chapter-1 - rrc-ne office address
TRANSCRIPT
1
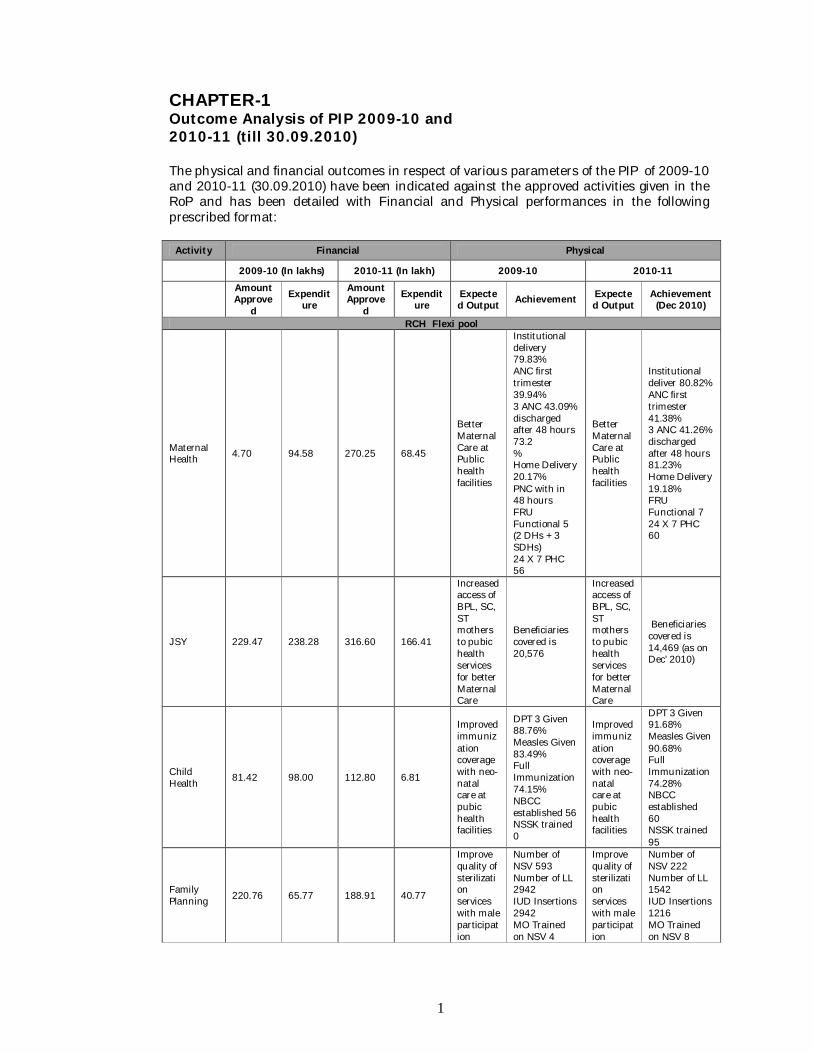
CHAPTER-1 Outcome Analysis of PIP 2009-10 and 2010-11 (till 30.09.2010) The physical and financial outcomes in respect of various parameters of the PIP of 2009-10 and 2010-11 (30.09.2010) have been indicated against the approved activities given in the RoP and has been detailed with Financial and Physical performances in the following prescribed format: Activity Financial Physical
2009-10 (In lakhs) 2010-11 (In lakh) 2009-10 2010-11
Amount Approve
d Expendit
ure Amount Approve
d Expendit
ure Expected Output Achievement Expecte
d Output Achievement (Dec 2010)
RCH Flexi pool
Maternal Health 4.70 94.58 270.25 68.45
Better Maternal Care at Public health facilities
Institutional delivery 79.83% ANC first trimester 39.94% 3 ANC 43.09% discharged after 48 hours 73.2 % Home Delivery 20.17% PNC with in 48 hours FRU Functional 5 (2 DHs + 3 SDHs) 24 X 7 PHC 56
Better Maternal Care at Public health facilities
Institutional deliver 80.82% ANC first trimester 41.38% 3 ANC 41.26% discharged after 48 hours 81.23% Home Delivery 19.18% FRU Functional 7 24 X 7 PHC 60
JSY 229.47 238.28 316.60 166.41
Increased access of BPL, SC, ST mothers to pubic health services for better Maternal Care
Beneficiaries covered is 20,576
Increased access of BPL, SC, ST mothers to pubic health services for better Maternal Care
Beneficiaries covered is 14,469 (as on Dec’ 2010)
Child Health 81.42 98.00 112.80 6.81
Improved immunization coverage with neo-natal care at pubic health facilities
DPT 3 Given 88.76% Measles Given 83.49% Full Immunization 74.15% NBCC established 56 NSSK trained 0
Improved immunization coverage with neo-natal care at pubic health facilities
DPT 3 Given 91.68% Measles Given 90.68% Full Immunization 74.28% NBCC established 60 NSSK trained 95
Family Planning 220.76 65.77 188.91 40.77
Improve quality of sterilization services with male participation
Number of NSV 593 Number of LL 2942 IUD Insertions 2942 MO Trained on NSV 4
Improve quality of sterilization services with male participation
Number of NSV 222 Number of LL 1542 IUD Insertions 1216 MO Trained on NSV 8
2
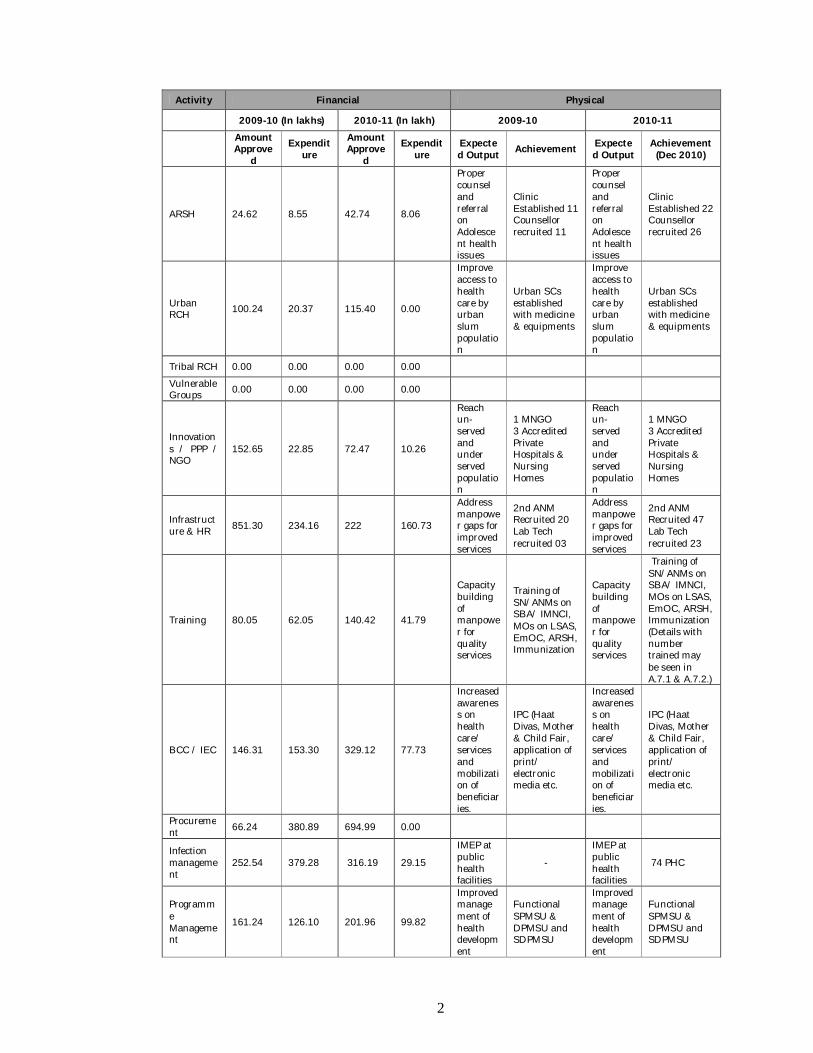
Activity Financial Physical
2009-10 (In lakhs) 2010-11 (In lakh) 2009-10 2010-11
Amount Approve
d Expendit
ure Amount Approve
d Expendit
ure Expected Output Achievement Expecte
d Output Achievement (Dec 2010)
ARSH 24.62 8.55 42.74 8.06
Proper counsel and referral on Adolescent health issues
Clinic Established 11 Counsellor recruited 11
Proper counsel and referral on Adolescent health issues
Clinic Established 22 Counsellor recruited 26
Urban RCH 100.24 20.37 115.40 0.00
Improve access to health care by urban slum population
Urban SCs established with medicine & equipments
Improve access to health care by urban slum population
Urban SCs established with medicine & equipments
Tribal RCH 0.00 0.00 0.00 0.00
Vulnerable Groups 0.00 0.00 0.00 0.00
Innovations / PPP / NGO
152.65 22.85 72.47 10.26
Reach un-served and under served population
1 MNGO 3 Accredited Private Hospitals & Nursing Homes
Reach un-served and under served population
1 MNGO 3 Accredited Private Hospitals & Nursing Homes
Infrastructure & HR 851.30 234.16 222 160.73
Address manpower gaps for improved services
2nd ANM Recruited 20 Lab Tech recruited 03
Address manpower gaps for improved services
2nd ANM Recruited 47 Lab Tech recruited 23
Training 80.05 62.05 140.42 41.79
Capacity building of manpower for quality services
Training of SN/ANMs on SBA/ IMNCI, MOs on LSAS, EmOC, ARSH, Immunization
Capacity building of manpower for quality services
Training of SN/ANMs on SBA/ IMNCI, MOs on LSAS, EmOC, ARSH, Immunization (Details with number trained may be seen in A.7.1 & A.7.2.)
BCC / IEC 146.31 153.30 329.12 77.73
Increased awareness on health care/ services and mobilization of beneficiaries.
IPC (Haat Divas, Mother & Child Fair, application of print/ electronic media etc.
Increased awareness on health care/ services and mobilization of beneficiaries.
IPC (Haat Divas, Mother & Child Fair, application of print/ electronic media etc.
Procurement 66.24 380.89 694.99 0.00
Infection management
252.54 379.28 316.19 29.15
IMEP at public health facilities
-
IMEP at public health facilities
74 PHC
Programme Management
161.24 126.10 201.96 99.82
Improved management of health development
Functional SPMSU & DPMSU and SDPMSU
Improved management of health development
Functional SPMSU & DPMSU and SDPMSU
3
Activity Financial Physical
2009-10 (In lakhs) 2010-11 (In lakh) 2009-10 2010-11
Amount Approve
d Expendit
ure Amount Approve
d Expendit
ure Expected Output Achievement Expecte
d Output Achievement (Dec 2010)
initiative initiative
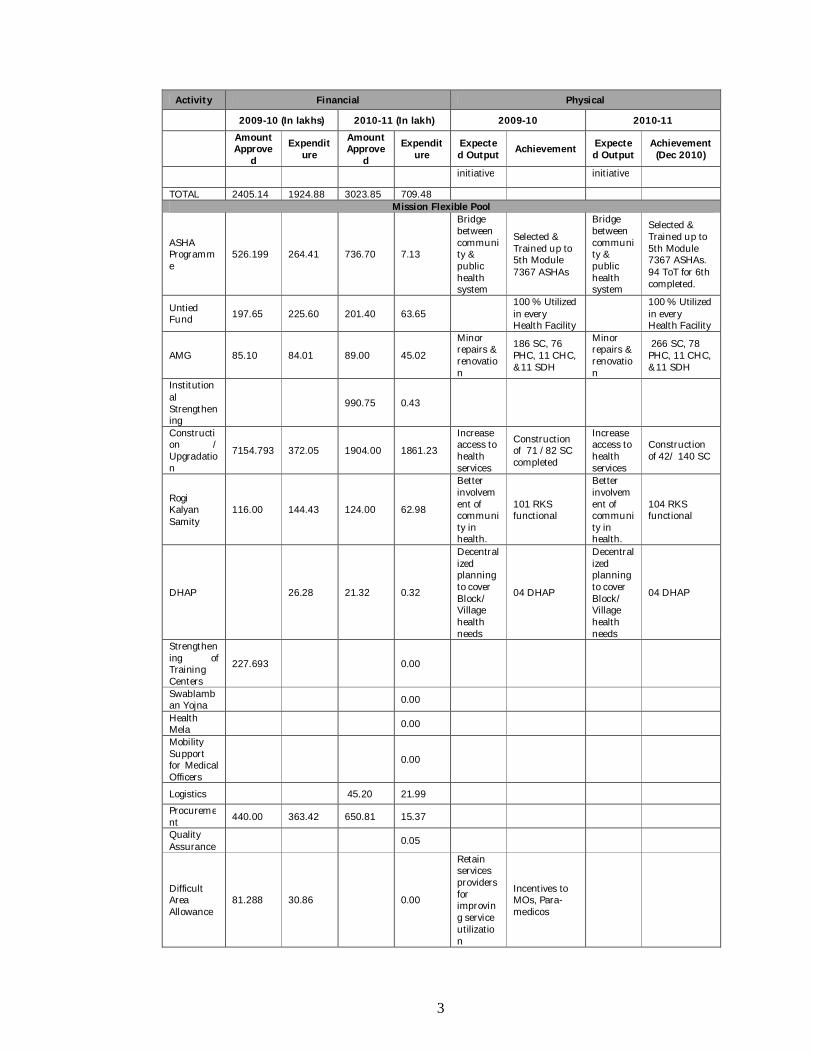
TOTAL 2405.14 1924.88 3023.85 709.48 Mission Flexible Pool
ASHA Programme
526.199 264.41 736.70 7.13
Bridge between community & public health system
Selected & Trained up to 5th Module 7367 ASHAs
Bridge between community & public health system
Selected & Trained up to 5th Module 7367 ASHAs. 94 ToT for 6th completed.
Untied Fund 197.65 225.60 201.40 63.65
100 % Utilized in every Health Facility
100 % Utilized in every Health Facility
AMG 85.10 84.01 89.00 45.02
Minor repairs & renovation
186 SC, 76 PHC, 11 CHC, &11 SDH
Minor repairs & renovation
266 SC, 78 PHC, 11 CHC, &11 SDH
Institutional Strengthening
990.75 0.43
Construction / Upgradation
7154.793 372.05 1904.00 1861.23
Increase access to health services
Construction of 71 /82 SC completed
Increase access to health services
Construction of 42/ 140 SC
Rogi Kalyan Samity
116.00 144.43 124.00 62.98
Better involvement of community in health.
101 RKS functional
Better involvement of community in health.
104 RKS functional
DHAP 26.28 21.32 0.32
Decentralized planning to cover Block/ Village health needs
04 DHAP
Decentralized planning to cover Block/ Village health needs
04 DHAP
Strengthening of Training Centers
227.693 0.00
Swablamban Yojna 0.00
Health Mela 0.00
Mobility Support for Medical Officers
0.00
Logistics 45.20 21.99
Procurement 440.00 363.42 650.81 15.37
Quality Assurance 0.05
Difficult Area Allowance
81.288 30.86 0.00
Retain services providers for improving service utilization
Incentives to MOs, Para-medicos
4
Activity Financial Physical
2009-10 (In lakhs) 2010-11 (In lakh) 2009-10 2010-11
Amount Approve
d Expendit
ure Amount Approve
d Expendit
ure Expected Output Achievement Expecte
d Output Achievement (Dec 2010)
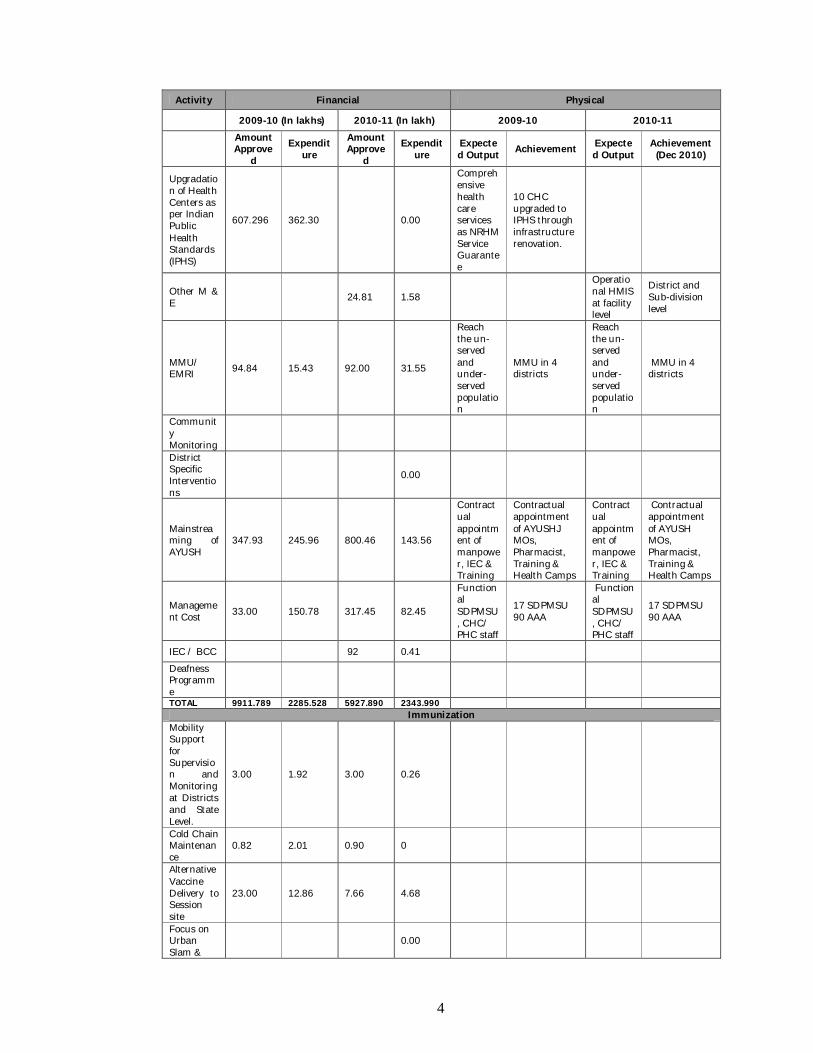
Upgradation of Health Centers as per Indian Public Health Standards (IPHS)
607.296 362.30 0.00
Comprehensive health care services as NRHM Service Guarantee
10 CHC upgraded to IPHS through infrastructure renovation.
Other M & E 24.81 1.58
Operational HMIS at facility level
District and Sub-division level
MMU/ EMRI 94.84 15.43 92.00 31.55
Reach the un-served and under-served population
MMU in 4 districts
Reach the un-served and under-served population
MMU in 4 districts
Community Monitoring
District Specific Interventions
0.00
Mainstreaming of AYUSH
347.93 245.96 800.46 143.56
Contractual appointment of manpower, IEC & Training
Contractual appointment of AYUSHJ MOs, Pharmacist, Training & Health Camps
Contractual appointment of manpower, IEC & Training
Contractual appointment of AYUSH MOs, Pharmacist, Training & Health Camps
Management Cost 33.00 150.78 317.45 82.45
Functional SDPMSU, CHC/ PHC staff
17 SDPMSU 90 AAA
Functional SDPMSU, CHC/ PHC staff
17 SDPMSU 90 AAA
IEC / BCC 92 0.41
Deafness Programme
TOTAL 9911.789 2285.528 5927.890 2343.990 Immunization
Mobility Support for Supervision and Monitoring at Districts and State Level.
3.00 1.92 3.00 0.26
Cold Chain Maintenance
0.82 2.01 0.90 0
Alternative Vaccine Delivery to Session site
23.00 12.86 7.66 4.68
Focus on Urban Slam &
0.00
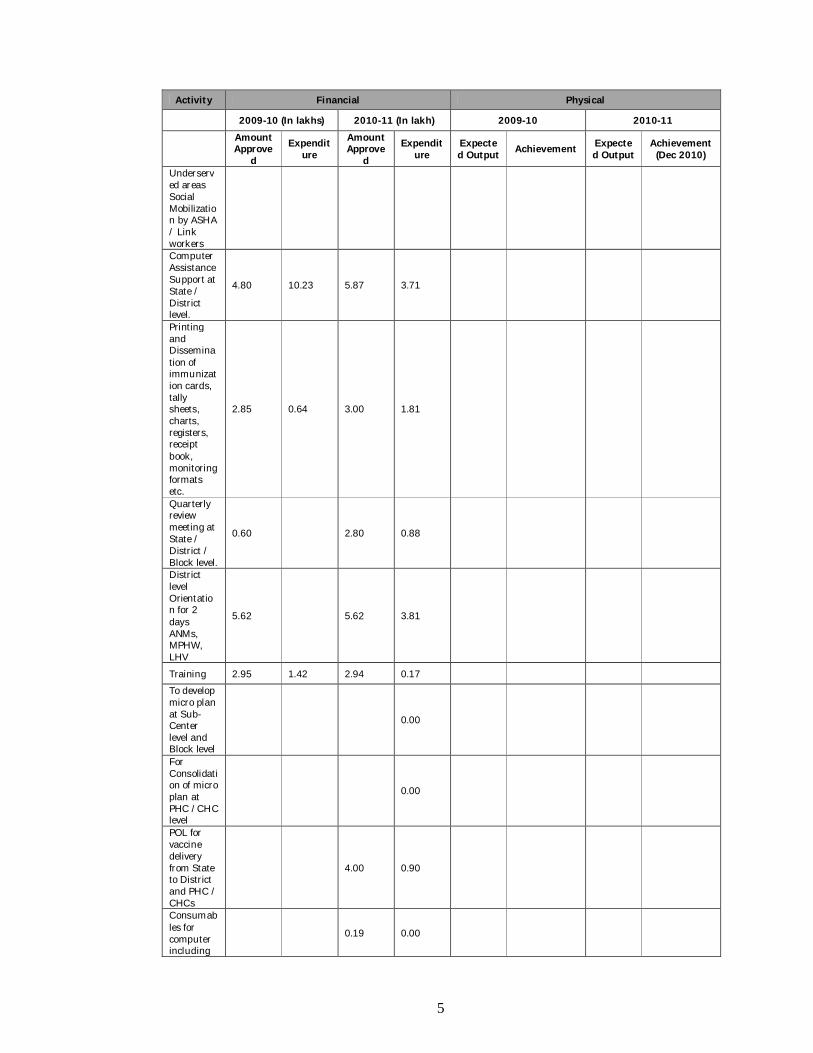
5
Activity Financial Physical
2009-10 (In lakhs) 2010-11 (In lakh) 2009-10 2010-11
Amount Approve
d Expendit
ure Amount Approve
d Expendit
ure Expected Output Achievement Expecte
d Output Achievement (Dec 2010)
Underserved areas Social Mobilization by ASHA / Link workers Computer Assistance Support at State / District level.
4.80 10.23 5.87 3.71
Printing and Dissemination of immunization cards, tally sheets, charts, registers, receipt book, monitoring formats etc.
2.85 0.64 3.00 1.81
Quarterly review meeting at State / District / Block level.
0.60 2.80 0.88
District level Orientation for 2 days ANMs, MPHW, LHV
5.62 5.62 3.81
Training 2.95 1.42 2.94 0.17 To develop micro plan at Sub-Center level and Block level
0.00
For Consolidation of micro plan at PHC /CHC level
0.00
POL for vaccine delivery from State to District and PHC / CHCs
4.00 0.90
Consumables for computer including
0.19 0.00
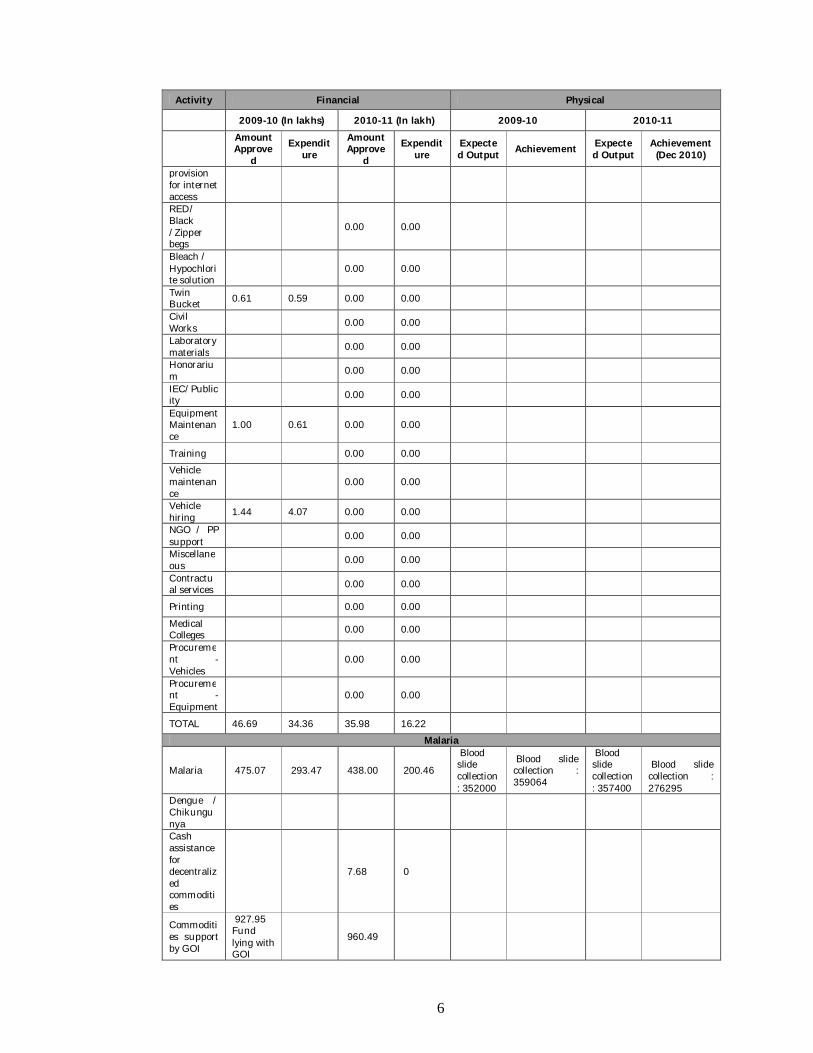
6
Activity Financial Physical
2009-10 (In lakhs) 2010-11 (In lakh) 2009-10 2010-11
Amount Approve
d Expendit
ure Amount Approve
d Expendit
ure Expected Output Achievement Expecte
d Output Achievement (Dec 2010)
provision for internet access RED/ Black /Zipper begs
0.00 0.00
Bleach / Hypochlorite solution
0.00 0.00
Twin Bucket 0.61 0.59 0.00 0.00 Civil Works 0.00 0.00 Laboratory materials 0.00 0.00 Honorarium 0.00 0.00 IEC/Publicity 0.00 0.00 Equipment Maintenance
1.00 0.61 0.00 0.00
Training 0.00 0.00 Vehicle maintenance
0.00 0.00
Vehicle hiring 1.44 4.07 0.00 0.00 NGO / PP support 0.00 0.00 Miscellaneous 0.00 0.00 Contractual services 0.00 0.00
Printing 0.00 0.00 Medical Colleges 0.00 0.00 Procurement - Vehicles
0.00 0.00
Procurement -Equipment
0.00 0.00
TOTAL 46.69 34.36 35.98 16.22 Malaria
Malaria 475.07 293.47 438.00 200.46
Blood slide collection : 352000
Blood slide collection : 359064
Blood slide collection : 357400
Blood slide collection : 276295
Dengue / Chikungunya
Cash assistance for decentralized commodities
7.68 0
Commodities support by GOI
927.95 Fund lying with GOI
960.49
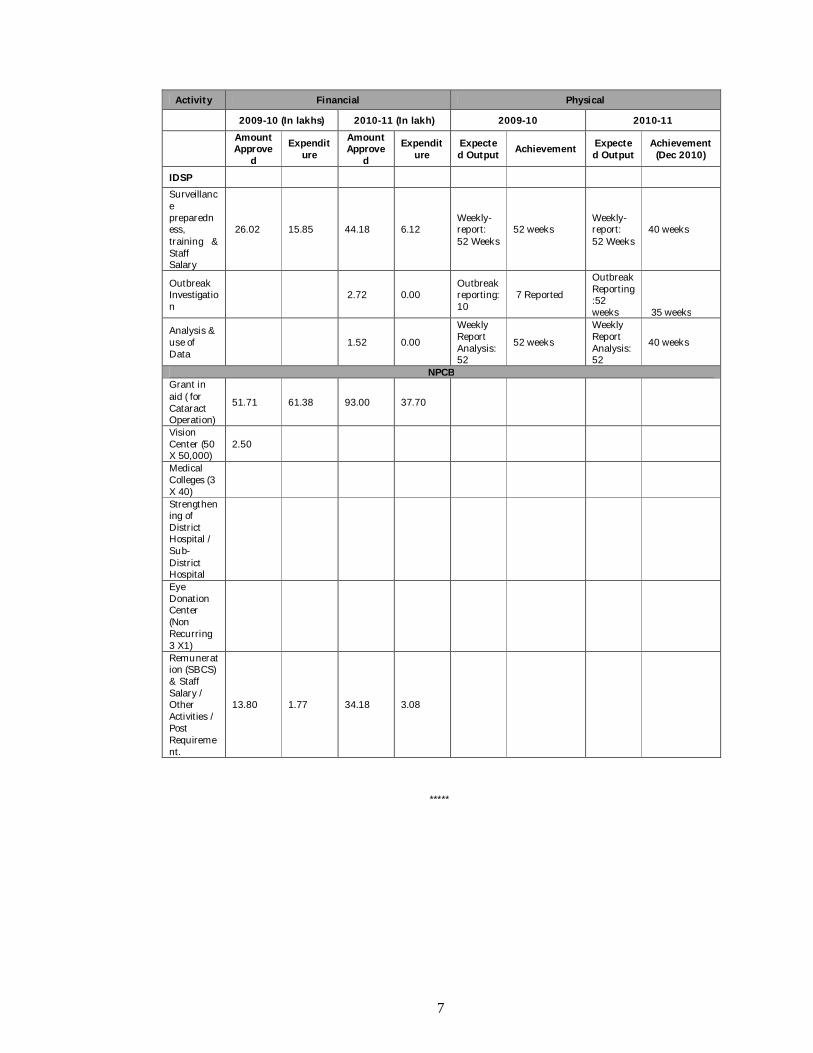
7
Activity Financial Physical
2009-10 (In lakhs) 2010-11 (In lakh) 2009-10 2010-11
Amount Approve
d Expendit
ure Amount Approve
d Expendit
ure Expected Output Achievement Expecte
d Output Achievement (Dec 2010)
IDSP Surveillance preparedness, training & Staff Salary
26.02 15.85 44.18 6.12 Weekly-report: 52 Weeks
52 weeks Weekly-report: 52 Weeks
40 weeks
Outbreak Investigation
2.72 0.00 Outbreak reporting: 10
7 Reported
Outbreak Reporting:52 weeks 35 weeks
Analysis & use of Data
1.52 0.00
Weekly Report Analysis: 52
52 weeks
Weekly Report Analysis: 52
40 weeks
NPCB Grant in aid ( for Cataract Operation)
51.71 61.38 93.00 37.70
Vision Center (50 X 50,000)
2.50
Medical Colleges (3 X 40)
Strengthening of District Hospital / Sub-District Hospital
Eye Donation Center (Non Recurring 3 X1)
Remuneration (SBCS) & Staff Salary / Other Activities / Post Requirement.
13.80 1.77 34.18 3.08
*****
8
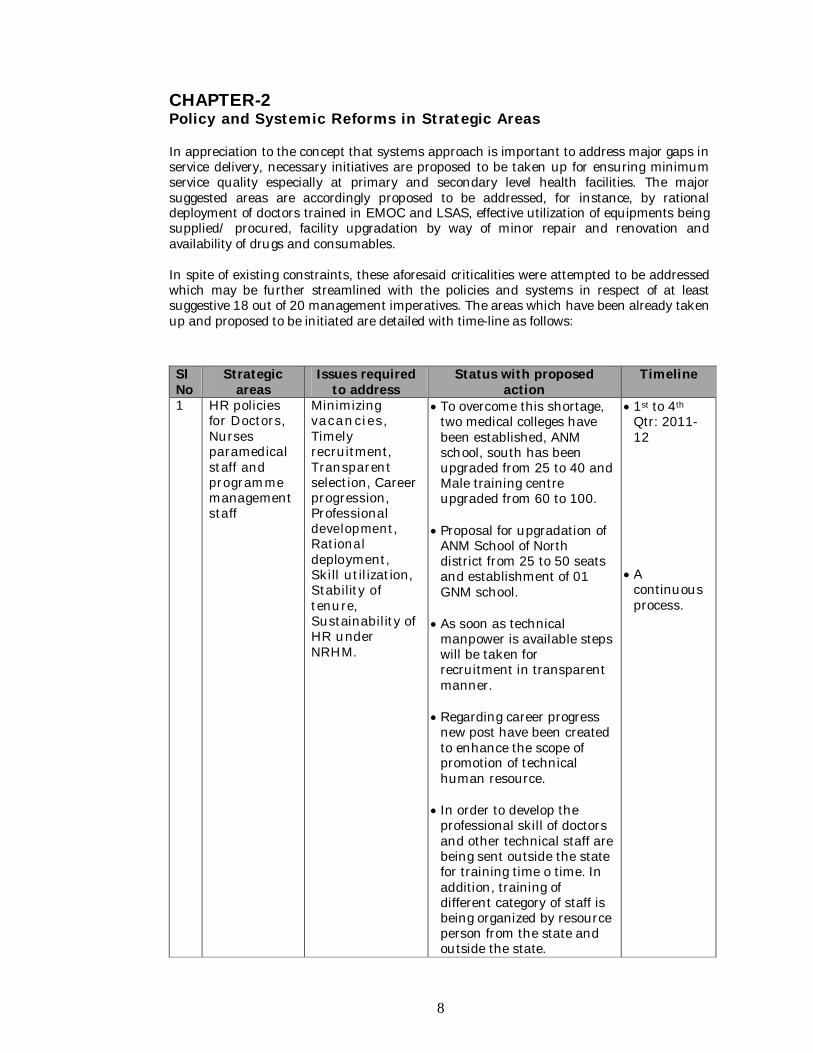
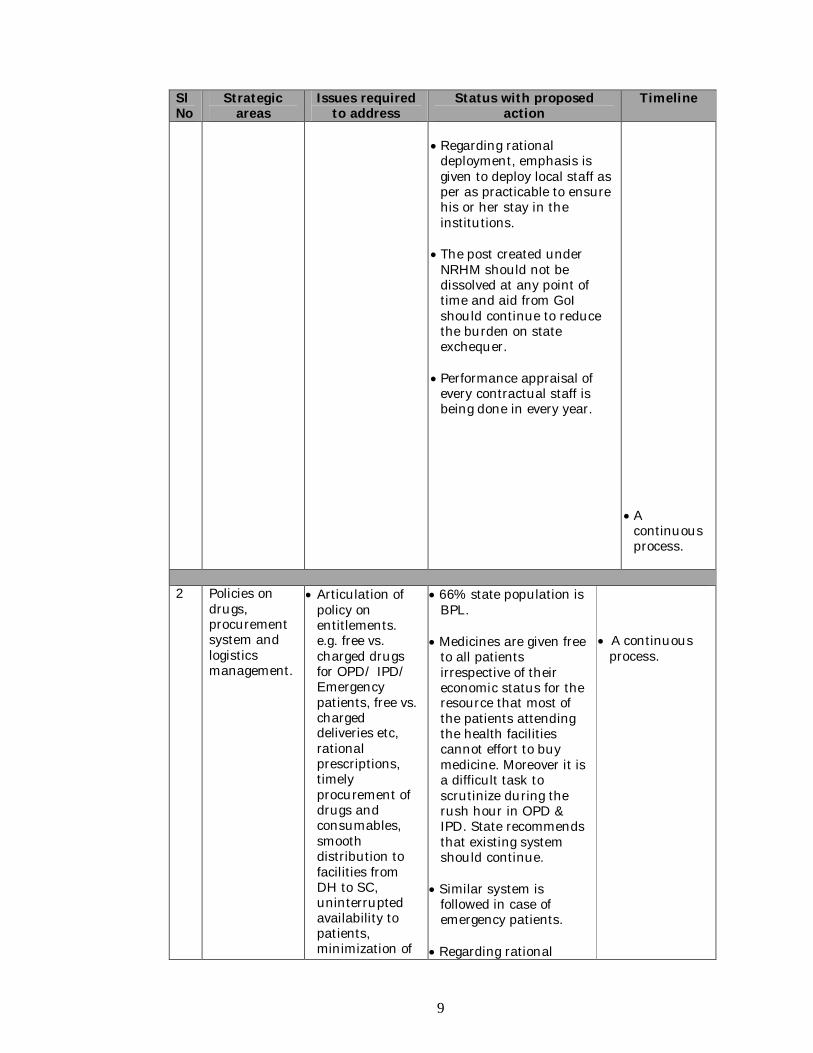
CHAPTER-2 Policy and Systemic Reforms in Strategic Areas In appreciation to the concept that systems approach is important to address major gaps in service delivery, necessary initiatives are proposed to be taken up for ensuring minimum service quality especially at primary and secondary level health facilities. The major suggested areas are accordingly proposed to be addressed, for instance, by rational deployment of doctors trained in EMOC and LSAS, effective utilization of equipments being supplied/ procured, facility upgradation by way of minor repair and renovation and availability of drugs and consumables. In spite of existing constraints, these aforesaid criticalities were attempted to be addressed which may be further streamlined with the policies and systems in respect of at least suggestive 18 out of 20 management imperatives. The areas which have been already taken up and proposed to be initiated are detailed with time-line as follows: Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
1 HR policies for Doctors, Nurses paramedical staff and programme management staff
Minimizing vacancies, Timely recruitment, Transparent selection, Career progression, Professional development, Rational deployment, Skill utilization, Stability of tenure, Sustainability of HR under NRHM.
To overcome this shortage, two medical colleges have been established, ANM school, south has been upgraded from 25 to 40 and Male training centre upgraded from 60 to 100.
Proposal for upgradation of
ANM School of North district from 25 to 50 seats and establishment of 01 GNM school.
As soon as technical
manpower is available steps will be taken for recruitment in transparent manner.
Regarding career progress
new post have been created to enhance the scope of promotion of technical human resource.
In order to develop the
professional skill of doctors and other technical staff are being sent outside the state for training time o time. In addition, training of different category of staff is being organized by resource person from the state and outside the state.
1st to 4th Qtr: 2011-12
A
continuous process.
9
Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
Regarding rational
deployment, emphasis is given to deploy local staff as per as practicable to ensure his or her stay in the institutions.
The post created under
NRHM should not be dissolved at any point of time and aid from GoI should continue to reduce the burden on state exchequer.
Performance appraisal of
every contractual staff is being done in every year.
A
continuous process.
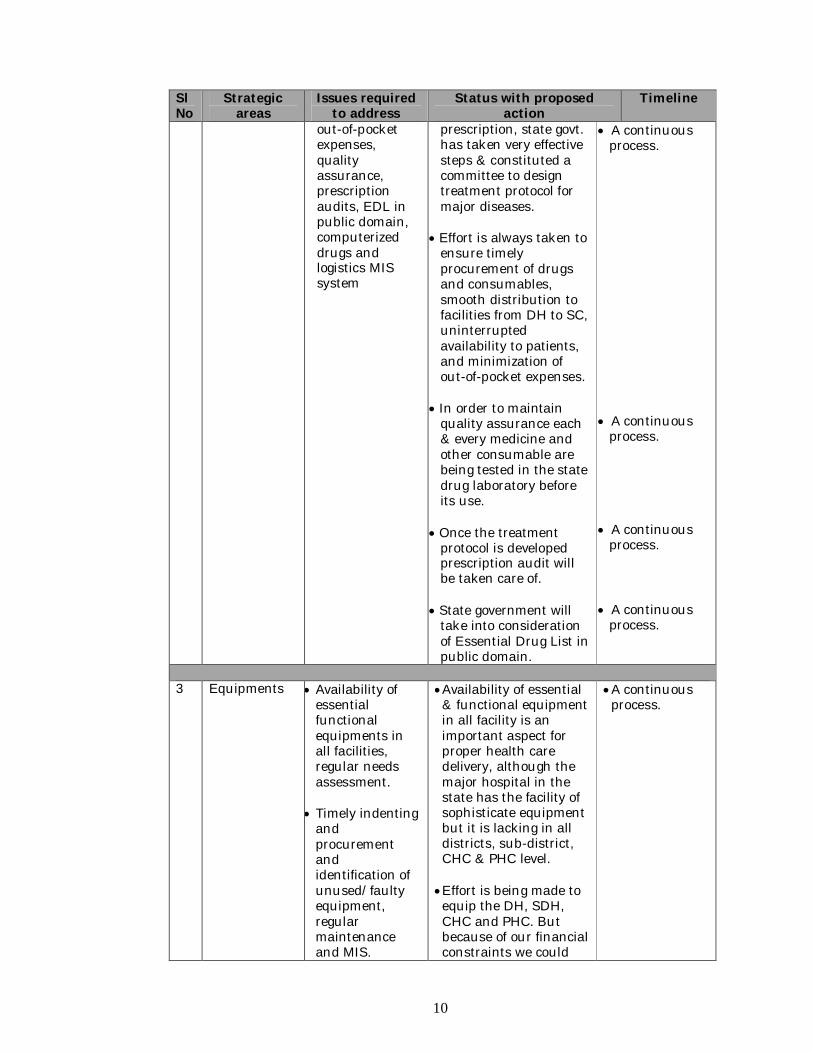
2 Policies on
drugs, procurement system and logistics management.
Articulation of policy on entitlements. e.g. free vs. charged drugs for OPD/ IPD/ Emergency patients, free vs. charged deliveries etc, rational prescriptions, timely procurement of drugs and consumables, smooth distribution to facilities from DH to SC, uninterrupted availability to patients, minimization of
66% state population is BPL.
Medicines are given free
to all patients irrespective of their economic status for the resource that most of the patients attending the health facilities cannot effort to buy medicine. Moreover it is a difficult task to scrutinize during the rush hour in OPD & IPD. State recommends that existing system should continue.
Similar system is
followed in case of emergency patients.
Regarding rational
A continuous
process.
10
Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
out-of-pocket expenses, quality assurance, prescription audits, EDL in public domain, computerized drugs and logistics MIS system
prescription, state govt. has taken very effective steps & constituted a committee to design treatment protocol for major diseases.
Effort is always taken to
ensure timely procurement of drugs and consumables, smooth distribution to facilities from DH to SC, uninterrupted availability to patients, and minimization of out-of-pocket expenses.
In order to maintain
quality assurance each & every medicine and other consumable are being tested in the state drug laboratory before its use.
Once the treatment
protocol is developed prescription audit will be taken care of.
State government will
take into consideration of Essential Drug List in public domain.
A continuous process.
A continuous
process. A continuous
process. A continuous
process.
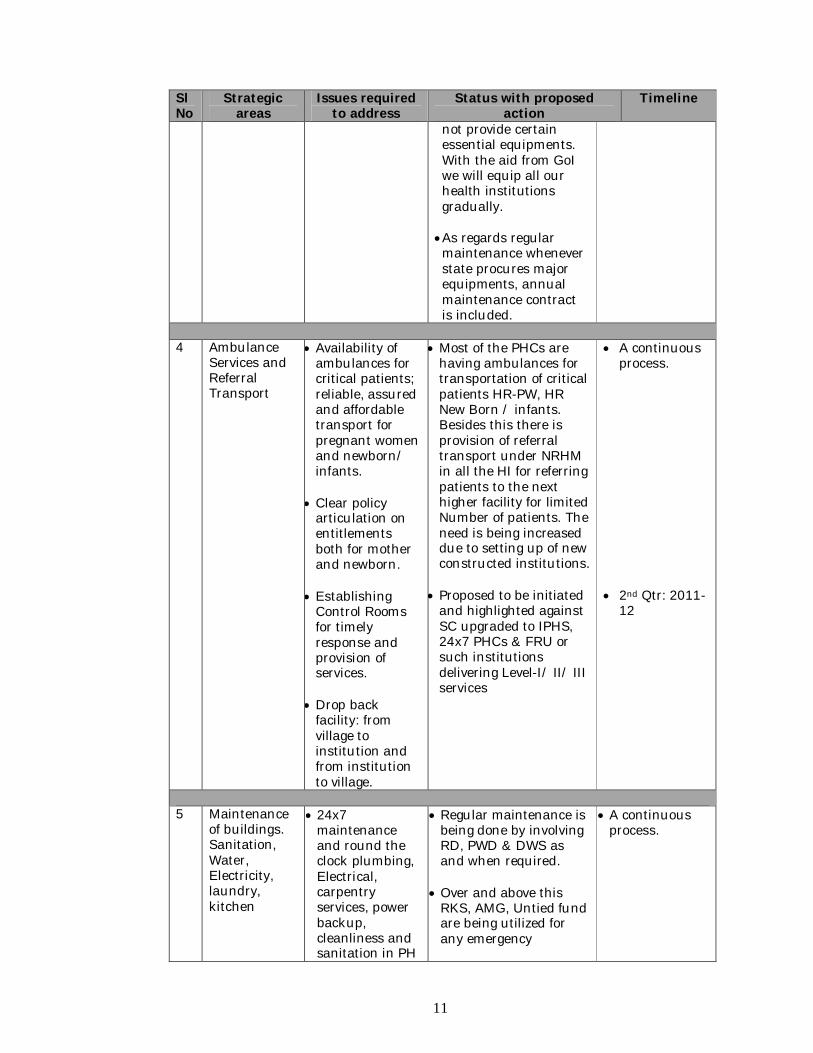
3 Equipments Availability of
essential functional equipments in all facilities, regular needs assessment.
Timely indenting
and procurement and identification of unused/faulty equipment, regular maintenance and MIS.
Availability of essential & functional equipment in all facility is an important aspect for proper health care delivery, although the major hospital in the state has the facility of sophisticate equipment but it is lacking in all districts, sub-district, CHC & PHC level.
Effort is being made to equip the DH, SDH, CHC and PHC. But because of our financial constraints we could
A continuous process.
11
Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
not provide certain essential equipments. With the aid from GoI we will equip all our health institutions gradually.
As regards regular maintenance whenever state procures major equipments, annual maintenance contract is included.
4 Ambulance
Services and Referral Transport
Availability of ambulances for critical patients; reliable, assured and affordable transport for pregnant women and newborn/ infants.
Clear policy
articulation on entitlements both for mother and newborn.
Establishing
Control Rooms for timely response and provision of services.
Drop back
facility: from village to institution and from institution to village.
Most of the PHCs are having ambulances for transportation of critical patients HR-PW, HR New Born / infants. Besides this there is provision of referral transport under NRHM in all the HI for referring patients to the next higher facility for limited Number of patients. The need is being increased due to setting up of new constructed institutions.
Proposed to be initiated
and highlighted against SC upgraded to IPHS, 24x7 PHCs & FRU or such institutions delivering Level-I/ II/ III services
A continuous process.
2nd Qtr: 2011-
12
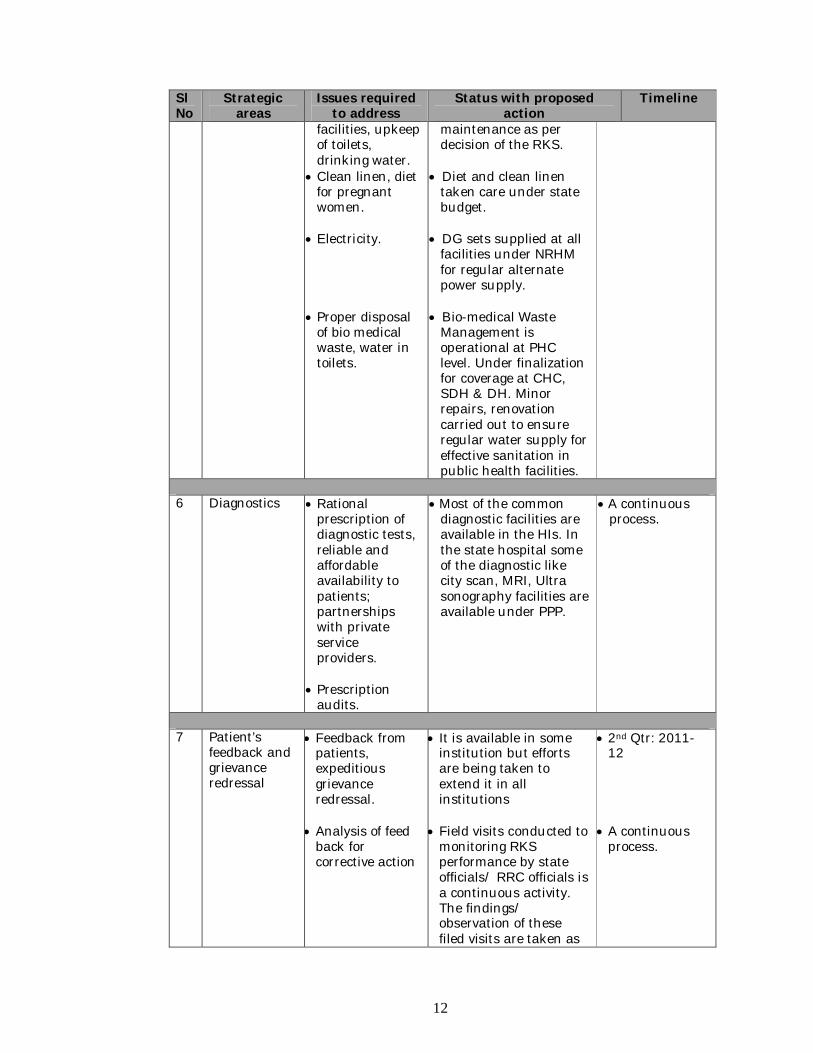
5 Maintenance
of buildings. Sanitation, Water, Electricity, laundry, kitchen
24x7 maintenance and round the clock plumbing, Electrical, carpentry services, power backup, cleanliness and sanitation in PH
Regular maintenance is being done by involving RD, PWD & DWS as and when required.
Over and above this
RKS, AMG, Untied fund are being utilized for any emergency
A continuous process.
12
Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
facilities, upkeep of toilets, drinking water.
Clean linen, diet for pregnant women.
Electricity.
Proper disposal
of bio medical waste, water in toilets.
maintenance as per decision of the RKS.
Diet and clean linen
taken care under state budget.
DG sets supplied at all
facilities under NRHM for regular alternate power supply.
Bio-medical Waste
Management is operational at PHC level. Under finalization for coverage at CHC, SDH & DH. Minor repairs, renovation carried out to ensure regular water supply for effective sanitation in public health facilities.
6 Diagnostics Rational
prescription of diagnostic tests, reliable and affordable availability to patients; partnerships with private service providers.
Prescription
audits.
Most of the common diagnostic facilities are available in the HIs. In the state hospital some of the diagnostic like city scan, MRI, Ultra sonography facilities are available under PPP.
A continuous process.
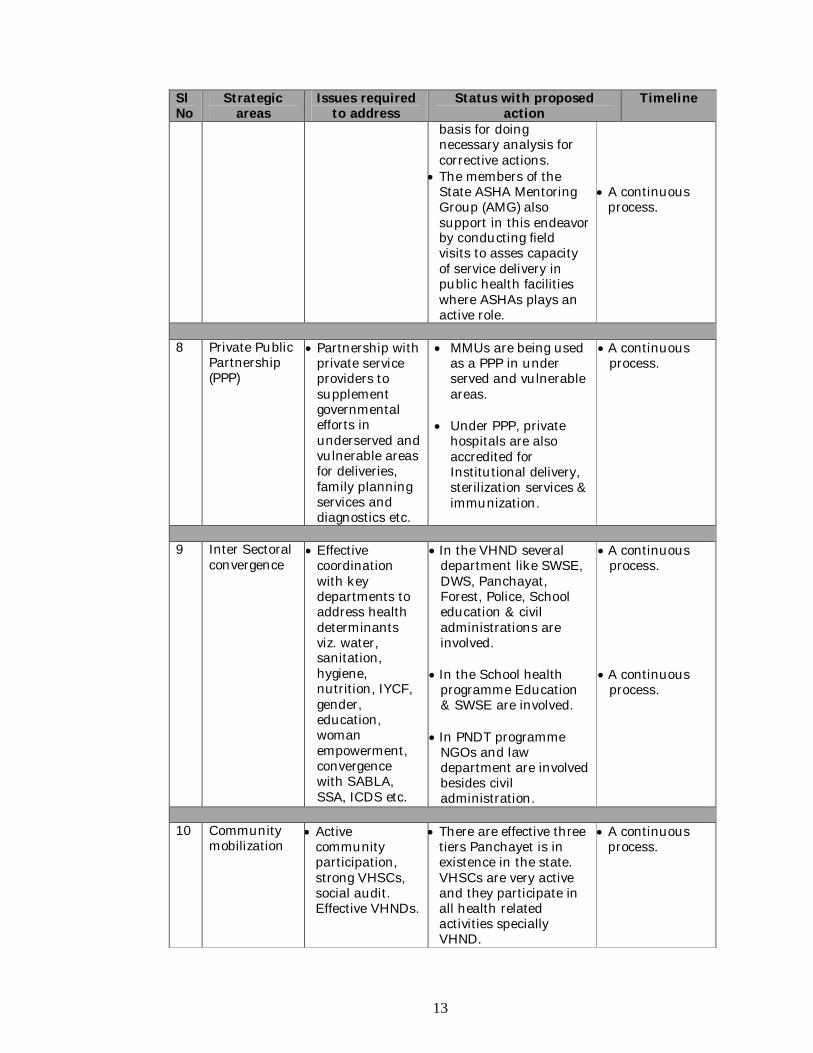
7 Patient’s
feedback and grievance redressal
Feedback from patients, expeditious grievance redressal.
Analysis of feed
back for corrective action
It is available in some institution but efforts are being taken to extend it in all institutions
Field visits conducted to
monitoring RKS performance by state officials/ RRC officials is a continuous activity. The findings/ observation of these filed visits are taken as
2nd Qtr: 2011-12
A continuous
process.
13
Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
basis for doing necessary analysis for corrective actions.
The members of the State ASHA Mentoring Group (AMG) also support in this endeavor by conducting field visits to asses capacity of service delivery in public health facilities where ASHAs plays an active role.
A continuous
process.
8 Private Public
Partnership (PPP)
Partnership with private service providers to supplement governmental efforts in underserved and vulnerable areas for deliveries, family planning services and diagnostics etc.
MMUs are being used as a PPP in under served and vulnerable areas.
Under PPP, private
hospitals are also accredited for Institutional delivery, sterilization services & immunization.
A continuous process.
9 Inter Sectoral
convergence Effective
coordination with key departments to address health determinants viz. water, sanitation, hygiene, nutrition, IYCF, gender, education, woman empowerment, convergence with SABLA, SSA, ICDS etc.
In the VHND several department like SWSE, DWS, Panchayat, Forest, Police, School education & civil administrations are involved.
In the School health
programme Education & SWSE are involved.
In PNDT programme
NGOs and law department are involved besides civil administration.
A continuous process.
A continuous
process.
10 Community
mobilization Active
community participation, strong VHSCs, social audit. Effective VHNDs.
There are effective three tiers Panchayet is in existence in the state. VHSCs are very active and they participate in all health related activities specially VHND.
A continuous process.
14
Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
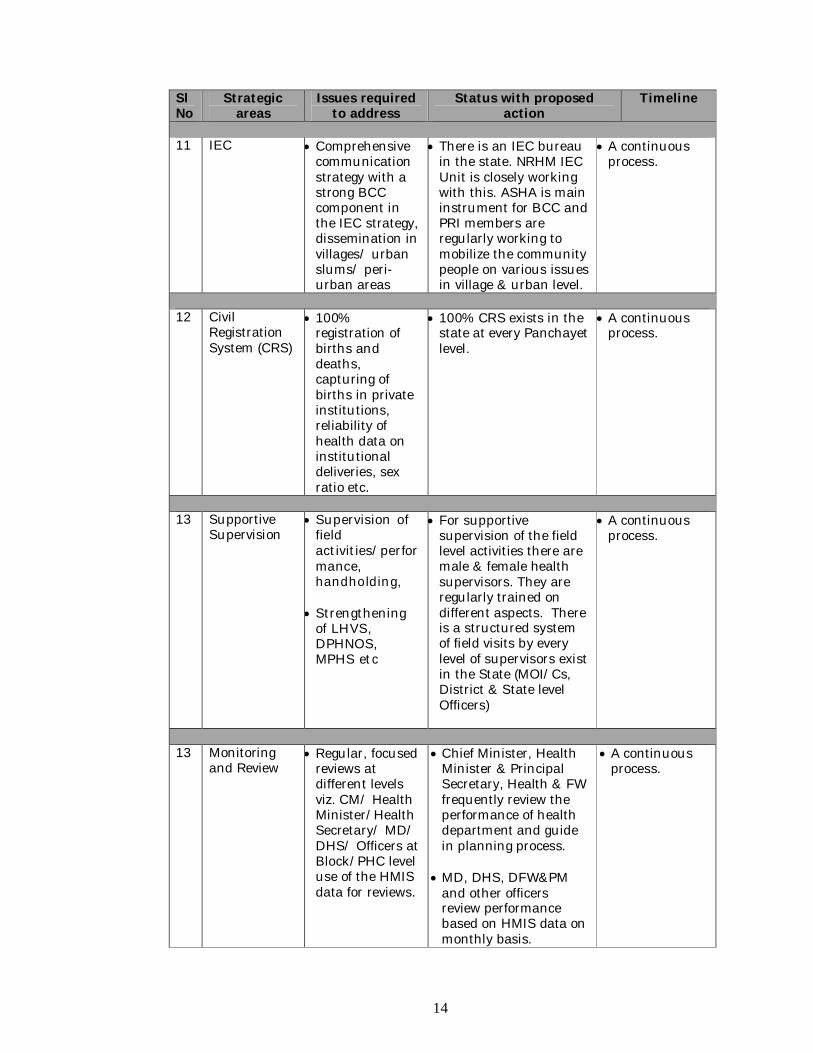
11 IEC Comprehensive
communication strategy with a strong BCC component in the IEC strategy, dissemination in villages/ urban slums/ peri-urban areas
There is an IEC bureau in the state. NRHM IEC Unit is closely working with this. ASHA is main instrument for BCC and PRI members are regularly working to mobilize the community people on various issues in village & urban level.
A continuous process.
12 Civil
Registration System (CRS)
100% registration of births and deaths, capturing of births in private institutions, reliability of health data on institutional deliveries, sex ratio etc.
100% CRS exists in the state at every Panchayet level.
A continuous process.
13 Supportive
Supervision Supervision of
field activities/performance, handholding,
Strengthening
of LHVS, DPHNOS, MPHS etc
For supportive supervision of the field level activities there are male & female health supervisors. They are regularly trained on different aspects. There is a structured system of field visits by every level of supervisors exist in the State (MOI/Cs, District & State level Officers)
A continuous process.
13 Monitoring
and Review Regular, focused
reviews at different levels viz. CM/ Health Minister/Health Secretary/ MD/ DHS/ Officers at Block/PHC level use of the HMIS data for reviews.
Chief Minister, Health Minister & Principal Secretary, Health & FW frequently review the performance of health department and guide in planning process.
MD, DHS, DFW&PM
and other officers review performance based on HMIS data on monthly basis.
A continuous process.
15
Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
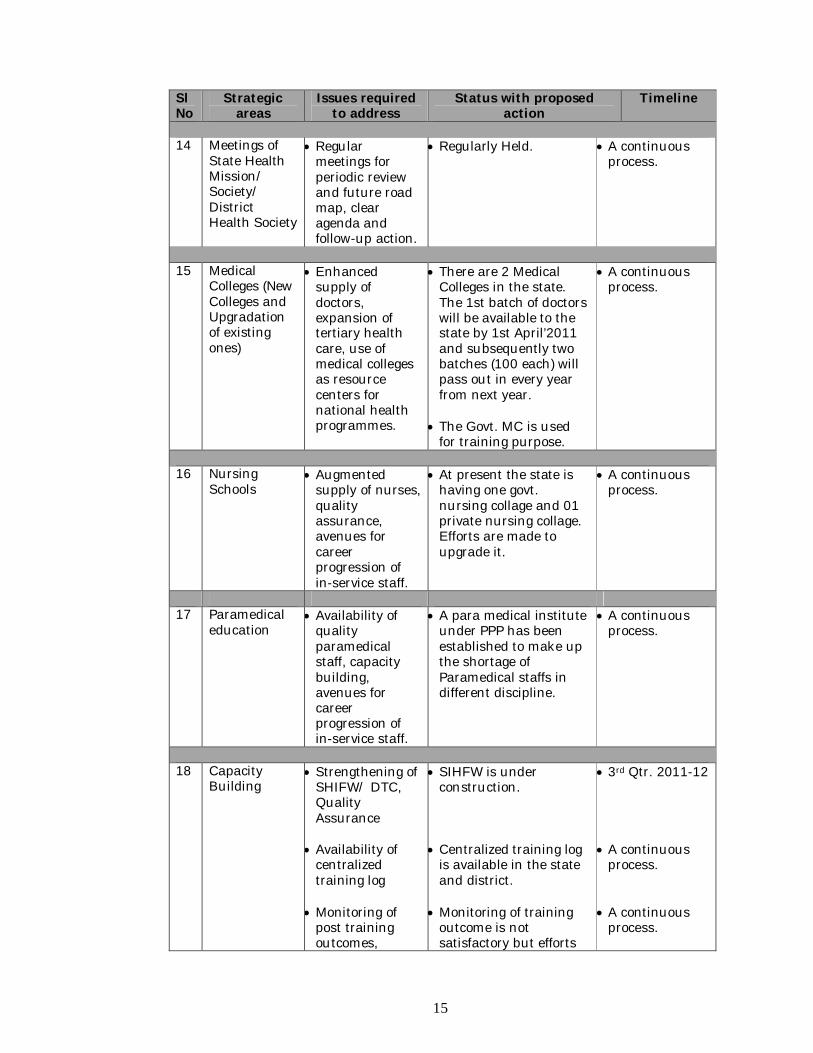
14 Meetings of
State Health Mission/ Society/ District Health Society
Regular meetings for periodic review and future road map, clear agenda and follow-up action.
Regularly Held.
A continuous process.
15 Medical
Colleges (New Colleges and Upgradation of existing ones)
Enhanced supply of doctors, expansion of tertiary health care, use of medical colleges as resource centers for national health programmes.
There are 2 Medical Colleges in the state. The 1st batch of doctors will be available to the state by 1st April’2011 and subsequently two batches (100 each) will pass out in every year from next year.
The Govt. MC is used
for training purpose.
A continuous process.
16 Nursing
Schools Augmented
supply of nurses, quality assurance, avenues for career progression of in-service staff.
At present the state is having one govt. nursing collage and 01 private nursing collage. Efforts are made to upgrade it.
A continuous process.
17 Paramedical
education Availability of
quality paramedical staff, capacity building, avenues for career progression of in-service staff.
A para medical institute under PPP has been established to make up the shortage of Paramedical staffs in different discipline.
A continuous process.
18 Capacity
Building Strengthening of
SHIFW/ DTC, Quality Assurance
Availability of
centralized training log
Monitoring of
post training outcomes,
SIHFW is under construction.
Centralized training log
is available in the state and district.
Monitoring of training
outcome is not satisfactory but efforts
3rd Qtr. 2011-12 A continuous
process. A continuous
process.
16
Sl No
Strategic areas
Issues required to address
Status with proposed action
Timeline
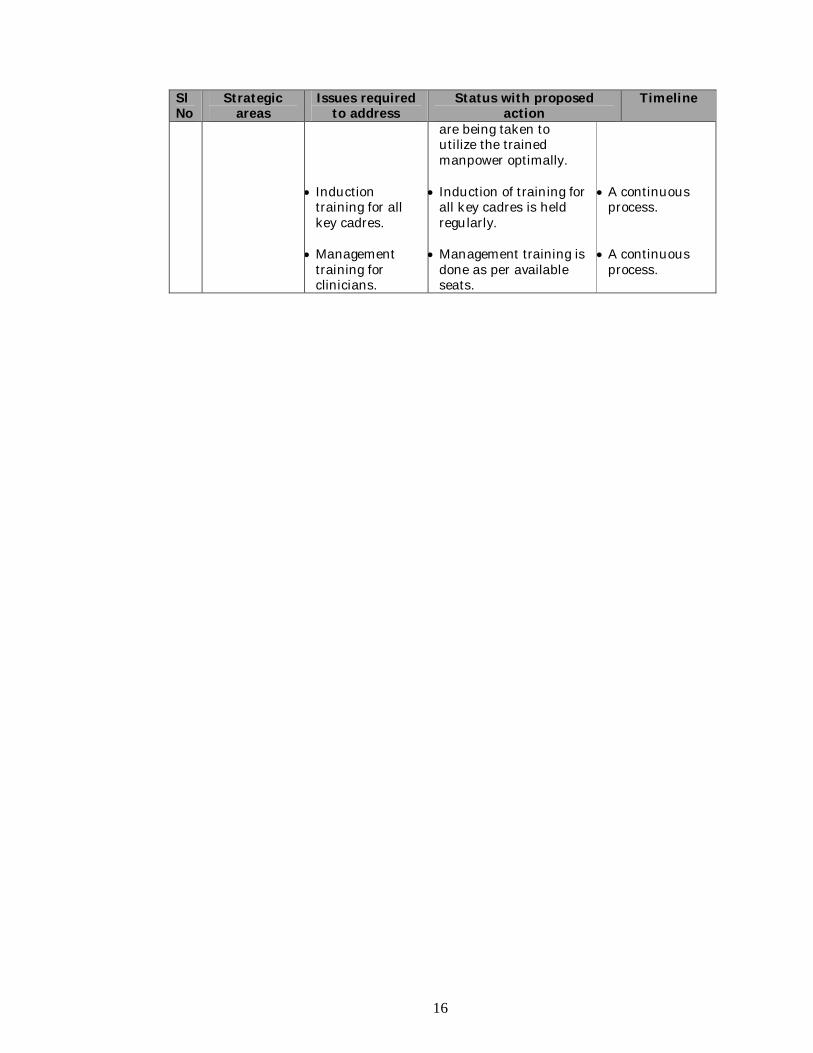
Induction
training for all key cadres.
Management
training for clinicians.
are being taken to utilize the trained manpower optimally.
Induction of training for
all key cadres is held regularly.
Management training is
done as per available seats.
A continuous
process. A continuous
process.
17
CHAPTER-3 Conditionalities As per instruction in the revised Framework for preparation of PIP for 2011-12 following conditionalities are required to be fulfilled in order to ensure non intermittent fund flow as under:- a) Pre-requisites fulfilled for release of first tranche of funds by GOI for PIP 2011- 12 are as under:
Mission Director for NRHM is in place as Chairman of State Programme Management Support Unit (SPMSU) of State Health & Family Welfare Society, Tripura having other additional charges from March 2011.
A full-time post of Chief Accounts Manager is created under State Health &
Family Welfare Society, Tripura to assist the financial management of SPMSU. The post has been filled-up by a retired Accounts Officer who had served in Audit General Office under State Finance Services. He does not hold any additional charge.
The State Plan Budget for 2011-12 would be increased by at least 10% over and
above and place 15% State share in the Bank A/C of State Health & Family Welfare Society, Tripura under NRHM.
b) Proposed action for release of second tranche of funds by GOI for PIP 2011-12 are as under:
HR POLICIES & SYSTEMS as mentioned at S.NO. 1 of the Management imperatives, measures is in practice to ensure rational deployment with stability of tenure by way of a clear transfer policy and facility based monitoring for results.
DRUG POLICY & SYSTEMS, procurement and logistics mechanism as
mentioned at S.NO. 3 of the Management Imperatives are under strengthening to the existing system by implementing ProMIS, so as to enable minimizing out-of-pocket expenses. Training of key personnels handling GOI supply of RCH, UIP, RNTCP, NVBDCP etc. have already being trained by Ministry officials. Infrastructure development is under process, required manpower has been engaged (Manager- Logistics, QA, Procurement, Bio-medical Engineer & MIS). IT appliances would be ensured to be in place on completion of infrastructural works.
The compliance status in respect of the 31 Conditionalities which was complied
during the year 2010-11 would also be ensured for 2011-12 also and is proposed in the prescribed format.
18
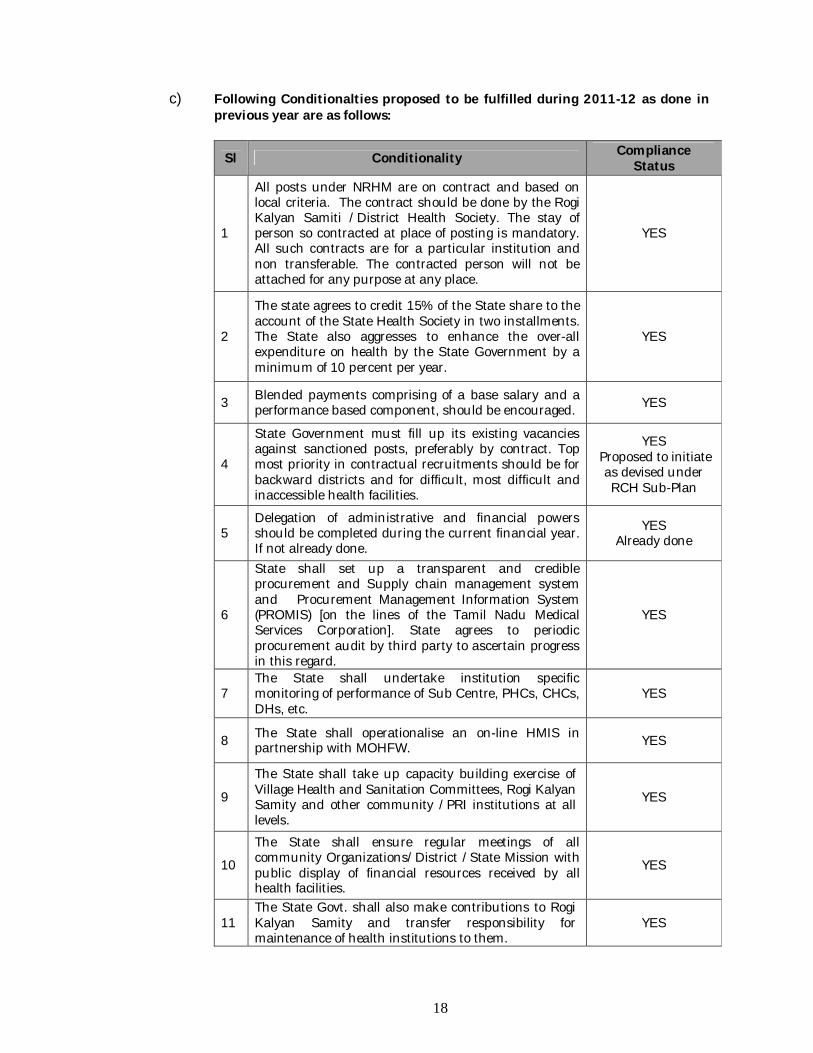
c) Following Conditionalties proposed to be fulfilled during 2011-12 as done in previous year are as follows:
Sl Conditionality Compliance Status
1
All posts under NRHM are on contract and based on local criteria. The contract should be done by the Rogi Kalyan Samiti /District Health Society. The stay of person so contracted at place of posting is mandatory. All such contracts are for a particular institution and non transferable. The contracted person will not be attached for any purpose at any place.
YES
2
The state agrees to credit 15% of the State share to the account of the State Health Society in two installments. The State also aggresses to enhance the over-all expenditure on health by the State Government by a minimum of 10 percent per year.
YES
3 Blended payments comprising of a base salary and a performance based component, should be encouraged. YES
4
State Government must fill up its existing vacancies against sanctioned posts, preferably by contract. Top most priority in contractual recruitments should be for backward districts and for difficult, most difficult and inaccessible health facilities.
YES Proposed to initiate as devised under RCH Sub-Plan
5 Delegation of administrative and financial powers should be completed during the current financial year. If not already done.
YES Already done
6
State shall set up a transparent and credible procurement and Supply chain management system and Procurement Management Information System (PROMIS) [on the lines of the Tamil Nadu Medical Services Corporation]. State agrees to periodic procurement audit by third party to ascertain progress in this regard.
YES
7 The State shall undertake institution specific monitoring of performance of Sub Centre, PHCs, CHCs, DHs, etc.
YES
8 The State shall operationalise an on-line HMIS in partnership with MOHFW. YES
9
The State shall take up capacity building exercise of Village Health and Sanitation Committees, Rogi Kalyan Samity and other community /PRI institutions at all levels.
YES
10
The State shall ensure regular meetings of all community Organizations/District /State Mission with public display of financial resources received by all health facilities.
YES
11 The State Govt. shall also make contributions to Rogi Kalyan Samity and transfer responsibility for maintenance of health institutions to them.
YES
19
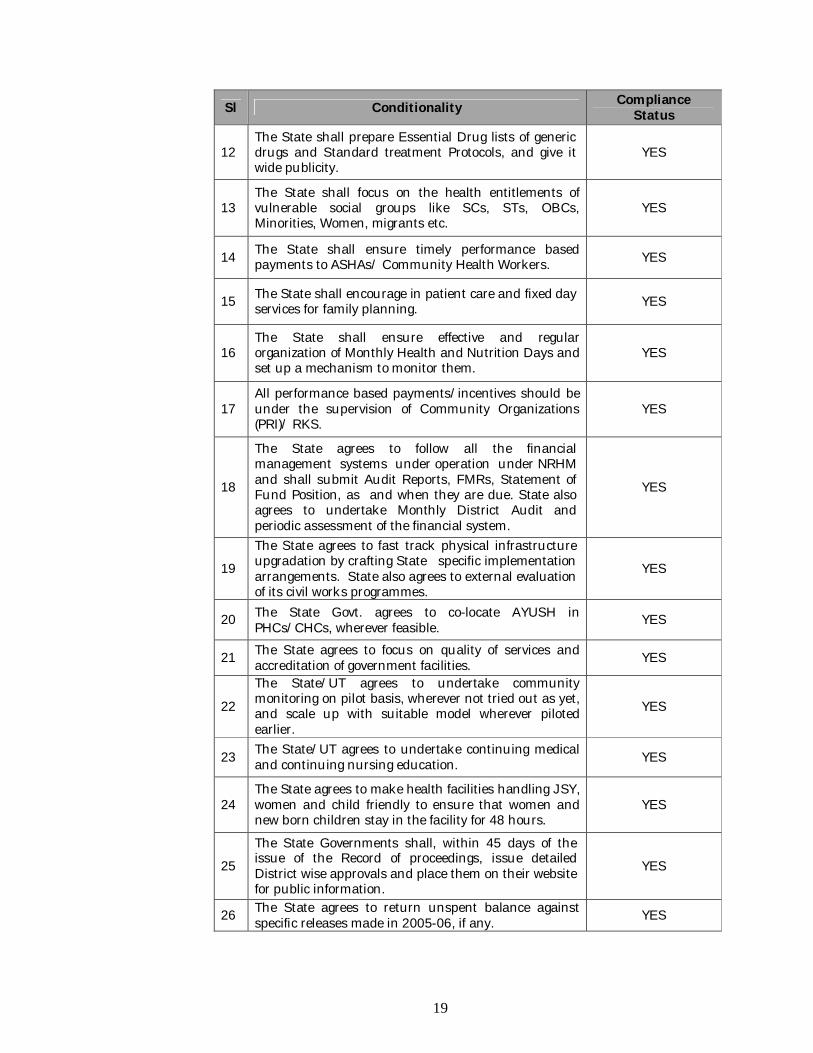
Sl Conditionality Compliance Status
12 The State shall prepare Essential Drug lists of generic drugs and Standard treatment Protocols, and give it wide publicity.
YES
13 The State shall focus on the health entitlements of vulnerable social groups like SCs, STs, OBCs, Minorities, Women, migrants etc.
YES
14 The State shall ensure timely performance based payments to ASHAs/ Community Health Workers. YES
15 The State shall encourage in patient care and fixed day services for family planning. YES
16 The State shall ensure effective and regular organization of Monthly Health and Nutrition Days and set up a mechanism to monitor them.
YES
17 All performance based payments/incentives should be under the supervision of Community Organizations (PRI)/ RKS.
YES
18
The State agrees to follow all the financial management systems under operation under NRHM and shall submit Audit Reports, FMRs, Statement of Fund Position, as and when they are due. State also agrees to undertake Monthly District Audit and periodic assessment of the financial system.
YES
19
The State agrees to fast track physical infrastructure upgradation by crafting State specific implementation arrangements. State also agrees to external evaluation of its civil works programmes.
YES
20 The State Govt. agrees to co-locate AYUSH in PHCs/CHCs, wherever feasible. YES
21 The State agrees to focus on quality of services and accreditation of government facilities. YES
22
The State/UT agrees to undertake community monitoring on pilot basis, wherever not tried out as yet, and scale up with suitable model wherever piloted earlier.
YES
23 The State/UT agrees to undertake continuing medical and continuing nursing education. YES
24 The State agrees to make health facilities handling JSY, women and child friendly to ensure that women and new born children stay in the facility for 48 hours.
YES
25
The State Governments shall, within 45 days of the issue of the Record of proceedings, issue detailed District wise approvals and place them on their website for public information.
YES
26 The State agrees to return unspent balance against specific releases made in 2005-06, if any. YES
20
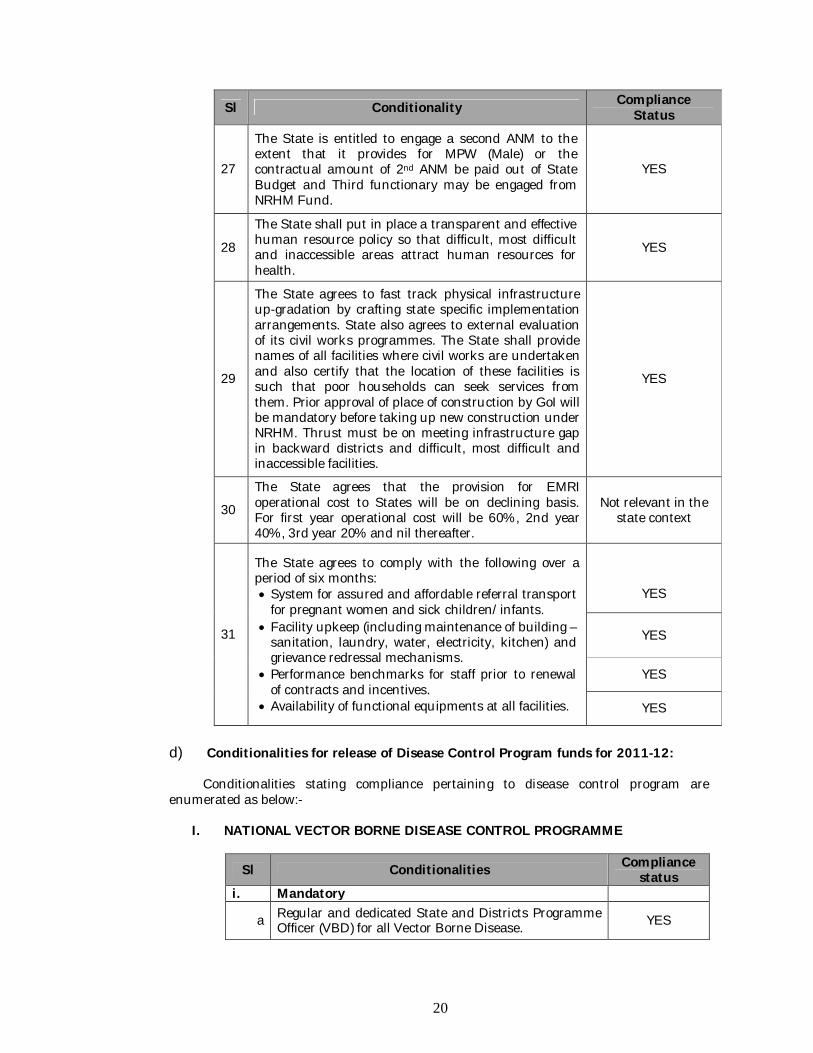
Sl Conditionality Compliance Status
27
The State is entitled to engage a second ANM to the extent that it provides for MPW (Male) or the contractual amount of 2nd ANM be paid out of State Budget and Third functionary may be engaged from NRHM Fund.
YES
28
The State shall put in place a transparent and effective human resource policy so that difficult, most difficult and inaccessible areas attract human resources for health.
YES
29
The State agrees to fast track physical infrastructure up-gradation by crafting state specific implementation arrangements. State also agrees to external evaluation of its civil works programmes. The State shall provide names of all facilities where civil works are undertaken and also certify that the location of these facilities is such that poor households can seek services from them. Prior approval of place of construction by GoI will be mandatory before taking up new construction under NRHM. Thrust must be on meeting infrastructure gap in backward districts and difficult, most difficult and inaccessible facilities.
YES
30
The State agrees that the provision for EMRI operational cost to States will be on declining basis. For first year operational cost will be 60%, 2nd year 40%, 3rd year 20% and nil thereafter.
Not relevant in the state context
31
The State agrees to comply with the following over a period of six months: System for assured and affordable referral transport
for pregnant women and sick children/infants. Facility upkeep (including maintenance of building –
sanitation, laundry, water, electricity, kitchen) and grievance redressal mechanisms.
Performance benchmarks for staff prior to renewal of contracts and incentives.
Availability of functional equipments at all facilities.
YES
YES
YES
YES
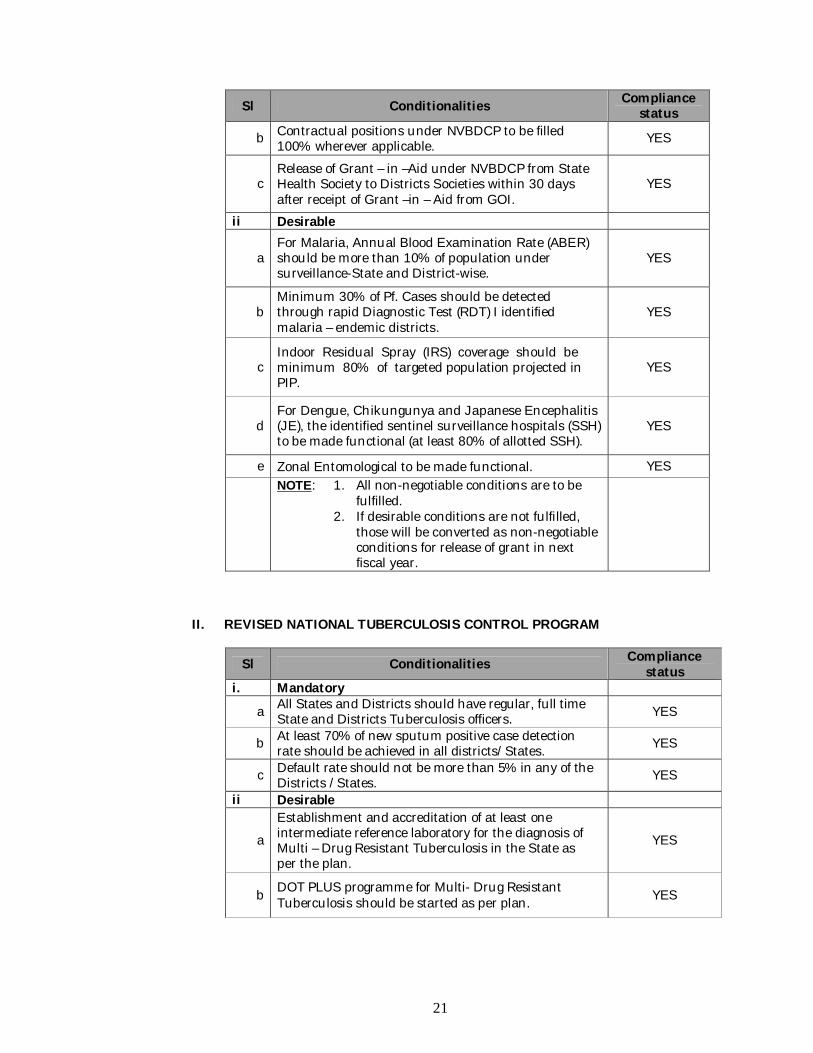
d) Conditionalities for release of Disease Control Program funds for 2011-12: Conditionalities stating compliance pertaining to disease control program are enumerated as below:-
I. NATIONAL VECTOR BORNE DISEASE CONTROL PROGRAMME
Sl Conditionalities Compliance status
i. Mandatory
a Regular and dedicated State and Districts Programme Officer (VBD) for all Vector Borne Disease. YES
21
Sl Conditionalities Compliance status
b Contractual positions under NVBDCP to be filled 100% wherever applicable. YES
c Release of Grant – in –Aid under NVBDCP from State Health Society to Districts Societies within 30 days after receipt of Grant –in – Aid from GOI.
YES
ii Desirable
a For Malaria, Annual Blood Examination Rate (ABER) should be more than 10% of population under surveillance-State and District-wise.
YES
b Minimum 30% of Pf. Cases should be detected through rapid Diagnostic Test (RDT) I identified malaria – endemic districts.
YES
c Indoor Residual Spray (IRS) coverage should be minimum 80% of targeted population projected in PIP.
YES
d For Dengue, Chikungunya and Japanese Encephalitis (JE), the identified sentinel surveillance hospitals (SSH) to be made functional (at least 80% of allotted SSH).
YES
e Zonal Entomological to be made functional. YES
NOTE: 1. All non-negotiable conditions are to be fulfilled.
2. If desirable conditions are not fulfilled, those will be converted as non-negotiable conditions for release of grant in next fiscal year.
II. REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAM
Sl Conditionalities Compliance status
i. Mandatory
a All States and Districts should have regular, full time State and Districts Tuberculosis officers. YES
b At least 70% of new sputum positive case detection rate should be achieved in all districts/States. YES
c Default rate should not be more than 5% in any of the Districts /States. YES
ii Desirable
a
Establishment and accreditation of at least one intermediate reference laboratory for the diagnosis of Multi – Drug Resistant Tuberculosis in the State as per the plan.
YES
b DOT PLUS programme for Multi- Drug Resistant Tuberculosis should be started as per plan. YES
22
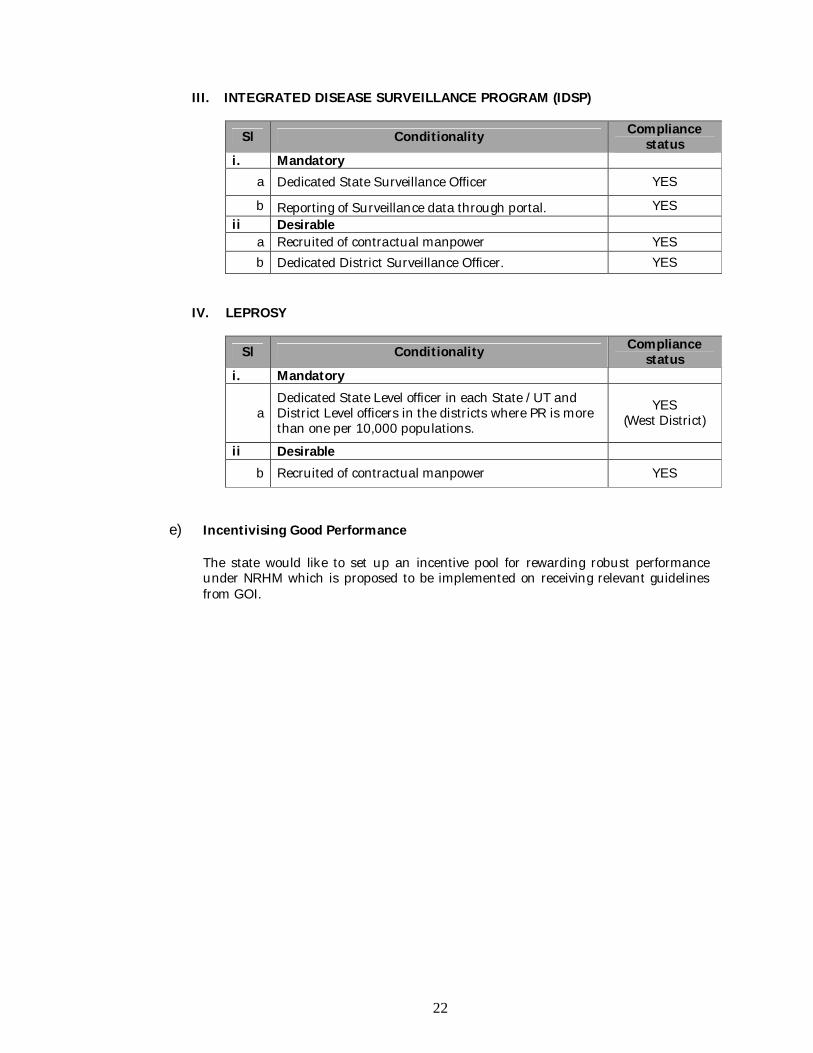
III. INTEGRATED DISEASE SURVEILLANCE PROGRAM (IDSP)
Sl Conditionality Compliance status
i. Mandatory a Dedicated State Surveillance Officer YES
b Reporting of Surveillance data through portal. YES ii Desirable
a Recruited of contractual manpower YES b Dedicated District Surveillance Officer. YES
IV. LEPROSY
Sl Conditionality Compliance status
i. Mandatory
a Dedicated State Level officer in each State /UT and District Level officers in the districts where PR is more than one per 10,000 populations.
YES (West District)
ii Desirable b Recruited of contractual manpower YES
e) Incentivising Good Performance The state would like to set up an incentive pool for rewarding robust performance under NRHM which is proposed to be implemented on receiving relevant guidelines from GOI.
23
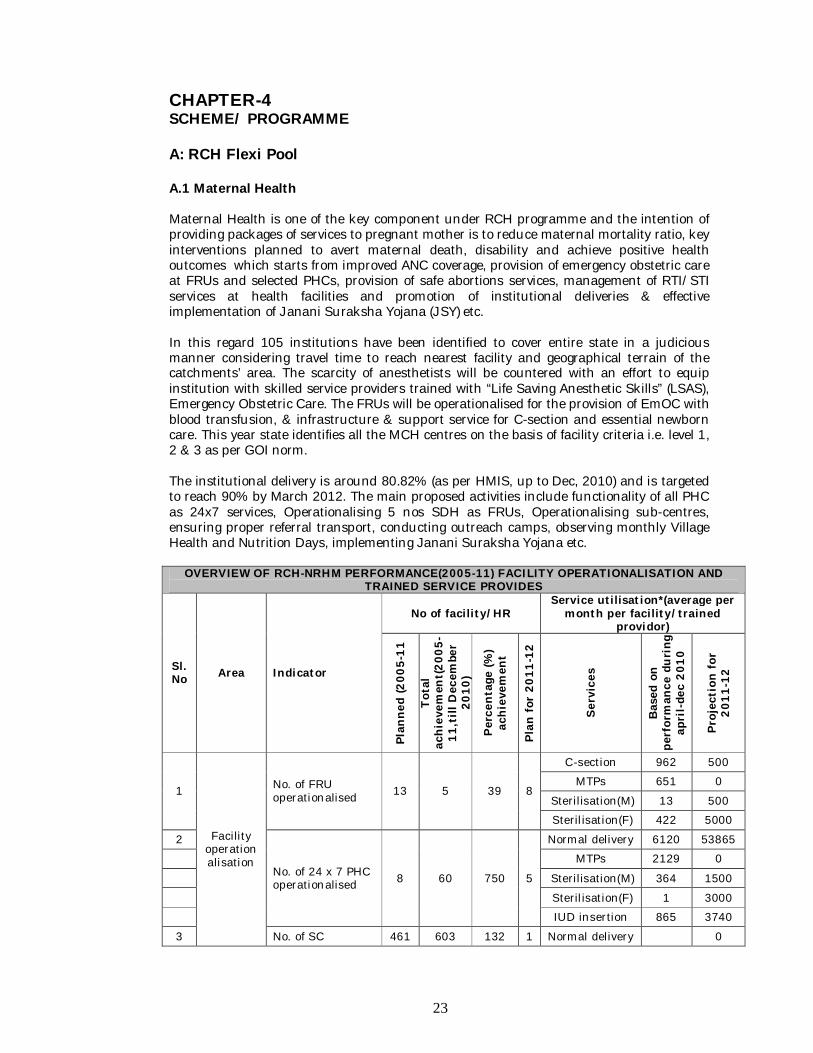
CHAPTER-4 SCHEME/ PROGRAMME A: RCH Flexi Pool A.1 Maternal Health Maternal Health is one of the key component under RCH programme and the intention of providing packages of services to pregnant mother is to reduce maternal mortality ratio, key interventions planned to avert maternal death, disability and achieve positive health outcomes which starts from improved ANC coverage, provision of emergency obstetric care at FRUs and selected PHCs, provision of safe abortions services, management of RTI/STI services at health facilities and promotion of institutional deliveries & effective implementation of Janani Suraksha Yojana (JSY) etc. In this regard 105 institutions have been identified to cover entire state in a judicious manner considering travel time to reach nearest facility and geographical terrain of the catchments’ area. The scarcity of anesthetists will be countered with an effort to equip institution with skilled service providers trained with “Life Saving Anesthetic Skills” (LSAS), Emergency Obstetric Care. The FRUs will be operationalised for the provision of EmOC with blood transfusion, & infrastructure & support service for C-section and essential newborn care. This year state identifies all the MCH centres on the basis of facility criteria i.e. level 1, 2 & 3 as per GOI norm. The institutional delivery is around 80.82% (as per HMIS, up to Dec, 2010) and is targeted to reach 90% by March 2012. The main proposed activities include functionality of all PHC as 24x7 services, Operationalising 5 nos SDH as FRUs, Operationalising sub-centres, ensuring proper referral transport, conducting outreach camps, observing monthly Village Health and Nutrition Days, implementing Janani Suraksha Yojana etc.
OVERVIEW OF RCH-NRHM PERFORMANCE(2005-11) FACILITY OPERATIONALISATION AND TRAINED SERVICE PROVIDES
Sl. No Area Indicator
No of facility/HR Service utilisation*(average per
month per facility/trained providor)
Plan
ned
(200
5-11
Tota
l ac
hiev
emen
t(20
05-
11,t
ill D
ecem
ber
2010
)
Perc
enta
ge (%
) ac
hiev
emen
t
Plan
for
201
1-12
Serv
ices
Bas
ed o
n pe
rfor
man
ce d
urin
g ap
ril-
dec
2010
Proj
ecti
on fo
r 20
11-1
2
1
Facility operationalisation
No. of FRU operationalised 13 5 39 8
C-section 962 500
MTPs 651 0
Sterilisation(M) 13 500
Sterilisation(F) 422 5000
2
No. of 24 x 7 PHC operationalised 8 60 750 5
Normal delivery 6120 53865
MTPs 2129 0
Sterilisation(M) 364 1500
Sterilisation(F) 1 3000
IUD insertion 865 3740
3 No. of SC 461 603 132 1 Normal delivery 0
24
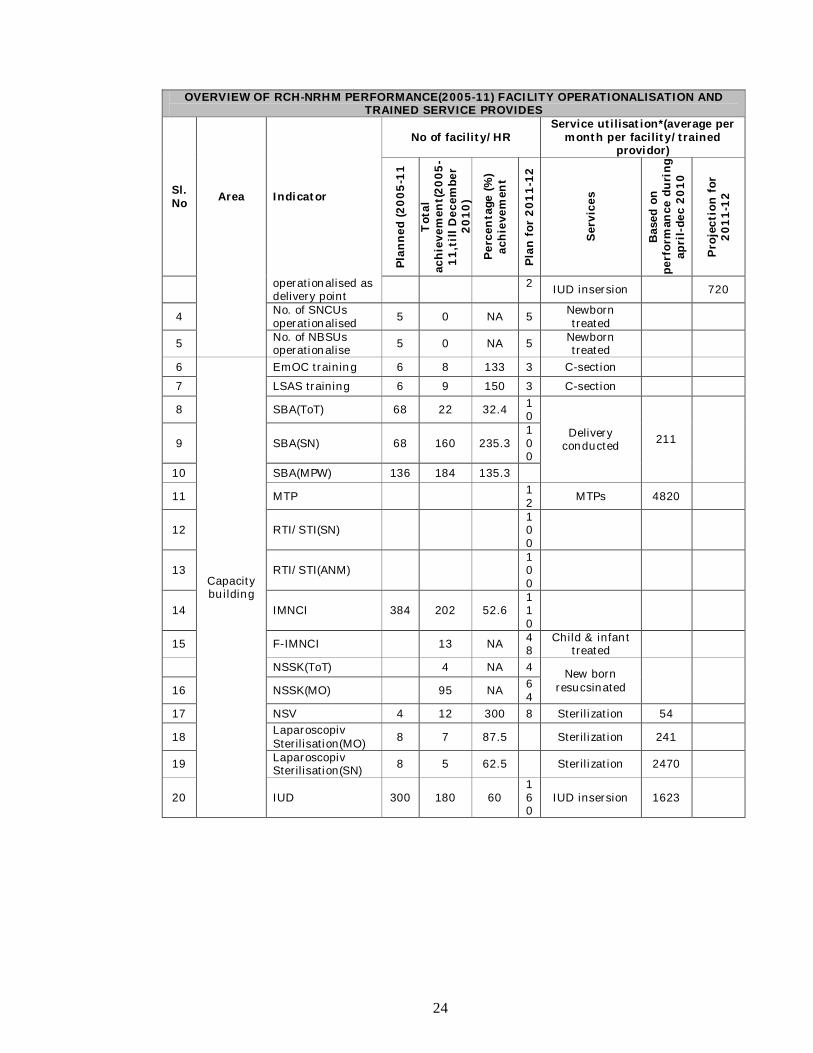
OVERVIEW OF RCH-NRHM PERFORMANCE(2005-11) FACILITY OPERATIONALISATION AND TRAINED SERVICE PROVIDES
Sl. No Area Indicator
No of facility/HR Service utilisation*(average per
month per facility/trained providor)
Plan
ned
(200
5-11
Tot
al
achi
evem
ent(
2005
-11
,till
Dec
embe
r 20
10)
Perc
enta
ge (%
) ac
hiev
emen
t
Plan
for
201
1-12
Serv
ices
Bas
ed o
n pe
rfor
man
ce d
urin
g ap
ril-
dec
2010
Proj
ecti
on f
or
2011
-12
operationalised as delivery point
2 IUD insersion 720
4 No. of SNCUs operationalised 5 0 NA 5 Newborn
treated
5 No. of NBSUs operationalise 5 0 NA 5 Newborn
treated
6
Capacity building
EmOC training 6 8 133 3 C-section
7 LSAS training 6 9 150 3 C-section
8 SBA(ToT) 68 22 32.4 10
Delivery conducted 211 9 SBA(SN) 68 160 235.3
100
10 SBA(MPW) 136 184 135.3
11 MTP 12 MTPs 4820
12 RTI/STI(SN) 100
13 RTI/STI(ANM) 100
14 IMNCI 384 202 52.6 110
15 F-IMNCI 13 NA 48
Child & infant treated
NSSK(ToT) 4 NA 4 New born resucsinated
16 NSSK(MO) 95 NA 64
17 NSV 4 12 300 8 Sterilization 54
18 Laparoscopiv Sterilisation(MO) 8 7 87.5 Sterilization 241
19 Laparoscopiv Sterilisation(SN) 8 5 62.5 Sterilization 2470
20 IUD 300 180 60 160
IUD insersion 1623
25
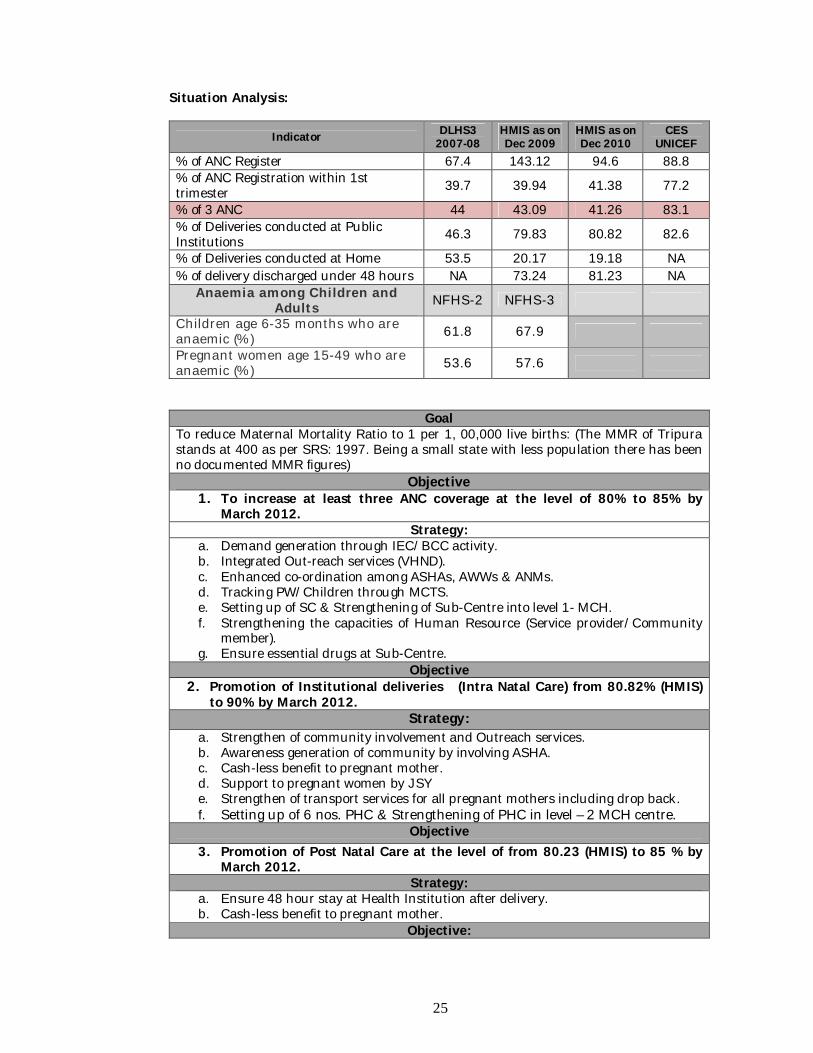
Situation Analysis:
Indicator DLHS3 2007-08
HMIS as on Dec 2009
HMIS as on Dec 2010
CES UNICEF
% of ANC Register 67.4 143.12 94.6 88.8 % of ANC Registration within 1st trimester 39.7 39.94 41.38 77.2
% of 3 ANC 44 43.09 41.26 83.1 % of Deliveries conducted at Public Institutions 46.3 79.83 80.82 82.6
% of Deliveries conducted at Home 53.5 20.17 19.18 NA % of delivery discharged under 48 hours NA 73.24 81.23 NA
Anaemia among Children and Adults NFHS-2 NFHS-3
Children age 6-35 months who are anaemic (%) 61.8 67.9
Pregnant women age 15-49 who are anaemic (%) 53.6 57.6
Goal To reduce Maternal Mortality Ratio to 1 per 1, 00,000 live births: (The MMR of Tripura stands at 400 as per SRS: 1997. Being a small state with less population there has been no documented MMR figures)
Objective 1. To increase at least three ANC coverage at the level of 80% to 85% by
March 2012. Strategy:
a. Demand generation through IEC/BCC activity. b. Integrated Out-reach services (VHND). c. Enhanced co-ordination among ASHAs, AWWs & ANMs. d. Tracking PW/Children through MCTS. e. Setting up of SC & Strengthening of Sub-Centre into level 1- MCH. f. Strengthening the capacities of Human Resource (Service provider/Community
member). g. Ensure essential drugs at Sub-Centre.
Objective 2. Promotion of Institutional deliveries (Intra Natal Care) from 80.82% (HMIS)
to 90% by March 2012. Strategy:
a. Strengthen of community involvement and Outreach services. b. Awareness generation of community by involving ASHA. c. Cash-less benefit to pregnant mother. d. Support to pregnant women by JSY e. Strengthen of transport services for all pregnant mothers including drop back. f. Setting up of 6 nos. PHC & Strengthening of PHC in level – 2 MCH centre.
Objective 3. Promotion of Post Natal Care at the level of from 80.23 (HMIS) to 85 % by
March 2012. Strategy:
a. Ensure 48 hour stay at Health Institution after delivery. b. Cash-less benefit to pregnant mother.
Objective:
26
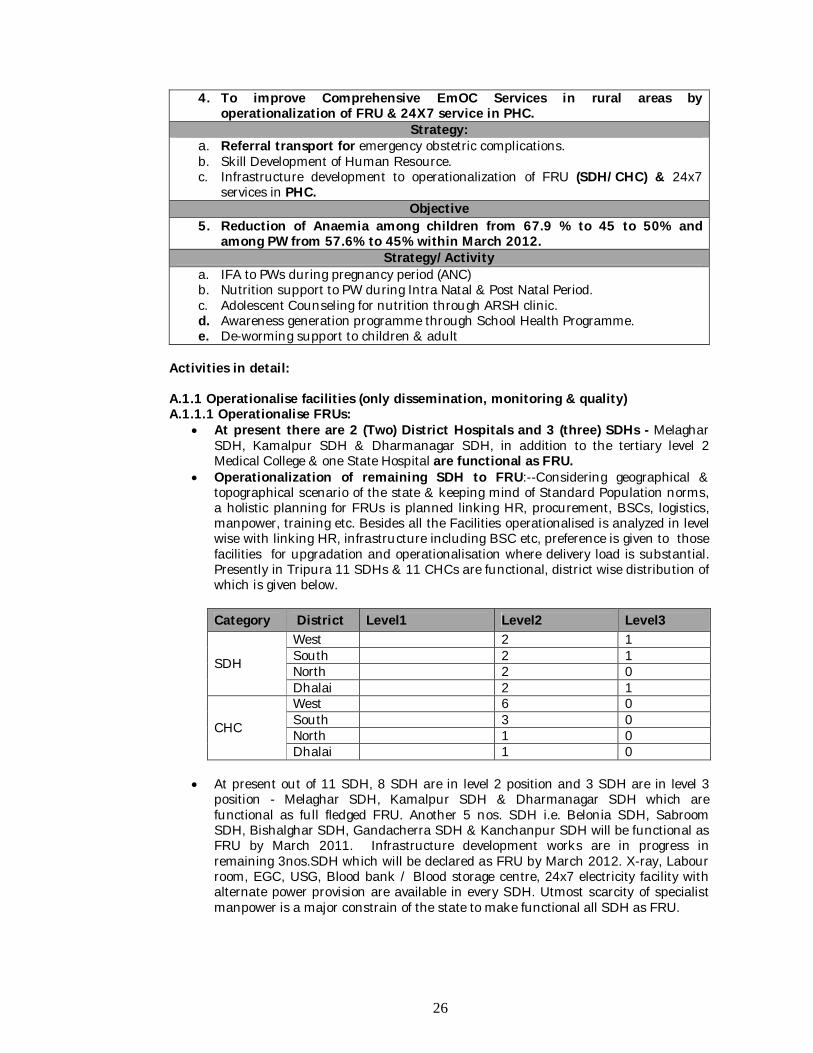
4. To improve Comprehensive EmOC Services in rural areas by operationalization of FRU & 24X7 service in PHC.
Strategy: a. Referral transport for emergency obstetric complications. b. Skill Development of Human Resource. c. Infrastructure development to operationalization of FRU (SDH/CHC) & 24x7
services in PHC. Objective
5. Reduction of Anaemia among children from 67.9 % to 45 to 50% and among PW from 57.6% to 45% within March 2012.
Strategy/Activity a. IFA to PWs during pregnancy period (ANC) b. Nutrition support to PW during Intra Natal & Post Natal Period. c. Adolescent Counseling for nutrition through ARSH clinic. d. Awareness generation programme through School Health Programme. e. De-worming support to children & adult
Activities in detail: A.1.1 Operationalise facilities (only dissemination, monitoring & quality) A.1.1.1 Operationalise FRUs:
At present there are 2 (Two) District Hospitals and 3 (three) SDHs - Melaghar SDH, Kamalpur SDH & Dharmanagar SDH, in addition to the tertiary level 2 Medical College & one State Hospital are functional as FRU.
Operationalization of remaining SDH to FRU:--Considering geographical & topographical scenario of the state & keeping mind of Standard Population norms, a holistic planning for FRUs is planned linking HR, procurement, BSCs, logistics, manpower, training etc. Besides all the Facilities operationalised is analyzed in level wise with linking HR, infrastructure including BSC etc, preference is given to those facilities for upgradation and operationalisation where delivery load is substantial. Presently in Tripura 11 SDHs & 11 CHCs are functional, district wise distribution of which is given below.
Category District Level1 Level2 Level3
SDH
West 2 1 South 2 1 North 2 0 Dhalai 2 1
CHC
West 6 0 South 3 0 North 1 0 Dhalai 1 0
At present out of 11 SDH, 8 SDH are in level 2 position and 3 SDH are in level 3
position - Melaghar SDH, Kamalpur SDH & Dharmanagar SDH which are functional as full fledged FRU. Another 5 nos. SDH i.e. Belonia SDH, Sabroom SDH, Bishalghar SDH, Gandacherra SDH & Kanchanpur SDH will be functional as FRU by March 2011. Infrastructure development works are in progress in remaining 3nos.SDH which will be declared as FRU by March 2012. X-ray, Labour room, EGC, USG, Blood bank / Blood storage centre, 24x7 electricity facility with alternate power provision are available in every SDH. Utmost scarcity of specialist manpower is a major constrain of the state to make functional all SDH as FRU.
27
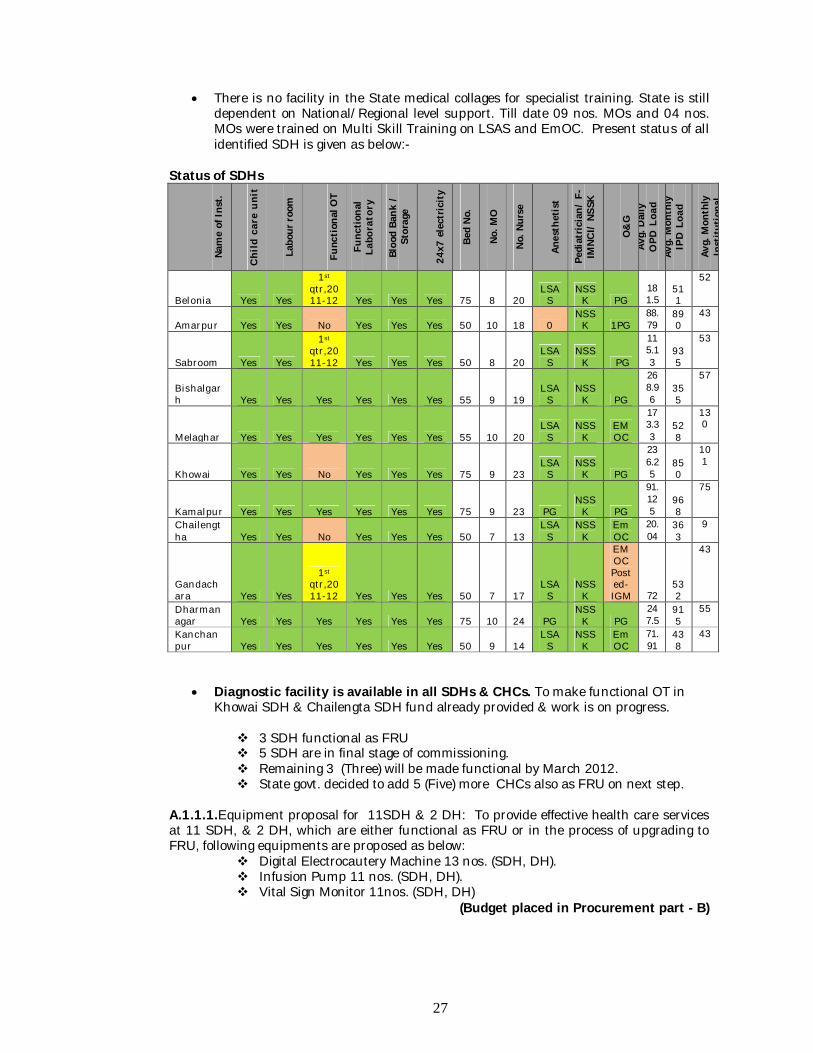
There is no facility in the State medical collages for specialist training. State is still dependent on National/Regional level support. Till date 09 nos. MOs and 04 nos. MOs were trained on Multi Skill Training on LSAS and EmOC. Present status of all identified SDH is given as below:-
Status of SDHs
Nam
e of
Inst
.
Chi
ld c
are
unit
Labo
ur r
oom
Func
tion
al O
T
Func
tiona
l La
bora
tory
Bloo
d Ba
nk /
St
orag
e
24x7
ele
ctric
ity
Bed
No.
No. M
O
No. N
urse
Anes
thet
ist
Pedi
atric
ian/
F-
IMNC
I/ N
SSK
O&
G Av
g. D
aily
O
PD L
oad
Avg.
Mon
thly
IP
D L
oad
Avg.
Mon
thly
In
stitu
tion
al
Belonia Yes Yes
1st qtr,2011-12 Yes Yes Yes 75 8 20
LSAS
NSSK PG
181.5
511
52
Amarpur Yes Yes No Yes Yes Yes 50 10 18 0 NSS
K 1PG 88.79
890
43
Sabroom Yes Yes
1st qtr,2011-12 Yes Yes Yes 50 8 20
LSAS
NSSK PG
115.13
935
53
Bishalgarh Yes Yes Yes Yes Yes Yes 55 9 19
LSAS
NSSK PG
268.96
355
57
Melaghar Yes Yes Yes Yes Yes Yes 55 10 20 LSA
S NSS
K EMOC
173.33
528
130
Khowai Yes Yes No Yes Yes Yes 75 9 23 LSA
S NSS
K PG
236.25
850
101
Kamalpur Yes Yes Yes Yes Yes Yes 75 9 23 PG NSS
K PG
91.125
968
75
Chailengtha Yes Yes No Yes Yes Yes 50 7 13
LSAS
NSSK
EmOC
20.04
363
9
Gandachara Yes Yes
1st qtr,2011-12 Yes Yes Yes 50 7 17
LSAS
NSSK
EMOC Posted-IGM 72
532
43
Dharmanagar Yes Yes Yes Yes Yes Yes 75 10 24 PG
NSSK PG
247.5
915
55
Kanchanpur Yes Yes Yes Yes Yes Yes 50 9 14
LSAS
NSSK
EmOC
71.91
438
43
Diagnostic facility is available in all SDHs & CHCs. To make functional OT in Khowai SDH & Chailengta SDH fund already provided & work is on progress. 3 SDH functional as FRU 5 SDH are in final stage of commissioning. Remaining 3 (Three) will be made functional by March 2012. State govt. decided to add 5 (Five) more CHCs also as FRU on next step.
A.1.1.1.Equipment proposal for 11SDH & 2 DH: To provide effective health care services at 11 SDH, & 2 DH, which are either functional as FRU or in the process of upgrading to FRU, following equipments are proposed as below:
Digital Electrocautery Machine 13 nos. (SDH, DH). Infusion Pump 11 nos. (SDH, DH). Vital Sign Monitor 11nos. (SDH, DH)
(Budget placed in Procurement part - B)
28
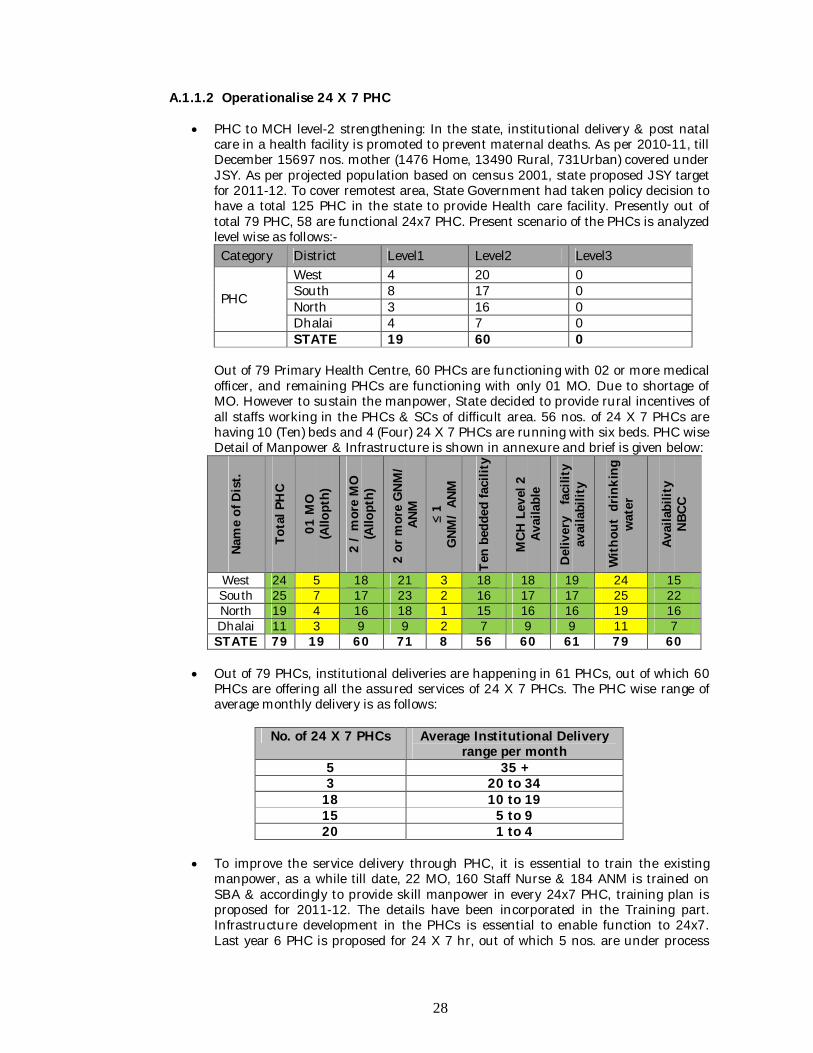
A.1.1.2 Operationalise 24 X 7 PHC
PHC to MCH level-2 strengthening: In the state, institutional delivery & post natal care in a health facility is promoted to prevent maternal deaths. As per 2010-11, till December 15697 nos. mother (1476 Home, 13490 Rural, 731Urban) covered under JSY. As per projected population based on census 2001, state proposed JSY target for 2011-12. To cover remotest area, State Government had taken policy decision to have a total 125 PHC in the state to provide Health care facility. Presently out of total 79 PHC, 58 are functional 24x7 PHC. Present scenario of the PHCs is analyzed level wise as follows:- Category District Level1 Level2 Level3
PHC
West 4 20 0 South 8 17 0 North 3 16 0 Dhalai 4 7 0
STATE 19 60 0
Out of 79 Primary Health Centre, 60 PHCs are functioning with 02 or more medical officer, and remaining PHCs are functioning with only 01 MO. Due to shortage of MO. However to sustain the manpower, State decided to provide rural incentives of all staffs working in the PHCs & SCs of difficult area. 56 nos. of 24 X 7 PHCs are having 10 (Ten) beds and 4 (Four) 24 X 7 PHCs are running with six beds. PHC wise Detail of Manpower & Infrastructure is shown in annexure and brief is given below:
Nam
e of
Dis
t.
Tota
l PH
C
01 M
O
(Allo
pth)
2 /
mor
e M
O
(Allo
pth)
2 or
mor
e G
NM/
ANM
≤ 1
GNM
/ AN
M
Ten
bedd
ed fa
cilit
y
MCH
Lev
el 2
Av
aila
ble
Del
iver
y f
acili
ty
avai
labi
lity
With
out
drin
king
w
ater
Avai
labi
lity
NB
CC
West 24 5 18 21 3 18 18 19 24 15 South 25 7 17 23 2 16 17 17 25 22 North 19 4 16 18 1 15 16 16 19 16 Dhalai 11 3 9 9 2 7 9 9 11 7 STATE 79 19 60 71 8 56 60 61 79 60
Out of 79 PHCs, institutional deliveries are happening in 61 PHCs, out of which 60
PHCs are offering all the assured services of 24 X 7 PHCs. The PHC wise range of average monthly delivery is as follows:
No. of 24 X 7 PHCs Average Institutional Delivery range per month
5 35 + 3 20 to 34 18 10 to 19 15 5 to 9 20 1 to 4
To improve the service delivery through PHC, it is essential to train the existing
manpower, as a while till date, 22 MO, 160 Staff Nurse & 184 ANM is trained on SBA & accordingly to provide skill manpower in every 24x7 PHC, training plan is proposed for 2011-12. The details have been incorporated in the Training part. Infrastructure development in the PHCs is essential to enable function to 24x7. Last year 6 PHC is proposed for 24 X 7 hr, out of which 5 nos. are under process
29
and regarding Garji PHC, decision is to be finalized by the state govt. The following listed PHCs are proposed to make functional as 24x7 Health Care Service: Budget: Sl.No Component Number Remarks
1. Establishment New PHC in difficult areas 6 Budgeted
under Part-B
2. Strengthening of PHC for making level -2 MCH centre 5
Budget under Infra & HR, Part-
A.
3.
5nos.PHC as 24x7 health care (Kanchanmala, Mungiakami in West & Machmara, Sanichera & Khedachera in North.) (As per District proposal)
5 Budget under
Infra & HR, Part-A.
A.1.1.3 Increase ANC coverage:
Provision of antenatal care, including at least three antenatal care visits, iron prophylaxis for pregnant and lactating mothers, two doses of tetanus Toxoid vaccine, detection and treatment of anaemia in mothers, and management and referral of high–risk pregnancies. To increase the coverage following activities undertaken:
SC to MCH level 1: To increase 3 ANC by Health professionals and involving ASHA as a motivator to render services at the grass root level. Presently in Tripura 627 Sub-centres are functional & by March, 2011, another 32 SC will be functional though all in below Level 1. In Dhalai District, which is one of the High focus District of Tripura, presently 5 SCs are strengthened in level 1 & required manpower also trained up. It has been found that GOI emphasized on SC level Delivery which may be considered as level 1 MCH centre. This refers to a delivery conducted by skilled birth attendant in all Sub-Centres and in some Primary Health Centres (PHCs) which have not yet reached the next level of “24 x 7 PHC & Newborn Care Corner in all facilities. Home deliveries assisted by a skilled birth attendant would also be included under safe deliveries at this level. State Government had taken policy decision to have a total 1040 Sub-Centre in the State to provide one Sub-Centre in each Gram Panchayat and ADC Village. In this regard strengthening of sub-centre facility in remote area by adding new sub-centre and development of SC infrastructure is one of the most important priorities. It is proposed to commission 100 new SCs in 2011-12. Besides establishment of new SC it is proposed to strengthen existing 12SC by upgrading as MCH-level-1 (IPHS standard) by ensuring 24 hr stay of ANM facility. Financial involvement is reflected in Infrastructure & HR of PART-A. The identified SCs are: West (Devipur SC, Kalikrishnanagar SC & Uttar Ramchandraghat SC) South (North Bharat Ch. Nagar SC, Bagmara SC & Kasko SC) North (Rangauti SC, Satsangam SC & Krishna Tilla SC) Dhalai (Amtali SC, Tuichakma SC & Gantacherra SC)
Skill development through Training: Training like Skill birth Attendant,
Immunization for Nurse/ANM/MPW, 6th & 7th module training of ASHA on HBNC etc also proposed to develop skill of Nurse, MPW/ANM, ASHA to provide quality service. (Budgeted in Training Part-A)
30
VH&ND: VHND is a platform for interfacing between the community and the health system is proposed in all 1040 GP/ADC twice in a month to increase ANC coverage. The roles of the ANM, ASHA, AWW & PRI members is to understand the needs of the community & fulfill their demands by sharing information & educating them on matters related to health. VHND can bring effective behavioral changes in the community, and can also induce health-seeking behavior in the community leading to better health outcomes. Services designed to be provided: All pregnant women are to be registered. Registered pregnant women are to be given ANC. Dropout pregnant women eligible for ANC are to be tracked and
services are to be provided to them. (Budgeted in Maternal Health)
Equipment Support: It is also essential for availability of instruments, such as BP
instrument, weighing machine, foetoscope, measuring tape, Haemoglobin meters and regular supply of essential drugs and proper use and maintenance of records and regular supply of essential drugs at health institutions (Kit-A & Kit-B).
Tracking of Pregnant Women and Children Operationalising MCTS: Through MCTS drop-outs of 3ANC can be identified in area wise where Health professional & ASHA can directly take initiative to motivate PW. NIC Tripura has customized the Mother & Children Tracking System Portal under the URL of http://nrhm-mcts-trp.nic.in. Mapping/Coding of Master database of all health facility has been completed. 1040 GP/ADC of the state are mapped under the health institution of Tripura as catchment area. In the year 2010-11, 3 GP namely Kaurikuli, Jalai and Gounagar under Jalai & Gournagar SC of Kanikamemorial PHC, North District has been taken as pilot basis for online MCTS data entry. in the meantime legacy information has collected by MCTS excel format provided by MoHFW. During Pilot phase, lots of corrective measure has taken by NIC for the MCTS portal. From April 2011, State will update the MCTS as regular manner. Accordingly plan is incorporated in PART-B.
Integrated Outreach RCH services: RCH Outreach camps in the identified 30 PHCs proposed to be conducted two times in a year to provide Anti Natal Care, Post Natal Care, Immunization, Family Planning services, Nutrition Education etc., RCH out reach camp is being organized, for the people residing in the rural remote areas usually not availing PHC services. (Budgeted in Maternal Health)
Generating awareness through IEC/BCC: To increase ANC coverage, Mother and Child Health Fair one in each 17 nos. Sub-Division @ Rs.90, 000, (to disseminate messages through speeches, leaflets. Slogan, Essay, drawing, quiz competition will be organized among the villagers through interactive stalls may be created in market places and exhibition will decorate the stall) is proposed.
(Budgeted in Part-B)
Activity Number Proposed
Rate Proposed
Remarks
Setting up of 100 new SC 100 1500000 Budgeted in
Part B Functioning of 12 Sc as level 1 MCH centre by ensuring stay of ANM 24 hrs.
12 780000
Budgeted in Part A,
Infrastructure & HR
31
A.1.2 Strengthening of referral transport services (Assured Referral Transport system):
Assured referral transport makes easier for high risk pregnant women to access a functional FRU in time and thus becomes an important factor to reduce MMR & IMR to achieve program objectives. In the state Tripura Referral Transportation System was in practice since beginning of the Health Service. With the support of NRHM, the system is strengthened for all health Institutions. Referred patients were benefitted under this system prioritising High Risk Pregnant Mothers & High Risk Babies.
Referral System is assured in the state by two ways, i.e.: a. By own vehicle of the concern institution: At present about 60%
Health Institution having own Vehicle (ambulances) which is also used for programme /outreach activities massively used for nearly 15 to 20 days of a month. Whenever the vehicle is available in the institution, patients are referred by this vehicle only.
b. By hiring process on contract basis through RKS: In emergency period referral system is made by hiring of vehicles called by respective health institution from the local Agency selected by RKS on contract basis with a pre-fixed rate. Hired vehicle collect the cheque by showing the referral slip from the referral unit after dropping the patients.
To reduce maternal morbidity and mortality, referral system needs to be
reformed & is also emphasized by GOI. Meanwhile it is mentionable that between facility service i.e. referral transport from facility to facility for high risk pregnant mother is included since 2006-07 and also proposed in 2011-12. This will ensure timely treatment during emergency cases. On the basis of performance during 2010-11 it is expected that around 5003 cases will need referral to higher centers for specialists’ care services. To reduce MMR & to ensure Institutional Delivery as decided in the
meeting of State Health Ministers & State Secretaries of Health & Medical Education under the chairmanship of Union Minister, Health & Family Welfare, Shri Gulam Nabi Azad Held during 11th – 13th January, 2011 at Hyderabad, Andhra Pradesh that, for general cases to & fro service i.e. home to facility & facility to home is incorporated as a new inclusion in 2011-12 PIP. Budget proposed by the sate @ Rs. 1000/- (will be paid as per actual).
There are few areas in the Dhalai district which is not connected (Tribal area &
Border connected area) by road. Experimental innovation of Doli service had given good response & demand increased for uncovered Tribal Villages. The area is under the coverage of “Doli” service to enable expecting mothers reach health institutions.
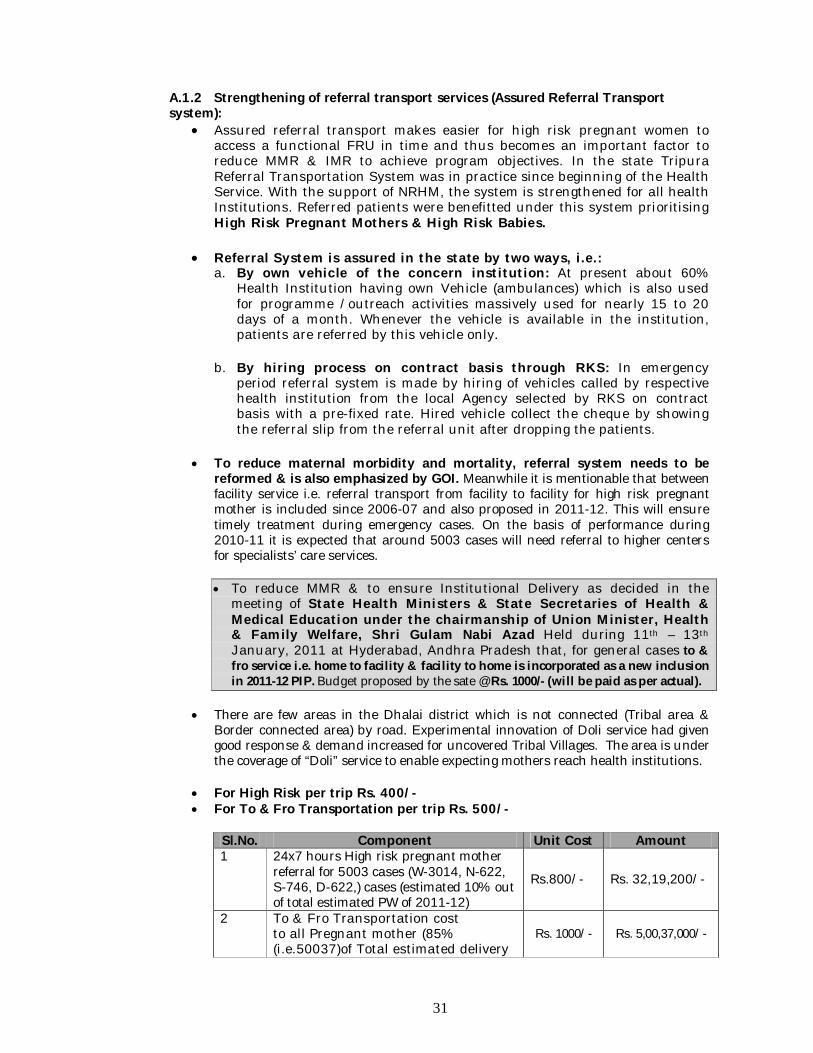
For High Risk per trip Rs. 400/- For To & Fro Transportation per trip Rs. 500/-
Sl.No. Component Unit Cost Amount 1 24x7 hours High risk pregnant mother
referral for 5003 cases (W-3014, N-622, S-746, D-622,) cases (estimated 10% out of total estimated PW of 2011-12)
Rs.800/- Rs. 32,19,200/-
2 To & Fro Transportation cost to all Pregnant mother (85% (i.e.50037)of Total estimated delivery
Rs. 1000/- Rs. 5,00,37,000/-
32
i.e. 58868)
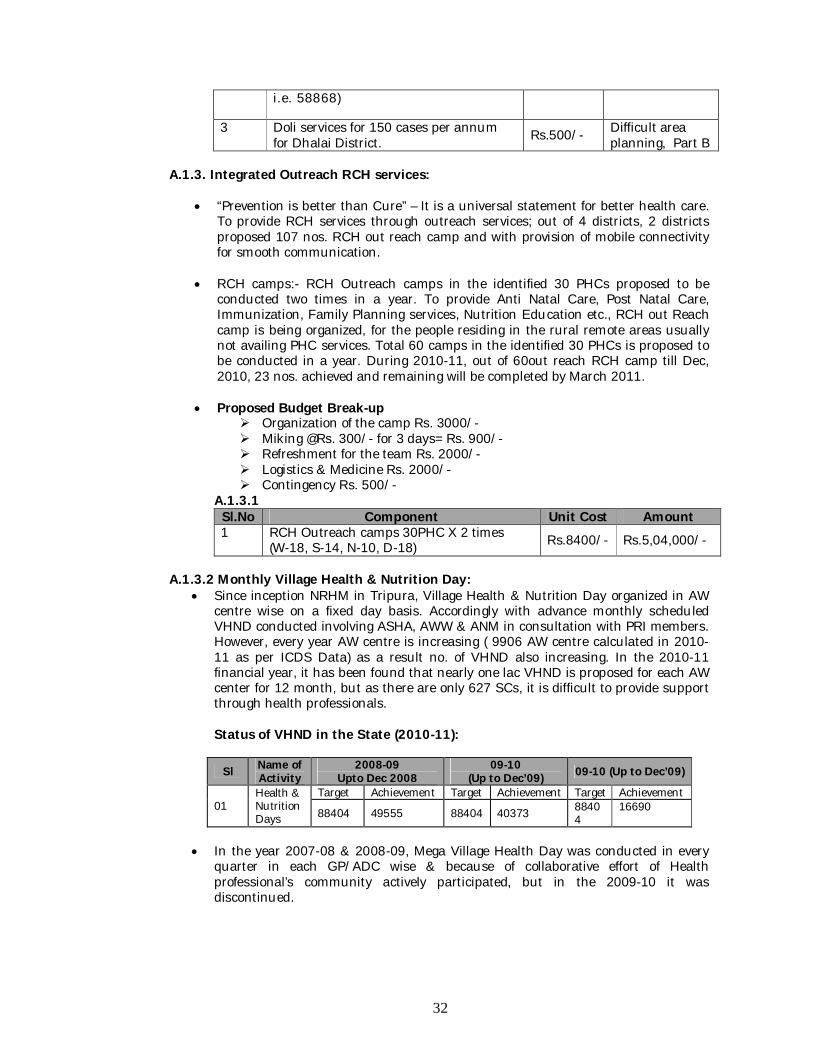
3 Doli services for 150 cases per annum for Dhalai District. Rs.500/- Difficult area
planning, Part B A.1.3. Integrated Outreach RCH services:
“Prevention is better than Cure” – It is a universal statement for better health care. To provide RCH services through outreach services; out of 4 districts, 2 districts proposed 107 nos. RCH out reach camp and with provision of mobile connectivity for smooth communication.
RCH camps:- RCH Outreach camps in the identified 30 PHCs proposed to be
conducted two times in a year. To provide Anti Natal Care, Post Natal Care, Immunization, Family Planning services, Nutrition Education etc., RCH out Reach camp is being organized, for the people residing in the rural remote areas usually not availing PHC services. Total 60 camps in the identified 30 PHCs is proposed to be conducted in a year. During 2010-11, out of 60out reach RCH camp till Dec, 2010, 23 nos. achieved and remaining will be completed by March 2011.
Proposed Budget Break-up Organization of the camp Rs. 3000/- Miking @Rs. 300/- for 3 days= Rs. 900/- Refreshment for the team Rs. 2000/- Logistics & Medicine Rs. 2000/- Contingency Rs. 500/-
A.1.3.1 Sl.No Component Unit Cost Amount 1 RCH Outreach camps 30PHC X 2 times
(W-18, S-14, N-10, D-18) Rs.8400/- Rs.5,04,000/-
A.1.3.2 Monthly Village Health & Nutrition Day:
Since inception NRHM in Tripura, Village Health & Nutrition Day organized in AW centre wise on a fixed day basis. Accordingly with advance monthly scheduled VHND conducted involving ASHA, AWW & ANM in consultation with PRI members. However, every year AW centre is increasing ( 9906 AW centre calculated in 2010-11 as per ICDS Data) as a result no. of VHND also increasing. In the 2010-11 financial year, it has been found that nearly one lac VHND is proposed for each AW center for 12 month, but as there are only 627 SCs, it is difficult to provide support through health professionals. Status of VHND in the State (2010-11):
Sl Name of Activity
2008-09 Upto Dec 2008
09-10 (Up to Dec’09) 09-10 (Up to Dec’09)
01 Health & Nutrition Days
Target Achievement Target Achievement Target Achievement
88404 49555 88404 40373 88404
16690
In the year 2007-08 & 2008-09, Mega Village Health Day was conducted in every
quarter in each GP/ADC wise & because of collaborative effort of Health professional’s community actively participated, but in the 2009-10 it was discontinued.
33
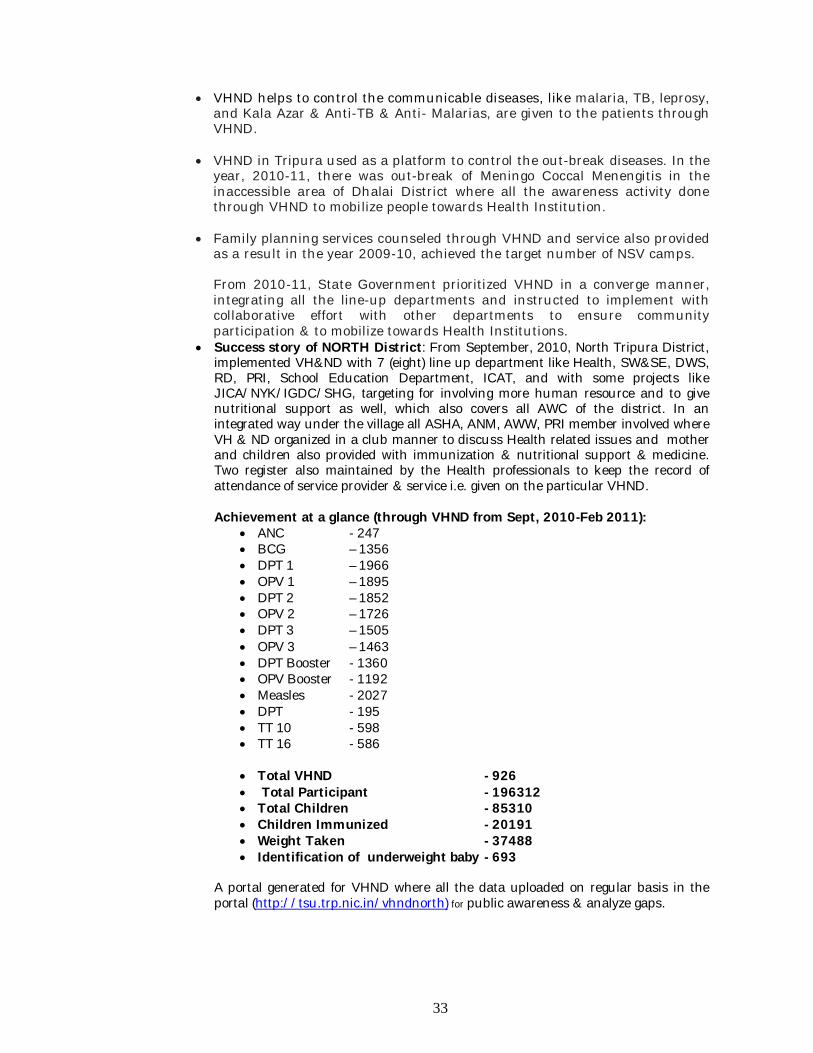
VHND helps to control the communicable diseases, like malaria, TB, leprosy, and Kala Azar & Anti-TB & Anti- Malarias, are given to the patients through VHND.
VHND in Tripura used as a platform to control the out-break diseases. In the year, 2010-11, there was out-break of Meningo Coccal Menengitis in the inaccessible area of Dhalai District where all the awareness activity done through VHND to mobilize people towards Health Institution.
Family planning services counseled through VHND and service also provided as a result in the year 2009-10, achieved the target number of NSV camps. From 2010-11, State Government prioritized VHND in a converge manner, integrating all the line-up departments and instructed to implement with collaborative effort with other departments to ensure community participation & to mobilize towards Health Institutions.
Success story of NORTH District: From September, 2010, North Tripura District, implemented VH&ND with 7 (eight) line up department like Health, SW&SE, DWS, RD, PRI, School Education Department, ICAT, and with some projects like JICA/NYK/IGDC/SHG, targeting for involving more human resource and to give nutritional support as well, which also covers all AWC of the district. In an integrated way under the village all ASHA, ANM, AWW, PRI member involved where VH & ND organized in a club manner to discuss Health related issues and mother and children also provided with immunization & nutritional support & medicine. Two register also maintained by the Health professionals to keep the record of attendance of service provider & service i.e. given on the particular VHND. Achievement at a glance (through VHND from Sept, 2010-Feb 2011):
ANC - 247 BCG – 1356 DPT 1 – 1966 OPV 1 – 1895 DPT 2 – 1852 OPV 2 – 1726 DPT 3 – 1505 OPV 3 – 1463 DPT Booster - 1360 OPV Booster - 1192 Measles - 2027 DPT - 195 TT 10 - 598 TT 16 - 586
Total VHND - 926 Total Participant - 196312 Total Children - 85310 Children Immunized - 20191 Weight Taken - 37488 Identification of underweight baby - 693
A portal generated for VHND where all the data uploaded on regular basis in the portal (http://tsu.trp.nic.in/vhndnorth) for public awareness & analyze gaps.
34
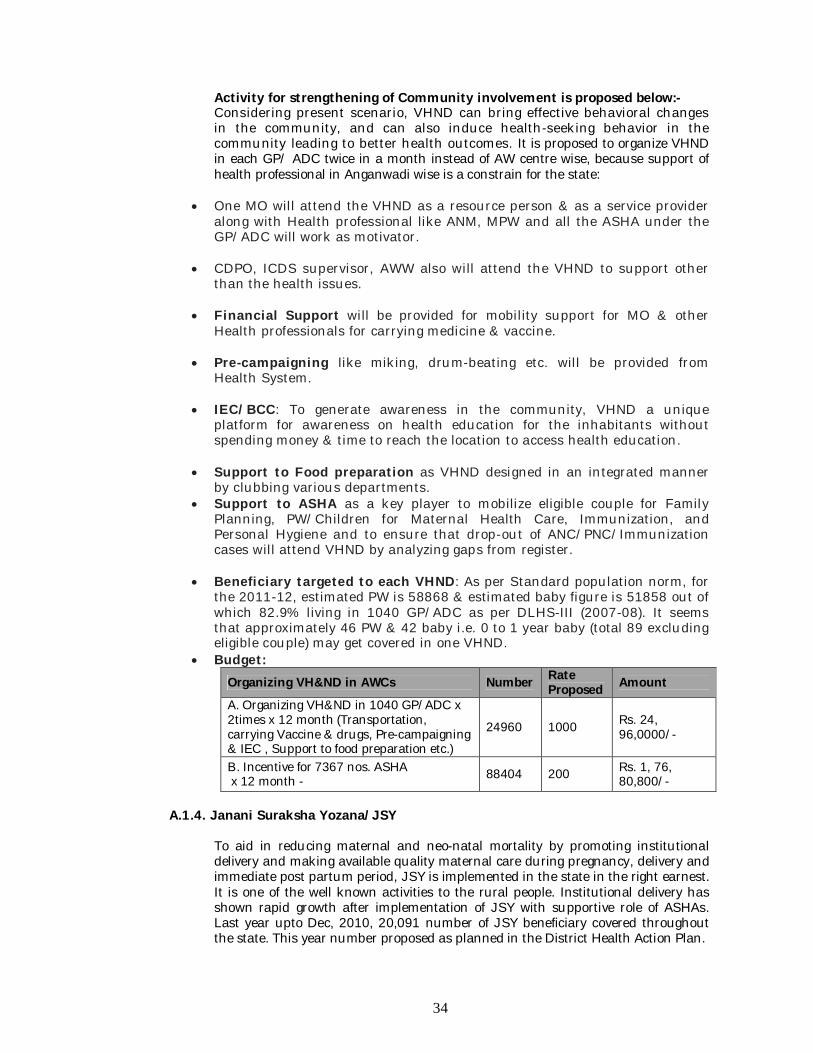
Activity for strengthening of Community involvement is proposed below:- Considering present scenario, VHND can bring effective behavioral changes in the community, and can also induce health-seeking behavior in the community leading to better health outcomes. It is proposed to organize VHND in each GP/ ADC twice in a month instead of AW centre wise, because support of health professional in Anganwadi wise is a constrain for the state:
One MO will attend the VHND as a resource person & as a service provider along with Health professional like ANM, MPW and all the ASHA under the GP/ADC will work as motivator.
CDPO, ICDS supervisor, AWW also will attend the VHND to support other than the health issues.
Financial Support will be provided for mobility support for MO & other Health professionals for carrying medicine & vaccine.
Pre-campaigning like miking, drum-beating etc. will be provided from Health System.
IEC/BCC: To generate awareness in the community, VHND a unique platform for awareness on health education for the inhabitants without spending money & time to reach the location to access health education.
Support to Food preparation as VHND designed in an integrated manner by clubbing various departments.
Support to ASHA as a key player to mobilize eligible couple for Family Planning, PW/Children for Maternal Health Care, Immunization, and Personal Hygiene and to ensure that drop-out of ANC/PNC/Immunization cases will attend VHND by analyzing gaps from register.
Beneficiary targeted to each VHND: As per Standard population norm, for the 2011-12, estimated PW is 58868 & estimated baby figure is 51858 out of which 82.9% living in 1040 GP/ADC as per DLHS-III (2007-08). It seems that approximately 46 PW & 42 baby i.e. 0 to 1 year baby (total 89 excluding eligible couple) may get covered in one VHND.
Budget: Organizing VH&ND in AWCs Number Rate
Proposed Amount
A. Organizing VH&ND in 1040 GP/ADC x 2times x 12 month (Transportation, carrying Vaccine & drugs, Pre-campaigning & IEC , Support to food preparation etc.)
24960 1000 Rs. 24, 96,0000/-
B. Incentive for 7367 nos. ASHA x 12 month - 88404 200 Rs. 1, 76,
80,800/- A.1.4. Janani Suraksha Yozana/JSY
To aid in reducing maternal and neo-natal mortality by promoting institutional delivery and making available quality maternal care during pregnancy, delivery and immediate post partum period, JSY is implemented in the state in the right earnest. It is one of the well known activities to the rural people. Institutional delivery has shown rapid growth after implementation of JSY with supportive role of ASHAs. Last year upto Dec, 2010, 20,091 number of JSY beneficiary covered throughout the state. This year number proposed as planned in the District Health Action Plan.
35
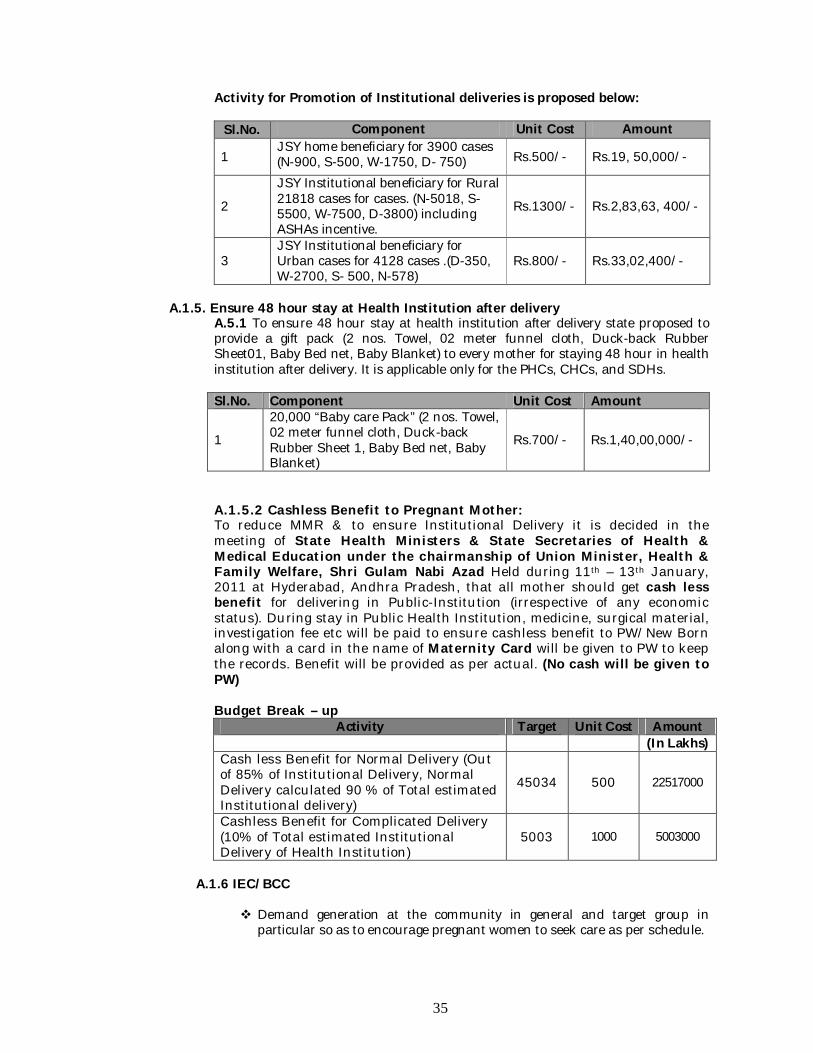
Activity for Promotion of Institutional deliveries is proposed below:
Sl.No. Component Unit Cost Amount
1 JSY home beneficiary for 3900 cases (N-900, S-500, W-1750, D- 750) Rs.500/- Rs.19, 50,000/-
2
JSY Institutional beneficiary for Rural 21818 cases for cases. (N-5018, S-5500, W-7500, D-3800) including ASHAs incentive.
Rs.1300/- Rs.2,83,63, 400/-
3 JSY Institutional beneficiary for Urban cases for 4128 cases .(D-350, W-2700, S- 500, N-578)
Rs.800/- Rs.33,02,400/-
A.1.5. Ensure 48 hour stay at Health Institution after delivery
A.5.1 To ensure 48 hour stay at health institution after delivery state proposed to provide a gift pack (2 nos. Towel, 02 meter funnel cloth, Duck-back Rubber Sheet01, Baby Bed net, Baby Blanket) to every mother for staying 48 hour in health institution after delivery. It is applicable only for the PHCs, CHCs, and SDHs.
Sl.No. Component Unit Cost Amount
1
20,000 “Baby care Pack” (2 nos. Towel, 02 meter funnel cloth, Duck-back Rubber Sheet 1, Baby Bed net, Baby Blanket)
Rs.700/- Rs.1,40,00,000/-
A.1.5.2 Cashless Benefit to Pregnant Mother: To reduce MMR & to ensure Institutional Delivery it is decided in the meeting of State Health Ministers & State Secretaries of Health & Medical Education under the chairmanship of Union Minister, Health & Family Welfare, Shri Gulam Nabi Azad Held during 11th – 13th January, 2011 at Hyderabad, Andhra Pradesh, that all mother should get cash less benefit for delivering in Public-Institution (irrespective of any economic status). During stay in Public Health Institution, medicine, surgical material, investigation fee etc will be paid to ensure cashless benefit to PW/New Born along with a card in the name of Maternity Card will be given to PW to keep the records. Benefit will be provided as per actual. (No cash will be given to PW) Budget Break – up
Activity Target Unit Cost Amount (In Lakhs)
Cash less Benefit for Normal Delivery (Out of 85% of Institutional Delivery, Normal Delivery calculated 90 % of Total estimated Institutional delivery)
45034 500 22517000
Cashless Benefit for Complicated Delivery (10% of Total estimated Institutional Delivery of Health Institution)
5003 1000 5003000
A.1.6 IEC/BCC
Demand generation at the community in general and target group in particular so as to encourage pregnant women to seek care as per schedule.
36
Generate community awareness on importance and necessity of institutional deliveries.
Provide consultation and information to families to improve the affordability
of maternal care.
Specific activity proposed for IEC/ BCC under Maternal Health are: Mother and Child Health Fair one in each 17 nos. Sub-Division @
Rs.90,000. Interactive stalls may be created in market places and exhibition will decorate the stall. The messages will be disseminated through speeches, leaflets. Slogan, Essay, drawing, quiz competition will be organized among the villagers.
Radio Jingles is already available with State Health & FW Society and it will be aired through All India Radio (15 seconds duration) in Bengali, Kokborak through Agartala Station. Jingles will be aired from July 2011 – February 2012 and 240 times in 240 days in each station @ Rs. 1200/- per unit cost. Radio Jingles is already available with State Health & FW Society and it will be aired through All India Radio (15 seconds duration) in Bengali, Kokborak through Belonia and Kailashahar Station. Jingles will be aired from July 2011 – February 2012 and 240 times in 240 days in each station @ Rs. 800/- per unit cost.
Janani Suraksha Yojana: ‘Swasthya Haat Mela ‘ a comprehensive programme consisting of Puppet show, street drama, quiz competition etc. may be organized in each block in a popular market day focusing on maternal health issue.
(Budget is reflected in IEC-BCC part of RCH-II) A.1.7. Human Resource Development:
Skill development programme is one of the needs to prevent maternal mortality and morbidity. Last year SBA for ANM, LSAS, EmOC training is planned and achievement status is shown in Training part. As per requirement for the newly established health institutions and also to ensure functional FRUs & 24 X 7 health care services in the state; LSAS, EmOC, B-EmOC, SBA, RTI/STI training is proposed. Following training is proposed for skill development of human resource & quality service:
Status of RTI /STI service in Health Institution: STI & RTI services are provided in the below mentioned institutions through STD (Sexually Transmitted Disease) Clinics. Consultation & provision of medicines for STI/RTI clients are free of cost with the support of NACO. AGMC & GBP Hospital RGM Hospital, Kailasahar TSD Hospital ,Udaipur Amarpur S.D Hospital . Belonia S.D Hospital Sabroom S.D Hospital Bishalghar S.D Hospital Khowai S.D Hospital Melaghar S.D Hospital
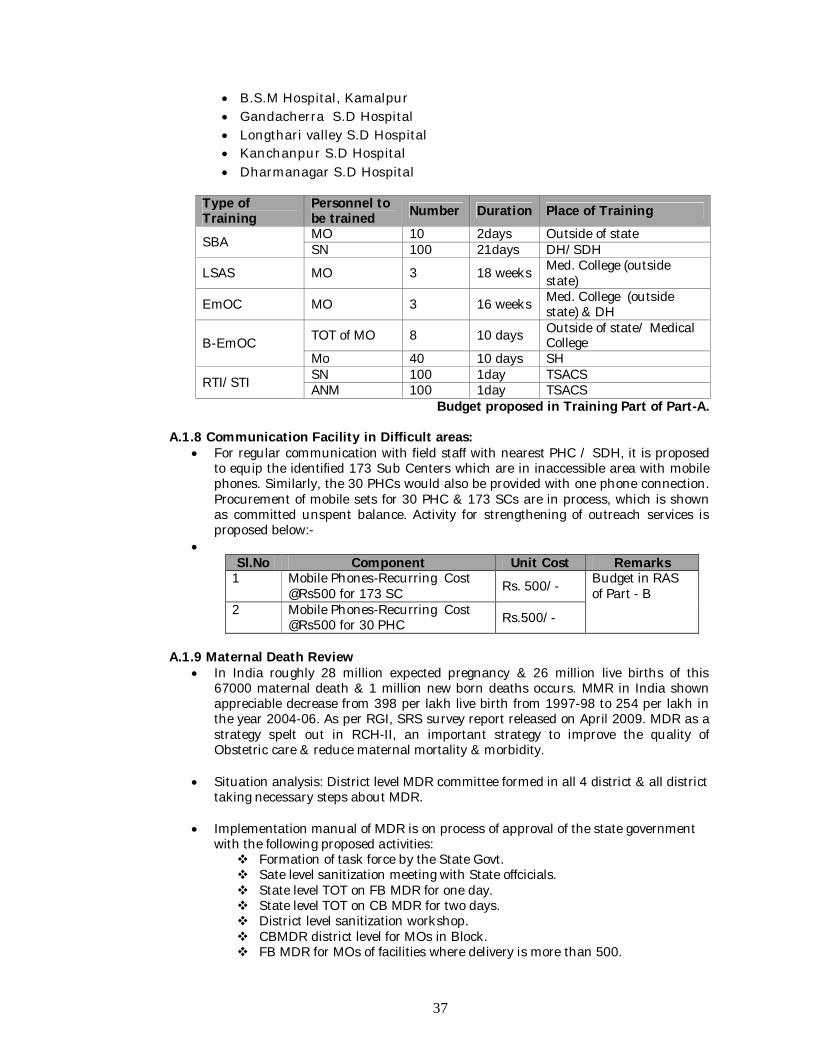
37
B.S.M Hospital, Kamalpur Gandacherra S.D Hospital Longthari valley S.D Hospital Kanchanpur S.D Hospital Dharmanagar S.D Hospital
Type of Training
Personnel to be trained Number Duration Place of Training
SBA MO 10 2days Outside of state SN 100 21days DH/SDH
LSAS MO 3 18 weeks Med. College (outside state)
EmOC MO 3 16 weeks Med. College (outside state) & DH
B-EmOC TOT of MO 8 10 days Outside of state/ Medical College
Mo 40 10 days SH
RTI/STI SN 100 1day TSACS ANM 100 1day TSACS
Budget proposed in Training Part of Part-A. A.1.8 Communication Facility in Difficult areas:
For regular communication with field staff with nearest PHC / SDH, it is proposed to equip the identified 173 Sub Centers which are in inaccessible area with mobile phones. Similarly, the 30 PHCs would also be provided with one phone connection. Procurement of mobile sets for 30 PHC & 173 SCs are in process, which is shown as committed unspent balance. Activity for strengthening of outreach services is proposed below:-
Sl.No Component Unit Cost Remarks
1 Mobile Phones-Recurring Cost @Rs500 for 173 SC Rs. 500/- Budget in RAS
of Part - B 2 Mobile Phones-Recurring Cost
@Rs500 for 30 PHC Rs.500/-
A.1.9 Maternal Death Review
In India roughly 28 million expected pregnancy & 26 million live births of this 67000 maternal death & 1 million new born deaths occurs. MMR in India shown appreciable decrease from 398 per lakh live birth from 1997-98 to 254 per lakh in the year 2004-06. As per RGI, SRS survey report released on April 2009. MDR as a strategy spelt out in RCH-II, an important strategy to improve the quality of Obstetric care & reduce maternal mortality & morbidity.
Situation analysis: District level MDR committee formed in all 4 district & all district
taking necessary steps about MDR.
Implementation manual of MDR is on process of approval of the state government with the following proposed activities: Formation of task force by the State Govt. Sate level sanitization meeting with State offcicials. State level TOT on FB MDR for one day. State level TOT on CB MDR for two days. District level sanitization workshop. CBMDR district level for MOs in Block. FB MDR for MOs of facilities where delivery is more than 500.
38
Block level orientation. Block level training for investigators. Printing of materials like MDR manuals & formats.
Strategy/activity: Community based maternal death Review Facility based maternal death Review Confidential enquiries on maternal death. Survey of severe morbidity. Clinical audit.
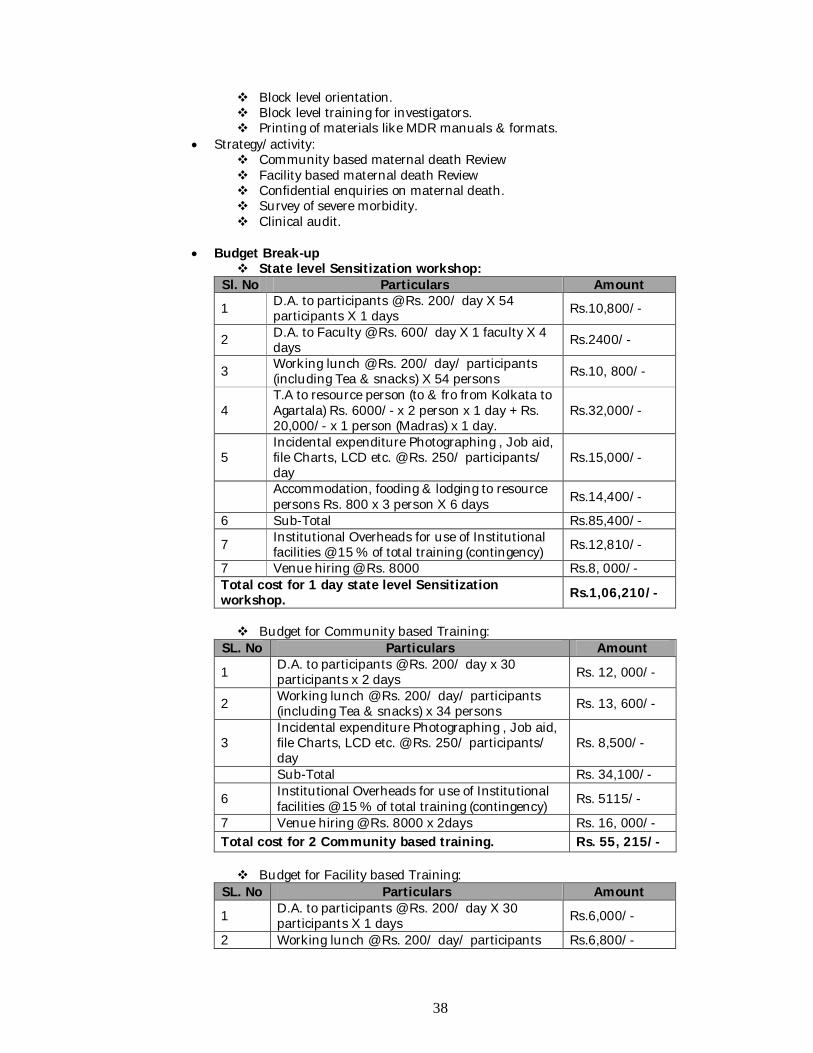
Budget Break-up
State level Sensitization workshop: Sl. No Particulars Amount
1 D.A. to participants @ Rs. 200/ day X 54 participants X 1 days Rs.10,800/-
2 D.A. to Faculty @ Rs. 600/ day X 1 faculty X 4 days Rs.2400/-
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 54 persons Rs.10, 800/-
4 T.A to resource person (to & fro from Kolkata to Agartala) Rs. 6000/- x 2 person x 1 day + Rs. 20,000/- x 1 person (Madras) x 1 day.
Rs.32,000/-
5 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/ participants/ day
Rs.15,000/-
Accommodation, fooding & lodging to resource persons Rs. 800 x 3 person X 6 days Rs.14,400/-
6 Sub-Total Rs.85,400/-
7 Institutional Overheads for use of Institutional facilities @ 15 % of total training (contingency) Rs.12,810/-
7 Venue hiring @ Rs. 8000 Rs.8, 000/- Total cost for 1 day state level Sensitization workshop. Rs.1,06,210/-
Budget for Community based Training:
SL. No Particulars Amount
1 D.A. to participants @ Rs. 200/ day x 30 participants x 2 days Rs. 12, 000/-
2 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) x 34 persons Rs. 13, 600/-
3 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/ participants/ day
Rs. 8,500/-
Sub-Total Rs. 34,100/-
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training (contingency) Rs. 5115/-
7 Venue hiring @ Rs. 8000 x 2days Rs. 16, 000/- Total cost for 2 Community based training. Rs. 55, 215/-
Budget for Facility based Training:
SL. No Particulars Amount
1 D.A. to participants @ Rs. 200/ day X 30 participants X 1 days Rs.6,000/-
2 Working lunch @ Rs. 200/ day/ participants Rs.6,800/-
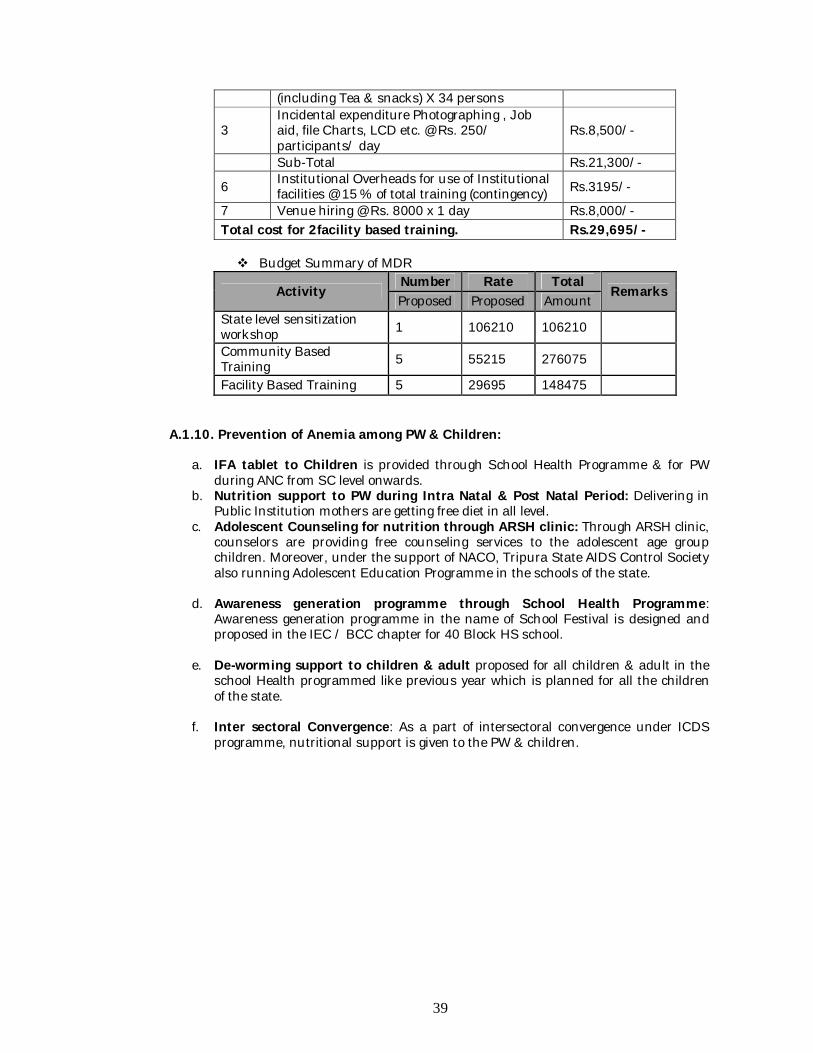
39
(including Tea & snacks) X 34 persons
3 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/ participants/ day
Rs.8,500/-
Sub-Total Rs.21,300/-
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training (contingency) Rs.3195/-
7 Venue hiring @ Rs. 8000 x 1 day Rs.8,000/- Total cost for 2facility based training. Rs.29,695/-
Budget Summary of MDR
Activity Number Rate Total
Remarks Proposed Proposed Amount
State level sensitization workshop 1 106210 106210
Community Based Training 5 55215 276075
Facility Based Training 5 29695 148475 A.1.10. Prevention of Anemia among PW & Children:
a. IFA tablet to Children is provided through School Health Programme & for PW during ANC from SC level onwards.
b. Nutrition support to PW during Intra Natal & Post Natal Period: Delivering in Public Institution mothers are getting free diet in all level.
c. Adolescent Counseling for nutrition through ARSH clinic: Through ARSH clinic, counselors are providing free counseling services to the adolescent age group children. Moreover, under the support of NACO, Tripura State AIDS Control Society also running Adolescent Education Programme in the schools of the state.
d. Awareness generation programme through School Health Programme: Awareness generation programme in the name of School Festival is designed and proposed in the IEC / BCC chapter for 40 Block HS school.
e. De-worming support to children & adult proposed for all children & adult in the school Health programmed like previous year which is planned for all the children of the state.
f. Inter sectoral Convergence: As a part of intersectoral convergence under ICDS programme, nutritional support is given to the PW & children.
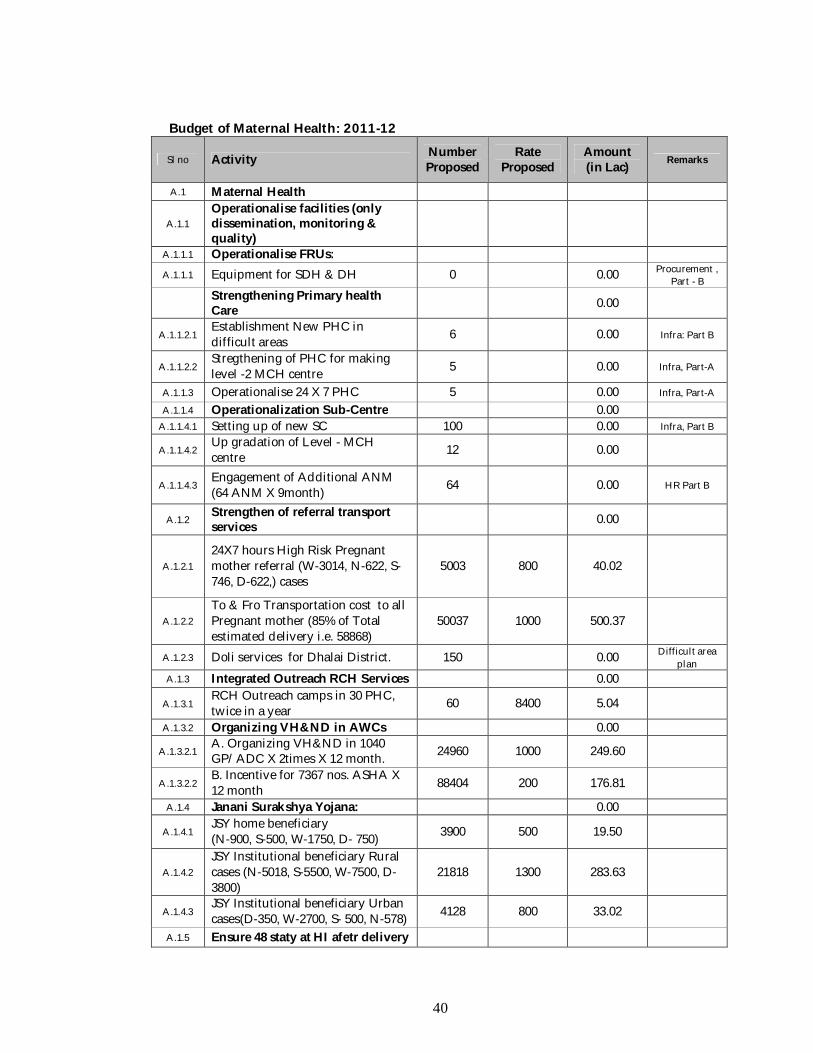
40
Budget of Maternal Health: 2011-12
Sl no Activity Number Proposed
Rate Proposed
Amount (in Lac) Remarks
A.1 Maternal Health
A.1.1 Operationalise facilities (only dissemination, monitoring & quality)
A.1.1.1 Operationalise FRUs:
A.1.1.1 Equipment for SDH & DH 0 0.00 Procurement , Part - B
Strengthening Primary health Care 0.00
A.1.1.2.1 Establishment New PHC in difficult areas 6 0.00 Infra: Part B
A.1.1.2.2 Stregthening of PHC for making level -2 MCH centre 5 0.00 Infra, Part-A
A.1.1.3 Operationalise 24 X 7 PHC 5 0.00 Infra, Part-A
A.1.1.4 Operationalization Sub-Centre 0.00 A.1.1.4.1 Setting up of new SC 100 0.00 Infra, Part B
A.1.1.4.2 Up gradation of Level - MCH centre 12 0.00
A.1.1.4.3 Engagement of Additional ANM (64 ANM X 9month) 64 0.00 HR Part B
A.1.2 Strengthen of referral transport services 0.00
A.1.2.1 24X7 hours High Risk Pregnant mother referral (W-3014, N-622, S-746, D-622,) cases
5003 800 40.02
A.1.2.2 To & Fro Transportation cost to all Pregnant mother (85% of Total estimated delivery i.e. 58868)
50037 1000 500.37
A.1.2.3 Doli services for Dhalai District. 150 0.00 Difficult area plan
A.1.3 Integrated Outreach RCH Services 0.00
A.1.3.1 RCH Outreach camps in 30 PHC, twice in a year 60 8400 5.04
A.1.3.2 Organizing VH&ND in AWCs 0.00
A.1.3.2.1 A. Organizing VH&ND in 1040 GP/ADC X 2times X 12 month. 24960 1000 249.60
A.1.3.2.2 B. Incentive for 7367 nos. ASHA X 12 month 88404 200 176.81
A.1.4 Janani Surakshya Yojana: 0.00
A.1.4.1 JSY home beneficiary (N-900, S-500, W-1750, D- 750) 3900 500 19.50
A.1.4.2 JSY Institutional beneficiary Rural cases (N-5018, S-5500, W-7500, D-3800)
21818 1300 283.63
A.1.4.3 JSY Institutional beneficiary Urban cases(D-350, W-2700, S- 500, N-578) 4128 800 33.02
A.1.5 Ensure 48 staty at HI afetr delivery
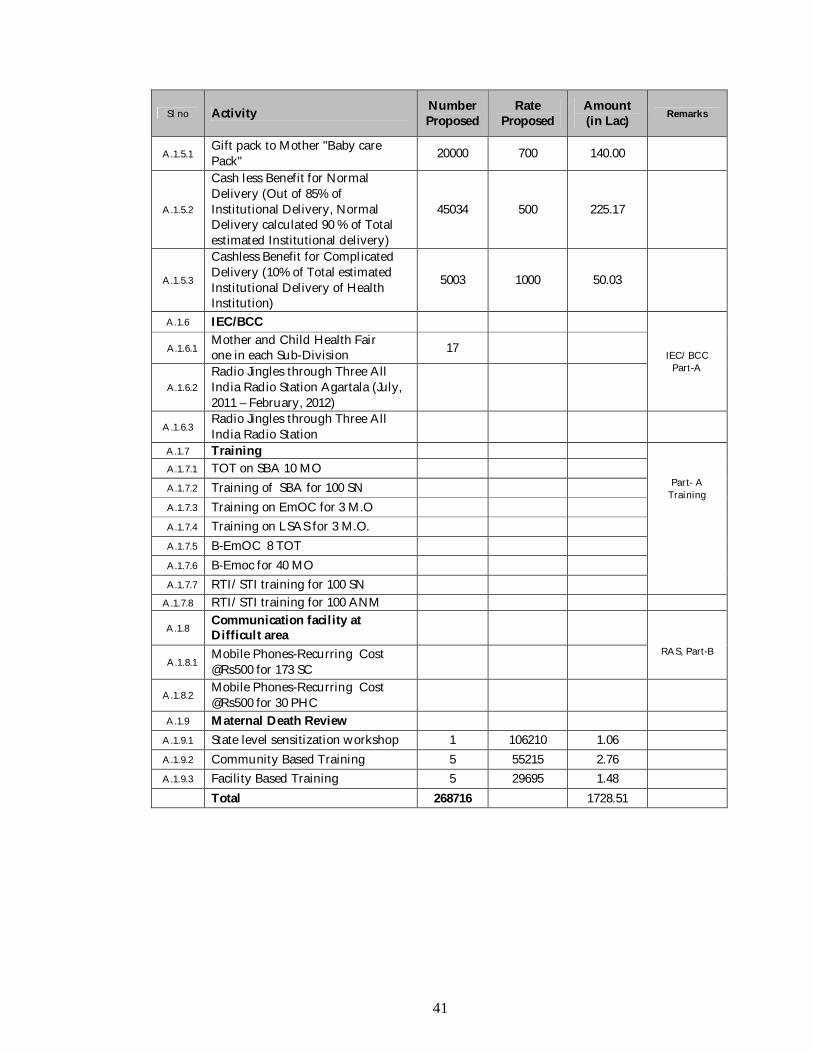
41
Sl no Activity Number Proposed
Rate Proposed
Amount (in Lac) Remarks
A.1.5.1 Gift pack to Mother "Baby care Pack" 20000 700 140.00
A.1.5.2
Cash less Benefit for Normal Delivery (Out of 85% of Institutional Delivery, Normal Delivery calculated 90 % of Total estimated Institutional delivery)
45034 500 225.17
A.1.5.3
Cashless Benefit for Complicated Delivery (10% of Total estimated Institutional Delivery of Health Institution)
5003 1000 50.03
A.1.6 IEC/BCC
IEC/BCC Part-A
A.1.6.1 Mother and Child Health Fair one in each Sub-Division 17
A.1.6.2 Radio Jingles through Three All India Radio Station Agartala (July, 2011 – February, 2012)
A.1.6.3 Radio Jingles through Three All India Radio Station
A.1.7 Training
Part- A Training
A.1.7.1 TOT on SBA 10 MO A.1.7.2 Training of SBA for 100 SN A.1.7.3 Training on EmOC for 3 M.O A.1.7.4 Training on LSAS for 3 M.O. A.1.7.5 B-EmOC 8 TOT A.1.7.6 B-Emoc for 40 MO A.1.7.7 RTI/STI training for 100 SN
A.1.7.8 RTI/STI training for 100 ANM
A.1.8 Communication facility at Difficult area
RAS, Part-B
A.1.8.1 Mobile Phones-Recurring Cost @Rs500 for 173 SC
A.1.8.2 Mobile Phones-Recurring Cost @Rs500 for 30 PHC
A.1.9 Maternal Death Review
A.1.9.1 State level sensitization workshop 1 106210 1.06
A.1.9.2 Community Based Training 5 55215 2.76
A.1.9.3 Facility Based Training 5 29695 1.48
Total 268716 1728.51
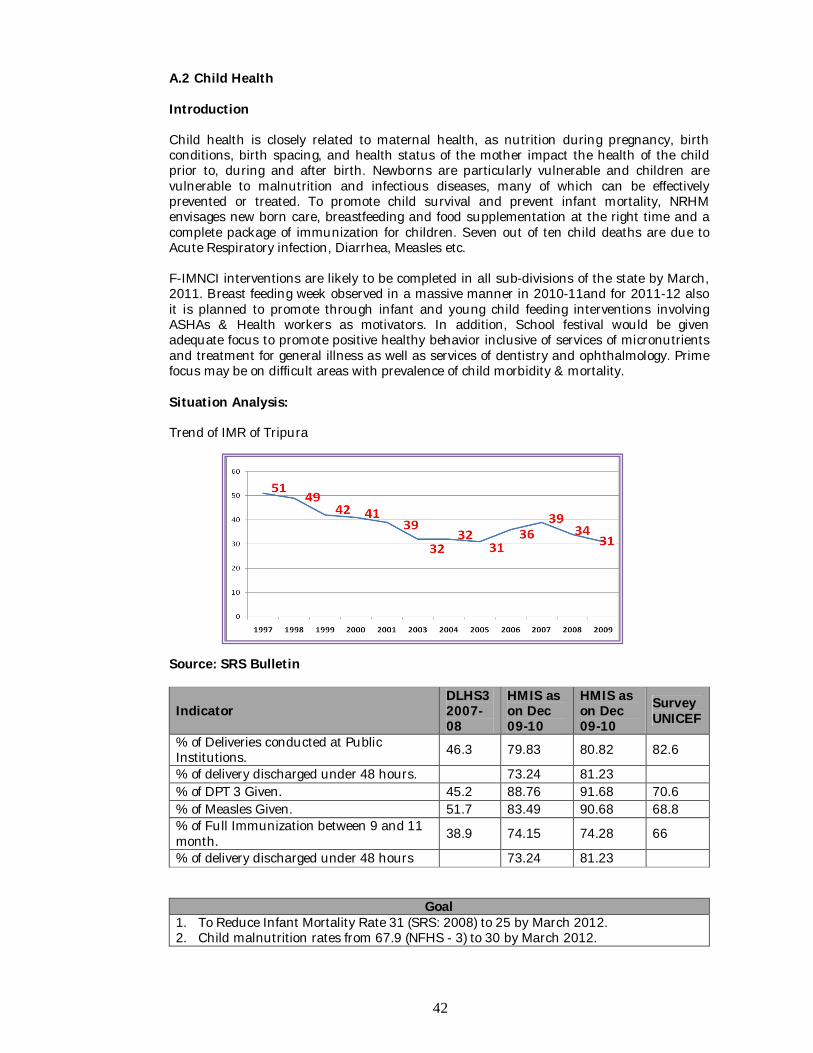
42
A.2 Child Health Introduction Child health is closely related to maternal health, as nutrition during pregnancy, birth conditions, birth spacing, and health status of the mother impact the health of the child prior to, during and after birth. Newborns are particularly vulnerable and children are vulnerable to malnutrition and infectious diseases, many of which can be effectively prevented or treated. To promote child survival and prevent infant mortality, NRHM envisages new born care, breastfeeding and food supplementation at the right time and a complete package of immunization for children. Seven out of ten child deaths are due to Acute Respiratory infection, Diarrhea, Measles etc. F-IMNCI interventions are likely to be completed in all sub-divisions of the state by March, 2011. Breast feeding week observed in a massive manner in 2010-11and for 2011-12 also it is planned to promote through infant and young child feeding interventions involving ASHAs & Health workers as motivators. In addition, School festival would be given adequate focus to promote positive healthy behavior inclusive of services of micronutrients and treatment for general illness as well as services of dentistry and ophthalmology. Prime focus may be on difficult areas with prevalence of child morbidity & mortality. Situation Analysis: Trend of IMR of Tripura Source: SRS Bulletin
Indicator DLHS3 2007-08
HMIS as on Dec 09-10
HMIS as on Dec 09-10
Survey UNICEF
% of Deliveries conducted at Public Institutions. 46.3 79.83 80.82 82.6
% of delivery discharged under 48 hours. 73.24 81.23 % of DPT 3 Given. 45.2 88.76 91.68 70.6 % of Measles Given. 51.7 83.49 90.68 68.8 % of Full Immunization between 9 and 11 month. 38.9 74.15 74.28 66
% of delivery discharged under 48 hours 73.24 81.23
Goal 1. To Reduce Infant Mortality Rate 31 (SRS: 2008) to 25 by March 2012. 2. Child malnutrition rates from 67.9 (NFHS - 3) to 30 by March 2012.
43
Objective 1. To increase institutional deliveries 80% to 85 % by March 2012
Strategy a. Comprehensive IEC /BCC for Exclusive Breast Feeding Week
Objective 2. Managing New Born Complications
Strategy a. To improve the New Born care by operationalsing NICU/ NBSU at all FRUs. b. Facility to Sick New Born “30 Days Life under NRHM. c. Capacity Building of Service provider (NSSK, F-IMNCI/IMNCI). d. Increase the percentage of fully immunized children before 12 months of age. e. To reduce the incidence of ARI & ADD & controlling mortality. f. Community awareness through ASHA on Home based Neonatal Care.
Objective 3. Increase full immunization
Strategy a. Strategy developed under Part-C, Immunization
Objective 4. To reduce low birth weight babies at the level of 30 % by March 2012.
Strategy a. Management of ARI & Diarrhoea. b. Care of malnourished children.
Activities in details A.2.1 Skill Development of Human Resource (IMNCI/ F-IMNCI, NSSK)
Scarcity of specialist doctor is a major crisis for the State. There is only 04 Sub-Divisional Hospital functioning with Child Specialist. There is no facility in state medical college for specialist training. IMNCI is the first training for child care which has been taken-up by the state with right earnest. Till date 40 MO and 70 ANM has been trained on IMNCI. 04 MO from the state has been trained on F-IMNCI as state level trainer. Till date state does not get any scope for multi skilling training on pediatric. Skill development on child care is most important for prevention of neo-natal death. Activity for skill development is proposed below:-
Type of Training Personnel to be trained Number Duration Place of
Training
F-IMNCI Specialist 4 11/5days Delhi MO 48 11days AGMC SN 48 11 days AGMC
IMNCI ANM 110 8days AGMC
TOT of NSSK MO 4 2days Delhi/ Guwahati
NSSK training MO 64 10days AGMC (Budget proposed in Training Part of A)
A.2.2. Facility Based New Born Care/FBNC: Improve the quality of service delivery: Considering geographical & topographical of the state & keeping mind of Standard Population norms, a holistic planning for FRUs is planned linking HR, procurement, BSCs, logistics, manpower, training etc. Besides all the Facilities operational is analyzed in level wise & preference is given to those facilities for upgradation and operationalisation where delivery load is substantial. Presently in Tripura there are 79 PHC, 11SDH & 11 CHC is functional & district wise status is given below.
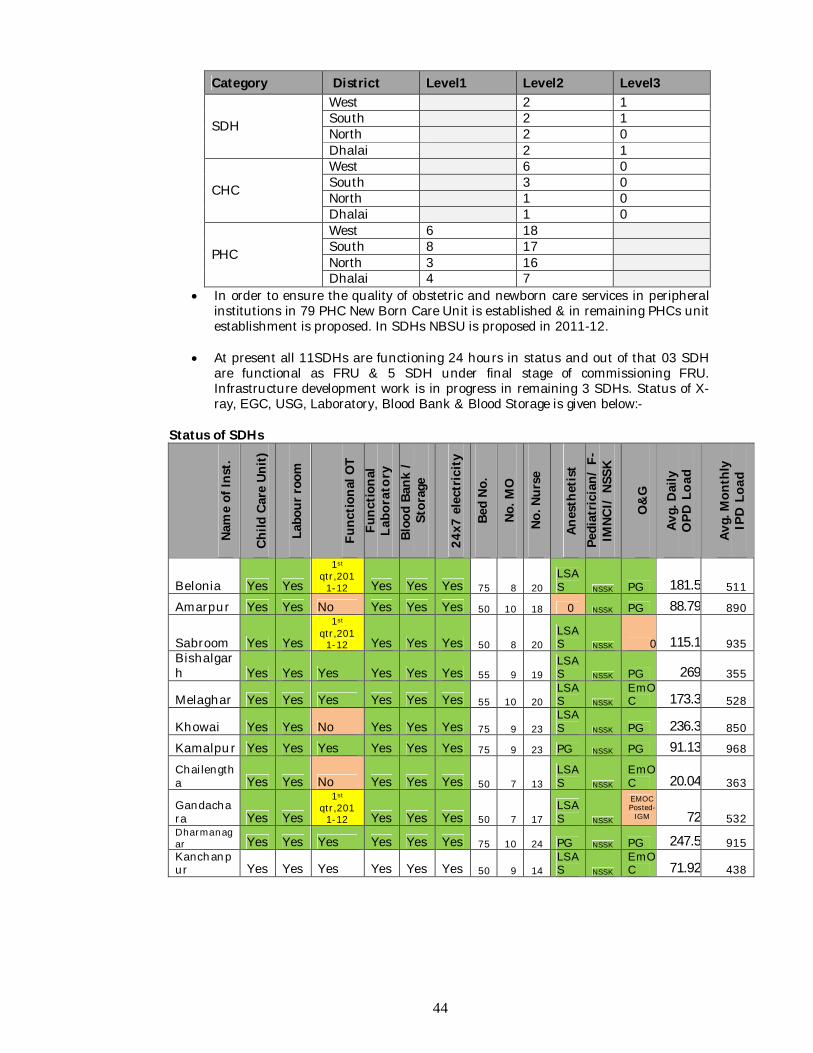
44
Category District Level1 Level2 Level3
SDH
West 2 1 South 2 1 North 2 0 Dhalai 2 1
CHC
West 6 0 South 3 0 North 1 0 Dhalai 1 0
PHC
West 6 18 South 8 17 North 3 16 Dhalai 4 7
In order to ensure the quality of obstetric and newborn care services in peripheral institutions in 79 PHC New Born Care Unit is established & in remaining PHCs unit establishment is proposed. In SDHs NBSU is proposed in 2011-12.
At present all 11SDHs are functioning 24 hours in status and out of that 03 SDH are functional as FRU & 5 SDH under final stage of commissioning FRU. Infrastructure development work is in progress in remaining 3 SDHs. Status of X-ray, EGC, USG, Laboratory, Blood Bank & Blood Storage is given below:-
Status of SDHs
Nam
e of
Inst
.
Child
Car
e Un
it)
Labo
ur ro
om
Func
tiona
l OT
Func
tiona
l La
bora
tory
Bl
ood
Bank
/
Stor
age
24x7
ele
ctric
ity
Bed
No.
No. M
O
No. N
urse
Anes
thet
ist
Pedi
atric
ian/
F-
IMNC
I/ N
SSK
O&
G
Avg.
Dai
ly
OPD
Loa
d
Avg.
Mon
thly
IP
D L
oad
Belonia Yes Yes
1st qtr,201
1-12 Yes Yes Yes 75 8 20 LSAS NSSK PG 181.5 511
Amarpur Yes Yes No Yes Yes Yes 50 10 18 0 NSSK PG 88.79 890
Sabroom Yes Yes
1st qtr,201
1-12 Yes Yes Yes 50 8 20 LSAS NSSK 0 115.1 935
Bishalgarh Yes Yes Yes Yes Yes Yes 55 9 19
LSAS NSSK PG 269 355
Melaghar Yes Yes Yes Yes Yes Yes 55 10 20 LSAS NSSK
EmOC 173.3 528
Khowai Yes Yes No Yes Yes Yes 75 9 23 LSAS NSSK PG 236.3 850
Kamalpur Yes Yes Yes Yes Yes Yes 75 9 23 PG NSSK PG 91.13 968
Chailengtha Yes Yes No Yes Yes Yes 50 7 13
LSAS NSSK
EmOC 20.04 363
Gandachara Yes Yes
1st qtr,201
1-12 Yes Yes Yes 50 7 17 LSAS NSSK
EMOC Posted-
IGM 72 532 Dharmanagar Yes Yes Yes Yes Yes Yes 75 10 24 PG NSSK PG 247.5 915 Kanchanpur Yes Yes Yes Yes Yes Yes 50 9 14
LSAS NSSK
EmOC 71.92 438
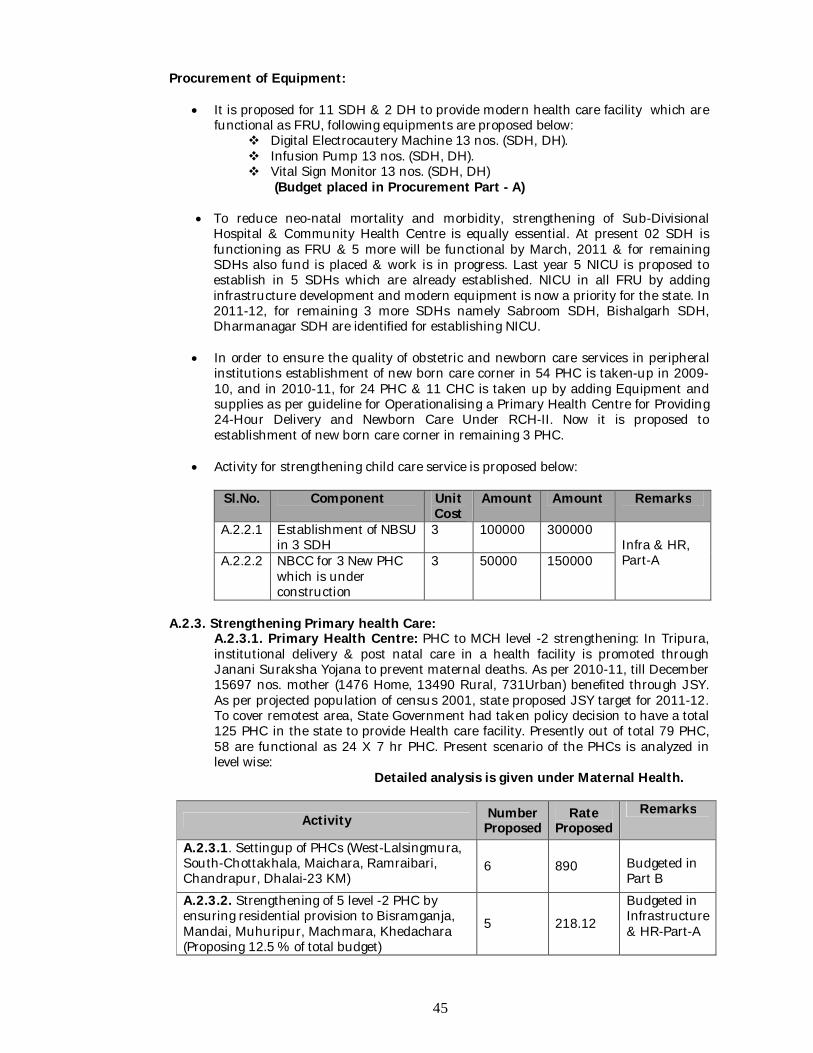
45
Procurement of Equipment:
It is proposed for 11 SDH & 2 DH to provide modern health care facility which are functional as FRU, following equipments are proposed below:
Digital Electrocautery Machine 13 nos. (SDH, DH). Infusion Pump 13 nos. (SDH, DH). Vital Sign Monitor 13 nos. (SDH, DH)
(Budget placed in Procurement Part - A)
To reduce neo-natal mortality and morbidity, strengthening of Sub-Divisional Hospital & Community Health Centre is equally essential. At present 02 SDH is functioning as FRU & 5 more will be functional by March, 2011 & for remaining SDHs also fund is placed & work is in progress. Last year 5 NICU is proposed to establish in 5 SDHs which are already established. NICU in all FRU by adding infrastructure development and modern equipment is now a priority for the state. In 2011-12, for remaining 3 more SDHs namely Sabroom SDH, Bishalgarh SDH, Dharmanagar SDH are identified for establishing NICU.
In order to ensure the quality of obstetric and newborn care services in peripheral
institutions establishment of new born care corner in 54 PHC is taken-up in 2009-10, and in 2010-11, for 24 PHC & 11 CHC is taken up by adding Equipment and supplies as per guideline for Operationalising a Primary Health Centre for Providing 24-Hour Delivery and Newborn Care Under RCH-II. Now it is proposed to establishment of new born care corner in remaining 3 PHC.
Activity for strengthening child care service is proposed below:
Sl.No. Component Unit
Cost Amount Amount Remarks
A.2.2.1 Establishment of NBSU in 3 SDH
3 100000 300000 Infra & HR, Part-A A.2.2.2 NBCC for 3 New PHC
which is under construction
3 50000 150000
A.2.3. Strengthening Primary health Care:
A.2.3.1. Primary Health Centre: PHC to MCH level -2 strengthening: In Tripura, institutional delivery & post natal care in a health facility is promoted through Janani Suraksha Yojana to prevent maternal deaths. As per 2010-11, till December 15697 nos. mother (1476 Home, 13490 Rural, 731Urban) benefited through JSY. As per projected population of census 2001, state proposed JSY target for 2011-12. To cover remotest area, State Government had taken policy decision to have a total 125 PHC in the state to provide Health care facility. Presently out of total 79 PHC, 58 are functional as 24 X 7 hr PHC. Present scenario of the PHCs is analyzed in level wise:
Detailed analysis is given under Maternal Health.
Activity Number Proposed
Rate Proposed
Remarks
A.2.3.1. Settingup of PHCs (West-Lalsingmura, South-Chottakhala, Maichara, Ramraibari, Chandrapur, Dhalai-23 KM)
6 890 Budgeted in Part B
A.2.3.2. Strengthening of 5 level -2 PHC by ensuring residential provision to Bisramganja, Mandai, Muhuripur, Machmara, Khedachara (Proposing 12.5 % of total budget)
5 218.12
Budgeted in Infrastructure & HR-Part-A
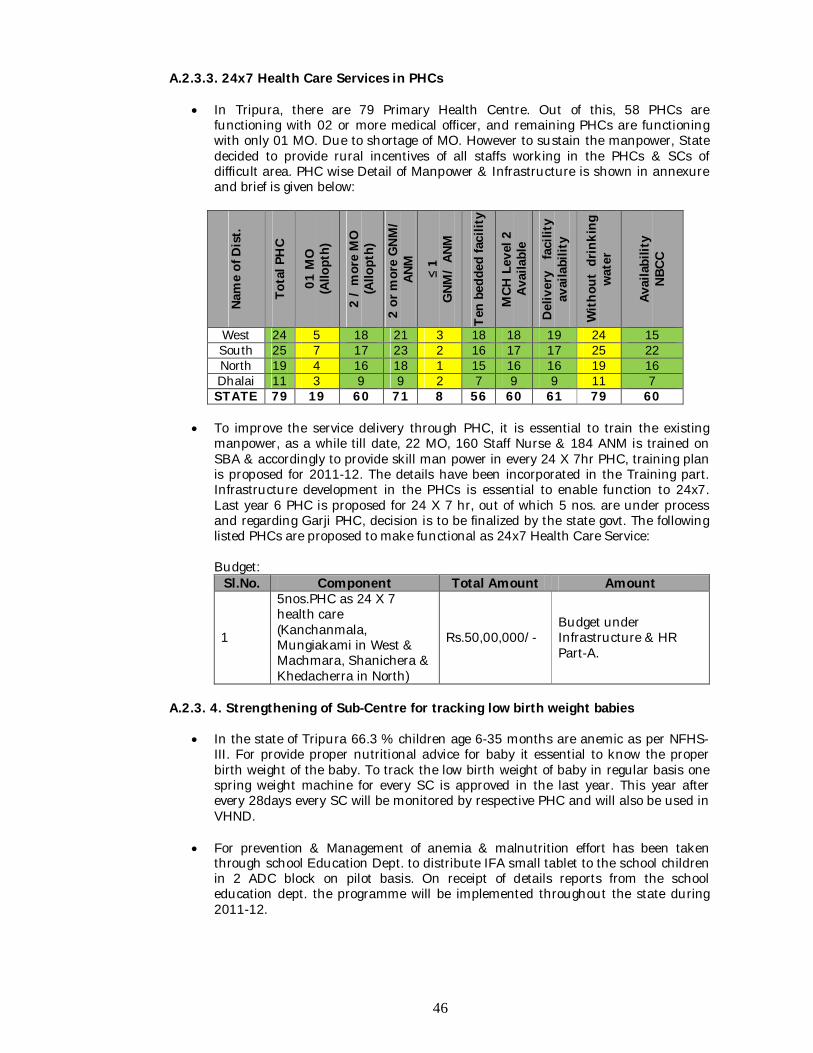
46
A.2.3.3. 24x7 Health Care Services in PHCs
In Tripura, there are 79 Primary Health Centre. Out of this, 58 PHCs are functioning with 02 or more medical officer, and remaining PHCs are functioning with only 01 MO. Due to shortage of MO. However to sustain the manpower, State decided to provide rural incentives of all staffs working in the PHCs & SCs of difficult area. PHC wise Detail of Manpower & Infrastructure is shown in annexure and brief is given below:
Nam
e of
Dis
t.
Tota
l PH
C
01 M
O
(Allo
pth)
2 /
mor
e M
O
(Allo
pth)
2 or
mor
e G
NM/
ANM
≤ 1
GNM
/ AN
M
Ten
bedd
ed fa
cilit
y
MCH
Lev
el 2
Av
aila
ble
Del
iver
y f
acili
ty
avai
labi
lity
With
out
drin
king
w
ater
Avai
labi
lity
NB
CC
West 24 5 18 21 3 18 18 19 24 15 South 25 7 17 23 2 16 17 17 25 22 North 19 4 16 18 1 15 16 16 19 16 Dhalai 11 3 9 9 2 7 9 9 11 7 STATE 79 19 60 71 8 56 60 61 79 60
To improve the service delivery through PHC, it is essential to train the existing
manpower, as a while till date, 22 MO, 160 Staff Nurse & 184 ANM is trained on SBA & accordingly to provide skill man power in every 24 X 7hr PHC, training plan is proposed for 2011-12. The details have been incorporated in the Training part. Infrastructure development in the PHCs is essential to enable function to 24x7. Last year 6 PHC is proposed for 24 X 7 hr, out of which 5 nos. are under process and regarding Garji PHC, decision is to be finalized by the state govt. The following listed PHCs are proposed to make functional as 24x7 Health Care Service:
Budget:
Sl.No. Component Total Amount Amount
1
5nos.PHC as 24 X 7 health care (Kanchanmala, Mungiakami in West & Machmara, Shanichera & Khedacherra in North)
Rs.50,00,000/- Budget under Infrastructure & HR Part-A.
A.2.3. 4. Strengthening of Sub-Centre for tracking low birth weight babies
In the state of Tripura 66.3 % children age 6-35 months are anemic as per NFHS-III. For provide proper nutritional advice for baby it essential to know the proper birth weight of the baby. To track the low birth weight of baby in regular basis one spring weight machine for every SC is approved in the last year. This year after every 28days every SC will be monitored by respective PHC and will also be used in VHND.
For prevention & Management of anemia & malnutrition effort has been taken
through school Education Dept. to distribute IFA small tablet to the school children in 2 ADC block on pilot basis. On receipt of details reports from the school education dept. the programme will be implemented throughout the state during 2011-12.
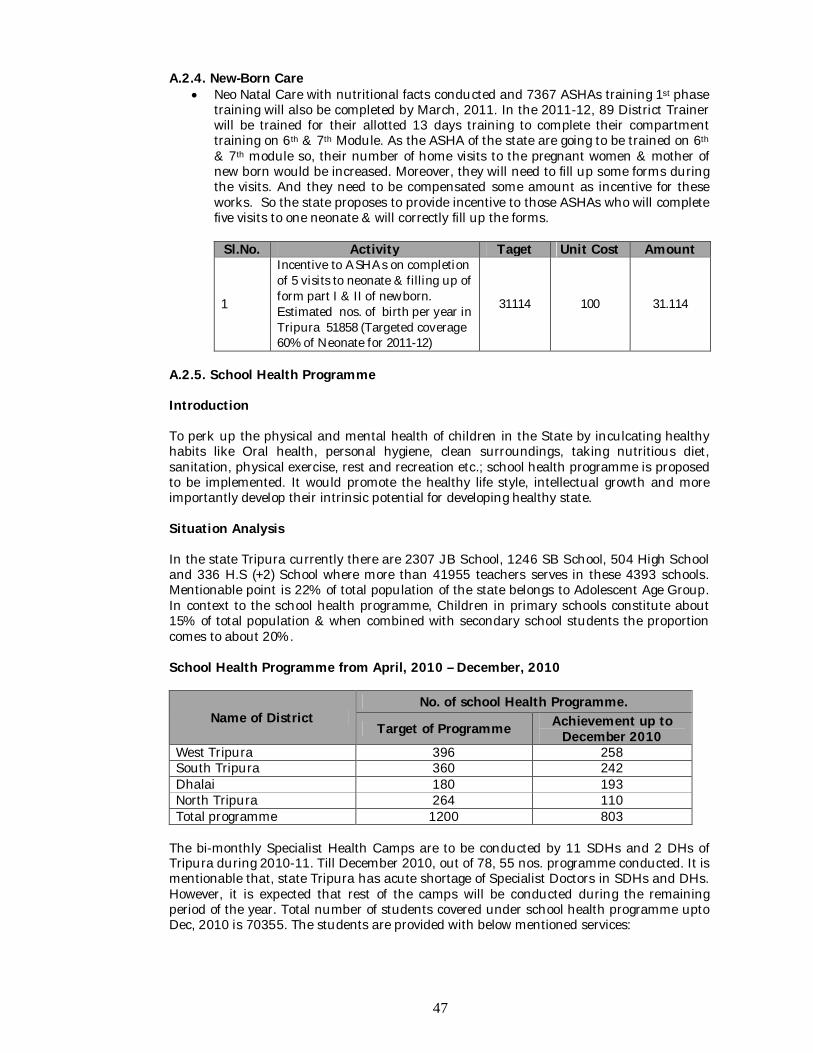
47
A.2.4. New-Born Care Neo Natal Care with nutritional facts conducted and 7367 ASHAs training 1st phase
training will also be completed by March, 2011. In the 2011-12, 89 District Trainer will be trained for their allotted 13 days training to complete their compartment training on 6th & 7th Module. As the ASHA of the state are going to be trained on 6th & 7th module so, their number of home visits to the pregnant women & mother of new born would be increased. Moreover, they will need to fill up some forms during the visits. And they need to be compensated some amount as incentive for these works. So the state proposes to provide incentive to those ASHAs who will complete five visits to one neonate & will correctly fill up the forms.
Sl.No. Activity Taget Unit Cost Amount
1
Incentive to ASHAs on completion of 5 visits to neonate & filling up of form part I & II of newborn. Estimated nos. of birth per year in Tripura 51858 (Targeted coverage 60% of Neonate for 2011-12)
31114 100 31.114
A.2.5. School Health Programme Introduction To perk up the physical and mental health of children in the State by inculcating healthy habits like Oral health, personal hygiene, clean surroundings, taking nutritious diet, sanitation, physical exercise, rest and recreation etc.; school health programme is proposed to be implemented. It would promote the healthy life style, intellectual growth and more importantly develop their intrinsic potential for developing healthy state. Situation Analysis In the state Tripura currently there are 2307 JB School, 1246 SB School, 504 High School and 336 H.S (+2) School where more than 41955 teachers serves in these 4393 schools. Mentionable point is 22% of total population of the state belongs to Adolescent Age Group. In context to the school health programme, Children in primary schools constitute about 15% of total population & when combined with secondary school students the proportion comes to about 20%. School Health Programme from April, 2010 – December, 2010
Name of District No. of school Health Programme.
Target of Programme Achievement up to December 2010
West Tripura 396 258 South Tripura 360 242 Dhalai 180 193 North Tripura 264 110 Total programme 1200 803
The bi-monthly Specialist Health Camps are to be conducted by 11 SDHs and 2 DHs of Tripura during 2010-11. Till December 2010, out of 78, 55 nos. programme conducted. It is mentionable that, state Tripura has acute shortage of Specialist Doctors in SDHs and DHs. However, it is expected that rest of the camps will be conducted during the remaining period of the year. Total number of students covered under school health programme upto Dec, 2010 is 70355. The students are provided with below mentioned services:
48
Diarrhea cases 1951 Fever cases- 2440 Warm Infestation- 6958 Dental cases – 4497 Skin Diseases – 2143 Eye Cases – 13403 Refractive Error – 815 Spectacles supplied – 179 IFA given – 3367 students Albendazole tablet supplied through the districts.
Number of patient treated in the specialist camp is included along with the above mentioned. Transportation for serious cases is provided by the ambulance. Super speciality care also provided by referring through state medical board. For school health check up programme medical team is consists of Medical Officer, Dentist, MPS, MPW, Pharmacist etc. Health card given by the Education Department & referral card will be given by the health Department. The approved fund for school, health programme for the year 2010-11 was 101.8 lakh, & expenditure incurred up to Dec, 2010, is 52.53L.
Goals: Physical & Mental Development of School Students.
Objective: Promotion of Positive Health Prevention of Diseases Early Diagnosis & Treatment. Awakening Health consciousness in children. Provision of Healthful environment Provision of Good Dental Health. Target Groups: Primary, Secondary & Higher Secondary school going children.
Aspects to be covered under School Health Programme: Health education. Remedial measures. Prevention & cure of Communicable diseases. Prevention of Non Communicable diseases. Healthy environment. Nutritional services. First aid & Emergency care. Mental, Dental & Eye health. Education of handicapped children. Health appraisal of School children & school personnel. Proper maintenance and use of school health records (School Health Card for all
children). Strategy: Every Health Institution i.e. SDHs/ CHCs/ PHCs shall visit the school under their jurisdiction for health checkup of the student every week. The visit is proposed to be made on fixed days of every month. The second Medical Officer/AYUSH Medical Officer of the PHC/CHC/SDH would be responsible for health checkup of school students. Each institution would prepare a calendar plan of visit indicating the name of the school for the entire calendar year in consultation with District Education Officer/Inspector of Schools and submit it in advance to the Chief Medical Officer with a copy to Mission Director, NRHM, Tripura and District Education Officer. A monthly report would also be submitted
49
to the CMOs by 2nd working day of the next month. The CMOs shall compile report of the entire district and forward it to Mission Director, NRHM, Tripura. Director of Family Welfare & P.M. would be procured and supply of medicine, blood grouping reagent and equipment for PHCs and CHCs and Director of Health Services would be procured and supply of the same to SDHs . State Programme Management Support Unit (SPMSU) shall prepare IEC materials like posters, leaflets, booklets etc. This would be supplied to the CMOs for distribution among the health institutions for further distribution to the beneficiaries. The process would be completed in 2 month time. Activities: A.2.5.1 Medical Officer with their teams will examine all school going children on date as per Micro plan @ Rs. 800/- (POL cost/ contingency) x 2 times in a month x 12 months x 101 institutions (79 PHCs/ 11 CHCs/ 11 SDHs) = Rs.19,39,200/- A.2.5.2 Procurement and supply of blood groupings reagent and equipment for PHCs/ CHCs/ SDHs = Rs.6,24,000/-
A.2.5.3 Preparation of IEC materials for Teachers, students & parents in the form of posters, leaflets, booklets etc. (@ Rs.300/- X 4393schools) = Rs.13,17,900/-
A.2.5.4 Specialist services will be made available for all referred school children at Sub-divisional hospitals and District Hospitals by organizing specialists’ camps on fixed date where children will be treated by different experts of Ophthalmic Surgeon, Physician, and Pediatrician, Dentist, Skin specialist and E.N.T. One camp on alternate month in two DHs and 1 camp on alternate month in 11 SDHs are proposed to be organized @ Rs. 1000/- as contingency. Budget: 2 DHs x 6 times x Rs. 1000/- = Rs. 12,000/- 11 SDHs x 6 times x Rs. 1000/- = Rs. 66,000/- Total = Rs. 78,000/- A.2.5.5 In Tripura, there are 2307 nos. of Primary / JB Schools having student capacity of 4, 44, 516 students and 1246 nos S.B. Schools having students’ capacity of 2, 19, 303, & 504 High Schools having student capacity of 106841 and Higher Secondary Schools having students’ capacity of 40739. It is proposed to provide micro-nutrient in the form of Iron Folic Acid (IFA) to each student to prevent anemia of the school children. Total involvement of fund will be as: for IFA tablet 811399 students X @ Rs. 9.26/per100 tablet = 75, 13, 555/-. The IFA tablets are proposed to be given to school authorities for distribution to the children. A.2.5.6 It is also proposed to De-worm 811399 students by providing Albendazole tablets @ 2 tablets per student in a gap of 7 days. The net total involvement will be 811399 x Rs.2.50 / per two tablet = Rs.20, 28,498/-
A.2.5.7. IEC-BCC: Generation of awareness in community.
Community awareness on signs and symptoms of anemia, better diet, hygiene and prevention of malaria.
Provide consultation and information to young children and their families and to child care providers to improve the affordability of child care.
Observance of Breast Feeding Week (1st August to 7th August): Rally by ASHA, Health Workers in the prominent places of Gram Panchayat and ADC villages
50
during 1st August to 7th August in all Health Institutions (Total 101) throughout the State District Media Expert, SDPM will ensure the programme. An action plan with date and place should be sent to BO, IEC in advance. Total: Rs.5,00,000/-.
Group meeting with target groups (Mothers, Guardians and eligible couple): The financial involvement for organizing the meeting Rs.11000/- for each Block.
Docu drama on Home Based Neonatal Care & Navajat Sishu Suraksha Karyakram will be prepared by state for wide publicity in Mother & Child Fair & also will be broadcasted & telecasted in local TV & FM channel. Budget: 100000/- (Budget proposed in IEC/BCC plan).
Activity Target Unit Cost
Total Amount Remarks
School health check-up visit 2424 800 19.39 Blood grouping & laboratory Reagents & equipment etc. Proc., Part -
A IEC materials for Teachers, students & parents 4393 300 13.19
Organization of Specialist health Camps at 11 SDH & 2DH (6times) 78 1000 0.78
Micro-nutrient in the form of Iron Folic Acid (IFA) to each student. 811399 9.26 75.14
De-worming of students by providing Albendazole tab. 811399 2.5 20.28
Sub-Total 128.77
A.2.6 Care of Sick children & severe Malnutrition A.2.5.1. To reduce IMR & to ensure Institutional Delivery it is decided in the meeting of State Health Ministers & State Secretaries of Health & Medical Education under the chairmanship of Union Minister, Health & Family Welfare, Shri Gulam Nabi Azad Held during 11th – 13th January, 2011 at Hyderabad, Andhra Pradesh, that Sick New Born Children will be facilitated first 30 days of Life Under NRHM, to ensure management support i.e. drugs, consumables, surgical support, neo-natal care, supplementary nutrition, miscellaneous expenses will be provided to the new-born. To ensure 48 hour stay at health institution after delivery state proposed to provide a gift pack (Big size towel, 02 meter funnel cloth, Duck-back Rubber Sheet01, Baby Bed net, Blanket) to every mother for staying 48 hour in health institution after delivery. It is applicable only for the PHCs, CHCs, and SDHs. Sl.No. Component Unit Cost Remarks
1
Management Support (Medicine, Supplementary Nutrition & logistic support) to Sick New Born First 30 days “Life under NRHM” (Estimated live birth in a year i.e. 51858 X 10 %)
2000 103.70
2
20,000 “Baby care Pack” (Big size towel, 02 meter funnel cloth, Duck-back Rubber Sheet01, Baby Bed net, Blanket)
Rs. 700/- Budgeted under Maternal Health, Part-A
51
A.2.7. Strengthen of Referral System
Specialist care for neo-born babies is not available in all Sub-divisional hospital. To reducing the neo-natal mortality in rural areas it is essential to provide referral transportation service in every health institution. Diarrhea and malarial is a common problem for the state. Every year few child deaths are found to this reason. Many times it is difficult to bring the child to the nearest health institution due to the inaccessible and difficult geographical terrain. Meanwhile as per decision taken in the monthly meeting of State Health Ministers & secretaries with Union Health Minister in Hyderabad, proposal extended Rs 800 to Rs.1500/- to provide referral transportation facility from identified difficult and inaccessible sub-centre to PHC including drop back (per trip 750/-) (No cash provided to beneficiary). Methodology mentioned in Assured referral transport system under Maternal Health. There are few areas in the Dhalai district which is not connected (Tribal area &
Border connected area) by road. Experimental innovation of Doli service had given good response & demand increased for uncovered Tribal Villages. The area is under the coverage of “Doli” service to enable expecting mothers reach health institutions. This component will not be overlapping the referral transport under JSY scheme. The unit cost has been calculated on the basis of average rate of transport in different parts of the state. Proposals incorporated in a separate chapter under NRHM Part-B.
Sl.No.
Component Unit Cost Amount
1 Extended Referral Transportation cost for high risk babies (Sick New Born, Life Under NRHM) (Estimated live birth in a year i.e. 51858 X 10 %)
1500 77.775
A.2.8. Malnourished baby Unit for North Tripura District Introduction: Geographically & topographically Kanchanpur sub-division of the North district is one of the most difficult sub-division in the state of Tripura in terms of accessibility and development. It becomes daunting task to deliver health care services to communities door step. Provision of essential services in these remote pockets is one of the biggest challenges before the district administration. Situation analysis Kanchanpur Sub Division of North District is having 4 ADC Blocks (Tribal belt) with completely hilly terrain. The total population of the Sub Division is approximately 1, 91,564. It covers 6 Reang Refugee Camps having approximate population of 25,625 and 55 ADC villages. The referral system prevailing in the sub division as well as in the entire district is from the health institution to the nearest FRU. But the geographical condition of the Sub Division is such that it is very difficult to reach to the nearest health institution in time due to lack of communication. Due to this difficult terrain and lack of communication a very sad incident took place in Kangrai, an ADC village under Dasda Block. 24 deaths took place in Kangrai ADC village of Kanchanpur Sub division due to infectious disease. Most of the deaths took place in the month of June 2010 and out of these 19 were children below 5 years most of whom were suffering from malnutrition. Unfortunately the information reached to the SDM office,
52
which is just located 15 Kms. away from the village of Kangrai on 19th June 2010, even though 14 children had already died. This indicates clear-cut failure of the communication and information between the community and various service provider and administration. Objective: To reduce the incidence of death due to Malnourishment of children. Strategy / Activity Therefore activity designed to deliver health care service to the door step of the inhabitant of hilly area. Referral service planned from household to SC and PHC to SDH with support to ASHA & other supporting manpower as well. Special emphasis given on mal nourished children by providing nutritional support. Budget:
Malnourished care unit Number proposed
Unit Cost
Amount (Fig. in Rs.)
Remarks
Monthly Honorarium to ASHA 500 200 1,00,000 Provision for baby’s diet 500 350 1,75,000 Provision for mother’s diet 500 350 1,75,000 Provision for mother’s wages 500 700 3,50,000 Transportation cost from Home to Hospital 500 200 1,00,000
Sub-Total 9,00,000 A.2.9. Newborn Care Interventions /Management of ARI & Diarrhea State targeted to increase acceptance of ORS from 61% (DLHS-III) to 70% by March, 2012, and increase the rate of seeking treatment for ARI from 73.5% (DLHS-III) to 85% by March, 2012.
Reduce morbidity and mortality among infants due to diarrhea, ARI & &
Communicable Diseases is very much essential. Supply of ORS will be ensured and would be made available in all depots. The ASHA drug kit will have ORS and Cotrimoxazole tablets, which will be replenished as per need. Anganwadi centers will also be given ORS. Orientation of ASHA for identification of symptoms of diarrhea and ARI and their treatment is proposed to be carried out during the bi-monthly periodic retraining. Identification of danger signs and time for prompt transportation of sick child will also be taught to ASHAs.
To Manage diarrhea, ARI & Communicable diseases an amount of Rs.10, 00,000/-
is proposed. A. 2. 10. Other strategies / activities
Child Immunization State level coverage as per District Level Household Survey-3, Coverage Evaluation
Survey 2009 & Reported coverage for 2009-10, 2010-11 till Nov’ 10 are as follows:
Vaccines DLHS-3 (2007-08)
CES (2008-09)
Reported Coverage 2009-10 2010-11
DPT-3 47.3 70.6 46395 (75%) 27983(77%) OPV-3 51.2 66.0 45968 (74%) 28081(77%) BCG 69.8 66.0 51083 (82%) 30294(83%) Measles 51.7 68.8 43640 (70%) 28170(78%) TT-10 Yrs - - 30252 (58%) 18370(54%) TT-16 Yrs - - 27435 (54%) 15346(48%) Vitamin-A 53.6 68.0 33435 (54%) 24257(67%) Full Immunization 38.5 66.0 38759 (62%) 22491(62%)
53
To reduce infant mortality rate immunization is one of the most cost effective public
health interventions as it is a preventable disease. Reported immunization coverage for fully vaccinated children has shown an increase from 19% in NFHS -1 to 41 % in NFHS -2 and 49.7% in NFHS - 3. But as per the State HMIS the full immunization coverage is 74.28 % in 2010-11 ( upto December ). 100% coverage needs to cover the difficult tarrains, though neglegency of gurdian, and traditional feeling is also a constrain. ASHAs involvements to accompany the children increased the percentage of full immunization in comparison to last year. ASHA will accompany children in SC, PHC, CHC, SDH, DH or in out reach camp for immunization. Incentive for ASHA for this purpose is proposed.
Activity for Child Immunization is proposed below:
Sl.No. Component Unit Cost Amount
01 Incentive to ASHA for full immunization of 0-1 yr old infant Rs.150/- Budget
under Part B
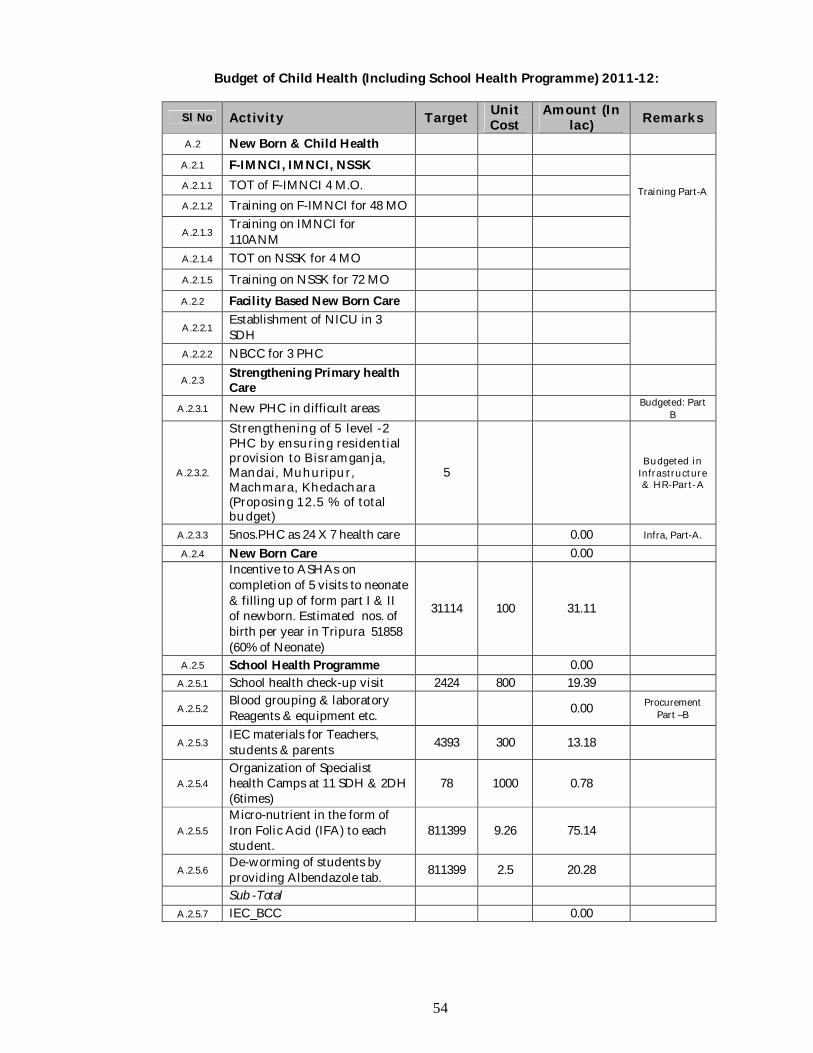
54
Budget of Child Health (Including School Health Programme) 2011-12:
Sl No Activity Target Unit Cost
Amount (In lac) Remarks
A.2 New Born & Child Health
A.2.1 F-IMNCI, IMNCI, NSSK
Training Part-A
A.2.1.1 TOT of F-IMNCI 4 M.O. A.2.1.2 Training on F-IMNCI for 48 MO
A.2.1.3 Training on IMNCI for 110ANM
A.2.1.4 TOT on NSSK for 4 MO A.2.1.5 Training on NSSK for 72 MO A.2.2 Facility Based New Born Care
A.2.2.1 Establishment of NICU in 3 SDH
A.2.2.2 NBCC for 3 PHC
A.2.3 Strengthening Primary health Care
A.2.3.1 New PHC in difficult areas Budgeted: Part B
A.2.3.2.
Strengthening of 5 level -2 PHC by ensuring residential provision to Bisramganja, Mandai, Muhuripur, Machmara, Khedachara (Proposing 12.5 % of total budget)
5 Budgeted in
Infrastructure & HR-Part-A
A.2.3.3 5nos.PHC as 24 X 7 health care 0.00 Infra, Part-A.
A.2.4 New Born Care 0.00
Incentive to ASHAs on completion of 5 visits to neonate & filling up of form part I & II of newborn. Estimated nos. of birth per year in Tripura 51858 (60% of Neonate)
31114 100 31.11
A.2.5 School Health Programme 0.00
A.2.5.1 School health check-up visit 2424 800 19.39
A.2.5.2 Blood grouping & laboratory Reagents & equipment etc. 0.00 Procurement
Part –B
A.2.5.3 IEC materials for Teachers, students & parents 4393 300 13.18
A.2.5.4 Organization of Specialist health Camps at 11 SDH & 2DH (6times)
78 1000 0.78
A.2.5.5 Micro-nutrient in the form of Iron Folic Acid (IFA) to each student.
811399 9.26 75.14
A.2.5.6 De-worming of students by providing Albendazole tab. 811399 2.5 20.28
Sub -Total
A.2.5.7 IEC_BCC 0.00
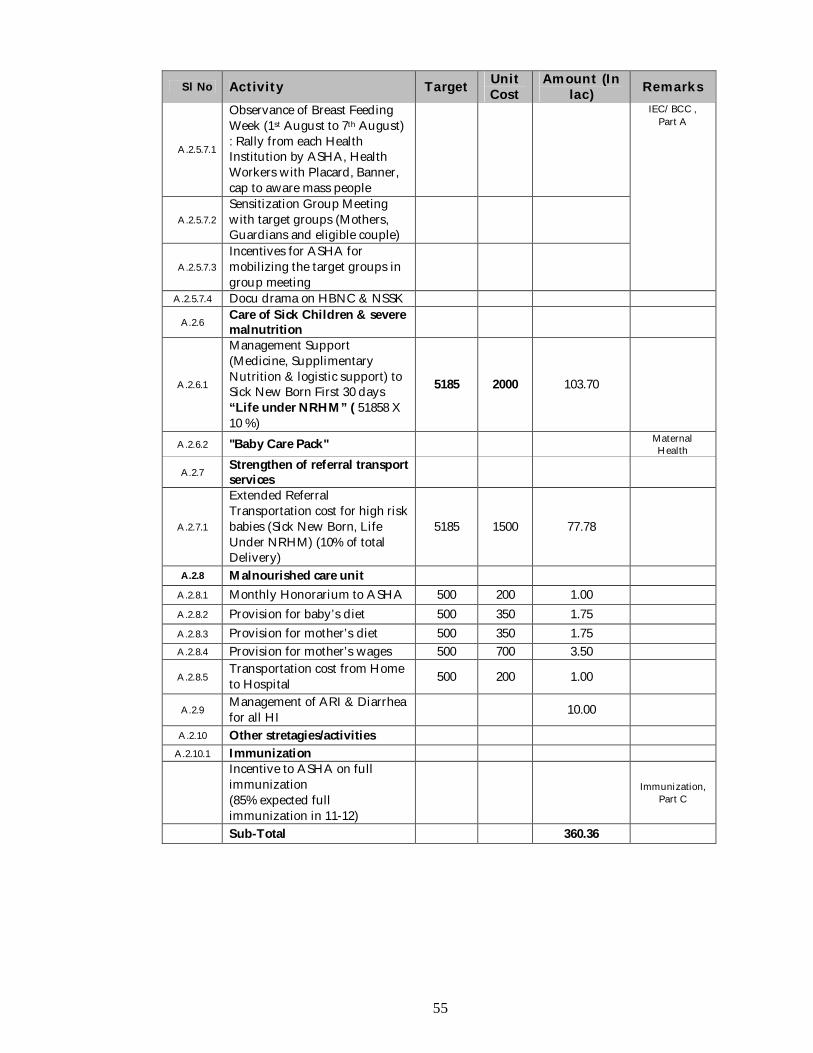
55
Sl No Activity Target Unit Cost
Amount (In lac) Remarks
A.2.5.7.1
Observance of Breast Feeding Week (1st August to 7th August) : Rally from each Health Institution by ASHA, Health Workers with Placard, Banner, cap to aware mass people
IEC/BCC , Part A
A.2.5.7.2 Sensitization Group Meeting with target groups (Mothers, Guardians and eligible couple)
A.2.5.7.3 Incentives for ASHA for mobilizing the target groups in group meeting
A.2.5.7.4 Docu drama on HBNC & NSSK
A.2.6 Care of Sick Children & severe malnutrition
A.2.6.1
Management Support (Medicine, Supplimentary Nutrition & logistic support) to Sick New Born First 30 days “Life under NRHM” ( 51858 X 10 %)
5185 2000 103.70
A.2.6.2 "Baby Care Pack" Maternal Health
A.2.7 Strengthen of referral transport services
A.2.7.1
Extended Referral Transportation cost for high risk babies (Sick New Born, Life Under NRHM) (10% of total Delivery)
5185 1500 77.78
A.2.8 Malnourished care unit
A.2.8.1 Monthly Honorarium to ASHA 500 200 1.00
A.2.8.2 Provision for baby’s diet 500 350 1.75
A.2.8.3 Provision for mother’s diet 500 350 1.75
A.2.8.4 Provision for mother’s wages 500 700 3.50
A.2.8.5 Transportation cost from Home to Hospital 500 200 1.00
A.2.9 Management of ARI & Diarrhea for all HI 10.00
A.2.10 Other stretagies/activities
A.2.10.1 Immunization
Incentive to ASHA on full immunization (85% expected full immunization in 11-12)
Immunization, Part C
Sub-Total 360.36
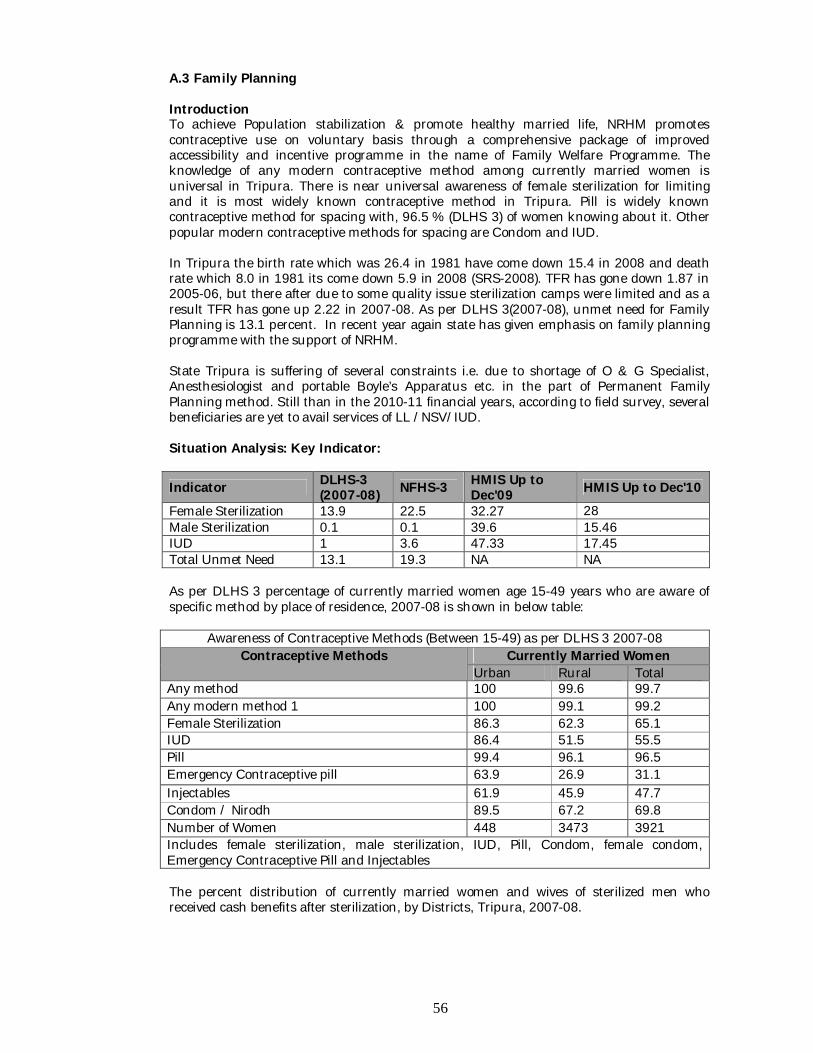
56
A.3 Family Planning Introduction To achieve Population stabilization & promote healthy married life, NRHM promotes contraceptive use on voluntary basis through a comprehensive package of improved accessibility and incentive programme in the name of Family Welfare Programme. The knowledge of any modern contraceptive method among currently married women is universal in Tripura. There is near universal awareness of female sterilization for limiting and it is most widely known contraceptive method in Tripura. Pill is widely known contraceptive method for spacing with, 96.5 % (DLHS 3) of women knowing about it. Other popular modern contraceptive methods for spacing are Condom and IUD. In Tripura the birth rate which was 26.4 in 1981 have come down 15.4 in 2008 and death rate which 8.0 in 1981 its come down 5.9 in 2008 (SRS-2008). TFR has gone down 1.87 in 2005-06, but there after due to some quality issue sterilization camps were limited and as a result TFR has gone up 2.22 in 2007-08. As per DLHS 3(2007-08), unmet need for Family Planning is 13.1 percent. In recent year again state has given emphasis on family planning programme with the support of NRHM. State Tripura is suffering of several constraints i.e. due to shortage of O & G Specialist, Anesthesiologist and portable Boyle’s Apparatus etc. in the part of Permanent Family Planning method. Still than in the 2010-11 financial years, according to field survey, several beneficiaries are yet to avail services of LL /NSV/IUD. Situation Analysis: Key Indicator:
Indicator DLHS-3 (2007-08) NFHS-3 HMIS Up to
Dec'09 HMIS Up to Dec'10
Female Sterilization 13.9 22.5 32.27 28 Male Sterilization 0.1 0.1 39.6 15.46 IUD 1 3.6 47.33 17.45 Total Unmet Need 13.1 19.3 NA NA As per DLHS 3 percentage of currently married women age 15-49 years who are aware of specific method by place of residence, 2007-08 is shown in below table:
Awareness of Contraceptive Methods (Between 15-49) as per DLHS 3 2007-08 Contraceptive Methods Currently Married Women
Urban Rural Total Any method 100 99.6 99.7 Any modern method 1 100 99.1 99.2 Female Sterilization 86.3 62.3 65.1 IUD 86.4 51.5 55.5 Pill 99.4 96.1 96.5 Emergency Contraceptive pill 63.9 26.9 31.1 Injectables 61.9 45.9 47.7 Condom / Nirodh 89.5 67.2 69.8 Number of Women 448 3473 3921 Includes female sterilization, male sterilization, IUD, Pill, Condom, female condom, Emergency Contraceptive Pill and Injectables The percent distribution of currently married women and wives of sterilized men who received cash benefits after sterilization, by Districts, Tripura, 2007-08.
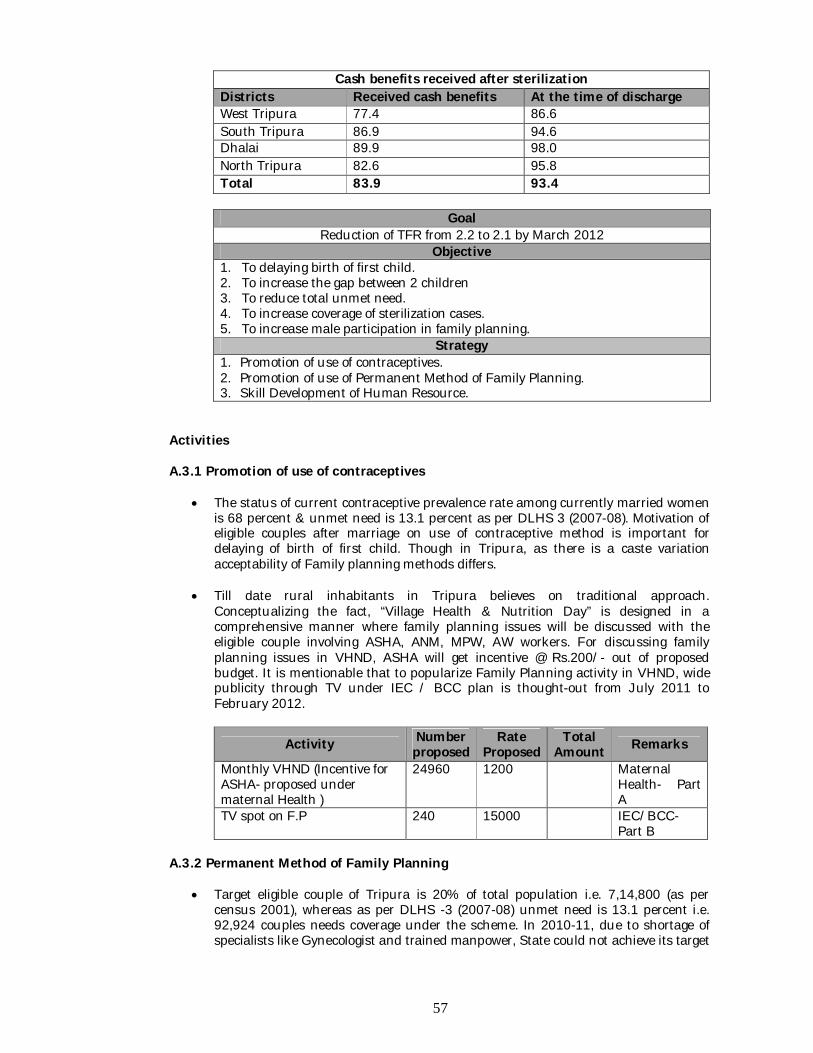
57
Cash benefits received after sterilization Districts Received cash benefits At the time of discharge West Tripura 77.4 86.6 South Tripura 86.9 94.6 Dhalai 89.9 98.0 North Tripura 82.6 95.8 Total 83.9 93.4
Goal
Reduction of TFR from 2.2 to 2.1 by March 2012 Objective
1. To delaying birth of first child. 2. To increase the gap between 2 children 3. To reduce total unmet need. 4. To increase coverage of sterilization cases. 5. To increase male participation in family planning.
Strategy 1. Promotion of use of contraceptives. 2. Promotion of use of Permanent Method of Family Planning. 3. Skill Development of Human Resource.
Activities A.3.1 Promotion of use of contraceptives
The status of current contraceptive prevalence rate among currently married women is 68 percent & unmet need is 13.1 percent as per DLHS 3 (2007-08). Motivation of eligible couples after marriage on use of contraceptive method is important for delaying of birth of first child. Though in Tripura, as there is a caste variation acceptability of Family planning methods differs.
Till date rural inhabitants in Tripura believes on traditional approach. Conceptualizing the fact, “Village Health & Nutrition Day” is designed in a comprehensive manner where family planning issues will be discussed with the eligible couple involving ASHA, ANM, MPW, AW workers. For discussing family planning issues in VHND, ASHA will get incentive @ Rs.200/- out of proposed budget. It is mentionable that to popularize Family Planning activity in VHND, wide publicity through TV under IEC / BCC plan is thought-out from July 2011 to February 2012.
Activity Number proposed
Rate Proposed
Total Amount Remarks
Monthly VHND (Incentive for ASHA- proposed under maternal Health )
24960 1200 Maternal Health- Part A
TV spot on F.P 240 15000 IEC/BCC- Part B
A.3.2 Permanent Method of Family Planning
Target eligible couple of Tripura is 20% of total population i.e. 7,14,800 (as per census 2001), whereas as per DLHS -3 (2007-08) unmet need is 13.1 percent i.e. 92,924 couples needs coverage under the scheme. In 2010-11, due to shortage of specialists like Gynecologist and trained manpower, State could not achieve its target
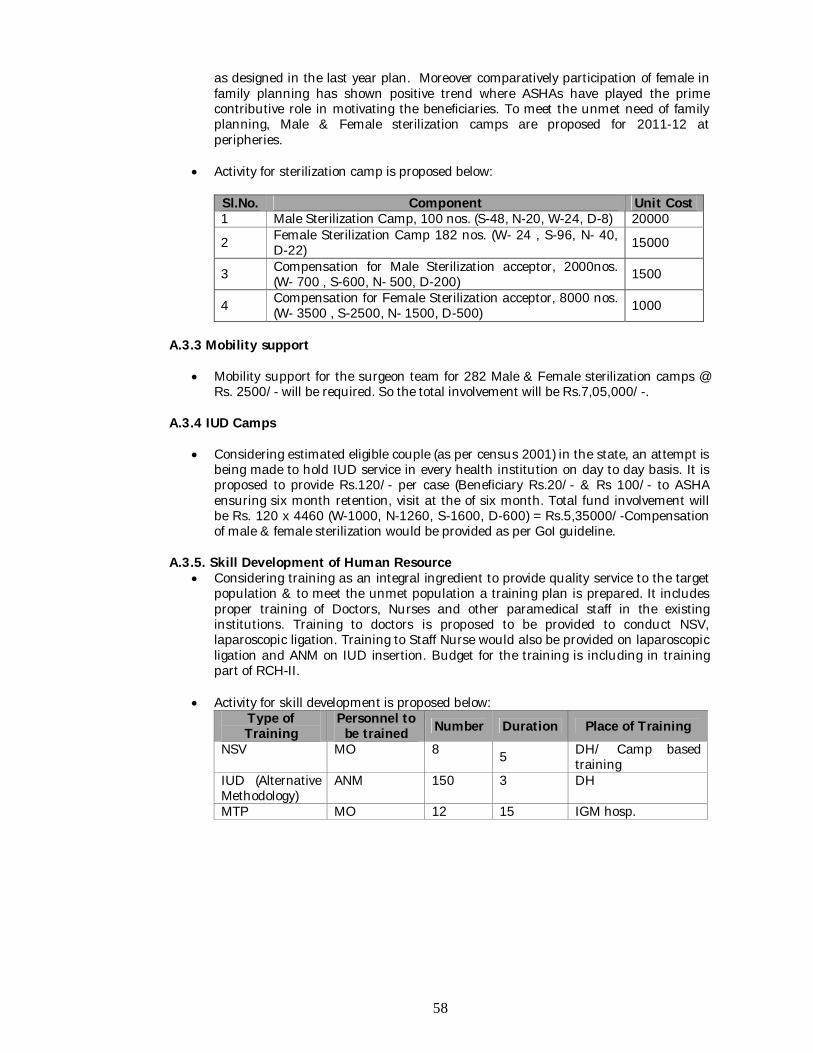
58
as designed in the last year plan. Moreover comparatively participation of female in family planning has shown positive trend where ASHAs have played the prime contributive role in motivating the beneficiaries. To meet the unmet need of family planning, Male & Female sterilization camps are proposed for 2011-12 at peripheries.
Activity for sterilization camp is proposed below:
Sl.No. Component Unit Cost 1 Male Sterilization Camp, 100 nos. (S-48, N-20, W-24, D-8) 20000
2 Female Sterilization Camp 182 nos. (W- 24 , S-96, N- 40, D-22) 15000
3 Compensation for Male Sterilization acceptor, 2000nos. (W- 700 , S-600, N- 500, D-200) 1500
4 Compensation for Female Sterilization acceptor, 8000 nos. (W- 3500 , S-2500, N- 1500, D-500) 1000
A.3.3 Mobility support
Mobility support for the surgeon team for 282 Male & Female sterilization camps @ Rs. 2500/- will be required. So the total involvement will be Rs.7,05,000/-.
A.3.4 IUD Camps
Considering estimated eligible couple (as per census 2001) in the state, an attempt is being made to hold IUD service in every health institution on day to day basis. It is proposed to provide Rs.120/- per case (Beneficiary Rs.20/- & Rs 100/- to ASHA ensuring six month retention, visit at the of six month. Total fund involvement will be Rs. 120 x 4460 (W-1000, N-1260, S-1600, D-600) = Rs.5,35000/-Compensation of male & female sterilization would be provided as per GoI guideline.
A.3.5. Skill Development of Human Resource Considering training as an integral ingredient to provide quality service to the target
population & to meet the unmet population a training plan is prepared. It includes proper training of Doctors, Nurses and other paramedical staff in the existing institutions. Training to doctors is proposed to be provided to conduct NSV, laparoscopic ligation. Training to Staff Nurse would also be provided on laparoscopic ligation and ANM on IUD insertion. Budget for the training is including in training part of RCH-II.
Activity for skill development is proposed below: Type of Training
Personnel to be trained Number Duration Place of Training
NSV MO 8 5 DH/ Camp based training
IUD (Alternative Methodology)
ANM 150 3 DH
MTP MO 12 15 IGM hosp.
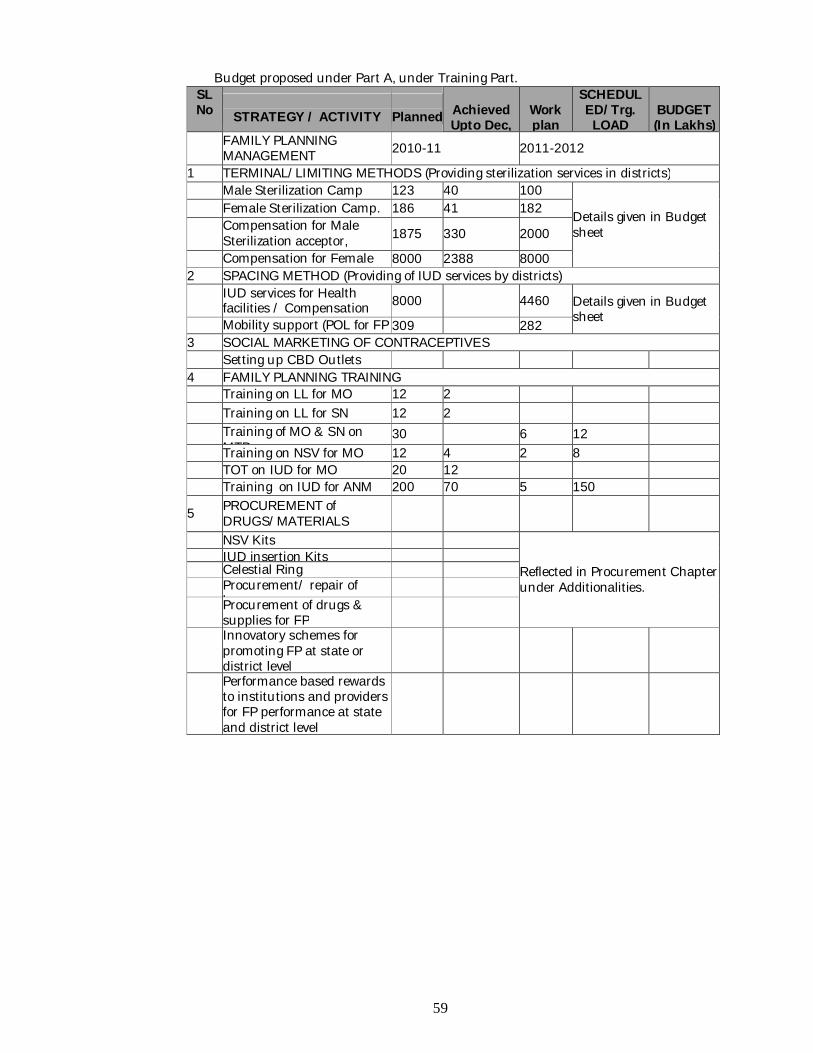
59
Budget proposed under Part A, under Training Part. SL No
STRATEGY / ACTIVITY
Planned
Achieved Upto Dec,
Work plan
SCHEDUL ED/Trg. LOAD
BUDGET (In Lakhs)
FAMILY PLANNING MANAGEMENT 2010-11 2011-2012
1 TERMINAL/LIMITING METHODS (Providing sterilization services in districts) Male Sterilization Camp 123 40 100
Details given in Budget sheet
Female Sterilization Camp. 186 41 182
Compensation for Male Sterilization acceptor, 2000nos.
1875 330 2000
Compensation for Female Sterilization acceptor,
8000 2388 8000 2 SPACING METHOD (Providing of IUD services by districts)
IUD services for Health facilities / Compensation 8000 4460 Details given in Budget
sheet Mobility support (POL for FP
/ Others) 309 282
3 SOCIAL MARKETING OF CONTRACEPTIVES Setting up CBD Outlets 4 FAMILY PLANNING TRAINING Training on LL for MO 12 2 Training on LL for SN 12 2 Training of MO & SN on
MTP 30 6 12
Training on NSV for MO 12 4 2 8 TOT on IUD for MO 20 12 Training on IUD for ANM 200 70 5 150
5 PROCUREMENT of DRUGS/MATERIALS
NSV Kits
Reflected in Procurement Chapter under Additionalities.
IUD insertion Kits Celestial Ring Procurement/ repair of
laparoscopes
Procurement of drugs & supplies for FP
Innovatory schemes for promoting FP at state or district level
Performance based rewards to institutions and providers for FP performance at state and district level
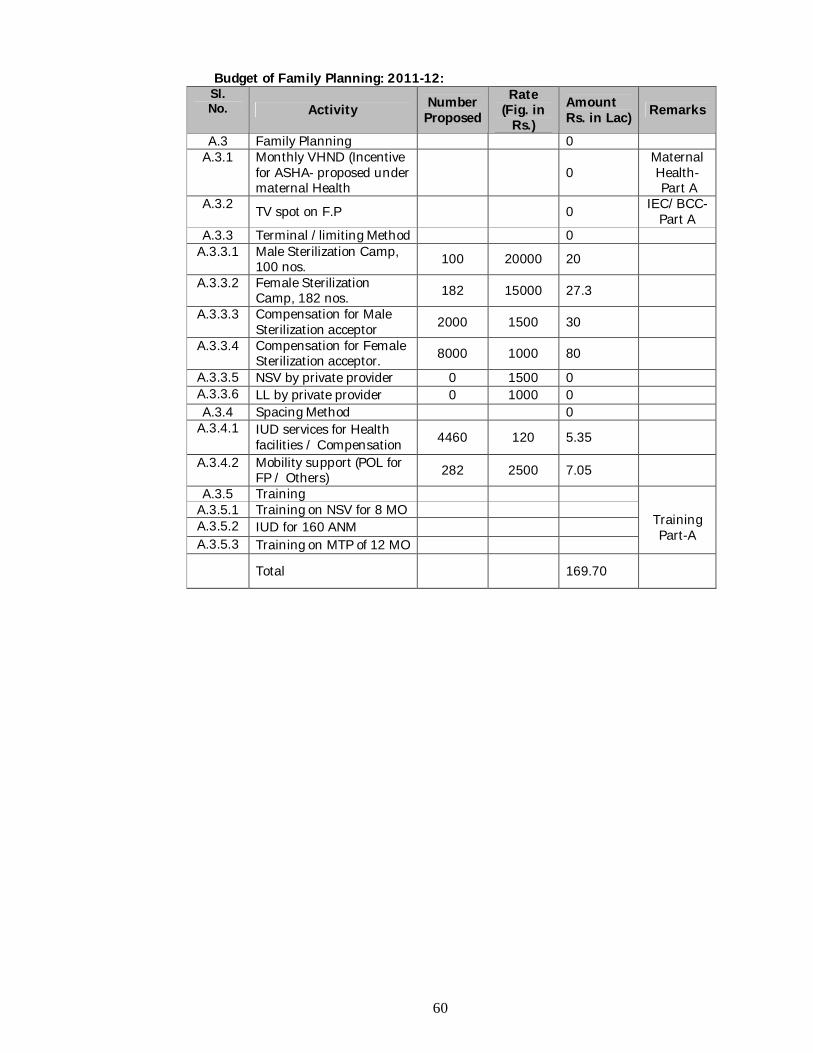
60
Budget of Family Planning: 2011-12: Sl. No. Activity Number
Proposed Rate
(Fig. in Rs.)
Amount Rs. in Lac) Remarks
A.3 Family Planning 0 A.3.1 Monthly VHND (Incentive
for ASHA- proposed under maternal Health
0 Maternal Health- Part A
A.3.2 TV spot on F.P 0 IEC/BCC- Part A
A.3.3 Terminal /limiting Method 0 A.3.3.1 Male Sterilization Camp,
100 nos. 100 20000 20
A.3.3.2 Female Sterilization Camp, 182 nos. 182 15000 27.3
A.3.3.3 Compensation for Male Sterilization acceptor 2000 1500 30
A.3.3.4 Compensation for Female Sterilization acceptor. 8000 1000 80
A.3.3.5 NSV by private provider 0 1500 0 A.3.3.6 LL by private provider 0 1000 0 A.3.4 Spacing Method 0
A.3.4.1 IUD services for Health facilities / Compensation 4460 120 5.35
A.3.4.2 Mobility support (POL for FP / Others) 282 2500 7.05
A.3.5 Training
Training Part-A
A.3.5.1 Training on NSV for 8 MO A.3.5.2 IUD for 160 ANM A.3.5.3 Training on MTP of 12 MO
Total 169.70
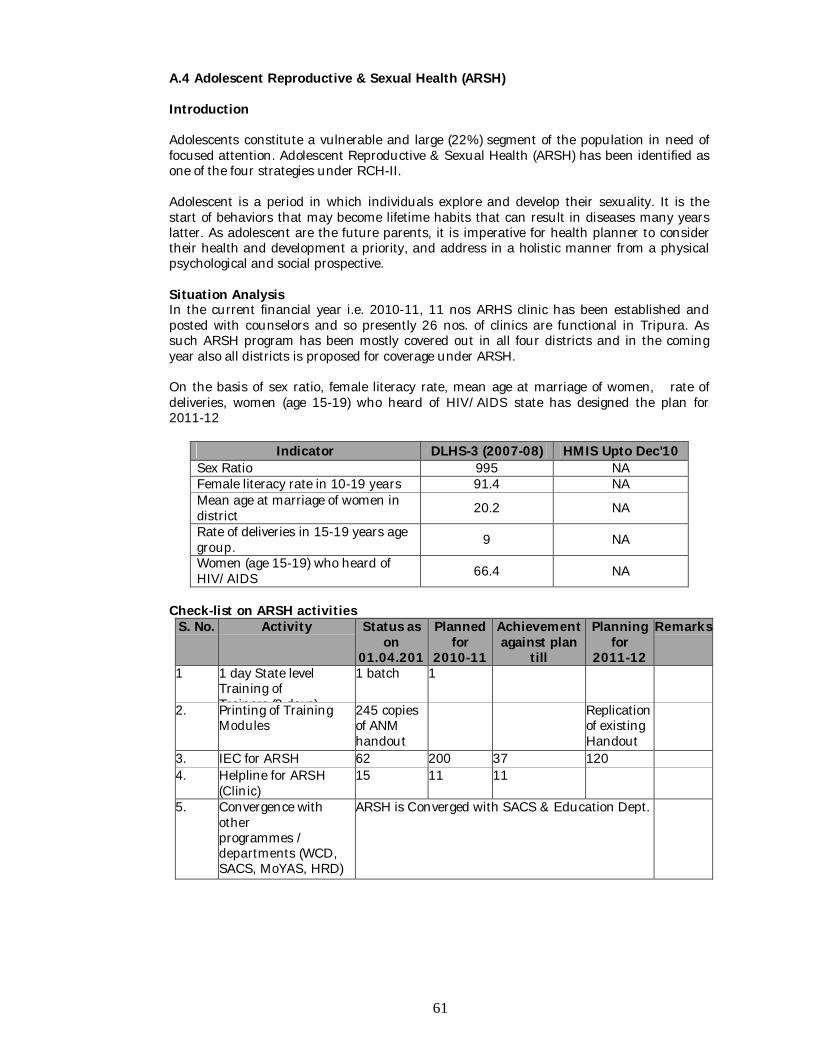
61
A.4 Adolescent Reproductive & Sexual Health (ARSH) Introduction Adolescents constitute a vulnerable and large (22%) segment of the population in need of focused attention. Adolescent Reproductive & Sexual Health (ARSH) has been identified as one of the four strategies under RCH-II. Adolescent is a period in which individuals explore and develop their sexuality. It is the start of behaviors that may become lifetime habits that can result in diseases many years latter. As adolescent are the future parents, it is imperative for health planner to consider their health and development a priority, and address in a holistic manner from a physical psychological and social prospective. Situation Analysis In the current financial year i.e. 2010-11, 11 nos ARHS clinic has been established and posted with counselors and so presently 26 nos. of clinics are functional in Tripura. As such ARSH program has been mostly covered out in all four districts and in the coming year also all districts is proposed for coverage under ARSH. On the basis of sex ratio, female literacy rate, mean age at marriage of women, rate of deliveries, women (age 15-19) who heard of HIV/AIDS state has designed the plan for 2011-12
Indicator DLHS-3 (2007-08) HMIS Upto Dec'10 Sex Ratio 995 NA Female literacy rate in 10-19 years 91.4 NA Mean age at marriage of women in district 20.2 NA
Rate of deliveries in 15-19 years age group. 9 NA
Women (age 15-19) who heard of HIV/AIDS 66.4 NA
Check-list on ARSH activities
S. No. Activity Status as on
01.04.2010
Planned for
2010-11
Achievement against plan
till 31.12.2010
Planning for
2011-12
Remarks
1 1 day State level Training of Trainers (3 days)
1 batch 1
2. Printing of Training Modules
245 copies of ANM handout
Replication of existing Handout
3. IEC for ARSH 62 200 37 120 4. Helpline for ARSH
(Clinic) 15 11 11
5. Convergence with other programmes / departments (WCD, SACS, MoYAS, HRD)
ARSH is Converged with SACS & Education Dept.
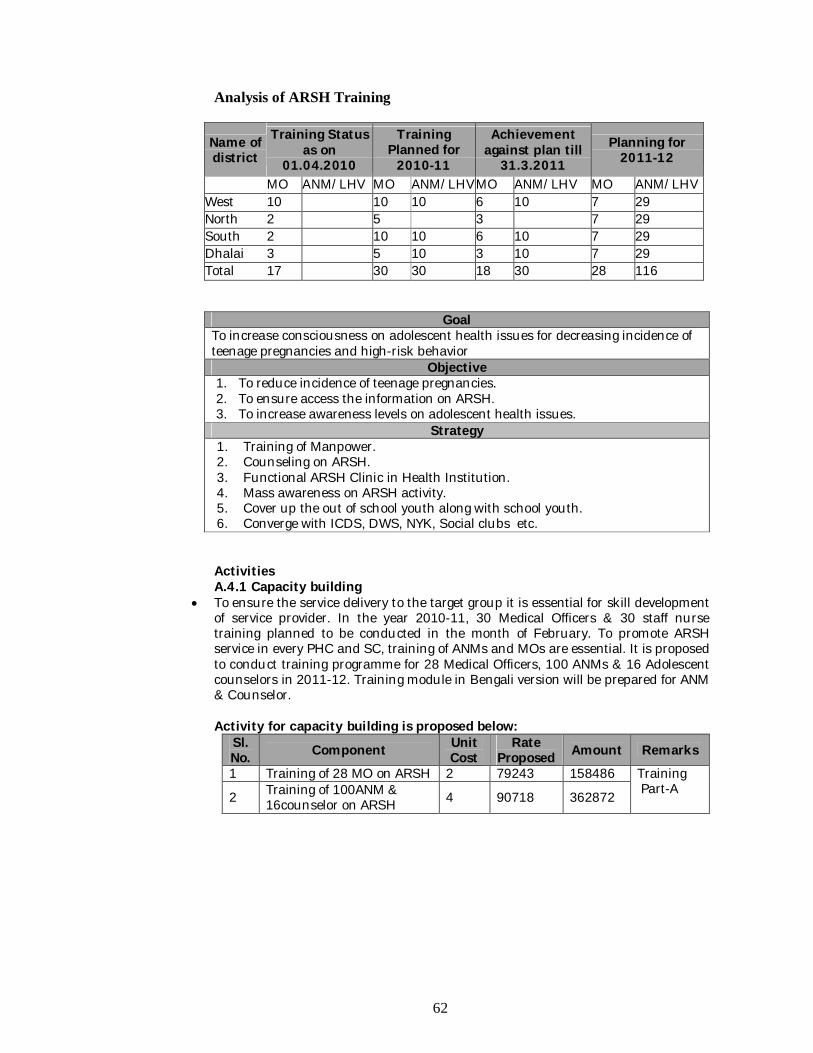
62
Analysis of ARSH Training
Name of district
Training Status as on
01.04.2010
Training Planned for
2010-11
Achievement against plan till
31.3.2011 Planning for
2011-12
MO ANM/LHV MO ANM/LHV MO ANM/LHV MO ANM/LHV West 10 10 10 6 10 7 29 North 2 5 3 7 29 South 2 10 10 6 10 7 29 Dhalai 3 5 10 3 10 7 29 Total 17 30 30 18 30 28 116
Goal To increase consciousness on adolescent health issues for decreasing incidence of teenage pregnancies and high-risk behavior
Objective 1. To reduce incidence of teenage pregnancies. 2. To ensure access the information on ARSH. 3. To increase awareness levels on adolescent health issues.
Strategy 1. Training of Manpower. 2. Counseling on ARSH. 3. Functional ARSH Clinic in Health Institution. 4. Mass awareness on ARSH activity. 5. Cover up the out of school youth along with school youth. 6. Converge with ICDS, DWS, NYK, Social clubs etc.
Activities A.4.1 Capacity building
To ensure the service delivery to the target group it is essential for skill development of service provider. In the year 2010-11, 30 Medical Officers & 30 staff nurse training planned to be conducted in the month of February. To promote ARSH service in every PHC and SC, training of ANMs and MOs are essential. It is proposed to conduct training programme for 28 Medical Officers, 100 ANMs & 16 Adolescent counselors in 2011-12. Training module in Bengali version will be prepared for ANM & Counselor.
Activity for capacity building is proposed below:
Sl. No. Component Unit
Cost Rate
Proposed Amount Remarks 1 Training of 28 MO on ARSH 2 79243 158486 Training
Part-A 2 Training of 100ANM & 16counselor on ARSH 4 90718 362872
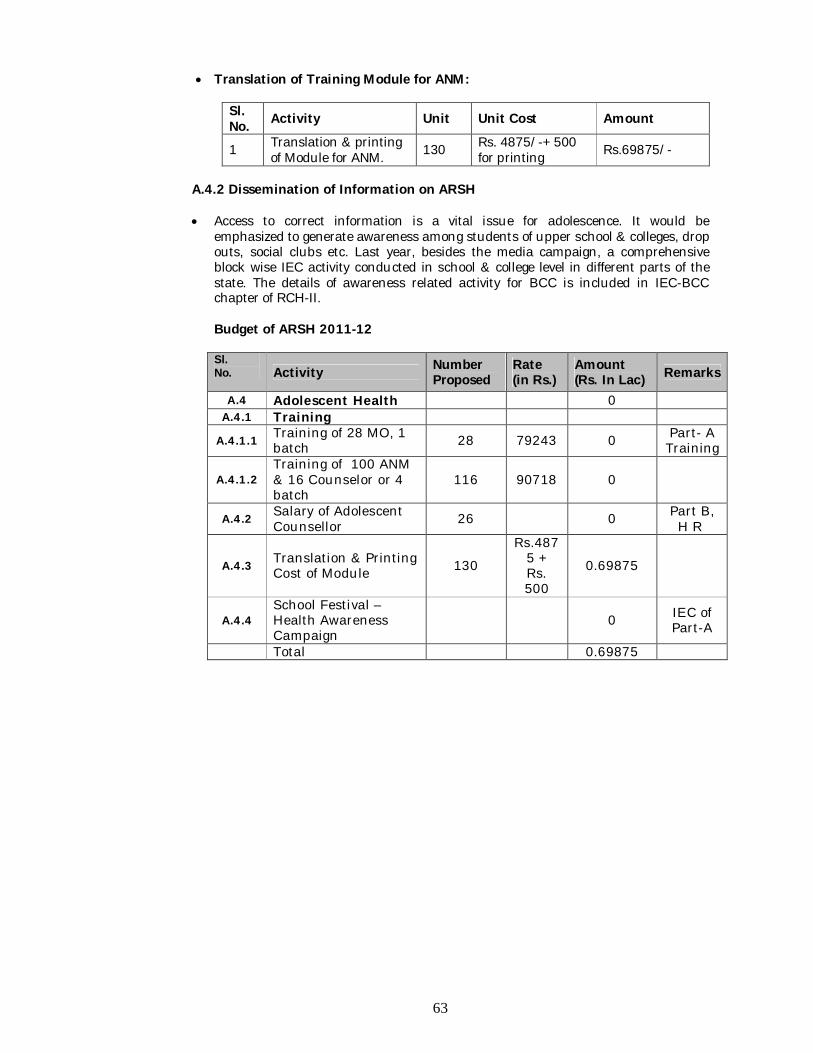
63
Translation of Training Module for ANM:
Sl. No. Activity Unit Unit Cost Amount
1 Translation & printing of Module for ANM. 130 Rs. 4875/-+ 500
for printing Rs.69875/-
A.4.2 Dissemination of Information on ARSH
Access to correct information is a vital issue for adolescence. It would be
emphasized to generate awareness among students of upper school & colleges, drop outs, social clubs etc. Last year, besides the media campaign, a comprehensive block wise IEC activity conducted in school & college level in different parts of the state. The details of awareness related activity for BCC is included in IEC-BCC chapter of RCH-II.
Budget of ARSH 2011-12
Sl. No. Activity Number
Proposed Rate (in Rs.)
Amount (Rs. In Lac) Remarks
A.4 Adolescent Health 0 A.4.1 Training
A.4.1.1 Training of 28 MO, 1 batch 28 79243 0 Part- A
Training
A.4.1.2 Training of 100 ANM & 16 Counselor or 4 batch
116 90718 0
A.4.2 Salary of Adolescent Counsellor 26 0 Part B,
H R
A.4.3 Translation & Printing Cost of Module 130
Rs.4875 + Rs. 500
0.69875
A.4.4 School Festival – Health Awareness Campaign
0 IEC of Part-A
Total 0.69875
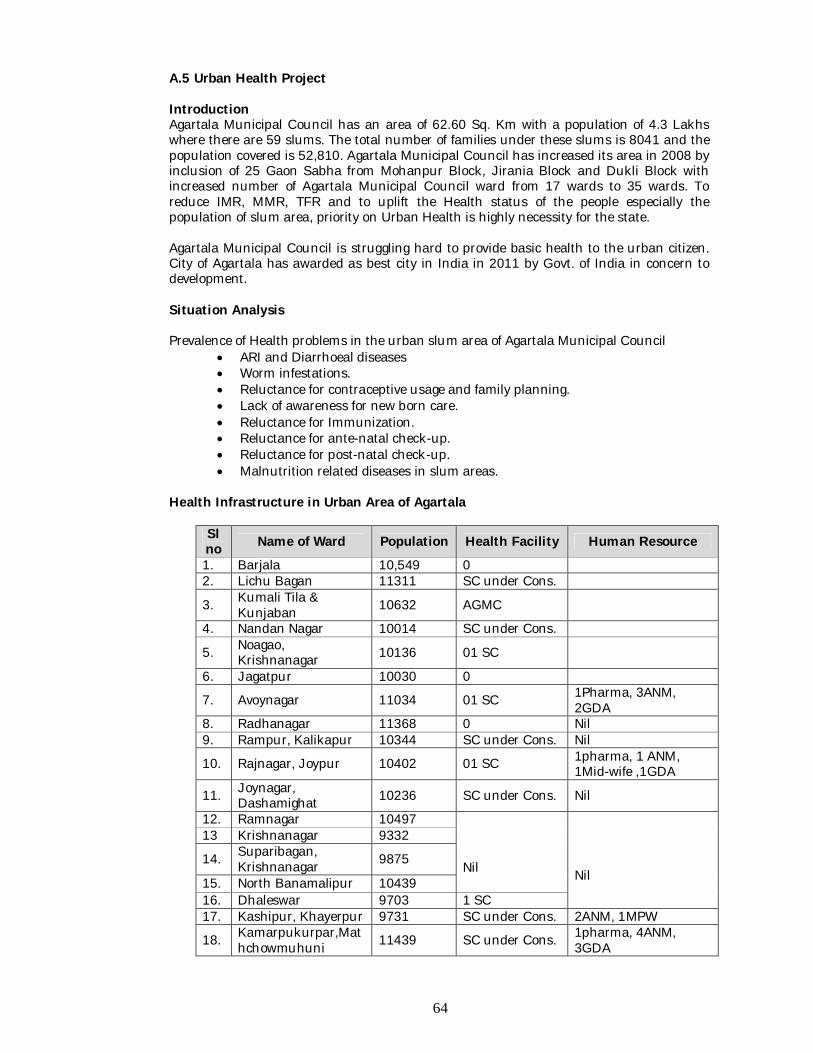
64
A.5 Urban Health Project Introduction Agartala Municipal Council has an area of 62.60 Sq. Km with a population of 4.3 Lakhs where there are 59 slums. The total number of families under these slums is 8041 and the population covered is 52,810. Agartala Municipal Council has increased its area in 2008 by inclusion of 25 Gaon Sabha from Mohanpur Block, Jirania Block and Dukli Block with increased number of Agartala Municipal Council ward from 17 wards to 35 wards. To reduce IMR, MMR, TFR and to uplift the Health status of the people especially the population of slum area, priority on Urban Health is highly necessity for the state. Agartala Municipal Council is struggling hard to provide basic health to the urban citizen. City of Agartala has awarded as best city in India in 2011 by Govt. of India in concern to development. Situation Analysis Prevalence of Health problems in the urban slum area of Agartala Municipal Council
ARI and Diarrhoeal diseases Worm infestations. Reluctance for contraceptive usage and family planning. Lack of awareness for new born care. Reluctance for Immunization. Reluctance for ante-natal check-up. Reluctance for post-natal check-up. Malnutrition related diseases in slum areas.
Health Infrastructure in Urban Area of Agartala
Sl no Name of Ward Population Health Facility Human Resource
1. Barjala 10,549 0 2. Lichu Bagan 11311 SC under Cons.
3. Kumali Tila & Kunjaban 10632 AGMC
4. Nandan Nagar 10014 SC under Cons.
5. Noagao, Krishnanagar 10136 01 SC
6. Jagatpur 10030 0
7. Avoynagar 11034 01 SC 1Pharma, 3ANM, 2GDA
8. Radhanagar 11368 0 Nil 9. Rampur, Kalikapur 10344 SC under Cons. Nil
10. Rajnagar, Joypur 10402 01 SC 1pharma, 1 ANM, 1Mid-wife ,1GDA
11. Joynagar, Dashamighat 10236 SC under Cons. Nil
12. Ramnagar 10497 Nil
Nil
13 Krishnanagar 9332
14. Suparibagan, Krishnanagar 9875
15. North Banamalipur 10439 16. Dhaleswar 9703 1 SC 17. Kashipur, Khayerpur 9731 SC under Cons. 2ANM, 1MPW
18. Kamarpukurpar,Mathchowmuhuni 11439 SC under Cons. 1pharma, 4ANM,
3GDA
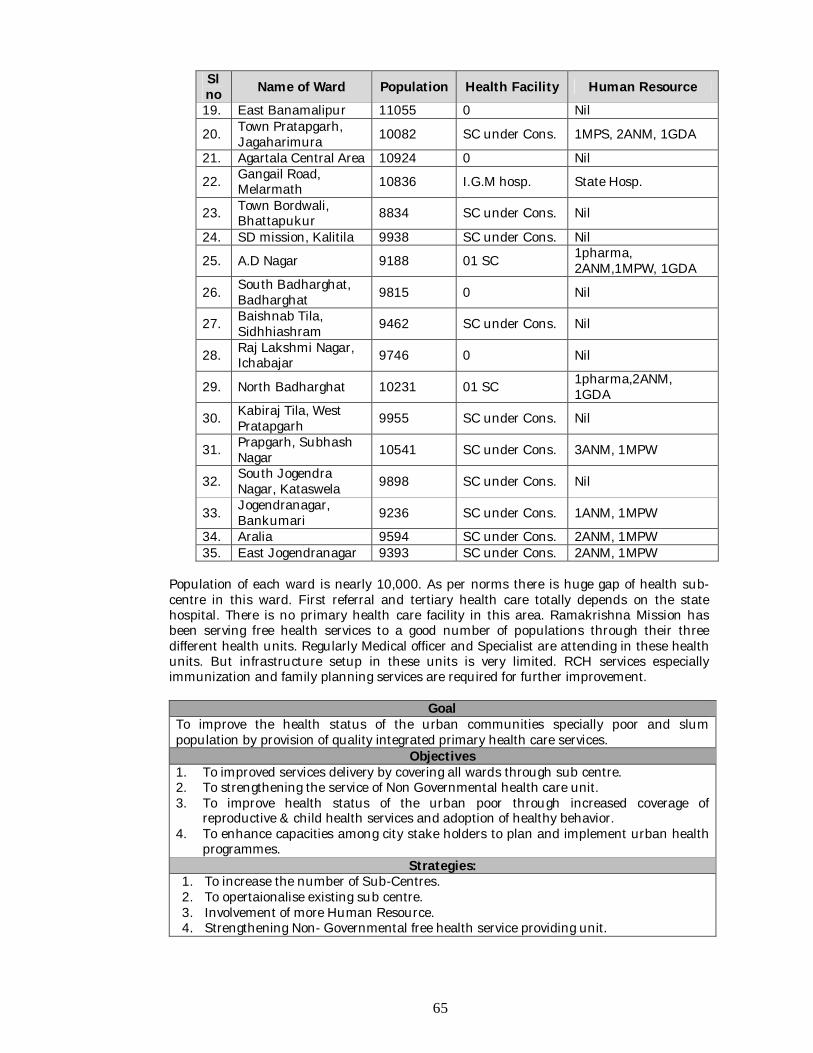
65
Sl no Name of Ward Population Health Facility Human Resource 19. East Banamalipur 11055 0 Nil
20. Town Pratapgarh, Jagaharimura 10082 SC under Cons. 1MPS, 2ANM, 1GDA
21. Agartala Central Area 10924 0 Nil
22. Gangail Road, Melarmath 10836 I.G.M hosp. State Hosp.
23. Town Bordwali, Bhattapukur 8834 SC under Cons. Nil
24. SD mission, Kalitila 9938 SC under Cons. Nil
25. A.D Nagar 9188 01 SC 1pharma, 2ANM,1MPW, 1GDA
26. South Badharghat, Badharghat 9815 0 Nil
27. Baishnab Tila, Sidhhiashram 9462 SC under Cons. Nil
28. Raj Lakshmi Nagar, Ichabajar 9746 0 Nil
29. North Badharghat 10231 01 SC 1pharma,2ANM, 1GDA
30. Kabiraj Tila, West Pratapgarh 9955 SC under Cons. Nil
31. Prapgarh, Subhash Nagar 10541 SC under Cons. 3ANM, 1MPW
32. South Jogendra Nagar, Kataswela 9898 SC under Cons. Nil
33. Jogendranagar, Bankumari 9236 SC under Cons. 1ANM, 1MPW
34. Aralia 9594 SC under Cons. 2ANM, 1MPW 35. East Jogendranagar 9393 SC under Cons. 2ANM, 1MPW
Population of each ward is nearly 10,000. As per norms there is huge gap of health sub-centre in this ward. First referral and tertiary health care totally depends on the state hospital. There is no primary health care facility in this area. Ramakrishna Mission has been serving free health services to a good number of populations through their three different health units. Regularly Medical officer and Specialist are attending in these health units. But infrastructure setup in these units is very limited. RCH services especially immunization and family planning services are required for further improvement.
Goal To improve the health status of the urban communities specially poor and slum population by provision of quality integrated primary health care services.
Objectives 1. To improved services delivery by covering all wards through sub centre. 2. To strengthening the service of Non Governmental health care unit. 3. To improve health status of the urban poor through increased coverage of
reproductive & child health services and adoption of healthy behavior. 4. To enhance capacities among city stake holders to plan and implement urban health
programmes. Strategies:
1. To increase the number of Sub-Centres. 2. To opertaionalise existing sub centre. 3. Involvement of more Human Resource. 4. Strengthening Non- Governmental free health service providing unit.
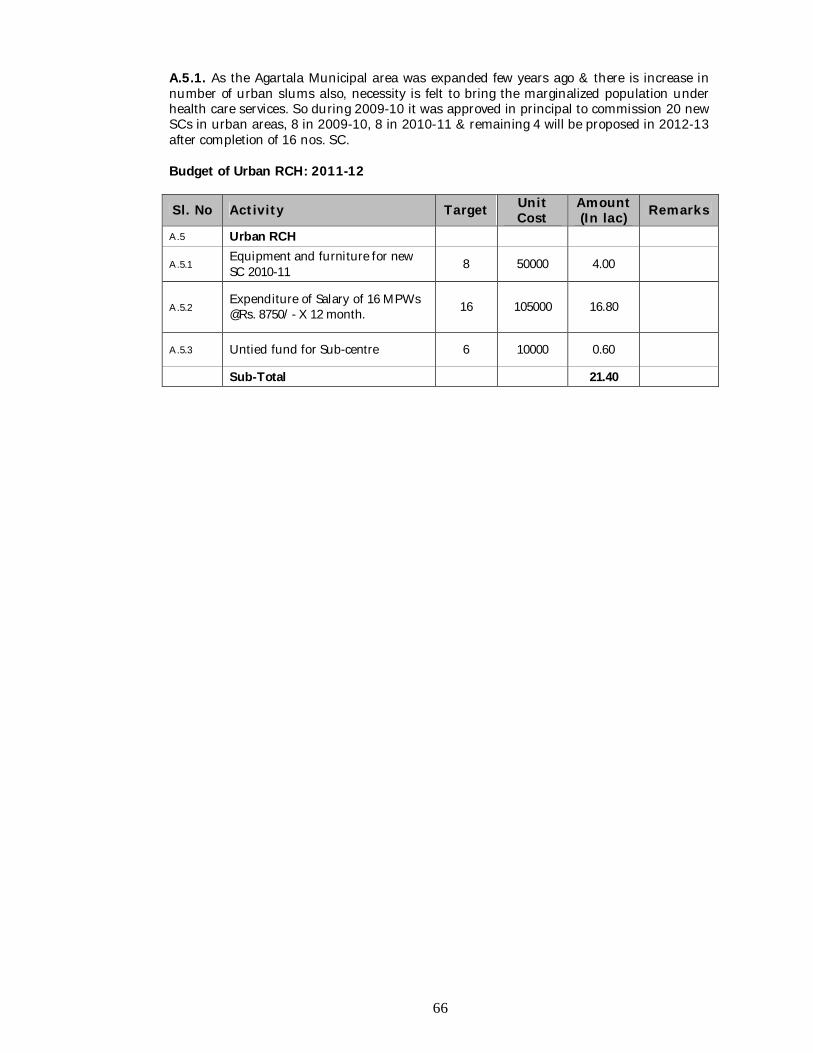
66
A.5.1. As the Agartala Municipal area was expanded few years ago & there is increase in number of urban slums also, necessity is felt to bring the marginalized population under health care services. So during 2009-10 it was approved in principal to commission 20 new SCs in urban areas, 8 in 2009-10, 8 in 2010-11 & remaining 4 will be proposed in 2012-13 after completion of 16 nos. SC. Budget of Urban RCH: 2011-12
Sl. No Activity Target Unit Cost
Amount (In lac) Remarks
A.5 Urban RCH
A.5.1 Equipment and furniture for new SC 2010-11 8 50000 4.00
A.5.2 Expenditure of Salary of 16 MPWs @Rs. 8750/- X 12 month. 16 105000 16.80
A.5.3 Untied fund for Sub-centre 6 10000 0.60
Sub-Total 21.40
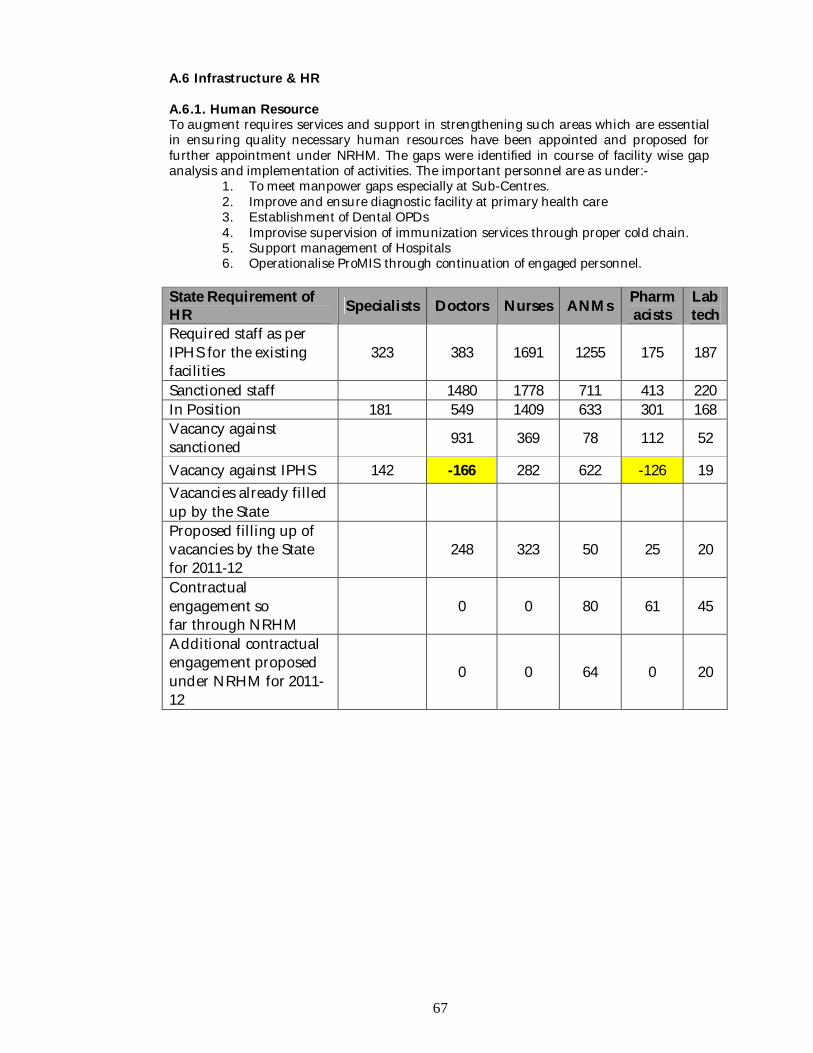
67
A.6 Infrastructure & HR A.6.1. Human Resource To augment requires services and support in strengthening such areas which are essential in ensuring quality necessary human resources have been appointed and proposed for further appointment under NRHM. The gaps were identified in course of facility wise gap analysis and implementation of activities. The important personnel are as under:-
1. To meet manpower gaps especially at Sub-Centres. 2. Improve and ensure diagnostic facility at primary health care 3. Establishment of Dental OPDs 4. Improvise supervision of immunization services through proper cold chain. 5. Support management of Hospitals 6. Operationalise ProMIS through continuation of engaged personnel.
State Requirement of HR Specialists Doctors Nurses ANMs Pharm
acists Lab tech
Required staff as per IPHS for the existing facilities
323 383 1691 1255 175 187
Sanctioned staff 1480 1778 711 413 220 In Position 181 549 1409 633 301 168 Vacancy against sanctioned 931 369 78 112 52
Vacancy against IPHS 142 -166 282 622 -126 19 Vacancies already filled up by the State
Proposed filling up of vacancies by the State for 2011-12
248 323 50 25 20
Contractual engagement so far through NRHM
0 0 80 61 45
Additional contractual engagement proposed under NRHM for 2011-12
0 0 64 0 20
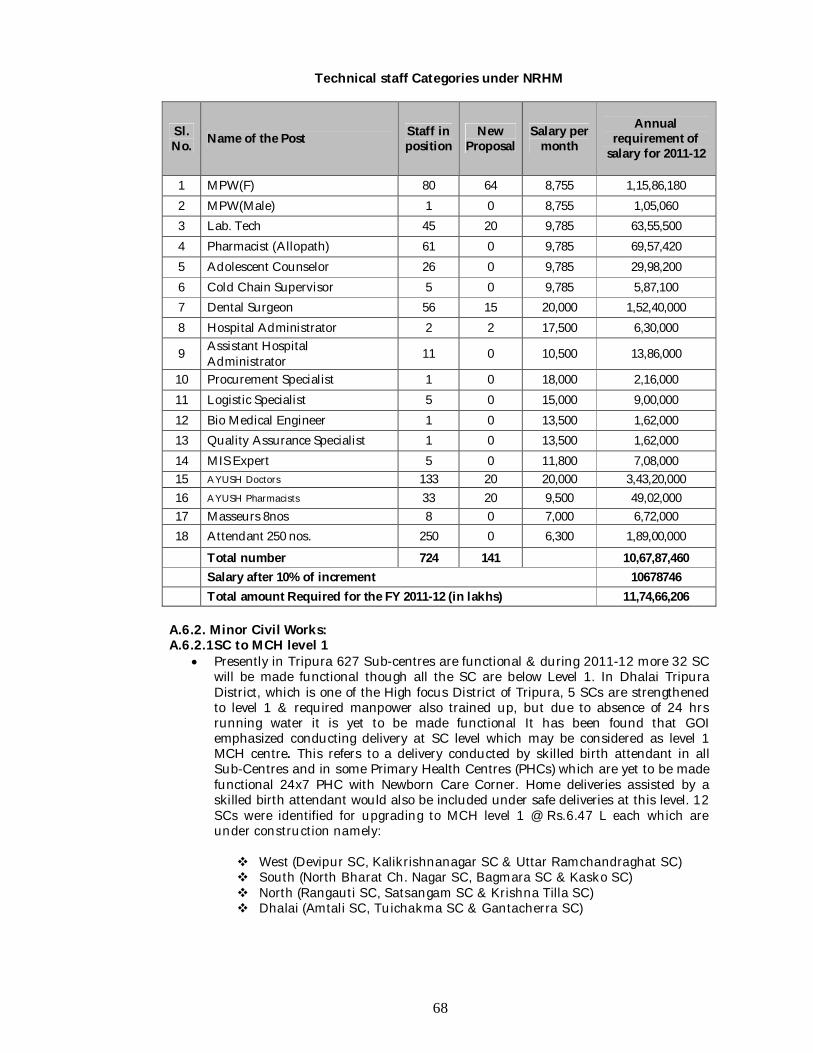
68
Technical staff Categories under NRHM
Sl. No. Name of the Post Staff in
position New
Proposal Salary per
month
Annual requirement of
salary for 2011-12
1 MPW(F) 80 64 8,755 1,15,86,180 2 MPW(Male) 1 0 8,755 1,05,060 3 Lab. Tech 45 20 9,785 63,55,500 4 Pharmacist (Allopath) 61 0 9,785 69,57,420 5 Adolescent Counselor 26 0 9,785 29,98,200 6 Cold Chain Supervisor 5 0 9,785 5,87,100 7 Dental Surgeon 56 15 20,000 1,52,40,000 8 Hospital Administrator 2 2 17,500 6,30,000
9 Assistant Hospital Administrator 11 0 10,500 13,86,000
10 Procurement Specialist 1 0 18,000 2,16,000 11 Logistic Specialist 5 0 15,000 9,00,000 12 Bio Medical Engineer 1 0 13,500 1,62,000 13 Quality Assurance Specialist 1 0 13,500 1,62,000 14 MIS Expert 5 0 11,800 7,08,000 15 AYUSH Doctors 133 20 20,000 3,43,20,000 16 AYUSH Pharmacists 33 20 9,500 49,02,000 17 Masseurs 8nos 8 0 7,000 6,72,000 18 Attendant 250 nos. 250 0 6,300 1,89,00,000
Total number 724 141 10,67,87,460 Salary after 10% of increment 10678746 Total amount Required for the FY 2011-12 (in lakhs) 11,74,66,206
A.6.2. Minor Civil Works: A.6.2.1SC to MCH level 1
Presently in Tripura 627 Sub-centres are functional & during 2011-12 more 32 SC will be made functional though all the SC are below Level 1. In Dhalai Tripura District, which is one of the High focus District of Tripura, 5 SCs are strengthened to level 1 & required manpower also trained up, but due to absence of 24 hrs running water it is yet to be made functional It has been found that GOI emphasized conducting delivery at SC level which may be considered as level 1 MCH centre. This refers to a delivery conducted by skilled birth attendant in all Sub-Centres and in some Primary Health Centres (PHCs) which are yet to be made functional 24x7 PHC with Newborn Care Corner. Home deliveries assisted by a skilled birth attendant would also be included under safe deliveries at this level. 12 SCs were identified for upgrading to MCH level 1 @ Rs.6.47 L each which are under construction namely: West (Devipur SC, Kalikrishnanagar SC & Uttar Ramchandraghat SC) South (North Bharat Ch. Nagar SC, Bagmara SC & Kasko SC) North (Rangauti SC, Satsangam SC & Krishna Tilla SC) Dhalai (Amtali SC, Tuichakma SC & Gantacherra SC)
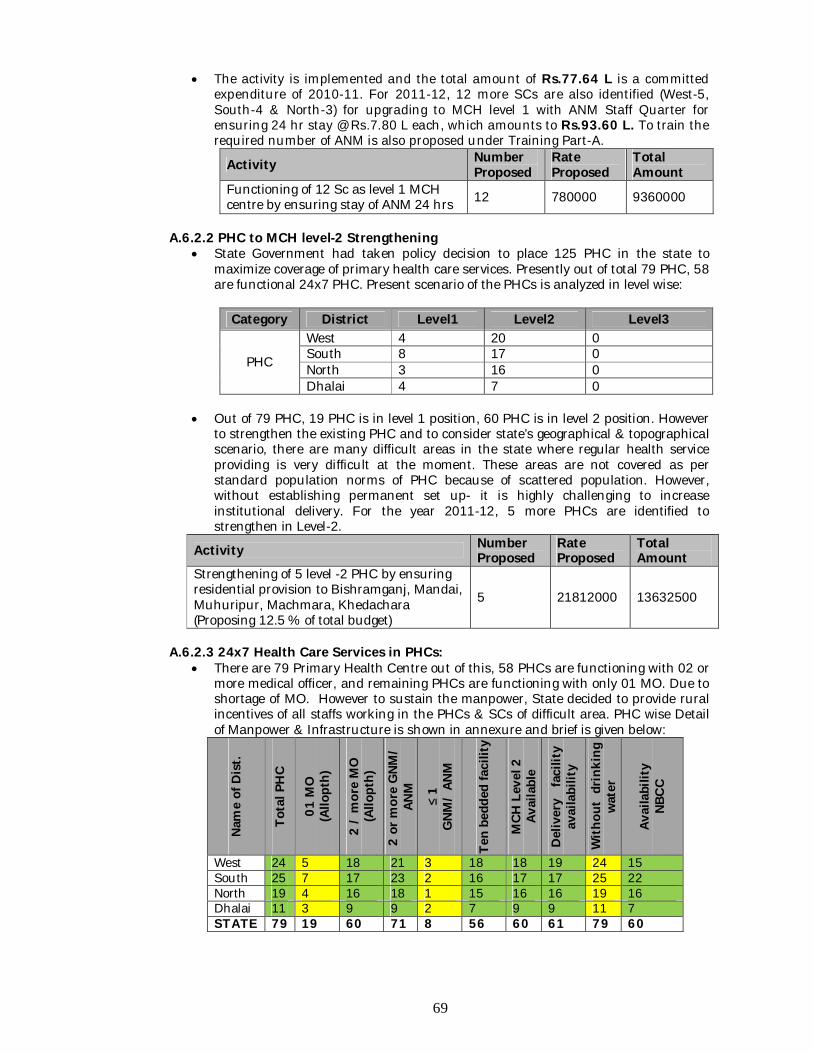
69
The activity is implemented and the total amount of Rs.77.64 L is a committed expenditure of 2010-11. For 2011-12, 12 more SCs are also identified (West-5, South-4 & North-3) for upgrading to MCH level 1 with ANM Staff Quarter for ensuring 24 hr stay @ Rs.7.80 L each, which amounts to Rs.93.60 L. To train the required number of ANM is also proposed under Training Part-A.
Activity Number Proposed
Rate Proposed
Total Amount
Functioning of 12 Sc as level 1 MCH centre by ensuring stay of ANM 24 hrs 12 780000 9360000
A.6.2.2 PHC to MCH level-2 Strengthening
State Government had taken policy decision to place 125 PHC in the state to maximize coverage of primary health care services. Presently out of total 79 PHC, 58 are functional 24x7 PHC. Present scenario of the PHCs is analyzed in level wise:
Category District Level1 Level2 Level3
PHC
West 4 20 0 South 8 17 0 North 3 16 0 Dhalai 4 7 0
Out of 79 PHC, 19 PHC is in level 1 position, 60 PHC is in level 2 position. However
to strengthen the existing PHC and to consider state’s geographical & topographical scenario, there are many difficult areas in the state where regular health service providing is very difficult at the moment. These areas are not covered as per standard population norms of PHC because of scattered population. However, without establishing permanent set up- it is highly challenging to increase institutional delivery. For the year 2011-12, 5 more PHCs are identified to strengthen in Level-2.
Activity Number Proposed
Rate Proposed
Total Amount
Strengthening of 5 level -2 PHC by ensuring residential provision to Bishramganj, Mandai, Muhuripur, Machmara, Khedachara (Proposing 12.5 % of total budget)
5 21812000 13632500
A.6.2.3 24x7 Health Care Services in PHCs:
There are 79 Primary Health Centre out of this, 58 PHCs are functioning with 02 or more medical officer, and remaining PHCs are functioning with only 01 MO. Due to shortage of MO. However to sustain the manpower, State decided to provide rural incentives of all staffs working in the PHCs & SCs of difficult area. PHC wise Detail of Manpower & Infrastructure is shown in annexure and brief is given below:
Nam
e of
Dis
t.
Tota
l PH
C
01 M
O
(Allo
pth)
2 /
mor
e M
O
(Allo
pth)
2 or
mor
e G
NM/
ANM
≤ 1
GNM
/ AN
M
Ten
bedd
ed fa
cilit
y
MCH
Lev
el 2
Av
aila
ble
Del
iver
y f
acili
ty
avai
labi
lity
With
out
drin
king
w
ater
Avai
labi
lity
NB
CC
West 24 5 18 21 3 18 18 19 24 15 South 25 7 17 23 2 16 17 17 25 22 North 19 4 16 18 1 15 16 16 19 16 Dhalai 11 3 9 9 2 7 9 9 11 7 STATE 79 19 60 71 8 56 60 61 79 60
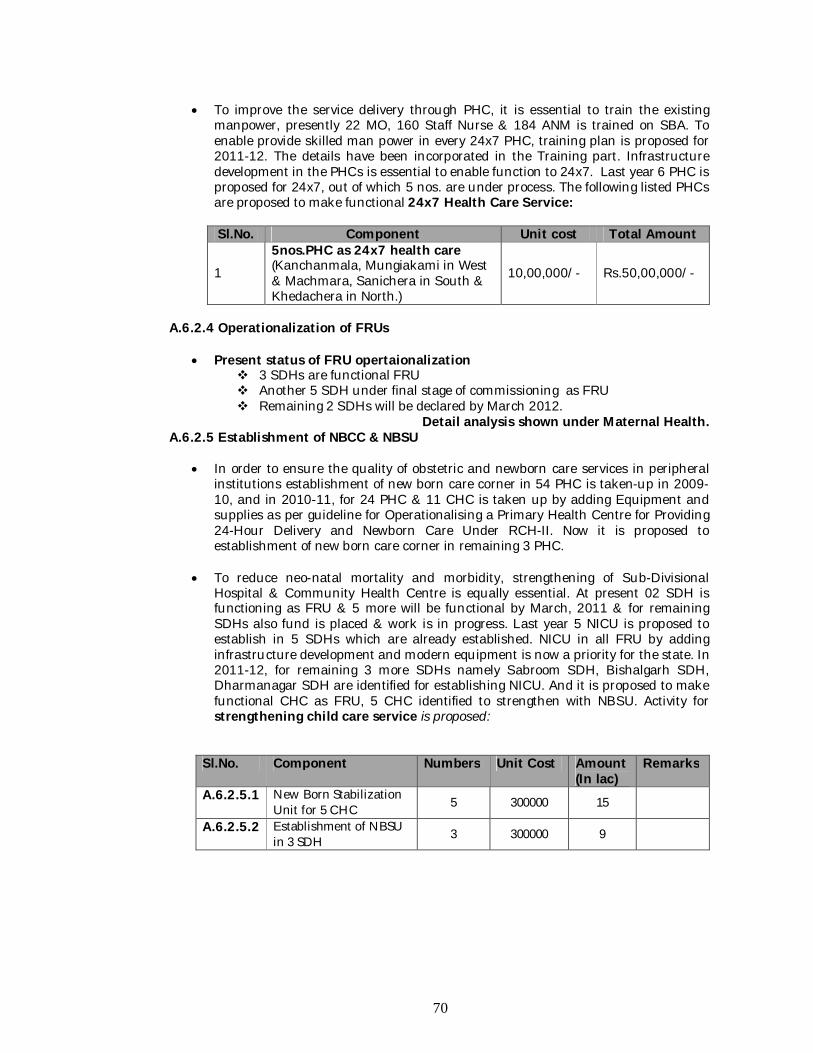
70
To improve the service delivery through PHC, it is essential to train the existing manpower, presently 22 MO, 160 Staff Nurse & 184 ANM is trained on SBA. To enable provide skilled man power in every 24x7 PHC, training plan is proposed for 2011-12. The details have been incorporated in the Training part. Infrastructure development in the PHCs is essential to enable function to 24x7. Last year 6 PHC is proposed for 24x7, out of which 5 nos. are under process. The following listed PHCs are proposed to make functional 24x7 Health Care Service: Sl.No. Component Unit cost Total Amount
1
5nos.PHC as 24x7 health care (Kanchanmala, Mungiakami in West & Machmara, Sanichera in South & Khedachera in North.)
10,00,000/- Rs.50,00,000/-
A.6.2.4 Operationalization of FRUs
Present status of FRU opertaionalization 3 SDHs are functional FRU Another 5 SDH under final stage of commissioning as FRU Remaining 2 SDHs will be declared by March 2012.
Detail analysis shown under Maternal Health. A.6.2.5 Establishment of NBCC & NBSU
In order to ensure the quality of obstetric and newborn care services in peripheral institutions establishment of new born care corner in 54 PHC is taken-up in 2009-10, and in 2010-11, for 24 PHC & 11 CHC is taken up by adding Equipment and supplies as per guideline for Operationalising a Primary Health Centre for Providing 24-Hour Delivery and Newborn Care Under RCH-II. Now it is proposed to establishment of new born care corner in remaining 3 PHC.
To reduce neo-natal mortality and morbidity, strengthening of Sub-Divisional Hospital & Community Health Centre is equally essential. At present 02 SDH is functioning as FRU & 5 more will be functional by March, 2011 & for remaining SDHs also fund is placed & work is in progress. Last year 5 NICU is proposed to establish in 5 SDHs which are already established. NICU in all FRU by adding infrastructure development and modern equipment is now a priority for the state. In 2011-12, for remaining 3 more SDHs namely Sabroom SDH, Bishalgarh SDH, Dharmanagar SDH are identified for establishing NICU. And it is proposed to make functional CHC as FRU, 5 CHC identified to strengthen with NBSU. Activity for strengthening child care service is proposed:
Sl.No. Component Numbers Unit Cost Amount (In lac)
Remarks
A.6.2.5.1 New Born Stabilization Unit for 5 CHC 5 300000 15
A.6.2.5.2 Establishment of NBSU in 3 SDH 3 300000 9
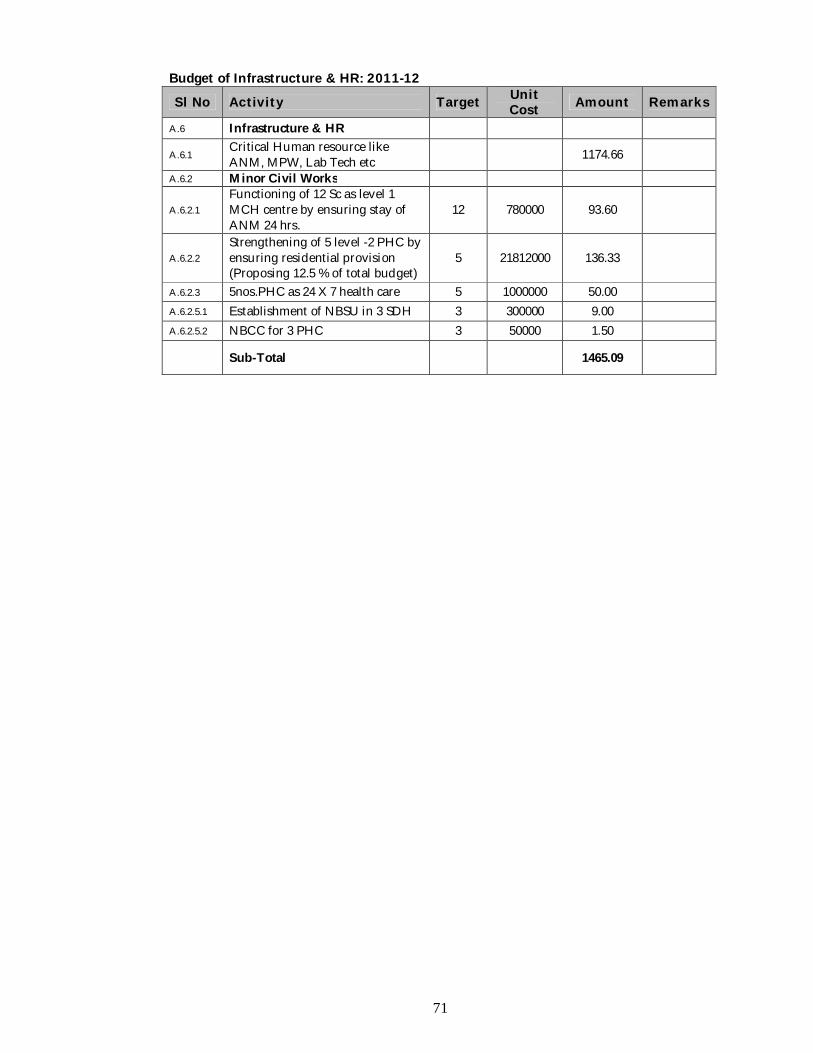
71
Budget of Infrastructure & HR: 2011-12
Sl No Activity Target Unit Cost Amount Remarks
A.6 Infrastructure & HR
A.6.1 Critical Human resource like ANM, MPW, Lab Tech etc 1174.66
A.6.2 Minor Civil Works
A.6.2.1 Functioning of 12 Sc as level 1 MCH centre by ensuring stay of ANM 24 hrs.
12 780000 93.60
A.6.2.2 Strengthening of 5 level -2 PHC by ensuring residential provision (Proposing 12.5 % of total budget)
5 21812000 136.33
A.6.2.3 5nos.PHC as 24 X 7 health care 5 1000000 50.00
A.6.2.5.1 Establishment of NBSU in 3 SDH 3 300000 9.00
A.6.2.5.2 NBCC for 3 PHC 3 50000 1.50
Sub-Total 1465.09
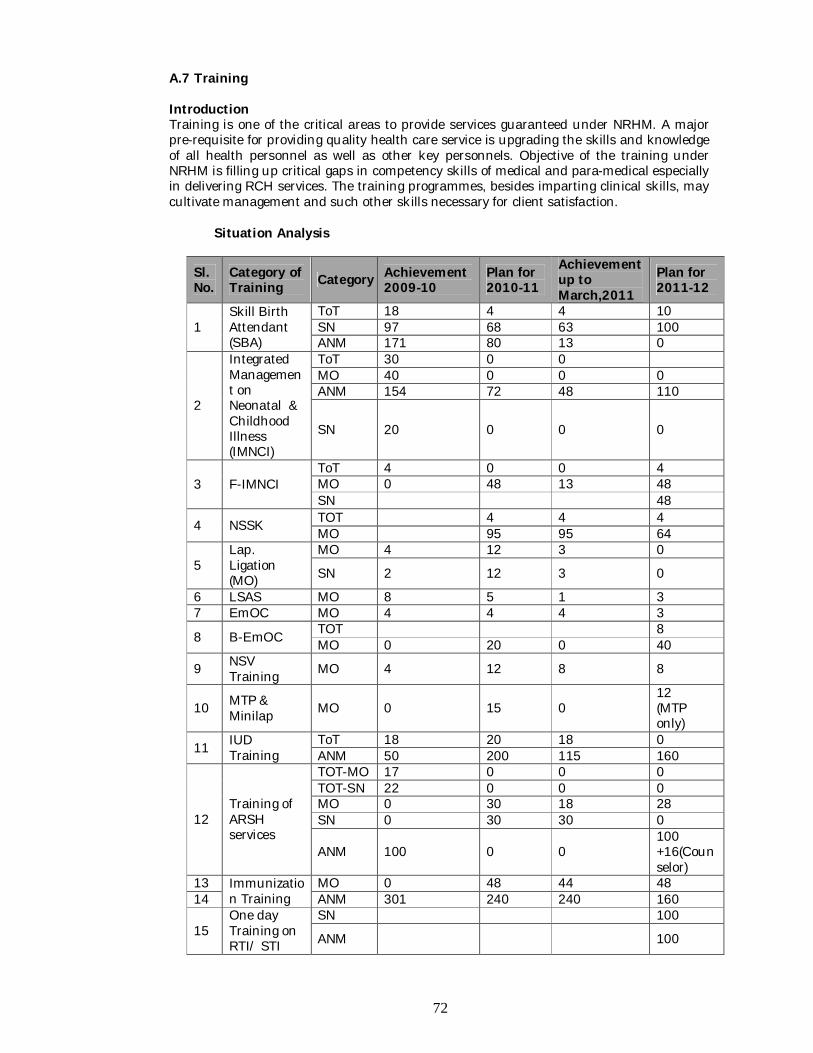
72
A.7 Training
Introduction Training is one of the critical areas to provide services guaranteed under NRHM. A major pre-requisite for providing quality health care service is upgrading the skills and knowledge of all health personnel as well as other key personnels. Objective of the training under NRHM is filling up critical gaps in competency skills of medical and para-medical especially in delivering RCH services. The training programmes, besides imparting clinical skills, may cultivate management and such other skills necessary for client satisfaction.
Situation Analysis
Sl. No.
Category of Training Category Achievement
2009-10 Plan for 2010-11
Achievement up to March,2011
Plan for 2011-12
1 Skill Birth Attendant (SBA)
ToT 18 4 4 10 SN 97 68 63 100 ANM 171 80 13 0
2
Integrated Management on Neonatal & Childhood Illness (IMNCI)
ToT 30 0 0 MO 40 0 0 0 ANM 154 72 48 110
SN 20 0 0 0
3 F-IMNCI ToT 4 0 0 4 MO 0 48 13 48 SN 48
4 NSSK TOT 4 4 4 MO 95 95 64
5 Lap. Ligation (MO)
MO 4 12 3 0
SN 2 12 3 0
6 LSAS MO 8 5 1 3 7 EmOC MO 4 4 4 3
8 B-EmOC TOT 8 MO 0 20 0 40
9 NSV Training MO 4 12 8 8
10 MTP & Minilap MO 0 15 0
12 (MTP only)
11 IUD Training
ToT 18 20 18 0 ANM 50 200 115 160
12 Training of ARSH services
TOT-MO 17 0 0 0 TOT-SN 22 0 0 0 MO 0 30 18 28 SN 0 30 30 0
ANM 100 0 0 100 +16(Counselor)
13 Immunization Training
MO 0 48 44 48 14 ANM 301 240 240 160
15 One day Training on RTI/ STI
SN 100
ANM 100
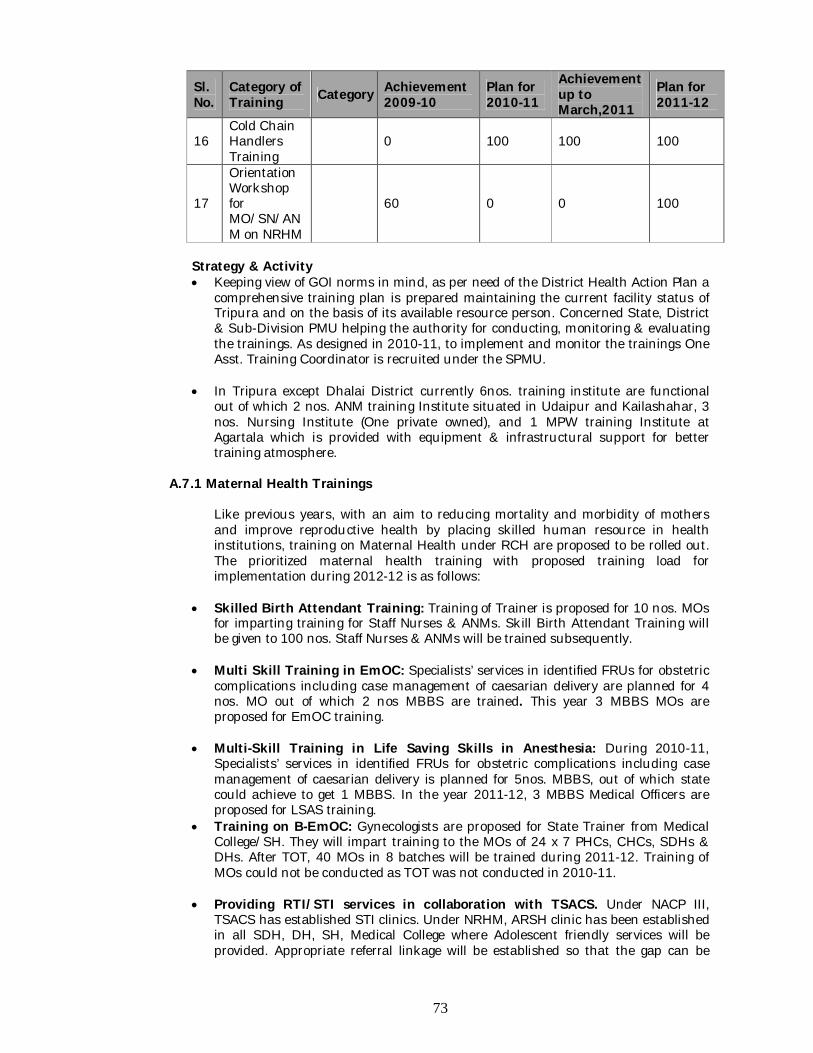
73
Sl. No.
Category of Training Category Achievement
2009-10 Plan for 2010-11
Achievement up to March,2011
Plan for 2011-12
16 Cold Chain Handlers Training
0 100 100 100
17
Orientation Workshop for MO/SN/ANM on NRHM
60 0 0 100
Strategy & Activity Keeping view of GOI norms in mind, as per need of the District Health Action Plan a
comprehensive training plan is prepared maintaining the current facility status of Tripura and on the basis of its available resource person. Concerned State, District & Sub-Division PMU helping the authority for conducting, monitoring & evaluating the trainings. As designed in 2010-11, to implement and monitor the trainings One Asst. Training Coordinator is recruited under the SPMU.
In Tripura except Dhalai District currently 6nos. training institute are functional out of which 2 nos. ANM training Institute situated in Udaipur and Kailashahar, 3 nos. Nursing Institute (One private owned), and 1 MPW training Institute at Agartala which is provided with equipment & infrastructural support for better training atmosphere.
A.7.1 Maternal Health Trainings
Like previous years, with an aim to reducing mortality and morbidity of mothers and improve reproductive health by placing skilled human resource in health institutions, training on Maternal Health under RCH are proposed to be rolled out. The prioritized maternal health training with proposed training load for implementation during 2012-12 is as follows:
Skilled Birth Attendant Training: Training of Trainer is proposed for 10 nos. MOs
for imparting training for Staff Nurses & ANMs. Skill Birth Attendant Training will be given to 100 nos. Staff Nurses & ANMs will be trained subsequently.
Multi Skill Training in EmOC: Specialists’ services in identified FRUs for obstetric complications including case management of caesarian delivery are planned for 4 nos. MO out of which 2 nos MBBS are trained. This year 3 MBBS MOs are proposed for EmOC training.
Multi-Skill Training in Life Saving Skills in Anesthesia: During 2010-11, Specialists’ services in identified FRUs for obstetric complications including case management of caesarian delivery is planned for 5nos. MBBS, out of which state could achieve to get 1 MBBS. In the year 2011-12, 3 MBBS Medical Officers are proposed for LSAS training.
Training on B-EmOC: Gynecologists are proposed for State Trainer from Medical College/SH. They will impart training to the MOs of 24 x 7 PHCs, CHCs, SDHs & DHs. After TOT, 40 MOs in 8 batches will be trained during 2011-12. Training of MOs could not be conducted as TOT was not conducted in 2010-11.
Providing RTI/STI services in collaboration with TSACS. Under NACP III, TSACS has established STI clinics. Under NRHM, ARSH clinic has been established in all SDH, DH, SH, Medical College where Adolescent friendly services will be provided. Appropriate referral linkage will be established so that the gap can be
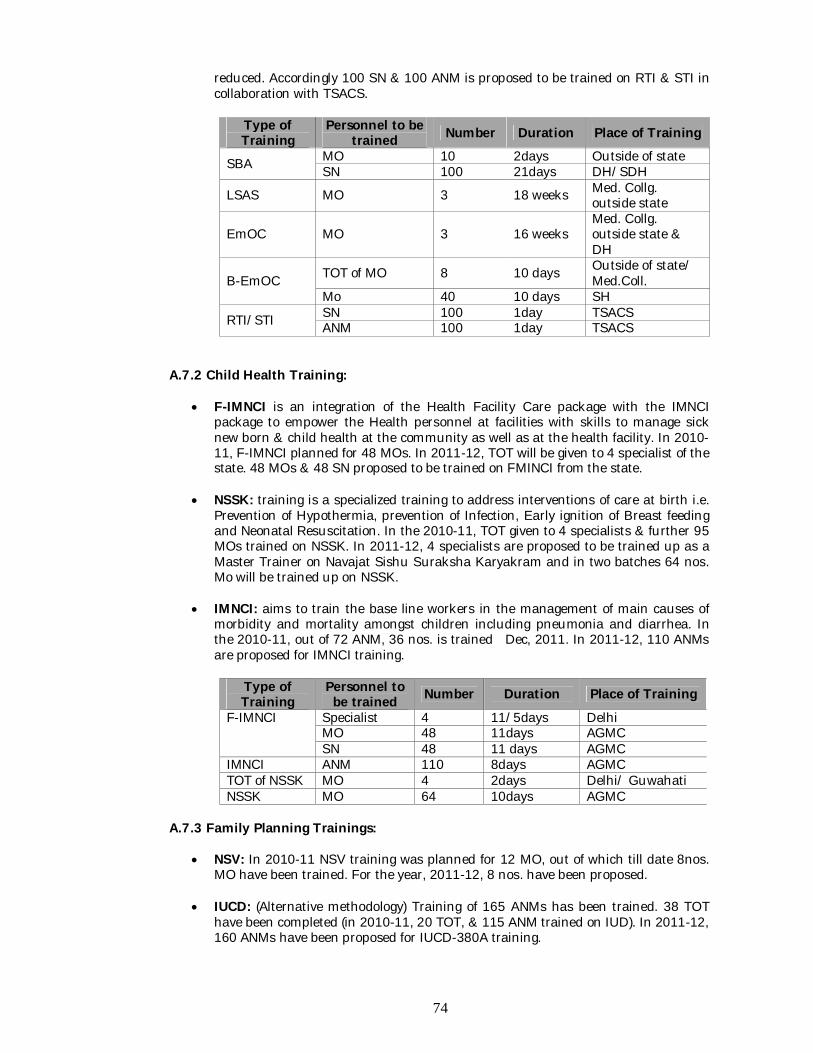
74
reduced. Accordingly 100 SN & 100 ANM is proposed to be trained on RTI & STI in collaboration with TSACS.
Type of Training
Personnel to be trained Number Duration Place of Training
SBA MO 10 2days Outside of state SN 100 21days DH/SDH
LSAS MO 3 18 weeks Med. Collg. outside state
EmOC MO 3 16 weeks Med. Collg. outside state & DH
B-EmOC TOT of MO 8 10 days Outside of state/ Med.Coll.
Mo 40 10 days SH
RTI/STI SN 100 1day TSACS ANM 100 1day TSACS
A.7.2 Child Health Training:
F-IMNCI is an integration of the Health Facility Care package with the IMNCI package to empower the Health personnel at facilities with skills to manage sick new born & child health at the community as well as at the health facility. In 2010-11, F-IMNCI planned for 48 MOs. In 2011-12, TOT will be given to 4 specialist of the state. 48 MOs & 48 SN proposed to be trained on FMINCI from the state.
NSSK: training is a specialized training to address interventions of care at birth i.e. Prevention of Hypothermia, prevention of Infection, Early ignition of Breast feeding and Neonatal Resuscitation. In the 2010-11, TOT given to 4 specialists & further 95 MOs trained on NSSK. In 2011-12, 4 specialists are proposed to be trained up as a Master Trainer on Navajat Sishu Suraksha Karyakram and in two batches 64 nos. Mo will be trained up on NSSK.
IMNCI: aims to train the base line workers in the management of main causes of morbidity and mortality amongst children including pneumonia and diarrhea. In the 2010-11, out of 72 ANM, 36 nos. is trained Dec, 2011. In 2011-12, 110 ANMs are proposed for IMNCI training.
Type of Training
Personnel to be trained Number Duration Place of Training
F-IMNCI Specialist 4 11/5days Delhi MO 48 11days AGMC SN 48 11 days AGMC
IMNCI ANM 110 8days AGMC TOT of NSSK MO 4 2days Delhi/ Guwahati NSSK MO 64 10days AGMC
A.7.3 Family Planning Trainings:
NSV: In 2010-11 NSV training was planned for 12 MO, out of which till date 8nos. MO have been trained. For the year, 2011-12, 8 nos. have been proposed.
IUCD: (Alternative methodology) Training of 165 ANMs has been trained. 38 TOT have been completed (in 2010-11, 20 TOT, & 115 ANM trained on IUD). In 2011-12, 160 ANMs have been proposed for IUCD-380A training.
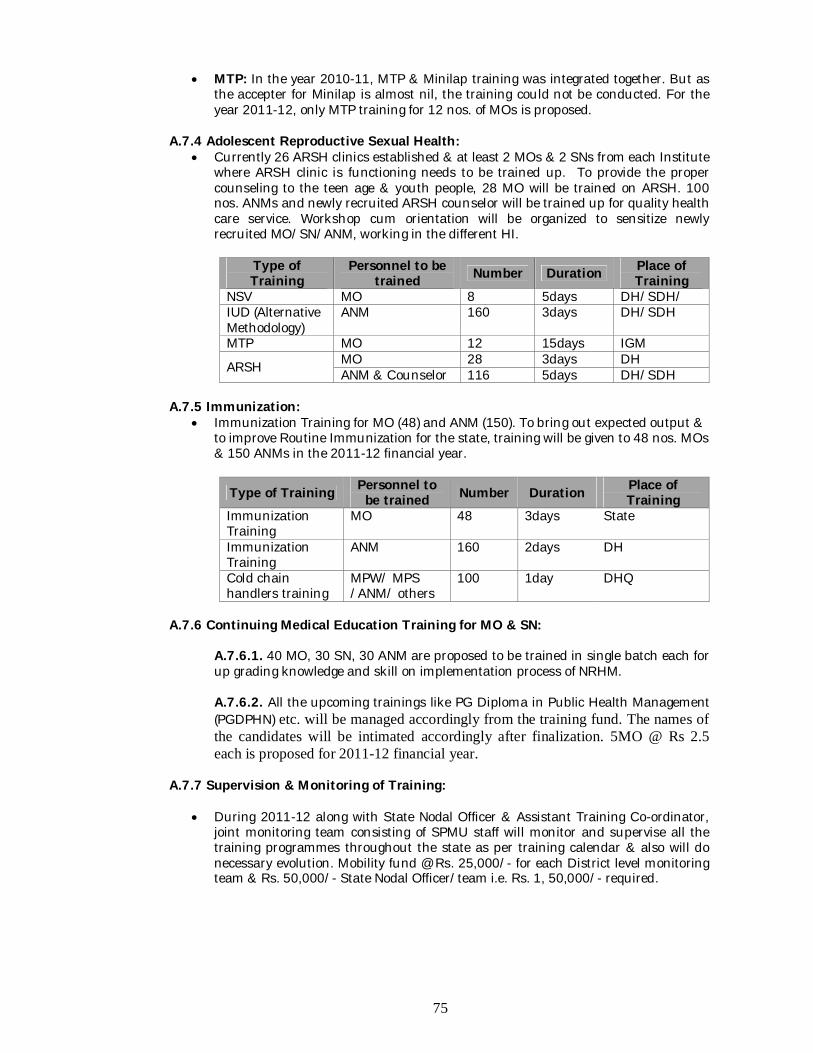
75
MTP: In the year 2010-11, MTP & Minilap training was integrated together. But as the accepter for Minilap is almost nil, the training could not be conducted. For the year 2011-12, only MTP training for 12 nos. of MOs is proposed.
A.7.4 Adolescent Reproductive Sexual Health:
Currently 26 ARSH clinics established & at least 2 MOs & 2 SNs from each Institute where ARSH clinic is functioning needs to be trained up. To provide the proper counseling to the teen age & youth people, 28 MO will be trained on ARSH. 100 nos. ANMs and newly recruited ARSH counselor will be trained up for quality health care service. Workshop cum orientation will be organized to sensitize newly recruited MO/SN/ANM, working in the different HI.
Type of Training
Personnel to be trained Number Duration Place of
Training NSV MO 8 5days DH/SDH/ IUD (Alternative Methodology)
ANM 160 3days DH/SDH
MTP MO 12 15days IGM
ARSH MO 28 3days DH ANM & Counselor 116 5days DH/SDH
A.7.5 Immunization:
Immunization Training for MO (48) and ANM (150). To bring out expected output & to improve Routine Immunization for the state, training will be given to 48 nos. MOs & 150 ANMs in the 2011-12 financial year.
Type of Training Personnel to be trained Number Duration Place of
Training Immunization Training
MO 48 3days State
Immunization Training
ANM 160 2days DH
Cold chain handlers training
MPW/ MPS /ANM/ others
100 1day DHQ
A.7.6 Continuing Medical Education Training for MO & SN:
A.7.6.1. 40 MO, 30 SN, 30 ANM are proposed to be trained in single batch each for up grading knowledge and skill on implementation process of NRHM. A.7.6.2. All the upcoming trainings like PG Diploma in Public Health Management (PGDPHN) etc. will be managed accordingly from the training fund. The names of the candidates will be intimated accordingly after finalization. 5MO @ Rs 2.5 each is proposed for 2011-12 financial year.
A.7.7 Supervision & Monitoring of Training:
During 2011-12 along with State Nodal Officer & Assistant Training Co-ordinator, joint monitoring team consisting of SPMU staff will monitor and supervise all the training programmes throughout the state as per training calendar & also will do necessary evolution. Mobility fund @ Rs. 25,000/- for each District level monitoring team & Rs. 50,000/- State Nodal Officer/team i.e. Rs. 1, 50,000/- required.
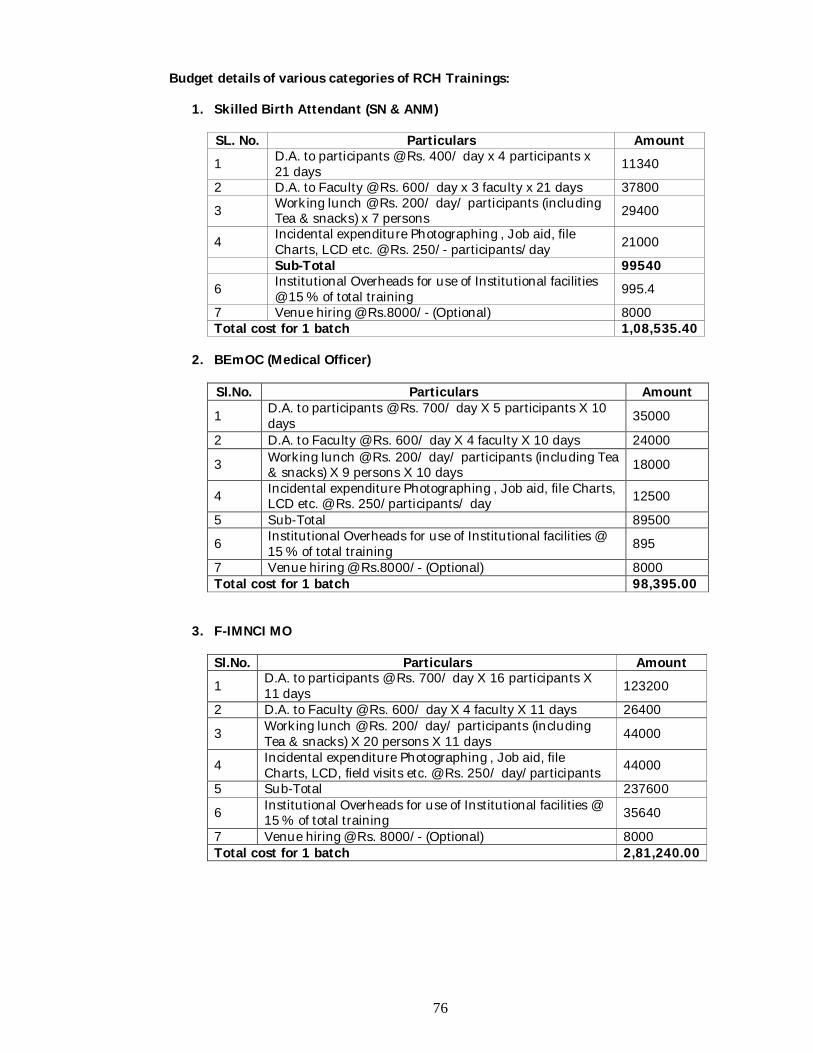
76
Budget details of various categories of RCH Trainings:
1. Skilled Birth Attendant (SN & ANM) SL. No. Particulars Amount 1 D.A. to participants @ Rs. 400/ day x 4 participants x
21 days 11340
2 D.A. to Faculty @ Rs. 600/ day x 3 faculty x 21 days 37800
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) x 7 persons 29400
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/- participants/day 21000
Sub-Total 99540 6 Institutional Overheads for use of Institutional facilities
@ 15 % of total training 995.4
7 Venue hiring @ Rs.8000/- (Optional) 8000 Total cost for 1 batch 1,08,535.40
2. BEmOC (Medical Officer)
Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 700/ day X 5 participants X 10 days 35000
2 D.A. to Faculty @ Rs. 600/ day X 4 faculty X 10 days 24000
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 9 persons X 10 days 18000
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/ day 12500
5 Sub-Total 89500
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 895
7 Venue hiring @ Rs.8000/- (Optional) 8000 Total cost for 1 batch 98,395.00
3. F-IMNCI MO Sl.No. Particulars Amount 1 D.A. to participants @ Rs. 700/ day X 16 participants X
11 days 123200
2 D.A. to Faculty @ Rs. 600/ day X 4 faculty X 11 days 26400
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 20 persons X 11 days 44000
4 Incidental expenditure Photographing , Job aid, file Charts, LCD, field visits etc. @ Rs. 250/ day/participants 44000
5 Sub-Total 237600
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 35640
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 2,81,240.00
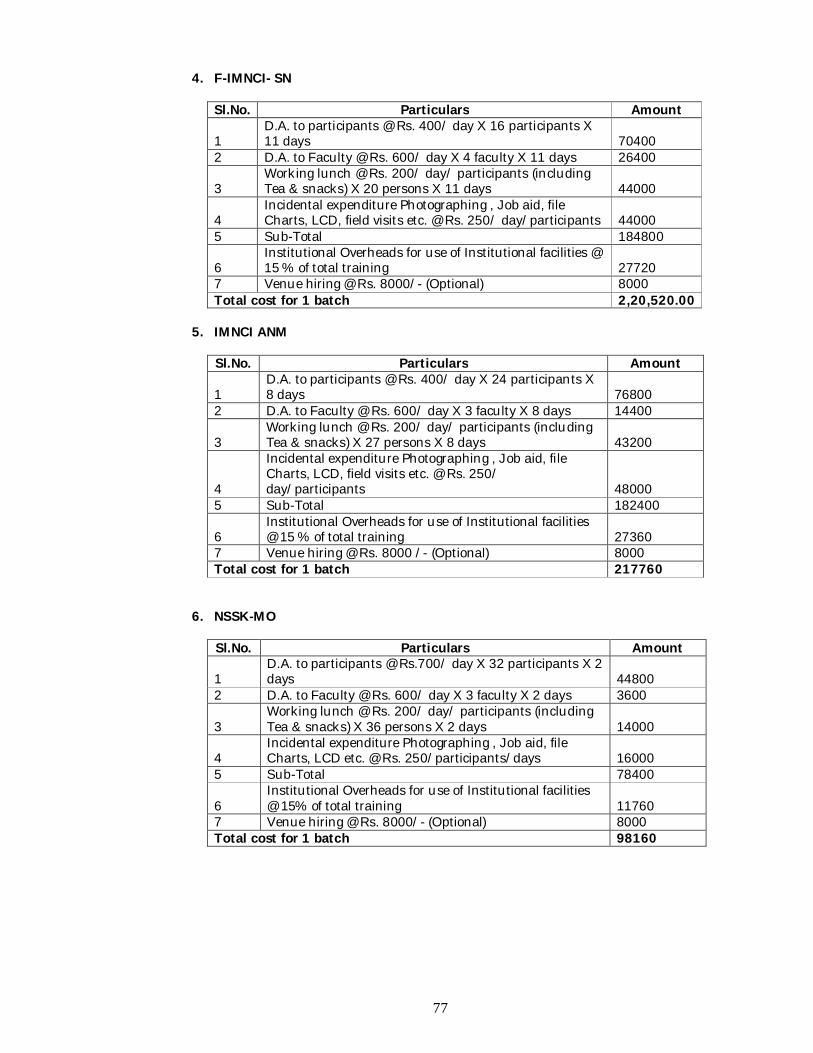
77
4. F-IMNCI- SN Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 400/ day X 16 participants X 11 days 70400
2 D.A. to Faculty @ Rs. 600/ day X 4 faculty X 11 days 26400
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 20 persons X 11 days 44000
4 Incidental expenditure Photographing , Job aid, file Charts, LCD, field visits etc. @ Rs. 250/ day/participants 44000
5 Sub-Total 184800
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 27720
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 2,20,520.00
5. IMNCI ANM
Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 400/ day X 24 participants X 8 days 76800
2 D.A. to Faculty @ Rs. 600/ day X 3 faculty X 8 days 14400
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 27 persons X 8 days 43200
4
Incidental expenditure Photographing , Job aid, file Charts, LCD, field visits etc. @ Rs. 250/ day/participants 48000
5 Sub-Total 182400
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 27360
7 Venue hiring @ Rs. 8000 /- (Optional) 8000 Total cost for 1 batch 217760
6. NSSK-MO Sl.No. Particulars Amount
1 D.A. to participants @ Rs.700/ day X 32 participants X 2 days 44800
2 D.A. to Faculty @ Rs. 600/ day X 3 faculty X 2 days 3600
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 36 persons X 2 days 14000
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/days 16000
5 Sub-Total 78400
6 Institutional Overheads for use of Institutional facilities @ 15% of total training 11760
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 98160
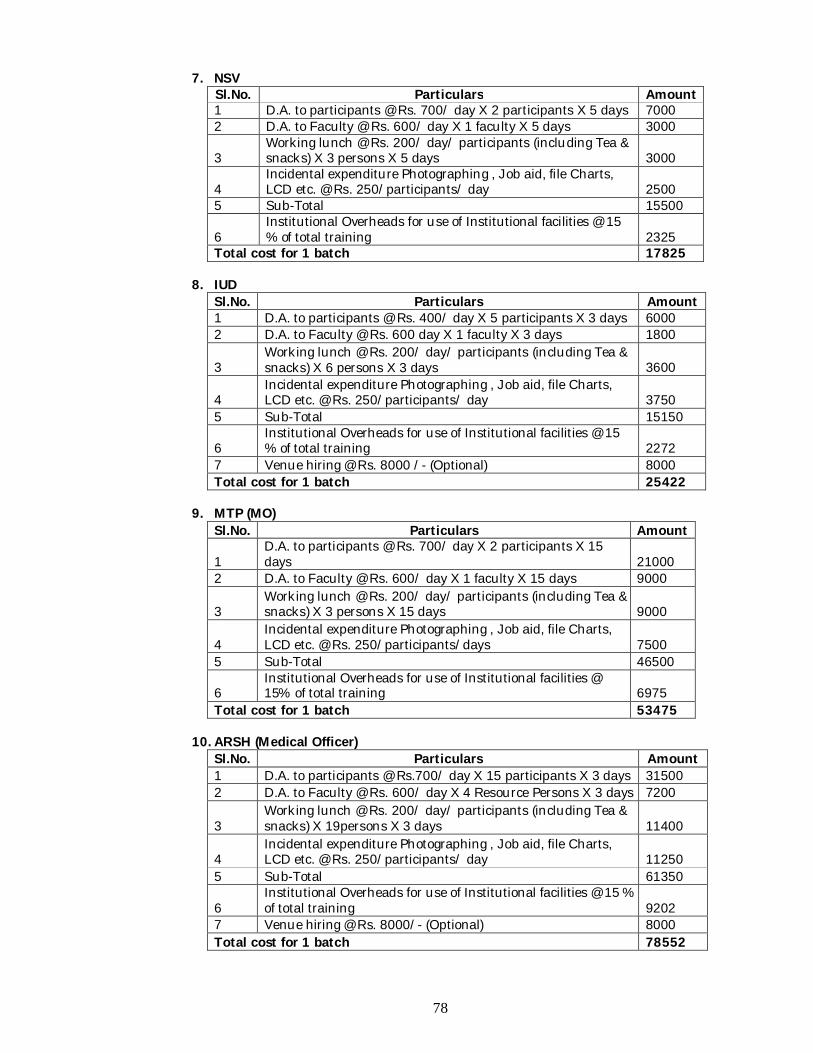
78
7. NSV Sl.No. Particulars Amount 1 D.A. to participants @ Rs. 700/ day X 2 participants X 5 days 7000 2 D.A. to Faculty @ Rs. 600/ day X 1 faculty X 5 days 3000
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 3 persons X 5 days 3000
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/ day 2500
5 Sub-Total 15500
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 2325
Total cost for 1 batch 17825
8. IUD Sl.No. Particulars Amount 1 D.A. to participants @ Rs. 400/ day X 5 participants X 3 days 6000 2 D.A. to Faculty @ Rs. 600 day X 1 faculty X 3 days 1800
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 6 persons X 3 days 3600
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/ day 3750
5 Sub-Total 15150
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 2272
7 Venue hiring @ Rs. 8000 /- (Optional) 8000 Total cost for 1 batch 25422
9. MTP (MO)
Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 700/ day X 2 participants X 15 days 21000
2 D.A. to Faculty @ Rs. 600/ day X 1 faculty X 15 days 9000
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 3 persons X 15 days 9000
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/days 7500
5 Sub-Total 46500
6 Institutional Overheads for use of Institutional facilities @ 15% of total training 6975
Total cost for 1 batch 53475
10. ARSH (Medical Officer) Sl.No. Particulars Amount 1 D.A. to participants @ Rs.700/ day X 15 participants X 3 days 31500 2 D.A. to Faculty @ Rs. 600/ day X 4 Resource Persons X 3 days 7200
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 19persons X 3 days 11400
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/ day 11250
5 Sub-Total 61350
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 9202
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 78552
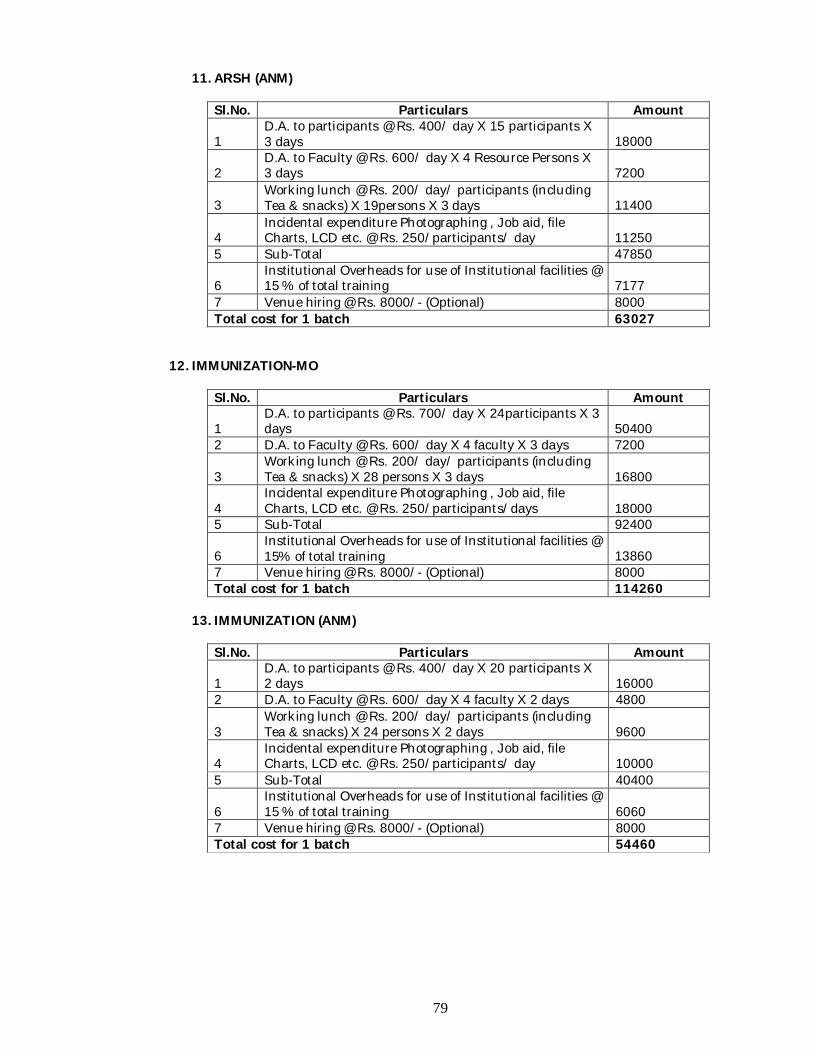
79
11. ARSH (ANM) Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 400/ day X 15 participants X 3 days 18000
2 D.A. to Faculty @ Rs. 600/ day X 4 Resource Persons X 3 days 7200
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 19persons X 3 days 11400
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/ day 11250
5 Sub-Total 47850
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 7177
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 63027
12. IMMUNIZATION-MO
Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 700/ day X 24participants X 3 days 50400
2 D.A. to Faculty @ Rs. 600/ day X 4 faculty X 3 days 7200
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 28 persons X 3 days 16800
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/days 18000
5 Sub-Total 92400
6 Institutional Overheads for use of Institutional facilities @ 15% of total training 13860
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 114260
13. IMMUNIZATION (ANM)
Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 400/ day X 20 participants X 2 days 16000
2 D.A. to Faculty @ Rs. 600/ day X 4 faculty X 2 days 4800
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 24 persons X 2 days 9600
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/ day 10000
5 Sub-Total 40400
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 6060
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 54460
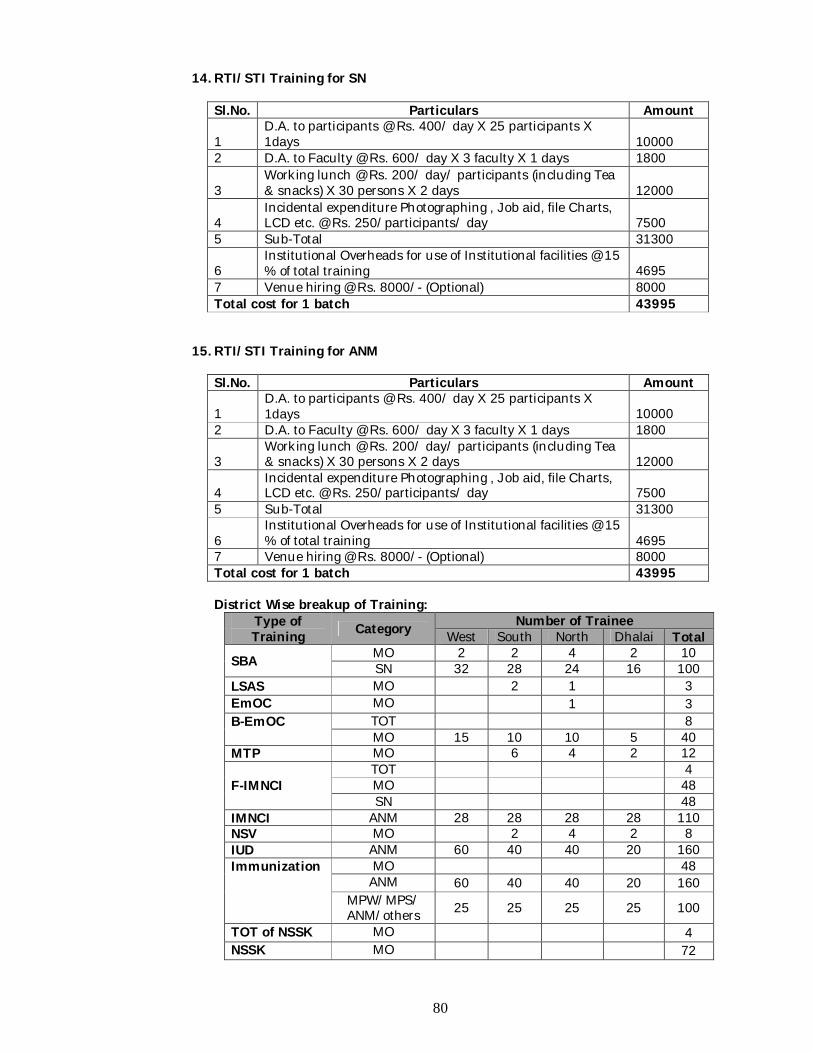
80
14. RTI/STI Training for SN Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 400/ day X 25 participants X 1days 10000
2 D.A. to Faculty @ Rs. 600/ day X 3 faculty X 1 days 1800
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 30 persons X 2 days 12000
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/ day 7500
5 Sub-Total 31300
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 4695
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 43995
15. RTI/STI Training for ANM Sl.No. Particulars Amount
1 D.A. to participants @ Rs. 400/ day X 25 participants X 1days 10000
2 D.A. to Faculty @ Rs. 600/ day X 3 faculty X 1 days 1800
3 Working lunch @ Rs. 200/ day/ participants (including Tea & snacks) X 30 persons X 2 days 12000
4 Incidental expenditure Photographing , Job aid, file Charts, LCD etc. @ Rs. 250/participants/ day 7500
5 Sub-Total 31300
6 Institutional Overheads for use of Institutional facilities @ 15 % of total training 4695
7 Venue hiring @ Rs. 8000/- (Optional) 8000 Total cost for 1 batch 43995
District Wise breakup of Training:
Type of Training Category Number of Trainee
West South North Dhalai Total
SBA MO 2 2 4 2 10 SN 32 28 24 16 100
LSAS MO 2 1 3 EmOC MO 1 3 B-EmOC TOT 8
MO 15 10 10 5 40 MTP MO 6 4 2 12
F-IMNCI TOT 4 MO 48 SN 48
IMNCI ANM 28 28 28 28 110 NSV MO 2 4 2 8 IUD ANM 60 40 40 20 160 Immunization MO 48
ANM 60 40 40 20 160 MPW/MPS/ ANM/others 25 25 25 25 100
TOT of NSSK MO 4 NSSK MO 72
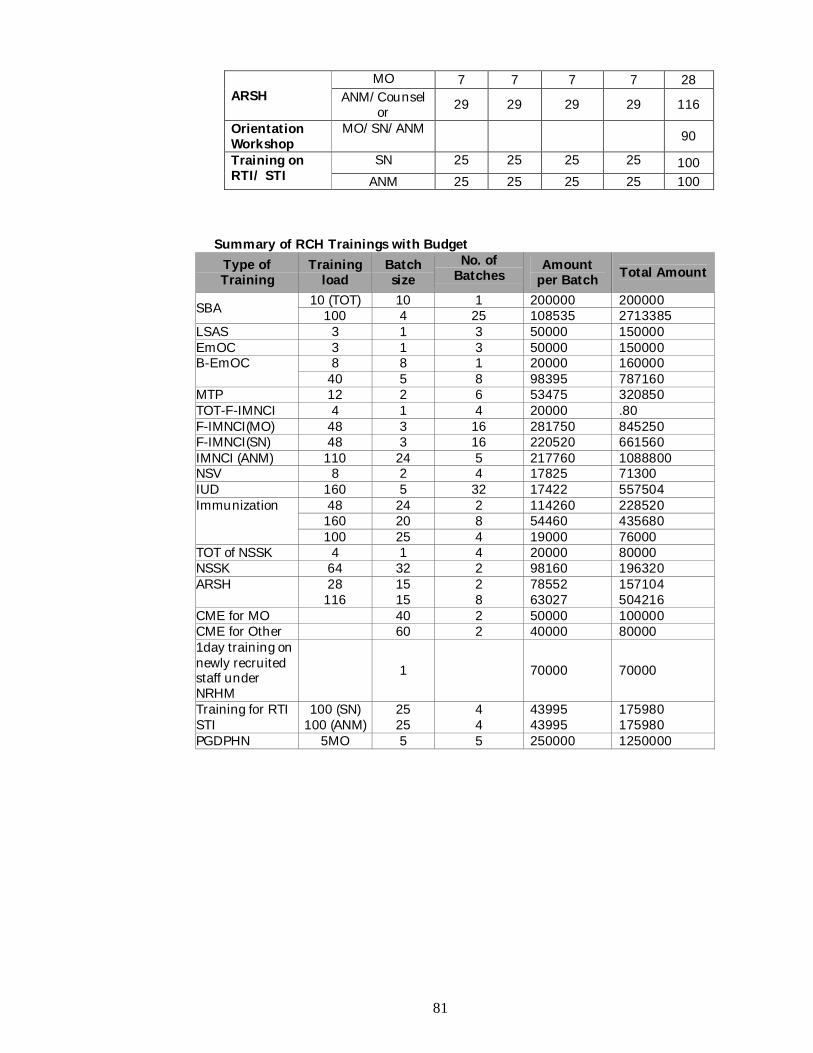
81
ARSH MO 7 7 7 7 28
ANM/Counselor 29 29 29 29 116
Orientation Workshop
MO/SN/ANM 90
Training on RTI/ STI
SN 25 25 25 25 100 ANM 25 25 25 25 100
Summary of RCH Trainings with Budget Type of Training
Training load
Batch size
No. of Batches
Amount per Batch Total Amount
SBA 10 (TOT) 10 1 200000 200000 100 4 25 108535 2713385
LSAS 3 1 3 50000 150000 EmOC 3 1 3 50000 150000 B-EmOC 8 8 1 20000 160000
40 5 8 98395 787160 MTP 12 2 6 53475 320850 TOT-F-IMNCI 4 1 4 20000 .80 F-IMNCI(MO) 48 3 16 281750 845250 F-IMNCI(SN) 48 3 16 220520 661560 IMNCI (ANM) 110 24 5 217760 1088800 NSV 8 2 4 17825 71300 IUD 160 5 32 17422 557504 Immunization 48 24 2 114260 228520
160 20 8 54460 435680 100 25 4 19000 76000
TOT of NSSK 4 1 4 20000 80000 NSSK 64 32 2 98160 196320 ARSH 28 15 2 78552 157104
116 15 8 63027 504216 CME for MO 40 2 50000 100000 CME for Other 60 2 40000 80000 1day training on newly recruited staff under NRHM
1
70000 70000
Training for RTI STI
100 (SN) 25 4 43995 175980 100 (ANM) 25 4 43995 175980
PGDPHN 5MO 5 5 250000 1250000
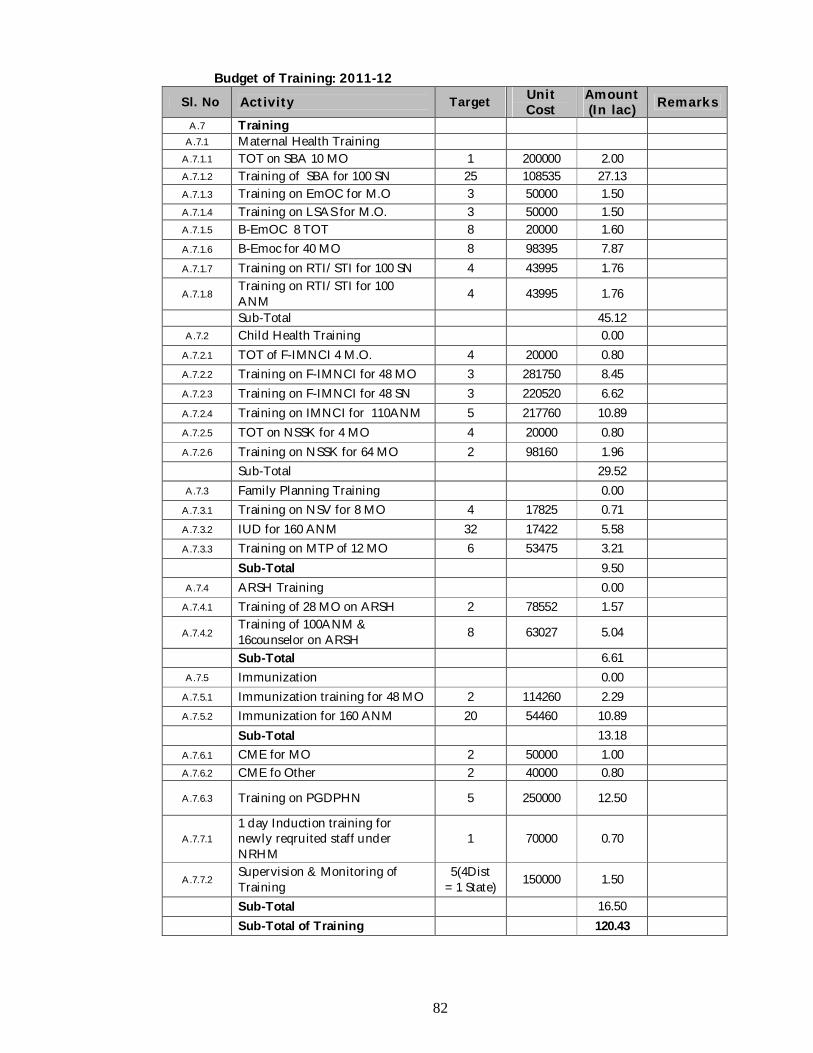
82
Budget of Training: 2011-12
Sl. No Activity Target Unit Cost
Amount (In lac) Remarks
A.7 Training A.7.1 Maternal Health Training
A.7.1.1 TOT on SBA 10 MO 1 200000 2.00
A.7.1.2 Training of SBA for 100 SN 25 108535 27.13
A.7.1.3 Training on EmOC for M.O 3 50000 1.50
A.7.1.4 Training on LSAS for M.O. 3 50000 1.50
A.7.1.5 B-EmOC 8 TOT 8 20000 1.60
A.7.1.6 B-Emoc for 40 MO 8 98395 7.87
A.7.1.7 Training on RTI/STI for 100 SN 4 43995 1.76
A.7.1.8 Training on RTI/STI for 100 ANM 4 43995 1.76
Sub-Total 45.12
A.7.2 Child Health Training 0.00
A.7.2.1 TOT of F-IMNCI 4 M.O. 4 20000 0.80
A.7.2.2 Training on F-IMNCI for 48 MO 3 281750 8.45
A.7.2.3 Training on F-IMNCI for 48 SN 3 220520 6.62
A.7.2.4 Training on IMNCI for 110ANM 5 217760 10.89
A.7.2.5 TOT on NSSK for 4 MO 4 20000 0.80
A.7.2.6 Training on NSSK for 64 MO 2 98160 1.96
Sub-Total 29.52
A.7.3 Family Planning Training 0.00
A.7.3.1 Training on NSV for 8 MO 4 17825 0.71
A.7.3.2 IUD for 160 ANM 32 17422 5.58
A.7.3.3 Training on MTP of 12 MO 6 53475 3.21
Sub-Total 9.50
A.7.4 ARSH Training 0.00
A.7.4.1 Training of 28 MO on ARSH 2 78552 1.57
A.7.4.2 Training of 100ANM & 16counselor on ARSH 8 63027 5.04
Sub-Total 6.61
A.7.5 Immunization 0.00
A.7.5.1 Immunization training for 48 MO 2 114260 2.29
A.7.5.2 Immunization for 160 ANM 20 54460 10.89
Sub-Total 13.18
A.7.6.1 CME for MO 2 50000 1.00
A.7.6.2 CME fo Other 2 40000 0.80
A.7.6.3 Training on PGDPHN 5 250000 12.50
A.7.7.1 1 day Induction training for newly reqruited staff under NRHM
1 70000 0.70
A.7.7.2 Supervision & Monitoring of Training
5(4Dist = 1 State) 150000 1.50
Sub-Total 16.50
Sub-Total of Training 120.43
83
A.8 Programme Management
Introduction For better execution of projected schemes/ programmes, Programme Managements have been established at State and District level under NRHM. Further to this, there are Sub-divisional Programme Management Units in each 17 Sub-divisions as well as Assistants in each PHC/ CHC of the state. Like previous years it is proposed for their continuation of engagement to implement NRHM activities effectively. Programme Management Units and its structure with requisition for the FY: 2011-12 is proposed for strengthening accordingly.
Goal Strengthening the State & District & Sub-district management units
Objectives 1. Contractual engagement of personnel and their continuation of services at
SPMSU, DPMSU, SDPMSU and at PHC/ CHC. 2. Support operationalising the State & District & Sub-district offices with articles/
equipments and vehicle hiring. Strategies & Activities A.8.1 State Programme Management Support Unit (SPMSU) The State Health & Family Welfare Society, Tripura has been constituted with an aim to provide additional technical and managerial capacity to Health & Family Welfare Department under NRHM. In course of time, State Health & Family Welfare Society, Tripura assessed the need for additional manpower to the existing Programme Manager, Manager-MIS, Finance & Accounts, Mass Media & NGO Coordinator and few Office Assistants for timely execution of projected activities as well as better functioning of the SPMSU. To strengthen SPMSU, functioning under State Health & Family Welfare Society & to facilitate in advancing systemic changes in health sector and support the planning process & implementation process to meet the goals and objectives of the Society some expert hands recruited from different backgrounds. Followings are the ranks:
Sl. No. Name of the Post Staff in
position Remarks
1 Medical Officer RCH and Family Welfare 1 Budgeted
under SPMU 2 Consultant SH&FWS 1 3 Consultant Adolescent Coordinator 1
Proposed Major Terms of Reference of SPMSU
Support strengthening the SPMSU which is the Secretariat to the State Health & Family Welfare Society, Tripura as well as State Rural Health Mission by organizing its half yearly review meetings.
Compare and contrast best practices in other states for adoption. Advancing systemic changes in health sector through continuous Research &
Evaluation of the ongoing and past programmes implemented under NRHM. Other Proposed Ancillary Activities of SPMSU
To function as State FMG. Secretarial function to the Society. Documentation of special projects and schemes.
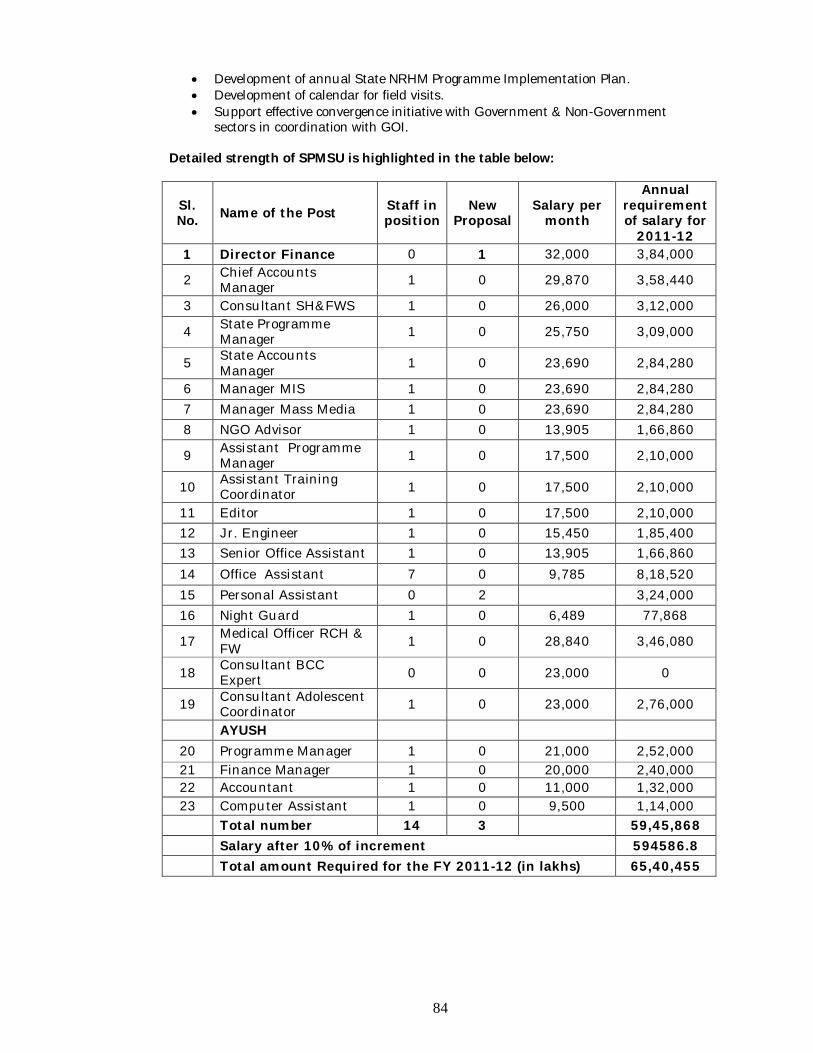
84
Development of annual State NRHM Programme Implementation Plan. Development of calendar for field visits. Support effective convergence initiative with Government & Non-Government
sectors in coordination with GOI. Detailed strength of SPMSU is highlighted in the table below:
Sl. No. Name of the Post Staff in
position New
Proposal Salary per
month
Annual requirement of salary for
2011-12 1 Director Finance 0 1 32,000 3,84,000
2 Chief Accounts Manager 1 0 29,870 3,58,440
3 Consultant SH&FWS 1 0 26,000 3,12,000
4 State Programme Manager 1 0 25,750 3,09,000
5 State Accounts Manager 1 0 23,690 2,84,280
6 Manager MIS 1 0 23,690 2,84,280 7 Manager Mass Media 1 0 23,690 2,84,280 8 NGO Advisor 1 0 13,905 1,66,860
9 Assistant Programme Manager 1 0 17,500 2,10,000
10 Assistant Training Coordinator 1 0 17,500 2,10,000
11 Editor 1 0 17,500 2,10,000 12 Jr. Engineer 1 0 15,450 1,85,400 13 Senior Office Assistant 1 0 13,905 1,66,860 14 Office Assistant 7 0 9,785 8,18,520 15 Personal Assistant 0 2 3,24,000 16 Night Guard 1 0 6,489 77,868
17 Medical Officer RCH & FW 1 0 28,840 3,46,080
18 Consultant BCC Expert 0 0 23,000 0
19 Consultant Adolescent Coordinator 1 0 23,000 2,76,000
AYUSH 20 Programme Manager 1 0 21,000 2,52,000 21 Finance Manager 1 0 20,000 2,40,000 22 Accountant 1 0 11,000 1,32,000 23 Computer Assistant 1 0 9,500 1,14,000 Total number 14 3 59,45,868 Salary after 10% of increment 594586.8 Total amount Required for the FY 2011-12 (in lakhs) 65,40,455
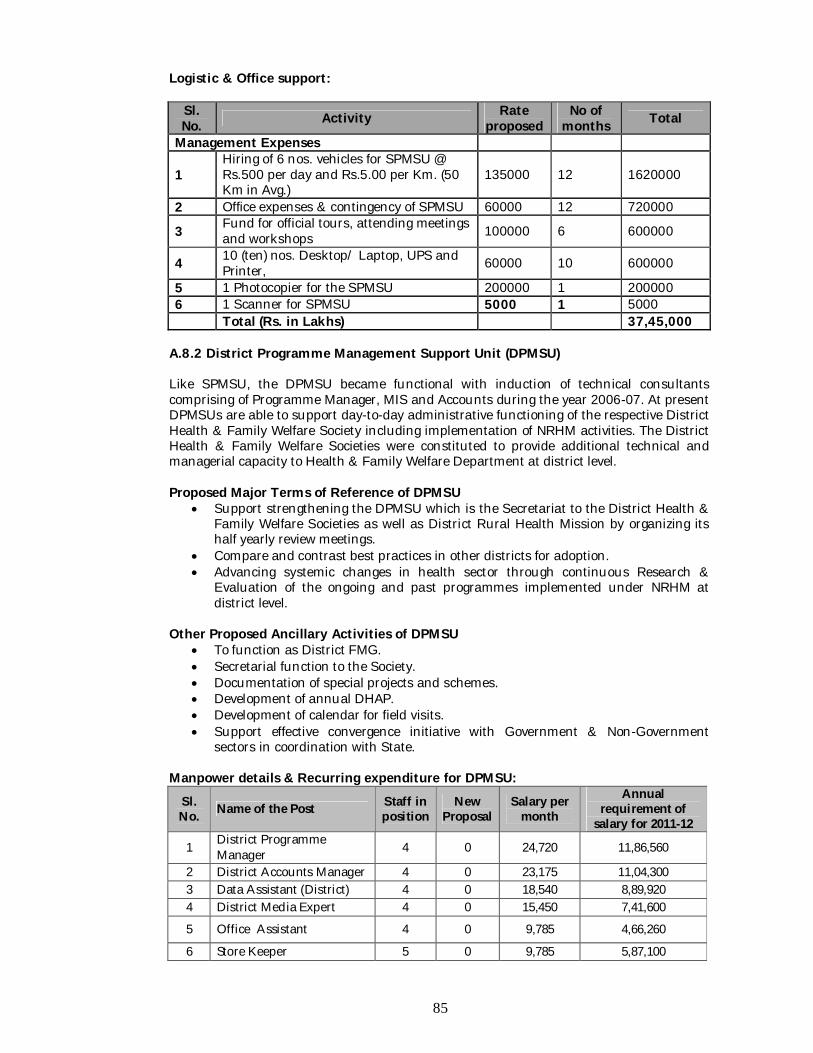
85
Logistic & Office support:
Sl. No. Activity Rate
proposed No of
months Total
Management Expenses
1 Hiring of 6 nos. vehicles for SPMSU @ Rs.500 per day and Rs.5.00 per Km. (50 Km in Avg.)
135000 12 1620000
2 Office expenses & contingency of SPMSU 60000 12 720000
3 Fund for official tours, attending meetings and workshops 100000 6 600000
4 10 (ten) nos. Desktop/ Laptop, UPS and Printer, 60000 10 600000
5 1 Photocopier for the SPMSU 200000 1 200000 6 1 Scanner for SPMSU 5000 1 5000 Total (Rs. in Lakhs) 37,45,000
A.8.2 District Programme Management Support Unit (DPMSU) Like SPMSU, the DPMSU became functional with induction of technical consultants comprising of Programme Manager, MIS and Accounts during the year 2006-07. At present DPMSUs are able to support day-to-day administrative functioning of the respective District Health & Family Welfare Society including implementation of NRHM activities. The District Health & Family Welfare Societies were constituted to provide additional technical and managerial capacity to Health & Family Welfare Department at district level. Proposed Major Terms of Reference of DPMSU
Support strengthening the DPMSU which is the Secretariat to the District Health & Family Welfare Societies as well as District Rural Health Mission by organizing its half yearly review meetings.
Compare and contrast best practices in other districts for adoption. Advancing systemic changes in health sector through continuous Research &
Evaluation of the ongoing and past programmes implemented under NRHM at district level.
Other Proposed Ancillary Activities of DPMSU
To function as District FMG. Secretarial function to the Society. Documentation of special projects and schemes. Development of annual DHAP. Development of calendar for field visits. Support effective convergence initiative with Government & Non-Government
sectors in coordination with State. Manpower details & Recurring expenditure for DPMSU:
Sl. No. Name of the Post Staff in
position New
Proposal Salary per
month
Annual requirement of
salary for 2011-12
1 District Programme Manager 4 0 24,720 11,86,560
2 District Accounts Manager 4 0 23,175 11,04,300 3 Data Assistant (District) 4 0 18,540 8,89,920 4 District Media Expert 4 0 15,450 7,41,600
5 Office Assistant 4 0 9,785 4,66,260
6 Store Keeper 5 0 9,785 5,87,100
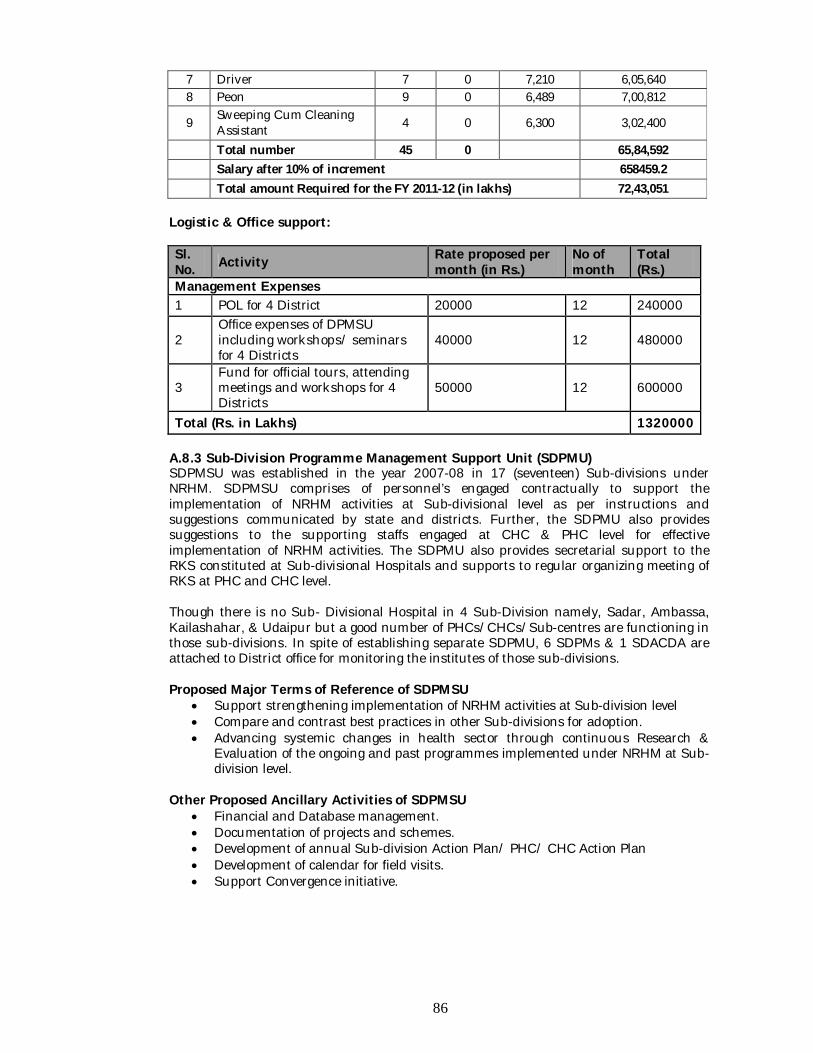
86
7 Driver 7 0 7,210 6,05,640 8 Peon 9 0 6,489 7,00,812
9 Sweeping Cum Cleaning Assistant 4 0 6,300 3,02,400
Total number 45 0 65,84,592 Salary after 10% of increment 658459.2 Total amount Required for the FY 2011-12 (in lakhs) 72,43,051
Logistic & Office support: Sl. No. Activity Rate proposed per
month (in Rs.) No of month
Total (Rs.)
Management Expenses 1 POL for 4 District 20000 12 240000
2 Office expenses of DPMSU including workshops/ seminars for 4 Districts
40000 12 480000
3 Fund for official tours, attending meetings and workshops for 4 Districts
50000 12 600000
Total (Rs. in Lakhs) 1320000 A.8.3 Sub-Division Programme Management Support Unit (SDPMU) SDPMSU was established in the year 2007-08 in 17 (seventeen) Sub-divisions under NRHM. SDPMSU comprises of personnel’s engaged contractually to support the implementation of NRHM activities at Sub-divisional level as per instructions and suggestions communicated by state and districts. Further, the SDPMU also provides suggestions to the supporting staffs engaged at CHC & PHC level for effective implementation of NRHM activities. The SDPMU also provides secretarial support to the RKS constituted at Sub-divisional Hospitals and supports to regular organizing meeting of RKS at PHC and CHC level. Though there is no Sub- Divisional Hospital in 4 Sub-Division namely, Sadar, Ambassa, Kailashahar, & Udaipur but a good number of PHCs/CHCs/Sub-centres are functioning in those sub-divisions. In spite of establishing separate SDPMU, 6 SDPMs & 1 SDACDA are attached to District office for monitoring the institutes of those sub-divisions. Proposed Major Terms of Reference of SDPMSU
Support strengthening implementation of NRHM activities at Sub-division level Compare and contrast best practices in other Sub-divisions for adoption. Advancing systemic changes in health sector through continuous Research &
Evaluation of the ongoing and past programmes implemented under NRHM at Sub-division level.
Other Proposed Ancillary Activities of SDPMSU
Financial and Database management. Documentation of projects and schemes. Development of annual Sub-division Action Plan/ PHC/ CHC Action Plan Development of calendar for field visits. Support Convergence initiative.
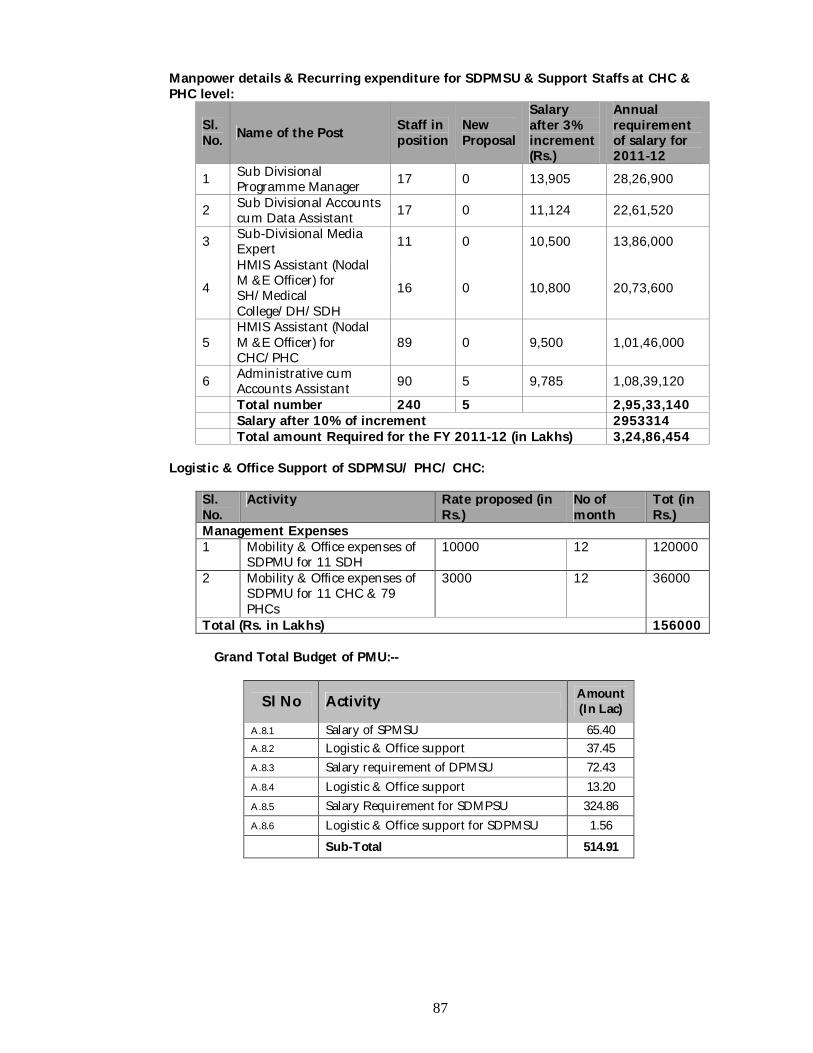
87
Manpower details & Recurring expenditure for SDPMSU & Support Staffs at CHC & PHC level:
Sl. No. Name of the Post Staff in
position New Proposal
Salary after 3% increment (Rs.)
Annual requirement of salary for 2011-12
1 Sub Divisional Programme Manager 17 0 13,905 28,26,900
2 Sub Divisional Accounts cum Data Assistant 17 0 11,124 22,61,520
3 Sub-Divisional Media Expert 11 0 10,500 13,86,000
4
HMIS Assistant (Nodal M &E Officer) for SH/Medical College/DH/SDH
16 0 10,800 20,73,600
5 HMIS Assistant (Nodal M &E Officer) for CHC/PHC
89 0 9,500 1,01,46,000
6 Administrative cum Accounts Assistant 90 5 9,785 1,08,39,120
Total number 240 5 2,95,33,140 Salary after 10% of increment 2953314 Total amount Required for the FY 2011-12 (in Lakhs) 3,24,86,454
Logistic & Office Support of SDPMSU/ PHC/ CHC:
Sl. No.
Activity Rate proposed (in Rs.)
No of month
Tot (in Rs.)
Management Expenses 1 Mobility & Office expenses of
SDPMU for 11 SDH 10000 12 120000
2 Mobility & Office expenses of SDPMU for 11 CHC & 79 PHCs
3000 12 36000
Total (Rs. in Lakhs) 156000
Grand Total Budget of PMU:--
Sl No Activity Amount (In Lac)
A.8.1 Salary of SPMSU 65.40 A.8.2 Logistic & Office support 37.45 A.8.3 Salary requirement of DPMSU 72.43 A.8.4 Logistic & Office support 13.20 A.8.5 Salary Requirement for SDMPSU 324.86 A.8.6 Logistic & Office support for SDPMSU 1.56 Sub-Total 514.91
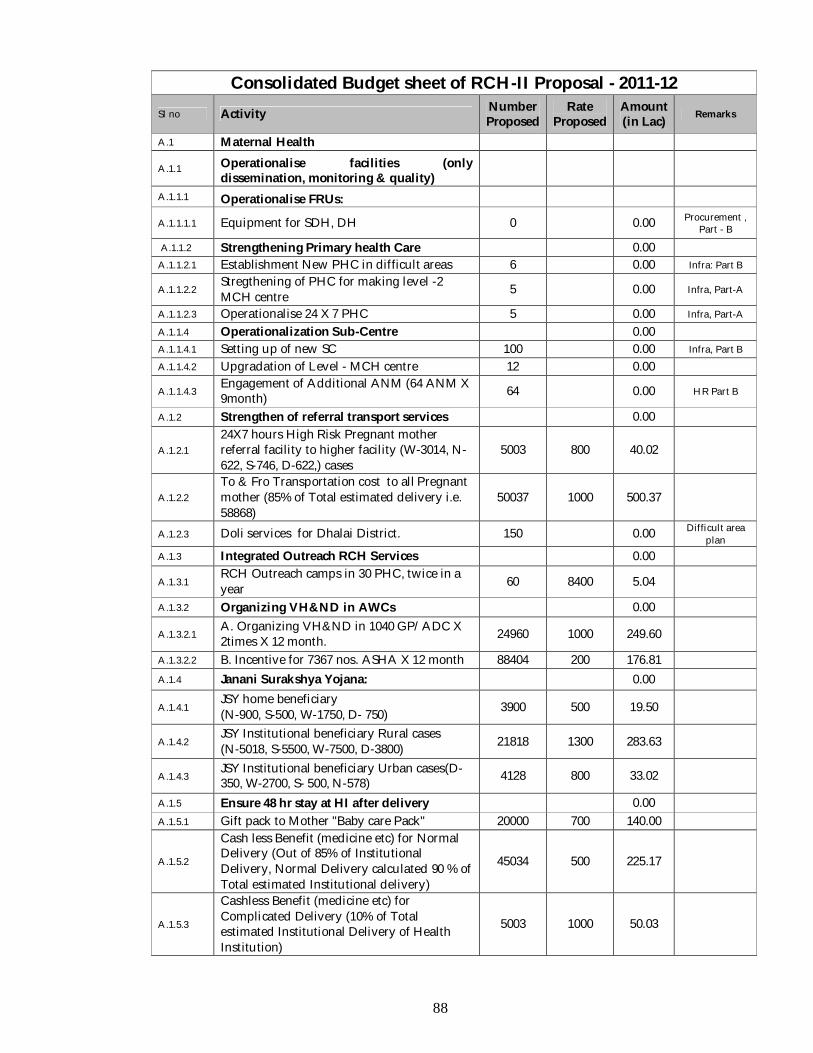
88
Consolidated Budget sheet of RCH-II Proposal - 2011-12 Sl no Activity Number
Proposed Rate
Proposed Amount (in Lac) Remarks
A.1 Maternal Health
A.1.1 Operationalise facilities (only dissemination, monitoring & quality)
A.1.1.1 Operationalise FRUs:
A.1.1.1.1 Equipment for SDH, DH 0 0.00 Procurement , Part - B
A.1.1.2 Strengthening Primary health Care 0.00
A.1.1.2.1 Establishment New PHC in difficult areas 6 0.00 Infra: Part B
A.1.1.2.2 Stregthening of PHC for making level -2 MCH centre 5 0.00 Infra, Part-A
A.1.1.2.3 Operationalise 24 X 7 PHC 5 0.00 Infra, Part-A
A.1.1.4 Operationalization Sub-Centre 0.00
A.1.1.4.1 Setting up of new SC 100 0.00 Infra, Part B
A.1.1.4.2 Upgradation of Level - MCH centre 12 0.00
A.1.1.4.3 Engagement of Additional ANM (64 ANM X 9month) 64 0.00 HR Part B
A.1.2 Strengthen of referral transport services 0.00
A.1.2.1 24X7 hours High Risk Pregnant mother referral facility to higher facility (W-3014, N-622, S-746, D-622,) cases
5003 800 40.02
A.1.2.2 To & Fro Transportation cost to all Pregnant mother (85% of Total estimated delivery i.e. 58868)
50037 1000 500.37
A.1.2.3 Doli services for Dhalai District. 150 0.00 Difficult area plan
A.1.3 Integrated Outreach RCH Services 0.00
A.1.3.1 RCH Outreach camps in 30 PHC, twice in a year 60 8400 5.04
A.1.3.2 Organizing VH&ND in AWCs 0.00
A.1.3.2.1 A. Organizing VH&ND in 1040 GP/ADC X 2times X 12 month. 24960 1000 249.60
A.1.3.2.2 B. Incentive for 7367 nos. ASHA X 12 month 88404 200 176.81
A.1.4 Janani Surakshya Yojana: 0.00
A.1.4.1 JSY home beneficiary (N-900, S-500, W-1750, D- 750) 3900 500 19.50
A.1.4.2 JSY Institutional beneficiary Rural cases (N-5018, S-5500, W-7500, D-3800) 21818 1300 283.63
A.1.4.3 JSY Institutional beneficiary Urban cases(D-350, W-2700, S- 500, N-578) 4128 800 33.02
A.1.5 Ensure 48 hr stay at HI after delivery 0.00
A.1.5.1 Gift pack to Mother "Baby care Pack" 20000 700 140.00
A.1.5.2
Cash less Benefit (medicine etc) for Normal Delivery (Out of 85% of Institutional Delivery, Normal Delivery calculated 90 % of Total estimated Institutional delivery)
45034 500 225.17
A.1.5.3
Cashless Benefit (medicine etc) for Complicated Delivery (10% of Total estimated Institutional Delivery of Health Institution)
5003 1000 50.03
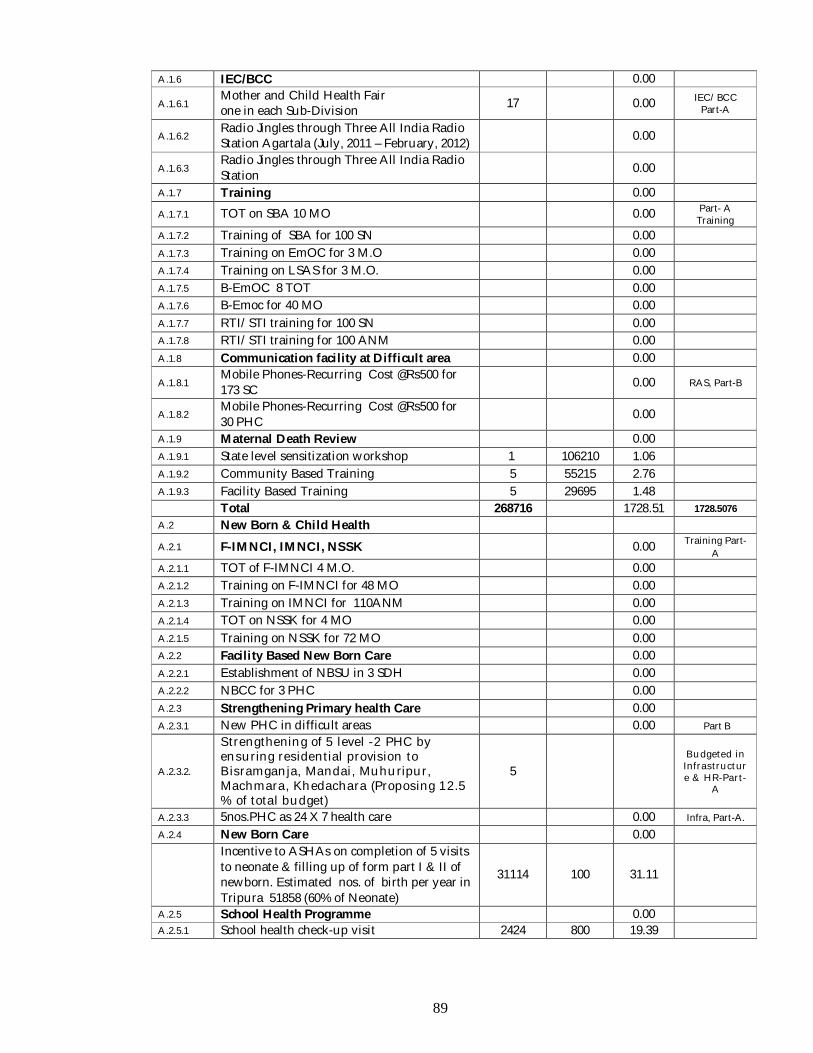
89
A.1.6 IEC/BCC 0.00
A.1.6.1 Mother and Child Health Fair one in each Sub-Division 17 0.00 IEC/BCC
Part-A
A.1.6.2 Radio Jingles through Three All India Radio Station Agartala (July, 2011 – February, 2012) 0.00
A.1.6.3 Radio Jingles through Three All India Radio Station 0.00
A.1.7 Training 0.00
A.1.7.1 TOT on SBA 10 MO 0.00 Part- A Training
A.1.7.2 Training of SBA for 100 SN 0.00
A.1.7.3 Training on EmOC for 3 M.O 0.00
A.1.7.4 Training on LSAS for 3 M.O. 0.00
A.1.7.5 B-EmOC 8 TOT 0.00
A.1.7.6 B-Emoc for 40 MO 0.00
A.1.7.7 RTI/STI training for 100 SN 0.00
A.1.7.8 RTI/STI training for 100 ANM 0.00
A.1.8 Communication facility at Difficult area 0.00
A.1.8.1 Mobile Phones-Recurring Cost @Rs500 for 173 SC 0.00 RAS, Part-B
A.1.8.2 Mobile Phones-Recurring Cost @Rs500 for 30 PHC 0.00
A.1.9 Maternal Death Review 0.00
A.1.9.1 State level sensitization workshop 1 106210 1.06
A.1.9.2 Community Based Training 5 55215 2.76
A.1.9.3 Facility Based Training 5 29695 1.48
Total 268716 1728.51 1728.5076 A.2 New Born & Child Health
A.2.1 F-IMNCI, IMNCI, NSSK 0.00 Training Part-A
A.2.1.1 TOT of F-IMNCI 4 M.O. 0.00
A.2.1.2 Training on F-IMNCI for 48 MO 0.00
A.2.1.3 Training on IMNCI for 110ANM 0.00
A.2.1.4 TOT on NSSK for 4 MO 0.00
A.2.1.5 Training on NSSK for 72 MO 0.00
A.2.2 Facility Based New Born Care 0.00
A.2.2.1 Establishment of NBSU in 3 SDH 0.00
A.2.2.2 NBCC for 3 PHC 0.00
A.2.3 Strengthening Primary health Care 0.00
A.2.3.1 New PHC in difficult areas 0.00 Part B
A.2.3.2.
Strengthening of 5 level -2 PHC by ensuring residential provision to Bisramganja, Mandai, Muhuripur, Machmara, Khedachara (Proposing 12.5 % of total budget)
5 Budgeted in Infrastructure & HR-Part-
A
A.2.3.3 5nos.PHC as 24 X 7 health care 0.00 Infra, Part-A.
A.2.4 New Born Care 0.00
Incentive to ASHAs on completion of 5 visits to neonate & filling up of form part I & II of newborn. Estimated nos. of birth per year in Tripura 51858 (60% of Neonate)
31114 100 31.11
A.2.5 School Health Programme 0.00 A.2.5.1 School health check-up visit 2424 800 19.39
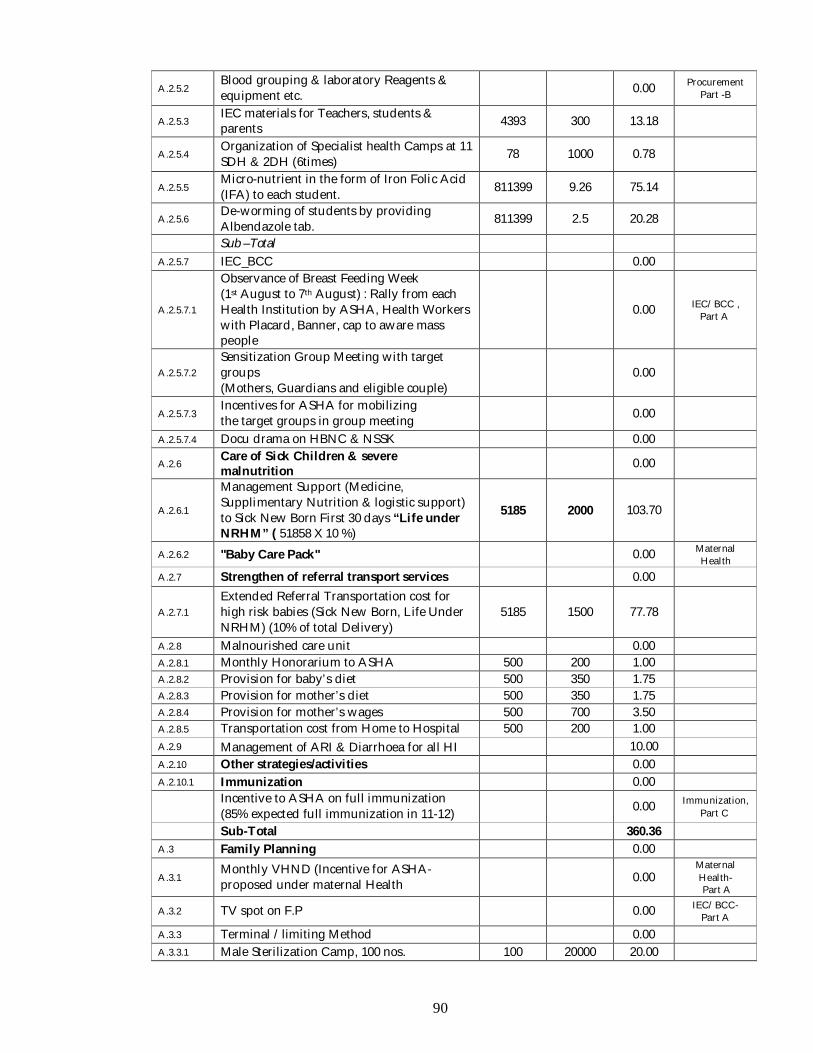
90
A.2.5.2 Blood grouping & laboratory Reagents & equipment etc. 0.00 Procurement
Part -B
A.2.5.3 IEC materials for Teachers, students & parents 4393 300 13.18
A.2.5.4 Organization of Specialist health Camps at 11 SDH & 2DH (6times) 78 1000 0.78
A.2.5.5 Micro-nutrient in the form of Iron Folic Acid (IFA) to each student. 811399 9.26 75.14
A.2.5.6 De-worming of students by providing Albendazole tab. 811399 2.5 20.28
Sub –Total
A.2.5.7 IEC_BCC 0.00
A.2.5.7.1
Observance of Breast Feeding Week (1st August to 7th August) : Rally from each Health Institution by ASHA, Health Workers with Placard, Banner, cap to aware mass people
0.00 IEC/BCC , Part A
A.2.5.7.2 Sensitization Group Meeting with target groups (Mothers, Guardians and eligible couple)
0.00
A.2.5.7.3 Incentives for ASHA for mobilizing the target groups in group meeting 0.00
A.2.5.7.4 Docu drama on HBNC & NSSK 0.00
A.2.6 Care of Sick Children & severe malnutrition 0.00
A.2.6.1
Management Support (Medicine, Supplimentary Nutrition & logistic support) to Sick New Born First 30 days “Life under NRHM” ( 51858 X 10 %)
5185 2000 103.70
A.2.6.2 "Baby Care Pack" 0.00 Maternal Health
A.2.7 Strengthen of referral transport services 0.00
A.2.7.1 Extended Referral Transportation cost for high risk babies (Sick New Born, Life Under NRHM) (10% of total Delivery)
5185 1500 77.78
A.2.8 Malnourished care unit 0.00
A.2.8.1 Monthly Honorarium to ASHA 500 200 1.00 A.2.8.2 Provision for baby’s diet 500 350 1.75 A.2.8.3 Provision for mother’s diet 500 350 1.75 A.2.8.4 Provision for mother’s wages 500 700 3.50 A.2.8.5 Transportation cost from Home to Hospital 500 200 1.00
A.2.9 Management of ARI & Diarrhoea for all HI 10.00
A.2.10 Other strategies/activities 0.00
A.2.10.1 Immunization 0.00
Incentive to ASHA on full immunization (85% expected full immunization in 11-12) 0.00 Immunization,
Part C
Sub-Total 360.36
A.3 Family Planning 0.00
A.3.1 Monthly VHND (Incentive for ASHA- proposed under maternal Health 0.00
Maternal Health- Part A
A.3.2 TV spot on F.P 0.00 IEC/BCC- Part A
A.3.3 Terminal /limiting Method 0.00
A.3.3.1 Male Sterilization Camp, 100 nos. 100 20000 20.00
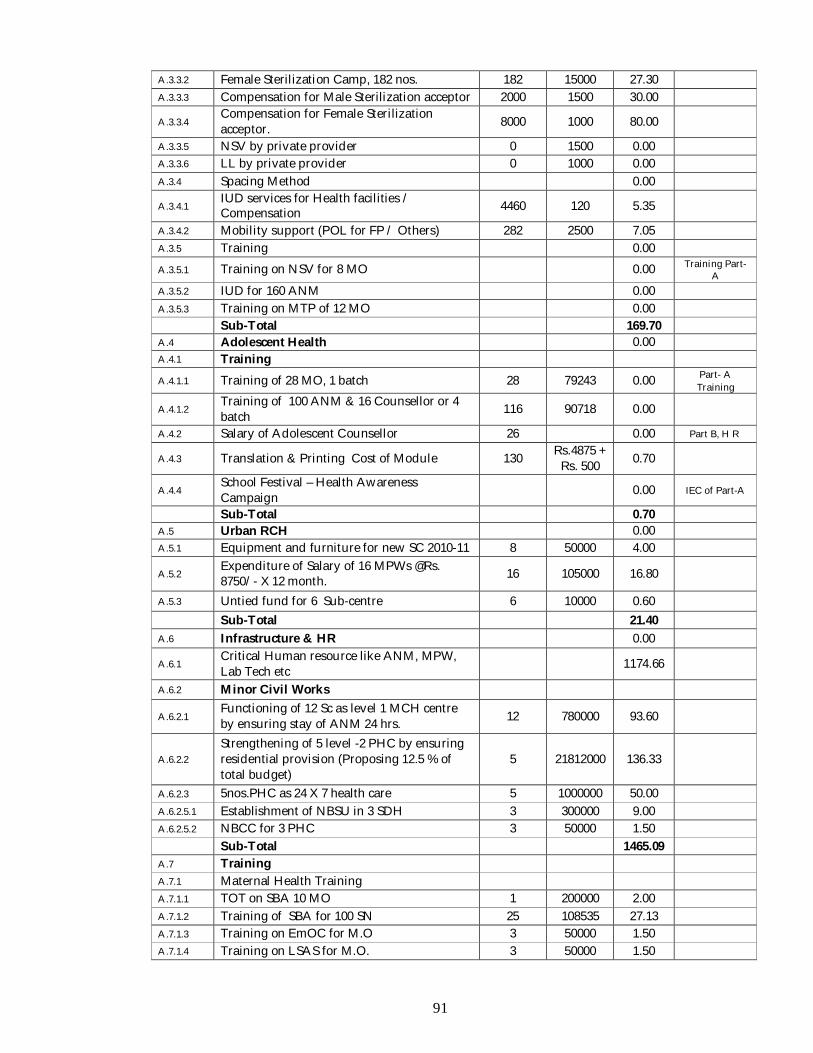
91
A.3.3.2 Female Sterilization Camp, 182 nos. 182 15000 27.30
A.3.3.3 Compensation for Male Sterilization acceptor 2000 1500 30.00
A.3.3.4 Compensation for Female Sterilization acceptor. 8000 1000 80.00
A.3.3.5 NSV by private provider 0 1500 0.00
A.3.3.6 LL by private provider 0 1000 0.00
A.3.4 Spacing Method 0.00
A.3.4.1 IUD services for Health facilities / Compensation 4460 120 5.35
A.3.4.2 Mobility support (POL for FP / Others) 282 2500 7.05
A.3.5 Training 0.00
A.3.5.1 Training on NSV for 8 MO 0.00 Training Part-A
A.3.5.2 IUD for 160 ANM 0.00
A.3.5.3 Training on MTP of 12 MO 0.00 Sub-Total 169.70
A.4 Adolescent Health 0.00
A.4.1 Training
A.4.1.1 Training of 28 MO, 1 batch 28 79243 0.00 Part- A Training
A.4.1.2 Training of 100 ANM & 16 Counsellor or 4 batch 116 90718 0.00
A.4.2 Salary of Adolescent Counsellor 26 0.00 Part B, H R
A.4.3 Translation & Printing Cost of Module 130 Rs.4875 + Rs. 500 0.70
A.4.4 School Festival – Health Awareness Campaign 0.00 IEC of Part-A
Sub-Total 0.70
A.5 Urban RCH 0.00
A.5.1 Equipment and furniture for new SC 2010-11 8 50000 4.00
A.5.2 Expenditure of Salary of 16 MPWs @Rs. 8750/- X 12 month. 16 105000 16.80
A.5.3 Untied fund for 6 Sub-centre 6 10000 0.60
Sub-Total 21.40
A.6 Infrastructure & HR 0.00
A.6.1 Critical Human resource like ANM, MPW, Lab Tech etc 1174.66
A.6.2 Minor Civil Works
A.6.2.1 Functioning of 12 Sc as level 1 MCH centre by ensuring stay of ANM 24 hrs. 12 780000 93.60
A.6.2.2 Strengthening of 5 level -2 PHC by ensuring residential provision (Proposing 12.5 % of total budget)
5 21812000 136.33
A.6.2.3 5nos.PHC as 24 X 7 health care 5 1000000 50.00
A.6.2.5.1 Establishment of NBSU in 3 SDH 3 300000 9.00
A.6.2.5.2 NBCC for 3 PHC 3 50000 1.50
Sub-Total 1465.09
A.7 Training
A.7.1 Maternal Health Training
A.7.1.1 TOT on SBA 10 MO 1 200000 2.00
A.7.1.2 Training of SBA for 100 SN 25 108535 27.13
A.7.1.3 Training on EmOC for M.O 3 50000 1.50
A.7.1.4 Training on LSAS for M.O. 3 50000 1.50
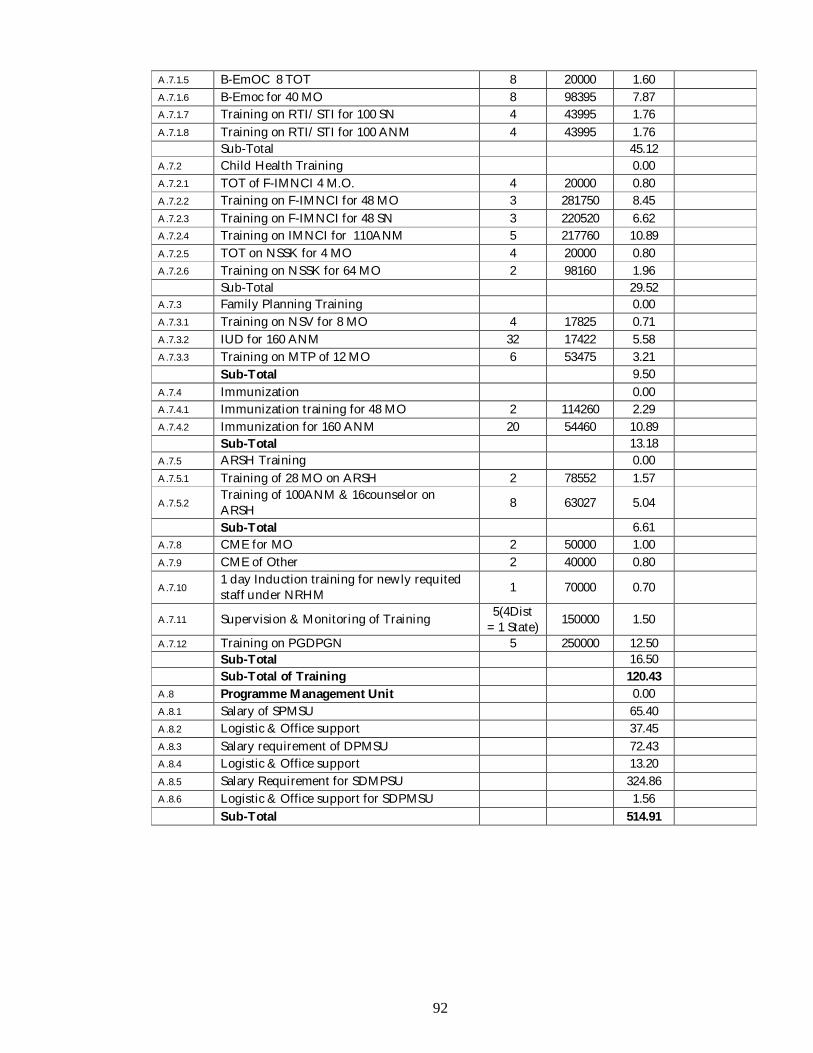
92
A.7.1.5 B-EmOC 8 TOT 8 20000 1.60
A.7.1.6 B-Emoc for 40 MO 8 98395 7.87
A.7.1.7 Training on RTI/STI for 100 SN 4 43995 1.76
A.7.1.8 Training on RTI/STI for 100 ANM 4 43995 1.76 Sub-Total 45.12
A.7.2 Child Health Training 0.00
A.7.2.1 TOT of F-IMNCI 4 M.O. 4 20000 0.80
A.7.2.2 Training on F-IMNCI for 48 MO 3 281750 8.45
A.7.2.3 Training on F-IMNCI for 48 SN 3 220520 6.62
A.7.2.4 Training on IMNCI for 110ANM 5 217760 10.89
A.7.2.5 TOT on NSSK for 4 MO 4 20000 0.80
A.7.2.6 Training on NSSK for 64 MO 2 98160 1.96
Sub-Total 29.52 A.7.3 Family Planning Training 0.00
A.7.3.1 Training on NSV for 8 MO 4 17825 0.71
A.7.3.2 IUD for 160 ANM 32 17422 5.58
A.7.3.3 Training on MTP of 12 MO 6 53475 3.21
Sub-Total 9.50
A.7.4 Immunization 0.00
A.7.4.1 Immunization training for 48 MO 2 114260 2.29
A.7.4.2 Immunization for 160 ANM 20 54460 10.89
Sub-Total 13.18
A.7.5 ARSH Training 0.00
A.7.5.1 Training of 28 MO on ARSH 2 78552 1.57
A.7.5.2 Training of 100ANM & 16counselor on ARSH 8 63027 5.04
Sub-Total 6.61
A.7.8 CME for MO 2 50000 1.00
A.7.9 CME of Other 2 40000 0.80
A.7.10 1 day Induction training for newly requited staff under NRHM 1 70000 0.70
A.7.11 Supervision & Monitoring of Training 5(4Dist = 1 State) 150000 1.50
A.7.12 Training on PGDPGN 5 250000 12.50 Sub-Total 16.50
Sub-Total of Training 120.43
A.8 Programme Management Unit 0.00
A.8.1 Salary of SPMSU 65.40
A.8.2 Logistic & Office support 37.45
A.8.3 Salary requirement of DPMSU 72.43
A.8.4 Logistic & Office support 13.20
A.8.5 Salary Requirement for SDMPSU 324.86
A.8.6 Logistic & Office support for SDPMSU 1.56
Sub-Total 514.91
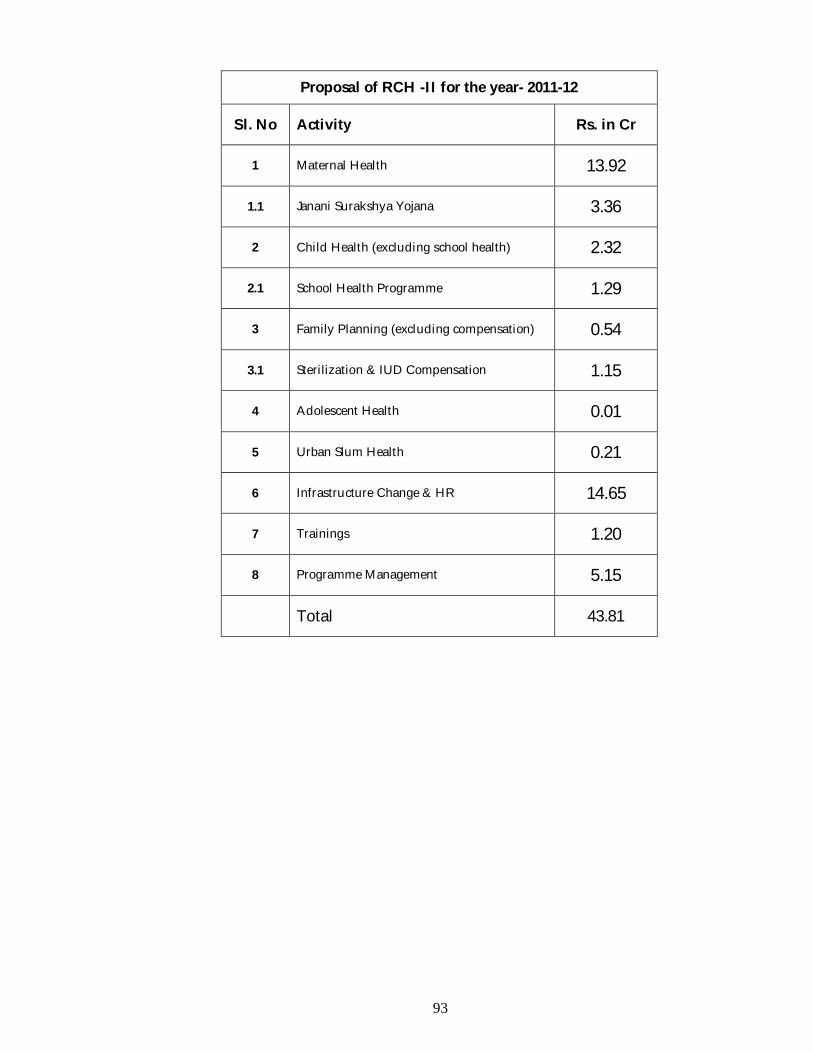
93
Proposal of RCH -II for the year- 2011-12
Sl. No Activity Rs. in Cr
1 Maternal Health 13.92
1.1 Janani Surakshya Yojana 3.36
2 Child Health (excluding school health) 2.32
2.1 School Health Programme 1.29
3 Family Planning (excluding compensation) 0.54
3.1 Sterilization & IUD Compensation 1.15
4 Adolescent Health 0.01
5 Urban Slum Health 0.21
6 Infrastructure Change & HR 14.65
7 Trainings 1.20
8 Programme Management 5.15
Total 43.81
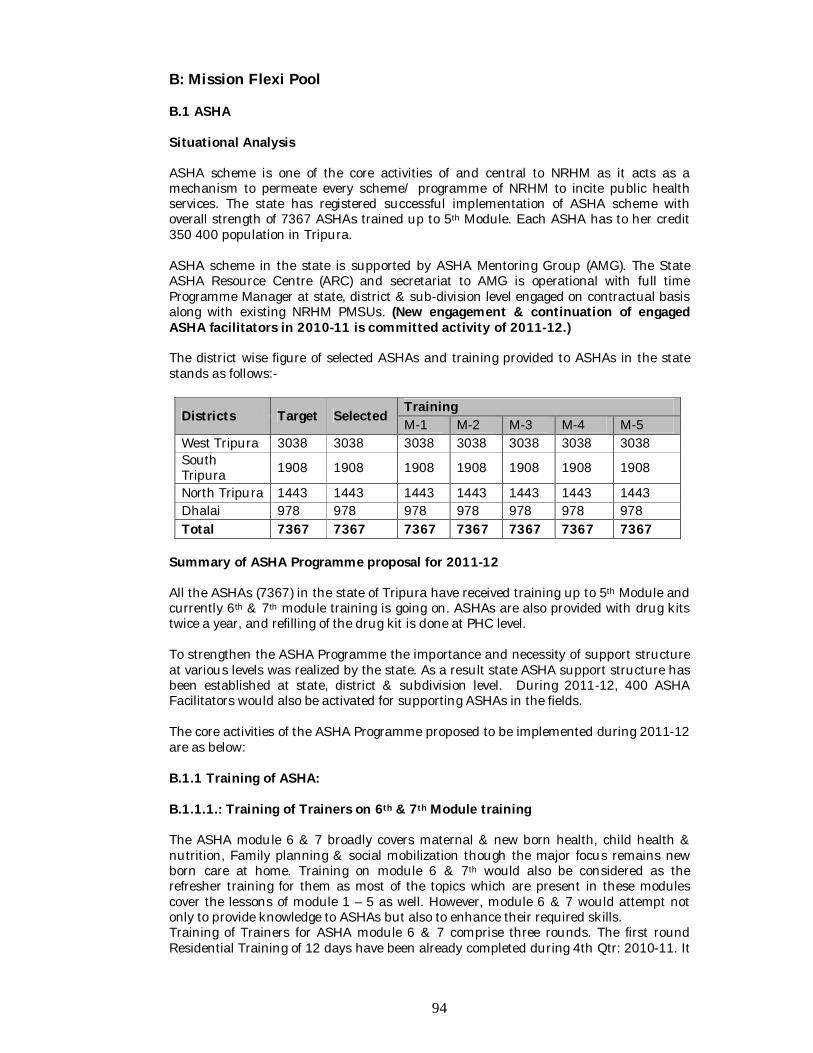
94
B: Mission Flexi Pool B.1 ASHA Situational Analysis ASHA scheme is one of the core activities of and central to NRHM as it acts as a mechanism to permeate every scheme/ programme of NRHM to incite public health services. The state has registered successful implementation of ASHA scheme with overall strength of 7367 ASHAs trained up to 5th Module. Each ASHA has to her credit 350 400 population in Tripura. ASHA scheme in the state is supported by ASHA Mentoring Group (AMG). The State ASHA Resource Centre (ARC) and secretariat to AMG is operational with full time Programme Manager at state, district & sub-division level engaged on contractual basis along with existing NRHM PMSUs. (New engagement & continuation of engaged ASHA facilitators in 2010-11 is committed activity of 2011-12.) The district wise figure of selected ASHAs and training provided to ASHAs in the state stands as follows:-
Districts Target Selected Training M-1 M-2 M-3 M-4 M-5
West Tripura 3038 3038 3038 3038 3038 3038 3038 South Tripura 1908 1908 1908 1908 1908 1908 1908
North Tripura 1443 1443 1443 1443 1443 1443 1443 Dhalai 978 978 978 978 978 978 978 Total 7367 7367 7367 7367 7367 7367 7367
Summary of ASHA Programme proposal for 2011-12 All the ASHAs (7367) in the state of Tripura have received training up to 5th Module and currently 6th & 7th module training is going on. ASHAs are also provided with drug kits twice a year, and refilling of the drug kit is done at PHC level. To strengthen the ASHA Programme the importance and necessity of support structure at various levels was realized by the state. As a result state ASHA support structure has been established at state, district & subdivision level. During 2011-12, 400 ASHA Facilitators would also be activated for supporting ASHAs in the fields. The core activities of the ASHA Programme proposed to be implemented during 2011-12 are as below: B.1.1 Training of ASHA: B.1.1.1.: Training of Trainers on 6th & 7th Module training The ASHA module 6 & 7 broadly covers maternal & new born health, child health & nutrition, Family planning & social mobilization though the major focus remains new born care at home. Training on module 6 & 7th would also be considered as the refresher training for them as most of the topics which are present in these modules cover the lessons of module 1 – 5 as well. However, module 6 & 7 would attempt not only to provide knowledge to ASHAs but also to enhance their required skills. Training of Trainers for ASHA module 6 & 7 comprise three rounds. The first round Residential Training of 12 days have been already completed during 4th Qtr: 2010-11. It
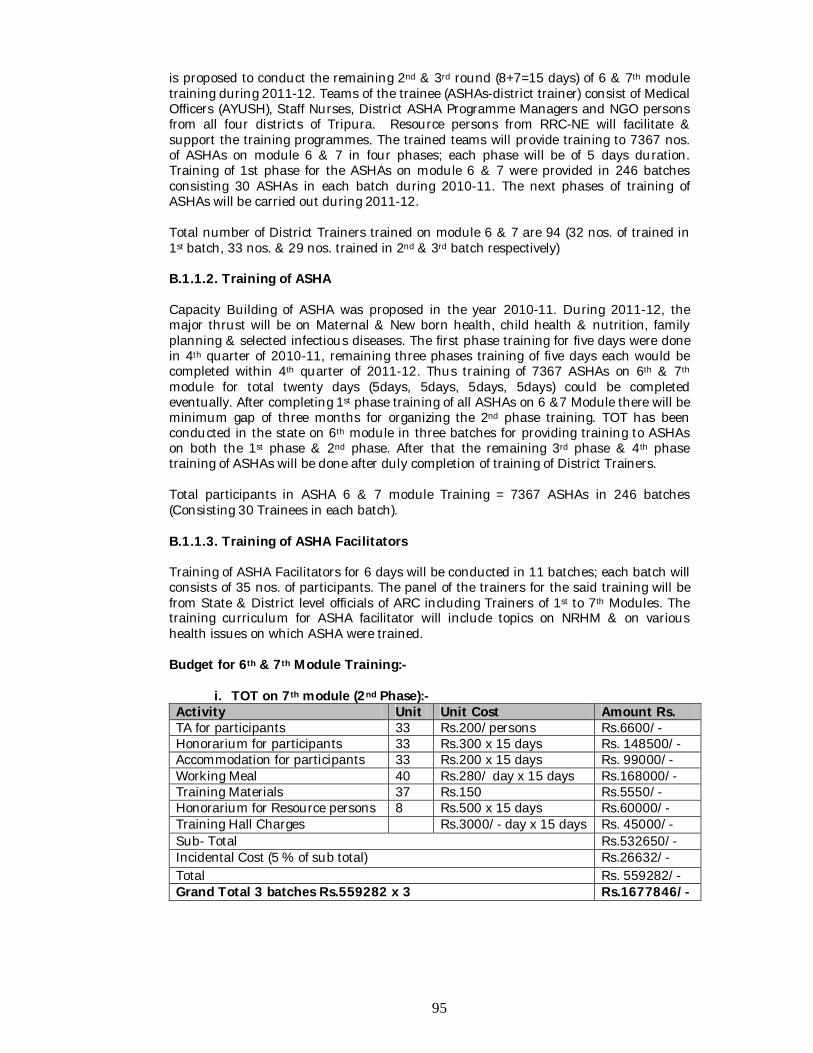
95
is proposed to conduct the remaining 2nd & 3rd round (8+7=15 days) of 6 & 7th module training during 2011-12. Teams of the trainee (ASHAs-district trainer) consist of Medical Officers (AYUSH), Staff Nurses, District ASHA Programme Managers and NGO persons from all four districts of Tripura. Resource persons from RRC-NE will facilitate & support the training programmes. The trained teams will provide training to 7367 nos. of ASHAs on module 6 & 7 in four phases; each phase will be of 5 days duration. Training of 1st phase for the ASHAs on module 6 & 7 were provided in 246 batches consisting 30 ASHAs in each batch during 2010-11. The next phases of training of ASHAs will be carried out during 2011-12. Total number of District Trainers trained on module 6 & 7 are 94 (32 nos. of trained in 1st batch, 33 nos. & 29 nos. trained in 2nd & 3rd batch respectively) B.1.1.2. Training of ASHA Capacity Building of ASHA was proposed in the year 2010-11. During 2011-12, the major thrust will be on Maternal & New born health, child health & nutrition, family planning & selected infectious diseases. The first phase training for five days were done in 4th quarter of 2010-11, remaining three phases training of five days each would be completed within 4th quarter of 2011-12. Thus training of 7367 ASHAs on 6th & 7th module for total twenty days (5days, 5days, 5days, 5days) could be completed eventually. After completing 1st phase training of all ASHAs on 6 &7 Module there will be minimum gap of three months for organizing the 2nd phase training. TOT has been conducted in the state on 6th module in three batches for providing training to ASHAs on both the 1st phase & 2nd phase. After that the remaining 3rd phase & 4th phase training of ASHAs will be done after duly completion of training of District Trainers. Total participants in ASHA 6 & 7 module Training = 7367 ASHAs in 246 batches (Consisting 30 Trainees in each batch). B.1.1.3. Training of ASHA Facilitators Training of ASHA Facilitators for 6 days will be conducted in 11 batches; each batch will consists of 35 nos. of participants. The panel of the trainers for the said training will be from State & District level officials of ARC including Trainers of 1st to 7th Modules. The training curriculum for ASHA facilitator will include topics on NRHM & on various health issues on which ASHA were trained. Budget for 6th & 7th Module Training:-
i. TOT on 7th module (2nd Phase):- Activity Unit Unit Cost Amount Rs. TA for participants 33 Rs.200/persons Rs.6600/- Honorarium for participants 33 Rs.300 x 15 days Rs. 148500/- Accommodation for participants 33 Rs.200 x 15 days Rs. 99000/- Working Meal 40 Rs.280/ day x 15 days Rs.168000/- Training Materials 37 Rs.150 Rs.5550/- Honorarium for Resource persons 8 Rs.500 x 15 days Rs.60000/- Training Hall Charges Rs.3000/- day x 15 days Rs. 45000/- Sub- Total Rs.532650/- Incidental Cost (5 % of sub total) Rs.26632/- Total Rs. 559282/- Grand Total 3 batches Rs.559282 x 3 Rs.1677846/-
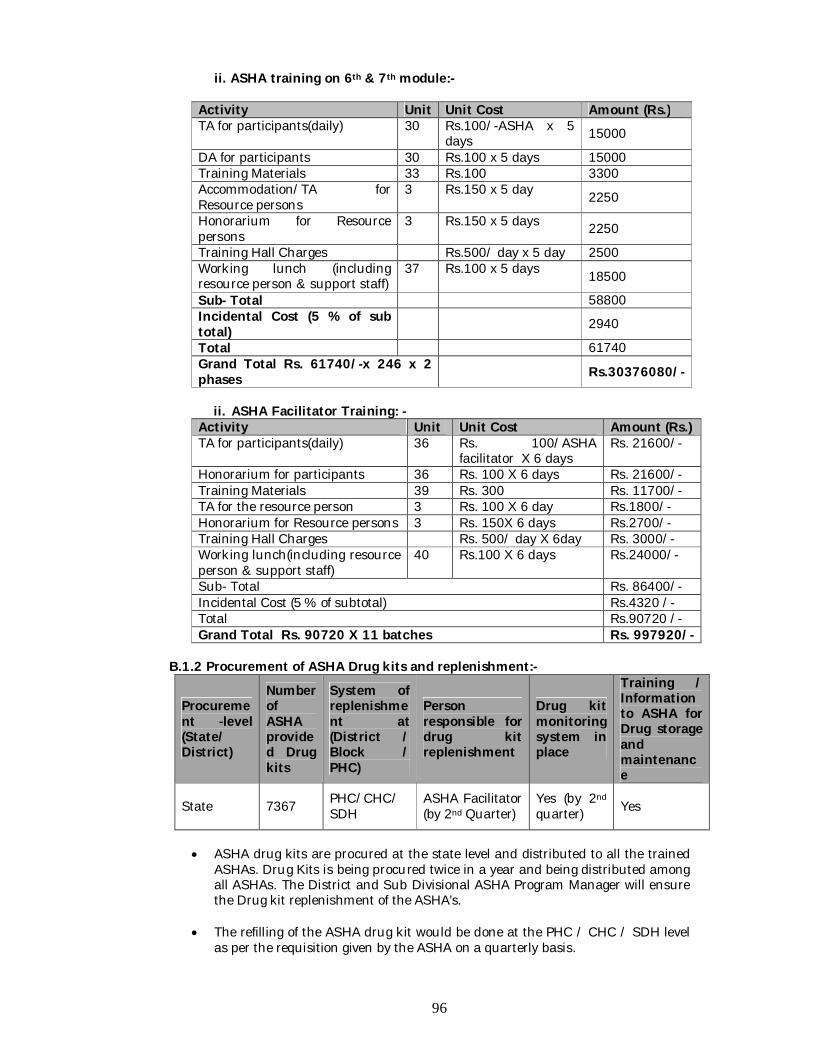
96
ii. ASHA training on 6th & 7th module:-
Activity Unit Unit Cost Amount (Rs.) TA for participants(daily) 30 Rs.100/-ASHA x 5
days 15000
DA for participants 30 Rs.100 x 5 days 15000 Training Materials 33 Rs.100 3300 Accommodation/TA for Resource persons
3 Rs.150 x 5 day 2250
Honorarium for Resource persons
3 Rs.150 x 5 days 2250
Training Hall Charges Rs.500/ day x 5 day 2500 Working lunch (including resource person & support staff)
37 Rs.100 x 5 days 18500
Sub- Total 58800 Incidental Cost (5 % of sub total)
2940
Total 61740 Grand Total Rs. 61740/-x 246 x 2 phases
Rs.30376080/-
ii. ASHA Facilitator Training: - Activity Unit Unit Cost Amount (Rs.) TA for participants(daily) 36 Rs. 100/ASHA
facilitator X 6 days Rs. 21600/-
Honorarium for participants 36 Rs. 100 X 6 days Rs. 21600/- Training Materials 39 Rs. 300 Rs. 11700/- TA for the resource person 3 Rs. 100 X 6 day Rs.1800/- Honorarium for Resource persons 3 Rs. 150X 6 days Rs.2700/- Training Hall Charges Rs. 500/ day X 6day Rs. 3000/- Working lunch(including resource person & support staff)
40 Rs.100 X 6 days Rs.24000/-
Sub- Total Rs. 86400/- Incidental Cost (5 % of subtotal) Rs.4320 /- Total Rs.90720 /- Grand Total Rs. 90720 X 11 batches Rs. 997920/-
B.1.2 Procurement of ASHA Drug kits and replenishment:-
Procurement -level (State/ District)
Number of ASHA provided Drug kits
System of replenishment at (District / Block / PHC)
Person responsible for drug kit replenishment
Drug kit monitoring system in place
Training / Information to ASHA for Drug storage and maintenance
State 7367 PHC/CHC/ SDH
ASHA Facilitator (by 2nd Quarter)
Yes (by 2nd quarter) Yes
ASHA drug kits are procured at the state level and distributed to all the trained
ASHAs. Drug Kits is being procured twice in a year and being distributed among all ASHAs. The District and Sub Divisional ASHA Program Manager will ensure the Drug kit replenishment of the ASHA’s.
The refilling of the ASHA drug kit would be done at the PHC / CHC / SDH level as per the requisition given by the ASHA on a quarterly basis.
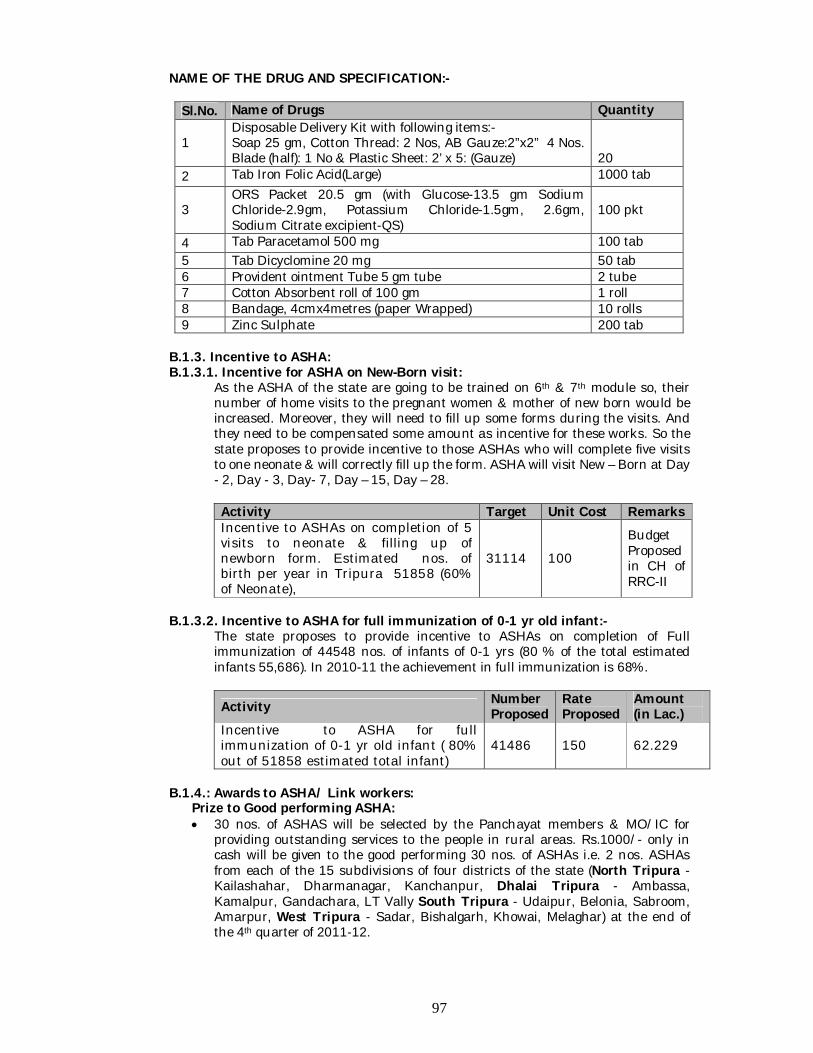
97
NAME OF THE DRUG AND SPECIFICATION:-
Sl.No. Name of Drugs Quantity
1 Disposable Delivery Kit with following items:- Soap 25 gm, Cotton Thread: 2 Nos, AB Gauze:2”x2” 4 Nos. Blade (half): 1 No & Plastic Sheet: 2’ x 5: (Gauze)
20
2 Tab Iron Folic Acid(Large) 1000 tab
3 ORS Packet 20.5 gm (with Glucose-13.5 gm Sodium Chloride-2.9gm, Potassium Chloride-1.5gm, 2.6gm, Sodium Citrate excipient-QS)
100 pkt
4 Tab Paracetamol 500 mg 100 tab 5 Tab Dicyclomine 20 mg 50 tab 6 Provident ointment Tube 5 gm tube 2 tube 7 Cotton Absorbent roll of 100 gm 1 roll 8 Bandage, 4cmx4metres (paper Wrapped) 10 rolls 9 Zinc Sulphate 200 tab
B.1.3. Incentive to ASHA: B.1.3.1. Incentive for ASHA on New-Born visit:
As the ASHA of the state are going to be trained on 6th & 7th module so, their number of home visits to the pregnant women & mother of new born would be increased. Moreover, they will need to fill up some forms during the visits. And they need to be compensated some amount as incentive for these works. So the state proposes to provide incentive to those ASHAs who will complete five visits to one neonate & will correctly fill up the form. ASHA will visit New – Born at Day - 2, Day - 3, Day- 7, Day – 15, Day – 28. Activity Target Unit Cost Remarks Incentive to ASHAs on completion of 5 visits to neonate & filling up of newborn form. Estimated nos. of birth per year in Tripura 51858 (60% of Neonate),
31114 100
Budget Proposed in CH of RRC-II
B.1.3.2. Incentive to ASHA for full immunization of 0-1 yr old infant:-
The state proposes to provide incentive to ASHAs on completion of Full immunization of 44548 nos. of infants of 0-1 yrs (80 % of the total estimated infants 55,686). In 2010-11 the achievement in full immunization is 68%.
Activity Number Proposed
Rate Proposed
Amount (in Lac.)
Incentive to ASHA for full immunization of 0-1 yr old infant ( 80% out of 51858 estimated total infant)
41486 150 62.229
B.1.4.: Awards to ASHA/ Link workers:
Prize to Good performing ASHA: 30 nos. of ASHAS will be selected by the Panchayat members & MO/IC for
providing outstanding services to the people in rural areas. Rs.1000/- only in cash will be given to the good performing 30 nos. of ASHAs i.e. 2 nos. ASHAs from each of the 15 subdivisions of four districts of the state (North Tripura - Kailashahar, Dharmanagar, Kanchanpur, Dhalai Tripura - Ambassa, Kamalpur, Gandachara, LT Vally South Tripura - Udaipur, Belonia, Sabroom, Amarpur, West Tripura - Sadar, Bishalgarh, Khowai, Melaghar) at the end of the 4th quarter of 2011-12.
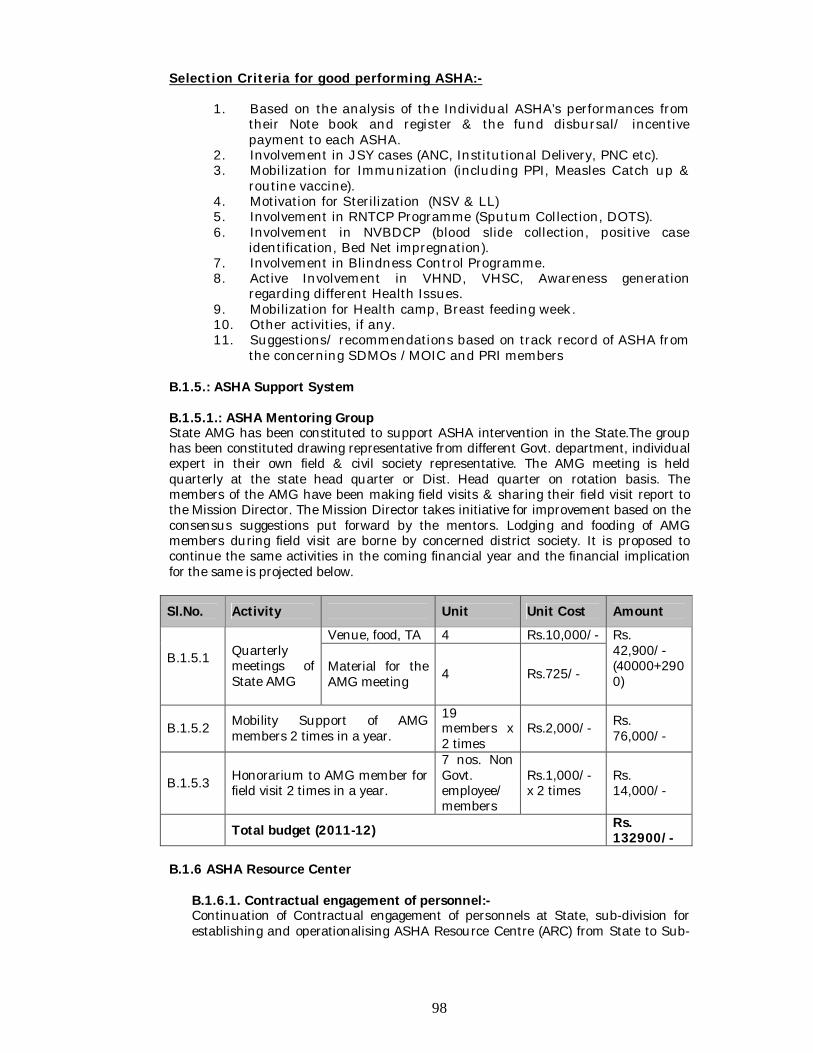
98
Selection Criteria for good performing ASHA:-
1. Based on the analysis of the Individual ASHA’s performances from their Note book and register & the fund disbursal/ incentive payment to each ASHA.
2. Involvement in JSY cases (ANC, Institutional Delivery, PNC etc). 3. Mobilization for Immunization (including PPI, Measles Catch up &
routine vaccine). 4. Motivation for Sterilization (NSV & LL) 5. Involvement in RNTCP Programme (Sputum Collection, DOTS). 6. Involvement in NVBDCP (blood slide collection, positive case
identification, Bed Net impregnation). 7. Involvement in Blindness Control Programme. 8. Active Involvement in VHND, VHSC, Awareness generation
regarding different Health Issues. 9. Mobilization for Health camp, Breast feeding week. 10. Other activities, if any. 11. Suggestions/ recommendations based on track record of ASHA from
the concerning SDMOs /MOIC and PRI members B.1.5.: ASHA Support System B.1.5.1.: ASHA Mentoring Group State AMG has been constituted to support ASHA intervention in the State.The group has been constituted drawing representative from different Govt. department, individual expert in their own field & civil society representative. The AMG meeting is held quarterly at the state head quarter or Dist. Head quarter on rotation basis. The members of the AMG have been making field visits & sharing their field visit report to the Mission Director. The Mission Director takes initiative for improvement based on the consensus suggestions put forward by the mentors. Lodging and fooding of AMG members during field visit are borne by concerned district society. It is proposed to continue the same activities in the coming financial year and the financial implication for the same is projected below.
Sl.No. Activity Unit Unit Cost Amount
B.1.5.1
Quarterly meetings of State AMG
Venue, food, TA 4 Rs.10,000/- Rs. 42,900/- (40000+2900)
Material for the AMG meeting 4 Rs.725/-
B.1.5.2 Mobility Support of AMG members 2 times in a year.
19 members x 2 times
Rs.2,000/- Rs. 76,000/-
B.1.5.3 Honorarium to AMG member for field visit 2 times in a year.
7 nos. Non Govt. employee/members
Rs.1,000/- x 2 times
Rs. 14,000/-
Total budget (2011-12) Rs. 132900/-
B.1.6 ASHA Resource Center
B.1.6.1. Contractual engagement of personnel:- Continuation of Contractual engagement of personnels at State, sub-division for establishing and operationalising ASHA Resource Centre (ARC) from State to Sub-
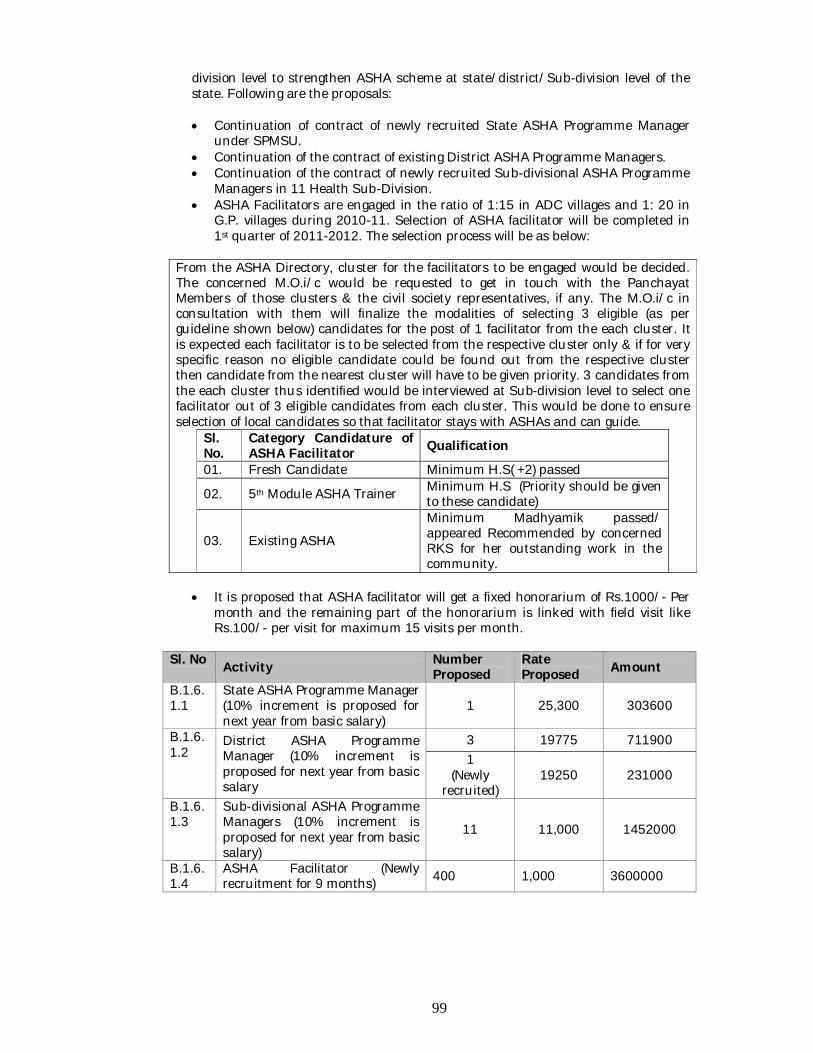
99
division level to strengthen ASHA scheme at state/district/Sub-division level of the state. Following are the proposals:
Continuation of contract of newly recruited State ASHA Programme Manager
under SPMSU. Continuation of the contract of existing District ASHA Programme Managers. Continuation of the contract of newly recruited Sub-divisional ASHA Programme
Managers in 11 Health Sub-Division. ASHA Facilitators are engaged in the ratio of 1:15 in ADC villages and 1: 20 in
G.P. villages during 2010-11. Selection of ASHA facilitator will be completed in 1st quarter of 2011-2012. The selection process will be as below:
From the ASHA Directory, cluster for the facilitators to be engaged would be decided. The concerned M.O.i/c would be requested to get in touch with the Panchayat Members of those clusters & the civil society representatives, if any. The M.O.i/c in consultation with them will finalize the modalities of selecting 3 eligible (as per guideline shown below) candidates for the post of 1 facilitator from the each cluster. It is expected each facilitator is to be selected from the respective cluster only & if for very specific reason no eligible candidate could be found out from the respective cluster then candidate from the nearest cluster will have to be given priority. 3 candidates from the each cluster thus identified would be interviewed at Sub-division level to select one facilitator out of 3 eligible candidates from each cluster. This would be done to ensure selection of local candidates so that facilitator stays with ASHAs and can guide.
Sl. No.
Category Candidature of ASHA Facilitator Qualification
01. Fresh Candidate Minimum H.S( +2) passed
02. 5th Module ASHA Trainer Minimum H.S (Priority should be given to these candidate)
03. Existing ASHA
Minimum Madhyamik passed/ appeared Recommended by concerned RKS for her outstanding work in the community.
It is proposed that ASHA facilitator will get a fixed honorarium of Rs.1000/- Per
month and the remaining part of the honorarium is linked with field visit like Rs.100/- per visit for maximum 15 visits per month.
Sl. No Activity Number Proposed
Rate Proposed Amount
B.1.6.1.1
State ASHA Programme Manager (10% increment is proposed for next year from basic salary)
1 25,300 303600
B.1.6.1.2
District ASHA Programme Manager (10% increment is proposed for next year from basic salary
3 19775 711900 1
(Newly recruited)
19250 231000
B.1.6.1.3
Sub-divisional ASHA Programme Managers (10% increment is proposed for next year from basic salary)
11 11,000 1452000
B.1.6.1.4
ASHA Facilitator (Newly recruitment for 9 months) 400 1,000 3600000
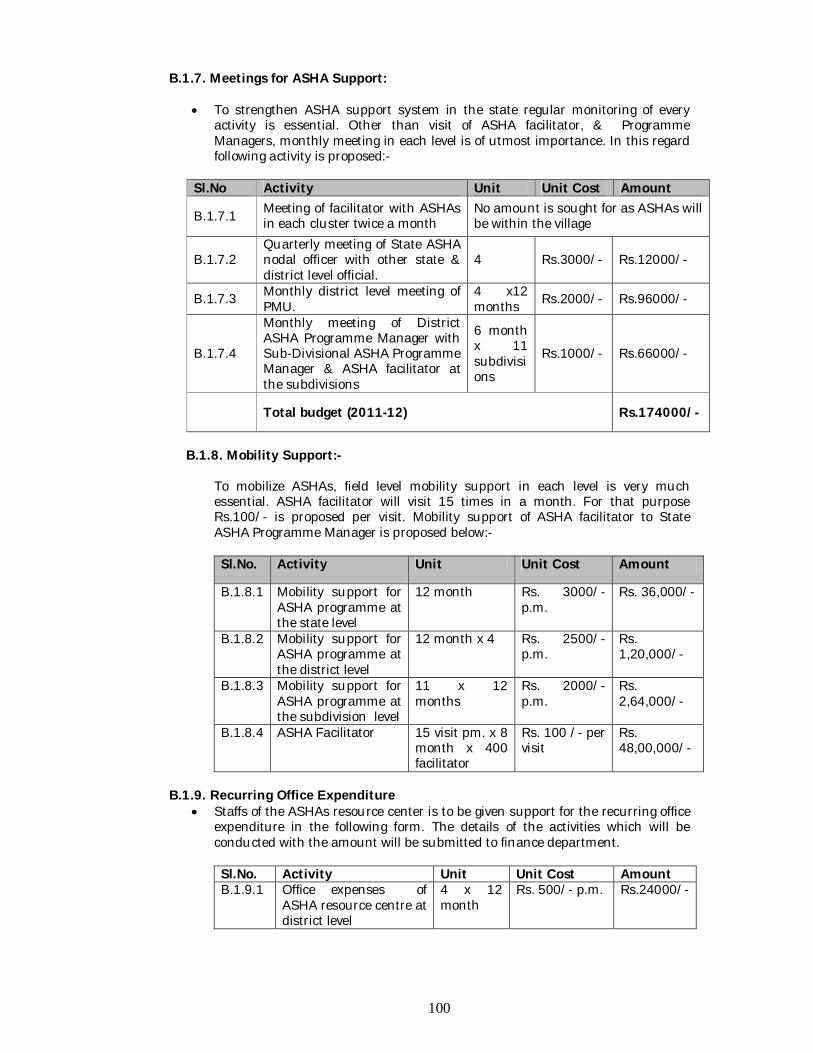
100
B.1.7. Meetings for ASHA Support: To strengthen ASHA support system in the state regular monitoring of every
activity is essential. Other than visit of ASHA facilitator, & Programme Managers, monthly meeting in each level is of utmost importance. In this regard following activity is proposed:-
Sl.No Activity Unit Unit Cost Amount
B.1.7.1 Meeting of facilitator with ASHAs in each cluster twice a month
No amount is sought for as ASHAs will be within the village
B.1.7.2 Quarterly meeting of State ASHA nodal officer with other state & district level official.
4 Rs.3000/- Rs.12000/-
B.1.7.3 Monthly district level meeting of PMU.
4 x12 months Rs.2000/- Rs.96000/-
B.1.7.4
Monthly meeting of District ASHA Programme Manager with Sub-Divisional ASHA Programme Manager & ASHA facilitator at the subdivisions
6 month x 11 subdivisions
Rs.1000/- Rs.66000/-
Total budget (2011-12) Rs.174000/-
B.1.8. Mobility Support:-
To mobilize ASHAs, field level mobility support in each level is very much essential. ASHA facilitator will visit 15 times in a month. For that purpose Rs.100/- is proposed per visit. Mobility support of ASHA facilitator to State ASHA Programme Manager is proposed below:- Sl.No. Activity Unit Unit Cost Amount
B.1.8.1 Mobility support for ASHA programme at the state level
12 month Rs. 3000/- p.m.
Rs. 36,000/-
B.1.8.2 Mobility support for ASHA programme at the district level
12 month x 4 Rs. 2500/- p.m.
Rs. 1,20,000/-
B.1.8.3 Mobility support for ASHA programme at the subdivision level
11 x 12 months
Rs. 2000/- p.m.
Rs. 2,64,000/-
B.1.8.4 ASHA Facilitator 15 visit pm. x 8 month x 400 facilitator
Rs. 100 /- per visit
Rs. 48,00,000/-
B.1.9. Recurring Office Expenditure
Staffs of the ASHAs resource center is to be given support for the recurring office expenditure in the following form. The details of the activities which will be conducted with the amount will be submitted to finance department. Sl.No. Activity Unit Unit Cost Amount B.1.9.1 Office expenses of
ASHA resource centre at district level
4 x 12 month
Rs. 500/- p.m. Rs.24000/-
101
B.1.9.2 Office expenses ASHA resource centre at Subdivision Level.
11 x 12 month
Rs. 500/- p.m. Rs.66000/-
B. 1.10. : “ASHA-r- VAROSA DIVAS” – an immediate support initiative to
ASHA:-
For the first time in Tripura the concept of “ASHA- VAROSA DIVAS” will be introduced. Varosha is an immediate support initiative to ASHAs, who will be directly facilitated at the monthly meeting of Sub-divisional ASHA Programme Manager with ASHAs & ASHA facilitators at the concern subdivisions in 2 batches. In the said meeting ASHA can clarify all their confusions concerning activities in the field & pending problems of incentives. ASHA will require to fill format which will include their respective activities & status of incentive including pending status & to bring it to the said meetings so that SDAPM can record it & can intimate these reports to the districts & states. In each of the said meetings two resource persons (PRI members/MO/IC/SAPM/DAPM/SAPM/trainees of 1st – 7th module) will make their valuable discussion on the topics related to 1st – 7th module & ASHAs will be oriented on different field level issues so that they can improve their performances in the filed.
Budget breakup for ASHA VAROSA Divas- Monthly meeting of DAPM/SDAPM with ASHA & ASHA facilitators. Sl no. Activity Unit Unit cost Amount
1. Honorarium to ASHA 7367 Rs.100/- x 10 months 7367000
2. Refreshment to ASHA & others (resource person, ASHA facilitators & organizers)
7367 Rs. 40/- x 10 months 2946800
3.
Honorarium for resource persons (one Resource person per meeting & total 100 health facilities in 10 months )
1 100 x 10 x 100 100000
Total budget (2011-12) 10413800
B.1.11. Other Activities B.1.11.1.: ASHA Help Desk & Rest room (ASHA-r-Ghar)
One of the important objectives of NRHM is to increase institutional deliveries with a view to bring about reduction in MMR and IMR. To motivate the mother to be able to reach to an institution for delivery, ASHA has been assigned the task of accompanying pregnant lady to the health facility for delivery. Often ASHA reaches the health institution with the pregnant women after covering a lot of distance. The pregnant woman after delivery is expected to stay in the health facility for at least 48 hr. for observation before she is discharged. It is desirable though not mandatory for ASHAs accompanying the pregnant lady need to stay in the health facility with her. Therefore, it is essential for ASHA to have her stay arrangement within the campus of the health facility. A help desk to provide required information/support to ASHAs & patients referred by her is also needed.
The facility will offer reasonable accommodation (a room with provision of at least two beds) exclusively to be used by ASHA for her stay while she comes to
102
the health facility accompanying pregnant lady for delivery (for at least 48hrs to 72 hrs). ASHAs should be allowed to stay for longer duration. The room should be neat and clean, safe, with basic requirements of stay such as, beds, bed sheets, pillows, drinking water etc. and have easy access to bathroom/toilet. The room should be available for 24x7.
It is proposed to establish the Rest room / ASHA-r–Ghar in 15 nos. of Health facilities (11 Sub Divisional Hospital, 2 District Hospitals, 1 State Hospital & 1 Medical College& Hospital). However, if it is not feasible in any of the mentioned facilities then alternate options will be opted to select the other health facilities where it will be feasible. Rogi Kalyan Samiti of the health institution will do the overall management of the ASHA-r–Ghar.
The state proposes to run ASHA help desk at all the health institutions. For this purpose the concern health facility will appoint one of its existing staffs as nodal person. Once the ASHA facilitators are recruited they will be engaged in the said work B.1.11.2.: ASHA Notebook
In 2011-12 the state proposes to provide ASHA & ASHA Facilitator note book to all the ASHAs for recording regular activities. The diary will include space for recording her regular activities & home visit forms in relevant local dialect.
B.1.11.2. District Level ASHA Convention:-
State proposes to organize one day district level ASHA Convention at four districts of the state. 15 % of all the ASHAs from each district may join the convention. There will be an open discussion on different activities and issues related to ASHAs in presence of Officials from District Administration, Health and Family Welfare, Social Welfare & Social Education, members of PRI and Civil Societies. West Tripura:- B.1.11.3. Digital Thermometer:- It is decided to provide a digital thermometer to all ASHAs as a digital thermometer can be used for many years. Budget breakup: - Rs. 5, 89,600/- @ Rs.80/- per thermometer for total 7367 nos. of ASHAs (total 7370 nos. of thermometers required, extra 3 nos).
Activity Unit Cost ( Fig.in Rs.)
Physical Target
Required fund under NRHM (Rs. In Lakhs)
ASHA note book 50 per note book 7800 Rs.390000/-
Activity West Tripura South Tripura
North Tripura
Dhalai Tripura
Venue Charge 10000 3000 3000 2000 Hall Decoration 1000 1000 1000 1000 Honorarium for ASHA( @ Rs.100/- per ASHA for 15 % ASHA)
45500 28600 21600 14600
Lunch 45500 28600 21600 14600 Mis. Cost 4000 3000 3000 3000 TOTAL 106000 64200 50200 35200 Grand Total Rs. 255600/- (Rupees Two Lakh Fifty Five
Thousand Six Hundred)

103
B.1.11.4. Printing of ASHA 7th Module:- The state proposes to procure 7th module in Bengali through NHSRC, New Delhi for providing training to ASHAs (7367 nos ) and ASHA facilitator (400 nos.) Budget breakup: - Rs. 4, 90,000/- for total 8000 copies (for ASHAs and ASHA facilitators) B.1.11.5. Flip Chart for ASHA:-The state proposes to Procure a flip chart containing messages in Bengali on health using pictures developed by NHSRC for providing to each ASHA and ASHA facilitator. And it will be very effective in making awareness among the pregnant women & mothers in the village. Approximate cost of per flip chart is Rs. 43.50/-. The total requirement of fund will be = Rs. 3, 48,000 /- (8000 X 43.50)/- ( i.e. Rupees Three Lakh Forty Eight Thousand) only. The state proposes to incur the required fund from the allotted fund (uncommitted expenditure) for 2010-11.
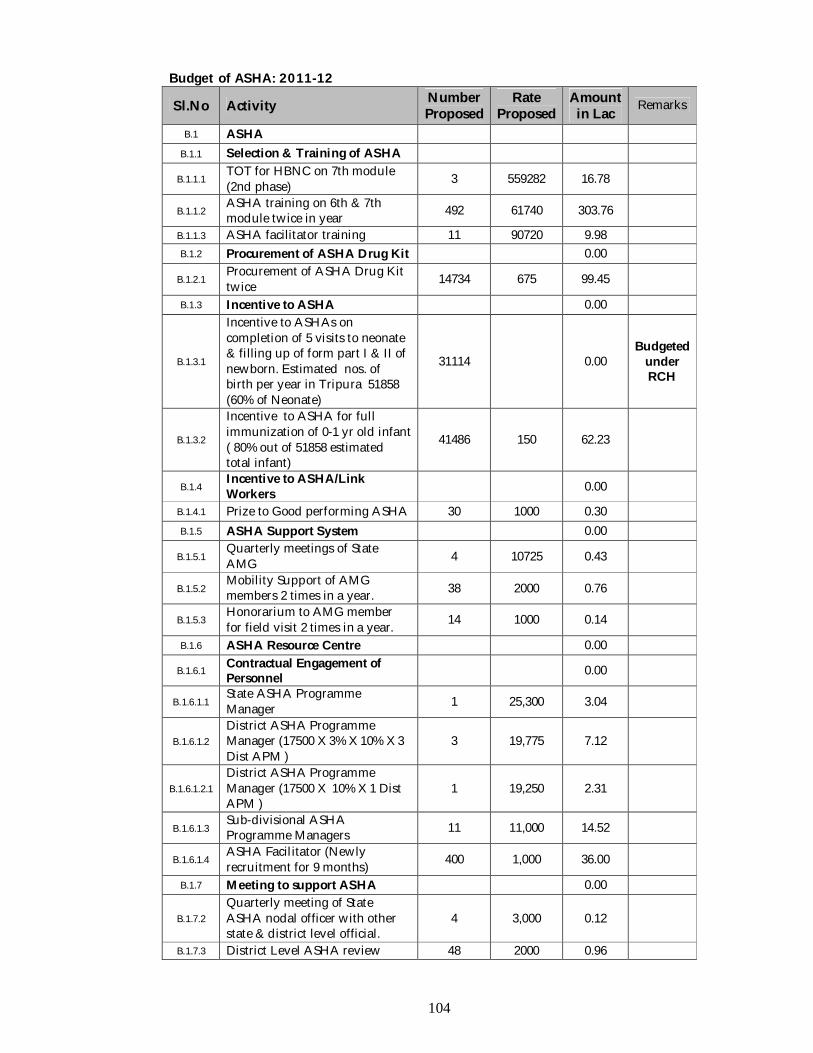
104
Budget of ASHA: 2011-12
Sl.No Activity Number Proposed
Rate Proposed
Amount in Lac Remarks
B.1 ASHA B.1.1 Selection & Training of ASHA
B.1.1.1 TOT for HBNC on 7th module (2nd phase) 3 559282 16.78
B.1.1.2 ASHA training on 6th & 7th module twice in year 492 61740 303.76
B.1.1.3 ASHA facilitator training 11 90720 9.98 B.1.2 Procurement of ASHA Drug Kit 0.00
B.1.2.1 Procurement of ASHA Drug Kit twice 14734 675 99.45
B.1.3 Incentive to ASHA 0.00
B.1.3.1
Incentive to ASHAs on completion of 5 visits to neonate & filling up of form part I & II of newborn. Estimated nos. of birth per year in Tripura 51858 (60% of Neonate)
31114 0.00 Budgeted
under RCH
B.1.3.2
Incentive to ASHA for full immunization of 0-1 yr old infant ( 80% out of 51858 estimated total infant)
41486 150 62.23
B.1.4 Incentive to ASHA/Link Workers 0.00
B.1.4.1 Prize to Good performing ASHA 30 1000 0.30 B.1.5 ASHA Support System 0.00
B.1.5.1 Quarterly meetings of State AMG 4 10725 0.43
B.1.5.2 Mobility Support of AMG members 2 times in a year. 38 2000 0.76
B.1.5.3 Honorarium to AMG member for field visit 2 times in a year. 14 1000 0.14
B.1.6 ASHA Resource Centre 0.00
B.1.6.1 Contractual Engagement of Personnel 0.00
B.1.6.1.1 State ASHA Programme Manager 1 25,300 3.04
B.1.6.1.2 District ASHA Programme Manager (17500 X 3% X 10% X 3 Dist APM )
3 19,775 7.12
B.1.6.1.2.1 District ASHA Programme Manager (17500 X 10% X 1 Dist APM )
1 19,250 2.31
B.1.6.1.3 Sub-divisional ASHA Programme Managers 11 11,000 14.52
B.1.6.1.4 ASHA Facilitator (Newly recruitment for 9 months) 400 1,000 36.00
B.1.7 Meeting to support ASHA 0.00
B.1.7.2 Quarterly meeting of State ASHA nodal officer with other state & district level official.
4 3,000 0.12
B.1.7.3 District Level ASHA review 48 2000 0.96
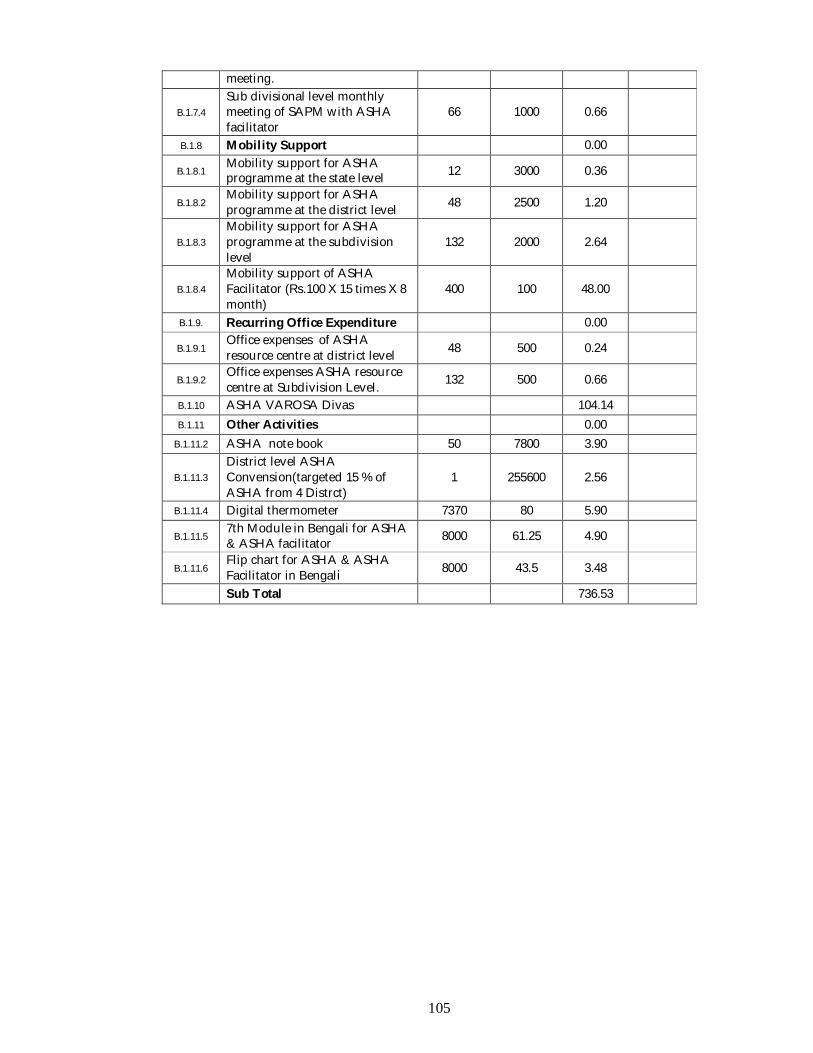
105
meeting.
B.1.7.4 Sub divisional level monthly meeting of SAPM with ASHA facilitator
66 1000 0.66
B.1.8 Mobility Support 0.00
B.1.8.1 Mobility support for ASHA programme at the state level 12 3000 0.36
B.1.8.2 Mobility support for ASHA programme at the district level 48 2500 1.20
B.1.8.3 Mobility support for ASHA programme at the subdivision level
132 2000 2.64
B.1.8.4 Mobility support of ASHA Facilitator (Rs.100 X 15 times X 8 month)
400 100 48.00
B.1.9. Recurring Office Expenditure 0.00
B.1.9.1 Office expenses of ASHA resource centre at district level 48 500 0.24
B.1.9.2 Office expenses ASHA resource centre at Subdivision Level. 132 500 0.66
B.1.10 ASHA VAROSA Divas 104.14 B.1.11 Other Activities 0.00
B.1.11.2 ASHA note book 50 7800 3.90
B.1.11.3 District level ASHA Convension(targeted 15 % of ASHA from 4 Distrct)
1 255600 2.56
B.1.11.4 Digital thermometer 7370 80 5.90
B.1.11.5 7th Module in Bengali for ASHA & ASHA facilitator 8000 61.25 4.90
B.1.11.6 Flip chart for ASHA & ASHA Facilitator in Bengali 8000 43.5 3.48
Sub Total 736.53
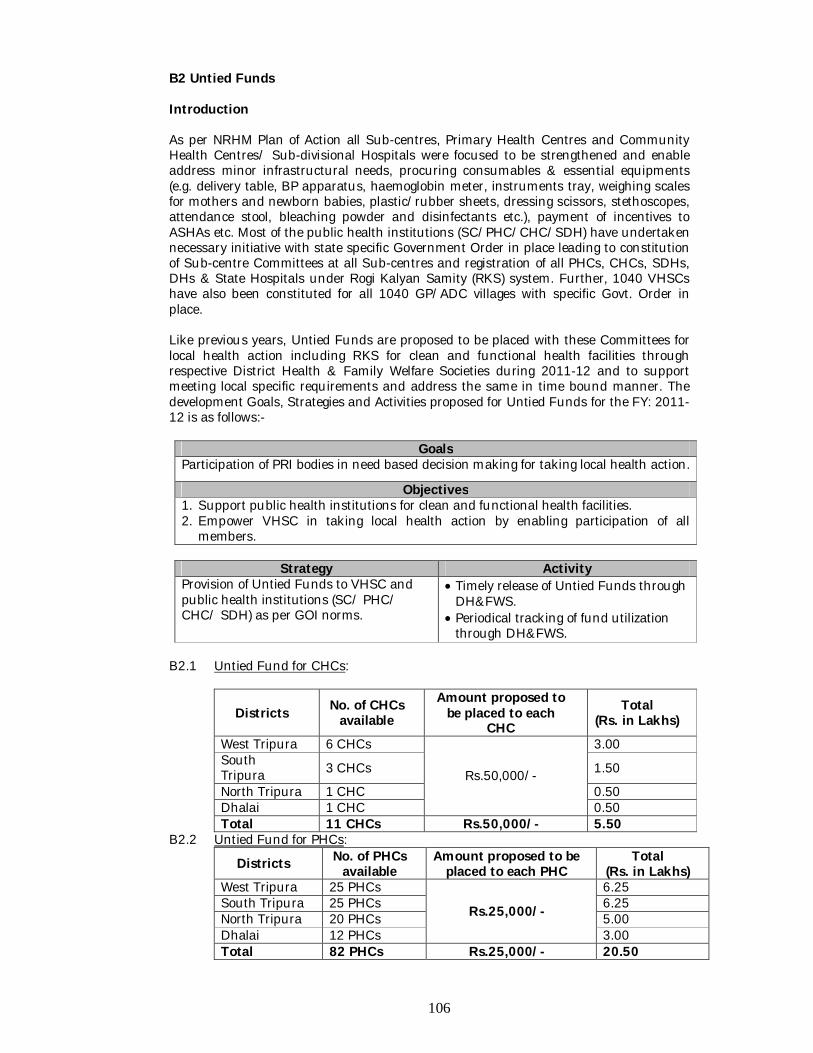
106
B2 Untied Funds Introduction As per NRHM Plan of Action all Sub-centres, Primary Health Centres and Community Health Centres/ Sub-divisional Hospitals were focused to be strengthened and enable address minor infrastructural needs, procuring consumables & essential equipments (e.g. delivery table, BP apparatus, haemoglobin meter, instruments tray, weighing scales for mothers and newborn babies, plastic/rubber sheets, dressing scissors, stethoscopes, attendance stool, bleaching powder and disinfectants etc.), payment of incentives to ASHAs etc. Most of the public health institutions (SC/PHC/CHC/SDH) have undertaken necessary initiative with state specific Government Order in place leading to constitution of Sub-centre Committees at all Sub-centres and registration of all PHCs, CHCs, SDHs, DHs & State Hospitals under Rogi Kalyan Samity (RKS) system. Further, 1040 VHSCs have also been constituted for all 1040 GP/ADC villages with specific Govt. Order in place. Like previous years, Untied Funds are proposed to be placed with these Committees for local health action including RKS for clean and functional health facilities through respective District Health & Family Welfare Societies during 2011-12 and to support meeting local specific requirements and address the same in time bound manner. The development Goals, Strategies and Activities proposed for Untied Funds for the FY: 2011-12 is as follows:-
Goals Participation of PRI bodies in need based decision making for taking local health action.
Objectives 1. Support public health institutions for clean and functional health facilities. 2. Empower VHSC in taking local health action by enabling participation of all
members.
Strategy Activity Provision of Untied Funds to VHSC and public health institutions (SC/ PHC/ CHC/ SDH) as per GOI norms.
Timely release of Untied Funds through DH&FWS.
Periodical tracking of fund utilization through DH&FWS.
B2.1 Untied Fund for CHCs:
Districts No. of CHCs available
Amount proposed to be placed to each
CHC Total
(Rs. in Lakhs)
West Tripura 6 CHCs
Rs.50,000/-
3.00 South Tripura 3 CHCs 1.50
North Tripura 1 CHC 0.50 Dhalai 1 CHC 0.50 Total 11 CHCs Rs.50,000/- 5.50
B2.2 Untied Fund for PHCs:
Districts No. of PHCs available
Amount proposed to be placed to each PHC
Total (Rs. in Lakhs)
West Tripura 25 PHCs
Rs.25,000/-
6.25 South Tripura 25 PHCs 6.25 North Tripura 20 PHCs 5.00 Dhalai 12 PHCs 3.00 Total 82 PHCs Rs.25,000/- 20.50
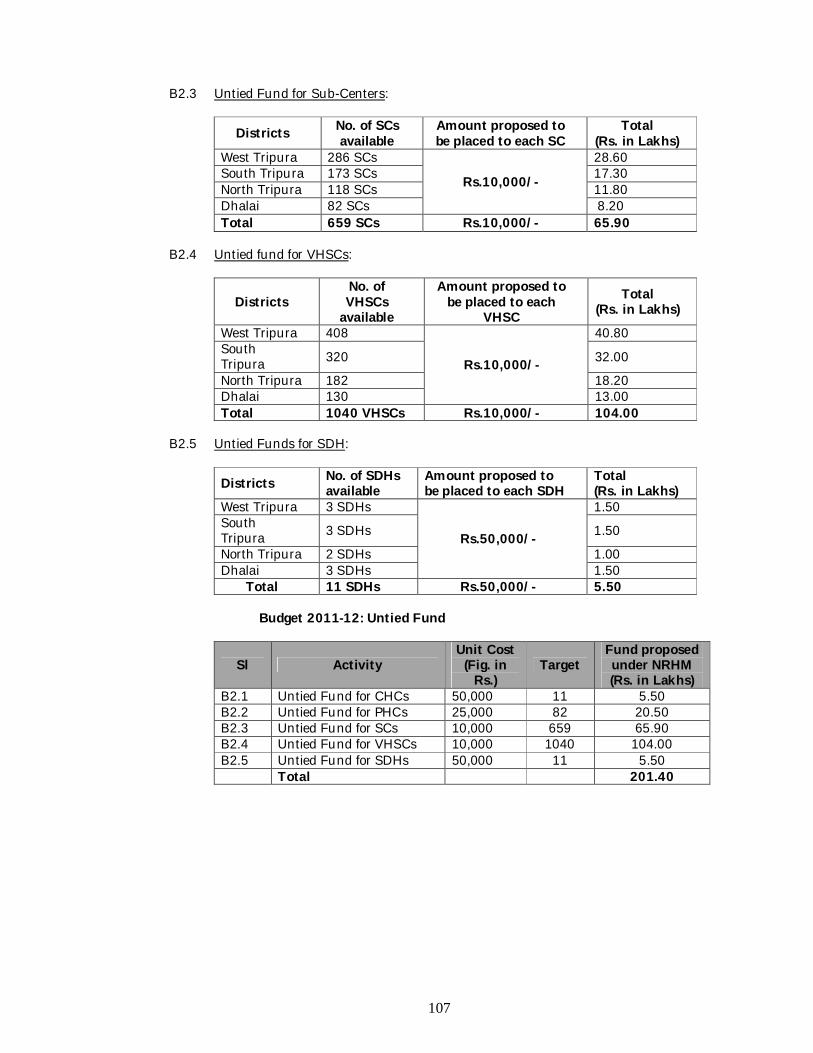
107
B2.3 Untied Fund for Sub-Centers:
Districts No. of SCs available
Amount proposed to be placed to each SC
Total (Rs. in Lakhs)
West Tripura 286 SCs
Rs.10,000/-
28.60 South Tripura 173 SCs 17.30 North Tripura 118 SCs 11.80 Dhalai 82 SCs 8.20 Total 659 SCs Rs.10,000/- 65.90
B2.4 Untied fund for VHSCs:
Districts No. of VHSCs
available
Amount proposed to be placed to each
VHSC Total
(Rs. in Lakhs)
West Tripura 408
Rs.10,000/-
40.80 South Tripura 320 32.00
North Tripura 182 18.20 Dhalai 130 13.00 Total 1040 VHSCs Rs.10,000/- 104.00
B2.5 Untied Funds for SDH:
Districts No. of SDHs available
Amount proposed to be placed to each SDH
Total (Rs. in Lakhs)
West Tripura 3 SDHs
Rs.50,000/-
1.50 South Tripura 3 SDHs 1.50
North Tripura 2 SDHs 1.00 Dhalai 3 SDHs 1.50
Total 11 SDHs Rs.50,000/- 5.50 Budget 2011-12: Untied Fund
Sl Activity Unit Cost (Fig. in
Rs.) Target
Fund proposed under NRHM (Rs. in Lakhs)
B2.1 Untied Fund for CHCs 50,000 11 5.50 B2.2 Untied Fund for PHCs 25,000 82 20.50 B2.3 Untied Fund for SCs 10,000 659 65.90 B2.4 Untied Fund for VHSCs 10,000 1040 104.00 B2.5 Untied Fund for SDHs 50,000 11 5.50 Total 201.40
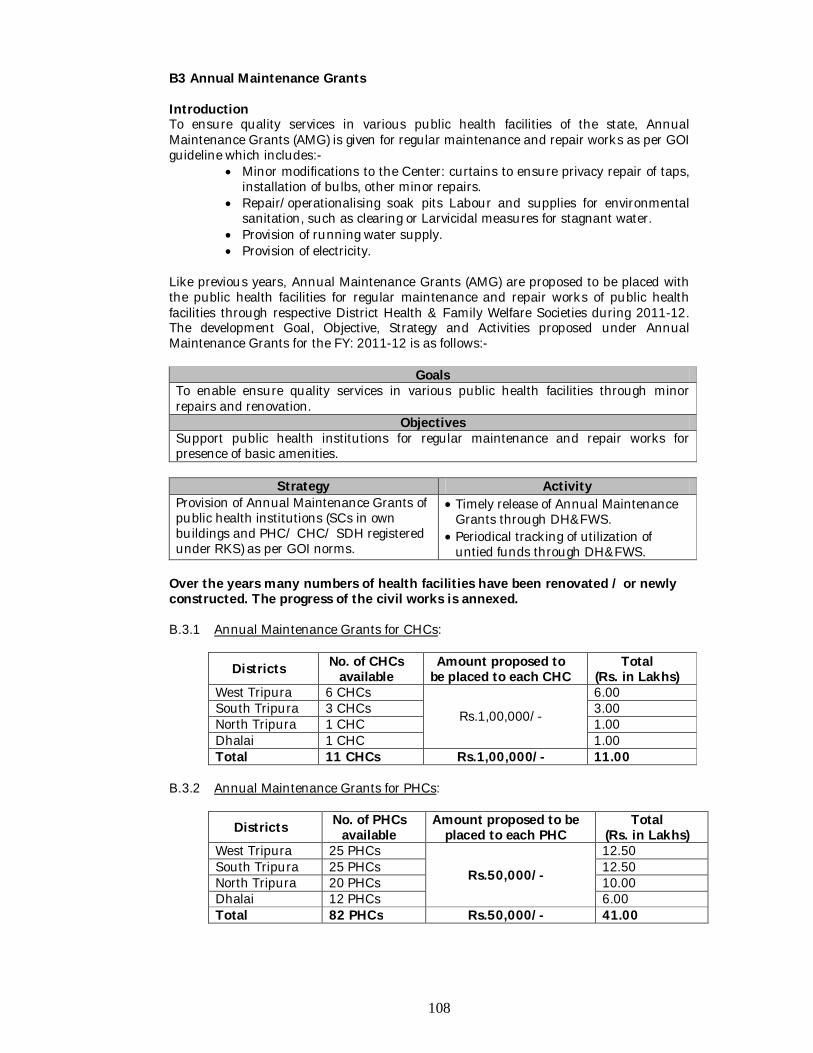
108
B3 Annual Maintenance Grants Introduction To ensure quality services in various public health facilities of the state, Annual Maintenance Grants (AMG) is given for regular maintenance and repair works as per GOI guideline which includes:-
Minor modifications to the Center: curtains to ensure privacy repair of taps, installation of bulbs, other minor repairs.
Repair/operationalising soak pits Labour and supplies for environmental sanitation, such as clearing or Larvicidal measures for stagnant water.
Provision of running water supply. Provision of electricity.
Like previous years, Annual Maintenance Grants (AMG) are proposed to be placed with the public health facilities for regular maintenance and repair works of public health facilities through respective District Health & Family Welfare Societies during 2011-12. The development Goal, Objective, Strategy and Activities proposed under Annual Maintenance Grants for the FY: 2011-12 is as follows:-
Goals To enable ensure quality services in various public health facilities through minor repairs and renovation.
Objectives Support public health institutions for regular maintenance and repair works for presence of basic amenities.
Strategy Activity
Provision of Annual Maintenance Grants of public health institutions (SCs in own buildings and PHC/ CHC/ SDH registered under RKS) as per GOI norms.
Timely release of Annual Maintenance Grants through DH&FWS.
Periodical tracking of utilization of untied funds through DH&FWS.
Over the years many numbers of health facilities have been renovated / or newly constructed. The progress of the civil works is annexed. B.3.1 Annual Maintenance Grants for CHCs:
Districts No. of CHCs available
Amount proposed to be placed to each CHC
Total (Rs. in Lakhs)
West Tripura 6 CHCs
Rs.1,00,000/-
6.00 South Tripura 3 CHCs 3.00 North Tripura 1 CHC 1.00 Dhalai 1 CHC 1.00 Total 11 CHCs Rs.1,00,000/- 11.00
B.3.2 Annual Maintenance Grants for PHCs:
Districts No. of PHCs available
Amount proposed to be placed to each PHC
Total (Rs. in Lakhs)
West Tripura 25 PHCs
Rs.50,000/-
12.50 South Tripura 25 PHCs 12.50 North Tripura 20 PHCs 10.00 Dhalai 12 PHCs 6.00 Total 82 PHCs Rs.50,000/- 41.00
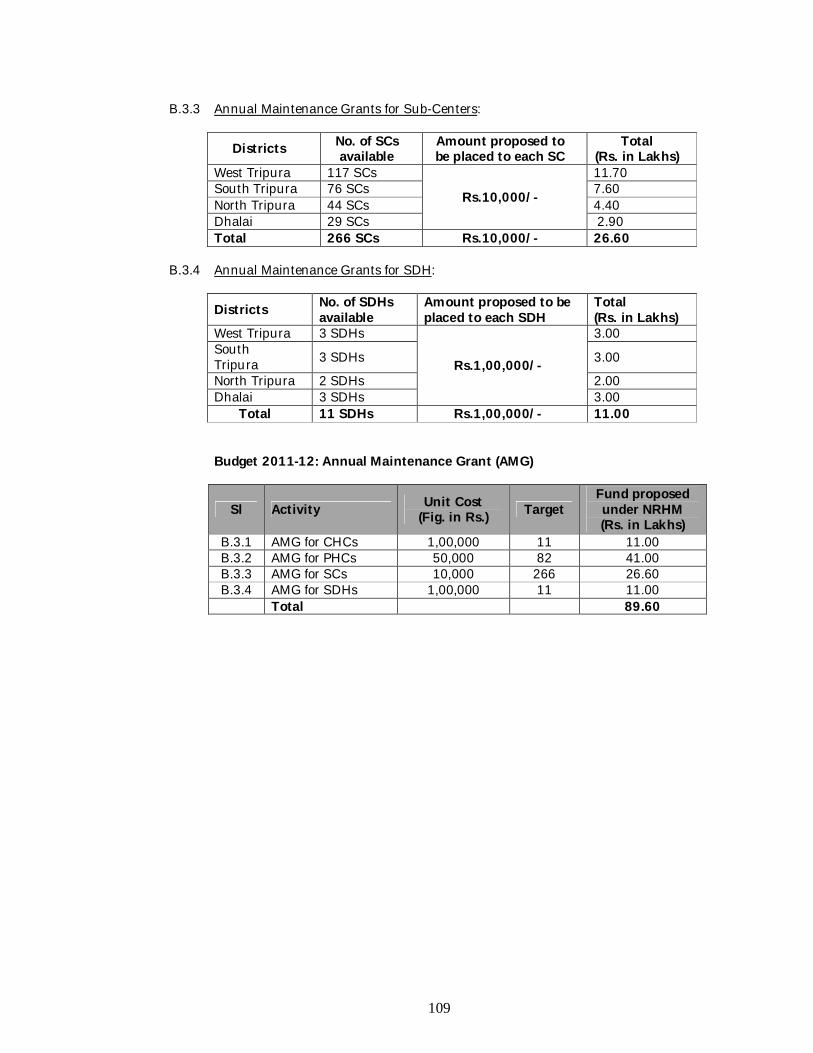
109
B.3.3 Annual Maintenance Grants for Sub-Centers:
Districts No. of SCs available
Amount proposed to be placed to each SC
Total (Rs. in Lakhs)
West Tripura 117 SCs
Rs.10,000/-
11.70 South Tripura 76 SCs 7.60 North Tripura 44 SCs 4.40 Dhalai 29 SCs 2.90 Total 266 SCs Rs.10,000/- 26.60
B.3.4 Annual Maintenance Grants for SDH:
Districts No. of SDHs available
Amount proposed to be placed to each SDH
Total (Rs. in Lakhs)
West Tripura 3 SDHs
Rs.1,00,000/-
3.00 South Tripura 3 SDHs 3.00
North Tripura 2 SDHs 2.00 Dhalai 3 SDHs 3.00
Total 11 SDHs Rs.1,00,000/- 11.00 Budget 2011-12: Annual Maintenance Grant (AMG)
Sl Activity Unit Cost (Fig. in Rs.) Target
Fund proposed under NRHM (Rs. in Lakhs)
B.3.1 AMG for CHCs 1,00,000 11 11.00 B.3.2 AMG for PHCs 50,000 82 41.00 B.3.3 AMG for SCs 10,000 266 26.60 B.3.4 AMG for SDHs 1,00,000 11 11.00
Total 89.60
110
B.4. Hospital Strengthening B.4.1 Upgradation of SC, CHCs, PHCs, SDHs, District Hospitals to IPHS Situation Analysis Infrastructure strengthening under NRHM has been taken as a crucial part to ensure service quality across the state. Although minor repairs and renovation is maintained through Annual Maintenance Grant (AMG) support under RKS System at SC/ PHC/ CHC/ SDH, there are few institutions which require further renovation works to ensure service quality especially in the un-served & underserved areas of the districts. All construction works are proposed to be RCC Frame Structure with RCC Roof including electrification and Sanitation. As such, series of activities have been undertaken by the state to renovate the identified health infrastructures under NRHM by undertaking repairs, renovation/ minor alteration, expansion and construction of staff quarters leading to enable rendering services as per Indian Public Health Standards (IPHS) in a gradual manner. Although the progress towards matching with the desired objective has been partially retarded due to felt need of presence of desired number of skilled manpower (RCH/ RNTCP/ NVBDCP/ NBCP/ NLEP), timely drug distribution and most importantly system strengthening of the executing/ implementing agencies identified for completing infrastructural works in time, the minimum services have however got enhanced. For instance, all 11 CHCs and 58 out of 79 PHCs are providing 24x7 services in the areas of maternal and child health with well equipped OT/ Labour Room, Laboratory, water supply, sanitation etc. In line with MCH services, all 24x7 PHCs have NBCC with trained NSSK Medical Officers while 30% to 40% of the 24x7 PHCs have SBA trained SNs/ANMs. The two existing District Hospitals have been upgraded to IPHS by doing infrastructural development/ renovation with one time grant of Rs.100.0 L sanctioned by GOI during 2007-08. The development Goal, Objective, Strategy & Activity under Infrastructure Strengthening for 2011-12 is as under:-
Goal Strengthening SC, CHC, PHC, SDHs & District Hospitals to render services at par with Indian Public Health Standards (IPHS).
Objective Support public health institutions (PHC/CHC) in addressing infrastructure gaps to enhance service delivery with requisite skilled manpower, equipments and drugs for RCH as well as Disease Control Programmes laid down in NRHM service guarantees for SCs, PHCs, CHCs, SDHs and DH
Strategy Activity
B.4.1 Upgradation of PHC to SDH (On going Construction).
During 2009-10, Shantirbazar PHC of South Tripura district was proposed to upgrade to 100 bedded Sub-divisional Hospital (SDH) with projected cost of Rs.2757.01 L (Estimated Cost). Out of this, fund amounting Rs.1001.70 L was approved as 1st installment and the activity against the 1st installment is completed. UCs have been received accordingly. During 2011-12, 25% fund of its 2nd installment Rs.1755.31 L amounting Rs. Rs.438.827L is proposed.
B.4.2 Fund for on-going construction works at
8 new PHCs were undertaken by the Health Dept. for new construction which was approved during 2009-10 as follows:-
111
Strategy Activity PHCs (continuation of 2009-10 activity)
New PHCs 1. West Tripura (Ratanpur) 2. South Tripura (Paikhola) 3. North Tripura (Haluicherra) 4. Dhalai (Nepaltilla)
New Building in existing PHC
1. South Tripura (Karbook & Baikhora) 2. Dhalai (Ambassa & Manikpur)
The activity is assigned to PWD/ District authorities/ Directorate of Family Welfare and is in progress. 87.5% (Rs.360.50 L) sanctioned for each PHC, remaining 12.5% @ Rs.51.50 L each is proposed for 2011-12 which amounts to Rs.412.00 Lakhs
Budget 2011-12: Hospital Strengthening
Sl No Activity Target Unit Cost Amount (In lac) Remarks
B.4 Hospital Strengthening 0
B.4.1
Upgradation of PHC to SDH (2009-10 activity) Santirbazar Rs.1001.70 L approved as 1st installment during 2009-10. 25% fund of its 2nd installment Rs.1755.31 L amounting Rs.438.827 proposed for 2011-12.
1 275701000 438.8275
B.4.2
Construction of new PHCs (Activity of 2009-10). Remaining 12.5% @ Rs.51.50 L each is proposed for 2011-12
8 5150000 412
Sub Total 850.83
112
B.5. New Constructions/ Renovation and Setting up Introduction Setting up of new public health facilities to reach the un-served and under served population is prioritized under NRHM. Necessary steps have been taken towards achieving this end in line with state’s plan/ requirement. The population norm while planning to establish new health institution is taken into account by correlating with RHS-2009 statistics. Besides setting up of public health infrastructures, new construction are also taken up in the areas of strengthening training infrastructure to ensure adequate presence of skilled manpower in near future. All construction works are proposed to be RCC Frame Structure with RCC Roof including electrification and Sanitation. It is to further mention that, Bio-medical Waste Management (BWM) under IMEP is implemented as an ancillary activity of upgrading to IPHS since 2007-08. So far, 74 PHCs have been covered. Remaining facilities viz. 4 PHCs, 11 CHCs, 11 SDHs & 2 DHs were attempted for coverage during 2010-11. Tender/EOI was floated but agency could not the finalized as their proposals to implement Bio-medical management did not match with Department and State Pollution Control Board’s requirement in state’s context. Moreover, there is policy issue to be considered, if Bio-medical Waste Management Strategy is going to be implemented based on Central Treatment Facility (CTF) or Facility specific. However, it has been decided to outsource the activity of continuing implementation at 74 PHCs and activating at 8 PHCs, 11 CHCs, 11 SDHs & 2 DHs to a single agency for better implementation, monitoring and output. Therefore, the activity is proposed to be revalidated for 2011-12 with its associated approved budget and implementation by addressing strategic issues. The development Goal, Objective, Strategy and Activities of 2011-12 under new construction/renovation and setting up are as follows:-
Goal To set up new health infrastructure to meet service gaps and enable access to quality services by rural population.
Objective 1. Enable to supplement setting up new PHC/SC to meet service gaps as projected in
the state plan/ requirements. 2. Support existing public health institutions in undertaking major renovation works as
well as Civil Works for Opertaionalization of Infection Management & Environment Plan.
Strategy Activity
B.5.1
On going activity of construction of PHC
Construction of 8 new PHCs with Staff Quarters (RCC Frame Structure Building with electrification & sanitation) @ Rs.630.00 L (PWD SoR) each were proposed as follows:-
- West Tripura – Taxapara - South Tripura – Baishnabpur & Ratanpur - North Tripura – Rajkandi, Muruaibari &
Bhaterbazar - Dhalai Tripura – Lalcharra & Masli
One third of 630.00 L @ Rs.210.0 L for each PHC was sought and GOI had approved Rs.12.00 L against the demand of 30% as 1st installment for 8 PHCs amounting Rs.1680.00 L.
113
Strategy Activity Considering the price escalation and transportation cost of materials in NE Region, the estimated cost in DPR of each PHC may be considered for kind approval. Copies of the DPR have been shared with GOI for appraisal. Fund approved earlier of Rs.12.00 Lakhs is proposed for revalidation and consolidation with 12.5% demand @ Rs.78.75 L each PHC as 1st installment of 2011-12 which amounts to Rs.630.00 Lakhs. PWD is the authorized implementing agency.
B.5.2 New construction for existing 2 nos. PHC
building
Two functional PHCs namely Dayarampara PHC of West Tripura, Kalacherra PHC of South Tripura is proposed to be provided with new PHC building (RCC Frame Structure Building with electrification & sanitation) during 2011-12 with following features:-
i. New PHC building - (Single storied with double storied provision).
ii. Staff quarters [4 nos. Type-I (Twin) Triple Storied; 4 nos. Type-II (Twin) Triple Storied 2 nos. Type-IV (Twin) Double Storied)
Preliminary Estimated Cost (2011-12) Sl Particulars No. of
Unit Amount (Rs. in Lakhs)
1 PHC Building (Single storied with double storied provision) – 1230 sqr meter – building area.
1 Rs.491.00
2 Type-I (Twin) Double Storied
4 Rs. 69.49
3 Type-II (Twin) Double Storied
4 Rs. 83.42
4 Type-III (Twin) Single Storied
2 Rs. 58.21
5 Site Development Rs.31.00 TOTAL Rs.733.12 6 Add @ 3%
Contingencies Rs.21.99
GRAND TOTAL Rs.755.11 SAY Rs.755.00
Fund to the tune of Rs.755.00 L per PHC including Staff Quarters as per PWD SoR is provisioned. 12.5% of Rs.755.00 L of each PHC comes to Rs.94.37 L. The fund required against total project cost of Rs.1510.00 L is Rs.188.75 L which may be considered for implementation during 2011-12
Further, 6 new PHCs are proposed to be constructed (RCC Frame Structure Building with electrification & Sanitation) during 2011-12 in the state. West: Lalgsinghmura.
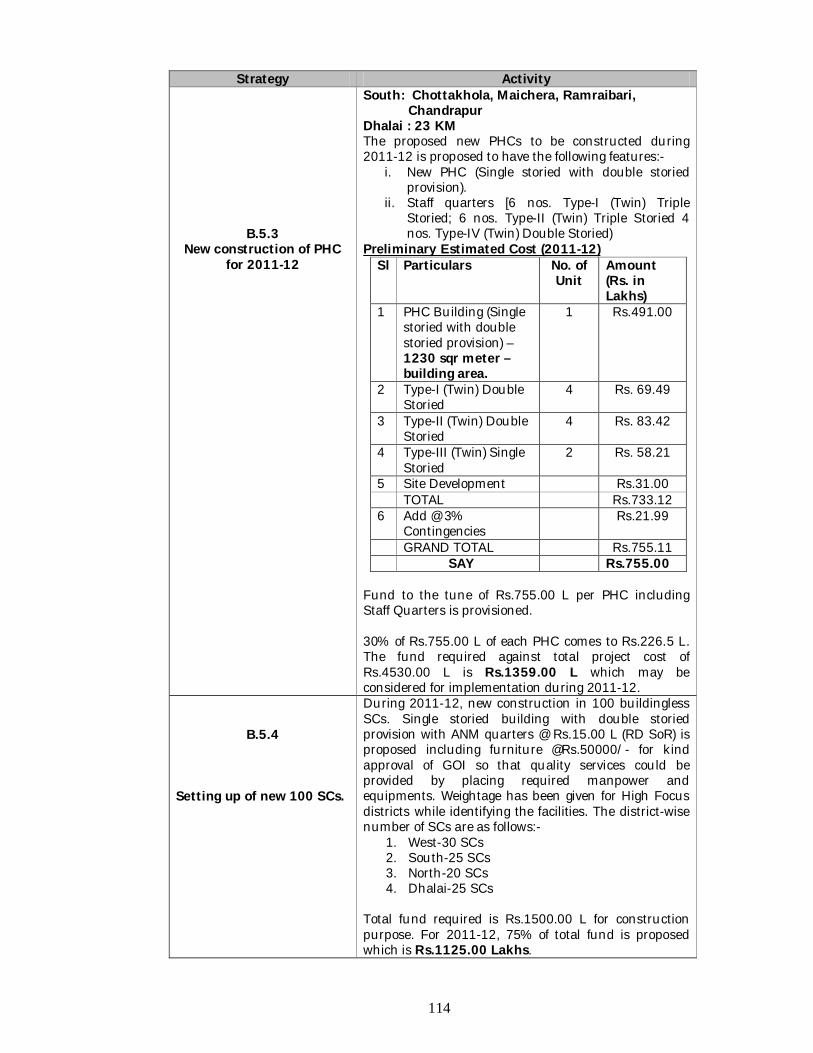
114
Strategy Activity
B.5.3 New construction of PHC
for 2011-12
South: Chottakhola, Maichera, Ramraibari, Chandrapur Dhalai : 23 KM The proposed new PHCs to be constructed during 2011-12 is proposed to have the following features:-
i. New PHC (Single storied with double storied provision).
ii. Staff quarters [6 nos. Type-I (Twin) Triple Storied; 6 nos. Type-II (Twin) Triple Storied 4 nos. Type-IV (Twin) Double Storied)
Preliminary Estimated Cost (2011-12) Sl Particulars No. of
Unit Amount (Rs. in Lakhs)
1 PHC Building (Single storied with double storied provision) – 1230 sqr meter – building area.
1 Rs.491.00
2 Type-I (Twin) Double Storied
4 Rs. 69.49
3 Type-II (Twin) Double Storied
4 Rs. 83.42
4 Type-III (Twin) Single Storied
2 Rs. 58.21
5 Site Development Rs.31.00 TOTAL Rs.733.12 6 Add @ 3%
Contingencies Rs.21.99
GRAND TOTAL Rs.755.11 SAY Rs.755.00
Fund to the tune of Rs.755.00 L per PHC including Staff Quarters is provisioned. 30% of Rs.755.00 L of each PHC comes to Rs.226.5 L. The fund required against total project cost of Rs.4530.00 L is Rs.1359.00 L which may be considered for implementation during 2011-12.
B.5.4 Setting up of new 100 SCs.
During 2011-12, new construction in 100 buildingless SCs. Single storied building with double storied provision with ANM quarters @ Rs.15.00 L (RD SoR) is proposed including furniture @Rs.50000/- for kind approval of GOI so that quality services could be provided by placing required manpower and equipments. Weightage has been given for High Focus districts while identifying the facilities. The district-wise number of SCs are as follows:-
1. West-30 SCs 2. South-25 SCs 3. North-20 SCs 4. Dhalai-25 SCs
Total fund required is Rs.1500.00 L for construction purpose. For 2011-12, 75% of total fund is proposed which is Rs.1125.00 Lakhs.
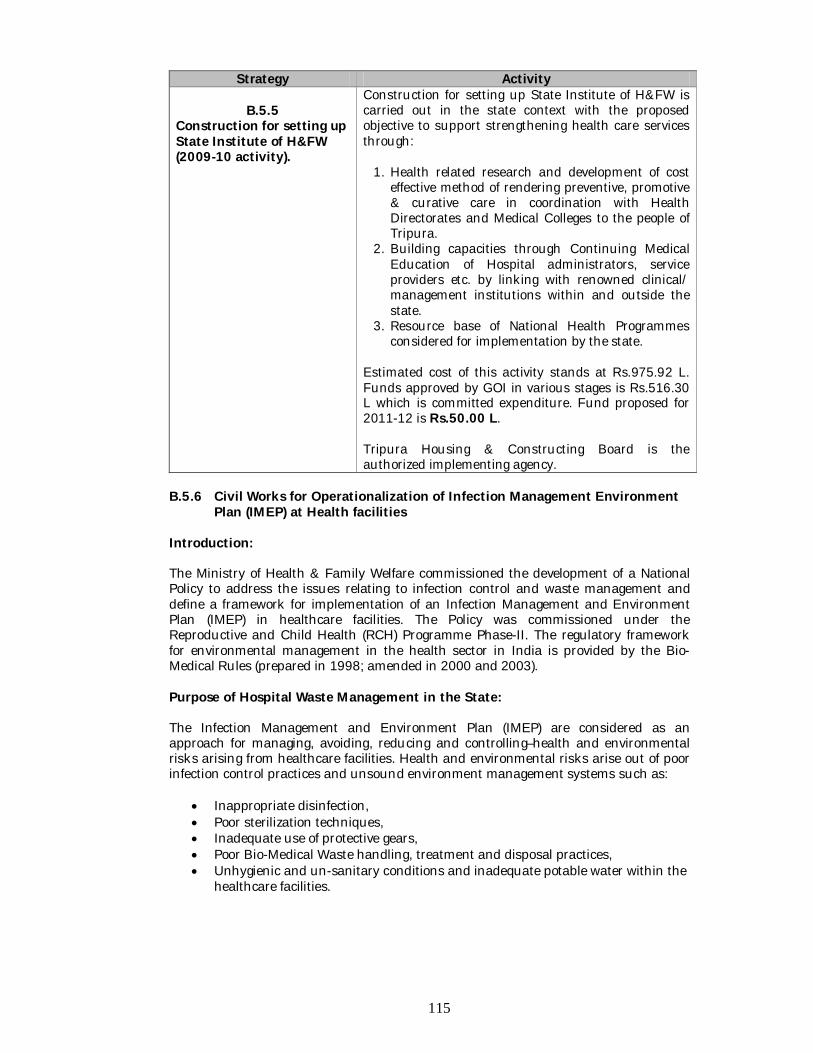
115
Strategy Activity
B.5.5 Construction for setting up State Institute of H&FW (2009-10 activity).
Construction for setting up State Institute of H&FW is carried out in the state context with the proposed objective to support strengthening health care services through:
1. Health related research and development of cost effective method of rendering preventive, promotive & curative care in coordination with Health Directorates and Medical Colleges to the people of Tripura.
2. Building capacities through Continuing Medical Education of Hospital administrators, service providers etc. by linking with renowned clinical/ management institutions within and outside the state.
3. Resource base of National Health Programmes considered for implementation by the state.
Estimated cost of this activity stands at Rs.975.92 L. Funds approved by GOI in various stages is Rs.516.30 L which is committed expenditure. Fund proposed for 2011-12 is Rs.50.00 L. Tripura Housing & Constructing Board is the authorized implementing agency.
B.5.6 Civil Works for Operationalization of Infection Management Environment Plan (IMEP) at Health facilities Introduction: The Ministry of Health & Family Welfare commissioned the development of a National Policy to address the issues relating to infection control and waste management and define a framework for implementation of an Infection Management and Environment Plan (IMEP) in healthcare facilities. The Policy was commissioned under the Reproductive and Child Health (RCH) Programme Phase-II. The regulatory framework for environmental management in the health sector in India is provided by the Bio-Medical Rules (prepared in 1998; amended in 2000 and 2003). Purpose of Hospital Waste Management in the State: The Infection Management and Environment Plan (IMEP) are considered as an approach for managing, avoiding, reducing and controlling–health and environmental risks arising from healthcare facilities. Health and environmental risks arise out of poor infection control practices and unsound environment management systems such as:
Inappropriate disinfection, Poor sterilization techniques, Inadequate use of protective gears, Poor Bio-Medical Waste handling, treatment and disposal practices, Unhygienic and un-sanitary conditions and inadequate potable water within the
healthcare facilities.
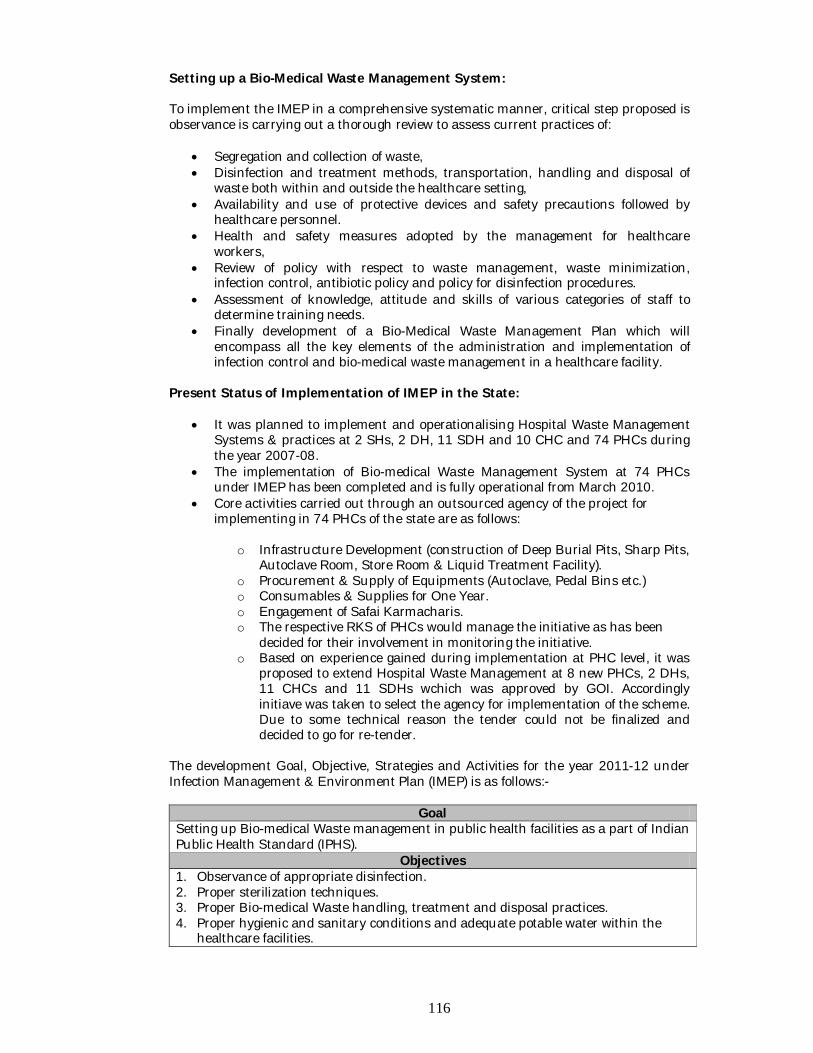
116
Setting up a Bio-Medical Waste Management System: To implement the IMEP in a comprehensive systematic manner, critical step proposed is observance is carrying out a thorough review to assess current practices of:
Segregation and collection of waste, Disinfection and treatment methods, transportation, handling and disposal of
waste both within and outside the healthcare setting, Availability and use of protective devices and safety precautions followed by
healthcare personnel. Health and safety measures adopted by the management for healthcare
workers, Review of policy with respect to waste management, waste minimization,
infection control, antibiotic policy and policy for disinfection procedures. Assessment of knowledge, attitude and skills of various categories of staff to
determine training needs. Finally development of a Bio-Medical Waste Management Plan which will
encompass all the key elements of the administration and implementation of infection control and bio-medical waste management in a healthcare facility.
Present Status of Implementation of IMEP in the State:
It was planned to implement and operationalising Hospital Waste Management Systems & practices at 2 SHs, 2 DH, 11 SDH and 10 CHC and 74 PHCs during the year 2007-08.
The implementation of Bio-medical Waste Management System at 74 PHCs under IMEP has been completed and is fully operational from March 2010.
Core activities carried out through an outsourced agency of the project for implementing in 74 PHCs of the state are as follows:
o Infrastructure Development (construction of Deep Burial Pits, Sharp Pits, Autoclave Room, Store Room & Liquid Treatment Facility).
o Procurement & Supply of Equipments (Autoclave, Pedal Bins etc.) o Consumables & Supplies for One Year. o Engagement of Safai Karmacharis. o The respective RKS of PHCs would manage the initiative as has been
decided for their involvement in monitoring the initiative. o Based on experience gained during implementation at PHC level, it was
proposed to extend Hospital Waste Management at 8 new PHCs, 2 DHs, 11 CHCs and 11 SDHs wchich was approved by GOI. Accordingly initiave was taken to select the agency for implementation of the scheme. Due to some technical reason the tender could not be finalized and decided to go for re-tender.
The development Goal, Objective, Strategies and Activities for the year 2011-12 under Infection Management & Environment Plan (IMEP) is as follows:-
Goal Setting up Bio-medical Waste management in public health facilities as a part of Indian Public Health Standard (IPHS).
Objectives 1. Observance of appropriate disinfection. 2. Proper sterilization techniques. 3. Proper Bio-medical Waste handling, treatment and disposal practices. 4. Proper hygienic and sanitary conditions and adequate potable water within the
healthcare facilities.
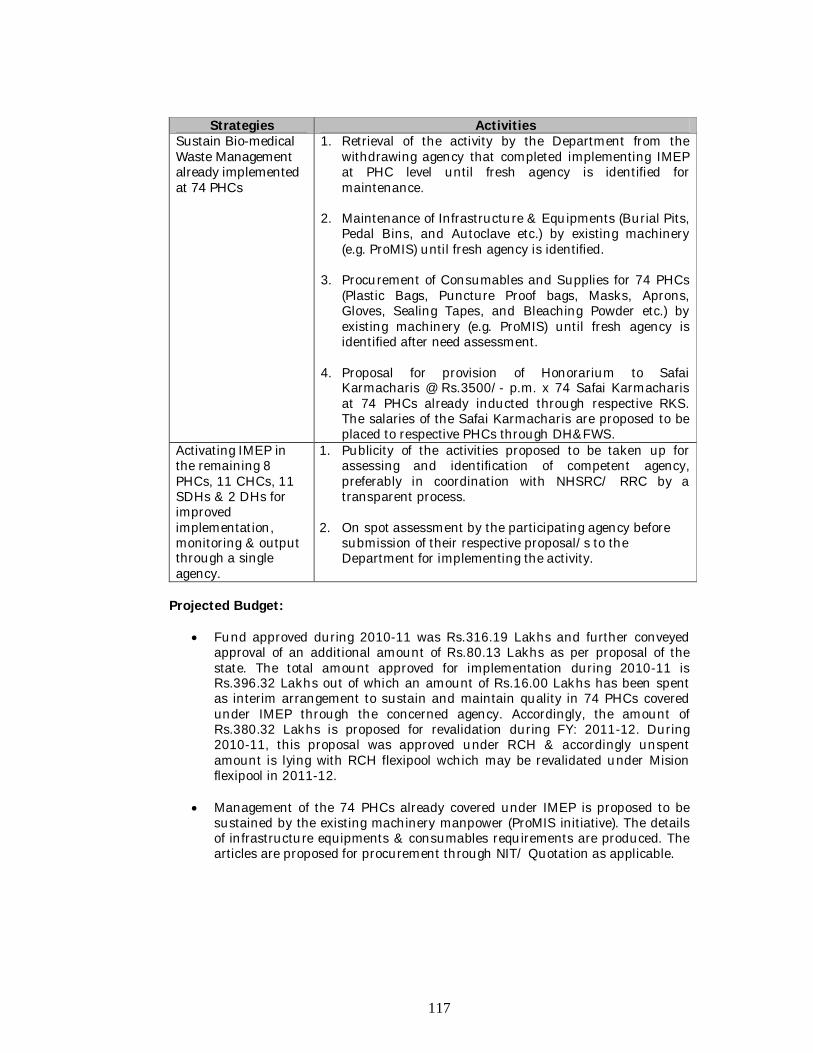
117
Strategies Activities Sustain Bio-medical Waste Management already implemented at 74 PHCs
1. Retrieval of the activity by the Department from the withdrawing agency that completed implementing IMEP at PHC level until fresh agency is identified for maintenance.
2. Maintenance of Infrastructure & Equipments (Burial Pits,
Pedal Bins, and Autoclave etc.) by existing machinery (e.g. ProMIS) until fresh agency is identified.
3. Procurement of Consumables and Supplies for 74 PHCs
(Plastic Bags, Puncture Proof bags, Masks, Aprons, Gloves, Sealing Tapes, and Bleaching Powder etc.) by existing machinery (e.g. ProMIS) until fresh agency is identified after need assessment.
4. Proposal for provision of Honorarium to Safai
Karmacharis @ Rs.3500/- p.m. x 74 Safai Karmacharis at 74 PHCs already inducted through respective RKS. The salaries of the Safai Karmacharis are proposed to be placed to respective PHCs through DH&FWS.
Activating IMEP in the remaining 8 PHCs, 11 CHCs, 11 SDHs & 2 DHs for improved implementation, monitoring & output through a single agency.
1. Publicity of the activities proposed to be taken up for assessing and identification of competent agency, preferably in coordination with NHSRC/ RRC by a transparent process.
2. On spot assessment by the participating agency before submission of their respective proposal/s to the Department for implementing the activity.
Projected Budget:
Fund approved during 2010-11 was Rs.316.19 Lakhs and further conveyed approval of an additional amount of Rs.80.13 Lakhs as per proposal of the state. The total amount approved for implementation during 2010-11 is Rs.396.32 Lakhs out of which an amount of Rs.16.00 Lakhs has been spent as interim arrangement to sustain and maintain quality in 74 PHCs covered under IMEP through the concerned agency. Accordingly, the amount of Rs.380.32 Lakhs is proposed for revalidation during FY: 2011-12. During 2010-11, this proposal was approved under RCH & accordingly unspent amount is lying with RCH flexipool wchich may be revalidated under Mision flexipool in 2011-12.
Management of the 74 PHCs already covered under IMEP is proposed to be sustained by the existing machinery manpower (ProMIS initiative). The details of infrastructure equipments & consumables requirements are produced. The articles are proposed for procurement through NIT/ Quotation as applicable.
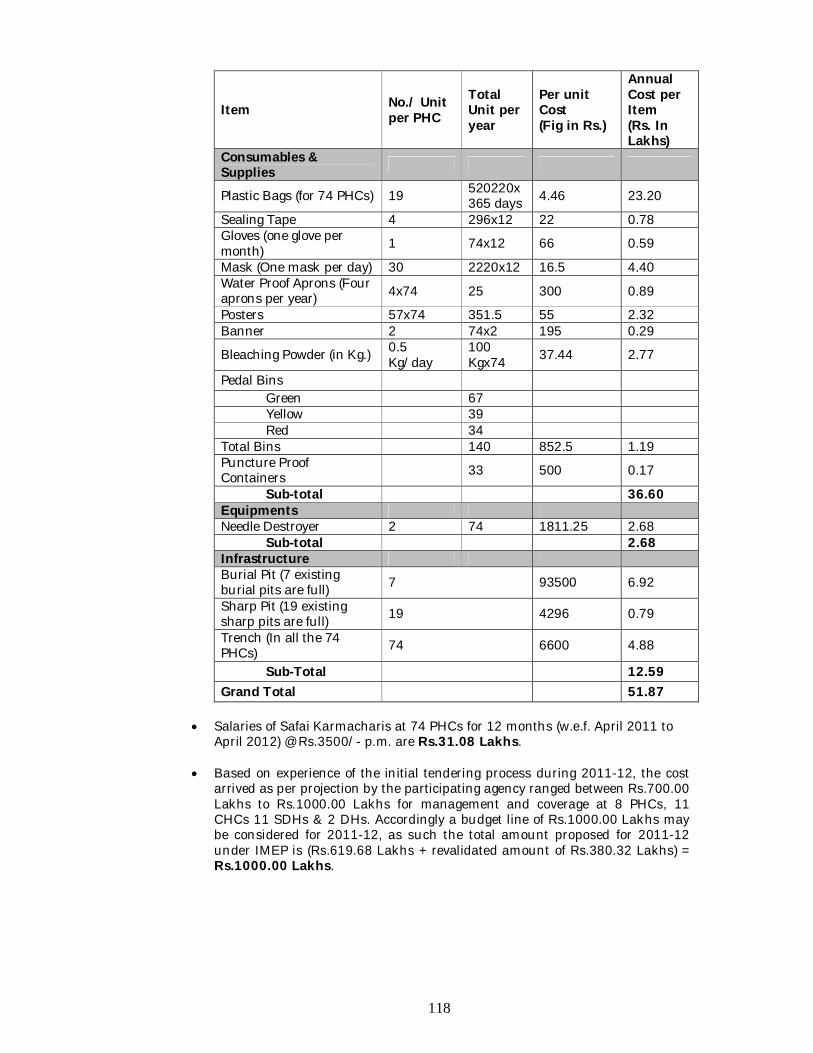
118
Item No./ Unit per PHC
Total Unit per year
Per unit Cost (Fig in Rs.)
Annual Cost per Item (Rs. In Lakhs)
Consumables & Supplies
Plastic Bags (for 74 PHCs) 19 520220x365 days 4.46 23.20
Sealing Tape 4 296x12 22 0.78 Gloves (one glove per month) 1 74x12 66 0.59
Mask (One mask per day) 30 2220x12 16.5 4.40 Water Proof Aprons (Four aprons per year) 4x74 25 300 0.89
Posters 57x74 351.5 55 2.32 Banner 2 74x2 195 0.29
Bleaching Powder (in Kg.) 0.5 Kg/day
100 Kgx74 37.44 2.77
Pedal Bins Green 67 Yellow 39 Red 34 Total Bins 140 852.5 1.19 Puncture Proof Containers 33 500 0.17
Sub-total 36.60 Equipments Needle Destroyer 2 74 1811.25 2.68 Sub-total 2.68 Infrastructure Burial Pit (7 existing burial pits are full) 7 93500 6.92
Sharp Pit (19 existing sharp pits are full) 19 4296 0.79
Trench (In all the 74 PHCs) 74 6600 4.88
Sub-Total 12.59 Grand Total 51.87
Salaries of Safai Karmacharis at 74 PHCs for 12 months (w.e.f. April 2011 to
April 2012) @ Rs.3500/- p.m. are Rs.31.08 Lakhs.
Based on experience of the initial tendering process during 2011-12, the cost arrived as per projection by the participating agency ranged between Rs.700.00 Lakhs to Rs.1000.00 Lakhs for management and coverage at 8 PHCs, 11 CHCs 11 SDHs & 2 DHs. Accordingly a budget line of Rs.1000.00 Lakhs may be considered for 2011-12, as such the total amount proposed for 2011-12 under IMEP is (Rs.619.68 Lakhs + revalidated amount of Rs.380.32 Lakhs) = Rs.1000.00 Lakhs.
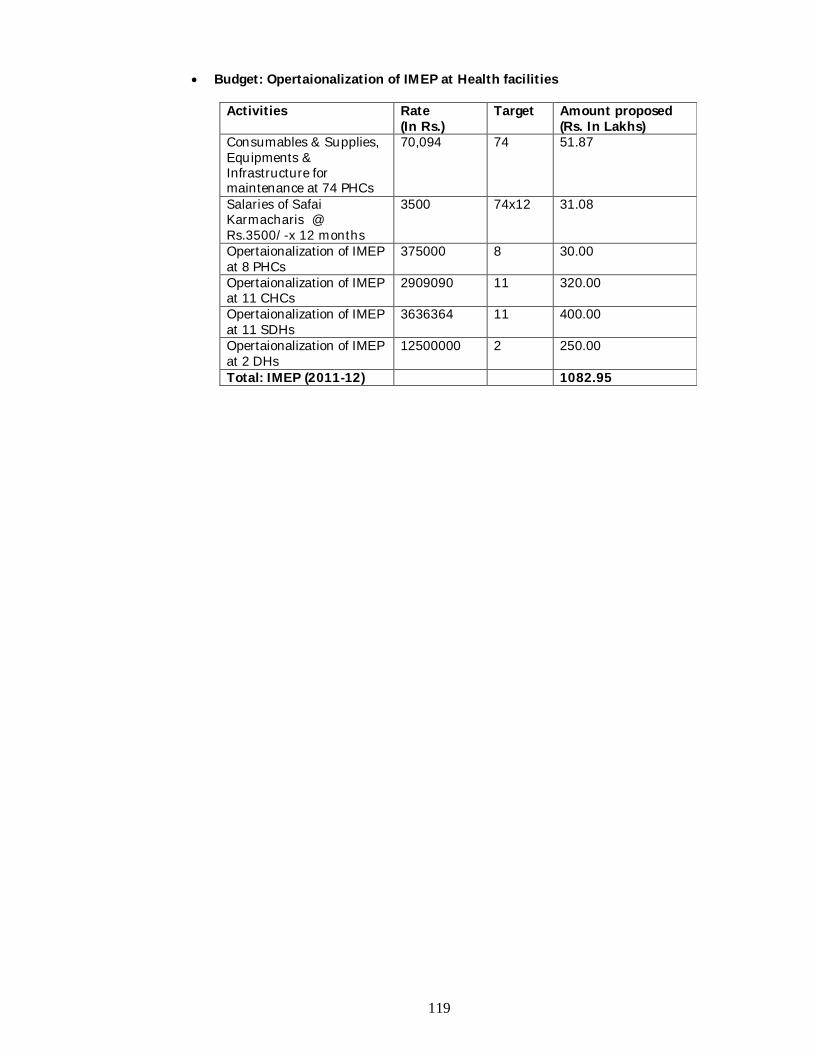
119
Budget: Opertaionalization of IMEP at Health facilities
Activities Rate (In Rs.)
Target Amount proposed (Rs. In Lakhs)
Consumables & Supplies, Equipments & Infrastructure for maintenance at 74 PHCs
70,094 74 51.87
Salaries of Safai Karmacharis @ Rs.3500/-x 12 months
3500 74x12 31.08
Opertaionalization of IMEP at 8 PHCs
375000 8 30.00
Opertaionalization of IMEP at 11 CHCs
2909090 11 320.00
Opertaionalization of IMEP at 11 SDHs
3636364 11 400.00
Opertaionalization of IMEP at 2 DHs
12500000 2 250.00
Total: IMEP (2011-12) 1082.95
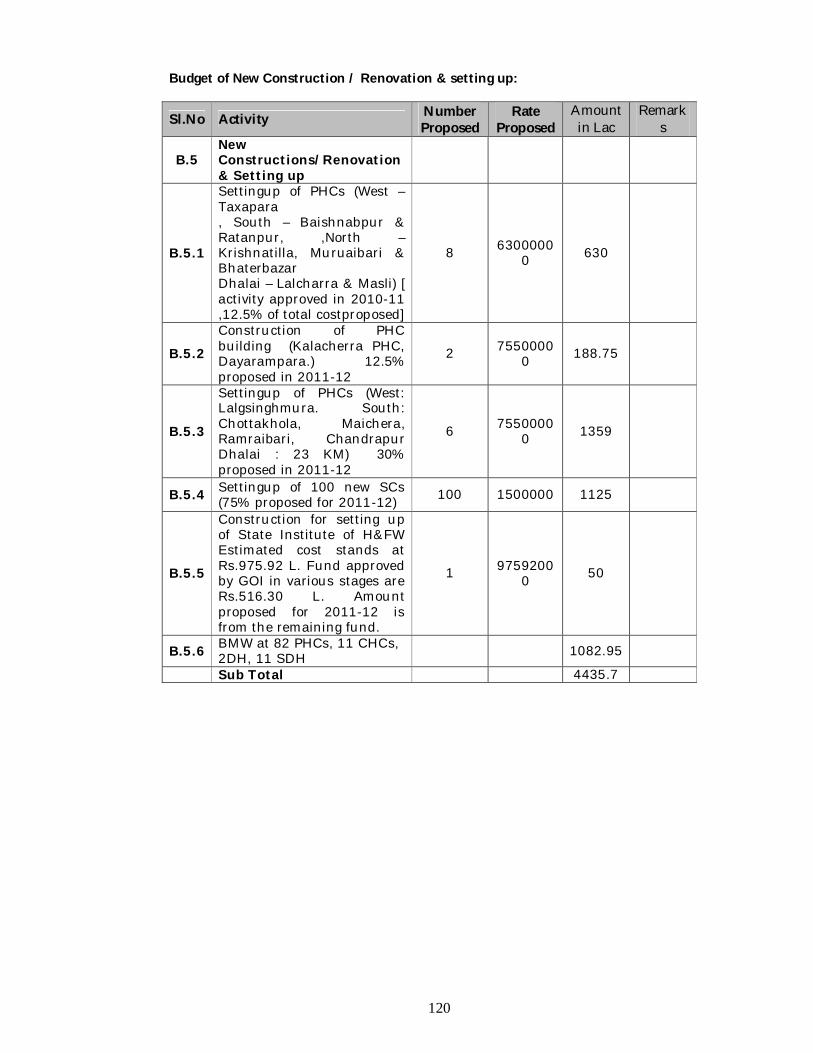
120
Budget of New Construction / Renovation & setting up:
Sl.No Activity Number Proposed
Rate Proposed
Amount in Lac
Remarks
B.5 New Constructions/Renovation & Setting up
B.5.1
Settingup of PHCs (West – Taxapara , South – Baishnabpur & Ratanpur, ,North – Krishnatilla, Muruaibari & Bhaterbazar Dhalai – Lalcharra & Masli) [ activity approved in 2010-11 ,12.5% of total costproposed]
8 63000000 630
B.5.2 Construction of PHC building (Kalacherra PHC, Dayarampara.) 12.5% proposed in 2011-12
2 75500000 188.75
B.5.3
Settingup of PHCs (West: Lalgsinghmura. South: Chottakhola, Maichera, Ramraibari, Chandrapur Dhalai : 23 KM) 30% proposed in 2011-12
6 75500000 1359
B.5.4 Settingup of 100 new SCs (75% proposed for 2011-12) 100 1500000 1125
B.5.5
Construction for setting up of State Institute of H&FW Estimated cost stands at Rs.975.92 L. Fund approved by GOI in various stages are Rs.516.30 L. Amount proposed for 2011-12 is from the remaining fund.
1 97592000 50
B.5.6 BMW at 82 PHCs, 11 CHCs, 2DH, 11 SDH 1082.95
Sub Total 4435.7
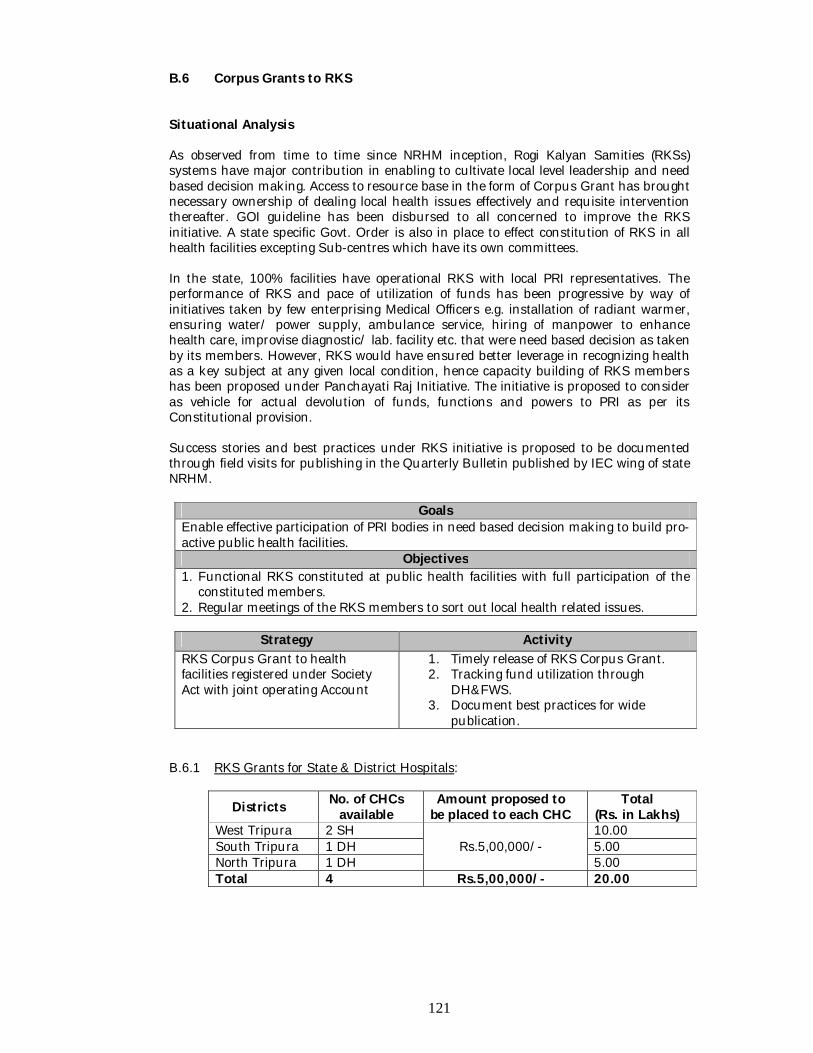
121
B.6 Corpus Grants to RKS Situational Analysis As observed from time to time since NRHM inception, Rogi Kalyan Samities (RKSs) systems have major contribution in enabling to cultivate local level leadership and need based decision making. Access to resource base in the form of Corpus Grant has brought necessary ownership of dealing local health issues effectively and requisite intervention thereafter. GOI guideline has been disbursed to all concerned to improve the RKS initiative. A state specific Govt. Order is also in place to effect constitution of RKS in all health facilities excepting Sub-centres which have its own committees.
In the state, 100% facilities have operational RKS with local PRI representatives. The performance of RKS and pace of utilization of funds has been progressive by way of initiatives taken by few enterprising Medical Officers e.g. installation of radiant warmer, ensuring water/ power supply, ambulance service, hiring of manpower to enhance health care, improvise diagnostic/ lab. facility etc. that were need based decision as taken by its members. However, RKS would have ensured better leverage in recognizing health as a key subject at any given local condition, hence capacity building of RKS members has been proposed under Panchayati Raj Initiative. The initiative is proposed to consider as vehicle for actual devolution of funds, functions and powers to PRI as per its Constitutional provision.
Success stories and best practices under RKS initiative is proposed to be documented through field visits for publishing in the Quarterly Bulletin published by IEC wing of state NRHM.
Goals
Enable effective participation of PRI bodies in need based decision making to build pro-active public health facilities.
Objectives 1. Functional RKS constituted at public health facilities with full participation of the
constituted members. 2. Regular meetings of the RKS members to sort out local health related issues.
Strategy Activity
RKS Corpus Grant to health facilities registered under Society Act with joint operating Account
1. Timely release of RKS Corpus Grant. 2. Tracking fund utilization through
DH&FWS. 3. Document best practices for wide
publication. B.6.1 RKS Grants for State & District Hospitals:
Districts No. of CHCs available
Amount proposed to be placed to each CHC
Total (Rs. in Lakhs)
West Tripura 2 SH Rs.5,00,000/-
10.00 South Tripura 1 DH 5.00 North Tripura 1 DH 5.00 Total 4 Rs.5,00,000/- 20.00
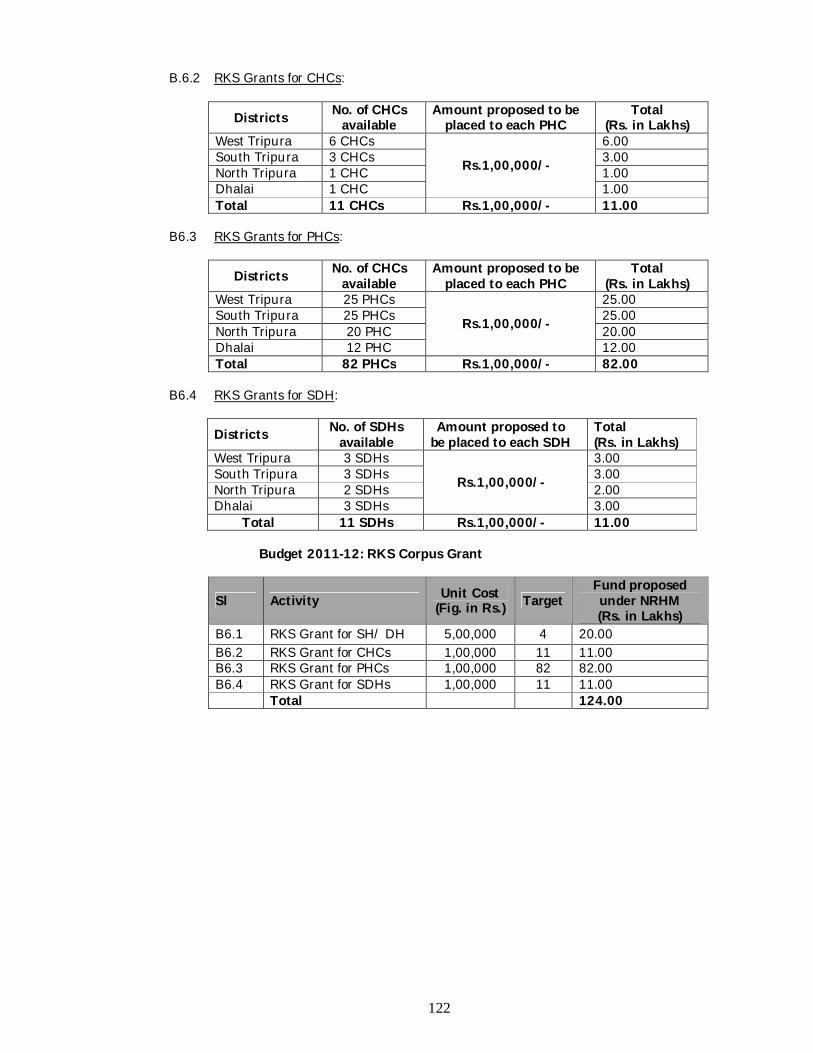
122
B.6.2 RKS Grants for CHCs:
Districts No. of CHCs available
Amount proposed to be placed to each PHC
Total (Rs. in Lakhs)
West Tripura 6 CHCs
Rs.1,00,000/-
6.00 South Tripura 3 CHCs 3.00 North Tripura 1 CHC 1.00 Dhalai 1 CHC 1.00 Total 11 CHCs Rs.1,00,000/- 11.00
B6.3 RKS Grants for PHCs:
Districts No. of CHCs available
Amount proposed to be placed to each PHC
Total (Rs. in Lakhs)
West Tripura 25 PHCs
Rs.1,00,000/-
25.00 South Tripura 25 PHCs 25.00 North Tripura 20 PHC 20.00 Dhalai 12 PHC 12.00 Total 82 PHCs Rs.1,00,000/- 82.00
B6.4 RKS Grants for SDH:
Districts No. of SDHs available
Amount proposed to be placed to each SDH
Total (Rs. in Lakhs)
West Tripura 3 SDHs
Rs.1,00,000/-
3.00 South Tripura 3 SDHs 3.00 North Tripura 2 SDHs 2.00 Dhalai 3 SDHs 3.00
Total 11 SDHs Rs.1,00,000/- 11.00 Budget 2011-12: RKS Corpus Grant
Sl Activity Unit Cost (Fig. in Rs.) Target
Fund proposed under NRHM (Rs. in Lakhs)
B6.1 RKS Grant for SH/ DH 5,00,000 4 20.00 B6.2 RKS Grant for CHCs 1,00,000 11 11.00 B6.3 RKS Grant for PHCs 1,00,000 82 82.00 B6.4 RKS Grant for SDHs 1,00,000 11 11.00 Total 124.00
123
B.7 District Action Plans (including Block, Village) Introduction District Action Plans (DAPs) under NRHM forms an important constituent for planning purposes especially in the context for decentralized planning involving the PRIs. In the state’s context PRI has got a strong base with operational three tier Panchayat system i.e. Gram Panchayet, Block Panchayet and Zilla Parishad. From planning and management perspective, adequate importance of involving the age long institution has been considered at all levels in the state. Situational Analysis Since 2005-06, RCH.II/ NRHM is implemented which have resulted the constitution of Sub-centre Committee, Village Health & Sanitation Committee (VHSC) & Rogi Kalyan Samity (RKS) involving the PRI for improving ownership, functional & clean facilities and local health action. Since then, the preparation of Village Health Action Plan, Facility (PHC/ CHC) Plan, Sub-divisional Health Action Plan, District Health Action Plan and finally State Health Action Plan has been a refining process. It was an attempt to ensure participation at all levels in the planning process for which the programmes were structured. However, resources were scarce and it has been pertinent to prioritize the activities to be carried out at village, blocks and the districts in terms of intervening disease burden, improving infrastructures, strengthening manpower etc. under all National Health Programmes. Allocation of resources from state to district and from district to blocks was required to ensure arriving at consensus decision of the choices being made. The important issues and challenges are finally projected in the PIPs for addressal with required provision for monitoring tools and systems for implementation of the activity smoothly. State has inducted adequate human resource under NRHM and so it is proposed to establish planning units at Blocks, Sub-division, districts and state in line with Block Resource Group, Sub-divisional Resource Groups, District Resource Groups and State Resource Groups as per NRHM approaches. The Development Goal, Objective, Strategy & Activities for 2011-12 under District Action Plans are as follows:-
Goals Development of comprehensive State/ District/ Block Annual Action Plan for Health sector.
Objectives 1. Improving major health index of the state to achieve State specific vision. 2. Improve vital rates and other health indicators.
Strategy Activity
Block Programme Management Unit Block PMU/ Establishment of Block Resource Group
There are 40 Blocks in the state and it is proposed to establish a Block PMU/ Block Resource Group by grouping the available human resources in each Block as follows: 1. All Administrative cum Accounts Assistants of the PHC/
CHC available in a Block. 2. All HMIS Assistants of PHC/ CHC available in a Block. Proposal: 1. In line with NRHM approaches, the BRG is proposed to
function as resource base for planning and management on local specific health issues of all villages falling under a particular Block. The resource group would support crucial
124
Strategy Activity areas of NRHM as:- ASHA scheme. Village Health & Sanitation Committee. Rogi Kalyan Samiti. Identification of disease burden in the block/ villages. Capacity Building/ workshop. Annual Block Action Plan
2. To opertaionalise the Group, the PHC/ CHC situated nearest
to the Block HQ may be considered as Block Resource Centre. All ASHA Facilitators, HMIS Assistants and the Administrative cum Accounts Assistants of all PHC/CHC under the Block may be the human resources. The MO I/C of that identified PHC/ CHC would act as Block Resource Officer for Health. Information pertaining to disease outbreak, RKS meeting, status of schemes under implementation etc. would be collated for further analysis for appropriate intervening by a process of monthly interaction under the leadership of the Block Resource Officer
3. Block Resource Group would act as planning unit of that particular Block. As such, each Sub-division would convey resource size to each Block so that the Blocks are able to project their prioritized activities leading to formulation of 40 nos. Annual Block Plan accommodating the village level health needs.
Budget: The human resources are already engaged under NRHM with operational expenses; therefore, no separate budget is provisioned. However, fund for few planning visits, organizing FGD, drafting etc. by the team is proposed for each Block Resource Group which may be required during 3rd & 4th Qtr: 2011-12 phases. An amount of Rs.20,000/- per Block may be considered which is Rs.20,000/- x 40 = Rs.8,00,000/-
Sub-divisional Programme Management Units/ Sub-divisional Resource Group
There are 17 Sub-divisions in the state and for each sub-division there are 17 Sub-divisional Programme Management Units (SDPMUs) to support plan, implementation and monitoring at Sub-divisional level with the following existing Human Resource engaged under NRHM:
i. Sub-divisional Programme Manager. ii. Sub-divisional Accounts cum Data Assistant.
Proposal: 1. Each Sub-division covers on an average have 2-3 Blocks. It is
proposed to consider each SDPMU as a constituent of Resource Group in state’s context. Like Block Resource Group, this group would also support to enhance crucial areas of NRHM as:- RCH & Immunization. ASHA scheme at Sub-division level. Rogi Kalyan Samiti (RKS). JSY. Capacity Building/ workshop. Update programme implementation status by application
of MIS tools/ Finance Management tools etc.
125
Strategy Activity Develop local based innovation/ projects.
2.To operationalised the Group, newly inducted Human
Resource is proposed to be pooled in addition to above as: (i) Sub-divisional HMIS Assistants, (ii) Sub-divisional ASHA Programme Manager & (iii) Sub-divisional Media Expert wherever available in the Sub-division. The SDMO of that Sub-division would act as Sub-division Resource Officer for Health. Information pertaining to disease outbreak, RKS meeting, status of schemes under implementation etc. would be collated for further analysis for appropriate intervening by a process of monthly interaction under the leadership of Sub-division Resource Officer.
3.Sub-division Resource Group would act as planning unit of that particular Sub-division. As such, Districts are proposed to convey resource size so that each Sub-division is able to project their prioritized activities leading to formulation of 17 Annual Sub-divisional Plans by accommodating the health needs of Blocks and Villages.
Budget: The required human resources are already engaged under NRHM with operational expenses; therefore, no separate budget is provisioned. However fund for few planning visits, organizing FGD, drafting etc. by the team is proposed for each Sub-division Resource Group which may be required during 3rd & 4th Qtr: 2011-12 phases. An amount of Rs.20,000/- per Sub-division may be considered which is Rs.20,000/- x 17 = Rs.3,40,000/-.
District Programme Management Unit/ District Resource Group (DRG)
There are 4 districts in the state and for each districts there are 4 District Programme Management Support Units (DPMSUs) to support planning, implementation and monitoring at District level with the following existing Human Resource known by District Programme Management Support Units (DPMSU) engaged under RC.II/NRHM:-
i. District Programme Manager. ii. District Accounts Manager. iii. District Data Assistants.
Proposal: 1. Each district covers on an average 3-5 Sub-divisions. It is
proposed to consider each DPMSU as a constituent of Resource Group at District level. Like Sub-divisional Resource Group, this group would also support to enhance crucial areas of NRHM as:-
RCH & Immunization ASHA scheme at Sub-division level. JSY Rogi Kalyan Samiti (RKS). Capacity Building/ workshop. Develop procurement system for Drugs & Equipments in
line with ProMIS. Update programme implementation status by
application of MIS tools/ Finance Management tools etc. Develop innovation/ cost-effective mechanisms. Build effective public private partnership/ NGOs/ private
126
Strategy Activity service providers as per existing guideline.
2. To operationalised the Group, newly inducted Human Resource is proposed to be pooled in addition to above as:- (i) HMIS of District Hospitals, (ii) District ASHA Programme Manager & (iii) District Media Expert available in the District. The Chief Medical Officer (CMO) of the district may be considered as District Resource Officer for Health. Updated information that pertains to disease profile of Blocks & villages, RKS functioning, updated status of schemes under implementation, document best practices under the district etc. would be collated for further analysis for appropriate intervening by a process of monthly interaction under the leadership of District Resource Officer. Development of District Resource Group may act as refining process to the functioning of District Health & Family Welfare Society constituted as NRHM Institution.
3. District Resource Group would act as planning unit of that particular District. As such, State is proposed to convey resource size so that each district is able to project their prioritized activities leading to formulation of 4 Annual District Plans by accommodating health needs of Sub-division, Blocks and Villages.
Budget: The required human resources are already engaged under RCH.II/NRHM with operational expenses; therefore, no separate budget is provisioned. However fund for few planning visits, organizing FGD, drafting etc. by the team is proposed for each District that may be required during 3rd & 4th Qtr: 2011-12 phases. An amount of Rs.50,000/- per District may be considered which is Rs.50,000/- x 4 = Rs.2,00,000/-.
State Programme Management Unit/ State Resource Group (SRG)
There is functional State Programme Management Support Unit (SPMSUs) to support planning, implementation and monitoring at state level with the following existing Human Resource engaged under RC.II/NRHM:-
i. State Programme Manager ii. State MIS Manager iii. State Accounts Manager iv. State Mass Media Manager v. State NGO Coordinator
Proposal: 1. The state has four districts. It is proposed to consider SPMSU
as a constituent of Resource Group for State level. Like District Resource Group, this group would also support to enhance crucial areas of NRHM as:-
RCH & Immunization ASHA scheme. JSY Rogi Kalyan Samiti (RKS). Capacity Building/ workshop. Develop procurement system for Drugs & Equipments in
line with ProMIS. Update/ improve programme implementation by
application of MIS/ Finance Management tools etc.
127
Strategy Activity Develop innovation/ cost-effective mechanisms. Build effective public private partnership/ NGOs/ private
service providers as per existing guideline.
2. To operationalised the Group, newly inducted Human Resource is proposed to be pooled in addition to above as:- (i) Consultant, SH&FWS (ii) Asst. Programme Manager (iii) State ASHA Programme Manager (iii) State BCC Consultant, (iv) Asst. Training Coordinator and (v) Technical Experts of RRC-NES (Public Health Planning & Community Processes). The State Mission Director may be considered as State Resource Officer for Health. Updated information that pertains to disease profile of Sub-division, Blocks & Villages, RKS functioning, updated status of schemes under implementation, document best practices etc. would be collated for further analysis for appropriate intervening by a process of monthly interaction under the leadership of State Resource Officer. Development of State Resource Group may act as refining process to the functioning of State Health & Family Welfare Society constituted as NRHM Institution.
3. State Resource Group would act as planning unit in the state. As such, resources conveyed by Centre may be allocated to able to project prioritized activities leading to formulation of State Action Plan by accommodating health needs of Districts, Sub-divisions, Blocks and Villages for implementation across the state.
Budget: The required human resources are already engaged under RCH.II/NRHM with operational expenses; therefore, no separate budget is provisioned. However fund for few planning visits, organizing FGD, drafting etc. by the team is proposed that may be required during 3rd & 4th Qtr: 2011-12 phases. An amount of Rs.60,000/- may be considered. A Govt. Order is proposed to be put in place mentioning the involvement of important stakeholders in NRHM context to affect the proposed structure from Block to State.
Budget 2011-12: District Action Plan
Sl Activity Unit Cost (Fig. in Rs.) Target
Fund proposed under NRHM (Rs. in Lakhs)
B.7.1 Block Health Action Plan 20,000 40 8.00
B.7.2 Sub-division Health Action Plan 20,000 17 3.40
B.7.3 District Action Plan 50,000 4 2.00 B.7.4 State Action Plan 60,000 1 0.60 Total 14.00
128
B.8 Panchayati Raj Initiative Introduction As per NRHM Implementation Framework it is imminent that the Schemes/ Programmes NRHM are implemented involving the Panchayati Raj Institution (PRI). As highlighted, the three tiers PRI is in place as an integral part of grass-root level planning and implementation of Health Programmes. Accordingly there is existing three tiers viz. Zilla Parishad at District level, Panchayat Samity/ Block Advisory Committee (in tribal areas) at Block level and Gram Panchayat/ ADC Villages (in tribal areas) at village level. From 1994 onwards, the State Govt. has been delegating different powers and responsibilities with the 3-tier of the Panchayati Raj Institution. The Panchayat (Administration) Rules 1994 and the Tripura Panchayat (Election of office bearers) Rules 1994 have been framed for effective decentralization of development activities and determination of the responsibilities of Panchayat. Therefore, in state’s context, Department of Panchayat is strongly involved as evident from the existing State Govt. Orders pertaining to VHSC, Sub-Centre Committees, RKS and constitution of DH&FWS & SH&FWS.
Level Name of the Functionaries/Committee GP/ ADC at village level Village Health & Sanitation Committee (VH&SC) Panchayat Samity at Block level Rogi Kalyan Samity at PHC/ CHC/ SDH
District level Rogi Kalyan Samity at District Hospitals/ District Society
The main concept of VH&SC/ Rogi Kalyan Samity (RKS) at different level is a simple yet effective management structure. This committee which is a Registered Society except VHSC acts as a group of trustees for the different health institution to manage the affairs of the people or society. It consists of members from local Panchayati Raj Institutions (PRIs), NGOs, local elected representatives and officials from Government sector who are responsible for proper functioning and management of the SHC/ CHC / PHC/ SDH/ DH/ SH/FRUs. These bodies are proposed to prescribe freely, generate and use the funds with it as per its best judgment for smooth functioning and maintaining the quality of services. The development Goal, Objective, Strategy & Activity for 2011-12 under Panchayati Raj Initiative is as follows:-
Goals Generate involvement of people’s representative for Health Sector improvement.
Objectives 1. Enhance people’s participation in decision making related to health. 2. Obtain critical inputs of prevailing local specific health issues for designing and
reflection in the Block/ Sub-division/ District/ State Action Plan. 3. Improve awareness in cultivating determinants of health as a means to achieve
holistic public health goals.
Strategy Activity Organize one day capacity building workshop for all PRI representatives associated with Health.
One Day Capacity Development Programme of PRI representatives.
Participants Number of participants
Batch Size
No. of Batch
Place of Training
Members of VH&SC
3120 (3 members of each VH&SC
30 35 batches State HQ
129
RKS members
303 (3 members of PHC/ CHC/ SDH)
30 10 batches
District HQ
District Rural Health Mission
20 (5 members each) 20 1 batch State HQ
Proposed Implementation Procedure: I. Training of VH&SC Members:
Proposed to be imparted in coordination of Department of Panchayet through its existing institution Panchayet Raj Training Institute (PRTI) at state HQ. Resource person would be arranged by State Health & Family Welfare Society of Health Department as follows: Member Secretary, NRHM Branch Officer, NRHM Consultants and Programme Managers under
SPMSU A training calendar (District/wise/ Block wise) proposed to
be formulated for rolling out one-day training of VHSC members at State HQ and also shared with Department of Panchayat/ Institution
DH&FWS may provide the list of the eligible members (3 members from each VHSC) to participate in the training. Their to and fro movement from village to state shall be managed by the concerning DH&FWS.
Time-line: 2nd Qtr: 2011-12 onwards. II. Training of RKS Members (PHC/ CHC/ SDH/DH)
Training modalities/ contents/ guidelines aligning with GOI guideline of RKS proposed to be developed at state HQ and disseminated to the DH&FWS for organizing the training through Resource person would be arranged by State Health & Family Welfare Society of Health Department as follows: Member Secretary, NRHM Branch Officer, NRHM Consultants and Programme Managers under
SPMSU A training calendar (District/wise/ Block wise) proposed to
be formulated for rolling out one-day training of RKS members by DH&FWS.
DH&FWS may sort out list of the eligible members (one each from concern Health institution, PRI representative and Administration) to participate in the training. Their to and fro movement may be managed by the concerning DH&FWS.
Time-line: 1st Qtr: 2011-12 (3rd month) III. Training of District Rural Health Mission Members
Training proposed to be organized at state level to disseminate the principles and progresses made under NRHM since inception. The participants for attending the workshop/ Training would be finalized by Chairman of District Health Mission/ Zilla Parishad.
The workshop is proposed to be organized by State Health & Family Welfare Society, Tripura under the Chairmanship of Vice Chairman, State Rural Health Mission.
Time-line: 1st Qtr: 2011-12 (2nd month)
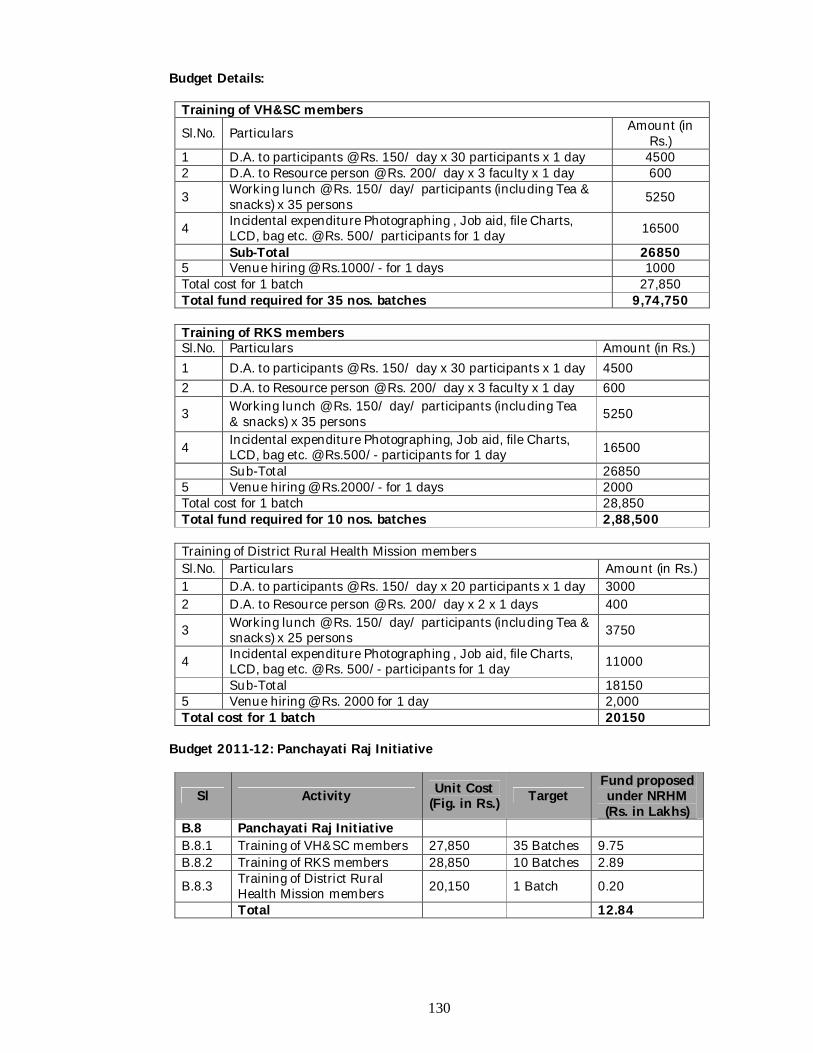
130
Budget Details:
Training of VH&SC members Sl.No. Particulars Amount (in
Rs.) 1 D.A. to participants @ Rs. 150/ day x 30 participants x 1 day 4500 2 D.A. to Resource person @ Rs. 200/ day x 3 faculty x 1 day 600
3 Working lunch @ Rs. 150/ day/ participants (including Tea & snacks) x 35 persons 5250
4 Incidental expenditure Photographing , Job aid, file Charts, LCD, bag etc. @ Rs. 500/ participants for 1 day 16500
Sub-Total 26850 5 Venue hiring @ Rs.1000/- for 1 days 1000 Total cost for 1 batch 27,850 Total fund required for 35 nos. batches 9,74,750
Training of RKS members Sl.No. Particulars Amount (in Rs.) 1 D.A. to participants @ Rs. 150/ day x 30 participants x 1 day 4500 2 D.A. to Resource person @ Rs. 200/ day x 3 faculty x 1 day 600
3 Working lunch @ Rs. 150/ day/ participants (including Tea & snacks) x 35 persons 5250
4 Incidental expenditure Photographing, Job aid, file Charts, LCD, bag etc. @ Rs.500/- participants for 1 day 16500
Sub-Total 26850 5 Venue hiring @ Rs.2000/- for 1 days 2000 Total cost for 1 batch 28,850 Total fund required for 10 nos. batches 2,88,500
Training of District Rural Health Mission members Sl.No. Particulars Amount (in Rs.) 1 D.A. to participants @ Rs. 150/ day x 20 participants x 1 day 3000 2 D.A. to Resource person @ Rs. 200/ day x 2 x 1 days 400
3 Working lunch @ Rs. 150/ day/ participants (including Tea & snacks) x 25 persons 3750
4 Incidental expenditure Photographing , Job aid, file Charts, LCD, bag etc. @ Rs. 500/- participants for 1 day 11000
Sub-Total 18150 5 Venue hiring @ Rs. 2000 for 1 day 2,000 Total cost for 1 batch 20150
Budget 2011-12: Panchayati Raj Initiative
Sl Activity Unit Cost (Fig. in Rs.) Target
Fund proposed under NRHM (Rs. in Lakhs)
B.8 Panchayati Raj Initiative B.8.1 Training of VH&SC members 27,850 35 Batches 9.75 B.8.2 Training of RKS members 28,850 10 Batches 2.89
B.8.3 Training of District Rural Health Mission members 20,150 1 Batch 0.20
Total 12.84
131
B9 Mainstreaming of AYUSH Introduction The National Rural Health Mission (NRHM) has been launched with a view to bringing about dramatic improvement in the health system and the health status of people, especially those who live in the rural areas of the country. The Mission seeks to provide universal access to equitable, affordable and quality health care which is accountable at the same time responsive to the needs of the people, reduction of child and maternal deaths as well as population stabilization, gender and demographic balance. One of the visions of NRHM is to revitalize local health traditions and mainstream AYUSH into the public health system thereby improve access to rural people, especially poor women and children to equitable, affordable, accountable and effective primary health care. In the State’s context, AYUSH is being administered under Directorate of Health Services of Health & Family Welfare Department. The State of Tripura has special emphasis for strengthening AYUSH, as it is practiced both conventionally and unconventionally in almost all parts of the State. The State has its own richness in traditional healing methods, herbs etc. which facilitates the rural poor to take preventive & curative measures of ailments. The local treatment methods is proposed to be enhanced by application of well-researched AYUSH medicines by state/national level experts and strengthen existing infrastructures by renovation, new creation, establish AYUSH Hospitals and develop of skilled human resource. The development Goals, Objective, Strategy & Activity under Mainstreaming of AYUSH for 2011-12 is as follows:
Goal Revitalize local health traditions and Mainstream AYUSH into the public health system.
Objective Strengthening OPD services through posting/ appointment of contractual AYUSH MOs and collocation at PHC/ CHC/ SDH.
Strategy Activities
Contractual appointment of AYUSH MOs/ Paramedics and strengthening AYUSH Programme Managements Units (PMUs).
Continuing existing and new appointment of AYUSH MOs, Pharmacists, Masseurs & Attendants.
Strengthening of AYUSH Programme Management Units (PMUs)
AYUSH Training Training of AYUSH MOs
Training of Paramedics on AYUSH Training of ASHAs on AYUSH
IEC/ BCC on AYUSH Wide publicity by application of print & electronic
media Organization of Health Fair
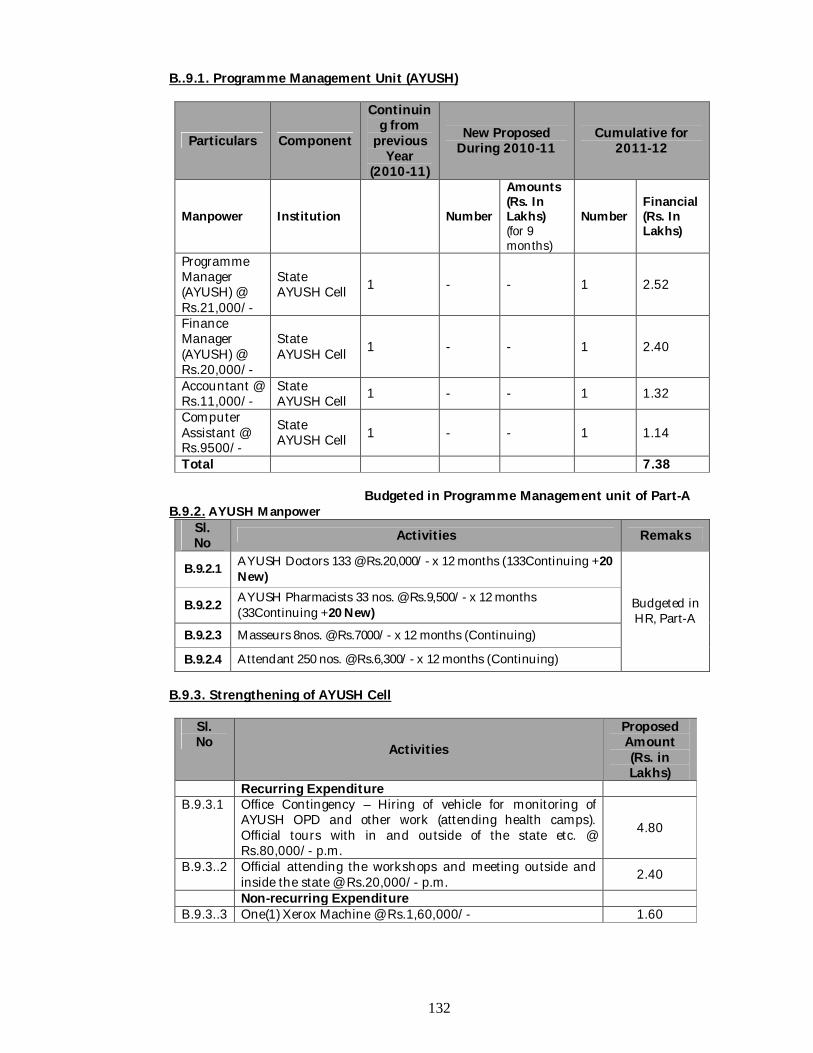
132
B..9.1. Programme Management Unit (AYUSH)
Particulars Component
Continuing from
previous Year
(2010-11)
New Proposed During 2010-11
Cumulative for 2011-12
Manpower Institution Number
Amounts (Rs. In Lakhs) (for 9 months)
Number Financial (Rs. In Lakhs)
Programme Manager (AYUSH) @ Rs.21,000/-
State AYUSH Cell 1 - - 1 2.52
Finance Manager (AYUSH) @ Rs.20,000/-
State AYUSH Cell 1 - - 1 2.40
Accountant @ Rs.11,000/-
State AYUSH Cell 1 - - 1 1.32
Computer Assistant @ Rs.9500/-
State AYUSH Cell 1 - - 1 1.14
Total 7.38
Budgeted in Programme Management unit of Part-A B.9.2. AYUSH Manpower
Sl. No Activities Remaks
B.9.2.1 AYUSH Doctors 133 @ Rs.20,000/- x 12 months (133Continuing +20 New)
Budgeted in HR, Part-A
B.9.2.2 AYUSH Pharmacists 33 nos. @ Rs.9,500/- x 12 months (33Continuing +20 New)
B.9.2.3 Masseurs 8nos. @ Rs.7000/- x 12 months (Continuing)
B.9.2.4 Attendant 250 nos. @ Rs.6,300/- x 12 months (Continuing) B.9.3. Strengthening of AYUSH Cell
Sl. No Activities
Proposed Amount (Rs. in Lakhs)
Recurring Expenditure B.9.3.1 Office Contingency – Hiring of vehicle for monitoring of
AYUSH OPD and other work (attending health camps). Official tours with in and outside of the state etc. @ Rs.80,000/- p.m.
4.80
B.9.3..2 Official attending the workshops and meeting outside and inside the state @ Rs.20,000/- p.m. 2.40
Non-recurring Expenditure B.9.3..3 One(1) Xerox Machine @ Rs.1,60,000/- 1.60
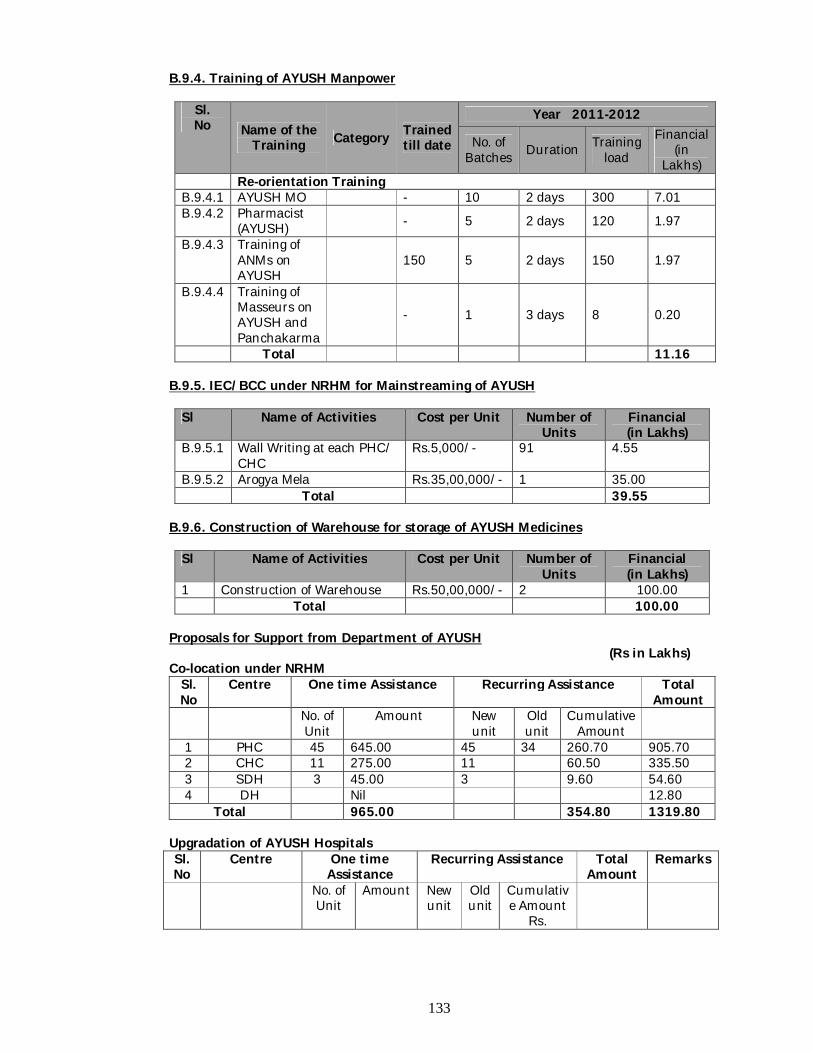
133
B.9.4. Training of AYUSH Manpower
Sl. No Name of the
Training Category Trained till date
Year 2011-2012
No. of Batches Duration Training
load
Financial (in
Lakhs) Re-orientation Training B.9.4.1 AYUSH MO - 10 2 days 300 7.01 B.9.4.2 Pharmacist
(AYUSH) - 5 2 days 120 1.97
B.9.4.3 Training of ANMs on AYUSH
150 5 2 days 150 1.97
B.9.4.4 Training of Masseurs on AYUSH and Panchakarma
- 1 3 days 8 0.20
Total 11.16 B.9.5. IEC/BCC under NRHM for Mainstreaming of AYUSH
Sl Name of Activities Cost per Unit Number of Units
Financial (in Lakhs)
B.9.5.1 Wall Writing at each PHC/ CHC
Rs.5,000/- 91 4.55
B.9.5.2 Arogya Mela Rs.35,00,000/- 1 35.00 Total 39.55
B.9.6. Construction of Warehouse for storage of AYUSH Medicines
Sl Name of Activities Cost per Unit Number of Units
Financial (in Lakhs)
1 Construction of Warehouse Rs.50,00,000/- 2 100.00 Total 100.00
Proposals for Support from Department of AYUSH
(Rs in Lakhs) Co-location under NRHM
Sl. No
Centre One time Assistance Recurring Assistance Total Amount
No. of Unit
Amount New unit
Old unit
Cumulative Amount
1 PHC 45 645.00 45 34 260.70 905.70 2 CHC 11 275.00 11 60.50 335.50 3 SDH 3 45.00 3 9.60 54.60 4 DH Nil 12.80
Total 965.00 354.80 1319.80
Upgradation of AYUSH Hospitals Sl. No
Centre One time Assistance
Recurring Assistance Total Amount
Remarks
No. of Unit
Amount New unit
Old unit
Cumulative Amount
Rs.
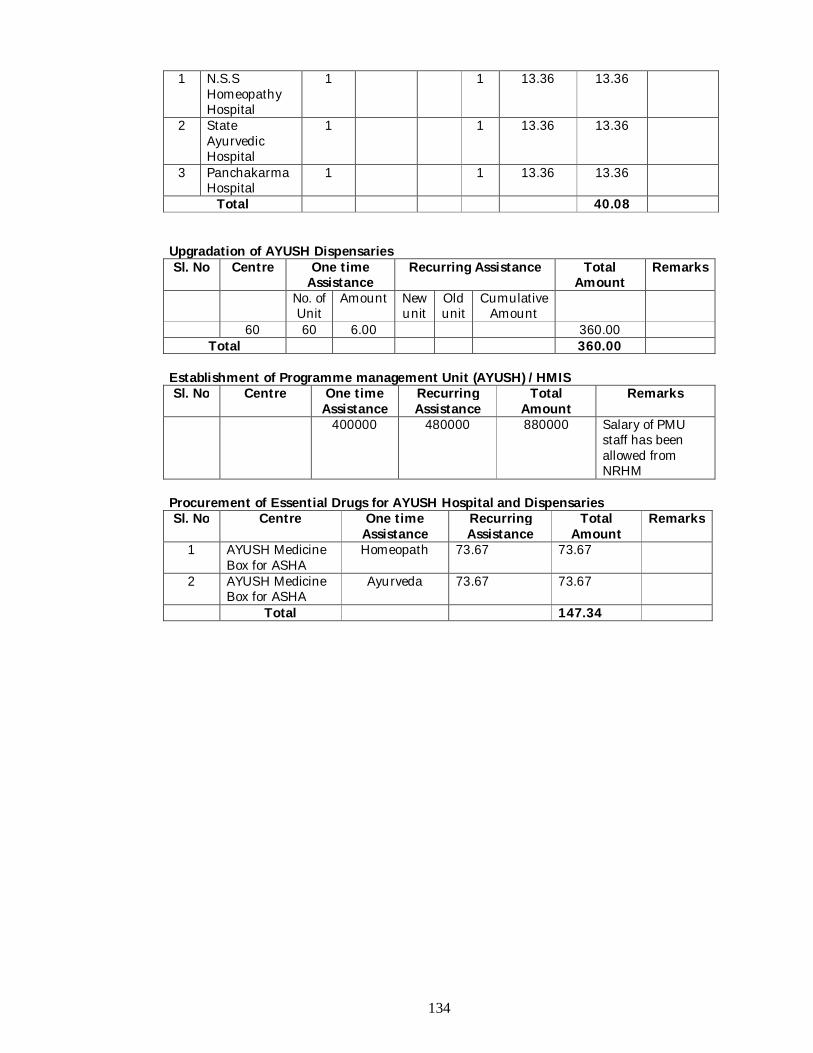
134
1 N.S.S Homeopathy Hospital
1 1 13.36 13.36
2 State Ayurvedic Hospital
1 1 13.36 13.36
3 Panchakarma Hospital
1 1 13.36 13.36
Total 40.08
Upgradation of AYUSH Dispensaries Sl. No Centre One time
Assistance Recurring Assistance Total
Amount Remarks
No. of Unit
Amount New unit
Old unit
Cumulative Amount
60 60 6.00 360.00 Total 360.00
Establishment of Programme management Unit (AYUSH) /HMIS Sl. No Centre One time
Assistance Recurring Assistance
Total Amount
Remarks
400000 480000 880000 Salary of PMU staff has been allowed from NRHM
Procurement of Essential Drugs for AYUSH Hospital and Dispensaries Sl. No Centre One time
Assistance Recurring Assistance
Total Amount
Remarks
1 AYUSH Medicine Box for ASHA
Homeopath 73.67 73.67
2 AYUSH Medicine Box for ASHA
Ayurveda 73.67 73.67
Total 147.34
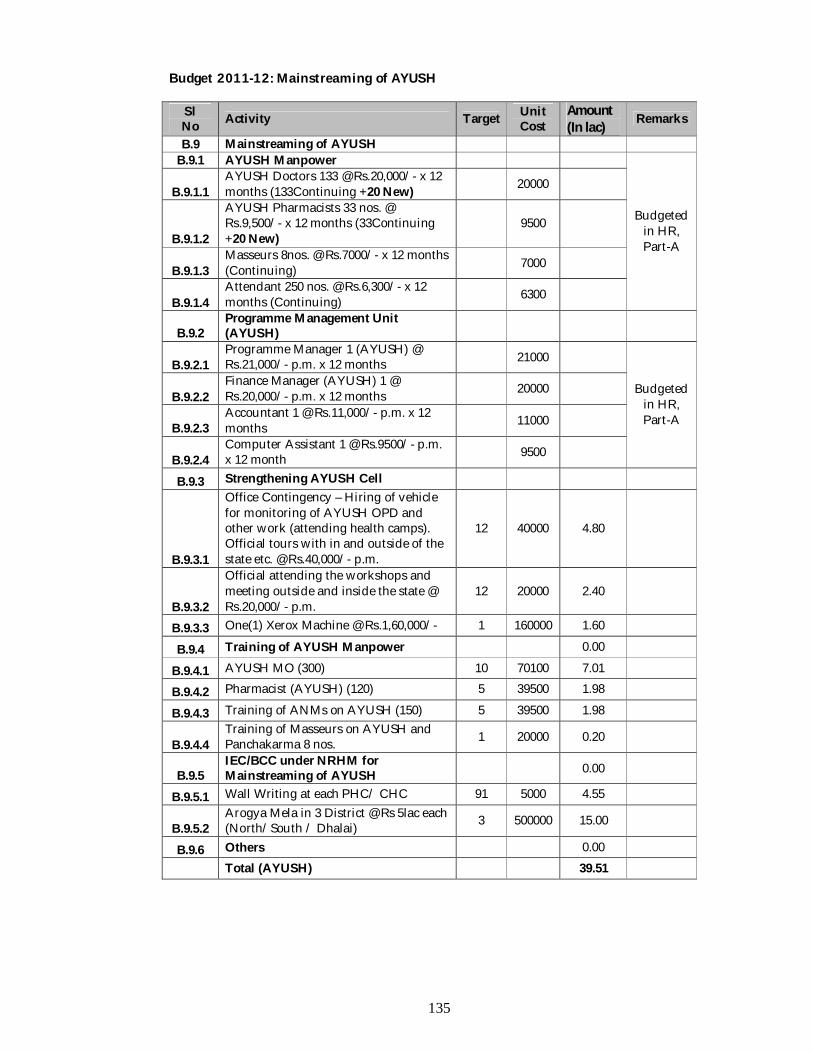
135
Budget 2011-12: Mainstreaming of AYUSH
Sl No Activity Target Unit
Cost Amount (In lac)
Remarks
B.9 Mainstreaming of AYUSH B.9.1 AYUSH Manpower
Budgeted in HR, Part-A
B.9.1.1 AYUSH Doctors 133 @ Rs.20,000/- x 12 months (133Continuing +20 New) 20000
B.9.1.2
AYUSH Pharmacists 33 nos. @ Rs.9,500/- x 12 months (33Continuing +20 New)
9500
B.9.1.3 Masseurs 8nos. @ Rs.7000/- x 12 months (Continuing) 7000
B.9.1.4 Attendant 250 nos. @ Rs.6,300/- x 12 months (Continuing) 6300
B.9.2 Programme Management Unit (AYUSH)
B.9.2.1 Programme Manager 1 (AYUSH) @ Rs.21,000/- p.m. x 12 months 21000
Budgeted in HR, Part-A
B.9.2.2 Finance Manager (AYUSH) 1 @ Rs.20,000/- p.m. x 12 months 20000
B.9.2.3 Accountant 1 @ Rs.11,000/- p.m. x 12 months 11000
B.9.2.4 Computer Assistant 1 @ Rs.9500/- p.m. x 12 month 9500
B.9.3 Strengthening AYUSH Cell
B.9.3.1
Office Contingency – Hiring of vehicle for monitoring of AYUSH OPD and other work (attending health camps). Official tours with in and outside of the state etc. @ Rs.40,000/- p.m.
12 40000 4.80
B.9.3.2
Official attending the workshops and meeting outside and inside the state @ Rs.20,000/- p.m.
12 20000 2.40
B.9.3.3 One(1) Xerox Machine @ Rs.1,60,000/- 1 160000 1.60 B.9.4 Training of AYUSH Manpower 0.00
B.9.4.1 AYUSH MO (300) 10 70100 7.01 B.9.4.2 Pharmacist (AYUSH) (120) 5 39500 1.98 B.9.4.3 Training of ANMs on AYUSH (150) 5 39500 1.98
B.9.4.4 Training of Masseurs on AYUSH and Panchakarma 8 nos. 1 20000 0.20
B.9.5 IEC/BCC under NRHM for Mainstreaming of AYUSH 0.00
B.9.5.1 Wall Writing at each PHC/ CHC 91 5000 4.55
B.9.5.2 Arogya Mela in 3 District @ Rs 5lac each (North/South / Dhalai) 3 500000 15.00
B.9.6 Others 0.00 Total (AYUSH) 39.51
136
B10. IEC-BCC NRHM Introduction Behaviour change communication (BCC) is an interactive process for encouraging and sustaining positive and appropriate behaviours. A carefully planned and managed BCC strategy ensures that the behaviour identified for change is feasible within the social and cultural context in which people live. The purpose of planning the implementation strategy of BCC is to provide a framework for planning, designing, implementing and supporting strategic health communication activities for RCH Programme in the State’s context IEC/BCC activities play a very important and strategic role in development communications. Strategic IEC/ BCC programmes use a systematic process to understand people’s behavior and influences. A successful IEC/ BCC plan would help in refuting myths and misunderstandings prevalent in the society and will lead to a demand for the various health services being provided, thus bringing about a behavioral change among individuals and the community at large. Any comprehensive IEC/BCC strategy should basically accomplish the following objectives:
Address underlying causes of identified health problems and issues and create an enabling environment at household, community and policy levels.
Follow a structured communications plan with audience research, segmentation, objectives, pre-tests, communication mix, detailed implementation plans and monitoring and evaluation modules.
Define and segment the audience, tailor messages and materials to the interests of audience with readiness to change messages as per feedback
Link shared understanding including ownership, implementation and monitoring of initiatives and activities among various stakeholders to achieve the desired objectives
Build local capacities through education, training, work partnerships to create need specific BCC interventions
Create demand for services and healthy behaviors and help ensure quality services
AMG members visited all districts and demand increased IEC/BCC activities to achieve target
Situation Analysis The State of Tripura is represented by 68% BPL population and implementation of IEC/ BCC strategy to promote health intervention especially under NRHM is of profound importance. The target groups being of vulnerable population, the goals of achieving NRHM in the State has been started by few initiatives like inclusion in syllabus of Panchayati Raj Training Institution by Panchayat Department PRI members trainings, Village Health Days, application of print & electronic media etc. The institutional capacity is proposed to be brought in a formidable position by rolling out capacity building initiatives while at the community level component wise IEC/ BCC is proposed to be continued to reach the target groups.
Goal Demand Generation for Health Services and Change the Behavior of People for Good Health.
Objective To catalyze improving maternal health, child health, family planning and ARSH activities of RCH.II/NRHM
137
Strategies
Application of development communication through utilization of information technologies.
Application of IPC methods to promote MCH related awareness. Develop effective partnership with voluntary/ community based organization.
Activities
B.10.1.IEC Initiative for Maternal Health B.10.1.1.: Mother and Child Health Fair one in each 17 nos. Sub-Division @ Rs.90,000. Interactive stalls may be created in market places and exhibition will decorate the stall. The messages will be disseminated through speeches, leaflets. Slogan, Essay, drawing, quiz competition will be organized among the villagers.
Budget
Sl. No. Activity Unit Unit Cost
Amount (In Rs.)
1 Theme Pavilion and Cultural Stage:- (Construction & Decoration)
1 1
20000 6000
20000 6000
2 Stalls (Construction & Decoration)
05 05
3000 3000
15000 15000
3 Cultural Programme 6 Programme 2000 12000 4 Quiz & Prize Distributions 1 5000 5000 5 Arrangement and Materials for
Ancillary Services 2 (since it is proposed for two days)
5000 10000
6 Miscellaneous (Refreshment, Hiring vehicles, contingencies )
1 7000 7000
Total 90, 000.00
Total Rs. 90,000/- x 17 Sub-Division = Rs. 15, 30, 000
B.10.1.2.: Radio Jingles is already available with State Health & FW Society and it will be aired through All India Radio (15 seconds duration) in Bengali, kokborak through Agartala Station. Jingles will be aired from July 2010 – February 2012 and 240 times in 240 days in each station @ Rs. 1200/- per unit cost.
Total Budget Rs.1200 x 240 Nos = Rs. 2, 88,000/-
B.10.1.3: Radio Jingles is already available with State Health & FW Society and it will be aired through All India Radio (15 seconds duration) in Bengali, kokborak through Belonia and Kailasahar Station. Jingles will be aired from July 2010 – February 2012 and 240 times in 240 days in each station @ Rs. 800/- per unit cost.
Total Budget Rs. 800 x 480 nos. = Rs. 3, 84,000/-
B.10.2: IEC Initiative for New Born & Child Health Observance of Breast Feeding Week (1st August to 7th August): Rally by ASHA, Health Workers in the prominent places of Gram Panchayat and ADC villages during 1st August to 7th August in all Health Institutions (Total 101) through out the State District Media Expert, SDPM will ensure the programme. An action plan with date and place should be sent to BO, IEC in advance. Total: Rs.5,00,000/-.
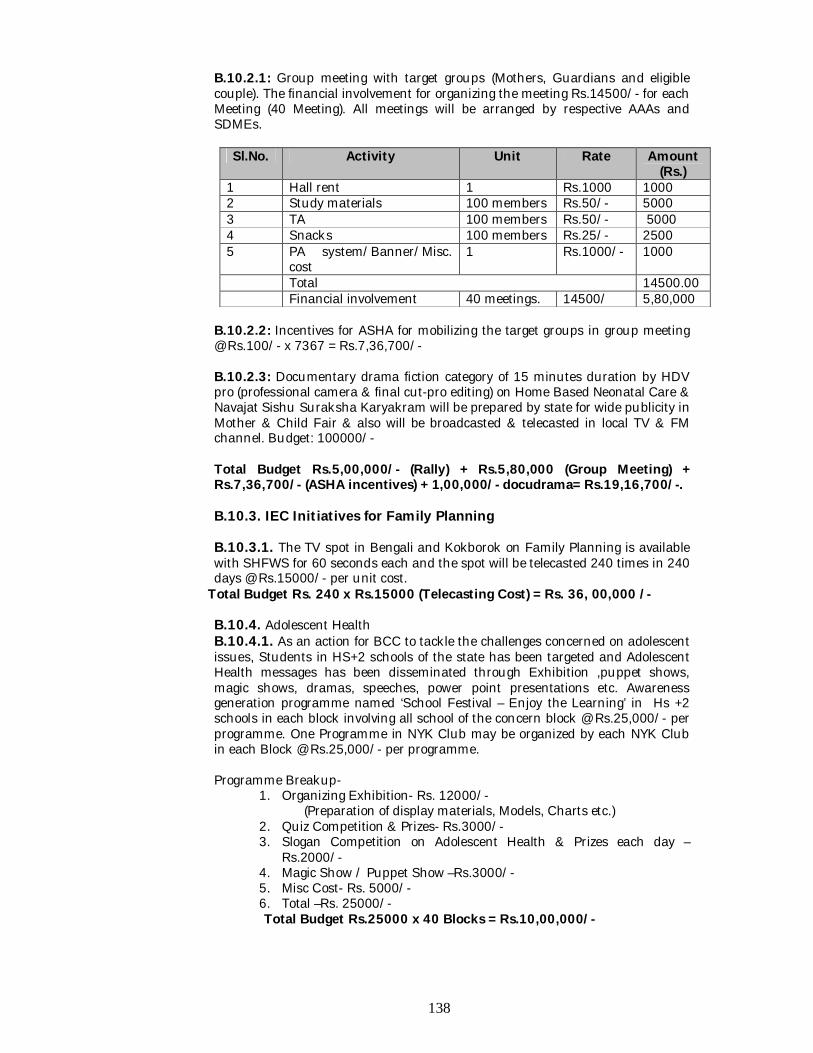
138
B.10.2.1: Group meeting with target groups (Mothers, Guardians and eligible couple). The financial involvement for organizing the meeting Rs.14500/- for each Meeting (40 Meeting). All meetings will be arranged by respective AAAs and SDMEs.
Sl.No. Activity Unit Rate Amount (Rs.)
1 Hall rent 1 Rs.1000 1000 2 Study materials 100 members Rs.50/- 5000 3 TA 100 members Rs.50/- 5000 4 Snacks 100 members Rs.25/- 2500 5 PA system/Banner/Misc.
cost 1 Rs.1000/- 1000
Total 14500.00 Financial involvement 40 meetings. 14500/ 5,80,000
B.10.2.2: Incentives for ASHA for mobilizing the target groups in group meeting @ Rs.100/- x 7367 = Rs.7,36,700/- B.10.2.3: Documentary drama fiction category of 15 minutes duration by HDV pro (professional camera & final cut-pro editing) on Home Based Neonatal Care & Navajat Sishu Suraksha Karyakram will be prepared by state for wide publicity in Mother & Child Fair & also will be broadcasted & telecasted in local TV & FM channel. Budget: 100000/- Total Budget Rs.5,00,000/- (Rally) + Rs.5,80,000 (Group Meeting) + Rs.7,36,700/- (ASHA incentives) + 1,00,000/- docudrama= Rs.19,16,700/-.
B.10.3. IEC Initiatives for Family Planning B.10.3.1. The TV spot in Bengali and Kokborok on Family Planning is available with SHFWS for 60 seconds each and the spot will be telecasted 240 times in 240 days @ Rs.15000/- per unit cost.
Total Budget Rs. 240 x Rs.15000 (Telecasting Cost) = Rs. 36, 00,000 /-
B.10.4. Adolescent Health B.10.4.1. As an action for BCC to tackle the challenges concerned on adolescent issues, Students in HS+2 schools of the state has been targeted and Adolescent Health messages has been disseminated through Exhibition ,puppet shows, magic shows, dramas, speeches, power point presentations etc. Awareness generation programme named ‘School Festival – Enjoy the Learning’ in Hs +2 schools in each block involving all school of the concern block @ Rs.25,000/- per programme. One Programme in NYK Club may be organized by each NYK Club in each Block @ Rs.25,000/- per programme.
Programme Breakup-
1. Organizing Exhibition- Rs. 12000/- (Preparation of display materials, Models, Charts etc.) 2. Quiz Competition & Prizes- Rs.3000/- 3. Slogan Competition on Adolescent Health & Prizes each day –
Rs.2000/- 4. Magic Show / Puppet Show –Rs.3000/- 5. Misc Cost- Rs. 5000/- 6. Total –Rs. 25000/- Total Budget Rs.25000 x 40 Blocks = Rs.10,00,000/-
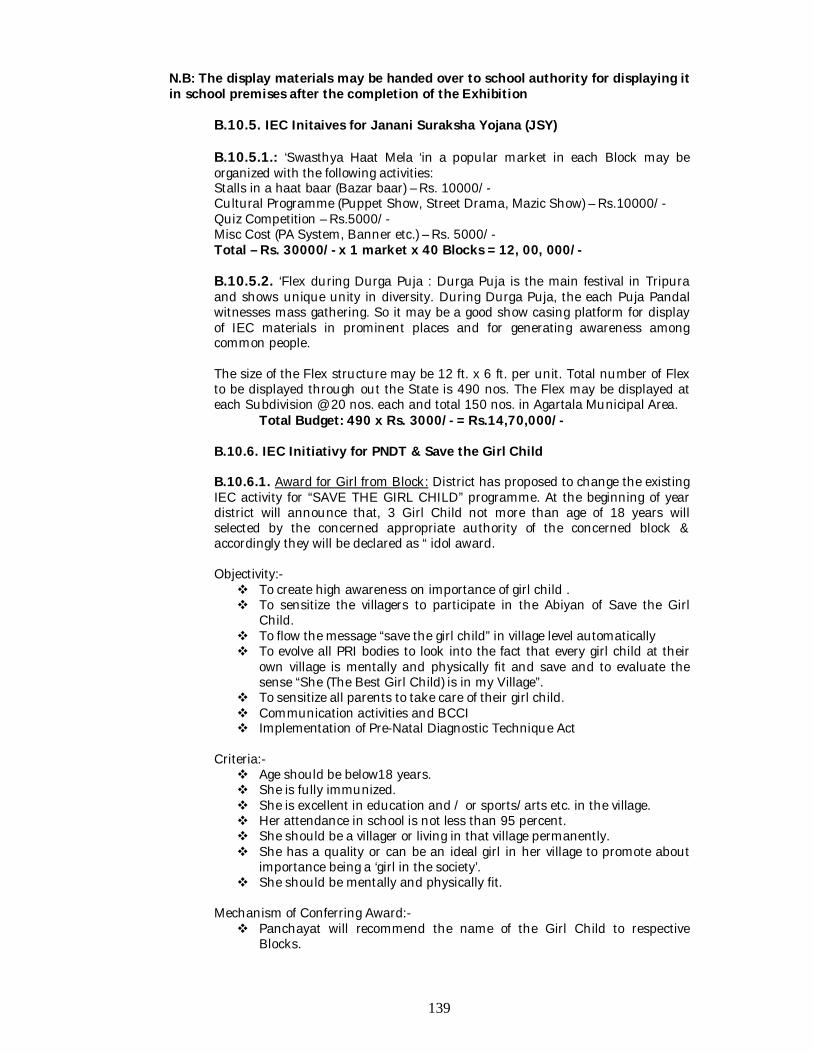
139
N.B: The display materials may be handed over to school authority for displaying it in school premises after the completion of the Exhibition
B.10.5. IEC Initaives for Janani Suraksha Yojana (JSY) B.10.5.1.: ‘Swasthya Haat Mela ‘in a popular market in each Block may be organized with the following activities: Stalls in a haat baar (Bazar baar) – Rs. 10000/- Cultural Programme (Puppet Show, Street Drama, Mazic Show) – Rs.10000/- Quiz Competition – Rs.5000/- Misc Cost (PA System, Banner etc.) – Rs. 5000/-
Total – Rs. 30000/- x 1 market x 40 Blocks = 12, 00, 000/-
B.10.5.2. ‘Flex during Durga Puja : Durga Puja is the main festival in Tripura and shows unique unity in diversity. During Durga Puja, the each Puja Pandal witnesses mass gathering. So it may be a good show casing platform for display of IEC materials in prominent places and for generating awareness among common people. The size of the Flex structure may be 12 ft. x 6 ft. per unit. Total number of Flex to be displayed through out the State is 490 nos. The Flex may be displayed at each Subdivision @ 20 nos. each and total 150 nos. in Agartala Municipal Area. Total Budget: 490 x Rs. 3000/- = Rs.14,70,000/-
B.10.6. IEC Initiativy for PNDT & Save the Girl Child B.10.6.1. Award for Girl from Block: District has proposed to change the existing IEC activity for “SAVE THE GIRL CHILD” programme. At the beginning of year district will announce that, 3 Girl Child not more than age of 18 years will selected by the concerned appropriate authority of the concerned block & accordingly they will be declared as “ idol award. Objectivity:- To create high awareness on importance of girl child . To sensitize the villagers to participate in the Abiyan of Save the Girl
Child. To flow the message “save the girl child” in village level automatically To evolve all PRI bodies to look into the fact that every girl child at their
own village is mentally and physically fit and save and to evaluate the sense “She (The Best Girl Child) is in my Village”.
To sensitize all parents to take care of their girl child. Communication activities and BCCI Implementation of Pre-Natal Diagnostic Technique Act
Criteria:- Age should be below18 years. She is fully immunized. She is excellent in education and / or sports/arts etc. in the village. Her attendance in school is not less than 95 percent. She should be a villager or living in that village permanently. She has a quality or can be an ideal girl in her village to promote about
importance being a ‘girl in the society’. She should be mentally and physically fit.
Mechanism of Conferring Award:- Panchayat will recommend the name of the Girl Child to respective
Blocks.
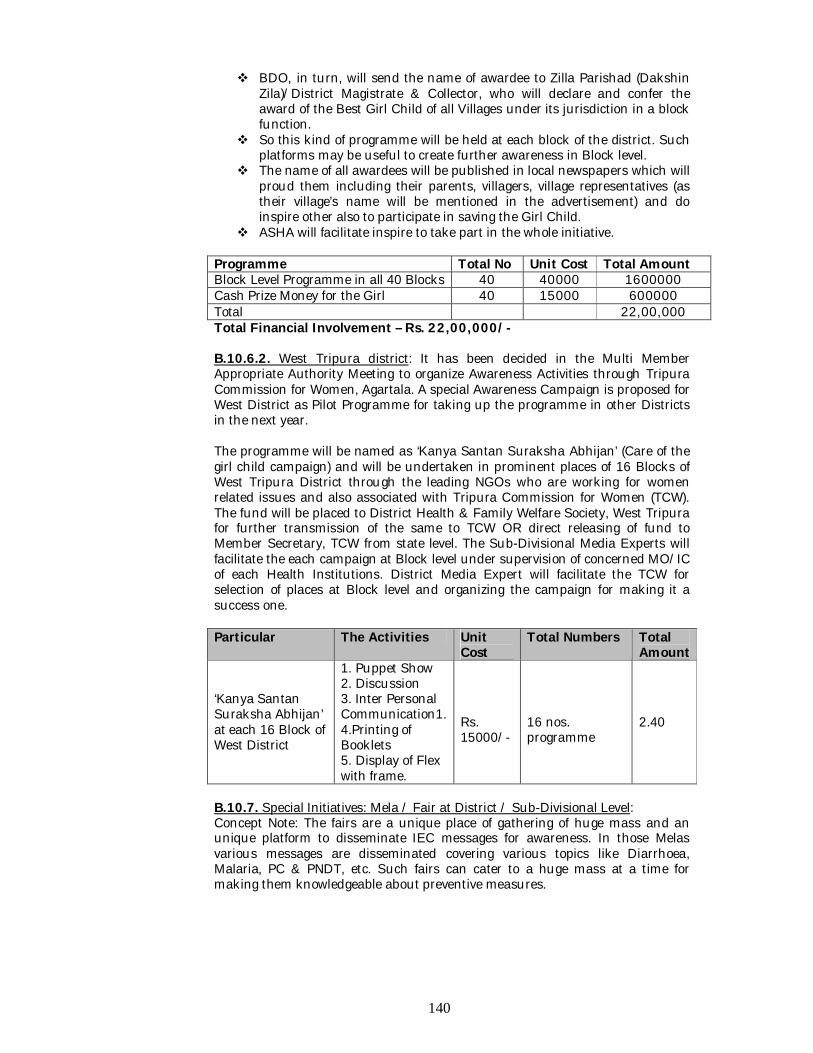
140
BDO, in turn, will send the name of awardee to Zilla Parishad (Dakshin Zila)/District Magistrate & Collector, who will declare and confer the award of the Best Girl Child of all Villages under its jurisdiction in a block function.
So this kind of programme will be held at each block of the district. Such platforms may be useful to create further awareness in Block level.
The name of all awardees will be published in local newspapers which will proud them including their parents, villagers, village representatives (as their village’s name will be mentioned in the advertisement) and do inspire other also to participate in saving the Girl Child.
ASHA will facilitate inspire to take part in the whole initiative.
Programme Total No Unit Cost Total Amount Block Level Programme in all 40 Blocks 40 40000 1600000 Cash Prize Money for the Girl 40 15000 600000 Total 22,00,000 Total Financial Involvement – Rs. 22,00,000/-
B.10.6.2. West Tripura district: It has been decided in the Multi Member Appropriate Authority Meeting to organize Awareness Activities through Tripura Commission for Women, Agartala. A special Awareness Campaign is proposed for West District as Pilot Programme for taking up the programme in other Districts in the next year. The programme will be named as ‘Kanya Santan Suraksha Abhijan’ (Care of the girl child campaign) and will be undertaken in prominent places of 16 Blocks of West Tripura District through the leading NGOs who are working for women related issues and also associated with Tripura Commission for Women (TCW). The fund will be placed to District Health & Family Welfare Society, West Tripura for further transmission of the same to TCW OR direct releasing of fund to Member Secretary, TCW from state level. The Sub-Divisional Media Experts will facilitate the each campaign at Block level under supervision of concerned MO/IC of each Health Institutions. District Media Expert will facilitate the TCW for selection of places at Block level and organizing the campaign for making it a success one. Particular The Activities Unit
Cost Total Numbers Total
Amount
‘Kanya Santan Suraksha Abhijan’ at each 16 Block of West District
1. Puppet Show 2. Discussion 3. Inter Personal Communication1. 4.Printing of Booklets 5. Display of Flex with frame.
Rs. 15000/-
16 nos. programme
2.40
B.10.7. Special Initiatives: Mela / Fair at District / Sub-Divisional Level: Concept Note: The fairs are a unique place of gathering of huge mass and an unique platform to disseminate IEC messages for awareness. In those Melas various messages are disseminated covering various topics like Diarrhoea, Malaria, PC & PNDT, etc. Such fairs can cater to a huge mass at a time for making them knowledgeable about preventive measures.
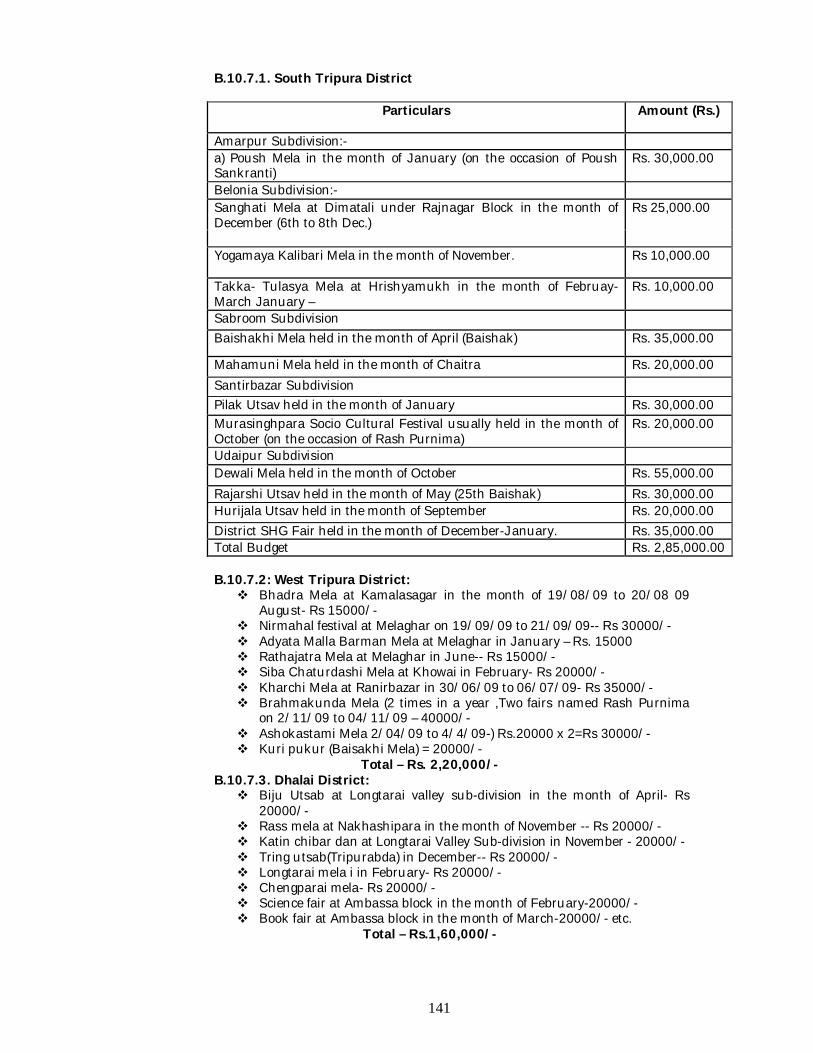
141
B.10.7.1. South Tripura District
Particulars Amount (Rs.)
Amarpur Subdivision:- a) Poush Mela in the month of January (on the occasion of Poush Sankranti)
Rs. 30,000.00
Belonia Subdivision:- Sanghati Mela at Dimatali under Rajnagar Block in the month of December (6th to 8th Dec.)
Rs 25,000.00
Yogamaya Kalibari Mela in the month of November. Rs 10,000.00
Takka- Tulasya Mela at Hrishyamukh in the month of Februay- March January –
Rs. 10,000.00
Sabroom Subdivision Baishakhi Mela held in the month of April (Baishak) Rs. 35,000.00
Mahamuni Mela held in the month of Chaitra Rs. 20,000.00 Santirbazar Subdivision Pilak Utsav held in the month of January Rs. 30,000.00 Murasinghpara Socio Cultural Festival usually held in the month of October (on the occasion of Rash Purnima)
Rs. 20,000.00
Udaipur Subdivision Dewali Mela held in the month of October Rs. 55,000.00 Rajarshi Utsav held in the month of May (25th Baishak) Rs. 30,000.00 Hurijala Utsav held in the month of September Rs. 20,000.00 District SHG Fair held in the month of December-January. Rs. 35,000.00 Total Budget Rs. 2,85,000.00
B.10.7.2: West Tripura District: Bhadra Mela at Kamalasagar in the month of 19/08/09 to 20/08 09
August- Rs 15000/- Nirmahal festival at Melaghar on 19/09/09 to 21/09/09-- Rs 30000/- Adyata Malla Barman Mela at Melaghar in January – Rs. 15000 Rathajatra Mela at Melaghar in June-- Rs 15000/- Siba Chaturdashi Mela at Khowai in February- Rs 20000/- Kharchi Mela at Ranirbazar in 30/06/09 to 06/07/09- Rs 35000/- Brahmakunda Mela (2 times in a year ,Two fairs named Rash Purnima
on 2/11/09 to 04/11/09 – 40000/- Ashokastami Mela 2/04/09 to 4/4/09-) Rs.20000 x 2=Rs 30000/- Kuri pukur (Baisakhi Mela) = 20000/-
Total – Rs. 2,20,000/- B.10.7.3. Dhalai District:
Biju Utsab at Longtarai valley sub-division in the month of April- Rs 20000/-
Rass mela at Nakhashipara in the month of November -- Rs 20000/- Katin chibar dan at Longtarai Valley Sub-division in November - 20000/- Tring utsab(Tripurabda) in December-- Rs 20000/- Longtarai mela i in February- Rs 20000/- Chengparai mela- Rs 20000/- Science fair at Ambassa block in the month of February-20000/- Book fair at Ambassa block in the month of March-20000/- etc.
Total – Rs.1,60,000/-
142
B.10.7.4. North District: Total Financial Involvement for different Mela at South District -Rs. 1,
60,000/- (North District) Total Budget of 4 District: Rs. 2, 85,000/- + Rs. 2, 20,000/- + Rs.1,
60,000/- + Rs.1, 60,000/- = Rs.8,25,000/- B.10.7.5. Other IEC Activities (Printing of Quarterly Bulletin / Calendar / Folder/ Leaflets/ Publication of IEC Materials) Publication of Quarterly Bulletin in Kakborok – Rs. 1,50,000/- Publication of Quarterly Bulletin in Bengali – Rs. 3,00,000/- Publication of Album – Rs. 50,000/- Publication of Compendium– Rs. 1,50,000/- Publication of wall calendar at State Level – Rs. 1,00,000/- Publication of Desktop Calendar at State level – Rs. 1,00,000/- Publication of Advertisements in Souvenirs – Rs. 1,50,000/- Publication of Leaflets / Folders/ Posters / Booklets – Rs. 10,00,000/- Publication of Newspaper Advertisements at District level @ Rs. 50,000/-
each = Rs. 2,00,000/- Publication of Advertisements in Newspapers at State level –
Rs.2,00,000/- Publication of Bi-annual Newsletter on NRHM in English – Rs.1,50,000/-
Total Budget –Rs.24, 00,000/-
B.10.7.6. Broadcasting of ASHA–R KATHA through All India Radio from Agartala, Belonia and Kailashahar Kendra (@Rs.5000 per programme for total 60 nos. programmes) – Rs. 300000/-
B.10.7.7. Tableaux on 26th January at Agartala – A tableaux on a theme on NRHM will be carried out on 26th January, 2011 from Assam Rifles Ground. Total cost may be Rs. 60000/-.
B.10.7.8. Hiring of Vehicles for monitoring and supervision of IEC activities: West District – Rs. 75,000/- South District – Rs. 75,000/- South District –Rs. 50, 000/- North District – Rs.50, 000/- State level – Rs. 2, 00,000/- Total Budget –Rs. 4, 50,000/-
B.10.7.9. Capacity building and training of manpower: State Level IEC Workshop at Agartala: One State level IEC Workshop may be organized at State level for two days during 1st quarter of financial year. The total participants may be approx 60 person.
The Financial Break-up is shown below:
Component Unit Cost Total Cost Stationary Articles Rs.125 Rs.125 x 60= 7500 Lunch/ Tea-Snacks Rs.200 RS.200 x 60 x 2= 24000 Hall Rent Rs.10000 20000 Honorarium of Resource Persons (GOI , RRC, Professional agency / Institute)
Rs.1000 per head Rs.1000 x 3 = 2000
Accommodation and fooding of 3 Resource Persons (3 days)
Rs.1500/- per day
Rs.1500 x 3 x 3 =13500
Honorarium of local Resource Rs. 300 per head Rs. 300 x 10 = Rs.3000/-
143
Component Unit Cost Total Cost Person including programme divisions
for 10 person
Hiring of Vehicles (2 nos.) for 2 days
Rs.1000/- Rs.4000/-
Certificate, Badge, Flower Bouquet etc
--------- Rs.2000/-
Backdrop Banner Rs.4000/- Misc. Cost -------- Rs.7000 TOTAL Rs. 85000/-
Total Budget for State Level Workshop: Rs. 85,000/- B.10.7.10. District level IEC workshop
West District:
Participants: One IEC personal from each PHC / CHC (32 nos) & 2 from sub-divisional
level IEC wings(4nos) Resource persons 4nos Official from State, district & Sub divisional level (14 nos) Representative of NGO-12 Representative of different IEC related agencies-10 Budget:
Hall rent-Rs1000/- Study materials @ Rs.50/- x 80 =Rs.4000/- Lunch @Rs.100/-x 80 = Rs.8,000/- PA system/Banner/Misc. cost- Rs.5000/- Honorarium for resource person @ Rs 300/- x 4= Rs1200/- Honorarium for participants @ Rs 200/- x 76= Rs 15200/-
Total Rs. 45200/- (West District)
B.10.7.11. Dhalai District: Participants:
One IEC personal from each PHC / CHC (12 nos) & 2 from sub-divisional level IEC wings(3nos)
Resource persons 4nos Official from State, district & Sub divisional level (10nos) Representative of NGO-8 Representative of different IEC related agencies-5 Break-up:
Hall rent-Rs1000/- Study materials @ Rs.50/- x 45 =Rs.2250/- Lunch @Rs.100/-x 45 = Rs.45,00/- PA system/Banner/Misc. cost- Rs.5000/- Honorium for resource person @ Rs 300/- x 4= Rs1200/- Honorium for participants @ Rs 200/- x 41= Rs 8200/- Total Rs. 22150/- (Dhalai District)
B.10.7.12. North District Participants:
One IEC personal from each PHC / CHC (23 nos) &2 from sub-divisional level IEC wings(2nos)
Resource persons 4nos Official from State, district & Sub divisional level (10nos)
144
Representative of NGO-8 Representative of different IEC related agencies-6 Break-up:
Hall rent-Rs1000/- Study materials @ Rs.50/- x 55 =Rs.2750/- Lunch @Rs.100/-x 55 = Rs.5500/- PA system/Banner/Misc. cost- Rs.5000/- Honorium for resource person @ Rs 300/- x 4= Rs1200/- Honorium for participants @ Rs 200/- x 51= Rs 10200/- Total Rs.25650/- (North District)
B.10.7.13. South District: Total Financial Involvement for District level Workshop: Rs.30,900/- (South District)
Total Budget: Rs. 45,200/- (West District) + Rs. 22150/- (Dhalai District) + Total Rs.25650/- (North District) + Rs. 30900 (South District) = Rs.1, 23,900/- B.10.7.14. Evaluation Survey: The impact survey of Health Awareness programmes and the programmes of RCH related issues is vital for assessing the need for planning of the IEC/BCC programmes. A household survey at each District level will be carried out for the each district so that the district may have the evaluation survey report for making plan for next year. The District Evaluation survey will be carried out at GP/ADC village level. The detailed questionnaire and sampling methods will be chalked out after selecting the nodal agency for the task following all codal formalities by the district. The Total cost may be Rs. 10 Lakhs approx. for the four districts @ Rs.2, 50,000/- for each district.
B.10.7.15. IEC activities on Immunization:-
Sl. NO.
Activity Remarks
1 ‘Swasthya Haat Mela’ in a popular market day in all Blocks
The said activity is designed in an integrated manner under Maternal Health.
2 Mother and Child Health Fair one in each Sub-Division
B.10.7.16. Purpose: To intensify the IEC activities under RNTCP
Introduction: IEC is an important tool of community health. It involves the transmission to the people in matters of health and disease so that they live healthier lives. TB is a major public health problem. In order to control TB there is need for dissemination of information about the Tuberculosis (signs & symptoms), its causes detection and treatment thereby empowering individuals, families and communities to be responsible for behavioural change to achieve cure of people suffering from Tuberculosis. So, strengthening the existing IEC approach, it is proposed to introduce “Yakshma Niyantran Rath” ( Chariot ) for campaign of RNTCP throughout the State especially remote areas. It is well known fact that Success of any health communication strategy for health development depends largely on the close interaction and coordination between communities & Service provider. The State TB Cell, Tripura plans to advocate and generate awareness level through its IEC wing to improve case detection & cure rate in the remote places of all the districts. In this situation RNTCP Chariot van will
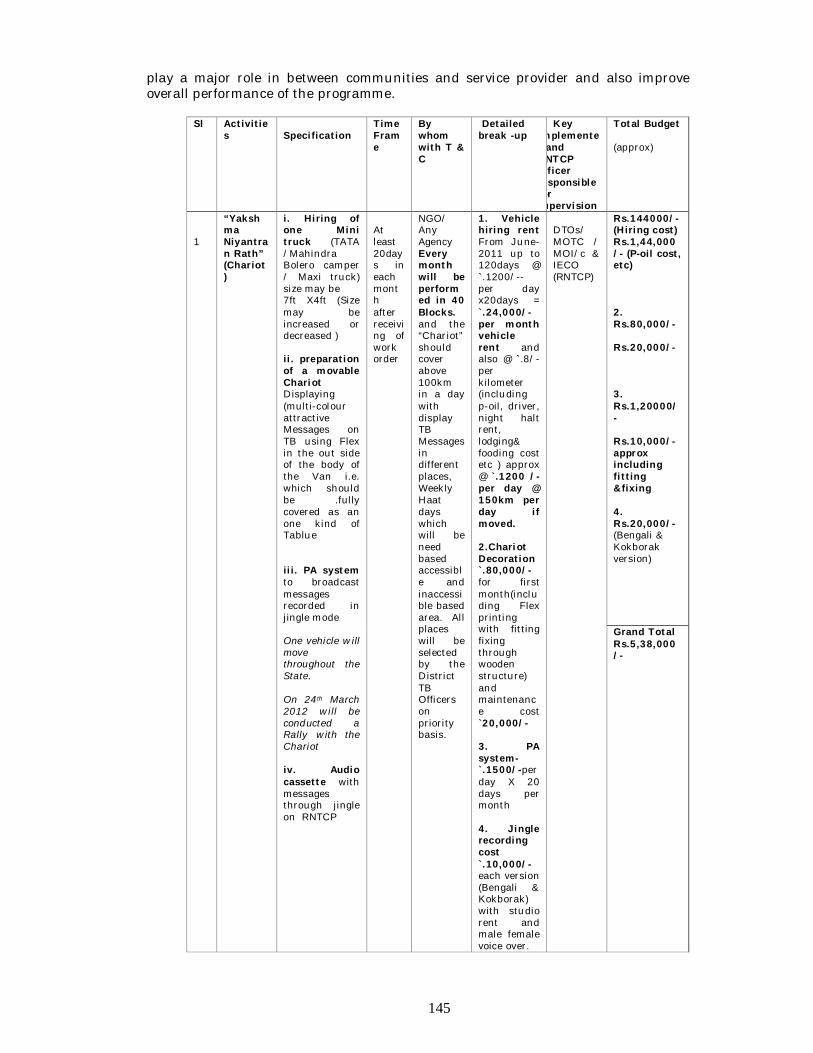
145
play a major role in between communities and service provider and also improve overall performance of the programme.
Sl Activities
Specification
Time Frame
By whom with T & C
Detailed break -up
Key implementer and RNTCP officer responsible for supervision
Total Budget (approx)
1
“Yakshma Niyantran Rath” (Chariot )
i. Hiring of one Mini truck (TATA /Mahindra Bolero camper / Maxi truck) size may be 7ft X4ft (Size may be increased or decreased ) ii. preparation of a movable Chariot Displaying (multi-colour attractive Messages on TB using Flex in the out side of the body of the Van i.e. which should be .fully covered as an one kind of Tablue iii. PA system to broadcast messages recorded in jingle mode One vehicle will move throughout the State. On 24th March 2012 will be conducted a Rally with the Chariot iv. Audio cassette with messages through jingle on RNTCP
At least 20days in each month after receiving of work order
NGO/ Any Agency Every month will be performed in 40 Blocks. and the “Chariot” should cover above 100km in a day with display TB Messages in different places, Weekly Haat days which will be need based accessible and inaccessible based area. All places will be selected by the District TB Officers on priority basis.
1. Vehicle hiring rent From June-2011 up to 120days @ `.1200/-- per day x20days = `.24,000/- per month vehicle rent and also @ `.8/- per kilometer (including p-oil, driver, night halt rent, lodging& fooding cost etc ) approx @ `.1200 /- per day @ 150km per day if moved. 2.Chariot Decoration `.80,000/- for first month(including Flex printing with fitting fixing through wooden structure) and maintenance cost `20,000/- 3. PA system-`.1500/-per day X 20 days per month 4. Jingle recording cost `.10,000/- each version (Bengali & Kokborak) with studio rent and male female voice over.
DTOs/ MOTC / MOI/c & IECO (RNTCP)
Rs.144000/- (Hiring cost) Rs.1,44,000/- (P-oil cost, etc) 2. Rs.80,000/- Rs.20,000/- 3. Rs.1,20000/- Rs.10,000/- approx including fitting &fixing 4. Rs.20,000/- (Bengali & Kokborak version)
Grand Total Rs.5,38,000/-
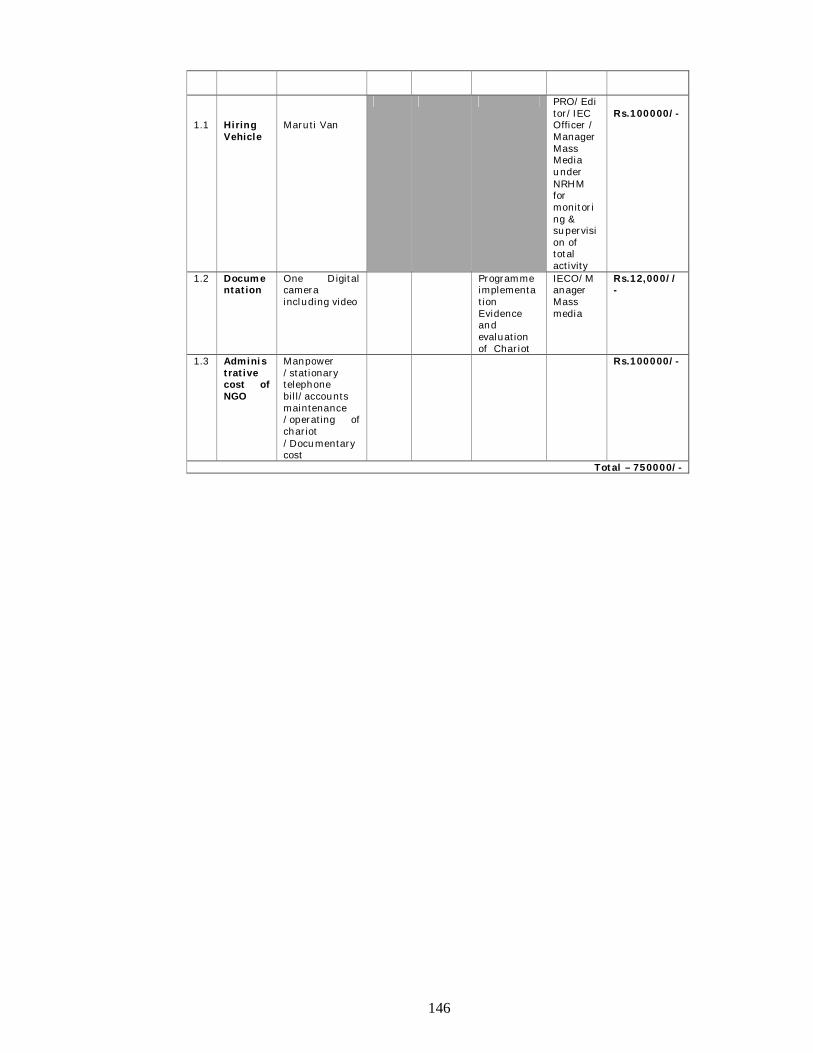
146
1.1
Hiring Vehicle
Maruti Van
PRO/Editor/IEC Officer / Manager Mass Media under NRHM for monitoring & supervision of total activity
Rs.100000/-
1.2 Documentation
One Digital camera including video
Programme implementation Evidence and evaluation of Chariot
IECO/Manager Mass media
Rs.12,000//-
1.3 Administrative cost of NGO
Manpower /stationary telephone bill/accounts maintenance /operating of chariot /Documentary cost
Rs.100000/-
Total – 750000/-
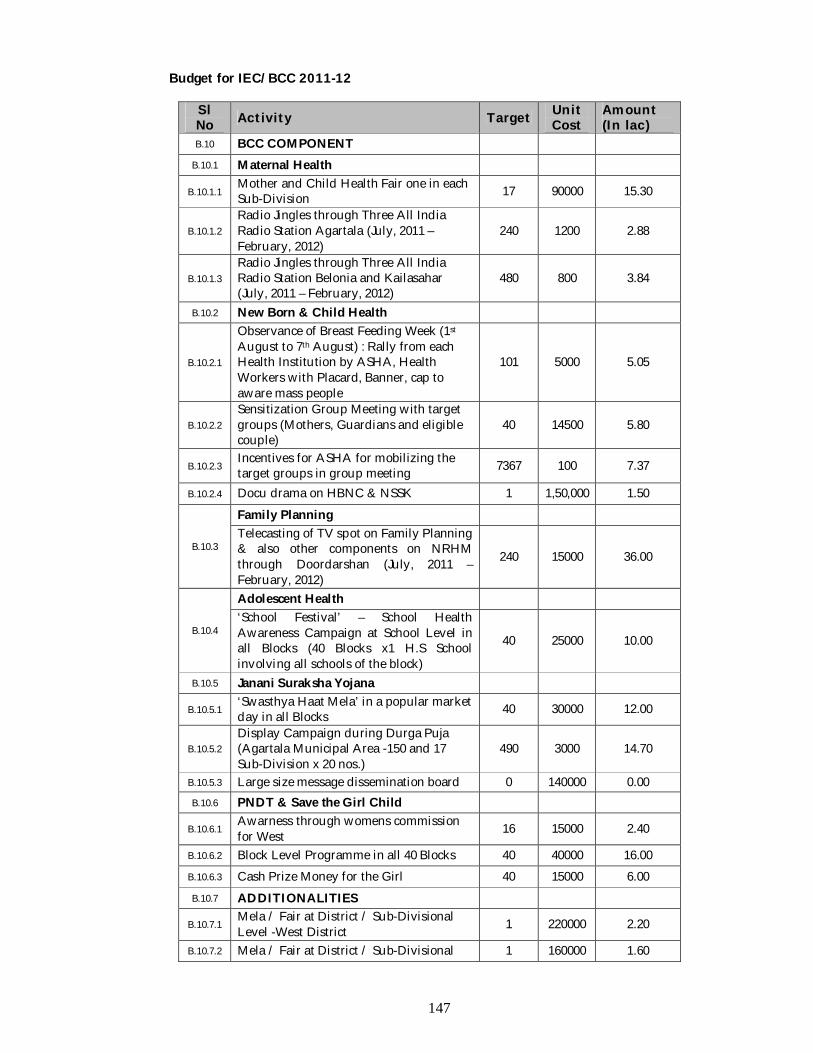
147
Budget for IEC/BCC 2011-12
Sl No Activity Target Unit
Cost Amount (In lac)
B.10 BCC COMPONENT B.10.1 Maternal Health
B.10.1.1 Mother and Child Health Fair one in each Sub-Division 17 90000 15.30
B.10.1.2 Radio Jingles through Three All India Radio Station Agartala (July, 2011 – February, 2012)
240 1200 2.88
B.10.1.3 Radio Jingles through Three All India Radio Station Belonia and Kailasahar (July, 2011 – February, 2012)
480 800 3.84
B.10.2 New Born & Child Health
B.10.2.1
Observance of Breast Feeding Week (1st August to 7th August) : Rally from each Health Institution by ASHA, Health Workers with Placard, Banner, cap to aware mass people
101 5000 5.05
B.10.2.2 Sensitization Group Meeting with target groups (Mothers, Guardians and eligible couple)
40 14500 5.80
B.10.2.3 Incentives for ASHA for mobilizing the target groups in group meeting 7367 100 7.37
B.10.2.4 Docu drama on HBNC & NSSK 1 1,50,000 1.50
B.10.3
Family Planning Telecasting of TV spot on Family Planning & also other components on NRHM through Doordarshan (July, 2011 – February, 2012)
240 15000 36.00
B.10.4
Adolescent Health ‘School Festival’ – School Health Awareness Campaign at School Level in all Blocks (40 Blocks x1 H.S School involving all schools of the block)
40 25000 10.00
B.10.5 Janani Suraksha Yojana
B.10.5.1 ‘Swasthya Haat Mela’ in a popular market day in all Blocks 40 30000 12.00
B.10.5.2 Display Campaign during Durga Puja (Agartala Municipal Area -150 and 17 Sub-Division x 20 nos.)
490 3000 14.70
B.10.5.3 Large size message dissemination board 0 140000 0.00 B.10.6 PNDT & Save the Girl Child
B.10.6.1 Awarness through womens commission for West 16 15000 2.40
B.10.6.2 Block Level Programme in all 40 Blocks 40 40000 16.00 B.10.6.3 Cash Prize Money for the Girl 40 15000 6.00 B.10.7 ADDITIONALITIES
B.10.7.1 Mela / Fair at District / Sub-Divisional Level -West District 1 220000 2.20
B.10.7.2 Mela / Fair at District / Sub-Divisional 1 160000 1.60
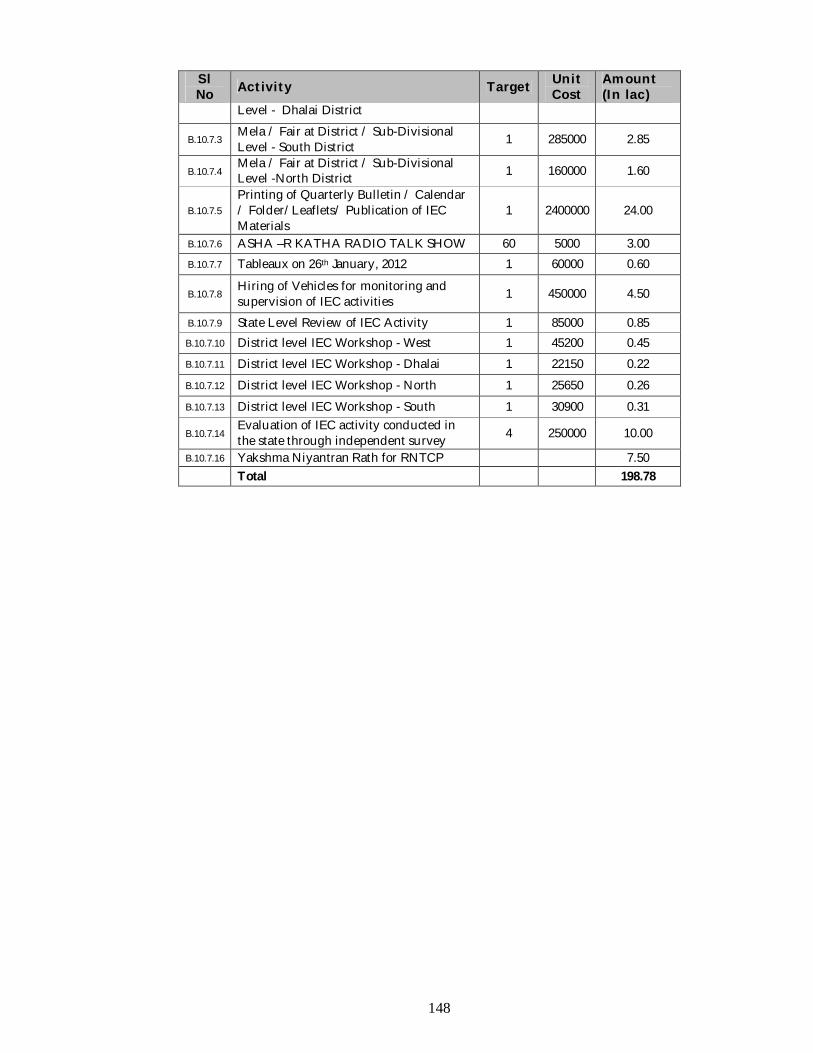
148
Sl No Activity Target Unit
Cost Amount (In lac)
Level - Dhalai District
B.10.7.3 Mela / Fair at District / Sub-Divisional Level - South District 1 285000 2.85
B.10.7.4 Mela / Fair at District / Sub-Divisional Level -North District 1 160000 1.60
B.10.7.5 Printing of Quarterly Bulletin / Calendar / Folder/Leaflets/ Publication of IEC Materials
1 2400000 24.00
B.10.7.6 ASHA –R KATHA RADIO TALK SHOW 60 5000 3.00 B.10.7.7 Tableaux on 26th January, 2012 1 60000 0.60
B.10.7.8 Hiring of Vehicles for monitoring and supervision of IEC activities 1 450000 4.50
B.10.7.9 State Level Review of IEC Activity 1 85000 0.85 B.10.7.10 District level IEC Workshop - West 1 45200 0.45 B.10.7.11 District level IEC Workshop - Dhalai 1 22150 0.22 B.10.7.12 District level IEC Workshop - North 1 25650 0.26 B.10.7.13 District level IEC Workshop - South 1 30900 0.31
B.10.7.14 Evaluation of IEC activity conducted in the state through independent survey 4 250000 10.00
B.10.7.16 Yakshma Niyantran Rath for RNTCP 7.50 Total 198.78
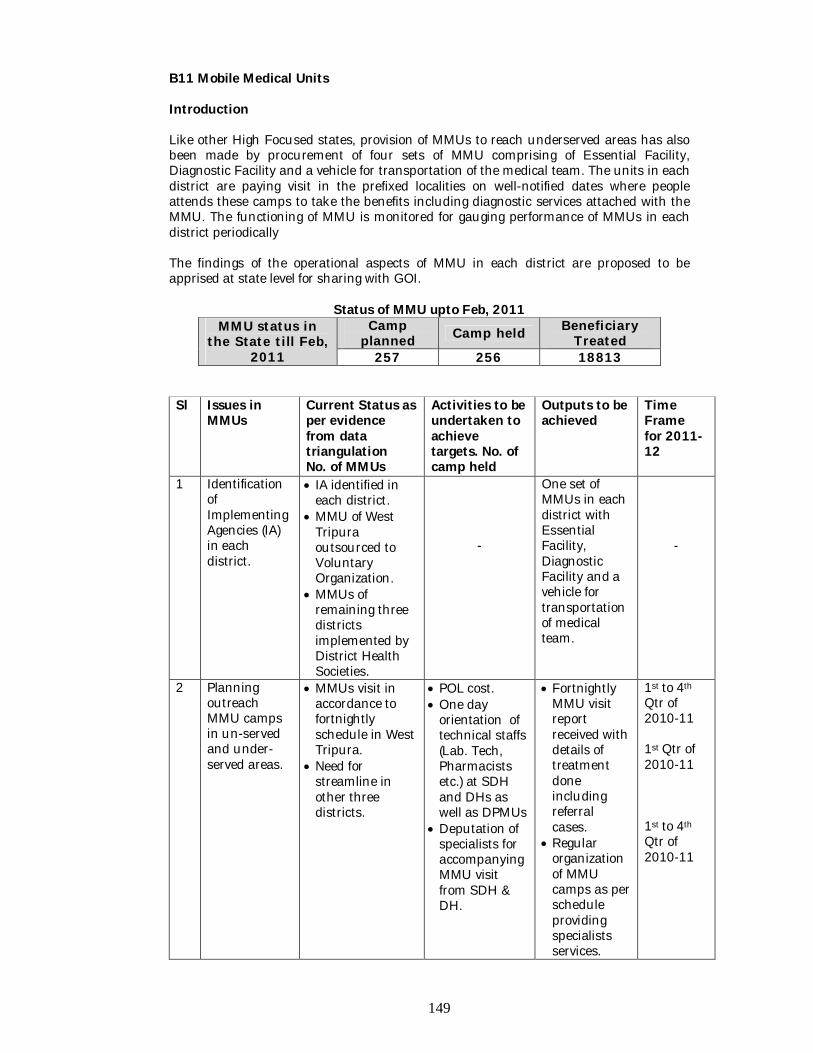
149
B11 Mobile Medical Units Introduction Like other High Focused states, provision of MMUs to reach underserved areas has also been made by procurement of four sets of MMU comprising of Essential Facility, Diagnostic Facility and a vehicle for transportation of the medical team. The units in each district are paying visit in the prefixed localities on well-notified dates where people attends these camps to take the benefits including diagnostic services attached with the MMU. The functioning of MMU is monitored for gauging performance of MMUs in each district periodically
The findings of the operational aspects of MMU in each district are proposed to be apprised at state level for sharing with GOI.
Status of MMU upto Feb, 2011 MMU status in
the State till Feb, 2011
Camp planned Camp held Beneficiary
Treated 257 256 18813
Sl Issues in
MMUs Current Status as per evidence from data triangulation No. of MMUs
Activities to be undertaken to achieve targets. No. of camp held
Outputs to be achieved
Time Frame for 2011-12
1 Identification of Implementing Agencies (IA) in each district.
IA identified in each district.
MMU of West Tripura outsourced to Voluntary Organization.
MMUs of remaining three districts implemented by District Health Societies.
-
One set of MMUs in each district with Essential Facility, Diagnostic Facility and a vehicle for transportation of medical team.
-
2 Planning outreach MMU camps in un-served and under-served areas.
MMUs visit in accordance to fortnightly schedule in West Tripura.
Need for streamline in other three districts.
POL cost. One day
orientation of technical staffs (Lab. Tech, Pharmacists etc.) at SDH and DHs as well as DPMUs
Deputation of specialists for accompanying MMU visit from SDH & DH.
Fortnightly MMU visit report received with details of treatment done including referral cases.
Regular organization of MMU camps as per schedule providing specialists services.
1st to 4th Qtr of 2010-11 1st Qtr of 2010-11 1st to 4th Qtr of 2010-11
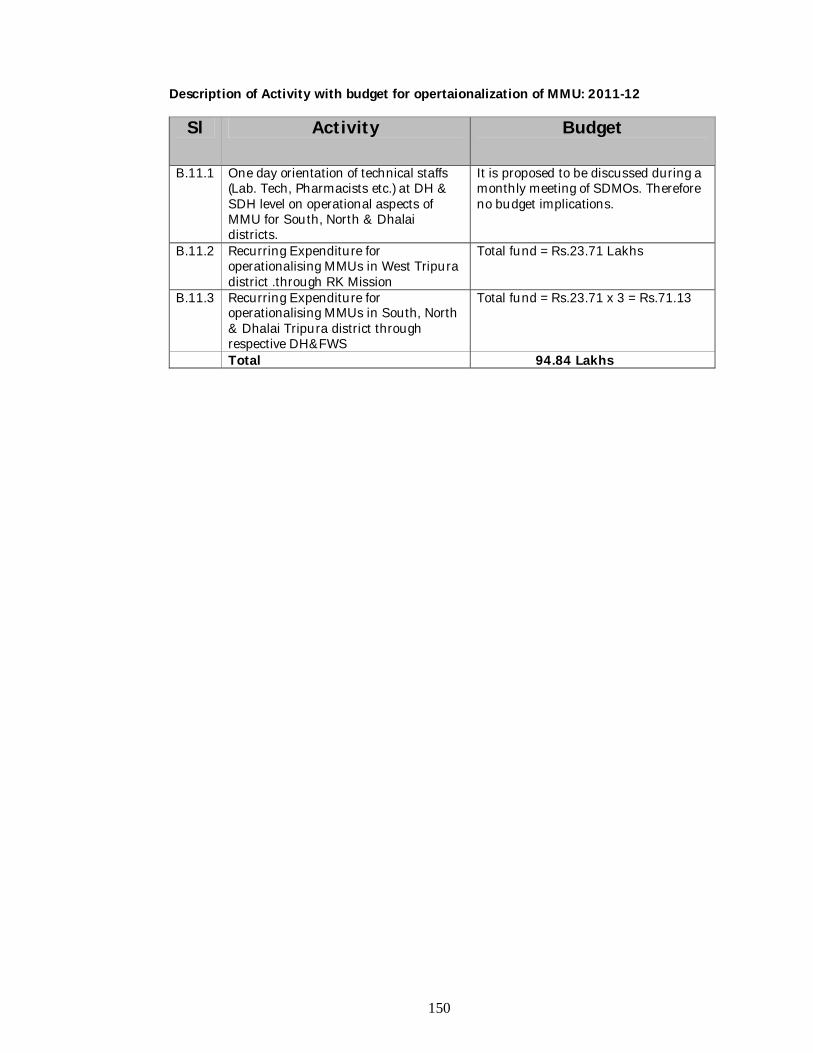
150
Description of Activity with budget for opertaionalization of MMU: 2011-12
Sl Activity Budget
B.11.1 One day orientation of technical staffs (Lab. Tech, Pharmacists etc.) at DH & SDH level on operational aspects of MMU for South, North & Dhalai districts.
It is proposed to be discussed during a monthly meeting of SDMOs. Therefore no budget implications.
B.11.2 Recurring Expenditure for operationalising MMUs in West Tripura district .through RK Mission
Total fund = Rs.23.71 Lakhs
B.11.3 Recurring Expenditure for operationalising MMUs in South, North & Dhalai Tripura district through respective DH&FWS
Total fund = Rs.23.71 x 3 = Rs.71.13
Total 94.84 Lakhs
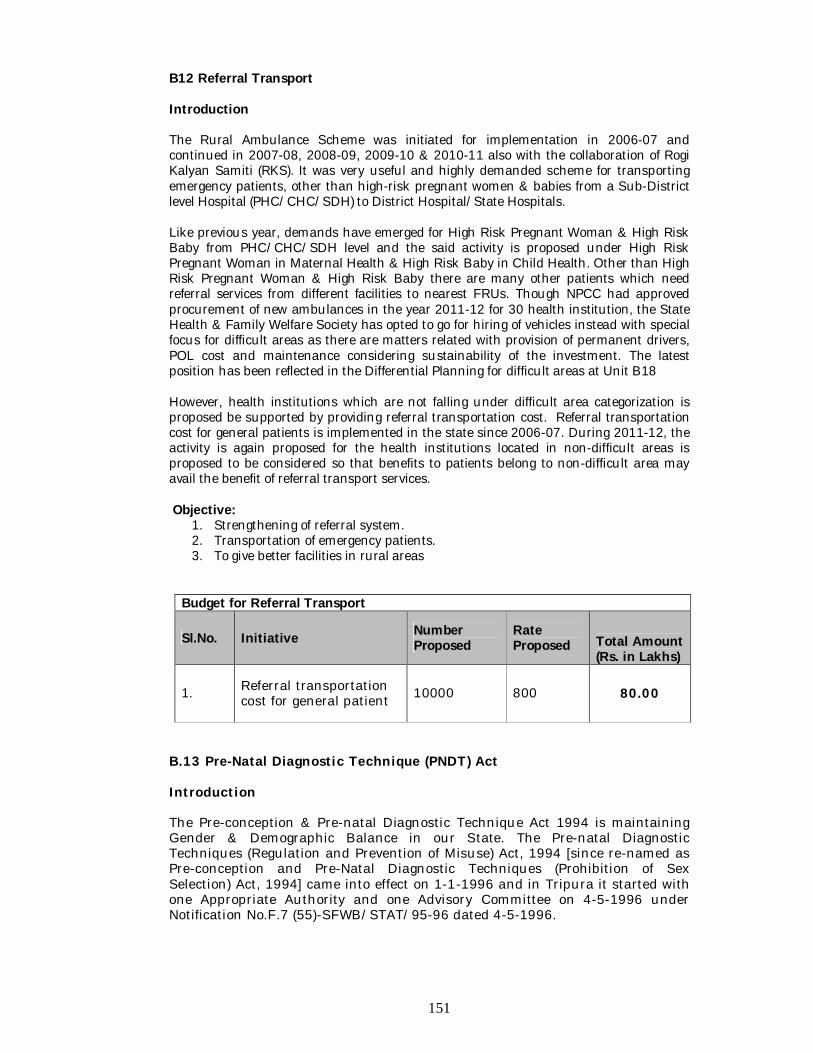
151
B12 Referral Transport Introduction The Rural Ambulance Scheme was initiated for implementation in 2006-07 and continued in 2007-08, 2008-09, 2009-10 & 2010-11 also with the collaboration of Rogi Kalyan Samiti (RKS). It was very useful and highly demanded scheme for transporting emergency patients, other than high-risk pregnant women & babies from a Sub-District level Hospital (PHC/CHC/SDH) to District Hospital/State Hospitals. Like previous year, demands have emerged for High Risk Pregnant Woman & High Risk Baby from PHC/CHC/SDH level and the said activity is proposed under High Risk Pregnant Woman in Maternal Health & High Risk Baby in Child Health. Other than High Risk Pregnant Woman & High Risk Baby there are many other patients which need referral services from different facilities to nearest FRUs. Though NPCC had approved procurement of new ambulances in the year 2011-12 for 30 health institution, the State Health & Family Welfare Society has opted to go for hiring of vehicles instead with special focus for difficult areas as there are matters related with provision of permanent drivers, POL cost and maintenance considering sustainability of the investment. The latest position has been reflected in the Differential Planning for difficult areas at Unit B18 However, health institutions which are not falling under difficult area categorization is proposed be supported by providing referral transportation cost. Referral transportation cost for general patients is implemented in the state since 2006-07. During 2011-12, the activity is again proposed for the health institutions located in non-difficult areas is proposed to be considered so that benefits to patients belong to non-difficult area may avail the benefit of referral transport services. Objective:
1. Strengthening of referral system. 2. Transportation of emergency patients. 3. To give better facilities in rural areas
Budget for Referral Transport
Sl.No. Initiative Number Proposed
Rate Proposed Total Amount
(Rs. in Lakhs)
1. Referral transportation cost for general patient 10000 800 80.00
B.13 Pre-Natal Diagnostic Technique (PNDT) Act Introduction The Pre-conception & Pre-natal Diagnostic Technique Act 1994 is maintaining Gender & Demographic Balance in our State. The Pre-natal Diagnostic Techniques (Regulation and Prevention of Misuse) Act, 1994 [since re-named as Pre-conception and Pre-Natal Diagnostic Techniques (Prohibition of Sex Selection) Act, 1994] came into effect on 1-1-1996 and in Tripura it started with one Appropriate Authority and one Advisory Committee on 4-5-1996 under Notification No.F.7 (55)-SFWB/STAT/95-96 dated 4-5-1996.
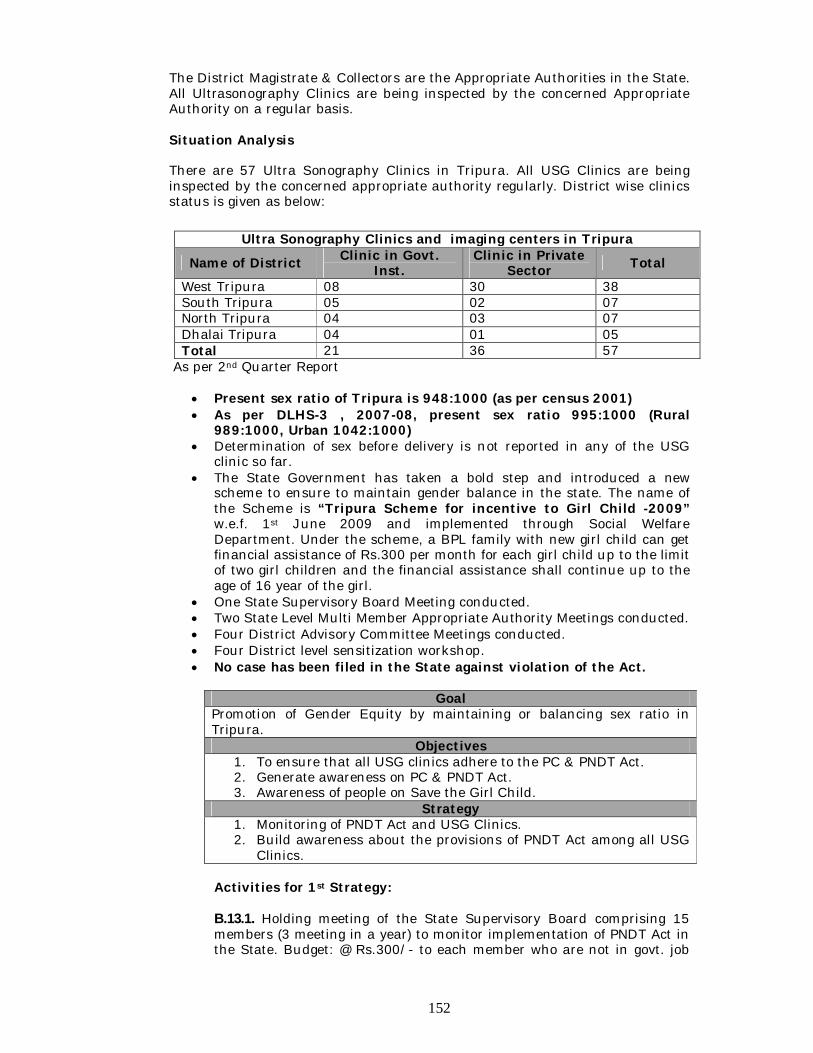
152
The District Magistrate & Collectors are the Appropriate Authorities in the State. All Ultrasonography Clinics are being inspected by the concerned Appropriate Authority on a regular basis. Situation Analysis There are 57 Ultra Sonography Clinics in Tripura. All USG Clinics are being inspected by the concerned appropriate authority regularly. District wise clinics status is given as below:
As per 2nd Quarter Report
Present sex ratio of Tripura is 948:1000 (as per census 2001) As per DLHS-3 , 2007-08, present sex ratio 995:1000 (Rural
989:1000, Urban 1042:1000) Determination of sex before delivery is not reported in any of the USG
clinic so far. The State Government has taken a bold step and introduced a new
scheme to ensure to maintain gender balance in the state. The name of the Scheme is “Tripura Scheme for incentive to Girl Child -2009” w.e.f. 1st June 2009 and implemented through Social Welfare Department. Under the scheme, a BPL family with new girl child can get financial assistance of Rs.300 per month for each girl child up to the limit of two girl children and the financial assistance shall continue up to the age of 16 year of the girl.
One State Supervisory Board Meeting conducted. Two State Level Multi Member Appropriate Authority Meetings conducted. Four District Advisory Committee Meetings conducted. Four District level sensitization workshop. No case has been filed in the State against violation of the Act.
Goal
Promotion of Gender Equity by maintaining or balancing sex ratio in Tripura.
Objectives 1. To ensure that all USG clinics adhere to the PC & PNDT Act. 2. Generate awareness on PC & PNDT Act. 3. Awareness of people on Save the Girl Child.
Strategy 1. Monitoring of PNDT Act and USG Clinics. 2. Build awareness about the provisions of PNDT Act among all USG
Clinics.
Activities for 1st Strategy: B.13.1. Holding meeting of the State Supervisory Board comprising 15 members (3 meeting in a year) to monitor implementation of PNDT Act in the State. Budget: @ Rs.300/- to each member who are not in govt. job
Ultra Sonography Clinics and imaging centers in Tripura
Name of District Clinic in Govt. Inst.
Clinic in Private Sector Total
West Tripura 08 30 38 South Tripura 05 02 07 North Tripura 04 03 07 Dhalai Tripura 04 01 05 Total 21 36 57
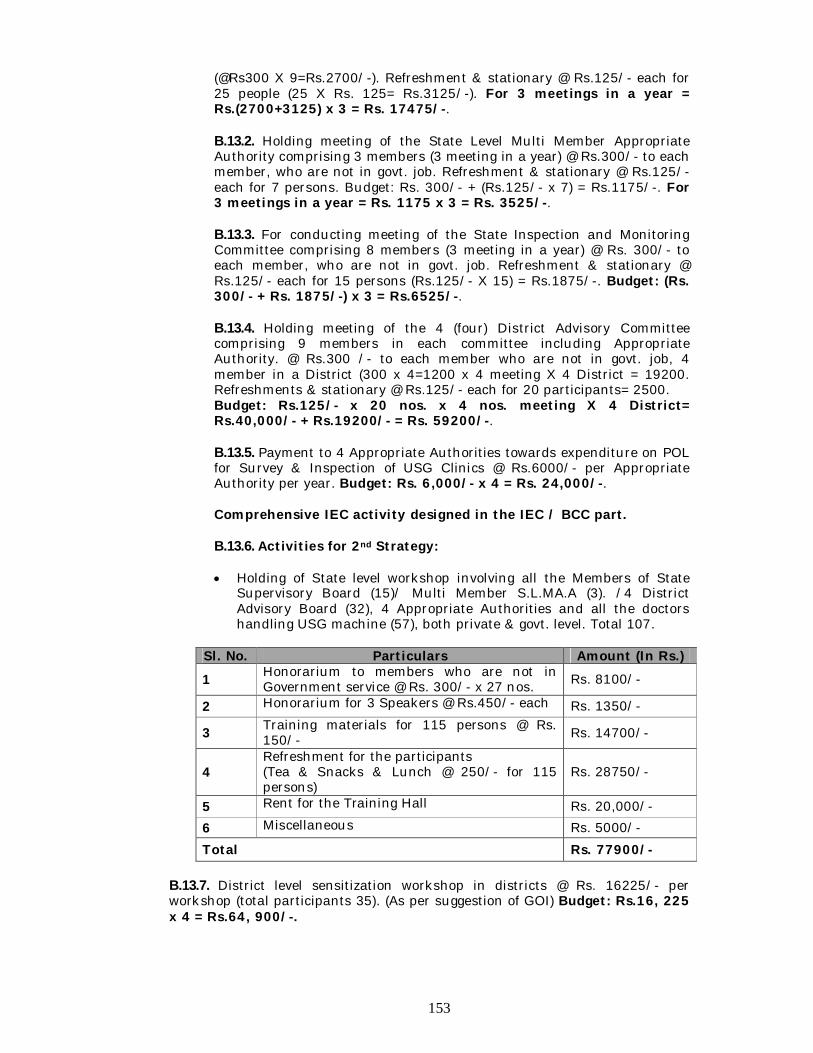
153
(@Rs300 X 9=Rs.2700/-). Refreshment & stationary @ Rs.125/- each for 25 people (25 X Rs. 125= Rs.3125/-). For 3 meetings in a year = Rs.(2700+3125) x 3 = Rs. 17475/-.
B.13.2. Holding meeting of the State Level Multi Member Appropriate Authority comprising 3 members (3 meeting in a year) @ Rs.300/- to each member, who are not in govt. job. Refreshment & stationary @ Rs.125/- each for 7 persons. Budget: Rs. 300/- + (Rs.125/- x 7) = Rs.1175/-. For 3 meetings in a year = Rs. 1175 x 3 = Rs. 3525/-. B.13.3. For conducting meeting of the State Inspection and Monitoring Committee comprising 8 members (3 meeting in a year) @ Rs. 300/- to each member, who are not in govt. job. Refreshment & stationary @ Rs.125/- each for 15 persons (Rs.125/- X 15) = Rs.1875/-. Budget: (Rs. 300/- + Rs. 1875/-) x 3 = Rs.6525/-. B.13.4. Holding meeting of the 4 (four) District Advisory Committee comprising 9 members in each committee including Appropriate Authority. @ Rs.300 /- to each member who are not in govt. job, 4 member in a District (300 x 4=1200 x 4 meeting X 4 District = 19200. Refreshments & stationary @ Rs.125/- each for 20 participants= 2500. Budget: Rs.125/- x 20 nos. x 4 nos. meeting X 4 District= Rs.40,000/- + Rs.19200/- = Rs. 59200/-. B.13.5. Payment to 4 Appropriate Authorities towards expenditure on POL for Survey & Inspection of USG Clinics @ Rs.6000/- per Appropriate Authority per year. Budget: Rs. 6,000/- x 4 = Rs. 24,000/-.
Comprehensive IEC activity designed in the IEC / BCC part. B.13.6. Activities for 2nd Strategy:
Holding of State level workshop involving all the Members of State
Supervisory Board (15)/ Multi Member S.L.MA.A (3). /4 District Advisory Board (32), 4 Appropriate Authorities and all the doctors handling USG machine (57), both private & govt. level. Total 107.
Sl. No. Particulars Amount (In Rs.)
1 Honorarium to members who are not in Government service @ Rs. 300/- x 27 nos. Rs. 8100/-
2 Honorarium for 3 Speakers @ Rs.450/- each Rs. 1350/-
3 Training materials for 115 persons @ Rs. 150/- Rs. 14700/-
4 Refreshment for the participants (Tea & Snacks & Lunch @ 250/- for 115 persons)
Rs. 28750/-
5 Rent for the Training Hall Rs. 20,000/-
6 Miscellaneous Rs. 5000/-
Total Rs. 77900/-
B.13.7. District level sensitization workshop in districts @ Rs. 16225/- per workshop (total participants 35). (As per suggestion of GOI) Budget: Rs.16, 225 x 4 = Rs.64, 900/-.
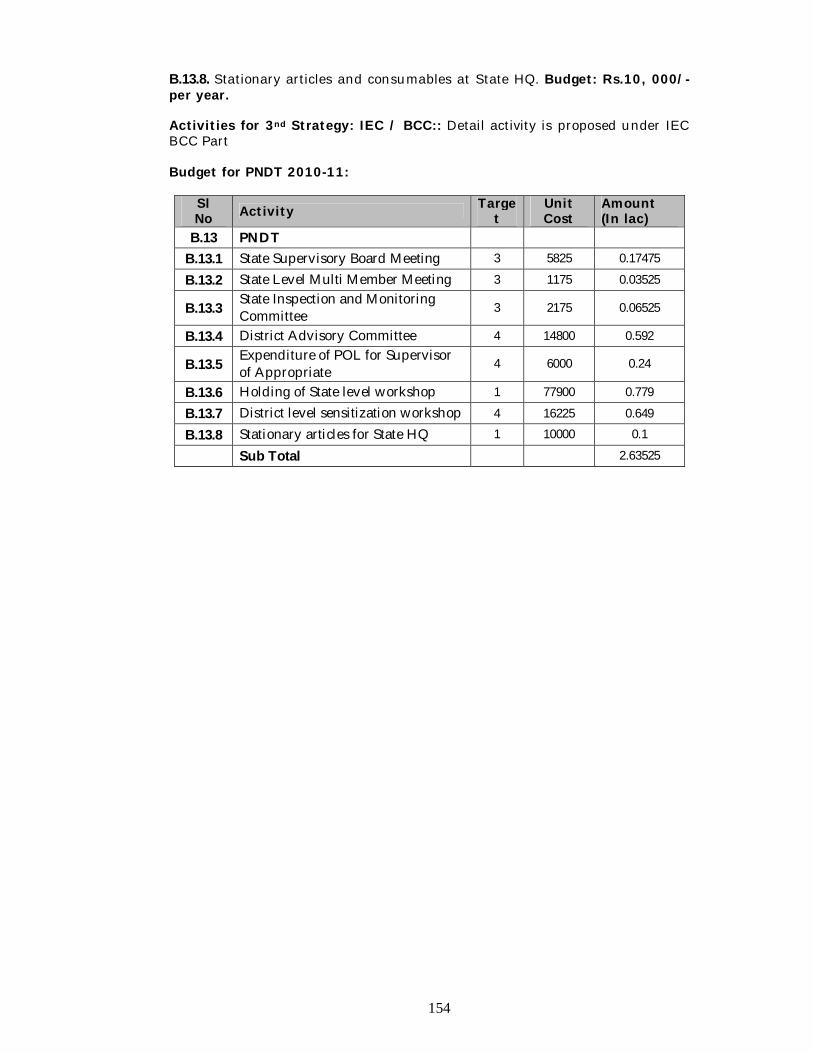
154
B.13.8. Stationary articles and consumables at State HQ. Budget: Rs.10, 000/- per year.
Activities for 3nd Strategy: IEC / BCC:: Detail activity is proposed under IEC BCC Part
Budget for PNDT 2010-11:
Sl No Activity Targe
t Unit Cost
Amount (In lac)
B.13 PNDT
B.13.1 State Supervisory Board Meeting 3 5825 0.17475
B.13.2 State Level Multi Member Meeting 3 1175 0.03525
B.13.3 State Inspection and Monitoring Committee 3 2175 0.06525
B.13.4 District Advisory Committee 4 14800 0.592
B.13.5 Expenditure of POL for Supervisor of Appropriate 4 6000 0.24
B.13.6 Holding of State level workshop 1 77900 0.779
B.13.7 District level sensitization workshop 4 16225 0.649
B.13.8 Stationary articles for State HQ 1 10000 0.1
Sub Total 2.63525
155
B.14 NGO Programme (MNGO & PPP) Introduction With an aim to give boost to the implementation of various activities through RCH.II under NRHM, partnership with private hospitals has been initiated for implementing JSY, newborn care services and family welfare program. The payment mechanism is as per the guidelines of GoI. Regular supervision and monitoring of these accredited institutions/hospitals will be done as per the revised accreditation guideline. I. Accreditation of Private Hospital
The accredited private hospitals and nursing homes in Agartala city under West Tripura district are as follows:-
Sl Name of the Private Hospital Location of the Private Hospital/ Nursing Home
1 Tripura Medical College & Dr. B. R. Ambedkar Memorial Teaching Hospital
Hapania, Agartala
2 Sarkar Nursing Home H.G. Basak Road, Agartala 3 Bhowmik Polyclinic & Nursing
Homes H.G. Basak Road, Agartala
The service delivery as per the capacity of the facility is proposed to be
categorized either MCH Level-1 or MCH Level-2 by performing facility survey/ analysis with the help of State/ District Quality Assurance Committee with reference to the latest accreditation guideline published by the Ministry.
Activities proposed to be carried out by the accredited institutions are as follows:- 1. Immunization: Immunization of all children 0-1 years of age as per the
national Immunization Schedule as well as pregnant women.
2. Pulse polio booths.
3. Monthly reporting to the office of the CMO (West).
4. Promotion of NSV, female sterilization, IUD insertion is to be initiated. Rates of payments will be as per GoI norms and State memorandum.
5. Beneficiaries under JSY will be allowed financial benefits as per the
guidelines issued by the Government of Tripura.
Performance report of the accredited institutions is proposed to be shared with GOI on quarterly basis to FP, MH & Immunization Division, Ministry of Health & Family Welfare, Govt. of India as per prescribed proforma.
II. Mother NGO Scheme
In pursuance of efforts towards population stabilization and Reproductive & Child Health, aiming at sustainable development and inculcating a meaningful partnership with Non-Governmental Organizations (NGOs) as one of the strategic themes, envisaged in the National Population Policy – 2000, the Mother NGO Scheme is implemented under RCH.II Programme of NRHM.
156
As per revised Guideline for selection of MNGOs, each district is to be
allotted with one MNGO with 3-4 Field NGOs (FNGOs). In state’s context, one MNGO has been identified in North Tripura. Similarly for identification of MNGOs in the remaining districts viz. West, South & Dhalai districts, wide publicity have been done Proposals were received from all interested NGOs of the three districts. Statuses of the three districts are:-
1. Dhalai district have send the Field appraisal report of NGOs by DM &
Collector, Dhalai of the short listed NGOs. A meeting of the State NGO Committee is scheduled during 2nd month of 4th Qtr: 2010-11 for final selection of one MNGO.
2. West Tripura district is in process of sending the Field appraisal report of NGOs scrutinized at State HQ by the district authority. On receiving the report another MNGO for West Tripura districts may be kindly considered for final selection by State NGO Committee during 4th Qtr: 2010-11.
3. Regarding South Tripura district, no NGOs have fulfilled the criteria for
considering field appraisals by District authority under the present publicity.
4. Under MNGO scheme, it is proposed to have at least 4 (four) FNGOs
which would be identified by the selected MNGO in a transparent process with specific allotted areas (Administrative Blocks). The activity is proposed to promote advancing community participation, awareness and to ensure outreach of services etc. Progress report of the MNGOs performance is proposed to be shared with GOI on quarterly basis to Apex Resource Cell, NGO Division, Ministry of Health & Family Welfare, Govt. of India.
Goal Supplementation of RCH service delivery in underserved areas/ Blocks of the State by improving quality and outreach. Objectives 1. Improve access of BPL/ SC/ ST population access to quality ANC/
Institutional delivery/ PNC of urban areas. 2. Improve outreach MCH services in the un served and under served areas
Strategy Activities
Accreditation of private hospitals and nursing homes as per latest GOI guideline.
Conduct facility survey to enable categorizes either MCH Level-1 or MCH Level-2 service.
Releasing funds to the accredited institutions through the respective District Health & Family Welfare Societies as per terms & conditions of the MoU and approved physical targets.
Identification of MNGO as per existing GOI guideline.
Support identified MNGO of West Tripura & Dhalai district to attend Capacity Building workshop as per schedule of Regional Resource Centre for NE States for MNGOs-Voluntary Health Association of Assam (VHAA).
Enable new identified MNGOs to conduct Baseline Survey after attending Capacity Building Workshop.
Grant-in-aid for functional MNGOs and new MNGOs
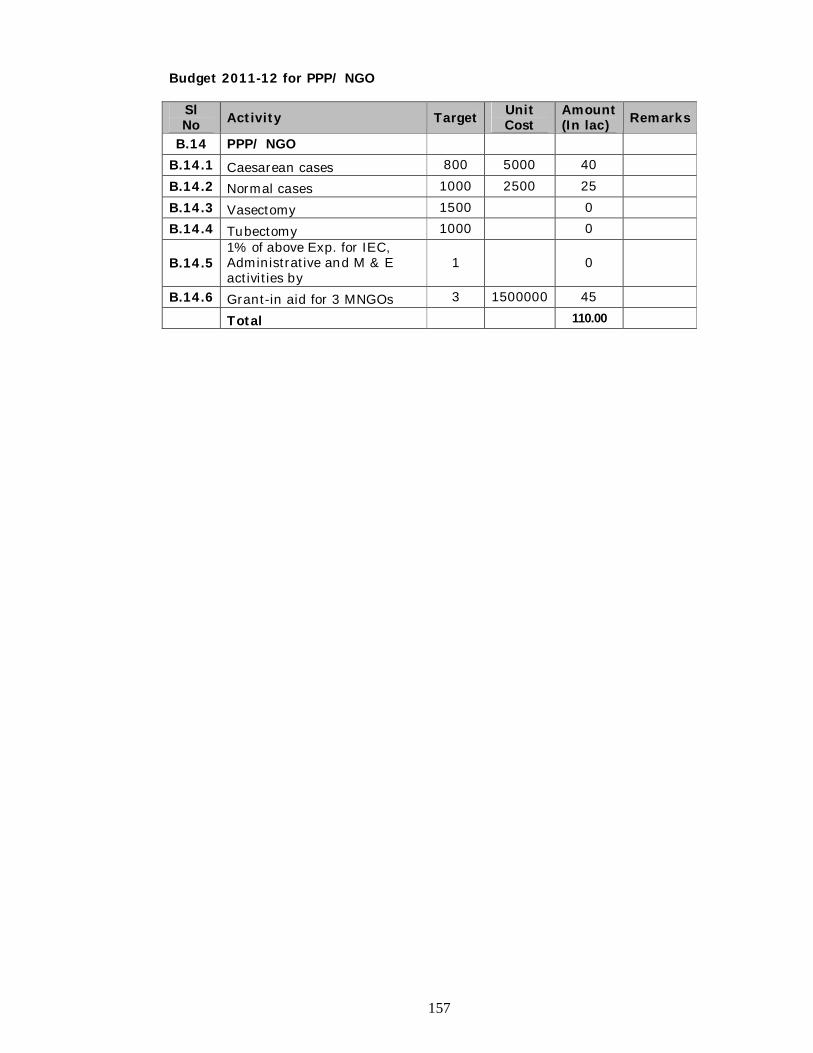
157
Budget 2011-12 for PPP/ NGO
Sl No Activity Target Unit
Cost Amount (In lac) Remarks
B.14 PPP/ NGO B.14.1 Caesarean cases 800 5000 40
B.14.2 Normal cases 1000 2500 25
B.14.3 Vasectomy 1500 0 B.14.4 Tubectomy 1000 0
B.14.5 1% of above Exp. for IEC, Administrative and M & E activities by
1 0
B.14.6 Grant-in aid for 3 MNGOs 3 1500000 45 Total 110.00
158
B.15. Monitoring & Evaluation Introduction An effective health management information system (HMIS) is an important instrument to plan and monitor health interventions and facilitate overall surveillance of the health condition of a population. Situation Analysis 1. HMIS Portal
i. Facility level online data entry and Sub-division level analysis has been
implemented in the State of Tripura. Facility wise information for the year 2010-11 is already available in the HMIS portal. Data from the Private Institution is already been updated into the HMIS portal.
ii. State has appointed the HMIS Assistant in each facility (PHC/CHC/SDH/DH), which will be acting as Nodal Information Officer for collection, compilation, filled up HMIS formats of all other health related information and to upload data on the HMIS web portal.
iii. Once HMIS portal is committable with capturing the information related to Disease Control Programme, State has capable to report the information from facility level into the Web portal.
iv. Facility wise Infrastructure details and facility survey reports will be uploaded in to the Web portal from April 2011 onwards by the State.
v. Ministry develops the FMR format for uploading to the Web portal. Once the FMR format (Provided by FMG and made available with the HMIS Portal) becomes uniform, it will be uploaded regularly. MoHFW may make a provision for monthly facility wise SOE as it would be convenient for the state to implement.
2. MCTS Portal
2.1 Customization of MCTS: NIC Tripura has customized the MCTS Portal under the URL of http://nrhm-mcts-trp.nic.in Mapping/Coding of Master database of all health facility has been completed. 1040 GP/ADC of the state are mapped under the health institution of Tripura as catchment area. In the year 2010-11, 3 GP namely Kaurikuli, Jalai and Gounagar under Jalai & Gournagar SC of Kanika Memorial PHC, North District has been taken as pilot basis for online MCTS data entry in this meantime, legacy information has collected by MCTS excel format provided by MoHFW. During Pilot phase, lots of corrective measure has taken by NIC for the MCTS portal. From April 2011, State will updated the MCTS as regular manner.
2.2 Integration of Monitoring & Evaluation activities across the programmes: Proposed that State is to be integrated the Monitoring & Evaluation activities vide developing a State MIS Cell which comprises by the Team leader of Manager – MIS followed by Data Manager of NVBDCP, NLEP, RNTCP, and IDSP. Accordingly District MIS Cell may comprise by the Team leader of District Data Manager.
159
Action Plan for the Year 2011-12: Strategies
1. Strengthening the HMIS/M&E activity and MCTS system in the facility level. 2. Monthly, Quarterly Review 3. Capacity building for Health Staffs and HMIS Asst (Nodal &E Officer)
Activities: 2.1 Strengthening of HMIS/M&E/MCTS 2.1.1 Salaries
Particulars Cost (Rs.) Amount (Rs) Salary of State/District Hospitals/SDH level HMIS Asst (Nodal M&E Officer) with 10% increment of present salary.
@ Rs. 11,880/- for 12 months for 16 persons
Budget under Programme Management Unit of Part-A
Salary of PHC/CHC level HMIS Asst (Nodal M&E Officer) with 10% increment of present salary.
@ Rs. 10,450/- for 12 months for 89 persons
Salary of Districts Data Manager with 10% increment of present salary
@ Rs. 20,394/- for 12 months for 4 persons
Salary of State MIS Manager with 10% increment of present salary
@ Rs. 26,059/- for 12 months for 1 person
2.1.2 Mobility Cost for State MIS Manager, District Data Manager & HMIS Asst (Nodal M & E Officers). It is proposed that PHCs/CHCs level HMIS Asst to be visited in Health
Sub- centres/VHND/to attend the review meeting/to utilization of CSC/ cyber café/any other monitoring visit of 48 times (4 times in a month) in a year
SDH level HMIS Assistant to be visited in HSC/PHC/CHC/VHND to attend the review meeting/to utilize the CSC/ cyber café/any other monitoring visit of 48 time (4 times in a month) in a year.
District Nodal M & E Officer (District Data Manager) to be visited in HSC/PHC/CHC/SDH /DH/ VHND/to attend the review meeting/to utilize the CSC/ any other monitoring visit of 72 times (6 times in a month) in a year.
State Nodal M & E Officer (State MIS Manager) to be visited in HSC/PHC/CHC/SDH/DH/VHND/to attend the review meeting/to utilize the CSC/ any other monitoring visit as well as other activities according to requirement of the Society.
Financial Involvement for mobility cost of Nodal M&E Officer is:
Particulars Cost (Rs.) Amount (Rs.) To be visited in Health Sub- centres of 40 times (4 times in a month) by PHCs/CHCs level Nodal M&E Officer (HMIS Asst) for 10 months.
Rs. 500/- for 89 PHCs/CHCs for 40 times
17,80,000.00
160
2.1.3 Workshop/Training for HMIS Asst (Nodal M & E Officer) 2.1.3.1 Two days Refresher Workshop/Training on HMIS Portal (HMIS formats,
Data Entry, Data Uploading, Report generation by) is proposes to be organized for 110 Number HMIS Asst and Districts Data Manager. Financial Involvement on Workshop/Training on HMIS Portal for 110 HMIS Asst (Nodal M & E Officers).
Particulars Cost (Rs.) Amount (Rs) Rent for Computer Lab with Internet facilities
6000/- for 2 days 12,000.00
Rent of LCD Projector 3000/- for 2 days 6,000.00 Breakfast, Lunch, Tea & Snacks and Dinner
200/- for 2 days for 17 person
6,800.00
Rent of Dinning hall 600/- for 2 day 1,200.00 Writing Pad, Pen, Study Materials, Beg etc
500/- for 17 sets 8,500.00
Hiring cost of vehicle 1000/- for 2 days 2,000.00 TA and Accommodation Cost 500/- for 17 Nos 8,500.00 Overhead expenditure (10%) 3,650.00 Sub Total 40,150.00 Cost of 2 Days Training for 17 person x 7 batch for @ Rs. 40,150/- per batch = Rs.2,81,050.00
2.1.3.2 Two days training on data validation for HMIS and MCTS are proposes to be
organized for 110 Number Nodal M & E Officers. Financial Involvement on Workshop/Training on HMIS Portal and MCTS for 110 Nodal M & E Officers.
Particulars Cost (Rs.) Amount (Rs) Rent for Computer Lab with Internet facilities
6000/- for 2 days 12,000.00
Rent of LCD Projector 3000/- for 2 days 6,000.00 Breakfast, Lunch, Tea & Snacks and Dinner
200/- for 2 days for 17 person
6,800.00
Rent of Dining hall 600/- for 2 day 1,200.00 Writing Pad, Pen, Study Materials, Bag 500/- for 17 sets 8,500.00
To be visited in HSC/PHC/CHC of 40 time (4 times in a month) by SDH level Nodal M&E Officer (HMIS Asst) for 10 month
Rs. 750/- for 15 SDH for 40 times
4,50,000.00
To be visited in HSC/PHC/CHC/ SDH/DH of 80 time (8 times in a month) by Nodal M&E Officer. (District Data Manager) for 10 months.
Rs. 1200/- for 4 District HQ for 80 times
3,84,000.00
To be visited in HSC/PHC/ CHC/SDH /DH in a year by State Nodal M & E Officer (State MIS Manager) and Communication with others organization/ CMO/SDM other than regular monitoring programme A vehicle may hire on monthly rent basis @ Rs. 600/- per day and Rs. 6/- per KM basis for 10 months.
Rs. 21,600/- per month for 10 months
2,16,000.00
Total 28,30,000.00 Total Mobility Cost of the Nodal M & E Officers is Rs. 28,30,000.00
161
etc Hiring cost of vehicle 1000/- for 2 days 2,000.00 TA and Accommodation Cost 500/- for 17 Nos 8,500.00 Overhead expenditure (10%) 3,650.00
Sub Total 40,150.00 Cost of 2 Days Training for 17 person X 7 batch for @ Rs 40,150/- per batch = Rs. 2,81050.00
2.2 Procurement 2.2.1 Procurement of Internet Connectivity: It is proposed to procure the data
card (USB) and reimbursement the monthly rent, for State MIS Manager and Districts Data Manager (Four) for the purpose of HMIS and MCTS.The Financial involvement for network strengthening is:
Component Cost (Rs.) Amount (Rs.)
Cost of the data card (USB) @ Rs. 2500/- for 5 Nos 12,500.00
Rent for 10 month @ Rs. 750/- per month for 5 Nos for 10 months 37,500.00
Total (Rs.) 50,000.00 Total cost of network strengthening is Rs.50,000.00
2.2.2 Annual Maintenance Cost: The Annual Maintenance Cost are propose for 33 Computers which are procured for West District of Tripura. The Financial involvement of the AMC is:
Component Cost (Rs.) Amount (Rs.) Annual Maintenance Cost for 33 Computers for West Districts of Tripura
@ Rs. 1600/- for 33 Nos 52,800.00
Total (Rs.) 52,800.00 Total Cost involved for AMC is Rs. 52,800.00
2.2.3 Operational Costs (Consumable etc): Day to day consumable is to be
required as printing & stationeries for the all health institution, Districts & State Head quarters for the year 2011-12 The Financial involvement of the Printing & Computer Stationeries is:
Component Cost (Rs.) Amount (Rs.)
Printing & Computer Stationeries @ Rs. 5000/- per annum for 110 nos institution
5,50,000.00
Total (Rs.) 5,50,000.00 Total cost of the Printing & Computer Stationeries is Rs. 5,50,000.00
2.3 Operationalising HMIS at Facility level 2.3.1 Sensitization to Medical Officers (PHC/CHC/SDH) on MCTS and Data
quality: It is proposed that sensitization on MCTS and data quality to be organized by the State for validate & quality data transmission through HMIS and MCTS. Financial Involvement for the Sensitization are:
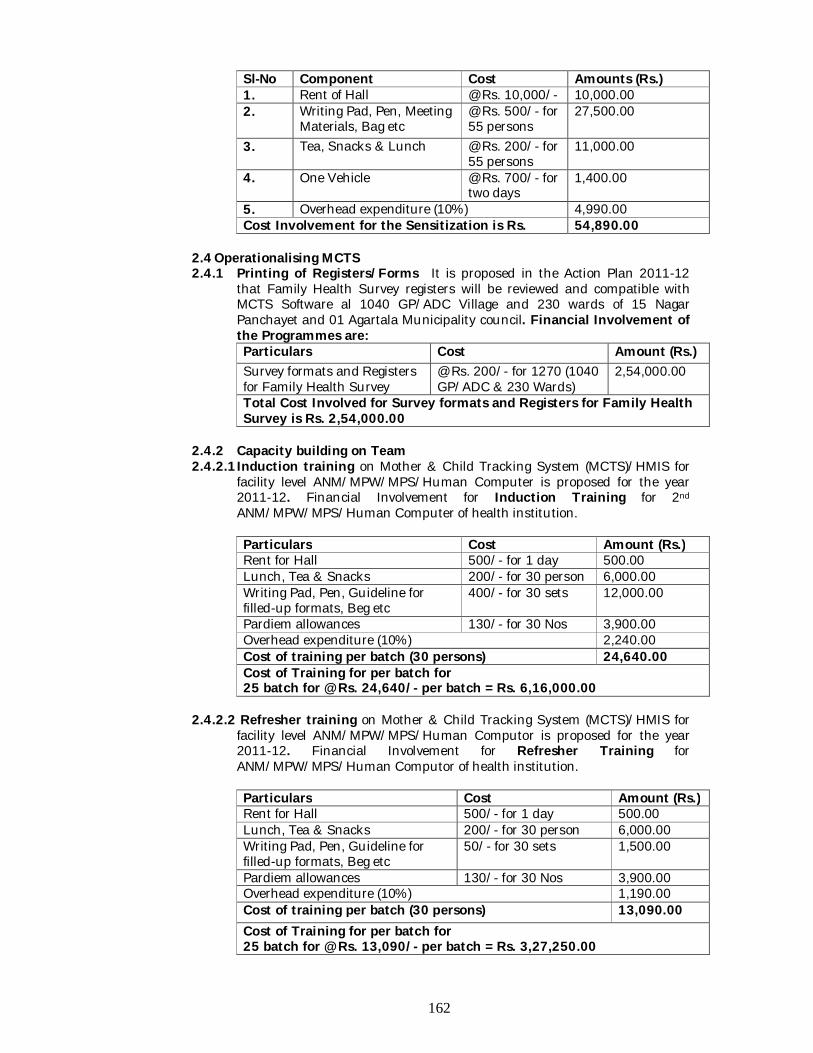
162
Sl-No Component Cost Amounts (Rs.) 1. Rent of Hall @ Rs. 10,000/- 10,000.00 2. Writing Pad, Pen, Meeting
Materials, Bag etc @ Rs. 500/- for 55 persons
27,500.00
3. Tea, Snacks & Lunch @ Rs. 200/- for 55 persons
11,000.00
4. One Vehicle @ Rs. 700/- for two days
1,400.00
5. Overhead expenditure (10%) 4,990.00 Cost Involvement for the Sensitization is Rs. 54,890.00
2.4 Operationalising MCTS 2.4.1 Printing of Registers/Forms It is proposed in the Action Plan 2011-12
that Family Health Survey registers will be reviewed and compatible with MCTS Software al 1040 GP/ADC Village and 230 wards of 15 Nagar Panchayet and 01 Agartala Municipality council. Financial Involvement of the Programmes are: Particulars Cost Amount (Rs.) Survey formats and Registers for Family Health Survey
@ Rs. 200/- for 1270 (1040 GP/ADC & 230 Wards)
2,54,000.00
Total Cost Involved for Survey formats and Registers for Family Health Survey is Rs. 2,54,000.00
2.4.2 Capacity building on Team 2.4.2.1 Induction training on Mother & Child Tracking System (MCTS)/HMIS for
facility level ANM/MPW/MPS/Human Computer is proposed for the year 2011-12. Financial Involvement for Induction Training for 2nd ANM/MPW/MPS/Human Computer of health institution.
Particulars Cost Amount (Rs.) Rent for Hall 500/- for 1 day 500.00 Lunch, Tea & Snacks 200/- for 30 person 6,000.00 Writing Pad, Pen, Guideline for filled-up formats, Beg etc
400/- for 30 sets 12,000.00
Pardiem allowances 130/- for 30 Nos 3,900.00 Overhead expenditure (10%) 2,240.00 Cost of training per batch (30 persons) 24,640.00 Cost of Training for per batch for 25 batch for @ Rs. 24,640/- per batch = Rs. 6,16,000.00
2.4.2.2 Refresher training on Mother & Child Tracking System (MCTS)/HMIS for
facility level ANM/MPW/MPS/Human Computor is proposed for the year 2011-12. Financial Involvement for Refresher Training for ANM/MPW/MPS/Human Computor of health institution.
Particulars Cost Amount (Rs.) Rent for Hall 500/- for 1 day 500.00 Lunch, Tea & Snacks 200/- for 30 person 6,000.00 Writing Pad, Pen, Guideline for filled-up formats, Beg etc
50/- for 30 sets 1,500.00
Pardiem allowances 130/- for 30 Nos 3,900.00 Overhead expenditure (10%) 1,190.00 Cost of training per batch (30 persons) 13,090.00 Cost of Training for per batch for 25 batch for @ Rs. 13,090/- per batch = Rs. 3,27,250.00
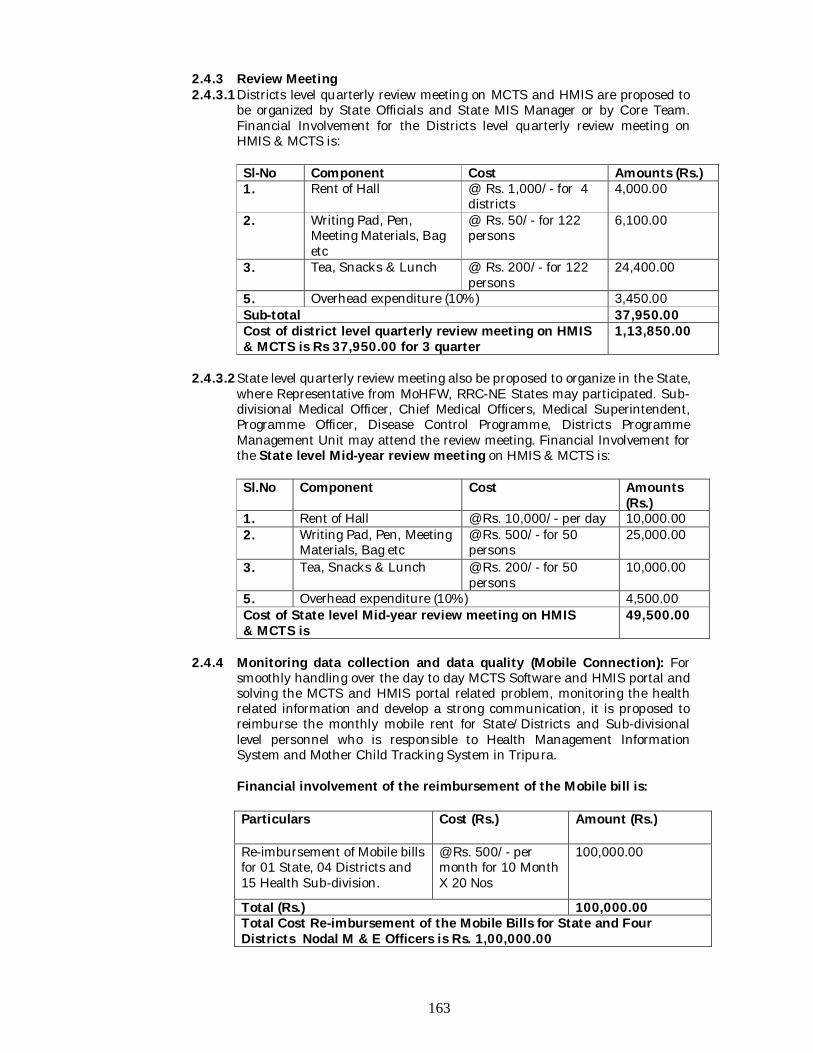
163
2.4.3 Review Meeting 2.4.3.1 Districts level quarterly review meeting on MCTS and HMIS are proposed to
be organized by State Officials and State MIS Manager or by Core Team. Financial Involvement for the Districts level quarterly review meeting on HMIS & MCTS is:
Sl-No Component Cost Amounts (Rs.) 1. Rent of Hall @ Rs. 1,000/- for 4
districts 4,000.00
2. Writing Pad, Pen, Meeting Materials, Bag etc
@ Rs. 50/- for 122 persons
6,100.00
3. Tea, Snacks & Lunch @ Rs. 200/- for 122 persons
24,400.00
5. Overhead expenditure (10%) 3,450.00 Sub-total 37,950.00 Cost of district level quarterly review meeting on HMIS & MCTS is Rs 37,950.00 for 3 quarter
1,13,850.00
2.4.3.2 State level quarterly review meeting also be proposed to organize in the State,
where Representative from MoHFW, RRC-NE States may participated. Sub-divisional Medical Officer, Chief Medical Officers, Medical Superintendent, Programme Officer, Disease Control Programme, Districts Programme Management Unit may attend the review meeting. Financial Involvement for the State level Mid-year review meeting on HMIS & MCTS is:
Sl.No Component Cost
Amounts (Rs.)
1. Rent of Hall @ Rs. 10,000/- per day 10,000.00 2. Writing Pad, Pen, Meeting
Materials, Bag etc @ Rs. 500/- for 50 persons
25,000.00
3. Tea, Snacks & Lunch @ Rs. 200/- for 50 persons
10,000.00
5. Overhead expenditure (10%) 4,500.00 Cost of State level Mid-year review meeting on HMIS & MCTS is
49,500.00
2.4.4 Monitoring data collection and data quality (Mobile Connection): For
smoothly handling over the day to day MCTS Software and HMIS portal and solving the MCTS and HMIS portal related problem, monitoring the health related information and develop a strong communication, it is proposed to reimburse the monthly mobile rent for State/Districts and Sub-divisional level personnel who is responsible to Health Management Information System and Mother Child Tracking System in Tripura.
Financial involvement of the reimbursement of the Mobile bill is: Particulars Cost (Rs.) Amount (Rs.)
Re-imbursement of Mobile bills for 01 State, 04 Districts and 15 Health Sub-division.
@ Rs. 500/- per month for 10 Month X 20 Nos
100,000.00
Total (Rs.) 100,000.00 Total Cost Re-imbursement of the Mobile Bills for State and Four Districts Nodal M & E Officers is Rs. 1,00,000.00
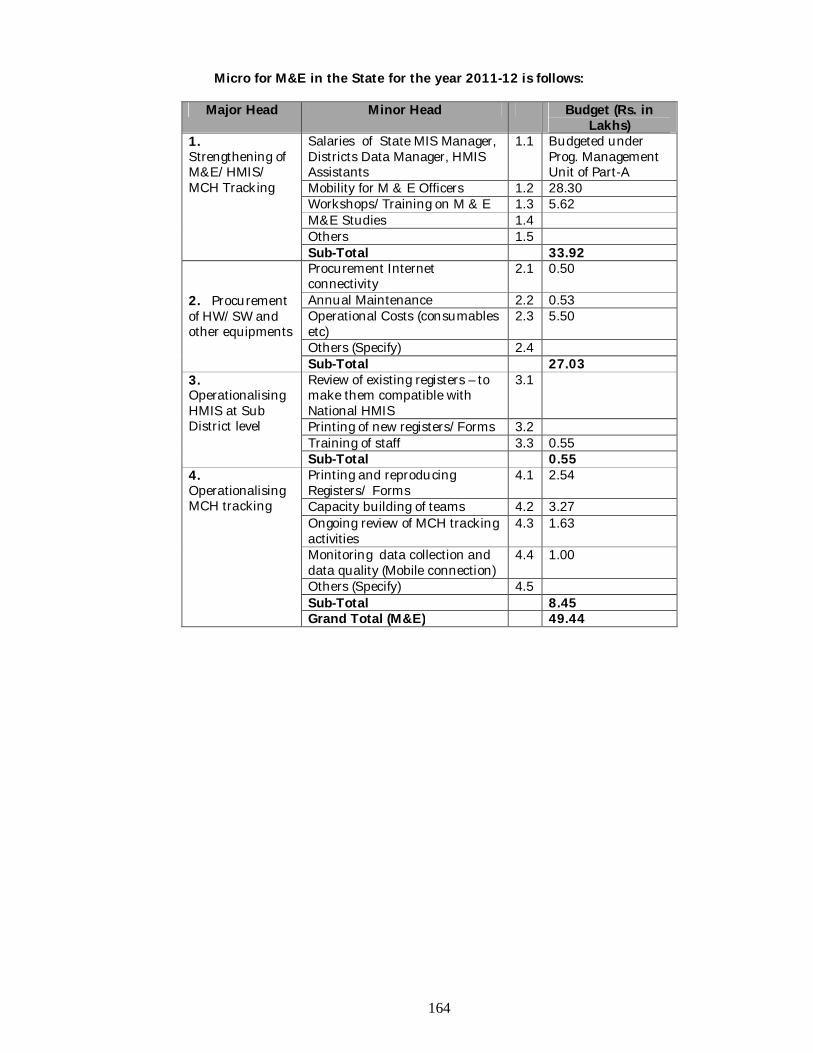
164
Micro for M&E in the State for the year 2011-12 is follows:
Major Head Minor Head Budget (Rs. in Lakhs)
1. Strengthening of M&E/HMIS/ MCH Tracking
Salaries of State MIS Manager, Districts Data Manager, HMIS Assistants
1.1 Budgeted under Prog. Management Unit of Part-A
Mobility for M & E Officers 1.2 28.30 Workshops/Training on M & E 1.3 5.62 M&E Studies 1.4 Others 1.5 Sub-Total 33.92
2. Procurement of HW/SW and other equipments
Procurement Internet connectivity
2.1 0.50
Annual Maintenance 2.2 0.53 Operational Costs (consumables etc)
2.3 5.50
Others (Specify) 2.4 Sub-Total 27.03
3. Operationalising HMIS at Sub District level
Review of existing registers – to make them compatible with National HMIS
3.1
Printing of new registers/Forms 3.2 Training of staff 3.3 0.55 Sub-Total 0.55
4. Operationalising MCH tracking
Printing and reproducing Registers/ Forms
4.1 2.54
Capacity building of teams 4.2 3.27 Ongoing review of MCH tracking activities
4.3 1.63
Monitoring data collection and data quality (Mobile connection)
4.4 1.00
Others (Specify) 4.5 Sub-Total 8.45 Grand Total (M&E) 49.44
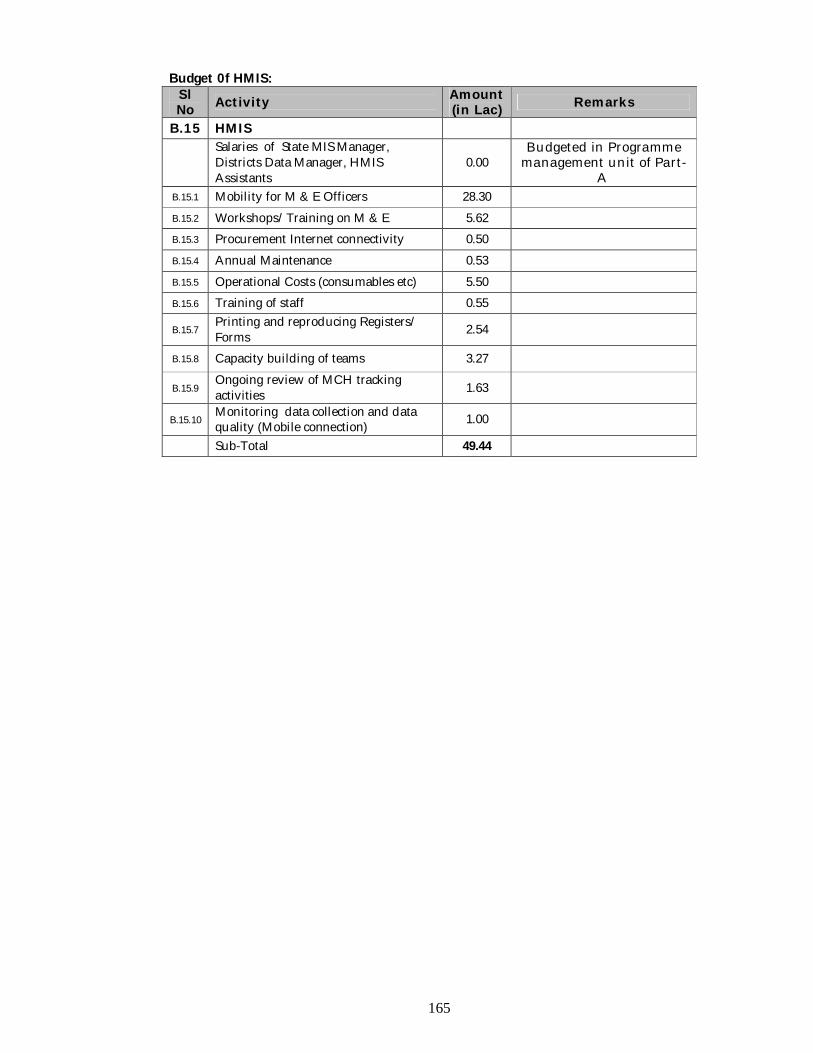
165
Budget 0f HMIS: Sl No Activity Amount
(in Lac) Remarks
B.15 HMIS
Salaries of State MIS Manager, Districts Data Manager, HMIS Assistants
0.00 Budgeted in Programme
management unit of Part-A
B.15.1 Mobility for M & E Officers 28.30 B.15.2 Workshops/Training on M & E 5.62 B.15.3 Procurement Internet connectivity 0.50 B.15.4 Annual Maintenance 0.53 B.15.5 Operational Costs (consumables etc) 5.50 B.15.6 Training of staff 0.55
B.15.7 Printing and reproducing Registers/ Forms 2.54
B.15.8 Capacity building of teams 3.27
B.15.9 Ongoing review of MCH tracking activities 1.63
B.15.10 Monitoring data collection and data quality (Mobile connection) 1.00
Sub-Total 49.44
166
B.16 Procurement of Drugs and supplies Situation Analysis Under RCH, to deliver MCH care, Child health care & family planning services, the foremost primary need is to make available the modern equipments. By March 2011, in Tripura, 5 more SDH will be declared as FRU. To render services through all PHC, CHC, SDH, some equipments are necessary and along with that, supply of essential Medicine to the respective health institutions in time is required. It has been decided by GOI that fund for essential drugs for Maternal Health, Child Health, RTI/STI for PHCs, CHCs, FRUs, SDHs & DHs would be supplied centrally. Objective To provide RCH services to pregnant mother, sick infants & children and Men & Women of Reproductive age group in time through PHC, CHC, SDHs & DHs Strategies & Activities B16.1. KIT- A & B will be supplied by GOI. B.16.2. Equipment proposal for the Year 2011-12.: To provide modern health care facility in 11 SDH, 5 CHC & 2 DH, which are functional as FRU, following equipments are proposed below:
Digital Electrocautery Machine 13 nos. (SDH, DH) Infusion Pump 13 nos. (SDH, DH). Vital Sign Monitor 13 nos. (SDH, DH) X – Ray machine 5 nos. (CHC).
Equipment specification in detail:
B.16.2.1. Electrocautery Machine -Digital (FOR SD HOSP) i. Electro surgical unit with Mono-polar, Bipolar & Under water cutting
facility. Digital display facility for power setting should be available. ii. Patient plate testing function should be available. iii. Explosion protected foot switch & Silicon rubber Patient Plate iv. Maximum Power Output:
a) Mono-polar Cutting Power at least 400 Watts b) Mono-polar TUR Power: 300 W. c) Bipolar Coagulation maximum up to 60 Watts
v. Separate Monopolar & Bipolar Generator to be provided in the unit to ensure proper patient safety.
vi. Auto Power output switch off facility for both Monopolar & Bipolar should be available.
vii. Auto start facility in bipolar mode should be available. viii. Haemostatic adjustment up to 4 steps should be available. ix. Power adjustment facility in Monopolar & Bipolar mode should be
available. x. Volume control facility should be available. xi. Should be supplied with explosion protected foot switch & min. 03 types of
electrodes. xii. Machine to meet the design & safety standards of international standards
(i.e. as per IEC 60601).
B.16.2.2. Infusion Pump (FOR SDH & DH): i. Machine should be Syringe infusion pump. ii. Syringe acceptability – 10, 20, 30, 50/60 ml for all standard Indian and
Foreign brand Syringes. Also can be programmed for other syringes as per customer’s requirements.
167
iii. Dual display LED & LCD. Flow rate in LED enable user to look from distance.
iv. Drug name display. Up to 100 drugs library (Minimum 50 stored). v. Front Loading of Syringe to protect unwanted pilferage of fluid inside the
machine. vi. Delivery Rate Range: 0.1 –200 ml/hr, and 0.1 – 1000.0 ml/hr for high flow
requirements. Bolus Rate Range up to 1000 ml/hr. vii. Delivery Rate Range: 0.1 –200 ml/hr, and 0.1 – 1000.0 ml/hr for high flow
requirements. Bolus Rate Range up to 1000 ml/hr. viii. Delivery Rate Range: 0.1 –200 ml/hr, and 0.1 – 1000.0 ml/hr for high flow
requirements. Bolus Rate Range up to 1000 ml/hr. ix. Accuracy of Infusion +2%. x. KVR/KVO facility for patient safety. Prevents syringes from clogging. xi. All possible alarms along with user selectable alarms. xii. Data locking for precision infusions. xiii. Stacking facility for max. up to 8 pumps on a single pole with normal or
optional single power cord. xiv. KOR/KVO function to prevent needle from clogging. xv. Bolus facility both manual and automatic setting. xvi. Auto power off and wide range of alarms including preventive maintenance
alarm. xvii. Alarm facility for following options should be available.
a. Battery Low. b. Occlusion c. KOR/KVO d. Syringe displaced. e. Power failure f. End of Infusions time.
Machine will be supplied with: Battery, Power Cable & Operating manual B.16.2.3. VITAL SIGN MONITOR (For SDH & DH)
i. 8 channel monitor with 12.1” high resolution TFT display. ii. Neonatal, Adult & Pediatric modes should be available. iii. 3/5 lead ECG is available. HR range is 20-350BPM iv. NIBP v. Pulse Oximetry (spo2). vi. Micro stream Capnography with display of CO2 wave form & digital values
of EtCO2 is available vii. Respiration, Dual Temperature, IBP etc. viii. CE & US FDA Approved. ix. In built Dual Channel Recorder. x. In built cautery & defibrillator protection. xi. ST& Arrhythmia analysis. xii. 72 hrs/200 patients’ tabular & graphical trend. xiii. Colour coded (RED & YELLOW) alarm facility
B.16.9. Anti Rabies Vaccine: Rabies is a major public health problem in India. Dogs are the major source of infection and are responsible for 96% of human rabbis and rest 4% are other animals for Rabbis. Keeping in view that once developed human rabiss is 100% fatal It is very effectively preventable and is the only disease where vaccination is given after a person has been exposed. In this respect Govt., of Tripura adopted a policy to provide prophylaxis treatment to the BPL categories patients having original BPL ration card at free of cost. No of patient (BPL+APL) attended in anti rabies clinic, IGM hospital, Agartala:
Status upto 1st January to 31st December
168
Year No. of Beneficiary 2008 3556 2009 3126 2010 3101
Utilization status of anti rabies vaccine .Number of vial utilized in A R Clinic IGM hospital Agartala upto 1st January to 31st December.
Year No. of Beneficiary 2008 4097 vials 2009 3406 vials 2010 2340 vials
Number of vials (vaccine) supplied to other peripheral Health Institution
of Tripura upto 1st January to 31st December. Year No. of Beneficiary 2008 17570 vials 2009 18914 vials 2010 16832 vials
Present requirement of vaccine for the year 2011 to 2012 financial year =30,000 vials Cost of per vial (govt. rate) =Rs.210.00
Budget: (Procurement & Supplies)
Sl No Activity Target Unit Cost
Amount (In lac)
B.16 Procurement & Supplies
B.16.1 Kit -A, Kit - B twice in a year for 680 SC (659 in rural area & 21 in urban area (AMC).
680 0 0.00
B.16.2 Digital Electrocautery Machine ( 11SDH) 13 175000 22.75
B.16.3 Infusion Pump (5CHC, 11SDH) 13 55000 7.15 B.16.4 Vital Sign Monitor (11SDH) 13 420000 54.60 B.16.5 Drugs for 79 PHC 79 300000 237.00 B.16.6 Drugs for 11 CHC 11 500000 55.00 B.16.7 Drugs for 11 SDH 11 500000 55.00 B.16.8 Drugs for 2 DH 2 1000000 20.00 B.16.9 Procurement of Minilap kits 20 1500 0.30
B.16.10 Blood groupings, reagent, & equipments (PHC, CHC, SDH) 104 6000 6.24
B.16.11 Anti Rabbis Vaccine 30000 210 63.00
B.16.12 Vitamin- A 6.32
B.16.13 Purchase of drugs & Medicine for Sub- centre 21 16500 3.47
Sub Total 530.83
169
B.17 Implementation the Pro-MIS Introduction Information Technology is already boosting the efficiency in health care administration. Procurement Management Information System (ProMIS) has been introduced at MoHFW in order to computerize the complete procurement process, from procurement planning to final delivery to end user i.e. complete logistics chain. Pro MIS is a web based scalable and technically versatile model to bring about increased transparency, competitiveness, timely supplies, record keeping, complaints handling, and informed decision making. 1. Human Resource For Successful implementation of Pro-MIS in the state, State Health & Family Welfare Society, NRHM, Tripura has recruited Procurement Manager/ Logistic Manager/ Bio-Medical Engineer/ Quality Assurance Specialist/ MIS Expert through Walk-in Interview on contractual basis. Their salary cost has been budgeted under Infrastructure & Human Resource of Part-A: RCH 2. Training/Workshop for Pro-MIS personnel:
Two days workshop/training programme was successfully completed by the state in the year 2010-11 by the Resource person from Ministry of Health & Family Welfare, Govt. of India
Sl.No Programme
Division Category of Personnel
Number of trainee
Duration of Training
1 Nodal Officer MO/DIO/Drug inspector
3
2 Days
2 RCH Pharmacist/Store- keeper
4
3 RNTCP Pharmacist 5 4 UIP MPW/Cold Chain
Supervisor 5
5 District Store Personnel
Pharmacist 6
Total 23
Two days Workshop/Training on Pro MIS warehouse Information System for recruited staffs is proposed to be organized in the year 2011-12.
Financial Involvement on Workshop/Training on Pro MIS warehouse
Information System:
Particulars Cost (Rs.) Amount (Rs) Rent for Computer Lab with Internet facilities
6000/- for 2 days 12000.00
T.A for Resource Person.(Air fair to and fro journey)
@10000/-for2 person. 20000.00
Honorarium for Resource person
@ 1000/- for 2 person for 2days.
4000.00-
Boarding and Lodging @ 1000/- for 3 days for 2 person.
6000.00
Rent of LCD Projector 3000/- for 2 days 6000.00 Breakfast, Lunch, Tea & Snacks and Dinner
200/- for 2 days for 12 person
48000.00
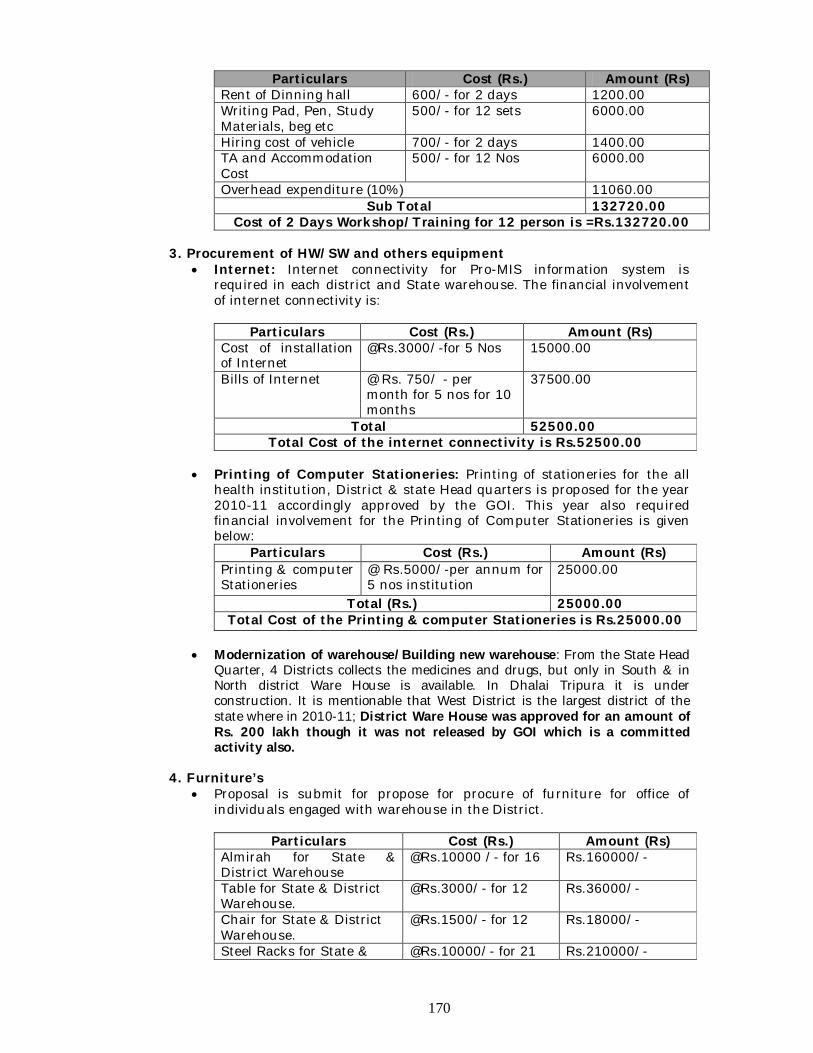
170
Particulars Cost (Rs.) Amount (Rs) Rent of Dinning hall 600/- for 2 days 1200.00 Writing Pad, Pen, Study Materials, beg etc
500/- for 12 sets 6000.00
Hiring cost of vehicle 700/- for 2 days 1400.00 TA and Accommodation Cost
500/- for 12 Nos 6000.00
Overhead expenditure (10%) 11060.00 Sub Total 132720.00
Cost of 2 Days Workshop/Training for 12 person is =Rs.132720.00 3. Procurement of HW/SW and others equipment
Internet: Internet connectivity for Pro-MIS information system is required in each district and State warehouse. The financial involvement of internet connectivity is:
Particulars Cost (Rs.) Amount (Rs)
Cost of installation of Internet
@Rs.3000/-for 5 Nos 15000.00
Bills of Internet @ Rs. 750/ - per month for 5 nos for 10 months
37500.00
Total 52500.00 Total Cost of the internet connectivity is Rs.52500.00
Printing of Computer Stationeries: Printing of stationeries for the all
health institution, District & state Head quarters is proposed for the year 2010-11 accordingly approved by the GOI. This year also required financial involvement for the Printing of Computer Stationeries is given below:
Particulars Cost (Rs.) Amount (Rs) Printing & computer Stationeries
@ Rs.5000/-per annum for 5 nos institution
25000.00
Total (Rs.) 25000.00 Total Cost of the Printing & computer Stationeries is Rs.25000.00
Modernization of warehouse/Building new warehouse: From the State Head
Quarter, 4 Districts collects the medicines and drugs, but only in South & in North district Ware House is available. In Dhalai Tripura it is under construction. It is mentionable that West District is the largest district of the state where in 2010-11; District Ware House was approved for an amount of Rs. 200 lakh though it was not released by GOI which is a committed activity also.
4. Furniture’s
Proposal is submit for propose for procure of furniture for office of individuals engaged with warehouse in the District.
Particulars Cost (Rs.) Amount (Rs)
Almirah for State & District Warehouse
@Rs.10000 /- for 16 Rs.160000/-
Table for State & District Warehouse.
@Rs.3000/- for 12 Rs.36000/-
Chair for State & District Warehouse.
@Rs.1500/- for 12 Rs.18000/-
Steel Racks for State & @Rs.10000/- for 21 Rs.210000/-
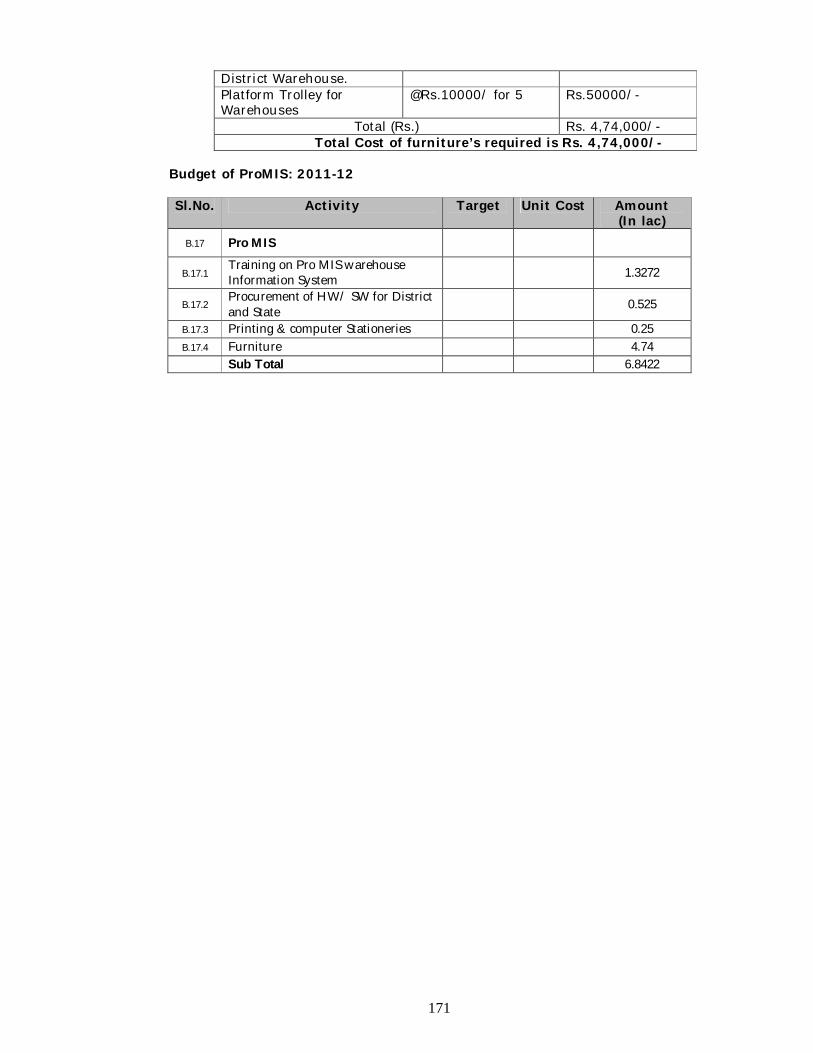
171
District Warehouse. Platform Trolley for Warehouses
@Rs.10000/ for 5 Rs.50000/-
Total (Rs.) Rs. 4,74,000/- Total Cost of furniture’s required is Rs. 4,74,000/-
Budget of ProMIS: 2011-12 Sl.No. Activity Target Unit Cost Amount
(In lac) B.17 Pro MIS
B.17.1 Training on Pro MIS warehouse Information System 1.3272
B.17.2 Procurement of HW/ SW for District and State 0.525
B.17.3 Printing & computer Stationeries 0.25 B.17.4 Furniture 4.74
Sub Total 6.8422
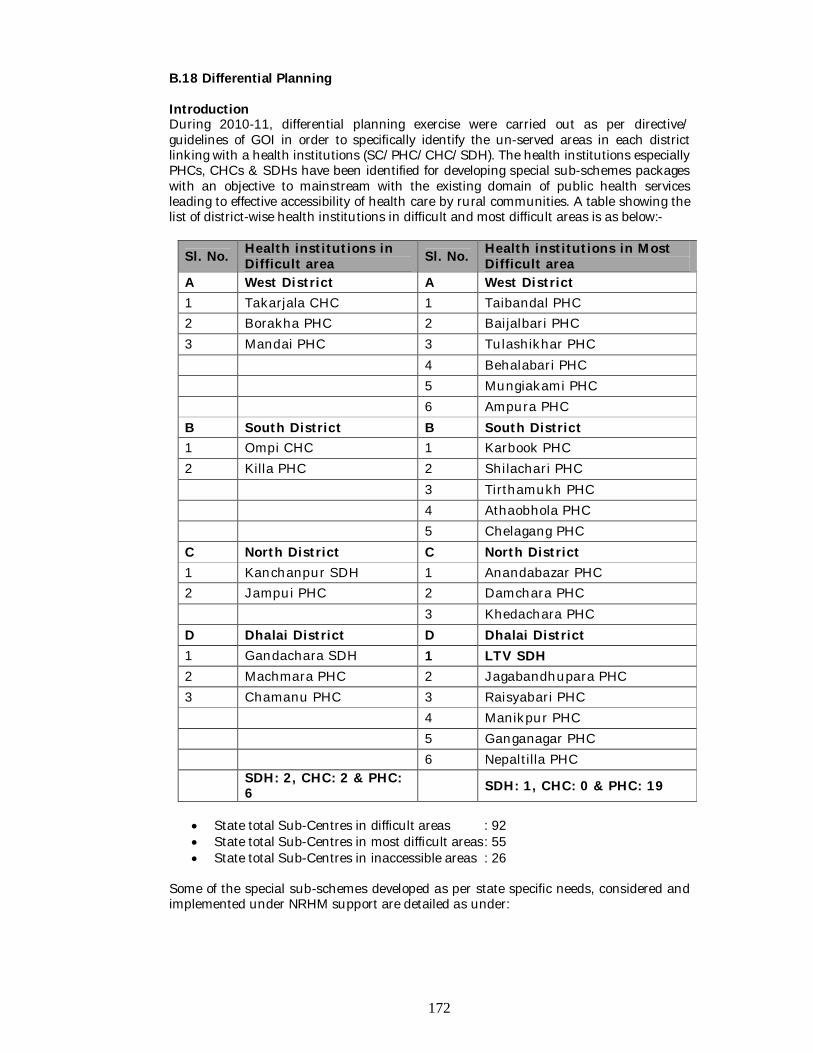
172
B.18 Differential Planning Introduction During 2010-11, differential planning exercise were carried out as per directive/ guidelines of GOI in order to specifically identify the un-served areas in each district linking with a health institutions (SC/PHC/CHC/SDH). The health institutions especially PHCs, CHCs & SDHs have been identified for developing special sub-schemes packages with an objective to mainstream with the existing domain of public health services leading to effective accessibility of health care by rural communities. A table showing the list of district-wise health institutions in difficult and most difficult areas is as below:-
Sl. No. Health institutions in Difficult area Sl. No. Health institutions in Most
Difficult area A West District A West District 1 Takarjala CHC 1 Taibandal PHC 2 Borakha PHC 2 Baijalbari PHC 3 Mandai PHC 3 Tulashikhar PHC 4 Behalabari PHC 5 Mungiakami PHC 6 Ampura PHC B South District B South District 1 Ompi CHC 1 Karbook PHC 2 Killa PHC 2 Shilachari PHC 3 Tirthamukh PHC 4 Athaobhola PHC 5 Chelagang PHC C North District C North District 1 Kanchanpur SDH 1 Anandabazar PHC 2 Jampui PHC 2 Damchara PHC 3 Khedachara PHC D Dhalai District D Dhalai District 1 Gandachara SDH 1 LTV SDH 2 Machmara PHC 2 Jagabandhupara PHC 3 Chamanu PHC 3 Raisyabari PHC 4 Manikpur PHC 5 Ganganagar PHC 6 Nepaltilla PHC
SDH: 2, CHC: 2 & PHC: 6 SDH: 1, CHC: 0 & PHC: 19
State total Sub-Centres in difficult areas : 92 State total Sub-Centres in most difficult areas : 55 State total Sub-Centres in inaccessible areas : 26
Some of the special sub-schemes developed as per state specific needs, considered and implemented under NRHM support are detailed as under:
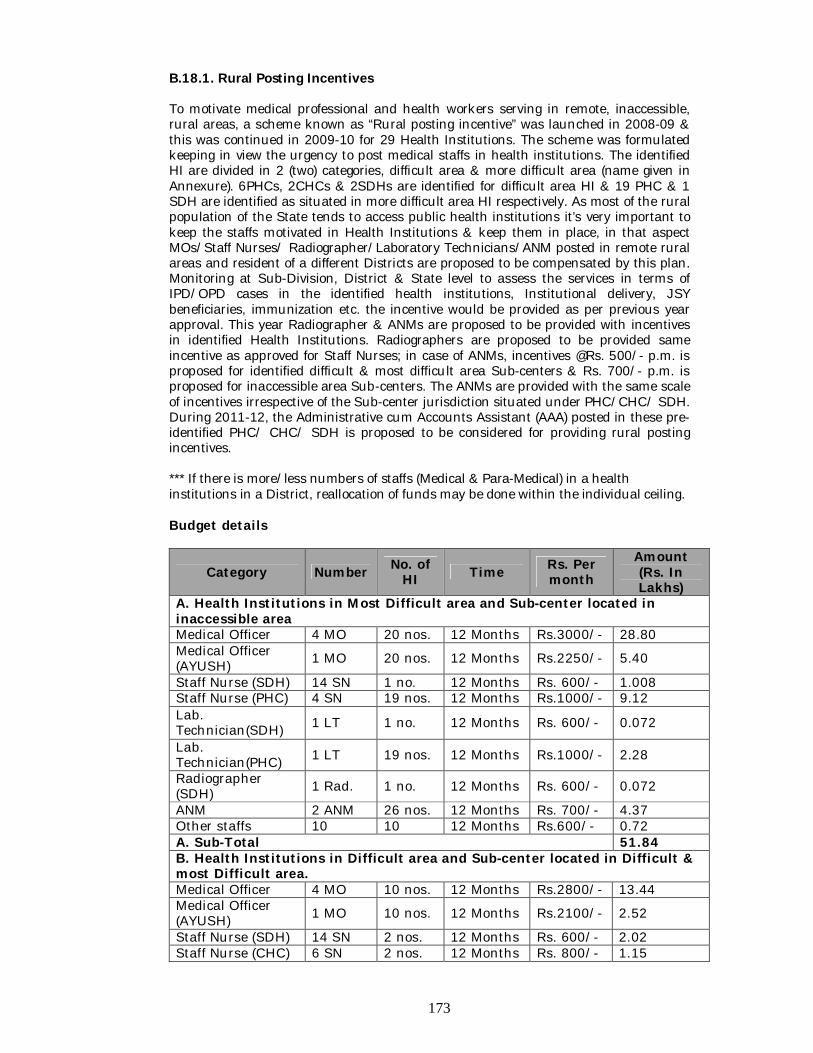
173
B.18.1. Rural Posting Incentives To motivate medical professional and health workers serving in remote, inaccessible, rural areas, a scheme known as “Rural posting incentive” was launched in 2008-09 & this was continued in 2009-10 for 29 Health Institutions. The scheme was formulated keeping in view the urgency to post medical staffs in health institutions. The identified HI are divided in 2 (two) categories, difficult area & more difficult area (name given in Annexure). 6PHCs, 2CHCs & 2SDHs are identified for difficult area HI & 19 PHC & 1 SDH are identified as situated in more difficult area HI respectively. As most of the rural population of the State tends to access public health institutions it’s very important to keep the staffs motivated in Health Institutions & keep them in place, in that aspect MOs/Staff Nurses/ Radiographer/Laboratory Technicians/ANM posted in remote rural areas and resident of a different Districts are proposed to be compensated by this plan. Monitoring at Sub-Division, District & State level to assess the services in terms of IPD/OPD cases in the identified health institutions, Institutional delivery, JSY beneficiaries, immunization etc. the incentive would be provided as per previous year approval. This year Radiographer & ANMs are proposed to be provided with incentives in identified Health Institutions. Radiographers are proposed to be provided same incentive as approved for Staff Nurses; in case of ANMs, incentives @Rs. 500/- p.m. is proposed for identified difficult & most difficult area Sub-centers & Rs. 700/- p.m. is proposed for inaccessible area Sub-centers. The ANMs are provided with the same scale of incentives irrespective of the Sub-center jurisdiction situated under PHC/CHC/ SDH. During 2011-12, the Administrative cum Accounts Assistant (AAA) posted in these pre-identified PHC/ CHC/ SDH is proposed to be considered for providing rural posting incentives.
*** If there is more/less numbers of staffs (Medical & Para-Medical) in a health institutions in a District, reallocation of funds may be done within the individual ceiling. Budget details
Category Number No. of HI Time Rs. Per
month Amount (Rs. In Lakhs)
A. Health Institutions in Most Difficult area and Sub-center located in inaccessible area Medical Officer 4 MO 20 nos. 12 Months Rs.3000/- 28.80 Medical Officer (AYUSH) 1 MO 20 nos. 12 Months Rs.2250/- 5.40
Staff Nurse (SDH) 14 SN 1 no. 12 Months Rs. 600/- 1.008 Staff Nurse (PHC) 4 SN 19 nos. 12 Months Rs.1000/- 9.12 Lab. Technician(SDH) 1 LT 1 no. 12 Months Rs. 600/- 0.072
Lab. Technician(PHC) 1 LT 19 nos. 12 Months Rs.1000/- 2.28
Radiographer (SDH) 1 Rad. 1 no. 12 Months Rs. 600/- 0.072
ANM 2 ANM 26 nos. 12 Months Rs. 700/- 4.37 Other staffs 10 10 12 Months Rs.600/- 0.72 A. Sub-Total 51.84 B. Health Institutions in Difficult area and Sub-center located in Difficult & most Difficult area. Medical Officer 4 MO 10 nos. 12 Months Rs.2800/- 13.44 Medical Officer (AYUSH) 1 MO 10 nos. 12 Months Rs.2100/- 2.52
Staff Nurse (SDH) 14 SN 2 nos. 12 Months Rs. 600/- 2.02 Staff Nurse (CHC) 6 SN 2 nos. 12 Months Rs. 800/- 1.15
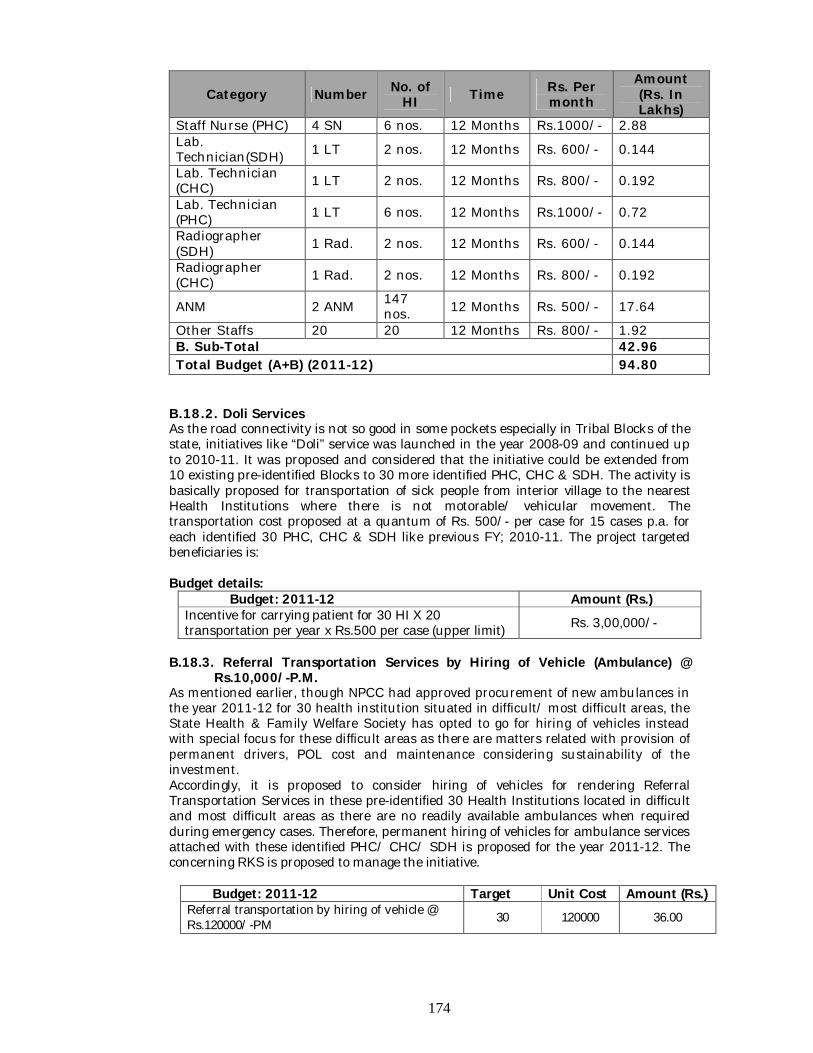
174
Category Number No. of HI Time Rs. Per
month Amount (Rs. In Lakhs)
Staff Nurse (PHC) 4 SN 6 nos. 12 Months Rs.1000/- 2.88 Lab. Technician(SDH) 1 LT 2 nos. 12 Months Rs. 600/- 0.144
Lab. Technician (CHC) 1 LT 2 nos. 12 Months Rs. 800/- 0.192
Lab. Technician (PHC) 1 LT 6 nos. 12 Months Rs.1000/- 0.72
Radiographer (SDH) 1 Rad. 2 nos. 12 Months Rs. 600/- 0.144
Radiographer (CHC) 1 Rad. 2 nos. 12 Months Rs. 800/- 0.192
ANM 2 ANM 147 nos. 12 Months Rs. 500/- 17.64
Other Staffs 20 20 12 Months Rs. 800/- 1.92 B. Sub-Total 42.96 Total Budget (A+B) (2011-12) 94.80
B.18.2. Doli Services As the road connectivity is not so good in some pockets especially in Tribal Blocks of the state, initiatives like “Doli” service was launched in the year 2008-09 and continued up to 2010-11. It was proposed and considered that the initiative could be extended from 10 existing pre-identified Blocks to 30 more identified PHC, CHC & SDH. The activity is basically proposed for transportation of sick people from interior village to the nearest Health Institutions where there is not motorable/ vehicular movement. The transportation cost proposed at a quantum of Rs. 500/- per case for 15 cases p.a. for each identified 30 PHC, CHC & SDH like previous FY; 2010-11. The project targeted beneficiaries is:
Budget details:
Budget: 2011-12 Amount (Rs.) Incentive for carrying patient for 30 HI X 20 transportation per year x Rs.500 per case (upper limit) Rs. 3,00,000/-
B.18.3. Referral Transportation Services by Hiring of Vehicle (Ambulance) @ Rs.10,000/-P.M. As mentioned earlier, though NPCC had approved procurement of new ambulances in the year 2011-12 for 30 health institution situated in difficult/ most difficult areas, the State Health & Family Welfare Society has opted to go for hiring of vehicles instead with special focus for these difficult areas as there are matters related with provision of permanent drivers, POL cost and maintenance considering sustainability of the investment. Accordingly, it is proposed to consider hiring of vehicles for rendering Referral Transportation Services in these pre-identified 30 Health Institutions located in difficult and most difficult areas as there are no readily available ambulances when required during emergency cases. Therefore, permanent hiring of vehicles for ambulance services attached with these identified PHC/ CHC/ SDH is proposed for the year 2011-12. The concerning RKS is proposed to manage the initiative.
Budget: 2011-12 Target Unit Cost Amount (Rs.)
Referral transportation by hiring of vehicle @ Rs.120000/-PM 30 120000 36.00
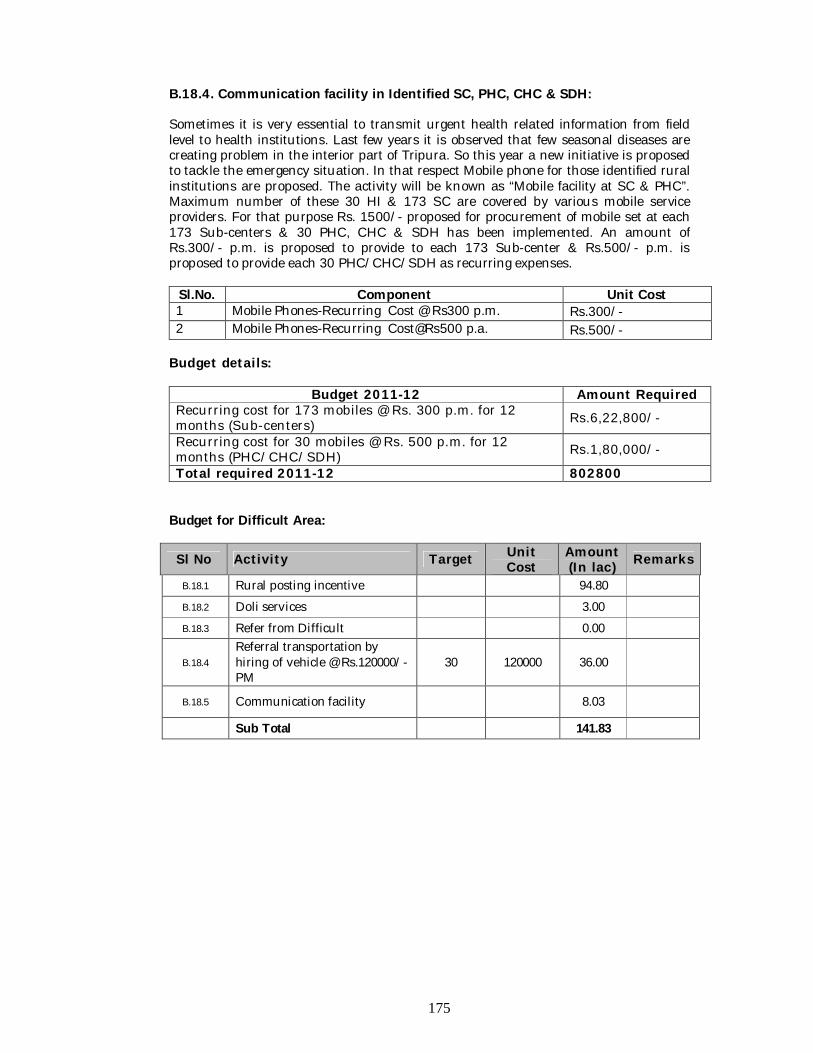
175
B.18.4. Communication facility in Identified SC, PHC, CHC & SDH:
Sometimes it is very essential to transmit urgent health related information from field level to health institutions. Last few years it is observed that few seasonal diseases are creating problem in the interior part of Tripura. So this year a new initiative is proposed to tackle the emergency situation. In that respect Mobile phone for those identified rural institutions are proposed. The activity will be known as “Mobile facility at SC & PHC”. Maximum number of these 30 HI & 173 SC are covered by various mobile service providers. For that purpose Rs. 1500/- proposed for procurement of mobile set at each 173 Sub-centers & 30 PHC, CHC & SDH has been implemented. An amount of Rs.300/- p.m. is proposed to provide to each 173 Sub-center & Rs.500/- p.m. is proposed to provide each 30 PHC/CHC/SDH as recurring expenses.
Sl.No. Component Unit Cost 1 Mobile Phones-Recurring Cost @ Rs300 p.m. Rs.300/- 2 Mobile Phones-Recurring Cost@Rs500 p.a. Rs.500/-
Budget details:
Budget 2011-12 Amount Required Recurring cost for 173 mobiles @ Rs. 300 p.m. for 12 months (Sub-centers) Rs.6,22,800/-
Recurring cost for 30 mobiles @ Rs. 500 p.m. for 12 months (PHC/CHC/SDH) Rs.1,80,000/-
Total required 2011-12 802800 Budget for Difficult Area:
Sl No Activity Target Unit Cost
Amount (In lac) Remarks
B.18.1 Rural posting incentive 94.80
B.18.2 Doli services 3.00
B.18.3 Refer from Difficult 0.00
B.18.4 Referral transportation by hiring of vehicle @ Rs.120000/-PM
30 120000 36.00
B.18.5 Communication facility 8.03
Sub Total 141.83
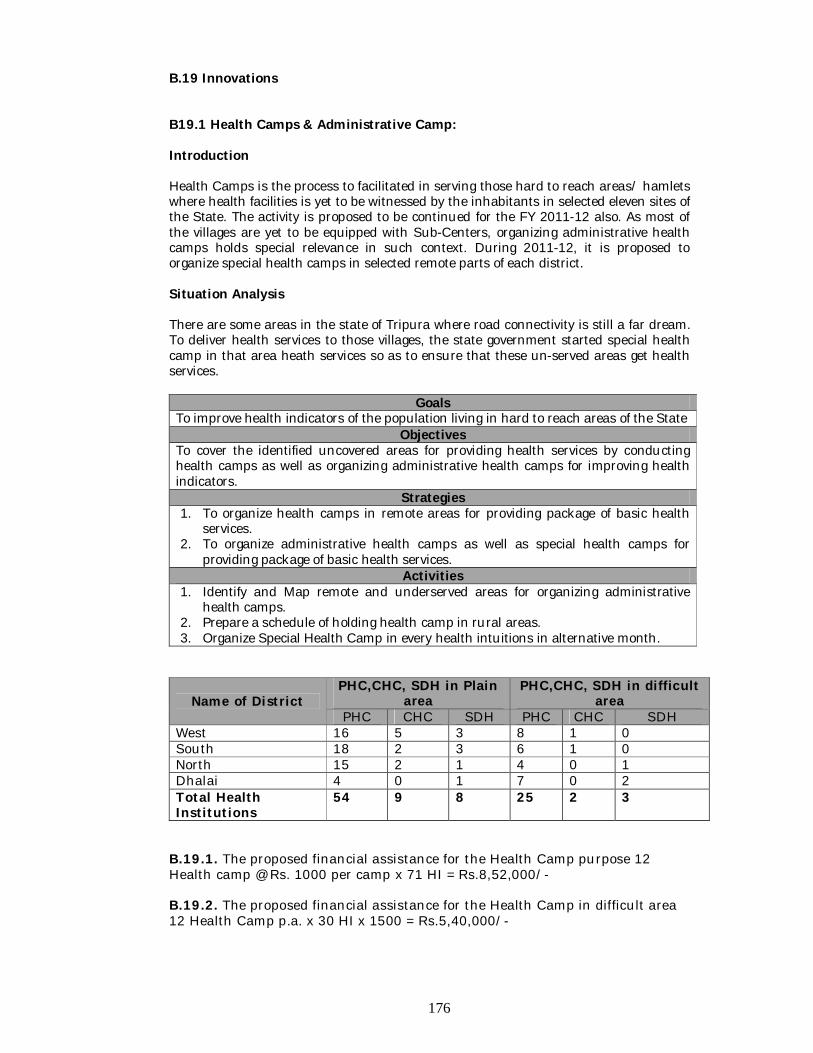
176
B.19 Innovations B19.1 Health Camps & Administrative Camp: Introduction Health Camps is the process to facilitated in serving those hard to reach areas/ hamlets where health facilities is yet to be witnessed by the inhabitants in selected eleven sites of the State. The activity is proposed to be continued for the FY 2011-12 also. As most of the villages are yet to be equipped with Sub-Centers, organizing administrative health camps holds special relevance in such context. During 2011-12, it is proposed to organize special health camps in selected remote parts of each district. Situation Analysis There are some areas in the state of Tripura where road connectivity is still a far dream. To deliver health services to those villages, the state government started special health camp in that area heath services so as to ensure that these un-served areas get health services.
Goals To improve health indicators of the population living in hard to reach areas of the State
Objectives To cover the identified uncovered areas for providing health services by conducting health camps as well as organizing administrative health camps for improving health indicators.
Strategies 1. To organize health camps in remote areas for providing package of basic health
services. 2. To organize administrative health camps as well as special health camps for
providing package of basic health services. Activities
1. Identify and Map remote and underserved areas for organizing administrative health camps.
2. Prepare a schedule of holding health camp in rural areas. 3. Organize Special Health Camp in every health intuitions in alternative month.
Name of District PHC,CHC, SDH in Plain
area PHC,CHC, SDH in difficult
area PHC CHC SDH PHC CHC SDH
West 16 5 3 8 1 0 South 18 2 3 6 1 0 North 15 2 1 4 0 1 Dhalai 4 0 1 7 0 2 Total Health Institutions
54 9 8 25 2 3
B.19.1. The proposed financial assistance for the Health Camp purpose 12 Health camp @ Rs. 1000 per camp x 71 HI = Rs.8,52,000/- B.19.2. The proposed financial assistance for the Health Camp in difficult area 12 Health Camp p.a. x 30 HI x 1500 = Rs.5,40,000/-
177
B.19.3. Strategy: To organize health camps in remote areas by helicopter service for providing package of basic health services Health camp through Helicopter: Health Camps by Helicopter Service is an approved activity since 2006-07. The process has facilitated in serving those hard to reach areas/ hamlets including immunization services to the children of targeted age group where health facilities is yet to be witnessed by the inhabitants in selected eleven sites of the State. Situation analysis (a) Necessity of Helicopter Health Camp : There are many difficult interior/hilly areas in Tripura, Particular in West,
North and Dhalai Districts of the State which can not be reached by Motor/Vehicle and access to those areas by on foot walking requires a lot of time. In these areas, health camp through Helicopter service is the only mean to provide health care services to the inhabitants. Initially Health Camps by Helicopter service use to cater the health need of people of the 17 (Seventeen) locations. Over the years, with expansion of the health network in the state along with improvement in the road network six locations have been deleted from the list.
Health care through Helicopter service is the only mean to provide health service in those areas in cases of extreme emergency health situation without losing much of time.
Health Sub-Centre can not yet be made functional properly in those areas and here again, health camp through Helicopter service becomes essential.
Health Camp through Helicopter service is one of the several activities in PART-B NRHM INITIATIVE.
(b) Area of Implementation : North District * Kanchanpur Sub-Division i) S.K. Serhmun G.P. and its adjacent areas, ii) Bhandarima G.P. and its adjacent areas, Dhalai District * Longtarai Valley Sub-Division - i) Gobindabari G.P. and its adjacent areas, ii) Garjanpassa G.P. and its adjacent areas, iii) Tuipaibari G.P. and its adjacent areas, * Gandacharra Sub-Division i) M.K. Para and its adjacent areas, ii) B.R. Para and its adjacent areas, iii) J.B. Para and its adjacent areas, iv) Dalapati Para and its adjacent areas, West District * Teliamura Sub-Division i) Nonacharra Village and its adjacent area, ii) Kakracharra Village and its adjacent areas, (c) Comparative Nos. of beneficiary :
o Nos. of Total Patients treated in 2009-2010 (April 2009 to March 2010) Covered by General Camp - 268115 Nos. Covered by Helicopter Camp in 2009 - 3695 Nos.
o Nos. of Total Patients treated in 2010-2011 (April 2009 to March 2010)
Covered by General Camp - 239476 Nos. (Up to February) Covered by Helicopter Camp in 2010 -3947 Nos
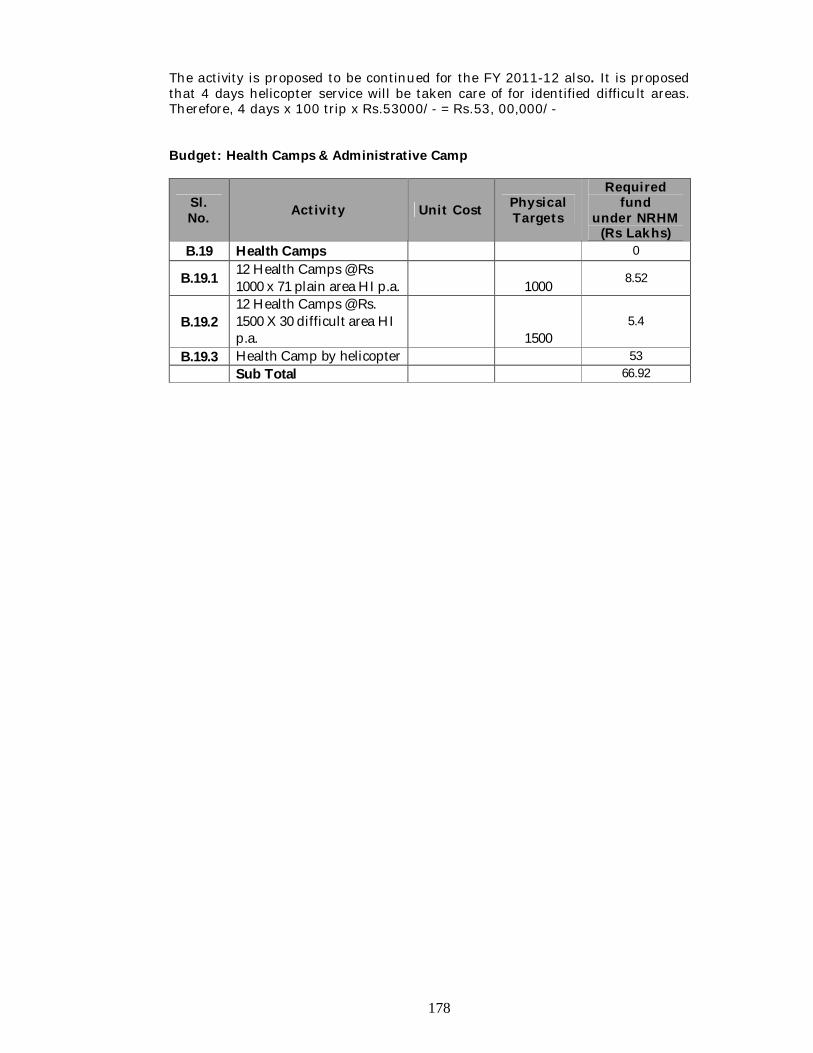
178
The activity is proposed to be continued for the FY 2011-12 also. It is proposed that 4 days helicopter service will be taken care of for identified difficult areas. Therefore, 4 days x 100 trip x Rs.53000/- = Rs.53, 00,000/- Budget: Health Camps & Administrative Camp
Sl. No. Activity Unit Cost Physical
Targets
Required fund
under NRHM (Rs Lakhs)
B.19 Health Camps 0
B.19.1 12 Health Camps @ Rs 1000 x 71 plain area HI p.a. 1000 8.52
B.19.2 12 Health Camps @ Rs. 1500 X 30 difficult area HI p.a.
1500
5.4
B.19.3 Health Camp by helicopter 53 Sub Total 66.92
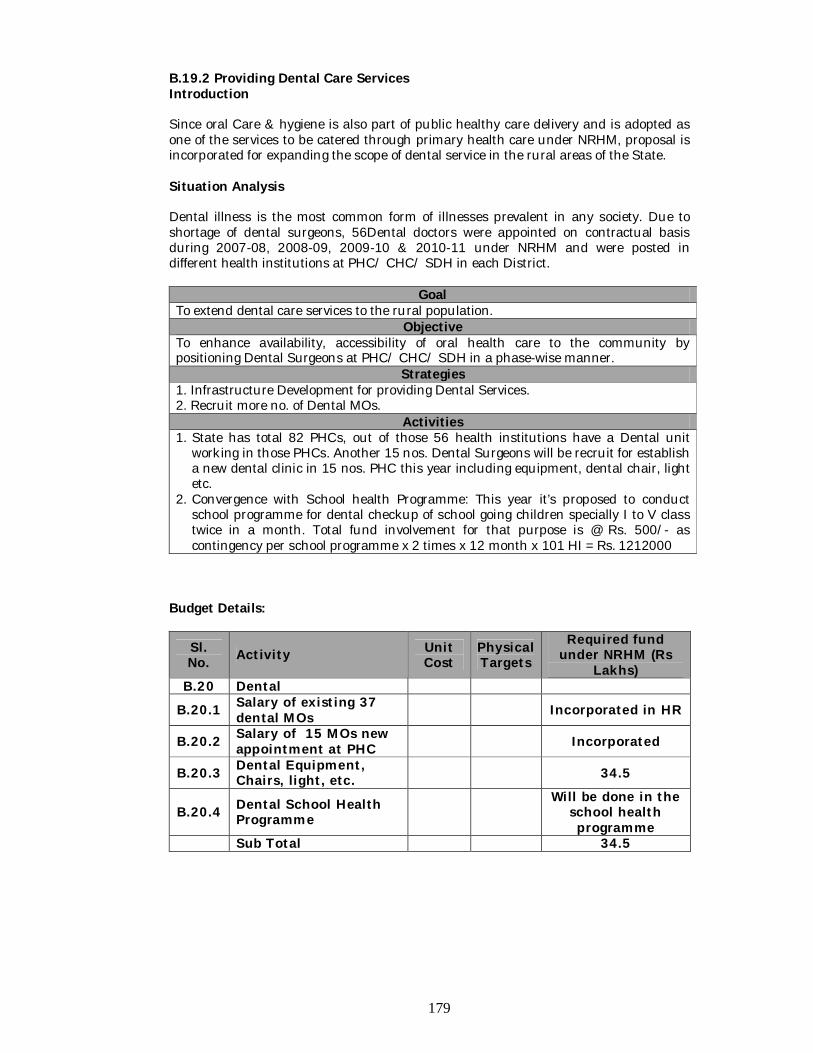
179
B.19.2 Providing Dental Care Services Introduction Since oral Care & hygiene is also part of public healthy care delivery and is adopted as one of the services to be catered through primary health care under NRHM, proposal is incorporated for expanding the scope of dental service in the rural areas of the State. Situation Analysis Dental illness is the most common form of illnesses prevalent in any society. Due to shortage of dental surgeons, 56Dental doctors were appointed on contractual basis during 2007-08, 2008-09, 2009-10 & 2010-11 under NRHM and were posted in different health institutions at PHC/ CHC/ SDH in each District.
Goal To extend dental care services to the rural population.
Objective To enhance availability, accessibility of oral health care to the community by positioning Dental Surgeons at PHC/ CHC/ SDH in a phase-wise manner.
Strategies 1. Infrastructure Development for providing Dental Services. 2. Recruit more no. of Dental MOs.
Activities 1. State has total 82 PHCs, out of those 56 health institutions have a Dental unit
working in those PHCs. Another 15 nos. Dental Surgeons will be recruit for establish a new dental clinic in 15 nos. PHC this year including equipment, dental chair, light etc.
2. Convergence with School health Programme: This year it’s proposed to conduct school programme for dental checkup of school going children specially I to V class twice in a month. Total fund involvement for that purpose is @ Rs. 500/- as contingency per school programme x 2 times x 12 month x 101 HI = Rs. 1212000
Budget Details:
Sl. No. Activity Unit
Cost Physical Targets
Required fund under NRHM (Rs
Lakhs) B.20 Dental
B.20.1 Salary of existing 37 dental MOs Incorporated in HR
B.20.2 Salary of 15 MOs new appointment at PHC Incorporated
B.20.3 Dental Equipment, Chairs, light, etc. 34.5
B.20.4 Dental School Health Programme
Will be done in the school health programme
Sub Total 34.5
180
B.19.3. Telemedicine Introduction The advances of Communication and Information technology on one side and Medical science and Biomedical engineering on the other side have opened up wide opportunities for improved health care. Telemedicine, defined as the use of Communication and Information technology to provide health care when distance separates the patients and the doctors, can play a significant role to revolutionize the health care systems particularly in a developing country like India. To provide the basic minimum healthcare to the population is one of the top priorities of the Government all along. The National Health Policy –2002 of Government of India emphasizes that overriding importance would be given to ensuring a more equitable access to health services across the social and geographical expanse of the country. In a geographically backward state like Tripura in the North Eastern Region with infrastructural and different other bottlenecks which restricted the fast economical growth of the state, the introduction of Telemedicine in different areas has enabled the health care service providers to deliver the specialized health care facility to the people of the state. All these constraints are also coupled with huge shortage of specialist manpower in the State. It is to be emphasized that despite of multifarious problems, the state government is committed to deliver Health and Family Welfare services to the doorsteps of all segments of population and also provide better health care facility to the people of the state. Recognizing the advances in the provision of health care through use of Telemedicine, Government of Tripura has taken public health initiatives on the deployment of Telemedicine in different Govt. Hospitals of the state. The State Government has decided to implement Telemedicine Projects, in phases, in all District, Sub Divisional Hospitals and Community Health Centers / Primary Health Centers to improve the quality of health care delivery systems in the rural, remote, hilly and tribal areas, particularly for the poor and under-served people. One of the important landmarks in the State’s journey towards e- governance was the launching of the Telemedicine Projects on:
1. “Setting up of Telemedicine Facilities in Tripura” with the Approval of the Dept. of IT, Govt. of India in March 2004, with a grant-in-aid of Rs.287 lakhs, the project on
2. “Deployment of Telemedicine in Tripura” with the Approval of the Dept. of IT, Govt. of India in March 2006, with a grant-in-aid of Rs.282 lakhs and
3. “Deployment of Telemedicine at Remote CHC/PHC in Tripura” with the Approval of the Dept. of IT, Govt. of India in February 2009, with a grant-in-aid of Rs.296 lakhs.
In the 1st phase of the Telemedicine project, the telemedicine facilities have been set up at two Referral centers (G.B. Pant Hospital and IGM Hospital at Agartala) connected to five Nodal centers (Sub Division Hospitals at Amarpur, Kanchanpur, Chailengta, Gandacherra and PHC at Kathalia) and the project has already been handed over to the Dept. of H & FW, Govt. of Tripura. In the 2nd phase of the approved project, the telemedicine facilities have been set up at six Nodal Centers (Sabroom SDH, Belonia SDH, Melaghar SDH, Kumarghat CHC, Kulai DH and Natunbazar PHC) and the 3rd phase of Telemedicine Project were to be setup at six Nodal Centers (Khowai SDH, Takarjala PHC, Ompinagar PHC, Hrishyamukh PHC, Chawmanu PHC, Khedacherra PHC). All these centers the communication links used are 512 Kbps leased lines provided by BSNL. The systems are in operation and so far about 17000 patients have
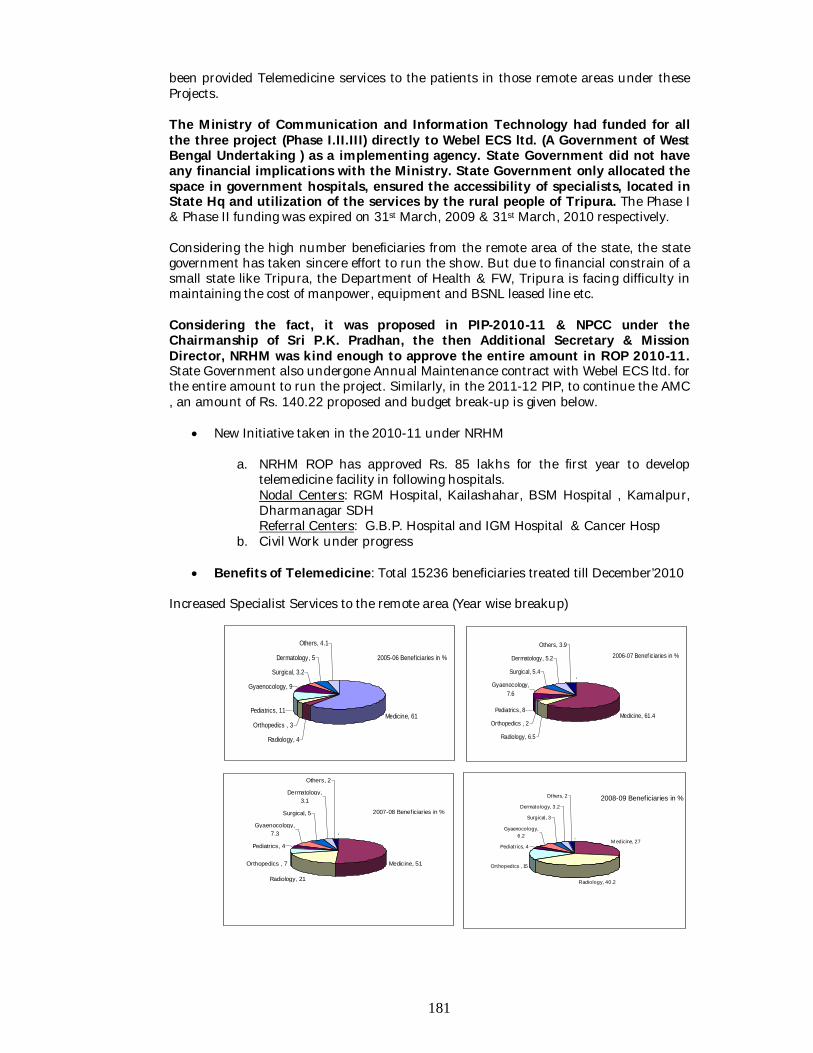
181
2005-06 Benef iciaries in %
Medicine, 61
Radiology, 4
Orthopedics , 3
Pediatrics, 11
Gyaenocology, 9
Surgical, 3.2
Dermatology, 5
Others, 4.1
2006-07 Benef iciaries in %
,
Medicine, 61.4
Radiology, 6.5
Orthopedics , 2
Pediatrics, 8
Gyaenocology, 7.6
Surgical, 5.4
Dermatology, 5.2
Others, 3.9
2007-08 Beneficiaries in %
,
Medicine, 51
Radiology, 21
Orthopedics , 7
Pediatrics, 4
Gyaenocology, 7.3
Surgical, 5
Dermatology, 3.1
Others, 2
2008-09 Beneficiaries in %
, M edicine, 27
Radiology, 40.2
Orthopedics , 15
Pediatrics, 4
Gyaenocology, 6.2
Surgical, 3
Dermatology, 3.2
Others, 2
been provided Telemedicine services to the patients in those remote areas under these Projects. The Ministry of Communication and Information Technology had funded for all the three project (Phase I.II.III) directly to Webel ECS ltd. (A Government of West Bengal Undertaking ) as a implementing agency. State Government did not have any financial implications with the Ministry. State Government only allocated the space in government hospitals, ensured the accessibility of specialists, located in State Hq and utilization of the services by the rural people of Tripura. The Phase I & Phase II funding was expired on 31st March, 2009 & 31st March, 2010 respectively. Considering the high number beneficiaries from the remote area of the state, the state government has taken sincere effort to run the show. But due to financial constrain of a small state like Tripura, the Department of Health & FW, Tripura is facing difficulty in maintaining the cost of manpower, equipment and BSNL leased line etc. Considering the fact, it was proposed in PIP-2010-11 & NPCC under the Chairmanship of Sri P.K. Pradhan, the then Additional Secretary & Mission Director, NRHM was kind enough to approve the entire amount in ROP 2010-11. State Government also undergone Annual Maintenance contract with Webel ECS ltd. for the entire amount to run the project. Similarly, in the 2011-12 PIP, to continue the AMC , an amount of Rs. 140.22 proposed and budget break-up is given below.
New Initiative taken in the 2010-11 under NRHM
a. NRHM ROP has approved Rs. 85 lakhs for the first year to develop telemedicine facility in following hospitals.
Nodal Centers: RGM Hospital, Kailashahar, BSM Hospital , Kamalpur, Dharmanagar SDH Referral Centers: G.B.P. Hospital and IGM Hospital & Cancer Hosp b. Civil Work under progress
Benefits of Telemedicine: Total 15236 beneficiaries treated till December’2010
Increased Specialist Services to the remote area (Year wise breakup)
182
528 798
3303
4058 4134
0
500
1000
1500
2000
2500
3000
3500
4000
4500
2005-06 2006-07 2007-08 2008-09 2009-2010
BENEFICIARIES YEAR WISE
TELEMEDICINE UNIT OF AGMC & GBP HOSPITAL/IGM HOSPITAL & CANCER REGIONAL HOSPITAL FROM 9th June’05 to 31st December 10. TELEMEDICINE CENTRES TOTAL Amarpur SDH 1507 Kanchanpur SDH 882 Gandacharra SDH 2035 Chailengta SDH 394 Kathalia PHC 1161 Belonia SDH 2187 Melaghar SDH 5380 Sabroom SDH 708 Kumarghat CHC 804 Natun Bazar RH 91 Khowai SDH 87 Total NO. of Patient 15236
B.21 Telemadicine Budget (In lac)
B.21.1 AMC for Phase-I Telemedicine Project from 1st April 2011 to 31st March 2012 60.16865
B.21.2 AMC for Phase-II Telemedicine Project from 1st April 2011 to 31st March 2012 54.808
B.21.3 2nd Year recurring charge for the three nodal centers 25.25
Sub Total 140.22665
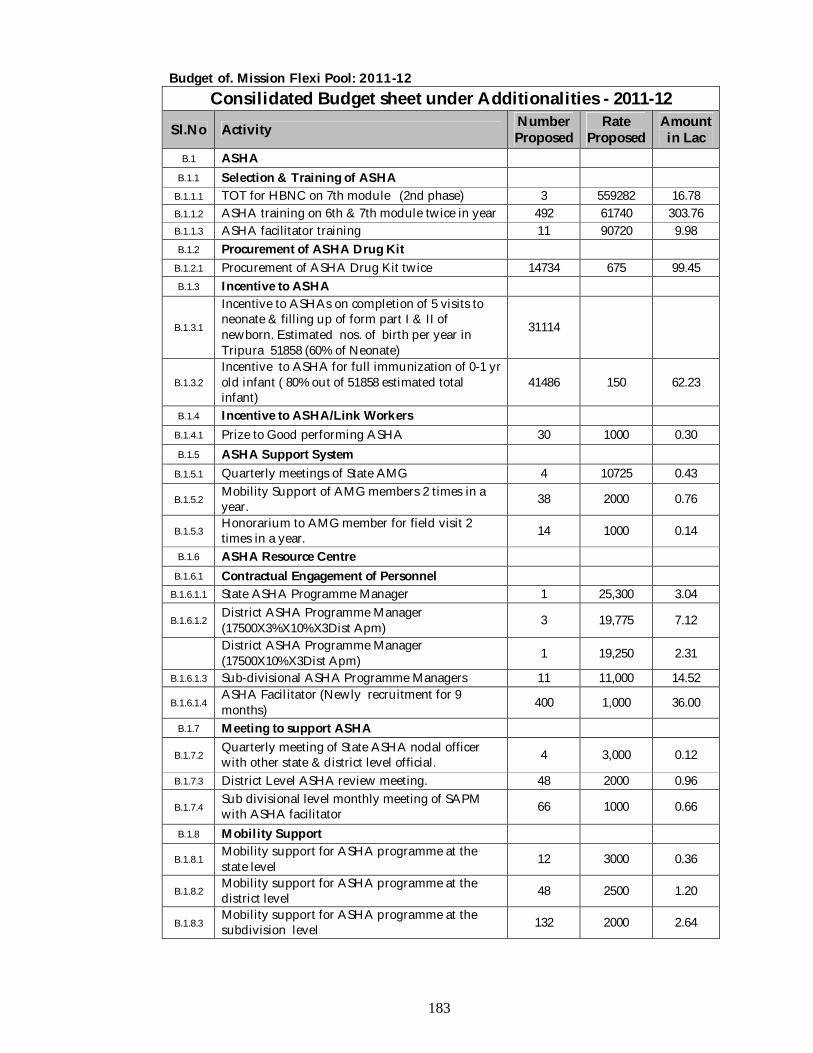
183
Budget of. Mission Flexi Pool: 2011-12 Consilidated Budget sheet under Additionalities - 2011-12
Sl.No Activity Number Proposed
Rate Proposed
Amount in Lac
B.1 ASHA B.1.1 Selection & Training of ASHA
B.1.1.1 TOT for HBNC on 7th module (2nd phase) 3 559282 16.78 B.1.1.2 ASHA training on 6th & 7th module twice in year 492 61740 303.76 B.1.1.3 ASHA facilitator training 11 90720 9.98 B.1.2 Procurement of ASHA Drug Kit
B.1.2.1 Procurement of ASHA Drug Kit twice 14734 675 99.45 B.1.3 Incentive to ASHA
B.1.3.1
Incentive to ASHAs on completion of 5 visits to neonate & filling up of form part I & II of newborn. Estimated nos. of birth per year in Tripura 51858 (60% of Neonate)
31114
B.1.3.2 Incentive to ASHA for full immunization of 0-1 yr old infant ( 80% out of 51858 estimated total infant)
41486 150 62.23
B.1.4 Incentive to ASHA/Link Workers B.1.4.1 Prize to Good performing ASHA 30 1000 0.30 B.1.5 ASHA Support System
B.1.5.1 Quarterly meetings of State AMG 4 10725 0.43
B.1.5.2 Mobility Support of AMG members 2 times in a year. 38 2000 0.76
B.1.5.3 Honorarium to AMG member for field visit 2 times in a year. 14 1000 0.14
B.1.6 ASHA Resource Centre B.1.6.1 Contractual Engagement of Personnel
B.1.6.1.1 State ASHA Programme Manager 1 25,300 3.04
B.1.6.1.2 District ASHA Programme Manager (17500X3%X10%X3Dist Apm) 3 19,775 7.12
District ASHA Programme Manager (17500X10%X3Dist Apm) 1 19,250 2.31
B.1.6.1.3 Sub-divisional ASHA Programme Managers 11 11,000 14.52
B.1.6.1.4 ASHA Facilitator (Newly recruitment for 9 months) 400 1,000 36.00
B.1.7 Meeting to support ASHA
B.1.7.2 Quarterly meeting of State ASHA nodal officer with other state & district level official. 4 3,000 0.12
B.1.7.3 District Level ASHA review meeting. 48 2000 0.96
B.1.7.4 Sub divisional level monthly meeting of SAPM with ASHA facilitator 66 1000 0.66
B.1.8 Mobility Support
B.1.8.1 Mobility support for ASHA programme at the state level 12 3000 0.36
B.1.8.2 Mobility support for ASHA programme at the district level 48 2500 1.20
B.1.8.3 Mobility support for ASHA programme at the subdivision level 132 2000 2.64
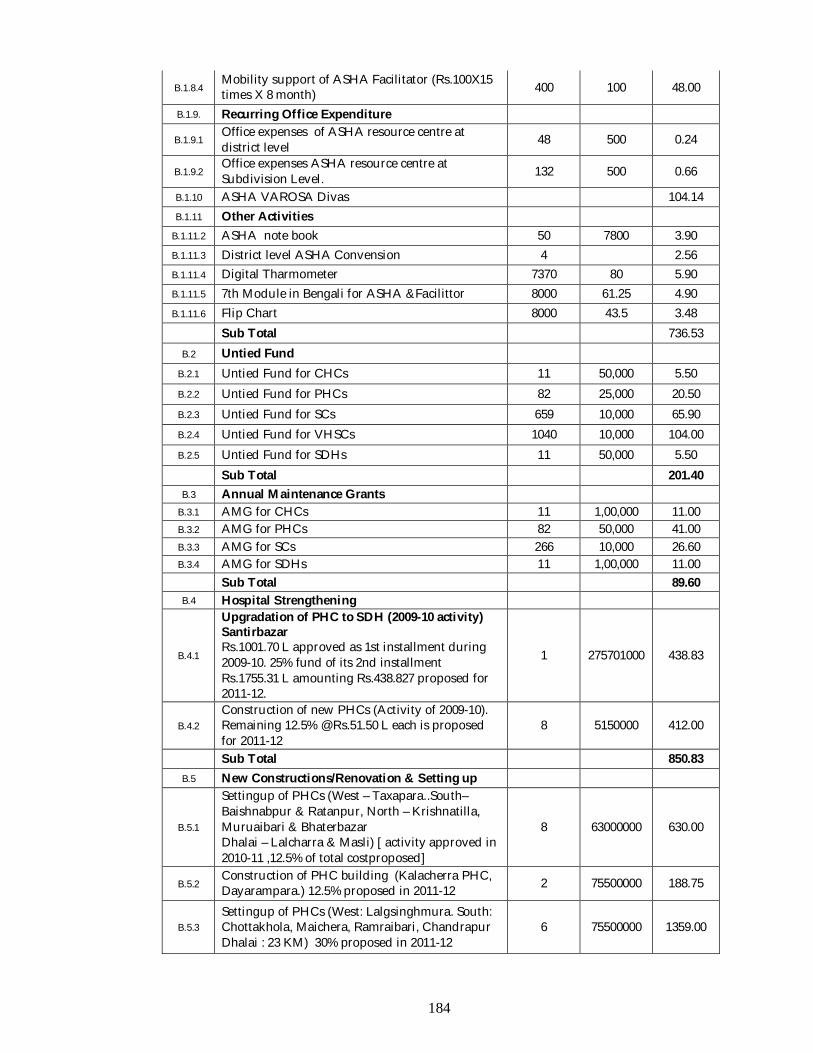
184
B.1.8.4 Mobility support of ASHA Facilitator (Rs.100X15 times X 8 month) 400 100 48.00
B.1.9. Recurring Office Expenditure
B.1.9.1 Office expenses of ASHA resource centre at district level 48 500 0.24
B.1.9.2 Office expenses ASHA resource centre at Subdivision Level. 132 500 0.66
B.1.10 ASHA VAROSA Divas 104.14 B.1.11 Other Activities
B.1.11.2 ASHA note book 50 7800 3.90 B.1.11.3 District level ASHA Convension 4 2.56 B.1.11.4 Digital Tharmometer 7370 80 5.90 B.1.11.5 7th Module in Bengali for ASHA &Facilittor 8000 61.25 4.90 B.1.11.6 Flip Chart 8000 43.5 3.48
Sub Total 736.53 B.2 Untied Fund
B.2.1 Untied Fund for CHCs 11 50,000 5.50 B.2.2 Untied Fund for PHCs 82 25,000 20.50 B.2.3 Untied Fund for SCs 659 10,000 65.90 B.2.4 Untied Fund for VHSCs 1040 10,000 104.00 B.2.5 Untied Fund for SDHs 11 50,000 5.50
Sub Total 201.40 B.3 Annual Maintenance Grants
B.3.1 AMG for CHCs 11 1,00,000 11.00 B.3.2 AMG for PHCs 82 50,000 41.00 B.3.3 AMG for SCs 266 10,000 26.60 B.3.4 AMG for SDHs 11 1,00,000 11.00
Sub Total 89.60 B.4 Hospital Strengthening
B.4.1
Upgradation of PHC to SDH (2009-10 activity) Santirbazar Rs.1001.70 L approved as 1st installment during 2009-10. 25% fund of its 2nd installment Rs.1755.31 L amounting Rs.438.827 proposed for 2011-12.
1 275701000 438.83
B.4.2 Construction of new PHCs (Activity of 2009-10). Remaining 12.5% @ Rs.51.50 L each is proposed for 2011-12
8 5150000 412.00
Sub Total 850.83 B.5 New Constructions/Renovation & Setting up
B.5.1
Settingup of PHCs (West – Taxapara..South–Baishnabpur & Ratanpur, North – Krishnatilla, Muruaibari & Bhaterbazar Dhalai – Lalcharra & Masli) [ activity approved in 2010-11 ,12.5% of total costproposed]
8 63000000 630.00
B.5.2 Construction of PHC building (Kalacherra PHC, Dayarampara.) 12.5% proposed in 2011-12 2 75500000 188.75
B.5.3 Settingup of PHCs (West: Lalgsinghmura. South: Chottakhola, Maichera, Ramraibari, Chandrapur Dhalai : 23 KM) 30% proposed in 2011-12
6 75500000 1359.00
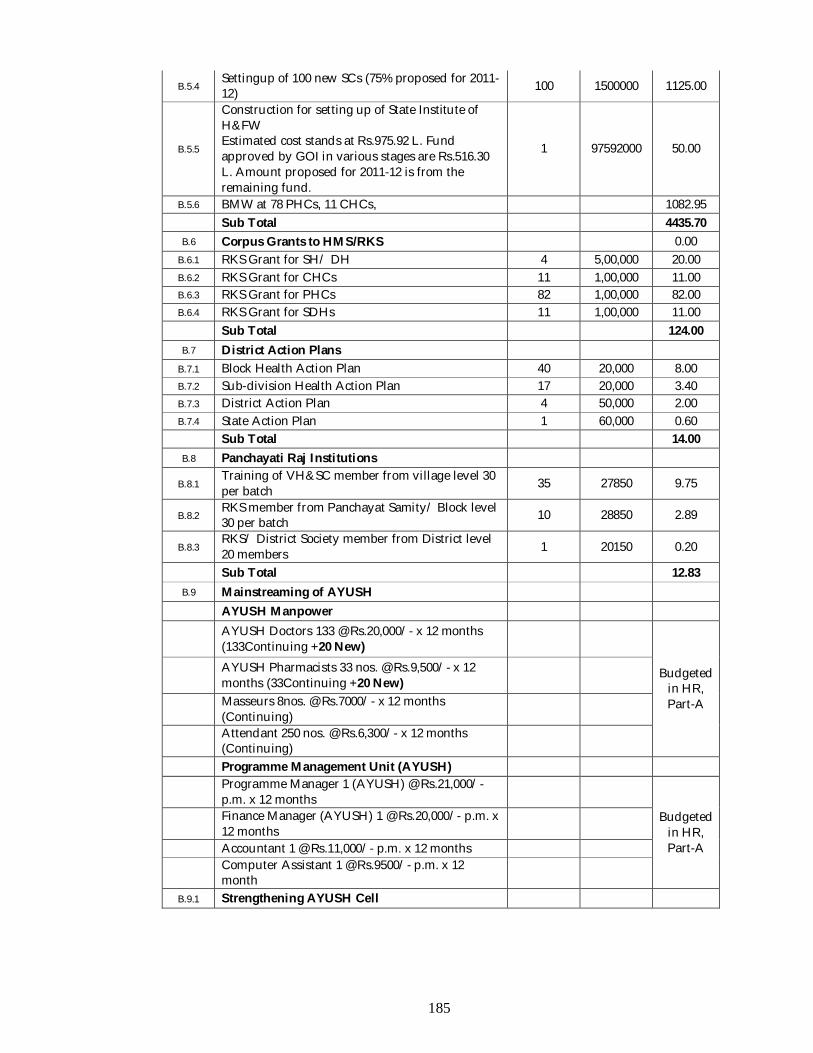
185
B.5.4 Settingup of 100 new SCs (75% proposed for 2011-12) 100 1500000 1125.00
B.5.5
Construction for setting up of State Institute of H&FW Estimated cost stands at Rs.975.92 L. Fund approved by GOI in various stages are Rs.516.30 L. Amount proposed for 2011-12 is from the remaining fund.
1 97592000 50.00
B.5.6 BMW at 78 PHCs, 11 CHCs, 1082.95 Sub Total 4435.70
B.6 Corpus Grants to HMS/RKS 0.00 B.6.1 RKS Grant for SH/ DH 4 5,00,000 20.00 B.6.2 RKS Grant for CHCs 11 1,00,000 11.00 B.6.3 RKS Grant for PHCs 82 1,00,000 82.00 B.6.4 RKS Grant for SDHs 11 1,00,000 11.00
Sub Total 124.00 B.7 District Action Plans
B.7.1 Block Health Action Plan 40 20,000 8.00 B.7.2 Sub-division Health Action Plan 17 20,000 3.40 B.7.3 District Action Plan 4 50,000 2.00 B.7.4 State Action Plan 1 60,000 0.60
Sub Total 14.00 B.8 Panchayati Raj Institutions
B.8.1 Training of VH&SC member from village level 30 per batch 35 27850 9.75
B.8.2 RKS member from Panchayat Samity/ Block level 30 per batch 10 28850 2.89
B.8.3 RKS/ District Society member from District level 20 members 1 20150 0.20
Sub Total 12.83 B.9 Mainstreaming of AYUSH
AYUSH Manpower
AYUSH Doctors 133 @ Rs.20,000/- x 12 months (133Continuing +20 New)
Budgeted in HR, Part-A
AYUSH Pharmacists 33 nos. @ Rs.9,500/- x 12 months (33Continuing +20 New)
Masseurs 8nos. @ Rs.7000/- x 12 months (Continuing)
Attendant 250 nos. @ Rs.6,300/- x 12 months (Continuing)
Programme Management Unit (AYUSH)
Programme Manager 1 (AYUSH) @ Rs.21,000/- p.m. x 12 months
Budgeted in HR, Part-A
Finance Manager (AYUSH) 1 @ Rs.20,000/- p.m. x 12 months
Accountant 1 @ Rs.11,000/- p.m. x 12 months
Computer Assistant 1 @ Rs.9500/- p.m. x 12 month
B.9.1 Strengthening AYUSH Cell
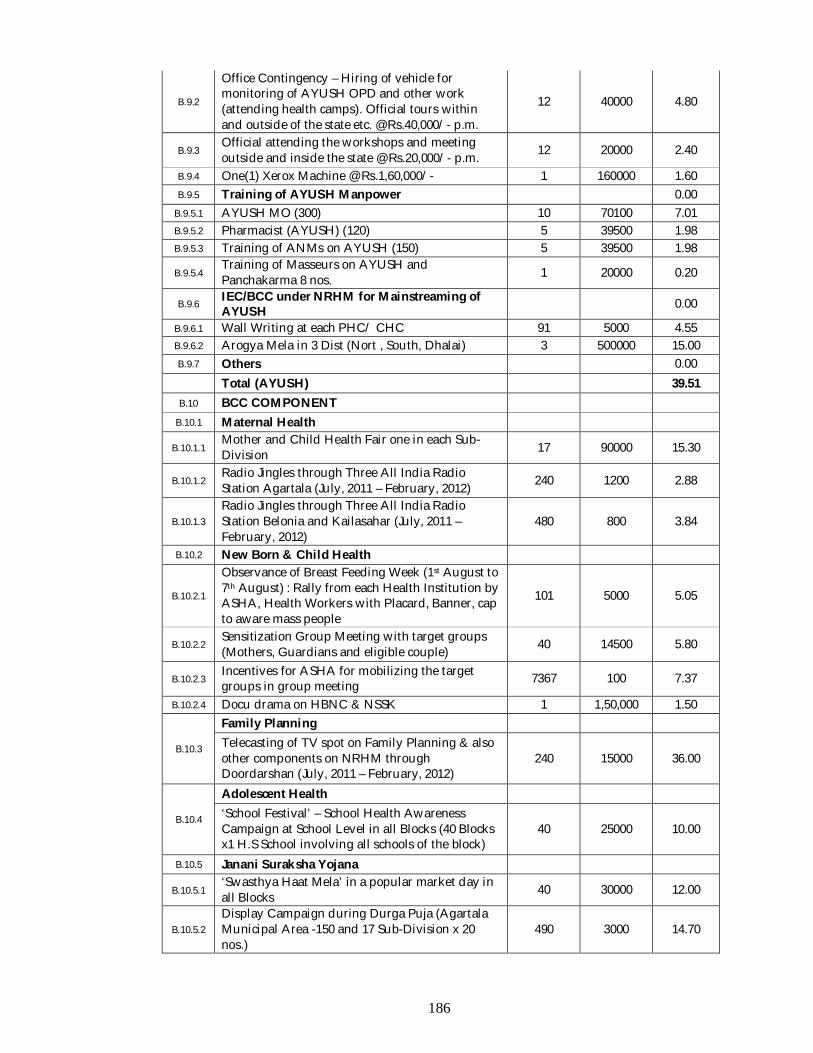
186
B.9.2
Office Contingency – Hiring of vehicle for monitoring of AYUSH OPD and other work (attending health camps). Official tours within and outside of the state etc. @ Rs.40,000/- p.m.
12 40000 4.80
B.9.3 Official attending the workshops and meeting outside and inside the state @ Rs.20,000/- p.m. 12 20000 2.40
B.9.4 One(1) Xerox Machine @ Rs.1,60,000/- 1 160000 1.60 B.9.5 Training of AYUSH Manpower 0.00
B.9.5.1 AYUSH MO (300) 10 70100 7.01 B.9.5.2 Pharmacist (AYUSH) (120) 5 39500 1.98 B.9.5.3 Training of ANMs on AYUSH (150) 5 39500 1.98
B.9.5.4 Training of Masseurs on AYUSH and Panchakarma 8 nos. 1 20000 0.20
B.9.6 IEC/BCC under NRHM for Mainstreaming of AYUSH 0.00
B.9.6.1 Wall Writing at each PHC/ CHC 91 5000 4.55 B.9.6.2 Arogya Mela in 3 Dist (Nort , South, Dhalai) 3 500000 15.00 B.9.7 Others 0.00
Total (AYUSH) 39.51 B.10 BCC COMPONENT
B.10.1 Maternal Health
B.10.1.1 Mother and Child Health Fair one in each Sub-Division 17 90000 15.30
B.10.1.2 Radio Jingles through Three All India Radio Station Agartala (July, 2011 – February, 2012) 240 1200 2.88
B.10.1.3 Radio Jingles through Three All India Radio Station Belonia and Kailasahar (July, 2011 – February, 2012)
480 800 3.84
B.10.2 New Born & Child Health
B.10.2.1
Observance of Breast Feeding Week (1st August to 7th August) : Rally from each Health Institution by ASHA, Health Workers with Placard, Banner, cap to aware mass people
101 5000 5.05
B.10.2.2 Sensitization Group Meeting with target groups (Mothers, Guardians and eligible couple) 40 14500 5.80
B.10.2.3 Incentives for ASHA for mobilizing the target groups in group meeting 7367 100 7.37
B.10.2.4 Docu drama on HBNC & NSSK 1 1,50,000 1.50
B.10.3
Family Planning Telecasting of TV spot on Family Planning & also other components on NRHM through Doordarshan (July, 2011 – February, 2012)
240 15000 36.00
B.10.4
Adolescent Health ‘School Festival’ – School Health Awareness Campaign at School Level in all Blocks (40 Blocks x1 H.S School involving all schools of the block)
40 25000 10.00
B.10.5 Janani Suraksha Yojana
B.10.5.1 ‘Swasthya Haat Mela’ in a popular market day in all Blocks 40 30000 12.00
B.10.5.2 Display Campaign during Durga Puja (Agartala Municipal Area -150 and 17 Sub-Division x 20 nos.)
490 3000 14.70
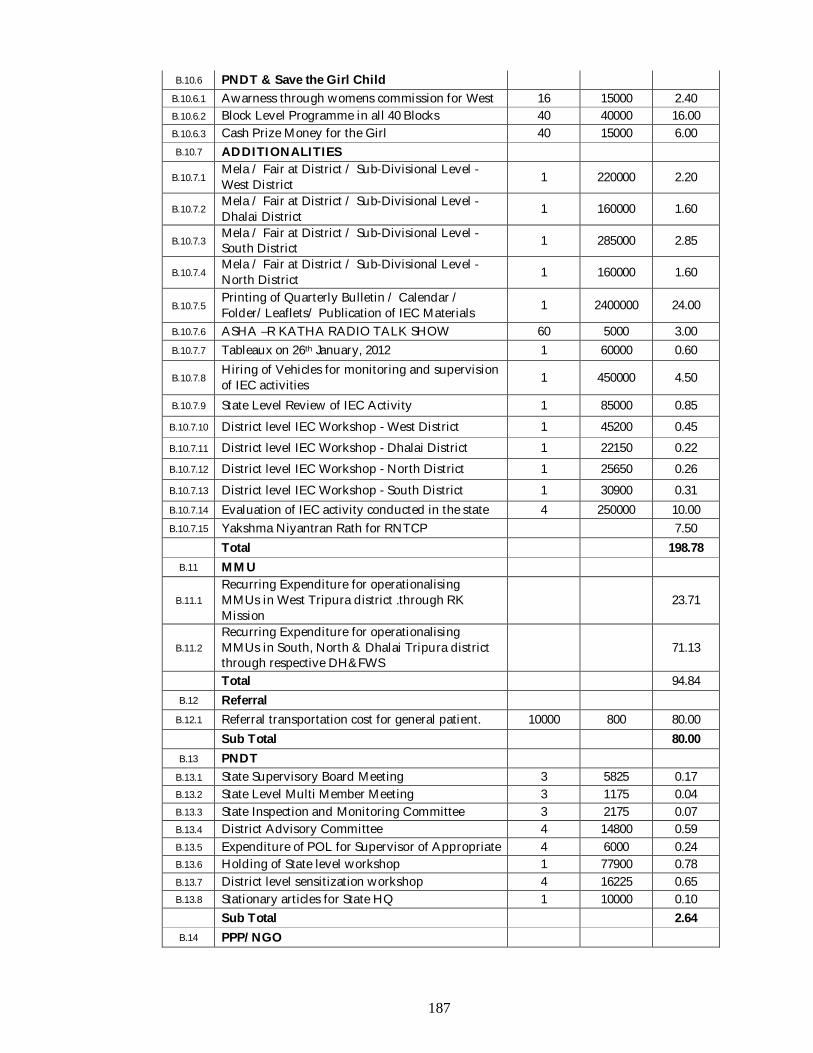
187
B.10.6 PNDT & Save the Girl Child B.10.6.1 Awarness through womens commission for West 16 15000 2.40 B.10.6.2 Block Level Programme in all 40 Blocks 40 40000 16.00 B.10.6.3 Cash Prize Money for the Girl 40 15000 6.00 B.10.7 ADDITIONALITIES
B.10.7.1 Mela / Fair at District / Sub-Divisional Level -West District 1 220000 2.20
B.10.7.2 Mela / Fair at District / Sub-Divisional Level - Dhalai District 1 160000 1.60
B.10.7.3 Mela / Fair at District / Sub-Divisional Level - South District 1 285000 2.85
B.10.7.4 Mela / Fair at District / Sub-Divisional Level -North District 1 160000 1.60
B.10.7.5 Printing of Quarterly Bulletin / Calendar / Folder/Leaflets/ Publication of IEC Materials 1 2400000 24.00
B.10.7.6 ASHA –R KATHA RADIO TALK SHOW 60 5000 3.00 B.10.7.7 Tableaux on 26th January, 2012 1 60000 0.60
B.10.7.8 Hiring of Vehicles for monitoring and supervision of IEC activities 1 450000 4.50
B.10.7.9 State Level Review of IEC Activity 1 85000 0.85 B.10.7.10 District level IEC Workshop - West District 1 45200 0.45 B.10.7.11 District level IEC Workshop - Dhalai District 1 22150 0.22 B.10.7.12 District level IEC Workshop - North District 1 25650 0.26 B.10.7.13 District level IEC Workshop - South District 1 30900 0.31 B.10.7.14 Evaluation of IEC activity conducted in the state 4 250000 10.00 B.10.7.15 Yakshma Niyantran Rath for RNTCP 7.50
Total 198.78 B.11 MMU
B.11.1 Recurring Expenditure for operationalising MMUs in West Tripura district .through RK Mission
23.71
B.11.2 Recurring Expenditure for operationalising MMUs in South, North & Dhalai Tripura district through respective DH&FWS
71.13
Total 94.84 B.12 Referral
B.12.1 Referral transportation cost for general patient. 10000 800 80.00 Sub Total 80.00
B.13 PNDT B.13.1 State Supervisory Board Meeting 3 5825 0.17 B.13.2 State Level Multi Member Meeting 3 1175 0.04 B.13.3 State Inspection and Monitoring Committee 3 2175 0.07 B.13.4 District Advisory Committee 4 14800 0.59 B.13.5 Expenditure of POL for Supervisor of Appropriate 4 6000 0.24 B.13.6 Holding of State level workshop 1 77900 0.78 B.13.7 District level sensitization workshop 4 16225 0.65 B.13.8 Stationary articles for State HQ 1 10000 0.10
Sub Total 2.64 B.14 PPP/ NGO
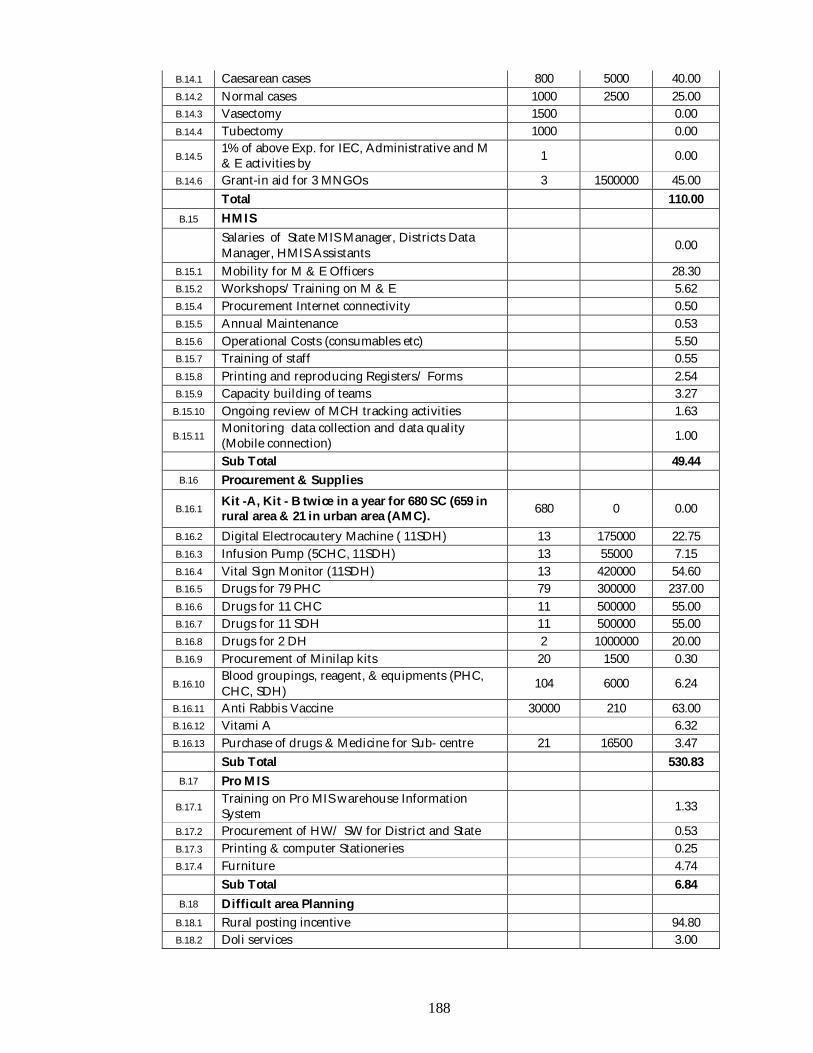
188
B.14.1 Caesarean cases 800 5000 40.00 B.14.2 Normal cases 1000 2500 25.00 B.14.3 Vasectomy 1500 0.00 B.14.4 Tubectomy 1000 0.00
B.14.5 1% of above Exp. for IEC, Administrative and M & E activities by 1 0.00
B.14.6 Grant-in aid for 3 MNGOs 3 1500000 45.00 Total 110.00
B.15 HMIS
Salaries of State MIS Manager, Districts Data Manager, HMIS Assistants 0.00
B.15.1 Mobility for M & E Officers 28.30 B.15.2 Workshops/Training on M & E 5.62 B.15.4 Procurement Internet connectivity 0.50 B.15.5 Annual Maintenance 0.53 B.15.6 Operational Costs (consumables etc) 5.50 B.15.7 Training of staff 0.55 B.15.8 Printing and reproducing Registers/ Forms 2.54 B.15.9 Capacity building of teams 3.27
B.15.10 Ongoing review of MCH tracking activities 1.63
B.15.11 Monitoring data collection and data quality (Mobile connection) 1.00
Sub Total 49.44 B.16 Procurement & Supplies
B.16.1 Kit -A, Kit - B twice in a year for 680 SC (659 in rural area & 21 in urban area (AMC). 680 0 0.00
B.16.2 Digital Electrocautery Machine ( 11SDH) 13 175000 22.75 B.16.3 Infusion Pump (5CHC, 11SDH) 13 55000 7.15 B.16.4 Vital Sign Monitor (11SDH) 13 420000 54.60 B.16.5 Drugs for 79 PHC 79 300000 237.00 B.16.6 Drugs for 11 CHC 11 500000 55.00 B.16.7 Drugs for 11 SDH 11 500000 55.00 B.16.8 Drugs for 2 DH 2 1000000 20.00 B.16.9 Procurement of Minilap kits 20 1500 0.30
B.16.10 Blood groupings, reagent, & equipments (PHC, CHC, SDH) 104 6000 6.24
B.16.11 Anti Rabbis Vaccine 30000 210 63.00 B.16.12 Vitami A 6.32 B.16.13 Purchase of drugs & Medicine for Sub- centre 21 16500 3.47
Sub Total 530.83 B.17 Pro MIS
B.17.1 Training on Pro MIS warehouse Information System 1.33
B.17.2 Procurement of HW/ SW for District and State 0.53 B.17.3 Printing & computer Stationeries 0.25 B.17.4 Furniture 4.74
Sub Total 6.84 B.18 Difficult area Planning
B.18.1 Rural posting incentive 94.80 B.18.2 Doli services 3.00
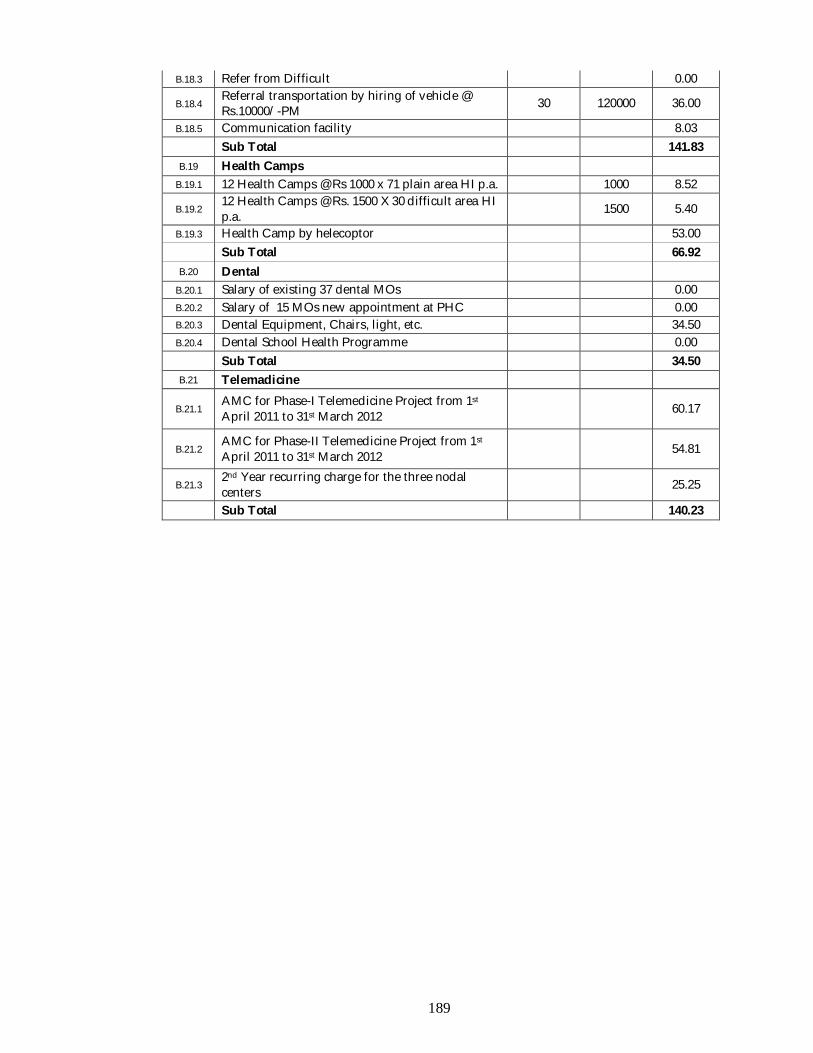
189
B.18.3 Refer from Difficult 0.00
B.18.4 Referral transportation by hiring of vehicle @ Rs.10000/-PM 30 120000 36.00
B.18.5 Communication facility 8.03 Sub Total 141.83
B.19 Health Camps B.19.1 12 Health Camps @ Rs 1000 x 71 plain area HI p.a. 1000 8.52
B.19.2 12 Health Camps @ Rs. 1500 X 30 difficult area HI p.a. 1500 5.40
B.19.3 Health Camp by helecoptor 53.00 Sub Total 66.92
B.20 Dental B.20.1 Salary of existing 37 dental MOs 0.00 B.20.2 Salary of 15 MOs new appointment at PHC 0.00 B.20.3 Dental Equipment, Chairs, light, etc. 34.50 B.20.4 Dental School Health Programme 0.00
Sub Total 34.50 B.21 Telemadicine
B.21.1 AMC for Phase-I Telemedicine Project from 1st April 2011 to 31st March 2012 60.17
B.21.2 AMC for Phase-II Telemedicine Project from 1st April 2011 to 31st March 2012 54.81
B.21.3 2nd Year recurring charge for the three nodal centers 25.25
Sub Total 140.23
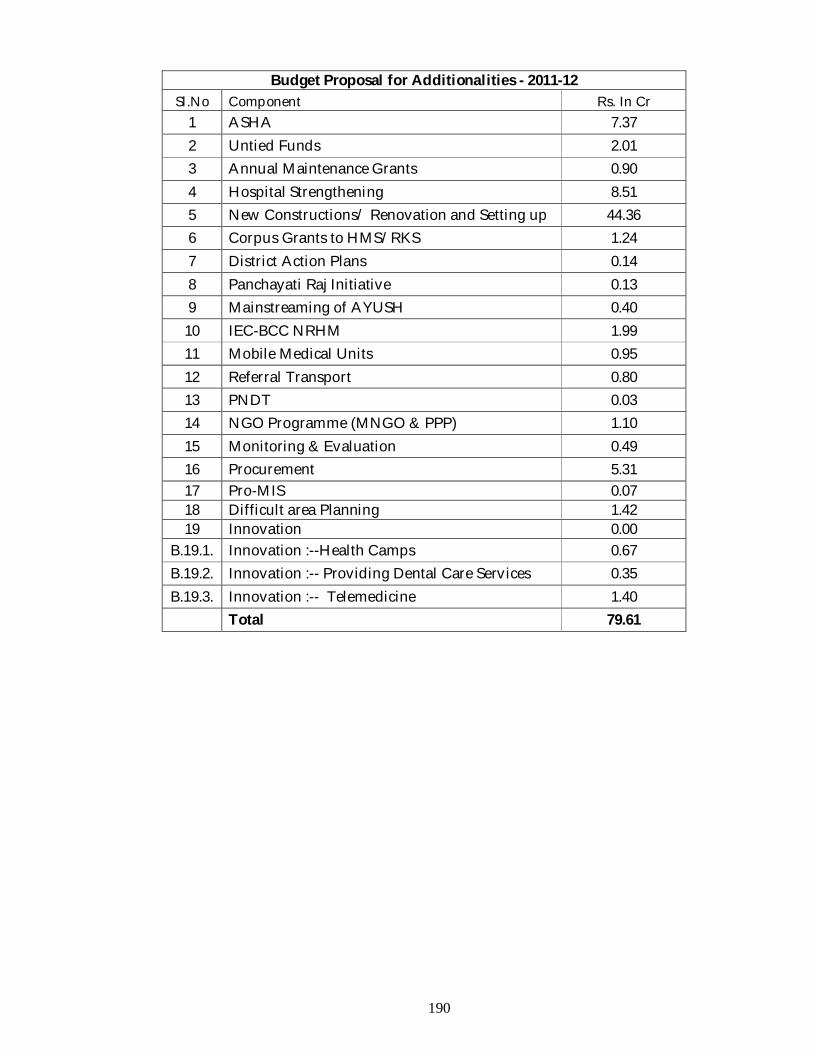
190
Budget Proposal for Additionalities - 2011-12 Sl.No Component Rs. In Cr
1 ASHA 7.37 2 Untied Funds 2.01 3 Annual Maintenance Grants 0.90 4 Hospital Strengthening 8.51 5 New Constructions/ Renovation and Setting up 44.36 6 Corpus Grants to HMS/RKS 1.24 7 District Action Plans 0.14 8 Panchayati Raj Initiative 0.13 9 Mainstreaming of AYUSH 0.40
10 IEC-BCC NRHM 1.99 11 Mobile Medical Units 0.95 12 Referral Transport 0.80 13 PNDT 0.03 14 NGO Programme (MNGO & PPP) 1.10 15 Monitoring & Evaluation 0.49 16 Procurement 5.31 17 Pro-MIS 0.07 18 Difficult area Planning 1.42 19 Innovation 0.00
B.19.1. Innovation :--Health Camps 0.67 B.19.2. Innovation :-- Providing Dental Care Services 0.35 B.19.3. Innovation :-- Telemedicine 1.40
Total 79.61
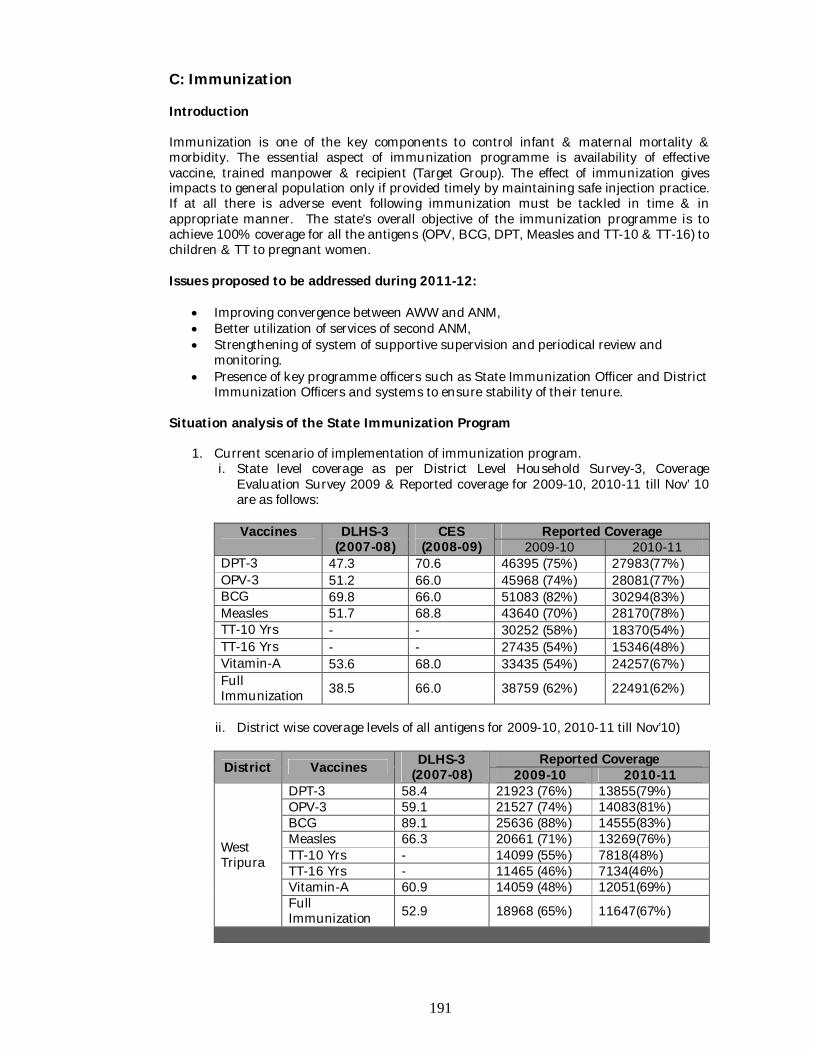
191
C: Immunization Introduction Immunization is one of the key components to control infant & maternal mortality & morbidity. The essential aspect of immunization programme is availability of effective vaccine, trained manpower & recipient (Target Group). The effect of immunization gives impacts to general population only if provided timely by maintaining safe injection practice. If at all there is adverse event following immunization must be tackled in time & in appropriate manner. The state’s overall objective of the immunization programme is to achieve 100% coverage for all the antigens (OPV, BCG, DPT, Measles and TT-10 & TT-16) to children & TT to pregnant women. Issues proposed to be addressed during 2011-12:
Improving convergence between AWW and ANM, Better utilization of services of second ANM, Strengthening of system of supportive supervision and periodical review and
monitoring. Presence of key programme officers such as State Immunization Officer and District
Immunization Officers and systems to ensure stability of their tenure. Situation analysis of the State Immunization Program
1. Current scenario of implementation of immunization program. i. State level coverage as per District Level Household Survey-3, Coverage
Evaluation Survey 2009 & Reported coverage for 2009-10, 2010-11 till Nov’ 10 are as follows:
Vaccines DLHS-3
(2007-08) CES
(2008-09) Reported Coverage
2009-10 2010-11 DPT-3 47.3 70.6 46395 (75%) 27983(77%) OPV-3 51.2 66.0 45968 (74%) 28081(77%) BCG 69.8 66.0 51083 (82%) 30294(83%) Measles 51.7 68.8 43640 (70%) 28170(78%) TT-10 Yrs - - 30252 (58%) 18370(54%) TT-16 Yrs - - 27435 (54%) 15346(48%) Vitamin-A 53.6 68.0 33435 (54%) 24257(67%) Full Immunization 38.5 66.0 38759 (62%) 22491(62%)
ii. District wise coverage levels of all antigens for 2009-10, 2010-11 till Nov’10)
District Vaccines DLHS-3 (2007-08)
Reported Coverage 2009-10 2010-11
West Tripura
DPT-3 58.4 21923 (76%) 13855(79%) OPV-3 59.1 21527 (74%) 14083(81%) BCG 89.1 25636 (88%) 14555(83%) Measles 66.3 20661 (71%) 13269(76%) TT-10 Yrs - 14099 (55%) 7818(48%) TT-16 Yrs - 11465 (46%) 7134(46%) Vitamin-A 60.9 14059 (48%) 12051(69%) Full Immunization 52.9 18968 (65%) 11647(67%)
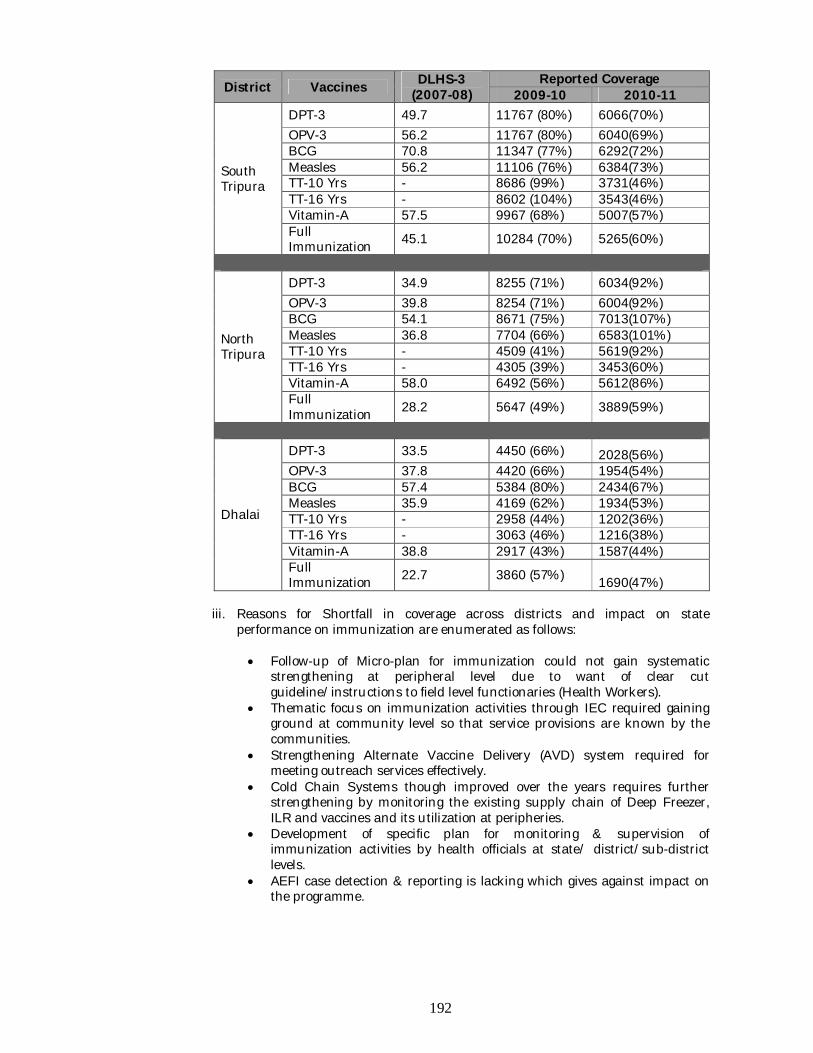
192
District Vaccines DLHS-3 (2007-08)
Reported Coverage 2009-10 2010-11
South Tripura
DPT-3 49.7 11767 (80%) 6066(70%) OPV-3 56.2 11767 (80%) 6040(69%) BCG 70.8 11347 (77%) 6292(72%) Measles 56.2 11106 (76%) 6384(73%) TT-10 Yrs - 8686 (99%) 3731(46%) TT-16 Yrs - 8602 (104%) 3543(46%) Vitamin-A 57.5 9967 (68%) 5007(57%) Full Immunization 45.1 10284 (70%) 5265(60%)
North Tripura
DPT-3 34.9 8255 (71%) 6034(92%) OPV-3 39.8 8254 (71%) 6004(92%) BCG 54.1 8671 (75%) 7013(107%) Measles 36.8 7704 (66%) 6583(101%) TT-10 Yrs - 4509 (41%) 5619(92%) TT-16 Yrs - 4305 (39%) 3453(60%) Vitamin-A 58.0 6492 (56%) 5612(86%) Full Immunization 28.2 5647 (49%) 3889(59%)
Dhalai
DPT-3 33.5 4450 (66%) 2028(56%) OPV-3 37.8 4420 (66%) 1954(54%) BCG 57.4 5384 (80%) 2434(67%) Measles 35.9 4169 (62%) 1934(53%) TT-10 Yrs - 2958 (44%) 1202(36%) TT-16 Yrs - 3063 (46%) 1216(38%) Vitamin-A 38.8 2917 (43%) 1587(44%) Full Immunization 22.7 3860 (57%) 1690(47%)
iii. Reasons for Shortfall in coverage across districts and impact on state
performance on immunization are enumerated as follows: Follow-up of Micro-plan for immunization could not gain systematic
strengthening at peripheral level due to want of clear cut guideline/instructions to field level functionaries (Health Workers).
Thematic focus on immunization activities through IEC required gaining ground at community level so that service provisions are known by the communities.
Strengthening Alternate Vaccine Delivery (AVD) system required for meeting outreach services effectively.
Cold Chain Systems though improved over the years requires further strengthening by monitoring the existing supply chain of Deep Freezer, ILR and vaccines and its utilization at peripheries.
Development of specific plan for monitoring & supervision of immunization activities by health officials at state/ district/sub-district levels.
AEFI case detection & reporting is lacking which gives against impact on the programme.
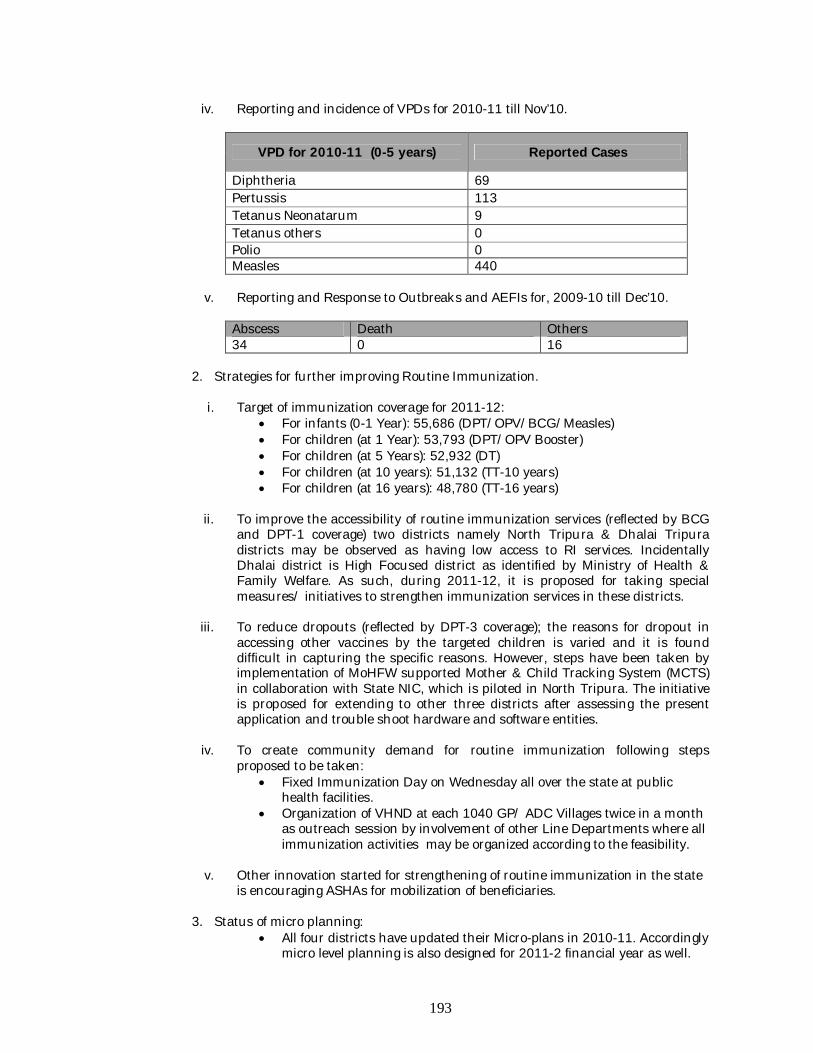
193
iv. Reporting and incidence of VPDs for 2010-11 till Nov’10.
VPD for 2010-11 (0-5 years) Reported Cases
Diphtheria 69 Pertussis 113 Tetanus Neonatarum 9 Tetanus others 0 Polio 0 Measles 440
v. Reporting and Response to Outbreaks and AEFIs for, 2009-10 till Dec’10.
Abscess Death Others 34 0 16
2. Strategies for further improving Routine Immunization.
i. Target of immunization coverage for 2011-12:
For infants (0-1 Year): 55,686 (DPT/OPV/BCG/Measles) For children (at 1 Year): 53,793 (DPT/OPV Booster) For children (at 5 Years): 52,932 (DT) For children (at 10 years): 51,132 (TT-10 years) For children (at 16 years): 48,780 (TT-16 years)
ii. To improve the accessibility of routine immunization services (reflected by BCG
and DPT-1 coverage) two districts namely North Tripura & Dhalai Tripura districts may be observed as having low access to RI services. Incidentally Dhalai district is High Focused district as identified by Ministry of Health & Family Welfare. As such, during 2011-12, it is proposed for taking special measures/ initiatives to strengthen immunization services in these districts.
iii. To reduce dropouts (reflected by DPT-3 coverage); the reasons for dropout in
accessing other vaccines by the targeted children is varied and it is found difficult in capturing the specific reasons. However, steps have been taken by implementation of MoHFW supported Mother & Child Tracking System (MCTS) in collaboration with State NIC, which is piloted in North Tripura. The initiative is proposed for extending to other three districts after assessing the present application and trouble shoot hardware and software entities.
iv. To create community demand for routine immunization following steps
proposed to be taken: Fixed Immunization Day on Wednesday all over the state at public
health facilities. Organization of VHND at each 1040 GP/ ADC Villages twice in a month
as outreach session by involvement of other Line Departments where all immunization activities may be organized according to the feasibility.
v. Other innovation started for strengthening of routine immunization in the state
is encouraging ASHAs for mobilization of beneficiaries.
3. Status of micro planning: All four districts have updated their Micro-plans in 2010-11. Accordingly
micro level planning is also designed for 2011-2 financial year as well.
194
4. In the state of Tripura there is one ANM & one MPW (M) posted in most of the SHC,
but all the SHC have at least one ANM or one MPW male. 5. Presently, there are 1040 VH&SC in all the GP/ ADC villages. All kind of problems
regarding health & others issues of the village is shorted out in the VH&SC meeting which is held at every month.
6. Status of Cold Chain Equipment-
i. ILRs, DF, Voltage stabilizers.
a. Plan for replacement of all condemned or non-serviceable equipment, which is beyond repair. 22 Nos. of ILR & 32 Nos. of DFs are beyond repair. GOI should replace through new equipment.
b. Expansion: - Need based depending on the setting up of New PHC/ cold
chain points. At present there is 134 cold chain points. But under 11th plan and under NRHM another 21 Nos. of institutions will be extended. Hence additional equipment is to be provided.
ii. Cold boxes, Vaccine carriers - replacement plan for expansion or replacement of
condemn equipment.
iii. Mechanism for cold chain maintenance and repairs- HR structure, AMC (if any) etc. State does not have any mechanism for repairing in district level. All major repairing is done in state HQ through local agencies. However to reduce BREAK DOWN TIME state required vehicle to replace damaged equipment of periphery with fresh stock of Hq and the repair the equipment in HQ. An amount of Rs. 10000/- per month as transportation & loading unloading charges of CC equipment may be provided
7. Status of implementation of Procurement Management Information System (Pro
MIS) : Details may be seen at ProMIS chapter under Additionalities.
8. IEC plan for strengthening UIP; however the budget for IEC is to be provisioned under RCH : Budget for IEC has been provisioned under IEC/BCC chapter under Additionalities.
9. Infrastructural and manpower requirements that are essential for implementation
of UIP but not admissible under Part C (Immunization) may be provisioned under the NRHM/RCH heads. (e.g; Refrigerator mechanics, renovation of stores etc.) This should include district level need for go down for vaccine/logistics. Helper 5 nos. at cold chain store.
Basic information of the State/UT related to Immunization Programme
Position Name & Designation Contact No./Email
State Immunization Officer
1. Dr. Asish Dasgupta State Programme Officer (FW&RCH cum Immunization) Directorate of FW & PM Government of Tripura
9436120238 [email protected]
State Cold Chain Officer
Er. Rajat Bhattacharyya Cold Chain Officer, Directorate of FW & PM, Government of Tripura
9436126417 [email protected]
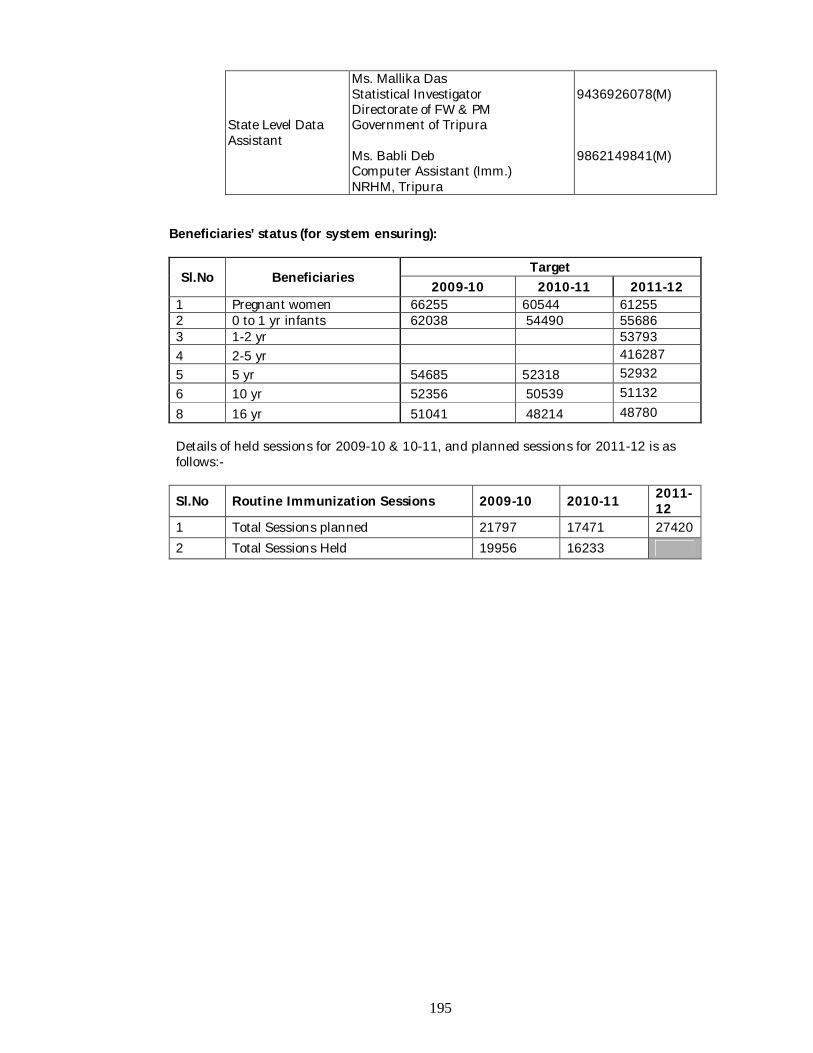
195
State Level Data Assistant
Ms. Mallika Das Statistical Investigator Directorate of FW & PM Government of Tripura Ms. Babli Deb Computer Assistant (Imm.) NRHM, Tripura
9436926078(M) 9862149841(M)
Beneficiaries’ status (for system ensuring):
Sl.No Beneficiaries Target
2009-10 2010-11 2011-12 1 Pregnant women 66255 60544 61255 2 0 to 1 yr infants 62038 54490 55686 3 1-2 yr 53793 4 2-5 yr 416287 5 5 yr 54685 52318 52932 6 10 yr 52356 50539 51132 8 16 yr 51041 48214 48780 Details of held sessions for 2009-10 & 10-11, and planned sessions for 2011-12 is as follows:-
Sl.No Routine Immunization Sessions 2009-10 2010-11 2011-12
1 Total Sessions planned 21797 17471 27420 2 Total Sessions Held 19956 16233
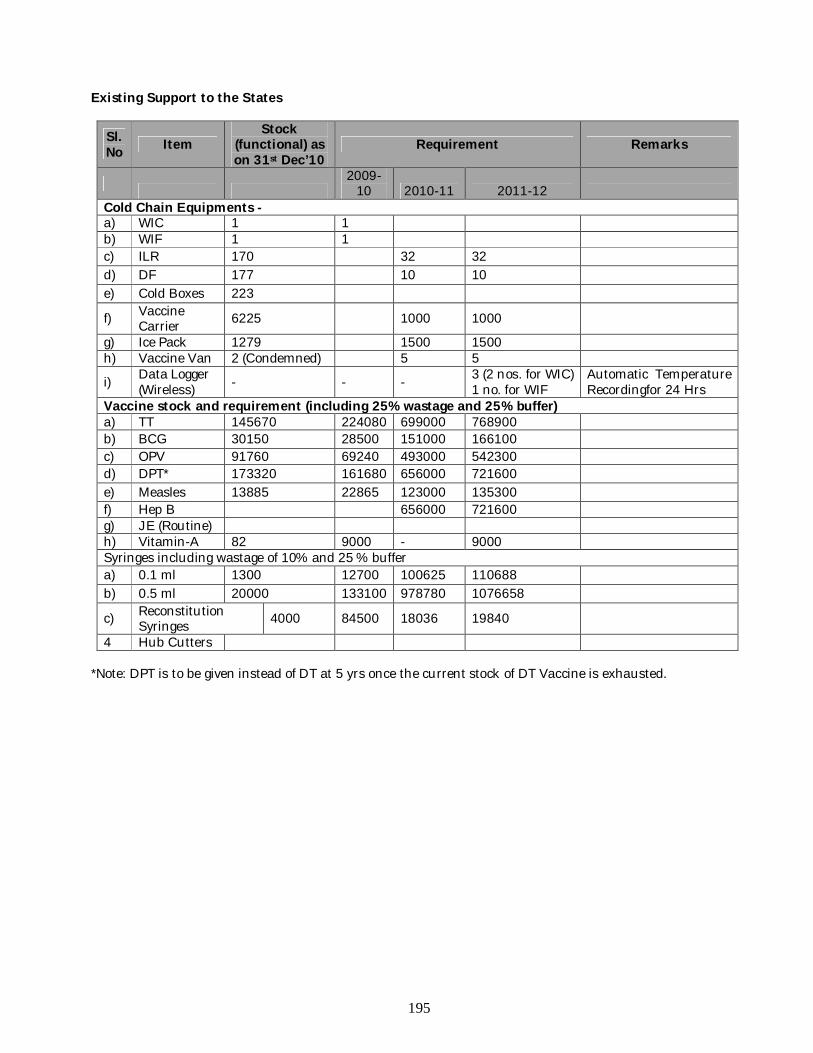
195
Existing Support to the States
Sl. No Item
Stock (functional) as on 31st Dec’10
Requirement Remarks
2009-
10 2010-11 2011-12 Cold Chain Equipments - a) WIC 1 1 b) WIF 1 1 c) ILR 170 32 32 d) DF 177 10 10 e) Cold Boxes 223
f) Vaccine Carrier 6225 1000 1000
g) Ice Pack 1279 1500 1500 h) Vaccine Van 2 (Condemned) 5 5
i) Data Logger (Wireless) - - - 3 (2 nos. for WIC)
1 no. for WIF Automatic Temperature Recordingfor 24 Hrs
Vaccine stock and requirement (including 25% wastage and 25% buffer) a) TT 145670 224080 699000 768900 b) BCG 30150 28500 151000 166100 c) OPV 91760 69240 493000 542300 d) DPT* 173320 161680 656000 721600 e) Measles 13885 22865 123000 135300 f) Hep B 656000 721600 g) JE (Routine) h) Vitamin-A 82 9000 - 9000 Syringes including wastage of 10% and 25 % buffer a) 0.1 ml 1300 12700 100625 110688 b) 0.5 ml 20000 133100 978780 1076658
c) Reconstitution Syringes 4000 84500 18036 19840
4 Hub Cutters *Note: DPT is to be given instead of DT at 5 yrs once the current stock of DT Vaccine is exhausted.
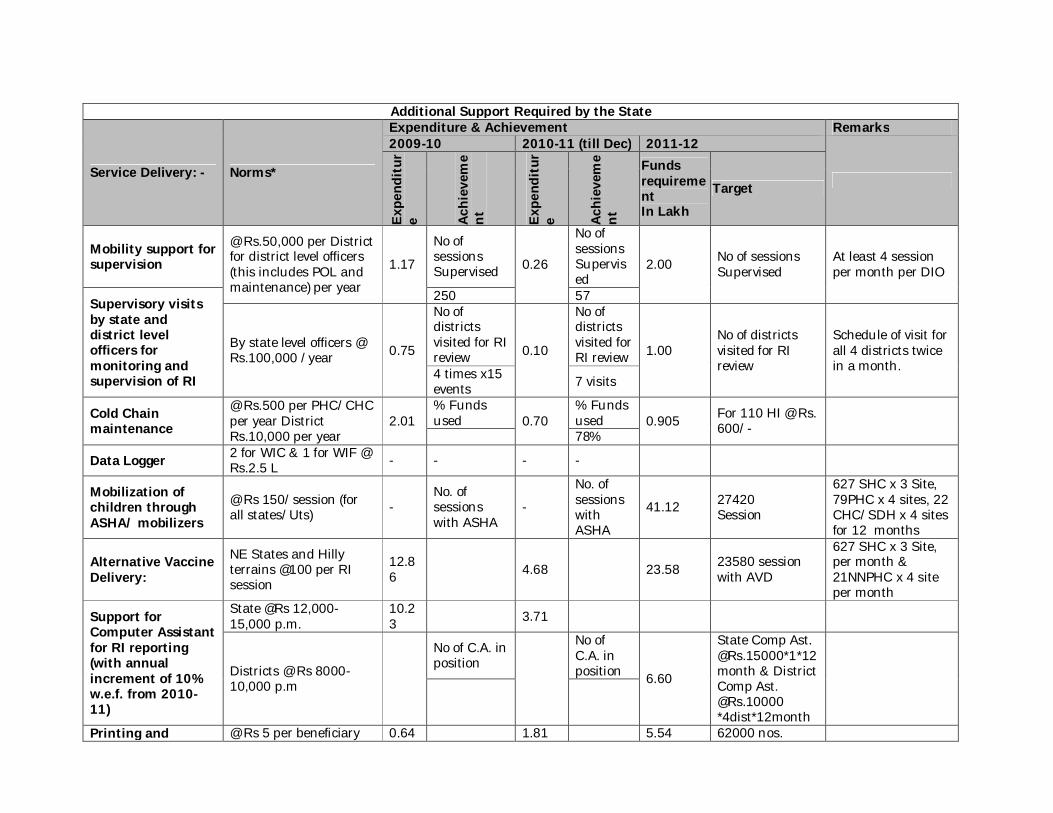
Additional Support Required by the State
Service Delivery: - Norms*
Expenditure & Achievement Remarks 2009-10 2010-11 (till Dec) 2011-12
Expe
ndit
ure Ac
hiev
eme
nt
Expe
ndit
ure Ac
hiev
eme
nt
Funds requirement In Lakh
Target
Mobility support for supervision
@ Rs.50,000 per District for district level officers (this includes POL and maintenance) per year
1.17
No of sessions Supervised 0.26
No of sessions Supervised
2.00 No of sessions Supervised
At least 4 session per month per DIO
Supervisory visits by state and district level officers for monitoring and supervision of RI
250 57
By state level officers @ Rs.100,000 /year 0.75
No of districts visited for RI review 0.10
No of districts visited for RI review 1.00
No of districts visited for RI review
Schedule of visit for all 4 districts twice in a month. 4 times x15
events 7 visits
Cold Chain maintenance
@ Rs.500 per PHC/CHC per year District Rs.10,000 per year
2.01 % Funds used 0.70
% Funds used 0.905 For 110 HI @ Rs.
600/- 78%
Data Logger 2 for WIC & 1 for WIF @ Rs.2.5 L - - - -
Mobilization of children through ASHA/ mobilizers
@ Rs 150/session (for all states/Uts) -
No. of sessions with ASHA
-
No. of sessions with ASHA
41.12 27420 Session
627 SHC x 3 Site, 79PHC x 4 sites, 22 CHC/SDH x 4 sites for 12 months
Alternative Vaccine Delivery:
NE States and Hilly terrains @100 per RI session
12.86 4.68 23.58 23580 session
with AVD
627 SHC x 3 Site, per month & 21NNPHC x 4 site per month
Support for Computer Assistant for RI reporting (with annual increment of 10% w.e.f. from 2010-11)
State @Rs 12,000- 15,000 p.m.
10.23
3.71
Districts @ Rs 8000- 10,000 p.m
No of C.A. in position
No of C.A. in position 6.60
State Comp Ast. @Rs.15000*1*12 month & District Comp Ast. @Rs.10000 *4dist*12month
Printing and @ Rs 5 per beneficiary 0.64 1.81 5.54 62000 nos.
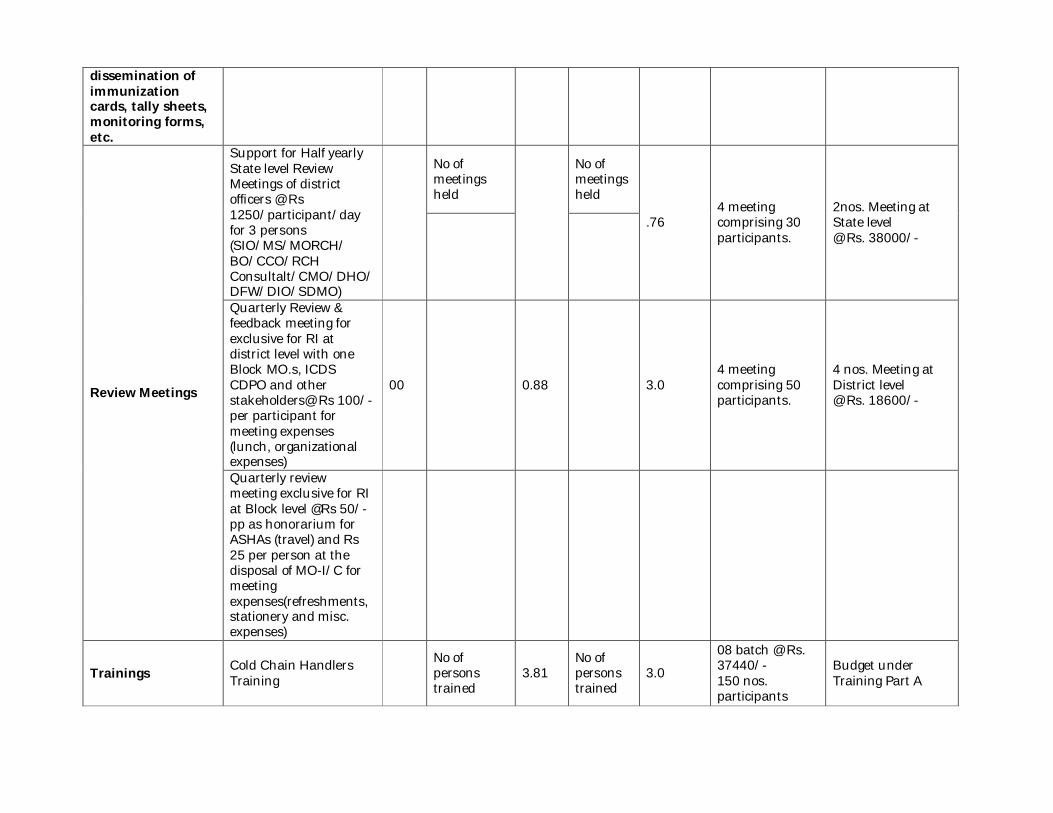
dissemination of immunization cards, tally sheets, monitoring forms, etc.
Review Meetings
Support for Half yearly State level Review Meetings of district officers @ Rs 1250/participant/day for 3 persons (SIO/MS/MORCH/ BO/CCO/RCH Consultalt/CMO/DHO/DFW/DIO/SDMO)
No of meetings held
No of meetings held
.76 4 meeting comprising 30 participants.
2nos. Meeting at State level @ Rs. 38000/-
Quarterly Review & feedback meeting for exclusive for RI at district level with one Block MO.s, ICDS CDPO and other stakeholders@ Rs 100/- per participant for meeting expenses (lunch, organizational expenses)
00 0.88 3.0 4 meeting comprising 50 participants.
4 nos. Meeting at District level @ Rs. 18600/-
Quarterly review meeting exclusive for RI at Block level @Rs 50/-pp as honorarium for ASHAs (travel) and Rs 25 per person at the disposal of MO-I/C for meeting expenses(refreshments, stationery and misc. expenses)
Trainings Cold Chain Handlers Training
No of persons trained
3.81 No of persons trained
3.0
08 batch @ Rs. 37440/- 150 nos. participants
Budget under Training Part A
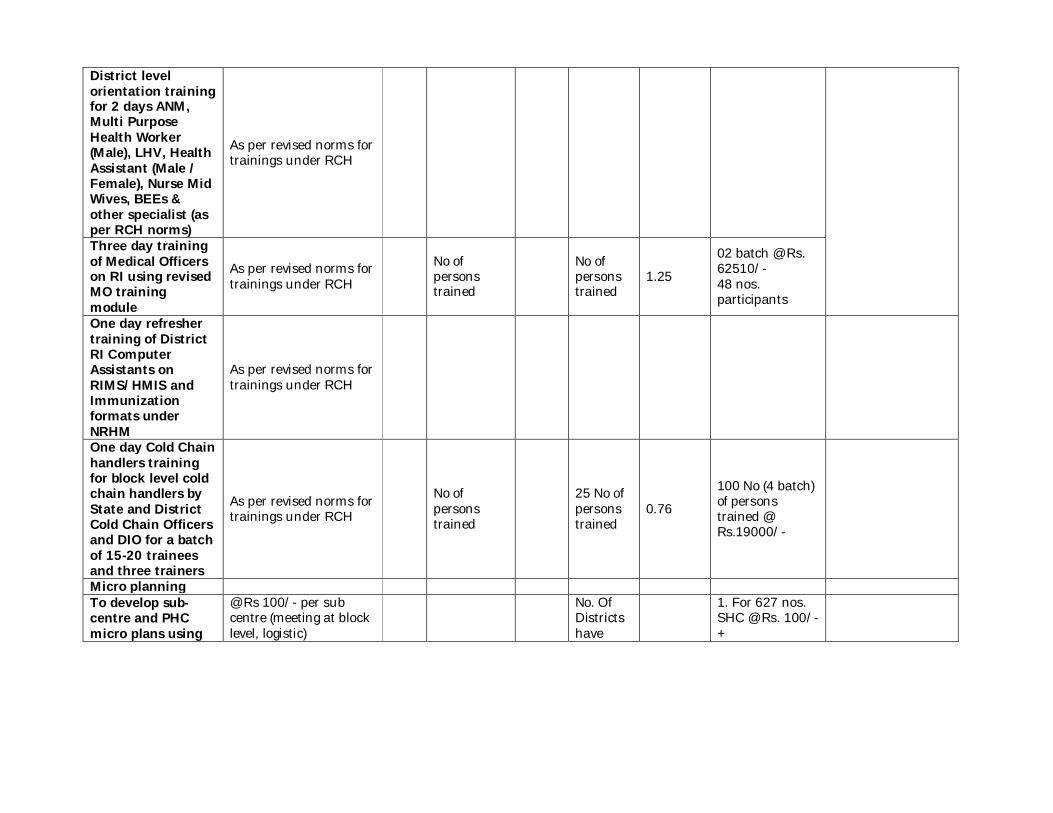
District level orientation training for 2 days ANM, Multi Purpose Health Worker (Male), LHV, Health Assistant (Male / Female), Nurse Mid Wives, BEEs & other specialist (as per RCH norms)
As per revised norms for trainings under RCH
Three day training of Medical Officers on RI using revised MO training module
As per revised norms for trainings under RCH
No of persons trained
No of persons trained
1.25
02 batch @ Rs. 62510/- 48 nos. participants
One day refresher training of District RI Computer Assistants on RIMS/HMIS and Immunization formats under NRHM
As per revised norms for trainings under RCH
One day Cold Chain handlers training for block level cold chain handlers by State and District Cold Chain Officers and DIO for a batch of 15-20 trainees and three trainers
As per revised norms for trainings under RCH
No of persons trained
25 No of persons trained
0.76
100 No (4 batch) of persons trained @ Rs.19000/-
Micro planning To develop sub-centre and PHC micro plans using
@ Rs 100/- per sub centre (meeting at block level, logistic)
No. Of Districts have
1. For 627 nos. SHC @ Rs. 100/- +
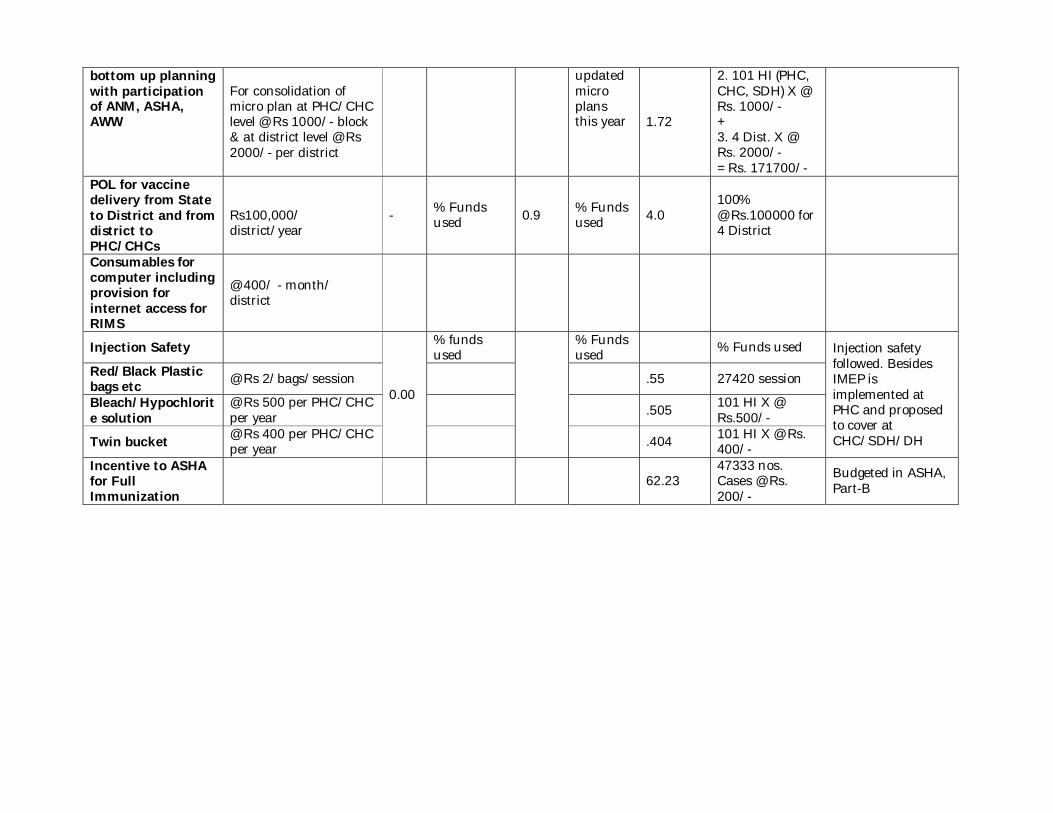
bottom up planning with participation of ANM, ASHA, AWW
For consolidation of micro plan at PHC/CHC level @ Rs 1000/- block & at district level @ Rs 2000/- per district
updated micro plans this year 1.72
2. 101 HI (PHC, CHC, SDH) X @ Rs. 1000/- + 3. 4 Dist. X @ Rs. 2000/- = Rs. 171700/-
POL for vaccine delivery from State to District and from district to PHC/CHCs
Rs100,000/ district/year
- % Funds used 0.9 % Funds
used 4.0 100% @ Rs.100000 for 4 District
Consumables for computer including provision for internet access for RIMS
@ 400/ - month/ district
Injection Safety
0.00
% funds used
% Funds used % Funds used Injection safety
followed. Besides IMEP is implemented at PHC and proposed to cover at CHC/SDH/DH
Red/Black Plastic bags etc @ Rs 2/bags/session .55 27420 session
Bleach/Hypochlorite solution
@ Rs 500 per PHC/CHC per year .505 101 HI X @
Rs.500/-
Twin bucket @ Rs 400 per PHC/CHC per year .404 101 HI X @ Rs.
400/- Incentive to ASHA for Full Immunization
62.23 47333 nos. Cases @ Rs. 200/-
Budgeted in ASHA, Part-B
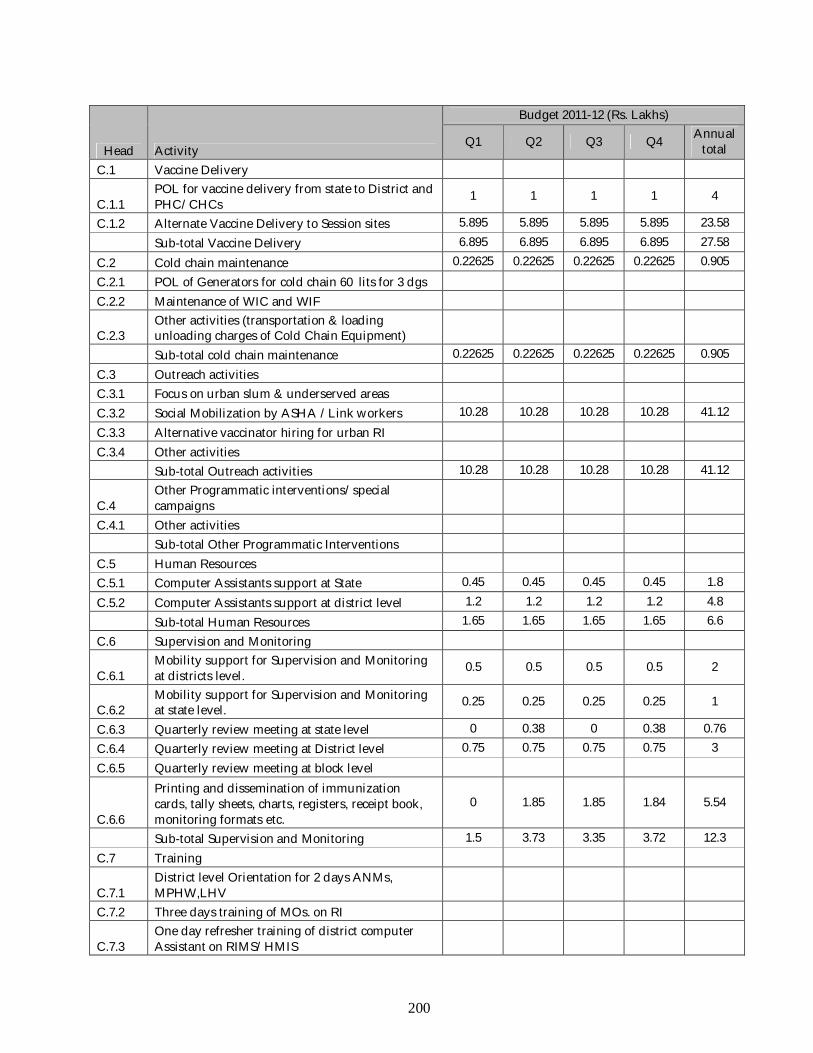
200
Head Activity
Budget 2011-12 (Rs. Lakhs)
Q1 Q2 Q3 Q4 Annual total
C.1 Vaccine Delivery
C.1.1 POL for vaccine delivery from state to District and PHC/CHCs
1 1 1 1 4
C.1.2 Alternate Vaccine Delivery to Session sites 5.895 5.895 5.895 5.895 23.58 Sub-total Vaccine Delivery 6.895 6.895 6.895 6.895 27.58 C.2 Cold chain maintenance 0.22625 0.22625 0.22625 0.22625 0.905 C.2.1 POL of Generators for cold chain 60 lits for 3 dgs C.2.2 Maintenance of WIC and WIF
C.2.3 Other activities (transportation & loading unloading charges of Cold Chain Equipment)
Sub-total cold chain maintenance 0.22625 0.22625 0.22625 0.22625 0.905 C.3 Outreach activities C.3.1 Focus on urban slum & underserved areas C.3.2 Social Mobilization by ASHA /Link workers 10.28 10.28 10.28 10.28 41.12 C.3.3 Alternative vaccinator hiring for urban RI C.3.4 Other activities Sub-total Outreach activities 10.28 10.28 10.28 10.28 41.12
C.4 Other Programmatic interventions/special campaigns
C.4.1 Other activities Sub-total Other Programmatic Interventions C.5 Human Resources C.5.1 Computer Assistants support at State 0.45 0.45 0.45 0.45 1.8 C.5.2 Computer Assistants support at district level 1.2 1.2 1.2 1.2 4.8 Sub-total Human Resources 1.65 1.65 1.65 1.65 6.6 C.6 Supervision and Monitoring
C.6.1 Mobility support for Supervision and Monitoring at districts level.
0.5 0.5 0.5 0.5 2
C.6.2 Mobility support for Supervision and Monitoring at state level.
0.25 0.25 0.25 0.25 1
C.6.3 Quarterly review meeting at state level 0 0.38 0 0.38 0.76 C.6.4 Quarterly review meeting at District level 0.75 0.75 0.75 0.75 3 C.6.5 Quarterly review meeting at block level
C.6.6
Printing and dissemination of immunization cards, tally sheets, charts, registers, receipt book, monitoring formats etc.
0 1.85 1.85 1.84 5.54
Sub-total Supervision and Monitoring 1.5 3.73 3.35 3.72 12.3 C.7 Training
C.7.1 District level Orientation for 2 days ANMs, MPHW,LHV
C.7.2 Three days training of MOs. on RI
C.7.3 One day refresher training of district computer Assistant on RIMS/HMIS
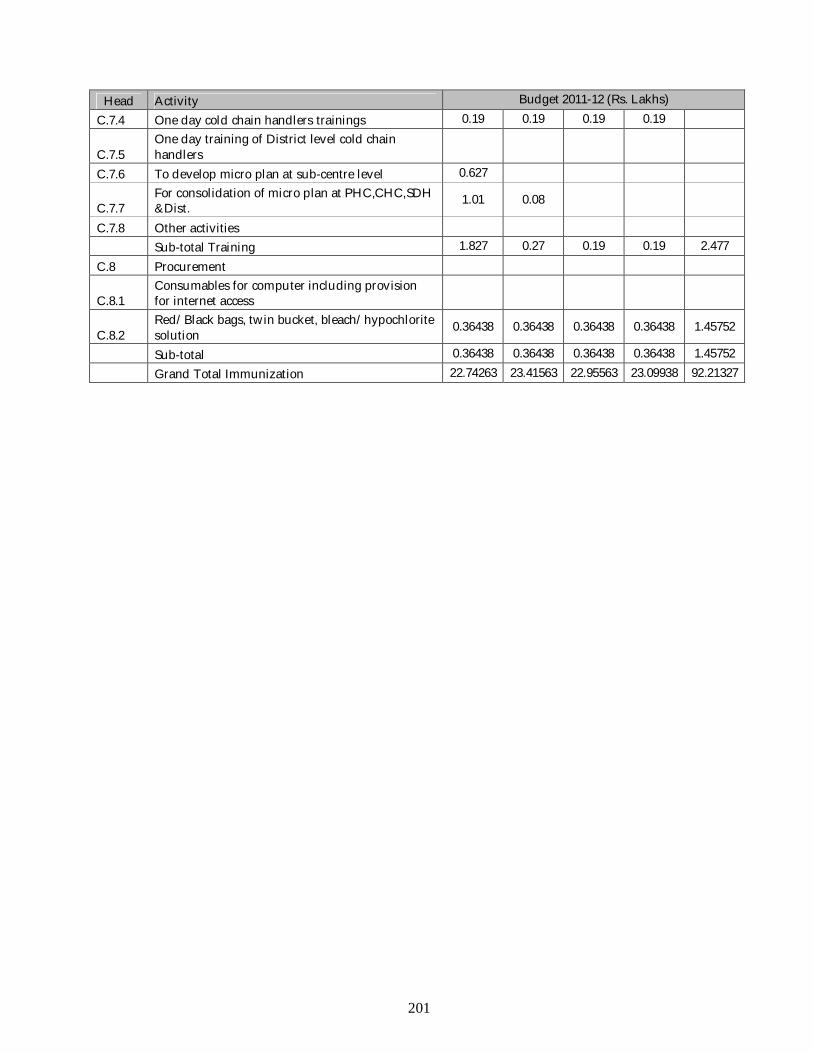
201
Head Activity Budget 2011-12 (Rs. Lakhs) C.7.4 One day cold chain handlers trainings 0.19 0.19 0.19 0.19
C.7.5 One day training of District level cold chain handlers
C.7.6 To develop micro plan at sub-centre level 0.627
C.7.7 For consolidation of micro plan at PHC,CHC,SDH &Dist.
1.01 0.08
C.7.8 Other activities Sub-total Training 1.827 0.27 0.19 0.19 2.477 C.8 Procurement
C.8.1 Consumables for computer including provision for internet access
C.8.2 Red/Black bags, twin bucket, bleach/hypochlorite solution
0.36438 0.36438 0.36438 0.36438 1.45752
Sub-total 0.36438 0.36438 0.36438 0.36438 1.45752 Grand Total Immunization 22.74263 23.41563 22.95563 23.09938 92.21327