alcohol-related cues potentiate alcohol impairment of behavioral control in drinkers
TRANSCRIPT
Psychology of Addictive Behaviors
Alcohol-Related Cues Potentiate Alcohol Impairment ofBehavioral Control in DrinkersJessica Weafer and Mark T. FillmoreOnline First Publication, August 18, 2014. http://dx.doi.org/10.1037/adb0000013
CITATIONWeafer, J., & Fillmore, M. T. (2014, August 18). Alcohol-Related Cues Potentiate AlcoholImpairment of Behavioral Control in Drinkers. Psychology of Addictive Behaviors. Advanceonline publication. http://dx.doi.org/10.1037/adb0000013

Alcohol-Related Cues Potentiate Alcohol Impairment of BehavioralControl in Drinkers
Jessica Weafer and Mark T. FillmoreUniversity of Kentucky
The acute impairing effects of alcohol on inhibitory control are well-established, and these disinhibitingeffects are thought to play a role in its abuse potential. Alcohol impairment of inhibitory control istypically assessed in the context of arbitrary cues, yet drinking environments are comprised of an arrayof alcohol-related cues that are thought to influence drinking behavior. Recent evidence suggests thatalcohol-related stimuli reduce behavioral control in sober drinkers, suggesting that alcohol impairment ofinhibitory control might be potentiated in the context of alcohol cues. The current study tested thishypothesis by examining performance on the attentional-bias behavioral activation (ABBA) task thatmeasures the degree to which alcohol-related stimuli can reduce inhibition of inappropriate responses ina between-subjects design. Social drinkers (N � 40) performed the task in a sober condition, and thenagain following placebo (0.0 g/kg) and a moderate dose of alcohol (0.65 g/kg) in counterbalanced order.Inhibitory failures were greater following alcohol images compared to neutral images in sober drinkers,replicating previous findings with the ABBA task. Moreover, alcohol-related cues exacerbated alcoholimpairment of inhibitory control as evidenced by more pronounced alcohol-induced disinhibitionfollowing alcohol cues compared to neutral cues. Finally, regression analyses showed that greateralcohol-induced disinhibition following alcohol cues predicted greater self-reported alcohol consump-tion. These findings have important implications regarding factors contributing to binge or “loss ofcontrol” drinking. That is, the additive effect of disrupted control mechanisms via both alcohol cues andthe pharmacological effects of the drug could compromise an individual’s control over ongoing alcoholconsumption.
Keywords: alcohol, inhibition, behavioral control, alcohol cues, cued go/no-go task
The link between impaired inhibitory control and problematicalcohol consumption has been recognized for some time. Limitingone’s alcohol consumption necessarily requires a certain degree ofbehavioral control, and thus deficits in inhibitory mechanisms arethought to compromise the ability to control one’s drinking. Stud-ies have tested this association using inhibitory control tasks thatrequire participants to respond as quickly as possible to go signals,but inhibit their responses when stop or no-go signals occasionallyappear (e.g., stop signal and go/no-go tasks). As hypothesized,heavy drinkers and alcoholics display deficits in response inhibi-tion compared to social-drinking controls (Bjork, Hommer, Grant,& Danube, 2004; Henges & Marczinski, 2012; Lawrence, Luty,
Bogdan, Sahakian, & Clark, 2009; Rubio et al., 2008), and longi-tudinal studies show that deficits in response inhibition can predictgreater alcohol use later in life (Nigg et al., 2006; Rubio et al.,2008). Alcohol consumption acutely impairs performance on thesetasks as well (de Wit, Crean, & Richards, 2000; Dougherty et al.,1999; Fillmore & Vogel-Sprott, 1999; Marczinski & Fillmore,2003), and initial evidence suggests an association betweenalcohol-induced impairment of inhibitory control and excessive,binge-like consumption. For instance, binge drinkers are moresensitive to the disinhibiting effects of the drug (Marczinski,Combs, & Fillmore, 2007), and individual differences in sensitiv-ity to the disinhibiting effects of alcohol predict ad lib consump-tion (Gan et al., 2014; Weafer & Fillmore, 2008). In sum, there isa wealth of evidence demonstrating an association between im-paired control and excessive alcohol consumption in both soberand intoxicated drinkers.
The majority of evidence implicating impaired behavioral con-trol in alcohol abuse has assessed response inhibition to arbitrarycues (e.g., colors, geometric shapes, and simple auditory tones).However, drinking environments are comprised of a rich array ofdiscrete and contextual cues that are reliably associated with theconsumption of alcohol (e.g., beer bottles, wine glasses, neon barsigns, bar rooms), and these cues are thought to play an influentialrole in drinking behavior. According to the incentive-sensitization theory, drug cues come to be associated with drugtaking and the rewarding effects of the drug, causing the cues tobecome increasingly salient for the drug user, and to acquire
Jessica Weafer and Mark T. Fillmore, Department of Psychology, Uni-versity of Kentucky.
Jessica Weafer is now at the Department of Psychiatry and BehavioralNeuroscience, University of Chicago.
This research was supported by National Institute on Alcohol Abuse andAlcoholism Grant R01 AA018274 and National Institute on Drug AbuseGrant F32 DA033756. The content is solely the responsibility of theauthors and does not necessarily represent the official views of the NationalInstitute on Alcohol Abuse and Alcoholism, the National Institute on DrugAbuse, or the National Institutes of Health.
Correspondence concerning this article should be addressed to Mark T.Fillmore, Department of Psychology, 115 Kastle Hall, University of Ken-tucky, Lexington KY 40506-0044. E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Psychology of Addictive Behaviors © 2014 American Psychological Association2014, Vol. 28, No. 3, 000 0893-164X/14/$12.00 http://dx.doi.org/10.1037/adb0000013
1

incentive-motivational properties that promote drug seeking anddrug taking (Robinson & Berridge, 1993, 2001). In terms ofalcohol abuse, individuals with a history of heavy drinking showan attentional bias toward alcohol-related stimuli, and this isthought to be indicative of enhanced incentive-salience of alcoholcues (Ceballos, Komogortsev, & Turner, 2009; Fadardi & Cox,2008; Field, Christiansen, Cole, & Goudie, 2007; Miller & Fill-more, 2010; Murphy & Garavan, 2011; Sharma, Albery, & Cook,2001; Tibboel, De Houwer, & Field, 2010; Townshend & Duka,2001; Weafer & Fillmore, 2013). It is important to note that thereis also evidence that attention toward alcohol-related stimuli isassociated with increased craving (Field & Cox, 2008; Field,Munafo, & Franken, 2009).
Recent models of drug addiction emphasize the reciprocal in-fluence of incentive-motivational properties of drug-related cuesand impaired inhibitory control over drug taking (Dawe & Loxton,2004; Feil et al., 2010; Goldstein & Volkow, 2002; Jentsch &Taylor, 1999). These models cite neuroanatomical evidence im-plicating frontostriatal circuitry dysfunction in both salience attri-bution and response inhibition, and propose that the intense mo-tivation elicited by drug-associated cues could serve to directlyimpair control mechanisms necessary to inhibit the cue-inducedimpulse. In terms of alcohol abuse, attention directed towardalcohol cues could thus serve to acutely disrupt mechanisms ofinhibitory control in heavy drinkers. We tested this hypothesis ina recent study by modifying the traditional cued go/no-go task toassess inhibitory control following both alcohol-related and neutralcues (Weafer & Fillmore, 2012). The modified task is called theattentional bias-behavioral activation (ABBA) task and presentseither a test condition in which alcohol-related images signal thata response is required or a test condition in which neutral imagessignal that a response is required. The cues serve to increaseresponse activation and make inhibition difficult on the occasionalinstances when the response must be suddenly inhibited. In accordwith the hypothesis that alcohol cues should impair control mech-anisms necessary to inhibit the cue-induced impulse, we showedthat inhibitory control was disrupted to a greater degree followingalcohol cues compared with neutral cues (Weafer & Fillmore,2012). Similar results have since been reported from other labo-ratories using similarly modified cued go/no-go tasks (Fleming &Bartholow, 2013; Kreusch, Vilenne, & Quertemont, 2013). Takentogether, these findings provide preliminary evidence for a disrup-tive effect of alcohol-related stimuli on the ability to inhibit pre-potent (i.e., instigated) responses (although see Nederkoorn, Bal-tus, Guerrieri, & Wiers, 2009).
Given the evidence that inhibitory control can be compro-mised by the presence of alcohol-related stimuli in the imme-diate environment, it is important to consider this disruptiveeffect in the intoxicated individual. Alcohol is well-known forits ability to acutely impair inhibitory control over prepotentresponses in laboratory tasks, such as the cued go/no-go model(for a review see, Fillmore & Weafer, 2013). Such acute im-pairment of inhibitory control could be especially pronouncedin the context of alcohol-related environmental stimuli that alsodisrupt response inhibition. Such potential additive or overaddi-tive impairments could be particularly important for under-standing associations between alcohol-induced disinhibitionand binge drinking. As termination of a drinking episode likelyoccurs in the context of alcohol-related stimuli, greater sensi-
tivity to the acute disinhibiting effects of alcohol in the pres-ence of such stimuli could further disrupt the ability to stopdrinking. To our knowledge, only two studies to date havesought to examine the degree to which alcohol effects oninhibition might be exacerbated following alcohol-related im-ages (Adams, Ataya, Attwood, & Munafo, 2013; Rose & Duka,2008). These studies examined performance on alcohol shiftingtasks, where participants shifted between responding to alcohol-related or neutral images following consumption of alcohol orplacebo. However, neither study reported a significant maineffect of alcohol on disinhibition (regardless of cue type), thusprecluding analyses regarding the potentially exacerbating ef-fects of alcohol cues on alcohol-induced disinhibition. Thefailure to observe a general disinhibiting effect of alcohol inthese studies is likely due to limitations of the shifting task asa measure of inhibitory control. In typical go/no-go models,strong response prepotency is established by making the goresponse dominant, with no-go targets appearing only occasion-ally. This makes inhibition difficult when a no-go signal unex-pectedly occurs. By contrast, the alcohol-shifting task requiresparticipants to shift between responding to alcohol-related orneutral images. Because the go target continually shiftsthroughout the test, a strong prepotent response is less likely tobe established, thus limiting the ability to detect alcohol oralcohol-cue effects on inhibition.
For the current study, we compared the magnitude of alcohol-induced disinhibition following alcohol-related versus neutralcues on the ABBA task in a sample of nondependent, socialdrinkers. The ABBA task was adapted from a cued go/no-gomodel in which sensitivity to the disinhibiting effects of alcoholhas been well-documented (Fillmore & Weafer, 2013). Further,we have previously demonstrated that alcohol images elicit astrong prepotent response tendency on the ABBA task, asevidenced by significantly disrupted inhibitory control follow-ing alcohol cues (Weafer & Fillmore, 2012). To replicate ourprevious findings, participants first performed the task in asober state. They then completed a placebo-controlled test ofthe acute effect of 0.65 g/kg alcohol on their inhibitory controlin the context of alcohol-related versus neutral cues. We hy-pothesized that the ability to inhibit responses would be gen-erally poorer when tested in the context of alcohol cues com-pared with neutral cues, and that alcohol would impairinhibitory control overall. Moreover, we expected an additiveeffect of alcohol cues and alcohol intoxication, such that dis-inhibition would be most pronounced following alcohol con-sumption in the context of alcohol cues versus neutral cues. Toexamine the degree to which disrupted inhibitory control fol-lowing alcohol cues is associated with excessive alcohol con-sumption, we also tested associations of drinkers’ self-reporteddrinking habits with their inhibitory failures following alcoholand neutral cues. We hypothesized that greater disinhibitionwould be associated with greater alcohol consumption, and thatthis association would be stronger for inhibitory failures fol-lowing alcohol cues. That is, individuals who experience themost difficulty inhibiting responses to alcohol cues were ex-pected to report more excessive drinking patterns, perhaps dueto difficulty inhibiting consumption in the presence of suchcues.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
2 WEAFER AND FILLMORE
Method
Participants
Forty adult beer drinkers (11 women and 29 men) between theages of 21 and 29 years (mean age � 23.3, SD � 2.8) wererecruited to participate in this study. Screening measures wereconducted to determine medical history and current and past drugand alcohol use. Any volunteers who self-reported head trauma,psychiatric disorder, or substance abuse disorder were excludedfrom participation. Volunteers who reported alcohol dependence,as determined by a score of 5 or higher on the Short-MichiganAlcoholism Screening Test (S-MAST; Selzer, Vinokur, & vanRooijen, 1975), were also excluded. Volunteers were recruited vianotices placed on community bulletin boards and by universitynewspaper advertisements. The University of Kentucky MedicalInstitutional Review Board approved the study, and participantswere compensated for their participation.
Materials and Measures
Attentional Bias-Behavioral Activation (ABBA) task. TheABBA task (Weafer & Fillmore, 2012), a modified cued go/no-goreaction time (RT) task, was operated using E-prime experimentgeneration software (Psychology Software Tools, Pittsburgh, PA)and was performed on a PC. A trial involved the followingsequence of events: (a) presentation of a fixation point (�) for 800
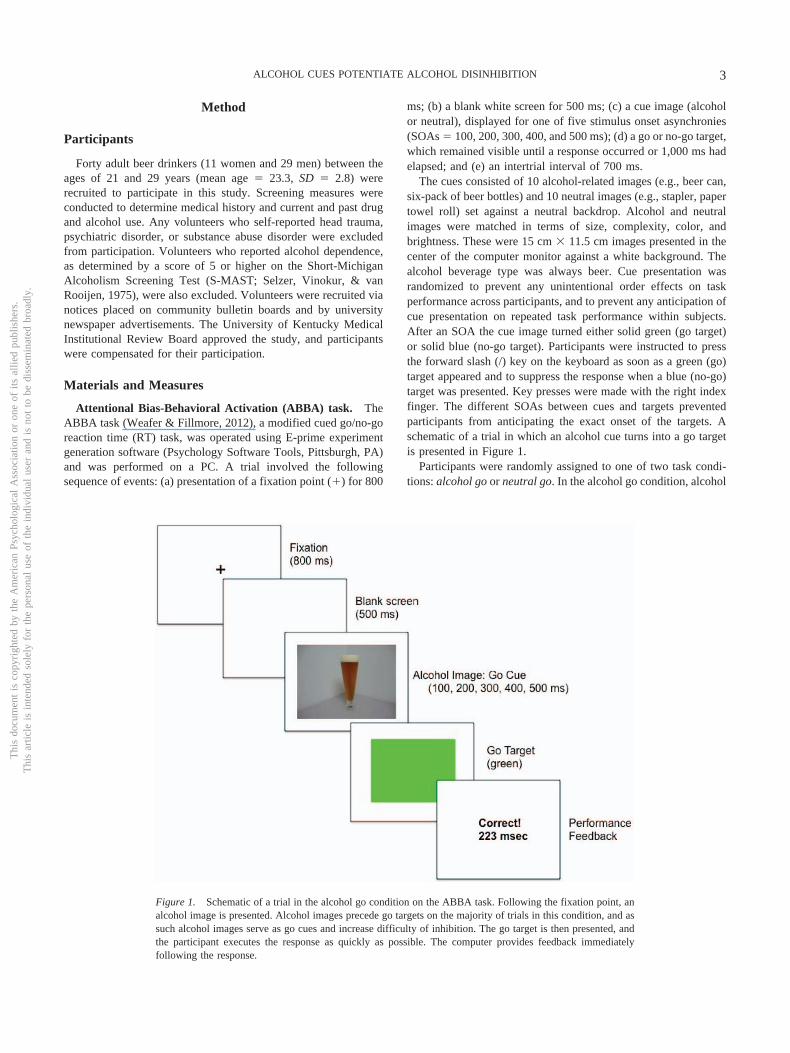
ms; (b) a blank white screen for 500 ms; (c) a cue image (alcoholor neutral), displayed for one of five stimulus onset asynchronies(SOAs � 100, 200, 300, 400, and 500 ms); (d) a go or no-go target,which remained visible until a response occurred or 1,000 ms hadelapsed; and (e) an intertrial interval of 700 ms.
The cues consisted of 10 alcohol-related images (e.g., beer can,six-pack of beer bottles) and 10 neutral images (e.g., stapler, papertowel roll) set against a neutral backdrop. Alcohol and neutralimages were matched in terms of size, complexity, color, andbrightness. These were 15 cm � 11.5 cm images presented in thecenter of the computer monitor against a white background. Thealcohol beverage type was always beer. Cue presentation wasrandomized to prevent any unintentional order effects on taskperformance across participants, and to prevent any anticipation ofcue presentation on repeated task performance within subjects.After an SOA the cue image turned either solid green (go target)or solid blue (no-go target). Participants were instructed to pressthe forward slash (/) key on the keyboard as soon as a green (go)target appeared and to suppress the response when a blue (no-go)target was presented. Key presses were made with the right indexfinger. The different SOAs between cues and targets preventedparticipants from anticipating the exact onset of the targets. Aschematic of a trial in which an alcohol cue turns into a go targetis presented in Figure 1.
Participants were randomly assigned to one of two task condi-tions: alcohol go or neutral go. In the alcohol go condition, alcohol
Figure 1. Schematic of a trial in the alcohol go condition on the ABBA task. Following the fixation point, analcohol image is presented. Alcohol images precede go targets on the majority of trials in this condition, and assuch alcohol images serve as go cues and increase difficulty of inhibition. The go target is then presented, andthe participant executes the response as quickly as possible. The computer provides feedback immediatelyfollowing the response.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
3ALCOHOL CUES POTENTIATE ALCOHOL DISINHIBITION

images turned into the go target on 80% of trials and turned intothe no-go target on only 20% of trials. Therefore, alcohol imagesoperated as go cues, based on the high probability that they wouldsignal go targets. As such, these images should speed RT to the gotargets, but also increase failures to inhibit the response when theno-go target is occasionally presented. By contrast, in the neutralgo condition the opposite cue image-target pairings were pre-sented. Therefore, in this condition neutral images serve as gocues, producing faster RT to go targets, but more inhibitory fail-ures to the occasional presentation of no-go targets. By comparingthe alcohol go condition and neutral go condition (between-subjects), the task measures the degree to which alcohol-related gocues elicit poorer response inhibition compared to neutral go cues.
A test consisted of 250 trials, presented as five blocks of 50trials each, with each individual cue presented 12 or 13 times. Foreach trial, the computer recorded whether a response occurred and,if so, the RT in milliseconds was measured from the onset of thetarget until the key was pressed. To encourage quick and accurateresponding, the computer presented feedback to the participantduring the intertrial interval by displaying the words correct orincorrect along with the RT in milliseconds. Omission errors(when participants failed to respond to go targets) were alsorecorded. These were infrequent and occurred on less than 0.005%of go target trials (i.e., less than one trial per test). Each blockrequired approximately 2.5 min to complete and blocks wereseparated by 30-s breaks, for a total test time of approximately 15min.
Barratt Impulsiveness Scale (BIS). Participants completedthe BIS (Patton, Stanford, & Barratt, 1995) to provide a self-reportmeasure of the personality dimension of impulsivity. Impulsivity isthought to contribute to the risk of behavioral disinhibition underalcohol, as well as risk for alcoholism (Boyatzis, 1975; Cloninger,1987; Finn, Kessler, & Hussong, 1994; Sher & Trull, 1994).Participants indicate how typical each of 30 statements (e.g., “I amself-controlled”) is for them on a 4-point Likert scale. Higherscores indicated greater total levels of impulsiveness. This measurewas included to ensure that groups did not differ in terms ofimpulsive personality.
Time Line Follow-Back (TLFB; Sobell & Sobell, 1992).Participants completed a retrospective time line calendar of theiralcohol consumption for the past 3 months to assess daily patternsof drinking, including number of binge episodes. The measure uses“anchor points” to structure and facilitate participants’ recall ofpast drinking episodes. For each day, participants estimated thenumber of standard drinks they consumed and the number of hoursthey spent drinking. This information, along with gender and bodyweight, was used to estimate the resultant BAC obtained for eachdrinking day. This was done using well-established, validanthropometric-based BAC estimation formulae that assume anaverage clearance rate of 15 mg/dl per hour (McKim, 2007;Watson, Watson, & Batt, 1981). These formulae have been used inprevious studies and have been shown to yield high correlationswith actual resultant BACs obtained under laboratory conditions(Fillmore, 2001). Any day in which the estimated resultant BACwas 80 mg/100 ml or higher was classified as a binge episode(NIAAA, 2004). The TLFB provided three measures of drinkinghabits over the past 3 months: (a) drinking days (total number ofdays alcohol was consumed); (b) binge days (total number of binge
episodes); and (c) total drinks (total number of drinks consumedover the three months).
Subjective intoxication. Degree of subjective intoxicationwas measured on a visual analogue scale that has been used inprevious research on acute alcohol tolerance (e.g., Ostling &Fillmore, 2010). Participants rated their degree of subjective in-toxication by placing a vertical line at the point representing theextent to which they “feel intoxicated” on a 100-mm horizontalline ranging from 0 mm not at all to 100 mm very much.
Procedure
Interested volunteers responded to study advertisements by call-ing the laboratory to participate in an intake-screening interviewconducted by a research assistant. At that time, they were informedthat the purpose of the study was to examine the effects of alcoholon behavioral tasks. Volunteers were asked to report their pre-ferred alcoholic beverage (beer, wine, or liquor). Because allalcohol-related stimuli presented in the ABBA task consisted ofbeer images, only volunteers reporting beer as their preferredbeverage were eligible for study participation. All sessions wereconducted in the Behavioral Pharmacology Laboratory of theDepartment of Psychology and testing began between 10 a.m. and6 p.m. All participants were tested individually. Sessions werescheduled at least 24 hr apart and were completed within 3 weeks.Participants were instructed to fast for 4 hr prior to each alcoholsession, as well as to refrain from consuming alcohol or anypsychoactive drugs or medications for 24 hr before all sessions.Prior to each session, participants provided urine samples that weretested for drug metabolites, including amphetamine, barbiturates,benzodiazepines, cocaine, opiates, and tetrahydrocannabinol (ONtrakTesTstiks, Roche Diagnostics Corporation, Indianapolis, IN)and, in women, HCG, to verify that they were not pregnant(Mainline Confirms HGL, Mainline Technology, Ann Arbor, MI).Breath samples were also provided and analyzed by an Intoxilyzer,Model 400 (CMI, Inc., Owensboro, KY) at the beginning of eachsession to verify a zero breath alcohol content (BrAC).
Part 1: Sober baseline performance. All participants firstcompleted a sober assessment of their performance on the ABBAtask to replicate our previous findings that showed inhibitorycontrol was poorer in the context of alcohol-related versus neutralstimuli (Weafer & Fillmore, 2012). Upon arrival to the laboratory,participants provided informed consent for participation and werefamiliarized with study protocol and procedures. Participants’heights and weights were measured, and questionnaire measureswere completed. Men and women were randomly assigned toeither the alcohol go or the neutral go task condition such thatgender make-up was equivalent across conditions. Participantsthen performed the ABBA task to provide a measure of sober taskperformance.
Part 2: Dose-challenge sessions. Part 2 of the study wasdesigned to test the degree to which alcohol-related stimuli exac-erbate the acute disinhibiting effects of a moderate dose of alcoholin a placebo-controlled design. ABBA task performance was testedfollowing placebo (0.0 g/kg) and a moderate dose of alcohol (0.65g/kg). The 0.65 g/kg dose was reduced to 87% for women toachieve equivalent BrACs for men and women (Fillmore, 2001;Mulvihill, Skilling, & Vogel-Sprott, 1997). Each dose was admin-istered on a separate test session, and dose order was counterbal-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
4 WEAFER AND FILLMORE

anced across conditions. Sessions were separated by a minimum of1 day and a maximum of 1 week. Participants were told that theywould receive alcohol on each session, and that the dose would notnecessarily be the same each session. Alcohol doses were calcu-lated on the basis of body weight and administered as absolutealcohol mixed with three parts carbonated soda. The 0.65 g/kgalcohol dose produces an average peak BAC of 80 mg/100 ml(Fillmore, Marczinski, & Bowman, 2005). The placebo dose (0.0g/kg) consisted of a volume of carbonated mix that matched thetotal volume of the 0.65 g/kg alcohol drink. A small amount (3 ml)of alcohol was floated on the surface of the beverage. It wassprayed with an alcohol mist that resembled condensation andprovided a strong alcoholic scent as the beverage was consumed.Previous research has shown that individuals report that this bev-erage contains alcohol (Fillmore & Vogel-Sprott, 1999). All drinkswere consumed in 6 min.
Participants completed the subjective intoxication measure, fol-lowed by the ABBA task at 30 min after drinking. Participantsperformed the same task condition (alcohol go or neutral go) as inPart 1 following both the placebo and active dose in Part 2. Breathsamples were obtained immediately prior to subjective measuresand immediately following the ABBA task to measure partici-pants’ BrACs. Once testing was finished, participants remained atleisure in the lounge area until their BrACs, which were monitoredat 20-min intervals, reached 20 mg/100 ml or below. Participantswere provided a meal during this leisure time and were allowed towatch movies and read magazines. Transportation home was pro-vided as needed. Upon completing the final session, participantswere paid and debriefed.
Data Analyses
For Part 1, independent-groups t tests (alcohol go vs. neutral go)tested the degree to which alcohol images disrupted responseinhibition (proportion [p] of inhibitory failures) and increasedresponse activation (i.e., speeded RT) relative to neutral imagesduring sober ABBA task performance. For Part 2, p-inhibitoryfailures and RT during the dose-challenge sessions were analyzedindividually by 2 condition (alcohol go vs. neutral go) � 2 dose(0.0 g/kg vs. 0.65 g/kg) mixed-design analyses of variance(ANOVAs) in which dose was the within-subjects factor and
condition was the between-subjects factor. Significant interactionswere followed up with paired samples t tests comparing perfor-mance following placebo and 0.65 g/kg alcohol separately in eachcondition. For both parts of the study, we conducted hierarchicallinear regression analyses to examine the extent to which individ-ual differences in response inhibition predicted self-reported alco-hol consumption as measured by the TLFB across conditions, andto test whether this relation differed according to cue condition.We hypothesized that poorer inhibitory control would predictgreater alcohol consumption, and that this effect would be morepronounced in the alcohol go condition.
Results
Demographics, Trait Impulsivity, and DrinkingHabit Measures
Table 1 summarizes demographic data, trait impulsivity, anddrinking habit measures for participants in the alcohol go andneutral go conditions. The groups did not differ significantly ingender make-up, age, BIS scores, or alcohol consumption over thepast 90 days as reported on the TLFB (ps � .10). The table showsthat participants in both groups were frequent drinkers who regu-larly engaged in binge drinking episodes. These self-reporteddrinking patterns provide confirmation of participants’ frequentmoderate to heavy alcohol consumption.
Part 1: Sober Baseline ABBA Performance
To first demonstrate that inhibitory control is impaired in thecontext of alcohol-related cues as well as replicate our initialfindings with the ABBA task (Weafer & Fillmore, 2012), wecompared task performance in the alcohol go and neutral goconditions when participants were in the sober state in Part 1 of thestudy. Figure 2 presents mean p-inhibitory failures (left panel) andmean RT (right panel) following go cues for the two conditions.The figure shows greater p-inhibitory failures following alcoholimages compared to neutral images. A between-groups t testconfirmed that mean p-inhibitory failures were greater in thealcohol go condition compared to the neutral go condition, t(38) �
Table 1Mean Demographics, Trait Impulsivity, and Drinking Habits by Condition
Condition
Alcohol go Neutral go Contrasts
M SD M SD Sig Cohen’s d
Gender (F:M) 6:14 5:15 nsAge 23.4 3.3 23.2 2.4 ns .07Barratt Impulsiveness Scale 60.2 7.5 62.5 9.9 ns .26TLFB (past 90 days)
Drinking days 35.4 18.9 28.6 15.5 ns .39Binge days 16.6 12.6 11.0 8.7 ns .52Total drinks 190.1 123.6 165.0 128.1 ns .19
Mean BrAC during testing 80.9 11.9 86.8 11.0 ns .51
Note. Group contrasts were tested by between-groups t tests. ns indicates p � .05. Effect size is indicated byCohen’s d.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
5ALCOHOL CUES POTENTIATE ALCOHOL DISINHIBITION
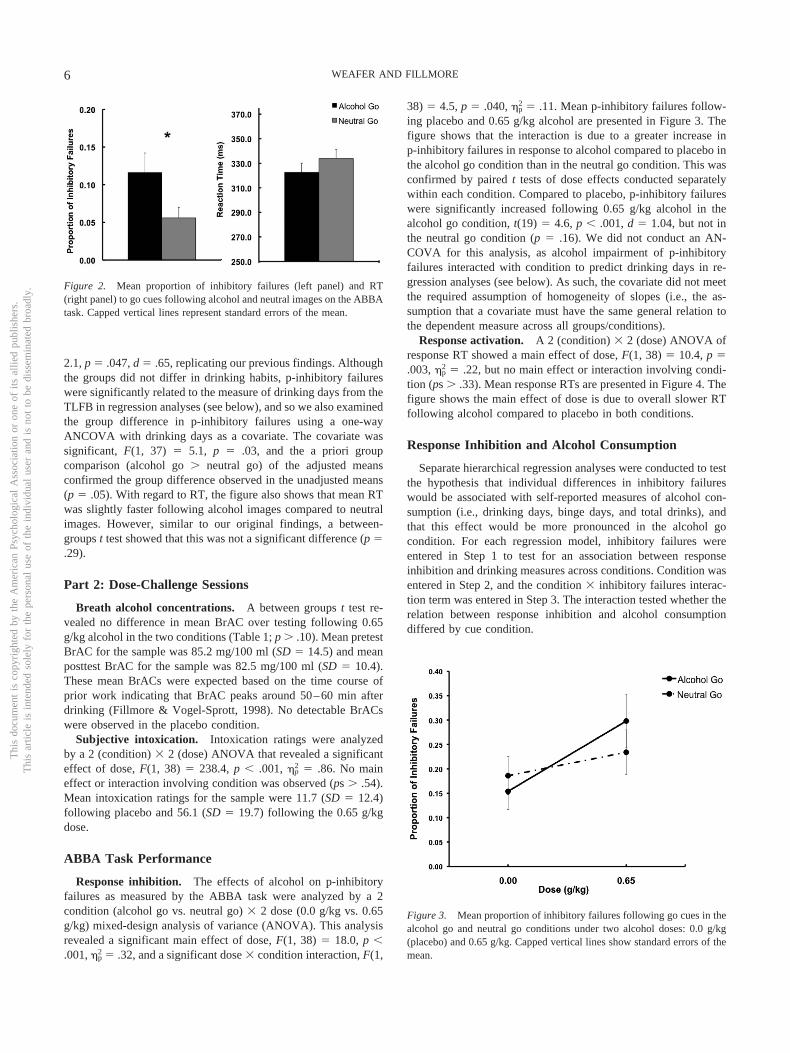
2.1, p � .047, d � .65, replicating our previous findings. Althoughthe groups did not differ in drinking habits, p-inhibitory failureswere significantly related to the measure of drinking days from theTLFB in regression analyses (see below), and so we also examinedthe group difference in p-inhibitory failures using a one-wayANCOVA with drinking days as a covariate. The covariate wassignificant, F(1, 37) � 5.1, p � .03, and the a priori groupcomparison (alcohol go � neutral go) of the adjusted meansconfirmed the group difference observed in the unadjusted means(p � .05). With regard to RT, the figure also shows that mean RTwas slightly faster following alcohol images compared to neutralimages. However, similar to our original findings, a between-groups t test showed that this was not a significant difference (p �.29).
Part 2: Dose-Challenge Sessions
Breath alcohol concentrations. A between groups t test re-vealed no difference in mean BrAC over testing following 0.65g/kg alcohol in the two conditions (Table 1; p � .10). Mean pretestBrAC for the sample was 85.2 mg/100 ml (SD � 14.5) and meanposttest BrAC for the sample was 82.5 mg/100 ml (SD � 10.4).These mean BrACs were expected based on the time course ofprior work indicating that BrAC peaks around 50–60 min afterdrinking (Fillmore & Vogel-Sprott, 1998). No detectable BrACswere observed in the placebo condition.
Subjective intoxication. Intoxication ratings were analyzedby a 2 (condition) � 2 (dose) ANOVA that revealed a significanteffect of dose, F(1, 38) � 238.4, p � .001, �p
2 � .86. No maineffect or interaction involving condition was observed (ps � .54).Mean intoxication ratings for the sample were 11.7 (SD � 12.4)following placebo and 56.1 (SD � 19.7) following the 0.65 g/kgdose.
ABBA Task Performance
Response inhibition. The effects of alcohol on p-inhibitoryfailures as measured by the ABBA task were analyzed by a 2condition (alcohol go vs. neutral go) � 2 dose (0.0 g/kg vs. 0.65g/kg) mixed-design analysis of variance (ANOVA). This analysisrevealed a significant main effect of dose, F(1, 38) � 18.0, p �.001, �p
2 � .32, and a significant dose � condition interaction, F(1,
38) � 4.5, p � .040, �p2 � .11. Mean p-inhibitory failures follow-
ing placebo and 0.65 g/kg alcohol are presented in Figure 3. Thefigure shows that the interaction is due to a greater increase inp-inhibitory failures in response to alcohol compared to placebo inthe alcohol go condition than in the neutral go condition. This wasconfirmed by paired t tests of dose effects conducted separatelywithin each condition. Compared to placebo, p-inhibitory failureswere significantly increased following 0.65 g/kg alcohol in thealcohol go condition, t(19) � 4.6, p � .001, d � 1.04, but not inthe neutral go condition (p � .16). We did not conduct an AN-COVA for this analysis, as alcohol impairment of p-inhibitoryfailures interacted with condition to predict drinking days in re-gression analyses (see below). As such, the covariate did not meetthe required assumption of homogeneity of slopes (i.e., the as-sumption that a covariate must have the same general relation tothe dependent measure across all groups/conditions).
Response activation. A 2 (condition) � 2 (dose) ANOVA ofresponse RT showed a main effect of dose, F(1, 38) � 10.4, p �.003, �p
2 � .22, but no main effect or interaction involving condi-tion (ps � .33). Mean response RTs are presented in Figure 4. Thefigure shows the main effect of dose is due to overall slower RTfollowing alcohol compared to placebo in both conditions.
Response Inhibition and Alcohol Consumption
Separate hierarchical regression analyses were conducted to testthe hypothesis that individual differences in inhibitory failureswould be associated with self-reported measures of alcohol con-sumption (i.e., drinking days, binge days, and total drinks), andthat this effect would be more pronounced in the alcohol gocondition. For each regression model, inhibitory failures wereentered in Step 1 to test for an association between responseinhibition and drinking measures across conditions. Condition wasentered in Step 2, and the condition � inhibitory failures interac-tion term was entered in Step 3. The interaction tested whether therelation between response inhibition and alcohol consumptiondiffered by cue condition.
Figure 2. Mean proportion of inhibitory failures (left panel) and RT(right panel) to go cues following alcohol and neutral images on the ABBAtask. Capped vertical lines represent standard errors of the mean.
Figure 3. Mean proportion of inhibitory failures following go cues in thealcohol go and neutral go conditions under two alcohol doses: 0.0 g/kg(placebo) and 0.65 g/kg. Capped vertical lines show standard errors of themean.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
6 WEAFER AND FILLMORE

Results from the regression analyses predicting drinking habitsfrom inhibitory failures during sober baseline ABBA performance(Part 1) are presented in Table 2. Mean inhibitory failures for thesample were positively skewed, and so the square root transfor-mation was entered in these analyses. The table shows a maineffect of inhibitory failures in the model predicting drinking days,indicating that greater inhibitory failures were associated withgreater number of drinking days across cue conditions. No signif-icant effects were observed in the models predicting binge days ortotal drinks.
Results from hierarchical regression models testing the relation-ship between alcohol impairment of inhibitory control (Part 2) andself-reported alcohol consumption are presented in Table 3. Alco-hol impairment scores were calculated by subtracting inhibitoryfailures in the placebo session from inhibitory failures in thealcohol session, such that greater values indicated greater alcohol-
induced impairment of inhibitory control. These alcohol impair-ment scores were then entered into the hierarchical regressionanalyses described above. Table 3 shows a significant condition �inhibitory failures interaction in the model predicting drinkingdays. This interaction was probed with bivariate correlationalanalyses of inhibitory failures and drinking days conducted sepa-rately for each condition. Results showed a significant associationbetween greater alcohol impairment of inhibitory failures andgreater number of drinking days in the alcohol go condition (r �.47, p � .038), but not in the neutral go condition (p � .27). Nosignificant effects were observed in the models predicting bingedays or total drinks.
Discussion
This study examined the degree to which alcohol images dis-rupted inhibitory control on the ABBA task in both sober andintoxicated drinkers. In Part 1, participants performed the task in asober state to replicate our previous findings with this task (Weafer& Fillmore, 2012). In Part 2, participants performed the taskfollowing placebo and 0.65 g/kg alcohol to examine the degree towhich alcohol impairment of inhibitory control was potentiated inthe context of alcohol-related compared to neutral cues. We thenconducted regression analyses to determine if task performancewas related to typical drinking habits. Results from Part 1 repli-cated our previous findings, again showing greater disinhibitionfollowing alcohol-related compared to neutral cues in sober drink-ers. Moreover, results from Part 2 showed that alcohol-related cuesexacerbated alcohol impairment of inhibitory control as evidencedby more pronounced alcohol-induced disinhibition following al-cohol cues compared to neutral cues. Finally, regression analysesshowed that in sober drinkers, greater disinhibition in both cueconditions predicted greater number of drinking days over the past90 days. By contrast, the association between alcohol-induceddisinhibition and greater number of drinking days was observedfollowing alcohol cues only.
To our knowledge, this is the first study to show that alcohol-induced disinhibition is exacerbated in the context of alcohol-
Figure 4. Mean RT following go cues in the alcohol go and neutral goconditions under two alcohol doses: 0.0 g/kg (placebo) and 0.65 g/kg.Capped vertical lines show standard errors of the mean.
Table 2Regresssion Models Predicting Alcohol Consumption MeasuresFrom Inhibitory Failures on the ABBA Task During SoberBaseline Performance (Part 1)
Alcoholconsumption measure Beta �R2 �F
Drinking daysStep 1 P-Failures 0.36 0.13 5.82�
Step 2 Condition 0.09 0.01 0.29Step 3 P-Failures�Condition 0.57 0.02 0.81
Binge daysStep 1 P-Failures 0.24 0.06 2.39Step 2 Condition 0.20 0.04 1.44Step 3 P-Failures�Condition 0.93 0.05 2.08
Total drinksStep 1 P-Failures 0.24 0.06 2.32Step 2 Condition 0.03 0.00 0.03Step 3 P-Failures�Condition 0.71 0.03 1.15
Note. P-Failures � the proportion of inhibitory failures (square roottransformation).� indicates a significance value of p � .05.
Table 3Regresssion Models Predicting Alcohol Consumption MeasuresFrom Alcohol Impairment of Inhibitory Failures on the ABBATask (Part 2)
Alcoholconsumption measure Beta �R2 �F
Drinking DaysStep 1 P-Failures (impairment) 0.18 0.03 1.31Step 2 Condition 0.15 0.02 0.82Step 3 P-Failures�Condition 1.31 0.14 6.04�
Binge DaysStep 1 P-Failures (impairment) 0.19 0.03 1.35Step 2 Condition 0.22 0.04 1.73Step 3 P-Failures�Condition 0.32 0.01 0.31
Total DrinksStep 1 P-Failures (impairment) 0.21 0.04 1.71Step 2 Condition 0.04 0.00 0.05Step 3 P-Failures�Condition 0.19 0.00 0.10
Note. P-Failures (impairment) � inhibitory failures following placebosubtracted from inhibitory failures following 0.65 g/kg alcohol.� indicates a significance value of p � .05.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
7ALCOHOL CUES POTENTIATE ALCOHOL DISINHIBITION

related images. This finding could have potentially importantimplications for understanding factors contributing to excessive,undercontrolled alcohol consumption. Alcohol’s impairing effectson inhibitory control are well documented (Fillmore & Weafer,2013), and previous studies have demonstrated associations be-tween greater sensitivity to alcohol impairment of inhibitory con-trol and heavy drinking (Gan et al., 2014; Marczinski et al., 2007;Weafer & Fillmore, 2008). Together, these findings suggest thatacute alcohol-induced disinhibition might directly influence ongo-ing consumption by reducing an individual’s ability to stop orcontrol drinking (Fillmore, 2003). It is important to note that theseprior studies all assessed inhibitory control following neutral stim-uli (e.g., geometric shapes). To the extent that the magnitude ofalcohol-induced disinhibition is exacerbated in the context ofalcohol-related cues, as indicated by the current findings, suchdisinhibition might result in greater impairment of control overdrinking within real-world drinking contexts. That is, the additiveeffect of disrupted control mechanisms via both alcohol-cues in theenvironment and the pharmacological effects of the drug couldserve to severely compromise an individual’s control over ongoingalcohol consumption once a drinking episode is initiated.
The current findings replicated previous findings from our laband others (Fleming & Bartholow, 2013; Kreusch et al., 2013;Weafer & Fillmore, 2012) showing that, as expected, alcohol-related images disrupt inhibitory control in sober drinkers. It isimportant to note that studies are beginning to address the extent towhich this finding generalizes to other drugs of abuse. For in-stance, Pike, Stoops, Fillmore, and Rush (2013) modified theABBA task by replacing alcohol-related with cocaine-related im-ages, and tested the degree to which these images disrupted inhib-itory control in cocaine users. Results showed greater disinhibitionfollowing cocaine images relative to neutral images, suggestingthat cue-induced disinhibition is not specific to alcohol-relatedcues. Together, these findings suggest that drug- and alcohol-related cues disrupt inhibitory mechanisms necessary to refrainfrom initiating drinking or drug-taking episodes. This is likely animportant mechanism through which such cues serve to increaserelapse in individuals attempting to abstain. That is, in addition toincreasing desire for drugs or alcohol (i.e., craving), drug-relatedcues also likely disrupt an individual’s ability to control drug-seeking behavior in response to such cue-induced craving.
These findings provide support for drug addiction models thatemphasize the interplay between enhanced salience attribution todrug-related cues and impaired behavioral control in perpetuatingongoing drug abuse (Goldstein & Volkow, 2002; Jentsch & Tay-lor, 1999). These models propose that the incentive-motivationalproperties of such cues could directly impair inhibitory mecha-nisms necessary to control drug-taking urges. It is important thatthe attribution of such incentive salience to drug-related cues isthought to result from conditioning processes that occur over ahistory of heavy drug use (Robinson & Berridge, 2001). As theseconditioned cue responses become “sensitized” over continuedperiods of heavy use, drug-related cues become stronger andstronger motivators of behavior, thus increasing the difficulty incontrolling drug use in the face of such cues. Thus, individualswith more extensive experience with heavy alcohol or drug usewould be expected to have stronger incentive-motivational re-sponses to drug cues, and perhaps greater cue-induced disinhibi-tion as well. Indeed, the regression analyses in the current study
showed that greater alcohol-induced disinhibition following alco-hol cues (but not neutral cues) was associated with greater fre-quency of self-reported alcohol consumption. Although it is notpossible to infer causal relations from these analyses, it could bethat heavier drinkers have stronger conditioned associations toalcohol-related stimuli, which lead to greater cue-induced urges forconsumption, as well as greater cue-induced disruption of inhibi-tory control. In turn, such enhanced cue-induced disinhibitionlikely serves as a risk factor for continued alcohol consumption (asdiscussed above), thus perpetuating the cycle of excessive, binge-like drinking or drug use.
Evidence that alcohol cues disrupt inhibitory control and that themagnitude of disruption is directly related to excessive alcohol usesuggests that retraining of inhibitory control in the context ofalcohol-related cues could be a potential treatment strategy forlowering alcohol consumption. Initial studies testing this hypoth-esis have provided promising results. For example, Houben andcolleagues conducted two studies in which participants weretrained on an alcohol go/no-go task to either inhibit responses toalcohol cues (alcohol no-go) or to respond to alcohol cues (alcoholgo; Houben, Havermans, Nederkoorn, & Jansen, 2012; Houben,Nederkoorn, Wiers, & Jansen, 2011). Although inhibition trainingdid not affect ad lib alcohol consumption immediately followingtraining, those trained to inhibit to alcohol cues consumed signif-icantly less alcohol over the week following the training in bothstudies. In a similar study, participants were trained to eitherinhibit or respond to alcohol cues using the stop signal paradigm,in which participants are required to respond to go signals asquickly as possible, but to inhibit their response on the occasionaltrial when a stop signal (i.e., an auditory tone) is sounded (Jones &Field, 2013). Here, participants trained to inhibit to alcohol pic-tures drank less alcohol in a taste-test procedure immediatelyfollowing the training compared to those trained to inhibit toneutral cues, but this effect did not extend to self-reported drinkingover the next week. Together, these studies provide promisingresults regarding the potential effects of inhibition training onlowering alcohol consumption. It will be important for futurestudies to examine the extent to which such retraining might alsoreduce cue-induced disinhibition in intoxicated individuals.
There are some limitations to the current study. The between-subjects design could be a potential limitation, as it is possible thatthe groups differed in baseline levels of inhibitory control. How-ever, we chose this design to limit any switching between “go”targets (alcohol vs. neutral) that might serve to reduce the prepo-tency of the “go” response and thus limit our ability to observeinhibitory failures on this task. Additionally, it is important to notethat all participants were recruited from the same population ofyoung adults and randomly assigned to conditions, and the groupsdid not differ in terms of gender make-up, drinking habits, impul-sive personality, or BrACs following alcohol administration. Asecond potential limitation is the gender make-up of our sample(25% female), which precluded analyses of sex differences in thecurrent study. Our decision to include more men than women wasbased on logistical difficulties in recruiting moderate to heavyfemale drinkers who report beer as their most frequently consumedbeverage. It will be important for future studies to extend thesefindings to larger samples comprising equal numbers of men andwomen.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
8 WEAFER AND FILLMORE

In sum, the current study showed that alcohol-related imagesdisrupt inhibitory control in sober and intoxicated drinkers, andthat individual differences in cue-induced disinhibition are asso-ciated with individual differences in typical drinking habits. Thesefindings have important implications regarding the significance ofdrug-related cues and disinhibition in promotion of ongoing, ex-cessive alcohol consumption, and suggest directions for futureresearch. For instance, the potential role of cue-induced disinhibi-tion in binge drinking could be assessed more directly in futurestudies by comparing ABBA task performance in binge and non-binge drinkers, or by examining the degree to which alcoholimpairment on this task predicts laboratory measures of alcoholconsumption. Additionally, modified versions of the task, such asthat developed by Pike et al. (2013), could be used to assess thedegree to which alcohol impairment of inhibitory control is poten-tiated in drug users in the context of other drug-related stimuli.This type of study would provide important information regardingfactors influencing the coadministration of alcohol and otherdrugs.
References
Adams, S., Ataya, A. F., Attwood, A. S., & Munafo, M. R. (2013). Effectsof alcohol on disinhibition towards alcohol-related cues. Drug andAlcohol Dependence, 127, 137–142. doi:10.1016/j.drugalcdep.2012.06.025
Bjork, J. M., Hommer, D. W., Grant, S. J., & Danube, C. (2004). Impul-sivity in abstinent alcohol-dependent patients: Relation to control sub-jects and type 1-/type 2-like traits. Alcohol, 34, 133–150. doi:10.1016/j.alcohol.2004.06.012
Boyatzis, R. E. (1975). The predisposition toward alcohol-related interper-sonal aggression in men. Journal of Studies on Alcohol, 36, 1196–1207.
Ceballos, N. A., Komogortsev, O. V., & Turner, G. M. (2009). Ocularimaging of attentional bias among college students: Automatic andcontrolled processing of alcohol-related scenes. Journal of Studies onAlcohol and Drugs, 70, 652–659.
Cloninger, C. R. (1987). Recent advances in family studies of alcoholism.Progress in Clinical and Biological Research, 241, 47–60.
Dawe, S., & Loxton, N. J. (2004). The role of impulsivity in the develop-ment of substance use and eating disorders. Neuroscience and Biobe-havioral Reviews, 28, 343–351.
de Wit, H., Crean, J., & Richards, J. B. (2000). Effects of d-amphetamineand ethanol on a measure of behavioral inhibition in humans. BehavioralNeuroscience, 114, 830–837. doi:10.1037/0735-7044.114.4.830
Dougherty, D. M., Moeller, F. G., Steinberg, J. L., Marsh, D. M., Hines,S. E., & Bjork, J. M. (1999). Alcohol increases commission error ratesfor a continuous performance test. Alcoholism: Clinical and Experimen-tal Research, 23, 1342–1351. doi:10.1111/j.1530-0277.1999.tb04356.x
Fadardi, J. S., & Cox, W. M. (2008). Alcohol-attentional bias and moti-vational structure as independent predictors of social drinkers’ alcoholconsumption. Drug and Alcohol Dependence, 97, 247–256. doi:10.1016/j.drugalcdep.2008.03.027
Feil, J., Sheppard, D., Fitzgerald, P. B., Yucel, M., Lubman, D. I., &Bradshaw, J. L. (2010). Addiction, compulsive drug seeking, and therole of frontostriatal mechanisms in regulating inhibitory control. Neu-roscience and Biobehavioral Reviews, 35, 248–275. doi:10.1016/j.neubiorev.2010.03.001
Field, M., Christiansen, P., Cole, J., & Goudie, A. (2007). Delay discount-ing and the alcohol Stroop in heavy drinking adolescents. Addiction,102, 579–586. doi:10.1111/j.1360-0443.2007.01743.x
Field, M., & Cox, W. M. (2008). Attentional bias in addictive behaviors:A review of its development, causes, and consequences. Drug andAlcohol Dependence, 97, 1–20. doi:10.1016/j.drugalcdep.2008.03.030
Field, M., Munafo, M. R., & Franken, I. H. (2009). A meta-analyticinvestigation of the relationship between attentional bias and subjectivecraving in substance abuse. Psychological Bulletin, 135, 589–607. doi:10.1037/a0015843
Fillmore, M. T. (2001). Cognitive preoccupation with alcohol and bingedrinking in college students: Alcohol-induced priming of the motivationto drink. Psychology of Addictive Behaviors, 15, 325–332. doi:10.1037/0893-164X.15.4.325
Fillmore, M. T. (2003). Drug abuse as a problem of impaired control:Current approaches and findings. Behavioral and Cognitive Neurosci-ence Reviews, 2, 179–197. doi:10.1177/1534582303257007
Fillmore, M. T., Marczinski, C. A., & Bowman, A. M. (2005). Acutetolerance to alcohol effects on inhibitory and activational mechanisms ofbehavioral control. Journal of Studies on Alcohol, 66, 663–672.
Fillmore, M. T., & Vogel-Sprott, M. (1998). Behavioral impairment underalcohol: Cognitive and pharmacokinetic factors. Alcoholism: Clinicaland Experimental Research, 22, 1476–1482.
Fillmore, M. T., & Vogel-Sprott, M. (1999). An alcohol model of impairedinhibitory control and its treatment in humans. Experimental and Clin-ical Psychopharmacology, 7, 49–55. doi:10.1037/1064-1297.7.1.49
Fillmore, M. T., & Weafer, J. (2013). Behavioral inhibition and addiction.In J. MacKillop & H. de Wit (Eds.), The Wiley-Blackwell handbook ofaddiction psychopharmacology (pp. 135–164). West Sussex, UK: Wileyand Sons Limited. doi:10.1002/9781118384404.ch6
Finn, P. R., Kessler, D. N., & Hussong, A. M. (1994). Risk for alcoholismand classical conditioning to signals for punishment: Evidence for aweak behavioral inhibition system? Journal of Abnormal Psychology,103, 293–301. doi:10.1037/0021-843X.103.2.293
Fleming, K. A., & Bartholow, B. D. (2013). Alcohol cues, approach bias,and inhibitory control: Applying a dual process model of addiction toalcohol sensitivity. Psychology of Addictive Behaviors, 28, 85–96. doi:10.1037/a0031565
Gan, G., Guevara, A., Marxen, M., Neumann, M., Junger, E., Kobiella, A.,. . . Smolka, M. N. (2014). Alcohol-induced impairment of inhibitorycontrol is linked to attenuated brain responses in right fronto-temporalcortex. Biological Psychiatry. Advance online publication. doi:10.1016/j.biopsych.2013.12.017
Goldstein, R. Z., & Volkow, N. D. (2002). Drug addiction and its under-lying neurobiological basis: Neuroimaging evidence for the involvementof the frontal cortex. The American Journal of Psychiatry, 159, 1642–1652. doi:10.1176/appi.ajp.159.10.1642
Henges, A. L., & Marczinski, C. A. (2012). Impulsivity and alcoholconsumption in young social drinkers. Addictive Behaviors, 37, 217–220. doi:10.1016/j.addbeh.2011.09.013
Houben, K., Havermans, R. C., Nederkoorn, C., & Jansen, A. (2012). Beera no-go: Learning to stop responding to alcohol cues reduces alcoholintake via reduced affective associations rather than increased responseinhibition. Addiction, 107, 1280–1287. doi:10.1111/j.1360-0443.2012.03827.x
Houben, K., Nederkoorn, C., Wiers, R. W., & Jansen, A. (2011). Resistingtemptation: Decreasing alcohol-related affect and drinking behavior bytraining response inhibition. Drug and Alcohol Dependence, 116, 132–136. doi:10.1016/j.drugalcdep.2010.12.011
Jentsch, J. D., & Taylor, J. R. (1999). Impulsivity resulting from frontos-triatal dysfunction in drug abuse: Implications for the control of behaviorby reward-related stimuli. Psychopharmacology, 146, 373–390. doi:10.1007/PL00005483
Jones, A., & Field, M. (2013). The effects of cue-specific inhibitiontraining on alcohol consumption in heavy social drinkers. Experimentaland Clinical Psychopharmacology, 21, 8–16. doi:10.1037/a0030683
Kreusch, F., Vilenne, A., & Quertemont, E. (2013). Response inhibitiontoward alcohol-related cues using an alcohol go/no-go task in problemand non-problem drinkers. Addictive Behaviors, 38, 2520–2528. doi:10.1016/j.addbeh.2013.04.007
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
9ALCOHOL CUES POTENTIATE ALCOHOL DISINHIBITION

Lawrence, A. J., Luty, J., Bogdan, N. A., Sahakian, B. J., & Clark, L.(2009). Impulsivity and response inhibition in alcohol dependence andproblem gambling. Psychopharmacology, 207, 163–172. doi:10.1007/s00213-009-1645-x
Marczinski, C. A., Combs, S. W., & Fillmore, M. T. (2007). Increasedsensitivity to the disinhibiting effects of alcohol in binge drinkers.Psychology of Addictive Behaviors, 21, 346–354. doi:10.1037/0893-164X.21.3.346
Marczinski, C. A., & Fillmore, M. T. (2003). Preresponse cues reduce theimpairing effects of alcohol on the execution and suppression of re-sponses. Experimental and Clinical Psychopharmacology, 11, 110–117.doi:10.1037/1064-1297.11.1.110
McKim, W. A. (2007). Drugs and behavior: An introduction to behavioralpharmacology (6th ed.). Upper Saddle River, NJ: Pearson Prentice Hall.
Miller, M. A., & Fillmore, M. T. (2010). The effect of image complexityon attentional bias towards alcohol-related images in adult drinkers.Addiction, 105, 883–890. doi:10.1111/j.1360-0443.2009.02860.x
Mulvihill, L. E., Skilling, T. A., & Vogel-Sprott, M. (1997). Alcohol andthe ability to inhibit behavior in men and women. Journal of Studies onAlcohol, 58, 600–605.
Murphy, P., & Garavan, H. (2011). Cognitive predictors of problemdrinking and AUDIT scores among college students. Drug and AlcoholDependence, 115, 94–100. doi:10.1016/j.drugalcdep.2010.10.011
National Institute on Alcohol Abuse and Alcoholism. (2004). NIAAAcouncil approves definition of binge drinking. NIAAA Newsletter, Win-ter 2004(3), 3.
Nederkoorn, C., Baltus, M., Guerrieri, R., & Wiers, R. W. (2009). Heavydrinking is associated with deficient response inhibition in women butnot in men. Pharmacology Biochemistry and Behavior, 93, 331–336.doi:10.1016/j.pbb.2009.04.015
Nigg, J. T., Wong, M. M., Martel, M. M., Jester, J. M., Puttler, L. I., Glass,J. M., . . . Zucker, R. A. (2006). Poor response inhibition as a predictorof problem drinking and illicit drug use in adolescents at risk foralcoholism and other substance use disorders. Journal of the AmericanAcademy of Child & Adolescent Psychiatry, 45, 468–475. doi:10.1097/01.chi.0000199028.76452.a9
Ostling, E. W., & Fillmore, M. T. (2010). Tolerance to the impairingeffects of alcohol on the inhibition and activation of behavior. Psycho-pharmacology, 212, 465–473. doi:10.1007/s00213-010-1972-y
Patton, J. H., Stanford, M. S., & Barratt, E. S. (1995). Factor structure ofthe Barratt impulsiveness scale. Journal of Clinical Psychology, 51,768 –774. doi:10.1002/1097-4679(199511)51:6�768::AID-JCLP2270510607�3.0.CO;2-1
Pike, E., Stoops, W. W., Fillmore, M. T., & Rush, C. R. (2013). Drug-related stimuli impair inhibitory control in cocaine abusers. Drug andAlcohol Dependence, 133, 768–771. doi:10.1016/j.drugalcdep.2013.08.004
Robinson, T. E., & Berridge, K. C. (1993). The neural basis of drugcraving: An incentive-sensitization theory of addiction. Brain ResearchReviews, 18, 247–291. doi:10.1016/0165-0173(93)90013-P
Robinson, T. E., & Berridge, K. C. (2001). Incentive-sensitization andaddiction. Addiction, 96, 103–114. doi:10.1046/j.1360-0443.2001.9611038.x
Rose, A. K., & Duka, T. (2008). Effects of alcohol on inhibitory processes.Behavioural Pharmacology, 19, 284–291.
Rubio, G., Jiménez, M., Rodríguez-Jiménez, R., Martinez, I., Ávila, C.,Ferre, F., . . . Palomo, T. (2008). The role of behavioral impulsivity inthe development of alcohol dependence: A 4-year follow-up study.Alcoholism: Clinical and Experimental Research, 32, 1681–1687. doi:10.1111/j.1530-0277.2008.00746.x
Selzer, M. L., Vinokur, A., & van Rooijen, L. (1975). A self-administeredShort Michigan Alcoholism Screening Test (SMAST). Journal of Stud-ies on Alcohol, 36, 117–126.
Sharma, D., Albery, I. P., & Cook, C. (2001). Selective attentional bias toalcohol related stimuli in problem drinkers and non-problem drinkers.Addiction, 96, 285–295. doi:10.1046/j.1360-0443.2001.96228512.x
Sher, K. J., & Trull, T. J. (1994). Personality and disinhibitory psychopa-thology: Alcoholism and antisocial personality disorder. Journal ofAbnormal Psychology, 103, 92–102. doi:10.1037/0021-843X.103.1.92
Sobell, L. C., & Sobell, M. B. (1992). Timeline follow-back: A techniquefor assessing self-reported alcohol consumption. In R. Z. Litten & J. P.Allen (Eds.), Measuring alcohol consumption: Psychosocial and bio-chemical methods (pp. 41–72). Totowa, NJ: Humana Press. doi:10.1007/978-1-4612-0357-5_3
Tibboel, H., De Houwer, J., & Field, M. (2010). Reduced attentional blinkfor alcohol-related stimuli in heavy social drinkers. Journal of Psycho-pharmacology, 24, 1349–1356. doi:10.1177/0269881109106977
Townshend, J., & Duka, T. (2001). Attentional bias associated with alcoholcues: Differences between heavy and occasional social drinkers. Psy-chopharmacology, 157, 67–74. doi:10.1007/s002130100764
Watson, P. E., Watson, I. D., & Batt, R. D. (1981). Prediction of bloodalcohol concentrations in human subjects. Updating the Widmark Equa-tion. Journal of Studies on Alcohol, 42, 547–556.
Weafer, J., & Fillmore, M. T. (2008). Individual differences in acutealcohol impairment of inhibitory control predict ad libitum alcoholconsumption. Psychopharmacology, 201, 315–324. doi:10.1007/s00213-008-1284-7
Weafer, J., & Fillmore, M. T. (2012). Alcohol-related stimuli reduceinhibitory control of behavior in drinkers. Psychopharmacology, 222,489–498. doi:10.1007/s00213-012-2667-3
Weafer, J., & Fillmore, M. T. (2013). Acute alcohol effects on attentionalbias in heavy and moderate drinkers. Psychology of Addictive Behaviors,27, 32–41. doi:10.1037/a0028991
Received February 19, 2014Revision received June 6, 2014
Accepted June 9, 2014 �Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
10 WEAFER AND FILLMORE