hormonal contraceptive. The copper acts as a spermicide and prevents the union of sperm and egg.
Cost minimization analysis: Economic analysis in which the costs are expressed in monetary units and the health effects are identical.
Cost-utility analysis: Economic analysis in which the costs are expressed in monetary units and the benefi ts in QALY (years of quality-adjusted life). The result, expressed as a cost/QALY ratio, can be used to compare different interventions.
C-Peptide: peptide secreted in equimolar amounts with insulin, which is used as a marker for the role of the cells.
DTSQ (Diabetes Treatment Satisfaction Questionnaire): questionnaire assessing the quality of life for people with diabetes
Embase: European Database (Dutch) created by Excerpta Médica containing clinical medicine and pharmacology.
Endomysial antibody: immunoglobulin A antibodies which act directly against the interfi brillar substance of the smooth muscle (endomysium).
FDA: Food and Drug Administration (USA).
Formal Education: that which is based on regulated or structured programs
Glucagon: contra-insular hormone with a hyperglycaemic effect.
Glucose real time reading systems: Data generated from an initial latency period and the fi rst calibration. It includes alarm systems in case of hypoglycaemia and hyperglycaemia, and some models have predictive alarms. The “real time” information is used by the patient (previously trained) interactively. This information is downloaded by the patient himself; these devices are designed to be used by the patient.
Glucose retrospective reading systems (Holter): Glucose data are downloaded to the end of the record using all the calibration points for its adjustment; they are placed by physicians/nurses, are blind to the patient and the data is downloaded afterwards so that the appropriate changes can be decided on.
296 SNS CLINICAL PRACTICE GUIDELINES
Glycated haemoglobin (also glycosylated haemoglobin) refl ects the percentage of glucose binding to haemoglobin. Higher blood glucose levels are associated with higher glycated haemoglobin levels. Taking into account the average life of the erythrocyte, this measurement refl ects the elevation of blood glucose over a period of approximately 3 months.
Heterogeneity: See ‘Homogeneity’.
HLA (human leukocyte antigen region): group of localised genes in the major histocompatibility complex on chromosome 6p21.
Homogeneity: means ‘similarity’. Some studies are considered homogeneous if the results do not vary among themselves more than what can be expected by chance. The opposite of homogeneity is heterogeneity.
Intensive therapy: elements that are part of intensive therapy in DM1:
1. Multiple doses of insulin.
2. Careful balance between food intake, physical activity and insulin doses.
3. Daily monitoring of blood glucose.
4. Self-adjustment plan in the treatment (diet, exercise, insulin).
5. Defi ne optimum glucose levels for each patient.
6. Frequent visits to the monitoring team.
7. Patient and health care team education and motivation.
8. Psychological support.
9. Quarterly assessment of HbA1c
levels.
Ketonemia: presence of ketones in the blood.
Ketonuria: presence of urine ketones (acetone, beta-hydroxybutyric acid and acetoacetic acid).
LNG-IUD: levonorgestrel-releasing intrauterine device for birth control used by producing endometrial atrophy, also acting on the cervical mucus and the ovary, preventing fertilization and the progressive decrease of bleeding.
Medline: Predominantly clinical database produced by the US National Library of Medicine.
Meta-analysis: A statistical technique used to integrate the results of different studies (studies of diagnostic tests, clinical trials, cohort studies, etc.) in a single endpoint, giving more importance to the results obtained in larger studies.
MODY diabetes (Maturity-onset diabetes of the young) adult diabetes that appears early in life and which nowadays tends to be included in the group of monogenic diabetes.
NICE: Part of the NHS (National Health Service, UK). Its role is to provide physicians, patients and the general public with the best evidence available, primarily in the form of clinical guidelines.
Non-mydriatic camera: a camera that can take pictures of the retina and generally of the fundus of the eye without inducing mydriasis.
Odds Ratio (OR): Is a measure of the effectiveness of a treatment. If equal to 1, the effect of the treatment does not differ from that of the control effect. If the OR is greater (or smaller) than 1, the treatment effect is higher (or lower) than the control effect. It must be noted that the effect being measured may be adverse (e.g., death, disability) or desirable (e.g. quit smoking).
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 297
Ophthalmoscope: An optical instrument with a special lighting system used to observe the position of the eye, particularly the retina and its components e. g. vessels, parenchyma and optic nerve.
Ophthalmoscopy or fundus of the eye check-up: is the process of exploration of the retina. It can be done by direct or indirect ophthalmoscopy or with different lenses such as the Goldaman lenses, Bayadi lens, Hurbi lens, among others.
Prefi lled syringes or prefi lled pens: insulin injection systems with a capacity of 300 IU, p en-shaped and which includes the possibility of fractionated dosing and scale variations of 1 or 2 IU.
Randomized clinical trial: a study design in which people are randomly assigned to two groups: one (the experimental group) receives the treatment that is being tested and the other (comparison or control group) receives the standard treatment (or sometimes placebo). The two groups are monitored to observe any difference in the results. This is how the effi cacy of a treatment is assessed.
Refractory arterial hypertension: lack of adequate control of blood pressure despite using a treatment with three drugs at maximum doses.
Relative Risk (RR): The ratio between the event rate in the treatment group and the control group. Its value follows the same interpretation as the OR.
SIGN: Scottish multidisciplinary agency that develops clinical practice guidelines based on evidence and on methodological documents about their design.
Sliding scales or phased demand: Managing fast acting insulin before meals or every 4-6 hours depending on the blood glucose levels.
Specifi city: the proportion (or percentage) of really healthy people who obtain a negative result in the test. That is, the proportion of true negatives.
Spontaneous Remission: period that may appear after the diagnosis of DM1 that leads to a reduction in the need for exogenous insulin at doses lower than 0.3 IU/kg/day with improved metabolic control in HbA
1c levels at 6% or less (36 mmol/mol).
Starch: food reserve polysaccharide predominant in plants, consisting of amylose and amylopectin.
Structured or regulated educational program: one that provides knowledge and skills through a planned and progressive program, which includes coherent objectives, is fl exible in content, covers the individual clinical and psychological needs, and is adaptable to the cultural context.
Sucrose: (table sugar) disaccharide of glucose and fructose.
Survival Education: initial acquisition of the basic knowledge and skills by the person with diabetes that make him/her able to cope with the diseases, by applying the care and treatment effectively.
Systematic review (SR): A review, in which the evidence on an issue has been systematically identifi ed, evaluated and summarized according to predetermined criteria. It can include the meta-analysis or not.
298 SNS CLINICAL PRACTICE GUIDELINES
Appendix 13. Abbreviations
21-OH: 21-hydroxylase Ac. Anti-Tg: thyroglobulin antibodies Ac. Anti-TPO: thyroid peroxidase antibodies Anti-ZnT8: zinc antibodies antiporter ACA: adrenocortical antibodies ACE: angiotensin converting enzyme inhibitorsADA: American Diabetes Association AMI: AMI Anti-IA2: anti tyrosine phosphatase antibodies BMI: body mass index CD: celiac disease CGM: Continuous Glucose Monitoring CH: carbohydrates CIBERDEM: Biomedical Research Centre in Diabetes and Associated Metabolic Disorders CPG: Clinical Practice Guidelines CPR: Clinical prediction rule CRF: Chronic renal failure CSII: Continuous subcutaneous insulin infusion CV: cardiovascular DCCT: Diabetes Control and Complication Trial DESIGN: erectile dysfunction 1. Diabetes mellitus Type 1 2. Diabetes mellitus Type 2 DM: diabetes mellitus DN: diabetic neuropathy DR: Diabetic Retinopathy DTSQ: Diabetes Treatment Satisfaction Questionnaire DVC: Vacuum devices EAG: Estimated average glucose EMA: endomysial antibodiesEMEA: European Medicines Agency GADA: glutamic acid decarboxylase antibodies GCK: glucokinase GEG: Group to create the Clinical Practice Guideline GF: glomerular fi ltration GIK: glucose, insulin and potassium infusionHbAIC: Glycosylated haemoglobin IAA: insulin antibodiesICA: islet cell antibodies ICI: intracavernous injection
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 299
ICU: intensive care unit IFCC: International Federation of Clinical Chemistry and Laboratory Medicine IgA: Immunoglobulin A IIC: intracavernous injection IIEF: International Index of Erectile Function IM: intramuscular ISPAD: International Society of Paediatric and Adolescent Diabetes IUDs: intrauterine device IV: intravenous JAS/JSCC: Japanese Diabetes Society/Japanese Society for Clinical Chemistry JDRF: Juvenile Diabetes Research Foundation LDL: low-density lipoprotein LMP: lidocaine plaster MA: meta-analysis MDI: multiple doses of insulin MODY: Maturity Onset Diabetes of the Young NEFA: non-esterifi ed fatty acidsNGSP: National Glycohemoglobin Standardization Program NICE: National Institute for Clinical Excellence (UK) NNH: number of patients needed to be treated for one patient to suffer an adverse
event. NNT: number of cases to try to get a unit of effectiveness PCP: preconception care program PDE5: phosphodiesterase QALY: years of quality-adjusted life RCT: randomized SBP: Systolic blood pressure SC: subcutaneous SD: standard deviation SEP: Sexual Encounter Profi le SFQ: sexual function questionnaire SR: spontaneous remission SR: systematic review SSRIs: selective serotonin reuptake inhibitorsUAEN: specialized care units nephrology WBQ: Well-Being Questionnaire WMD: weighted mean difference

Appendix 14. Declaration of interest
They following people have declared no confl icts of interest:
David Cantero Gonzalez, Ignacio Conget Donlo, Lorea Cañibano Garcia, Ricardo V. Garcia-Mayor, John Adrian Girbés Borrás, Alberto Goday Arno, Itziar Güemes Careaga, Virginia Guillen Cañas, M. Iruretagoiena Luisa Sánchez, Paloma Jimenez Huertas, Pedro Mª García Latorre, Argumedo Marta Lopez, Eduardo Millán Ortuondo, Ana M.ª Pedrueza Ortiz, M. Dolores González Ramírez, Mercedes Rigual Rodriguez, Jose Ramon Santos Martinez Rueda, Joseba Soloeta Eraso, Jorge Taboada Gomez, Gemma Villanueva Hernandez.
Manuel Aguilar Diosdado has received funding support from Almirall for meetings and con-ferences or when attending courses and fees as a speaker.
M ª Ángeles Anton Miguel has received funding support from Novo Nordisk, Sanofi Aventis, Pfi zer, Almirall and GSK for meetings and conferences, when attending courses or fees as a speaker.
Beatriz Santiago Corcóstegui has received funding support from Sanofi Aventis, Esteve, Abbott, Wyeth and Bristol for conferences or meetings and attending courses.
Alicia Galarza Cortazar has received funding support from Lilly, Novo-Nordisk and Almirall for meetings and conferences or attending courses and Glaxo and MSD for fees as a speaker.
Peace Gallego Saiz has received funding support from the Foundation Beta, Bayer, Braun, Roche, Abbott, Pfi zer and Sanofi Aventis for conferences or meetings and attending courses.
Gaztambide Sonia Saenz has received funding support from Lilly, Ipsen Pharma, Novartis, NovoNordisk, BMS and Sanofi Aventis for meetings and conferences or attending courses and Novartis, Lilly and Otsuka for fees as a speaker.
Antonio Hernández Mijares has received funding support from Novo Nordisk, Lilly, Sanofi Aventis, for meetings and conferences or attending courses and Novonordisk, Lilly, Pfi zer, Abbott, Sanofi Aventis for fees as a speaker.
Briñas Oscar Lopez Ortega has received funding support from Abbott for conferences or meetings and attending courses.
Edelmiro Menendez Torre has received funding support from Sanofi Aventis for meetings and conferences or attending courses and Novo Nordisk for fees as a speaker.
Itxaso Rica Echevarría has received funding support from Novo Nordisk, Lilly, Pfi zer, Senofi , Aventis and Serono as funding for conferences or meetings and attending courses.
Jose Antonio Vazquez Garcia has received funding support from Lilly, Pfi zer and GSK for meetings and conferences or attending courses, from MSD to fi nance courses and participate in research and consultancy work for Pfi zer.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 301
Clotilde Martinez Vazquez has received funding support from Lilly for meetings and con-ferences or attending courses and from Sanofi Aventis for fees as a speaker, from MAPFRE for funding educational programs or courses and has been hired by Nestlé as dietician.
Federico Vazquez San Miguel has received funding support from Novo Nordisk, MSD, Lilly, GSK, Sanofi Aventis and Novartis for meetings and conferences or attending courses, from Novo Nordisk, MSD, Lilly, GSK, Sanofi Aventis for fees as a speaker and from Novo Nordisk, MSD, Lilly, GSK, Sanofi Aventis, Roche and Medtronic for educational programs.
Yoldi Alfredo Arrieta has received funding support from Novo Nordisk and Novartis for meetings and conferences or attending courses and from Novo and Sanofi Aventis in with the concept of fees as a speaker.
302 SNS CLINICAL PRACTICE GUIDELINES
Bibliography
1. Scottish Intercollegiate Guidelines Network. A guideline developers’ handbook. Edinburgh: Scottish Intercollegiate Guidelines Network 2008;Sign 50.
2. Instituto Aragonés de Ciencias de la Salud-I+CS. Grupo de trabajo sobre GPC. Elaboración de Guías de Práctica Clínica en el Sistema Nacional de Salud. Manual Metodológico. Madrid: Plan Nacional para el SNS del MSC. Guías de Práctica Clínica en el SNS: I+CS Nº 2006/01 2007.
3. National Institute for Health and Clinical Excellence (January 2009). The guidelines manu-al. London: national Institute for Health and Clinical Excellence. Available from: www.nice.org.uk
4. Soriguer F, Goday A, Bosch-Comas A, Bordiú E, Calle A, Carmena R, et al. Prevalence of diabetes mellitus and impaired glucose regulation in Spain. Diabetes Study Diabetología (Journal of the European Association for the Study of Diabetes) (EASD) en prensa 2010.
5. Estrategia en diabetes del Sistema Nacional de Salud. Ministerio de Sanidad y Consumo. Agencia Española del Medicamento y Productos Sanitarios Madrid 2007.
6. Etxeberria A, Rotaeche R, Lekue I, Callén B, Merino M, Villar Mea. Descripción de la metodología de elaboración-adaptación-actualización empleada en la guía de práctica clínica sobre asma de la CAPV. Proyecto de Investigación Comisionada Vitoria-Gasteiz Departamento de Sanidad Gobierno Vasco 2005 Informe nº: Osteba D-05-03 2005.
7. National Institute for Health and Clinical Excellence. Diagnosis and management of type 1 diabetes in children, young people and adults. Clinical Guideline 15 2004 Jul.
8. ADAPTE.Manual for Guideline Adaptation. Version 1. 0. ADAPTE Collaboration 2007.
9. NICE. Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus. NICE technology appraisal guidance 151. Review of technology appraisal guidance 57 2008.
10. The AGREE Collaboration. Appraisal of Guidelines for Research & Evaluation (AGREE). www agreecollaboration org 2001 Sep.
11. Scottish Intercollegiate Guidelines Network. Management of diabetes. A national clinical guideline. SIGN Publication 2001;Nº 55.
12. Oxford. Levels of Evidence and Grades of Recommendation. Oxford Centre for Evidencebased Medicine [sitio web] 2001.
13. Schmidt KD, Valeri C, Leslie RD. Autoantibodies in Type 1 diabetes. Clin Chim Acta 2005 Apr;354(1-2):35-40.
14. Leslie D, Lipsky P, Notkins AL. Autoantibodies as predictors of disease. J Clin Invest 2001 Nov;108(10):1417-22.
15. World Health Organization. Defi nition, diagnosis and classifi cation of diabetes mellitus and its complications. Report of a WHO consultation. Part I: Diagnosis and classifi cation of dia-betes mellitus. Geneva WHO 1999.
16. International Society for Pediatric and Adolescent Diabetes (ISPAD). Consensus guidelines 2000. ISPAD consensus guidelines for the management of type 1 diabetes mellitus in chil-dren and adolescents. Zeist: Medical Forum International 2000.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 303
17. Bingley PJ. Clinical applications of Diabetes antibody testing. J Clin Endocrinol Metab 2010;95:25-33.
18. Turner R, Stratton I, Horton V, Manley S, Zimmet P, Mackay IR, et al. UKPDS 25: autoan-tibodies to islet-cell cytoplasm and glutamic acid decarboxylase for prediction of insulin requirement in type 2 diabetes. UK Prospective Diabetes Study Group. Lancet 1997 Nov 1;350(9087):1288-93.
19. Bober E, Dundar B, Buyukgebiz A. Partial remission phase and metabolic control in type 1 diabetes mellitus in children and adolescents. J Pediatr Endocrinol Metab 2001;14:435-41.
20. Heinze E, Thon A. Honeymoon period in insulin-dependent diabetes mellitus. Pediatrician 1985;12:208-12.
21. Muhammad BJ, Swift PG, Raymond NT, Botha JL. Partial remission phase of diabetes in children younger than age 10 years. Arch Dis Child 1999 Apr;80(4):367-9.
22. Bonfati R, Bazzigaluppi E, Calori G, Riva MC, Viscardi M, Bognetti E, et al. Parameters associated with residual insulin secretion during the fi rst year of disease in children and ado-lescents with Type 1 diabetes mellitus. Diabet Med 1998;15:844-50.
23. Lombardo F, Valenzise M, WasniewsCAD M, Messina MF, Ruggeri C, Arrigo T, et al. Two year prospective evaluation of the factors affecting honeymoon frequency and duration in children with insulin dependent diabetes mellitus: The key-role of at diagnosis. Diabetes Nutr Metab 2002;15:246-51.
24. Bonfanti R, Bazzigaluppi E, Calori G, Riva MC, Viscardi M, Bognetti E, et al. Parameters associated with residual insulin secretion during the fi rst year of disease in children and ado-lescents with Type 1 diabetes mellitus. Diabet Med 1998 Oct;15(10):844-50.
25. Knip M, PuukCAD R, CADar ML, Akerblom HK. Remission phase, endogenous insulin secretion and metabolic control in diabetic children. Acta Diabetol Lat 1982;19:243-51.
26. Standards of medical care in diabetes—2010. Diabetes Care 2010 Jan;33 Suppl 1:S11-S61.
27. Weedon MN, Frayling TM. Insights on pathogenesis of type 2 diabetes from MODY genet-ics. Curr Diab Rep 2007;7(2):131-8.
28. Raeder H, Johansson S, Holm PI, Haldorsen IS, Mas E, Sbarra V, et al. Mutations in the CEL VNTR cause a syndrome of diabetes and pancreatic exocrine dysfunction. Nature Genetics 2006 Jan;54-62.
29. Estalella I, Rica I, Perez DN, Bilabo JR, Vazquez JA, San Pedro JI, et al. Mutations in GCK and HNF-1alpha explain the majority of cases with clinical diagnosis of MODY in Spain. Clin Endocrinol 2007;67(4):538-46.
30. Costa A, Bescos M, Velho G, Chevre J, Vidal J, Sesmilo G, et al. Genetic and clinical char-acterisation of maturity-onset diabetes of the young in Spanish families. Eur J Endocrinol 2000;142(4):380-6.
31. Barrio R, Bellanne-Chantelot C, Moreno JC, Morel V, Calle H, Alonso M, et al. Nine novel mutations in maturity-onset diabetes of the young (MODY) candidate genes in 22 Spanish families. J Clin Endocrinol Metab 2002;87(6):2532-9.
32. Ellard S, Bellanné-Chantelot C, Hattersley AT. European Molecular Genetics Quality Network (EMQN) MODY group. Best practice guidelines for the molecular genetic diagno-sis of maturity-onset diabetes of the young. Diabetol 2008;51:546-53.
33. Barker JM. Clinical review: Type 1 diabetes-associated autoimmunity: natural history, ge-netic associations, and screening. J Clin Endocrinol Metab 2006 Apr;91(4):1210-7.
304 SNS CLINICAL PRACTICE GUIDELINES
34. Kordonouri O, Maguire AM, Knip M, Schober E, Lorini R, Holl RW, et al. ISPAD Clinical Practice Consensus Guidelines 2006-2007. Other complications and associated conditions. Pediatr Diabetes 2007;8:171-6.
35. De Graaff LCG, Smit JWA, Radder JK. Prevalence and clinical signifi cance of organ-specif-ic autoantibodies in type 1 diabetes mellitus. Net J Med 2007;65(7):235-47.
36. Fröhlich-Reiterer EE, Hofer S, Kaspers S, Herbst A, Kordonouri O, Schwarz H-P, et al. Screening frequency for celiac disease and autoimmune thyroiditis in children and adoles-cents with type 1 diabetes mellitus-data from a German/Austrian multicentre survey. Pediatr Diabetes 2008;9:546-53.
37. Nóvoa Y, López-Capapé M, Lara E, Alonso M, camarero C, Barrio R. Impacto del diag-nóstico de la enfermedad celíaca en el control metabólico de la diabetes tipo 1. An Pediatr (Barc) 2008;68(1):13-7.
38. Poulain C, Johanet C, Delcroix C, Lévy-Marchal C, Tubiana-Rufi N. Prevalence and clinical features of celiac disease in 950 children with type 1 diabetes in France. Diabetes Metab 33 2007;453-8.
39. Larsson K, Carlsson A, Cederwall E, Jönsson B, Neiderud J, Jonsson B, et al. Annual screen-ing detects celiac disease in children with type 1 diabetes. Pediatr Diabetes 2008;9(Part II):354-9.
40. ISPAD Clinical Practice Consensus Guidelines 2009 Compendium. Pediatric Diabetes 2009;10(Suppl. 12): 1-2 doi: 10.1111/j.1399-5448.2009.00577.x © 2009 John Wiley & Sons A/S.
41. Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al. Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: a systematic review. Health Technol Assess 2001;5:1-79.
42. De Weerdt I, Visser AP, Kok GJ, et al. Randomized controlled multicentre evaluation of an education programme fi r insulin-treated diabetic patients: effects on metabolic control, qual-ity of life and costs of therapy. Diabet Med 1991;8:338-45.
43. Lennon GM, Taylor KG, Debney I, Bailey CJ. Knowledge, attitudes, technical competences, and blood glucose control of Type 1diabetic patients during and after an educational pro-gramme. Diabet Med 1990;7:825-32.
44. Couch R, Jetha M, Dryden DM, Hooton N, Liang Y, Durect T, et al. Diabetes Education for Children with Type 1 Diabetes Mellitus and Their Families. Evidence Report/Technology Assessment No.166.(Prepared by the University of Alberta/Capital Health Evidence-based Practice Center under Contract No.290-02-0023) AHRQ Publication No.08-E011. Rockville,MD:Agency for Healthcare Research and Quality 2008.
45. Zhang X, Norris SL, Chowdhury FM, et al. The Effects of Interventions on Health-Related Quality of Life Among Persons With Diabetes A Systematic Review. Med Care 2007;45: 820-34.
46. Murphy HR, Wadham C, Rayman G, Skinner TC. Approaches to integrating paediatric diabetes care and structured education: experiences from the Families, Adolescents, and Children’s Teamwork Study (FACTS). Diabet Med 2007;24:1261-8.
47. Hermanns N, Kulzer B, Kubiak T, Krichbaum M, Haak T. The effect of an education pro-gramme (HyPOS) to treat hypoglycaemia problems in patients with type 1 diabetes. Diabetes Metab Res Rev 2007;23:528-38.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 305
48. Training in fl exible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised controlled trial. BMJ 2002 Oct 5;325(7367):746-51.
49. Swift PGF. ISPAD Clinical Practice Consensus Guidelines 2006-2007. Diabetes Educ 2007;8:103-9.
50. Court JM, Cameron FJ, Berg-Kelly K, Swift PGF. ISPAD Clinical Practice Consensus Guidelines 2006-2007.Diabetes in adolescence. Pediatr Diabetes 2008;9(PartI):255-62.
51. American Diabetes Association (ADA). Standards of Medical Care in Diabetes. Diabetes Care 2008;31(S1).
52. Funell MM, Brown TL, Childs BP, Hass LB, Hosey GM, Jensen B, et al. National Standards for Diabetes Self-Management Education. Diabetes Care 2008;31(Sup 1).
53. Checklist for therapeutic patient education. DESG Teaching Letter Number 11 2009.
54. Patient Education. DESG Teaching Letter Number 7 2009.
55. Bailey BJ, Kahn A. Apportioning illness management authority: how diabetic individu-als evaluate The DAWN (Diabetes Attitudes, Wishes and Needs) Study. Pract Diab Int 2002;19:22a-4a.
56. Hanson CL, Henggeler SW, Burghen GA. Social competence and parental support as media-tors of the link between stress and metabolic control in adolescents with insulin-dependent diabetes mellitus. J Consulting Clin Psychol 1987;55:529-33.
57. Schafer LC, McCaul KD, Glasgow RE. Supportive and nonsupportive family behaviours: relationships to adherence and metabolic control in persons with type I diabetes. Diabetes Care 1986;9:179-85.
58. Norris SL, Nichols PJ, Caspersen CJ, et al. The Task Force on Community Preventive Services. Am J Prev Med 2002;22(4S):39.
59. Karaguzel G, Bircan I, Erisir S, Bundak R. Metabolic control and educational status in chil-dren with type 1 diabetes: effects of a summer camp and intensive insulin treatment. Acta Diabetologica 2005 Dec;42(4):156-61.
60. Gunasekera H, Ambler G. Safety and effi cacy of blood glucose management practices at a diabetes camp. Journal of Paediatrics & Child Health 42(10):643-8, 2006 Oct.
61. Garcia-Perez L, Perestelo-Perez L, Serrano-Aguilar P, Del MT-M. Effectiveness of a psy-choeducative intervention in a summer camp for children with type 1 diabetes mellitus. Diabetes Educator 2010 Mar;36(2):310-7.
62. Wang YC, Stewart S, Tuli E, White P. Improved glycemic control in adolescents with type 1 diabetes mellitus who attend diabetes camp. Pediatric Diabetes 2008 Feb;9(1):29-34.
63. Santiprabhob J, Likitmaskul S, Kiattisakthavee P, Weerakulwattana P, Chaichanwattanakul K, Nakavachara P, et al. Glycemic control and the psychosocial benefi ts gained by patients with type 1 diabetes mellitus attending the diabetes camp. Patient Education & Counseling 2008 Oct;73(1):60-6.
64. Franz MJ, Powers MA, Leontos C, Holzmeister LA, Kulkarni K, Monk A, et al. The evi-dence for medical nutrition therapy for type 1 and type 2 diabetes in adults. J Am Diet Assoc 2010 Dec;110(12):1852-89.
65. Boden G, Sargrad K, Homko C, Mozzoli M, Stein TP. Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. Ann Intern Med 2005 Mar 15;142(6):403-11.
306 SNS CLINICAL PRACTICE GUIDELINES
66. Nielsen JV, Jonsson E, Ivarsson A. A low carbohydrate diet in type 1 diabetes: clinical expe-riencea brief report. Ups J Med Sci 2005;110(3):267-73.
67. Wolever TM, Hamad S, Chiasson JL, Josse RG, Leiter LA, Rodger NW, et al. Day-to-day consistency in amount and source of carbohydrate intake associated with improved blood glucose control in type 1 diabetes. J Am Coll Nutr 1999 Jun;18(3):242-7.
68. DCCT. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. New England Journal of Medicine 1993 Sep 30;329(14):977-86.
69. Lowe J, Linjawi S, Mensch M, James K, Attia J. Flexible eating and fl exible insulin dosing in patients with diabetes: Results of an intensive self-management course. Diabetes Res Clin Pract 2008 Jun;80(3):439-43.
70. Garg A, Bantle JP, Henry RR, Coulston AM, Griver KA, Raatz SK, et al. Effects of varying carbohydrate content of diet in patients with non-insulin-dependent diabetes mellitus. JAMA 1994 May 11;271(18):1421-8.
71. Gerhard GT, Ahmann A, Meeuws K, McMurry MP, Duell PB, Connor WE. Effects of a low-fat diet compared with those of a high-monounsaturated fat diet on body weight, plas-ma lipids and lipoproteins, and glycemic control in type 2 diabetes. Am J Clin Nutr 2004 Sep;80(3):668-73.
72. Komiyama N, Kaneko T, Sato A, Sato W, Asami K, Onaya T, et al. The effect of high carbo-hydrate diet on glucose tolerance in patients with type 2 diabetes mellitus. Diabetes Res Clin Pract 2002 Sep;57(3):163-70.
73. Xu J, Eilat-Adar S, Loria CM, Howard BV, Fabsitz RR, Begum M, et al. Macronutrient in-take and glycemic control in a population-based sample of American Indians with diabetes: the Strong Heart Study. Am J Clin Nutr 2007 Aug;86(2):480-7.
74. Delahanty LM, Nathan DM, Lachin JM, Hu FB, Cleary PA, Ziegler GK, et al. Association of diet with glycated haemoglobin during intensive treatment of type 1 diabetes in the Diabetes Control and Complications Trial. Am J Clin Nutr 2009 Feb;89(2):518-24.
75. Chantelau EA, Gosseringer G, Sonnenberg GE, Berger M. Moderate intake of sucrose does not impair metabolic control in pump-treated diabetic out-patients. Diabetologia 1985 Apr;28(4):204-7.
76. Peterson DB, Lambert J, Gerring S, Darling P, Carter RD, Jelfs R, et al. Sucrose in the diet of diabetic patients—just another carbohydrate? Diabetologia 1986 Apr;29(4):216-20.
77. Bantle JP, Laine DC, Thomas JW. Metabolic effects of dietary fructose and sucrose in types I and II diabetic subjects. JAMA 1986 Dec 19;256(23):3241-6.
78. Buysschaert M, Sory R, Mpoy M, Lambert AE. Effect of the addition of simple sugars to mixed meals on the glycemic control of insulin treated diabetic patients. Diabete Metab 1987 Nov;13(6):625-9.
79. Cooper PL, Wahlqvist ML, Simpson RW. Sucrose versus saccharin as an added sweetener in non-insulin-dependent diabetes: short- and medium-term metabolic effects. Diabet Med 1988 Oct;5(7):676-80.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 307
80. Santacroce G, Forlani G, Giangiulio S, Galuppi V, Pagani M, Vannini P. Long-term effects of eating sucrose on metabolic control of type 1 (insulin-dependent) diabetic outpatients. Acta Diabetol Lat 1990 Oct;27(4):365-70.
81. Loghmani E, Rickard K, Washburne L, Vandagriff J, Fineberg N, Golden M. Glycemic re-sponse to sucrose-containing mixed meals in diets of children of with insulin-dependent diabetes mellitus. J Pediatr 1991 Oct;119(4):531-7.
82. Bantle JP, Swanson JE, Thomas W, Laine DC. Metabolic effects of dietary sucrose in type II diabetic subjects. Diabetes Care 1993 Sep;16(9):1301-5.
83. Schwingshandl J, Rippel S, Unterluggauer M, Borkenstein M. Effect of the introduction of dietary sucrose on metabolic control in children and adolescents with type I diabetes. Acta Diabetol 1994 Dec;31(4):205-9.
84. Malerbi DA, Paiva ES, Duarte AL, Wajchenberg BL. Metabolic effects of dietary sucrose and fructose in type II diabetic subjects. Diabetes Care 1996 Nov;19(11):1249-56.
85. Nadeau J, Koski KG, Strychar I, Yale JF. Teaching subjects with type 2 diabetes how to in-corporate sugar choices into their daily meal plan promotes dietary compliance and does not deteriorate metabolic profi le. Diabetes Care 2001 Feb;24(2):222-7.
86. Coulston AM, Hollenbeck CB, Donner CC, Williams R, Chiou YA, Reaven GM. Metabolic effects of added dietary sucrose in individuals with noninsulin-dependent diabetes mellitus (NIDDM). Metabolism 1985 Oct;34(10):962-6.
87. Maran A, Crazzolara D, Nicoletti M, Costa S, Dal Pos M, Tiengo A, et al. A randomized crosso-ver study to compare continuous subcutaneous insulin infusion (CSII) with multiple daily injec-tion (MDI) in type 1 diabetic patients previously treated with CSII. Diabetologia 2005;48:A328.
88. Mezitis NH, Maggio CA, Koch P, Quddoos A, Allison DB, Pi-Sunyer FX. Glycemic effect of a single high oral dose of the novel sweetener sucralose in patients with diabetes. Diabetes Care 1996 Sep;19(9):1004-5.
89. Grotz VL, Henry RR, McGill JB, Prince MJ, Shamoon H, Trout JR, et al. Lack of effect of sucralose on glucose homeostasis in subjects with type 2 diabetes. J Am Diet Assoc 2003 Dec;103(12):1607-12.
90. Reyna NY, Cano C, Bermudez VJ, Medina MT, Souki AJ, Ambard M, et al. Sweeteners and beta-glucans improve metabolic and anthropometrics variables in well controlled type 2 diabetic patients. Am J Ther 2003 Nov;10(6):438-43.
91. Mackenzie T, Brooks B, O’Connor G. Beverage intake, diabetes, and glucose control of adults in America. Ann Epidemiol 2006 Sep;16(9):688-91.
92. Barriocanal LA, Palacios M, Benitez G, Benitez S, Jimenez JT, Jimenez N, et al. Apparent lack of pharmacological effect of steviol glycosides used as sweeteners in humans. A pilot study of repeated exposures in some normotensive and hypotensive individuals and in Type 1 and Type 2 diabetics. Regul Toxicol Pharmacol 2008 Jun;51(1):37-41.
93. Maki KC, Curry LL, Reeves MS, Toth PD, McKenney JM, Farmer MV, et al. Chronic con-sumption of rebaudioside A, a steviol glycoside, in men and women with type 2 diabetes mellitus. Food Chem Toxicol 2008 Jul;46 Suppl 7:S47-S53.
94. Murillo S. CIBER de Diabetes y Enfermedades Metabólicas Asociadas. Hospital Clinic de Barcelona 2008.
308 SNS CLINICAL PRACTICE GUIDELINES
95. Bantle JP. Dietary fructose and metabolic syndrome and diabetes. J Nutr 2009 Jun;139(6):1263S8S.
96. Hallfrisch J, Reiser S, Prather ES. Blood lipid distribution of hyperinsulinemic men consum-ing three levels of fructose. Am J Clin Nutr 1983 May;37(5):740-8.
97. Reiser S, Powell AS, Scholfi eld DJ, Panda P, Ellwood KC, Canary JJ. Blood lipids, lipo-proteins, apoproteins, and uric acid in men fed diets containing fructose or high-amylose cornstarch. Am J Clin Nutr 1989 May;49(5):832-9.
98. Wolever TM, Jenkins DJ, Jenkins AL, Josse RG. The glycemic index: methodology and clinical implications. Am J Clin Nutr 1991 Nov;54(5):846-54.
99. Fontvieille AM, Rizkalla SW, Penfornis A, Acosta M, Bornet FR, Slama G. The use of low glycaemic index foods improves metabolic control of diabetic patients over fi ve weeks. Diabet Med 1992 Jun;9(5):444-50.
100. Wolever TM, Nguyen PM, Chiasson JL, Hunt JA, Josse RG, Palmason C, et al. Determinants of diet glycemic index calculated retrospectively from diet records of 342 individuals with non-insulin-dependent diabetes mellitus. Am J Clin Nutr 1994 Jun;59(6):1265-9.
101. Gilbertson HR, Brand-Miller JC, Thorburn AW, Evans S, Chondros P, Werther GA. The effect of fl exible low glycemic index dietary advice versus measured carbohydrate exchange diets on glycemic control in children with type 1 diabetes. Diabetes Care 2001 Jul;24(7):1137-43.
102. Gilbertson HR, Thorburn AW, Brand-Miller JC, Chondros P, Werther GA. Effect of low-glycemic-index dietary advice on dietary quality and food choice in children with type 1 diabetes. Am J Clin Nutr 2003 Jan;77(1):83-90.
103. Buyken AE, Toeller M, Heitkamp G, Karamanos B, Rottiers R, Muggeo M, et al. Glycemic index in the diet of European outpatients with type 1 diabetes: relations to glycated hemo-globin and serum lipids. Am J Clin Nutr 2001 Mar;73(3):574-81.
104. Brand-Miller J, Hayne S, Petocz P, Colagiuri S. Low-glycemic index diets in the man-agement of diabetes: a meta-analysis of randomized controlled trials. Diabetes Care 2003 Aug;26(8):2261-7.
105. Burani J, Longo PJ. Low-glycemic index carbohydrates: an effective behavioral change for glycemic control and weight management in patients with type 1 and 2 diabetes. Diabetes Educ 2006 Jan;32(1):78-88.
106. Thomas D, Elliott EJ. Low glycaemic index, or low glycaemic load, diets for diabetes mel-litus. Cochrane Database Syst Rev 2009;(1):CD006296.
107. Nansel TR, Gellar L, McGill A. Effect of varying glycemic index meals on blood glucose control assessed with continuous glucose monitoring in youth with type 1 diabetes on basal-bolus insulin regimens. Diabetes Care 2008 Apr;31(4):695-7.
108. Rovner AJ, Nansel TR, Gellar L. The effect of a low-glycemic diet vs a standard diet on blood glucose levels and macronutrient intake in children with type 1 diabetes. J Am Diet Assoc 2009 Feb;109(2):303-7.
109. Chandalia M, Garg A, Lutjohann D, von BK, Grundy SM, Brinkley LJ. Benefi cial effects of high dietary fi ber intake in patients with type 2 diabetes mellitus. N Engl J Med 2000 May 11;342(19):1392-8.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 309
110. Hagander B, Asp NG, Efendic S, Nilsson-Ehle P, Schersten B. Dietary fi ber decreases fast-ing blood glucose levels and plasma LDL concentration in noninsulin-dependent diabetes mellitus patients. Am J Clin Nutr 1988 May;47(5):852-8.
111. Giacco R, Parillo M, Rivellese AA, Lasorella G, Giacco A, D’Episcopo L, et al. Long-term dietary treatment with increased amounts of fi ber-rich low-glycemic index natural foods improves blood glucose control and reduces the number of hypoglycemic events in type 1 diabetic patients. Diabetes Care 2000 Oct;23(10):1461-6.
112. Kinmonth AL, Angus RM, Jenkins PA, Smith MA, Baum JD. Whole foods and increased dietary fi bre improve blood glucose control in diabetic children. Arch Dis Child 1982 Mar;57(3):187-94.
113. Del TE, Lintas C, Clementi A, Marcelli M. Soluble and insoluble dietary fi bre in diabetic diets. Eur J Clin Nutr 1988 Apr;42(4):313-9.
114. Riccardi G, Rivellese A, Pacioni D, Genovese S, Mastranzo P, Mancini M. Separate infl u-ence of dietary carbohydrate and fi bre on the metabolic control in diabetes. Diabetologia 1984 Feb;26(2):116-21.
115. Story L, Anderson JW, Chen WJ, Karounos D, Jefferson B. Adherence to high-carbohy-drate, high-fi ber diets: long-term studies of non-obese diabetic men. J Am Diet Assoc 1985 Sep;85(9):1105-10.
116. Lindsay AN, Hardy S, Jarrett L, Rallison ML. High-carbohydrate, high-fi ber diet in children with type I diabetes mellitus. Diabetes Care 1984 Jan;7(1):63-7.
117. McCulloch DK, Mitchell RD, Ambler J, Tattersall RB. A prospective comparison of ‘con-ventional’ and high carbohydrate/high fi bre/low fat diets in adults with established type 1 (insulindependent) diabetes. Diabetologia 1985 Apr;28(4):208-12.
118. Buyken AE, Toeller M, Heitkamp G, Vitelli F, Stehle P, Scherbaum WA, et al. Relation of fi bre intake to HbA
1c and the prevalence of severe ketoacidosis and severe hypoglycaemia.
EURODIAB IDDM Complications Study Group. Diabetologia 1998 Aug;41(8):882-90.
119. Shimakawa T, Warram JH, Herrera-Acena MG, Krolewski AS. Usual dietary intake and hemoglobin A1 level in patients with insulin-dependent diabetes. J Am Diet Assoc 1993 Dec;93(12):1409-12, 1415.
120. Van HL, McCoin M, Kris-Etherton PM, Burke F, Carson JA, Champagne CM, et al. The evidence for dietary prevention and treatment of cardiovascular disease. J Am Diet Assoc 2008 Feb;108(2):287-331.
121. Nordt TK, Besenthal I, Eggstein M, Jakober B. Infl uence of breakfasts with different nutri-ent contents on glucose, C peptide, insulin, glucagon, triglycerides, and GIP in non-insulin-dependent diabetics. Am J Clin Nutr 1991 Jan;53(1):155-60.
122. Gannon MC, Nuttall JA, Damberg G, Gupta V, Nuttall FQ. Effect of protein ingestion on the glucose appearance rate in people with type 2 diabetes. J Clin Endocrinol Metab 2001 Mar;86(3):1040-7.
123. Parker B, Noakes M, Luscombe N, Clifton P. Effect of a high-protein, high-monounsaturat-ed fat weight loss diet on glycemic control and lipid levels in type 2 diabetes. Diabetes Care 2002 Mar;25(3):425-30.
310 SNS CLINICAL PRACTICE GUIDELINES
124. Luscombe ND, Clifton PM, Noakes M, Parker B, Wittert G. Effects of energy-restricted di-ets containing increased protein on weight loss, resting energy expenditure, and the thermic effect of feeding in type 2 diabetes. Diabetes Care 2002 Apr;25(4):652-7.
125. Nuttall FQ, Gannon MC, Saeed A, Jordan K, Hoover H. The metabolic response of subjects with type 2 diabetes to a high-protein, weight-maintenance diet. J Clin Endocrinol Metab 2003 Aug;88(8):3577-83.
126. Gannon MC, Nuttall FQ, Saeed A, Jordan K, Hoover H. An increase in dietary protein im-proves the blood glucose response in persons with type 2 diabetes. Am J Clin Nutr 2003 Oct;78(4):734-41.
127. Brinkworth GD, Noakes M, Parker B, Foster P, Clifton PM. Long-term effects of advice to consume a high-protein, low-fat diet, rather than a conventional weight-loss diet, in obese adults with type 2 diabetes: one-year follow-up of a randomised trial. Diabetologia 2004 Oct;47(10):1677-86.
128. Robertson L, Waugh N, Robertson A. Protein restriction for diabetic renal disease. Cochrane Database Syst Rev 2007;(4):CD002181.
129. Pan Y, Guo LL, Jin HM. Low-protein diet for diabetic nephropathy: a meta-analysis of ran-domized controlled trials. Am J Clin Nutr 2008 Sep;88(3):660-6.
130. Raal FJ, Kalk WJ, Lawson M, Esser JD, Buys R, Fourie L, et al. Effect of moderate dietary protein restriction on the progression of overt diabetic nephropathy: a 6-mo prospective study. Am J Clin Nutr 1994 Oct;60(4):579-85.
131. Hansen HP, Christensen PK, Tauber-Lassen E, Klausen A, Jensen BR, Parving HH. Lowprotein diet and kidney function in insulin-dependent diabetic patients with diabetic nephropathy. Kidney Int 1999 Feb;55(2):621-8.
132. Dussol B, Iovanna C, Raccah D, Darmon P, Morange S, Vague P, et al. A randomized trial of low-protein diet in type 1 and in type 2 diabetes mellitus patients with incipient and overt nephropathy. J Ren Nutr 2005 Oct;15(4):398-406.
133. Meloni C, Morosetti M, Suraci C, Pennafi na MG, Tozzo C, Taccone-Gallucci M, et al. Severe dietary protein restriction in overt diabetic nephropathy: benefi ts or risks? J Ren Nutr 2002 Apr;12(2):96-101.
134. Hansen HP, Tauber-Lassen E, Jensen BR, Parving HH. Effect of dietary protein restriction on prognosis in patients with diabetic nephropathy. Kidney Int 2002 Jul;62(1):220-8.
135. Azadbakht L, Shakerhosseini R, Atabak S, Jamshidian M, Mehrabi Y, Esmaill-Zadeh A. Benefi ciary effect of dietary soy protein on lowering plasma levels of lipid and improving kidney function in type II diabetes with nephropathy. Eur J Clin Nutr 2003 Oct;57(10):1292-4.
136. Meloni C, Tatangelo P, Cipriani S, Rossi V, Suraci C, Tozzo C, et al. Adequate protein di-etary restriction in diabetic and nondiabetic patients with chronic renal failure. J Ren Nutr 2004 Oct;14(4):208-13.
137. Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005 Dec 22;353(25):2643-53.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 311
138. Mayer-Davis EJ, Levin S, Marshall JA. Heterogeneity in associations between macronutri-ent intake and lipoprotein profi le in individuals with type 2 diabetes. Diabetes Care 1999 Oct;22(10):1632-9.
139. Orchard TJ, Forrest KY, Kuller LH, Becker DJ. Lipid and blood pressure treatment goals for type 1 diabetes: 10-year incidence data from the Pittsburgh Epidemiology of Diabetes Complications Study. Diabetes Care 2001 Jun;24(6):1053-9.
140. Mukamal KJ, Nesto RW, Cohen MC, Muller JE, Maclure M, Sherwood JB, et al. Impact of diabetes on long-term survival after acute myocardial infarction: comparability of risk with prior myocardial infarction. Diabetes Care 2001 Aug;24(8):1422-7.
141. Faulkner MS, Chao WH, Kamath SK, Quinn L, Fritschi C, Maggiore JA, et al. Total homo-cysteine, diet, and lipid profi les in type 1 and type 2 diabetic and nondiabetic adolescents. J Cardiovasc Nurs 2006 Jan;21(1):47-55.
142. Buccino J, Murray K, Farmer S, Assor E, Daneman D. Systematic review of the dietary man-agement of children with type 1 diabetes. Canadian Journal of Diabetes 2004;28:219-25.
143. Goksen D, Darcan S, Buyukinan M, Kose T, Erermis S, Coker M. The effect of insulin glar-gine and nutritional model on metabolic control, quality of life and behavior in children and adolescents with type 1 diabetes mellitus. Acta Diabetol 2008 Mar;45(1):47-52.
144. Kalergis M, Pacaud D, Strychar I, Meltzer S, Jones PJ, Yale JF. Optimizing insulin delivery: assessment of three strategies in intensive diabetes management. Diabetes Obes Metab 2000 Oct;2(5):299-305.
145. Campaigne BN, Gilliam TB, Spencer ML, Lampman RM, Schork MA. Effects of a physical activity program on metabolic control and cardiovascular fi tness in children with insulin-dependent diabetes mellitus. Diabetes Care 1984 Jan;7(1):57-62.
146. Huttunen NP, Lankela SL, Knip M, Lautala P, Kaar ML, Laasonen K, et al. Effect of once-aweek training program on physical fi tness and metabolic control in children with IDDM. Diabetes Care 1989 Nov;12(10):737-40.
147. Ruzic L, Sporis G, Matkovic BR. High volume-low intensity exercise camp and glycemic control in diabetic children. J Paediatr Child Health 2008 Mar;44(3):122-8.
148. Herbst A, Bachran R, Kapellen T, Holl RW. Effects of regular physical activity on control of glycemia in pediatric patients with type 1 diabetes mellitus. Arch Pediatr Adolesc Med 2006 Jun;160(6):573-7.
149. Laaksonen DE, Atalay M, Niskanen LK, Mustonen J, Sen CK, Lakka TA, et al. Aerobic exercise and the lipid profi le in type 1 diabetic men: a randomized controlled trial. Med Sci Sports Exerc 2000 Sep;32(9):1541-8.
150. Lehmann R, Kaplan V, Bingisser R, Bloch KE, Spinas GA. Impact of physical activity on cardiovascular risk factors in IDDM. Diabetes Care 1997 Oct;20(10):1603-11.
151. Schneider SH, Khachadurian AK, Amorosa LF, Clemow L, Ruderman NB. Ten-year experi-ence with an exercise-based outpatient life-style modifi cation program in the treatment of diabetes mellitus. Diabetes Care 1992 Nov;15(11):1800-10.
152. Ligtenberg PC, Blans M, Hoekstra JB, van dT, I, Erkelens DW. No effect of long-term physi-cal activity on the glycemic control in type 1 diabetes patients: a cross-sectional study. Neth J Med 1999 Aug;55(2):59-63.
312 SNS CLINICAL PRACTICE GUIDELINES
153. Conn VS, Hafdahl AR, Lemaster JW, Ruppar TM, Cochran JE, Nielsen PJ. Meta-analysis of health behavior change interventions in type 1 diabetes. Am J Health Behav 2008 May;32(3):315-29.
154. Pedersen BK, Saltin B. Evidence for prescribing exercise as therapy in chronic disease. Scand J Med Sci Sports 2006 Feb;16 Suppl 1:3-63.
155. Wasserman DH, Zinman B. Exercise in individuals with IDDM. Diabetes Care 1994 Aug;17(8):924-37.
156. Veves A, Saouaf R, Donaghue VM, Mullooly CA, Kistler JA, Giurini JM, et al. Aerobic exercise capacity remains normal despite impaired endothelial function in the micro- and macrocirculation of physically active IDDM patients. Diabetes 1997 Nov;46(11):1846-52.
157. Wallberg-Henriksson H, Gunnarsson R, Henriksson J, Ostman J, Wahren J. Infl uence of physical training on formation of muscle capillaries in type I diabetes. Diabetes 1984 Sep;33(9):851-7.
158. Yki-Jarvinen H, DeFronzo RA, Koivisto VA. Normalization of insulin sensitivity in type I diabetic subjects by physical training during insulin pump therapy. Diabetes Care 1984 Nov;7(6):520-7.
159. Wallberg-Henriksson H, Gunnarsson R, Rossner S, Wahren J. Long-term physical training in female type 1 (insulin-dependent) diabetic patients: absence of signifi cant effect on gly-caemic control and lipoprotein levels. Diabetologia 1986 Jan;29(1):53-7.
160. Kavookjian J, Elswick BM, Whetsel T. Interventions for being active among individuals with diabetes: a systematic review of the literature. Diabetes Educ 2007 Nov;33(6):962-88.
161. Carral F, Gutierrez JV, Ayala C, Garcia C, Silva JJ, Aguilar M. Impacto de la actividad física sobre el control metabólico y el desarrollo de complicaciones crónicas en pacientes con dia-betes mellitus tipo 1. Endocrinol Nutr 2010; 57:268-76 - vol 57 núm 06 2010.
162. Nielsen PJ, Hafdahl AR, Conn VS, Lemaster JW, Brown SA. Meta-analysis of the effect of exercise interventions on fi tness outcomes among adults with type 1 and type 2 diabetes. Diabetes Res Clin Pract 2006 Nov;74(2):111-20.
163. Marrone S, Plume JW, Kerr P, Pignol A, Vogeltanz-Holm N, Holm J, et al. The role of free-play physical activity in healthy blood glucose maintenance in children with type 1 diabetes mellitus. Psychol Health Med 2009 Jan;14(1):48-52.
164. Durak EP, Jovanovic-Peterson L, Peterson CM. Randomized crossover study of effect of resistance training on glycemic control, muscular strength, and cholesterol in type I diabetic men. Diabetes Care 1990 Oct;13(10):1039-43.
165. Ramalho AC, de Lourdes LM, Nunes F, Cambui Z, Barbosa C, Andrade A, et al. The effect of resistance versus aerobic training on metabolic control in patients with type-1 diabetes mellitus. Diabetes Res Clin Pract 2006 Jun;72(3):271-6.
166. Delahanty L, Simkins SW, Camelon K. Expanded role of the dietitian in the Diabetes Control and Complications Trial: implications for clinical practice. The DCCT Research Group. J Am Diet Assoc 1993 Jul;93(7):758-64, 767.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 313
167. EDIC. Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group.[Erratum appears in N Engl J Med 2000 May 4;342(18):1376]. New England Journal of Medicine 2000 Feb 10;342(6):381-90.
168. Stettler C, Allemann S, Juni P, Cull CA, Holman RR, Egger M, et al. Glycemic control and macrovascular disease in types 1 and 2 diabetes mellitus: Meta-analysis of randomized tri-als. Am Heart J 2006 Jul;152(1):27-38.
169. Shankar A, Klein R, Klein BE, Moss SE. Association between glycosylated hemoglobin level and cardiovascular and all-cause mortality in type 1 diabetes. Am J Epidemiol 2007 Aug 15;166(4):393-402.
170. Saleem T, Mohammad KH, bdel-Fattah MM, Abbasi AH. Association of glycosylated hae-moglobin level and diabetes mellitus duration with the severity of coronary artery disease. Diab Vasc Dis Res 2008 Sep;5(3):184-9.
171. Goberna R, Aguilar Diosdado M, Santos Rey K, Mateo J. Documento de consenso para la armonización de resultados de HbA
1c en España. Av Diabetol Publisher ahead of Print
Publisher online ahead of print 2009 2009.
172. American Diabetes Association. Consensus statement on the worldwide standardisation of the HbA
1c measurement. European Association for the Study of Diabetes,International
Federation of Clinical Chemistry and Laboratory Medicine,and the International Diabetes Federation Consensus Committee American Diabetes Association 2007;Diabetología 2007; DOI 0.1007/s00125-007-0789-7.
173. Gabriely I, Wozniak R, Mevorach M, Kaplan J, Aharon Y, Shamoon H. Transcutaneous glucose measurement using near-infrared spectroscopy during hypoglycemia. Diabetes Care 1999 Dec;22(12):2026-32.
174. Muller UA, Mertes B, Fischbacher C, Jageman KU, Danzer K. Non-invasive blood glucose monitoring by means of near infrared spectroscopy: methods for improving the reliability of the calibration models. International Journal of Artifi cial Organs 1997;(20):285-90.
175. Uemura T, Nishida K, Sakakida M, Ichinose K, Shimoda S, Shichiri M. Non-invasive blood glucose measurement by Fourier transform infrared spectroscopic analysis through the mu-cous membrane of the lip: application of a chalcogenide optical fi ber system. Frontiers of Medical and Biological Engineering 1999;9:137-53.
176. Garg S, Zisser H, Schwartz S, Bailey T, Kaplan R, Ellis S, et al. Improvement in glycemic excursions with a transcutaneous, real-time continuous glucose sensor: a randomized con-trolled trial. Diabetes Care 2006 Jan;29(1):44-50.
177. Monsod TP, Flanagan DE, Rife F, Saenz R, Caprio S, Sherwin RS, et al. Do sensor glucose levels accurately predict plasma glucose concentrations during hypoglycemia and hyperin-sulinemia? Diabetes Care 2002 May;25(5):889-93.
178. Gross TM, Bode BW, Einhorn D, Kayne DM, Reed JH, White NH, et al. Performance evaluation of the MiniMed continuous glucose monitoring system during patient home use. Diabetes Technology & Therapeutics 2(1):49-56, 2000.
314 SNS CLINICAL PRACTICE GUIDELINES
179. Chetty VT, Almulla A, Odueyungbo A, Thabane L. The effect of continuous subcutaneous glucose monitoring (CGMS) versus intermittent whole blood fi nger-stick glucose monitor-ing (SBGM) on hemoglobin A1c (HBA
1c) levels in Type I diabetic patients: a systematic
review. Diabetes Res Clin Pract 2008 Jul;81(1):79-87.
180. Golicki DT, Golicka D, Groele L, Pankowska E. Continuous Glucose Monitoring System in children with type 1 diabetes mellitus: a systematic review and meta-analysis. Diabetologia 2008 Feb;51(2):233-40.
181. Chico A, Vidal-Rios P, Subira M, Novials A. The continuous glucose monitoring system is useful for detecting unrecognized hypoglycemias in patients with type 1 and type 2 diabetes but is not better than frequent capillary glucose measurements for improving metabolic con-trol. Diabetes Care 2003 Apr;26(4):1153-7.
182. Murphy HR, Rayman G, Lewis K, Kelly S, Johal B, Duffi eld K, et al. Effectiveness of continuous glucose monitoring in pregnant women with diabetes: randomised clinical trial. BMJ 2008;337:a1680.
183. Hirsch IB, Abelseth J, Bode BW, Fischer JS, Kaufman FR, Mastrototaro J, et al. Sensoraugmented insulin pump therapy: results of the fi rst randomized treat-to-target study. Diabetes Technol Ther 2008 Oct;10(5):377-83.
184. Tamborlane WV, Beck RW, Bode BW, Buckingham B, Chase HP, Clemons R, et al. Continuous glucose monitoring and intensive treatment of type 1 diabetes. N Engl J Med 2008 Oct 2;359(14):1464-76.
185. Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group. The Effect of Continuous Glucose Monitoring in Well-Controlled Type 1 Diabetes. Diabetes Care 2009 Aug;32 no.8:1378-83.
186. Clar C, Waugh N, Thomas S. Hospitalización sistemática versus atención ambulatoria o domiciliaria de niños con diagnóstico de diabetes mellitus tipo 1 (Revisión Cochrane tradu-cida). Biblioteca Cochrane Plus 2008;Numero 2.
187. Chase HP, Crews KR, Garg S, Crews MJ, Cruickshanks KJ, Klingensmith G, et al. Outpatient management vs in-hospital management of children with new-onset diabetes. Clinical Pediatrics 31(8):450-6, 1992 Aug.
188. Dougherty GE, Soderstrom L, Schiffrin A. An economic evaluation of home care for chil-dren with newly diagnosed diabetes: results from a randomized controlled trial. Medical Care 36(4):586-98, 1998 Apr.
189. Simell T, Putto-Laurila A, Näntö-Salonen K, Salomaa P, Piekkala P, Hakalax J, et al. Randomized prospective trial of ambulatory treatment and one-week hospitalisation of chil-dren with newly diagnosed IDDM. Diabetes 1995;Suppl 1:162A.
190. Srinivasan S, Craig ME, Beeney L, Hayes R, Harkin N, Ambler GR, et al. An ambulatory stabilisation program for children with newly diagnosed type 1 diabetes. Medical Journal of Australia 180(6):277-80, 2004 Mar 15.
191. Siminerio LM, Charron-Prochownik D, Banion C, Schreiner B. Comparing outpatient and inpatient diabetes education for newly diagnosed pediatric patients. Diabetes Educator 25(6):895-906, 1999 Nov;-Dec.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 315
192. Galatzer A, Amir S, Gil R, Karp M, Laron Z. Crisis intervention program in newly diag-nosed diabetic children. Diabetes Care 5(4):414-9, 1982 Jul;-Aug.
193. Spaulding RH, Spaulding WB. The diabetic day-care unit. II. Comparison of patients and costs of initiating insulin therapy in the unit and a hospital. Can Med Assoc J 1976 May 8;114(9):780-3.
194. Anderson JH, Jr., Brunelle RL, Koivisto VA, Pfutzner A, Trautmann ME, Vignati L, et al. Reduction of postprandial hyperglycemia and frequency of hypoglycemia in IDDM pa-tients on insulinanalog treatment. Multicenter Insulin Lispro Study Group. Diabetes 1997 Feb;46(2):265-70.
195. Ciofetta M, Lalli C, Del Sindaco P, Torlone E, Pampanelli S, Mauro L, et al. Contribution of postprandial versus interprandial blood glucose to HbA
1c in type 1 diabetes on physiologic
intensive therapy with lispro insulin at mealtime. Diabetes Care 1999;22:795-800.
196. Garg SK, Carmain JA, Braddy KC, Anderson JH, Vignati L, Jennings MK, et al. Pre-meal insulin analogue insulin lispro vs Humulin R insulin treatment in young subjects with type 1 diabetes. Diabet Med 1996 Jan;13(1):47-52.
197. Heller SR, Amiel SA, Mansell P. Effect of the fast-acting insulin analog lispro on the risk of nocturnal hypoglycemia during intensifi ed insulin therapy. U.K. Lispro Study Group. Diabetes Care 1999 Oct;22(10):1607-11.
198. Janssen MM, Snoek FJ, Masurel N, Hoogma RP, Deville WL, Popp-Snijders C, et al. Optimized basal-bolus therapy using a fi xed mixture of 75% lispro and 25% NPL insulin in type 1 diabetes patients: no favorable effects on glycemic control, physiological responses to hypoglycemia, well-being, or treatment satisfaction. Diabetes Care 2000 May;23(5):629-33.
199. Lalli C, Ciofetta M, Del Sindaco P, Torlone E, Pampanelli S, Compagnucci P. Long-term intensive treatment of type 1 diabetes with the short-acting insulin analog lispro in variable combination with NPH insulin at mealtime. Diabetes Care 1999;22:468-77.
200. Valle D, Santoro D, Bates P, Scarpa L, Italian Multicentre Lispro Study Group. Italian mul-ticentre study of intensive therapy with insulin lispro in 1184 patients with Type 1 diabetes. Diabetes, Nutrition & Metabolism - Clinical & Experimental 14(3):126-32, 2001 Jun.
201. Vignati L, Anderson JH, Brunelle RL, Jefferson FL, Richardson M. Improvement of glyce-mic control with the rapidly absorbed lispro insulin analog in type 1 diabetes. Diabetologia 1994;37(Suppl 1):A78.
202. Home PD, Lindholm A. Insulin aspart vs. human insulin in the management of long-term blood glucose control in Type 1 diabetes mellitus: a randomized controlled trial. Diabet Med 2000;17:762-70.
203. Raskin P, Guthrie RA, Leiter L, Riis A, Jovanovic L. Use of insulin aspart, a fast-acting insulin analog, as the mealtime insulin in the management of patients with type diabetes. Diabetes Care 2000;53:583-8.
204. Tamas G, Marre M, Astorga R, Dedov I, Jacobsen J, Lindholm A, et al. Glycaemic control in type 1 diabetic patients using optimised insulin aspart or human insulin in a randomised multinational study. Diabetes Res Clin Pract 2001;54:105-14.
316 SNS CLINICAL PRACTICE GUIDELINES
205. Annuzzi G, Del Prato S, Arcari R, Bellomo DA, Benzi L, Bruttomesso D, et al. Preprandial combination of lispro and NPH insulin improves overall blood glucose control in type 1 diabetic patients: a multicenter randomized crossover trial. Nutr Metab Cardiovasc Dis 2001;11:168-75.
206. Caixas A, Perez A, Payes A, Otal C, Carreras G, Ordonez-Llanos J, et al. Effects of a short-acting insulin analog (Insulin Lispro) versus regular insulin on lipid metabolism in insu-lindependent diabetes mellitus. Metabolism: Clinical and Experimental 1998;47:371-6.
207. Ferguson SC, Strachan MW, Janes JM, Frier BM. Severe hypoglycaemia in patients with type 1 diabetes and impaired awareness of hypoglycaemia: a comparative study of insulin lispro and regular human insulin. Diabetes Metab Res Rev 2001;17:285-91.
208. Gale EA. A randomized, controlled trial comparing insulin lispro with human soluble insulin in patients with Type 1 diabetes on intensifi ed insulin therapy.The UK Trial Group. Diabet Med 2000;17:209-14.
209. Holleman F, Schmitt H, Rottiers R, Rees A, Symanowski S, Anderson JH, et al. Reduced frequency of severe hypoglycemia and coma in well-controlled IDDM patients treated with insulin lispro. Diabetes Care 1997;20:1827-32.
210. Pfutzner A, Kustner E, Forst T, Schulze-Schleppinghoff B, Trautmann ME, Haslbeck M, et al. Intensive insulin therapy with insulin lispro in patients with type 1 diabetes reduces the frequency of hypoglycemic episodes. Exp Clin Endocrinol Diabetes 1996;104(1):25-30.
211. Provenzano C, Vero R, Oliva A, Leto G, Puccio L, Vecci E, et al. Lispro insulin in type 1 diabetic patients on a Mediterranean or normal diet: a randomized, cross-over comparative study with regular insulin. Diabetes Nutr Metab 2001;14:133-9.
212. Vignati L, Anderson JH, Iversen PW. Effi cacy of insulin lispro in combination with NPH human insulin twice per day in patients with insulin-dependent or non-insulin-dependent diabetes mellitus. Clin Ther 1997;19:1408-21.
213. Banerjee S, Tran K, Li H, Cimon K, Daneman D, Simpson S, et al. Short-acting insulin analogues for diabetes mellitus: meta-analysis of clinical outcomes and assesssment of cost effectiveness. Otawa: Canadian Agency for drugs and Technologies in Health 2007.
214. Siebenhofer A, Plank J, Berghold A, Narath M, Gfrerer R, Pieber TR. Short acting insu-lin analogues versus regular human insulin in patients with diabetes mellitus. Cochrane Database Syst Rev 2006;(4):CD003287.
215. Siebenhofer A, Plank J, Berghold A, Horvath K, Sawicki PT, Beck P, et al. Meta-analysis of short acting insulin analogues in adult patients with type 1 diabetes: continuous subcutane-ous insulin infusion versus injection theraphy38. Diabetologia 2004;47(11):1895-905.
216. Plank J, Siebenhofer A, Berghold A, Jeitler K, Horvath K, Mrak P, et al. Systematic review and metaanalysis of short-acting insulin analogues in patients with diabetes mellitus. Arch Intern Med 2005;165(12):1337-44.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 317
217. Colquitt J, Royle P, Waug N. Are analogue insulins better than soluble in continuous subcuta-neous insulina infusion? Results of a meta-analysis. Diabet Med 2003;20(10):863-6.
218. Brunelle BL, Llewelyn J, Anderson JH, Gale EA, Koivisto VA. Meta-analysis of the effect of insulin lispro on severe hypoglycemia in patients with type 1 diabetes. Diabetes Care 1998;21(10):1726-31.
219. Jacobsen IB, Henriksen JE, Hother-Nielsen O, Vach W, Beck-Nielsen H. Evidence-based insulin treatment in type 1 diabetes mellitus. Diabetes Res Clin Pract 2009 Oct;86(1):1-10.
220. Chen JW, Lauritzen T, Bojesen A, Christiansen JS. Multiple mealtime administration of biphasic insulin aspart 30 versus traditional basal-bolus human insulin treatment in patients with type 1 diabetes. Diabetes Obes Metab 2006;8(6):682-9.
221. Singh SR, Ahmad F, Lal A, Yu C, Bai Z, Bennett H. Effi cacy and safety of insulin analogues for the management of diabetes mellitus: a meta-analysis. CMAJ 2009 Feb 17;180(4):385-97.
222. Anderson JH, Jr., Brunelle RL, Koivisto VA, Trautmann ME, Vignati L, DiMarchi R. Improved mealtime treatment of diabetes mellitus using an insulin analogue. Multicenter Insulin Lispro Study Group. Clin Ther 1997 Jan;19(1):62-72.
223. Bode B, Weinstein R, Bell D, McGill J, Nadeau D, Raskin P, et al. Comparison of insulin aspart with buffered regular insulin and insulin lispro in continuous subcutaneous insulin infusion: a randomized study in type 1 diabetes. Diabetes Care 2002 Mar;25(3):439-44.
224. Del SP, Ciofetta M, Lalli C, Perriello G, Pampanelli S, Torlone E, et al. Use of the shortact-ing insulin analogue lispro in intensive treatment of type 1 diabetes mellitus: importance of appropriate replacement of basal insulin and time-interval injection-meal. Diabet Med 1998 Jul;15(7):592-600.
225. Garg SK, Rosenstock J, Ways K. Optimized Basal-bolus insulin regimens in type 1 diabetes: insulin glulisine versus regular human insulin in combination with Basal insulin glargine. Endocr Pract 2005 Jan;11(1):11-7.
226. Renner R, Pfutzner A, Trautmann M, Harzer O, Sauter K, Landgraf R. Use of insulin lis-pro in continuous subcutaneous insulin infusion treatment. Results of a multicenter trial. German Humalog-CSII Study Group. Diabetes Care 1999 May;22(5):784-8.
227. Schmauss S, Konig A, Landgraf R. Human insulin analogue [LYS(B28), PRO(B29)]: the ideal pump insulin? Diabet Med 1998 Mar;15(3):247-9.
228. Bradley C, Lewis KS. Measures of psychological well-being and treatment satisfaction developed from the responses of people with tablet-treated diabetes. Diabet Med 1990 Jun;7(5):445-51.
229. Bradley C. A guide to psychological measurement in diabetes research and practice. Handbook of Psychology and Diabetes Routledge 1994.
230. Cox DJ, Irvine A, Gonder-Frederick L, Nowacek G, Butterfi eld J. Fear of hypoglycemia: quantifi cation, validation, and utilization. Diabetes Care 1987 Sep;10(5):617-21.
231. Bott U, Muhlhauser I, Overmann H, Berger M. Validation of a diabetes-specifi c quality-of-life scale for patients with type 1 diabetes. Diabetes Care 1998 May;21(5):757-69.
318 SNS CLINICAL PRACTICE GUIDELINES
232. Reliability and validity of a diabetes quality-of-life measure for the diabetes control and com-plications trial (DCCT). The DCCT Research Group. Diabetes Care 1988 Oct;11(9):725-32.
233. Tubiana-Rufi N, Coutant R, Bloch J, Munz-Licha G, Delcroix C, Montaud-ragideau N, et al. Special management of insulin lispro in continuous subcutaneous insulin infusion in young diabetic children: a randomized cross-over study. Horm Res 2004;62:265-71.
234. Johansson UB, Adamson UCK, Lins PES, Wredling RAM. Improved blood glucose vari-ability, HBA
1C Insuman Infusat and less insulin requirement in IDDM patients using in-
sulin lispro in CSII. The Swedish multicenter lispro insulin study Diabetes Metabolism 2000;26(3):192-6.
235. Jeitler K, Horvath K, Berghold A, Gratzer TW, Neeser K, Pieber TR, et al. Continuous sub-cutaneous insulin infusion versus multiple daily insulin injections in patients with diabetes mellitus: systematic review and meta-analysis. Diabetologia 2008;51(6):941-51.
236. Deeb LC, Holcombe JH, Brunelle R, Zalani S, Brink S, Jenner M, et al. Insulin lispro lowers postprandial glucose in prepubertal children with diabetes. Pediatrics 2001;108:1175-9.
237. Ford-Adams ME, Murphy NP, Moore EJ, Edge JA, Ong KL, Watts AP, et al. Insulin lispro: a potential role in preventing nocturnal hypoglycaemia in young children with diabetes mel-litus. Diabet Med 2003;20:656-60.
238. Tupola S, Komulainen J, Jääskeläinen J, Sipilä I. Post-prandial insulina lispro vs. human reg-ular insulin in prepubertal children with Type diabetes mellitus. Diabet Med 2001;18:654-8.
239. Danne T, Rastam J, Odendahl R, Näke A, Schimmel U, Szczepanski R, et al. Parental pref-erence of prandial insulin aspart compared with prepandial human insulin in a basal-bolus scheme with NPH insulin in a 12-wk crossover study of preschool children with type 1 dia-betes. Pediatr Diabetes 2007;8(5):278-85.
240. Holcombe JH, Zalani S, Arora VK, Mast CJ. Comparison of insulin lispro with regular hu-man insulin for the treatment of type 1 diabetes in adolescents. Clin Ther 2002;24(4):626-38.
241. Mortensen H, Kocova M, Teng LY, Keiding J, Bruckner I, Philotheou A. Biphasic insulin as-part vs. human insulin in adolescents with type diabetes on multiple daily insulin injections. Pediatr Diabetes 2006;7(1):4-10.
242. Persson B, Swahn ML, Hjertberg R, Hanson U, Nord E, Nordlander E, et al. Insulin lis-pro theraphy in pregnancies complicated by type diabetes mellitus. Diabetes Res Clin Pract 2002;58:115-21.
243. Mathiesen ER, Kinsley B, Amiel SA, Heller S, McCance D, Duran S, et al. Insulin Apart Pregnancy Study Group. Maternal Glycemic control and hypoglycemia in type 1 diabetic pregnancy: a randomized trial of insulin aspart versus human insulin in 322 pregnant wom-en. Diabetes Care 2007;30(4):771-6.
244. Lapolla A, Dalfra MG, Fedele D. Insulin therapy in pregnancy complicated by diabetes: are insulin analogs a new tool? Diabetes Metab Res Rev 2005 May;21(3):241-52.
245. Hod M, Damm P, Kaaja R, Visser GH, Dunne F, Demidova I, et al. Fetal and perinatal out-comes in type 1 diabetes pregnancy: a randomized study comparing insulin aspart with hu-man insulin in 322 subjects. Am J Obstet Gynecol 2008 Feb;198(2):186-7.
246. Torlone E, Di CG, Mannino D, Lapolla A. Insulin analogs and pregnancy: an update. Acta Diabetol 2009 Sep;46(3):163-72.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 319
247. Tran K, Banerjee S, Li H, Cimon K, Daneman D, simpson SH, et al. Long-acting insulin analogues for diabetes mellitus: meta-analysis of clinical outcomes and assessment of cost effectiveness. Otawa: Canadian Agency for drugs and Technologies in Health 2007.
248. Vardi M, Jacobson E, Nini A, Bitterman H. Insulina de acción intermedia versus insulina de acción prolongada para la diabetes mellitus tipo 1 (Revisión Cochrane traducida). (Traducida de The Cochrane Library, 2008 Issue 3 Chichester, UK: John Wiley & Sons, Ltd) 2008.
249. Monami M, Marchionni N, Mannucci E. Long-acting insulin analogues vs. NPH human insulin in type 1 diabetes. A meta-analysis. Diabetes Obes Metab 2009 Apr;11(4):372-8.
250. Kudva YC, Basu A, Jenkins GD, Pons GM, Quandt LL, Gebel JA, et al. Randomized con-trolled clinical trial of glargine versus ultralente insulin in the treatment of type 1 diabetes. Diabetes Care 2005;28(1):10-4.
251. Witthaus E, Stewart J, Bradley C. Treatment satisfaction and psychological well-being with insulina glargine compared with NPH in patients with type 1 diabetes. Diabet Med 2001;18(8):619-25.
252. Colhoun HM, SDRN Epidemiology Group. Use of insulin glargine and cancer incidence in Scotland: a study from the Scottish Diabetes Research Network Epidemilogy Group. Diabetologia 2009;52:1755-65.
253. Jonasson JM, Ljung R, Talbäck M, Haglund B, Gudbjörnsdóttir S, Steineck G. Insulin glar-gine use and short-term incidence of malignancies a population-based follow-up study in Sweden. Diabetologia 2009;52:1732-44.
254. Hemkens LG, Grouven U, Bender R, Günster C, Gutschmidt S, Selke GW, et al. Risk of malignancies in patients with diabetes treated with human insulin or insulin analogues: a cohort study. Diabetologia 2009;52:1732-44.
255. Currie CJ, Poole CD, Gale EAM. The infl uence of glucose lowering therapies on cancer risk in type 2 diabetes. Diabetologia 2009;52:1766-77.
256. Mianowska B, Szadkowska A, Czerniawska E, Pietrzak I, Bodalski J. Insulin glargine im-proves fasting blood glucose levels in prepubertal children with unsatisfactorily controlled type 1 diabetes. Endokrynol Diabetol Chor Przemiany Materii Wieku Rozw 2007;13(4):189-93.
257. Hassan K, Rodriguez LM, Johnson SE, Tadlock S, Heptulla RA. A randomized, controlled trial comparing twice-a-day unsulin glargine mixed with rapid-acting insulin analogs versus standard neutral protamine Hagedorn (NPH) therapy in newly diagnosed type 1 diabetes. Pediatrics 2008;121(3):e466-72.
258. Schober E, Schoenle E, Van Dyk J, Wernicke-Panten K. Comparative trial between insulin glargine and NPH insulin in children and adolescents with type 1 diabetes mellitus. J Pediatr Endocrinol Metab 2002;15(4):369-76.
259. Karges B, Kapellen T, Neu A, Hofer SE, Rohrer T, Rosenbauer J, et al. Long-acting insu-lin analogs and the risk of diabetic ketoacidosis in children and adolescents with type 1 diabetes: a prospective study of 10,682 patients from 271 institutions. Diabetes Care 2010 May;33(5):1031-3.
260. Robertson KJ, Schoenle E, Gucev Z, Mordhorst L, Gall MA, Ludvigsson J. Insulin determir compared with NPH insulin in children and adolescents with type 1 diabetes. Diabet Med 2007;24(1):27-34.
320 SNS CLINICAL PRACTICE GUIDELINES
261. Pieber TR, Treichel HC, Hompesch B, Philotheou A, Mordhorst L, Gall MA, et al. Comparison of insulin determir and insulin glargine in subjects with type 1 diabetes using intensive insulin theraphy. Diabet Med 2007;24(6):635-42.
262. Heller S, Koenen C, Bode B. Comparison of insulin detemir and insulin glargine in a basal-bolus regimen, with insulin aspart as the mealtime insulin, in patients with type 1 diabetes: a 52-week, multinational, randomized, open-label, parallel-group, treat-to-target noninferior-ity trial. Clin Ther 2009 Oct;31(10):2086-97.
263. Porcellati F, Rossetti P, Busciantella NR, Marzotti S, Lucidi P, Luzio S, et al. Comparison of pharmacokinetics and dynamics of the long-acting insulin analogs glargine and detemir at steady state in type 1 diabetes: a double-blind, randomized, crossover study. Diabetes Care 2007 Oct;30(10):2447-52.
264. Cummins E, Royle P, Snaith A, Greene A, Robertson L, McIntyre L, et al. Clinical effec-tiveness and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes: systematic review and economic evaluation. Health Technol Assess 2010 Feb;14(11):iii-xvi, 1.
265. Fatourechi MM, Kudva YC, Murad MH, Elamin MB, Tabini CC, Montori VM. Hypoglycemia with intensive insulin therapy: a systematic review and meta-analyses of randomized trials of continuous subcutaneous insulin infusion versus multiple daily injections. J Clin Endocrinol Metab 2009;94(3):729-40.
266. Misso ML, Egberts KJ, Page M, O’Connor D, Shaw J. Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus. Cochrane Database Syst Rev 2010;(1):CD005103.
267. Bruttomesso D, Crazzolara D, Maran A, Costa S, Dal Pos M, Girelli A, et al. In Type 1 diabetic patients with good glycaemic control, blood glucose variability is lower during continuous subcutaneous insulin infusion than during multiple daily injections with insulin glargine. Diabet Med 2008;25(3):326-32.
268. DeVries JH, Snoek FJ, Kostense PJ, Masurel N, Heine RJ. A randomised trial of continuous subcutaneous insulin infusion and intensive injection therapy in type 1 diabetes for patients with longstanding poor glycemic control. Diabetes Care 2002;25:2074-80.
269. Hanaire-Broutin H, Melki V, Bessieres-Lacombe S, Tauber JP. Comparison of continuous subcutaneous insulin infusion and multiple daily injection regimens using insulin lispro in type 1 diabetic patients on intensifi ed treatment: a randomized study. The Study Group for the Development of Pump Therapy in Diabetes. Diabetes Care 2000 Sep;23(9):1232-5.
270. Home PD, Capaldo B, Burrin JM, Worth R, Alberti KG. A crossover comparison of con-tinuous subcutaneous insulin infusion (CSII) against multiple insulin injections in insulin-dependent diabetic subjects: improved control with CSII. Diabetes Care 1982 Sep;5(5):466-71.
271. Hoogma RP, Hammond PJ, Gomis R, et al. Comparison of the effects of continuous subcu-taneous insulin infusion (CSII) and NPH-based multiple daily insulin injections (MDI) on glycaemic control and quality of life: results of the 5-nations trial. Diab Med 2005;23:141-7.
272. Lepore G, Dodesini AR, Nosari I, Trevisan R. Both continuous subcutaneous insulin in-fusion and a multiple daily insulin injection regimen with glargine as basal insulin are equally better than traditional multiple daily insulin injection treatment. Diabetes Care 2003 Apr;26(4):1321-2.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 321
273. Nathan DM, Lou P, Avruch J. Intensive conventional and insulin pump therapies in adult type I diabetes. A crossover study. Ann Intern Med 1982 Jul;97(1):31-6.
274. Nosadini R, Velussi M, Fioretto P, et al. Frequency of hypoglycaemic and hyperglycaemick-etotic episodes during convencional and subcutaneous continuous insulin infusion therapy in IDDM. Diabetes Nutr Metab 1988;1:289-96.
275. Dahl-Jorgensen K, Brinchmann-Hansen O, Hanssen KF, Sandvik L, Aagenaes O. Rapid tightening of blood glucose control leads to transient deterioration of retinopathy in in-sulin dependent diabetes mellitus: the Oslo study. Br Med J (Clin Res Ed) 1985 Mar 16;290(6471):811-5.
276. Dahl-Jorgensen K, Brinchmann-Hansen O, Hanssen KF, Ganes T, Kierulf P, Smeland E, et al. Effect of near normoglycaemia for two years on progression of early diabetic retin-opathy, nephropathy, and neuropathy: the Oslo study. Br Med J (Clin Res Ed) 1986 Nov 8;293(6556):1195-9.
277. Brinchmann-Hansen O, hl-Jorgensen K, Sandvik L, Hanssen KF. Blood glucose concentra-tions and progression of diabetic retinopathy: the seven year results of the Oslo study. BMJ 1992 Jan 4;304(6818):19-22.
278. Saurbrey N, Arnold-Larsen S, Moller-Jensen B, Kuhl C. Comparison of continuous subcu-taneous insulin infusion with multiple insulin injections using the NovoPen. Diabet Med 1988;5:150-3.
279. Schmitz A, Christiansen JS, Christensen CK, Hermansen K, Mogensen CE. Effect of pump versus pen treatment on glycaemic control and kidney function in long-term uncomplicated insulin-dependent diabetes mellitus (IDDM). Dan Med Bull 1989;36:176-8.
280. Tsui E, Barnie A, Ross S, Parkes R, Zinman B. Intensive insulin therapy with insulin lispro, a randomised trial of continuous subcutaneous insulin infusion versus multiple daily insulin injection. Diabetes Care 2001;24:1722-7.
281. Torres I, Ortego J, Valencia I, Garcia-Palacios MV, guilar-Diosdado M. Benefi ts of continu-ous subcutaneous insulin infusion in type 1 diabetes previously treated with multiple daily injections with once-daily glargine and pre-meal analogues. Exp Clin Endocrinol Diabetes 2009 Sep;117(8):378-85.
282. Bergenstal RM, Tamborlane WV, Ahmann A, Buse JB, Dailey G, Davis SN, et al. Effectiveness of sensor-augmented insulin-pump therapy in type 1 diabetes. N Engl J Med 2010 Jul 22;363(4):311-20.
283. Bolli GB, Kerr D, Thomas R, Torlone E, Sola-Gazagnes A, Vitacolonna E, et al. Comparison of a multiple daily insulin injection regimen (basal once-daily glargine plus mealtime lispro) and continuous subcutaneous insulin infusion (lispro) in type 1 diabetes: a randomized open parallel multicenter study. Diabetes Care 2009 Jul;32(7):1170-6.
284. Doyle EA, Weinzimer SA, Steffen AT, Ahern JA, Vincent M, Tamborlane WV. A rand-omized, prospective trial comparing the effi cacy of continuous subcutaneous insulin infu-sion with multiple daily injections using insulin glargine. Diabetes Care 2004;27:1554-8.
285. Schottenfeld-Naor Y, Galatzer A, Karp M, Josefsberg Z, Laron Z. Comparison of metabolic and psychological parameters during continuous subcutaneous insulin infusion and intensi-fi ed conventional insulin treatment in type I diabetic patients. Isr J Med Sci 1985;21:822-8.
322 SNS CLINICAL PRACTICE GUIDELINES
286. Ziegler D, Dannehl K, Koschinsky T, Toeller M, Gries FA. Comparison of continuous sub-cutaneous insulin infusion and intensifi ed conventional therapy in the treatment of type I diabetes: a two-year randomized study. Diabetes Nutr Metab 1990;3:203-13.
287. Hoogma RP SD. Safety of insulin glulisine when given by continuous subcutaneous infusion using an external pump in patients with type 1 diabetes. Horm Metab Res 2006;38(6):429-33.
288. Barnard KD, Lloyd CE, Skinner TC. Systematic literature review: quality of life associated with insulin pump use in Type 1 diabetes. Diabet Med 2007;24(6):607-17.
289. Thomas RM, Aldibbiat A, Griffi n W, Cox MA, Leech NJ, Shaw JA. A randomized pilot study in Type 1 diabetes complicated by severe hypoglycaemia, comparing rigorous hypo-glycaemia avoidance with insulin analogue therapy, CSII or education alone. Diabet Med 2007;24(7): 778-83.
290. Conget I, Serrano D, Rodríguez JM, Levy I, Castell C, Roze S. Análisis coste-utilidad de las bombas de insulina frente a múltiples dosis diarias en pacientes con diabetes Mellitus tipo 1 en España. Rev Esp Salud pública 2006;80(6):679-95.
291. Pankowska E, Blazik M, Dziechciarz P, Szypowska A, Szajewska H. Continuous subcu-taneous insulin infusion vs. multiple daily injections in children with type 1 diabetes: a systematic review and meta-analysis of randomized control trials. Pediatr Diabetes 2009 Feb;10(1):52-8.
292. De Beaufort CE, Houtzagers CM, Bruining GJ, Aarsen RS, Den Boer NC, Grose WF, et al. Continuous subcutaneous insulina infusion (CSII) versus conventional injection therapy in newly diagnosed diabetic children: two-year follow-up of a randomized, prospective trial. Diabet Med 1989;6:766-71.
293. Perlman K, Ehrlich RM, Filler RM, Albisser AM. Sustained normoglycemia in newly di-agnosed type I diabetic subjects. Short-term effects and one-year follow-up. Diabetes 1984;33:995-1001.
294. Edelmann E, Walter H, Biermann E, Schleicher E, Bachmann W, Mehnert H. Sustained nor-moglycemia and remission phase in newly diagnosed type I diabetic subjects. Comparison between continuous subcutaneous insulin infusion and conventional therapy during a one year follow-up. Horm Metab Res 1987;19:419-21.
295. Opipari-Arrigan L, Fredericks EM, Burkhart N, Dale L, Hodge M, Foster C. Continuous subcutaneous insulin infusion benefi ts quality of life in preschool-age children with type 1 diabetes mellitus. Pediatr Diabetes 2007;8(6):377-83.
296. Wilson DM, Buckingham BA, Kunselman EL, Sullivan MM, Paguntalan HU, Gitelman SE. A two-center randomized controlled feasibility trial of insulin pump therapy in young chil-dren with diabetes. Diabetes Care 2005;28:15-9.
297. Cohen D, Weintrob N, Benzaquen H, Galatzer A, Fayman G, Phillip M. Continuous subcuta-neous insulin infusion versus multiple daily injections in adolescents with type I diabetes mel-litus: a randomized open crossover trial. J Pediatr Endocrinol Metab 2003 Sep;16(7):1047-50.
298. Meschi F, Beccaria L, Vanini R, Szulc M, Chiumello G. Short-term subcutaneous insulin infusion in diabetic children. Comparison with three daily insulin injections. Acta Diabetol Lat 1982 Oct;19(4):371-5.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 323
299. Nuboer R, Borsboom GJ, Zoethout JA, Koot HM, Bruining J. Effects of insulin pump vs. injection treatment on quality of life and impact of disease in children with type 1 diabe-tes mellitus in a randomized, prospective comparison. Pediatr Diabetes 2008 Jul 28;9(4 Pt 1):291-6.
300. Pozzilli P, Crino A, Schiaffi ni R, Manfrini S, Fioriti E, Coppolino G, et al. A 2-year pilot trial of continuous subcutaneous insulin infusion versus intensive insulin therapy in patients with newly diagnosed type 1 diabetes (IMDIAB 8). Diabetes Technol Ther 2003;5(6):965-74.
301. Skogsberg L, Fors H, Hanas R, Chaplin JE, Lindman E, Skogsberg J. Improved treatment satisfaction but no difference in metabolic control when using continuous subcutaneous in-sulin infusion vs. multiple daily injections in children at onset of type 1 diabetes mellitus. Pediatr Diabetes 2008;9(5):472-9.
302. Weintrob N, Schechter A, Benzaquen H, Shalitin S, Lilos P, Galatzer A, et al. Glycemic patterns detected by continuous subcutaneous glucose sensing in children and adolescents with type 1 diabetes mellitus treated by multiple daily injections vs continuous subcutaneous insulin infusion. Arch Pediatr Adolesc Med 2004 Jul;158(7):677-84.
303. Schiffrin A, Desrosiers M, Moffat M, Belmonte MM. Feasibility of strict diabetes control in insulin-dependent diabetic adolescents. J Pediatr 1983;103:522-7.
304. Weintrob N, Benzaquen H, Galatzer A, Shalitin S, Lazar L, Fayman G, et al. Comparison of continuous subcutaneous insulin infusion and multiple daily injection regimens in children with type 1 diabetes: a randomized open crossover trial. Pediatrics 2003;112:559-64.
305. Fox LA, Buckloh LM, Smith SD, Wysocki T, Mauras N. A randomised controlled trial of insulin pump therapy in young children with type 1 diabetes. Diabetes Care 2005;28:1277-81.
306. Farrar D, Tufnell DJ, West J. Continuous subcutaneous insulin infusion versus multiple daily injections of insulin for pregnant women with diabetes. Cochrane Databases Syst Rev 2007;18(3).
307. Nosari I, Maglio ML, Lepore G, Cortinovis F, Pagani G. Is continuous subcutaneous insu-lin infusion more effective than intensive convencional insulin therapy in the treatment of pregnant diabetic women? Diabetes, Nutrition & Metabolism - Clinical & Experimental 1993;6:33-7.
308. Carta Q, Meriggi E, Trossarelli GF, Catella G, Dal Molin V, Menato G, et al. Continuous subcutaneous insulin infusion versus intensive convencional insulin therapy in type I and type II diabetic pregnancy. Diabete et Metabolisme 1986;12:121-9.
309. Murray DP, Keenan P, Gayer E, Salmon P, Tomkin GH, Drury MI, et al. A randomized trial of the effi cacy and acceptability of a pen injector. Diabet Med 1988 Nov;5(8):750-4.
310. Kolendorf K, Beck-Nielsen H, Oxenboll B. Clinical experience with NovoPen II and insulin Protaphane HM Penfi ll. Postgrad Med J 1988;64 Suppl 3:14-6.
311. Jorgensen JO, Flyvbjerg A, Jorgensen JT, Sorensen HH, Johansen BR, Christiansen JS. NPH insulin administration by means of a pen injector. Diabet Med 1988 Sep;5(6):574-6.
312. Chen HS, Hwu CM, Kwok CF, Yang HJ, Shih KC, Lin BJ, et al. Clinical response and pa-tient acceptance of a prefi lled, disposable insulin pen injector for insulin-treated diabetes. Zhonghua Yi Xue Za Zhi (Taipei) 1999 Jul;62(7):455-60.
324 SNS CLINICAL PRACTICE GUIDELINES
313. Engström LHK. Insulin pen for administration of isophane insulin. Pract Diab Int 1990;7(4): 162-4.
314. Korytkowski M, Bell D, Jacobsen C, Suwannasari R. A multicenter, randomized, open-label, comparative, two-period crossover trial of preference, effi cacy, and safety profi les of a pre-fi lled, disposable pen and conventional vial/syringe for insulin injection in patients with type 1 or 2 diabetes mellitus. Clin Ther 2003 Nov;25(11):2836-48.
315. Shelmet J, Schwartz S, Cappleman J, Peterson G, Skovlund S, Lytzen L, et al. Preference and resource utilization in elderly patients: InnoLet versus vial/syringe. Diabetes Res Clin Pract 2004 Jan;63(1):27-35.
316. Stockl K, Ory C, Vanderplas A, Nicklasson L, Lyness W, Cobden D, et al. An evaluation of patient preference for an alternative insulin delivery system compared to standard vial and syringe. Curr Med Res Opin 2007 Jan;23(1):133-46.
317. Molife C, Lee LJ, Shi L, Sawhney M, Lenox SM. Assessment of patient-reported outcomes of insulin pen devices versus conventional vial and syringe. Diabetes Technol Ther 2009 Aug;11(8):529-38.
318. Asche CV, Shane-McWhorter L, Raparla S. Health economics and compliance of vials/syringes versus pen devices: a review of the evidence. Diabetes Technol Ther 2010 Jun;12 Suppl 1:S101-S108.
319. Costa B, Estopa A, Borras J, Sabate A. Diabetes and pharmacoeconomics. Effi ciency of insulin injection methods available in Spain. Aten Primaria 1995 Oct 31;16(7):391-6.
320. Perry LJ. A multicentre study of the acceptability and convenience of a disposable pen injec-tion device (preloaded pen) in children and adolescents. Novo Nordisk [unpublished] 1993.
321. Arslanoglu I, Saka N, Bundak R, Gunoz H, Darendeliler F. A comparison of the use of pre-mixed insulins in pen-injectors with conventional patient-mixed insulin treatment in chil-dren and adolescents with IDDM. Is there a decreased risk of night hypoglycemia? J Pediatr Endocrinol Metab 2000 Mar;13(3):313-8.
322. Valk NK, Cerny G, Sieber J, Lytzen L, Berg B. Effi cacy and safety performance of the Innovo insulin doser. Diabetes Technol Ther 2004 Feb;6(1):53-8.
323. Vidal M, Colungo C, Jansà M. Update on insulin administration techniques and devices (I). Av Diabetol 2008;24 (2):175-9.
324. Henriksen JE, Djurhuus MS, Vaag A, Thye-Ronn P, Knudsen D, Hother-Nielsen O, et al. Impact of injection sites for soluble insulin on glycaemic control in type 1 (insulin-depend-ent) diabetic patients treated with a multiple insulin injection regimen. Diabetologia 1993 Aug;36(8):752-8.
325. Koivisto VA, Felig P. Alterations in insulin absorption and in blood glucose control associated with varying insulin injection sites in diabetic patients. Ann Intern Med 1980 Jan;92(1):59-61.
326. Bantle JP, Weber MS, Rao SM, Chattopadhyay MK, Robertson RP. Rotation of the anatomic regions used for insulin injections and day-to-day variability of plasma glucose in type I diabetic subjects. JAMA 1990 Apr 4;263(13):1802-6.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 325
327. Bantle JP, Neal L, Frankamp LM. Effects of the anatomical region used for insulin injections on glycemia in type I diabetes subjects. Diabetes Care 1993 Dec;16(12):1592-7.
328. Frid A, Hirsch L, Gaspar R, Hicks D, Kreugel G, Liersch J, et al. New injection recommen-dations for patients with diabetes. Diabetes Metab 2010 Sep;36 Suppl 2:S3-18.
329. Frid A, Hirsch L, Gaspar R, Hicks D, Kreugel G, Liersch J, et al. The Third Injection Technique Workshop in Athens (TITAN). Diabetes Metab 2010 Sep;36 Suppl 2:S19-S29.
330. Strauss K. Insulin injection techniques. Report from the 1st International Insulin Injection Technique Workshop, Strasbourg, FranceΓÇöJune 1997. Pract Diab Int 1998;15(6):181-4.
331. Davis ED, Chesnaky P. Site rotation: an old practice gains new currency in light of todays research. Diabetes Forecast 1992;3:54-6.
332. Frid A, Linden B. Where do lean diabetics inject their insulin? A study using computed to-mography. Br Med J (Clin Res Ed) 1986 Jun 21;292(6536):1638.
333. Engstrom L, Bergman A. A new injection technique for insulin treatment, simpler to use and as effective? Scand J Caring Sci 1993;7(1):57-9.
334. Birkebaek NH, Solvig J, Hansen B, Jorgensen C, Smedegaard J, Christiansen JS. A 4-mm needle reduces the risk of intramuscular injections without increasing backfl ow to skin sur-face in lean diabetic children and adults. Diabetes Care 2008 Sep;31(9):e65.
335. Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at sites used for insulin injections: implications for needle length recommendations. Curr Med Res Opin 2010 Jun;26(6):1519-30.
336. Hofman PL, Lawton SA, Peart JM, Holt JA, Jefferies CA, Robinson E, et al. An angled in-sertion technique using 6-mm needles markedly reduces the risk of intramuscular injections in children and adolescents. Diabet Med 2007 Dec;24(12):1400-5.
337. Fleming DR, Jacober SJ, Vandenberg MA, Fitzgerald JT, Grunberger G. The safety of inject-ing insulin through clothing. Diabetes Care 1997 Mar;20(3):244-7.
338. Schwartz S, Hassman D, Shelmet J, Sievers R, Weinstein R, Liang J, et al. A multicenter, open-label, randomized, two-period crossover trial comparing glycemic control, satisfac-tion, and preference achieved with a 31 gauge x 6 mm needle versus a 29 gauge x 12.7 mm needle in obese patients with diabetes mellitus. Clin Ther 2004 Oct;26(10):1663-78.
339. Hirsch LJ, Gibney MA, Albanese J, Qu S, Kassler-Taub K, Klaff LJ, et al. Comparative gly-cemic control, safety and patient ratings for a new 4 mm x 32G insulin pen needle in adults with diabetes. Curr Med Res Opin 2010 Jun;26(6):1531-41.
340. Kreugel G, Beijer HJM, Kerstens MN, Ter Maaten JC, Sluiter WJ, Boot BS. Infl uence of needle size for SC insulin administration on metabolic control and patient acceptance. Europ Diab Nursing 2007 2007;4:1-5.
341. Ross SA, Jamal R, Leiter LA, Josse RG, Parkes JL, Qu S, et al. Evaluation of 8 mm insulin pen needles in people with type 1 and type 2 diabetes. Pract Diab Int 1999;16(5):145-8.
342. Tubiana-Rufi N, Belarbi N, Du Pasquier-Fediaevsky L, Polak M, Kakou B, Leridon L, et al. Short needles (8 mm) reduce the risk of intramuscular injections in children with type 1 diabetes. Diabetes Care 1999 Oct;22(10):1621-5.
326 SNS CLINICAL PRACTICE GUIDELINES
343. Hamilton J, Cummings E, Zdravkovic V, Finegood D, Daneman D. Metformin as an adjunct therapy in adolescents with type 1 diabetes and insulin resistance: a randomized controlled trial. Diabetes Care 2003 Jan;26(1):138-43.
344. Sarnblad S, Kroon M, Aman J. Metformin as additional therapy in adolescents with poorly controlled type 1 diabetes: randomised placebo-controlled trial with aspects on insulin sen-sitivity. Eur J Endocrinol 2003 Oct;149(4):323-9.
345. Vella S, Buetow L, Royle P, Livingstone S, Colhoun HM, Petrie JR. The use of metformin in type 1 diabetes: a systematic review of effi cacy. Diabetologia 2010 May;53(5):809-20.
346. Abdelghaffar S, Attia AM. Metformin added to insulin therapy for type 1 diabetes mellitus in adolescents. Cochrane Database Syst Rev 2009;(1):CD006691.
347. Cohen DJ, St ML, Christensen LL, Bloom RD, Sung RS. Kidney and pancreas transplanta-tion in the United States, 1995-2004. Am J Transplant 2006;6(5 Pt 2):1153-69.
348. Venstrom JM, McBride MA, Rother KI, Hirshberg B, Orchard TJ, Harlan DM. Survival af-ter pancreas transplantation in patients with diabetes and preserved kidney function. JAMA 2003 Dec 3;290(21):2817-23.
349. Nathan DM. Isolated pancreas transplantation for type 1 diabetes: a doctor’s dilemma. JAMA 2003 Dec 3;290(21):2861-3.
350. Gruessner RW, Sutherland DE, Gruessner AC. Mortality assessment for pancreas trans-plants. Am J Transplant 2004 Dec;4(12):2018-26.
351. Pozza G, Traeger J, Dubernard JM, Secchi A, Pontiroli AE, Bosi E, et al. Endocrine respons-es of type 1 (insulin-dependent) diabetic patients following successful pancreas transplanta-tion. Diabetologia 1983 Apr;24(4):244-8.
352. Katz H, Homan M, Velosa J, Robertson P, Rizza R. Effects of pancreas transplantation on postprandial glucose metabolism. N Engl J Med 1991 Oct 31;325(18):1278-83.
353. Diem P, Abid M, Redmon JB, Sutherland DE, Robertson RP. Systemic venous drainage of pancreas allografts as independent cause of hyperinsulinemia in type I diabetic recipients. Diabetes 1990 May;39(5):534-40.
354. Osei K, Henry ML, O’Dorisio TM, Tesi RJ, Sommer BG, Ferguson RM. Physiological and pharmacological stimulation of pancreatic islet hormone secretion in type I diabetic pan-creas allograft recipients. Diabetes 1990 Oct;39(10):1235-42.
355. Elahi D, Clark BA, oon-Dyke M, Wong G, Brown R, Shapiro M, et al. Islet cell responses to glucose in human transplanted pancreas. Am J Physiol 1991 Dec;261(6 Pt 1):E800-E808.
356. Robertson RP, Diem P, Sutherland DE. Time-related, cross-sectional and prospective fol-lowup of pancreatic endocrine function after pancreas allograft transplantation in type 1 (insulindependent) diabetic patients. Diabetologia 1991 Aug;34 Suppl 1:S57-S60.
357. Landgraf R, Nusser J, Riepl RL, Fiedler F, Illner WD, Abendroth D, et al. Metabolic and hormonal studies of type 1 (insulin-dependent) diabetic patients after successful pancreas and kidney transplantation. Diabetologia 1991 Aug;34 Suppl 1:S61-S67.
358. Secchi A, Dubernard JM, La RE, LeFrancois N, Melandri M, Martin X, et al. Endocrinometabolic effects of whole versus segmental pancreas allotransplantation in dia-betic patients--a two-year follow-up. Transplantation 1991 Mar;51(3):625-9.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 327
359. Barrou Z, Seaquist ER, Robertson RP. Pancreas transplantation in diabetic humans normal-izes hepatic glucose production during hypoglycemia. Diabetes 1994 May;43(5):661-6.
360. Kendall DM, Rooney DP, Smets YF, Salazar BL, Robertson RP. Pancreas transplantation re-stores epinephrine response and symptom recognition during hypoglycemia in patients with long-standing type I diabetes and autonomic neuropathy. Diabetes 1997 Feb;46(2):249-57.
361. Cottrell DA, Henry ML, O’Dorisio TM, Tesi RJ, Ferguson RM, Osei K. Hypoglycemia after successful pancreas transplantation in type I diabetic patients. Diabetes Care 1991 Nov;14(11):1111-3.
362. Redmon JB, Teuscher AU, Robertson RP. Hypoglycemia after pancreas transplantation. Diabetes Care 1998 Nov;21(11):1944-50.
363. Robertson RP, Sutherland DE, Kendall DM, Teuscher AU, Gruessner RW, Gruessner A. Metabolic characterization of long-term successful pancreas transplants in type I diabetes. J Investig Med 1996 Dec;44(9):549-55.
364. Robertson RP. Pancreas and islet transplants for patients with diabetes: taking positions and making decisions. Endocr Pract 1999 Jan;5(1):24-8.
365. Bohman SO, Tyden G, Wilczek H, Lundgren G, Jaremko G, Gunnarsson R, et al. Prevention of kidney graft diabetic nephropathy by pancreas transplantation in man. Diabetes 1985 Mar;34(3):306-8.
366. Bilous RW, Mauer SM, Sutherland DE, Najarian JS, Goetz FC, Steffes MW. The effects of pancreas transplantation on the glomerular structure of renal allografts in patients with insulin-dependent diabetes. N Engl J Med 1989 Jul 13;321(2):80-5.
367. Fioretto P, Steffes MW, Sutherland DE, Goetz FC, Mauer M. Reversal of lesions of diabetic nephropathy after pancreas transplantation. N Engl J Med 1998 Jul 9;339(2):69-75.
368. Navarro X, Kennedy WR, Loewenson RB, Sutherland DE. Infl uence of pancreas transplan-tation on cardiorespiratory refl exes, nerve conduction, and mortality in diabetes mellitus. Diabetes 1990 Jul;39(7):802-6.
369. Navarro X, Kennedy WR, Sutherland DE. Autonomic neuropathy and survival in diabetes mellitus: effects of pancreas transplantation. Diabetologia 1991 Aug;34 Suppl 1:S108-S112.
370. Navarro X, Sutherland DE, Kennedy WR. Long-term effects of pancreatic transplantation on diabetic neuropathy. Ann Neurol 1997 Nov;42(5):727-36.
371. Aridge D, Reese J, Niehoff M, Carney K, Lindsey L, Chun HS, et al. Effect of success-ful renal and segmental pancreatic transplantation on peripheral and autonomic neuropathy. Transplant Proc 1991 Feb;23(1 Pt 2):1670-1.
372. Allen RD, Al-Harbi IS, Morris JG, Clouston PD, O’Connell PJ, Chapman JR, et al. Diabetic neuropathy after pancreas transplantation: determinants of recovery. Transplantation 1997 Mar 27;63(6):830-8.
373. Gaber AO, Cardoso S, Pearson S, Abell T, Gaber L, Hathaway D, et al. Improvement in autonomic function following combined pancreas-kidney transplantation. Transplant Proc 1991 Feb;23(1 Pt 2):1660-2.
374. Fiorina P, La RE, Venturini M, Minicucci F, Fermo I, Paroni R, et al. Effects of kidney-pancreas transplantation on atherosclerotic risk factors and endothelial function in patients with uremia and type 1 diabetes. Diabetes 2001 Mar;50(3):496-501.

328 SNS CLINICAL PRACTICE GUIDELINES
375. Piper M, Seidenfeld J, Aronson N. Islet transplantation in patients with type 1 diabetes mel-litus. Evid Rep Technol Assess (Summ) 2004 Jul;(98):1-6.
376. ECRI. Islet cell transplantation for the treatment of type 1 diabetes. Plymouth Meeting, PA: ECRI 2005; 72 2005.
377. Guo B, Harstall C, Corabian P. Islet Cell Transplantation for the Treatment of Non-uremic Type 1 Diabetic Patients with Severe Hypoglycemia. Alberta Heritage Foundation for Medical Researc HTA 31 Health Technology Assessment 2003 Apr.
378. Hirshberg B, Rother KI, Digon BJ, III, Lee J, Gaglia JL, Hines K, et al. Benefi ts and risks of solitary islet transplantation for type 1 diabetes using steroid-sparing immunosuppression: the National Institutes of Health experience. Diabetes Care 2003 Dec;26(12):3288-95.
379. Hering BJ, Kandaswamy R, Ansite JD, Eckman PM, Nakano M, Sawada T, et al. Single-donor, marginal-dose islet transplantation in patients with type 1 diabetes. JAMA 2005 Feb 16;293(7):830-5.
380. Shapiro AM, Ricordi C, Hering BJ, Auchincloss H, Lindblad R, Robertson RP, et al. International trial of the Edmonton protocol for islet transplantation. N Engl J Med 2006 Sep 28;355(13):1318-30.
381. Ryan EA, Paty BW, Senior PA, Bigam D, Alfadhli E, Kneteman NM, et al. Five-year fol-lowup after clinical islet transplantation. Diabetes 2005 Jul;54(7):2060-9.
382. Froud T, Ricordi C, Baidal DA, Hafi z MM, Ponte G, Cure P, et al. Islet transplantation in type 1 diabetes mellitus using cultured islets and steroid-free immunosuppression: Miami experience. Am J Transplant 2005 Aug;5(8):2037-46.
383. Hering BJ, Kandaswamy R, Harmon JV, Ansite JD, Clemmings SM, Sakai T, et al. Transplantation of cultured islets from two-layer preserved pancreases in type 1 diabetes with antiCD3 antibody. Am J Transplant 2004 Mar;4(3):390-401.
384. Lee TC, Barshes NR, O’Mahony CA, Nguyen L, Brunicardi FC, Ricordi C, et al. The effect of pancreatic islet transplantation on progression of diabetic retinopathy and neuropathy. Transplant Proc 2005 Jun;37(5):2263-5.
385. Maffi P, Bertuzzi F, De TF, Magistretti P, Nano R, Fiorina P, et al. Kidney function after islet transplant alone in type 1 diabetes: impact of immunosuppressive therapy on progression of diabetic nephropathy. Diabetes Care 2007 May;30(5):1150-5.
386. Keymeulen B, Gillard P, Mathieu C, Movahedi B, Maleux G, Delvaux G, et al. Correlation between beta cell mass and glycemic control in type 1 diabetic recipients of islet cell graft. Proc Natl Acad Sci U S A 2006 Nov 14;103(46):17444-9.
387. Badet L, Benhamou PY, Wojtusciszyn A, Baertschiger R, Milliat-Guittard L, Kessler L, et al. Expectations and strategies regarding islet transplantation: metabolic data from the GRAGIL 2 trial. Transplantation 2007 Jul 15;84(1):89-96.
388. O’Connell PJ, Hawthorne WJ, Holmes-Walker DJ, Nankivell BJ, Gunton JE, Patel AT, et al. Clinical islet transplantation in type 1 diabetes mellitus: results of Australia’s fi rst trial. Med J Aust 2006 Mar 6;184(5):221-5.
389. Shapiro AM, Lakey JR, Ryan EA, Korbutt GS, Toth E, Warnock GL, et al. Islet transplanta-tion in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosup-pressive regimen. N Engl J Med 2000 Jul 27;343(4):230-8.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 329
390. Barshes NR, Vanatta JM, Mote A, Lee TC, Schock AP, Balkrishnan R, et al. Health-related quality of life after pancreatic islet transplantation: a longitudinal study. Transplantation 2005 Jun 27;79(12):1727-30.
391. Fung MA, Warnock GL, Ao Z, Keown P, Meloche M, Shapiro RJ, et al. The effect of medical therapy and islet cell transplantation on diabetic nephropathy: an interim report. Transplanttion 2007 Jul 15;84(1):17-22.
392. Frank A, Deng S, Huang X, Velidedeoglu E, Bae YS, Liu C, et al. Transplantation for type I diabetes: comparison of vascularized whole-organ pancreas with isolated pancreatic islets. Ann Surg 2004 Oct;240(4):631-40.
393. Furnary AP, Zerr KJ, Grunkemeier GL, Starr A. Continuous intravenous insulin infusion re-duces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg 1999;67(2):352-60.
394. Christiansen CL, Schurizek BA, Malling B, Knudsen L, Alberti KG, Hermansen K. Insulin treatment of the insulin-dependent diabetic patient undergoing minor surgery. Continuous intravenous infusion compared with subcutaneous administration. Anaesth 1988;43(7):533-7.
395. Pezzarossa A, Taddei F, Cimicchi MC, Rossini E, Contini S, Bonora E, et al. Perioperative management of diabetic subjects. Subcutaneous versus intravenous insulin administration during glucose-potassium infusion. Diabetes Care 1988;11(1):52-8.
396. Simmons D, Morton K, Laughton SJ, Scott DJ. A comparison of two intravenous insulin regimens among surgical patients with insulin-dependent diabetes mellitus. Diabetes Educ 1994;20(5):422-7.
397. Furnary AP, Gao G, Grunkemeier GL, Wu Y, ZAerr KL, Bookin SO, et al. Continuous insu-lin infusion reduces mortality in patients with diabetes under-going coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003;125:1007-21.
398. Gandhi GY, Murad MH, Flynn DN, Erwin PJ, Cavalcante AB, Bay NH, et al. Effect of perioperative insulin infusion on surgical morbidity and mortality: systematic review and metaanalysis of randomized trials.7. Mayo Clin Proc 2008;83(4):418-30.
399. Malmberg K, Ryden L, Efendic S, et al. Randomized trial of insulin-glucose infusion fol-lowed by subcutaneous insulin treatment in diabetic patients with acute myocardial infarc-tion (DIGAMI study): effects on mortality at 1 year. J Am Coll Cardiol 1995;26:57-65.
400. Malmberg KA, Efendic S, Ryden LE. Feasibility of insulin-glucose infusion in diabetic patients with acute myocardial infarction. A report from the multicenter trial: DIGAMI. Diabetes Care 1994;17:1007-14.
401. Dazzi D, Taddei F, Gavarini A, Uggeri E, Negro R, Pezzarossa A. The control of blood glucose in the critical diabetic patient: a neuro-fuzzy method. J Diabetes Complications 2001;15(2):80-7.
402. Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med 2001;345:1359-67.
403. Krinsley JS. Effect of an intensive glucose management protocol on the mortality of criti-cally ill adult patients.[Erratum appears in Mayo Clin Proc. 2005 Aug;80(8):1101]. Mayo Clinic Proceedings 79(8):992-1000, 2004 Aug.
330 SNS CLINICAL PRACTICE GUIDELINES
404. Wiener RS, Wiener DC, Larson RJ. Benefi ts and risk of tight glucose control in critically ill adults: a meta-analysis. JAMA 2008;300:933-44.
405. NICE-SUGAR Stdy Investigators, Finfer S, Chittock DR, Su SY, Blair D, Foster D, et al. 73. N Engl J Med 2009;360:1283-97.
406. Malmberg K, DIGAMI (Diabetes Mellitus IGIiAMISG. Prospective randomised study of intensive insulin treatment on long term survival after acute myocardial infarction in patients with diabetes mellitus. BMJ 1997;314:1512-5.
407. Van den Berghe G, Wilmer A, Hermans G, Meersseman W, Wouters PJ, Milants I, et al. Intensive insulin therapy in the medical ICU. N Engl J Med 2006;354:449-61.
408. Devos P, Preiser JC, Me´lot C. Impact of tight glucose control by intensive insulin theraphy on ICU mortality and the rate of poglycaemia: fi nal results of the Glucontrol study. Intensive Care Med 2007;33(Suppl2):S189.
409. Umpierrez GE, Smiley D, Zisman A, Prieto LM, Palacio A, Ceron M, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT2trial). Diabetes Care 2007;30:2181-6.
410. American Diabetes Association. Standards of medical care in diabetes.VIII. Diabetes care in specifi c settings. Diabetes Care 2009;32:S41-8.
411. Perez PA, Conthe GP, Aguilar DM, Bertomeu M, V, Galdos AP, Garcia de CG, et al. Hospital management of hyperglycemia. [64 refs] [Spanish][Reprint in Endocrinol Nutr. 2009 Jun-Jul;56(6):303-16; PMID: 19695512]. Medicina Clinica 132(12):465-75, 2009 Apr 4.
412. Australasian Paediatric Endocrine Group for the Department of Health and Ageing. Type 1 diabetes in children and adolescents. Australian Government National Health and Medical Research Council 2005.
413. Brink S, Laffel L, Likitmaskul S, Liu L, Maguire AM, Olsen B, et al. Sick day management in children and adolescents with diabetes. Pediatric Diabetes 10 Suppl 12:146-53, 2009 Sep.
414. Patrick AW, Collier A, Hepburn DA, Steedman DJ, Clarke BF, Robertson C. Comparison of intramuscular glucagon and intravenous dextrose in the treatment of hypoglycaemic coma in an accident and emergency department. Archives of Emergency Medicine 7(2):73-7, 1990 Jun.
415. Collier A, Steedman DJ, Patrick AW, Nimmo GR, Matthews DM, MacIntyre CC, et al. Comparison of intravenous glucagon and dextrose in treatment of severe hypoglycemia in an accident and emergency department. Diabetes Care 10(6):712-5, 1987 Nov;-Dec.
416. Haymond MW, Schreiner B. Mini-dose glucagon rescue for hypoglycemia in children with type 1 diabetes. Diabetes Care 24(4):643-5, 2001 Apr.
417. Silverstein J, Klingensmith G, Copeland K, Plotnick L, Kaufman F, Laffel L, et al. Care of children and adolescents with type 1 diabetes: a statement of the American Diabetes Association. Diabetes Care 28(1):186-212, 2005 Jan.
418. Lawrenson R, Williams J. Antidepressant use in people with diabetes. Diabetes Primary Care 2001;3:70-4.
419. Anderson RJ, Freesland KE, Cluse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 24(6):1069-78, 2001 Jun.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 331
420. Barnard KD, Skinner TC, Preveler R. The prevalence of co-morbid depression in adults with type 1 diabetes: systematic literature review. Diabetic Medicine 23(4):445-8, 2006 Apr.
421. Kanner S, Hamrin V, Grey M. Depression in adolescentes with diabetes. J Child Adolesc Psychiatri Nurs 2003;16(1):15-24.
422. Kessing LV, Nilsson FM, Siersma V, Andersen PK. No increased risk of developing depres-sion in diabetes compared to other chronic illness. Diabetes Res Clin Pract 2003;62(2):113-21.
423. Petrack F, Hardt J, Wittchen HU, Kulzer B, Hisch A, Hentzel F, et al. Prevalence of psychi-atric disorders in an onset cohort of adults with type 1 diabetes. Diabetes Metab Res Rev 2003;19:216-22.
424. Shaban MC, Fosbury J, Kerr D, Cavan DA. The prevalence of depression and anxiety in adults with type 1 diabetes. Diabet Med 2006;23:1381-4.
425. Hermanns N, Kulzer B, Krichbaum M, Kubiak T, Haak T. Affective and anxiety disorders in a German sample of diabetics: prevalence, comorbidity and risk factors. Diabet Med 2005;22:293-300.
426. AI-Ghamdi. A high prevalence of depression among diabetic patients at a teaching hospital in Western Saudi Arabia. Neurosci 2004;9(2):108-12.
427. Khamseh ME, Baradaram HR, Rajabali H. Depression and diabetes in Iranian patients: a comparative study. Int Journal Psychiatry in Medicine 2007;37(1):81-6.
428. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of co-morbid depres-sion in adults with type 2 diabetes: a systematic review and meta-analysis. Diabet Med 2006;23:1165-73.
429. Hislop AL, Fegan PG, Schlaeppi MJ, Duck M, Yeap BB. Prevalence and associations of psychological distress in young adults with Type 1 diabetes. Diabetic Medicine 25(1):91-6, 2008 Jan.
430. Bryden KS, Neil A, Mayou RA, et al. Eating habits, body weight, and insulin misuse. A longitudinal study of teenagers and young adults with type 1 diabetes. Diabetes Care 22(12):1956- 60, 1999 Dec.
431. Nielsen S. Eating disorders in females with type 1 diabetes: an update of a meta-analysis. Eur Eat Disord Rev 2002;10:241.
432. Herpertz S, Wagener R, Albus C, Kocnar M, Wagner R, Best F, et al. Diabetes mellitus and eating disorders: a multicenter study on the comorbidity of the two diseases. Journal of Psychosomatic Research 44(3-4):503-15, 1998.
433. Jones JM, Lawson ML, Daneman D, Olmsted MP, Rodin G. Eating disorders in adolescent females with and without type 1 diabetes: cross sectional study. BMJ 320(7249):1563-6, 2000 Jun 10.
434. Rydall AC, Rodin GM, Olmsted MP, Devenyi RG, Daneman D. Disordered eating behavior and microvascular complications in young women with insulin-dependent diabetes mellitus. New England Journal of Medicine 336(26):1849-54, 1997 Jun 26.
332 SNS CLINICAL PRACTICE GUIDELINES
435. Goebel-Fabbri AE, Fikkan J, Franko DL, Pearson K, Anderson BJ, Weinger K. Insulin re-striction and associated morbidity and mortality in women with type 1 diabetes. Diabetes Care 31(3):415-9, 2008 Mar.
436. Grylli V, Hafferl-Gattermayer A, Schober E, Karwautz A. Prevalence and clinical manifes-tations of eating disorders in Austrian adolescents with type 1 diabetes. Wiener Klinische Wochenschrift 116(7-8):230-4, 2004 Apr 30.
437. Pinar R. Disordered eating behaviors among turkish adolescents with and without type 1 diabetes. J Pediatr Nurs 2005;20(5):383-8.
438. Cameron F. Teenagers with diabetes-management challenges. Aust Fam Physician 2006;35(6): 386-90.
439. Safyer AW, Hauser ST, Jacobson AM, Bliss R. The impact of the family on diabetes adjust-ment: a developmental perspective. Chile and Adolescent Social Work Journal 1993;10:123-40.
440. Bruno G, Cerutti F, Merletti F, Novelli G, Panero F, Zucco C, et al. Short-term mortality risk in children and young adults with type 1 diabetes: The population-based Registry of the Province of Turin,Italy. Nutr Metab Cardiovasc Dis 2009;19(5):340-4.
441. Whittemore R, Kanner S, Singleton S, Hamrin V, Chiu J, Grey M. Correlates of depressive symptoms in adolescents with type 1 diabetes. Pediatr Diabetes 2002;3:135-43.
442. Lawler MK. Individual and family factors impacting diabetic control in the adolescent: A preliminary study. Matern Chl Nurs J 1990;19:331-45.
443. Korbel CD, Wiebe DJ, Berg CA, Palmer DL. Gender differences in adherence to type 1 dia-betes management across adolescence: The mediating role of depression. Child Health Care 2007;26(3):83-98.
444. Lawrence JM, Standiford DA, Loots B, Klingensmith GJ, Wiliams DE, Ruggiero A, et al. Prevalence and correlates of depressed mood among youth with diabetes: The SEARCH for diabetes in youth study. Pediatr 2006;117(4):1348-58.
445. Stewart SM, Rao U, Emslie GJ, Klein D, White PC. Depressive symptoms predict hospitali-zation for adolescents with type 1 diabetes mellitus. Pediatr 2005;115(5):1315-9.
446. Morris AD, Boyle DI, McMahon AD, Greene SA, MacDonald TM, Newton RW. Adherence to insulin treatment, glycaemic control, and ketoacidosis in insulin-dependent diabetes mel-litus. The DARTS/MEMO Collaboration. Diabetes Audit and Research in Tayside Scotland. Medicine Monitoring Unit. Lancet 1997;350:1505-10.
447. Naar-King S, Idalski A, Ellis D, Frey M, Templin T, Cunningham PB, et al. Gender Differences in Adherence and Metabolic Control in Urban Youth with Poorly Controlled Type 1 Diabetes: The Mediating Role of Mental Health Symptoms. Journal of Pediatric Psychology 2006;13(8):793-802.
448. Borus JS, Laffel L. Adherence challenges in the management of type 1 diabetes in adoles-cents: prevention and intervention. Curr Opin Pediatr 2010 Aug;22(4):405-11.
449. Confi dential Inquiry into Maternal and Child Health. Diabets in pregnancy: are we providing the best care? Finding of a national enquiry: England, Wales and Northerm Ireland. London: CEMACH 2007.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 333
450. Ray JG, Vermeulen MJ, Shapiro JL, Kenshole AB. Maternal and neonatal outcomes in pregestational and gestational diabetes mellitus, and the infl uence of maternal obesity and weight gain: the DEPOSIT study. Diabetes Endocrine Pregnancy Outcome Study in Toronto. QMJ 2001;94(7):347-56.
451. McElvy SS, Miodovnik M, Rosenn B, Khoury JC, Siddiqi T, Dignan PS, et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces peri-natal mortality and malformation rates to general population levels. J Matern Fetal Med 2000;9(1):14-20.
452. Kitzmiller JL, Wallerstein R, Correa A, Kwan S. Preconception care for women with diabe-tes and prevention of major congenital malformations. Birth Defects Res A Clin Mol Teratol 2010 Oct;88(10):791-803.
453. Robertson H, Pearson DW, Gold AE. Severe hypoglycaemia during pregnancy in women with Type 1 diabetes is common and planning pregnancy does not decrease the risk. Diabetic Medicine 26(8):824-6, 2009 Aug.
454. Yogev Y, Chen R, Ben-Haroush A, Hod M, Bar J. Maternal overweight and pregnancy out-come in women with Type-1 diabetes mellitus and different degrees of nephropathy. Journal of Maternal-Fetal & Neonatal Medicine 23(9):999-1003, 2010 Sep.
455. Wahabi HA, Alzeidan RA, Bawazeer GA, Alansari LA, Esmaeil SA. Preconception care for diabetic women for improving maternal and fetal outcomes: a systematic review and metaanalysis. BMC Pregnancy & Childbirth 10:63, 2010.
456. The Diabetes Control and Complications Trial Research Group. Effect of pregnancy on mi-crovascular complications in the diabetes control and complications trial. Diabetes Care 2000;23(8):1084-91.
457. Axer-Siegel R, Hod M, Fink-Cohen S, Kramer M, Weinberger D, Schindel B, et al. Diabetic retinopathy during pregnancy. Ophthalmology 1996;103(11):1815-9.
458. Rosenn B, Miodovnik M, Kranias G, Khoury J, Combs CA, Mimouni F, et al. Progression of diabetic retinopathy in pregnancy: association with hypertension in pregnancy. Am J Obstet Gynecol 1992;166(4):1214-8.
459. Suhonen L, HIilesmaa V, Teramo K. Glycaemic control during early pregnancy and fetal malformations in women with type I diabetes mellitus. Diabetologia 2000;43(1):79-82.
460. Boulot P, chabbert-Buffet N, dÉrcole C, Floriot M, Fontaine P, Fournier A, et al. French mul-ticentric survey of outcome of pregnancy in women with pregestational diabetes. Diabetes Care 2003;26(11):2990-3.
461. Dicker D, Feldberg D, Samuel N, Yeshaya A, Karp M, Goldman JA. Spontaneous abortion in patients with insulin-dependent diabetes mellitus: the effect of preconceptional diabetic control. Am J Obstet Gynecol 1988;158(5):1161-4.
462. Fuhrmann K, reiher H, Semmler K, Glockner E. The effect of intensifi ed conventional in-sulin therapy before and during pregnancy on the malformation rate in offspring of diabetic mothers. Exp Clin Endocrinol 1984;83(2):173-7.
463. Gold AE, Reilly R, Little J, Walker JD. The effect of glycemic control in the preconception period and early pregnancy on birth weight in women with IDDM. Diabetes Care 1998;21(4): 535-8.
334 SNS CLINICAL PRACTICE GUIDELINES
464. Goldman JA, Dicker D, Feldberg D, Yeshaya A, Samuel N, Karp M. Pregnancy outcome in patients with insulin-dependent diabetes mellitus with preconceptional diabetic control: a comparative study. Am J Obstet Gynecol 1986;155(2):293-7.
465. Jensen DM, Damm P, Molested-Pedersen L, Ovesen P, Westergaard JG, Moeller M, et al. Outcomes in type 1 diabetic pregnancies: a nationwide, population-based study. Diabetes Care 2004;27(12):2819-23.
466. Key TC, Giuffrida R, Moore TR. Predictive value of early pregnancy glycohemoglobin in the insulin-treated diabetic patient. Am J Obstet Gynecol 1987;156(5):1096-100.
467. Kitzmiller JL, Gavin LA, Gin GD, Jovanovic-Peterson L, Main EK, Zigrang WD. Preconception care of diabetes. Glycemic control prevents congenital anomalies. JAMA 1991;265(6):731-6.
468. Miodovnik M, Skillman C, Holroyde JC, Butler JB, Wendel JS, Siddiqi TA. Elevated mater-nal glycohemoglobin in early pregnancy and spontaneous abortion among insulin-dependent diabetic women. Am J Obstet Gynecol 1985;153(4):439-42.
469. Miodovnik M, Mimouni F, Tsang RC, Ammar E, Kaplan L, Siddiqi TA. Glycemic con-trol and spontaneous abortion in insulin-dependent diabetic women. Obstet Gynecol 1986;68(3):366-9.
470. Miller E, Hare JW, Cloherty JP, Dunn PJ, Gleason RE, Soeldner JS, et al. Elevated maternal hemoglobin A1c in early pregnancy and major congenital anomalies in infants of diabetic mothers. N Eng J Med 1981;304(22):1331-4.
471. Rosenn B, Miodovnik M, Combs CA, Khoury J, Siddiqi TA. Glycemic thresholds for spon-taneous abortion and congenital malformations in insulin-dependent diabetes mellitus. Obstet Gynecol 1994;84(4):515-20.
472. Schafer-Graf UM, Buchanan TA, Xiang A, Songster G, Montoro M, Kjos SL. Patterns of congenital anomalies and relationship to initial maternal fasting glucose levels in pregnan-cies complicated by type 2 and gestational diabetes. Am J Obstet Gynecol 2000;182(2):313-20.
473. Rosenn BM, Miodovnik M, Holcberg G, Khoury JC, Siddiqi TA. Hypoglycemia: the price of intensive insulin therapy for pregnant women with insulin-dependent diabetes mellitus. Obstet Gynecol 1995;85(3):417-22.
474. Greene MF, Hare JW, Cloherty JP, Benacerraf BR, Soeldner JS. First-trimester hemo-globin A1 and risk for major malformation and spontaneous abortion in diabetic pregnancy. Teratology 1989;39(3):225-31.
475. Mills JL, Simpson JL, Driscoll SG, Jovanovic-Peterson L, Van AM, Aaron JH, et al. Incidence of spontaneous abortion among normal women and insulin-dependent diabetic women whose pregnancies were identifi ed within 21 days of conception. N Eng J Med 1988;319(25):1617-23.
476. Ylinen K, Aula P, Stenman UH, Kesaniemi-Kuokkanen T, Teramo K. Risk of minor and ma-jor fetal malformations in diabetics with high haemoglobin A1c values in early pregnancy. Br Med J (Clin Res Ed) 1984;289(6441):345-6.
477. Lucas MJ, Leveno KJ, Williams ML, Raskin P, Whalley PJ. Early pregnancy glyco-sylated hemoglobin, severity of diabetes, and fetal malformations. Am J Obstet Gynecol 1989;161(2):426-31.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 335
478. Rosenn B, Miodovnik M, Combs CA, Khoury J, Siddiqi TA. Pre-conception manage-ment of insulin-dependent diabetes: improvement of pregnancy outcome. Obstet Gynecol 1991;77(6): 846-9.
479. Steel JM, Johnstone FD, Hepburn DA, Smith AF. Can prepregnancy care of diabetic women reduce the risk of abnormal babies? BMJ 1990;301(6760):1070-4.
480. Pregnancy outcomes in the Diabetes Control and Complications Trial. Am J Obstet Gynecol 1996;174(4):1343-53.
481. Inkster ME, Fahey TP, Donnan PT, Leese GP, Mires GJ, Murphy DJ. The role of modifi able pre-pregnancy risk factors in preventing adverse fetal outcomes among women with type 1 and type 2 diabetes. Acta Obstet Gynecol Scand 2009;88(10):1153-7.
482. Middleton P, Crowther CA, Simmonds L, Muller P. Different intensities of glycaemic control for pregnant women with pre-existing diabetes. Cochrane Database of Systematic Reviews (9):CD008540, 2010.
483. Visser J, Snel M, Van Vliet HA. Hormonal versus non-hormonal contraceptives in women with diabetes mellitus type 1 and 2. Cochrane Database Syst Rev 2006;(4):CD003990.
484. Medical eligibility criteria for contraceptive use (article online). Third edition,2005.World Health Organization. Avaliable from: URL: www who int/reproductive-health 2005.
485. Diabetes y Ramadán.FICHAS DE CONSULTA RÁPIDA. Sociedad Valenciana de Medicina Familiar y Comunitaria 2009.
486. Al-Arouj M, Bouguerra R, Buse J, Hafez S, Hassanein M, Ibrahim MA, et al. Recommendations for management of diabetes during Ramadan. Diabetes Care 28(9):2305-11, 2005 Sep.
487. Mucha GT, Merkel S, Thomas W, Bantle JP. Fasting and insulin glargine in individuals with type 1 diabetes. Diabetes Care 27(5):1209-10, 2004 May.
488. Kadiri A, Al-Nakhi A, El-Ghazali S, Jabbar A, Al AM, Akram J, et al. Treatment of type 1 diabetes with insulin lispro during Ramadan. Diabetes & Metabolism 27(4 Pt 1):482-6, 2001 Sep.
489. Kassem HS, Zantout MS, Azar ST. Insulin therapy during Ramadan fast for Type 1 diabetes patients. Journal of Endocrinological Investigation 28(9):802-5, 2005 Oct.
490. Azar ST, Khairallah WG, Merheb MT, Zantout MS, Fliti F. Insulin therapy during Ramadan fast for patients with type 1 diabetes mellitus. Journal Medical Libanais - Lebanese Medical Journal 56(1):46, 2008 Jan;-Mar.
491. Canadian Diabetes Association. Clinical Practice Guiddelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2008;32(S1-S201).
492. Defi ning and reporting hypoglycemia in diabetes: a report from the American Diabetes Association Workgroup on Hypoglycemia. Diabetes Care 2005 May;28(5):1245-9.
493. Machnica L, Osior A, Jarosz-Chobot P, Deja G, Polanska J, Otto-Buczkowska E. An analy-sis of the prevalence of thyroid autoantibodies: thyroid peroxidase antibodies (ATA) and thyroglobulin antibodies (ATG) in children with newly diagnosed diabetes mellitus type 1 during 2000-2004 in the Upper Silesia region, Poland. Acta Diabetol 2008;45:37-40.
494. Wiethop BV, Cryer PE. Alanine and terbutaline in treatment of hypoglycemia in IDDM. Diabetes Care 1993 Aug;16(8):1131-6.
336 SNS CLINICAL PRACTICE GUIDELINES
495. Slama G, Traynard PY, Desplanque N, Pudar H, Dhunputh I, Letanoux M, et al. The search for an optimized treatment of hypoglycemia. Carbohydrates in tablets, solutin, or gel for the correction of insulin reactions. Arch Intern Med 1990 Mar;150(3):589-93.
496. Carstens S, Sprehn M. Prehospital treatment of severe hypoglycaemia: a comparison of in-tramuscular glucagon and intravenous glucose. Prehosp Disaster Med 1998 Apr;13(2-4):44-50.
497. MacCuish AC, Munro JF, Duncan LJ. Treatment of hypoglycaemic coma with glucagon, intravenous dextrose, and mannitol infusion in a hundred diabetics. Lancet 1970 Nov 7;2(7680):946-9.
498. Namba M, Hanafusa T, Kono N, Tarui S. Clinical evaluation of biosynthetic glucagon treatment for recovery from hypoglycemia developed in diabetic patients. The GL-G Hypoglycemia Study Group. Diabetes Res Clin Pract 1993 Feb;19(2):133-8.
499. Aman J, Wranne L. Hypoglycaemia in childhood diabetes. II. Effect of subcutaneous or intra-muscular injection of different doses of glucagon. Acta Paediatr Scand 1988 Jul;77(4):548-53.
500. Stenninger E, Aman J. Intranasal glucagon treatment relieves hypoglycaemia in children with type 1 (insulin-dependent) diabetes mellitus. Diabetologia 1993 Oct;36(10):931-5.
501. Slama G, Alamowitch C, Desplanque N, Letanoux M, Zirinis P. A new non-invasive method for treating insulin-reaction: intranasal lyophylized glucagon. Diabetologia 1990 Nov;33(11):671-4.
502. Pontiroli AE, Calderara A, Pajetta E, Alberetto M, Pozza G. Intranasal glucagon as remedy for hypoglycemia. Studies in healthy subjects and type I diabetic patients. Diabetes Care 1989 Oct;12(9):604-8.
503. Hvidberg A, Christensen NJ, Hilsted J. Counterregulatory hormones in insulin-treated di-abetic patients admitted to an accident and emergency department with hypoglycaemia. Diabet Med 1998 Mar;15(3):199-204.
504. Monsod TP, Tamborlane WV, Coraluzzi L, Bronson M, Yong-Zhan T, Ahern JA. Epipen as an alternative to glucagon in the treatment of hypoglycemia in children with diabetes. Diabetes Care 2001 Apr;24(4):701-4.
505. Moore C, Woollard M. Dextrose 10% or 50% in the treatment of hypoglycaemia out of hos-pital? A randomised controlled trial. Emerg Med J 2005 Jul;22(7):512-5.
506. Kinsley BT, Weinger K, Bajaj M, Levy CJ, Simonson DC, Quigley M, et al. Blood glucose awareness training and epinephrine responses to hypoglycemia during intensive treatment in type 1 diabetes. Diabetes Care 1999 Jul;22(7):1022-8.
507. Schachinger H, Hegar K, Hermanns N, Straumann M, Keller U, Fehm-Wolfsdorf G, et al. Randomized controlled clinical trial of Blood Glucose Awareness Training (BGAT III) in Switzerland and Germany. J Behav Med 2005 Dec;28(6):587-94.
508. Cox DJ, Kovatchev B, Koev D, Koeva L, Dachev S, Tcharaktchiev D, et al. Hypoglycemia anticipation, awareness and treatment training (HAATT) reduces occurrence of severe hypo-glycemia among adults with type 1 diabetes mellitus. Int J Behav Med 2004;11(4):212-8.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 337
509. Grupo de trabajo de la Guía de Práctica Clínica sobre Diabetes tipo 2. Guía de Práctica Clínica sobre Diabetes tipo 2. Madrid: Plan Nacional para el SNS del MSC Agencia de Evaluación de Tecnologías Sanitarias del País Vasco 2008;Guías de Práctica Clínica en el SNS: OSTEBA Nº 2006/08.
510. Hu G, Jousilahti P, Qiao Q, Peltonen M, Katoh S, Tuomilehto J. The gender-specifi c impact of diabetes and myocardial infarction at baseline and during follow-up on mortality from all causes and coronary heart disease. J Am Coll Cardiol 2005 May 3;45(9):1413-8.
511. Juutilainen A, Kortelainen S, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Gender differ-ence in the impact of type 2 diabetes on coronary heart disease risk. Diabetes Care 2004 Dec;27(12):2898-904.
512. Natarajan S, Liao Y, Cao G, Lipsitz SR, McGee DL. Sex differences in risk for coronary heart disease mortality associated with diabetes and established coronary heart disease. Arch Intern Med 2003 Jul 28;163(14):1735-40.
513. Whiteley L, Padmanabhan S, Hole D, Isles C. Should diabetes be considered a coronary heart disease risk equivalent?: results from 25 years of follow-up in the Renfrew and Paisley survey. Diabetes Care 2005 Jul;28(7):1588-93.
514. Vaccaro O, Eberly LE, Neaton JD, Yang L, Riccardi G, Stamler J. Impact of diabetes and previous myocardial infarction on long-term survival: 25-year mortality follow-up of pri-mary screenees of the Multiple Risk Factor Intervention Trial. Arch Intern Med 2004 Jul 12;164(13):1438-43.
515. Hu FB, Manson JE, Stampfer MJ, Colditz G, Liu S, Solomon CG, et al. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N Engl J Med 2001 Sep 13;345(11):790-7.
516. Wannamethee SG, Shaper AG, Lennon L. Cardiovascular disease incidence and mortality in older men with diabetes and in men with coronary heart disease. Heart 2004 Dec;90(12):1398-403.
517. McGin T, Guyatt G. Diagnosis. Clinical prediction Rules.User’s Guides to the Medical Literature. A manual for evidence-based clinical practice. American Medical Association 2002.
518. Marrugat J, D’Agostino R, Sullivan L, Elosua R, Wilson P, Ordovas J, et al. An adaptation of the Framingham coronary heart disease risk function to European Mediterranean areas. J Epidemiol Community Health 2003 Aug;57(8):634-8.
519. Marrugat J, Solanas P, D’Agostino R, Sullivan L, Ordovas J, Cordon F, et al. [Coronary risk estimation in Spain using a calibrated Framingham function]. Rev Esp Cardiol 2003 Mar;56(3):253-61.
520. Marrugat J, Subirana I, Comin E, Cabezas C, Vila J, Elosua R, et al. Validity of an adapta-tion of the Framingham cardiovascular risk function: the VERIFICA Study. J Epidemiol Community Health 2007 Jan;61(1):40-7.
521. Mohamed Q, Gillies MC, Wong TY. Management of diabetic retinopathy: a systematic re-view. JAMA 2007 Aug 22;298(8):902-16.
522. Lachin JM, Genuth S, Nathan DM, Zinman B, Rutledge BN. Effect of glycemic exposure on the risk of microvascular complications in the diabetes control and complications trial--revisited. Diabetes 2008 Apr;57(4):995-1001.
338 SNS CLINICAL PRACTICE GUIDELINES
523. Chaturvedi N, Porta M, Klein R, Orchard T, Fuller J, Parving HH, et al. Effect of candesartan on prevention (DIRECT-Prevent 1) and progression (DIRECT-Protect 1) of retinopathy in type 1 diabetes: randomised, placebo-controlled trials. Lancet 2008 Oct 18;372(9647):1394-402.
524. Lopes de Jesus CC, Atallah AN, Valente O, Moça Trevisani VF. Pentoxifi lina para la retin-opatía diabética (Revisión Cochrane traducida). Biblioteca Cochrane Plus 2008;4.
525. Ribeiro ML, Seres AI, Carneiro AM, Stur M, Zourdani A, Caillon P, et al. Effect of calcium dobesilate on progression of early diabetic retinopathy: a randomised double-blind study. Graefes Arch Clin Exp Ophthalmol 2006 Dec;244(12):1591-600.
526. Wang PH, Lau J, Chalmers TC. Meta-analysis of effects of intensive blood-glucose control on late complications of type I diabetes. Lancet 1993 May 22;341(8856):1306-9.
527. Wang PH, Lau J, Chalmers TC. Metaanalysis of the effects of intensive glycemic control on late complications of type I diabetes mellitus. Online J Curr Clin Trials 1993 May 21;Doc No 60:5023.
528. White NH, Sun W, Cleary PA, Tamborlane WV, Danis RP, Hainsworth DP, et al. Effect of prior intensive therapy in type 1 diabetes on 10-year progression of retinopathy in the DCCT/ EDIC: comparison of adults and adolescents. Diabetes 2010 May;59(5):1244-53.
529. Blood glucose control and the evolution of diabetic retinopathy and albuminuria. A pre-liminary multicenter trial. The Kroc Collaborative Study Group. N Engl J Med 1984 Aug 9;311(6):365-72.
530. Reichard P, Berglund B, Britz A, Cars I, Nilsson BY, Rosenqvist U. Intensifi ed convention-al insulin treatment retards the microvascular complications of insulin-dependent diabetes mellitus (IDDM): the Stockholm Diabetes Intervention Study (SDIS) after 5 years. J Intern Med 1991 Aug;230(2):101-8.
531. Weinrauch LA, Sun J, Gleason RE, Boden GH, Creech RH, Dailey G, et al. Pulsatile inter-mittent intravenous insulin therapy for attenuation of retinopathy and nephropathy in type 1 diabetes mellitus. Metabolism 2010 Oct;59(10):1429-34.
532. Chaturvedi N, Sjolie AK, Stephenson JM, Abrahamian H, Keipes M, Castellarin A, et al. Effect of lisinopril on progression of retinopathy in normotensive people with type 1 dia-betes. The EUCLID Study Group. EURODIAB Controlled Trial of Lisinopril in Insulin-Dependent Diabetes Mellitus. Lancet 1998 Jan 3;351(9095):28-31.
533. Mauer M, Zinman B, Gardiner R, Suissa S, Sinaiko A, Strand T, et al. Renal and retinal ef-fects of enalapril and losartan in type 1 diabetes. N Engl J Med 2009 Jul 2;361(1):40-51.
534. Bergerhoff K, Clar C, Richter B. Aspirin in diabetic retinopathy. A systematic review. Endocrinol Metab Clin North Am 2002 Sep;31(3):779-93.
535. Clinical study of ticlopidine in diabetic retinopathy. Belgian Ticlopidine Retinopathy Study Group (BTRS). Ophthalmologica 1992;204(1):4-12.
536. Ticlopidine treatment reduces the progression of nonproliferative diabetic retinopathy. The TIMAD Study Group. Arch Ophthalmol 1990 Nov;108(11):1577-83.
537. Pagani A, Greco G, Tagliaferro V, Marena S, Pagano G. Dipyridamole administration in insulin-dependent diabetics with background retinopathy: a 36-month follow-up. Current Therapeutic Research, Clinical and Experimental 1989;45:469-75.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 339
538. Esmatjes E, Maseras M, Gallego M, Coves MJ, Conget I. Effect of treatment with an inhibi-tor of platelet aggregation on the evolution of background retinopathy: 2 years of follow-up. Diabetes Res Clin Pract 1989 Nov 6;7(4):285-91.
539. Cummins E, Facey K, Macpherson K, Morris A, Reay L, Slattery J. Health Technology Assessment of Organization of Services for Diabetic Retinopathy Screening (project). Glasgow: Health Technology Board for Scotland 2001.
540. Scottish Intercollegiate Guidelines Network. Management of diabetes: a national clinical guideline. SIGN Publication 2010;No 116(Edinburgh: SIGN).
541. Khalaf SS, Al-Bdour MD, Al-Till MI. Clinical biomicroscopy versus fl uorescein angiogra-phy: effectiveness and sensitivity in detecting diabetic retinopathy. Eur J Ophthalmol 2007 Jan;17(1):84-8.
542. Hutchinson A, McIntosh A, Peters J, O’Keeffe C, Khunti K, Baker R, et al. Effectiveness of screening and monitoring tests for diabetic retinopathy--a systematic review. Diabet Med 2000 Jul;17(7):495-506.
543. Kinyoun J, Barton F, Fisher M, Hubbard L, Aiello L, Ferris F, III. Detection of diabetic mac-ular edema. Ophthalmoscopy versus photography--Early Treatment Diabetic Retinopathy Study Report Number 5. The ETDRS Research Group. Ophthalmology 1989 Jun;96(6):746-50.
544. Leese GP, Tesfaye S, gler-Harles M, Laws F, Clark DI, Gill GV, et al. Screening for diabetic eye disease by optometrists using slit lamps. J R Coll Physicians Lond 1997 Jan;31(1):65-9.
545. Vujosevic S, Benetti E, Massignan F, Pilotto E, Varano M, Cavarzeran F, et al. Screening for diabetic retinopathy: 1 and 3 nonmydriatic 45-degree digital fundus photographs vs 7 stand-ard early treatment diabetic retinopathy study fi elds. Am J Ophthalmol 2009 Jul;148(1):111-8.
546. Sharp PF, Olson J, Strachan F, Hipwell J, Ludbrook A, O’Donnell M, et al. The value of digital imaging in diabetic retinopathy. Health Technol Assess 2003;7(30):1-119.
547. Cummings E, Facey K, Macpherson K, Morris A, Reay L, Slattery J. Organisation of Services for Diabetic Retinopathy Screening. Health Technology Assessement Report 1 2002;Glasgow: Health Technology Board for Scotland.
548. Donaghue KC, Fairchild JM, Chan A, Hing SJ, Howard NJ, Silink M. Diabetes complication screening in 937 children and adolescents. J Pediatr Endocrinol Metab 1999 Mar;12(2):185-92.
549. Younis N, Broadbent DM, Harding SP, Vora JP. Incidence of sight-threatening retinopathy in Type 1 diabetes in a systematic screening programme. Diabet Med 2003 Sep;20(9):758-65.
550. Olafsdottir E, Stefansson E. Biennial eye screening in patients with diabetes without retin-opathy: 10-year experience. Br J Ophthalmol 2007 Dec;91(12):1599-601.
551. Vazquez JA, Hernaez MC, Natividad M, Soto E. Incidencia de retinopatía diabética a partir de un programa de despistaje en cámara no midriática empleado en pacientes diabéticos de la Comunidad Autonoma del País Vasco (CAPV). Investigación comisionada Vitoria-Gasteiz Departamento de Sanidad Gobierno Vasco 2003;Informe n.º Osteba D-06-03.
340 SNS CLINICAL PRACTICE GUIDELINES
552. Obrador GT, Pereira BJ. Early referral to the nephrologist and timely initiation of renal replacement therapy: a paradigm shift in the management of patients with chronic renal failure. Am J Kidney Dis 1998 Mar;31(3):398-417.
553. Gorriz JL, Beltrán S. Cambios inducidos por la enfermedad renal crónica en los pacientes con diabetes. Av Diabetol. 2010;26:235-41. Av Diabetol 2010;26:235-41.
554. Lameire N, Wauters JP, Teruel JL, Van BW, Vanholder R. An update on the referral pattern of patients with end-stage renal disease. Kidney Int Suppl 2002 May;(80):27-34.
555. Gallego E, Lopez A, Lorenzo I, Lopez E, Llamas F, Illescas ML, et al. [Infl uence of early or late referral to nephrologist over morbidity and mortality in hemodialysis]. Nefrologia 2003;23(3):234-42.
556. Winkelmayer WC, Owen WF, Jr., Levin R, Avorn J. A propensity analysis of late versus early nephrologist referral and mortality on dialysis. J Am Soc Nephrol 2003 Feb;14(2):486-92.
557. Jones C, Roderick P, Harris S, Rogerson M. Decline in kidney function before and after nephrology referral and the effect on survival in moderate to advanced chronic kidney dis-ease. Nephrol Dial Transplant 2006 Aug;21(8):2133-43.
558. Lopez RK, Garcia Lopez FJ, de Alvaro MF, Alonso J. Perceived mental health at the start of dialysis as a predictor of morbidity and mortality in patients with end-stage renal disease (CALVIDIA Study). Nephrol Dial Transplant 2004 Sep;19(9):2347-53.
559. Jungers P, Choukroun G, Robino C, Massy ZA, Taupin P, Labrunie M, et al. Epidemiology of end-stage renal disease in the Ile-de-France area: a prospective study in 1998. Nephrol Dial Transplant 2000 Dec;15(12):2000-6.
560. Lameire N, Van BW. The pattern of referral of patients with end-stage renal disease to the nephrologist—a European survey. Nephrol Dial Transplant 1999;14 Suppl 6:16-23.
561. Mora-Fernandez C, Muros M, Jarque A, Gonzalez-Cabrera F, Garcia-Perez J, Navarro J. [Characteristics of the diabetic patients referred for the fi rst time to the nephrologist]. Nefrologia 2007;27(2):154-61.
562. Kanter J, Puerta CM, Goicoechea M, Garcia DS, Gomez-Campdera F, Luno J. What fea-tures show patients referred for the fi rst time to an outpatient nephrology clinic? Nefrologia 2005;25 Suppl 4:4-6.
563. Garber AJ, Moghissi ES, Bransome ED, Clark NG, Clement S, Cobin RH, et al. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Pract 2004;10:4-9.
564. Burden R, Tomson C. Identifi cation, management and referral of adults with chronic kidney disease: concise guidelines. Clin Med 2005 Nov;5(6):635-42.
565. Alcazar R, Egocheaga MI, Orte L, Lobos JM, Gonzalez PE, Alvarez GF, et al. [SEN-SEMFYC consensus document on chronic kidney disease]. Nefrologia 2008;28(3):273-82.
566. The ACE Inhibitors in Diabetic Nephropathy Trialist Group. Should all patients with type 1 diabetes mellitus and microalbuminuria receive angiotensin-converting enzyme inhibitors? A meta-analysis of individual patient data. Ann Intern Med 2001 Mar 6;134(5):370-9.
CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 341
567. Jerums G, Allen TJ, Campbell DJ, Cooper ME, Gilbert RE, Hammond JJ, et al. Long-term comparison between perindopril and nifedipine in normotensive patients with type 1 diabe-tes and microalbuminuria. Am J Kidney Dis 2001 May;37(5):890-9.
568. Tarnow L, Rossing P, Jensen C, Hansen BV, Parving HH. Long-term renoprotective effect of nisoldipine and lisinopril in type 1 diabetic patients with diabetic nephropathy. Diabetes Care 2000 Dec;23(12):1725-30.
569. Kopf D, Schmitz H, Beyer J, Frank M, Bockisch A, Lehnert H. A double-blind trial of perindopril and nitrendipine in incipient diabetic nephropathy. Diabetes Nutr Metab 2001 Oct;14(5):245-52.
570. Giorgino F, Laviola L, Cavallo PP, Solnica B, Fuller J, Chaturvedi N. Factors associated with progression to macroalbuminuria in microalbuminuric Type 1 diabetic patients: the EURODIAB Prospective Complications Study. Diabetologia 2004 Jun;47(6):1020-8.
571. Ficociello LH, Perkins BA, Silva KH, Finkelstein DM, Ignatowska-Switalska H, Gaciong Z, et al. Determinants of progression from microalbuminuria to proteinuria in patients who have type 1 diabetes and are treated with angiotensin-converting enzyme inhibitors. Clin J Am Soc Nephrol 2007 May;2(3):461-9.
572. Ciavarella A, Silletti A, Forlani G, Morotti L, Borgnino LC, D’Apote M, et al. A screening test for microalbuminuria in type 1 (insulin-dependent) diabetes. Diabetes Res Clin Pract 1989 Nov 6;7(4):307-12.
573. Ahn CW, Song YD, Kim JH, Lim SK, Choi KH, Kim KR, et al. The validity of random urine specimen albumin measurement as a screening test for diabetic nephropathy. Yonsei Med J 1999 Feb;40(1):40-5.
574. Microvascular and acute complications in IDDM patients: the EURODIAB IDDM Complications Study. Diabetologia 1994 Mar;37(3):278-85.
575. National Kidney Foundation. KDOQITM Clinical Practice Guidelines and Clinical Practice Recommendations for Diabetes and Chronic Kidney Disease. Am J Kidney Dis 49 2007;sup-pl 2:S1-S180.
576. McCabe CJ, Stevenson RC, Dolan AM. Evaluation of a diabetic foot screening and protec-tion programme. Diabet Med 1998 Jan;15(1):80-4.
577. Lavery LA, Wunderlich RP, Tredwell JL. Disease management for the diabetic foot: effec-tiveness of a diabetic foot prevention program to reduce amputations and hospitalizations. Diabetes Res Clin Pract 2005 Oct;70(1):31-7.
578. Anichini R, Zecchini F, Cerretini I, Meucci G, Fusilli D, Alviggi L, et al. Improvement of dia-betic foot care after the Implementation of the International Consensus on the Diabetic Foot (ICDF): results of a 5-year prospective study. Diabetes Res Clin Pract 2007 Feb;75(2):153-8.
579. American Diabetes Association. Standards of medical care in diabetes--2009. Diabetes Care 2009 Jan;32 Suppl 1:S13-S61.
580. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA 2005 Jan 12;293(2):217-28.
581. Mayfi eld JA, Sugarman JR. The use of the Semmes-Weinstein monofi lament and other threshold tests for preventing foot ulceration and amputation in persons with diabetes. J Fam Pract 2000 Nov;49(11 Suppl):S17-S29.
342 SNS CLINICAL PRACTICE GUIDELINES
582. Oyer DS, Saxon D, Shah A. Quantitative assessment of diabetic peripheral neuropathy with use of the clanging tuning fork test. Endocr Pract 2007 Jan;13(1):5-10.
583. Nather A, Neo SH, Chionh SB, Liew SC, Sim EY, Chew JL. Assessment of sensory neu-ropathy in diabetic patients without diabetic foot problems. J Diabetes Complications 2008 Mar;22(2):126-31.
584. NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993 Jul 7;270(1):83-90.
585. Martin-Morales A, Sanchez-Cruz JJ, Saenz dT, I, Rodriguez-Vela L, Jimenez-Cruz JF, Burgos-Rodriguez R. Prevalence and independent risk factors for erectile dysfunction in Spain: results of the Epidemiologia de la Disfuncion Erectil Masculina Study. J Urol 2001 Aug;166(2):569-74.
586. Setter SM, Iltz JL, Fincham JE, Campbell RK, Baker DE. Phosphodiesterase 5 inhibitors for erectile dysfunction. Ann Pharmacother 2005 Jul;39(7-8):1286-95.
587. Vardi M, Nini A. Phosphodiesterase inhibitors for erectile dysfunction in patients with dia-betes mellitus. Cochrane Database Syst Rev 2007;(1):CD002187.
588. Nehra A. Erectile dysfunction and cardiovascular disease: effi cacy and safety of phosphodi-esterase type 5 inhibitors in men with both conditions. Mayo Clin Proc 2009 Feb;84(2):139-48.
589. Hatzimouratidis K. Erectile dysfunction and diabetes mellitus. Insulin 2009;4(2):114-22.
590. Apomorphine for erectile dysfunction. Bandolier Journal 2007.
591. Dula E, Keating W, Siami PF, Edmonds A, O’neil J, Buttler S. Effi cacy and safety of fi xed-dose and dose-optimization regimens of sublingual apomorphine versus placebo in men with erectile dysfunction. The Apomorphine Study Group. Urology 2000 Jul;56(1):130-5.
592. Dula E, Bukofzer S, Perdok R, George M. Double-blind, crossover comparison of 3 mg apomorphine SL with placebo and with 4 mg apomorphine SL in male erectile dysfunction. Eur Urol 2001 May;39(5):558-3.
593. Von Keitz AT, Stroberg P, Bukofzer S, Mallard N, Hibberd M. A European multicentre study to evaluate the tolerability of apomorphine sublingual administered in a forced dose-escala-tion regimen in patients with erectile dysfunction. BJU Int 2002 Mar;89(4):409-15.
594. Gontero P, D’Antonio R, Pretti G, Fontana F, Panella M, Kocjancic E, et al. Clinical ef-fi cacy of Apomorphine SL in erectile dysfunction of diabetic men. Int J Impot Res 2005 Jan;17(1):80-5.
595. Eardley I, Wright P, MacDonagh R, Hole J, Edwards A. An open-label, randomized, fl exible-dose, crossover study to assess the comparative effi cacy and safety of sildenafi l citrate and apomorphine hydrochloride in men with erectile dysfunction. BJU Int 2004 Jun;93(9):1271-5.
596. Perimenis P, Markou S, Gyftopoulos K, Giannitsas K, Athanasopoulos A, Liatsikos E, et al. Effi cacy of apomorphine and sildenafi l in men with nonarteriogenic erectile dysfunction. A comparative crossover study. Andrologia 2004 Jun;36(3):106-10.
597. Afi f-Abdo J, Teloken C, Damiao R, Koff W, Wroclawski E, Yamasaki R, et al. Comparative cross-over study of sildenafi l and apomorphine for treating erectile dysfunction. BJU Int 2008 Sep;102(7):829-34.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 343
598. Porst H, Behre HM, Jungwirth A, Burkart M. Comparative trial of treatment satisfaction, effi cacy and tolerability of sildenafi l versus apomorphine in erectile dysfunction--an open, randomized cross-over study with fl exible dosing. Eur J Med Res 2007 Feb 26;12(2):61-7.
599. Giammusso B, Colpi GM, Cormio L, Ludovico G, Soli M, Ponchietti R, et al. An open-label, randomized, fl exible-dose, crossover study to assess the comparative effi cacy and safety of sildenafi l citrate and apomorphine hydrochloride in men with erectile dysfunction. Urol Int 2008;81(4):409-15.
600. Maclennan KM, Boshier A, Wilton LV, Shakir SA. Examination of the safety and use of apo-morphine prescribed in general practice in England as a treatment for erectile dysfunction. BJU Int 2006 Jul;98(1):125-31.
601. Atienza G. La prótesis de pene en el tratamiento de la disfunción eréctil. Santiago de Compostela: Axencia de Avaliación de Tecnoloxías Sanitarias de Conselleria de Sanidade Serie Avaliación de tecnologías Informes de Avaliación Galicia, avalia-t Subdirección Xeral de Aseguramento e Planifi cación Sanitaria 2005;INF2005/02.
602. Natali A, Olianas R, Fisch M. Penile implantation in Europe: successes and complications with 253 implants in Italy and Germany. J Sex Med 2008 Jun;5(6):1503-12.
603. Tang Y, Wen J, Jiang X, Yang J, Huang K, Tang J, et al. Intracavernous injection of alo-prostadil sterile power (prostaglandin E 1,caverject) for treatment of erectile dysfunction: A 8-years experience. Chinese Journal of Andrology 2007;21(9):16-8+25.
604. Melnik T, Soares BG, Nasselo AG. Psychosocial interventions for erectile dysfunction. Cochrane Database Syst Rev 2007;(3):CD004825.
605. Nunez MC, Rios GE, Martinez-Pineiro LL, Julve VE, Pastor AT, Cortes GR, et al. [Treatment of erectile dysfunction with vacuum devices]. Arch Esp Urol 2000 Nov;53(9):819-25.
606. Chen J, Sofer M, Kaver I, Matzkin H, Greenstein A. Concomitant use of sildenafi l and a vac-uum entrapment device for the treatment of erectile dysfunction. J Urol 2004 Jan;171(1):292-5.
607. Israilov S, Shmuely J, Niv E, Engelstein D, Livne P, Boniel J. Evaluation of a progressive treatment program for erectile dysfunction in patients with diabetes mellitus. Int J Impot Res 2005 Sep;17(5):431-6.
608. Chen J, Mabjeesh NJ, Greenstein A. Sildenafi l versus the vacuum erection device: patient preference. J Urol 2001 Nov;166(5):1779-81.
609. Linet OI, Ogrinc FG. Effi cacy and safety of intracavernosal alprostadil in men with erectile dysfunction. The Alprostadil Study Group. N Engl J Med 1996 Apr 4;334(14):873-7.
610. Colli E, Calabro A, Gentile V, Mirone V, Soli M. Alprostadil sterile powder formulation for intracavernous treatment of erectile dysfunction. Eur Urol 1996;29(1):59-62.
611. Eastman RC, Chase HP, Buckingham B, Hathout EH, Fuller-Byk L, Leptien A, et al. Use of the GlucoWatch biographer in children and adolescents with diabetes. Pediatric Diabetes 3(3):127-34, 2002 Sep.
612. Tsai YS, Lin JS, Lin YM. Safety and effi cacy of alprostadil sterile powder (S. Po., CAVERJECT) in diabetic patients with erectile dysfunction. Eur Urol 2000 Aug;38(2):177-83.
344 SNS CLINICAL PRACTICE GUIDELINES
613. Heaton JP, Lording D, Liu SN, Litonjua AD, Guangwei L, Kim SC, et al. Intracavernosal alprostadil is effective for the treatment of erectile dysfunction in diabetic men. Int J Impot Res 2001 Dec;13(6):317-21.
614. Dominguez M, Gutierrez A, Blasco P, Vega P, et al. El test de inyección intracavernosa con pge1 en la disfunción eréctil: nuestra experiencia. Actas Urol Esp 2000;24(10):796-800.
615. Helme R. Drug treatment of neuropathic pain. Austr Prescr 2006;29:72-5.
616. Actualización en el tratamiento del dolor neuropático. Infac 2007;15(Nº 3).
617. Wong MC, Chung JW, Wong TK. Effects of treatments for symptoms of painful diabetic neuropathy: systematic review. BMJ 2007 Jul 14;335(7610):87.
618. Adriaensen H, Plaghki L, Mathieu C, Joffroy A, Vissers K. Critical review of oral drug treatments for diabetic neuropathic pain-clinical outcomes based on effi cacy and safety data from placebocontrolled and direct comparative studies. Diabetes Metab Res Rev 2005 May;21(3):231-40.
619. Wiffen PJ, McQuay HJ, Edwards JE, Moore RA. Gabapentin for acute and chronic pain. Cochrane Database Syst Rev 2005;(3):CD005452.
620. Wiffen PJ, McQuay HJ, Moore RA. Carbamazepine for acute and chronic pain. Cochrane Database Syst Rev 2005;(3):CD005451.
621. Hollingshead J, Duhmke RM, Cornblath DR. Tramadol for neuropathic pain. Cochrane Database Syst Rev 2006;3:CD003726.
622. Eisenberg E, McNicol ED, Carr DB. Effi cacy and safety of opioid agonists in the treatment of neuropathic pain of nonmalignant origin: systematic review and meta-analysis of rand-omized controlled trials. JAMA 2005 Jun 22;293(24):3043-52.
623. Jose VM, Bhansali A, Hota D, Pandhi P. Randomized double-blind study comparing the effi cacy and safety of lamotrigine and amitriptyline in painful diabetic neuropathy. Diabet Med 2007 Apr;24(4):377-83.
624. Raskin J, Smith TR, Wong K, Pritchett YL, D’Souza DN, Iyengar S, et al. Duloxetine versus routine care in the long-term management of diabetic peripheral neuropathic pain. J Palliat Med 2006 Feb;9(1):29-40.
625. Gilron I, Bailey JM, Tu D, Holden RR, Weaver DF, Houlden RL. Morphine, gabapentin, or their combination for neuropathic pain. N Engl J Med 2005 Mar 31;352(13):1324-34.
626. Chou R, Carson S, Chan KS. Garbapentin versus tricyclic antidepressants for diabetic neu-ropathy and post-herpetic neuralgia: discrepancies between direct and indirect meta-analysis of randomized controlled trials. J Gen Intern Med 2008;24(2):178-88.
627. Quilici S, Chancello J, Löthgren M, Simon D, Said G, Le T, et al. Meta-analysis of dulox-etine and gabapentin in the treatment of diabetic peripheral neuropatic pain. 2009;9:6-19. BMC Neurology 2009;9:6-19.
628. Sultan A, Gaskell H, Derry S, Moore RA. Duloxetine for painful diabetic neuropathy and fi bromyalgia pain: systematic review of randomised controlled trials. BMC Neurology 2008;8:29-37.

CLINICAL PRACTICE GUIDELINE FOR DIABETES MELLITUS TYPE 1 345
629. Wolff RF, Bala MM, Westwood M, Kessels AG, Kleijnen J. 5% lidocaine medicated plaster in painful diabetic peripheral neuropathy (DPN): a systematic review. Swiss Med Wkly 2010 May 29;140(21-22):297-306.
630. Agrawal RP, Goswami J, Jain S, Kochar DK. Management of diabetic neuropathy by sodi-um valproate and glyceryl trinitrate spray: a prospective double-blind randomized placebo-controlled study. Diabetes Res Clin Pract 2009 Mar;83(3):371-8.
631. Hanna M, O’Brien C, Wilson MC. Prolonged-release oxycodone enhances the effects of existing gabapentin therapy in painful diabetic neuropathy patients. Eur J Pain 2008 Aug;12(6):804-13.
632. Kadiroglu AK, Sit D, Kayabasi H, Tuzcu AK, Tasdemir N, Yilmaz ME. The effect of ven-lafaxine HCl on painful peripheral diabetic neuropathy in patients with type 2 diabetes mel-litus. J Diabetes Complications 2008 Jul;22(4):241-5.
633. Datta J. Moving up with Diabetes: The Transition from Paediatric to Adult Care. National Children´s Bureau Books 2003.
634. Jefferson IG, Swift PG, Skinner TC, Hood GK. Diabetes services in the UK: third national survey confi rms continuing defi ciencies. Arch Dis Child 2003 Jan;88(1):53-6.
635. Kipps S, Bahu T, Ong K, Ackland FM, Brown RS, Fox CT, et al. Current methods of transfer of young people with Type 1 diabetes to adult services. Diabet Med 2002 Aug;19(8):649-54.
636. Pacaud D, McConnell B, Huot C, Aebi C, Yale J. Transition from pediatric care to adult care for insulin-dependent diabetes patients. Canadian Journal of Diabetes Care 1996;20:14-20.
637. Court JM. Issues of transition to adult care. J Paediatr Child Health 1993;29 Suppl 1:S53-S55.
638. Eiser C, Flynn M, Green E, Havermans T, Kirby R, Sandeman D, et al. Coming of age with diabetes: patients’ views of a clinic for under-25 year olds. Diabet Med 1993 Apr;10(3):285-9.
639. Salmi J, Huupponen T, Oksa H, Oksala H, Koivula T, Raita P. Metabolic control in ado-lescent insulin-dependent diabetics referred from pediatric to adult clinic. Ann Clin Res 1986;18(2):84-7.
640. Vanelli M, Caronna S, Adinolfi B, Chiari G, Gugliotta M, Arsenio L. Effectiveness of an uninterrupted procedure to transfer adolescents with Type 1 diabetes from the Paediatric to the Adult Clinic held in the same hospital: eight-year experience with the Parma protocol. Diabetes Nutr Metab 2004 Oct;17(5):304-8.
641. Busse FP, Hiermann P, Galler A, Stumvoll M, Wiessner T, Kiess W, et al. Evaluation of pa-tients’ opinion and metabolic control after transfer of young adults with type 1 diabetes from a pediatric diabetes clinic to adult care. Horm Res 2007;67(3):132-8.
642. Holmes-Walker DJ, Llewellyn AC, Farrell K. A transition care programme which improves diabetes control and reduces hospital admission rates in young adults with Type 1 diabetes aged 15-25 years. Diabetic Medicine 24(7):764-9, 2007 Jul.
643. European Diabetes Policy Group. A Desktop Guide To Type 1 (Insulin-dependent) Diabetes Mellitus. International Diabetes Federation (Europe), Brussels 1998.
644. A WHO Family Planning Cornerstone. Medica l elegibility criteria for contraceptive use. World Health Organization 2009;Fourth edition.

MINISTERIODE ECONOMÍAY COMPETITIVIDAD
MINISTERIODE SANIDAD, SERVICIOS SOCIALESE IGUALDAD