anatomic relationships between disc hemorrhage and parapapillary atrophy
TRANSCRIPT

●
ot●
●
opTboTBvo●
wiat�gFgCtdo●
go7
Glio
A
IRYMJC
1
0d
Anatomic Relationships between Disc Hemorrhage andParapapillary Atrophy
NATHAN M. RADCLIFFE, JEFFREY M. LIEBMANN, ILYA ROZENBAUM, ZAHER SBEITY,
SHLOMIT F. SANDLER, CELSO TELLO, AND ROBERT RITCHlnp
awo((atstatprwhfada
tzdia�avtmogm
ieofirln
PURPOSE: Parapapillary atrophy (PPA) and disc hem-rrhage (DH) are associated with glaucoma. We soughto determine whether they are anatomically related.
DESIGN: Retrospective study.METHODS: All digital optic nerve stereophotographs
btained over a one-year period were screened for theresence of DH. Only patients with DH were included.he location of the greatest � zone PPA width as definedy the radial distance between the scleral rim and theuter border of the � zone was compared in each patient.he clock hour location of the DH was determined.aseline central corneal thickness, intraocular pressure,ertical cup-to-disc ratio, and visual field indices werebtained.RESULTS: Photographs from 1,559 glaucoma patientsere evaluated and 46 eyes with unilateral DH were
dentified; 42 (91.3%) had � zone PPA and 38 eyes hadsymmetric PPA width. DH occurred more frequently inhe eye with the greater PPA width (29/38 eyes [76.3%];
� 0.611; P < .001). The DH fell on the point ofreatest PPA width in 10 (23.9%) of 42 eyes (P < .05,isher exact test) and within two clock hours of thereatest PPA width in 31 (73.8%) of 42 eyes (P < .001,hi-square test). Logistic regression analysis determined
hat greater PPA width (odds ratio, 17.16; 95% confi-ence interval, 5.34 to 55.12; P < .001) was the onlycular characteristic to predict the laterality of the DH.CONCLUSIONS: DHs tend to occur in the eye with the
reatest PPA width and usually are found within the regionf its greatest width. (Am J Ophthalmol 2008;146:35–740. © 2008 by Elsevier Inc. All rights reserved.)
LAUCOMATOUS OPTIC NEUROPATHY MAY BE DE-
tected by stereoscopic examination of the opticnerve at the slit-lamp with a hand-held indirect
ens, by optic nerve photography, or by computerizedmaging technologies. Clinical features of glaucomatousptic neuropathy include atrophy of the retinal nerve fiber
ccepted for publication Jun 17, 2008.From the Einhorn Clinical Research Center, New York Eye and Ear
nfirmary, New York, New York (N.M.R., J.M.L., I.R., Z.S., S.F.S., C.T.,.R.); the Department of Ophthalmology, New York University, Nework, New York (N.M.R., J.M.L.); the Department of Ophthalmology,anhattan Eye, Ear and Throat Hospital, New York, New York (N.M.R.,
.M.L.); and the Department of Ophthalmology, The New York Medicalollege, Valhalla, New York (R.R.).
fInquiries to Jeffrey M. Liebmann, 310 East 14th Street, New York, NY
0003; e-mail: [email protected]
© 2008 BY ELSEVIER INC. A002-9394/08/$34.00oi:10.1016/j.ajo.2008.06.018
ayer (RNFL), focal or diffuse narrowing of the neuroreti-al rim, optic disc splinter hemorrhage (DH), and para-apillary atrophy (PPA).1–3
Disc hemorrhages are a risk factor for the developmentnd progression of glaucomatous optic neuropathy4–11 andere associated with an increased risk of conversion fromcular hypertension to primary open-angle glaucomaPOAG) in the Ocular Hypertension Treatment StudyOHTS).12 These hemorrhages occur within the RNFLnd most often are visible adjacent to, or in contact with,he disc rim, although they can occur within the rim or cuplope.13,14 In patients with localized RNFL defects, DHends to be located adjacent to or within these defects,15
nd a DH is likely to occur superiorly and inferiorly ratherhan in the horizontal meridian.16,17 Although DH has arevalence of 0.2% in patients without glaucoma, it isoughly 20 times more common (4% to 5.7%) in patientsith glaucomatous optic neuropathy8,14,18,19 and is evenigher in patients with normal-tension glaucoma.20 There-
ore, DH is highly specific for glaucomatous optic neurop-thy. Other conditions associated with DH includeiabetes mellitus, anticoagulation use, age, female gender,nd recent posterior vitreous detachment.17,21,22
Parapapillary atrophy is a form of chorioretinal atrophyhat abuts the optic disc and can be divided into � and �ones. Because this atrophy most often lies adjacent to butoes not completely surround the nerve, the term parapap-
llary atrophy may be preferable to peripapillary atrophy,lthough they are used interchangeably in the literature. In
zone PPA, the retinal pigment epithelium (RPE) isbsent, large choroidal vessels are present, and the sclera isisible.23,24 In � zone PPA, there is irregular hypopigmen-ation and hyperpigmentation of the RPE. The � zone isore peripheral than the � zone. Both the � and � zones
f PPA are larger and occur more frequently in eyes withlaucoma than in normal eyes, although � zone PPA isore specific for glaucoma.25–32
Parapapillary atrophy has been reported to be helpfuln differentiating between normal and glaucomatousyes.25–30,33 The incorporation of PPA assessment intoptic nerve evaluation increases the sensitivity and speci-city for glaucoma detection.1 In areas where the neuro-etinal rim is focally narrow, � zone PPA tends to bearger.31 Because � zone PPA is present in 15% to 20% oformal eyes, its presence is less specific for glaucoma than
or DH.12 The spatial distribution of PPA differs in
LL RIGHTS RESERVED. 735
gntfPse6h
coTsamdsb
A
taaDbe�gdtwt
ldetwwpTswsmfD
tubw
Fphwm
7
laucoma, with PPA being present nasally in 1.2% oformal patients and in 15% to 53% of glaucoma pa-ients.29,31 PPA most commonly is located temporally,ollowed by inferotemporally and then superotemporally.34
PA increases in size as glaucoma progresses and is notpecific to the mechanism of glaucoma.32 In one report ofyes with progressive cupping, the area of PPA enlarged in4%, as opposed to 17% of eyes with glaucoma that did notave progressive cupping.35
In addition to being more common in eyes with glau-oma, both PPA and DH tend to occur in regions of theptic nerve where the neuroretinal rim is damaged.36
herefore, one may expect to find an anatomic relation-hip between PPA and DH within the same eye. Annatomic relationship between PPA, DH, and glaucomaay imply a cause-and-effect situation with respect to the
evelopment of glaucomatous optic neuropathy. Weought to determine if an anatomic relationship existsetween PPA and DH.
METHODS
LL DIGITAL OPTIC NERVE STEREOPHOTOGRAPHS OB-
ained in the glaucoma referral practices of three of theuthors (R.R., J.M.L., and C.T.) between October 1, 2006nd September 30, 2007, were screened for the presence ofH. Only patients with DH were included. Each of theseilateral sets of optic nerve stereophotographs were thenvaluated for the presence, extent, and location of DH and
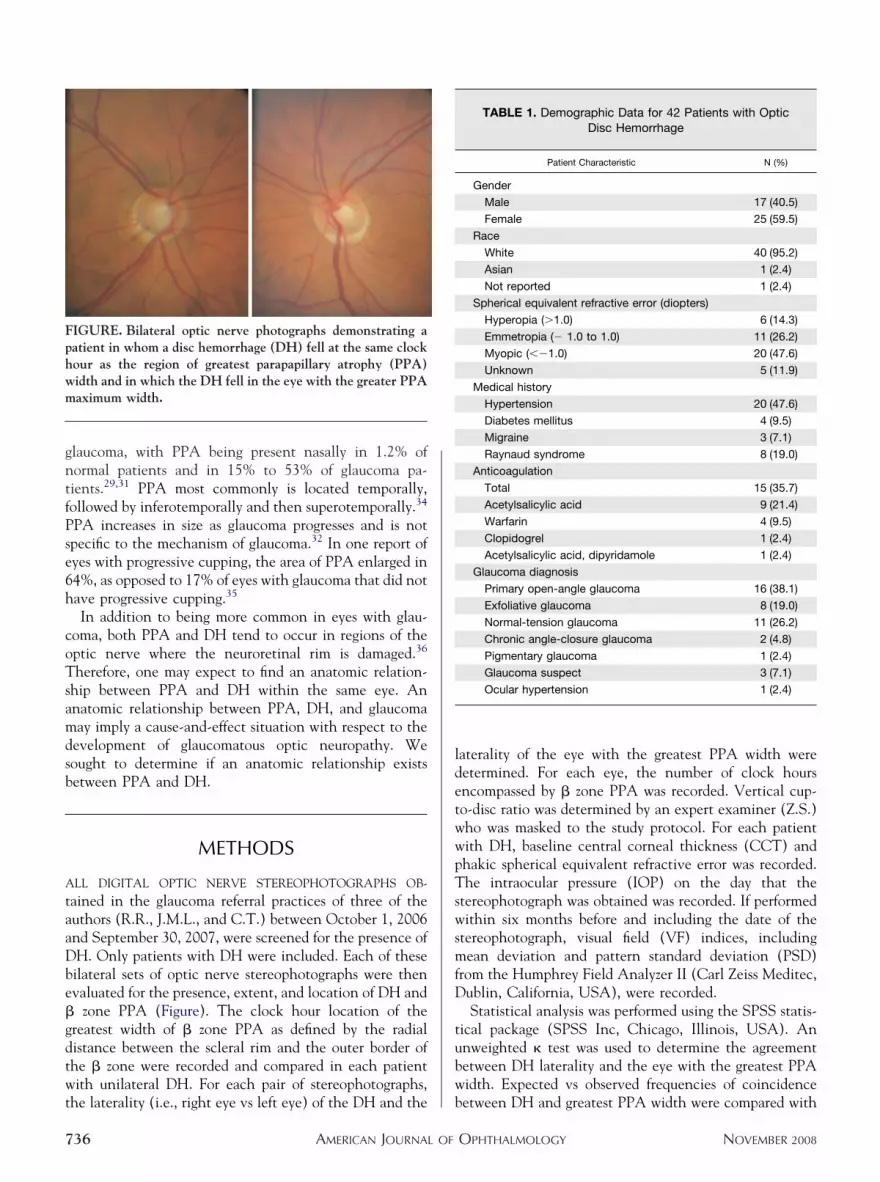
zone PPA (Figure). The clock hour location of thereatest width of � zone PPA as defined by the radialistance between the scleral rim and the outer border ofhe � zone were recorded and compared in each patientith unilateral DH. For each pair of stereophotographs,
IGURE. Bilateral optic nerve photographs demonstrating aatient in whom a disc hemorrhage (DH) fell at the same clockour as the region of greatest parapapillary atrophy (PPA)idth and in which the DH fell in the eye with the greater PPAaximum width.
he laterality (i.e., right eye vs left eye) of the DH and the b
AMERICAN JOURNAL OF36
aterality of the eye with the greatest PPA width wereetermined. For each eye, the number of clock hoursncompassed by � zone PPA was recorded. Vertical cup-o-disc ratio was determined by an expert examiner (Z.S.)ho was masked to the study protocol. For each patientith DH, baseline central corneal thickness (CCT) andhakic spherical equivalent refractive error was recorded.he intraocular pressure (IOP) on the day that the
tereophotograph was obtained was recorded. If performedithin six months before and including the date of the
tereophotograph, visual field (VF) indices, includingean deviation and pattern standard deviation (PSD)
rom the Humphrey Field Analyzer II (Carl Zeiss Meditec,ublin, California, USA), were recorded.Statistical analysis was performed using the SPSS statis-
ical package (SPSS Inc, Chicago, Illinois, USA). Annweighted � test was used to determine the agreementetween DH laterality and the eye with the greatest PPAidth. Expected vs observed frequencies of coincidence
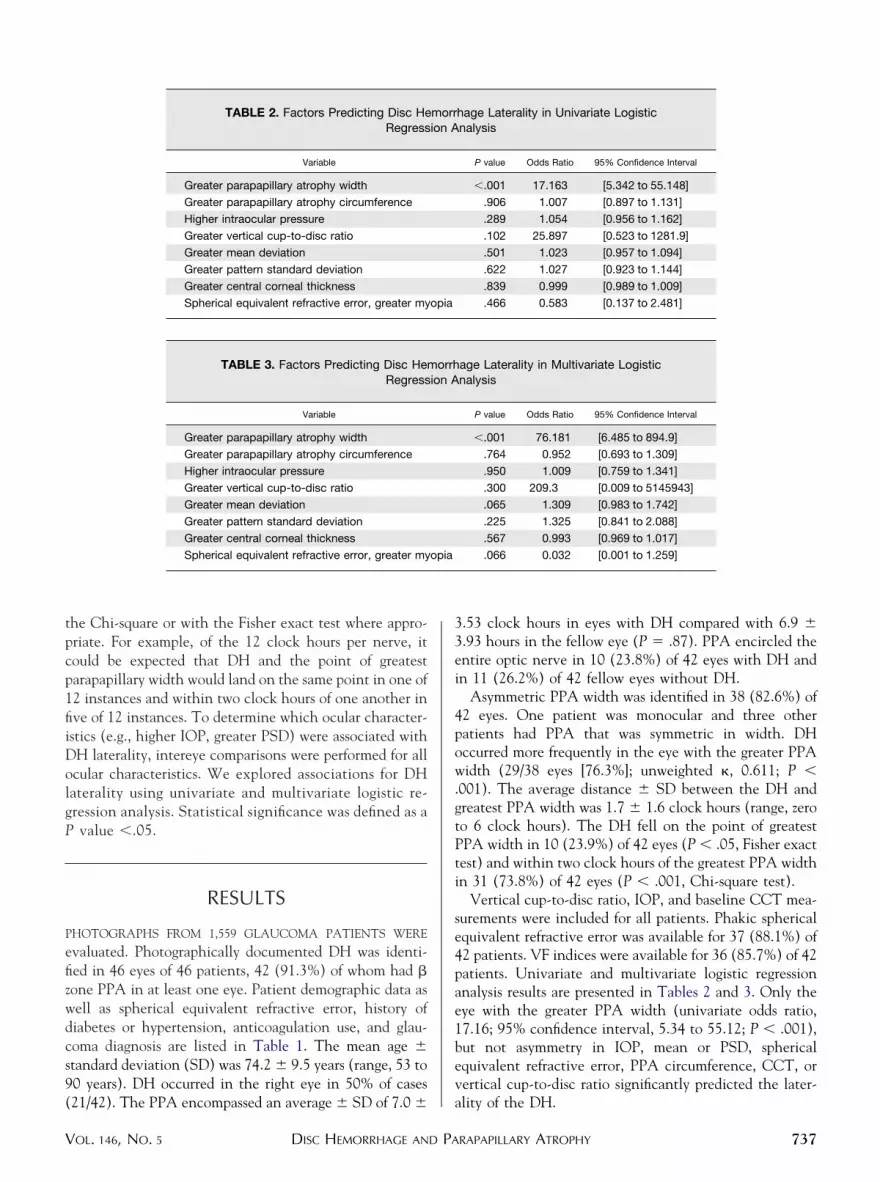
TABLE 1. Demographic Data for 42 Patients with OpticDisc Hemorrhage
Patient Characteristic N (%)
Gender
Male 17 (40.5)
Female 25 (59.5)
Race
White 40 (95.2)
Asian 1 (2.4)
Not reported 1 (2.4)
Spherical equivalent refractive error (diopters)
Hyperopia (�1.0) 6 (14.3)
Emmetropia (� 1.0 to 1.0) 11 (26.2)
Myopic (��1.0) 20 (47.6)
Unknown 5 (11.9)
Medical history
Hypertension 20 (47.6)
Diabetes mellitus 4 (9.5)
Migraine 3 (7.1)
Raynaud syndrome 8 (19.0)
Anticoagulation
Total 15 (35.7)
Acetylsalicylic acid 9 (21.4)
Warfarin 4 (9.5)
Clopidogrel 1 (2.4)
Acetylsalicylic acid, dipyridamole 1 (2.4)
Glaucoma diagnosis
Primary open-angle glaucoma 16 (38.1)
Exfoliative glaucoma 8 (19.0)
Normal-tension glaucoma 11 (26.2)
Chronic angle-closure glaucoma 2 (4.8)
Pigmentary glaucoma 1 (2.4)
Glaucoma suspect 3 (7.1)
Ocular hypertension 1 (2.4)
etween DH and greatest PPA width were compared with
OPHTHALMOLOGY NOVEMBER 2008
tpcp1fiiDolgP
P
efizwdcs9(
33ei
4pow.gtPti
se4pae1bev
opia
opia
V
he Chi-square or with the Fisher exact test where appro-riate. For example, of the 12 clock hours per nerve, itould be expected that DH and the point of greatestarapapillary width would land on the same point in one of2 instances and within two clock hours of one another inve of 12 instances. To determine which ocular character-stics (e.g., higher IOP, greater PSD) were associated withH laterality, intereye comparisons were performed for allcular characteristics. We explored associations for DHaterality using univariate and multivariate logistic re-ression analysis. Statistical significance was defined as avalue �.05.
RESULTS
HOTOGRAPHS FROM 1,559 GLAUCOMA PATIENTS WERE
valuated. Photographically documented DH was identi-ed in 46 eyes of 46 patients, 42 (91.3%) of whom had �one PPA in at least one eye. Patient demographic data asell as spherical equivalent refractive error, history ofiabetes or hypertension, anticoagulation use, and glau-oma diagnosis are listed in Table 1. The mean age �tandard deviation (SD) was 74.2 � 9.5 years (range, 53 to0 years). DH occurred in the right eye in 50% of cases
TABLE 2. Factors Predicting Disc HeRegress
Variable
Greater parapapillary atrophy width
Greater parapapillary atrophy circumference
Higher intraocular pressure
Greater vertical cup-to-disc ratio
Greater mean deviation
Greater pattern standard deviation
Greater central corneal thickness
Spherical equivalent refractive error, greater my
TABLE 3. Factors Predicting Disc HemRegress
Variable
Greater parapapillary atrophy width
Greater parapapillary atrophy circumference
Higher intraocular pressure
Greater vertical cup-to-disc ratio
Greater mean deviation
Greater pattern standard deviation
Greater central corneal thickness
Spherical equivalent refractive error, greater my
21/42). The PPA encompassed an average � SD of 7.0 � a
DISC HEMORRHAGE AND PAOL. 146, NO. 5
.53 clock hours in eyes with DH compared with 6.9 �
.93 hours in the fellow eye (P � .87). PPA encircled thentire optic nerve in 10 (23.8%) of 42 eyes with DH andn 11 (26.2%) of 42 fellow eyes without DH.
Asymmetric PPA width was identified in 38 (82.6%) of2 eyes. One patient was monocular and three otheratients had PPA that was symmetric in width. DHccurred more frequently in the eye with the greater PPAidth (29/38 eyes [76.3%]; unweighted �, 0.611; P �
001). The average distance � SD between the DH andreatest PPA width was 1.7 � 1.6 clock hours (range, zeroo 6 clock hours). The DH fell on the point of greatestPA width in 10 (23.9%) of 42 eyes (P � .05, Fisher exactest) and within two clock hours of the greatest PPA widthn 31 (73.8%) of 42 eyes (P � .001, Chi-square test).
Vertical cup-to-disc ratio, IOP, and baseline CCT mea-urements were included for all patients. Phakic sphericalquivalent refractive error was available for 37 (88.1%) of2 patients. VF indices were available for 36 (85.7%) of 42atients. Univariate and multivariate logistic regressionnalysis results are presented in Tables 2 and 3. Only theye with the greater PPA width (univariate odds ratio,7.16; 95% confidence interval, 5.34 to 55.12; P � .001),ut not asymmetry in IOP, mean or PSD, sphericalquivalent refractive error, PPA circumference, CCT, orertical cup-to-disc ratio significantly predicted the later-
hage Laterality in Univariate Logisticnalysis
P value Odds Ratio 95% Confidence Interval
�.001 17.163 [5.342 to 55.148]
.906 1.007 [0.897 to 1.131]
.289 1.054 [0.956 to 1.162]
.102 25.897 [0.523 to 1281.9]
.501 1.023 [0.957 to 1.094]
.622 1.027 [0.923 to 1.144]
.839 0.999 [0.989 to 1.009]
.466 0.583 [0.137 to 2.481]
age Laterality in Multivariate Logisticnalysis
P value Odds Ratio 95% Confidence Interval
�.001 76.181 [6.485 to 894.9]
.764 0.952 [0.693 to 1.309]
.950 1.009 [0.759 to 1.341]
.300 209.3 [0.009 to 5145943]
.065 1.309 [0.983 to 1.742]
.225 1.325 [0.841 to 2.088]
.567 0.993 [0.969 to 1.017]
.066 0.032 [0.001 to 1.259]
morrion A
orrhion A
lity of the DH.
RAPAPILLARY ATROPHY 737

I
wiwtcg
taigIpotsa(taoip
arvttclldopidrdpbhatcunrtptg
sa
zPahe6lafplwmas
bebwoChbsetr
LbPnacwlhrcihgpotrfs
Cd
7
DISCUSSION
N THIS SERIES OF 46 PATIENTS WITH UNILATERAL DH, PPA
as associated anatomically with DH, by intereye compar-son as well as within the eye with DH. The eye with theidest PPA was the eye that contained the DH in more
han three quarters of cases, and in the same number ofases, the DH fell within two clock hours of the point ofreatest width of PPA.
Several prior studies have examined relationships be-ween glaucoma, PPA, and DH.13,14,18,37,38 Sugiyama andssociates reported that PPA is more prevalent and is largern normal-tension glaucoma patients with DH than in aroup of normal-tension glaucoma patients without DH.39
n a group of healthy patients, DH occurred more often inatients with PPA, even if they did not have glauc-ma.14,18 Ahn and associates reviewed 44 glaucoma pa-ients with unilateral DH and found that rim area wasmaller and � zone PPA was larger in the hemorrhagic eyes measured by confocal scanning laser ophthalmoscopySLO).13 In multivariate analysis, only PPA area predictedhe laterality of the hemorrhage. Whereas Jonas andssociates found that � zone of PPA was larger in a groupf patients with DH than in those without, in a multivar-ate analysis, only neuroretinal rim area was a significantredictor of DH.38
In our univariate, intereye analysis, only PPA width wassignificant predictor of DH laterality, a finding previously
eported using confocal SLO.14 Although mean IOP andertical cup-to-disc ratios were greater in the eye with DHhan its fellow eye, the regression analysis indicated thathe laterality of the eye with higher IOP or greater verticalup-to-disc ratio was not a reliable predictor of DHaterality. Jonas and associates previously reported that DHaterality is statistically independent of CCT intereyeifferences, although decreased CCT was related to theccurrence of DH in the OHTS.4,12 In a large study of 99atients with DH and POAG, there were no significantntereye differences in IOP, PPA, disc size, or blood vesseliameter between the DH eye and the fellow eye.37 In aecent evaluation of patients with DH, IOP, and cup-to-isc ratio did not predict DH laterality.19 Furthermore,revious investigations have not found a relationshipetween DH and VF indices.13,40 Neuroretinal rim areaas been associated with DH laterality in a multivariatenalysis that included PPA,38 and this finding may reflecthe superiority of neuroretinal rim area over verticalup-to-disc ratio (used in our analysis) in glaucoma eval-ation, because DH tends to occur adjacent to focal rimotches.36 Given that glaucoma and DH are closelyelated, it is somewhat surprising that in our analysis and inhat of others,14 PPA was the sole ocular characteristic toredict DH laterality. However, it is interesting to notehat PPA and DH also are associated in eyes without
laucomatous-appearing optic nerves,14,18 raising the pos- wAMERICAN JOURNAL OF38
ibility that relationships between PPA and DH are medi-ted by anatomy, rather than by a glaucomatous process.
A large number of patients in our study (91.3%) had �one PPA in at least one eye. In their study of DH andPA, Ahn and associates reported PPA in 84%.13 Law andssociates found preexisting PPA in 79% of patients whoad a unilateral DH.36 The prevalence of PPA in appar-ntly healthy subjects with DH has been reported to be6.7%,39 whereas in POAG eyes without DH, the preva-ence was reported to be 60%.31 Our rate of PPA is highnd likely reflects the advanced nature of the glaucomaound in patients with DH as well as the tertiary referralractice where these patients were managed. It is alsoikely that patients with advanced glaucoma, most ofhom have PPA, are followed up more closely and thusay have had more opportunities to have a DH detected
nd may therefore be represented disproportionately in ourtudy.
This study is limited by its retrospective nature andecause the presence of DH could not be masked whilevaluating PPA. Whereas a masked observer could haveeen used to determine the clock hour of the greatest PPAidth, visible DHs in the photograph still could skew thebserver’s determinations of PPA location and laterality.onfocal SLO has been used to define � zone PPA13;owever, this does not entirely eliminate the potential forias because contour lines still must be drawn and DH istill visible. Because there was no difference in refractiverror in hemorrhagic vs nonhemorrhagic eyes, it is unlikelyhat optical artifacts in PPA measurement affected theseesults.
The mechanisms of DH and PPA remain elusive.ocalized vascular insufficiency has been implicated inoth PPA41 and DH.42,43 Both increase with age.4,21,36,44
arapapillary vasoconstriction, including diffuse arteriolararrowing, is associated with glaucomatous optic neurop-thy and has been reported to exist in the region of greatestupping in up to 91% of glaucoma patients and in theidest region of PPA in 87% of glaucoma patients.45 DH
ong has been associated with normal-tension glaucoma;owever, Tezel and associates found that DH, focal arte-iolar narrowing, and � zone PPA were significantly moreommon in patients with normal-tension glaucoma thann those with ocular hypertension, although not all studiesave found PPA to be larger in eyes with normal-tensionlaucoma.46,47 DH also has been described in patients withrimary vascular dysregulation, a syndrome of decreasedcular perfusion and systemic blood pressure.48 Alterna-ively, DH may not represent a primary vascular event, butather, it may result from secondary vessel damage incurredrom mechanical collapse of underlying optic nervetructure.
The data regarding IOP and DH are mixed. In theollaborative Normal-Tension Glaucoma Study, DH in-icated a reduced likelihood that IOP-lowering therapy
ould reduce VF progression, suggesting that DH may beOPHTHALMOLOGY NOVEMBER 2008

roDIaimped
poP(sPuDaioemP
P
sebdfctteeesf
mptawcescssl
TIfir(Jw
V
elated to pressure-independent glaucoma mechanisms,ne of which may be ocular blood flow.49 In the OHTS,H was a powerful predictor of progression, but baseline
OP was not related to development of DH.12 Both DH12
nd PPA50 have been shown in prospective trials involv-ng ocular hypertensive patients to predict the develop-ent of future optic nerve or VF damage. Whether IOP
lays a role in the development of DH awaits furthervidence elucidating the underlying mechanisms of thisisease process.Parapapillary atrophy has been evaluated in DH by its
revalence,13,14,39 total area,13,18,37–38 angular extent,13,39
r width,39 or by whether the DH fell within the area ofPA.36 We chose the greatest width of � zone PPAmeasured by visual inspection) because this method isimple, fast, and does not require expensive technology.revious studies of PPA and DH relationships either havesed intereye comparisons13,37 or have compared eyes withH with those without DH.14,18,38 Although Law and
ssociates reported that DH occurs within the area of PPAn 79% of eyes with a DH, in our study, almost one-quarterf eyes with a DH had 360 degrees of PPA, and on average,yes in this study had approximately seven hours of PPA,aking it probable that DH would fall within the area ofPA in half of cases.36
This study evaluated relationships between DH and
PA within the same eye. Because our methodology tsion of glaucoma. Ophthalmology 1996;103:1014–1024.
1
1
1
1
DISC HEMORRHAGE AND PAOL. 146, NO. 5
pecifically determined a clock hour location of the great-st width of PPA and its relationship to DH, the proba-ility that these two points will coincide by chance wasecreased. Surprisingly, PPA greatest width not only wasound more frequently in the eye with the DH on intereyeomparison, but it also was found to be in close proximityo the DH within the hemorrhagic eye. In this manner,his analysis of PPA both confirms previously found inter-ye relationships between PPA and DH13,14,18,38 andxtends emerging evidence that this relationship alsoxists within the hemorrhagic eye.36 Our data suggest thatimply evaluating the greatest width of PPA may deserveurther consideration in optic nerve evaluation.
We used largest width or radial extent of PPA aseasured by visual inspection, a technique that can be
erformed at the slit-lamp using a hand-held lens. Al-hough not as quantitative as optic nerve morphometricnalysis, the evaluation we used can be performed quicklyhile viewing digital images or on clinical evaluation. DHan be difficult to detect on nondilated optic nervexamination, whereas dilated optic nerve photography isignificantly more sensitive.12 However, the latter is timeonsuming and less convenient for the patient. Perhaps byearching for DH near the greatest width of PPA, theensitivity of the nondilated optic nerve examination forocating DH can be increased, allowing for better detec-
ion of patients who are at risk of progression.HIS STUDY WAS SUPPORTED BY THE LOWELL HARWOOD RESEARCH FUND OF THE NEW YORK GLAUCOMA RESEARCHnstitute and the Manhattan Eye, Ear, and Throat Hospital Glaucoma Education and Research Fund, New York, New York. The authors indicate nonancial conflict of interest. Involved in conception and design (N.M.R., J.M.L., I.R.); analysis (N.M.R., J.M.L., Z.S.); writing (N.M.R., J.M.L.); criticalevision (N.M.R., J.M.L., I.R., S.F.S., R.R.); final approval (N.M.R., J.M.L.); data collection (N.M.R., J.M.L., I.R., Z.S., S.F.S.); provision of materialsN.M.R., J.M.L., C.T., R.R.); statistical expertise (N.M.R., J.M.L., R.R.); obtaining funding (N.M.R., J.M.L., C.T., R.R.); literature search (N.M.R.,.M.L., I.R., S.S.); and administrative support (N.M.R., J.M.L.). Approval for this Health Insurance Portability and Accountability Act-compliant studyas obtained from the New York Eye and Ear Infirmary Institutional Review Board.
The authors thank Praveen Nirmalan of Prashasa, Hyderabad, India, for statistical consultation and assistance.
REFERENCES
1. Harper R, Reeves B. The sensitivity and specificity of directophthalmoscopic optic disc assessment in screening forglaucoma: a multivariate analysis. Graefes Arch Clin ExpOphthalmol 2000;238:949–955.
2. Theodossiades J, Murdoch I. What optic disc parameters aremost accurately assessed using the direct ophthalmoscope?Eye 2001;15:283–287.
3. Jonas JB, Budde WM, Panda-Jonas S. Ophthalmoscopicevaluation of the optic nerve head. Surv Ophthalmol 1999;43:293–320.
4. Jonas JB, Stroux A, Oberacher-Velten IM, Kitnarong N,Jünemann A. Central corneal thickness and development ofglaucomatous optic disk hemorrhages. Am J Ophthalmol2005;140:1139–1141.
5. Drance SM, Fairclough M, Butler DM, Kottler MS. Theimportance of disc hemorrhage in the prognosis of chronicopen-angle glaucoma. Arch Ophthalmol 1977;95:226–228.
6. Siegner SW, Netland PA. Optic disc hemorrhages and progres-
7. Ishida K, Yamamoto T, Sugiyama K, Kitazawa Y. Disk hemor-rhage is a significantly negative prognostic factor in normal-tension glaucoma. Am J Ophthalmol 2000;129:707–714.
8. Jonas JB, Xu L. Optic disk hemorrhages in glaucoma. Am JOphthalmol 1994;118:1–8.
9. Airaksinen PJ, Mustonen E, Alanko HI. Optic disc hemor-rhages precede retinal nerve fiber layer defects in ocular hyper-tension. Acta Ophthalmol (Copenh) 1981;59:627–641.
0. Jonas JB, Schiro D. Localised wedge shaped defects of theretinal nerve fiber layer in glaucoma. Br J Ophthalmol1994;78:285–290.
1. Leske MC, Heijl A, Hyman L, Bengtsson B, Dong L, Yang Z,EMGT Group. Predictors of long-term progression in the earlymanifest glaucoma trial. Ophthalmology 2007;114:1965–1972.
2. Budenz DL, Anderson DR, Feuer WJ, et al, Ocular Hyper-tension Treatment Study Group. Detection and prognosticsignificance of optic disc hemorrhages during the OcularHypertension Treatment Study. Ophthalmology 2006;113:2137–2143.
3. Ahn JK, Kang JH, Park KH. Correlation between a disc
hemorrhage and peripapillary atrophy in glaucoma patientsRAPAPILLARY ATROPHY 739

1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
7
with a unilateral disc hemorrhage. J Glaucoma 2004;13:9–14.
4. Sugiyama K, Tomita G, Kawase K, et al. Disc hemorrhageand peripapillary atrophy in apparently healthy subjects.Acta Ophthalmol Scand 1999;77:139–142.
5. Sugiyama K, Uchida H, Tomita G, Sato Y, Iwase A,Kitazawa Y. Localized wedge-shaped defects of retinal nervefiber layer and disc hemorrhage in glaucoma. Ophthalmology1999;106:1762–1767.
6. Healey PR, Mitchell P, Smith W, Wang JJ. Optic dischemorrhages in a population with and without signs ofglaucoma. Ophthalmology 1998;105:216–223.
7. Yamamoto T, Iwase A, Kawase K, Sawada A, Ishida K. Opticdisc hemorrhages detected in a large-scale eye disease screen-ing project. J Glaucoma 2004;13:356–360.
8. Hayakawa T, Sugiyama K, Tomita G, et al. Correlation ofthe peripapillary atrophy area with optic disc cupping anddisc hemorrhage. J Glaucoma 1998;7:306–311.
9. Lan YW, Wang IJ, Hsiao YC, Sun FJ, Hsieh JW. Character-istics of disc hemorrhage in primary angle-closure glaucoma.Ophthalmology. Forthcoming.
0. Krupin T, Liebmann JM, Greenfield DS, Rosenberg LF,Ritch R, Yang JW, Low-Pressure Glaucoma Study Group.The Low-Pressure Glaucoma Treatment Study (LoGTS)study design and baseline characteristics of enrolled patients.Ophthalmology 2005;112:376–385.
1. Soares AS, Artes PH, Andreou P, Leblanc RP, Chauhan BC,Nicolela MT. Factors associated with optic disc hemorrhagesin glaucoma. Ophthalmology 2004;111:1653–1657.
2. Roberts TV, Gregory-Roberts JC. Optic disc hemorrhages inposterior vitreous detachment. Aust N Z J Ophthalmol1991;19:61–63.
3. Kubota T, Jonas JB, Naumann GO. Direct clinico-histolog-ical correlation of parapapillary chorioretinal atrophy. Br JOphthalmol 1993;77:103–106.
4. Jonas JB, Naumann GO. Parapapillary chorioretinal atrophyin normal and glaucoma eyes. II. Correlations. Invest Oph-thalmol Vis Sci 1989;30:919–926.
5. Primrose J. The incidence of the peripapillary halo glauco-matosus. Trans Ophthalmol Soc U K 1970;89:585–587.
6. Wilensky JT, Kolker AE. Peripapillary changes in glaucoma.Am J Ophthalmol 1976;81:341–345.
7. Daugeliene L, Yamamoto T, Kitazawa Y. Risk factors forvisual field damage progression in normal-tension glaucomaeyes. Graefes Arch Clin Exp Ophthalmol 1999;237:105–108.
8. Rockwood EJ, Anderson DR. Acquired peripapillary changesand progression in glaucoma. Graefes Arch Clin Exp Oph-thalmol 1988;226:510–515.
9. Jonas JB, Nguyen XN, Gusek GC, Naumann GO. Parapap-illary chorioretinal atrophy in normal and glaucoma eyes. I.Morphometric data. Invest Ophthalmol Vis Sci 1989;30:908–918.
0. Jonas JB, Naumann GO. Parapapillary chorioretinal atrophyin normal and glaucoma eyes. II. Correlations. Invest Oph-thalmol Vis Sci 1989;30:919–926.
1. Uhm KB, Lee DY, Kim JT, Hong C. Peripapillary atrophy innormal and primary open-angle glaucoma. Korean J Oph-
thalmol 1998;12:37–50.AMERICAN JOURNAL OF40
2. Xu L, Wang Y, Yang H, Jonas JB. Differences in parapapillaryatrophy between glaucomatous and normal eyes: the BeijingEye Study. Am J Ophthalmol 2007;144:541–546.
3. Jonas JB. Clinical implications of peripapillary atrophy inglaucoma. Curr Opin Ophthalmol 2005;16:84–88.
4. Heltzer JM. Progression of peripapillary atrophy. Ophthal-mology 1999;106:857.
5. Uchida H, Ugurlu S, Caprioli J. Increasing peripapillaryatrophy is associated with progressive glaucoma. Ophthal-mology 1998;105:1541–1545.
6. Law SK, Choe R, Caprioli J. Optic disk characteristics beforethe occurrence of disk hemorrhage in glaucoma patients.Am J Ophthalmol 2001;132:411–413.
7. Jonas JB, Martus P, Budde WM. Inter-eye differences inchronic open-angle glaucoma patients with unilateral dischemorrhages. Ophthalmology 2002;109:2078–2083.
8. Jonas JB, Martus P, Budde WM, Hayler J. Morphologic predic-tive factors for development of optic disc hemorrhages inglaucoma. Invest Ophthalmol Vis Sci 2002;43:2956–2961.
9. Sugiyama K, Tomita G, Kitazawa Y, Onda E, Shinohara H,Park KH. The associations of optic disc hemorrhage with retinalnerve fiber layer defect and peripapillary atrophy in normal-tension glaucoma. Ophthalmology 1997;104:1926–1933.
0. Gazzard G, Morgan W, Devereux J, et al. Optic dischemorrhage in Asian glaucoma patients. J Glaucoma 2003;12:226–231.
1. Raitta C, Sarmela T. Fluorescein angiography of the opticdisc and the peripapillary area in chronic glaucoma. ActaOphthalmol (Copenh) 1970;48:303–308.
2. Jonas JB, Budde WM, Németh J, Gründler AE, MistlbergerA, Hayler JK. Central retinal vessel trunk exit and locationof glaucomatous parapapillary atrophy in glaucoma. Oph-thalmology 2001;108:1059–1064.
3. Flammer J. The vascular concept of glaucoma. Surv Oph-thalmol 1994;38:S3–S6.
4. Xu L, Wang Y, Yang H, Jonas JB. Differences in parapapillaryatrophy between glaucomatous and normal eyes: the BeijingEye Study. Am J Ophthalmol 2007;144:541–546.
5. Rader J, Feuer WJ, Anderson DR. Peripapillary vasoconstric-tion in the glaucomas and the anterior ischemic opticneuropathies. Am J Ophthalmol 1994;117:72–80.
6. Tezel G, Kass MA, Kolker AE, Wax MB. Comparative opticdisc analysis in normal pressure glaucoma, primary open-angle glaucoma, and ocular hypertension. Ophthalmology1996;103:2105–2113.
7. Jonas J. Biomorphometry and histomorphometry of the opticdisc with special reference to the parapapillary region. BullSoc Belge Ophtalmol 1992;244:45–60.
8. Grieshaber MC, Terhorst T, Flammer J. The pathogenesis ofoptic disc splinter hemorrhages: a new hypothesis. ActaOphthalmol Scand 2006;84:62–68.
9. Anderson DR, Drance SM, Schulzer M, CollaborativeNormal-Tension Glaucoma Study Group. Factors that pre-dict the benefit of lowering intraocular pressure in normal-tension glaucoma. Am J Ophthalmol 2003;136:820–829.
0. Tezel G, Kolker AE, Kass MA, Wax MB, Gordon M,Siegmund KD. Parapapillary chorioretinal atrophy in pa-tients with ocular hypertension. I. An evaluation as apredictive factor for the development of glaucomatous dam-
age. Arch Ophthalmol 1997;115:1503–1508.OPHTHALMOLOGY NOVEMBER 2008
DBIGm
V
Biosketch
r Jeffrey M. Liebmann completed his residency at the State University of New York/Downstate Medical Center,rooklyn, New York in 1987 and his glaucoma fellowship at the New York Eye and Ear Infirmary, New York, New York.
n addition to serving on the governing boards of the American Glaucoma Society, the Glaucoma Foundation, and Worldlaucoma Association, he is the principal investigator for two NIH-sponsored clinical trials and has authored over 450edical and scientific papers and book chapters in the field of glaucoma.
DISC HEMORRHAGE AND PARAPAPILLARY ATROPHYOL. 146, NO. 5 740.e1

DEoo
7
Biosketch
r Nathan M. Radcliffe was chief resident during his ophthalmology residency at New York University and Manhattanye, Ear and Throat Hospital, New York, New York. His fellowship training in glaucoma was performed under the tutelagef Drs Robert Ritch, Jeffrey Liebmann, and Celso Tello at the New York Eye and Ear Infirmary. Dr Radcliffe is currentlyn the faculty at Weill Cornell Medical College and New York Hospital.
AMERICAN JOURNAL OF OPHTHALMOLOGY40.e2 NOVEMBER 2008