biomarkers in burnout: a systematic review
TRANSCRIPT

Journal of Psychosomatic Research xx (2010) xxx–xxx
Review article
Biomarkers in burnout: A systematic review
Marie Bernardine Danhof-Ponta,⁎, Tineke van Veenb, Frans G. Zitmanb
aDepartment of Health, Safety, and Environment, Leiden University Medical Center and Leiden University, RC Leiden, The NetherlandsbDepartment of Psychiatry, Leiden University Medical Center, RC Leiden, The Netherlands
Received 10 February 2010; received in revised form 26 October 2010; accepted 26 October 2010
Abstract
Background: Burnout is a stress state characterized by symp-toms of mental exhaustion and physical fatigue, detachment fromwork, and feelings of diminished competence. Several biomarkershave been tested for association with burnout, but the results areconflicting. Aim: The objective of this review was to identifypotential biomarkers for burnout. Methods: We carried out asystematic review of studies comparing biomarkers in individualswith burnout and healthy controls, or individuals with low scoresand those with high scores on burnout questionnaires. Literaturesearches in MEDLINE and EMBASE were performed. We describebiomarkers on which at least three studies were available. Whereappropriate, a meta-analysis was carried out.Results:We identified31 studies on 38 biomarkers involved in the hypothalamus–pituitary–adrenal axis, autonomic nervous system, immune system,metabolic processes, antioxidant defense, hormones, and sleep. At
⁎ Corresponding author. Department of Safety, Health, and Environ-ment, Leiden University Medical Center and Leiden University, Poortge-bouw Zuid, P.O. Box 9600, 2300 RC Leiden, The Netherlands. Tel.: +31 (0)71 5268015; fax +31 (0)71 5261052.
E-mail address: [email protected] (M.B. Danhof-Pont).
0022-3999/10/$ – see front matter © 2010 Elsevier Inc. All rights reserved.doi:10.1016/j.jpsychores.2010.10.012
least 3 studies were available for cortisol in saliva and blood, bloodpressure, heart rate, cholesterol, dehydroepiandrosterone sulfate,(numbers or activity of) natural killer cells, C-reactive protein, andprolactin. The comparability of studies was limited, due todifferences in the methods used to characterize patients and controls,to assess biomarkers, and to control for confounders. Furthermore,burnout was operationalized in different ways. Meta-analysesshowed no differences for cortisol awakening response and cortisolawakening response after administration of dexamethasone, cortisolin blood, and blood pressure.Conclusions:No potential biomarkersfor burnout were found, largely due to the incomparability of studies.We emphasize the need for a dimensional and longitudinal approachin future research to account for the heterogeneity of burnout.© 2010 Elsevier Inc. All rights reserved.
Keywords: Burnout; Biomarkers; HPA axis
Introduction
Burnout is a stress state characterized by such symptomsas mental exhaustion and physical fatigue, detachment fromwork, diminished competence, loss of energy, increasedirritability and sleep, and concentration problems that canoccur irrespective of the type of profession [1]. Yearly,approximately 10%–15% of the working population inThe Netherlands suffers from burnout [2]. In 2008, 17% ofall reported occupational diseases concerned work-related
psychological problems [3]. In The Netherlands, the welfareof the employees who yearly report ill because of stress atwork costs 1.7 billion Euros [4]. Therefore, it is importantto prevent and treat burnout effectively.
Risk factors include a high workload, monotonoustasks, conflict with superiors or colleagues, and exposureto aggressive behavior of customers [5]. According to thewidely used demand–control model, the risk of develop-ing burnout is higher if there is a combination of highpsychological demands and poor job resources [6]. How-ever, it remains unclear why some people developburnout, whereas others do not. Furthermore, psycholog-ical treatment, consisting of relaxation therapy, cognitivetherapy, learning of coping skills, and reactivation, canreduce complaints effectively. However, individuals differwidely in the rate of recovery. It is largely unknown

Table 1Search strategy and terms used to identify studies on burnout and biomarkers
1 ((“Diagnostic Techniques, Neurological” [MeSH] OR “DiagnosticTests, Routine” [MeSH] OR “Diagnostic Techniques and Procedures”[MeSH] OR “Diagnostic Imaging” [MeSH] OR “Mental Disorders”[MeSH] OR “diagnostic use” [Subheading] OR “Clinical ChemistryTests” [MeSH] OR “Clinical Laboratory Techniques” [MeSH] OR“Biological Markers” [MeSH] OR “Psychological Techniques” [MeSH]OR “Psychiatry” [MeSH] OR “Chemistry, Clinical” [MeSH] OR“blood” [Subheading]))
2 Burnout3 1 AND 2Direct keywords or MeSH terms4 “Cortisol”5 “antioxidant enzymes”6 “immune variables”7 “leukocyte adhesiveness/aggregation”8 “blood pressure”9 “heart rate”10 “tumor necrosis factor alpha”11 “prolactine”12 “pituitary–adrenal hormones”13 “leucocyte”14 “C-reactive protein”15 “antioxidants”16 “pituitary hormones”17 (2) AND (4) OR (2) AND (5) OR (2) AND (6) OR (2) AND (7) OR (2)
AND (8) OR (2) AND (9) OR (2) AND (10) OR (2) AND (11) OR (2)AND (12) OR (2) AND (13) OR (2) AND (14) OR (2) AND (15) OR(2) AND (16)
The search was continued in PUBMED and EMBASE using “burnout” incombination with these biomarkers.
2 M.B. Danhof-Pont et al. / Journal of Psychosomatic Research xx (2010) xxx–xxx
which factors influence treatment refractoriness. Asburnout is a stress state, it has been hypothesized thatthe autonomous nervous system (ANS) and the hypothal-amus–pituitary–adrenal axis (HPA axis) are involved.Most studies on the behavior of these systems focused onacute stress. During acute stress, the sympathetic part ofthe ANS is activated and the parasympathetic part isdown-regulated. These are reflected in peripheral blood bythe release of catecholamines via the ANS and by releaseof cortisol via the HPA axis. There is an increase in bothheart rate and blood pressure. The immune system istemporarily suppressed, and metabolism becomes catabol-ic. Among patients with burnout, an increased incidenceof common cold, flu-like illness, and gastroenteritis hasbeen reported [7]. Therefore, several studies haveinvestigated if biomarkers involved in the immuneresponse were associated with burnout.
After stress, all processes return to normal. It is hypo-thesized that in burnout the ANS and HPA axis havebecome exhausted due to prolonged or recurrent stress. Ithas been postulated that, as a consequence, burnout will beaccompanied by abnormal (low) blood levels of adrenalineand cortisol and their metabolites. In addition, vitalfunctions, such as heart rate and blood pressure, areexpected to remain overactivated and metabolism and theimmune system to be compromised. These dysfunctionswould be responsible for the symptom of physical fatigue.However, it is unlikely that these biological changes areresponsible for the other symptoms of burnout [i.e.,feelings of emotional exhaustion (EE), detachment fromwork, and diminished competence].
In order to investigate the evidence for a role of ANS,the HPA axis, and the vital functions mentioned above,we reviewed the literature until December 2008 on studiesof biomarkers in burnout.
Subjects and methods
Search strategy
Articles published until December 2008 were identifiedthrough a search of PUBMED (http://www.ncbi.nlm.nih.gov/entrez/query.fcgi) and EMBASE (http://www.ovid.com). An overview of the search strategy is given inTable 1.
The inclusion criteria were as follows: (1) publishedclinical trials and observational studies; (2) studies thatcompared biological markers between healthy individualsand participants who suffered from burnout, or biologicalmarkers between individuals with high scores and thosewith low scores on a burnout scale; and (3) articles in theDutch, English, or German language. The absence of areference group was an exclusion criterion. The full textof relevant articles was obtained. The references of thesearticles were manually reviewed for additional studies.
Data extraction
For each eligible study, detailed information wascollected (by one investigator) on year, country of study,sample size, definition of burnout, severity of burnout, andconfounders adjusted for. Authors of primary studies werecontacted to obtain data when articles did not provide therequired information.
Methodological quality
For assessment of the quality of observational studies,to assess the risk of bias, we extracted additional dataregarding the recruitment of cases and controls, responserate, selection of subjects, similarity of baseline charac-teristics, and appropriate control for confounding.
Statistical analysis
We chose to perform a meta-analysis on biomarkersfor which at least three studies in which the biomarkerwas assessed in the same body fluid were available. Forcomparable studies, the differences of the means ofbiomarker levels were calculated with accompanying 95%confidence intervals. Random-effects models were madeto allow for different effects in the studies. Theseanalyses were conducted using Review Manager [8].
3M.B. Danhof-Pont et al. / Journal of Psychosomatic Research xx (2010) xxx–xxx
Multilevel meta-analyses were carried out for the cortisolawakening response (CAR) and the CAR after dexameth-asone, which consist of measurements at the time ofawakening and 15, 30, and 45 min thereafter. For thisanalysis, Proc Mixed of SAS 9.1.3 for multilevelmodeling (SAS Institute, Cary, NC, USA) was used[9,10]. In order to select an appropriate covariance matrixfor this analysis, we inspected correlation matrices of twodata sets of the CAR (Klaassens et al. [11]; Langelaan etal. [12]). On the basis thereof, and as the number ofstudies was small, compound symmetry covariance matrixwas selected. In the meta-analysis, the data showedreasonable fit with the (conservative) assumption of aconstant correlation of 0.8 between intra-individualcortisol measurements. Sensitivity analyses with correla-tions of 0.7 and 0.9 were carried out. P values b.05 wereconsidered statistically significant.
Results
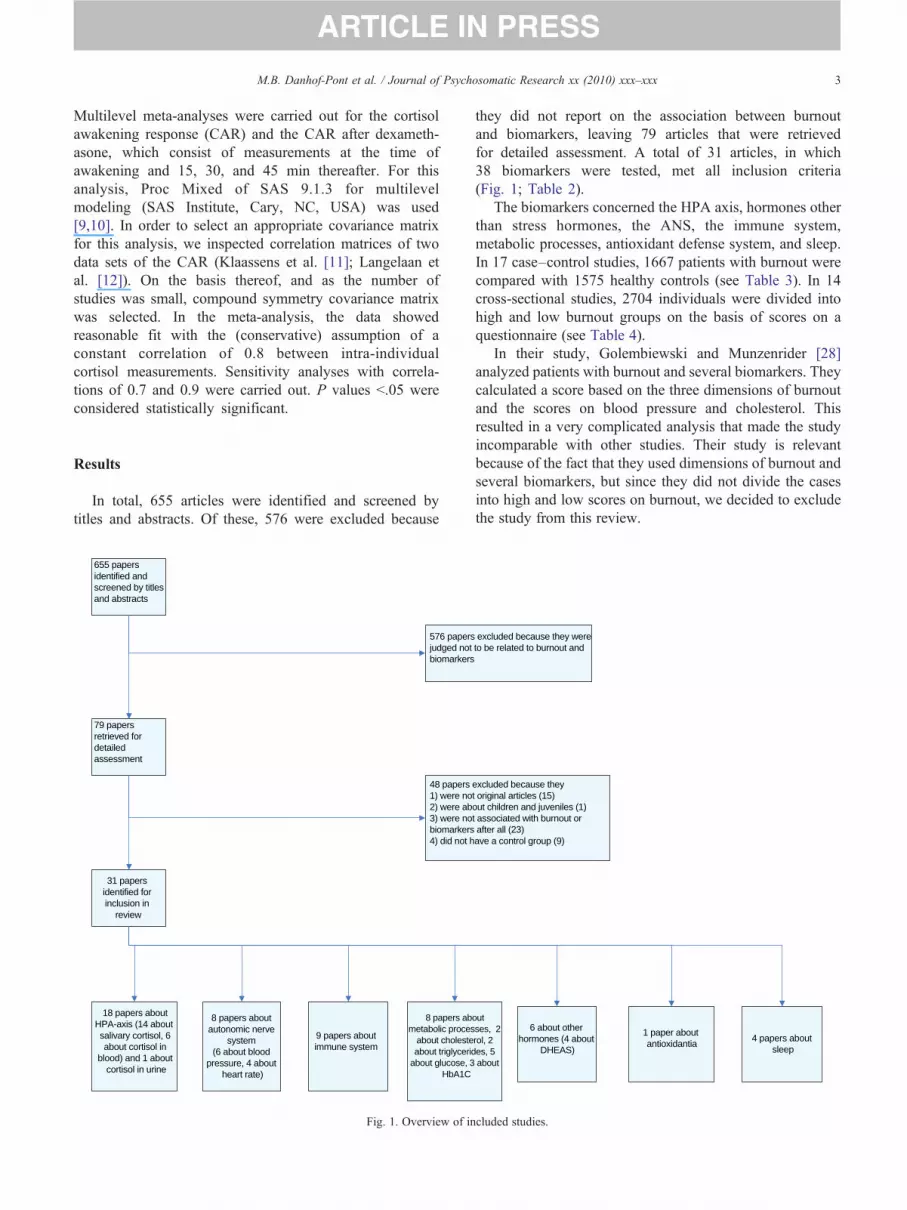
In total, 655 articles were identified and screened bytitles and abstracts. Of these, 576 were excluded because
655 papers identified and screened by titles and abstracts
79 papers retrieved for detailed assessment
18 papers about HPA-axis (14 about salivary cortisol, 6 about cortisol in
blood) and 1 about cortisol in urine
8 papers about autonomic nerve
system (6 about blood
pressure, 4 about heart rate)
9 papers about immune system
8 papers abmetabolic proces
about cholesteabout triglyceri
about glucose, 3HbA1C
31 papers identified for inclusion in
review
576 papersjudged notbiomarkers
48 papers 1) were no2) were ab3) were nobiomarkers4) did not h
Fig. 1. Overview of in
they did not report on the association between burnoutand biomarkers, leaving 79 articles that were retrievedfor detailed assessment. A total of 31 articles, in which38 biomarkers were tested, met all inclusion criteria(Fig. 1; Table 2).
The biomarkers concerned the HPA axis, hormones otherthan stress hormones, the ANS, the immune system,metabolic processes, antioxidant defense system, and sleep.In 17 case–control studies, 1667 patients with burnout werecompared with 1575 healthy controls (see Table 3). In 14cross-sectional studies, 2704 individuals were divided intohigh and low burnout groups on the basis of scores on aquestionnaire (see Table 4).
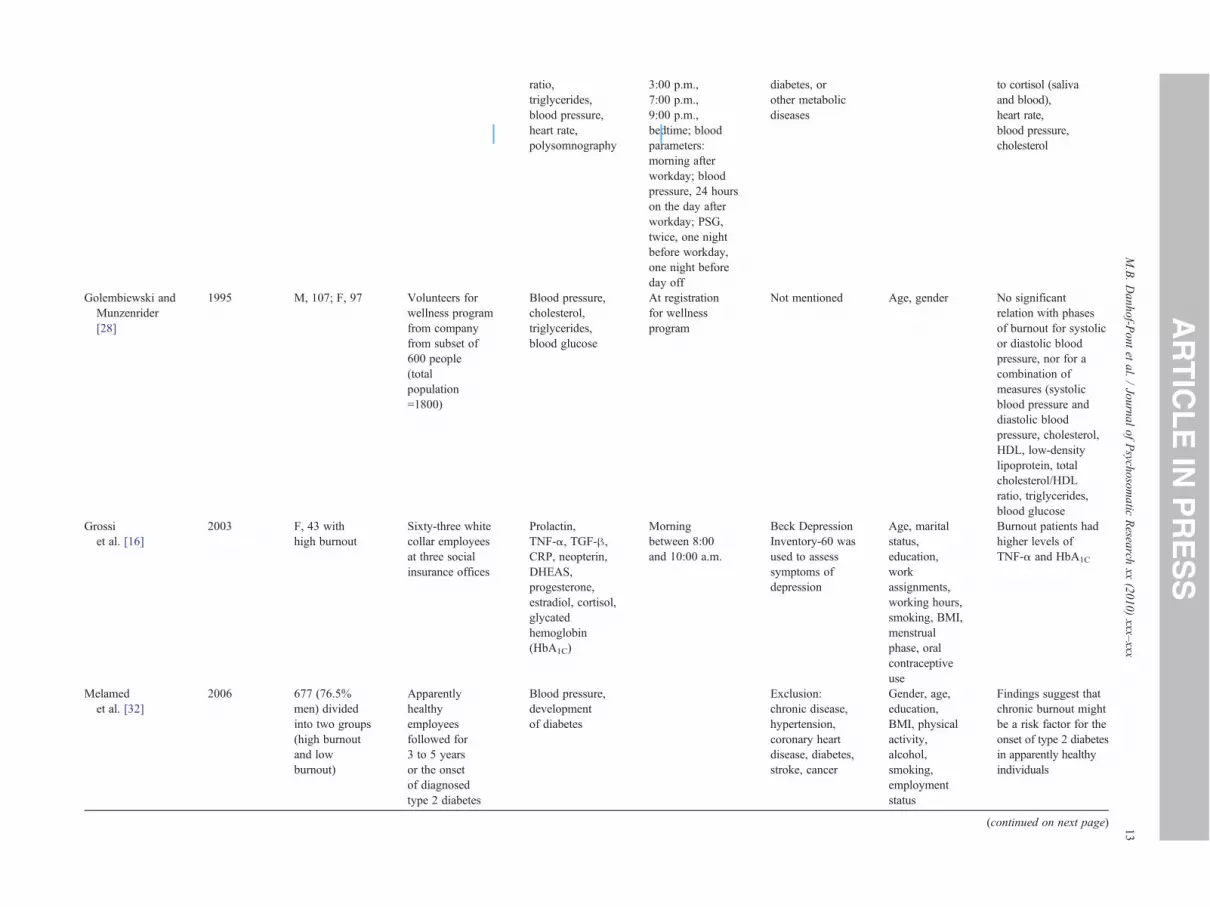
In their study, Golembiewski and Munzenrider [28]analyzed patients with burnout and several biomarkers. Theycalculated a score based on the three dimensions of burnoutand the scores on blood pressure and cholesterol. Thisresulted in a very complicated analysis that made the studyincomparable with other studies. Their study is relevantbecause of the fact that they used dimensions of burnout andseveral biomarkers, but since they did not divide the casesinto high and low scores on burnout, we decided to excludethe study from this review.
out ses, 2 rol, 2 des, 5 about
6 about other hormones (4 about
DHEAS)
1 paper about antioxidantia
excluded because they were to be related to burnout and
excluded because they t original articles (15)out children and juveniles (1)t associated with burnout or after all (23)ave a control group (9)
4 papers about sleep
cluded studies.
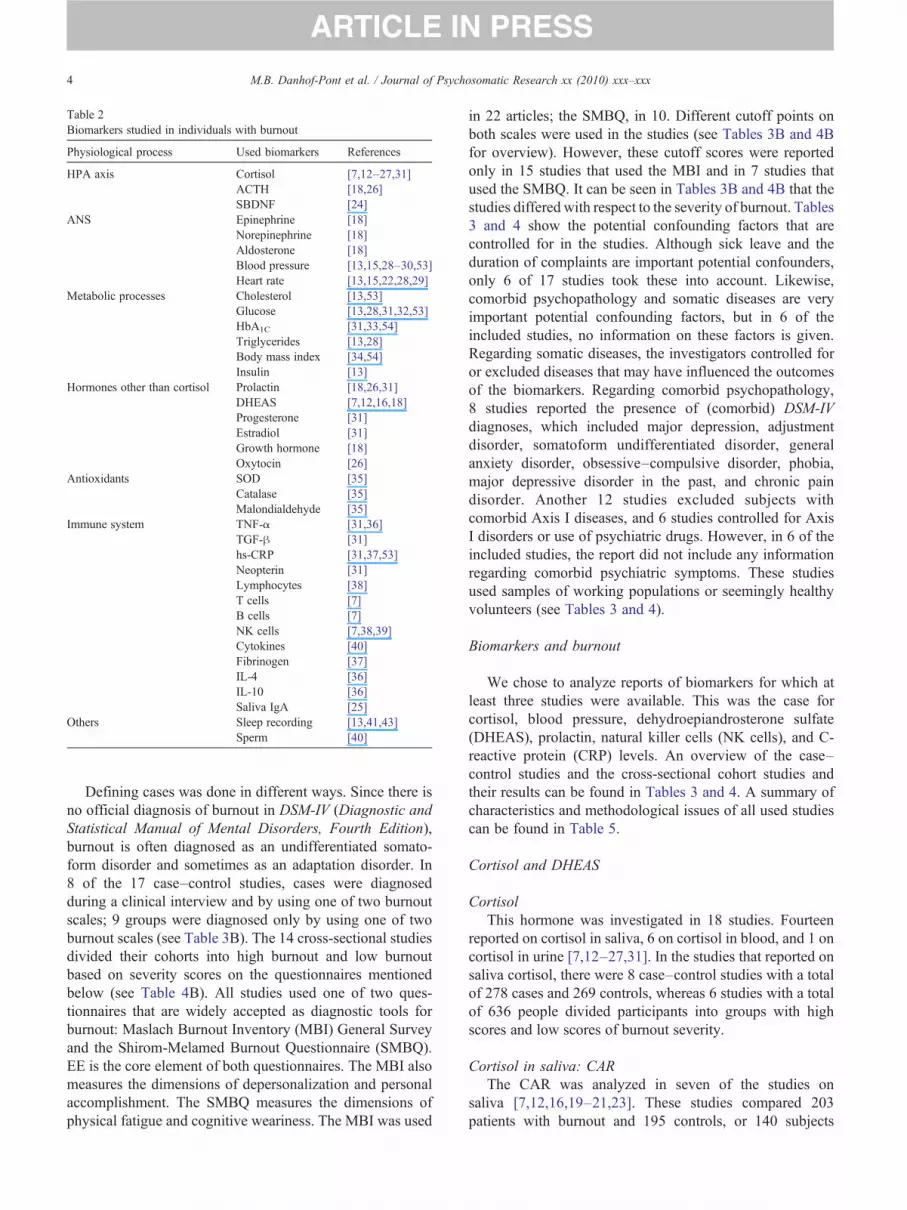
Table 2Biomarkers studied in individuals with burnout
Physiological process Used biomarkers References
HPA axis Cortisol [7,12–27,31]ACTH [18,26]SBDNF [24]
ANS Epinephrine [18]Norepinephrine [18]Aldosterone [18]Blood pressure [13,15,28–30,53]Heart rate [13,15,22,28,29]
Metabolic processes Cholesterol [13,53]Glucose [13,28,31,32,53]HbA1C [31,33,54]Triglycerides [13,28]Body mass index [34,54]Insulin [13]
Hormones other than cortisol Prolactin [18,26,31]DHEAS [7,12,16,18]Progesterone [31]Estradiol [31]Growth hormone [18]Oxytocin [26]
Antioxidants SOD [35]Catalase [35]Malondialdehyde [35]
Immune system TNF-α [31,36]TGF-β [31]hs-CRP [31,37,53]Neopterin [31]Lymphocytes [38]T cells [7]B cells [7]NK cells [7,38,39]Cytokines [40]Fibrinogen [37]IL-4 [36]IL-10 [36]Saliva IgA [25]
Others Sleep recording [13,41,43]Sperm [40]
4 M.B. Danhof-Pont et al. / Journal of Psychosomatic Research xx (2010) xxx–xxx
Defining cases was done in different ways. Since there isno official diagnosis of burnout in DSM-IV (Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition),burnout is often diagnosed as an undifferentiated somato-form disorder and sometimes as an adaptation disorder. In8 of the 17 case–control studies, cases were diagnosedduring a clinical interview and by using one of two burnoutscales; 9 groups were diagnosed only by using one of twoburnout scales (see Table 3B). The 14 cross-sectional studiesdivided their cohorts into high burnout and low burnoutbased on severity scores on the questionnaires mentionedbelow (see Table 4B). All studies used one of two ques-tionnaires that are widely accepted as diagnostic tools forburnout: Maslach Burnout Inventory (MBI) General Surveyand the Shirom-Melamed Burnout Questionnaire (SMBQ).EE is the core element of both questionnaires. The MBI alsomeasures the dimensions of depersonalization and personalaccomplishment. The SMBQ measures the dimensions ofphysical fatigue and cognitive weariness. The MBI was used
in 22 articles; the SMBQ, in 10. Different cutoff points onboth scales were used in the studies (see Tables 3B and 4Bfor overview). However, these cutoff scores were reportedonly in 15 studies that used the MBI and in 7 studies thatused the SMBQ. It can be seen in Tables 3B and 4B that thestudies differed with respect to the severity of burnout. Tables3 and 4 show the potential confounding factors that arecontrolled for in the studies. Although sick leave and theduration of complaints are important potential confounders,only 6 of 17 studies took these into account. Likewise,comorbid psychopathology and somatic diseases are veryimportant potential confounding factors, but in 6 of theincluded studies, no information on these factors is given.Regarding somatic diseases, the investigators controlled foror excluded diseases that may have influenced the outcomesof the biomarkers. Regarding comorbid psychopathology,8 studies reported the presence of (comorbid) DSM-IVdiagnoses, which included major depression, adjustmentdisorder, somatoform undifferentiated disorder, generalanxiety disorder, obsessive–compulsive disorder, phobia,major depressive disorder in the past, and chronic paindisorder. Another 12 studies excluded subjects withcomorbid Axis I diseases, and 6 studies controlled for AxisI disorders or use of psychiatric drugs. However, in 6 of theincluded studies, the report did not include any informationregarding comorbid psychiatric symptoms. These studiesused samples of working populations or seemingly healthyvolunteers (see Tables 3 and 4).
Biomarkers and burnout
We chose to analyze reports of biomarkers for which atleast three studies were available. This was the case forcortisol, blood pressure, dehydroepiandrosterone sulfate(DHEAS), prolactin, natural killer cells (NK cells), and C-reactive protein (CRP) levels. An overview of the case–control studies and the cross-sectional cohort studies andtheir results can be found in Tables 3 and 4. A summary ofcharacteristics and methodological issues of all used studiescan be found in Table 5.
Cortisol and DHEAS
CortisolThis hormone was investigated in 18 studies. Fourteen
reported on cortisol in saliva, 6 on cortisol in blood, and 1 oncortisol in urine [7,12–27,31]. In the studies that reported onsaliva cortisol, there were 8 case–control studies with a totalof 278 cases and 269 controls, whereas 6 studies with a totalof 636 people divided participants into groups with highscores and low scores of burnout severity.
Cortisol in saliva: CARThe CAR was analyzed in seven of the studies on
saliva [7,12,16,19–21,23]. These studies compared 203patients with burnout and 195 controls, or 140 subjects

5M.B. Danhof-Pont et al. / Journal of Psychosomatic Research xx (2010) xxx–xxx
with high vs. low scores on burnout severity. All studiesadjusted for possible effects on cortisol of age, gender,smoking, and oral anticonceptives. One study analyzed 74cases before and 62 cases after treatment (Mommersteeg et al.[19]). As these data were paired, we did not include this studyin the meta-analysis.
Within the six included studies, the typical shape of theCAR was present. However, the baseline levels variedwidely between studies. Forest plots were used to investigatethe origin of these differences. Clinical features (severity ofdisease, confounders controlled for) or methodologicalfeatures (case–control vs. cross-sectional, sample size) didnot explain this statistical heterogeneity. Differences inabsolute values may be due to different protocols inlaboratories (Garde and Hansen [44]) or to selection ofsubjects. Although the mean severity of burnout in groupswas not related to cortisol levels, the healthy control groupselected by Grossi et al. [16] had cortisol levels far lowerthan those of the cases. In the other studies, there was morebetween-study variation than within-study variation. There-fore, the results of the meta-analysis need to be interpretedwith caution. We pooled the results from the six studies onCAR in a multilevel meta-analysis and used random-effectsmodels to account for heterogeneity in effects. There was nodifference in CAR between patients with burnout andcontrols. (See Fig. 2).
Cortisol in saliva: CAR after dexamethasoneThe CAR was measured after administration of dexa-
methasone in the evening in five studies [7,12,19,21,23].Dexamethasone is a cortisol analogue that has difficultycrossing the blood–brain barrier. In the used dose of 0.25mg, dexamethasone suppressed mainly the ACTH release inthe pituitary gland where the blood–brain barrier is missing.Thus, dexamethasone suppression of the CAR is anindication of the sensitivity of the HPA axis for negativefeedback [7]. The between-study variability was consider-ably lower than for the CAR. Three of the studies comparedpeople who sought medical help for burnout with healthycontrols (Mommersteeg et al. [7,21]; Langelaan et al. [12]).Pruessner et al. [23] divided 66 teachers in a group thatscored high on burnout and a group that scored low onburnout, and Mommersteeg et al. [19] followed 74 clients ofa psychotherapy outpatient clinic. They all used the samemethod in the sampling and measurement of cortisol. Theseverity of the burnout symptoms differed between the fivestudies. Only Pruessner et al. found higher suppression ofcortisol after dexamethasone. The multilevel meta-analysisrevealed no significant differences between patients withburnout and controls (see Fig. 3). More studies are necessaryto see if the association of CAR after dexamethasone withdimensions of burnout can be replicated.
Cortisol in saliva: other assessmentsThere were one report on saliva cortisol measurements at
only one time point [24] and another at two time points [25]
in the morning. In these reports, no associations of burnoutwith cortisol levels were observed. However, as cortisollevels follow a diurnal pattern, it is essential to measurecortisol on time points with reference to the moment ofawakening. In conclusion, these two studies are notinformative on the association between cortisol and burnout.
Blood cortisolWe found six articles that reported on blood cortisol
levels [13,18,22,24,26,31]. In these studies, single fastingblood samples were taken between 8:00 and 10:00 a.m.One hundred ninety cases were compared with 60 healthycontrols. One study divided a population of 41 soldiersinto those with high scores on burnout and those withlow scores [22]. No differences were found betweenpatients and controls in a fasting blood sample takenbetween 8:00 and 10:00 a.m. [18,31], although Moch etal. [18] found that patients had a significantly lower meanserum cortisol level only after 4 months of therapy. Atbaseline, after 1 and 2 months, no differences were found.Sertoz et al. [24] found normal cortisol levels in patientsand controls. Tops et al. [26] used a different approach;they treated nine female burnout subjects and nine controlswith 35 mg of cortisol and placebo and found that thepeople with a low dopaminergic function improved fromcortisol replacement.
We did not carry out a meta-analysis as we deemed thestudies incomparable.
In summary, observations on blood cortisol levels areconflicting. As mentioned in Cortisol in saliva: otherassessments, there is a diurnal pattern in the level of cortisol.Therefore, the time of awakening should be mentioned inthese studies to be able to find associations between cortisoland burnout.
DheasDHEAS is a steroid hormone with an immunomodulatory
function opposite to cortisol. Four articles compared levelsof DHEAS, with a total of 164 cases with burnout and 113controls [7,12,16,18]. Two studies assessed blood levels ofDHEAS. They did not find differences between patients withburnout and healthy controls [16,18]. The other two studiesmeasured saliva levels of DHEAS [7,12]. In one of these,DHEAS levels were higher in burnout cases. In this study,only healthy managers with few burnout symptoms wereincluded [12]. The other study reported no associationbetween DHEAS and burnout. In summary, the studies couldnot be pooled, and evidence is inconclusive. Further study isneeded to investigate if DHEAS is elevated in (a subgroupof) patients with burnout.
The ANSBlood pressure. Four studies reported on blood pressure
in burnout [15,29,32,53]. One of these reported only meanblood pressure and was not included in the meta-analysis ofsystolic or diastolic blood pressure [29]. The studies by

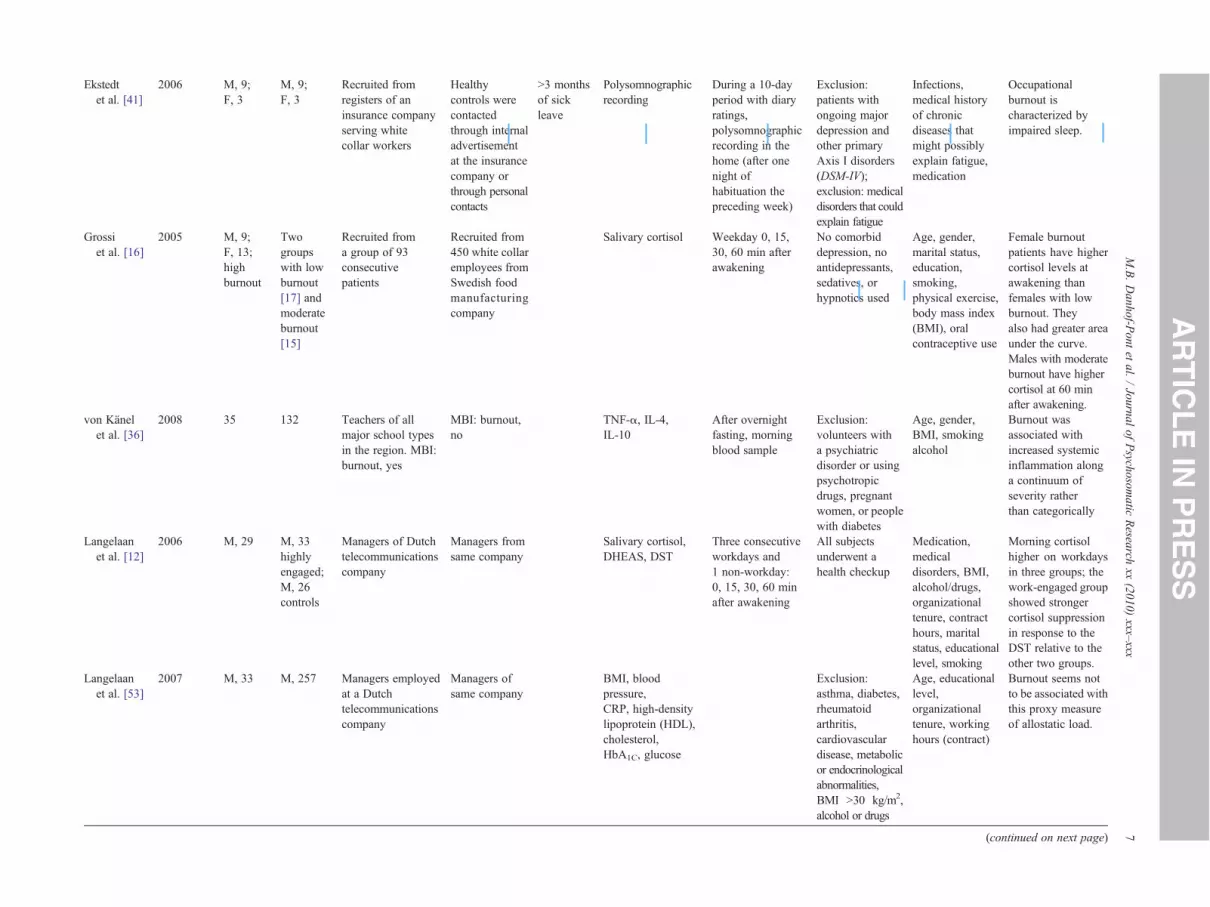
Table 3Characteristics of used studies (patients vs. controls)
A. Overview
AuthorsYear ofpublication
No. ofpatients
No. ofcontrols
Characteristicsof patients
Characteristicsof controls
Meanduration ofcomplaintsat intake
Biomarkersused
Time ofmeasurement
Psychopathologyor somatic illness
Controlledvariables Results
Moragonet al. [42]
2005 M, 69;F, 42
80 Healthy workersof a prehospitalaryemergency servicein Spain
Eighty age-matchedhealthyindividualsof both sexes
Antioxidantenzymes: SODand catalase
Not mentioned;healthy workers
Gender, age,place of birth,marital status,lifestyle,smoking, alcohol,coffee, workshifts, workingconditions
No significantvariations withrespect to sex andlevels of burnout.Significantdifferences in SODactivity between thecontrol group andworkers were found.SOD activity washigher in workers onnight and eveningshifts.
CasadoMoragon,LucasGarcia[35]
2006 M 69;F42(samegroup asstudy 4)
80 (samegroup asotherstudy oftheseauthors)
healthy workersof a prehospitalaryemergency servicein Spain
80 age-matchedhealthyindividualsof both sexes
malondialdehyde(end product oflipid peroxidation
psychopathologynot mentioned,subjects had noother somaticillness
gender, age, placeof birth, maritalstatus, lifestyle,smoking, alcohol,coffee, workshifts,professionalcategories,workingconditions
A positivecorrelationbetweenmalondialdehydeand occupationalstress, as estimatedby elements of theMBI, andoxidative stress.
De Venteet al. [15]
2003 M, 14;F, 8
M, 10;F, 13
Recruited throughoccupational healthpractitioners
Recruitedthrough flyersin libraries andother publicplaces andstudents
46%between6 and12 months;36% morethan12 months
Salivary cortisol,heart rate, bloodpressure
Saliva cortisol: 0,30, 60 min afterawakening,12:00 p.m.; fivetimes duringlaboratorysession; bloodpressure and heartrate continuousfinger bloodpressure duringstress test
Exclusion:primary axisdisorders;exclusion: historyof medicaldisease, suchas diabetes
Gender, age,smoking, type ofoccupation,medicaldisorders,primary axisdisorders
Burnout: higherresting HR;burnout patientsshowed elevatedcortisol levelsduring the firsthour afterawakening.
6M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx
Ekstedtet al. [41]
2006 M, 9;F, 3
M, 9;F, 3
Recruited fromregisters of aninsurance companyserving whitecollar workers
Healthycontrols werecontactedthrough internaladvertisementat the insurancecompany orthrough personalcontacts
N3 monthsof sickleave
Polysomnographicrecording
During a 10-dayperiod with diaryratings,polysomnographicrecording in thehome (after onenight ofhabituation thepreceding week)
Exclusion:patients withongoing majordepression andother primaryAxis I disorders(DSM-IV);exclusion: medicaldisorders that couldexplain fatigue
Infections,medical historyof chronicdiseases thatmight possiblyexplain fatigue,medication
Occupationalburnout ischaracterized byimpaired sleep.
Grossiet al. [16]
2005 M, 9;F, 13;highburnout
Twogroupswith lowburnout[17] andmoderateburnout[15]
Recruited froma group of 93consecutivepatients
Recruited from450 white collaremployees fromSwedish foodmanufacturingcompany
Salivary cortisol Weekday 0, 15,30, 60 min afterawakening
No comorbiddepression, noantidepressants,sedatives, orhypnotics used
Age, gender,marital status,education,smoking,physical exercise,body mass index(BMI), oralcontraceptive use
Female burnoutpatients have highercortisol levels atawakening thanfemales with lowburnout. Theyalso had greater areaunder the curve.Males with moderateburnout have highercortisol at 60 minafter awakening.
von Känelet al. [36]
2008 35 132 Teachers of allmajor school typesin the region. MBI:burnout, yes
MBI: burnout,no
TNF-α, IL-4,IL-10
After overnightfasting, morningblood sample
Exclusion:volunteers witha psychiatricdisorder or usingpsychotropicdrugs, pregnantwomen, or peoplewith diabetes
Age, gender,BMI, smokingalcohol
Burnout wasassociated withincreased systemicinflammation alonga continuum ofseverity ratherthan categorically
Langelaanet al. [12]
2006 M, 29 M, 33highlyengaged;M, 26controls
Managers of Dutchtelecommunicationscompany
Managers fromsame company
Salivary cortisol,DHEAS, DST
Three consecutiveworkdays and1 non-workday:0, 15, 30, 60 minafter awakening
All subjectsunderwent ahealth checkup
Medication,medicaldisorders, BMI,alcohol/drugs,organizationaltenure, contracthours, maritalstatus, educationallevel, smoking
Morning cortisolhigher on workdaysin three groups; thework-engaged groupshowed strongercortisol suppressionin response to theDST relative to theother two groups.
Langelaanet al. [53]
2007 M, 33 M, 257 Managers employedat a Dutchtelecommunicationscompany
Managers ofsame company
BMI, bloodpressure,CRP, high-densitylipoprotein (HDL),cholesterol,HbA1C, glucose
Exclusion:asthma, diabetes,rheumatoidarthritis,cardiovasculardisease, metabolicor endocrinologicalabnormalities,BMI N30 kg/m2,alcohol or drugs
Age, educationallevel,organizationaltenure, workinghours (contract)
Burnout seems notto be associated withthis proxy measureof allostatic load.
(continued on next page) 7M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx
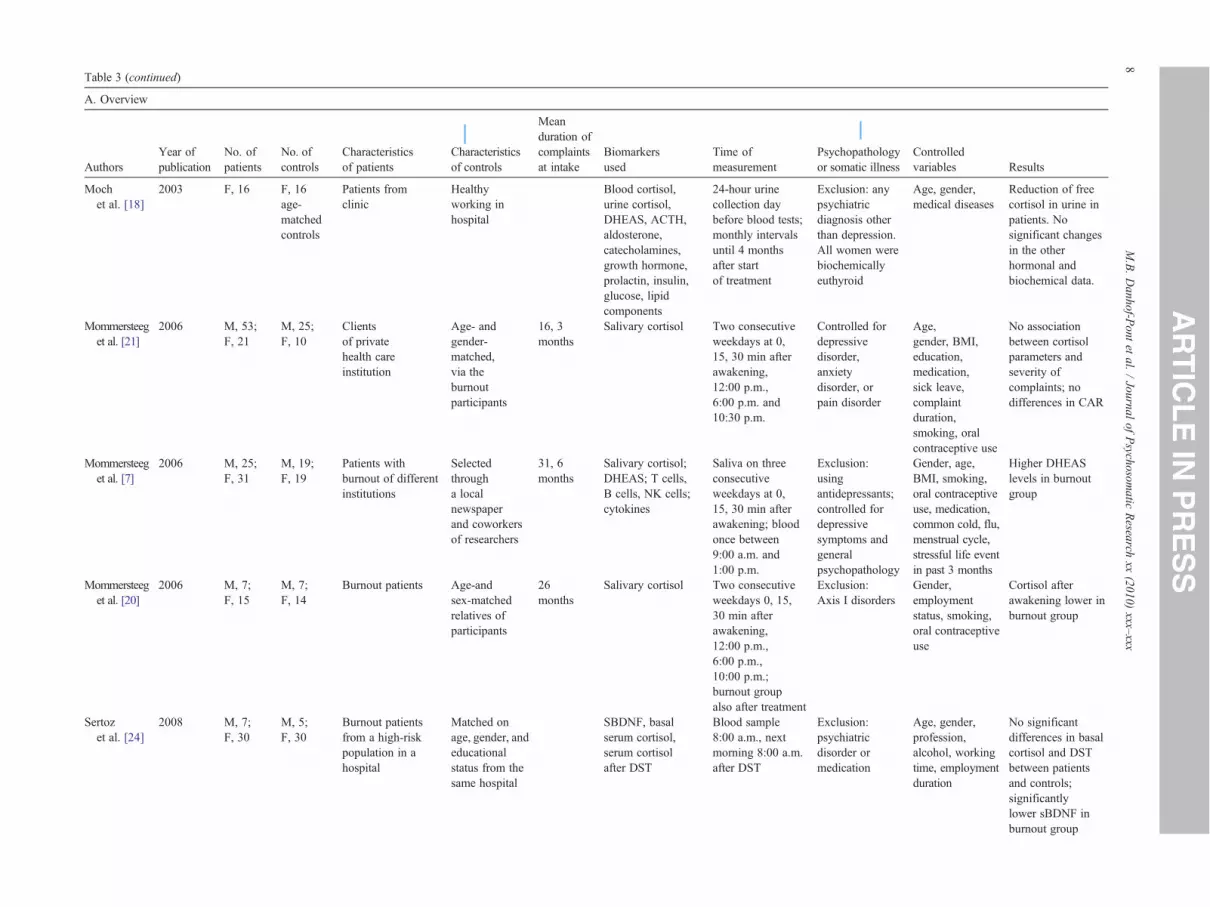
Table 3 (continued)
A. Overview
AuthorsYear ofpublication
No. ofpatients
No. ofcontrols
Characteristicsof patients
Characteristicsof controls
Meanduration ofcomplaintsat intake
Biomarkersused
Time ofmeasurement
Psychopathologyor somatic illness
Controlledvariables Results
Mochet al. [18]
2003 F, 16 F, 16age-matchedcontrols
Patients fromclinic
Healthyworking inhospital
Blood cortisol,urine cortisol,DHEAS, ACTH,aldosterone,catecholamines,growth hormone,prolactin, insulin,glucose, lipidcomponents
24-hour urinecollection daybefore blood tests;monthly intervalsuntil 4 monthsafter startof treatment
Exclusion: anypsychiatricdiagnosis otherthan depression.All women werebiochemicallyeuthyroid
Age, gender,medical diseases
Reduction of freecortisol in urine inpatients. Nosignificant changesin the otherhormonal andbiochemical data.
Mommersteeget al. [21]
2006 M, 53;F, 21
M, 25;F, 10
Clientsof privatehealth careinstitution
Age- andgender-matched,via theburnoutparticipants
16, 3months
Salivary cortisol Two consecutiveweekdays at 0,15, 30 min afterawakening,12:00 p.m.,6:00 p.m. and10:30 p.m.
Controlled fordepressivedisorder,anxietydisorder, orpain disorder
Age,gender, BMI,education,medication,sick leave,complaintduration,smoking, oralcontraceptive use
No associationbetween cortisolparameters andseverity ofcomplaints; nodifferences in CAR
Mommersteeget al. [7]
2006 M, 25;F, 31
M, 19;F, 19
Patients withburnout of differentinstitutions
Selectedthrougha localnewspaperand coworkersof researchers
31, 6months
Salivary cortisol;DHEAS; T cells,B cells, NK cells;cytokines
Saliva on threeconsecutiveweekdays at 0,15, 30 min afterawakening; bloodonce between9:00 a.m. and1:00 p.m.
Exclusion:usingantidepressants;controlled fordepressivesymptoms andgeneralpsychopathology
Gender, age,BMI, smoking,oral contraceptiveuse, medication,common cold, flu,menstrual cycle,stressful life eventin past 3 months
Higher DHEASlevels in burnoutgroup
Mommersteeget al. [20]
2006 M, 7;F, 15
M, 7;F, 14
Burnout patients Age-andsex-matchedrelatives ofparticipants
26months
Salivary cortisol Two consecutiveweekdays 0, 15,30 min afterawakening,12:00 p.m.,6:00 p.m.,10:00 p.m.;burnout groupalso after treatment
Exclusion:Axis I disorders
Gender,employmentstatus, smoking,oral contraceptiveuse
Cortisol afterawakening lower inburnout group
Sertozet al. [24]
2008 M, 7;F, 30
M, 5;F, 30
Burnout patientsfrom a high-riskpopulation in ahospital
Matched onage, gender, andeducationalstatus from thesame hospital
SBDNF, basalserum cortisol,serum cortisolafter DST
Blood sample8:00 a.m., nextmorning 8:00 a.m.after DST
Exclusion:psychiatricdisorder ormedication
Age, gender,profession,alcohol, workingtime, employmentduration
No significantdifferences in basalcortisol and DSTbetween patientsand controls;significantlylower sBDNF inburnout group
8M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx

Sheineret al. [40]
2002 M, 106 M, 66 Patients of a fertilityclinic with a maleinfertility problem
Patients of afertility clinicwith a femaleinfertilityproblem
Sperm assessment Detailed medicalhi was taken
Age, ethnicorigin, education,partner employed,economic status,smoking,physical activity
Male infertilitywas independentlyassociated withindustry andconstruction jobs, aswell as job burnout.
Tokeret al. [37]
2005 M, 933 F, 630 Apparently healthymen who underwentperiodic healthexamination
Apparentlyhealthy womenwho underwentperiodic healthexamination
CRP,fibrinogen
Ex ion: mentalcr medication:an ressants,se es,an chotics;ex ion:in matory,ca vascular,rh atic,pe eral blooddi , cancer,str medication
Age, BMI,moking, exercise,DL, fastinglucose, bloodressure,riglycerides,ormoneeplacementherapy,epression,anxiety
Burnout, depression,and anxiety aredifferentiallyassociated withmicro inflammationbiomarkers,dependenton gender.
Tops,et al. [26]
2006 F, 9 F, 9 Burnout patients,premenopausal(advertisement);less than 4 weeksof absencefrom work
Healthypremenopausalwomen
b4 weeksof sickleave, notherapy
Prolactin, oxytocin,blood cortisol (afteradministratingcortisol or placebo),ACTH
70 min aftercapsule (35 mgof hydrocortisoneor placebo) intake
Ex ion:sy tricdi ers, no useof chotropiced on;ex ion:ch c healthpr ms, drugor hol abuse,ex ive smokingor eine
Gender, age,sorders, dication,smoking, alcohol/drugs, coffee
Burnout subjectsdisplayed extremedistribution of basalprolactin levels,higher or lower thancontrols. Lowprolactin burnoutsubjects had lowattachment scores.High prolactinburnout subjectstended to showcortisol-induceddecreased prolactin.
Zanstraet al. [29]
2006 M, 18;F, 21
M, 13;F, 27
Patients withburnout fromuniversityoutpatientclinic
Healthycontrolsrecruited bymeans ofadvertisementsin localnewspapers
Blood pressure,heart rate
Finger cuff aroundmiddle finger,continuousregistration; ECG
Ex ion: Axis Iiso rs;ex ion:ed on,ca vascularco aints,im e disease,di ic or otherm alco ions
Medication,cardiovascularcomplaints,immune disease,other diseases
No differences atpretest; controlgroup showsdecrease in bloodpressure andrespiratory sinusarrhythmia activityduring test, whereasburnout groupdoes not
9M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx
story
clusisis,tidepdativtipsyclusflamrdioeumriphseaseoke,cluschiasordpsyicaticlusronioblealcocesscaff
clusrdeclusicatirdiomplmunabetedicndit
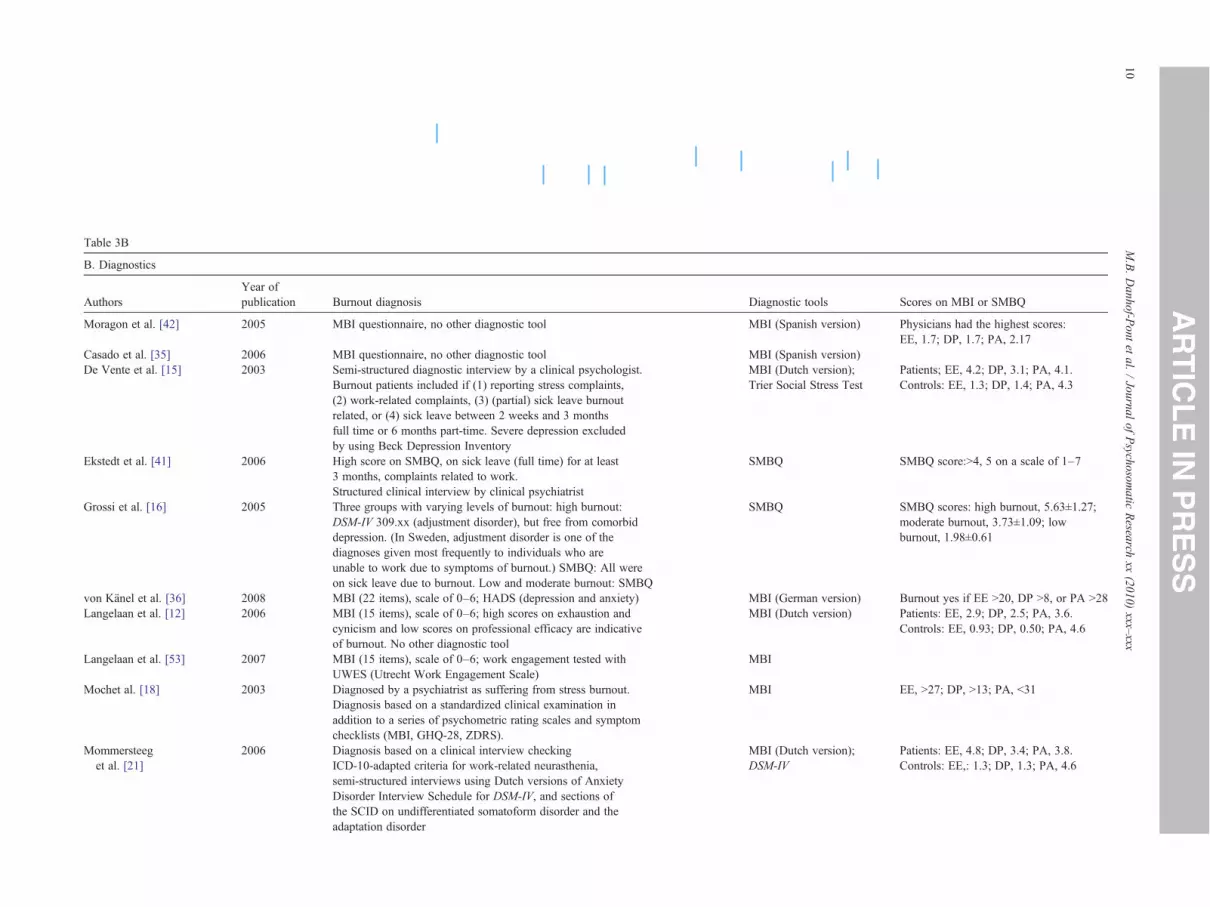
Table 3B
B. Diagnostics
AuthorsYear ofpublication Burnout diagnosis Diagnostic tools Scores on MBI or SMBQ
Moragon et al. [42] 2005 MBI questionnaire, no other diagnostic tool MBI (Spanish version) Physicians had the highest scores:EE, 1.7; DP, 1.7; PA, 2.17
Casado et al. [35] 2006 MBI questionnaire, no other diagnostic tool MBI (Spanish version)De Vente et al. [15] 2003 Semi-structured diagnostic interview by a clinical psychologist.
Burnout patients included if (1) reporting stress complaints,(2) work-related complaints, (3) (partial) sick leave burnoutrelated, or (4) sick leave between 2 weeks and 3 monthsfull time or 6 months part-time. Severe depression excludedby using Beck Depression Inventory
MBI (Dutch version);Trier Social Stress Test
Patients; EE, 4.2; DP, 3.1; PA, 4.1.Controls: EE, 1.3; DP, 1.4; PA, 4.3
Ekstedt et al. [41] 2006 High score on SMBQ, on sick leave (full time) for at least3 months, complaints related to work.Structured clinical interview by clinical psychiatrist
SMBQ SMBQ score:N4, 5 on a scale of 1–7
Grossi et al. [16] 2005 Three groups with varying levels of burnout: high burnout:DSM-IV 309.xx (adjustment disorder), but free from comorbiddepression. (In Sweden, adjustment disorder is one of thediagnoses given most frequently to individuals who areunable to work due to symptoms of burnout.) SMBQ: All wereon sick leave due to burnout. Low and moderate burnout: SMBQ
SMBQ SMBQ scores: high burnout, 5.63±1.27;moderate burnout, 3.73±1.09; lowburnout, 1.98±0.61
von Känel et al. [36] 2008 MBI (22 items), scale of 0–6; HADS (depression and anxiety) MBI (German version) Burnout yes if EE N20, DP N8, or PA N28Langelaan et al. [12] 2006 MBI (15 items), scale of 0–6; high scores on exhaustion and
cynicism and low scores on professional efficacy are indicativeof burnout. No other diagnostic tool
MBI (Dutch version) Patients: EE, 2.9; DP, 2.5; PA, 3.6.Controls: EE, 0.93; DP, 0.50; PA, 4.6
Langelaan et al. [53] 2007 MBI (15 items), scale of 0–6; work engagement tested withUWES (Utrecht Work Engagement Scale)
MBI
Mochet al. [18] 2003 Diagnosed by a psychiatrist as suffering from stress burnout.Diagnosis based on a standardized clinical examination inaddition to a series of psychometric rating scales and symptomchecklists (MBI, GHQ-28, ZDRS).
MBI EE, N27; DP, N13; PA, b31
Mommersteeget al. [21]
2006 Diagnosis based on a clinical interview checkingICD-10-adapted criteria for work-related neurasthenia,semi-structured interviews using Dutch versions of AnxietyDisorder Interview Schedule for DSM-IV, and sections ofthe SCID on undifferentiated somatoform disorder and theadaptation disorder
MBI (Dutch version);DSM-IV
Patients: EE, 4.8; DP, 3.4; PA, 3.8.Controls: EE,: 1.3; DP, 1.3; PA, 4.6
10M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx
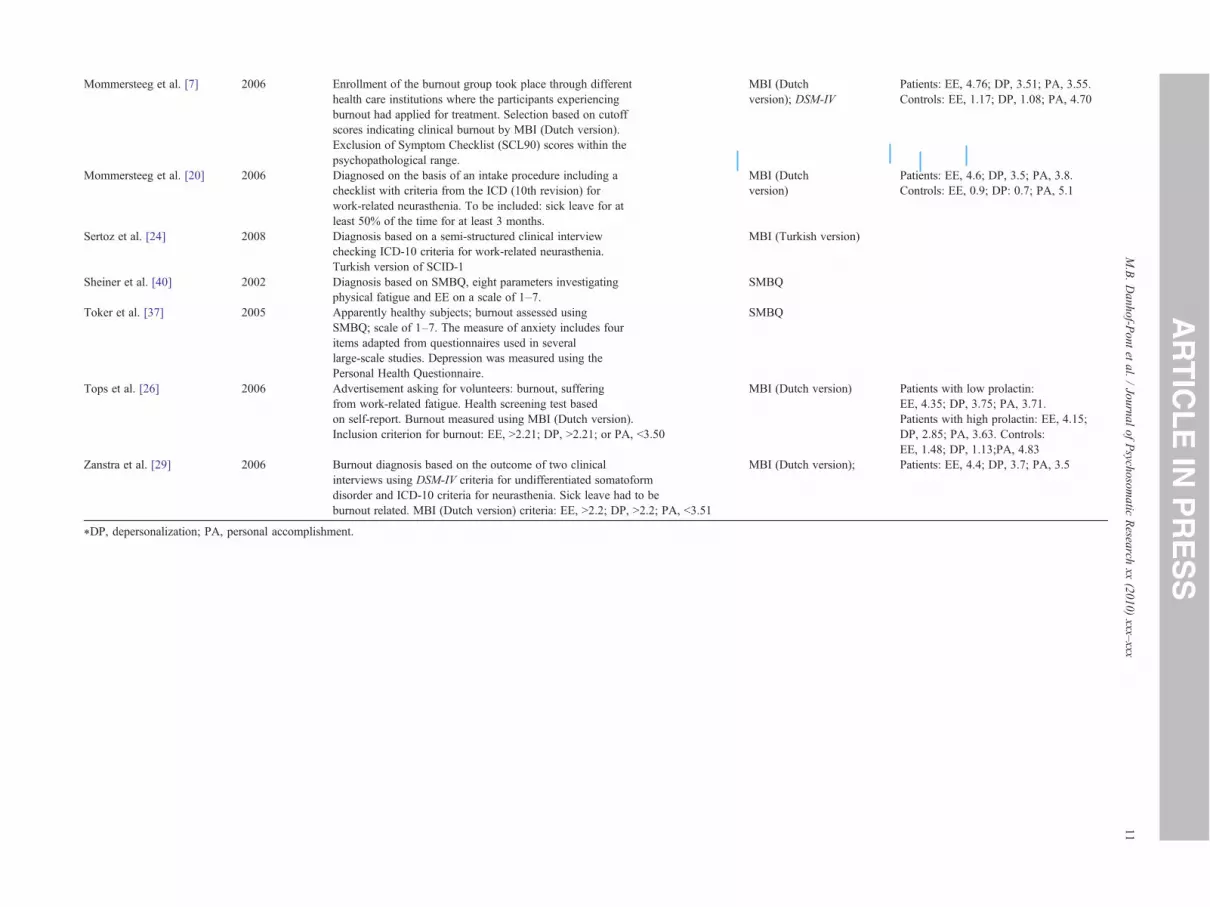
Mommersteeg et al. [7] 2006 Enrollment of the burnout group took place through differenthealth care institutions where the participants experiencingburnout had applied for treatment. Selection based on cutoffscores indicating clinical burnout by MBI (Dutch version).Exclusion of Symptom Checklist (SCL90) scores within thepsychopathological range.
MBI (Dutchversion); DSM-IV
Patients: EE, 4.76; DP, 3.51; PA, 3.55.Controls: EE, 1.17; DP, 1.08; PA, 4.70
Mommersteeg et al. [20] 2006 Diagnosed on the basis of an intake procedure including achecklist with criteria from the ICD (10th revision) forwork-related neurasthenia. To be included: sick leave for atleast 50% of the time for at least 3 months.
MBI (Dutchversion)
Patients: EE, 4.6; DP, 3.5; PA, 3.8.Controls: EE, 0.9; DP: 0.7; PA, 5.1
Sertoz et al. [24] 2008 Diagnosis based on a semi-structured clinical interviewchecking ICD-10 criteria for work-related neurasthenia.Turkish version of SCID-1
MBI (Turkish ve n)
Sheiner et al. [40] 2002 Diagnosis based on SMBQ, eight parameters investigatingphysical fatigue and EE on a scale of 1–7.
SMBQ
Toker et al. [37] 2005 Apparently healthy subjects; burnout assessed usingSMBQ; scale of 1–7. The measure of anxiety includes fouritems adapted from questionnaires used in severallarge-scale studies. Depression was measured using thePersonal Health Questionnaire.
SMBQ
Tops et al. [26] 2006 Advertisement asking for volunteers: burnout, sufferingfrom work-related fatigue. Health screening test basedon self-report. Burnout measured using MBI (Dutch version).Inclusion criterion for burnout: EE, N2.21; DP, N2.21; or PA, b3.50
MBI (Dutch vers ) Patients with low prolactin:EE, 4.35; DP, 3.75; PA, 3.71.Patients with high prolactin: EE, 4.15;DP, 2.85; PA, 3.63. Controls:EE, 1.48; DP, 1.13;PA, 4.83
Zanstra et al. [29] 2006 Burnout diagnosis based on the outcome of two clinicalinterviews using DSM-IV criteria for undifferentiated somatoformdisorder and ICD-10 criteria for neurasthenia. Sick leave had to beburnout related. MBI (Dutch version) criteria: EE, N2.2; DP, N2.2; PA, b3.51
MBI (Dutch vers ); Patients: EE, 4.4; DP, 3.7; PA, 3.5
⁎DP, depersonalization; PA, personal accomplishment.
11M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx
rsio
ion
ion
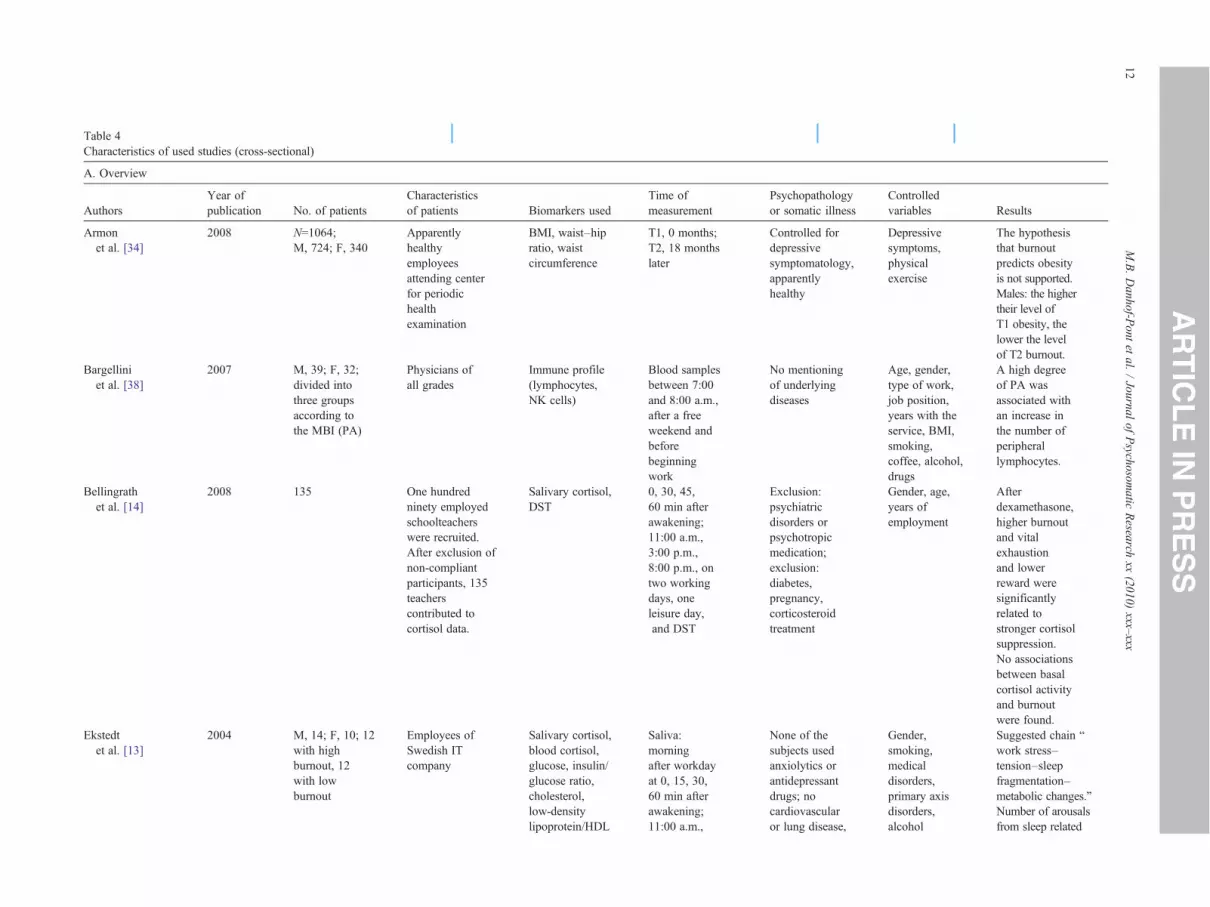
Table 4Characteristics of used studies (cross-sectional)
A. Overview
AuthorsYear ofpublication No. of patients
Characteristicsof patients Biomarkers used
Time ofmeasurement
Psychopathologyor somatic illness
Controlledvariables Results
Armonet al. [34]
2008 N=1064;M, 724; F, 340
Apparentlyhealthyemployeesattending centerfor periodichealthexamination
BMI, waist–hipratio, waistcircumference
T1, 0 months;T2, 18 monthslater
Controlled fordepressivesymptomatology,apparentlyhealthy
Depressivesymptoms,physicalexercise
The hypothesisthat burnoutpredicts obesityis not supported.Males: the highertheir level ofT1 obesity, thelower the levelof T2 burnout.
Bargelliniet al. [38]
2007 M, 39; F, 32;divided intothree groupsaccording tothe MBI (PA)
Physicians ofall grades
Immune profile(lymphocytes,NK cells)
Blood samplesbetween 7:00and 8:00 a.m.,after a freeweekend andbeforebeginningwork
No mentioningof underlyingdiseases
Age, gender,type of work,job position,years with theservice, BMI,smoking,coffee, alcohol,drugs
A high degreeof PA wasassociated withan increase inthe number ofperipherallymphocytes.
Bellingrathet al. [14]
2008 135 One hundredninety employedschoolteacherswere recruited.After exclusion ofnon-compliantparticipants, 135teacherscontributed tocortisol data.
Salivary cortisol,DST
0, 30, 45,60 min afterawakening;11:00 a.m.,3:00 p.m.,8:00 p.m., ontwo workingdays, oneleisure day,and DST
Exclusion:psychiatricdisorders orpsychotropicmedication;exclusion:diabetes,pregnancy,corticosteroidtreatment
Gender, age,years ofemployment
Afterdexamethasone,higher burnoutand vitalexhaustionand lowerreward weresignificantlyrelated tostronger cortisolsuppression.No associationsbetween basalcortisol activityand burnoutwere found.
Ekstedtet al. [13]
2004 M, 14; F, 10; 12with highburnout, 12with lowburnout
Employees ofSwedish ITcompany
Salivary cortisol,blood cortisol,glucose, insulin/glucose ratio,cholesterol,low-densitylipoprotein/HDL
Saliva:morningafter workdayat 0, 15, 30,60 min afterawakening;11:00 a.m.,
None of thesubjects usedanxiolytics orantidepressantdrugs; nocardiovascularor lung disease,
Gender,smoking,medicaldisorders,primary axisdisorders,alcohol
Suggested chain “work stress–tension–sleepfragmentation–metabolic changes.”Number of arousalsfrom sleep related
12M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx
ratio,triglycerides,blood pressure,heart rate,polysomnography
3:00 p.m.,7:00 p.m.,9:00 p.m.,bedtime; bloodparameters:morning afterworkday; bloodpressure, 24 hourson the day afterworkday; PSG,twice, one nightbefore workday,one night beforeday off
diabetes, orother metabolicdiseases
to cortisol (salivaand blood),heart rate,blood pressure,cholesterol
Golembiewski andMunzenrider[28]
1995 M, 107; F, 97 Volunteers forwellness programfrom companyfrom subset of600 people(totalpopulation=1800)
Blood pressure,cholesterol,triglycerides,blood glucose
At registrationfor wellnessprogram
Not mentioned Age, gender No significantrelation with phasesof burnout for systolicor diastolic bloodpressure, nor for acombination ofmeasures (systolicblood pressure anddiastolic bloodpressure, cholesterol,HDL, low-densitylipoprotein, totalcholesterol/HDLratio, triglycerides,blood glucose
Grossiet al. [16]
2003 F, 43 withhigh burnout
Sixty-three whitecollar employeesat three socialinsurance offices
Prolactin,TNF-α, TGF-β,CRP, neopterin,DHEAS,progesterone,estradiol, cortisol,glycatedhemoglobin(HbA1C)
Morningbetween 8:00and 10:00 a.m.
Beck DepressionInventory-60 wasused to assesssymptoms ofdepression
Age, maritalstatus,education,workassignments,working hours,smoking, BMI,menstrualphase, oralcontraceptiveuse
Burnout patients hadhigher levels ofTNF-α and HbA1C
Melamedet al. [32]
2006 677 (76.5%men) dividedinto two groups(high burnoutand lowburnout)
Apparentlyhealthyemployeesfollowed for3 to 5 yearsor the onsetof diagnosedtype 2 diabetes
Blood pressure,developmentof diabetes
Exclusion:chronic disease,hypertension,coronary heartdisease, diabetes,stroke, cancer
Gender, age,education,BMI, physicalactivity,alcohol,smoking,employmentstatus
Findings suggest thatchronic burnout mightbe a risk factor for theonset of type 2 diabetesin apparently healthyindividuals
(continued on next page) 13M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx
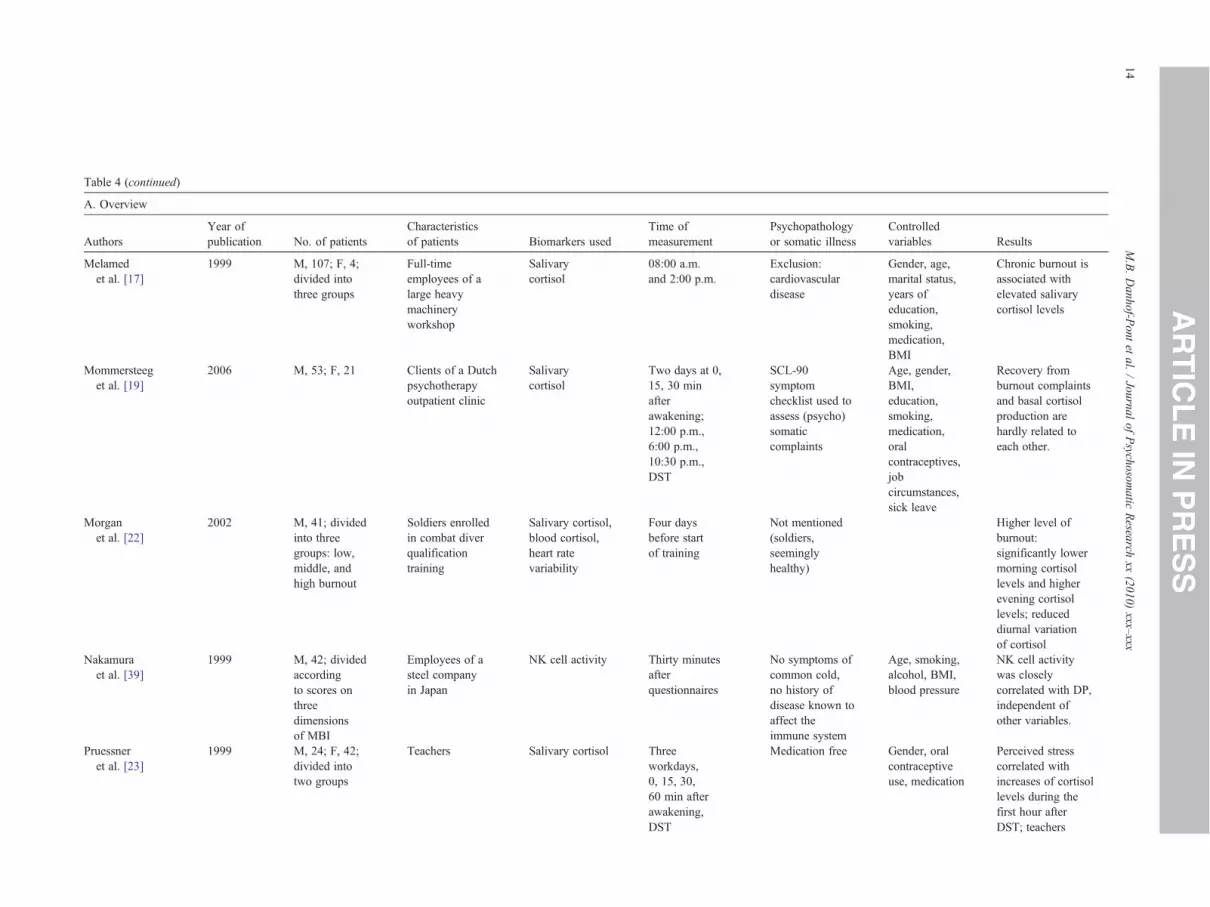
Table 4 (continued)
A. Overview
AuthorsYear ofpublication No. of patients
Characteristicsof patients Biomarkers used
Time ofmeasurement
Psychopathologyor somatic illness
Controlledvariables Results
Melamedet al. [17]
1999 M, 107; F, 4;divided intothree groups
Full-timeemployees of alarge heavymachineryworkshop
Salivarycortisol
08:00 a.m.and 2:00 p.m.
Exclusion:cardiovasculardisease
Gender, age,marital status,years ofeducation,smoking,medication,BMI
Chronic burnout isassociated withelevated salivarycortisol levels
Mommersteeget al. [19]
2006 M, 53; F, 21 Clients of a Dutchpsychotherapyoutpatient clinic
Salivarycortisol
Two days at 0,15, 30 minafterawakening;12:00 p.m.,6:00 p.m.,10:30 p.m.,DST
SCL-90symptomchecklist used toassess (psycho)somaticcomplaints
Age, gender,BMI,education,smoking,medication,oralcontraceptives,jobcircumstances,sick leave
Recovery fromburnout complaintsand basal cortisolproduction arehardly related toeach other.
Morganet al. [22]
2002 M, 41; dividedinto threegroups: low,middle, andhigh burnout
Soldiers enrolledin combat diverqualificationtraining
Salivary cortisol,blood cortisol,heart ratevariability
Four daysbefore startof training
Not mentioned(soldiers,seeminglyhealthy)
Higher level ofburnout:significantly lowermorning cortisollevels and higherevening cortisollevels; reduceddiurnal variationof cortisol
Nakamuraet al. [39]
1999 M, 42; dividedaccordingto scores onthreedimensionsof MBI
Employees of asteel companyin Japan
NK cell activity Thirty minutesafterquestionnaires
No symptoms ofcommon cold,no history ofdisease known toaffect theimmune system
Age, smoking,alcohol, BMI,blood pressure
NK cell activitywas closelycorrelated with DP,independent ofother variables.
Pruessneret al. [23]
1999 M, 24; F, 42;divided intotwo groups
Teachers Salivary cortisol Threeworkdays,0, 15, 30,60 min afterawakening,DST
Medication free Gender, oralcontraceptiveuse, medication
Perceived stresscorrelated withincreases of cortisollevels during thefirst hour afterDST; teachers
14M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx

scoring high onburnout showedlower overallcortisol secretionon all samplingdays.
Soderstromet al. [27]
2006 M, 10; F,14; dividedinto two groups
IT companyemployees
Salivary cortisol;polysomnography
Two days: oneworkday at 0,15,30, 60 minafterawakening;11:00 a.m.,3:00 p.m.,7:00 p.m.,9:00 p.m.,11:00 p.m.
Not mentioned Age, gender,menstrualcycle phase,oralcontraceptiveuse, sick leave,smoking,alcohol,exercise
High burnoutgroup: higherawakening cortisolduring workdaythan weekend,higher frequencyof arousals duringsleep associatedwith a higherdiurnal amplitudeand an earlierdiurnal peak ofcortisol duringthe workday
Wright [25] 2008 N=98; M, 43;F, 55
Direct-caredisability workersfrom adulttraining andsupport servicesand communityresidential units
Saliva cortisol;saliva IgA
0, 30 min afterawakening; onthe same day30 min afterawakening
Exclusion;diabetes,psychiatricdiseases,neuroendocrinediseases or eatingdisorders, or useof corticosteroids
Gender,neuroendocrinediseases,medication
The job demand–control–supportmodel successfullyfitted with the dataand was able topredictphysiologicaloutcomes. SalivaryIgA can bepredicted better bythe job strain modeland the jobdemand–control–support model thansaliva cortisol.
15M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx
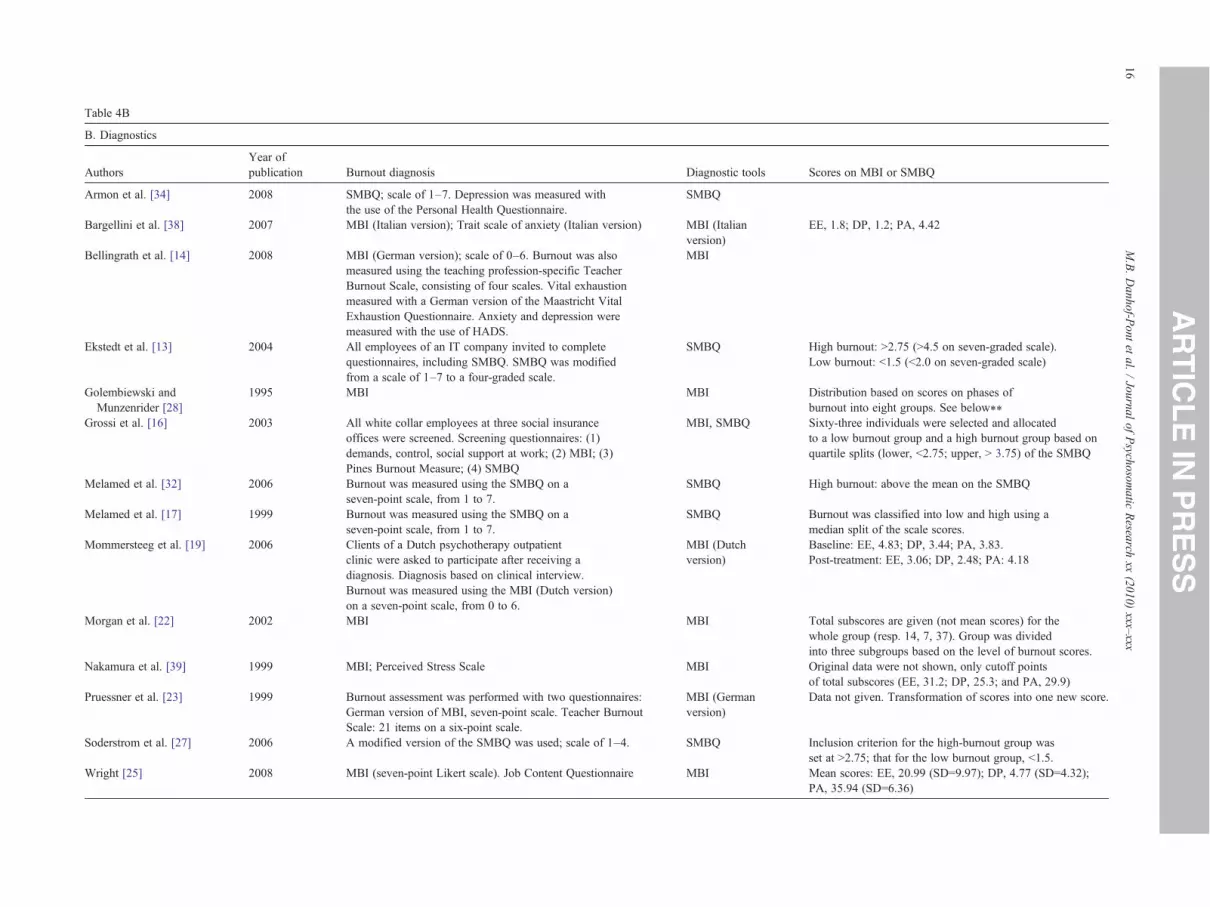
Table 4B
B. Diagnostics
AuthorsYear ofpublication Burnout diagnosis Diagnostic tools Scores on MBI or SMBQ
Armon et al. [34] 2008 SMBQ; scale of 1–7. Depression was measured withthe use of the Personal Health Questionnaire.
SMBQ
Bargellini et al. [38] 2007 MBI (Italian version); Trait scale of anxiety (Italian version) MBI (Italianversion)
EE, 1.8; DP, 1.2; PA, 4.42
Bellingrath et al. [14] 2008 MBI (German version); scale of 0–6. Burnout was alsomeasured using the teaching profession-specific TeacherBurnout Scale, consisting of four scales. Vital exhaustionmeasured with a German version of the Maastricht VitalExhaustion Questionnaire. Anxiety and depression weremeasured with the use of HADS.
MBI
Ekstedt et al. [13] 2004 All employees of an IT company invited to completequestionnaires, including SMBQ. SMBQ was modifiedfrom a scale of 1–7 to a four-graded scale.
SMBQ High burnout: N2.75 (N4.5 on seven-graded scale).Low burnout: b1.5 (b2.0 on seven-graded scale)
Golembiewski andMunzenrider [28]
1995 MBI MBI Distribution based on scores on phases ofburnout into eight groups. See below⁎⁎
Grossi et al. [16] 2003 All white collar employees at three social insuranceoffices were screened. Screening questionnaires: (1)demands, control, social support at work; (2) MBI; (3)Pines Burnout Measure; (4) SMBQ
MBI, SMBQ Sixty-three individuals were selected and allocatedto a low burnout group and a high burnout group based onquartile splits (lower, b2.75; upper, N 3.75) of the SMBQ
Melamed et al. [32] 2006 Burnout was measured using the SMBQ on aseven-point scale, from 1 to 7.
SMBQ High burnout: above the mean on the SMBQ
Melamed et al. [17] 1999 Burnout was measured using the SMBQ on aseven-point scale, from 1 to 7.
SMBQ Burnout was classified into low and high using amedian split of the scale scores.
Mommersteeg et al. [19] 2006 Clients of a Dutch psychotherapy outpatientclinic were asked to participate after receiving adiagnosis. Diagnosis based on clinical interview.Burnout was measured using the MBI (Dutch version)on a seven-point scale, from 0 to 6.
MBI (Dutchversion)
Baseline: EE, 4.83; DP, 3.44; PA, 3.83.Post-treatment: EE, 3.06; DP, 2.48; PA: 4.18
Morgan et al. [22] 2002 MBI MBI Total subscores are given (not mean scores) for thewhole group (resp. 14, 7, 37). Group was dividedinto three subgroups based on the level of burnout scores.
Nakamura et al. [39] 1999 MBI; Perceived Stress Scale MBI Original data were not shown, only cutoff pointsof total subscores (EE, 31.2; DP, 25.3; and PA, 29.9)
Pruessner et al. [23] 1999 Burnout assessment was performed with two questionnaires:German version of MBI, seven-point scale. Teacher BurnoutScale: 21 items on a six-point scale.
MBI (Germanversion)
Data not given. Transformation of scores into one new score.
Soderstrom et al. [27] 2006 A modified version of the SMBQ was used; scale of 1–4. SMBQ Inclusion criterion for the high-burnout group wasset at N2.75; that for the low burnout group, b1.5.
Wright [25] 2008 MBI (seven-point Likert scale). Job Content Questionnaire MBI Mean scores: EE, 20.99 (SD=9.97); DP, 4.77 (SD=4.32);PA, 35.94 (SD=6.36)
16M.B.Danhof-P
ontet
al./Journal
ofPsychosom
aticResearch
xx(2010)
xxx–xxx

Table 5Characteristics of studies included in the systematic review
Total study population 31 (100)ComparisonCase–control 17 (55)Survey (cross-sectional) 14 (45)Sample sizeMedian (interquartile range) 79 (44–170)Methodological issuesResponse rate reported 31 (100)Age reported 27 (87)Gender reported 31 (100)Disease duration reported 7 (23)Psychiatric comorbidity reported (including excluded) 18 (58)Confounding variables reported 31 (100)Burnout severity/group definition based onMBI (1/22 used both MBI and SMBQ) 22 (71)SMBQ 10 (32)
Data are given as n (%) unless otherwise noted.
Meta-analysis CAR with dexamethason
9
17M.B. Danhof-Pont et al. / Journal of Psychosomatic Research xx (2010) xxx–xxx
Langelaan et al. [53] and De Vente et al. [15] found nosignificant differences in resting blood pressure betweenpatients and controls. Melamed et al. [32] followed 677employed men and women for 3 to 5 years. They found thatpersons with burnout had significantly lower systolic bloodpressures compared with persons without burnout. In a meta-analysis (see Figs. 4 and 5), we observed a lower systolicblood pressure in patients with burnout than in controls. Nooverall effect on diastolic blood pressure was found.
Immune factorsChronic psychological stress has been suggested to alter
several immunological processes [45].
Crp. CRP is used as a measure of inflammation. Threearticles on CRP in burnout were found [31,37,53]. Samplesizes ranged from 63 to 1563, with a total of 1029 patientsand 887 controls. In two of the three studies, nodifferences in CRP levels were found between burnoutcases and controls [31,53]. Grossi [31] studied onlywomen, whereas Langelaan et al. [53] studied only men.In a third study [37], CRP was positively associated withburnout scores in women but not in men. Toker et al. [37]dichotomized the CRP levels as elevated (N3.0 mg/L) and
Meta-analysis without dexamethason
0
5
10
15
20
25
0 15 30 60
time (minutes after awakening)
mea
n c
ort
iso
l (S
EM
)
control
burnout
Fig. 2. Meta-analysis of CAR in patients with burnout vs. controls.
normal; therefore, quantitative analysis of the study datawas not possible. Thus, putative gender-specific effectsremain to be verified.
NK cells. Three articles on NK cells were found[7,38,39]. Sample sizes ranged from 42 to 94, with atotal of 169 patients and 38 controls. In 42 male workers,Nakamura et al. [39] found that a higher score on thedepersonalization scale of the MBI was associated with alower NK cell activity. No association was found with EE.Two studies found no relation between burnout andnumber of NK cells [7,38]. In these articles, putativeassociations of NK cells with dimensions of burnout werenot assessed. We did not perform a meta-analysis sincetwo articles addressed numbers of NK cells and one articleaddressed NK cell activity.
Other hormonesProlactin. Although not consistently, a few studies have
reported elevations of prolactin plasma levels in men andwomen in response to different stress factors (examinationstress [46,47], in anticipation of surgical intervention [48], orduring unemployment [49]). Three articles on prolactin inburnout were found [18,26,31]. Sample sizes ranged from 18to 63, with a total of 88 cases and 25 controls. Moch et al.[18] compared 16 patients with burnout from a clinic with 16age-matched healthy women working in a hospital. Theyfound no differences in prolactin levels before, during, andafter 4 months of treatment. Grossi [31] found no differencesbetween 43 women with high burnout and 20 women withlow burnout. The groups in these studies were relativelyhealthy and did not differ significantly in sociodemographic,lifestyle, and gynecological variables. In a small study, Topset al. [26] compared 9 burnout patients with 9 controls andreported that 4 patients had low and another 4 had highprolactin levels. Data on the ninth patient were not given.Because of the missing data in the last study, no meta-analysis was carried out. Taken together, the studies suggest
0
1
2
3
4
5
6
7
8
0 15 30 60time (minutes after awakening)
mea
n c
ort
iso
l (S
EM
)
control
burnout
Fig. 3. Meta-analysis of CAR with dexamethasone in patients with burnoutvs. controls.

Study or Subgroup
De Vente et al. 2003Langelaan et al., 2007Melamed et al., 2006
Total (95% CI)
Heterogeneity: Tau2 = 5.57; Chi2 = 3.78, df = 2 (P = 0.15); I2 = 47%Test for overall effect: Z = 1.36 (P = 0.17)
Mean
138.55142.6
119
SD
18.0313.613.4
Total
2233
348
403
Mean
132.25146.2
123
SD
16.6916
14.7
Total
23257329
609
Weight
11.8%31.4%56.8%
100.0%
IV, Random, 95% CI
6.30 [-3.86, 16.46]-3.60 [-8.64, 1.44]
-4.00 [-6.12, -1.88]
-2.66 [-6.49, 1.17]
Experimental Control Mean Difference Mean DifferenceIV, Random, 95% CI
-20 -10 0 10 20Lower in burnout lower in control
Fig. 4. Forest plot of meta-analysis of systolic blood pressure in patients with burnout vs. controls.
18 M.B. Danhof-Pont et al. / Journal of Psychosomatic Research xx (2010) xxx–xxx
that no overall differences in prolactin level exist betweenburnout patients and controls.
Discussion
In our review of the literature, we found 31 articles thatfulfilled our inclusion criteria. Together, these articlesinvestigated 38 potential biomarkers covering manyphysiological processes. For some parameters, the numberand quality of the studies permitted a meta-analysis. Thiswas the case with the CAR assessed in saliva, systolicblood pressure, and diastolic blood pressure. No relation-ship with burnout was found. For the other biomarkers, thenumber of studies was too small for a meta-analysis. Ingeneral, it can be concluded that we did not find aconvincing relationship between any of these biomarkersand burnout.
Several factors may have contributed to these negativefindings. The first one is the way burnout was defined. Allincluded articles used the MBI or SMBQ to assess burnout.However, they used different cutoff scores for the diagnosis,and sometimes dimensions were analyzed, which may haveled to heterogeneity in the patient groups. In addition, theremay have been differences in the patients who qualified foran assessment and thus in the selection of subjects for thestudies, as countries and cultures differ in the symptoms thattrigger the suspicion of a burnout diagnosis. Burnout asdefined by MBI has been related to increased anxiety,depression, sleep disturbances, somatic symptoms, andimpaired health. In contrast, burnout as defined by theSMBQ focuses on the chronic depletion of energeticresources and resembles the chronic fatigue syndrome and“vital exhaustion,” a state characterized by unusual fatigue,
Study or Subgroup
Langelaan et al., 2007Melamed et al., 2006De Vente et al. 2003
Total (95% CI)
Heterogeneity: Tau2 = 0.00; Chi2 = 0.05, df = 2 (P = 0.98); I2 = 0%Test for overall effect: Z = 1.17 (P = 0.24)
Mean
88.674.3
78.52
SD
9.99.5
8.27
Total
3334822
403
Mean
89.175.179.8
SD
11.29.6
13.17
Total
25732923
609
Weight
12.9%82.9%4.2%
100.0%
Burnout Control
Fig. 5. Forest plot of meta-analysis of diastolic blood
increased irritability, and feelings of demoralization. Vitalexhaustion often precedes cardiac events [31]. Both scalesmeasure burnout, are used frequently, and are validated.However, since they do not measure exactly the same thing,it is very difficult to compare the severity of burnout betweenstudies that use different scales. Analyzing dimensions ofburnout makes comparison more reliable.
The second factor is the way the potential biomarkerswere assessed. This appeared to be different for mostparameters assessed in more than one study. For instance,differences in the body fluids used for assessments (blood,saliva, or urine) in the assays and the outcome measurements(blood pressure vs. mean blood pressure) made a systematiccomparison of the study results impossible. The third factorconcerns differences in the exclusion criteria and potentialconfounders. The differences in studies assessing the sameparameters are large enough to hamper a comparison of thestudies (see Tables 3 and 4). Several important confoundingfactors (for instance, duration of complaints, whetherpatients were on sick leave or not, and psychopathology/somatic diseases) were not mentioned by some authors. It islikely that different types of symptoms are associated withdifferent biomarkers. If psychopathology other than burnoutis present and not controlled for, this may confoundassociations of burnout with biomarkers.
Different levels of chronic stress may have led to thefinding that baseline levels of the biological markers varybetween the studies. Studies do not mention data on thisimportant factor; for instance, if there is only one stressor(i.e., the work stress) or if there are other stress factors inworking or private life.
Notwithstanding the face validity for the hypothesis thatthe stress system is involved in burnout, none of thepostulated biological characteristics of burnout, such as
IV, Random, 95% CI
-0.50 [-4.14, 3.14]-0.80 [-2.24, 0.64]-1.28 [-7.68, 5.12]
-0.78 [-2.09, 0.53]
Year
200720062003
Mean Difference Mean DifferenceIV, Random, 95% CI
-20 -10 0 10 20Lower in burnout lower in control
pressure in patients with burnout vs. controls.

19M.B. Danhof-Pont et al. / Journal of Psychosomatic Research xx (2010) xxx–xxx
elevated cortisol levels and lower blood pressure, could besubstantiated. However, because of the many problems withthe interpretation of the findings discussed above, it is tooearly to say that no relationship of burnout with the stresssystem and associated factors exist. A definite answer canonly be given with methodologically more sound andcomparable studies. This implies, in the first place, theinclusion of well-defined patient groups. It might be morefruitful to dissect the clinical diagnosis in the componentparts (for instance, symptom dimensions). Recently, a fewassociations of biomarkers with dimensions of burnout havebeen reported [25,49]. In the second place, we suggest alongitudinal approach, as it is more powerful in detectingcausal relationships. For instance, assessments of biomarkersbefore and after treatment could help clarify the relationshipbetween symptoms and biomarkers.
We did not include studies that were written in languagesother than English, German, and Dutch. However, to assessselection bias, we did look for studies in other languages. Wefound three articles in other languages (Spanish, French, andChinese). The Spanish article [50] investigated the relationbetween sleep quality and burnout. Burnout was tested withthe Spanish version of the MBI. Sleep quality was testedwith a questionnaire and reported as good, normal, or bad. Inour review, this would have been the only study on sleepquality, and it was therefore not discussed. Miro et al. [50]did find significant associations between sleep quality andburnout. The French article was an overview of the literatureand would therefore not have been included in our review[51]. The authors of the Chinese article, Lian et al. [52], didnot define cases as suffering from burnout; therefore, theirstudy would not have been included in the review. Theinformation was retrieved from the English abstract. Thearticle itself could not be used because of language problems.In conclusion, no bias has been introduced by using languageas an inclusion criterion.
In conclusion, we have not identified clinical relevancefor biomarkers in occupational health practice. Even if allresearchers had used the same methods in, for example,patients/controls, techniques in measuring, and confounders,it is likely that still a great variety in results would have beenfound. This is caused by the fact that burnout is not ahomogenous entity, and there are great intra-individual andinter-individual varieties.
Acknowledgments
We thank Prof. Theo Stijnen and Dr. Massoud Boroujerdifor their statistical assistance.
References
[1] Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol2001;52:397–422.
[2] van Doornen LJ. [Work-stress and cortisol; measurements and results].Tijdschr Psychiatr 2009;51:587–94.
[3] NCvB and Coronel Instituut voor Arbeid en Gezondheid AMC/UVA.Beroepsziekten in cijfers 2009. 2009.
[4] Blatter B., Houtman I. and others. Gezondheidsschade en kosten alsgevolg van RSI en psychosociale arbeidsbelasting in Nederland. TNOreport august 2005. 2005.
[5] Klink JJL, van der Terluin B. Psychische problemen en werk,Handboek voor een activerende begeleiding door huisarts en bed-rijfsarts. Bohn: Stafleu van Loghum., 2005.
[6] Karasek RA, Theorell T. Healthy work: stress, productivity and thereconstruction of working life. New York: Basic Books, 1990.
[7] Mommersteeg PM, Heijnen CJ, Kavelaars A, van Doornen LJ.Immune and endocrine function in burnout syndrome. PsychosomMed2006;68:879–86.
[8] The Nordic Cochrane Centre, The Cochrane Collaboration. RevManVersion 5.0 Copenhagen. 2008.
[9] van Houwelingen HC, Arends LR, Stijnen T. Advanced methods inmeta-analysis: multivariate approach and meta-regression. Stat Med2002;21:589–624.
[10] Cnaan A, Laird NM, Slasor P. Using the general linear mixed model toanalyse unbalanced repeated measures and longitudinal data. Stat Med1997;16:2349–80.
[11] Klaassens ER, van Noorden MS, Giltay EJ, van PJ, van VT, ZitmanFG. Effects of childhood trauma on HPA-axis reactivity in women freeof lifetime psychopathology. Prog Neuropsychopharmacol BiolPsychiatry 2009;33:889–94.
[12] Langelaan S, Bakker AB, Schaufeli WB, van Rhenen W, van DoornenLJ. Do burned-out Zand work-engaged employees differ in thefunctioning of the hypothalamic–pituitary–adrenal axis? Scand JWork Environ Health 2006;32:339–48.
[13] Ekstedt M, Akerstedt T, SoderstromM. Microarousals during sleep areassociated with increased levels of lipids, cortisol, and blood pressure.Psychosom Med 2004;66:925–31.
[14] Bellingrath S, Weigl T, Kudielka BM. Cortisol dysregulation in schoolteachers in relation to burnout, vital exhaustion, and effort–reward-imbalance. Biol Psychol 2008;78:104–13.
[15] De Vente W, Olff M, Van Amsterdam JG, Kamphuis JH, EmmelkampPM. Physiological differences between burnout patients and healthycontrols: blood pressure, heart rate, and cortisol responses. OccupEnviron Med 2003;60(Suppl 1):i54–61.
[16] Grossi G, Perski A, Ekstedt M, Johansson T, Lindstrom M, Holm K.The morning salivary cortisol response in burnout. J Psychosom Res2005;59:103–11.
[17] Melamed S, Ugarten U, Shirom A, Kahana L, Lerman Y, Froom P.Chronic burnout, somatic arousal and elevated salivary cortisol levels.J Psychosom Res 1999;46:591–8.
[18] Moch SL, Panz VR, Joffe BI, Havlik I, Moch JD. Longitudinalchanges in pituitary–adrenal hormones in South African women withburnout. Endocrine 2003;21:267–72.
[19] Mommersteeg PM, Heijnen CJ, Verbraak MJ, van Doornen LJ. Alongitudinal study on cortisol and complaint reduction in burnout.Psychoneuroendocrinology 2006;31:793–804.
[20] Mommersteeg PM, Keijsers GP, Heijnen CJ, Verbraak MJ, vanDoornen LJ. Cortisol deviations in people with burnout beforeand after psychotherapy: a pilot study. Health Psychol 2006;25:243–8.
[21] Mommersteeg PM, Heijnen CJ, Verbraak MJ, van Doornen LJ.Clinical burnout is not reflected in the cortisol awakeningresponse, the day-curve or the response to a low-dose dexameth-asone suppression test. Psychoneuroendocrinology 2006;31:216–25.
[22] Morgan CA, Cho T, Hazlett G, Coric V, Morgan J. The impact ofburnout on human physiology and on operational performance: aprospective study of soldiers enrolled in the combat diver qualificationcourse. Yale J Biol Med 2002;75:199–205.
[23] Pruessner JC, Hellhammer DH, Kirschbaum C. Burnout, perceivedstress, and cortisol responses to awakening. Psychosom Med 1999;61:197–204.
20 M.B. Danhof-Pont et al. / Journal of Psychosomatic Research xx (2010) xxx–xxx
[24] Sertoz OO, Binbay IT, Koylu E, Noyan A. The role of BDNF and HPAaxis in the neurobiology of burnout syndrome. Prog Neuropsycho-pharmacol Biol Psychiatry 2008;32:1459–65.
[25] Wright BJ. Comparing the job strain and job demand–control–supportmodels in direct-care diability workers: support for support. J OccupEnviron Med 2008;50:316–23.
[26] Tops M, Boksem MA, Wijers AA, van Duinen H, Den Boer JA,Meijman TF, et al. The psychobiology of burnout: are there twodifferent syndromes? Neuropsychobiology 2007;55:143–50.
[27] SöderströmM, EkstedtM, Akerstedt T.Weekday andweekend patternsof diurnal cortisol, activation and fatigue among people scoring high forburnout. Scand J Work Environ Health 2006(Suppl 2):35–40.
[28] Golembiewski RT, Munzenrider RF. Blood-chemistry covariants ofphases of burnout: a pilot study. Journal of Health and Human ServicesAdministration 17(3)()(pp 265–283), 1995 Date of Publication: 19951995;(3):265–83.
[29] Zanstra YJ, Schellekens JM, Schaap C, Kooistra L. Vagal andsympathetic activity in burnouts during a mentally demandingworkday. Psychosom Med 2006;68:583–90.
[30] Melamed S, Kushnir T, Shirom A. Burnout and risk factors forcardiovascular diseases. Behav Med 1992;18:53–60.
[31] Grossi G. Physiological correlates of burnout among women, 2003.[32] Melamed S, Shirom A, Toker S, Shapira I. Burnout and risk of type 2
diabetes: a prospective study of apparently healthy employed persons.Psychosom Med 2006;68:863–9.
[33] Han TY. A biopsychosocial perspective to the burnout of Koreanworkers with diabetes. Am J Health Behav 2008;32:741–53.
[34] Armon G, Shirom A, Berliner S, Shapira I, Melamed S. A prospectivestudy of the association between obesity and burnout among apparentlyhealthy men and women. J Occup Health Psychol 2008;13:43–57.
[35] Casado A, De Lucas N, Lopez-Fernandez E. Lipid peroxidation,occupational stress and aging in workers of a prehospital emergencyservice. Eur J Emerg Med 2006;13:165–71.
[36] von Känel R, Bellingrath S, Kudielka BM. Association betweenburnout and circulating levels of pro- and anti-inflammatory cytokinesin schoolteachers. J Psychosom Res 2008;65:51–9.
[37] Toker S, Shirom A, Shapira I, Berliner S, Melamed S. The associationbetween burnout, depression, anxiety, and inflammation biomarkers:C-reactive protein and fibrinogen in men and women. J Occup HealthPsychol 2005;10:344–62.
[38] Bargellini A, Barbieri A, Rovesti S, Vivoli R, Roncaglia R, Borella P.Relation between immune variables and burnout in a sample ofphysicians. Occup Environ Med 2000;57:453–7.
[39] Nakamura H, Nagase H, Yoshida M, Ogino K. Natural killer (NK) cellactivity and NK cell subsets in workers with a tendency of burnout. JPsychosom Res 1999;46:569–78.
[40] Sheiner EK, Sheiner E, Carel R, Potashnik G, Shoham-Vardi I.Potential association between male infertility and occupationalpsychological stress. J Occup Environ Med 2002;44:1093–9.
[41] Ekstedt M, Soderstrom M, Akerstedt T, Nilsson J, Sondergaard HP,Aleksander P. Disturbed sleep and fatigue in occupational burnout.Scand J Work Environ Health 2006;32:121–31.
[42] Moragon AC, De Lucas GN, Encarnacion Lopez FM, Rodriguez-Manzaneque AS, Jimenez Fraile JA. Antioxidant enzymes, occupa-tional stress and burnout in workers of a prehospitalary emergencyservice. Eur J Emerg Med 2005;12:111–5.
[43] Söderström M, Ekstedt M, Akerstedt T, Nilsson J, Axelsson J. Sleepand sleepiness in young individuals with high burnout scores. Sleep2004;27.
[44] Garde AH, Hansen AM. An inter-laboratory comparison for determi-nation of cortisol in saliva. Accred Qual Assur 2003;2003:16–20.
[45] O'Leary A. Stress, emotion, and human immune function. PsycholBull 1990;108:363–82.
[46] Johansson GG, Karonen SL, Laakso ML. Reversal of an elevatedplasma level of prolactin during prolonged psychological stress. ActaPhysiol Scand 1983;119:463–4.
[47] Meyerhoff JL, Oleshansky MA, Mougey EH. Psychologic stressincreases plasma levels of prolactin, cortisol, and POMC-derivedpeptides in man. Psychosom Med 1988;50:295–303.
[48] Demyttenaere K, Nijs P, Evers-Kiebooms G, Koninckx PR. Coping,ineffectiveness of coping and the psychoendocrinological stressresponses during in-vitro fertilization. J Psychosom Res 1991;35:231–43.
[49] Brenner SO, Levi L. Long-term unemployment among women inSweden. Soc Sci Med 1987;25:153–61.
[50] Miro E, Solanes A, Martinez P, Sanchez AI, Rodriguez MJ.[Relationship between burnout, job strain, and sleep characteristics].Psicothema 2007;19:388–94.
[51] Poirier MF. [Biology of states of burnout]. Ann Med Psychol (Paris)1985;143:761–8.
[52] Lian YL, Liu JW, Tan WG, Zeng H, Wang H. [Effects of occupationalstress on immunological function, glucose and blood lipid of femaleworkers in oil-field]. Wei Sheng Yan Jiu 2005;34:469–71.
[53] Langelaan S, Bakker AB, Schaufeli W, van Rhenen W, van DoornenLJP. [Is burnout related to allostatic load?]. Int J Behav Med 2007;14:213–21.