abstracts from hip international vol. 1 no. 1-4 - citeseerx
TRANSCRIPT

S1
Hip International / Vol. 11 S-1, 2001 / pp. S1-S10 ©by Wichtig Editore, 2001
A new look at the forces acting on the hip joint
R. BOMBELLI 1, N. KULLER 2, M. BOMBELLI 3
1 Department of Orthopaedic Surgery, General Hospital, Busto Arsizio (Va) - Italy 2 Ellis Hospital, Schenectady, New York - USA3 Department of Traumatology and Reconstructive Surgery, University of Ulm, Ulm - Germany
ABSTRACT: A simple diagram of coronal plane forces about the hip is used to describe pathomechanics of coxavara, coxa valga, coxarthrosis, femoral neck fracture, congenital coxa vara, slipped capital epiphysis, disloca-tion of the femoral head and acetabular loosening in total hip replacement. A common pattern of abnormality isseen to be excessive shear against a cranio-laterally oblique plane with consequent cranio-lateral migration ofthe structure distal to that plane. As soon as the plane is made horizontal with surgical treatment, the shearingforces disappear and the vertical compressive forces achieve healing. (Hip International 1991; 1: 7-16)
KEY WORDS: Hip biomechanics, Hip arthroprosthesis
Exchange arthroplasty best for infected total hip replacement
D.J. THOMAS, G. BANNISTER
Winford Orthopaedic Hospital, Bristol - UK
ABSTRACT: Thirty-seven patients with infected total hip replacements, treated by either exchange hip replace-ment with antibiotic loaded acrylic cement, or excision arthroplasty, were assessed after an average of fiveyears. Recurrence of infection was comparable in both groups but exchange arthroplasty gave supenor func-tional results. The success of exchange arthroplasty in the hands of general orthopaedic surgeons was similarto that of tertiary referral centres specialising in hip surgery. When technically possible, exchange seems to bepreferable to excision arthroplasty in infected hip replacement. (Hip International 1991: 1: 17-20)
KEY WORDS: Infected, Hip, Arthroplasty, Exchange, Excision
Long term results of Charnley low-friction arthroplasty A thirteen-year average follow-up study
G. STRINGA, G. V. Dl MURIA, M. MARCUCCI, R.P. PITTO
Department of Orthopaedics and Traumatic Surgery, University of Firenze, Florence - Italy
ABSTRACT: Of the first 127 consecutive patients who had had a Charnley total hip replacement at the FirstOrthopaedic Clinic, University of Florence, between 1970 and 1977, 74 (76 hips) were re-evaluated eleven toeighteen years post-operatively by clinical examination and roentgenograms. In this group we identified 8failures (3 mechanical loosening and 5 septic loosening). All failed cases were revised. At 13 years averagefollow-up, the incidence of radiological aseptic loosening was 19.1% for the acetabular component and 17.6%
Abstracts from Hip International Vol. 1 No. 1-4

S2
for the femoral component; nevertheless in most of these cases, the clinical status was excellent or good. Acetabular component wear was found to be a significant problem. (Hip International 1991; 1: 21-7)
KEY WORDS: Hip arthroplasty
Cementless revision operations of loosened cemented hip arthroplasties:ten years experience
R. WEINHART, T.H. BUCHOLZ, P. RINDERLE, R. PARHOFER
Stadtkrankenhaus Memmingen- Germany
ABSTRACT: We report on ten years' experience with cementless hip arthroplasty in revision-operations of loos-ened cemented hip arthroplasties. In about 25 percent of cases admitted to our hospital, patients had beenpreviously operated on more than once, and nearly 9 percent had a bacteriologically proven infection. Thereconstruction of acetabulum and femur for implantation of a cementless prosthesis is performed by meansof homologous bonegraft stored in a bonebank. The bone is stored at -70 to -80 °C. A condition of an ade-quate ingrowth to both autologous or homologous bonegraft is that the implant is resting well in its bedding.With the aid of examples the results of the above technique are shown. Since April 1987 the stem is coatedwith Titanium powder in the proximal part. Since 1987 several methods have been utilized to minimize ho-mologous blood transfusions (i. e. plasmapheresis, preoperative haemodilution; intra- and postoperative cell-saving). (Hip International 1991; 1: 28-38)
KEY WORDS: THR-revision-operations, Cementless implantation, Homologous bonegraft, Autologous blood-transfusion
The "elliptical" femoral prosthesis
F. PIPINO, L. MOLFETTA
1st Orthopaedic Clinic, University of Bari, Bari - Italy
ABSTRACT: The elliptical femoral prosthesis was designed for solving the problem of the relationship be-tween the prosthetic head and the anatomical acetabulum and to minimize the incidence of cotyloiditis, i.e.acetabular wear-protrusion and pain. Long -term clinical tests have been performed using the Cathcart pros-thesis, which is the most advanced technological design. Its basic feature lies in the ellipticity of the headand its development was based on the anatomy and biomechanics of the hip: the femoral head is, in fact,naturally elliptical. The acetabulum is a "deformable"structure, the facies lunata being a stress contact andbearing area, whereas the trabecular system of a "gothic arch”, the "sourcil” and the ileum cortical laminaeserve as a load distribution and carrying structure. Clinical results have shown a very low percentage of "coty-loiditis" (1-3%), thanks to the optimal relationship between the prosthetic head and the antomical acetabu-lum, which guarantees improved distribution of the lubrication stresses and nourishment of the articular car-tilage. (Hip International 1991; 1: 39-44)
KEY WORDS: Hip femoral prosthesis, Cotyloiditis

S3
Computerized evaluation of the articular loads on the normal dynamichuman hip: a study of biomechanics
A. SURACE, A.M. PREVITERA, C. MICALE, G. MINEO
Department of Orthopaedics and Traumatology, University of Milano, Milan - Italy
ABSTRACT: Since the beginning of this century hip biomechanics has been widely studied. This subject is ofgreat interest to the orthopaedic surgeon, especially regarding dismorphic and degenerative pathology, andtrauma. Biomechanical evaluation is one of the key points in the setting-up of various surgical methodolo-gies (osteotomies, arthroplasties, osteosyntheses, etc). Calculations referring to this subject are complex andalmost impossible to do manually, as so hip operations orthopaedics base themselves on theoretical notions,empirically applied to individual cases and to personal experience. To obviate such inconveniences a com-puterized procedure has been realized to effect a biomechanical evaluation of the hip for each single sub-ject. The Author describe their own computerized procedure for a biomechanical analysis of normal hip. (HipInternational 1991; 1: 45-58)
KEY WORDS: Hip biomechanics, Biomechanical analysis
Cementless hip arthroplasty in primary procedures: ten years experience
P. RINDERLE, R. WEINHART, T.H. BUCHOLZ, R. PARHOFER
Stadtkrankenhaus Chirurg Klinic, Memmingen - Germany
ABSTRACT: The Authors report on 10 years of experience with cementless PM-Hip-Arthroplasty in primaryprocedures, 1500 prostheses of this type having been implanted during the past decade. Our report is limit-ed to the prosthesis design and operative technique as well as to the indications for implanting a cementlesship arthroplasty. The major problem of cementless hip arthroplasty is located in the shaft and causes of pos-sible failures are presented and discussed. In patients with clinical symptoms characteristic radiological changesare almost always present. It is clear that particularly in cementless hip arthroplasty, the precise operativetechnique is of paramount importance. (Hip International 1991; 1: 59-66)
KEY WORDS: Hip arthroplasty, Cementless implantation, PM prosthesis
Selective arterial embolization in aneurysmal bone cyst
M. MISASI, F. COZZOLINO, D. MARINO
Locomotor System and Surgery Institute,University of Napoli, Second Medicine and Surgery Faculty, Napoli - Italy
ABSTRACT:After brief discussion of the method and technique of selective arterial embolization (S.A.E.), theAuthors report their experience in the treatment of aneurysmal bone cyst (A. B. C.), presenting particular lo-calization and extension, using this kind of therapeutical embolization (S.A. E.). (Hip International 1991; 1:67-9)
KEY WORDS: Aneurysmal bone cyst, Arterial embolization

S4
Reconstructive hip prosthesis surrounded by allografts
D. POITOUT, G. GAUJOUX, P. O'ZOUX, C.L. FILIPPI, M. LEMPIDAKIS
Hospital Center North, University of Aix-Marseille ll, Marseille - France
ABSTRACT: Autologous grafts, unlike allogenic grafts, have an important osteogenic potential. But, as the pro-curement volume is limited, they do not permit bone or joint reconstruction where there has been partial or totalresection as a result of either a bone tumor or post-traumatic lack of substance. For this reason, we have electedsince 1976 to use fresh allogenic bone grafts and since 1981 deep-frozen allogenic grafts to rebuild the skeleton(421 cases, 1976-1990). Deep-freezing alone allows the preservation of even large bone pieces in satisfactory con-ditions of sterilization. This type of preservation keeps the bone architecture in an optimal biological and biome-chanical state. With the bone cells destroyed and the bone being recolonized by the host's own cells, there is noimmunological risk of inadequate blood and leukocyte compatibility between donor and recipient. If the bone is tobe totally or partially integrated by the skeleton within a few years, the functional value of the cartilaginous sur-faces can be altered after a massive osteocartilaginous graft. At the hip therefore we prefer to use a massive pros-thesis surrounded by allografts. Reconstructive hip prosthesis surrounded by deep-frozen preserved bone has sev-eral advantages: easy fixation of the muscles on the graft; close tightening of the muscles; increasing of the bonemass; rapid loading. Since 1983, 103 hips have been rebuilt with cortico-spongious allografts (femoral heads, to-tal hemipelvis or acetabulum) associated with total hip prosthesis. To reconstruct the upper part of the femur weused a mega hip prosthesis surrounded by allograft. The reconstructive mega hip prosthesis has to have the innershape of the femur with its two sagittal curves to permit cementless fixation at the upper part of the prosthesiswhich is placed into the allograft and cemented fixation of the lower part of the stem which is fixed into the receiverbone. When great precautions are taken during surgical procurement and grafting (sterility, stability, and appropri-ate muscular surrounding) the long-term results are excellent in 80% of cases. (Hip International 1991;1:70-8).
KEY WORDS: Megaprosthesis, Massive bone allograft, Deep-frozen bone, Bone tumor, Hip reconstruction,Acetabulum reconstruction
Factors associated with the development of heterotopic ossification intwo different types of hip prosthesis
M. PARRINI 1, F. LAZZARO 2, L. PARRINI 2
1 5th and 2 1st Department of Orthopaedic Surgery, University of Milano Medical School, Milan - Italy
ABSTRACT: The Authors evaluated the incidence and the dimensions of heterotopic ossifications (HO) in twogroups of patients in which two different types of prosthesis were implanted. The first group of 31 patients hadreceived an alumina-alumina Rosenthal-SAMO total hip replacement, while the second group (79 patients) hada metal-polyethylene Charnley low friction arthroplasty. While the total incidence of HO was similar, the HO weresignificantly smaller in the first group (all grade I according to Brooker) (3). The patients' clinical files were ret-rospectively examined, but it was not possible to find any significant difference for the following parameters: age,sex, side, previous homolateral surgery, diagnosis, operating team, operating time, type of anaesthesia, and bloodloss during surgery. The only difference was in the number of suction drains positioned: two in the first groupand one in the second. Even if it is impossible to draw a definite conclusion, we postulate that the decrease involume and duration of the periprosthetic haematoma, and the smaller amount of debris caused by the alumina-alumina coupling, could be of protective value. (Hip International 1991; 1:79-82)
KEY WORDS: Total hip replacement, Ossification, Haematoma, Alumina

S5
Morphology and biomechanics of the hip. Study I: the normal hip
F. SPECCHIULLI, R. LAFORGIA, L. NITTI, N. PELLICANI, G. SAVINO, N. MASTROSIMONE, G. SOLARINO
2nd Institute of Clinical Orthopedics, University of Bari, Bari - Italy
ABSTRACT: With the aim of defining the roentgenographic characteristics of a "normal" hip - meaning anarticulation able to fully respond to static and dynamic stress without wear, we examined 60 hips of peo-ple over 70 years old from a population of Southern Italy. The parameters considered were: width of WBS,inclination of WBS, height of Gothic Arch, width of Gothic Arch, α angle of aperture of Gothic Arch, α an-gle of Gothic Arch, diameter of femoral head, CE angle of Wiberg, neck-shaff angle, offset, angle of aper-ture of spherichal sector (SS), surface area of SS, volume of SS, radius of the spherical bowl, height ofthe spherical bowl, distance from the "tear drop " image of the fundus acetabuli. The main findings are:a) the WBS is horizontal; b) the gothic arch is orthogonal to the WBS; c) the spherical sector presentswide individual oscillations; d) the female hip has specific characteristics, being mainly smaller. (Hip In-ternational 1991; 1: 83-94)
KEY WORDS: Hip biomechanics
Vascularized Lage-Napoli hip shelf procedure: a new technique
M.M.M. NAPOLI, J.A. LAGE, R.C. COSTA, R. BASILE, L.A.A. LAGE, L.A. LAGE
Institute of Orthopaedics and Traumatology (IOT) - University of Sao Paulo School of Medicine,Sao Paulo - Brazil
ABSTRACT: The difficulty of stabilizing hips with pathological dislocation or dysplasias, mainly in the se-quelae of pyoarthritis where destruction of the head and neck of femur occurs with upward dislocation ofthe femur, is well known. In such cases, the stabilization methods for the hip are free bone grafts that of-ten fail due to bone resorption and subsequent hip instability, and so arthrodesis is the only method ofchoice. Using our method good stabilization of the hip was achieved and mobility of the joint was pre-served. In this series of 35 cases with a follow-up of eight years after surgery, the Authors propose a newtechnique for the treatment of unstable hips with the use of a vascularized muscle pedicled bone graff.This technique can also be used in cases of Legg-Perthes disease, where the femoral head tends to par-tially dislocate. (Hip Intemational 1991; 1: 95-101)
KEY WORDS: Hip, Pathologic dislocation, Congenital dislocation, Dysplasia, Vascularized hip shelf
Long-term evaluation of hip arthroplasty (Mid-thigh pain, limp, loose-ning and failures)
A. SURACE, G. MINEO, C. MICALE, G. DE GIOVANNI, A.M. PREVITERA
3rd Orthopedic Department, University of Milano, Milan - Italy
ABSTRACT: Two hundred and fifty arthroplasties performed from February 1982 to June 1990 at the 3rdOrthopedic Department of the University of Milan, were evaluated in the long term after operation. All pa-tients were rated by a personal scoring system based on the analysis of hip motion. Twenty-one patients

S6
who had received cementless arthroplasties were examined by bony scintigraphy to check the time courseof prosthetic fixation on the basis of bone metabolic state. The excellent clinical results strongly supportthe correctness of the concept of arthroplasty, but various aspects of surgical technique must be studiedand further improvements made in components. (Hip International 1991; 1:102-7)
KEY WORDS: Hip arthroplasty, Cementless hip arthroplasty, Complications in hip arthroplasty
HN cementless HIP system. Results on 320 cases with average 2 yearfollow-up
F. HENRY 1, J. NEGRE 2
1 Clinique de la Présentation, Fleury les Aubrais2 Clinique de l'Archette, Olivet - France
ABSTRACT: The study of any cementless hip system is essentially based on three concepts: initial stability,secondary biological stability and factors regarding the reliability of this stability. Initial Stability relies on op-timal bone fill with press-fit support on the cortical bone. For the acetabular component, this is best achievedwith a hemispherical form. Femoral support is assured by a triple cortical contact in the metaphyseal zone.A triple support requires a stem with a sagittal bow. Secondary stability must account for a compromise be-tween fixation and extractability. The sand-blasted titanium surface provides this possibility. Bone on-growthproduces a sheath around the metal, similar to cement, from the fourth week onwards. Reliability. Reliabestability of the acetabular cup is favored by the hemispherical form of the shell and the ample thickness ofpolyethylene which distribute adverse forces. Femur stability is provided through pure metaphyseal fixation.Metaphysodiaphyseal fixation often becomes plain diaphyseal fixation with all its inherent problems. Initialresults with a minimum follow-up of one year (320 cases with an average follow-up of 2 years) seem to con-firm the efficient nature of the biological fixation by the total absence of pain. Only the future will tell us if ourconcepts are entirely effective. (Hip International 1991; 1: 111-7)
KEY WORDS: Impacted acetabular component, Press-fit, Metaphyseal fixation, Sagittal bow, Titanium
Mechanical evaluation of a wire mesh cup acetabulum reinforcement
R. CAVALIERI COSTA, J.D.M.B. ALVARENGA ROSSI, M.M.M. NAPOLI, T. PUGA LEIVAS, L. DE AZEVEDOLAGE, E. KUKEN TERUYA, H.A. MITSUI
Institute of Orthopaedics and Traumatology (IOT), University of Sao Paulo School of Medicine, Sao Paulo -Brazil
ABSTRACT: Eight acetabula obtained from cadavers were studied to assess axial force strenght. Four of themwere reinforced by a wire mesh and four others were tested without this reinforcement. We observed a sig-nificant increase in strength in the group reinforced by wire mesh. (Hip lnternational 1991; 1: 118-22)
KEY WORDS: Hip biomechanics, Hip arthroplasty

S7
Ender nailing versus nail-plate fixation in the treatment of trochantericfemoral fractures
F. GRECO 1, L. DE PALMA 2, N. SPECCHIA 2, L. RIZZI 2, A. GIGANTE 2
1 Department of Orthopedics, University of Ancona, School of Medicine, Ancona2 Department of Orthopedics, Catholic University of the Sacred Heart, School of Medicine, Roma - Italy
ABSTRACT: The increasing incidence of lateral fractures of the femoral neck, which is related to increased longevity andincidence of osteoporosis, has renewed the need to investigate the problems involved in the treatment of these frac-tures and their complications. A retrospective study was carried out with the aim of comparing the results of two meth-ods used in the treatment of trochanteric fractures: Ender nailing and Jewett nail-plate fixation. The results showed thatoutcome and survival are related to the state of health of the patient. A greater failure rate was observed in patientstreated with Ender nailing than in patients treated with nail-plate fixation. Complications are mainly due to insufficiencyof mechanical synthesis and erroneous surgical techniques. The results of this study confirm the need to focus on thebiological aspects of treatment rather than the mechanical aspects of the fracture. (Hip International 1991; 1: 123-30)
KEY WORDS: Ender nailing, Trochanteric fractures
Morphology and biomechanics of the hip. Study II: the hip at risk
F. SPECCHIULLI 1, R. LAFORGIA 1, L. NITTI 2, N. PELLICANI 1, G. SAVINO 1, N. MASTROSIMONE 1, G. SOLARINO 1
1 2nd Institute of Clinical Orthopedics, University of Bari, Bari2 Institute of Physical-Medical School, University of Bari, Bari - Italy
ABSTRACT: The aim of this study was to establish the point at which a hip is at risk of developing osteoarthritisand the percentage of hips which run such a risk. 253 hips of 164 adults (average age 43) suffering frompathologies not involving the coxofemoral joint were examined. The most important data were: The WBS pre-sented a greater obliquity than the medio-normal; the S. S. surface was narrower; all parameters presentedconsiderable standard deviation. A hip was considered "at risk" when at least two parameters were outsidethe "normal" limits established in our previous study. (Hip International 1991; 1:131-7)
KEY WORDS: Hip biomechanics
Mathematical evaluation of inclination angle in hip osteotomies
C. SIMONE 1, F. DELVECCHIO 2, C. MACCAGNANO, P. DE RUVO 1, P. PACIULLO 1
1 Department of Locomotor Pathology, Faculty of Medicine, University of Bari, Bari2 School of Statistics, Faculty of Economy and Commerce, University of Bari, Bari - Italy
ABSTRACT: When planning an osteotomy reproduction of a bidimensional radiographical femoral image isfundamental. The authors show that radiographical measurement of the inclination angle on X-ray (β1) andon segment (β) differs according to the correlation between β, β1, and the anteversion angle (α) and thus anosteotomy plan must be rigorously mathematical. (Hip International 1991; 1: 138-47)
KEY WORDS: Hip biomechanics, Hip osteotomies

S8
Running and degenerative osteoarthritis of the hip: a morphobiomechanic study
R. LAFORGIA 1, F. SPECCHIULLI 1, L. NITTI 2, M. DE CANDIA 1, M. SOLARINO 3, N. PELLICANI 1, G. SOLARINO 1
1 Department of Clinical Orthopedics, University of Bari Polyclinic, Bari 2 Institute of Physical-Medical School, University of Bari, Bari 3 Department of Radiology, Traumathological Center, Bari - Italy
ABSTRACT: The Authors studied the possible development of degenerative changes in 60 hips of 30 ex-dis-tance runners and ex-long-jumpers who had competed at a national level and had given up competitive sportat least 25 years previously. Careful clinical and radiological examination was carried out with particular at-tention to certain radiographic parameters. The Authors conclude that intensive, long-term sports activitycontributes in no way to degenerative hip disease, and that the origin of so-called primary degenerative arthri-tis of the hip must be sought in morphological changes seen in hip radiographs which may be evaluated bylinear and angular parameters. They suggest that the continuous joint movement might have delayed the oc-currence of a degenerative process which would inevitably have arisen due to mechanical changes within thejoint. (Hip International 1991; 1: 148-52)
KEY WORDS: Sport, Osteoarthritis, Hip, Radiographic parameters
Bipolar prosthetic replacement for the management of intertrochanterichip fractures
A. SURACE, G. MINEO, C. MICALE, A.M. PREVITERA
Orthopedic Surgery Department, University of Milano, Medical School, Milan - Italy
ABSTRACT: To promote early weight bearing and rapid rehabilitation, 55 patients with intertrochanteric hipfractures were treated with bipolar prosthetic replacement. If performed shortly after injury, this procedureallows the restoration of correct limb length and almost nullifies the classic complications of osteosynthesisas well as mortality during or after surgery. (Hip International 1991; 1: 153-6)
KEY WORDS: Hip arthroplasty
Magnetic resonance imaging in the treatment of congenital dislocation ofthe hip in infants
G.U. EXNER 1, R. HALDEMANN 2, J. HODLER 2, A. SCHREIBER 1
1 Department of Orthopedics 2 Department of Medical Radiology, University of Zürich, Zürich - Switzerland
ABSTRACT: In 11 children (aged 4 weeks to 8 months) with congenital dysplasia of the hip and complete dis-locations of the femoral head, magnetic resonance imaging was performed after closed reduction. Gradientecho sequences allowing for a short examination time are well suited for imaging of the articular cartilageand documentation of the position of the femoral head. The use of magnetic resonance imaging decreasesthe risk that incompletely reduced or redislocated hips after closed or open reduction are retained in this po-
S9
sition. Magnetic resonance imaging can be recommended for postreduction assessment of congenital dislo-cation of the hip in infants and may significantly reduce the need for arthrography. (Hip International 1991;1: 161-7)
KEY WORDS: Magnetic resonance imaging, Congenital dislocation of the hip
Aggressive granulomatosis lesions after hip arthroplasty. Revisionarthroplasty with bias total hip system (5 cases)
M. ULIVI, M. GERMANI, K. MOTAVALLI, G.A. BENIGNI, C. OTTAVIANI
Il Orthopaedic Clinic, University of Milano, Milan - Italy
ABSTRACT: Researchers have shown few cases of aggressive granulomatosis appeared after the hip ce-mented arthroplasty. The histopathologic aspects of this disease have been considered, distinguishing it fromthe most common aseptic cemented arthroplasty. In conclusion, the use of a non-cemented titanium arthro-plasty for the surgical treatment of these cases has proved efficient. (Hip International 1991; 1: 168-74)
KEY WORDS: Aggressive granulomatosis, Hip arthroplasty, Non-cemented revision
Morphology and biomechanics of the hip. Study III: the diseased hip
F. SPECCHIULLI, R. LAFORGIA, L. NITTI, G SAVINO, N. MASTROSIMONE, N. PELLICANI, G. SOLARINO
2nd Institute of Clinical Orthopedics, University of Bari, Bari - Italy
ABSTRACT: The aim of this study was to define the characteristics of the diseased hip through a series ofroentgenographic parameters measured on X-rays taken from a group of patients suffering from primary os-teoarthritis. The arthritic hips were divided into three groups: superolateral OA, concentric OA, and medialOA. In light of the anatomo-roentgenographic characteristics this study proposes a new classification of os-teoarthritis based on the direction of migration of the femoral head. Analysis of the data has highlighted theextreme polymorphism which characterizes the course and evolution of osteoarthritis and the serious modi-fications brought about in the hip-joint region. The clinical impression at the conclusion of this study is of adirect correlation between primary alterations of parameters of the hip and development of osteoarthritis.(Hip International 1991; 1: 175-84)
KEY WORDS: Hip biomechanics
New treatment of idiopathic necrosis of the femoral head
N. MARCHETTI 1, A. FALDINI 2, E. BARBIERI 1, M. SCAGLIONE 1, G. PUNZI 1
1 ll Orthopaedic Clinic of Pisa University, Pisa2 I Orthopaedic Clinic of Pisa University, Pisa - Italy
ABSTRACT: The etiology of idiopathic necrosis of the femoral head is surveyed from the literature and a newsurgical treatment is proposed. This treatment aims to create a new blood flow in the necrotic area. The
S10
necrotic area, which lies between normal bone tissue and non-vascularized tissue, is broken by means of per-cutaneous nails. In this paper, treatment strategies are discussed, as well as failures and surgical mistakes.The results obtained with this technique seem to confirm the theoretical assumptions. (Hip International 1991;1: 185-95)
KEY WORDS: Idiopathic necrosis, Femoral head, Percutaneous nails
Mid-thigh pain in cementless arthroplasty: Pathogenetic hypotheses
A. SURACE, L. PIETROGRANDE, G. MINEO
lll Orthopaedic Department, University of Milano, Milan - Italy
ABSTRACT: Mid Thigh Pain (MTP), i.e. a continuous dull pain in the thigh present after prolonged weight-bearing, is a common experience in hip arthroplasties. Since its origin is not clear, the Authors try to explainits etiology and pathogenesis through an analysis of a selection of their cases and of the literature. MTP seemsto be a signal of bone overloading at the interface with the prosthesis; the overloading causes biochemicalchanges in the fibrous tissue surrounding the femoral component, which, in turn, provokes a bone resorptionenhancing movements and overloading. If not treated with unloading, MTP may result in stem loosening. (HipInternational 1991; 1: 196-203)
KEY WORDS: Mid-thigh pain, Cementless arthroplasty
The morphobiomechanics of the hip
R. LAFORGIA, F. SPECCHIULLI, G. SOLARINO, L. NITTI, N. MASTROSIMONE, G. SAVINO, N. PELLICANI
2nd Institute of Clinical Orthopedics, University of Bari, Bari - Italy
ABSTRACT: In this first, introductory study we established the parameters with which to develop an in-depthstudy of the mechanical interpretation of roentgenographic images of osteoarthritic hips. Our choice of pa-rameters, and in fact our whole approach, parted from the theories of morphobiomechanics advanced byPauwels and by Bombelli (Hip International 1992; 2: 1-10)
KEY WORDS: Hip biomechanics, Hip osteoarthritis
Therapeutic considerations on spastic hip treatment in children
F. MOTTA, G. SELVA
Orthopaedic Clinic II, University of Milano, Milan - Italy
Abstracts from Hip International Vol. 2 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S10-S15 ©by Wichtig Editore, 2001
S11
ABSTRACT: The most recent international literature concerning the natural evolution of the hip in pediatriccerebral palsy has been reviewed by the Authors. Therefore a description of the surgical protocol used bythem and other Authors for the prevention and treatment of hip luxation has been performed. From the clin-ical data, a high incidence of subluxation in cerebral palsy has been pointed out. The importance of or-thopaedic screening for this pathology has been underlined. (Hip International 1992; 2: 11-6)
KEY WORDS: Children’s spastic hip, Pediatric pathology of hip
Proposal for hip prosthesis with stress-breaker
A. SURACE, A.M. PREVITERA
Orthopaedic Surgery and Trauma Department, University of Milano, School of Medicine, San Paolo HospitalMilan - Italy
ABSTRACT: The Authors, taking into account the fact that hip prosthetic implant mobilization frequently oc-curs due to excessive stress exerted on bone-prosthesis interface, suggest using prosthesis having stress-breakers, capable in reducing the loads exerted on the implant. There are some hip prosthesis in design whichhave a descharge force system in the cotyloid, in the neck and in the prosthetic stem. Some technical prob-lems are not yet solved, expecially concerning the wear and tear, the friction and the lubrication of the stress-breakers. (Hip International 1992; 2: 17-20).
KEY WORDS: Hip biomechanics
Arthroplasty revision for aseptic failure. Our experience
A. SURACE, L. PIETROGRANDE, M. SARTORIS
Orthopaedic Surgery and Trauma Department, University of Milano, School of Medicine, San PaoloHospital Milan - Italy
ABSTRACT: 35 cases of arthroplasty revision are reviewed with mean follow-up time of 56 m. (range 24 to107), by clinical and radiographic study. The results were satisfactory, having only one case of secondary fail-ure (2.8%), also in comparison with other studies. The reason of this probably lies in the adaptability of ourtechnique: in fact we use without preconcepts both cement and cementless fixations with many types ofstems and cotyles; this allows us to obtain a stable fixation also taking in consideration the bone character-istics of each case. (Hip International, 1992; 2: 21-6)
KEY WORDS: Arthroplasty revision, Arthroplasty aseptic failure
Bone-prosthesis implant relation in total cementless hip arthroprosthesis
E. DE SANTIS, G. GASPARINI, A. PAOLI, S. CUDONI
Orthopaedic Clinic, University of Sassari, Sassari - Italy
ABSTRACT: The best relation between bone and prosthetic implant occurs when an adequate bone surface

S12
preparation and a correct implant placing ensure wide interface contact, with homogeneous load distribution(primary stability). This is necessary premise to achieve osteointegration (secondary stability) which is con-ditioned by factors connected with the implant (materials, surface work, lining) and with the hosting bone(pathological onset, sex, age). The evolution of bone-implant relation leads to the formation of fibrous or os-seous interface; the stimulus which act on the interface (in relation with primary stability, distance betweensurfaces, bony heritage, etc...) infact determine a fibroblastic or osteoblastic evolution of mesenchymal ele-ments colonizing the interface during the initial phases. In successive phases the prevailing apposition (hy-perthropy) or resorption (focal or diffuse atrophy) processes are equally conditioned by mechanical factors(the position and dimension of the implant). (Hip International 1992; 2: 27-34).
KEY WORDS: Hip arthroplasty, Histology of hip arthroplasty
Isoelastic cementless total hip replacement in rheumatoid arthritis. Long-term results
U. FUSCO 1, R. CAPELLI 1, A. AVAI 1, M. GERUNDINI 1, L. COLOMBINI 1, W. REDFORD 2
1 Orthopaedic Department, Busto Arsizio Hospital, Busto Arsizio (VA) - Italy 2 Queen Mary’s Robempton Hospital London, London - UK
ABSTRACT: Between 1980 and 1987 we have implanted 46 isoelastic cementless THR in 40 patients affect-ed with rheumatoid arthritis. We have reviewed 38 hips clinically and by X-ray. The mean follow-up was 8.5years. Harris hip scores ranged from 30.6 pre operatively to 73.4 post-operatively when reviewed. While onthe other hand Merle D'Aubigné hip scores ranged from 7.06 pre-operatively to 15.59 post-operatively. Allpatients have been satisfied, and X-rays showed an improvement for both Charnely and Gruen X-ray score.(Hip International 1992; 2: 43-6)
KEY WORDS: Total hip replacement, Isoelastic prosthesis, Rheumatoid arthritis
Greater trochanteric transfer in children
P. GUARNIERO, W.P. BUNNELL, G.D. MACEWEN
Alfred I, Dupont Institute, Wilmington, Delaware - USA
ABSTRACT: Fifteen patients who were treated at the Alfred I DuPont Institute with greater trochanter overgrowth were reviewed to investigate the results of a surgical procedure for greater trochanteric transfer. Theaim of the paper is to present the clinical findings, X-Ray evaluation, pre and post-operative measurementsbased on pain, limp, Trendelemburg sign, hip abduction power and hip joint motion. The surgical procedureitself is relatively easy to perform and does not often result in complications. The greater trochanteric trans-fer is indicated for older children (about ten years of age) and can offer good results in patients who requireelongation of the lever arm in hip abductor muscles. (Hip International 1992; 2: 47-52)
KEY WORDS: Hip salvage procedure, Greater trochanteric transfer, Children and childhood hip surgery
S13
Multiple revision of total hip arthroplasty
A. SURACE, G. MINEO, C. MICALE, A.M. PRIVITERA, L. PIETROGRANDE
Orthopaedic Surgery and Trauma Department, University of Milano, School of Medicine, San Paolo Hospital,Milan - Italy
ABSTRACT: The Authors present 85 cases of multiple reimplantation of total hip arthroplasty (THA), analyz-ing the complex problems connected to this type of intervention, and putting in evidence primary objectivesrelated technical procedures. (Hip International 1992; 2: 53-62)
KEY WORDS: Total hip arthroplasty, Multiple reimplantation of THA
Our experience with hydroxyapatite ceramic coated Furlong mod. Hipprosthesis
A. SURACE, G. MINEO, C. MICALE
Orthopaedic Surgery and Trauma Department, University of Milano, School of Medicine, San Paolo Hospital,Milan - Italy
ABSTRACT: The Authors present the results of their two years experience in hip arthroplasty with a hydrox-yapatite coated Furlong mod. prosthesis. The deducible considerations taken from these results represent alogic evolution of a new philosophical conceptuality on every suggested usage for hip arthroplasty (Hip In-ternational 1992; 2: 63-7)
KEY WORDS: Hip arthroplasty, Hydroxyapatite ceramic coated hip prosthesis
The self-locking Balgrist hip socket for cementless fixation. Biomechanical principles and clinical results
A. SCHREIBER, H.A.C. JACOB, R. HAUSER, S. KERN
Department of Orthopaedic Surgery, University of Zürich/Balgrist, Zürich - Switzerland
ABSTRACT: The Authors illustrate the biomechanical principles that have governed the production of theirBalgrist hip socket and present the clinical results up to the end of 1991 with 717 implants. By virtue of thespecific design and the tightening mechanism, this socket lends itself particularly well for use in dysplasticacetabuli or in revision hip surgery, where bone grafts are required to fill cavities that have resulted from se-vere bone loss. (Hip International 1992; 2: 71-8)
KEY WORDS: Biomechanical principles of hip arthroplasty, Hip socket
S14
Lateral or valgus shift: a mode of failure of cementless stems
U.E. PAZZAGLIA 1, F. GHISELLINI 2, M. CIOTTI 3, G. ZATTI 1, P. CHERUBINO 1
1 Orthopaedic Clinic, Faculty of Medicine and Surgery of the University of Pavia, F. Del Ponte Hospital, Varese2 Department of Orthopaedics, Hospital della Carità, Novara3 Department of Orthopaedics, Cittiglio Hospital, Varese - Italy
ABSTRACT: Two cases of unusual valgus and lateral stem displacement in cementless total hip replacementare reported. A certain number of mechanical conditions must have been present to cause this unusual pros-thesis displacement. The Authors suggest that the stem's design was one of these factors. (Hip Internation-al 1992; 2: 79-81)
KEY WORDS: Cementless hip arthroplasty, Failure of hip arthroprostheses
Cementless arthroprostheses: case result
M. CANIGGIA, P. FERRATA, P. MANISCALCO, L. BOCCHI
Orthopaedic Surgery and Trauma Department, University of Siena, Siena - Italy
ABSTRACT: The Authors analyse the cases treated with cementless hip endo- arthroprostheses from 1983 tothe present at the Orthopaedic and Traumatology Department of the University of Siena, Italy. They review,in chronological order, the cases treated with three different types of cementless hip prosthesis: the GCO,the PCA and the Omnifit prosthesis. (Hip International 1992; 2: 82-7)
KEY WORDS: Hip arthroplasty
Two cases of ochronotic arthropathy
A. ANDREACCHIO 1, G. P. MOLINARl 2, P.L. ORESTE 3
1 Orthopaedic Surgery and Trauma Department, University of Milano, School of Medicine, San Paolo Hospital,1 Milan2 2nd Division of the Galeazzi Orthopaedic Institute, Milan3 Pathological Anatomy Institute, Ca' Granda Niguarda Hospital, Milan - Italy
ABSTRACT: Phenylketonuria is a congenital inborn error of metabolism of phenylalanine hydroxylase. Char-acteristic arthrosis called ochronotic arthropathy is localized at main joints. The Authors present two casesof ochronotic arthropathy. Clinical and radiological features are described. (Hip International 1992; 2: 88-93)
KEY WORDS: Phenylketonuria, Arthrosis, Ochronotic arthropathy

S15
Congenital hip dislocation relationship between echography and treatment: our experience
W. ALBISETTI 1, B. CARBONE 1, R. FACCHINI 1, F. ROSSETTI 1, S. SERANTONI 2
1 Clinical Orthopaedic Institute, University of Milano, Milan2 Radiology Service, lOPM M. Melloni, Milan - Italy
ABSTRACT: The Authors consider that hip echography plays a fundamental role in the diagnosis of congen-ital hip dislocation in the perinatal age group and that this methodic provides accurate information. The ab-sence of risk to the patient allows its utilization in the screening protocol. The aim of the research was notonly to confirm echography utility in diagnosis, but also to plan and to promote its uniform use as a prog-nostic instrument in predicting and guiding a more accurate therapeutic approach. (Hip International 1992;2: 94-8)
KEY WORDS: Echography hip, Congenital hip dislocation
The treatment of femoral neck fractures in elderly patientsCurrent guide-lines
A. SURACE, G. MINEO, C. MICALE
Orthopaedic Surgery and Trauma Department, University of Milano, Medical School, San PaoloHospital, Milan - Italy
ABSTRACT: The most important goal of femoral neck fracture treatment in elderly patients must be a speedyfunctional recovery which reduces the pathological conditions associated with bed-ridden patients and en-sures an easier family insertion. In this report the Authors present the results of a 48 h post traumatic eventin elderly patients who underwent surgical treatment for femoral neck fractures. Immediately following surgeryall patients were entered in rehabilitation programs. (Hip International 1992; 2: 99-103)
KEY WORDS: Femoral neck fracture treatment, Hip arthroplasty
Post-operative treatment with synthetic salmon calcitonin in patients whounderwent hip endo- and arthroprosthesis implantation
M. CANIGGIA, P. FERRATA, P. MANISCALCO, L. OSTI
Orthopaedic and Traumatological Clinic Institute, University of Siena, Siena - Italy
ABSTRACT: Authors present their results with the use of synthetic salmon calcitonin to treat 21 patients whounderwent implantation of hip endo- or arthroprosthesis. Clinical data as well as laboratory, radiographic andscintigraphic documentation are presented. (Hip International 1993; 3: 1-5)
KEY WORDS: Salmon calcitonin, Post-operative hip arthroplasty
Abstracts from Hip International Vol. 3 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S15-S19 ©by Wichtig Editore, 2001

S16
Bilateral avulsion of iliac spines
F. SPECCHIULLI 1, R. LAFORGIA 1, L. MIOLLA 2, N. MASTROSIMONE 1
1 II Orthopaedic Clinic, University of Bari2 IV Division C.T.O. of Bari, Bari - Italy
ABSTRACT: It is the first time that a case of simultaneous and bilateral avulsion of the iliac spines is describedin the international orthopaedic literature. The X-ray diagnosis was made by means of traditional techniques and tridimensional CT. (Hip International1993; 3: 6-8)
KEY WORDS: Iliac spines fracture
Treatment of femoral neck lateral fractures with the D.H.S. sliding screwplate
A. ANDREACCHIO 1, F. DE MARCHI 2, G.P. MOLINARI 2
1 Orthopaedic Surgery and Trauma Department, University of Milano, Medical School, San Paolo Hospital, 1 Milan2 Galeazzi Orthopaedic Institute, Milan - Italy
ABSTRACT: Authors examine the case report of pertrochanteric femoral fractures treated with the D.H S. screwplate at 135° in three years (from june 1987 to august 1990) at the Istituto Ortopedico Galeazzi of Milan. During this period of time 92 patients have been operated, and 38 have been clinically controlled with midfollow-up of 54 months.Authors describe characteristics of this synthesis means comparing it with others (Thorton nail-plate, Endernails, etc.) commonly used. Finally, they compare the obtained results with those mentioned in literature. (Hip International 1993; 3: 9-16)
KEY WORDS: Femoral neck lateral fractures, Osteosynthesis of femoral neck fractures
Hip arthrodesis: present evaluations
A. ANDREACCHIO 1, F. BASSI 2
1 Orthopaedic Surgery and Trauma Department, University of Milano, Medical School San Paolo Hospital, Milan2 Galeazzi, Orthopaedic Institute, Milan - Italy
ABSTRACT: Authors examine the case-report of hip arthrodesis of the Istituto Ortopedico Galeazzi of Milan. 32 cases have been examined with mid follow-up of more than 31 years. Authors reconsider advantages and disadvantages of a surgical technique that now is almost abandoned,emphasizing the possible effectiveness of this surgical procedure in the light of knowledges of the prosthet-ic hip surgery. (Hip International 1993; 3: 17-25)
KEY WORDS: Arthrodesis, Hip
S17
Endurance and future of total hip replacement: 10 years of experience
G. MINEO, A. SURACE
Orthopaedic Surgery and Trauma Department, University of Milano, Medical School, San Paolo Hospital,Milan - Italy
ABSTRACT: The Authors have revaluated 613 primary THA implants performed in a ten year period from 1982to 1992, with respect to age, gender, diagnosis, kind of prosthesis, surgical and fixation technique. In thisgroup, considering the failure of THA with exchange of one or both prosthetic components or permanent pros-thesis extraction, 19 THA were revised. (Hip International 1993; 3: 26-30)
KEY WORDS: Total hip replacement, THA failure
Centralization of the femoral component in THR. Biomechanical considerations and method
G. KRAKOVITS, L. SASS
Department of Orthopaedic Surgery and Traumatology, Szent Jànos Kòràz, Budapest - Hungary
ABSTRACT: The correct implacement of the femoral component is decisive in the longevity of the total hipreplacement (THR). The stem has to be placed along the anatomical axis of the femur and accomodated tothe internal wall of the femoral canal to prevent tilting, subsidence, torsion movement and its clinical disad-vantages. The author discusses the biomechanical consideration as well as the operative method. (Hip In-ternational 1993; 3: 33-8)
KEY WORDS: Hip arthroplasty, Femoral component, Operation technique
Ultrasonographic screening of deep venous thrombosis in patientsundergoing total hip replacement
F. RAVASI, V. SANSONE, P. GIFUNI
IV Orthopaedic Department, University of Milano, IRCCS San Raffaele, Milan - Italy
ABSTRACT: The incidence of deep venous thrombosis (DVT) after total hip replacement is estimated to beup to 45%. Venography is widely accepted as the gold standard procedure for diagnosis of DVT. With thepurpose of detecting the presence of DVT in asymptomatic patients operated on for primary hip replace-ment, we adopted Real-time B-Mode ultrasonography in order to evaluate its specificity and sensitivity in68 patients. A venography was performed in all the cases in order to obtain a gold standard to comparewith sonography. Sensitivity and specificity of sonography for femoral thrombosis were 71.4% and 97.6%respectively. Ultrasounds were not able to detect thrombosis of the calf veins but the risk of an evolutionto worse pulmonary embolism is quite insignificant at this level. We suggest the use of B-mode ultra-sonography for DVT screening of lower limbs in all the patients undergoing total hip replacement. (Hip In-ternational 1993; 3: 39-45)
KEY WORDS: Venous thrombosis, Hip arthroplasty, Ultrasonography

S18
A histological evaluation of the bone-implant interface failure in total hiparthroplasty due to aseptic loosening
O. MORESCHINI, F. MARGHERITINI
II Orthopaedic Department, University "La Sapienza", Roma - Italy
ABSTRACT: We report a study on how the bone-implant interface of 20 T.H.A. failed because of aseptic loos-ening. The aim of this study was to look for the mechanism that promotes the activation of the cell-popula-tion located in the tissues at the interface. We have demonstrated, with the help of cytochemical and enzy-matic techniques, that cell-activation can be supported by similar agents for every type of implant (cement-ed or cementless). We believe that these agents could be identified with Iymphokines, particularly with In-terleukin 1 (IL-1), and that the production of these factors is stimulated by mechanical factors. These resultsevidence the importance of debris, in addition to micromotion, at the beginning of the process of asepticloosening. (Hip International 1993; 3: 46-50)
KEY WORDS: Hip revision, Aseptic loosening, Cell-activation
Joint replacement failure: error of inevitable event
G. MINEO, L. PIETROGRANDE, M. SURACE
Orthopaedic Surgery and Trauma Department, University of Milano, Medical School, San Paolo Hospital, Milan - Italy
ABSTRACT: It has been a matter of debate as to when a hip prosthesis can be said to have failed. Pain, limpand functional impairment are considered clinical signs of failure while radiolucent lines, subside, bone reab-sorption and gross mobilitation are considered radiological sing. But many times, the patients without signs,free of pain and well functioning, show radiological signs of failure and the patients without radiological signsshow clinical signs of failure. In the revision of 613 hip arthroplasties performed since 1983, the authors havepointed out 19 failures of their patients and 36 failures of the implants done in other hospitals. Moreover, theyhave observed on 15 cases radiological signs of failure without clinical sings. (Hip International 1993; 3: 51-6)
KEY WORDS: Failure of T.H.A.
Immunophenotypic analysis of mononuclear phagocyte antigens in thearthritic synovium of the hip joint
N.A. ATHANASOU
University of Oxford, Nuffield Department of Pathology & Bacteriology, John Radcliffe Hospital, Department of Pathology, Nuffield Orthopaedic Centre, Oxford - UK
ABSTRACT: The antigenic phenotype of lining and subintimal mononuclear phagocytes (MPs) of the synoviumin osteoarthritis (OA) and rheumatoid arthritis (RA) was characterised, using monoclonal antibodies directedagainst a range of monocyte/macrophage associated antigens, in order to determine the role of MPs in thepathobiology of OA and RA of the hip. A major proportion of synovial lining cells (SLCs) and subintimal cells inRA and OA consisted of CD68 positive MPs which expressed a wide range of macrophage-associated antigens.
S19
The monocyte marker, CD14, was downregulated on SLCs in RA while OA and early markers of MP activationpredominated in the OA synovium which was independent of the level of inflammation. In contrast, synovial MPsin RA showed increased expression of activation, maturation and functional antigens such as CD11a, CD11b,CD11c, CD16, CD32, CD54, CD64. Moreover, MP recruitment did not correlate with the degree of Iymphocyticinfiltration in RA. Thus, synovial MPs in RA are rapidly and fully activated with upregulation of activation, dif-ferentiation, and functional antigens occurring in situ. There was also no difference in antigenic phenotype ofsynovial MPs in inflammatory and non-inflammatory OA. (Hip International 1993; 3: 67-74)
KEY WORDS: Macrophage, Rheumatoid arthritis, Osteoarthritis, Hip joint, Synovium
Is the RM-uncemented coated acetabular cup a reliable component intotal hip replacement?
A. AVAI, M. BOMBELLI
Department of Traumatologic, Orthopaedic Surgery General Hospital, Busto Arsizio (Va) - Italy
ABSTRACT: From August 1987 to the 1st of March 1993 1,477 RM-isoelastic, uncemented cup components(257 HA, 1,220 Titanium coated) were inserted for T.H.R., matched with the RM- isoelastic and isotitan stemcomponents. At a 4 year mean follow-up (7-1 years) 1,302 cups were clinically and radiographically assessed; 6.2% of cupscould not be controlled, because at follow-up time the patients had died; 5.6% could not be traced. All the cups were fixed with 3.2 mm peripheral screws (mean number of screws: 6). The cups more than 60mm in diameter were fixed with 2 additional cancellous (6.5 mm) screws. The Charnley score is: - 9 - (97.5%) - 8- (2.43%); 1 cup was removed because of infection (0.07%); 3 cups were revised because of malposition and reinserted in proper position. The results with a similar number of RM-uncoated cups, fixed with only one or two screws from 1979 to 1985,at a mean 4 year follow-up were: 7% revision and 9% im pending loosening. Even bone reaction at the bone-cup interface signifies no osteolisis, neither around the cup nor around the screws. The satisfactory clinicalresults suggest to proceed with the use of this cup (Hip International 1993; 3: 75-83).
KEY WORDS: Total hip replacement, Acetabular replacement
Radio-lucent line: interpretation and clinical correspondence in T.H.A.
G. MINEO, L. PIETROGRANDE, M. SURACE
Orthopaedic Surgery and Trauma Department University of Milano, Medical School, San Paolo Hospital, Milan - Italy
ABSTRACT: The Authors have re-evaluated 84 cementless total hip arthroprostheses out of 700 hip arthro-plasties carried out in their department from January 1982 to December 1992. The aim was to find a corre-lation between the radio-lucent line and the clinical signs of prosthetic loosening. On the basis of the resultsof this study and reports in the literature, the Authors conclude that a very poor correlation exists. (Hip In-ternational 1993; 3: 85-8)
KEY WORDS: Radio-lucent line, Hip arthroplasty failure - Radiological signs
S20
Medium-term clinical and radiological results of the uncemented total hipprosthesis PM
A. REICHELT, H. BOTTERER
Orthopaedic Department, University Hospital Freiburg, Freiburg - Germany
ABSTRACT: Medium term results of 114 cementfree hip joint endoprostheses type PM implanted until mid -1986 are presented. The clinical evaluation was based on the methods of Merle d'Aubigné and Harris. The mean Merle d'Aubigné score increased from 9.15 to 13.95 points and the Harris score from 44.13 to 75.60points. After a mean in situ period of 7.6 years only 35.96% of the operated hips were totally painfree. Twenty-sev-en prostheses (23.68%) did not need any support when walking (5.62% pre-op). Patients with forty-eightprostheses (42.11 %) were able to walk without limitation (18.42% pre-op). Of the operated hip joints 93.9%were judged subjectively as improved. Eighty-four patients were very satisfied (73.7%), twenty-seven werefairly satisfied (23.6%) and three were not at all satisfied (2.6%). Radiographically, 61% of the stems showed a change of position, whereas only 8% of the acetabular com-ponents shifted. In 71.4% of the cases, a radiolucent line around the stem was seen in zone 14. Approxi-mately two thirds of the cups showed this radiolucency. Atrophy of the cortex was noticed in 37.8% of thecases in zone 6. Periosteal reactions appeared only around the tip of the femoral shaft (26.5%).Seventy-eight femora showed a bony consolidation around the stem-tip. Ectopic ossifications were detected at seventy-three joints altogether. In three cases, Brooker-stage IV wasreached. The statistical evaluation showed a low significant correlation between atrophy of cortex in various zones andappearance of pain. The survival-analysis showed for primary implanted PM prostheses a survival rate of 90.5% (Confidence in-terval 86.3%-94.6%) after a five year period and of 73.3% (Confidence interval 60.3%-36.4%) after a ten yearperiod in situ. (Hip International 1994; 4: 1-9)
KEY WORDS: Uncemented total hip prosthesis, Medium term results, Statistical analysis
C.D.H. in the pre- and post-sonographic era
R. BOMBELLI 1, C.H. TSCHAUNER 2, M. BOMBELLI 3
1 Department of Orthopedics, Busto Arsizio General Hospital, Busto Arsizio - Italy2 Department of Orthopedics, Landeskrankenhause Stolzalpe, Stolzalpe - Austria3 Droitwich Knee Clinic, Droitwich - UK
ABSTRACT: The young generation of orthopedic Surgeons, entering the sonographic era, are more aware ofthe importance of the early diagnosis of hip development dysplasia (D.D.H.). In time, probably during the next decades, D.D.H. sequelae will no longer be one of the most frequent rea-sons for surgical hip treatments. Early sonographic investigation indicates that about 41% of newborn hips still have not reached normal maturationat the time of birth (physiological immaturity) and 0.66% of dislocatable or dislocated hips elude pure clinical tests.
Abstracts from Hip International Vol. 4 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S20-S27 ©by Wichtig Editore, 2001
S21
Prevention and, when necessary, early treatment, which limit the suffering of both patients and parents, achievefirst rate results and help contain costs for Society. However, for those cases detected later, either closed oropen reposition-retention is still necessary. From the fundamental contributions of the past, we can now compare the results of the pre- and post-sono-graphic experience. (Hip International 1994; 4: 10-34)
KEY WORDS: Hip, Sonography, Pathogenesis, Biomechanics, Therapy
The use of image intensification as an aid to femoral cement extraction inrevision hip surgery
R. SPENCER JONES, F.M. ISSA
Warrington District General Hospital, Mersey Region - UK
ABSTRACT: Revision hip surgery for a loose or infected prosthesis is becoming more common as increasingnumbers of total hip replacement are performed each year. The use of the image intensifier to aid in the re-moval of the femoral cement is described, and the results of eighteen cases perfomed in this fashion report-ed. (Hip International 1994; 4: 35-40)
KEY WORDS: Image intensifier, Cement
The continuing development of vibration arthrometry as a screeningmethod in developmental dysplasia of the hip
W.G. KERNOHAN 1, B. TRAINOR 2, P. HAUGH 2, A. JOHNSTON 2, I. TURNER 1, R.A.B. MOLLAN 1
1 The Queen's University of Belfast, Department of Orthopaedic Surgery, Musgrave Park Hospital, Belfast2 Musgrave Park Regional Orthopaedic Service, Green Park Healthcare Trust, Belfast - Northern Ireland
ABSTRACT: As part of the continuing development of a non-invasive, objective screening method to achieveefficient early detection of developmental dysplasia of the hip (DDH), we determined the diagnostic sensitiv-ity of an experienced nurse examiner and vibration arthrometry in the range of pathological anatomy of thedisease. A cohort of 25 children were studied prior to commencement of their treatment. The hips were clas-sified into four categories by an experienced paediatric orthopaedic surgeon with all diagnostic modalitiesavailable ("normal", "stable but dysplastic", "unstable and reducible" or "irreducible"). Of the 28 hips identi-fied as abnormal, two hips were classified as stable dysplastic, 11 were unstable/reducible and 15 were ir-reducible hips. The experienced nurse examiner identified eight out of 11 unstable-reducible hips and re-ported clinical signs of abnormality in another 18 cases. Vibration arthrometry identified nine out of 11 un-stable-reducible dislocations and detected abnormal signals from three irreducible hips. Vibration arthrome-try may be of value in detecting abnormality in unstable-reducible and clicking hips. The low detection ratein the irreducible and dysplastic hips by vibration arthrometry was due to the absence of detectable vibra-tion from mechanical events as the hips were manoeuvred. Examination by an experienced clinical examin-er continues to be necessary if all degrees of mechanical abnormality in DDH are to be detected. Further de-velopment is required to achieve an objective non-invasive system of detecting all stages in the pathology ofDDH. (Hip International 1994; 4: 41-9)
KEY WORDS: Vibration arthrometry, Developmental dysplasia, Screening, Accelerometer
S22
Extracapsular hip fractures treated with the titanium captured hip screwsystem
M. CANIGGIA, P. MANISCALCO, A. PICINOTTI, L. BOCCHI
Università degli Studi di Siena, Istituto di Clinica Ortopedica e Traumatologica, Siena - Italy
ABSTRACT: The Authors discuss their experience with the titanium captured hip screw system for extracap-sular fractures. The present review of the results is based on a case group of 93 patients treated with thismethod at the Orthopedic and Trauma Clinic of the University of Siena, Italy, from March 1991 to August 1993.(Hip International 1994; 4: 50-2)
KEY WORDS: Extracapsular hip fractures, Hip screw system
Acetabular growth potential in the dysplastic and normal hip. A long-termfollow-up
F. SPECCHIULLI 1, L. SCIALPI 1, G. SOLARINO Jr 1, L. BATTELLI 2, L. NITTI 3
1 Clinica Ortopedica Università di Bari, Bari2 Ospedale Pediatrico Giovanni XXIII, Bari3 Istituto Fisica Medica Università di Bari, Bari - Italy
ABSTRACT: In CHD (Congenital Hip Dislocation), the elements which determine the degree and quality of ac-etabular growth are not clear. This has caused a great deal of controversy on the capability of developmentof the cotyloid cavity, hence on the indications to reconstructive surgical treatment. In order to study the behavior of che cotyloid cavity, two groups of patients were taken into consideration:normal subjects and subjects with CHD. In normal subjects the median value of the Hingelreiner angle was 19°-4'± 1° (normal limit), at 1 year old. Theacetabular index decreases rapidly until becoming stable at adult values at the age of 8-10 years of age. The distinctive characteristics of the hip with spontaneous recovery from cotyloid dysplasia could be definedas follows: a) the higher critical value on average is reached after 24 months of treatment; b) once the borderline is reached, the dislocated hip evolves in the same way as the healthy hip; c) the earlier treatment is started, the sooner correction of the H angle is obtained; d) the cotyloid cavity continues to develop even after 5 years from reduction. In CHD with terminal residual dysplasia, an initial correction of the H angle is followed by a sudden interrup-tion in acetabular development, which remains inadequate and will never reach normal values. These data allow not only the definition of the acetabular growth potential, but also the establishment of moreprecise indications for reconstructive surgical treatment. (Hip International 1994; 4: 53-8)
KEY WORDS: Acetabular growth, Hip
S23
Partial weight bearing after total hip arthroplasty. What does the patientreally do? A prospective randomized gait analysis
W. E. SIEBERT
Orthopaedic Clinic Kassel, Kassel - Germany
ABSTRACT: We investigated whether the instruction to bear full or partial weight is accurately followedby the patient after total hip arthroplasty. The investigation was made with a measuring insole. It wasrevealed that the patient is able to follow the order only if he receives training with and is controlledby an acoustic and/or optical biofeedback system with every step he takes. Training, even very inten-sive repeated training, with only a scale is futile. The patients' strides are made with either a full weightload, when they should not do so or with only a partial weight load, when they should bear full weight.(Hip International 1994; 4: 61-8)
KEY WORDS: Gait analysis, Total hip replacement, Partial weight bearing
The porous-coated anatomic (PCA) total hip prosthesis. Two-eight year follow-up studies of 30 cases
P. FARSETTI 1, R. CATERINI 1, V. BARLETTA 2, A.E. GUARNIERI 3, E. IPPOLITO 2
1 Department of Orthopaedic Surgery, University of Reggio Calabria, Catanzaro2 Department of Orthopaedic Surgery, University of Roma "Tor Vergata", Roma3 Ars Medica Hospital, Roma - Italy
ABSTRACT: Thirty uncemented porous-coated anatomic (PCA) total hip prostheses were implanted in27 patients. The average age at the time of surgery was 54 years, and the average follow-up was 4.5years. The average hip rating score was 88 points. Three patients had thigh pain at follow-up and fifteen hada mild limp, related to a weakness of the gluteus medius and minimus. On radiographic examination,we observed a good bone ingrowth of the implant in all patients. No aseptic loosening was radiographicallydemonstrated. No relationship was found between pain in the thigh and the various radiographic pa-rameters studied (radiodense lines, sclerosis, varus position of the stem). (Hip International 1994; 4:69-74)
KEY WORDS: Prosthesis, Radiodense lines, Thigh pain
Protrusio socket technique in total hip arthroplasty in chronicallydislocated hips
J. LAKATOS 1, M. SHAFER 2, A. ZIMMERMANN 2, L. BUCSI 1
1 Department of Orthopaedics, Semmelweis Medical University, Budapest2 Department of Orthopaedics, Haynal Imre Postgraduate Medical University, Budapest - Hungary
ABSTRACT: The Authors give a description of a protrusio socket technique, applied since 1987 as aroutine method for arthroplasty in CDH. This method gives good bony coverage of the acetabular com-
S24
ponent, with achievement of good stability, and acetabular roof grafting is becoming unnecessary. Thismethod has been performed in 90 cases, 42 of which have a minimum follow-up of 2 years. The latterhave been reviewed, the results being excellent. (Hip International 1994; 4: 75-9)
KEY WORDS: Revision THR, CDH, Protrusio socket technique
Problems seen after Olerud acetabular augmentation for recurrentdislocation of total hip arthroplasty
B. COHEN 1, R.E. FIELD 1, W.F.G. MUIRHEAD-ALLWOOD 2, N. RUSHTON 1, J.E. SCOTT 3
1 The Orthopaedic Research Unit, University of Cambridge, Cambridge 2 The Whittington Hospital, Highgate Hill, London3 The Westminster Hospital, London - UK
ABSTRACT: In 1985 Olerud and Karlstrom described a procedure for treating recurrent dislocation after to-tal hip arthroplasty. We report our results, using this procedure, in nine patients and discuss the mechanismsof its failure in four cases. (Hip International 1994; 4: 80-4)
KEY WORDS: T.H.R., Dislocation, Acetabular augmentation
Protrusio acetabuli, an unwelcome result in hip hemiarthroplasty
M. SANFELIU, J.L. PARRA, J.M. APARICI, J. FENOLLOSA
Servicio de Cirugia Ortopedica y Traumatologia, Hospital Dr. Peset, Valencia - Spain
ABSTRACT: We report 140 patients with subcapital fractures of the femur, treated by hemiarthroplasty. Weused self locking Muller stems Trilock® with modular heads as well as Thompson prostheses, all being ce-mented. The self locking stems were of Ti-6A1-4V, the Thompsons of chrome-cobalt alloy and the modularheads of stainless steel. Having found 14% to develop protrusio acetabuli, we retrospectively studied the main variables: age, sex,presence or absence of osteoarthritis, osteoporosis, length of the prosthetic neck, disparity of diameters be-tween the head of the femur and the prosthetic head, the type of hemiarthroplasty and the degree of inde-pendence of the patients. Patients in their seventies suffered protrusio more than those in their eighties(p=0.0004), as did those with an independent life, in contrast with dependent patients (p<0.05). The modu-lar Muller Trilock® prostheses, with stainless steel heads, protruded in greater number than the Thompsonchrome-cobalt type. (Hip International 1994; 4: 85-90)
KEY WORDS: Neck of femur fractures, Hemiarthroplasty, Surgical treatment, Elderly
The X-ray magnification of the hip for preoperative planning: a newtechnique
A. DALLERA 1, E.M. BRACH DEL PREVER 1, G. BASILE 2, M. FORTI 1, P. GALLINARO 1
1 I Clinica Ortopedica dell'Università di Torino
S25
2 Consiglio Nazionale delle Ricerche, Istituto di Metrologia "G. Colonnetti", Turin - Italy
ABSTRACT: Precise pre-op planning is fundamental for surgical precision in fit and fil l of uncementedprostheses, and reliable and comparable radiographs are necessary for the early diagnosis of loosening.All this can be obtained with a given X-ray magnification factor. The Authors prove that the routinely usedmethods are misleading and suggest a new technique to obtain a uniform and/or measurable magnifica-tion in the A.P. radiograms of the hip. The method gives accurate measurements within a few tenths of amillimetre. It is based on the knowledge of the femoral position in relation to the X-ray film, obtained witha lateral radiographic view, and on mathematical calculation to obtain the X-ray focus height and posi-tion. Also in the case of a flexed and externally rotated hip, the non-uniform longitudinal and transversemagnifications can be measured. (Hip International 1994; 4: 91-8)
KEY WORDS: X-ray magnification, Hip arthroplasty, Pre-op planning, Radiographic control, Uncementedhip prosthesis
Intertrochanteric corrective osteotomy as a joint-saving surgical treatment for femoral head necrosis
B.T. BERENDSEN 1, C.J. WIRTH 1, H.V.D. BOOM 2
1 Orthopaedic Clinic, Hannover Medical School, Hannover 2 Orthopaedic Clinic, St.-Josef-Stift, Sendenhorst - Germany
ABSTRACT: Forty-seven intertrochanteric osteotomies were performed in 9 years on 40 patients with femoralhead necrosis in Arlet and Ficat stages II and III in the Orthopaedic Department of the Medical School,Hannover. With an average follow up of 5.9 years (minimum 2.3 years, maximum 9.3 years), the studyshows only 46% of the patients with satisfactory, good and very good results. After the joint saving op-eration, 26% of treated patients with pre-operative employment went into premature retirement. The av-erage postoperative non-working period was 11 months (7-18 months). Clinical relevance: The results after the joint-saving operation were better when the operation was per-formed at an early stage of the disease with only a small area of necrosis. Although the operation will notprevent a progression of necrosis and a secondary arthrosis, we recommend that the joint-saving opera-tion be performed during stages I and II to prolong the period before a total hip joint replacement be-comes necessary. During stage III a total hip joint replacement may be preferable depending on clinicalsymptoms, patient age and the radiological findings (necrosis angle > 180°). (Hip International 1994; 4:101-14)
KEY WORDS: Femoral head necrosis, Intertrochanteric osteotomy
Factors affecting the design of the head and neck segment of a contemporary total hip prosthesis
B. ZICAT 1, Y. KUKITA 2, S. GRANDIA 3, C. ENGH 4
1 Cremorne, New South Wales - Australia 2 Hokkaido - Japan 3 Orthopaedic Surgeon, Frederick, MD 4 Anderson Orthopaedic Research Institute, Arlington, VA - USA

S26
ABSTRACT: Anthropometric investigation of femoral sizes and femoral pelvic relationships was performed ina group of unilateral total hip arthroplasty patients. Standardized radiographs were used to perform the mea-surements. The non-operated, contralateral side was used as a standard for endosteal anatomy and the nor-mal femoral pelvic relationship. Analysis of endosteal shape reveals a spectrum ranging from the stove pipeshape of the aged bone that has undergone diaphyseal expansion, to the trumpet shaped proximal femurfound in younger patients. There is also a relationship between this shape and the relative varus or valgusposition of the head and neck of the femur. Implants can be designed with head and neck geometry corre-sponding to these relationships. These implants would reconstruct normal anatomy more accurately. Ce-mentless, acetabula placed in a more medial and proximal position should be matched to femoral componentswith longer neck-length options than cemented acetabular components. (Hip International 1994; 4: 115-26)
KEY WORDS: Total hip arthroplasty, Femoral component, Implant design
Extruding synovitis of the hip in childhood: a case report
G. VAVALLE, L. MOLFETTA, M. CAPOZZI, C. SIMONE
Institute ll of Clinical Orthopaedics, University of Bari, Bari - Italy
ABSTRACT: The authors describe an unusual case of extrusive synovitis of the hip that they believe is ananatomo-clinical variant of transient synovitis of the infantile hip. Transient synovitis of the hip (TSH) is a benign pathology of the hip with complete healing within a few daysafter onset of the disease. The case reported distinguishes itself for the expulsive tendency of the femoralhead from the acetabular cavity with potential ischemic disturbances due to an increased pressure inside thearticular joint causing stretching of the circumflex vessels supplying the femoral head. (Hip International 1994;4: 127-32)
KEY WORDS: Synovitis, Extrusion, Hip, Childhood
The snapping hip
M. PECINA, I. BOJANIC, M. HASPL
Department of Orthopaedic Surgery, School of Medicine, University of Zagreb, Zagreb - Croatia
ABSTRACT: The snapping hip syndrome is a symptom complex characterized by an audible snapping sen-sation usually, but not necessarily, associated with hip pain during certain movements of the hip joint. A num-ber of different aetiologies, both intraarticular and extraarticular have been described. Intraarticular causesfor the snapping hip include loose bodies, osteocartilaginous exostosis, osteochondromatosis and subluxa-tion of the hip. Extraarticular causes for the snapping hip are described in this paper (Tab. I). Due to local-ization of the causes, three different syndromes are described: the medial (internal), the lateral (external), andthe posterior snapping hip syndrome. The authors describe diagnosis, differential diagnosis, and treatmentof these syndromes. Successful results in the treatment of lateral snapping hip syndrome with the iliotibialtract fenestration method are also reported. (Hip International 1994; 4: 133-6)
KEY WORDS: Snapping hip, Extraarticular causes, Treatment
S27
Clinical results and radiologic findings four to eight years after total hipreplacement with the Link RS endoprosthesis system
S. SAVILAHTI, I. MYLLYNEVA, K.J.J. PAJAMÄKI, J. NEVALAINEN, T.S. LINDHOLM
Department of Clinical Medicine, University of Tampere, and Department of Orthopaedics and Traumatology,Tampere University Hospital, Tampere - Finland
ABSTRACT: A total of 102 uncemented Link Rippen System (RS) total hip prostheses were implanted in 100patients whose mean age was 57 years. The Merle d'Aubigné hip score was 9.3 preoperatively and 15.3 atthe latest follow-up. The thigh was painful in 56 per cent; 5 per cent had moderate or severe pain. Forty-fiveper cent of patients had a slight limp and 9 per cent a severe limp at the most recent follow-up. Fifteen percent still needed a cane. A Kaplan-Meier survivorship analysis revealed a 74 per cent probability of survival at 6 years. Serial radiographic evaluations revealed that 16 per cent of patients (non-revised hips) had acetabular com-ponent migration, 10 per cent had continuous femoral radiolucencies, 14 per cent had subsidence and 31 percent progressive varus migration. (Hip International 1994; 4: 137-42)
KEY WORDS: Hip prosthesis, Radiography, Hip diseases, Clinical results
How often are custom implants actually needed in hip revision surgery?
M.D. NORTHMORE-BALL
Unit for Joint Reconstruction, The Robert Jones & Agnes Hunt Orthopaedic Hospital, Oswestry, Shropshire - UK
ABSTRACT: The implants used in a series of 230 consecutive hip replacement revisions have been analysedand divided into those in which the implant was already available in the hospital (Group A), those in which animplant had to be specially brought in, but which was, nevertheless, in production (Group B), and a third groupin which an implant had to be specially made (Group C). Ninety-four per cent of the series were in Group A,3% in Group B, and 3% in Group C. The types of case requiring a Group C or true "custom" implant are dis-cussed. (Hip International 1995; 5: 1-7)
KEY WORDS: Revision hip arthroplasty, Custom implants
Osteoblast activity around failed total hip replacements: synovial fluidlevels of osteocalcin and alkaline phosphatase
P.J. MILLETT, A. SABOKBAR, M.J. ALLEN, B. MYER, N. RUSHTON
University of Cambridge Orthopaedic Research Unit, Addenbrooke's Hospital Cambridge - UK
ABSTRACT: An understanding of the pathogenesis of aseptic loosening is critical to its prevention. Though
Abstracts from Hip International Vol. 5 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S27-S34 ©by Wichtig Editore, 2001
S28
many studies have focused on the increase in bone resorption, few have examined osteoblastic activity inloosened arthroplasties. In this study, alkaline phosphatase and osteocalcin, two well-described osteoblastmarkers, were measured in synovial fluid samples from patients with either primary osteoarthrosis (OA) orfailed hip replacements. Osteocalcin levels were significantly reduced in failed arthroplasties as compared toprimary OA (p < 0.05) with mean (SEM) values of 3.13 ng/ml (0.874) and 6.84 ng/ml (1.24) respectively. Themean (SEM) alkaline phosphatase activity was 0.436 mol/ml/15min (0.127) in revisions and 0. 712 (0.199) inprimary OA (NS). There was poor correlation between osteocalcin concentration and alkaline phosphataseactivity (r=0.16, p>0.05) These data suggest that in addition to enhanced bone resorption, osteoblastic boneformation may also be reduced in periprosthetic bone and as such may play a key role in the pathogenesisof aseptic loosening. (Hip International 1995; 5: 8-14)
KEY WORDS: Total hip replacement, Aseptic loosening, Osteoblast, Synovial fluid, Osteocalcin, Alkaline phosphatase
Short-term clinical results with an elliptical femoral prosthesis
C. SIMONE, V. PATELLA, B. MORETTI, L. MOLFETTA, V. PESCE, G. VAVALLE
II Orthopaedic Clinic, University of Bari, Bari - Italy
ABSTRACT: The biomechanics of an elliptical-head femoral prosthesis, considered in relation to the physiol-ogy of the coxo-femoral joint, can be taken as the rationale for its use in the treatment of medial fractures ofthe neck of the femur. Short-term results based on clinical variables (Harris's evaluation method) and X-rayfindings show a functional joint and good preservation of radiographic relations between the prosthetic epi-physis and the acetabulum, and between the stem and femoral metadiaphysis. These findings confirm thevalidity of the biomechanical concepts underlying the design of the elliptical-head femoral prosthesis. It isan "etiological" solution for patients with medial fractures of the neck of the femur since it fits in with thecoxo-femoral physiology without interfering with the normal anatomical/biomechanical relations between thetwo joint components. (Hip International 1995; 5: 15-9)
KEY WORDS: Neck of the femur, Medial fractures, Elliptical femoral prosthesis
Periprosthetic fractures of the hip: the Mennen clasp plate
A.H.N. ROBINSON 1, A. AYLLON-GARCIA 2, J.P. HALLETT 1, B.F. MEGGITT 2
1 Department of Trauma and Orthopaedics Surgery, The Ipswich Hospital N.H.S. Trust, Ipswich2 Department of Trauma and Orthopaedics Surgery, Addenbrooke's Hospital, Cambridge - UK
ABSTRACT: Fractures around upper femoral prostheses are difficult to treat. The Mennen plate is a new formof treatment. In this paper 14 cases treated with this plate and a postoperative cast-brace are discussed. Wealso describe the use of screws to supplement the fixation. Of the 14 patients, 12 survived to follow up, of whom 11 went on to unite at an average of 14 weeks. All 11of these patients went on to an excellent or satisfactory result at follow-up.One patient with a non-union had two plate breakages.We conclude that this plate, used in conjunction with a cast-brace, is a useful method of treatment for frac-tures around upper femoral prostheses (Hip International 1995; 5: 20-4)
KEY WORDS: Mennen plate, Fracture, Hip prosthesis

S29
Hip arthroplasty for femoral head osteonecrosis in Gaucher's disease
P. GRIGORIS 1, M.J. GRECULA 2, H.C. AMSTUTZ 3
1 Birmingham Orthopaedic Service, Nuffield Hospital, Birmingham - UK2 Department of Orthopaedics, University of Texas, Medical Branch at Galveston, Texas3 Joint Replacement Institute, Orthopaedic Hospital, Los Angeles, CA - USA
ABSTRACT: Seven Gaucher patients were treated with a hip arthroplasty from 1973 to 1990. The average ageat initial operation was 29.5 years. There were five primary total hip replacements, three surface replace-ments, and one revision. Clinical results were favorable although there was a high rate of postoperative com-plications. Two surface replacements were converted to total hip replacements, and two stemmed arthro-plasties required revision for aseptic loosening. As we are approaching a cure for the underlying disease anddespite the high potential for complications, cemented or hybrid total hip arthroplasty provides predictablesymptomatic relief for this difficult patient group. (Hip International 1995; 5: 25-30)
KEY WORDS: Gaucher's disease, Hip arthroplasty
Clinical results after 2-4 years with a new MMA/DMA/IBMA bone cementused for fixation of the femoral stem
J. STEEN JENSEN 1, S. BØDTKER 1, M. KRAMHØFT 1, P.B. THOMSEN 2, D. PETERSEN 3, K. NIELSEN 3
1 Departments of Orthopaedic Surgery, Rigshospitalet, University of Copenhagen, Copenhagen, and the 1 Central Hospitals 2 Holstebro, and 3 Randers - Denmark
ABSTRACT: A series of 190 consecutive patients were followed 30 (24-44) months after fixation of the femoralstem with a new MMA/DMA/IBMA bone cement at total hip arthroplasty. Clinically, the patients performed astraditionally reported with cemented implants. Revision surgery for loosening had been undertaken in 2%,and a further 2% were assessed as loose. Polished Exeter® stems subsided 3+ mm in every fifth case, ascould be expected, but any other radiological changes were rarely found. The short term results with this newproduct is considered acceptable. (Hip International 1995; 5: 31 -6)
KEY WORDS: New bone cement, Total hip replacement
Nailing the femoral neck may cause femoral head necrosis
A. LAZZERINI 1, C. GRISPIGNI 1, L. GALLI 2, N. PORTINARO 1, 3, D. W. MURRAY 3
1 Department of Orthopaedics and Traumatology2 Unit of Epidemiology and Medical Statistics, Ospedale S. Raffaele, Milan - Italy3 Nuffield Department of Orthopaedics, Oxford - UK
ABSTRACT: Intra-articular pressure, measured in the hip joints of seven patients treated by nailing for subcapi-tal femoral neck fracture, was increased after closed reduction and nailing of the fracture. The difference betweenpre- and postoperative pressure was significant (p=0.016). In five of the patients pressure after surgery was morethan 20% higher than before surgery. (Hip International 1995; 5: 37-9)
KEY WORDS: Femoral head, Nailing, Necrosis
S30
Snapping hip: anatomy, clinical features and an effective operation
S.T. DONELL, C.F. BRADISH, H. PHILLIPS
Department of Orthopaedics, Norfolk and Norwich Hospital, Norwich - UK
ABSTRACT: A new operation for treating snapping of the hip due to the vertical fibres of the iliotibial tractcatching on the greater trochanter is described. A "V"-shaped proximally based flap of fascia lata that di-vides the vertical fibres of the iliotibial is rotated anteriorly. It preserves the function of the iliotibial tract bymaintaining its integrity and length. It preserves the function of the gluteus maximus, and covers the greatertrochanter with soft tissue; the muscle fibres of the gluteus maximus. The results of the operation in ten pa-tients with eleven affected hips are presented. There was one minor wound infection, otherwise all patientswere cured of pain and snapping. All patients had a negative Trendelenburg test at a minimum of two yearsafter the operation. (Hip International 1995; 5: 47-51)
KEY WORDS: Snapping hip, Iliotibial band, Operation
The rationale for CAD-CAM uncemented custom hips: an interim assessment
J. HUA 1, P.S. WALKER 1, W. MUIRHEAD-ALLWOOD 1, G. BENTLEY 1, C.J. McCULLOUGH 2
1 Department of Biomedical Engineering, Institute of Orthopaedics, University College London, Royal National1 Orthopaedic Hospital Trust, Stanmore, Middlesex2 Northwick Park Hospital, Harrow, Middlesex - England
ABSTRACT: The purpose of this paper is to examine whether the rationale for CAD-CAM Custom Hips is re-alised in clinical practice. Previous studies demonstrated that custom uncemented stems, with a close fitproximally and a sliding fit distally, produced stresses closer to normal than for other stem types, which shouldresult in the preservation of proximal bone. Custom stems showed less micromotion, especially in torsionalloading, and hence should demonstrate interface osseointegration. The hips are designed and manufacturedusing specially written software. The standard design includes proximal macro-grooves with HA coating, ananterior flare, a lateral flare, a collar, and a smooth distal stem for a sliding fit. Elective features are addedsuch as proximal stem twist and neck retroversion in CDH, increased stem length to bypass defects, curva-tures in AP and ML views, and distal cutting flutes when extra torsional stability is required. From 1989 to1994, 411 cases were carried out, approximately one-third in each of the categories of OA, JCA/CDH, andrevision. Studies were made of the available radiographs at yearly intervals, while DEXA scans were taken ofthe RNOHT patients pre-operatively, at 6 months and then yearly. There were four failures requiring revision,three of the early primary design without HA coating, and one a revision design. The radiographs in primaryhips showed complete proximal bone-implant apposition in 81% of all cases. The DEXA scans showed thatthe mean bone mass after two years for all seven Gruen zones was greater than 90%. It was concluded thatthe CAD-CAM HA-coated Custom Hips showed bone and interface stability up to this time. The hip has playeda useful role in providing the ideal stem for each particular case, which may result in an improvement of long-term results, compared with the use of off-the-shelf implants. (Hip International 1995; 5: 52-62)
KEY WORDS: Custom hip, Total hip, Uncemented hip, HA coating, DEXA scanning
S31
Dysplasia epiphysealis capitis femoris: two long-term observations
B. MORETTI, V. PATELLA, G. MASTRORILLO, V. PESCE, G. LO BIANCO, C. SIMONE
II Orthopaedics and Traumatology Institute, University of Bari, Bari - Italy
ABSTRACT: Two patients with Meyer's dysplasia epiphysealis capitis femoris were followed, and the clinicaland radiological findings are described. The importance of early diagnosis is underlined, and of differentiat-ing Meyer's disease from Perthes disease, particularly in children under the age of four years, who presentno true clinical signs. The utility of monitoring ossification of the femoral head is illustrated (Hip International1995; 5: 63-8)
KEY WORDS: Dysplasia capitis femoris, Meyer, Long-term observation
Does acute urinary retention after total joint replacement predispose todeep vein thrombosis?
D.W. MURRAY, C.L.M.H. GIBBONS, S.J. GREGG-SMITH
The Nuffield Orthopaedic Centre, Oxford - UK
ABSTRACT: Deep vein thrombosis (DVT) and acute urinary retention are both common complications of totalhip replacement. Previous experimental studies have demonstrated that bladder distension obstructs the il-iac veins causing a decrease in venous outflow from the legs, and that after hip replacement a decrease invenous outflow is associated with the development of DVT. This suggests that acute urinary retention afterjoint replacement predisposes to DVT and that routine catheterisation would reduce the risk of DVT. The aim of the study was to determine, using strain gauge venous plethysmography, whether acute urinaryretention after joint replacement causes a decrease in venous outflow from the legs. It was found that acuteretention did not significantly alter the venous outflow. We therefore conclude that acute urinary retention af-ter joint replacement does not predispose to DVT. (Hip International 1995; 5: 69-71)
KEY WORDS: Acute urinary retention, Total joint replacement, Deep vein thrombosis
Avascular necrosis in congenital dislocation of the hip: long-term resultsand proposed new classification
F. SPECCHIULLI, L. SCIALPI, G. SOLARINO Jr., R. LAFORGIA
I Orthopaedic Clinic, University of Bari, Bari - Italy
ABSTRACT: A new classification is proposed for post-reduction necrosis of the femoral epiphysis based onretrospective analysis of 54 cases with a mean follow-up of 15 years. Necrosis can be divided under two main headings: A) partial, involving only the epiphysis B) total, involving the metaphyseal cartilage. Four total forms have been identified: B1: eventually resulting in coxa valga B2: eventually resulting in a short stubby neck, oval head and coxa magna
S32
B3: eventually resulting in coxa vara and severe acetabular dysplasia B4: eventually resulting in hypoplasia of the whole hip joint. This classification system comprises all the aspects of necrosis, while at the same time providing guidelinesfor treatment and long-term planning. (Hip International 1995; 5: 72-81)
KEY WORDS: Avascular necrosis, Congenital dislocation of the hip
Arthroplasty of the hip. Experiences over more than thirty years
H.G. WILLERT 1, M. SEMLITSCH 2
1 Orthopaedic Department, University of Göttingen, Göttingen - Germany 2 Sulzer Medical Technology, Winterthur - Switzerland
ABSTRACT: After a short historical introduction several factors which may in the long run influence the results ofjoint replacements are listed. Amongst these, the topics fixation and materials are discussed in more detail. By dis-cussion of various experiences of success and failure, the progress and improvements, but also considerable set-backs which have come about in the field of hip replacement are illustrated. (Hip Internation al 1995; 5: 91-101)
KEY WORDS: History, Artificial hip joint replacement, Fixation biomaterials, Failure modes
The effect of surgical technique on cement mantle strength in total hiparthroplasty
J.M. WEBB 1, A.J. MAHAJAN 1, G.C. BANNISTER 1, R.C. HAYNES 2, A.W. MILES 2
1 University Department of Orthopaedics, Southmead Hospital, Bristol 2 School of Mechanical Engineering, University of Bath, Bath - UK
ABSTRACT: A tapered aluminium model was designed to simulate the internal geometry of the reamed femoralmedullary cavity. The surface of the model was coated with blood and then polymethylmethacrylate cement(Simplex P, Howmedica UK) was inserted retrograde, prograde, prograde with a venting tube, prograde witha perforated distal cement restrictor, all with a cement gun; and manually by thumbing with a venting tube. Casts were examined radiographically, weighed, measured and tested to failure in compression. Using thesame cementing techniques, both concentric and eccentric mantles were produced by insertion of a pros-thesis, with or without spacers, and tested to failure in hoop tension. Cast weight correlated with cement strength per unit weight and volume. Casts produced by the retrogradetechnique were heaviest and those produced by prograde with a venting and thumbed mantles the weakest.Concentric mantles were stronger than eccentric. Incomplete spacers ensured concentricity but weakenedthe mantle such that no benefit was gained. Complete precast spacers also ensured concentricity and a min-imum mantle thickness but did not compromise mantle strength. The best method of inserting cement in the femur during total hip arthroplasty is retrograde with a completeprecast spacer. (Hip International 1995; 5: 102-7)
KEY WORDS: Hip, Arthroplasty, Failure, Cement, Surgical technique
S33
Chiari osteotomy of the pelvis for residual hip dysplasia in adults
M. INNOCENTI, A. CAPONE, R. PASSALACQUA, G. SCOCCIANTI
II Orthopaedic Unit, University of Firenze, Florence - Italy
ABSTRACT: The treatment of residual hip dysplasia can be carried out using different methods which range from T.H.R.to the various kinds of osteotomy. Among these, Chiari osteotomy still holds a prominent position, although new tech-niques have decreased its indication. Following the results of 13 years' experience with this procedure, the Authorsconfirm that Chiari osteotomy permits the reduction of the acetabular inclination and a wider articular coverage of thefemoral head on all planes. Nowadays, this long experience together with an accurate knowledge of the biomechan-ical effects of the procedure should be able to guide the orthopaedic surgeon, with adequate accuracy, to the choiceand the indications of this complex but effective procedure. (Hip International 1995; 5: 108-12)
KEY WORDS: Chiari osteotomy, Hip dysplasia
The relationship between femoral morphotype and femoral componentdesign
G. MINEO, A.M. PREVITERA, G. DE GIOVANNI, M. SURACE
Orthopaedic Surgery and Trauma Department, University of Milano, Medical School, S. Paolo Hospital, Milan - Italy
ABSTRACT: The shape of the femoral canal is variable, much more so than most contemporary designs offemoral components would suggest or can accommodate. In the face of this variability, line-to-line or sur-face-to-surface contact is not expected between the cementless implant and much of the endosteal surface.It is also apparent that changes in implant design are still needed if the normal biomechanics of the hip jointare to be restored in each patient and if component fixation is to be optimized. Most cementless componentsaim to achieve proximal load transfer to the femoral canal. However, increasing clinical evidence suggeststhat distal filling of the femur is also necessary to minimize the incidence of postoperative symptoms, par-ticularly in revision procedures. If this is indeed the case, more accommodating designs of femoral compo-nents are needed that will permit proximal and distal fitting at the femoral canal so that stable fixation maybe achieved regardless of variations in bone geometry. (Hip International 1995; 5: 113-20)
KEY WORDS: Femoral component design, Anatomy of proximal femur
Chondromalacia coxae
F.H. NORMAN-TAYLOR, S.J. MANNION, R.N. VILLAR
Department of Orthopaedic and Trauma Surgery, Addenbrooke's Hospital, NHS Trust, Cambridge, England - UK
ABSTRACT: A new arthroscopic finding of chondromalacia of the femoral head is reported in five patients un-dergoing hip arthroscopy for undiagnosed hip pain. The term chondromalacia coxae is used to describe thecondition, and its similarity to chondromalacia patellae is discussed. (Hip International 1995; 5: 121-3)
KEY WORDS: Chondromalacia, Hip, Arthroscopy

S34
The in vitro measurement of bone-cement interface pressures and shearstrengths in the femur: a comparison of two cementation methods
A.J. WARD 1, E.J. SMITH 2, J.W. BARLOW 3, A. POWELL 3, M. HALAWA 4, I.D. LEARMONTH 2
1 Department of Orthopaedic Surgery, Frenchay NHS Healthcare Trust, Frenchay, Bristol 2 University of Bristol, Department of Orthopaedic Surgery, Avon Orthopaedic Centre, Southmead General 1 Hospital, Westbury-on-Trym, Bristol 3 School of Manufacturing, Materials and Mechanical Engineering, University of Plymouth, Plymouth 4 Department of Orthopaedic Surgery, Mount Gould Hospital, Plymouth - UK
ABSTRACT: Two differing cementation methods were investigated in an in vitro simulation of hip arthroplasty. The bone-cement interface pressures were recorded during cement injection and stem insertion in matchedpairs of fresh cadaveric femora. Reduced viscosity cement injected with a cement gun and proximal seal wascompared with injection of high viscosity cement and finger-packing in each pair. The resultant shear strengthof the bone-cement interface was measured by push-out tests. Results were analysed using the Wilcoxonranked sum test for paired samples. The Exeter method of cementation produced significantly higher mean and maximum pressures above thebleeding pressure of femoral bone at all interface levels during cement injection. This was associated withsignificantly greater mean shear strengths. The authors conclude that the Exeter pressurization system forcementation overcomes the effect of femoral bone bleeding and improves the quality of the bone-cement in-terface. This may contribute to reduction in the incidence of loosening in cement hip arthroplasty. (Hip In-ternational 1995; 5: 124-30)
KEY WORDS: Cement, Interface pressure, Shear strength, Femur
Groin pain from cement extrusion in total hip arthroplasty
A.J.R. GRAY 1, B.F. MEGGITT 2
1 Department of Orthopaedic and Trauma Surgery, The Ipswich Hospital, Ipswich 2 Department of Orthopaedic and Trauma Surgery, Addenbrooke's Hospital, Cambridge - UK
ABSTRACT: Bone cement pressurisation is considered to be an advance in bone microlock fixation of the ac-etabular and femoral components of total hip arthroplasty. We have identified a previously unreported com-plication of this technique in which the pressurised cement extruded through an anterior pubic anchor drillhole giving early and persistent anterior groin pain. This paper reports on the condition, its incidence andtreatment in four cases. (Hip International 1995; 5: 131-4)
KEY WORDS: Arthroplasty, Hip, Complications, Extrusion, Cement
S35
Hypercoagulability after total hip replacement
M.A. McNALLY 1, A. KYLE 2, W.R.G. MacDONALD 2, E. MAYNE 2, R.A.B. MOLLAN 1
1 Department of Orthopaedic Surgery, The Queen's University of Belfast, Musgrave Park Hospital, Belfast2 Department of Haematology, Institute of Clinical Science, Royal Victoria Hospital, Belfast - Northern Ireland
ABSTRACT: Changes in blood coagulation are believed to be involved in the aetiology of postoperative throm-boembolism. Antithrombin III (AT III) is the most important natural inhibitor of thrombin activation and hencethrombogenesis. This study investigated the nature of a hypercoagulable state in total hip replacement bymeasurement of AT III in the perioperative period, giving a quantitative assessment of coagulation. AntithrombinIII levels fell in all patients after surgery. However, the degree of the fall and the timing of the fall were vari-able. Eight percent of patients had abnormally low AT III prior to operation, indicating that this proportion ofour patients are in a procoagulant state even before surgery. One third of patients had a clinically significantreduction (below 70% of normal) in AT III level after surgery. In this group the fall in AT III was maximal at 2hours after division of the femoral neck. Careful correction for haemodilution provided new evidence for ac-tive consumption of antithrombin III in the perioperative period. By 24 hours after surgery the level of AT IIIwas not significantly different from preoperative levels (p>0. 7), even in the group with a clinically importantreduction. These findings support only a transient period of hypercoagulability after total hip replacement.The "at-risk"period of venous thrombosis has been shown to be at least several weeks after surgery and thetransient nature of the fall in AT lll suggests that venous thrombosis is unlikely to be due to hypercoagulabil-ity alone. (Hip International 1996; 6: 1-6)
KEY WORDS: Hip arthroplasty, Thromboembolism, Antithrombin lll, Coagulation
Five year results of 113 bipolar, cementless "Bateman" hip replacementsfor degenerative hip disease
A.H.N. ROBINSON, A. AYLLON-GARCIA, J.P. HALLETT
Department of Trauma and Orthopaedics, The Ipswich Hospital NHS Trust, Ipswich - UK
ABSTRACT: 113 Bateman UPF II arthroplasties with a straight, non-cemented, non fenestrated, Moore typestem were used in 106 patients with degenerative hip disease. The patients were followed for a mean of 5years and 8 months (range 48-102 months). 20 patients had died. There were therefore 93 hips available forreview. Of these 91 were contacted. Of the 91 hips, 15 had been revised for stem loosening, and 6 more hadgross radiological evidence of stem loosening in the absence of symptoms. In contrast to the stem failures,the bipolar acetabular component of this prosthesis gave no clinical problems. Radiologically there were 5patients who showed evidence of acetabular migration, but in all of these cases the migration was 4 mil-limetres or less. (Hip International 1996; 6: 7-12)
KEY WORDS: Bateman, Non-cemented, Arthroplasty, Bipolar, Osteoarthritis
Abstracts from Hip International Vol. 6 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S35-S46 ©by Wichtig Editore, 2001

S36
Chiari's pelvic osteotomy in the adult. A long term clinical, radiologicaland statistical evaluation
F. BENAZZO, L. PEDROTTI, L. GIORGI, R. MORA, L. CECILIANI
Istituto di Clinica Ortopedica e Traumatologica, Università degli Studi di Pavia, IRCCS PoliclinicoS. Matteo, Pavia- Italy
ABSTRACT: Chiari’s pelvic osteotomy, conceived for the surgical correction of congenital dysplasia of thehip, is indicated by some authors for juvenile patient: 16 years of age: Graham et al (7); 18 years of age: Hoghand Macnicol (9); 19.8 years of age: Calvert et al (1), while others do not identify any age limit (2, 11). Retro-spectively reviewing a series of adult patients, we tried to determine the optimum age range of Chiari’s os-teotomy, and to evaluate the relative importance of surgical and radiological parameters of the results. Wereviewed 74 patients, mean age 38.5 years, for a total number of 80 operations; 72.6% were aged between31 and 60 years. The follow-up interval ranged from 1.8 to 15 years - mean 6.6, 180 months. The results,based on a mathematical evaluation of pain, walking, joint mobility, limping and Trendelenburg’s sign, were:31 excellent (38.8%), 25 good (31.3%), 18 fair (22.5%), and 6 poor (7.5%). The best results were numerical-ly concentrated in the 41 - 50 age group, in terms of percentages, we found a constant decrease of the goodresults in the different decades. Pain was absent in 61 of 80 cases. Clinical and radiological data, plus thestatistical correlation of the different data (17 parameters), showed that Chiari’s osteotomy is valid for thetreatment of CDH even in older patients, although the best results are obtained in the 21-50 age group. (HipInternational 1996; 6: 13-23)
KEY WORDS: Chiari’s pelvic osteotomy, Hip dysplasia
Treatment of the infected total hip arthroplasty with a temporary gentamicin spacer
L.P. MØLLER, S. SOLGAARD, M.B. PETERSEN, J.B. RETPEN
Department of Orthopaedics, Hillerod Hospital, Hillerod - Denmark
ABSTRACT: We report a series of 11 two-stage exchange arthroplasties for infected hip prostheses. The in-termediate period was managed by using a gentamicin loaded cement spacer. At follow-up after 18-33 months,there was one recurrent infection. The spacer provides greater patient comfort and mobility, and may deliv-er high levels of antibiotics into the periprosthetic tissue. The second stage of revision has been simplifiedand there have been no serious complications. (Hip International 1996; 6: 24-8)
KEY WORDS: Revision hip arthroplasty, Infection, Two-stage reimplantation, Cement spacer
Peritrochanteric fractures of the femur: a comparison between the Endernail, Gamma nail and Dynamic Hip Screw
J.A. DE PEDRO 1, J. REY 1, R. LOPEZ-CASERO 1, A.J. PEREZ-CABALLER 1, I. DOMINGUEZ 1, L. DURAN 2, J HURTADO 2, L. LOPEZ-DURAN 1
1 Department of Surgery, Trauma Division2 Department of Anesthesiology, Hospital "San Carlos", Complutense University of Madrid, Madrid - Spain
S37
ABSTRACT: Surgical fixation, early weight-bearing, and bony union remain a challenge in the treatment ofperitrochanteric femur fractures, especially if the fractures are comminuted or unstable. A randomized prospec-tive study of 154 fractures treated by either the Gamma nail (43), Dynamic Hip Screw (DHS) (30) or Ender'snail (81) is reported. The average follow-up for Ender's nails was 36.7 months; for DHS 39.4 months and forGamma nails 37.3 months. The Ender's nails required a significantly (p<0.001) shorter operation time of 42±13.4min. The Gamma nail group required a higher mean duration of screening, 193±92 sec. Few screws in eithergroup were in a bad position, but 12 (32%), in the Gamma nail group, and 2 (10%) in the DHS were placedsuperiorly in the head. From this experience, the Gamma nail appears to allow for early patient ambulationregardless of the fracture configuration with good clinical results, but the potential advantages of the Gam-ma nail are still unclear in these already compromised patients. (Hip International 1996; 6: 29-39)
KEY WORDS: Hip, Trochanteric fractures, Surgical procedures in hip fractures
A clinical and electromyographic review of the lateral and postero-lateralapproaches to the hip after prosthetic replacement
O. MORESCHINI 1, M.C. GIORDANO 1, F. MARGHERITINI 1, R. CHIATTI 2
1 Department of Orthopaedics and Traumatic Surgery2 Department of Physical and Rehabilitative Medicine, University "La Sapienza" of Roma, Roma - Italy
ABSTRACT: The Authors carried out a clinical and electromyographic study on two groups of patients un-dergoing total hip replacement with two different surgical approaches, evaluating the evolution of the clini-cal results at three and fifteen months after operation and comparing the same to the electromyographic re-sults of the muscles involved during surgical exposure. They found differences in the post-operative func-tional changes in the two groups of patients and the reliability of the clinical and electromyographic resultsin the critical evaluation of the two different approaches. (Hip International 1996; 6: 40-7)
KEY WORDS: Hip replacement, Electromyography
Micromotion at the bone-stem interface during the gait cycle aftercementless total hip replacement: influence of stem design and loadinglevel
N.A. RAMANIRAKA 1, P.F. LEYVRAZ 2, L.R. RAKOTOMANANA 1,2, P.J. RUBIN 3, P.K. ZYSSET 1
1 Ecole Polytechnique Fédérale, Lausanne2 Clinical Department of Orthopaedics and Traumatology CHUV, Hopital Orthopédique de la Suisse Romande, 2 Lausanne3 Symbios Orthopédie, Yverdon - Switzerland
ABSTRACT: The micromotion distribution of a cementless stem relative to femoral bone and the stress trans-fer were calculated with a three dimensional model including bone non-homogeneity, anisotropy and dis-continuity of the bone-implant interface. Two implant designs (anatomical, straight) were investigated to pointout the geometry effects. Micromotion distributions were calculated over the entire interface during a com-plete gait cycle taking into account the hip musculature forces. Different loading levels (from 20% to 100%of total load) were stimulated. For the two implants, peak values of distractive and shear micromotions weremaximal at the Single Limb Stance phase. The implant geometry had no sensible effects on distractive mi-
S38
cromotion magnitude. Conversely, the implant design had noticeable influences on shear micromotions. Re-garding the effects of loading levels, at 20% of the full load, interface shear micromotions were lower than30 µm over the entire interface allowing bony ingrowth and expected to ensure initial stability for both im-plants. At 40%, shear micromotions exceeding 30 µm appeared and were located differently according to thestem design. (Hip International 1996; 6: 51-8)
KEY WORDS: Hip replacement, Micromotions, Stem design
Intertrochanteric femoral fractures: optimal screw position and bonedensity determined by computer tomography
N. LEVI 1,2, A. INGLES Jr. 3, H. KLYVER 2, B.F. IVERSEN 2,3
1 Department of Surgery, Hammersmith Hospital, University of London Royal Postgraduate Medical School, 1 London - UK 2 Department of Orthopaedic Surgery, Frederiksberg Hospital, University of Copenhagen - Denmark 3 Department of Biomedical Engineering, Institute of Orthopaedics, University College London, Stanmore, 1 Middlesex - UK
ABSTRACT: The bone density of five proximal femora from female cadavers was measured with computer to-mography using a pixel size of 1.2 mm. A three-dimensional reconstruction was performed along 4 axes. Theregion of maximum relative bone density correlated well with previous reports of an optimal position for thescrew when treating an intertrochanteric femoral fracture. (Hip International 1996; 6: 59-62)
KEY WORDS: Bone density, Hip fracture, Computer tomography
Three-year results with the cementless Bicontact total hip arthroplastyfemoral component
M.l. GUSSO, L. PISO, B. CADDEO, A. CAPONE, C. PINTUS, F. NICOLA
Orthopaedic Department, University of Cagliari, Cagliari - Italy
ABSTRACT: Between 1990 and 1993, 65 consecutive primary total hip arthroplasties were performed usingthe cementless Bicontact femoral component. Of these, 56 hips in 51 patients were clinically and radiologi-cally reviewed at an average follow-up of 35.4 months (24-53 m). The patients’ mean age was 65.9 years.There were three revision procedures (5.4%) with an average time to failure of 13.2 months. Using the Hos-pital for Special Surgery hip rating system, 67.9% of the hips were rated excellent, 17.9% as good, 10.7%as fair and 1.8% as poor at final evaluation. At follow-up four patients (12.5%) had mid-thigh pain and 38hips (67.9%) were free from any observable limp. Radiolucent lines greater than 2 mm were identified in sev-en femora (12.5%) and stress shielding was seen in nine (16.1%). Using the fixation scale assessment of Engh the femoral component was classified as fixed by bone ingrowth or stable fibrous fixation in 87.5% ofhips. Retrospective analysis of these results showed the efficacy of the Bicontact cementless stem and con-firmed the importance of patient's age and femur morpho-cortical index in clinical and radiographic resultswith the cementless total hip. (Hip International 1996; 6: 63-8)
KEY WORDS: Cementless total hip arthroplasty, Porous coated femoral component, Age
S39
Cementless revision for failed cemented total hip arthroplasty
J.G. HUSSELL 1, E.J. SMITH 2, I.D. LEARMONTH 2
1 Department of Orthopaedic Surgery, Princess Margaret Hospital, Swindon 2 Department of Orthopaedic Surgery, University of Bristol, Bristol - UK
ABSTRACT: Sixty-two consecutive revision hip arthroplasties were carried out in 57 patients between 1986and 1990 using the long stem Porous Coated Anatomic (PCA) prosthesis. Fifty-two hips were available forclinical and radiological review. The remainder had either died or were lost to follow-up. The average follow-up was 4.8 years (range 3-7.8 years) and the mean age was 56 years (range 25-77 years). Using the HarrisHip Score, 38/53 (73%) were regarded as good/excellent, 6/52 (11.5%) as fair and 8/52 (15.5%) as poor. Theincidence of femoral component subsidence (31/52 - 60%) was a cause of concern, and accounted for twocases of late dislocation. Of the remaining six hips regarded as failures, two had been revised for acetabulargraft resorption and migration of the cup while four had moderate persistent pain despite fair hip function.The authors are unable to recommend the long stem PCA prosthesis for routine use in revision hip arthro-plasty. (Hip International 1996; 2: 69-74)
KEY WORDS: Revision, Cementless, Total hip replacement
A study of pre-operative planning in CLS total hip arthroplasty
C.G. SCHIZAS 1, B. PARKER 2, P-F. LEYVRAZ 3
1 Oberarzt Orthopädie, Schulthess Klinik, Zürich - Switzerland2 Consultant Orthopaedic Surgeon, Kingston Hospital, Kingston, Surrey - UK3 Médecin Adjoint, Orthopaedic Department, University Hospital, Lausanne - Switzerland
ABSTRACT: This study involved 200 cementless primary total hip arthroplasties of which 100 had formal pre-operative planning as recommended by the manufacturer using standardised radiographs, templates and trac-ing paper. The remaining 100 had no formal pre-operative planning. The operations were performed by twodifferent groups of surgeons using different surgical exposures. The variables measured included radiologi-cal magnification, component sizing, intra-operative lengthening, positioning of the centre of the femoral headand femoral component fit and fill. Clinical data was obtained from a questionnaire. The results indicate animproved position of the centre of rotation and better leg length equalisation in the planned group. There wasno significant difference in the number of intra-operative fractures among the two groups. No correlation wasfound between femoral fit and upper femoral morphology nor between fit and the surgeon's seniority. Therewas no significant difference in the incidence of thigh pain in the two groups at an average follow-up of 28months. The more striking finding was the poorer femoral fit and fill encountered in the unplanned group. (HipInternational 1996; 6: 75-81)
KEY WORDS: Hip arthroplasty, Uncemented hip prosthesis, Planning, Leg length inequality

S40
Pyomyositis in babies presenting with painful hip: clinical and radiographic course of two cases
U.E PAZZAGLIA 1, S. BINDA 2, G. ZATTI 1, V. SESSA 3
1 Clinica Ortopedica, 2a Facoltà di Medicina e Chirurgia dell'Università di Pavia, Pavia2 Clinica Pediatrica, 2a Facoltà di Medicina e Chirurgia dell'Università di Pavia, Pavia3 Divisione di Radiologia, Ospedale F. Del Ponte, Varese - Italy
ABSTRACT: Two cases of pyomyositis in babies, one in the ilio-psoas muscle, the other in the quadriceps,are reported. The presenting sign was a painful hip in both, suggesting osteomyelitis of the proximal femuror arthritis. Pyomyositis is unusual in western countries and in healthy, well-nourished children, but thesecases suggest considering this pathology in the differential diagnosis of a painful hip in babies. In the firstcase an upper respiratory tract infection was followed by haematogenous spread to the ilio-psoas muscle; inthe second an injection of vaccine in the quadriceps played a determinant role. The latter case was compli-cated by secondary osteomyelitis; a metaphyseal radiolucent band just below the growth plate appeared inthe early stage together with metaphyseal osteopenia and was interpreted as a consequence of altered bloodflow in the metaphysis, not specific osteomyelitis, but indicative of some disturbance of the growth plate-metaphyseal complex. (Hip International 1996; 6: 82-5)
KEY WORDS: Pyomyositis, Osteomyelitis, Painful hip
Hip arthroplasty in osteopetrosis. Case report
C. CASTELLI, G. ZATTI, A. FERRARIO
Istituto di Clinica Ortopedica e Traumatologica "Mario Boni", II Facoltà di Medicina e Chirurgia, Universitàdegli Studi di Pavia, Varese - Italy
ABSTRACT: The authors report a rare case of hip osteoarthritis in osteopetrosis, where the patient underwenttotal hip arthroplasty. The aim of this paper is firstly to report the experience with an operation which, in thisparticular case, required special technical skill and caution; and secondly to discuss the role osteopetrosisplays in the pathogenesis of hip osteoarthritis. (Hip International 1996; 6: 86-9)
KEY WORDS: Osteopetrosis, Osteoarthritis, Total hip arthroplasty
Muscular activity and the biomechanics of the hip
R.S.M. LING 1,3, J.J. O'CONNOR 2, TUNG-WU LU 2, A.J.C. LEE 3
1 Princess Elizabeth Orthopaedic Hospital, Exeter, Devon2 Oxford Orthopaedic Engineering Centre, University of Oxford, Nuffield Orthopaedic Centre, Headington, Oxford3 School of Engineering, University of Exeter, Exeter, Devon - UK
ABSTRACT: The interactions between the forces transmitted by the muscles and by the bones are central tothe understanding of load transmission in the musculo-skeletal system. A reasonable concept of the biome-
S41
chanics of the hip can only be grasped when the activities of all the major muscle groups acting across thehip and proximal femur are considered. (Hip International 1996; 6: 91-105)
KEY WORDS: Hip, Muscular activity, Biomechanics
Outcome of primary total hip replacement in patients less than 50 years old
O. MASBAH 1, S.P.F. HUGHES 2
1 Department of Orthopaedics & Traumatology Faculty of Medicine, University Kebangsaan Malaysia, Kuala 1 Lumpur, Malaysia2 Orthopaedic Surgery, Royal Postgraduate Medical School, Hammersmith Hospital, London - UK
ABSTRACT: We reviewed 33 primary total hip replacements in 24 patients younger than 50 years old. Themean age was 39.5 years and the follow-up averaged 6.1 years. There were 15 men and 9 women. Twenty-five hip replacements were cemented and 8 were uncemented. The most common hip pathology was os-teonecrosis of the femoral head (36%), followed by rheumatoid arthritis (27%) and osteoarthritis (21%). Goodpain relief was obtained in 70% of hips. Thigh pain developed in 2 uncemented hips and an other had in-creasing hip pain. Function was good in 64% and 67% had good hip mobility. The best results were obtainedin osteonecrosis of the femoral head, followed by osteoarthritis and rheumatoid arthritis. The commonest in-dication for revision was loosening of the acetabular component. Survival analysis of the 25 cemented hipsshowed a failure of 35% at 6 years and 9.1% at 8 years. Total hip replacement in young patients providesgood pain relief and function although there is a limited time expectancy for good results. (Hip International1996; 6: 106-11)
KEY WORDS: Total hip replacement, Outcome, Young patient
Boneloc versus Simplex cement for fixation of femoral components. An interim report of a prospective randomized study of THRs with a 2.5year mean follow-up time
H. KLYVER, K. JACOBSEN, H. KOFOED
Department of Orthopaedics, Frederiksberg Hospital, University Hospital of Copenhagen, Copenhagen - Denmark
ABSTRACT: A prospective randomized study of femoral stem fixation comparing Boneloc and Simplex ce-ments was carried out. A collarless double-tapered femoral component was used in all cases. The materialconsisted of 94 patients representing 97 THRs (3 bilateral cases). Their mean age was 76 years (range 58-88). Clinico-radiographic follow-ups were carried out after 3 months, 12 months and 2 to 3 years. The meanfollow up time was 2.5 years. Clinically there was no difference between the groups. Radiolucencies at thebone-cement interface and metal-cement interface, cement cracks, and subsidence of the femoral compo-nent were compared. No significant differences could be proven between the fixation patterns of the bonecements during this short-term follow-up. (Hip International 1996; 6: 112-8)
KEY WORDS: Bone cement (Boneloc versus Simplex), total hip replacement, Randomized prospective study

S42
Computerized tomography and magnetic resonance imaging in treatmentof congenital luxation of the hip
D. LAZOVIC, J. FRANKE, C.J. WIRTH
Department of Orthopaedic Surgery, Medical School Hannover, Hannover - Germany
ABSTRACT: In treatment of congenital dislocation of the hip, a main aim is to achieve concentricity of reduction. Control by plain x-ray lacks accuracy in determining antero posterior position. Arthrography andsonography cannot be used when a spica cast is in place. After April 1988, therefore, as an alternative in 16hips, we have used computed tomography to determine femoral head position, acetabular angle, and extentand integrity of posterior rim. However, the presence of any metallic artefacts, unossified cartilage and thegeneral poor-quality imaging of soft tissue associated with the technique reduce its use fulness. Since Jan-uary 1990, we have instead used magnetic resonance imaging to control treatment. This technique, in 34 hips,proved accurate in determinating the femoral head position. MRI also gave better images than computed to-mography of osseous and cartilaginous structures of the acetabulum and the surrounding soft tissue. Spicacasting does not affect the quality of imaging. The effect of metal artefacts can be minimized by using, wherenecessary, implants of titanium alloy. (Hip International 1996; 6: 119-23)
KEY WORDS: Computerized tomography, Magnetic resonance imaging, Congenital luxation of the hip, Control of treatment
Results of trochanteric wire removal surgery and its relation to revisionhip arthroplasty
S.C. DESHMUKH, J.C.M. MURPHY, H.R. CASSERLY, L. MARCOVIC
Centre for Hip Surgery, Wrightington Hospital, Appley Bridge, Lancashire - England
ABSTRACT: Local trochanteric symptoms can occur after Total Hip Arthroplasty through any approach butare said to be more common after the transtrochanteric approach. Most of these symptoms subside sponta-neously or after a local anaesthetic and steroid injection. Unremitting symptoms can be indicative of persis-tent trochanteric bursitis, septic loosening or aseptic loosening. In cases of hip arthroplasties performedthrough a transtrochanteric approach, the trochanteric wires are commonly incriminated as a cause of per-sistent trochanteric pain. In this retrospective study of 92 patients who underwent trochanteric wire removalsurgery, 32 patients (34.78%) had an unsatisfactory result. 24 patients (26.09%) underwent revision surgeryat an average of 36.75 months after wire removal surgery. This study suggests that signs of early looseningneed to be carefully looked for and ruled out before advising trochanteric wire removal for persistent trochantericdiscomfort. (Hip International 1996; 6: 124-6)
KEY WORDS: Total hip replacement, Trochanteric bursitis, Trochanteric wire removal surgery, Revision hip re-placement surgery
S43
Cup deformation during total hip replacement: a brief report
D.l. WISE 1, S.J. CALDER 1, B. DERBYSHIRE 2
1 Department of Orthopaedic Surgery, Huddersfield Royal Infirmary, Lindley, Huddersfield 2 Research Fellow, Department of Mechanical Engineering, Leeds University, Leeds - UK
ABSTRACT: Cup deformation is demonstrated to be significantly greater using an 8 mm than a 22 mm push-er. Deformation may lead to increased polyethylene wear and late prosthetic failure. Use of a 22 mm pusheris recommended in Charnley total hip replacement. (Hip International 1996; 6: 127-8).
KEY WORDS: Hip, Arthroplasty, Technique
Extrapelvic compression of the femoral nerve: an uncommon cause of hip pain
H. STALDER 1, J. ROMERO 1, V. DIETZ 2
1 University Hospital Balgrist, Unit for Hip Surgery, Zürich2 Swiss Paraplegic Center, University Hospital, Balgrist, Zürich - Switzerland
ABSTRACT: The case of a patient with short history of unilateral hip pain due to compression of the lumbarplexus by a cyst arising from the hip joint is reported. Radiologically there were only mild signs of osteoarthritisof the affected hip but severe degenerative changes were found in the lumbar spine. There was atrophy ofthe quadriceps muscle of the affected limb with subsequent giving-way during gait and sensory loss on thelateral aspect of the thigh. The neurological and electromyographical examination suggested compression ofthe lumbar plexus. By sonography, computerized tomography and contrast radiographs, a finger shaped cystwas identified going from the ventromedial aspect of the hip joint between the iliopsoas, the pectineus, andthe iliacus muscles respectively. After excision of the cyst, hip pain ceased and the signs of neural com-pression disappeared almost completely within 12 weeks. Histologically the specimen showed synovial tis-sue with cartilaginous debris. In cases of hip pain without sufficient radiological and clinical signs of os-teoarthritis, femoral nerve compression should be excluded by neurological examination. To our knowledge,this is the first report about compression of the femoral nerve by an isolated extrapelvic cyst arising from thehip joint. (Hip International 1996; 6: 129-33)
KEY WORDS: Hip pain, Femoral nerve compression, Cyst of the hip joint
How to correct increased anteversion of the femoral neck during THR
E. MORSCHER
Orthopadische Universitätsklinik, Felix Platter-Spital, Basel - Switzerland
ABSTRACT: In the great majority of the cases the "Anteversion Angle" (AVA) is in the normal range (10-20°)and on insertion the femoral stem follows automatically the direction of the femoral neck. There are basical-ly 5 means of correcting an increased AVA: 1) The smaller the diameter of the endoprosthetic stem and themore its cross section is circular the easier it is to modify the rotational position. 2) The lower the resectionof the femoral neck the greater the freedom of correction of the anteversion. 3) A custom-made femoral en-doprosthesis. 4) A non-cemented endoprosthesis with a stem circular in cross section - such as the conical

S44
stem of Wagner - can easily be positioned in a great variety of rotational positions. 5) To correct an AVA ofthe femur of more than 45 degrees an inter- or sub-trochanteric derotational osteotomy of the femur is indi-cated. With this not only is the AVA corrected but also the greater trochanter is brought from its posterior po-sition to a more lateral one and the functional lever arm of the abductors is lengthened. To stabilize the os-teotomy the use of a femoral endo-prosthesis with a non-cemented stem which is stable in rotation all alongits length is recommended. (Hip International 1996; 6: 135-9)
KEY WORDS: Hip joint anatomy, Anteversion, Total hip replacement, Intertrochanteric osteotomy
A practical screener for deep vein thrombosis after total hip replacement
M.A. McNALLY, M.D. CRONE, R.A.B. MOLLAN
Department of Orthopaedic Surgery, The Queen’s University of Belfast and Musgrave Park Hospital,Belfast- Northern Ireland
ABSTRACT: A new non-invasive screener for the detection of proximal deep vein thrombosis was evaluatedin two consecutive series of patients undergoing primary total hip replacement. The system, which utilisescomputerised strain gauge venous occlusion plethysmography, was simple to use and allowed serial screen-ing of large numbers of patients without complication. Comparison with venography in 112 patients gave aspecificity of 96% (106/1 10) and a sensitivity of 100% (2/2) for clinically important proximal DVT. Based onthis study, a larger management study was performed. After total hip replacement, 516 patients were serial-ly screened and all were followed to at least four months (mean 7.6 months) from surgery. Venography wasonly requested after a positive screening test. The screener correctly identified proximal and major calf throm-bi in this group allowing early treatment. There were no fatal pulmonary emboli. This initial assessment sug-gests that computerised strain gauge plethysmography may be useful in identifying those patients with silentvenous thrombosis after total replacement. (Hip International 1996; 6: 140-8)
KEY WORDS: Total hip replacement, Deep vein thrombosis, Screening, Plethysmography, Cost effectiveness
The Charnley-Hastings hemiarthroplasty for fractures of the femoral neckwith special reference to complications
S. BENGTSON, C. OLSSON
Department of Orthopaedics, Central Hospital, Växjö - Sweden
ABSTRACT: We report a retrospective study of the incidence of major complications following Charnley-Hast-ings bipolar hemiarthroplasty in 117 patients with 120 fractures of the femoral neck. Primary hemiarthroplasty(n=40) was used for irreducible or old fractures and secondary hemiarthroplasty (n=80) for fractures with dis-turbed healing. The mean age was 80 (54-95) years. The mean follow-up was 34 (0-149) months. There wasno major complication in 87.2 percent. Mortality was 10.3 percent after 6 months and 13.7 percent after oneyear. Dislocation occurred in 7.5 percent, prosthetic loosening in 4.2 percent, acetabular fracture and deepinfection in 0.8 percent respectively. Reoperation was required in 7.5 percent: open reduction after disloca-tion (2.5 percent), conversion to a Charnley total hip arthroplasty (3.3 percent), Girdlestone arthroplasty (0.8percent) and exchange of a loose femoral component (0.8 percent). We conclude that the selective use of

S45
bipolar hemiarthroplasty for fractures of the femoral neck carries few major complications. Patient selectionmust be strict in order to reduce the risk of dislocation. (Hip International 1996; 6: 149-54)
KEY WORDS: Fractures of the femoral neck, Bipolar hemiarthroplasty, Complications
The mechanical cement extractor: an original device for cement extraction in total hip arthroplasty revision
J. P. VIDALAIN
Artro Group, Clinique Du Lac, Annecy - France
ABSTRACT: A variety of instruments and techniques have been developed to facilitate cement removal in THArevisions. Many of these methods can lead to femoral fractures or uncontrolled cortical perforation, increas-ing bone damage. The purpose of this brief report is to present a new device that particularly facilitates theextraction of the cement plug from the femoral canal. The basic characteristic of this system is to guide dif-ferent specific tools, with a high reliability, through the middle of the cement plug. In our experience, this de-vice has always permitted femoral cement extraction without serious complications. (Hip International 1996;6: 155-8)
KEY WORDS: Arthroplasty, Hip, Cement, Loosening, Revision
Fractures of the femoral head
G.C. TRAINA 1, L MASSARI 1, A. SCHIAVI 1, R. MARROCCO 1, L. PROSPERI 1, F. VITA 2
1 Orthopaedics and Traumatology Section 2 Radiology Section, Department of Biomedical Sciences and Advanced Therapies, University of Ferrara, 2 Ferrara - Italy
ABSTRACT: Fractures of the femoral head are not frequent and are almost always combined with dislocationof the hip. We reviewed 43 cases of femoral head fractures (33 men, 10 women), mean age 38. 6 years. Us-ing Pipkin’s classification there were 13 type 1 cases, 5 type 2 and 25 type 4. Twenty-nine patients (67.4%)were seen again after a minimum of two years. Overall, there were ten excellent results, nine good, four fairand six poor. Complications were three cases of ischemic necrosis, eleven secondary arthritis, and three cas-es of heterotopic ossification. CT is an extremely useful method for assessing these lesions, especially incases with small intra-articular fragments (Pipkin 1 and 4). Therapeutic indications obtained from this studywere a non-invasive approach for Pipkin type 1 lesions, except those with a large intra-articular fragment,surgery for Pipkin type 2 cases, with osteosynthesis of the fragments, mainly using Herbert screws, andsurgery particularly for Pipkin type 4, especially for osteosynthesis of the fragments of acetabular wall. (HipInternational 1996; 6: 159-65)
KEY WORDS: Femoral head, Fractures

S46
The initial stability of femoral impaction grafting
E.J. SMITH 1, J.B. RICHARDSON 2, I.D. LEARMONTH 1, G.P. EVANS 3, K. NELSON 3, R. LEE 3, J. DYSON 3
1 Department of Orthopaedic Surgery, University of Bristol, Bristol 2 Institute of Orthopaedics, Robert Jones and Agnes Hunt Orthopaedic Hospital, Oswestry 3 AEA Technology, Harwell - UK
ABSTRACT: Aseptic loosening is the major cause of failure in primary total hip re placements. Loss of bonestock occurs in both cementless and cemented implants. Impaction of morsellised allograft represents a ma-jor advance in the restoration of bone loss at revision hip surgery. This study was designed to test the earlystability of the femoral impaction construct. Polished double tapered stems were inserted into neo medullarycanals within impacted allograft in fibreglass femora. Subsidence was measured during cyclical loading. Fourmethods of impaction grafting were tested: allograft alone; allograft and heparinised blood; allograft/cement/heparinisedblood; allograft/cement/clotted blood. Uncemented impaction grafting failed at low loads and few cycles. Thecemented technique supported higher loads. Heparinised blood reduced the strength of the composite. Ini-tial stability was achieved with allograft, cement and clotted blood. There is need for caution in the early post-operative period due to the wide variation in initial stability of the allograft composite. The reliability of thistechnique has been increased by the use of specialised instruments. Experimental studies and clinical ex-perience suggest that this approach to revision surgery is technique dependent. (Hip International 1996; 6:166-72)
KEY WORDS: Impaction grafting, Stability, Femoral component
Total hip arthroplasty in athetoid cerebral palsy
N.J. HARRIS, M. UTUKURI, M.J. ROBSON, M.J. BELL
Departments of Orthopaedic SurgeryRoyal Hallamshire Hospital, Sheffield and Rotherham District Hospital, Rotherham - UK
ABSTRACT: Total hip replacement is one alternative in the management of refractory coxarthrosis in patientswith cerebral palsy. There are however concerns regarding both loosening and dislocation especially in theathetoid variant. We report two successful cases of total hip replacement in athetoid cerebral palsy and con-clude that total hip replacement offers the only real chance of improving the patient’s symptoms while at thesame time maintaining or improving mobility in this group. (Hip International 1996; 6: 173-5)
KEY WORDS: Hip arthroplasty, Athetoid cerebral palsy, Hip surgery
S47
Proximal femoral reconstruction for revision hip arthroplasty with severebone loss: a new technique using autologous bone graft and a proximallyloading femoral component
J. ALFARO ADRIAN, M. EMERTON, D.W. MURRAY, P. MCLARDY-SMITH
Nuffield Department of Orthopaedic Surgery, University of Oxford, Nuffield Orthopaedic Centre, Oxford - UK
ABSTRACT: We report the results of a new method of reconstructing the femur in 22 patients with severe boneloss having revision hip arthroplasty. The calcar and metaphysis were reconstructed with cortico-cancellousautograft around a new modular hip replacement. The metaphyseal portion of the implant is free to slide onthe stem and therefore loads the graft and, we believe, encourages bone graft incorporation. The stem gainscementless fixation distal to the area of bone loss, thus preventing fractures and allowing the areas of boneloss to heal. At the time of review at a mean of 3 years follow-up there had been no revisions (since then there has beenone re-revision due to recurrence of infection). The modified D'Aubigné and Postel hip score improved from7.3 to 15. In 17 patients the graft has incorporated, in 5 it has partially resorbed but the prosthesis remainssecure. We conclude that this is a relatively simple and successful technique for overcoming the problem of majorfemoral bone loss. (Hip International 1997; 7: 3-10)
KEY WORDS: Revision hip arthroplasty, Bone loss, Bone graft, Proximal loading
Hydroxyapatite-coated threaded acetabular prostheses. A five-yearfollow-up radiographic study
G. LOUPASIS, S.J. BIRTWISTLE, I.D. HYDE
Department of Orthopaedics, County Hospital, Lincoln - England
ABSTRACT: We have reviewed 83 consecutive cementless Furlong hydroxyapatite (HA)-coated threaded ac-etabular components which were inserted in 75 patients. The mean age of the patients at the operation was54 years (range 31 to 67years) and the mean follow-up period was 61 months (range 40 to 82 months). Largesize gaps at the implant -bone interface (attributed to failure to achieve bone-prosthesis contact), were pre-sent in 89% of the cases on the initial radiographs. At the last follow-up, the gaps were either no longer vis-ible or had decreased in 95% of the cases. Radiolucencies were absent in well-fixed components. Three ac-etabular components were considered to be loose and are awaiting revision, giving a 3.6% aseptic loosen-ing rate. The remainder of the cups were radiographically stable with positive evidence of bone ingrowth andno signs of impending loosening. (Hip International 1997; 7: 11-6)
KEY WORDS: HA-coated threaded acetabular components, Aseptic loosening
Abstracts from Hip International Vol. 7 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S47-S54 ©by Wichtig Editore, 2001
S48
Revision of failed cemented total hip arthroplasty using the Charnleytechnique and implants
G. CH. BABIS, TH. PANTAZOPOULOS, TH. IOANNIDIS, G. HARTOFILAKIDIS
Orthopaedic Department, University of Athens Medical School, KAT Hospital, Athens - Greece
ABSTRACT: The authors present the results of 57 revisions in 54 patients performed for aseptic loosening ofcemented total hip arthroplasties. The Charnley technique and implants were used in all cases. The mean fol-low-up was 8 years and 6 months with a minimum of 5 years. The failure rate for the femoral component was15% and for the acetabular component it was 19.1%. The cumulative success rate at 8 years was 81. 7% forthe femoral component and 83.4% for the acetabular component. The Charnley technique and implants were found efficient for revision of cemented total hip arthroplasties inthe long term, but there are limitations to their use in the presence of severely compromised bone stock. (HipInternational 1997; 7: 17-27)
KEY WORDS: Total hip replacement, Revision, Cemented hip
Efficacy of two types of femoral cement restrictor in total hip arthroplasty
J.A. JEFFERY
Orthopaedic Registrar, The Royal Free Hospital, London - UK
ABSTRACT: Distal occlusion of the femoral canal in total hip arthroplasty is important for cement pressurisa-tion. Failure to adequately restrict cement may result in earlier prosthetic loosening and a longer column ofdistal cement which may make revision surgery more difficult. A standard plastic restrictor (Hardinge type) wascompared with a bone plug restriction method in a randomised, prospective trial of 50 patients. Both types ofrestrictor failed to adequately restrict cement in over 50% of cases. (Hip International 1997; 7: 28-33)
KEY WORDS: Cement restrictor, Leakage, Slippage, Pressurisation
Radiological assessment of bone graft in revision acetabular arthroplasty
I. ABOLS 1, H. OLIVIER 2
1 Département d'Imagerie Médicale2 Département de Chirurgie Orthopédique, Hopital Saint-Michel, Paris - France
ABSTRACT: The purpose of this study was to describe the radiological appearance of moulded cancellousbone graft used for acetabular reconstruction in revision arthroplasty of the hip. We reviewed retrospectively 48 cases with a mean follow-up of 3.5 years. The radiological study was basedon: the density of the graft, the delineation line between the graft and the host bone or the presence of tra-becular continuity between the graft and the acetabular bone, and the position of the cup.Increasing density of the graft was observed in 35 cases.Trabecular continuity between the graft and the host bone appeared in 9 cases, in Zone 1, with a mean de-lay of 2.6 years. This finding was associated with the disappearance of the dense line separating the graft
S49
from the acetabular bone in 8 hips (16.6%). At a mean follow-up of 2.5 years, 4 patients showed migrationof the cup; this was secondary to graft resorption in 3 cases. Only one of these patients had been reoperat-ed on. From these observations we have made an attempt to describe the evolving appearance of the bone graftand the radiological signs that may be used to assess graft incorporation. (Hip International 1997; 7: 34-8)
KEY WORDS: Revision acetabular arthroplasty, Acetabular bone grafting
Orthopaedic consequences of slipped capital femoral epiphysis in adults
D. LAZOVIC, G. PETERS
Orthopaedic Hospital, Hannover Medical School, Hannover - Germany
ABSTRACT: Slipping of the femoral head usually occurs at the beginning of puberty. With sexual hormonedeficiency the growth plates remain open with the danger of a Slipped Capital Femoral Epiphysis (SCFE) be-yond the normal age of growth. In several endocrine disorders such as hypothyroidism or growth hormonedeficiency, and especially during supplemental therapy with hormones, SCFE can occur. SCFE can occur evenif the hormonal replacement therapy has stopped. Since 1984 we have seen and treated 7 adult patients (6male, 1 female) with SCFE. They were between 17 and 36 years old. Due to the lack of sexual hormones threepatients had severe osteoporosis which caused difficulties in surgical treatment. From the orthopaedic pointof view regular clinical and radiological check-ups are necessary in patients with open physes beyond thenormal growth age - especially in patients with endocrine dysfunction and hormonal supplement therapy.These reviews have to be continued until the growth plates are closed because SCFE occur even after hor-monal replacement has been stopped for years. Prophylactic screwing of the opposite hip is also recom-mended in high risk patients. (Hip International 1997; 7: 49-56)
KEY WORDS: Slipped capital femoral epiphysis (SCFE) in adults, Orthopaedic consequences of SCFE
Reinforcement rings for deficient acetabular bone in revision surgery:long-term results
E. GARCIA-CIMBRELO, J. ALONSO-BIARGE, J. CORDERO-AMPUERO
Department of Orthopaedics, Hospital "La Paz", Universidad Autónoma de Madrid, Madrid - Spain
ABSTRACT: This study analyzes the long-term results of 23 metal ring supports used in revision surgery since1979. Only a metallic ring and a cemented cup were used in this series. Bone grafts and cementless cupswere excluded from this study. One deep infection was excluded from the follow-up study. In the 22 casesanalyzed, the mean follow-up period was 10 years for all cases and 12.2 years for unrevised cases. Bone de-fects according to the AAOS classification were: Grade 1, 1 case, Grade 2, 1 case, Grade 3, 10 cases, andGrade 4, 10 cases. A Müller ring was indicated in an anterior or medial wall defect (12 cases) and a Burch-Schneider ring was indicated in an anterior or posterior column defect or in pelvic discontinuity (10 cases).The clinical results were good in 8 cases, fair in 8 cases, and poor in 6 cases. Six cases were rerevised or re-moved, resulting in a total cumulative probability of rerevison or removal of 23.8% after 10 years accordingto the Kaplan-Meier analysis. Postoperatively, 18 cases had neutral rings, 2 cases had horizontal rings, and2 cases had vertical rings. Radiological cup migration was found in 12 cases, resulting in a total cumulativeprobability of migration of 56.8% after 13 years according to the Kaplan-Meier analysis. Changes in the ac-

S50
etabular angle were present in 2 cases, vertical migration in 12 cases, and medial migration in 10 cases. Ourdata suggest that the metal ring and cemented cup alone could be used for salvage surgery in elderly pa-tients and in low-demand patients. Possibly, adding bone graft could improve these results. (Hip International1997; 7: 57-64)
KEY WORDS: Hip, Revision surgery, Reinforcement ring
Patterns of osteolysis in two different cementless total hip arthroplasties
M.J. HUBBLE 1, J.D. ELDRIDGE 1, E.J. SMITH 1, I.D. LEARMONTH 1, W.H. HARRIS 2
1 The University Department of Orthopaedic Surgery, Avon Orthopaedic Centre, Bristol - UK2 The Department of Orthopaedic Surgery, Massachusetts General Hospital and Harvard Medical School, Boston, 2 MA - USA
ABSTRACT: The incidence and pattern of distribution of osteolysis around two different cementless total hiparthroplasties, the Harris Galante Porous (HGP) and the Porous Coated Anatomic (PCA), were compared. TheHGP femoral component has a straight, collared, titanium alloy stem with non circumferential titanium meshpads. The PCA has a collarless cobalt chrome stem with an anatomical bow and a circumferential proximalporous coating. Ninety-four HGPs and 104 PCAs were followed for an average of four and a half years. Bothgroups were well matched for age, sex and primary diagnosis. Each group was operated on at seperate, sin-gle, institutions by a single surgeon at each centre. The incidence of osteolysis around the acetabular components (1%) was the same. The incidence of femoralosteolysis was 31% with the HGP and 23% with the PCA. The pattern of femoral osteolysis was very differ-ent, being predominantly around the mid and distal stem with the HGP, and restricted to the proximal withthe PCA. The presence of osteolysis was clinically silent unless the femoral component was also loose. Prosthetic design, in particular the presence or absence of a circumferential ingrowth mesh or porous coat-ing, will influence the effective joint space and the distribution of wear debris particles. This may explain theprosthesis specific pattern of osteolysis seen. (Hip International 1997; 7: 65-9)
KEY WORDS: Osteolysis, Cementless total hip arthroplasty
A new procedure for revision for fracture of the stem in total hip replacement
S. HOUSHIAN, I. HVASS, P. RIEGELS-NIELSEN
Department of Orthopaedic Surgery T, Centralsygehuset i Esbjerg, Esbjerg - Denmark
ABSTRACT: A new system for antegrade removal of fractured femoral stems, the Anspach Extractor III®, isdescribed. A conical hole is made in the fracture surface of the stem with a high speed drill. An extractor rodis then fixed into the hole with a malleable sleeve. We have used the system in eight cases of a broken Charn-ley stem and removed the distal hip in 6 cases without problems. 2 cases were unsuccessful and neededfemoral fenestration for retrograde removal. This system is easy to use and we have found it to shorten operation time in case of broken stem revision.(Hip International 1997; 7: 70-4)
KEY WORDS: Stem, Fracture, Revision
S51
Intrapelvic dislocation of the femoral head after central acetabular andfemoral neck fracture
A. CEBALLOS MESA, R. BALMASEDA MANENT, R. PUENTE RODRIGUEZ, M. PEDROSO CANTO
Department of Orthopaedics. CIMEQ (Centro de Investigaciones Médico Quirúrgicas), Havana- Cuba
ABSTRACT: Central fracture-dislocation of the hip associated with fracture of the femoral neck and intrapelvicintrusion of the femoral head is a very rare condition. The treatment of choice consists of open reduction ofthe dislocation and internal fixation of both fractures, but this is often not possible in delayed cases. In ourpatient, a young female, operated on six months after the trauma by partial resection of the femoral head anda cementless total hip arthroplasty, a good clinical result was achieved. (Hip International 1997; 7: 75-7)
KEY WORDS: Hip, Intrapelvic dislocation of femoral head
A lethal arterial injury associated with total hip replacement
G. TSELENTAKIS, V. PATEL, D.W. PARSONS
St. Helier Hospital, Wrythe Lane, Surrey - UK
ABSTRACT: We report a case of vascular damage to the profunda femoris artery following total hip replace-ment. Arterial injury usually presents with acute haemorrhage but on this occasion the presentation was de-layed (16 days). Arterial damage should always be considered when swelling persists or increases. (Hip In-ternational 1997; 7: 78-9)
KEY WORDS: Total hip replacement, Profunda femoris artery, Post operative bleeding
Fat embolism in hip arthroplasty
S. HOFMANN 1, M. SALZER 2
1 Department Orthopaedic Danube Hospital2 Department Orthopaedic Herz-Jesu Hospital, Vienna - Austria
ABSTRACT: Since 1970 cardiorespiratory deterioration has been a well recognised complication during ce-mented Total Hip Arthroplasty (THA). Originally this effect was attributed to chemical and thermal effects ofbone cement. There is evidence from several animal and clinical studies that these cardiorespiratory changesare caused by fat embolism to the lung, and high intramedullary pressure (IMP) is the main causative factorfor this fatty marrow release into the circulation. Fat embolism syndrome (FES) as a rare but severe periop-erative complication represents the clinical manifestation of severe fat embolism. It is of clinical importancethat surgeons have a better understanding on this syndrome. In this review a new pathophysiological modelfor FES is presented. As there is no causal therapy for FES, several modified surgical techniques are dis-cussed in relation to their efficiency in preventing fat embolism during endoprosthetic surgery of the hip. Theanaesthetic contribution to prophylaxis is also described and a therapeutic concept for the symptomatic treat-ment of FES is proposed. (Hip International 1997; 7: 89-100)
KEY WORDS: Fat embolism, Hip arthroplasty, Surgical techniques, Pathophysiology, Intramedullary pressure

S52
Prognosis of the Müller straight stem
C.J.M. OOSTERBOS, A.J. TONINO
Department of Orthopaedic Surgery, De Wever Hospital, Heerlen - The Netherlands
ABSTRACT: 214 primary total hip arthroplasties in 208 patients with the Müller straight stem using the sec-ond generation cementing technique were performed between 1979 and 1983. 149 hips were assessed clin-ically and 134 hips radiographically after a minimum of 10 years of follow-up. 55 patients had died and 10hips had been revised, 4 for infection and 6 for aseptic loosening. In the remaining 139 patients the clinicalresults were very satisfactory (Merle d'Aubigné score). According to Harris' radiographic and subsidence cri-teria there were 13.2% stem loosenings at 10 years. Stress shielding induced bone resorption of the proxi-mal part of the femur was noted in 61.2% of the hips. Survival analysis of the stem showed a success rateat 10 years of 89.2% while the cumulative survival rate was 91.22% which compares well with the "gold stan-dard" (Charnley's THA). It is suggested that there is a correlation between "physiological" subsidence andstress shielding induced bone resorption, which may lead to an elevated level of stem loosening after 10years. (Hip International 1997; 7: 101-9)
KEY WORDS: Hip arthroplasty, Müller, Cemented
Biomechanical aspects of modular inlay fixation
W. BLÖMER
Aesculap, Research and Development, Tuttlingen - Germany
ABSTRACT: Based on positive clinical experience with the taper lock of ceramic heads in total hip replace-ment, conical fixation was also chosen for modular cup inlays made of alumina ceramic and polyethylene.For a comparative assessment of inlay fixation, new ceramic and polyethylene inlays with a taper lock werebiomechanically tested and compared with clinically proven system with a snap lock mechanism. With regardto the prevention of dislocation and relative movements the same level of safety was found. Measurementsof the damping characteristic of the acetabulum replacement showed that there is no considerable shock-absorption for a metal backed polyethylene inlay and there are no differences in this respect between ce-ramic and polyethylene inlays. (Hip International 1997; 7: 110-20)
KEY WORDS: Acetabular cup, Ceramic/ceramic coupling, Modular inlay, Inlay testing, Shock absorption
Leg length discrepancy after total hip replacement
P.P. SARANGI, G.C. BANNISTER
University Department of Orthopaedic Surgery, Southmead Hospital, Westbury on Trym, Bristol - UK
ABSTRACT: Leg length differential in 110 patients with unilateral hip arthritis was measured on supine AP ra-diographs before and after hip arthroplasty, and compared with subjective sensation of leg length discrep-ancy at that time. Eight percent of limbs were of equal length, 60% were within 0.5 cm. and 9% demonstrateda discrepancy greater than 1 cm. Shortening was tolerated better than lengthening. No patient with true short-ening of less than 6 mm or lengthening of less than 4 mm perceived discrepancy. Shortening of over 10 mm

S53
and lengthening of over 6 mm was perceived universally. Shortening of between 6 mm and 10 mm wasperceived by 55% of patients, and lengthening between 4 mm and 6 mm by 26%. (Hip International 1997;7: 121-24)
KEY WORDS: Leg length discrepancy, Patient perception, Templating
Displacement of femoral stem during closed reduction of total hip arthroplasty
J. CORDES, K. SPERLING, M. KRAMHØFT
Department of Orthopaedics, Hvidovre Hospital, Copenhagen - Denmark
ABSTRACT: In the literature, only one case of displacement of a cemented femoral stem from its cement bedduring closed reduction of a dislocation has been reported. In that case, it was suggested that the stem de-sign may in part be the explanation for the displacement.Another case with a cemented Müller straight stem is now presented, emphasizing the use of image intensi-fication if reduction proves difficult. (Hip International 1997; 7: 125-7)
KEY WORDS: Arthroplasty (cemented), Dislocation, Complication, Reduction
Femoral perforation during cement removal in revision hip arthroplasty
P.R. WILLIAMS, M.V.S. MAHESON
Cardiff Royal Infirmary, Cardiff - UK
ABSTRACT: Eighty two cemented femoral revision hip arthroplasties were reviewed to assess the incidenceof intra-operative perforation of the femur and subsequent periprosthetic fracture using a high speed pneu-matic burr for the removal of acrylic bone cement with an extensile exposure. There was one case of intra-operative femoral perforation; this patient did not go onto fracture postoperatively. There were no cases ofintraoperative femoral fracture. There were 3 cases of periprosthetic femoral fracture all of which occurredmore than 12 months after their impaction grafted femoral revision arthroplasty using a standard length ce-mented stem. The pneumatic high speed burr was extremely effective in the removal of acrylic bone cement in femoral re-vision arthroplasty. The incidence of subsequent femoral fracture in the impaction grafted revised populationwas low and did not appear to be related to intraoperative femoral perforation. (Hip International 1997; 7:153-7)
KEY WORDS: Revision hip arthroplasty, Cement removal, Femoral perforation, Periprosthetic fracture

S54
Evidence for induction of cardiorespiratory and vascular complications bymethylmethacrylate monomer in hip replacement surgery. Laboratory and animal investigations
O.E. DAHL 1, T. ASPELIN 1, I.E. RUYTER 2, T. LYBERG 1
1 Research Forum, Ullevaal University Hospital2 Scandinavian Institute of Dental Materials, Oslo - Norway
ABSTRACT: Hip replacement surgery (HRS) using acrylic cement for prosthetic fixation is associated with periop-erative cardiorespiratory dysfunction. Large amounts of thrombin are generated locally and systemically in the pul-monary microcirculation during traumatization of bone. Hypercoagulation is rapidly followed by maximal central ve-nous blood concentrations of methylmethacrylate monomer (MMA) released during impaction of bone cement in-to the femoral shaft. In vitro and in vivo studies have shown that MMA in different ways contribute to activation ofcoagulation. In addition, MMA per se is cytotoxic and may in clinically relevant concentrations cause disintegra-tion of vascular and blood cells with potential release of proteolytic enzymes and exposure of subendothelial con-stituents. The present experimental studies showed that implantation of cement and prosthesis into the femoralshaft or injection of MMA into a femoral vein caused a marked increase in mean pulmonary arterial blood pressure(MPAP) and a transient fall in mean arterial blood pressure (MAP) followed by a compensatory increase. To avoidadmixed reactions by other elements than MMA alone, MMA in different concentrations was injected directly intoa pulmonary artery. MPAP increased and MAP decreased in a clear dose response relationship. Analyses of bloodMMA concentrations following injection of 5 ml MMA (200 mg/ml) into a femoral vein, revealed a ten to hundredfold reduced MMA concentration at the moment blood entered the pulmonary capillaries and additionally ten timesreduction when the blood had passed the lungs. This may indicate that the MMA concentrations recorded in cen-tral venous and mixed venous blood of earlier reports only reflect a small fraction of the actual concentrations invein blood close to cemented areas. This rapid decrease of MMA concentrations by passage of blood from thefemoral vein to the pulmonary artery is mainly due to dilution but also underlines the highly lipophilic character ofMMA. In areas of high concentrations MMA rapidly penetrates and destroys cell membranes and may potentiallycontribute to development of local deep vein thrombosis. In addition, systemic effects of MMA may superimposeon existing disturbances of the thrombohaemorrhagic balance during hip replacement surgery and cause haemo-dynamic alterations which occasionally may be fatal. (Hip International 1997; 7: 158-68)
KEY WORDS: Bone cement toxicity
Sport after total hip replacement
F. MARGHERITINI, A. ZERI, P. BELLI, A. GIULIANTE
II Orthopedics Department University of Roma, "La Sapienza", Roma - Italy
ABSTRACT: The scientific literature is scant on the possibility of mild sport after hip replacement. To analyse theeffect of sport on the outcome of uncemented total hip arthroplasty we studied 72 patients who had undergonehip replacement, with at least 20 months follow-up, with maximum age 60 years at surgery. Patients were checkedclinically and radiologically and were asked to respond to a questionnaire about the type, level and frequency ofsports before and after surgery. The findings suggest that intelligent low-impact sporting activities can improvethe outcome of hip replacement surgery with time though it is advisable to avoid high-stress sports that can wearjoint components and loosen the prostheses. (Hip International 1997; 7: 169-73)
KEY WORDS: Hip prostheses, Sports, Rehabilitation, Loosening
S55
Standardised audit of hip fracture in Europe (SAHFE)
M.J. PARKER 1, C.T. CURRIE 2, J.A. MOUNTAIN 2, K.-G. THORNGREN 3
1 Orthopaedic Research Fellow, Peterborough District Hospital, Peterborough2 Department of Medicine, University of Edinburgh, Edinburgh - UK3 Department of Orthopaedics, University Hospital, Lund - Sweden
ABSTRACT: The Standardization Audit of Hip Fracture in Europe (SAHFE) project aims to encourage centresin Europe to participate in hip fracture audit. It defines a data set consisting of a core of 34 questions whichincludes outcome measures at 120 days from injury. In addition there is a larger number of optional questions.It is envisaged that each participating centre will collect and analyse its own data, with national centres toprovide comparative data. Because the data are standardised, international comparisons can be made, the-reby assisting in defining the optimal method of treatment and rehabilitation for this common condition. (HipInternational 1998; 8: 10-5)
KEY WORDS: Audit, Hip fracture
Effect of pelvic tilt on radiographic migration and wear measurements after total hip arthroplasty
T. ILCHMANN 1, U. KESTERIS 2, H. WINGSTRAND 2
1 BG Trauma Centre, University of Tubingen, Tubingen - Germany2 Department of Orthopaedics, University Hospital, Lund - Sweden
ABSTRACT: Tilt effects on radiographic measurements after total hip arthroplasty should be studied. A newcomputerized method for measurement, called EBRA, making three dimensional calculations and intended toidentify tilted radiographs was evaluated for its clinical usefulness. In an experimental set-up repeated ra-diographs were taken with a human pelvis tilted gradually around its horizontal and vertical axes. Migrationand wear were measured with the EBRA method and the results were compared with those made using stan-dard methods. Tilted radiographs were identified and excluded from analysis by the EBRA method, signifi-cantly reducing the maximum error of measurement. A systematic error of measurement was found in the pre-sence of consecutively changing tilt in a single direction. Wear measurements were only slightly affected bypelvic tilt. A pelvic tilt can cause considerable errors in the measurement of cup migration-i.e. up to 8.2 mm.The EBRA method improves the accuracy of measurements by taking the effects of tilt into account. (Hip In-ternational 1998; 8: 16-23)
KEY WORDS: Total hip arthroplasty, Migration, Wear, EBRA, Measurement, Tilt
Abstracts from Hip International Vol. 8 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S55-S85 ©by Wichtig Editore, 2001
S56
The biomechanics of the dysplastic hip
R. BOMBELLI
Emeritus Director of the Orthopaedic Department of the General Hospital of Busto Arsizio - Italy
The biomechanical effect of the forces produced by the abductors, the ilio-psoas, the gluteus maximus, theadductors, the ischio-tibial muscles in the normal hip, both in standing and in dynamic phases, is to centrethe femoral head in the acetabulum. In lying position of the new born baby the muscles are relawed due tothe flexed abudcted hips and to the flexed knees, but they achieve the same effect.Any time the physiological flexed, abducted, externally-rotated hips of the new born baby are erroneouslyforced in adduction and extension, and the knees are extended the muscular force dislocates the femoralhead antero-cranio-laterally, hindering a normal development of the cranio-lateral part of the sourcil.Sonographic investigations in the early stage of dysplasia detects the pathologic position of the head in theacetabulum and the abonormal inclination of the soft tissue components of the sourcil. Sonography pointsout 41% of cases the immaturity of new born hips and 0,66% of dislocatable or dislocated hips, which areundetectable through the clinical screening (R. Graf, Ch. Tschauner).
Heterotopic ossification in hip surgery: Aetiopathogenesis, classificationand clinical pictures
L. ROMANINI, S. RIPANTI, A. GIULIANTE
II Chair of Orthopaedics and Traumatology, “La Sapienza” University, Roma - Italy
The presence of heterotopic ossification (HO) during orthopaedic surgery has always aroused interest, even whenit creates no real clinical problems for the patient. Reviewed brifly here is the current state of knowledge aboutthe aetiopathogenesis and classification of these cases, with reference to some personal experience.HO is the term used when lamellar bone structure, with haversian canals and haematopoietic bone marrowwith marked metabolic activity is found at extraskeletal sites. HO must not be confused with calcification -caused simply by precipitation of calcium phosphate crystals as a result of altered local pH (inflammation) -whose structure is unorganized, and always outside the skeleton.HO consequent to hip surgery (joint replacement to deal with various pathologies) has an incidence of 15-90% depending on the amount of periarticular bone tissue present, according to published reports. It usual-ly appears about two weeks after surgery, stabilizing at around one year. Although its pathogenesis is still notclear, the surgical trauma to soft tissues is sometimes considered causal.The initial stimulus deriving from the surgery activates two cell lines; the DOPC are mesenchymal bone pre-cursor cells, needed for development of the cartilaginous and bone cell lines, and are found in the bone mar-row. The IOPC are also mesenchymal bone precursor cells but are non-specific, and can be stimulated; theyare found in connective tissue and muscle. They are stimulated to transform by various factors, some un-derstood better now, such as BMP and PGE2, but also by the degree of tissue damage, and - finally - by in-dividual predisposition.Various classification systems have been proposed to standardize descriptions of HO, all based on the amountof newformed periarticular bone tissue, leading to more or less complete joint blockage (ankylosis). Theseinclude Hamblen’s classification (1971), DeLee-Charnley’s (1976) and Brooker’s (1973), used by most inves-
ABSTRACTS FROM II MEETING OF THE ITALIAN HIP SOCIETY (COXA) - BOLOGNA, ITALY, 28 NOVEMBER, 1997 (HIP INTERNATIONAL 1998; 8: 31-37)

S57
tigators in this field. Factors that may increase the risk of HO after hip surgery include sex, previous surgery,factors closely linked to the surgical method; patients with ankylosing spondylitis or hypertrophic joint dis-ease are certainly at high risk.Confirming published reports, our caselist too shows HO in patients with abundant hyper-active bone tissue(osteophytosis), with previous fractures of the acetabulum or femoral neck, and such patients should receiveappropriate prophylaxis.
Femoral neck preservation in young patients: the Thrust Plate Prosthesis
F. BIGGI, G. COSTACURTA, F. FRANCHI, C. GIOS, E. SCALCO
Orthopaedic and Trauma Department, Azienda ULSS 3, Asiago - Italy
Hip surgery in young patients, even now, has problems concerning mechanical and biological factors, withdifficulties in long-term prognosis because of aseptic loosening, which means, often, revision surgery. Manystudies, starting in early 1970’s, have been carried on, trying to identify new prosthesis designs for maximumbone-stock preservation, both in the acetabulum and in femur. Focusing on femoral component, the so-called“femoral neck preservation philosophy” has been developed by some Authors, Paltrinieri and Pipino for theItalian school, Wagner and Huggler for the European, Townley for the American.Looking at the Zurich Balgrist University experience (Huggler A.H., Jacob H.A.C.: Long term results with theuncemented Thrust Plate Prosthesis - TPP - Acta Orthopaedica Belgica, Vol. 59 Suppl. 1: 215-223, 1993), in1995 we started our clinical application. The Thrust Compression Plate is a totally uncemented implant man-ufactured in Protasul-100; its application needs a good femoral neck without varus-valgus deformities; femoralmedullary cavity is entirely respected; primary stability is obtained by the screwbolt, inserted in the shortplate fixed against the cilindrical cortical bone of the femoral neck; furthermore, a small cortical plate lashadds antirotational stability; finally, this system permits a metal-on-metal coupling with acetabular compo-nent.We treated 20 cases, and early results are encouraging, confirming previous reports.
Cementless porous hemispherical acetabula for hip replacement
A. MANUNTA, G. RINONAPOLI, D. FARRIS, G. PIGA, P.D. MULAS, A. DEMONTIS, C. MOSCARITOLO
Institute of Orthopaedics, Sassari - Italy
We made a clinical and radiographic study of 300 cementless hip replacements.Materials. from 1990-6 we implanted 300 press-fit hemispherical acetabula, made of titanium with polytheneinserts, in 270 patients aged 38-92 years. One or two screws were needed to ensure stabilization in 25% ofcases. We clinically reviewed 210 patients.Methods. Clinical assessment was made using Harris’ scoring system, considering excellent or good scores(81-100) satisfactory. We recorded subjective signs, especially groin pain. Radiographic parameters (orien-tation, containment, positioning of the acetabulum) were checked immediately after surgery, using Pupparoand Engh’s criteria (1991); other parameters, such as radiolucent and radioopaque lines, osteolysis, slcero-sis and migration were assessed during follow-up. The mean score, 34.9 before surgery, rose to 93 duringpostoperative follow-up. A very high percentage of satisfactory outcomes was achieved (95%). Radiograph-ic checks during follow-up indicated that 95% of the implants were stable, with good bone anchorage andone case presented aseptic mobilization.

S58
Clinico-radiographic evaluation of femoral stems coated or not with hydroxyapatite
G. RINONAPOLI, A. DEMONTIS, G. PIGA, D. FARRIS, P.D. MULAS, C. MOSCARITOLO
Institute of Orthopaedics, Sassari - Italy
This study regards a clinico-radiographic assessment of prosthetic hip stems with different metaphyseal sur-faces (smooth, porous, grooved), coated or not with hydroxyapatite.Materials. Clinical/radiographic examinations were made before surgery, immediately after, at two and sixmonths, one year and annually thereafter. Clinical assessments were made using Harris’s scoring system.Good or excellent results were rated as “satisfactory”, moderate or poor outcomes as “unsatisfactory”. Ra-diographic examinations were done using standard projections and the postoperative parameters were con-sidered according to initial positioning, fill and fit. At longer postoperative intervals we checked for changesat the bone-implant interface and bone changes induced by the implant. Subsidence was considered signif-icant when it exceeded 3 mm.Clinical results. The mean score rose from 42 before surgery to 87.6 at six years. Scores for coated implantswere higher. Results were satisfactory in 88% of cases; 7% complained pain in the thigh.Radiographic findings. Fit was excellent in 92% of cases, fill adequate in 97%. Radiolucency lines were vis-ible in 11%. Applying Engh’s criteria for stem stability we found for the uncoated stems bone stability in 89%,fibrous stability in 7%, unstable implants in 4%; the respective values for the hydroxyapatite-coated hipswere stable. Distal cortical hypertrophy was seen in 13% of cases. proximal bone atrophy as an adaptivestress-shielding response was observed in 35% of cases, cortical atrophy in 6%. Eight percent had osteol-ysis. In seven patients the stem migrated.Conclusions. On the whole our results were satisfactory. Coated stems gave a lower percentage of radiolu-cent lines and greater periprosthetic bone density. Atrophy and distal cortical hypertrophy are functional adap-tations made by the bone to the implanted hip.
The Polar® acetabular component
R. GIACOMETTI CERONI, L. ZAGRA, F. RANDELLI
Galeazzi Institute of Orthopaedics, Milan - Italy
The present study regards a clinical and radiographic evaluation of a consecutive series of 50 patients op-erated with total hip replacement by the same surgeon, using the Polar® cup. The outside of this cup is hemi-spherical so it can be implanted after removal of only the osteophytes and acetabular cartilage. The twocolumns of compact bone ensuring the mechanical strength of the acetabular bone are thus spared. The Po-lar cup has no macrostructuring on its surface so it imposes no limits to the acetabulum. The only anchor-age point is in the postero-superior area of the cavity, which is relatively stable, and requires two 6-mm di-ameter pins.We employed the parameters set out in the DOVAC documentation to assess the out-come. At a mean fol-low-up of six years (range 5.25 yrs - 6.5 yrs) there was only one case of late loosening of the cup in a patientwith a Charcot hip. No clinical or radiographic signs of migration of the acetabular component were seen withthe other 49 implants. We found no cortical dystrophy, no areas of resorption, and no atrophy. To date thecups with a 32-mm head insert have given results comparable to those with the 28-mm head insert.The frequent radiolucent lines in the Gruen B zone and especially the C zone can be considerd normal forthis type of cup with its smooth surface, as no bone integration is sought with the pubic or ischiatic zones.

S59
Indications and technique of total hip arthroplasties in hip dysplasia
P. CALDERONI 1, D. DALLARI 1, A. FERRUZZI 1, I. GUALTIERI 2, G. GUALTIERI 1, S. GNUDI 3
1 IV Division, Rizzoli Orthopaedic Institute, Bologna2 Orthopaedics Division, Bufalini Hospital, Cesena3 General Medicine, Rizzoli Orthopaedic Institute, Bologna - Italy
In this study we examined dysplastic hips treated with different prostheses at the Rizzoli Orthopaedics In-stitute from 1977 to 1991, in order to evalate the results and to compare them with those reported in the lit-erature. The aim of our study was to select the appropriate surgical technique, type of fixation and prostheticdesign according to the pathologic anatomy of the hip and the clinical conditions of the patient.Congenital hip dysplasia is one of the main causes of secondary hip arthritis. Especially in severe forms, thesurgeon has to face remarkable technical problems when planning hip arthroplasty, both on the acetabularand on the femoral side.Our series consists of 288 total hip arthroplasties in dysplastic hips, which were classified according toEftekhar. The results were rated excellent or good in 61% of the cases, fair in 30% and poor in 9%. At radi-ographic evaluation, 64% of the implants were judged to be stable, while 12% showed marked signs of loos-ening and the remaining 24% were considered “at risk”.On the basis of our experience, we now believe that the acetabular rotation center should be placed in itsoriginal site, even though this makes the surgical technique more demanding and the chances of neurologi-cal complications higher.It is our opinion that the femoral stem should be straight and that the femoral osteotomy should be performedclose to the lesser trochanter, in order to remove most of the metaphyseal anatomical dysmorphism.
The ceramic-ceramic hip prosthesis: 1000 implants in ten years
S. TERZI, A. TONI, A. SUDANESE, G. BARBANTI-BRODANO, S. PADERNI, G. BIANCHI, A. GIUNTI
Rizzoli Orthopaedic Institute Bologna - Italy
Material and Methods. Between 1987 and 1996 were implanted 1018 ceramic-ceramic primary hip prosthe-ses. up to 1994 we used an AnCA model with anatomically shaped 13-cm chrome-cobalt stem, entirely coat-ed with ceramic (alumina or hydroxyapatite) and with porous coating on the medial, anterior and posteriorsides of the proximal half. The 32-mm diameter alumina (BIOLOX) head is coupled on a truncated-conicalneck of the stem. The acetabulum is high-density alumina (BIOLOX) covered by a cup of titanium alloy (TiAl6Va4)ring screwed on. The dome of the cup is coated with porous alumina.Since 1994 we have gradually replaced this model with a press-fit version (AnCA Fit), which has an aluminainsert. Since 1995, for cementless implants we have been using the AnCA Fit stem, with a modular neck.Two of the 1018 implants had to be removed and a Girdlestone procedure performed because of septic loos-ening (one 22 days and the other eight months after implantation). There were three immediate postopera-tive deaths (two from cardiovascular collapse, one from acute respiratory syndrome). Fifty-seven patientswere lost to follow-up. We can therefore describe 956 primary prostheses, 644 of them cementless, 312 hy-brid (cemented stem). The decision whether to cement the stem or not depends on the femoral bone miner-al content. Of the 644 cementless hips, 111 were alumina-coated, and 533 hydroxyapatite.Results. The rate of revision was 2.6% (25 cases). Three needed global reimplant, 11 reimplant of the ac-etabular component, 11 the stem. None of the cemented stems needed revision. Among the cementless pros-theses that needed revision 7/111 were alumina-coated (6.3%) and 7/533 hydroxyapatite (0.8%). None of the956 Biolox alumina heads ever broke.

S60
Histological examination of periprosthetic tissues sampled at reimplant showed scant ceramic detritus, main-ly measuring 0.1-1.0 microns, except where there was massive wear due to recurrent luxation of the pros-thesis, and little or no cellular reaction. Using the logistic regression method, we studied the risk of radiolucency at the bone-implant interface in re-lation to the time and type of coating on cementless stems. The risk of osteolysis at the interface at variousintervals after surgery was close to zero from the ceramic-ceramic implant.
Luxation of the proximal femoral head with acetabular fracture
L. PONZIANI, R. PASCARELLA
Rizzoli Orthopaedic Institute, Bologna - Italy
Fractures of the acetabulum are combined with luxation of the proximal femoral epiphysis in about 40% ofour patients. The luxation may be anterior in fractures involving the anterior wall, central with transverse frac-tures or both bone columns, posterior with fractures of the posterior wall or column. From 1980-95 at the Riz-zoli Orthopedic Institute III Division 507 cases of acetabular fracture were treated: 209 had luxation of theproximal femoral epiphysis. Of these cases, 115 were admitted directly to this Institute, and the remaining392 were first seen in another hospital. The mean time between injury and admission for these latter patientswas 9.6±6.0 days.Five cases presented anterior luxation, 41 central and 163 posterior. Two years after surgery 36 cases hadnecrosis of the femoral head: two after fracture of the two columns, 11 fractures of the posterior wall, 18transverse+posterior wall fractures, 5 posterior-column+wall fractures. In 34 cases the luxation was posteri-or, in two central. It is worth noting that only 12 out of the 36 patients with femoral head necrosis had un-dergone reduction of the hip immediately after the accident. Fourteen patients received a hip replacement,and two became infected.
Wagner’s periacetabular osteotomy: a review of cases with at least fiveyear follow-up
R. GIACOMETTI CERONI, L. ZAGRA
Galeazzi Institute of Orthopaedics, Milan - Italy
Between 1979 and the first half of 1997 at the Galeazzi Orthopaedic Institute in Milan 138 periacetabular os-teotomies according to Wagner were performed. A series of cases with at least five year follow-up, operatedby the same surgeon (RGC) has been reviewed: 74 hips in 57 patients (47 women and 10 men), mean age 26(range 11-49 years), 37 right and 37 left. The preoperative diagnosis comprised: 54 dysplastic hips, and 20with varying degrees of arthrosis (classified according to Tonnis in three grades).Seventy-two cases were operated according to Wagner’s type I and two cases with type III osteotomy. Twochanges have been made to the original technique: the first is the use of Kirschner wires for synthesis of theosteotomy, and the second a convergent osteotomy in cases with lateral subluxation in order to medializethe center of rotation of the head.We assessed clinical parameters (degree, site and occurrence of pain, hip mobility, Trendelenburg sign and limp),and radiographic variables (CE angle, joint ratios, morphology of the acetabulum and head, articular rim), be-fore and after surgery, classifying the patients as dysplastic or arthritic. Complications were recorded.Fifty-five patients (72 hips) were followed up for a mean of 9.5 yrs (range 5-17 years); one was lost to follow-up, and one died in a traffic accident.

S61
The review of cases operated according to Wagner shows that the method achieves satisfactory terapeuticeffects with an acceptable rate of complications.The treatment, when indicated for pure dysplastic hips with acetabular deficiency, achieves better resultsthan when an osteoarthritic process is in progress.
Total hip arthroplasty in rheumatoid arthritis
F. TURBACCI, M.F. CAPORALE, G. MAGLIOCCHETTI, D. DALL’ACQUA
Institute of Orthopaedic, Sacro Cuore Catholic University, Roma - Italy
The hip joint is not an early affection in rheumatoid arhritis. However, once the hip is involved, the symptomsquickly worsen.If the initial treatment fails, the patients have to undergo a total hip arthroplasty, cemented oruncemented. The planning must take into account the associated eventual deformity and the quality of thebone left. When wide bone loss had taken place, it is highly necessary to use bonegrafts.Between 1988 and 1996, 20 patients with rheumatoid arthritis underwent total hip arthroplasty: 12 hips hada cemented implant and 8 an uncemented implant. The age of patients ranged from 34 to 68 years (average47 years). The average follow-up was 5 years and 4 months. The average Harris hip scores were 84 for thecemented implants and 55 for the uncemented, respectively. The incidence of migration of the acetabularcomponent (4 cases, 2 in the cemented and 2 in the uncemented hips) was not affected by compenent fixa-tion.The authors’ first choice would be the uncemented prosthesis, particularly when the joint geometry or thebone deficiency do not allow a correct positioning of the components.
Megaprosthesis of the hip and proximal third of the femur for primary andsecondary oncological pathology: personal experience and improvementsin reconstructive techniques
M.A. ROSA, A. LAUDATI, M. GALLI
Institute of Orthopaedics, Sacro Cuore Catholic University, Roma - Italy
Morphological and structural alterations to the hip joint are frequent complications in patients with primaryor secondary bone tumors. The hip is usually involved. The orthopedic surgeon treating patients with exten-sive primary and/or secondary tumoral bone lesions seeks to restore the continuity of the skeleton and tosave the limb. Often amputation can be avoided by resection with ample margins, followed later by recon-struction with modular prostheses. Besides ensuring a better prognosis, this method achieves good func-tional recovery, leaving the hip joint function.Surgical criteria for resection must always take into account the need for radical intervention, because am-ple margins are essential to minimize the rate of local recurrences. Using modular prostheses long bone seg-ments can be rebuilt to the same length of the other limb. Using modern hip implants the surgeon can large-ly restore the joint’s physiological range of movement. This immediate improvement gives the patient an eas-ier social life, and his overall quality of life.The main complications with a megaprosthesis are mobilization breakage infections, and recurrent tumor. Theexperience regards 22 modular prostheses used for reconstructive techniques, in patients with extensive neo-plastic lesions of the hip joint, followed for up to eight years after surgery.

S62
Finite element analysis applied to bone remodelling in revision arthroplasty of the femur using morselized allograft and cement
J.P. SIMON 1, J. VANDER SLOTEN 2, R.VAN AUDEKERCKE 2, G.VAN DER PERRE 2, R.S.M. LING 3, G.A. GIE 3, G. FABRY 1
1 Department of Orthopaedics, Faculty of Medicine, University Hospital Pellenberg, Katholieke UniversiteitLeuven - Belgium
2 Division of Biomechanics and Engineering Design, Faculty of Applied Sciences, Katholieke Universiteit Leu-ven - Belgium
3 Princess Elizabeth Orthopaedic Hospital, Exeter, Devon - England
ABSTRACT: Finite element models have extensively been developed and reported for primary cemented anduncemented total hip replacement, but not for revision arthroplasty of the hip. A two-dimensional equivalentthickness model was developed of the proximal femur with bone grafts, a thin but uniform cement layer and astandard femoral component. This model represents the reconstructed femoral revision setting described byGie et al (1). The effects of surface texture, cement-stem friction, cement creep and stem malplacement wereevaluated. Within the range of coefficients of friction which was investigated in this study (0.03, 0.136 and 0.3)it was observed that the influence of the value of the coefficient upon the stresses in the bone-implant struc-ture are less than 5%. Also static cement creep and certain stem malalignments which were simulated showeda relatively small influence upon the stress distribution within this structure. An agreement between trabecu-lar orientations in the remodeled bone allograft and the principal stress orientations in this structure was ob-served in the calcar region. It was concluded that the remodelling which occurs in the bone allografts followsWolff’s law of optimal material use in the trabecular structure. (Hip International 1998; 8: 51-61)
KEY WORDS: Finite element analysis, Revision arthroplasty, Allograft
Proximal cementing for revision hip arthroplasty
J. ALFARO-ADRIAN, R.W. CRAWFORD, A. WULKE, D.W. MURRAY, P. MCLARDY-SMITH
Nuffield Department of Orthopaedic Surgery, University of OxfordNuffield Orthopaedic Centre - Oxford - UK
ABSTRACT: We report the results of a new technique of proximal cement fixation in 41 patients having revi-sion hip arthroplasty using the Oxford modular femoral component. This consists of two parts, a metaphisedwedge and a stem. The metaphyseal wedge is cemented and applies the load proximally to encourage bonehealing. The wedge is free to slide on an uncemented stem that gains fixation distal to areas of bone loss,with the intention of reducing the risk of fracture. The clinical and radiographic follow-up ranged from a min-imum of 3 years to 7 years. There have been no re-revisions. Ninety percent of the patients had pain or slightpain. Despite a relatively high rate of early subsidence, we feel that our results are encouraging, and justifythe continued use of this component in hip revision surgery. (Hip International 1998; 8: 62-9)
KEY WORDS: Revision hip arthroplasty, Proximal cementing, Modular hip
S63
Osteonecrosis of the femoral head (Part 1)
Early pathophysiology of osteonecrosis
J.P. JONES, Jr.
Diagnostic Osteonecrosis Center and Research FoundationKelseyville, California - USA
ABSTRACT: Current concepts regarding the early pathophysiology of osteonecrosis (ON) are reviewed. Trau-matic ON appears to result from arterial severance, an acute ischaemic event. Intravascular coagulation ofthe intraosseous microcirculation (capillaries and venous sinusoids) progressing to generalized venous throm-bosis, and less commonly retrograde arterial occlusion, now appears to be the genesis of nontraumatic ON.However, a coagulopathy is only an intermediary event, which is always activated by some underlying aetio-logical risk factor(s). Conditions capable of triggering intravascular coagulation include familial thrombophil-ia (resistance to activated protein C, decreased protein C, protein S, or antithrombin III), hyperlipaemia andembolic lipid (alcoholism and hypercortisonism), hypersensitivity reactions (allograft organ rejection, immunecomplexes, and antiphospholipid antibodies), bacterial endotoxic (Shwartzman) reactions and various viralinfections, proteolytic enzymes (pancreatitis), tissue factor release (inflammatory bowel disease, malignan-cies, neurotrauma, and pregnancy), and other prethrombotic and hypofibrinolytic conditions. In order to ex-ceed the ischaemic threshold and produce ON, significant residual fibrin-platelet microthrombi must remainwithin the intraosseous vasculature for a minimum of two to six hours, and not be immediately removed byendogenous fibrinolysis. Hypofibrinolysis with increased plasminogen activator inhibitor has been found inpatients with ON. The thrombotic threshold may be decreased in those hypercoagulable patients with hered-itary thrombophilia, antiphospholipid antibodies, or hyperlipaemia. Subsequent exposure to an additional fac-tor should facilitate intraosseous thrombosis and ON. It is also conceivable that fractional subchondral ONcan cause both degenerative disc disease and “primary” osteoarthritis of aging and obesity. (Hip Interna-tional 1998; 8: 71-9)
KEY WORDS: Pathophysiology, Osteonecrosis, Coagulopathy, Hyperlipaemia, Thrombosis, Revasculariza-tion, Hypofibrinolysis, Thrombophilia
Histomorphology-correlated imaging of osteonecrosis
S. HOFMANN 1, M. URBAN 2, J. KRAMER 3, H. PLENK4 Jr .
1 Dept. Orthopaedics, Danube Hospital, Vienna2 Radiology Dept., Danube Hospital, Vienna3 MR-Institute, University Vienna and Inst. for CT and MRI, Linz4 Dept. Biomaterial Research Lab, Inst. of Histology and Embryology Univ., Vienna - Austria
ABSTRACT: Early diagnosis and proper staging is of crucial clinical importance for osteonecrosis (ON). Tobetter understand the different imaging patterns, the underlying pathophysiological sequence has to be known.The initial stage 0 is less understood and all routine imaging modalities are negative. In stage I, the bone mar-row changes can be visualised by bone scintigraphy and MRI only, but a sufficiently effective repair mecha-nism can make the lesion reversible. In stage II an insufficient repair process demarcates the necrotic lesionfrom the viable bone. At this “point of no return” the lesion becomes irreversible and on MRI the demarca-tion border appears as a “reactive interface” with a “double-line sign”. In this early stage II plain radiographs

S64
and computed tomography (CT) are normal or show only non-specific changes. In the late stage II the insuf-ficient repair process leads to typical patchy subchondral radiolucencies mixed with sclerotic changes in thenecrotic area surrounded by a sclerotic rim on radiographs and CT. In stage III the repair mechanism and theloading stress produce the subchondral fracture which can be best visualised as a “crescent sign” by radi-ographs or CT. In stage IV mechanical instability leads to flattening of the femoral head followed by late sec-ondary joint destruction. Nevertheless in ON plain radiographs remain the first diagnostic step and allow ex-clusion of most of the differential diagnoses for hip joint pain. However, CT is very helpful for early detectionof a possible subchondral fracture. Although bone scintigraphy is very sensitive in the early onset of the dis-ease, it remains non-specific in most of the cases. MRI is the modality of choice for a proper diagnosis andstaging in early ON. (Hip International 1998; 8: 80-91)
KEY WORDS: Osteonecrosis, Histomorphology, Imaging, Postphysiology, Staging
Natural history and conservative treatment of osteonecrosis (ON) of thefemoral head
B. MAZIÈRES, M. LAROCHE, A. CANTAGREL
Department of RheumatologyUniversity Hospital of Rangueil, Toulose - France
ABSTRACT: Until now the natural history of nontraumatic osteonecrosis of the femoral head (ON) has beenpoorly understood. The spontaneous course of ON with radiographic changes (even asymptomatic) is re-garded as poor with progression in 50-80% of the cases within two years. In contrast, stabilisation or dis-appearance of the lesions on MRI can occur in early ON with normal radiographs (stage 1), leading to the de-finition of a purely “magnetic ON”. Furthermore MRI allows us to study the volume of the necrotic area, whichseems to be the most important prognostic factor in early ON. If this volume is less than 20% of the femoralhead, the percentage of spontaneous progression is very low. The natural history of ON, especially in the ear-ly onset of the disease, has been redefined by MR imaging studies.Conservative treatment in ON is generally regarded as not very successful. Discontinuing weightbearing hasshown to be ineffective in numerous studies. Pulsed electromagnetic fields have given promising results insome studies, but the value of this approach is still controversial. Vasoactive drugs have been shown to re-duce pain significantly in ON and there might be a possible role for treating early cases. Some other ON dis-ease modifying drugs may be helpful in carefully selected patients in the future. Nevertheless so far no con-servative or surgical therapeutic method has been shown to heal the necrotic lesion. Therefore prevention isthe only way which may prevent collapse in patients with a high ON risk, other than treatable aetiological fac-tors. (Hip International 1998; 8: 92-8)
KEY WORDS: Osteonecrosis, Femoral head, Natural history, Conservative treatment
The steps in the evaluation of a new implant - from the inventor to theorthopaedic community
K. LUNSJÖ
Department of Orthopaedics, Helsingborg Hospital, Helsingborg - Sweden
ABSTRACT: New implants are constantly being introduced to the orthopaedic community. Their steps from

S65
invention to general clinical use vary. Some devices have not been evaluated scientifically, others have under-gone assessment in case series, and a few have been critically reviewed in randomized controlled trials. The rea-sons for these variations are discussed and a practical example is presented. (Hip International 1998; 8: 102-4)
KEY WORDS: Randomized controlled trials, Evaluation, Case series
Short to medium-term results with two types of proximally porous-coatedlong-stemmed femoral components in revision surgery
E. GARCIA-CIMBRELO, J. CORDERO, J. ALONSO-BIARGE
Orthopaedic Department, Hospital La Paz, Universidad Autónoma de Madrid - Spain
ABSTRACT: Results using 30 long-stemmed femoral components in revision surgery were analyzed. Therewere 15 PCA (Howmedica) and 15 BIAS (Zimmer). The mean age was 50 years (range, 23 to 65 years) for thePCA group and 61 years (range, 35 to 75 years) for the BIAS group. The mean follow-up was 5.2 years (range,2.5 to 10 years). Using the Endoklinik classification, there were 2 cases of Grade 1 bone defects, 16 casesof Grade 2, and 12 cases of Grade 3. Morcellized graft was used in 21 cases. A Kaplan-Meier survivorshipanalysis was carried out. The probabilities of re-revision, clinical failure, and loosening were 23%, 32% and80% at eight years. Subsidence was very common, with means of 15mms in the PCA group and 19mms inthe BIAS group. In the grafted cases, minor resorption was found in 17 cases and major resorption in 4 cas-es. Because of the frequency of poor results using these prostheses, due to failure to obtain bone ingrowth,even in femora with a good bone stock, we do not recommend their use in revision surgery. The results forthe PCA and BIAS group were similar. (Hip International 1998; 8: 121-8)
KEY WORDS: Total hip replacement, Revision, Cementless stem
Cement within cement revision hip arthroplasty. A minimum 5 year follow-up study
J.P. HOLLAND1, F.A. WEBER2
1 Consultant Orthopaedic Surgeon, The Freeman Hospital, Newcastle-upon-Tye - UK2 Consultant Orthopaedic Surgeon, Sandton Medi-Clinic, Johannesburg - RSA Republic of South Africa
ABSTRACT: Complete removal of femoral shaft cement during revision hip surgery is a difficult task prone to compli-cations. If the cement bone interface is intact however, is there a place for its preservation and re-use with a new ce-mented stem? The results are reported of 51 cement within cement femoral stem revisions carried out between 1984and 1991 with a minimum of 5 years’ follow-up, and a mean of 7.8 years. Excluding patients lost or deceased, 39 hipsin 38 patients were reviewed clinically and radiologically. Eighty-two percent of these were still functioning in situ,72% were excellent or good using the HSS scoring system and 97% had no radiological evidence of loosening. Femoralstem failure due to aseptic loosening occurred in 4 cases (10%) between 4 and 12 years after revision.Comparing this series to a previous revision hip series by the senior author, there appears to be no deterio-ration in long term results using this technique, and a better long term radiological outcome. (Hip Interna-tional 1998; 8: 129-37)
KEY WORDS: Cement within cement, Hip, Arthroplasty
S66
Treatment of femoral fractures associated with stem loosening followingtotal hip arthroplasty
B. ERDEMLI, I. GURKAN, B. GUZEL, I. CETIN
Department of Orthopaedics and Traumatology, Ibni Sina Hospital, University of Ankara, Faculty of Medicine,Ankara - Turkey
ABSTRACT: We report the results of Kent hip revision arthroplasties performed in 5 patients with fractures ofthe femur associated with femoral loosening following total hip arthroplasty. The fractures occurred at an av-erage of 40.4 months following the primary hip arthroplasty. The system of Merle D’Aubigné and Postel, asmodified by Charnley, was used for the clinical evaluation. One to four years (mean, 2.6 years) after the re-vision operation, the clinical and radiographic results were satisfactory. With the help of the transfixion screwsthe Kent Hip prosthesis provides stable fixation and facilitates early mobilization, with its attendant advan-tages. (Hip International 1998; 8: 138-44)
KEY WORDS: Hip arthroplasty, Femoral fracture
Osteonecrosis of the femoral head (Part 2)
Core decompression
M.E. STEINBERG
Department of Orthopaedic Surgery, University of Pennsylvania School of Medicine, Philadelphia - USA
ABSTRACT: Although there is no completely effective treatment for osteonecrosis (ON), core decompressionis one of the more popular methods used to promote healing and retard progression. However, there has beenconsiderable controversy about its safety and effectiveness. Published reports have indicated clinical suc-cess which has varied from 40 to 90 percent. We performed core decompression with supplementary can-cellous bone grafting on 406 hips with ON. There were five complications in the entire series, including twohip fractures resulting from falls. Of 297 hips with a two to fourteen year follow-up, total hip replacement wasrequired in only 36 percent of treated hips as compared to 77 percent of non-operated controls. The outcomewas correlated with both the stage and the size of the necrotic lesion. Only 22 percent of the hips with smalllesions required total hip replacement as compared to 39 percent with intermediate or large lesions. Therewas no correlation between outcome and the amount of pain present prior to surgery.Various modifications of core decompression have also been used to treat ON. These have included the useof supplementary grafts of various types, electrical stimulation, decalcified bone matrix, and bone morphogenicprotein. Early results in limited series have been encouraging, but some of those techniques remain experi-mental.At the present time we feel that core decompression, with or without bone grafting, is a simple, safe, and es-tablished technique which is our first choice for the treatment of patients with earlier stages of ON. The roleof vascularized fibular grafts is promising and the place of other new techniques is currently being evaluat-ed. (Hip International 1998; 8: 145-53)
KEY WORDS: Osteonecrosis (ON), Avascular necrosis (AVN), Core decompression, Bone grafting, Electricalstimulation

S67
Treatment of osteonecrosis: treatment by femoral osteotomy
F. MENSCHIK, K.D. SCHATZ, R. KOTZ
Department of Orthopaedics, University of Vienna, Vienna - Austria
ABSTRACT: The purpose of the use of an osteotomy for the treatment of osteonecrosis (ON) of the femoralhead is to move the necrotic segment away from the major load-transmitting area of the acetabulum and toredistribute the weight-bearing forces to articular cartilage that is supported by healthy bone. The most com-mon osteotomies are the varus, valgus, flexion, rotational (Sugioka), and combined osteotomies. Their longterm outcome, reported in the literature, is quite controversial. We found a decreasing frequency of flexionosteotomies between 1986 and 1996 performed at our department. In 1977 we started with the Sugioka os-teotomy in special cases of femoral head ON (necrotic angle in the AP-view about 90 degree) resulting in atotal of 51 cases. Forty-one of them have been analyzed regarding complications, reoperations and HarrisHip Scores. Seventeen of 41 patients developed complications and underwent reoperation. Nevertheless theresults according to the Harris Hip Score were satisfactoy (excellent and good in 24 patients fair in 10 andpoor only in 7 cases). Independently from the size of the necrosis total hip arthroplasties have been performedin 8 cases. The survival curve of 41 Sugioka osteotomies shows a 50% decrease at 6 years. Due to this factand the regression in the number of osteotomies of the femur in cases of ON of the hip joint we find in ourmaterial that the importance of osteotomies has dramatically decreased in contrast to the excellent resultsof total hip arthroplasty. (Hip International 1998; 8: 154-8)
KEY WORDS: Osteonecrosis, Femoral osteotomy, Sugioka
Treatment of osteonecrosis by joint replacement
J.W.M. GARDENIERS
Orthopaedic Surgery, Akademisch Ziekenhuis Nijmege, Nijmegen - The Netherlands
Osteonecrosis (ON) is an increasing phenomenon, because of an increasing number of transplant recipients,patients treated with corticosteroids, alcoholism, hyperlipaemia, and long term survival with a better qualityof life of patients with chronic diseases such as rheumatism, SLE or Gaucher’s disease. This means that moreand more patients with ON are younger with a longer life expectancy. It is therefore of the utmost importancethat an orthopaedic surgeon who is treating patients with ON knows the many treatment options available forthis disease. (Hip International 1998; 8: 159-66)
KEY WORDS: Osteonecrosis, Joint replacement

S68
The history of allograft
A.J. MILLER
Mayday, University Hospital, Croydon - UK
The history of allograft goes back to antiquity. The patron saints were Cosmos and Damian, twins born in Silicia who weresaintly doctors practising in Syria. They performed many miracles while alive and were beheaded in a.D. 287 by the Ro-man Emperior Dioclecian. After torment, which included being whipped, thrown off a cliff and attempts to burn them andfire arrows at them, they were given the honour, in those days only afforded to Roman citizens and that was to be de-capitated by the sword. They performed their most famous miracle, the miracle of the black leg, posthumously 300 yearslater. A church warden was dying of gangrene in a crypt in the Basilica in Rome, in his sleep the two saints arrived, am-putated the leg and replaced it with the leg of an Abbysinian who died the same day. This is the first recorded allograft.In 1668, Jon van Meekeren grafted a soldier’s cranium with bone from a dog’s skull. This is the first record-ed xenograft. In the 17th and early 18th century Ollier and others studied the structure of bone and callousand in the 19th century Phemister talked about creeping substitution.In 1820 Philip von Walter described the first clinical autograft, reconstructing the skull of a patient following trephining.In 1880 W. MacEwan from Scotland performed the first recorded modern allograft, reconstructing an infect-ed humerus of a four year old boy, doing it with a tibia from a child, presumably that had died of rickets.In 1915 Albee talked about autogenecity of bone grafts and grafting.Coming more up to date, Harris from Boston in 1980 wrote “The inescapable crucial element in reconstruc-tion of a failed hip replacement is bone. The problem is of mounting frequency and usual complexity and in-creasing importance”. He performed a series of bulk allograft operations which took him a great length oftime, on average six and a half hours, caused a great amount of blood loss and with multiple complications.He noted however that all the grafts united and this did make subsequent operations easier. He eventuallyconcluded that the procedure was untenable because of the high complication rate and the fact that some50% of the acetabular component became loose over a period of ten years. Subsequent operations of fur-ther revisions were of course then more easy as the bone was of better quality and substance.
Development of bone banking in the United Kingdom
R. VILLAR
Addenbrooke’s Hospital, Cambridge - UK
Musculoskeletal transplantation is a big business, with more than 300,000 procedures being annually performed in theUSA, 25,000 annually in Germany. The ideal musculoskeletal transplantation service requires three things: (1) Donor, (2)Recipient, (3) Somewhere to store the tissue. The storage and acquisition of tissue in the United Kingdom has, until re-cently, been a cottage industry affair. There is an “opt in” donor policy, rather than an “opt out”, with donors now in veryshort supply. Nationally, the major source of bone is the femoral head taken at hip replacement. Cadaveric sources pro-vide greater quantities, and are more predictable. Contamination is a problem, with more than 35% of specimens beinglost in the early days of bone banking. Sterilisation is now widely undertaken, using irradiation, ethylene oxide, auto-clavation, and other methods. It is essential to adhere to strict ethical guidelines whilst eduction of staff is vital. Bonebanks are at variable temperatures. The lower the temperature the longer tissue may be stored. Banks should be lock-able, with access limited to key staff members. Ideally, a bone bank should be managed by professionally-trained staff.
ABSTRACTS FROM II MEETING OF THE ANGLO-ITALIAN REVISION HIP GROUP - CROYDON, UK,10-11 OCTOBER 1997 (HIP INTERNATIONAL 1998; 8: 167-85)
S69
The management and problems of bone banking and sterilisation
J. FOREMAN
East Anglia Tissue Bank, Tissue Services, NBS, London and South East Zone - UK
The increased need for tissue together with more stringent donor selection criteria, virology screening, quar-antining and storage of tissue has led, in recent years, to the establishment and development of purpose builttissue banks.Prior to this, in the United Kingdom, the banking of bone was mainly carried out in Orthopaedic Departmentswith individual surgeons collecting surgical bone and storing it for their own use in a –20°C freezer. A work-ing party of the British Orthopaedic Association, in 1992, recognised that this “cottage industry” approachshould be abandoned and that a centralised scheme be administered through the Blood Transfusion Serviceor equivalent organisation.Although the Blood Service has no formal national role in the co-ordination of bone banking, many centreswithin the Service are active in bone banking, indeed in Scotland this activity is carried out exclusively with-in the Blood Service.There are many good reasons for basing tissue banks within a Blood Centre. The Service has establishedlinks with hospitals and has gained a professional confidence in its activities, particularly among surgeonswho will also use the services of a bone bank. The Service has medical/technical expertise in donor selec-tion, microbiology, quality control/assurance and data handling and although the procedures may be differ-ent the need for this experience is as great for tissues as it is for blood.Having said this there are, in this country, experienced and respected tissue banks operating outside the Na-tional Blood Service.The East Anglia Tissue Bank, based in the Blood Centre in Cambridge, began operations in 1993 providing aservice for the procurement, processing and issue of bone and heart valves. Skin has recently been addedto the tissues that can be provided. The Bank also provides support to the Regional Bone Marrow TransplantProgram by the cryopreservation and storage of cells. The North London Tissue Bank, part of the North Lon-don Blood Centre, was established in 1994 for the procurement, processing and issue of bone, cord bloodcollection and storage and bone marrow/PBSC cryopreservation. In 1996, following reorganisation within theBlood Service, the two banks amalgamated to provide an integrated tissue service.Some bone banks only store and supply surgical bone removed during primary hip operations and femoralcondyles and tibial plateau from knee operations. In the United Kingdom, the majority of bone banks providethis service. There are, currently, five banks which also collect bone from cadaver donors and, therefore, areable to provide tissue for a wider range of applications. All banks are involved with procedures related todonor selection, procurement, testing, storage, documentation and issue of tissue but not all process thebone to produce individual tissue grafts.Individual surgeons vary in their requirements for bone graft material, for example, some prefer to use un-processed femoral heads for their revision surgery while others opt for washed, ground, frozen or freeze-driedtissue. Processed bone does offer some advantages: through various washing stages and subsequent ter-minal sterilisation of the bone the risk of bacterial contamination is virtually eliminated, a reduction in thewastage of bone by the appropriate graft being provided for each operation, grafts are more easily trans-ported and there is a reduction of time spent in theatre. Washing the bone and removing blood and marrowfrom a graft will reduce the possibility of HIV transmission and other viral transmissions.Prior to collection of tissue, consent is obtained directly in the case of a living donor and through the next ofkin for cadaver donors.Selection of a donor with a minimal risk of transmitting disease to the recipient is one of the major responsi-bilities of the tissue bank. Suitability of the donor should be determined by means of the medical history re-view, physical examination and laboratory screening which must include testing for HIV 1 and 2 antibodies,hepatitis B and C and syphilis. Nurse co-ordinators are employed by tissue banks whose role is to carry out

S70
the consent procedure and obtain the medical information relating to a donor. This may be done by a combi-nation of interview and referral to hospital notes and GPs. In the case of cadaver donors, when a post mortemis being performed a copy of the report will be requested. In addition, the Department of Health requires thatliving donors are retested, for HIV and hepatitis, at least 180 days following donation.Bone is stored, in a quarantined tissue freezer, at –80°C, pending a review of the medical history and labo-ratory tests by a Medical Officer of the tissue bank.It is standard practice, in this country, to terminally sterilise bone that has been processed to minimise therisk of bacterial contamination of allografts. Many methods of sterilisation have been used. The most frequentmethods currently used for sterilisation include heat, ethylene oxide and gamma-irradiation.Heating bone above 60°C will denature and degrade collagen which affects the biomechanical properties ofthe bone. Boiling bone will result in a loss of osteoinductive properties. Recent interest in the use of heat hasfocused on the fact that HIV is known to be inactivated by heat. However, hepatitis B is known to be muchmore heat stable. Ethylene oxide has been shown to be an effective method for sterilising bone allografts.There have been conflicting reports regarding residual amounts of ethylene oxide, ethylene chlorhydrine andethylene glycol remaining in the tissue. In our experience there are no detectable residues following a steril-isation and aeration cycle. There is insufficient evidence to comment as to whether ethylene oxide impairsthe osteoinductive capacity of bone. Ethylene oxide sterilisation is used following the freeze-drying of bone.Gamma-irradiation has been reported to affect the osteoinductive and biomechanical properties of bone.However, this effect has been shown to be dose-dependent. Most banks use an irradition dose of 25 kGy, alevel that is used for catheters and implant materials. It has been shown that doses in excess of 60 kGy arerequired to eliminate HIV virus; at this level bone becomes brittle and unsuitable for clinical use. Gamma-ir-radiation should therefore only be considered for bacteriological sterilisation of tissues. Lower doses of irra-diation should therefore be employed to irradicate likely levels of bacteria and fungal infection, thereby fur-ther reducing the effect of irradiation on the properties of bone.Standardisation of procedures has become more widespread with the stablishment of guidelines from tissuebanking organisations; in this country the British Association of Tissue Banks produced a Technical Manual forMusculoskeletal Tissues in 1996. However, membership of tissue banking organisations and therefore adher-ence to standards is voluntary. In 1996, the Committee on Microbiological Safety of Blood and Tissues for Trans-plantation (MSBT), on behalf of the Department of Health, published guidelines to minimise the risk of trans-mitting disease through tissues and organs. The tissue banking community would welcome and recognise someform of regulation is necessary for the future. The Department of Health has recently conducted a review of tis-sue banks in the United Kingdom and we await the outcome and regulation of some tissue banking activities.
Strength of allograft
A.J. HAMER, R.A. ELSON, I. STOCKLEY
Northern General Hospital, Sheffield - UK
The use of allograft bone in revision arthroplasty surgery is now regarded by many as being standard surgicalpractice. However, there are many, unanswered questions.One of the main dilemmas is: should bone be secondarily sterilised? Doing so allows for the retrieval of bonefrom a semi-sterile bone harvest. Femoral heads with positive bacteriology swabs can be sterilised ratherthan be discarded. However, there are conflicting reports concerning the effects of the material properties ofcortical allograft bone on gamma-irradiation.We used a new method of comparative bone strength measurement to investigate the effects of irradiation atstandard dose (28 kGy) on 233 bone samples from 6 patients. We also investigated the effects of increasingdoses from 6.8 to 60 kGy (n = 132). No treatment had any effect on the elastic behaviour of the samples, butthere was a dose-dependent reduction in strength and plastic deformation. The plastic properties of bone re-
S71
late to the composition of the bone matrix. We therefore examined bone collagen in two ways to determine theeffects of gamma-irradiation. Collagen crosslinks are responsible for the maintenance of collagen’s structur-al integrity in vivo. Pyridinoline (Pyr) and deoxypyridinoline (Dpyr) are stable, mature crosslinks. High perfor-mance liquid chromatography was used to determine Pyr and Dpyr concentrations in the bone collagen. Therewas no difference in the crosslink concentration between control and irradiated groups at 28 kGy, but therewas a reduction in Pyr and Dpyr of 12% and 13% respectively, at 60 kGy (p < 0.01). Increasing doses of irra-diation led to a rise in the percentage of denatured collagen. This suggests that embrittlement of bone is pri-marily due to damage to the collagen triple helix or alpha chains, which is dose-dependent, and that at high-er doses crosslink damage occurs.In clinical practice, as long as the allografts are subject to “normal” loadings and loading rates, so that theloads are within the elastic region of their behaviour, and then graft collapse or fracture will probably not oc-cur. High bending loads applied to cortical struts, for example, should be avoided, as this mode of loadingmay exceed the elastic limit of the graft in bending. The biological behaviour of such large allografts is poor-ly understood, and it is not yet clear how radiation affects graft incorporation.
The Italian experience of bone banks with frozen femoral heads
G. ANARRATONE1, P. BARTOLOZZI 2, P. CHERUBINO 3, F. PIPINO 4, V. SALVI 5
1 Gradenigo Orthopaedic Hospital, Turin - Italy2 Clinica Ortopedica, University of Verona - Italy3 Clinica Ortopedica, University of Varese - Italy4 Clinica Ortopedica, University of Genoa - Italy5 Maria Adelaide Orthopaedic Hospital, Turin - Italy
The purpose of this contribution is to present the experience made by a group of Italian orthopaedic centreswith bone banks using frozen preserved femoral heads.A questionaire consisting of the statistical data reported below has been sent to each member of the G.I.R.(Gruppo Italiano di Riprotesizzazione).Five orthopaedic centres have replyed: three were university centres and two were hospital centres.
The technique of taking allografts and preserving themThe femoral head is taken at primary hip arthroplasty. Donors selection follows a protocol established in 1990by the Italian Society for Orthopaedics and Traumatology.The most important points to emphasize are:- donors should respond to the anamnestic criteria established by the American Association of Tissue Banks;- serology tests in donors have been done as follows: Rh, HBV, HCV, HIV, VDRL. The HIV test is repeated six
months after taking the head: only after this test should the head be used.- the heads are obviously taken in the strictly aseptic conditions guaranteed by the operation; specimens
from the head are taken for aerobic and anaerobic culture.- the heads are stored in double sterile glass jars and preserved in a freezer whose temperature varies from
–73 to –80°C.
Statistical dataThe oldest experience started 16 years ago (Clinica Ortopedica - Genova), the most recent one year ago (Clin-ica Ortopedica - Verona). Statistical data concerning the figures for the harvested, used and eliminated headsper year are shown in Table I.
S72
Table I
min 25Number of heads harvested per year: average 77 max 160Percentage of heads used per year: 70%Percentage of heads eliminated per year: 2% - 5%
Use of allograftsWhen implanted, the femoral head allografts have been used in the following way: head en bloc, head en blocdecorticated, morselized mixed cortical and cancellous, and morselized cancellous. Morselized allograftshave been the most frequently used. The use in different types of surgery is reported in Table II.
Table II
Hip revision 60% - 90%Bone tumour 5% - 25%Various 6% - 25%Knee revision 3%
ComplicationsNone of the users had major complications: particularly no local infections related to the allograft or trans-mission of general infection have been noted.
Graft integrationNo specific clinical investigations have been done in this study to find out the integration of the allograft.The surgeons have been asked however to give their impressions about the capacity of osteointegration ofthe allograft: 70% - 100% of morselized grafts are considered to have the capacity to integrate with the hostbone.
ConclusionsWe believe that this study may allow the following conclusions:- a bone bank preserving in freezer femoral heads harvested in primary hip arthroplasty covers widely the
needs of any orthopaedic centre doing joint revision surgery or bone tumour surgery;- it is safe regarding local and general infections;- the morselized allograft seems to have high rate of osteointegration.
Massive allografts in femoral reconstruction
R. VILLAR
Adderbrooke’s Hospital, Cambridge - UK
There are many ways to reconstruct a femur at revision surgery. Massive allografting, initially used for tumoursurgery, has its place in the orthopaedic armamentarium, though it relies on the existence of a well-run tissuebank. Massive grafting is often used in conjunction with other techniques, e.g impaction grafting or customcomponents. Massive grafts are classified as: (1) Strut, (2) Calcar, (3) Proximal femur. Reconstruction is per-formed in two phases: (1) Distal fix, (2) Proximal reconstruction.The ideal recipient should be emotionally and physically stable before surgery: treat the patient, not the x-ray.Surgery requires two operators: Operator 1 - recipient preparation; Operator 2 - graft preparation. Results for

S73
47 consecutive cases performed for aseptic loosening are as follows: Union rate 94%; Infection 4%; Disloca-tion 6%; Revision rate at four years 15%; Fracture rate 0%; Mean operating time 3.4 hours. Massive allo-grafting is a demanding, yet useful addition to the revisionist’s repertoire.
Impaction grafting
R. LING
Princess Elizabeth Orthopaedic Hospital, Exeter - UK
Impaction cancellous grafting was first reported by Professor Tom Slooff and his colleagues from Nijmegenin 1984 in relation to the management of primary acetabular protrusio and acetabular protrusio secondary tofailure of total hip arthroplasty.The first case of femoral impaction grafting done in Exeter was carried out in 1985. In this case, cement wasnot used. Though the patient was relieved of her symptoms, the femoral component subsided gradually in-side the graft. She refused further surgery. Impaction grafting in the femur with cement was first performedat the Princess Elizabeth Orthopaedic Hospital of Bone and Joint Surgery in 1993. Since then, over 400 im-paction graftings with cement have been done at the Princess Elizabeth by multiple surgeons. The indica-tions for the operation are not yet fully established, since, although one can be confident of a satisfactory re-sult in a case with moderate to severe bone stock loss, increasingly complex cases are now being under-taken and for these the longer term outlook is uncertain. The x-ray appearances that are frequently seen aredemonstrated in these five cases and the appearances that one may see with a more severe type of problemare demonstrated in these two cases.The technique of the operation is in evolution and in the original cases done at the Princess Elizabeth thetechnique was crude without dedicated instrumentation. Dedicated packing instruments are now available toimprove the stability that can be achieved of the new implant and also the reproducibility of the operation.It is important to emphasise that stability in impaction grafting is achieved first of all by containment of thegraft and secondly by impaction of the graft. It cannot be over-emphasised that satisfactory results in thisprocedure depend on attention to the details of the operative technique.The primary key to a satisfactory operation is exposure. This procedure cannot be performed through a lim-ited exposure and trying to do this greatly increases the problems that one may encounter with, for example,intra-operative fracture of the femur, so exposure is the primary key followed by the establishment of con-tainment for the graft and then impaction of the graft. The aim is to achieve stability and a bone-coated im-plant.In the acetabulum, the basis for producing containment is to convert segmental defects to cavitary defectsby the appropriate use of wire meshes and then, once having produced the cavitary defect, simply to impactthe graft vigorously in the usual way and then fix the new cup in position using acrylic cement, aiming to bringthe cup down to the original anatomical position by adequate use of graft. Similarly, in the femur, areas of di-aphyseal bone loss, wherever they are, are dealt with using femoral meshes applied appropriately and fixedwith cerclage. For segmental diaphyseal defects, cables must be used rather than cerclage wire. Impactionand cementing then follows, utilising pressurisation techniques.As far as the latest results are concerned from the original series from Exeter, the follow-up now in these cas-es is between 6 and 9.5 years. There are 2 or 3 patients who, if they had survived, would have now exceed-ed 10 years. The average age to operation was 67, the range being 46-85. The original report was in 1991 on56 survivors and we now report on 42 who are alive though 3 have not yet been seen. Thirty-nine have beenexamined so far and the x-rays of 44 have been seen. The clinical assessment of these patients has beencarried out by Dr. Lars Linder from Gavle in Sweden.From the technical standpoint, it is important to recognise that no special instrumentation was used in thesecases. The technique was basically freehand. The grafts were all fresh frozen femoral heads that were un-

S74
washed. There were 11 different operators and 10 of the patients were under the age of 60 at the time of op-eration. Graft impaction was achieved by plug sizers distally and by using oversized trial stems proximally.Since 1991, more patients have moved from category A to category C as might be expected with advancingyears, but the clinical gradings for pain and function have changed very little since 1991. Twenty-one out ofthe 39 patients are graded 6 for pain, i.e. are totally pain-free and 10 out of 39 are graded 5 for pain.As far as the x-ray analysis is concerned, radiolucent lines continue to be very uncommon and are really on-ly seen significantly where the graft packing has been so bad as to allow the cement to go right through thegraft to the endosteal surface of the femur. Subsidence of the stem within the cement occurs when utilisingstems of the Exeter type and may be important as far as loading the graft is concerned. Subsidence haschanged very little in the last 3 years. Cortical healing was seen in 34 cases, trabecular incorporation in 33,trabecular remodelling in 23, no change in 4 and failure in 1 patient though this is a radiological failure andto date is not a clinical failure; this patient actually had an intra-operative fracture which was rather inade-quately fixed and she now has a fibrous union but is entirely asymptomatic. No patient so far has shown en-dosteal bone lysis and no patient has been re-operated on for recurrent aseptic loosening. Some more x-rayexamples are shown.The complications include 2 intra-operative femoral fractures, 1 femoral component that was driven out throughthe shaft of the femur at the original operation (this was corrected a month later and the patient had no fur-ther trouble), and 3 dislocations of which 1 required open reduction and 1 post-operative femoral fracture.There were in addition 1 CVA post-operatively and 1 case of DIC.There have been 5 re-operations to date: 2 for femoral fracture non-unions, 1 open reduction of a disloca-tion, 1 malposition of the stem and 1 re-revision of a socket that was unfortunately originally revised with ametal-backed cup.The major problem after this procedure is post-operative femoral fracture. There are 11 cases to date out ofall those that have been done in Exeter. These patients are usually elderly, with lysis near the tip of the stem.We know now that this complication can be prevented by either reinforcing the femur with a plate or a strutgraft or using a longer stem or a combination of these three, so that this complication is likely to be muchless common in the future.In conclusion, what can be said is that the clinical and radiological results have been maintained to date inthe original series. There is an enormous amount to be learned about the basic biology of this operation andat the moment its limitations are uncertain. It is certainly technique-sensitive. Overall, an attitude of guard-ed optimism is justified for the future.
The cement mantle with impaction grafting: an in vitro study
J.W.S. TICE, S.H. BRIDLE
St. George’s Hospital, London - UK
The use of impaction bone grafting with a cemented femoral stem is one method of revision to restore bonestock. The cement and bone graft are not clearly distinguishable on the radiographs so it is impossible to as-sess the integrity or thickness of the cement mantle. The aims of this study were: 1) To look closely at thecement mantle and its interface with the bone graft; 2) To establish which impactor size gives a completemantle of at least 1 mm thickness.Method: Impaction grafting procedures were carried out on plastic model femurs using milled cancellousbone, cannulated impactors, low viscosity cement and plastic dummy Protek MS-30 prostheses. We usedfour different set ups with the impactors, which come in sizes identical to the stems: a) oversize by one, b)oversize by two, c) as a + overinsertion by 1 cm, d) as b + overinsertion by 1 cm. The femora were then sec-tioned longitudinally and transversely into 8 mm slices which were inspected microscopically and measure-ments made to give a maximum, minimum and mean cement mantle thickness for each Gruen zone.

S75
Results: In all femora the cement mantle was complete with no significant voids or displaced graft. There wasgood bone cement contact at the interface with micro-interlock of 1-2 mm. The most uniform mantle with ad-equate thickness in all zones was achieved with setup b. There was no advantage in overinserting the im-pactor, as this led to proximal collapse of the graft.Conclusions: In our model a complete cement mantle without voids was consistently achieved. The mantletended to be thicker in the mid zones, probably due to poor impaction. The use of the impactor two sizeslarger than the prosthesis resulted in a mantle thickness of at least 1 mm throughout. The apparent need touse an impactor larger than anticipated is partly due to the elasticity of the morsellized bone.
Allograft reconstruction of the acetabulum in revision of total hip arthroplasty
M.F. CAPORALE, F. TURBACCI, G. MAGLIOLOTTI LOMBI
Istituto di Clinica Ortopedica, Università Cattolica S. Cuore, Roma - Italia
Revision surgery of the acetabulum may be extremely easy, but is often extremely difficult and requires a longsurgical procedure.There are essentially three objectives, all related:1. to implant a new acetabulum with good primary stability, required for secondary stability;2. to re-establish a centre of rotation that is as physiological as possible, required for good range of motionand correct load transfer;3. to reintegrate “bone stock”, that is often severely impoverished.We are supporters of cementless revision surgery and it is our belief that loss of bone tissue must only bereintegrated with bone tissue, auto- or allografting, associated with methods aimed at facilitating regenera-tion by using material such as hydroxyapatite or bioglass, perhaps even BMP in the future. We also believethat it is a good rule to minimize the use of metal instrumentation that could alter local trophism that is al-ready compromised. The bone graft must not cover more than 40% of original acetabulum. We use bone graftin three forms: massive, morsellized and crushed. Bone graft gives a good result only if it is used correctly.This means: limited quantities and thicknesses and submitted to limited loading in compression. Allograft willhave to be positioned in an acetabulum that has previously been cleaned, and such as to provide it with rigidstability, that may secondarily be improved with screws.Thus, it will be necessary to implant large acetabula so as to obtain adequate contact with live bone and dis-tribute load on wide surfaces, reduce the thickness of the grafts, and improve the press fit.Our experience is based on 214 cementless revisions performed from 1986 to 1996. Bone grafts were usedin 141 patients (66%). There were 139 females (65%) and 75 males (35%). Mean age was 69 (range from 39to 84). The Paprosky classification of bone loss in loosened prostheses is particularly useful because it re-lates well to surgical indications.In the first 6 years we used PCA porous coated acetabulum, in the next 4 years acetabulum coated with hy-droxyapatite.We are able to observe the effectiveness of 70% of grafts after 5 years and 60% after 7 years. Also in casesof partial graft resorption clinical results are good.

S76
Acetabular reconstruction in Croydon using the McMinn stemmed aceta-bular prosthesis. An early report on a series of 103 patients
A.J. MILLER
Mayday U.H., Croydon - UK
This is a District General Hospital serving a population of 330,000 people. We perform roughly 200 hip re-placements and 100 knee replacements every year and approximately 40 revisions. One in every five opera-tions are therefore revisions and this number is increasing. The 1970s and 1980s was the era of hip joint re-placement and the 1990s is the era of the revision arthroplasty.The problems encountered are of bone loss in the femur and in the acetabulum caused either by cement dis-ease, high density polyethylene disease or possibly the rasping effect of a loose prosthesis and of course in-fection.The requirements of a revision arthroplasty are that the operation should be quick, easy, safe and repro-ducible, giving instant stability preferably without the use of cement. In practice, revision arthroplasty is time-consuming, difficult, costly and less rewarding than the primary procedure. In the past I have performed ex-cision arthroplasty which gets a surgeon out of trouble, but not the patient. I have used Müller and Schnei-der rings with bone graft and on occasions almost a cement replacement of the hemipelvis. These operationsare long, difficult and in my hands unreliable and carry the potential for early failure.The operation I propose to talk about was developed by Derek McMinn from Birmingham as a modificationof Peter Ring's acetabular implant. The prosthesis is inserted through a posterior approach and the most im-portant instrument is the finger, which is placed in the greater sciatic notch. Various instruments are used,but provided the finger is in the sciatic notch, penetration of the bone by the guide wire or drills will be de-tected and repositioning can be carried out. The prosthesis is inserted into the strong bar of bone which goesup alongside the sacroiliac joint. The acetabular stem I almost always use is 8.5 cm long and the cup either45 mm or 50 mm outside diameter.I have now carried out 103 acetabular reconstructions in Croydon from 1993 to 1996. Twenty-two of the cas-es have been primary and 81 for revision hips. I have used no bone graft on 23 occasions, coral on 11, morsel-lized graft on 28 and a whole head allograft on 19 occasions.The primary cases are an interesting group, which I will now demonstrate briefly. I have used the McMinnprosthesis in patients who have had acetabular fractures, patients with metastatic deposits in the pelvis, withacetabular dysplasia and protrusio, and on a patient with a fractured hip whose pin had cut out and destroyedthe superior acetabulum.As regards revisions, I have now performed 81 revisions using the McMinn prosthesis; nearly all cases hadserious bone loss.The McMinn prosthesis, with its long stem, is very suited for use with a bulk allograft, the bulk allograft be-ing a prepared whole femoral head. The technique which I developed with Professor Garosi is to prepare theacetabulum using a reamer, to match the acetabulum with a femoral head prepared to the same size and toput a McMinn prosthesis through the middle of the femoral head.I will now describe the Croydon classification of acetabular defects based on the use of the McMinn pros-thesis. Type I defect has an intact supporting rim with mild osteolysis and virtually any prosthesis can beused. Type II has a deficient rim with a ballooned acetabulum and superior and medial bone loss, but with anintact posterior column. This seems to the commonest form of acetabular defect I have come across and isvery suitable for a McMinn cup with morsellized graft. Type III has a deficient rim, a ballooned acetabulumwith superior medial and posterior bone loss and no posterior column. It is this group of patients which re-quired a whole lead allograft. Type IV is acetabular dissociation, which I believe requires at least a two-stageprocedure.The age range of my 81 revision hip replacements is from 30 to 92 years, the average being 68.9 and mostbeing female. The interval between primary and revision, on average, is 8.8 years. Many of these patients had

S77
multiple operations. The average length of stay in hospital is 12.9 days, ranging frm 7 to 59 days. The aver-age blood loss is 1.7 litres. There is not much difference in operation time or blood loss between the Wagn-er transfemoral approach and an intramedullary approach to replacing the femoral component.There have, of course, been many complications, which one would expect in this type of surgery. I have had2 deaths, one immediately post-operatively from a myocardial infarct and one at two weeks from a pulmonaryembolus.Local complications have included 2 patients with dislocation, both of which were reduced and gave no fur-ther problems. I have had 4 nerve palsies, all though to be stretching of the sciatic nerve or femoral nerve,3 of which have recovered and one, a sciatic palsy, is slowly recovering at two years. Three patients havehad fracture of the ilium, 2 united without any trouble, one was infected at revision with very porotic boneinto which the McMinn prosthesis sank and further revision proved necessary. Two patients have complainedof back pain, one because of penetration of the sacroiliac joint by the McMinn stem peroperatively, andthough her hip gives no trouble I think I may well have to revise this prosthesis. The second patient alwayshad a high stem and although the hip gave no trouble, the tip of the stem irritated one of the lumbar nerveroots and the prosthesis had to be revised. In 7 patients there has been infection. All these, I believe, wererevisions with pre-existing infection present.The only complication, therefore, that could be directly attributed to the technique of using a stemmed ac-etabular component is back pain caused by penetration of the sacroiliac joint or irritating the lumbar plexus.These complications can be avoided.In conclusion, the McMinn cup gives instant stability in the presence of massive bone loss. It allows the in-corporation of structural allograft or morsellized allograft. The insertion depends on the integrity of the ileo-pubic bar of bone. The operation is quick, easy, safe and reproducible. In my series of 103 McMinn hips Ihave had complications in 13 patients which represents some 12%. Most of the failures were associated withinfection.
Treatment of bone loss with oblong cup with or without bone graft
C. CASTELLI
Del Ponte Orthopaedic Hospital, Varese - Italy
The Authors present their preliminary experience on hip revision arthroplasty for acetabular loosening withan oblong uncemented revision cup (L.O.R., Allopro of Sulzer Orthopaedics, CH) with or without bone graft.From February 1995 to February 1997, 29 patients (34% of all revision arthoplasty for acetabular looseningdone in the same period) underwent acetabular revision with this cup. Homologous bone chips graft was em-ployed in 21 up to 29 cases. No case was treated with acetabular substitution and bulk bone graft becausethe principle of this acetabular cup is to fill the defect anchoring to the host bone.No loosening or migration were observed.The mean follow-up presented here is 11.5 months.Although good clinical and radiographic results have been obtained up to now, a longer follow-up is neces-sary for a more reliable results analysis.

S78
Revision in infected cases
R.A. ELSON
Northern General Hospital, Sheffield - UK
The principles of exchange arthroplasty for infection are well known. Direct exchange is undoubtedly an op-tion giving about 80% chance of eradication of the infection and a useful function. My experience followsteaching from the EndoKlinik in Hamburg and until about 1990 the majority of our operations performed inSheffield were of this type. In broad terms we could expect a 12% failure from re-infection. We recognisedthat the failure was less likely following a two-stage exchange with an interval of several months (now muchshortened) before re-implantation: 4%. While accepting this fact the impossible comparison between a high-er failure rate and the disadvantage of two major procedures was always a problem.Two factors have led to a marked swing towards the two-stage procedure:1. The increase in resistant organisms, notably the Coagulase negative cocci which are now in many casessensitive only to vancomycin. The one-stage operation was heavily dependent upon the use of antibioticloaded acrylic cement and especially when it was possible to obtain lincomycin powder and other suitableantibiotics, we were confident of a suitable outcome with acceptable risk. Now that is not possible. Whetherwe have encouraged the emergence of resistant strains due to overuse of these agents is debatable althoughthe widening use of vancomycin for prophylaxis is of concern and perhaps unwise. Previously it was the dif-ficult group of organisms (Group D Streptococcus, Proteus, Pseudomonas) that made us cautious: now it isthe resistant Coagulase negative coccus and the likely presence of multiple strains that is the problem.2. The increased use of bone grafting for impoverished bone stock, although reports are appearing that con-firm the successful use of allograft in previously infected cases. Universally, a two-stage procedure is em-ployed, the first stage optimising the likely sterilization of the field.Many aspects remain open to question: the use of antibiotic-acrylic pellets during the interval phase, the du-ration of this interval, the place for operative histology in diagnosis, the use of antibiotic-loaded cement bothprophylactically and for second stage implantation and also the alarming prospect of our having no usefulantibiotic for the highly resistant CNS.One of our greatest problems relates to the difficulty in comparing results of management conducted in dif-ferent centres. This is being currently addressed by interested parties in the UK and perhaps our Italian col-leagues could be persuaded to co-operate in a standardisation exercise.
Strategies in revision of infected cases
K. ZWEYMÜLLER, K. PERNER
Abteilung Des Orthopadischen, Wien - Austria
Our operating procedure in early infection (1-3 months) is the x-ray-controlled aspiration, debridement, andsuction-irrigation drainage. The implants remain in situ. A polyethylene inlay in a metalbacked cup has al-ways to be changed. Antibiotic therapy has to be used up to 3 months after surgery. A good diagnostic helpis the MRI for the visualisation of soft tissue abscesses and joint effusions. In most of the cases with a lateinfection (more than 3 months post-operatively) the implants have to be removed and the hip remains as aGirdlestone resection. No Gentamycin-Palacos-beads or Sulmycin mesh etc. are used. Clinical controls, ESR,CRP as well as scintimetric controls are made. The re-implantation is performed after 3-9 months. Our aimis to use cementless implants at the revision. This gives the chance for osteointegration of the implant alsoin severe atrophic bone, provided that all bone cement and granulation tissue had been removed. Accordingto our experience there is no need for cemented refixation in the re-implantation. A one-stage revision is al-

S79
so under discussion. One of us (K.P.) has analysed a series of 26 one-stage revisions. In 12 cases the or-ganism was Staphylococcus aureus, followed by Coagulase negative Staph. and Serratia. There had been anaverage of 2.46 ranging from 1 to 13 previous operations. The average follow-up time was 44.6 months (4-101). In 6 cases an early and in 20 cases a late infection had been treated. In 16 infections a cementless andin 10 infections an implant with bone cement was revised. The necrosis’ areas are intraoperatively stainedwith methylene-blue, the debridement has been made exactly as in an oncological procedure. If necessary,a spongioplasty is performed. During three days a suction-irrigation drainage with up to 20 liters a day andbacteriological control of the irrigation fluid is the routine procedure. At follow-up in 24 cases (one patientdied, one was not available for review) there was no recurrence in 18 cases, no recurrence occured after an-other revision in 4 cases and there was a recurrence in 2 cases, where up to now no further surgery has beennecessary. These results are a good argument, that a one-stage cementless revision in infected cases couldbe a good alternative to the well-known two-stage method.
Xenograft
F.H. NORMAN-TAYLOR
Immutran Laboratories, University of Cambridge, Cambridge - UK
The immune response adversely affects bone graft incorporation. The strength of the immune response elicit-ed by a xenograft is determined by whether donor and recipient are concordant or discordant. Hence, theideal donors of grafts to humans would be other primates. Clearly, there are ethical problems with this, andfarmed animals such as the cow or pig are generally considered more suitable.Calf bone is available, but in order to reduce its immunogenicity sufficiently its protein content has to be re-moved or denatured to such an extent that the strength of the graft is reduced. Matrix protein is not onlystructurally important but also osteoinductive, and osteoinductive proteins demonstrate profound cross-specieshomology. A bone xenograft in which the matrix proteins are intact may thus have some advantages. Theproblem is that bound to the matrix protein are a-galactosyl sugar residues which act as antigens. The serumof a discordant host carries naturally-occurring xenoreactive antibodies to these antigens. On binding theyactivate complement and initiate the immune response.In Cambridge, we have studied such a graft from transgenic pigs, which have been bred to express in theirtissues a human protein which inhibits the human complement cascade. This protein is called Decay Accel-erating Factor or DAF. It is found in all tissues including bone and is species-specific. Human DAF is foundin trasgenic pig bone even after processing and irradiation. We studied this bone in a primate model and com-pared it with non-transgenic bone graft. We measured mineralisation rates during the 8th week after graftingusing the fluorochrome Calcein, and found that there was an average increase in mineralisation rate of over50% in the presence of the transgenic graft, compared with almost no increase with the non-transgenic graft.
Hydroxyapatite: experimental data, clinical results and some aspects inrevision hip surgery
C.M. MÜLLER-MAI, C. VOIGHT, U. GROSS*, R. RAHMANZADEH
Dept. of Traumatology and Reconstructive Surg., *Inst. of Pathology, Universitätsklinikum Benjamin Franklin,FU Berlin, Berlin - Germany
Introduction: Since 1971, when L.L. Hench developed Bioglass® and described its behaviour after implan-tation into bone, bone bonding to biomaterials is known (1). Today several materials are used clinically, e.g.
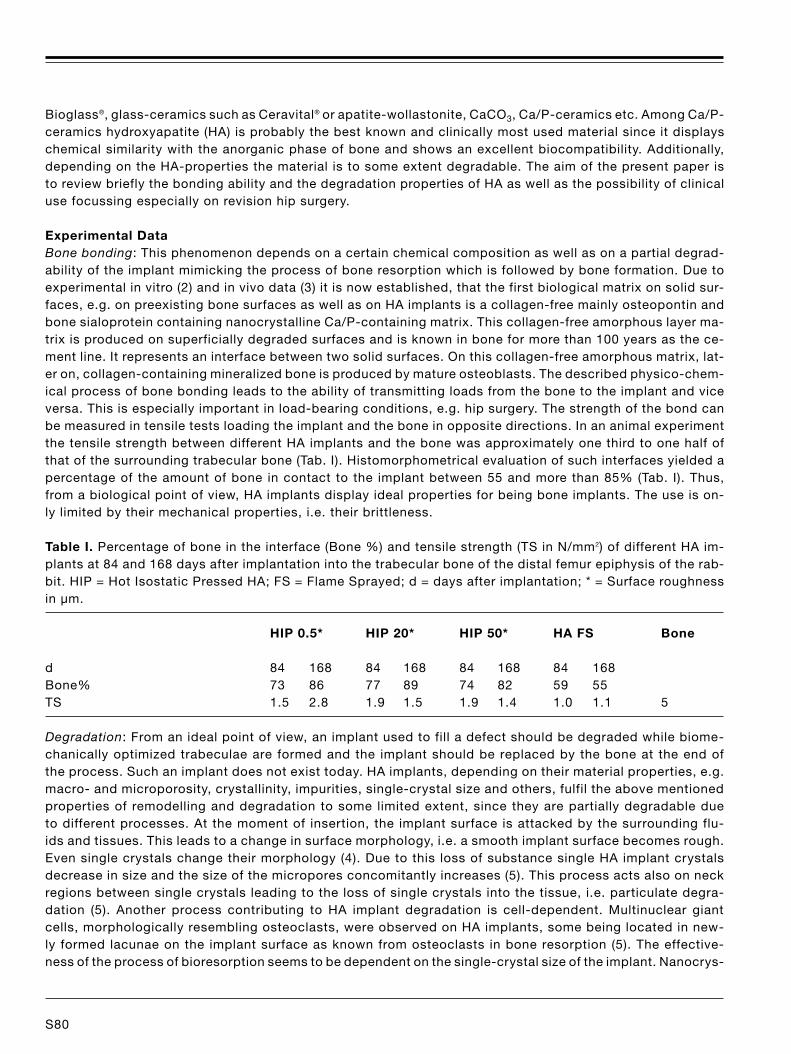
S80
Bioglass®, glass-ceramics such as Ceravital® or apatite-wollastonite, CaCO3, Ca/P-ceramics etc. Among Ca/P-ceramics hydroxyapatite (HA) is probably the best known and clinically most used material since it displayschemical similarity with the anorganic phase of bone and shows an excellent biocompatibility. Additionally,depending on the HA-properties the material is to some extent degradable. The aim of the present paper isto review briefly the bonding ability and the degradation properties of HA as well as the possibility of clinicaluse focussing especially on revision hip surgery.
Experimental DataBone bonding: This phenomenon depends on a certain chemical composition as well as on a partial degrad-ability of the implant mimicking the process of bone resorption which is followed by bone formation. Due toexperimental in vitro (2) and in vivo data (3) it is now established, that the first biological matrix on solid sur-faces, e.g. on preexisting bone surfaces as well as on HA implants is a collagen-free mainly osteopontin andbone sialoprotein containing nanocrystalline Ca/P-containing matrix. This collagen-free amorphous layer ma-trix is produced on superficially degraded surfaces and is known in bone for more than 100 years as the ce-ment line. It represents an interface between two solid surfaces. On this collagen-free amorphous matrix, lat-er on, collagen-containing mineralized bone is produced by mature osteoblasts. The described physico-chem-ical process of bone bonding leads to the ability of transmitting loads from the bone to the implant and viceversa. This is especially important in load-bearing conditions, e.g. hip surgery. The strength of the bond canbe measured in tensile tests loading the implant and the bone in opposite directions. In an animal experimentthe tensile strength between different HA implants and the bone was approximately one third to one half ofthat of the surrounding trabecular bone (Tab. I). Histomorphometrical evaluation of such interfaces yielded apercentage of the amount of bone in contact to the implant between 55 and more than 85% (Tab. I). Thus,from a biological point of view, HA implants display ideal properties for being bone implants. The use is on-ly limited by their mechanical properties, i.e. their brittleness.
Table I. Percentage of bone in the interface (Bone %) and tensile strength (TS in N/mm2) of different HA im-plants at 84 and 168 days after implantation into the trabecular bone of the distal femur epiphysis of the rab-bit. HIP = Hot Isostatic Pressed HA; FS = Flame Sprayed; d = days after implantation; * = Surface roughnessin µm.
HIP 0.5* HIP 20* HIP 50* HA FS Bone
d 84 168 84 168 84 168 84 168Bone% 73 86 77 89 74 82 59 55TS 1.5 2.8 1.9 1.5 1.9 1.4 1.0 1.1 5
Degradation: From an ideal point of view, an implant used to fill a defect should be degraded while biome-chanically optimized trabeculae are formed and the implant should be replaced by the bone at the end ofthe process. Such an implant does not exist today. HA implants, depending on their material properties, e.g.macro- and microporosity, crystallinity, impurities, single-crystal size and others, fulfil the above mentionedproperties of remodelling and degradation to some limited extent, since they are partially degradable dueto different processes. At the moment of insertion, the implant surface is attacked by the surrounding flu-ids and tissues. This leads to a change in surface morphology, i.e. a smooth implant surface becomes rough.Even single crystals change their morphology (4). Due to this loss of substance single HA implant crystalsdecrease in size and the size of the micropores concomitantly increases (5). This process acts also on neckregions between single crystals leading to the loss of single crystals into the tissue, i.e. particulate degra-dation (5). Another process contributing to HA implant degradation is cell-dependent. Multinuclear giantcells, morphologically resembling osteoclasts, were observed on HA implants, some being located in new-ly formed lacunae on the implant surface as known from osteoclasts in bone resorption (5). The effective-ness of the process of bioresorption seems to be dependent on the single-crystal size of the implant. Nanocrys-

S81
talline implants, i.e. implants with particle sizes in the range of human bone crystals, were much faster and ef-fectively resorbed as implants with higher crystal size (6). Due to the degradative processes described above,HA implants are partially involved in the process of bone remodelling by being degraded to some extent.Clinical Results: Due to the properties described above HA implants were used in many surgical applica-tions. Several different implant types, i.e. bulk materials, porous materials, particulates and others wereused e.g. to fill defects, such as bone cysts as well as defects after impression fractures in the epiphysealregion. Special requirements have to be fulfilled in hip surgery since loads are transmitted. Therefore, coat-ings of the brittle material HA were used to cover stems and cups. Such implants now work sufficient formore than 10 years without any sign of migration in the case of acetabular components (7). If large bonedefects exist in primary hip surgery, the autologous femoral head can be used to fill the defect as a bonetransplant. In a revision operation an additional operation site has to be created to harvest autologous bonee.g. from the iliac crest. This leads to more pain and weakening of the pelvis. On the other hand, homolo-gous bone has the risk of transmitting e.g. viral diseases. Furthermore, not every hospital has a bone bankbecause of the costs and legal problems. Buying bone from e.g. Eurotransplant can also not exclude therisk of infection. Therefore, the use of HA implants becomes more important. HA implants are available indifferent shapes as described above. We recommend if ever possible the use of bioactive implant squares,e.g. made from HA. If a macroporous material is used it should be loaded with the bone/blood mixture ob-tained by milling the acetabulum. In case of acetabular defects blocks allowing load-transmission to someextent can be placed between the bone and the acetabular component of the prosthesis and the gap be-tween blocks can be filled with granular material. Such a procedure ensures a fast and sufficient mineral-ization leading to a proper implant fixation within 5-6 weeks. In case of defects of the femur cavity and useof cement-free components the use of bioactive implants, e.g. HA as a filling material helps integrating thestem within a few weeks.
References1. LL Hench et al. J Biomed Mater Res 1971; 2: 117.2. JE Davies. Anat Rec 1996; 245: 426.3. H Kawaguchi et al. Cells & Mater 1993; 3: 337.4. J Zhang et al. J Mater Sci 1994; 5: 243.5. CM Müller-Mai et al. Scanning Microsc 1990; 4: 613.6. CM Müller-Mai et al. J Biomed Mater Res 1996; 29: 9.7. CM Müller-Mai et al. Transactions, Vol 1, 5th World Biomat Congress, Int Liaison
Committee (Ed.), University of Toronto Press, Toronto, Canada, 268.
Are allografts really necessary?
K. ZWEYMÜLLER
Abteilung Des Orthopädischen, Wien - Austria
The reconstruction of femoral bone loss - resulting from loosening of hip endoprostheses’ stems - is an issue tosolve which many different materials and constructions have been used. As a further use of bone cement oftenis not possible because it would not fulfill the requirements of modern cementing technique, today attention ismore and more directed to a restoration of the joint function with cementless implants. We would like to reportabout 85 revisions, made between September 1991 and September 1996, where a special revision stem has beenused. We had 30 male and 55 female patients with an age between 49 and 91 years. The mean age was 76 years.According to the classification of Engelbrecht and Heinert 20% were in grade I, 40% in grade II and 30% in gradeIII. This stem consists of a titanium alloy with a rectangular cross section and is implanted into the osseous bedprepared with the aid of a sharp cutting rasp with exactly the implant’s dimension. Our aim is to achieve a pri-

S82
mary stable fixation and durable incorporation due to osseous integration. We abandoned ever additional pro-cedure such as the implantation of large allografts. In several cases, however, a bone graft was used in order tofill up large defects and not with regard to the stability, as the implant has been anchored in the pre-existing bonestock in all cases. In 40% of the cases we had to make a fenestration of the diaphysis, which enabled us to re-move the cement quickly and protect for the surrounding diaphysis. Until now we had no spontaneous fracturedue to fenestrations. In 2 cases we had to do revisions due to loosening of the implant. 3 cases have to be clas-sified as loose from a radiological point of view. In practically all of the cases without radiological signs of loos-ening, newly formed bone tissue could be identified radiologically, in 4 patients an additional atrophy in position1 and 7 and in 21 patients in position 2 and 6 was noted. Due to our results with this method we would like toconclude as follows: 1. Femoral fenestrations are no risk with regard to post-operative fractures. 2. There is thepossibility of osseous integration of a titanium stem in revision surgery. 3. In the course of years formation of newbone around the implant can be assured, often however with atrophy of other parts due to stress shielding. 4.Large allografts are not necessary.
If skeletal augmentation is not essential can long-term success beachieved with cement alone?
M.D. NORTHMORE-BALL
The Robert Jones & Agnes Hunt Orthopaedic Hospital, Oswestry, Shropshire - UK
In this talk, illustrative examples are first given of types of grafting techniques, described by other lecturersearlier in the meeting, taken from the author’s own experience. It is acknowledged that these techniques (with,for example, sound fixation, restoration of hip centre, and correction of severe skeletal loss) are excellent.The questions is, however: Are techniques of this kind necessary in all cases (especially, for example, if abone bank happens not to be available)?The author considers that there are two separate questions:1. How the implants are going to be fixed and2. Whether, in a patient with severe bone destruction and young enough possibly to be going to need anotherrevision later, skeletal augmentation by bone grafting is desirable. Put differently, all implants have to be fixed,but do we also need to try to “put the clock back”?These two questions overlap, but are fundamentally completely different.Hence the title of the talk. Can good long-lasting results be achieved with cement alone? Many papers havebeen published showing that the answer is “No”, but the author’s experience is that it can be made to work,provided a number of details are attended to.The results of a consecutive series of 150 hip revisions carried out by the author are then given (Journal ofBone & Joint Surgery, 76B, 24-39, 1994). These were bad cases, about a third having had at least one pre-vious revision, and about one-third also having a proven deep infection at the time of revision. The great ma-jority of the hips were treated using Charnley components (132) with purely cemented fixation and this is thejustification for giving the results of this study in this lecture now. Of the relatively small number (27) that didhave grafts, 9 were in association with the RM-Isoelastic stem and these, in fact, had poor results.Clinical and radiological survival curves are then shown. Taking clinical survival as retention of the implant,there was a clinical survival of 95% at ten years. The functional result was also very good, as measured byD’aubigné & Postel’s scoring, but time does not permit inclusion of this data. Of more significance is the ra-diological survival. Hips were classified into three radiological grades on the basis of serial x-rays. Those show-ing good interfaces with no detectable change over a period of two years, though perhaps including a smalllocalised non-progressive defect seen on the immediate post-operative film, were called Grade I; those show-ing a small radiolucent area not present on the post-operative film, but with no subsequent progression, werecalled Grade II; those with serial radiographs showing progressive increase in radiolucency or component mi-

S83
gration, or both, were classified as Grade III. The hip was considered to be a survivor radiologically if in Grades Ior II. When the RM-Isoelastic cementless THRs were excluded, the radiological survival was 90% at ten years. Thestriking finding is the horizontal nature of the survival curve in the later years, suggesting that no later catastroph-ic fall-off in results is likely. This study was completed about four years ago, but the author’s conclusions remainvery much the same. The answer to the question posed by the title is, therefore, “Yes”, in the author’s opinion.Technical details are then given, relating to the two essential details for successful cemented fixation in revisionsurgery, namely:1. Creating a closed cavity (acetabulum or femur) by effective blocking of defects and by the use of standard vis-cosity cement. Examples are given of good and less successful methods of blocking acetabular perforations, ex-amples of femoral perforations, and the author briefly reports on a very simple technique he uses for preventingplastic plugs migrating down the femur (Journal of Arthroplasty 1991; 6, (3): 199-210).2. Cement pressurization is briefly mentioned, and as an example a late result following conversion from a Girdle-stone in a patient with two previous revisions is shown, there being no radiolucencies.It is acknowledged that in the acetabulum, cemented fixation in revision does have its limitations, as describedby Wroblewski (Journal of Bone & Joint Surgery, 1996; 78A: 1853-6). The author’s practice has been to use AOrings particularly if, after making the acetabulum into a closed cavity, very little host bone will be available forpurely cemented fixation, and if the shape of the mouth of acetabulum is such that it cannot be sealed by anyavailable pressurizer. Time does not permit discussion of this subject, unfortunately. Rings, however, were onlyused in 18 cases. A series of examples are then given, many showing late (10 years+) results.The author concludes that, in his experience, while bone grafting is very effective and often highly desirable,it is not a “sine qua non” of lasting success. This can be achieved with cement, provided that certain detailsare attended to.
Surface replacement: the hip replacement of the future?
H.C. AMSTUTZ, E.A. SPARLING, P. GRIGORIS, P.A. CAMPBELL, F.J. DOREY
Joint Replacement Institute at Orthopaedic Hospital Los Angeles, California - USA
ABSTRACT: Surface replacement is a significant development in the evolution of hip arthroplasty. Unlike con-ventional total hip arthroplasty, surface replacement does not require resection of the femoral head; thus, itpresents a potentially effective, bone-conserving alternative to conventional replacements. Moreover, con-version to total hip replacement can be made readily, if necessary, with fewer complicating factors than withtotal hip revision surgery. It offers the greatest potential benefit to patients who are young and physically ac-tive. Previous surface replacement used metal-on-polyethylene devices; however, the large ball size of thefemoral component contributed to high volumes of polyethylene wear. For some patients, osteolysis occurreddue to tissue reaction to polyethylene debris, resulting in aseptic component loosening. Recent advances intechnology have allowed metal-on-metal implants to be manufactured with great precision. Hybrid and all ce-mentless fixation, have both shown good early results without the prevalence of loosening seen with poly-ethylene bearings. Metal-on-metal surface replacement has proved to be quite successful. Results from pa-tients with metal-on-metal devices, especially those with ConservePlusTM implants, show no complications;moreover, there has been an absence of pain and a return to high functional levels, including participation insports. Due to the large ball size, metal-on-metal devices offer high stability and low dislocation rates. Hemisur-face replacement of the femoral head has also proved to be successful in patients with osteonecrosis withor without collapse of the femoral head, when the acetabulum remains relatively normal. For this type ofsurgery, some acetabular articular cartilage must be preserved. With high survivorship over time, it has emergedas the treatment of choice for this patient group. (Hip International 1998; 8: 187-207)
KEY WORDS: Metal-on-metal surface hip replacement
S84
Non-cemented hip replacement using a conical screw-in cup and a straight press-fit stem. A six to eight-year clinical and radiological follow-up study
G. KÖSTER, S. LEIB, H.-G. WILLERT
Orthopaedic Department, Georg-August-Universität, Göttingen - Germany
ABSTRACT: Noncemented hip replacement using a conical titanium metal-backed screw-in cup to be im-planted with precutting of the threads (TITAN-METAL-BACKED, AlloPro, Baar, Switzerland), in combinationwith a straight conical press-fit stem (ZWEYMÜLLER-“hochgezogen”, AlloPro, Baar, Switzerland) was evalu-ated clinically and radiologically in 64 consecutive primary arthroplasties with an average 7.2 year follow-up.The clinical results compare very favourably with other cementless systems. The Harris hip score revealed animprovement from 45 to 84. The Merle d’Aubigné index showed an increase during the case-control periodfrom 16 to 26. Thigh pain was practically absent except in one patient. A radiographic appearance of boneingrowth around the acetabular component was found in nearly all cases. Only one cup migrated in a patientwith a large cystic lesion in the acetabular roof, which was not grafted, with no other signs of loosening. Ad-ditionally this patient had chemotherapy. In all other cases there were no signs of cup migration, significantradiolucency, osteolysis or definite cup loosening. Around the stem, primary cortical contact was mainly lo-cated in the distal zones. Radiolucent lines appeared only proximally, with few exceptions, and were, exceptin four cases, always smaller than 2 mm. They were never circumferential and usually combined with scle-rotic lines. Only one stem subsided, but the patient remained asymptomatic. There was a high incidence ofproximal bone atrophy, distal cortical thickening and endosteal bone formation, not correlating with radio-logical loosening or clinical symptoms. Signs of femoral osteolysis were absent. No patient had to be revised.(Hip International 1998; 8: 208-18)
KEY WORDS: Noncemented hip replacement, Screw-in cup, Press-fit stem
Vacuum loading of the femoral cement gun: the effect on mantle porosity
P. KENNY 1, J. RICE 1, B. MCCORMACK 2, S.K. O’ROURKE 1
1 Department of Orthopaedic Surgery, Cappagh Orthopaedic Hospital, Finglas, Dublin2 The Bioengineering Centre, Dept. of Mechanical Engineering, University College Dublin - Ireland
ABSTRACT: The femoral cement mantle was reproduced in a laboratory model. This model consisted of rigidplastic tubing, 10 cm long, with an internal diameter of 2.5 cm. One end of the tube was sealed to simulate anintramedullary plug. A wooden model was used to simulate the femoral component of a total hip arthroplasty.Bone cement was mixed in a glass bowl with a steel spatula in a standardised manner for two minutes. In all cases the model femur was filled with bone cement and a regular mantle around the wooden “femoralstem” was observed. Pores were present on the cut surface of all of the specimens. The pore density (No. ofpores per unit area) was measured using an NIH image programme and was found to be dramatically reducedin the experimental cement mantles, when compared to the control specimens. The porosity in the cement mantles produced by vacuum loading the gun was significantly lower (p< 0.001)than that in the mantles produced by the manually loaded guns. (Hip International 1998; 8: 219-22)
KEY WORDS: Cement mantle, Cement gun, Vacuum vs manual loading, Porosity
S85
Transient osteoporosis and avascular necrosis of the hip in the samepatient
A. PEIRÓ, M. SALOM, J. E. AROCA
Service of Traumatology and Orthopedic SurgeryUniversity Hospital “La Fe”, Valencia - Spain
ABSTRACT: We present a case of a 45-year-old woman who developed a transient osteoporosis in her righthip that resolved spontaneously after four months. Three years after she developed an avascular necrosis ofher left hip. It is controversial if transient osteoporosis and avascular necrosis are two separate clinical enti-ties or if they are different grades of the same disease. We describe both entities and discuss these two the-ories based on the findings of our case. (Hip International 1998; 8: 226-30)
KEY WORDS: Avascular necrosis, Transient osteoporosis, Hip
Simultaneous bilateral central acetabular fracture-dislocations followingan epileptic seizure in a patient with chronic renal failure
A.G. PAPANIKOLAOU, D.D. AKTIPIS, A.G. GIOTA, N.C. ANTONIOU
Department of Orthopedics, Red Cross Hospital, Athens - Greece
ABSTRACT: We report on a rare injury in a 60-year old diabetic lady suffering from chronic renal insufficien-cy. She sustained bilateral central acetabular fracture-dislocations following an epileptic seizure. (Hip Inter-national 1998; 8: 231-2)
KEY WORDS: Hip, Central fracture-dislocation, Renal insufficiency, Epileptic seizure
Initial stability of two different hip revision concepts. A biomechanicalstudy
L. PALM, I. IVARSSON, S.-A. JACOBSSON
Department of Orthopaedics, University Hospital, Linköping - Sweden
ABSTRACT: Two fundamentally different revision concepts, a standard stem cemented in a bed of firmly im-pacted morselized bone graft, and an uncemented long stem implanted with proximal bone grafting, werecompared in terms of initial stability under torsional load immediately after implantation. A stem cementedwithout bone graft was used as a baseline reference. The stems were implanted in identically prepared com-posite femora inclined at 45° and loaded vertically. During 9 individual tests of each concept, the stems dis-placed into retroversion with no detectable axial displacement. At a load of 1000 N the average displacementin retroversion of the prosthetic head was 3.9° ± 2.6° for the uncemented long stem and 9.1° ± 2.6° for thestem cemented in impacted morselized bone graft (P < 0.001). Both revision concepts displaced rather dra-
Abstracts from Hip International Vol. 9 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S85-S117 ©by Wichtig Editore, 2001

S86
matically compared to the stem cemented without bone grafting. The magnitude of displacement may indi-cate insufficient initial rotational stability of both concepts particularly with the stem cemented in impactedmorselized bonegraft. (Hip International 1999; 9: 7-13)
KEY WORDS: Hip revision, Mechanical testing, Stability
Assessment of supero-lateral bulk bone grafts in total hips using radiographs and scintigraphy
C.A. BUSCH, K.J. DRABU
Sir John Charnley Research Fellow, Joint Replacement Unit, East Surrey Hospital, Redhill, Surrey - UK
ABSTRACT: Incorporation of autologous bulk grafts in dysplastic acetabula may be difficult to confirm radio-logically. In our series twelve consecutive patients (fifteen hip replacements) were assessed between two andseven years from the time of surgery. All the femoral heads used for bulk autografting showed radiological ev-idence of cross trabeculation in the load bearing zone of the acetabulum. To confirm the radiological impres-sion of incorporation and consolidation scintigraphy was carried out on 11 out of 12 patients. 5 patients alsohad tomograms of their graft-host interface. Radiologically resorption of these bulk grafts occurred at the lat-eral non-weight bearing edge of the graft in a number of patients. Scintigraphy confirmed block graft incor-poration in all patients. Tomograms were not found to be a useful assessment of the incorporation of the su-pero-lateral bulk graft. An indirect measurement of acetabular migration showed no significant migration ofthe acetabular component over the period of follow up in all patients. (Hip International 1999; 9: 14-19)
KEY WORDS: Hip arthroplasty, Dysplastic acetabuli, Autologous femoral bulk grafts, Scintigraphy, Tomo-grams
The histology of impacted cancellous allograft in acetabular reconstruction
G.C. SINGER 1, S.K. MUIRHEAD-ALLWOOD 2
1 St. Mary’s Hospital NHS Trust, Praed St, London - UK2 The Royal National Orthopaedic Hospital NHS Trust, Brockley Hill, Stanmore, Middlesex - UK
ABSTRACT: Reconstruction of the acetabulum in the presence of severe bone loss presents challenging prob-lems. Ideally, the acetabulum should be reconstructed with a stable component placed in the anatomical po-sition with reconstitution of bone stock. The clinical and radiological results of using impacted morselised al-lograft for acetabular reconstruction appear satisfactory in the short term but there is little histological evi-dence in humans that the bone chips are revascularised and incorporated into the host.We present two cases of histology of retrieved bone samples, obtained at two years and three years follow-ing impaction allografting of the acetabulum. Both samples were taken from cases of aseptic failure, and wereobtained during the revision surgery. It showed that the bone was viable, and undergoing the process of creep-ing substitution, where new bone was being laid down on dead bone. At three years this process was not yetcomplete, which indicates that the process is significantly slower than that described by Sloof in his animalexperiments. (Hip International 1999; 9: 20-24)
KEY WORDS: Histology, Impaction, Cancellous, Allograft

S87
The Wagner uncemented long-stemmed revision prosthesis: medium-termresults for proximal femoral osteolysis
I.A. KARNEZIS, K.E. DRETAKIS, T.J.S. CHESSER, M.B. LEE, I.D. LEARMONTH
University Department of Orthopaedic Surgery, Bristol Royal Infirmary, Bristol - UK
ABSTRACT: This paper presents a clinical and radiological review of nineteen hips that were revised usingthe uncemented long stem Wagner prosthesis. All the hips were symptomatic and demonstrated proximalfemoral osteolysis. The mean follow-up was 61 months: there were four hips with a follow-up of more than 4years, eight hips with a follow-up of more than 5 years, three hips with a follow-up of over 6 years, while therewere two hips with a follow-up of above 7 years. Only two hips had a follow-up of less than 4 years. The clin-ical results were satisfactory. 95% of patients had mild, occasional or no pain, and 90% minimal or no limi-tations of mobility. Radiographically, significant restoration of the proximal femoral bone stock (Pak and Pa-prosky classification) occurred in 42% of cases. No stems were radiographically loose. 89% of stems showedsubsidence of less than 4mm. There were no re-revisions at the time of follow-up. These medium-term re-sults support the use of the Wagner uncemented distal load bearing femoral prosthesis for difficult revisioncases in the presence of symptomatic proximal femoral bone resorption. Significant stem subsidence wasnot encountered. (Hip International 1999; 9: 25-30)
KEY WORDS: Hip, Osteolysis, Revision arthroplasty, Uncemented prosthesis
ORTHOPAEDIC SURGERY AND THE DEVELOPING HIP JOINT
INTRODUCTION
Appropriate management of pathological conditions of the hip joint in infants and adolescents such as DDH,septic arthritis, the epiphyseal dysplasias, Perthes’ disease and Slipped Upper Femoral Epiphysis (SUFE) maysignificantly reduce the long term morbidity and lessen the need for premature joint replacement. To understand the working of the hip joint in health and more importantly in disease, it is helpful to knowsomething of the embryology of the hip joint together with its normal anatomy, if for no other reason than thatto know the aetiologies and timing of failure in maturation of the joint will assist in planning and executing re-constructive procedures.The following article will discuss the history and the ongoing controversies in Developmental Dysplasia of theHip (DDH), and three subsequent articles will focus on embryology, normal and pathological anatomy.
N.M.A. Portinaro
Developmental dysplasia of the hip
N.M.A. PORTINARO
Clinica Ortopedica dell’Ospedale San Raffaele, Università degli Studi, Milano - ItalyRoyal Hospital for Sick Children, Bristol - UK
ABSTRACT: This historical review highlights the uncertainty about the aetiology, diagnosis and managementof developmental dysplasia and dislocation of the hip joint. On that account to optimize the management of this condition, we have to consider the importance of thenormal embryology of he hip joint and to be aware of the basic anatomy of the hip joint at birth to promptlydetect and treat most of its structural anomaly.

S88
Embryology of the human hip
N.M.A. PORTINARO 1, F.G. BONIFORTI 2, M.F. GARGAN 3
1 Clinica Ortopedica IV, Università degli Studi di Milano, Ospedale S.Raffaele, Milan - Italy2 Clinica Ortopedica II, Università degli Studi di Milano, Istituto Ortopedico “G.Pini”, Milan - Italy1-3 Department of Orthopaedic Surgery, Royal Hospital for Sick Children, Bristol - UK
ABSTRACT: The origin and development of the hip joint can be divided into two main periods, namely, theembryonic and the foetal. The embryonic period inlcudes the first trimester of pregnancy, when the embryoreaches an average crown-rump lenght of 5 centimetres. The major joint components, the acetabulum andthe femoral head, and surrounding structures separate from a single mesenchymal mass to become differententities and gain their topographical relationships (1, 2). At the end of this period, the hip joint is essentiallyformed and closely resembles the configuration of the adult joint.The second period starts at the end of he first trimester and ends with the delivery. This second phase com-prises an increase in size and volume of each of the joint components (2).
Ender nails compared with nail or screw plate devices for trochantericfemoral fractures: a meta-analysis of randomised trials
M.J. PARKER1, H.H.G. HANDOLL2, S. BHONSLE1, W.J. GILLESPIE3
1 Peterborough District Hospital, Thorpe Road, Peterborough - UK2 Princess Margaret Rose Orthopaedic Hospital, Fairmilehead, Edinburgh - UK3 Dean of Dundean Medical School, Dundean - New Zealand
ABSTRACT: A systematic review of all randomised trials comparing the use of Ender nails with alter-native implants for the reconstruction of extracapsular fractures of the proximal femur has been con-ducted. Wherever possible the results for the 1.570 patients in the 10 trials identified were pooled. Ap-parent advantages of Ender nails were reduced deep wound sepsis rate, shorter duration of surgeryand lower operative blood loss, but they were associated with an increased risk of re-operation andfracture of the femur. Ender nails were also associated with an increased risk of cut-out of the implantfrom the femoral head when compared with a sliding hip screw, although not when compared with afixed nail plate. Additional problems associated with Ender nails included backing out of the nail, short-ening of the leg, external rotation deformity and residual pain. The continued use of Ender nails in thefixation of proximal femoral fracture is inappropriate. (Hip International 1999; 9: 41-48)
KEY WORDS: Hip fracture, Femoral fracture, Ender nails, Nail plates, Sliding hip screw
S89
The use of pulsed lavage with integral suction in total hip replacement
T. D. TENNENT, E. TELLO, J.S. BLACKBURNE
Orthopaedic Department, Barnet General Hospital, Wellhouse Lane Barnet, Herts - UK
ABSTRACT: Both pulsatile lavage and distal femoral plugs are used routinely in preparation of the femoralcanal prior to cementing. Using an in-vitro model, two types of pulsed lavage irrigation systems were testedto assess their relative abilities to clear the femoral canal of the polethylene vanes which commonly becomedetached from the Hardinge type of cement restrictor during insertion. The narrower tipped system, whichdid not incorporate an integral suction system, performed significantly better. Surgeons should be aware ofthis potential problem when preparing the femoral canal. (Hip International 1999; 9: 49-51)
KEY WORDS: Pulsatile lavage, Cement restrictor, Femoral canal preparation
Sciatic nerve pain from proximal femoral mesh in revision hip arthroplasty
T.J.S. CHESSER, I.D. LEARMONTH
University Department of Orthopaedic Surgery, Bristol Royal Infirmary, Bristol - UK
ABSTRACT: Sciatic nerve damage is a serious complication of revision hip arthroplasty. We report a case ofsevere posterior thigh pain produced by sciatic nerve irritation from stainless steel mesh used to reconstructthe proximal femur. The symptoms were not associated with any neurological deficit or electromyographicchanges. Surgeons should be aware that nerve compression or irritation is one cause of pain after hip arthro-plasty, and the neurological presentation may be atypical. (Hip International 1999; 9: 52-54)
KEY WORDS: Sciatic nerve, Revision arthroplasty, Femoral reconstruction
The MRL stem: a decade of follow-up of 100 primary implants
L. RAVAGLIA, M. ZUCCHI
Divisione di Ortopedia e Traumatologia Ospedale di Lugo, Azienda U.S.L. di Ravenna, Ravenna - Italy
ABSTRACT: The Authors report the results with the MRL prosthesis in 100 hips, reviewed on the basis of spe-cific chronological parameters, with a mean follow-up of 11 years and 6 months, range 10-14 years. Resultswere excellent or good in 97%. A valgus cervicodiaphyseal angle of the stem constitutes a relative contraindicationin some cases of coxa vara. We recommend widening the range to include stems with greater lateralizing effectand a physiological cervicodiaphyseal angle. (Hip International 1999; 9: 55-58)
KEY WORDS: Hip prosthesis, Acrylic cement, Mechanical stress

S90
The repeatability of EBRA in migration and wear analysis
T. ILCHMANN
BG Trauma Centre, University of Tübingen - Germany
ABSTRACT: The new computerized EBRA method should be tested for its usefulness in multicentre studies.One patient was followed wlth roentgen-stereophotogrammetry for three years after THA. Ten clinical pelvicradiographs were taken over a period of nine years and analysed with EBRA at four different centres inde-pendently. The maximum difference in repeated measurements after nine years was 2.2 mm for migration and0.7 mm for wear. The error of measurement (two standard deviations) was 0.36 mm for horizontal and 0.62mm for vertical migration. For wear it was 0.06 mm and 0.16 mm respectively. The results with EBRA weresimilar to the corresponding roentgen-stereophotogrammetric results. EBRA proved to be useful for multi-centre studies, reducing the error of measurement. It might detect prosthetic failure at a more early stage.(Hip International 1999; 9: 63-66)
KEY WORDS: Total hip arthroplasty, Migration, Wear, EBRA
A comparison of the survival of total hip replacement inserted over twosequential time periods
S.L. WHITEHOUSE, O.A. GABBAR, I.D. LEARMONTH
Department of Orthopaedic Surgery, University of Bristol, Winford Unit, Avon Orthopaedic Centre, Westburyon Trym, Bristol - UK
ABSTRACT: Modifications in design and surgical technique have been directed at improving the long-termsurvival of total hip replacement. This study examines the failure rate, with revision as endpoint, of two largecohorts of primary total hip replacement carried out over consecutive six-year intervals. The intention of thestudy was not to compare specific prostheses or techniques, but to examine failure rates between two timeperiods which embraced significant changes of practice. At one specialised centre in Bristol, 2747 primarytotal hip replacements were performed between 1980 and 1986. Seventy-six failed within 5 years (2.8%) with23 of these failing in the first year (0.8%). Between 1987 and 1992, 3232 primary total hip replacements werecarried out, with 98 hips requiring revision within 5 years (3.0%), 21 of these in the first year (0.6%). Therewas no statistical difference in the incidence of failure between these two time periods; however, the failurerate for the more recent time period was marginally higher. This indicates that, although techniques and pros-thetic design have changed significantly, the anticipated reduction in incidence of failure has not materialised.There is undoubtedly a need for ongoing review to ensure that changes in technique and component designare producing the desired long-term effect. (Hip International 1999; 9: 67-70)
KEY WORDS: THR, Comparison, Failure rate

S91
The effect of a lateral flare feature on uncemented hip stems
P.S. WALKER1, S.G. CULLIGAN1, J. HUA1, S.K. MUIRHEAD-ALLWOOD 1,2, G. BENTLEY3
1 Centre for Biomedical Engineering, University College London, The Royal National Orthopaedic Hospital,Trust, Stanmore - UK
2 The Whittington Hospital, Hampstead, London - UK3 Institute of Orthopaedics, The Royal National Orthopaedic Hospital, Trust, Stanmore - UK
ABSTRACT: Ideal goals for a primary uncemented femoral stem prosthesis are to transmit the loads to thefemur proximally, and to minimise the interface migration. It has been proposed that the addition of a lateralflare which loads the lower region of the greater trochanter will contribute positively to these goals. Analyti-cal and radiographic studies were used to study the load transfer between the stem and the bone, and themigration. A comparison was made between a straight stem, and a straight stem with the addition of a lat-eral flare. The finite element study showed that the straight stem migrated down the canal approximately fourmillimeters before stabilisation was reached. The forces were transmitted on to the proximal-medial femurand around the lower half of the stem. When the lateral flare was added, there was only one millimeter of mi-gration to reach stability. The loads were transferred by a wedging effect between the proximal-medial femurand the around the lateral flare, with little force transfer from the stem. In a radiographic follow-up of an HA-coated lateral flare stem, trabeculae could be seen attaching to the lateral flare. The axial migration was sig-nificantly less for this stem design compared with that from a series of previously reported cemented stems.This study suggested that the lateral flare contributed positively to the goals of uncemented stem design,and that the stems could be made shorter than designs not incorporating the lateral flare feature. (Hip Inter-national 1999; 9: 71-80)
KEY WORDS: Hip stem, Lateral flare, Bone stresses, Migration, Interface stresses
Diagnostic imaging in transient osteoporosis of the hip
M.A. ROSA, G. MACCAURO, M. D’ARIENZO
Istituto di Clinica OrtopedicaUniversità Cattolica del S. Cuore, Roma - Italy
ABSTRACT: The clinical aspects, imaging and therapy of Transient Osteoporosis of the Hip (TOH) were ex-amined. Eleven patients, three during pregnancy, were observed. Our conclusion is that magnetic resonance(MR) has a very important role in the diagnosis monitoring of this pathology. (Hip International 1999; 9: 81-85)
KEY WORDS: Osteoporosis, Hip, Imaging

S92
Rehabilitation following proximal femoral fracture: a comparative audit oftwo different regimens
A.B. DUNKLEY, M. BOULD, E. PINCH, G.C. BANNISTER
Department of Orthopaedics, Southmead Hospital, Westbury on Trym, Bristol - UK
ABSTRACT: The objective of this study was to investigate the effect of rehabilitation policy following proxi-mal femoral fracture at two adjacent hospitals. Patients transferred to a dedicated orthogeriatric rehabilita-tion unit had a significantly shorter length of stay compared with patients transferred to an elective orthopaedicward at a distant site. 93% of patients returned to their previous accommodation from the rehabilitation unit,and 66% from the orthopaedic ward. Early discharge planning and co-ordination between members of thehealth care team are crucial in maximising the efficiency of rehabilitation following hip fractures in the elder-ly. (Hip International 1999; 9: 86-89)
KEY WORDS: Femoral neck fractures, Rehabilitation, Audit, Length of stay
Fatigue fracture of gamma nail
S. HOUSHIAN1, K.G. FREUND1, J.H. PEDERSEN 2
1 Department of Orthopaedic Surgery, Esbjerg County Hospital2 Department of Electron Microscopy, Aalborg University Esbjerg - Denmark
ABSTRACT: We report a case of a fatigue fracture of a Gamma nail in a patient with an unstable oblique sub-trochanteric fracture, together with scanning electron microscopy analysis of the fracture surface. In contrastto other published cases, the fracture was in the part of the nail distal to the insertion point of the lag screw.(Hip International 1999; 9: 90-93)
KEY WORDS: Gamma nail, Fracture
Spontaneous assembly of the acetabular component in an alumina-alumina hip arthroplasty
A. PEIRÓ, M. SALOM, J.E. AROCA, F. BAIXAULI
Department of Traumatology and Orthopaedic Surgery, La Fe University Hospital, Valencia - Spain
ABSTRACT: The use of modular designs of hip prostheses introduces the risk of post-operative disassemblyof the components. We report on two cases of alumina-alumina hip arthroplasty in which a spontaneous as-sembly of the acetabular component occurred. A review of the literature on such complications is also pre-sented. (Hip International 1999; 9: 94-98)
KEY WORDS: Hip prosthesis, Prosthesis design, Modularity
S93
Normal anatomy of the hip joint at birth
N.M.A. PORTINARO1,3, F.G. BONIFORTI2, M.J. HUBBLE 3, M.F. GARGAN 3
1 Clinica Ortopedica IV, Università degli Studi di Milano, Ospedale S.Raffaele, Milan - Italy2 Clinica Ortopedica I, Università degli Studi di Milano, Istituto Ortopedico “G.Pini”, Milan - Italy3 Department of Orthopaedic Surgery, Bristol Hospital for Sick Children, Bristol - UK
ABSTRACT: The unusual anatomy of the hip joint at birth is outlined below. The morphology, blood supply,growth and orientation of the acetabulum and proximal femur are described and the interdependence of thevarious components on subsequent development are discussed. (Hip International 1999; 9: 99-103)
KEY WORDS: Anatomy, Hip joint, Infantile
MIGRATION, SUBSIDENCE AND WEAR AFTER HIP REPLACEMENT
Contamination of polyethylene cups with polymethylmethacrylate particles.An experimental study
U. KESTERIS 1, J. LAUSMAA 2, L. CARLSSON 1, L. LIDGREN 1, H. WINGSTRAND 1, R. ÖNNERFÄLT 1
1 Dept. of Orthopaedics, Lund University Hospital, Sweden; 2 Swedish National Testing and Research Insti-1 tute, Boras - Sweden
We investigated whether exposure of ultra-high-weight-molecular polyethylene (UHWMP) acetabular cups tocuring polymethylmethacrylate (PMMA) bone cement causes PMMA contamination and/or mechanical dam-ages on the articulating surface, a possible source of early “third-body” wear.Six cups, made from the same batch and consecutively machined from the same UHWMP rod, were ex-posed to curing bone cement. Half the inner surface was covered with a silicone inlay, and this protectedarea was used as reference. Cement was prechilled at 4°C and brought into the cups 3 minutes after mix-ing, then placed in 37°C for 10 minutes. The areas 10 mm from the centre of the cup was chosen for scan-ning electron microscope (SEM) analysis. Two images at 200 and 2000 times magnification from each spec-imen were examined.No signs of debris or defects were observed on any of the unexposed surfaces. Varying amounts of PMMA par-ticles were found on the exposed portions of five cups. Four of these specimens showed the same patternof surface contamination, with particles sizes from tenths of a micrometre to nearly 10 micrometres. The par-ticles appeared to be well adherent to the UHMWP surfaces. On one specimen, large areas, mainly within themachining grooves, were coated with a thin layer of cement.Conclusions: bone cement left in UHWMP cups during polymerisation can contaminate the articulating sur-face with PMMA particles. Cups contaminated with PMMA during surgery might wear out faster due to thepresence of this “third-body” wear already present post-operatively.
ABSTRACTS OF THE THIRD EBRA-MEETING - TÜBINGEN, GERMANY, 27-28 NOVEMBER 1998 (HIP INTERNATIONAL 1999; 9: 104-111)

S94
The MAXIMA hip technique
K. HARDINGE
Centre for hip surgery, Wrightington Hospital, Wigan - UK
Orthopaedic research frequently involves angular and linear measurement on plain radiographs. Standardis-ation of projection and exposure is difficult and manual techniques for measurement are lengthy and highlysubjective.The Manchester X-ray Image Analysis Technique (MAXIMA) is an image analysis system which measures mul-tiple parameters of radiographs of patients with total hip replacements, either automatically, by computer orinteractively, by the user and the computer together. All measurements are under the control of the comput-er software, so that they are defined explicitly and made objectively: the software can be used on inexpen-sive personal computers.The MAXIMA system consists of a personal computer, qa light box, a video camera and a high resolutionmonochrome television monitor. The heart of the system is a frame grabber contained within the personalcomputer. The radiograph is placed on a back lit l ight box and the camera contained above on a stand. Theanalogue camera output is fed into the frame grabber which, under software control, converts it into a digi-tal image.
Radiological assessment of socket wear using EBRA and a new comput-erised, automatic edge detection aided software
A. RODRIGUEZ, N. BOUABDALLAH, P. GEORIS, G. KARAA, R. LEMAIRE
Dept. of Orthopaedics, University Hospital Sart-Tilman, Liège - Belgium
Classical methods to measure socket wear, such as the Livermore method, lack both precision and accura-cy. The EBRA method permits the measurement of selected films, based on their comparability, leading to animprovement in accuracy.We have developed a new image analysis module, using IMAGlKA® software, to study linear wear on digitisedfilms. The software determines automatically the centres of the socket and of the prosthetic head by an au-tomatic edge detecting device based on the analysis of a gray scale. The program measures the distance ofthe two centres. The evolution of this distance over time is seen as linear wear.In a preliminary clinical retrospective study of different implants, EBRA and IMAGIKA® were used and com-pared on 5 groups of RM uncemented cups: 10 all-polyethylene cups with good clinical and radiological out-come over 10 - 14 years; 10 all-polyethylene cups which required later revision for aseptic loosening; 10 hy-droxyapatite (HA) -coated cups (10 years follow-up); 10 HA-coated cups revised for femoral osteolysis with-out loosening of the cup; 10 titanium (Ti) -coated cups with good clinical and radiological results (8 - 13 years).Cups revised for aseptic loosening showed higher wear-rates than non-revised cups. Direction and magni-tude of the socket wear may be influenced by migration of the cup. HA-coated cups revised for femoral os-teolysis showed a wear-rate of 0.1 mm / year (as measured with both methods), HA-coated cups without re-vision 0.08 mm/year with EBRA and 0.04 mm/year with IMAGIKA®. Ti-coated cups had a wear rate of 0.03mm/year (both methods).Conclusions: In these preliminary tests the new method appears very rapid and reliable and it shows higherprecision than EBRA. This might be due to the automatic edge detection analysis, reducing the inter- and in-traobserver variability. At the present time we are working to validate this new method.
S95
Cup migration of metal-metal and polyethylene-ceramic articulations usingthe EBRA method
C. HELFRICH, P. FERRAT, P.E. OCHSNER
Dept. of Orthopaedics, Kantonsspital, Liestal - Switzerland
We investigated the migration pattern of a single design acetabular cup with two different bearing surfaces.One hundred thirty-one total hip replacements with a Müller SL-cup were assessed with a minimum of 2 yearsfollow-up. 70 of these hips had a polyethylene-ceramic articulation and 61 had a metal-metal articulation(Metasul). Migration was measured with the EBRA method.Nine cups (13%) showed a measurable migration in the polyethylene group, and 18 cups (30°) in the metal- met-al group. The cups with polyethylene-ceramic articulation showed cranial and medial migration, the cups withthe metal-metal articulation migrated in no specific direction.Conclusion: The migration behaviour of one type of cup may depend on the material of the inlay.
Two year migration results of the Duraloc cup
B. STÖCKL, M. SANDOW, M. KRISMER, R. BIEDERMANN
Dept. of Orthopaedics, University of Innsbruck - Austria
Seventy-one primary total hip arthroplasties using the porous coated, hemispherical press fit DURALOC/100Series cup were implanted in 68 consecutive patients; 61 combined with the CLS and 10 with the cemented Lu-binus SP ll stem. Underreaming of 2 mm was used to achieve press fit. Sixty-nine of 71 hips (97.1%) underwentfollow-up after a mean of 2.4 years.The clinical outcome was very good. Migration analysis was performed using the EBRA method with an ac-curacy of 1 mm. Horizontal migration of 1 mm or more within 24 months correlated significantly with the pres-ence of radiolucencies around the cup postoperatively (p = 0.002). Mean total migration after 24 months was1.13 mm.Defining loosening as total migration of 1 mm within 24 months post-operatively 30 of 63 cups (48%) have tobe regarded as loose. Therefore, the long term result of the DURALOC cup might be worse.
Migration measurement of two acetabular components
A. ECKARDT, M. SCHWITALLE, C. HEISEL, C. SEELEITNER
Dept. of Orthopaedics, University Hospital, Mainz - Germany
In previous studies, Krismer et al showed the predictive value of acetabular cup migration within the first twoyears for late loosening of hip sockets. We measured two different sockets to evaluate the possible outcomeof these implants.Seventy-four spherical HA-coated ABG-cups and 50 conical and threaded Zweymueller cups were followedclinically and radiologically. Migration was measured with EBRA, using a digitizing table. All radiographs weremeasured by a single person to minimize the methodological error.Fourteen (19%) of the spherical cups and 7 (14%) of the screwed cups showed migration of more than 1 mmwithin the first two years. Single-case analysis showed important features for clinical practice: Patients withinflammatory disease or with steroid induced demineralisation of the pelvis, that means patients with a poor
S96
acetabular bone stock, tended to show early migration. For the spherical cup, perforation of the inner pelviccortex and severe dysplasia seemed to be causes for early migration.Conclusions: Patients with steroid induced osteoporosis should be followed carefully after implantation of acementless hip prosthesis. Spherical press-fit cups must be implanted without penetration on the inner cor-tex, a high inclination angle and lateral non-coverage of the socket must be avoided. By using the EBRAmethod, we were able to improve our operative results and know about a population at risk which has to beobserved carefully.
Difficulties in the examination of the migratory behaviour of an acetabularcup in a multicentre study
P.E. OCHSNER
Dept. of Orthopaedics, Kantonsspital, Liestal - Switzerland
A multicentre study was performed at 5 Swiss hospitals to investigate the migration behaviour of acetabularcups with a metal-metal articulation (Metasul). A standard radiographic protocol was developed, determin-ing the technique for taking an ap radiograph and the timing of follow-up. Staff of the participating hospitalsattended a training program at one of the hospitals to get the follow-up more standardised. After 2 years, mi-gration should be measured with the EBRA method on a serie of four standard pelvis radiographs of each pa-tient.At the beginning of evaluation, problems appeared with missing or delayed radiographs and varying qualityof the Radiographs (tilting, rotation, exposure), partially depending on the hospital. Out of 131 series of ra-diographs, in 94 (72%) migration could be analysed in two directions. 36 series could only be analysed in thex-axis. The percentage of comparable radiographs varied between the hospitals (35% - 91%). Conclusions: a precise instruction for taking standardised radiographs must be performed by the involvedradiological institutes and the follow-ups have to be in time. Otherwise, too many radiographs get lost for anEBRA analysis.
Which factors influence the migratory behaviour of the cup?
M. SCHAFROTH, P.E. OCHSNER
Dept. of Orthopaedics, Kantonsspital, Liestal - Switzerland
The migration behaviour of a cup is determined by various factors: the cup design, the type of anchorage andthe implantation technique, as well as patient specific factors. Little is known about the acetabular bonestock, where to place the cup. The histological quality of the bone should be compared with eventual mi-gration of the cup, as measured with EBRA. During primary hip replacement, 110 bone biopsies were taken prospectively from the acetabular roof andanalysed histologically with a non-decalcifying technique. Three types of cups were used: non-cementedMüller SL-cup (85%), Müller Acetabular Reinforcement Ring (14%) and the Burch-Schneider ReinforcementCage (1%). There was standardised radiographic follow-up at 4 months, 1 year and 2 years. Migration wasmeasured with the EBRA-method on all radiographs. Histology was divided into 4 groups: 1. Normal: 25% (mean age 67.7 yrs);2. Increased sclerosis: 22% (66.3 yrs);3. “restless bone” i.e. bone destruction and bone reconstruction at the same time: 25% (68.8 yrs);
S97
4. Bone destruction: 28% (72.3 yrs). We found no migration in 71%, slight migration (1 to 2 mm) in 21%, moderate migration (>2mm) in 8%. In thegroup with slight migration, 13% showed a normal bone stock, 43% increased sclerosis, 25% “restless bone”and 19% bone destruction. In the group with moderate migration there was no case of normal bone stock, 25%increased sclerosis, 25% “restless bone” and 50% bone destruction. The tendency to migrate increased withthe degree of bone destruction.Conclusions: the quality of the acetabular bone stock influences the stability of the implanted cup. The bone stockshould be carefully analysed on the pre-operative radiographs to avoid insufficient anchorage of the cup.
On the comparability of femoral component radiographs
P. MAYRHOFER
Institute for Mathematics and Geometry, University of Innsbruck, Innsbruck - Austria
Several methods for migration measurement of the femoral component are known, but only two (Müller andFCA) analyse the comparability of the radiographs to enhance the accuracy. For the other methods, various reference lines are suggested, assumed to be little affected by rotation of the leg. The aim of thisstudy is to assess the expected theoretical accuracy of such measurements by comparison of measurementsin a real radiographic series with those generated in a mathematical model. Two different stem designs could be compared (Müller straight stem MEM and PCA stem). A series of 116 stems(59 MEM and 57 PCA) with a total number of 1087 standard pelvic radiographs (mean 9 per patient) were mea-sured. After processing with the FCA-method the data files were analysed statistically with respect to the para-meters of comparability. For each type of implant the ranges (min-max) of the comparability parameters were cal-culated. The mean and standard deviation of the ranges was calculated for each implant, providing informationon the prosthetic contours distortion, caused by projection differences on the radiographs. In a mathematicalmodel, combined rotations around all axes of a Cartesian coordinate system were calculated, simulating variousradiographic projections. For that purpose the prosthetic stem was simplified by a triangle, consisting of headcentre, tip and shoulder of the stem. The lengths of its sides corresponded with a middle-sized shaft of the stud-ied prosthesis. The results from the clinical measurements were compared with the mathematical model.The data showed that rotations may not only be considered separately for each axis but in combination. Theamount of femoral rotations in the real patient series exceeded the limits of most experimental studies. Witha combination of 0° to 25° flexion, 10° internal to 50° external rotation and ±7° abduction, ±2 SD of the meanvalues, measured in the real patient series, could be reached. For the worst among 27 studied marker posi-tions in the greater trochanter the theoretical error ranges were +0.6/-3.6mm (MEM) and –0.5/11.8mm (PCA).Using a limit of comparability of 3 mm with the FCA method, the errors could be reduced to +0.2/-2.4 mm(MEM) and 2.5/-8.5mm (PCA).For a landmark in the centre of the zone concerned the errors were reduced to +0.1/-0.3 mm (MEM) and +0.1/-1.5 mm (PCA), respectively.

S98
Precision of femoral component migration following total hip arthroplastyusing the EBRA-FCA digital system
J.M. WILKINSON 1, A.J. HAMER 2, N.F.A. PEEL 1, R. ELSON 2, I. STOCKLEY 2, R. EASTELL 1
1 Bone Metabolism Group, Section of Medicine, Division of Clinical Sciences (NGHT), University of Sheffield2 Lower Limb Arthroplasty Unit, Dept. of Orthopaedics, Northern General Hospital, Sheffield - UK
Manual methods of measuring femoral component migration from 2 dimensional radiographs lack sufficient pre-cision to enable their reliable use in clinical practice. Roentgen stereophotogrammetric analysis offers a highlyprecise alternative, but requires specialised, expensive radiographic equipment, the intra-operative placementof marker beads, and cannot be applied retrospectively. The EBRA-FCA System allows measurements of femoralcomponent migration from plain radiographs, does not rely on beads, and can be applied retrospectively pro-vided radiographs of the correct size are taken. The aim of the study was to evaluate the precision of this sys-tem in clinical practice. Twenty-nine subjects (17 men, 12 women) who had undergone total hip arthroplasty (THA) using a cement-ed, double tapered, polished femoral stem were studied. Duplicate 35x43 cm radiographs of the hip wereperformed on the same day after repositioning, and digitised using a Lumisys 200 laser digitiser. Medial andlateral femoral stem migration was measured at four sites along the femoral shaft. Femoral component sub-sidence was measured using the prosthetic head centre or shoulder as the prosthetic landmark, and thegreater or lesser trochanter as the bony landmark, giving rise to four combinations of measurement values.The prosthetic stem / femoral shaft angle was derived by the software from landmarks recorded in the pre-ceding measurements. Precision was expressed as 95% confidence limits of the mean (+/- 1.96 standard de-viation).
Results:
Stem Migration (mm) Site 1 Site 2 Site 3 Site 4Medial ± 0.57 ± 0.45 ± 0.53 ± 0.53Lateral ± 0.45 ± 0.47 ± 0.34 ± 0.51
Subsidence (mm) GT-SS GT-HC LT-SS LT-HC± 0.58 ±0.78 ± 1.76 ± 1.69
(GT = greater trochanter, LT = lesser trochanter, HC = head centre, SS = stem shoulder).The precision for prosthetic stem / femoral shaft angle was found to be ±0.38 degrees. Conclusions: Precise measurements of femoral stem migration may be made using the EBRA-FCA Dig-ital system. Subsidence of the femoral stem is most precisely measured between the greater trochanterand the stem shoulder. Use of the lesser trochanter as a landmark is associated with poorer precision. Useof this system may enable prospective and retrospective assessment of femoral component migrationin individuals following total hip arthroplasty.The authors would like to thank The Royal College of Surgeons of England, The British Orthopeadic Associ-ation, and The John Charnley Trust for supporting this work.
S99
Migration measurement of femoral components in total hip arthroplasty. Accuracy of EBRA-FCA
R. BIEDERMANN 1, M. KRISMER 1, P. MAYRHOFER 2, B. STÖCKL 1, E. ORNSTEIN 3, H. FRANZÉN 4
1 Dept. of Orthopaedics, University of Innsbruck - Austria; 2 Dept. of Geometry, University of Innsbruck, Innsbruck -Austria; 3 Dept. of Orthopaedics, Hässleholm-Kristianstad Hospitals, Hässleholm - Sweden; 4 Dept. of Orthopaedics,University Hospital Lund - Sweden
Occurrence of early migration of stems and cups above a certain level has been reported to predict pros-thetic failure. This necessitates the development of methods for migration measurement. The aim of this studywas to identify the most accurate reference points and reference lines, respectively, to determine the accu-racy of the EBRA-FCA method and to prove its accuracy with several independent methods. Four different reference lines were chosen for migration measurement. Accuracy has been evaluated by the useof three different methods: 1. Comparison of x-ray pairs taken within one month, 2. Measurement of simulatedupward migration, and 3. Comparison of the EBRA-FCA results with the RSA method. The interobserver varia-tion of the results was also tested.The most accurate reference line for migration measurement of the femoral component is between greatertrochanter and stem shoulder. The accuracy of EBRA-FCA depends on the method of assessment: it is -1.1 mmto +0.8 mm (method 1, range), 0.9 mm (method 2; 95% percentile) and +1.5 mm to -1.2 mm (method 3; 95%percentile), respectively; thus an accuracy better than ±1.5 mm can be estimated. EBRA-FCA has a specificityof 100% and a sensitivity of 78% to detect real migration of more than one millimeter.Conclusion: EBRA-FCA is accurate enough to detect significant migration and to assess the stability of theprosthesis.
Early clinical results using the FCA-method on tantalum marked femora
M. LÜEM
Dept. of Orthopaedics, Kantonsspital, Liestal - Switzerland
Since July 1996 we have been performing a randomised, prospective study, comparing the Virtec versus theMuller Straight Stem in primary hip replacement. All femora, were marked with tantalum balls in the greaterand lesser trochanters. For 2 years, 12 patients were studied with a standardised follow-up including four radiographs. The radiographswere digitised and analysed with the Femoral Component Analysis system (FCA) for possible subsidence. Mea-surements on hard copies (‘manually’) were also made. Subsidence was measured as the distance of the greater trochanter or the tantalum marker to the shoulderof the prosthesis. Furthermore, subsidence was determined as the distance of the lesser trochanter to thehead centre and the shoulder, respectively. To make the FCA outcome comparable with the manual mea-surements, the same time-range was used and the magnification of the radiographs calculated. From the 12 patients, 8 could be evaluated by FCA, but each had only two comparable radiographs. One stemsubsided between the 4-months and 1-year follow-up, it was stable afterwards. The results were similar whenmeasuring on the hard copies. Measurements related to the bone structure of the greater or lesser trochantershowed significant errors. Measuring the distance from the shoulder of the prosthesis to the tantalum mark-er, the results were similar for the FCA and manual measurements. Conclusions: Subsidence can be determined easily and accurately on a radiograph if tantalum markersare placed in the greater trochanter near the shoulder of the prosthesis.

S100
Prediction of femoral component failure by early migration
M. KRISMER, R. BIEDERMANN, B. STÖCKL, C.H. HAID
Dept. of Orthopaedics, University Hospital, Innsbruck - Austria
The clinical value of stem subsidence is not well established. Some authors believe that subsidence alwaysindicates loosening, and others that especially uncemented stems should subside initially. We hypothesisedthat secondary stabilisation after initial migration as well as late onset of subsidence can occur, and wantedto establish the percentage of both. Furthermore, we wanted to evaluate whether different subsidence pat-terns are associated with different survival rates. We report on ten year results of 240 femoral components. Subsidence was measured in plain radiographs taken at regular intervals. Migration patterns could be de-termined in 158 hips (66%). Out of those, 108 stems (68%) were always stable, and five (3%) started to mi-grate after a median of fifty-four months. Forty-five stems (29%) showed initial migration of at least 1 mmduring the first two years. Seventy-three percent of those stems showed secondary stabilisation. Seventeenstems were revised due to aseptic loosening, and twelve due to other reasons. Twenty-nine percent of thestems showing continuous migration were revised after ten years, and 40% of the stems with late onset ofmigration, in contrast to 2% of the non-migrating stems and 6% of the stems with stabilisation following aninitial period of subsidence.Conclusions: Stabilisation after initial subsidence can occur, and this migration pattern is associated with favourablemigration curves. Late onset of migration after a stable period of at least 2 years was observed as well, althoughonly in porous coated anatomic stems. This migration pattern had a incidence of revision.
Bernese periacetabular osteotomy: technical aspects and clinical results
M. LEUNIG, K.A. SIEBENROCK, M.N. MAHOMED, R. GANZ
Department of Orthopaedic Surgery, University of Bern Inselspital, Bern - Switzerland
ABSTRACT: The Bernese periacetabular osteotomy is a joint preserving procedure used in young adults toimprove acetabular coverage and stabilize the femoral head. This juxta-articular osteotomy respects the vas-cular blood supply to the acetabular fragment. It facilitates extensive acetabular reorientation and can becombined with a femoral osteotomy. All acetabular osteotomy steps are performed using the modified Smith-Petersen approach. Anterior joint inspection provides information on acetabular rim pathology and allowscontrol of an impingement free range of motion. The posterior column remains mechanically intact allowingminimal internal fixation and early mobilisation. The dimensions of the true pelvis remain unchanged permit-ting vaginal delivery. Over 700 pelvic osteotomies have been performed since the introduction of the Berneseperiacetabular osteotomy. A greater than 10 year follow-up of the first 75 osteotomies revealed hip jointpreservation in 82% of cases with a good to excellent result in 73%. Poor results correlated with increasedage, pre-existing arthritis, labral pathology and the amount of correction. Treatment of the labral lesions wasperformed only if unstable and included either refixation or resection. (Hip International 1999; 9: 119-126)
KEY WORDS: Hip, Dysplasia, Acetabulum, Osteotomy

S101
Fibrin sealant reduces blood loss in total hip arthroplasty
R.W. CRAWFORD1, P. GIANGRANDE2, D. MURRAY1
1 Nuffield Orthopaedic Centre, Windmill Road, Headington, Oxford - UK2 Oxford Haemophilia Centre, Churchill Hospital, Oxford - UK
ABSTRACT: The purpose of this study was to investigate the influence of a new fibrin glue spray, QuixilTM, onblood loss and blood transfusion requirements in patients undergoing total hip replacement. This fibrin sealantis derived from human cryoprecipitate. It imitates the final stages of coagulation and when sprayed over awound it prevents bleeding. Thirteen patients received sealant, which was applied at different stages duringthe surgical procedure. Treatment patients were compared with 12 control patients who were selected ac-cording to the same criteria. The average total blood loss of the treatment group was 587 ml, a highly sig-nificant reduction in blood loss in comparison with the controls which had an average loss of 1016 ml (p=0.001).No patients in the treatment group needed a blood transfusion, whereas in the control group 5 patients weretransfused with a total of 10 units of blood (p=0.015). We conclude that QuixilTM is an effective means of re-ducing blood loss and blood requirements in total hip arthroplasty surgery. (Hip International 1999; 9: 127-132)
KEY WORDS: Hip, Arthroplasty, Blood loss, Fibrin sealant
Radiographic evaluation of the “conus” uncemented stem
C.C. CASTELLI, F. D’ANGELO, M. MOLINA, A. FERRARIO, P. CHERUBINO
Institute of Orthopaedics and Traumatology “M. Boni”, University of Varese, Varese - Italy
ABSTRACT: The purpose of this study was to evaluate 54 “Conus” uncemented stems both clinically and ra-diologically. The radiological evaluation was carried out to verify the stability of this rounded cross-sectionstem in terms of bone ingrowth and axial subsidence. Clinically, 39 hips (72%) were rated excellent, 13 (24%)were rated good, 2 (4%) were rated fair or poor. The average Harris Hip Score increased from 53 before op-eration to 93 at the time of the last follow-up (average FU 22.5 months). None was reoperated. Radiologi-cally, 13 stems (24%) were judged to have subsided using a method described by Loudon and Charnley (6).Calcar modification, observed in 22 hips (41%), consisted of a slight rounding off of the proximal medial edgeat the cut femoral neck. These results encourage the use of this versatile stem which revealed good primaryand secondary stability, with good load distribution along the femur. (Hip International 1999; 9: 133-138)
KEY WORDS: Total hip replacement, Cementless stem, Radiographic evaluation, Subsidence

S102
Early subsidence of the Exeter femoral stem within the cement mantle inprimary arthroplasties and in revisions using impacted allografts andcement: a roentgen stereophotogrammetric analysis
E. ORNSTEIN1, H. FRANZÉN3, R. JOHNSSON2, T. LÖFQVIST1, A. STEFÁNSDÓTTIR1, M. SUNDBERG1
1 Departments of Orthopaedics, Hassleholm - Kristianstad Hospital, Hässleholm - Sweden 2 Lund University Hospital - Sweden3 Lund and Ängelholm Hospital, Ängelholm - Sweden
ABSTRACT: In five primary hip arthroplasties and in six revisions with impacted, morselized allografts andcement, roentgen stereophotogrammetric analysis (RSA) was planned to be used to measure the subsidenceof the polished and double-tapered Exeter femoral stem, relative both to the cement and the femur. Only intwo primary arthroplasties and in two revisions could the tantalum markers be adequately imaged for RSAevaluation. The stems in the primary arthroplasties subsided 1.4 to 2.0 mm and all the subsidence occurredwithin the cement mantle. The two revisions subsided 1.9 to 3.1 mm within the cement mantle, but there wasalso a slight subsidence of the cement in relation to the femur, 0.5 to 0.4 mm, respectively. No radiographicsigns of stem loosening were found in any of the hips. Our findings of subsidence of the Exeter femoral stemwithin the cement mantle with no radiographic signs of loosening are in accordance with those reported bythe Exeter group. The present technique using tantalum markers in the medioproximal aspect of the cementmantle must be considered as difficult. (Hip International 1999; 9: 139-143)
KEY WORDS: Hip, Primary, Revision, Subsidence, Allografts, RSA
Steel’s triple pelvic osteotomy in the treatment of acetabular dysplasia
N. SENER 1, C. SEN 2, I.R. TÖZÜN 3, B. BOYNUK 3
1 SSK Göztepe Hospital, Istanbul - Turkey2 PTT Hospital, Istanbul - Turkey3 Istanbul Medical Faculty, Istanbul - Turkey
ABSTRACT: Arthrosis is inevitable in patients with acetabular dysplasia. A pelvic osteotomy can prevent sec-ondary degenerative changes in these hips. We have carried out a retrospective review of 12 hips after tripleosteotomy with an average follow-up of 6.5 years (5 to 8). In 92% of the patients there was pain improve-ment, but 42% continued to limp. Radiographic assessment showed improvement of the average centre-edgeangle by 24.6 degrees, anterior centre-edge angle by 26.25 degrees and correction of the acetabular indexby 16.3 degrees. The degree of osteoarthritis improved in six hips over a period of six years. We observedsuperficial infection in two patients. In two patients the correction was lost because of insufficient osteosynthesisand additional surgery was performed for reosteosynthesis. In general triple osteotomy can achieve enoughcorrection and coverage. This type of osteotomy is easier than other periacetabular osteotomies. However,it has disadvantages such as acetabular lateralization, pelvic asymmetry and difficulties in correcting the ac-etabular coverage and stable osteotomy fixation. (Hip International 1999; 9: 144-147)
KEY WORDS: Osteotomy, Pelvic, Triple, Dysplasia, Arthrosis

S103
The effect of legislation on discharge from hospital of patients withproximal femoral fractures 1990-1997
M.A.A. CROWTHER, G.C. BANNISTER, J.H. DIXON
Southmead Hospital, Bristol and Weston General Hospital - UK
ABSTRACT: In 1993, legislation (The Community Care Act) was passed requiring that patients be assessedby social workers before discharge from hospital back to the community. The effect of the Care in the Com-munity Act on the discharges from Weston General Hospital of patients, with fractures of the femoral neck,was studied comparing prospective data from 1990 three years before implementation of the Act, and datafrom February 1996-l997. Length of hospital stay and distribution of placement after admission from homewere compared. There was a 13% rise in bed occupancy caused by a significant increase in time to dischargefor patients newly placed in nursing homes as well as a rise in average inpatient stay for patients dischargedhome. (Hip International 1999; 9: 148-150)
KEY WORDS: Fracture, Proximal femur, Community Care Act, Hospital stay, Discharge, Destination
Cemented hip replacements in patients younger than 50 years: 16-24 yearresults
I.J. LANGDON1, G.C. BANNISTER2
1 University of Bristol, South West Region - UK2 Southmead Hospital - UK
ABSTRACT: Although specialist centres have recorded a 75% survivorship of hip arthroplasty after 20 years(1), results in general orthopaedic units are unreported. Thirty-four patients with 45 primary cemented totalhip arthroplasties implanted by “first generation” cementing techniques were reviewed after a mean of 20years, documenting revision, occupation, and function. Twenty of the 35 (57%) hips were revised after a meanof 12 (2 to 21) years and reviewed after a mean of 7.6 years. Three hips had been subsequently re-revised.Seven out of nine (78%) hip arthroplasties in males failed, compared with 13 of 26 (50%) in females. Eighty-five percent failed by aseptic loosening. Five of nine employed patients had retired or changed profession.The mean Harris Hip Score was 73% (unrevised), 75% (revised), and 64% (re-revised). These results justifycontinuing efforts to improve technique and prosthetic design. Over a quarter of our patients were lost to fol-low up despite repeated contact over the previous 18 years, which mirrors the world literature. To adequatelyassess modern designs and techniques, we must improve retrieval. A national database would assist this.(Hip International 1999; 9: 151-153)
KEY WORDS: Hip, Arthroplasty, Revision, Survivorship
S104
Ilio-psoas bursitis presenting as deep vein thrombosis
M. K. KENAAN 2, C. H. WYNN-JONES 2, V.N. CASSAR-PULLICINO 1
1 Department of Trauma and Orthopaedics, North Staffordshire Royal Infirmary, Stoke-on-Trent* - UK2 Department of Diagnostic Imaging, The Robert Jones & Agnes Hunt Orthopaedic Hospital, Oswestry - UK
ABSTRACT: Para-articular communicating cysts of the hip joint can uncommonly cause secondary compres-sion of neighbouring neurovascular structures. We report two patients with ilio-psoas bursitis in whom deepvein thrombosis of the lower extremity and an inguinal mass were the mode of presentation. (Hip International1999; 9: 154-157)
KEY WORDS: Bursa, Ilio-psoas, Venous thrombosis
Pathological anatomy of developmental dysplasia of the hip joint
N.M.A. PORTINARO1-2, R.D. CASE2, M.F. GARGAN2
1 Clinica Ortopedica, Ospedale San Raffaele, Milano - Italy2 Bristol Children Hospital, St.Michael’s Hill, Bristol - UK
ABSTRACT: The pathology of developmental dysplasia of the hip (DDH) is reviewed using post-mortem ma-terial and observations at operation. Different patterns of dysplasia, found macroscopically and microscop-ically, are related to the different stages of foetal maldevelopment. We believe that an understanding of themorbid anatomy and histology is the cornerstone from which a rational treatment protocol can be developed.(Hip International 1999; 9: 158-162)
KEY WORDS: DDH, Pathology
I LABRAL LESIONS OF THE HIP
Biomechanics and pathomorphology of labral lesions in the hip joint
C. TSCHAUNER (CONVENOR)
Orthopaedic Dept. LKH, Stolzalpe - Austria
The capsular-labral complex consists of the capsule and the triangular fibrocartilaginous labrum, which isfixed at the bony acetabular rim (limbus) and supported by the ligamentum transversum acetabuli in the cau-dal part. The capsule is separated from the labrum by a gap (recessus perilimbicus). No gap occurs betweenthe articular side of the labrum and the joint cartilage of the lunate surface in the anterolateral part. There are two basic mechanisms for labral lesions of the hip joint:1) major (rotational) trauma or recurrent microtrauma in the post-traumatic group;2) chronic mechanical overloading due to instability in acetabular dysplasia impingement due to mal-torsion
ABSTRACTS FROM THE SPECIALITY DAY DURING THE FOURTH EFORT CONGRESS - BRUSSELS,BELGIUM, 6 JUNE 1999 (HIP INTERNATIONAL 1999; 9: 163-171)

S105
of the femoral neck, and/or mal-version of the acetabulum.In the “dysplastic” acetabulum, the femoral head is poorly covered by the pathologically orientated acetab-ulum: its lunate surface is sloping in an antero-supero-lateral direction, leading to micro-instability with ten-sion and shear forces on the antero-supero-lateral capsular-labrum complex. As a compensation mechanism,the capsular-labrum complex is hypertrophied (Type “IB” in MRA-classification) and becomes a secondarystabiliser (a “guide rail”) for the decentering femoral head. Progressive mechanical decompensation of thecapsular-labral complex leads to tears (Type “IIB” or complete avulsions (Type “IIIB”) of the labrum.In post-traumatic lesions with normal biomechanics of the hip joint, partial resection of the labral lesion seemsto be appropriate. As the majority of labral lesions are caused by residual hip dysplasia, the basic therapeu-tic principle is a corrective (“redirecting”) acetabular osteotomy.
Diagnosis and imaging of acetabular labral lesions
S. HOFMANN (CONVENOR)
Orthopaedic Dept LKH, Stolzalpe - Austria
Labral lesions are common findings in chronic hip joint pain in patients with residual hip dysplasia or aftertrauma. Clinical signs have been described as the “acetabular rim syndrome” in 1991 but conventional imag-ing including arthrography and MRI are not sufficient for diagnosis. Recently MR-arthrography has shown anexcellent accuracy of over 90% to detect these lesions; so far, however, clinical signs, radiological diagno-sis and therapeutic consequences are not well known. In a prospective study, patients with suspected labi-al lesions were evaluated using a standard clinical protocol, including history, clinical signs, radiography andMR-arthrography. Clinical signs were evaluated in six criteria and two provocation tests. In 11% patients clin-ical suspicion was wrong. Best agreement was with MR-arthrography and with clinical features:- “knife-sharp”groin pain (100%), impingement test (100%) and painful giving way (83%). Thirty five per cent of patientsshowed minor (grade 2) and 52% severe (grade 3 and 4) dysplasia. Independent from grade of dysplasia, noor only slight arthrosis (grade 0 and 1) was found in 64% of patients. In 16% a single acetabular cyst couldbe detected on radiographs, which all could be identified as intra-osseous ganglia on MR-arthrography. Labrallesions type A (post traumatic) were found in 23% of the patients with only no or minor dysplasia (grade 1and 2), whereas labral lesions type B (dysplastic) were found in 67% of the patients with severe dysplasia(grade 3 and 4).In conclusion clinical signs for labral lesions are typical but can also be observed in other pathologies of thehip joint. Radiographs remain the first diagnostic step for differential diagnosis and staging of dysplasia andosteoarthritis. Conventional arthrography can only detect large lesions without further staging and location.Computer tomography should be restricted for malrotation problems of the proximal femur, malversion of theacetabulum or planning of difficult cases. MR-arthrography is the imaging modality of choice. Based on thefindings of this study, we recommend radiographic evaluation for dysplasia and MR-arthrography in patientswith suspected labral lesions of the hip joint.
The Bernese therapeutical concept in the treatment of labral lesions of thehip joint
M. LEUNIG
Inselspital, Berne - Switzerland
The acetabular rim syndrome, characterised by recurrent episodes of sharp groin pain and painful acetabu-

S106
lar impingement frequently in patients with dysplasia of the hip has increasingly been recognised by or-thopaedic surgeons. This pathology, e.g. hypertrophy, degeneration, and/or tears of the labrum as a conse-quence of the abnormal acetabular load has been identified as an early sign of osteoarthritis of the hip joint.To prevent or at least delay severe articular alterations of the hip early addressing of the underlying patho-mechanical problem is recommended. The Bernese peri-acetabular osteotomy is a joint preserving treatmentmodality used in young adults after closure of the growth plate with residual hip dysplasia to improve the ac-etabular coverage and to stabilise the femoral head. If required it can be combined with a femoral osteoto-my. This polygonal, juxta-articular osteotomy preserving the vascular blood supply to the acetabular frag-ment facilitates an extensive acetabular reorientation with improvement of the insufficient coverage of thefemoral head including eventually required medial displacement of the fragment. All osteotomies are per-formed by one approach, the modified Smith-Petersen, allowing an anterior capsulotomy. The joint inspec-tion not only provides information on acetabular rim pathologies but also facilitates the control of impinge-ment free range of motion after the correction. The posterior column remains partially intact, allowing mini-mal internal fixation of the acetabular fragment and early mobilisation similar to that after an intertrochantericosteotomy. Moreover the dimensions of the true pelvis remain unchanged providing unimpeded child deliv-ery in women. Since the introduction of the Bernese peri-acetabular osteotomy more than 15 years ago ap-proximately 700 pelvic osteotomies have been performed. A more than ten years follow-up of the first 75 os-teotomies revealed that the hip joint remained preserved in 87% of treated hips and a good to excellent re-sult in 73% of these patients. Poor results were correlated with an increased age of patients, the pre-exis-tence of arthritis or labral pathologies and the amount of corrections of the femoral deficiency. Treatment oflabral lesions was performed only as a supplementary measure if the labrum was unstable and included ei-ther refixation or resection.
The torn acetabular labrum
R. VILLAR
Cambridge - UK
With advances in diagnostic techniques and minimally invasive surgery, the acetabular labral tear is becom-ing increasingly diagnosed, and understood. Five hundred hip arthroscopies were reviewed retrospectively,from which 76 labral tears were identified as the arthroscopist’s primary diagnosis. Of the 76 patients, 58 hadsufficient data to be included in the study, all patients having undergone partial acetabular labrectomy, thelabral margin being taken back to a stable margin with a power shaver.Mean age of patient was 36.7 years, 25 being male and 33 being female. Chondral damage was present in48% of cases, as well as the primary labral tear. Patients were reviewed simply, by being asked the question“Are you happy with your hip?”. Thirty nine (67.3%) replied “Yes” and 19 (32.7%) replied “No”. Those whowere happy with their postoperative result remained so for a minimum of four years. All those who were un-happy had chondral damage visible at arthroscopy, though no patient became worse within a year of surgery.It is concluded that it is worthwhile undertaking arthroscopic acetabular labrectomy, assuming the skills ex-ist in the relevant orthopaedic unit. If performed, there is an approximately 67% chance the patient will im-prove.

S107
II PLASTIC CONTRIBUTIONS TO HIP SURGERY
V. HEPPERT
BG Unfallklinik, Ludwigshafen - Germany
The development of flaps has revolutioned the possibilities of reconstructive surgery. With these techniquesit is easy to close soft tissue defects in trauma and tumour surgery. Debridement is the most important factorfor therapy success in those subjects of orthopaedic surgery. There is clinical evidence that the quality of de-bridement is better if the surgeon has some experience with plastic surgery, because he knows how to closethe defects. Another very important function - especially of muscle flaps - is the filling of infected cavities inosteitis therapy. In the hip region we rarely need free flaps, because there are so many pedicled muscles witha wide arc of rotation to solve most problems. The most important flaps are: rectus abdominis, TFL, rectusfemoris, vastus lateralis. Vastus lateralis muscle seems to be the best choice. It is easy to harvest, has a greatmuscle volume, a wide arc of rotation and a neglectable donor site morbidity. We use it with great success es-pecially in chronic recalcitrant hip infections after resection arthroplasty.A still unsolved problem for hip surgeons is the avascular necrosis of the femoral head. Once x-ray changesare apparent, osteonecrosis generally follows a rapid course of femoral head collapse and joint incongruity.The patients usually are young adults. Therefore the main goal of therapy is to preserve, not replace, thefemoral head as long as possible. Bone grafts have been used for years to reach that challenging goal. Mostimportant with these techniques is the mechanical support for the cartilage. Literature shows nearly the samelong term results, whether you use a vascularised or a normal bone transplant. But the studies are mostly ofsmall numbers and not comparable due to different classifications and different aetiologies of the necrosis.Pathologists have demonstrated that there is up to now no revascularisation of necrotic bone by a vascularpedicled graft. But the viable cortical strut will be incorporated more quickly and the survival for the trans-plant is safer. The free fibula, through a transtrochanteric canal, is nowadays, the transplant of choice, caus-ing no harm to the anterior or posterior capsule of the hip joint. Success rates are reported up to 90% andseem to be only slightly better than core decompression or correction osteotomy.The combination of plastic surgery and hip surgery brings benefit for patient and doctor, if the available fas-cinating techniques are weighed critically in each individual case.
III PAEDIATRIC HIP CONTRIBUTIONS TO ADULT HIP SURGERY
The assessment of the painful hip in adolescence
A. CATTERALL
Royal National Orthopaedic Hospital, London - UK
Unfortunately many people reach adolescence or young adult life with the residue of previous hip surgery,not all of which has been successful. When assessing these patients it is essential to establish the overall di-agnosis of the problem. Although a primary diagnosis such as Perthes’ disease or acetabular dysplasia maybe apparent, this may be complicated by the problems of avascular change, or possibly neurological deficit,and it is essential that the diagnosis covers all aspects of the problem.The potential for long-term remodelling of the hip establishes the need for surgical treatment. This potentialis related to a number of factors. The first is a horizontal acetabulum, with a wide sourcil or loadbearing sur-face. This should be horizontally orientated for the best transmission of load. The outer 20% of the load-bearing area is formed as the result of the fusion of the lateral acetabular epiphysis and failure of this to oc-cur results in an unstable lateral segment. This piece of the acetabulum which includes the labrum is liable,

S108
if unstable, to degenerative change and the labrum itself may become detached or torn. The next essentialrequirement for normal function is a congruous relationship between femoral head and acetabulum in the po-sition in which the patient stands. Femoral head deformity may be present but provided that the head is sta-ble in the neutral position of weightbearing, good long-term function can be expected. It is a principle oftreatment to establish stable movement in the position of weightbearing. The third important factor is the im-pact of leg length difference and the range of abduction. For normal gait only a few degrees of abduction arerequired, but this is increased if there is shortening at the rate of ten degrees of abduction for each centimetreof leg length difference. It should be a principle of management, therefore, to achieve equal leg lengths asthe result of surgical treatment with an adequate range of abduction to cope with any inequality. A final prob-lem related to hip joint development is the development of avascular necrosis of the upper femoral epiph-ysis, either primarily as in Perthes’ disease, or secondary to treatment as in slipped upper femoral epiphysisor the residue of developmental dysplasia of the hip joint.When assessing the patients, an adequate clinical history and examination are essential. The fixed deformi-ties around the hip must be carefully assessed together with the range of movement, particularly abduction,and any leg length inequality. An extension of clinical examination is the dynamic arthrogram which exam-ines the shape of the femoral head and the stability of the joint on dynamic movement. On the basis of thisexamination the movement may be found to be either stable or possibly eccentric. The latter is related withunstable lateral segment. Where the femoral head is displaced, the subluxation may either be reducible orirreducible. Where the subluxation is reducible, the principle of management will be realignment eitherabove or below the hip in the form of innominate or femoral osteotomy. Where the subluxation is irre-ducible, the acetabulum must be enlarged by a lateral shelf acetabuloplasty of the Chiari procedure.Unstable movement in the form of hinge abduction is a good indication for a valgus extension osteoto-my, which may in addition require a trochanteric transfer to improve the normal biomechanics of the hipjoint. If the involved leg is long the femur must be shortened at the time of the realignment so that the leglengths are equal as the result of the surgery.If all these factors are taken into account, it is possible to recognise indications for all the commonly usedsurgical procedures used in the management of these patients and to plan protocols of treatment to improvefunction.
IV UPDATE ON THE EUROPEAN IMPLANTS REGISTER
J. LEVALLE
Ottignies-LLN - Belgium
At the meeting of the European Hip Society in Beaune last year it was decided that a list of the minimum datarequired for a European Implant Register should be composed by a working group (The European Implants Reg-ister Committee - (EIRC) and that support for this would come from the Maurice Müller Foundation. This com-mittee was confronted with many problems.It appeared that if the majority of European orthopaedic surgeons were to contribute, the exchange of dataand quality control would be forthcoming. We believe that such an improvement is a “must” nowadays. If wedo not voluntarily contribute to a register ourselves, it is likely to be enforced by governments and this maybe in a manner difficult for orthopaedic surgeons and certainly less effective for patient care.We have been recently informed that the EU has entrusted its “Institute for Health and Consumers Protec-tion” to study the implications of an implant register as part of its Fifth Framework Programme.Our present information indicates that if the EIRC of the European Hip Society wishes to participate in theprogramme of the European Community Register it is essential “to single out a list of possible members fromeach EU member state- set up a steering committee;
S109
- agree on and submit a common proposal by October 11th 1999.If the programme is accepted the resources granted by the EU for the EIR could be substantial.The working group of the EIRC suggests the following:- re-assess the data list according to the new programme;- identify a list of members;- submit a common proposal by the 11th October.For countries where a national register is already in operation the person charge should be the delegate onthe committee. For those existing registers, the data that they have recorded, could be sent directly to theEuropean Register Study Centre and be entered into the European register.For countries not having a register the centre will be able to help them to organise a national register ac-cording to the data list.One of our main concerns will be that the use of the register should be easy and not time consuming for thesurgeons participating.It should be noted that several attempts are now being made with a view to create implant registers and thatsome of these appear to be attempted in isolation. Thus European Hip Society through the EIRC has to en-quire about the different projects and registers that are being attempted in this way. If this is not done, or-thopaedic surgeons might find themselves required to fill in several forms for different registers.These concepts, if achieved, will allow informed exchange of information between orthopaedic departmentsand every orthopaedic surgeon to obviously great advantage.
V CURRENT CONCEPTS OF BULK AND PARTICULATE ALLOGRAFT
H. WINKLER (CONVENOR)
Danube Hospital, Vienna - Austria
Allografts in femoral revision surgery
P. POILVACHE
Université Catholique de Louvain, Brussels - Belgium
During the past decade the use of allograft bone for femoral reconstruction has considerably increased dueto the rising numbers of complex revision procedures. In order to reconstruct the femur, allograft bone may be used in a variety of forms: massive or morsellised,cortical or cancellous, frozen or freeze-dried, and sterilised or sterile procured. An ideal bone graft shouldprovide four elements: an osteoconductive matrix, osteoinductive factors, osteogeneic cells, and structuralintegrity. Allogeneic bone is osteoconductive, but its osteoinductive capacity is clearly inferior to the one ofautogeneous bone, and it lacks the osteoprogenitor cells of autologous bone graft. It evokes specific immuneresponse, which is reduced by deep freezing and by freeze-drying. The remodelling observed during graft in-corporation is analogous to intact bone homeostasis and fracture healing, and depends on a cascade of cir-culating systemic factors and molecular signals, notably the bone morphogenetic proteins and transforminggrowth factor - beta molecules. Addition of autogenous cancellous bone or bone marrow to allograft bonecan provide osteogeneic cells and facilitate the incorporation of the graft.Morsellised grafts are adequate for treating cavitary defects, while massive allografts are needed to repairsegmental defects.Non-circumferential cortical defects can be treated by means of strut grafts, but when there is circumferen-tial bone loss proximal allografts may be introduced into the host femur. The residual host femur should not

S110
be removed or devascularised. The surgical exposure should be wide. The implant should be cemented in theallograft. All the bony defects should be bridged. Rigid fixation must be achieved between allograft and host,and the junction should be autografted. The femoral length should be restored, and the abductor mechanismrepaired. Using the abductor tendons left attached to the trochanter of the graft can help to achieve this goal.In the future the efficiency of allografts could be improved by modifying their processing, by using combina-tion grafts, and by adding bone marrow, autologous mesenchymal stem cells, or recombinant bone morpho-genetic protein to the graft.
Morsellised graft
I.D. LEARMONTH
Bristol Royal Infirmary, Bristol - UK
Morsellised graft has been used as a filler for many years. However it is only recently that it has been im-pacted and used as a “structural graft” at revision surgery. The technique was initially used in the acetabu-lum by Sloof (1984) and then applied to the femur by Simon (1991). The use of impaction grafting at revisionsurgery represents a significant advance.Impaction grafting is a technique-dependent procedure. However, there are various factors which will affectthe structural integrity of the graft. It is clearly important that the graft is impacted into a contained space.Tight impaction is essential, but there is currently no mechanism of objectively assessing whether adequateaxial and rotational stability has been achieved.Various biological and mechanical factors may influence graft stability. Thus the addition of heparin reducesthe composite graft strength, while the addition of blood enhances it. Larger sized bone chips have beenshown to provide better stability than small chips - particularly in the acetabulum. However, soil mechanicsstudies suggest that a mixture of large and small chips may optimise the strength of the impacted bone.It has been shown that all the allograft does not necessarily revascularise, incorporate and remodel. Pros-thetic design considerations will affect the environmental stresses which may significantly influence the propen-sity for neovascularisation and continued stability.There are limitations on the availability of allograft. In addition the method of sterilisation (i.e. irradiation) maycompromise the structural integrity of the bone. Bioactive bone substitutes (ceramics, coraline, etc.) are avail-able but further research is required to characterise the biomechanical and biological properties of these ma-terials that will ensure that stability is maintained, both initially and following bone ingrowth.
Endomedullary femoral reconstruction with massive femoral allograft
M. KERBOULL
Hôpital Cochin, Paris - France
Endomedullary femoral reconstruction with a massive femoral allograft, the so-called double sheath tech-nique, aims at repairing (with cortical bone), femoral cortices where they are destroyed, inside the medullarycanal. Its main indication is extensive femoral osteolysis due to an aggressive granulomatosis that has thinneddown cortices, widening the medullary canal and loosening the femoral component.The principle of the technique is relatively simple: it is to repair the femoral cortex inside the medullary canalby lining it with a femoral cortical allograft. After prosthesis and cement removal, reaming and cleaning themedullary canal, a massive proximal femoral allograft is introduced through the cervical orifice. Of course,the graft has to be carefully shaped so that it exactly and tightly fits the medullary canal and goes down be-
S111
yond the pathologic area without splitting thin cortices. Then a standard femoral component can be cementedinto the graft. The femoral allograft is a sheath for the prosthesis and the widened proximal part of the femura sheath for the graft. This technique requires a bone bank well supplied with proximal femoral allografts.This is relatively rare, and the main limitation of the procedure is the difficulty finding a suitable graft.Radiological bone union between the graft and host femoral cortices has been regularly obtained within ayear after surgery. Demarcation between graft and host bone visible in the immediate postoperative time hasprogressively disappeared, the gap being filled with new bone. Three or four years post-operatively we canhardly distinguish the graft from the host bone.The outcome of this type of femoral reconstruction was studied in a series of 27 femoral reconstructionsperformed from 1987 to September 1998 on 26 patients, 17 females and nine males, of an average age of67 years at the time of revision. They had 24 mechanical and three septic loosenings. Femoral bone loss,classified according to SICOT grading, was type III (17), type IV (10), and according to the AAOS systemall cases were classified type III on the level II (9) or III (18). After surgery patients were seen for physicaland radiological examination at six weeks, three months, six months, one year, then every one or twoyears. Four patients died between two and six years postoperatively; none was lost to follow-up. The meanfollow-up duration of the series is five years (6m, to 10 years). Complications were as follows: of threetrochanteric non-unions, two were revised, only one has united; one late and recurrent dislocation; onefemoral fracture below the tip of graft and stem united after plating; one fatigue fracture has spontaneouslyunited.Clinical results, rated according to d’Aubigné scale, were satisfying with a mean postoperative score of 17.4(vs 12 pre-operatively); 23 out of 27 were classified as excellent or very good, one good, two fair and onepoor.Radiologically 25 were successful (graft-host bone union, no resorption of the graft, no loosening of the stem),one was a potential failure (partial resorption of the graft without loosening of the prosthesis) and one an ac-tual failure (partial resorption of the graft and stem loosening).Despite these failures, this reconstruction procedure seems to be valuable and reliable enough to allow us toextend this short series.
VI MANAGEMENT OF SEVERE FEMORAL BONE LOSS WITHOUT BONE GRAFTING
J. WITVOET (CONVENOR)
Hôpital Lariboisière, Paris - France
Upper femoral intramedullary replacement
C. PICAULT
Hôpital Cochin, Paris - France
Since 1991, in severe THR femoral failures, we use a curved revision stem proximally HAP coated, implant-ed with transfemoral approach and distally locked with two screws. A rigorous pre-operative plan must berespected in order to cut and lift the classical pedicled flap, comprising the whole greater trochanter massifand the lateral part of the femoral cortex down to the distal end of the implant. Additional pedicled flap maybe elevated from the linea aspera region in order to safely enlarge the exposure and to provide a supple-mentary zone of consolidation. After the completion of the preparation and cleaning the region, the stem ofa diameter smaller than the femoral canal diameter is introduced and locked. An exact, tight osteosynthesismust bring into close contact bone to bone and bone to stem at the femoral isthmus with control of the greater
S112
trochanter height and lateralisation. The callus of consolidation sets off endocortical as well as subperiostealbone apposition which will spontaneously repair the bone defects (neither bone graft nor substitutes are need-ed). Histological sections made with a prosthesis in situ (in dogs) clearly demonstrate the mechanism of newliving and highly adapted bone ensuring the stem osseointegration without any fibrous tissue interposition.The full documented study of a series of 104 patients (56% from second to eighth revision; from two to sixyear follow-up) demonstrates very satisfactory clinical and radiological results with a two level assessment.With regard to previous bone defects there was not one failure in the bone stock restoration which was con-stantly obtained. Considering stem stability, because of failure of osseointegration, four cases went to alocked stem removal easily performed and immediately followed by a classical replacement with a standardstem implanted in a rebuilt femur; two cases were definitely left in resection; unsatisfactory results were not-ed in seven out of 104 patients.The transfemoral approach regularly carried out illustrates not only a mechanical but also a biological conceptpermitting spontaneous improvement, both in quantity and quality of the femoral bone stock. The distal lock-ing which is only a simple vertical stabilisation and has no distal wedging effect is well tolerated without anyadverse effects on the diaphysis if the proximal stem osseointegration is achieved. This technique is repro-ducible as demonstrated by homogenous results obtained by 24 surgeons in these really difficult cases.
Results of femoral reconstruction in revision total hip arthroplasty using theWagner stem
M. WEBER (PRESENTER), A. HEMPFING, R. ORLER, R. GANZ
Inselspital, Berne - Switzerland
This retrospective study reports the mid-term results of a consecutive series of 39 patients with 40 revisionhip arthroplasties in whom femoral reconstruction was performed using the Wagner stem for loss of struc-tural integrity of a segment of the proximal femur due to aseptic or septic loosening of the femoral compo-nent. The main intra-operative complications were fractures in the shell-like osteolytic proximal femur, withno consequences as to the ultimate outcome. The most frequent postoperative complications were disloca-tions, related to poor soft tissue quality and patient compliance, but not to mild or moderate subsidence. Thelimited off-set of the prosthetic head to the shaft can lead to trochanteric impingement which may act as ahinge for dislocation. This has to be addressed intra-operatively. Clinical improvement was best for pain.Once the stem was osteo-integrated, the clinical and radiological result remained stable for up to nine years.
Total femoral replacement
K. STEINBRINK
Ev. Krankenhaus, Alsterdorf, Hamburg - Germany
The design of the total femoral prosthesis originated from a custom-made prosthesis (St. Georg Hospital,Hamburg), which was later developed into a modular system at the Endo-Klinik, Hamburg. It has been usedmore frequently for failures in revision surgery of total hip and knee prostheses than for tumour cases. Theindications were: loss of bone stock after revision (64 cases), infection (40 cases), history of infection (27 cas-es), tumour (14 cases).
S113
The complications
In this group of 145 patients we had aseptic and septic complications.Among the aseptic complications there were:- 21 dislocations- 4 acetabular loosenings- 1 tibial loosening and- 4 fractures of material, two of these at the hip component when undersized.Of 145 patients, 81 were evaluated according to the Enneking System with an overall survival rate of 60% af-ter ten years. If disarticulation became necessary it was not because the prosthetic design had failed, butbecause of either infection or recurrence of tumour. The final rating was: excellent n = 12, good n = 29, fairn = 30 and poor n = 10.This operation remains a rare procedure. The indication accounts for only 1.4% of all our revision cases.
Results of saddle prosthesis (ENDO-MODELL) in hip revision
C. FRIESECKE
EndoKlinik, Hamburg - Germany
The ENDO-Modell saddle prosthesis has been designed as a simple alternative to other methods of hip re-construction. A saddle-shaped proximal finish of a femoral stem articulates directly against the bone. The in-dication is strictly confined to the irreparable acetabulum after failed THR or after acetabular resection fortumour.The purpose of this study was to investigate the function of the saddle prosthesis ENDO-Modell and fre-quency of complications after implantation. Seventy three saddle prostheses were implanted at the ENDO-Klinik from 1987 to 1991 in cases where bony reconstruction of the acetabulum and re-implantation of an ac-etabular cup was no longer possible. At the time of operation 45 cases were aseptic, 28 were infected. Theimplants were: 13 saddles with standard stems, 51 with a proximal and nine with a total femur replacement.The infected cases underwent one-stage exchange arthroplasty and antibiotic-loaded cement was used tofix the new implant in position.After a postoperative follow-up period of one to five years (average 25.5 months) the functional results were
evaluated according to the Enneking scheme and the implant related and unrelated complications investi-gated. Cases with primary and persisting infection were excluded from the functional evaluation as the re-sulting problems interfered with assessment of the function of the saddle. Mobility, pain, stability, strength,deformity, emotional acceptance and functional activities were graded pre- and postoperatively as very good,good, moderate or poor. The parameters pain and emotional acceptance attained the best results - both wereconsidered postoperatively to be “good”.The complications not related to the saddle were ten persisting and six primary infections, two cases of femoralloosening and two of peroneal nerve palsy.The saddle-related complications among the aseptic cases at the time of follow-up were seven dislocations,one cracked iliac bearing, one iliac wing fracture and three cases of progressive upward migration. All othersaddles migrated only minimally in the initial period after implantation or not at all. Formation of new bonearound the saddle horns was always a sign of the stability of the implant.
Conclusion
The saddle prosthesis is small and modular. The operation is simple. Leg length can be preserved or restored.The saddle can be immediately subjected to full weightbearing. Function depends on the condition of the re-

S114
maining muscles. The indication should be very strict because the procedure can lead to serious complica-tions. It is a useful implant for cases in which reconstruction of the acetabulum by homologous bone graft-ing is no longer possible. In these cases, it is then possible to save the limb.
Failure of migration by injected polyethylene particles around press fitimplants: an experimental study in rabbits
J. FRØKJÆR, S. OVERGAARD, M. LIND, C. BÜNGER, K. SØBALLE
Biomechanics Laboratory and Department of Orthopaedic Surgery, Aarhus University Hospital, Aarhus - Denmark
ABSTRACT: In a rabbit model, we wanted to study the migration of polyethylene particles into the interfacebetween implant and bone, the effect of these wear particles on periimplant tissue, and whether hydroxyap-atite coating inhibited particle migration. Non weight bearing implants were inserted into the distal femur ofboth knees in 14 rabbits. Hydroxyapatite coated implants were inserted on the right side and non coated,polished titanium implants on the left side. Three, four and five weeks after surgery, group 1 (n=7) had bi-lateral intraarticular knee injections of polyethylene particles, group 2 (n=7) had bilateral sham injections. His-tological analysis after six weeks revealed no osteolysis and showed no difference in bone ingrowth betweenthe two groups, but a significantly higher bone ingrowth around hydroxyapatite coated implants. Around im-plants in both groups, only trace numbers of polyethylene particles were found in the interface close to thejoint surface, and no specific inflammatory reaction could be verified. The tip of all implants, against the jointsurface were covered by a massive fibrocartilaginous overgrowth. Synovial tissue contained scattered poly-ethylene particles in group 1, but histology was similar to group 2. The press fit situation and fibrocartilagi-nous overgrowth most likely closed the entrance to the interface. (Hip International 1999; 9: 173-7)
KEY WORDS: Polyethylene particles, Hydroxyapatite coating, Rabbit study
The effect of interleukin-1β, tumour necrosis factor α and particle phagocytosis on monocyte-osteoclast differentiation
W. WANG1, A. SABOKBAR1, A.H.R.W. SIMPSON1, N.A. ATHANASOU 1,2
1 Nuffield Department of Orthopaedic Surgery2 Department of Pathology, Nuffield Orthopaedic Centre, Oxford - UK
ABSTRACT: Interleukin-1 (IL-1) and tumour necrosis factor (TNF) are inflammatory cytokines which are knownto influence osteoclastic bone resorption. To determine the effect of these cytokines on inflammatory macrophage-osteoclast differentiation, we added IL-1ß and TNFα to long term co-cultures of mouse monocytes and os-teoblastic cells. IL-1ß (10 & 100 pg/ml) stimulated osteoclast formation as measured by expression of TRAPand the extent of lacunar bone resorption whereas TNFα (10 & 100 ng/ml) inhibited macrophage-osteoclastdifferentiation and bone resorption. Particle phagocytosis (which is known to stimulate the release of thesecytokines) did not influence the extent of osteoclast formation. IL-1ß stimulation of osteoclast formation mayin part account for the increase in bone resorption associated with this inflammatory cytokine; TNFα inhibi-tion of osteoclast formation may be due to interruption of the interaction between osteoblasts and osteoclastprecursors. (Hip International 1999; 9: 178-85)
KEY WORDS: Particle phagocytosis, Osteoclast differentiation, Bone resorption, Cytokines

S115
Capsular closure to prevent posterior dislocation after primary total hiparthroplasty through the posterior approach
M. DE BUTTET 1, G. PASQUIER 2
1 Clinique Saint Jean, Roubaix - France2 Centre Hospitalier, Roubaix - France
ABSTRACT: Posterior dislocation remains the most frequent early complication after Total Hip Arthroplasty(THA) carried out through a posterior approach. In our experience, the preservation of the capsule and itsclosure after insertion of the prosthetic components significantly reduced our rate of posterior dislocation.We compared 2 groups of patients similar in size (186 versus 174 cases) and characteristics: all cases weredone by one surgeon, with the same surgical technique, the same implants and the same post-operative care.The only difference between the 2 groups was the capsulectomy in the group 1 and the capsular closure inthe group 2. In this retrospective study, 22 dislocations were noted in group 1 (capsulectomy), but only onedislocation in group 2 (capsular closure). This additional technique preventing posterior dislocation after THAseemed to be efficient. (Hip International 1999; 9: 186-93)
KEY WORDS: Total hip replacement, Dislocation, Posterior approach
Detection of asymptomatic venous thrombosis following hip replacementsurgery
Retrospective evaluation of routine screening by duplex ultrasonography based on 286 cases
E. DE THOMASSON 1, C. STRAUSS 2, P. GIRARD 3, I. CAUX, O. GUINGAUD 1, C. MAZEL 1
1 Orthopaedic and Trauma Department, Institut Mutualiste Montsouris, Paris - France2 Medical Imaging Department3 Chest Disease Department
ABSTRACT: This study evaluates a pragmatic approach using duplex ultrasonography (US) for detecting ve-nous thromhosis (VT) after total hip arthroplasty (THA).Venous B-mode and colour duplex US examination of both legs including a systematic evaluation of calf veinswas performed twice during hospitalisation in 286 consecutive patients. VT was diagnosed in 31 patients(12%). Thrombosis was asymptomatic in 28 patients (90%), and was bilateral or concerned the non-operat-ed leg in 6 patients (19.4%). No clinical pulmonary embolism occurred during hospitalisation. Prior phlebitisand age over 70 were identified as statistically significant risk-factors (p<0.02 and p<0.04 respectively). Allpatients were seen at three months. Four patients (1.6%) developed VT between hospital discharge and the3-month follow-up visit.Venous US performed twice after THA detected VT in 31 patients, 90% of these were asymptomatic. This ap-proach might explain the absence of pulmonary embolism (PE) in our series, and support a systematic eval-uation of the vein of the lower limb with ultrasonography after THA. (Hip International 1999; 9: 194-9)
KEY WORDS: Postoperative deep vein thrombosis, Duplex ultrasonography, Complications of THA

S116
Wear and migration of Harris-Galante II acetabular cups 29 cases followed for 3-6 years
A. OLOFSSON, U. KESTERIS, R. ÖNNERFÄLT
Department of Orthopaedics, Lund University Hospital, Lund - Sweden
ABSTRACT: We performed a 3-6 years radiographic follow-up of 28 patients (29 hips) operated on with a Har-ris-Galante II uncemented acetabular component and a cemented ScanHip® femoral stem. The patients av-erage age when operated on was 50 (36-59) years. The primary aim was to measure wear of the plastic lin-er, but migration and radiolucency were also evaluated. In all hips the mean linear wear rate was 0.17 mm/year and the mean volumetric wear rate was 116 mm3/year.The wear rates in hips with a 28 mm head (n=6) were 0.14 mm/year and 83 mm3/year, and in hips with a 32mm head (n=22) the rates were 0.18 mm/year and 130 mm3/year. The total volumetric wear was significantlyhigher in hips with 32 mm head than in hips with a 28 mm head. No acetabular component was radiograph-ically loose, but 3 femoral components were radiographically loose and in need of revision. (Hip Internation-al 1999; 9: 200-5)
KEY WORDS: Hip arthroplasty, Metal-backing, Harris-Galante, Wear
Positioning the infant for a pelvic radiograph
F.G. BONIFORTI 1, G. FUJII 2, M.K.D. BENSON 3
1 Divisione di Ortopedia e Traumatologia, Ospedale Treviglio-Caravaggio, Treviglio (BG) - Italy2 Department of Orthopaedic Surgery, Tohoku University School of Medicine, Sendai - Japan3 Nuffield Orthopaedic Centre, Oxford - England
ABSTRACT: It can be difficult to take reproducible radiographs of infants’ hips. We have compared antero-posterior pelvic radiographs when the infant’s hips are held in flexion or extension. One hundred and fifty ra-diographs of infants aged 3 to 12 months have been analysed. Radiographic indicators for the diagnosis ofdevelopmental dysplasia of the hip and alignment pelvic indicators have been assessed. There were signifi-cant differences using the Student t-test analysis for the symphysis-os ischium angle (p<0.0001) and thepelvic tilt index (p=0.0017) between the positions of the infants’ hips on the x-ray table. Twenty degrees ofhip flexion increases the pelvic tilt backward (decreased lumbar lordosis). When positioning infants over 3months old on the x-ray table the neutral antero posterior position is preferable. The pelvic position is moreneutral when the hips are extended. (Hip International 1999; 9: 206-11)
KEY WORDS: DDH, Pelvic radiograph, Hip flexion contracture
Pigmented villonodular synovitis of the hip
T. BOUDOURIS, A.P. FORTIS , A. PASTROUDIS , A. VARATSOS
Orthopaedic Department, Panarkadian Hospital “Evagelistria”, Arcadia, Tripolis - Greece
ABSTRACT: Pigmented villonodular synovitis of the hip is a quite rare entity characterised by minimal or nosymptoms, until severe pressure into the hip joint leads the patient to seek medical care. A 64 year-old woman
S117
presented with spontaneous hip pain and, except for a cystic lesion of the femoral lead on the x-rays, thelaboratory investigations were normal. During the operation a bleeding mass eroding the femoral head, withminimal acetabular involvement, was found and histological examination revealed pigmented villonodular syn-ovitis. A total hip replacement was performed and the patient was clinically satisfactory 5 years later. (Hip In-ternational 1999; 9: 212-3)
KEY WORDS: Pigmented villonodular synovitis, Hip
Progressive osteolysis after porous-coated anatomic (PCA) uncementedtotal hip arthroplasty Ten-year results in 32 consecutive cases
P. REVALD, P. KJAERSGAARD-ANDERSEN, U. LUCHT
Section for Hip SurgeryDepartment of Orthopaedic SurgeryAarhus University Hospital, Aarhus - Denmark
ABSTRACT: Thirty-two primary non-cemented first generation Porous-Coated Anatomic (PCA) total hip pros-theses in 31 patients were followed prospectively. The average follow-up period was 10.3 years. The medi-an age at surgery was 53 years (range 21-65). All operations were performed by one surgeon. Preoperatively, all cases had a poor Harris Hip Score. Ten years after surgery, 95% were rated good or ex-cellent. Progressive roentgenographical changes were observed. In particular there was severe femoral osteolysis inzones 1, 2 and 7, and extensive wear of the polyethylene liner at the two latest follow-up examinations. Wearof the polyethylene liner, up to 0.4 mm/year, was significantly correlated with osteolysis after seven years(p=0.003). Aseptic cup loosening was the reason for six of the eight failures. At 10.3 years after surgery thesurvival with revision as end-point was 72%.We stopped using the 1st generation PCA prosthesis after five years due to worrying roentgenographic changes.The seven and ten years results have confirmed that this prosthesis cannot be recommended for implanta-tion. (Hip International 1999; 9: 214-20)
KEY WORDS: Porous Coated Anatomic, Hip prosthesis, Osteolysis, Polyethylene wear, Implant failure
Impaction grafting in primary total hip arthroplasty: a pilot study
A. BLOM, I.D. LEARMONTH
University Department of Orthopaedic Surgery, Bristol Royal Infirmary, Bristol - UK
ABSTRACT: The quality of bone encountered in the proximal femur at primary total hip arthroplasty variesconsiderably. It would be advantageous to improve the bone stock quality of patients who are likely to re-quire subsequent revision. Impaction grafting with morsellised autograft was performed at primary total hiparthroplasty on seven patients who had poor proximal femoral bone stock. Minimum follow-up was 33 months.
Abstracts from Hip International Vol. 10 No. 1-4
Hip International / Vol. 11 S-1, 2001 / pp. S117-S192 ©by Wichtig Editore, 2001

S118
One patient died 5 weeks post-operatively. Radiographic assessment showed improved bone stock in fivehips with little or no improvement in one hip. There was no evidence of prosthetic subsidence. Impactiongrafting at primary total hip arthroplasty is a viable method of improving bone stock in patients with poorproximal femoral bone quality. The technique would be of particular benefit in the younger patient present-ing for total hip arthroplasty with poor bone stock in the proximal femur. (Hip International 2000; 10: 11-15)
KEY WORDS: Impaction grafting, Primary total hip arthroplasty, Bone stock loss
Changes in bone turnover and bone density after total hip arthroplasty
N.J. HARRIS 1, A. LOWMAN 1, L. WOLSEY 1, R. HANNON 2, T.W.D. SMITH 1, R. EASTELL 2
1 Department of Orthopaedics2 Bone Metabolism Group, Section of Medicine, Division of Clinical Sciences (NGHT), University of 2 Sheffield, Northern General Hospital, Sheffield - UK
ABSTRACT: The purpose of this study was to relate changes in bone mineral density postoperatively arounda cemented femoral prosthesis with changes in bone turnover. This might allow appropriate timing of antire-sorptive therapies in the prevention of aseptic loosening. We recruited ten patients and evaluated both boneturnover, by measurement of urinary N-telopeptide of collagen type I, bone specific alkaline phosphatase andosteocalcin, and bone mineral density following total hip arthroplasty. Bone formation markers decreased sig-nificantly postoperatively (p<0.001). Bone resorption markers increased postoperatively and were maximal at6 weeks (p<0.05). There was a 5-15% decrease in bone mineral density at the proximal femur by 6 months(p<0.01). The changes in bone mineral density confirm the pattern of reduced stress in the proximal femur.The early decrease in bone formation markers was unexpected and could relate to enoxaparin therapy. Theoptimal time to administer antiresorptive therapy might be 6-12 weeks post-operatively. (Hip International2000; 10: 16-20)
KEY WORDS: Bone turnover, Bone density, Total hip arthroplasty
The role of osteoporosis and fracture comminution in the outcome ofanatomically reduced and adequately fixed intertrochanteric femoralfractures
E. PANAGIOTOPOULOS, A.P. FORTIS, M. TYLLIANAKIS, A. ARMONIS, E. LAMBIRIS
Orthopaedic Clinic, Patras University Rion, Patras - Greece
ABSTRACT: To assess the role of osteoporosis and fracture comminution in the migration of the tip of thesliding screw within the femoral head, as well as the fracture collapse in anatomically reduced and adequatelyfixed intertrochanteric fractures, 151 patients, whose intertrochanteric fractures had been treated surgicallywith anatomic reduction and a centrally placed Dynamic Hip Screw (Protek Synthes, Switzerland), were re-viewed with an average follow-up of 6 months after the fracture had healed (mean 9 months after fracture fix-ation). Osteoporosis was determined using the Singh scale, whereas fracture comminution was classified us-ing the Tronzo criteria. Vertical and horizontal screw migration as well as fracture collapse (screw retrolis-thesis) were measured in immediate anterioposterior post-operative roentgenograms and in roentgenogramsat the end of the treatment. Failure in osteosynthesis occurred in 2.65% of the cases. Osteoporosis is strong-ly related to vertical (P = 0.00001), and horizontal (P = 0.0125) migration of the tip of the screw within the
S119
femoral head and less so to fracture collapse. On the other hand, fracture comminution is strongly related tofracture collapse (P = 0.0124) but not to the migration of the screw within the femoral head. The successfuloutcome of treating patients with intertrochanteric fractures depends on both adequate biology (no severeosteoporosis) and adequate mechanics (proper implant and surgical technique). Anatomic reduction and cen-tral placement of the sliding screw must be performed as a routine. Modifications to decrease the loading ofthe fractured hip (medial displacement and valgus osteotomy) should only be considered in exceptional cas-es in the presence of significant osteoporosis, thus avoiding the expected severe vertical and horizontal mi-gration of the tip of the screw as well as fracture collapse. (Hip International 2000; 10: 21-25)
KEY WORDS: Intertrochanteric fractures, Osteoporosis, Fracture collapse, Sliding screw migration
The long term results of Charnley low-friction arthroplasty in patientswith juvenile chronic rheumatoid arthritis
D. H. SOCHART, M. L. PORTER
The Centre for Hip Surgery, Wrightington Hospital, Hall Lane, Appley Bridge, Lancashire - UK
ABSTRACT: Eighty Charnley low-friction arthroplasties, performed on 49 patients with juvenile chronic rheuma-toid arthritis, between 1966 and 1986, were followed-up for an average duration of 217 months (18.1 years;26 to 366 months). There were 10 male patients (17 arthroplasties) and 39 females (63 arthroplasties) whoseaverage age at time of operation was 28.5 years (18 to 35 years). A total of 14 patients (24 arthroplasties) haddied, at an average of 208 months (17.3 years, 26 to 339 months) following operation.All patients had marked improvement in levels of pain, function and range of movement of the joint, with 88%(43 patients, 70 arthroplasties) being completely free of pain and all but one of the remainder experiencingonly minimal discomfort. Fourteen acetabular components (18%) were revised at an average of 148 months(12.3 years: 26 to 252 months) from the time of operation. Three were revised for deep sepsis, four for ex-cessive wear, and seven for aseptic loosening (9%). Three acetabular components are currently loose andthe total aseptic loosening rate was therefore 13% (10 hips). The average acetabular wear rate was 0.11 mil-limeters per year for the entire series. Twelve femoral components were revised at an average of 153.8 months(12.8 years; 26 to 231 months), three for deep sepsis, five for aseptic loosening (6%) and three following frac-ture of the implant. One component was revised, although not actually loose, during an operation to replacea loose acetabular component. One of the surviving implants is currently loose and the total rate of mechanicalfailure of the femoral implant was therefore 11% (9 hips). Acetabular component survivorship was 94% (95%C.I.: 88 - 99%) at 10 years and 79% (69 - 89%) at 25 years, with the survivorship of the femoral implant be-ing 95% (90 - 100%) and 81% (70 - 91%) respectively. (Hip International 1999; 9: 26-37)
KEY WORDS: Charnley arthroplasty, Cement, Juvenile chronic rheumatoid arthritis
Early aseptic loosening in one design (3M-capital) of cemented total hipreplacement
H.G. PANDIT 1, C.J. HAND 1, J.L. RAMOS 2, N.S. PRADHAN 1, N.J. HOBBS 1
1 St. Mary’s Hospital, Isle of Wight, England - UK2 Queen Alexandra Hospital, Portsmouth, England - UK
ABSTRACT: This is a retrospective study of one particular design of cemented hip (the 3M - Capital) used

S120
in Great Britain in the early 90’s. The study included 224 primary THRs performed over a period of 5 years(average follow-up: 38.4 months) using either monobloc (31) or modular (193) stems the former made of stain-less steel and the latter of titanium alloy. A high incidence of early loosening of the femoral component wasnoticed with both types of stem (12.5% definite loosening, 11.16% possible loosening). Possible aetiologiesare discussed. Thirty-five patients (15.6%) were listed for revision. Early failure with the use of the stainlesssteel implants version of this prosthesis is so far unreported. Patients with early loosening were heavier thanthose without loosening over the same period of follow up, which was statistically significant. Histologicalfindings at the time of revision are also discussed. In early 1998 a national audit was initiated to locate all thepatients with Capital hip implant and these are the results of the study at one of these centres. The need fora national arthroplasty register in a country where more than 40,000 hip replacements are performed annu-ally has become more obvious with failure of the Capital hip. (Hip International 2000; 10: 38-42)
KEY WORDS: Capital hip, Early failure, National register for THR
Acetabular revision with morsellized allograft and the Harris Galanteporous cup. Two to ten year results
M.J. HUBBLE, J.D. ELDRIDGE, M.B. LEE, S.L. WHITEHOUSE, E.J. SMITH, I.D. LEARMONTH
University Department of Orthopaedic Surgery, Avon Orthopaedic Centre, Bristol - UK
ABSTRACT: Sixty eight cementless acetabular revisions were performed using impacted morsellized bonegraft and the Harris Galante 1 porous coated component (HGP 1). Acetabular defects were graded accord-ing to the American Association of Orthopaedic Surgeons classification. Twenty nine (43%) were contained(Type 2 cavitatory) and thirty nine (57%) uncontained (Types 1 or 3 - segmental or combined) defects. Thepatients were followed prospectively for a mean of five years (range two to ten years). Radiological evidenceof graft remodelling was seen in twenty two hips. Progressive radiolucent lines were present in eight cases(12%). Two screws broke. There were two cases of deep infection. Radiological failure, with a change in cupangle of greater than 5 degrees or migration of greater than 5 mm, was seen in six cases (9%). All six haduncontained defects (segmental or combined). Gratifying medium term results have been obtained after re-construction of contained acetabular defects using impacted morsellized bone graft and the cementless HGP1 cup. Inadequate graft support in uncontained defects resulted in six cases of failure. (Hip International2000; 10: 43-48)
KEY WORDS: Revision hip arthroplasty, Bone graft, Acetabulum
Fracture of ceramic components in total hip arthroplasty
A. TONI, S. TERZI, A. SUDANESE, G. BIANCHI
Orthopaedic Clinic of Bologna University, Rizzoli Orthopaedic Institute, Bologna - Italy
ABSTRACT: The authors experienced two cases of alumina prosthetic components fracture among the 2879implanted in 10 years; these components were part of 1484 prosthetic implants. In both cases ceramic frac-ture was the result of a surgical technical error: in the first case a 32 mm alumina head was replaced in thesame tapered neck with a 28 mm one during cup revision without removing the stem; after 9 months the newhead failed. In the second case the prosthesis presented recurrent sub-dislocations causing alumina cup lin-er chipping. Fracture of a ceramic component is actually an episodic complication (0,08% in our experience),

S121
often caused by an uncorrect surgical technique, and shall not limit the use of this material. (Hip International2000; 10: 49-56)
KEY WORDS: Ceramic, Fracture, Total hip arthroplasty, Complication
DDH treatment with Pavlik harness: weekly ultrasound monitoring forstability
C.J. HAND 1, N.M. PORTINARO 2, R.H. RICHARDS 1
1 Trauma and Orthopaedic Surgery, Queen Alexandra Hospital Portsmouth, Hants - UK2 Trauma and Orthopaedic Surgery, Bristol Children Hospital, Bristol - UK
ABSTRACT: Normal development of the infantile hip joint relies upon the congruent and stable relationshipof the femoral head and the acetabulum. Treatment with dynamic bracing for instability of the hip joint is ac-cepted, but the duration of treatment required and the timing of follow up is of current debate. The aim ofthis study was to determine the outcome of Pavlik Harness treatment in children with early presenting ultra-sonographically unstable and dislocated hips, independently of morphological appearance of the joint. Chil-dren suspected of having or to be high risk for DDH were assessed by clinical and ultrasound examination.Ultrasonographically unstable and dislocated hips were treated in the Pavlik harness and reviewed weeklywith ultrasound. Once reduction had been maintained for six consecutive weeks weaning from the harnessover the following 5 weeks was started. Thirty three children (37 hips) were treated. The mean follow up timewas 2.9 years (6 weeks – 5.3 years). Six hips failed to remain reduced. There was no statistical difference inage at commencement of Pavlik harness treatment between the successfully and unsuccessfully treated groups(p>0.1). Evaluation of the duration of splintage required to achieve reduction of the hip compared against theage of the child at the commencement of splintage revealed no statistically significant correlation (p>0.1) tobe present. Early treatment of hip instability within the first weeks of life, even with an apparent normal mor-phology of the acetabular socket, results in normal joint development, decreasing the need for prolongedcompliance with treatment. It may also reduce the incidence of late presentation, without increasing the rateof complications (0 in our series). (Hip International 2000; 1: 57-61)
KEY WORDS: Pavlik harness, Hip instability
Down-hill skiing after a total hip replacement?
P. KLOEN, H.R. DE MAN, R.K. MARTI
Department of Orthopaedic Surgery, Academic Medical Centre, Amsterdam - The Netherlands
ABSTRACT: This paper presents data on a group of 9 patients (12 hips) who underwent a total hip arthroplastyand subsequently engaged in down-hill skiing. Average follow-up was 6.4 years (range 1-13 years). Average timeto return to skiing was 10.3 months after surgery. None of the patients reported difficulties during their skiing ac-tivities. Only one acetabular and one femoral component developed grade 2 loosening. None of the hips need-ed revision. The acetabular wear rate (0.16 mm/year) was comparable to those reported in the literature, althoughhigher than another on average less active group treated with the same prosthesis by the same surgeon. A re-view of the literature on athletics after hip arthroplasty is given. Based on our early results and the literature, wefeel that down-hill skiing is feasible for the THR patient, but they should be advised to ski with long turns ongroomed slopes. Longer term follow-up studies are needed to address the issue of athletics after hip arthro-

S122
plasties in general, and more specifically, of downhill-skiing. (Hip International 2000; 10: 77-82)
KEY WORDS: Total hip arthroplasty, Down-hill skiing, Athletics, Wear
Precision of dual energy X-ray absorptiometry in determining periprosthetic bone mineral density of the hydroxyapatite coated hip prosthesis
A.I.A. RAHMY 1, A.J. TONINO 2, W. TAN 1, G. TER RIET 3
1 Department of Nuclear Medicine, Atrium Medical Centre Heerlen - The Netherlands2 Department of Orthopaedic Surgery, Atrium Medical Centre Heerlen - The Netherlands3 Department of Epidemiology, Maastricht University, Maastricht - The Netherlands
ABSTRACT: The objectives of this study were to demonstrate the potential usefulness of dual-energy X-rayabsorptiometry (DEXA) in the assessment of dynamic changes in bone mineral density (BMD) around thefemoral stem of non cemented hydroxyapatite-coated hip prostheses and to establish our procedures by de-termining the variabilities associated with error introduced by the machine, operator, and/or subject. Methods: Regional BMD were measured twice by DEXA for 27 patients. All scans were analysed twice by ap-plying large size regions of interest (ROI’s), 7 in total, defined by ‘modified’ Gruen zones. The data of 27 pa-tients were analysed for the second time using smaller size ROI’s, 14 in total, 7 small ROI’s on each of themedial and lateral sides of the prosthesis. Three patients, all of whom exhibited intense ectopic ossification,were scanned twice. The variation associated with rotation of the femur was assessed by scanning six pa-tients first in neutral rotation, thereafter by ± 15° in internal and external rotation position. Results: The overall coefficient of variation (CV) using ‘modified’ Gruen zones was 2.40% and varied accordingto the zone assessed. When smaller zones were used, the overall CV was 3.42%. The overall CV in the patientswith ectopic ossification was 7.56%. When the leg was rotated by ± 15° externally or internally, the overall CVwas approximately 10%. Conclusions: Patient positioning is probably the most variable condition in the clinical setting. Using large ROI’ssuch as ‘modified’ Gruen zones yields significantly better overall precision than using smaller ROI’s. Patients withintense ectopic ossification are not suitable candidates for longitudinal study. (Hip International 2000; 10: 83-90)
KEY WORDS: Hydroxyapatite, Total hip arthroplasty, Dual-energy x-ray absorptiometry
The effect of in-stem versus around-stem centralizers on cement mantlethickness and stem alignment in total hip arthroplasty
J.M. WRIGHT 1, K. J. SALEH 2, E. T. TOLO 1, M.P.G. BOSTROM 1, P. PELLICCI 1, E.A. SALVATI 1
1 The Hospital for Special Surgery, New York - USA2 Department of Orthopaedic Surgery, University of Minnesota Delaware St.S.E., Minneapolis, Minnesota -USA
ABSTRACT: The long term success of cemented total hip arthroplasty has been attributed to the presenceof a well pressurized, thick cement mantle around a properly designed stem that has been placed in neutralalignment. Femoral centralizers were developed to achieve this goal more consistently.While some centralizers fit into the distal tip, others fit around the tip of the prosthesis. We undertook a studyto compare the effect of an into-distal-tip (IDT) centralizer versus around-distal-tip (ADT) one. A retrospec-

S123
tive review of three groups of primary total hip arthroplasty (THA) patients was performed. Group I consisted ofa control population of the last 100 consecutive cases performed with no distal centralizer. Group ll consistedof the first 100 consecutive cases performed with the IDT design. Group lll consisted of 51 consecutive patientsperformed using an ADT centralizer. All cases were performed with similar cementing technique by the samesenior surgeon (E.S.). Our results show that, while adequate mantles can be obtained, either with or without theuse of a centralizer, an around-stem centralizer on a tapered distal stem consistently gave a more neutral stemalignment and a thicker, concentric cement mantle. (Hip International 2000; 10: 91-97)
KEY WORDS: Alignment, Cement thickness, Centralizers, Hip Arthroplasty
The use of PLLA screws for the fixation of bone graft in total hip arthroplasty
K. ANDO, T. YAMAJI, T. UKAI, K. NAKAGAWA
Department of Orthopaedic Surgery, Fujita Health University School of Medicine, Toyoake City - Japan
ABSTRACT: We used Poly-L-lactic Acid (PLLA) screws for fixation of bone graft during THA operation in 22patients (22 hips) with terminal stage coxarthrosis accompanied by marked acetabular dysplasia. Fixationwith PLLA screws alone was performed in 6 of the first 7 cases. A metal washer was also used for better sta-bility in one hip in which the bone graft was soft. In order to achieve adequate fixation between graft boneand acetabulum, a PLLA washer was produced and used at the time of PLLA screw fixation in the other 15cases. Good bone union and good remodelling of the graft bone were observed in all hips. Since the follow-up period was short, the long term state of the grafted bone in the absorption process of the PLLA screws isstill unclear. However, at present, PLLA screws appear to be a promising material that can replace metal orceramic screws which may have some problems. (Hip International 2000; 10: 98-101)
KEY WORDS: Poly-L-lactic acid, Bone graft, Total hip arthroplasty, Acetabular dysplasia
Aseptic loosening of Boneloc cemented Exeter total hip replacement. A 5 year follow-up of the first 100 hips
P.B. THOMSEN, S. BØVLING, B. JACOBY, T.B. HANSEN
Department of Orthopaedics Holstebro Central Hospital, Holstebro - Denmark
ABSTRACT: To evaluate the midterm performance of Boneloc cemented primary Exeter hip arthroplasty we ex-amined the first 100 hips in 93 patients, who were alive at a median 56.6 (50-62) months after the operation. Dur-ing the follow-up period 2 femoral stems and 2 acetabular cups were revised because of aseptic loosening from3-5 years after the operation. A third acetabular cup was revised at the same time as a loose femoral stem, butwas not found loose. The 5-year survival of both the stem and the cup was 98 per cent and for the surviving 98hips the average Harris Hip Score was 87.6 (43-100) and the average pain score was 42.2 (10-44). Eighty nineper cent of patients were very satisfied or satisfied with their hip prosthesis and the patients’ own evaluationscorrelated well with the Harris Hip Scores. Follow-up radiographs revealed definite loosening of 3 stems and 2cups, probably loosening of one stem and 2 cups, and possibly loosening of 2 stems and one cup. The Exeterstem subsided significantly within the cement mantle by median 3.3 (0-19) mm. In a subgroup of patients subsi-dence diminished significantly from the first 28 months compared to the last 31 months. Subsidence at the ce-ment bone interface was only seen in 4 hips, where cement fractures had developed. Poor quality cementation,
S124
and valgus position of the femoral stem, significantly increased the risk of aseptic loosening, as did osteolysisand cement fracture. Poor cementing technique and continuous radiolucent lines at follow-up radiographs werepositively correlated with acetabular cup loosening. The rather good midterm results with the Exeter femoral stemcan probably be ascribed to the collarless, polished, double tapered stem design. (Hip International 2000; 10:102-107)
KEY WORDS: Total hip arthroplasty, Exeter hip, Boneloc cement, Aseptic loosening
Age and surgical management determine quality of life after trochantericfracture
F. GUILLEMIN 1, M.M. CAO 1, J.P. DELAGOUTTE 2, D. MAINARD 2
1 Service d’Epidémiologie et Évaluation Cliniques, Hôpital Marin, CHU de Nancy - France2 Service de Chirurgie Orthopédique et Traumatologie, Hôpital Central, CHU de Nancy - France
ABSTRACT: Purpose: The aim of the study was to determine factors influencing functional ability and quality of lifesix months after trochanteric fracture treated surgically.Patients and method: A multicentre cohort included 459 patients (356 females and 103 males, mean age 80 years)in Eastern France. Sixty-two percent of the fractures were stable and 38% were unstable. Determinants of functionalability assessed by the Merle d’Aubigné and Harris scores, of quality of life by the Duke Health profile, and of returnto home at 6 months after surgery were considered using logistic regression analyses.Result: Older age was the most prominent factor predicting bad functional ability (p<.001) and quality of life (p<.05).The material for surgery predicted 6-month poor functional ability (p<.001), probably through the different strategiesfor care management involved. The quality of fracture reduction assessed on lateral radiographs, as well as post-operative complications were predictors of a better functional ability (p<.001) and less frequent return to home(p<.001).Conclusion: Age and surgical management procedure are determinants of outcome at 6 month after trochantericfracture. (Hip International 2000; 10: 108-115)
KEY WORDS: Hip fracture, Prognosis, Quality of life
A tissue retractor for hip fracture surgery
M.J. PARKER, R.J. PATTERSON
Orthopaedic Department, Peterborough District Hospital, Peterborough - UK
ABSTRACT: A tissue retractor is described for use during insertion of a sliding hip screw in hip fracture surgery.The retractor enables an unassisted surgeon to have good operative exposure whilst causing minimal tissuedamage. (Hip International 2000; 10: 116-117)
KEY WORDS: Hip fracture, Sliding hip screw, Instruments
S125
Confirmation of the reduction and containment of the femoral head withCT or MRI scans in DDH: The need for repeated scans
R.D. CASE, M.F. GARGAN, D. GRIER, N.M.A. PORTINARO
Bristol Royal Hospital for Sick Children, St. Michael’s Hill, Bristol - UK
ABSTRACT: The accuracy of reduction of the femoral head in the acetabulum after the application of plastercasts in open and closed reduction was retrospectively assessed by means of CT or MRI scan in 59 patientsand 67 hips. Scanning after the first plaster application showed that the position was not maintained in thehip spica in 1 out of 37 patients (3%), who had undergone open reduction, and 8 out of 30 (27%), who hadundergone closed reduction. All hips shown to be reduced and contained at the time of the first scan, andheld in a spica remained reduced on subsequent scans. This study shows that the hip is vulnerable to redisplacement, especially after closed reduction, but stabilisesafter the first 6 to 8 weeks in plaster. This suggests therefore that repeating the scan after each plaster changewas not necessary, and that resources could be conserved.This study has also shown that all the 113 CT scans clearly defined the anatomy but 6 out of the 33 MRI scanswere blurred and needed repeating. (Hip International 2000; 10: 118-122)
KEY WORDS: Developmental dislocation of the hip, CT scan, MRI scan
Fragmentation of the polyethylene cement restrictor in total hip arthroplasty
O.A. GABBAR, R.W. WILLIAMS, R.F. SPENCER
Weston General Hospital, Weston-Super-Mare - UK
ABSTRACT: The presence of polyethylene wear particles at the bone-cement interface after joint re-placement is considered a major cause of prosthetic loosening. Nevertheless, many surgeons contin-ue to use winged Hardinge polyethylene restrictor of which fragments are frequently seen to detachduring insertion into the femoral canal, and to emerge during medullary lavage. The extent to whichsuch fragments may be retained in the femoral cement mantle is not clear, and there is obvious con-cern that such fragments may result in polyethylene granuloma formation. We reviewed 89 post-oper-ative X-rays after hip replacement employing the Hardinge restrictor. The following issues were exam-ined: 1. Dimensions and number of distal radiolucencies in the cement and their correspondence with thewing size of the restrictor, 2. Method of suction used during pressurised lavage,3. Proximal and distal canal diameter and amount of taper, 4. Gruen zone location of radiolucencies. Linear lucencies corresponding exactly to the wings of the restrictor were found on 14 X-rays (15.7%),7 were seen out of 54 cases in which distal suction was used during lavage, and 7 were seen in 35 cas-es in which proximal suction only was employed. There was no statistical difference between these twomethods of suction in limiting the number of retained fragments of restrictor (P= 0.156). There was nocorrelation between the likelihood of fragment detachment and canal taper or distal diameter. A totalof (17) detached fragments were identified, distributed in the following Gruen zones; 3 (35.3%), 4 (38.2%),5 (26.5%). We suggest that the above observations should alert surgeons who wish to use this type ofrestrictor to the importance of meticulous femoral preparation, preferably under direct vision, to en-
S126
sure that no fragments of restrictor become detached (Hip International 2000; 10: 123-126)
KEY WORDS: Hip replacement, Polyethylene particles, Aseptic loosening, Bone-cement interface, Cement restrictor
Mechanisms of bacterial resistance in implant infection
J. CORDERO, E. GARCÍA-CIMBRELO
Orthopaedic Department, Hospital La Paz, Madrid - Spain
ABSTRACT: Although prophylaxis has cut down the infection rate in any type of implant to an average of 2.3%(0.38%-10%), the increased number of orthopaedic implants worldwide results in an extremely high numberof cases yearly. Infection is also one of the most serious complications of implant surgery: it provokes life-long clinical sequelae, and greatly increases the difficulty and cost of treatment. Most bacterial infections respond to antibiotics alone, but implant infections do not. Most of the hypothesesdeveloped over the last 40 years have been confirmed in clinical practice, and the most recent ones have notreplaced earlier ones. (Hip International 2000; 10: 139-144)
KEY WORDS: Bacterial resistance, Implant infection
Acetabular revision with a roof reinforcement ring and impacted allograftbone
P. WONG 1, K.J. SALEH 2, A. KING 1, A.E. GROSS 1
1 Division of Orthopedics, Mount Sinai Hospital Toronto University, Toronto, Ontario - USA2 Department of Orthopedics University of Minnesota and Clinical Outcome Research Center, Minneapolis, 2 Minnesota - USA
ABSTRACT: A series of 43 acetabular revisions treated with impacted allograft bone and a roof reinforcementring were reviewed. The average follow-up was 5 years (2-15). The mean age was 70 years. The position ofthe hip center, and the orientation of the ring and cup were digitized and measured.The average inclinationof the roof ring with respect to the horizontal was 44° (22°-60°) early post-operatively. The cup inclinationwas 33° (21°- 49°). These figures did not change significantly at the latest follow-up. Definite loosening wasdefined as migration of the components or breakage of the screws. Four components were definitely loose.Two other patients had continuous radiolucent lines, but no migration of the components at the bone-implantinterface. The radiographic success rate was 86%. Pre- and post-operative Harris Hip Score were 34.1 (18 -65) and 71.6 (36 - 90) respectively. The study supports the use of impacted morsellized allograft bone and aroof reinforcement ring for cavitary acetabular defects. (Hip International 2000; 10: 145-150)
KEY WORDS: Acetabulum, Hip reconstruction, Allograft, Reinforcement rings

S127
Histological investigation of polyethylene particles in total hip replace-ment: ceramic versus metal heads
I. BOS
Institute of Pathology, Medical University of Lübeck, Lübeck - Germany
ABSTRACT: Pseudocapsules and interface membranes around hip prostheses with ceramic- and metal poly-ethylene combinations from 128 revision cases and 40 autopsy cases were histomorphologically analysed,including a semiquantitative grading of the wear particles and histological changes. The amount of wear par-ticles increased with increasing implant duration.Comparing the revision cases with metal-on-polyethylene combinations and ceramic-on polyethylene com-binations 4 to 8 years in situ, more than twice as many polyethylene wear particles were produced from pros-theses with metallic heads. In the autopsy cases with stable prostheses 3 times more polyethylene wear wasfound. The synovial layer was found to be thicker in the metal-polyethylene couplings, the villous transfor-mation of the synovial surface and the scar-like fibrosis of the pseudocapsules appeared to be more pro-nounced too. Differences between the different types of prostheses with metal-polyethylene combinationswere not apparent with the exception of the bipolar prostheses, which showed markedly increased polyeth-ylene wear. (Hip International 2000; 10: 151-160)
KEY WORDS: Hip prosthesis, Polyethylene wear, Ceramic-polyethylene couples, Metal polyethylene couples,Foreign body reaction
Depth of insertion and radiographic fate of non-holed cementless metalbacked acetabular components
J. WRIGHT, M. BOSTROM, P. PELLICCI, E. SALVATI
The Hospital for Special Surgery, New York - USA
ABSTRACT: A retrospective radiographic review of 48 non-holed, factory assembled, cementless metal backedacetabular components, implanted in 45 patients, was performed. Post operative anteroposterior radiographsof the hips were compared to the radiographs at one year follow-up. In addition, measurements were madeon 100 post-operative radio-graphs from patients implanted during the same time period with multiple holedacetabular components whose polyethylene liner was assembled after final impaction of the metal shell. Thenon-holed cups were implanted at a greater distance from Kohler’s line than the multiple holed acetabularcomponents (1.45 ± 1.83 mm [ range 0 - 7.89 mm ] vs. 0.69 ± 1.70 mm [range 0 -15.26 mm], p = 0.018). Alarger percentage of non-holed cups had gaps between the metal shell and the bone bed (67% vs. 17.5%).Impaction through the polyethylene liner of the non-holed acetabular components leads to a higher incidenceof radiographic gaps between the metal shell and the bone bed as well as lateralization of the component,since there were no holes to assess the proper seating at surgery. These radiographic findings did not ap-pear to be detrimental, however, as the cups remained radiographically stable at one year follow-up. (Hip In-ternational 2000; 10: 161-165)
KEY WORDS: Acetabulum, Total hip arthroplasty, Non-cemented, Insertion depth

S128
A little too close to the bone? Risk of sciatic nerve injury during hiparthroplasty
W.T.M. MASON, B.M. BURGESS, R.N. VILLAR
Department of Anatomy, University of Cambridge, Cambridge - UK
ABSTRACT: Sciatic nerve palsy is an uncommon but potentially disabling complication of total hip arthro-plasty and may be a cause for litigation. At operation, the location of the nerve appears to be extremely vari-able. In this study, the position of the sciatic nerve in relation to the femoral head, the greater trochanter andthe ischial tuberosity was measured in thirty-nine cadavers. The distance between the nerve and the femoralhead varied from 15 to 32 mm (mean 23 mm). This distance was unrelated to patient size or sex. Its positionbetween the ischial tuberosity and the greater trochanter was also variable. In view of its variable and un-predictable position, it is recommended that the sciatic nerve is identified in all hip arthroplasties when a pos-terior approach is used. (Hip International 2000; 10: 166-169)
KEY WORDS: Sciatic nerve palsy, Total hip arthroplasty, Litigation
The Windsweep Index: a method of evaluating pelvic asymmetry andmonitoring the efficacy of treatment in cerebral palsy
N.M.A. PORTINARO, K. OWERS, J. PYMAN, M.F. GARGAN
The Royal Hospital for Sick Children, Bristol - UK
ABSTRACT: Progressive asymmetry of the pelvis is frequently observed in total body involved cerebral pal-sy (CP) children, when opposite contractures and deformities affect the two sides of the body. This asym-metry is important in terms of difficulty in standing and seating stability and if untreated can lead to bilater-al dislocation of the hip. The visual term “Windsweep” has been used to describe this deformity. We presentan equation to determine the extent of this asymmetry - the “Windsweep” Index (WSI). This can be used asa numerical assessment of the deformity and to assess the efficacy of treatment. (Hip International 2000; 10:170-173)
KEY WORDS: Windsweep index, Cerebral palsy, Pelvic asymmetry
Ipsilateral fractures of the hip, femoral shaft, distal femur and patella
J. BARTONÍCEK, J. STEHLÍK, P. DOUSA
Department of Orthopaedics and Traumatology, 3rd Medical Faculty of Charles University, Prague - CzechRepublic
ABSTRACT: The case reports unusual ipsilateral fracture of the femur, i.e. intertrochanteric fracture, diaphy-seal fracture, intra-articular fracture of the distal femur and cominuted fracture of the patella. The fracture ofthe femur was succesfully treated by the long gamma nail and angled condylar plate, the fracture of the patel-la by tension wiring. (Hip International 2000; 10: 174-177)
KEY WORDS: Ipsilateral fractures of the femur, Long gamma nail
S129
I CEMENTLESS TOTAL HIP ARTHROPLASTY: LONG-TERM RESULTS (PART I)
Long-term results of different first-generation cementless hemisphericalporous-coated cups
E. GARCIA-CIMBRELO
Hospital la Paz, Madrid - Spain
We analyse the long-term results of 236 first-generation hemispherical porous-coated cups implanted between1984 and 1991. Ninety-three were Harris-Galante I (HGP I) cups, 103 were PCA, and 40 were ACS polyethy-lene liners associated to 19 Trilock and 21 Profile shells. The mean follow-up was 12.7 years for the HGP Igroup, 12.6 for the PCA group, and 9.0 years for the ACS group.Radiographic loosening was present in 8 HGP I cups and 30 PCA (40% at 16 years according to Kaplan andMeier), but not in ACS liners (p<0.001). However, polyethylene liner rupture occurred in one HGP I cup, 2 PCA,and 9 ACS cups (29% at 11 years according to Kaplan and Meier) (p<0.001). There were 6 revisions of the HGP I cups, 31 of the PCA cups and 9 ACS liners ruptured. Due to polyethyle-ne wear, 5 HGP I polyethylene liners were also changed during a femoral stem revision.Mean polyethylene wear, excluding the cases with rupture of the polyethylene liner, was 0.17 mm/year for theHGP I group, and 0.16 mm/year each for the PCA and ACS groups. Osteolytic cavities around the cup wereseen in 2 HGP I cups, in 24 PCA cups, and in 8 ACS cups that had a ruptured polyethylene liner.In conclusion, radiographic osseointegration was more frequent in cups made in titanium (HGP I and ACS [Trilock andProfile shells]). There was 40% of radiographic loosening in the PCA group (made in chrome-cobalt). The rupture of thepolyethylene liner was more frequent in the ACS group. Fewer HGP I cups required revision than the other designs,although the incidence was higher than in other published series. Polyethylene wear was similar in the three groups.
Cementless acetabular component in primary THA. Long-term results
J. SANCHEZ-SOTELO
Mayo Clinic, Rochester, Minnesota - USA
This study analyses four different designs used in our institution: PCA; Acetabular Reconstruction Compo-nent; Osteonics Dual Geometry, Dual Radius and Threaded; and Harris-Galante.A. Porous Coated Anatomic. Loosening and osteolysis were frequent (539 PCA cups). After 10 years, 13.2%of the cups had been revised, and 17.8% had loosening. The percentage of surviving cups without looseningor osteolysis was 61%.B. Acetabular Reconstruction Component. 71 cups are analysed after 10 to 13.3 years. There was a 4% in-cidence of loosening and osteolysis. C. Osteonics. Polyethylene wear and osteolysis were frequent. Loosening was also frequent in cases with hy-droxyapatite coating.D. Harris-Galante. Loosening was uncommon, but acetabular wear and osteolysis were frequent. No case wasrevised for loosening. Five cases were revised for osteolysis and/or dissociation (2.6%).Conclusions: 1) Osseointegrtion is obtained in cementless acetabular cups, even in young patients. 2) Osteoly-sis, associated with polyethylene liner wear, was frequent in the first generation designs.
ABSTRACTS FROM THE INTERNATIONAL MEETING ON TOTAL HIP ARTHROPLASTY - MADRID, SPAIN,6-8 APRIL 2000 (HIP INTERNATIONAL 2000; 10: 178-190)

S130
Indications and results of the cone hip prostheses
H. WAGNER
Schwarzenbruck, Nuremberg - Germany
The shape of the proximal femur was taken into account when implanting a cementless prothesis. Nume-rous prostheses are available for a "trumpet-shaped" morphology. However, the femur often has a nar-row, more cylindrical configuration, as is frequently seen in dysplastic hip joints. Conventional femoralprostheses with a proximal transverse oval or rectangular cross-section often can only be incorrectly po-sitioned, because they can fracture the more narrow bones. In many cases, a pathological anteversion at-tachment cannot be adequately corrected. The cone prosthesis is ideal for these cases when pre-operati-ve planning indicates good contact between the cortex and the middle third of the prosthetic stem. The ta-pered anchorage of the cone stem in the medullary cavity reamed to a cone shape promotes primary stabi-lity, which is a fundamental pre-requisite for the osseointegration of a coarse blasted titanium implant. Thesharp longitdinal ridges of the stem, which tend to cut into the bone, ensure good rotational stability, and ex-plains why thigh pain is not associated with the cone prosthesis.
Results of ceramic on ceramic bearings in patients younger than 40 yearsof age
P. BIZOT, R. NIZARD, L. BANALLEC, L. SEDEL
Hôpital Lariboisière, Paris - France
As alumina on alumina was originally designed to avoid wear debris generation, we analyzed the results ofthe hips in patients younger than 40 years of age operated from 1978 to 1994 (128 hips in 116 patients).During this period, four methods of acetabular component fixation were used. The cemented cup (41 hips) was a plain alumina socket fixed with a conventional cementing technique. The press-fit cementlessplain alumina socket (Cerapress, 32 hips) was introduced in a 2 mm under-reamed cavity. The screw-ring (22hips) was a smooth titanium conical ring with an alumina liner. The press-fit cementless titanium shell withan alumina liner was made of a titanium alloy core covered with pure titanium mesh in order to allow bone in-growth (Cerafit, Ceraver, 33 hips). The femoral component was a smooth cemented titanium alloy stem forthe 128 hips (Ceraver). In all cases a 32-mm diameter surgical grade alumina head was used. An acetabulargraft was necessary in 22 hips.At the end of the study, 16 hips had been revised, 8 patients (11 hips) had died and 101 hips are still func-tioning.Survival analysis. When revision was considered as the end-point, the cumulative survival was 84% at 10years and 81% at 15 years. When mechanical failure was considered as the end-point, the respective survi-vorships at 10 and 15 years were 85% and 81%. The survival of the femoral component was 95% at 10 yearsand 85% at 15 years. The respective 10 years survival rates were 63% for the grafted acetabular cups and 90% for the non-grafted acetabular cups (p=0.004). The survival rates for the cemented cups was95% at 5 years, 91% at 7 years, 88% at 10 years, and 77% at 15 years. For screw-in cups the rates were95% at 5 years, 89% at 7 years and 89% at 10 years. For the Cerapress cups the rates were 100% at 5 yearsand 95% at 7 years.For the Cerafit cups the rates were 100% at 5 years and 94% at 7 years.The mid-term results with either Cerapress and Cerafit systems need long-term confirmation. The absence of osteolysis created a favorable situation for revision surgery.
S131
II CEMENTLESS TOTAL HIP ARTHROPLASTY: LONG-TERM RESULTS (PART II)
Three different cementless femoral stems: Long-term results
A. CRUZ
Hospital la Paz, Madrid - Spain
We analyzed three different cementless femoral stems: Harris-Galante I (HGP I, 93 stems), PCA (91 stems),and Zweymüller (104 stems). The mean follow-up was 10.2 years for the HGP I group, 8 years for the PCAgroup, and 7.7 years for the Zweymüller group.According to Kaplan-Meier survivorship analysis, at 13 years there was revision of the HGP I stem in 23% ofthe cases, and loosening in 18.5%. Thirteen stems were revised, 10 for aseptic loosening and 3, which we-re osseointegrated, for osteolysis and thigh pain.At 14 years, 9% of the PCA stems were revised. There was loosening in 6 stems (17.3% at the same time).At the end of the follow-up none of the Zweymüller stems had been revised. Thirteen stems showed radio-graphic loosening Type of fixation. In the HGP I group there was radiographic osseointegration in 54 stems, fibrous-stable fixa-tion in 24 stems, and unstable fixation in 15 stems. Unstable fixation was more frequent in patients youngerthan 50 years, hips with a poor canal filling, or those with stem subsidence of more than 5 mm. In the PCA group, there was osseointegration in 57 stems, stable fibrous fixation in 22 stems, and unstablefixation in 12 stems. Unstable fixation was more frequent in cases with poor canal filling and >5mm stem sub-sidence.In the Zweymüller group, osseointegration was seen in 83 stems, stable fibrous fixation in 8 stems, and un-stable fixation in 13 stems, more frequently in cases with a poor canal filling.Thigh pain was more frequent in the HGP I group. Osteolysis was seen in 24 femora (25.8%) from the HGP Igroup, in 50 (55%) from the PCA group, and in 20 (19%) from the Zweymüller group.
Cementless femoral stem in primary THA: Long-term results
J. SANCHEZ SOTELO
Mayo Clinic, Rochester, Minnesota - USA
Thigh pain was more frequent in PCA and Harris-Galante I stems, intermediate in stems with distal fixation(AML), and less frequent in stems with proximal porous fixation (Trilok, Omnifit) and in stems with hydroxyapatite coating (Omnifit). The mechanism of the thigh pain is unknown.Stress shielding is more frequent in distally fixed stems made of chrome-cobalt. The significance is also unknown after 10 years.Distal osteolysis was frequent in stems with a non-circumferential proximal porous coating (Harris-Galante I,Omniflex).Results: A. Harris-Galante I. At 10 years there was revision in 20% of cases, loosening in 11%, and osteolysis in 60%.B. Porous Coated Anatomic. Revision was seen in 10% of the cases, and osteolysis in 50%.C. Trilok. At 10 years, loosening was seen in 5% and osteolysis in 3.2% of the cases.D. Omnifit (Porous Coated). Osteolysis was very frequent.E. Antomic Medullary Locking. Engh reported osteolysis in 39%, thigh pain in 8%, and osteopenia in 23% ofthe stems.F. Omnifit (HA). Mechanical failure occurred in 0.3% at 10 years and osteolysis was seen in 28% of the cases.
S132
In fact, in the Mayo Clinc the femoral designs more frequently used are stems with proximal HA coating foryoung patients, and stems with an extensive porous coating for older and/or inactive patients.
Clinical and radiographic analysis of the Zweymüller prostheses implanted between 1986 and 1988
M. MARTÍNEZ GRANDE
Hospital Virgen del Camino, Pamplona - Spain
One hundred and nineteen Zweymüller stems were implanted in 1988 and 1889. Seventy were Hg stems, and69 SL stems. The mean follow-up was 12.3 years. 27 patients were lost during the follow-up.Good clinical results were seen in 92% of the cases, while 6 stems showed subsidence greater than 4 mm.Radiolucent lines in Gruen zones 1 and 7 were seen in 60%, but had no clinical relevance in most of the hips.
Cementless anatomical femoral prosthesis with resorbable centralizer
J. AEBI J, C. CHAIX, C. WEISANG
La Tour Raynalde, Rodez - France
Primary fixation is the key to secondary fixation. Some femoral implants have introduced a metallic distal centralizer to enhance distal stability, but corrosion may still lead to debris, osteolysis and loosening.We have developed an anatomical cementless stem, proximally hydroxyapatite coated with an absorbablecentralizer. The centralizer was made of polylactic acid with 0.9 to 1.1 of viscosity. Resorption began at 6 months and was completed at 2 years. Experimental studies had been conducted in sheep.This prosthesis was implanted in 87 patients in 1995. Seventy hips form the basis of the follow-up study with a 4-yearfollow-up. Clinically, the average Harris Hip Score was 92. Only 2 patients showed pain related to the arthroplasty.No femoral stem was loose. Subsidence was detected in 5 stems, and ranged from 2 to 4 mm; one case hadsubsidence of 6 mm. In all cases, subsidence was non progressive after one year. Calcar resorption was seenin 26 hips (39.4%). No osteolysis was observed at the 4-year follow-up after resorption of the centralizer.
Principles and planning of cementless THA with conical stems
H. WAGNER
Schwarzenbruck - Germany
The most important function of preoperative planning is selection of the correct stem length and the requi-red stem diameter. Preoperative planning facilitates the actual procedure and improves the quality of the sur-gery, because the individual stages involved do not have to be considered and "attempted" during the ope-ration. All details are available at the start of the surgery, since they were planned in advance.The basis of preoperative planning consists of radiographs with a magnification of 1.15:1. The planning tem-plates are adapted to this and the most suitable prosthesis can then be selected. In revision cases, the stemextends 10 cm (minimum 7 cm) distal to the old prosthetic bed into the intact medullary cavity.The stem diameter required is determined at the same time as the distal segment. The outline of the pro-sthesis on the template will overlap the inner outline of the cortex by 1 mm on both sides, because it is ne-
S133
cessary to take into account the bone substance that will be removed during conical reaming and the cuttingof the longitudinal ribs into the bone.The planning of a primary cone prosthesis is similar. The cone prosthesis is designed for a particular morecylindrical morphology of the femur and is not suitable for a "trumpet" shaped femur.
III HYDROXYAPATITE COATING IN TOTAL HIP ARTHROPLASTY
The role of hydroxyapatite coating in the primary and revision setting inanimal and human studies
K. SØBALLE
Department of Orthopaedics, University Hospital of Aarhus - Denmark
Introduction: The present studies were performed in order to investigate the effect of the hydroxyapatite coa-ting and growth factors on bone ingrowth into cementless implants when subjected to pathological and me-chanical conditions mimicking the clinical results Material, Methods and Results: Hydroxyapatite (HA) and titanium alloy (Ti) coated implants were inserted in-to femoral condyles in mature dogs. The observation period ranged from 4 to 16 weeks and the results wereevaluated by a mechanical push-out test and histomorphometric analysis.First, the significance of a gap of 1 and 2 mm between bone and implant was studied and compared withpress fit insertion. The HA coating had a superior effect on bone ingrowth compared to Ti when surroundedby a gap whereas no effect was found in the press fit situation. Arthritic bone changes (osteopoenia), weake-ned the anchorage of Ti implants as compared with control bone; this weakening was eliminated when theHA coating was used.A bone graft model was developed in order to investigate incorporation of bone graft material around Ti andHA coated implants. Allogenic bone graft packed around the implant, enhanced the anchorage of Ti implants,but an HA coating alone without bone graft offered almost the same improvement in anchorage in 2mm defects.Only a minor improvement was obtained when bone graft was used together with HA.Another study showed that HA coating could prevent polyethylene particles from migration around the im-plant by creating a seal of bony ingrowth.The effect of surface texture of the metal implant was studied. It was found that the HA coating on a poroussurface resulted in significantly stronger fixation than did the HA coating on a grist blasted surface.Micromovements of 500 um and 150 um between bone and implant prevented bony ingrowth and resulted in development of a fibrous membrane. In a long-term study (16 weeks), the motion-induced fibrousmembrane around HA implants was replaced by bone.The effect of growth factors (BMP-7) was investigated in a newly developed experimental model which showed that they enhanced incorporation of allogenec bone graft in a revision situation as comparedto a control without BMP-7.A clinical study (using RSA) of total hip arthroplasty showed that HA coated femoral components were stable 3 months after surgery, whereas migration of Ti coated components continued resulting in si-gnificantly less migration of HA coated components at 60 months.
S134
Two HA coated femoral stems: A 5-10 year study
J. CORDERO
Hospital La Paz, Madrid - Spain
Ninety standard (Omnifit) and 92 anatomic (Profile DePuy) HA-coated stems were implanted between 1988 and1996. The mean-follow-up was 7.6 years. Good clinical results were seen in almost all cases in both series. Two Omnifit stems and one Profile stem were revised, due to mechanical failure of the cup. In these stems,the hydroxyapatite had disappeared. Osseointegration was seen in all stems, even in osteopoenic and cylindri-cal femora. Osteolysis was seen only in proximal zones. Proximal osteoporosis was frequent in both series.
ABG prosthesis experience (International Group)
C. GARCIA ARAUJO, J. FERNÁNDEZ GONZÁLEZ
Hospital La Princesa, Madrid - Spain
Six hundred and thirty-seven ABG prostheses were included in an international multicentre study. Thepre-operative Merle D'Abigné and Postel score was 8.5 points, and the post-operative score reached17.5 points at 8 years. Thigh pain was reported in 4% of the hips. There was proximal ostopoenia after3 years, but without clinical relevance. Ossointegration was shown in most cases. Distal osteolysis wasnot found in this series.
Seven-twelve year results of a randomised prospective trial to comparethe functional results of the Charnley prosthesis with the HA coatedFurlong prosthesis
J. BRADLEY
Scarborough Hospital, Yorkshire - UK
We report a clinical trial comparing the Furlong pros-thesis with the Charnley prosthesis. The mean follow-up was 8.5 years. The patients were randomised by year of birth. There were 125 hips in the Furlong groupand 97 hips in the Charnley group. Function has been satisfactory in all respects in both groups.The Furlong group has had four complications. One stem came loose at four years, one ceramic head brokeat ten weeks post surgery, and at six years two polyethylene cups have worn out and broken. In the Charn-ley group, three stems have failed through aseptic loosening. In all cases where failure has occurred revisionsurgery has achieved excellent results.In summary, it is recognised that the Furlong HAC prosthesis with its biological fixation has matched upto the cemented Charnley prosthesis in respect to pain relief, functional results and in mid-term survival rates.
S135
Corail prosthesis. 12 years of experience
B. BALAY
Polyclinique de Beaujolais, Arnas - France
This study analyzes 6,700 Corail prostheses. The Kaplan-Meier analysis shows a survival of 97.7% at 10years. Sixty-three percent of the patients showed an excellent clinical result. The main problems arethe consequences of polyethylene wear.
Minimum 10 year results of hydroxyapatite-coated total hip replacement
R.G.T. GEESINK
University Hospital of Maastricht - The Netherlands
Patients and Methods: Results are discussed of the first 118 consecutive cases with primary hydroxya-patite coated hip (Osteonics) replacement implanted between 1986 and 1988. All patients were prospec-tively followed at 3, 6, 12 months and yearly thereafter.Clinical results. The average HHS was 94 at 6 months, 97 at 5 years, and 91 at 10-12 years. The rounded ave-rage Merle D'Aubigné scores were 6-6-5 at 10 years.Radiological results. Bone remodeling became evident at 3-6 months especially around the HA-coatedparts of the proximal femoral stem. Very few reactive lines were seen in bone around the HA-coated partsof the femoral stem. Reactive lines were regularly seen around the distal non-HA-coated part of the stem.Periosteal bone remodeling reactions increased with time and were stil l visible in 66% of cases at 10 yearsfollow-up. Also calcar remodeling increased over time and was mild to moderate at 10 years follow-up.Survival rate. The survival rate at 12 years for the HA-stem was 97% and 91% for the threaded cup.Reoperations. There were 9 cup revisions or head and insert exchanges because of polyethylene wear andimpingement. In 3 instances these were combined with a stem revision because of malposition with re-current dislocation or polyethylene wear. All stems had excellent bony fixation, as confirmed by retrievalhistology.Discussion: Mean 11 to 13 year results of hydroxyapatite coated total hip replacement in a younger agepopulation are very encouraging, especially for the stem. PE-wear in younger patients remains a problem.The revisions have been performed for severe PE-wear and not because of mechanical failure.
IV PRIMARY THA IN ACETABULAR BONE DEFICIENCIES
Acetabular cup in patients with acetabular deficiencies
E. GARCIA-CIMBRELO, A. DÍAZ-MARTÍN
Hospital La Paz and Hospital 12 de Octubre, Madrid - Spain
An acetabular bone deficiency is related to early loosening of the cemented cup, i.e.: congenital dysplasia ofthe hip, acetabular fractures, and acetabular protrusion.The femoral head has been recommended for reconstruction of a deficient acetabulum in CDH, when the bo-ne defect is greater than 30%. Any pelvic discontinuity, frequent in old acetabular fractures, must be reconstructed with osteosynthesis plates or with an anti-protrusio cage (Burch-Schneider) associa-
S136
ted with bone grafts. In acetabular protrusio, the use of impacted grafts taken from the femoral head favoursthe reconstruction of the deficient medial acetabular wall.
Acetabular fracture. Bone reconstruction or total hip arthroplasty in very severe cases
L. SEDEL, A. VEILL PICART
Hôpital Lariboisière, Paris - France
Severe acetabular fractures are difficult to treat. Even well operated on and stabilised, there is a major riskof secondary osteoarthrosis, due to bone necrosis, and/or cartilage surface damage.There are also intraoperative risks of neural damage: sciatic nerve as well gluteus nerve supply. On the otherhand, modern surgical technique, including an alumina against alumina bearing, could allow very long termsurvival without any activity limitation.A secondary procedure after a failed osteosynthesis provides statistically worse functional results than in pri-mary total hip arthroplasty. The surgery is difficult because of material retrieval difficulties, nerve dissection,bone reconstruction and remaining muscular dysfunction.We studied 80 patients who received a total hip for acetabular fracture. The results were clearly inferior to aregular total hip if an osteosynthesis had been performed previously. In contrast, a few cases who had firsthad conservative treatment, followed by a total hip arthroplasty some weeks later, experienced very good re-sults. Of course, for simple acetabular fracture with large displacement involvement of the posterior wall, onecolumn osteosynthesis is still recommended. For all other cases (comminuted, bicolumn, transverse displa-ced or fracture in the elderly) we recommend conservative treatment during the first days then a primary to-tal hip arthroplasty.
THA in congenital dislocation of the hip
M.E. CABANELA
Mayo Clinic, Rochester, Minnesota - USA
In CDH, the acetabulum is shallow, sloping, deficient superolaterally and anteriorly, with a poor bone quality. Thesolutions are an uncemented small component, and a 22 mm head is necessary if socket outer diameter is lessthan 50 mm. To restore the anatomic hip center, structural femoral head autograft may be needed.The femur has a narrow canal, anteversion, and a small or large deformed femoral head. Soft tissues are elon-gated with a thickened capsule requiring complete capsulotomy. Tenotomies of psoas, abductors and rectusfemoris could be needed. It is necessary to avoid >4 cm lengthening to avoid damaging short nerves and ves-sels.In conclusion, it is essential to know the altered anatomy, careful exposure, restoration of normal hip jointmechanics, resulting in a very satisfying procedure, that is not for beginner surgeons.
S137
Surgical treatment of CDH and acetabular dysplasia
K. SØBALLE
Department of Orthopaedics, University Hospital of Aarhus - Denmark
For CDH, an alternative to THA is a periacetabular osteotomy, which allows for a three-dimensional recon-struction of the acetabulum in order to delay or prevent the need for THA in the future. The Ganz periaceta-bular osteotomy was introduced in 1996 in our institution.Material and Methods. Sixty-eight Ganz osteotomies have been performed in 62 patients. Mean age was 28years. Five patients had both a periacetabular osteotomy as well as an intertrochanteric derotational osteo-tomy during the same procedure. The indication for surgery was pain in the hip, presence of acetabular dy-splasia, and grade 0, I, or II osteoarthrosis (Tönnis). Mean observation period was 19 months.Results: The preoperative HHS was 60 and 6 months postoperatively, the HHS improved significantly. Themean preoperative Centre Edge (CE) angle was 6 (-16 to 21) degrees. Postoperatively the CE angle was cor-rected to 34 (10 to 44) degrees. There was no infection, no deep venous thrombosis, no neurovascular com-plications and no heterotopic ossification. One patient developed delayed union of the iliac osteotomy andwas reoperated on.Conclusion: the Ganz osteotomy is a challenging operation, but early results are encouraging as a significantreduction in pain was demonstrated. The operation allows for a 3-D correction of the acetabulum, which mayprevent or at least delay further development of osteoarthrosis in these young patients.
Cementless total hip replacement in severe dysplastic osteoarthritis
K. ZWEYMÜLLER
Orthopädisches Krankenhaus, Wien - Austria
One hundred and eleven primary replacements were performed between 1993 and 1995 in patients with CDH.Mean follow-up was 4.1 years. The average age at surgery was 53 years. All the patients were managed witha conical threaded cup made of pure titanium. In 91 cases, the Standard version, designed for use in normalor in hard bone, was employed, while the Porosis type of cup, with a 46% greater thread surface area, waschosen in 20 cases. Conical cups are inserted with prestress, and do not, therefore, require additional fixa-tion with screws or lugs.Results: In 110 cases, the position of the cup had not changed during the follow-up period; in one case, cranial migration was seen. In stable implants, the extent of preoperative sclerosis around the cup wasmuch reduced following arthroplasty. The regression of sclerosis suggests that the implantation of the tita-nium cup results in an improvement of the periacetabular stress pattern. In 84 cases, there was evidence ofincreasing integration of the implant; in 22 cases, no bony response could be detected, i.e. there was neither apposition of new bone nor loss of existing bone stock.
S138
V REVISION SURGERY (PART I)
Revision surgery. La Paz Experience
E. GARCÍA-CIMBRELO
Hospital La Paz, Madrid - Spain
Patients without bone defects could be treated as primary surgery Acetabular component. In cases with an acetabular bone defect less than 30% (Paprosky types 1 and 2) we usea cementless hemispherical porous coated cup, made of titanium, associated with morsellized grafts.In patients with a bone defect greater than 30% (Paprosky type 3) we prefer impacted morsellized graft witha cemented cup (Slooff technique).Acetabular defects with pelvic discontinuity require acetabular stabilisation (anti-protrusio cage).Femoral component. In old and inactive patients with circumferential defects less than 2 m (calcar), we usecementless prosthesis with distal fixation.In young and active patients without a circumferential defect, we prefer impacted morsellized graft and ce-mented stem (Gie technique).In patients with a distal circumferential defect greater than 5 cm, a femoral segmental graft can be necessary.
Reconstruction without cement in severe acetabular defects. ARTROexperience
B. BALAY
Polyclinique du Beaujolais, Arnas - France
The author recommends the use of a metal ring (Octopus) in patients with acetabular bone defects, asso-ciated with grafts and a cementless acetabular cup. The ring is stabilised in the original bone bed.This study analyzes 49 "Octopus" rings implanted between 1989 to 1998. The mean follow-up was 4.2 years.Complications were frequent in revision surgery. Clinical results were good. Eighty one percent of the casesshowed radiographic incorporation of the grafts. The survival according to Kaplan and Meier was 86.4%.
The use of Titanium cup in revision surgery
K. ZWEYMÜLLER
Orthopädisches Krankenhaus, Wien - Austria
Since 1985 we have used a self cutting conical threaded cup made of pure titanium for revision surgery. Aprimary stable anchorage can also be achieved with the Bicon cup also in cases with large defects of theacetabulum.Patients and Methods: We analyzed 118 cup revisions operated between 1993 and 1996. The mean follow-up time was 3.7 years. Bone defects were classified according to the Endoklinik classification.Results. In 10 cases allograft had been used to fill large bone defects. In 48 of the cases we used cup type"Standard", in 70 cases cup type "Porosis". The radiological follow-up showed increasing incorporation ofthe cup in 96 cases (81.4%), and an indifferent osseous situation in 14 cases (11.9%), bone resorption (tu-berculosis) in one case, and migration with secondary stabilisation in 3 cases. One loosening, 3 cases were
S139
judged "at risk". The applicability of this implant also at large bone defects as well as the high percentage ofhips with osseointegration suggest that our management principle is sound.
Acetabular revision. Current attitude
M.E. CABANELA
Mayo Clinic, Rochester, Minnesota - USA
The goals of acetabular revision are: restore the hip's center of rotation, optimize the component coverage,optimize the component fixation, restore the continuity and bone stock, and optimize the component contactwith native bone.The alternatives are: cemented socket, bipolar prosthesis, threaded socket, press-fitted porous socket withscrews, ring or cage HDP cemented socket, and special sockets. Nevertheless, the hemispherical cementless sockets with screws are applicable to most situations with good results.Reinforcement rings: Failure of uncemented sockets in revision has been reported when limited native boneis available for fixation, particularly if the dome has been substituted with bone graft. Rates of 30-78% fai-lure have occurred with hemispherical sockets if segmental deficiencies were present.Acetabular reinforcement devices or rings have been used for a long time. Today some authors consider re-constructions using rings as cementless procedures, since cement is used only to attach the polyethylenesocket to the ring. The reinforement device is utilized to provide both support and a quiet, unloaded environ-ment for the bone graft (morsellized, particulate) to heal. Even if bulk grafts are necessary for reconstruction,the ring may protect them from collapse and avoid early migration. In cases with pelvic discontinuity with mas-sive bone loss, the APC or antiprotrusio cage of Burch-Schneider may prove useful.
VI REVISION SURGERY (PART II)
Impaction grafting with cemented component in revision surgery
A. MURCIA MAZÓN
Hospital de Cabueñes, Gijón - Spain
The main indication for impaction grafting is to augment bone support in patients with severe osteolysis. Wehave used this technique since 1994 in more than 200 cases.Our results confirm those described in other series.
Femoral side cementless HAC coated stem in revision surgery
J.G. BRADLEY, L. FUNK, G.S. RADCLIFFE, M. ANDREWS
Scarborough Hospital, Yorkshire - UK
To overcome the osteolysis in revision surgery, an alternative approach is to use a cementless prosthesis withhydroxyapatite coating, which is bio-compatible and achieves stability by initial press fit leading to osteo in-tegration. We analyzed 31 revision hip stems using the Furlong HAC revision system between 1991 and 1997.The mean follow-up was 3.5 years. Signs of osteo integration were noted in 29 cases. In 48% of the cases

S140
there was trabecular formation or re-orientation of the cone of the prosthesis and in 72% of the cases clo-sure of lucent lines or zones was found. In 2 cases (8%), where migration of the prosthesis was noted at 3months, stability was achieved by 12 months.In summary, it can be stated that the Furlong HAC revision stem can be safely and effectively used in revisionsurgery. There is good osteo integration of the prosthesis to the bone allowing for satisfactory painfree function.
HA coatings in femoral hip revision arthroplasty
R.G.T. GEESINK
Maastricht University Medical Center & Center for Biomaterials Research Maastricht - The Netherlands
This study evaluates the results of 60 cases of HA-coated exchange arthroplasty for loosening arthroplasty.Thirty-seven cases were multi-revisions. The mean follow-up was 9 years. The policy of exchange arthropla-sty with HA-coated implants is to provide restoration of proximal femoral bone-stock if necessary using au-to- or allograft bone transplants. For early bone ingrowth to occur, the HA-coating must be in contact withviable bone, usually in the area of the femur below the lesser trochanter. This will provide early stability, whe-reas the bone graft will provide increased bone stock over the long term. There were no complications rela-ted to the implant fixation method. The average Harris score was 93 at 2 years and longer up to 10 years.Pain incidence at 2 years is 4%. The pattern of radiological ingrowth in revision cases is more irregular ascompared to primary cases. The majority of cases have much better bone stock two years after revision sur-gery as compared to the pre-revision status. According to Engh's criteria all stems but two have confirmedosseointegration at two years and later. One autopsy retrieval of an HA-coated revision hip arthroplasty con-firms by histology the excellent implant fixation. The survival rates for femoral components is 94% at 9 years,and the mechanical failure rate for femoral component is 7%.In conclusion, HA-coated femoral exchange arthroplasty for mechanical loosening has very satisfying resultsand the restoration of bone stock is very promising for long-term implant survival. Bone grafting at the timeof revision arthroplasty is an important part of the reconstrution.
Femoral revision. Alternative Results
M.E. CABANELA
Mayo Clinic, Rochester, Minnesota - USA
The objectives for femoral revision are: restore anatomy (rebuild osseous defects), restore joint mechanics,and obtain satisfactory component fixation. The femoral reconstruction options are:1. Cemented revision is indicated in old patients with reasonable bone, post-infection reimplantation, femo-ral deformity, and/or metabolic disease.2. Cement-within-cement. It is essential to have an excellent bone-cement interface. This is indicated in ca-ses with fracture of the stem, and recurrent dislocation-stem malposition.3. Uncemented distal fixation. Indicated in patients with poor metaphyseal and good diaphyseal bone with acanal diameter <19.5 mm.4. Impaction grafting. Indicated in cavitary or combined metaphyseal defects. Small segmental defects aresolved with strut grafting, and a mesh of Co-Cr and circumferential cables.5. Allograft-prosthesis composite and Megaprosthesis. Indicated in patients with massive proximal femoraldefects (>5cm). Megaprostheses are indicated in old patients.
S141
VII THR IN DIFFICULT SITUATIONS
Bacterial survival mechanisms in THR
J. CORDERO
Hospital La Paz, Madrid - Spain
This paper has been printed in full elsewhere in this journal: Cordero J, García-Cimbrelo E. Mechanisms ofbacterial resistance in implant infection. Hip International 2000; 10: 139-144.
THA in proximal femoral deformity
M.E. CABANELA
Mayo Clinic, Rochester, Minnesota - USA
Proximal femoral deformity can be seen as the result of CDH, after previous intertrochanteric osteotomy, andafter previous THA.If the deformity is significant (altered mechanical limb axis), correction by osteotomy could be necessary atthe time of the THA. The use of THA with concomitant osteotomy is a demanding procedure. Pre-operativeplanning is essential. The use of a fully porous coated prosthesis is preferred today. Autogenous bone graf-ting at the osteotomy site is advisable. Stability of the osteotomy must be achieved.
Total hip arthroplasty in femoral deformities
H. WAGNER
Schwarzenbruck, Nuremberg - Germany
Osseous deformities of the proximal femur can create serious problems in the implantation of a THA. Deformities canoccur after fractures or osteotomies, sometimes also in metabolic skeletal disorders or inflammatory reactions. In the-se cases the preparation of the bone and the medullary cavity for the seat of the stem with conventional rasps canbe very difficult or even impossible. For the implantation of a conical revision stem or a conus prosthesis careful co-nical reaming of the proximal femur can be carried out without any problem to fit the conical prosthetic stem.In particular corrective osteotomies for proximal femoral deformities have to be performed at the same timeas the prosthesis is fitted. In these cases the revision stem can be used as a medullary pin to stabilize theosteotomy as well.
Use of computer navigation in hip implant surgery
R.G.T. GEESINK
Maastricht University Medical Center & Center for Biomaterials Research, Maastricht - The Netherlands
In a recently published prospective study it was proven that even with experienced surgeons and adequatesurgical technique, only a minority of acetabular components show a position that falls in a range described

S142
before as acceptable. Only 35% of primary THA had an acetabular orientation in space with less than 5º aber-ration from the ideal position of 45º abduction and 25º anteversion. Major component malpositions lead toearly problems such as recurrent dislocation, however minor rates of malposition do not lead to early pro-blems but by the process of impingement, do lead to enhanced PE-wear at intervals from 5 to 8 years po-stoperatively. Computer-navigation might be able to improve the accuracy of component positioning in THA.Together with Medivision a project was started to make the software, already available for use in spinal ap-plications, usable for acetabular and femoral component positioning in THA. The software for cup placementis now ready and the method and techniques will be demonstrated. Beginning with preoperative planningusing a CT-scan, definition of the landmarks to be used for matching during surgery are defined together withthe actual preparation and instrumentation of the acetabular component. Early experience with a still limitednumber of patients has shown that accurate planning and execution of this technique allows exact placementof the cup with an accuracy in space of a few degrees.
VIII NEW TECHNOLOGIES IN THR
From craft to biomechanics, from biomechanics to molecular biology
L. MUNUERA
Hospital La Paz, Madrid - Spain
Early operations on the hip were used before the experimental studies had confirmed the good results. On thecontrary, when Charnley developed the low-friction arthroplasty, he previously studied the designs and wear ofdifferent biomaterials in detail in the laboratory. Biomechanics was widely used for total hip replacement in theSeventies. In 1983 Mankin stated the importance of the biology and the study of the cell for total hip arthropla-sty. This introduced the era of "Tissue engineering". It will become very useful in the near future.
Osteogenic Protein I (BMP-7): An overview on background and currentstatus
L.R. GILTAIJ
Biotech. Doom - The Netherlands
The identification and production of recombinant human Osteogenic Protein-I (rhOP-I), also referredto as rhBMP-7, lead to identification of the body-compound responsible for inducing the process ofbone formation.In 1934 Levander showed that demineralized bone could reproduce mature bone. In 1965, Urist publi-shed on the sequential reproduction of the cellular events that occur in embryonic bone development andin adult bone fracture repair by implantation of demineralized bone matrix in an ectopic site.Sampath succeeded in extracting the osteogenic protein complex from the demineralized bone matrix in1981. One of the earliest identified proteins is OP-I. Currently several members of a closely related pro-teins family have been identified: the so called BMP-family. With new technologies becoming available,it may be possible to sequence OP-I from bovine origin. Identifying and isolating the human OP-I-genewill make it possible to manufacture the protein by Recombinant DNA-technology, resulting in rhOP-I re-combinant VP-I.Research has shown that the recombinant produced human CP-I initiated recruitment, attachment,proliferation and differentation of mesenchymal stem cells, leading to new bone containing fully func-

S143
tional bone-marrow components. OP-I containing devices could replace the conventionally employedautografts in repairing non-union diaphyseal bone fractures, cranio-facial defects and spinal fusionand could speed up healing of delayed union fractures. Such devices could even promote osseointe-gration of metal joints. In the event of massive bone loss, an OP-I containing device could also re-place allograft implants, while speeding the process of bone formation. Clinical experiences were pre-sented.
Alendronate prevents periprosthetic bone loss: 2 year results
A. LEUNG, B. SCAMMELL, A. LYONS, M. CZACHUR, J. GILBERT, D. FREEDHOLM, W. MALBECQ, C. MILLER,A. CARR, L. CHECKLEY
Rahway, NJ - USA; Nottingham - UK; Madison, WI - USA
Bone loss after THA occurs due to stress-shielding, and years later as a result of osteolysis and aseptic loo-sening. Maintenance of bone mass and prevention of osteolysis with alendronate (ALN) may benefit patientswith THA.Methods. Forty-nine patients with a Charnley prosthesis were enrolled into a clinical trial. Three groups we-re studied: patients soon after THA (acute, N = 16), those with THA >5 years and no clinical or radiologicalevidence of loosening (chronic, N = 17), and those with aseptic loosening awaiting revision surgery (revision,N = 16). Patients were randomized to either ALN 10mg/day orally or placebo (PBO) for one year. During thesecond year, 28 patients (14 from the acute group and 14 from the chronic group) received the same treat-ment. They were assessed at 18 and 24 months. All patients received calcium supplements (500 mg/day).The primary efficacy endpoint was periprosthetic bone mineral density (BMD) measured by dual-energy x-rayabsortiometry (lunar). Results. Overall, there was a significant mean percentage increase of 1.48 ±0.76% in BMD at month 24 in theALN group (p=0.05). PBO-treated patients demonstrated a mean percentage change in BMD of -0.45% atmonth 24. Chronic patients did not lose bone in either the PBO- or ALN- treated groups.Discussion: ALN appears to have a beneficial role in the prevention of early rapid bone loss due to stressshielding. The potential to reverse later bone loss due to established osteolysis has yet to be demon-strated in humans.
A new THA sliding couple: ceramized-coated metal with ceramized-coated metal: the "plasma-metal"
J.P. ARNAUD
Hôpital Universitaire Limoges - France
HDPE particle wear is today considered the most important reason for aseptic loosening of THA. Plasma-Me-tal is obtained by a plasma-spray procedure for CrO2 ceramic. The speed of the ceramic particles leaving theplasma-gun is 1800 m/sec at a temperature of 15000ºC. The cooling system permits hyper-hardening between15000ºC to 60ºC in 60 micro-seconds. The plasma splash performs a high hot fitting of hexagonal crystalswith a mechanical setting better than other common ceramic crystals. We tested the mechanical propertiesof this kind of coated ceramic. With static and dynamic tests we found very good anchorage (200 G pascals)and over all, no measurable wear after 8 million cycles. A comparative study with a metal-metal couple wasquite effective. Biocompatibility was also tested and perfect immunological tolerance was found.In 1990 we began a very short series of 8 cases, and after 7 years, there had been 7 survivals with very good

S144
clinical and radiographic results. Since 1995, we began the first large series and we report the first 60 cases with a minimum 4 year follow-up. The results are also good in this large series. The use of ce-ramic-coated metal in a sliding THA couple seems to provide all the advantages of a metal-metal couple butwith better wear results and without the disadvantages of an electrochemical couple. Only a 10 year follow-up can confirm these good results.
Future developments with calcium-phosphate coatings
R. GEESINK
University Hospital of Maastricht - The Netherlands
Current generations of HA-coatings are manufactured using the plasma-spray technique. Although cli-nical results are excellent for use on primary and revision type femoral components, the plasma-spraytechnique has some built-in limitations. One, since it is a "line-of-sight" process, it is unable to coatthree-dimensional surfaces such as porous coatings, because it would occlude the pore space andthereby inhibit bone ingrowth. Another limitation is the high temperature at which the coating is ma-nufactured, and prohibiting the addition of biologically active components to the coatings such asgrowth factors and/or antibiotics.Recent improvements in HA-coating technique make it possible to apply HA by different methods, withthe end result stil l being an HA-coating with known properties. The most promising is the precipitationtechnique.A thin Ca-P coating of 10-30 micron thickness can be applied using precipitation in fluid. The processtakes place at room temperature instead of at thousands of degrees Centrigrade. Still providing an HA-coating like the one with the plasma spray technique, it has several advantages associated with itsuse. To start with, the coating is of a micro-crystalline instead of macro-crystalline type. This providesenhanced bioactivity because the exposed surface area of a micro-crystalline surface is much greater.Secondly, it can coat irregular surfaces, including porous materials that can not be coated using con-ventional techniques because the pores would be clogged. Thirdly, it is possible to include biologicalfactors in the coating such as growth factors, BMP or antibiotics at the time of manufacture becausethe process takes place at room temperature. Experimental studies confirm these improvements andshow much enhanced bone apposition. Also the combination with growth factors or BMP's is attracti-ve, because it may reduce the need for bone graft materials especially in revision surgery. Several ex-perimental studies are currently ongoing and it is to be expected that these new enhanced coatingswill become clinically available in the near future.
The evolution of ceramics in total hip replacement
G. WILLMANN
CeramTec AG, Medical Products Division, Plochingen - Germany
ABSTRACT: Today’s THR systems have been developed in conjunction with feedback from clinical practice,i.e. by evolution. In the 70s and 80s ceramic stems, monolithic cups, monoblock components, and skirtedheads were used. Today, modular hip systems are offered, designed for ceramic heads, which articulateagainst ceramic or PE cups. The surgeon has the option of choosing a combination suitable to the specificsituation. About 70 cups with ceramic inserts have been developed. More than 200,000 ceramic inserts havebeen used since the mid 80s.

S145
The article discusses which combinations of head and cup inserts have been approved by government agen-cies and which combinations are not recommended (Hip International 2000; 10: 193-203)
KEY WORDS: Total hip replacement, Monolithic, Monoblock, Modular, Bioceramics, Ceramic wear couple
Influence of region size on bone mineral measurements along femoralstems in THA
P. M. GEHRCHEN 1, M.M. PETERSEN 1, P.K. NIELSEN 2, B. LUND 1
Departments of 1 Orthopaedics and 2 Nephrology, The National University Hospital, Rigshospitalet, Copenhagen - Denmark
ABSTRACT: The influence of regional size on the precision error in the evaluation of bone mineral changesalong femoral components in uncemented THA's was studied methodologically using Dual Energy X-ray Ab-sorptiometry (DEXA) and with a review of the literature. A significant negative relation between region sizeand precision error was found in experimental studies and the precision error was shown to vary with type ofDEXA scanner when reviewing the literature. When using Gruen's zones we found that the precision was bestat the tip and poorest in the proximal regions. Guidelines based upon calculations of the approximate per-centage changes necessary in a single individual to be statistically significant in a longitudinal study with95% probability were made for three different types of DEXA scanners. (Hip International 2000; 10: 204-8)
KEY WORDS: Bone mineral, Region size, THA, Precision, DEXA, Uncemented
Radionuclide bone scan appearances in asymptomatic patients followinghip hemiarthroplasty
A. KHALEEL 1, S. HARDEN 1, K.W.R. TUSON 1, J.J. FLANAGAN 2, B.G. CONRY 2
1 Department of Orthopaedics2 Department of Radiology, Kent and Sussex Hospital, Mount Ephriam, Tunbridge Wells, Kent - UK
ABSTRACT: We report the radionuclide bone scan appearances following hemiarthroplasty of the hip in 15asymptomatic, active patients at a mean of 14 months following surgery. All patients had a normal clinicalexamination, white cell count and erythrocyte sedimentation rates.Tracer activity was graded. Minimal tracer activity especially along the lateral stem and acetabulum were consistent findings. We conclude that this should be regarded as normal in this situation.(Hip International 2000; 10: 209-11)
KEY WORDS: Bone scan, Hip fracture, Hemiarthroplasty
S146
A simple method of planning and performing a proximal femoral varus-shortening-derotation osteotomy for hip dislocation in cerebralpalsy using a blade-plate
R.A. BROOKS, K. KIRBY, T.N. THEOLOGIS
Nuffield Orthopaedic Centre NHS Trust, Oxford - UK
ABSTRACT: Femoral varus, derotation and shortening osteotomy is part of the surgical treatment of hip sub-luxation and dislocation in children with cerebral palsy. In such cases, a post-operative neck-shaft angle of110-120º is desirable as well as 0-15º anteversion.Standard techniques of planning a femoral osteotomy require accurate knowledge of proximal femoral de-formity, but in cerebral palsy this may be difficult to measure owing to excessive anteversion and difficultieswith positioning for radiographs.We have developed and used a method that does not rely on preoperative radiographic measurements or theuse of the femoral diaphysis for reference. Our method is focused on achieving the desired postoperativeneck-shaft and anteversion angles mentioned above. The centre of the femoral neck is used as a referenceand the chisel for a blade plate is applied 20-30º varus to this neutral axis. Osteotomy cuts are then madeparallel to the chisel and perpendicular to the femoral shaft. The chisel is replaced with a 90º blade plateand the osteotomy is reduced, derotated and fixed to the femoral shaft. The final neck-shaft angle is there-fore 90º plus 20-30º, ie the desirable 110-120º. This position is achieved without knowledge of the angle ofthe wedge of bone removed by the osteotomy.This technique has been performed in 16 hips in 10 patients with cerebral palsy during one year. The finalneck shaft angle fell within the desired range in 12 hips (75%). We have found this technique to be a simpleand reliable means of achieving correction in patients in whom accurate preoperative estimate of the femoralneck shaft angle is not possible. (Hip International 2000; 10: 212-15)
KEY WORDS: Cerebral palsy, Hip dysplasia, Varus femoral osteotomy, Surgical technique
The difficulties of nutritional assessment in major hip surgery
M. COSTA, L. SHEPSTONE, S.T. DONELL
UEA Musculo-Skeletal Research Group, Institute of Orthopaedics, Norfolk and Norwich Hospital, Norwich - UK
ABSTRACT: There are many factors affecting the outcome of major hip surgery. One postulated factor is thepatient's peri-operative nutritional status. Several papers have confirmed the benefits of dietary supplementsfor malnourished patients. Despite this, there are currently no guidelines as to how best to assess nutritionin orthopaedic patients.The aim of this study was to find a simple diagnostic test that accurately reflects nutritional status in pa-tients undergoing major hip surgery. Twenty-five patients with fracture neck of femur and 25 total hip re-placement patients were assessed. Nutritional risk assessment scores, body mass index (BMI),anthropometricand biochemical tests were applied. The different indices were correlated. Length of hospital stay was usedas a measure of morbidity.The correlations between the individual indices of nutritional status were disappointingly low. The only sig-nificant correlations for the Total Hip Arthroplasty group were BMI to triceps skinfold thickness (rs=0.769,95%CI: 0.505 to 0.900, p=0.0001) and BMI to skeletal muscle mass (rs=0.501,95%CI: 0.092 to 0.766, p=0.018).The assessment of BMI is in practice very difficult in patients with fractures of the neck of the femur. Therewere no statistically significant correlations between any of the nutritional indices measured and post-oper-
S147
ative morbidity.This study was unable to accurately assess nutritional status in patients undergoing major hip surgery. A sim-ple nutritional assessment that can be used on a busy orthopaedic ward has not been identified. (Hip Inter-national 2000; 10: 216-20)
KEY WORDS: Nutrition assessment, Hip surgery
Selective arterial embolization for postoperative bleeding after total hiparthroplasty
C.H. COURT, P.H. BOISRENOULT, G. CHICK, J.Y. NORDIN
Service d’Orthopédie et Traumatologie, CHU de Bicêtre, Bicêtre – France
ABSTRACT: The Authors report a case of postoperative bleeding after total hip replacement revision, suc-cessfully stopped by the use of selective arterial embolization. Physio-pathology and treatment of postoper-ative bleeding after total hip arthroplasty are discussed. (Hip International 2000; 10: 221-4)
KEY WORDS: Postoperative bleeding, Embolization, Hip arthroplasty revision, Complications
Intraprosthetic disassembly of the Charnley-Hastings prosthesis
J.M. LUND, A.S. VINCE, S.T. DONELL
Orthopaedic and Trauma Department, Norfolk & Norwich Health Care NHS Trust, Norwich - UK
ABSTRACT: The Charnley-Hastings hip prosthesis is a hybrid bipolar hemiarthroplasty derived from a Hast-ings acetabular component and a Charnley stem. This report documents a presentation in which the ac-etabular component rotated in a medial fashion, resulting in an intra-acetabular dislocation of the Charnleyfemoral component. (Hip International 2000; 10: 225-7)
KEY WORDS: Charnley Hastings Prosthesis
OSTEOTOMY AND DDH
Periacetabular osteotomy in DDH management
A. DIAZ, J. CRUZ, J.C. ABRIL
Hospital Niño Jesús, Madrid - Spain
Introduction: Periacetabular osteotomy, Albee (1915) was modified by Dega cutting the ilium down to the triradiatecartilage. The osteotomy is then performed laterally and above the acetabulum and reaching the triradiate cartilage.
ABSTRACTS FROM THE 2000 EUROPEAN HIP SOCIETY MEETING - BRISTOL, UK 1-4 JUNE 2000 (HIP INTERNATIONAL 2000; 10: 228-258)

S148
Materials and Methods: Thirty two patients with periacetabular osteotomies were reviewed. Underlying orthopaedicconditions were DDH (24), cerebral palsy (5) and myelomeingocele (3). Mean age was 6.53 years (range, 3-12).Mean follow-up was 23.47 months. Complications included acute anaemia in six patients and TrendelenbergGait in one. There were no cases of epiphyseal necrosis. We measured acetabular, Sharp and Wiberg angles.Acetabular index was measured comparing the affected vs the contralateral non affected.Results: A significant improvement of 7.91° in the acetabular angle was recorded (SD 8.68; p=0 0130. Wiberg'sangle improved in 14.26° (SD 11.81; p=0 001). Sharp’s angle improved in 3.20° (SD 6.70; p-0.046). Acetabu-lar index improved from 0.9 (SD 0.24) to 1.0 (SD 0.30; p=0.001). An increase of 99.4 mm2 (p=0.014) in the sizeof the operated acetabulum was recorded.Conclusion: Supracetabular osteotomy provides good acetabular coverage decreasing the acetabular andSharp angles and increasing Wilberg's. Besides, it increases acetabular index thus diminishing the risk ofepiphyseal necrosis.
Sugioka’s transtrochanteric anterior rotational osteotomy for avascularnecrosis of the femoral head
L. REMZI TOZUN, N. SENER, U. TALU, O. SOYHAN
Istanbul Medical Faculty, Dept. of Orthopaedics and Traumatology, Istanbul - Turkey
Introduction: When avascular necrosis of the femoral head occurs in young patients joint realignment of thefemoral head can be a method of delaying total hip arthroplasty.Materials and Methods: From 1983 to 1995 Sugioka's osteotomy was used to treat 14 hips in 13 patients withavascular necrosis of the femoral head. Six hips were Ficat stage II and eight hips stage III. Follow up aver-aged 9.7 (5-17) years. In patients who did not require arthroplasty, it averaged 10.3 years. The average ageat surgery was 26.2 (18-34) years.At review 6 (42.8%) of the 14 hips had required total hip arthroplasty. The post operative Merle d'Aubignerating scale were 15 of 18 with 12.5% excellent and 50% good results. In these patients, 5 hips had loss ofjoint motion at some stage. There was radiological evidence of further collapse in 3 and 5 showed increasedjoint space narrowing. There were no cases of malunion or non-union.Conclusion: The results suggest that this procedure may be used to delay total hip arthroplasty but clinicalresults are not satisfactory. It does give early pain relief perhaps through joint denervation produced by cap-sulotomy but the procedure appears to increase both collapse of the femoral head and secondary degener-ative changes.
Surgical treatment of acetabular dysplasia
K. SØBALLE, S. OVERGAARD, F. MADSEN, P. K. ANDERSEN, U. LUCHT, I. HVID, B. CREVE
Department of Orthopaedics, Aarhus University Hospital Aarhus - Denmark
Introduction: Current treatment for acetabular dysplasia has been primarily limited to total hip arthroplasty(THA). However, results after THA in young and active patients are very poor with a high revision rate. An al-ternative to THA is a periacetabular osteotomy which allows for a three-dimensional reconstruction of the ac-etabulum in order to delay or prevent the need for THA in the future. The Ganz periacetabular osteotomy wasintroduced in Denmark in October 1996 by our institution.Patients and Methods: Thirty two Ganz osteotomies were performed in 30 patients. Mean age was 29 (16-45)years. There were 2 male and 28 female patients. Two patients were operated on bilaterally. Two patients had
S149
both a periacetabular osteotomy as well as an intertrochanteric derotational osteotomy during the same pro-cedure. All operations were done using epidural hypotensive anaesthesia. Mean operation time was 3 (2-4)hours and mean blood loss was 800 (350-3000) ml. The indication for surgery was pain in the hip, presenceof acetabular dysplasia and grade 0, I or II osteoarthrosis (Tonnis). Mean observation period was 13 (4-28)months.Results: Clinical results were evaluated using Harris Hip Score ( HHS). Preoperative HHS was 60 and 6 monthspostoperatively the HHS improved significantly. The mean preoperative Centre Edge (CE) angle was 5 (-16 to20) degrees. Postoperatively the CE angle was corrected to 33 (10-44). There was no infection, no deep ve-nous thrombosis, no neurovascular complication and no heterotopic ossification. One patient developed de-layed union of the iliac osteotomy requiring re-operation with a plate and has now united.Conclusion: The Ganz osteotomy is a challenging operation, and early results are encouraging as a signifi-cant reduction in pain was demonstrated. The operation allows for a 3-D correction of the acetabulum, whichmay prevent or at least delay further development of osteoarthrosis in young patients.
Lumbosacral sagittal plane avalysis in patients with developmentaldislocation of the hip joint after total hip replacement
B. ATILLA, H. ALI, A. MAZHAR TOKGÖZOGLU, M. YAZICI, A. MUMTAZ
Alpaslan Hacettepe University, Faculty of Medicine, Department of Orthopaedics and Traumatology, Saman-pazari, Ankara - Turkey
Introduction: Patients with high dislocated hips have altered standing balance and lumbopelvic alignment dueto increased lumbar lordosis. This leads to an increased incidence of degenerative spine problems.Our treatment protocol for high DDH includes restoration of hip biomechanics with shortening of the femurand placing the acetabular cup in the true acetabulum. Hypothetically these patients should benefit from nor-malised hip mechanics on their posture. Materials and Methods: We evaluated Crowe 3 and 4 hips on standing lateral radiographs to investigate thesagittal alignment of the lumbosacral spine. 15 patients with a minimum follow up of two years fulfilled thecriteria. All of them were female and their mean age was 45.5 years.Results: At the time of presentation mean Sacral Slope was 45°, mean total lordosis from Ll to Sl of 66° andLl to L5 was 53°. These parameters were 44° of Sacral Slope, 60° of Ll/Sl lordosis and 53° of Ll/L5 lordosisat the last follow-up. Statistical analysis revealed no significant changes before and after the follow-up.Discussion: The deformed sagittal alignment of the patients with high dislocated hips is already structural.Restoration of hip joint mechanics with a total hip prosthesis has no significant corrective influence on lum-bosacral sagittal alignment.
Total hip arthroplasty with subtrochanteric femoral shortening osteotomyfor the treatment of completely dislocated hips
A. BAKTIR, S. KABAK, M. HALICI, S. KARAOGLU, F. BALKAR
University of Erciyes, Faculty of Medicine, Department of Orthopaedics and Traumatology Kayseri - Turkey
Materials and Methods: We performed total hip anhroplasty (THA) on 28 hips in 26 patients with congenitalhigh hip dislocation. Mean age of our patients was 41 (26-41) years. Mean follow up time was 33(25-59)months. In 24 we carried out a subtrochanteric shortening osteotomy (average 3.8 cm). We performed uni-cortical internal fixation with a 3. 5 mm DCP on 21 hips after the osteotomy. All femoral components were

S150
cemented and both cemented and cementless components were used in acetabulum.Results: Twenty-three of 24 osteotomies (96%) demonstrated radiographic evidence of union at an averageof 6 months. ‘Superficial infection caused delay in wound healing in two and early dislocation in one. Tem-porary neurapraxia of femoral and sciatic nerve was observed in two patients. We obtained excellent andgood results in 24 patients (92.3%) according to the AAOS criteria. One patient had an asymptomatic nonunion of the osteotomy site but still had a good overall clinical result. One patient developed radiolucency atthe acetabular component. Revision was performed in one patient for deep infection.Conclusion: In completely dislocated hips, if subtrochanteric osteotomy is preferred during THA, greater trochantericosteotomy and proximal bone stock can be avoided and protected respectively. We believe that internal fixationwith a DCP leads to safer transverse osteotomy and easier correction of anteversion.
Total hip replacement for congenital hip dysplasia
V. STEDRY’, J. VACULIK
Orthopaedic Clinic of the Postgraduate Medical School, Bulovka Hospital, Prague - Czech Republic
Materials and Methods: We have used 10 different types of total hip implant systems in the treatment of de-generative arthritis secondary to congenital hip dysplasia from 1968 to 1995. Even short term experience withsome of the implant systems was bad. Using Zweymuller Bicon Plus hip implant system we have performed 102 total hip implants in patients withdegenerative arthritis secondary to congenital hip dysplasia from February 1995 to September 1996.Acetabular component sizes 58,55 and 61, femoral component sizes 3,4 and 5 were used most frequently.We made an effort to place the acetabular component medially within the true acetabulum in all patients withdysplasia. It was necessary to broaden severely dysplastic iliac bone mass by acetabular bone autograftingin two female patients and good primary stability was obtained in all cases.While implanting the femoral component we made an effort to obtain good contact between the distal stemand cortical bone of femoral diaphysis.Results: With post-operative x-rays we noted inadequate medial placement 14 times, cup valgus position ofmore than 55° in 4 patients and inadequate stem cortical contact in 7 patients. Dislocation of the implant andfemoral nerve palsy occurred in one case.Conclusion: Our experience with the Zweymuller Bicon Plus total hip implant system has been very good. Thesmall size of cups and stems enables treatment even in significantly morphologically changed hip joints.Arthritis secondary to congenital hip dysplasia is an excellent indication for this implant.
Fate of femoral head autografts in total hip arthroplasty for acetabulardysplasia
B. ATILLA, A. MAZHAR TOKGÖZOGLU, H. ALI, A. MÜMTAZ ALPASLAN
Hacettepe University Faculty of Medicine, Department of Orthopaedics and Traumatology, Samanpazari, Ankara - Turkey
Introduction: Reconstruction of severe bone deficiency with autogenous femoral head graft is controversialin total hip arthroplasty for developmental dislocation of the hip (DDH).Materials and Methods: We investigated 46 hips in 38 patients with DDH undergoing total hip arthroplastyand with acetabular components supported with autogenous strut grafts. Clinical assessments were doneusing the Merle d'Aubigne-Postel grading system. Radiological evaluations included assessment of the ini-

S151
tial position and coverage of the acetabular component, mechanical loading and resorption of the graft andmigration, loosening or revision of the cup at the latest follow-up.Results: All but one of the patients were female. The meanage at surgery was 42.4 years. The mean follow upperiod was 6 years. We revised 3 hips for acetabular loosening and 3 cups migrated more than 2mm. Con-solidation of the graft was inadequate in 4 cases and more than 10% of graft resorption occurred in patients.Discussion: After an average of 6 years the graft seemed to be a successful adjunct to the arthroplasty.
BASIC SCIENCE
Perioperative use of epoetin alfa in anaemic patients undergoing total hipreplacement
G.A. MACHERAS, K. TSIAMTSOURIS, A. KOUSTAKOS, N. POULLIS
Ika Hospital, Athens - Greece
Introduction: We present our experience in the perioperative use of r HuEPO in anaemic patients undergoingtotal hip replacement.Materials and Methods: Seventy patients scheduled for THR between 1997 to 1999 with low Hb levels in-cluded 45 females and 25 males, age 60-82, mean age 77 years. The criteria were: preoperative Hb level 9 -12mg/dl, age 50-85 years, ferritin equal or greater than 50ng/ml, body weight 50-80kg and normal iron lev-els. The exclusion criteria were: cardiopulmonary and neurological diseases, DVT, chronic anaemia, alcoholicsand drug users. The patients were divided in two matched groups of 35. Group A patients received 300RUper kg per day of r HuEPO and 200 mg/dl of iron per day starting 1 week preoperatively through the fourthpostoperative day. Group B patients received only 200mg/dl of iron per day.The diagnosis was OA (50), RA (7) and AVN (8) and CDH (5). We performed 52 uncemented and 18 cement-ed THR. Post operative blood and re-infusion (autotransfusion) was used in all patients. Haemoglobin levelswere measured seven and one days preoperatively and one and four days postoperatively.Results: In the intervention group the mean Hb level was 10.8mg/dl on the seventh pre-op., 13.4 mg/dl onthe pre-op. day, 10.1 mg/dl on the first post-op and 11.2 mg/dl on the fourth. In the control group the meanHb level was 11 mg/dl on the seventh pre-op day, 11 mg/dl on the pre-op day, 8.6 mg/dl on the first post-op day and 10.5 mg/dl on the fourth.We had no allergic reactions, no DVTs and no complications. In the intervention group 23 patients received300cc of allogeneic red blood cell transfusion, 7 received 600ccs and 5 received no transfusion. In the con-trol group 13 patients received 600ccs of allogeneic red blood cell transfusion and 22 received 900ccs.Conclusion: Our results suggest that the pre-operative use of r HuEPO is clinically safe and efffcient to re-duce allogeneic blood transfusion in patients undergoing major orthopaedic surgery.
Does hip resurfacing really conserve bone?
S.J. PALMER, J.A. WIMHURST, R.N. VILLAR
Addenbrookes Hospital, Cambridge - England
Introduction: The perceived purpose of resurfacing arthroplasty of the hip is to conserve bone. We wanted toestablish if this was truely the case. In order to compare the amount of bone resected for both resurfacingand hybrid total hip arthroplasties, femoral and pelvic ‘Sawbones’ were prepared for insertion of components.It was felt that artificial bone would allow more accurate standardised comparisons to be made.

S152
Results: Total bone resection is significantly greater at hybrid arthroplasty than at resurfacing arthroplasty(p=0.001) and insertion of a cemented femoral stem requires significantly more bone resection than resur-facing the femur (p<0.001 ). However inserting the acetabular component of a resurfacing arthroplasty re-quires significantly more bone to be removed than for the uncemented cup of a hybrid arthroplasty (p<0.001).Conclusion: We conclude that whilst reduced femoral bone resection may be advantageous, should patientscome to revision surgery, the increased amount of bone removed from the acetabulum may prove problematic.
Compaction of existing cancellous bone enhances implant fixation
K. SØBALLE, K. CHAREANCHOLVANICH, J.E. BECHTOLD, R.B. GUSTILO
Department of Orthopaedics, University of Aarhus, Aarhus - Denmark
Introduction: in situ compaction of existing cancellous bone in the primary setting may increase the long termsurvival of implants by creating a more durable construct with increased implant/bone interfacial shear strength.The integrity of the implant/bone interface is crucial to the stability of the construct and its long term sur-vival. In previous work, we have shown that in situ compaction of existing cancellous bone in the primary set-ting with both cemented and uncemented femoral components was significantly more stable than conven-tional broaching, in vitro. The goal of this in vivo study is to examine the biologic response to in situ com-paction of existing cancellous bone in the primary setting. We measured the two-and four-week interfacialshear strength of loaded cylindrical titanium implants in the canine knee. When the bone bed was preparedwith conventional methods (drilling), or with in situ compaction.Materials and Methods: 16 cylindrical plasma sprayed titanium implants (5.6mm diameter, 1.0cm length) wereinserted after either drilling or compaction bone preparation methods, into the medial and lateral condyles offour dogs. For each dog the treatments were balanced between medial and lateral condyles. Compaction wasachieved by sequential radial enlargement of the hole, beginning with an initial drill hole of 4.4mms, then ex-panding 4.7mms, then 5.2mms and finally 5.6mms. Drilled holes were directly drilledto 5.6mms. The implantswere press-fitted with equivalent force into each hole, and a polyethylene cap was attached. Implants wereloaded through the polyethylene cap while the animals were allowed full activity. The observation period was2 and 4 weeks. Fixation was determined by push-out test. Data were subjected to Analysis of Variance, withcategorical variables of treatment (drill, compaction), time (2, 4 weeks) condyle (medial lateral) and ID (1-4)and a significance level of p > 0.05.Results: When pooling the data per categorical variable, there was no statistical difference between individ-ual dogs, or between medial and lateral sides. There was a significant treatment effect (p=0.029), with meaninterfacial shear strength for compaction being higher than drilling (10.3 (SE= 1.2)vs. 6.1 (1.2) N/mm2). Therealso was a significant time effect (p=0.036), with mean interfacial shear strength at 4 weeks being higher than2 weeks. (4.7 (1.7) vs. 1 1.6 (1.7) N/mm2).Discussion and Conclusion: In situ compaction of existing cancellous bone has been shown to increase theinterfacial shear strength of plasma sprayed titanium implants as compared to conventional drilling tech-niques, at 2-and 4 week time points, in this in vivo study of loaded implants. This may be due in part to anincreased stability of the implant construct, as shown in our previous work, or may also be due to a local ef-fect, due to the compaction process. Because of these promising in vivo results at important early time points,longer term in vivo studies should be undertaken to continue to evaluate the compaction technique as a po-tential tool for improving implant survival and patient function.
S153
Distal locking of a femoral revision stem - a theoretical study
D. VAN DE VELDE, J. TABUTIN, L. BAUDEL
Centre Hospitalier De Cannes, Cannes - France
Introduction: Although distal locking of the femoral stem becomes more frequently used in total hip revision,the theo-retical basis of this concept had not been explored yet.Materials and Methods: The implant was a LINEA ANATOMIC REVISION stem no 6, the bone support was pur-posely not optimal (no metaphyseal stability, cortical thickness 8mm). A static load of 750 N was applied ver-tically on the femoral head. The resulting stresses on the interlocking screws, variable adjustment of the stemin medullary canal, use of different types of interlocking screws).Results: Cortical reactions were distributed asymmetrically, with lateral traction and medial compression.Bone reactions increase when cortice thickness decrease. Stresses in the locking system were inversely cor-related to the number of interlocking screws: use of a single screw could exceed the elastic limit of titaniumalloy. The influence of the stem diameter (close fitting of the stem to the medullary canal) seems secondary.Discussion: Design of interlocking screw is important: - if laterally threaded, stresses remain continuous andacceptable, within the metal elastic limit; - if medially threaded, stresses are discontinuous, increasing dras-tically at the shaft / thread junction, eventually higher than the elastic limit of titanium alloy; a cortical screwis the most unfavourable design: stresses are continuous but at a very high level, due to a small diameter.This theoretical model cannot give absolute values but shows how the system works and where problemsmay happen. Further studies are in process. Clinical relevance: When distally locking a femoral revision stem, we recommend the use of at least two lat-erally threaded interlocking screws (and not cortical screws), and stem adjustment to the medullary canal.
The aetiology of cement mantle voids
S.D. MÜLLER, S.M. GREEN, P.J. GREGG, A. W. McCASKIE
Department of Trauma and Orthopaedics, University of Newcastle upon Tyne, Newcastle - England
Introduction: To define the aetiology and behaviour of cement mantle voids we devised two related experi-ments.Experiment I - Materials and Methods: Initially, we instrumented air containing voids with thermocouples andpressure transducers and recorded temperature dependent high peak pressures (76-155KPa), void volumeincrease (26.1-35.7%)and final sub-atmospheric pressure (-18 to -44KPa).Results: Vaporisation and subsequent condensation of methyl methacrylate within the void accounts for themagnitude of these observations. Indeed calculations reveal that gaseous methyl methacrylate (MMA) con-tributes a significant proportion of the final void volume (45-62%).Experiment II - Materials and Methods: Secondly, peak polymerisation temperatures of three vacuum mixedcement specimens of differing volumes were recorded (79-112°C). Results: Sectioning of these specimens did not demonstrate any correlation between temperature and voidformation. There was a notable absence of voids in all specimens. This suggests that vaporisation of MMAis incapable of forming voids. Conclusion: There is a complex relationship between trapped air and vaporised MMA: vaporisation of MMAcannot occur in the absence of trapped air voids, however, when air is present, MMA forms a significant pro-portion of the final void volume. Furthermore, reservoirs of MMA within voids may impalr polymerisation inthe cement immediately adjacent to the void, thereby weakening the cement in this area of high stress con-centration.
S154
Permeability of thicknesses of PMMA cement to tissue fluid
B.F. SHAHGALDI, E.J. TAYLOR, J. COMPSON, R. BRUETON
Orthopaedic Academic Unit, Rayne Institute, St Thomas's Hospital, London - England
Introduction: Corrosion of cemented hip implants is frequently reported. For corrosion to occur fluid must bepresent at the implant cement interface. This study examined whether fluid can reach the interface throughan intact cement mantle. Materials and Methods: Eleven implants had been removed for aseptic loosening. These implants were ex-amined for corrosion and thickness of cement mantles.Results: Corrosion was found on three implants. The cement mantles had variable thickness ranging from 0.4to 12 mm.Materials and Methods: To examine the permeability of the PMMA cement, cement shells of thickness rang-ing from 0.3 to 2.0mm were made and filled with a solution of haemotoxylene stain. It was assumed that thisstain solution would penetrate bone cement the same way as body fluid.Results: Even after 24 hours no moisture or stain was found on the external surfaces of shells.Conclusion: This study showed that an intact cement mantle, thicker than 0.3 mm, is a good barrier to permeation byfluid. Passage of fluid through voids and cracks is the likely route on to an implant's metal-cement interface for cor-rosion to occur.
Corrosion of cemented hip implants
B.F. SHAHGALDI, E.J. TAYLOR, J. COMPSON, R. BRUETON
Orthopaedic Academic Unit, Rayne Institute, St Thomas's Hospital, London - England
Materials and Methods: Gross corrosion was seen on surfaces of 24 cemented hip implants that were re-moved for aseptic loosing. The implants were in place from 7 to 14 years. The implant materials were: mod-ern stainless steel alloys including Exeter (14); cobalt-chromium alloy (2); titanium alloy (7). The corroded sur-faces were further examined by scanning electron microscopy and the chemical compositions of corrosionproducts were determined using Energy Dispersive X - ray Analysis (EDXA).Results: Corrosion was of crevice type, although abrasion of metal surfaces had occurred away from the cor-rosion sites.Conclusion: Crevice corrosion occurs when a film of fluid is trapped at the metal cement interface. Cementmantle thickness, intactness and a complete coverage of metal surfaces by cement are important factors inpreventing corrosion.
The trans-iliac exposure of the hip, a modification of the Smith-Petersenapproach
R. GIACOMETTI CERONI
Istituto Ortopedico Galeazzi, Milan - Italy
Introduction: Since 1917, when Smith Petersen (SP) introduced “a new supra-articular subperiosteal approachto the hip joint”, the ilio-femoral technique has been widely used by the surgeons in order to expose the hipjoint and the ilium. This approach was usefully employed for hip arthroplasty (primary and revision), fusion,

S155
pelvic osteotomy, and in traumatology too. In time, many modifications were proposed by different Authors(Hueter, Callahan, Fahey, Judet, Salter etc) to improve the technique.Nevertheless, tensor fasciae and glutei muscle detachment from the iliac crest and wing remains a possiblecause of muscular weakness, due to the unreliability of the suture. A Trendelenburg sign or a limp can be thetemporary or permanent clinical effect.Materials and Methods: Since 1995 I have performed a modification of the classic SP approach splitting theiliac bone through a sagittal osteotomy starting from the anterior superior iliac spine backwards for 7-8 cen-timetres and extending distally for 3-4 centimetres. In this way muscles can be laterally reflected avoidingany detachment. At the end of the surgical procedure the two fragments of the osteotomy can be easily re-duced and fixed by means of two screws with washers. An excellent immediate mechanical stability is achievedso that the patient can start an early active mobilisation of the hip.Results: Thirty four patients underwent this procedure for 32 spherical periacetabular osteotomies, 1 fractureof the head of the femur and 1 acetabular fracture. The iliac osteotomy united in all cases within three monthsafter the operation. Two complications occurred. In one case refixation was necessary 4 days after the op-eration, because the screws cut out and in another case an intraoperative fracture of the iliac wing requiredadditional fixation.Conclusion: This technique is useful especially in abductor muscle lengthening for instance, during a THA ina high dislocated hip.
Gross contamination of grit-blasted hip implant surfaces with aluminaparticles
B.F. SHAHGALDI, E.J. TAYLOR, J. COMPSON
Orthopaedics Department, The Rayne Institute, St Thomas's Hospital, London - England
Introduction: Hip implants with textured surfaces are popular devices for uncemented hip arthroplasty.Materials and Methods: A group of twenty eight surgically retrieved titanium alloy (Ti-6AL-4V) specimens wereexamined.Results: We found large areas of osteolysis bordering or overlying surface particles of aluminum.These specimens had been in place for between four months to five years and were removed between 1996and 1998. The reasons for revision were aseptic loosening pain and protrusio (Austin Moore implants). Boneand soft tissue samples remaining attached to the metal were carefully removed from the metal and the sur-faces in contact with the metal were examined. Tissue samples from the acetabular region, joint capsule andfrom areas adjacent to the stems of eight implants were examined histologically and by electron microscopy.Scanning electron microscopy including microprobe X ray analysis was used for morphological determina-tion and chemical analysis (EDXA) of metal surfaces and tissues. Two newly manufactured grit-blasted pros-theses were used for controls.Aluminium containing particles were seen on the surface of both retrieved and newly manufactured speci-mens. The aluminium containing areas on the surface of the retrieved implants were often adjacent to areasof osteolysis. The tissues in contact with the prostheses also contained aluminium particles. The particles onthe surfaces of the controls and retrieved implants were identical as regards their morphology and X-ray peaksfor aluminium and associated oxygen.Conclusion: We are currently examining the chemical and biological affects of aluminium contamination ofhydroxyapatite coated surfaces.

S156
Ha-bone interface - a joint venture for longevity?
A. J. TONINO, A. I. RAHMY, M. THERIN, C. DOYLE
Atruim Medisch Centrum, Heerlen - The Netherlands
Introduction: As is already known from earlier histological studies, hydroxyapatite coating will be reabsorbedafter some time. The purpose of this study was to document the extent and pattern of bone apposition to ac-etabular cups in relation to the fate of the hydroxyapatite coating.Patients and Methods: We performed a histological and histomorphometric examination in 6 cadaver speci-mens of the femoral and acetabular components and the associated tissue which had been recovered be-tween 3.3 and 6.6 years after clinically successful primary total hip arthroplasty (THA) using a proximal hy-droxyapatite (HA) coated titanium alloy implant.Cups: None of the cups were implanted with screws. All the cups showed bone in growth with an averagebone-implant contact of 36.3% ± 13.5% mean and standard deviation without a fibrous interface. A positivecorrelation could be found between the percentage of bone implant contact and the bone density for the ac-etabular bone around the cup. The amount of HA residue was related to the age of the patient and the timeof implantation of the implant. In two sections, degradation and absorption of the HA was reflected by os-teoclasts and macrophages respectively. Polyethylene debris from the back surface of the liners was notedin half of the empty screw holes with sometimes a granulomatous reaction which showed a tendency to debondthe osseointegration.Conclusion: It has become clear that plasma-sprayed HA coatings do enhance fast and reliable osseointe-gration without a fibrous interface. The cell mediated degradation and resorption of HA is dependent on therate of bone remodelling, but also on the time of implantation. Nevertheless, even in the components wherethe HA-coating was fully absorbed, the bone implant contact ratio did not change much. This is a very im-portant observation, because it indicates that fixation of the component is not dependant on the HA residue.However the surface texture of the substrate is of paramount importance for continued fixation of the implantand therefore for longevity. Empty screw holes are a risk factor for spreading PE debris into the extendedjoint space.
Pharmocological prevention of periprosthetic bone loss after total hiparthroplasty: a randomised trial
J.M. WILKINSON, I. STOCKLEY, N. PEEL, A. HAMER, R. ELSON, N. BARRINGTON, R. EASTELL
Department of Orthopaedics, Department of Diagnostic Imaging, Northern General Hospital, Sheffield - England
Introduction: An acute phase of periprosthetic bone loss occurs following total hip arthroplasty. Peripros-thetic bone loss undermines implant support, may contribute to its failure, and complicates revision surgeryas allograft may be required to replace lost bone.Materials and Methods: We assessed the effect of a single 90mg dose of the biophosphonate pamidronate onearly periprosthetic bone mineral density (BMD), biomechanical markers of bone turnover, and clinical outcomein 47 men and women undergoing hybrid THA in a randomised, double blinded, placebo controlled trial.Results: The mean (+ 95% CI) differences in BMD (area under BMD change time curve) between those re-ceiving pamidronate and those receiving placebo was 0.91 (± 0.51) g.weeks/cm2 for the proximal femur (P=0.002),and 0.80 (± 0.60) g.weeks/cm2 for the pelvis (P=0.009). Patients in the pamidronate group had suppressionof all biochemical markers of bone turnover compared to placebo (P=0.05), except for urinary free deoxypyridinoline.Both treatment groups experienced similar improvement in Harris hip and SF-36 UK outcome scores. The fre-
S157
quency of adverse events was similar in each treatment group (placebo 7/24, pamidronate 8/23, P=0.05).Conclusion: Acute periprosthetic bone loss following THA is due to a transient increase in bone turnover. Asingle dose infusion of pamidronate in the early post-operative period significantly reduces this bone lossand is well tolerated.
Dual-energy X ray absorptiometry measurement of bone mineral densityaround cemented and cementless femoral prosthesis
S. KABAK, M. HALICI, S. KARAOGLU, A. BAKTIR
University of Erctyes, Faculty of Medicine, Department of Orthopaedics and Traumatology, Kayseri - Turkey
Introduction: The measurement of bone mineral density (BMD) in defined areas around metal implants hasimproved with the development of dual energy X-ray absorptiometry (DEXA). The purpose of this prospectivestudy was to investigate the course of the periprosthetic bone mass changes after implantation of unce-mented and cemented femoral implants over a 4 year period.Materials and Methods: A consecutive homogeneous group of 60 female patients with an average age of 58years was operated on for unilateral hip osteoarthritis. The types of prosthetic components used were thecemented Protec MS-30 and uncemented femoral stem. Periprosthetic bone mineral density was measuredin 7 different zones (Zones I to VII) in femoral components. BMD of the femoral components was measuredpreoperatively and one week, I year and 4 years post-operatively.Results: The stem of the Protec prosthesis induced bone mass reduction in the medial femoral calcar andthe lesser trochanter area (Zone VI-VII). The cementless femoral stem produced significant bone resorp-tion in the area of the lesser and greater trochanter (Zone I-VII) 4 years after. Cemented and uncementedfemoral stems induced bone mass increase in the greater trochanter (Zone I), and distal lateral femoralcortex (Zones III-IV). No correlation was found between the age of the patients and bone mineral densityvalues.Conclusion: These observations may be of much better prognostic value for aseptic loosening of total hiparthroplasty long before any radiographic or clinical signs of this complication are evident.
The microbiology of the infected total hip replacement
A. GAMBHIR, P. KAY, B. WROBLEWSKI
Centre for Hip Surgery Wrigtington Hospital, Wigan - England
Materials and Methods: We retrospectively analysed a series of 301 infected total hip replacements. Infec-tion was defined on pre and peri operative clinical findings.Results: Of these 57 cases demonstrated no bacterial growth after prolonged incubation of multiple sampleson enrichment media. The remaining 244 had proven bacteriological evidence of deep infection. Thirty sev-en cases grew 2 different organisms, the rest grew one, hence a total of 281 bacteriological isolates weregrown. Coagulase negative staphylococcus accounted for 54.8%, staphylococcus aureus 13.5%, gram pos-itive cocci 9.2%, streptococci 8.9%, Escherichia coli 6.1% and diptheroids 2.5%.These organisms were plated out in standard fashion against a variety of antimicrobial agents.We looked at 10 antibiotics and their sensitivity profiles against the spectrum of organisms demonstrated bythis series.Best antimicrobial coverage was afforded by fucidin (85.3%) and erythromycin (79.6%).Gentamicin was found to be sensitive to only 76.1% of the bacteria present at the time of revision surgery.
S158
Combining gentamicin with other antibiotics improved the theoretical coverage. A combination of gentamicinand fucidin demonstrated a 97.5% coverage. Gentamicin with erythromycin gave 95.2%.Conclusion: We would suggest that the combination of gentamicin with fucidin or erythromycin be stronglyconsidered when designing the next generation of antibiotic acrylic cements.
The microbiology of the primary joint replacement
A. GAMBHIR, A. CURRY, N. DAVIS, H. PANIGRAHI, E. WILKINS, M. WORSLEY, P. KAY
Bone Infection Group, University of Manchester, Manchester - England
Introduction: We prospectively assessed a consecutive series of 125 primary arthroplasties. Each case wasperformed in a clean air theatre with laminar flow. Prophylactic antibiotics were given at the time of induc-tion and standard waterproof theatre clothing was worn.Materials and Methods: From each case a series of microbiological swabs were described.Samples taken: surgeons glove tip, skin knife, inside knife sucker tip (if used), light handle (2 samples),collection bag (2 samples- hips only), surgeons gown.Each case generated between 5 and 9 samples. The study as a whole generated 867 microbiologicalspecimens. All samples were plated out on Robertson's cooked meat medium and incubated for 24 hours. Any re-sulting ecolonies were then subcultured on to blood agar (aerobic and anaerobic) and chocolate agar(aerobic). Standard laboratory methods were used to identify organisms.Results: 137 positive cultures (15.8%) were identified from 90 of the 125 cases (72%). Coagulase nega-tive staphylococcus accounted for 67.2%, with staphylococcus albus and diptheroids accounting for 18.3%.Sensitivity profiles were available on 87 of these 137 cultures. These were tested against penicillin, ery-thromycin, methacillin, fusidin, gentamicin, vancomycin, ciproxin and teicoplanin. The best coverage bya single antibiotic was achieved with vancomycin, ciprofloxacin and teicoplanin. Gentamicin showed acoverage of 94.2%.
Total hip arthroplasty infection following pneumonia
C.M. BACH, S. TROBOS, M. NOGLER, C. WIMMER, B. STOECKL
Department of Orthopaedic Surgery, University of Innsbruck, Innsbruck - Austria
Introduction: Infection of a total hip replacement was reported to range between 1 and 11 percent. Theincidence of Klebsiella infection in cases of prosthetic infection is reported to be 1 to 2 percent. Kleb-siella pneumoniae is a gram negative rod, found in the upper respiratory tract as well as in the gas-trointestinal tract. It may be involved in pneumonia, urinary tract infection and sepsis.Materials and Methods: In 1993 a left total joint replacement was done for severe osteoarthritis with goodresult until 1996. The patient then fell causing severe deterioration of her general health followed by twoepisodes of Klebsiella pneumoniae. Subsequently she experienced increasing left hip pain. Left hip jointaspiration documented infection with Klebsiella pneumoniae. Plain radiographs revealed that the left sock-et was moderately loose. Due to the poor general health condition, revision was not performed. In 1999rapid progression of prosthetic loosening was noted, requiring removal of implant.Discussion: Klebsiella pneumoniae infection must be considered to occur by hematogenous spread af-ter episodes of pneumoma or gastrointestinal infection. Therefore antibiotic prophylaxis should be con-sidered in older or impaired patients.

S159
Antibiotic elution from bone cement
M. ARMSTRONG, R. SPENCER, A. LOVERING, S. GHEDUZZI, T. MILES, I. LEARMONTH
Avon Orthopaedic Centre and Southmead Hospital, Bristol - England
Materials and Methods: The elution characteristics of gentamicin, vancomycin and flucloxacill in in vari-ous combinations from palacos LV, palacos R and CMW cement, were studied in vitro by creating cementrods of a defined size and immersing them in saline at 37°. The elution curves for the following cement/antibioticcombinations were determined: 1) CMW plus gentamicin, 2) palacos plus gentamicin, 3) palacos LV plusgentamicin, 4) CMW plus gentanlicin and vancomycin, 5) palacos plus gentamicin and vancomycin, 6)CMW plus gentamicin and flucloxacill in, 7) palacos plus gentamicin and flucloxacill in. At three weeks theabove combinations were the most commonly used in revision surgery. At three weeks the cement spec-imens were fractured and reimmersed causing a late antibiotic peak similar to that reported during revi-sion surgery after cement fracture. Results: Elution from palacos was found to be greater than from CMW and the elution chalacteristics ofboth gentamicin and vancomycin appeared satisfactory. It was possible to assay both flucloxacill in andits primary breakdown product Flucloxacill ic acid, which is microbiologically inactive. All the antibioticeluting from the cements after the first 4 days was in the form of this breakdown product.Conclusion: It was concluded that gentamicin and vancomycin are suitable additives to bone cement ei-ther alone or in combination, but both may be released late (eg at revision surgery), and antibiotic resis-tance may develop. Ourresults question the effectiveness of flucloxacill in as an additive to bone cementin revision surgery.
Monitoring prosthetic migration following total hip arthroplasty using theEBRA-digital radiograph analysis system
J. WILKINSON, A. HAMER, R. ELSON, N. PEEL, I. STOCKLEY, R. EASTELL
Department of Orthopaedics, Northern General Hospital, Sheffield - England
lntroduction: Implant migration of greater than 1mm per year over the first 2 years following total hiparthroplasty (THA) is associated with reduced implant survival. We aimed to assess whether the precisionof the EBRA-Digital software for measuring implant migration following THA in prospective clinical prac-tice is sufficient to identify individuals at risk of early failure.Materials and Methods: Seventeen men and 12 women following THA underwent duplicate, standardised,plain radiographic examinations of the hip on the same day after repositioning. The resulting radiographpairs were then digitised using 2 methods and analysed by 3 observers using the ENRA-Digital software.Precision was expressed as 95% confidence interval (95% Cl = ± 1.96 x Std.Dev.).All l inear migration measurements had a precision of better than ± 1 mm when measured by a single ob-server and were free from systematic error (paired t-test, P>0.05). The 95% CI for measurements madeby multiple observers were ±0.9mm to ±1.6mm for cup migration and ±0.7 to ±0.9mm for femoral com-ponent migration. Measurement precision was not strongly related to patient gender or digitisation method.Conclusion: The EBRA-Digital method has suffilcient precision to detect clinically relevant migration inprospective clinical practice, to allow individual patient monitoring following total hip arthroplasty.

S160
Is there amelioration of accuracy and precision in migration measurementof femoral components by use of bone markers? A study of conventional,measurements, EBRA-FC and RSA
R. BIEDERMANN, B. STOECKL, P. MAYRHOFER, M. KRISMER
Department of Orthopaedics, University of Innsbruck, Innsbruck - Austria
Introduction: The aim of this study was to find out whether tantalum markers improve accuracy and/orprecision in migration measurement in THR compared with conventional measurements without mathe-matical correction of data and also in EBRA-FCA with a correction by the computer.Materials and Methods: 13 series with a total of 88 RSA compatible x-rays were analysed by three ob-servers independently. Data were obtained from measurements in conventional radiographs, with EBRA-FCA and with the RSA method. All results were compared with RSA data. Also x-rays were examined toassess the number in which bone markers could be simulated. Results showed that tantalum markers im-prove reliability whereas accuracy is assisted less well by bone markers when considered with RSA at 24months, (median difference for bony reference point = 1.7, for tantalum marker =-1.1; p=0.1), EBRA-FCAis comparable to RSA (for bony reference point = -0.3, for tantalum marker= -0.4, p =0.1).Conclusion: We conclude that accuracy of stem mlgration measurement cannot be improved by use ofbone markers.
Biological reaction to wear debris: an histological, immunohistochemicaland ultra-structural study
M. CAPORALE, G. MACCAURO, P. PERANI, V. DE SANTIS, E. POLA, F. SILVI
Orthopaedic Department, Catholic University, Rome - Italy
Introduction: To assess the histological and ultrastructural host response to loosened implants, we analysed the mem-branes surrounding the failed implants using a specific protocol.Materials and Methods: In sixty five loosened implants (metal polyethylene, Alumina Alumina, Alumina polyethylene)the membranes were analysed for wear debris by histology, immunohistochemistry, scanning and transmission elec-tron microscopy. Image analysis was used to measure the dimension of granules.Results: Vessels and mononuclear cells were observed in the granulomatous reaction to metal and ceramicdebris (average size 1.75 µm2). The size of PE debris was more variable from submicroscopic to large parti-cles and giant cells were prevalent.Conclusion: Size of particles is crucial to the biological host response. The smaller ones may induce a directtoxic effect on mononuclear cells, the bigger are surrounded by giant cells and may induce a chronic in-flammatory response, which also contributes to failure. Immunohistochemistry confirmed the role of T Iym-phocyte in the response to debris. EDAX revealed, in the case of ceramic, the presence of traces, which mayreduce mechanical properties. We conclude that the biological host response is more dependent on the sizethan the chemical composition of particles released. Metal and Alumina debris are more active.

S161
Periprosthetic membrane around loose hip arthroplasties
B. ATILLA, A. MAZHAR TOKGÖZOGLU, P. ATILLA, A. NUR ÇAKAR, A. MUMTAZ ALPASLAN
Hacettepe University, Faculty of Medicine, Department of Orthopaedics and Traumatology, Ankara - Turkey
Introduction: In order to evaluate the cellular mechanisms responsible for the aseptic loosening of total hipreplacements, 20 periprosthetic membranes were collected during revision procedures.Materials and Methods: Arthroplasties with and without polyethylene components were subdivided into twoseparate groups. Immunohistochemical analysis performed with a number of monoclonal antibodies reactiveto certain cell surface antigens defined as CDs including: CD45 (Leukocyte common antigen), CD44 (Hermesantigen), CD98 (4F2 antigen), CD3 1 (PECAM-I: platelet endothelial cell adhesion molecule), CD26 (ADA bind-ing protein), CD71 (Transferrin receptor) and ki67 are used to distinguish certain cell types, leukocytes, anddistribution of the vasculature. Different morphological characteristics were observed in each group regard-ing the adjacent fibrosis, leukocyte activation, and immunologic response.Results: Although polyethylene particles appear to be involved with a more aggressive periprosthetic mem-brane formation characterised by a dense fibrous tissue and more active Iymphocytes, there is an obviousleukocyte activation and immunologic reaction leading to eventual bone resorption around the prosthesiswithout a polyethylene interface as well.Conclusions: These results indicate that there may be some other factors responsible for aseptic looseningand the two types of membranes utilise different cellular and molecular mechanisms.
Perioperative stress-reduction with video-tape preparation before totalhip replacement
H. BEHENSKY, S. DOERING, M. KRISMER, G. RUMPOLD, S. ROESSLER, B. HOFSTÖTTER, G. LUZ-KUEHBACHER
Department of Orthopaedic Surgery, University School of Medicine, Innsbruck - Austria
Materials and Methods: 100 patients scheduled for elective total hip replacement surgery for osteoarthritisof the hip were randomly assigned to a control (n=54) and an intervention group (n=46). The intervention groupwas shown the video tape on the evening before surgery. Anxiety and pain were assessed daily for five daysbeginning with the preoperative day by means of the Satte-Trait Anxiety-Inventory and a visual analogue scale.Intraoperative heart rate and blood pressure as well as postoperative intake of analgesics and sedatives wererecorded. Levels of cortisol, epinephrine and norepinephrine were determined in 12 hour night-urine collec-tions for five nights beginning with the preoperative night.Results: Compared to the controls patients of the intervention group showed significantly decreased anxietyon the morning before surgery (p=0.03) and the mornings of the two postoperative days (p1=0.02, p2=0.048)and significantly fewerof them had an intraoperative heart rate increase of more than 15% (p=0.01). Pain rat-ings did not differ significantly between the two groups, but prepared patients needed significantly less opi-ods (p=0.001) postoperatively. Patients of the preparation group showed a significantly lower cortisol excre-tion in the preoperative night (p=0.0001) and in the two postoperative nights (p1=0.01, p2=0.003). The ex-cretion of catecholamines did not differ between the two groups.Conclusion: We conclude that our video-tape preparation is well suited to decrease anxiety and stress in pa-tients undergoing total hip replacement surgery.
S162
Hip dislocation memory defects
M. EVANS, G. C. BANNISTER, R. BUCKINGHAM
Department of Orthopaedic Surgery, Southmead Hospital, Bristol - England
Introduction: Dislocation following total hip replacement occurs in between 0.5 and 8% of patients. Disloca-tion may result from lack of compliance in patients whose hip dislocates. This lack of compliance may be theresult of memory failure. Materials and Methods: Fifteen patients whose hips recurrently dislocated were compared with 15 age andsex matched controls. Short-term memory was examined by the Folstein test and long-term memory by theability of a patient to pick up an item from the floor, in the manner prescribed by the physiotherapist in thetreating unit.Results: There was no difference in the mean Folstein scores in patients who did and did not dislocate.Two of the 15 patients who dislocated ( 13%) and none of the stable hips adopted positions that risked dis-location in picking up low objects.Conclusion: This suggests that dislocations are not related to failure of short-term memory and only a smallproportion to non compliance with post-operative instructions.
FEMORAL REVISION - Session I
Revision arthroplasty with the ESLR revision schaft
J. LOEHR, U. SCHUTZU, U. MUNZINGER
Schulthess Clinic, Dept of Orthopaedics, Zürich - Switzerland
Introduction: The Zweymuller revision system was developed in 1991. The principal of the design is to allowan optimal distal fixation while allowing the bone to remodel in the proximal part. This study reviews the re-sults and relates the design of the implant to the outcome.Patients and Methods: Fifty one hip revisions were performed utilising the SLR shaft (Endo-Plus Orthopaedics)between 1995 and 1996. All patients are being followed prospectively. In 25 patients the left, and in 26 theright side was involved. The cause of revision was aseptic loosening in 90 % (46 patients). Six patients hadundergone more than one previous revision in this collective. In all cases either the polyethylene insert of theacetabulum or the acetabulum itself was changed as well. The follow-up clinical examination and X-ray re-view was performed in 46 patients by an independent observer. Five patients were living outside the coun-try, therefore follow up examination was only available through a questionnaire and X-rays taken by the localphysician. Clinical assessment used the Merle d'Aubigne score.Results: The preoperative pain sensation was severe to moderate in 92%. While postoperatively 73% of thepatients had no pain, 20% of the patients had slight hip pain with activities. Walking for more than 1 hourwithout a stick was recorded preoperatively in 11 patients 22%, and postoperatively in 28 (55%). Half the pa-tients (24) were able to walk without a limp postoperatively while 21 had a positive Trendelenburg sign. Therange of flexion reached over 90° in 3 cases, with 70% of the patients achieving between 70° and 90°. Thepreoperative Merle d'Aubigne score changed from 13.5 to 16.4. At X-ray review all stems were found to becentralised. Subsidence of the stem was found in 9 cases, with 8 cases subsiding more than 3mm and oneless. Resorption lines were found at the proximal end, although these corresponded with the osteolysis pre-sent at the time of change. In one case possible loosening was felt to be present and one patient has painbut has declined revision at the time of reporting. General complications consisted of 4 haematomas, 1 dis-
S163
location, 1 deep infection and I deep vein thrombosis.Conclusions: The SLR revision prosthesis is an excellent implant in revising femoral defects at revision arthro-plasty. Before selecting this device, the femoral shaft should still have sufficient bone stock to allow ade-quate distal fixation. This prevents subsidence and maintains rotational stability at the same time.
The use of the Furlong hydroxyapatite ceramic coated prosthesis inrevision hip arthroplasty
G. RADCLIFFE, L. FUNK, J. BRADLEY, C. ANDREWS
The Adela Shaw Orthopaedic Unit, Scarborough Hospital, Scarborough - England
Introduction: The purpose of this study is to analyse the clinical and radiological results of revision hip arthro-plasty using the 'Furlong HA-C' coated prosthesis.Materials and Methods: We retrospectively reviewed 37 hips in 33 patients for a mean of 3.5 years (range 1-7 years) following revision hip arthroplasty using the 'Furlong HA-C' coated prosthetic system. Clinical eval-uation was by a modification of the Harris Hip Score excluding the values for range of movement and defor-mity. Radiological evaluation used the AAOS system for pre operative films and a scoring system after Enghfor the post-operative films.Results: We found that the clinical outcome was good with a mean modified Harris Hip Score of 74.84 out ofa possible 91 (95%C>I> 69.07-80.61).Complication rates were comparable to previously reported ranges with a dislocation rate of 8.1% and a fur-ther revision rate of 10.8%. Two acetabular prostheses failed early where there were large medial wall defects pre-revision. One femoralprosthesis fractured 4 years postoperatively due to toggling of an unfixed proximal segment. Conclusions: We conclude that the Furlong HA-C coated prosthesis is suitable for implantation at revisionhip arthroplasty and can give good results in the short to medium term in selected patients.
Revision hip arthroplasty using cementelss extensively porous coatedfemoral stems
I. CARLUKE, J. SHER WANSBECK
General Hospital, Ashington, Northumberland - England
Introduction: The aim of this paper is to report the 2-8yr (mean 5yr) follow up on the medium term durabilityof 82 extensively porous coated Solution femoral stems used during revision hip arthroplasty in 79 patients.99 patients have had 103 hips implanted in 3 DGHs within the northern region of England since the intro-duction of the Solution femoral stem. There are currently 82 patients (85 hips) suIviving. Six have moved fromthe region and been lost to follow up.The remaining 76 patients (79 hips) have been independently assessed using radiographic criteria as de-scribed by Engh et al.Results: Age at surgery was mean 68.8yrs, range 41-89yrs. 70 femoral components were stable with 66 stemsshowing bone ingrowth and 4 stable fibrous union. Eight showed radiographic instability manifested by dis-tal migration of the femoral stem. Five are symptomatic with further revision planned Dislocation occurred in7 hips of which 6 are asymptomatic and radiographically stable. One remains chronically dislocated. Onedeep infection occurred. Mild to moderate stress shielding was observed in 22 hips but did not seem to besignificant.
S164
Conclusion: These results indicate that diaphyseal fixation using extensively porous coated cementless femoralstems can achieve satisfactory medium term stability in the difficult revision scenario when the proximal fe-mur is biologically or mechanically deficient. Early complications of surgery including proximal femoral frac-ture do not seem to have any adverse effect on the implant survival. Subsidence of the femoral stem, as seenin the unstable hip, tends to occur early and invariably progresses.
Management of femoral defects THR using a cementless modular system
E. DE SANTIS, M. CAPORALE, G. LOGROSCINO, E. ROMANINI, E. POLA, S. RIVELLI
Orthopaedic Department, Catholic University, Rome - Italy
Introduction: The revision of failed THA is a difficult challenge in reconstructive hip surgery due to severefemoral bone loss. Different options are available.Materials and Methods: This study describes our experience with modular cementless components. Results: Femoral defects were Paparosky type I (45%), with minimal bone loss; type II-III (38%) with more ex-tensive metaphyseal destruction and type IV (17%) with extensive metaphyseal and diaphyseal bone loss.Thirty-eight hips (M:F=13.25) type II-III IV underwent THR with a porous coated stem (S ROM) with proximalmultiple size sleeves to provide proximal fit and fill and avoid torsional strength mobilisation.All patients were evaluated clinically (HHS, WOMAC, SF-12) and radiologically with the Engh criteria. Themean follow-up was 24 months.HHS improved from 40-85. Stable fixation was present in 97%. Mechanical failure rate was 3%. We did not ob-serve significant complications. Minor fracture and dislocation occurred in 10% and deep infection in one pa-tient. Residual leg discrepancy more than 2cm was observed in 3%.Conclusion: Assessment of bone loss and residual bone stock before surgery is crucial to choose the implantable to achieve durable mechanical stability. No complications were attributable to the S-ROM implant. Thisdemonstrates it is effective in reducing pain and restoring hip function.
Management of late post operative peri-prosthetic fractures in the elderlywith a distally locked revision femoral component
G. CHARNLEY
Trauma Specialist Directorate Level 11, Derriford Hospital, Plymouth - England
Introduction: For the revision hip surgeon peri-prosthetic fractures around failing implants pose a significant challenge.Materials and Methods: A prospective, consecutive study of 16 patients (average age 77 years) over 4 1/2years is reported. The mean surviving follow up is 29 months. All patients were treated with a Cannulok im-plant with distal locking and proximal cemented impaction allografting.Due to implant failure, osteolysis and fracture patterns other forms of treatment were felt inappropriate. Wehave classified these problems using the Vives and Gruen scores and the Cook and Newman and Duncan andMasri classifications.Results: The mean inpatient stay was 26 days (7-107 days). Many patients had discharge delayed by co ex-isting orthopaedic, medical and social problems. They were all allowed immediate weight bearing.All fractures united by six months and all patients have improved bone stock on review of X-rays.Conclusion: We believe that the combination of secure initial fixation with a distally locked femoral compo-nent and proximal allografting allows early discharge and weightbearing and in the medium term satisfacto-ry radiological and clinical function.

S165
The treatment of periprosthetic fractures of the femur using cortical onlayallograft and long-stem femoral components
N. SENER, I. REMI TOZUN, M. ASIK, F. DIKICI
Istanbul Medical Faculty, Department of Orthopaedics and Traumatology, Istanbul - Turkey
Introduction: Periprosthetic femoral fractures present the problem of fracture management and prostheticstability. Various treatment options are recommended for managing these fractures.Materials and Methods: We treated 10 periprosthetic fractures between 1992 and 1999 All fractures were man-aged with revision to a long stem, porous coated prosthesis and augmented with cortical onlay strut allo-grafts. According to the Vancouver classification, there were six B1 fractures (associated with a well fixedprosthesis), two B2 fractures (associated with a loose stem), and four B3 fractures (associated with very poorproximal bone). Follow-up ranged from 6-84 months (mean 23 months). Three fractures occurred with minortrauma, four from falling down, two after traffic accidents and one intraoperatively.Results: All fractures healed and patient function increased dramatically. The postoperative Merle d'Aubignerating scale was 16.2 out of 18 with 82% excellent or good results. The average time to union of the fractureand allografts was 10.6 months. Complications consisted of loosening of one stem.Conclusion: We recommend revision with long stem, cementless implants in conjunction with circlage wiringor cable grips and strut grafts for the treatment of femoral fractures around loose femoral stems. Implant sta-bility distal to the fracture is emphasised.
Does freeze-dried allograft work in impaction grafting of the femur inrevision total hip arthroplasty?
A. MAZHAR TOKGÖZOGLU, H. SENARAN, B. ATILLA, A. MÜMTAZ ALPASLAN
Hacettepe University, Faculty of Medicine, Ankara - Turkey
Introduction: Impaction grafting of the femur in revision total hip arthroplasty (THA) has become a widely ac-cepted procedure for reconstructing the proximal femur. Morcelised fresh frozen femoral heads has been usedfor this since it is readily available. We have used freeze-dried cancellous allograft obtained from bone banksfor impaction grafting since fresh frozen femoral heads are not available in our institution. The purpose of thisstudy is to evaluate our experience of impaction grafting of the femur using freeze-dried allograft bone.Methods: We performed 40 impaction grafting procedures of the femur during revision THA. Freeze-dried al-lograft obtained from bone banks was used and vigorous impaction was performed during surgery. Twentyseven hips in twenty-five patients of this population with a minimum follow up of 24 months (average 29,range 24 to 45) were subjects of this study.Results: All patients demonstrated a significant improvement of their hip scores (average preoperative score55, postoperative 89, p=0.043). There was no loosening, radiographically detectable migration or subsidence.All patients demonstrated reconstitution of the proximal femur with incorporation of the allograft.Conclusion: In our opinion when vigorous impaction is used freeze-dried allograft is a suitable material forimpaction grafting of the femur in revision THA.

S166
ACETABULAR REVlSION
Acetabular reconstruction in revision surgery. Impaction grafting ontitanium mesh for severe bone deficiency
G. ULLMARK
Orthopaedic Department, Gävle Hospital, Gävle - Sweden
Materials and Methods: 28 hips in 27 patients were operated for acetabular revision, twenty-three had me-chanical loosening, 6 peri-prosthetic infection and one after fracture. All had combined cavity and segmen-tal deficiencies (type III AAOS classification). The segmental cortical defects were covered with a 0.5-0.8 mmTitanium mesh or Titanium Graft Cup (Waldemar Link GmbH & Co, Hamburg, Germany), anchored with mul-tiple screws. Morcelised and partly defatted allograft was firmly impacted in the cleaned bone defect, partlyagainst the mesh, using Acetabular Impactors (Waldemar Link GmbH & Co). In cases of a thick graft bed, aTitanium Graft Cup was anchored with screws on top of the impacted neo acetabulum. Finally a polyethyl-ene cup was cemented on the graft bed in a routine manner. The patients were mobilised with toe-touchweight bearing on the operated leg for 6 to 12 weeks. Twenty-six hips in 25 patients were examined clinical-ly and radiologically after 40 (31-52) months.Results: Two hips in two patients were failures after two and 20 months respectively. One had a persistentinfection, the other one had a mechanical failure. For 26 hips in 25 patients the clinically Merle d'Aubigne-Postel score was significantly improved at follow-up. At radiology two cups had migrated 6 and 9 mm re-spectively. Incomplete radiolucent lines were detected in three cases. New trabecular formation in the graft-ed areas could be assessed only in 14 of the hips, due to covering of the mesh. Ten of those showed newtrabecular formation. Histology on the two failures together with one of the other patients, showed ingrowthof living tissue and new bone formation inside the graft bed.Conclusion: This study suggests ímpaction grafting on Titanium Mesh to be a technically demanding butpromising method. In addition to a good clinical and radiological result the method seemed to result in arestoration of the bone stock, using standard prostheses. A longer follow-up will be done.
Management of polyethylene wear and pelvic osteolysis with cementlesscups
G. MAGLIOCCHETTI LOMBI, D. DALL'ACQUA, A. OPPI, R. BONDI, V. DE SANTIS, M.F. CAPORALE
Orthopaedic Department, Catholic University, Rome - Italy
Introduction: Loosening of the acetabular component remains a long-term problem of THA.Polyethylene wear induces debris release with a consequent granulomatous reaction and osteoclastic acti-vation. The end of this process is osteolysis and loosening of the acetabular component. We used the D'An-tonio (1989) AAOS classification of acetabular defects. The type of acetabular reconstruction utilized for thesedefects is based upon the extent of bone loss and the type of defect.In type 1 and 2 we prefer to use a large diameter cementless hemispherical cup, in type 3 a press fit hemi-spherical cup with additional screws of spikes of pegs fixations and in the other cases a jumbo oblong cup.Material and Methods: We studied a series of 340patients. Theywere 211 female and 129 male. The age ofpatient at the time of operation ranged between 44 to 82 years with an average of 63 (mean follow-up 5.3years). The pre-op diagnosis included aseptic loosening (74 cases), liner breakage (12 cases), post traumat-ic loosening (5 cases), dislocation (7 cases) and ceramic head breakage (2 cases). We used a large diametercementless hemispherical cup without screws in 44% of the cases, a cementless hemispherical cup with
S167
screws in 39%, threaded in 11% and an oblong cup in 6%.We assessed our patients by the Harris hip score and X-ray after 1, 3, 6 months and yearly post operatively.Discussion and Conclusions: Good results reported by other authors are confirmed in our study. We believethat threaded sockets, because of their design, determine a high localised concentration of stresses, re-sponsible for the high incidence for failure. Hemispheric cups, because of the optimised distribution of theforces and the optimal fit, do not require additional screws, and so, the absence of holes with the high con-gruence of the liner, determine a dramatic reduction of polyethylene wear at the inner interface. We avoid,when possible, the use of screws and grafts and threaded and oblong cups and prefer jumbo cups. We no-ticed better results with an early surgery. Patients followed after total hip arthroplasty, will have radiograph-ic evidence of early acetabular failure before of significant symptoms. They should not wait for the develop-ment of significant symptoms, but they should be encouraged to an early revision surgery, to minimise theproblems of a surgical reconstruction.
Total hip replacement with tantalum acetabular cup
M. CAPORALE, G. RINONAPOLI, E. ROMANINI, R. BONDI, P. PERANI, G. LOMBI MAGLIOCCHETTI
Orthopaedic Department, Catholic University, Rome - Italy
Introduction: Acetabular revision remains a cornmon problem in total hip replacement. Improvement of de-sign has significantly reduced the incidence of early stem loosening. For that reason, attention has been fo-cused on the acetabular component.Materials and Methods: The aim of the present study is to assess the validity of a new cup. It is elliptical andhas a size of over 60mm of diameter but the main characteristic is the new biomaterial by which it is made.It is commercially deposited into and about a carbon skeleton using a chemical vapour deposition/infiltrationprocess.Another characteristic is that the polyethylene insert is moulded into the carbon skeleton; this eliminates mi-cromotion, which therefore minimizes the amount of released wear debris. Several studies show that all theimplants with Tantulum have stable bone-implant interfaces. In the pores of the cup signs of bone ingrowthare found.We describe our experience of about 25 total hip replacements with a follow-up of 2 years and clinical andradiographic evaluation at 6 months and yearly thereafter.
Failure of acetabular revision with the Harris Galante I cup
J. TABUTIN, P. CAMBAS, F. VOGT
Centre Hospitalier, Cannes - France
Introduction: We have used the Harris Galante I cementless cup (hemispherical titanium alloy implant covered bypure titaniurn fibre mesh and fixed with screws) in more than 250 acetabular revlslons, whlch were satisfactoryafter at 2 and 10 years follow-up. However we had to re revise a few of them. We shall focus on those (apart fromrecurrent dislocations).Materials and Methods: 238 aseptic acetabular revisions were perforlned with the Harris Galante cup (21 sep-tic cases are excluded). We studied secondary loosening of the implant by ENGH and MASSlN's criteria (morethan 2mm or 5° of displacement).Results: Six cups in 6 patients (4 women, 2 men) have been revised again with a Harris Galante cup. One wasan acetabular granuloma which went to loosening. The other ones were high grade revisions (2 SOFCOT III,
S168
3 SOFCOT IV) having had a segmental graft. 31 segmental grafts (in the 238 patients) were performed usingcryopreserved femoral heads. In those five cases the secondary revision was not difficult (as in a grade II)and the outcome clinically and radiologically satisfactory.Discussion and Conclusion: The case with the granuloma underlines the necessity of a strict radio clinical fol-low-up which might have allowed a simple revision before extensive bone damage.Late migration after revision of high grade lesions with segmental allografting emphasises the limits of thistechnique. The grafts united to host bone but did not completely incorporate.With good mechanical properties of the allograft (donor selection) and the operative technique (press-fit, ori-entation of bone trabeculae), this technique does not merit its poor reputation.Conclusion: We now tend to add iliac crest autografts to allogenic bone chips for segmental defects and asbone substitutes for cavitary defects. At least 50% of the cup should come in contact with host bone and itshydroxyapatite coating should promote a better fixation.
Structural allografts of the acetabulum in cementless total hip revisionarthroplasty
J. TRILLAUD
Clinique Lamartine, Thonon Les Bains - France
Introduction: The use of massive allografts of bone stock in the acetabulum is a technique that allows ananatomical reconstruction of the lost bone stock. The aim of this study was to assess how these grafts de-velop with time.Materials and Methods: We reviewed 20 surgical cases performed between August 85 and August 94. Theprocedure consisted in filling in bone defects with frozen, unfragmented femoral heads, carefully adapted,screwed and then reamed in situ. Only cementless cups were implanted.Follow up time (after failure or last examination) was 56.5 months (5-140). Failure was defined by the collapseof the graft or by the mobility of the implant.Results: We were able to identify 7 failures that clearly appeared after 54 months (5-140). The survivorshipprobability (actuarial method) remains stable at 60% at I 1 years, but drops to 20% at 12 years.The age, the sex and the weight of the patients, the age, the sex and the hip disease of the graft donors wereanalysed: none of these factors were relevant.All these grafts are or appear to be solid. Three biopsies were carried out (at 5, 20 and 36 months) all showing necrot-ic bone.Conclusions: With these results, which were not encouraging, we decided to abandon this technique, whichwas however an interesting way to anatomically reconstruct the acetabulum.
Homologous reconstruction of the acetabulum in 447 cases of revisionhip arthroplasty: results after 10 years
C. FRIESECKE
Endo Klinik, Hamburg - Germany
Introduction: We perform about 1000 hip arthroplasties per year.Material and Methods: This retrospective study reports on 447 cases between 1983 and 1985 in which ho-mologous bone grafting was carried out to treat loss of acetabular bone stock in revision hip arthroplasty.Results: Aseptic loosening occurred in 59 (=13%) cases, and early and late in 17 (=3.8%). These 76 cups were

S169
exchanged. In 29 of these revised cases the graft was still completely or partially in situ.According to the Kaplan-Meier Method, the survival probability for aseptic cup loosening was 81% after 102months and 90% for the bone graft. For a comparative group of 102 cases in which lost bone was recon-structed with cement the swival probability was 72%. This shows clearly the advantage of homologous bonegrafting. The follow-up period was between 8.6 and 11.8 years, on average 10 years.
Late cup revision with the ABG hip system
A. TONINO, W. MEIJERS, M. VAN DER LINDE
Atrium Medisch Centrum, Heerlen - The Netherlands
Introduction: The problem of late aseptic and septic cup loosening is nearly always accompanied by impor-tant loss of acetabular bone stock, loss of leg length and loss of the anatomic centre of rotation again. Thereare two ways to overcome these problems; first by restoring all lost bone stock and using more or less thesame size of cup or secondly by using a much larger cup without restoring all lost bone stock. The advan-tages of the last method are immediate with restricted weight bearing, shorter operating time and lower cost.With the ABG hydroxyapatite coated cup we have opted for the second solution.Patient and Methods: Between 1990 and 1999 81 patients with an age between 40-80 years (mean age of 71.5years) were operated on for prosthetic hip loosening (6 cups and stems and 1 cup). 67 cups were revised (41previously cemented and 26 previously uncemented). The mean age at the index operation was 59.5 years andthe mean cup size was 52. Regardless of acetabular defect classifications all cups could be placed in a sta-ble position which was enhanced by screws in 31 cases. The mean size of the newly inserted cup was 64.Results: Follow-up was between one and nine years (mean 4.1 years). All cups osseointegrated and none hadto be revised for aseptic loosening. Two patients died from heart failure, one after two months and the otherafter two years. In both cases histology of the acetabulum was obtained. The first case showed sparse andpartial osseointegration while in the second case osseointegration was complete and no different from pri-mary cases.Conclusions: The concept of osseointegration and thereby of reliable fixation of HA coated implants provedalso valuable in late aseptic cup loosening. By using a much larger cup the need to replace all lost bone stockcan be bypassed and early stability could be achieved in host bone in 36/67 cups without the need for sup-plementaly screwfixation. A100% success of osseointegration could be achieved.
PROXIMAL FEMORAL FRACTURE
Conservative treatment of hip fractures in elderly patients
E. BAIXAULI, E. NAVARRETE, F. BAIXAULI Jr, F. BAIXAULI
La Fe University Hospital, Valencia - Spain
Introduction: The treatment of choice of hip fractures in elderly patients is surgical fixation or hip replace-ment but in some patients the surgical treatment is contraindicated.The aims of the study were to assess the magnitude of the problem, the mortality rate and the functional out-come in these patients.Material and Methods: Between January and December of 1998, 140 patients with hip fracture were treatedconservatively at our institution ( 17% of all hip fractures). Onehundred and thirteen patients were prospec-tively reviewed at 1, 3, 6 and 12 months or until death. The mean age was 85 years and 68% were women.
S170
Forty-seven fractures were intracapsular and 66 were extracapsular.Results: The mean pre-fracture score was 1.4 and after one year 3.1 (walk with a frame). Mental statusdid not deteriorate significantly. Ninety five % of patients returned to their own or their family's house.After one year mortality was 61%. Despite the functional deterioration and high mortality, conservativetreatment was highly acceptable to their families.
Mental state and oxygenation of patients with fractures of the proximalfemur
D. VERETTAS, A. ATHANASIOU, B. GALANIS, K. KAZAKOS
Department of Orthopaedics, Alexandroupolis Regional General Hospital, Alexandroupolis - Greece
Introduction: The mental state of elderly patients with fractures of the proximal end of the femur may frequently de-lay discharge and rehabilitation despite otherwise successful operative procedure.Aim: To study the possible relationship of the blood oxygenation of elderly patients with fractures of the proximal fe-mur, with their mental state pre operatively and again during the first and third post-operative days.Material and Methods: Forty four consecutive patients with 26 pertrochanteric and 18 cervical fractures of the prox-imal femur were included in our study. Thirty eight were women and 6 men and their ages ranged from 61-93, aver-age 75. Upon admission and the first and third post-operative day their blood oxygenation was assessed PO2, oxy-gen saturation and haemoglobin concentration. At the same time their mental state was assessed by completing aspecially designed score sheet (MMSE). A score of 30 was normal and below 20 the patient was considered demented.Results: The pre-operative PO2 ranged from 51 to 107 (average 70.6), oxygen saturation from 83 to 99% (average93.5%), their haemoglobin levels from 9.3 to 15.2g/dl (average 12g/dl) and their MMSE score ranged from 14 to 29(average 25). During the first post operative day the PO2 values ranged from 51 to 108 (average 68.3), the oxygensaturation from 85 to 99% (average 93.2%), their haemoglobin levels from 8.9 to 15d/dl (average 11.5g/dl) and theirMMSE score from 15 to 29 (average 25). On the third post-operative day the PO2 values ranged from 51 to 110 (av-erage 68.4), oxygen saturation from 89 to 99% (average 93.6%) haemoglobin levels from 9.3 to 15g/dl (average 11g/dl) and MMSE score from 14 to 29 (average 24.8).Conclusion: We conclude, from this study, that there is no correlation between the mental state of elderly patients,who have been admitted to hospital with fractures of the upper end of the femur and their blood oxygenation, andthat attempts to give oxygen to these patients, in the hope of avoiding the development of dementia, is probably notjustified in the absence of other indications.
Are early post operative radiographs necessary following thermal imagingduring DHS fixation?
G. PATTISON, C. HUGHES, R. SPENCER
Department of Orthopaedics, Weston General Hospital, Uphill Weston-Super-Mare - England
Introduction: This study aimed to determine if the thermal prints of intra-operative image intensifier imageswere of sufficient quality to allow accurate assessment of the DHS implant and if immediate post operativeradiographs added any further clinically relevant information.Material and Methods: The position of the screw within the head was measured using previously validatedmeasures:- the tip apex distance (TAD) (Baumgaertner 1995) and the ratio of the screw position in the APand lateral planes (Parker 1992). The proportion of the hip screw protruding from the barrel of the plate wascalculated in mm using the method of Lunsjo (1997). Blinded measurements were made on both the ther-

S171
mal prints and post operative radiographs. The measurements were compared using the paired t-test. Pa-tients, age, gender, fracture classification (Kyle 1979) and adequacy of imaging was noted.Results: Fifty five consecutive patients (38F: 17M) had a dynamic hip screw inserted for 56 intertrochantericfractures, the mean age was 83 years (range 56-98). In 20 patients (20 fractures) full measurements werenot possible:- 14 patients had lateral images of the hip of insufficient quality to allow measurement (9thermals and 5 radiographs), in 4 cases the thermal images were missing and in 2 cases radiographswere not taken.There was no significant difference in the TAD (18.8mm 18.7mm, p.0.5, CI - 1.2 to 2.0), AP ratio (48 6v47.4,p.0.1 .CI 3.4 to 0.82) or lateral ratio (44.6v42.0, p>0. 1, CI -5.0 to 0.26) of the screw position when measured onthe radiograph and the thermal image. On average the hip screw compressed 3.3mm between the intra oper-ative and post-operative imaging - a statistically significant difference (3 1 .4v34.7 mm, p<0.05, CI 1.9 to 8.8).Conclusion: Routine early post operative radiographs add no new information about the position of thescrew within the femoral head. They do demonstrate the small amount of collapse which occurs duringthis period but this is unlikely to be clinically significant. Post operative radiographs are uncomfortablefor the patient, may delay post operative mobilisation and utilise scarce resources. Their routine useshould be abandoned except when intra operative imaging is substandard.
Modular versus bipolar prosthesis: a prospective evaluation of functionaloutcome after femoral neck fracture
A. KAPTANOGLU, S. KARAOGLU, M. HALICI, A. BAKTIR
University of Erciyes, Faculty of Medicine, Department of Orthopaedics and Traumatology, Kayseri - Turkey
Introduction: The aim of this study was to compare the results of the patients treated with bipolar andmonopolar prosthesis for femoral neck fracture. Sixty three patients were used in this study. Forty threeof them were treated with bipolar endosprosthesis bipolar group and 20 with modular endoprosthesis.All patients were followed-up at least for 18 months. The average follow-up for the bipolar group (BP)was 27 months (18-42) and 29 months (19-41) for the monopolar group (MG). Sixty one percent of thebipolar group was female and 39% was male. Fifty four percent of the monopolar group was female and26% was male. Ninety five percent of fractures were Garden grade III-IV. Sixty five percent of the bipo-lar group and 55% of monopolar group has returned to the pre-injury state activity. The average Harrisscore for the bipolar group was 83 and 77 for the monopolar group. There was only one acetabular ero-sion (2.3%) in the bipolar group and three ( 15%) in the monopolar group.Conclusion: Prosthetic management of the fractures of the femoral neck in elderly patients is the treat-ment of choice because early mobilisation of the patients prevents a number of risk factors. Bipolar en-doprosthetic treatment in younger more active and longer life expecting patients, is preferred to pre-vent acetabular erosion and protrusio.
Intra-acetabular dislocation of a bipolar hip prosthesis
J. TABUTIN, A. DAMOTTE
Centre Hospitalier, Cannes - France
Introduction: Some complications are specific to bipolar prosthesis such as acetabular erosion or dis-sociation. Intra acetabular progressive dislocation has not been reported yet.Case reports: In four cases, after implantation of a bipolar prosthesis for a femoral neck fracture in an

S172
elderly women, we noticed the progressive superior migration of the metal-backed cup: the ball grad-ually dislocated into the acetabulum and began eroding it. This needed revision with a hemisphericalcup and grafting. The follow-up was then uneventful.Discussion: This phenomenon is different from the acute intra-acetabular dislocation that may followrupture of the locking polyethylene ring in the new models implant, or after a dissociation of the balland cup after closed reduction of a dislocation.We think the cause of this intra acetabular progressive dislocation is a poor design of the cup. If thecentres of the inner and outer spheres are superimposed, the cup has a natural tendency to drop intovalgus because of its weight. This is even worse if the centre of the outer sphere is medial to the ballcentre. The cup should be designed so that the centre of the outer sphere be lateral to the one of theinner sphere creating a varus torque for the cup.Conclusion: Designing a bipolar cup is not as simple a matter as it may seem. The rotation centres are important.
FEMORAL COMPONENT FIXATION
Eight to ten years results of Zweymüller alloclassic total hip replacement
G.A. MACHERAS, K. TSIAMTSOURIS, A. KOSTAKOS, N. POULLIS
Ika Hospital, Athens - Greece
Purpose: This study reports the minimum of 8 years follow up of our experience with the porous coated Zweymüller-Alloclassic total hip arthroplasty.Material and Methods: A total of ninety-five primary total hip replacements in ninety patients were performedbetween February 1989 and December 1992. The patients were relatively young (average age 61 yrs) andmost were female (64%). Six patients were lost to follow up and excluded from the study.Results: The Harris hip score was improved from a mean of 46 points preoperatively to mean of 97 at last fol-low up. Two undisplaced acetabular fractures during screwing the socket, three superficial wound infections,two deep vein thrombosis and two late deep infections were the complications. Five hips were revised: threebecause of aseptic loosening of the socket and two because of late hematogenous infection. Thigh pain waspresent in four patients. Five stems subsided more than 2mm. No stress shielding was observed. Cortical hy-pertrophy in Gruen zones 3,4,5 developed in nine cases. Periarticular ossification occurred in thirty five hips.Conclusion: These results suggest that the cementless Zweymüller-Allocentric total hip arthroplasty providesstable and long lasting fixation, a low incidence of thigh pain and no osteolysis.
Bone remodeling in a proximally hydroxyapatite coated anatomic femorastem: a 7.6-year follow-up prospective study
E. GARCIA CIMBRELO, J. CORDERO
Orthopaedic Department, Hospital La Paz, Madrid - Spain
Introduction: We analyse mid-term results in patients with a profile HA-coated anatomic stem (DePuy).Material and Methods: Ninety two Profile stems, implanted between 1988-1996, originally with an ACS poly-ethylene (PE) liner (34 hips) and, after 1992, with a Duracon cup (58 hips). There were no infections. The meanfollow-up was 7.6 years (4-11).

S173
Results: There was thigh pain in 3 hips. All stems osseointegrated. 8 cups were revised after fracture of theACS Liner; in one the stem required revision because of massive proximal osteolysis. Mean femoral fillingwas 93% with type A femur (funnel-shaped, 43 hips), 89% with type B (intermediate, 29 hips), and 81% withtype C (cylindrical, 20 hips). Cortical hypertrophy (34 hips with a mean canal filling of 92%) and proximal os-teoporosis (62 hips) were frequent. On the Engh scale, there were 18 grade 2 hips, 4 grade 3 hips, and 1 grade4 hip. Osteoporosis was associated with stem width(p<0.05). Proximal osteolysis (8 hips) was associated withrupture of the ACSS liner (3 hips) and with PE wear greater than 2mm (5 hips). No distal osteolysis was foundin this series.Conclusion: The Profile stem shows good mid-term results, even in osteopenic cylindrical femurs. Thigh painis uncommon. Optimal press-fit was frequent. Radiographic ingrowth was seen in all hips. Proximal osteo-porosis and cortical hypertrophy were frequent, and proximal osteolysis was associated to rupture or ex-cessive wear of the PE liner.
HA Coated vs porous coated straight stems in THR
E. DE SANTIS, G. LOGROSCINO, D. DALL'ACQUA, S. RIVELLI, G. MAGLIOCCHETTE LOMBI, G. GASPARINI
Orthopaedic Department, Catholic University, Rome - Italy
Purpose: Clinical and radiographic outcome of 245 consecutive cementless total hip arthroplasties were analysedfor osseointegration.Materials and Methods: Between October 1997 and December 1999, the senior surgeon performed 245 THA im-planting a cementless titanium stem and a cementless titanium cup. The features of the stem were as follows:tapered, straight, low-profile neck, 3 proximal grooves, metaphyseal and isthmic fit, proximal 1/3 HA coating in136 cases and titanium porous coating in 109 cases. The two types of stem were randomly implanted. The ac-etabular component was hemispheric and titanium porous coated. A 28 mm zirconia head was used.The age of patients ranged between 31 and 83 years with an average of 65. 53% were female. The diagno-sis was primary osteoarthritis (167 cases), congenital hip dysplasia (21), fracture (13), aseptic loosening (20),osteonecrosis (14), previous femoral osteotomy (8), previous pelvic osteotomy (2).Clinical objective assessment was based on the Harris hip score; this evaluation was obtained with self-ad-ministered questionnaires (WOMAC and SF12). Radiological assessment was based on the Hip Society cri-teria and on the Engh method.Results: The mean HHS score increased from 42 to 94 points (92 in PC stems and 96 in HA stems). The WOM-AC and SF 12 questionnaires showed a statistically significant improvement in health related quality of life.We did not observe significant general complications, deep infections or leg length discrepancy of more than1 cm. Intraoperative cracks occurred in 6 cases, postoperative dislocation in 2 and mid thigh pain in 9.Radiographic assessment of the stem showed consistent evidence of proximal bone ingrowth respectively in96% (HA) and 91% (PC), stable proximal fibrous in growth in 4% (HA) and 9% (PC). Osseointegration ap-peared earlier in HA. Radiolucent lines, pedestal signs osteolysis and subsidence were not identified.Discussion and Conclusions: The use of HA, according to our previous experimental and clinical studies,seems to improve osseointegration. New bone formation appears earlier and more consistently in HA coat-ed stems, even if this difference is not statistically significant. This study, despite the short follow-up, indi-cates that the straight stem and hemispheric cup that we used can achieve excellent early results. Patientoriented assessment confirms the reliability of this cementless prosthesis.
S174
Periprosthetic fractures in uncemented HA coated ABG hips
A. J. TONINO, M. VISCHJAGER, W.G.H. MEIJERS
Atrium Medisch Centrum, Heerlen - The Netherlands
Introduction: Periprosthetic fractures (PPF) around cemented hip prostheses are well known and mostly seenat the tip of the femoral component. PPF in uncemented THA are only sporadically mentioned in literature butno common guidance for treatment are given. We will describe 8 cases.Patients: From a consecutive series of 1000 uncemented proximal HA coated ABG prostheses (Howmedica,UK), eight patients (6 women and two men) sustained a PPF after an adequate trauma. The mean time be-tween the index operation and the fracture was 5.2 years (range 2.5-7 years). The mean age of the patientsat the time of fracture was 72.8 years (range 59-87). In 3 patients there was only a crack of the greatertrochanter with loosening of the greater trochantic complex. They could all be treated conservatively. In 5cases, the fracture was transtrochanteric with complete loosening of the stem in 2 cases which needed re-vision, while the other fracture could be reconstructed by internal fixation. In the remaining twotranstrochanteric fractures there was only loosening of the proximal bone fragment while the stem was stillosseointegrated in the distal bone fragment into the femoral medullary canal. These fractures could also betreated conservatively.Results: The 5 conservatively treated patients and the one with internal fixation all showed proximal re-os-seointegration within six months and full functional recovery after one year. The two revision cases managedwith uncemented stems and cable grip systems also recovered uneventfully.Discussion: Bone remodelling in the ABG stem has recently been described in two clinical series and one his-tological study. Because of proximal stress shielding, bone resorption develops late after implantation andan acute bone density gradient between the proximal Gruen zones and the middle Gruen zones is observedafter some years. When the patient falls on the operated hip a local or transtrochanteric fracture can developat that particular location with debonding of the proximal osseointegration. However when the stem is also dis-tally osseointegrated the fracture remains stable and can be treated conservatively. In all other cases osteosynthesisor revision with osteosynthesis is necessary.
The Exeter universal total hip replacement
M. O'BRIEN, G. BANNISTER
Southmead Hospital, Bristol - England
Introduction: The Exeter Universal Stem was developed from the original prosthesis that preserved proximalmedial bone stock. As modifications can alter the performance of a prosthesis, we reviewed the medium termresults of the Exeter Universal Stem clinically and radiologically.Material and Methods: Sixty patients underwent primary total hip replacement with the Exeter Universal Stemand a variety of cups using second generation cementing techniques.Results: After a minimum of 7 years the mean Harris hip score was 76. There were no stem but 2 cup revi-sions. Cementing technique was A or B in all patients, but the cement mantle was less than 3mm in one ormore zones in 48% of patients, predominantly on the lateral view. A radio-lucent line of 2mm was visible at thecement bone interface in 1 zone of 5 hips (9%) and 1% of all zones. There was no endosteal bone Iysis. Prox-imal medial cortical thinning occurred in 76%, stabilised after 2 years and was less when the proximal me-dial cement mantle was thicker and in patients with a high corticomedullary ratio.Conclusion: The Exeter Universal Stem is comparable to the original. Narrower stems that allow space formedial cement preserve bone stock better. Radiologically the cemented cup with a 26mm + head loosens.
S175
Fragmentation of polyethylene cement restrictor in total hip arthroplasty
O. GABBAR, R. WILLIAMS, R. SPENCER
Weston General Hospital, Weston-Super-Mare - England
Introduction: Polyethylene wear particles at the bone cement interface after joint replacement is a major causeof prosthetic loosening. Polyethylene medullary brushes have recently come under scrutiny in this regard.Nevertheless many surgeons continue to use winged Hardinge polyethylene restrictor of which fragments arefrequently seen to detach during insertion into the femoral canal and emerge during medullary lavage.The extent to which such fragments may be retained in the femoral cement mantle has not been determined.Concern exists that such fragments may result in polyethylene granuloma formation.Material and Methods: We reviewed 89 post operative X-rays after hip replacement employing the Hardingerestrictor. We recorded the dimensions and number of distal radiolucencies in the cement and their corre-spondence with wing size of the restrictor, method of suction used during pressurised lavage, proximal anddistal canal diameter and amount of taper and Gruen zone location of radiolucencies.Results: Linear lucencies corresponding exactly to the wings of the restrictor were found on 14 X-rays (15.7%),7/54 in which distal suction was used during lavage and 7/35 in which proximal suction only was employed.There was no correlation between the likelihood of fragment detachment and canal taper or distal diameter.A total of (17) detached fragments were identified, distributed in the following Gruen zones; 3 (35.3%), 4(38.2%), 5 (26.5%).Conclusion: We suggest that the above observations should alert surgeons who wish to use this type of re-strictor to the importance of meticulous femoral preparation, preferably under direct vision, to ensure that nodetached fragments of restrictor become incorporated in the cement mantle.
Comparison of femoral component in posterior approaches to the hip
J. WEBB, G. BANNISTER
Southmead Hospital, Bristol - England
Introduction: 72% of revisions in the Swedish Arthroplasty Survey are the result of aseptic loosening. The riskof revision is increased when the transgluteal direct lateral approach is used. The true axis of the proximal fe-mur is the piriform fossa, which is poorly accessed by the transgluteal direct lateral approach. Cement mantledefects in the A-P plane are associated with aseptic loosening and this principle should apply in the lateral. Material and Methods: The lateral radiographs of the first 100 consecutive total hip replacements carried outby the posterior and direct lateral approaches were examined for prosthetic alignment and cement mantledefect. Cement mantles of less than 3mm were deemed inadequate.Results: There were inadequate cement mantles in 60% of the stems inserted by the direct lateral approachand 35% by the posterior (P<0.001). Anteroposterior alignment from proximal to distal was present in 69%of direct lateral and 37% of posterior approaches (P<0.001). When the prosthesis was implanted from an-teroposterior alignment, 70% of the cement mantles were inadequate compared with 21% of those implant-ed in neutral (P<0.001).Conclusion: The cement mantle defects in the sagittal plane correlate closely to the relative risks of asepticloosening in the Swedish Arthroplasty Survey, and may explain the association with surgical approach.
S176
ACETABULAR FIXATION
Our experience with the Zweymüller cementless bicon cup
M. JANECEK, P. BUCEK
Trauma Centrum, Brno - Czech Republic
Introduction: The previous cementless conical titanium cup was used from 1985, both for primary hip re-placement and revision. Its major disadvantage was the larger bone resection because of its strictly conicalshape. For these reasons the cup was finished by bevelling in the frontal level and so the double cone emerges(Bicon cup) decreasing bone resection substantially.With the increasing cup diameter in particular sizes, its depth increases too, particularly in revision surgery,when larger acetabular defects have to be filled. The threads are produced in two versions. The Standard ver-sion is meant for normally dense or hard subchondral bone and the Porose for soft porotic bone. The highercutting ability of threads was achieved by making them thinner. In the Porose version the thread surface issignificantly larger than in the Standard version. With the increasing cup diameter the height of threads in-creases along with the anchorage surface. The cup surface is rough (mean roughness 3-5 µm) enhancing sec-ondary osseointegration. Threads on the cup bottom grip the medial cortex of the bone acetabulum and can-cellous bone. The cup is implanted at the angle 40-50° in the level of the bone acetabulum and at 10-15° ofanteversion. The insert for the own contact with the head of femoral part of the prosthesis is produced in thepolyethylene-on-ceramic, metal-on-metal or ceramic-on-ceramic combination.Clinical Experience: In years 1992-1999 together 462 Bicon cups were implanted in the Arthroplasty Centreof the Traumatology Hospital, Brno - the standard version in 403 cases and the Porose version in 59 cases.The prosthesis was inserted in 194 male and 268 female patients, right in 237 cases and left in 225 cases.Most patients were in the 6th and 7th decade of life ( 171 and 157 patients). The youngest patient was 17 and theoldest 81 years. 334 patients were treated for the diagnosis of primary osteoarthritis, 74 patients for post trau-matic osteoarthritis, 30 patients for post dysplastic arthritis and 24 patients for arthritis after avarcular necrosis.The most frequently used cup size was No 5 (147 cases) and No 4 (119 cases) in the Standard version, andNo 4 (20 cases) and No 3 (21 cases) in the Porose version. The polyethylene inserts were mostly No 5 (103cases) and No 4 (86 cases) in the Standard version, No 5 (32 cases), No 4 (23 cases) and No 3 (31 cases) inthe dysplasia version.Complications: There was one septic case one year after surgery treated by two-stage replantation and oneby one-stage exchange.Conclusion: Our middle term results of the cementless Bicon cup in the Standard and Porose version for pri-mary hip replacement are comparable with other systems. The primary fixation allows quick mobilisation ofthe patient and the secondary osseointegration with eventual remodelling of the cancellous bone guaranteeslong-term results. The biological fixation of the Bicon cup is long lasting and better than bone cement.
Harris Galante cementless acetabular replacement in avascular necrosis: a five to thirteen year prospective study
A.H. TAYLOR, M.B. LEE, S.L. WHITEHOUSE, I.D. LEARMONTH
Department of Orthopaedic Surgery, University of Bristol; Winford Unit Avon, Orthopaedic Centre, Westburyon Trym, Bristol - England
Purpose of the Study: To assess the clinical and radiological results of the Harris Galante Porous cup(Zimmer, Warsaw, Indiana) in patients with avascular necrosis of the femoral head.

S177
Patients and Materials: All Harris Galante (HGPI) cups inserted at our centre between 1986 and 1994were followed prospectively. Standardised radiographs were taken pre operatively and post opera-tively at 6 months, 12 months and annually there after. All patients were clinically assessed at annu-al review using the Harris Hip Score. Of a total of 1246 HGP cups, 78 HGPl cups in 65 patients hadAVN of the femoral head. Age at surgery was 19-80 years (mean 49.9), 51 hips in males and 27 in fe-males. The cup angle was measured on AP X-ray, with radiographic evaluation of horizontal and ver-tical migration performed using the technique described by Massin using the teardrop as the pelviclandmark. Radiolucent lines were measured on the anteroposterior radiograph in bones described byDe Lee and Charnley, and were defined as integrated, non-progressive or progressive. Screw osteol-ysis was recorded and heterotopic ossification was assessed using the Brooker classification.Results: Seventy-eight HGP 1 cups in 65 patients were included in the study. Four patients were lostto follow-up and three died (total of 7 hips), leaving 71 hips included in the study. The average lengthof follow-up was 7.6 years (range 5.3 to 13.5). Clinical: The mean Harris Hip Score preoperatively was 29 (range 0 to 65) and 94 (range 72 to 100) atlast review. Five cups (6.4%) have been revised, none for loosening, two liners were replaced for wear(13 years) and one for late dissociation of the insert (7.9 years). One patient with a cemented Sheehanstem, developed extensive femoral osteolysis in all zones and had femoral revision after 49 months.The acetabular component was firmly fixed with no apparent wear and the liner was not exchanged.There is apparent wear of the plastic insert in 5 other cups, which are being closely followed. Therewas no evidence of cup migration. The mean cup angle was 39° (range 12-62). Fifty cups were well in-tegrated, 27 had a non progressive radiolucent line (RLL) in Zones 1 or 2 (<2mm), 3 had progressiveRLL, and at last follow-up 2 had a complete RLL <2mm.Conclusions: The results show excellent rates of fixation for the HGP I cup in the medium term for thisgroup of patients.
A comparison of the first 100 cemented cups and first 100 hydroxyapatitecoated screw cups performed by one surgeon
E. J. TAYLOR, S. McNALLY, C. V. MANN, J.A.N. SHEPPERD
South Malling Cottage, Lindfield West Sussex, Hastings - England
Material and Methods: This study compares clinical and radiological results of the first one hundredhydroxyapatite coated screw cup prostheses and cemented cups performed by the same surgeon. Hy-droxyapatite coated JRI stems were used in all hips.Results: One hundred percent was obtained in both groups at a seven to ten year follow up. Nine ofthe screw cups have been revised, two for loosening, one for infection, three for wear and two for re-current dislocation. There is one patient who is awaiting revision for loosening (90% survival). Seven-teen hips have lucencies of 0.5mm or more in one or more zones of the cup, but do not require revi-sion clinically. Of the cemented cups three were revised, two for loosening and one for infection (97%survival). Twenty two of these hips have acetabular lucencies on X ray. This study shows a 3% rate orrevision for loosening in the hydroxyapatite coated screw cups and a 2% rate in the cemented cups,although the incidence of radiological lucencies in the cement group was higher.

S178
Hemispheric porous-coated acetabular component with and withoutscrew fixation
E. GIL GARAY, P. GOMEZ CARDERO, M. PELETEIRO PENSADO
Department of Orthopaedic Surgery, Hospital La Paz, Madrid - Spain
Introduction: Fixation of cementless acetabular components may be achieved by under-reaming/oversizingthe component, with or without several methods of supplementary fixation as pegs, spikes of screws. Emp-ty holes for screws have been considered as disadvantageous because they provide a pathway for wear par-ticles and osteolysis.Material and Methods: In this study the results of 49 hemispheric Vitalock Cluster acetabular components(Howmedica International) in 39 patients with a mean follow-up of 6 years (range 5 to 7) are reported. Screwswere used in 27 cases, and only press-fit type fixation without screws in 22. The mean age of patients whenthe operation was performed was 56 years (range 21 to 72).All the operations were performed by the same surgical team following the same technique, with under-ream-ing of 2mm or, in some cases, 1mm, oversizing the component to obtain a pressfit fixation. The use of screwsdepended on the surgeons preference.All the components were assessed radiographically for fixation, radiolucent lines, bone sclerosis, changes of an-gle, medial or proximal migration, osteolysis and polyethylene wear.No revision for loosening or other causes has been performed to date. No significant changes in acetabularposition were observed. In one patient an asymptomatic osteolytic lesion was present in zone II, near one ofthe screws; another patient showed a non progressive radiolucent line in zones I and II. Mean linear wear was0.18mm per year. No complications related to the use of screws was registered (bending, break etc.).Conclusions: These data suggest that fixation of this type of hemispheric acetabular component can be achievedwith and without screws, providing that a good initial stability is obtained under-reaming oversizing the com-ponent by 2mm as average. After 5 years and with only one case of osteolysis, no conclusion can be drawnabout the role of the empty holes as wear particle pathways.
Intrapelvic complications after total hip replacement - a meta-analysis
C.M. BACH, I. STEINGRUBER, C. WIMMER, M. NOGLER, B. STOECKL, M. KRISMER
Department of Radiology, University of Innsbruck, Innsbruck - Austria
Severe failure of a total hip arthroplasty with perforation of the medial acetabular wall may be asso-ciated with injuries of intrapelvic structures.In the years from 1971 to 1999, 81 cases of intrapelvic complications after primary or revision total hip re-placements were recorded in the English literature. During the last 10 years of total hip replacement surgeryat our department we recorded 7 intrapelvic complications.We detected urologic (29 cases) and vascular (22 cases) complications, intrapelvic infection (13 cases), coloninvolvement (11 cases), injury to nerves (7 patients) and intrapelvic cyst formation (5 cases).The most common complications were haemorrhage and development of a pseudoaneurysm, compression ofnerves or vessels leading to paralysis, ischaemia, haematuria, fistulas of the sigmoid colon, skin, abdominal cav-ity, rectum, bladder and ureter, perforation of vessels, bladder or sigmoid colon, herniation of intrapelvic organsthrough an acetabular defect, dyspareunia, infection of the psoas bursa or local effects of intrapelvic cysts.Complications were diagnosed 51.6 months after surgery and were most frequently due to intrapelvic migrationof the prosthetic cup, intrapelvically protruding cement, injury with prosthetic dislocation and debris from thepolyethylene inlay.
S179
Results of 14,880 cemented Charnley cups and 4,227 uncemented HA-coated cups from the Norwegian arthroplasty register
L.I. HAVELING, B. ESPEHAUG, L. B. ENGESÆTER
Department of Orthopaedic Surgery, Haukeland University Hospital, Bergen - Norway
Introduction: HA coating on implants has been shown to give a good primary fixation, and the short-term re-sults with HA-coating have been promising. The purpose of this study was to assess the mid-term results oftwo HA-coated cups, compared with a cemented cup.Material and Methods: With a follow-up of 0-10 years of 19,107 primary total hip replacements, we have as-sessed the survival results of the uncemented HA-coated cups Atoll (Depuy, France) and Trophic (Depuy,France). Their results were compared with Charnley cups (Depuy, England) fixed with high viscosity cement,by use of the Cox regression model with adjustment for age, gender and diagnosis.Results: The adjusted eight-year revision rate was 3.3% for the Charnley, 6.4% for the Tropic and 9.9% forthe Atoll cups. During the first 4 years of follow-up, the risk for revision was similar for the HA-coated cupsand the Charnley cup. Beyond 4 years of follow-up, compared to the Charnley cup, the risk for revision ofthe hemispheric HA-coated cup (Atoll, n=1,363) was 5.0 (95% confidence Interval (Cl): 3.0-8.2, p<0.001) timesincreased, and for the threaded HA coated cup (Tropic, n=2,864) 3.3 (95% CI: 2.3-4.8, p<0.001) times in-creased. Also when investigating revisions performed due to aseptic loosening, and when limiting the analy-ses to patient under or over the age of 60 years respectively, the HA coated cups were inferior to the Charn-ley cup.Conclusion: For these two uncemented HA-coated cups, both the risk for revision due to aseptic looseningand the revision due to other reasons were increased compared to cemented Charnley cups.
COMPLICATIONS PREVENTION AND OUTCOME
Early death following primary total hip replacement
G.T.R. PATTISON, S.L. WHITEHOUSE, A. TAYLOR, A. BLOM, G.C. BANNISTER
Winford Unit, Avon Orthopaedic Centre, Westbury on Trym, Bristol - England
Introduction: The purpose of this study was to determine the timing and cause of early deaths following to-tal hip replacement (THR). Analysis of these data will improve preventative measures against deaths and al-low informed consent to be accurately given to patients undergoing the procedure.Material and Method: Between 1993 and 1996, 1727 consecutive patients underwent single primary THR ina regional elective orthopaedic centre. Those patients thought to be still alive were sent a questionnaire ask-ing about the functioning of their THR. Those patients found to have died had their medical case notes, deathcertificates and, if appropriate, post-mortem reports examined. Follow up with regard to death was 100%.Results: Seventeen (6M:11F) patients (0.9%) died within 90 days of their procedure. Of these, 8 were aged70-79 years and 7 were aged 80 or over. The death rate for the under 70's was 2/882 = 0.2% for those aged70-79 was 8/626 = 1.3% for those aged over 80 the death rate was 7/279 = 2.5%. In 7 cases the cause ofdeath was ischaemic heart disease, in 4 cerebrovascular accidents (CVA), 2 patients died of malignant dis-ease and one patient each of peritonitis, pneurnonia and pulmonary embolism.Discussion: The most common causes of death in the early post operative period are heart attacks and strokes.Fatal pulmonary embolism is a rare event (1/1727= 0.06%). Thirteen of the observed early deaths were dueto vascular events and therefore were potentially preventable. In other settings anti-platelet drugs (ie aspirin)have reduced mortality from CVA and myocardial infarction. Further investigation should determine if this can

S180
reduce the early death rate in the over 70's.Conclusion: Patients under 70 can be reassured that early post operative death is unlikely (0.2%). Patientsin their 70's should be counselled that there is approximately a 1.5% chance that that will die within 90 daysof a primary THR. This risk increases to 2.5% for those over 80.
Safety and efficacy of enoxoparine Na for deep vein thrombosis prophy-laxis in total hip arthroplasty
H. SENARAN, R. EMRE ACAROGLU, B. ATILLA, A. MAZHAR TOKGÖZOGLU, A. SURAT
Hacettepe University, Faculty of Medicine, Department of Orthopaedics and Traumatology, Hacettepe, Ankara - Turkey
Aim: To compare efficacy and safety of enoxoparine Na with that of unfractionated heparin for deep veinthrombosis (DVT) prophylaxis in total hip arthroplasty (THA).Design: Prospective, randomised.Methods: One hundred patients were randomised into enoxoparine Na (40 milligrams daily) starting 12 hoursbefore surgery or heparin (5000U subcutaneously tid) starting 8 hours before surgery. Efficacy was evaluat-ed by clinical examination and Doppler utlrasonography at the seventh or eighth days. Measurements re-garding safety were hepatic enzymes, the amount of preoperative blood loss and the presence of haematomasand/or wound drainage.Results: Of eighty five patients who had complete Doppler data, DVT was detected in 3 patients in the he-parin group (314) and in no patients in the enoxoparine Na group (p=0.108). Additional complications (hepa-totoxicity, late DVT or haematoma formation) occurred in 7 patients (14 percent) in enoxoparine Na and 6 pa-tients ( 12 percent) in heparin group (p=139). Preoperative blood loss was similar (1016 ml vs. 1125 ml,p=0.379).Conclusion: This study demonstrated that enoxoparine Na appears to be as safe and as effective as unfrac-tionated heparin Na for DVT prophylaxis.
What would you let your patient do following a routine hip arthroplasty?
S.J. PALMER, C. DEANS, R.N. VILLAR
Addensbrookes Hospital, Cambridge - England
Introduction: The main function of a total hip replacement (THR) is to alleviate hip pain and improve the func-tional quality of life of the patient. Increasing numbers of young patients are undergoing THR and often they wishto participate in sporting activities that the elderly and more sedate patients do not perform. These activities of-ten place increased forces through the THR with subsequent increased risk of earlier failure of their THR. Wewanted to see what activities consultant orthopaedic surgeons would allow their patients to perform following aroutine primary total hip replacement.Material and Methods: A postal questionnaire was sent to 100 members of the European Hip Society askingthem whether they would recommend their patients perform the activities listed post THR.Results: There was in general an increase in the activities that surgeons recommended to their patients fol-lowing a THR in our series when compared to previous papers. There was unanimous agreement from all sur-geons that patients should be allowed to partake in activities of riding a bicycle, gardening, playing golf,dancing and sexual intercourse following their THR, but there was a wide variation when considering the re-sponses to other activities.

S181
Is patient satisfaction or their perception of their symptom improvementafter primary total hip replacement related to either the Merle d’Aubigneand postel hip score or their pain score?
E.J. TAYLOR, J.A.N. SHEPPERD
South Malling Cottage, Lindfield, West Sussex, Hastings - England
Introduction: The aim of this study was to assess whether patient satisfaction and improvement of symptomsafter primary total hip replacement were related more to the Merle, d'Aubigne and Postel hip score or to apain score.Material and Methods: Patients in a pre existing study had pain scores and Merle, d'Aubigne and Postel scoresmeasured before and after their primary total hip replacement. They were also asked to rate how much bet-ter their symptoms are as a result of the operation. The measures were compared to the postoperative painand hip scores as well as the change in these scores as a result of the operation.Results: Patient satisfaction did not always correlate with the scores. However, the patients own assessmentsymptomatic improvement as a result of the operation correlated well. By far the strongest correlation overallwas between the pain scores and the patient assessment of symptom improvement.Discussion: This suggests that the most important factors as far as the patient is concerned, in the outcome of a pri-mary total hip replacement, are the level of postoperative pain and the degree of improvement in their pain level.
Postal questionnaires - do they work?
A.H. TAYLOR, G. PATTISON, S.L. WHITEHOUSE, A. BLOM, G. BANNISTER
The Avon Orthopaedic Centre, Southmead Hospital, Westbury on Trym Bristol - England
Aims: In the B.O.A's "Total hip replacement: A guide to best practice" it is suggested that "best practice" re-quires patients to be followed up in the long terrn. One method would be the use of a postal questionnaire.We have looked at the feasibility of this and the results obtained.Method: All patients who had had a single primary THR at the Avon Orthopaedic Centre between 1993 and1996 were sent a postal questionnaire. The questionnaire was designed to ask about their post-operative re-covery, particularly any complications such as infection, dislocation, readmission to hospital and further sur-gical intervention pain maps were included and questions about patient’s perceived leg length. The OxfordHip Score (OHS) was used to assess their functional outcome. Those patients that did not return the ques-tionnaire were then contacted by phone or by being re-mailed (after checking their address with the FHSAcomputer). The returned questionnaires were then analysed for their completeness and accuracy of responses.Results: There were 1727 single primary THR performed in this period, of which 190 patients were found tobe deceased. There were 1171 forms returned (65 of these by repeat mail-shot). A further 201 were collect-ed by phone. One hundred and sixty five patients could not be contacted. Of these questionnaires returned238 were incomplete (20.3%). The questionnaire covered 5 sides of A4 paper, the last two sides being the 12questions of the OHS of the OHS question 1-6 were left blank in 44 forms(3.8%). The question relating tousual pain (1), limp (10), sudden pain (12) were commonly missed out. The most often left however was thequestion relating to walking time before pain (7), this was left blank in 167 forms (14.3%). On closer exami-nation, it was felt that a further 91 patients (7.8%) had incorrectly answered question 7, indicating that theycould not walk at all by showing good - excellent results for all other items.Conclusions: It is possible to get over a 90% response rate with a postal questionnaire. There are howeverproblems with this and patients have appeared to have found certain questions on the OHS either difficult tounderstand or were unable to answer due to other co-morbidity's that the score does not take into account.
S182
ROBOTIC SURGERY TECHNIQUE: COMPLICATIONS AND RESULTS
Gluteal function after ROBODOC total hip arthroplasty
C.M. BACH, M. NOGLER, P. WINTER, C. WIMMER, M. FISCHER, M. KRISMER
Department of Orthopaedic Surgery, University of Innsbruck, Innsbruck - Austria
Introduction: The ROBODOC (ISS, Davis, Ca) system has been introduced to increase precision total hip re-placement. This surgical procedure requires an extended exposure of the proximal femur. Prolonged fixationof the leg in adduction and external rotation may result in increased lengthening of the gluteal muscles ascompared to the standard procedure. Impairment of the hip abductors may cause gluteal insufficiency.Material and Methods: We tested a series of 25 patients which underwent total hip replacement using the RO-BODOC system (group 1) and a second series, treated by conventional total hip replacement (group II).The transgluteal approach was used in both groups. The results were compared with a healthy control group.All patients underwent 3D gait analysis (VICON System, Oxford Metrics) for dynamic assessment of pelvicand hip motion.Results: For the pelvis we did not record an increased drop in the frontal plane but a decrease of 7 degreesin the range of motion. In the sagittal plane pelvic tilt was reduced by about 6 degrees. Hip adduction wasnormal but a reduction of 6 degrees in hip adduction caused a decrease of range of motion.Conclusion: In conclusion we state that there is no gluteal insufficiency following ROBODOC total hip arthro-plasty.
Detection of the aerosol cloud produced by ROBODOC’S® high-speedbone burr - a contamination risk for the surgical team?
M. NOGLER, C. WIMMER, C. C. LASS-FLÖRL, E. MAYR, B. STAÖCKL, M. KRISMER
Universitätsklinik Für Orthopadie Leopold Franzens, Universität Innsbruck, Innsbruck - Austria
Introduction: During the cutting of the femoral cavity in the ROBODOC procedure we observed an aerosolcloud of irrigation fluid, blood and tissue debris. This cloud is potentially contaminated with bacterial and vi-ral vectors - an infection risk for the operative team.Material and Methods: Irrigation in the ROBODOC procedure was perforrned by a continuous flow through aniv-needle. Additional irrigation-fluid was added with a syringe towards the cutter's top. On top of the femurthe cutter moved through a basin formed by the bone filled with blood and irrigation fluid. We tested for a flatand a ball cutter in these standard situations. For macroscopical detection we used artificially coloured Ni-grosin solution. In a second experiment we exposed the cutter to a fluid, contaminated with staphylococcusaureus.Results: We detected the aerosol cloud in an area of 6 x 3.6m. Extension and concentration varied depend-ing on the irrigation situation. Cutting in a fluid basin was found to be the most extreme setting. The vectorconcentration in all settings was 1.6 x10 CFU/ml.Conclusion: ROBODOC's high speed cutter produces an aerosol cloud in an area in which all members of thesurgical team are affected. Water resistant clothing and face protection is therefore necessary for everybodyin the OR.
S183
Temperature measurements during the cutting of cement in the ROBODOC® hip-revision procedure
M. NOGLER, M. KRISMER, C.H. HAID, C. WIMMER, M. OGON, K. KHALIFA, S. SHIMBLES
Department of Orthopaedic Surgery, University of Innsbruck, Innsbruck - Austria
Introduction: The cutting of cement with ROBODOC® is a promising new method for cemented hiparthroplasty revisions. During the procedures we observed the melting of cement. In this study we mea-sured the temperature that occurred during the cutting of cement with the ROBODOC® high speed cut-ter and if irrigation could cool that temperatures down sufficiently.Material and Methods: We measured the temperature during cutting in blocks of cement with temper-ature sensors in defined distances to the cutting area from 0.5mm to 3mm. We tested for the typicalcutting parameters of the procedures. Cuts were performed in a cement mantle as well as in a solidcement cylinder.Results: We could show, that under cutting parameters given by the ROBODOC® revision procedure,temperatures between 60° and over 250° centigrade occurred in the area of cutting. These tempera-tures are high enough to damage tissue. We could also show that extensive irrigation does sufficient-ly cool down temperatures below 60°.Conclusion: We conclude that cutting cement with ROBODOC's high speed cutter contains a risk ofheat injuries to the bone tissue but it is secure if sufficient irrigation reaches the cutter top without anybreak.
The risk of nerve injury through ROBODOC’S distal pin in the medialfemoral condyle
M. NOGLER, M. KRISMER, H. MAURER, C. WIMMER, C. GEGENHUBER, C. BACH
Department of Orthopaedic Surgery, University of Innsbruck, Innsbruck - Austria
Introduction: The 2-pin-based ROBODOC® procedure requires a pin to be implanted into the patientsmedial femoral condyle in order to register the femur.Results: A number of patients reported severe pain. In twenty cadaver specimens a pin- a titaniumscrew, twelve 'millimetres in length, with a diameter of five millimetres - was implanted into the me-dial femoral condyle. We found injuries of three different nerves - the infrapatellar branch of the saphe-nous nerve, the saphenous nerve and anterior cutaneous branches of the femoral nerve- in 55 per-cent of the specimens, caused by cutting of the nerve or by the screw itself.Knee pain at the location of the distal pin after removal of that screw is a severe problem of RO-BODOC®'s pin based registration method. It was shown that in more than fifty percent of the cadav-er specimens, a nerve injury occurred. Over fifty percent of our patients reported severe knee pain.Due to the variations and density of the neural supply of the medial condyle it was not possible to de-fine a safe placement zone for the pin.Conclusion: It is therefore concluded that an anatomic region with fewer nerves should be chosen forthe distal pin in the ROBODOC® procedure.

S184
Revision of femoral component: cement removal by robot vs manualprocedure
M. KRISMER, M. NOGLER, C.H. KAUFMANN, M. OGON
University Clinic of Orthopaedic Surgery, Innsbruck - Austria
Introduction: In revision arthroplasty of a cemented femoral component, removal of the cement, es-pecially of a completely fil led femur at the tip of the prosthesis, can be surgically demanding, and of-ten requires a time consuming procedure, and sometimes either splitting or fenestration of the femur.Material and Methods: In this retrospective study, ten conventional revisions are compared with tencement removals done by the Robodoc. In preoperative planning the cement bone interface is iden-tified based on CT scans. Intra-operatively, the robot reams a cavity according to preop planning. Thehypothesis is that the reduced intra- operative exposure in the robot-procedure is associated withless blood loss and postoperative morbidity.Results: Median age at revision surgery was 72 (Robodoc) and 80 years (manual), and surgery tookplace 13 and 16 years after primary implantation, respectively. Surgery lasted 210 vs. 220 minutes.Median preop haemoglobin was 129 vs. 1 26g/l, and worst intra- operative haemoglobin amounted to92 vs. 96g/l (ns). The total amount of given blood units was 7.8 (std. Dev 5.8) vs. 4.6 (2.4) (ns). In thepostoperative course there was no significant difference in motion or in other clinical parameters.Conclusion: This preliminary report indicates that cement removal by a robot does perhaps reduceblood loss during revision arthroplasty.
HIP REGISTRIES
Total hip arthroplasty (THA) in Greece
EMM. K. DRETAKIS, K. EMM. DRETAKIS, K. STERIOPOULOS
Department of Orthopaedics, University Hospital, Herkalion, Crete - Greece
Material and Methods: We present data concerning THA performed in Greece during 1998. The data were ob-tained from the orthopaedic clinics of all state hospitals and from the largest private hospitals in Greece, fol-lowing a faxed questionnaire and a letter explaining the aim of the survey.The reply rate to our questionnaire was 100 per cent.Results: During 1998, 4,477 THA were performed in Greece, in 3200 women and in 1277 men. It is possiblethat some more hundreds of THA were done during 1998, by Orthopaedic surgeons working privately, main-ly in Athens. The mean age of the patients was 66. 5 years. About 10% of these operations were revisions.Osteoarthritis accounted for 74% of all cases, followed by intra-articular hip fracture (7%), unreduced con-genital dislocation of the hip in adults (5%), idiopathic osteonecrosis of the femoral head (5%), rheumatoidarthritis and ankylosing spondylitis (4%) and miscellaneous conditions (5%). Most of the THA were cement-less (53.5%), while in 26.5% cement and in 20% hybrid combinations were used.The mean hospitalisation time was 13 days. Antibiotics and anti-thrombotics were used prophylactically inall clinics, while anti-inflammatory drugs, for heterotopic ossification, were used in 50% of the clinics. Thir-teen of the 4,477 patients (0.29%) died post-operatively during hospitalisation and 31 (0.7%) developed deepwound infection.The first THA - a McKee-Farrar prosthesis - was carried out in Athens, in 1966. In 1970, a Charnley low fric-tion THA was also performed in Athens.
S185
Influence of bilateral total hip arthroplasty on the survivorship of theprosthesis in primary osteoarthrosis
T. VISURI, K.B. TURULA, P. PULKKINEN, J. NEVALAINEN
Central Military HospitalDepartment of Public Health, University of Helsinki National Agency for Medicines, Helsinki - Finland
Introduction: Walking needs symmetric use of both hips. Function of one hip depends on the other. The Ka-plan-Meier method is routinely used to show the survivorship of implants. Per prosthesis analysis may causebias compared to per patient study. We studied this effect on a large series of hip arthroplasties (THAs).Material and Methods: Study material consisted of 39,114 THAs from the Finnish Arthroplasty Registry op-erated on for primary osteoarthrosis in 1980-1998. Number of bilateral prostheses was 13,299. Cox multi-variate analysis was used to compare the survival of the unilateral and both bilateral THAs separately.Results: Fifteen year unadjusted survivorship for the unilateral prostheses was 68%, for the first bilateral 66%and for the second bilateral 74%. Adjusted survivorship of the second bilateral was significantly better (Oddsratio 0.88, 95% Cl 0.80-0.97) than that of the unilaterals. At any time during the first 6 years after surgerythe remaining survival of the first bilateral prostheses was significantly better, if the second hip wasoperated on within the next year (ORs 0.60-0.63).Conclusions: After adjustment of age and sex, survivorship of the second bilateral THA is better thanthat of the unilateral or the first bilateral. When indicated the second hip should be provided with aprosthesis as soon as possible after the first THA.
Organisation of the Hungarian hip arthroplasty register
M. SARUNGI, P. THAN, I. UDVARHELYI Jr.
O.R.F.I. Department of Orthopaedics Budapest, Budapest - Hungary
Purpose: The purpose of this study was to create a nation-wide, prospective, multi-centre study on totalhip replacements (THRs) performed in Hungary - to establish the Hungarian Hip Arthroplasty Register.Materials and Method: Consensus on data collection and development of computer software startedin 1997. The database was built according to intemational standards after collaboration with the Scan-dinavian registers.Results: To date 34 Hungarian centres (70% of all) joined the project voluntarily and the number is in-creasing. The register is under the aegis of the Hungarian Orthopaedic Association. Data collection start-ed in late 1998 after free distribution of the software, with the central database containing records of over3000 hip operations by November 1999. First analysis of over 3000 THRs data (patients, diagnosis, im-plants, fixation method, revision, complications) are introduced and discussed in the lecture.Conclusion: Our experience shows that early collaboration with the experienced Scandinavian regis-ters, voluntary participation facilitated by confidential information feedback to partner units, active in-volvement of the local profession (EHS, European Implant Register Committee), non-profit foundationfor co-ordination and finance, collaboration with industry - were the initial key steps to build up theHungarian Hip Register.

S186
The need for a personal hip arthroplasty registry
C. DELAUNAY
Clinique de l’Yvette, Longjumeau - France
Introduction: Influence of the Swedish Hip Arthroplasty Registry (SHAR) is unanimously acknowledgedworld wide. Nevertheless, the SHAR reported only about the total hip prostheses (THP) used in thatparticular country, and provides little information about the preferences of the Swedish Orthopaediccommunity regarding implants and fixation techniques (cemented versus cementless) used. A strikingparadox is that the most famous European Hip Registry (SHAR) provides no data about one of the mostpopular cementless THP used in Europe (>250,000 Zweymüller-Alloclassic hips since 1988).Purpose of the study: To compare survivorships available in the SHAR second-period (1987-1996, af-ter introduction of second generation cementing techniques) with that of a consecutive series of Zweymüller-Alloclassic THP from a personal hip arthroplasty registry (PHAR).Material: From 1987 to 1996, 96,196 primary total hip arthroplasties (THA) were entered in the Swedishdata base: 91.8% were cemented, 4.3% hybrids and 3.9% cementless (49 Zweymuller only). Duringthe same study period, 400 primary THAs were performed in our institution: I cemented, 8% hybridsand 92% cementless Zweymüller-Alloclassic.Methods: Survival analysis was conducted according to the SHAR study criteria: Primary THAs for on-ly osteoarthrosis (SHAR, 71,187 hips; PHAR, 267 hips) and 9-year survivorship (Dobbs Method) withrevision for aseptic loosening as the end point.Results: Nine-year survivals; SHAR: second generation cemented THAs (65,318), 95.5% (1st-genera-tion cementless THAs, 87.2%). PHAR: cementless Zweymüller Alloclassic (267), 99.4% (1 threaded cuprevised for aseptic loosening at 5.2 years). The difference between revision probabilities (4.5% versus6%) was significant (p=0.0002).Discussion: The 1998-SHAR indicated the Charnley prosthesis as the most popular THA used in Sweden(21,109 hips, 30% of all primary THAs), but no longer as the most successful (9 year survival, =94.1%) ac-knowledged, among the second-generation cemented THAs used in Sweden, a "group of excellence" in-cluding: the smooth Exeter THA (96%), the Stanmore (96.8%), the Müller "Straight" (97.2%), the Lubinus-SP (97.4%) and the Harris D-II, with the best 9-year survival (99.2%) but did not allow for comparison withlater generation cementless THAs, due to non inclusion (Alloclassic) or short term follow-up (ABG, CLS).Conclusions: Thus far, our personal HAR indicates a 9-year survivorship of the Zweymüller-Alloclassicprosthesis at least as good as the best results of second-generation cemented THAs reported in the SwedishHAR. This data pleads for continuous use of this cementless hip system. Conducting a personal THA sur-vey is an absolute requirement when using implants with no available results in a hip registry.
POSTERS DISPLAYED AT EUROPEAN HIP SOCIETY MEETING
The thrust plate prosthesis in patients with inflammatory arthritis
H. GUDERIAN, B. FINK, W. RUTHER
Orthopaedic Department, Clinic for Rheumatology, Bad; Bramstedt University Hospital, Hamburg Eppendorf,Bad Bramstedt - Germany
Introduction: The thrust plate prosthesis is an implant with metaphyseal fixation at the proximal femur whichleave the diaphyseal bone untouched. This implant is preferably used in younger patients. It is dependenton a good bone quality in the proximal femur. Because bone quality is reduced in patients with inflammato-

S187
ry arthritis, this kind of endoprosthesis may have a higher failure rate than conventional stemmed endopros-theses in these patients. Therefore patients with inflammatory arthritis, even short and midterm results of thethrust plate prosthesis may be of high importance.Material and Method: Forty seven thrust plate prostheses were implanted in 42 patients with inflammatoryarthritis (29 with rheumatoid arthritis, 6 with juvenile chronic arthritis and 7 patients with spondarthritis) andfollowed prospectively. The average age at the operation was 40.8 ± 10.7 years. Each patient was clinicallyand radiologically examined preoperatively, 3 and 6 months after the operation and at the end of each post-operative year. The mean follow up was 26.1 ± 10.7 months. The clinical findings were evaluated using theHarris Hip Score. Radiologically 8 different zones at the thrust plate prosthesis were analysed for radiolu-cencies.Results: During the first year the Harris Hip Score rose continuously from the preoperative average of 42.4 ±6.5 points to 78.8 ± 10.3 points 3 months postoperatively, 82.3 ± 9.8 points 6 months postoperatively and86.8 ± 10.1 points one year after the operation. The following examinations showed Harris Hip Scores at thesame level. Five patients (5 joints, 10.6%) had to undergo a revision of the thrust plate prosthesis due toaseptic loosening in 3 cases and septic loosening in 2 cases. Six prostheses (12.6%) showed radiolucencies,mostly below the thrust plate in zone 1 and 2. Two of these prostheses were certainly radiologically loosewhich raised the failure rate to 7 of 47 (14.8%).Conclusions: The thrust plate prosthesis improves function and pain in patients with inflammatory arthritis toa satisfactory degree. Concerning the failure rate in this type seems to yield slightly worse results than ce-mentless stemmed endoprostheses in the same patient group. Due to the preservation of the diaphyseal boneof the femur and the advantages in salvage surgery, the thrust plate prosthesis remains the implant of firstchoice in younger patients with inflammatory arthritis.
Septic femoral shaft non-union in hip prosthesis: two cases treated in twostage surgery and different technical solutions
E. GIL-GARAY, N. FEMANDEZ-BAILLO
Department of Orthopaedic Surgery, La Paz Hospital, Madrid - Spain
The cases of two patients with septic non-union of the femoral diaphysis, one after a fracture and one aftera diaphyseal osteotomy, are presented. In both the causative organism was Staph epidermidis.The surgical technique consisted of removal of septic bone and debridement of soft tissues, filling of the re-maining cavity and bone loss with antibiotic (Vancomycin) impregnated bone cement, the use of external fix-ation device to preserve leg length and i.v antibiotic therapy for six weeks. In a second procedure the cementwas removed and the bone defect was treated in two different ways, depending on location and severity ofthe bone defect. In the first case a composite of a massive femoral allograft with a cemented prosthesis (LFACharnley) and internal fixation to the distal femur was used. In the second case a long, cementless SL (Wag-ner) stem was used, with massive supply of morsellised bone graft, auto and allogenic. Post operatively bothpatients were kept on i.v. antibiotic therapy.At the last follow-up visit, five years after the procedure, both patients were ambulatory with crutches, ex-periencing slight and occasional pain. The allograft of the first patient was healed and still mechanically com-petent. The second patient non-union was healed and no shrinking of the femoral stem was observed.

S188
Clinical and radiological behaviour of a tantalum acetabular component
G. MACHERAS, K. TSIAMTOURIS, A. KOSTAKOS, N. POULIS
Ika Hospital, Athens - Greece
Purpose: This study evaluated the osseous response to a non-cemented metal backed acetabular compo-nent made of a new porous tantalum biomaterial (HEDROCEL) based on clinical and radiological findings.Patients and Methods: Thirty two uncemented THRs were performed between January 1998 and November l998using metal backed acetabular components made of porous tantalum biomaterial. Twenty three females and ninemales aged 40-75 (mean age 62.5. The diagnosis was OA 26, AVN 4 and CDH 2. Posterior approach wasused. Three doses of Cefuroxime and low molecular weight heparin were used. Press-fit technique wasused. PWB on the second postoperative day. FWB in four weeks. All patients were clinically and radio-logically evaluated in six weeks, three months and thereafter every six months. The mean, postoperativeHSS was 45.Results: Minimum follow-up was 12 months (range 12-24 months). We had no major complications intra and post-operatively. We report the difficulties we experience during insertion of the cup which are: 1) Adhesion of therough material to the surrounding soft tissue. 2) Anchorage of the component to the acetabular rim resulting toa gap between the component and the acetabular floor. Despite this fact the initial intraoperative stability wasconsidered very satisfactory.Clinical findings were excellent. All patients were asymptomatic through all follow-up and all patients returnedto their previous activities. The mean HSS was improved to 95 at last examination. Radiological evaluationrevealed a gap of 1-3mm in Charnley zones II and V in ten cases. Most of them were during the learning cur-vature period. This gap was closely followed-up and although the patients were asymptomatic the gap waspresent at the two year evaluation.Conclusion: This new biomaterial theorectically having better physical, mechanical and histological propertiesthan others, has a very good clinical behaviour in all cases. When good apposition of the socket was achievedto the acetabular wall, we observed good bone response without radiolucencies. When we had gaps the boneresponse was not as good as we expected forcing us to be more conscious of the proper use of this material.
Measuring bone mineral density of the pelvis and proximal femur aftertotal hip arthroplasty
J. WILKINSON, R. ELSON, N. PEEL, I. STOCKLEY, R. EASTELL
Bone Metabolism Group Department of Orthopaedics, Northern General Hospital, Sheffield - England
We aimed to evaluate the precision and longitudinal sensitivity of the pelvic bone mineral density (BMD) mea-surement and to determine the effect of bone cement on BMD measurement in femoral regions of interest(ROI) following total hip arthroplasty (THA).Twenty nine subjects underwent duplicate DXA scans of the hip after repositioning a median of 6 months af-ter THA. Pelvic analyses using 3 and 4 ROI models gave coefficient of variations (CV) of 2.4% to 3.6% and2.5 to 4.8% respectively. Repeat scans in 17 subjects one year later showed significant BMD change D% in 3 re-gions using the 4 ROI model, compared to change in only 1 region using the 3 ROI model (P<0.05).Manual exclusion of cement from femoral ROls increased the net CV from 1.6% to 3.6% (P=0.001), and decreasedthe measured BMD by 20% (t = 12.1, P<0.001). Studies of 2 cement BMD giving a measurement error of less than0.03g/cm2/year associated with cement inclusion in femoral ROIs.Changes in pelvic periprosthetic BMD are best detected using a 4 ROI model. Femoral ROI analysis is moreprecise without cement exclusion, although an awareness of its effect on BMD measurement is needed.

S189
Prevotella Loeschii infection of a total hip arthroplasty
C. BACH, C. WIMMER, M. NOGLER, S. TROBOS, I. STEINGRUBER, B. STOECKL
Department of Orthopaedic Surgery, University of Innsbruck, Innsbruck - Austria
Infection of total hip arthroplasties associated with a dental process are infrequently reported. Recent stud-ies propose that 6 % of all late infection cases may be due to a dental procedure. Due to the type of organ-isms isolated previously, an association between the joint infection and the dental process remained uncer-tain. We present the first case in the English literature of total hip arthroplasty infection with Prevotella loescheii,a pigmented bacteroides species that is detected in the human mouth.A 2 year old male patient underwent right total hip arthroplasty in 1983, after an accident. Four years laterthe cup revealed signs of moderate loosening. Joint aspirations excluded involvement of infection. In 1987the patient experienced increasing hip pain requiring revision of the socket identifying joint infection with Pre-votella loescheii. Medical records revealed multiple episodes of dental procedures in this period. Antibiotictreatment failed. In 1999 removal of all prosthetic components had to be performed.Organisms isolated in previous studies are part of the oral, cutaneous, intestinal or genitourinary tract flora. SincePrevotella loeschii is an inhabitant of the human mouth, the suggestion of prosthetic infection by haematoge-nous spreading from a dental process can be confirmed for the first time.
Slipped capital femoral epiphysis unresolved hip disorder
F. BAIXAULI Jr, F. BAIXAULI, E. BAIXAULI, R. GABARDA
La Fe University Hospital, Valencia - Spain
Introduction: In spite of the advances achieved in the management of the SCFP, there still remain unsolvedcontroversial matters. The purpose of this paper is to show our conduct in some of these matters.Pre-operative Management: In agreement with Fish, we have never applied traction pre-operatively. The pa-tient is placed on bed rest with the affected limb elevated on pillows and in a position of maximum capsularrelaxation: mild flexion, abduction and external rotation.Direction of the slip: The appearance of varus, as says Griffith and Nguyen et al, is probably an optical il-lusion due to parallax. Our own observations of patients with mild and moderate slips lend support tothese works.Pin Penetration: Several methods have been proposed to evaluate pin placement. From l991 we used two methodsfor this purpose: the"catheretism" authors' method and the fluoroscopy double "sweeping" as described by Rookset al. The "catheterism" consists of the introduction of a blunt Kirschner wire through a canulated screw; the fluo-roscopy vision and easy passage further up the tip of the screw, suggest penetration. Bilaterally: The incidence of bilateral slip varies according to different authors and the conduct to follow is still amatter of controversy. As a rule, we perform prophylactic pinning of the contralateral hip, except for patientsnearer to closure of the physis. This conduct is based on the high incidence of contralateral invovement, poten-tial risk of development of a slip in the contralateral hip after pinning (overload of the opposite hip), and the pos-sible shortening provoked by an early unilateral closure of the physis.

S190
Slipped capital femoral epiphysis algorhythm for treatment
F. BAIXAULI Jr, F. BAIXAULI, E. BAIXAULI, R. GABARDA
La Fe University Hospital, Valencia - Spain
Slipped capital femoral epiphysis (SCFE) is a disorder of unknown origin, but much is being investigated aboutits pathogenesis and natural history.This disease heals when the epiphyseal-plate cartilage closes, but with a residual deformity. The main com-plications of SCFE are not the consequences of the disease but of the therapeutic manoeuvres, so it is veryimportant to be cautious when treating SCFE.Under these concepts we propose a therapeutic algorhythm to treat SCFE. - No traction is applied on ad-mission, only bed rest with the affected leg on a pillow with the hip in mild abduction, flexion or external ro-tation. - For small and moderate slips (acute, acute on chronic and chronic with open physis), in situ fixationis recommended. - For severe slips (greater than 60°): - Acute and acute on chronic: reduction of the acutecomponent to reach a moderate slip, and after in situ fixation is done. - Chronic with open physis: intra-ar-ticular osteotomy (Fish). - Chronic with closed physis: trochanteric osteotomy.
Calcium phosphate deposition around metal debris in muscle tissuefollowing a failed dynamic hip screw
R. N. BRUETON, B. F. SHAHGALDI
Orthopaedic Academic Unit, Rayne Institute, St Thomas' Hospital, London - UK
A 55 year old lady was referred with an ununited sub-trochanteric fracture sustained fifteen months previ-ously. This had been treated initially with a dynamic hip screw and a subsequent unsuccessful bone graft.The plate had pulled away from the femur with screw breakage and the creation of a large bony cavity with-in the femoral head. Extensive radio-opaque material was seen within the soft tissues. The implant was re-moved and replaced with an intramedullary device and further bone graft.The dynamic hip screw and tissue from the adjacent muscle were examined by means of electron microscopyand histology to determine the origin of the radio opaque particles. The chemical composition of particleswas also determined using Energy Dispersive X-ray Analysis (EDXA) of the scanning electron microscope.Metal particles were demonstrated in the muscle and these were associated with crystals of calcium phosphate.The major sources of the metal particles were areas of wear at the proximal end of the lag screw, the screw headsand screw threads. Corrosion of the screw heads and their screw hold counterparts in the plate had also oc-curred. The radiolucent particles in the tissue were demonstrated to be a mixture of corrosion products togeth-er with fine wear particles of stainless steel alloy that were in close association with localised areas of calcifica-tion within the muscle tissue.

S191
Clinical and radiological results of Bernese pariacetabular osteotomy inacetabular dysplasia
B. ATILLA, A. MAZHAR TOKGÖZOGLU, A. ARIK, A. MÜMTAZ
Alpaslan Hacettepe University Faculty of Medicine, Department of Orthopaedics and Traumtology, Ankara -Turkey
Introduction: Hip dysplasia in adolescents and young adults leads to early arthritis due to altered hip me-chanics. Peri-acetabular osteotomies are aimed at solving this problem.Material and Methods: We have investigated the 2 l Ganz osteotomy of 19 patients. Clinical assessments weredone according to Matta Clinical Grading System. Radiological evaluations included the measurements ofthe Sharp angle, antero posterior and lateral CE angles, medial joint space opening and medialization of thehip joint. Labral tear or sub chondral cyst formations were assessed by MRI.Results: Among 19 patients, 18 were female. The mean age at the time of surgery was 25.5 years. A mean ra-diological correction of 12.8° lateral CE angle, 19.8° AP CE angle, 12 4° Sharp angle was obtained by surgery.(Student's test showed significant difference at p:0.05 level). Clinical grading scores showed a marked in-crease after the operation and remained high after a mean follow up of 25 months.Discussion: Before operation, patients mostly complained of groin pain or mild limping. Pain was mostly as-sociated wíth labral tears and surgery resulted in marked pain relief. In this series, bad results were due toinadequate technique or bad indications and observed in subluxated or multi operated hips.Conclusion: Bernese peri-acetabular osteotomy offers good results if realised in patients presenting with mildTonnis grade I osteoarthritis. Associated labral tears must be evaluated and properly treated. However, itspreventive effect for osteoarthritis requires longer follow-up in order to be proven.
Effect of pre-operative rehabilitative education on early function activitiesof patients undergoing total hip replacement
I. AKARCALI, N. TUGAY, Z. ERDEN, D. KAYA, A. MAZHAR TOKGÖZOGLU, B. ATILLA
Hacettepe University School of Physical Therapy and Rehabilitation and Faculty of Medicine; Department ofOrthopaedics and Traumatology, Hacettepe, Ankara - Turkey
Early mobilisation is important in preventing medical complications following primary total hip arthroplasty(THA). The purpose of this randomised-controlled study was to investigate the effect of patient education onthe post operative acute care in THA. For this purpose, 20 patients received two sessions of intensive pa-tient education on the day before operation. The patients were advised on activities of daily living and surgeryduring the first session and were instructed in walking with assisting devices, stair climbing, transfers andrange of motion and hip strengthening exercises during the second session. These patients were given an il-lustrated guide about THA and rehabilitation. Another 20 control patients were not given any rehabilitativeeducation except the attending surgeon's explanations in the pre-operative period. During the acute care pe-riod, a standard rehabilitation regimen was used for all patients. All subjects were assessed with the IowaLevel of Assistance Scale (ILAS) and Iowa Ambulation Velocity Scale (IAVS).Results: The educated group had a higher ILAS on the second pre-operative day (p<0.05). However the totalfunctional score (ILAS + LAVS) was similar in both groups on the sixth day.Pre-operative information about post-operative acute care encourages early ambulation of a THA patient andmay help to minimise medical complications.

S192
Revision hip arthroplasty in the octogenarian - is it worth it?
N. J. TALBOT, G.C. BANNISTER
Southmead Hospital, Westbury on Trym, Bristol - England
Materials and Method: We have retrospectively reviewed the clinical and patient-perceived results of 76 re-vision hip arthroplasties performed in 68 octogenarians since 1990. 59 hips were revised for aspetic loosen-ing, 8 for recurrent dislocation, 8 for periprosthetic fracture and 1 for deep infection.Results: 60% of patients reported a worthwhile reduction in pain but, in contrast to previous studies, only12% felt that their functional level improved. Mean modified Harris hip score rose from 44 to 65. The ma-jority of this difference was due to successful relief of pain. Pain scores rose from 19 to 36 with an increasein function score from only 21 to 24.The in-hospital mortality was 4%. 47% of patients suffered complications which were multiple in over a quar-ter. There was a 17% dislocation rate which was usually recurrent and rarely salvageable. 29% of patientsfelt that they gained no benefit from their operation and with the benefit of hindsight, 24% of patients wouldnot have consented to surgery from which they found recovery harder than their first operation.Conclusion: The indication for revision surgery in the octogenarian must be pain of sufficient severity to jus-tify these risks. The procedure is unlikely to improve function or independence.