a gastroesophageal electrode for electrophysiological studies
TRANSCRIPT

A Gastroesophageal Electrode forElectrophysiological Studies
DAVID J. MCENEANEY, OMAR ESCALONA, JOHN A. ANDERSON, andA.A. JENNIEER ADGEY
From tbeteegional Medical Cardiology Centre. Royal Victoria Hospital, Belfast,land tbeBioengineWing Centre. University of Ulster, Jorclanstown. Nijrtbern Ireland '~^ ^
MCENEANEY DJ., ET AL.: A Gastroesophageal Electrode for Electrophysiological Studies. A novel gas-troesophageal electrode has been developed capable of atrial and ventricular pacing. We performed elec-trophysiological studies using the gastroesophageal electrode (Esothoracic) and compared the results withthe standard endocardial approach. The flexible polythene gastroesophageal electrode wns passed intothe stomach under light sedation. Five ring electrodes, now positioned in the km'er esophagus were usedfor bipolar atriai pacing and recording. Ventricular pacing was performed using a cathodic point sourceon the gastroesophageal electrode tip: the indifferent electrode (anode) was a high impedance chest pad.Parameters of sinus and AV nodal function were obtained by atrial pacing. Programmed ventricular stim-ulation was performed using a standard protocol. These electrophysiological parameters were subse-quently determined using the endocardia! approach. There was close correlation between measurementsof sinus and AV node function using the two approaches in 48 subjects: sinus node recovery time (SNRT)r^ = 0.70, corrected sinus node recovery time (CSNRT) i^ = 0.37. AV Wenckebach cycle length (AVWCL)r^ - 0.97. Tho degree of agreement between the two approaches was estimated by the mean difference 5and standard deviation of the difference a (SNRT 8 = 40 ms, a = 257 ms: CSNRT a = 14 ms, 8 = 164 ms:AVWCL a = 7 ms, 8=16 ms). Programmed ventricular stimulation was performed in 15 of 48 subjectswith knoivn or suspected ventricular tachyarrhythmias. Seven had ventricular tachycardia induced usingboth esothoracic and endocardia} programmed ventricular stimulation. One subject was noninducible us-ing esothoracic programmed ventricular stimulation, but inducible at endocardial electrophysiologicalstudies. Another subject was inducible at esothoracic electrophysiological studies, but noninducible us-ing endocardial programmed ventricular stimulation. Six subjects were noninducible using both endo-cardial and esothoracic programmed ventricular stimulation.The gastroesophageal electrode permitsreliable atrial and ventricular pacing without transvenous catheterization or fluoroscopy. Electrophysio-logical parameters determined using this electrode are similar to those obtained using endocardial stim-ulation.^fACE 1999; 22:487-499)
gastroesophageal electrode, electrophysiological studies
The work descriheti in this paper received the runner up awardin thi! tiournand and Coiiiroe Yuung Investigator Competition,Amt:ric:;in Heart A.ssociation 67th Scientific; Sessions, Dallas,November 1994. (McEneiiney D.|. An esothoracic pacing sys-tem for atrial and ventricular pacing and electrophysiologicalstudies. Circulation 1994; 90(suppl,):R),]
This work was supported in part by a Royal Victoria HospitalResearch Fellowship.
Address for reprints: A,A. Jennifer Adgey, M.D,. FACC, Car-diac Unit. Royal Victoria Hospital. CJrosvenor Road, BelfastBT12 6BA. Northern Ireland, Fax; (+44) 1232-312907.
Received January 13, 199fi; revised May 7, 1998; accepted May28. 1998,
Introduction
The investigation of atrial or ventricular tach-yarrhythmias often requires an electrophysiologi-cal study. This procodure involves positioningolectrode catheters in the atria or ventricles andobserving the response to programmed stimula-tion. The requirement for transvenous catheteriza-tion and fluoroscopy are obvious drawbacks.
Our objective was to perform an electrophys-iological study without transvenous catheter-ization or fluoroscopy. The left atrium lies ante-rior to the lower third of the esophagus. It iswell known Ihat a bipolar electrode positioned
PACE, Vol. 22 March 1999 487

MCENEANEY, ET AL.
in the lower esophagus is capable of atrial pac-ing. Parameters of sinus and atrioventricular(AV) nodal function determined by esophagealatrial pacing are comparable with those obtainedby the endocardial approach.' Ventricular cap-ture using a bipolar esophageal electrode is un-usual, due to the more anterior location of theventricles. We have developed a gastroesopb-ageal electrode capable of reliable atrial and ven-tricular pacing.^"' In the present study, wecompare the outcome of electrophysiolog-ical studies performed using the gastroesoph-ageal electrode with that obtained using a trans-venous approach.
Methods
Esothoracic Pacing
Gastroesophageal Electrode
The gastroesophageal electrode was de-signed in-house and manufactured by MeridianMedical Technologies, Columbia, MD, USA. It isa flexible polythene tube 60 cm in length and 4.0mm in diameter containing a pulley system per-mitting tbe distal 6.0 cm to he angled from 180"(fully extended. Fig. lA) to 90° [Fig. IB). A 6.0-mm diameter gold plated brass spbere fixed totbe electrode tip is used as the cathode duringventricular pacing. Atrial pacing is performed
Figure 1. Gastroasophageal electrode. {A} ^ extendedto ISO": (B) = at 90" angle.
using five ring electrodes constructed of goldplated copper wire at 2.0 cm spacing positionedproximally on the gastroesopbageal electrode.We have previously established the optimumconfiguration for atrial and ventricular pacingusing the gastroesophageal electrode.^ Atrialpacing is optimum using pairs of proximal ringelectrodes (bipolar), while ventricular pac-ing is optimum using the tip electrode ascathode in conjunction with a high impedancecbest pad (anode) placed medial to the apex(unipolar).
EsothoracJc Pacing
Subjects were recruited from those patientsadmitted to tbe Regional Medical CardiologyCentre, Royal Victoria Hospital, Belfast for per-manent pacemaker implantation or electropbysi-ological studies. Patients with a history of dys-phagia, dyspepsia, or upper gastrointestinal tractdisorder were excluded. All studies were per-formed after overnight fast if possible. Dentureswere removed if present. A cannula was insertedin a peripheral vein.
The subject was placed in a reclining posi-tion with the bed angled at 30° to tbe horizontal.Standard monitoring leads were attached. Self-adhesive defihrillation/cardioversion electrodeswere positioned in tbe anteroapical chest posi-tions so as not to come into contact with the highimpedance chest pad used during esothoracicventricular pacing. Cardiac rhythm was continu-ously monitored using a Hewlett-Packard Moni-tor/Defibrillator HP43120A (Hewlett-Packard,Andover, MA, USA). Aliquots (2.5 mg) of di-azepam (Diazemuls) were administered untilmild sedation was achieved. Tbe gastroesoph-ageal electrode was lubricated with nonconduc-tive gel. With the electrode in the fully extendedconfiguration (180°, Fig. lA) the electrode tipwas placed on the patient's tongue. With the co-operation of the patient, the electrode was swal-lowed or gently passed into the stomach. The tipwas then angled to 90° using the internal pulleysystem and gently withdrawn until it met the re-sistance of the gastroesophageal junction (Fig.IB). The electrode tip was now positioned in the
488 March 1999 PACE, Vol. 22

GASTROESOPHAGEAL ELEGTRODE EP STUDIES
Left Ventricle
Chest Pad (+ve)
Ventricular PacingElectrode {-ve)
Left Atrium
Atrial Recording and— Pacing Electrodes
Gastro-OesophageiilJunction
Figure 2. Gastroesophageal electrode positioned foratrial and ventricular pacing.
fundus of the stomach. Thus, the five ring elec-trodes (1,2,3,4,5 [labeled superiorly to inferi-orlyl) were positioned in the lower esophagus,lying behind the left atrium (Fig. 2).
Programmable Stimulator Interface
Standard programmable stimulators for endo-cardial electrophysiological studies generate max-imum currents typically around 10 mA at a maxi-mum pulse duration of 10 ms. Thresholds foratrial and ventricular capture using tbe gastroe-sophageal electrode are typically 10—20 niA (pulseduration 9 ms) and 20-30 mA (pulse duration 40ms), respectively.**'̂ ' Thus, a purpose built inter-face was constructed to allow triggering hy astandard programmable stimulator (UHS 20,Biotronic, Lake Oswego, OR. USA). The output ofthe stimulator interface was a square waveformpulse with amplitude and pulse duration continu-ously variable. Constant current waveforms withamplitude 0-100 mA and pulse duration 3—40 mswere thus obtainable. Standard ECG leads wererecorded with a bipolar esophageal electrogramon a multichannel recorder (Siemens Elema Min-gograf 62, Siemens, Stockliolm, Sweden). The am-plified signals were filtered at 5-10 Hz to reducepacing artifact.
Electrophysiological Studies
Electrophysiological studies were performedin those subjects, where indicated, as a part oftheir routine clinical management.
Esothoracic Electrophysiological Studies
Sinus node recovery time (SNRT) was mea-sured by esothoracic bipolar atrial pacing at120/min (cycle length 500 ms) for 30 seconds andrecording the interval in ms hetween the last pac-ing artifact and appearance of the first sinus beatafter cessation of pacing. Corrected sinus noderecovery time (CSNRT) was calculated hy sub-tracting the average of ten sinus cycle lengthsfrom SNRT.
Incremental esothoracic atrial pacing wasused to determine the AV Wenckebach point.Esothoracic ventricular pacing and bipolaresophageal atrial electrogram recording wereused to evaluate retrograde ventriculoatrial (VA)conduction. Tbe values of SNRT and CSNRT ob-tained from esothoracic and endocardial ap-proaches were used to classify subjects as hav-ing normal or abnormal sinus node function. Val-ues of 525 and 1,500 ms wore chosen as theupper limits of normal for CSNRT and SNRT,respectively.^'^
Programmed esothoracic ventricular stimula-tion was performed according to a standard proto-col recommended by the North American Societyof Pacing and Electrophysiology." As stimulationduring esothoracic pacing is possible from onlyone ventricular site, a stimulation protocol requir-ing only one ventricular site was chosen to main-tain equivalence with the ondocardial approach.This consisted of delivering single, double, andtriple ventricular extrastimuli in sinus rhythmand after paced drive trains of 100/min (600-mscycle length), 120/min (500-ms cycle length), and150/min (400-ms cycle length). Programmedesothoracic ventricular stimulation at 5 mA abovethreshold was commenced with an initial ex-trastimulus in sinus rhythm. Sinus beats weresensed via standard lead II. Coupling intervals forextrastimuli were decremented by 20 ms. Cou-pling intervals below 200 ms were not used so asto avoid nonspecific responses. If ventriculartachycardia (VT) was induced the cycle length,morphology, bemodynamic stability, and stimula-tion protocol at induction were documented. Ifhemodynamically stable VT was induced, over-drive pacing or extrastimuli were used to restoresinus rhythm; if this was unsuccessful or if
PACE, Vol. 22 March 1999 489

MCENEANEY, ETAL.
the arrhythmia was hemodynamically unstable,cardioversion was performed.
Endocardial Electrophysiological Study
Endocardial studies were performed within24 hours of esothoracic electrophysiologicalstudy, with no change in cardiac medication.Bipolar or quadripolar electrode catheters (Cordis,France) were positioned in high right atrium,coronary sinus, His-bundle region, and right ven-tricular apex as appropriate, via the femoral vein.A 5 Fr sheath was placed in the femoral artery forpressure monitoring where appropriate.
Tbe programmable stimulator (Biotronik UHS20) was connected directly to the temporary pac-ing electrodes. Sinus node recovery time, AVWenckebach cycle length (AVWCX) and VA con-duction were determined by atrial pacing. Forventricular programmed stimulation, pulse dura-tion was 2 ms and pulse amplitude twice diastolicthreshold. Ventricular programmed stimulationwas performed according to the same protocol, us-ing a single ventricular site at tbe right ventricleapex with three drive cycles and up to three ex-trastimuli. Parameters of sinus and AV node func-tion and inducihility or otherwise of ventriculartachyarrhythmia during esothoracic and endocar-dial studies were compared. If VT was provokedby botb techniques, the cycle length, morphology,and hemodynamic consequences of the VT werecompared.
Statistical Analysis
Statistical analysis was performed on a Mi-croVax computer using Statistical Package for theSocial Sciences (SPSS) software. Discrete variableswere analyzed using the cbi-square test of associa-tion. The correlation between continuous variablesdetermined by two techniques was analyzed usingcorrelation coefficients. The agreement betweenIwo techniques measuring the same continuousvariable was analyzed using the method of Blandand Altman.^ Results are expressed as mean ± SD.A P value < 0.05 was considered significant.
Informed consent was obtained from all pa-tients. This study was approved by the EthicalCommittee, Queen's University, Belfast.
Results
Atrial and Ventricular Pacing Thresholds
Threshold current for atrial capture was 14.3± 2.4 mA (range 2.5-23.6) using pulse duration9 ms. Threshold current for ventricular capturewas 26.2 ± 8.3 mA (range 9-42) at 40-ms pulseduration.
Parameters of Sinus and AV Node Function
Forty-eight subjects (37 male; age 66.2 years ±SD 13.7; range 30-72) participated in the study.Previous history of myocardial infarction, cardiacsurgery, and rhythm abnormalities in the studypopulation are shown in Table I.
Table I.
Previous Myocardial Infarction and Cardiac Surgery, Rhythm Abnormalities in the Study Populationlor Comparing Esothoracic and Endocardial Electrophysiological Parameters
18.837.512.556.2
4.295.8
20.829.2
Previous Myocardial Infarction:AnteriorInferiorAnterior and inferiorNo myocardial infarction
Previous Cardiac Surgery:Coronary artery bypass surgeryNo cardiac surgery
Rhythm Abnormality:Sinus node dysfunctionPrior ventricular arrhythmia
Number
9186
. 5 ^
246
1014
Total 48 subjects (37 male).
490 March 1999 PACE, VoL 22
GASTROESOPHAGEAL ELEGTRODE EP STUDIES
Sinus Cycle Length After Insertion ofGastroesophageal Electrode Gompared withEndocardial Study
The sinus cycle length after insertion of thegastroesophageal electrode was 894 ms ± SD 188.The sinus cycle length after endocardial catheter-ization, whether at transfemoral catheterization orpermanent pacemaker implantation, was 950 ms± SD 249 (P< 0.01).
SNRT and GSNRT
Average endocardial SNRT did not differ sig-nificantly from the value ohtained at esothoracicstudy (esothoracic SNRT 1,340 ms ± standard er-ror of mean (SEM) 60; endocardial SNRT 1,344 ms± SEM 68, P = NS). There was a reasonable corre-lation (r̂ = 0.70) between esothoracic SNRT andendocardial SNRT. To estimate the degree ofagreement between esothoracic and endocardialSNRT, the variance of the difference between theesothoracic and endocardial measurements wascalculated. The degree of agreement between thetwo methods is measured by the mean difference5 and SD of the difference CT.^ For SNRT S - 40 msand a = 257 ms: 95% of the differences lie in theinterval 8 ± 1.96CT, or -463 ms to +543 ms. Thisimplies that in the majority of cases, the differencebetween esothoracic and endocardial measure-ments of SNRT will lie between these values.
SNRT is influenced by a number of factors,among which are the resting sinus cycle length(SCL). As noted above, heart rate tended to begreater during esothoracic electrophysiologicalstudy; this may account for some of the discrep-ancy between esothoracic and endocardial SNRT:those subjects with increased resting heart rateduring esothoracic electrophysiological study willhave shorter SNRT. most likely a reflection of in-creased sympathetic tone. To account for the ef-fect of heart rate on SNRT, the corrected SNRT(CSNRT) is often quoted, calculated as (SNRT— SCL). Average endocardial CSNRT did not differsignificantly from the value obtained at esotho-racic study (esothoracic CSNRT 459 ms ± SEM 57,endocardial CSNRT 450 ms ± SEM 66, P = NS).
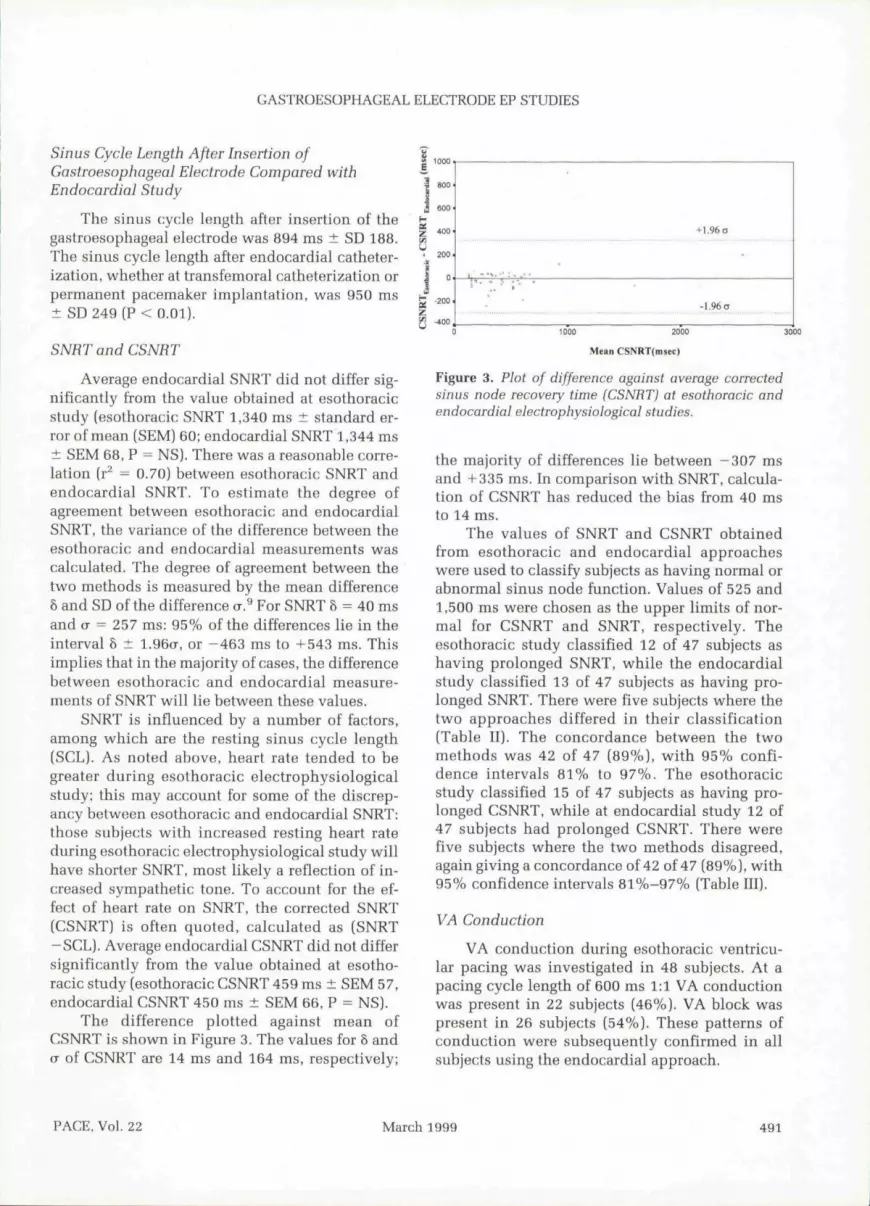
The difference plotted against mean ofCSNRT is shown in Figure 3. The values for 5 anda of CSNRT are 14 ms and 164 ms, respectively;
+1.96 (J
•1.96O
Mean
Figure 3. Plot of difference against average correctedsinus node recovery time (CSNHT) at esothoracic andendocardial electrophysioiogical studies.
the majority of differences lie between -307 msand -1-335 ms. In comparison with SNRT, calcula-tion of CSNRT has reduced the bias from 40 msto 14 ms.
The values of SNRT and CSNRT obtainedfrom esothoracic and endocardial approacheswere used to classify subjects as having normal orabnormal sinus node function. Values of 525 and1,500 ms were chosen as the upper limits of nor-mal for CSNRT and SNRT, respectively. Theesothoracic study classified 12 of 47 subjects ashaving prolonged SNRT, while the endocardialstudy classified 13 of 47 subjects as having pro-longed SNRT. There were five suhjects where thetwo approaches differed in their classification(Table II). The concordance between the twomethods was 42 of 47 (89%), with 95% confi-dence intervals 81% to 97%. The esothoracicstudy classified 15 of 47 subjects as having pro-longed CSNRT, while at endocardial study 12 of47 subjects had prolonged CSNRT. There werefive subjects where the two methods disagreed,again giving a concordance of 42 of 47 (89%), with95% confidence intervals 81%-97% (Tahle 111).
VA Gonduction
VA conduction during esothoracic ventricu-lar pacing was investigated in 48 subjects. At apacing cycle length of 600 ms 1:1 VA conductionwas present in 22 subjects (46%). VA block waspresent in 26 subjects (54%). These patterns ofconduction were subsequently confirmed in allsubjects using the endocardial approach.
PAGE. Vol. 22 March 1999 491

MCENEANEY, ETAL.
Table II.
Classification of Subjects as Having Normai (^ 1500 ms) or Abnormal (> 1500 ms) Sinus NodeRecovery Time (SNRT) from Esothoracic and Endocardiai Eiectrophysiological Studies
EndocardialSNRT
NormalAbnormal
Total
Esothoracic
Normal
323
35 (74.5)
SNRT
Abnormal
210
12(25.5)
Total
34 (72.3)13(27.7)47(100)
2 Tailed P 1 (McNemars Test)Concordance = 89% (95% confidence intervals 81% to 97%
Table III.
Classification of Subjects as Having Normal (^ 525 ms) or abnormal (> 525 ms) Corrected SinusNode Recovery Time (CSNRT) from Esothoracic and Endocardial Electrophysiological Studies
EndocardialCSNRT
NormalAbnormal
Total
Esothoracic CSNRT
Normal
311
32(68.1)
Abnormal
411
15(31,9)
Total
35 (74.5)12(25.5)47(100)
2 Tailed P = 0.375 (McNemars Test)Concordance = 89% (95% confidence intervals 81% to 97%)
=. 50
+1.96 o
-L96a
300 400 500 600 700
Mean AV Wenckebach cycle length (msec)
Figure 4. Plot of difference against average atrio-ventricular (A V) Wenckebach cycle length at vsothoracicand endocardial electrophysiological studies.
492 March 1999 PACE, Vol. 22

GASTROESOPHAGEAL ELECTRODE EP STUDIES
Table IV.
Classification of Subjects as Having Normal (< 400 ms) or Abnormal (> 400 ms) AV WenckebachCycle Length (AVWCL) from Esothoracic and Endocardial Electrophysiological Studies
Esothoracic AVWCL
Normal Abnormal Total
EndocardialAVWCL
Normal
Abnormal
19
1 26
21 (43.8)
27 (56.3)
Total 20(41.7) 28 (58.3) 48(100)
2 Tailed P = 1 (McNemars Test)Concordance = 94% (95% confidence intervals + 7%)
AV Wenckebach Gvcle Length
AVWCL was slightly shorter at esothoranicstudy than at endocardial (433 ms ± SEM 13 eso-thoracic vs 440 ms ± SEM 13 endocardial. t = 3.12,P = 0.003). There was a high degree of correlation(r̂ = 0.97) between the values obtained using thetwo methods. The difference in esothoracic and en-docardial AVWCL is plotted against moan AVWCLin Figure 4, In the difference plot S and a are 7 and16 ms, respectively. Thus, in most cases, the differ-ence in AVWCL as measured by esothoracic and en-docardial approaches will lie in the range -24.4 to+ 38.4 ms. These margins of error are less than thoseobtained for the parameters of sinus node function;thns there is more agreement between values ofAVWCL at esothoracic and endocardial electro-physiological study than for CSNRT. Subjects wereclassified as having "normal" AV conduction if AVconduction was intact at atrial pacing rates greaterthan 150/min (cycle length 400 ms) and "abnormal"AV conduction if Wenckebach block was presentbelow this rate. Using this criterion 27 (56.3%) sub-jects were classified as abnormal at endocardialstudy and 28 (58.3%) at esothoracic study (TahleIV). The concordance between the two techniqueswas 94%, with 95% confidence intervals ± 7%.
Programmed Ventricular Stimulation
In addition to determination of sinus and AVnode parameters, programmed ventricular stimu-lation was performed in 15 subjects. Endocardialelectrophysiological studies were performed us-ing the same stimulation protocol in these 15
subjects during the same hospital admission,usually within 24 hours of the esothoracic elec-trophysiological study. Antiarrhythmic medica-tions remained unaltered between esothoracicand endocardial electrophysiological studies.The medical history, clinical presentation, con-current antiarrhythmic therapy, and outcome ofendocardial and esothoracic electrophysiologicalstudies, inchiding programmed ventricular stim-ulation, are summarized in Table V. If VT was in-duced, the morphology, cycle length, hemody-namic stability, and coupling intervals at whichthe arrhythmia was induced are noted. An exam-ple of induction of VT induction is shown in Fig-
Figure 5. Induction of ventricular tachycardia (VT) atesothoracic electrophysiological study. After a paceddrive train (150/min) and two coupled frxtrastimuti VTrate 145/min is induced. Ventriculoatrial (VA) dissoc-iation is evident on the esophageal electrogram duringVT. Standard leads I. III. Vl with bipolar esophagealelectrogram (Es), Paper speed 25 mm/s.
PACE. Vol. 22 March 1999 493

Table V.
Summary of Esothoracic and Endocardial Electrophysiological Studies
Patient Age Sex History
Anti-ArrhythmicMedication ECG CSNRT AVW
VTESO
VES
YES
YES
YES
VTENDO
YES
YES
YES
NO
VTCL,MORPH,HEUO,(ESO)
Z70
RBBB
Stabie
310
RBBB
Stable
STB
RBBB
Stabie
W9
RBBB
iJnsiable
VTCL,MORPH,HEMO,(ENOO)
300
RBBB
Stabie
325
RBBB
Stable
400
RBBB
Stable
N/A
IND.ESO
D500
Cl 230
C2 240
D600
C1 270
C2 300
D400
C1 240
C2 320
D400
Cl 260
C2 280
C3 280
iND.ENDO
D500
CI300
02 260
C3 260
D500
C1 270
C2 300
D60G
Cl 280
C2 320
N/A
53
36
i^ype(1ensjon
Previous VT
Amiodarone
Mexileline
SR
LBBB
54
Previous repairol mitrai vaivepeoiapse withregurgilationPrevious VF
IHD, previousCABG, earty
LV aneurysm,EF 24%
Previous VT
Previousanterior Mi,ventricularaneurysm
Outolhospital VF,
Syncope,complex
ventricularectopy on
Holter
Previousanterior Ml,
EF 26%Out ot
hospital VF.
PreviousMl
sustainedVT
Dilatedcardio-
myopathynonsustained
VT
Previousmyocardialinfarctions,sustained
VT
ischaemicheart diseaseout of hospitai
VF
ischaemicheart diseaseout ot fiospitai
VF
Amiodarone
Mexiietine
Digoxin
Amiodarone
Mexiietine
Digoxin
Metoprolol
None
Atenolol
Amiodarone
Uexitetine
Digoxin
soiaioi
amiodarone
metoprolol
None
Mexiiitene
SR
SR
Anterior
Ml
SR
LBBB
SR
SR,
Anterior
M<
SR
antehor
Ml
SR
SRanterior
and
infenorMl
SR
Inferior
Ml
SR
LBBB
(A) 110 (A) 500 (A) 220
(B)130 (B)460 (B)280
(A) 160 (A) 520 (A) 280
(B)150 (B)545 (B)280
(A) 140 (A) 410 (A) 220
(B|155 (B)480 (B)300
(A) 130 (A) 365 (A) 280
(B)nO (B)350 (BJ300
(A) 120 (A) 500 (A) 240
(B)100 (B)520 (B)200
(A) 130 (A) 545 (A)260
(B) 120 (B| 500 (B)280
(A)130 (A)360 {A)240
{B)365 (B) 260
(A) 125 (A) 390 (A) 240
(B)135 (B)410 (B)200
(A)130 (A)375 (A)260
(B)150 IB) 390 (B)220
(A)105 (A) 415 (A) 320
(B) 130 (8)400 (B)300
(A) 130 (A) 440 |A]290
(B) 125 (B)445 (B) 300
NO NO N/A
300
YES YES RBBB
Unstable
NO YES N/A
NO NO N/A
YES YES HBBB
Stable
NO NO N/A
YES YES LBBB
unstable
300
RBBB
Unstable
310
RBBB
Stable
0 600
Cl 280
02 240
03 260
N/A
D400
Cl 280
02 240
C3 2B0
SR
01 300
C2 280
C3 260
N/A N/A
340
RBBB
Stable
D600
Cl 230
C2 300
D400
01 260
C2 220
C3 230
N/A N/A N/A
300 D 600 D 600
LBBB C1 290 Cl 320
unstable C2 240 C2 360
494 March 1999 PACE, Vol. 22

GASTROESOPHAGEAL ELEGTRODE EP STUDIES
Patient
L
M
N
0
Age
55
62
58
71
Sex
M
M
M
M
History
Previousanterior MlRecurrent
stableventricular
tachycardia.
Previousanterior Ml
Out of hospitalVF
Hype rlro phi ccardio-
myopathy,Syncope
Previousanterior Ml,
NonsustainedVT
Anti-ArrhythmicMedication
Amiodarone
Amiodarone
Amiodarone
Metoproiol
ECG
SR
Anterior
Ml
SR
Anterior Ml
Sfl, LVHwitti repolar-isaiionabnormality
SR LBBB
Table V.
(Continued)
CSNRT
(A) 130
(B) 120
(A)150
(B) 180
(A) 130
(6) 125
(A)125
(B) 135
AVW
(A) 400
(B)415
(A) •• 365
(B) • 365
(A) 440
(B)445
(A) 400
(B) 440
VRP
(A) 280
(B) 280
(A) 260
(B) 240
(A| 290
(B) 300
(A) 230
(B) 350
VTESO
YES
NO
NO
NO
VTENDO
YES
NO
NO
NO
VTCL,MORPH.HEMO,(ESO)
390
RBBB
Stable
N/A
N/A
N/A
VTCL.MORPH.HEMO,(ENDO)
390
RBBB
Stable
N/A
N/A
N/A
IND.ESO
SH
C1 320
C2 330
C3 360
N/A
N/A
N/A
IND,ENDO
D600
C1 300
C2 320
N/A
N/A
N/A
esottiofacic eiectrophysioiogical study; B ^ endocardiai electrophysiologic
ure 5. Of the 15 subjects evaluated, seven hadVT induced using both esothoracic and endo-cardial programmed ventricular stimulation.One suhject was nouinducible using esothor-acic programmed ventricular stimulation, hutinducible at endocardial electrophysiolog-ical study. Another subject was inducible atesothoracic electrophysiological study, but non-inducihle using endocardial programmed ven-tricular stimulation. Six subjects were non-inducible using both endocardial and eso-
thoracic programmed ventricular stimulation.Concordance is 87% hetween the two ap-proaches, alheit with wide confidence intervals(Tahle VI).
The induction sequence (i.e., pacing drive cy-cle length and coupling interval of extrastimuli)tended to vary between esothoracic and endocar-dial study when VT was induced at both (TahleV), The esothoracic and endocardial pacing drivecycle length and extrastimuli coupling intervals atinduction of VT were broadly similar in subjects
Table VI.
Inducibility of Ventricuiar Tachyarrhythmias During Endocardial and Esothoracic ProgrammedVentricular Stimulation
EndocardialProgrammedStimuiation
InducibleNoninducible
Total
Esothoracic Programmed Stimulation
Inducible Non-inducible
7 11 6
8(53.3) 7 (46.7)
Total
8 (53,3)7(46.7)
15(100)
Concordance = 87%; 95% confidence intervals ± 35%
PACE, Vol. 22 March 1999 495

MCENEANEY, ET AL.
450
400
350
300
250
.00
Esothoracic
^ stable
Endocardial
Unstable
Figure 6. Comparison of cycle lengths and hemo-dynomic consequences of ventriculartachycardia (VT) induced at esothoracic and endocardial electro-physiological studies.
B, C, and F. In subjects A, I, and L VT was inducedat a somewhat more aggressive stage of the proto-col using the endocardial approach. For example,suhject A had VT induced during esnthoracic elec-trophysiological study using a 500-ms drive cyclelength with two coupled extrastimuli at 230 msand 240 ms. At endocardial electrophysiologicalstudy VT was induced using the same 500-msdrive cycle length but in this instance requiringthree extrastimuli at 300, 280, and 260 ms. How-ever, when VT was induced using both esotho-racic and endocardial approaches, the morphol-ogy and hemodynamic consequences were similar(Table V, Fig. 6). Two subjects had VTs whichwere pace terminable using overdrive esothoracicventricular pacing.
The average dose of sedation administeredwas 7.6 mg (range 2.5^15 mg) diazepam (Di-azemuls). No complications were observed in thestudy group. There were no cases of diaphrag-matic stimulation.
Discussion
The aim of this investigation was to develop apacing system that would have potential use inclinical electrophysiology. We have previouslydemonstrated tbe feasibility of reliable atrial andventricular pacing using the gastroesophagealelectrode.^"^ The electrode has been effective inthe emergency management of acute hrad-yarrhythmias." In a comparison of esothoracic
ventricular pacing and external (transcutaneous]pacing, ventricular capture was more frequent andpacing threshold was lower using the esothoracicapproach.' In the present study, we compared tbeoutcome of electropbysiological testing using tbeesothoracic approach with results obtained via en-docardial stimulation.
Sinus Cycle Length During Esothoracic andEndocardial Electrophysiological Testing
Instrumentation of the upper gastrointestinaltract may he associated with arrhythmias includingsinus tachycardia.^" The resting heart rate duringesothoracic electrophysiological study was slightlygreater than that during endocardial electropbysio-logical study. Tbis would be consistent with agreater level of sympathetic tone following insertionof tbe gastroesopbageal electrode compared withtransvenous catheterization. In a study of 20 subjectsLe Heuzey et al.̂ ^ also detected a small but signifi-cant rise in beart rate after insertion of an esopbagealelectrode compared witb endocardial catheteriza-tion; this was interpreted as a reflection of sympa-thetic overactivity, Others have found no differencein resting sinus cycle length wben esophageal andendocardial methods were compared.^^
Sinus Node and AV Node Function
In tbe present study, there was close correla-tion between the values for SNRT and CSNRT ob-
496 March 1999 PACE, Vol. 22

GASTROESOPHAGEAL ELECTRODE EP STUDIES
tained using endocardial and esothoracic meth-ods. SNRT and CSNRT at esothoracic study ex-ceeded by an average of 40 and 14 ms, respec-tively, the values obtained at endocardial study.Esotboracic atrial pacing differs from the endocar-dial approach in several respects. First, atrial acti-vation during esopbageal pacing differs from thepattern observed with endocardial pacing. Duringendocardial stimulation the electrode is posi-tioned in the bigb right atrium close to the sinusnode. The gastroesopbageal electrode activatesthe left atrium first, followed by conductionacross the interatrial septum to tbe right atrium,and tben to the sinus node. Thus, the conductiontime of an esotboracic atrial pacing impulse fromesophagus to sinus node will be prolonged incomparison to the endocardial pacing stimulus.In addition, conduction hlock could occur at oneor more of several atrial structures prior to reach-ing tbe sinus node, which would in turn be re-flected in prolonged SNRT and CSNRT. Eso-phageal leads have been used to investigateintraatrial and interatrial conduction times. Thesestudies showed tbat normal interatrial conduc-tion time was approximately 40 ms, with prolon-gation to 90-lOOms in subjects with paroxysmalatrial arrhythmias, in particular atrial flutter.^'Thus, interatrial conduction time may account inpart for tbe prolongation of esotboracic SNRT andCSNRT compared witb endocardial values. As aconsequence of the greater distance hetween stim-ulation site and sinus node, prolongation of indi-rectly lueasured parameters of sinus node func-tion as determined by esothoracic atrial pacingmay be due to ahnormai intraatrial and interatrialconduction in addition to defective atriosinus andsinoatrial conduction and reduced sinus node au-tomaticity. Otber authors have reported variableeffects on sinus node parameters when esopha-geal and endocardial methods are compared. LeHeuzey et al.̂ ^ noted prolongation in hoth sino-atrial conduction time (SACT) and CSNRT usingthe esopbageal technique; tbey attributed this tothe greater delay inherent in conduction of theatrial activation wavefront from esophagus to si-nus node. Cebron et al.^'' found no significant dif-ference in CSNRT wben measured using the twoapproaches. In contrast, Blomstrom-Lundqvistand Edvardsson^^ found a trend toward a shorterSACT with esophageal stimulation. They at-
tributed tbis to sympathetic overactivity duringesopbageal pacing causing enbanced retrogradeand anterograde sinoatrial conduction. ^̂
When subjects were classified as having nor-mal or abnormal sinus node function based on thevalues of SNRT and CSNRT obtained at eso-thoracic and endocardial study tbere was goodconcordance (89%, 95% confidence intervals81%-97%) between the two approaches. Tberewas misclassification in only 5 of 47 subjects.
In addition to evaluating sinus node function,atrial pacing permits assessment of tbe functionalproperties of tbe AV node. The average cyclelength at which AV Wenckebach conduction oc-curred during esothoracic study was 433 ms,slightly less tban tbe value at endocardial study(440 ms). As already noted, tbe higber heart rateduring esothoracic studies may reflect increasedsympathetic tone: this could also influence the cy-cle length at wbicb AV Wenckebach conductionoccurs. One previous study reports AV Wencke-hach occurring at a slightly shorter cycle lengthwith esophageal atrial pacing than witb endocar-dial pacing'"*; however another reported no differ-ence between tbe techniques.^^ There was goodagreement between esotboracic and endocardialvalues of AVWCL, witb most of the difference inmeasurements in the range -24 to +38 ms (Fig. 4).When classified as "normal" or "ahnormai" ac-cording to Wenckebach cycle length above or be-low 400 ms (atrial pacing rate 150/min). 27(56.3%) subjects were abnormal at endocardialstudy and 28 (58.3%) abnormal at esotboracicstudy (concordance 94%). Given the otber limita-tions of the study, including tbe influence of auto-nomic tone during esothoracic stimulation, tbisdegree of agreement would appear satisfactory forclinical purposes. One limitation of tbe esotbo-racic approach is the ahsence of a His-hundle eiec-trogram allowing precise identification of the siteof AV block,
VA conduction is present in approximately30%-70% of subjects witb normal anterogradeAV conduction, depending on tbe populationstudied.'-'^ In this study 1:1 VA conduction waspresent in 21 subjects (45%) during ventricularpacing at 100/min. VA hlock was observed in 26subjects (55%). These patterns of conduction weresubsequently confirmed in all subjects using theendocardial approach.
PACE, Vol. 22 March 1999 497

MCENEANEY, ETAL.
Programmed Ventricular Stimulation
In 1972, Wellens et al.̂ ** descrihed the repro-ducible initiation and termination of ventriculartachyarrhytbmias using programmed ventricularstimulation. Since then, the technique bas beenextensively used in the evaluation of ventriculararrhythmias. In recent years, some doubt has beencast over the validity of programmed stimulationin certain situations, partitiularly in guiding an-tiarrhythmic therapy. Nonetheless, electropbysio-logical testing, in conjunction with clinical find-ings, still bas an important role to play in the riskstratification of patients with VT,̂ ^
Programmed atrial stimulation bas heen per-formed using a bipolar esophageal electrode, per-mitting induction and termination of supraventric-ular arrhythmias.' Induction and termination ofVT using programmed ventricular stimulation viaan esophageal electrode has not previously beenreported. Of tbe 15 subjects studied, seven had VTinduced using botb esothoracic and endocardialprogrammed ventricular stimulation. One subjectwas noninducible using esothoracic programmedventricular stimulation but was inducible at endo-cardial electropbysiological study. Anotber sub-ject was inducible at esotboracic electrophysiolog-ical study but noninducible using endocardialprogrammed ventricular stimulation. Six subjectswere noninducible using both methods. Two sub-jects had VTs that were pace terminable usingoverdrive esothoracic ventricular pacing.
Wbere VT was induced using hoth ap-proaches, tbe cycle length, morphology, andhemodynamic consequences were similar (TableV. Fig. 6). Tbis suggests thai ibe same anatomicalpathway for reentry during VT was used duringesothoracic and endocardial studies. The pacingdrive rate and coupling intervals for extrastimuliat which VT was induced during endocardial andesothoracic studies were not identical, but didtend to he at approximately the same stage of thestimulation protocol. Studies of the day to day re-producibility of endocardial programmed ventric-ular stinuilation have shown tbat tbe number ofextrastimuli required for VT induction varies by atleast one extrastimulus in over 70% of patients.^"In addition, the cardiac site of stimulation may in-fluence the coupling intervals necessary to pro-voke reentry. During the endocardial study, stim-ulation is performed at the right ventricular apex;
the exact site of ventricular activation duringesotboracic ventricular stimulation is uncertain,but the morphology of paced beats is dissimilarfrom endocardial paced heats. Tbis suggests tbatduring esotboracic pacing cardiac activation isinitiated at a different point, perhaps tbe inferiorsurface of the left ventricle. There is some evi-dence tbat autonomic tone is increased duringesotboracic pacing (e.g., the marginally bigherresting sinus rate). Altered autonomic tone mayalso affef:t Ibe cycle length of induced VT. Giventhese factors, it is thus unlikely that VT would beinduced using the identical protocol of extrastim-uli using the two approaches.
In terms of inducibility of VT, tbe concor-dance between esotboracic and endocardial pro-grammed stimulation in the present study was87%, although the small study group renders theconfidence intervals large. It is unlikely tbat thetwo approaches would give exactly tbe same out-come in terms of inducihility. For one reason, theday to day reproducibility of induction of VT atendocardial electrophysiology study may vary. Ifonly sustained monomorpbic VT is considered,most investigators report day to day reproducibil-ity of 80%-90%.''*'^" For otber ventricular ar-rbythmias, in particular polymorpbic VT and ven-tricular fihrillation, the day to day reproducibilityis usually lower.^^ In our present study, one sub-ject (D) bad VT induced by esothoracic hut not en-docardial stimulation. This suhject presentedwitb cardiac arrest (ventricular fibrillation) on abackground of chronic ischemic beart disease.Ventricular arrhythmia was induced at a relativelyaggressive stage of tbe protocol, using three cou-pled extrastimuli after a rapid (150/min) pacingdrive train. In a study of the day to day repro-ducibility of ventricular arrhythmias using endo-cardial programmed stimulation those subjects re-quiring multiple extrastimuli for induction bad alower reproducibility of arrhythmia induction.^^
Since Wellens et al.^'' described tbe inductionof arrhythmias using programmed stimulationover two decades ago, the technique has becomewidely accepted as a standard investigation in pa-tients with supraventricular and ventricular ar-rhythmias. In current cardiological practice, elec-trophysiological studies are performed usingtemporary pacing electrodes positioned using flu-oroscopy. Tbe requirement for sterile precautions
498 March 1999 PACE. Vol. 22

GASTROESOPHACEAL ELECTRODE EP STUDIES
and tbe potential hazards of transvenous catheter-ization necessitate skilled personnel. While it isrecognized that endocardial catheterization willbe necessary in some cases, tbere remains a largeproportion of electrophysiological studies wheretbe information required is relatively straightfor-ward, consisting of simple parameters of sinusand AV node function and tbe response to pro-grammed atrial and ventricular stimulation.
The esothoracic pacing system allows assess-ment of sinus and AV node function and pro-grammed stimulation. Transvenous catheteriza-tion and fluoroscopy are not required. Thetechnique may be useful as a screening electro-physiological investigation in suspected conduc-tion system disease and for programmed ventricu-lar stimulation in patients witb known orsuspected ventricular arrhythmias.
References
1. Santini M, Ansalono G, Cacciatore G, nt al, Trans-tisophageai pacing. PACE 1990; 13:1298-1323.
2. McEneanoy DJ, Cochrane DJ. Adgey AA). Use ofthe ga.stro-esophageal route for the rapid nstablish-mtmt of ventricular pacing, Int } Carcliol 1994;46:275-278.
3. McEneaney D). An esothoracic: pacing system foratrial and ventricular pacing and electrophysiolog-ical studies. Cournand and Comroe Young Investi-gator Finalist, American Heart Association 67thScientific Sessions, Dallas, November 1994, Circu-lation 1994; 90{Suppl,):I-(>.
4. McEneaney D, Adgey }, Anderson J. Optimum elec-trode configuration for a novel esothoranic pacingsystem, (abstract) PACE 1993; 16 (Pt, II):852.
5. McEneaney DJ, Cochrane D], Adgey AAI. t't al. Anovel gaslro-esophageal electrode for atrial andvontricular pacing. PACE 1997; 20:1815-1825.
6. Narula OS, Samet P, lavier RP. Significance of thesinns node recovery time. Circulation 1972; 45:140-157.
7. Fisher JD, Role of electrophysiologic testing in thediagnosis and treatment of' patients with knownand suspected bradycardias and tachycardias.Prog Cardiovasc Dis f981; 24:25-90.
8. Waldo AL, Akhtar M, Brugada P et al. The mini-mally appropriate electrophysiologic study for theinitial assessment of patients with documentedsustained monomorphic ventricuiar tachycardia. JAm Coll Cardiol 1985; 6:1174-1177.
9. Bland JM, Altman DG, Statistical methods for as-sessing agreement between two methods of clini-cal measurement. Lancet 1986; 1:307-310.
10, Lieberman DA, Wuerker CK, Katon RM. Car-diopulmonary risks of esophagogastro-duo-denoscopy. Gastroenterology 1985; 88:468-472,
11, Le Heuzey JY, Khaznadar G. Guize L. et al. Thestudy of sinus node function and nodal conduc-tion hy oesophageal recordings. Arch Mai Coeur1987; 80:28-35.
12, Blomstrom-Lundqvist C, Edvardsson N. Trans-cfsophageal versus intracardiac atrial stimulationin assessing eiectrophysiologic parameters of the
sinus and AV nodes and of the atrial myocardium.PACE 1987; 10:1081-1095.
13. LoiorCV, Meacham JA, Schaal SF. Prolonged atrialconduction—-A major predisposing factor for thedevelopment of atrial flutter. Circulation 1978;57:213-216.
14. Cebron IP, Brugada J. Gallay P, et al. Comparativestudy of transoesophageal and intracavity pacingfor the evaluation of sinus node and atrioventricu-lar node function. Arch Mai Coeur 1987; 80:170-175.
15. Akhtar M. Retrograde conduction in man. PACE1981; 4:548-562.
16. Wellens HJJ, Schuilenhurg RM, Durrer D. Electri-cal stimuiation of the heart in patients with ven-tricular tachycardia. Circulation 1972; 46:216-226,
17. Garratt C). Who needs ventricular stimulationstudies? Br Heart J 1994; 71:307-308.
18. Cooper MJ, Hunt LJ, Palmer KJ et al, Quantita-tion of day to day variability in mode of induc-tion of ventricular tachyarrhythmias by pro-grammed stimulation. J Am Coll Cardiol 1988;11:101-108,
19. Bigger IT, Reiffel JA, Livelli ED. et al. Sensitivity,specificity and reproducibility of programmedventricular stimulation. Circulation 1986; 73(Suppl. II):lI-73.
20. Roy D, Marchand E, Theroux P et al. Long term re-producihility and significance of provokahle ven-tricular arrhythmias after myocardial infarction. JAm Coll Cardiol 1986; 8:32-39.
21. McPherson CA, Rosenfeld LE, Batsford WP. Day today reproducibility of responses to right ventricu-lar programmed electrical stimulation: Implica-tions for serial drug testing. Am J Cardiol 1985;55:689-695.
22. Kudenchuk PJ, Kron J, Walance CC, et al. Repro-ducibility of arrhythmia induction with intracar-diac electrophysiologic testing: Patients with clin-ical sustained ventricular tachyarrhythmias. J AmColl Cardiol 1986; 7:819-828. '
PACE, Vol. 22 March 1999 499
