cervical carcinoma in southern mexico: human papillomavirus and cofactors
TRANSCRIPT
Cervical carcinoma in Southern Mexico: Human
papillomavirus and cofactors§
Berenice Illades-Aguiar PhDa,*, Enoc-Mariano Cortes-Malagon MSa,Veronica Antonio-Vejar MSa, Noelio Zamudio-Lopez MSa,
Luz del Carmen Alarcon-Romero PhDa, Gloria Fernandez-Tilapa PhDa,Daniel Hernandez-Sotelo MSa, Marco-Antonio Teran-Porcayo MDb,
Eugenia Flores-Alfaro MSa, Marco-Antonio Leyva-Vazquez PhDa
a Laboratorio de Biomedicina Molecular, Unidad Academica de Ciencias Quımico Biologicas,
Universidad Autonoma de Guerrero, Chilpancingo, Guerrero, Mexicob Instituto Estatal de Cancerologıa ‘‘Dr. Arturo Beltran Ortega’’, Acapulco, Guerrero, Mexico
Accepted 10 September 2008
Abstract
Background: This study was conducted to determine human papillomavirus (HPV) types in women with cervical cancer (CC) and normal
cervical cytology in the Southern region of Mexico, and to know the contribution of HPV types and cofactors in cervical cancer etiology.
Methods: A case–control study was performed in 133 women with CC and 256 controls. HPV detection was done by MY09/11 and GP5+/
GP6+ PCR systems and typing by restriction fragment length polymorphism or DNA sequencing. Results: HPV was found in 100% of CC and
35.5% of controls. The genotype distribution in CC was: HPV 16 (66.8%), 18 (9%), 31 (7.5%), 45 (4.5%), 58 (3.7%), 69 (3%), 52 (1.6%), 6,
11, 33, 56, and 67 (0.8% each). Among controls, HPV 33 followed by HPV 16 were the most frequent. Cervical cancer was associated with
HPV 16 (OR = 573.5), HPV 18 (OR = 804.4), and undetermined risk HPV (types 67 and 69) (OR = 434.3). Age at first intercourse<16 years
(OR = 9.6) and �3 births (OR = 16) were significant risk factors for CC. Conclusions: HPV 16, by far, is the most frequent type in CC, HPV
16 and 18 are responsible for 75.8% of the CC cases and high-risk HPV for 94.7%, which is useful data to take into account in vaccination
programs. HPV 33 is the most frequent type in controls and high-risk HPV are more common than low-risk HPV.
# 2008 Elsevier Ltd. All rights reserved.
Keywords: Human papillomavirus epidemiology in Mexico; Human papillomavirus genotypes in Mexico; Human papillomavirus and cervical cancer;
Cervical cancer in Mexico; Cervical cancer risk; Cervical cancer in Latin America; Cervical cancer co-factors; Human papillomavirus in normal cervix; HPV
typing; HPV PCR detection
www.elsevier.com/locate/cdp
Cancer Detection and Prevention 32 (2009) 300–307
1. Introduction
Cancer of the cervix uteri is the second most important
cancer among women worldwide with an estimated
§ Sources of support: This work was supported by Grants S-20 and
97SIBEJ-02-016 from the Sistema de Investigacion Benito Juarez-CON-
ACYT, Mexico.
* Corresponding author. Tel.: +52 747 4710901; fax: +52 747 4710901.
E-mail addresses: [email protected], [email protected]
(B. Illades-Aguiar).
0361-090X/$ – see front matter # 2008 Elsevier Ltd. All rights reserved.
doi:10.1016/j.cdp.2008.09.001
493,000 new cases and 274,000 deaths in 2002 [1]. More
than eighty percent of new cases are currently diagnosed in
developing countries [1], where there is a high incidence of
the disease because there are severe limitations in
screening programs as well as treatment facilities [2]. In
Latin America, a high incidence and mortality were
registered for cervical cancer (CC); by the year 2000, some
76,000 new cervical cancer cases and almost 30,000 deaths
were estimated for the whole region, which represent 16%
and 13% of the world burden, respectively. From Latin

B. Illades-Aguiar et al. / Cancer Detection and Prevention 32 (2009) 300–307 301
American countries, Mexico is seventh place in relative
incidence (age standardized rates – ASR – 40.5 per 100,000
women) and fifth in mortality (ASR 17.1 per 100,000
women [3].
In Mexico, cervical cancer is the most common type of
cancer among women [4]. Deaths due to cervical cancer
did not decrease during the 1990–2000 period; on the
contrary, there was a 0.76% yearly average increase.
Cervical cancer mortality shows heterogeneity in different
regions of the country. The Central region of Mexico,
where Mexico City is located, has the lowest mortality rate
and the lowest risk of death from cervical cancer, while the
Southern region has the highest mortality rate and the
highest mortality risk. The State of Guerrero, which is
located in the Southern region, is one of the states with the
highest rates of non-coverage by social security health
care services (47.7%), and one of the states with the
highest cervical cancer rates with the highest mortality
risk for this disease [5]. The State of Guerrero cervical
cancer mortality rate was 11 deaths per 100,000 women in
2005 [6].
Certain types of human papillomavirus (HPV) are the
central and necessary cause of cervical cancer worldwide
[7]. So far, nearly 100 HPV have been described [8] and
more than 50 different HPV types primarily infect the anal
and genital tracts. The IARC Monograph Working Group [9]
in 2005 concluded that human papillomavirus types 16, 18,
31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 66 are carcinogenic
for human beings and have been classified as high-risk or
oncogenic types. Munoz et al. consider that it is arbitrary to
classify HPV 66 as carcinogenic and they therefore propose
that HPV 66 as well as HPV 26, 53, 68, 73 and 82 should be
considered as probably carcinogenic [10]. HPV 6, 11, 13, 40,
42, 43, 44, 54, 61, 70, 72, 81, 89 are classified as low-risk
types. For HPV 2a, 3, 7, 10, 27, 28, 29, 30, 32, 34, 55, 57, 62,
67, 69, 71, 74, 77, 83, 84, 85, 86, 87, 90, 91 the risk of
cervical cancer is undetermined [10]. HPV 55 was
reclassified as a subtype of HPV 44 and is considered as
low-risk HPV type [11].
HPV 16 is the most prevalent type found in women with
cervical cancer worldwide and together with HPV 18, 31,
and 45 account for about 80% of invasive cervical cancer
collected from around the world [12].
Geographical variation in HPV type distribution is known
to occur in different regions of the world. Limited
information is available on the prevalence and distribution
of HPV types in cervical cancer in Southern Mexico. In
addition to this, there have been relatively few case–control
studies about invasive cervical carcinoma performed in
Mexico [13–17].
This study in the State of Guerrero, Mexico, was
undertaken to establish which HPV types are circulating in
women with cervical cancer and normal cervical cytology
from Southern Mexico, and to describe the contribution of
different HPV types and cofactors in cervical cancer
etiology.
2. Material and methods
2.1. Study population
The study was carried out in the Cancer Institute of the
State of Guerrero, a regional concentration Hospital located
in Acapulco, Guerrero, Mexico. The cases were 133
Mexican women with residence in Guerrero State, with
invasive cervical cancer recruited between 1997 and 2003.
Inclusion criteria for case subjects were that they had
histological confirmation of invasive cervical cancer
diagnosis, had not received any treatment, and that DNA
extracted from the biopsy samples was good quality. Of the
cases group, no exfoliated cells were obtained. Squamous
cell carcinoma (SCC) was diagnosed in 119 cases (89.5%)
and adeno/adenosquamous carcinoma (ADC/ADSC) in 14
(10.5%), by histological diagnosis, according to the
classification system of the International Federation of
Gynecology and Obstetrics (FIGO) [18]. The controls were
256 gynecological patients who attended the hospital
mentioned above for cytological screening with cytologi-
cally normal cervical epithelium according to the Bethesda
System [19]. Control women were selected to match the
expected age distribution of the case subjects and had to
fulfill the following inclusion criteria: negative diagnosis of
any kind of cancer, and to not have gone through cervical
conization or hysterectomy. The controls provide a cervical
scrape containing exfoliated cells from the cervix, from
which good quality DNA was confirmed to include them in
the study. Participants answered a standardized question-
naire on sexual behavior, reproductive history, smoking
habits, and socioeconomic background.
Informed consent was obtained from both cases and
control women. This study was approved by the ethical
committee of the Cancer Institute of the State of Guerrero.
2.2. Specimen collection
For cytological analysis and HPV detection, cervical
scrapes were collected by sampling the ectocervix with an
Ayre spatula and endocervix with a cytobrush, making sure
that tissue from the transformation zone was taken. Smears
were used for cytomorphological examination using
conventional Papanicolaou. For HPV detection, cytobrushes
with cervical scrapes were placed in lysis buffer (10 mM
Tris pH 8.0, 20 mM EDTA pH 8.0 and 0.5% sodium dodecyl
sulfate), and were removed after taking out cervical material
and stored at �20 8C until analysis. A tumor biopsy
specimen was also taken and was eluted in phosphate-
buffered saline (PBS), and stored at �70 8C until analysis.
2.3. HPV detection and typing
DNA was extracted according to the standard SDS–
proteinase K–phenol–chloroform method [20]. DNA
samples were tested by the MY09/11 PCR protocol
B. Illades-Aguiar et al. / Cancer Detection and Prevention 32 (2009) 300–307302
[21,22]. The consensus primers MY09 and MY11 target a
conserved 450-pb region of the HPV L1 gene. The reaction
mixtures (50 ml) contained 1 mg of target DNA, 0.8 mM of
each primer, 2 mM MgCl2, PCR buffer 1X, 150 mM of each
dNTP and 1.25 U of Ampli Taq GoldTM (Applied
Biosystems, Foster City, CA). DNA was amplified in a
GeneAmp PCR System 2400 (Applied Biosystems, Foster
City, CA) with the following steps: an initial step 10 min
denaturation at 95 8C, followed by 40 cycles of 95 8C for
1 min, 58 8C for 1 min, 72 8C for 1 min, and a final
extension at 72 8C for 10 min.
Integrity of DNA specimens was verified by amplifica-
tion of a 268-bp region of the human b-globin gene using
PC04 and GH20 primers [23]. HPV 16 plasmid, CaSki and
HeLa cells were used as positive controls, human DNA
without HPV DNA and water were used as negative
controls.
For HPV typing, amplified PCR products were digested
with restriction enzymes BamHI, DdeI, HaeIII, HinfI, PstI,
RsaI and Sau3AI (Invitrogen, Carlsbad, CA) and restriction
fragment length polymorphism (RFLP) analysis were
performed to identify more than 40 genital HPV types
[24]. Typing of HPVof randomly selected samples that were
positive for HPV 33 and HPV 16 was carried out by type-
specific PCR with primers designed for the E6 region of
these viral types [25,26] (see: Supplementary Data).
When samples analyzed with MY09/11 PCR protocol
were negative or the HPV could not be genotyped by
RFLP’s, the presence of HPV DNA was assessed using the
general GP5+/6+ PCR system [27]. PCR GP5+/GP6+
products were subjected to sequencing analysis. Briefly,
after the purification of PCR products using 75%
isopropanol and columns (Centri-Sep Spin Columns,
Applied Biosystems, Foster City, CA), these were sequenced
using Big Dye Terminator Chemistry Version 3 Cycle
Sequencing Kit (Applied Biosystems, Foster City, CA) in an
automated sequencer (310 ABI PRISM Genetic Analyzer,
Applied Biosystems, Foster City, CA). All the sequences
available for the HPV types were recovered from the NCBI
site [28]. HPV types were classified as high-risk versus low-
risk accordingly to Munoz et al. classification [10].
2.4. Statistical analysis
To estimate the relative risk of cervical cancer associated
with HPV types and other risk factors, odds ratios (ORs) and
95% confidence intervals (CIs) were calculated by using
logistic regression in non-adjusted models and adjusted
models for different risk factors. Statistical analysis was
performed using STATA software version 9.2.
3. Results
A total of 133 case patients with cervical cancer and 256
control subjects were included in this study. Of the cases,
119 (89.5%) were SCC and 14 (10.5%) were ADC/ADSC.
The average age of the cases was 52.2 years and of the
controls 50.5 ( p = 0.2). Fifty-three percent of the cervical
cancer cases occurred in women 50 years old or older, 41%
in women 35–49 years old, and 6% in women 34 years old or
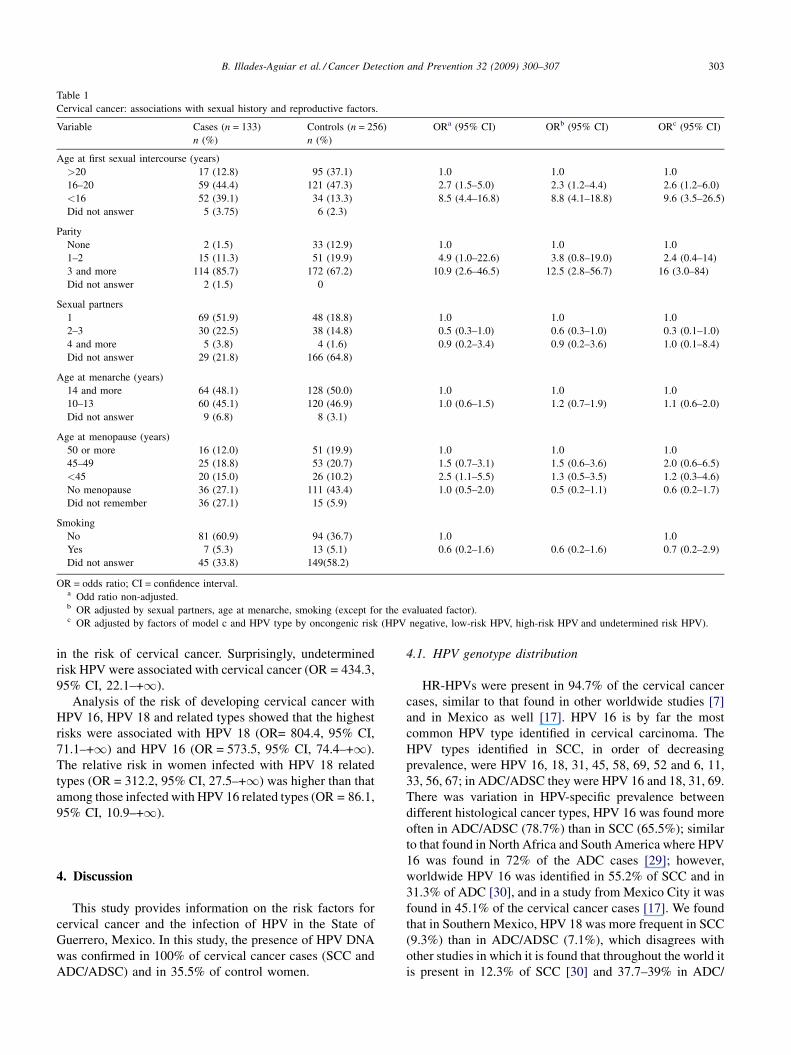
younger. Table 1 summarizes the main sexual history and
reproductive factors characteristics of study subjects by case
and control status and the association of these characteristics
with cervical carcinoma after various adjustments. In the
fully adjusted model, start of sexual activity before age 16
(OR = 9.6, 95% CI, 3.5–26.5) and having 3 or more births
(OR = 16, 95% CI, 3–84) showed statistically significant
associations with cervical cancer. In the non-adjusted model
for age, menopause in women younger than 45 years showed
an apparent association with the risk of developing cervical
cancer, however, after adjusting for HPV infection, number
of sexual partners, age at menarche and smoking habits, the
association was found to be not significant (OR = 1.2, 95%
CI, 0.3–4.6). Other characteristics that were examined and
found not to be associated with cervical cancer included
number of sexual partners, age at menarche and smoking. Of
the women that participated in this study, 64.8% did not
provide the number of sexual partners they have had and
58.2% did not say if they smoked or not.
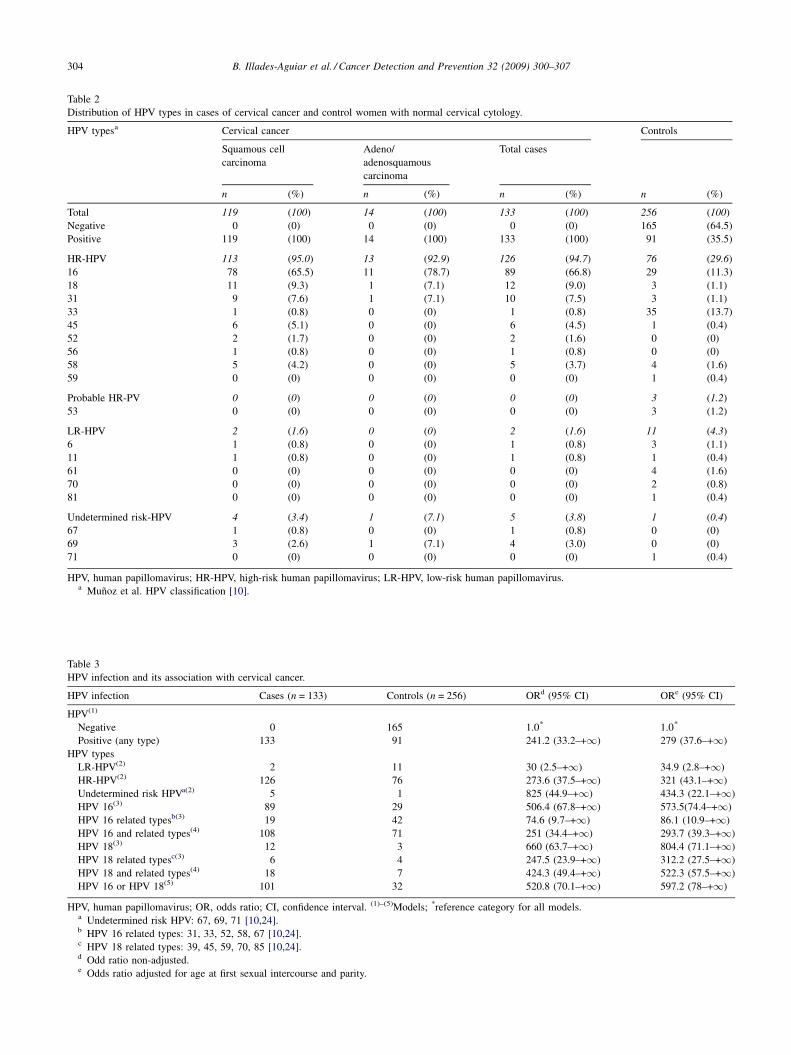
Among the 256 control women, specimens from 91
(35.5%) and all cases of SSC and ADC/ADSC were positive
for HPV DNA. Analysis of the HPV type-specific
distribution among cases and control women showed that
the most common HPV type in women with SCC was HPV
type 16 (65.5%) followed by HPV types 18 (9.3%), 31
(7.6%), 45 (5.1%), and 58 (4.2%). Two LR-HPV types (HPV
6 and 11) and two undetermined risk HPV types (HPV 67
and 69) were also detected. In women with ADC/ADSC,
HPV type 16 (78.7%) was the most frequent type followed
by HPV types 18 (7.1%), 31 (7.1%) and 69 (7.1%). In
control subjects, 76 (29.6%) were infected with high-risk
types and only 11 (4.3%) where infected with low-risk types.
It is important to note that in the control group HPV type 33
was the most recurrent (13.7%) followed by HPV types 16
(11.3%), 58 (1.6%) and 61 (1.6%). When we analyzed by
type-specific PCR, 5 samples with HPV 33 and 14 with HPV
16, they corresponded to the results obtained by MY-RFLPs.
Multiple infection was not found in either control or cases
(Table 2) (see: Supplementary Data).
HPV 16 phylogenetically related types found in this study
(a-9: HPV 31, 33, 52, 58, 67) were present in 14.4% of
cervical cancer cases and HPV 18 phylogenetically related
types (a-7: HPV 45) were present in 4.5% of cervical cancer.
The remainder 5.4% cases had a-5 (HPV 69), a-6 (HPV 56),
and a-10 (HPV 6 and 11) (Table 2).
The presence of HPV was associated with SCC (OR,
216.5; 95% CI, 56–+1) and with ADC/ADSC (OR, 27.1;
95% CI, 6.5–+1) (data not shown). Table 3 summarizes the
association of cervical cancer with HPV genotype infection
using five models and various adjustments. HPV infection
with any HPV type was associated with a 279-fold increase
B. Illades-Aguiar et al. / Cancer Detection and Prevention 32 (2009) 300–307 303
Table 1
Cervical cancer: associations with sexual history and reproductive factors.
Variable Cases (n = 133) Controls (n = 256) ORa (95% CI) ORb (95% CI) ORc (95% CI)
n (%) n (%)
Age at first sexual intercourse (years)
>20 17 (12.8) 95 (37.1) 1.0 1.0 1.0
16–20 59 (44.4) 121 (47.3) 2.7 (1.5–5.0) 2.3 (1.2–4.4) 2.6 (1.2–6.0)
<16 52 (39.1) 34 (13.3) 8.5 (4.4–16.8) 8.8 (4.1–18.8) 9.6 (3.5–26.5)
Did not answer 5 (3.75) 6 (2.3)
Parity
None 2 (1.5) 33 (12.9) 1.0 1.0 1.0
1–2 15 (11.3) 51 (19.9) 4.9 (1.0–22.6) 3.8 (0.8–19.0) 2.4 (0.4–14)
3 and more 114 (85.7) 172 (67.2) 10.9 (2.6–46.5) 12.5 (2.8–56.7) 16 (3.0–84)
Did not answer 2 (1.5) 0
Sexual partners
1 69 (51.9) 48 (18.8) 1.0 1.0 1.0
2–3 30 (22.5) 38 (14.8) 0.5 (0.3–1.0) 0.6 (0.3–1.0) 0.3 (0.1–1.0)
4 and more 5 (3.8) 4 (1.6) 0.9 (0.2–3.4) 0.9 (0.2–3.6) 1.0 (0.1–8.4)
Did not answer 29 (21.8) 166 (64.8)
Age at menarche (years)
14 and more 64 (48.1) 128 (50.0) 1.0 1.0 1.0
10–13 60 (45.1) 120 (46.9) 1.0 (0.6–1.5) 1.2 (0.7–1.9) 1.1 (0.6–2.0)
Did not answer 9 (6.8) 8 (3.1)
Age at menopause (years)
50 or more 16 (12.0) 51 (19.9) 1.0 1.0 1.0
45–49 25 (18.8) 53 (20.7) 1.5 (0.7–3.1) 1.5 (0.6–3.6) 2.0 (0.6–6.5)
<45 20 (15.0) 26 (10.2) 2.5 (1.1–5.5) 1.3 (0.5–3.5) 1.2 (0.3–4.6)
No menopause 36 (27.1) 111 (43.4) 1.0 (0.5–2.0) 0.5 (0.2–1.1) 0.6 (0.2–1.7)
Did not remember 36 (27.1) 15 (5.9)
Smoking
No 81 (60.9) 94 (36.7) 1.0 1.0
Yes 7 (5.3) 13 (5.1) 0.6 (0.2–1.6) 0.6 (0.2–1.6) 0.7 (0.2–2.9)
Did not answer 45 (33.8) 149(58.2)
OR = odds ratio; CI = confidence interval.a Odd ratio non-adjusted.b OR adjusted by sexual partners, age at menarche, smoking (except for the evaluated factor).c OR adjusted by factors of model c and HPV type by oncongenic risk (HPV negative, low-risk HPV, high-risk HPV and undetermined risk HPV).
in the risk of cervical cancer. Surprisingly, undetermined
risk HPV were associated with cervical cancer (OR = 434.3,
95% CI, 22.1–+1).
Analysis of the risk of developing cervical cancer with
HPV 16, HPV 18 and related types showed that the highest
risks were associated with HPV 18 (OR= 804.4, 95% CI,
71.1–+1) and HPV 16 (OR = 573.5, 95% CI, 74.4–+1).
The relative risk in women infected with HPV 18 related
types (OR = 312.2, 95% CI, 27.5–+1) was higher than that
among those infected with HPV 16 related types (OR = 86.1,
95% CI, 10.9–+1).
4. Discussion
This study provides information on the risk factors for
cervical cancer and the infection of HPV in the State of
Guerrero, Mexico. In this study, the presence of HPV DNA
was confirmed in 100% of cervical cancer cases (SCC and
ADC/ADSC) and in 35.5% of control women.
4.1. HPV genotype distribution
HR-HPVs were present in 94.7% of the cervical cancer
cases, similar to that found in other worldwide studies [7]
and in Mexico as well [17]. HPV 16 is by far the most
common HPV type identified in cervical carcinoma. The
HPV types identified in SCC, in order of decreasing
prevalence, were HPV 16, 18, 31, 45, 58, 69, 52 and 6, 11,
33, 56, 67; in ADC/ADSC they were HPV 16 and 18, 31, 69.
There was variation in HPV-specific prevalence between
different histological cancer types, HPV 16 was found more
often in ADC/ADSC (78.7%) than in SCC (65.5%); similar
to that found in North Africa and South America where HPV
16 was found in 72% of the ADC cases [29]; however,
worldwide HPV 16 was identified in 55.2% of SCC and in
31.3% of ADC [30], and in a study from Mexico City it was
found in 45.1% of the cervical cancer cases [17]. We found
that in Southern Mexico, HPV 18 was more frequent in SCC
(9.3%) than in ADC/ADSC (7.1%), which disagrees with
other studies in which it is found that throughout the world it
is present in 12.3% of SCC [30] and 37.7–39% in ADC/
B. Illades-Aguiar et al. / Cancer Detection and Prevention 32 (2009) 300–307304
Table 2
Distribution of HPV types in cases of cervical cancer and control women with normal cervical cytology.
HPV typesa Cervical cancer Controls
Squamous cell
carcinoma
Adeno/
adenosquamous
carcinoma
Total cases
n (%) n (%) n (%) n (%)
Total 119 (100) 14 (100) 133 (100) 256 (100)
Negative 0 (0) 0 (0) 0 (0) 165 (64.5
Positive 119 (100) 14 (100) 133 (100) 91 (35.5
HR-HPV 113 (95.0) 13 (92.9) 126 (94.7) 76 (29.6)
16 78 (65.5) 11 (78.7) 89 (66.8) 29 (11.3
18 11 (9.3) 1 (7.1) 12 (9.0) 3 (1.1)
31 9 (7.6) 1 (7.1) 10 (7.5) 3 (1.1)
33 1 (0.8) 0 (0) 1 (0.8) 35 (13.7
45 6 (5.1) 0 (0) 6 (4.5) 1 (0.4)
52 2 (1.7) 0 (0) 2 (1.6) 0 (0)
56 1 (0.8) 0 (0) 1 (0.8) 0 (0)
58 5 (4.2) 0 (0) 5 (3.7) 4 (1.6)
59 0 (0) 0 (0) 0 (0) 1 (0.4)
Probable HR-PV 0 (0) 0 (0) 0 (0) 3 (1.2)
53 0 (0) 0 (0) 0 (0) 3 (1.2)
LR-HPV 2 (1.6) 0 (0) 2 (1.6) 11 (4.3)
6 1 (0.8) 0 (0) 1 (0.8) 3 (1.1)
11 1 (0.8) 0 (0) 1 (0.8) 1 (0.4)
61 0 (0) 0 (0) 0 (0) 4 (1.6)
70 0 (0) 0 (0) 0 (0) 2 (0.8)
81 0 (0) 0 (0) 0 (0) 1 (0.4)
Undetermined risk-HPV 4 (3.4) 1 (7.1) 5 (3.8) 1 (0.4)
67 1 (0.8) 0 (0) 1 (0.8) 0 (0)
69 3 (2.6) 1 (7.1) 4 (3.0) 0 (0)
71 0 (0) 0 (0) 0 (0) 1 (0.4)
HPV, human papillomavirus; HR-HPV, high-risk human papillomavirus; LR-HPV, low-risk human papillomavirus.a Munoz et al. HPV classification [10].
Table 3
HPV infection and its association with cervical cancer.
HPV infection Cases (n = 133) Controls (n = 256) ORd (95% CI) ORe (95% CI)
HPV(1)
Negative 0 165 1.0* 1.0*
Positive (any type) 133 91 241.2 (33.2–+1) 279 (37.6–+1)
HPV types
LR-HPV(2) 2 11 30 (2.5–+1) 34.9 (2.8–+1)
HR-HPV(2) 126 76 273.6 (37.5–+1) 321 (43.1–+1)
Undetermined risk HPVa(2) 5 1 825 (44.9–+1) 434.3 (22.1–+1HPV 16(3) 89 29 506.4 (67.8–+1) 573.5(74.4–+1)
HPV 16 related typesb(3) 19 42 74.6 (9.7–+1) 86.1 (10.9–+1)
HPV 16 and related types(4) 108 71 251 (34.4–+1) 293.7 (39.3–+1HPV 18(3) 12 3 660 (63.7–+1) 804.4 (71.1–+1HPV 18 related typesc(3) 6 4 247.5 (23.9–+1) 312.2 (27.5–+1HPV 18 and related types(4) 18 7 424.3 (49.4–+1) 522.3 (57.5–+1HPV 16 or HPV 18(5) 101 32 520.8 (70.1–+1) 597.2 (78–+1)
HPV, human papillomavirus; OR, odds ratio; CI, confidence interval. (1)–(5)Models; *reference category for all models.a Undetermined risk HPV: 67, 69, 71 [10,24].b HPV 16 related types: 31, 33, 52, 58, 67 [10,24].c HPV 18 related types: 39, 45, 59, 70, 85 [10,24].d Odd ratio non-adjusted.e Odds ratio adjusted for age at first sexual intercourse and parity.
)
)
)
)
)
)
)
)
)

B. Illades-Aguiar et al. / Cancer Detection and Prevention 32 (2009) 300–307 305
ADSC [29,30]; however, in North Africa the frequency of
HPV 18 in ADC/ADSC is 13.6% and in South America
19.6% [29]. The fraction of SCC attributable to HPV 16 and
18 was 74.8% while that for ADC/ADSC was 85.8%, almost
the same as reported worldwide [10]. In this study LR-HPV
were absent in ADC and were only found in SCC and control
women.
4.2. HPV and cervical cancer
The presence of HPV was associated with SCC and with
ADC/ADSC, as reported in many studies worldwide
[10,29,30]. Three-fourths of invasive cervical cancers in
this study were associated with HPV 16 and HPV 18.
However, ten more types were also associated with invasive
cervical cancer. The most frequent HPV species associated
with cervical cancer was a-9 HPV followed by a-7 HPV.
Odd ratios linked to HPV types demonstrated very strong
associations (OR > 100) for total HR-HPV, HPV 16, HPV
18, and HPV 18 related types, and strong associations
(OR > 18) for HPV 16 related types like in other worldwide
studies [10]. It is interesting to address that undetermined
risk HPV (HPV 67 and HPV 69) [10] were very strongly
associated with cervical carcinoma, so these findings could
contribute to determining the association of these HPV types
in the development of cervical carcinoma.
It is important to take into account that HPV status in the
control group is variable because transient infections could
not be differentiated from persistent infections, which could
influence in the estimation of the risk in the cases in which
infection is persistent. Epidemiologically, a basal risk is
present in both cases and controls, assuming that an effect of
the transitory infections could be present in the calculation
of the ORs. However, it would be difficult to evaluate in this
type of studies. Because this is not a follow up study, the
change in infection status throughout time cannot be
evaluated. In cases and control studies, a single measure
is done that allows us to know the current HPV infection
status, without letting us know if the infection is transitory of
persistent.
The geographic distribution and prevalence of HPV types
in cervical cancer varies worldwide. In this study we found
12 types of HPV including types 67 and 69, different from
that reported by Munoz et al. [31], who found 26 types in a
multicentric worldwide study in which types 67 and 69 are
not reported. The prevalence we found for HPV types 16, 45,
52 and 6 is similar to that found in Northern Africa and the
prevalence for types 18, 31, 58, 56 and 11 is similar to that in
Central/South America. Knowledge of geographic distribu-
tion of HPV types in cervical cancer has implications for
cervical cancer prevention and screening regarding the
composition of prophylactic vaccines and screening cock-
tails. At present, two HPV vaccines are available, a bivalent
vaccine (Cervarix) against HPV 16 and 18, and a tetravalent
vaccine against HPV 6, 11, 16, and 18 (Gardasil). In the
south of Mexico, the bivalent vaccine in theory could
prevent 75.8% of cervical cancer cases; the tetravalent
vaccine could prevent 77.4% of cases, leaving 22.6%
unprotected. On the other hand, an effective vaccine against
the 5 most common HPV types (16, 18, 31, 45 and 58) could
prevent 91.5% of the cases of cervical cancer.
The prevalence of infection by HPV in population-based
studies carried out in different regions of the world is
variable; in Sub-Saharian Africa it is 25.6%, in Asia 8.7%, in
South America 14.3%, and in Europe 5.2% [32]. The use of
hospital controls, like in our study, has advantages such as
high participation and disadvantages like potential for
selection bias. This partially explains the high frequency of
HPV in the controls (35.5%). The most common HPV type
in controls was HPV 33, followed by HPV 16, 58, 61, 6, 18,
31, 53, 70, 11, 45, 59, 71, and 81. It is important to mention
that HR-HPVs are present in 29.6% of the controls while
LR-HPVs are only present in 4.3%.
In comparison to the south of Mexico, worldwide
distribution of HPV types in cytologically normal women
reported by the International Agency for Research on
Cancer HPV in 2005 [32] showed that HPV 16 was the most
common HPV type, followed by HPV 42, 58, 31, 18, 56, 81,
35, 33 and 45. Our population is different from others
regarding predominance of HPV 33 in women with normal
cytology, which is higher than that of HPV 16. Type-specific
PCR for HPV 33 carried out in 11% of the samples of normal
cervical cytology with HPV 33 and in the only cervical
cancer sample with the this viral type, that were previously
typed by MY-RFLPs, confirmed that our findings were real.
In Mexican women with normal cytology, Torroella-Kouri
et al. [13] did not find HPV 33 in Mexico City and Lazcano-
Ponce et al. [4] found it in 1% in the State of Morelos. The
heterogeneity of the HPV genotypes distribution in Mexico
is evident in the study by Gonzalez-Losa et al. [33] in which
they found that in women from the State of Yucatan, HPV 58
was the most frequent type found in LSIL and HSIL, and in
cervical cancer cases its frequency was the same as HPV 16
(see: Supplementary Data).
In this study multiple infections were not found in cases
or controls. This could be due to the methods employed for
typing (RFLPs or sequencing) which are not suitable for the
detection of infections with multiple HPV types; these are
less sensitive than hybridization methods and, in case of
being positive, these will usually give an uninterpretable
mix-up of digestion/sequence patterns [34]. On the other
hand, in studies carried out in Mexican women, the presence
of multiple infections in women with normal cervical
cytology is low (0–2.4%) [4,13,35], although in women with
cervical cancer the prevalence is greater [13,33].
A total of 18 HPV types were detected in this study, 12
HPV types in cervical cancer and 14 HPV types in normal
cervical cytology. From those, 9 were HR-HPV, 1 probable
HR-HPV, 5 LR-HPV, and 3 undetermined risk-HPV. The
presence of these HPV types was detected using MY09/11
and GP5+/6+ PCR systems. Combination of two PCR
detection systems increased HPV DNA detection in cervical
B. Illades-Aguiar et al. / Cancer Detection and Prevention 32 (2009) 300–307306
cancer from 97.8% using MY09/11 PCR system to 100% by
analyzing MY-PCR negative samples with GP5+/6+ PCR
system. We found a higher prevalence than the worldwide
prevalence found in other studies (83–89% [30], >95% [31]
and 99.7% [7]), which reflects significant differences in
HPV DNA detection.
Our findings indicate that the commercially available
Hybrid Capture II (Digene) assay that detects 13 HR-HPVand
5 LR-HPV [36], would not detect genotypes 67 and 69 that
were found in 3.8% of cervical cancer cases in this study. It
would also not detect genotypes 53, 61, 70, 71 and 81 which
were found in 4.4% of the controls. It would be important that
the composition of screening ‘‘cocktails’’ for HR-HPV and
LR-HPV types be revised as proposed by other studies [37].
4.3. Cofactors for cervical cancer
Because infection by HR-HPV is a necessary, but not a
sufficient, cause for cervical cancer [7], it has been assumed
that other factors contribute to modulate the risk of transition
from cervical HPV infection to cervical cancer. Even though
there are many studies performed worldwide that analyze
these factors, in Mexico very few exist. In 1995, Lazcano-
Ponce et al. [16] found that the main risk factors for cervical
cancer in women from Mexico City (Central region) are
multiparity and a history of many sexual partners. The risk
factors found by Castaneda-Iniguez et al. [15] in 1998 in
women from the State of Zacatecas (Central-Northern
Mexico) are multiparity, early start of sexual activity and the
use of oral contraceptives. In 2005, Tirado-Gomez et al. [17]
found as risk factors in women from the Central region
(Mexico City and Veracruz) and Southern region (Morelos)
of Mexico low education levels, lack of access to health
services, unfavorable socioeconomic condition, multiparity,
presence of vaginal infection, and early start of sexual
activity.
In this study, we found that in the State of Guerrero,
located in the Southern region of Mexico, the risk factors of
invasive cervical cancer are having three or more births and
start of sexual activity before 16 years of age. High parity
may increase the risk of cervical cancer because it maintains
the transformation zone of the exocervix for many years,
facilitating the direct exposure to HPV and possibly other
cofactors. Hormonal changes induced by pregnancy may
also modulate the immune response to HPV and influence
risk of persistence or progression. It has also been proposed
that the developing cervix, around peri-menarchy, or the
healing cervix are high-risk situations for an HPV infection
to reach the basal layer and establish a persistent infection
[38]. Age, smoking habits, and number of sexual partners
were not risk factors in the development of cervical cancer,
as reported in other World populations. In the State of
Guerrero, polygamy is not a frequent practice among
women, in this study 60% of the women said that they were
monogamous and in a study that we carried out in Nahuatl
indigenous women in the year 2000 over 90% reported they
were monogamous (unpublished data). However, polygamy
is a common practice among men from the State of
Guerrero. A study shows that 98% of men have had more
than one sexual partner, of which 60% is infected with HPV
[39]. So, even though the number of the sexual partners the
women had is not a risk factor in the development of cervical
cancer in this study, the high promiscuity of the men could
explain the high frequency of infection by HPV and shows
why the sexual behavior of the men is an important factor in
the development of cervical cancer.
Acknowledgments
We thank all of the Instituto Estatal de Cancerologıa
‘‘Dr. Arturo Beltran Ortega’’ and Secretarıa de Salud
personnel who helped with this study at the clinic sites. We
thank Vıctor Hugo Garzon for management of the patients
and specimen collection, and Marco Antonio Jimenez for
histological evaluation of all biopsy material. We also
thank technicians of Laboratorio de Biomedicina Molecular
for their excellent laboratory assistance. And we would also
like to thank Dinorah Leyva-Illades (Texas A&M Health
Science Center) for revising the English style of the
manuscript.
Appendix A. Supplementary data
Supplementary data associated with this article can be
found, in the online version, at doi:10.1016/j.cdp.2008.
09.001.
References
[1] Ferlay J, Bray F, Pisani P, Parkin DM. Globocan 2002 cancer
incidence. Mortality and prevalence worldwide. IARC CancerBase
No. 5 version 2.0. Lyon: IARC Press; 2004.
[2] Lazcano-Ponce EC, Najera-Aguilar P, Buiatti E, Alonso de Ruiz P,
Kuri P, Cantoral L, et al. The cervical cancer screening program in
Mexico: problems with access and coverage. Cancer Causes Control
1997; 8:698–704.
[3] Arrossi S, Sankaranarayanan R, Parkin DM. Incidence and mortality
of cervical cancer in Latin America. Salud Publica Mex 2003;
45:S306–14.
[4] Lazcano-Ponce E, Herrero R, Munoz N, Cruz A, Shah KV, Alonso P,
et al. Epidemiology of HPV infection among Mexican women with
normal cervical cytology. Int J Cancer 2001; 91:412–20.
[5] Palacio-Mejıa LS, Rangel-Gomez G, Hernandez-Avila M, Lazcano-
Ponce E. Cervical cancer, a disease of poverty: mortality differences
between urban and rural areas in Mexico. Salud Publica Mex 2003;
45:S315–25.
[6] Secretarıa de Salud. Direccion General de Informacion en Salud.
Mexico, 2006. Available from URL: http://sinais.salud.gob.mx/ [Last
accessed: 2007 May 8].
[7] Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA,
Shah KV, et al. Human papillomavirus is a necessary cause of invasive
cervical cancer worldwide. J Pathol 1999; 189:12–9.
B. Illades-Aguiar et al. / Cancer Detection and Prevention 32 (2009) 300–307 307
[8] de Villiers EM, Fauquet C, Broker TR, Bernard HU, zur Hausen H.
Classification of papillomaviruses. Virology 2004; 324:17–27.
[9] Cogliano V, et al. Carcinogenicity of human papillomavirus. Lancet
Oncol 2005; 6:204.
[10] Munoz N, Castellsague X, Berrington de Gonzalez A, Gissmann L.
HPV in the etiology of human cancer. Vaccine 2006; 24S3. S3/1–10.
[11] Calleja-Macıas IE, Kalantari M, Allan B, Williamson AL, Chung LP,
Collins RJ, et al. Papillomavirus subtypes are natural and old taxa:
phylogeny of human papillomavirus types 44 and 55 and 68a and–b. J
Virol 2005; 79:6565–9.
[12] Bosch FX, Manos MM, Munoz N, Sherman M, Jansen AM, Peto J,
et al. Prevalence of human papillomavirus in cervical cancer: a
worldwide perspective. International biological study on cervical
cancer (IBSCC) Study Group. J Natl Cancer Inst 1995; 87:796–802.
[13] Torroella-Kouri M, Morsberger S, Carrillo A, Mohar A, Meneses A,
Ibarra M, et al. HPV prevalence among Mexican women with neo-
plastic and normal cervixes. Gynecol Oncol 1998; 70:115–20.
[14] Hernandez-Hernandez DM, Garcıa-Carranca A, Guido-Jimenez MC,
Gonzalez-Sanchez JL, Cruz-Talonia F, Apresa-Garcıa T, et al. High-risk
human papillomavirus and cervical intraepithelial neoplasia in women
at 2 hospitals in Mexico City. Rev Invest Clin 2002; 54:299–306.
[15] Castaneda-Iniguez MS, Toledo-Cisneros R, Aguilera-Delgadillo M.
Risk factors for cervico-uterine cancer in women in Zacatecas. Salud
Publica Mex 1998; 40:330–8.
[16] Lazcano-Ponce EC, Hernandez-Avila M, Lopez-Carrillo L, Alonso de
Ruiz P, Torres-Lobaton A, Gonzalez-Lira G, et al. Reproductive risk
factors and sexual history associated with cervical cancer in Mexico.
Rev Invest Clin 1995; 47:377–85.
[17] Tirado-Gomez LL, Mohar-Betancourt A, Lopez-Cervantes M, Garcıa-
Carranca A, Franco-Marina F, Borges G. Risk factors in invasive
cervical cancer among Mexican women. Salud Publica Mex 2005;
47:342–50.
[18] FIGO Committee on Gynecologic Oncology. Staging classifications
and clinical practice guidelines of gynaecologic cancers. Int J Gynecol
Obst 2000; 70:207–312.
[19] Solomon D, Davey D, Kurman R, Moriarty A, O’Connor D, Prey M,
et al. The 2001 Bethesda System: terminology for reporting results of
cervical cytology. JAMA 2002; 287:2114–9.
[20] Leornard D, Michael K, James B. Basic methods in molecular biology,
2nd ed., Connecticut: Appleton & Lange, 1994.
[21] Bauer HM, Greer CE, Manos MM. Determination of genital human
papillomavirus infection by consensus PCR amplification. In: Her-
rington CS, McGee JO, eds. Diagnostic molecular pathology: a
practical approach. Oxford: Oxford University Press, 1992: 131–52.
[22] Bauer HM, Manos MM. PCR detection of genital human
papillomavirus. In: Persing DH, Smith TF, Tenover FC, White TJ,
eds. Diagnostic molecular microbiology, principles and applications.
Washington: American Society for Microbiology, 1993: 407–13.
[23] Vossler JL, Forbes BA, Adelson MD. Evaluation of the polymerase
chain reaction for the detection of human papillomavirus from urine. J
Med Virol 1995; 45:354–60.
[24] Bernard HU, Chan SY, Manos MM, Ong CK, Villa LL, Delius H, et al.
Identification and assessment of known and novel human papilloma-
virus by polymerase chain reaction amplification, restriction fragment
length polymorphisms, nucleotide sequence, and phylogenetic algo-
rithms. J Infect Dis 1994; 170:1077–85.
[25] Casas L, Galvan SC, Ordonez RM, Lopez N, Guido M, Berumen J.
Asian-American variants of human papillomavirus type 16 have
extensive mutations in the E2 gene and are highly amplified in cervical
carcinomas. Int J Cancer 1999; 83:449–55.
[26] Xin CY, Matsumoto K, Yoshikawa H, Yasugi T, Onda T, Nakagawa S,
et al. Analysis of E6 variants of human papillomavirus type 33, 52 and
58 in Japanese women with cervical intraepithelial neoplasia/cervical
cancer in relation to their oncogenic potential. Cancer Lett 2001;
170:19–24.
[27] de Roda Husman AM, Walboomers JM, van den Brule AJ, Meijer CJ,
Snijders PJ. The use of general primers GP5 and GP6 elongated at their
30 ends with adjacent highly conserved sequences improves human
papillomavirus detection by PCR. J Gen Virol 1995; 76:412–7.
[28] National Center for Biotechnology Information. U.S. National Library
of Medicine. Bethesda, MD. Available from URL: http://
www.ncbi.nlm.nih.gov/BLAST/ [Last accessed: 2007 May 8].
[29] Castellsague X, Dıaz M, Sanjose S, Munoz N, Herrero R, Franceschi
S, et al. Worldwide human papillomavirus etiology of cervical ade-
nocarcinoma and its cofactors: implications for screening and pre-
vention. J Natl Cancer Inst 2006; 98:303–15.
[30] Clifford GM, Smith JS, Plummer M, Munoz N, Franceschi S. Human
papillomavirus types in invasive cervical cancer worldwide: a meta-
analysis. Br J Cancer 2003; 88:63–73.
[31] Munoz N, Bosch FX, Castellsague X, Dıaz M, Sanjose S, Hammouda
D, et al. Against which human papillomavirus types shall we vaccinate
and screen? The international perspective. Int J Cancer 2004;
111:278–85.
[32] Clifford GM, Gallus S, Herrero R, Munoz N, Snijders PJF, Vaccarella
S, et al. Worldwide distribution of human papillomavirus types in
cytologically normal women in the International Agency for Research
on Cancer HPV prevalence surveys: a pooled analysis. Lancet 2005;
366:991–8.
[33] Gonzalez-Losa MR, Rosado-Lopez I, Valdez-Gonzalez N, Puerto-
Solis M. High prevalence of human papillomavirus type 58 in Mexican
colposcopy patients. J Clin Virol 2004; 29:202–5.
[34] Brink A, Snijders P, Meijer C. HPV detection methods. Dis Markers
2007; 23:273–81.
[35] Giuliano A, Papenfuss M, Brown de Galaz EM, Feng J, Abrahamsen
M, Denman C, et al. Risk factors for squamous intraepithelial lesions
(SIL) of the cervix among women residing at the US–Mexico border.
Int J Cancer 2004; 109:112–8.
[36] Poljak M, Fujs K, Seme K, Kocjan BJ, Vrtacnik-Bokal E. Retro-
spective and prospective evaluation of the amplicor HPV test for
detection of 13 high-risk human papillomavirus genotypes on 862
clinical samples. Acta Dermatoven APA 2005; 14:147–52.
[37] Munoz N, Bosch FX, de Sanjose S, Herrero R, Castellsague X, Shah
KV, et al. Epidemiologic classification of human papillomavirus
types associated with cervical cancer. N Engl J Med 2003; 348:
518–27.
[38] Castellsague X, Bosch X, Munoz N. Environmental co-factors in HPV
carcinogenesis. Virus Res 2002; 89:191–9.
[39] Illades-Aguiar B, Ortiz-Ortiz J, Cornejo-Ortega H, Zamudio-Lopez
N, Leyva-Vazquez MA, Barrientos-Garzon VH. Human papilloma-
virus infection in male from Southern of Mexico. In: 21st
International Conference Papillomavirus and Clinical Workshop.
2004. 205.