anesthetic management of children with upper respiratory tract infections
TRANSCRIPT
Instructor’s Guide Title: Anesthetic Management of Children with Upper Respiratory Tract Infections Authors: Ahsan Qadeer, Nadine Odo, Yi Hua; Anesthesiology and Perioperative Medicine, Medical College of Georgia, Georgia Regents University Description: We developed this resource for anesthesia faculty to train third- and fourth-year anesthesiology residents before they begin their pediatric rotation as well as medical students enrolled in an anesthesiology clerkship. This presentation will help them to determine whether a child with a current or recent upper respiratory tract infection (URI) should undergo a surgical procedure based on the specifics of his/her illness, the type of procedure being performed, and preexisting conditions, and will also provide guidance on which anesthetic to use. Resource Files
1. Instructor’s Guide: Outlines the purpose of the slide presentation. 2. Slides: PowerPoint presentation will help anesthesia faculty and residents to
familiarize themselves with the current guidelines related to anesthesia in children with URI. The slides facilitate lecture preparation.
3. Evaluation Form: Attendees will complete the evaluation form soon after the lecture to provide their feedback which will guide changes to the presentation.
4. Pre- and Post-Tests and Answer Key: The pre-test will be given just before the lecture and the post-test within a week of the lecture and the before and after scores will be compared. Additional training can be provided to those who have not mastered the content, after which the post-test will be retaken.
When, How and Order in Which to Use Each Resource File
The instructor’s guide gives an overview of the slide presentation and is to be read before reviewing the slide presentation, which is to be used by an anesthesiologist to prepare his/her lecture. We suggest reading Tait and Malviya’s 2005 article in Pediatric Anesthesia for a good overview of the topic. The evaluation should be completed within a month of the presentation. The pre-test will be given before the presentation and the post-test within a week of the lecture. Purpose of the Resource
This resource will help anesthesiologists to 1) decide, based on evidence-based medicine, whether to allow a child with a URI to undergo a surgical procedure under anesthesia, and 2) plan the pre-, peri-, and postoperative anesthetic management of the patient. At the end of the presentation, the attendee should be able to describe:
URI signs, symptoms and etiology Risk factors for anesthesia-related complications Preoperative evaluation and determining whether to proceed with surgery Peri- and postoperative management

Conceptual Background
Pediatric anesthesiologists and surgeons often find themselves in a difficult situation when a child presents for a procedure with a current or recent upper respiratory infection. The practitioner needs to balance patient safety with other concerns (e.g., logistic) when considering whether to proceed or postpone the surgery. If a procedure is canceled, then it must be decided when it should be rescheduled. On the other hand, if the decision is to proceed, questions arise as to which anesthetics and intubation techniques should be used. The slides are based on a presentation that Dr. Ahsan Qadeer has used at Georgia Regents University to train anesthesiology residents and medical students. For this submission, we included a more thorough review of the literature using MEDLINE, slightly revised an algorithm by Dr. Tait (Slide 24) which we are using with his permission, and obtained permission to use an image by Dr. Chamberlain (Slide 10). Practical Implementation Advice
The presentation will take 30-60 minutes, depending on the experience of the students and time spent in the question-and-answer period. Hands-on simulation training with a high fidelity mannequin could be accomplished during the same session. We suggest that this training occurs within two weeks of residents beginning their pediatric anesthesia rotation to ensure retention of the information learned. An evaluation form for this specific lecture was created to gain feedback and improve the lecture for future audiences. Successful Implementation
We have used this presentation to train faculty, residents, and medical students. In recent One45 feedback, 93% of the attendees rated the presentation “good” or “excellent.” One attendee noted that the presentation helped him/her to be more comfortable with the decision to proceed with surgery for a child with a URI. We have developed a pre- and post-test will be used in the future. Limitations of Resource and Ideas to Improve/Expand It
The presentation gives an overview of upper respiratory tract infections in children, decision making tools to determine whether to proceed with surgery, and if so, which anesthetics and intubation techniques to use. One limitation of the presentation is that most of the discussion focuses on URI in otherwise healthy children. Discussion of precautions to be taken in children with comorbidities such as Down syndrome, sickle cell disease, or obesity would strengthen this presentation, and we are planning a retrospective review of various patient populations at our institution to strengthen this area of the presentation. We also welcome comments from MedEdPORTAL readers.
References
1. Cohen MM, Cameron CB. Should you cancel the operation when a child has an upper respiratory tract infection? Anesth Analg 1991;72:282-8.
2. De Soto H, Patel RI, Soliman IE, Hannallah RS. Changes in oxygen saturation following general anesthesia in children with upper respiratory infection signs and symptoms undergoing otolaryngological procedures. Anesthesiology 1988;68:276-9.
3. Elwood T, Morris W, Martin LD, Nespeca M-K, Wilson DA, Fleisher LA, Robotham JL, Nichols DG. Bronchodilator premedication does not decrease respiratory adverse events in pediatric general anesthesia. Can J Anaesth 2003;50:277-84.
4. Hackel A, Badgwell JM, Binding RR, Dahm LS, Dunbar BS, Fischer CG, Geiduschek JM, Gunter JB, Gutierrez-Mazzora JF, Kain Z, Liu L, Means L, Myer P, Morray JP, Polaner DM, Striker TW. Guidelines for the pediatric anesthesia environment. American Academy of Pediatrics. Section on Anesthesiology. Pediatrics 1999;103(2):512-5.
5. Litman RS (2004). Pediatric anesthesia: The requisites in anesthesia. St. Louis: Elsevier Mosby.
6. Malviya S, Voepel-Lewis T, Stewart M, pandit UA, Riegger LQ, Tait AR. Risk factors for adverse postoperative outcomes in children presenting for cardiac surgery with upper respiratory tract infections. Anesthesiology 2003;98:628-32.
7. McGill WA, Coveler LA, Epstein BS. Subacute upper respiratory infection in small children. Anesth Analg 1979;58:331-3.
8. Minambres E, Buron J, Ballesteros MA, Llorca J, Munoz P, Gonzales-Castro A. Tracheal rupture after endotracheal intubation: a literature systematic review. Eur J Cardiothorac Surg 2009;35(6):1056-62.
9. Parnis SJ, Barker DS, Van Der Walt JH. Clinical predictors of anaesthetic complications in children with respiratory tract infections. Paediatr Anaesth 2001;11:29-40.
10. Silvanus M-T, Groeben H, Peters J. Corticosteroids and inhaled salbutamol in patients with reversible airway obstruction markedly decrease the incidence of bronchospasm after tracheal intubation. Anesthesiology 2004;100:1052-7.
11. Tait AR, Burke C, Voepel-Lewis T, Chiravuri D, Wagner D, Malviya S. Glycopyrrolate does not reduce the incidence of perioperative adverse events in children with upper respiratory tract infections. Anesth Analg 2007:104:265-70.
12. Tait AR, Malviya S. Anesthesia for the child with an upper respiratory tract infection: still a dilemma? Anesth Analg 2005;100(1):59-65.
13. Tait AR, Malviya S, Voepel-Lewis T, Munro HM, Stewert M, Pandit UA. Risk factors for perioperative adverse respiratory events in children with upper respiratory tract infections. Anesthesiology 2001;95:299-306.
14. Tait AR, Reynolds PI, Gutstein HB. Factors that influence an anesthesiologist’s decision to cancel elective surgery for the child with an upper respiratory tract infection. J Clin Anesth 1995;7:491-9.
15. Tait AR, Pandit UA, Voepel-Lewis T, Munro HM, Malviya S. Use of the laryngeal mask airway in children with upper respiratory tract infections: a comparison with endotracheal infection. Anesth Analg 1998;86:706-11.
16. Tait AR, Voepel-Lewis T, Munro HM, Gutstein HB, Reynolds PI. Cancellation of pediatric outpatient surgery: Economic and emotional implications for patients and their families. J Clin Anesth 1997;9:213-9.
17. von Ungern-Sternberg BS, Boda K, Schwab C, Sims C, Johnson C, Habre W. Laryngeal mask airway is associated with an increased incidence of adverse respiratory events in children with recent upper respiratory tract infections. Anesthesiology 2007;107(5):714-9.
Anesthetic Management of Children with Upper Respiratory Tract Infections
Ahsan Qadeer, MD, Nadine Odo, CCRC, and Yi Hua, MDDepartment of Anesthesiology and Perioperative MedicineMedical College of Georgia, Georgia Regents University, Augusta, Georgia
May 2013
Educational ObjectivesAfter this presentation, participants will be able to describe:
URI signs, symptoms and etiology Risk factors for anesthesia-related
complicationsPreoperative evaluationPeri- and postoperative management
OutlineURI signs, symptoms and etiology Risk factors for anesthesia-related
complications Literature reviewPreoperative evaluationPeri- and postoperative management Take-away points
Abbreviations ETT = Endotracheal tube Hx = History LMA = Laryngeal mask airway PONV = Postoperative nausea and
vomiting RSV = Respiratory syncytial virus URI = Upper respiratory tract infection
Children with URI Belief was that URIs increase risk of
perioperative respiratory complications (McGill case series was main impetus)
Were surgeries under anesthesia canceled unnecessarily? (Possibly)
Signs, Symptoms and Etiology

Signs and Symptoms Mild sore throat Mild malaise Sneezing Rhinorrhea Nasal congestion or stuffiness Non-productive cough Low-grade fever (< 101°F/38.3°C)
Rhinovirus (30–40%) Adenovirus Coronavirus Parainfluenza Respiratory syncytial virus
Etiology
URI Facts Children have 6-8 URIs/year 40% present for anesthesia with recent URI Some have noninfectious URI-like symptoms 95% of URIs are viral, most are self-limiting Airway hyperreactivity may last several
weeks after the infection Pulmonary function abnormalities possible
Tait AR, Malviya S. Anesth Analg 2005;100(1):59-65; von Ungern-Sternberg. Anesthesiology 2007;107:714-9.
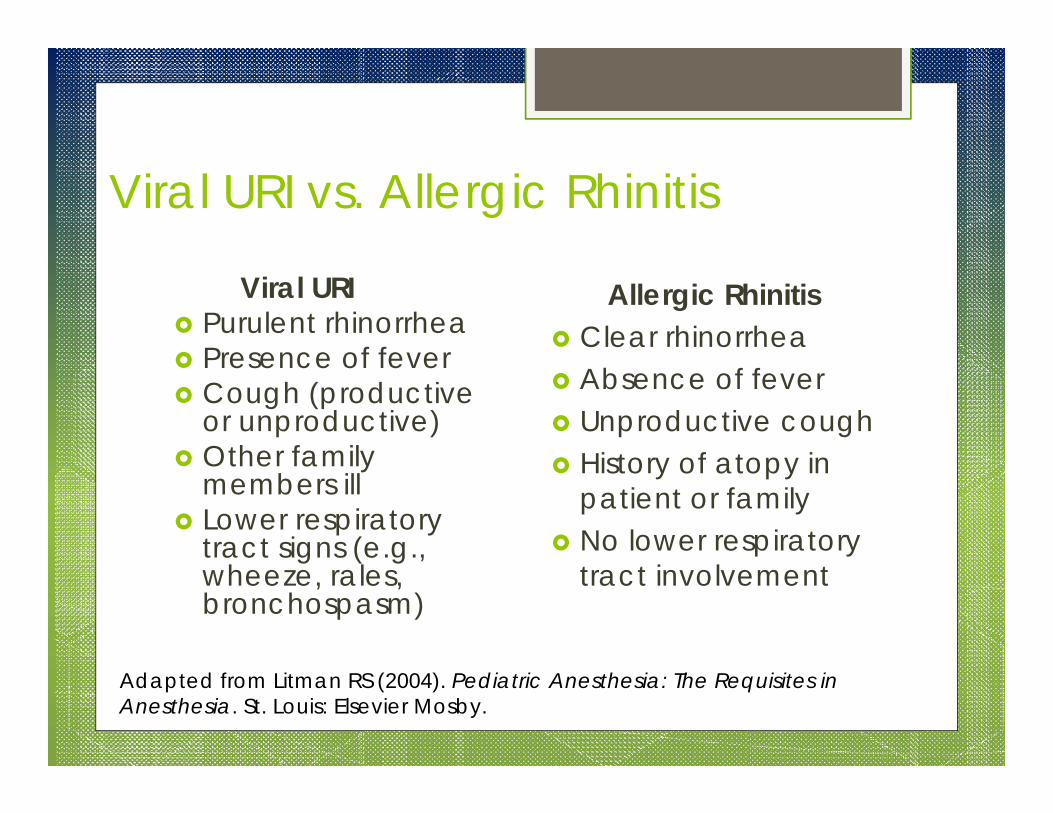
Viral URI vs. Allergic Rhinitis
Viral URI Purulent rhinorrhea Presence of fever Cough (productive
or unproductive) Other family
members ill Lower respiratory
tract signs (e.g., wheeze, rales, bronchospasm)
Allergic Rhinitis Clear rhinorrhea Absence of fever Unproductive cough History of atopy in
patient or family No lower respiratory
tract involvement
Adapted from Litman RS (2004). Pediatric Anesthesia: The Requisites in Anesthesia. St. Louis: Elsevier Mosby.
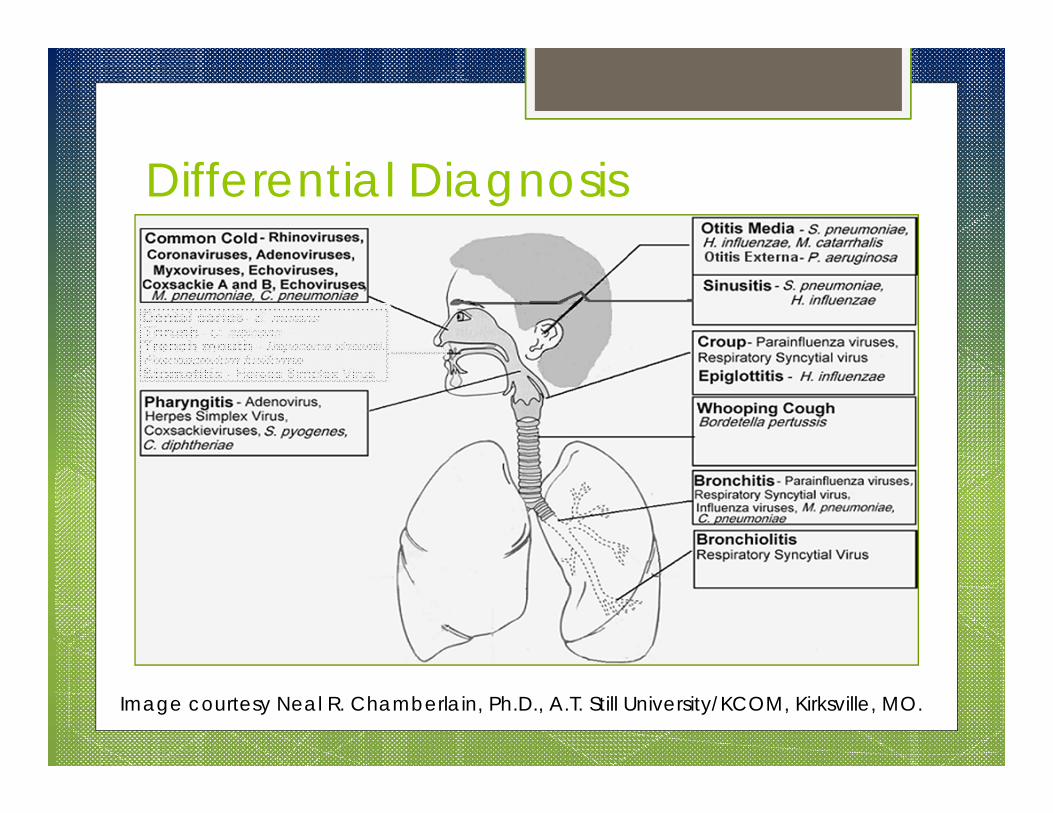
Differential Diagnosis
Image courtesy Neal R. Chamberlain, Ph.D., A.T. Still University/KCOM, Kirksville, MO.
Differential Diagnosis
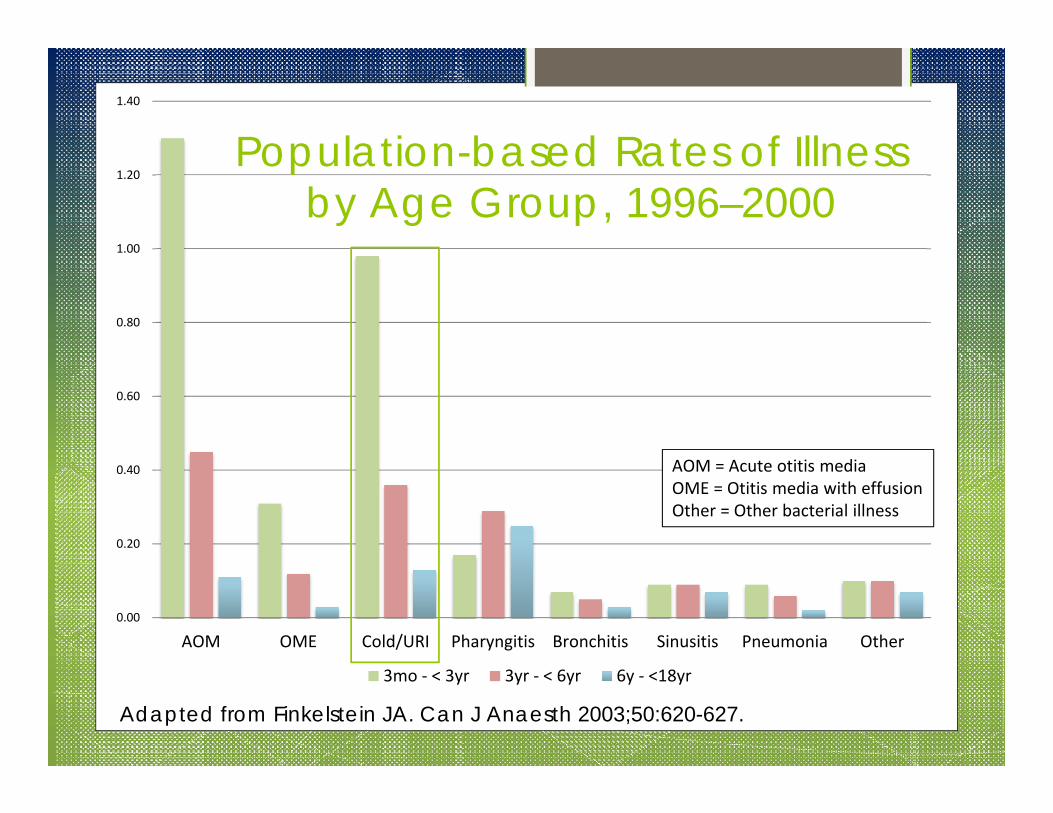
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
AOM OME Cold/URI Pharyngitis Bronchitis Sinusitis Pneumonia Other
3mo ‐ < 3yr 3yr ‐ < 6yr 6y ‐ <18yr
Adapted from Finkelstein JA. Can J Anaesth 2003;50:620-627.
AOM = Acute otitis mediaOME = Otitis media with effusionOther = Other bacterial illness
Population-based Rates of Illness by Age Group, 1996–2000

Airway Hyperreactivity Viral invasion may make airways sensitive
to secretions, irritant anesthetic gases Chemical mediators, neurologic reflexes
may play a role in bronchoconstriction Effects can persist 6 weeks after URI
Tait AR, Malviya S. Anesth Analg 2005;100(1):59-65.
Pulmonary Function Abnormalities Decrease forced vital capacity Decrease forced expiratory volume in 1
sec (FEV1) Decrease diffusion capacity

Literature Review
McGill Case Series Primary impetus for canceling surgery for
children with URI (all McGill patients were intubated for the procedure)
Suggested that practitioners: Seek URI symptom history over past month Obtain chest x-ray if unsure URI has resolved Postpone surgery if x-ray is positive
McGill WA. Anesth Analg 1979;58:331-3.
Surveys Pediatric anesthesiologists – wide range of
opinions/approaches How often cancel elective cases because of URI
“Never” (1%), “seldom” (34%), “occasionally” (25%), “frequently/usually” (37%), “always” (3%)
Those in practice >10 years more likely to cancel than those in practice <10 years (changing attitudes)
Tait AR. J Clin Anesth 1995;7:491-9.
Surveys Parents whose children’s elective surgeries
were canceled 35% of surgeries canceled because of URI 42% were canceled on day of surgery
Some parents missed work Ave. distance traveled: 159 miles roundtrip
Cancelling surgeries can be emotional and economic burden
Tait AR. J Clin Anesth 1997;9:213-219.
Registry/Chart Review What is added risk of child with URI?
Respiratory adverse events 2–7x more likelyin children with URI than without URI
For 5% with URI who were intubated, respiratory event risk increased 11-fold
Even without URI, respiratory events 5more likely when intubated than not intubated
Cohen MM, Cameron CB. Anesth Analg 1991;72:282-28.
Registry/Chart Review Respiratory or temperature regulation
problems 4 more likely perioperativelywith URI vs. without URI
Vomiting in recovery and postoperatively less likely with URI vs. without URI
Cohen MM, Cameron CB. Anesth Analg 1991;72:282-8.

Registry/Chart Review Risks related to age of child
1–5 year olds more likely to have URI vs. other age groups
Laryngospasm, coughing, O2 desaturation higher in young children with recent URI
As child ages, respiratory complication risk decreases
Cohen MM, Cameron CB. Anesth Analg 1991;72:282-8; von Ungern-Sternberg. Anesthesiology 2007;107:714-9.
Prospective Studies Facemask – perioperative complications
similar among children with or without URI LMA – complications similar with or
without URI
Tait AR. Anesthesiology 1987;67:930-5; von Ungern-Sternberg. Anesthesiology 2007;107:714-9.
Prospective Studies With intubation
More mild hypoxemia with URI vs. without URI
More major desaturation events (SpO2<90%) and total respiratory complications with ETT vs. LMA
Postop complications similar between groups
DeSoto H. Anesthesiology 1988;68:276-9; Tait AR. Anesth Analg 1998;86:706-11.
Review Paper No need to postpone surgery in children
with URI who are otherwise healthy Base final decision on risk-benefit ratio
Tait AR. Anesth Analg 2005;100:59-65.
Cardiac Surgery Children scheduled for cardiac surgery
(with URI vs. without URI) More respiratory and multiple postop
complications More bacterial infections Longer ICU stays BUT – no difference in overall postop
complications or overall hospital stay
Malviya S. Anesthesiology 2003;98:628-2.
Parnis and Tait Studies Two large-scale studies found minimal
morbidity related to URI and described risk factors for adverse events
Parnis SJ. Paediatr Anaesth 2001;11:29-40; Tait AR. Anesthesiology 2001;95:299-306.
Risk Factors – Patient History of asthma History of prematurity Child’s snoring (airway obstruction) Passive smoking (laryngospasm) Parent’s belief that child has a cold Moist or productive cough, nasal
congestion
Parnis SJ. Paediatr Anaesth 2001;11:29-40 ; Tait AR. Anesthesiology 2001;95:299-306.

Risk Factors – Surgery Surgery of airway Airway management (intubation vs.
facemask) Induction agent (thiopental vs. propofol) Anticholinergic
Parnis SJ. Paediatr Anaesth 2001;11:29-40; Tait AR. Anesthesiology 2001;95:299-306.
Preoperative Evaluation
History and Physical Ask about fever, productive cough, nasal
congestion, lethargy, allergies Ask parent if he/she thinks child has a cold Auscultate for crackles, rhonchi,
wheezing; check temperature Labs not cost effective
Continued next slide
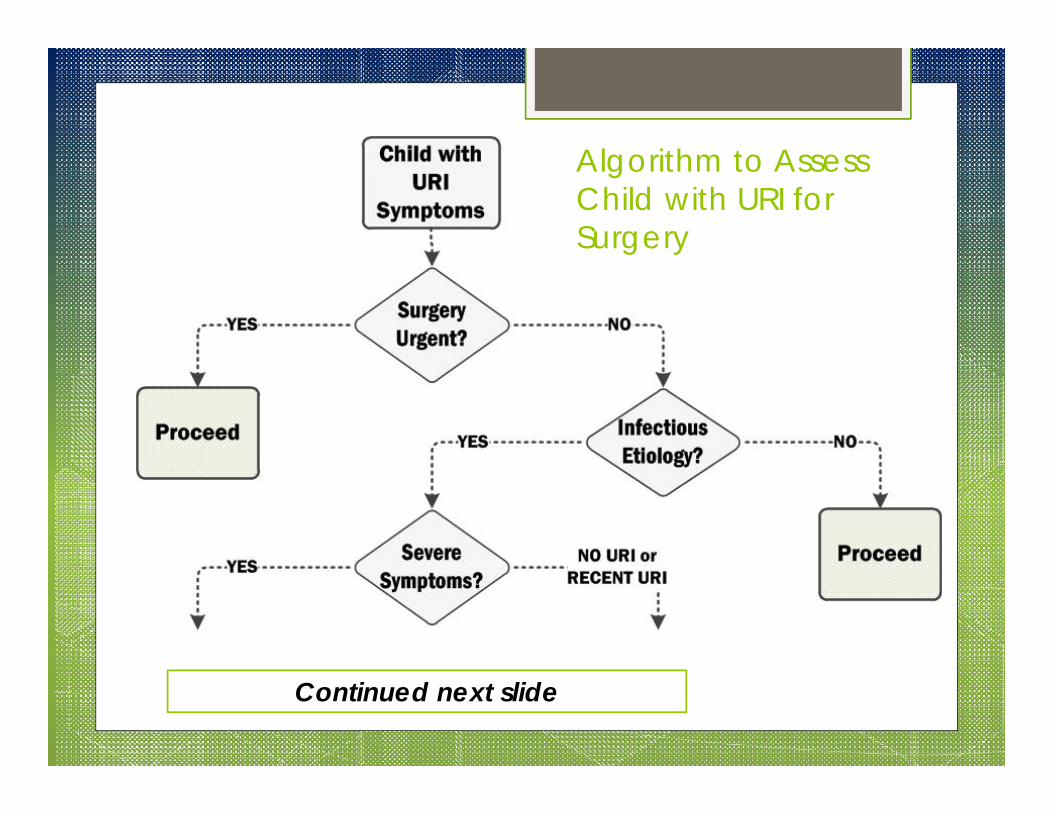
Algorithm to Assess Child with URI for Surgery
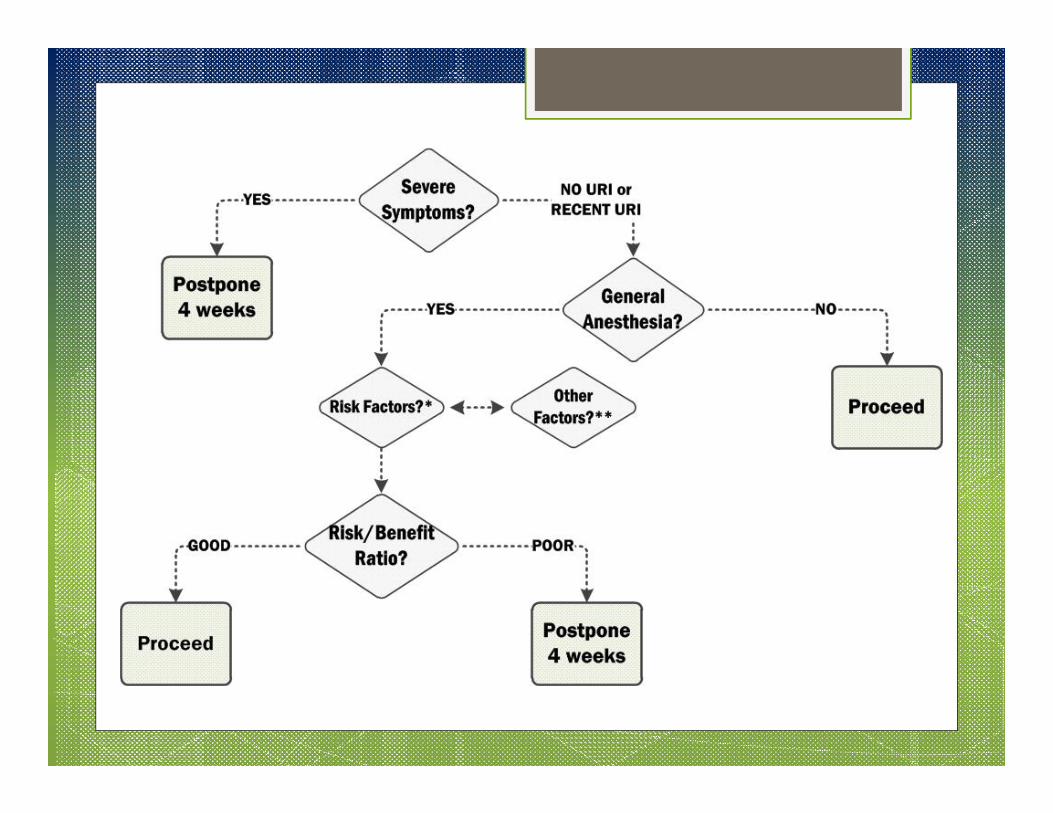
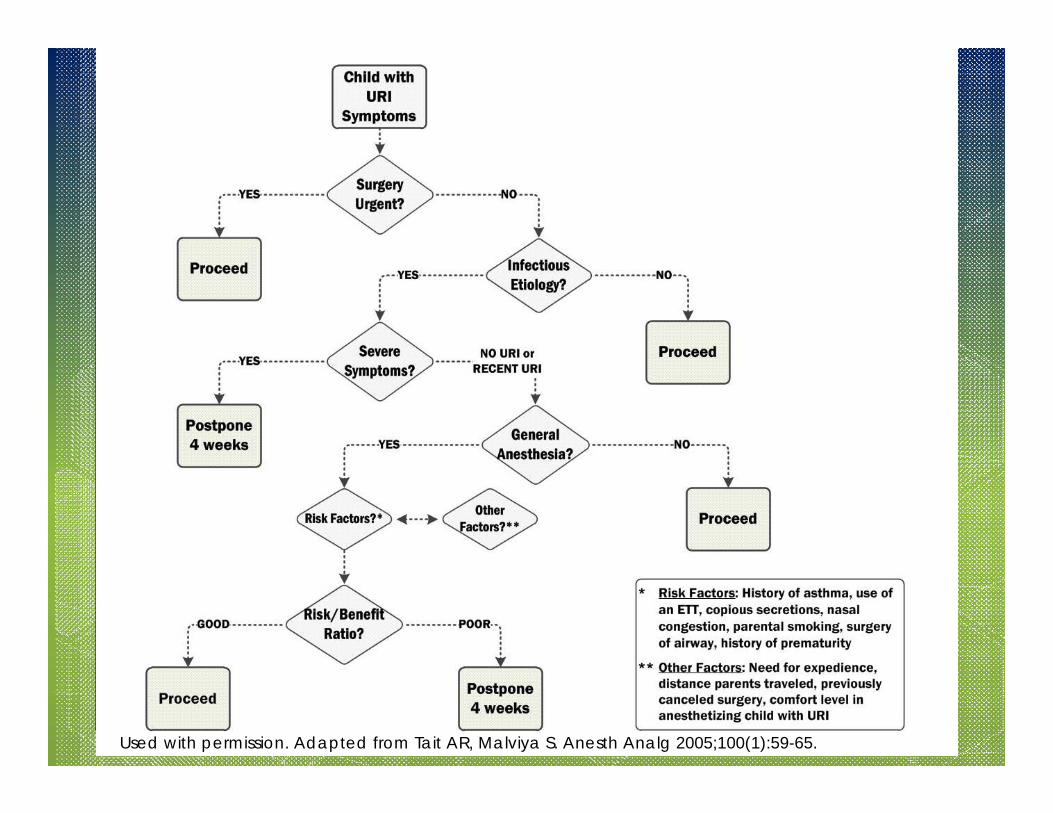
Used with permission. Adapted from Tait AR, Malviya S. Anesth Analg 2005;100(1):59-65.
Proceed or Cancel? Proceed if
Emergent/urgent surgery Mild URI (e.g., afebrile, clear secretions) Decision is more difficult if child has only a
few symptoms
Tait AR. Anesth Analg 2005;100:59-65.
Proceed or Cancel? Cancel if
Mucopurulent secretions Croupy cough Temperature >101°F/38.3°C Malaise Evidence of lower respiratory tract infection Suspected bacterial infection
Tait AR. Anesth Analg 2005;100:59-65.
Proceed or Cancel? Postponing surgery – avoids potential
complications, but emotional and economic burdens on parent/child
May not be practical in today’s health care environment
Tait AR. Anesth Analg 2005;100:59-65.
Deciding Case by Case Urgency of the surgery Child’s symptoms and age Risk factors, potential complications Comorbidities (e.g., asthma) URI frequency Type of surgery Difficulty in rescheduling surgery Emotional/economic burdens on parent Anesthesiologist’s comfort/experience
Reschedule When? No consensus Respiratory complications highest 3 days
after a URI, remain elevated for 6 weeks Uncomplicated nasopharyngitis – wait 1-2
weeks Severe symptoms – wait 4 weeks
Tait AR. J Clin Anesth 1995;7:491-9; Tait AR. Anesthesiology 2001;95:299-306.
Reschedule When? 4 weeks should be sufficient because
Airway hyperreactivity lasts 6 weeks Most patients present with 1-2 week-old
illness
What Do We Recommend for Children with URI? Children <1 year old – pediatric anesthesiologist Children 1-5 years old – weigh risks/benefits of
the procedure on an individual basis. Higher respiratory complication risk even without respiratory illness
Children >5 years old – lower rates of respiratory complications (risk decreases with age, possibly because of larger airways)
Hackel A. Pediatrics 1999;103(2):512-5; Cohen MM, Cameron CB. Anesth Analg1991;72:282-8.
Peri- and Postoperative Evaluation
Perioperative Management Minimize secretions Avoid stimulating a potentially sensitive
airway
Airway Management ETT – avoid
Increases airway complications If ETT is used, suction to remove excess
secretions LMA
Appears not to stimulate larynx Fewer major desaturations, respiratory
complications vs. ETT Face mask
Lowest incidence of complications May not be appropriate for all cases.
Tait AR. Anesth Analg 1998;86:706-11; Tait AR. Anesthesiology 2001;95:299-306.
Induction & Maintenance Avoid respiratory complications – deep
plane of anesthesia before intubation Propofol – probably safest for induction
(then sevoflurane, halothane, thiopental) Sevoflurane – better than halothane for
both induction and maintenance
Parnis SJ. Paediatr Anaesth 2001;11:29-40.
Perioperative Management Consider
IV hydration Facemask or LMA vs. ETT Deep plane of anesthesia before intubation Continuous monitoring (pulse oximetry, etc.) Bronchodilators? Humidification? Anticholinergics?
Perioperative Management IV Hydration – unless procedure is very
short Humidification
May help to minimize drying of secretions May maintain adequate ciliary clearance
mechanism Controlled trials data do NOT support its use
Tait AR. J Clin Anesth 1995;7:491-9.
Perioperative Management Anticholinergics
Residual neuromuscular block may have subtle effect on outcome
Reversing muscle relaxants – fewer adverse events
Glycopyrrolate does NOT reduce respiratory events, but does decrease PONV
Parnis SJ. Paediatr Anaesth 2001;11:29-40; Tait AR. Anesth Analg 2007:104:265-70.

Bronchodilator Premedication May reduce autonomically mediated
airway complications No effect on URI-related respiratory
complications (pediatric study) In adults with bronchial hyperreactivity,
corticosteroids plus salbutamol better than salbutamol alone
Elwood T. Can J Anaesth 2003;50:277-4; Silvanus M-T. Anesthesiology 2004;100:1052-7.
Extubation Depth of anesthesia (awake vs. deep)
when ETT/LMA was removed did not affect respiratory events
LMA and ETT – those with URI had worse respiratory complications vs. without URI
Removal of ETT in children with active URI – more breath holding, severe cough, major oxygen desaturation
Tait AR. Anesthesiology 2001;95:299-306.
Postoperative Management Postoperative complications
Laryngospasm (muscle relaxant) Hypoxia Stridor Post-extubation croup Apnea
Monitor continuously by pulse oximetry
Take-away Points Most children with mild or recent URI can
undergo surgery under anesthesia with proper management
Otherwise, postpone surgery 4 weeks Less airway irritation is better – LMA or
facemask rather than ETT Propofol and sevoflurane for induction
ANESTHESIOLOGY AND PERIOPERATIVE MEDICINE Version date 05.31.2013
Evaluation Form
Objectives: At the end of this activity, the participant should be able to describe the basic disease mechanisms and clinical implications relevant to anesthesiology; incorporate the new information in an evidence-based medical practice; enhance patient care, outcomes, and satisfaction; and improve the management of hospital resources in the perioperative setting.
Indicate agreement with each statement using this scale: 1=Definitely disagree, 2=Disagree, 3=Neither agree nor disagree, 4=Agree, 5=Definitely agree
Item 1 2 3 4 5 Overall content of the presentation was comprehensive Presentation was educational Presentation will change the way I care for my patients Presentation style was conducive to my learning
Answer each statement using this scale: 1=Very low, 2=Low, 3=Neither low nor high, 4=High, 5=Very high
Item 1 2 3 4 5 My level of understanding/mastery of the material before the activity My level of understanding/mastery of the material after the activity
How do you plan to use the information gained from this presentation in your practice?
May we contact you for a post-activity evaluation to determine educational effectiveness?
Yes No
Version date 06.19.2013 Page 1
PRE-Test for “Anesthetic Management of Children with Upper Respiratory Tract Infections”
Check the box beside the best answer for each question.
1. Which of the following signs and symptoms are most often associated with upper respiratory infection (URI)?
A. Sneezing, rhinorrhea, high fever
B. Productive cough, mild rash, mild sore throat
C. Mild malaise, rhinorrhea, non-productive cough
D. Nasal congestion, mild fever, wheezing
2. Which statement about URIs is TRUE?
A. A majority of URIs in children are of bacterial origin.
B. Airway hyperreactivity can persist for 6 weeks after the URI began.
C. Most viral URIs require medical intervention.
D. On average, children experience 12-15 URIs per year.
3. Which age group is most often diagnosed with URIs?
A. 4 months to less than 4 years old
B. 4 years old to less than 8 years old
C. 8 years old to less than 12 years old
D. 12 years old to less than18 years old
4. Which of the following risk factors are associated with adverse events in patients with URI?
A. Child’s history of asthma, parental smoking, parent’s belief that child has a cold
B. Child’s snoring, history of bedwetting, administration of an anticholinesterase
C. Nasal congestion, nearsightedness, surgery of airway
D. Parental alcohol use, history of prematurity, presence of copious secretions
5. Which statement about postponing surgical procedures because of a URI is FALSE?
A. Postpone for 1-2 weeks if a child has uncomplicated nasopharyngitis
B. Postpone for 4 weeks if a child has a severe URI symptoms
C. Postpone for 4 weeks if general anesthesia will be used and the practitioner determines that the risks of surgery under anesthesia outweigh the benefits
D. Postpone for 8 weeks if a child has severe URI symptoms
Version date 06.19.2013 Page 2
6. Under which circumstances should a physician proceed with surgery in child with URI?
A. Croupy cough and/or mucopurulent secretions
B. Emergent or urgent surgery or mild URI symptoms
C. Suspected bacterial infection
D. Temperature greater than 101°F/38.3°C
7. Which of the following practices is most appropriate during the perioperative period?
A. Use of facemask or laryngeal mask airway
B. Continuous monitoring by pulse oximetry
C. Intravenous hydration unless the procedure is short
D. All of the above
8. Which of the following statements regarding intubation and induction of anesthesia is FALSE?
A. A deep plane of anesthesia should be attained before intubation to avoid respiratory complications.
B. Halothane results in fewer complications than propofol when used for induction.
C. Propofol results in fewer complications than thiopental when used for induction.
D. Sevoflurane results in fewer complications than halothane, particularly when used for both induction and maintenance.
9. A child who has recovered or who is recovering from a URI is at increased risk for developing which of the following complications postoperatively?
A. Apnea
B. Croup
C. Laryngospasm
D. All of the above
10. Which statement about airway management of children with URI is WRONG?
A. Among children who are NOT intubated, those with URI are more likely to have respiratory events than those without URI.
B. Among children who are intubated, those with URI are more likely to have respiratory events than those without URI.
C. Laryngeal mask airway is associated with more respiratory complications than endotracheal tube intubation.
D. Suction should be used to remove excess secretions.
Version date 06.19.2013 Page 3
POST-Test for “Anesthetic Management of Children with Upper Respiratory Tract Infections”
Check the box beside the best answer for each question.
1. Which age group is most often diagnosed with URIs?
A. 4 months to less than 4 years old
B. 4 years old to less than 8 years old
C. 8 years old to less than 12 years old
D. 12 years old to less than18 years old
2. Which of the following risk factors are associated with adverse events in patients with URI?
A. Child’s history of asthma, parental smoking, parent’s belief that child has a cold
B. Child’s snoring, history of bedwetting, administration of an anticholinesterase
C. Nasal congestion, nearsightedness, surgery of airway
D. Parental alcohol use, history of prematurity, presence of copious secretions
3. Which of the following signs and symptoms are most often associated with upper respiratory infection (URI)?
A. Sneezing, rhinorrhea, high fever
B. Productive cough, mild rash, mild sore throat
C. Mild malaise, rhinorrhea, non-productive cough
D. Nasal congestion, mild fever, wheezing
4. Which statement about URIs is TRUE?
A. A majority of URIs in children are of bacterial origin.
B. Airway hyperreactivity can persist for 6 weeks after the URI began.
C. Most viral URIs require medical intervention.
D. On average, children experience 12-15 URIs per year.
5. Under which circumstances should a physician proceed with surgery in child with URI?
A. Croupy cough and/or mucopurulent secretions
B. Emergent or urgent surgery or mild URI symptoms
C. Suspected bacterial infection
D. Temperature greater than 101°F/38.3°C
Version date 06.19.2013 Page 4
6. Which of the following practices is most appropriate during the perioperative period?
A. Use of facemask or laryngeal mask airway
B. Continuous monitoring by pulse oximetry
C. Intravenous hydration unless the procedure is short
D. All of the above
7. Which of the following statements regarding intubation and induction of anesthesia is FALSE?
A. A deep plane of anesthesia should be attained before intubation to avoid respiratory complications.
B. Halothane results in fewer complications than propofol when used for induction.
C. Propofol results in fewer complications than thiopental when used for induction.
D. Sevoflurane results in fewer complications than halothane, particularly when used for both induction and maintenance.
8. Which statement about airway management of children with URI is WRONG?
A. Among children who are NOT intubated, those with URI are more likely to have respiratory events than those without URI.
B. Among children who are intubated, those with URI are more likely to have respiratory events than those without URI.
C. Laryngeal mask airway is associated with more respiratory complications than endotracheal tube intubation.
D. Suction should be used to remove excess secretions.
9. Which statement about postponing surgical procedures because of a URI is FALSE?
A. Postpone for 1-2 weeks if a child has uncomplicated nasopharyngitis
B. Postpone for 4 weeks if a child has a severe URI symptoms
C. Postpone for 4 weeks if general anesthesia will be used and the practitioner determines that the risks of surgery under anesthesia outweigh the benefits
D. Postpone for 8 weeks if a child has severe URI symptoms
10. A child who has recovered or who is recovering from a URI is at increased risk for developing which of the following complications postoperatively?
A. Apnea
B. Croup
C. Laryngospasm
D. All of the above
Version date 06.19.2013 Page 5
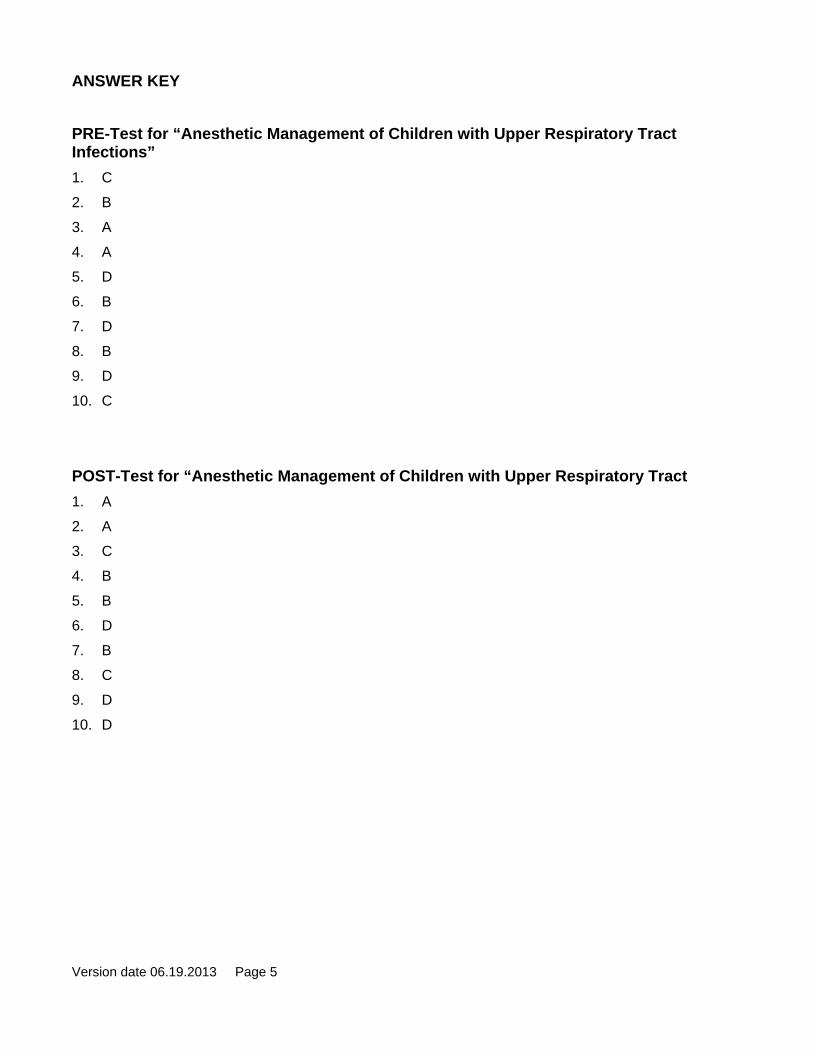
ANSWER KEY
PRE-Test for “Anesthetic Management of Children with Upper Respiratory Tract Infections”
1. C
2. B
3. A
4. A
5. D
6. B
7. D
8. B
9. D
10. C
POST-Test for “Anesthetic Management of Children with Upper Respiratory Tract
1. A
2. A
3. C
4. B
5. B
6. D
7. B
8. C
9. D
10. D