cd5 as a target for immune-based therapies
TRANSCRIPT
85
Critical Reviews™ in Immunology, 35(2): 85-115 (2015)
1040-8401/15/$35.00 © 2015 by Begell House, Inc.
CD5 as a Target for Immune-Based TherapiesMarta Consuegra-Fernández,a Fernando Aranda,a Inês Simões,a Marc Orta,a Adelaida Sarukhan,b & Francisco Lozanoa,c,d,*a Group of Immune Receptors of the Innate and Adaptive System, Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain; bInstitut National de la Santé et de la Recherche Médicale (INSERM), Paris, France; cDepartament de Biologia Cellular, Immunologia i Neurociències, Facultat de Medicina, Universitat de Barcelona, Barcelona, Spain; dServei d’Immunologia, Hospital Clínic de Barcelona, Barcelona, Spain
*Address correspondence to: Francisco Lozano, MD, PhD, Centre Esther Koplowitz, Roselló 149-153, 08036 Barcelona, Spain; Tel.: +34 932 275 400 ext. 4217; [email protected]
ABSTRACT: CD5 was one of the first surface receptors described for mouse and human T lymphocytes. Since then, it has been found to be highly expressed by regulatory T cells and a subpopulation of regulatory B cells, to be physically associated with the T- and B-cell antigen receptors, to negatively modulate TCR- and BCR-mediated signals, and to bind certain pathogen-associated molecular patterns. These findings position CD5 as an attractive target for developing immunotherapies aimed at either boosting or dampening ongoing immune responses. Here the available data on the function of CD5 and its involvement in the regulation of immune responses in health and disease are reviewed, as well as the evidence for and future challenges in developing therapeutic strategies aimed at targeting CD5 for autoimmune diseases, cancer, and infections.
KEY WORDS: scavenger receptor, CD5, autoimmunity, cancer, infection, immunotherapy
ABBREVIATIONS: AICD: activation-induced cell death; BCR: B-cell receptor; Breg: regulatory/supressor B cell; B-1a: CD5+ B-cell subset; DC: dendritic cell; EAE: experimental autoimmune encephalomyelitis; EAN: experimental autoimmune/allergic neuritis; GvHD: graft-versus-host disease; HCV: hepatitis C virus; Ig: immunoglobulin; IgAN: human IgA nephropathy; IL: in-terleukin; mAb: monoclonal antibody; MS: multiple sclerosis; RA: rheumatoid arthritis; RTA: ricin toxin A chain; sCD5: soluble CD5; SLE: systemic lupus erythematosus; SRCR: scavenger receptor cysteine-rich; TCR: T-cell receptor; TLR: Toll-like recep-tor; Treg: regulatory T cell; UC: ulcerative colitis
I. INTRODUCTION
The mouse and human CD5 glycoprotein was one of the first lymphocyte surface receptors reported, thanks to the technology of monoclonal antibodies (mAbs),1–3 and its official name was assigned during the first International Workshop and Conference on Human Leukocyte Differentiation Antigens (HLDA) held in Paris in 1982. However, CD5 was discovered much earlier (late 1960s) with the descrip-tion of the so-called mouse cell membrane allogenic determinants (CMADs) (Thy-1, Lyt-1, Lyt-2, Lyt-3, Lyt-4, Lyt-5, Lyt-6, etc.), which were used to distin-guish different functional subpopulations of T and B lymphocytes.4 In that context, the mouse Lyt-1 alloantigen (also known as Ly-A or Ly-1 and later known as CD5) emerged as one of the first clearly defined lymphocyte-specific antigenic systems.5 This
was achieved because of the generation of mouse alloantisera against irradiated murine leukemic T cells.6 The characterization of these alloantisera allowed the initial identification of CD5 expression in T cells from thymus, spleen, and lymph nodes. Later, immunization of mice with lymphocytes from different congenic strains led to the identification of diverse strain-specific polymorphisms of the Lyt-1 molecule (Lyt-1.1 and Lyt-1.2 allotypes).4
The advent of hybridoma technology in the late seventies and early eighties soon rendered the generation of the first rat (e.g., 53-7.3) and mouse (e.g., OKT1) mAbs against mouse and human CD5 molecules.3,7 These reagents led to the discovery that CD5 was not only a pan-T-cell marker but also a molecular signature for a small but functionally relevant subset of B cells (B-1a or CD5+ B cells) involved in the production of natural polyreactive

Critical Reviews™ in Immunology
Consuegra-Fernández et al.86
antibodies (e.g., isoagglutinins). Importantly, recent work demonstrated that this B-cell subset includes regulatory/suppressor B cells (Bregs), which are also known as B10 cells because they are a main source of interleukin (IL)-10. A myriad of early stud-ies with anti-CD5 mAbs came to the misleading conclusion that CD5 was a costimulatory molecule for T-cell activation and proliferation in mouse and human.8–10 This notion was later contradicted by data from CD5-deficient mice,11,12 and today there is broad consensus that CD5 is indeed a negative modulator of the activation signals delivered by the antigen-specific receptor expressed by T and B-1a cells. All of this, together with its physical association with such a relevant receptor, positions CD5 as an attractive target for developing novel immunotherapies aimed at potentiating or inhibit-ing ongoing immune responses. Aside from its role in lymphocyte activation, recent evidence indicates that CD5 may also work as a receptor for microbial surface structures present at least in fungi and viruses, which adds a further level of complexity to CD5’s function. The present report reviews basic informa-tion on CD5 physiology relevant to past, current, and future therapeutic interventions aimed at the immunomodulation of, among others, infectious, autoimmune, and neoplastic disorders.
II. CD5 STRUCTURE, EXPRESSION, AND FUNCTION
A. Structure
The CD5 receptor is a type-I membrane glycoprotein of 67 kDa structurally belonging to the ancient and highly conserved scavenger receptor cysteine-rich (SRCR) superfamily.13,14 This family is composed of more than 30 different membrane-bound and/or soluble receptors having in common the presence of at least one SRCR extracellular domain—a protein module of 90–110 amino acids (aas) homologous to the cysteine-rich C-terminal domain first reported for the macrophage type-I class-A scavenger receptor (SR-AI).15 Although there is no unifying biological function for the members of the SRCR superfam-
ily, some of them have been reported to play a role in homo- or heterotypical protein interactions and pathogen-associated molecular pattern (PAMP) rec-ognition16–22 as well as in the development and modu-lation of innate and adaptive immune responses.23
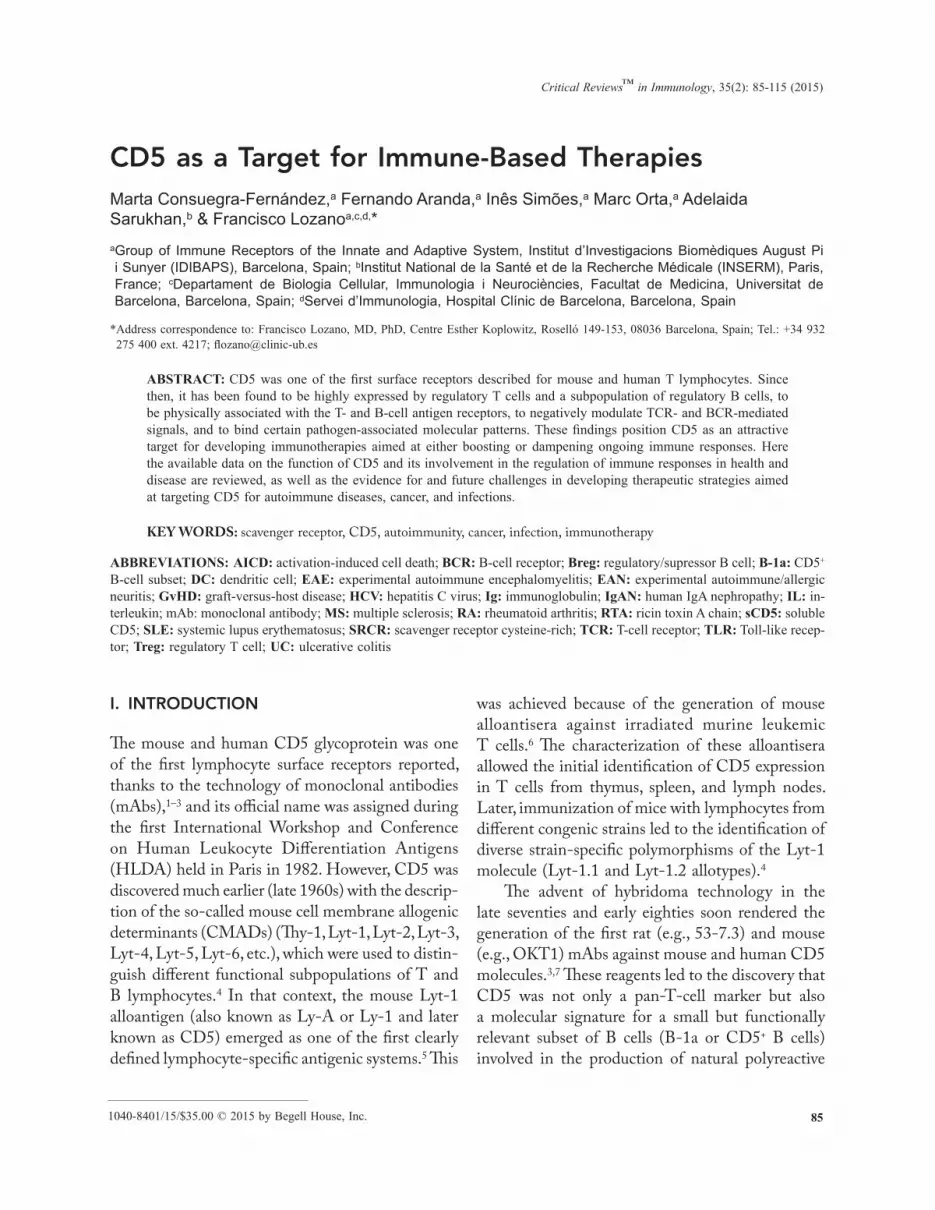
The CD5 gene maps to human chromosome 11 (chromosome 9 in mice) and is telomeric to another highly related SRCR superfamily member, CD6.24,25 CD5 codes for a surface receptor with an extracellular region composed exclusively of three SRCR domains in tandem (D1, D2, and D3), a transmembrane region, and an intracytoplasmatic region adapted to intracel-lular signaling transduction (Fig. 1).13 The N-terminal domains D1 and D2 are heavily N-glycosilated and spaced by a Pro-Ser-Thr–rich polypeptide with O-linked glycosylations (D3 is not glycosylated at all). Although not all of the extracellular region has been crystallized, three-dimensional structural information is already available on the D1 and D3 domains,26,27 showing no large discrepancies with other SRCR domains.28 The 94-aa-long intracytoplasmic region lacks intrinsic catalytic activity, but includes several 11 Ser, 4 Thr, and 4 Tyr residues suitable for phos-phorylation by protein Ser/Thr kinases [protein kinase C, Ca2+/calmodulin-dependent kinase II, and casein kinase 2 (CK2)]29–31 and protein Tyr kinases (Lck, Fyn).29,32 These residues are also suitable for further generation of downstream signaling events, including activation of phosphatidylcholine-specific phospholipase C,33 acidic sphingomyelinase, protein kinase C-ζ, mitogen-activated protein kinase kinase, and c-Jun NH2-terminal kinase.34
Interestingly, the cytoplasmic tail of CD5 pres-ents a pseudo-ITAM (immunoreceptor tyrosine–based activation motif ) that serves as a docking site for signaling mediators such as Lck, Fyn, Ras GTPase-activating protein (Ras-GAP), and c-Cbl29; it also presents a membrane-proximal pseudo-ITIM (immunoreceptor tyrosine–based inhibitory motif ) that interacts with SHP-1 (Src homology region 2 domain-containing phosphatase-1).35 Both of these motifs have been linked to the activating or inhibi-tory signaling properties attributed to CD5.36 Also, Y429 from the ITAM-like motif has been reported to be critical for binding the m2 subunit of the AP2 adaptor complex to CD5 and for the internaliza-

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 87
tion of the latter via clathrin-coated pits following monovalent or bivalent ligation.37
In addition to membrane-bound CD5, a circulat-ing soluble form (sCD5) is detected at a picomolar range in sera from healthy individuals as the result of proteolytic cleavage following lymphocyte activation.38 Furthermore, patients with lymphocyte hyperactivation
diseases, such as Sjögren’s syndrome, have increased levels of sCD5 in serum.39 The function of this soluble form is still unknown, but one hypothesis is that it may compete with membrane-bound CD5 for interaction with its ligand(s) and thus interfere with homeostatic lymphocyte responses. Recent data from transgenic mice expressing human sCD5 bear this out.40
FIG. 1: Schematic of the extracellular and intracellular interactions mediated by CD5. AP2: adaptor protein com-plex 2; BCR: B cell receptor; CaMK-IV: calcium/calmodulin-dependent protein kinase IV; c-Cbl: casitas b-lineage lymphoma–related protein; CK2: casein kinase 2; Fyn: proto-oncogene tyrosine-protein kinase Fyn; VHFR: framework region of immunoglobulin heavy chain variable domain; gp40-80: mouse glycoprotein 40-80 kDa; gp150: human glycoprotein 150 kDa; gp200: bovine glycoprotein 200 kDa; HCV: hepatitis C virus; IgVH: immunoglobulin vari-able heavy region; ITAM-like: immune receptor tyrosine-based activation-like motif; ITIM-like: immune receptor tyrosine-based inhibitory-like motif; Lck: lymphocyte specific tyrosine-protein kinase; PKC/G/A: protein kinase C, G, or A; Ras-GAP: GTP-binding proteins of the Ras superfamily; SHP-1: Src homology region 2 domain–containing phosphatase-1; Syk: spleen tyrosine kinase; TCR: T-cell receptor; ZAP70: zeta-chain-associated protein kinase 70.

Critical Reviews™ in Immunology
Consuegra-Fernández et al.88
B. Expression
CD5 is a highly specific lymphoid marker expressed by all mature T cells (both αβ and γδ) but only a small subset of mature B cells (B-1a cells). In thymocytes, it is expressed from the early stages (double negative, or DN) of thymocyte development in a T-cell recep-tor (TCR-) –regulated manner, and consequently its expression increases during the transition from DN to double positive (DP) and later from DP to single positive (SP).41 Moreover, CD5 expression is directly proportional to the avidity of the TCR–ligand interaction.41,42 In general, the expression levels found in peripheral T cells are higher than in B cells43 and are the highest in CD4+TCRαβ cells, followed by CD8+TCRαβ cells and then CD4–CD8–TCRγδ cells.44 Regarding the last, although most spleen γδT cells are CD5+, gut intraepithelial γδT cells are mostly CD5–.45 Interestingly, CD5 expression is found increased in T- and B-lymphocyte subsets with regulatory functions (both Tregs and Bregs); thus,46,47 CD5 overexpression (CD5hi) can be used as a marker of these cell populations. Similarly, anergic T and B cells resulting from chronic stimulation by endogenous or exogenous antigens are characterized by CD5 overexpression.48,49
B-1a cells (CD5+CD23–IgMhiIgDlow) are related to the production of natural polyreactive autoanti-bodies50 and are expanded in several autoimmune disorders such as rheumatoid arthritis,51 systemic lupus erythematosus,52 insulin-dependent diabetes mellitus),53 Graves’ thyroiditis,54 or Sjögren’s syn-drome,55 and chronic hepatitis C virus infection, as well as in some B-cell lymphoproliferative disorders (B-cell chronic lymphocytic leukemia, Mantle zone lymphoma, and hairy cell leukemia).56,57 CD5 is considered an activation marker for conventional mouse B2 cells (CD5–CD23+IgMlowIgDhi) because its expression can be induced following IgM cross-linking.58 This is not the case for human B cells.59 B-cell receptor (BCR-) –induced up-regulation of CD5 was shown to be dependent on nuclear factor of activated T cell (NFAT) binding to an enhancer located 2 kb upstream of the mouse cd5 gene.60 The transcriptional control of CD5 gene expression is, however, only partially known. It mainly involves
regulatory elements mapping to the 5′-flanking region of exon 1 and binding to, among others, members of the Ets family of transcription factors, which are also relevant for other lymphoid-specific genes (e.g., CD4, TCRα, TCRβ).61
C. Ligands
The ultimate nature of the endogenous CD5 ligand(s) is still a controversial matter. Several reported CD5 ligands have been questioned because of the inability of other groups to validate them. They include coun-ter-receptors expressed by B cells such as CD72,62 the framework region of IgVH,63 and gp20064; by B and T cells such as gp40-8065,66 and CD5 itself66; and by lymphoid, myelomonocytic, and epithelial cells such as gp150.68 Only some of these interac-tions have been mapped, and they involve the most amino-terminal domains—that is, D1 for CD5, D2 for the framework region of IgVH, and D1-D2 for gp150 (Fig. 1).
Recent evidence shows that exogenous ligands can also interact with the extracellular region of CD5. This is the case for β-D-glucans, a conserved constitutive component of fungal cell walls.21 The affinity of this interaction has been calculated (KD, 3.7 ± 0.2 nM) and is in the same range as that reported for dectin-1, which is the main known receptor of β-D-glucans in mammalian myeloid cells.69 All three CD5 individual extracellular domains can recognize β-D-glucans, and the interaction seems to be specific given that little or no binding to other conserved fungal (mannan) and bacterial (lipopolysaccharide, peptidoglycan) cell wall constituents is observed. Furthermore, exposure of CD5 transfectants to zymosan (a β-D-glucan–rich fungal particle) was shown to induce mitogen-activated protein kinase (MAPK) pathway activation and IL-8 secretion, which is dependent on the integrity of the CD5 cytoplasmic region. Interestingly, CD5-deficient mice are hypersensitive to zymosan-induced septic shock–like syndrome, as deduced from higher clini-cal scores and serum cytokine levels (Fenutria et.al., unpublished observations).
It was recently reported that CD5 is a relevant receptor for hepatitis C virus (HCV) entry into both

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 89
primary and leukemic human T cells.70 This explains the lymphoid reservoir reported for HCV and opens the possibility that CD5 may act as a receptor for other related and unrelated viruses. This is not surpris-ing because viral recognition is a property reported for other related members of the SRCR superfamily such as salivary agglutinin/DMBT1/gp340 [gp120 HIV-1 (human immunodeficiency virus type 1), influenza A virus)] and CD163 [porcine reproductive and respiratory syndrome virus (PRRSV), simian hemorrhagic fever virus (SHFV)].71–74
D. Polymorphism
The existence of a biallelic polymorphism for the extracellular region of CD5 has been reported in some mammalian species,4,75 with most of the nucleotide changes mapping to D1 in mouse.76 A number of nonsynonymous variants can be found for human CD5, with only two of them present at relatively high frequencies in Caucasians: rs2241002, involving a Pro to Leu substitution at position 224 in the extracellular D2 domain; and rs2229177, involving Ala to Val substitution at position 471 just C-terminal to the cytoplasmic ITAM-like motif (Fig. 1).77 Interestingly, the CD5 SNP rs2229177 was identified among the gene signatures for recent positive selection in human populations, particularly East Asians and Native Americans.78 Although the mechanism by which such a substitution would have been favored by selection remains unclear, evidence for its functional relevance comes from observed differences regarding CD5’s signaling capabilities and lymphocyte proliferative responses following zymosan exposure or CD3 cross-linking among Ala- and Val-expressing individuals.77,79
E. Function
1. Regulation of T- and B-Cell Activation
CD5 is physically associated with the antigen-specific receptor of T and B cells (TCR and BCR) and becomes part of the macromolecular complex in the central area of the mature immune synapse of T cells.80–82 This feature positions it as a potential
modulator of lymphocyte activation or cell death signals following antigen-specific binding.
CD5 has long been considered an accessory molecule involved in either positive or negative regulation of lymphocyte activation depending on cell type and maturation stage.36 An early myriad of in vitro studies using anti-CD5 mAbs, either alone or in combination with anti-CD3 or anti-CD28 mAbs, led to the notion that CD5 is a costimula-tory molecule for lymphocyte activation.8–10,83,84 This notion was later challenged by in vivo experiments with CD5-deficient mice that showed that CD5 acts as a negative modulator of activation and differentia-tion signals mediated by antigen-specific receptors in both thymocytes and B-1a cells.11,12 Accordingly, thymocytes from CD5-deficient mice are hyper-responsive to TCR/CD3 cross-linking, showing enhanced proliferative responses, intracellular Ca2+ mobilization, and tyrosine phosphorylation of PLC-γ1, TCRζ, LAT, and Vav.11 In turn, membrane IgM cross-linking of B-1a cells from the same mice also induces increased Ca2+ mobilization, resistance to apoptosis, and enhanced cell proliferation.12
The studies cited suggested that CD5 very likely influences the selection and maturation process of T and B-1a cells. Indeed, studies with TCR-transgenic mice showed that CD5 negatively modulates the development of CD4+ T cells.85 Further work also showed that developmental expression of CD5 paral-lels TCR signal intensity and avidity and that it plays a key role in the fine-tuning of TCR signaling.41,86 Thus, CD5-mediated signal inhibition during thy-mocyte selection increases when the avidity of the positively selecting TCR–ligand interaction (and TCR signal strength) is relatively high. Conversely, the requirement for CD5-mediated signal inhibition decreases when the avidity of the positively selecting TCR–ligand interaction (and TCR signal strength) is relatively low.86
Although CD5 expression correlates with self-reactivity and is highly expressed by regulatory and anergic T cells, two recent studies showed that CD5hi T cells are better positioned to respond to foreign antigens because of their enhanced antipathogen reactivity.87,88 A similar situation applies to B cells, in which membrane CD5 negatively regulates Ig

Critical Reviews™ in Immunology
Consuegra-Fernández et al.90
receptor signaling and inhibits autoimmune B-cell responses.49 Interestingly, a new role for IL-10–pro-ducing CD5+ B cells was recently proposed in which this cell subset inhibits IgE-mediated mast cell activa-tion and anaphylaxis in mice in an IL-10–dependent and cell-to-cell contact manner.89
2. Regulation of Survival
CD5 has been shown to function as a regulator of T- and B-1a-cell survival.90 In T cells, the mecha-nism by which CD5 mediates survival is not fully understood. Nevertheless, the PI3K/Akt and CK2 signaling pathways seem to be involved in CD5-mediated lymphocyte survival by inducing expres-sion of prosurvival molecules (Bcl-2 and Bcl-xl) or by inhibiting proteins associated with apoptotic pathways (caspases and Bid).91–93 In B cells, CD5 protects against apoptosis by stimulating IL-10 production upon BCR stimulation while reduc-ing the BCR-induced Ca2+ mobilization response that would eventually send death signals.94 Thus, membrane-bound CD5 might support survival and eventually maintain homeostasis of B-1a cells that are susceptible to activation-induced cell death (AICD).90
3. Tolerance Induction
CD5 plays a role in the establishment of immuno-logical tolerance.90 First, the CK2-binding region in the intracellular tail of CD5 was shown to be neces-sary for inducing antigen-specific unresponsiveness in a myelin oligodendrocyte glycoprotein (MOG-) –induced experimental allergic encephalomyelitis (EAE) model.95 The researchers proposed that CD5 contributes to tolerance by setting the threshold of T-cell responsiveness. In addition, the absence of CD5 results in increased Treg numbers and sup-pressive activity by mechanisms that remain to be defined.46,96
A recently published report on the role of CD5 in peripheral T-cell homeostasis proposed that CD5 promotes the development of extrathymic Treg cells by blocking mTOR-dependent signals induced by effector-differentiating cytokines to inhibit Treg
induction.97 Accordingly, CD5 would be determinant in T-cell fate by facilitating Treg cell conversion from T cells not only when recognizing high-affinity self-pMHC in the thymus but also when tolerizing antigens presented by DCs in the periphery.97
4. Pathogen Recognition
The fact that CD5 can recognize pathogen-associated structures present in fungi and viruses opens the question of its putative physiological relevance. The expression of pattern recognition receptors by cells outside the innate immune system, such as T and B lymphocytes, is well documented. This is the case with CD6, a closely related member of the SRCR superfamily that recognizes bacterial pathogen–asso-ciated molecular patterns (PAMPs) (LPS, LTA, and PGN).19,22 It is also the case with different Toll-like receptors (TLRs).98,99 Increasing evidence demon-strates that the binding of microbial components to Pattern Recognition Receptors (PRRs) expressed by lymphocytes modulates the latter’s functions.100–104 Although the ultimate consequences of such binding remain unknown, PAMP binding to surface CD5 (or CD6) engages intracellular signaling cascades.21,77 Based on these results, together with the role of CD5 in negative regulation of lymphocyte antigen receptor signaling, it has been hypothesized that sensing of the external milieu for microbial products by scavenger-like lymphocyte receptors (namely CD5) is beneficial because (1) it prevents autoimmune responses triggered by infectious agents (microbial binding to CD5 would provide inhibitory signals to low-affinity T/B-cell clones that could otherwise become autoreactive during infection) and (2) it optimizes antimicrobial immune responses (CD5 inhibitory signals would increase the threshold for activation of microbe-specific lympho-cytes, allowing expansion of high- but not low-affinity T/B clones).105 Another, nonexcluding, hypothesis is that CD5 may be expressed by nonlymphoid cell types and thus exert its pathogen-related effects through activation of innate immune responses. In line with this is the observation of CD5 expression on certain endothelial cells,106 macrophages, and peripheral blood and vaginal dendritic cell (DC) subsets.107–110

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 91
III. INVOLVEMENT OF CD5 IN CLINICAL AND EXPERIMENTAL DISORDERS AND ITS POTENTIAL IMMUNOTHERAPEUTIC USE
In view of the key role played by CD5 in modulat-ing T- and B1-a-cell responses, this report reviews the available information on the involvement of CD5hi cells in different immune disorders as well as the different therapeutic approaches based on CD5 targeting, all of which are summarized in Table 1.
A. Autoimmunity
Autoimmunity is defined as a pathological immune-based disorder caused by the peripheral activation of T and B cells against self-tissue components, in the absence or presence of infection, tissue injury, or other discernible origin. Even though failures in the mechanisms maintaining self-tolerance increase the risk of autoimmune diseases, disease progression is regulated by control mechanisms at so-called immunological tolerance checkpoints.111 In this context, both Treg and Breg subpopulations play an important role in the establishment and maintenance of peripheral tolerance. Intriguingly, both regulatory subpopulations express high levels of CD5.
In fact, early reports in mice showed that CD4+CD5hi cells have a suppressive effect on lym-phocyte activation.112 Later on, these cells were pheno-typically better characterized as CD4+CD25hiFoxP3+ and designated as Tregs.113 It was reported that the absence of Tregs increased autoimmunity whereas their adoptive transfer reversed it.114 In humans, Treg defects contribute to autoimmunity because genetic defects in FoxP3, for instance, can lead to autoimmunity (immunodysregulation polyendocrinopathy enteropa-thy X-linked syndrome, or IPEX).115 However, despite numerous studies there is very little evidence linking defects in Treg or Breg numbers to autoimmune disorders, except for systemic lupus erythematosus, in humans.116 It is thus likely that functional changes rather than alterations in Treg and/or Breg numbers are involved in the breakdown of self-tolerance and the progression to autoimmune disease.
1. Systemic Lupus Erythematosus
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder whose main features are B-cell hyperactivity, spontaneous lymphocyte proliferation, and production of pathogenic antibodies to self-antigens. B-cell abnormalities in SLE also include excess cytokine production, self-antigen presentation to T cells, and modulation of the functions of other immune cells.117 SLE is a very complex disorder that involves genetic and environmental factors, hormones, and immunological mechanisms. The precise origin of the disease is not known, although increased expression of genes regulated by type-I interferon (IFN), termed IFN signature, has been reported in patients with SLE as well as in those with other autoimmune disorders.118
SLE was traditionally treated with immunosup-pressive drugs, such as corticosteroids, mycophenolate, azathioprine, cyclophosphamide, and cyclosporine A, which eventually inhibit T- and B-cell prolifera-tion but cause several adverse side effects.119 More recent strategies focus on selective B-cell depletion, targeting specific B-cell surface receptors and cyto-kines. As an example, rituximab, a cytotoxic anti-CD20 mAb, causes selective short-term depletion of mature B cells and gives encouraging results in murine models, but a review found it to be unsuc-cessful in recent controlled trials.120 Also, the use of ocrelizumab (anti-CD20), epratuzumab (anti-CD22), and certain drugs targeting soluble mediators such as BlyS (B-lymphocyte stimulator) and APRIL (a proliferation-inducing ligand) to inhibit B-cell growth and function has yielded promising results, but needs further long-term clinical studies to discard potential side effects.121–123
Other novel therapies specifically targeting IL-6 and IFN-α are on the horizon, as well as the block-ing of costimulatory interactions between immune cells (CD40–CD40 ligand), interference with cell-signaling pathways, and even the targeting of anti-dsDNA mAbs.124,125
The contribution of CD5+ circulating B cells to autoantibody secretion in SLE has been much discussed and is still an open question, with some studies reporting increased numbers and others

Critical Reviews™ in Immunology
Consuegra-Fernández et al.92
Dis
ease
Trea
tmen
t or
Con
ditio
nC
othe
rapy
Phas
eO
bjec
tive
Succ
ess
/ Sid
e E
ffec
tsR
efer
ence
s
SLE
Zolim
omab
arit
ox (m
ouse
an
ti-C
D5
mA
b-RT
Aa )
No
Pilo
t (hu
man
)D
eple
te C
D5+
cell
subs
etYe
s (tr
ansi
ent)
/ Ye
s (c
ytot
oxic
)13
2,13
3
MS
Ado
ptiv
ely
trans
ferr
ed
CD
5+ CD
19+
B c
ells
Gla
tiram
er
acet
ate
Prec
linic
al
(mou
se)
Dow
n-re
gula
te in
flam
mat
ory
resp
onse
Yes
/ n.a
.b15
3
Imm
une
regu
latio
n15
4C
D5
KO
mic
eM
ouse
sC
D5
prot
ein
No
Prec
linic
al
(mou
se)
Atte
nuat
e si
gnal
s th
roug
h TC
R
and
regu
late
sig
nalin
g th
resh
old
Yes
/ no
155
Reg
ulat
ed s
urvi
val o
f act
ivat
ed
T ce
llsYe
s / n
.a.
CD
5-ΔC
K2
Tgc m
ice
Blo
ck T
cel
l apo
ptos
is a
nd
regu
late
sur
viva
l thr
ough
CK
2N
o / n
.a.
91
Ant
i-rat
OX
19 (m
ouse
) Pr
eclin
ical
(rat
)Ta
rget
CD
5Ye
s (ti
me
depe
nden
t) / n
.a.
156
Hum
an s
CD
5 Tg
mic
ePr
eclin
ical
(m
ouse
)B
lock
ade
bind
ing
of c
ell-
asso
ciat
ed C
D5
to it
s na
tura
l lig
and(
s)
No
/ No
40H
uman
reco
mbi
nant
sC
D5
prot
ein
(i.p.
d )N
o / n
.a.
RA
Zolim
omab
arit
ox (m
ouse
m
Ab-
RTA
)N
oPi
lot (
hum
an)
Inhi
bito
ry e
ffect
Yes
/ n.a
.18
2Im
mun
olog
ic e
ffect
s17
8 M
TXe a
nd/o
r A
ZTf
Phas
e II
Safe
ty a
nd a
ctiv
ityYe
s / N
o18
0
Rat
ant
i-mou
se C
D5
TIB
104
No
Prec
linic
al
(mou
se)
Find
pot
entia
l the
rape
utic
targ
ets
for R
A tr
eatm
ent m
odul
atin
g T-
cell
resp
onsi
vene
ss
Yes
/ n.a
.19
0
IDD
MM
ouse
ant
ihum
an C
D5-
Plus
®N
oPi
lot (
hum
an)
Dep
lete
T c
ells
and
pre
serv
e β-
cell
func
tion
Yes
/ No
193
Mou
se a
ntih
uman
CD
5 m
Ab-
RTA
Prot
ectio
nYe
s /n
.a19
4
a RTA
: ric
in t
oxin
A c
hain
; b n
.a.:
not
avai
lable;
c Tg:
tra
nsge
nic,
d i.p.
: in
trape
riton
eal;
e MT
X:
met
hotre
xate
; f A
ZT:
aza
thio
prin
e; g C
TL:
cyt
otox
ic T
lym
phoc
yte.
TAB
LE
1: S
umm
ary
of e
xper
imen
tal a
nd c
linic
al th
erap
eutic
inte
rven
tions
targ
etin
g C
D5

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 93
Dis
ease
Trea
tmen
t or
Con
ditio
nC
othe
rapy
Phas
eO
bjec
tive
Succ
ess
/ Sid
e E
ffec
tsR
efer
ence
s
Aut
oim
mun
e ne
phro
path
yM
ouse
ant
i-rat
CD
5 O
X19
Ant
i-CD
4,
anti-
CD
8 m
Ab,
or a
lone
Prec
linic
al
(mou
se)
Dep
lete
pan
-T c
ells
Yes
/ n.a
.19
9,20
0,20
2
Hum
an s
CD
5-Fc
No
Blo
ckad
e C
D5–
CD
5 lig
and
inte
ract
ion.
65
IBD
CD
5 K
O m
ice
No
Prec
linic
al
(mou
se)
Enha
nce
supp
ress
ive
activ
ity o
f C
D5–/
– Tre
g ce
llsYe
s / N
o96
Fung
al
infe
ctio
nH
uman
reco
mbi
nant
sC
D5
prot
ein
(i.p.
) N
oPr
eclin
ical
(m
ouse
)B
ind
and
aggr
egat
e fu
ngi
Yes
/ n.a
.21
GvH
DM
ouse
ant
ihum
an T
101
mA
b A
nti-C
D2
(35.
1) p
lus
anti-
CD
3 (U
CH
T-1)
Pilo
t (hu
man
)D
eple
te T
cel
lsYe
s / Y
es
(toxi
city
)23
8–24
2
Ant
ihum
an T
101-
RTA
or
Leu-
1 m
Ab
No
Yes
/ n.a
.24
6–24
9
Xom
aZym
e-H
65 (m
ouse
m
Ab-
RTA
)N
o / Y
es
(toxi
city
)25
0–25
5
Can
cer
Mou
se a
ntih
uman
CD
5 T1
01 m
Ab
No
Phas
e I
(hum
an)
Ant
itum
or c
ytot
oxic
ityYe
s (p
artia
l) /
Yes
275
90Y-
labe
led
mou
se
antih
uman
CD
5 T1
01
mA
b
Phas
e I
(hum
an)
Phar
mac
okin
etic
s an
d bi
odis
tribu
tion
Yes
(par
tial)
/ Ye
s27
6
Rat
non
depl
etin
g an
ti-m
ouse
Ly1
mA
bPr
eclin
ical
(m
ouse
)En
hanc
e im
mun
e re
spon
seYe
s / n
.a.
269
CD
5 K
O m
ice
Enha
nce
antit
umor
CTL
g re
spon
seYe
s (tr
ansi
ent)
/ No
273
Hum
an s
CD
5 Tg
mic
eB
lock
ade
CD
5–C
D5
ligan
d in
tera
ctio
nYe
s / N
o40
Hum
an re
com
bina
nt
sCD
5 pr
otei
n (i.
p.)
a RTA
: ric
in t
oxin
A c
hain
; b n
.a.:
not
avai
lable;
c Tg:
tra
nsge
nic,
d i.p.
: in
trape
riton
eal;
e MT
X:
met
hotre
xate
; f A
ZT:
aza
thio
prin
e; g C
TL:
cyt
otox
ic T
lym
phoc
yte.
TAB
LE
1: C
ontin
ued

Critical Reviews™ in Immunology
Consuegra-Fernández et al.94
not.55,126–128 Some researchers propose that increased levels of CD5+ B cells lead to augmented levels of autoantibodies by undergoing uncontrolled Ig VDJ recombination as a result of their expression of recom-bination activation genes (RAG 1 and 2).129,130 Other researchers support the idea that CD5+ cells exhibit an immunosuppressive function involving IL-21–mediated secretion of Granzyme B.131 Renaudineau and colleagues provided evidence for the pivotal role of CD5 in maintaining anergy in autoreactive B cells.132 The level of CD5 on the B-cell surface is determined by the relative level of two alternative CD5 isoforms: CD5-E1A, which is expressed on the membrane, and CD5-E1B, which is retained in the cytoplasm.133 B cells from SLE patients were shown to have decreased DNA methylation, leading to an increased expression of the truncated CD5-E1B form, which in turn results in reduced levels of membrane CD5.132 Because CD5 negatively regulates BCR-mediated signaling, the researchers proposed that lower levels of membrane CD5 can promote the activation and expansion of autoreac-tive B cells in SLE patients. Moreover, the observed DNA hypomethylation was further enhanced by IL-6, suggesting therapeutic benefits of anti-IL-6 treatment.132 Accordingly, the use of tocilizumab, a blocking anti-IL-6 receptor, was shown to improve abnormal B- and T-cell homeostasis and is being used in preliminary clinical trials.134,135
A few pilot studies in human SLE patients have been conducted using an immunoconjugate composed of a murine anti-CD5 mAb bound to ricin toxin A chain (RTA) (zolimomab aritox) to induce depletion of differenT cell subsets expressing CD5.136,137 This immunoconjugate induced modest T-cell depletion, which persisted for months, and a transient decrease in CD5+ B cells but no persistent depletion of total B-cell numbers. Unfortunately, the drug was not successful because of its powerful cytotoxic effect and multiple adverse reactions.
2. Multiple Sclerosis
Demyelinating diseases are characterized by degen-eration and loss of the myelin with a relative pres-ervation of axons.138 Among the many different
etiologies that can cause axonal demyelination, the focus here is on those resulting from inflamma-tory immune-mediated processes: multiple sclerosis (MS), postinfectious encephalomyelitis, and acute hemorrhagic leukoencephalitis. The relationship of CD5+ B-cell subsets and MS has been extensively investigated. Although their role in mediating MS’s inflammatory and degenerative processes is not well understood, it is broadly considered that CD5+ B cells are important in disease pathogenesis.
Given that autoantibodies appear to be involved in a major subgroup of patients with MS,139–141 stud-ies have addressed the contribution of CD5+ B cells with sometimes contradictory results.142 One study, for example, reported an increased percentage of CD5+ B cells in cerebrospinal fluid and associated it with a higher MS risk.143–145 In fact, another study proposed that a high percentage of CD5+ B cells in blood is predictive of earlier conversion to the dis-ease,146 and some studies have found an association between expression levels of CD5 in B cells and the occurrence and duration of relapsing-remitting MS.147–149 However, yet another study found CD5 expression on B cells to be decreased in patients with secondary progressive MS (a stage following relapsing-remitting MS).150 A later study described increased percentages of CD5– B cells and sug-gested that CD5+ B cells are associated with a lower prevalence of antimyelin antibody production.151 Because of such conflicting results, CD5 expression in B cells is considered a double-edged sword that can either worsen the course of MS or result in its lower prevalence. This “janus” facet to CD5 seems to hold true in animal models of MS as well.152–157
The experimental autoimmune/allergic neuritis (EAN) model has been used as an animal approach to inflammatory peripheral demyelinating neuropathy; the experimental autoimmune encephalomyelitis (EAE) model has been used as the corresponding disease model in the central nervous system. Both are considered CD4+ T-cell–mediated models of MS: CD4+ TH17 are the major effector cells, whereas TH2 and Treg cells have a protective role.91,158–160 Both models have been widely studied in rats and mice to determine the involvement of CD5 in MS pathogenesis. For example, a good amount of evidence points toward a protective

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 95
role for CD5 or CD5+ B cells in EAE—in one study, targeting myelin oligodendrocyte glycoprotein (MOG) at steady-state DC induced overexpression of CD5 on T cells and proliferative unresponsiveness to antigen rechallenge in vivo and in vitro.152
In a series of studies, adoptively transferred CD5+CD19+ B cells protected against EAE, an effect amplified by the addition of glatiramer acetate (a therapeutic treatment for relapsing MS).153 The cell transfer down-regulated inflammation through the increased production of immunoregulatory cytokines and the down-regulation of the CXCR5 chemo-kine receptor. Along the same lines, oral antibiotic treatment of mice at EAE induction resulted in an increased CD5+ B-cell population with regulatory features (e.g., IL-10 secretion) that conferred pro-tection against the disease. Furthermore, transfer of CD5+ B cells from antibiotic-treated mice conferred protection against EAE.154
Given the results just discussed, the outcome of EAE in CD5-deficient mice came as a surprise. Contrary to what was expected, in one study mice lacking CD5 exhibited significantly delayed EAE onset and decreased severity.155 The researchers pro-posed that this was due to the prosurvival activity of CD5 in T cells via engagement of the serine/kinase CK2 that binds to the receptor. Indeed, transgenic mice lacking the site of interaction between intra-cytoplasmic CD5 and CK2 were also resistant to EAE, which was attributed to increased AICD and decreased populations of cells coexpressing IFN-γ and IL-17.91 The same group later showed that the CK2-CD5 pathway is necessary for efficient differ-entiation of naïve CD4+ T cells to TH2 and TH17 and for induction of T cell anergy.95
Few studies have been conducted on the targeting of CD5 to treat EAE. In one, a mouse anti-CD5 mAb (OX19, IgG1) was used to treat rats showing clinical signs of EAN at different dosing schedules.156 The results indicated that OX19 given at the immu-nization time partly prevented clinical signs of EAN; when given shortly before the expected onset of the disease or during its height, however, OX19 drastically exaggerated disease symptoms. These results illustrate that anti-T/B-lymphocyte antibodies (OX19) might exert opposite effects on autoimmune diseases when
given at different phases of disease development, and they are in line with the results of more recent studies using anti-CD20 mAbs to deplete B cells.156 When given at disease initiation, treatment with anti-CD20 mAbs exacerbated EAE reportedly because of a decrease in CD5+IL-10+ Breg cells. In contrast, B-cell depletion during the disease phase suppressed symptoms. This was also seen in other studies using transgenic mice constitutively expressing a sCD5, which likely acted as a decoy receptor to block the interaction of CD5 and its natural ligand(s). EAE severity was enhanced in these mice, and the same effect was reproduced by repeated administration of recombinant human sCD5 from disease initiation.40
The results just discussed apparently contradict previous reports by Raman’s group showing that the infection of mice with adenovirus expressing CD5-immunoglobulin fusion protein (CD5-Fc) when clinical signs were apparent promoted recovery from EAE.155 It could be that differences in the time at which recombinant human sCD5 (day 0) and CD5-Fc (day 14) were administered were the reason for such contradictory outcomes. If confirmed, this would indicate that EAE may be improved by agonist targeting of CD5 during the disease initiation phases whereas CD5 blockade may be useful during symptomatic and more advanced phases.
3. Rheumatoid Arthritis
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by systemic inflammation and synovitis that eventually causes cartilage damage and bone loss as a result of unequal bone formation and resorption.157 Although the pathogenesis of the dis-ease remains unclear, both antibody- and cell-medi-ated immune responses, as well as many cytokines, chemokines, and growth factors, have been reported to be involved in its development. Genetic studies reveal that RA is a complex genetic disease involving the influences of a long list of risk loci shared with other autoimmune disorders.161 Interestingly, CD5 was identified among 14 new susceptibility loci for RA in populations of European ancestry,162 with the nonsynonymous SNP rs229177 (Ala471Val) being a strong candidate for the causal variant.

Critical Reviews™ in Immunology
Consuegra-Fernández et al.96
Although TNF-α, IL-6, and IL-17 have been reported to enhance bone resorption,163 tumor growth factor beta (TGF-b) seems to play a dual role in both bone resorption and formation.164 Treg cells appar-ently inhibit bone resorption (osteoclastogenesis), whereas the role of B cells (including Bregs) is not well understood. The contribution of CD5+ B cells to RA pathogenesis has been investigated for many years. One of the first reports showed increased percentages of CD5+ B cells in peripheral blood from 17 patients with RA compared to normal con-trols.165 Other reports showed increased CD5+ B cell numbers in patients with RA and spondylarthritis and concluded that activated CD5+ B cells could be responsible for autoantibody production.52,166,167 In these studies, higher levels of CD5+ B cells correlated with increased amounts of polyreactive antibodies, increased levels of rheumatoid factor (RF), and the clinical features of a severe disease.168 However, other studies failed to show a correlation between the percentages of CD5+ B cells and the levels of RF or C-reactive protein.169
It has been proposed that the number of CD5+ B lymphocytes reflects individual genetic back-grounds.170–172 Recent studies on Breg populations in RA not only support the idea of a negative cor-relation between Bregs and RA but suggest this cell subset as a potential target in future therapeutic strategies.173–175 Current therapies used in RA, the so-called disease-modifying anti-rheumatic drugs (DMARDs), involve immunosuppressants such as methotrexate, glucocorticoids, and blocking mAbs that target TNF-a, IL-6, or CD19, among many oth-ers, in order to block autoantibody production.176,177
Some RA clinical trials using depleting or block-ing anti-CD5 mAbs have been reported. Clinical studies performed with an anti-CD5 mAb linked to RTA revealed inhibition of IL-2–induced prolifera-tion of synovial-fluid T cells in some patients treated with this immunotoxin.178–182 Despite positive initial results, presumably obtained by the elimination of pathogenic B cells that contribute to inflammation, the use of depleting anti-CD5 mAbs was finally stopped when a wide double-blind placebo-controlled multicenter trial demonstrated no clinical benefits or significant differences between groups.183,184 More
recent studies have shown therapeutic benefits from depleting B cells with an anti-CD20 mAb (rituximab) in RA patients.185–189
Anti-CD5 mAbs have been tested in animal RA models, such as collagen-induced arthritis (CIA), which is the most common experimental mouse model for human RA. One relevant study showed benefits after the administration of a nondepleting anti-CD5 mAb190: a rat IgG2a mAb specific for CD5 (TIB104) was administered in DBA/1 mice that presented clinical arthritis after CIA induction. The results demonstrated a significant decrease in disease severity in 60% of the mice and supported a T-cell–mediated mechanism given that levels of circulating antibodies to native collagen II were unaltered and that the amelioration of disease sever-ity appeared six days after mAb treatment. Overall, this outcome suggests that the blockade of CD5+, rather than the depletion of CD5 populations, is a potential therapeutic strategy in RA that needs more investigation.
4. Insulin-Dependent Diabetes Mellitus
Insulin-dependent diabetes mellitus (IDDM) is an organ-specific autoimmune disease in which T-cell–mediated pancreatic β-cell destruction leads to absolute insulin deficiency.191 Specific autoanti-bodies to insulin (IAAs), glutamic acid decarboxylase (GADA/GAA), and protein tyrosine phosphatase IA2 (IA-2AA) have been related to IDDM.191 Although there is no definitive correlation between expanded CD5+ B lymphocytes and the presence of circulating ICA and IAA autoantibodies, increased proportions of this cell subset were reported in early IDDM phases.53,192
Two studies explored the therapeutic benefits of anti-CD5 mAbs conjugated to RTA in human and mouse autoimmune diabetes.193,194 In the first one, patients with recent-onset IDDM were subjected to anti-T-cell therapy with the immunoconjugate CD5-Plus® (anti-CD5 H65 mAbs bound to RTA). It was reported that the therapy was tolerated and resulted in reversible T-cell depletion together with a dose-dependent preservation of β-cell function.193 In the second study, mice undergoing low-dose streptozocin/

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 97
IFN-γ–induced autoimmune diabetes and treated with anti-Ly-1 mAbs linked to RTA were protected against diabetes onset in a dose-dependent manner requiring higher doses and a longer schedule than that required by an anti-CD3 RTA.194 Although the mechanisms underlying anti-CD5-RTA–mediated protection remain poorly defined, both studies show that anti-CD5 immunotoxins may be useful for the in vivo treatment of diabetes and other T-cell–medi-ated autoimmune diseases.
5. Autoimmune Nephropathy
Glomerulonephritis defines a group of kidney autoimmune diseases characterized by glomerular inflammation and leukocyte accumulation. T and B lymphocytes have been reported to play a relevant role in the pathogenesis of proliferative and nonpro-liferative nephritis.195–198 Although T cells are thought to enhance antibody production against glomerular structures and to mediate cellular cytotoxicity through macrophage activation, the precise mechanisms underlying glomerular injury and lymphocyte infiltra-tion are not fully understood. Experimental animal models, such as antiglomerular basement membrane (GBM) glomerulonephritis in rats, have been largely used as an approach to the human diseases. In the rat model, anti-CD5 mAb (OX19) was administered as a pan-T-cell–depleting treatment, in combination with anti-CD4 and anti-CD8 mAbs or even alone, and showed reduced proteinuria and ameliora-tion of glomerular lesions.199–202 Similar beneficial effects were reported for a CD5-Fc chimera in a murine model of antibody-mediated membranous glomerulonephritis.65 Infusion of CD5-Fc was found to abrogate disease development by interfering with the CD5–CD5 ligand interaction.
Regarding the involvement of CD5+ B cells, it has been reported that these cells contribute to the pathology of some human nephropathies such as steroid-dependent nephrotic syndrome, cryo-globulinemic glomerulonephropathy, and human IgA nephropathy (IgAN).203–206 For example, num-bers of CD19+CD5+ cells inversely correlated with response to treatment in IgAN, and CD19+CD5+ cells isolated from untreated patients expressed higher
levels of IgA and IFN-γ and were more resistant to CD95L-induced apoptosis. This suggests that CD5+ B cells play a prominent role in IgAN. Indeed, higher numbers of CD19+CD5+ cells have also been found in patients with IgAN.207
Targeted B-cell–depleting therapies, in particular rituximab, are increasingly being used for the treatment of a number of glomerular diseases.208,209 However, new treatments specifically targeting CD5+CD19+ cells, which should avoid long-term consequences of pan-B-cell–depleting mAbs, remain to be explored.
6. Inflammatory Bowel Disease
Ulcerative colitis (UC) and Crohn’s disease (CD) are inflammatory bowel diseases (IBDs) character-ized by mucosal inflammation due to exacerbated activation of the immune system that affects only the colon (UC) or any region of the intestinal tract (CD). Oral administration of dextran sulfate sodium (DSS) solution has largely been used as the mouse model that best mimics IBD in human UC patients. Although the precise mechanisms of the disease remain unknown, several studies point to the role of Breg and Treg subsets in its modulation.96,210 B cells and IL-10 have been reported to play important inhibitory roles in the development of colitis. For example, a genetic deficiency of IL-10 results in spontaneous UC while its mAbs-induced blockade causes increased severity of IBDs generally.211,212
A recent study observed that, in contrast to RA, an anti-CD20 mAb (rituximab) had deleteri-ous effects in UC by blocking IL-10–producing B cells and stressing the importance of their anti-inflammatory role over their proinflammatory role.213 This observation was experimentally supported by adoptive transfer assays showing that regulatory B10 cells (CD1dhiCD5+IL-10+) from wild-type mice reduced DSS-induced intestinal injury in an IL-10–dependent manner.210 DSS-induced colitis was also shown to be less severe in CD5-deficient mice, which was attributed to increased levels of FoxP3 mRNA in the mouse colon and the enhanced suppressive activity of CD5–/– Tregs.96 Based on these observations, the use of CD5 antagonists in delaying or attenuating human UC deserves further study.

Critical Reviews™ in Immunology
Consuegra-Fernández et al.98
B. Infection
1. Viral Infection
CD5 has often been mentioned in studies aimed at deciphering the mechanisms by which viruses invade immune cells and/or modulate immune responses. Examples are hepatitis C virus (HCV), hepatitis B virus (HBV), HIV-1, Epstein-Barr virus (EBV), and equine infectious anemia (EIA).214–218
HCV infection is a global health problem and one of the main causes of cirrhosis, chronic hepatitis, and liver cancer. HCV infects hepatocytes as well as other cell types, in particular the cells of the immune system such as lymphocytes, monocytes/macrophages, and DCs.219,220 Although the cell invasion mechanism remains incompletely understood, it has been proposed that several surface molecules act as viral receptors mediating virion internalization. In hepatocytes, human scavenger receptor class B type 1 (SR-B1), a lipoprotein receptor responsible for the uptake of cholesteryl esters from high-density lipoproteins, has been reported to mediate cell invasion through its interaction with the HCV E2 glycoprotein.
In addition to SR-B1, LDLr, CD81 tetraspanin, and a few other molecules have been found to be necessary for HCV entry in hepatocytes.221 Different receptors seem to be required for HCV entry into T cells, one of them being CD5.70,214 Only primary T cells and T-cell lines expressing CD5 are suscep-tible to HCV infection, suggesting that CD5 is an important molecule for HCV entry into primary human T lymphocytes.70 The authors70 propose that, while CD81 may contribute to broad recognition of cells by HCV, CD5 facilitates HCV tropism specifi-cally toward lymphocytes. The role of CD5 in HCV entry into B cells has not been established.
Although there is no reported evidence for direct interaction between CD5 and other known pathogenic viruses, CD5+ T- and B-cell subsets have been proposed to play a role in the progression of some viral infections. On the one hand, patients with HBV were reported to have increased numbers of CD5+ B cells and Treg cells compared to healthy donors.215,222 On the other hand, it was reported that a cytotoxic CD5–CD8+ T cell subpopulation
expanded in patients with HIV-1 and was also found in inflammatory infiltrates of patients undergoing HCV reinfection.216,223 Down-regulation of CD5 on activated CD8+ T cells has been proposed a diagnostic marker of dysregulated T cells in EBV-associated hemophagocytic lymphohistiocytosis as well.217,224,225
The efficacy of specifically depleting CD5+ T lymphocytes in vivo with a murine IgG2a mAb (HB19A) was tested for control of chronic EIA lentiviral infection.218 Horses given this mAb (25–50 mg/day intravenously for 11 days) showed sustained depletion of peripheral blood CD5+ T cells but still maintained a residual (~15%) CD5–CD2+ T-cell population (either CD4+ or CD8+). Following CD5+ T cell depletion, EIA-infected horses did not develop recrudescent viremia or disease, unlike horses receiving corticosteroids.218
2. Fungal Infection
Although most clinical cases of sepsis are caused by gram-positive bacteria followed by endotoxin-pro-ducing gram-negative bacteria, fungi can also cause septic shock. The most recent study on sepsis etiology in the United States noted the dramatic increase in fungal sepsis over the last years,226 with infection by Candida albicans still the most common.227,228 This increase may reflect the efficient bacterial treatments currently in place in contrast to current antifungal treatment regimens that require prolonged admin-istration of medications with significant toxicity. Research on new treatments has focused on the use of vaccines and/or immunotherapy for the active treatment or prevention of specific fungal pathogens.
The pathogen-binding capabilities of the CD5 ectodomain were found to be beneficial for the control of fungal-induced experimental septic shock.21 Thus, a recombinant sCD5 equivalent to the soluble variant present in human serum38,39 was efficient not only in binding but also in aggregating both pathogenic (Can-dida albicans, Cryptococcus neoformans) and saprophytic (Saccharomyces Pombe) fungi through recognition of β-D-glucans, which is a major component of fungal cell walls.21 Pretreatment of mice undergoing zymosan-induced septic shock–like syndrome with a single dose (1.25 mg/Kg, intraperitoneal) of recombinant sCD5

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 99
(but not recombinant sCD6 or bovine seroalbumin) induced significant reductions in mortality, toxicity score, serum levels of proinflammatory cytokines, and leukocyte infiltration. Importantly, the beneficial effects were still evident when recombinant sCD5 was administered 1–3 hours post-zymosan challenge. These results open the possibility of developing new antifungal biotherapies based on CD5 alone or in com-bination with other well-studied β-D-glucan receptors such as TLR2. Indeed, TLR2-deficient mice were shown to be more resistant to Candida albicans dis-semination because of an impaired anti-inflammatory response (decreased IL-10 secretion, enhanced IFN-γ secretion),229 while dectin-1–deficient mice became more susceptible to infection because of an impaired proinflammatory response.230 The combination of a TLR2-blocking therapy and recombinant sCD5 is a strategy that should be looked into.
Another issue to look at is the relevance of CD5 polymophisms in individual susceptibility to fungal infections. As demonstrated in a recent report, cells expressing the more recently derived V471 vari-ant showed enhanced IL-8 cytokine secretion and mitogen-activated protein kinase (MAPK) activation after zymosan exposure when compared with the ancestral A471 variant.77
Overall, the data show that the CD5 molecule is involved in the modulation of inappropriate immune responses during fungal infections.
C. Transplantation
1. Hemopoietic Stem Cell Transplantation
Hemopoietic stem cell transplantation is a potentially curative immunotherapy used in several hematologic malignancies. However, graft-versus-host disease (GvHD) continues to limit its success. Even minor donor–host differences in major histocompatibility complex (MHC) and/or non-MHC antigens can lead to T-cell alloreactivity, which is mainly responsible for the pathogenesis of acute or chronic GvHD.231 Donor T-cell alloactivation leads to secretion of Th1 cytokines such as IL-2 and IFN-γ, which eventually activate cytotoxic lymphocytes and effector B cells, and induce macrophage recruitment as well as clonal
expansion. Moreover, common chemotherapy/radio-therapy pretreatment of host tissues can activate host immune populations and increase the release of proinflammatory cytokines (TNF-a and IL-1) that increase the surface expression of MHC antigens. Regarding CD5, expansion of a small population of peripheral CD3+CD5– cytolytic T cells normally present in healthy individuals has been reported after bone marrow transplantation and correlates well with the incidence of GvHD.232,233
Therapeutic strategies used in both acute and chronic GvHD mainly involve immunosuppressive regimes, including cyclosporin A, corticosteroids, and methotrexate. Depleting treatments targeting T-cell or even B-cell receptors are also being consid-ered, as is the blocking of anti-TNF-α and anti-IL-2 receptor mAbs.234 Because most immunosuppressive drugs are reported to cause long-term side effects and are not efficient for chronic GvHD, the main purpose in transplantation now is to induce host-specific tolerance. In this regard, special interest in the specific populations that contribute to the maintenance of long-standing tolerance, such as T and B regulatory subsets and inhibitory cytokines, has emerged.
An increased number of B cells expressing CD5 and CD1d were found in patients who main-tained stable kidney graft function in the absence of immunosuppression as compared to patients with chronic rejection and healthy volunteers.235 Thus, this B-cell population is believed to display an inhibitory profile. In contrast, IL-10, a cytokine secreted by CD19+CD5+ B cells, has been reported to play a dual role: (1) inhibiting both proliferation of antigen-presenting-cell (APC-) –dependent T cells and production of IL-2 T cells236 and (2) accelerat-ing T-cell–mediated GvHD lethality in vivo in a dose-dependent manner.237 Given that both T and B regulatory populations express high levels of CD5 and may be crucial for inducing tolerance after allo-genic transplantation, CD5-based therapies may be a feasible approach to positively immunomodulating these populations and eventually stimulating long-term tolerance. Unfortunately, given that CD5 is a pan-T-cell marker, depleting anti-CD5 mAbs have mostly been used as immunosuppressive drugs.

Critical Reviews™ in Immunology
Consuegra-Fernández et al.100
The first uses of anti-CD5 mAbs in preventing GvHD were in humans 30 years ago. An anti-CD5 mAb (T101) was first used with anti-CD2 (35.1) and anti-CD3 (UCHT-1) mAbs in what was called the TUT cocktail.238 These reagents together inhibited T-cell proliferation in vitro more effectively than did any one of them alone. For this reason, researchers proposed the TUT cocktail as a potential T-cell–depleting therapy. To avoid side effects derived from toxic drugs used in vivo, the cocktail was developed to purge ex vivo GvHD-producing cells from bone marrow before allogeneic marrow engraftment.239–241 However, few beneficial effects were observed in clinical assays.242 Later on, T101 was conjugated to an immunotoxin (T101-IT) and optimized for T-cell depletion from human bone marrow grafts.239,243–245 Clinical studies using T101-IT in ex vivo bone mar-row transplantation in patients with acute leukemia showed not only low effectiveness in preventing GvHD but also increased severity in some cases.246–249
Despite the unsuccessful results reported in the use of ex vivo anti-CD5–depleting therapy, an anti-CD5-RTA conjugate was used in later clinical studies in vivo following bone marrow transplanta-tion. Not surprisingly, patients receiving the drug showed increased risk of rejections, higher morbidity and mortality associated with viral infections, and greater risk of developing post-transplant lympho-proliferative disorder derived from anti-CD5-RTA toxicity.250–255 Toxicities observed in preclinical and clinical trials were also seen in mice and rats receiv-ing anti-CD5-RTA against mouse and rat CD5, respectively, after GvHD induction.256–258
The effect of nondepleting CD5-based inter-ventions in GvHD on the modulation of B and T regulatory populations and host tolerance induction urgently requires investigation.
2. Solid Organ Transplantation
As far as is known, little has been done on the use of CD5-based therapies in solid organ transplanta-tion. Increased survival of renal allografts has been reported in recipients with high titers of pre-existing alloantibodies after preoperational treatment with anti-CD5 immunotoxin (a conjugate of anti-CD5
monoclonal antibody with RTA). In this case, additional pretreatment of renal transplants with anti-CD5-RTA caused a reduction in passenger lymphoid cells, which ultimately improved trans-plantation success.259
D. Cancer
The last decade has seen great progress in under-standing the cellular and molecular interrelationship of immune cells and tumor cells. This improved knowledge has led to the development of a wide range of immunotherapies with greater antitumor efficacy.260 Since Burnet and Thomas first proposed the hypothesis of immunosurveillance in cancer,261 the immune response has been considered to play a relevant role in eradication of tumors. However, tumor cells are usually poorly immunogenic and are able to create suppressive environments262–264 that promote the activation, proliferation, and migration of regulatory cells such as Tregs,265 myeloid-derived suppressor cells (MDSC), tumor-associated macro-phages (TAM), and other subtypes of mature and immature DCs that produce immunosuppressive cytokines (IL-10, IL-4, TGF-β).266 This tumor microenvironment suppresses the immune effector response against tumor cells.
The destruction of tumor cells by the immune system is controlled by receptors that tightly regulate, positively or negatively, T-cell effector functions. Some current immunotherapeutic strategies in cancer are based on blocking the inhibitory receptor for B7, cytotoxic T-lymphocyte antigen 4 (CTLA-4), whose role is to shut off responses against self-antigens.267 Very encouraging results were recently obtained in patients with different types of tumors by blocking another inhibitory receptor, programmed death-1 (PD-1), which prevents T-cell activation.268 Along this line, CD5 also behaves as a negative modulator of activation and differentiation signals mediated by the T-cell receptor, and it has been shown to contribute to the regulation of antitumor immune responses.11,12 An early study in mice reported that a nondepleting mAb against CD5 was efficacious in the treatment of lymphoid (EL-4 leukemia) and nonlymphoid (Lewis lung carcinoma) tumors.269 In

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 101
previous work, the researchers had demonstrated that anti-Lyt-1 mAbs augmented the production of IL-2, thus improving T-cell proliferation.270
Much more recently, a careful analysis of human tumor-infiltrating T lymphocytes (TILs) showed that CD5 expression is inversely related to TIL antitumor activity. In this study, certain T-cell clones obtained from human lung carcinoma TILs showed dramatically lower CD5 expression com-pared to peripheral blood lymphocytes from the same patients.271 Increased AICD in lymphocytes with low or undetectable levels of CD5 was also reported,272 suggesting that these lymphocytes are more activated than are their high-expressing coun-terparts and that CD5, much like PD-1 or CTLA-4, may hinder the activation or survival of anti-tumor T cells. This hypothesis was validated by studies in CD5-deficient mice, which showed slower tumor growth in a B16F10 melanoma model.273 The results are in full agreement with observations using trans-genic mice expressing sCD5, which was expected to act as a decoy receptor and to block the binding of cell-associated CD5 to its natural ligand(s).40 Using a nonorthotopic melanoma model (B16), the mice showed slower tumor growth when compared to their nontransgenic littermates. Similar results were achieved by repeated administration of recombinant human sCD5 protein to wild-type mice after tumor injection. The increased antitumor response observed was associated with a basal reduced proportion of Tregs and peritoneal IL-10–producing B cells and an increased percentage of natural killer T cells.40
The targeting of new immunological checkpoints such as CTLA-4 and PD-1/PD1 ligand in cancer has yielded promising results in clinical trials, especially in patients with metastatic melanoma.274 The avail-able data suggest that CD5 represents a new cancer checkpoint molecule, opening up new therapeutic possibilities based on neutralizing anti-CD5 mAbs or sCD5 proteins alone or in combination with other immunomodulatory treatments.
Early phase-I studies have demonstrated rapid but transient responses with the use of an unmodified anti-CD5 mAb (T101) in patients with cutaneous T-cell lymphoma and chronic lymphocytic leukemia with minimal toxicity.275 This has prompted further
phase I studies using radiolabeled (90Y) versions of the same mAb, in which similar partial and transient responses were observed.276
IV. CONCLUSION
Since its discovery more than 50 years ago, much progress has been made toward establishing CD5’s role in the fine-tuning of antigen-mediated responses by T and B cells. For this reason, it is clear that CD5 is an attractive target for developing novel immunotherapies aimed at potentiating or inhibit-ing ongoing immune responses. However, important gaps remain concerning the identification of CD5’s endogenous ligand(s), the role of its soluble form, and the functional consequences of its ligation by pathogen-associated molecular patterns. Further investigation will allow a better interpretation of the sometimes conflicting results concerning the role of CD5+ cells in different autoimmune, infectious, and neoplastic disorders. It will also permit researchers to go beyond initial strategies using pan-T-cell–deplet-ing CD5 antibodies to treat such disorders (e.g., autoimmunity, GvHD) and to design nondepleting reagents that target specific subpopulations to down-modulate self-reactive cells or boost regulatory cell functions. In this regard, attention should also be paid to the disease stage at which those therapies will be introduced to avoid absent or even unwanted effects.
Recent evidence obtained with experimental tumor models suggests that CD5 is a new check-point molecule that can be neutralized to enhance current immunotherapies for cancer. Furthermore, the recently described pathogen (fungal, viral) recognition capacities of CD5 open new venues in the treatment of either acute or chronic infections.
ACKNOWLEDGMENTS
The authors’ work is supported by grants from the Association for International Cancer Research (14-1275) and the Spanish Ministerio de Economía y Competitividad (Plan Nacional de I+D+i, SAF2010-19717 and SAF2013-46151-R), the Instituto de

Critical Reviews™ in Immunology
Consuegra-Fernández et al.102
Salud Carlos III (Spanish Network for Research in Infectious Diseases, REIPI RD06/0008/1013 and RD12/0015/0018), the Fundació La Marató TV3 (201319-30), and the Generalitat de Catalunya (2009SGR1101). IS is the recipient of a fellowship from the Portuguese Fundação para a Ciência e a Tec-nologia (SFRH/BD/75738/2011). MO is the recipi-ent of a FPI fellowship from the Spanish Ministerio de Economía y Competitividad. FL is ad honorem scientific advisor at ImmunNovative Developments, a spin-off company of the University of Barcelona.
REFERENCES
1. Jones NH, Clabby ML, Dialynas DP, Huang HJ, Herzenberg LA, Strominger JL. Isolation of complementary DNA clones encoding the human lymphocyte glycoprotein T1/Leu-1. Nature. 1986;323:346-9.
2. Huang HJ, Jones NH, Strominger JL, Herzenberg LA. Molecular cloning of Ly-1, a membrane glycoprotein of mouse T lymphocytes and a subset of B cells: molecular homology to its human counterpart Leu-1/T1 (CD5). Proc Natl Acad Sci U S A. 1987;84:204-8.
3. Ledbetter JA, Rouse R V, Micklem HS, Herzenberg LA. T cell subsets defined by expression of Lyt-1,2,3 and Thy-1 antigens. Two-parameter immunofluorescence and cytotoxicity analysis with monoclonal antibodies modifies current views. J Exp Med. 1980;152:280-95.
4. McKenzie IF, Potter T. Murine lymphocyte surface antigens. Adv Immunol. 1979;27:179-338.
5. Boyse EA, Old LJ, Stockert E. An approach to the mapping of antigens on the cell surface. Proc Natl Acad Sci U S A. 1968;60:886-93.
6. Kisielow P, Szkudlarek J, Wysocka M. Studies on cell surface antigens of mouse leukemic and normal lymphocytes. III. Preparation and characteristics of alloantisera to differentiation antigens of mouse T lymphocytes. Arch Immunol Ther Exp (Warsz). 1978;26:99-103.
7. Reinherz EL, Kung PC, Goldstein G, Schlossman SF. Further characterization of the human inducer T cell subset defined by monoclonal antibody. J Immunol. 1979;123:2894-6.
8. Hollander N, Pillemer E. Weissman IL. Effects of Lyt antibodies on T-cell functions: augmentation by
anti-Lyt-1 as opposed to inhibition by anti-Lyt-2. Proceed. Proc Natl Acad Sci U S A. 1981;78:1148-51.
9. Ceuppens JL, Baroja ML. Monoclonal antibodies to the CD5 antigen can provide the necessary second signal for activation of isolated resting T cells by solid-phase-bound OKT3. J Immunol. 1986;137:1816-21.
10. Alberola-Ila J, Places L, Cantrell DA, Vives J, Lozano F. Intracellular events involved in CD5-induced human T cell activation and proliferation. J Immunol. 1992;148:1287-93.
11. Tarakhovsky A, Kanner SB, Hombach J, Ledbetter JA, Müller W, Killeen N, Rajewsky K. A role for CD5 in TCR-mediated signal transduction and thymocyte selection. Science. 1995;269:535-7.
12. Bikah G, Carey J, Ciallella JR, Tarakhovsky A, Bondada S. CD5-mediated negative regulation of antigen receptor-induced growth signals in B-1 B cells. Science. 1996;274:1906-9.
13. Sarrias MR, Gronlund J, Padilla O, Madsen J, Holmskov U, Lozano F. The Scavenger Receptor Cysteine-Rich (SRCR) domain: an ancient and highly conserved protein module of the innate immune system. Crit Rev Immunol. 2004;24:1-38.
14. Martínez VG, Moestrup SK, Holmskov U, Mollenhauer J, Lozano F. The conserved scavenger receptor cysteine-rich superfamily in therapy and diagnosis. Pharmacol Rev. 2011;63:967-1000.
15. Freeman M, Ashkenas J, Rees DJ, Kingsley DM, Copeland NG, Jenkins NA, Krieger M. An ancient, highly conserved family of cysteine-rich protein domains revealed by cloning type I and type II murine macrophage scavenger receptors. Proc Natl Acad Sci U S A. 1990;87:8810-4.
16. Bowen MA, Bajorath J, Siadak AW, Modrell B, Malacko AR, Marquardt H, Nadler SG, Aruffo A. The amino-terminal immunoglobulin-like domain of activated leukocyte cell adhesion molecule binds specifically to the membrane-proximal scavenger receptor cysteine-rich domain of CD6 with a 1:1 stoichiometry. J Biol Chem. 1996;271:17390-6.
17. Brännström A, Sankala M, Tryggvason K, Pikkarainen T. Arginine residues in domain V have a central role for bacteria-binding activity of macrophage scavenger receptor MARCO. Biochem Biophys Res Commun. 2002;290:1462-9.
18. Sarrias M-R, Roselló S, Sánchez-Barbero F, Sierra JM, Vila J, Yélamos J, Vives J, Casals C, Lozano F. A role for human Sp alpha as a pattern recognition receptor. J Biol Chem. 2005;280:35391-8.

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 103
19. Sarrias M-R, Farnós M, Mota R, Sánchez-Barbero F, Ibáñez A, Gimferrer I, Vera J, Fenutría R, Casals C, Yélamos J, Lozano F. CD6 binds to pathogen-associated molecular patterns and protects from LPS-induced septic shock. Proc Natl Acad Sci U S A. 2007;104:11724-9.
20. Fabriek BO, van Bruggen R, Deng DM, Ligtenberg AJM, Nazmi K, Schornagel K, Vloet RP, Dijkstra CD, van den Berg TK. The macrophage scavenger receptor CD163 functions as an innate immune sensor for bacteria. Blood. 2009;113:887-92.
21. Vera J, Fenutría R, Cañadas O, Figueras M, Mota R, Sarrias M-R, Williams DL, Casals C, Yelamos J, Lozano F. The CD5 ectodomain interacts with conserved fungal cell wall components and protects from zymosan-induced septic shock-like syndrome. Proc Natl Acad Sci U S A. 2009;106:1506-11.
22. Martínez-Florensa M, Consuegra-Fernández M, Martínez VG, Cañadas O, Armiger-Borràs N, Bonet-Roselló L, Farrán A, Vila J, Casals C, Lozano F. Targeting of key pathogenic factors from gram-positive bacteria by the soluble ectodomain of the scavenger-like lymphocyte receptor CD6. J Infect Dis. 2014;209:1077-86.
23. Aruffo A, Bowen MA, Patel DD, Haynes BF, Starling GC, Gebe JA, Bajorath J. CD6-ligand interactions: a paradigm for SRCR domain function? Immunol Today. 1997;18:498-04.
24. Lecomte O, Bock JB, Birren BW, Vollrath D, Parnes JR. Molecular linkage of the mouse CD5 and CD6 genes. Immunogenetics. 1996;44:385-90.
25. Padilla O, Calvo J, Vilà JM, Arman M, Gimferrer I, Places L, Arias MT, Pujana MA, Vives J, Lozano F. Genomic organization of the human CD5 gene. Immunogenetics. 2000;51:993-1001.
26. Garza-Garcia A, Esposito D, Rieping W, Harris R, Briggs C, Brown MH, Driscoll PC. Three-dimensional solution structure and conformational plasticity of the N-terminal scavenger receptor cysteine-rich domain of human CD5. J Mol Biol. 2008;378:129-44.
27. Rodamilans B, Muñoz IG, Bragado-Nilsson E, Sarrias MR, Padilla O, Blanco FJ, Lozano F, Montoya G. Crystal structure of the third extracellular domain of CD5 reveals the fold of a group B scavenger cysteine-rich receptor domain. J Biol Chem. 2007;282:12669-77.
28. Ojala JRM, Pikkarainen T, Tuuttila A, Sandalova T, Tryggvason K. Crystal structure of the cysteine-rich domain of scavenger receptor MARCO reveals
the presence of a basic and an acidic cluster that both contribute to ligand recognition. J Biol Chem. 2007;282:16654-66.
29. Vilà JM, Calvo J, Places L, Padilla O, Arman M, Gimferrer I, Aussel C, Vives J, Lozano F. Role of two conserved cytoplasmic threonine residues (T410 and T412) in CD5 signaling. J Immunol. 2001;166:396-402.
30. Bauch A, Campbell KS, Reth M. Interaction of the CD5 cytoplasmic domain with the Ca2+/calmodulin-dependent kinase IIdelta. Eur J Immunol. 1998;28:2167-77.
31. Calvo J, Vildà JM, Places L, Simarro M, Padilla O, Andreu D, Campbell KS, Aussel C, Lozano F. Human CD5 signaling and constitutive phosphorylation of C-terminal serine residues by casein kinase II. J Immunol. 1998;161:6022-9.
32. Bamberger M, Santos AM, Gonçalves CM, Oliveira MI, James JR, Moreira A, Lozano F, Davis SJ, Carmo AM. A new pathway of CD5 glycoprotein-mediated T cell inhibition dependent on inhibitory phosphorylation of Fyn kinase. J Biol Chem. 2011;286:30324-36.
33. Simarro M, Pelassy C, Calvo J, Places L, Aussel C, Lozano F. The cytoplasmic domain of CD5 mediates both TCR/CD3-dependent and -independent diacylglycerol production. J Immunol. 1997;159:4307-15.
34. Simarro M, Calvo J, Vilà JM, Places L, Padilla O, Alberola-Ila J, Vives J, Lozano F. Signaling through CD5 involves acidic sphingomyelinase, protein kinase C-zeta, mitogen-activated protein kinase kinase, and c-Jun NH2-terminal kinase. J Immunol. 1999;162:5149-55.
35. Perez-Villar JJ, Whitney GS, Bowen MA, Hewgill DH, Aruffo AA, Kanner SB. CD5 negatively regulates the T-cell antigen receptor signal transduction pathway: involvement of SH2-containing phosphotyrosine phosphatase SHP-1. Mol Cell Biol. 1999;19:2903-12.
36. Lozano F, Simarro M, Calvo J, Vilà JM, Padilla O, Bowen MA, Campbell KS. CD5 signal transduction: positive or negative modulation of antigen receptor signaling. Crit Rev Immunol. 2000;20:347-58.
37. Lu X, Axtell RC, Collawn JF, Gibson A, Justement LB, Raman C. AP2 adaptor complex-dependent internalization of CD5: differential regulation in T and B cells. J Immunol. 2002;168:5612-20.
38. Calvo J, Places L, Espinosa G, Padilla O, Vilà JM, Villamor N, Ingelmo M, Gallart T, Vives J, Font J,

Critical Reviews™ in Immunology
Consuegra-Fernández et al.104
Lozano F. Identification of a natural soluble form of human CD5. Tissue Antigens. 1999;54:128-37.
39. Ramos-Casals M, Font J, García-Carrasco M, Calvo J, Places L, Padilla O, Cervera R, Bowen MA, Lozano F, Ingelmo M. High circulating levels of soluble scavenger receptors (sCD5 and sCD6) in patients with primary Sjögren’s syndrome. Rheumatology (Oxford). 2001;40:1056-9.
40. Fenutría R, Martinez VG, Simões I, Postigo J, Gil V, Martínez-Florensa M, Sintes J, Naves R, Cashman KS, Alberola-Ila J, Ramos-Casals M, Soldevila G, Raman C, Merino J, Merino R, Engel P, Lozano F. Transgenic expression of soluble human CD5 enhances experimentally-induced autoimmune and anti-tumoral immune responses. PLoS One. 2014;9:e84895.
41. Azzam HS, Grinberg A, Lui K, Shen H, Shores EW, Love PE. CD5 expression is developmentally regulated by T cell receptor (TCR) signals and TCR avidity. J Exp Med. 1998;188:2301-11.
42. Kassiotis G, Zamoyska R, Stockinger B. Involvement of avidity for major histocompatibility complex in homeostasis of naive and memory T cells. J Exp Med. 2003;197:1007-16.
43. Hardy RR, Hayakawa K. Development and physiology of Ly-1 B and its human homolog, Leu-1 B. Immunol Rev. 1986;93:53-79.
44. Cron RQ, Ezquerra A, Coligan JE, Houlden BA, Bluestone JA, Maloy WL. Identification of distinct T cell receptor (TCR)-gamma delta heterodimers using an anti-TCR-gamma variable region serum. J Immunol. 1989;143:3769-75.
45. Mizoguchi A, Mizoguchi E, de Jong YP, Takedatsu H, Preffer FI, Terhorst C, Bhan AK. Role of the CD5 molecule on TCR gammadelta T cell-mediated immune functions: development of germinal centers and chronic intestinal inflammation. Int Immunol. 2003;15:97-108.
46. Ordoñez-Rueda D, Lozano F, Sarukhan A, Raman C, Garcia-Zepeda EA, Soldevila G. Increased numbers of thymic and peripheral CD4+ CD25+Foxp3+ cells in the absence of CD5 signaling. Eur J Immunol. 2009;39:2233-47.
47. Matsushita T, Yanaba K, Bouaziz J-D, Fujimoto M, Tedder TF. Regulatory B cells inhibit EAE initiation in mice while other B cells promote disease progression. J Clin Invest. 2008;118:3420-30.
48. Stamou P, de Jersey J, Carmignac D, Mamalaki C, Kioussis D, Stockinger B. Chronic exposure to low levels of antigen in the periphery causes reversible
functional impairment correlating with changes in CD5 levels in monoclonal CD8 T cells. J Immunol. 2003;171:1278-84.
49. Hippen KL, Tze LE, Behrens TW. CD5 maintains tolerance in anergic B cells. J Exp Med. 2000;191:883-90.
50. Berland R, Wortis HH. Origins and functions of B-1 cells with notes on the role of CD5. Annu Rev Immunol. 2002;20:253-300.
51. Plater-Zyberk C, Maini RN, Lam K, Kennedy TD, Janossy G. A rheumatoid arthritis B cell subset expresses a phenotype similar to that in chronic lymphocytic leukemia. Arthritis Rheum. 1985;28:971-6.
52. Smith HR, Olson RR. CD5+ B lymphocytes in systemic lupus erythematosus and rheumatoid arthritis. J Rheumatol. 1990;17:833-5.
53. Muñoz A, Gallart T, Viñas O, Gomis R. Increased CD5-positive B lymphocytes in type I diabetes. Clin Exp Immunol. 1991;83:304-8.
54. Iwatani Y, Amino N, Kaneda T, Ichihara K, Tamaki H, Tachi J, Matsuzuka F, Fukata S, Kuma K, Miyai K. Marked increase of CD5 + B cells in hyperthyroid Graves’ disease. Clin Exp Immunol. 1989;78:196-200.
55. Dauphinée M, Tovar Z, Talal N. B cells expressing CD5 are increased in Sjögren’s syndrome. Arthritis Rheum. 1988;31:642-7.
56. Zuckerman E, Slobodin G, Kessel A, Sabo E, Yeshurun D, Halas K, Toubi E. Peripheral B-cell CD5 expansion and CD81 overexpression and their association with disease severity and autoimmune markers in chronic hepatitis C virus infection. Clin Exp Immunol. 2002;128:353-8.
57. Lydyard PM, Jewell AP, Jamin C, Youinou PY. CD5 B cells and B-cell malignancies. Curr Opin Hematol. 1999;6:30-6.
58. Bandyopadhyay RS, Teutsch MR, Wortis HH. Activation of B-cells by sIgM cross-linking induces accumulation of CD5 mRNA. Curr Top Microbiol Immunol. 1995;194:219-28.
59. Freedman DO, Nutman TB, Jamal S, Kumaraswami V, Ottesen EA. Selective up-regulation of endothelial cell class I MHC expression by cytokines from patients with lymphatic filariasis. J Immunol. 1989;142:653-8.
60. Berland R, Wortis HH. An NFAT-dependent enhancer is necessary for anti-IgM-mediated induction of murine CD5 expression in primary splenic B cells. J Immunol. 1998;161:277-85.

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 105
61. Arman M, Calvo J, Trojanowska ME, Cockerill PN, Santana M, López-Cabrera M, Vives J, Lozano F. Transcriptional regulation of human CD5: important role of Ets transcription factors in CD5 expression in T cells. J Immunol. 2004;172:7519-29.
62. Van de Velde H, von Hoegen I, Luo W, Parnes JR, Thielemans K. The B-cell surface protein CD72/Lyb-2 is the ligand for CD5. Nature. 1991;351:662-5.
63. Pospisil R, Silverman GJ, Marti GE, Aruffo A, Bowen MA, Mage RG. CD5 is a potential selecting ligand for B-cell surface immunoglobulin: a possible role in maintenance and selective expansion of normal and malignant B cells. Leuk Lymphoma. 2000;36:353-65.
64. Haas KM, Estes DM. The identification and characterization of a ligand for bovine CD5. J Immunol. 2001;166:3158-66.
65. Biancone L, Bowen MA, Lim A, Aruffo A, Andres G, Stamenkovic I. Identification of a novel inducible cell-surface ligand of CD5 on activated lymphocytes. J Exp Med. 1996;184:811-9.
66. Bikah G, Lynd FM, Aruffo AA, Ledbetter JA, Bondada S. A role for CD5 in cognate interactions between T cells and B cells, and identification of a novel ligand for CD5. Int Immunol. 1998;10:1185-96.
67. Brown MH, Lacey E. A ligand for CD5 is CD5. J Immunol. 2010;185:6068-74.
68. Calvo J, Places L, Padilla O, Vilà JM, Vives J, Bowen MA, Lozano F. Interaction of recombinant and natural soluble CD5 forms with an alternative cell surface ligand. Eur J Immunol. 1999;29:2119-29.
69. Adams EL, Rice PJ, Graves B, Ensley HE, Yu H, Brown GD, Gordon S, Monteiro MA, Papp-Szabo E, Lowman DW, Power TD, Wempe MF, Williams DL. Differential high-affinity interaction of dectin-1 with natural or synthetic glucans is dependent upon primary structure and is influenced by polymer chain length and side-chain branching. J Pharmacol Exp Ther. 2008;325:115-23.
70. Sarhan MA, Pham TNQ, Chen AY, Michalak TI. Hepatitis C virus infection of human T lymphocytes is mediated by CD5. J Virol. 2012;86:3723-35.
71. Wu Z, Lee S, Abrams W, Weissman D, Malamud D. The N-terminal SRCR-SID domain of gp-340 interacts with HIV type 1 gp120 sequences and inhibits viral infection. AIDS Res Hum Retroviruses. 2006;22:508-15.
72. White MR, Crouch E, van Eijk M, Hartshorn M, Pemberton L, Tornoe I, Holmskov U, Hartshorn KL. Cooperative anti-influenza activities of respiratory innate immune proteins and neuraminidase inhibitor. Am J Physiol Lung Cell Mol Physiol. 2005;288:L831-40.
73. Van Gorp H, Van Breedam W, Van Doorsselaere J, Delputte PL, Nauwynck HJ. Identification of the CD163 protein domains involved in infection of the porcine reproductive and respiratory syndrome virus. J Virol. 2010;84:3101-5.
74. Caì Y, Postnikova EN, Bernbaum JG, Yú SQ, Mazur S, Deiuliis NM, Radoshitzky SR, Lackemeyer MG, McCluskey A, Robinson PJ, Haucke V, Wahl-Jensen V, Bailey AL, Lauck M, Friedrich TC, O’Connor DH, Goldberg TL, Jahrling PB, Kuhn JH. Simian hemorrhagic fever virus cell entry is dependent on CD163 and uses a clathrin-mediated endocytosis-like pathway. J Virol. 2015;89:844-56.
75. Howard CJ, Morrison WI, Brown WC, Naessens J, Sopp P. Demonstration of two allelic forms of the bovine T cell antigen Bo5 (CD5) and studies of their inheritance. Anim Genet. 1989;20:351-9.
76. Starling GC, Llewellyn MB, Whitney GS, Aruffo A. The Ly-1.1 and Ly-1.2 epitopes of murine CD5 map to the membrane distal scavenger receptor cysteine-rich domain. Tissue Antigens. 1997;49:1--6.
77. Carnero-Montoro E, Bonet L, Engelken J, Bielig T, Martínez-Florensa M, Lozano F, Bosch E. Evolutionary and functional evidence for positive selection at the human CD5 immune receptor gene. Mol Biol Evol. 2012;29:811-23.
78. Moreno-Estrada A, Tang K, Sikora M, Marquès-Bonet T, Casals F, Navarro A, Calafell F, Bertranpetit J, Stoneking M, Bosch E. Interrogating 11 fast-evolving genes for signatures of recent positive selection in worldwide human populations. Mol Biol Evol. 2009;26:2285-97.
79. Cenit MC, Martínez-Florensa M, Consuegra M, Bonet L, Carnero-Montoro E, Armiger N, Caballero-Baños M, Arias MT, Benitez D, Ortego-Centeno N, de Ramón E, Sabio JM, García-Hernández FJ, Tolosa C, Suárez A, González-Gay MA, Bosch E, Martín J, Lozano F. Analysis of ancestral and functionally relevant CD5 variants in systemic lupus erythematosus patients. PLoS One. 2014;9:e113090.
80. Beyers AD, Spruyt LL, Williams AF. Multimolecular associations of the T-cell antigen receptor. Trends Cell Biol. 1992;2:253-5.

Critical Reviews™ in Immunology
Consuegra-Fernández et al.106
81. Brossard C, Semichon M, Trautmann A, Bismuth G. CD5 inhibits signaling at the immunological synapse without impairing its formation. J Immunol. 2003;170:4623-9.
82. Gimferrer I, Farnós M, Calvo M, Mittelbrunn M, Enrich C, Sánchez-Madrid F, Vives J, Lozano F. The accessory molecules CD5 and CD6 associate on the membrane of lymphoid T cells. J Biol Chem. 2003;278:8564-71.
83. Imboden JB, June CH, McCutcheon MA, Ledbetter JA. Stimulation of CD5 enhances signal transduction by the T cell antigen receptor. J Clin Invest. 1990;85:130-4.
84. Verwilghen J, Vandenberghe P, Wallays G, de Boer M, Anthony N, Panayi GS, Ceuppens JL. Simultaneous ligation of CD5 and CD28 on resting T lymphocytes induces T cell activation in the absence of T cell receptor/CD3 occupancy. J Immunol. 1993;150:835-46.
85. Peña-Rossi C, Zuckerman LA, Strong J, Kwan J, Ferris W, Chan S, Tarakhovsky A, Beyers AD, Killeen N. Negative regulation of CD4 lineage development and responses by CD5. J Immunol. 1999;163:6494-501.
86. Azzam HS, DeJarnette JB, Huang K, Emmons R, Park CS, Sommers CL, El-Khoury D, Shores EW, Love PE. Fine tuning of TCR signaling by CD5. J Immunol. 2001;166:5464-72.
87. Fulton RB, Hamilton SE, Xing Y, Best JA, Goldrath AW, Hogquist KA, Jameson SC. The TCR’s sensitivity to self peptide-MHC dictates the ability of naive CD8+ T cells to respond to foreign antigens. Nat Immunol. 2014;16:107-17.
88. Persaud SP, Parker CR, Lo W-L, Weber KS, Allen PM. Intrinsic CD4+ T cell sensitivity and response to a pathogen are set and sustained by avidity for thymic and peripheral complexes of self peptide and MHC. Nat Immunol. 2014;15:266-74.
89. Kim HS, Kim AR, Kim do K, Kim HW, Park YH, Jang GH, Kim B, Park YM, You JS, Kim HS, Beaven MA, Kim YM, Choi WS. Interleukin-10-producing CD5+ B cells inhibit masT cells during immunoglobulin E-mediated allergic responses. Sci Signal. 2015;8:ra28-ra28.
90. Soldevila G, Raman C, Lozano F. The immunomodulatory properties of the CD5 lymphocyte receptor in health and disease. Curr Opin Immunol. 2011;23:310-8.
91. Axtell RC, Xu L, Barnum SR, Raman C. CD5-CK2 binding/activation-deficient mice are resistant
to experimental autoimmune encephalomyelitis: protection is associated with diminished populations of IL-17-expressing T cells in the central nervous system. J Immunol. 2006;177:8542-9.
92. Dennehy KM, Broszeit R, Ferris WF, Beyers AD. Thymocyte activation induces the association of the proto-oncoprotein c-Cbl and ras GTPase-activating protein with CD5. Eur J Immunol. 1998;28:1617-25.
93. Perez-Chacon G, Vargas JA, Jorda J, Morado M, Rosado S, Martin-Donaire T, Losada-Fernandez I, Rebolleda N, Perez-Aciego P. CD5 provides viability signals to B cells from a subset of B-CLL patients by a mechanism that involves PKC. Leuk Res. 2007;31:183-93.
94. Gary-Gouy H, Harriague J, Bismuth G, Platzer C, Schmitt C, Dalloul AH. Human CD5 promotes B-cell survival through stimulation of autocrine IL-10 production. Blood. 2002;100:4537-43.
95. Sestero CM, McGuire DJ, De Sarno P, Brantley EC, Soldevila G, Axtell RC, Raman C. CD5-dependent CK2 activation pathway regulates threshold for T cell anergy. J Immunol. 2012;189:2918-30.
96. Dasu T, Qualls JE, Tuna H, Raman C, Cohen DA, Bondada S. CD5 plays an inhibitory role in the suppressive function of murine CD4(+) CD25(+) T(reg) cells. Immunol Lett. 2008;119:103-13.
97. Henderson JG, Opejin A, Jones A, Gross C, Hawiger D. CD5 instructs extrathymic regulatory T cell development in response to self and tolerizing antigens. Immunity. 2015;42:471-83.
98. Hornung V, Rothenfusser S, Britsch S, Krug A, Jahrsdörfer B, Giese T, Endres S, Hartmann G. Quantitative expression of toll-like receptor 1-10 mRNA in cellular subsets of human peripheral blood mononuclear cells and sensitivity to CpG oligodeoxynucleotides. J Immunol. 2002;168:4531-7.
99. Zarember KA, Godowski PJ. Tissue expression of human Toll-like receptors and differential regulation of Toll-like receptor mRNAs in leukocytes in response to microbes, their products, and cytokines. J Immunol. 2002;168:554-61.
100. Caron G, Duluc D, Frémaux I, Jeannin P, David C, Gascan H, Delneste Y. Direct stimulation of human T cells via TLR5 and TLR7/8: flagellin and R-848 up-regulate proliferation and IFN-gamma production by memory CD4+ T cells. J Immunol. 2005;175:1551-7.
101. Caramalho I, Lopes-Carvalho T, Ostler D, Zelenay S, Haury M, Demengeot J. Regulatory

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 107
T cells selectively express toll-like receptors and are activated by lipopolysaccharide. J Exp Med. 2003;197:403-11.
102. Krupnick AS, Gelman AE, Barchet W, Richardson S, Kreisel FH, Turka LA, Colonna M, Patterson GA, Kreisel D. Murine vascular endothelium activates and induces the generation of allogeneic CD4+25+Foxp3+ regulatory T cells. J Immunol. 2005;175:6265-70.
103. Liu H, Komai-Koma M, Xu D, Liew FY. Toll-like receptor 2 signaling modulates the functions of CD4+ CD25+ regulatory T cells. Proc Natl Acad Sci U S A. 2006;103:7048-53.
104. Sutmuller RP, den Brok MH, Kramer M, Bennink EJ, Toonen LW, Kullberg BJ, Joosten LA, Akira S, Netea MG, Adema GJ. Toll-like receptor 2 controls expansion and function of regulatory T cells. J Clin Invest. 2006;116:485-94.
105. Lenz LL. CD5 sweetens lymphocyte responses. Proc Natl Acad Sci U S A. 2009;106:1303-4.
106. Gogolin-Ewens K, Meeusen E, Lee CS, Brandon M. Expression of CD5, a lymphocyte surface antigen on the endothelium of blood vessels. Eur J Immunol. 1989;19:935-8.
107. Moreau MF, Thibaud JL, Miled LB, Chaussepied M, Baumgartner M, Davis WC, Minoprio P, Langsley G. Theileria annulata in CD5(+) macrophages and B1 B cells. Infect Immun. 1999;67:6678-82.
108. Borrello MA, Palis J, Phipps RP. The relationship of CD5+ B lymphocytes to macrophages: insights from normal biphenotypic B/macrophage cells. Int Rev Immunol. 2001;20:137-55.
109. Wood GS, Freudenthal PS. CD5 monoclonal antibodies react with human peripheral blood dendritic cells. Am J Pathol. 1992;141:789-95.
110. De Bernardis F, Lucciarini R, Boccanera M, Amantini C, Arancia S, Morrone S, Mosca M, Cassone A, Santoni G. Phenotypic and functional characterization of vaginal dendritic cells in a rat model of Candida albicans vaginitis. Infect Immun. 2006;74:4282-94.
111. Yurasov S, Wardemann H, Hammersen J, Tsuiji M, Meffre E, Pascual V, Nussenzweig MC. Defective B cell tolerance checkpoints in systemic lupus erythematosus. J Exp Med. 2005;201:703-11.
112. Sakaguchi S, Fukuma K, Kuribayashi K, Masuda T. Organ-specific autoimmune diseases induced in mice by elimination of T cell subset. I. Evidence for the active participation of T cells in natural self-tolerance; deficit of a T cell subset as a
possible cause of autoimmune disease. J Exp Med. 1985;161:72-87.
113. Kuniyasu Y, Takahashi T, Itoh M, Shimizu J, Toda G, Sakaguchi S. Naturally anergic and suppressive CD25(+)CD4(+) T cells as a functionally and phenotypically distinct immunoregulatory T cell subpopulation. Int Immunol. 2000;12:1145-55.
114. Sakaguchi S, Ono M, Setoguchi R, Yagi H, Hori S, Fehervari Z, Shimizu J, Takahashi T, Nomura T. Foxp3+ CD25+ CD4+ natural regulatory T cells in dominant self-tolerance and autoimmune disease. Immunol Rev. 2006;212:8-27.
115. Wildin RS, Smyk-Pearson S, Filipovich AH. Clinical and molecular features of the immunodysregulation, polyendocrinopathy, enteropathy, X linked (IPEX) syndrome. J Med Genet. 2002;39:537-45.
116. Long SA, Buckner JH. CD4+FOXP3+ T regulatory cells in human autoimmunity: more than a numbers game. J Immunol. 2011;187:2061-6.
117. Renaudineau Y, Pers J-O, Bendaoud B, Jamin C, Youinou P. Dysfunctional B cells in systemic lupus erythematosus. Autoimmun Rev. 2004;3:516-23.
118. Rönnblom L, Eloranta M-L. The interferon signature in autoimmune diseases. Curr Opin Rheumatol. 2013;25:248-53.
119. Francis L, Perl A. Pharmacotherapy of systemic lupus erythematosus. Expert Opin Pharmacother. 2009;10:1481-94.
120. Kamal A. The efficacy of novel B cell biologics as the future of SLE treatment: a review. Autoimmun Rev. 2014;
121. Mysler EF, Spindler AJ, Guzman R, Bijl M, Jayne D, Furie RA, Houssiau FA, Drappa J, Close D, Maciuca R, Rao K, Shahdad S, Brunetta P. Efficacy and safety of ocrelizumab in active proliferative lupus nephritis: results from a randomized, double-blind, phase III study. Arthritis Rheum. 2013;65:2368-79.
122. Strand V, Petri M, Kalunian K, Gordon C, Wallace DJ, Hobbs K, Kelley L, Kilgallen B, Wegener WA, Goldenberg DM. Epratuzumab for patients with moderate to severe flaring SLE: health-related quality of life outcomes and corticosteroid use in the randomized controlled ALLEVIATE trials and extension study SL0006. Rheumatology (Oxford). 2014;53:502-11.
123. Ginzler EM, Wallace DJ, Merrill JT, Furie RA, Stohl W, Chatham WW, Weinstein A, McKay JD, McCune WJ, Zhong ZJ, Freimuth WW, Petri MA, LBSL02/99 Study Group. Disease control and

Critical Reviews™ in Immunology
Consuegra-Fernández et al.108
safety of belimumab plus standard therapy over 7 years in patients with systemic lupus erythematosus. J Rheumatol. 2014;41:300-9.
124. Lo MS, Tsokos GC. Treatment of systemic lupus erythematosus: new advances in targeted therapy. Ann NY Acad Sci. 2012;1247:138-52.
125. Bosch X, Ramos-Casals M, Khamashta MA. The DWEYS peptide in systemic lupus erythematosus. Trends Mol Med. 2012;18:215-23.
126. Lee J, Kuchen S, Fischer R, Chang S, Lipsky PE. Identification and characterization of a human CD5+ pre-naive B cell population. J Immunol. 2009;182:4116-26.
127. Markeljević J, Batinić D, Uzarević B, Bozikov J, Cikes N, Babić-Naglić D, Horvat Z, Marusić M. Peripheral blood CD5+ B cell subset in the remission phase of systemic connective tissue diseases. J Rheumatol. 1994;21:2225-30.
128. Böhm I. Increased peripheral blood B-cells expressing the CD5 molecules in association to autoantibodies in patients with lupus erythematosus and evidence to selectively down-modulate them. Biomed Pharmacother. 2004;58:338-43.
129. Morbach H, Singh SK, Faber C, Lipsky PE, Girschick HJ. Analysis of RAG expression by peripheral blood CD5+ and CD5– B cells of patients with childhood systemic lupus erythematosus. Ann Rheum Dis. 2006;65:482-7.
130. Hillion S, Garaud S, Devauchelle V, Bordron A, Berthou C, Youinou P, Jamin C. Interleukin-6 is responsible for aberrant B-cell receptor-mediated regulation of RAG expression in systemic lupus erythematosus. Immunology. 2007;122:371-80.
131. Hagn M, Ebel V, Sontheimer K, Schwesinger E, Lunov O, Beyer T, Fabricius D, Barth TF, Viardot A, Stilgenbauer S, Hepp J, Scharffetter-Kochanek K, Simmet T, Jahrsdörfer B. CD5+ B cells from individuals with systemic lupus erythematosus express granzyme B. Eur J Immunol. 2010;40:2060-9.
132. Garaud S, Le Dantec C, Jousse-Joulin S, Hanrotel-Saliou C, Saraux A, Mageed RA, Youinou P, Renaudineau Y. IL-6 modulates CD5 expression in B cells from patients with lupus by regulating DNA methylation. J Immunol. 2009;182:5623-32.
133. Garaud S, Le Dantec C, Berthou C, Lydyard PM, Youinou P, Renaudineau Y. Selection of the alternative exon 1 from the CD5 gene down-regulates membrane level of the protein in B lymphocytes. J Immunol. 2008;181:2010-8.
134. Illei GG, Shirota Y, Yarboro CH, Daruwalla J, Tackey E, Takada K, Fleisher T, Balow JE, Lipsky PE. Tocilizumab in systemic lupus erythematosus: data on safety, preliminary efficacy, and impact on circulating plasma cells from an open-label phase I dosage-escalation study. Arthritis Rheum. 2010;62:542-52.
135. Shirota Y, Yarboro C, Fischer R, Pham T-H, Lipsky P, Illei GG. Impact of anti-interleukin-6 receptor blockade on circulating T and B cell subsets in patients with systemic lupus erythematosus. Ann Rheum Dis. 2013;72:118-28.
136. Wacholtz MC, Lipsky PE. Treatment of lupus nephritis with CD5 PLUS, an immunoconjugate of an anti-CD5 monoclonal antibody and ricin A chain. Arthritis Rheum. 1992;35: 837-9.
137. Stafford FJ, Fleisher TA, Lee G, Brown M, Strand V, Austin HA, Balow JE, Klippel JH. A pilot study of anti-CD5 ricin A chain immunoconjugate in systemic lupus erythematosus. J Rheumatol. 1994;21:2068-70.
138. Love S. Demyelinating diseases. J Clin Pathol. 2006;59:1151-9.
139. Andersson M, Alvarez-Cermeño J, Bernardi G, Cogato I, Fredman P, Frederiksen J, Fredrikson S, Gallo P, Grimaldi LM, Grønning M. Cerebrospinal fluid in the diagnosis of multiple sclerosis: a consensus report. J Neurol Neurosurg Psychiatry. 1994;57:897-902.
140. Lucchinetti CF, Brück W, Rodriguez M, Lassmann H. Distinct patterns of multiple sclerosis pathology indicate heterogeneity on pathogenesis. Brain Pathol. 1996;6:259-74.
141. Sellebjerg F, Jensen CV, Christiansen M. Intrathecal IgG synthesis and autoantibody-secreting cells in multiple sclerosis. J Neuroimmunol. 2000;108:207-15.
142. Youinou P, Renaudineau Y. CD5 expression in B cells from patients with systemic lupus erythematosus. Crit Rev Immunol. 2011;31:31-42.
143. Hardy RR, Hayakawa K. B cell development pathways. Annu Rev Immunol. 2001;19: 595-621.
144. Mix E, Olsson T, Correale J, Baig S, Kostulas V, Olsson O, Link H. B cells expressing CD5 are increased in cerebrospinal fluid of patients with multiple sclerosis. Clin Exp Immunol. 1990;79:21-7.
145. Correale J, Mix E, Olsson T, Kostulas V, Fredrikson S, Höjeberg B, Link H. CD5+ B cells and CD4-8-T cells in neuroimmunological diseases. J Neuroimmunol. 1991;32:123-32.

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 109
146. Villar LM, Espiño M, Roldán E, Marín N, Costa-Frossard L, Muriel A, Alvarez-Cermeño JC. Increased peripheral blood CD5+ B cells predict earlier conversion to MS in high-risk clinically isolated syndromes. Mult Scler. 2011;17:690-4.
147. Bongioanni P, Fioretti C, Vanacore R, Bianchi F, Lombardo F, Ambrogi F, Meucci G. Lymphocyte subsets in multiple sclerosis. A study with two-colour fluorescence analysis. J Neurol Sci. 1996;139:71-7.
148. Scott TF, McKolanis J, Rothfus W, Cottington E. Lymphocyte subsets in relapsing-remitting multiple sclerosis: a longitudinal study of B lymphocytes and T lymphocytes. Neurol Res. 1994;16:385-8.
149. Seidi OA, Semra YK, Sharief MK. Expression of CD5 on B lymphocytes correlates with disease activity in patients with multiple sclerosis. J Neuroimmunol. 2002;133:205-10.
150. Niino M, Fukazawa T, Minami N, Amino I, Tashiro J, Fujiki N, Doi S, Kikuchi S. CD5-positive B cell subsets in secondary progressive multiple sclerosis. Neurosci Lett. 2012;523:56-61.
151. Sellebjerg F, Jensen J, Jensen C V, Wiik A. Expansion of CD5 - B cells in multiple sclerosis correlates with CD80 (B7-1) expression. Scand J Immunol. 2002;56:101-7.
152. Hawiger D, Masilamani RF, Bettelli E, Kuchroo VK, Nussenzweig MC. Immunological unresponsiveness characterized by increased expression of CD5 on peripheral T cells induced by dendritic cells in vivo. Immunity. 2004;20:695-705.
153. Begum-Haque S, Christy M, Ochoa-Reparaz J, Nowak EC, Mielcarz D, Haque A, Kasper LH. Augmentation of regulatory B cell activity in experimental allergic encephalomyelitis by glatiramer acetate. J Neuroimmunol. 2011;232:136-44.
154. Ochoa-Repáraz J, Mielcarz DW, Haque-Begum S, Kasper LH. Induction of a regulatory B cell population in experimental allergic encephalomyelitis by alteration of the gut commensal microflora. Gut Microbes. 2010;1:103-8.
155. Axtell RC, Webb MS, Barnum SR, Raman C. Cutting edge: critical role for CD5 in experimental autoimmune encephalomyelitis: inhibition of engagement reverses disease in mice. J Immunol. 2004;173:2928-32.
156. Strigård K, Olsson T, Larsson P, Holmdahl R, Klareskog L. Modulation of experimental allergic neuritis in rats by in vivo treatment with monoclonal anti T cell antibodies. J Neurol Sci. 1988;83:283-91.
157. Engelmann R, Wang N, Kneitz C, Müller-Hilke B. Bone resorption correlates with the frequency of CD5+ B cells in the blood of patients with rheumatoid arthritis. Rheumatology (Oxford). 2014;54:545-53.
158. Chitnis T, Najafian N, Benou C, Salama AD, Grusby MJ, Sayegh MH, Khoury SJ. Effect of targeted disruption of STAT4 and STAT6 on the induction of experimental autoimmune encephalomyelitis. J Clin Invest. 2001;108:739-47.
159. Falcone M, Rajan AJ, Bloom BR, Brosnan CF. A critical role for IL-4 in regulating disease severity in experimental allergic encephalomyelitis as demonstrated in IL-4-deficient C57BL/6 mice and BALB/c mice. J Immunol. 1998;160:4822-30.
160. Kohm AP, Carpentier PA, Anger HA, Miller SD. Cutting edge: CD4+CD25+ regulatory T cells suppress antigen-specific autoreactive immune responses and central nervous system inflammation during active experimental autoimmune encephalomyelitis. J Immunol. 2002;169:4712-6.
161. Stahl EA, Raychaudhuri S, Remmers EF, Xie G, Eyre S, Thomson BP, Li Y, Kurreeman FA, Zhernakova A, Hinks A, Guiducci C, Chen R, Alfredsson L, Amos CI, Ardlie KG; BIRAC Consortium, Barton A, Bowes J, Brouwer E, Burtt NP, Catanese JJ, Coblyn J, Coenen MJ,Costenbader KH, Criswell LA, Crusius JB, Cui J, de Bakker PI, De Jager PL, Ding B, Emery P, Flynn E, Harrison P, Hocking LJ,Huizinga TW, Kastner DL, Ke X, Lee AT, Liu X, Martin P, Morgan AW, Padyukov L, Posthumus MD, Radstake TR, Reid DM, Seielstad M,Seldin MF, Shadick NA, Steer S, Tak PP, Thomson W, van der Helm-van Mil AH, van der Horst-Bruinsma IE, van der Schoot CE, van Riel PL, Weinblatt ME, Wilson AG, Wolbink GJ, Wordsworth BP; YEAR Consortium, Wijmenga C, Karlson EW, Toes RE, de Vries N, Begovich AB, Worthington J, Siminovitch KA, Gregersen PK, Klareskog L, Plenge RM. Genome-wide association study meta-analysis identifies seven new rheumatoid arthritis risk loci. Nat Genet. 2010;42:508-14.
162. Eyre S, Bowes J, Diogo D, Lee A, Barton A, Martin P, Zhernakova A, Stahl E, Viatte S, McAllister K, Amos CI, Padyukov L, Toes RE,Huizinga TW, Wijmenga C, Trynka G, Franke L, Westra HJ, Alfredsson L, Hu X, Sandor C, de Bakker PI, Davila S, Khor CC, Heng KK,Andrews R, Edkins S, Hunt SE, Langford C, Symmons

Critical Reviews™ in Immunology
Consuegra-Fernández et al.110
D; Biologics in Rheumatoid Arthritis Genetics and Genomics Study Syndicate, Wellcome Trust Case Control Consortium, Concannon P, Onengut-Gumuscu S, Rich SS, Deloukas P, Gonzalez-Gay MA, Rodriguez-Rodriguez L, Ärlsetig L, Martin J, Rantapää-Dahlqvist S, Plenge RM, Raychaudhuri S, Klareskog L, Gregersen PK, Worthington J. High-density genetic mapping identifies new susceptibility loci for rheumatoid arthritis. Nat Genet. 2012;44:1336-40.
163. Kotake S, Udagawa N, Takahashi N, Matsuzaki K, Itoh K, Ishiyama S, Saito S, Inoue K, Kamatani N, Gillespie MT, Martin TJ, Suda T. IL-17 in synovial fluids from patients with rheumatoid arthritis is a potent stimulator of osteoclastogenesis. J Clin Invest. 1999;103:1345-52.
164. Sato K, Suematsu A, Okamoto K, Yamaguchi A, Morishita Y, Kadono Y, Tanaka S, Kodama T, Akira S, Iwakura Y, Cua DJ, Takayanagi H. Th17 functions as an osteoclastogenic helper T cell subset that links T cell activation and bone destruction. J Exp Med. 2006;203:2673-82.
165. Hara M, Kitani A, Hirose T, Norioka K, Harigai M, Suzuki K, Tabata H, Kawakami M, Kawagoe M, Nakamura H. Stimulatory effect of CD5 antibody on B cells from patients with rheumatoid arthritis. Clin Immunol Immunopathol. 1988;49:223-30.
166. Burastero SE, Lo Pinto G, Goletti D, Cutolo M, Burlando L, Falagiani P. Rheumatoid arthritis with monoclonal IgE rheumatoid factor. J Rheumatol. 1993;20:489-94.
167. Cantaert T, Doorenspleet ME, Francosalinas G, Paramarta JE, Klarenbeek PL, Tiersma Y, van der Loos CM, De Vries N, Tak PP, Baeten DL. Increased numbers of CD5+ B lymphocytes with a regulatory phenotype in spondylarthritis. Arthritis Rheum. 2012;64:1859-68.
168. Burastero SE, Cutolo M, Dessì V, Celada F. Monoreactive and polyreactive rheumatoid factors produced by in vitro Epstein-Barr virus-transformed peripheral blood and synovial B lymphocytes from rheumatoid arthritis patients. Scand J Immunol. 1990;32:347-57.
169. Sowden JA, Roberts-Thomson PJ, Zola H. Evaluation of CD5-positive B cells in blood and synovial fluid of patients with rheumatic diseases. Rheumatol Int. 1987;7:255-9.
170. Kipps TJ, Vaughan JH. Genetic influence on the levels of circulating CD5 B lymphocytes. J Immunol. 1987;139:1060-4.
171. Jamin C, Magadur G, Lamour A, Mackenzie L, Lydyard P, Katsikis P, Youinou P. Cell-free CD5 in patients with rheumatic diseases. Immunol Lett. 1992;31:79-83.
172. Liu ST, Wang CR, Liu MF, Li JS, Lei HY, Chuang CY. The study of circulating CD5 positive B lymphocytes in Chinese patients with rheumatoid arthritis. Clin Rheumatol. 1996;15:250-3.
173. Cui D, Zhang L, Chen J, Zhu M, Hou L, Chen B, Shen B. Changes in regulatory B cells and their relationship with rheumatoid arthritis disease activity. Clin Exp Med. 2014;
174. Ma L, Liu B, Jiang Z, Jiang Y. Reduced numbers of regulatory B cells are negatively correlated with disease activity in patients with new-onset rheumatoid arthritis. Clin Rheumatol. 2014;33:187-95.
175. Daien CI, Gailhac S, Mura T, Audo R, Combe B, Hahne M, Morel J. Regulatory B10 cells are decreased in patients with rheumatoid arthritis and are inversely correlated with disease activity. Arthritis Rheumatol. 2014;66:2037-46.
176. Graudal N, Hubeck-Graudal T, Tarp S, Christensen R, Jürgens G. Effect of combination therapy on joint destruction in rheumatoid arthritis: a network meta-analysis of randomized controlled trials. PLoS One. 2014;9:e106408.
177. Anderson AE, Lorenzi AR, Pratt A, Wooldridge T, Diboll J, Hilkens CMU, Isaacs JD. Immunity 12 years after alemtuzumab in RA: CD5+ B-cell depletion, thymus-dependent T-cell reconstitution and normal vaccine responses. Rheumatology (Oxford). 2012;51:1397-406.
178. Cannon GW, Marble DA, Griffiths MM, Cole BC, McCall S, Schulman SF, Strand V. Immunologic assessment during treatment of rheumatoid arthritis with anti-CD5 immunoconjugate. J Rheumatol. 1995;22:207-13.
179. Fishwild DM, Strand V. Administration of an anti-CD5 immunoconjugate to patients with rheumatoid arthritis: effect on peripheral blood mononuclear cells and in vitro immune function. J Rheumatol. 1994;21:596-604.
180. Strand V, Lipsky PE, Cannon GW, Calabrese LH, Wiesenhutter C, Cohen SB, Olsen NJ, Lee ML, Lorenz TJ, Nelson B. Effects of administration of an anti-CD5 plus immunoconjugate in rheumatoid arthritis. Results of two phase II studies. The CD5 Plus Rheumatoid Arthritis Investigators Group. Arthritis Rheum. 1993;36:620-30.

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 111
181. Olsen NJ, Teal GP, Strand V. In vivo T cell depletion in rheumatoid arthritis is associated with increased in vitro IgM-rheumatoid factor synthesis. Clin Immunol Immunopathol. 1993;67:124-9.
182. Verwilghen J, Kingsley GH, Ceuppens JL, Panayi GS. Inhibition of synovial fluid T cell proliferation by anti-CD5 monoclonal antibodies. A potential mechanism for their immunotherapeutic action in vivo. Arthritis Rheum. 1992;35:1445-51.
183. Lorenz M, Kalden JR. Biological agents in rheumatoid arthritis: which ones could be used in combination? BioDrugs. 1998;9:303-24.
184. Olsen NJ, Brooks RH, Cush JJ, Lipsky PE, St Clair EW, Matteson EL, Gold KN, Cannon GW, Jackson CG, McCune WJ, Fox DA,Nelson B, Lorenz T, Strand V. A double-blind, placebo-controlled study of anti-CD5 immunoconjugate in patients with rheumatoid arthritis. The Xoma RA Investigator Group. Arthritis Rheum. 1996;39:1102-8.
185. Carbone J, del Pozo N, Gallego A, Sarmiento E. Immunological risk factors for infection after immunosuppressive and biologic therapies. Expert Rev Anti Infect Ther. 2011;9:405-13.
186. Bruzzese V. Therapeutic effectiveness of minimal doses of rituximab in a patient with rheumatoid arthritis. Int J Immunopathol Pharmacol. 24:265-7.
187. Edwards JCW, Szczepanski L, Szechinski J, Filipowicz-Sosnowska A, Emery P, Close DR, Stevens RM, Shaw T. Efficacy of B-cell-targeted therapy with rituximab in patients with rheumatoid arthritis. N Engl J Med. 2004;350:2572-81.
188. Popa C, Leandro MJ, Cambridge G, Edwards JCW. Repeated B lymphocyte depletion with rituximab in rheumatoid arthritis over 7 yrs. Rheumatology (Oxford). 2007;46:626-30.
189. Leandro MJ, Edwards JCW, Cambridge G. Clinical outcome in 22 patients with rheumatoid arthritis treated with B lymphocyte depletion. Ann Rheum Dis. 2002;61:883-8.
190. Plater-Zyberk C, Taylor PC, Blaylock MG, Maini RN. Anti-CD5 therapy decreases severity of established disease in collagen type II-induced arthritis in DBA/1 mice. Clin Exp Immunol. 1994;98:442-7.
191. Devendra D, Liu E, Eisenbarth GS. Type 1 diabetes: recent developments. BMJ. 2004;328:750-4.
192. Lorini R, Massa M, d’Annunzio G, Cortona L, De Benedetti F, Martini A, Severi F. CD5-positive B cells in type 1 (insulin-dependent) diabetic children. Diabetes Res Clin Pract. 1993;19:17-22.
193. Skyler JS, Lorenz TJ, Schwartz S, Eisenbarth GS, Einhorn D, Palmer JP, Marks JB, Greenbaum C, Saria EA, Byers V. Effects of an anti-CD5 immunoconjugate (CD5-plus) in recent onset type I diabetes mellitus: a preliminary investigation. The CD5 Diabetes Project Team. J Diabetes Complications. 1993;7:224-32.
194. Vallera DA, Carroll SF, Brief S, Blazar BR. Anti-CD3 immunotoxin prevents low-dose STZ/interferon-induced autoimmune diabetes in mouse. Diabetes. 1992;41:457-64.
195. Lowe MG, Holdsworth SR, Tipping PG. T lymphocyte participation in acute serum sickness glomerulonephritis in rabbits. Immunol Cell Biol. 1991;69(Pt 2):81-7.
196. Nolasco FE, Cameron JS, Hartley B, Coelho A, Hildreth G, Reuben R. Intraglomerular T cells and monocytes in nephritis: study with monoclonal antibodies. Kidney Int. 1987;31:1160-6.
197. Tipping PG, Neale TJ, Holdsworth SR. T lymphocyte participation in antibody-induced experimental glomerulonephritis. Kidney Int. 1985;27:530-7.
198. Hooke DH, Gee DC, Atkins RC. Leukocyte analysis using monoclonal antibodies in human glomerulonephritis. Kidney Int. 1987;31:964-72.
199. Tipping PG, Huang XR, Berndt MC, Holdsworth SR. P-selectin directs T lymphocyte-mediated injury in delayed-type hypersensitivity responses: studies in glomerulonephritis and cutaneous delayed-type hypersensitivity. Eur J Immunol. 1996;26:454-60.
200. Huang XR, Tipping PG, Apostolopoulos J, Oettinger C, D’Souza M, Milton G, Holdsworth SR. Mechanisms of T cell-induced glomerular injury in anti-glomerular basement membrane (GBM) glomerulonephritis in rats. Clin Exp Immunol. 1997;109:134-42.
201. Ikezumi Y, Kawachi H, Toyabe S, Uchiyama M, Shimizu F. An anti-CD5 monoclonal antibody ameliorates proteinuria and glomerular lesions in rat mesangioproliferative glomerulonephritis. Kidney Int. 2000;58:100-14.
202. Ikezumi Y, Kanno K, Karasawa T, Han GD, Ito Y, Koike H, Toyabe S, Uchiyama M, Shimizu F, Kawachi H. The role of lymphocytes in the experimental progressive glomerulonephritis. Kidney Int. 2004;66:1036-48.
203. Nagatani K, Yamaoka R, Tezuka Y, Hayashi M. Involvement of CD5+CD19+Cell in steroid-dependent nephrotic syndrome treated with B-cell targeting therapy. Pediatr Int. 2013;55:99-101.

Critical Reviews™ in Immunology
Consuegra-Fernández et al.112
204. Kim YL, Gong SJ, Hwang YH, Joo JE, Cho YU, Lee JA, Sung SA, Lee SY, Kim NY. Waldenstrom macroglobulinemia with CD5+ expression presented as cryoglobulinemic glomerulonephropathy: a case report. J Korean Med Sci. 2011;26:824-8.
205. Wu G, Peng YM, Liu H, Hou QD, Liu FY, Chen NL, Bi HX. Expression of CD19(+)CD5(+)B cells and IgA1-positive cells in tonsillar tissues of IgA nephropathy patients. Ren Fail. 2011;33:159-63.
206. Wang Y-Y, Zhang L, Zhao P-W, Ma L, Li C, Zou H-B, Jiang YF. Functional implications of regulatory B cells in human IgA nephropathy. Scand J Immunol. 2014;79:51-60.
207. Yuling H, Ruijing X, Xiang J, Yanping J, Lang C, Li L, Dingping Y, Xinti T, Jingyi L, Zhiqing T, Yongyi B, Bing X, Xinxing W, Youxin J, Fox DA, Lundy SK, Guohua D, Jinquan T. CD19+CD5+ B cells in primary IgA nephropathy. J Am Soc Nephrol. 2008;19:2130-9.
208. Perry M, Delarche A, Ribes D, Vergez F, Guilbeau-Frugier C, Laurent C, Huart A, Tavitian S, El Hachem H, Oberic L, Chauveau D, Michallet AS, Ysebaert L, Faguer S. Rituximab-cyclophosphamide-dexamethasone is highly effective in patients with monoclonal Ig deposit-related glomerulopathy and indolent non-Hodgkin lymphomas. Am J Hematol. 2014;89:969-73.
209. Iijima K. [Rituximab for the treatment of nephrotic syndrome]. Nihon Jinzo Gakkai Shi. 2014;56:471-7.
210. Yanaba K, Yoshizaki A, Asano Y, Kadono T, Tedder TF, Sato S. IL-10-producing regulatory B10 cells inhibit intestinal injury in a mouse model. Am J Pathol. 2011;178:735-43.
211. Mizoguchi A, Mizoguchi E, Takedatsu H, Blumberg RS, Bhan AK. Chronic intestinal inflammatory condition generates IL-10-producing regulatory B cell subset characterized by CD1d upregulation. Immunity. 2002;16:219-30.
212. Kühn R, Löhler J, Rennick D, Rajewsky K, Müller W. Interleukin-10-deficient mice develop chronic enterocolitis. Cell. 1993;75:263-74.
213. Goetz M, Atreya R, Ghalibafian M, Galle PR, Neurath MF. Exacerbation of ulcerative colitis after rituximab salvage therapy. Inflamm Bowel Dis. 2007;13:1365-8.
214. Sarhan MA, Chen AY, Michalak TI. Differential expression of candidate virus receptors in human T lymphocytes prone or resistant to infection with patient-derived hepatitis C virus. PLoS One. 2013;8:e62159.
215. Sun H, Lv J, Tu Z, Hu X, Yan H, Pan Y, Xu D, Lian Z, Chi X, Niu J. Antiviral treatment improves disrupted peripheral B lymphocyte homeostasis in chronic hepatitis B virus-infected patients. Exp Biol Med (Maywood). 2013;238:1275-83.
216. Penney SJ, Gallant ME, Grant MD. Greater frequency of CD5-negative CD8(+) T cells against human immunodeficiency virus type 1 than other viruses is consistent with adaptation to antigenic variation. AIDS Res. Ther. 2014;11:30.
217. Karandikar NJ, Kroft SH, Yegappan S, Rogers BB, Aquino VM, Lee K-M, Kumar V, Guenaga FJ, Jaffe ES, Douek DC, McKenna RW. Unusual immunophenotype of CD8+ T cells in familial hemophagocytic lymphohistiocytosis. Blood. 2004;104:2007-9.
218. Tumas DB, Hines MT, Perryman LE, Davis WC, McGuire TC. Corticosteroid immuno-suppression and monoclonal antibody-mediated CD5+ T lymphocyte depletion in normal and equine infectious anaemia virus-carrier horses. J Gen Virol. 1994;75( Pt 5):959-68.
219. Navas M-C, Fuchs A, Schvoerer E, Bohbot A, Aubertin A-M, Stoll-Keller F. Dendritic cell susceptibility to hepatitis C virus genotype 1 infection. J Med Virol. 2002;67:152-61.
220. Lerat H, Rumin S, Habersetzer F, Berby F, Trabaud MA, Trépo C, Inchauspé G. In vivo tropism of hepatitis C virus genomic sequences in hematopoietic cells: influence of viral load, viral genotype, and cell phenotype. Blood. 1998;91:3841-9.
221. Bartosch B, Vitelli A, Granier C, Goujon C, Dubuisson J, Pascale S, Scarselli E, Cortese R, Nicosia A, Cosset FL. Cell entry of hepatitis C virus requires a set of co-receptors that include the CD81 tetraspanin and the SR-B1 scavenger receptor. J Biol Chem. 2003;278:41624-30.
222. Wang L, Qiu J, Yu L, Hu X, Zhao P, Jiang Y. Increased numbers of CD5+CD19+CD1dhighIL-10+ Bregs, CD4+Foxp3+ Tregs, CD4+CXCR5+Foxp3+ follicular regulatory T (TFR) cells in CHB or CHC patients. J Transl Med. 2014;12:251-62.
223. Ziarkiewicz-Wróblewska B, Wróblewski T, Ciszek M, Kalinowski P, Malejczyk J. Change in composition of inflammatory infiltrate in the course of hepatitis C reinfection and concomitant acute rejection after orthotopic liver transplantation. Ann Transplant. 2014;19:41-50.
224. Toga A, Wada T, Sakakibara Y, Mase S, Araki R, Tone Y, Toma T, Kurokawa T, Yanagisawa

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 113
R, Tamura K, Nishida N, Taneichi H, Kanegane H, Yachie A. Clinical significance of cloned expansion and CD5 down-regulation in Epstein-Barr virus (EBV)-infected CD8+ T lymphocytes in EBV-associated hemophagocytic lymphohistiocytosis. J Infect Dis. 2010;201:1923-32.
225. Wada T, Sakakibara Y, Nishimura R, Toma T, Ueno Y, Horita S, Tanaka T, Nishi M, Kato K, Yasumi T, Ohara O, Yachie A. Down-regulation of CD5 expression on activated CD8+ T cells in familial hemophagocytic lymphohistiocytosis with perforin gene mutations. Hum Immunol. 2013;74:1579-85.
226. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546-54.
227. Tortorano AM, Dho G, Prigitano A, Breda G, Grancini A, Emmi V, Cavanna C, Marino G, Morero S, Ossi C, Delvecchio G, Passera M, Cusumano V, David A, Bonaccorso G, Corona A, Favaro M, Vismara C, Garau MG, Falchi S, Tejada MR; ECMM-FIMUA Study Group. Invasive fungal infections in the intensive care unit: a multicentre, prospective, observational study in Italy (2006-2008). Mycoses. 2012;55:73-9.
228. Bougnoux M-E, Kac G, Aegerter P, d’Enfert C, Fagon J-Y. Candidemia and candiduria in critically ill patients admitted to intensive care units in France: incidence, molecular diversity, management and outcome. Intensive Care Med. 2008;34:292-9.
229. Netea MG, Sutmuller R, Hermann C, Van der Graaf CAA, Van der Meer JWM, van Krieken JH, Hartung T, Adema G, Kullberg BJ. Toll-like receptor 2 suppresses immunity against Candida albicans through induction of IL-10 and regulatory T cells. J Immunol. 2004;172:3712-8.
230. Taylor PR, Tsoni SV, Willment JA, Dennehy KM, Rosas M, Findon H, Haynes K, Steele C, Botto M, Gordon S, Brown GD. Dectin-1 is required for beta-glucan recognition and control of fungal infection. Nat Immunol. 2007;8:31-8.
231. Jaglowski SM, Devine SM. Graft-versus-host disease: why have we not made more progress? Curr Opin Hematol. 2014;21:141-7.
232. Bierer BE, Nishimura Y, Burakoff SJ, Smith BR. Phenotypic and functional characterization of human cytolytic T cells lacking expression of CD5. J Clin Invest. 1988;81:1390-7.
233. Bierer BE, Burakoff SJ, Smith BR. A large proportion of T lymphocytes lack CD5 expression
after bone marrow transplantation. Blood. 1989;73:1359-66.
234. Dhir S, Slatter M, Skinner R. Recent advances in the management of graft-versus-host disease. Arch Dis Child. 2014;
235. Pallier A, Hillion S, Danger R, Giral M, Racapé M, Degauque N, Dugast E, Ashton-Chess J, Pettré S, Lozano JJ, Bataille R, Devys A,Cesbron-Gautier A, Braudeau C, Larrose C, Soulillou JP, Brouard S. Patients with drug-free long-term graft function display increased numbers of peripheral B cells with a memory and inhibitory phenotype. Kidney Int. 2010;78:503-13.
236. De Waal Malefyt R, Yssel H, de Vries JE. Direct effects of IL-10 on subsets of human CD4+ T cell clones and resting T cells. Specific inhibition of IL-2 production and proliferation. J Immunol. 1993;150:4754-65.
237. Blazar BR, Taylor PA, Panoskaltsis-Mortari A, Narula SK, Smith SR, Roncarolo MG, Vallera DA. Interleukin-10 dose-dependent regulation of CD4+ and CD8+ T cell-mediated graft-versus-host disease. Transplantation. 1998;66:1220-9.
238. Vallera DA, Ash RC, Zanjani ED, Kersey JH, LeBien TW, Beverley PC, Neville DM Jr, Youle RJ. Anti-T-cell reagents for human bone marrow transplantation: ricin linked to three monoclonal antibodies. Science. 1983;222:512-5.
239. Siena S, Villa S, Bonadonna G, Bregni M, Gianni AM. Specific ex-vivo depletion of human bone marrow T lymphocytes by an anti-pan-T cell (CD5) ricin A-chain immunotoxin. Transplantation. 1987;43:421-6.
240. Uckun FM, Azemove SM, Myers DE, Vallera DA. Anti-CD2 (T, p50) intact ricin immunotoxins for GVHD-prophylaxis in allogeneic bone marrow transplantation. Leuk Res. 1986;10:145-53.
241. Uckun FM, Gajl-Peczalska K, Meyers DE, Ramsay NC, Kersey JH, Colvin M, Vallera DA. Marrow purging in autologous bone marrow transplantation for T-lineage acute lymphoblastic leukemia: efficacy of ex vivo treatment with immunotoxins and 4-hydroperoxycyclophosphamide against fresh leukemic marrow progenitor cells. Blood. 1987;69:361-6.
242. Filipovich AH, Vallera DA, Youle RJ, Haake R, Blazar BR, Arthur D, Neville DM Jr, Ramsay NK, McGlave P, Kersey JH. Graft-versus-host disease prevention in allogeneic bone marrow transplantation from histocompatible siblings.
Critical Reviews™ in Immunology
Consuegra-Fernández et al.114
A pilot study using immunotoxins for T cell depletion of donor bone marrow. Transplantation. 1987;44:62-9.
243. Siena S, Bregni M, Formosa A, Martineau D, Lappi DA, Bonadonna G, Gianni AM. Evaluation of antihuman T lymphocyte saporin immunotoxins potentially useful in human transplantation. Transplantation. 1988;46:747-53.
244. Derocq JM, Laurent G, Casellas P, Vidal H, Poncelet P, Fauser A, Demur C, Jansen F. Rationale for the selection of ricin A-chain anti-T immunotoxins for mature T cell depletion. Transplantation. 1987;44:763-9.
245. Preijers FW, De Witte T, Rijke-Schilder GP, Tax WJ, Wessels JM, Haanen C, Capel PJ. Human T lymphocyte differentiation antigens as target for immunotoxins or complement-mediated cytotoxicity. Scand J Immunol. 1988;28:185-94.
246. Bregni M, Siena S, Subar M, Villa S, Bonadonna G, Dalla-Favera R, Gianni AM. Detection of occult leukemic cells in the autologous bone marrow graft of a patient with T-cell acute lymphoblastic leukemia by a highly specific and sensitive assay. Haematologica. 1989;74:11-4.
247. Filipovich AH, Vallera D, McGlave P, Polich D, Gajl-Peczalska K, Haake R, Lasky L, Blazar B, Ramsay NK, Kersey J. T cell depletion with anti-CD5 immunotoxin in histocompatible bone marrow transplantation. The correlation between residual CD5 negative T cells and subsequent graft-versus-host disease. Transplantation. 1990;50:410-5.
248. Longmore G, Guinan EC, Weinstein HJ, Gelber RD, Rappeport JM, Antin JH. Bone marrow transplantation for myelodysplasia and secondary acute nonlymphoblastic leukemia. J Clin Oncol. 1990;8:1707-14.
249. Antin JH, Bierer BE, Smith BR, Ferrara J, Guinan EC, Sieff C, Golan DE, Macklis RM, Tarbell NJ, Lynch E. Selective depletion of bone marrow T lymphocytes with anti-CD5 monoclonal antibodies: effective prophylaxis for graft-versus-host disease in patients with hematologic malignancies. Blood. 1991;78:2139-49.
250. Weisdorf D, Filipovich A, McGlave P, Ramsay N, Kersey J, Miller W, Blazar B. Combination graft-versus-host disease prophylaxis using immunotoxin (anti-CD5-RTA [Xomazyme-CD5]) plus methotrexate and cyclosporine or prednisone after unrelated donor marrow transplantation. Bone Marrow Transplant. 1993;12:531-6.
251. Koehler M, Hurwitz CA, Krance RA, Coustan-Smith E, Williams LL, Santana V, Ribeiro RC, Brenner MK, Heslop HE. XomaZyme-CD5 immunotoxin in conjunction with partial T cell depletion for prevention of graft rejection and graft-versus-host disease after bone marrow transplantation from matched unrelated donors. Bone Marrow Transplant. 1994;13:571-5.
252. Przepiorka D, LeMaistre CF, Huh YO, Luna M, Saria EA, Brown CT, Champlin RE. Evaluation of anti-CD5 ricin A chain immunoconjugate for prevention of acute graft-vs.-host disease after HLA-identical marrow transplantation. Ther Immunol. 1994;1:77-82.
253. Henslee-Downey PJ, Parrish RS, MacDonald JS, Romond EH, Marciniak E, Coffey C, Ciocci G, Thompson JS. Combined in vitro and in vivo T lymphocyte depletion for the control of graft-versus-host disease following haploidentical marrow transplant. Transplantation. 1996;61:738-45.
254. Micallef IN, Chhanabhai M, Gascoyne RD, Shepherd JD, Fung HC, Nantel SH, Toze CL, Klingemann HG, Sutherland HJ, Hogge DE,Nevill TJ, Le A, Barnett MJ. Lymphoproliferative disorders following allogeneic bone marrow transplantation: the Vancouver experience. Bone Marrow Transplant. 1998;22:981-7.
255. Przepiorka D, Chan KW, Champlin RE, Culbert SJ, Petropoulos D, Ippoliti C, Khouri I, Huh YO, Vreisendorp H, Deisseroth AB. Prevention of graft-versus-host disease with anti-CD5 ricin A chain immunotoxin after CD3-depleted HLA-nonidentical marrow transplantation in pediatric leukemia patients. Bone Marrow Transplant. 1995;16:737-41.
256. Vallera DA, Carroll SF, Snover DC, Carlson GJ, Blazar BR. Toxicity and efficacy of anti-T-cell ricin toxin A chain immunotoxins in a murine model of established graft-versus-host disease induced across the major histocompatibility barrier. Blood. 1991;77:182-94.
257. Clark CL, Smith GJ, Crane PW, Price BA, Lear PA, Fabre JW, Wood RF. Reduction of graft-versus-host reactivity after small bowel transplantation: ex vivo treatment of intestinal allografts with an anti-T cell immunotoxin. Clin Exp Immunol. 1992;88:220-5.
258. Neipp M, Exner BG, Maru D, Haber M, Gammie JS, Pham SM, Ildstad ST. T-cell depletion of allogeneic bone marrow using anti-alphabeta TCR monoclonal antibody: prevention of graft-versus-host disease

Volume 35, Number 2, 2015
CD5-Based Immunotherapies 115
without affecting engraftment potential in rats. Exp Hematol. 1999;27:860-7.
259. Alexeev LP, Toptygin AY, Korenkova EV, Yan G, Moisiuk Y, Muromtseva IB, Tonevitsky AG, Dolbin AG, Sechkin AV, Shumakov VI,Vasilov RG, Khaitov RM. Pretreatment of kidney allografts with anti-CD5 immunotoxin: a new chance for high responder recipients. Transplant Proc. 1997;29:3605-6.
260. Galluzzi L, Vacchelli E, Bravo-San Pedro J-M, Buqué A, Senovilla L, Baracco EE, Bloy N, Castoldi F, Abastado JP, Agostinis P, Apte RN, Aranda F, Ayyoub M, Beckhove P, Blay JY, Bracci L, Caignard A, Castelli C, Cavallo F, Celis E,Cerundolo V, Clayton A, Colombo MP, Coussens L, Dhodapkar MV, Eggermont AM, Fearon DT, Fridman WH,Fučíková J, Gabrilovich DI, Galon J, Garg A, Ghiringhelli F, Giaccone G, Gilboa E, Gnjatic S, Hoos A, Hosmalin A,Jäger D, Kalinski P, Kärre K, Kepp O, Kiessling R, Kirkwood JM, Klein E, Knuth A, Lewis CE, Liblau R, Lotze MT, Lugli E, Mach JP, Mattei F, Mavilio D, Melero I, Melief CJ, Mittendorf EA, Moretta L, Odunsi A, Okada H, Palucka AK, Peter ME, Pienta KJ, Porgador A, Prendergast GC, Rabinovich GA, Restifo NP, Rizvi N, Sautès-Fridman C, Schreiber H, Seliger B, Shiku H, Silva-Santos B, Smyth MJ, Speiser DE, Spisek R, Srivastava PK, Talmadge JE, Tartour E, Van Der Burg SH, Van Den Eynde BJ, Vile R, Wagner H, Weber JS, Whiteside TL, Wolchok JD,Zitvogel L, Zou W, Kroemer G. Classification of current anticancer immunotherapies. Oncotarget. 2014;5:12472-508.
261. Vesely MD, Kershaw MH, Schreiber RD, Smyth MJ. Natural innate and adaptive immunity to cancer. Annu Rev Immunol. 2011;29:235-71.
262. Zitvogel L, Tesniere A, Kroemer G. Cancer despite immunosurveillance: immunoselection and immunosubversion. Nat Rev Immunol. 2006;6:715-27.
263. Senovilla L, Vacchelli E, Galon J, Adjemian S, Eggermont A, Fridman WH, Sautès-Fridman C, Ma Y, Tartour E, Zitvogel L, Kroemer G,Galluzzi L. Trial watch: prognostic and predictive value of the immune infiltrate in cancer. Oncoimmunology. 2012;1:1323-43.
264. Senovilla L, Galluzzi L, Zitvogel L, Kroemer G. Immunosurveillance as a regulator of tissue homeostasis. Trends Immunol. 2013;34:471-81.
265. Sakaguchi S, Wing K, Onishi Y, Prieto-Martin P, Yamaguchi T. Regulatory T cells: how do they suppress immune responses? Int Immunol. 2009;21:1105-11.
266. Medina-Echeverz J, Aranda F, Berraondo P. Myeloid-derived cells are key targets of tumor immunotherapy. Oncoimmunology. 2014;3:e28398.
267. Callahan MK, Postow MA, Wolchok JD. CTLA-4 and PD-1 pathway blockade: combinations in the clinic. Front Oncol. 2014;4:385.
268. Aranda F, Vacchelli E, Eggermont A, Galon J, Fridman WH, Zitvogel L, Kroemer G, Galluzzi L. Trial watch: immunostimulatory monoclonal antibodies in cancer therapy. Oncoimmunology. 2014;3:e27297.
269. Hollander N. Immunotherapy of lymphoid and nonlymphoid tumors with monoclonal anti-Lyt-1 antibodies. J Immunol. 1984;133:2801-5.
270. Hollander N. Effects of anti-Lyt antibodies on T-cell functions. Immunol Rev. 1982;68:43-66.
271. Dorothée G, Vergnon I, El Hage F, Le Maux Chansac B, Ferrand V, Lécluse Y, Opolon P, Chouaib S, Bismuth G, Mami-Chouaib F. In situ sensory adaptation of tumor-infiltrating T lymphocytes to peptide-MHC levels elicits strong antitumor reactivity. J Immunol. 2005;174:6888-97.
272. Friedlein G, El Hage F, Vergnon I, Richon C, Saulnier P, Lécluse Y, Caignard A, Boumsell L, Bismuth G, Chouaib S, Mami-Chouaib F. Human CD5 protects circulating tumor antigen-specific CTL from tumor-mediated activation-induced cell death. J Immunol. 2007;178:6821-7.
273. Tabbekh M, Franciszkiewicz K, Haouas H, Lécluse Y, Benihoud K, Raman C, Mami-Chouaib F. Rescue of tumor-infiltrating lymphocytes from activation-induced cell death enhances the antitumor CTL response in CD5-deficient mice. J Immunol. 2011;187:102-9.
274. Simeone E, Ascierto PA. Immunomodulating antibodies in the treatment of metastatic melanoma: the experience with anti-CTLA-4, anti-CD137, and anti-PD1. J Immunotoxicol. 9:241-7.
275. Dillman RO, Shawler DL, Dillman JB, Royston I. Therapy of chronic lymphocytic leukemia and cutaneous T-cell lymphoma with T101 monoclonal antibody. J Clin Oncol. 1984;2:881-91.
276. Foss FM, Raubitscheck A, Mulshine JL, Fleisher TA, Reynolds JC, Paik CH, Neumann RD, Boland C, Perentesis P, Brown MR,Frincke JM, Lollo CP, Larson SM, Carrasquillo JA. Phase I study of the pharmacokinetics of a radioimmunoconjugate, 90Y-T101, in patients with CD5-expressing leukemia and lymphoma. Clin Cancer Res. 1998;4:2691-700.
