an experimental test of medical disclosure and consent documentation: assessing patient...
TRANSCRIPT
This article was downloaded by: [University of Texas Libraries]On: 10 September 2014, At: 14:12Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Communication MonographsPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rcmm20
An Experimental Test of MedicalDisclosure and Consent Documentation:Assessing Patient Comprehension, Self-Efficacy, and UncertaintyErin E. Donovan, Brittani Crook, Laura E. Brown, Angie E.Pastorek, Camille A. Hall, Michael S. Mackert & Keri K. StephensPublished online: 30 Jan 2014.
To cite this article: Erin E. Donovan, Brittani Crook, Laura E. Brown, Angie E. Pastorek, CamilleA. Hall, Michael S. Mackert & Keri K. Stephens (2014) An Experimental Test of Medical Disclosureand Consent Documentation: Assessing Patient Comprehension, Self-Efficacy, and Uncertainty,Communication Monographs, 81:2, 239-260, DOI: 10.1080/03637751.2013.876059
To link to this article: http://dx.doi.org/10.1080/03637751.2013.876059
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
An Experimental Test of MedicalDisclosure and Consent Documentation:Assessing Patient Comprehension,Self-Efficacy, and UncertaintyErin E. Donovan, Brittani Crook, Laura E. Brown,Angie E. Pastorek, Camille A. Hall, Michael S. Mackert &Keri K. Stephens
Effectively conveying risks and hazards in medical disclosure and informed consentdocumentation is a crucial type of communication. However, existing protocols typicallydo not meet the needs of patients or practitioners. In the present study, we advance areconceptualization of obtaining written informed consent by analyzing it as a process ofuncertainty management rather than a matter of document readability and recall. Resultsof this randomized trial indicated that patients who reviewed a simplified consentdocument reported greater comprehension of medico-legal terminology and loweruncertainty about the document, although they did not evince greater self-efficacy. Healthliteracy was a significant moderator of the relationship between consent form version andcomprehension.
Keywords: Informed Consent; Disclosure; Uncertainty; Health Literacy
The process of obtaining written informed consent is a cornerstone of providingethical, legal, and patient-centered care (Schenker, Fernandez, Sudore, & Schillinger,
Erin Donovan (PhD, University of Illinois at Urbana-Champaign) is an assistant professor in the Department ofCommunication Studies at the University of Texas at Austin, where Brittani Crook (MA, Texas State University),Laura E. Brown (MA,University of Illinois at Urbana-Champaign), Angie E. Pastorek (MS, Illinois StateUniversity,MA, DePaul University), and Camille A. Hall (MA, University of North Texas) are doctoral candidates and Keri K.Stephens (PhD, University of Texas at Austin) is an associate professor. Michael Mackert (PhD, Michigan StateUniversity) is an associate professor in the Department of Advertising and Public Relations at the University ofTexas at Austin and in the University of Texas Health Science Center at Houston School of Public Health. Theauthors extend their appreciation toHeidi Shalev for her assistance at the recruitment site. Correspondence to: ErinDonovan, 2504 Whitis Avenue (A1105), Austin TX 78712, USA. Email: [email protected]
Communication MonographsVol. 81, No. 2, June 2014, pp. 239–260
ISSN 0363-7751 (print)/ISSN 1479-5787 (online) © 2014 National Communication Associationhttp://dx.doi.org/10.1080/03637751.2013.876059
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
2011). In the United States, in particular, the communication of medical disclosureand consent information is meant to accomplish two important objectives. First, ithelps to protect patients’ constitutionally protected right to privacy, which includesthe right to accept or decline medical care. Second, it helps healthcare providersprotect themselves from malpractice lawsuits that have arisen when patients were notproperly informed about the potential consequences of treatment (Osman, 2001).Current research indicates that if these goals are to be met, then the medicaldisclosure and informed consent process needs to be improved.
In the present study, we tested a prototype of a revised medical disclosure andconsent document (MDCD) to evaluate some best practices for communicating thepossible risks of a cardiac procedure. In the following sections, we review literaturethat demonstrates the inadequacies of the informed consent process in healthcaresettings. Then we describe our project, which was grounded in Uncertainty in IllnessTheory and Uncertainty Management Theory and designed with two purposes inmind: (1) to advance research on informed consent by extending the conceptualapproaches that have guided scholarship on this topic and (2) to assist stakeholderswho are currently working to revise MDCDs.
Background and Warrant for the Present Study
There is ample evidence to suggest that MDCDs do not sufficiently accomplish thetasks of (1) informing patients about reasonable expectations of an upcomingprocedure and (2) equipping them to make knowledgeable decisions about their care(e.g. Davis, Williams, Marin, Parker, & Glass, 2002; Katz, 1984; Krumholz, 2010;Schenker et al., 2011). Research from the National Quality Forum (2005) suggeststhat the majority of patients who sign MDCDs do not understand the informationthat is communicated therein and that many people might be unmotivated to readthe material for that reason. Patients appear to have difficulties interpreting vitalpieces of information in the documents, such as risks, benefits, and even the purposeand nature of the procedure itself (Byrne, Napier, & Cuschieri, 1988; NationalQuality Forum, 2005). This constitutes a problem, because when the material thatpatients receive is not clear enough, then their ability to provide truly informedconsent is compromised.
A primary reason why people struggle with these forms is that the descriptions ofprocedures and their associated risks are presented in ways that are too complex forthe majority of patients to understand (Institute of Medicine Committee on HealthLiteracy, 2004). The concepts in MDCDs often contain medical and legal jargon thatis highly confusing to a lay audience (Davis et al., 2002; Jubelirer, 1991). Manypatients are unable to explain important medical terms or make sense of thelikelihood of the risks to which they are susceptible (Davis et al., 2001, 2002). Basedon numerous studies, the American Medical Association has warned that there is aserious disconnect between typical patient abilities and the skills needed tounderstand MDCDs (Doak, Doak, Friedell, & Meade, 1998). Consequently, patientadvocacy groups have finally begun work to improve MDCDs in order to address the
240 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

ethical, legal, and practical dilemmas stemming from their incomprehensibility (e.g.Minnesota Literacy Council, 2007).
Because barriers to effective consent exist at a systemic level, a worthwhile meansof addressing them is to improve the comprehensibility of existing MDCDs, so thatprevailing legal directives are met but not at the expense of patients’ informedinvolvement in their care. The current project was designed to contribute to an effortin Texas to overhaul the MDCDs that are approved for use in healthcareorganizations throughout the state. Our investigation was part of an ongoingprogram of translational research about the barriers to effective disclosure andconsent communication in healthcare settings. We collaborated with the TexasMedical Disclosure Panel, a board of medical practitioners and attorneys chargedwith the responsibility of making recommendations to the Texas state legislatureabout improving patient safety and care while adequately regulating providerliability.
Advancing Research on Communication and Informed Consent
Given that signing MDCDs prior to medical procedures is customary, this taskrepresents a primary point of communication during which patient understandingcould be maximized. A recent systematic review of medical disclosure and informedconsent interventions (N = 44) indicated that many efforts to improve the medicalconsent process have focused on providing patients with additional writteninformation, such as a brief booklet, to accompany the signing of forms or theconversation that a patient would have with a healthcare practitioner (see Schenkeret al., 2011). Most of those studies have resulted in somewhat improved compre-hension of risks of medical procedures. Although any improvement in patientcomprehension is valuable, the small effect sizes and marginal practical benefitsoffered by this corpus of research suggest that there is more work yet to be done andthat rethinking some assumptions about effective communication during informedconsent is warranted.
Our own analysis of the literature suggests four opportunities for extending theaforementioned body of work. First, the research evaluating written informationabout risks of medical procedures has tended to focus merely on including extramaterial, rather than improving the quality of the existing written material (e.g.Brown, Massoud, & Bance, 2003). Second, much of the previous research hasemphasized patients’ recall of key points from the MDCDs as the dependent variable(e.g. Graham, 2003; Langdon, Hardin, & Learmonth, 2002). We propose thatadvancing theory about communication and informed consent requires broadeningthe outcomes of interest. Third, we believe that although readability formulae havetheir place in judging the adequacy of communication in informed consent (e.g.Paasche-Orlow, Taylor, & Brancati, 2003), their utility is limited. Finally, the researchexamining informed consent has rarely taken into account patient characteristics thatare likely to be relevant to the process of achieving informed consent, namely healthliteracy. In fact, few studies even report such information as part of their sample
Medical Disclosure Uncertainty 241
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
descriptions, let alone factor it into their designs (Schenker et al., 2011). We elaborateon all of these propositions and introduce our corresponding hypotheses next.
Informed Consent as Uncertainty Management
A general premise of informed consent interventions is that giving patients moreinformation is a key component to improving the consent process (e.g. Graham,2003; Inglis & Farnill, 1993). We would argue that effective disclosure and informedconsent hinges on providing sufficient amounts of high-quality, usable information—in other words, patients need better, rather than just more, information. This logic isgrounded in our contention that because the practice of disclosing medical risks andproviding informed consent tends to involve interacting with complex and unclearinformation, it is fundamentally a process of communication and uncertaintymanagement.
Mishel’s (1988) Uncertainty in Illness Theory (UIT) and Brashers’s (2001)Uncertainty Management Theory (UMT) have guided much of the scholarship onuncertainty in health contexts. According to UIT and UMT, uncertainty is aninability to make sense of health- or illness-related information or events (Brashers,2001; Mishel, 1988). Both theories contend that people are likely to experienceuncertainty when they are confronted with ambiguous or inadequate information.UMT built upon many of the central assumptions of UIT and stressed thatcommunication has the potential to arouse and reduce uncertainty and that throughcommunication, uncertainty can be reduced, maintained, or even increased(Brashers, 2001; Hogan & Brashers, 2009). Notably, these perspectives recognizethat people might experience uncertainty because they have too little information orbecause they have too much information (Brashers, 2001; Brashers, Goldsmith, &Hsieh, 2002; Brashers, Neidig, & Goldsmith, 2004; Mishel, 1988). In the informedconsent context, patients might feel uncertain because they have not received enoughinformation about the potential risks of a procedure, but might likewise experienceuncertainty if they receive extensive risk information that feels overwhelming orseems contradictory. In contrast with many informed consent studies, we proposethat according to uncertainty management theories, greater quantities of informationmay be inadvisable.
Previous research grounded in uncertainty theories has identified four mainsources of uncertainty that patients report after reviewing medical disclosure andconsent forms. These are uncertainty about (1) medical, technical, and legalterminology; (2) risks and hazards; (3) what will occur during the procedure; and(4) implications of the document format (Donovan-Kicken, Mackert, Guinn,Tollison, & Breckinridge, 2013). Consistent with UIT and UMT, our recent workhas also indicated that patients are critical of MDCDs that not only seem to skimp ondetail but also seem too lengthy (Donovan-Kicken et al., 2013). One reason whypeople might struggle with additional information, even if it is designed to be helpful,is that their information-processing capabilities might be compromised due to illness,pain, or the stress of being in the hospital (Mishel, 1988). Therefore, the approach we
242 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
took in the present study was distinct from many other informed consentinterventions. Specifically, rather than providing supplemental information tomitigate the confusion aroused by consent forms, we focused on simplifying thematerial within the form itself. Our research strategy conformed with existingliterature indicating that the quality of health information vis-à-vis uncertaintydepends on how ambiguous, consistent, and complex the information is (Babrow,Kasch, & Ford, 1998; Hurley, Kosenko, & Brashers, 2011). As Hurley et al. (2011)noted: “Unclear messages, such as those that are exceedingly complex or laden inmedical jargon, can convey or create uncertainty because they do not contribute tomeaning making” (p. 373).
An uncertainty management framework enhances the study of medical disclosureand informed consent because it suggests the relevance of multiple dimensions ofpatient information–processing outcomes. As previous scholarship on informedconsent has demonstrated, it is important to test patients’ understanding of theconsent material with objective measures of comprehension (Inglis & Farnill, 1993;Livesley & Rider, 1993). This knowledge acquisition outcome is crucial, and itprovides relatively unbiased information about the effectiveness of informed consentprocedures. Additionally, consistent with UIT and UMT’s prioritization of indivi-duals’ perceptions of how much they understand, it is worthwhile to consider moresubjective measures of patients’ ability to use informed consent materials.
Other research has found that patient self-efficacy—self-reported confidence inone’s ability to describe and evaluate the risks of a medical procedure—is a proximalpredictor of how satisfied patients are with the extent to which they have beenadequately informed (Donovan-Kicken et al., 2012). And self-reports of uncertaintyare likely to add insight to findings about comprehension, because even if patientssatisfactorily complete tests designed to gauge their understanding of certain consentform elements, they may yet experience confusion about other aspects of theinformed consent process. The present investigation was designed to take a multi-dimensional approach to evaluating MDCD adequacy, by studying how changes incommunicating informed consent information might result not only in improvedcomprehension but also in higher self-efficacy and lower overall uncertainty.Studying informed consent communication through a lens of uncertainty manage-ment provides a means of addressing the aforementioned gaps in the consentliterature, one of which is an over-emphasis on readability formulae.
Moving Beyond Readability Scores
From health promotion materials to legal contracts to instruction manuals, atraditional strategy for simplifying written information has been to improve adocument’s readability score. Readability is an attribute of text that refers to how easyit is to read and understand in comparison to other texts (Dubay, 2004). Severalword- and sentence-level attributes influence how difficult it is to understand adocument’s content; for example, having shorter sentences, shorter words, fewerpolysyllabic words, and fewer adverbs tends to enhance readability (Dubay, 2004;
Medical Disclosure Uncertainty 243
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

Hull, 1979; Klare, 1976). Many readability indices rely on such metrics to produce aquantified score representing the difficulty of understanding a given text, such as theFlesch-Kincaid grade level and Flesch reading ease score (Kincaid, Fishburne, Rogers,& Chissom, 1975), the Gunning Fog index (Laubach & Koschnick, 1977), and theSMOG index (McLaughlin, 2008). If a document is rated as 11 on the Flesch-Kincaidscale, for instance, then a person would require approximately an 11th-gradeeducation to read and understand it.
We contend that a tension exists between the goals for readability and the realitiesof the medical disclosure and consent process. On the one hand, readability scholarspropose that materials designed for general public consumption, such as healthinformation, should be conveyed in a manner that makes them easily understandablefor the majority of people (Chall & Dale, 1995). This seems to be an appropriate goal.MDCDs, which are typically written at a college reading level (Doak et al., 1998), arelikely too difficult for the average American, who reads at around an eighth-gradelevel, and they are almost certainly incomprehensible to the 17% of Americans whoread at only a fifth-grade level or lower (Grundner, 1980). Furthermore, even personswith above-average reading skills say that they prefer health materials that are easy toread and understand (Minnesota Literacy Council, 2007). On the other hand,however, patients report wanting detailed information about risks before consentingto care (Faden, Becker, Lewis, Freeman, & Faden, 1981; Inglis & Farnill, 1993).
Our proposed solution is to emphasize comprehensibility (based on formativeresearch) over readability (based on scores from text analysis formulae). From apragmatic standpoint, it is unrealistic to eliminate all of the elements of MDCDs thatwould contribute to their having lower readability—for instance, a certain number ofpolysyllabic medical terms is likely to be necessary for the disclosures to be accurateand precise. To meet the standards of valid informed consent, patients must receiveinformation that is thorough enough to enable them to make a knowledgeable choiceabout whether to receive the treatment or undergo the procedure. However, it shouldbe possible to improve the comprehensibility of the information, notwithstanding thereadability scores that might remain relatively difficult. Previous research hasproposed simple changes such as adding brief explanations of medical terms orsignposting plain language definitions with parentheses or phrases such as “Whatthis means is that …” (Donovan-Kicken, Mackert, Guinn, Tollison, & Breckinridge,2011). In sum, we do not anticipate that readability levels are as important ascommunicating the information in a more straightforward and accessible manner.
Thus, the primary goal of the present investigation is to test how simplifyingMDCDs improves the adequacy of information patients receive without substantiallychanging the readability scores of the text itself. We predicted that improving thecommunication of information about risks and hazards of a cardiac procedure wouldmake the information easier to understand. Specifically, we expected the following:patients who review a simplified MDCD will demonstrate higher comprehension ofmedico-legal terminology than patients who review the original form (H1). Patientswho review a simplified MDCD will report higher self-efficacy in evaluating the risksof the procedure than patients who review the original form (H2). Finally, patients
244 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

who review a simplified MDCD will express lower uncertainty about the content ofthe document than patients who review the original form (H3).
The Role of Health Literacy
Health literacy is defined as the ability of individuals to obtain, process, and actappropriately on health information (Ad Hoc Committee on Health Literacy, 1999;Nielsen-Bohlman, Panzer, & Kindig, 2004). Low health literacy is a widespread issue,as between one-third and one-half of adults in the United States struggle with healthinformation, and certain groups—the elderly, ethnic minorities, and those of lowersocioeconomic status—are particularly likely to have inadequate health literacy (AdHoc Committee on Health Literacy, 1999; National Center for Education Statistics,2003; Nielsen-Bohlman et al., 2004). Individuals with low health literacy have morefrequent and longer hospitalizations and greater difficulties managing chronic healthconditions and essentially do not have the requisite skills to navigate the healthcaresystem (Howard, Gazmararian, & Parker, 2005; Schloman, 2003; Weiss &Palmer, 2004).
Theoretically, health literacy fits into the uncertainty framework guiding thepresent investigation because it represents an individual-level construct that couldenhance or undermine how well patients can use health-related information.According to UIT (Mishel, 1988), a number of personal and situational factorsinfluence the extent to which people experience uncertainty in health contexts.Referred to as structure providers, these factors, which include education and socialsupport, influence how well patients can comprehend uncertainty-arousing stimuli.People with lower levels of education, for example, tend to find it more difficult tofigure out the meaning of information and events such as symptom patterns andrecommendations from physicians (Clayton, Mishel, & Belyea, 2006; Mishel, 1988).Likewise, we hypothesized that health literacy would serve as a structure providerthat will influence patients’ subjective and objective abilities to make sense ofmaterial in a MDCD. Not only is this position consistent with the premises of UIT,but empirical evidence already exists for a positive association between health literacyand self-efficacy in informed consent contexts (Donovan-Kicken et al., 2012).Patients who are relatively high in health literacy should demonstrate significantlyhigher comprehension of medical terminology, greater self-efficacy in understandingand using the consent form, and less uncertainty about the form than patients whoare relatively low in health literacy. In other words, we expect that health literacy ispositively associated with comprehension of medico-legal terminology (H4),positively associated with patient self-efficacy (H5), and inversely associated withoverall level of uncertainty (H6).
Finally, we believe that health literacy is also a relevant moderating factor toconsider when studying patients’ grasp of informed consent material, because healthliteracy is itself a predictor of an individual’s ability to understand and useinformation in medical documents (MacDougall, Connor, & Johnstone, 2012). It ispossible, for example, that simplified language in a consent document would be
Medical Disclosure Uncertainty 245
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

especially easy to understand for persons with relatively high levels of health literacy.Alternatively, perhaps both the more complicated and the simplified version of aMDCD would be equally comprehensible for people with high health literacy.Therefore, we planned to investigate the possibility that there might be an interactionbetween the version of the consent form patients review and their levels of healthliteracy.
Methods
Participants and Procedures
Recruitment. Participants were recruited from the lobbies of regional health careclinics in central Texas and were paid $15 for their participation. To be eligible,participants had to be at least 18 years of age, residents of Texas, and fluent inEnglish. The research team asked clinic patients if they were interested inparticipating in a survey of people’s opinions about medical forms. We explainedthat we were university researchers and that their participation had no bearing ontheir medical care with the healthcare organizations where we were collecting data.Procedures were approved by the university IRB and by clinic supervisors.
Interview procedures. Data were collected through structured face-to-face indi-vidual interviews. Members of the research team were trained extensively (e.g. viarecorded interviews with practice participants) so that all interviews would be asconsistent as possible. Research assistants drew a paper interview packet for eachparticipant from a stack of packets that contained a random distribution of originalMDCDs, revised MDCDs, and materials related to a different study. Participantswere asked to imagine that they were about to undergo treatment of a cardiaccatheterization, and they were given the MDCD and asked to read over it as thoughthey might be signing it before the procedure. Afterward, we asked participantsquestions about their self-efficacy in using the form. Participants were then asked topoint out areas of confusion where they found the document difficult to understandand to translate some of the medico-legal terminology on the form into everydaylanguage. Finally, the interviewers administered a health literacy measure andgathered demographic information. Interviews ranged from 15 to 30 minutes,typically lasting approximately 20 minutes.
Stimulus material. We revised and tested a prototypical MDCD in order toaddress some prominent comprehensibility concerns that were raised by patients inour formative research (Donovan-Kicken et al., 2013). The original consent form weused was based upon the MDCD template approved by the state legislature for usethroughout Texas. The overall template for the form is standardized, and details areadded to summarize the relevant risks and hazards of particular procedures. Wefocused our revisions on simplifying complex sentences and providing explanationsof medico-legal terms. For instance, “allergic sensitivity reaction to injected contrastmedia” was changed to “allergic reaction at injection site” and “acute myocardial
246 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

infarction” was changed to “acute myocardial infarction, commonly known as a heartattack.” This strategy adhered to the US Food and Drug Administration’s (2013)guide to informed consent for research studies, which requires that “technical andscientific terms are adequately explained or that common terms are substituted.” Weworked with the Texas Medical Disclosure Panel to retain essential medical and legalinformation. The readability scores of each document appear in Table 1.
Description of sample. Two hundred seventy-eight adults participated; 188 (67.6%)were female and 88 (31.7%) were male. Participants ranged in age from 18 to 88years (M = 37.8 years, SD = 15.08) and described themselves as African American(14.1%), American Indian (2.9%), Asian (8.3%), Caucasian (56.1%), Hispanic/Latino(a) (24.5%), Middle Eastern (1.4%), and multi-racial (3.2%). Education levels rangedfrom some high school (5%) to a graduate degree (6.1%), with the majority ofparticipants having earned a high-school diploma (16.5%), attended some college(38.1%), or completed a bachelor’s degree (29.5%). A majority of the participantsreported full-time (56.5%) or part-time (8.6%) employment; the rest indicated thatthey were students (13.3%), stay-at-home parents (4.3%), retired (5.8%), currentlyunemployed (4.3%), or other (5.8%). One hundred and twenty-eight participantsreceived the original version of the consent form (control condition) and 150 peoplereceived the revised consent form.
Measures
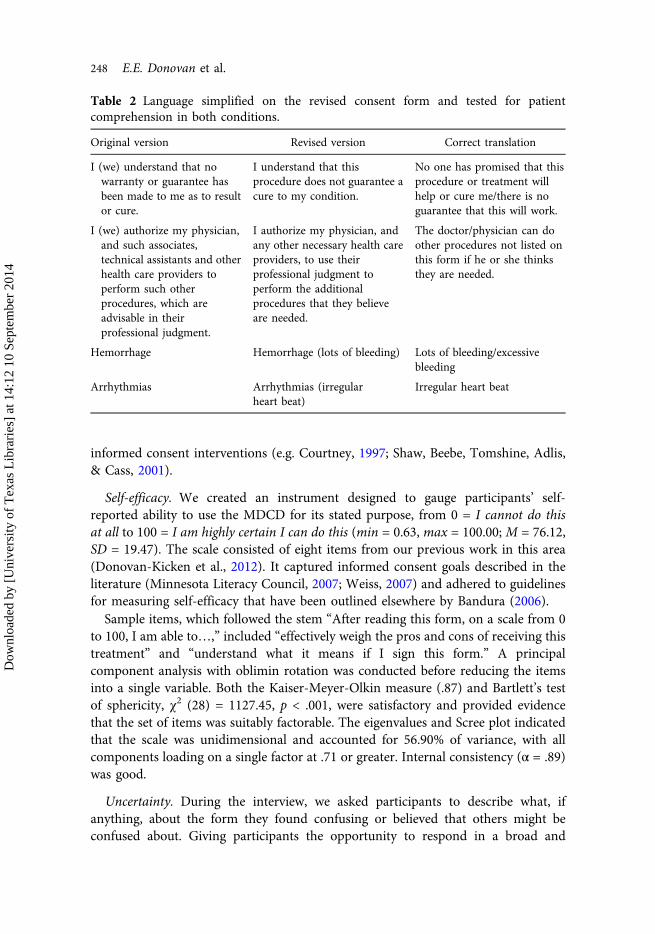
Comprehension of medico-legal terminology. We measured patient comprehensionof four medico-legal terms and phrases that were modified in the revised version ofthe MDCD (see Table 2). The physicians on the Panel attested that these were keypieces of information that patients ought to understand if they were to provideproper informed consent for a cardiac catheterization. Interviewers asked partici-pants to translate each of the terms into everyday language. We consulted with thePanel to determine what an accurate definition of each term or phrase would be. Forexample, the correct translation of “arrhythmia” was “irregular heart beat.” Wecategorically coded participant responses to indicate whether they provided anaccurate definition for each term (1 = yes, 0 = no) and then summed these codes tocreate an index of comprehension. Scores ranged from 0 to 4 (M = 2.52, SD = 1.35).Operationalizing comprehension as the number of correct responses to a short list ofquestions about procedural knowledge coheres with the approaches taken in other
Table 1 Readability scores of original consent form (control condition) and revisedconsent form.
Flesh-Kincaid grade level Gunning Fog SMOG index
Original version 11.6 15.3 11.7Revised version 11.9 14.4 12.0
Medical Disclosure Uncertainty 247
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
informed consent interventions (e.g. Courtney, 1997; Shaw, Beebe, Tomshine, Adlis,& Cass, 2001).
Self-efficacy. We created an instrument designed to gauge participants’ self-reported ability to use the MDCD for its stated purpose, from 0 = I cannot do thisat all to 100 = I am highly certain I can do this (min = 0.63, max = 100.00; M = 76.12,SD = 19.47). The scale consisted of eight items from our previous work in this area(Donovan-Kicken et al., 2012). It captured informed consent goals described in theliterature (Minnesota Literacy Council, 2007; Weiss, 2007) and adhered to guidelinesfor measuring self-efficacy that have been outlined elsewhere by Bandura (2006).
Sample items, which followed the stem “After reading this form, on a scale from 0to 100, I am able to…,” included “effectively weigh the pros and cons of receiving thistreatment” and “understand what it means if I sign this form.” A principalcomponent analysis with oblimin rotation was conducted before reducing the itemsinto a single variable. Both the Kaiser-Meyer-Olkin measure (.87) and Bartlett’s testof sphericity, χ2 (28) = 1127.45, p < .001, were satisfactory and provided evidencethat the set of items was suitably factorable. The eigenvalues and Scree plot indicatedthat the scale was unidimensional and accounted for 56.90% of variance, with allcomponents loading on a single factor at .71 or greater. Internal consistency (α = .89)was good.
Uncertainty. During the interview, we asked participants to describe what, ifanything, about the form they found confusing or believed that others might beconfused about. Giving participants the opportunity to respond in a broad and
Table 2 Language simplified on the revised consent form and tested for patientcomprehension in both conditions.
Original version Revised version Correct translation
I (we) understand that nowarranty or guarantee hasbeen made to me as to resultor cure.
I understand that thisprocedure does not guarantee acure to my condition.
No one has promised that thisprocedure or treatment willhelp or cure me/there is noguarantee that this will work.
I (we) authorize my physician,and such associates,technical assistants and otherhealth care providers toperform such otherprocedures, which areadvisable in theirprofessional judgment.
I authorize my physician, andany other necessary health careproviders, to use theirprofessional judgment toperform the additionalprocedures that they believeare needed.
The doctor/physician can doother procedures not listed onthis form if he or she thinksthey are needed.
Hemorrhage Hemorrhage (lots of bleeding) Lots of bleeding/excessivebleeding
Arrhythmias Arrhythmias (irregularheart beat)
Irregular heart beat
248 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
somewhat impersonal way, rather than emphasizing “what is confusing to youpersonally,” was a deliberate linguistic strategy designed to make the interviewprocess less face-threatening (Brown & Levinson, 1987; Lim & Bowers, 1991). We didthis in part because we expected that some of our participants would have limitedhealth literacy, which could affect their confidence in responding. This approach wasalso consistent with patient-oriented standards for informed consent, whichencourage stakeholders to prioritize what an average, reasonable patient is believedto consider as relevant information in a particular medical situation (Lo, 2000).
Interviewers wrote down participants’ responses. Four coders organized theresponses into 1568 discrete thought units (Hatfield & Weider-Hatfield, 1978). First,they coded a random subset of 20% of the data. We calculated Guetzkow’s U toestablish their unitization reliability, which was excellent at 0.01. Following that, thecoders divided the remainder of the dataset and unitized it. We calculateduncertainty by summing the number of units that each participant identified asconfusing. Uncertainty ranged from 0 to 35 (M = 5.64, SD = 4.56).
Health literacy. The Newest Vital Sign (NVS; Weiss et al., 2005) was used as anassessment of health literacy. The NVS includes a facsimile of an ice cream containernutrition label and six questions about the meanings of the information on the label(e.g. calculating how many calories a person would consume after eating severalservings). Individuals who answer fewer than four questions correctly are consideredto have low/limited health literacy. Summed scores ranged from 0 to 6 (M = 4.34, SD= 1.79), with 29% of the sample demonstrating low/limited health literacy. Toperform the analyses in the present study, we relied on conventions of the NVS todivide the sample into participants who had relatively low health literacy (n = 80)and those who had relatively high health literacy (n = 188).
Previous experience. Finally, we gathered information to control for the possibilitythat patients’ prior experience receiving healthcare would influence the results,guided by prior research indicating that people demonstrate greater understanding ofconsent materials in research studies when they have familiarity with the process(Cortes, Drainoni, Henault, & Paasche-Orlow, 2010). This logic is consistent withscholarship suggesting that situation-specific experience should enhance feelings ofself-efficacy (Bandura, 1977) and comports with the proposition of UIT that greaterknowledge is inversely associated with uncertainty. We asked participants, “Howmuch personal experience would you say you have receiving health care in Texas?”from 1 = none to 4 = a lot (M = 3.22, SD = 0.81).
Results
Preliminary analyses were performed to establish that sociodemographic character-istics were equivalent between the control and experimental groups. Importantly,there was no evidence that participants in either condition had significantly differentlevels of health literacy, F(1, 265) = 3.19, p = .06. There was also no evidence that theconditions differed in mean age, F(1, 268) = 3.37, p = .07, in the proportion of
Medical Disclosure Uncertainty 249
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
participants who were female versus male, χ2(275) = .52, p = .60, V = .04, or in theproportion of people who were White compared to non-White, χ2(275) = .44, p =.47, V = .05.
Main Effects of Consent Form Version
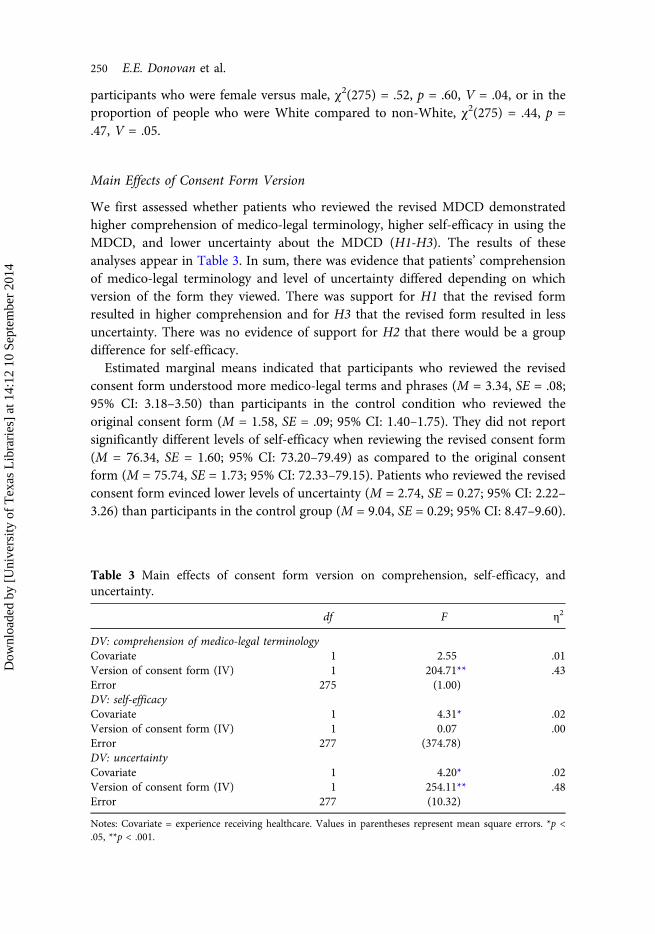
We first assessed whether patients who reviewed the revised MDCD demonstratedhigher comprehension of medico-legal terminology, higher self-efficacy in using theMDCD, and lower uncertainty about the MDCD (H1-H3). The results of theseanalyses appear in Table 3. In sum, there was evidence that patients’ comprehensionof medico-legal terminology and level of uncertainty differed depending on whichversion of the form they viewed. There was support for H1 that the revised formresulted in higher comprehension and for H3 that the revised form resulted in lessuncertainty. There was no evidence of support for H2 that there would be a groupdifference for self-efficacy.
Estimated marginal means indicated that participants who reviewed the revisedconsent form understood more medico-legal terms and phrases (M = 3.34, SE = .08;95% CI: 3.18–3.50) than participants in the control condition who reviewed theoriginal consent form (M = 1.58, SE = .09; 95% CI: 1.40–1.75). They did not reportsignificantly different levels of self-efficacy when reviewing the revised consent form(M = 76.34, SE = 1.60; 95% CI: 73.20–79.49) as compared to the original consentform (M = 75.74, SE = 1.73; 95% CI: 72.33–79.15). Patients who reviewed the revisedconsent form evinced lower levels of uncertainty (M = 2.74, SE = 0.27; 95% CI: 2.22–3.26) than participants in the control group (M = 9.04, SE = 0.29; 95% CI: 8.47–9.60).
Table 3 Main effects of consent form version on comprehension, self-efficacy, anduncertainty.
df F η2
DV: comprehension of medico-legal terminologyCovariate 1 2.55 .01Version of consent form (IV) 1 204.71** .43Error 275 (1.00)DV: self-efficacyCovariate 1 4.31* .02Version of consent form (IV) 1 0.07 .00Error 277 (374.78)DV: uncertaintyCovariate 1 4.20* .02Version of consent form (IV) 1 254.11** .48Error 277 (10.32)
Notes: Covariate = experience receiving healthcare. Values in parentheses represent mean square errors. *p <.05, **p < .001.
250 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

Associations between Health Literacy and Outcome Variables
The zero-order correlations among continuous variables are listed in Table 4. Healthliteracy was positively associated with comprehension, providing support for H4.However, contrary to the expectations set forth in H5 and H6, there was no evidencethat health literacy was correlated with patient self-efficacy, and although there was asignificant association between health literacy and uncertainty, it was in the oppositedirection as anticipated. Whereas we hypothesized that persons with higher healthliteracy would report lower uncertainty, we observed that higher health literacy wasactually associated with higher levels of uncertainty.
Interaction Effects of Consent Form Version and Health Literacy
Comprehension of medico-legal terminology. A 2 (revised consent form vs originalconsent form) × 2 (low health literacy vs high health literacy) between-subjectsANCOVA revealed a significant main effect of consent form version on compre-hension of medico-legal terminology, F(1, 261) = 234.62, p < .001, partial η2 = .47,with patients who reviewed the revised consent form correctly translating a highernumber of terms and phrases (M = 3.24, SE = 0.09) than patients who saw theoriginal consent form (M = 1.30, SE = 0.09). A main effect was found for healthliteracy, F(1, 261) = 38.72, p < .001, partial η2 = .13, such that patients having highhealth literacy correctly translated more medico-legal terms and phrases (M = 2.67,SE = 0.07) than patients with low health literacy (M = 1.88, SE = 0.12). The covariate,experience receiving healthcare, was significantly related to comprehension, F(1, 261)= 5.42, p < .05, partial η2 = .02.
There was also evidence of an interaction between MDCD version and healthliteracy, F(1, 261) = 15.22, p < .001, partial η2 = .06. The interaction effect suggestedthe following: patients in both the low and high health literacy groups exhibitedhigher comprehension of medico-legal terminology when reviewing the revisedconsent form, when compared to those in the control condition who reviewed theoriginal form. Yet although individuals in the control group demonstrated noticeablydifferent levels of comprehension depending on their levels of health literacy, peoplein both health literacy groups evinced rather similar levels of comprehension in the
Table 4 Bivariate correlations among main study variables.
Healthliteracy
Experiencereceiving Comprehension
Self-efficacy Uncertainty
Health literacy – −.08 .24** .06 .24**Experience receiving – .21** .13* −.23**Comprehension – .10 −.39**Self-efficacy – −.17**Uncertainty –
*p < .05, **p < .01.
Medical Disclosure Uncertainty 251
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
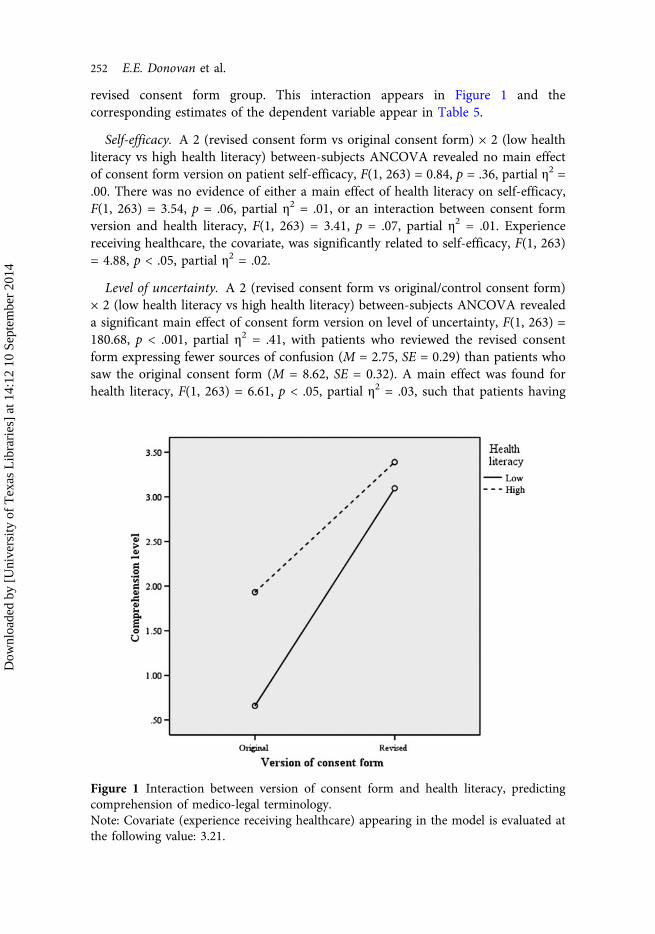
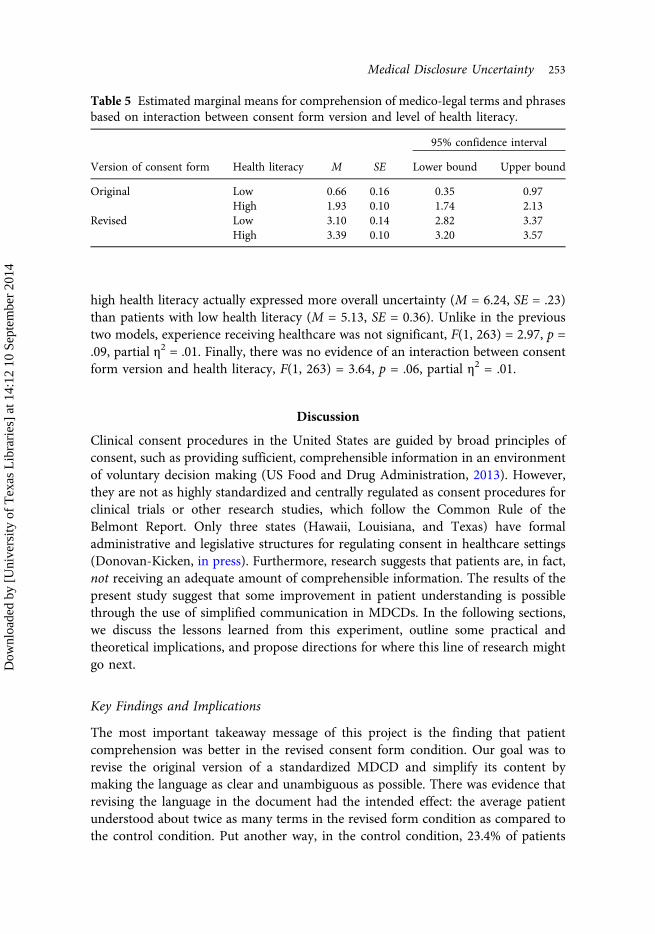
revised consent form group. This interaction appears in Figure 1 and thecorresponding estimates of the dependent variable appear in Table 5.
Self-efficacy. A 2 (revised consent form vs original consent form) × 2 (low healthliteracy vs high health literacy) between-subjects ANCOVA revealed no main effectof consent form version on patient self-efficacy, F(1, 263) = 0.84, p = .36, partial η2 =.00. There was no evidence of either a main effect of health literacy on self-efficacy,F(1, 263) = 3.54, p = .06, partial η2 = .01, or an interaction between consent formversion and health literacy, F(1, 263) = 3.41, p = .07, partial η2 = .01. Experiencereceiving healthcare, the covariate, was significantly related to self-efficacy, F(1, 263)= 4.88, p < .05, partial η2 = .02.
Level of uncertainty. A 2 (revised consent form vs original/control consent form)× 2 (low health literacy vs high health literacy) between-subjects ANCOVA revealeda significant main effect of consent form version on level of uncertainty, F(1, 263) =180.68, p < .001, partial η2 = .41, with patients who reviewed the revised consentform expressing fewer sources of confusion (M = 2.75, SE = 0.29) than patients whosaw the original consent form (M = 8.62, SE = 0.32). A main effect was found forhealth literacy, F(1, 263) = 6.61, p < .05, partial η2 = .03, such that patients having
Figure 1 Interaction between version of consent form and health literacy, predictingcomprehension of medico-legal terminology.Note: Covariate (experience receiving healthcare) appearing in the model is evaluated atthe following value: 3.21.
252 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
high health literacy actually expressed more overall uncertainty (M = 6.24, SE = .23)than patients with low health literacy (M = 5.13, SE = 0.36). Unlike in the previoustwo models, experience receiving healthcare was not significant, F(1, 263) = 2.97, p =.09, partial η2 = .01. Finally, there was no evidence of an interaction between consentform version and health literacy, F(1, 263) = 3.64, p = .06, partial η2 = .01.
Discussion
Clinical consent procedures in the United States are guided by broad principles ofconsent, such as providing sufficient, comprehensible information in an environmentof voluntary decision making (US Food and Drug Administration, 2013). However,they are not as highly standardized and centrally regulated as consent procedures forclinical trials or other research studies, which follow the Common Rule of theBelmont Report. Only three states (Hawaii, Louisiana, and Texas) have formaladministrative and legislative structures for regulating consent in healthcare settings(Donovan-Kicken, in press). Furthermore, research suggests that patients are, in fact,not receiving an adequate amount of comprehensible information. The results of thepresent study suggest that some improvement in patient understanding is possiblethrough the use of simplified communication in MDCDs. In the following sections,we discuss the lessons learned from this experiment, outline some practical andtheoretical implications, and propose directions for where this line of research mightgo next.
Key Findings and Implications
The most important takeaway message of this project is the finding that patientcomprehension was better in the revised consent form condition. Our goal was torevise the original version of a standardized MDCD and simplify its content bymaking the language as clear and unambiguous as possible. There was evidence thatrevising the language in the document had the intended effect: the average patientunderstood about twice as many terms in the revised form condition as compared tothe control condition. Put another way, in the control condition, 23.4% of patients
Table 5 Estimated marginal means for comprehension of medico-legal terms and phrasesbased on interaction between consent form version and level of health literacy.
95% confidence interval
Version of consent form Health literacy M SE Lower bound Upper bound
Original Low 0.66 0.16 0.35 0.97High 1.93 0.10 1.74 2.13
Revised Low 3.10 0.14 2.82 3.37High 3.39 0.10 3.20 3.57
Medical Disclosure Uncertainty 253
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

understood zero medico-legal terms and 3.9% understood all four terms. In contrast,in the revised condition, 0.7% of patients understood zero terms and 57.4%understood all four terms. Considering that our objective was to make theinformation in this MDCD more accessible and comprehensible to patients, webelieve that this main effect represents a success.
It is notable that comprehension was better when reviewing the revised form forpeople at both high and low levels of health literacy, but the magnitude of thedifference varied. Results indicated that although a simplified consent form hasbenefits for most patients, individuals with relatively low health literacy seem tomake especially great strides in their level of understanding. This finding underscoresthe potential for communicating effectively with as many patients as possible.Guidelines already exist for simple, effective oral and written communicationmaterials targeted at less-health-literate patients (National Cancer Institute, 2003;Weiss, 2003). It is important to note, however, that other interventions developedspecifically to meet the needs of less-health-literate audiences have been deemedengaging and acceptable for broader audiences (Mackert, Whitten, & Garcia, 2008).This suggests that a focus on simplifying medical information will have broaderbenefits than helping only the less-health-literate populations. From a practicalstandpoint, it is most economical and efficient to produce a single version of aMDCD, rather than trying to develop and disseminate multiple versions that areadapted to different levels of health literacy.
Patients’ levels of uncertainty also differed by condition. We anticipated thatpatients would cite fewer sources of uncertainty and confusion when reading therevised form, and this expectation was confirmed. Theoretically, it is reasonable thatthe act of reading a MDCD prior to a medical procedure could either reduce orincrease uncertainty (Mishel, 1988; Brashers, 2001)—for example, about theprocedure itself, the possible risks, the desire to follow through with the course ofaction, and the individual’s own ability to use the information presented in the form.Recent theorizing about uncertainty management has emphasized that receivinggreater amounts of health information has the potential to increase uncertainty, evenamong people who are actively seeking information to reduce their uncertainty (e.g.Brashers et al., 2004; Bylund et al., 2012). The results of the present experiment dosuggest that fewer questions about the consent form content were stimulated whenpatients reviewed simplified material.
There was no evidence that people who reviewed different versions of the consentform differed in their subsequent levels of self-efficacy. In general, participants in ourstudy felt moderately confident about their ability to understand and use theinformation contained in the MDCD, regardless of whether they were viewingrelatively complicated or relatively simplified material. This was despite the fact thatactual ratings of their comprehension level varied significantly by condition. It is alsoworth pointing out that self-efficacy and comprehension level were not significantlycorrelated with one another. It may be that in the context of informed consent, self-reported perceptions of ability are not as informative as objective measures ofcomprehension. This null result contradicts previous empirical evidence suggesting
254 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

that health literacy is moderately and positively correlated with self-efficacy; it alsochallenges some of our earlier recommendations that it might be useful to drawpatients’ attention to their levels of self-efficacy, in order to help establish whetherthe informed consent process has been adequate (Donovan-Kicken et al., 2012).Perhaps patients’ evaluations of their own knowledge are not as reliable as we hadearlier suspected.
An important theoretical implication of this project is that readability scores arenot necessarily the most useful means of evaluating how effectively medicaldisclosure and consent information is being communicated. The original and revisedversions of the document tested in the present study were very similar in terms oftraditional readability index scores, having nearly the same number of words andsyllables per word. In part, this was a natural consequence of the medical and legalmandates that require the inclusion of certain terms and phrases; our ability to makechanges that would have drastically modified readability scores was limited.Ultimately, though, we see this constraint as advantageous, because it allowed us tofocus on changes that were not geared around readability. Patients understood moreof the document content in our simplified version, even though the purportedreadability had not changed significantly. Conducting formative research prior to thisstudy enabled us to make revisions that were based on patients’ reported sources ofuncertainty, rather than simply submitting the text to a readability gauge until wecould attest that the desired reading level had been attained.
From both a theoretical and an applied perspective, the results of this studyprovided support for the UIT and UMT premise that sufficiency and quality ofinformation are as important to consider as quantity, if not more so. We would arguethat if it seems as though additional material is needed to augment a MDCD, thenthe MDCD itself needs work. Although replication and elaboration of our findingsare advised, our preliminary recommendation for applying the lessons of this studyis this: there is evidence that it is possible to decrease complexity without increasingthe volume or lowering the readability score of medical disclosure and consentinformation. Our changes amounted to retaining only the essential pieces ofinformation regarding risks and hazards and providing simple explanations ofmedical terms in everyday language. As stated previously, this is in line withthe FDA’s recommendations to explain and/or substitute common terms fortechnical language. The impetus to improve the comprehensibility of MDCDs isalso representative of broader currents that exist in guidelines on writing formultinational constituencies (European Commission, 2013), information access-ibility for persons with disabilities (Culnan, 1985), and textbooks on socialscientific questionnaire design that advise researchers to write simple surveyquestions with no unfamiliar or ambiguous words (Schwarz, 1999). Furthermore,our approach corresponds with the aims of the Plain Writing Act (2010), a USstatute designed to improve communication by requiring that materials publishedby federal agencies be clear, concise, well organized, and otherwise accessible to thelay public.
Medical Disclosure Uncertainty 255
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

Strengths, Limitations, and Directions for Future Research
Some strengths of this project are noteworthy. Ours was one of the largestrandomized studies of consent form comprehension to date, with effect sizes farexceeding the majority of published work on this topic (cf. Schenker et al., 2011). Weare encouraged by the results that suggest that patient comprehension can, in fact, beimproved. Furthermore, a reform of this nature would be relatively straightforwardand inexpensive for healthcare providers and lawmakers to carry out. Although itwould be inaccurate to minimize the amount of labor that went into researching,implementing, and testing the revisions to this consent document, the changes thatwe ultimately made were fairly simple and replicable. Given recent researchgrounded in UMT suggesting that people are likely to avoid health-relatedinformation when it is viewed as defective and unusable (Barbour, Rintamaki,Ramsey, & Brashers, 2012), replacing confusing language with common terms maybe a step in the right direction to overcome the public’s tendency to skip the step ofcarefully reading through consent forms.
As with many experiments, the drawbacks to this design amounted to tradeoffsbetween external and internal validity. Although much of the material on thisconsent form is standardized statewide and would be present on documents for otherhealth conditions and procedures, we tested a form that pertained only to a cardiaccatheterization. Second, we were not working with participants who were actuallyundergoing the procedure. This may have resulted in deflated or inflated self-reportsof self-efficacy or uncertainty, although it is unlikely to have seriously affected thecomprehension scores. Given the applied nature of this project, the experimentaldesign is not as tidy as it might have been otherwise. For example, we changedseveral elements of the form to improve the overall content and layout of thedocument, such as reorganizing some bulleted lists of risks. This means that theresults (especially, perhaps, those pertaining to uncertainty more so than compre-hension) cannot definitively be attributed to the isolation of a single, discrete consentform element. We felt that this disadvantage was outweighed by the merits ofconducting translational communication research that is serving the needs of thesecond most populous state in the United States, but it is worth mentioningnonetheless.
An opportunity for building upon the present investigation involves furtherpinpointing verbal and visual elements that consistently produce greater uncertaintyand lower comprehension of MDCDs. In recent years, interpersonal and masscommunication scholars have been engaging with research problems that focus onthe discursive features of health messages that both convey and arouse uncertainty(Bylund et al., 2012; Donovan, Brown, LeFebvre, Zaitchik, & Love, in press; Gill &Babrow, 2007; Hurley et al., 2011; Jensen, 2008). The experiment reported herefocused on the clarity of a MDCD and was developed according to the assumptionthat clearer communication—characterized by less ambiguous and less complexinformation—would facilitate patients’ comprehension. To advance theory onuncertainty, communication, and informed consent, it would be useful to design
256 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

future interventions that make finer distinctions among message features that reflectambiguity versus complexity, in both explicit and implicit ways (see Hurley et al.,2011), to test the relative effects of each. Likewise, it will be important to triangulateour measure of uncertainty, which did not capture certain dimensions of uncertaintythat exist in the literature, such as inability to make sense of statistical probabilitiesand difficulty in assigning value to an event or risk (see Babrow et al., 1998). Takingany or all of these steps will yield additional empirically and theoretically drivenscaffolding for the building of tools that could be used by practitioners to createaccessible MDCDs and to administer more successful informed consent.
Finally, although written consent interventions constitute the most prominent typeof study design in the literature (and the most cost-effective in practice), we recognizethe value of pursuing more interactive communication strategies in future research.There is some evidence that audiovisual and multimedia channels are associated withhigher levels of comprehension about risks, benefits, and alternatives to treatment, ascompared to written information (Shaw et al., 2001). For example, a brief educationalvideo or interactive e-health application, accompanying or in lieu of a consentdocument, could significantly enhance patient knowledge and satisfaction with theconsent process. However, there is limited evidence that verbal counseling alone (i.e.extended discussions with a healthcare practitioner) improves patient understandingof the risks of medical procedures (Schenker et al., 2011), so we contend that writtencommunication (with or without the addition of interactive media) should remain aprimary focus of future studies and of ongoing consent procedures.
References
Ad Hoc Committee on Health Literacy. (1999). Health literacy: Report of the Council on ScientificAffairs. Journal of the American Medical Association, 281, 552–557. doi:10.1001/jama.281.6.552
Babrow, A. S., Kasch, C. R., & Ford, L. A. (1998). The many meanings of uncertainty in illness:Toward a systematic accounting. Health Communication, 10, 1–23. doi:10.1207/s15327027hc1001_1
Bandura, A. (1977). Self-efficacy: The exercise of control. New York, NY: W. H. Freeman.Bandura, A. (2006). Guide for constructing self-efficacy scales. In F. Pajares & T. Urdan (Eds.),
Self-efficacy beliefs of adolescents (pp. 307–337). Greenwich, CT: Information AgePublishing.
Barbour, J. B., Rintamaki, L. S., Ramsey, J. R., & Brashers, D. E. (2012). Avoiding health information.Journal of Health Communication, 17, 212–229. doi:10.1080/10810730.2011.585691
Brashers, D. E. (2001). Communication and uncertainty management. Journal of Communication,51, 477–497. doi:10.1111/j.1460-2466.2001.tb02892.x
Brashers, D. E., Goldsmith, D. J., & Hsieh, E. (2002). Information seeking and avoiding in healthcontexts. Human Communication Research, 28, 258–271. doi:10.1111/j.1468-2958.2002.tb00807.x
Brashers, D. E., Neidig, J. L., & Goldsmith, D. J. (2004). Social support and the managementof uncertainty for people living with HIV or AIDS. Health Communication, 16, 305–331.doi:10.1207/S15327027HC1603_3
Brown, P., & Levinson, S. (1987). Politeness: Some universals in language use. Cambridge, MA:University Press.
Brown, T. F., Massoud, E., & Bance, M. (2003). Informed consent in otologic surgery: Prospectivestudy of risk recall by patients and impact of written summaries of risk. The Journal ofOtolaryngology, 32, 368–372. doi:10.2310/7070.2003.13987
Medical Disclosure Uncertainty 257
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
Bylund, C. L., Fisher, C. L., Brashers, D., Edgerson, S., Glogowski, E. A., Boyar, S. R., … Kissane, D.(2012). Sources of uncertainty about daughters’ breast cancer risk that emerge duringgenetic counseling consultations. Journal of Genetic Counseling, 21, 292–304. doi:10.1007/s10897-011-9400-y
Byrne, D. J., Napier, A., & Cuschieri, A. (1988). How informed is signed consent? British MedicalJournal, 296, 839–840. doi:10.1136/bmj.296.6625.839
Chall, J. S., & Dale, E. (1995). Readability revisited: The new Dale-Chall readability formula.Cambridge, MA: Brookline Books.
Clayton, M.F., Mishel, M.H., & Belyea, M. (2006). Testing a model of symptoms, communication,uncertainty, and well-being, in older breast cancer survivors. Research in Nursing & Health,29, 18–39. doi:10.1002/nur.20108
Cortes, D. E., Drainoni, M., Henault, L. E., & Paasche-Orlow, M. K. (2010). How to achieveinformed consent for research from Spanish-speaking individuals with low literacy:A qualitative report. Journal of Health Communication, 15, 172–182. doi:10.1080/10810730.2010.499990
Courtney, M. J. (1997). The effect of a preanaesthetic information booklet on patientunderstanding and satisfaction. The New Zealand Medical Journal, 110, 212–214.
Culnan, M. J. (1985). The dimensions of perceived accessibility to information: Implications for thedelivery of information systems and services. Journal of the American Society forInformation Science, 36, 302–308. doi:10.1002/asi.4630360504
Davis, T. C., Dolan, N. C., Ferreira, M. R., Tomori, C., Green, K. W., Sipler, A. M., & Bennett, C. L.(2001). The role of inadequate health literacy skills in colorectal cancer screening. CancerInvestigation, 19, 193–200. doi:10.1081/CNV-100000154
Davis, T. C., Williams, M. V., Marin, E., Parker, R. M., & Glass, J. (2002). Health literacy andcancer communication. CA: A Journal for Clinicians, 52(3), 134–149. doi:10.3322/canjclin.52.3.134
Doak, C. C., Doak, L. G., Friedell, G. H., & Meade, C. D. (1998). Improving comprehension forcancer patients with low literacy skills: Strategies for clinicians. CA: A Cancer Journal forClinicians, 48, 151–162. doi:10.3322/canjclin.48.3.151
Donovan, E. E., Brown, L. E., LeFebvre, L., Zaitchik, S., & Love, B. (in press). “The uncertainty iswhat is driving me crazy”: The tripartite model of uncertainty in the adolescent and youngadult cancer context. Health Communication.
Donovan-Kicken, E. (in press). Disclosure and informed consent. In T. L. Thompson (Ed.),Encyclopedia of health communication. Thousand Oaks, CA: Sage.
Donovan-Kicken, E., Mackert, M., Guinn, T. D., Tollison, A. C., & Breckinridge, B. (2011,November). Sources and predictors of patient uncertainty when reviewing medical disclosureand consent documentation. Paper presented at the annual convention of the NationalCommunication Association, New Orleans, LA.
Donovan-Kicken, E., Mackert, M., Guinn, T. D., Tollison, A. C., & Breckinridge, B. (2013). Sourcesof patient uncertainty when reviewing medical disclosure and consent documentation.Patient Education and Counseling, 90, 254–260. doi:10.1016/j.pec.2012.10.007
Donovan-Kicken, E., Mackert, M., Guinn, T. D., Tollison, A. C., Breckinridge, B., & Pont, S. J.(2012). Health literacy, self-efficacy, and patients’ assessment of medical disclosure andconsent documentation. Health Communication, 27, 581–590. doi:10.1080/10410236.2011.618434
Dubay, W. H. (2004). The principles of readability. Costa Mesa, CA: Impact Information.European Commission. (2013). How to write clearly. Retrieved from http://ec.europa.eu/transla-
tion/writing/clear_writing/how_to_write_clearly_en.pdf.Faden, R. R., Becker, C., Lewis, C., Freeman, J., & Faden, A. I. (1981). Disclosure of information
to patients in medical care. Medical Care, 19, 718–733. doi:10.1097/00005650-198107000-00003
Gill, E., & Babrow, A. S. (2007). To hope or to know: Coping with uncertainty and ambivalence inwomen’s magazine breast cancer articles. Journal of Applied Communication Research, 35,133–155. doi:10.1080/00909880701263029
Graham, P. (2003). Type of consent does not influence patient recall of serious potential radiationtoxicity of adjuvant breast radiotherapy. Australasian Radiology, 47, 416–421. doi:10.1046/j.1440-1673.2003.01212.x
258 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14
Grundner, T. M. (1980). On the readability of surgical consent forms. The New England Journal ofMedicine, 302, 900–902. doi:10.1056/NEJM198004173021606
Hatfield, J. D., & Weider-Hatfield, D. (1978). The comparative utility of three types of behavioralunits for interaction analysis. Communication Monographs, 45, 44–50. doi:10.1080/03637757809375950
Hogan, T. P., & Brashers, D. E. (2009). The theory of communication and uncertaintymanagement: Implications from the wider realm of information behavior. In T. D. Afifi &W. A. Afifi (Eds.), Uncertainty, information management, and disclosure decisions (pp. 45–66). New York, NY: Routledge.
Howard, D., Gazmararian, J., & Parker, R. (2005). The impact of low health literacy on the medicalcosts of Medicare managed care enrollees. The American Journal of Medicine, 118, 371–377.doi:10.1016/j.amjmed.2005.01.010
Hull, L. C. (1979). Measuring the readability of technical writing. In Proceedings of the 26thInternational Technical Communications Conference (pp. E79–E84). Los Angeles,CA: ITCC.
Hurley, R. J., Kosenko, K. A., & Brashers, D. (2011). Uncertain terms: Message features of onlinecancer news. Communication Monographs, 78, 370–390. doi:10.1080/03637751.2011.565061
Inglis, S., & Farnill, D. (1993). The effects of providing preoperative statistical anaesthetic-riskinformation. Anaesthesia and Intensive Care, 21, 799–805.
Institute of Medicine Committee on Health Literacy. (2004). Health literacy: A prescription to endconfusion. Washington, DC: National Academy Press.
Jensen, J. D. (2008). Scientific uncertainty in news coverage of cancer research: Effects of hedgingon scientists’ and journalists’ credibility. Human Communication Research, 34, 347–369.doi:10.1111/j.1468-2958.2008.00324.x
Jubelirer, S. J. (1991). Levels of reading difficulty in educational pamphlets and informed consentdocuments for cancer patients. West Virginia Medical Journal, 87, 554–557.
Katz, J. (1984). The silent world of doctor and patient. New York, NY: Free Press.Kincaid, J. P., Fishburne, R. P., Rogers, R. L., & Chissom, B. S. (1975). Derivation of new
readability formulas (Automated readability index, fog count, and flesch reading easeformula) for Navy enlisted personnel. Research Branch report 8–75. Memphis, TN: NavalAir Station.
Klare, G. R. (1976). A second look at the validity of the readability formulas. Journal of ReadingBehavior, 8, 159–152. doi:10.1080/10862967609547171
Krumholz, H. M. (2010). Informed consent to promote patient-centered care. Journal of theAmerican Medical Association, 303, 1190–1191. doi:10.1001/jama.2010.309
Langdon, I. J., Hardin, R., & Learmonth, I. D. (2002). Informed consent for total hip arthroplasty:Does a written information sheet improve recall by patients? Annals of the Royal College ofSurgeons of England, 84, 404–408. doi:10.1308/003588402760978201
Laubach, R., & Koschnick, K. (1977). Using readability: Formulas for easy adult materials. Syracuse,NY: New Readers Press.
Lim, T., & Bowers, J. W. (1991). Facework: Solidarity, approbation, and tact. HumanCommunication Research, 17, 415–450. doi:10.1111/j.1468-2958.1991.tb00239.x
Livesley, P. J., & Rider, M. A. (1993). Joint replacement and patient education. InternationalOrthopaedics, 17, 34–36. doi:10.1007/BF00195221
Lo, B. (2000). Resolving ethical dilemmas: A guide for clinicians (2nd ed.). Philadelphia, PA:Lippincott Williams & Wilkins.
MacDougall, D. S., Connor, U. M., & Johnstone, P. A. (2012). Comprehensibility of patient consentforms for radiation therapy of cervical cancer. Gynecologic Oncology, 125, 600–603.doi:10.1016/j.ygyno.2012.02.030
Mackert, M., Whitten, P., & Garcia, A. (2008). Interventions for low health literate audiences.Journal of Computer-Mediated Communication, 13, 504–515. doi:10.1111/j.1083-6101.2008.00407.x
McLaughlin, G.H. (2008). SMOG: Simple measure of gobbledygook. Retrieved from: http://www.harrymclaughlin.com/SMOG
Minnesota Literacy Council. (2007). Statewide informed consent process: Background andrecommendations for health care from the Minnesota Health Literacy Partnership. Retrievedfrom http://healthliteracymn.org/downloads/Informed-Consent-white-paper.pdf.
Medical Disclosure Uncertainty 259
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14

Mishel, M. H. (1988). Uncertainty in illness. Image: Journal of Nursing Scholarship, 20, 225–232.doi:10.1111/j.1547-5069.1988.tb00082.x
National Cancer Institute. (2003). Clear & simple: Developing effective print materials for low-literate readers. Retrieved from http://www.cancer.gov/cancertopics/cancerlibrary/clear-and-simple/AllPages.
National Center for Education Statistics. (2003). National assessment of adult literacy. Retrievedfrom http://nces.ed.gov/naal/kf_demographics.asp.
National Quality Forum. (2005). Implementing a national voluntary consensus standard forinformed consent: A user’s guide for healthcare professionals. Washington, DC: NationalQuality Forum.
Nielsen-Bohlman, L., Panzer, A., & Kindig, D. (Eds.). (2004). Health literacy: A prescription to endconfusion. Washington, DC: National Academy of Sciences.
Osman, H. (2001). History and development of the doctrine of informed consent. TheInternational Electronic Journal of Health Education, 4, 41–47.
Paasche-Orlow, M. K., Taylor, H. A., & Brancati, F. L. (2003). Readability standards for informed-consent forms as compared with actual readability. The New England Journal of Medicine,348, 721–726. doi:10.1056/NEJMsa021212
Plain Writing Act of 2010. (2010). Pub. L. No. 111–274 § 2, 124 Stat. 2861.Schenker, Y., Fernandez, A., Sudore, R., & Schillinger, D. (2011). Interventions to improve patient
comprehension in informed consent for medical and surgical procedures: A systematicreview. Medical Decision Making, 31, 151–173. doi:10.1177/0272989X10364247
Schloman, B. (2003). Quality of health information of the web: Where are we now? Online Journalof Issues in Nursing, 8(1), 26–34.
Schwarz, N. (1999). Self-reports: How the questions shape the answers. American Psychologist,54(2), 93–105. doi:10.1037/0003-066X.54.2.93
Shaw, M. J., Beebe, T. J., Tomshine, P. A., Adlis, S. A., & Cass, O. W. (2001). A randomized,controlled trial of interactive, multimedia software for patient colonoscopy education.Journal of Clinical Gastroenterology, 32, 142–147. doi:10.1097/00004836-200102000-00010
US Food and Drug Administration. (2013). Regulatory information: A guide to informed consentinformation sheet. Retrieved from http://www.fda.gov/RegulatoryInformation/Guidances/ucm126431.htm.
Weiss, B. D. (2003). Health literacy: A manual for clinicians. Chicago, IL: American MedicalAssociation Foundation.
Weiss, B. D. (2007). Health literacy and patient safety: Help patients understand (Manual forclinicians) (2nd ed.). Chicago, IL: American Medical Association Foundation.
Weiss, B. D., Mays, M. Z., Martz, W., Castro, K. M., DeWalt, D. A., Pignone, M. P. … Hale, F. A.(2005). Quick assessment of literacy in primary care: The Newest Vital Sign. Annals ofFamily Medicine, 3, 514–522. doi:10.1370/afm.405
Weiss, B. D., & Palmer, R. (2004). Relationship between health care costs and very low literacyskills in a medically needy and indigent Medicaid population. The Journal of the AmericanBoard of Family Practice, 17, 44–47. doi:10.3122/jabfm.17.1.44
260 E.E. Donovan et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
exas
Lib
rari
es]
at 1
4:12
10
Sept
embe
r 20
14