cbm current
TRANSCRIPT

1 23
Current Fungal Infection Reports ISSN 1936-3761 Curr Fungal Infect RepDOI 10.1007/s12281-012-0116-8
Chromoblastomycosis in the ClinicalPractice
Flavio Queiroz-Telles & DanielW. C. L. Santos

1 23
Your article is protected by copyright and all
rights are held exclusively by Springer Science
+Business Media New York. This e-offprint is
for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.

EPIDEMIOLOGICAL ASPECTS OF FUNGAL INFECTIONS (T CHILLER AND J BADDLEY, SECTION EDITORS)
Chromoblastomycosis in the Clinical Practice
Flavio Queiroz-Telles & Daniel W. C. L. Santos
# Springer Science+Business Media New York 2012
Abstract Chromoblastomycosis is one of the most impor-tant implantation (subcutaneous) mycoses in the world. Inrecent years, the most significant advances against thisdisease have been made on the molecular taxonomy of theetiologic agents with an increase of the reported cases fromMainland China and South America. This article outlinesthe actual microbiologic, eco-epidemiologic and clinico-pathologic aspects of the disease, as well as recent thera-peutic tolls to treat patients with different severity of chro-moblasomycosis lesions.
Keywords Implantationmycoses . Subcutaneous mycoses .
Chromomycosis . Black fungi . Melagnized fungi .
Dematiaceous . Fonsecaea sp.Cladophialophora sp.Verrucous .Muriform .Sclerotic .Antifungals . Itraconazole .
Posaconazole . Terbinafine . Photodynamic therapy
Introduction
Fungal propagule may infect human hosts across differentportals for entry. The implantation mycoses encompass agroup of unrelatedmycotic diseases where the etiologic agentsare transported from their saprobiotic life in soil to thecutaneous tegument through transcutaneous wounds. The list
of implantation mycoses includes sporotrichosis, eumyce-toma, chromoblastomycosis (CBM), phaeohyphomycosis,entomophtoramycosis (subcutaneous zygomycosis), and laca-ziosis (lobomycosis). They are also known as “subcutaneousmycoses” but this term seems to be inadequate because someof these infections may also involve other sites like lymphaticvessels, muscles, fascia, cartilage and bones, beyond the skinand the subcutaneous tissues [1–3, 4••, 6]. Chromoblastomy-coses is one of the commonest implantation mycoses and it isalso the most frequent human disease caused by melanizedfungi. [4••, 5–8, 9••, 10••, 11••, 12••] This disease presents thefollowing characteristics: primary lesion beginning at the siteof inoculation; chronic involvement of cutaneous and subcu-taneous tissues associated with a granulomatous, purulent andfibrotic tissular response and a nonprotective humoral im-mune reaction [10••, 12••]. The disease is caused by severalspecies of melanized (Dematiaceous) fungi, most belonging tothe Herpotrichiellaceaea family which are ubiquitouos inplant and soil [7, 10••, 11••, 12••].
In tissues all the etiologic agents present as muriform(sclerotic) cells, the hallmark of this disease.These are con-sidered as a biological adaptation leading the agents tosurvive in the hostility of the tissue host environment[12••]. Muriform cells are fundamental fungal elements todifferentiate CBM and phaeohyphomycosis [13–15].
Chromoblastomycosis is mainly an occupational diseaseof adult males involved in rural labor without appropriatefootwear or clothing. It is found worldwide, but most clin-ical reports are from tropical and subtropical climates [10••,16–18], Clinically, the CBM lesions are polymorphic lead-ing to a diverse spectrum of differential diagnosis and if notdiscovered early, they may be very difficult to treat [4••, 19].
Etiologic Agents
Over time, many fungi have been related to the CBMetiology, dating back to the publication of the first cases
F. Queiroz-Telles (*)Department of Public Health, Federal University of Parana,Curtiba, PR, Brazile-mail: [email protected]
D. W. C. L. SantosSpecial Mycology Laboratory-LEMI, Department of Medicine,Federal University of São Paulo,São Paulo, Brazile-mail: [email protected]
D. W. C. L. SantosInstitute of Infectious Diseases Emílio Ribas,São Paulo, Brazil
Curr Fungal Infect Rep
DOI 10.1007/s12281-012-0116-8
Author's personal copy

by Rudolph, in 1914 [20, 21]. Nowadays there is agreementthat several melanized fungi of Herpotrichiellaceae familycause CBM. However the exact number remains uncertain,especially after molecular tools have been added to fungaltaxonomy. The main species, according to the taxonomicproposal, can be grouped into four genera: Fonsecaea, Cla-dophialophora, Phialophora, Rhinocladiella and Exophiala
[4••, 10••, 22–24] All the genera mentioned belong to phy-lum Ascomycota, order Chaetothyriales and the Herpotri-
chiellaceae family. They have the common feature ofpresenting a mycelia aspect in saprobiotic life and muriformcorpuscles in parasitic life. The identification of genus andspecies is based on studies of micromorphology of threetypes of conidiophores and nowadays based on the molec-ular sequence of specific genes [24, 25].
Fonsecaea spp. is the main agent of CBM in the world.Although this agent is considered to have a worldwidedistribution, it’s mostly found in rotten wood, soil anddecomposing plants in tropical areas, where the weather ishot and humid, especially in South America [10••, 26–29].Based on limitations of morphological characterization andin the broad spectrum of diseases seen by this agent, molec-ular studies were realized in this scenario. The genus Fon-secaea presently contains three species, which all arepotential etiologic agents of human CBM. Fonsecaea
pedrosoi is distributed mainly in Central and South America(>90 %) [4••, 8, 26–29]. Environmental isolation of F.
pedrosoi has been reported and the main clinical manifesta-tion caused by this agent is CBM [30–33]. The second mostfrequent specie of this genus is F. monophora. Most of theisolates of F. monophora came from cases of deep seatedphaeohyphomycosis (cerebral abscess, adenopathy) andfrom CBM, found in an environment without the use ofmammal bait [33, 34, 35••]. F. monophora is found notablyin China (>50 %) and in a minor proportion in SouthAmerica and other countries [18]. F. nubica is the third mostcommon species of this genus which originated fromChina and South America. Similar to F. pedrosoi, F.
nubica is an exclusive agent of CBM [25, 34, 36•,37]. New species of the genus Fonsecaea has beendescribed as pathogens of animal diseases. A novelfungal species was described originating from the leftoccipital lobe of the cerebrum of the cat. It was namedFonsecaea multimorphosa. Lethargic Crab Disease iscommon in mangrove land and it is caused by an exoticblack yeast named Fonsecaea brasiliensis. These agentsaren’t pathogenic for humans. [35••, 36•, 37–39].
Species of Cladophialophora genus can cause phaeohy-phomicosis (keratitis, onychomycosis, subcutaneous infec-tions, pulmonary and brain infections) and sinusitis. It’sfound in the air, rotting material and frequently as a con-taminant of food [26, 39, 40]. Cladophialophora carrionii,formerly known as Cladosporium carrionii, is the second
agent isolated from lesions of CBM. Similar to Fonsecaea,Cladophialophora carrionii was reclassified based on mo-lecular studies. Different populations within C. carrionii
were recognized on a molecular basis, one of which wasglobal, one Austropacific, and one Chinese. This agenthas a closely related, environmental counterpart, C.
yegresii [26, 39–41]. Other less frequent CBM agents,where patients were reported with muriform cells intissue, include Phialophora verrucosa, Rhinocladiella aqua-
spersa, Exophiala jeanselmei E. dermatitidis, E. spinifera,Rhytidhysteron rufulum [1, 10••, 23, 24, 34, 42].
Although the list of agents of CBM is increasing,they share common characteristics in their parasitic life.There is no distinction in clinical manifestations between thedifferent agents cited.
Epidemiology and Mode of Infection
It is believed that the CBM etiologic agents are soil and/orplant saprobes. It is accepted that these melanized fungithrive in tropical and subtropical environments worldwide.The highest prevalence of the disease is within a zonebetween 30° latitude North and 30° latitude South, coincid-ing with most of the tropical and subtropical climates [16].The most causative agents, i.e.: F. pedrosoi and C. carionii,
predominates in humid and dry regions, respectively[4••, 10••, 12••, 16, 17].
Although CBM has no compulsory notification, gathereddata from published case reports and surveys shows thatincidence rates may range from 1:6,800 (Madagascar) to 1/8,625,000 (USA) [16, 17]. Most of the reported cases occurin Latin America, the Caribbean, Asia, Africa and Australia[4••, 6, 7, 16]. Madagascar, Brazil, Mexico, DominicanRepublic, Venezuela, India and Southern China contributewith the majority of cases [9••]. The disease is less frequentin the North Hemisphere, including USA and Europeancountries [6, 16]. Because CBM is a implantation mycoses,a person’s occupation seems to play an important role on theincidence of this disease. [4••, 16]. The majority of lesionsare observed on the extremities of outdoor workers, mainlymale rural workers. The initial lesion is related to a transcu-taneous trauma that may lead to the transfer of the agent’sinfective propagule from its environmental saprobe life to aparasitic adaptation in the host cutaneous tegument [12••].The main risk factors associated with CBM infection are:adult, male rural workers or outdoor activities, lack ofprotective shoes, gloves or garments, and poor nutritionand hygienic habits [16, 43]. Although the list of risk factorsare frequently in the endemic areas and because the etiologicagents are ubiquitary in nature, a genetic susceptibility wasalso suggested as an individual risk for developing CBMclinically, indicating that a continuous exposition to the
Curr Fungal Infect Rep
Author's personal copy

etiologic agent implantation may also be important to pro-gression from infection to disease [44, 45]. In a series of 100patients reported from the Brazilian South region, there wasa predominance of male patients (4:1) whose ages rangedfrom 50 to 59 years, with lesions on their lower limbs [46].In another casuistic study enrolling 325 cases in the Brazil-ian Amazon region, the main age group affected by thediseases ranged from 41 to 70 years-old, 86.1 % of thepatients were agricultural-workers, 93.2 % of them weremales and 80.7 % showed lesions on the lower limbs (feetand legs) [29]. On the other hand, a series of cases inchildren and adolescents patients ranging from 2 to 19 yearsold have been reported in an endemic Venezuelan semi-aridzone. Infection was related to C. carrionii , probably trans-mitted by cacataceae thorn implantation [47].
The mode of disease transmission in CBM is the inocu-lation of soil or plant material contaminated by melanizedfungi through several types of occupational or recreationaltrauma and other nonconventional methods of transmission[4••, 16, 48] Table 1 depicts a collection of trauma that mayinitiate CBM lesions in geographically different patients.
Mechanisms of Immunity and Immunopathogeny
of Chromoblastomycosis
The knowledge of immunology of CBM is poorly under-stood because to date there areno reproducible animal mod-els. The innate immune response is important for controllingthe growth of microorganisms. Neutrophils and macro-phages produce nitric oxide (NO) which control the disease.Its chronicity is related to the inhibition of NO synthesis bymelanised fungus infected macrophages [50]. As in otherchronic fungal infections, patients with CBM produce spe-cific antibodies, including specific IgG1, IgM and IgA, butthey are not protectors against the progression of the disease[51, 52]. On the other hand, the cell-mediated immuneresponse has also been shown to have a key role in theclinical forms of the disease. The mixed tissular responsein CBM, shows a granulomatous reaction associated withmicroabscesses, suggesting ineffective phagocytosis of
muriform cells and the chronification of the disease [53,54]. The CBM clinical forms seem to be associated withthe cytokine cellular mediated immune response. Severeclinical forms are characterized by the production of IL-10and TNF-alpha. These cytokines, associated with low IFN-gamma and lymphocyte proliferation levels, could result ina depressed cellular immune response and severe manifes-tation of the disease. On the other hand, patients with themild form might represent the opposite pole, in which highIFN-gamma production parallels with lymphocyte prolifer-ation, in addition to very low levels of IL-10. Clinicalimplications of these studies are important, including immu-notherapy strategies with cytokine agonists or antagonists,alone or in combination with antifungal drugs [55].
Genetic aspects may be also important to the develop-ment of clinical manifestations.
Tsuneto et al., studied 32 Brazilian patients with chromo-blastomycosis and they found that susceptibility to the dis-ease could be conferred by a gene located on chromosomesix. So, they determined that HLA-A29 can cause suscepti-bility to CBM with a risk 10-fold higher [44]. Yegres-Rodríguez et al., suggested a genetic susceptibility to dis-ease when they conducted a study of family factors thatpromoted susceptibility to chromoblastomycosis in the pop-ulation of the endemic area of Falcon State, Venezuela [45].In respect to the CBM agent’s virulence factor, severalmolecular and immunological studies seek to clarify thehost immune response to the presence of the melanizedfungi in subcutaneous tissues. On the other hand, severalvirulence factors of CBM agents aren’t well known. Enzy-matic activities have been reported, particularly esterase,phospholipase and lipases. However, these findings havebeen observed in animal models and investigations inhumans are required. [56, 57]. Although melanin carries akey role in virulence of the pathogen, it can provide aninteraction of F. pedrosoi with phagocytes, resulting inhigher levels of fungal internalization and destruction byhost cells. These results indicate that melanin from F. pedro-
soi is an immunologically active fungal structure that acti-vates humoral and cellular responses that could help thecontrol of CBM by host defences [53].
Clinical Manifestations
The period between inoculation and the onset of the initiallesion is uncertain and some patients may not refer to it. Theinitial lesion may be a solitary and unilateral macular lesion.With time, it may progress to a papular shape lesion with apink smooth-surface that gradually increases over a fewweeks and then may have a scaly surface. The initial skinlesion may progress and evolve to polymorphic clinicalaspects. To better describe the CBM clinical aspects, several
Table 1 Different types of trauma associated to with the implantationof chromoblastomycosis agents
Type of trauma References
Plants associated: Wood, straw, grass, thorns,
palm trees, bamboo, coconut shells,
cacatacea
[10••, 32, 33, 47, 48, 58]
Animal associated: Insect stings, stomp cow,
buck rear, cock spine, caterpillar contact
[10••, 59]
Agricultural tools: Hoes, axes, knive, mills, [10••, 60]
Other: Bricks, fall, car crash, shoes [10••, 49]
Curr Fungal Infect Rep
Author's personal copy
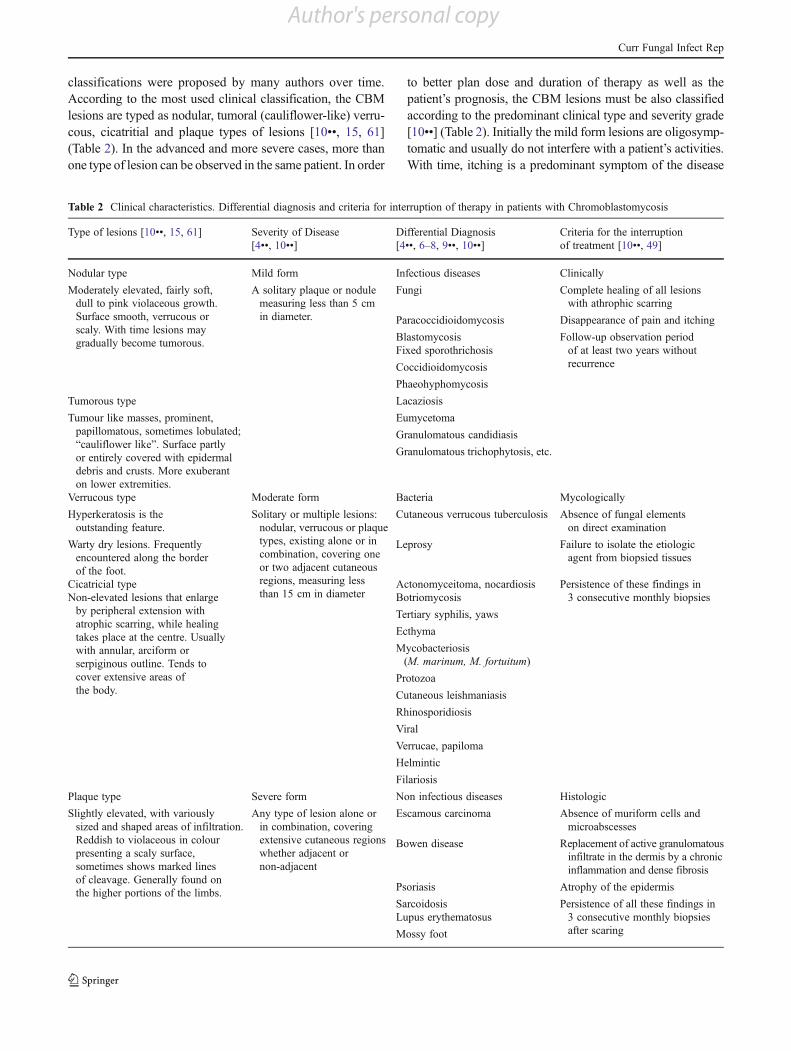
classifications were proposed by many authors over time.According to the most used clinical classification, the CBMlesions are typed as nodular, tumoral (cauliflower-like) verru-cous, cicatritial and plaque types of lesions [10••, 15, 61](Table 2). In the advanced and more severe cases, more thanone type of lesion can be observed in the same patient. In order
to better plan dose and duration of therapy as well as thepatient’s prognosis, the CBM lesions must be also classifiedaccording to the predominant clinical type and severity grade[10••] (Table 2). Initially the mild form lesions are oligosymp-tomatic and usually do not interfere with a patient’s activities.With time, itching is a predominant symptom of the disease
Table 2 Clinical characteristics. Differential diagnosis and criteria for interruption of therapy in patients with Chromoblastomycosis
Type of lesions [10••, 15, 61] Severity of Disease
[4••, 10••]
Differential Diagnosis
[4••, 6–8, 9••, 10••]
Criteria for the interruption
of treatment [10••, 49]
Nodular type Mild form Infectious diseases Clinically
Moderately elevated, fairly soft,
dull to pink violaceous growth.
Surface smooth, verrucous or
scaly. With time lesions may
gradually become tumorous.
A solitary plaque or nodule
measuring less than 5 cm
in diameter.
Fungi Complete healing of all lesions
with athrophic scarring
Paracoccidioidomycosis Disappearance of pain and itching
Blastomycosis Follow-up observation period
of at least two years without
recurrence
Fixed sporothrichosis
Coccidioidomycosis
Phaeohyphomycosis
Tumorous type Lacaziosis
Tumour like masses, prominent,
papillomatous, sometimes lobulated;
“cauliflower like”. Surface partly
or entirely covered with epidermal
debris and crusts. More exuberant
on lower extremities.
Eumycetoma
Granulomatous candidiasis
Granulomatous trichophytosis, etc.
Verrucous type Moderate form Bacteria Mycologically
Hyperkeratosis is the
outstanding feature.
Solitary or multiple lesions:
nodular, verrucous or plaque
types, existing alone or in
combination, covering one
or two adjacent cutaneous
regions, measuring less
than 15 cm in diameter
Cutaneous verrucous tuberculosis Absence of fungal elements
on direct examination
Warty dry lesions. Frequently
encountered along the border
of the foot.
Leprosy Failure to isolate the etiologic
agent from biopsied tissues
Cicatricial type Actonomyceitoma, nocardiosis Persistence of these findings in
3 consecutive monthly biopsiesNon-elevated lesions that enlarge
by peripheral extension with
atrophic scarring, while healing
takes place at the centre. Usually
with annular, arciform or
serpiginous outline. Tends to
cover extensive areas of
the body.
Botriomycosis
Tertiary syphilis, yaws
Ecthyma
Mycobacteriosis
(M. marinum, M. fortuitum)
Protozoa
Cutaneous leishmaniasis
Rhinosporidiosis
Viral
Verrucae, papiloma
Helmintic
Filariosis
Plaque type Severe form Non infectious diseases Histologic
Slightly elevated, with variously
sized and shaped areas of infiltration.
Reddish to violaceous in colour
presenting a scaly surface,
sometimes shows marked lines
of cleavage. Generally found on
the higher portions of the limbs.
Any type of lesion alone or
in combination, covering
extensive cutaneous regions
whether adjacent or
non-adjacent
Escamous carcinoma Absence of muriform cells and
microabscesses
Bowen disease Replacement of active granulomatous
infiltrate in the dermis by a chronic
inflammation and dense fibrosis
Psoriasis Atrophy of the epidermis
Sarcoidosis Persistence of all these findings in
3 consecutive monthly biopsies
after scaring
Lupus erythematosus
Mossy foot
Curr Fungal Infect Rep
Author's personal copy

which in the moderate forms, is intense and may be accom-panied by local pain. As severity increases, edema and bacte-rial secondary infections may lead to limitation or incapacityto labor routinely. Because the CBM lesions are very pruritic,It is accepted that the disease dissemination usually occurs byautoinoculation and contiguous lymphatic spread. In veryadvanced cases, chronic lymphedema, ankylosis and malig-nant transformation may occur [10••, 12••, 62–64, 65•]. Mostof the patients with CBM are otherwise healthy individualsand infection is limited to cutaneous and subcutaneous tissues.The earlier reports of systemic “chromoblastomicotic or chro-momicotic” infections in immunocompromised hosts are bet-ter referred to as phaeohyphomycosis nowadays, becauseusually hyphae, vesicular or yeast cells were observed intissue but not typical muriform cells [10••, 15, 66, 67].
Because CBM lesions are clinically polymorphic, thedifferential diagnosis may present a wide spectrum includ-ing infectious and noninfectious diseases (Table 2). Diagno-sis must always be confirmed by histopathological and/ormycological exams.
Laboratorial Diagnosis
The diagnosis of CBM requires the visualization of chestnut torounded brown pigmented structures with both transversal andlongitudinal cross septation resembling a brick wall and mea-suring 5 to 12 mm in diameter [10••, 14, 15]. Occasionally,near the cutaneous surface, the muriform cells may germinateand undergo dimorphic transformation displaying filamentousforms [68]. Fungal elements are easily found at the lesion’ssurface resembling black dots which are small hematic crustswith cellular debris and fungal structures, resulting from theirtransepithelial elimination [69, 70] (Fig. 1).
These areas are the main sites for collection of biologicmaterial because the visualization of the agent is easilyperformed. Skin scrapings, crusts, aspirated debris and tis-sue fragments can be analyzed. The direct examination ofthese with 10–40 % potassium hydroxide (KOH) can beperformed to detect the presence of dark brown muriformcells. The sensitivity of the direct exam ranges from 90 to100 % [70].
Although the direct visualization can be a fast exam,there are advantages in performing biopsies of lesions torealize histological studies with hematoxylin-eosin stain:contamination with aerobic bacteria is low and we canassess the immune response of the host and the healingprocess. In general, special stains (PAS and Grocott) arenot required for the diagnosis. Biopsies are also fundamentalto establish criteria for treatment interruption (Table 2)[10••, 49, 71]. CBM lesions are characterized histologicallyby pseudoepitheliomatous epidermal hyperplasia, hyperker-atosis, irregular acanthosis, alternating with areas of atrophyand collection of inflammatory cells forming epidermicabscesses. Granulomatous reaction with different grades offibrosis can be found at the dermal level. Muriform cellsmay be observed among these structures or inside Langer-hans giant cells [6, 7, 49, 72].
All the CBM agents present slow growing in culture.Initially the colonies are deep green, depicting a velvetydark aspect with time. Their correct identification has tradi-tionally been made through microscopic examination of theasexual reproductive structures. However, advances in mo-lecular taxonomy showed that the sequencing of specificgenes is necessary for correct identification at species level.As these techniques are not available in most centers, apractical identification method has been developed and con-sists of a rolling circle amplification technique [37, 40].
Therapy
Chromoblastomycosis lesions are recalcitrant and very dif-ficult to treat. Over time, several therapeutic regimens havebeen tried, including physical methods: surgery, thermo,laser and photodynamic therapies [3, 8, 9••, 10••, 12••, 71,73–78, 79•]. These therapeutic modalities are only indicatedat the early stages of the disease. They can also be associ-ated to systemic antifungal therapy. Initially the mild formsof CBM lesions can be treated by surgical excision butunfortunately most of the patients present with moderate tosevere forms, leading to long term courses of systemicantifungal drugs [71]. As in other neglected fungal infec-tions, comparative clinical trials are lacking in CBM. Hence,there is no treatment of choice for this mycosis, but rather aseries of therapeutic options. Neither in vitro sensibility testsare standard for the filamentous and the parasitic
Fig. 1 A nodular plaque lesion of chromoblastomycosis with several“black dots”(arrows) (a). Pathognomonic muriform cells are observedin KOH wet mount (b) and in HE sections (c)
Curr Fungal Infect Rep
Author's personal copy

(muriform), nor have experimental models been successful-ly developed for the therapy of the disease. Thus, it isaccepted that the most used drugs are itraconazole andterbinafine at the daily dose of 200–400 mg and 250–500 mg, respectively [8, 9••, 10••, 12••, 71, 73–75]. Inrefractory cases, the combination of these two drugs canbe tried [77]. Other effective treatments include posacona-zole, 800 mg per day and the combination of itraconazolewith 5-flucytosine [76, 78, 80••]. The association of thelatter with posaconazole may play an important role in thetherapy of this disease. The duration of therapy must bebased on clinical, mycological and histopathological cri-teria (Table 2). According to published data, cure rateswith terbinafine or itraconazole vary from 15 to 80 %,depending on the severity of the disease. As expected, insevere forms the cure rates are low and relapses are high[10••, 73–75].
Conclusions
The major recent advances in CBM were mainly achievedby the employment of molecular methods in the taxonomyof the etiologic agents and the epidemiology of this disease.This scientific progress did not seem to impact on themanagement of patients around the world. Patients withCBM still represent a true therapeutic challenge for clini-cians. Early clinical suspicion and adequate therapy are stillfundamental for therapeutic successes.
Disclosure F. Queiroz-Telles: none; D. W. de C. L. Santos: none
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Queiroz-Telles F, Mc Ginnis MR, Salkin I, Graybill JR. Subcuta-neous mycoses. Infect Dis Clin North Am. 2003;17:59–85.
2. Pang KR, Wu JJ, Huang DB, Tyring SK. Subcutaneous fungalinfections. Dermatol Ther. 2004;17:523–31.
3. Lupi O, Tyring SK, McGinnis MR. Tropical dermatology: fungaltropical diseases. J Am Acad Dermatol. 2005;53:931–51.
4. •• Queiroz-Telles F, Nucci M, Colombo AL, et al. Mycoses ofimplantation in Latin America: an overview of epidemiology, clinicalmanifestations, diagnosis and treatment. Med Mycol. 2011;49:225–36. This paper summarizes the most relevant casuistic reports and
suggests the use of the term “mycoses of implantation” instead of
“subcutaneous mycoses” for chromoblastomycosis and other similar
fungal infections.5. Errol Reiss H, Shadomy HJ, Marshall Lyon III. Mycoses of im-
plantation: fundamental Medical Mycology, In: John Wiley &Sons, Inc editor, Wiley-Blackwell, 2012. p475.
6. La Hoz RM, Baddley JW. Subcutaneous Fungal Infections CurrInfect Dis Rep, 2012; published on line 19 July 2012.
7. Rippon JW. Chromoblastomycosis and related dermal infectionscaused by dematiaceous fungi. In: Rippon JW, editor. MedicalMycology. The Pathogenic Fungi and the Pathogenic Actinomy-cetes. 2nd ed. Philadelphia: WB Saunders; 1982. p. 249–76.
8. Bonifaz A, Carrasco-Gerard E, Saul A. Chromoblastomycosis:clinical and mycologic experience of 51 cases. Mycoses. 2001;44(1–2):1–7.
9. •• Ameen M. Chromoblastomycosis: clinical presentation and man-agement. Clin Exp Dermatol. 2009;34:849–54. This paper shows anupdated approach for the management of chromoblastomycosis.
10. •• Queiroz-Telles F, Esterre P, Perez-Blanco M, et al. Chromoblas-tomycosis: an overview of clinical manifestations, diagnosis andtreatment. Med Mycol. 2009;47:3–15. This paper is a complete
review of the clinical, epidemiological, diagnostic and therapeutic
aspects of chromoblastomycosis.11. •• Revankar SG, Sutton DA. Melanized fungi in human disease.
Clin Microbiol Rev. 2010;23:884–928. This paper offers an exten-
sive review of the principal mycoses due to melanized fungi.12. •• Esterre P, Queiroz-Telles F. Management of chromoblastomycosis:
novel perspectives. Curr Opin Infect Dis. 2006;19:148–52. Thispaper reports the actual immunopathology of chromoblastomycosis.
13. Ajello L, Georg LK, Steilbigel RT, Wang K. A case of phaeohy-phomycosis caused by a new species of Phialophora. Mycologia.1974;66:490–8.
14. Matsumoto T, Matsuda T, McGinnis MR, Ajello L. Clinical andmycological spectra of Wangiella dermatitidis infections. Mycoses.1993;36:145–55.
15. McGinnis MR. Chromoblastomycosis and phaeohyphomycosis:new concepts, diagnosis, and mycology. J Am Acad Dermatol.1983;8:1–16.
16. Al-Doory Y. Chromomycosis In: Di Salvo, A.F. Occupational my-coses, 95–21. Ed.Lea & Febiger. Philadelphia. 1983, p. 95–121
17. Esterre P, Andriantsimahavandy A, et al. Forty years of chromoblasto-mycosis in Madagascar: a review. AmJTrop Med Hyg. 1996;55:45–7.
18. Xi L, Sun J, Lu C, et al. Molecular diversity of Fonsecaea(Chaetothyriales) causing chromoblastomycosis in Southern Chi-na. Med Mycol. 2009;47:27–33.
19. Garnica M, Nucci M, Queiroz-Telles F. Difficult mycoses of theskin: advances in the epidemiology and management of eumyce-toma, phaeohyphomycosis and chromoblastomycosis. Curr OpinInfect Dis. 2009;22:559–63.
20. Rudolph M. Über die brasilianische “Figueira” (Vorläufige Mittei-lung). Archiev Schiffs Tropen-Hyg. 1914;18:498–9.
21. Castro RM, Castro LGM. On the priority of description chromo-mycosis. Mykosen. 1987;30:397–403.
22. Borelli D. Acrotheca aquaspersa nova, new species agent of chro-momycosis. Acta Cient Venez. 1972;23:193–6.
23. Barba-Gomez JF, Mayorga J, McGinnis MR, Gonzalez-MendozaA. Chromoblastomycosis caused by Exophiala spinifera. J AmAcad Dermatol. 1992;26:367–70.
24. Naka W, Harada T, Nishikawa T, Fukushiro R. A case of chromo-blastomycosis: with special reference to the mycology of theisolated Exophiala jeanselmei. Mykosen. 1986;29:445–52.
25. de Hoog GS, Attili-Angelis D, Vicente VA, Van Den Ende AH,Queiroz-Telles F. Molecular ecology and pathogenic potential ofFonsecaea species. Med Mycol. 2004;42:405–16.
26. de Hoog GS, Nishikaku AS, Fernandez-Zeppenfeldt G, et al.Molecular analysis and pathogenicity of the Cladophialophora
carrionii complex, with the description of a novel species. StudMycol. 2007;58:219–34.
27. Silva ACC Me, Serra Neto A, Galvao CES, et al. Fonsecaeapedrosoi-caused chromoblastomycosis in the state of Maranhao.I. The clinical, epidemiological and evolutionary aspects. Rev SocBras Med Trop. 1992;25:37–44.
Curr Fungal Infect Rep
Author's personal copy

28. Pires CAA, Simões JA, Quaresma BR, et al. Clinical, epidemiologicalandmycological report on 65 patients from the Eastern Amazon regionwith chromoblastomycosis. An Bras Dermatol. 2012;87:555–60.
29. Silva JP, de Souza W, Rozental S. Chromoblastomycosis: a retro-spective study of 325 cases on Amazonic Region (Brazil). Myco-pathologia. 1998;143:171–5.
30. Gezuele E, Mackinnon JE, Conti-Diaz IA. The frequent isolationof Phialophora verrucosa and Phialophora pedrosoi from naturalsources. Sabouraudia. 1972;10:266–73.
31. Vicente AP, Attili DA, Queiroz-Telles F, et al. Isolation of Herpo-trichiellacious fungi from the environment. Braz J Microbiol.2001;32:47–51.
32. Salgado CG, da Silva JP, Diniz JAP, et al. Isolation of Fonsecaeapedrosoi from thorns ofMimosa pudica, a probable natural source ofChromoblastomycosis. Rev Inst Med Trop S Paulo. 2004;46:33–6.
33. Marques SG, Silva SMP, Saldanha PC, et al. Isolation of Fonse-caea pedrosoi from the shell of Babassu coconut (Orbignya pha-lerata Martius) in the Amazon Region of Maranhao, Brazil. Jpn JMed Mycol. 2006;47:305–3011.
34. Kondo M, Hiruma M, Nishioka Y, et al. A case of chromo-mycosis caused by Fonsecaea pedrosoi and a review ofreported cases of dematiaceous fungal infection in Japan.Mycoses. 2005;48:221–5.
35. •• Najafzadeh MJ, Gueidan C, Badali H, van den Ende AH, Xi L,de Hoog GS. Genetic diversity and species delimitation in theopportunistic genus Fonsecaea. Med Mycol. 2009;47:17–25. Thispaper uses molecular tools to describe several species of genus
Fonsecaea.36. • Vicente VA, Orélis-Ribeiro R, Najafzadeh MJ, Sun J, et al. Black
yeast-like fungi associated with Lethargic Crab Disease (LCD) inthe mangrove-land crab, Ucides cordatus (Ocypodidae). VetMicrobiol. 2012;158:109–22. This paper describes a new species
of melanized fungi which is pathogenic for crabs.37. Najafzadeh MJ, Sun J, Vicente V, Xi L, van den Ende AH, de Hoog
GS. Fonsecaea nubica sp. nov, a new agent of human chromoblasto-mycosis revealed using molecular data. Med Mycol. 2010;48:800–6.
38. Najafzadeh MJ, Vicente VA, Sun J, Meis JF, de Hoog GS. Fonsecaeamultimorphosa sp. nov, a new species of Chaetothyriales isolatedfrom a feline cerebral abscess. Fungal Biol. 2011;115:1066–76.
39. Guarro J, Gené J, Stchigel AM. Developments in fungal taxonomy.Clin Microbiol Rev. 1999;12:454–500.
40. Badali H, Gueidan C, Najafzadeh MJ, et al. Biodiversity of thegenus Cladophialophora. Stud Mycol. 2008;61:175–91.
41. Vitale RG, Perez-Blanco M, De Hoog GS. In vitro activity ofantifungal drugs against Cladophialophora species associated withhuman chromoblastomycosis. Med Mycol. 2009;47:35–40.
42. Chowdhary A, Guarro J, Randhawa HS, Gené J, Cano J, Jain RK,Kumar S, Khanna G. A rare case of chromoblastomycosis in arenal transplant recipient caused by a non-sporulating species ofRhytidhysteron. Med Mycol. 2008;46:163–6.
43. Londero AT, Ramos CD. Chromomycosis: a clinical and myco-logic study of thirty-five cases observed in the hinterland of RioGrande do Sul, Brazil. AmJTrop Med Hyg. 1976;25:132–5.
44. Tsuneto LT, Arce-Gomez B, Petzl-Erler ML, Queiroz-Telles F.HLA-A29 and genetic susceptibility to chromoblastomycosis. JMed Vet Mycol. 1989;27:181–5.
45. Yeguez-Rodriguez J, Richard-Yegres N, Yegres F, Rodriguez-Lerralde A. Cromomicosis: susceptibilidad genetica en gruposfamiliares de la zona endémica en Venezuela. Acta CientíficaVenezolana. 1992;43:98–102.
46. Minotto R, Bernardi CD, Mallmann LF, Edelweiss MI, ScrofernekerML. Chromoblastomycosis: a review of 100 cases in the state of RioGrande do Sul, Brazil. J Am Acad Dermatol. 2001;44:585–92.
47. Perez-Blanco M, Herna´ndez Valles R, Garcia-Humbria L, Yegres F.Chromoblastomycosis in children and adolescents in the endemicarea of the Falcon State, Venezuela. Med Mycol. 2006;44:467–471.
48. Tschen JA, Knox JM, McGavran MH, Duncan C. Chromomyco-sis. Association of fungal elements and wood splinters. ArchDermatol. 1974;120:107–8.
49. Bayles MA. Chromomycosis. In: Hay RJ, editor. Baillie’re’s clin-ical tropical medicine and comunicable diseases. Tropical fungalinfections. London: WB Saunders; 1986. p. 45–70.
50. BoccaAL, Brito PP, Figueiredo F, Tosta CE. Inhibition of nitric oxideproduction by macrophages in chromoblastomycosis: a role for Fon-secaea pedrosoi melanin. Mycopathologia. 2006;161:195–203.
51. Esterre P, Jahevitra M, Andriantsimahavandy A. Humoral immuneresponse in Chromoblastomycosis during and after therapy. ClinDiagn Lab Immunol. 2000;7:497–500.
52. Vidal MS, Castro LG, Cavalcante SC, Lacaz CS. Highly specificand sensitive, immunoblot-detected 54 kDa antigen from Fonse-caea pedrosoi. Med Mycol. 2004;42:511–5.
53. Alviano DS, Franzen DJ, Travassos LR, et al. Melanin fromFonsecaea pedrosoi induces production of human antifungal anti-bodies and enhances the antimicrobial efficacy of phagocytes.Infect Immun. 2004;72:229–37.
54. Esterre P, Peyrol S, Sainte-Marie D, et al. Granulomatous reactionand tissue remodelling in the cutaneous lesions of chromomycosis.Pathol Res Pract. 1993;422:285–91.
55. Mazo FGV, Da Gloria DS, Ferreira KS, et al. Cytokines andlymphocyte proliferation in patients with different clinical formsof chromoblastomycosis. Microbes Infect. 2005;7:708–13..
56. Souza TF, Scroferneker ML, Costa JM, Carissimi M, Corbellini VA.Secretion of five extracellular enzymes by strains of chromoblasto-mycosis agents. Rev Inst Med Trop Sao Paulo. 2008;50:269–72.
57. Palmeira VF, Kneipp LF, Alviano CS, dos Santos AL. Phospholipaseand esterase production by clinical strains of Fonsecaea pedrosoi andtheir interactions with epithelial cells. Mycopathologia. 2010;170:31–7.
58. Yew CC. Chromoblastomycosis: preliminary report case observedin China. Chin Med J. 1951;69:476.
59. Simsom FW, Harington C, Barnetson J. Chromoblastomycosis: areport of six cases. J Pathol Bacteriol. 1943;55:191–8.
60. Costello NJ, Defeo CP, Littman ML. Chromoblastomycosis treatedwith local infiltration of amphotericin B solution. Arch Dermatol.1959;79:184.
61. Carrion AL. Chromoblastomycosis. Ann NY Acad Sci.1950;50:1255–82.
62. Foster HM, Harris TJ. Malignant change (esquamous carcinoma) inchronic chromoblastomycosis. Aust N Z J Surg. 1987;57:775–59.
63. Paul C, Dupont B, Pialoux G, Avril MF, Pradinaud R. Chromo-blastomycosis with malignant transformation and cutaneous-synovial secondary localization. The potential therapeutic role ofitraconazole. J Med Vet Mycol. 1991;29:313–6.
64. Esterre P, Pecarrère JL, Raharisolo C, Huerre M. Squamous cellcarcinoma arising from chromomycosis. Report of two cases. AnnPathol. 1999;19(6):516–20.
65.• Jamil A, Lee YY, Thevarajah S. Invasive squamous cell carcino-ma arising from chromoblastomycosis. Med Mycol. 2012;50(1):99–102. This paper reports the malignant transformation of
a chromoblastomycosis lesion.66. Harada S, Ueda T, Kusunoki T. Systemic chromomycosis. J Der-
matol. 1976;3:13–7.67. Wackym PA, Gray Jr GF, Richie RE, Gregg CR. Cutaneous
chromomycosis in renal transplant recipients. Successful manage-ment in two cases. Arch Intern Med. 1985;145:1036–7.
68. Lee MW, Hsu S, Rosen T. Spores and mycelia in cutaneouschromomycosis. J Am Acad Dermatol. 1998;39:850–2.
69. Zaias N. Chromomycosis. J Cutan Pathol. 1978;5:155–64.70. Zaias N, Rebell G. A simple and accurate diagnostic method in
chromoblastomycosis. Arch Dermatol. 1973;108:545–6.71. Queiroz-Telles F, Purim KS, Fillus JN, et al. Itraconazole in the
treatment of chromoblastomycosis due to Fonsecaea pedrosoi. IntJ Dermatol. 1992;31:805–12.
Curr Fungal Infect Rep
Author's personal copy

72. Salfelder K, de Liscano TR, Sauerteig E. Atlas of fungal patholo-gy. Dordrecht: Kluwer; 1990. p. 145–50.
73. Restrepo A, Gonzalez A, Gomez I, Arango M, de Bedout C.Treatment of chromoblastomycosis with itraconazole. Ann N YAcad Sci. 1988;544:504–16.
74. Bonifaz A, Saul A, Paredes-Solis V, Araiza J, Fierro-Arias L.Treatment of chromoblastomycosis with terbinafine: experiencewith four cases. J Dermatolog Treat 2005; 16: 47_51.
75. Esterre P, Inzan CK, Rtasioharana M, et al. A multicenter trialof terbinafine in patients with chromoblastomycosis: effects onclinical and biological criteria. J Dermatol Treat. 1998;9:529–34.
76. Pradinaud R, Bolzinger T. Treatment of chromoblastomycosis. JAm Acad Dermatol. 1991;25:869–70.
77. Gupta AK, Taborda PR, Sanzovo AD. Alternate week and combina-tion itraconazole and terbinafine therapy for chromo- blastomycosis
caused by Fonsecaea pedrosoi in Brazil. Med Mycol. 2002;40:529–34.
78. Negroni R, Tobon A, Bustamante B, et al. Posaconazole treatmentof refractory eumycetoma and chromoblastomycosis. Rev InstMed Trop Sao Paulo. 2005;47:9–346.
79. • Lyon JP, Azevedo CMPS, Moreira LM, Lima CG, Resende MA.Photodynamic antifungal therapy against chromoblastomycosis.Mycopathologia. 2011;172:293–7. This paper reports a new phys-
ical method to be combined with antifungals for the therapy of
chromoblastomycosis.80. •• Antonello VS, Appel da Silva MC, Cambruzzi DA, Santos BR,
Queiroz-Telles F. Treatment of severe chromoblastomycosis withitraconazole and 5-flucytosine association. Rev Inst Med Trop SaoPaulo. 2010;52:329–31. This is a case report of one of the best
therapeutic approaches for patients needing antifungal therapy for
chromoblastomycosis.
Curr Fungal Infect Rep
Author's personal copy