animal experimental study on repairing alveolar clefts by using rectilinear distraction osteogenesis
TRANSCRIPT
Journal of Plastic, Reconstructive & Aesthetic Surgery (2009) 62, 1573e1579
Animal experimental study on repairing alveolarclefts by using rectilinear distraction osteogenesis
Li-shu Liao a,b, Zhi Tan c, Qian Zheng a,b,*, Jun Wu a,b, Bing Shi a,b,Xing He a,b, Tian Meng a,b, Da-wei Lu a,b, Yan Wang a,b, Sheng Li a,b
a Department of Cleft Lip and Palate, West China Stomatological Hospital, Sichuan University,Chengdu, People’s Republic of Chinab State Key Laboratory of Oral Diseases, Sichuan University, Chengdu, People’s Republic of Chinac Division of the oral and maxillofacial surgery, North Sichuan Medical College
Received 16 January 2008; accepted 16 June 2008
KEYWORDSRectilinear distractionosteogenesis;Alveolar cleft;Histology;Cat
* Corresponding author. Address: DeNo. 14, Section 3, Ren Min Nan Road,85502570.
E-mail addresses: susanna821209@
1748-6815/$ - see front matter ª 2008 Pdoi:10.1016/j.bjps.2008.06.068
Summary The aim of this study was to evaluate the clinical applicability of rectilineardistraction osteogenesis for repairing alveolar cleft models. Alveolar process distractionsurgery to produce bilateral clefts was performed on six adult cats. In our study, the left sidewith the distraction device was the experimental side, and the other side without a distractiondevice was the control side. After a 6-day latent period, animals underwent gradual distractionat a rate of 0.6 mm per day (distraction was performed twice each day, at a rate of 0.3 mmeach time), until the tissue on the two sides of the cleft touched, then the distraction strengthwas maintained for 2 days. Two cats were sacrificed at 2 weeks, 6 weeks and 10 weeks post-operatively. Gross anatomical, histological and radiographical analyses were performed afterthe animals were sacrificed. In addition, the arch width was measured both before setting thedistraction device and after distraction was complete. Two weeks after the distraction wascomplete, the soft tissue of the two sides of the cleft region on the experimental side touched,and it began to coalesce. The extremities of the two sides of the cleft region on all the exper-imental sides drew close to each other, but there was no bony conjunction. New bone forma-tion appeared in the distraction region. The arch width at the front of the maxillary bone onthe distraction side after distraction was smaller than before distraction. The alveolar cleftcould be closed by rectilinear distraction osteogenesis. Two sides of the cleft touched eachother and only soft tissue coalesced, but we did not observe bone coalescing. This phenom-enon suggested that it might be difficult to achieve complete bony repair by rectilinear
partment of Oral and Maxillofacial Surgery, West China College of Stomatology, Sichuan University,Chengdu 610041, People’s Republic of China. Tel.: þ86 28 61153199, þ86 13036670410; fax: þ86 28
163.com, [email protected] (Q. Zheng).
ublished by Elsevier Ltd on behalf of British Association of Plastic, Reconstructive and Aesthetic Surgeons.
1574 L.-shu Liao et al.
Figure 1 Distract
distraction osteogenesis. However, rectilinear distraction osteogenesis can minimise the sizeof the alveolar cleft and make bone grafting advisable for those patients who are not suitablefor bone grafting before distraction osteogenesis.ª 2008 Published by Elsevier Ltd on behalf of British Association of Plastic, Reconstructive andAesthetic Surgeons.
Secondary autogenous cancellous bone grafting is a classicmethod for the treatment of alveolar clefts. Successfulconditions for bone grafting include sufficient bone massand soft tissue overlay. However, graft failure sometimesoccurs due to inadequate covering with the surroundingsoft tissue and marked scar formation, or large clefts. Inaddition, some patients are not suitable to undergo bonegrafting.1
Distraction osteogenesis (DO) was introduced by Codi-villa in 1905. In 1992, McCarthy used DO to correct hypo-plasia of the mandible for the first time. After this, thestudy and application of DO in the field of maxillofacialsurgery developed quickly.2,3 Various studies have shownthat there are many advantages to using DO, such as, smalloperation perturbation, few scars, and the exact effect ofthe new bone formation.2 Success is easily obtained byusing DO at the alveolar process, because of the abundantblood supply. There are already many reports on success-fully increasing the height of the alveolar crest by usingDO.4e7 However, at present, the distraction device moveslinearly, and the transport disk can only be moved ina straight line. We wondered if it was possible to usea rectilinear distraction device in a curved dental arch.
Materials and methods
Distraction device
The distraction device, made in the State Key Laboratory ofOral Disease, Sichuan University, was made up of two guiderods, one screw rod, two fixing plates and one sliding board.There is a lag spike on one side of the screw rod, which canbe swivelled by a screwdriver bit. With every circle ofswivel, the sliding board moves 0.3 mm. The largestdistance is 12 mm (Figure 1). There are four retentive holes
ion device.
in the fixing plate and sliding board. The distraction devicecan be fixed to the alveolar bone with lag spikes. The slidingboard can drive the bone transfer disk to the medial side.
Animals
All experiments were performed in accordance withSichuan University Animal Care and Use Committee guide-lines. Six healthy cats (Department of ExperimentalAnimals, Sichuan University) of both sexes were used in thisstudy. The animals were between 1 and 2 years of age andweighed between 3 and 5 kg. All animals were randomisedinto three groups based on the time of sacrificing: 2, 6 and10 weeks postoperatively. The study adopts its own control.All of the six cats were given a bilateral cleft; the cleft onthe left side with the distracter was the experimental side,and the cleft on the other side without a distracter was thecontrol side.
Surgery
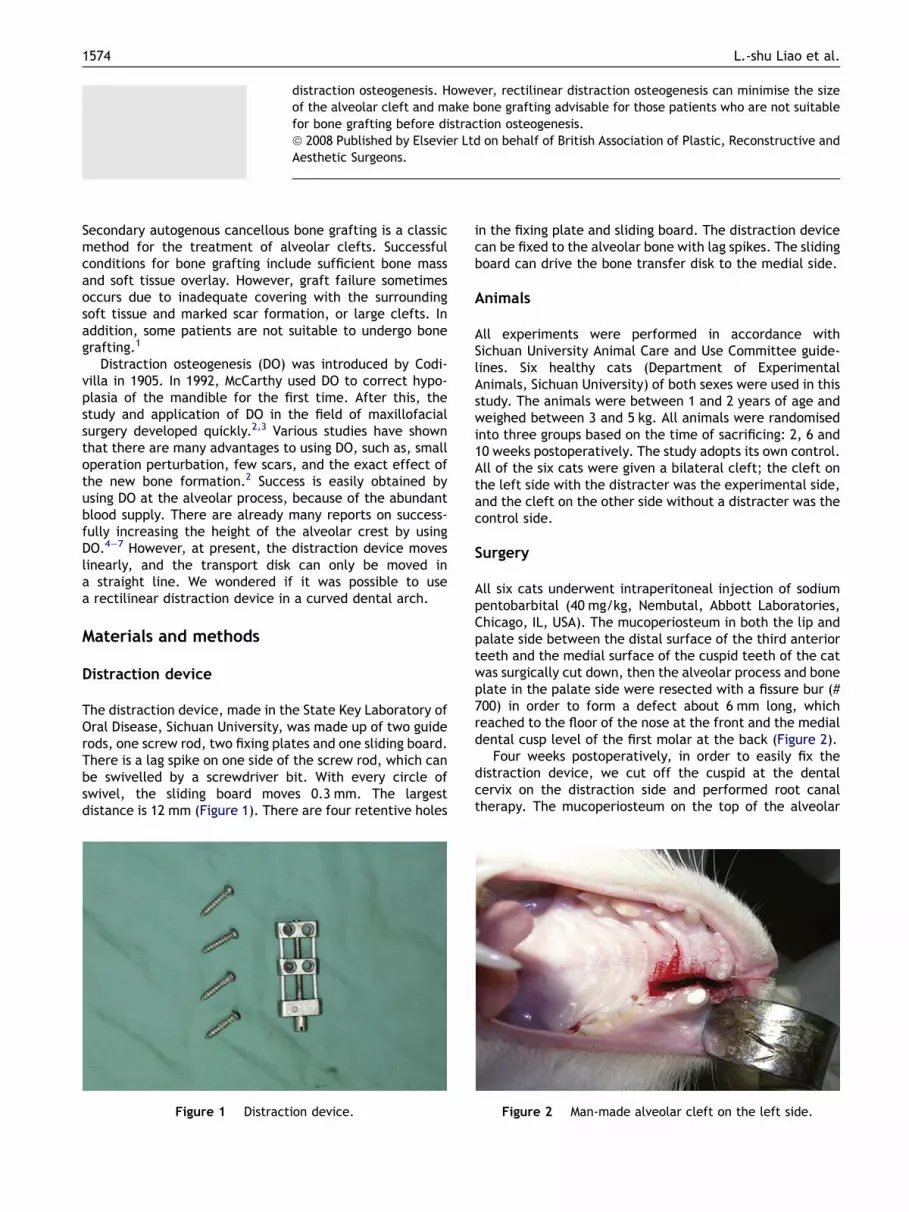
All six cats underwent intraperitoneal injection of sodiumpentobarbital (40 mg/kg, Nembutal, Abbott Laboratories,Chicago, IL, USA). The mucoperiosteum in both the lip andpalate side between the distal surface of the third anteriorteeth and the medial surface of the cuspid teeth of the catwas surgically cut down, then the alveolar process and boneplate in the palate side were resected with a fissure bur (#700) in order to form a defect about 6 mm long, whichreached to the floor of the nose at the front and the medialdental cusp level of the first molar at the back (Figure 2).
Four weeks postoperatively, in order to easily fix thedistraction device, we cut off the cuspid at the dentalcervix on the distraction side and performed root canaltherapy. The mucoperiosteum on the top of the alveolar
Figure 2 Man-made alveolar cleft on the left side.
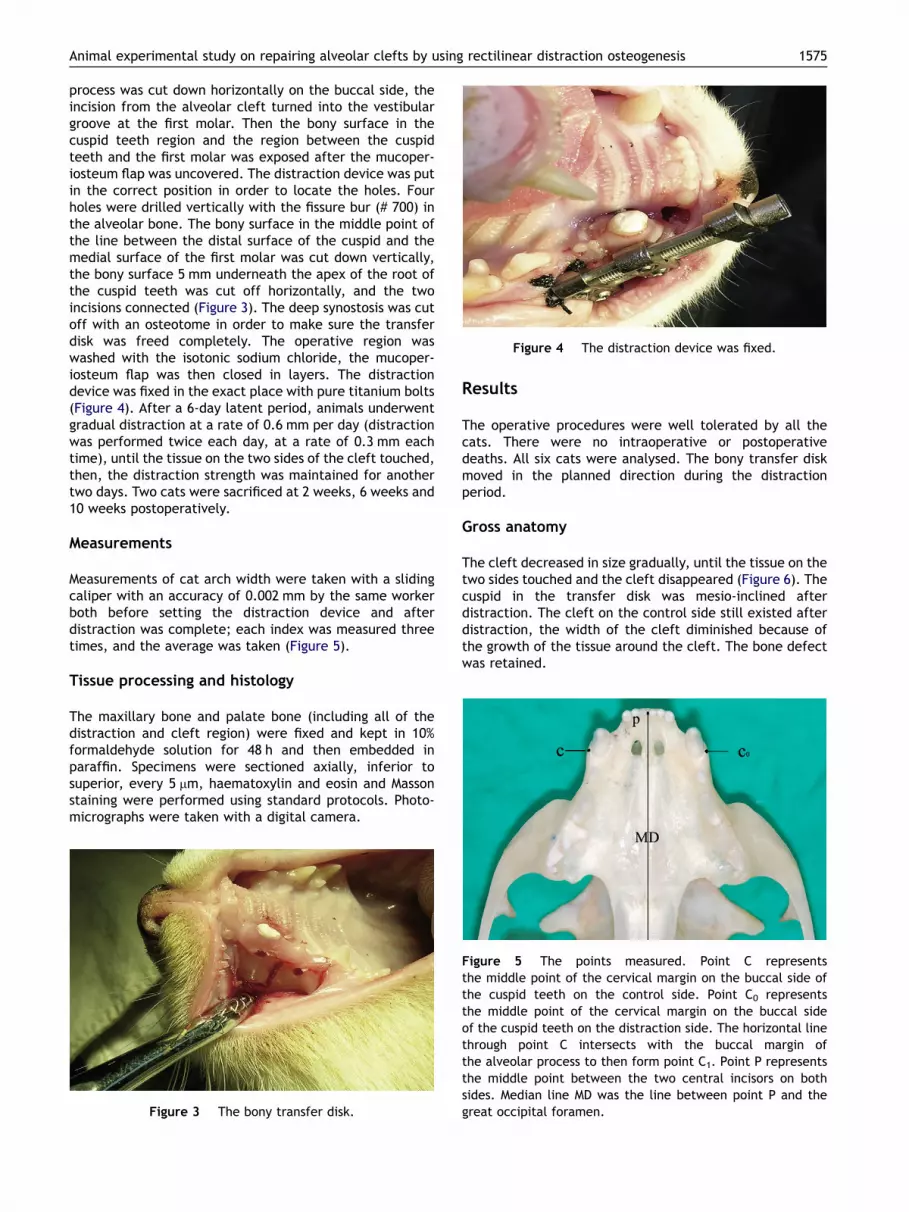
Figure 4 The distraction device was fixed.
Animal experimental study on repairing alveolar clefts by using rectilinear distraction osteogenesis 1575
process was cut down horizontally on the buccal side, theincision from the alveolar cleft turned into the vestibulargroove at the first molar. Then the bony surface in thecuspid teeth region and the region between the cuspidteeth and the first molar was exposed after the mucoper-iosteum flap was uncovered. The distraction device was putin the correct position in order to locate the holes. Fourholes were drilled vertically with the fissure bur (# 700) inthe alveolar bone. The bony surface in the middle point ofthe line between the distal surface of the cuspid and themedial surface of the first molar was cut down vertically,the bony surface 5 mm underneath the apex of the root ofthe cuspid teeth was cut off horizontally, and the twoincisions connected (Figure 3). The deep synostosis was cutoff with an osteotome in order to make sure the transferdisk was freed completely. The operative region waswashed with the isotonic sodium chloride, the mucoper-iosteum flap was then closed in layers. The distractiondevice was fixed in the exact place with pure titanium bolts(Figure 4). After a 6-day latent period, animals underwentgradual distraction at a rate of 0.6 mm per day (distractionwas performed twice each day, at a rate of 0.3 mm eachtime), until the tissue on the two sides of the cleft touched,then, the distraction strength was maintained for anothertwo days. Two cats were sacrificed at 2 weeks, 6 weeks and10 weeks postoperatively.
Measurements
Measurements of cat arch width were taken with a slidingcaliper with an accuracy of 0.002 mm by the same workerboth before setting the distraction device and afterdistraction was complete; each index was measured threetimes, and the average was taken (Figure 5).
Tissue processing and histology
The maxillary bone and palate bone (including all of thedistraction and cleft region) were fixed and kept in 10%formaldehyde solution for 48 h and then embedded inparaffin. Specimens were sectioned axially, inferior tosuperior, every 5 mm, haematoxylin and eosin and Massonstaining were performed using standard protocols. Photo-micrographs were taken with a digital camera.
Figure 3 The bony transfer disk.
Results
The operative procedures were well tolerated by all thecats. There were no intraoperative or postoperativedeaths. All six cats were analysed. The bony transfer diskmoved in the planned direction during the distractionperiod.
Gross anatomy
The cleft decreased in size gradually, until the tissue on thetwo sides touched and the cleft disappeared (Figure 6). Thecuspid in the transfer disk was mesio-inclined afterdistraction. The cleft on the control side still existed afterdistraction, the width of the cleft diminished because ofthe growth of the tissue around the cleft. The bone defectwas retained.
Figure 5 The points measured. Point C representsthe middle point of the cervical margin on the buccal side ofthe cuspid teeth on the control side. Point C0 representsthe middle point of the cervical margin on the buccal sideof the cuspid teeth on the distraction side. The horizontal linethrough point C intersects with the buccal margin ofthe alveolar process to then form point C1. Point P representsthe middle point between the two central incisors on bothsides. Median line MD was the line between point P and thegreat occipital foramen.
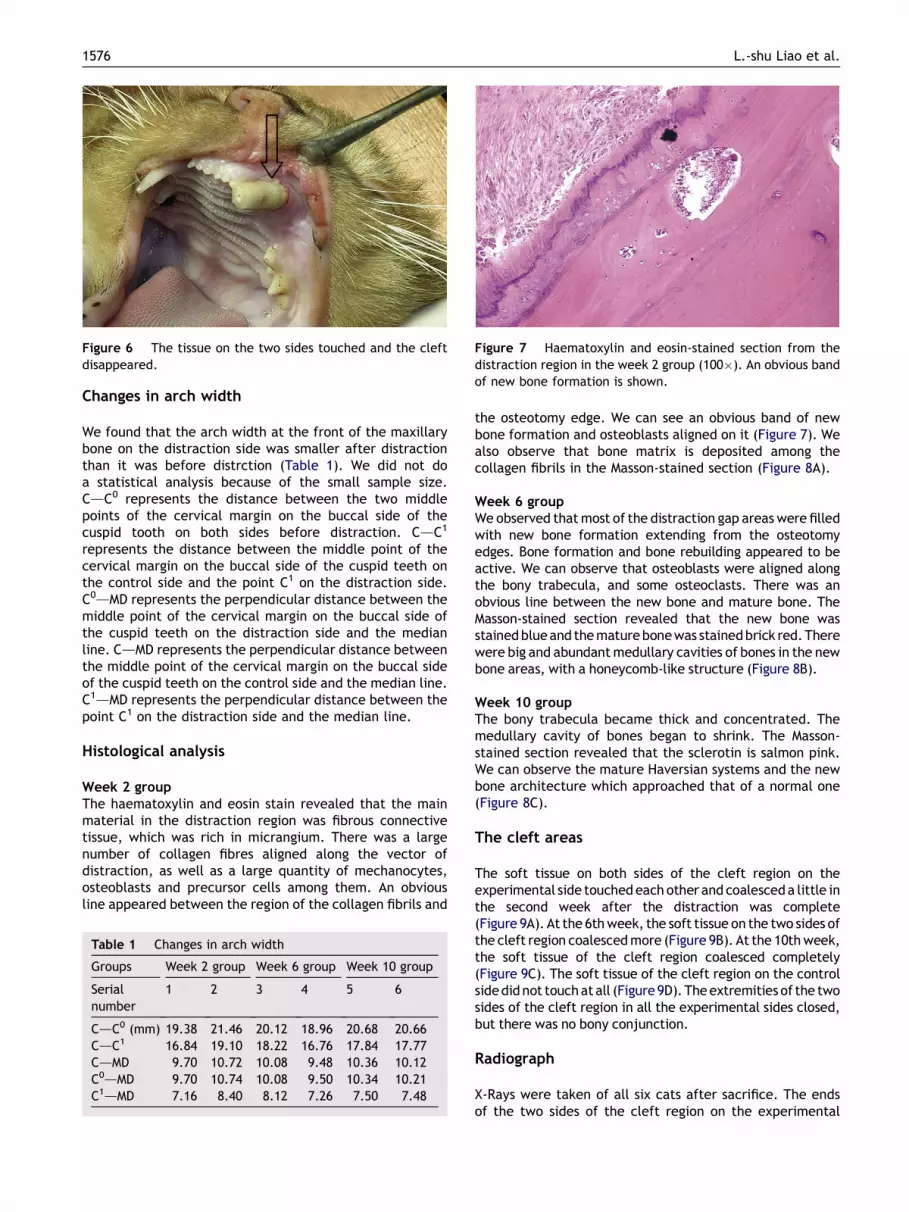
Figure 6 The tissue on the two sides touched and the cleftdisappeared.
Figure 7 Haematoxylin and eosin-stained section from thedistraction region in the week 2 group (100�). An obvious bandof new bone formation is shown.
1576 L.-shu Liao et al.
Changes in arch width
We found that the arch width at the front of the maxillarybone on the distraction side was smaller after distractionthan it was before distrction (Table 1). We did not doa statistical analysis because of the small sample size.CdC0 represents the distance between the two middlepoints of the cervical margin on the buccal side of thecuspid tooth on both sides before distraction. CdC1
represents the distance between the middle point of thecervical margin on the buccal side of the cuspid teeth onthe control side and the point C1 on the distraction side.C0dMD represents the perpendicular distance between themiddle point of the cervical margin on the buccal side ofthe cuspid teeth on the distraction side and the medianline. CdMD represents the perpendicular distance betweenthe middle point of the cervical margin on the buccal sideof the cuspid teeth on the control side and the median line.C1dMD represents the perpendicular distance between thepoint C1 on the distraction side and the median line.
Histological analysis
Week 2 groupThe haematoxylin and eosin stain revealed that the mainmaterial in the distraction region was fibrous connectivetissue, which was rich in micrangium. There was a largenumber of collagen fibres aligned along the vector ofdistraction, as well as a large quantity of mechanocytes,osteoblasts and precursor cells among them. An obviousline appeared between the region of the collagen fibrils and
Table 1 Changes in arch width
Groups Week 2 group Week 6 group Week 10 group
Serialnumber
1 2 3 4 5 6
CdC0 (mm) 19.38 21.46 20.12 18.96 20.68 20.66CdC1 16.84 19.10 18.22 16.76 17.84 17.77CdMD 9.70 10.72 10.08 9.48 10.36 10.12C0dMD 9.70 10.74 10.08 9.50 10.34 10.21C1dMD 7.16 8.40 8.12 7.26 7.50 7.48
the osteotomy edge. We can see an obvious band of newbone formation and osteoblasts aligned on it (Figure 7). Wealso observe that bone matrix is deposited among thecollagen fibrils in the Masson-stained section (Figure 8A).
Week 6 groupWe observed that most of the distraction gap areas were filledwith new bone formation extending from the osteotomyedges. Bone formation and bone rebuilding appeared to beactive. We can observe that osteoblasts were aligned alongthe bony trabecula, and some osteoclasts. There was anobvious line between the new bone and mature bone. TheMasson-stained section revealed that the new bone wasstained blueand the maturebonewas stainedbrick red.Therewere big and abundant medullary cavities of bones in the newbone areas, with a honeycomb-like structure (Figure 8B).
Week 10 groupThe bony trabecula became thick and concentrated. Themedullary cavity of bones began to shrink. The Masson-stained section revealed that the sclerotin is salmon pink.We can observe the mature Haversian systems and the newbone architecture which approached that of a normal one(Figure 8C).
The cleft areas
The soft tissue on both sides of the cleft region on theexperimental side touched each other and coalesceda little inthe second week after the distraction was complete(Figure 9A). At the 6th week, the soft tissue on the two sides ofthe cleft region coalesced more (Figure 9B). At the 10th week,the soft tissue of the cleft region coalesced completely(Figure 9C). The soft tissue of the cleft region on the controlsidedid not touchatall (Figure9D).Theextremities of the twosides of the cleft region in all the experimental sides closed,but there was no bony conjunction.
Radiograph
X-Rays were taken of all six cats after sacrifice. The endsof the two sides of the cleft region on the experimental
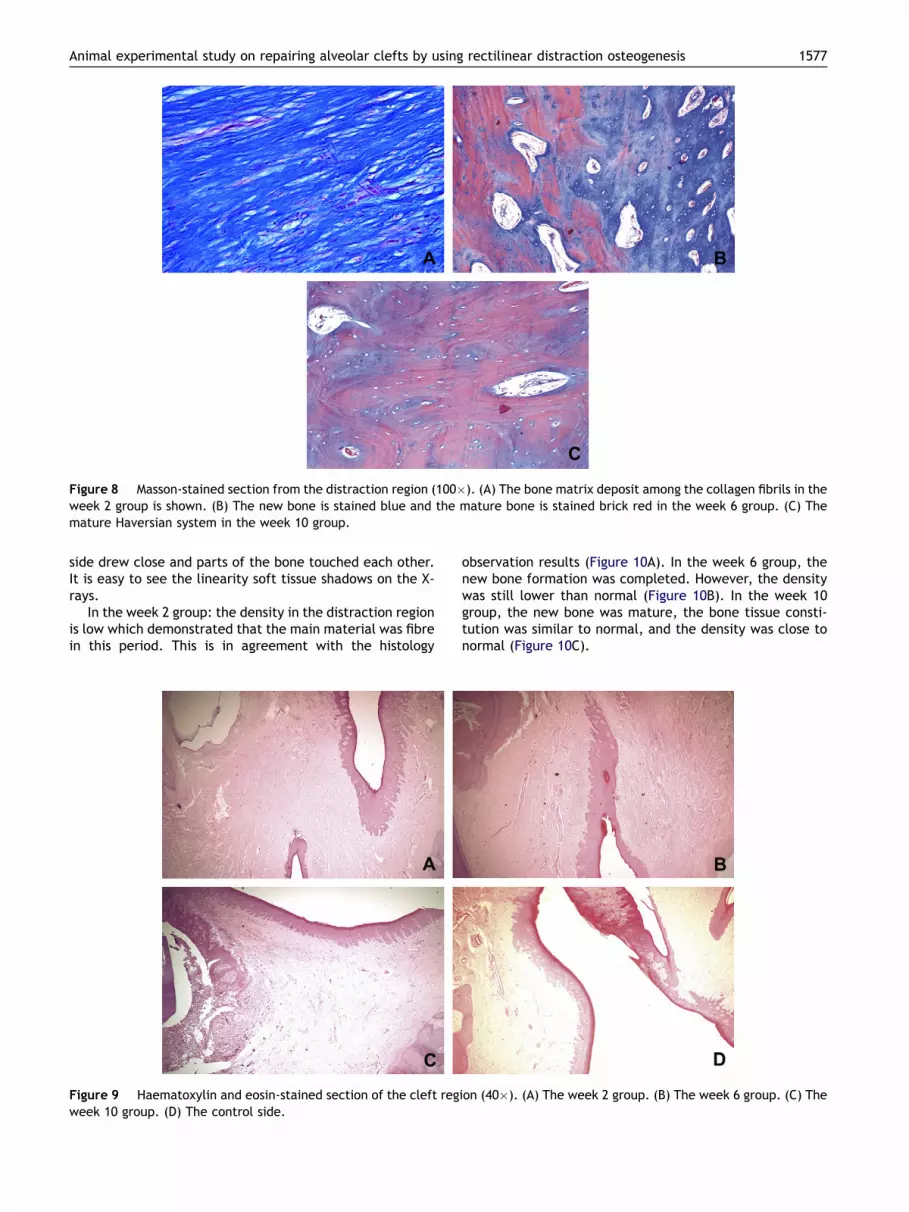
Figure 8 Masson-stained section from the distraction region (100�). (A) The bone matrix deposit among the collagen fibrils in theweek 2 group is shown. (B) The new bone is stained blue and the mature bone is stained brick red in the week 6 group. (C) Themature Haversian system in the week 10 group.
Animal experimental study on repairing alveolar clefts by using rectilinear distraction osteogenesis 1577
side drew close and parts of the bone touched each other.It is easy to see the linearity soft tissue shadows on the X-rays.
In the week 2 group: the density in the distraction regionis low which demonstrated that the main material was fibrein this period. This is in agreement with the histology
Figure 9 Haematoxylin and eosin-stained section of the cleft regweek 10 group. (D) The control side.
observation results (Figure 10A). In the week 6 group, thenew bone formation was completed. However, the densitywas still lower than normal (Figure 10B). In the week 10group, the new bone was mature, the bone tissue consti-tution was similar to normal, and the density was close tonormal (Figure 10C).
ion (40�). (A) The week 2 group. (B) The week 6 group. (C) The

Figure 10 X-Ray of the cleft and distraction region. (A) The week 2 group. (B) The week 6 group. (C) The week 10 group.
1578 L.-shu Liao et al.
Discussion
In the 1990s, Siegel and Mooney’s study showed that humanbeings are more similar to cats than primates and otheranimals in the type and growth patterns of craniofacialbone.8e10 Compared with the dog and goat, the cat’smaxillary bone is short and small, in addition the radian ofthe maxillary arch is similar to that of humans. There isa natural edentulous area in the front of the cat’s maxillarybone. It is just right for making the alveolar cleft. In thisstudy, we chose the adult cat whose growth and develop-ment have stopped, making it easier to observe the effectof bone formation by DO.
It is necessary to carefully monitor the size of the arti-ficially-created defect of the bony tissue, as some researchhas reported that any experimental bony defect must belong or wide enough to avoid spontaneous healing. Wecalled the critical defective bone mass CSD (critical sizedefect), which means that the bony defect cannot healspontaneously when the defect has formed and thedefective bone mass is greater than the CSD. In this study,the size of the defect created was 6 mm, the thickness ofthe cat’s alveolar process is about 3 mm. The membranamucosa and periosteum in the defective region wereexcised at the same time. We found that defects made inthis way cannot recover spontaneously.
Previously, we wanted to use the curved distractiondevice considering the morphology of the dental arch.However, the size and the morphology of the dental archare different in patients of different ages and with indi-vidual variation. A distraction device with individual vari-ation is needed. There are some reports on the use ofa three-dimensional distraction device, but this kind ofdevice is too big to use on the alveolar process. The
rectilinear distraction device used in this study is easy to fixon the alveolar process.
In this study, the arch width seemed to diminish afterdistraction. It is possible that the direction of distractionchanged to inward because of the pressure from the softtissue of the lip and buccal division. However, the width ofthe dental arch did not change once distraction wascomplete. This result indicates that the arch width didincrease by using rectilinear DO. Usually in pathologicalclefts there is often major distortion of the anterior archrelationships requiring alignment and restoration. Thus, weconsider whether we can correct the anterior arch rela-tionships with distraction. According to clinical observa-tions, we found that adult cleft lip and palate patients havejaw deformities of different degrees because of the surgeryto repair the cleft lip and palate. Most of them also need tohave orthognathic surgery to improve face type. Therefore,correcting the anterior arch relationships together withdistraction before alveolar process bone grafting will notonly make the distraction process more complex, but willalso aggravate the jaw deformity. In addition, doing theorthognathic surgery operation after growth and develop-ment arrest can be effective, and the need for feweroperations benefits patients.
After rectilinear distraction, the relationship betweenthe transfer disk and the mandibula has obviously changed.The major changes are the anteroposterior position and theexterior and interior positions. There are no obviouschanges in vertical direction because of the rectilineardistraction. We found an interesting phenomenon throughanimal experiments, which is that the anterior dental archdid not move along the rectilinear direction but did move ina curve along the dental arch. This suggested that recti-linear distraction can be used on the curved dental arch forDO. We measured the symmetry between transfer disk and

Animal experimental study on repairing alveolar clefts by using rectilinear distraction osteogenesis 1579
dental arch on the uninjured side in order to observethe movement of the transfer disk in a level direction. Theteeth on the transfer disk moved naturally following thealveolar process. Therefore the occlusal relationshipbetween upper and lower dentition changed. Through theobservation we found that only the cuspid on the transferdisk was slightly mesio-inclined without cinch. Most of thecleft lip and palate patients have severe malocclusion, andneed long-term orthodontic treatment. Therefore, even ifDO distorts occlusion, it can be rectified by later treatment.
The jaw bone is different from long bone in some aspects.Such as, embryo origin, the method of the blood supply andanatomic structure. The way that new bone is formed in DOis different. The histological observation suggested that themajor method is membrane bone formation. In the initialstage, the collagen fibrils were aligned along the vector ofdistraction in the distraction region. Then, osteoblastsdifferentiated among the collagen fibrils and bone matrixwas deposited. Finally, new bone gradually became maturebone during a period of remodelling.
According to the report, as long as vascular periosteumis present, osteogenesis is active11. So, we conjecturedthat there would be bone coalescing in the cleft regionafter distraction. It is interesting that radiographic andhistologic observations suggested the soft tissues in thetwo sides coalesced after the cleft closed, but we did notobserve bone coalescing in all cats. Mitsugi has alsoobserved this phenomenon.1 This phenomenon suggestedthat the alveolar cleft can be closed by DO. But there wasno complete bone closure. However, DO can diminish thesize of the bone defect of the cleft and make bonegrafting advisable. More research is needed to find outwhether the two extremities will coalesce throughkeeping the distraction device in place after distraction iscomplete.
This study demonstrated that transport distractionosteogenesis along the curve of the dental arch is ideal.Alveolar bone was transported in the planned directionusing a rectilinear distraction device. The morphology ofthe dental arch did not change much after distraction. Thismethod can be regarded as tissue engineering to expandbone tissue. It can be safely performed not only in patientsundergoing initial treatment for alveolar clefts but also inpatients in whom bone grafting has failed.
Some scholars have suggested that bone grafting afterDO, using new bone with high activity in the distraction
region, might be successful.1 In this study, we observed thatnewly formed bone in the distraction area appeared active;bone architecture resembled that of cancellated bone.Choosing the newly formed bone as the source of a bonegraft could be successful and avoid further operations.
Acknowledgements
The distraction devices were supplied by the State KeyLaboratory of Oral Disease, Sichuan University.
References
1. Mitsugi Masaharu, Ito Osamu, Alcalde Rafael E. Maxillary bonetransportation in alveolar cleftdtransport distraction osteo-genesis for treatment of alveolar cleft repair. Br J Plast Surg2005;58:619e25.
2. Swennen G, Schliephake H, Dempf R, et al. Craniofacialdistraction osteogenesis: a review of the literature: Part I:clinical studies. Int J Oral Maxillofac Surg 2001;30:89e103.
3. Annino Jr DJ, Goguen LA, Karmody CS. Distraction osteogenesisfor reconstruction of mandibular symphyseal defects. ArchOtolaryngol Head Neck Surg 1994;120:911e6.
4. Oda T, Sawaki Y, Ueda M. Alveolar ridge augmentation bydistraction osteogenesis using titanium implants: an experi-mental study. Int J Oral Maxillofac Surg 1999;28:151e6.
5. Oda T, Sawaki Y, Ueda M. Experimental alveolar ridgeaugmentation by distraction osteogenesis using a simple devicethat permits secondary implant placement. Int J Oral Max-illofac Implants 2000;15:95e102.
6. Gaggl A, Schultes G, Karcher H. Distraction implants: a newoperative technique for alveolar ridge augmentation. J Cra-niomaxillofac Surg 1999;27:214e21.
7. Gaggl A, Schultes G, Regauer S, et al. Healing process afteralveolar ridge distraction in sheep. Oral Surg Oral Med OralPathol Oral Radiol Endod 2000;90:420e9.
8. Siegel MI, Mooney MP. Appropriate animal models for cranio-facial biology. Cleft Palate J 1990;27:18e25.
9. Siegel MI, Mooney MP, Eichberg JW, et al. Septopremaxillaryligament resection and midfacial growth in a chimpanzeemodel. J Craniofac Surg 1990;1:182e6.
10. Losken A, Mooney MP, Siegel MI. A comparative study ofmandibular growth patterns in seven animal models. J OralMaxillofac Surg 1992;50:490e5.
11. Estrada JIC, Saulacic N, Vazquez L, et al. Periosteal distractionosteogenesis: preliminary experimental evaluation in rabbitsand dogs. Br J Oral Maxillofac Surg 2007;45:402e5.