auto-stigmatisation dans les troubles psychiques sévères et
TRANSCRIPT

HAL Id: tel-03336583https://tel.archives-ouvertes.fr/tel-03336583
Submitted on 7 Sep 2021
HAL is a multi-disciplinary open accessarchive for the deposit and dissemination of sci-entific research documents, whether they are pub-lished or not. The documents may come fromteaching and research institutions in France orabroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, estdestinée au dépôt et à la diffusion de documentsscientifiques de niveau recherche, publiés ou non,émanant des établissements d’enseignement et derecherche français ou étrangers, des laboratoirespublics ou privés.
Auto-stigmatisation dans les troubles psychiques sévèreset persistantsJulien Dubreucq
To cite this version:Julien Dubreucq. Auto-stigmatisation dans les troubles psychiques sévères et persistants. Neuro-sciences. Université de Lyon, 2020. Français. �NNT : 2020LYSE1074�. �tel-03336583�
Page 1
N°d’ordre NNT : 2020LYSE1074
THESE de DOCTORAT DE L’UNIVERSITE DE LYON opérée au sein de
l’Université Claude Bernard Lyon 1
Ecole Doctorale N° 476
Neurosciences et Cognition
Spécialité de doctorat :
Discipline: Physiologie et biologie des organismes - populations - interactions
Soutenue publiquement le 07/05/2020, par :
Julien DUBREUCQ
Auto-stigmatisation dans les troubles psychiques sévères et persistants
Devant le jury composé de :
MASSOUBRE Catherine, PU-PH, Université St Etienne Présidente
LLORCA Pierre-Michel, PU-PH, Université Clermont Auvergne Rapporteur PACHOUD Bernard, PU-PH, Université Paris Sorbonne Rapporteur MASSOUBRE Catherine, PU-PH, Université St Etienne Examinatrice DEMILY Caroline, PU-PH, Université Lyon 1 Examinatrice D’AMATO Thierry, PU-PH, Université Lyon 1 Examinateur CELLARD Caroline, Professeure agrégée, Université Laval Québec Examinatrice FRANCK, Nicolas, PU-PH, Université Claude Bernard Lyon 1 Directeur de thèse
Page 2
Page 3
Résumé
L’auto-stigmatisation est fréquente chez les personnes avec Troubles Psychiques Sévères et
Persistants (TPSP), dont elle altère le devenir clinique et fonctionnel. L’objectif ce travail était de
définir plus précisément l’auto-stigmatisation dans les TPSP et de mieux identifier les moyens d’y
faire face. Il comporte plusieurs étapes : i) une 1ère revue systématique de littérature pour mieux
appréhender les mécanismes cognitifs et neurobiologiques potentiels sous-tendant les effets de la
stigmatisation; ii) une 2nde revue systématique de littérature sur la prévalence, les prédicteurs et les
conséquences de l’auto-stigmatisation dans les TPSP ; iii) l’étude de la fréquence de l’auto-
stigmatisation et de la résistance à la stigmatisation et des corrélats d’une auto-stigmatisation ou
d’une résistance élevée à la stigmatisation dans la cohorte nationale des centres référents de
réhabilitation psychosociale (REHABase), décrite dans un 1er article ; iv) l’adaptation française du
programme de thérapie cognitive et de renforcement narratif (NECT) et un essai randomisé contrôlé
évaluant son efficacité sur le fonctionnement social dans les TPSP, débutant au 1er trimestre 2020.
L’auto-stigmatisation est un problème majeur de santé publique, et ce quelque soit l’aire
géographique et culturelle, la pathologie ou le stade évolutif considérés. Environ 1/3 des
participants de la cohorte REHABase ont une auto-stigmatisation élevée, celle-ci étant associée aux
stades précoces du rétablissement et à un bien être et une satisfaction dans les relations sociales
altérés. La résistance à la stigmatisation concerne plus de 50% des participants et est favorisée par
la satisfaction dans les relations familiales. Ce travail a plusieurs implications cliniques et pour la
recherche, discutées de façon approfondie.
Mots-clés : auto-stigmatisation ; troubles psychiques sévères ; réhabilitation psychosociale ;
résistance à la stigmatisation ; rétablissement

Page 4
Abstract
Self-stigma is highly prevalent in persons with Serious Mental Illness (SMI) and is associated with
poor patient’s outcomes. Our objectives were a better understanding of self-stigma and how to
reduce it trough improved clinical practice. This PhD dissertation has four steps : i) first, we
reviewed the potential cognitive and neurobiological mechanisms underlying stigma and self-
stigma ; ii) then we reviewed the prevalence, prédictors and correlates of self-stigma in SMI ; iii)
we assessed the frequency of self-stigma and stigma resistance in the French national network of
centres for psychiatric rehabilitation (REHABase), described in a previous article ; iv) we adapted
in French Narrative Enhancement and Cognitive Therapy (NECT) self-stigma reduction program
and initiated a stepped-wedge randomised control trial assessing its effectiveness in improving
social function in SMI. Self-stigma is a major public health issue, affecting people in all
geographical areas, all SMI conditions and all stages of the illness including at-risk states and early
disorders. Elevated self-stigma concerned roughly one third of the participants included in the
REHABase cohort. It was negatively associated with personal recovery, wellbeing and satisfaction
in interpersonal relationships. Elevated stigma resistance concerned more than 50% of the
participants and was positively associated with satisfaction in family relationships. The present
dissertation has several implications for research and clinical practice, discussed thoroughly.
Keywords : Self-stigma, Serious Mental Illness, Psychiatric rehabilitation ; Stigma resistance ;
Recovery
Page 5
Remerciements
A M. le Professeur Nicolas Franck,
Merci infiniment de m’avoir fait l’honneur de diriger mon travail de thèse. Merci également pour ta
confiance, ta disponibilité, tes encouragements et ton soutien lors de ce travail. J’ai beaucoup
apprécié de travailler à ton contact, depuis maintenant plusieurs années. Trouve ici l’expression de
ma reconnaissance et de mon profond respect.
A M. le Professeur Pierre-Michel Lllorca,
Merci beaucoup d’avoir accepté d’être rapporteur de ce travail de thèse. Merci pour vos conseils,
votre soutien et de m’avoir fait bénéficier de votre expérience. J’ai beaucoup apprécié de travailler à
votre contact, depuis maintenant plusieurs années. Veuillez trouver ici le témoignage de ma
gratitude et de mon profond respect.
A M. le Professeur Bernard Pachoud,
Merci beaucoup d’avoir accepté d’être rapporteur de ce travail de thèse. J’ai beaucoup apprécié nos
échanges autour de l’emploi accompagné, de la réhabilitation psychosociale et du rétablissement.
Trouve ici le témoignage de ma gratitude et de mon profond respect.
A Mme le Professeur Catherine Massoubre
Merci beaucoup d’avoir accepté de juger cette thèse. J’ai beaucoup apprécié de travailler à ton
contact et à celui de l’équipe de RehaCoor 42, depuis maintenant plusieurs années. Merci également
pour ta disponibilité, ton soutien et tes encouragements. Trouve ici l’expression de ma
reconnaissance et de mon profond respect.
Page 6
A Mme le Professeur Caroline Demily
Merci beaucoup d’avoir accepté de juger cette thèse. Merci également pour tes conseils, ton soutien
et tes encouragements lors des comités de suivi de thèse. J’ai beaucoup apprécié nos échanges et
collaborations autour de la réhabilitation psychosociale, du rétablissement et de l’autisme. Trouve
ici l’expression de ma reconnaissance et de mon profond respect.
A M le Professeur Thierry D’Amato
Merci beaucoup d’avoir accepté de juger cette thèse. J’ai beaucoup apprécié de travailler à ton
contact, depuis maintenant plusieurs années, au sein des centres experts et autour des programmes
RemedRugby et ProFamille. Trouve ici l’expression de ma gratitude et de mon profond respect.
A Mme le Professeur Caroline Cellard
Merci beaucoup d’avoir accepté de juger cette thèse. Ce fut un plaisir de te rencontrer, d’échanger
autour de la réhabilitation psychosociale, de la pair-aidance et du rétablissement, et de pouvoir
collaborer à l’ouvrage « pair aidance en santé mentale » que tu coordonnes avec Nicolas. Trouve
ici l’expression de ma gratitude et de mon profond respect.
Merci aussi mille fois au Dr Isabelle Amado et au Pr Mircea Polosan pour leurs conseils, leur
soutien et leurs encouragements lors des comités de suivi de thèse.
Merci infiniment au Dr Elisabeth Giraud Baro pour sa confiance, ses conseils, son soutien et ses
encouragements depuis le début de mon parcours en réhabilitation psychosociale. Merci aussi au Dr
Patrice Baro pour ses conseils et ses encouragements.
Page 7
Merci infiniment à toute l’équipe du C3R, des Centres Experts Schizophrénie et Asperger et du
Réseau Handicap Psychique, avec qui j’ai le plaisir de travailler depuis maintenant plusieurs
années. Merci plus particulièrement à Franck, Julien, Mégane, Marie, Patricia, Anne, Thomas,
Thierry, Fanny pour tout le travail autour de RemedRugby, NECT et tous les projets que nous
avons conduits ensemble et sur lesquels nous travaillons au quotidien.
Merci beaucoup à l’équipe du CRR, et plus particulièrement à Julien Plasse pour les analyses
statistiques et à Floriane Todoroff pour l’organisation de la journée de formation NECT avec Philip
Yanos
Merci aux médecins responsables et aux équipes des centres participant au réseau national des
Centres Référents de Réhabilitation psychosociale et de Remédiation cognitive ou au réseau
national des Centres Experts Schizophrénie et Asperger. Merci plus particulièrement aux docteurs
Céline Roussel, Isabelle Chéreau, Motassem Bakri, Emilie Legros Lafarge, Lucia Fiegl, Romain
Rey, Romain Pommier, Nathalie Guillard-Bouhet, Clélia Quiles, Hélène Richard-Lepouriel pour
nos collaborations autour de RemedRugby, NECT et de plusieurs autres projets. Merci aussi aux
professeurs Fabrice Berna, Franck Schurhoff et Marion Leboyer pour leur confiance et les projets
mis en œuvre au sein du réseau des Centres Experts.
Page 8
Liste des publications
Articles en rapport avec le travail de thèse
- Articles originaux :
-Dubreucq J, Plasse J, Gabayet F, Faraldo M, Blanc O, Chereau I, Cervello S, Couhet G, Demily C, Guillard-Bouhet N, Gouache B, Jaafari N, Legrand G, Legros-Lafarge E, Pommier R, Quilès C, Straub D, Verdoux H, Vignaga F, Massoubre C, REHABAse network* and Franck N. Self-stigma in Serious Mental Illness and Autism Spectrum Disorder: results from the REHABase national psychiatric rehabilitation cohort. Eur Psychiatry. https://doi.org/10.1192/j.eurpsy.2019.12
-Dubreucq J, Plasse J, Gabayet F, Faraldo M, Blanc O, Chereau I, Cervello S, Couhet G, Demily C, Guillard-Bouhet N, Gouache B, Jaafari N, Legrand G, Legros-Lafarge E, Pommier R, Quilès C, Straub D, Verdoux H, Vignaga F, Massoubre C, REHABAse network* and Franck N. Stigma Resistance in Serious Mental Illness and Autism Spectrum Disorder: results from the RehaBASE national psychiatric rehabilitation cohort. Soc Psychiatry Psychiatr Epidemiol. In
review -Dubreucq J, Faraldo M, Abbes M, Ycart B, Richard-Lepouriel H, Favre S, Jermann F,
Attal J, Bakri M, Cohen T, Cervello C, Chereau I, Cognard C, De Clercq M, Douasbin A, Giordana, JY, Giraud-Baro E, Guillard-Bouhet N, Legros-Lafarge E, Martin B, Polosan M, PouchonA, Rolland M, Rainteauk N, Roussel C, Wangermez C, Yanos PT, Lysaker PH, Franck N. Narrative Enhancement and Cognitive Therapy (NECT) and social function in Serious Mental Illness: study protocol for a stepped-wedge randomized controlled trial. Trials. Revised
-Franck N, Bon L, Dekerle M, Plasse J, Massoubre C, Pommier R, Legros-Lafarge E, Jaafari N, Guillard-Bouhet N, Quilès C, Couhet G, Verdoux H, Gouache B, Martin B, Cervello S, Demily C, Dubreucq J. Satisfaction and Needs in Serious Mental Illness and Autism Spectrum Disorder: The REHABase Psychosocial Rehabilitation Project. Psychiatr Serv. 2019 Apr 1;70(4):316-323. - Revues de littérature :
-Dubreucq J, Franck N. Neural and cognitive correlates of stigma and social rejection in individuals with Serious Mental Illness (SMI): A systematic review of the literature. Psychiatry Res. 2019 Apr; 274:146-158. doi: 10.1016/j.psychres.2019.02.023.
-Dubreucq J, Franck N. Internalized Stigma in Serious Mental Illness (SMI): a systematic review of prevalence, predictors and correlates. J affect disord. Revised Autres articles
-Dubreucq J, Ycart B, Gabayet F, et al., FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Towards an improved access to psychiatric rehabilitation: availability and effectiveness at 1-year follow-up of psychoeducation, cognitive remediation therapy, cognitive behaviour therapy and social skills training in the FondaMental Advanced Centers of Expertise-Schizophrenia (FACE-SZ) national cohort. Eur Arch Psychiatry Clin Neurosci. 2019 - Dubreucq J, Gabayet F, Ycart B, Faraldo M, Melis F, Lucas T, Arnaud B, Bacconnier M, Bakri M, Cambier G, Carmona F, Chereau I, Challe T, Pires S, Roussel C, Lamy P, Legrand G, Pages E, Pommier R, Rey R, Souchet Y, the RemedRugby group*, Llorca PM and Massoubre C. Improving social function with ecological social-cognitive remediation in SZ: results from the RemedRugby controlled trial. Eur Psychiatry. In review
Page 9
-Dubreucq J., Delorme C., Roure R. Metacognitive therapy focused on psychosocial function in psychosis. J Contemp Psychother 2016; 46: 197. doi: 10.1007/s10879-016-9334-7
-Dubreucq M, Jourdan S, Poizat A, Dubreucq J. Midwives' feelings about the post-partum care of women with severe mental illness: A qualitative analysis. Encephale. 2019 Sep 12.pii: S0013-7006(19)30243-X.
-Brunet-Gouet E, Urbach M, Ramos V, Ehrminger M, Aouizerate B, Brunel L, Capdevielle D, Chereau I, Dubertret C, Dubreucq J, Fond G, Lançon C, Leignier S, Mallet J, Misdrahi D, Pires S, Schneider P, Schürhoff F, Yazbek H, Zinetti-Bertschy A, Bazin N, Passerieux C, Roux P. Assessing metacognitive and help-seeking strategies in schizophrenia: design and psychometric validation of the Versailles Metacognitive Strategies Evaluation Questionnaire . Clin Rehabil. 2019 Dec 4:269215519888784
-Brunet-Gouet E, Myszkowski N, Ehrminger M, Urbach M, Aouizerate B, Brunel L, Capdevielle D, Chereau I, Dubertret C, Dubreucq J, Fond G, Lançon C, Leignier S, Mallet J, Misdrahi D, Pires S, Schneider P, Schurhoff F, Yazbek H, Zinetti-Bertschy A, Bazin N, Passerieux C, Zenasni F, Roux P. Confirmation of a Two-Factor Solution to the Questionnaire of Cognitive and Affective Empathy in a French Population of Patients With Schizophrenia Spectrum Disorders.Front Psychiatry. 2019 Oct 25;10:751.
-Verdoux H, Quiles C, Cervello S, Dubreucq J, et al. Functioning and cognitive characteristics of clozapine users referred to psychosocial rehabilitation centers: A REHABase cohort study. Psychiatry Res. 2019 Nov; 281:112543.
-Favrod J, Nguyen A, Tronche AM, Blanc O, Dubreucq J, Chereau-Boudet I, Capdevielle D, Llorca PM. Impact of Positive Emotion Regulation Training on Negative Symptoms and Social Functioning in Schizophrenia: A Field Test. Front Psychiatry. 2019 Jul 26; 10:532.
- Fond G, Godin O, Dumontaud M, Faget C, Schürhoff F, Berna F, Aouizerate B, Capdevielle D, Chereau I, D'Amato T, Dubertret C, Dubreucq J, Leignier S, Mallet J, Misdrahi D, Passerieux C, Rey R, Schandrin A, Szoke A, Urbach M, Vidailhet P, Leboyer M, Lançon C, Boyer L, Llorca PM; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Sexual dysfunctions are associated with major depression, chronic inflammation and anticholinergic consumption in the real-world schizophrenia FACE-SZ national cohort. Prog Neuropsychopharmacol Biol Psychiatry. 2019 Aug 30; 94:109654.
- Pignon B, Lajnef M, Godin O, Geoffray MM, Rey R, Mallet J, Dubertret C, Roux P, Passerieux C, Marulaz L, Brunel L, Dubreucq J, Leignier S, Capdevielle D, André M, Aouizerate B, Misdrahi D, Berna F, Vidailhet P, Chereau I, Llorca PM, Fond G, Lançon C, Leboyer M, Schürhoff F; FondaMental Academic Centers of Expertise for Schizophrenia (FACE-SZ) collaborators. Relationship between childhood trauma and level of insight in schizophrenia: A path-analysis in the national FACE-SZ dataset. Schizophr Res. 2019; pii: S0920-9964(19)30129-X
-Misdrahi D, Tessier A, Daubigney A, Meissner WG, Schurhoff F, Boyer L, Godin O, Bulzacka E, Aouizerate B, Andrianarisoa M, Berna F, Capdevielle D, Chereau-Boudet I, D'Amato T, Dubertret C, Dubreucq J, Faget-Agius C, Lançon C, Mallet J, Passerieux C, Rey R, Schandrin A, Urbach M, Vidailhet P, Llorca PM, Fond G; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) Group. Prevalence of and Risk Factors for Extrapyramidal Side Effects of Antipsychotics: Results From the National FACE-SZ Cohort. J Clin Psychiatry. 2019; 80(1).
-Godin O, Fond G, Bulzacka E, Schürhoff F, Boyer L, Myrtille A, Andrianarisoa M, Aouizerate B, Berna F, Capdevielle D, Chereau I, Dorey JM, Dubertret C, Dubreucq J, Faget C, Lancon C, Leignier S, Mallet J, Misdrahi D, Passerieux C, Rey R, Roux P, Vidailhet P, Costagliola D; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group, Leboyer M, Llorca PM. Validation and refinement of the clinical staging model in a French cohort of outpatient with schizophrenia (FACE-SZ). Prog Neuropsychopharmacol Biol Psychiatry. 2019; 92:226-234.
Page 10
-Fond G, Bulzacka E, Boucekine M, Schürhoff F, Berna F, Godin O, Aouizerate B, Capdevielle D, Chereau I, D'Amato T, Dubertret C, Dubreucq J, Faget C, Leignier S, Lançon C, Mallet J, Misdrahi D, Passerieux C, Rey R, Schandrin A, Urbach M, Vidailhet P, Leboyer M; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group, Boyer L, Llorca PM. Machine learning for predicting psychotic relapse at 2 years in schizophrenia in the national FACE-SZ cohort. Prog Neuropsychopharmacol Biol Psychiatry. 2019 Jun 8;92:8-18.
-Roux P, Urbach M, Fonteneau S, Berna F, Brunel L, Capdevielle D, Chereau I, Dubreucq
J, Faget-Agius C, Fond G, Leignier S, Perier CC, Richieri R, Schneider P, Schürhoff F, Tronche AM, Yazbek H, Zinetti-Bertschy A; FondaMental Advanced Centers of Expertise in Schizophrenia (FACE-SCZ) Collaborators, Passerieux C, Brunet-Gouet E. Screening for cognitive deficits with the Evaluation of Cognitive Processes involved in Disability in Schizophrenia scale. Clin Rehabil. 2019 Jan;33(1):113-119.
-Fond G, Godin O, Schürhoff F, Berna F, Aouizerate B, Capdevielle D, Chereau I, D'Amato T, Dubertret C, Dubreucq J, Faget C, Leignier S, Lançon C, Mallet J, Marulaz L, Misdrahi D, Passerieux C, Rey R, Schandrin A, Urbach M, Vidailhet P, Leboyer M; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group, Boyer L, Llorca PM. Inflammatory DEpression Advances in Schizophrenia (IDEAS): A precision medicine approach of the national FACE-SZ cohort. J Affect Disord. 2019 Feb 15;245:468-474.
-Schürhoff F, Fond G, Berna F, Bulzacka E, Godin O, Boyer L, Misdrahi D, Andrianarisoa M, Brunel L, Coulon N, Aouizerate B, Capdevielle D, Chereau I, D'Amato T, Dubertret C, Dubreucq J, Faget C, Gabayet F, Mallet J, Rey R, Lancon C, Passerieux C, Schandrin A, Urbach M, Vidailhet P, Leboyer M, Llorca PM; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. The 10-year findings from the FondaMental Academic Center of Expertise for Schizophrenia (FACE-SZ): Review and recommendations for clinical practice. Encephale. 2019 Feb;45(1):9-14. doi
-Schandrin A, Norton J, Raffard S, Aouizerate B, Berna F, Brunel L, Chereau-Boudet I, D'Amato T, Denizot H, Dubertret C, Dubreucq J, Faget C, Fond G, Gabayet F, Llorca PM, Mallet J, Misdrahi D, Passerieux C, Rey R, Schurhoff F, Urbach M, Bonnet S, Capdevielle D; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. A multi-dimensional approach to the relationship between insight and aggressiveness in schizophrenia: Findings from the FACE-SZ cohort. Schizophr Res. 2019 Feb;204:38-45
-Schandrin A, Norton J, Raffard S, Aouizerate B, Berna F, Brunel L, Chereau-Boudet I, D'Amato T, Denizot H, Dubertret C, Dubreucq J, Faget C, Fond G, Gabayet F, Llorca PM, Mallet J, Misdrahi D, Passerieux C, Rey R, Schurhoff F, Urbach M, Bonnet S, Capdevielle D; FACE-SZ group. A multi-dimensional approach to the relationship between insight and aggressiveness in schizophrenia: Findings from the FACE-SZ cohort. Schizophr Res. 2019 Feb;204:38-45.
-Fond G, Godin O, Boyer L, Berna F, Andrianarisoa M, Coulon N, Brunel L, Bulzacka E, Aouizerate B, Capdevielle D, Chereau I, D'Amato T, Dubertret C, Dubreucq J, Faget C, Leignier S, Lançon C, Mallet J, Misdrahi D, Passerieux C, Rey R, Schandrin A, Urbach M, Vidailhet P, Llorca PM, Schürhoff F, Leboyer M; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) Group. Chronic low-grade peripheral inflammation is associated with ultra resistant schizophrenia. Results from the FACE-SZ cohort. Eur Arch Psychiatry Clin Neurosci. 2019 Dec;269(8):985-992.
-Godin O, Leboyer M, Schürhoff F, Llorca PM, Boyer L, Andre M, Andrianarisoa M, Aouizerate B, Berna F, Capdevielle D, Chereau I, Dorey JM, Dubertret C, Dubreucq J, Faget C, Lancon C, Leignier S, Mallet J, Misdrahi D, Passerieux C, Rey R, Roux P, Vidailhet P, Costagliola D, Fond G; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) Group. Metabolic Syndrome and Illness Severity Predict Relapse at 1-Year Follow-Up in Schizophrenia: The FACE-SZ Cohort. J Clin Psychiatry. 2018 Sep 18;79(6). pii: 17m12007.
Page 11
-Roux P, Urbach M, Fonteneau S, Berna F, Brunel L, Capdevielle D, Chereau I, Dubreucq
J, Faget-Agius C, Fond G, Leignier S, Perier CC, Richieri R, Schneider P, Schürhoff F, Tronche AM, Yazbek H, Zinetti-Bertschy A; FondaMental Advanced Centers of Expertise in Schizophrenia (FACE-SCZ) Collaborators, Passerieux C, Brunet-Gouet E. Psychiatric disability as mediator of the neurocognition-functioning link in schizophrenia spectrum disorders: SEM analysis using the Evaluation of Cognitive Processes involved in Disability in Schizophrenia (ECPDS) scale. Schizophr Res. 2018 Nov;201:196-203.
-Fond G, Boyer L, Berna F, Godin O, Bulzacka E, Andrianarisoa M, Brunel L, Aouizerate B, Capdevielle D, Chereau I, Coulon N, D'Amato T, Dubertret C, Dubreucq J, Faget C, Leignier S, Lançon C, Mallet J, Misdrahi D, Passerieux C, Rey R, Schandrin A, Urbach M, Vidailhet P, Leboyer M, Schürhoff F, Llorca PM; FACE-SZ group. Remission of depression in patients with schizophrenia and comorbid major depressive disorder: results from the FACE-SZ cohort . Br J Psychiatry. 2018 Aug;213(2):464-470.
-Fond G, Boyer L, Schürhoff F, Berna F, Godin O, Bulzacka E, Andrianarisoa M, Brunel L, Aouizerate B, Capdevielle D, Chereau I, Coulon N, D'Amato T, Dubertret C, Dubreucq J, Faget C, Lançon C, Leignier S, Mallet J, Misdrahi D, Passerieux C, Rey R, Schandrin A, Urbach M, Vidailhet P, Llorca PM, Leboyer M; FACE-SZ group, Andrianarisoa M, Aouizerate B, Bazin N, Berna F, Blanc O, Brunel L, Bulzacka E, Capdevielle D, Chereau-Boudet I, Chesnoy-Servanin G, Coulon N, Danion JM, D'Amato T, Deloge A, Denizot H, Dorey JM, Dubertret C, Dubreucq J, Faget C, Fluttaz C, Fond G, Fonteneau S, Gabayet F, Giraud-Baro E, Jarroir M, Leignier S, Lacelle D, Lançon C, Laouamri H, Leboyer M, Le Gloahec T, Le Strat Y, Llorca PM, Mallet J, Metairie E, Misdrahi D, Offerlin-Meyer I, Passerieux C, Peri P, Pires S, Portalier C, Ramet L, Rey R, Roman C, Schandrin A, Schürhoff F, Tessier A, Tronche AM, Urbach M, Vaillant F, Vehier A, Vidailhet P, Vilà E, Yazbek H, Zinetti-Bertschy A. Latent toxoplasma infection in real-world schizophrenia: Results from the national FACE-SZ cohort. Schizophr Res. 2018 Nov; 201:373-380.
-Roux P, Misdrahi D, Capdevielle D, Aouizerate B, Berna F, Brunel L, Chereau I, Dorey JM, Dubertret C, Dubreucq J, Faget-Agius C, Fonteneau S, Gabayet F, Llorca PM, Mallet J, Rey R, Richieri R, Schandrin A, Schürhoff F, Tessier A, Vidailhet P, Passerieux C, Urbach M; FACE-SZ Group. Mediation Analyses of Insight, Quality of Life, Depression, and Suicidality: Results From the FACE-SZ Cohort. J Clin Psychiatry. 2018 May/Jun;79(3). pii: 17m11638.
-Fond G, Boyer L, Andrianarisoa M, Godin O, Bulzacka E, Berna F, Brunel L, Coulon N, Aouizerate B, Capdevielle D, Chereau I, D'amato T, Denizot H, Dubertret C, Dubreucq J, Faget C, Leignier S, Mallet J, Misdrahi D, Rey R, Lancon C, Passerieux C, Schandrin A, Urbach M, Vidailhet P, Leboyer M, Schurhoff F, Llorca PM; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Self-reported pain in patients with schizophrenia. Results from the national first-step FACE-SZ cohort. Prog Neuropsychopharmacol Biol Psychiatry 2018 Jul 13;85:62-68.
-Mallet J, Le Strat Y, Schürhoff F, Mazer N, Portalier C, Andrianarisoa M, Aouizerate B, Berna F, Brunel L, Capdevielle D, Chereau I, D'Amato T, Dubreucq J, Faget C, Gabayet F, Honciuc RM, Lançon C, Llorca PM, Misdrahi D, Rey R, Roux P, Schandrin A, Urbach M, Vidailhet P, Fond G, Dubertret C; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Tobacco smoking is associated with antipsychotic medication, physical aggressiveness, and alcohol use disorder in schizophrenia: results from the FACE-SZ national cohort. Eur Arch Psychiatry Clin Neurosci. 2019 Jun; 269(4):449-457.
-Laidi C, Prigent A, Plas A, Leboyer M, Fond G, Chevreul K; FACE-SCZ Group. Factors associated with direct health care costs in schizophrenia: Results from the FACE-SZ French dataset. Eur Neuropsychopharmacol. 2018; 28(1): 24-36
-Fond G, Resseguier N, Schürhoff F, Godin O, Andrianarisoa M, Brunel L, Bulzacka E, Aouizerate B, Berna F, Capdevielle D, Chereau I, D'Amato T, Dubertret C, Dubreucq J, Faget C, Gabayet F, Lançon C, Llorca PM, Mallet J, Misdrahi D, Passerieux C, Rey R, Schandrin A, Urbach
Page 12
M, Vidailhet P, Boyer L, Leboyer M; FACE-SZ group. Relationships between low-grade peripheral inflammation and psychotropic drugs in schizophrenia: results from the national FACE-SZ cohort. Eur Arch Psychiatry Clin Neurosci. 2018 Sep; 268(6):541-553.
-Fond G, Boyer L, Leboyer M, Godin O, Llorca PM, Andrianarisoa M, Berna F, Brunel L, Aouizerate B, Capdevielle D, Chereau I, D'Amato T, Dubertret C, Dubreucq J, Faget C, Gabayet F, Mallet J, Misdrahi D, Rey R, Lancon C, Passerieux C, Roux P, Vidailhet P, Yazbek H, Schürhoff F, Bulzacka E; FACE-SZ group. Influence of Venus and Mars in the cognitive sky of schizophrenia. Results from the first-step national FACE-SZ cohort. Schizophr Res. 2018 May; 195:357-365.
-Fond G, Boyer L, Andrianarisoa M, Godin O, Brunel L, Bulzacka E, Coulon N, Llorca PM, Berna F, Aouizerate B, Capdevielle D, D'Amato T, Dubertret C, Dubreucq J, Faget C, Gabayet F, Mallet J, Misdrahi D, Rey R, Richieri R, Roux P, Passerieux C, Schandrin A, Tronche AM, Vidailhet P, Leboyer M, Schürhoff F; FACE-SZ group. Risk factors for increased duration of untreated psychosis. Results from the FACE-SZ dataset. Schizophr Res 2018 May; 195:529-533.
-Fond G, Berna F, Boyer L, Godin O, Brunel L, Andrianarisoa M, Aouizerate B, Capdevielle D, Chereau I, Danion JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Le Gloahec T, Llorca PM, Mallet J, Misdrahi D, Rey R, Richieri R, Passerieux C, Portalier C, Roux P, Vehier A, Yazbek H, Schürhoff F, Bulzacka E; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Benzodiazepine long-term administration is associated with impaired attention/working memory in schizophrenia: results from the national multicentre FACE-SZ data set. Eur Arch Psychiatry Clin Neurosci. 2018; 268(1):17-26
-Fond G, Godin O, Schürhoff F, Berna F, Bulzacka E, Andrianarisoa M, Brunel L, Aouizerate B, Capdevielle D, Chereau I, Coulon N, D'Amato T, Dubertret C, Dubreucq J, Faget C, Lançon C, Leignier S, Mallet J, Misdrahi D, Passerieux C, Rey R, Schandrin A, Urbach M, Vidailhet P, Leboyer M, Boyer L, Llorca PM; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Hypovitaminosis D is associated with depression and anxiety in schizophrenia: Results from the national FACE-SZ cohort. Psychiatry Res. 2018 Dec;270:104-110.
-Andrianarisoa M, Boyer L, Godin O, Brunel L, Bulzacka E, Aouizerate B, Berna F, Capdevielle D, Dorey JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Llorca PM, Mallet J, Misdrahi D, Rey R, Richieri R, Passerieux C, Schandrin A, Tronche AM, Urbach M, Vidailhet P, Schürhoff F, Fond G; FACE-SCZ Group. Childhood trauma, depression and negative symptoms are independently associated with impaired quality of life in schizophrenia. Results from the national FACE-SZ cohort. Schizophr Res. 2017; 185:173-181.
-Fond G, Boyer L, Boucekine M, Aden LA, Schürhoff F, Tessier A, Andrianarisoa M, Berna F, Brunel L, Capdevielle D, Chereau I, Mallet J, Denizot H, Dorey JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Rey R, Richieri R, Passerieux C, Schandrin A, Urbach M, Vidailhet P, Llorca PM, Misdrahi D; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Validation study of the Medication Adherence Rating Scale. Results from the FACE-SZ national dataset. Schizophr Res. 2017; 182:84-89
-Fond G, Berna F, Andrianarisoa M, Godin O, Leboyer M, Brunel L, Aouizerate B, Capdevielle D, Chereau I, D'Amato T, Denizot H, Dubertret C, Dubreucq J, Faget C, Gabayet F, Llorca PM, Mallet J, Misdrahi D, Passerieux C, Richieri R, Rey R, Schandrin A, Urbach M, Vidailhet P, Boyer L, Schürhoff F; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Chronic low-grade peripheral inflammation is associated with severe nicotine dependence in schizophrenia: results from the national multicentric FACE-SZ cohort. Eur Arch Psychiatry Clin Neurosci. 2017; 267(5): 465-472
-Godin O, Leboyer M, Schürhoff F, Boyer L, Andrianarisoa M, Brunel L, Bulzacka E, Aouizerate B, Berna F, Capdevielle D, D'Amato T, Denizot H, Dubertret C, Dubreucq J, Faget C, Gabayet F, Llorca PM, Mallet J, Misdrahi D, Passerieux C, Rey R, Richieri R, Schandrin A, Urbach
Page 13
M, Vidailhet P, Costagliola D, Fond G; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Predictors of rapid high weight gain in schizophrenia: Longitudinal analysis of the French FACE-SZ cohort. J Psychiatr Res. 2017 Nov; 94:62-69.
-Mallet J, Le Strat Y, Schürhoff F, Mazer N, Portalier C, Andrianarisoa M, Aouizerate B, Berna F, Brunel L, Capdevielle D, Chereau I, D'Amato T, Denizot H, Dubreucq J, Faget C, Gabayet F, Lançon C, Llorca PM, Misdrahi D, Rey R, Roux P, Schandrin A, Urbach M, Vidailhet P, Fond G, Dubertret C; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Cigarette smoking and schizophrenia: a specific clinical and therapeutic profile? Results from the FACE-Schizophrenia cohort. Prog Neuropsychopharmacol Biol Psychiatry. 2017 Oct 3; 79(Pt B):332-339.
-Fond G, Godin O, Boyer L, Llorca PM, Andrianarisoa M, Brunel L, Aouizerate B, Berna F, Capdevielle D, D'Amato T, Denizot H, Dubertret C, Dubreucq J, Faget C, Gabayet F, Mallet J, Misdrahi D, Passerieux C, Rey R, Richieri R, Schandrin A, Urbach M, Vidailhet P, Leboyer M, Bulzacka E, Schürhoff F; FACE-SZ group. Advanced paternal age is associated withearlier schizophrenia onset in offspring. Results from the national multicentric FACE-SZ cohort. Psychiatry Res. 2017; 254:218-223.
-Rey R, D'Amato T, Boyer L, Brunel L, Aouizerate B, Berna F, Capdevielle D, Chereau I, Chesnoy-Servanin G, Denizot H, Dorey JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Lancon C, Mallet J, Misdrahi D, Passerieux C, Schandrin A, Schürhoff F, Urbach M, Vidailhet P, Llorca PM, Fond G; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Nicotine dependence is associated with depression and childhood trauma in smokers with schizophrenia: results from the FACE-SZ dataset. Eur Arch Psychiatry Clin Neurosci. 2017; 267(6):567-577.
-Fond G, Bulzacka E, Boyer L, Llorca PM, Godin O, Brunel L, Andrianarisoa MG, Aouizerate B, Berna F, Capdevielle D, Chereau I, Denizot H, Dorey JM, Dubertret J, Dubreucq J, Faget C, Gabayet F, Le Strat Y Micoulaud-Franchi JA, Misdrahi D, Rey R, Richieri R, Roger M, Passerieux C, Schandrin A, Urbach M, Vidalhet P, Schürhoff F, Leboyer M. Birth by cesarean section and schizophrenia: results from the multicenter FACE-SZ data-set. Eur Arch Psychiatry Clin Neurosci. 2017 Sep;267(6):587-594.
-Baudin G, Godin O, Lajnef M, Aouizerate B, Berna F, Brunel L, Capdevielle D, Chereau I, Dorey JM, Dubertret C, Dubreucq J, Faget C, Fond G, Gabayet F, Laouamri H, Lancon C, Le Strat Y, Tronche AM, Misdrahi D, Rey R, Passerieux C, Schandrin A, Urbach M, Vidalhet P, Llorca PM, Schürhoff F; FondaMental Academic Centers of Expertise for Schizophrenia (FACE-SZ) Collaborators. Differential effects of childhood trauma and cannabis use disorders in patients suffering from schizophrenia. Schizophr Res. 2016; 175(1-3):161-167
-Misdrahi D, Tessier A, Swendsen J., Berna F, Brunel L, Capdevielle D, Chereau I, Danion JM, De Pradier M, Dorey JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Rey R, Richieri R, Passerieux C, Schandrin A, Schurhoff F, Tronche AM, Urbach M, Llorca PM, Fond G. and the FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Determination of adherence profiles in schizophrenia using self-reported adherence: Results from the FACE-SZ data-set. Journal of Clinical Psychiatry 2016; 77(9):e1130-e1136
-Fond G., Godin O., Brunel L., Aouizerate B., Berna F., Bulzacka E., Capdevielle D., Chereau I., Dorey J.M., Dubertret C., Dubreucq J., Faget C., Gabayet F., Le Strat Y., Micoulaud-Franchi J.M., Misdrahi D., Reya R., Richieri R., Passerieux C., Schandrin A., Schürhoff F., Tronche
A.M., Urbach M., Vidalhet P., Llorca P.M., Leboyer M., the FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Peripheral sub-inflammation is associated with antidepressant consumption in schizophrenia. Results from the multi-center FACE-SZ data set. J Affect Disord. 2016 Feb;191:209-15.
Page 14
-Bulzacka E, Boyer L, Schürhoff F, Godin O, Berna F, Brunel L, Andrianarisoa M, Aouizerate B, Capdevielle D, Chéreau-Boudet I, Chesnoy-Servanin G, Danion JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Le Gloahec T, Llorca PM, Mallet J, Misdrahi D, Rey R, Richieri R, Passerieux C, Roux P, Yazbek H, Leboyer M, Fond G; FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) Group. Chronic peripheral inflammation is associated with cognitive impairment in schizophrenia. Results from the multicentric FACE-SZ dataset. Schizophrenia Bulletin. 2016; 42(5):1290-302
-Roux P, Urbach M., Fonteneau S., Aouizerate B., Berna F., Brunel L., Capdevielle D., Chereau I., Danion J.M., Dorey J, Dubertret C., Dubreucq J., Faget C., Gabayet F., Llorca P.M., Mallet J., Misdrahi D., Rey R., Richieri R., Schurhoff F., Yazbek H., Passerieux C., Brunet Gouet E. The EVACO Project: A new battery for assessing social cognition disorders and related psychiatric disability in schizophrenia. European Psychiatry. 2016;33:S78
-Fond G, Boyer L, Favez M, Brunel L, Aouizerate B, Berna F, Capdevielle D, Chereau I, Dorey JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Lancon C, Le Strat Y, Misdrahi D, Rey R, Passerieux C, Schandrin A, Schurhoff F, Tronche AM, Urbach M, Vidalhet P, Llorca PM, Pelissolo A. And the FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group. Medication and aggressiveness in real-world schizophrenia. Results from the FACE-SZ dataset. Psychopharmacology 2016; 233 (4) : 571-578
-Lysaker PH, Kukla M, Dubreucq J, Gumley A, McLeod H, Buck KD, Vohs J, Minor KM, Luther L, Leonhardt BL, Belanger EA, Popolo R, Dimaggio G. Metacognitive deficits predict future levels of negative symptoms in schizophrenia controlling for neurocognition, affect recognition, and self-expectation of goal attainment. Schizophrenia Research 2015; 168 (1-2) : 267-72
-Godin O, Leboyer M, Gaman A, Aouizerate B, Berna F, Brunel L, Capdevielle D, Chereau I, Dorey JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Le Strat Y, Llorca PM, Misdrahi D, Rey R, Richieri R, Passerieux C, Schandrin A, Schurhoff F, Urbach M, Vidalhet P, Girerd N, Fond G, And the FACE-SZ group*. Metabolic Syndrome, abdominal obesity and hyperuricemia in Schizophrenia: Results From the FACE-SZ cohort. Schizophrenia Research 2015; 168(1-2): 388-394.
-Fond G, Godin O, Brunel L, Aouizerate B, Berna F, Bulzacka E, Capdevielle D, Chereau I, Dorey JM, Dubertret Ca, Dubreucq J, Faget C, Gabayet F, Le Strat Y, Micoulaud-Franchi JM, , Misdrahi D, Rey R, Richieri R, Passerieux C, Schandrin A, Schurhoff F, Tronche AM, Urbach M, Vidalhet P, Llorca PM, Leboyer M. And the FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group Abnormal C-reactive protein (CRP) levels in schizophrenia and schizoaffective disorders. Results from the FACE-SZ dataset. European Psychiatry 2015; 30(S8) : S112
-Berna F, Misdrahi D, Boyer L Aouizerate B, Brunel L, Capdevielle D, Chereau I, Danion JM, Dorey JM, Dubertret C, Dubreucq J, Faget C, Gabayet F, Lancon C, Mallet J, Rey R, Passerieux C, Schandrin A, Schurhoff F, Tronche AM, Urbach M, Vidailhet P, Llorca PM, Fond G, and the FACE-SZ (FondaMental Academic Centers of Expertise for Schizophrenia) group*. Akathisia: prevalence and risk factors in a community-dwelling sample of patients with schizophrenia. Results from the FACE-SZ dataset. Schizophrenia Research 2015; 169(1-3): 255-261
-Schürhoff F, Fond G, Berna F, Bulzacka E, Vilain J, Capdevielle D, Misdrahi D, Leboyer M, Llorca PM; FondaMental Academic Centers of Expertise for Schizophrenia (FACE-SZ) collaborators. A National network of schizophrenia expert centres: An innovative tool to bridge the research-practice gap. Eur Psychiatry. 2015 ; 30(6):728-35
Page 15
Articles en préparation
-Dubreucq M, Plasse J, Gabayet F, Blanc O, Chereau I, Cervello S, Couhet G, Demily C, Guillard-Bouhet N, Gouache B, Jaafari N, Legrand G, Legros-Lafarge E, Pommier R, Quilès Cm, Straub D, Verdoux H, Vignaga F, Massoubre C, REHABAse network*, Franck N and Dubreucq J. Parents with Serious Mental Illness or Autism Spectrum Disorder: results from the RehaBASE national psychiatric rehabilitation cohort
-Dubreucq M, Besnard M, Revil-Signorat K, Abbes M, Cohen T, Favre-Reguillon L, Guy C, Tonnot B, Dubreucq J. Recovery-oriented supported intimate relationships and parenthood in Severe Mental Illness: development of a new intervention
- Dubreucq J, Martin A, Gabayet F, Plasse J, Quiles C, Bralet MC, Lysaker PH, Franck N. Comparing metacognition in schizophrenia and autism spectrum disorders
Ouvrages collectifs
Publications pédagogiques :
-Dubreucq J. Entrainement des compétences sociales chez les adultes avec troubles du spectre de l’autisme, EMC Psychiatrie (prévu pour 2020)
-Roman C, Guy C, Gobbo J, Dubreucq J. Décloisonner l’offre de soins et services, Santé mentale n°217 (mars 2017)
-Roussel C, Dubreucq J, Lucas T, Fernandez E. Retour à l’emploi et Psychoéducation, Santé
Mentale n°164 (janvier 2014), p 68-72. -Cambier G, Viezzoli D, Dubreucq J, Giraud Baro E. Autisme de haut niveau : une pratique de
réhabilitation, Santé mentale n°192 (janvier 2014), p 14-19
Chapitres de livres :
-Dubreucq J, Revil K, Lucas T, Fernandez E, Gabayet F, Roussel C. Les représentations du travail et leur utilisation dans la réinsertion professionnelle In : Franck N. (Ed) Outils de la réhabilitation en psychiatrie Elsevier, Paris, 2016.
-Dubreucq J, Gabayet F, Lucas T. (2016). Lutter contre la stigmatisation par la remédiation cognitive. In : Franck N. (Ed) Outils de la réhabilitation en psychiatrie Elsevier, Paris, 2016.
-Dubreucq J, Gobbo J, Roman C, Giraud Baro E. Le modèle des Équipes Spécialisées d’Évaluation du Handicap Psychique (ESEHP) et du Réseau Handicap Psychique (RéHPsy). In : Franck N. (Ed) Traité de réhabilitation psychosociale ; Elsevier, 2018
-Guy C, Lagasse S, Dubreucq J. Comment le case management contribue-t-il au rétablissement ? In : Franck N. (Ed) Traité de réhabilitation psychosociale ; Elsevier, 2018
-Dubreucq J, Leignier S, Viezzoli D, Fulachier D, Berthe L, Lagasse S. Réhabilitation psychosociale chez les personnes avec syndrome d’Asperger. In : Franck N. (Ed) Traité de réhabilitation psychosociale ; Elsevier, 2018
-Dubreucq J, Pennel L, Dematteis M. Réhabilitation psychosociale chez les personnes avec une addiction. In : Franck N. (Ed) Traité de réhabilitation psychosociale ; Elsevier, 2018
-Dubreucq J, Jobert E, Lucas T, Gabayet F, Revil K, Bogey A, Roussel C. Représentations du travail et réinsertion professionnelle In : Franck N. (Ed) Traité de réhabilitation en psychiatrie Elsevier, Paris, 2018.
-Dubreucq J, Gabayet F, Lucas T, Melis F, Faraldo M (2018). Réduire l’auto-stigmatisation et les symptômes négatifs par la remédiation cognitive. In : Franck N. (Ed) Outils de la réhabilitation en psychiatrie Elsevier, Paris, 2018.

Page 16
-Dematteis M, Pennel L, Dubreucq J, Giraud Baro E, Brousse G. Addiction : entre stratégies d'adaptation et pathologie - Place d'une réadaptation cognitivo-émotionnelle et sociale. In : Franck N. (Ed) Traité de réhabilitation psychosociale ; Elsevier, 2018
-Dubreucq J. Coordination de parcours et pair-aidance. In : N. Franck. Pair-Aidance en santé mentale. A paraître (juin 2020)

Page 17
Abréviations
TPSP: Troubles Psychiques Sévères et Persistants
TSA-SDI: Troubles du Spectre de l'Autisme sans Déficience Intellectuelle
Page 18
Liste des figures
-Figure 1. Les différentes formes de stigmatisation…………………………………………….…p22
-Figure 2. Les stéréotypes les plus courants concernant les troubles psychiques………………....p23
-Figure 3. Perception des personnes présentant des troubles psychiques en Europe………….…..p25
-Figure 4. Évolution des attributions causales pour la schizophrénie et la dépression ..….............p26
-Figure 5. Évolution de l’acceptation sociale des personnes avec schizophrénie ou dépression…………………………………………………………………………………………p27
-Figure 6. Évolution de 1996 à 2018 de la perception de la dangerosité potentielle des personnes avec schizophrénie et du soutien aux soins sous contrainte aux USA…………………………....p28
-Figure 7. Effets de la stigmatisation perçue sur les personnes avec TPSP…….……….………..p31
-Figure 8. Prévalence de la discrimination expérimentée chez les usagers des services de santé mentale en Angleterre en 2012…………………………………………………………..………..p32
-Figure 9. Discrimination expérimentée et anticipée du fait d’un diagnostic de schizophrénie- étude INDIGO, site France………………………………………...........................................................p33
-Figure 10. Les réponses possibles face à la stigmatisation…………...........................................p37
-Figure 11. Modèle de l’identité-maladie………….......................................................................p38
-Figure 12. Le « why try effect » …………………………………………………………..…….p39
-Figure 13. Le processus de réhabilitation psychosociale, centré sur la personne………………..p52
-Figure 14. Stratégies pour réduire la stigmatisation publique………….......................................p54
-Figure 15. Le processus de rétablissement personnel…………....................................................p57
-Figure 16. Programmes de réduction de l’auto-stigmatisation…………......................................p60
-Figure 17. Modèle théorique des mécanismes conduisant à la stigmatisation dans les services de santé mentale, selon la théorie de l’étiquetage modifiée (MLT)…………....................................p191
-Figure 18. Réactions émotionnelles négatives suite à une hospitalisation sous contrainte, stress lié à la stigmatisation et auto-stigmatisation…………..........................................................................p192
Page 19
Table des matières
Partie I. Auto-stigmatisation, réhabilitation psychosociale et rétablissement………..……...p21
Chapitre 1. La stigmatisation en santé mentale…………………………………………..…....p22
1.1 La stigmatisation publique……………………………………………………………….…p23
1.2 La stigmatisation structurelle…………………………………………………………….…p29
1.3 La stigmatisation perçue, expérimentée et anticipée……………………………………....p30
1.4 Le stress lié à la stigmatisation et les réactions possibles………………………….………p35
1.5 L’auto-stigmatisation et la résistance à la stigmatisation……………………………........p38
1.6 La stigmatisation de courtoisie………………………………………………………...........p40
Chapitre 2. Stigmatisation et neurosciences………………………………………………..…..p41
Chapitre 3. Mesurer les effets de la stigmatisation………………………………………….....p44
Chapitre 4. Réduire la stigmatisation et l’auto-stigmatisation………………...……………...p49
4.1. Réduire la stigmatisation structurelle…………………………………………………..…p49 4.1.1. Des maladies mentales au handicap psychique : un préalable indispensable à la
réduction de la stigmatisation…………………………………………………………...p49 4.1.2. Du handicap psychique au rétablissement : place de la lutte contre la
stigmatisation……………………………………………………………………………..p51 4.2. Réduire la stigmatisation publique…………………………………………………………p53 4.3. Réduire l’auto-stigmatisation……………………………………………………………….p55 4.3.1 Auto-stigmatisation et rétablissement……………………………………………..p55 4.3.2 Auto-stigmatisation et réhabilitation psychoociale……………………………….p58
Problématique principale et objectifs du travail de thèse……………………………………..p61
Partie II. L’auto-stigmatisation : mécanismes cognitifs et neurobiologiques identifiés dans la
littérature…………………………………………………………………………………………p64
Partie III. L’auto-stigmatisation dans la littéraure : prévalence, prédicteurs et
conséquences……………………………………………………………………………………...p78
Partie IV. L’auto-stigmatisation et la résistance à la stigmatisation en France…….………p120
Partie V. Discussion générale et perspectives…………………………………………………p182
Chapitre 1. Synthèse des résultats principaux………………………………………………..p183
1.1. L’auto-stigmatisation, une caractéristique fréquente et associée à de multiples effets
négatifs…………………………………………………………………………………………..p184 1.2. L’auto-stigmatisation, un paramètre sous l’influence de facteurs environementaux…p185 1.3. L’auto-stigmatisation, un prédicteur longitudinal du devenir des personnes avec
TPSP…………………………………………………………………………………………….p186 1.4.La réhabilitation psychosociale, un levier pour réduire l’auto-stigmatisation?............p187 1.5. Auto-stigmatisation et résistance à la stigmatisation…………………………………...p188
Page 20
Chapitre 2. Implcations cliniques et pour la recherche……………………………….……p188
2.1. Réduire la stigmatisation publique………………………………………………….…..p189 2.2. Diffuser les pratiques orientées vers le rétablissement dans les services de santé
mentale………………………………………………………………………………………...p190 2.3. Intervenir précocément auprès des personnes concernées et de leurs proches………p193
Chapitre 3. Limites……………………………………………………………………………p195
Chapitre 4. Perspectives………………………………………………………………………p196
Bibliographie………………………………………………..……..…………………………..p199 Bilbiographie des figures………………………………………………………………………p217
Annexes…………………………………………………………………………………………p219

Page 21
Partie I. Auto-stigmatisation, réhabilitation psychosociale et rétablissement
“I perceived myself, quite accurately, unfortunately, as having a serious mental illness and therefore as
having been relegated to what I called “the social garbage heap.” I tortured myself with the persistent and
repetitive thought that people I would encounter, even total strangers, did not like me and wished that
mentally ill people like me did not exist. Thus, I would do things such as standing away from others at bus
stops and hiding and cringing in the far corners of subway cars. Thinking of myself as garbage, I would even
leave the sidewalk in what I thought as exhibiting the proper deference to those above me in social class. The
latter group, of course, included all other human beings” (Kathleen Gallo, Self-stigmatized; Schizophrenia
Bulletin, 1994). [1]
Page 22
Chapitre 1. La stigmatisation en santé mentale
Décrite pour la 1ère fois par Irving Goffman en 1963, la stigmatisation (du grec « stigma », utilisé
pour décrire les marques d’infamie infligées dans l’Antiquité aux personnes d’un statut social
inférieur) peut être définie comme un « attribut ou une caractéristique évoquant une identité sociale
dévaluée dans un contexte particulier » [2]. Si elle a pu renvoyer à une identité positive à certaines
époques (par exemple, les « stigmates » du Christ), elle est principalement associée dans le domaine
de la santé mentale à des représentations sociales négatives et à une discrimination dans l’ensemble
des sphères de la vie quotidienne. Cinq étapes ont été décrites dans le processus de stigmatisation
d’un groupe social : i) la distinction et l’étiquetage de différences entre deux groupes sociaux; ii)
l’association de ces différences à des stéréotypes négatifs; iii) la séparation en deux groupes
distincts (« nous » et « eux ») ; iv) la perte du statut social et v) la discrimination [3]. La
stigmatisation survient lorsque les préjugés relatifs aux troubles psychiques sont associés à des
réactions émotionnelles négatives et à des comportements discriminants envers les personnes
présentant des troubles psychiques sévères et persistants (TPSP) [4]. Elle peut revêtir plusieurs
formes : i) la stigmatisation publique, ou les croyances négatives et attitudes discriminantes du
grand public envers les personnes présentant des troubles psychiques ; ii) la stigmatisation
structurelle, ou la restriction des droits et opportunités des personnes avec des troubles psychiques
par le corps social et les pouvoirs publics ; iii) la stigmatisation perçue par les personnes avec
troubles psychiques ; iv) la stigmatisation expérimentée ou anticipée par les personnes avec troubles
psychiques ; v) l’auto-stigmatisation ; vi) la stigmatisation vécue par les proches de la personne
avec troubles psychiques.
Page 23
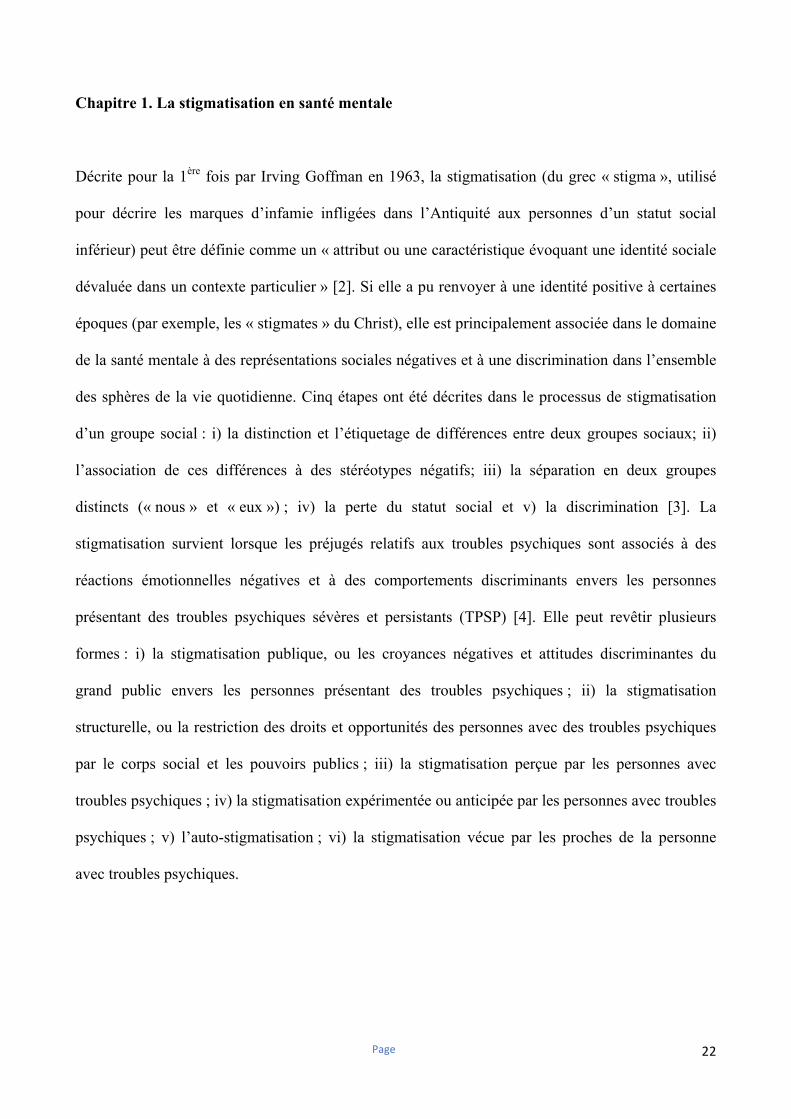
Figure 1. Les différentes formes de stigmatisationI
1.1 La stigmatisation publique
Très étudiée dans la littérature depuis les années 1970 (22 articles en 1980 pour 1008 articles parus
entre 2010 et 2016 ; [5]), la stigmatisation publique concerne les préjugés négatifs et attitudes
discriminantes relatifs aux troubles psychiques et aux personnes qui les présentent. Les préjugés
concernant les personnes avec TPSP peuvent être regroupés en trois catégories principales : i) la
dangerosité pour soi ou les autres ; ii) l’incapacité à s’occuper d’elles mêmes et à apporter une
contribution significative à la société ; iii) le caractère permanent des troubles, sans possibilité de
guérison ou de rétablissement [6].
Page 24
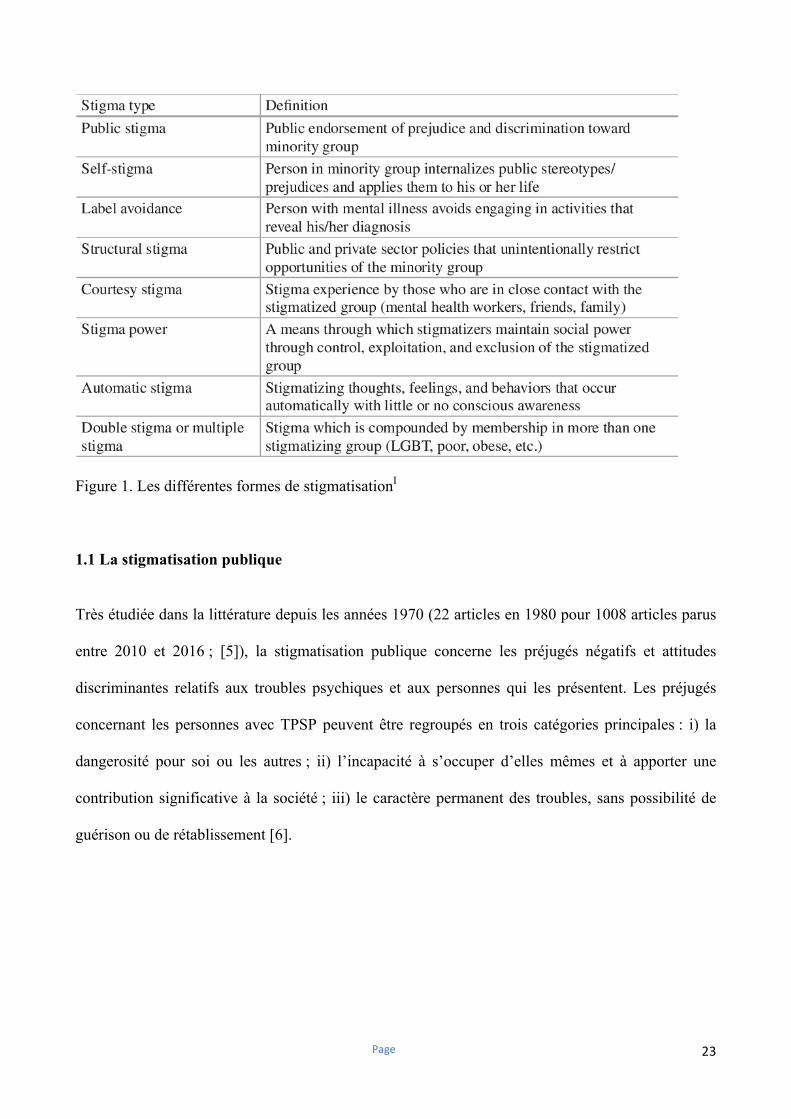
Figure 2. Les stéréotypes les plus courants concernant les troubles psychiquesII
Ces préjugés semblent présents dans toutes les aires géographiques et culturelles, comme le montre
l’étude « The Stigma in a Global Context- Mental Health Study » réalisée sur plus de 6000
participants issus de 16 pays dans le monde [6]. Ils concernent tous les TPSP, même si la
schizophrénie semble être la pathologie la plus stigmatisée [6]. Les personnes interrogées dans cette
étude décrivaient les personnes avec schizophrénie ou dépression comme imprévisibles
(respectivement 70% et 55%), potentiellement dangereuses pour elles mêmes (76% et 68%) ou les
autres (53% et 35%), moins productives que les autres (51% et 46%) et incapables de s’occuper
d’enfants (85% et 77%). Ces préjugés sont associés à des réactions émotionnelles négatives, comme
la pitié, la peur ou la colère conduisant souvent à des attitudes discriminantes, comme le rejet ou la
volonté de mise à distance les personnes présentant des TPSP [5]. Les domaines de vie les plus
stigmatisés sont le fait de s’occuper d’enfants (85% pour la garde de leurs enfants ; 58% pour
exercer en tant qu’enseignant), l’intégration dans une belle-famille (68%) ou encore d’exercer une
position d’autorité (58% pour occuper des fonctions managériales) [6]. Il existe des variations selon
les aires géographiques et culturelles étudiées, la stigmatisation publique étant plus marquée en
Europe de l’Est et du Sud et en Asie du Sud-Est [6], [7]. La stigmatisation publique en France est
dans la moyenne des pays Européens [7], [8].
Page 25
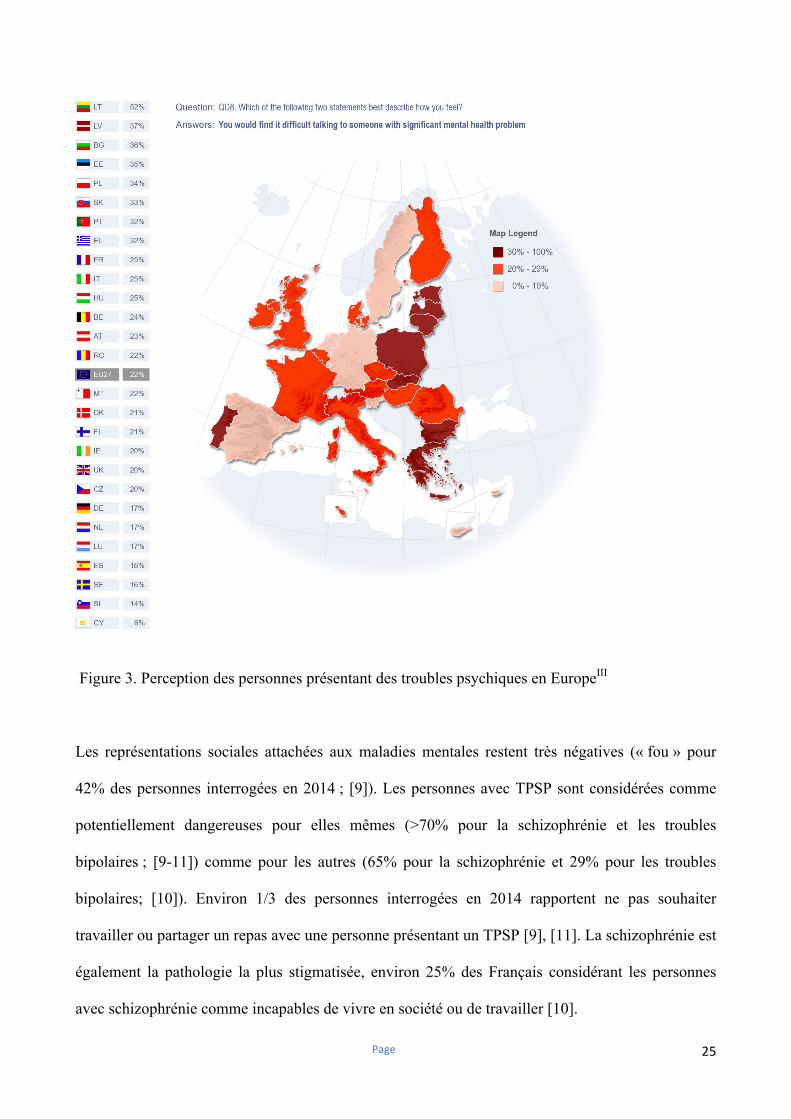
Figure 3. Perception des personnes présentant des troubles psychiques en EuropeIII
Les représentations sociales attachées aux maladies mentales restent très négatives (« fou » pour
42% des personnes interrogées en 2014 ; [9]). Les personnes avec TPSP sont considérées comme
potentiellement dangereuses pour elles mêmes (>70% pour la schizophrénie et les troubles
bipolaires ; [9-11]) comme pour les autres (65% pour la schizophrénie et 29% pour les troubles
bipolaires; [10]). Environ 1/3 des personnes interrogées en 2014 rapportent ne pas souhaiter
travailler ou partager un repas avec une personne présentant un TPSP [9], [11]. La schizophrénie est
également la pathologie la plus stigmatisée, environ 25% des Français considérant les personnes
avec schizophrénie comme incapables de vivre en société ou de travailler [10].
Page 26
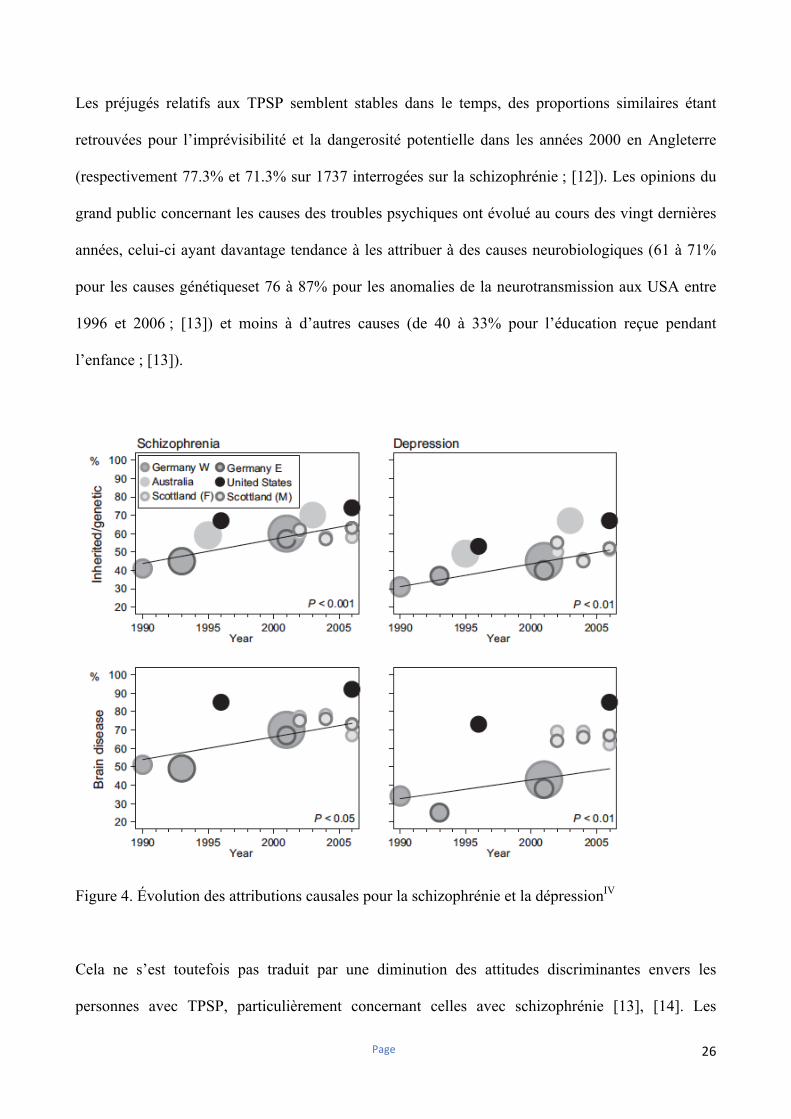
Les préjugés relatifs aux TPSP semblent stables dans le temps, des proportions similaires étant
retrouvées pour l’imprévisibilité et la dangerosité potentielle dans les années 2000 en Angleterre
(respectivement 77.3% et 71.3% sur 1737 interrogées sur la schizophrénie ; [12]). Les opinions du
grand public concernant les causes des troubles psychiques ont évolué au cours des vingt dernières
années, celui-ci ayant davantage tendance à les attribuer à des causes neurobiologiques (61 à 71%
pour les causes génétiqueset 76 à 87% pour les anomalies de la neurotransmission aux USA entre
1996 et 2006 ; [13]) et moins à d’autres causes (de 40 à 33% pour l’éducation reçue pendant
l’enfance ; [13]).
Figure 4. Évolution des attributions causales pour la schizophrénie et la dépressionIV
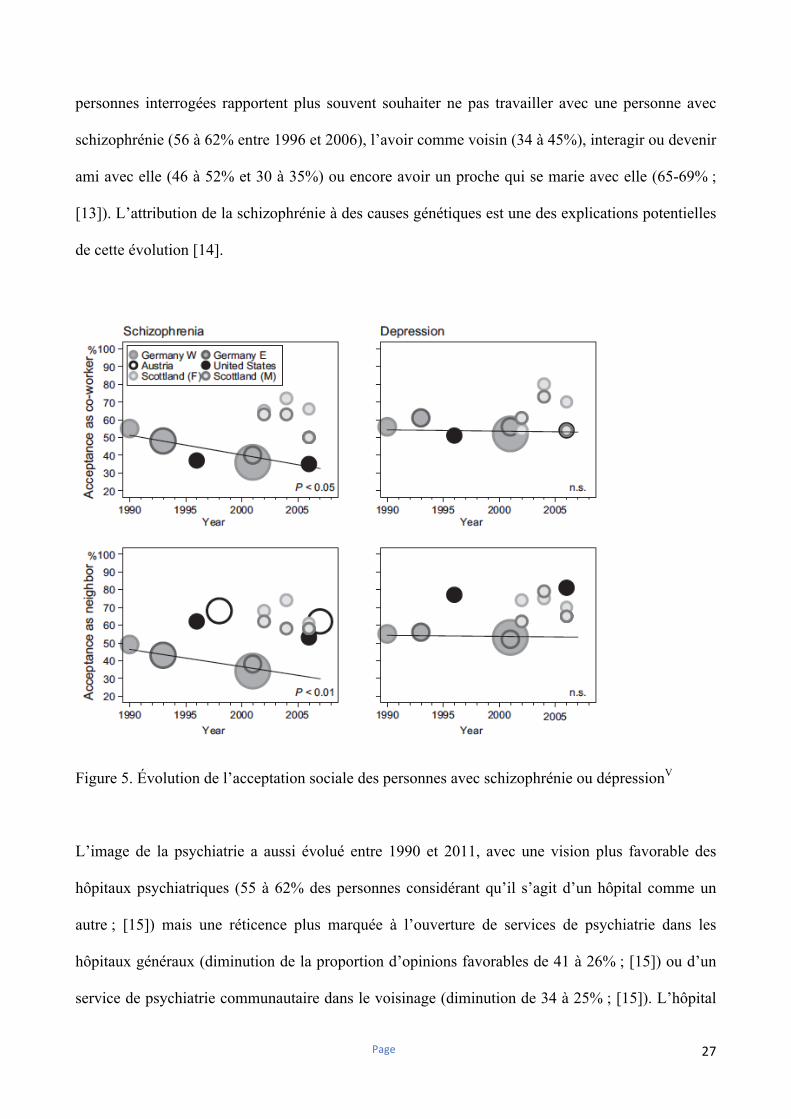
Cela ne s’est toutefois pas traduit par une diminution des attitudes discriminantes envers les
personnes avec TPSP, particulièrement concernant celles avec schizophrénie [13], [14]. Les
Page 27
personnes interrogées rapportent plus souvent souhaiter ne pas travailler avec une personne avec
schizophrénie (56 à 62% entre 1996 et 2006), l’avoir comme voisin (34 à 45%), interagir ou devenir
ami avec elle (46 à 52% et 30 à 35%) ou encore avoir un proche qui se marie avec elle (65-69% ;
[13]). L’attribution de la schizophrénie à des causes génétiques est une des explications potentielles
de cette évolution [14].
Figure 5. Évolution de l’acceptation sociale des personnes avec schizophrénie ou dépressionV
L’image de la psychiatrie a aussi évolué entre 1990 et 2011, avec une vision plus favorable des
hôpitaux psychiatriques (55 à 62% des personnes considérant qu’il s’agit d’un hôpital comme un
autre ; [15]) mais une réticence plus marquée à l’ouverture de services de psychiatrie dans les
hôpitaux généraux (diminution de la proportion d’opinions favorables de 41 à 26% ; [15]) ou d’un
service de psychiatrie communautaire dans le voisinage (diminution de 34 à 25% ; [15]). L’hôpital
Page 28
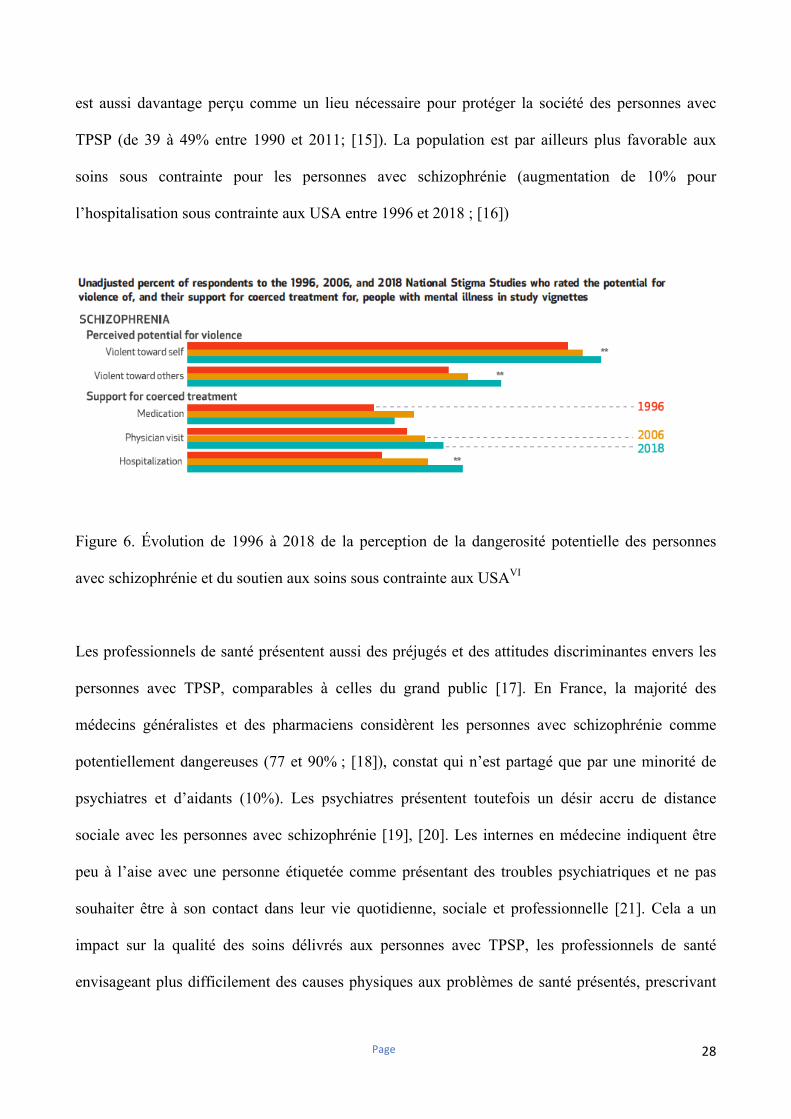
est aussi davantage perçu comme un lieu nécessaire pour protéger la société des personnes avec
TPSP (de 39 à 49% entre 1990 et 2011; [15]). La population est par ailleurs plus favorable aux
soins sous contrainte pour les personnes avec schizophrénie (augmentation de 10% pour
l’hospitalisation sous contrainte aux USA entre 1996 et 2018 ; [16])
Figure 6. Évolution de 1996 à 2018 de la perception de la dangerosité potentielle des personnes
avec schizophrénie et du soutien aux soins sous contrainte aux USAVI
Les professionnels de santé présentent aussi des préjugés et des attitudes discriminantes envers les
personnes avec TPSP, comparables à celles du grand public [17]. En France, la majorité des
médecins généralistes et des pharmaciens considèrent les personnes avec schizophrénie comme
potentiellement dangereuses (77 et 90% ; [18]), constat qui n’est partagé que par une minorité de
psychiatres et d’aidants (10%). Les psychiatres présentent toutefois un désir accru de distance
sociale avec les personnes avec schizophrénie [19], [20]. Les internes en médecine indiquent être
peu à l’aise avec une personne étiquetée comme présentant des troubles psychiatriques et ne pas
souhaiter être à son contact dans leur vie quotidienne, sociale et professionnelle [21]. Cela a un
impact sur la qualité des soins délivrés aux personnes avec TPSP, les professionnels de santé
envisageant plus difficilement des causes physiques aux problèmes de santé présentés, prescrivant
Page 29
moins d’examens complémentaires et adressant moins fréquemment les patients vers des
spécialistes [22]. Cela contribue notamment à une utilisation plus restreinte des soins somatiques,
tardive et souvent en urgence (+113%, [23]) et in fine à une perte d’espérance de vie pouvant aller
jusqu’à 12 ans dans les troubles bipolaires, jusqu’à 25 ans dans la schizophrénie et jusqu’à 40 ans
dans les troubles borderline [24-26]. Les professionnels de santé mentale ont quant à eux des
attitudes paternalistes envers les personnes avec TPSP, les associent peu aux décisions les
concernant et les orientent encore rarement vers des dispositifs de réinsertion professionnelle dans
l’objectif de les protéger contre un risque éventuel de rechute [22]. Les patients présentant un
trouble de personnalité borderline figurent parmi les plus stigmatisés par les professionnels de santé
et rapportent souvent avoir été discriminés lors d’un passage aux urgences ou au cours d’une
hospitalisation en psychiatrie [22], [26], [27]. Les professionnels de santé rapportent se sentir peu à
l’aise avec les personnes avec troubles de personnalité borderline, souvent perçues comme
manipulatrices et incapables de se rétablir [22], [26], [27]. Ils expriment aussi plus fréquemment
souhaiter éviter de les prendre en charge que des personnes présentant d’autres problèmes de santé
mentale [28].
1.2 La stigmatisation structurelle
La stigmatisation publique envers les personnes avec TPSP s’accompagne souvent d’une forme
structurelle de discrimination [29]. Celle-ci peut se traduire par des lois restreignant la liberté des
personnes avec TPSP (droit de vote, de siéger dans un jury, d’exercer des responsabilités ou encore
d’avoir la garde de ses enfants ; [29], [30], [31]) ou par un budget moindre accordé au domaine de
la santé mentale en comparaison des autres problématiques de santé [3], [29]. C’est notamment le
cas au Royaume-Uni et en France, même si le budget accordé à la recherche en santé mentale est en
augmentation [32], [33]. L’opinion publique est par ailleurs souvent peu encline à préserver les
ressources allouées à la santé mentale des restrictions budgétaires en cas de crise financière (10%
Page 30
des personnes interrogées en Allemagne entre 2001 pour la schizophrénie et la dépression contre
80% pour le cancer ; [34]). Le traitement médiatique des TPSP est souvent négatif (40% sur 11 000
articles parus dans la presse Canadienne entre 2005 et 2010 les associaient à une dangerosité
potentielle ; [35]; 58% des articles parus entre 2011 et 2015 dans la presse quotidienne et régionale
en France associaient schizophrénie et dangerosité ; [36]) et contribue à la stigmatisation
structurelle. Il semble toutefois sensible aux programmes de réduction de la stigmatisation
(diminution entre 2005 et 2015 d’un tiers du nombre d’articles au contenu stigmatisant parus dans
la presse Canadienne et augmentation de 50% de ceux présentant un contenu positif sur les TPSP ;
[37]).
1.3 La stigmatisation perçue, expérimentée et anticipée
« Tout ce que je connaissais, c’était les stéréotypes que j'avais vus à la télévision ou dans les films. Pour
moi, les maladies mentales, c’était le Dr Jekyll et M. Hyde, les tueurs en série psychopathes, l’asile de fous,
les imbéciles, les schizos, les dingues, les cinglés, la camisole et les fous délirants. C’était tout ce que je
savais sur les maladies mentales, et ce qui m'a effrayée, c'est que les professionnels disaient que j’étais l'une
d'entre eux. » (Deegan, 1993) [38] Les stéréotypes sur les TPSP constituent une construction sociale précoce, acquise avant le début
des troubles et largement partagée par les personnes présentant des troubles psychiques sévères
débutants ou plus installés [5], [39]. Les personnes avec TPSP sont majoritairement conscientes des
stéréotypes négatifs concernant leur pathologie, anticipant d’être discriminés pour cette raison
(69.4% sur 1229 participants avec schizophrénie et 71.6 % des 1182 participants avec troubles de
l’humeur inclus dans l’étude GAMIAN-Europe ; [40], [41]). La stigmatisation perçue peut survenir
avant la pose d’un diagnostic psychiatrique, par exemple chez les personnes dites à ultra-haut risque
de transition psychotique, et contribue alors à augmenter le stress lié à la stigmatisation [42]. Elle
est influencée par la stigmatisation publique [43] et par le fait de se sentir contraint ou non lors d’un
programme de soins ambulatoires sous contrainte [44]. Elle est associée à de multiples effets
négatifs, et ce dès le 1er épisode psychotique : allongement de la durée de psychose non traitée,
Page 31
symptômes psychiatriques plus sévères, fonctionnement psychosocial et bien être altérés et
perception d’être moins rétabli [45], [46]. Elle contribue à la stigmatisation anticipée et à un recours
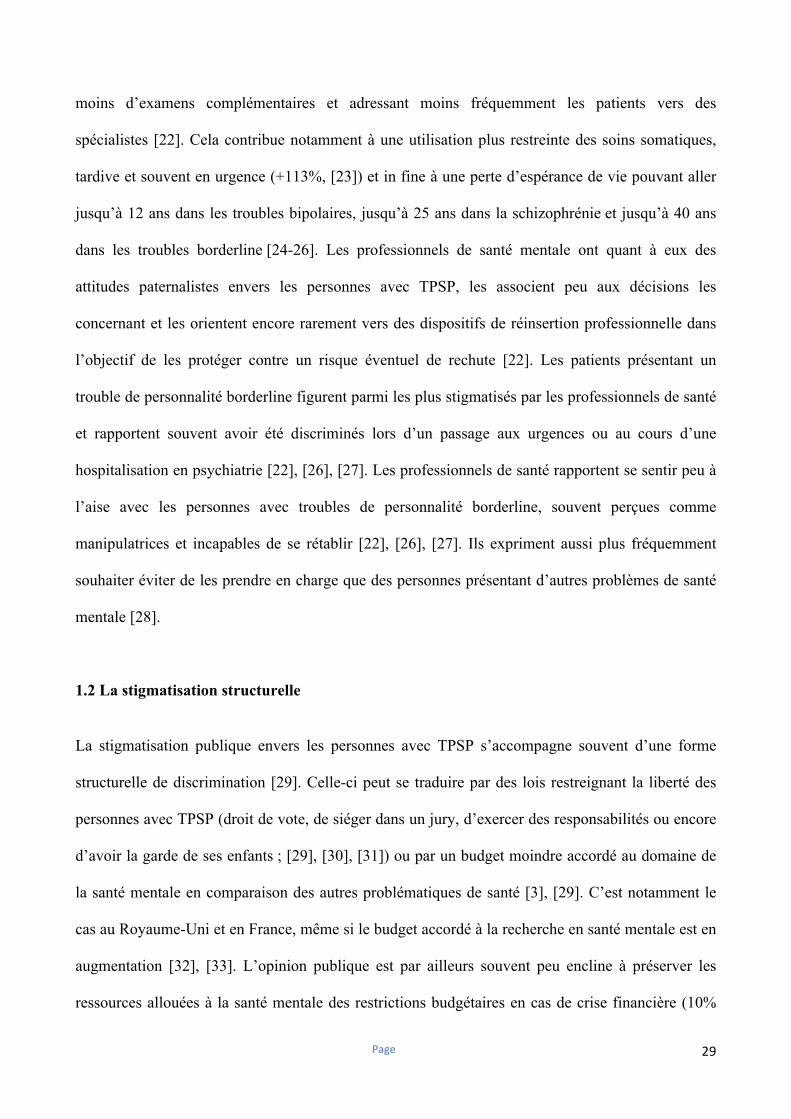
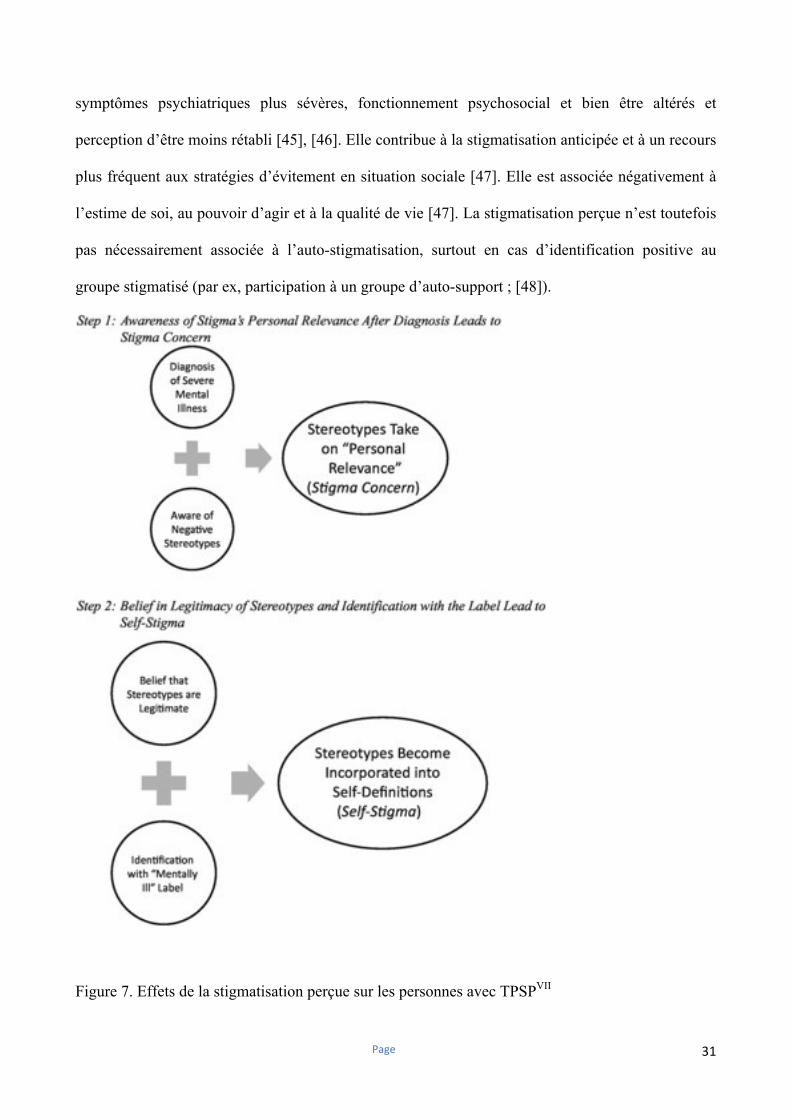
plus fréquent aux stratégies d’évitement en situation sociale [47]. Elle est associée négativement à
l’estime de soi, au pouvoir d’agir et à la qualité de vie [47]. La stigmatisation perçue n’est toutefois
pas nécessairement associée à l’auto-stigmatisation, surtout en cas d’identification positive au
groupe stigmatisé (par ex, participation à un groupe d’auto-support ; [48]).
Figure 7. Effets de la stigmatisation perçue sur les personnes avec TPSPVII
Page 32
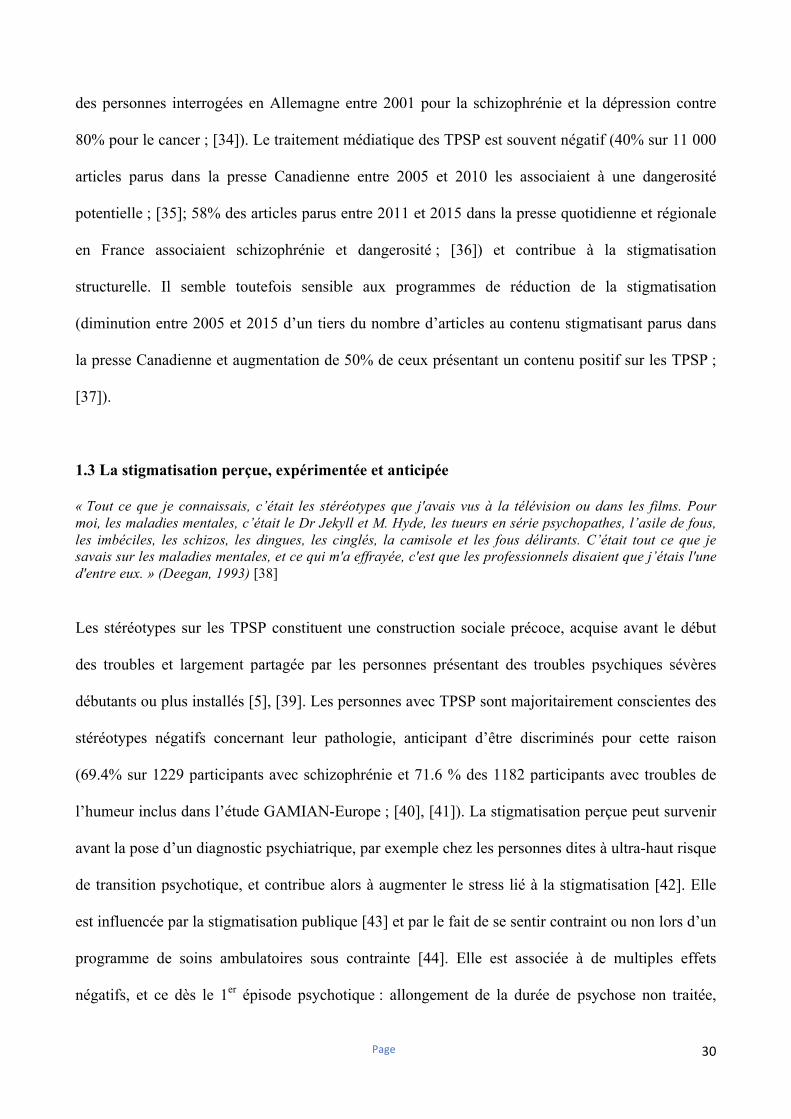
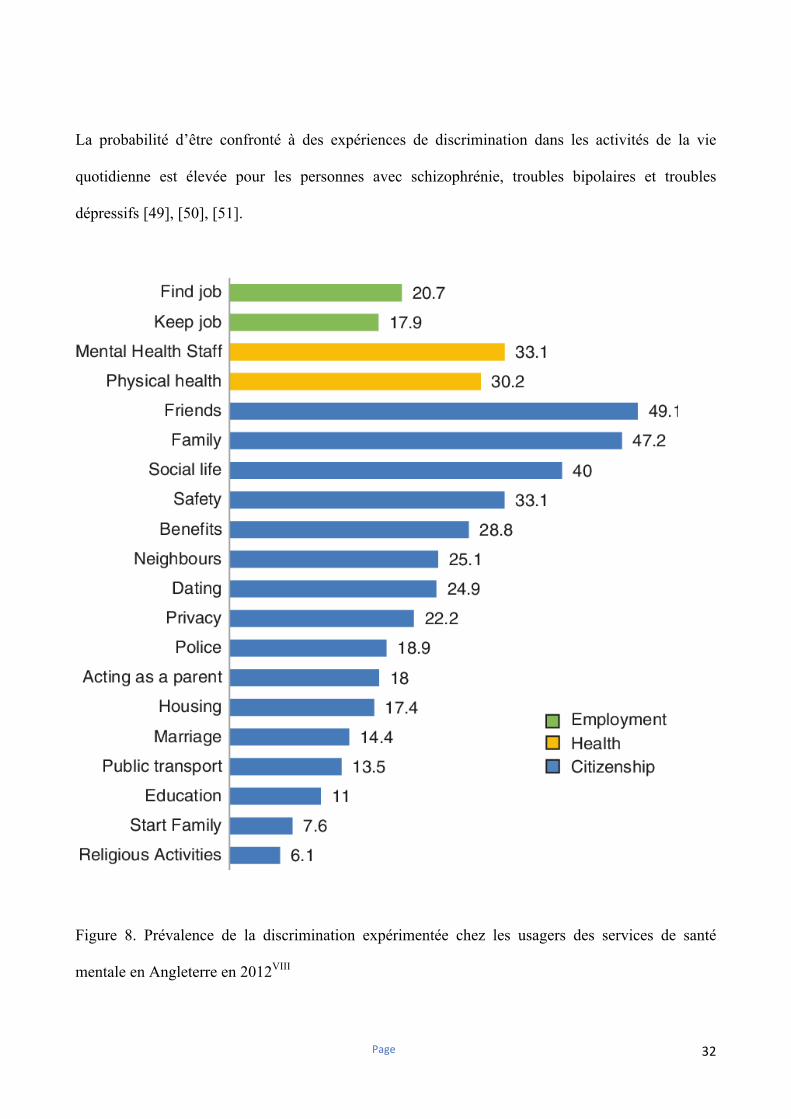
La probabilité d’être confronté à des expériences de discrimination dans les activités de la vie
quotidienne est élevée pour les personnes avec schizophrénie, troubles bipolaires et troubles
dépressifs [49], [50], [51].
Figure 8. Prévalence de la discrimination expérimentée chez les usagers des services de santé
mentale en Angleterre en 2012VIII
Page 33
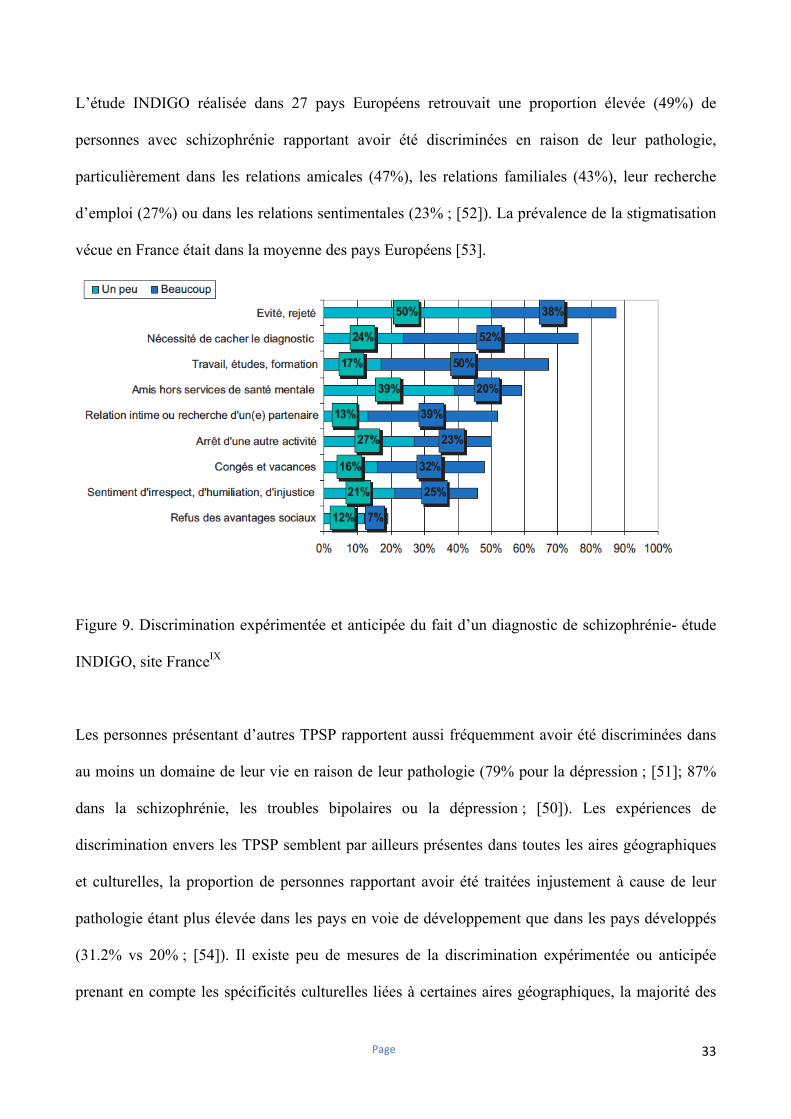
L’étude INDIGO réalisée dans 27 pays Européens retrouvait une proportion élevée (49%) de
personnes avec schizophrénie rapportant avoir été discriminées en raison de leur pathologie,
particulièrement dans les relations amicales (47%), les relations familiales (43%), leur recherche
d’emploi (27%) ou dans les relations sentimentales (23% ; [52]). La prévalence de la stigmatisation
vécue en France était dans la moyenne des pays Européens [53].
Figure 9. Discrimination expérimentée et anticipée du fait d’un diagnostic de schizophrénie- étude
INDIGO, site FranceIX
Les personnes présentant d’autres TPSP rapportent aussi fréquemment avoir été discriminées dans
au moins un domaine de leur vie en raison de leur pathologie (79% pour la dépression ; [51]; 87%
dans la schizophrénie, les troubles bipolaires ou la dépression ; [50]). Les expériences de
discrimination envers les TPSP semblent par ailleurs présentes dans toutes les aires géographiques
et culturelles, la proportion de personnes rapportant avoir été traitées injustement à cause de leur
pathologie étant plus élevée dans les pays en voie de développement que dans les pays développés
(31.2% vs 20% ; [54]). Il existe peu de mesures de la discrimination expérimentée ou anticipée
prenant en compte les spécificités culturelles liées à certaines aires géographiques, la majorité des
Page 34
échelles utilisées dans la littérature étant des adaptations d’outils développés en Europe ou en
Amérique du Nord [55].
La stigmatisation expérimentée est associée à un risque suicidaire plus élevé [50]. Elle se manifeste
aussi dans l’accès aux soins (17% d’expériences de discrimination chez un professionnel de santé
dans l’étude INDIGO ; [56]), la décision de fonder une famille (22.5% ; [57]) ou dans le rôle de
parent (28.3% ; [57]). Elle peut souvent prendre des formes plus subtiles (ou « micro-agressions »)
comme par exemple des attitudes paternalistes de l’entourage, un changement dans l’attitude de
l’interlocuteur en cas de divulgation des troubles ou encore l’exposition à des opinions
stigmatisantes sur les réseaux sociaux [58], [59]. Ces « micro-agressions », comme les expériences
plus franches de discrimination, peuvent contribuer à anticiper d’être discriminé en situation sociale
[51], [58], [60]. Environ un tiers des personnes avec TPSP rapportent que certains proches se sont
éloignés d’elles après la divulgation de leur pathologie [58].
La majorité des personnes avec schizophrénie de l’étude INDIGO indique toutefois anticiper d’être
discriminée en cas de divulgation des troubles et souhaiter pour cette raison les cacher à leur
entourage familial, amical ou professionnel (72% ; [49]). La stigmatisation anticipée concerne la
plupart des domaines de vie, mais est particulièrement marquée dans la recherche d’emploi ou les
relations sentimentales (64 et 55% ; [49]) et peut aussi survenir en l’absence d’expérience préalable
de discrimination (33% ; [49]). La stigmatisation anticipée contribue à l’utilisation de stratégies
d’évitement des situations sociales, à un moindre recours aux soins psychiatriques et à l’auto-
stigmatisation [60], [61].
La stigmatisation concerne aussi les personnes présentant des troubles psychiatriques débutants:
21% des adolescents hospitalisés en psychiatrie anticipaient d’être discriminés par leurs pairs après
leur sortie [62], 70% rapportant des expériences de discrimination après un suivi de six mois [63].
Page 35
Environ la moitié des personnes ayant présenté un 1er épisode psychotique se sentaient stigmatisées
ou rejetées socialement [64] et un quart rapportait des expériences de discrimination [65]. Celles-ci
étaient associées à une altération de l’estime de soi et de la qualité de vie [65]. Les expériences de
discrimination vécues ou anticipées par les personnes présentant des troubles psychiatriques
débutants sont déterminantes, car elles peuvent limiter la possibilité de recourir à des stratégies
adaptatives efficaces et l’adhésion aux soins [42], [66], [67]
1.4 Le stress lié à la stigmatisation et les réactions possibles
Rusch et al. ont décrit un modèle stress-vulnérabilité-compétences appliqué aux effets de la
stigmatisation [68], [69]. Dans ce modèle, le stress lié à la stigmatisation (« stigma stress ») survient
lorsque le préjudice lié à celle-ci excède les ressources d’une personne avec TPSP pour y faire face
[68], [69]. La stigmatisation perçue, la sensibilité au rejet social, le fait de considérer la
discrimination concernant les TPSP comme légitime ou non et l’identification positive ou négative
au groupe stigmatisé sont des prédicteurs du niveau de stress lié à la stigmatisation [68]. Celui-ci
influence en retour les réactions émotionnelles et comportementales d’un individu face à la
stigmatisation [69]. Un stress lié à la stigmatisation élevé conduit dans ce modèle à : i) un sentiment
de honte ; ii) une anxiété sociale plus marquée ; iii) un recours plus fréquent à des stratégies
d’évitement en situation sociale ; iv) une perte d’estime de soi et un sentiment de désespoir ; v) une
altération du fonctionnement social [69]. Le stress lié à la stigmatisation peut contribuer à l’auto-
stigmatisation [70], [71]. Chaque personne réagit de façon très personnelle face à la stigmatisation,
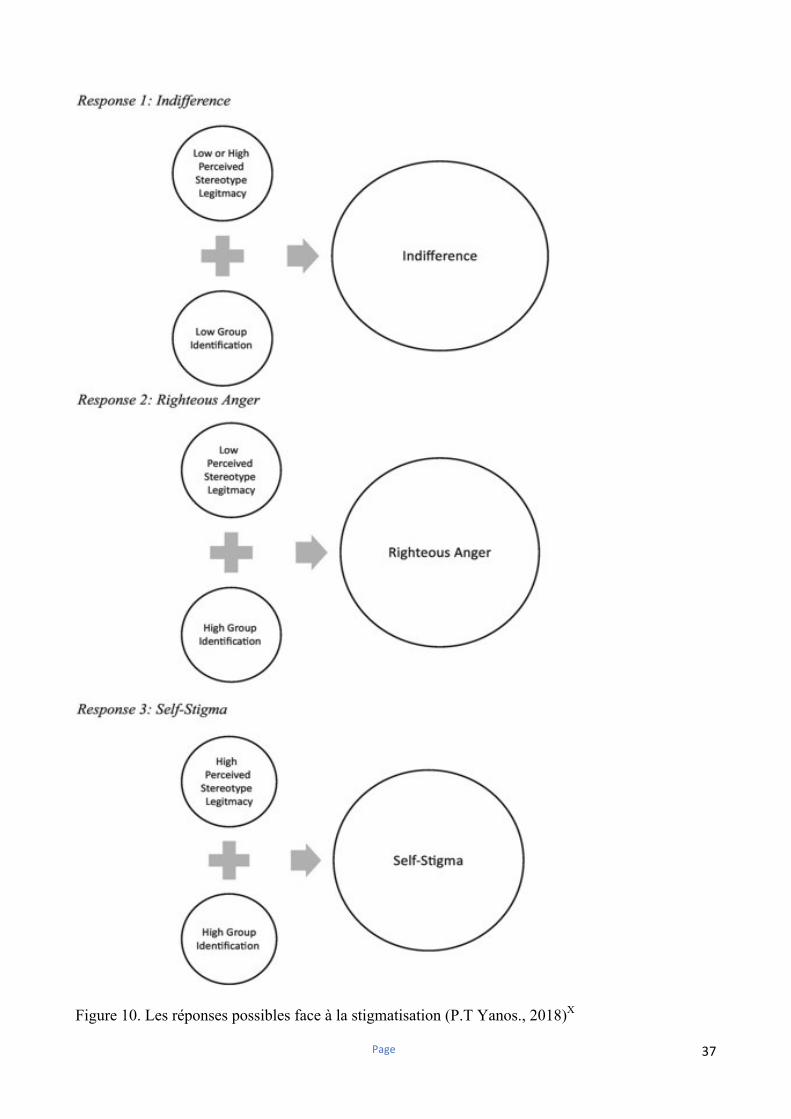
plusieurs réponses étant possibles : l’auto-stigmatisation, l’indifférence ou la juste colère [4]. La
façon dont un individu va réagir à la stigmatisation dépend principalement de deux facteurs,
l’identification au groupe stigmatisé et l’acceptation des stéréotypes négatifs concernant les TPSP
comme légitimes pour le décrire [4], [72]. Certaines personnes vont réagir avec indifférence face à
Page 36
la stigmatisation, soit par manque d’insight concernant les troubles ou en parvenant à s’en distancier
(« Cela ne me décrit pas », [73]). Les personnes réagissant par la juste colère s’identifient au groupe
social stigmatisé, mais perçoivent les stéréotypes négatifs concernant les TPSP comme injustes et
non pertinents pour les décrire [4]. Les personnes susceptibles de développer une auto-
stigmatisation sont celles s’identifiant fortement au groupe social stigmatisé, mais considérant les
stéréotypes négatifs concernant les TPSP comme vrais et s’appliquant donc à elles mêmes [4]. Il
s’agit souvent de personnes avec un insight préservé, une auto-stigmatisation élevée, des
symptômes dépressifs, un recours fréquent à des stratégies d’évitement, une estime de soi et une
qualité de vie altérée (le paradoxe de l’insight ; [74]). Certains facteurs renforcent la légitimité
perçue de la stigmatisation, comme les réactions implicites de honte [75], le fait d’avoir été en
contact avec d’autres personnes présentant un TPSP au cours d’une hospitalisation en psychiatrie
(« le fait d’être dans le service toute la journée avec 50 autres « malades mentaux » - c’est eux qui
vous apprennent ce que c’est que d’être malade » ; [76]), la manière d’annoncer le diagnostic
(« mon avenir avait été réduit à un pronostic funeste » ; [38]) ou encore le fait de bénéficier au long
cours de prestations de compensation du handicap [77].
Page 37
Figure 10. Les réponses possibles face à la stigmatisation (P.T Yanos., 2018)X
Page 38
1.5 L’auto-stigmatisation et la résistance à la stigmatisation
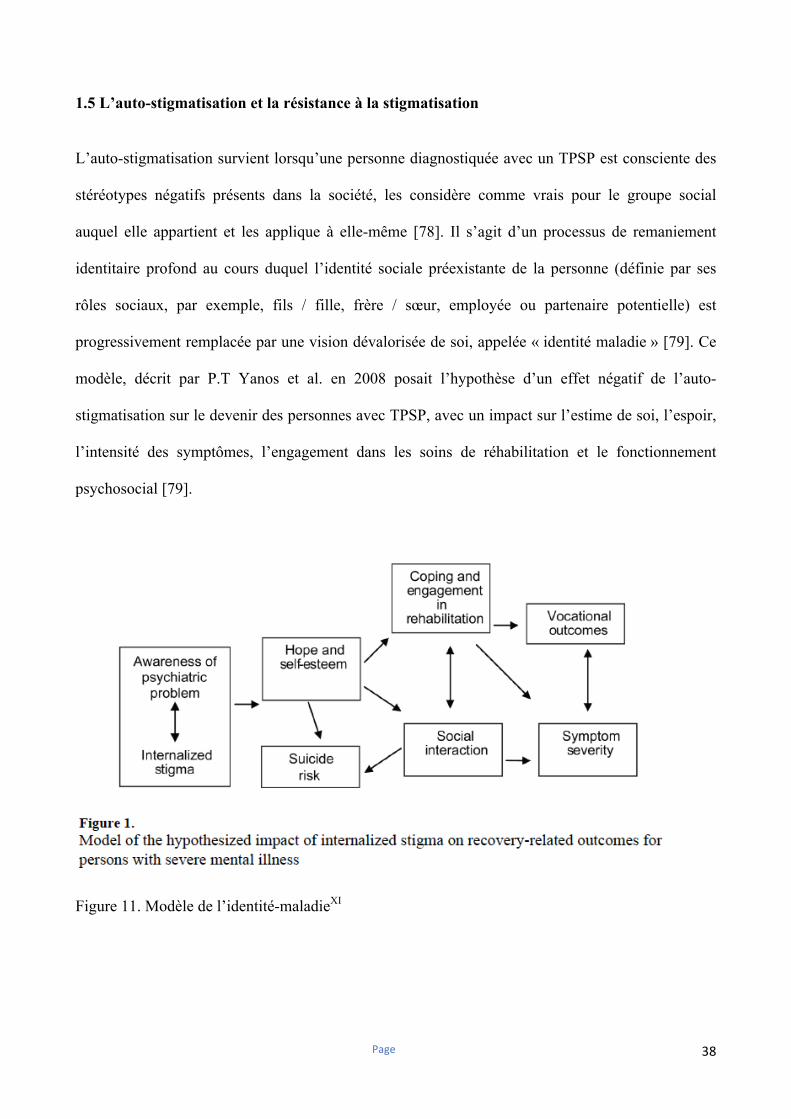
L’auto-stigmatisation survient lorsqu’une personne diagnostiquée avec un TPSP est consciente des
stéréotypes négatifs présents dans la société, les considère comme vrais pour le groupe social
auquel elle appartient et les applique à elle-même [78]. Il s’agit d’un processus de remaniement
identitaire profond au cours duquel l’identité sociale préexistante de la personne (définie par ses
rôles sociaux, par exemple, fils / fille, frère / sœur, employée ou partenaire potentielle) est
progressivement remplacée par une vision dévalorisée de soi, appelée « identité maladie » [79]. Ce
modèle, décrit par P.T Yanos et al. en 2008 posait l’hypothèse d’un effet négatif de l’auto-
stigmatisation sur le devenir des personnes avec TPSP, avec un impact sur l’estime de soi, l’espoir,
l’intensité des symptômes, l’engagement dans les soins de réhabilitation et le fonctionnement
psychosocial [79].
Figure 11. Modèle de l’identité-maladieXI
Page 39
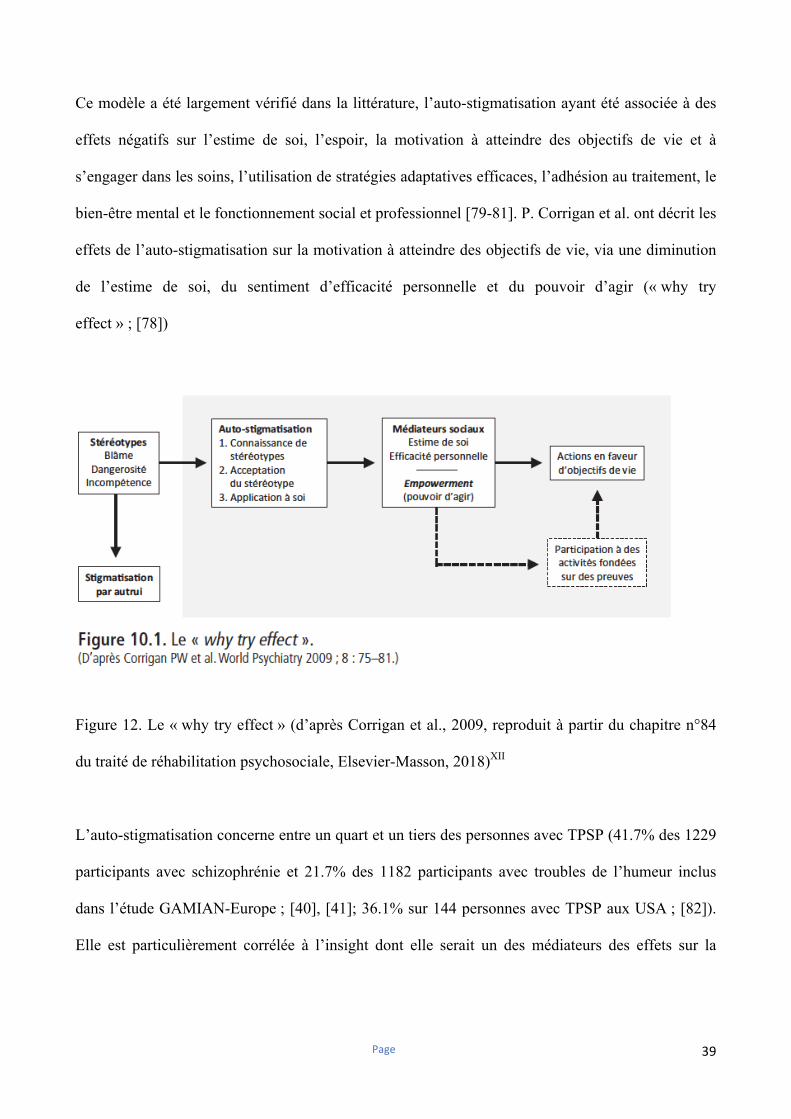
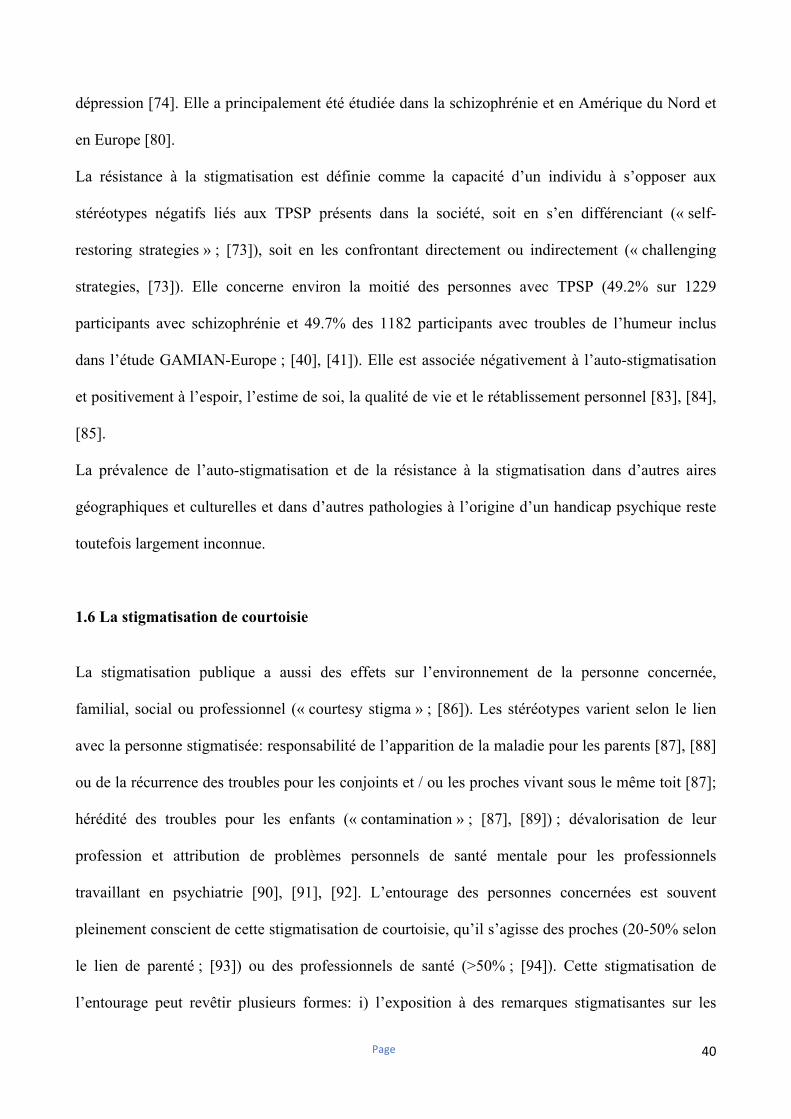
Ce modèle a été largement vérifié dans la littérature, l’auto-stigmatisation ayant été associée à des
effets négatifs sur l’estime de soi, l’espoir, la motivation à atteindre des objectifs de vie et à
s’engager dans les soins, l’utilisation de stratégies adaptatives efficaces, l’adhésion au traitement, le
bien-être mental et le fonctionnement social et professionnel [79-81]. P. Corrigan et al. ont décrit les
effets de l’auto-stigmatisation sur la motivation à atteindre des objectifs de vie, via une diminution
de l’estime de soi, du sentiment d’efficacité personnelle et du pouvoir d’agir (« why try
effect » ; [78])
Figure 12. Le « why try effect » (d’après Corrigan et al., 2009, reproduit à partir du chapitre n°84
du traité de réhabilitation psychosociale, Elsevier-Masson, 2018)XII
L’auto-stigmatisation concerne entre un quart et un tiers des personnes avec TPSP (41.7% des 1229
participants avec schizophrénie et 21.7% des 1182 participants avec troubles de l’humeur inclus
dans l’étude GAMIAN-Europe ; [40], [41]; 36.1% sur 144 personnes avec TPSP aux USA ; [82]).
Elle est particulièrement corrélée à l’insight dont elle serait un des médiateurs des effets sur la
Page 40
dépression [74]. Elle a principalement été étudiée dans la schizophrénie et en Amérique du Nord et
en Europe [80].
La résistance à la stigmatisation est définie comme la capacité d’un individu à s’opposer aux
stéréotypes négatifs liés aux TPSP présents dans la société, soit en s’en différenciant (« self-
restoring strategies » ; [73]), soit en les confrontant directement ou indirectement (« challenging
strategies, [73]). Elle concerne environ la moitié des personnes avec TPSP (49.2% sur 1229
participants avec schizophrénie et 49.7% des 1182 participants avec troubles de l’humeur inclus
dans l’étude GAMIAN-Europe ; [40], [41]). Elle est associée négativement à l’auto-stigmatisation
et positivement à l’espoir, l’estime de soi, la qualité de vie et le rétablissement personnel [83], [84],
[85].
La prévalence de l’auto-stigmatisation et de la résistance à la stigmatisation dans d’autres aires
géographiques et culturelles et dans d’autres pathologies à l’origine d’un handicap psychique reste
toutefois largement inconnue.
1.6 La stigmatisation de courtoisie
La stigmatisation publique a aussi des effets sur l’environnement de la personne concernée,
familial, social ou professionnel (« courtesy stigma » ; [86]). Les stéréotypes varient selon le lien
avec la personne stigmatisée: responsabilité de l’apparition de la maladie pour les parents [87], [88]
ou de la récurrence des troubles pour les conjoints et / ou les proches vivant sous le même toit [87];
hérédité des troubles pour les enfants (« contamination » ; [87], [89]) ; dévalorisation de leur
profession et attribution de problèmes personnels de santé mentale pour les professionnels
travaillant en psychiatrie [90], [91], [92]. L’entourage des personnes concernées est souvent
pleinement conscient de cette stigmatisation de courtoisie, qu’il s’agisse des proches (20-50% selon
le lien de parenté ; [93]) ou des professionnels de santé (>50% ; [94]). Cette stigmatisation de
l’entourage peut revêtir plusieurs formes: i) l’exposition à des remarques stigmatisantes sur les
Page 41
personnes avec TPSP (65% pour les familles ; [95]) ou le fait de travailler dans le domaine de la
santé mentale (58% en Belgique ; [96]) ; ii) un changement dans l’attitude de leur interlocuteur
pouvant aller jusqu’au rejet social (25-50% pour les familles [93], [97]; 30% pour les professionnels
[96]). Elle est associée à de multiples effets négatifs pour les familles : sentiment de honte pour 20 à
50% des proches [62], [97-99]; augmentation du fardeau lié aux TPSP, particulièrement en cas de
recours à des stratégies adaptatives inefficaces (auto-dévalorisation, déni, désengagement ; [100]) ;
niveau plus élevé d’émotions exprimées [101]; évitement des contacts sociaux [97]. La
stigmatisation de courtoisie peut aussi contribuer à la survenue d’un burnout chez les professionnels
de santé mentale [96], [102], qui pourrait influencer les réactions des usagers face à la
stigmatisation [96]. L’impact de la stigmatisation de courtoisie sur l’auto-stigmatisation des
familles et des personnes concernées reste toutefois encore peu connu.
Chapitre 2. Stigmatisation et neurosciences
La stigmatisation est de plus en plus étudiée dans la littérature scientifique, mais peu de liens ont été
faits avec les neurosciences. Dans cette perspective, une définition possible de la stigmatisation
publique pourrait être la réaction automatique cognitive, émotionnelle, physique et
comportementale déclenchée chez une personne « lambda » au cours d’une interaction sociale, par
un indice renvoyant à une caractéristique associée à un groupe stigmatisé [103]. Elle se traduit alors
de façon implicite, c’est-à-dire de façon automatique et non influencée par les biais de désirabilité
sociale [104]. Le test des associations implicites (IAT ; [104]) est un outil populaire en psychologie
sociale, évaluant la force des associations entre différents concepts par la mesure de la latence de
réponse pendant une tâche de catégorisation sur ordinateur entre certains attributs et concepts-
cibles. Une réponse plus rapide indique alors une association forte entre deux concepts (par
Page 42
exemple, « mental illness » et « blameworthy» ; [105]) et représente les attitudes implicites du
participant. Plusieurs études en imagerie fonctionnelle ont rapporté l’activation de plusieurs aires
cérébrales (amygdale, insula, cortex cingulaire antérieur et cortex préfrontal latéral) lors de tâches
d’évaluation implicites d’un groupe social stigmatisé, comme par exemple, les personnes sans abri
[106], [107]. Il n’existe toutefois pas d’étude de ce type dans le champ de la santé mentale. La
stigmatisation publique implicite a été étudiée dans le grand public et chez les professionnels de
santé mentale. Les étudiants en psychologie interrogés sur leur représentation des personnes avec
TPSP présentaient des niveaux élevés de stigmatisation explicite mais aussi implicite (association
entre « mental illness » et « bad », « blameworthy » ou « helpless » ; [105]). Chez les professionnels
de santé mentale, la stigmatisation implicite a été associée à un sur-diagnostic des troubles
psychiatriques [108]. Les attitudes implicites des professionnels de santé mentale (« automatic
stigma ») envers les personnes présentant des TPSP ont aussi été évaluées dans deux équipes aux
pratiques orientées rétablissement [109], [110]. Si les professionnels de ces équipes exprimaient
majoritairement des attitudes explicites positives envers les personnes avec TPSP, certains
présentaient aussi des attitudes stigmatisantes implicites (association entre les mots « bad » et «
mental illness » ; [109]; entre les mots « awful » et « schizophrenia » ou « bipolar disorder »;
[110]). Celles-ci étaient associées à des réactions émotionnelles négatives, un désir moindre de
venir en aide aux personnes avec TPSP et à une pratique moins orientée vers le rétablissement
[109], [110]. Le test des associations implicites a aussi pu être utilisé pour mesurer l’auto-
stigmatisation implicite et ses corrélations avec d’autres variables [105], [111], [112].
D’autres modèles populaires en psychologie sociale ont été utilisés pour décrire les processus
conduisant à la stigmatisation publique et ceux sous-tendant ses effets sur les personnes concernées.
L’étiquetage comme présentant un TPSP ou la présence de symptômes résiduels lors d’une
interaction sociale peuvent en effet modifier la perception que l’on a de son interlocuteur: si l’on est
Page 43
informé de son diagnostic de schizophrénie, l’interlocuteur est alors perçu comme plus agressif et
moins fiable, l’interaction étant vécue comme plus anxiogène par le participant [113]. La présence
de symptômes résiduels au cours d’une interaction sociale peut également altérer la perception de
son interlocuteur, et ce même lorsqu’elle n’est pas associée à la présence d’un diagnostic
psychiatrique [114], [115]. Ainsi la présence de symptômes négatifs ou de difficultés dans les
interactions sociales peut provoquer chez l’interlocuteur un sentiment d’étrangeté se traduisant par
un désir augmenté de distance sociale [114]. Le modèle du « stereotype threat », ou « menace du
stéreotype », est un paradigme expérimental couramment utilisé en psychologie sociale pour décrire
les effets de la stigmatisation sur les personnes concernées : un individu appartenant à un groupe
stigmatisé est placé dans une situation où ses actions peuvent confirmer ou non les stéréotypes
négatifs relatifs à celui-ci [116]. Ce modèle a été notamment utilisé pour décrire les effets des
stéréotypes de genre ou raciaux sur les personnes concernées [116], [117]. Il a pu être utilisé dans
les TPSP pour mesurer les effets de la stigmatisation sur le fonctionnement cognitif et social [118],
[119].
Les effets du rejet social sur les personnes concernées peuvent aussi être modélisés
expérimentalement, le paradigme du « cyberball » étant un des modèles les plus couramment
utilisés pour mesurer les réactions émotionnelles suivant l’exclusion ou la ré-inclusion sociale
[120]. Il s’agit d’un jeu de lancer de balle sur ordinateur au cours duquel les participants croient
jouer avec d’autres humains, alors qu’ils sont confrontés à des joueurs contrôlés par l’ordinateur et
placés dans différentes conditions expérimentales (exclusion, inclusion, sur-inclusion sociale ;
[120]). Ce modèle a permis d’identifier les corrélats en imagerie fonctionnelle de la douleur sociale
(activation de l’insula et du cortex cingulaire antérieur ; [121-123]) et les mécanismes de régulation
émotionnelle permettant d’y répondre (activation du cortex préfrontal médial, du précuneus et du
cortex cingulaire postérieur ; [121-123]).
Page 44
Le rejet social chronique (> 3 mois ; [124], [125]) a été étudié de façon expérimentale chez des
personnes qui y sont confrontées, mais ne présentant pas de TPSP. Il renforce la sensibilité à
l’exclusion sociale, provoque des sentiments de résignation, de désespoir, d’être sans valeur et
conduit au final à un sentiment d’aliénation sociale et à la survenue d’une dépression [124], [125]
(Williams et al., 2009 ; Riva et al., 2014). L’exposition à la stigmatisation - hors santé mentale - a
été associée en IRM fonctionnelle à une activité spontanée plus marquée de l’amygdale cérébrale et
à une connectivité accrue entre l’insula, l’amygdale et le cortex cingulaire antérieur [126]. Dans le
domaine de la santé mentale, il s’agit d’un paradigme principalement utilisé pour modéliser les
effets de l’exclusion sociale chez les personnes avec troubles de personnalité borderline.
Le lien entre neurosciences et auto-stigmatisation chez les personnes avec TPSP était peu clair et
aucune revue de littérature n’avait été conduite sur ce sujet.
Chapitre 3. Mesurer les effets de la stigmatisation
De multiples outils ont été développés pour mesurer les effets de la stigmatisation sur les personnes
avec TPSP. Ils présentent toutefois une grande hétérogénéité et ne mesurent pas tous les mêmes
aspects de la stigmatisation, bien qu’ils soient parfois indifféremment utilisés dans la littérature. La
stigmatisation perçue est principalement mesurée avec l’échelle de Dévalorisation et Discrimination
Perçue (82% des études inclues dans une revue de littérature en 2010 ; [127]). Il s’agit d’une échelle
évaluant la perception du participant des opinions de la majorité du grand public sur les personnes
avec TPSP [128]. Elle peut toutefois être évaluée par certaines dimensions d’autres instruments de
mesure, comme par exemple la sous-échelle « conscience des stéréotypes » de l’échelle de mesure
de l’auto-stigmatisation (SSMIS ; [129]) ou celle « sentiment d’être stigmatisé » du questionnaire
de mesure de l’estime de soi et de la stigmatisation [130] qui en sont des adaptations [127].
Page 45
L’inventaire des expériences de stigmatisation (ISE ; [131]) et l’échelle d’auto-stigmatisation dans
la dépression (DSS ; [132]) contiennent plusieurs items mesurant la stigmatisation perçue [40].
L’échelle de stigmatisation mesure quant à elle la façon dont le participant pense avoir été
personnellement perçu ou traité par la société [133].
Dix échelles permettent de mesurer la stigmatisation expérimentée ou anticipée, une des plus
couramment utilisées étant l’échelle de discrimination et de stigmatisation développée pour l’étude
INDIGO (DISC ; [49]). L’échelle de stigmatisation de King, validée en version française en 2013,
mesure les aspects positifs et négatifs de la discrimination vécue par la personne et ses réticences
éventuelles concernant la divulgation de ses troubles [134], [135]. L’inventaire des expériences de
stigmatisation mesure la discrimination vécue par les usagers et l’impact que celle-ci a eu sur leur
vie [131]. L’échelle d’auto-stigmatisation dans la dépression [132] et le sous-score «expériences de
discrimination » de l’échelle de mesure du stigma internalisé (ISMI ; [136]) mesurent la
stigmatisation vécue. Il existe également cinq autres échelles de mesure de la discrimination
expérimentée [127].
Le stress lié à la stigmatisation est mesuré avec une échelle en 8 items, mesurant la perception de la
stigmatisation comme potentiellement dommageable pour soi et la perception des ressources
disponibles pour y faire face [69]. Les items allant de 1 à 7 sont additionnés pour obtenir deux sous-
scores, le score total étant calculé par une soustraction entre les deux.
Il existait cinq échelles évaluant l’auto-stigmatisation en 2010 [40], quatorze autres échelles ayant
été développées depuis. L’échelle de mesure de la stigmatisation internalisée (ISMI ; [136]) et
l’échelle d’auto-stigmatisation (SSMI-S ; [129]) sont les plus couramment utilisées. L’ISMI est un
auto-questionnaire de 29 items, traduit dans 14 langues et adapté dans un large panel de pathologies
(schizophrénie, dépression, troubles de l’usage de substances, troubles du comportement
Page 46
alimentaire, épilepsie, lèpre ; [137]). Il existe également une version pour les proches de personnes
avec TPSP et une version abrégée en 10 items [137]. Cette échelle mesure l’expérience personnelle
de la stigmatisation, avec un score total et cinq sous-échelles en évaluant différents aspects : le
sentiment d’aliénation (ou d’être un membre dévalorisé de la société) ; l’accord avec les stéréotypes
négatifs concernant les TPSP ; les expériences de discrimination ; le retrait social comme stratégie
adaptative ; la résistance à la stigmatisation. Un score total supérieur ou égal à 2.5 indique un
niveau élevé d’auto-stigmatisation [40]. Cette échelle a montré une cohérence interne (alpha=0.80-
0.92 ; [137]) et des propriétés test-retest satisfaisantes (0.92 ; [137]). Le sous-score résistance à la
stigmatisation est généralement exclu des études sur l’auto-stigmatisation, car il est faiblement
corrélé aux autres dimensions évaluées (alpha=0.56 dans une méta-analyse de 2016 ; [83]). La
SSMI-S est un auto-questionnaire en 40 items, évaluant les quatre étapes du processus d’auto-
stigmatisation : conscience des stéréotypes négatifs concernant les TPSP ; accord avec ces
stéréotypes ; application à soi ; diminution de l’estime de soi liée à l’auto-stigmatisation [129]. Un
sous-score est calculé pour chaque étape, un score plus élevé indiquant un accord plus marqué avec
la dimension mesurée. Les deux dernières étapes de l’auto-stigmatisation (application et diminution
de l’estime de soi) sont celles qui entraînent une altération du rétablissement dans ses aspects
objectifs et subjectifs [138]. Les propriétés psychométriques de l’échelle sont satisfaisantes (0.72-
0.89 ; [129]) et il en existe une version abrégée, à 20 items [139]. L’utilisation de stratégies de non-
divulgation des troubles par crainte d’être stigmatisé (« secrecy ») est pour certains auteurs une
composante du processus d’auto-stigmatisation mais pour d’autres, il s’agit plutôt d’une mesure de
la discrimination anticipée [127]. Elle est évaluée dans trois instruments de mesure, l’échelle
d’auto-stigmatisation dans la dépression [132], l’inventaire des expériences de stigmatisation [131]
et l’échelle de stigmatisation de King [134], [135]. L’équipe de W.W.S Mak à Hong-Kong a
développé deux auto-questionnaires complémentaires, l’un mesurant les composantes cognitives,
émotionnelles et comportementales de l’auto-stigmatisation (échelle de mesure de l’auto-
Page 47
stigmatisation en 48 items, une version abrégée en 9 items ayant été développée par la suite; [140],
[141]) et l’autre l’automaticité et la répétition des pensées auto-stigmatisantes (STARS ; [142]). Les
deux échelles ont montré des propriétés psychométriques satisfaisantes (alpha=0.91 et 0.89 ; [143]).
Le questionnaire d’auto-stigmatisation [144] est une auto-évaluation en 42 items couvrant trois
périodes de vie - avant le début des troubles, pendant et après la phase aigue – et 8 dimensions dont
3 directement en lien avec l’auto-stigmatisation. Certaines échelles ont été créées spécifiquement
pour les personnes présentant des troubles psychiatriques débutants : l’échelle de mesure de la honte
internalisée, un auto-questionnaire en 30 items [145] ; l’échelle révisée des croyances personnelles à
propos de la maladie, un auto-questionnaire en 29 items avec des composantes cognitives et
émotionnelles (la honte ; le sentiment d’être piégé ; le contrôle sur la maladie ; la marginalisation
sociale / l’adaptation au groupe ; [146]) ; l’échelle des croyances personnelles à propos des
expériences inhabituelles, un auto-questionnaire en 13 items et 3 facteurs principaux (attentes
pessimistes, honte externalisée et internalisée, internalisation d’un statut dévalorisé ; [147]) ; une
version adaptée aux adolescents en 5 items de l’échelle d’auto-stigmatisation d’Austin mesurant le
sentiment de honte, de gêne et la crainte du regard des autres sur leurs difficultés [148] ; l’échelle de
la stigmatisation attachée à l’étiquette « troubles psychiatriques » pour les personnes à ultra-haut
risque de transition psychotique [149], en 42 items mesurant la conscience des stéréotypes, l’accord
avec ceux-ci, les réactions émotionnelles associées au fait de suivre un traitement (honte, embarras,
espoir), l’utilisation de stratégies de non-divulgation des troubles par crainte d’être stigmatisé et la
discrimination expérimentée. Plusieurs autres échelles de mesure de l’auto-stigmatisation ont été
développées pour les besoins d’une étude donnée : échelle d’auto-stigmatisation de Link en 8 items
mesurant les croyances et émotions consécutives au fait de développer un TPSP ou d’être
hospitalisé (honte, tristesse, sentiment d’être différent ou d’être « un raté » ; [150]) ; échelle d’auto-
stigmatisation en 4 items mesurant l’accord avec les stéréotypes, la culpabilité et le sentiment d’être
« un raté » [60] ; échelle de mesure des stratégies d’évitement de l’étiquette « troubles
Page 48
psychiatriques » dans la dépression [151] ; échelle de mesure de l’auto-stigmatisation de la
dépression en 16 items [152] ; échelle de mesure de la stigmatisation de la sexualité en 27 items
évaluant les expériences de discrimination, la stigmatisation structurelle, le sentiment d’être dévalué
dans leur sexualité, le sentiment d’être moins attirant pour les autres du fait de sa pathologie et
l’impression de devoir renoncer au contrôle de sa sexualité pour avoir des relations avec les autres
[153]. La résistance à la stigmatisation est principalement mesurée avec la sous-échelle spécifique
de l’ISMI en 7 items, un score supérieur ou égal à 2.5 indiquant un niveau élevé de résistance à la
stigmatisation [40], [41]. Il existe toutefois d’autres échelles, dont l’une mesure l’utilisation de
stratégies de distanciation ou de lutte contre la stigmatisation [154]. L’échelle de résistance à la
stigmatisation, un auto-questionnaire en 20 items développé en 2017, est un nouvel instrument
mesurant cinq dimensions: la capacité à se différencier des attitudes d’autrui ; l’identité personnelle
en dehors de la maladie mentale ; les stratégies utilisées pour se distancier des pensées négatives en
lien avec la stigmatisation ; le désir d’utiliser sa propre expérience pour aider d’autres usagers à
lutter contre la stigmatisation ; les stratégies utilisées par les personnes concernées pour faire face à
la stigmatisation [155].
Ces différentes formes de stigmatisation sont souvent peu différenciées dans la littérature et les
outils de mesure, alors qu’elles renvoient à des concepts distincts (43.9% des 127 études inclues
dans la méta-analyse de Livingston et Boyd en 2010 sur l’auto-stigmatisation utilisaient en fait des
échelles de mesure de la stigmatisation perçue ou expérimentée ; [80]). Il est donc particulièrement
difficile de distinguer les effets spécifiques de l’auto-stigmatisation sur les aspects objectifs et
subjectifs du rétablissement et de bien appréhender les relations entre ces différentes composantes
de la stigmatisation. Il est aussi difficile de mesurer l’impact des pratiques orientées rétablissement
sur les différents aspects de la stigmatisation des personnes concernées. Il n’existait encore aucune
revue de littérature s’intéressant spécifiquement à l’auto-stigmatisation.
Page 49
Chapitre 4. Réduire la stigmatisation et l’auto-stigmatisation
4.1 Réduire la stigmatisation structurelle
« For 650 million persons around the world living with disabilities, today promises to be the dawn of a new
era- an era in which disabled people will no longer have to endure the discriminatory practices and attitudes
that have been permitted to prevail for all too long (Kofi Annan’s statement, UN, 2006) [156]
4.1.1. Des maladies mentales au handicap psychique : un préalable indispensable à la
réduction de la stigmatisation
Le passage d’un modèle médical (« les maladies mentales ») à un modèle social du handicap est
souvent une étape clé dans la réduction de la stigmatisation structurelle, permettant de se focaliser
davantage sur les conséquences fonctionnelles des troubles et les moyens d’y remédier que sur les
symptômes résiduels. Cette conception a conduit aux USA, au Royaume-Uni, comme en France à
remplacer le terme « maladies mentales chroniques », associé à une vision pessimiste de l’évolution
des troubles, par ceux « Troubles Psychiques Sévères et Persistants » (Serious Mental Illness) et
« Handicap Psychique » (« psychiatric disability »).
Les Troubles Psychiques Sévères et Persistants (TPSP) sont définis par « la présence actuelle ou au
cours de l’année écoulée de troubles mentaux, comportementaux ou émotionnels (hors troubles du
spectre de l’autisme et troubles de l’usage des substances) pendant une durée suffisante pour
correspondre aux critères diagnostiques spécifiés par le DSM IV ou la CIM 11 pour certaines
pathologies (schizophrénie, troubles bipolaires, troubles de la personnalité borderline, troubles
anxieux ou troubles dépressifs sévères et invalidants) et à l’origine d’un retentissement fonctionnel
avec altération significative d’un ou plusieurs domaines de vie majeurs (relations interpersonnelles,
autonomie et accès au logement, accès à l’emploi, loisirs) » ; [157].
Page 50
Le terme Handicap Psychique (« psychiatric disability ») est apparu aux USA en 1990 dans
l’American with Disabilities Act (ADA) [158] prohibant la discrimination envers les personnes
handicapées dans tous les domaines de la vie. La même définition du handicap (« une altération
d’une fonction physique ou mentale limitant de façon substantielle la participation d’une personne
dans un ou plusieurs domaines majeurs de la vie ») a été reprise au Royaume-Uni en 1995 dans le
Disabilities Discrimination Act (DDA) [159]. En France, la Loi 2005-102 [160] pour l'égalité des
droits et des chances, la participation et la citoyenneté des personnes handicapées a introduit la
notion de handicap psychique : « Constitue un handicap, au sens de la présente loi, toute limitation
d'activité ou restriction de participation à la vie en société subie dans son environnement par une
personne en raison d'une altération substantielle, durable ou définitive d'une ou plusieurs fonctions
physiques, sensorielles, mentales, cognitives ou psychiques, d'un polyhandicap ou d'un trouble de
santé invalidant ».
Ces dispositions ont été renforcées par la Convention des Nations Unies pour le droit des personnes
en situation de handicap, signée en 2006 [161] par 151 pays à travers le monde, qui vise à
« promouvoir, protéger et assurer la pleine et égale jouissance de tous les droits de l’homme et de
toutes les libertés fondamentales par les personnes handicapées et de promouvoir le respect de leur
dignité intrinsèque » (article n°1, résolution 61/106). Elle mentionne dans son article n°8 la
nécessité de lutter contre la stigmatisation par : i) des campagnes mettant en lumière les forces et
capacités préservées des personnes en situation de handicap, par exemple à exercer un emploi ou
contribuer utilement à la société ; ii) des campagnes auprès du grand public, des enfants ou
adolescents et des médias incitant à adopter une attitude respectant leurs droits ; iii) des actions
auprès des personnes en situation de handicap pour les informer de leurs droits. La réduction de la
stigmatisation structurelle des personnes en situation de handicap est un objectif figurant dans
Page 51
plusieurs articles, qui rappellent le droit des personnes à exercer leur capacité juridique dans tous les
domaines de leur vie (article n°12), celui d’être inclus dans la communauté (article n°19), de se
marier et de fonder une famille (article n°23), d’accéder à des soins de qualité similaires à ceux
reçus par les personnes non handicapées (article n°25), d’exercer un emploi et une citoyenneté
pleine et entière (articles n°27 et 29).
4.1.2. Du handicap psychique au rétablissement : place de la lutte contre la stigmatisation
Un point clé de l’article n°8 de la Convention des Nations Unies pour le droit des personnes
handicapées [161] est l’accent mis sur les forces et capacités préservées des personnes concernées
plus que sur les limitations liées à leur pathologie dans les campagnes de lutte contre la
stigmatisation. Elle rejoint en cela le modèle du rétablissement dans la conception de R.P
Lieberman, où il existe un équilibre entre les ressources personnelles et environnementales d’une
personne avec TPSP et les difficultés liées à la pathologie ou à la stigmatisation, les soins de
réhabilitation psychosociale pouvant faciliter le dépassement de la situation de handicap et son
rétablissement [162], [163]. La réhabilitation psychosociale regroupe un large panel de soins et
services visant à favoriser le rétablissement des personnes avec TPSP, incluant l’amélioration de la
santé physique, du fonctionnement cognitif et social, du bien-être mental, de la qualité de vie, la
réduction des symptômes et de la stigmatisation et l’accompagnement vers le réinvestissement de
rôles sociaux significatifs pour elles [164].
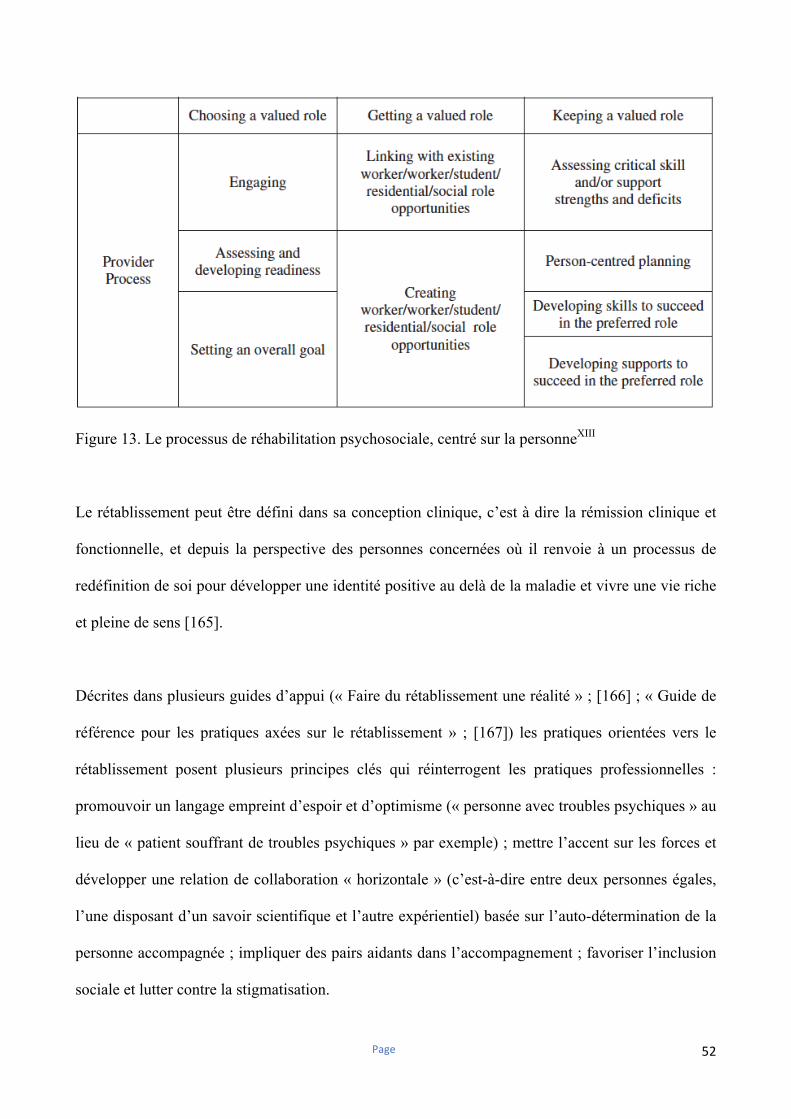
Page 52
Figure 13. Le processus de réhabilitation psychosociale, centré sur la personneXIII
Le rétablissement peut être défini dans sa conception clinique, c’est à dire la rémission clinique et
fonctionnelle, et depuis la perspective des personnes concernées où il renvoie à un processus de
redéfinition de soi pour développer une identité positive au delà de la maladie et vivre une vie riche
et pleine de sens [165].
Décrites dans plusieurs guides d’appui (« Faire du rétablissement une réalité » ; [166] ; « Guide de
référence pour les pratiques axées sur le rétablissement » ; [167]) les pratiques orientées vers le
rétablissement posent plusieurs principes clés qui réinterrogent les pratiques professionnelles :
promouvoir un langage empreint d’espoir et d’optimisme (« personne avec troubles psychiques » au
lieu de « patient souffrant de troubles psychiques » par exemple) ; mettre l’accent sur les forces et
développer une relation de collaboration « horizontale » (c’est-à-dire entre deux personnes égales,
l’une disposant d’un savoir scientifique et l’autre expérientiel) basée sur l’auto-détermination de la
personne accompagnée ; impliquer des pairs aidants dans l’accompagnement ; favoriser l’inclusion
sociale et lutter contre la stigmatisation.
Page 53
Le décret 2017-1200 [168], relatif au projet territorial de santé mentale, contribue à réduire la
stigmatisation structurelle des personnes avec TPSP, dans ses articles R. 3224-6.-I sur l’accès le
plus précoce possible aux soins de réhabilitation psychosociale et à des services facilitant l’accès au
logement, aux études, à l’emploi et à la vie sociale pour favoriser le rétablissement et l’inclusion
sociale des personnes concernées et R. 3224-9.-I. sur le respect et de la promotion des droits des
personnes présentant des troubles psychiques, du renforcement de leur pouvoir de décider et d’agir
et de la lutte contre la stigmatisation. L’instruction N°DGOS/R4/2019/10 [169] relative au
développement des soins de réhabilitation psychosociale sur les territoires et les décrets n°2016-
1940 [170] relatif au dispositifs d’appartements de coordination thérapeutique « Un chez-soi
d’abord » et n°2016-1889 [171] relative à la mise en œuvre du dispositif d’emploi accompagné
contribuent également à la réduction de la stigmatisation structurelle des personnes avec TPSP.
4.2. Réduire la stigmatisation publique
De façon générale, il existe principalement trois types de stratégies pour réduire la stigmatisation
publique : la protestation des personnes concernées, des aidants familiaux ou des professionnels de
santé, suite à un discours ou une émission à caractère stigmatisant ; l’éducation du grand public
pour corriger les stéréotypes négatifs et réduire les attitudes discriminantes envers les personnes
avec TPSP ; le contact direct avec des personnes concernées à l’occasion de campagnes de dé-
stigmatisation [172]. La protestation produit généralement des effets immédiats (par exemple, le
retrait du contenu stigmatisant ; [172]). Les stratégies d’éducation et de contact ont un effet positif
sur les réactions émotionnelles et les attitudes du grand public bien que de taille limitée [172],
[173]. L’éducation serait plus efficace chez les publics jeunes, alors que le contact avec des
personnes concernées aurait une effet plus important chez un public adulte [172]. Les campagnes
sur des médias locaux, régionaux ou nationaux auraient un effet positif modéré sur les attitudes du
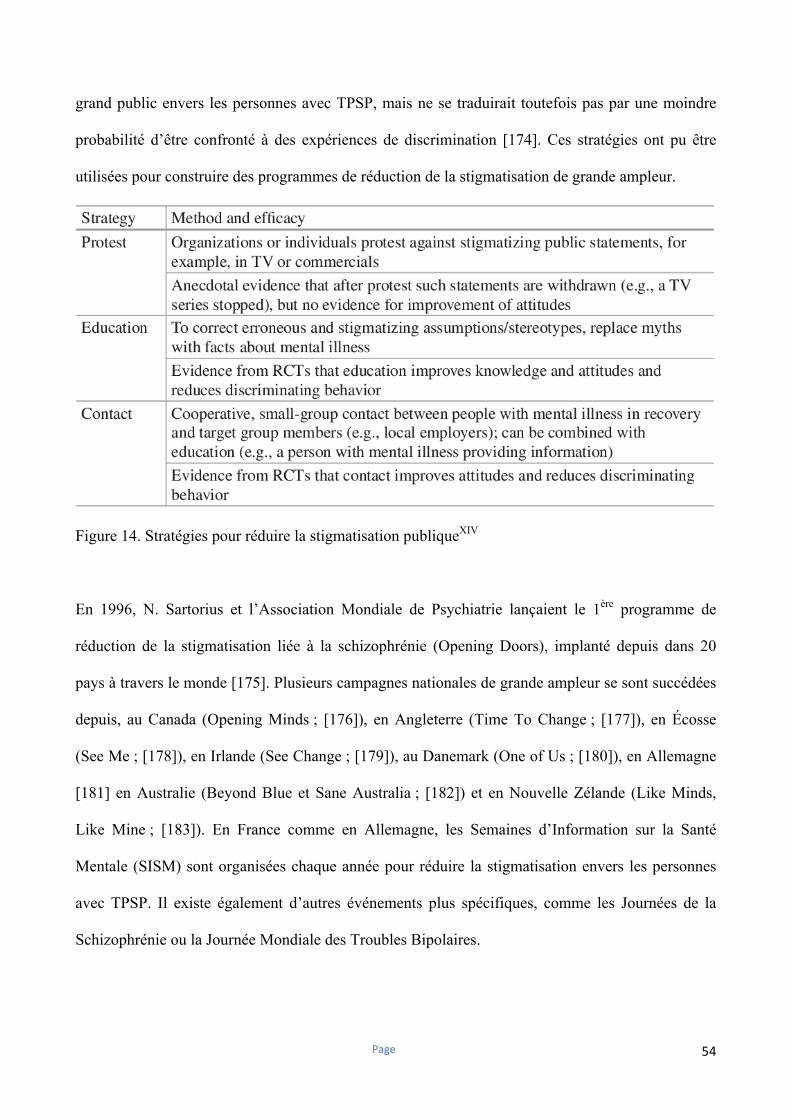
Page 54
grand public envers les personnes avec TPSP, mais ne se traduirait toutefois pas par une moindre
probabilité d’être confronté à des expériences de discrimination [174]. Ces stratégies ont pu être
utilisées pour construire des programmes de réduction de la stigmatisation de grande ampleur.
Figure 14. Stratégies pour réduire la stigmatisation publiqueXIV
En 1996, N. Sartorius et l’Association Mondiale de Psychiatrie lançaient le 1ère programme de
réduction de la stigmatisation liée à la schizophrénie (Opening Doors), implanté depuis dans 20
pays à travers le monde [175]. Plusieurs campagnes nationales de grande ampleur se sont succédées
depuis, au Canada (Opening Minds ; [176]), en Angleterre (Time To Change ; [177]), en Écosse
(See Me ; [178]), en Irlande (See Change ; [179]), au Danemark (One of Us ; [180]), en Allemagne
[181] en Australie (Beyond Blue et Sane Australia ; [182]) et en Nouvelle Zélande (Like Minds,
Like Mine ; [183]). En France comme en Allemagne, les Semaines d’Information sur la Santé
Mentale (SISM) sont organisées chaque année pour réduire la stigmatisation envers les personnes
avec TPSP. Il existe également d’autres événements plus spécifiques, comme les Journées de la
Schizophrénie ou la Journée Mondiale des Troubles Bipolaires.
Page 55
Ces programmes nationaux ou internationaux partagent certaines caractéristiques : utilisation de
stratégies d’éducation ou de contact, parfois combinée avec des campagnes de grande ampleur dans
les médias et public cible diversifié (jeunes, médias, professionnels de santé et monde du travail). Il
existe toutefois des spécificités, comme par exemple, l’adaptation du programme néo-zélandais au
contexte culturel Maori [183]. Ces programmes auraient un effet sur la stigmatisation publique,
mais de durée limitée [184]. Ils permettraient par ailleurs d’améliorer le traitement médiatique des
personnes avec TPSP, en augmentant le nombre de contenus positifs et en diminuant celui de
contenus stigmatisants [37], [52]. La réalisation en Allemagne de campagnes de dé-stigmatisation
entre 1990 et 2011 aurait permis de réduire la stigmatisation perçue par les personnes avec TPSP, ce
qui contraste avec les changements limités de la stigmatisation publique sur cette même période
[34]. Le programme le plus évalué, Times To Change, permettrait par ailleurs de réduire la
discrimination vécue de 11% sur une période de 3 ans [185]. Les effets des campagnes de dé-
stigmatisation sur l’auto-stigmatisation sont toutefois encore inconnus.
4.3. Réduire l’auto-stigmatisation
4.3.1. Auto-stigmatisation et rétablissement
Le rétablissement personnel, défini par l’usager, implique: 1) de trouver et garder espoir ; 2) la
redéfinition d’une identité positive au-delà de la pathologie ; 3) l’auto-détermination et la reprise du
pouvoir d’agir ; 4) le réengagement dans une vie riche et dotée de sens [165], [166].
Il s’agit d’un processus non linéaire, pouvant être modélisé selon R. Andresen en cinq stades, le
stade moratoire (déni, désespoir), celui de prise de conscience de la possibilité du rétablissement,
celui de préparation où la personne fait l’inventaire de ses ressources et vulnérabilités et bénéficie le
plus des stratégies de réhabilitation psychosociale, celui de reconstruction au cours duquel la
Page 56
personne réinvestit activement des rôles sociaux significatifs et celui de croissance caractérisé par
une autogestion des troubles et un sentiment de bien-être [186]. Patricia Deegan illustre cette phase
de la façon suivante, « Le rétablissement, c’est une attitude, une façon d’aborder la journée et les
difficultés qu’on y rencontre. Cela signifie que je sais que j’ai certaines limitations et qu’il y a des
choses que je ne peux pas faire. Mais plutôt que de laisser ces limitations être une occasion de
désespoir, une raison de laisser tomber, j’ai appris qu’en sachant ce que je ne peux pas faire, je
m’ouvre aussi aux possibilités liées à toutes les choses que je peux faire.» [187].
Le rétablissement implique un remaniement identitaire profond au cours duquel la personne évolue
dans son rapport avec sa pathologie, s’en distancie pour retrouver une identité positive à laquelle
celle-ci est intégrée, mais ne la définit pas [188]. Il a été illustré de la façon suivante : « Le
rétablissement implique de remplacer une vision de soi-même centrée sur le handicap psychique par
une perception de soi comme une personne complète confrontée à des défis, renforçant ainsi son
récit de vie par la transformation d’une expérience douloureuse en un événement marquant de vie »
[189]).
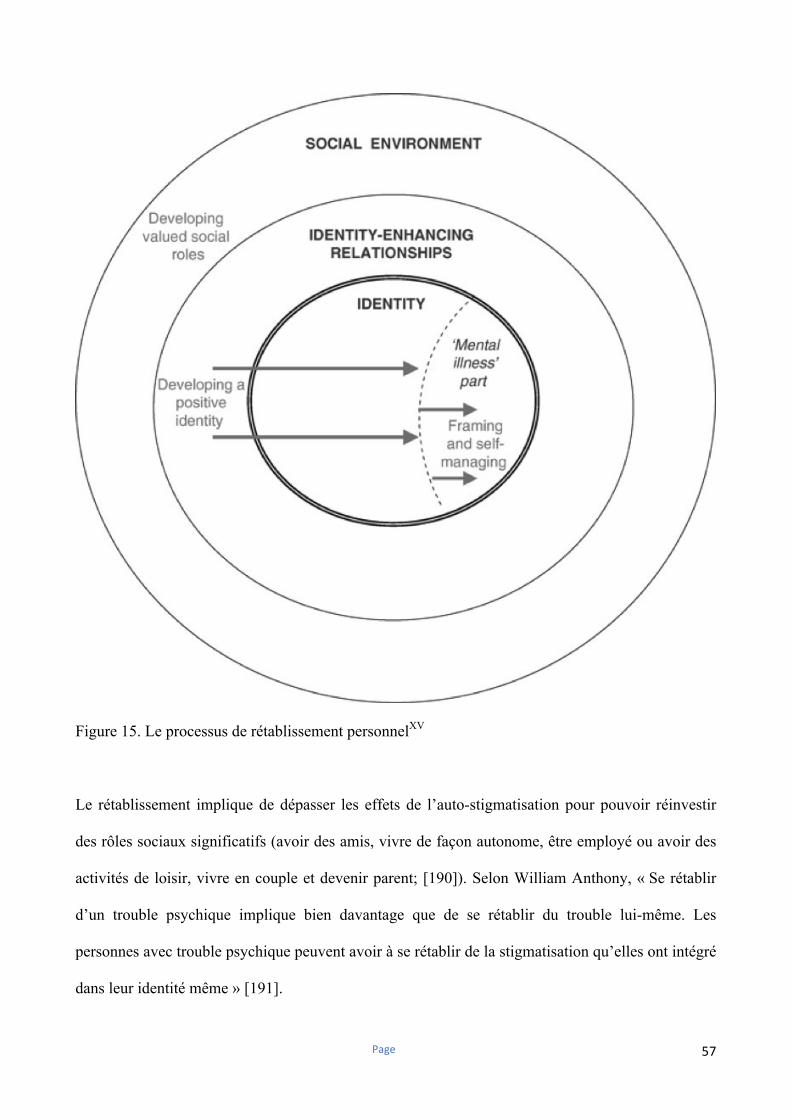
Page 57
Figure 15. Le processus de rétablissement personnelXV
Le rétablissement implique de dépasser les effets de l’auto-stigmatisation pour pouvoir réinvestir
des rôles sociaux significatifs (avoir des amis, vivre de façon autonome, être employé ou avoir des
activités de loisir, vivre en couple et devenir parent; [190]). Selon William Anthony, « Se rétablir
d’un trouble psychique implique bien davantage que de se rétablir du trouble lui-même. Les
personnes avec trouble psychique peuvent avoir à se rétablir de la stigmatisation qu’elles ont intégré
dans leur identité même » [191].
Page 58
4.3.2. Auto-stigmatisation et réhabilitation psychosociale
Le rétablissement – dans ses aspects objectifs (« rétablissement fonctionnel et social ») comme dans
ses aspects plus subjectifs (« rétablissement personnel ») – est l’objectif final de tout
accompagnement en réhabilitation psychosociale [164], [165]. Il peut être soutenu dans ses
différentes dimensions par la mise en place de soins de réhabilitation psychosociale et par la
diffusion large des pratiques orientées vers le rétablissement dans les secteurs sanitaires, sociaux et
médico-sociaux. Celles-ci n’impliquent pas nécessairement la mise en place de techniques
spécialisées mais nécessite la création d’un environnement favorable au rétablissement, c’est-à-dire
porteur d’espoir, focalisé sur les ressources préservées plus que sur les difficultés liées à la
pathologie et soutenant l’auto-détermination et le contrôle de sa vie par l’usager [166], [192]. La
mise en place de pratiques orientées vers le rétablissement au sein des services de santé mentale
pourrait réduire la stigmatisation et l’auto-stigmatisation, bien que cela n’aie pas encore été évalué.
Plusieurs interventions spécifiques ont été développées pour réduire l’auto-stigmatisation à partir de
la fin des années 2000, principalement aux USA, mais aussi à Hong Kong et au Royaume-Uni
[184], [193]. Il s’agit pour la plupart de programmes couplant de la psychoéducation destinée à
remettre en cause les préjugés relatifs aux personnes avec TPSP et de la restructuration cognitive
visant à prendre du recul par rapport aux biais cognitifs relatifs à l’auto-stigmatisation (par exemple,
« je ne suis pas quelqu’un de fiable »). C’est notamment le cas des programmes Ending Self-Stigma
(9 séances ; [194], [195]), Self-stigma Reduction (16 séances ; [196]) et Narrative Enhancement and
Cognitive Therapy (NECT) (20 séances ; [197]). Le programme NECT a comme spécificité une
partie consacrée à la narration de soi pour aider les participants à donner un sens à leurs expériences
en lien avec la maladie et renforcer leurs capacités à se dégager de « l’identité-maladie » pour
parvenir à une conception plus intégrée d’eux mêmes [197]. Ces programmes ont tous montré une
efficacité sur la réduction de l’auto-stigmatisation, bien que parfois non durable dans le temps
Page 59
[102], [195], [196], [198], [199]. Le programme NECT a déjà été adapté en Israël et en Suède, une
adaptation étant en cours à Singapour. Il a fait l’objet de trois essais randomisés contrôlés,
retrouvant des effets positifs sur l’auto-stigmatisation, l’espoir et l’estime de soi, persistants après
six mois de suivi [102], [198], [199]. Le programme NECT aurait également des effets sur le retrait
social en lien avec l’auto-stigmatisation et l’utilisation de stratégies d’évitement des situations
sociales, mais son efficacité sur le fonctionnement social des participants est encore inconnu [102].
L’accompagnement à la divulgation contrôlée des troubles, stratégie associée à la reprise du pouvoir
d’agir et l’amélioration de l’estime de soi, fait l’objet d’un programme en 3 séances (Honest, Open
and Proud ; [200], [201]) en cours d’adaptation en Suisse francophone. Il a montré une efficacité sur
la réduction du stress lié à la stigmatisation et de l’auto-stigmatisation chez des adolescents et
adultes avec TPSP [200], [201]. Il existe également d’autres types d’intervention : un programme
combinant psychoéducation et photo-expression animé par des pairs aidants (PhotoVoice ; [202]) ;
un programme basé sur les thérapies d’acceptation et d’engagement développé pour les personnes
avec troubles de l’usage de substances [203] ; des thérapies cognitives et comportementales
individuelles ciblant les biais cognitifs relatifs à l’auto-stigmatisation et renforçant l’utilisation de
stratégies adaptatives efficaces pour faire face à la stigmatisation [204], [205] ; des programmes
d’auto-support entièrement gérés par les usagers, sans assistance de la part de professionnels [206].
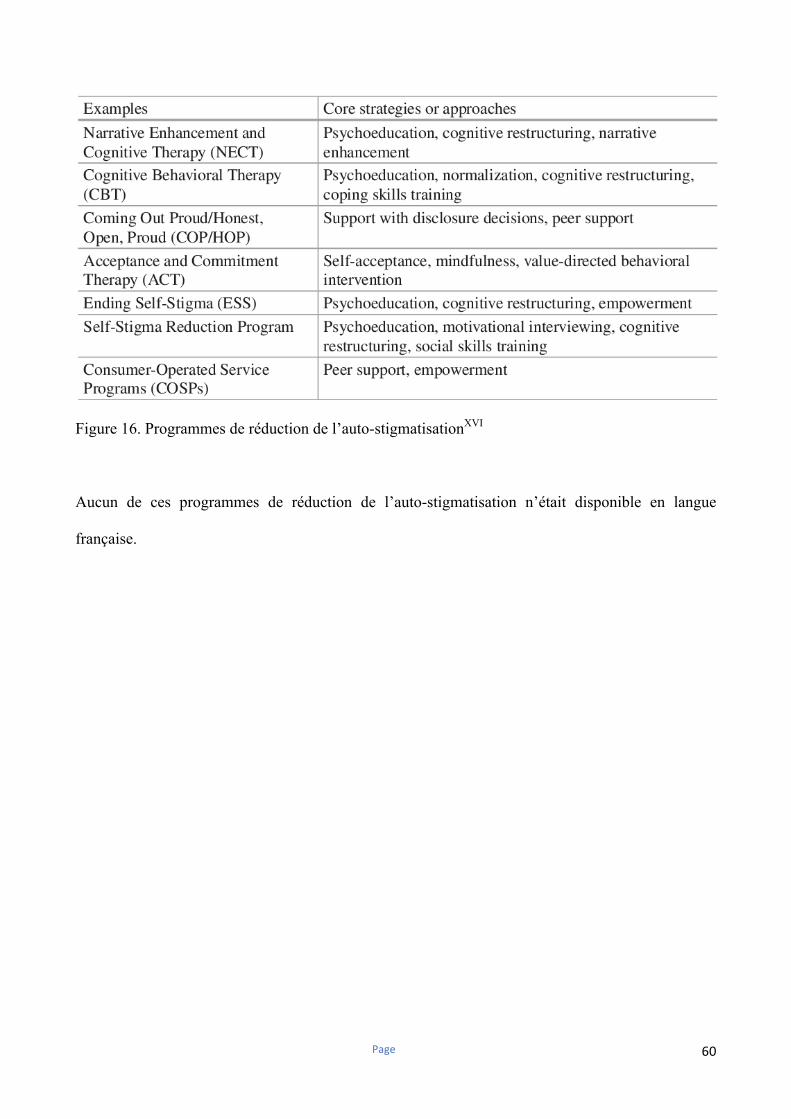
Page 60
Figure 16. Programmes de réduction de l’auto-stigmatisationXVI
Aucun de ces programmes de réduction de l’auto-stigmatisation n’était disponible en langue
française.
Page 61
Problématique et objectifs du travail de thèse
L’auto-stigmatisation est fréquente chez les personnes avec Troubles Psychiques Sévères et
Persistants, dont elle altère le devenir clinique et fonctionnel. Elle est toutefois encore peu étudiée
du point de vue des neurosciences et sur un plan expérimental. L’auto-stigmatisation a
principalement été étudiée de façon transversale, dans la schizophrénie et en Europe ou en
Amérique du Nord. Sa prévalence dans d’autres aires géographiques et culturelles et dans d’autres
pathologies à l’origine d’un handicap psychique reste encore peu connue. Elle a fréquemment été
évaluée avec des échelles mesurant d’autres aspects de la stigmatisation (stigmatisation perçue,
expérimentée ou anticipée) et il est donc difficile d’en discerner les prédicteurs et effets spécifiques.
L’auto-stigmatisation, comme la résistance à la stigmatisation, n’ont pas encore été étudiées en
France, où leur fréquence et les caractéristiques qui y sont associées restent donc largement
inconnues. Elles ont par ailleurs été peu étudiées dans des cohortes de réhabilitation psychosociale,
où la réduction de l’auto-stigmatisation et le renforcement des capacités à y faire face pourraient
être des objectifs thérapeutiques majeurs. Aucun programme de réduction de l’auto-stigmatisation
n’est disponible en langue française.
Le présent travail est composé de deux revues systématiques de la littérature, l’une sur les corrélats
neurobiologiques de l’auto-stigmatisation et l’autre sur sa prévalence, ses prédicteurs et ses
corrélats cliniques et fonctionnels dans les TPSP. Il comprend également trois articles originaux
issus de la base nationale des centres référents de réhabilitation psychosociale et de remédiation
cognitive (REHABase) et le protocole d’un essai randomisé contrôlé en stepped-wedge portant sur
l’évaluation de l’efficacité de la version française du programme de thérapie cognitive et de
renforcement narratif (NECT) sur le fonctionnement social chez des personnes avec TPSP.
Page 62
La première revue systématique de littérature avait pour objectifs de : i) recenser les études ayant
évalué l’auto-stigmatisation ou des concepts proches, comme le rejet social, d’un point de vue
expérimental ; ii) mieux appréhender les mécanismes cognitifs et neurobiologiques sous-tendant les
effets de la stigmatisation sur les personnes avec TPSP ; iii) dégager des pistes de recherches pour
une modélisation expérimentale de l’auto-stigmatisation pouvant être utilisée comme variable
d’intérêt dans des essais cliniques.
La seconde revue systématique de littérature avait pour objectifs de : i) recenser les études sur la
prévalence, les prédicteurs et les conséquences de l’auto-stigmatisation chez les personnes avec
TPSP ; ii) dégager les implications pour la pratique clinique ; iii) identifier les forces et limites des
connaissances existantes et de nouvelles pistes de recherche sur le sujet.
Le 1er article issu de REHABase avait pour objectifs : i) la description de la cohorte nationale des
centres référents de réhabilitation psychosociale et de remédiation cognitive ; ii) la présentation des
premiers résultats décrivant les caractéristiques des personnes avec TPSP ou troubles du spectre
autistique sans déficience intellectuelle (TSA-SDI), leur bien-être, leur satisfaction dans différents
domaines de la vie, leurs demandes d’aide et leur rétablissement personnel ; iii) dégager des pistes
d’analyses transversales et longitudinales ultérieures.
Le 2nd article issu de REHABase avait pour objectifs : i) d’identifier la fréquence de l’auto-
stigmatisation dans les TPSP et les TSA-SDI au sein de la cohorte nationale des centres référents de
réhabilitation psychosociale et de remédiation cognitive ; ii) d’identifier les facteurs associés à une
auto-stigmatisation élevée avec leurs implications thérapeutiques.
Page 63
Le 3ème article issu de REHABase avait pour objectifs : i) d’identifier la fréquence de la résistance à
la stigmatisation dans les TPSP et les TSA-SDI au sein de la cohorte nationale des centres référents
de réhabilitation psychosociale et de remédiation cognitive ; ii) d’identifier les facteurs associés à
une résistance élevée à la stigmatisation avec leurs implications thérapeutiques.
La dernière étude présente le protocole d’un essai randomisé contrôlé en stepped-wedge sur
l’efficacité de la version française du programme NECT, dont le début est prévu en janvier 2020.
Les objectifs de cet essai sont d’évaluer : i) l’efficacité de NECT sur le fonctionnement social chez
des participants avec TPSP ; ii) l’efficacité de NECT sur l’auto-stigmatisation, les symptômes
psychiatriques, la dépression, le bien-être, la qualité de vie et le rétablissement personnel ; iii) si
l’amélioration éventuelle observée pendant les visites de suivi est prédite par l’insight et le
fonctionnement cognitif à l’évaluation initiale ; iv) si les effets sur les objectifs principaux et
secondaires persistent lors des visites de suivi, à 6 et 12 mois.

Page 64
Partie II. L’auto-stigmatisation : mécanismes cognitifs et neurobiologiques identifiés dans la
littérature

Page 65
Contents lists available at ScienceDirect
Psychiatry Research
journal homepage: www.elsevier.com/locate/psychres
Review article
Neural and cognitive correlates of stigma and social rejection in individualswith Serious Mental Illness (SMI): A systematic review of the literature
Dubreucq J.a,b,c,⁎, Franck N.a,d,e,f
a Centre de Neurosciences Cognitive, UMR 5229, CNRS & Université Lyon 1, Franceb Centre Référent de Réhabilitation Psychosociale et de Remédiation Cognitive (C3R), Centre Hospitalier Alpes Isère, 1 place du Conseil National de la Résistance, Grenoble,38400 Saint Martin d'Hères, Francec Fondation FondaMental, Créteil, Franced Réseau Handicap Psychique, Grenoble, Francee Centre Référent Lyonnais de Réhabilitation Psychosociale et de Remédiation Cognitive (CL3R), Centre Hospitalier Le Vinatier, Francef Centre Ressource de Réhabilitation Psychosociale et de Remédiation Cognitive, Centre Hospitalier Le Vinatier, France
A R T I C L E I N F O
Keywords:Cognitive neuroscienceSelf-stigmaStigmaSocial rejectionSevere mental illness
A B S T R A C T
Stigma and self-stigma are major issues for people with Serious Mental Illness (SMI). This review's aims were todetermine the cognitive and neural processes underlying the effects of stigma and social rejection in people with SMI.A stepwise systematic literature review (PRISMA) was conducted by searching PubMed, Medline and Web of
Science using the following keywords: “cyberball” OR “stereotype threat” OR “implicit association test” AND“mental illness”. The articles included met the following criteria: (a) reporting on social rejection, stigma or self-stigma (b) diagnosis of SMI (c) available data on the underlying mechanisms.Our search on July 31th 2018 found in 955 articles on PubMed and 3,362 on Web of Science. Hypersensitivity
to acute social rejection was found and associated with more self-related negative emotions and more dys-functional emotion regulation strategies. People with SMI under-performed in cognitive tasks when confrontedwith stigma. Stigma resistance was described with its neural correlates. Psychiatric symptoms, duration of illnessand baseline non-specific distress influenced the response to acute social rejection or stigma. The samples,methods, and reported outcomes were heterogeneous and difficult to compare. Future studies should investigatethe associations between self-stigma and responses to acute and chronic social rejection.
1. Introduction
Stereotypes can be defined as common social knowledge shared bypeople from the same cultural background. They make it possible torapidly identify and categorize the individuals with whom one interactsand contribute to understanding social situations and shaping beha-vioral responses (Krendl et al., 2006). Stigma occurs when stereotypesgenerate negative emotional responses and behaviors towards themembers of a group – or towards oneself in the case of self-stigma(Corrigan and Watson, 2002). Self-stigma - or Internalized Stigma (IS) -is an identity transformation process wherein a person's previously heldsocial identity (defined by social roles such as son, brother, sister,friend, employee or potential partner) is progressively replaced by adevalued and stigmatized view of oneself termed “illness identity”(Yanos et al., 2008). Stigma Resistance (SR) is defined as one's ability todeflect or challenge stigmatizing beliefs (Thoits, 2011).
According to the US Substance Abuse and Mental Health ServicesAdministration, individuals with “Serious Mental Illness” (SMI) are“persons aged 18 or older who currently or at any time in the past yearhave had a diagnosable mental, behavioral, or emotional disorder(excluding developmental and substance use disorders) of sufficientduration to meet diagnostic criteria specified within DSM-IV that hasresulted in serious functional impairment, which substantially inter-feres with or limits one or more major life activities such as maintaininginterpersonal relationships, activities of daily living, self-care, em-ployment, and recreation”. Serious Mental Illnesses (SMI;SAMSAH, 2014) include schizophrenia (SZ), bipolar disorder (BD), andborderline personality disorder (BPD), as well as Major DepressiveDisorder (MDD) and Anxiety Disorders that cause severe and persistentfunctional impairments. SMI are frequent (1% for SZ; 1.5% for BD;1.5% for BPD) and heavily stigmatized (Angermeyer et al., 2013;Ellison et al., 2013). People with SZ, BD or MDD are more likely to
https://doi.org/10.1016/j.psychres.2019.02.023Received 18 November 2018; Received in revised form 9 February 2019; Accepted 9 February 2019
⁎ Corresponding author at: Centre Référent de Réhabilitation Psychosociale et de Remédiation Cognitive (C3R), Centre Hospitalier Alpes Isère, 1 place du ConseilNational de la Résistance, Grenoble, 38400 Saint Martin d'Hères, France.E-mail address: [email protected] (D. J.).
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.

Page 66
experience discrimination in a range of aspects of their daily life(Thornicroft et al., 2009; Farrelly et al., 2014; Lasalvia et al., 2013).They frequently expect to be discriminated in social contexts even whenthey have no previous experience of discrimination (Thornicroft et al.,2009; Farrelly et al., 2014; Lasalvia et al; 2013). Internalized Stigma(IS) is frequent (41.7% of the 1229 participants with SZ and 21.7% ofthe 1182 participants with BD in the 2010 GAMIAN-Europe study hadmoderate to high levels of self-stigma; Brohan et al., 2010, 2011) andassociated with multiple negative consequences: lower therapeuticadherence, self-efficacy, self-esteem, empowerment and hope and agreater intensity of depressive symptoms and suicidal ideation(Livingston and Boyd, 2010; Ellison et al., 2013). Stigma resistanceconcerns a wide range of people with SMI (49.2% of the 1229 partici-pants with SZ and 49.7% of the 1182 participants with BD in the 2010GAMIAN-Europe study had moderate to high levels of self-stigma;Brohan et al., 2010, 2011). It was associated with higher levels ofmetacognitive abilities, self-efficacy, self-esteem, empowerment, hope,personal recovery and subjective quality of life (Nabors, 2014;Firmin et al., 2016). Several psychosocial interventions (mainly com-binations of psychoeducation and Cognitive Behavior Therapy (CBT))have been designed to reduce IS and its impact on clinical and func-tional outcomes, with preliminary results on IS, insight, and self-effi-cacy. Their impact on functional brain connectivity remains unknownto date.
Public stigma, i.e. the relatively automatic cognitive and behavioralresponse in a social context cued by a characteristic related to a stig-matized group (Krendl et al., 2006), is the most documented area in theliterature (Krendl et al., 2013; Reihl et al., 2015). The processes leadingto negative or stigmatizing attitudes towards individuals with SMI wereinvestigated and showed the role of the SZ diagnosis, persistent nega-tive symptoms, and functional impairments (mostly on social skills)play in participants’ emotional reactions when interacting with peoplethey believed to have SZ (Penn et al., 2000; Heenan et al., 2014). Moresevere negative symptoms and poorer social skills were associated withhigher perceived strangeness and desire for social distance when in-teracting with individuals with SZ (Penn et al., 2000).
In contrast with public stigma (or endorsement of negative beliefsand discriminating attitudes by the general population), personalstigma refers to the beliefs experiences and attitudes towards mentalillness endorsed by the members of a stigmatized group, in this casepeople with SMI (Gerlinger et al., 2013). It includes perceived stigma(or one's beliefs and anticipations about the perception and attitudes ofthe general population towards persons with mental illness), experi-enced stigma (or the actual experiences of social discrimination lived bythe persons with mental illness) and self-stigma. In a recent study an-ticipated social discrimination mediated the relationships between ex-perienced stigma and self-stigma (Quinn et al., 2015), showing thatthese concepts may be interrelated. Three experimental paradigms wereused in the literature to investigate the cognitive and neural mechan-isms underlying personal stigma. Implicit association tests(Greenwald et al., 2009) and stereotype threat conditions directly ad-dressed stigma or self-stigma and the cyberball game was used to in-vestigate social exclusion, a stigma-related concept.
Implicit association tests (IAT) are commonly used to assess implicitself-associations, emotional reactions and attitudes towards a conceptor a population, as they are less influenced than explicit measures bysocial desirability biases and have good psychometric properties(Greenwald et al., 2009). IAT assess the strength of association betweenconcepts by measuring response latencies during computerized cate-gorization tasks: the quicker the stimuli are classified, the more likelythey are to match the respondent's associations with a target concept(Greenwald et al., 2009). IAT are particularly well-suited to in-vestigating automatically activated reactions towards stigmatized in-dividuals, as these reactions can influence outcomes, and because de-liberately endorsed stereotypes and negative attitudes towardsstigmatized individuals have become less acceptable (Greenwald et al.,
2009). IAT was used to assess automatic stereotyping and negativeemotional reactions towards individuals with SMI in the general po-pulation (Peris et al., 2008; Heenan et al., 2014), in mental healthprofessionals (Stull et al., 2013), and in participants diagnosed with SZor BD (Teachman et al., 2006; Rusch et al., 2010a, 2011a).
The stereotype threat (ST) model is a popular experimental para-digm in social psychiatry that has been used in numerous studies con-cerning discriminated populations and minorities (Derks et al., 2008).The ST paradigm refers to situations where one individual is at risk ofconfirming by his/her actions his/her negative stereotypes aboutthemselves or his/her social group (Derks et al., 2008). As an individualcan suffer simultaneously from various forms of discrimination, Shapiroand Neuberg created a multi-threat framework. In this model, self andgroup concept threats imply endorsement by an individual of negativebeliefs about oneself or about one's social group, respectively. Own andgroup reputation threats correspond to one's fear of being identified aspossessing stigmatizing attributes and therefore reinforce negative be-liefs about his/her own social group (Shapiro and Neuberg, 2007).Given the proximity of these concepts to stigma and self-stigma, thenumber of studies using ST in individuals with SMI is surprisinglylimited (Henry et al., 2010; Moritz et al., 2018; Shapiro, 2011).
Social rejection models recreate stigma-related environments underexperimental conditions. The most popular paradigm is the cyberballgame, a ball-tossing game in which participants believe they areplaying with fellow participants, but are in fact randomly assigned toinclusion, exclusion and sometimes over-inclusion conditions and playwith computer-controlled players. Cyberball is considered to be anecologically valid paradigm for evaluating emotional reactions fol-lowing social inclusion or exclusion, and was used in numerous studiesinvolving healthy individuals (Hartgerink et al., 2015). The neuralcorrelates of acute social exclusion/inclusion in healthy controls (HC)are well known (Bolling et al., 2011; Moor et al., 2012 Kawamoto et al.,2012). Enhanced activation of the insula and of the dorsal and ventralanterior cingulate cortex (ACC) during social exclusion was associatedwith self-reported experience of rejection (Bolling et al., 2011; Mooret al., 2012). Enhanced activation of the medio-prefrontal cortex(mPFC), the precuneus and the posterior cingulate cortex during socialexclusion were identified as a potential protective mechanism mod-ulating the affective response to acute social rejection (Bolling et al.,2011; Moor et al., 2012 Kawamoto et al., 2012). Cyberball was used inindividuals with SMI, mostly BPD (Lawrence et al., 2011; Staebler et al.,2011; Domsalla et al., 2014; De Panfilis, 2015; Brown et al., 2017; Euleret al., 2018; Ernst et al., 2018; Weinbrecht et al., 2018).
In summary, the clinical and functional correlates of stigma in in-dividuals with SMI are well known and several strategies have beenrecently developed to reduce stigma and self-stigma (Griffiths, 2015;Wood, 2016). In contrast, there appears to be surprisingly little cogni-tive neuroscience research into mental illness stigma. Only a few stu-dies directly addressed the cognitive and neural processes underlyingself-stigma or stigma resistance in individuals with SMI (Rusch 2010a,2010b, 2011; Raij et al., 2014; Moritz et al., 2018). These mechanismsremain therefore unclear as the data are heterogeneous and come fromvarious sources and different experimental paradigms (some of whichnot even directly related to stigma or self-stigma). To our knowledge,no literature review has yet been conducted on this particular topic.
The present review has two objectives: (i) to review the cognitiveand neural processes underlying the effects of stigma, discriminationand social rejection in individuals with SMI; (ii) to evaluate thestrengths and limits of the current evidence in order to guide futureresearch.
2. Methods
A stepwise systematic literature review (PRISMA guidelines) wasconducted by searching PubMed, Medline and Web of Science forpublished, peer-reviewed papers using the following keywords:
D. J. and F. N.
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.
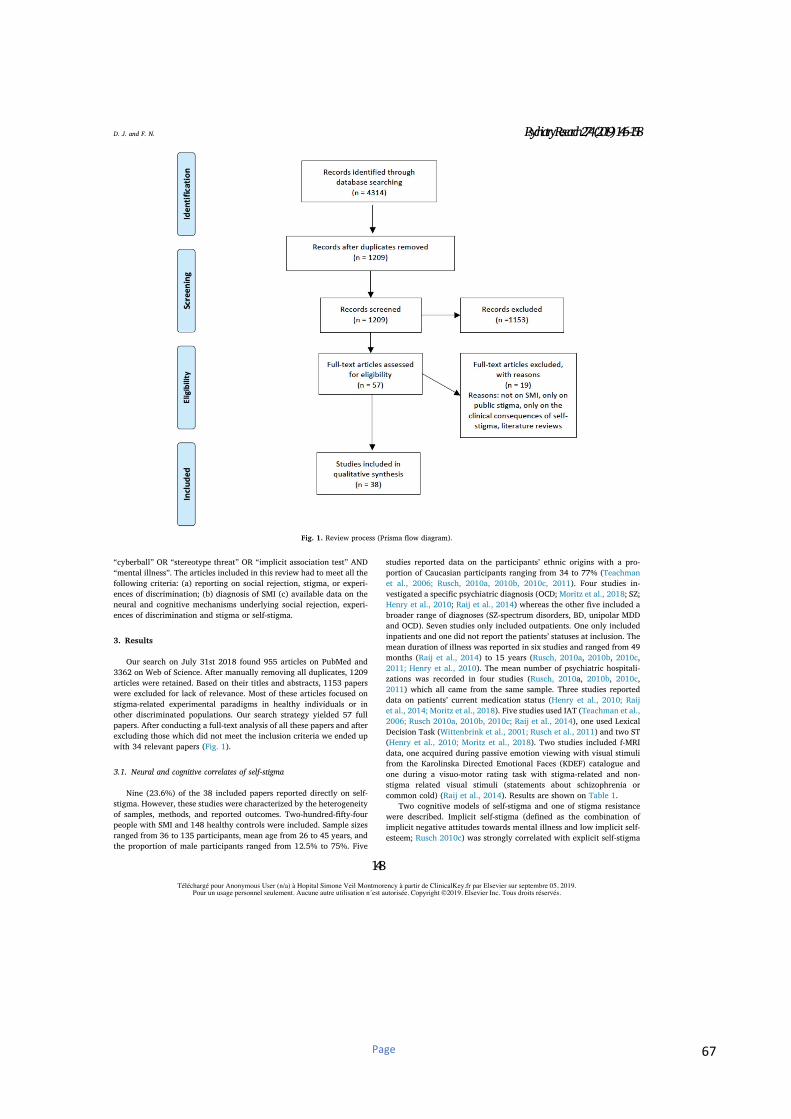
Page 67
“cyberball” OR “stereotype threat” OR “implicit association test” AND“mental illness”. The articles included in this review had to meet all thefollowing criteria: (a) reporting on social rejection, stigma, or experi-ences of discrimination; (b) diagnosis of SMI (c) available data on theneural and cognitive mechanisms underlying social rejection, experi-ences of discrimination and stigma or self-stigma.
3. Results
Our search on July 31st 2018 found 955 articles on PubMed and3362 on Web of Science. After manually removing all duplicates, 1209articles were retained. Based on their titles and abstracts, 1153 paperswere excluded for lack of relevance. Most of these articles focused onstigma-related experimental paradigms in healthy individuals or inother discriminated populations. Our search strategy yielded 57 fullpapers. After conducting a full-text analysis of all these papers and afterexcluding those which did not meet the inclusion criteria we ended upwith 34 relevant papers (Fig. 1).
3.1. Neural and cognitive correlates of self-stigma
Nine (23.6%) of the 38 included papers reported directly on self-stigma. However, these studies were characterized by the heterogeneityof samples, methods, and reported outcomes. Two-hundred-fifty-fourpeople with SMI and 148 healthy controls were included. Sample sizesranged from 36 to 135 participants, mean age from 26 to 45 years, andthe proportion of male participants ranged from 12.5% to 75%. Five
studies reported data on the participants’ ethnic origins with a pro-portion of Caucasian participants ranging from 34 to 77% (Teachmanet al., 2006; Rusch, 2010a, 2010b, 2010c, 2011). Four studies in-vestigated a specific psychiatric diagnosis (OCD; Moritz et al., 2018; SZ;Henry et al., 2010; Raij et al., 2014) whereas the other five included abroader range of diagnoses (SZ-spectrum disorders, BD, unipolar MDDand OCD). Seven studies only included outpatients. One only includedinpatients and one did not report the patients’ statuses at inclusion. Themean duration of illness was reported in six studies and ranged from 49months (Raij et al., 2014) to 15 years (Rusch, 2010a, 2010b, 2010c,2011; Henry et al., 2010). The mean number of psychiatric hospitali-zations was recorded in four studies (Rusch, 2010a, 2010b, 2010c,2011) which all came from the same sample. Three studies reporteddata on patients’ current medication status (Henry et al., 2010; Raijet al., 2014; Moritz et al., 2018). Five studies used IAT (Teachman et al.,2006; Rusch 2010a, 2010b, 2010c; Raij et al., 2014), one used LexicalDecision Task (Wittenbrink et al., 2001; Rusch et al., 2011) and two ST(Henry et al., 2010; Moritz et al., 2018). Two studies included f-MRIdata, one acquired during passive emotion viewing with visual stimulifrom the Karolinska Directed Emotional Faces (KDEF) catalogue andone during a visuo-motor rating task with stigma-related and non-stigma related visual stimuli (statements about schizophrenia orcommon cold) (Raij et al., 2014). Results are shown on Table 1.
Two cognitive models of self-stigma and one of stigma resistancewere described. Implicit self-stigma (defined as the combination ofimplicit negative attitudes towards mental illness and low implicit self-esteem; Rusch 2010c) was strongly correlated with explicit self-stigma
Fig. 1. Review process (Prisma flow diagram).
D. J. and F. N.
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.
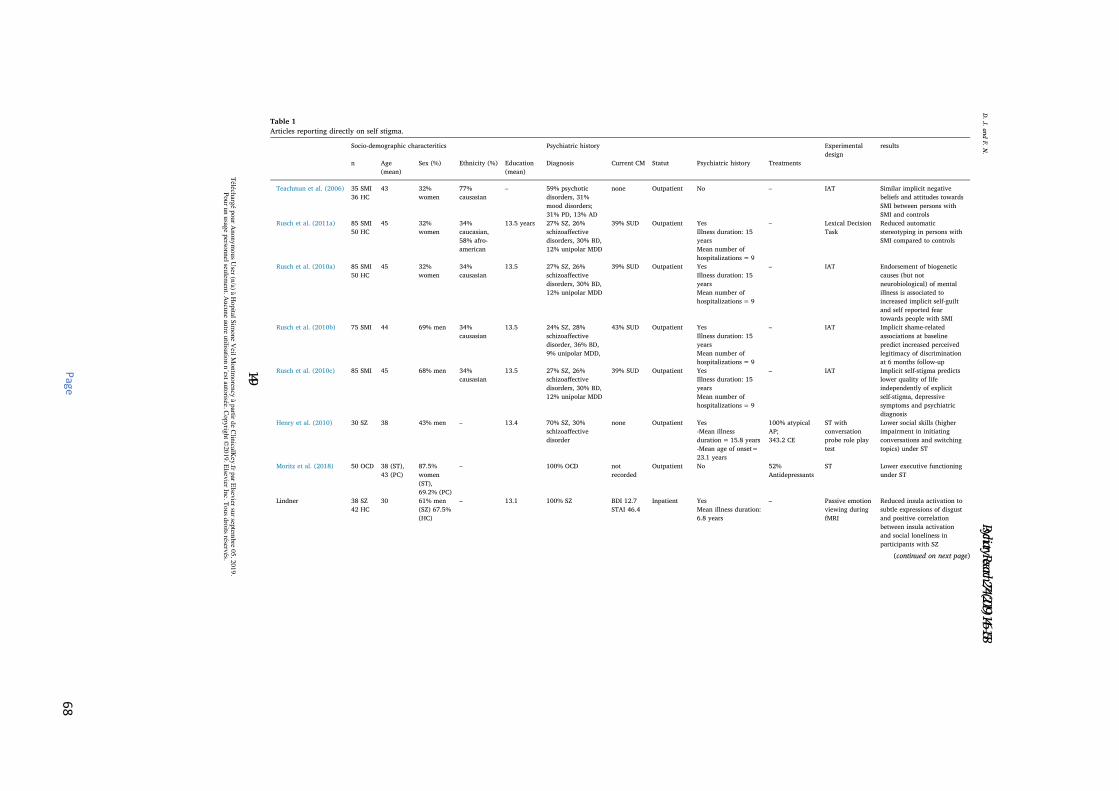
Page
68
Table 1
Articles reporting directly on self stigma.
Socio-demographic characteritics Psychiatric history Experimentaldesign
results
n Age(mean)
Sex (%) Ethnicity (%) Education(mean)
Diagnosis Current CM Statut Psychiatric history Treatments
Teachman et al. (2006) 35 SMI36 HC
43 32%women
77%causasian
– 59% psychoticdisorders, 31%mood disorders;31% PD, 13% AD
none Outpatient No – IAT Similar implicit negativebeliefs and attitudes towardsSMI between persons withSMI and controls
Rusch et al. (2011a) 85 SMI50 HC
45 32%women
34%caucasian,58% afro-american
13.5 years 27% SZ, 26%schizoaffectivedisorders, 30% BD,12% unipolar MDD
39% SUD Outpatient YesIllness duration: 15yearsMean number ofhospitalizations= 9
– Lexical DecisionTask
Reduced automaticstereotyping in persons withSMI compared to controls
Rusch et al. (2010a) 85 SMI50 HC
45 32%women
34%causasian
13.5 27% SZ, 26%schizoaffectivedisorders, 30% BD,12% unipolar MDD
39% SUD Outpatient YesIllness duration: 15yearsMean number ofhospitalizations= 9
– IAT Endorsement of biogeneticcauses (but notneurobiological) of mentalillness is associated toincreased implicit self-guiltand self reported feartowards people with SMI
Rusch et al. (2010b) 75 SMI 44 69% men 34%causasian
13.5 24% SZ, 28%schizoaffectivedisorder, 36% BD,9% unipolar MDD,
43% SUD Outpatient YesIllness duration: 15yearsMean number ofhospitalizations= 9
– IAT Implicit shame-relatedassociations at baselinepredict increased perceivedlegitimacy of discriminationat 6 months follow-up
Rusch et al. (2010c) 85 SMI 45 68% men 34%causasian
13.5 27% SZ, 26%schizoaffectivedisorders, 30% BD,12% unipolar MDD
39% SUD Outpatient YesIllness duration: 15yearsMean number ofhospitalizations= 9
– IAT Implicit self-stigma predictslower quality of lifeindependently of explicitself-stigma, depressivesymptoms and psychiatricdiagnosis
Henry et al. (2010) 30 SZ 38 43% men – 13.4 70% SZ, 30%schizoaffectivedisorder
none Outpatient Yes-Mean illnessduration=15.8 years-Mean age of onset=23.1 years
100% atypicalAP;343.2 CE
ST withconversationprobe role playtest
Lower social skills (higherimpairment in initiatingconversations and switchingtopics) under ST
Moritz et al. (2018) 50 OCD 38 (ST),43 (PC)
87.5%women(ST),69.2% (PC)
– 100% OCD notrecorded
Outpatient No 52%Antidepressants
ST Lower executive functioningunder ST
Lindner 38 SZ42 HC
30 61% men(SZ) 67.5%(HC)
– 13.1 100% SZ BDI 12.7STAI 46.4
Inpatient YesMean illness duration:6.8 years
– Passive emotionviewing duringfMRI
Reduced insula activation tosubtle expressions of disgustand positive correlationbetween insula activationand social loneliness inparticipants with SZ
(continued on next page)
D.J.andF.N.
Téléch
argé p
our A
nonym
ous U
ser (n/a) à H
opital S
imone V
eil Montm
oren
cy à p
artir de C
linicalK
ey.fr p
ar Elsev
ier sur sep
tembre 0
5, 2
019.
Pour u
n u
sage p
ersonnel seu
lemen
t. Aucu
ne au
tre utilisatio
n n
´est auto
risée. Copyrig
ht ©
2019. E
lsevier In
c. Tous d
roits réserv
és.
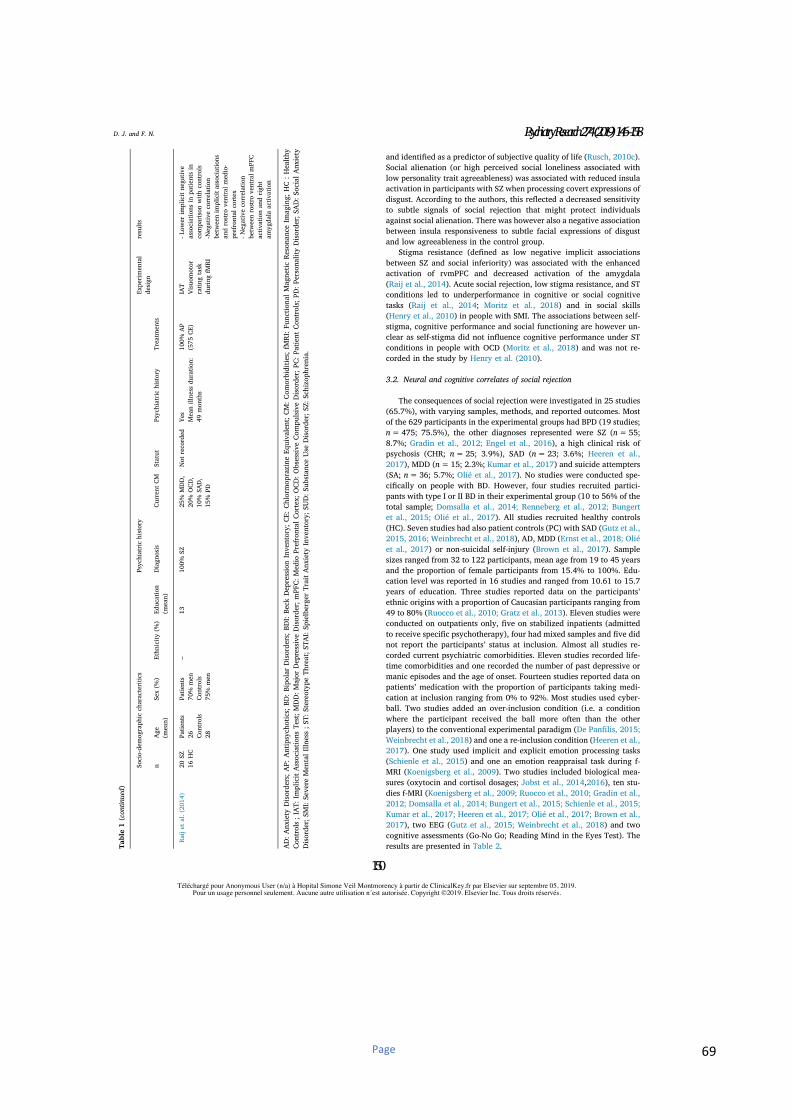
Page 69
and identified as a predictor of subjective quality of life (Rusch, 2010c).Social alienation (or high perceived social loneliness associated withlow personality trait agreeableness) was associated with reduced insulaactivation in participants with SZ when processing covert expressions ofdisgust. According to the authors, this reflected a decreased sensitivityto subtle signals of social rejection that might protect individualsagainst social alienation. There was however also a negative associationbetween insula responsiveness to subtle facial expressions of disgustand low agreeableness in the control group.
Stigma resistance (defined as low negative implicit associationsbetween SZ and social inferiority) was associated with the enhancedactivation of rvmPFC and decreased activation of the amygdala(Raij et al., 2014). Acute social rejection, low stigma resistance, and STconditions led to underperformance in cognitive or social cognitivetasks (Raij et al., 2014; Moritz et al., 2018) and in social skills(Henry et al., 2010) in people with SMI. The associations between self-stigma, cognitive performance and social functioning are however un-clear as self-stigma did not influence cognitive performance under STconditions in people with OCD (Moritz et al., 2018) and was not re-corded in the study by Henry et al. (2010).
3.2. Neural and cognitive correlates of social rejection
The consequences of social rejection were investigated in 25 studies(65.7%), with varying samples, methods, and reported outcomes. Mostof the 629 participants in the experimental groups had BPD (19 studies;n=475; 75.5%), the other diagnoses represented were SZ (n=55;8.7%; Gradin et al., 2012; Engel et al., 2016), a high clinical risk ofpsychosis (CHR; n=25; 3.9%), SAD (n=23; 3.6%; Heeren et al.,2017), MDD (n=15; 2.3%; Kumar et al., 2017) and suicide attempters(SA; n=36; 5.7%; Olié et al., 2017). No studies were conducted spe-cifically on people with BD. However, four studies recruited partici-pants with type I or II BD in their experimental group (10 to 56% of thetotal sample; Domsalla et al., 2014; Renneberg et al., 2012; Bungertet al., 2015; Olié et al., 2017). All studies recruited healthy controls(HC). Seven studies had also patient controls (PC) with SAD (Gutz et al.,2015, 2016; Weinbrecht et al., 2018), AD, MDD (Ernst et al., 2018; Oliéet al., 2017) or non-suicidal self-injury (Brown et al., 2017). Samplesizes ranged from 32 to 122 participants, mean age from 19 to 45 yearsand the proportion of female participants from 15.4% to 100%. Edu-cation level was reported in 16 studies and ranged from 10.61 to 15.7years of education. Three studies reported data on the participants’ethnic origins with a proportion of Caucasian participants ranging from49 to 80% (Ruocco et al., 2010; Gratz et al., 2013). Eleven studies wereconducted on outpatients only, five on stabilized inpatients (admittedto receive specific psychotherapy), four had mixed samples and five didnot report the participants’ status at inclusion. Almost all studies re-corded current psychiatric comorbidities. Eleven studies recorded life-time comorbidities and one recorded the number of past depressive ormanic episodes and the age of onset. Fourteen studies reported data onpatients’ medication with the proportion of participants taking medi-cation at inclusion ranging from 0% to 92%. Most studies used cyber-ball. Two studies added an over-inclusion condition (i.e. a conditionwhere the participant received the ball more often than the otherplayers) to the conventional experimental paradigm (De Panfilis, 2015;Weinbrecht et al., 2018) and one a re-inclusion condition (Heeren et al.,2017). One study used implicit and explicit emotion processing tasks(Schienle et al., 2015) and one an emotion reappraisal task during f-MRI (Koenigsberg et al., 2009). Two studies included biological mea-sures (oxytocin and cortisol dosages; Jobst et al., 2014,2016), ten stu-dies f-MRI (Koenigsberg et al., 2009; Ruocco et al., 2010; Gradin et al.,2012; Domsalla et al., 2014; Bungert et al., 2015; Schienle et al., 2015;Kumar et al., 2017; Heeren et al., 2017; Olié et al., 2017; Brown et al.,2017), two EEG (Gutz et al., 2015; Weinbrecht et al., 2018) and twocognitive assessments (Go-No Go; Reading Mind in the Eyes Test). Theresults are presented in Table 2.T
able1(continued)
Socio-demographiccharacteritics
Psychiatrichistory
Experimental
design
results
nAge(mean)
Sex(%)
Ethnicity(%)
Education
(mean)
Diagnosis
CurrentCM
Statut
Psychiatrichistory
Treatments
Raijetal.(2014)
20SZ
16HC
Patients
26Controls
28
Patients
70%men
Controls
75%men
–13
100%SZ
25%MDD,
20%OCD,
10%SAD,
15%PD
Notrecorded
YesMeanillnessduration:
49months
100%AP
(575CE)
IAT
Visuom
otor
ratingtask
duringfMRI
-Lowerimplicitnegative
associationsinpatientsin
comparison
withcontrols
-Negativecorrelation
betweenimplicitassociations
androstroventralmedio-
prefrontalcortex
-Negativecorrelation
betweenrostroventralmPFC
activation
andright
amygdalaactivation
AD:AnxietyDisorders;AP:Antipsychotics;BD:BipolarDisorders;BDI:BeckDepressionInventory;CE:ChlormoprazineEquivalent;CM:Com
orbidities;fMRI:FunctionalMagneticResonanceImaging;HC:Healthy
Controls;IAT:ImplicitAssociationsTest;MDD:MajorDepressiveDisorder;mPFC:MedioPrefrontalCortex;OCD:ObsessiveCom
pulsiveDisorder;PC:PatientControls;PD:PersonalityDisorder;SAD:SocialAnxiety
Disorder;SM
I:SevereMentalIllness;ST:StereotypeThreat;STAI:SpielbergerTraitAnxietyInventory;SUD:SubstanceUseDisorder;SZ:Schizophrenia.
D. J. and F. N.
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.
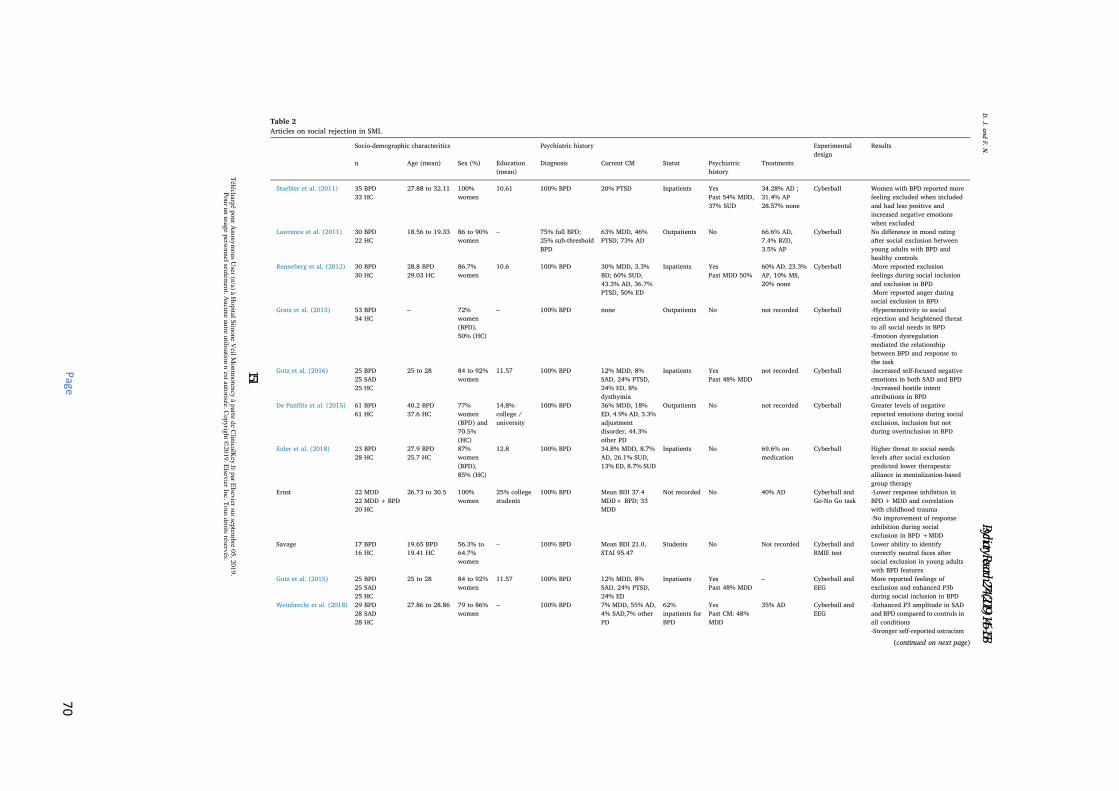
Page
70
Table 2
Articles on social rejection in SMI.
Socio-demographic characteritics Psychiatric history Experimentaldesign
Results
n Age (mean) Sex (%) Education(mean)
Diagnosis Current CM Statut Psychiatrichistory
Treatments
Staebler et al. (2011) 35 BPD33 HC
27.88 to 32.11 100%women
10.61 100% BPD 20% PTSD Inpatients YesPast 54% MDD,37% SUD
34.28% AD ;31.4% AP28.57% none
Cyberball Women with BPD reported morefeeling excluded when includedand had less positive andincreased negative emotionswhen excluded
Lawrence et al. (2011) 30 BPD22 HC
18.56 to 19.33 86 to 90%women
– 75% full BPD;25% sub-thresholdBPD
63% MDD, 46%PTSD; 73% AD
Outpatients No 66.6% AD,7.4% BZD,3.5% AP
Cyberball No difference in mood ratingafter social exclusion betweenyoung adults with BPD andhealthy controls
Renneberg et al. (2012) 30 BPD30 HC
28.8 BPD29.03 HC
86.7%women
10.6 100% BPD 30% MDD, 3.3%BD; 60% SUD,43.3% AD, 36.7%PTSD, 50% ED
Inpatients YesPast MDD 50%
60% AD, 23.3%AP, 10% MS,20% none
Cyberball -More reported exclusionfeelings during social inclusionand exclusion in BPD-More reported anger duringsocial exclusion in BPD
Gratz et al. (2013) 53 BPD34 HC
– 72%women(BPD),50% (HC)
– 100% BPD none Outpatients No not recorded Cyberball -Hypersensitivity to socialrejection and heightened threatto all social needs in BPD-Emotion dysregulationmediated the relationshipbetween BPD and response tothe task
Gutz et al. (2016) 25 BPD25 SAD25 HC
25 to 28 84 to 92%women
11.57 100% BPD 12% MDD, 8%SAD, 24% PTSD,24% ED, 8%dysthymia
Inpatients YesPast 48% MDD
not recorded Cyberball -Increased self-focused negativeemotions in both SAD and BPD-Increased hostile intentattributions in BPD
De Panfilis et al. (2015) 61 BPD61 HC
40.2 BPD37.6 HC
77%women(BPD) and70.5%(HC)
14.8%college /university
100% BPD 36% MDD, 18%ED, 4.9% AD, 3.3%adjustmentdisorder, 44.3%other PD
Outpatients No not recorded Cyberball Greater levels of negativereported emotions during socialexclusion, inclusion but notduring overinclusion in BPD
Euler et al. (2018) 23 BPD28 HC
27.9 BPD25.7 HC
87%women(BPD),85% (HC)
12.8 100% BPD 34.8% MDD, 8.7%AD, 26.1% SUD,13% ED, 8.7% SUD
Inpatients No 69.6% onmedication
Cyberball Higher threat to social needslevels after social exclusionpredicted lower therapeuticalliance in mentalization-basedgroup therapy
Ernst 22 MDD22 MDD+BPD20 HC
26.73 to 30.5 100%women
25% collegestudents
100% BPD Mean BDI 37.4MDD+ BPD; 33MDD
Not recorded No 40% AD Cyberball andGo-No Go task
-Lower response inhibition inBPD+MDD and correlationwith childhood trauma-No improvement of responseinhibition during socialexclusion in BPD +MDD
Savage 17 BPD16 HC
19.65 BPD19.41 HC
56.3% to64.7%women
– 100% BPD Mean BDI 21.0,STAI 95.47
Students No Not recorded Cyberball andRMIE test
Lower ability to identifycorrectly neutral faces aftersocial exclusion in young adultswith BPD features
Gutz et al. (2015) 25 BPD25 SAD25 HC
25 to 28 84 to 92%women
11.57 100% BPD 12% MDD, 8%SAD, 24% PTSD,24% ED
Inpatients YesPast 48% MDD
– Cyberball andEEG
More reported feelings ofexclusion and enhanced P3bduring social inclusion in BPD
Weinbrecht et al. (2018) 29 BPD28 SAD28 HC
27.86 to 28.86 79 to 86%women
– 100% BPD 7% MDD, 55% AD,4% SAD,7% otherPD
62%inpatients forBPD
YesPast CM: 48%MDD
35% AD Cyberball andEEG
-Enhanced P3 amplitude in SADand BPD compared to controls inall conditions-Stronger self-reported ostracism
(continued on next page)
D.J.andF.N.
Téléch
argé p
our A
nonym
ous U
ser (n/a) à H
opital S
imone V
eil Montm
oren
cy à p
artir de C
linicalK
ey.fr p
ar Elsev
ier sur sep
tembre 0
5, 2
019.
Pour u
n u
sage p
ersonnel seu
lemen
t. Aucu
ne au
tre utilisatio
n n
´est auto
risée. Copyrig
ht ©
2019. E
lsevier In
c. Tous d
roits réserv
és.
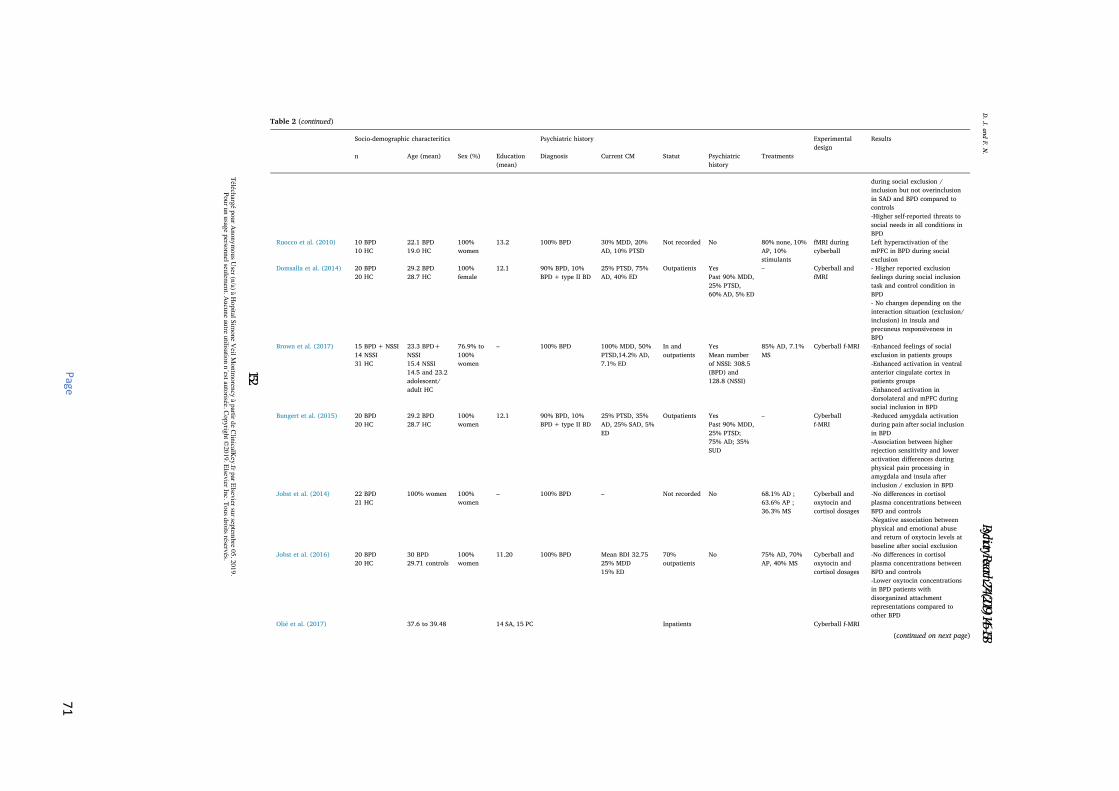
Page
71
Table 2 (continued)
Socio-demographic characteritics Psychiatric history Experimentaldesign
Results
n Age (mean) Sex (%) Education(mean)
Diagnosis Current CM Statut Psychiatrichistory
Treatments
during social exclusion /inclusion but not overinclusionin SAD and BPD compared tocontrols-Higher self-reported threats tosocial needs in all conditions inBPD
Ruocco et al. (2010) 10 BPD10 HC
22.1 BPD19.0 HC
100%women
13.2 100% BPD 30% MDD, 20%AD, 10% PTSD
Not recorded No 80% none, 10%AP, 10%stimulants
fMRI duringcyberball
Left hyperactivation of themPFC in BPD during socialexclusion
Domsalla et al. (2014) 20 BPD20 HC
29.2 BPD28.7 HC
100%female
12.1 90% BPD, 10%BPD+ type II BD
25% PTSD, 75%AD, 40% ED
Outpatients YesPast 90% MDD,25% PTSD,60% AD, 5% ED
– Cyberball andfMRI
- Higher reported exclusionfeelings during social inclusiontask and control condition inBPD- No changes depending on theinteraction situation (exclusion/inclusion) in insula andprecuneus responsiveness inBPD
Brown et al. (2017) 15 BPD+NSSI14 NSSI31 HC
23.3 BPD+NSSI15.4 NSSI14.5 and 23.2adolescent/adult HC
76.9% to100%women
– 100% BPD 100% MDD, 50%PTSD,14.2% AD,7.1% ED
In andoutpatients
YesMean numberof NSSI: 308.5(BPD) and128.8 (NSSI)
85% AD, 7.1%MS
Cyberball f-MRI -Enhanced feelings of socialexclusion in patients groups-Enhanced activation in ventralanterior cingulate cortex inpatients groups-Enhanced activation indorsolateral and mPFC duringsocial inclusion in BPD
Bungert et al. (2015) 20 BPD20 HC
29.2 BPD28.7 HC
100%women
12.1 90% BPD, 10%BPD+ type II BD
25% PTSD, 35%AD, 25% SAD, 5%ED
Outpatients YesPast 90% MDD,25% PTSD;75% AD; 35%SUD
– Cyberballf-MRI
-Reduced amygdala activationduring pain after social inclusionin BPD-Association between higherrejection sensitivity and loweractivation differences duringphysical pain processing inamygdala and insula afterinclusion / exclusion in BPD
Jobst et al. (2014) 22 BPD21 HC
100% women 100%women
– 100% BPD – Not recorded No 68.1% AD ;63.6% AP ;36.3% MS
Cyberball andoxytocin andcortisol dosages
-No differences in cortisolplasma concentrations betweenBPD and controls-Negative association betweenphysical and emotional abuseand return of oxytocin levels atbaseline after social exclusion
Jobst et al. (2016) 20 BPD20 HC
30 BPD29.71 controls
100%women
11.20 100% BPD Mean BDI 32.7525% MDD15% ED
70%outpatients
No 75% AD, 70%AP, 40% MS
Cyberball andoxytocin andcortisol dosages
-No differences in cortisolplasma concentrations betweenBPD and controls-Lower oxytocin concentrationsin BPD patients withdisorganized attachmentrepresentations compared toother BPD
Olié et al. (2017) 37.6 to 39.48 14 SA, 15 PC Inpatients Cyberball f-MRI
(continued on next page)
D.J.andF.N.
Téléch
argé p
our A
nonym
ous U
ser (n/a) à H
opital S
imone V
eil Montm
oren
cy à p
artir de C
linicalK
ey.fr p
ar Elsev
ier sur sep
tembre 0
5, 2
019.
Pour u
n u
sage p
ersonnel seu
lemen
t. Aucu
ne au
tre utilisatio
n n
´est auto
risée. Copyrig
ht ©
2019. E
lsevier In
c. Tous d
roits réserv
és.
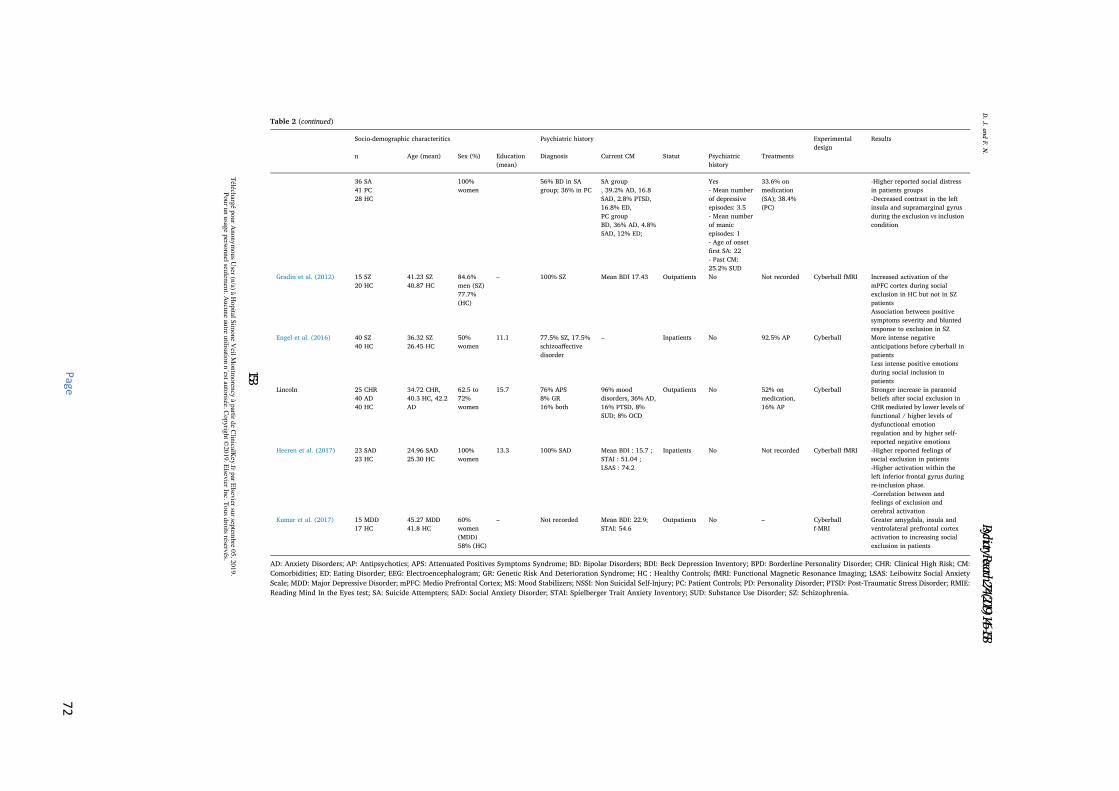
Page
72
Table 2 (continued)
Socio-demographic characteritics Psychiatric history Experimentaldesign
Results
n Age (mean) Sex (%) Education(mean)
Diagnosis Current CM Statut Psychiatrichistory
Treatments
36 SA41 PC28 HC
100%women
56% BD in SAgroup; 36% in PC
SA group, 39.2% AD, 16.8SAD, 2.8% PTSD,16.8% ED,PC groupBD, 36% AD, 4.8%SAD, 12% ED;
Yes- Mean numberof depressiveepisodes: 3.5- Mean numberof manicepisodes: 1- Age of onsetfirst SA: 22- Past CM:25.2% SUD
33.6% onmedication(SA); 38.4%(PC)
-Higher reported social distressin patients groups-Decreased contrast in the leftinsula and supramarginal gyrusduring the exclusion vs inclusioncondition
Gradin et al. (2012) 15 SZ20 HC
41.23 SZ40.87 HC
84.6%men (SZ)77.7%(HC)
– 100% SZ Mean BDI 17.43 Outpatients No Not recorded Cyberball fMRI Increased activation of themPFC cortex during socialexclusion in HC but not in SZpatientsAssociation between positivesymptoms severity and bluntedresponse to exclusion in SZ
Engel et al. (2016) 40 SZ40 HC
36.32 SZ26.45 HC
50%women
11.1 77.5% SZ, 17.5%schizoaffectivedisorder
– Inpatients No 92.5% AP Cyberball More intense negativeanticipations before cyberball inpatientsLess intense positive emotionsduring social inclusion inpatients
Lincoln 25 CHR40 AD40 HC
34.72 CHR,40.3 HC, 42.2AD
62.5 to72%women
15.7 76% APS8% GR16% both
96% mooddisorders, 36% AD,16% PTSD, 8%SUD; 8% OCD
Outpatients No 52% onmedication,16% AP
Cyberball Stronger increase in paranoidbeliefs after social exclusion inCHR mediated by lower levels offunctional / higher levels ofdysfunctional emotionregulation and by higher self-reported negative emotions
Heeren et al. (2017) 23 SAD23 HC
24.96 SAD25.30 HC
100%women
13.3 100% SAD Mean BDI : 15.7 ;STAI : 51.04 ;LSAS : 74.2
Inpatients No Not recorded Cyberball fMRI -Higher reported feelings ofsocial exclusion in patients-Higher activation within theleft inferior frontal gyrus duringre-inclusion phase.-Correlation between andfeelings of exclusion andcerebral activation
Kumar et al. (2017) 15 MDD17 HC
45.27 MDD41.8 HC
60%women(MDD)58% (HC)
– Not recorded Mean BDI: 22.9;STAI: 54.6
Outpatients No – Cyberballf-MRI
Greater amygdala, insula andventrolateral prefrontal cortexactivation to increasing socialexclusion in patients
AD: Anxiety Disorders; AP: Antipsychotics; APS: Attenuated Positives Symptoms Syndrome; BD: Bipolar Disorders; BDI: Beck Depression Inventory; BPD: Borderline Personality Disorder; CHR: Clinical High Risk; CM:Comorbidities; ED: Eating Disorder; EEG: Electroencephalogram; GR: Genetic Risk And Deterioration Syndrome; HC : Healthy Controls; fMRI: Functional Magnetic Resonance Imaging; LSAS: Leibowitz Social AnxietyScale; MDD: Major Depressive Disorder; mPFC: Medio Prefrontal Cortex; MS: Mood Stabilizers; NSSI: Non Suicidal Self-Injury; PC: Patient Controls; PD: Personality Disorder; PTSD: Post-Traumatic Stress Disorder; RMIE:Reading Mind In the Eyes test; SA: Suicide Attempters; SAD: Social Anxiety Disorder; STAI: Spielberger Trait Anxiety Inventory; SUD: Substance Use Disorder; SZ: Schizophrenia.
D.J.andF.N.
Téléch
argé p
our A
nonym
ous U
ser (n/a) à H
opital S
imone V
eil Montm
oren
cy à p
artir de C
linicalK
ey.fr p
ar Elsev
ier sur sep
tembre 0
5, 2
019.
Pour u
n u
sage p
ersonnel seu
lemen
t. Aucu
ne au
tre utilisatio
n n
´est auto
risée. Copyrig
ht ©
2019. E
lsevier In
c. Tous d
roits réserv
és.
Page 73
The relationships between acute social rejection and self-stigma arestill largely unknown. However, acute social exclusion results in greatersocial distress, more negative emotions (i.e. self-blame, more internalattributions, decreased feeling of control) and less use of functionalemotion regulation strategies in people with SMI (Staebler et al., 2011;Gratz et al., 2013; Olié et al., 2017). The response to social rejectionwas influenced by the psychiatric diagnosis and might be stigma-re-lated. In people with SZ, the results are controversial. Some studiessupported the hypothesis that reduced sensitivity to social rejectionmight be related to social cognition deficits (Gradin et al., 2012) andprotect against social alienation. However, another study found similarnegative emotions during social exclusion, less positive emotionsduring social inclusion and increased negative expectations before thetask (Engel et al., 2016). According to the authors, the decrease inpositive emotions during inclusion was related to social anhedonia andincreased negative expectations before exclusion, due to higher an-ticipatory social anxiety (Engel et al., 2016). Hypersensitivity to socialrejection and increased paranoid beliefs during social exclusion werefound in people with CHR and were mediated by difficulties withemotion regulation and self-blaming. The potential role of self-stigmaand of experienced or anticipated discrimination cannot be determined,as these variables were not recorded.
Almost all studies of BPD participants found a hypersensitivity tosocial rejection during both social exclusion and social inclusion. Thishypersensitivity was associated in some studies with enhanced P3amplitudes and with enhanced activation within the salience network(dorsal anterior cingulate cortex (dACC), dorsal medio prefrontal cortex(dmPFC) and precuneus), supporting the hypothesis of an alteredmodulation of the affective response to social rejection in people withBPD (Gutz et al., 2015; Weinbrecht et al., 2018; Ruocco et al., 2010;Domsalla et al., 2014; Brown et al., 2017). Participants with BPDshowed an enhanced activation of the amygdala when processing dis-gusted faces, this activation being associated with self-disgust. Emotionregulation difficulties were also found in people with BPD with loweramygdala deactivation and lower recruitment of the brain areas in-volved in cognitive reappraisal in HC (Koenigsberg et al., 2009). Self-stigma, anticipated social discrimination and stigma resistance mighttherefore play a role in the response to social rejection in people withBPD, but their potential role remains unknown to date. Hypersensitivityto social rejection was also found in people with MDD and SAD, withincreased difficulties recovering from social rejection in those withSAD. There were no direct correlations with stigma or self-stigma.
3.3. Predictors of the response to stigma and social rejection
Socio-demographic characteristics (age, sex, ethnicity, educationlevel), current and past psychiatric comorbidities, current psychotropicmedication, insight into illness and global functioning did not appear toinfluence the cognitive mechanisms underlying the effects of stigma orsocial rejection on people with SMI (Rusch, 2007; 2010a, 2010b, 2010c,2011a,2011b; Ruocco et al., 2010; Staebler et al., 2011; Lawrence et al.,2011; Gratz et al., 2013; Raij et al., 2014; Brown et al., 2017; Ernstet al., 2018; Euler et al., 2018). Group identification, implicit shame-related self-associations and implicit self-guilt did however contributeto self-stigma and to a lesser ability to resist stigma (Rusch, 2010a,2010b, 2010c). The endorsement of genetic causal attributions aboutmental illness increased implicit self-guilt in individuals with SMI(Rusch 2010a) which has implications when designing anti-stigmacampaigns or psychoeducation interventions for people with SMI(Rusch, 2010a). The psychiatric diagnosis did not influence implicitstigma-related self-negative associations in people with SMI (Rusch2010a, 2010b, 2010c, 2011a). It did however influence the response tosocial rejection (Rusch, 2007; Staebler et al., 2011; Renneberg et al.,2012; Gratz et al., 2013; Gutz et al., 2015, 2016; Domsalla et al., 2014;De Panfilis, 2015; Engel et al., 2016; Weinbrecht et al., 2018). Thisconcurs with the literature on explicit self-stigma, which is more
frequent in people with SZ (Brohan et al., 2010,2011) but affects clin-ical and psychosocial outcomes in all people with SMI (Livingston andBoyd, 2010). Psychiatric symptoms influenced self-perceptions assymptomatic BD participants had more implicit negative self-associa-tions (Jabben et al., 2014). The number of BPD features influencedsocial-cognitive performance after social rejection in people with BPDand the severity of positive symptoms affected the response to socialrejection in participants with SZ (Gradin et al., 2012). Illness durationaffected negatively stigma resistance (Raij et al., 2014). There were nosignificant differences between inpatients and outpatients with SZ intheir response to social rejection (Engel et al., 2016). The participants’social networks did not influence the response to social exclusion inpeople with BPD (Gratz et al., 2013). Baseline non-specific distress wasassociated with elevated distress during social exclusion (Gratz et al.,2013) suggesting that chronic social rejection might affect the responseto acute social rejection and contribute to social alienation (Gutz et al.,2016). A history of trauma influenced the biological and behaviouralresponse to social rejection (Jobst et al., 2015, 2016; Ernst et al., 2018)and was associated with more shame-related self-associations in peoplewith BPD (Rusch et al., 2011a). However, emotion processing whenconfronted with disgusted faces (Schienle et al., 2015) and when dis-tancing from negative social cues (Koenigsberg et al., 2009) were notaffected by a history of trauma. A history of suicidal acts influenced theresponse to social rejection in people with SMI (Olié et al., 2017).
4. Discussion
Overall, the results of the present review can be summarized asfollows: Acute social rejection and its consequences on individuals withSMI were the most documented area (25 studies). Hypersensitivity toacute social rejection was found in almost all the studies includingpeople with SMI and was associated with more self-related negativeemotions and with the use of less functional and more dysfunctionalemotion regulation strategies. Enhanced activation within the saliencenetwork was associated with hypersensitivity to acute social rejection.Hypersensitivity to social rejection resulted in an increase in paranoidbeliefs in people with CHR. Reduced sensitivity to acute social rejectionand reduced activation within the salience network were, however,found in people with SZ and could be related to social cognition deficitsor act as a protection mechanism against social alienation. Individualswith SMI under-performed in cognitive and social cognitive tasks whenplaced in stigma-related environments. Stigma resistance was asso-ciated with enhanced activation of the rostro-ventral medio prefrontalcortex (rvmPFC) and decreased activation of the amygdala in peoplewith SZ. Psychiatric symptoms, illness duration and baseline non-spe-cific distress influenced the response to acute social rejection or stigma.The potential role of chronic social discrimination and its effects onpeople with SMI should be further investigated.
The existing body of research on the cognitive neuroscience ofstigma in individuals with SMI has several limitations. Only a fewstudies directly addressed the consequences of self-stigma on peoplewith SMI. The samples, methods, experimental paradigms and reportedoutcomes used in the studies were heterogeneous and therefore difficultto compare. The results mostly came from individual studies that havenot yet been replicated. The cognitive and neural correlates of personalstigma remain largely unknown and should therefore be further in-vestigated. Neuroimaging studies may add to the knowledge about theneural mechanisms underlying personal stigma and stigma resistance.Personal stigma is however a complex construct difficult to modelprecisely in cognitive neuroscience. Studying the effects of experiencedand anticipated social discrimination on brain functional connectivityand biological inflammatory response in persons with SMI might im-prove the understanding of the mechanisms underlying personal stigmabut future research will be needed.
D. J. and F. N.
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.
Page 74
4.1. Relationships between acute social discrimination and self-stigma
The relationships between acute social rejection and self-stigma areunclear, as most studies did not record self-stigma. Implicit and explicitself-stigma predicted subjective quality of life (Rusch, 2010c;Livingston and Boyd, 2010). As expected, individuals with SMI under-performed in cognitive and social cognitive tasks under stigma-relatedconditions (stereotype threat or acute social rejection). This supportsprevious findings that explicit self-stigma is associated with lowercognitive, social and vocational functioning (Yanos et al., 2010;Hill and Startup, 2013). Individuals with SMI showed higher rejectionexpectancy and anticipatory anxiety before social exclusion. They hadalso more self-related negative emotions during social exclusion and anincreased tendency to use avoidant strategies after being excludedwhen compared with HC (Gratz et al., 2013; Gutz et al., 2015,2016;Engel et al., 2016). This may back up previous research where antici-pated social discrimination mediated the relationship between experi-enced discrimination and self-stigma in individuals with SMI(Quinn et al., 2015), and where self-stigma predicted social anxiety inpeople with SZ (Lysaker et al., 2010) and was associated with avoidantcoping strategies (Vauth et al., 2007). Anticipated social discriminationand self-stigma may influence the response to social rejection and theirpotential role should therefore be investigated further. In people withCHR, social exclusion was associated with hypersensitivity to acutesocial rejection and increased paranoid beliefs that were mediated byemotion regulation difficulties and self-blaming. This might be relatedto self-stigma, associated with hypersensitivity to social rejection andparanoid delusions in a cognitive model of self-stigma in psychosis(Wood et al., 2017). Two studies found reduced sensitivity to socialrejection and reduced activation within the salience network in peoplewith SZ (Gradin et al., 2012). This might relate to social cognitiondeficits (Gradin et al., 2012) and protect against social alienation. Itmight, however, also more generally reflect the salience network dys-function described in people with SZ (Palaniyappan et al., 2012). The“insight paradox” described by P. Lysaker (association between de-pression and good insight) and its relationships with social cognitionand emotion regulation abilities might also explain the differencesobserved in people with SZ (Lysaker et al., 2007,2013). The presence(or the absence) of metacognitive deficits impeding one's abilities todeflect negative beliefs about oneself can also be a potential explainingfactor (Nabors et al., 2014). The relationships between social cognition,metacognitive abilities, self-stigma and the response to acute socialrejection should therefore be further investigated.
Although very few studies reported on self-stigma in BPD, there issome evidence supporting its potential role in moderating the responseto acute social rejection. Participants with BPD showed an enhancedactivation of the amygdala when processing disgusted faces, this acti-vation being associated with self-disgust. As implicit self-disgust con-tributed to self-stigma by increasing the perceived legitimacy of dis-crimination and by decreasing the ability to resist stigma(Rusch, 2010b), this hypersensitivity to social rejection in people withBPD might be stigma-related. Emotion regulation difficulties in peoplewith BPD were associated with lower deactivation of the amygdala andlower recruitment of the brain areas involved in cognitive reappraisal inHC (Koenigsberg et al., 2009). Although affect dysregulation is a keyfeature of BPD, it has been suggested that this mechanism might also berelated to the internalization of psychiatric disorders or early-life mal-treatment (Gunderson et al., 2018). In contrast stigma resistance wasassociated with preserved cognitive performance in people with SZ. Thef-MRI showed SR to be associated with enhanced activation of therostro-ventral medio prefrontal cortex (rvmPFC) and decreased amyg-dala activation in people with SZ after controlling for global func-tioning, insight and depressive symptoms (Raij et al., 2014). As thervmPFC was identified as a regulator of the affective response to socialexclusion (Eisenberger, 2004) this could be one of the mechanismsbehind stigma resistance (Raij et al., 2014). Self-stigma, anticipated
social discrimination, stigma resistance, and social cognition andemotion regulation ability might influence the response to acute socialrejection and their potential role should be investigated in future stu-dies.
4.2. Implications for future research
Several predictors of the response to stigma or acute social rejectionwere identified. Self-stigma was influenced by group identification,implicit shame-related self-associations and implicit self-guilt, but notby psychiatric diagnosis, psychiatric comorbidities or socio-demo-graphic characteristics. The association between implicit shame-relatedself-associations and self-stigma is also found in a previous study whereexplicit shame-proneness was identified as a mediator between insightand self-stigma (Hasson-Ohayon et al., 2012). Stigma resistance wasnegatively affected by illness duration in accordance with previousresults (Sibitz et al., 2011a). The response to social rejection was notinfluenced by the participants’ status or social network in people withSZ and BPD (Gratz et al., 2013; Engel et al., 2016). Further investigationis however needed, as inpatient status and reduced social network wereassociated with decreased stigma resistance in people with SZ(Sibitz et al., 2011a,2011b). The role of the psychiatric diagnosis inmoderating the response to acute social rejection remains unclear, as allthe studies were diagnosis-specific. The severity of the psychiatricsymptoms influenced the response to acute social rejection. The numberof BPD features influenced social-cognitive performance after socialrejection in people with BPD and the severity of positive symptomsaffected the response to social rejection in participants with SZ(Gradin et al., 2012). This might be stigma-related as self-blaming,social threat processing dysfunctions and self-stigma can underpinparanoid beliefs in people with psychosis (Corlett et al., 2010;Wood et al., 2017) and explicit self-stigma is associated with increasedseverity of positive and depressive symptoms (Livingston and Boyd,2010; Cerit et al., 2012).
Baseline non-specific distress was associated with elevated distressduring social exclusion (Gratz et al., 2013) suggesting that chronic so-cial rejection might affect the response to acute social rejection andcontribute to the development of social alienation (Gutz, 2016). How-ever, research on chronic social rejection is extremely limited in HC andnon-existent in people with SMI. Chronic social rejection was in-vestigated in people without SMI, but confronted with prolonged os-tracism (social rejection > 3-months; Williams, 2009; Riva et al.,2014). In contrast to acute social rejection, chronic social rejection wasassociated with feelings of resignation, helplessness, unworthiness andlow self-worth and ultimately with social alienation and depression(Williams, 2009; Riva et al., 2014). An increased sensitivity to acutesocial exclusion was also found in people suffering from chronic socialrejection (Williams, 2009; Riva et al., 2014). In people at risk of beingostracized, enhanced spontaneous amygdala resting-state activity andincreased connectivity with the salience network were associated with agreater exposure to discrimination, independently of ethnicity, sex orcurrent psychiatric comorbidities. Elevated pro-inflammatory cytokines(Il-6 and TNF-alpha) were associated with enhanced dorsal ACC andanterior insula activation after acute social rejection in HC(Slavich et al., 2010). Exposure to everyday social stressors and to so-cial rejection was associated in HC with elevated inflammatory activityand with MDD (Slavich et al., 2010, 2014; Beatty et al., 2014; VanDyke, 2017). Elevated CRP levels were found in people with SZ, BD orMDD (Miller et al., 2014; Horsdal et al., 2017) and associated withmore severe depressive symptoms in people with SZ (Faugere et al.,2018). However, the correlations between inflammatory activity, ex-periences of discrimination and self-stigma in people with SMI have notbeen investigated to date. Future research should therefore investigatethe potential role of current, past and anticipated social discriminationin the modulation of biological and neural responses to stigma or acutesocial rejection in people with SMI.
D. J. and F. N.
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.
Page 75
In conclusion, the studies conducted in the last decade have im-proved our understanding of the cognitive and neural correlates ofstigma, self-stigma and acute social rejection in people with SMI.Several potential mechanisms and predictors have been identified andshould be further documented. Future research should investigate theassociations between self-stigma, performance under ST conditions andthe responses to acute and chronic social rejection in people with SMI.Chronic social rejection in people with mental illness and its cognitive,biological and neural correlates should also be further investigated.
Acknowledgement
The authors would like to thank Mrs. Kim Barrett for proofreadingthe manuscript.
Role of the funding source
This research did not receive any specific grant from fundingagencies in the public, commercial, or not-for-profit sectors.
Conflicts of interests
None.
References
Angermeyer, M.C., Millier, A., Rémuzat, C., Refaï, T., Toumi, M., 2013. Attitudes andbeliefs of the French public about schizophrenia and major depression: results from avignette-based population survey. BMC Psychiatry 13, 313. https://doi.org/10.1186/1471-244X-13-313.
Beatty, D.L., Matthews, K.A., Bromberger, J.T., Brown, C., 2014. Everyday discriminationprospectively predicts inflammation across 7-Years in racially diverse midlife women:study of women's health across the nation. J. Soc. Issues 70 (2), 298–314.
Bolling, D.Z., Pitskel, N.B., Deen, B., Crowley, M.J., McPartland, J.C., Kaiser, M.D., Wyk,B.C., Wu, J., Mayes, L.C., Pelphrey, K.A., 2011. Enhanced neural responses to ruleviolation in children with autism: a comparison to social exclusion. Dev. Cogn.Neurosci. 1 (3), 280–294. https://doi.org/10.1016/j.dcn.2011.02.002.
Brohan, E., Elgie, R., Sartorius, N., Thornicroft, G., GAMIAN-Europe Study Group., 2010.Self-stigma, empowerment and perceived discrimination among people with schi-zophrenia in 14 European countries: the GAMIAN-Europe study. Schizophr. Res. 122(1–3), 232–238. https://doi.org/10.1016/j.schres.2010.02.1065.
Brohan, E., Gauci, D., Sartorius, N., Thornicroft, G., GAMIAN-Europe Study Group., 2011.Self-stigma, empowerment and perceived discrimination among people with bipolardisorder or depression in 13 European countries: the GAMIAN-Europe study. J.Affect. Disord. 129 (1–3), 56–63. https://doi.org/10.1016/j.jad.2010.09.001.
Brown, R.C., Plener, P.L., Groen, G., Neff, D., Bonenberger, M., Abler, B., 2017.Differential neural processing of social exclusion and inclusion in adolescents withnon-suicidal self-injury and young adults with borderline personality disorder. Front.Psychiatry. 8, 267. https://doi.org/10.3389/fpsyt.2017.00267.
Bungert, M., Koppe, G., Niedtfeld, I., Vollstädt-Klein, S., Schmahl, C., Lis, S., Bohus, M.,2015. Pain processing after social exclusion and its relation to rejection sensitivity inborderline personality disorder. PLoS One 10 (8), e0133693. https://doi.org/10.1371/journal.pone.013369.
Cerit, C., Filizer, A., Tural, Ü., Tufan, A.E., 2012. Stigma: a core factor on predictingfunctionality in bipolar disorder. Compr. Psychiatry 53 (5), 484–489. https://doi.org/10.1016/j.comppsych.2011.08.010. Epub 2011 Oct 27.
Corlett, P.R., Taylor, J.R., Wang, X.J., Fletcher, P.C., Krystal, J.H., 2010. Toward a neu-robiology of delusions. Prog. Neurobiol. 92, 345–369.
Corrigan, P.W., Watson, A.C., 2002. Understanding the impact of stigma on people withmental illness. World Psychiatry 1 (1), 16–20.
De Panfilis, C., Riva, P., Preti, E., Cabrino, C., Marchesi, C., 2015. When social inclusion isnot enough: implicit expectations of extreme inclusion in borderline personalitydisorder. . Personal. Disord. Theory Res. Treat. 6 (4), 301–309 1949-2715/15/$12.00.
Derks, B., Inzlicht, M., Kang, S., 2008. The neuroscience of stigma and stereotype threat.Group Process. Intergroup Relat. 11 (2), 163–181. https://doi.org/10.1177/1368430207088036.
Domsalla, M., Koppe, G., Niedtfeld, I., Vollstädt-Klein, S., Lis, S., 2014. Cerebral proces-sing of social rejection in patients with borderline personality disorder. Scan 9,1789–1797. https://doi.org/10.1093/scan/nst176.
Eisenberger, N.I., Lieberman, M.D., 2004. Why rejection hurts: a common neural alarmsystem for physical and social pain. Trends Cogn. Sci. 8 (7), 294–300. https://doi.org/10.1016/j.tics.2004.05.010.
Ellison, N., Mason, O., Scior, K., 2013. Bipolar disorder and stigma: a systematic review ofthe literature. J. Affect. Disord. 151 (3), 805–820. https://doi.org/10.1016/j.jad.2013.08.014.
Engel, M., Fritzsche, A., Lincoln, T.M., 2016. Anticipation and experience of emotions inpatients with schizophrenia and negative symptoms. An experimental study in a
social context. Schizophr. Res. 170 (1), 191–197. https://doi.org/10.1016/j.schres.2015.11.028.
Ernst, M., Mohr, H.M., Schhött, M., Rickmeyer, C., Fischmann, T., Leuzinger-Bohleber,M., Weiß, H., Grabhorn, R., 2018. The effects of social exclusion on response in-hibition in borderline personality disorder and major depression. Psychiatry. Res.262, 333–339. https://doi.org/10.1016/j.psychres.2017.03.034.
Euler, S., Wrege, J., Busmann, M., Lindenmeyer, H.J., Sollberger, D., Lang, U.E., Gaab, J.,Walter, M., 2018. Exclusion-proneness in borderline personality disorder inpatientsimpairs alliance in mentalization-based group therapy. Front. Psychol. 9, 824.https://doi.org/10.3389/fpsyg.2018.00824.
Farrelly, S., Clement, S., Gabbidon, J., Jeffery, D., Dockery, L., Lassman, F., Brohan, E.,Henderson, R.C., Williams, P., Howard, L.M., Thornicroft, G., MIRIAD study group.,2014. Anticipated and experienced discrimination amongst people with schizo-phrenia, bipolar disorder and major depressive disorder: a cross sectional study. BMCPsychiatry 14, 157. https://doi.org/10.1186/1471-244X-14-157.
Faugere, M., Micoulaud-Franchi, J.A., Faget-Agius, C., Lançon, C., Cermolacce, M.,Richieri, R., 2018. High C-reactive protein levels are associated with depressivesymptoms in schizophrenia. J. Affect. Disord. 225, 671–675. https://doi.org/10.1016/j.jad.2017.09.004.
Firmin, R.L., Luther, L., Lysaker, P.H., Minor, K.S., Salyers, M.P., 2016. Stigma resistanceis positively associated with psychiatric and psychosocial outcomes: a meta-analysis.Schizophr. Res. 175 (1–3), 118–128. https://doi.org/10.1016/j.schres.2016.03.008.
Gerlinger, G., Hauser, M., De Hert, M., Lacluyse, K., Wampers, M., Correll, C.U., 2013.Personal stigma in schizophrenia spectrum disorders: a systematic review of pre-valence rates, correlates, impact and interventions. World Psychiatry 12 (2),155–164. https://doi.org/10.1002/wps.20040.
Gradin, V.B., Waiter, G., Kumar, P., Stickle, C., Milders, M., Matthews, K., Reid, I., Hall,J., Steele, J.D., 2012. Abnormal neural responses to social exclusion in schizophrenia.PLoS One 7 (8), e42608. https://doi.org/10.1371/journal.pone.0042608.
Gratz, K.L., Dixon-Gordon, K.L., Breetz, A., Tull, M., 2013. A laboratory-based examina-tion of responses to social rejection in borderline personality disorder: the mediatingrole of emotion dysregulation. J. Pers. Disord. 27 (3), 426. https://doi.org/10.1521/pedi.2013.27.2.157.
Greenwald, A.G., Poehlman, T.A., Uhlmann, E.L., Banaji, M.R., 2009. Understanding andusing the Implicit Association Test: III. Meta-analysis of predictive validity. J. Pers.Soc. Psychol. 97 (1), 17–41. https://doi.org/10.1037/a0015575.
Gunderson, J.G., Herpertz, S.C., Skodol, A.E., Torgersen, S., Zanarini, M.C., 2018.Borderline personality disorder. Nat. Rev. Dis. Primers 4, 18029. https://doi.org/10.1038/nrdp.2018.29.
Gutz, L., Renneberg, B., Roepke, S., Niedeggen, M., 2015. Neural processing of socialparticipation in borderline personality disorder and social anxiety disorder. J.Abnorm. Psychol. 124 (2), 421–431. https://doi.org/10.1037/a0038614.
Gutz, L., Roepke, S., Renneberg, B., 2016. Cognitive and affective processing of socialexclusion in borderline personality disorder and social anxiety disorder. Behav. Res.Ther. 87, 70–75. https://doi.org/10.1016/j.brat.2016.08.020.
Hartgerink, C.H., van Beest, I., Wicherts, J.M., Williams, K.D., 2015. The ordinal effects ofostracism: a meta-analysis of 120 Cyberball studies. PLoS One 10 (5), e0127002.https://doi.org/10.1371/journal.pone.0127002.
Hasson-Ohayon, I., Ehrlich-Ben Or, S., Vahab, K., Amiaz, R., Weiser, M., Roe, D., 2012.Insight into mental illness and self-stigma: the mediating role of shame proneness.Psychiatry Res. 200 (2–3), 802–806. https://doi.org/10.1016/j.psychres.2012.07.038.
Heenan, A., Best, M.W., Ouellette, S.J., Meiklejohn, E., Troje, N.F., Bowie, C.R., 2014.Assessing threat responses towards the symptoms and diagnosis of schizophreniausing visual perceptual biases. Schizophr. Res. 159 (1), 238–242. https://doi.org/10.1016/j.schres.2014.07.024.
Heeren, A., Dricot, L., Billieux, J., Philippot, P., Grynberg, D., de Timary, P., Maurage, P.,2017. Correlates of social exclusion in social anxiety disorder: an fMRI study. Sci.Rep. 7 (1), 260. https://doi.org/10.1038/s41598-017-00310-9.
Henry, J.D., von Hippel, C., Shapiro, L., 2010. Stereotype threat contributes to socialdifficulties in people with schizophrenia. Br. J. Clin. Psychol. 49 (1), 31–41. https://doi.org/10.1348/014466509x421963.
Hill, K., Startup, M., 2013. The relationship between internalized stigma, negativesymptoms and social functioning in schizophrenia: the mediating role of self-efficacy.Psychiatry. Res. 206 (2–3), 151–157. https://doi.org/10.1016/j.psychres.2012.09.056.
Horsdal, H.T., Köhler-Forsberg, O., Benros, M.E., Gasse, C., 2017. C-reactive protein andwhite blood cell levels in schizophrenia, bipolar disorders and depression - associa-tions with mortality and psychiatric outcomes: a population-based study. Eur.Psychiatry. 44, 164–172. https://doi.org/10.1016/j.eurpsy.2017.04.012.
Jabben, N., de Jong, P.J., Kupka, R.W., Glashouwer, K.A., Nolen, W.A., Penninx, B.W.,2014. Implicit and explicit self-associations in bipolar disorder: a comparison withhealthy controls and unipolar depressive disorder. Psychiatry Res. 215 (2), 329–334.https://doi.org/10.1016/j.psychres.2013.11.030.
Jobst, A., Albert, A., Bauriedl-Schmidt, C., Mauer, M.C., Renneberg, B., Buchheim, A.,Sabass, L., Falkai, P., Zill, P., Padberg, F., 2014. Social exclusion leads to divergentchanges of oxytocin levels in borderline patients and healthy subjects. Psychother.Psychosom. 83 (4), 252–254. https://doi.org/10.1159/000358526.
Jobst, A., Sabass, L., Palagyi, A., Bauriedl-Schmidt, C., Mauer, M.C., Sarubin, N.,Buchheim, A., Renneberg, B., Falkai, P., Zill, P., Padberg, F., 2015. Effects of socialexclusion on emotions and oxytocin and cortisol levels in patients with chronic de-pression. J. Psychiatr. Res. 60, 170–177. https://doi.org/10.1016/j.jpsychires.2014.11.001.
Jobst, A., Padberg, F., Mauer, M.C., Daltrozzo, T., Bauriedl-Schmidt, C., Sabass, L.,Sarubin, N., Falkai, P., Renneberg, B., Zill, P., Gander, M., Buchheim, A., 2016. LowerOxytocin Plasma Levels in Borderline Patients with Unresolved Attachment
D. J. and F. N.
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.
Page 76
Representations. Front. Hum. Neurosci. 10, 125. https://doi.org/10.3389/fnhum.2016.00125.
Kawamoto, T., Onoda, K., Nakashima, K., Nittono, H., Yamaguchi, S., Ura, M., 2012. Isdorsal anterior cingulate cortex activation in response to social exclusion due toexpectancy violation? An fMRI study. Front. Evol. Neurosci. 4, 11. https://doi.org/10.3389/fnevo.2012.00011.
Koenigsberg, H.W., Fan, J., Ochsner, K.N., Lui, X., Guise, K.G., Pizzarello, S., Dorantes, C.,Guerreri, S., Tecuta, L., Goodman, M., New, A., Siever, L.J., 2009. Neural correlatesof the use of psychological distancing to regulate responses to negative social cues: astudy of patients with borderline personality disorder. Biol. Psychiatry 66 (9),854–863. https://doi.org/10.1016/j.biopsych.2009.06.010.
Krendl, A.C., Macrae, C.N., Kelley, W.M., Fugelsang, J.A., Heatherton, T.F., 2006. Thegood, the bad, and the ugly: an fMRI investigation of the functional anatomic cor-relates of stigma. Soc. Neurosci. 1 (1), 5–15. https://doi.org/10.1080/17470910600670579.
Krendl, A.C., Moran, J.M., Ambady, N., 2013. Does context matter in evaluations ofstigmatized individuals? An fMRI study. Soc. Cogn. Affect. Neurosci. 8 (5), 602–608.https://doi.org/10.1093/scan/nss037.
Kumar, P., Waiter, G.D., Dubois, M., Milders, M., Reid, I., Steele, J.D., 2017. Increasedneural response to social rejection in major depression. Depress. Anxiety. 34 (11),1049–1056. https://doi.org/10.1002/da.22665.
Lasalvia, A., Zoppei, S., Van Bortel, T., Bonetto, C., Cristofalo, D., Wahlbeck, K., Bacle,S.V., Van Audenhove, C., van Weeghel, J., Reneses, B., Germanavicius, A., Economou,M., Lanfredi, M., Ando, S., Sartorius, N., Lopez-Ibor, J.J., Thornicroft, G., ASPEN/INDIGO Study Group., 2013. Global pattern of experienced and anticipated dis-crimination reported by people with major depressive disorder: a cross-sectionalsurvey. Lancet 381, 55–62.
Lawrence, K.A., Chanen, A.M., Allen, J.S., 2011. The effect of ostracism upon mood inyouth with Borderline Personality Disorder. J. Personal. Disord. 25 (5), 702–714.https://doi.org/10.1521/pedi.2011.25.5.702.
Livingston, J.D., Boyd, J.E., 2010. Correlates and consequences of internalized stigma forpeople living with mental illness: a systematic review and meta-analysis. Soc. Sci.Med. 71 (12), 2150–2161. https://doi.org/10.1016/j.socscimed.2010.09.030.
Lysaker, P.H, Roe, D., Yanos, P.T., 2007. Toward understanding the insight paradox:internalized stigma moderates the association between insight and social functioning,hope, and self-esteem among people with schizophrenia spectrum disorders.Schizophr. Bull. 33 (1), 192–199.
Lysaker, P.H., Yanos, P.T., Outcalt, J., Roe, D., 2010. Association of stigma, self-esteem,and symptoms with concurrent and prospective assessment of social anxiety inschizophrenia. Clin. Schizophr. Relat. Psychoses 4 (1), 41–48. https://doi.org/10.3371/CSRP.4.1.3.
Lysaker, P.H., Vohs, J., Hasson-Ohayon, I., Kukla, M., Wierwille, J., Dimaggio, G., 2013.Depression and insight in schizophrenia: comparisons of levels of deficits in socialcognition and metacognition and internalized stigma across three profiles. Schizophr.Res. 148 (1–3), 18–23. https://doi.org/10.1016/j.schres.2013.05.025.
Miller, B.J., Culpepper, N., Rapaport, M.H., 2014. C-reactive protein levels in schizo-phrenia: a review and meta-analysis. Clin. Schizophr. Relat. Psychoses. 7 (4),223–230. https://doi.org/10.3371/CSRP.MICU.020813.
Moor, B.G., Güroğlu, B., Op de Macks, Z.A., Serge, A.R.B., Rombouts, S.A.R.B., Van derMolen, M.W., Crone, E.A., 2012. Social exclusion and punishment of excluders:neural correlates and developmental trajectories. NeuroImage 59 (2012), 708–717.https://doi.org/10.1016/j.neuroimage.2011.07.02814.
Moritz, S., Spirandelli, K., Happach, I., Lion, D., Berna, F., 2018. Dysfunction by dis-closure? Stereotype threat as a source of secondary neurocognitive malperformancein obsessive-compulsive disorder. J. Int. Neuropsychol. Soc. 24 (6), 584–592. https://doi.org/10.1017/S1355617718000097.
Nabors, L.M., Yanos, P.T., Roe, D., Hasson-Ohayon, I., Leonhardt, B.L., Buck, K.D.,Lysaker, P.H., 2014. Stereotype endorsement, metacognitive capacity, and self-es-teem as predictors of stigma resistance in persons with schizophrenia. Compr.Psychiatry 55, 792–798. https://doi.org/10.1016/j.comppsych.2014.01.011.
Olié, E., Jollant, F., Deverdun, J., de Champfleur, N.M., Cyprien, F., Le Bars, E., Mura, T.,Bonafé, A., Courtet, P., 2017. The experience of social exclusion in women with ahistory of suicidal acts: a neuroimaging study. Sci. Rep. 7 (1), 89. https://doi.org/10.1038/s41598-017-00211-x.
Palaniyappan, L., White, T.P., Liddle, P.F., 2012. The concept of salience network dys-function in schizophrenia: from neuroimaging observations to therapeutic opportu-nities. Curr. Top. Med. Chem. 12 (21), 2324–2338.
Penn, D.L., Kohlmaier, J.R., Corrigan, P.W., 2000. Interpersonal factors contributing tothe stigma of schizophrenia: social skills, perceived attractiveness, and symptoms.Schizophr. Res. 45 (1–2), 37–45.
Peris, T.S., Teachman, B.A., Nosek, B.A., 2008. Implicit and explicit stigma of mentalillness: links to clinical care. J. Nerv. Ment. Dis. 196 (10), 752–760. https://doi.org/10.1097/NMD.0b013e3181879dfd.
Quinn, D.M., Williams, M.K., Weisz, B.M., 2015. From discrimination to internalizedmental illness stigma: the mediating roles of anticipated discrimination and antici-pated stigma. Psychiatr. Rehabil. J. 38 (2), 103–108. https://doi.org/10.1037/prj0000136.
Raij, T.T., Korkeila, J., Joutsenniemi, K., Saarni, S.I., Riekki, T.J., 2014. Association ofstigma resistance with emotion regulation - functional magnetic resonance imagingand neuropsychological findings. Compr. Psychiatry. 55 (3), 727–735. https://doi.org/10.1016/j.comppsych.2013.10.010.
Reihl, K.M., Hurley, R.A., Taber, K.H., 2015. Neurobiology of implicit and explicit bias:implications for clinicians. J. Neuropsychiatr. Clin. Neurosci. 27 (4), A6–253. https://doi.org/10.1176/appi.neuropsych.15080212.
Renneberg, B., Herm, K., Hahn, A., Staebler, K., Lammers, C.H., Roepke, S., 2012.Perception of social participation in borderline personality disorder. Clin. Psychol.
Psychother. 19, 473–480. https://doi.org/10.1002/cpp.772.Riva, P., Wesselmann, E.D., Wirth, J.H., Carter-Sowell, A.R., Williams, K.D., 2014. When
pain does not heal: the common antecedents and consequences of chronic social andphysical pain. Basic Appl. Soc. Psychol. 36, 329–346. https://doi.org/10.1080/01973533.2014.917975.
Ruocco, A.C., Medaglia, J.D., Tinker, J.R., Ayaz, H., Forman, E.M., Newman, C.F.,Williams, J.M., Hillary, F.G., Platek, S.M., Onaral, B., Chute, D.L., 2010. Medialprefrontal cortex hyperactivation during social exclusion in borderline personalitydisorder. Psychiatry Res. Neuroimag. 181 (3), 233–236. https://doi.org/10.1016/j.pscychresns.2009.12.001.
Rüsch, N., Lieb, K., Göttler, I., Hermann, C., Schramm, E., Richter, H., Jacob, G.A.,Corrigan, P.W., Bohus, M., 2007. Shame and implicit self-concept in women withborderline personality disorder. Am. J. Psychiatry. 164 (3), 500–508. https://doi.org/10.1176/ajp.2007.164.3.500.
Rüsch, N., Todd, A.R., Bodenhausen, G.V., Olschewski, M., Corrigan, P.W., 2010a.Automatically activated shame reactions and perceived legitimacy of discrimination:a longitudinal study among people with mental illness. J. Behav. Ther. Exp.Psychiatry 41 (1), 60–63. https://doi.org/10.1016/j.jbtep.2009.10.002.
Rüsch, N., Todd, A.R., Bodenhausen, G.V., Corrigan, P.W., 2010b. Biogenetic models ofpsychopathology, implicit guilt, and mental illness stigma. Psychiatry Res. 179 (3),328–332. https://doi.org/10.1016/j.psychres.2009.09.010.
Rüsch, N., Corrigan, P.W., Todd, A.R., Bodenhausen, G.V., 2010c. Implicit self-stigma inpeople with mental illness. J. Nerv. Ment. Dis. 198 (2), 150–153. https://doi.org/10.1097/NMD.0b013e3181cc43b5.
Rüsch, N., Schulz, D., Valerius, G., Steil, R., Bohus, M., Schmahl, C., 2011a. Disgust andimplicit self-concept in women with borderline personality disorder and posttrau-matic stress disorder. Eur. Arch. Psychiatry Clin. Neurosci. 261 (5), 369–376. https://doi.org/10.1007/s00406-010-0174-2.
Rüsch, N., Corrigan, P.W., Todd, A.R., Bodenhausen, G.V., 2011b. Automatic stereotypingagainst people with schizophrenia, schizoaffective and affective disorders. PsychiatryRes. 186 (1), 34–39. https://doi.org/10.1016/j.psychres.2010.08.024.
Schienle, A., Wabnegger, A., Schöngassner, F., Leutgeb, V., 2015. Effects of personal spaceintrusion in affective contexts: an fMRI investigation with women suffering fromborderline personality disorder. Soc. Cogn. Affect. Neurosci. 10 (10), 1424–1428.https://doi.org/10.1093/scan/nsv034.
Shapiro, J.R., Neuberg, S.L., 2007. From stereotype threat to stereotype threats: im-plications of a multi-threat framework for causes, moderators, mediators, con-sequences, and interventions. Pers. Soc. Psychol. Rev. 11 (2), 107–130. https://doi.org/10.1177/1088868306294790.
Shapiro, J.R., 2011. Different groups, different threats: a multi-threat approach to theexperience of stereotype threats. Pers. Soc. Psychol. Bull. 37 (4), 464–480. https://doi.org/10.1177/0146167211398140.
Sibitz, I., Amering, M., Unger, A., Seyringer, M.E., Bachmann, A., Schrank, B., Benesch,T., Schulze, B., Woppmann, A., 2011a. The impact of the social network, stigma andempowerment on the quality of life in patients with schizophrenia. Eur. Psychiatry 26(1), 28–33. https://doi.org/10.1016/j.eurpsy.2010.08.010.
Sibitz, I., Unger, A., Woppmann, A., Zidek, T., Amering, M., 2011b. Stigma resistance inpatients with schizophrenia. Schizophr. Bull. 37 (2), 316–323. https://doi.org/10.1093/schbul/sbp048.
Slavich, G.M., Way, B.M., Eisenberger, N.I., Taylor, S.E., 2010. Neural sensitivity to socialrejection is associated with inflammatory responses to social stress. Proc. Natl. Acad.Sci. USA. 107 (33), 14817–14822. https://doi.org/10.1073/pnas.1009164107.
Slavich, G.M., Irwin, M.R., 2014. From stress to inflammation and major depressivedisorder: a social signal transduction theory of depression. Psychol. Bull. 140 (3),774–815. https://doi.org/10.1037/a0035302.
Staebler, K., Renneberg, B., Stopsack, M., Fiedler, P., Weiler, M., Roepke, S., 2011. Facialemotional expression in reaction to social exclusion in borderline personality dis-order. Psychol. Med. 41 (9), 1929–1938. https://doi.org/10.1017/S0033291711000080.
Stull, L.G., McGrew, J.H., Salyers, M.P., Ashburn-Nardo, L., 2013. Implicit and explicitstigma of mental illness: attitudes in an evidence-based practice. J. Nerv. Ment. Dis.201 (12), 1072–1079. https://doi.org/10.1097/NMD.0000000000000056.
Substance Abuse and Mental Health Services Administration (SAMHSA), 2014. Resultsfrom the 2013 National Survey on Drug Use and Health: mental Health Findings.NSDUH Series H-49, HHS Publication No. (SMA) 14-4887. Substance Abuse andMental Health Services Administration, Rockville, MD.
Teachman, B.A., Wilson, J.G., Komarovskaya, I., 2006. Implicit and explicit stigma ofmental illness in diagnosed and healthy samples. J. Soc. Clin. Psychol. 25 (1), 75–95.
Thoits, P.A., 2011. Mechanisms linking social ties and support to physical and mentalhealth. J. Health. Soc. Behav. 52 (2), 145–161. https://doi.org/10.1177/0022146510395592.
Thornicroft, G., Brohan, E., Rose, D., Sartorius, N., Leese, M., INDIGO Study Group, 2009.Global pattern of experienced and anticipated discrimination against people withschizophrenia: a cross-sectional survey. Lancet 373 (9661), 408–415. https://doi.org/10.1016/S0140-6736(08)61817-6.
Van Dyke, M.E., Vaccarino, V., Dunbar, S.B., Pemu, P., Gibbons, G.H., Quyyumi, A.A.,Lewis, T.T., 2017. Socioeconomic status discrimination and C-reactive protein inAfrican–American and White adults. Psychoneuroendocrinology 82, 9–16. https://doi.org/10.1016/j.psyneuen.2017.04.009.
Vauth, R., Kleim, B., Wirtz, M., Corrigan, P.W., 2007. Self-efficacy and empowerment asoutcomes of self-stigmatizing and coping in schizophrenia. Psychiatry Res. 150 (1),71–80.
Weinbrecht, A., Niedeggen, M., Roepke, S., Renneberg, B., 2018. Feeling excluded nomatter what? Bias in the processing of social participation in borderline personalitydisorder. Neuroimage Clin. 19, 343–350. https://doi.org/10.1016/j.nicl.2018.04.031.
D. J. and F. N.
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.
Page 77
Williams, K.D., 2009. Ostracism: a temporal need-threat model. Adv. Exp. Soc. Psychol.41, 275–314.
Wittenbrink, B., Judd, C.M., Park, B., 2001. Evaluative versus conceptual judgments inautomatic stereotyping and prejudice. J. Exp. Soc. Psychol. 37, 244–252.
Wood, L., Byrne, R., Varese, F., Morrison, A.P., 2016. Psychosocial interventions for in-ternalised stigma in people with a schizophrenia-spectrum diagnosis: a systematicnarrative synthesis and meta-analysis. Schizophr. Res. 176 (2–3), 291–303. https://doi.org/10.1016/j.schres.2016.05.001.
Wood, L., Byrne, R., Burke, E., Enache, G., Morrison, A.P., 2017. The impact of stigma on
emotional distress and recovery from psychosis: the mediatory role of internalisedshame and self-esteem. Psychiatry Res. 255, 94–100. https://doi.org/10.1016/j.psychres.2017.05.016.
Yanos, P.T., Roe, D., Markus, K., Lysaker, P.H., 2008. Pathways between internalizedstigma and outcomes related to recovery in schizophrenia spectrum disorders.Psychiatr. Serv. 59 (12), 1437–1442. https://doi.org/10.1176/appi.ps.59.12.1437.
Yanos, P.T., Lysaker, P.H., Roe, D., 2010. Internalized stigma as a barrier to improvementin vocational functioning among people with schizophrenia-spectrum disorders.Psychiatry Res. 178 (1), 211–213. https://doi.org/10.1016/j.psychres.2010.01.003.
D. J. and F. N.
Téléchargé pour Anonymous User (n/a) à Hopital Simone Veil Montmorency à partir de ClinicalKey.fr par Elsevier sur septembre 05, 2019.Pour un usage personnel seulement. Aucune autre utilisation n´est autorisée. Copyright ©2019. Elsevier Inc. Tous droits réservés.

Page 78
Partie III. L’auto-stigmatisation dans la littéraure : prévalence, prédicteurs et conséquences
Page 79
Internalized Stigma in Serious Mental Illness (SMI): a systematic review of prevalence, predictors and
correlates
Running title: Prevalence and correlates of self-stigma in serious mental illness
AUTHORS
Dubreucq Ja,b,c,d
, Franck Na,e,f
a Centre de Neurosciences Cognitive, UMR 5229, CNRS & Université Lyon 1
b Centre référent de réhabilitation psychosociale et de Remédiation Cognitive (C3R), Centre Hospitalier Alpes Isère, Grenoble
c Fondation FondaMental, Créteil, France
d Réseau Handicap Psychique, Grenoble France
e Centre Ressource de Réhabilitation Psychosociale et de Remédiation cognitive, Centre Hospitalier Le Vinatier
f Centre Référent Lyonnais de Réhabilitation Psychosociale et de Remédiation Cognitive (CL3R), Centre
Hospitalier Le Vinatier
Page 80
Abstract
Background: Self-stigma is associated with poor clinical and functional outcomes in Serious Mental Illness
(SMI). There has been no review of self-stigma prevalence and predictors in diverse cultural areas and SMI.
Aims: i) to review the prevalence, correlates, and consequences of self-stigma in individuals with SMI; ii) to
evaluate the strengths and limitations of the current body of evidence to guide future research.
Methods: A systematic electronic database search (PubMed, Web of Science) following PRISMA guidelines
was conducted on July 4th 2019 on the prevalence, predictors and correlates of self-stigma in SMI.
Results: Of 220 papers, 66 (30%) reported on prevalence rates (n=17 623), 139 (63%) on cross-sectional or
longitudinal predictors of self-stigma and 146 (66%) on the correlates and consequences of self-stigma. On
average 31.5% of SMI patients reported high self-stigma, with the highest prevalence in South East Asia
(39.7%) and the Middle East (39%). High self-stigma was more prevalent in schizophrenia (SZ) (39.3%).
Socio-demographic and illness-related predictors yielded mixed results. Perceived and experienced stigma -
including from mental health providers - predicted self-stigma, which supports the need to develop anti-
stigma campaigns and recovery-oriented practices. Increased transition to psychosis and poor clinical and
functional outcomes are both associated with self-stigma.
Limitations: Excluding studies where self-stigma was not the main focus could have limited the
comprehension of stigma effects on people with SMI
Conclusion: Psychiatric rehabilitation and recovery-oriented early interventions are effective in reducing
self-stigma and should be better integrated into public policy.
Keywords: self-stigma, serious mental illness, prevalence, correlates, psychiatric rehabilitation
Page 81
Introduction
Schizophrenia, Bipolar Disorder (BD), Borderline Personality Disorder (BPD), major depression (MDD) and
severe anxiety disorders are all Serious Mental Illnesses (SMI), as defined by the US Substance Abuse and
Mental Health Services Administration: “persons aged 18 or older who currently or at any time in the past
year have had a diagnosable mental, behavioral, or emotional disorder (…) that has resulted in serious
functional impairment”1. SMI are frequent (1% schizophrenia; 1.5% BD; 1.5% BPD) and heavily
stigmatized2,3. People with BPD are prone to self-criticism and feelings of shame that can render them more
vulnerable to self-stigma 4. They face high levels of stigma, not only from the general public but also from
mental health professionals5. For a long time, research on stigma in psychiatric disorders focused on public
stigma, or the endorsement of negative beliefs and discriminating attitudes towards individuals by the
general population. Over the last two decades, attention has shifted towards the effects of stigma on
individuals. Perceived stigma is defined as one’s beliefs about the attitudes of the general public towards
people with Severe Mental Illness (SMI). Experienced stigma refers to the experiences of discrimination
individuals with SMI have had or expect to have. Self-stigma- or internalized stigma describes the
transformation process wherein a person’s previous social identity (defined by social roles such as son,
brother, sister, friend, employee or potential partner) is progressively replaced by a devalued and stigmatized
view of one self, known as “illness identity”6. The “illness identity model”6 proposed that self-stigma can
have pervasive effects on outcomes related to recovery from SMI, including self-esteem, hopefulness, social
interaction, employment, and symptom severity. The evidence consistently supports many of this model’s
predictions, including that self-stigma is negatively associated with self-esteem, hope, motivation to achieve
personal life goals, the use of adaptive coping strategies, adherence into treatment, well-being, quality of life,
personal recovery and social function.2,3,6 Self-stigma occurs when a person moves beyond mere awareness
of public stigma to actually agree with it and apply it to themselves7. The stress-coping model or self-stigma
proposed that perceived stigma, rejection sensitivity and negative in-group identification (i.e identification
with one’s stigmatized group) are associated with stigma stress, shame, social anxiety, secrecy and social
withdrawal8,9. Stigma Resistance is defined as a person’s ability to deflect or challenge stigmatizing beliefs
and is positively associated with patient’s outcomes10,11.
Page 82
There is a growing body of evidence - including meta-analyses - on self-stigma in SMI2,3,12-15. Studies on
internalized stigma have mostly been conducted in Europe or North America (77.5% of the 127 articles2,
schizophrenia being the most common diagnosis (54.3%2). The prevalence of internalized stigma was high in
Europe (41.7% of the 1,229 participants with schizophrenia and 21.7% of the 1,182 participants with mood
disorders had moderate to high levels of internalized stigma in the GAMIAN-Europe study12,13) and North
America (36.1% out of 144 people with SMI 16). Less is known about internalized stigma prevalence in other
geographic areas. The level of self-stigma might vary according to socio-demographic or cultural factors
(e.g. causal attributions of mental illness). The effectiveness of anti-stigma campaigns and self-stigma
reduction interventions could be influenced by cultural factors17,18. The results concerning the socio-
demographic predictors of self-stigma are mixed2,3. Few studies compared internalized stigma at different
stages of illness3 and it is still unclear whether self-stigma is greater in cases of prolonged psychosis
compared to early psychosis, at-risk stages or other SMI diagnoses. To date, there have been no literature
reviews comparing self-stigma prevalence and predictors in different geographical and cultural areas
(Europe, North America, South America, Middle East, South Asia, South-East Asia and Oceania). Similarly,
to our knowledge no literature review has been conducted comparing internalized stigma in at-risk stages,
schizophrenia, BD, MDD, BPD and anxiety disorders. Self-stigma was negatively associated with self-
esteem, self-efficacy, quality of life (QoL) and clinical and functional outcomes2. However, it is difficult to
disentangle the specific effects of self-stigma, as measures of perceived or experienced stigma are often used
to assess the correlates of internalized stigma (43.9% of the 127 studies 2). Most studies were cross-sectional
(86.7% of 127 studies2). The longitudinal effects of self-stigma remain largely unknown. Several
interventions (combinations of psychoeducation and cognitive restructuring in most cases, strategic
disclosure in others) have been designed to reduce self-stigma and its impact on patient’s outcomes, with
preliminary results on self-stigma, insight, self-efficacy, hope, social withdrawal and personal
recovery18,19,20,21,22. Psychiatric rehabilitation brings together a wide range of recovery-oriented
interventions23. Psychiatric rehabilitation could indirectly reduce self-stigma (e.g. through improved
psychiatric symptoms, self-esteem, cognitive, social and vocational functioning) although this remains to be
investigated.

Page 83
In summary, three reviews have been conducted on self-stigma since 2010, in schizophrenia3 and BD14,15.
One meta-analysis investigated correlates of stigma resistance in SMI11. Several predictors, correlates, and
consequences were identified. To our knowledge, there has been no review of self-stigma prevalence and
predictors in diverse cultural areas and SMI conditions; nor any specific review of self-stigma, excluding
explicitly perceived or experienced stigma. The effects of non-specific recovery-oriented practices on self-
stigma remain largely unknown. The present review has two objectives: i) to review the prevalence,
correlates, and consequences of self-stigma in individuals with SMI; ii) to evaluate the strengths and
limitations of the current body of evidence to guide future research.
Methods
A stepwise systematic literature review (PRISMA guidelines)24 was conducted by searching PubMed,
Medline and Web of Science for published and peer-reviewed papers using the following keywords:
“schizophrenia” / “bipolar disorder” / “borderline personality disorder” / “major depression” / “anxiety
disorder” / “serious mental illness” AND “stigma” / “self-stigma”. No time restriction was set. Only the
published papers in English or French were included in the review. The reference list of three meta-
analyses2,11,19 and three literature reviews3,14,15 on stigma and schizophrenia or BD were screened for
additional relevant articles. To be included in this review articles had to meet all the following criteria: a)
reporting explicitly on self-stigma (i.e papers on public stigma or using measures of perceived or
experienced stigma were excluded); b) a diagnosis of schizophrenia, bipolar disorder, borderline personality
disorder, major depression or anxiety disorders; c) quantitative data available on the prevalence, correlates or
consequences of internalized stigma or stigma resistance. The first author applied eligibility criteria and
screened the records to select the included studies. The last author checked all the decisions made. Disputed
items were solved discussing together and reading further the paper to reach a final decision. Means and
percentages were weighted for the number of cases per study to obtain prevalence data. Weighted scores
were calculated using proportions of rating scale scores. The prevalence of self-stigma is frequently

Page 84
measured using Internalized Stigma of Mental Illness Scale25. A score above the midpoint indicates a
moderate to high level of self-stigma12,25. Stigma resistance is often measured using ISMI stigma resistance
subscale, which shows variable internal consistency (0.56 in Firmin et al 2016 meta-analysis11). Only the
studies reporting internal consistency above 0.50 were considered for extracting the correlates of stigma
resistance. The study protocol was registered on PROSPERO database on July 4th 2019 (ID 141282).
Results
Our search on July 5th 2019 resulted in 3215 articles from PubMed and 11,472 from Web of Science. After
manually removing all duplicates there were 3,824 remaining references. Based on their titles and abstracts,
3,495 papers were excluded for lack of relevance. Most of these articles focused on public stigma, perceived
or experienced stigma or to self-stigma in other discriminated populations. Our search strategy yielded 329
full-text articles. After conducting a full-text analysis of all these papers and excluding those which did not
meet the inclusion criteria we ended up with 220 relevant papers (figure 1).
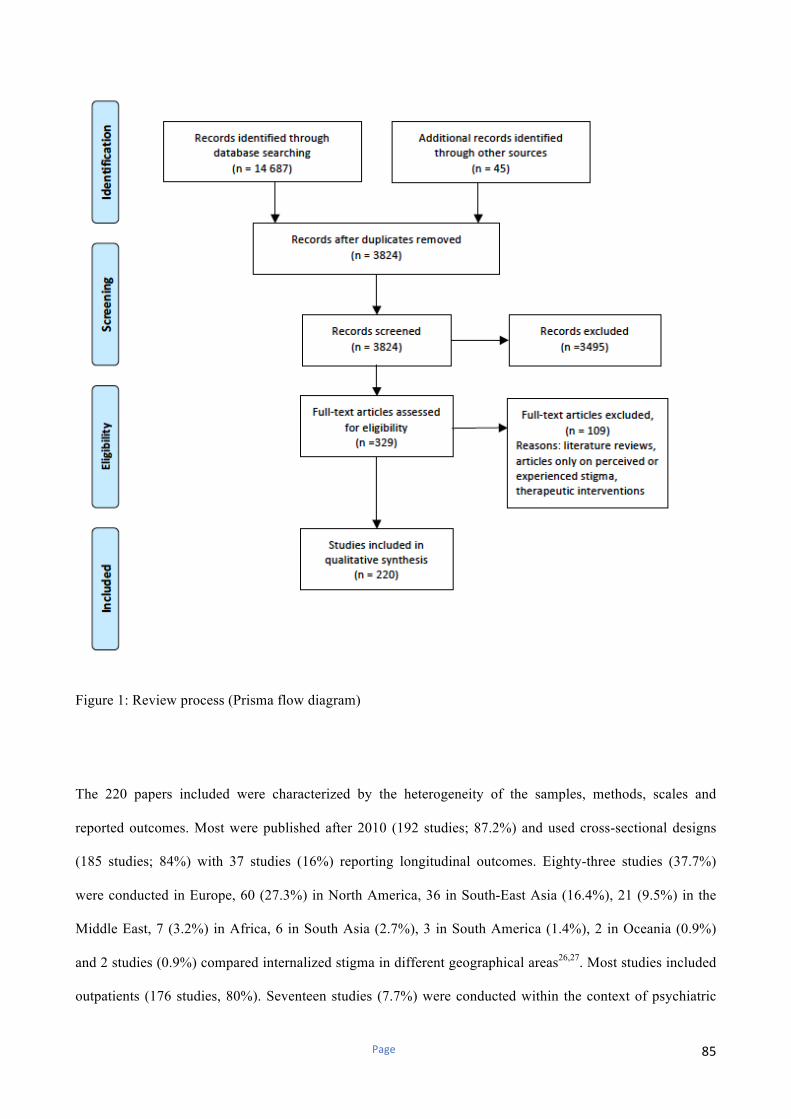
Page 85
Figure 1: Review process (Prisma flow diagram)
The 220 papers included were characterized by the heterogeneity of the samples, methods, scales and
reported outcomes. Most were published after 2010 (192 studies; 87.2%) and used cross-sectional designs
(185 studies; 84%) with 37 studies (16%) reporting longitudinal outcomes. Eighty-three studies (37.7%)
were conducted in Europe, 60 (27.3%) in North America, 36 in South-East Asia (16.4%), 21 (9.5%) in the
Middle East, 7 (3.2%) in Africa, 6 in South Asia (2.7%), 3 in South America (1.4%), 2 in Oceania (0.9%)
and 2 studies (0.9%) compared internalized stigma in different geographical areas26,27. Most studies included
outpatients (176 studies, 80%). Seventeen studies (7.7%) were conducted within the context of psychiatric

Page 86
rehabilitation (recovery-oriented day care28-30), vocational rehabilitation16,31-34, inpatient35 or community-
based psychiatric rehabilitation services36-43, one study (0.45%) in an advocacy group44,and five studies
(2.3%) in prison settings45-49.
Ninety-five studies (43.2%) concerned schizophrenia, 11 (5%) BD, 12 (5.4%) MDD and 10 (4.5%) at-risk
stages or first episode psychosis, two (0.9%) anxiety disorders, one obsessive-compulsive disorder (0.5%)
and two (0.9%) personality disorders. Eighty-seven studies (39.6%) looked at SMI. There were large
variations in the definition of SMI. Twenty-eight studies (12.6%) defined SMI as schizophrenia, BD or
MDD. Thirty studies (13.6%) used a broad definition of SMI and included participants with anxiety
disorders (AD, n=19), obsessive-compulsive disorder (n=9), post-traumatic stress disorder (n=7), personality
disorders (7 studies), substance use disorders (n=3) attention deficit and hyperactive disorder (ADHD, n=2)
and eating disorders (n=1). Twelve studies (5.4%) investigated self-stigma in schizophrenia and BD (n=9),
schizophrenia and MDD (n=2) and in mood disorders (n=1), and 16 studies (7.2%) did not specify the
different forms of SMI. There were large variations in the proportion of participants with schizophrenia (1.8
to 98.1%), BD (1.9 to 63%), MDD (2.6% to 85%), AD (3.7% to 36.1%), obsessive-compulsive disorder
(1.7% to 21.8%) and personality disorders (6.3% to 34%) included in SMI studies. Most studies included
young (18-34 years old; 47 studies (21.4%)) or middle-aged participants (35-50 years old; 149 studies
(67.7%)). Four studies (1.8%) included participants under 18 years old, 13 (5.9%) participants above the age
of 50 years old and 7 (3.1%) used mixed samples. One hundred and forty-four studies (65%) used the
Internalized Stigma of Mental Illness25 scale to measure internalized stigma and 31 studies (14%) the Self-
Stigma of Mental Illness Scale50 (SSMI). Forty-five studies (21%) measured self-stigma with other scales.
The results are shown in Table 1.
Internalized stigma prevalence
Sixty-six papers (30%) reported data on internalized stigma extent in SMI, or on the proportion of
individuals with moderate to high internalized stigma, or on both outcomes. Twenty-one studies were
conducted in Europe, 13 studies in North America, 12 in South East Asia, 21 in, 6 in Africa, 7 in Middle
Page 87
East, 4 in South Asia, one in South America, one in Australia and one in Austria and Japan. Nine studies
compared the prevalence of internalized stigma in different countries12,13,26,51,52, cities53, or settings16,45,46. The
samples were mostly constituted of individuals with schizophrenia (30 studies; 45%) or SMI (27 studies;
41%). The results are shown in Table 2.
Thirty-three papers reported on the proportion of moderate to high internalized stigma (ISMI >2.5 or above
the midpoint on other scales) in a total of 10,728 participants (5,457 SMI, 4,332 schizophrenia, 1,339 BD,
955 MDD). Sixty papers documented internalized stigma extent (ISMI mean total score) in 17,623
participants (8,442 with SMI, 7,799 with schizophrenia, 1,538 with BD, 1,545 with MDD, 358 with AD, 52
with BPD). Self-stigma prevalence was higher in schizophrenia (39.35%) than in SMI (31.5%). Higher
prevalence was found in South-East Asia and the Middle East for SMI, and in North America, Europe and
Africa for schizophrenia. There were significant country-related differences in the proportion of self-
stigmatized SMI patients in Europe (from 15.2% in Sweden12 to 57% in Croatia51), North America (from 9%
in Canada46 to 37% in USA29) and in South-East Asia (from 8.1% in South Korea54 to 50% in Taiwan55).
Setting-related differences were also found16,53. Similar variations were found for schizophrenia, BD (1.93 in
Europe to 2.26 in India; 18.5% Turkey56 in remitted BD; 26% USA57 in non-adherent BD), MDD (2.15 in
Europe to 2.44 in South East Asia), obsessive-compulsive disorder and anxiety disorders.
Predictors of internalized stigma
One hundred and thirty-two studies (60%) reported on cross-sectional internalized stigma predictors. The
most common diagnosis was schizophrenia (n=60; 45.4%), followed by BD (n=7; 5.3%) at-risk states (n=5;
3.7%) and early psychosis (n=4; 3%). Fifty-six studies (42.4%) concerned SMI. Predictors were illness-
related (n=95 studies; 71.9%), socio-demographic (n=60; 45.4%) or related to participant’s environment (n=
45; 34%). The results are shown in Table 3.
Few socio-demographic characteristics correlated significantly with internalized stigma. Being the income
earner58, immigrant status, history of incarceration or homelessness45,59, rural residence60-62, parenting status
(mothers > fathers63), shame proneness, and avoidant or self-defeating personality traits64-68 predicted higher
Page 88
IS. The results were contrasted for all other socio-demographic variables (age, gender, education level,
employment, marital status, income, disability status). Other personal characteristics (attachment style, self-
compassion and mindfulness abilities) did not predict internalized stigma69-71. Insight into illness10,54,65,72-81,
parental insight76, self-perception of clinical severity82-84, hopelessness53,54 and attributions of personal
responsibility80 predicted internalized stigma. Impairments in cognitive metacognitive and psychosocial
function85-94, decreased well-being53, and avoidant coping strategies95-99, predicted higher internalized stigma.
Conversely preserved cognitive abilities49,100,101, empowerment, self-efficacy, self-agency and stigma
resistance protected against internalized stigma12,13,44,102. Comorbid post-traumatic stress disorder29 and an
increased number of drug side effects60 predicted self-stigma in single studies. Residual psychiatric
symptomatology, positive and negative symptoms for schizophrenia and depressive symptoms for BD
predicted internalized stigma in most studies (up to 90% significance). Mixed results were found for all other
illness-related predictors (age of onset, psychiatric diagnosis, illness duration, history of suicide attempts,
inpatient status, past psychiatric admission and the number of hospitalizations). Internalized stigma was
equally severe in participants with ultra-high risk and established psychosis103. Public stigma59 and other
dimensions of personal stigma predicted self-stigma (perceived stigma, n= 14 studies; perceived stigma from
mental health providers104, n=1; experienced stigma, n=9; anticipated stigma; n=3). Cultural factors such as
attributing mental illness to supernatural causes60,105, a history of traditional treatment60, and loss of face in
Eastern countries26,53,106 determined internalized stigma. Concerns about losing face (or the fear of losing
face because of being diagnosed with SMI) mediated the relationship between perceived stigma and
internalized stigma106. Stigma stress42,107,108 and negative emotional reactions to involuntary psychiatric
admission42,107 were significant predictors of internalized stigma, in contrast with compulsory community
treatment46, forensic status45 and the number of involuntary admissions42,107,109. Ingroup-value (i.e how people
with SMI see their own group110), social network and support, membership of an advocacy group, and family
support protected against self-stigma12,13,28,35,44,51,96,111-113.
Page 89
Predictors of change in internalized stigma
The longitudinal predictors of change in internalized stigma over time were reported in 15 studies (6.8%)
mostly conducted in North America (n=8) with middle-aged participants (n=8). Ten were conducted in
psychiatric rehabilitation settings (recovery-oriented day-care28-30,38, or interventions to prevent compulsory
readmission42,114, vocational rehabilitation32-34, early intervention programs115). The results are shown in
Table 3. Residual psychiatric symptoms38,114-116, negative emotional reactions to involuntary
hospitalization42,114, and emotional distress33,38 were the most significant baseline predictors of internalized
stigma at follow-up. Duration of untreated psychosis115 and baseline coping strategies117 predicted
internalized stigma in single studies. Mixed results were found for internalized stigma stability over time
with no specific intervention32,117-119. Attending psychiatric rehabilitation predicted significant reductions in
internalized stigma extent (from a mean total ISMI score of 2.31 on admission to 1.96 at discharge29; 2.36 to
2.2033; 2.11 to 1.9630; 2.1 to 2.0428; 1.80 to 1.50 in participants having worked in the past year without being
discriminated against34) and in the proportion of participants with high internalized stigma (ISMI>2.5 from
37% to 13.7%29; reduction in ISMI levels at follow up > 25% in 38% of the participants with mean
internalized stigma>232). Receiving no disability benefits during psychiatric rehabilitation predicted a higher
reduction in internalized stigma29.
Correlates of internalized stigma
Cross-sectional correlates of internalized stigma were reported in 127 studies (57.7%). Most participants
were middle-aged (n=88; 69.2%) and diagnosed with schizophrenia (n=51; 40.1%) or SMI (n=52; 40.9%).
The results are shown in Table 4.
In general self-stigma was positively associated with depressive symptoms (n=26) and suicidal ideation
(n=9) and negatively correlated with hope (n=13), help seeking (n=3), attitudes towards psychiatric
medication (n=3) and treatment adherence (n=9). Single studies found negative associations with therapeutic
alliance120 and shared decision making121. Insight into illness75,78,100,122-125, avoidant personality traits64, and
coping strategies99, loneliness126 and resilience127 moderated the relationship with depression and self-esteem
Page 90
mediated internalized stigma effects on hope128. Internalized stigma mediated the effects of perceived
cognitive dysfunction and experienced stigma on suicidality118,129 and QoL130. Self-stigma was negatively
associated with QoL (n=29), self-esteem (n=22), self-efficacy (n=6), well-being (n=4), life satisfaction
(n=3), empowerment (n=3), resilience (n=5), stigma resistance (n=2) and personal recovery (n=15).
Internalized stigma positively correlated with the “why try effect”131 and later stages of self-stigma with a
higher impact on hope, self-esteem, psychosocial function and personal recovery41,131. Participants in the late
stages of self-stigma reported more reasons to not disclose their psychiatric diagnosis, in contrast with those
in the early stages who reported greater benefits from being “out”39. Self-stigma was negatively associated
with global functioning (n=17) and social participation (n=6). Higher demoralization and decreased
resilience mediated the relationship between internalized stigma and psychosocial function75,132. Self-
stigmatized participants reported more dysfunctional attitudes133 and an increased use of avoidant coping
strategies (n=5). Single studies reported negative associations with activity134, self-rated physical health30,
perceived social support135, self-reported attractiveness136, capacity for intimacy137, relational satisfaction56
and self-reported parenting experiences63,138. Internalized stigma positively correlated with sense of
loneliness126,139, fear of intimate relationships56, and self-stigma on parenting abilities for mothers living
without their child63. Psychiatric symptoms (n=4), anxiety (n=3), social anxiety140, distress from sub-
threshold psychotic symptoms141 were positively correlated with self-stigma. Stigma stress- a predictor of
self-stigma in several studies42,107,108, was positively associated with transition to psychosis142.
Internalized stigma as a predictor of outcome
Twenty-seven studies (12.3%) reported longitudinal outcomes associated with internalized stigma. Studies
included mostly middle-aged (n=17; 63%) participants with SMI (n=12; 44.4%) or schizophrenia (n=9;
33.3%). Three studies were about at-risk states (11%). Eight studies included young participants (<18, n=1;
18-35, n=7; 29.6%) and two individuals over 50 years old (7.4%). The duration of follow-up ranged from 6
weeks143 to 2 years144. The results are shown in Table 4.

Page 91
Self-stigma at baseline predicted increased positive symptoms145, emotional discomfort116, social anxiety146,
depression147,148, suicidal ideation144, and an increased risk of psychiatric hospitalization149 at follow-up.
Participants with high self-stigma reported reduced self-esteem148, decreased life satisfaction150, lower
personal recovery151, less use of adaptive coping strategies117, and lower treatment adherence152 at follow-up.
Baseline internalized stigma predicted poorer social and vocational functioning145,153 at follow-up, and less
benefits from vocational rehabilitation31. Change in internalized stigma during follow-up predicted
depression, increases in internalized stigma being associated with more depressive symptoms145 and higher
suicidality114,154 and decreases in internalized stigma with less depression30,119. Increased internalized stigma
predicted more negative attitudes towards psychiatric medication155, poorer social function156, reduced self-
esteem114, and lower personal recovery151. Reduced internalized stigma predicted decreased subjective
clinical severity30, higher self-esteem33, and improved global functioning30. Baseline internalized stigma did
not predict QoL at follow-up46, decreased internalized stigma during follow-up did however predict
improvements in QoL30 during psychiatric rehabilitation.
Internalized stigma and stigma resistance
Twenty-nine studies (13.2%) reported data on stigma resistance prevalence in SMI. The results are shown in
Table 5. Stigma resistance was higher in mood disorders (59.7%13) than in schizophrenia (53.1%; n=5).
Stigma resistance in schizophrenia varied within Europe (from 49.2%12 to 63% 157 and Africa (from 49.4% in
Ethiopia158 to 72.7% in Nigeria159). Stigma resistance was negatively correlated with internalized stigma in
Austria26,157, Croatia160, Nigeria159 and South Africa44. In some countries internalized stigma and stigma
resistance were both high (USA57, Turkey, Ethiopia158, India, Bolivia52, Peru52, Chile52, China58) and in
Canada these were both low45,46. Metacognitive abilities161-163, social network43,157, social power111, self-
compassion43, psychological flexibility43, fear of negative evaluation161, perceived stigma110,149, negative
symptoms163 and coping strategies95,162 predicted stigma resistance.
Page 92
Discussion
Overall, the main results of the present review can be summarized as follows: research on self-stigma in SMI
has considerably progressed over the past decade (192 articles since 2010 / 28 studies published prior to
this2). Self-stigma was more frequent in SZ (39.3%) compared to other SMI. Self-stigma was present in all
geographical areas in South-East Asia and the Middle East for SMI (>39%) and in North America, Europe,
South America and Africa for schizophrenia (>38%). Schizophrenia led to high self-stigma in all
geographical areas (36.8% to 44.2%). Self-stigma differed according to the geographical area in other SMI
(internalized stigma extent ranging from 1.93 to 2.26 in BD, 1.9 to 2.31 in anxiety and 2.15 to 2.44 in MDD).
Variations in patterns of stigma according to the cultural area might explain these differences. Internalized
stigma extent appeared higher in BPD (2.42) but this is based on a small number of studies with small
sample sizes. Large country and setting-related variations were found. Socio-demographic and illness-related
predictors yielded mixed results in accordance with previous reviews2,3. Internalized stigma was equally
severe in the at-risk stages as in psychosis147. Further research will however be necessary to confirm this
result. Self-stigma was positively associated with insight into illness, psychiatric symptoms, impaired
cognitive and psychosocial functioning and avoidant personality traits and coping strategies. Recovery-
oriented psychoeducation, cognitive remediation, group cognitive behavior therapy and social skills training
might contribute to self-stigma reduction, trough improved symptoms and functioning23,100. Several potential
predictors were identified in single studies that have not yet been replicated. Anti-stigma campaigns
contribute to reducing public and perceived stigma and should be reinforced59, taking into consideration
cultural factors26,53,60,105,106. Self-stigma reduction interventions should take into consideration cultural factors
(e.g. cost / benefits of strategic disclosure in a specific cultural context18). Self-stigma was closely associated
with perceived and experienced stigma. These concepts are however distinct and should be better
differentiated between, as stereotype awareness and self-labelling do not necessarily imply stereotype
agreement, self-application and increased internalized stigma131,164. Self-support groups and recovery-
oriented services promoting positive group identification28-30,44,110,165 should therefore be further developed to
prevent or reduce self-stigma. Reducing self-stigma implies targeting explicitly negative views about the self
that are related to being diagnosed with SMI.
Page 93
Strategic disclosure of one’s diagnosis of SMI appears particularly effective for adolescents or people in the
early stages of self-stigma22,39. Patients in the late stages of self-stigma often need to participate to group
interventions combining psychoeducation to counteract SMI stereotypes and cognitive restructuring to
challenge dysfunctional attitudes about the self20,42. Interventions should be proposed to each individual
according to his/her personal needs and level of self-stigma. The development of recovery-oriented practices
in mental health facilities should be encouraged as it might reduce perceived stigma, stigma stress42,107,109,
and the negative emotional reactions to involuntary admissions42,107,109. Peer-supported self-management
interventions, Joint Crisis Plans, “No Force First” policies and selective disclosure programs could improve
self-stigma through reduced stigma stress and perceived coercion22,166-168. Recovery-oriented training
programs for mental health professionals improve personal recovery in people with SMI169. Their
effectiveness in reducing self-stigma should be investigated.
Given the potential relationships with stigma stress142, duration of untreated psychosis115, distress from sub-
threshold psychotic symptoms141, and transition to psychosis142, the effects of recovery-oriented early
interventions on self-stigma and its consequences should be further investigated. Strategic disclosure
improves stigma stress and self-stigma in adolescents with SMI22 and should be integrated in recovery-
oriented early intervention services. As expected2,3, self-stigma was negatively associated with self-esteem,
self-efficacy, QoL, global functioning, treatment adherence and personal recovery, and positively associated
with depression, social anxiety, and positive symptoms. Self-stigma correlated negatively with therapeutic
alliance, help-seeking, intimate relationships, parenting, wellbeing, life satisfaction, empowerment, resilience
and stigma resistance. Dysfunctional attitudes, avoidant coping strategies and suicidality positively
correlated with internalized stigma. Further research will be needed as some results come from single
studies56,134,137,162. Insight into illness was the most significant moderator of internalized stigma. Other
potential moderators or mediators were identified and should be further investigated. Perceived cognitive
dysfunction, perceived and experienced stigma had indirect effects on clinical and functional outcomes via
self-stigma55,118,129,130,170. Baseline internalized stigma predicted depression, social anxiety, self-esteem,
treatment adherence and psychosocial function at follow-up3. Self-stigma at baseline also predicted positive
symptoms, suicidal ideation, coping strategies, benefits from vocational rehabilitation life satisfaction, and

Page 94
personal recovery at follow-up117,144,145,150,151,153. Change in internalized stigma predicted changes in
depression, suicidality, attitudes towards medication, self-esteem, QoL and social function at follow-
up30,114,116,119,145,151,155,156. Reducing self-stigma through psychiatric rehabilitation or specific interventions
might improve clinical and functional outcomes and should therefore be a primary objective in public
policies. Stigma resistance and internalized stigma predicted each other11 but with different patterns. As
previously suggested, internalized stigma and stigma resistance are distinct constructs and should be
measured with more specific scales11.
Limitations
There are some limitations to this review, due to the heterogeneity in the definition of SMI and in the
samples, settings, methods, scales and reported outcomes. Few papers reported longitudinal outcomes with a
limited number of studies conducted in psychiatric rehabilitation. This review excluded studies where self-
stigma was not the main focus possibly meaning that stigma (i.e. perceived, experienced or anticipated
stigma and self-stigma) could have wider effects on people with SMI. The focus on self-stigma in this review
allows however a more accurate comprehension of its effects on people with SMI. The heterogeneity of the
samples, methods, scales and reported outcomes in the included papers limited the possibilities to extract
comparable data. The large number of studies included in this review and the range of countries represented
is however a considerable strength. The underreporting of negative or non-significant results due to
publication bias and the exclusion of unpublished studies from this review might have limited the accuracy
of the synthesis.
Conclusions
In summary, self-stigma is a severe problem in all SMI conditions - including the at-risk stages - and all
geographical areas and is associated with poor clinical and functional outcomes. The levels of public,
perceived and experienced stigma (including from mental health providers) are significant predictors of
Page 95
internalized stigma, pleading for the reinforcement of anti-stigma campaigns and the development of
recovery-oriented practices in mental health settings. The respective associations between duration of
untreated psychosis, internalized stigma and transition to psychosis support the development of recovery-
oriented early intervention programs. Psychiatric rehabilitation is effective on internalized stigma reduction
and should therefore be further developed in public policies.
Acknowledgements
The authors would like to thank Mrs. Kim Barrett for proofreading the manuscript.
Role of the funding source: This research did not receive any specific grant from funding agencies in the
public, commercial, or not-for-profit sectors.
Author contribution statement: The two authors had full access to the data in the study and take the
responsibility for the integrity of the data and the accuracy of the data analysis. Dr Julien Dubreucq drafted
the article. Dr Julien Dubreucq and Pr Nicolas Franck made the literature review. Pr Nicolas Franck critically
revised the article. Both authors were involved in the collection and analysis of the data. Both authors
contributed to and have approved the final manuscript
Conflicts of interests : none
References
1-Substance Abuse and Mental Health Services Administration (SAMHSA). Results from the 2013 National Survey on Drug Use and Health: Mental
Health Findings. NSDUH Series H-49, HHS Publication No. (SMA) 14-4887. Rockville, MD: Substance Abuse and Mental Health Services
Administration, 2014.
2-Livingston JD, Boyd JE. Correlates and consequences of internalized stigma for people living with mental illness: A systematic review and meta-
analysis. Soc Sci Med 2010;71:2150-61.
3-Gerlinger G, Hauser M, De Hert M, et al. Personal stigma in schizophrenia spectrum disorders: a systematic review of prevalence rates, correlates,
impact and interventions. Word Psychiatry 2013;12:155-64
Page 96
4-Rüsch N, Hölzer A, Hermann C, et al. Self-stigma in women with borderline personality disorder and women with social phobia. J Nerv Ment Dis
2006;194:766-73.
5-Gunderson JG, Herpertz SC, Skodol AE, et al. Borderline personality disorder. Nat Rev Dis Primers. 2018 ;4:18029.
6-Yanos PT, Roe D, Markus K, et al. Pathways between internalized stigma and outcomes related to recovery in schizophrenia spectrum disorders.
Psychiatr Serv 2008;59:1437-42.
7-Corrigan PW., Larson JE., Rüsch N. Self-stigma and the “why try” effect: impact on life goals and evidence-based practices. World Psychiatry
2009;8:75-81
8-Rüsch N, Corrigan PW, Wassel A, et al. A stress-coping model of mental illness stigma: I. Predictors of cognitive stress appraisal. Schizophr Res.
2009 ;110(1-3):59-64.
9-Rüsch N, Corrigan PW, Powell K, et al. A stress-coping model of mental illness stigma: II. Emotional stress responses, coping behavior and
outcome. Schizophr Res. 2009 ;110(1-3):65-71.
10- Thoits PA. Resisting the stigma of mental illness. Soc Psychol Q 2011;74(1):6-28.
11- Firmin RL, Luther L, Lysaker PH, and al. Stigma resistance is positively associated with psychiatric and psychosocial outcomes: A meta-analysis.
Schizophr Res. 2016;175(1-3):118-28.
12-Brohan E, Elgie R, Sartorius N, et al; GAMIAN-Europe Study Group. Self-stigma, empowerment and perceived discrimination among people
with schizophrenia in 14 European countries: the GAMIAN-Europe study. Schizophr Res 2010;122:232-8.
13-Brohan E, Gauci D, Sartorius N, et al.; GAMIAN-Europe Study Group. Self-stigma, empowerment and perceived discrimination among people
with bipolar disorder or depression in 13 European countries: the GAMIAN-Europe study. J Affect Disord 2011;129:56-63.
14-Ellison N, Mason O, Scior K. Bipolar disorder and stigma: a systematic review of the literature. J Affect Disord 2013;151:805-20
15-Hawke LD, Parikh SV, Machalak EE. Stigma and bipolar disorder: a review of the literature. J Affec Disord 2013;150:181-91
16-West ML, Yanos PT, Smith SM, et al. Prevalence of Internalized Stigma among Persons with Severe Mental Illness. Stigma Res Action 2011;1:3-
10.
17-Xu Z, Rüsch N, Huang F, et al . Challenging mental health related stigma in China: Systematic review and meta-analysis. I. Interventions among
the general public. Psychiatry Res. 2017 ;255:449-56.
18-Xu Z, Huang F, Kösters M, et al. Challenging mental health related stigma in China: Systematic review and meta-analysis. II. Interventions among
people with mental illness. Psychiatry Res. 2017 ;255:457-464.
19-Wood L, Byrne R, Varese F, et al. Psychosocial interventions for internalized stigma in people with schizophrenia-spectrum diagnosis: A
systematic narrative synthesis and meta-analysis. Schizophr Res 2015;176:291-303
Page 97
20-Yanos PT, Lucksted A, Drapalski AL, et al. Interventions targeting mental health self-stigma: A review and comparison. Psychiatr Rehabil J. 2015
;38(2):171-178.
21-Corrigan PW, Larson JE, Michaels PJ, et al. Diminishing the self-stigma of mental illness by coming out proud. Psychiatry Res. 2015 ;229(1-
2):148-54.
22-Mulfinger N, Müller S, Böge I, et al. Honest, Open, Proud for adolescents with mental illness: pilot randomized controlled trial. J Child Psychol
Psychiatry. 2018 ;59(6):684-691.
23-Franck N, Bon L, Dekerle M, et al. Satisfaction and Needs in Serious Mental Illness and Autism Spectrum Disorder: The REHABase Psychosocial
Rehabilitation Project. Psychiatr Serv. 2019 ;70(4):316-323.
24-Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement.
Syst Rev 2015;4:1.
25-Ritsher Boyd JB, Otilingam PG, Grajales M. Internalized stigma of mental illness: psychometric properties of a new measure. Psychiatry Res
2003;121:31e49.
26-Hofer A, Mizuno Y, Frajo-Apor B, et al. Resilience, internalized stigma, self-esteem, and hopelessness among people with schizophrenia: Cultural
comparison in Austria and Japan. Schizophr Res 2016;171:86-91.
27-Mileva VR, Vázquez GH, Milev R. Effects, experiences, and impact of stigma on patients with bipolar disorder. Neuropsychiatr Dis Treat
2013;9:31-40.
28-Sibitz I, Provaznikova K, Lipp M, et al. The impact of recovery-oriented day clinic treatment on internalized stigma: preliminary report.
Psychiatry Res 2013;209:326-32
29-Harris JI, Farchmin L, Stull L, et al. Prediction of changes in self-stigma among veterans participating in partial psychiatric hospitalization: The
role of disability status and military cohort. Psychiatr Rehabil J 2015;38:179-85.
30-Pearl RL, Forgeard MJC, Rifkin L, et al. Internalized stigma of mental illness: Changes and associations with treatment outcomes. Stigma Health
2017;2:2-15.
31-Yanos PT, Lysaker PH, Roe D. Internalized stigma as a barrier to improvement in vocational functioning among people with schizophrenia-
spectrum disorders. Psychiatry Res 2010;178:211-3.
32-Lysaker PH, Tunze C, Yanos PT, et al. Relationships between stereotyped beliefs about mental illness, discrimination experiences, and distressed
mood over 1 year among persons with schizophrenia enrolled in rehabilitation. Soc Psychiatry Psychiatr Epidemiol 2012;47:849-55.
33-Lysaker PH, Roe D, Ringer J, et al. Change in self-stigma among persons with schizophrenia enrolled in rehabilitation: associations with self-
esteem and positive and emotional discomfort symptoms. Psychol Serv 2012;9:240-7.
34-Rüsch N, Nordt C, Kawohl W, et al. Work-related discrimination and change in self-stigma among people with mental illness during supported
employment. Psychiatr Serv 2014;65:1496-8.
Page 98
35-Hsiao CY, Lu HL, Tsai YF. Effect of family sense of coherence on internalized stigma and health-related quality of life among individuals with
schizophrenia. Int J Ment Health Nurs 2018;27:138-46.
36-Muñoz M, Sanz M, Pérez-Santos E, et al. Proposal of a socio-cognitive-behavioral structural equation model of internalized stigma in people with
severe and persistent mental illness. Psychiatry Res 2011;186:402-8.
37-Tang IC, Wu HC. Quality of life and self-stigma in individuals with schizophrenia. Psychiatr Q 2012;83:497-507.
38-Ben-Zeev D, Frounfelker R, Morris SB, et al. Predictors of Self-Stigma in Schizophrenia: New Insights Using Mobile Technologies. J Dual Diagn
2012;8:305-14.
39-Corrigan PW, Michaels PJ, Powell K, et al. Who Comes Out With Their Mental Illness and How Does It Help? J Nerv Ment Dis 2016;204:163-8.
40-Treichler EBH, Lucksted AA. The role of sense of belonging in self-stigma among people with serious mental illnesses. Psychiatr Rehabil J
2017;41:149-52.
41-Cunningham KC, Lucksted A. Social cognition, internalized stigma, and recovery orientation among adults with serious mental illness. Psychiatr
Rehabil J 2017;40:409-11.
42-Xu Z, Lay B, Oexle N, et al. Involuntary psychiatric hospitalization, stigma stress and recovery: a 2-year study. Epidemiol Psychiatr Sci
2018;31:1-8.
43-Chan KKS, Lee CWL, Mak WWS. Mindfulness Model of Stigma Resistance Among Individuals with Psychiatric Disorders. Mindfullness
2018;9:1433-42.
44-Sorsdahl KR, Kakuma R, Wilson Z, et al. The internalized stigma experienced by members of a mental health advocacy group in South Africa. Int
J Soc Psychiatry 2012;58:55-61
45-Livingston JD, Rossiter KR, Verdun-Jones SN. 'Forensic' labeling: an empirical assessment of its effects on self-stigma for people with severe
mental illness. Psychiatry Res 2011;188:115-22.
46-Livingston J. Self-stigma and quality of Life among people with Mental illness who receive Compulsory community treatment services. J
Community Psychol 2012;40:699-714
47-Dequelson A, Saloppé X, Bandinelli A. Insight, Sigma and Self-stigma: The personal conviction applied to schizophrenia patients hospitalized in
forensic hospital. Ann Med Psychol 2015;173:913-5
48-West ML, Vayshenker B, Rotter M, et al. The influence of mental illness and criminality self-stigmas and racial self-concept on outcomes in a
forensic psychiatric sample. Psychiatr Rehabil J 2015;38:150-7.
49-West ML, Mulay AL, DeLuca JS, et al. Forensic psychiatric experiences, stigma, and selfconcept: a mixed-methods study. J Forens Psychiatry
Psychol 2018;29:574-96.
50-Corrigan P, Watson A, Barr L. The self-stigma of mental illness: implications for self-esteem and self-efficacy. J Soc Clin Psychol
2006;25:875e884.
Page 99
51-Krajewski C, Burazeri G, Brand H. Self-stigma, perceived discrimination and empowerment among people with a mental illness in six countries:
Pan European stigma study. Psychiatry Res 2013;210:1136-46.
52-Caqueo-Urízar A, Boyer L, Urzúa A, et al. Self-stigma in patients with schizophrenia: a multicentric study from three Latin-America countries.
Soc Psychiatry Psychiatr Epidemiol 2019;54(8):905-9.
53-Young DK, Ng PY. The prevalence and predictors of self-stigma of individuals with mental health illness in two Chinese cities. Int J Soc
Psychiatry 2016;62:176-85
54-Kim WJ, Song YJ, Ryu HS, et al. Internalized stigma and its psychosocial correlates in Korean patients with serious mental illness. Psychiatry Res
2015;225:433-9.
55-Kao YC, Lien YJ, Chang HA, et al. Evidence for the indirect effects of perceived public stigma on psychosocial outcomes: The mediating role of
self-stigma. Psychiatry Res 2016;240:187-95.
56- Sarısoy G, Kaçar ÖF, Pazvantoğlu O, et al. Internalized stigma and intimate relations in bipolar and schizophrenic patients: a comparative study.
Compr Psychiatry 2013;54:665-72.
57-Howland M, Levin J, Blixen C, et al. Mixed-methods analysis of internalized stigma correlates in poorly adherent individuals with bipolar
disorder. Compr Psychiatry 2016;70:174-80.
58-Ran MS, Zhang TM, Wong IY, et al; CMHP Study Group. Internalized stigma in people with severe mental illness in rural China. Int J Soc
Psychiatry 2018;64:9-16.
59-Evans-Lacko S, Brohan E, Mojtabai R, et al. Association between public views of mental illness and self-stigma among individuals with mental
illness in 14 European countries. Psychol Med 2012;42:1741-52.
60-Girma E, Tesfaye M, Froeschl G, et al. Facility based cross-sectional study of self-stigma among people with mental illness: towards patient
empowerment approach. Int J Ment Health Syst 2013;7:21.
61-Assefa D, Shibre T, Asher L, et al. Internalized stigma among patients with schizophrenia in Ethiopia: a cross-sectional facility-based study. BMC
Psychiatry 2012;12:239
62-Grover S, Avasthi A, Singh A, et al. Stigma experienced by patients with severe mental disorders: A nationwide multicentric study from India.
Psychiatry Res 2017;257:550-58.
63-Lacey M, Paolini S, Hanlon MC, et al. Parents with serious mental illness: Differences in internalized and externalized mental illness stigma and
gender stigma between mothers and fathers. Psychiatry Res 2015;225:723-33.
64-Aukst-Margetić B, Jakšić N, Boričević Maršanić V, et al. Harm avoidance moderates the relationship between internalized stigma and depressive
symptoms in patients with schizophrenia. Psychiatry Res 2014;219:92-4.
65-Hasson-Ohayon I, Ehrlich-Ben Or S, Vahab K, et al. Insight into mental illness and self-stigma: the mediating role of shame proneness. Psychiatry
Res 2012;200:802-6.
Page 100
66-Bassirnia A, Briggs J, Kopeykina I, et al. Relationship between personality traits and perceived internalized stigma in bipolar patients and their
treatment partners. Psychiatry Res 2015;230:436-40.
67-Ociskova M, Prasko J, Kamaradova D, et al. Individual correlates of self-stigma in patients with anxiety disorders with and without comorbidities.
Neuropsychiatr Dis Treat 2015;11:1767-79.
68-Borecki L, Gozdzik-Zelazny A, Pokorski M. Personality and perception of stigma in psychiatric patients with depressive disorders. Eur J Med Res
2010;15(Suppl. 2):10-6.
69-Bradstreet S, Dodd A, Jones S. Internalized stigma in mental health: An investigation of the role of attachment style. Psychiatry Res
2018;270:1001-9.
70-Døssing M, Nilsson KK, Svejstrup SR, et al. Low self-compassion in patients with bipolar disorder. Compr Psychiatry 2015;60:53-8.
71-Mersh L, Jones F, Oliver J. Mindfulness, self-stigma and social functioning in first episode psychosis: A brief report. Psychosis 2015;7:1-4
72-Adewuya AO, Owoeye AO, Erinfolami AO, et al. Correlates of self-stigma among outpatients with mental illness in Lagos, Nigeria. Int J Soc
Psychiatry 2011;57:418-27.
73-Schrank B, Amering M, Hay AG, et al. Insight, positive and negative symptoms, hope, depression and self-stigma: a comprehensive model of
mutual influences in schizophrenia spectrum disorders. Epidemiol Psychiatr Sci 2014;23:271-9.
74-Sharaf AY, Ossman LH, Lachine OA. A cross-sectional study of the relationships between illness insight, internalized stigma, and suicide risk in
individuals with schizophrenia. Int J Nurs Stud 2012;49:1512-20.
75-Cavelti M, Kvrgic S, Beck EM, et al. Self-stigma and its relationship with insight, demoralization, and clinical outcome among people with
schizophrenia spectrum disorders. Compr Psychiatry 2012;53:468-79.
76-Gaziel M, Hasson-Ohayon I, Morag-Yaffe M, et al. Insight and satisfaction with life among adolescents with mental disorders: assessing
associations with self-stigma and parental insight. Eur Psychiatry 2015;30:329-33.
77-Lien YJ, Chang HA, Kao YC, et al. The impact of cognitive insight, self-stigma, and medication compliance on the quality of life in patients with
schizophrenia. Eur Arch Psychiatry Clin Neurosci 2018;268:27-38.
78-Lien YJ, Chang HA, Kao YC, et al. Insight, self-stigma and psychosocial outcomes in Schizophrenia: a structural equation modelling approach.
Epidemiol Psychiatr Sci 2018;27:176-85.
79-Lu Y, Wang X. Correlation between insight and internalized stigma in patients with schizophrenia. Shanghai Arch Psychiatry 2012;24:91-8.
80-Mak WW, Wu CF. Cognitive insight and causal attribution in the development of self-stigma among individuals with schizophrenia. Psychiatr
Serv 2006;57:1800-2.
81-Pruß L, Wiedl KH, Waldorf M. Stigma as a predictor of insight in schizophrenia. Psychiatry Res 2012;198:187-93.
Page 101
82-Grambal A, Prasko J, Kamaradova D, et al. Self-stigma in borderline personality disorder - cross-sectional comparison with schizophrenia
spectrum disorder, major depressive disorder, and anxiety disorders. Neuropsychiatr Dis Treat 2016;12:2439-48.
83-Vrbova K, Prasko J, Holubova M, et al. Self-stigma and schizophrenia: a cross-sectional study. Neuropsychiatr Dis Treat 2016;12:3011-20
84-Holubova M, Prasko J, Ociskova M, et al. Self-stigma and quality of life in patients with depressive disorder: a cross-sectional study.
Neuropsychiatr Dis Treat 2016;2016:2677-87
85-Pal A, Sharan P, Chadda RK. Internalized stigma and its impact in Indian outpatients with bipolar disorder. Psychiatry Res 2017;258:158-65
86-Chan SKW, Kao SYS, Leung SL, et al. Relationship between neurocognitive function and clinical symptoms with self-stigma in patients with
schizophrenia-spectrum disorders. J Ment Health 2017;23:1-6.
87-Lysaker PH, Buck KD, Taylor AC, et al. Associations of metacognition and internalized stigma with quantitative assessments of self-experience in
narratives of schizophrenia. Psychiatry Res 2008;157:31-8.
88-Lysaker PH, Vohs JL, Tsai J. Negative symptoms and concordant impairments in attention in schizophrenia: associations with social functioning,
hope, self-esteem and internalized stigma. Schizophr Res 2009;110:165-72.
89-Galderisi S, Rossi A, Rocca P, et al; Italian Network For Research on Psychoses. The influence of illness-related variables, personal resources and
context-related factors on real-life functioning of people with schizophrenia. World Psychiatry 2014;13:275-87.
90-Firmin RL, Lysaker PH, Luther L, et al. Internalized stigma in adults with early phase versus prolonged psychosis. Early Interv Psychiatry 2018.
91-Hasson-Ohayon I, Mashiach-Eizenberg M, Elhasid N, et al. Between self-clarity and recovery in schizophrenia: reducing the self-stigma and
finding meaning. Compr Psychiatry 2014;55:675-80
92-Hasson-Ohayon I, Mashiach-Eizenberg M, Lysaker PH, et al. Self-clarity and different clusters of insight and self-stigma in mental illness.
Psychiatry Res 2016;240:308-13.
93-Singh A, Mattoo SK, Grover S. Stigma and its correlates in patients with schizophrenia attending a general hospital psychiatric unit. Indian J
Psychiatry. 2016;58:291-300.
94-Surmann M, Gruchalla LV, Falke S, et al. The importance of strengthening competence and control beliefs in patients with psychosis to reduce
treatment hindering self-stigmatization. Psychiatry Res 2017;255:314-20.
95-O'Connor LK, Yanos PT, Firmin RL. Correlates and moderators of stigma resistance among people with severe mental illness. Psychiatry Res
2018;270:198-204.
96-Chronister J, Chou CC, Liao HY. The role of stigma coping and social support in mediating the effect of societal stigma on internalized stigma,
mental health recovery, and quality of life among people with serious mental illness. J community psychol 2013;41:582-600
97-Thoits PA, Link BG. Stigma Resistance and Wellbeing among People in Treatment for Psychosis. Soc. Ment Health 2016;6:1-20
Page 102
98-Holubova M, Prasko J, Hruby R, et al. Coping strategies and self-stigma in patients with schizophrenia-spectrum disorders. Patient Prefer
Adherence 2016;10:1151-8.
99-Espinosa R, Valiente C, Rigabert A, et al. Recovery style and stigma in psychosis: the healing power of integrating. Cogn Neuropsychiatry
2016;21:146-55.
100-Lysaker PH, Vohs J, Hasson-Ohayon I, et al. Depression and insight in schizophrenia: comparisons of levels of deficits in social cognition and
metacognition and internalized stigma across three profiles. Schizophr Res 2013;148:18-23.
101-Chan RCH, Mak WWS. Common sense model of mental illness: Understanding the impact of cognitive and emotional representations of mental
illness on recovery through the mediation of self-stigma. Psychiatry Res 2016;246:16-24.
102-Chiu MY, Davidson L, Lo WT, et al. Modeling self-agency among people with schizophrenia: empirical evidence for consumer-based recovery.
Psychopathology 2013;46:413-20.
103-Pyle M, Morrison AP. Internalised stereotypes across ultra-high risk of psychosis and psychosis populations. Psychosis 2017;9:1-9
104-Wang K, Link BG, Corrigan PW, et al. Perceived provider stigma as a predictor of mental health service users' internalized stigma and
disempowerment. Psychiatry Res 2018;259:526-31.
105-Makanjuola V, Esan Y, Oladeji B, et al. Explanatory model of psychosis: impact on perception of self-stigma by patients in three sub-saharan
African cities. Soc Psychiatry Psychiatr Epidemiol 2016;51:1645-54.
106-Chen ES, Chang WC, Hui CL, et al. Self-stigma and affiliate stigma in first-episode psychosis patients and their caregivers. Soc Psychiatry
Psychiatr Epidemiol 2016;51:1225-31.
107-Rüsch N, Müller M, Lay B, et al. Emotional reactions to involuntary psychiatric hospitalization and stigma-related stress among people with
mental illness. Eur Arch Psychiatry Clin Neurosci 2014;264:35-43
108-Farrelly S, Jeffery D, Rüsch N, et al. The link between mental health-related discrimination and suicidality: service user perspectives. Psychol
Med 2015;45:2013-22.
109-Chang CC, Wu TH, Chen CY, et al. Comparing Self-stigma Between People With Different Mental Disorders in Taiwan. J Nerv Ment Dis
2016;204:547-53
110-Rüsch N, Corrigan PW, Wassel A, et al. Ingroup perception and responses to stigma among persons with mental illness. Acta Psychiatr Scand
2009;120:320-8.
111-Campellone TR, Caponigro JM, Kring AM. The power to resist: the relationship between power, stigma, and negative symptoms in
schizophrenia. Psychiatry Res 2014;215:280-5.
112-Lanfredi M, Zoppei S, Ferrari C, et al; ASPEN Study group. Self-stigma as a mediator between social capital and empowerment among people
with major depressive disorder in Europe: the ASPEN study. Eur Psychiatry 2015;30:58-64.
Page 103
113-Cullen BA, Mojtabai R, Bordbar E, et al. Social network, recovery attitudes and internal stigma among those with serious mental illness. Int J
Soc Psychiatry 2017;63:448-58.
114-Xu Z, Müller M, Lay B, et al. Involuntary hospitalization, stigma stress and suicidality: a longitudinal study. Soc Psychiatry Psychiatr Epidemiol
2018;53:309-12.
115-Ho RWH, Chang WC, Kwong VWY, et al. Prediction of self-stigma in early psychosis: 3-Year follow-up of the randomized-controlled trial on
extended early intervention. Schizophr Res 2018;195:463-8.
116-Lysaker PH, Davis LW, Warman DM, et al. Stigma, social function and symptoms in schizophrenia and schizoaffective disorder: associations
across 6 months. Psychiatry Res 2007;149:89-95.
117-Moses T. Coping strategies and self-stigma among adolescents discharged from psychiatric hospitalization: a 6-month follow-up study. Int J Soc
Psychiatry 2015;61:188-97.
118-Stip E, Caron J, Tousignant M, et al. Suicidal Ideation and Schizophrenia: Contribution of Appraisal, Stigmatization, and Cognition. Can J
Psychiatry 2017;62:726-34.
119-Lagger N, Amering M, Sibitz I, et al. Stability and mutual prospective relationships of stereotyped beliefs about mental illness, hope and
depressive symptoms among people with schizophrenia spectrum disorders. Psychiatry Res 2018;268:484-9
120-Kvrgic S, Cavelti M, Beck EM, et al. Therapeutic alliance in schizophrenia: the role of recovery orientation, self-stigma, and insight. Psychiatry
Res 2013;209:15-20.
121-Hamann J, Bühner M, Rüsch N. Self-Stigma and Consumer Participation in Shared Decision Making in Mental Health Services. Psychiatr Serv
2017;68:783-8.
122-Lysaker PH, Roe D, Yanos PT. Toward understanding the insight paradox: internalized stigma moderates the association between insight and
social functioning, hope, and self-esteem among people with schizophrenia spectrum disorders. Schizophr Bull 2007;33:192-9.
123-Valiente C, Provencio M, Espinosa R, et al. Insight in paranoia: The role of experiential avoidance and internalized stigma. Schizophr Res
2015;164:214-20.
124-Bouvet C, Bouchoux A. Exploring the relationship between internalized stigma, insight and depression for inpatients with schizophrenia.
Encephale 2015;41:435-43.
125-MacDougall AG, Vandermeer MR, Norman RM. Negative future self as a mediator in the relationship between insight and depression in
psychotic disorders. Schizophr Res 2015;165:66-9.
126-Świtaj P, Grygiel P, Anczewska M, et al. Loneliness mediates the relationship between internalised stigma and depression among patients with
psychotic disorders. Int J Soc Psychiatry 2014;60(8):733-40
127-Rossi A, Galderisi S, Rocca P, et al; Italian Network for Research on Psychoses. Personal resources and depression in schizophrenia: The role of
self-esteem, resilience and internalized stigma. Psychiatry Res 2017;256:359-64.
Page 104
128-Mashiach-Eizenberg M, Hasson-Ohayon I, Yanos PT, et al. Internalized stigma and quality of life among persons with severe mental illness: the
mediating roles of self-esteem and hope. Psychiatry Res 2013;208:15-20.
129-Oexle N, Waldmann T, Staiger T, et al. Mental illness stigma and suicidality: the role of public and individual stigma. Epidemiol Psychiatr Sci
2018;27:169-75
130-Shin YJ, Joo YH, Kim JH. Self-perceived cognitive deficits and their relationship with internalized stigma and quality of life in patients with
schizophrenia. Neuropsychiatr Dis Treat 2016;12:1411-7.
131-Corrigan PW, Bink AB, Schmidt A, et al. What is the impact of self-stigma? Loss of self-respect and the "why try" effect. J Ment Health
2016;25:10-5.
132- Galderisi S, Rucci P, Kirkpatrick B, et al; Italian Network for Research on Psychoses. Interplay Among Psychopathologic Variables, Personal
Resources, Context-Related Factors, and Real-life Functioning in Individuals With Schizophrenia: A Network Analysis. JAMA Psychiatry
2018;75:396-404.
133- Park SG, Bennett ME, Couture SM, et al. Internalized stigma in schizophrenia: relations with dysfunctional attitudes, symptoms, and quality of
life. Psychiatry Res 2013;205:43-7.
134- Moriarty A, Jolley S, Callanan MM, et al. Understanding reduced activity in psychosis: the roles of stigma and illness appraisals. Soc Psychiatry
Psychiatr Epidemiol 2012;47:1685-93.
135- Cerit C, Filizer A, Tural Ü, et al. Stigma: a core factor on predicting functionality in bipolar disorder. Compr Psychiatry 2012;53:484-9.
136- Wainberg ML, Cournos F, Wall MM, et al. Mental illness sexual stigma: Implications for health and recovery. Psychiatr Rehabil J 2016;39:90-6.
137- Segalovich J, Doron A, Behrbalk P, et al. Internalization of stigma and self-esteem as it affects the capacity for intimacy among patients with
schizophrenia. Arch Psychiatr Nurs 2013;27:231-4.
138- Chan SYY, Ho GWK, Bressington D. Experiences of self-stigmatization and parenting in Chinese mothers with severe mental illness. Int J Ment
Health Nurs 2019;28:527-37.
139-Yildirim T, Kavak Budak F. The relationship between internalized stigma and loneliness in patients with schizophrenia. Perspect Psychiatr Care
2019. doi: 10.1111/ppc.12399.
140-Aydemir O, Akkaya C. Association of social anxiety with stigmatisation and low self-esteem in remitted bipolar patients. Acta Neuropsychiatr
2011;23:224-8.
141-Denenny D, Thompson E, Pitts SC, et al. Subthreshold psychotic symptom distress, self-stigma, and peer social support among college students
with mental health concerns. Psychiatr Rehabil J 2015;38:164-70.
142-Rüsch N, Heekeren K, Theodoridou A, et al. Stigma as a stressor and transition to schizophrenia after one year among young people at risk of
psychosis. Schizophr Res 2015;166:43-8.
Page 105
143-Prasko J, Ociskova M, Grambal A et al. Personality features, dissociation, self-stigma, hope, and the complex treatment of depressive disorder.
Neuropsychiatr Dis Treat 2016;12:2539-52.
144-Oexle N, Rüsch N, Viering S, et al. Self-stigma and suicidality: a longitudinal study. Eur Arch Psychiatry Clin Neurosci 2017;267:359-61.
145-Cavelti M, Rüsch N, Vauth R. Is living with psychosis demoralizing? Insight, self-stigma, and clinical outcome among people with schizophrenia
across 1 year. J Nerv Ment Dis 2014;202:521-9.
146-Lysaker PH, Yanos PT, Outcalt J, et al. Association of stigma, self-esteem, and symptoms with concurrent and prospective assessment of social
anxiety in schizophrenia. Clin Schizophr Relat Psychoses 2010;4:41-8.
147-Pyle M, Stewart SL, French P, et al. Internalized stigma, emotional dysfunction and unusual experiences in young people at risk of psychosis.
Early Interv Psychiatry 2015;9:133-40.
148-Ritsher JB, Phelan JC. Internalized stigma predicts erosion of morale among psychiatric outpatients. Psychiatry Res 2004;129:257-65.
149-Rüsch N, Corrigan PW, Wassel A, et al. Self-stigma, group identification, perceived legitimacy of discrimination and mental health service use.
Br J Psychiatry 2009;195:551-2.
150-Chio FHN, Mak WWS, Chan RCH, et al. Unraveling the insight paradox: One-year longitudinal study on the relationships between insight, self-
stigma, and life satisfaction among people with schizophrenia spectrum disorders. Schizophr Res 2018;pii:S0920-9964(18)30034-3.
151-Oexle N, Müller M, Kawohl W, et al. Self-stigma as a barrier to recovery: a longitudinal study. Eur Arch Psychiatry Clin Neurosci
2018;268:209-12.
152-Campbell DG, Bonner LM, Bolkan CR, et al. Stigma Predicts Treatment Preferences and Care Engagement Among Veterans Affairs Primary
Care Patients with Depression. Ann Behav Med 2016;50:533-44.
153-Berry C, Greenwood K. Direct and indirect associations between dysfunctional attitudes, self-stigma, hopefulness and social inclusion in young
people experiencing psychosis. Schizophrenia Research 2018;193:197–203
154-Xu Z, Mayer B, Müller M, et al. Stigma and suicidal ideation among young people at risk of psychosis after one year. Psychiatry Res
2016;243:219-24.
155-Xu Z, Müller M, Heekeren K, et al. Self-labelling and stigma as predictors of attitudes towards help-seeking among people at risk of psychosis:
1-year follow-up. Eur Arch Psychiatry Clin Neurosci 2016;266:79-82.
156-Yanos PT, West ML, Gonzales L, et al. Change in internalized stigma and social functioning among persons diagnosed with severe mental
illness. Psychiatry Res 2012;200:1032-4.
157- Sibitz I, Unger A, Woppmann A, et al. Stigma resistance in patients with schizophrenia. Schizophr Bull 2011;37:316-23.
158-Bifftu BB, Dachew BA, Tiruneh BT. Stigma resistance among people with schizophrenia at Amanuel Mental Specialized Hospital Addis Ababa,
Ethiopia: a cross-sectional institution based study. BMC Psychiatry 2014;14:259.
Page 106
159- Mosanya TJ, Adelufosi AO, Adebowale OT, et al. Self-stigma, quality of life and schizophrenia: An outpatient clinic survey in Nigeria. Int J Soc
Psychiatry 2014;60:377-86.
160-Vidović D, Brecić P, Vilibić M, et al. Insight and self-stigma in patients with schizophrenia. Acta Clin Croat 2016;55:23-8.
161-Firmin RL, Luther L, Salyers MP, et al. Greater Metacognition and Lower Fear of Negative Evaluation: Potential Factors Contributing to
Improved Stigma Resistance among Individuals Diagnosed with Schizophrenia. Isr J Psychiatry Relat Sci 2017;54(1):50-4.
162-Kao YC, Lien YJ, Chang HA,et al. Stigma Resistance in Stable Schizophrenia: The Relative Contributions of Stereotype Endorsement, Self-
Reflection, Self-Esteem, and Coping Styles. Can J Psychiatry 2017;62:735-44.
163-Nabors LM, Yanos PT, Roe D, et al. Stereotype endorsement, metacognitive capacity, and self-esteem as predictors of stigma resistance in
persons with schizophrenia. Compr Psychiatry 2014;55:792-8.
164-Yang LH, Link BG, Ben-David S, et al. Stigma related to labels and symptoms in individuals at clinical high-risk for psychosis. Schizophr Res
2015;168:9-15.
165-Watson AC, Corrigan P, Larson JE, et al. Self-stigma in people with mental illness. Schizophr Bull 2007;33:1312-8
166-Johnson S, Lamb D, Marston L, et al. Peer-supported self-management for people discharged from a mental health crisis team: a randomised
controlled trial. Lancet. 2018 ;392(10145):409-418.
167-Thornicroft G, Farrelly S, Szmukler G, et al. Clinical outcomes of Joint Crisis Plans to reduce compulsory treatment for people with psychosis: a
randomised controlled trial. Lancet. 2013 ;381(9878):1634-41.
168-Ashcraft L, Bloss M, Anthony WA. Best practices: The development and implementation of "no forcefirst" as a best practice. Psychiatr Serv.
2012;63(5):415-7.
169-Meadows G, Brophy L, Shawyer F, et al. REFOCUS-PULSAR recovery-oriented practice training in specialist mental health care: a stepped-
wedge cluster randomised controlled trial. Lancet Psychiatry. 2019 ;6(2):103-114.
170-Picco L, Lau YW, Pang S, et al. Subramaniam M. Mediating effects of self-stigma on the relationship between perceived stigma and
psychosocial outcomes among psychiatric outpatients: findings from a cross-sectional survey in Singapore. BMJ Open 2017;7:e018228.
171-Kamaradova D, Latalova K, Prasko J, et al. Connection between self-stigma, adherence to treatment, and discontinuation of medication. Patient
Prefer Adherence 2016;10:1289-98.
172-Sibitz I, Amering M, Unger A, et al. The impact of the social network, stigma and empowerment on the quality of life in patients with
schizophrenia. Eur Psychiatry 2011;26:28-33.
173-Rossi A, Amore M, Galderisi S, et al; Italian Network for Research on Psychoses. The complex relationship between self-reported 'personal
recovery' and clinical recovery in schizophrenia. Schizophr Res 2018;192:108-12.
174-Post F, Pardeller S, Frajo-Apor B, et al. Quality of life in stabilized outpatients with bipolar I disorder: Associations with resilience, internalized
stigma, and residual symptoms. J Affect Disord 2018;238:399-404.
Page 107
175-Moritz S, Spirandelli K, Happach I, et al. Dysfunction by Disclosure? Stereotype Threat as a Source of Secondary Neurocognitive
Malperformance in Obsessive-Compulsive Disorder. J Int Neuropsychol Soc 2018;24:584-92.
176-Livingston J, Patel N, Bryson S, et al. Stigma associated with mental illness among Asian men in Vancouver, Canada. Int J Soc Psychiatry
2018;64:679-89.
177-Boyd JE, Juanamarga J, Hashemi P. Stigma of taking psychiatric medications among psychiatric outpatient veterans. Psychiatr Rehabil J
2015;38:132-4.
178-Drapalski AL, Lucksted A, Perrin PB, et al. A model of internalized stigma and its effects on people with mental illness. Psychiatr Serv
2013;64:264-9.
179-Link BG, Wells J, Phelan JC, et al. Understanding the importance of "symbolic interaction stigma": How expectations about the reactions of
others adds to the burden of mental illness stigma. Psychiatr Rehabil J 2015;38:117-24.
180-Hill K, Startup M. The relationship between internalized stigma, negative symptoms and social functioning in schizophrenia: the mediating role
of self-efficacy. Psychiatry Res 2013;206:151-7.
181-Grover S, Hazari N, Aneja J, et al. Stigma and its correlates among patients with bipolar disorder: A study from a tertiary care hospital of North
India. Psychiatry Res 2016;244:109-16.
182-Picco L, Pang S, Lau YW, et al. Internalized stigma among psychiatric outpatients: Associations with quality of life, functioning, hope and self-
esteem. Psychiatry Res 2016;246:500-6.
183-Lv Y, Wolf A, Wang X. Experienced stigma and self-stigma in Chinese patients with schizophrenia. Gen Hosp Psychiatry 2013;35:83-8.
184-Li J, Guo YB, Huang YG, et al. Stigma and discrimination experienced by people with schizophrenia living in the community in Guangzhou,
China. Psychiatry Res 2017;255:225-31.
185-Ghanean H, Nojomi M, Jacobsson L. Internalized Stigma of Mental Illness in Tehran, Iran. Stigma Research and Action 2011;1:11-7
186-Çapar M, Kavak F. Effect of internalized stigma on functional recovery in patients with schizophrenia. Perspect Psychiatr Care 2019;55:103-11.
187-Olçun Z, Şahin Altun Ö. The Correlation Between Schizophrenic Patients' Level of Internalized Stigma and Their Level of Hope. Arch Psychiatr
Nurs 2017;31:332-7
188-Karakaş SA, Okanlı A, Yılmaz E. The Effect of Internalized Stigma on the Self Esteem in Patients with Schizophrenia. Arch Psychiatr Nurs
2016;30:648-52.
189-Yilmaz E, Okanlı A. The Effect of Internalized Stigma on the Adherence to Treatment in Patients With Schizophrenia. Arch Psychiatr Nurs
2015;29:297-301.
190-Aukst-Margetić BA, Jakovljević M, Ivanec D, et al. Relations of internalized stigma with temperament and character in patients with
schizophrenia. Compr Psychiatry 2010;51:603-6.

Page 108
191-Chuang SP, Wu JYW, Wang CS. Self-perception of mental illness, and subjective and objective cognitive functioning in people with
schizophrenia. Neuropsychiatr Dis Treat. 2019;15:967-76.
192-Wood L, Byrne R, Burke E, et al. The impact of stigma on emotional distress and recovery from psychosis: The mediatory role of internalised
shame and self-esteem. Psychiatry Res 2017;255:94-100.
193-Rüsch N, Corrigan PW, Heekeren K, et al. Well-being among persons at risk of psychosis: the role of self-labeling, shame, and stigma stress.
Psychiatr Serv 2014;65:483-9.
194-Stolzenburg S, Freitag S, Schmidt S, et al. Associations between causal attributions and personal stigmatizing attitudes in untreated persons with
current mental health problems. Psychiatry Res 2018;260:24-9.
195-Moses T. Self-labeling and its effects among adolescents diagnosed with mental disorders. Soc Sci Med 2009;68:570-8.
196-Korkmaz G, Küçük L. Internalized Stigma and Perceived Family Support in Acute Psychiatric In-Patient Units. Arch Psychiatr Nurs 2016;30:55-
61
197-Nagai K, Kajita E. "Coming Out" with a Mental Disorder in Japan: How Self-Stigma and Empowerment Affect this Decision. Issues Ment
Health Nurs 2018;39:215-25.
198-Ho WW, Chiu MY, Lo WT, et al. Recovery components as determinants of the health-related quality of life among patients with schizophrenia:
structural equation modelling analysis. Aust N Z J Psychiatry 2010;44:71-84.
199-Lazowski L, Koller M, Stuart H, et al. Stigma and discrimination in people suffering with a mood disorder: a cross-sectional study. Depress Res
Treat 2012;2012:724848.
200-Quinn DM, Williams MK, Weisz BM. From discrimination to internalized mental illness stigma: The mediating roles of anticipated
discrimination and anticipated stigma. Psychiatr Rehabil J 2015;38:103-8.
201- Szcześniak D, Kobyłko A, Wojciechowska I, et al. Internalized stigma and its correlates among patients with severe mental illness.
Neuropsychiatr Dis Treat 2018;14:2599-608
202-Jahn DR, Leith J, Muralidharan A, et al. The influence of experiences of stigma on recovery: Mediating roles of internalized stigma, self-esteem,
and self-efficacy. Psychiatr Rehabil J 2019. doi: 10.1037/prj0000377
203-Horsselenberg EM, van Busschbach JT, Aleman A, et al. Self-Stigma and Its Relationship with Victimization, Psychotic Symptoms and Self-
Esteem among People with Schizophrenia Spectrum Disorders. PLoS One 2016;11:e0149763.
204-Al-Khouja MA, Corrigan PW. Self-Stigma, Identity, and Co-Occurring Disorders. Isr J Psychiatry Relat Sci 2017;54:56-60
205-Busby Grant J, Bruce CP, Batterham PJ. Predictors of personal, perceived and self-stigma towards anxiety and depression. Epidemiol Psychiatr
Sci 2016;25:247-54.
206-Hofer A, Post F, Pardeller S, et al. Self-stigma versus stigma resistance in schizophrenia: Associations with resilience, premorbid adjustment, and
clinical symptoms. Psychiatry Res 2019;271:396-401.
Page 109
207-Kalisova L, Michalec J, Hadjipapanicolaou D, et al. Factors influencing the level of self-stigmatisation in people with mental illness. Int J Soc
Psychiatry 2018;64:374-80.
208-Au CH, Wong CS, Law CW, et al. Self-stigma, stigma coping and functioning in remitted bipolar disorder. Gen Hosp Psychiatry 2019;57:7-12.
209-Werner P, Aviv A, Barak Y. Self-stigma, self-esteem and age in persons with schizophrenia. Int Psychogeriatr 2008;20:174-87.
210-Werner P, Stein-Shvachman I, Heinik J. Perceptions of self-stigma and its correlates among older adults with depression: a preliminary study. Int
Psychogeriatr 2009;21:1180-9.
211-Morgades-Bamba CI, Fuster-Ruizdeapodaca MJ, Molero F. The impact of internalized stigma on the well-being of people with Schizophrenia.
Psychiatry Res 2019;271:621-7.
212-Holubova M, Prasko J, Matousek S, et al. Comparison of self-stigma and quality of life in patients with depressive disorders and schizophrenia
spectrum disorders - a cross-sectional study. Neuropsychiatr Dis Treat 2016;12:3021-30.
213-Świtaj P, Chrostek A, Grygiel P, et al. Exploring Factors Associated with the Psychosocial Impact of Stigma Among People with Schizophrenia
or Affective Disorders. Community Ment Health J 2016;52:370-8.
214-Karidi MV, Vassilopoulou D, Savvidou E, et al. Bipolar disorder and self-stigma: A comparison with schizophrenia. J Affect Disord
2015;184:209-15
215-Gaudiano BA, Miller IW. Self-stigma and attitudes about treatment in depressed patients in a hospital setting. Int J Soc Psychiatry 2013;59:586-
91.
216-Chan KK, Mak WW. The mediating role of self-stigma and unmet needs on the recovery of people with schizophrenia living in the community.
Qual Life Res 2014;23:2559-68.
217-Aakre JM, Klingaman EA, Docherty NM. The relationship between stigma sentiments and self-identity of individuals with schizophrenia.
Psychiatr Rehabil J 2015;38:125-31.
218-Collett N, Pugh K, Waite F, et al. Negative cognitions about the self in patients with persecutory delusions: An empirical study of self-
compassion, self-stigma, schematic beliefs, self-esteem, fear of madness, and suicidal ideation. Psychiatry Res 2016;239:79-84
219-Yoo T, Kim SW, Kim SY, et al. Relationship between Suicidality and Low Self-esteem in Patients with Schizophrenia. Clin Psychopharmacol
Neurosci. 2015;13:296-301.
220-Rossi A, Galderisi S, Rocca P, et al; Italian Network for Research on Psychoses. The relationships of personal resources with symptom severity
and psychosocial functioning in persons with schizophrenia: results from the Italian Network for Research on Psychoses study. Eur Arch Psychiatry
Clin Neurosci 2017;267:285-94.
221-Vazquez G, Kapczinski F, Magalhaes P, et al. Stigma and functioning in patients with bipolar disorder. J Affect Disord 2011;130:323-7.
222-Corrigan PW, Powell KJ, Rüsch N. How does stigma affect work in people with serious mental illnesses? Psychiatr Rehabil J. 2012
Sep;35(5):381-4.

Page 110
223-Elkington KS, Hackler D, Walsh TA, et al. Perceived mental illness stigma, intimate relationships and sexual risk behavior in youth with mental
illness. J Adolesc Res 2013;28:378-404.
224-Corrigan PW, Rafacz J, Rüsch N. Examining a progressive model of self-stigma and its impact on people with serious mental illness. Psychiatry
Res 2011;189:339-43.
225-Vrbova K, Prasko J, Ociskova M, et al. Suicidality, self-stigma, social anxiety and personality traits in stabilized schizophrenia patients - a cross-
sectional study. Neuropsychiatr Dis Treat 2018;14:1415-24.
226-Boerema AM, Kleiboer A, Beekman AT, et al. Determinants of help-seeking behavior in depression: a cross-sectional study. BMC Psychiatry
2016;16:78.
227-Schomerus G, Auer C, Rhode D, et al. Personal stigma, problem appraisal and perceived need for professional help in currently untreated
depressed persons. J Affect Disord 2012;139:94-7.
228-Uhlmann C, Kaehler J, Harris MS, et al. Negative impact of self-stigmatization on attitude toward medication adherence in patients with
psychosis. J Psychiatr Pract 2014;20:405-10.
229-Tsang HW. Stages of change, self-stigma, and treatment compliance among Chinese adults with severe mental illness. Hong Kong Med J
2013;19(Suppl. 9):4-8.
230-Fung KMT, Tsang HWH, Corrigan PW. Self-stigma of people with schizophrenia as predictor of their adherence to psychosocial treatment.
Psychiatr Rehabil J 2008;32:95-104.
231-Świtaj P, Grygiel P, Chrostek A, et al. The relationship between internalized stigma and quality of life among people with mental illness: are self-
esteem and sense of coherence sequential mediators? Qual Life Res 2017;26:2471-8.
232-Rüsch N, Corrigan PW, Todd AR, et al. Implicit self-stigma in people with mental illness. J Nerv Ment Dis 2010;198:150-3.
233-Corrigan PW, Sokol KA, Rüsch N. The impact of self-stigma and mutual help programs on the quality of life of people with serious mental
illnesses. Community Ment Health J 2013;49:1-6.
234-Vrbova K, Prasko J, Ociskova M, et al. Quality of life, self-stigma, and hope in schizophrenia spectrum disorders: a cross-sectional study.
Neuropsychiatr Dis Treat 2017 23;13:567-76.
235-Oliveira SE, Carvalho H, Esteves F. Internalized stigma and quality of life domains among people with mental illness: the mediating role of self-
esteem. J Ment Health 2016;25:55-61.
236-Caqueo-Urízar A, Urzúa A, Habib J, and al. Relationships between social stigma, stigma experience and self-stigma and impaired quality of life
in schizophrenia across three Latin-American countries. Eur Arch Psychiatry Clin Neurosci 2019. doi: 10.1007/s00406-019-01035-8
237-Xu Z, Müller M, Heekeren K, et al. Pathways between stigma and suicidal ideation among people at risk of psychosis. Schizophr Res
2016;172(1-3):184-8.

Page 111
238-Vass V, Sitko K, West S, et al. How stigma gets under the skin: the role of stigma, self-stigma and self-esteem in subjective recovery from
psychosis. Psychosis 2017;9:235-44.
239-Oliveira SE, Esteves F, Carvalho H. Clinical profiles of stigma experiences, self-esteem and social relationships among people with
schizophrenia, depressive, and bipolar disorders. Psychiatry Res 2015;229:167-73.
240-Mizuno Y, Hofer A, Suzuki T, et al. Clinical and biological correlates of resilience in patients with schizophrenia and bipolar disorder: A cross-
sectional study. Schizophr Res 2016;175:148-53.
241-Pérez-Garín D, Molero F, Bos AE. Internalized mental illness stigma and subjective well-being: The mediating role of psychological well-being.
Psychiatry Res 2015;228:325-31.
242-Norman RM, Windell D, Lynch J, et al. Parsing the relationship of stigma and insight to psychological well-being in psychotic disorders.
Schizophr Res 2011;133:3-7.
243-Ehrlich-Ben Or S, Hasson-Ohayon I, Feingold D, et al. Meaning in life, insight and self-stigma among people with severe mental illness. Compr
Psychiatry 2013;54:195-200.
244-Grover S, Hazari N, Aneja J, et al. Recovery and its correlates among patients with bipolar disorder: A study from a tertiary care centre in North
India. Int J Soc Psychiatry 2016;62:726-36.
245-Ociskova M, Prasko J, Vrbova K, et al. Self-stigma and treatment effectiveness in patients with anxiety disorders - a mediation analysis.
Neuropsychiatr Dis Treat 2018;14:383-92
246-Lau YW, Picco L, Pang S, et al. Stigma resistance and its association with internalised stigma and psychosocial outcomes among psychiatric
outpatients. Psychiatry Res 2017;257:72-8.
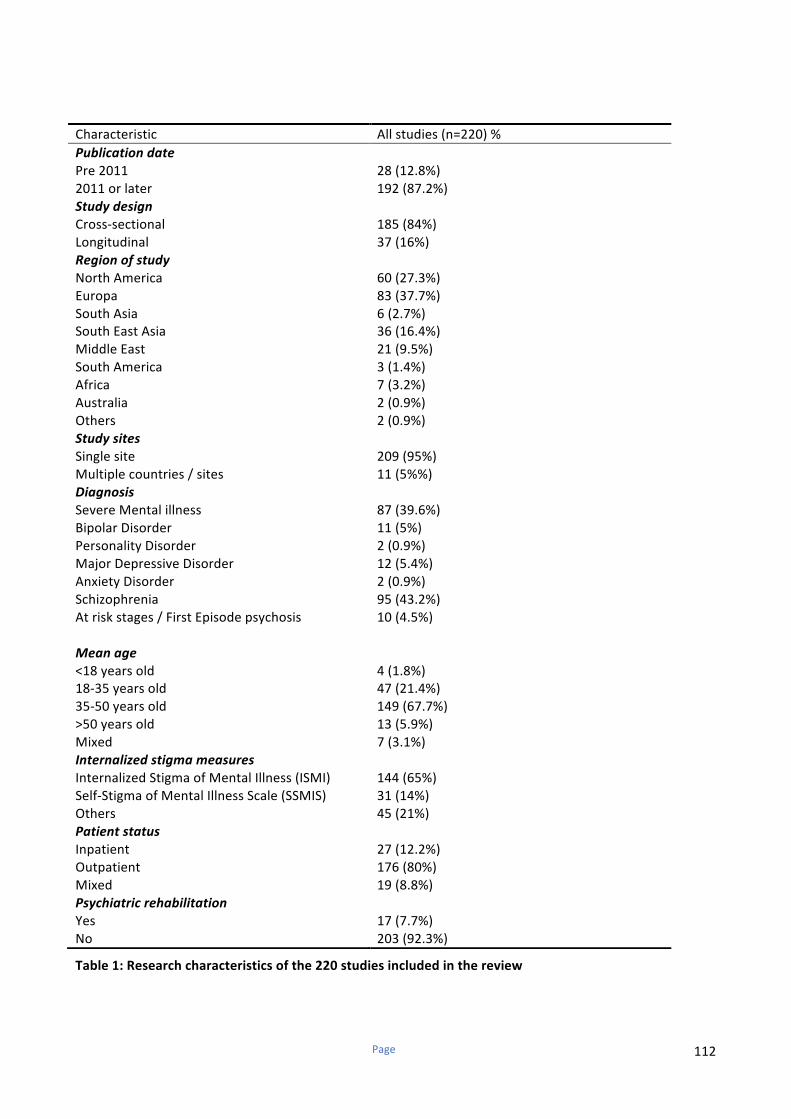
Page 112
Table1:Researchcharacteristicsofthe220studiesincludedinthereview
Characteristic Allstudies(n=220)%
Publicationdate
Pre2011 28(12.8%)
2011orlater 192(87.2%)
Studydesign
Cross-sectional 185(84%)
Longitudinal 37(16%)
Regionofstudy
NorthAmerica 60(27.3%)
Europa 83(37.7%)
SouthAsia
SouthEastAsia
6(2.7%)
36(16.4%)
MiddleEast 21(9.5%)
SouthAmerica 3(1.4%)
Africa 7(3.2%)
Australia
Others
2(0.9%)
2(0.9%)
Studysites
Singlesite 209(95%)
Multiplecountries/sites 11(5%%)
Diagnosis
SevereMentalillness 87(39.6%)
BipolarDisorder 11(5%)
PersonalityDisorder 2(0.9%)
MajorDepressiveDisorder 12(5.4%)
AnxietyDisorder 2(0.9%)
Schizophrenia 95(43.2%)
Atriskstages/FirstEpisodepsychosis 10(4.5%)
Meanage
<18yearsold 4(1.8%)
18-35yearsold 47(21.4%)
35-50yearsold 149(67.7%)
>50yearsold 13(5.9%)
Mixed 7(3.1%)
Internalizedstigmameasures
InternalizedStigmaofMentalIllness(ISMI) 144(65%)
Self-StigmaofMentalIllnessScale(SSMIS) 31(14%)
Others 45(21%)
Patientstatus
Inpatient 27(12.2%)
Outpatient 176(80%)
Mixed 19(8.8%)
Psychiatricrehabilitation
Yes
No
17(7.7%)
203(92.3%)
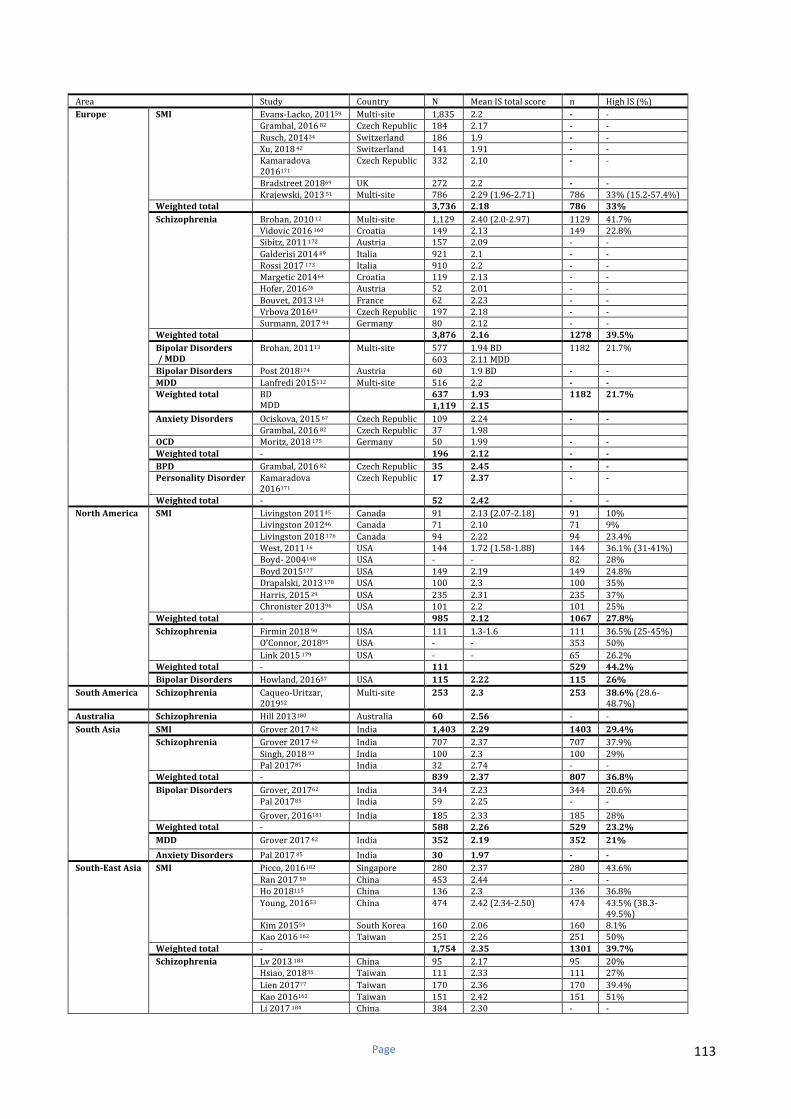
Page 113
Area Study Country N MeanIStotalscore n HighIS(%)
Europe
SMI
Evans-Lacko,201159 Multi-site 1,835 2.2 - -
Grambal,201682 CzechRepublic 184 2.17 - -
Rusch,201434 Switzerland 186 1.9 - -
Xu,201842 Switzerland 141 1.91 - -
Kamaradova
2016171CzechRepublic 332 2.10 - -
Bradstreet201869 UK 272 2.2 - -
Krajewski,201351 Multi-site 786 2.29(1.96-2.71) 786 33%(15.2-57.4%)
Weightedtotal 3,736 2.18 786 33%
Schizophrenia Brohan,201012 Multi-site 1,129 2.40(2.0-2.97) 1129 41.7%
Vidovic2016160 Croatia 149 2.13 149 22.8%
Sibitz,2011172 Austria 157 2.09 - -
Galderisi201489 Italia 921 2.1 - -
Rossi2017173 Italia 910 2.2 - -
Margetic201464 Croatia 119 2.13 - -
Hofer,201626 Austria 52 2.01 - -
Bouvet,2013124 France 62 2.23 - -
Vrbova201683 CzechRepublic 197 2.18 - -
Surmann,201794 Germany 80 2.12 - -
Weightedtotal 3,876 2.16 1278 39.5%
BipolarDisorders
/MDD
Brohan,201113 Multi-site 577 1.94BD 1182 21.7%
603 2.11MDD
BipolarDisorders Post2018174 Austria 60 1.9BD - -
MDD Lanfredi2015112 Multi-site 516 2.2 - -
Weightedtotal BD
MDD
637 1.93 1182
21.7%
1,119 2.15
AnxietyDisorders Ociskova,201567 CzechRepublic 109 2.24 - -
Grambal,201682 CzechRepublic 37 1.98
OCD Moritz,2018175 Germany 50 1.99 - -
Weightedtotal - 196 2.12 - -
BPD Grambal,201682 CzechRepublic 35 2.45 - -
PersonalityDisorder Kamaradova
2016171CzechRepublic 17 2.37 - -
Weightedtotal - 52 2.42 - -
NorthAmerica
SMI
Livingston201145 Canada 91 2.13(2.07-2.18) 91 10%
Livingston201246 Canada 71 2.10 71 9%
Livingston2018176 Canada 94 2.22 94 23.4%
West,201116 USA 144 1.72(1.58-1.88) 144 36.1%(31-41%)
Boyd-2004148 USA - - 82 28%
Boyd2015177 USA 149 2.19 149 24.8%
Drapalski,2013178 USA 100 2.3 100 35%
Harris,201529 USA 235 2.31 235 37%
Chronister201396 USA 101 2.2 101 25%
Weightedtotal - 985 2.12 1067 27.8%
Schizophrenia Firmin201890 USA 111 1.3-1.6 111 36.5%(25-45%)
O’Connor,201895 USA - - 353 50%
Link2015179 USA - - 65 26.2%
Weightedtotal - 111 529 44.2%
BipolarDisorders Howland,201657 USA 115 2.22 115 26%
SouthAmerica Schizophrenia Caqueo-Uritzar,
201952Multi-site 253 2.3 253 38.6%(28.6-
48.7%)
Australia Schizophrenia Hill2013180 Australia 60 2.56 - -
SouthAsia SMI Grover201762 India 1,403 2.29 1403 29.4%
Schizophrenia Grover201762 India 707 2.37 707 37.9%
Singh,201893 India 100 2.3 100 29%
Pal201785 India 32 2.74 - -
Weightedtotal - 839 2.37 807 36.8%
BipolarDisorders Grover,201762 India 344 2.23 344 20.6%
Pal201785 India 59 2.25 - -
Grover,2016181 India 185 2.33 185 28%
Weightedtotal - 588 2.26 529 23.2%
MDD Grover201762 India 352 2.19 352 21%
AnxietyDisorders Pal201785 India 30 1.97 - -
South-EastAsia
SMI Picco,2016182 Singapore 280 2.37 280 43.6%
Ran201758 China 453 2.44 - -
Ho2018115 China 136 2.3 136 36.8%
Young,201653 China 474 2.42(2.34-2.50) 474 43.5%(38.3-
49.5%)
Kim201554 SouthKorea 160 2.06 160 8.1%
Kao2016162 Taiwan 251 2.26 251 50%
Weightedtotal - 1,754 2.35 1301 39.7%
Schizophrenia Lv2013183 China 95 2.17 95 20%
Hsiao,201835 Taiwan 111 2.33 111 27%
Lien201777 Taiwan 170 2.36 170 39.4%
Kao2016162 Taiwan 151 2.42 151 51%
Li2017184 China 384 2.30 - -
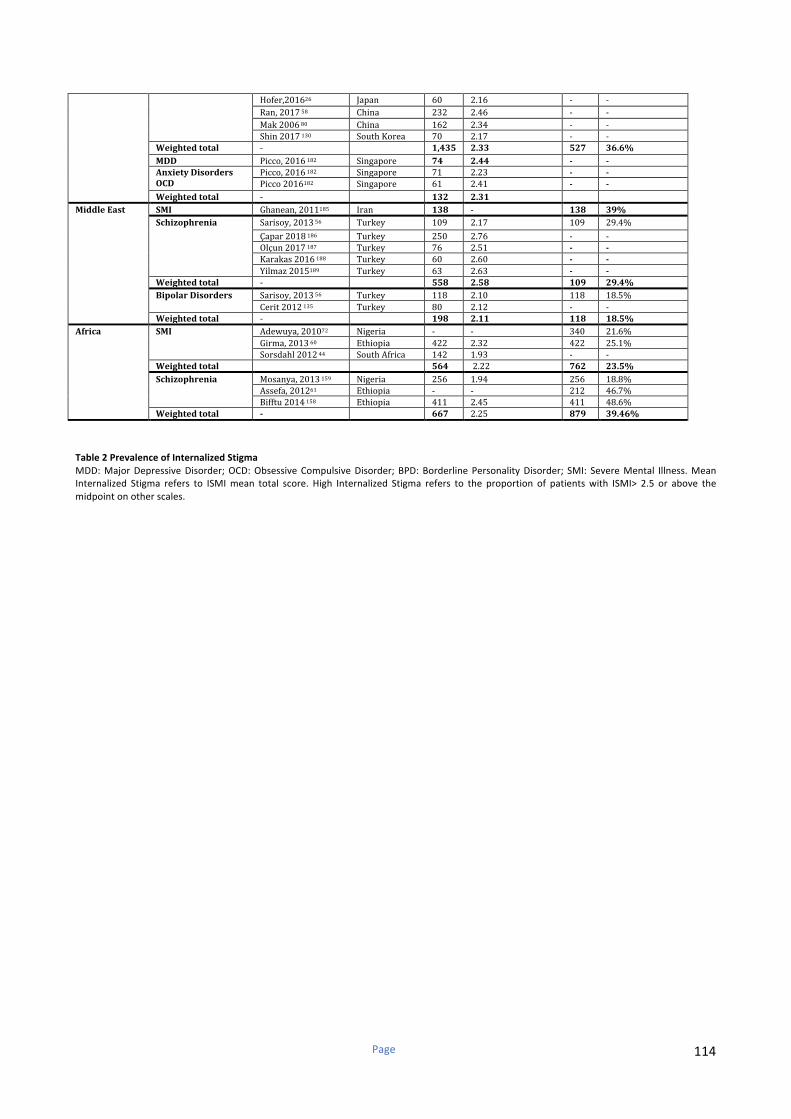
Page 114
Hofer,201626 Japan 60 2.16 - -
Ran,201758 China 232 2.46 - -
Mak200680 China 162 2.34 - -
Shin2017130 SouthKorea 70 2.17 - -
Weightedtotal - 1,435 2.33 527 36.6%
MDD Picco,2016182 Singapore 74 2.44 - -
AnxietyDisorders
OCD
Picco,2016182 Singapore 71 2.23 - -
Picco2016182 Singapore 61 2.41 - -
Weightedtotal - 132 2.31
MiddleEast
SMI Ghanean,2011185 Iran 138 - 138 39%
Schizophrenia Sarisoy,201356 Turkey 109 2.17 109 29.4%
Çapar2018186 Turkey 250 2.76 - -
Olçun2017187 Turkey 76 2.51 - -
Karakas2016188 Turkey 60 2.60 - -
Yilmaz2015189 Turkey 63 2.63 - -
Weightedtotal - 558 2.58 109 29.4%
BipolarDisorders Sarisoy,201356 Turkey 118 2.10 118 18.5%
Cerit2012135 Turkey 80 2.12 - -
Weightedtotal - 198 2.11 118 18.5%
Africa
SMI Adewuya,201072 Nigeria - - 340 21.6%
Girma,201360 Ethiopia 422 2.32 422 25.1%
Sorsdahl201244 SouthAfrica 142 1.93 - -
Weightedtotal 564 2.22 762 23.5%
Schizophrenia Mosanya,2013159 Nigeria 256 1.94 256 18.8%
Assefa,201261 Ethiopia - - 212 46.7%
Bifftu2014158 Ethiopia 411 2.45 411 48.6%
Weightedtotal - 667 2.25 879 39.46%
Table2PrevalenceofInternalizedStigma
MDD:MajorDepressiveDisorder;OCD:ObsessiveCompulsiveDisorder;BPD:BorderlinePersonalityDisorder; SMI: SevereMental Illness.Mean
Internalized Stigma refers to ISMImean total score. High Internalized Stigma refers to the proportion of patientswith ISMI> 2.5 or above the
midpointonotherscales.
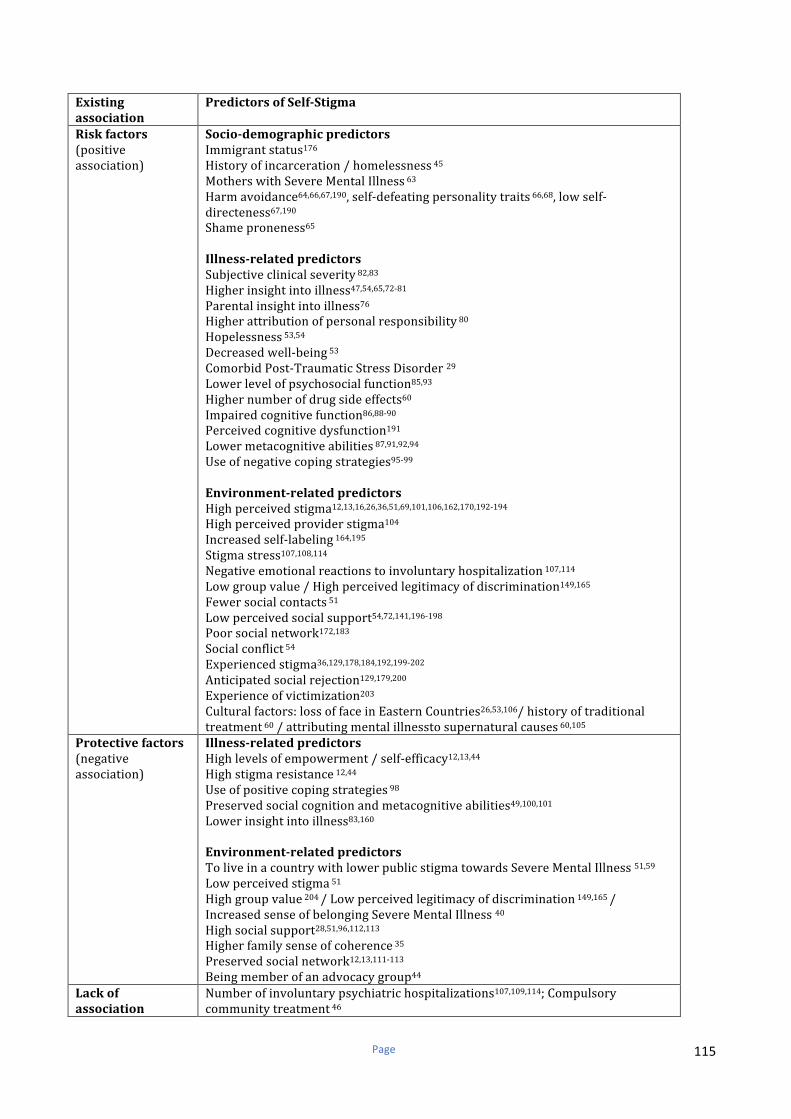
Page 115
Existing
association
PredictorsofSelf-Stigma
Riskfactors
(positive
association)
Socio-demographicpredictors
Immigrantstatus176
Historyofincarceration/homelessness45
MotherswithSevereMentalIllness63
Harmavoidance64,66,67,190,self-defeatingpersonalitytraits66,68,lowself-
directeness67,190
Shameproneness65
Illness-relatedpredictors
Subjectiveclinicalseverity82,83
Higherinsightintoillness47,54,65,72-81
Parentalinsightintoillness76
Higherattributionofpersonalresponsibility80
Hopelessness53,54
Decreasedwell-being53
ComorbidPost-TraumaticStressDisorder29
Lowerlevelofpsychosocialfunction85,93
Highernumberofdrugsideeffects60
Impairedcognitivefunction86,88-90
Perceivedcognitivedysfunction191
Lowermetacognitiveabilities87,91,92,94
Useofnegativecopingstrategies95-99
Environment-relatedpredictors
Highperceivedstigma12,13,16,26,36,51,69,101,106,162,170,192-194
Highperceivedproviderstigma104
Increasedself-labeling164,195
Stigmastress107,108,114
Negativeemotionalreactionstoinvoluntaryhospitalization107,114
Lowgroupvalue/Highperceivedlegitimacyofdiscrimination149,165
Fewersocialcontacts51
Lowperceivedsocialsupport54,72,141,196-198
Poorsocialnetwork172,183
Socialconflict54
Experiencedstigma36,129,178,184,192,199-202
Anticipatedsocialrejection129,179,200
Experienceofvictimization203
Culturalfactors:lossoffaceinEasternCountries26,53,106/historyoftraditional
treatment60/attributingmentalillnesstosupernaturalcauses60,105
Protectivefactors
(negative
association)
Illness-relatedpredictors
Highlevelsofempowerment/self-efficacy12,13,44
Highstigmaresistance12,44
Useofpositivecopingstrategies98
Preservedsocialcognitionandmetacognitiveabilities49,100,101
Lowerinsightintoillness83,160
Environment-relatedpredictors
ToliveinacountrywithlowerpublicstigmatowardsSevereMentalIllness51,59
Lowperceivedstigma51
Highgroupvalue204/Lowperceivedlegitimacyofdiscrimination149,165/
IncreasedsenseofbelongingSevereMentalIllness40
Highsocialsupport28,51,96,112,113
Higherfamilysenseofcoherence35
Preservedsocialnetwork12,13,111-113
Beingmemberofanadvocacygroup44
Lackof
association
Numberofinvoluntarypsychiatrichospitalizations107,109,114;Compulsory
communitytreatment46

Page 116
Forensicpatientstatus45
ComorbidSubstanceUseDisorder46
Attachmentstyle69
Highermindfulness71/LowSelf-compassion70
Stageofillness103
Mixedresults
Socio-demographicpredictors
Age:16,29,30,36,46,51,57,58,60,62,72,78,80,82,86,87,109,124,125,130,171,176,178,181,182,186,201,205-211
Maritalstatus:29,53,60,61,78,82-84,130,171,178,181,182,186,207
Gender:16,30,34,40,53,54,57,58-60,62,72,77,78,80,82,84,86,94,115,124,125,130,171,172,178,181,182,186,190,201,206-
208,211
Educationlevel:13,36,57,59,60,63,78,80,82-85,87,124,130,135,159,171,172,178,181-183,196,201,206,208,210
Employment:12,13,51,54,59,72,82,112,159,176,178,181-183,201,206,207,212
Income:58,62,72,85,159,181,186,210
Incomeassistance/Disabilitystatus29,46,83,207,208
Ruralresidence60-62/Farmers60
Veteranstatus16,29
Illness-relatedpredictors
Ageofonset6,16,57,62,77,78,109,171,172,206
Illnessduration36,46,57,62,72,77,78,80,90,130,172,183,201,207,211
Diagnosis4,13,29,30,34,36,51,53,54,56,58,59,62,67,72,82,85,109,162,170,171,178,182,196,201,207,212-214
Numberofpsychiatrichospitalizations6,16,54,60,78,82,83,87,109,112,135,171,172,183,190,201,208
Pastpsychiatricadmission:30,77,109,112,115,182,196
LongerdurationofdepressiveepisodesBipolarDisorders181/lowerremission
duration181
Inpatientstatus54,94,137,201,213,214
Severityofpsychiatricsymptoms45,54,57,67,80,159,178,215-217
Positive38,61,73,78,90,115,120,125,183,203,218andnegative
symptoms73,78,88,89,101,132,133,180,203,210
Residualdepressive/manicsymptoms57,62,135
Historyofsuicideattempt109,201,219
Self-esteem51,54,60,85,184
Existing
association
PredictorsofchangeinSelf-Stigma
Riskfactors
(positive
association)
Socio-demographicpredictors
Femalegender115
Illness-relatedpredictors
Priorpsychiatrichospitalization115
LongerDurationofUntreatedPsychosis115
Baselinepsychiatric114andpositivesymptoms38,115,116
Shame,self-contemptandstigmastress42,114
Emotionaldistress33,38
Lessadaptivecopingstrategiesatbaseline117
Protectivefactors
(negative
association)
Environment-relatedpredictors
Attendingtoarecovery-orienteddaycareprogram28-30/tovocational
rehabilitation33
Receivingnodisabilitybenefitsduringpsychiatricrehabilitation29
Workwithoutexperiencingdiscrimination34
Lackof
association
Comingoutandcomingoutassertiveness197
Mixedresults InternalizedStigmastabilityovertime32,117-119
Table3Cross-sectionalandlongitudinalpredictorsofInternalizedstigma
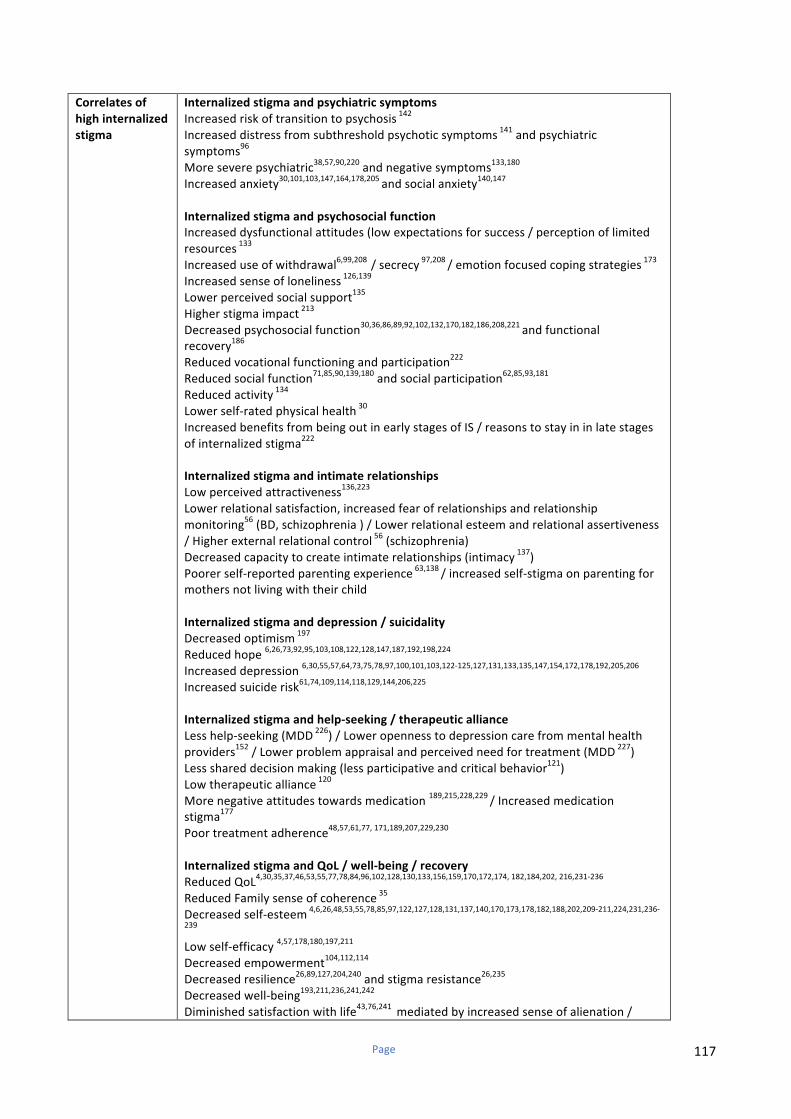
Page 117
Correlatesof
highinternalized
stigma
Internalizedstigmaandpsychiatricsymptoms
Increasedriskoftransitiontopsychosis142
Increaseddistressfromsubthresholdpsychoticsymptoms141
andpsychiatric
symptoms96
Moreseverepsychiatric38,57,90,220
andnegativesymptoms133,180
Increasedanxiety30,101,103,147,164,178,205
andsocialanxiety140,147
Internalizedstigmaandpsychosocialfunction
Increaseddysfunctionalattitudes(lowexpectationsforsuccess/perceptionoflimited
resources133
Increaseduseofwithdrawal6,99,208
/secrecy97,208
/emotionfocusedcopingstrategies173
Increasedsenseofloneliness126,139
Lowerperceivedsocialsupport135
Higherstigmaimpact213
Decreasedpsychosocialfunction30,36,86,89,92,102,132,170,182,186,208,221
andfunctional
recovery186
Reducedvocationalfunctioningandparticipation222
Reducedsocialfunction71,85,90,139,180
andsocialparticipation62,85,93,181
Reducedactivity134
Lowerself-ratedphysicalhealth30
IncreasedbenefitsfrombeingoutinearlystagesofIS/reasonstostayininlatestages
ofinternalizedstigma222
Internalizedstigmaandintimaterelationships
Lowperceivedattractiveness136,223
Lowerrelationalsatisfaction,increasedfearofrelationshipsandrelationship
monitoring56(BD,schizophrenia)/Lowerrelationalesteemandrelationalassertiveness
/Higherexternalrelationalcontrol56(schizophrenia)
Decreasedcapacitytocreateintimaterelationships(intimacy137
)
Poorerself-reportedparentingexperience63,138
/increasedself-stigmaonparentingfor
mothersnotlivingwiththeirchild
Internalizedstigmaanddepression/suicidality
Decreasedoptimism197
Reducedhope6,26,73,92,95,103,108,122,128,147,187,192,198,224
Increaseddepression6,30,55,57,64,73,75,78,97,100,101,103,122-125,127,131,133,135,147,154,172,178,192,205,206
Increasedsuiciderisk61,74,109,114,118,129,144,206,225
Internalizedstigmaandhelp-seeking/therapeuticalliance
Lesshelp-seeking(MDD226
)/Loweropennesstodepressioncarefrommentalhealth
providers152/Lowerproblemappraisalandperceivedneedfortreatment(MDD
227)
Lessshareddecisionmaking(lessparticipativeandcriticalbehavior121)
Lowtherapeuticalliance120
Morenegativeattitudestowardsmedication189,215,228,229
/Increasedmedication
stigma177
Poortreatmentadherence48,57,61,77,171,189,207,229,230
InternalizedstigmaandQoL/well-being/recovery
ReducedQoL4,30,35,37,46,53,55,77,78,84,96,102,128,130,133,156,159,170,172,174,182,184,202,216,231-236
ReducedFamilysenseofcoherence35
Decreasedself-esteem4,6,26,48,53,55,78,85,97,122,127,128,131,137,140,170,173,178,182,188,202,209-211,224,231,236-
239
Lowself-efficacy4,57,178,180,197,211
Decreasedempowerment104,112,114
Decreasedresilience26,89,127,204,240
andstigmaresistance26,235
Decreasedwell-being193,211,236,241,242
Diminishedsatisfactionwithlife43,76,241
mediatedbyincreasedsenseofalienation/
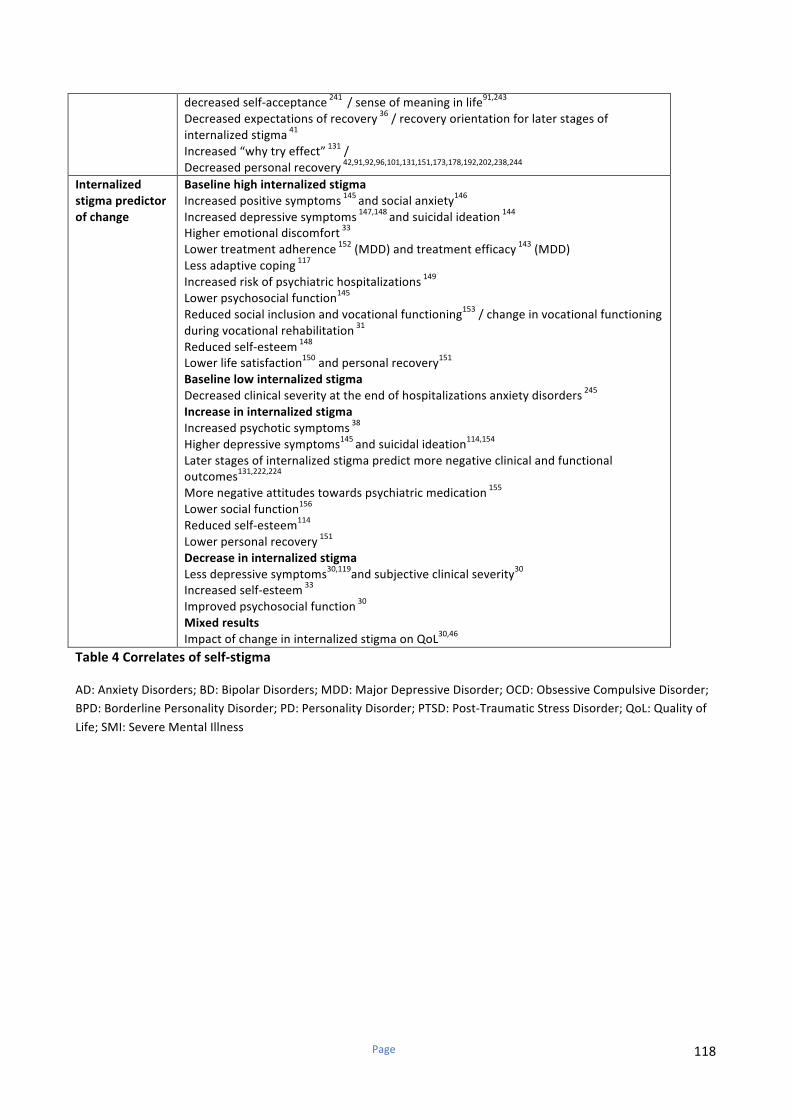
Page 118
decreasedself-acceptance241
/senseofmeaninginlife91,243
Decreasedexpectationsofrecovery36/recoveryorientationforlaterstagesof
internalizedstigma41
Increased“whytryeffect”131
/
Decreasedpersonalrecovery42,91,92,96,101,131,151,173,178,192,202,238,244
Internalized
stigmapredictor
ofchange
Baselinehighinternalizedstigma
Increasedpositivesymptoms145
andsocialanxiety146
Increaseddepressivesymptoms147,148
andsuicidalideation144
Higheremotionaldiscomfort33
Lowertreatmentadherence152
(MDD)andtreatmentefficacy143
(MDD)
Lessadaptivecoping117
Increasedriskofpsychiatrichospitalizations149
Lowerpsychosocialfunction145
Reducedsocialinclusionandvocationalfunctioning153/changeinvocationalfunctioning
duringvocationalrehabilitation31
Reducedself-esteem148
Lowerlifesatisfaction150andpersonalrecovery
151
Baselinelowinternalizedstigma
Decreasedclinicalseverityattheendofhospitalizationsanxietydisorders245
Increaseininternalizedstigma
Increasedpsychoticsymptoms38
Higherdepressivesymptoms145
andsuicidalideation114,154
Laterstagesofinternalizedstigmapredictmorenegativeclinicalandfunctional
outcomes131,222,224
Morenegativeattitudestowardspsychiatricmedication155
Lowersocialfunction156
Reducedself-esteem114
Lowerpersonalrecovery151
Decreaseininternalizedstigma
Lessdepressivesymptoms30,119
andsubjectiveclinicalseverity30
Increasedself-esteem33
Improvedpsychosocialfunction30
Mixedresults
ImpactofchangeininternalizedstigmaonQoL30,46
Table4Correlatesofself-stigma
AD:AnxietyDisorders;BD:BipolarDisorders;MDD:MajorDepressiveDisorder;OCD:ObsessiveCompulsiveDisorder;
BPD:BorderlinePersonalityDisorder;PD:PersonalityDisorder;PTSD:Post-TraumaticStressDisorder;QoL:Qualityof
Life;SMI:SevereMentalIllness
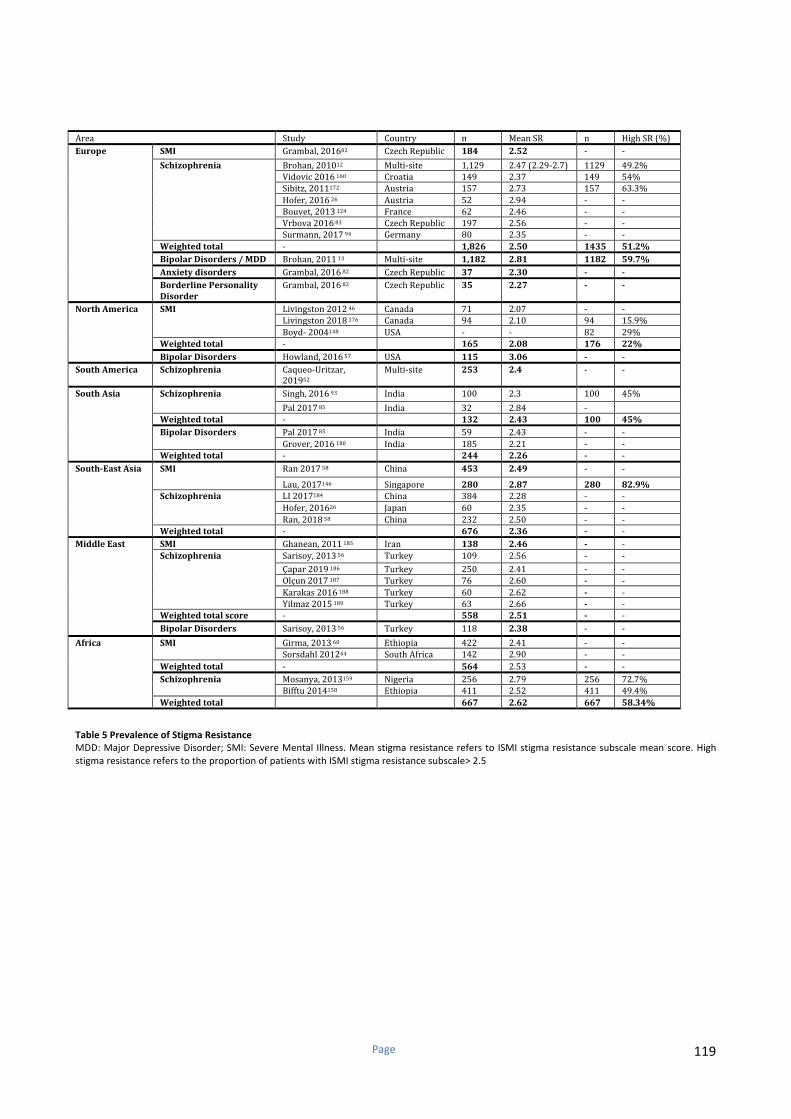
Page 119
Area Study Country n MeanSR n HighSR(%)
Europe
SMI Grambal,201682 CzechRepublic 184 2.52 - -
Schizophrenia
Brohan,201012 Multi-site 1,129 2.47(2.29-2.7) 1129 49.2%
Vidovic2016160 Croatia 149 2.37 149 54%
Sibitz,2011172 Austria 157 2.73 157 63.3%
Hofer,201626 Austria 52 2.94 - -
Bouvet,2013124 France 62 2.46 - -
Vrbova201683 CzechRepublic 197 2.56 - -
Surmann,201794 Germany 80 2.35 - -
Weightedtotal - 1,826 2.50 1435 51.2%
BipolarDisorders/MDD Brohan,201113 Multi-site 1,182 2.81 1182 59.7%
Anxietydisorders Grambal,201682 CzechRepublic 37 2.30 - -
BorderlinePersonality
Disorder
Grambal,201682 CzechRepublic 35 2.27 - -
NorthAmerica
SMI
Livingston201246 Canada 71 2.07 - -
Livingston2018176 Canada 94 2.10 94 15.9%
Boyd-2004148 USA - - 82 29%
Weightedtotal - 165 2.08 176 22%
BipolarDisorders Howland,201657 USA 115 3.06 - -
SouthAmerica Schizophrenia Caqueo-Uritzar,
201952
Multi-site 253 2.4 - -
SouthAsia Schizophrenia Singh,201693 India 100 2.3 100 45%
Pal201785 India 32 2.84 -
Weightedtotal - 132 2.43 100 45%
BipolarDisorders Pal201785 India 59 2.43 - -
Grover,2016180 India 185 2.21 - -
Weightedtotal - 244 2.26 - -
South-EastAsia SMI Ran201758 China 453 2.49 - -
Lau,2017146 Singapore 280 2.87 280 82.9%
Schizophrenia
LI2017184 China 384 2.28 - -
Hofer,201626 Japan 60 2.35 - -
Ran,201858 China 232 2.50 - -
Weightedtotal - 676 2.36 - -
MiddleEast
SMI Ghanean,2011185 Iran 138 2.46 - -
Schizophrenia
Sarisoy,201356 Turkey 109 2.56 - -
Çapar2019186 Turkey 250 2.41 - -
Olçun2017187 Turkey 76 2.60 - -
Karakas2016188 Turkey 60 2.62 - -
Yilmaz2015189 Turkey 63 2.66 - -
Weightedtotalscore - 558 2.51 - -
BipolarDisorders Sarisoy,201356 Turkey 118 2.38 - -
Africa
SMI Girma,201360 Ethiopia 422 2.41 - -
Sorsdahl201244 SouthAfrica 142 2.90 - -
Weightedtotal - 564 2.53 - -
Schizophrenia Mosanya,2013159 Nigeria 256 2.79 256 72.7%
Bifftu2014158 Ethiopia 411 2.52 411 49.4%
Weightedtotal 667 2.62 667 58.34%
Table5PrevalenceofStigmaResistance
MDD:MajorDepressiveDisorder;SMI:SevereMental Illness.MeanstigmaresistancereferstoISMIstigmaresistancesubscalemeanscore.High
stigmaresistancereferstotheproportionofpatientswithISMIstigmaresistancesubscale>2.5

Page 120
Partie IV. L’auto-stigmatisation et la résistance à la stigmatisation en France
Page 121
Satisfaction and Needs in Serious Mental Illness and
Autism Spectrum Disorder: The REHABase
Psychosocial Rehabilitation Project
Nicolas Franck, M.D., Ph.D., Laura Bon, M.Sc., Marie Dekerle, Ph.D., Julien Plasse, M.Sc., Catherine Massoubre, M.D., Ph.D.,
Romain Pommier, M.D., Emilie Legros-Lafarge, M.D., Nemat Jaafari, M.D., Ph.D., Nathalie Guillard-Bouhet, M.D.,
Clélia Quilès, M.D., Ph.D., Geoffroy Couhet, M.D., Hélène Verdoux, M.D., Ph.D., Benjamin Gouache, M.D.,
Brice Martin, M.D., Ph.D., Sophie Cervello, M.D., Caroline Demily, M.D., Ph.D., Julien Dubreucq, M.D.
Objective: The REHABase project is a French observational,
prospective, and multicenter cohort study of serious men-
tal illness and autism spectrum disorder (ASD), launched
in 2016 for a planned minimum duration of 15 years. The
aim is to characterize the care and quality-of-life needs of
participants. This article presents initial results from data
collection.
Methods: Psychosocial, cognitive, and functional data
were collected at baseline, annually, and after rehabil-
itation care. Data from the baseline evaluation on diag-
noses, medications, well-being, insight, life satisfaction,
and care needs are presented. The clinical profiles of
REHABase participants with serious mental illness or
ASD were assessed in relation to their level of satisfaction
with life and well-being in nine life dimensions and their
needs, according to their stage of recovery in a five-stage
model.
Results: Baseline data were collected for 1,397 participants
between January 2016 and August 2018. Main diagnoses
were schizophrenia spectrum disorder (49%); ASD (13%); and
personality (12%), bipolar (9%), and major depressive (6%)
disorders. More than 50% of participants reported needs for
care or interventions in four of nine dimensions: employ-
ment, cognitive functioning, symptom management, and
interpersonal relationships. Nearly half of participants were
not in the active stages of recovery (stages 4 and 5), and even
those considered to have reached the final stage continued
to require help in several areas.
Conclusions: Most participants had already received psych-
iatric care for several years, and most remained dissatisfied
with their social and emotional life and their psycholog-
ical well-being.
Psychiatric Services in Advance (doi: 10.1176/appi.ps.201800420)
In 2018, the World Health Organization highlighted that the
burden of mental illness continues to grow. This not only has
a significant impact on health but also has major social,
human rights, and economic consequences for countries all
over the world. Serious mental illness is defined as “a di-
agnosable mental, behavioral, or emotional disorder . . . that
has resulted in severe functional impairment” (1). It includes
schizophrenia, bipolar disorder, and borderline personality
disorder, as well as major depression and anxiety disorders
that cause severe and persistent functional impairment.
Autism spectrum disorder (ASD) is also associated with per-
sistent and significant social and communication impair-
ments (2, 3).
Access to a comprehensive standardized evaluation,
leading to personalized recovery-oriented care and to psy-
chosocial rehabilitation interventions, remains extremely
limited for individuals with schizophrenia and is almost
nonexistent for those with borderline personality disorder
or ASD (4). In France, a national network of rehabilitation
centers was set up under the French decree on the territory
HIGHLIGHTS
• The REHABase project is a French cohort study that aims
to characterize the rehabilitation needs of people with
serious mental illness and autism spectrum disorder (ASD).
• Most participants with serious mental illness and ASD
asked for help with employment, cognitive functioning,
symptom management, and interpersonal relationships.
• The level of dissatisfaction with life and well-being of
people with serious mental illness differed according to
the stage of recovery.
• Participants with serious mental illness considered to
have reached the final stage of their recovery process
continued to require help.
PS in Advance ps.psychiatryonline.org 1
ARTICLES

Page 122
national mental health plan for recovery-focused care. In-
dividuals who have serious mental illness or ASD (disorders
that present similar difficulties and rehabilitation needs) and
who are engaged in ongoing treatment delivered in public or
private mental health establishments are referred by their
psychiatrists to third-line rehabilitation centers for com-
plementary, customized evaluations and care. The REHA-
Base database project is a result of this national network.
Psychiatric rehabilitation helps people with serious
mental illness to “be successful and satisfied in the living,
working, learning, and social environments of their choice”
(5) by designing customized, recovery-oriented rehabil-
itation plans based on their perceived difficulties, re-
sources, needs for care, objectives, and preferred and valued
roles. Evaluations in psychiatric rehabilitation are used to
design individualized recovery-oriented intervention plans,
and to assess their effectiveness on clinical and functional
outcomes. However, rather than being regarded as as ther-
apeutic outcomes, these components are generally used to
describe a population; for example, investigators often ex-
amine the predictors of subjective quality of life (6) or job
satisfaction (7) or participants’ perception of the suitability
of services received in relation to their care needs (8).
Rehabilitation brings together a wide range of recovery-
oriented interventions. They include strengths-based case
management, improvements in physical and mental health
and well-being, low-dose psychotropic medication, cogni-
tive remediation, cognitive-behavioral therapy, psycho-
education, social skills training, stigma reduction, family
support, supported housing, and supported employment (5,
9, 10). Combining interventions is the key to effective ther-
apy. For instance, case management is more effective when
combined with other therapies (11, 12). Psychosocial re-
habilitation has demonstrated significant positive effects on
hospitalization rates (13), symptoms, and social aspects of
schizophrenia (14, 15). It has also shown effectiveness in the
treatment of bipolar disorder (16), borderline personality
disorder (17), and ASD (18). Today, although these inter-
ventions figure in international guidelines, they are not
widely used in routine clinical practice, and not all patients
have access to a comprehensive evaluation. Psychosocial
impairments are still underdetected and underestimated,
and thus they remain untreated, leading to poorer functional
outcomes and quality of life.
Quantitative research on recovery among individuals
with serious mental illness has been conducted from a
clinical perspective (i.e., focusing more on clinical and
functional outcomes than on empowerment, autonomy, and
agency, which are key to personal recovery) (19). Recovery
rates remain low to moderate, depending on the definition of
clinical recovery. For example, Salzer et al. (20), who defined
recovery as absence of substantial interference or limitation
in major life activities in the past 12 months, found a rate of
approximately one-third among 2,401 participants with a
lifetime serious mental illness. In a review and meta-
analysis, Jääskeläinen et al. (21), who defined recovery as
clinical remission and social recovery for at least 2 years,
found a rate of 13.5% in a sample of persons with
schizophrenia.
Subjective recovery does not perfectly fit the medical
definition of recovery. Therefore, it depends on a person’s
life goals (22). Supporting personal recovery (defined as “a
deeply personal, unique process of changing one’s attitudes,
values, feelings, goals, skills and/or roles . . . a way of living a
satisfying, hopeful and contributing life even with the limi-
tations caused by illness” [23]) is therefore one of the major
objectives of psychiatric rehabilitation (5). Andresen and
colleagues (24) defined five stages of recovery on which they
later based the STORI (STage Of Recovery Instrument),
which is part of the REHABase assessment. The first stage is
the moratorium, during which the person is overwhelmed
by his or her disability. The second stage is awareness, when
hope returns. The person starts developing skills during the
third stage, preparation. Then comes rebuilding, where re-
covery truly starts, with steps forward and steps back, and
finally growth, which is considered as the end goal of re-
covery. Individuals now have faith in their abilities and can
handle any setbacks. Of interest, all these stages were found
to correlate with other scales that evaluate hope or with
recovery-based scales that use other theoretical models.
However, the authors suggested that the five stages might
overlap, because only three consistent clusters were found
in a cluster analysis. This lack of specificity might also be
explained by the nonlinear aspect of the recovery process.
The rehabilitation centers in France offer personal-
ized cognitive remediation, psychoeducation, and cognitive-
behavioral therapy to help participants implement their
life plans according to their strengths and weaknesses (25)
for a limited duration (2–3 years of follow-up). The centers
aim to help participants develop strategies they can use on
their own. Service users also have representative commit-
tees and participate in writing presentation documents. In
this article, we present initial data on the clinical profiles,
requests, and recovery stages of persons with serious men-
tal illness or ASD participating in the REHABase project.
We hypothesized that participants’ requests for help would
differ according to their recovery stage.
METHODS
The REHABase project is an observational, prospective, and
multicenter cohort study launched in 2016 for a planned
minimum duration of 15 years. REHABase is supported by
the French Regional Health Agencies of Auvergne-Rhône-
Alpes and Nouvelle-Aquitaine. Since 2016, five support–
psychosocial rehabilitation centers have contributed to the
data collection: Lyon, Grenoble, and Saint-Etienne since
January 2016 and Bordeaux and Limoges/Poitiers since
December 2017. The centers selected to participate in the
REHABase network were previously involved in psychoso-
cial rehabilitation and recovery-oriented care. Regular group
meetings were held to select the instruments used for the
2 ps.psychiatryonline.org PS in Advance
SATISFACTION AND NEEDS IN SERIOUS MENTAL ILLNESS AND AUTISM SPECTRUM DISORDER
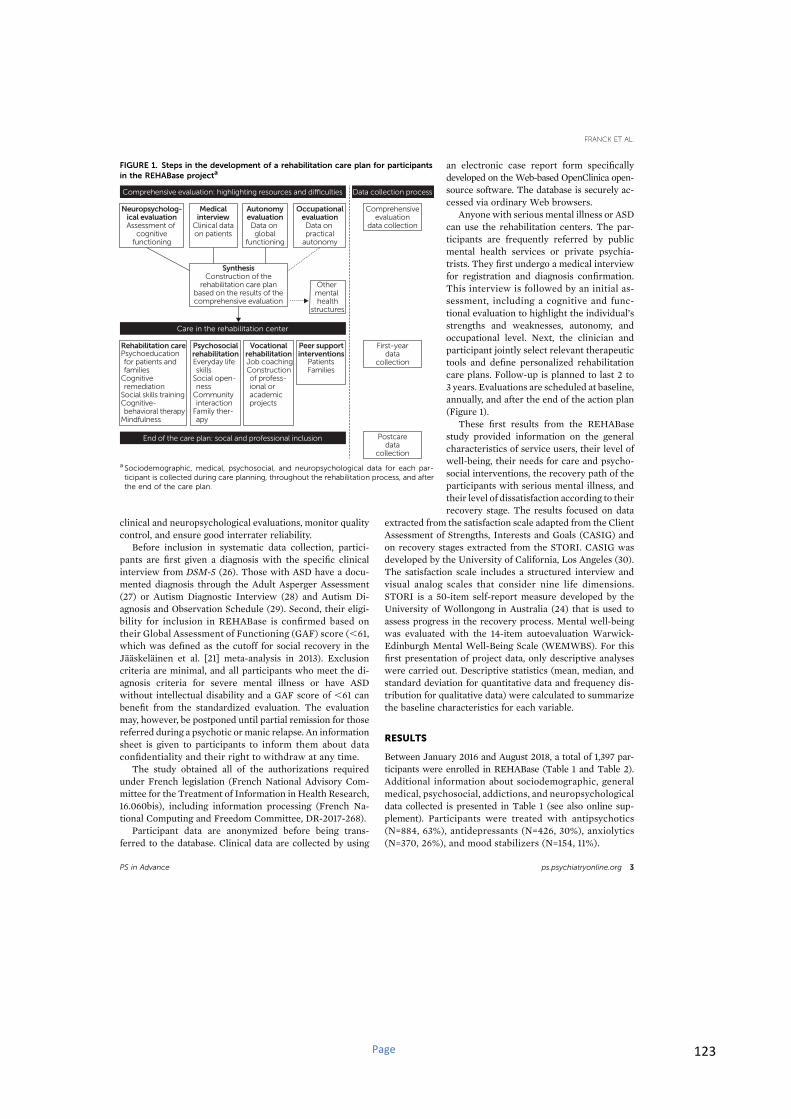
Page 123
clinical and neuropsychological evaluations, monitor quality
control, and ensure good interrater reliability.
Before inclusion in systematic data collection, partici-
pants are first given a diagnosis with the specific clinical
interview from DSM-5 (26). Those with ASD have a docu-
mented diagnosis through the Adult Asperger Assessment
(27) or Autism Diagnostic Interview (28) and Autism Di-
agnosis and Observation Schedule (29). Second, their eligi-
bility for inclusion in REHABase is confirmed based on
their Global Assessment of Functioning (GAF) score (,61,
which was defined as the cutoff for social recovery in the
Jääskeläinen et al. [21] meta-analysis in 2013). Exclusion
criteria are minimal, and all participants who meet the di-
agnosis criteria for severe mental illness or have ASD
without intellectual disability and a GAF score of ,61 can
benefit from the standardized evaluation. The evaluation
may, however, be postponed until partial remission for those
referred during a psychotic ormanic relapse. An information
sheet is given to participants to inform them about data
confidentiality and their right to withdraw at any time.
The study obtained all of the authorizations required
under French legislation (French National Advisory Com-
mittee for the Treatment of Information in Health Research,
16.060bis), including information processing (French Na-
tional Computing and Freedom Committee, DR-2017-268).
Participant data are anonymized before being trans-
ferred to the database. Clinical data are collected by using
an electronic case report form specifically
developed on the Web-based OpenClinica open-
source software. The database is securely ac-
cessed via ordinary Web browsers.
Anyone with serious mental illness or ASD
can use the rehabilitation centers. The par-
ticipants are frequently referred by public
mental health services or private psychia-
trists. They first undergo a medical interview
for registration and diagnosis confirmation.
This interview is followed by an initial as-
sessment, including a cognitive and func-
tional evaluation to highlight the individual’s
strengths and weaknesses, autonomy, and
occupational level. Next, the clinician and
participant jointly select relevant therapeutic
tools and define personalized rehabilitation
care plans. Follow-up is planned to last 2 to
3 years. Evaluations are scheduled at baseline,
annually, and after the end of the action plan
(Figure 1).
These first results from the REHABase
study provided information on the general
characteristics of service users, their level of
well-being, their needs for care and psycho-
social interventions, the recovery path of the
participants with serious mental illness, and
their level of dissatisfaction according to their
recovery stage. The results focused on data
extracted from the satisfaction scale adapted from the Client
Assessment of Strengths, Interests and Goals (CASIG) and
on recovery stages extracted from the STORI. CASIG was
developed by the University of California, Los Angeles (30).
The satisfaction scale includes a structured interview and
visual analog scales that consider nine life dimensions.
STORI is a 50-item self-report measure developed by the
University of Wollongong in Australia (24) that is used to
assess progress in the recovery process. Mental well-being
was evaluated with the 14-item autoevaluation Warwick-
Edinburgh Mental Well-Being Scale (WEMWBS). For this
first presentation of project data, only descriptive analyses
were carried out. Descriptive statistics (mean, median, and
standard deviation for quantitative data and frequency dis-
tribution for qualitative data) were calculated to summarize
the baseline characteristics for each variable.
RESULTS
Between January 2016 and August 2018, a total of 1,397 par-
ticipants were enrolled in REHABase (Table 1 and Table 2).
Additional information about sociodemographic, general
medical, psychosocial, addictions, and neuropsychological
data collected is presented in Table 1 (see also online sup-
plement). Participants were treated with antipsychotics
(N=884, 63%), antidepressants (N=426, 30%), anxiolytics
(N=370, 26%), and mood stabilizers (N=154, 11%).
FIGURE 1. Steps in the development of a rehabilitation care plan for participants
in the REHABase projecta
Data collection processComprehensive evaluation: highlighting resources and difficulties
Neuropsycholog-ical evaluationAssessment of
cognitivefunctioning
SynthesisConstruction of the
rehabilitation care planbased on the results of thecomprehensive evaluation
Medicalinterview
Clinical dataon patients
AutonomyevaluationData on global
functioning
OccupationalevaluationData on practical
autonomy
Care in the rehabilitation center
End of the care plan: socal and professional inclusion
Rehabilitation care Vocationalrehabilitation
Peer supportinterventions
Other mental health
structures
Comprehensiveevaluation
data collection
First-yeardata
collection
Postcaredata
collection
Psychoeducationfor patients andfamilies
Cognitive remediation
Social skills trainingCognitive-behavioral therapy
Mindfulness
PsychosocialrehabilitationEveryday lifeskills
Social open-ness
Communityinteraction
Family ther-apy
Job coachingConstructionof profess-ional oracademicprojects
PatientsFamilies
a Sociodemographic, medical, psychosocial, and neuropsychological data for each par-
ticipant is collected during care planning, throughout the rehabilitation process, and after
the end of the care plan.
PS in Advance ps.psychiatryonline.org 3
FRANCK ET AL.
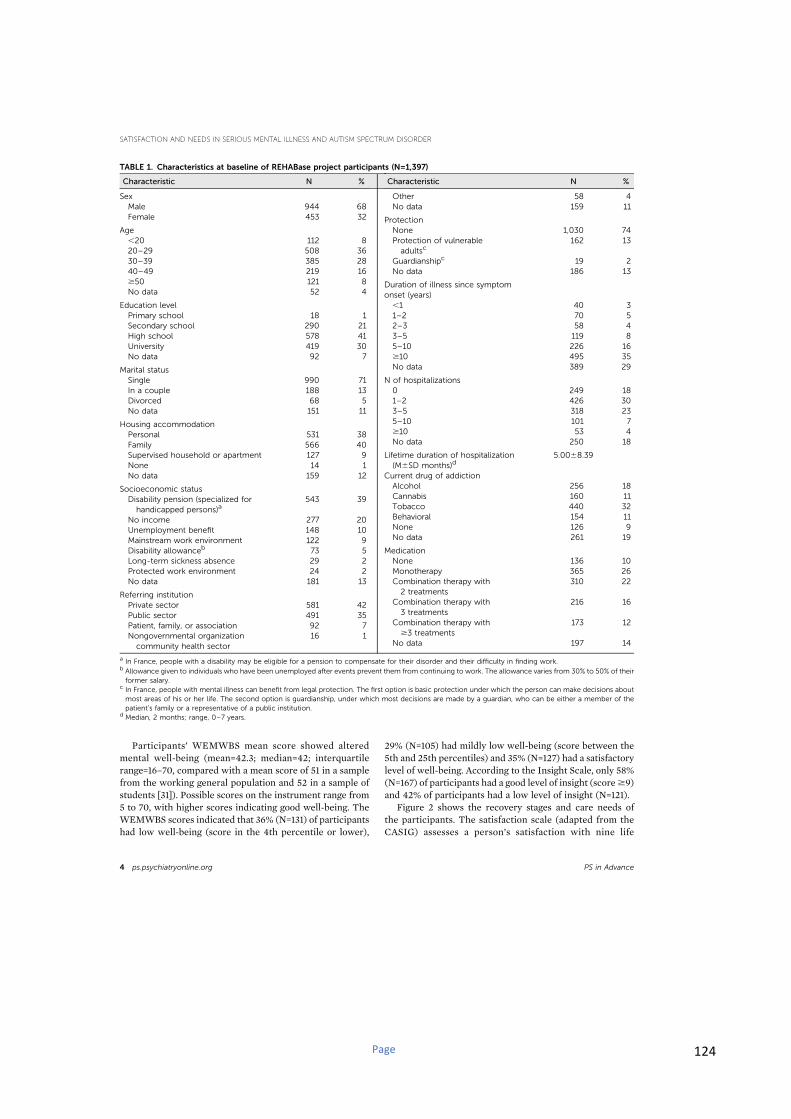
Page 124
Participants’ WEMWBS mean score showed altered
mental well-being (mean=42.3; median=42; interquartile
range=16–70, compared with a mean score of 51 in a sample
from the working general population and 52 in a sample of
students [31]). Possible scores on the instrument range from
5 to 70, with higher scores indicating good well-being. The
WEMWBS scores indicated that 36% (N=131) of participants
had low well-being (score in the 4th percentile or lower),
29% (N=105) had mildly low well-being (score between the
5th and 25th percentiles) and 35% (N=127) had a satisfactory
level of well-being. According to the Insight Scale, only 58%
(N=167) of participants had a good level of insight (score$9)
and 42% of participants had a low level of insight (N=121).
Figure 2 shows the recovery stages and care needs of
the participants. The satisfaction scale (adapted from the
CASIG) assesses a person’s satisfaction with nine life
TABLE 1. Characteristics at baseline of REHABase project participants (N=1,397)
Characteristic N %
Sex
Male 944 68
Female 453 32
Age
,20 112 8
20–29 508 36
30–39 385 28
40–49 219 16
$50 121 8
No data 52 4
Education level
Primary school 18 1
Secondary school 290 21
High school 578 41
University 419 30
No data 92 7
Marital status
Single 990 71
In a couple 188 13
Divorced 68 5
No data 151 11
Housing accommodation
Personal 531 38
Family 566 40
Supervised household or apartment 127 9
None 14 1
No data 159 12
Socioeconomic status
Disability pension (specialized for
handicapped persons)a543 39
No income 277 20
Unemployment benefit 148 10
Mainstream work environment 122 9
Disability allowanceb 73 5
Long-term sickness absence 29 2
Protected work environment 24 2
No data 181 13
Referring institution
Private sector 581 42
Public sector 491 35
Patient, family, or association 92 7
Nongovernmental organization
community health sector
16 1
Characteristic N %
Other 58 4
No data 159 11
Protection
None 1,030 74
Protection of vulnerable
adultsc162 13
Guardianshipc 19 2
No data 186 13
Duration of illness since symptom
onset (years)
,1 40 3
1–2 70 5
2–3 58 4
3–5 119 8
5–10 226 16
$10 495 35
No data 389 29
N of hospitalizations
0 249 18
1–2 426 30
3–5 318 23
5–10 101 7
$10 53 4
No data 250 18
Lifetime duration of hospitalization
(M6SD months)d5.0068.39
Current drug of addiction
Alcohol 256 18
Cannabis 160 11
Tobacco 440 32
Behavioral 154 11
None 126 9
No data 261 19
Medication
None 136 10
Monotherapy 365 26
Combination therapy with
2 treatments
310 22
Combination therapy with
3 treatments
216 16
Combination therapy with
$3 treatments
173 12
No data 197 14
a In France, people with a disability may be eligible for a pension to compensate for their disorder and their difficulty in finding work.b Allowance given to individuals who have been unemployed after events prevent them from continuing to work. The allowance varies from 30% to 50% of their
former salary.c In France, people with mental illness can benefit from legal protection. The first option is basic protection under which the person can make decisions about
most areas of his or her life. The second option is guardianship, under which most decisions are made by a guardian, who can be either a member of the
patient’s family or a representative of a public institution.d Median, 2 months; range, 0–7 years.
4 ps.psychiatryonline.org PS in Advance
SATISFACTION AND NEEDS IN SERIOUS MENTAL ILLNESS AND AUTISM SPECTRUM DISORDER
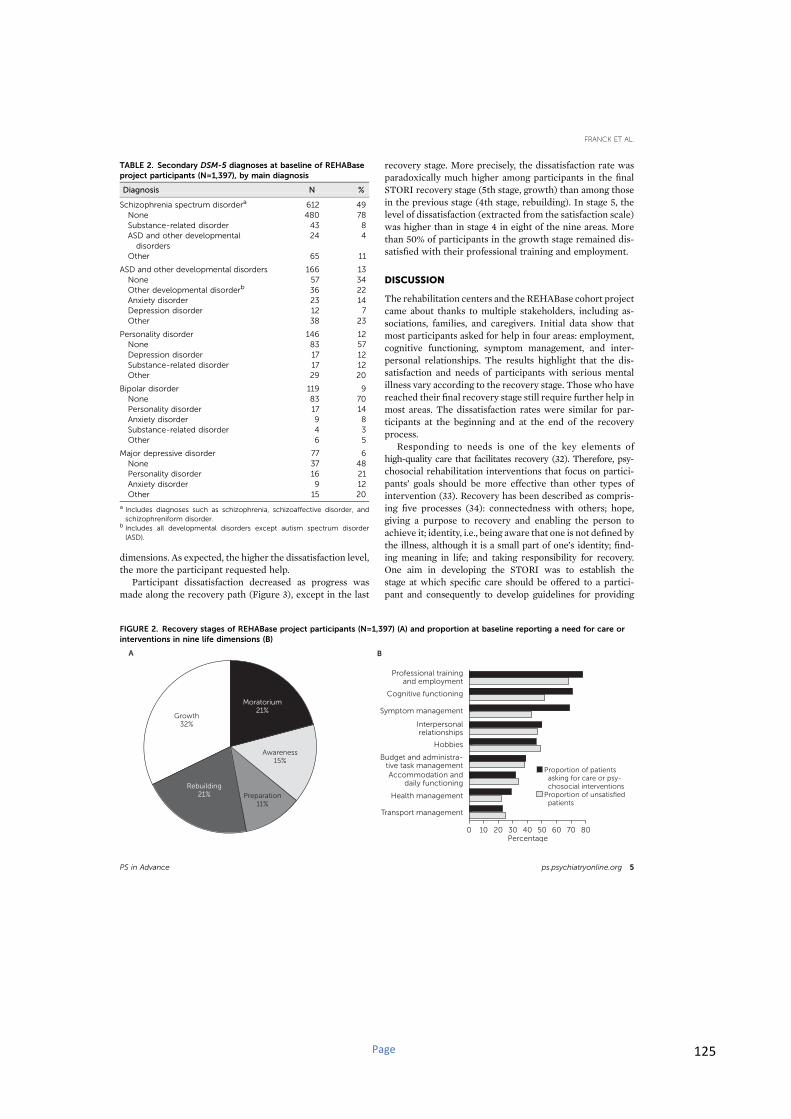
Page 125
dimensions. As expected, the higher the dissatisfaction level,
the more the participant requested help.
Participant dissatisfaction decreased as progress was
made along the recovery path (Figure 3), except in the last
recovery stage. More precisely, the dissatisfaction rate was
paradoxically much higher among participants in the final
STORI recovery stage (5th stage, growth) than among those
in the previous stage (4th stage, rebuilding). In stage 5, the
level of dissatisfaction (extracted from the satisfaction scale)
was higher than in stage 4 in eight of the nine areas. More
than 50% of participants in the growth stage remained dis-
satisfied with their professional training and employment.
DISCUSSION
The rehabilitation centers and the REHABase cohort project
came about thanks to multiple stakeholders, including as-
sociations, families, and caregivers. Initial data show that
most participants asked for help in four areas: employment,
cognitive functioning, symptom management, and inter-
personal relationships. The results highlight that the dis-
satisfaction and needs of participants with serious mental
illness vary according to the recovery stage. Those who have
reached their final recovery stage still require further help in
most areas. The dissatisfaction rates were similar for par-
ticipants at the beginning and at the end of the recovery
process.
Responding to needs is one of the key elements of
high-quality care that facilitates recovery (32). Therefore, psy-
chosocial rehabilitation interventions that focus on partici-
pants’ goals should be more effective than other types of
intervention (33). Recovery has been described as compris-
ing five processes (34): connectedness with others; hope,
giving a purpose to recovery and enabling the person to
achieve it; identity, i.e., being aware that one is not defined by
the illness, although it is a small part of one’s identity; find-
ing meaning in life; and taking responsibility for recovery.
One aim in developing the STORI was to establish the
stage at which specific care should be offered to a partici-
pant and consequently to develop guidelines for providing
TABLE 2. Secondary DSM-5 diagnoses at baseline of REHABase
project participants (N=1,397), by main diagnosis
Diagnosis N %
Schizophrenia spectrum disordera 612 49
None 480 78
Substance-related disorder 43 8
ASD and other developmental
disorders
24 4
Other 65 11
ASD and other developmental disorders 166 13
None 57 34
Other developmental disorderb 36 22
Anxiety disorder 23 14
Depression disorder 12 7
Other 38 23
Personality disorder 146 12
None 83 57
Depression disorder 17 12
Substance-related disorder 17 12
Other 29 20
Bipolar disorder 119 9
None 83 70
Personality disorder 17 14
Anxiety disorder 9 8
Substance-related disorder 4 3
Other 6 5
Major depressive disorder 77 6
None 37 48
Personality disorder 16 21
Anxiety disorder 9 12
Other 15 20
a Includes diagnoses such as schizophrenia, schizoaffective disorder, and
schizophreniform disorder.b Includes all developmental disorders except autism spectrum disorder
(ASD).
FIGURE 2. Recovery stages of REHABase project participants (N=1,397) (A) and proportion at baseline reporting a need for care or
interventions in nine life dimensions (B)
0 10 20 30 40 50 60 70 80
Professional trainingand employment
Cognitive functioning
Symptom management
Interpersonalrelationships
Accommodation anddaily functioning
Budget and administra-tive task management
Health management
Transport management
Hobbies
Percentage
Proportion of patients asking for care or psy- chosocial interventionsProportion of unsatisfied patients
Awareness15%
Preparation11%
Growth32%
Moratorium21%
Rebuilding21%
A B
PS in Advance ps.psychiatryonline.org 5
FRANCK ET AL.

Page 126
appropriate care based on an individual’s needs. Given the
nonlinear nature of personal recovery, such a goal may be
overly ambitious at this time, and future research will be
needed to determine whether the recovery process includes
five distinct stages or only three, as documented in other
models (35–38). Despite these limitations, the STORI is useful
in clinical practice, because identifying a patient’s current
stage of personal recovery can informclinical decisionmaking
about the most appropriate intervention (38).
Fifty-three percent of the REHABase participants were
already actively engaged in recovery (rebuilding phase, 21%;
growth phase, 32%). Less than a quarter were still in the
moratorium phase, and according to the stages established
by Andresen et al. (24), these participants might still be
looking for hope. The REHABase project could help de-
termine the effects of psychiatric rehabilitation on an in-
dividual’s progress through recovery in comparison with
improvements in clinical and functional outcomes. The
data collected in the REHABase project could also be used
to suggest a refinement of the stage model proposed by
Andresen et al. (24). The REHABase project may contribute
to shifting the culture of care toward more recovery-
oriented practices by introducing personal recovery into
clinical decision making about psychosocial interven-
tions (38).
Compared with samples in previous studies and control
populations, the REHABase project has a high proportion of
participants with relatively low well-being scores. Whereas
Tennant et al. (39) showed that the medianWEMWBS score
was 50 in a student sample and 51 in a general population
sample, with interquartile ranges of 45–55 and 45–56, re-
spectively, the REHABase participants had amedian score of
42, with an interquartile range of 16–70. This result reflects
the overall altered life satisfaction and self-realization in
severe mental illness and ASD.
Initial data on participant employment indicated that
only 10% of participants worked in a mainstream environ-
ment, 68% were dissatisfied with their professional situa-
tion, and 78% expressed a need for help in this area. This
finding is consistent with data from previous research—work
plays a central role in the recovery process (40). It is thus
necessary to assess a participant’s needs in terms of re-
habilitation interventions (41, 42). In France, persons with
schizophrenia have more difficulties accessing employment
(employment rate of 11.5%), compared with their counter-
parts in other countries, such as Germany (employment rate
of 30.3%) (43). Graduating from a university and accessing
competitive employment are also challenging for people
with ASD. A Swedish sample of 50 participants with ASD
who were prospectively followed for 20 years had a gradu-
ation rate of 14% and employment rates of 33% or 27%,
depending on the presence of psychiatric comorbidities (44).
Professional training or competitive employment was a
major life goal for 78% of the participants included in
REHABase, and these individuals identified vocational re-
habilitation as their primary care need.
REHABase includes various scales that measure a par-
ticipant’s most unsatisfying dimensions, goals, and life pri-
orities. For example, in the satisfaction scale adapted from
CASIG, the care needs and priorities are evaluated in nine
dimensions. As expected, the proportion of unsatisfied par-
ticipants decreased during the recovery process. However,
surprisingly, it increased again in the final stage of recovery
(i.e., growth) for all the dimensions assessed. This result
needs to be interpreted carefully given the cyclical nature of
personal recovery and its potential correlations with other
FIGURE 3. Proportion of REHABase project participants (N=1,397) reporting dissatisfaction with nine life dimensions at baseline, by
stage of recovery
0
10
20
30
40
50
60
70
80
Part
icip
an
ts (
%)
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Mo
rato
riu
m
Aw
are
ne
ss
Pre
para
tio
n
Re
bu
ild
ing
Gro
wth
Symptommanagement
Professionaltraining andemployment
Interpersonalrelationships
Cognitivefunctioning
Budget andadministrative
taskmanagement
Hobbies Transportmanagement
Healthmanagement
Accommo-dation
6 ps.psychiatryonline.org PS in Advance
SATISFACTION AND NEEDS IN SERIOUS MENTAL ILLNESS AND AUTISM SPECTRUM DISORDER

Page 127
variables, such as low insight (45) and self-stigma (46). In-
dividuals who are in the growth stage at the beginning of
psychiatric rehabilitation and who have low insight into
their illness might consider themselves as both recovered
from mental illness and dissatisfied with one or more major
life activities. Therefore, the effects of psychiatric re-
habilitation on personal recovery should be investigated
taking into account the fact that such effects will be influ-
enced by the simultaneous changes in insight into illness and
self-stigma during the follow-up period. Finally, it is im-
portant to note that the study was cross-sectional, and no
causal statements can be extracted from the data.
CONCLUSIONS
Participants’ needs were not met in several major life ac-
tivities, and further research is needed to better characterize
these needs. Indeed, improving the fit between needs and
the care available, which could reduce both the duration and
the cost of care, should be a priority, considering the large
numbers of individuals affected by serious mental illness
and ASD and the need to optimize the use of public funds.
Improving our understanding of the trajectories of illness
and the effects of psychosocial rehabilitation remains a major
challenge. To our knowledge, REHABase is the first national
project to collect transnosographic data on psychiatric ser-
vice users, promoting care strategies based on participants’
self-determination (empowerment). The two main focuses
of this project are the functional impact of the disorder on
participants’ daily lives and the impact of the psychosocial
therapies provided by the psychosocial rehabilitation cen-
ters. Future results should improve our understanding of
the recovery process.
Furthermore, the REHABase data will be used to study
factors that determine or hinder recovery (e.g., self-stigma)
(47, 48). The impact of personalized psychosocial reha-
bilitation will be reported for several variables: psychosocial
condition, cognitive processes, well-being, social inclu-
sion, interpersonal relationships, and professional situa-
tion. Finally, by recording the effectiveness of personalized
rehabilitation action plans, the REHABase project may be
key to improving the quality of care and to developing
guidelines.
AUTHOR AND ARTICLE INFORMATION
Centre Ressource de Réhabilitation Psychosociale et de Remédia-
tion Cognitive (CRR), Hôpital Le Vinatier, Centre National de la
Recherche Scientifique (CNRS) et Université de Lyon, Lyon, France
(Franck, Bon, Dekerle, Plasse, Cervello); Centre Référent Lyonnais de
Réhabilitation Psychosociale (CL3R), Centre Hospitalier Le Vinatier, Lyon
(Franck, Martin); REHALise, Centre Hospitalier Universitaire de Saint-
Etienne, Saint-Etienne, France (Massoubre, Pommier); Centre Référent
de Réhabilitation Psychosociale de Limoges (C2RL), Limoges, France
(Legros-Lafarge); CREATIV & URC Pierre Deniker, Centre Hospitalier
Laborit, Poitiers, France (Jaafari, Guillard-Bouhet); Centre Référent de
Réhabilitation Psychosociale (C2RP), Centre Hospitalier Charles Perrens,
Pôle Universitaire de Psychiatrie Adulte, Bordeaux, France (Quilès,
Verdoux); Centre Référent de Réhabilitation Psychosociale (C2RP), Pôle
De Réhabilitation Psychosociale, Bruges, France (Couhet); Centre Réf-
érent de Réhabilitation Psychosociale (C3R), Centre Hospitalier Alpes
Isère, Grenoble, France (Gouache, Dubreucq); Centre de Référence
Maladies Rares Génopsy, Centre Hospitalier Le Vinatier, CNRS et Uni-
versité de Lyon, Lyon (Demily). Send correspondence to Dr. Franck
This work was funded by Auvergne-Rhône-Alpes and Nouvelle-
Aquitaine regional health agencies. The authors thank Kim Barrett for
editorial assistance; Floriane Todoroff for her contribution to the figures;
Emmanuel Gauthier and Mara Conil for data management; and the
members of the REHABase Network (the following teams have all par-
ticipated in developing the study: C2RL, Limoges; C2RP, Bordeaux; C3R,
Grenoble; CL3R, Lyon; CREATIV & URC Pierre Deniker, Poitiers; and
REHALise, Saint-Etienne). The funding source had no role in the data-
base creation and the data analysis or interpretation.
The authors report no financial relationships with commercial interests.
Received September 8, 2018; revisions received October 23 and
November 22, 2018; accepted December 7, 2018; published online
January 29, 2019.
REFERENCES
1. Hedden SL, Kennet J, Lipari R, et al: Behavioral Health Trends in
the United States: Results From the 2014 National Survey on Drug
Use and Health. Rockville, MD, Substance Abuse and Mental
Health Services Administration, 2014
2. Gillberg IC, Helles A, Billstedt E, et al: Boys with Asperger syn-
drome grow up: psychiatric and neurodevelopmental disorders
20 years after initial diagnosis. J Autism Dev Disord 2016; 46:74–82
3. Buescher AVS, Cidav Z, Knapp M, et al: Costs of autism spectrum
disorders in the United Kingdom and the United States. JAMA
Pediatr 2014; 168:721–728
4. Pincus HA, Spaeth-Rublee B, Sara G, et al: A review of mental
health recovery programs in selected industrialized countries. Int
J Ment Health Syst 2016; 10:73
5. Anthony WA, Farkas MD: The Essential Guide to Psychiatric Re-
habilitation Practice. Boston, Boston University, Center for Psychi-
atric Rehabilitation, 2012
6. Blenkiron P, Hammill CA: What determines patients’ satisfaction
with their mental health care and quality of life? Postgrad Med J
2003; 79:337–340
7. Villotti P, Corbiere M, Zaniboni S, et al: Evaluating the motivation
to obtain and sustain employment in people with psychiatric dis-
abilities. Psicol Soc 2015
8. Fleury M-J, Grenier G, Bamvita J-M, et al: Variables associated
with perceived unmet need for mental health care in a Canadian
epidemiologic catchment area. Psychiatr Serv 2016; 67:78–85
9. Dixon L, Perkins C, Calmes C: Guideline Watch (Sept 2009):
Practice Guideline for the Treatment of Patients With Schizo-
phrenia. Arlington, VA, American Psychiatric Association, 2009
10. Ramon S: The Strengths Model: A Recovery Oriented Approach
to Mental Health Services: CA Rapp and RJ Goscha (book rev).
Am J Psychiatr Rehabil 2013; 16:232–233
11. D’Ercole A, Struening E, Curtis JL, et al: Effects of diagnosis,
demographic characteristics, and case management on rehospi-
talization. Psychiatr Serv 1997; 48:682–688
12. Björkman T, Hansson L: Case management for individuals with a
severe mental illness: a 6-year follow-up study. Int J Soc Psychi-
atry 2007; 53:12–22
13. Xia J, Merinder LB, Belgamwar MR: Psychoeducation for schizo-
phrenia. Cochrane Database Syst Rev 2011; (6):CD002831
14. Wykes T, Newton E, Landau S, et al: Cognitive remediation
therapy (CRT) for young early onset patients with schizophrenia:
an exploratory randomized controlled trial. Schizophr Res 2007;
94:221–230
PS in Advance ps.psychiatryonline.org 7
FRANCK ET AL.
Page 128
15. Morin L, Franck N: Rehabilitation interventions to promote re-
covery from schizophrenia: a systematic review. Front Psychiatry
2017; 8:100
16. Oud M, Mayo-Wilson E, Braidwood R, et al: Psychological inter-
ventions for adults with bipolar disorder: systematic review and
meta-analysis. Br J Psychiatry 2016; 208:213–222
17. Bateman AW, Gunderson J, Mulder R: Treatment of personality
disorder. Lancet 2015; 385:735–743
18. Tobin MC, Drager KDR, Richardson LF: A systematic review of
social participation for adults with autism spectrum disorders:
support, social functioning, and quality of life. Res Autism Spectr
Disord 2014; 8:214–229
19. Drake RE, Whitley R: Recovery and severe mental illness: de-
scription and analysis. Can J Psychiatry 2014; 59:236–242
20. Salzer MS, Brusilovskiy E, Townley G: National estimates of
recovery-remission from serious mental illness. Psychiatr Serv
2018; 69:523–528
21. Jääskeläinen E, Juola P, Hirvonen N, et al: A systematic review
and meta-analysis of recovery in schizophrenia. Schizophr Bull
2013; 39:1296–1306
22. Jose D, Ramachandra, Lalitha K, et al: Consumer perspectives on
the concept of recovery in schizophrenia: a systematic review.
Asian J Psychiatr 2015; 14:13–18
23. Anthony WA: Recovery from mental illness: the guiding vision of
the mental health service system in the 1990s. Psychosoc Rehabil J
1993; 16:11–23
24. Andresen R, Caputi P, Oades L: Stages of Recovery Instrument:
development of a measure of recovery from serious mental illness.
Aust N Z J Psychiatry 2006; 40:972–980
25. Franck N, Laforcade M: Responding to the needs of the population
suffering from severe mental disorders by a multifaceted territorial
approach: reorganization of the French mental health system.
Perspect Psychiatr Care 2018; 54:527–529
26. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.
Arlington, VA, American Psychiatric Association, 2013
27. Baron-Cohen S, Wheelwright S, Robinson J, et al: The Adult
Asperger Assessment (AAA): a diagnostic method. J Autism Dev
Disord 2005; 35:807–819
28. Lord C, Rutter M, Le Couteur A: Autism Diagnostic Interview–
Revised: a revised version of a diagnostic interview for caregivers
of individuals with possible pervasive developmental disorders.
J Autism Dev Disord 1994; 24:659–685
29. Lord C, Risi S, Lambrecht L, et al: The Autism Diagnostic Obser-
vation Schedule–Generic: a standard measure of social and com-
munication deficits associated with the spectrum of autism. J
Autism Dev Disord 2000; 30:205–223
30. Wallace CJ, Lecomte T, Wilde J, et al: CASIG: a consumer-
centered assessment for planning individualized treatment and
evaluating program outcomes. Schizophr Res 2001; 50:105–119
31. Trousselard M, Steiler D, Dutheil F, et al: Validation of the
Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) in
French psychiatric and general populations. Psychiatry Res 2016;
245:282–290
32. Green CA, Perrin NA, Leo MC, et al: Recovery from serious mental
illness: trajectories, characteristics, and the role of mental health
care. Psychiatr Serv 2013; 64:1203–1210
33. Sanches SA, van Busschbach JT, Michon HWC, et al: The role of
working alliance in attainment of personal goals and improvement
in quality of life during psychiatric rehabilitation. Psychiatr Serv
2018; 69:903–909
34. Leamy M, Bird V, Le Boutillier C, et al: Conceptual framework for
personal recovery in mental health: systematic review and narra-
tive synthesis. Br J Psychiatry 2011; 199:445–452
35. Young SL, Ensing DS: Exploring recovery from the perspective
of people with psychiatric disabilities. Psychiatr Rehabil J 1999; 22:
219–231
36. Baxter EA, Diehl S: Emotional stages: consumers and family
members recovering from the trauma of mental illness. Psychiatr
Rehabil J 1998; 21:349–355
37. Pettie D, Triolo AM: Illness as evolution: the search for identity
and meaning in the recovery process. Psychiatr Rehabil J 1999; 22:
255–262
38. Weeks G, Slade M, Hayward M: A UK validation of the Stages of
Recovery Instrument. Int J Soc Psychiatry 2011; 57:446–454
39. Tennant R, Hiller L, Fishwick R, et al: The Warwick-Edinburgh
Mental Well-Being Scale (WEMWBS): development and UK val-
idation. Health Qual Life Outcomes 2007; 5:63
40. Roe D, Werbeloff N, Gelkopf M: Do persons with severe mental
illness who consume the psychiatric rehabilitation basket of ser-
vices in Israel have better outcomes than those who do not? Isr J
Psychiatry Relat Sci 2010; 47:166–170
41. Barrowclough C, Tarrier N, Lewis S, et al: Randomised controlled
effectiveness trial of a needs-based psychosocial intervention ser-
vice for carers of people with schizophrenia. Br J Psychiatry 1999;
174:505–511
42. Alanen YO, Lehtinen K, Räkköläinen V, et al: Need-adapted
treatment of new schizophrenic patients: experiences and results
of the Turku Project. Acta Psychiatr Scand 1991; 83:363–372
43. Marwaha S, Johnson S, Bebbington PE, et al: Predictors of em-
ployment status change over 2 years in people with schizophrenia
living in Europe. Epidemiol Psichiatr Soc 2009; 18:344–351
44. Helles A, Wallinius M, Gillberg IC, et al: Asperger syndrome in
childhood—personality dimensions in adult life: temperament,
character and outcome trajectories. BJPsych Open 2016; 2:210–216
45. Giusti L, Ussorio D, Tosone A, et al: Is personal recovery in
schizophrenia predicted by low cognitive insight? Community
Ment Health J 2015; 51:30–37
46. Hasson-Ohayon I, Mashiach-Eizenberg M, Elhasid N, et al: Be-
tween self-clarity and recovery in schizophrenia: reducing the self-
stigma and finding meaning. Compr Psychiatry 2014; 55:675–680
47. Livingston JD, Boyd JE: Correlates and consequences of inter-
nalized stigma for people living with mental illness: a systematic
review and meta-analysis. Soc Sci Med 2010; 71:2150–2161
48. Boyd JE, Adler EP, Otilingam PG, et al: Internalized Stigma of
Mental Illness (ISMI) scale: a multinational review. Compr Psy-
chiatry 2014; 55:221–231
8 ps.psychiatryonline.org PS in Advance
SATISFACTION AND NEEDS IN SERIOUS MENTAL ILLNESS AND AUTISM SPECTRUM DISORDER

Page 129

Page 130

Page 131
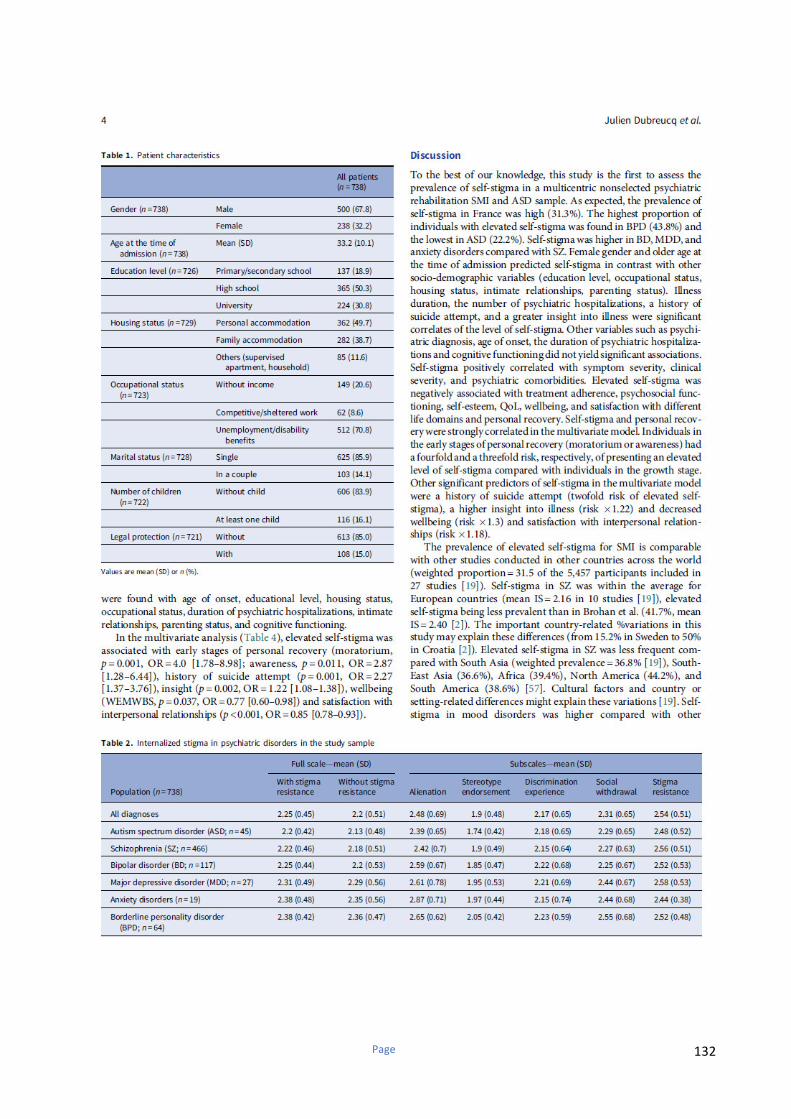
Page 132
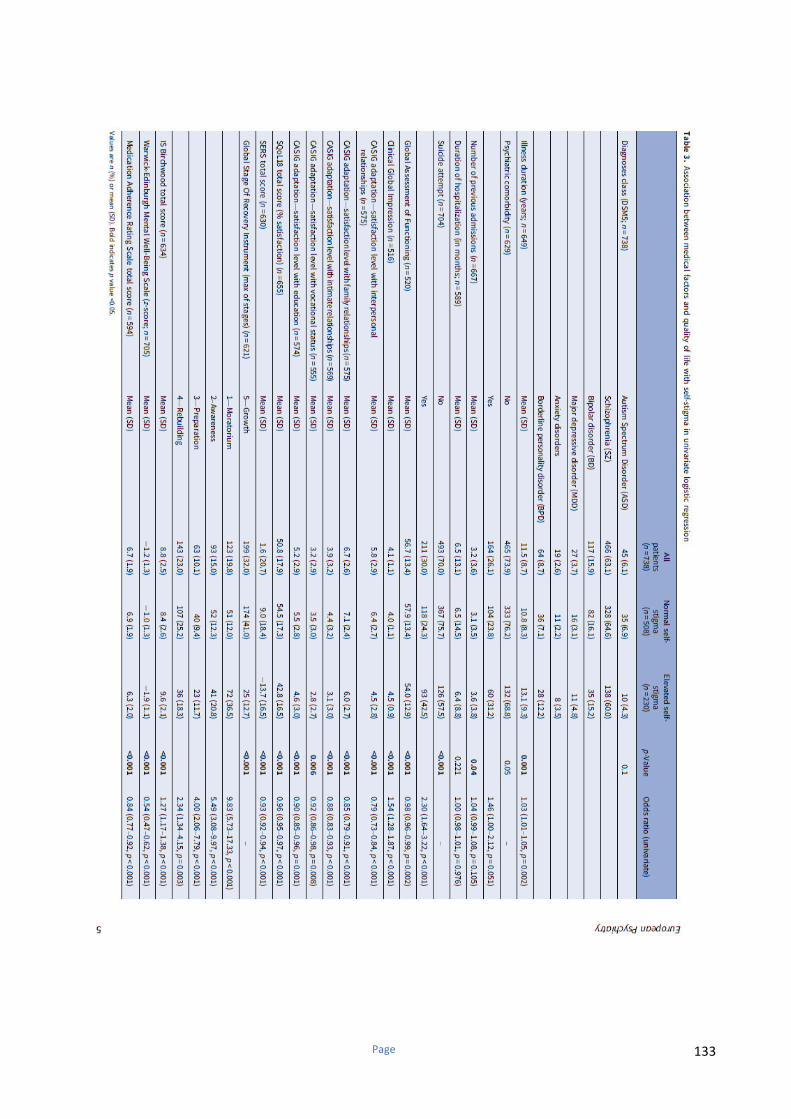
Page 133
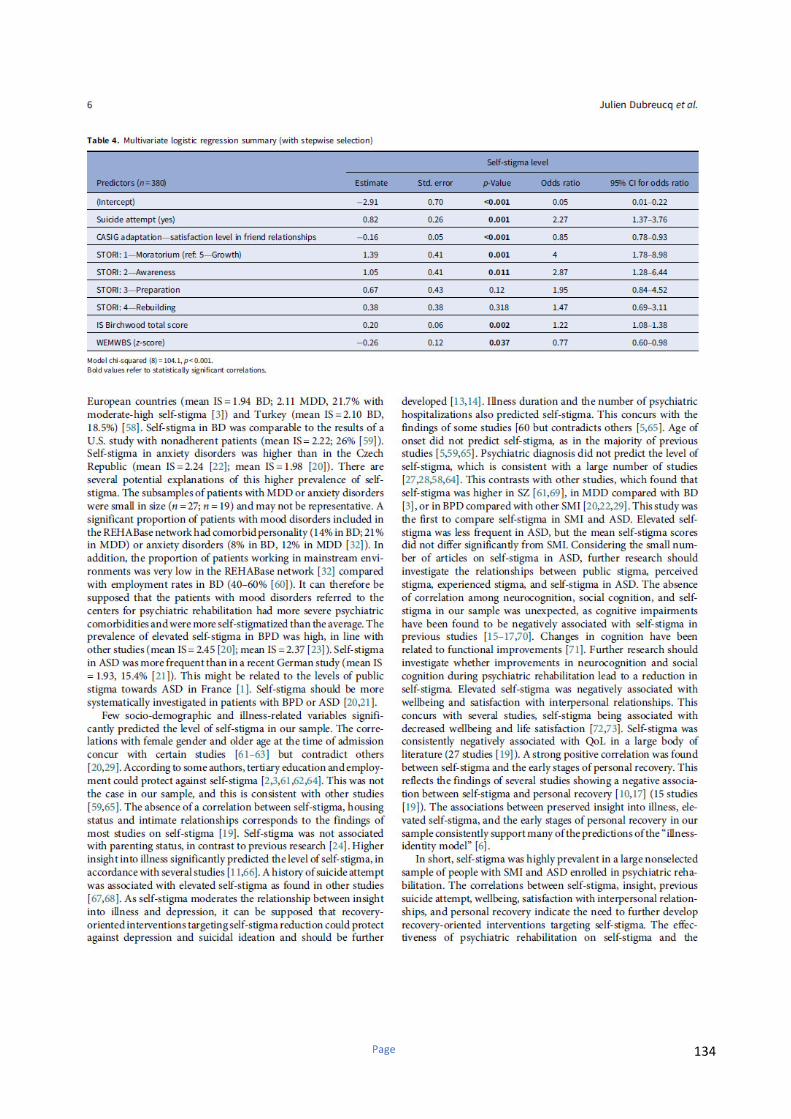
Page 134

Page 135
Page 136

Page 137

Page 138
Stigma Resistance in Serious Mental Illness and Autism Spectrum Disorder: results from the
RehaBASE national psychiatric rehabilitation cohort
Running title: Stigma Resistance in Serious Mental Illness and Autism Spectrum Disorder
AUTHORS
Dubreucq Ja,b,c,d
, Plasse Jh,i
, Gabayet Fb,c
, Faraldo Mb,c
, Blanc Of, Chereau I
c,f, Cervello S
a, h,i,, Couhet
Gn, Demily C
a,j, Guillard-Bouhet N
l, Gouache B
b, Jaafari N
l, Legrand G
g, Legros-Lafarge E
k,
Pommier Re, Quilès C
m, Straub D
i, Verdoux H
m, Vignaga F
j, Massoubre C
e , REHABAse network*and
Franck Na,h,i
a Centre de Neurosciences Cognitive, UMR 5229, CNRS & Université Lyon 1
b Centre référent de réhabilitation psychosociale et de Remédiation Cognitive (C3R), Centre Hospitalier Alpes Isère, Grenoble
c Fondation FondaMental, Créteil, France
d Réseau Handicap Psychique, Grenoble France
e REHALise, CHU de Saint-Etienne
f CMP B, CHU, EA 7280 Faculté de Médecine, Université d'Auvergne, BP 69 63003 Clermont-Ferrand Cedex 1, France.
g Centre Hospitalier Sainte Marie de Clermont Ferrand, 33 rue Gabriel Péri, CS 9912, 63037 Clermont-Ferrand Cedex 1
h Centre ressource de réhabilitation psychosociale et de remédiation cognitive, Hôpital Le Vinatier, UMR 5229, CNRS & Université Lyon 1, Université de Lyon
i Centre référent lyonnais de réhabilitation psychosociale CL3R, centre hospitalier Le Vinatier, Lyon j Centre de référence maladies rares Génopsy, pôle ADIS, centre hospitalier Le Vinatier, UMR 5229, CNRS & Université Lyon 1, Université de Lyon k Centre Référent de Réhabilitation Psychosociale de Limoges C2RL, CH Esquirol, Limoges
l CREATIV & URC Pierre Deniker, CH Laborit, Poitiers
Page 139
m Centre référent de réhabilitation psychosociale C2RP Nouvelle Aquitaine Sud, Pôle universitaire de psychiatrie adulte, centre hospitalier Charles Perrens, Bordeaux& Univ. Bordeaux, Inserm, Bordeaux Population Health Research Center, team pharmacoepidemiology, UMR 1219, F-33000 Bordeaux, France
n Centre référent de réhabilitation psychosociale C2RP Nouvelle-Aquitaine Sud, Pôle de réhabilitation psychosociale, Centre de la Tour de Gassies, Bruges
i Centre de Réhabilitation Psychosociale, Centre Hospitalier de Roanne j Dispositif de Soins de Réhabilitation Psychosociale, Centre Psychothérapeutique de l’Ain
* Correspondence should be sent to: Julien DUBREUCQ
Centre référent de réhabilitation psychosociale et de Remédiation Cognitive (C3R), CH Alpes Isère, 1 place
du Conseil National de la Résistance, 38400 Saint Martin d’Hères, France
Tel: (33 4) 56 58 88 00, e-mail: [email protected]
Page 140
Abstract
Purpose: Stigma resistance (SR) is defined as one’s ability to deflect or challenge stigmatizing beliefs. SR is
positively associated with patient’s outcomes in Serious Mental Illness (SMI). SR appears as a promising
target for psychiatric rehabilitation as it might facilitate personal recovery. The objectives of the present
study are: (i) to assess the frequency of stigma resistancein a multicentric non-selected psychiatric
rehabilitation SMI and Autism Spectrum Disorder (ASD) sample; (ii) to investigate the correlates of low
stigma resistance in different SMI and in ASD
Methods: 738 SMI or ASD outpatients were recruited fromthe French National Centers of Reference for
Psychiatric Rehabilitation cohort (REHABase). Evaluation included standardized scales for clinical severity,
quality of life, satisfaction with life, wellbeing, and personal recovery, a large cognitive battery, and daily
functioning assessment. SR was measured using Internalized Stigma of Mental Illness- SR subscale.
Results: 54.1% of the total sample had elevated SR. The highest frequency (59.3%) was found in major
depression and the lowest (36.8%) in anxiety disorders. In the multivariate analysis, elevated stigma
resistance was best predicted by satisfaction with family relationships (p<0.002, OR=1.18[1.05-1.33]).
Conclusion: The present study has indicated the importance of addressing stigma resistance in patients
enrolled in psychiatric rehabilitation. Cognitive remediation, family psychoeducation and recovery-oriented
psychoeducation might improve SR. The effectiveness of psychiatric rehabilitation on SR and the potential
mediating effects of changes in SR on treatment outcomes should be further investigated.
Keywords: stigma resistance, serious mental illness, autism spectrum disorder, prevalence, psychiatric
rehabilitation
Page 141
1. Introduction
Public stigma refers to the endorsement of negative stereotypes and discriminating attitudes about Serious
Mental Illness (SMI) or Autism Spectrum Disorder (ASD) by the general population [1]. The effects of
stigma on individuals (or personal stigma) include perceived, experienced and self-stigma. Self-stigma
occurs when someone moves beyond awareness of stigma to accepting the negative stereotypes about SMI or
ASD as true to describe him/herself [1]. Self-stigma is associated with decreased hope, wellbeing, quality of
life, motivation to achieve life goals and poorer recovery-related outcomes [2]. Some people with SMI will
however respond to awareness of stigma with indifference or righteous anger [1]. Stigma Resistance (SR) is
defined as one’s ability to deflect or challenge stigmatizing beliefs [3]. SR concerns a wide range of people
with SMI (49.2% of the 1,229 participants with schizophrenia (SZ) and 49.7% of the 1,182 participants with
mood disorders in a 2010 European study had moderate to high levels of stigma resistance [4] [5]). SR has
been associated negatively with self-stigma in a 2016 meta-analysis composed of 48 studies [6]. SR was
positively associated with self-efficacy, self-esteem, empowerment, hope, social function, personal recovery
and subjective quality of life in SMI [6], [7], [8]. Metacognitive abilities [9][10][11], outpatient treatment
[12], lower stereotype endorsement [8][9][10], insight into illness [6], social network [12], [13],[14], social
power [15] self-compassion [14], psychological flexibility [14], fear of negative evaluation [11] perceived
stigma [16], negative symptoms[9] and coping strategies [8][10] were significant cross-sectional correlates
of SR. Given its strong association with recovery-related outcomes, promoting SR in patients enrolled in
psychiatric rehabilitation appears promising [6]. Its potential role as a predictor of treatment outcome and the
effectiveness of recovery-oriented interventions on SR remain largely unknown.
Compared with self-stigma, SR was under-studied. Most studies concern people with schizophrenia (63.5%
of the participants in a 2016 meta-analysis [6]). Considerably less is known about SR in mood disorders [5],
[17], [18], [19], [20]. SR in borderline personality disorder (BPD) and in anxiety disorders remains largely
unknown. No study to our knowledge investigated SR and its correlates in ASD. ASD has been associated
with dangerousness to self and inability to work in over 20% of the 1000 respondents of a 2012 French
population survey [21]. The reactions of ASD patients confronted to stigma remain largely unknown. Self-
stigma is less frequent in ASD than in SMI (22.1% out of 45 patients from the REHABase network [22];
Page 142
15.4% out of 149 participants in a 2019 German study [23]). Compensation strategies (defined by the
discrepancy between observable social difficulties and actual underlying social-cognitive abilities [24]) have
been associated in ASD patients with better global functioning but also with poorer mental health [24].
Modulating the use of compensation strategies could reduce the probability to experience discrimination in
social contexts and increase SR. Unsuccessful compensation strategies might in contrast be associated with
greater self-stigma and SR.
In summary stigma resistance could be a key target for improving treatment outcome during psychiatric
rehabilitation. SR was studied in cross-sectional studies including mostly people with SZ. Its frequency and
correlates in patients enrolled in psychiatric rehabilitation or being diagnosed with other SMI or ASD remain
largely unknown. The role of socio-demographic (age, gender, education level, occupational, marital or
parenting status) and illness-related (insight, cognitive functioning) variables as correlates of SR in SMI
could be further investigated. The objectives of the present study were: (i) to assess the frequency of stigma
resistance in a multicentric non-selected psychiatric rehabilitation SMI and ASD sample; (ii) to investigate
the correlates of elevated stigma resistance in SMI and in ASD
2. Material and Methods
2.1 Study population
The REHABase cohort is made up of patients from a French network of psychiatric rehabilitation centers
that has been extensively described in a previous article [25]. Patients are referred to these centers by their
general practitioner or psychiatrist, who remains in charge of routine care and treatment. The inclusion
criteria are: i) a diagnosis of serious mental illness (i.e. schizophrenia, bipolar disorder, borderline
personality disorder, major depression or severe anxiety disorders, according to the SAMSAH 2013
definition [26]) or autism spectrum disorder (DMS-5 criteria [27]); ii) a score below the cut-off scores for
social recovery according to Jaaskelainen et al. in 2013 (a score of less than 61 on the Global Assessment of
Page 143
Functioning (GAF) scale [28]). A comprehensive clinical, functional and cognitive assessment is performed
to establish the individual’s strengths and weaknesses, autonomy, and occupational level. Therapeutic tools
are selected based on the participant’s personal life goals as part of an individualized psychiatric
rehabilitation action plan. The action plan can include psychoeducation, joint crisis plans, cognitive
remediation, cognitive behavior therapy, social skills training, peer-delivered interventions and supported
employment [25]. Follow-up is planned to last for 2 to 3 years. Evaluations are scheduled at baseline,
annually, and after the action plan is completed. The action plan can begin before the evaluation when
clinically relevant to support patient’s engagement in mental health care or psychiatric rehabilitation. This is
for instance the case for strengths-based case management in early psychosis and supported employment,
housing or parenting. Two thousand and fifty three patients were included in the eight REHABase sites
between January 2016 and April 2019. Seven hundred and thirty eight (35.9%) were effectively evaluated at
the time of extraction. The study obtained the authorizations required under French legislation (French
National Advisory Committee for the Treatment of Information in Health Research, 16.060bis; French
National Computing and Freedom Committee, DR-2017-268). All participants gave their informed consent.
2.2 Site selection and training
Site selection and training have been described in a previous article [25]. Since this first study, three new
sites have joined the REHABase network. The eight sites (Lyon, Grenoble, Saint-Etienne, Limoges/Poitiers,
Bordeaux, Clermont-Ferrand, Roanne and Bourg-en-Bresse) opened in France were already actively
involved in the treatment of patients with SMI (pharmacological and non-pharmacological), as well as
research on psychiatric rehabilitation and recovery-oriented practices. Each center has accepted and been
trained to use the same package of assessment tools for the baseline visit and follow-up. Clinical team
members have regular group meetings to monitor quality control and ensure good inter-rater reliability.
Page 144
2.3 Data collected
General information on education, marital status, economic status, illness onset and trajectory and
comorbidities was recorded. Stigma resistance was assessed using the Internalized Stigma of Mental Illness
scale (ISMI [4] [29]), a 29-item self-report measure designed to assess one’s personal experience of stigma
related to mental disorders and is rated on a 4-point Likert scale. Items are summed to provide a mean total
score and five subscale scores (alienation or feeling of being a devaluated member of the society; stereotype
endorsement or agreement with the negative attitudes about SMI; discrimination experience; social
withdrawal as a coping strategy and stigma resistance). Stigma resistance was analysed independently of
self-stigma, these constructs having been identified as independent from each other [6]. A higher score
reflects a higher level of stigma resistance. A score above 2.5 indicates a moderate to high level of stigma
resistance [6]. Satisfaction in four life dimensions (social, familial and intimate relationships, occupational
status) was measured using visual analogue scales and a structured interview adapted from the Client
Assessment of Strengths, Interests and Goals (CASIG [30]). Illness severity was assessed using the Positive
and Negative Syndrome (PANSS [31]) and the Clinical Global Impression (CGI [32]) scales. Insight and
treatment adherence were measured with self-reported measures (Birchwood Insight Scale; BIS [33];
Medication Adherence Rating Scale; MARS [34]). General Functioning was measured with the Global
Assessment of Functioning scale (GAF [35]). Quality of Life was evaluated with the self-reported Quality of
Life scale (S-QoL [36]) and wellbeing using the Warwick-Edinburgh Mental Well-being Scale (WEMWBS
[37]). Self-esteem was assessed with the Self-Esteem Rating Scale-Short Form (SERS-SF [38]) and personal
recovery was measured using the self-reported Stage of Recovery Instrument (STORI [39]). Baseline
neuropsychological cognitive assessments include the Wechsler Adult Intelligence Scale-4th edition [40]
(WAIS-IV) subscale assessing short-term and working memory, the California Verbal Learning Test
(CVLT) [41] or RL/RI-16 [42] for global verbal memory, d2-R for selective attention, concentration and
speed of processing [43] and shopping test [44] or Six Element Test [45] for planning abilities. Theory of
mind was assessed using the Movie for the Assessment of Social Cognition (MASC) [46] and attribution
style with the Ambiguous Intentions and Hostility Questionnaire (AIHQ) [47].

Page 145
2.4 Statistical analysis
Data are presented as the mean and SD for continuous variables and number and percentage for categorical
variables. A one-way analysis of variance was performed and the p-values adjusted for multiple comparisons
using Tukey’s method. The internal consistency of the ISMI total scale and subscales was measured using
Cronbach's alpha (α).
Patients’ baseline characteristics were analyzed to identify factors associated with elevated stigma resistance.
Categorical variables were analyzed using Chi-square analysis or Fisher’s exact test as appropriate, and
continuous variables were analyzed using Student’s t test or Wilcoxon’s test for non-normal variables.
Logistic regression was used to calculate OR with 95% CI. Finally, a multivariate logistic regression with
stepwise selection was performed on all predictors to investigate the factors independently associated with
the level of stigma resistance. The collinearity was checked using the variance inflation factor (VIF). P-
values <0.05 were considered significant. All statistical analyses were performed using R (R Foundation for
Statistical Computing, Vienna, Austria; https://www.R-project.org/) [48].
3. Results
Seven hundred and thirty-eight clinically stabilized patients were recruited from the REHABase network.
They had been included in this cohort study between January 2016 and April 2019. SZ was the most
represented diagnosis with 466 patients (63.1%). Other diagnoses were BD (117, 15.9%), BPD (64, 8.7%),
ASD (45, 6.1%), major depression (MDD) (27, 3.7%) and anxiety disorders (19, 2.5%). Baseline sample
characteristics are shown on Table 1.
3.1 Frequency of stigma resistance
The internal consistency for the 24-item ISMI was α=0.90. The SR subscale had an internal consistency of α
=0.49. The following values were found for the 4 other subscales: alienation α=0.81, stereotype endorsement
α=0.69, discrimination experiences α=0.78, social withdrawal α=0.78. A strong negative association was

Page 146
found between SR, ISMI total score and the 4 other subscales (data not shown). Elevated stigma resistance
was found in 54.1% of the total sample (55.4% in SZ, 52.1% in BD, 59.3% in MDD, 36.8% in anxiety
disorders, 51.6% in BPD and 53.3% in ASD).
3.2 Correlates of elevated stigma resistance
Table 2 presents the results of the univariate analyses for the correlates of elevated stigma resistance.
Elevated SR was positively associated with wellbeing (WEWMBS; p<0.001, OR=1.38 [1.22-1.56]), self-
esteem (SERS; p<0.001, OR=1.02 [1.01-1.03]), quality of life (S-QoL; p<0.001, OR= 1.03 [1.02-1.04]) and
satisfaction with life (interpersonal relationships, p=0.047, OR=1.06 [1.00-1.12]); familial relationships,
p=0.05, OR=1.07 [1.00-1.14]; vocational status, p=0.011, OR=1.07 [1.01-1.14]). Elevated SR was negatively
associated with personal recovery (p<0.001). Compared with participants in the moratorium stage of
personal recovery, those in later stages showed significantly higher levels of SR (awareness, OR=1.19 [0.69-
2.06]; preparation OR=1.37 [0.74-2.54]; rebuilding, OR=2.28 [1.40-3.75]; growth OR=2.78 [1.76-4.45]).
Elevated SR was negatively associated with impaired executive functioning (working memory, p=0.049,
OR=0.38 [0.13-0.99]; planning abilities, p=0.049, OR=0.63 [0.39-1.00]), psychiatric comorbidities (p=0.034;
OR=0.68 [0.47-0.97]), clinical severity (CGI; p=0.03, OR=0.83 [0.71-0.97]), and greater insight into illness
(BIS; p=0.007, OR=0.93 [0.87-0.99]). No significant correlations were found with socio-demographic
variables, age of onset, psychiatric diagnosis, illness duration, inpatient status, number and duration of
psychiatric hospitalizations, history of suicide attempt, social cognition and psychosocial function. Table 3
presents the result of the multivariate analysis. In the multivariate analysis, elevated stigma resistance was
best predicted by satisfaction with family relationships (p<0.002, OR=1.18 [1.05-1.33]).
Discussion
To our knowledge this study is the first assessing the frequency of stigma resistance in a multicentric non-
selected psychiatric rehabilitation SMI and ASD sample. SR in SMI was within the average of European
Page 147
countries (54.1% with elevated SR). The highest proportion of individuals with elevated stigma resistance
was found in MDD (59.3%) and the lowest in anxiety disorders (36.8%). SR was lower in anxiety disorders
compared with other conditions. Socio-demographic variables did not yield significant associations with SR.
Impaired executive functioning, greater insight into illness, clinical severity and psychiatric comorbidities
were negatively associated with elevated SR in contrast with most illness-related variables (psychiatric
diagnosis, age of onset, illness duration, the number and duration of psychiatric hospitalizations, inpatient
status, history of suicide attempt). Elevated stigma resistance was positively associated with self-esteem,
QoL, wellbeing, satisfaction with different life domains and personal recovery. Individuals in the late stages
of personal recovery (rebuilding or growth) had a two-fold and a three-fold likelihood, respectively of
presenting a high level of stigma resistance compared with those in the moratorium stage. Elevated SR was
best predicted in the multivariate model by satisfaction with familial relationships (risk x 1.18).
SR in SMI (2.54) was below the level reported by Firmin et al 2016 meta-analysis (2.7 out of 48 studies) [6].
SR was similar to the levels found in the Czech Republic (2.52; [49]), in China (2.49; [50]), Iran (2.46; [51])
and Ethiopia (2.41; [52]). SR was higher in France compared with North America (weighted mean=2.08,
weighted elevated SR=22%; [2]). This could be explained by the low frequency of self-stigma in North
America [2]. Elevated stigma resistance for SZ was comparable with other studies across the world
(weighted proportion=53.1% of the 2202 participants included in 6 studies; [2]). SR was within the average
for European countries for SZ (mean SR=2.50 in 8 studies; [2]). Compared with the 2010 GAMIAN-Europe
study, SR was more frequent (49.2%, mean IS=2.47; [4]) and self-stigma less frequent (29.8%, [22]; 41.7%,
[4]). The important country-related variations in this study may explain these differences (from 2.29 in
Greece to 2.70 in Lituania; [4]). SR for SZ was lower in France than in Austria (2.73, 63.3% with elevated
SR) or Nigeria (2.79; 72.7% with elevated SR; [53]). SR was comparable with Turkey (weighted mean=2.51
in 5 studies; [2]) and Ethiopia (2.52, 49.4% with elevated self-stigma; [54]). SR was higher than in India
(weighted mean= 2.43 in 2 studies), South East Asia (weighted mean=2.36 in 3 studies; [2]) and South
America (mean SR=2.4; [55]). SR in mood disorders was lower compared with other European countries
(mean SR=2.81; 59.7% with elevated SR; [5]). Elevated self-stigma was more frequent in France for people
Page 148
with BD compared with other European countries (29.9%, [22]; 21.7%, [5]). SR in BD was lower than in the
USA (mean SR=3.06; [18]) but higher than in India (weighted mean=2.43 in 2 studies) or Turkey (mean
SR=2.38; [17]). Cultural factors and country or setting-related differences might explain these variations [2].
SR in anxiety disorders was lower in France than in the Czech Republic (mean SR=2.3; [49]). The higher
levels of self-stigma in mood and anxiety disorders [22] might explain the lower SR. It can also be
hypothesized that the patients with mood disorders referred to the centers for psychiatric rehabilitation had
more severe psychiatric comorbidities, are more self-stigmatized and have less abilities for resisting stigma
than the average [22]. SR in BPD was higher than in the Czech Republic (2.27; [49]) in spite of elevated
self-stigma in both countries [22]. It can be supposed that people with BPD are more self-stigmatized than
those with other SMI but have preserved abilities for resisting stigma. Further research will be necessary to
better characterize SR in anxiety disorders and BPD. Elevated SR was frequent in ASD (53.3%), while self-
stigma was less frequent in ASD compared to SMI (respectively 22.2% and 31.2%; [22]). The level of SR in
ASD was lower than in SZ or MDD but higher than in BD, BPD and anxiety disorders. This is the first study
assessing SR in ASD. Further research will be necessary to better understand SR in this population.
All socio-demographic and most illness-related variables were not significantly associated with the level of
SR. This contrasts with Firmin et al 2016 meta-analysis where age and education moderated the effects of
SR on functional outcomes [6]. Marital status was not associated with SR in contrast with some studies [7]
[12]. The absence of correlation between SR and psychiatric diagnosis concurs with a 2016 meta-analysis [6]
but contradicts other studies [7] [13]. Outpatient status did not predict SR in contrast with Sibitz et al [12].
Satisfaction with interpersonal and family relationships was positively associated with stigma resistance.
This concurs with several studies showing a positive relationship between SR and social support [12] [13]
[14]. Family psychoeducation has shown effectiveness in improving clinical and functional outcomes in
people with SZ [56]. Family psychoeducation could therefore improve SR through increased satisfaction
with familial relationships. Future research should investigate its potential effects on self-stigma and SR.
Insight into illness was negatively associated with SR, in contrast with Firmin et al. [6]. The relationships
between insight into illness and SR are still unclear. SR could contribute to improved insight instead of being
Page 149
a prerequisite for resisting stigma [6]. Insight into illness predicts and compounds the effects of self-stigma
on depression and suicidal ideation [2], [57], [58], [22], [59]. Recovery-oriented psychoeducation targeting
improvements in self-stigma and SR could therefore protect against insight-related depression and should be
further developed [58]. Stigma resistance was negatively associated with self-stigma in accordance with
other studies [6]. This subscale showed however poor internal consistency. As suggested previously self-
stigma and stigma resistance are distinct constructs and should be measured with more specific scales [6].
Impaired executive functioning was associated with lower SR. Cognitive impairments were negatively
associated with the use of adaptive coping strategies [60], which predicted SR in previous research [8] [10].
SR was associated with resilience [61], which has been identified as a potential mediator of the effects of
cognitive impairments on self-stigma and psychosocial function [62]. Cognitive remediation could therefore
be effective on SR through improved executive functioning and increased use of adaptive coping strategies
[63]. Considering the positive association between metacognitive abilities and SR [9] [11], improving
metacognition during psychiatric rehabilitation with cognitive remediation or specific interventions could
improve SR. This remains however to be investigated. SR was not associated with social cognition or
negative symptoms in contrast with several studies [6] [9] [58]. SR was negatively associated with clinical
severity and psychiatric comorbidities in line with previous research showing an association between general
psychopathology and SR [6] [61]. Stigma resistance was not associated with psychosocial function in
contrast with previous research [8]. Elevated stigma resistance was positively associated with self-esteem,
QoL, wellbeing, satisfaction with different life domains and personal recovery. This is in line with several
studies showing positive associations between self-esteem, subjective quality of life and satisfaction with
life, personal recovery and stigma resistance [6] [7] [8] [14]. Improving SR could facilitate personal recovery
by developing a positive social identity extending beyond mental illness [6]. Further research should
investigate whether psychiatric rehabilitation improves SR and the potential effects of improved SR on
personal recovery.
In short, elevated stigma resistance was frequent in a large non-selected sample of people with SMI and ASD
enrolled in psychiatric rehabilitation. The correlations between stigma resistance, clinical severity, cognitive
Page 150
functioning, insight, wellbeing, self-esteem, satisfaction with life and personal recovery suggest to design
specific interventions targeting SR. The effectiveness of psychiatric rehabilitation on SR after one-year of
follow-up and the potential mediating role of changes in stigma resistance on treatment outcomes should be
further investigated.
Limits: Although the REHABase network covers a large proportion of the French territory, it cannot be
definitively asserted that its database constitutes a representative sample of the French population of SMI and
ASD patients. The REHABase database is composed of participants enrolled in psychiatric rehabilitation and
might therefore not be representative of all patients with SMI or ASD. However, some sample characteristics
(including sex ratio, age at illness onset, comorbidities) suggest that the present sample is comparable to the
general community-dwelling SMI population.
Strengths. The present study has some clear strengths: a large non-selected sample of community-dwelling
SMI and ASD outpatients, the use of a large bundle of standardized evaluation scales, and the inclusion of a
large number of potential confounding factors in the multivariate analysis.
Acknowledgements
This work was funded by Auvergne-Rhône-Alpes and Nouvelle-Aquitaine regional health agencies. The
authors thank Emmanuel Gauthier and Mara Conil for data management; and the members of the REHABase
Network (the following teams have all participated in developing the study and collecting the data: C2RL,
Limoges; C2RP, Bordeaux; C3R, Grenoble; CL3R, Lyon; CREATIV & URC Pierre Deniker, Poitiers; CMP
B CHU Clermont-Ferrand, CH Roanne, DSRP Bourg en Bresse and REHALise, Saint-Etienne).
Page 151
Role of the funding source: This work was funded by Auvergne-Rhône-Alpes and Nouvelle-Aquitaine
regional health agencies. The funding source had no role in the database creation and the data analysis or
interpretation.
Conflicts of interests : none
References
[1]-Corrigan PW, Watson AC.Understanding the impact of stigma on people with mental illness. World Psychiatry. 2002;1(1):16-20
[2]-Dubreucq J, Franck N. Internalized Stigma in Serious Mental Illness (SMI): a systematic review of prevalence, predictors and correlates. In revision
[3]-Thoits PA. Resisting the stigma of mental illness. Soc Psychol Q 2011;74(1):6-28.
[4]-Brohan E, Elgie R, Sartorius N, Thornicroft G, GAMIAN-Europe Study Group. Self-stigma, empowerment and perceived discrimination among people with schizophrenia in 14 European countries: the GAMIAN-Europe study. Schizophr Res. 2010;122(1-3):232-238.
[5]-Brohan E, Gauci D, Sartorius N, Thornicroft G, GAMIAN-Europe Study Group. Self-stigma, empowerment and perceived discrimination among people with bipolar disorder or depression in 13 European countries: the GAMIAN-Europe study. J Affect Disord. 2011;129(1-3):56-63.
[6]-Firmin RL, Luther L, Lysaker PH, Minor KS, Salyers MP. Stigma resistance is positively associated with psychiatric and psychosocial outcomes: A meta-analysis. Schizophr Res. 2016;175(1-3):118-128.
[7]-Lau YW, Picco L, Pang S, Jeyagurunathan A, Satghare P, Chong SA, Subramaniam M. Stigma resistance and its association with internalised stigma and psychosocial outcomes among psychiatric outpatients. Psychiatry Res 2017;257:72-8.
[8]-O'Connor LK, Yanos PT, Firmin RL. Correlates and moderators of stigma resistance among people with severe mental illness. Psychiatry Res. 2018;270:198-204.
[9]-Nabors LM, Yanos PT, Roe D, Hasson-Ohayon I, Leonhardt BL, Buck KD, Lysaker PH. Stereotype endorsement, metacognitive capacity, and self-esteem as predictors of stigma resistance in persons with schizophrenia. Compr Psychiatry. 2014;55:792-8.
[10]-Kao YC, Lien YJ, Chang HA, Wang SC, Tzeng NS, Loh CH. Evidence for the indirect effects of perceived public stigma on psychosocial outcomes: The mediating role of self-stigma. Psychiatry Res. 2016;240:187-195.
[11]-Firmin RL, Luther L, Salyers MP, Buck KD, Lysaker PH. Greater Metacognition and Lower Fear of Negative Evaluation: Potential Factors Contributing to Improved Stigma Resistance among Individuals Diagnosed with Schizophrenia. Isr J Psychiatry Relat Sci. 2017;54(1):50-54.
Page 152
[12]-Sibitz I, Amering M, Unger A, Seyringer ME, Bachmann A, Schrank B, Benesch T, Schulze B, Woppmann A. The impact of the social network, stigma and empowerment on the quality of life in patients with schizophrenia. Eur Psychiatry. 2011;26: 28-33.
[13]-Thoits PA, Link BG. Stigma Resistance and Wellbeing among People in Treatment for Psychosis. Soc Ment Health. 2016;6:1-20
[14]-Chan KKS, Lee CWL, Mak WWS. Mindfulness Model of Stigma Resistance Among Individuals with Psychiatric Disorders. Mindfullness. 2018;9:1433-1442.
[15]-Campellone TR, Caponigro JM, Kring AM. The power to resist: the relationship between power, stigma, and negative symptoms in schizophrenia. Psychiatry Res. 2014;215:280-285.
[16]-Rüsch N, Corrigan PW, Wassel A, Michaels P, Olschewski M, Wilkniss S, Batia K. Ingroup perception and responses to stigma among persons with mental illness. Acta PsychiatrScand 2009;120:320-8.
[17]-Sarısoy G, Kaçar ÖF, Pazvantoğlu O, Korkmaz IZ, Öztürk A, Akkaya D, Yılmaz S, Böke Ö, Sahin AR. Internalized stigma and intimate relations in bipolar and schizophrenic patients: a comparative study. Compr Psychiatry.2013;54:665-672.
[18]-Howland M, Levin J, Blixen C, Tatsuoka C, Sajatovic M. Mixed-methods analysis of internalized stigma correlates in poorly adherent individuals with bipolar disorder. Compr Psychiatry. 2016;70:174-180.
[19]-Grover S, Hazari N, Aneja J, Chakrabarti S, Sharma S, Avasthi A. Recovery and its correlates among patients with bipolar disorder: A study from a tertiary care centre in North India. Int J Soc Psychiatry. 2016;62:726-36.
[20]-Pal A, Sharan P, Chadda RK. Internalized stigma and its impact in Indian outpatients with bipolar disorder. Psychiatry Res. 2017;258:158-65
[21]-Durand-Zaleski I, Scott J, Rouillon F, Leboyer M. A first national survey of knowledge, attitudes and behaviours towards schizophrenia, bipolar disorders and autism in France. BMC Psychiatry. 2012;12:128.
[22]-Dubreucq J, Plasse J, Gabayet F, Faraldo M, Blanc O, Chereau I, Cervello S, Couhet G, Demily C,Guillard-Bouhet N, Gouache B, Jaafari N, Legrand G, Legros-Lafarge E, , Pommier R, Quilès C, Straub D, Verdoux H, Vignaga F, Massoubre C, REHABAse network and Franck N. Self-stigma in Serious Mental Illness and Autism Spectrum Disorder: results from the REHABase national psychiatric rehabilitation cohort. Eur Psychiatry. Accepted for publication.
[23]-Bachmann CJ, Höfer J, Kamp-Becker I, Küpper C, Poustka L, Roepke S, Roessner V, Stroth S, Wolff N, Hoffmann F. Internalised stigma in adults with autism: A German multi-center survey. Psychiatry Res. 2019;276:94-99.
[24]-Livingston LA, Shah P, Happé F. Compensatorystrategiesbelowthebehaviouralsurfaceinautism:a
qualitativestudy. Lancet Psychiatry. 2019;6(9):766-777.
[25]-Franck N, Bon L, Dekerle M, Plasse J, Massoubre C, Pommier R, Legros-Lafarge E, Jaafari N, Guillard-Bouhet N, Quilès C, Couhet G, Verdoux H, Gouache B, Martin B, Cervello S, Demily C, Dubreucq J. Satisfaction and Needs in Serious Mental Illness and Autism Spectrum Disorder: The REHABase Psychosocial Rehabilitation Project. Psychiatr Serv. 2019;70(4):316-323
Page 153
[26]-Substance Abuse and Mental Health Services Administration (SAMHSA). Results from the 2013 National Survey on Drug Use and Health: Mental Health Findings. NSDUH Series H-49, HHS Publication No. (SMA) 14-4887. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2014.
[27]-American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM5), 5th ed. Washington, DC: American Psychiatric Press. 2013.
[28]-Jääskeläinen E, Juola P, Hirvonen N, McGrath JJ, Saha S, Isohanni M, Veijola J, Miettunen J . A systematic review and meta-analysis of recovery in schizophrenia. Schizophr Bull. 2013;39:1296–1306.
[29]-Boyd Ritsher J, Otilingam PG, Grajales M. Internalized Stigma of Mental Illness: psychometric properties of a new measure. Psychiatry Res. 2003;121:31-49.
[30]-Wallace CJ, Lecomte T, Wilde J, Liberman RP. CASIG: a consumer-centered assessment for planning individualized treatment and evaluating program outcomes. Schizophr Res. 2001;50(1-2):105-119.
[31]-Kay S, Fiszbein A, Opler L. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull1. 1987;3(2):261-276.
[32]-Haro JM, Kamath SA, Ochoa S, Novick D, Rele K, Fargas A, Rodríguez MJ, Rele R, Orta J, Kharbeng A, Araya S, Gervin M, Alonso J, Mavreas V, Lavrentzou E, Liontos N, Gregor K, Jones PB; SOHO Study Group. The clinical global impression-schizophrenia scale: a simple instrument to measure the diversity of symptoms present in schizophrenia. Acta Psychiatr Scand.2003;107(416):16-23
[33]-Birchwood M, Smith J, Drury V, Healy J, Macmillan F, Slade M. A self-report Insight Scale for psychosis: reliability, validity and sensitivity to change. Acta Psychiatr Scand. 1994;89(1):62-7.
[34]-Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (MARS) for the psychoses. Schizophr Res. 2000;42(3):241-247.
[35]-Startup M, Jackson MC, Bendix S. The concurrent validity of the Global Assessment of Functioning (GAF). Br J Clin Psychol.2002;41(Pt 4):417–422.
[36]-Auquier P, Simeoni MC, Sapin C, Reine G, Aghababian V, Cramer J, Lançon C. Development and validation of a patient-based health-related quality of life questionnaire in schizophrenia: the S-QoL. Schizophr Res. 2003;63(1–2):137-149.
[37]-Tennant R, Hiller L, Fishwick R, et al. The Warwick-Edinburgh Mental Well-being Scale 19 (WEMWBS): development and UK validation. Health Qual Life Outcomes. 2007;5:63.
[38]-Lecomte T, Corbière M, Laisné F. Investigating self-esteem in individuals with schizophrenia: Relevance of the Self-Esteem Rating Scale-Short Form. Psychiatry Res. 2006;143(1):99-108.
[39]-Andresen R, Caputi P, Oades LG. Stages of recovery instrument: development of a measure of recovery from serious mental illness. Aust NZ J Psychiatry. 2006;40:972-980.
[40]-Wechsler D. WAIS IV Nouvelle version de l’échelle d’intelligence de Weschler pour adultes. 4th ed. Paris : Edition de Centre de Psychologie Appliquée.2011.
[41]-Woods SP, Delis DC, Scott JC, Kramer JH, Holdnack JA. The California Verbal Learning Test – second edition: Test-retest reliability, practice effects, and reliable change indices for the standard and alternate forms. Arch Clin Neuropsychol. 2006;21(5):413-420.
Page 154
[42]-Van der Linden M, Coyette F, Poitrenaud J, et al. L’épreuve de rappel libre / rappel indice à 16 items (RL/RI-16). In: L’Évaluation Des Troubles de La Mémoire: Présentation de Quatre Tests de Mémoire Épisodique Avec Leur Étalonnage. 2004 ;25-47.
[43]-Brickenkamp R, Schmidt-Atzert L, Liepmann D. D2-R : Test d’attention concentrée révisé. Paris: Editions Hogrefe. 2015
[44]-Pelletier Y, Lemoine L, Gros C, et al. Test des commissions révisé. GREMOIRE II Tests et échelles des maladies neurologiques avec symptomatologie cognitive. Paris : De Boeck-Solal; 2009
[45]-Murakami H, Owan Y, Oguchi T, et al. Modified Six Elements Test: Earlier diagnosis of the correlation between motor and executive dysfunction in Parkinson’s disease without dementia. Neurol Clin Neurosci. 2015;3(6):209-214.
[46]-Dziobek I, Fleck S, Kalbe E, Rogers K, Hassenstab J, Brand M, Kessler J, Woike JK, Wolf OT, Convit A. Introducing MASC: a movie for the assessment of social cognition. J Autism Dev Disord. 2006;36(5):623-636.
[47]-Combs DR, Penn DL, Wicher M,Waldheter E. The Ambiguous Intentions Hostility Questionnaire (AIHQ): a new mesure for evaluating hostile social-cognitive biases in paranoia. Cogn Neuropsychiatry. 2007;12(2):128-143
[48]-R Core Team. R: A Language and Environment for Statistical Computing, R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/. 2015
[49]-Grambal A, Prasko J, Kamaradova D, Latalova K, Holubova M, Marackova M, Ociskova M, Slepecky M. Self-stigma in borderline personality disorder - cross-sectional comparison with schizophrenia spectrum disorder, major depressive disorder, and anxiety disorders. Neuropsychiatr Dis Treat. 2016; 12:2439-48.
[50]-Ran MS, Zhang TM, Wong IY, Yang X, Liu CC, Liu B, Luo W, Kuang WH, Thornicroft G, Chan CL; CMHP Study Group. Internalized stigma in people with severe mental illness in rural China. Int J Soc Psychiatry. 2018;64(1):9-16.
[51]-Ghanean H, Nojomi M, Jacobsson L. Internalized Stigma of Mental Illness in Tehran, Iran. Stigma Research and Action 2011; 1(1): 11-17
[52]-Girma E, Tesfaye M, Froeschl G, Möller-Leimkühler AM, Dehning S, Müller N. Facility based cross-sectional study of self-stigma among people with mental illness: towards patient empowerment approach. Int J Ment Health Syst. 2013;7(1):21.
[53]-Mosanya TJ, Adelufosi AO, Adebowale OT, Ogunwale A, Adebayo OK. Self-stigma, quality of life and schizophrenia: An outpatient clinic survey in Nigeria. Int J Soc Psychiatry. 2014;60(4):377-86.
[54]-Bifftu BB, Dachew BA, Tiruneh BT. Stigma resistance among people with schizophrenia at Amanuel Mental Specialized Hospital Addis Ababa, Ethiopia: a cross-sectional institution based study. BMC Psychiatry. 2014;14:259.
[55]-Caqueo-Urízar A, Boyer L, Urzúa A, Williams DR. Self-stigma in patients with schizophrenia: a multicentric study from three Latin-America countries. Soc Psychiatry Psychiatr Epidemiol. 2019;54(8):905-909
Page 155
[56]-Harvey C. Family psychoeducation for people living with schizophrenia and their families. BJPsych Advances. 201824: 9-19
[57]-Schrank B, Amering M, Hay AG, Weber M, Sibitz I. Insight, positive and negative symptoms, hope, depression and self-stigma: a comprehensive model of mutual influences in schizophrenia spectrum disorders. Epidemiol Psychiatr Sci. 2014;23(3):271-279.
[58]-Lysaker PH, Vohs J, Hasson-Ohayon I, Kukla M, Wierwille J, Dimaggio G. Depression and insight in schizophrenia: comparisons of levels of deficits in social cognition and metacognition and internalized stigma across three profiles. Schizophr Res.2013;148(1-3):18-23
[59]-Oexle N, Waldmann T, Staiger T, Xu Z, Rüsch N. Mental illness stigma and suicidality: the role of public and individual stigma. Epidemiol Psychiatr Sci. 2018;27(2):169-175
[60]-Lysaker PH, Davis LW, Lightfoot J, Hunter N, Stasburger A. Association of neurocognition, anxiety, positive and negative symptoms with coping preference in schizophrenia spectrum disorders.Schizophr Res. 2005;80(2-3):163-71. [61]-Hofer A, Post F, Pardeller S, Frajo-Apor B, Hoertnagl CM, Kemmler G, Fleischhacker WW. Self-stigma versus stigma resistance in schizophrenia: Associations with resilience, premorbid adjustment, and clinical symptoms. Psychiatry Res. 2019;271:396-401.
[62]-Galderisi S, Rossi A, Rocca P, Bertolino A, Mucci A, Bucci P, Rucci P, Gibertoni D, Aguglia E, Amore M, Bellomo A, Biondi M, Brugnoli R, Dell'Osso L, De Ronchi D, Di Emidio G, Di Giannantonio M, Fagiolini A, Marchesi C, Monteleone P, Oldani L, Pinna F, Roncone R, Sacchetti E, Santonastaso P, Siracusano A, Vita A, Zeppegno P, Maj M; Italian Network For Research on Psychoses. The influence of illness-related variables, personal resources and context-related factors on real-life functioning of people with schizophrenia. World Psychiatry2014;13(3):275-287.
[63]-Wykes T, Spaulding WD. Thinking about the future cognitive remediation therapy-what works and could we do better? Schizophr Bull. 2011;37 Suppl 2):S80-90.
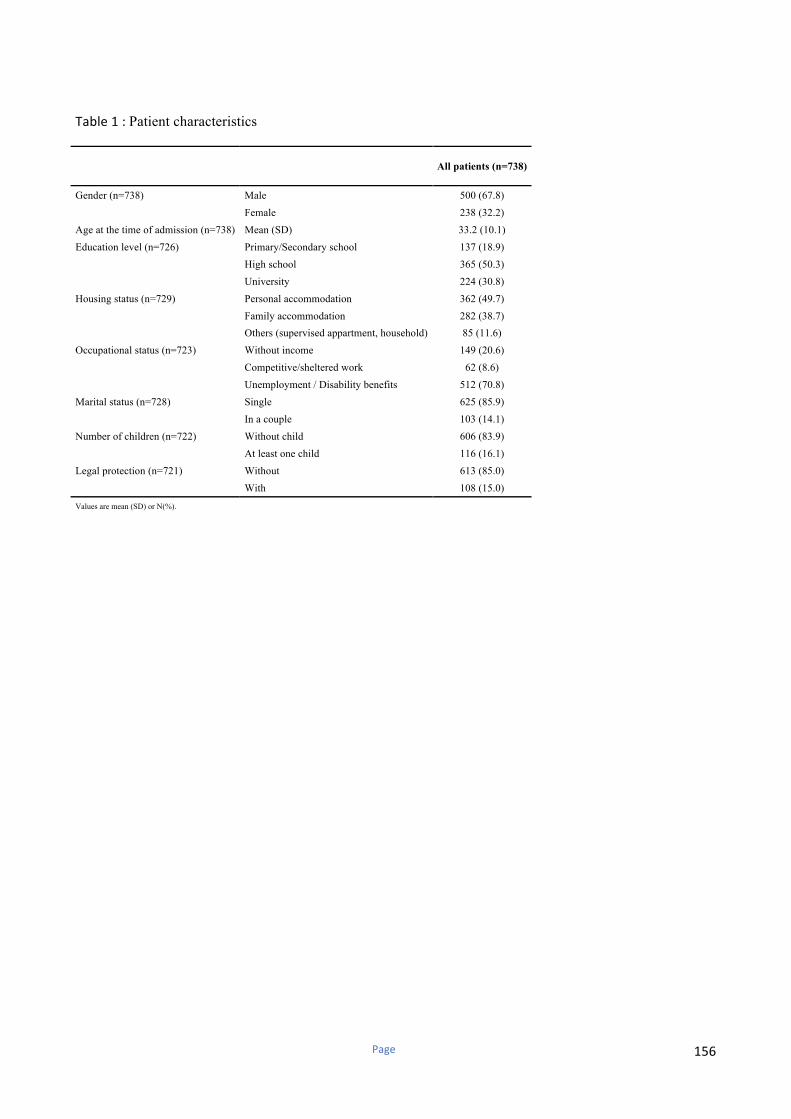
Page 156
Table1:Patient characteristics
All patients (n=738)
Gender (n=738) Male 500 (67.8)
Female 238 (32.2)
Age at the time of admission (n=738) Mean (SD) 33.2 (10.1)
Education level (n=726) Primary/Secondary school 137 (18.9)
High school 365 (50.3)
University 224 (30.8)
Housing status (n=729) Personal accommodation 362 (49.7)
Family accommodation 282 (38.7)
Others (supervised appartment, household) 85 (11.6)
Occupational status (n=723) Without income 149 (20.6)
Competitive/sheltered work 62 (8.6)
Unemployment / Disability benefits 512 (70.8)
Marital status (n=728) Single 625 (85.9)
In a couple 103 (14.1)
Number of children (n=722) Without child 606 (83.9)
At least one child 116 (16.1)
Legal protection (n=721) Without 613 (85.0)
With 108 (15.0)
Values are mean (SD) or N(%).
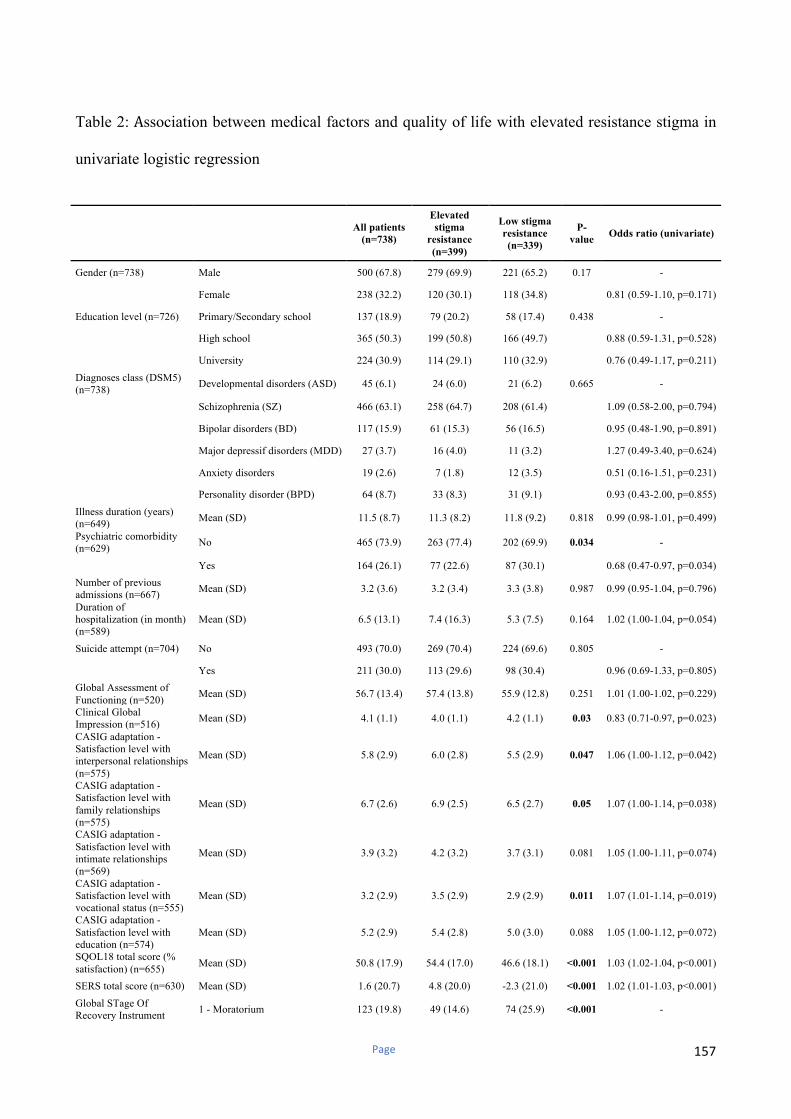
Page 157
Table 2:Association between medical factors and quality of life with elevated resistance stigma in
univariate logistic regression
All patients
(n=738)
Elevated
stigma
resistance
(n=399)
Low stigma
resistance
(n=339)
P-
value Odds ratio (univariate)
Gender (n=738) Male 500 (67.8) 279 (69.9) 221 (65.2) 0.17 -
Female 238 (32.2) 120 (30.1) 118 (34.8)
0.81 (0.59-1.10, p=0.171)
Education level (n=726) Primary/Secondary school 137 (18.9) 79 (20.2) 58 (17.4) 0.438 -
High school 365 (50.3) 199 (50.8) 166 (49.7)
0.88 (0.59-1.31, p=0.528)
University 224 (30.9) 114 (29.1) 110 (32.9)
0.76 (0.49-1.17, p=0.211)
Diagnoses class (DSM5) (n=738)
Developmental disorders (ASD) 45 (6.1) 24 (6.0) 21 (6.2) 0.665 -
Schizophrenia (SZ) 466 (63.1) 258 (64.7) 208 (61.4)
1.09 (0.58-2.00, p=0.794)
Bipolar disorders (BD) 117 (15.9) 61 (15.3) 56 (16.5)
0.95 (0.48-1.90, p=0.891)
Major depressif disorders (MDD) 27 (3.7) 16 (4.0) 11 (3.2)
1.27 (0.49-3.40, p=0.624)
Anxiety disorders 19 (2.6) 7 (1.8) 12 (3.5)
0.51 (0.16-1.51, p=0.231)
Personality disorder (BPD) 64 (8.7) 33 (8.3) 31 (9.1)
0.93 (0.43-2.00, p=0.855)
Illness duration (years) (n=649)
Mean (SD) 11.5 (8.7) 11.3 (8.2) 11.8 (9.2) 0.818 0.99 (0.98-1.01, p=0.499)
Psychiatric comorbidity (n=629)
No 465 (73.9) 263 (77.4) 202 (69.9) 0.034 -
Yes 164 (26.1) 77 (22.6) 87 (30.1)
0.68 (0.47-0.97, p=0.034)
Number of previous admissions (n=667)
Mean (SD) 3.2 (3.6) 3.2 (3.4) 3.3 (3.8) 0.987 0.99 (0.95-1.04, p=0.796)
Duration of hospitalization (in month) (n=589)
Mean (SD) 6.5 (13.1) 7.4 (16.3) 5.3 (7.5) 0.164 1.02 (1.00-1.04, p=0.054)
Suicide attempt (n=704) No 493 (70.0) 269 (70.4) 224 (69.6) 0.805 -
Yes 211 (30.0) 113 (29.6) 98 (30.4)
0.96 (0.69-1.33, p=0.805)
Global Assessment of Functioning (n=520)
Mean (SD) 56.7 (13.4) 57.4 (13.8) 55.9 (12.8) 0.251 1.01 (1.00-1.02, p=0.229)
Clinical Global Impression (n=516)
Mean (SD) 4.1 (1.1) 4.0 (1.1) 4.2 (1.1) 0.03 0.83 (0.71-0.97, p=0.023)
CASIG adaptation - Satisfaction level with interpersonal relationships (n=575)
Mean (SD) 5.8 (2.9) 6.0 (2.8) 5.5 (2.9) 0.047 1.06 (1.00-1.12, p=0.042)
CASIG adaptation - Satisfaction level with family relationships (n=575)
Mean (SD) 6.7 (2.6) 6.9 (2.5) 6.5 (2.7) 0.05 1.07 (1.00-1.14, p=0.038)
CASIG adaptation - Satisfaction level with intimate relationships (n=569)
Mean (SD) 3.9 (3.2) 4.2 (3.2) 3.7 (3.1) 0.081 1.05 (1.00-1.11, p=0.074)
CASIG adaptation - Satisfaction level with vocational status (n=555)
Mean (SD) 3.2 (2.9) 3.5 (2.9) 2.9 (2.9) 0.011 1.07 (1.01-1.14, p=0.019)
CASIG adaptation - Satisfaction level with education (n=574)
Mean (SD) 5.2 (2.9) 5.4 (2.8) 5.0 (3.0) 0.088 1.05 (1.00-1.12, p=0.072)
SQOL18 total score (% satisfaction) (n=655)
Mean (SD) 50.8 (17.9) 54.4 (17.0) 46.6 (18.1) <0.001 1.03 (1.02-1.04, p<0.001)
SERS total score (n=630) Mean (SD) 1.6 (20.7) 4.8 (20.0) -2.3 (21.0) <0.001 1.02 (1.01-1.03, p<0.001)
Global STage Of Recovery Instrument
1 - Moratorium 123 (19.8) 49 (14.6) 74 (25.9) <0.001 -
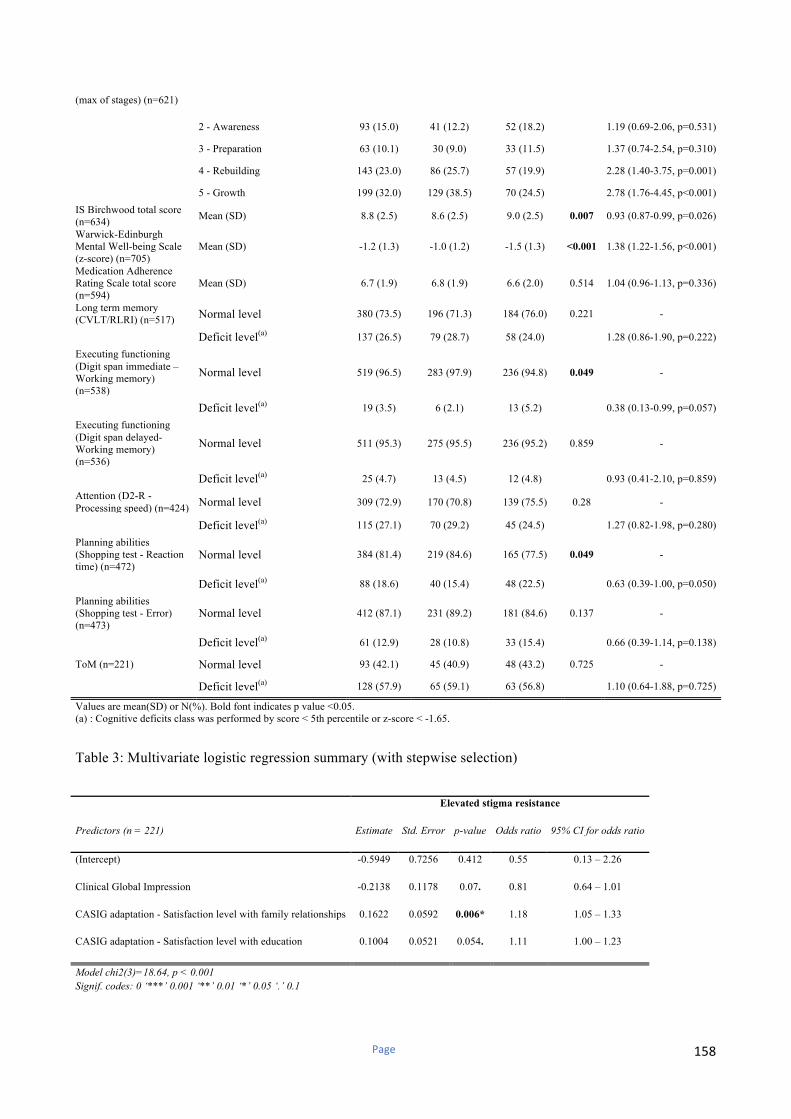
Page 158
(max of stages) (n=621)
2 - Awareness 93 (15.0) 41 (12.2) 52 (18.2)
1.19 (0.69-2.06, p=0.531)
3 - Preparation 63 (10.1) 30 (9.0) 33 (11.5)
1.37 (0.74-2.54, p=0.310)
4 - Rebuilding 143 (23.0) 86 (25.7) 57 (19.9)
2.28 (1.40-3.75, p=0.001)
5 - Growth 199 (32.0) 129 (38.5) 70 (24.5)
2.78 (1.76-4.45, p<0.001)
IS Birchwood total score (n=634)
Mean (SD) 8.8 (2.5) 8.6 (2.5) 9.0 (2.5) 0.007 0.93 (0.87-0.99, p=0.026)
Warwick-Edinburgh Mental Well-being Scale (z-score) (n=705)
Mean (SD) -1.2 (1.3) -1.0 (1.2) -1.5 (1.3) <0.001 1.38 (1.22-1.56, p<0.001)
Medication Adherence Rating Scale total score (n=594)
Mean (SD) 6.7 (1.9) 6.8 (1.9) 6.6 (2.0) 0.514 1.04 (0.96-1.13, p=0.336)
Long term memory (CVLT/RLRI) (n=517) Normal level 380 (73.5) 196 (71.3) 184 (76.0) 0.221 -
Deficit level(a) 137 (26.5) 79 (28.7) 58 (24.0)
1.28 (0.86-1.90, p=0.222)
Executing functioning (Digit span immediate – Working memory) (n=538)
Normal level 519 (96.5) 283 (97.9) 236 (94.8) 0.049 -
Deficit level(a) 19 (3.5) 6 (2.1) 13 (5.2)
0.38 (0.13-0.99, p=0.057)
Executing functioning (Digit span delayed- Working memory) (n=536)
Normal level 511 (95.3) 275 (95.5) 236 (95.2) 0.859 -
Deficit level(a) 25 (4.7) 13 (4.5) 12 (4.8)
0.93 (0.41-2.10, p=0.859)
Attention (D2-R - Processing speed) (n=424) Normal level 309 (72.9) 170 (70.8) 139 (75.5) 0.28 -
Deficit level(a) 115 (27.1) 70 (29.2) 45 (24.5)
1.27 (0.82-1.98, p=0.280)
Planning abilities (Shopping test - Reaction time) (n=472)
Normal level 384 (81.4) 219 (84.6) 165 (77.5) 0.049 -
Deficit level(a) 88 (18.6) 40 (15.4) 48 (22.5)
0.63 (0.39-1.00, p=0.050)
Planning abilities (Shopping test - Error) (n=473)
Normal level 412 (87.1) 231 (89.2) 181 (84.6) 0.137 -
Deficit level(a) 61 (12.9) 28 (10.8) 33 (15.4)
0.66 (0.39-1.14, p=0.138)
ToM (n=221) Normal level 93 (42.1) 45 (40.9) 48 (43.2) 0.725 -
Deficit level(a) 128 (57.9) 65 (59.1) 63 (56.8) 1.10 (0.64-1.88, p=0.725)
Values are mean(SD) or N(%). Bold font indicates p value <0.05. (a) : Cognitive deficits class was performed by score < 5th percentile or z-score < -1.65.
Table 3: Multivariate logistic regression summary (with stepwise selection)
Elevated stigma resistance
Predictors (n = 221) Estimate Std. Error p-value Odds ratio 95% CI for odds ratio
(Intercept) -0.5949 0.7256 0.412 0.55 0.13 – 2.26
Clinical Global Impression -0.2138 0.1178 0.07. 0.81 0.64 – 1.01
CASIG adaptation - Satisfaction level with family relationships 0.1622 0.0592 0.006* 1.18 1.05 – 1.33
CASIG adaptation - Satisfaction level with education 0.1004 0.0521 0.054. 1.11 1.00 – 1.23
Model chi2(3)=18.64, p < 0.001
Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1
Page 159
Narrative Enhancement and Cognitive Therapy (NECT) to improve social functioning in
people with Serious Mental Illness: study protocol for a stepped-wedge randomized controlled
trial
Running title: NECT and social function: study protocol
AUTHORS
Dubreucq Ja,b,c,d
, Faraldo Mb,c
, Abbes Mbc
, Ycart Bg, Richard-Lepouriel H
h, Favre S
h, Jermann F
h,
Attal Jk, Bakri M
i, Cohen T
b,c Cervello C
e,f , Chereau I
c,j, Cognard C
n, De Clercq M
o, Douasbin A
n,
Giordana J.Yp, Giraud-Baro E
r, Guillard-Bouhet N
m, Legros-Lafarge E
l, Polosan M
q, Pouchon A
q,
Rolland Me,f
, Rainteauk N, Roussel C
o, Wangermez C
m, Yanos PT, Lysaker PH, Franck N
a,e,f
a Centre de Neurosciences Cognitive, UMR 5229, CNRS & Université Lyon 1
b Centre référent de réhabilitation psychosociale et de Remédiation Cognitive (C3R), Centre Hospitalier Alpes Isère, Grenoble
c Fondation FondaMental, Créteil, France
d Réseau Handicap Psychique, Grenoble France
e Centre Ressource de Réhabilitation Psychosociale et de Remédiation cognitive, Centre Hospitalier Le Vinatier
f Centre Référent Lyonnais de Réhabilitation Psychosociale et de Remédiation Cognitive (CL3R), Centre
Hospitalier Le Vinatier
g Laboratoire Jean Kuntzmann, CNRS UMR 5224, Université Grenoble-Alpes, France
h Geneva University Hospital, Department of Psychiatry, Mood disorders Unit, 20bis rue de Lausanne, CH-1201 Geneva
i Centre de Réhabilitation Psychosociale et de Remédiation Cognitive (C2R), CH Drôme Vivarais
j CMP B, CHU, EA 7280 Faculté de Médecine, Université d'Auvergne, BP 69 63003 Clermont-Ferrand Cedex 1, France.
k Service Universitaire de Psychiatrie Adulte, Hôpital la Colombière, CHRU Montpellier, Université Montpellier 1, Inserm 1061, Montpellier, France.
l Centre Référent de Réhabilitation Psychosociale de Limoges C2RL, CH Esquirol, Limoges
m CREATIV & URC Pierre Deniker, CH Laborit, Poitiers
Page 160
n Unité Ariane de rehabilitation psychosociale, EPSM Caen
o Centre départemental de réhabilitation psychosociale des Glières, 219 chemin des bois des Fornets, 74800
La Roche sur Foron
p Centre Hospitalier Sainte Marie de Nice, 87 Avenue Joseph Raybaud, 06100 Nice
q Centre Expert Troubles Bipolaires, Service Universitaire de Psychiatrie, CHU de Grenoble et des Alpes,
CS10217, F-38043 Grenoble, France
r Clinique du Dauphiné- Groupe Sinoué, 252 Route de Saint-Nizier, 38180 Seyssins
* Correspondence should be sent to: Julien DUBREUCQ
Centre référent de réhabilitation psychosociale et de Remédiation Cognitive (C3R), CH Alpes Isère, 1 place
du Conseil National de la Résistance, 38400 Saint Martin d’Hères, France
Tel: (33 4) 56 58 88 00, e-mail: [email protected]
Page 161
Background: Self-stigma is highly prevalent in Serious Mental Illness (SMI) and is associated with poorer
clinical and functional outcomes. Narrative Enhancement and Cognitive Therapy (NECT) is a group-based
intervention combining psychoeducation, cognitive restructuring and story-telling exercises to reduce self-
stigma and its impact on recovery-related outcomes. Despite evidence of its effectiveness on self-stigma in
schizophrenia-related disorders, it is unclear whether NECT can impact social functioning.
Methods: This is a 12 centre stepped-wedge randomized controlled trial of NECT effectiveness on social
functioning in SMI, compared to treatment as usual. One hundred and twenty participants diagnosed with
schizophrenia, bipolar disorder or borderline personality disorder will be recruited across the 12 sites.
Participants will be randomized into two groups: one group (Group 1) receiving the intervention at the
beginning of the study (T0), one group (Group 2) treated as a control group for the first 6 months and then
receiving the intervention after (T1). Outcomes will be compared in both groups at T0 and T1, 6-month and
12-month outcomes for Groups 1 and 2 will be measured without a control group at T2 (to evaluate the
stability of the effects over time). Evaluations will be conducted by assessors blind to treatment allocation.
The primary outcome is personal and social performance compared across randomization groups. Secondary
outcomes include self-stigma, self-esteem, wellbeing, quality of life, illness severity, depressive symptoms
and personal recovery.
Discussion: NECT is a promising intervention for reducing self-stigma and improving recovery-related
outcomes in SMI. If shown to be effective in this trial, it is likely that NECT will be implemented in
psychiatric rehabilitation services with subsequent implications for routine clinical practice.
Trial registration number : Clinical Trials NCT03972735

Page 162
Introduction
Mental illness stigma refers to the negative beliefs, emotional reactions, and attitudes towards people with
Serious Mental Illness (SMI) endorsed by the general population (also referred to as public stigma1). People
with SMI are generally acutely aware of public stigma and expect to be rejected by others (69.4% of the
1,229 participants with schizophrenia (SZ) and 71.6% of the 1,182 participants with mood disorders in the
GAMIAN-Europe study had high perceived stigma2,3). Self-stigma occurs when someone moves beyond
awareness of stigma to accepting the negative stereotypes about SMI as true to describe him/herself.1 Self-
stigma refers to the process whereby a person’s previously held social identity (defined by social roles such
as son, brother, sister, friend, employee or potential partner) is progressively replaced by a devalued and
stigmatised view of oneself. Self-stigma is highly frequent in Europe (41.7% in SZ and 21.7% in mood
disorders2,3) and the USA (36.1% out of 144 people with SMI4). The “illness identity model”5 proposed that
self-stigma can have pervasive effects on outcomes related to recovery from SMI, including self-esteem,
hopefulness, social interaction, employment, and symptom severity. The evidence consistently supports
many of the model’s predictions, including that self-stigma is negatively associated with self-esteem,
motivation to achieve personal life goals, shared-decision making, adherence into treatment, well-being,
quality of life, personal recovery and social function.6-14 People with elevated self-stigma report more
dysfunctional attitudes, social withdrawal, depressive symptoms and increased suicidal ideation.5,15-21 High
insight into illness directly predicts and compounds the effects of self-stigma on depression.15,17,22-24
Impairments in cognitive functioning, metacognition and social cognition predict increased self-stigma.12,24-29
Several psychosocial interventions have been designed to reduce self-stigma and its impact on patient’s
outcomes, with preliminary results on self-stigma, insight, and self-efficacy.30 Narrative Enhancement and
Cognitive Therapy (NECT) is a structured, 20 session group-based approach which combines
psychoeducation to counteract SMI stereotypes, cognitive restructuring to challenge dysfunctional attitudes
about the self, and story-telling exercises to enhance meaning-making and the person’s ability to move
beyond their illness-identity to a more integrated sense of self.31 NECT is manualized and can be
implemented with fidelity in routine treatment settings.31 Four controlled studies, including three randomized
controlled trials (RCT) in three different countries (USA, Israel, Sweden) have been published to date in
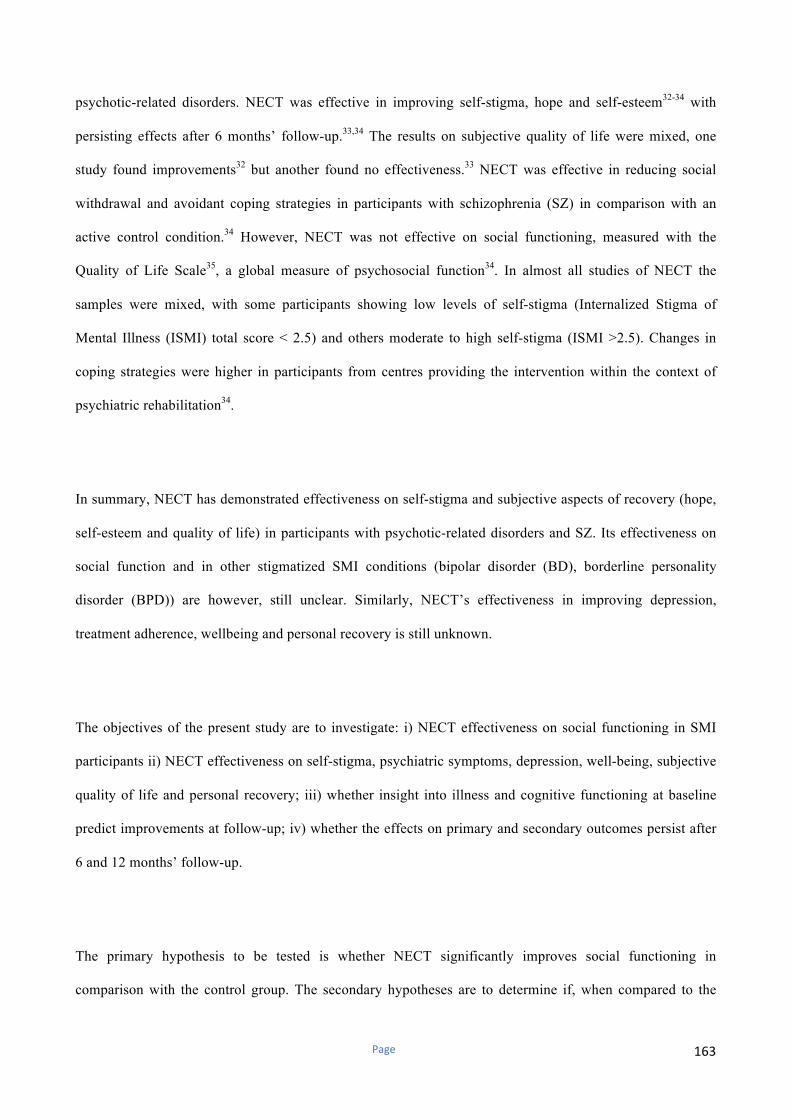
Page 163
psychotic-related disorders. NECT was effective in improving self-stigma, hope and self-esteem32-34 with
persisting effects after 6 months’ follow-up.33,34 The results on subjective quality of life were mixed, one
study found improvements32 but another found no effectiveness.33 NECT was effective in reducing social
withdrawal and avoidant coping strategies in participants with schizophrenia (SZ) in comparison with an
active control condition.34 However, NECT was not effective on social functioning, measured with the
Quality of Life Scale35, a global measure of psychosocial function34. In almost all studies of NECT the
samples were mixed, with some participants showing low levels of self-stigma (Internalized Stigma of
Mental Illness (ISMI) total score < 2.5) and others moderate to high self-stigma (ISMI >2.5). Changes in
coping strategies were higher in participants from centres providing the intervention within the context of
psychiatric rehabilitation34.
In summary, NECT has demonstrated effectiveness on self-stigma and subjective aspects of recovery (hope,
self-esteem and quality of life) in participants with psychotic-related disorders and SZ. Its effectiveness on
social function and in other stigmatized SMI conditions (bipolar disorder (BD), borderline personality
disorder (BPD)) are however, still unclear. Similarly, NECT’s effectiveness in improving depression,
treatment adherence, wellbeing and personal recovery is still unknown.
The objectives of the present study are to investigate: i) NECT effectiveness on social functioning in SMI
participants ii) NECT effectiveness on self-stigma, psychiatric symptoms, depression, well-being, subjective
quality of life and personal recovery; iii) whether insight into illness and cognitive functioning at baseline
predict improvements at follow-up; iv) whether the effects on primary and secondary outcomes persist after
6 and 12 months’ follow-up.
The primary hypothesis to be tested is whether NECT significantly improves social functioning in
comparison with the control group. The secondary hypotheses are to determine if, when compared to the

Page 164
control condition, NECT results in significant improvements in self-stigma, psychiatric symptoms,
depression, wellbeing, self-esteem, subjective quality of life and personal recovery.
Methods and design
Design
This randomized controlled study is multi-centric, prospective, interventional and exploratory.
For ethical purposes, we have chosen a stepped wedge cluster randomized trial design, with a waiting list
type control group. Previous research from the French national REHABase network showed that: i) most
patients were dissatisfied with their interpersonal relationships at the time of admission and asked for
interventions improving social function36; ii) elevated self-stigma was frequent (31.2% of the 738
participants37) and was negatively associated with recovery-related outcomes. Self-stigma has been
negatively associated with patient’s longitudinal outcomes and to lower benefits from psychiatric
rehabilitation38. Providing NECT to all participants aims at not excluding participants from interventions
improving social function (e.g. social skills training or social-cognitive remediation) during the follow-up
period without proposing them a credible therapeutic alternative (i.e. self-stigma reduction). This also aims at
reducing potential deception bias and dropouts in participants allocated to the control group. In stepped-
wedge RCTs, all clusters are evaluated before and after providing the intervention and each cluster switches
from control to become exposed, but not at the same point in time39,40. The participants who agree to join the
study will be randomized into two groups: one group (Group 1) receiving the intervention at the beginning of
the study (T0), one group (Group 2) being a control group for the first 6 months and receiving the
intervention after (T1). The stepped-wedge design of this 2-cluster trial can be seen on Figure 1.
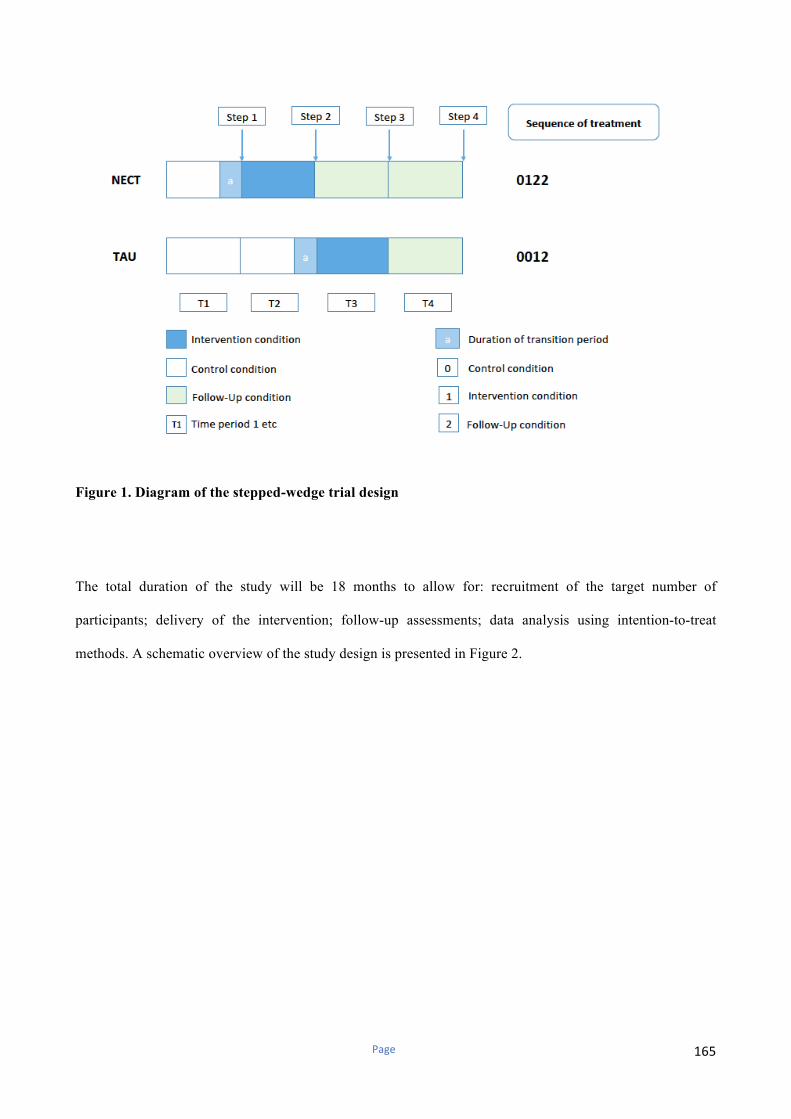
Page 165
Figure 1. Diagram of the stepped-wedge trial design
The total duration of the study will be 18 months to allow for: recruitment of the target number of
participants; delivery of the intervention; follow-up assessments; data analysis using intention-to-treat
methods. A schematic overview of the study design is presented in Figure 2.
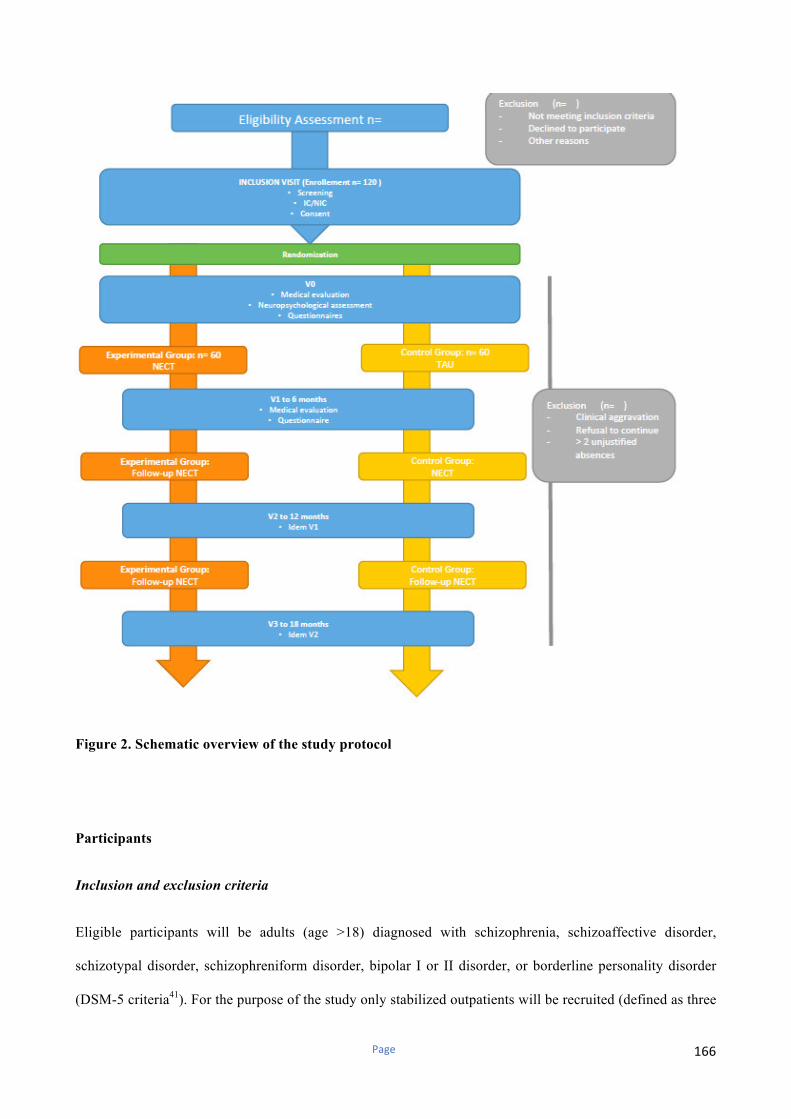
Page 166
Figure 2. Schematic overview of the study protocol
Participants
Inclusion and exclusion criteria
Eligible participants will be adults (age >18) diagnosed with schizophrenia, schizoaffective disorder,
schizotypal disorder, schizophreniform disorder, bipolar I or II disorder, or borderline personality disorder
(DSM-5 criteria41). For the purpose of the study only stabilized outpatients will be recruited (defined as three

Page 167
months of clinical stability and no changes in pharmacological treatment in the past three months).
Participants unable to give informed consent or with a comorbid intellectual disability will be excluded.
Participation in other programs having an impact on social function or self-stigma (social cognitive
remediation, social skills training) will be prohibited during the follow-up period.
Recruitment and randomization
Patients diagnosed with schizophrenia, bipolar disorder or borderline personality disorder (DSM-5 criteria41)
will be recruited through six Rehabase psychiatric rehabilitation network centres36, three FondaMental
Academic Centres of Expertise (FACE) for SZ or BD,42,43 one unit specialized in mood disorders at the
Geneva university hospital, one psychiatric day-care clinic specialized in mood and personality disorders in
Grenoble, and one psychiatric rehabilitation centre located in the psychiatric hospital in Caen. The selected
sites are already actively involved in treating patients with SZ, BD or BPD and have previous research
experience in the field of psychiatric rehabilitation. Regular group meetings will be organized to monitor
quality control and ensure good inter-rater reliability. A list of eligible participants will be generated under
the supervision of the coordinating centre clinical research officer. Each eligible patient will be approached
by a trained member of the research team and invited to participate in the study, thereby eliminating
selection biases. Eligible patients will be given a leaflet describing the program and the research. Informed
consent will be taken during a medical interview with one of the investigators. The clinical research officer
of the coordinating centre (Grenoble) will be in charge of the randomization process for participants from all
centres. Randomization using Clinsight software will be stratified by centre, gender, age and diagnosis with
an allocation ratio of 1:1. Outcomes will be compared in all groups at T0 and T1 (duration of intervention= 6
months). 6-month and 12-month outcomes for Group 1 and 2 will be measured at T2 (18 months after T0) to
evaluate the stability of the effects over time. A 7-point improvement in social functioning measured using
Personal and Social Performance Scale44 (PSP) is generally considered as clinically significant. The sample
size was calculated taking into consideration the cluster and time effects found in stepped-wedge RCT
designs. In order to ensure significance with an alpha error = 5% and an expected statistical power of 90%,
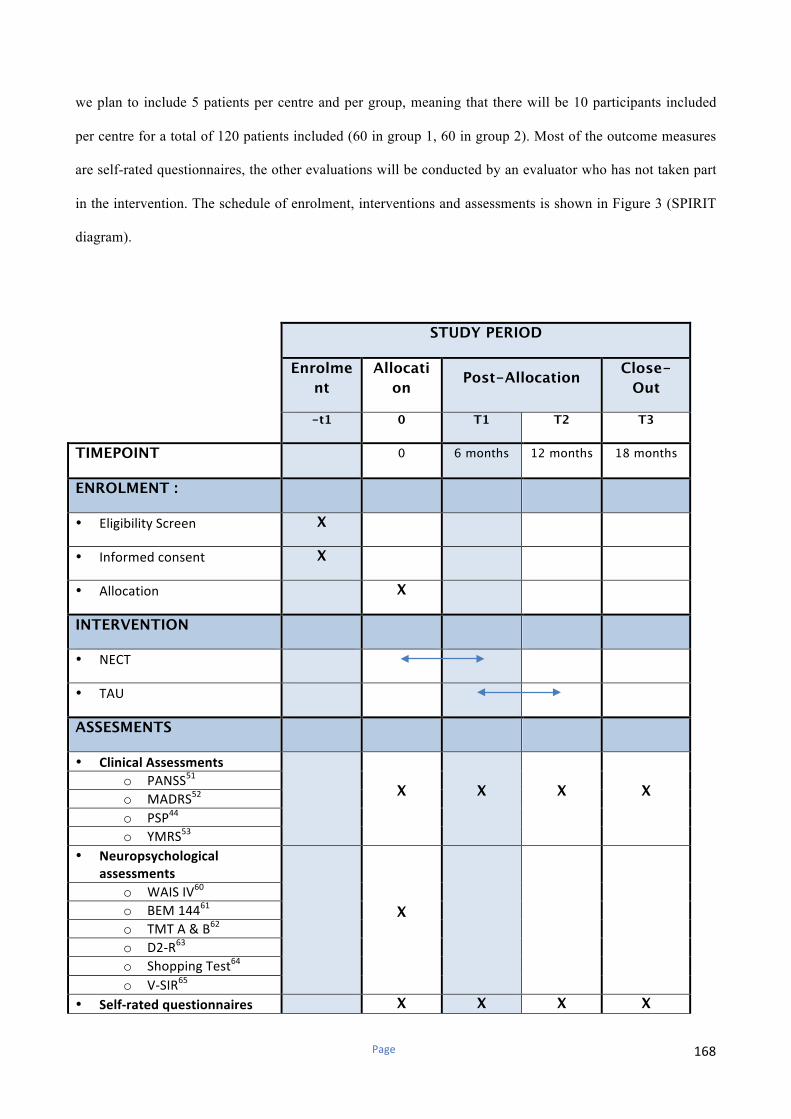
Page 168
we plan to include 5 patients per centre and per group, meaning that there will be 10 participants included
per centre for a total of 120 patients included (60 in group 1, 60 in group 2). Most of the outcome measures
are self-rated questionnaires, the other evaluations will be conducted by an evaluator who has not taken part
in the intervention. The schedule of enrolment, interventions and assessments is shown in Figure 3 (SPIRIT
diagram).
STUDY PERIOD
Enrolme
nt
Allocati
on Post-Allocation
Close-
Out
-t1 0 T1 T2 T3
TIMEPOINT 0 6 months 12 months 18 months
ENROLMENT :
• EligibilityScreen X
• Informedconsent X
• Allocation X
INTERVENTION
• NECT
• TAU
ASSESMENTS
• ClinicalAssessments
X X X X o PANSS
51
o MADRS52
o PSP44
o YMRS53
• Neuropsychological
assessments
X
o WAISIV60
o BEM14461
o TMTA&B62
o D2-R63
o ShoppingTest64
o V-SIR65
• Self-ratedquestionnaires X X X X

Page 169
o ISMI50
o STORI59
o SERS-SF58
o S-qol56
o WEWMBS57
o BIS54
o MARS55
Figure 3. Schedule of enrolment, interventions and assessments (SPIRIT diagram)
BIS: Birchwood Insight Scale; ISMI: Internalized Stigma of Mental Illness; MARS: Medication Adherence Rating Scale; NECT: Narrative Enhancement and Cognitive Therapy; PSP: Personal and Social Performance Scale; S-QoL: Subjective-Quality of Life; TAU: Treatment as Usual; TMT: Trail Making Test; V-SIR: Versailles-Situational Intention Reading; WAIS IV: Wechsler Adult Intelligence Scale-4th edition; WEWMBS: Warwiwk Edinburgh Mental WellBeing Scale; YMRS: Young Mania Rating Scale
NECT
Translation procedure
A consistent translation and cross-cultural adaptation procedure was realized by two independent research
teams (JD, MF and MA in Grenoble; HRL, SF and FJ in Geneva). All materials were translated from English
into French, the first language of all translators. Each team reviewed the material translated by the other team
so all translations were crosschecked. Regular group meetings between the two teams were conducted to
discuss any problematic translations and resolve any disputed items, in line with established translation
methods.
Training and fidelity monitoring
All the clinicians involved will attend a 1-day NECT training session, delivered by the creators of the
program (Yanos PT, Roe D). Training will include discussion and role-playing exercises, with corrective
feedback from the trainers. Regular group supervisions will be organized to ensure treatment fidelity. NECT
fidelity will be monitored using the NECT Fidelity Scale, developed by Yanos et al34.

Page 170
The experimental intervention
The French adaptation of NECT is a manualized, structured, 12-session, group-based intervention conducted
by two facilitators. The number of sessions was reduced in the French adaptation and their duration extended
to match the typical duration of psychosocial interventions in French-speaking countries (up to 15 sessions).
Figure 3 provides an overview of the NECT topics. The 2-hour sessions are divided into three main parts: 1)
psychoeducation about stigma, self-stigma, and myths about mental disorders; 2) cognitive restructuring
targeting negative thoughts about the self and dysfunctional attitudes; 3) story-telling exercises in which
participants tell stories about themselves, receive feedback from other group members and facilitators and
are invited to apply the cognitive restructuring skills learnt in the previous sessions to their personal life
narratives. At-home practice exercises are carried out between the sessions.
Figure 3 Structure of NECT topics
The control condition
Page 171
The control condition refers to the group receiving current standard care during the first six months of the
study before attending NECT after T1. There is no definition of standard care. The association of
pharmacological treatment with psychiatric rehabilitation is however recommended in all the international
guidelines on SMI45-47. All participants will attend day-care recovery-oriented services offering several forms
of psychiatric rehabilitation (group CBT on positive symptoms, general psychoeducation, cognitive
remediation, vocational rehabilitation, supported employment). Information about the interventions received
during the follow-up period (with their duration and the number of sessions) will be systematically collected
by the clinical research officer and taken into account when analysing the results.
Assessments
At baseline and at follow-up, socio-demographic and illness-related information (education level,
employment and marital status, psychiatric diagnosis, age of onset, illness duration, current pharmacological
treatment) will be collected. All outcome measures listed below are part of routine clinical evaluations in the
national REHABase and FACE networks for SZ and BD36,42,43 approved by the relevant ethical committees.
Primary outcome
Social function will be assessed with the Personal and Social Performance Scale44 (PSP), a clinician-reported
measure of social dysfunction using six-point severity scale in four life domains (socially useful activities,
personal and social relationships, self-care, and disturbing or aggressive behaviours). PSP provides an
overall rating score ranging from 1 to 100, higher scores representing better personal and social functioning.
PSP showed acceptable internal consistency48, excellent inter-rater reliability49, and a satisfactory ability to
detect changes44. A seven-point improvement during clinical trials is considered to be clinically significant44.
Secondary outcomes
Self-stigma will be assessed using the Internalized Stigma of Mental Illness scale (ISMI2,50), a 29-item self-
report measure designed to assess a person’s personal experience of stigma related to mental disorders and is
Page 172
rated on a four-point Likert scale. Items are summed to provide a mean total score and five subscale scores
(alienation or feeling of being a devalued member of the society; stereotype endorsement or agreement with
the negative attitudes about SMI; discrimination experience; social withdrawal as a coping strategy and
stigma resistance). Stigma resistance is generally excluded because of poor correlations with other
subscales32,34. Higher scores reflect higher levels of self-stigma. Scores above 2.5 indicate moderate to high
levels of self-stigma2,3. Illness severity will be assessed in patients with SZ using the Positive and Negative
Syndrome51 (PANSS) scales. Current depressive symptoms were evaluated using the Montgomery Asberg
Depression Rating Scale52 (MADRS) and current manic symptoms with theYoung Mania Rating Scale53
(YMRS). Insight and treatment adherence will be assessed with self-reported measures (Birchwood Insight
Scale (BIS)54; Medication Adherence Rating Scale (MARS)55). Quality of Life will be evaluated with the
self-reported Subjective Quality of Life scale56 (S-QoL) and wellbeing using the Warwick-Edinburgh Mental
Well-being Scale57 (WEMBS). Self-esteem will be measured with the Self-Esteem Rating Scale58 (SERS)
and personal recovery using the self-reported Stage of Recovery Instrument59 (STORI). Baseline
neuropsychological cognitive assessments include Wechsler Adult Intelligence Scale-4th edition60 (WAIS-
IV) subscales assessing working memory, verbal abstraction and hypothetico-deductive reasoning, BEM-144
story subtest for auditive-verbal memory61, Trail Making Test A and B (TMT-A or B)62 respectively for
speed of processing and reactive mental flexibility, D2-R for selective attention, concentration, and speed of
processing63, and shopping test for planning abilities64. Theory of mind will be assessed at baseline using the
Versailles-Situational Intention Reading Test65 (V-SIR).
Statistical Analysis
Intention-to-treat analyses will be conducted in the first instance. The analyses will be conducted using
parametric tests for normal distributed data (Student’s t and covariance analysis with repeat measures
ANCOVA) and with non-parametric tests (Mann-Whitney U and Kruskal-Wallis test) in case of significant
deviations from the normal distribution. The statistical analysis will be done using the R software, version
3.2.366. The psych package version 1.5.8, will be used67. Effect Size (Cohen's d) will be calculated using the

Page 173
effsize package67. Size effects inferior to 0.20 will be considered as negligible, from 0.20 to 0.40 as small,
from 0.40 to 0.60 as moderate, and superior to 0.60 as strong67. The leaps package version 2.9 will be used
for variable selection68. The level of confidence intervals will be set at 0.95, and the significance level of
tests at 0.05.
Trial status
The present trial has not yet started. The recruitment will begin on 2019/09/01 with an estimated study
completion date is 2023/04/03. Protocol version 1.5 was written on 2019/04/02 and approved by the relevant
ethical committee (CPP Nord-Ouest I) on 2019/04/26.
Discussion and conclusion
NECT has shown effectiveness in reducing self-stigma in patients with psychotic-related disorders in a range
of contexts in previous research. Considering the prevalence of moderate to high self-stigma in SMI and its
impact on functional outcomes, NECT appears to be a promising intervention to complete the basket of
services proposed by psychiatric rehabilitation centres (cognitive and social cognitive remediation,
psychoeducation, social skills training, group cognitive behaviour therapy, vocational rehabilitation, peer-
support36). If shown to be effective on social function and for different SMI, it is likely that NECT will have
widespread implications for clinical practice.
Ethics approval and consent to participate: The present study obtained all the authorizations required
under French regulations and was approved by the relevant ethical committee (CPP Nord-Ouest I) on
2019/04/26. Informed written consent will be systematically sought for all participants.
Author contribution statement: The authors had full access to the data in the study and take the
responsibility for the integrity of the data and the accuracy of the data analysis. Dr Julien Dubreucq drafted

Page 174
the article and made the literature review. Mrs Megane Faraldo, Mrs Marie Abbes, Mr Thomas Cohen, Pr
Paul Lysaker, Pr Philip Yanos and Pr Nicolas Franck contributed to design the study protocol and critically
revised the article. All the authors will be involved in the collection and analysis of the data. All authors
contributed to and have approved the final manuscript.
Author’s information: a Centre de Neurosciences Cognitive, UMR 5229, CNRS & Université Lyon 1 ; b
Centre référent de réhabilitation psychosociale et de Remédiation Cognitive (C3R), Centre Hospitalier Alpes Isère, Grenoble ; c Fondation FondaMental, Créteil, France ; d Réseau Handicap Psychique, Grenoble France ; e Centre Ressource de Réhabilitation Psychosociale et de Remédiation cognitive, Centre Hospitalier Le Vinatier ; f Centre Référent Lyonnais de Réhabilitation Psychosociale et de Remédiation Cognitive (CL3R), Centre Hospitalier Le Vinatier : g Laboratoire Jean Kuntzmann, CNRS UMR 5224, Université Grenoble-Alpes, France ; h Geneva University Hospital, Department of Psychiatry, Mood disorders Unit, 20bis rue de Lausanne, CH-1201 Geneva ; i Centre de Réhabilitation Psychosociale et de Remédiation Cognitive (C2R), CH Drôme Vivarais ; j CMP B, CHU, EA 7280 Faculté de Médecine, Université d'Auvergne, BP 69 63003 Clermont-Ferrand Cedex 1, France. ; k Service Universitaire de Psychiatrie Adulte, Hôpital la Colombière,
CHRU Montpellier, Université Montpellier 1, Inserm 1061, Montpellier, France ; lCentre Référent de
RéhabilitationPsychosocialedeLimogesC2RL,CHEsquirol,Limoges;mCREATIV&URCPierreDeniker,CH
Laborit, Poitiers;nUnité Ariane de rehabilitation psychosociale, EPSM Caen; oCentre départemental de
réhabilitation psychosociale des Glières, 219 chemin des bois des Fornets, 74800 La Roche sur Foron ; p
Centre Hospitalier Sainte Marie de Nice, 87 Avenue Joseph Raybaud, 06100 Nice ; q Centre Expert Troubles Bipolaires, Service Universitaire de Psychiatrie, CHU de Grenoble et des Alpes, CS10217, F-38043 Grenoble, France ; r Clinique du Dauphiné- Groupe Sinoué, 252 Route de Saint-Nizier, 38180 Seyssins
Availability of data and materials: The study protocol is available online on Clinical Trials:
https://clinicaltrials.gov/ct2/show/NCT03972735?term=nect&rank=1
Consent for publication: not applicable
Role of the funding source: This research did not receive any specific grants from funding bodies in the
public, private, or not-for-profit sectors. This trial will be conducted in day-care community services funded
by the Auvergne-Rhône-Alpes, Nouvelle-Aquitaine and Normandie regional health agencies
Conflicts of interests : none
Page 175
References :
1. Corrigan P.W., Watson A . C. Understanding the impact of stigma on people with mental illness. World
Psychiatry. 2002;1(1):16-20
2. Brohan E, Elgie R, Sartorius N, Thornicroft G, GAMIAN-Europe Study Group. Self-stigma,
empowerment and perceived discrimination among people with schizophrenia in 14 European countries: the
GAMIAN-Europe study. Schizophr Res. 2010;122(1-3):232-8.
3. Brohan E, Gauci D, Sartorius N, Thornicroft G, GAMIAN-Europe Study Group. Self-stigma,
empowerment and perceived discrimination among people with bipolar disorder or depression in 13
European countries: the GAMIAN-Europe study. J Affect Disord. 2011;129(1-3):56-63.
4. West ML, Yanos PT, Smith SM, Roe D, Lysaker PH. Prevalence of Internalized Stigma among Persons
with Severe Mental Illness. Stigma Res Action. 2011;1(1):3-10.
5. Yanos PT, Roe D, Markus K, Lysaker PH. Pathways between internalized stigma and outcomes related to
recovery in schizophrenia spectrum disorders. Psychiatr Serv. 2008;59(12):1437-42.
6. Gerlinger G, Hauser M, De Hert M, Lacluyse K, Wampers M, Correll CU. Personal stigma in
schizoprhenia spectrum disorders: a systematic review of prevalence rates, correlates, impact and
interventions. Word Psychiatry 2013;12:155-64
7. Corrigan P.W., Larson J.E., Rüsch N. Self-stigma and the “why try” effect: impact on life goals and
evidence-based practices. World Psychiatry. 2009;8:75-81
8. Hamann J, Bühner M, Rüsch N. Self-Stigma and Consumer Participation in Shared Decision Making in
Mental Health Services. Psychiatr Serv. 2017;68(8):783-8.
9. Hill K, Startup M. The relationship between internalized stigma, negative symptoms and social
functioning in schizophrenia: the mediating role of self-efficacy. Psychiatry Res. 2013;206(2-3):151-7
10. Cerit C, Filizer A, Tural Ü, Tufan AE. Stigma: a core factor on predicting functionality in bipolar
disorder. Compr Psychiatry. 2012;53(5):484-9.
Page 176
11. Mersh L, Jones F, Oliver J. Mindfulness, self-stigma and social functioning in first episode psychosis: A
brief report. Psychosis. 2015;7(3):1-4
12. Firmin RL, Lysaker PH, Luther L, Yanos PT, Leonhardt B, Breier A, et al. Internalized stigma in adults
with early phase versus prolonged psychosis. Early Interv Psychiatry. 2019;13(4):745-51
13. Xu Z, Lay B, Oexle N, Drack T, Bleiker M, Lengler S, et al. Involuntary psychiatric hospitalisation,
stigma stress and recovery: a 2-year study. Epidemiol Psychiatr Sci. 2018;31:1-8.
14. Oexle N, Müller M, Kawohl W, Xu Z, Viering S, Wyss C, et al. Self-stigma as a barrier to recovery: a
longitudinal study. Eur Arch Psychiatry Clin Neurosci. 2018;268(2):209-12.
15. Schrank B, Amering M, Hay AG, Weber M, Sibitz I. Insight, positive and negative symptoms, hope,
depression and self-stigma: a comprehensive model of mutual influences in schizophrenia spectrum
disorders. Epidemiol Psychiatr Sci. 2014;23(3):271-9.
16. Park SG, Bennett ME, Couture SM, Blanchard JJ. Internalized stigma in schizophrenia: relations with
dysfunctional attitudes, symptoms, and quality of life. Psychiatry Res. 2013;205(1-2):43-7.
17. Valiente C, Provencio M, Espinosa R, Duque A, Everts F. Insight in paranoia: The role of experiential
avoidance and internalized stigma. Schizophr Res. 2015;164(1-3):214-20.
18. Oexle N, Rüsch N, Viering S, Wyss C, Seifritz E, Xu Z, et al. Self-stigma and suicidality: a longitudinal
study. Eur Arch Psychiatry Clin Neurosci. 2017;267(4):359-61.
19. Oexle N, Waldmann T, Staiger T, Xu Z, Rüsch N. Mental illness stigma and suicidality: the role of
public and individual stigma. Epidemiol Psychiatr Sci. 2018;27:169-75
20. Espinosa R, Valiente C, Rigabert A, Song H. Recovery style and stigma in psychosis: the healing power
of integrating. Cogn Neuropsychiatry. 2016;21(2):146-55.
21. Au CH, Wong CS, Law CW, Wong MC, Chung KF. Self-stigma, stigma coping and functioning in
remitted bipolar disorder. Gen Hosp Psychiatry. 2019;57:7-12.
Page 177
22. Cavelti M, Kvrgic S, Beck EM, Rüsch N, Vauth R. Self-stigma and its relationship with insight,
demoralization, and clinical outcome among people with schizophrenia spectrum disorders. Compr
Psychiatry. 2012;53(5):468-79.
23. Lysaker PH, Roe D, Yanos PT. Toward understanding the insight paradox: internalized stigma moderates
the association between insight and social functioning, hope, and self-esteem among people with
schizophrenia spectrum disorders. Schizophr Bull. 2007;33(1):192-9
24. Lysaker PH, Vohs J, Hasson-Ohayon I, Kukla M, Wierwille J, Dimaggio G. Depression and insight in
schizophrenia: comparisons of levels of deficits in social cognition and metacognition and internalized
stigma across three profiles. Schizophr Res. 2013;148(1-3):18-23.
25. Lysaker PH, Buck KD, Taylor AC, Roe D. Associations of metacognition and internalized stigma with
quantitative assessments of self-experience in narratives of schizophrenia. Psychiatry Res. 2008;157(1-3):31-
8.
26. Lysaker PH, Vohs JL, Tsai J. Negative symptoms and concordant impairments in attention in
schizophrenia: associations with social functioning, hope, self-esteem and internalized stigma. Schizophr
Res. 2009;110(1-3):165-72.
27. Galderisi S, Rossi A, Rocca P, Bertolino A, Mucci A, Bucci P, et al. The influence of illness-related
variables, personal resources and context-related factors on real-life functioning of people with
schizophrenia. World Psychiatry. 2014;13(3):275-87.
28. Hasson-Ohayon I, Mashiach-Eizenberg M, Elhasid N, Yanos PT, Lysaker PH, Roe D. Between self-
clarity and recovery in schizophrenia: reducing the self-stigma and finding meaning. Compr Psychiatry.
2014;55(3):675-80
29. Hasson-Ohayon I, Mashiach-Eizenberg M, Lysaker PH, Roe D. Self-clarity and different clusters of
insight and self-stigma in mental illness. Psychiatry Res. 2016;240:308-13.
Page 178
30. Wood L, Byrne R, Burke E, Enache G, Morrison AP. The impact of stigma on emotional distress and
recovery from psychosis: The mediatory role of internalised shame and self-esteem. Psychiatry Res.
2017;255:94-100.
31. Yanos PT, Lysaker PH, Roe D. Internalized stigma as a barrier to improvement in vocational functioning
among people with schizophrenia-spectrum disorders. Psychiatry Res. 2010;178(1):211-3.
32. Roe D, Hasson-Ohayon I, Mashiach-Eizenberg M, Derhy O, Lysaker PH, Yanos PT. Narrative
enhancement and cognitive therapy (NECT) effectiveness: a quasi-experimental study. J Clin Psychol.
2014;70(4):303-12.
33. Hansson L, Lexén A, Holmén J. The effectiveness of narrative enhancement and cognitive therapy: a
randomized controlled study of a self-stigma intervention. Soc Psychiatry Psychiatr Epidemiol.
2017;52(11):1415-23
34. Yanos PT, Lysaker PH, Silverstein SM, Vayshenker B, Gonzales L, West ML, et al. A randomized-
controlled trial of treatment for self-stigma among persons diagnosed with schizophrenia-spectrum disorders.
Soc Psychiatry Psychiatr Epidemiol. 2019; doi: 10.1007/s00127-019-01702-0.
35. Heinrichs DW, Hanlon TE, Carpenter WT. The quality of life scale: an instrument for assessing the
schizophrenic deficit syndrome. Schizophr Bull. 1984;10:388-96
36. Franck N, Bon L, Dekerle M, Plasse J, Massoubre C, Pommier R, et al. Satisfaction and Needs in Serious
Mental Illness and Autism Spectrum Disorder: The REHABase Psychosocial Rehabilitation Project.
Psychiatr Serv. 2019;70(4):316-23
37. Dubreucq J, Plasse J, Gabayet F, Faraldo M et al. Self-stigma in Serious Mental Illness and Autism
Spectrum Disorder: results from the REHABase national psychiatric rehabilitation cohort. Eur Psychiatry.
Accepted for publication.
38. Dubreucq J, Franck N. Internalized Stigma in Serious Mental Illness (SMI): a systematic review of
prevalence, predictors and correlates. Journal of Affective Disorders, revised
Page 179
39. Hemming K, Haines TP, Chilton PJ, Girling AJ, Lilford RJ. The stepped wedge cluster randomised trial:
Rationale, design, analysis, and reporting. BMJ [Internet]. 2015 [cited 2019 Jul 17];350. Available from:
https://www . Bmj . Com/content/350/bmj.h391.long
40. Hemming K, Taljaard M, McKenzie JE, Hooper R, Copas A, Thompson JA, et al. Reporting of stepped
wedge cluster randomised trials: Extension of the CONSORT 2010 statement with explanation and
elaboration. BMJ [Internet] https://www . Bmj . Com/content/363/bmj.k1614
41. American Psychiatric Association. Diagnostic And Statistical Manual Of Mental Disorders, fifth edition
(DSM-5). 5th ed. Washington: DC Author; 2013
42. Schürhoff F, Fond G, Berna F, Bulzacka E, Vilain J, Capde-vielle D, et al. A National network of
schizophrenia expert centres: an innovative tool to bridge the research-practice gap. Eur Psychiatry.
2015;30(6):728-35.
43. Henry C, Etain B, Mathieu F, Raust A, Vibert JF, Scott J, et al. A French network of bipolar expert
centres: a model to close the gap between evidence-based medicine and routine practice. J Affect Disord.
2011;131(1-3):358-63.
44. Nasrallah H, Morosini PL, Gagnon DD. Reliability, validity and ability to detect change of the Personal
and Social Performance Scale in patients with stable schizophrenia. Psychiatry Res. 2008;161:213-24
45. Dixon LB, Dickerson F, Bellack AS, Bennett M, Dickinson D, Goldberg RW, et al. (2009) The 2009
schizophrenia PORT psychosocial treatment recommendations and summary statements. Schizophr Bull.
2010;36(1):48-70.
46. Vieta E, Berk M, Schulze TG, Carvalho AF, Suppes T, Calabrese JR, et al. Bipolar Disorders. Nat Rev
Dis Primers. 2018;4:18008.
47. Gunderson JG, Herpertz SC, Skodol AE, Torgersen S, Zanarini MC. Borderline personality disorder. Nat
Rev Dis Primers. 2018;4:18029.
Page 180
48. Kawata AK, Revicki DA. Psychometric properties of the Personal and Social Performance scale (PSP)
among individuals with schizophrenia living in the -community. Qual Life Res. 2008;17(10):1247-56.
49. Patrick DC, Burns T, Morosini P, Rothman M, Gagnon DD, Wild D, et al. Reliability, validity and ability
to detect change of the clinician-rated Personal and Social Performance scale in patients with acute
symptoms of schizophrenia. Curr Med Res Opin. 2009;25(2):325–35.
50. Boyd Ritsher J, Otilingam PG, Grajales M. Internalized Stigma of Mental Illness: psychometric
properties of a new measure. Psychiatry Res. 2003;121:31-49.
51. Kay S, Fiszbein A, Opler L. The positive and negative syndrome scale (PANSS) for schizophrenia.
Schizophr Bull. 1987;13(2):261-76.
52. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Brit J
Psychiatry. 1979;134:382-9
53. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and
sensitivity. Br J Psychiatry. 1978;133:429-35
54. Birchwood M, Smith J, Drury V, Healy J, Macmillan F, Slade M. A self-report Insight Scale for
psychosis: reliability, validity and sensitivity to change. Acta Psychiatr Scand. 1994;89(1):62-7.
55. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating
Scale (MARS) for the psychoses. Schizophr Res. 2000;42(3):241-7.
56. Auquier P, Simeoni MC, Sapin C, Reine G, Aghababian V, Cramer J, et al. Development and validation
of a patient-based health-related quality of life questionnaire in schizophrenia: the S-QoL. Schizophr Res.
2003;63(1–2):137-49.
57. Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick-Edinburgh Mental
Well-being Scale 19 (WEMWBS): development and UK validation. Health Qual Life Outcomes. 2007;5:63.
58. Lecomte T, Corbière M, Laisné F. Investigating self-esteem in individuals with schizophrenia: Relevance
of the Self-Esteem Rating Scale-Short Form. Psychiatry Res. 2006;143(1),99–108.
Page 181
59. Andresen R, Caputi P, Oades LG. Stages of recovery instrument: development of a measure of recovery
from serious mental illness. Aust NZ J Psychiatry. 2006;40:972-80.
60. Wechsler, D. WAIS IV Nouvelle version de l’échelle d’intelligence de Weschler pour adultes. 4th ed.
Paris : Edition de Centre de Psychologie Appliquée; 2011
61. Signoret JL. Batterie d’efficience mnésique BEM 144. Paris : Elsevier ; 1991
62. Godefroy O, GREFEX (Groupe de Réflexion pour l’Evaluation des Fonctions Exécutives). Fonctions
exécutives et pathologies neurologiques et psychiatriques. Evaluation en pratique clinique. Marseille : Solal ;
2008
63. Brickenkamp R, Schmidt-Atzert L, Liepmann D. D2-R : Test d’attention concentrée révisé. Paris:
Editions Hogrefe; 2015
64. Pelletier Y, Lemoine L, Gros C, Fournet N. Test des commissions révisé. GREMOIRE II Tests et
échelles des maladies neurologiques avec symptomatologie cognitive. Paris : De Boeck-Solal; 2009
65. Bazin N, Brunet-Gouet E, Bourdet C, Kayser N, Falissard B, Hardy-Baylé MC, et al. Quantitative
assessment of attribution of intentions to others in schizophrenia using an ecological video-based task: a
comparison with manic and depressed patients. Psychiatry Res. 2009;167:28-35.
66. R Core Team. R: A Language and Environment for Statistical Computing, R Foundation for Statistical
Computing, Vienna, Austria, 2015. https ://www.R-project.org/
67. Revelle W. Psych: Procedures for Psychological, Psychometric, and Personality Research, Northwestern
University, Evanston, Illinois, R package; 2015
68. Lumley T. Leaps: regression subset selection. 2009. https://CRAN.R-project.org/package=leaps

Page 182
Partie V. Discussion générale et perspectives
Page 183
Chapitre 1. Synthèse des résultats principaux
Ce travail de thèse a permis d’approfondir les connaissances existantes sur l’auto-stigmatisation
dans les TPSP, objet d’un nombre croissant de publications au cours des dernières années. Celle-ci
est fréquente et associée à un devenir clinique et fonctionnel altéré, et ce quelque soit l’aire
géographique et culturelle, la pathologie ou le stade évolutif considérés. Elle semble toutefois plus
prononcée en Asie du Sud-Est et dans la schizophrénie. Elle est peu étudiée du point de vue des
neurosciences, une modélisation expérimentale des mécanismes conduisant à l’auto-stigmatisation
et sous-tendant ses effets sur les personnes avec TPSP étant néanmoins possible et potentiellement
contributive pour la clinique et la recherche sur le sujet. La base de données nationale des centres
référents de réhabilitation psychosociale et de remédiation cognitive (REHABase) est un outil
prometteur pour mieux identifier les besoins de réhabilitation des personnes avec TPSP et évaluer
de façon longitudinale l’efficacité des interventions qui leurs sont proposées. Elle a permis de
recueillir les premières données françaises sur la satisfaction et les souhaits en termes
d’accompagnement des personnes avec TPSP dans plusieurs domaines de vie, leur bien-être, leur
rétablissement personnel et leur niveau d’auto-stigmatisation et de résistance à la stigmatisation.
Environ un tiers des participants inclus dans la cohorte REHABase présentait un niveau élevé
d’auto-stigmatisation, celle-ci étant associée à un risque supérieur d’être dans un stade précoce du
rétablissement (x 4 pour le stade moratoire et x3 pour le stade conscience) et à un bien être et une
satisfaction dans les relations sociales altérés. La résistance à la stigmatisation, élevée chez plus de
la moitié des personnes inclues dans la cohorte REHABase, était positivement associée à la
satisfaction dans les relations familiales. Le présent travail a permis la traduction française du
programme NECT, en collaboration avec l’équipe d’Hélène Richard-Lepouriel aux Hôpitaux
Universitaires de Genève et les concepteurs originaux du programme, Philip T. Yanos de
l’université de New York, Paul H. Lysaker, de l’université d’Indianapolis et David Roe, de
l’université de Haïfa. Cette étape a été suivie par la conception et la mise en œuvre d’un essai
Page 184
randomisé contrôlé sur 12 sites en France et en Suisse pour évaluer l’efficacité de ce programme sur
le fonctionnement social des personnes avec TPSP, dont le début est prévu au 1er trimestre 2020.
1.1. L’auto-stigmatisation, une caractéristique fréquente et associée à de multiples effets
négatifs
L’auto-stigmatisation affecte environ un tiers des personnes avec TPSP (31.2% en France, 31.5%
dans le monde). Elle est présente partout dans le monde, en contradiction avec les premiers travaux
sur le sujet la concevant comme un produit des sociétés occidentales plus industrialisées et moins
soutenantes pour les individus [4] [207], [208]. L’auto-stigmatisation est toutefois plus marquée en
Asie du Sud-Est et au Moyen-Orient (> 39%) envers les personnes avec TPSP et en Amérique du
Sud et en Afrique envers celles avec schizophrénie (>38%). Cela peut en partie être expliqué par
des facteurs culturels, comme par exemple la peur de perdre la face en Asie [209-211] ou
l’attribution de la pathologie à des causes surnaturelles en Afrique ou au Moyen-Orient [212],
[213]. La stigmatisation publique et l’auto-stigmatisation en France sont dans la moyenne des pays
Européens [7], [8], [214]. L’auto-stigmatisation est plus marquée en Europe de l’Est et du Sud
comparativement au reste de l’Europe (15.2% en Suède à 50% en Croatie pour la schizophrénie ;
[40]). Ces variations sont cohérentes avec les résultats d’études internationales retrouvant une
stigmatisation publique plus marquée dans ces aires géographiques et culturelles [6], [7], elle même
associée à un niveau supérieur d’auto-stigmatisation [43]. Plus spécifiquement, les pays où la
stigmatisation perçue et l’auto-stigmatisation sont les moins marquées seraient aussi ceux où il est
le plus simple d’accéder à des informations concernant la façon de faire face à un problème de santé
mentale et où la consommation d’anti-dépresseurs est la plus élevée [43]. L’influence du diagnostic
psychiatrique sur l’auto-stigmatisation est controversée, celle-ci étant plus marquée chez les
personnes avec schizophrénie ou avec dépression dans certaines études, mais pas dans d’autres
Page 185
[215]. L’auto-stigmatisation dans les TPSP hors schizophrénie apparaît par ailleurs plus prononcée
en Asie du Sud et du Sud-Est [216-218]. L’auto-stigmatisation semble affecter plus
particulièrement les personnes avec troubles de personnalité borderline (43.8% en France ; [214]),
ce qui est cohérent avec deux études réalisées en République Tchèque [219], [220]. La forte
stigmatisation publique attachée à cette pathologie et les biais cognitifs rendant ces personnes plus
vulnérables à l’auto-stigmatisation en sont des explications potentielles [26], [221], [222]. La
présence de comorbidités psychiatriques, comme un trouble anxieux, un trouble de personnalité ou
un état de stress post-traumatique associés, renforce par ailleurs l’auto-stigmatisation chez les
personnes avec TPSP [214], [223], [224]. Cela peut expliquer en partie l’auto-stigmatisation plus
marquée dans les TPSP hors schizophrénie retrouvée en France et en République Tchèque,
comparativement à d’autres pays Européens [214].
L’auto-stigmatisation est particulièrement associée à la dépression et au risque suicidaire [215]. Elle
altère l’estime de soi, le bien-être, l’adhésion aux soins, le fonctionnement psychosocial, la qualité
de vie, le pouvoir d’agir, la résistance à la stigmatisation et est un frein majeur au processus de
rétablissement [214], [215].
1.2. L’auto-stigmatisation, un paramètre sous l’influence de facteurs environnementaux
L’auto-stigmatisation est peu influencée par la majorité des variables socio-démographiques ou en
lien avec la pathologie [215]. Elle est aussi marquée chez des personnes à ultra-haut risque de
transition vers la psychose que chez des personnes présentant une pathologie plus installée et ne
dépend ni de la durée de la maladie ni du nombre d’hospitalisations, même celles sous contrainte
[70], [147], [215], [225]. L’insight, la présence de troubles cognitifs et métacognitifs et l’utilisation
de stratégies d’évitement des situations sociales contribuent à la survenue de l’auto-stigmatisation
Page 186
[215], [226], [227]. Ces facteurs renforcent aussi le stress lié à la stigmatisation et limitent les
capacités à y faire face [68], [228].
L’auto-stigmatisation est largement influencée par des facteurs environnementaux, parmi lesquels le
soutien social et familial mais aussi l’attitude des professionnels de santé mentale envers les
personnes avec TPSP ont un rôle majeur [215], [229]. L’insight parental peut contribuer à l’auto-
stigmatisation chez des adolescents avec troubles psychiatriques débutants [230]. Un soutien social
et familial préservé et une satisfaction élevée dans les relations familiales protège au contraire de
l’auto-stigmatisation en renforçant la résistance à la stigmatisation [215], [228], [229]. La
perception d’attitudes stigmatisantes chez les professionnels de santé par les personnes avec TPSP
est associée à une diminution du pouvoir d’agir, cet effet étant à la fois direct et indirect via l’auto-
stigmatisation [231]. La stigmatisation perçue et l’identification négative au groupe social
stigmatisé renforcent le stress lié à la stigmatisation [68]. Celui-ci contribue à l’auto-stigmatisation
suite à une hospitalisation sous contrainte, surtout si celle-ci est associée à des réactions
émotionnelles négatives (honte, mépris de soi ; [70]). L’identification positive au groupe stigmatisé,
par exemple en participant à un groupe d’auto-support, contribue au contraire à réduire l’auto-
stigmatisation [48], [206]. La stigmatisation vécue et anticipée renforce la probabilité d’utilisation
de stratégies d’évitement et de survenue de l’auto-stigmatisation [60], [63], [232], [233].
1.3. L’auto-stigmatisation, un prédicteur longitudinal du devenir des personnes avec TPSP
L’auto-stigmatisation altère significativement le pronostic clinique et fonctionnel des personnes
avec TPSP [215]. Elle majore les symptômes positifs, l’anxiété sociale, la dépression, le risque
suicidaire et altére l’estime de soi, le bien-être et le rétablissement [71], [234-237]. Elle limite aussi
les bénéfices d’un accompagnement à la réinsertion professionnelle [238]. L’auto-stigmatisation
Page 187
renforce la détresse associée aux expériences inhabituelles, l’anxiété sociale, la dépression et le
risque suicidaire chez les personnes présentant des troubles psychiatriques débutants [239]. Elle
altère le bien-être et limite la possibilité de recourir à des stratégies adaptatives efficaces et
l’adhésion aux soins [42], [63], [240]. Il pourrait s’agir d’un facteur de risque de transition
psychotique, via le stress lié à la stigmatisation [241]. L’auto-stigmatisation diminue l’espoir et
altère l’inclusion sociale et l’insertion professionnelle des personnes ayant fait un 1er épisode
psychotique [242].
L’auto-stigmatisation est sensible au changement [243]. Une aggravation se traduit par des
symptômes dépressifs plus sévères, davantage d’idées suicidaires et une estime de soi et un
fonctionnement social altérés [71], [197], [232], [235], [237]. Une réduction de l’auto-
stigmatisation s’accompagne au contraire d’une amélioration de l’humeur, de l’estime de soi et du
fonctionnement psychosocial [197], [243], [244]. Elle se traduit également par un amélioration plus
marquée de la qualité de vie pendant un parcours de réhabilitation psychosociale [244].
1.4 La réhabilitation psychosociale, un levier pour réduire l’auto-stigmatisation?
Les soins de réhabilitation psychosociale permettent de réduire significativement l’auto-
stigmatisation [224], [244-248]. L’auto-stigmatisation diminue chez les personnes accompagnées
vers l’emploi si elles ne sont pas confrontées à des expériences de discrimination en milieu
professionnel [248]. La réduction de l’auto-stigmatisation était par ailleurs plus sensible pour les
personnes avec TPSP n’ayant pas bénéficié de prestations de compensation du handicap pendant la
période de suivi [224]. La réduction de l’intensité des symptômes, l’amélioration du fonctionnement
cognitif, la reprise du pouvoir d’agir ou encore l’acquisition de stratégies adaptatives efficaces pour
gérer le stress ou interagir avec autrui expliquent potentiellement cet effet non-spécifique des soins
Page 188
de réhabilitation psychosociale [224], [244-248]. La mise en place précoce de soins orientés vers le
rétablissement pourrait prévenir l’auto-stigmatisation, en réduisant la durée de psychose non traitée
et en acquérant des stratégies adaptatives efficaces facilitant la réinsertion sociale [63], [249].
1.5 Auto-stigmatisation et résistance à la stigmatisation
La résistance à la stigmatisation est un construit distinct de l’auto-stigmatisation, même si ces deux
entités sont fortement corrélées [83]. Elle concerne plus de la moitié des personnes avec TPSP
inclues dans la cohorte REHABase (54.1% ; [228]. Elle est dans la moyenne des pays Européens
dans la schizophrénie et moindre dans les autres TPSP, ce qui peut être expliqué par une auto-
stigmatisation plus prononcée pour ces pathologies et par la présence de comorbidités
psychiatriques [214], [228]. Elle est influencée notamment par l’insight, les capacités cognitives et
métacognitives, les stratégies adaptatives et le soutien social et familial [83], [85], [155], [227],
[228]. La résistance à la stigmatisation est associée au rétablissement dans ses aspects objectifs et
subjectifs et constitue une cible thérapeutique à part entière en réhabilitation psychosociale [83],
[215], [228].
Chapitre 2. Implications cliniques et pour la recherche
La prévention de l’auto-stigmatisation est un objectif thérapeutique majeur pour améliorer le
devenir clinique et fonctionnel des personnes avec TPSP. Elle peut se réaliser de plusieurs
manières, avec des campagnes auprès du grand public ou des médias mais aussi des actions plus
spécifiques en direction des professionnels de santé mentale, des aidants familiaux ou des personnes
concernées.
Page 189
Ce travail de thèse présente plusieurs applications cliniques pour prévenir ou réduire l’auto-
stigmatisation: la réduction de la stigmatisation publique, l’adoption de pratiques orientées vers le
rétablissement dans les services de santé mentale, le développement de la pair-aidance et des
dispositifs facilitant une identification groupale positive et la prise en compte de l’auto-
stigmatisation dans les dispositifs d’intervention précoce et dans les programmes de
psychoéducation familiale.
2.1. Réduire la stigmatisation publique
Les campagnes de déstigmatisation n’ont pas entraîné un changement majeur dans l’opinion
publique concernant les personnes avec TPSP [34], [250]. Elles ont toutefois permis de réduire la
stigmatisation perçue et expérimentée [34], [185]. Cet effet pourrait s’expliquer par l’amélioration
du traitement médiatique des TPSP suite à ces campagnes, soulignant l’intérêt d’un travail régulier
auprès des médias pour promouvoir des contenus plus positifs, orientés vers le rétablissement [37],
[52]. Une conception neurobiologique des TPSP peut chez le grand public, renforcer le désir de
distance sociale [250], et chez les personnes concernées provoquer des sentiments de culpabilité
implicites contribuant à l’auto-stigmatisation [251]. Il pourrait être pertinent de développer des
campagnes de déstigmatisation intégrant la perspective du rétablissement à destination d’un public
varié, avec des lycéens, des étudiants, des employeurs, des journalistes, mais aussi des
professionnels de santé [15], [22], [188], [250]. Une campagne de ce type, basée sur les
témoignages d’une personne rétablie et d’un pair-aidant, a été réalisée à l’automne 2018 auprès de
134 étudiants en école de commerce, avec un effet positif sur leurs croyances et attitudes à propos
des personnes avec schizophrénie [252]. Les attitudes stigmatisantes sont toutefois largement
automatiques et implicites [112]. Les campagnes de déstigmatisation pourraient être évaluées par
l’évolution des attitudes implicites des journalistes, du grand public, des personnes concernées et de
Page 190
leurs proches et par leur efficacité sur la stigmatisation perçue, expérimentée, anticipée et
internalisée [15], [112], [184], [250].
La promotion dans les médias de témoignages de personnes rétablies ou de pairs-aidants et des
pratiques orientées vers le rétablissement pourrait également prévenir l’auto-stigmatisation et
faciliter l’accès aux soins en facilitant une identification positive au groupe social précedemment
stigmatisé [75], [253].
2.2. Diffuser les pratiques orientées vers le rétablissement dans les services de santé mentale
La prévention de l’auto-stigmatisation repose aussi sur la transformation des pratiques au sein des
services de santé mentale. La mise en place de pratiques orientées vers le rétablissement pourrait
réduire la stigmatisation perçue, expérimentée, anticipée et internalisée [215], [231]. La
stigmatisation dans les services de santé mentale est multifactorielle, sous-tendue principalement
par la différence de statut social et de pouvoir entre les professionnels et les usagers, qui se traduit
dans leurs croyances et attitudes respectives et dans l’organisation des soins et des locaux [254].
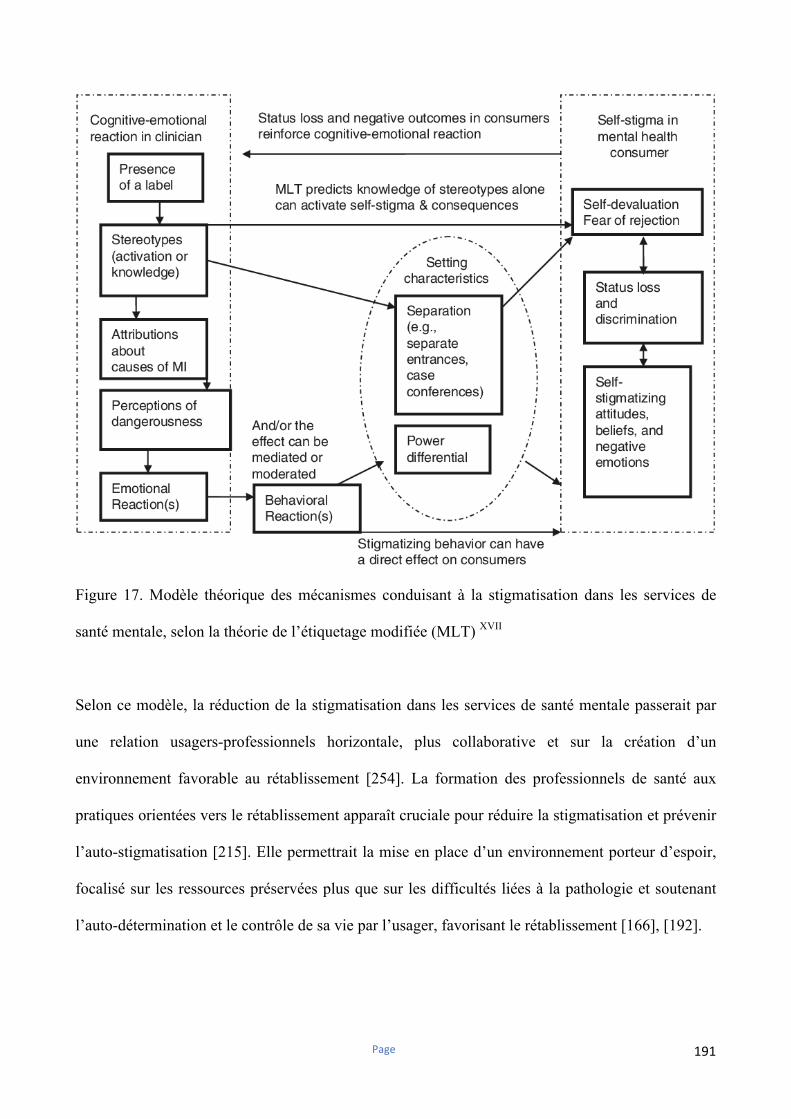
Page 191
Figure 17. Modèle théorique des mécanismes conduisant à la stigmatisation dans les services de
santé mentale, selon la théorie de l’étiquetage modifiée (MLT) XVII
Selon ce modèle, la réduction de la stigmatisation dans les services de santé mentale passerait par
une relation usagers-professionnels horizontale, plus collaborative et sur la création d’un
environnement favorable au rétablissement [254]. La formation des professionnels de santé aux
pratiques orientées vers le rétablissement apparaît cruciale pour réduire la stigmatisation et prévenir
l’auto-stigmatisation [215]. Elle permettrait la mise en place d’un environnement porteur d’espoir,
focalisé sur les ressources préservées plus que sur les difficultés liées à la pathologie et soutenant
l’auto-détermination et le contrôle de sa vie par l’usager, favorisant le rétablissement [166], [192].
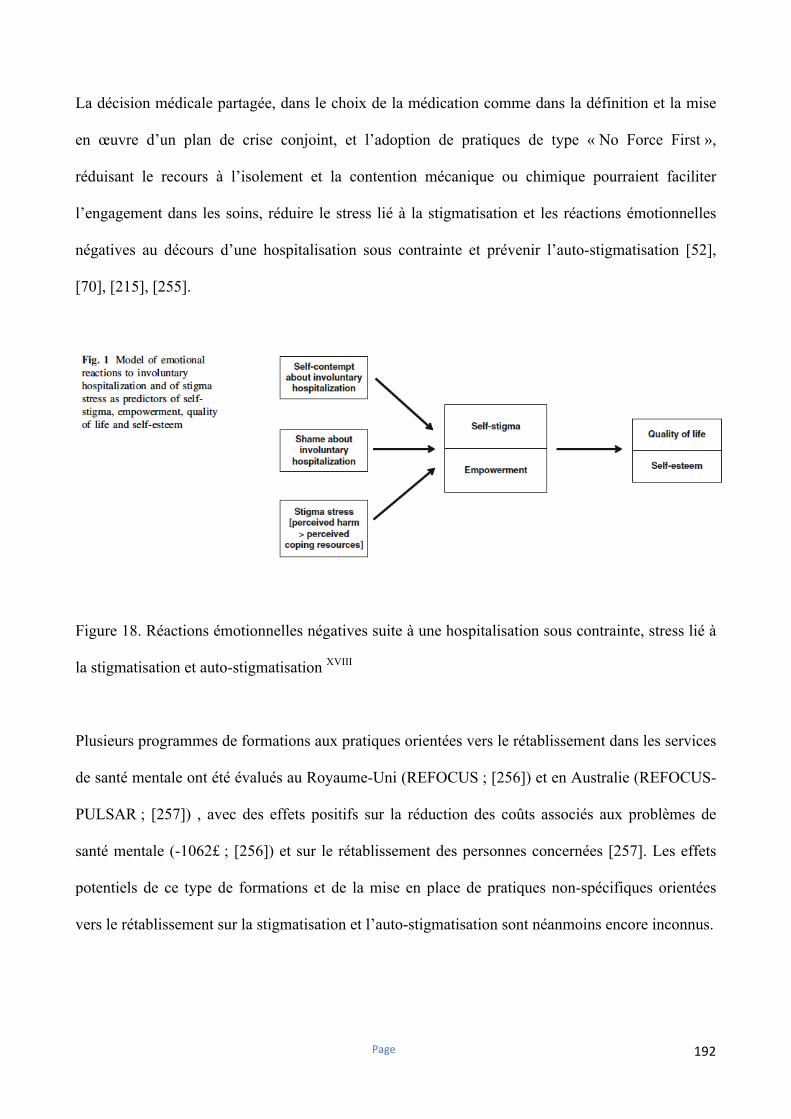
Page 192
La décision médicale partagée, dans le choix de la médication comme dans la définition et la mise
en œuvre d’un plan de crise conjoint, et l’adoption de pratiques de type « No Force First »,
réduisant le recours à l’isolement et la contention mécanique ou chimique pourraient faciliter
l’engagement dans les soins, réduire le stress lié à la stigmatisation et les réactions émotionnelles
négatives au décours d’une hospitalisation sous contrainte et prévenir l’auto-stigmatisation [52],
[70], [215], [255].
Figure 18. Réactions émotionnelles négatives suite à une hospitalisation sous contrainte, stress lié à
la stigmatisation et auto-stigmatisation XVIII
Plusieurs programmes de formations aux pratiques orientées vers le rétablissement dans les services
de santé mentale ont été évalués au Royaume-Uni (REFOCUS ; [256]) et en Australie (REFOCUS-
PULSAR ; [257]) , avec des effets positifs sur la réduction des coûts associés aux problèmes de
santé mentale (-1062£ ; [256]) et sur le rétablissement des personnes concernées [257]. Les effets
potentiels de ce type de formations et de la mise en place de pratiques non-spécifiques orientées
vers le rétablissement sur la stigmatisation et l’auto-stigmatisation sont néanmoins encore inconnus.
Page 193
Il serait pertinent d’évaluer l’efficacité de ces programmes de formation sur les attitudes explicites,
mais aussi implicites, des professionnels de santé mentale envers les personnes avec TPSP, car
celles ci peuvent persister même dans des équipes orientées rétablissement [109], [110], [254].
L’intégration de pairs-aidants dans les équipes de soins permet de prévenir la réhospitalisation en
psychiatrie après un épisode aigu (29% à 1 an contre 38% dans le groupe contrôle ; [258]), de
renforcer le pouvoir d’agir et l’estime de soi des usagers et de favoriser leur rétablissement [259-
261]. Elle a des effets positifs pour les pairs-aidants et facilite l’orientation des pratiques vers le
rétablissement dans les services de santé mentale [260]. Les pairs-aidants pourraient prévenir ou
réduire l’auto-stigmatisation, en étant vecteurs d’espoir et d’identification positive à une personne
rétablie, et en renforçant le pouvoir d’agir et l’estime de soi des usagers [260]. La participation à
des groupes d’entraide mutuelle ou d’auto-support contribue à réduire l’auto-stigmatisation [206],
[262]. L’efficacité d’interventions réalisées par des pairs-aidants sur la stigmatisation perçue,
expérimentée, anticipée et internalisée n’a toutefois pas encore été évaluée.
La prévention du burnout chez les soignants, associée à la stigmatisation de courtoisie et pouvant
contribuer à l’auto-stigmatisation des usagers, est aussi indispensable pour réduire la stigmatisation
dans les services de santé mentale [96], [102].
2.3. Intervenir précocément auprès des personnes concernées et de leurs proches
Prévenir l’auto-stigmatisation est un enjeu thérapeutique majeur dans les troubles psychiatriques
débutants, car cela permettrait de renforcer l’adhésion aux soins, de faciliter le recours à des
stratégies adaptatives efficaces et de réduire les risques de transition psychotique et de désinsertion
sociale, scolaire et professionnelle [215]. Il serait pertinent d’évaluer l’auto-stigmatisation chez
l’ensemble des personnes présentant des troubles psychiatriques débutants, au décours d’un passage
Page 194
aux urgences ou d’une hospitalisation pour un 1er épisode psychotique. Le repérage des adolescents
ou jeunes adultes à risque d’auto-stigmatisation, c’est-à-dire présentant des réactions automatiques
de honte, de mépris de soi ou de culpabilité, pourrait être conduit avec des tests d’association
implicites permettant ainsi la réalisation précoce d’interventions spécifiques [263]. Ces tests
pourraient par ailleurs permettre d’évaluer l’efficacité des stratégies thérapeutiques qui leur seraient
proposées [184], [263].
L’auto-stigmatisation est un des médiateurs entre un insight préservé et la survenue d’une
dépression [74], [264-268]. De même, l’insight en lien avec la présence de troubles cognitifs
contribuerait, via l’auto-stigmatisation, à un risque suicidaire accru et à une altération de la qualité
de vie [232], [269], [270]. La réalisation précoce de programmes de psychoéducation orientés vers
le rétablissement (TIPP ; [271] ; TCC-P ; [272]) pourrait permettre de réduire le stress lié à la
stigmatisation et de prévenir l’auto-stigmatisation [42], [241]. Leur efficacité sur ces paramètres n’a
toutefois pas encore été évaluée. La présence de troubles cognitifs et l’utilisation de stratégies
d’évitement en situation sociale peuvent contribuer à l’auto-stigmatisation et réduire la résistance à
la stigmatisation [214], [215], [228]. Certaines stratégies de réhabilitation psychosociale, comme la
remédiation cognitive, les thérapies cognitives et comportementales ou encore l’entraînement des
compétences sociales, pourraient également permettre de réduire l’auto-stigmatisation [215]. Le
programme RemedRugby, une intervention de remédiation de la cognition sociale couplée à la
pratique d’une activité sportive, comprend un volet dédié à la déstigmatisation dans les relations
sociales et avec les médias locaux [273], [274]. Il a fait l’objet d’une étude multicentrique quasi-
expérimentale de 2015 à 2018, retrouvant entre autres une efficacité modérée sur l’auto-
stigmatisation [274].
Page 195
Parmi les programmes spécifiques, le programme HOP (Honest, Open and Proud ; [200], [201])
semble particulièrement efficace chez les adolescents avec troubles psychiatriques débutants. Il
permettrait la réduction du recours aux stratégies d’évitement, du stress lié à la stigmatisation, de
l’auto-stigmatisation et l’amélioration des symptômes dépressifs et de la qualité de vie [201]. La
divulgation contrôlée des troubles serait une des stratégies thérapeutiques les plus pertinentes dans
les stades précoces de l’auto-stigmatisation [201], [275]. La participation à un programme plus
structuré comme NECT s’avére au contraire nécessaire pour les personnes déjà auto-stigmatisées,
ce type d’intervention complétant utilement l’offre de soins et services des centres de réhabilitation
psychosociale [193], [215], [276]. Le programme NECT est d’ailleurs en cours d’adaptation pour
les personnes avec troubles psychiatriques débutants [77].
L’implication précoce des familles est également indispensable pour prévenir l’auto-stigmatisation
[215]. Celle-ci est en effet liée à l’insight parental chez des adolescents avec troubles psychiatriques
débutants [230], ce qui plaide pour la mise en place précoce de programmes de psychoéducation
familiale intégrant la prévention de la stigmatisation et de l’auto-stigmatisation (BREF ; [277] ;
AVEC ; [272]). La psychoéducation familiale (BREF ; [277]; AVEC ; [272]; ProFamille ; [278])
pourrait par ailleurs renforcer la résistance à la stigmatisation, liée à la satisfaction dans les relations
familiales [228]. Il serait par ailleurs pertinent de mesurer l’efficacité de ces interventions sur
l’auto-stigmatisation des aidants familiaux et d’étudier si celle-ci influence leurs effets sur la
dépression des proches et le devenir des personnes concernées.
Chapitre 3. Limites
Ce travail de thèse présente plusieurs limites. L’hétérogénéité dans la définition des TPSP, des
échantillons, des paradigmes expérimentaux, des échelles d’évaluation et des variables d’intérêt
Page 196
recueillies a compliqué les comparaisons inter-études dans les deux revues de littérature sur l’auto-
stigmatisation [215], [279]. Celle-ci est par ailleurs peu étudiée d’un point de vue expérimental, en
raison de la difficulté à créer un paradigme pertinent pour mesurer un construit aussi complexe que
l’identité d’un individu ou au contraire son sentiment d’aliénation [279]. Le nombre limité d’études
longitudinales sur l’auto-stigmatisation et les biais de publication constituent aussi des limites
potentielles [215].
Le réseau national des centres référents de réhabilitation psychosociale couvre une grande partie du
territoire national. Il n’est toutefois constitué que de personnes consultant dans un centre de
réhabilitation psychosociale et ne peut donc pas être considéré comme représentatif de l’ensemble
de la population avec TPSP [214], [228].
Chapitre 4. Perspectives
Ce travail de thèse a permis de dégager plusieurs pistes de recherche, dont un essai randomisé
contrôlé en stepped-wedge évaluant l’efficacité du programme NECT sur le fonctionnement social
des personnes avec TPSP [276]. Cet essai comporte par ailleurs une étude ancillaire franco-suisse,
dont les objectifs sont : i) de modéliser d’un point de vue expérimental les liens entre auto-
stigmatisation, rejet social chronique et sensibilité au rejet social ; ii) d’évaluer l’efficacité du
programme NECT sur la sensibilité au rejet social aigu dans les TPSP. Cette étude ancillaire a fait
l’objet d’une lettre d’intention auprès de la Fondation d’Harcourt (en annexe).
La cohorte REHABase ouvre de nombreuses possibilités de recherche, transversales et
longitudinales. Plusieurs analyses sont en cours ou prévues prochainement, portant notamment sur
les caractéristiques des parents avec TPSP, sur celles des personnes exerçant un emploi compétitif,
Page 197
ou encore celles des femmes présentant un trouble de personnalité borderline ou un trouble du
spectre de l’autisme. Une évaluation longitudinale des effets de la réhabilitation psychosociale sur
l’auto-stigmatisation à deux ans est prévue dans les prochaines années. L’emploi accompagné IPS
(Individual Placement and Support ; [280]) est déployé dans plusieurs centres participant au réseau
national REHABase. Son efficacité pourrait être potentialisée en y associant des interventions de
réhabilitation psychosociale [281-283]. Le programme IPS intégré (IPS-I), développé au centre
référent de réhabilitation psychosociale de Grenoble, comprend un module de TCC en 8 séances sur
la motivation à retrouver un emploi et un module de 12 séances d’entraînement des compétences
sociales en milieu professionnel réalisés simultanément à l’emploi accompagné IPS [284]. Il a fait
l’objet de dépôt de lettres d’intention et d’un protocole expérimental lors de l’appel à projet PRME
2018 et 2019.
L’auto-stigmatisation a également un impact sur les relations sentimentales, la vie de couple et la
décision de devenir ou non parent [215]. Sa réduction dans ce contexte est abordée dans un groupe
de réhabilitation psychosociale en 21 séances, construit sur la base de focus groups et dont la
validation scientifique est prévue prochainement [285].
Ce travail a par ailleurs montré que l’auto-stigmatisation affecte aussi les personnes avec troubles
du spectre de l’autisme sans déficience intellectuelle, bien que de façon plus modérée [214]. La
stigmatisation publique, perçue, expérimentée et internalisée a été très peu étudiée dans cette
population et devrait être investiguée de façon plus approfondie [10], [214], [286].
Ce travail ouvre plusieurs autres pistes de recherche pertinentes : i) l’étude de l’auto-stigmatisation
chez les familles ; ii) l’évaluation de l’efficacité de la psychoéducation familiale sur l’auto-
stigmatisation des usagers et de leurs proches ; iii) l’étude de l’auto-stigmatisation dans les troubles
psychiatriques débutants et l’évaluation de l’efficacité des programmes d’intervention précoce sur

Page 198
la réduction de l’auto-stigmatisation ; iv) l’évaluation de l’impact de programmes de formation aux
pratiques orientées rétablissement sur les attitudes implicites et explicites des professionnels de
santé mentale et l’auto-stigmatisation des usagers.
Page 199
Bibliographie
[1]-GalloK.Self-stigmatized.SchizophreniaBulletin,1994
[2]-CrockerJ,MajorB,SteeleC.1998.Socialstigma.InTheHandbookofSocialPsychology,ed.DTGilbert,
STFiske,2:504–53.Boston,MA:McGraw-Hill
[3]-LinkBG,PhelanJ.Stigmapower.SocSciMed2001;103:24-32
[4]-Corrigan PW,Watson AC. Understanding the impact of stigma on peoplewithmental illness.World
Psychiatry.2002;1(1):16-20
[5]-Corrigan PW. Lessons learned from unintended consequences about erasing the stigma of mental
illness.WorldPsychiatry.2016;15(1):67-73.
[6]-PescosolidoBA,MedinaTR,Martin JK,etal. The "backbone"of stigma: identifying theglobal coreof
publicprejudiceassociatedwithmentalillness.AmJPublicHealth.2013;103(5):853-60.
[7]-Special Eurobarometer n°248. Mental Well-being. 2006. Available from URL:
https://ec.europa.eu/health/ph_information/documents/ebs_248_en.pdf
[8]-Special Eurobarometer n°345. Mental Health. 2010. Available from URL:
https://ec.europa.eu/commfrontoffice/publicopinion/archives/ebs/ebs_345_en.pdf
[9]-IPSOS-FondaMental. Perceptions et représentations des maladies mentales: rapport. 2014. Available
fromURL:https://www.fondation-fondamental.org/sites/default/files/rapport_ipsos_fondamental_1.pdf
[10]-Durand-ZaleskiI,ScottJ,RouillonF,etal.Firstnationalsurveyofknowledge,attitudesandbehaviours
towardsschizophrenia,bipolardisordersandautisminFrance.BMCPsychiatry.2012;12:128.
[11]-IPSOS-FondaMental.Perceptionetreprésentationsdesmaladiesmentales.2009.AvailablefromURL:
https://www.fondation-fondamental.org/sites/default/files/rapport_ipsos_fondamental_2009_0.pdf
[12]-Crisp AH, GelderMG, Rix S, and al. Stigmatisation of people withmental illnesses. Br J Psychiatry.
2000;177:4-7.
[13]-Pescosolido BA,Martin JK, Long JS, et al. "A disease like any other"? A decade of change in public
reactionstoschizophrenia,depression,andalcoholdependence.AmJPsychiatry.2010;167(11):1321-30.
[14]-Schomerus G, Schwahn C, Holzinger A, et al. Evolution of public attitudes about mental illness: a
systematicreviewandmeta-analysis.ActaPsychiatrScand.2012;125(6):440-52.
[15]-SchomerusG, AngermeyerMC. Changes of Stigmaover Time. In:GaebelW, RösslerW, SartoriusN
(Eds).TheStigmaofMentalIllness–EndoftheStory?SpringerInternationalPublishing.Switzerlan.2017.
p.157-172
[16]-Pescosolido BA,Manago B,Monahan J. Evolving Public Views On The Likelihood Of Violence From
PeopleWithMentalIllness:StigmaAndItsConsequences.HealthAff(Millwood).2019;38(10):1735-1743.
[17]-Reavley NJ, Mackinnon AJ, Morgan AJ, et al. Stigmatising attitudes towards people with mental
disorders: a comparison of Australian health professionals with the general community. Aust N Z J
Psychiatry.2014;48(5):433-41.
Page 200
[18]-UNAFAM(UnionNAtionaledeFamillesetAmisdepersonnesMaladeset/ouhandicapéespsychiques).
Le baromètre de la schizophrénie. 2018. Available from: URL: http://www.unafam13.org/le-barometre-de-la-schizophrenie/
[19]-Nordt C, Rössler W, Lauber C. Attitudes of mental health professionals toward people with
schizophreniaandmajordepression.SchizophrBull.2006;32(4):709-14.
[20]-Loch AA, Hengartner MP, Guarniero FB, et al. The more information, the more negative stigma
towardsschizophrenia:Braziliangeneralpopulationandpsychiatristscompared.PsychiatryRes2013;205:
185–91.
[21]-NeauportA,RodgersRF,SimonNM,etal.Effectsofapsychiatriclabelonmedicalresidents'attitudes.
IntJSocPsychiatry.2012;58(5):485-7.28.
[22]-Henderson RC, Corker E, Hamilton S, et al. Viewpoint survey of mental health service users'
experiencesofdiscriminationinEngland2008-2012.SocPsychiatryPsychiatrEpidemiol.2014;49(10):1599-
608.
[23]-Gervais J, Haour G, Michel M, et al. Impact of mental illness on care for somatic comorbidities in
France:anation-widehospital-basedobservationalstudy.EpidemiologyandPsychiatricSciences2018;1-
13.
[24]-Tiihonen J, Lönnqvist J, Wahlbeck K, et al. 11-year follow-up of mortality in patients with
schizophrenia:apopulation-basedcohortstudy(FIN11study).Lancet.2009;374(9690):620-7.
[25]-KessingLV,VradiE,McIntyreRS,etal.Causesofdecreasedlifeexpectancyoverthelifespaninipolar
disorder.JAffectDisord.2015;180:142-7.
[26]-Gunderson JG, Herpertz SC, Skodol AE, et al. Borderline personality disorder. Nat Rev Dis Primers.
2018;4:18029.
[27]-Lawn S, McMahon J. Experiences of care by Australians with a diagnosis of borderline personality
disorder.JPsychiatrMentHealthNurs.2015;22(7):510-21.
[28]-BlackDW,PfohlB,BlumN,andal.Attitudestowardborderlinepersonalitydisorder:asurveyof706
mentalhealthclinicians.CNSSpectr.2011Mar;16(3):67-74.
[29]-CorriganPW,MarkowitzFE,WatsonAC.Structural levelsofmental illnessstigmaanddiscrimination.
SchizophrBull.2004;30(3):481-91.
[30]-CorriganPW,WatsonAC,HeyrmanML, and al. Structural stigma in state legislation. Psychiatr Serv.
2005;56(5):557-63.
[31]-Lightfoot E, Hill K, LaLiberte T. The inclusion of disability as a condition for termination of parental
rights.ChildAbuseNegl.2010;34(12):927-34.
[32]-HazoJB,GandréC,LeboyerM,etal.National funding formentalhealthresearch inFinland,France,
SpainandtheUnitedKingdom.EurNeuropsychopharmacol.2017;27(9):892-899.
[33]-Gandré C, Prigent A, KemelML, et al. Evolution of public and non-profit funding formental health
researchinFrancebetween2007and2011.EurNeuropsychopharmacol.2015;25(12):2339-48.
Page 201
[34]-AngermeyerMC,MatschingerH,CartaMG,andal.Changesintheperceptionofmentalillnessstigma
inGermanyoverthelasttwodecades.EurPsychiatry.2014a;29(6):390-5.
[35]-Whitley R, Berry S. Trends in newspaper coverage of mental illness in Canada: 2005-2010. Can J
Psychiatry.2013;58(2):107-12.
[36]-GiordanaGY, Caria A, Arfeuillère S et al. Stigmatisation et déstigmatisation. In: FranckN. Traité de
RéhabiltationPsychosociale.ElsevierMasson.2018.P807-821
[37]-WhitleyR,WangJ.GoodNews?ALongitudinalAnalysisofNewspaperPortrayalsofMental Illness in
Canada2005to2015.CanJPsychiatry.2017;62(4):278-285.
[38]-Deegan PE. Recovering our sense of value after being labeled mental ill. Journal of psychosocial
nursingandmentalhealthservices,1993;31:7-11
[39]-Giordana JY. La stigmatisation en psychiatrie et en santé mentale. Congrès de sychiatrie et de
NeurobiologiedeLangueFrançaise.ElsevierMasson2009
[40]-BrohanE,ElgieR,SartoriusN,andal.Self-stigma,empowermentandperceiveddiscriminationamong
people with schizophrenia in 14 European countries: the GAMIAN-Europe study. Schizophr Res.
2010;122(1-3):232-8.
[41]-BrohanE,GauciD,SartoriusN,andal.Self-stigma,empowermentandperceiveddiscriminationamong
peoplewithbipolardisorderordepression in13Europeancountries: theGAMIAN-Europestudy. JAffect
Disord.2011;129(1-3):56-63.
[42]-RüschN,CorriganPW,HeekerenK,etal.Well-beingamongpersonsat riskofpsychosis: the roleof
self-labeling,shame,andstigmastress.PsychiatrServ.2014;65(4):483-9.
[43]-Evans-LackoS,BrohanE,MojtabaiR,etal.Associationbetweenpublicviewsofmentalillnessandself-
stigmaamongindividualswithmentalillnessin14Europeancountries.PsycholMed.2012;42:1741-52.
[44]-LinkB,CastilleDM,Stuber J. Stigmaandcoercion in thecontextofoutpatient treatment forpeople
withmentalillnesses.SocSciMed.2008;67(3):409-19.
[45]-Mueser KT, DeTore NR, Kredlow MA, et al. Clinical and demographic correlates of stigma in first-
episodepsychosis:theimpactofdurationofuntreatedpsychosis.ActaPsychiatrScand2019:1–10
[46]-ZäskeH, LindenM,DegnerD, et al. Stigmaexperiences andperceived stigma in patientswith first-
episodeschizophreniainthecourseof1yearaftertheirfirstin-patienttreatment.EurArchPsychiatryClin
Neurosci.2019;269(4):459-468.
[47]-VauthR,RushN,WirtzM,etal.Self-efficacyandempowermentasoutcomesofself-stigmatizingand
copinginschizophrenia.PsychiatryRes.2007;150:71-80
[48]-SorsdahlKR,KakumaR,WilsonZ,etal.Theinternalizedstigmaexperiencedbymembersofamental
healthadvocacygroupinSouthAfrica.IntJSocPsychiatry.2012;58(1):55-61
[49]-ThornicroftG,BrohanE,RoseD,etal.Globalpatternofexperiencedandanticipateddiscrimination
againstpeoplewithschizophrenia:across-sectionalsurvey.Lancet.2009;373(9661):408-15.
Page 202
[50]-Farrelly S, Clement S,Gabbidon J et al. Anticipated and experienceddiscrimination amongst people
with schizophrenia, bipolar disorder and major depressive disorder: a cross sectional study. BMC
Psychiatry.2014;14:157.
[51]-LasalviaA,ZoppeiS,VanBortelT,etal.Globalpatternofexperiencedandanticipateddiscrimination
reportedbypeoplewithmajordepressivedisorder:across-sectionalsurvey.Lancet.2013;381(9860):55-62.
[52]-ThornicroftA,GouldenR,SheferG,etal.NewspapercoverageofmentalillnessinEngland2008-2011.
BrJPsychiatrySuppl.2013;55:s64-9.
[53]-DaumerieN,VasseurBacleS,GiordanaJY,andal.Discriminationperceivedbypeoplewithadiagnosis
of schizophrenicdisorders. INternational studyofDIscriminationand stiGmaOutcomes (INDIGO): French
results.Encephale.2012Jun;38(3):224-31.
[54]-Alonso J, Buron A, Bruffaerts R, and al;WorldMental Health Consortium. Association of perceived
stigma and mood and anxiety disorders: results from theWorld Mental Health Surveys. Acta Psychiatr
Scand.2008Oct;118(4):305-14.
[55]-Yang LH, Chen FP, Sia KJ, et al. "Whatmatters most:" a cultural mechanismmoderating structural
vulnerabilityandmoralexperienceofmentalillnessstigma.SocSciMed.2014;103:84-93.
[56]-HarangozoJ,RenesesB,BrohanE,etal.Stigmaanddiscriminationagainstpeoplewithschizophrenia
relatedtomedicalservices.IntJSocPsychiatry.2014;60(4):359-66.
[57]-JefferyD,ClementS,CorkerE,etal.Discriminationinrelationtoparenthoodreportedbycommunity
psychiatricserviceusersintheUK:aframeworkanalysis.BMCPsychiatry.2013;13:120.
[58]-Gonzales L, Davidoff KC, Nadal KL, et al. Micro aggressions experienced by persons with mental
illnesses:Anexploratorystudy.PsychiatrRehabilJ2015;38(3):234-41.
[59]-Joseph AJ, Tandon N, Yang LH, et al. #Schizophrenia: Use and misuse on Twitter. Schizophr Res.
2015;165(2-3):111-5.
[60]-Quinn DM,WilliamsMK,Weisz BM. From discrimination to internalizedmental illness stigma: The
mediatingrolesofanticipateddiscriminationandanticipatedstigma.PsychiatrRehabilJ.2015;38(2):103-8.
[61]-CorriganPW,DrussBG,PerlickDA.TheImpactofMentalIllnessStigmaonSeekingandParticipatingin
MentalHealthCare.PsycholSciPublicInterest.2014;15(2):37-70.
[62]-MosesT.Stigmaapprehensionamongadolescentsdischargedfrombriefpsychiatrichospitalization.J
NervMentDis.2011;199(10):778-89
[63]-Moses T. Determinants of mental illness stigma for adolescents discharged from psychiatric
hospitalization.SocSciMed.2014;109:26-34.
[64]-TarrierN, Khan S, Cater J, et al. The subjective consequences of suffering a first episode psychosis:
traumaandsuicidebehaviour.SocPsychiatryPsychiatrEpidemiol.2007;42(1):29-35.
[65]-ZäskeH,DegnerD,Jockers-ScherüblM,etal.Experiencesofstigmaanddiscriminationinpatientswith
first-episodeschizophrenia.DerNervenarzt2016;87:82–87
[66]-Moses T. Coping strategies and self-stigma among adolescents discharged from psychiatric
hospitalization:a6-monthfollow-upstudy.IntJSocPsychiatry.2015;61(2):188-97
Page 203
[67]-Clement S,Williams P, Farrelly S, and al.Mental health-related discrimination as a predictor of low
engagementwithmentalhealthservices.PsychiatrServ.2015;66(2):171-6.
[68]-RüschN,CorriganPW,WasselA,etal.Astress-copingmodelofmentalillnessstigma:I.Predictorsof
cognitivestressappraisal.SchizophrRes.2009a;110(1-3):59-64.
[69]-RüschN, CorriganPW, Powell K, et al. A stress-copingmodel ofmental illness stigma: II. Emotional
stressresponses,copingbehaviorandoutcome.SchizophrRes.2009b;110(1-3):65-71
[70]-Rüsch N, Müller M, Lay B, et al. Emotional reactions to involuntary psychiatric hospitalization and
stigma-relatedstressamongpeoplewithmentalillness.EurArchPsychiatryClinNeurosci.2014;264(1):35-
43
[71]-XuZ,MüllerM,LayB,OexleN,DrackT,BleikerM,LenglerS,BlankC,VetterS,RösslerW,RüschN.
Involuntary hospitalization, stigma stress and suicidality: a longitudinal study. Soc Psychiatry Psychiatr
Epidemiol.2018b;53(3):309-312.
[72]-Watson AC, Corrigan P, Larson JE, et al. Self-stigma in people with mental illness. Schizophr Bull.
2007;33(6):1312-8.
[73]-Thoits PA. Mechanisms linking social ties and support to physical and mental health. J Health Soc
Behav,2011;52(2):145-61
[74]-Lysaker PH, Roe D, Yanos PT. Toward understanding the insight paradox: internalized stigma
moderates the association between insight and social functioning, hope, and self-esteem among people
withschizophreniaspectrumdisorders.SchizophrBull.2007;33(1):192-9
[75]-Rüsch N, Corrigan PW, Wassel A, et al. Self-stigma, group identification, perceived legitimacy of
discriminationandmentalhealthserviceuse.BrJPsychiatry.2009;195(6):551-2.
[76]-HermanNJ.Returntosender:Reintegrativestigma-managementstrategiesofex-psychiatricpatients.
JournalofContemporaryEthnography1993;22:295-330
[77]-Yanos PT. Written off: mental health stigma and the loss of human potential. New York, N.Y:
CambridgeUniversityPress,2018
[78]-Corrigan PW, Larson JE, Rüsch N. Self-stigma and the “why try” effect: impact on life goals and
evidence-basedpractices.WorldPsychiatry.2009;8:75-81
[79]-Yanos PT, Roe D,Markus K, et al. Pathways between internalized stigma and outcomes related to
recoveryinschizophreniaspectrumdisorders.PsychiatrServ.2008;59(12):1437-42.
[80]-Livingston JD, Boyd JE. Correlates and consequences of internalized stigma for people living with
mentalillness:Asystematicreviewandmeta-analysis.SocSciMed2010;71(12):2150-61
[81]-Gerlinger G, Hauser M, De Hert M, et al. Personal stigma in schizoprhenia spectrum disorders: a
systematicreviewofprevalencerates,correlates,impactandinterventions.WordPsychiatry2013;12:155-
64
[82]-WestML, Yanos PT, Smith SM, et al. Prevalence of Internalized Stigma among Personswith Severe
MentalIllness.StigmaResAction.2011;1(1):3-10.
Page 204
[83]-FirminRL, Luther L, LysakerPH, et al. Stigma resistance is positively associatedwithpsychiatric and
psychosocialoutcomes:Ameta-analysis.SchizophrRes.2016;175(1-3):118-128.
[84]-Lau YW, Picco L, Pang S, et al. Stigma resistance and its association with internalised stigma and
psychosocial outcomes among psychiatric outpatients. Psychiatry Res. 2017;257:72-78. doi:
10.1016/j.psychres.2017.07.027.Epub2017Jul14.
[85]-O'ConnorLK,YanosPT,FirminRL.Correlatesandmoderatorsofstigmaresistanceamongpeoplewith
severementalillness.PsychiatryRes.2018;270:198-204.
[86]-Goffman E. Stigma: notes on themanagement of spoiled identity. Prentice-Hall, Engglewoog Cliffs.
1963
[87]-CorriganPW,WatsonAC,Miller FE. Blame, shame, and contamination: the impact ofmental illness
anddrugdependencestigmaonfamilymembers.JFamPsychol.2006;20(2):239-46.
[88]-MukoloA,HeflingerCA.Factorsassociatedwithattributionsaboutchildhealthconditionsandsocial
distancepreference.CommunityMentHealthJ.2011;47(3):286-99.
[89]-Koschade JE, Lynd-Stevenson RM. The stigma of having a parent with mental illness: Genetic
attributionsandassociativestigma.AustralianJournalofPsychology2011;63(2):93–99.
[90]-StuartH,SartoriusN,LiinamaaT,etal. Imagesofpsychiatryandpsychiatrists.ActaPsychiatrScand.
2015;131(1):21-8.
[91]-Sebbane D. Les internes de psychiatrie vus par leurs confrères : jugés de près mais préjugés....
L’Informationpsychiatrique2015;91:417-26doi:10.1684/ipe.2015.1349
[92]-EbsworthSJ, Foster JLH.Publicperceptionsofmentalhealthprofessionals: stigmabyassociation? J
MentHealth.2017;26(5):431-441.
[93]-OstmanM, Kjellin L. Stigma by association: psychological factors in relatives of peoplewithmental
illness.BrJPsychiatry.2002;181:494-8.
[94]-Vayshenker BA, DeLuca J, Bustle T, et al. “As soon as people hear that word…”: associative stigma
among cliniciansworkingwith peoplewith seriousmental illness. Journal of PublicMentalHealth 2018;
17(1):20-28,https://doi.org/10.1108/JPMH-12-2016-0055
[95]-Angermeyer MC, Schulze B, Dietrich S. Courtesy stigma- a focus group study of relatives of
schizophreniapatients.SocPsychiatryPsychiatrEpidemiol.2003;38(10):593-602.
[96]-Verhaeghe M, Bracke P. Associative stigma among mental health professionals: implications for
professionalandserviceuserwell-being.JHealthSocBehav.2012;53(1):17-32.
[97]-MakWW,WuCF. Cognitive insight and causal attribution in thedevelopmentof self-stigmaamong
individualswithschizophrenia.PsychiatrServ.2006;57(12):1800-2.
[98]-Wong C, Davidson L, Anglin D, and al. Stigma in families of individuals in early stages of psychotic
illness:familystigmaandearlypsychosis.EarlyIntervPsychiatry.2009;3(2):108-15.
[99]-Krupchanka D, Katliar M. The role of insight in moderating the association between depressive
symptomsinpeoplewithschizophreniaandstigmaamongtheirnearestrelatives:apilotstudy.Schizophr
Bull2016;42(3):600–607
Page 205
[100]-VanderSandenRL,BosAE,StutterheimSE,etal.Experiencesofstigmabyassociationamongfamily
membersofpeoplewithmentalillness.RehabilPsychol.2013;58(1):73-80.
[101]-Gupta N, Mohanty S. Stigma and expressed emotion in spouses of schizophrenic patients. Indian
JournalofCommunityPsychology2016;12:98-106
[102]-YanosPT,LysakerPH,SilversteinSM,etal.Arandomized-controlledtrialoftreatmentforself-stigma
among persons diagnosed with schizophrenia-spectrum disorders. Soc Psychiatry Psychiatr Epidemiol.
2019;doi:10.1007/s00127-019-01702-0.
[103]-KrendlAC,MacraeCN,KelleyWM,etal.Thegood,thebad,andtheugly:AnfMRIinvestigationofthe
functionalanatomiccorrelatesofstigma.SocNeurosci.2006;1(1):5-15.doi:10.1080/17470910600670579.
[104]-Greenwald AG, Poehlman TA,Uhlmann EL, et al. Understanding and using the Implicit Association
Test:III.Meta-analysisofpredictivevalidity.JPersSocPsychol2009;97(1):17-41.
[105]-TeachmanBA,WilsonJG,KomarovskayaI.Implicitandexplicitstigmaofmentalillnessindiagnosed
andhealthysamples.JournalofSocialandClinicalPsychology2006;25(1):75-95
[106]-KrendlAC,KensingerEA,AmbadyN.Howdoesthebrainregulatenegativebiastostigma?SocCogn
AffectNeurosci.2012;7(6):715-26.doi:10.1093/scan/nsr046.
[107]-KrendlAC,MoranJM,AmbadyN.Doescontextmatterinevaluationsofstigmatizedindividuals?An
fMRIstudy.SocCognAffectNeurosci.2013;8(5):602-8.doi:10.1093/scan/nss037.
[108]-PerisTS,TeachmanBA,NosekBA.Implicitandexplicitstigmaofmentalillness:linkstoclinicalcare.J
NervMentDis.2008;196(10):752-60.
[109]-StullLG,McGrewJH,SalyersMP,etal. Implicitandexplicitstigmaofmental illness:attitudes inan
evidence-basedpractice.JNervMentDis.2013;201(12):1072-9.
[110]-BrenerL,RoseG,vonHippelC,andal.Implicitattitudes,emotions,andhelpingintentionsofmental
healthworkerstowardtheirclients.JNervMentDis.2013;201(6):460-3.
[111]-RüschN,CorriganPW,ToddAR,etal.Implicitself-stigmainpeoplewithmentalillness.JNervMent
Dis.2010c;198(2):150-3.
[112]-Rüsch N, Corrigan PW, Todd AR, et al. Automatic stereotyping against people with schizophrenia,
schizoaffectiveandaffectivedisorders.PsychiatryRes.2011;186(1):34-9.
[113]-ImhoffR.ZeroinginontheEffectoftheSchizophreniaLabelonStigmatizingAttitudes:ALarge-scale
Study.SchizophrBull.2016;42(2):456-63.
[114]-Penn DL, Kohlmaier JR, Corrigan PW. Interpersonal factors contributing to the stigma of
schizophrenia:socialskills,perceivedattractiveness,andsymptoms.SchizophrRes.2000;45(1-2):37-45.
[115]-Heenan A, Best MW, Ouellette SJ, et al. Assessing threat responses towards the symptoms and
diagnosisofschizophreniausingvisualperceptualbiases.SchizophrRes.2014;159(1):238-42.
[116]-DerksB, InzlichtM,KangS.TheNeuroscienceofStigmaandStereotypeThreat.GroupProcesses&
IntergroupRelations2008;11(2):163-181.
Page 206
[117]-ShapiroJR,NeubergSL.Fromstereotypethreattostereotypethreats:implicationsofamulti-threat
framework for causes, moderators, mediators, consequences, and interventions. Pers Soc Psychol Rev.
2007;11(2):107-30.
[118]-HenryC,EtainB,MathieuF,etal.AFrenchnetworkofbipolarexpertcentres:amodeltoclosethe
gapbetweenevidence-basedmedicineandroutinepractice.JAffectDisord.2011;131(1-3):358-63.
[119]-MoritzS,SpirandelliK,HappachI,etal.DysfunctionbyDisclosure?StereotypeThreatasaSourceof
Secondary Neurocognitive Malperformance in Obsessive-Compulsive Disorder. J Int Neuropsychol Soc.
2018;24(6):584-592.
[120]-HartgerinkCH,vanBeestI,WichertsJM,etal.Theordinaleffectsofostracism:ameta-analysisof120
Cyberballstudies.PLoSOne.2015;10(5):e0127002.
[121]-BollingDZ,PitskelNB,DeenB,andal.EnhancedNeuralResponsestoRuleViolationinChildrenwith
Autism: A Comparison to Social Exclusion. Dev Cogn Neurosci. 2011; 1(3):280–94.
Doi:10.1016/j.dcn.2011.02.002.
[122]-MoorBG,GüroğluB,OpdeMacks ZA, et al. Social exclusionandpunishmentof excluders:Neural
correlatesanddevelopmentaltrajectories.NeuroImage2012;59:708–717.
[123]-KawamotoT,OnodaK,NakashimaK,etal.Isdorsalanteriorcingulatecortexactivationinresponseto
socialexclusionduetoexpectancyviolation?AnfMRIstudy.FrontEvolNeurosci.2012;4:11.
[124]-WilliamsL,HuangJY,BarghJA.TheScaffoldedMind:Highermentalprocessesaregroundedinearly
experienceofthephysicalworld.EurJSocPsychol.2009;39(7):1257-67.
[125]-Riva P,Wesselmann ED,Wirth JH, et al.When PainDoesNotHeal:The CommonAntecedents and
ConsequencesofChronicSocialandPhysicalPain.Basicandappliedsocialpsychology2014;36:329–346.
[126]-Clark US,Miller ER, Hegde RR. Experiences of Discrimination Are AssociatedWith Greater Resting
AmygdalaActivityandFunctionalConnectivity.BiolPsychiatryCognNeurosciNeuroimaging.2018;3(4):367-
378.
[127]-Brohan E, SladeM, Clement S, Thornicroft G. Experiences of mental illness stigma, prejudice and
discrimination:areviewofmeasures.BMCHealthServRes.2010b;10:80.
[128]-LinkGB.Understandinglabelingeffectsintheareaofmentaldisorders:anassessmentoftheeffects
ofexpectationsofrejection.AmSociolRev1987;52:96-112
[129]-CorriganP,WatsonA,BarrL.Theself-stigmaofmentalillness:implicationsforself-esteemandself-
efficacy.JournalofSocialandClinicalPsychology2006;25(8):875e884.
[130]-Hayward P,Wong G, Bright JA, et al. Stigma and self-esteem inmanic depression: an exploratory
study.JournalofAffectiveDisorders2002;69:61–67.
[131]-StuartH,MilevR,KollerM.TheInventoryofStigmatizingExperiences:itsdevelopmentandreliability.
WorldPsychiatry2005;4(1):35-9.
[132]-KanterJW,RuschLC,BrondinoMJ.Depressionself-stigma:anewmeasureandpreliminaryfindings.J
NervMentDis.2008;196(9):663-70.
Page 207
[133]-Bagley C, King M. Exploration of three stigma scales in 83 users of mental health services:
Implicationsforcampaignstoreducestigma.JournalofMentalHealth2005;14:343–355.
[134]-KingM, Dinos S, Shaw J, et al. The Stigma Scale: development of a standardisedmeasure of the
stigmaofmentalillness.BrJPsychiatry.2007;190:248-54.
[135]-MorandiS,GibelliniManettiS,ZimmermannG,etal.Frenchtranslation,validationandadaptationof
theStigmaScale.Encephale.2013;39(6):408-15.
[136]-Boyd Ritsher J, Otilingam PG, Grajales M. Internalized Stigma of Mental Illness: psychometric
propertiesofanewmeasure.PsychiatryRes2003;121:31-49.
[137]-Boyd JE, Adler EP, Otilingam PG, and al. Internalized Stigma of Mental Illness (ISMI) scale: a
multinationalreview.ComprPsychiatry.2014Jan;55(1):221-31.
[138]-Corrigan PW, Rafacz J, Rüsch N. Examining a progressive model of self-stigma and its impact on
peoplewithseriousmentalillness.PsychiatryRes.2011;189(3):339-43
[139]-CorriganPW,MichaelsPJ,VegaE,etal.Self-stigmaofmentalillnessscale--shortform:reliabilityand
validity.PsychiatryRes.2012;199(1):65-9.
[140]-MakWW,CheungRY.Self-stigmaamongconcealableminoritiesinHongKong:conceptualizationand
unifiedmeasurement.AmJOrthopsychiatry.2010;80(2):267-81.
[141]-Chang CC,Wu TH, Chen CY, and al. Comparing Self-stigmaBetween PeopleWithDifferentMental
DisordersinTaiwan.JNervMentDis.2016;204(7):547-53
[142]-Chan KKS,MakWWS. The content and process of self-stigma in people withmental illness. Am J
Orthopsychiatry.2017;87(1):34-43.
[143]-ChioFHN,MakWWS,ChanRCH,andal.Unravelingtheinsightparadox:One-yearlongitudinalstudy
on the relationships between insight, self-stigma, and life satisfaction among peoplewith schizophrenia
spectrumdisorders.SchizophrRes.2018.pii:S0920-9964(18)30034-3.
[144]-Karidi MV, Stefanis CN, Theleritis C, et al. Perceived social stigma, self-concept, and self-
stigmatizationofpatientwithschizophrenia.ComprPsychiatry.2010;51(1):19-30.
[145]-Wood L, Byrne R, Burke E, et al. The impact of stigma on emotional distress and recovery from
psychosis:Themediatoryroleofinternalisedshameandself-esteem.PsychiatryRes.2017;255:94-100
[146]-BirchwoodM,JacksonC,BrunetK,andal.Personalbeliefsaboutillnessquestionnaire-revised(PBIQ-
R):reliabilityandvalidationinafirstepisodesample.BrJClinPsychol.2012Nov;51(4):448-58
[147]-Pyle M, Morrison AP. Internalised stereotypes across ultra-high risk of psychosis and psychosis
populations.PsychosisPsychological,SocialandIntegrativeApproaches2017;9(2):1-9
[148]-Moses T. Self-labeling and its effects among adolescents diagnosedwithmental disorders. Soc Sci
Med.2009;68(3):570-8.
[149]-YangLH,LinkBG,Ben-DavidS,etal.Stigmarelatedtolabelsandsymptomsinindividualsatclinical
high-riskforpsychosis.SchizophrRes.2015;168(1-2):9-15.
Page 208
[150]-Link BG,Wells J, Phelan JC, et al. Understanding the importance of "symbolic interaction stigma":
How expectations about the reactions of others adds to the burden of mental illness stigma. Psychiatr
RehabilJ.2015;38(2):117-24.
[151]-Campbell DG, Bonner LM, Bolkan CR, and al. Stigma Predicts Treatment Preferences and Care
Engagement Among Veterans Affairs Primary Care Patients with Depression. Ann Behav Med.
2016;50(4):533-44.
[152]-Barney LJ, Griffiths KM, Christensen H, Jorm AF. The Self-Stigma of Depression Scale (SSDS):
development and psychometric evaluation of a new instrument. Int J Methods Psychiatr Res.
2010;19(4):243-54.
[153]-ElkingtonKS,HacklerD,WalshTA,etal.Perceivedmental illnessstigma, intimaterelationshipsand
sexualriskbehaviorinyouthwithmentalillness.JAdolescRes.2013;28(3):378-404.
[154]-Thoits PA. “I’mNotMentally Ill”: Identity Deflection as a Form of Stigma Resistance. J Health Soc
Behav.2016;57(2):135-51
[155]-FirminRL,LysakerPH,McGrewJH,andal.TheStigmaResistanceScale:Amulti-samplevalidationofa
newinstrumenttoassessmentalillnessstigmaresistance.PsychiatryRes.2017;258:37-43.
[156]-StatementofKofiAnnan,UnitedNationSecretary-General,ontheoccasionofthepassageoftheUN
Convention on the Rights of Persons with Disabilities, 13 December 2006. Full Text Available at
http://www.un.org/News/Press/Docs//2006/sgsm10797.doc.htm.
[157]-SAMHSA:SubstanceAbuseandMentalHealthServicesAdministration (SAMHSA).Results from the
2013NationalSurveyonDrugUseandHealth:MentalHealthFindings.NSDUHSeriesH-49,HHSPublication
No.(SMA)14-4887.Rockville,MD:SubstanceAbuseandMentalHealthServicesAdministration,2014.
[158]-AmericanwithDisabilitiesAct(ADA).1990.Availablefrom:URL:https://www.ada.gov/pubs/ada.htm
[159]-Disabilities Discrimination Act (DDA). UK. 1995. Available from: URL:
http://www.legislation.gov.uk/ukpga/1995/50/contents/enacted
[160]-Loi2005-102pourl'égalitédesdroitsetdeschances,laparticipationetlacitoyennetédespersonnes
handicapées. Journal Officiel de la République Française n°36 du 12 Février 2005. Available from: URL:
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000000809647&categorieLien=id
[161]-ConventiondesNationsUniesrelativeauxDroitsdesPersonnesHandicapées.2006.Availablefrom:
URL:https://www.un.org/disabilities/documents/convention/convoptprot-f.pdf
[162]-Liberman RP. Recovery from disability: Manual of psychiatric Rehabilitation, American Psychiatric
Pub.2008
[163]-PachoudB.Laperspectivedurétablissement:sortirduhandicappsychiqueplutôtqu’enattendrela
compensation. In: Boucherat-Hue V, Leguay D, Pachoud B, Plagnol A, Weber F. Handicap psychique:
questionsvives.EdErès.2016.p.103-124
[164]-Farkas M, Anthony WA. Psychiatric rehabilitation interventions: a review. Int Rev Psychiatry.
2010;22(2):114-29.
[165]-RoeD,Maschiasch-EisenbergM,LysakerPH.Therelationbetweenobjectiveandsubjectivedomains
ofrecoveryamongpersonswithschizophrenia-relateddisorders.SchizophrRes2011;131:133-8
Page 209
[166]-ShepherdG,BoardmanJ,SladeM.Fairedurétablissementuneréalité,SainsburyCentreforMental
Health,London.Traductionen2012dudocumentMakingRecoveryaReality,Institutuniversitairedesanté
mentale Douglas, Montréal. 2007. Available from:
http://www.douglas.qc.ca/publications/220/file_fr/faire_du_retablissement_une_realite_2012.pdf
[167]-Mental Health Commission of Canada. “Guide de référence pour des pratiques axées sur le
rétablissement: espoir, dignité, citoyenneté », Ottawa (Ontario) 2012. Available from: URL:
https://www.mentalhealthcommission.ca/sites/default/files/MHCC_RecoveryGuidelines_FRE_0.pdf
[168]-Décretn°2017-1200du27juillet2017relatifauprojetterritorialdesantémentale.Availablefrom:
URL:https://www.legifrance.gouv.fr/eli/decret/2017/7/27/SSAH1710848D/jo/texte
[169]-Instruction N° DGOS/R4/2019/10 du 16 janvier 2019 relative au développement des soins de
réhabilitation psychosociale sur les territoires. Available from: URL:
http://circulaires.legifrance.gouv.fr/pdf/2019/01/cir_44293.pdf
[170]-Décret n° 2016-1940 du 28 décembre 2016 relatif aux dispositifs d'appartements de coordination
thérapeutique « Un chez-soi d'abord ». JORF n°0303 du 30 Décembre 2016. Available from : URL :
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000033735512&categorieLien=id
[171]-Décret n° 2016-1899 du 27 décembre 2016 relatif à la mise en œuvre du dispositif d'emploi
accompagné et au financement du compte personnel de formation des travailleurs handicapés. JORF
n°0302 du 29 décembre 2016. Available from: URL:
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000033719277&categorieLien=id
[172]-Corrigan PW,Morris SB,Michaels PJ, Rafacz JD, Rüsch N. Challenging the public stigma ofmental
illness:ameta-analysisofoutcomestudies.PsychiatrServ.2012;63(10):963-73.
[173]-Griffith JL,KohrtBA.ManagingStigmaEffectively:WhatSocialPsychologyandSocialNeuroscience
CanTeachUs.AcadPsychiatry.2016;40(2):339-47.
[174]-ClementS,LassmanF,BarleyE,andal.Massmediainterventionsforreducingmentalhealth-related
stigma.CochraneDatabaseSystRev.2013Jul23;(7):CD009453.
[175]-Stuart H, Sartorius N. Opening Doors: The Global Programme to Fight Stigma and Discrimination
BecauseofSchizophrenia.In:GaebelW,RösslerW,SartoriusN(Eds).TheStigmaofMentalIllness–Endof
theStory?SpringerInternationalPublishing.Switzerlan.2017.p.227-236
[176]-ChenSP,DobsonK,KirshB,andal.FightingstigmainCanada:OpeningMindsAnti-StigmaInitiative.
In: Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer
InternationalPublishing.Switzerlan.2017.p.237-261
[177]-HendersonC, Evans-LackoS, ThornicroftG. TheTimeToChangeProgramme to reduce Stigmaand
DiscriminationinEnglandandItsWiderContext.In:GaebelW,RösslerW,SartoriusN(Eds).TheStigmaof
MentalIllness–EndoftheStory?SpringerInternationalPublishing.Switzerlan.2017.p.339-356
[178]-Robertson,J.SeeMe:ScotlandCaseStudy.In:GaebelW,RösslerW,SartoriusN(Eds).TheStigmaof
MentalIllness–EndoftheStory?SpringerInternationalPublishing.Switzerlan.2017.p.379-404
[179]-CoyleK,LowryS,SaundersJ.SeeChange:TheNationalMentalHealthStigmaReductionPartnership
in Ireland.In: GaebelW, RösslerW, Sartorius N (Eds). The Stigma ofMental Illness – End of the Story?
SpringerInternationalPublishing.Switzerlan.2017.p.357-378
Page 210
[180]-BratboJ,VedelsbyAK.OneofUs:Thenationalcampaignforanti-stigmainDenmark. In:GaebelW,
RosslerW,SartoriusN(Eds.).Thestigmaofmentalillness–endofthestory?Basel:SpringerInternational.
2017.p.317-338
[181]-GaebelW, BaumannAE. Interventions to reduce the stigma associatedwith severemental illness:
experiencesfromtheopenthedoorsprograminGermany.CanJPsychiatry2003;48:657–662.
[182]-HarmanG,HeathJ.AustralianCountryPerspective:TheWorkofbeyondblueandSANEAustralia.In:
Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer
InternationalPublishing.Switzerlan.2017.p.289-316
[183]-CunninghamR,PetersonD,CollingsS.LikeMinds,LikeMine:SeventeenyearsofCounteringStigma
and Discrimination Against People with Experience of Mental Distress in New Zealand.In: Gaebel W,
Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer International
Publishing.Switzerlan.2017.p.263-288
[184]-RuschN,XuZ.StrategiestoReduceMentalIllnessStigma.In:GaebelW,RösslerW,SartoriusN(Eds).
TheStigmaofMentalIllness–EndoftheStory?SpringerInternationalPublishing.Switzerlan.2017.p.451-
468
[185]-Corker E, Hamilton S, Robinson E, and al. Viewpoint survey of mental health service users'
experiencesofdiscriminationinEngland2008-2014.ActaPsychiatrScand.2016;134(S446):6-13.
[186]-Andresen R, Caputi P, Oades LG. Stages of recovery instrument: development of a measure of
recoveryfromseriousmentalillness.AustNZJPsychiatry2006;40:972-80.
[187]-Deegan PE. «Recovery: the lived experience of rehabilitation», Psychosocial Rehabilitation
Journal1988;11:11-19
[188]-SladeM.PersonalRecoveryandMentalIllness.AGuideforMentalHealthProfessionals.Cambridge
UniversityPress2009
[189]-Onken SJ, Craig CM, Ridgway P, et al. An analysis of the definitions and elements of recovery: a
reviewoftheliterature.PsychiatrRehabilJ.2007;31(1):9-22.
[190]-LeamyM,BirdV,LeBoutillierC,etal.Conceptualframeworkforpersonalrecoveryinmentalhealth:
systematicreviewandnarrativesynthesis.BrJPsychiatry.2011;199(6):445-52.
[191]-AnthonyWA:Recoveryfrommentalillness:theguidingvisionofthementalhealthservicesystemin
the1990s.PsychosocRehabilJ1993;16:11–23
[192]-Roberts G, Boardman J. Becoming a recovery-oriented practitioner. Advances in psychiatric
treatment,2014;20:37–47
[193]-YanosPT,LuckstedA,DrapalskiA,etal. Interventionstargetingmentalhealthself-stigma:areview
andcomparison.PsychiatrRehabJ2015;38:171–178
[194]-LuckstedA,DrapalskiA,CalmesC,etal.Endingself-stigma:pilotevaluationofanewinterventionto
reduceinternalizedstigmaamongpeoplewithmentalillnesses.PsychiatrRehabilJ.2011;35(1):51-54.
[195]-LuckstedA,DrapalskiAL,BrownCH,etal.OutcomesofaPsychoeducationalInterventiontoReduce
InternalizedStigmaAmongPsychosocialRehabilitationClients.PsychiatrServ.2017;68(4):360-367.
Page 211
[196]-FungKM,TsangHW,CheungWM.Randomizedcontrolledtrialoftheself-stigmareductionprogram
amongindividualswithschizophrenia.PsychiatryRes.2011;189(2):208-14.
[197]-Yanos PT, Roe D, Lysaker PH. Narrative enhancement and cognitive therapy: a new group-based
treatmentforinternalizedstigmaamongpersonswithseverementalillness.IntJGroupPsychother2011;
61:577–59
[198]-RoeD,Hasson-OhayonI,Mashiach-EizenbergM,etal.Narrativeenhancementandcognitivetherapy
(NECT)effectiveness:aquasi-experimentalstudy.JClinPsychol.2014;70(4):303-12.
[199]-HanssonL,LexénA,HolménJ.Theeffectivenessofnarrativeenhancementandcognitivetherapy:a
randomized controlled study of a self-stigma intervention. Soc Psychiatry Psychiatr Epidemiol.
2017;52(11):1415-23
[200]-CorriganPW,LarsonJE,MichaelsPJ,andal.Diminishingtheself-stigmaofmental illnessbycoming
outproud.PsychiatryRes.2015;229(1-2):148-54.
[201]-MulfingerN,Müller S,Böge I, et al.Honest,Open,Proud for adolescentswithmental illness:pilot
randomizedcontrolledtrial.JChildPsycholPsychiatry.2018;59(6):684-691.
[202]-Russinova Z, Rogers ES, Gagne C, et al. A randomized controlled trial of a peer-run antistigma
photovoiceintervention.PsychiatrServ.2014;65(2):242-6.
[203]-LuomaJB,KohlenbergBS,HayesSC,etal.Slowandsteadywinstherace:arandomizedclinicaltrialof
acceptanceandcommitment therapy targeting shame in substanceusedisorders. JConsultClinPsychol.
2012;80(1):43-53.
[204]-WoodL,ByrneR,MorrisonAP.An IntegrativeCognitiveModelof InternalizedStigma inPsychosis.
BehavCognPsychother.2017;45(6):545-560.
[205]-Wood L, ByrneR, EnacheG, et al. A brief cognitive therapy intervention for internalised stigma in
acute inpatients who experience psychosis: A feasibility randomised controlled trial. Psychiatry Res.
2018;262:303-310.
[206]-SegalSP,SilvermanCJ,TemkinTL.Self-stigmaandempowermentincombined-CMHAandconsumer-
runservices:twocontrolledtrials.PsychiatrServ.2013;64(10):990-6.
[207]-Cooper J, Sartorius N. Cultural and temporal variations in schizophrenia: a speculation on the
importanceofindustrialization.BrJPsychiatry1977;130:50-55
[208]-Littlewood R. Cultural variation in the stigmatisation of mental illness. Lancet. 1998 Sep
26;352(9133):1056-7.
[209]-ChenES,ChangWC,HuiCL,andal.Self-stigmaandaffiliatestigmainfirst-episodepsychosispatients
andtheircaregivers.SocPsychiatryPsychiatrEpidemiol.2016;51(9):1225-31.
[210]-HoferA,MizunoY,Frajo-AporB,etal.Resilience,internalizedstigma,self-esteem,andhopelessness
amongpeoplewith schizophrenia: Cultural comparison inAustria and Japan. Schizophr Res. 2016;171(1-
3):86-91.
[211]-Young DK, Ng PY. The prevalence and predictors of self-stigma of individuals with mental health
illnessintwoChinesecities.IntJSocPsychiatry.2016;62(2):176-85
Page 212
[212]-GirmaE,TesfayeM,FroeschlG,etal.Facilitybasedcross-sectionalstudyofself-stigmaamongpeople
withmentalillness:towardspatientempowermentapproach.IntJMentHealthSyst.2013;7(1):21.
[213]-MakanjuolaV,EsanY,OladejiB,etal.Explanatorymodelofpsychosis:impactonperceptionofself-
stigma by patients in three sub-saharan African cities. Soc Psychiatry Psychiatr Epidemiol.
2016;51(12):1645-1654.
[214]-Dubreucq J, Plasse J, Gabayet F, and al. Self-stigma in seriousmental illness and autism spectrum
disorder:ResultsfromtheREHABasenationalpsychiatricrehabilitationcohort.EuropeanPsychiatry2019b
https://doi.org/10.1192/j.eurpsy.2019.12
[215]-Dubreucq J, Franck N. Internalized Stigma in Serious Mental Illness (SMI): a systematic review of
prevalence,predictorsandcorrelates.JAffDisord2020,revised
[216]-PiccoL,PangS,LauYW,etal. Internalizedstigmaamongpsychiatricoutpatients:Associationswith
qualityoflife,functioning,hopeandself-esteem.PsychiatryRes.2016;246:500-506.
[217]-GroverS,HazariN,AnejaJ,etal.Stigmaand itscorrelatesamongpatientswithbipolardisorder:A
studyfromatertiarycarehospitalofNorthIndia.PsychiatryRes.2016;244:109-16.
[218]-GroverS,AvasthiA,SinghA,etal.Stigmaexperiencedbypatientswithseverementaldisorders:A
nationwidemulticentricstudyfromIndia.PsychiatryRes.2017;257:550-558.
[219]-Grambal A, Prasko J, Kamaradova D, et al. Self-stigma in borderline personality disorder - cross-
sectional comparison with schizophrenia spectrum disorder, major depressive disorder, and anxiety
disorders.NeuropsychiatrDisTreat.2016;12:2439-48.
[220]-KamaradovaD,LatalovaK,PraskoJ,etal.Connectionbetweenself-stigma,adherencetotreatment,
anddiscontinuationofmedication.PatientPreferAdherence.2016;10:1289-98.
[221]-RüschN,HölzerA,HermannC,etal.Self-stigmainwomenwithborderlinepersonalitydisorderand
womenwithsocialphobia.JNervMentDis.2006;194(10):766-73.
[222]-Sheehan L, Nieweglowski K, Corrigan P. The Stigma of Personality Disorders. Curr Psychiatry Rep.
2016;18(1):11.
[223]-OciskovaM,PraskoJ,KamaradovaD,etal.Individualcorrelatesofself-stigmainpatientswithanxiety
disorderswithandwithoutcomorbidities.NeuropsychiatrDisTreat.2015;11:1767-79.
[224]-HarrisJI,FarchminL,StullL,etal.Predictionofchangesinself-stigmaamongveteransparticipatingin
partial psychiatric hospitalization: The role of disability status and military cohort. Psychiatr Rehabil J.
2015;38(2):179-185.
[225]-Firmin RL, Lysaker PH, Luther L, and al. Internalized stigma in adults with early phase versus
prolongedpsychosis.EarlyIntervPsychiatry.2019;13(4):745-751.
[226]-ChronisterJ,ChouCC,LiaoHY.Theroleofstigmacopingandsocialsupportinmediatingtheeffectof
societal stigma on internalized stigma, mental health recovery, and quality of life among people with
seriousmentalillness.Journalofcommunitypsychology2013;41(5):582-600
[227]-NaborsLM,YanosPT,RoeD,etal.Stereotypeendorsement,metacognitivecapacity,andself-esteem
aspredictorsofstigmaresistanceinpersonswithschizophrenia.ComprPsychiatry.2014;55(4):792-8.
Page 213
[228]-Dubreucq J, Plasse J, Gabayet F, and al. Stigma Resistance in Serious Mental Illness and Autism
SpectrumDisorder:resultsfromtheRehaBASEnationalpsychiatricrehabilitationcohort.SocialPsychiatry
andpsychiatricepidemiology,2020b.Inreview
[229]-Sibitz I,AmeringM,UngerA,etal.The impactofthesocialnetwork,stigmaandempowermenton
thequalityoflifeinpatientswithschizophrenia.EurPsychiatry.2011;26(1):28-33.
[230]-GazielM,Hasson-OhayonI,Morag-YaffeM,etal.Insightandsatisfactionwithlifeamongadolescents
with mental disorders: assessing associations with self-stigma and parental insight. Eur Psychiatry.
2015;30(2):329-33.
[231]-WangK,LinkBG,CorriganPW,etal.Perceivedproviderstigmaasapredictorofmentalhealthservice
users'internalizedstigmaanddisempowerment.PsychiatryRes.2018;259:526-531.
[232]-OexleN,MüllerM,KawohlW,etal.Self-stigmaasabarriertorecovery:alongitudinalstudy.EurArch
PsychiatryClinNeurosci.2018;268(2):209-212
[233]-JahnDR,LeithJ,MuralidharanA,etal.Theinfluenceofexperiencesofstigmaonrecovery:Mediating
roles of internalized stigma, self-esteem, and self-efficacy. Psychiatr Rehabil J 2019. doi:
10.1037/prj0000377
[234]-Lysaker PH, Yanos PT, Outcalt J, et al. Association of stigma, self-esteem, and symptoms with
concurrentandprospectiveassessmentofsocialanxiety inschizophrenia.ClinSchizophrRelatPsychoses.
2010;4(1):41-8.
[235]-CaveltiM,RüschN,VauthR. Is livingwithpsychosis demoralizing? Insight, self-stigma, and clinical
outcomeamongpeoplewithschizophreniaacross1year.JNervMentDis.2014;202(7):521-9.
[236]-OexleN,RüschN,VieringS,etal.Self-stigmaandsuicidality:alongitudinalstudy.EurArchPsychiatry
ClinNeurosci.2017;267(4):359-361.
[237]-XuZ,LayB,OexleN,etal.Involuntarypsychiatrichospitalisation,stigmastressandrecovery:a2-year
study.EpidemiolPsychiatrSci.2018a;31:1-8.
[238]-Yanos PT, Lysaker PH, Roe D. Internalized stigma as a barrier to improvement in vocational
functioningamongpeoplewithschizophrenia-spectrumdisorders.PsychiatryRes.2010;178(1):211-3.
[239]-Pyle M, Stewart SL, French P, et al. Internalized stigma, emotional dysfunction and unusual
experiencesinyoungpeopleatriskofpsychosis.EarlyIntervPsychiatry.2015;9(2):133-40.
[240]-XuZ,MüllerM,HeekerenK,etal.Pathwaysbetweenstigmaandsuicidal ideationamongpeopleat
riskofpsychosis.SchizophrRes.2016;172(1-3):184-8.
[241]-RüschN,HeekerenK,TheodoridouA,etal.Stigmaasastressorandtransitiontoschizophreniaafter
oneyearamongyoungpeopleatriskofpsychosis.SchizophrRes.2015;166(1-3):43-8.
[242]-BerryC,GreenwoodK.Directandindirectassociationsbetweendysfunctionalattitudes,self-stigma,
hopefulness and social inclusion in young people experiencing psychosis. Schizophrenia Research. 2018;
193:197–203
[243]-Lagger N, AmeringM, Sibitz I, et al. Stability andmutual prospective relationships of stereotyped
beliefs aboutmental illness,hopeanddepressive symptomsamongpeoplewith schizophrenia spectrum
disorders.PsychiatryRes.2018;268:484-489
Page 214
[244]-PearlRL,ForgeardMJC,RifkinL,etal.Internalizedstigmaofmentalillness:Changesandassociations
withtreatmentoutcomes.StigmaandHealth.2017;2(1):2-15.
[245]-LysakerPH,TunzeC,YanosPT,etal.Relationshipsbetweenstereotypedbeliefsaboutmentalillness,
discriminationexperiences,anddistressedmoodover1yearamongpersonswithschizophreniaenrolledin
rehabilitation.SocPsychiatryPsychiatrEpidemiol.2012;47(6):849-55.
[246]-LysakerPH,RoeD,RingerJ,etal.Changeinself-stigmaamongpersonswithschizophreniaenrolledin
rehabilitation: associations with self-esteem and positive and emotional discomfort symptoms. Psychol
Serv.2012;9(3):240-247
[247]-Sibitz I, Provaznikova K, Lipp M, et al. The impact of recovery-oriented day clinic treatment on
internalizedstigma:preliminaryreport.PsychiatryRes.2013;209(3):326-32
[248]-Rüsch N, Nordt C, KawohlW, et al.Work-related discrimination and change in self-stigma among
peoplewithmentalillnessduringsupportedemployment.PsychiatrServ.2014;65(12):1496-8
[249]-HoRWH,ChangWC,KwongVWY,etal.Predictionofself-stigmainearlypsychosis:3-Yearfollow-up
oftherandomized-controlledtrialonextendedearlyintervention.SchizophrRes.2018;195:463-468.
[250]-SchomerusG,MatschingerH,AngermeyerMC.Causalbeliefsofthepublicandsocialacceptanceof
personswithmentalillness:acomparativeanalysisofschizophrenia,depressionandalcoholdependence.
PsycholMed.2014;44(2):303-14.
[251]-RüschN,ToddAR,BodenhausenGV,etal.Biogeneticmodelsofpsychopathology,implicitguilt,and
mentalillnessstigma.PsychiatryRes2010b;179(3):328-32.
[252]-GinetC,CoricAM,SorumA,etal.UnpackingStigma:ChallengingPreconceptionsonSchizophrenia.A
experimentalStudyonbusinessschoolstudentsinFrance.Inpreparation
[253]-Al-KhoujaMA,CorriganPW.Self-Stigma, Identity,andCo-OccurringDisorders. Isr JPsychiatryRelat
Sci.2017;54(1):56-60.
[254]-FlanaganE,PavloA,DavidsonL.StigmaandRecovery.In:GaebelW,RösslerW,SartoriusN(Eds).The
StigmaofMentalIllness–EndoftheStory?SpringerInternationalPublishing.Switzerlan.2017.p.551-570
[255]-AshcraftL,BlossM,AnthonyWA.Bestpractices:Thedevelopmentandimplementationof"noforce
first"asabestpractice.PsychiatrServ.2012;63(5):415-7.
[256]-Slade M, Bird V, Clarke E, et al. Supporting recovery in patients with psychosis through care by
community-basedadultmentalhealthteams(REFOCUS):amultisite,cluster,randomised,controlledtrial.
LancetPsychiatry.2015;2(6):503-14.
[257]-Meadows G, Brophy L, Shawyer F, et al. REFOCUS-PULSAR recovery-oriented practice training in
specialist mental health care: a stepped-wedge cluster randomised controlled trial. Lancet Psychiatry.
2019;6(2):103-114.
[258]-JohnsonS,LambD,MarstonL,etal.Peer-supportedself-managementforpeopledischargedfroma
mentalhealthcrisisteam:arandomisedcontrolledtrial.Lancet.2018;392(10145):409-418.
[259]-RepperJ,CarterT.Areviewoftheliteratureonpeersupportinmentalhealthservices.JMentHealth
2011;20:392–411.
Page 215
[260]-Shepherd G, Repper J. Empowerment and Inclusion: The Introduction of Peer Workers into the
Workforce. Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story?
SpringerInternationalPublishing.Switzerlan.2017.p.591-612
[261]-Davidson L, BellamyC,GuyK, and al. Peer support amongpersonswith severemental illnesses: a
reviewofevidenceandexperience.WorldPsychiatry.2012;11(2):123-8.
[262]-CorriganPW,SokolKA,RüschN.Theimpactofself-stigmaandmutualhelpprogramsonthequality
oflifeofpeoplewithseriousmentalillnesses.CommunityMentHealthJ.2013;49(1):1-6.
[263]-RüschN, ToddAR,BodenhausenGV, et al.Automatically activated shame reactions andperceived
legitimacy of discrimination: A longitudinal study among people with mental illness. J Behav Ther Exp
Psychiatry.2010;41(1):60-3.
[264]-LysakerPH,VohsJ,Hasson-OhayonI,etal.Depressionandinsight inschizophrenia:comparisonsof
levels of deficits in social cognition and metacognition and internalized stigma across three profiles.
SchizophrRes.2013;148(1-3):18-23.
[265]-SchrankB,AmeringM,HayAG,etal.Insight,positiveandnegativesymptoms,hope,depressionand
self-stigma:acomprehensivemodelofmutual influences in schizophrenia spectrumdisorders. Epidemiol
PsychiatrSci.2014;23(3):271-9.
[266]-ValienteC,ProvencioM,EspinosaR,etal.Insightinparanoia:Theroleofexperientialavoidanceand
internalizedstigma.SchizophrRes.2015;164(1-3):214-20
[267]-MacDougallAG,VandermeerMR,NormanRM.Negativefutureselfasamediatorintherelationship
betweeninsightanddepressioninpsychoticdisorders.SchizophrRes.2015;165(1):66-9.
[268]-LienYJ,ChangHA,KaoYC,etal. Insight,self-stigmaandpsychosocialoutcomes inSchizophrenia:a
structuralequationmodellingapproach.EpidemiolPsychiatrSci.2018;27(2):176-185
[269]-Shin YJ, Joo YH, Kim JH. Self-perceived cognitive deficits and their relationship with internalized
stigmaandqualityoflifeinpatientswithschizophrenia.NeuropsychiatrDisTreat.2016;12:1411-7.
[270]-StipE,Caron J, TousignantM,et al. Suicidal IdeationandSchizophrenia:ContributionofAppraisal,
Stigmatization,andCognition.CanJPsychiatry.2017;62(10):726-734.
[271]-Favrod J,CrespiS,Faust J,andal.Apsychoeducation tool forpatientswith first-episodepsychosis.
ActaNeuropsychiatrica2011;23(2):75-77.doi:10.1111/j.1601-5215.2011.00529.
[272]-LecomteTGroupCBTforpsychosis:aguidebookforclinicians.Oxford;New-York:OxfordUniversity
Press.2016.
[273]-Dubreucq J, Gabayet F, Lucas T, and al. (2018). Réduire l’auto-stigmatisation et les symptômes
négatifs par la remédiation cognitive. In : FranckN. (Ed) Traitéde réhabilitationpsychosociale ; Elsevier,
2018
[274]-Dubreucq J, Gabayet F, Ycart B, and al. Improving social function with ecological social-cognitive
remediationinSZ:resultsfromtheRemedRugbycontrolledtrial.EurPsychiatry,2020c.InReview
[275]-CorriganPW,MichaelsPJ,PowellK,andal.WhoComesOutWithTheirMentalIllnessandHowDoes
ItHelp?JNervMentDis.2016;204(3):163-8.
Page 216
[276]-DubreucqJ,FaraldoM,AbbesM,andal.NarrativeEnhancementandCognitiveTherapy(NECT)and
social function inSeriousMental Illness:studyprotocol forastepped-wedgerandomizedcontrolledtrial.
Trails,2020d.Revised
[277]-ReyR,LouriouxC,d’AmatoT.Chapitre15:commentaider lesproches? In:Troublespsychotiques:
protocolesd’interventionprécoce.ElsevierMasson.2019
[278]-HodéY,KrychowskiR,BeckNetal.Moodimprovementinafamilyofschizophrenicpatientsaftera
psychoeducationalprogram.JTherComportCogn2008;18:104–7
[279]-Dubreucq J, FranckN. Neural and cognitive correlates of stigma and social rejection in individuals
withSeriousMentalIllness(SMI):Asystematicreviewoftheliterature.PsychiatryRes.2019;274:146-158.
[280]-BondGR,DrakeRE,BeckerDR.GeneralizabilityoftheIndividualPlacementandSupport(IPS)model
ofsupportedemploymentoutsidetheUS.WorldPsychiatry.2012;11(1):32-9.
[281]-Kinoshita Y, FurukawaTA,KinoshitaK, et al. Supportedemployment for adultswith severemental
illness.The Cochrane Database of Systematic Reviews,2013; 9:CD008297.
http://doi.org/10.1002/14651858.CD008297.pub2
[282]-Boycott N, Schneider J, McMurran M. Additional interventions to enhance the effectiveness of
individualplacementandsupport:arapidevidenceassessment.RehabilResPract.2012;2012:382420.
[283]-Lecomte T, Corbière M, Giguère CE, et al. Group cognitive behaviour therapy for supported
employment - Results of a randomized controlled cohort trial. Schizophr Res. 2019; pii: S0920-
9964(19)30498-0.
[284]-Dubreucq J, Fernandez E, Lucas T, and al. Représentation du travail et réinsertion professionnelle.
2018.In:FranckN.Traitéréhabilitationpsychosociale.Elsevier.2018b.p.701-712
[285]-DubreucqM,BesnardM,Revil-SignoratK,andal.Recovery-orientedsupportedintimaterelationships
andparenthoodinSevereMentalIllness:developmentofanewintervention.Inpreparation.
[286]-Bachmann CJ, Höfer J, Kamp-Becker I, et al. Internalised stigma in adults with autism: A German
multi-centersurvey.PsychiatryRes.2019;276:94-99.
Page 217
Bibliographie des figures
I Sheehan L, Nieweglowski K, Corrigan PW. Structures and types of Stigma? Table 3.3 “Types of Stigma”. In: Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer International Publishing. Switzerlan. 2017. p. 51
II Sheehan L, Nieweglowski K, Corrigan PW. Structures and types of Stigma? Table 3.1 “Common stereotypes of mental illness”. In: Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer International Publishing. Switzerlan. 2017. p. 45
III Special Eurobarometer n°345. p34. Mental Health. 2010. Available from URL: https://ec.europa.eu/commfrontoffice/publicopinion/archives/ebs/ebs_345_en.pdf
IVSchomerus G, Schwahn C, Holzinger A, et al. Evolution of public attitudes about mental illness:
a systematic review and meta-analysis. Fig.1. “Evolution of causal explanations for schizophrenia and depression. Results from representative, national trend studies using unlabelled case vignettes”. Acta Psychiatr Scand. 2012;125(6):440-52.
V Schomerus G, Schwahn C, Holzinger A, et al. Evolution of public attitudes about mental illness: a systematic review and meta-analysis. Fig. 3. “Evolution of social acceptance of persons with schizophrenia or depression. Results from representative, national trend studies using unlabelled case vignettes”. Acta Psychiatr Scand. 2012;125(6):440-52.
VIPescosolido BA, Manago B, Monahan J. Evolving Public Views On The Likelihood Of Violence
From People With Mental Illness: Stigma And Its Consequences. Health Aff (Millwood). 2019;38(10):1735-1743.
VII Yanos PT. Written off : mental health stigma and the loss of human potential. Figure 9 “odel for how awareness of stigma impacts people with mental illness. New York, N.Y: Cambridge University Press, 2018. p. 92
VIII Henderson C, Evans-Lacko S, Thornicroft G. The Time To Change Programme to reduce Stigma and Discrimination in England and Its Wider Context. Figure 18.1 “Prevalence of experienced discrimination among secondary mental health service users across life domains of employment, health, and citizenship in England (2012). In: Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer International Publishing. Switzerlan. 2017. p.344
IX Daumerie N, Vasseur Bacle S, Giordana JY, and al. Discrimination perceived by people with a diagnosis of schizophrenic disorders. INternational study of DIscrimination and stiGma Outcomes (INDIGO): French results. Figure 1 « Types de discrimination vécue et anticipée du fait d’un diagnostic de schizophrénie (site France) ». Encephale. 2012 Jun;38(3):224-31.
X Yanos PT. Written off : mental health stigma and the loss of human potential. Figure 11 “Possibly identity responses to stigma” New York, N.Y: Cambridge University Press, 2018. p.104
XI Yanos PT. Written off : mental health stigma and the loss of human potential. Figure 12 “The illness identity model” New York, N.Y: Cambridge University Press, 2018. p.119
Page 218
XII Dubreucq J, Gbayet F, Lucas T, et al. Réduire l’autostigmatisation et les symptômes négatifs par la remédiation cognitive. Figure 84.1 « Why try effect », (d’après Corrigan et al., 2009). In : Franck N. Traité de réhabilitation psychosociale. Elsevier Masson, 2018.
XIII Farkas M, Anthony WA. Psychiatric rehabilitation interventions: a review. Figure 1. “Process framework for psychiatric rehabilitation, person level process”. Int Rev Psychiatry. 2010;22(2):114-29.
XIV Rusch N, Xu Z. Strategies to Reduce Mental Illness Stigma. Table 24.1 “Strategies for challenging public stigma”. In: Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer International Publishing. Switzerlan. 2017. p. 453
XV Slade M. The personal Recovery Framework. Figure 9.1 “The personal Recovery Framework”. In: Personal Recovery and Mental Illness. A Guide for Mental Health Professionals. Cambridge University Press 2009. p.90
XVI Rusch N, Xu Z. Strategies to Reduce Mental Illness Stigma. Table 24.2 “Self-stigma reduction programs”. In: Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer International Publishing. Switzerlan. 2017. p. 458
XVII Flanagan E, Pavlo A, Davidson L. Stigma and Recovery. Figure 31.1 “conceptual mode for the mechanisms of stigma within mental health settings”. In: Gaebel W, Rössler W, Sartorius N (Eds). The Stigma of Mental Illness – End of the Story? Springer International Publishing. Switzerlan. 2017. p. 551-570
XVIII Rüsch N, Müller M, Lay B, et al. Emotional reactions to involuntary psychiatric hospitalization and stigma-related stress among people with mental illness. Figure 1 “Model of emotional reactions to involuntary hospitalization and of stigma stress as predictors of self-stigma, empowerment, quality of life and self-esteem”. Eur Arch Psychiatry Clin Neurosci. 2014;264(1):35-43
Page 219
Annexe
ConceptNoteTemplateConceptNotescanbesentbyemailtoinfo@fondationdharcourt.org
NameofORGANIZATION:FondationFondamentalSuisse
Legalstatus(Association,NGO,UN,Foundation,etc.):Foundation
Address:RueduNant8,1207Geneva
Website:www.fondamental-suisse.org
AnnualReportifavailable(URL):N/A
Contactperson:AliceSilvestre
Position:Fundraisingmanager
PhoneNumber:0786145979
E-mailaddress:[email protected]
TITLE OF THE PROJECT:Narrative Enhancement and Cognitive Therapy (NECT) to reduce self-stigma in Serious Mental Illness: preliminary effectiveness on response to acute social rejection and on chronic peripheral inflammation ProjectLocation(Pleasespecifyvillageorcity,regioncountry):
The co-coordination of this Swiss-French bi-national project will be Geneva-Grenoble (Dr Hélène Richard-Lepouriel, Dr Julien Dubreucq). This project will involve partners from the University of Geneva (Indrit Begue, Swann Pichon), the University Hospital Grenoble Alpes (Pr Mircea Polosan) and the University of Lyon 1 (Pr Nicolas Franck).
Durationoftheproject(months):36 months (January 2020- January 2023)
Briefdescriptionofthecontextandneeds-basedassessment:
Mental illness stigma refers to the negative beliefs, emotional reactions, and attitudes towards people with Serious Mental Illness (SMI) endorsed by the general population (also referred to as public stigma1). People with SMI are generally acutely aware of public stigma and expect to be rejected by others (69.4% of the 1,229 participants with schizophrenia (SZ) and 71.6% of the 1,182 participants with mood disorders in the GAMIAN-Europe study had high perceived stigma2,3). In a recent study, borderline personality participants reported higher ISMI score than participants living from bipolar disorder23. People with SMI are more likely to experience discrimination in a range of aspects of their daily life. They frequently expect to be discriminated in social contexts even when they have no previous experience of discrimination. Stereotype awareness and self-labelling with SMI can be associated with agreement with these stereotypes, and application to describe oneself, leading to self-stigma.1 Self-stigma refers to the process whereby a person’s previously held social identity is progressively replaced by a devalued and stigmatised view of oneself. Self-stigma is highly prevalent in Europe (41.7% in SZ and 21.7% in mood disorders2,3) and in France (31.2% in SMI26). Self-stigma can have pervasive effects on outcomes related to recovery from SMI, including self-esteem, hopefulness, social interaction, employment, and symptom severity4. Self-stigma is negatively associated with self-esteem, motivation to achieve personal life goals, shared-decision making, adherence into treatment, well-being, quality of life, personal recovery and social function.5-7People with elevated self-stigma report more dysfunctional attitudes and social withdrawal.7 Impairments in cognitive functioning,

Page 220
metacognition and social cognition predict increased self-stigma.7 Self-stigma can be deconstructed 24. Self-destigmatization is a personal and inter-relational process that deconstructs self-stigmatization and leads to an assumed and attuned individuality25. Narrative Enhancement and Cognitive Therapy (NECT) is a structured, 20 session group-basedapproach which combines psychoeducation to counteract SMI stereotypes, cognitive restructuring to challenge dysfunctional attitudes about the self, and story-telling exercises to enhance meaning-making and the person’s ability to move beyond their illness-identity to a more integrated sense of self.8 NECT showed effectiveness in improving self-stigma, hope and self-esteem9-11 with persisting effects after 6 months’ follow-up.8-10 NECT showed effectiveness in reducing social withdrawal and avoidant coping strategies in participants with schizophrenia (SZ) in comparison with an active control condition.10
CBT targeting positive symptoms has shown effectiveness in improving functional connectivity to social threat in SZ11.
Two cognitive models of self-stigma and one of stigma resistance were described in the literature6. Implicit self-stigma (defined as the combination of implicit negative attitudes towards mental illness and low implicit self-esteem) was strongly correlated with explicit self-stigma and identified as a predictor of subjective quality of life6. Social alienation (or high perceived social loneliness associated with low personality trait agreeableness) was associated with reduced insula activation in participants with SZ when processing covert expressions of disgust6. It has been suggested that a decreased sensitivity to subtle signals of social rejection that might protect individuals against social alienation6. Stigma resistance (defined as low negative implicit associations between SZ and social inferiority) was associated with the enhanced activation of rostro-ventral-medio prefrontal cortex and decreased activation of the amygdala6. Social rejection models recreate stigma-related environments under experimental conditions. The most popular paradigm is the cyberball game, a ball-tossing game in which participants believe they are playing with fellow participants, but are in fact randomly assigned to inclusion, exclusion and sometimes over-inclusion conditions and play with computer-controlled players. Cyberball is considered to be an ecologically valid paradigm for evaluating emotional reactions following social inclusion or exclusion, and was used in numerous studies involving healthy individuals and people with SMI6. Acute social rejection, low stigma resistance, and stereotype threat conditions led to underperformance in cognitive or social cognitive tasks and in social skills in people with SMI6. The associations between self-stigma, cognitive performance and social functioning are however still unclear6. Psychiatric symptoms, illness duration and baseline non-specific distress influenced the response to acute social rejection or stigma.
Chronic social rejection was investigated in people without SMI, but confronted with prolonged ostracism (social rejection > 3-months). 12-14 In contrast to acute social rejection, chronic social rejection was associated with feelings of resignation, helplessness, unworthiness and low self-worth and ultimately with social alienation and depression12-14. An increased sensitivity to acute social exclusion was also found in people suffering from chronic social rejection12-14. In people at risk of being ostracized, enhanced spontaneous amygdala resting-state activity and increased connectivity within the salience network were associated with a greater exposure to discrimination, independently of ethnicity, sex or current psychiatric comorbidities15. Elevated pro-inflammatory cytokines (Il-6 and TNF-alpha) were associated with enhanced dorsal anterior cingulate cortex and anterior insula activation after acute social rejection in healthy controls (HC16). Exposure to everyday social stressors and to social rejection was associated in HC with elevated inflammatory activity and with major depression17-18. Elevated CRP levels were found in people with SZ or BD18 and associated with more severe depressive symptoms in people with SZ18. Research on chronic social rejection is extremely limited in HC and non-existent in people with SMI. The correlations between inflammatory activity, experiences of discrimination and self-stigma in people with SMI have not been investigated to date.
Page 221
This project aims at comparing the response to acute social rejection in SMI patients with elevated self-stigma and with low self-stigma. This collaborative project has also for objective to assess whether self-stigma reduction through specific cognitive behavior therapy improves the response to acute social rejection and chronic peripheral inflammation in SMI patients with elevated self-stigma.
Project objectives:
• Aim 1: To compare the response to acute social rejection in SMI patients with elevated self-stigma and with low self-stigma
• Aim 2: To investigate the relationships between experienced stigma, self-stigma, acute social rejection and inflammatory activity in people with SMI
• Aim 3: To investigate whether self-stigma reduction with NECT improves the response to acute social rejection and chronic peripheral inflammation
Project Activities and indicative timeline (Please identify indicators for each activity): Our project is based on two independent work packages (WP).
In WP 1 (3 months) we will design a Cyberball paradigm modeling acute social rejection in experimental conditions. We will investigate the cross-sectional (at T0) associations between self-stigma (measured with Internalized Stigma of Mental Illness (ISMI19), experienced and anticipated stigma using Discrimination and Stigma Scale (DISC 1220), acute social rejection, social anxiety with Leibowitz Social Anxiety Scale (LSAS), cognitive functioning with a large battery, metacognitive abilities using Metacognition Assessment Scale (MAS-A), social functioning with Personal and Social Performance Scale (PSP21) and chronic peripheral inflammation (CRP). Cognitive evaluation will include Wechsler Adult Intelligence Scale-4th edition (WAIS-IV) subscales assessing working memory, verbal abstraction and hypothetico-deductive reasoning, UPPS for the self-assessment of impulsivity, BEM-144 story subtest for auditive-verbal memory, Trail Making Test A and B (TMT-A or B) respectively for speed of processing and reactive mental flexibility, Stroop test and GoNogo for inhibition abilities, TAP for cognitive flexibility D2-R for selective attention, concentration, and speed of processing, shopping test for planning abilities and Versailles-Situational Intention Reading Test61 (V-SIR) for Theory of Mind (ToM).
In WP 2 (18 months), we will perform an ancillary trial to the primary study conducted by our group on NECT effectiveness on social function in SMI22. This randomized controlled study is multi-centric, prospective, interventional and exploratory. For ethical purposes, we have chosen a stepped wedge cluster randomized trial design, with a waiting list type control group. The total duration of the study will be 24 months to allow for: recruitment of the target number of participants; delivery of the intervention; follow-up assessments; data analysis using intention-to-treat methods. The participants who agree to join the study will then be randomized into two groups: one group (Group 1) receiving the intervention at the beginning of the study (T0), one group (Group 2) being a control group for the first 6 months and receiving the intervention after (T1). Outcomes will be compared in all groups at T0 and T1 (duration of intervention= 6 months). 6-month and 12-month outcomes for Group 1 and 2 will be measured without a control group at T2 (18 months after T0) to evaluate the stability of the effects over time. This proof of concept trial will investigate whether the NECT intervention improves social anxiety, social withdrawal, the response to acute social rejection, inhibition abilities, cognitive flexibility and chronic peripheral inflammation.
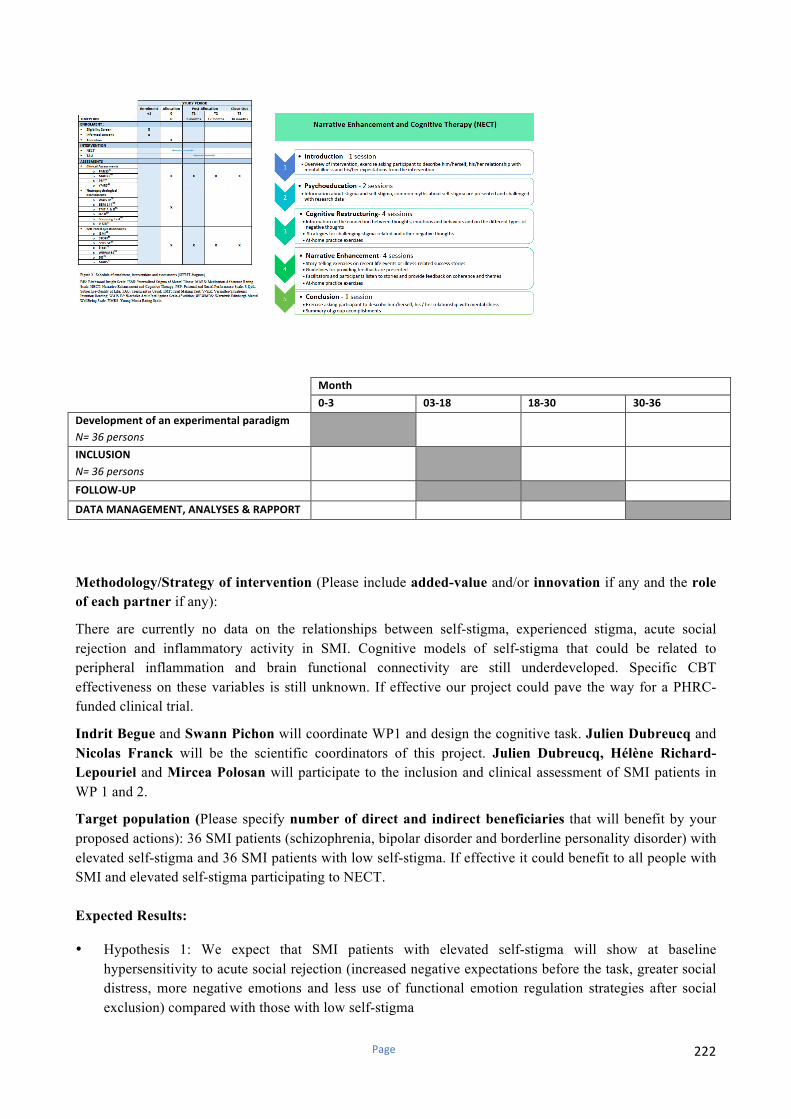
Page 222
Month
0-3 03-18 18-30 30-36
Developmentofanexperimentalparadigm
N=36persons
INCLUSION
N=36persons
FOLLOW-UP
DATAMANAGEMENT,ANALYSES&RAPPORT
Methodology/Strategy of intervention (Please include added-value and/or innovation if any and the role
of each partner if any):
There are currently no data on the relationships between self-stigma, experienced stigma, acute social rejection and inflammatory activity in SMI. Cognitive models of self-stigma that could be related to peripheral inflammation and brain functional connectivity are still underdeveloped. Specific CBT effectiveness on these variables is still unknown. If effective our project could pave the way for a PHRC-funded clinical trial.
Indrit Begue and Swann Pichon will coordinate WP1 and design the cognitive task. Julien Dubreucq and Nicolas Franck will be the scientific coordinators of this project. Julien Dubreucq, Hélène Richard-
Lepouriel and Mircea Polosan will participate to the inclusion and clinical assessment of SMI patients in WP 1 and 2.
Target population (Please specify number of direct and indirect beneficiaries that will benefit by your proposed actions): 36 SMI patients (schizophrenia, bipolar disorder and borderline personality disorder) with elevated self-stigma and 36 SMI patients with low self-stigma. If effective it could benefit to all people with SMI and elevated self-stigma participating to NECT. Expected Results:
• Hypothesis 1: We expect that SMI patients with elevated self-stigma will show at baseline hypersensitivity to acute social rejection (increased negative expectations before the task, greater social distress, more negative emotions and less use of functional emotion regulation strategies after social exclusion) compared with those with low self-stigma
Page 223
• Hypothesis 2: We expect that SMI patients with elevated self-stigma will have at baseline increased social anxiety, impaired cognitive, metacognitive and social functioning and higher CRP levels compared with those with low self-stigma
• Hypothesis 3: We expect that the intervention (NECT) will improve social anxiety, social withdrawal, cognitive flexibility, sensitivity to acute social rejection and chronic peripheral inflammation in patients with elevated self-stigma
Monitoring and evaluation of the project: The main endpoint is the sensitivity to acute social rejection within 12 months of inclusion: improved negative expectations, negative emotions and use of functional emotion regulation strategies after social exclusion Sustainability of the project: This project is an ancillary study to a trial that has already been approved by the relevant ethical committee in France (CPP Nord-Ouest I) on 2019/04/26. The study protocol has also been submitted to the ethical committee in Switzerland. The recruitment will begin on 2019/09/01 with an estimated study completion date is 2023/04/03. Our project and will benefit from clinical data and biological samples already collected within the frame of the network of Expert Centers for Schizophrenia and Bipolar Disorder. The clinicians involved in our project are recognized leaders in their field of expertise, which include social psychiatry and cognitive neuroscience.
Total Budget per year (CHF): 100 000 CHF Requested funding from Fondation d’Harcourt per year (CHF): 33 000 CHF (100 000 CHF after 3 years) Detailed budget: Development of the cognitive task: 15 000 CHF Statistics / data management: 15 000 CHF Clinical Study: 70 000 CHF Name(s) of other donor(s) funding the project: Searches in progress
Referencesrelatedtotheproject
1. Corrigan et al (2002) World Psychiatry;1(1):16-20 2. Brohan et al. (2010) Schizophr Res. 2010;122(1-3):232-8 3. Brohan et al. (2011) J Affect Disord.;129(1-3):56-63 4. Yanos et al. (2008) Psychiatr Serv.;59(12):1437-42. 5. Gerlinger et al. (2013) Word Psychiatry; 12:155-64 6. Dubreucq et al. (2019) Psychiatry Res. Apr;274:146-158. 7. Dubreucq et al. (2019) J Affect Disord. in review 8. Roe et al. (2014) J Clin Psychol. ;70(4):303-12. 9. Hansson et al. (2007) Soc Psychiatry Epidemiol.
2017;52(11):1415-23 10. Yanos et al. (2019) Soc Psychiatry Psychiatr Epidemiol.; doi:
10.1007/s00127-019-01702-0 11. Mason et al. (2016) Schizophr Bull; 42(3): 684–692. 12. Williams, et al (2009). Advances in Experimental Social
Psychology. 41, 275–314. 13. Riva et al. (2014) Basic and applied social psychology. 36,
329–346. DOI: 10.1080/01973533.2014.917975
14. Riva et al (2017). Journal of Social and Personal Relationships. 34(4), 1-24. DOI: 10.1177/0265407516644348
15. Clark et al. Biol. Psychiatry Cogn. Neurosci. Neuroimaging. 3(4), 367-378. doi: 10.1016/j . Bpsc.2017.11.011..
16. Slavich et al. (2010) Proc. Natl. Acad. Sci. U. S. A. 107(33), 14817-22. doi: 10.1073/pnas.1009164107.
17. Slavich et al. (2014) Psychol. Bull. 140(3), 774-815 18. Horsdal et al (2017) Eur. Psychiatry. 44, 164-172. doi:
10.1016/j.eurpsy.2017.04.012 19. Boyd et al (2003) Psychiatry Res 121:31-49 20. Brohan et al (2013) Psychiatr Res, 208(1):33–40. 21. Nasrallah H et al. (2008) Psychiatry Research; 161: 213-224 22. Dubreucq et al . (2019) BMC Trials, in review 23. Filion Quenneville et al. (2019) J Affect Disorder. in review 24. Richard-Lepouriel (2017). JTCC, 27(4), 177-183. 25. Richard-Lepouriel et al. (2019) J Affect Disord. in review 26. Dubreucq et al (2019). European Psychiatry, in rev

224