an approach to the retrieval of thoracic organs for transplantation
TRANSCRIPT

FEBRUARY 1996, VOL 63, NO 2 LloydJones Wheeldon Smith
Potter Wallwork Large
An Approach to the Retrieval of Thoracic Organs for Transplantation m he demand for thoracic organs for transplanta-
tion significantly outweighs the supply of avail- able organs. There are more than 50,000 US patients awaiting cardiac transplantation, but 1 hearts are procured from only 2,500 organ
donors each year.' A similar shortage exists in Europe.* Many factors contribute to the imbalance between donor organ supply and demand. Medical, legal, cul- tural, and religious issues affect people's understanding of organ donation and their attitudes toward consent for organ donation. Many health care personnel are unaware of the altered physiology in patients with lethal brainstem injuries and are not skilled in its man- agement..' The application of rigid or unsubstantiated donor organ acceptance criteria, which rarely consider proposed recipients, also hinders objective decision making and appropriate use of donor organs.
The recovery of thoracic donor organs for trans- plantation usually is part of a multiorgan surgical
retrieval procedure that involves several surgical teams. These surgical procedures demand perioperative team members who are skilled, flexible, cooperative, and diplomatic. This article describes the organ donor man- agement program at Papworth Hospital, National Health Service Trust, Cambridge, United Kingdom, that has alleviated many of the factors contributing to the shortage of thoracic donor organs in our referral area. This article describes our standardized approach that permits optimal management of donors and bene- fits patients with end-stage cardiopulmonary diseases. The article also addresses ethical issues related to organ donation and donor management.
DONOR ORGAN REI'RIEVAL Donor organ retrieval begins with a telephone call
from a regional donor transplant coordinator who con- veys the potential donor's anatomical and physiologi- cal data (Table 1) to a surgical member of the Pap-
A B S T R A C T A critical, worldwide shortage of thoracic organs exists. The
donor management program at Papworth Hospital, National Health Service Trust, Cambridge, United Kingdom, allows satisfactory trans- plantation of thoracic organs that initially appear unsuitable. The peri- operative organ retrieval team members assess the cardiovascular status of all potential donors and manage suboptimal hemodynamics with hormonal replacement therapy consisting of triiodothyronine, antidiuretic hormone, epinephrine, and insulin. These donors' cardio- vascular and pulmonary functions must be wlthln acceptable limits at the time of organ excision. Our standardized approach facilitates objective decision making regarding the appropriate use of donor organs and has increased the number of available donor organs at Papworth Hospital by 30%. Morbidity and mortality rates in thoracic organ recipients have not increased since the authors developed the standardized approach, and more patients have benefited from tho- racic organ transplantation. AORN ./ 63 (Feb 1996) 41 6-426.
worth Hospital transplant unit. Potential organ donors with appar- ent suboptimal cardiopulmonary function are not disqualified as donors automatically, because our donor management regimen often can correct organ dysfunction before organ retrieval. Absolute contraindications to accepting donor organs at the time of notifi- cation include uncontrolled sys- temic sepsis, severe organ trauma, extracranial malignancy, HIV, and hepatitis B or C virus. Additional contraindications for thoracic organ donation are evidence of car- diac toxicity and age greater than 65 years. Subsequent acceptance depends on logistics and the ability
H . LLOYD-JONES; D . R . W H E E L D O N ; J . A . SMITH; C . 11. 0. POTTER; J . W A L L W O R K ; S . R . L A R G E
416 AORN JOURNAL

FEBRUARY 1996, VOL 63, NO 2 8 Lloyd-Jones 9 Wheeldon Smith
Potter 9 Wallwork Large
Time
Table 1 CHECKLIST FOR THE POTENTIAL THORACIC ORGAN DONOR
Donor hospital: Contact: Telephone: Date: Organs offered: heart/lung heart right lung left lung Age: - yrs Sex: M/F Blood group: - Rh factor:+ - Weight: - kg Cause of death: Status: Admission: : hr / / Ventilated : hr / /
height __ cm Virology tests: HIV, hepatitis B, C, cytornegalovirus
MAP* CVP* Rate FIO,* pO,* pH No* K* Ca* Glu* Hgb* lnotropes
Trauma History
Head Cardiac arrest Thorax Cardiac Abdominal Hypertension Upper limbs Diabetes Lower limbs Renal
Blood products received Malignancy Central nervous system
Urine output: __ mulast hr - mulast 24 hr Endotracheal aspiration: Access lines: arterial venous Infection: yes/no/source Medications: Procedures :
Chest x-ray: Electrocardiogram:
History
Asthma Smoking Alcohol Substance abuse
*MAP = mean arterial pressure; CVP = central venous pressure; FlO, = fraction of inspired oxygen; PO, = partial pres- sure of oxygen (artery); Na = serum sodium; K = serum potassium; Ca = serum calcium; Glu = plasma glucose; Hgb = hemoglobin
to match the donor organs with recipients. Matching criteria include compatible blood group; height; weight; and, for lung transplantation, comparable cyto- megalovirus antibody status. Early institution of hor- monal replacement therapy is necessary in donors with apparent suboptimal cardiovascular hemodynamics.
Transport and preliminary preparation. The Papworth Hospital donor organ retrieval team con- sists of a cardiac surgeon, an assistant/trainee sur- geon, an anesthesiologist, a perioperative nurse, and a surgical technologist (ST). All surgical instruments, monitoring and perfusion equipment, and medica- tions needed for organ retrieval are prepackaged and stored at Papworth Hospital. The donor organ
retrieval team members transport this equipment to reduce the use of resources at the donor hospital.
Roles and responsibilities. On arrival at the donor hospital, the donor organ retrieval team mem- bers introduce themselves to donor hospital staff members. All team members wear name badges to facilitate communication among the many people involved in the organ retrieval process. Each donor organ retrieval team member has a defined role, and team members work cooperatively to achieve satis- factory outcomes.
The ST contacts the Papworth Hospital trans- plant coordinator and provides regular updates on the progress of the procurement procedure.
417 AORN JOURNAL

FEBRUARY 1996, VOL 63, NO 2 Lloyd-Jones Wheeldon Smith
Potter Wallwork Large
The surgeons confer with surgical team members from the donor hospital. The anesthesiologist goes to the intensive care unit (ICU) to review the donor’s status. The retrieval team perioperative nurse functions as the liaison between the Papworth Hospital donor organ retrieval team and the donor hospi- tal’s perioperative staff members who assist in preparing the organ retrieval instruments and equipment. The donor hospital’s perioperative nurses are not required to scrub on the organ retrieval procedures, but they do participate in sponge and instrument counts. At the end of the organ retrieval procedure, the organ retrieval team nurse disposes of all sharps and rubbish, thanks the donor hospital’s staff members for their assis- tance, and takes all dirty instruments back to Pap- worth Hospital for cleaning and sterilization.
The donor hospital’s perioperative staff members are responsible for providing routine surgical equipment and supplies.
Sensitivity. Donor organ retrieval is a unique aspect of health care because it involves performing procedures on one patient solely to benefit other patients. Although this practice is legal on patients who are certified brain-dead, it is imperative that donor organ retrieval team members act with the utmost sensitivity toward the donor hospital’s staff members and with due respect for donors. This is especially important when students and junior staff members are present, as some of them may have par- ticipated in the care of the recently deceased donor.
The perioperative nurse from the donor organ retrieval team is responsible for establishing rapport with the donor hospital’s perioperative nurses and for providing information to all staff members who are unfamiliar with organ donation. This interaction is an excellent opportunity to offset the negative aspects of donor organ retrieval procedures. The retrieval team nurse may review anatomy, offer one of the donor hospital perioperative nurses the opportunity to scrub on the organ retrieval procedure, or offer a donor hospital nurse the opportunity to accompany the donor organ retrieval team members back to Pap- worth Hospital to witness the organ transplantation. The donor organ retrieval team nurse also warns the donor hospital’s staff members that the donor organs may not prove suitable for transplantation. Although this is disappointing, team members may be reas- sured that their interventions maximized the potential organs’ suitability for transplantation.
DONOR MANAGEMENT
includes Preoperative care of the potential organ donor
maintaining the patient’s mean blood pressure between 55 mm Hg and 75 mm Hg with a mini- mum central venous pressure (CVP) < 12 mm Hg; ventilating the patient to achieve arterial oxygen saturation levels greater than 98% on minimum inspired oxygen; performing frequent endotracheal (ET) tube suctioning; monitoring and treating abnormal blood bio- chemistry values; maintaining the patient’s hemoglobin between 9 g/dL and 12 g/dL; maintaining a normal to high colloid osmotic pressure by restricting the patient’s crystalloid volume replacement; and treating diabetes insipidus with antidiuretic hor- mone (ADH [Pitressin]).
The donor organ retrieval team surgeons and anesthesiologist assess the donor in the ICU. They review the potential donor’s chest x-ray and electro- cardiogram and confirm the donor’s blood group by visually inspecting the blood cross-match form. They transport the donor to the OR where the donor organ retrieval team members assume responsibility for the donor’s management.
Organ donor management protocol. After reading reports in the literature of the metabolic con- sequences of brain death in experimental animals: we conducted clinical studies to assess the efficacy of hormone replacement therapy in brain-dead organ don01-s.~ The results of these studies led us to adopt a protocol that provides a standardized approach to organ donor management.
Optimum organ donor management requires comprehensive invasive monitoring. Failure to pro- vide adequate physiological support to potential organ donors accounts for at least 25% of lost donor organs.6 For this reason, an anesthesiologist with advanced training in cardiology is a member of the donor organ retrieval team.
These invasive monitoring lines are required because of the nature of the thoracic dissection and the need for reliable hemodynamic measurements:
a pulmonary artery catheter introduced through the right internal jugular vein; a right-sided, triple-lumen catheter in the internal jugular vein; and
418 AORN JOURNAL

FEBRUARY 1996, VOL 63, NO 2 8 Lloyd-Jones 8 Wheeldon Smith
Potter 8 Wallwork Large
Table 2 DIVISION OF POTENTIAL CARDIAC DONORS INTO THREE GROUPS BASED ON HEMODYNAMIC CRITERIA
Measurement Standard Hormone Cardiopulmonary support Cardiac index (Urnin/m2) > 2.6
< 10
Pulmonary capillary wedge pressure (mm Hg) < 10
Left ventricular stroke work (g-m) > 15 I notropes (p/kg/m i n) none
Central venous pressure (rnm Hg)
a left radial or brachial arterial line. If these lines are not already in place, the donor organ retrieval team members insert these invasive monitoring lines in the ICU or in the OR.
Our organ donor management protocol divides potential heart donors into three management approach groups (Table 2). The data, which are derived after a potential organ donor is stabilized and has had optimal IV fluid therapy, dictate the fol- lowing management approaches.
Standard management. The standard management approach consists of maintaining the donor’s mean arterial pressure between 55 mm Hg and 75 mm Hg with low cardiac filling pressures. We use a nomogram (Figure 1, Table 3) to guide this therapy.’ We adminis-
< 2.5 < 2.0
> 10 > 15 > 10 > 15 < 14 < 12 > 1.0 > 8.0
ter crystalloid and colloid IV solutions to replace uri- nary and intraoperative fluid losses and adjust the heart’s preload pressures.8 We administer packed red blood cells or whole blood as needed to maintain a hematocrit level of 30%. Regular ET tube suctioning ensures a clear airway, and use of a ventilator main- tains the donor’s arterial blood gases and oxygen satu- ration levels in the desired ranges. We monitor the organ donor’s serum potassium, calcium, and blood glucose levels and adjust the preoperative therapy to maintain these blood chemistries within normal limits.
Hormone replacement therapy. This manage- ment approach consists of administering IV infusions of triiodothyronine, ADH, epinephrine, and insulin, individually or in combination. The thyroid hormone
Mean arterial pressure minus central venous pressure (mm Hg)
normalize preload
0 1 2 3
I
reduce inotropes and reduce preload
vasodilate
vasoconsh‘ct, norma
vasoconshict and
vasoconsh‘ct, normalize preload, and increase , inotropes
L 4 5 6 7 Cardiac output (Llmin)
Figure 1 The donor organ retrieval team members use this nomogram to guide the donor‘s preop- erative man- agement.
419 AORN JOURNAL

FEBRUARY 1996, VOL 63, NO 2 Lloyd-Jones Wheeldon Smith
Potter 8 Wallwork 8 Large
augments myocardial metabolism in the presence of the “sick euthy- roid” stateg that exists in brain- dead organ donors. The ADH and epinephrine produce peripheral vasoconstriction that counters low systemic vascular resistance.1° Insulin normalizes catecholamine- induced hyperglycemia and facili- tates the provision of chemical fuel to cells.II
After an adequate period of hormone replacement therapy, a potential heart donor must achieve the following minimum criteria:
left ventricular stroke work greater than 15 g-m, left preload pressures less than 12 mm Hg, and inotrope medication doses of less than 5 p/kg/min.
A prospective organ donor who does not meet these criteria is considered unsuitable as a heart donor. Potential heart donors with
Table 3 GLOSSARY
Nomogram. Graphic representation of the relationship between variables. Hematocrit, Volume percentage of erythrocytes in whole blood. Catecholamine. Compound having a sympathomimetic action. lnotrope. Agent affecting the force of cardiac contraction. Pneumoplegio. Solution used to preserve lung tissue. Cardioplegia. Solution used to arrest and preserve the heart.
Beneficence. To do good. Nonmaleficence. To do no harm.
Deontological. Duty- based. Preload. Loading pressure to the ventricle (ie, central venous pressure for the right ventricle, left atrial pressure for the left ventricle). Ahflood. Pressure load that the ventricle works against (ie, mean pul- monary arterial pressure for the right ventricle, mean arterial pressure for the left ventricle). Systemic vascular resistance. Vascular system’s overall resistance to blood flow. l e t ventricular stroke work. Amount of work performed by the ventricle per beat (ie, composite of cardiac output and developed pressure).
congenital anomalies, coronary artery disease, or ventricular hypertrophy also are rejected even if their preoperative cardiac functions are adequate.
Cardiopulmonary support. We institute car- diopulmonary support (CPS) after stabilizing the prospective organ donor and initiating hormone replacement therapy. Cardiopulmonary support con- sists of a centrifugal blood pump, a hollow-fiber oxygenator with heat exchanger, and cannulas in the right atrium and aorta. The object of this manage- ment approach is to restore optimum blood flow, normothermia, and optimal oxygen delivery to all organs while reducing the workload of the heart. We withdraw CPS measures temporarily at hourly inter- vals to evaluate the organ donor’s cardiac function, and we continue CPS for up to three hours if improved cardiac function is evident.I2 Immediately before removing the donor organs, we can use CPS measures to initiate total body cooling.
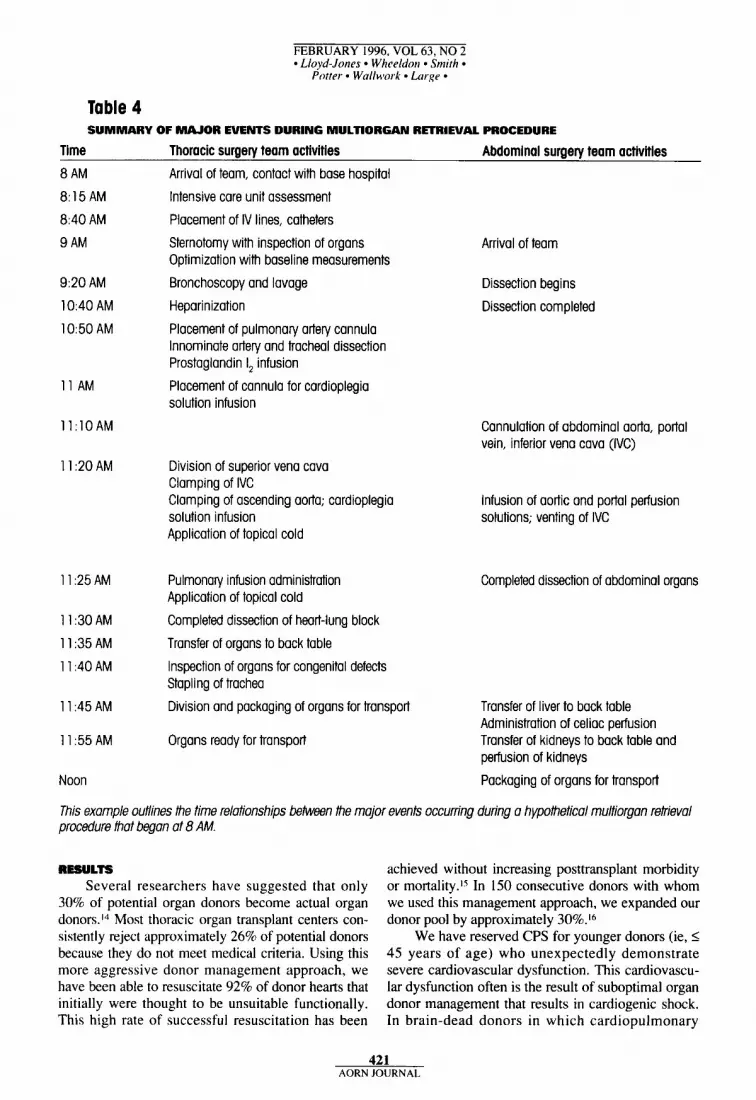
SURGICAL PROCEDURE We employ an organ retrieval procedure sched-
ule that is similar to those described by other organ retrieval teams (Table 4).13 The cardiac surgeon opens the organ donor’s chest and inspects the heart
and lungs. This surgeon performs preliminary dis- section and mobilization of the great vessels. The abdominal surgery team members dissect the liver and kidneys and also dissect the pancreas and small bowel, if these organs are to be transplanted.
The thoracic surgery team members perform flexible bronchoscopy during this time, if the lungs are to be dissected and transplanted. Bronchoscopy allows direct visualization of the organ donor’s major bronchi and detection of foreign matter. Any foreign matter or mucus that is present and obstructing gas exchange can be removed under direct visualization.
The team members use chest x-rays and arterial blood gas data to determine suitability of the organ donor’s lungs for transplantation. They administer 30 IU/kg heparin IV, place cannulas in the pulmonary artery for infusion of prostaglandin I, and pneumo- plegia solution, and place cannulas i n the ascending aorta for cardioplegia delivery. They also cannulate the abdominal vessels. After infusing the pneumople- gia and cardioplegia solutions, the thoracic surgery team members excise the thoracic organs and transfer them to the back table (Figures 2, 3, 4, 5 , and 6), where they are inspected, packaged, and stored for transport to Papworth Hospital.
420 AORN JOURNAL
FEBRUARY 1996, VOL 63, NO 2 Lloyd-Jones Wheeldon 9 Smith
Potter Wallwork Large
Table 4 SUMMARY OF MAJOR EVENTS DURING MULTIORGAN RECRIEVAL PROCEDURE
Time Thoracic surgery team activities Abdominal surgery team activities 8 AM
8:15 AM
8:40 AM
9 AM
9:20 AM
10:40 AM
10:50 AM
1 1 AM
11:lOAM
1 1 :20 AM
1 1 :25 AM
1 1 :30 AM
1 1 :35 AM
1 1 :40 AM
1 1 :45 AM
1 1 :55 AM
Noon
Arrival of team, contact with base hospital
Intensive care unit assessment
Placement of IV lines, catheters
Sternotomy with inspection of organs Optimization with baseline measurements
Bronchoscopy and lavage
Heparinization
Placement of pulmonary artery cannula Innominate artery and tracheal dissection Prostaglandin l2 infusion
Placement of cannula for cardioplegia solution infusion
Division of superior vena cava Clamping of IVC Clamping of ascending aorta; cardioplegia solution infusion Application of topical cold
Pulmonary infusion administration Application of topical cold
Completed dissection of heart-lung block
Transfer of organs to back table Inspection of organs for congenital defects Stapling of trachea
Division and packaging of organs for transport
Organs ready for transport
Arrival of team
Dissection begins
Dissection completed
Cannulation of abdominal aorta, portal vein, inferior vena cava (IVC)
Infusion of aortic and portal perfusion solutions; venting of IVC
Completed dissection of abdominal organs
Transfer of liver to back table Administration of celiac perfusion Transfer of kidneys to back table and perfusion of kidneys
Packaging of organs for transport
This example outlines the time relationships between the major events occurring during a hypothetical multiorgan retrieval procedure that began at 8 AM.
RESULTS Several researchers have suggested that only
30% of potential organ donors become actual organ donors.I4 Most thoracic organ transplant centers con- sistently reject approximately 26% of potential donors because they do not meet medical criteria. Using this more aggressive donor management approach, we have been able to resuscitate 92% of donor hearts that initially were thought to be unsuitable functionally. This high rate of successful resuscitation has been
achieved without increasing posttransplant morbidity or mortality.l5 In 150 consecutive donors with whom we used this management approach, we expanded our donor pool by approximately 30%.16
We have reserved CPS for younger donors (ie, I 45 years of age) who unexpectedly demonstrate severe cardiovascular dysfunction. This cardiovascu- lar dysfunction often is the result of suboptimal organ donor management that results in cardiogenic shock. In brain-dead donors in which cardiopulmonary
421 AORN JOURNAL

FEBRUARY 1996, VOL 63, NO 2 Lloyd-Jones Wheeldon Smith 9
Potter Wallwork Large
Figure 2 The heart-lung block is perfused before excision. excised heart-lung block. of excised heart-lung block.
Figure 3 Surgeon examines the Figure 4 Surgeon staples bronchus
Figure 5 Sur- geon removes
heart from heart-lung
block. Heart will be transplanted
separately.
dysfunction is exacerbated by low peripheral resis- tance, hypothermia, and reduced gas exchange, CPS provides a method of breaking the downward spiral by reestablishing normal blood flow, oxygen satura- tion, and core temperature while resting the heart. Young, previously healthy donors generally respond rapidly to CPS.
DISCUSSION AND ECIIICAL ISSUES There are a number of reports in the literature
that discuss the retrieval of multiple organs for trans- plantation.” Our method differs from other reported donor management methods because we perform objective, functional evaluations of and use a rigor- ous assessment and management regimen for poten- tial organ donors. In our program, the thoracic surgery organ retrieval team members assume com- plete responsibility for the organ donor’s preopera- tive and intraoperative management. These team members arrive at the donor hospital as soon as pos- sible to establish appropriate vascular access, ensure optimal ventilation and fluid management, obtain baseline measurements, and initiate appropriate resuscitative therapy.
The success and proliferation of organ trans- plantation programs has created a demand for donor organs that exceeds the available supply. Technolog-
Figure 6 Staff member inspects exclsed heart before packag- ing It for transport.
ical and surgical developments have surpassed soci- ety’s ability or willingness to resolve the many moral and philosophical issues that relate to every aspect of organ transplantation. When formulating ethical guidelines for organ donation and transplantation, health care professionals must consider the compet- ing moral principles of utilitarianism and duty. As there are several comprehensive textbooks on this subject,I8 we are restricting our discussion to the jus- tifications for the organ donor management protocol used at Papworth Hospital.
As less than 20% of established medical proce- dures have been subjected to the rigors of prospec- tive, randomized trials,Iy it is not surprising that many of the techniques and therapies associated with organ transplantation also are untested. A recent international survey revealed that 37% of organ transplantation centers use 14 different donor pre- treatment regimens.*” The most variable and contro- versial aspects of donor pretreatment regimens are organ donation and preservation.
In the early years of organ transplantation, tho- racic organ donors were transported to recipient hospitals where donor organ retrieval procedures occurred in an OR adjoining the recipient’s OR. Although the practice of transporting organ donors to recipient hospitals does not transgress any ethical
422 AORN JOURNAL

FEBRUARY 1996, VOL 63, NO 2 Lloyd-Jones Wheeldon Smith
Potter 9 Wullw~ork * Large
principle, it does conflict with the cultural sensitivi- ties of individuals who find it unacceptable to trans- port organ donors’ bodies to centers that are distant from grieving relatives and staffed by health care providers who are unfamiliar with the donors’ pre- disposing conditions. Advances in organ preserva- tion have made it unnecessary to transport organ donors to distant transplantation centers.
Institutional review boards traditionally have evaluated and given ethical approval to donor organ management and preservation regimens. As new donor management methods are developed, investi- gators and clinicians are unsure of whom to approach for informed consent. If the potential organ donor is legally dead, is there a need to discuss the issue of organ donation with the donor’s relatives? This may be prudent if unusual organ preservation techniques (eg, whole body freezing) are envisaged. Should investigators and clinicians seek consent from potential organ transplant recipients? This is a logistical problem in cases in which one multiorgan donor may supply organs for more than 10 recipi- ents, some of whom will be identified only after organ retrieval and tissue matching.
Before establishing the strategy used at Papworth Hospital for multiorgan donation and retrieval, we reviewed the literature and conducted carefully con- trolled, monitored pilot studies. Although our institu- tional review board approved these studies and we obtained organ donation consents, we did not seek informed consent for specific therapies that we used with donors. None of the methods we use (eg, pul- monary artery cannulation, hormone replacement ther- apy, medication infusions, CPS) is an unusual form of intensive therapy. We rigorously assess, manage, and reassess potential organ donors, which means that all organs that are retrieved and transplanted conform to specific criteria. We reject organs that are suboptimal at the time of surgical excision. Our management approach to organ donation has increased the number of organs available to Papworth Hospital patients awaiting transplants.”
Utilitarianism is a theory that promotes maximal welfare and the greatest good for the greatest num- ber. To achieve this goal, society’s resources are shared so that the maximum number of individuals benefit. In the context of organ transplantation, patients’ needs are compared so that the best results can be obtained and the best use of a scarce resource can be made. Our use of organs from patients who initially are judged to be medically unsuitable as
The principles of beneficence
and nonmaleficence underpin
Papworth Hospital’s organ
donor management program.
donors supports the utilitarian approach of expanding the pool of potential donor organs and providing ben- efits to a greater number of patients. The end result, however beneficial, does not justify the use of uneth- ical means. Medical utilitarianism is therefore sub- jected to principles that reflect deontological (ie, duty-based) theory.
Duty-based ethics hold that the consequences of an action do not altogether determine whether the action is right or wrong. Accordingly, decision mak- ing must consider the principles of beneficence, nonmaleficence, autonomy, and justice. Basing health care decisions on these principles avoids compromising patients’ or staff members’ integri- ty.?* The clinician’s duty does not lie entirely with the organ recipient but also with the organ donor, the value placed on organs offered for transplanta- tion, and the social system that has provided funding and skills training.
The principles of beneficence and nonmalefi- cence underpin the organ donor management pro- gram and protocol that we use at Papworth Hospital. The success of our program demonstrates that patients who receive “treated” organs are not at increased risks for complications or early death. As more patients are able to undergo organ transplanta- tion, the list of waiting patients is reduced.
Consulting surgeons assess potential organ recip- ients at Papworth Hospital before putting them on the waiting list for transplantation. The surgeons discuss the shortage of organ donors and the random nature of organ referral with these patients but do not pro- vide any information about the organ donors (eg, functional status of an organ before its retrieval). The patients and surgeons create an unwritten contract when they agree on a treatment plan; the patients trust that the surgeons will act in their best interests, and
423 AORN JOURNAL

FEBRUARY 1996. VOL 63, NO 2 Lloyd-Jones Wheeldon Smith
Potter 9 Wallwork 9 Large.
the surgeons have a duty to do so. Informed consent is composed of disclosure,
understanding, voluntaxiness, competence, and deci- sion.?’ Disclosing all details related to organ trans- plantation would be misleading, although it is essen- tial to disclose risk:benefit ratios. Surgeons answer patients’ questions truthfully, but experience has shown that revealing information about organ donors may cause recipients to experience unwarranted emotional anguish.24 Although this approach may be considered medical paternalism, truth-telling may conflict with the principle of nonmaleficence. A sur- geon may choose to compromise a patient’s autono- my to maintain beneficence. These ethical principles are not absolute and may ovemde each other in spe- cific situations, all of which demand that surgeons act in patients’ best interests.
Technological advances soon will enable sur- geons to transplant almost all donor organs and tis- sues. There is an urgent need for informed public debate and international accord on the bioethical issues of organ donat ion and t ransplantat ion. Improved public education and confidence in organ transplantation programs undoubtedly will increase the pool of prospective organ donors. Although alter- natives to human organ transplantation (eg, artificial devices,*S xenografts) offer a wider range of choices, ethical dilemmas remain. Medical technology contin- ues to outpace society’s ability or willingness to sup
NOTES 1. J D Hosenpud et al, “The reg-
istry of the International Society for Heart and Lung Transplantation: Eleventh official report-1 994,” Journal of Heart and Lung Trans- plantation 13 (July/August 1994)
2. B Cohen, “Introduction and 561-570
statistics,” Eurotransplant Newslet- ter 118 (September 1994) 1-2.
3. R C Mackersie, 0 L Brons- ther, S R Shackford, “Organ pro- curement in patients with fatal head injuries: The fate of the potential donor,” Annals of Surgery 2 13 (February 1991) 143-150.
4. D K C Cooper et al, “Electro- cardiographic, hemodynamic, and endocrine changes occumng during experimental brain death in the chacma baboon,” Journal of Heart Transplantation 4 (November 1984)
ply adequate sources of transplantable organs. Health care professionals and the public will need to have a clear understanding of the ethical basis for decision making and will be forced to make profound choices regarding organ donation and transplantation. A
Heather Lloyd-Jones, RN, BSc (Hons), is an operating room sister, Papworth Hospital, National Health Service Trust, Cambridge, United Kingdom.
Dereck R. Wheeldon, MiBiol, is a scient8c officer for the transplant unit, Papworth Hospital, National Health Service Trust, Cambridge, United Kingdom.
Julian A. Smith, MS, FRACS, is a cardiothoracic sur- geon, Alfred Healthcare Group, Prahran, Victoria, Australia.
Charles D. 0. Potter, PhD, is a scientific ofJicer for the transplant unit, Papworth Hospital, National Health Ser- vice Trust, Cambridge. United Kingdom.
John Wallwork, MBChB, FRCS (E) , is a consultant car- diothoracic surgeon and the director of the transplant unit, Papworth Hospital, National Health Service Trust, Cambridge, United Kingdom.
Stephen R. Large, MRCP. FRCS, is a consultant cardio- thoracic surgeon, Papworth Hospital, National Health Service Trust, Cambridge, United Kingdom.
63-69; W N Wincomb et al, “The effects of brain death and 24 hours’ storage by hypothermic perfusion on donor heart function in the pig,” Journal of Thoracic and Cardiovas- cular Surgery 91 (June 1986) 896- 909; B Shivalkar et al, “Variable effects of explosive or gradual increase of intracranial pressure on myocardial structure and function,” Circulation 87 (January 1993) 230- 239.
5 . D R Wheeldon et al, “Man- agement of organ donors,” abstract presented at The British Transplan- tation Society, Glasgow, Scotland, 14 April 1992; D R Wheeldon et al, “Transplantation of ‘unsuitable’ organs?” Transplantation Proceed- ings 25 (December 1993) 3104- 3105.
Oduro, “Multi-organ transplanta- 6. J A Pickett, D R Wheeldon, A
tion: Donor management,” Current Opinion in Anaesthesiology 7 no 1 (1994) 80-83.
7. C D 0 Potter, D R Wheeldon, J Wallwork, “Functional assessment and management of heart donors: A rationale for characterization and a guide to therapy,” Journal of Heart and Lung Transplantation 14 (Janu- arypebruary 1995) 59-65.
8. J L Canivet et al, “Fluid man- agement and plasma renin activity in organ donors,” Transplant Inter- national 2 (October 1989) 129-132.
9. M A Samuels, “Neurogenic heart disease: A unifying hypothe- sis,” American Journal of Cardiolo- g y 60 (Dec 28, 1987) 155-195.
10. T Yoshioka et al, “Prolonged hemodynamic maintenance by the combined administration of vaso- pressin and epinephrine in brain death: A clinical study,” Neurosurgery 18
425 AORN JOURNAL
FEBRUARY 1996. VOL 63, NO 2 Lloyd-Jones 9 Wheeldon Smith 9
Potter Wallwork Large
(May 1986) 565-567. 1 I . T A Howlett et al, “Anterior
and posterior pituitary function in brain-stem-dead donors: A possible role for hormone replacement thera- py,” Transplantation 47 (May
12. D R Wheeldon et al, “Haemodynamic correction in mul- tiorgan donation,” (Letter) The Lancet 339 (May 9, 1992) 1175; D R Wheeldon et al, “Multiorgan donor resuscitation: Practical tech- niques,” Perfusion 7 no 3 (1992)
13. D C Drinkwater, H Laks, “Thoracic organ donor procure- ment, management, and opera- tion,” in A S Kapoor, H Laks, eds, Atlas of Heart-Lung Transplanta- tion (New York: McGraw-Hill
Haverich, D Novitzky, D K C Cooper, “Selection of the donor, excision and storage of donor organs,” in The Transplantation and Replacement of Thoracic Organs: The Present Status of Bio- logical and Mechanical Replace- ment, ed D K C Cooper, D Novitzky (Dordrecht, Netherlands: Kluwer Academic Publishers, 1990) 273-282; R K Hardesty, B P Griffith, “Procurement for com- bined heart-lung transplantation: Bilateral thoracotomy with sternal transection, cardiopulmonary
1989) 828-834.
213-216.
Book CO, 1994) 37-48; A
bypass, and profound hypother- mia,” Journal of Thoracic and Cardiovascular Surgery 89 (May 1985) 795-799.
14. C E Nygaard, R N Townsend, D L Diamond, “Organ donor man- agement and organ outcome: A six- year review from a level I trauma center,” Journal of Trauma 30 (June 1990) 728-732; S M Gore, C J Hinds, A J Rutherford, “Organ donation from intensive care units in England,” BMJ 299 (November
15. D R Wheeldon et al, “Using ‘unsuitable’ hearts for transplanta- tion,” European Journal of Cardio- thoracic Surgery 8 (January 1994)
16. D R Wheeldon et al, “Trans- plantation of marginal donor organs,” (abstract) Journal of Heart and Lung Transplantation 13 no 1 suppl( 1994) 55 1.
17. S W Jamieson et al, “Opera- tive technique for heart-lung trans- plantation,” Journal of Thoracic and Cardiovascular Surgery 87 (June 1984) 930-935; J S Ladows- ki, R L Hardesty, B P Griffith, “Protection of the heart-lung allo- graft during procurement: Cooling of the lungs with extracorporeal circulation or pulmonary artery flush,” Heart Transplantation 3 no
18. H S Schwartz, “Bioethical
11, 1989) 1193-1 197.
7-11.
4 (1984) 351-353.
and legal considerations in increas- ing the supply of transplantable organs: From UAGA to baby Fae,” American Journal of Law and Med- icine 10 (Winter 1985) 397-437; D Lamb, Organ Transplants and Ethics (New York: Routledge, 1990).
19. S Kingman, “Quality control for medicine,” New Scientist (Sept
20. D R Wheeldon et al, “Donor heart preservation survey,” Journal of Heart and Lung Transplantation 11 (September/October 1992) 986- 993.
tion of marginal donor organs,” 551.
ical Ethics (New York: J Wiley & Sons, 1986) 21.
23. T L Beauchamp, J F Chil- dress, Principles of Biomedical Ethics (New York: Oxford Univer- sity Press, 1989) 78.
24. B Bunzel, G Wollenek, A Grundbock, “Living with a donor heart: Feelings and attitudes of patients toward the donor and the donor organ,” Journal of Heart and Lung Transplantation 1 1 (Novem- ber/December 1992) 1151-1 155.
25. S J Quaal, Cardiac Mechani- cal Assistance Beyond Balloon Pumping (St Louis: Mosby-Year Book, Inc, 1993).
17, 1994) 22-26.
2 1. Wheeldon et al, “Transplanta-
22. R Gillon, Philosophical Med-
Researchers Using Cryotherapy to Treat Breast Cancer Cryotherapy has been used to treat unwanted cell growths on skin, eyes, and cervical tissues for decades. It also has been used to treat prostate, liver, and kidney cancers. Researchers now are using cryotherapy to freeze and destroy malignant breast tumors, according to an article in the October 1995 Rush-Presbyterian-St Luke’s Medical Center News Tips.
The procedure is performed on an outpatient
basis and takes approximately 90 minutes. The sur- geon uses ultrasound technology to insert a pensized probe into the tumor. They cryoprobe procedure requires only local anesthetic, and patients requrie no pain medication postoperatively, the article states.
P Redd, A S Heinrich, D Modica, ‘New approach to breast cancer trealment: Deep fmzing, Rush-Presbyterian-% Luke’s Medical Center News Tips (October 1995).
426 AORN JOURNAL