a hyperlipidemic rabbit model provides new insights into pulmonary zinc exposure effects on...
TRANSCRIPT

A Hyperlipidemic Rabbit Model Provides New Insightsinto Pulmonary Zinc Exposure Effects on Cardiovascular Health
Adriana J. LaGier Æ Nick D. Manzo Æ Alex P. Carll ÆRichard H. Jaskot Æ Ralph Slade Æ Judy H. Richards ÆDarrell W. Winsett Æ Aimen K. Farraj Æ Janice A. Dye
Published online: 25 October 2008
� Humana Press 2008
Abstract This study ascertains the effects of zinc, a
major component of particulate matter, on pulmonary and
systemic endpoints using hyperlipidemic rabbits to model
diet-induced human atherosclerosis. New Zealand White
rabbits were fed a normal or cholesterol-enriched diet and
then were intratracheally instilled 19/week for 4 weeks with
saline or 16 lg/kg of zinc, equal parts sulfate and oxide.
Physiologic responses, blood after each exposure, and ter-
minal bronchoalveolar lavage (BAL) were assessed. Rabbits
fed a cholesterol-rich diet developed hyperlipidemia and
had consistently higher circulating leukocyte counts than
rabbits fed normal chow. Within minutes after zinc instil-
lation, saturation of peripheral oxygen was decreased in
hyperlipidemic rabbits and heart rate was increased in
hyperlipidemic rabbits with total serum cholesterol levels
greater than 200 mg/dl. Total circulating leukocytes levels
were increased 24 h after the first zinc instillation, but upon
repeated exposures this effect was attenuated. After repeated
zinc exposures, BAL fluid (BALF) N-acetylglucosaminidase
activity was increased regardless of hyperlipidemic state.
Hyperlipidemic rabbits had an increase in BALF-oxidized
glutathione and a decrease in serum nitrite. The study elu-
cidates mechanisms by which the zinc metal component of
PM drives cardiovascular health effects, as well as the pos-
sible susceptibility induced by hyperlipidemia. Furthermore,
the study exemplifies the benefits of monitoring circulatory
physiology during exposure as well as after exposure.
Keywords Zinc � Rabbit � Cardiovascular �Particulate matter � Hyperlipidemia
Introduction
Increases in particulate air pollution are associated with
elevated cardiovascular hospital admissions and mortality
(reviewed in [33]). Patients with existing cardiovascular
disease (CVD) are more strongly affected than other
patients [41]. These data indicate that individuals with pre-
existing cardiovascular disease are at increased risk from
particulate matter (PM) exposure. In addition, the pul-
monary inflammation initiated by repeated PM insults may
sustain sub-clinical systemic inflammation, which has a
pivotal role in the development of atherosclerosis. Hence,
chronic PM exposure could contribute to the development
of cardiovascular disease [26].
Animal models of atherosclerosis have been used to
study pulmonary PM exposure effects on this disease [4, 6,
This article was reviewed by the National Health and Environmental
Effects Research Laboratory, U.S. Environmental Protection Agency,
and approved for publication. Approval does not signify that the
contents necessarily reflect the views and policies of the agency, nor
does mention of trade names or commercial products constitute
endorsement or recommendation for use.
A. P. Carll and N. D. Manzo supported by EPA-CT82947101 and
EPA-CT826512010, respectively.
A. J. LaGier (&) � R. H. Jaskot � R. Slade �J. H. Richards � D. W. Winsett � A. K. Farraj � J. A. Dye
Experimental Toxicology Division, National Health and
Environmental Effects Research Laboratory, Office of Research
and Development, U.S. Environmental Protection Agency,
109 TW Alexander Drive, MD: B143-01, Research Triangle
Park, NC 27711, USA
e-mail: [email protected]
N. D. Manzo
Department of Molecular Biomedical Sciences, North Carolina
State University, Raleigh, NC 27606, USA
A. P. Carll
School of Public Health, ENVR, University of North Carolina,
Chapel Hill, NC 27599, USA
Cardiovasc Toxicol (2008) 8:195–206
DOI 10.1007/s12012-008-9028-9

29]. The models used to date have some limitations in
terms of mimicking human disease because they are largely
based on genetic defects, i.e. the apolipoprotein E knockout
(ApoE-/-) mouse [44] or the Watanabe heritable hyper-
lipidemic (WHHL) rabbit that has a natural defect in low-
density lipoprotein (LDL) receptors [42]. These genetic
defects lead to alterations in cholesterol clearance and
spontaneous increases in total serum cholesterol levels that
are unlike humans with diet-mediated atherosclerosis.
To better represent the at-risk hypercholesterolemia-
induced atherosclerotic human population as a whole, the
study presented here used a diet-induced rabbit model of
hyperlipidemia and atherosclerosis. In this model, total
serum cholesterol levels and the nature of the target lesions
are controlled, at least in part, by adjusting dietary cho-
lesterol intake [25, 38]. Additionally, these animals
develop transitional atherosclerotic plaques comprised
predominantly of foamy macrophages [25], which are
important for PM-induced progression of atherosclerosis
[36, 43].
One of the common PM-associated elements found in
ambient air, especially PM samples collected near indus-
trial sources [10], is zinc, a transition metal. Past reports
have suggested that the zinc content of PM samples is
responsible for the responses to inhaled particulates [2, 23].
In fact, zinc oxide fume inhalation causes metal fume
fever, an occupational health hazard. In addition, zinc is
one of the largest metal fractions of EHC-93 [2], the
ambient PM sample that reportedly increased atheroscle-
rotic plaque volume in WHHL rabbits [36].
Using zinc as a plausible driver of PM toxicity, we
hypothesize that PM exposure in the hyperlipidemic rabbits
will elicit a greater adverse cardiovascular health outcome
than the non-lipemic rabbits. In addition, we propose that
these responses will be influenced by the degree of
hyperlipidemia. Finally, by monitoring immediate physio-
logic responses, changes in systemic biomarkers and
terminal pulmonary endpoints, we evaluate the potential
utility of hyperlipidemic rabbits as a model to assess PM
exacerbation of existing cardiovascular disease.
Materials and Methods
Animals
Male New Zealand White rabbits were used in all experi-
ments (Charles River Laboratory, Wilmington, MA).
Animals were housed in an isolated animal room in an
AAALAC-approved facility (21 ± 1�C, 50 ± 5% relative
humidity, 12 h light–dark cycle) and allowed free access to
water. Rabbits weighed between 1.8 and 2.1 kg prior to
start of diet-induction phase and were 36 weeks old with
weights between 3.6 and 4.5 kg at the start of the intra-
tracheal instillation regimen. All protocols were approved
by the Institutional Animal Care and Use Committee of the
U.S. EPA.
Diet
Rabbits were randomized by body weight into two groups
(N = 6 per group). One group (normal) was fed certified
high fiber rabbit diet 2031C and the other group (hyper-
lipidemic) was fed this rabbit diet supplemented with 0.2%
cholesterol (Harlan Teklad, Madison, WI). Based on the
diet’s mineral content, rabbits ingested approximately
7 mg zinc per day. A 0.2% cholesterol-supplemented diet
for at least 16 weeks increases total plasma cholesterol
levels and induces aortic lesions similar to atherosclerotic
plaques [38]. The diet-induction phase was administered
beyond this time point as prolonged ingestion of a cho-
lesterol-rich diet leads to more fibrous and less cellular
plaques [1] suggestive of human lesions prone to fissure,
hematoma, and/or thrombus.
Body Weight, Temperature, and Identification
Animals were weighed weekly during the diet-induction
phase and prior to, 24 and 48 h after instillations on an
ES50L standard electronic balance (Ohaus, Pine Brook,
NJ). Identification and temperature were monitored using
Implantable Programmable Temperature Transponder-
200TM (Biomedic Data Systems, Seaford, DE) that was
inserted subcutaneously as per manufacturer’s instructions.
Core temperatures were determined with a rectal
thermometer.
Blood Collection and Analysis
Blood was collected biweekly during the diet-induction
phase, 24 h after each instillation, and at necropsy. Because
of the known diurnal variation in total white blood counts,
all samples were obtained in the morning after an overnight
fast. Rabbits were sedated with 0.5 mg/kg acepromazine
IM (Henry Schein, Melville, NY). Blood was drawn from
the central ear artery and aliquots were collected into
additive-free or EDTA-treated BD vacutainers (Becton
Dickinson (BD), Franklin Lakes, NJ).
Aliquots of additive-free blood were centrifuged at
3000 9 g at room temperature and the serum was collected
into separate tubes. Using commercially available kits
modified and adapted for use on the KONELAB 30 clinical
chemistry analyzer (Thermo Clinical Labsystems, Espoo,
Finland), serum was analyzed for total cholesterol, low-
density lipoprotein (LDL), high-density lipoprotein (HDL),
and triglyceride content (ThermoElectron Corp., Melbourne,
196 Cardiovasc Toxicol (2008) 8:195–206

Australia). In addition, serum C-reactive protein (CRP) and
nitrite was assessed as per manufacturer’s instructions by a
rabbit-specific ELISA (American Laboratory Products Co.,
Windham, NH) and by a Griess reagent kit (Molecular
Probes, Invitrogen, Carlsbad, CA), respectively. Colori-
metric assays were read and analyzed on a Thermomax�
plate reader outfitted with Softmax Pro� v2.6.1 software
(Molecular Devices Corp., Menlo Park, CA).
Aliquots of EDTA-collected blood were analyzed for
complete blood counts (CBC), which included white blood
cell (WBC) counts and hematocrit, with an AcT blood
analyzer (Beckman-Coulter Inc., Fullerton, CA) and for
differential cell determination ([200 cells counted per
slide) from air-dried blood smear preparations stained with
LeukoStat (Fisher Scientific Co., Pittsburgh, PA). A post-
instillation/baseline ratio was calculated by dividing the
total WBC count 24 h post-instillation by the average pre-
instillation WBC count from week 14–36 of the diet-
induction phase.
Intratracheal Zinc Instillation
We designed the present study to experimentally resemble
a study by Suwa et al. [36] that used Watanabe rabbits to
conclude that exposure to ambient PM led to progression of
atherosclerosis. In this regard, we chose intratracheal
instillation as an exposure method. Based on total choles-
terol levels at the end of the diet-induction phase, we chose
to diverge from our original 2 9 2 experimental matrix
(±diet, ±zinc) in order to assess whether the degree of
hyperlipidemia was correlated to the risk of adverse health
outcome following the same zinc exposure. Rabbits were
assigned to groups for instillation of control saline (n = 3)
or zinc (n = 3 each for rabbits with normal (N), moderate
(M) or high (H) lipid levels). Zinc oxide (ZnO) and zinc
sulfate heptahydrate (ZnSO4) (Sigma Chemical Co., St.
Louis, MO) were added to pyrogen-free sterile saline,
probe sonicated for 1 min (Microson Ultrasonic cell dis-
ruptor, Misonix, Farmingdale, NY), vortexed, and instilled
intratracheally (IT) at a total dose of 16 lg/kg of zinc,
containing equal parts of ZnO and ZnSO4, in a volume of
2 ml (0.5 ml/kg). Control rabbits were instilled with
0.5 ml/kg sterile saline.
The zinc instillate was prepared fresh for each instilla-
tion and contained 50% soluble zinc (i.e. sulfate) and 50%
insoluble zinc (i.e. oxide), similar to the zinc content of
EHC-93 [2]. The 16 lg/kg dose of zinc given per instil-
lation approximates the amount of zinc contained in the
1.56 mg/kg of EHC-93 used in comparable rabbit studies
[29, 36] (approximately 10.4 lg zinc per mg EHC-93 [2]
times 1.56 mg/kg equals 16 lg zinc/kg body weight). An
initial dose–response pilot experiment in rabbits, which
received a single instillation of saline or 8, 16, or 32 lg/kg
of the zinc sulfate–oxide (50:50) instillate confirmed
that the 16 lg/kg dose resulted in mild pulmonary
inflammation.
For the instillations, rabbits were pre-medicated with
1 mg/kg midazolam IM, given 0.05 mg/kg atropine IM
and anesthetized by inhalation of vaporized isoflurane
via face mask to allow transoral intubation. Two appli-
cations, at least 3 min apart, of a topical anesthetic,
cetacaine (14.0% benzocaine), were applied to the larynx
with a cotton-tipped applicator. All pharmaceuticals were
purchased from Henry Schein (Melville, NY). Anesthe-
tized rabbits were placed in sternal recumbency on a
circulating warm water blanket and intubated with a
2.5 mm ID, 10FR, 14 cm long, uncuffed, Murphy oral/
nasal ET tube (Hudson RCI, Temecula, CA). Placement
was confirmed by visualizing a breathing pattern on a
SurgiVet� V9400 capnograph (Smiths Medical PM Inc.,
Waukesha, WI), which was attached to the ET tube
during placement. A 5FR feeding tube (Henry Schein) cut
to a length of 34 cm was passed through the endotracheal
tube to the level of the carina. The saline or zinc sus-
pension was instilled via the feeding tube, as two separate
1 ml boluses, followed by 20 ml of air to extrude any
instillate remaining in the tubing.
Vital signs were monitored for at least 10 min before,
during, and for at least 10 min after instillations. In addi-
tion to monitoring lung sounds, rabbits were instrumented
with a capnograph (Smiths Medical PM Inc) to monitor
end-tidal CO2 and respiratory rate (RR). Saturation of
peripheral oxygen (SpO2) was determined at 2 min inter-
vals with an Ohmeda Biox340 pulse oximeter (DRE Inc.,
Louisville, KY) attached between the footpads. Heart rate
was determined by way of auscultation and during the third
and fourth instillation via electrocardiogram (ECG). ECG
were recorded continuously (beginning 5 min prior to and
ending 10 min after instillation) with a radiotelemetry
transmitter (Model TA11CTA-F40; Data Sciences Inter-
national Inc., St. Paul, MN) attached externally with
alligator clips to shaved skin moistened with conductive
gel. Signals were transmitted to a receiver placed beneath
the animal, electronically recorded at a rate of 1,000 Hz on
a 54 mV scale and analyzed with ECG-Auto v1.5.12.48
(EMKA Technologies, Falls Church, VA). A minimum of
50 waveforms were analyzed per 1 min segment. Absolute
area of T represents the absolute value of the area under the
curve between the ECG trace and the isoelectric line.
BAL Fluid and Analyses
Two days after the fourth instillation, a time point used in
comparable rabbit studies [29], rabbits were weighed,
anesthetized as described above and bronchoalveolar
lavage (BAL) was performed, followed by euthanasia with
Cardiovasc Toxicol (2008) 8:195–206 197
Euthanosol (250 ll/kg, IV). BAL was performed similar
to procedures recommended for clinical use in small
companion animals [18] and optimized for use in the
laboratory rabbit [11]. Briefly, lungs were lavaged with a
volume of sterile 0.9% NaCl (Braun Medical, Inc., Irvine,
CA) equal to 10 ml/kg body weight. The entire volume
was instilled through the pre-placed endotracheal tube and
was aspirated back a single time. The BAL fluid was
quantified, examined grossly for evidence of surfactant,
hemorrhage, mucus strands, or cloudiness and kept on ice
for further analysis.
Total white cell counts were determined from analyses
of aliquots of whole BALF using a Coulter counter
(Coulter Inc., Miami, FL). Differential cell determinations
([200 cells counted per slide) were made from air-dried
cytospin preparations (Shandon, Pittsburgh, PA) stained
with LeukoStat (Fisher Scientific Co., Pittsburgh, PA). The
remaining BAL fluid was centrifuged at 1500 9 g to
remove cells. Using commercially available kits modified
and adapted for use on the KONELAB 30 clinical chem-
istry analyzer (Thermo Clinical Labsystems, Espoo,
Finland), cell-free BAL fluid was analyzed for albumin
(Diasorin, Saluggia, Italy), total protein content (Coo-
massie Plus Protein assay kit, Pierce, Rockford, IL with
BSA standards from Sigma, St. Louis, MO), lactate
dehydrogenase (LDH) activity (ThermoElectron, Corp.),
and N-acetyl-b-D-glucosaminidase (NAG) activity (Roche
Diagnostics, Indianapolis, IN). In addition, reduced (GSH)
and oxidized (GSSG) glutathione was labeled with dansyl
chloride [21] and analyzed by HPCL using a modification
of a previously described method [13].
Statistics
The data were analyzed by analysis of variance (ANOVA),
or where appropriate, a Student’s t-test, and by Bonfer-
roni’s corrections for multiple comparisons, using Prism 4
(GraphPad Software Inc., San Diego, CA). Statistical sig-
nificance was stated when P value of B0.05 was reached.
Correlations were determined using the Excel 2003 data
analysis tool (Microsoft Corp., Redmond, WA).
Results
Diet-Induction Phase
During the 36 weeks of the diet-induction phase (prior to
zinc instillation), all rabbits were serially monitored
(Fig. 1). Serum was assessed for lipid profile changes (total
cholesterol, LDL, HDL, triglyceride). Physical parameters,
i.e. temperature and weight, were measured and CBCs
were determined.
Lipid Profile
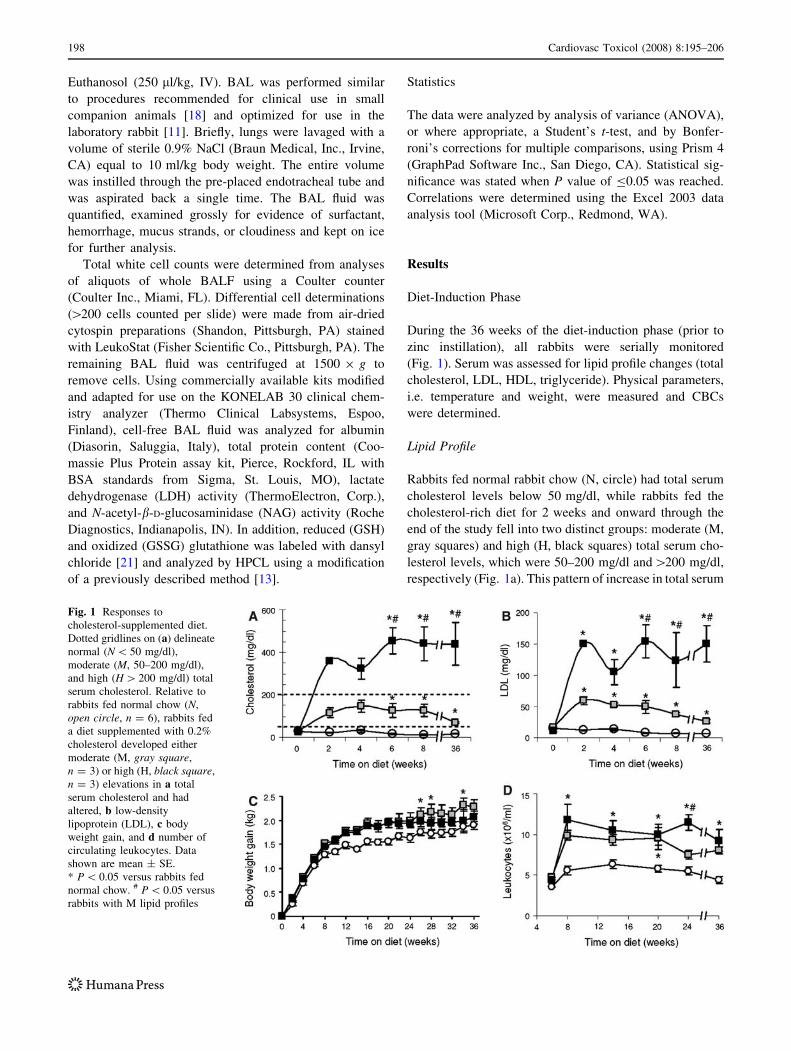
Rabbits fed normal rabbit chow (N, circle) had total serum
cholesterol levels below 50 mg/dl, while rabbits fed the
cholesterol-rich diet for 2 weeks and onward through the
end of the study fell into two distinct groups: moderate (M,
gray squares) and high (H, black squares) total serum cho-
lesterol levels, which were 50–200 mg/dl and[200 mg/dl,
respectively (Fig. 1a). This pattern of increase in total serum
Fig. 1 Responses to
cholesterol-supplemented diet.
Dotted gridlines on (a) delineate
normal (N \ 50 mg/dl),
moderate (M, 50–200 mg/dl),
and high (H [ 200 mg/dl) total
serum cholesterol. Relative to
rabbits fed normal chow (N,
open circle, n = 6), rabbits fed
a diet supplemented with 0.2%
cholesterol developed either
moderate (M, gray square,
n = 3) or high (H, black square,
n = 3) elevations in a total
serum cholesterol and had
altered, b low-density
lipoprotein (LDL), c body
weight gain, and d number of
circulating leukocytes. Data
shown are mean ± SE.
* P \ 0.05 versus rabbits fed
normal chow. # P \ 0.05 versus
rabbits with M lipid profiles
198 Cardiovasc Toxicol (2008) 8:195–206

cholesterol was correlated linearly with the increase in LDL
(r2 [ 0.95 at 2–36 weeks on diet) or hyperlipidemia
(Fig. 1b). HDL and triglyceride levels were not different
between groups, except at 14 weeks on diet, when the rab-
bits in group H had higher triglyceride levels (188 ± 32 mg/
dl) than rabbits in group N (54 ± 9 mg/dl) or M
(19 ± 1 mg/dl) (P \ 0.05, ANOVA).
Physical Parameters
No significant differences were noted in body temperatures
by way of subcutaneous transponders. After 8 weeks on
diet, the overall body weight gain was 0.23 ± 0.12 kg and
0.17 ± 0.03 kg higher in M and H hyperlipidemic rabbits,
respectively, when compared to N normolipidemic rabbits.
However, the weight difference between groups was always
\0.5 kg. Weight gain reached a plateau at approximately
16 weeks. Therefore, the diet-induction phase did not
cause the animals to become overtly obese or cachectic
(Fig. 1c). In general, all the rabbits appeared healthy and
did not show outward signs of poor health, e.g. appetite
loss or behavioral changes.
CBC
As previously reported [12], the rabbits with moderate (M)
and high (H) hyperlipidemia had elevated circulating leu-
kocytes when compared to rabbits with normal (N) lipid
levels. The leukocytosis in the hyperlipidemic rabbits was
noted consistently throughout the diet-induction phase
(Fig. 1d). Hematocrit levels were not different amongst
groups. Differential cell counts revealed that leukocytosis
was not driven by a single cell type, but rather reflected
increased lymphocytes, monocytes, and heterophils. (Het-
erophils in the rabbit represent neutrophils found in other
species.) However, total monocyte numbers correlated
linearly with total heterophil numbers (r2 = 0.98, 0.99, and
0.96, at 8, 10, and 14 weeks on diet, respectively), indic-
ative of the chronic inflammatory processes that
purportedly beget atherosclerosis.
Zinc Instillation Studies
Pilot Zinc Dose–Response Study in Normolipidemic
Rabbits
Past reports suggested that PM-associated zinc content is
an important causal component involved in acute lung and
sub-acute cardiac responses to inhaled particulates [2, 10,
24]. To ensure that these previous findings, which utilized
rodent models to implicate zinc, could be extended to the
rabbit species, we conducted an exploratory study to
examine the acute pulmonary effects of instilled zinc in
rabbits. All rabbits used in this dose–response study had
normal total serum cholesterol levels, \50 mg/dl.
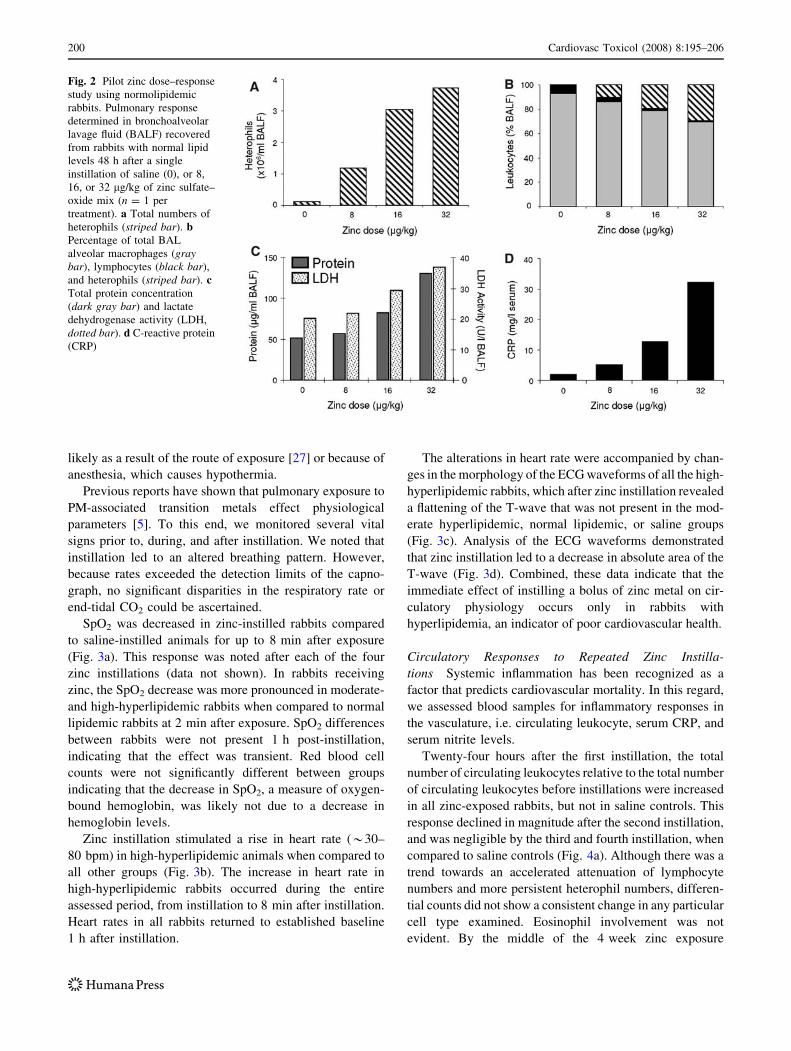
Acute lung injury was assessed 48 h after instillation of
a single bolus of saline; or 8, 16, or 32 lg/kg zinc, com-
posed of half zinc sulfate and half zinc oxide (see
‘‘Materials and Methods’’). In a dose-dependent manner,
the total number of heterophils in BAL increased in zinc-
exposed rabbits compared with rabbits exposed to saline
(Fig. 2a). The percentage of lavageable macrophages and
lymphocytes decreased in zinc-exposed rabbits compared
with rabbits exposed to saline (Fig. 2b). Based on dose,
BAL fluid levels of LDH and total protein were elevated in
zinc-exposed rabbits in comparison to rabbits exposed to
saline (Fig. 2c). When compared to saline control, a slight
increase in NAG activity was noted after zinc instillation,
but this was not dose-dependent (data not shown). In
addition, serum levels of CRP, a purportedly sensitive
biomarker of systemic inflammation and vascular disease,
were increased as zinc dose increased (Fig. 2d). These data
indicate that zinc induced an acute, dose-dependent lung,
and systemic inflammatory response in rabbits that was
similar to previous reports in zinc-exposed rodents.
We also observed that a dose of 32 lg/kg zinc was not
well tolerated in that immediately after instillation the
subject developed tachypnea associated with depressed
SpO2. Hence, for the formal repeated zinc instillation
study, we utilized a dose of 16 lg/kg zinc (sulfate–oxide)
because it (1) was well-tolerated acutely, (2) was compa-
rable to that used in previous hyperlipidemic rabbit studies
[36], and (3) caused a detectable lung response character-
ized by moderate neutrophilic inflammation and only
minor lung injury.
Repeated Zinc Instillation Study in Rabbits with Normal,
Moderate or High Lipid Levels
Based on our pilot dose–response study and on the previous
study in WHHL rabbits [36], in the formal zinc instillation
study, we instilled normal (N), moderate (M), and high (H)
hyperlipidemic rabbits with saline or 16 lg/kg zinc sul-
fate–oxide (50:50) once a week for 4 weeks. We assumed
the weekly dosing regimen allowed the rabbits time for
clearance as most soluble and insoluble zinc clears the lung
2 days after instillation [20, 39]. We assessed immediate
physiologic responses at the time of each instillation, blood
biomarkers 24 h after each exposure, and terminal end-
points, e.g. BAL fluid indices.
Immediate Physiological Response to Zinc Expo-
sure Because zinc oxide inhalation has been associated
with metal fume fever, we monitored the rabbits for body
temperature before and after instillation. No significant
alteration in temperature was evident between groups,
Cardiovasc Toxicol (2008) 8:195–206 199
likely as a result of the route of exposure [27] or because of
anesthesia, which causes hypothermia.
Previous reports have shown that pulmonary exposure to
PM-associated transition metals effect physiological
parameters [5]. To this end, we monitored several vital
signs prior to, during, and after instillation. We noted that
instillation led to an altered breathing pattern. However,
because rates exceeded the detection limits of the capno-
graph, no significant disparities in the respiratory rate or
end-tidal CO2 could be ascertained.
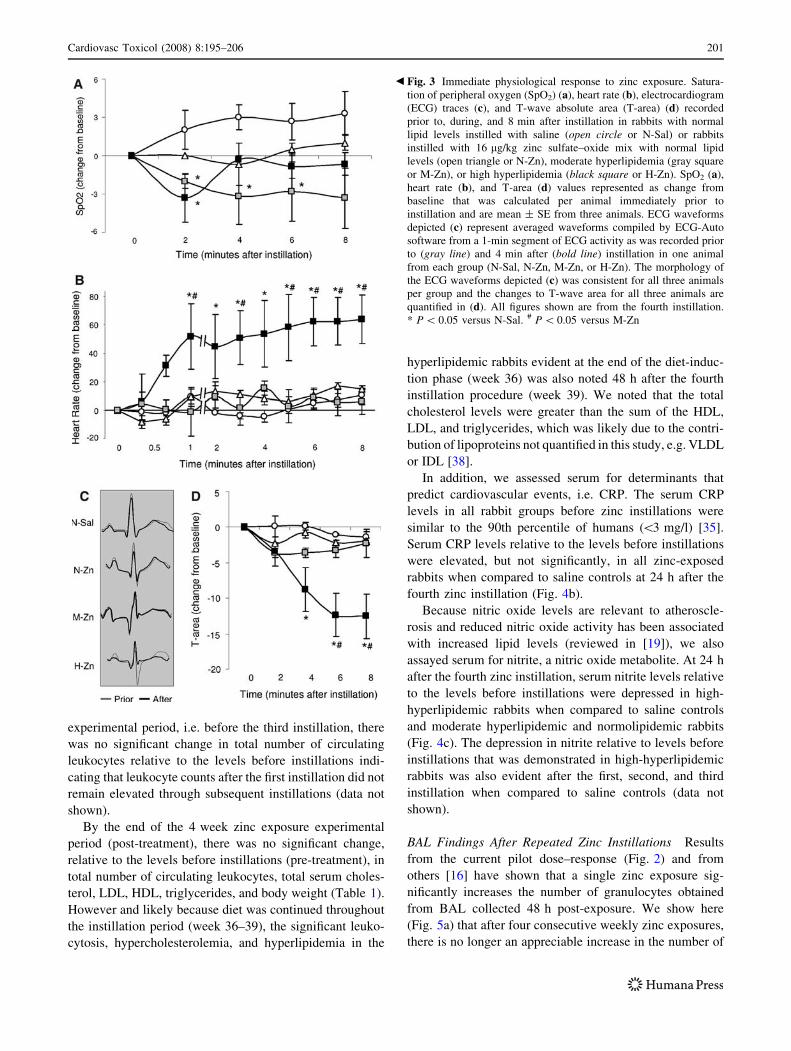
SpO2 was decreased in zinc-instilled rabbits compared
to saline-instilled animals for up to 8 min after exposure
(Fig. 3a). This response was noted after each of the four
zinc instillations (data not shown). In rabbits receiving
zinc, the SpO2 decrease was more pronounced in moderate-
and high-hyperlipidemic rabbits when compared to normal
lipidemic rabbits at 2 min after exposure. SpO2 differences
between rabbits were not present 1 h post-instillation,
indicating that the effect was transient. Red blood cell
counts were not significantly different between groups
indicating that the decrease in SpO2, a measure of oxygen-
bound hemoglobin, was likely not due to a decrease in
hemoglobin levels.
Zinc instillation stimulated a rise in heart rate (*30–
80 bpm) in high-hyperlipidemic animals when compared to
all other groups (Fig. 3b). The increase in heart rate in
high-hyperlipidemic rabbits occurred during the entire
assessed period, from instillation to 8 min after instillation.
Heart rates in all rabbits returned to established baseline
1 h after instillation.
The alterations in heart rate were accompanied by chan-
ges in the morphology of the ECG waveforms of all the high-
hyperlipidemic rabbits, which after zinc instillation revealed
a flattening of the T-wave that was not present in the mod-
erate hyperlipidemic, normal lipidemic, or saline groups
(Fig. 3c). Analysis of the ECG waveforms demonstrated
that zinc instillation led to a decrease in absolute area of the
T-wave (Fig. 3d). Combined, these data indicate that the
immediate effect of instilling a bolus of zinc metal on cir-
culatory physiology occurs only in rabbits with
hyperlipidemia, an indicator of poor cardiovascular health.
Circulatory Responses to Repeated Zinc Instilla-
tions Systemic inflammation has been recognized as a
factor that predicts cardiovascular mortality. In this regard,
we assessed blood samples for inflammatory responses in
the vasculature, i.e. circulating leukocyte, serum CRP, and
serum nitrite levels.
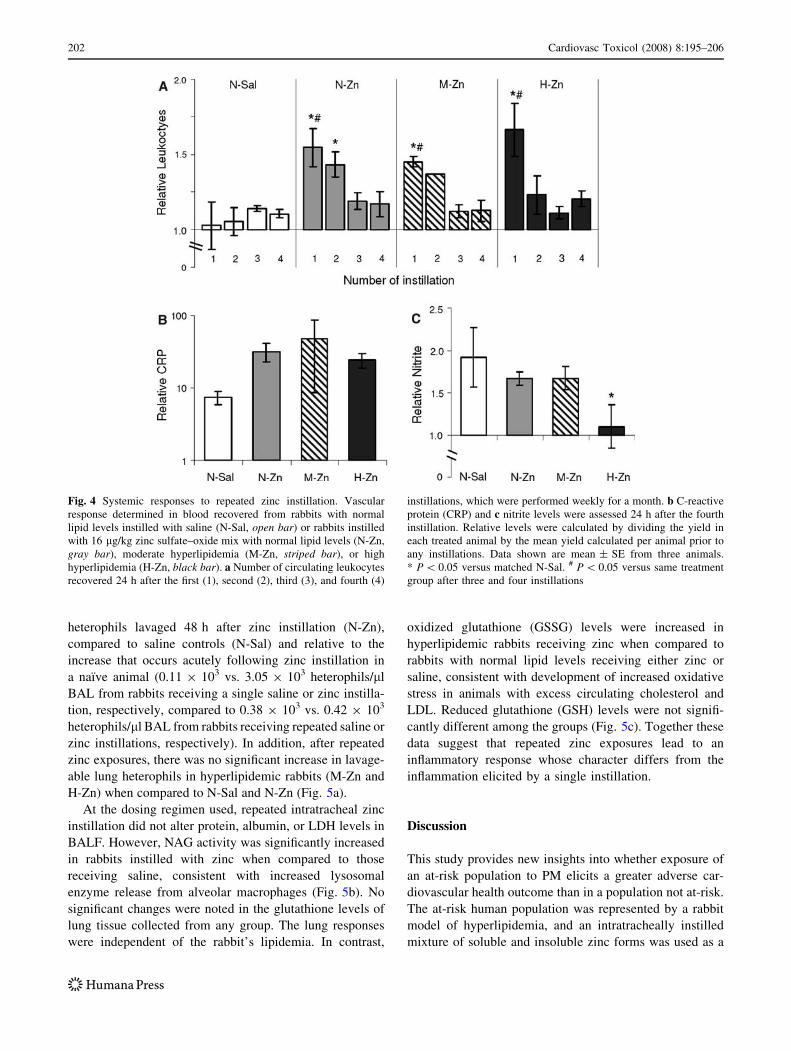
Twenty-four hours after the first instillation, the total
number of circulating leukocytes relative to the total number
of circulating leukocytes before instillations were increased
in all zinc-exposed rabbits, but not in saline controls. This
response declined in magnitude after the second instillation,
and was negligible by the third and fourth instillation, when
compared to saline controls (Fig. 4a). Although there was a
trend towards an accelerated attenuation of lymphocyte
numbers and more persistent heterophil numbers, differen-
tial counts did not show a consistent change in any particular
cell type examined. Eosinophil involvement was not
evident. By the middle of the 4 week zinc exposure
Fig. 2 Pilot zinc dose–response
study using normolipidemic
rabbits. Pulmonary response
determined in bronchoalveolar
lavage fluid (BALF) recovered
from rabbits with normal lipid
levels 48 h after a single
instillation of saline (0), or 8,
16, or 32 lg/kg of zinc sulfate–
oxide mix (n = 1 per
treatment). a Total numbers of
heterophils (striped bar). bPercentage of total BAL
alveolar macrophages (graybar), lymphocytes (black bar),
and heterophils (striped bar). cTotal protein concentration
(dark gray bar) and lactate
dehydrogenase activity (LDH,
dotted bar). d C-reactive protein
(CRP)
200 Cardiovasc Toxicol (2008) 8:195–206
experimental period, i.e. before the third instillation, there
was no significant change in total number of circulating
leukocytes relative to the levels before instillations indi-
cating that leukocyte counts after the first instillation did not
remain elevated through subsequent instillations (data not
shown).
By the end of the 4 week zinc exposure experimental
period (post-treatment), there was no significant change,
relative to the levels before instillations (pre-treatment), in
total number of circulating leukocytes, total serum choles-
terol, LDL, HDL, triglycerides, and body weight (Table 1).
However and likely because diet was continued throughout
the instillation period (week 36–39), the significant leuko-
cytosis, hypercholesterolemia, and hyperlipidemia in the
hyperlipidemic rabbits evident at the end of the diet-induc-
tion phase (week 36) was also noted 48 h after the fourth
instillation procedure (week 39). We noted that the total
cholesterol levels were greater than the sum of the HDL,
LDL, and triglycerides, which was likely due to the contri-
bution of lipoproteins not quantified in this study, e.g. VLDL
or IDL [38].
In addition, we assessed serum for determinants that
predict cardiovascular events, i.e. CRP. The serum CRP
levels in all rabbit groups before zinc instillations were
similar to the 90th percentile of humans (\3 mg/l) [35].
Serum CRP levels relative to the levels before instillations
were elevated, but not significantly, in all zinc-exposed
rabbits when compared to saline controls at 24 h after the
fourth zinc instillation (Fig. 4b).
Because nitric oxide levels are relevant to atheroscle-
rosis and reduced nitric oxide activity has been associated
with increased lipid levels (reviewed in [19]), we also
assayed serum for nitrite, a nitric oxide metabolite. At 24 h
after the fourth zinc instillation, serum nitrite levels relative
to the levels before instillations were depressed in high-
hyperlipidemic rabbits when compared to saline controls
and moderate hyperlipidemic and normolipidemic rabbits
(Fig. 4c). The depression in nitrite relative to levels before
instillations that was demonstrated in high-hyperlipidemic
rabbits was also evident after the first, second, and third
instillation when compared to saline controls (data not
shown).
BAL Findings After Repeated Zinc Instillations Results
from the current pilot dose–response (Fig. 2) and from
others [16] have shown that a single zinc exposure sig-
nificantly increases the number of granulocytes obtained
from BAL collected 48 h post-exposure. We show here
(Fig. 5a) that after four consecutive weekly zinc exposures,
there is no longer an appreciable increase in the number of
Fig. 3 Immediate physiological response to zinc exposure. Satura-
tion of peripheral oxygen (SpO2) (a), heart rate (b), electrocardiogram
(ECG) traces (c), and T-wave absolute area (T-area) (d) recorded
prior to, during, and 8 min after instillation in rabbits with normal
lipid levels instilled with saline (open circle or N-Sal) or rabbits
instilled with 16 lg/kg zinc sulfate–oxide mix with normal lipid
levels (open triangle or N-Zn), moderate hyperlipidemia (gray square
or M-Zn), or high hyperlipidemia (black square or H-Zn). SpO2 (a),
heart rate (b), and T-area (d) values represented as change from
baseline that was calculated per animal immediately prior to
instillation and are mean ± SE from three animals. ECG waveforms
depicted (c) represent averaged waveforms compiled by ECG-Auto
software from a 1-min segment of ECG activity as was recorded prior
to (gray line) and 4 min after (bold line) instillation in one animal
from each group (N-Sal, N-Zn, M-Zn, or H-Zn). The morphology of
the ECG waveforms depicted (c) was consistent for all three animals
per group and the changes to T-wave area for all three animals are
quantified in (d). All figures shown are from the fourth instillation.
* P \ 0.05 versus N-Sal. # P \ 0.05 versus M-Zn
b
Cardiovasc Toxicol (2008) 8:195–206 201
heterophils lavaged 48 h after zinc instillation (N-Zn),
compared to saline controls (N-Sal) and relative to the
increase that occurs acutely following zinc instillation in
a naı̈ve animal (0.11 9 103 vs. 3.05 9 103 heterophils/ll
BAL from rabbits receiving a single saline or zinc instilla-
tion, respectively, compared to 0.38 9 103 vs. 0.42 9 103
heterophils/ll BAL from rabbits receiving repeated saline or
zinc instillations, respectively). In addition, after repeated
zinc exposures, there was no significant increase in lavage-
able lung heterophils in hyperlipidemic rabbits (M-Zn and
H-Zn) when compared to N-Sal and N-Zn (Fig. 5a).
At the dosing regimen used, repeated intratracheal zinc
instillation did not alter protein, albumin, or LDH levels in
BALF. However, NAG activity was significantly increased
in rabbits instilled with zinc when compared to those
receiving saline, consistent with increased lysosomal
enzyme release from alveolar macrophages (Fig. 5b). No
significant changes were noted in the glutathione levels of
lung tissue collected from any group. The lung responses
were independent of the rabbit’s lipidemia. In contrast,
oxidized glutathione (GSSG) levels were increased in
hyperlipidemic rabbits receiving zinc when compared to
rabbits with normal lipid levels receiving either zinc or
saline, consistent with development of increased oxidative
stress in animals with excess circulating cholesterol and
LDL. Reduced glutathione (GSH) levels were not signifi-
cantly different among the groups (Fig. 5c). Together these
data suggest that repeated zinc exposures lead to an
inflammatory response whose character differs from the
inflammation elicited by a single instillation.
Discussion
This study provides new insights into whether exposure of
an at-risk population to PM elicits a greater adverse car-
diovascular health outcome than in a population not at-risk.
The at-risk human population was represented by a rabbit
model of hyperlipidemia, and an intratracheally instilled
mixture of soluble and insoluble zinc forms was used as a
Fig. 4 Systemic responses to repeated zinc instillation. Vascular
response determined in blood recovered from rabbits with normal
lipid levels instilled with saline (N-Sal, open bar) or rabbits instilled
with 16 lg/kg zinc sulfate–oxide mix with normal lipid levels (N-Zn,
gray bar), moderate hyperlipidemia (M-Zn, striped bar), or high
hyperlipidemia (H-Zn, black bar). a Number of circulating leukocytes
recovered 24 h after the first (1), second (2), third (3), and fourth (4)
instillations, which were performed weekly for a month. b C-reactive
protein (CRP) and c nitrite levels were assessed 24 h after the fourth
instillation. Relative levels were calculated by dividing the yield in
each treated animal by the mean yield calculated per animal prior to
any instillations. Data shown are mean ± SE from three animals.
* P \ 0.05 versus matched N-Sal. # P \ 0.05 versus same treatment
group after three and four instillations
202 Cardiovasc Toxicol (2008) 8:195–206

plausible driver of PM toxicity. Herein, we demonstrated
that immediately upon instillation of zinc, severely
hyperlipidemic rabbits had altered cardiovascular physiol-
ogy, characterized by a decrease in SpO2, an increase in
heart rate, and an alteration in the morphology of the ECG
waveforms, i.e. T-wave flattening. In addition, after repe-
ated zinc instillations, serum nitrite levels were depressed
and BALF-oxidized glutathione levels were increased in
high-hyperlipidemic rabbits when compared to all other
groups. These findings are consistent with our hypothesis
that hyperlipidemic subjects (similar to humans with ath-
erosclerosis) are at an increased risk for developing
untoward CVD health indices after repeated PM, i.e. zinc,
exposures and that these responses are influenced by the
degree of hyperlipidemia.
We also evaluated the potential utility of hyperlipidemic
rabbits as a model to assess air pollutant health effects on
populations susceptible to cardiovascular disease. By using
the rabbit model, we could non-invasively detect several
physiologic parameters and serially monitor a variety of
serum determinants. In this regard, we were able to detect
immediate changes in circulatory physiology and to deter-
mine that repeated intratracheal exposures to a mixture
of soluble and insoluble zinc forms resulted in attenuated
leukocyte increase. In this regard, this diet-induced hyper-
lipidemic rabbit model appears to be an ideal model with
Fig. 5 BAL findings after repeated zinc instillations. Pulmonary
response determined in bronchoalveolar lavage (BAL) recovered 48 h
after the fourth instillation in rabbits with normal lipid levels instilled
with saline (N-Sal) or rabbits instilled with 16 lg/kg zinc sulfate–
oxide mix with normal lipid levels (N-Zn), moderate hyperlipidemia
(M-Zn), or high hyperlipidemia (H-Zn). a Numbers of BAL
heterophils and b N-acetyl-b-D-glucosaminidase (NAG), [N-Sal (openbar), N-Zn (gray bar), M-Zn, (striped bar), H-Zn (black bar)]. cReduced (GSH, open bar) and oxidized (GSSG, gray bar) glutathi-
one. Data shown are mean ± SE from three animals. * P \ 0.05
versus N-Sal. # P \ 0.05 versus GSH
Table 1 Systemic response per treatment group before the first zinc
instillation and terminally, 48 h after the fourth zinc instillation
Before
instillations
After 4th
instillationa,b
Leukocytes (106/ml) N-Sal 5.2 ± 0.4 5.3 ± 0.8
N-Zn 3.6 ± 0.3 4.9 ± 0.7
M-Zn 7.6 ± 0.3 6.3 ± 0.7
H-Zn 9.3 ± 1.4*^ 11.4 ± 1.8*^
Cholesterol (mg/dl) N-Sal 16 ± 2 9 ± 6
N-Zn 19 ± 1 12 ± 3
M-Zn 70 ± 6*^ 97 ± 2*^
H-Zn 439 ± 101*^# 746 ± 254*^#
LDL (mg/dl) N-Sal 7 ± 0 13 ± 2
N-Zn 7 ± 1 13 ± 1
M-Zn 18 ± 1*^ 30 ± 2*^
H-Zn 150 ± 29*^# 249 ± 70*^#
HDL (mg/dl) N-Sal 9 ± 1 14 ± 3
N-Zn 7 ± 2 13 ± 1
M-Zn 12 ± 2 16 ± 2
H-Zn 19 ± 4 14 ± 1
Triglycericides (mg/dl) N-Sal 44 ± 5 39 ± 1
N-Zn 82 ± 35 59 ± 14
M-Zn 32 ± 5 21 ± 4
H-Zn 103 ± 51 111 ± 62
Weight (kg) N-Sal 4.0 ± 0.1 4.0 ± 0.1
N-Zn 3.8 ± 0.1 3.8 ± 0.1
M-Zn 4.2 ± 0.1 4.2 ± 0.0
H-Zn 3.9 ± 0.1 3.8 ± 0.1
Values are mean ± SE (n = 3 per group)a No significant differences versus before instillationsb All values from 48 h after fourth instillation, terminus of study
* P \ 0.05 versus N-Sal at matched time
^ P \ 0.05 versus N-Zn at matched time# P \ 0.05 versus M-Zn at matched time
Cardiovasc Toxicol (2008) 8:195–206 203

which to assess PM health effects in susceptible populations,
particularly when pathophysiology is involved.
Our findings are consistent with previous findings that
pulmonary exposure to the metal component of PM elicits
a cardiopulmonary inflammatory response. In this regard,
inhalation of heavy metal oxide, in particular zinc oxide,
leads acutely to metal fume fever, an occupational health
disease that in humans is accompanied by increased heart
rate [17] and leukocytosis [9]. Both of these metal fume-
induced effects were noted in our zinc-exposed hyperlipi-
demic rabbits.
Previous reports indicate that repeated exposure to zinc
fume leads to ‘pulmonary tolerance’, which is defined as the
lung’s ability to withstand the detrimental effects of a toxic
compound following multiple exposures [40]. We report
here that repeated instillation of zinc likely leads to more
global ‘tolerance’ as assessed by the blunting of zinc-
induced circulating leukocyte increases. Diminished leu-
kocyte increases could occur as a consequence of reduced
cellular production. However, reduction in production is not
indicated by a recent study demonstrated that increased
marrow production occurs in PM-exposed hyperlipidemic
rabbits [43].
In this study, we demonstrated that when leukocyte
infiltrate was reduced, i.e. after the fourth instillation,
serum CRP was elevated, serum nitrite was reduced, and
oxidized glutathione in airways was increased. Taking this
data into consideration, leukocyte numbers were likely
affected by cell influx because leukocyte migration is
modulated by CRP [22], nitric oxide [3], and oxidative
stress [28]. Furthermore, the anti-inflammatory milieu
established to terminate the first zinc-induced inflammatory
response would likely inhibit the influx of leukocytes
responding to successive zinc exposures. In addition to
production and cell influx, other causes of leukocytosis,
such as delayed apoptosis, altered clearance, or a shift from
marginating pools to circulating compartments, should be
considered for further study.
Systemic inflammation in combination with T-wave
changes on ECG traces has been previously shown to be
predictive of cardiovascular disease mortality [30]. This
study demonstrated that PM, i.e. zinc, initiated systemic
inflammation and altered the circulatory physiology of
hyperlipidemic rabbits, predicting deleterious cardiovas-
cular disease health effects in subjects with atherosclerosis.
In particular, we determined that zinc instillation led to an
immediate decrease in SpO2 and increase in heart rate in
the high-hyperlipidemic rabbits. Our data are consistent
with reports in humans with cardiovascular disease that
pulmonary PM exposure alters oxygen saturation [8], heart
rate [32], and ECG waveforms [31].
The altered SpO2 and heart rate that was noted in
hyperlipidemic subjects immediately upon pulmonary zinc
exposure could occur as a consequence of modified vascular
tone [34, 37]. We demonstrated that severely hyperlipidemic
rabbits had depressed levels of serum nitrite, tentatively
suggesting a reduction in the vasodilator activity of nitric
oxide and an alteration in vascular tone. Decreased nitric
oxide activity, as suggested by depressed levels of serum
nitrite, has also been associated with oxidative stress [14],
which is along with PM exposure involved with athero-
genesis [26]. In this regard, we showed as assessed
terminally with an increase in BALF-oxidized glutathione
that the airways in zinc-exposed hyperlipidemic rabbits had
an increase in oxidative stress. Combined these data suggest
that after repeated exposure to instilled zinc, hyperlipidemic
rabbits may have diminished antioxidant capacity and that
susceptibility to PM, i.e. zinc, may relate to being less able to
respond to the repeated oxidative stress associated with
continued zinc exposure.
Physiological effects elicited in already susceptible
cardiovasculature may lead to late-onset adverse effects
possibly modulating by decreased nitric oxide activity and
increased oxidative stress. The immediacy of the changes
in circulatory physiology suggests that the zinc-induced
pathophysiology is likely mediated by a neural reflex. In
this regard, atherosclerosis in combination with reduced
nitric oxide levels and increased oxidative stress have been
associated with reduced sensitivity of the baroreflex, which
detects and corrects changes in vascular tone [15]. Recent
evidence indicates that repeated activation of the barore-
ceptor reflex results in risk for late-onset cardiovascular
mortality [7].
In conclusion, using a diet-induced rabbit model of
hyperlipidemia, we present data that pulmonary instillation
of zinc induces both pulmonary and systemic inflammatory
responses whose character changes upon repeated instilla-
tions. Furthermore, the intratracheal instillation of zinc to
an already susceptible cardiovascular system likely leads to
immediate pathophysiology, decreased systemic nitric
oxide activity, and increased pulmonary oxidative stress.
These data may explain why sensitive groups exposed to
particle pollution experience heart-related health effects
after breathing polluted air.
Acknowledgments The authors thank Henry Daes, Allen Ledbetter,
and the animal staff for excellent technical assistance. We also thank
Dr. David Kurtz, Dr. Urmila Kodavanti, Dr. Gary Hatch, and Dr.
MaryJane Selgrade for critical review of the manuscript.
References
1. Adams, C. W., Miller, N. E., Morgan, R. S., & Rao, S. N. (1982).
Lipoprotein levels and tissue lipids in fatty-fibrous atherosclerosis
induced in rabbits by two years’ cholesterol feeding at a low
level. Atherosclerosis, 44, 1–8. doi:10.1016/0021-9150(82)90
047-8.
204 Cardiovasc Toxicol (2008) 8:195–206
2. Adamson, I. Y., Prieditis, H., Hedgecock, C., & Vincent, R. (2000).
Zinc is the toxic factor in the lung response to an atmospheric
particulate sample. Toxicology and Applied Pharmacology, 166,
111–119. doi:10.1006/taap.2000.8955.
3. Belenky, S. N., Robbins, R. A., & Rubinstein, I. (1993). Nitric
oxide synthase inhibitors attenuate human monocyte chemotaxis
in vitro. Journal of Leukocyte Biology, 53, 498–503.
4. Campen, M. J., McDonald, J. D., Reed, M. D., & Seagrave, J.
(2006). Fresh gasoline emissions, not paved road dust, alter
cardiac repolarization in ApoE-/- mice. Cardiovascular Toxi-cology, 6, 199–210. doi:10.1385/CT:6:3:199.
5. Campen, M. J., Nolan, J. P., Schladweiler, M. C., Kodavanti, U.
P., Evansky, P. A., Costa, D. L., et al. (2001). Cardiovascular and
thermoregulatory effects of inhaled PM-associated transition
metals: A potential interaction between nickel and vanadium
sulfate. Toxicological Sciences, 64, 243–252. doi:10.1093/toxsci/
64.2.243.
6. Chen, L. C., & Nadziejko, C. (2005). Effects of subchronic
exposures to concentrated ambient particles (CAPs) in mice. V.
CAPs exacerbate aortic plaque development in hyperlipidemic
mice. Inhalation Toxicology, 17, 217–224. doi:10.1080/0895837
0590912815.
7. De Ferrari, G. M., Sanzo, A., Bertoletti, A., Specchia, G., Vanoli,
E., & Schwartz, P. J. (2007). Baroreflex sensitivity predicts long-
term cardiovascular mortality after myocardial infarction even in
patients with preserved left ventricular function. Journal of theAmerican College of Cardiology, 50, 2285–2290. doi:10.1016/j.
jacc.2007.08.043.
8. DeMeo, D. L., Zanobetti, A., Litonjua, A. A., Coull, B. A.,
Schwartz, J., & Gold, D. R. (2004). Ambient air pollution and
oxygen saturation. American Journal of Respiratory and CriticalCare Medicine, 170, 383–387. doi:10.1164/rccm.200402-244OC.
9. Drinker, P., Thomson, R. M., & Finn, J. L. (1927). Metal fume
fever: II. Resistance acquired by inhalation of zinc oxide on two
successive days. Journal of Industrial Hygiene, 9, 98–105.
10. Dye, J. A., Lehmann, J. R., McGee, J. K., Winsett, D. W., Led-
better, A. D., Everitt, J. I., et al. (2001). Acute pulmonary toxicity
of particulate matter filter extracts in rats: Coherence with epi-
demiologic studies in Utah Valley residents. EnvironmentalHealth Perspectives, 109(Suppl 3), 395–403. doi:10.2307/343
4787.
11. Dye, J. A., Slade, R., Jaskot, R. H., Richards, J. H., Manzo, N.,
Taylor, G. M., & LaGier, A. J. (2008). Use of repeated bron-
choalveolar lavage in rabbits to assess pollutant-induced lung
changes in an animal model of cardiovascular (CV) disease.
American Thoracic Society International Conference, Toronto,
A426.
12. Feldman, D. L., Mogelesky, T. C., Liptak, B. F., & Gerrity, R. G.
(1991). Leukocytosis in rabbits with diet-induced atherosclerosis.
Arteriosclerosis and Thrombosis, 11, 985–994.
13. Gan, J., Harper, T. W., Hsueh, M. M., Qu, Q., & Humphreys, W.
G. (2005). Dansyl glutathione as a trapping agent for the quan-
titative estimation and identification of reactive metabolites.
Chemical Research in Toxicology, 18, 896–903. doi:10.1021/
tx0496791.
14. Ganafa, A. A., Socci, R. R., Eatman, D., Silvestrova, N., Abu-
khalaf, I. K., & Bayorh, M. A. (2002). Acute inhibition of
glutathione biosynthesis alters endothelial function and blood
pressure in rats. European Journal of Pharmacology, 454, 217–
223. doi:10.1016/S0014-2999(02)02500-1.
15. Gianaros, P. J., Jennings, J. R., Olafsson, G. B., Steptoe, A.,
Sutton-Tyrrell, K., Muldoon, M. F., et al. (2002). Greater intima-
media thickness in the carotid bulb is associated with reduced
baroreflex sensitivity. American Journal of Hypertension, 15,
486–491. doi:10.1016/S0895-7061(02)02923-0.
16. Gilmour, P. S., Nyska, A., Schladweiler, M. C., McGee, J. K.,
Wallenborn, J. G., Richards, J. H., et al. (2006). Cardiovascular
and blood coagulative effects of pulmonary zinc exposure. Tox-icology and Applied Pharmacology, 211, 41–52. doi:10.1016/j.
taap.2005.06.002.
17. Hassaballa, H. A., Lateef, O. B., Bell, J., Kim, E., & Casey, L.
(2005). Metal fume fever presenting as aseptic meningitis with
pericarditis, pleuritis and pneumonitis. Occupational Medicine(Oxford, England), 55, 638–641. doi:10.1093/occmed/kqi141.
18. Hawkins, E. C., & Berry, C. R. (1999). Use of a modified
stomach tube for bronchoalveolar lavage in dogs. Journal of theAmerican Veterinary Medical Association, 215, 1635–1639.
1620.
19. Henry, P. D., Cabello, O. A., & Chen, C. H. (1995). Hypercho-
lesterolemia and endothelial dysfunction. Current Opinion inLipidology, 6, 190–195.
20. Hirano, S., Higo, S., Tsukamoto, N., Kobayashi, E., & Suzuki, K.
T. (1989). Pulmonary clearance and toxicity of zinc oxide
instilled into the rat lung. Archives of Toxicology, 63, 336–342.
doi:10.1007/BF00278649.
21. Jones, D. P., Carlson, J. L., Samiec, P. S., Sternberg, P., Jr.,
Mody, V. C., Jr., Reed, R. L., et al. (1998). Glutathione mea-
surement in human plasma. Evaluation of sample collection,
storage and derivatization conditions for analysis of dansyl
derivatives by HPLC. Clinica Chimica Acta, 275, 175–184. doi:
10.1016/S0009-8981(98)00089-8.
22. Kew, R. R., Hyers, T. M., & Webster, R. O. (1990). Human
C-reactive protein inhibits neutrophil chemotaxis in vitro: Pos-
sible implications for the adult respiratory distress syndrome. TheJournal of Laboratory and Clinical Medicine, 115, 339–345.
23. Kodavanti, U. P., Schladweiler, M. C., Gilmour, P. S., Wallen-
born, J. G., Mandavilli, B. S., Ledbetter, A. D., et al. (2008). The
role of particulate matter-associated zinc in cardiac injury in rats.
Environmental Health Perspectives, 116, 13–20.
24. Kodavanti, U. P., Schladweiler, M. C., Ledbetter, A. D., Hauser,
R., Christiani, D. C., Samet, J. M., et al. (2002). Pulmonary and
systemic effects of zinc-containing emission particles in three rat
strains: Multiple exposure scenarios. Toxicological Sciences, 70,
73–85. doi:10.1093/toxsci/70.1.73.
25. Kolodgie, F. D., Katocs, A. S., Jr., Largis, E. E., Wrenn, S. M.,
Cornhill, J. F., Herderick, E. E., et al. (1996). Hypercholesterol-
emia in the rabbit induced by feeding graded amounts of low-
level cholesterol. Methodological considerations regarding indi-
vidual variability in response to dietary cholesterol and
development of lesion type. Arteriosclerosis, Thrombosis, andVascular Biology, 16, 1454–1464.
26. Kunzli, N., & Tager, I. B. (2005). Air pollution: From lung to
heart. Swiss Medical Weekly, 135, 697–702.
27. Mori, T., Akashi, S., & Nukada, A. (1975). Effects of the inha-
lation of catalytically active metallic oxide fumes on rabbits.
International Archives of Occupational and EnvironmentalHealth, 36, 29–39. doi:10.1007/BF01267849.
28. Moutet, M., d’Alessio, P., Malette, P., Devaux, V., & Chaudiere,
J. (1998). Glutathione peroxidase mimics prevent TNFalpha- and
neutrophil-induced endothelial alterations. Free Radical Biologyand Medicine, 25, 270–281. doi:10.1016/S0891-5849(98)000
38-0.
29. Mukae, H., Hogg, J. C., English, D., Vincent, R., & van Eeden, S.
F. (2000). Phagocytosis of particulate air pollutants by human
alveolar macrophages stimulates the bone marrow. The AmericanJournal of Physiology, 279, L924–L931.
30. Okin, P. M., Roman, M. J., Best, L. G., Lee, E. T., Galloway, J.
M., Howard, B. V., et al. (2005). C-reactive protein and elec-
trocardiographic ST-segment depression additively predict
mortality: The Strong Heart Study. Journal of the American
Cardiovasc Toxicol (2008) 8:195–206 205

College of Cardiology, 45, 1787–1793. doi:10.1016/j.jacc.
2005.02.072.
31. Pekkanen, J., Peters, A., Hoek, G., Tiittanen, P., Brunekreef, B.,
de Hartog, J., et al. (2002). Particulate air pollution and risk of
ST-segment depression during repeated submaximal exercise
tests among subjects with coronary heart disease: The Exposure
and Risk Assessment for Fine and Ultrafine Particles in Ambient
Air (ULTRA) study. Circulation, 106, 933–938. doi:
10.1161/01.CIR.0000027561.41736.3C.
32. Peters, A., Perz, S., Doring, A., Stieber, J., Koenig, W., &
Wichmann, H. E. (1999). Increases in heart rate during an air
pollution episode. American Journal of Epidemiology, 150,
1094–1098.
33. Pope, C. A., III, & Dockery, D. W. (2006). Health effects of fine
particulate air pollution: Lines that connect. Journal of the Air &Waste Management Association (1995), 56, 709–742.
34. Sartori, C., Lepori, M., & Scherrer, U. (2005). Interaction
between nitric oxide and the cholinergic and sympathetic nervous
system in cardiovascular control in humans. Pharmacology andTherapeutics, 106, 209–220. doi:10.1016/j.pharmthera.2004.11.
009.
35. Shine, B., de Beer, F. C., & Pepys, M. B. (1981). Solid phase
radioimmunoassays for human C-reactive protein. Clinica Chi-mica Acta, 117, 13–23. doi:10.1016/0009-8981(81)90005-X.
36. Suwa, T., Hogg, J. C., Quinlan, K. B., Ohgami, A., Vincent, R., &
van Eeden, S. F. (2002). Particulate air pollution induces pro-
gression of atherosclerosis. Journal of the American College ofCardiology, 39, 935–942. doi:10.1016/S0735-1097(02)01715-1.
37. Talke, P., & Stapelfeldt, C. (2006). Effect of peripheral vaso-
constriction on pulse oximetry. Journal of Clinical Monitoringand Computing, 20, 305–309. doi:10.1007/s10877-006-9022-3.
38. Thomas, L. J., Picard, M. D., Miller, D. P., Adari, H., Beattie, D.
T., Emmett, C. D., et al. (2003). Modifications of the cholesterol-
fed rabbit model of atherosclerosis using diets with different
levels of cholesterol supplementation. Preclinica, 1, 60–69.
39. Wallenborn, J. G., McGee, J. K., Schladweiler, M. C., Ledbetter,
A. D., & Kodavanti, U. P. (2007). Systemic translocation of
particulate matter-associated metals following a single intratra-
cheal instillation in rats. Toxicological Sciences, 98, 231–239.
doi:10.1093/toxsci/kfm088.
40. Wesselkamper, S. C., Chen, L. C., & Gordon, T. (2005). Quan-
titative trait analysis of the development of pulmonary tolerance
to inhaled zinc oxide in mice. Respiratory Research, 6, 73. doi:
10.1186/1465-9921-6-73.
41. Wichmann, H. E., Mueller, W., Allhoff, P., Beckmann, M.,
Bocter, N., Csicsaky, M. J., et al. (1989). Health effects during a
smog episode in West Germany in 1985. Environmental HealthPerspectives, 79, 89–99. doi:10.2307/3430534.
42. Yamamoto, T., Bishop, R. W., Brown, M. S., Goldstein, J. L., &
Russell, D. W. (1986). Deletion in cysteine-rich region of LDL
receptor impedes transport to cell surface in WHHL rabbit. Sci-ence, 232, 1230–1237. doi:10.1126/science.3010466.
43. Yatera, K., Hsieh, J., Hogg, J. C., Tranfield, E., Suzuki, H., Shih,
C. H., et al. (2008). Particulate matter air pollution exposure
promotes the recruitment of monocytes into atherosclerotic pla-
ques. American Journal of Physiology. Heart and CirculatoryPhysiology, 294, H944–H953.
44. Zhang, S. H., Reddick, R. L., Piedrahita, J. A., & Maeda, N.
(1992). Spontaneous hypercholesterolemia and arterial lesions in
mice lacking apolipoprotein E. Science, 258, 468–471. doi:
10.1126/science.1411543.
206 Cardiovasc Toxicol (2008) 8:195–206