a change to electronic medication
TRANSCRIPT
University of West LondonTheoretical Assessment Submission by TurnItin
NOTE TO ALL STUDENTS: Please complete section 1 of thisform as indicated. Please ensure that all relevant boxesare completed, otherwise assignments cannot be processedefficiently.
Section 1 (Student to complete) Please type clearly in the boxes provided
AssignmentTitle A Change to Electronic Medication in Mental
Health Hospitals using Kurt Lewin’s Change Management Theory
Student No 21183883
Module TitleDeveloping Innovative Practice
Module Code Module 3: AY2013-2014
Attempt 1st X 2nd
Programme Post graduate Diploma in Mental Health
Branch (IfApplicable)
Paragon House London
Intake September 2012 Group PGDip
Tutor Deborah Taylor
Word Count 3 3 3 2 Due Date 2 3 0 6 1 4
ExtensionAgreed
Yes No X (If YES provide Reference Number below)
Date ofextension
Student with Yes No X (If YES provide Reference Number below)Disability
Declaration: I confirm that I understand theUniversity's policy on plagiarism and I understand that Iwill be penalised if this assignment infringes that policy.I am also aware of the regulations governing claims formitigation, which should normally be submitted within 10
1
X
working days of the date of the examination/submission. Iunderstand it is my responsibility to keep a copy of thework submitted (Please refer to student Handbook for furtherdetails).I also accept that by my act of Submitting this of assignment, I agree with above Declaration
A change to Electronic Medication in MentalHealth Hospitals
Using Lewin’s Change Management Theory
Introduction Technological revolution in the area of computer
electronic services has changed the way healthcare
services are being delivered. The introduction of the
computer and computer networking system in health care
services have meant that the traditional paper works and
paper filing systems are giving way to electronic
services in the healthcare system. One obvious reason
why some areas of the healthcare services are reluctant
to embrace technological changes is the challenges it
will pose to the healthcare practitioners during
implementation. There is a hidden fear that a switch to
the digital system could produce anxiety which can lead
to resistance to adopt the new changes. Electronic
medication system will reduce medication errors which
often lead to fatal consequences. There are a surveys
that shows that nurses spent more than thirty minutes of
every hour of patient care on paper work
(PricewaterhouseCoopers, , 2001) and another that says
2
that three hours of a nurse shift is spent on documenting
clinical information (Poissant et al. 2005). Electronic
Medication system will save time that can be spent on
other areas of patient’s care delivery. Electronic
medication will also reduce the possibility of lost or
damaged to information which is common in manual
documentation (Curtis, 2011) and will facilitate
information transfer between professional without the
need to schedule meetings for the purpose of exchanging
documents. (Saranto & Kinnunen, 2008). This essay will
show how electronic medication system can be implemented
in our mental health hospitals using the framework of
Kurt Lewin’s “change management theory”.
Medication errors in our hospitals include: being
administered the wrong type or dose of medicine, placing
a patient on the same medication for too long,
administration of a medication for which a patient is
allergic to, prescription of a group of medication that
should not be taken together, giving a medication meant
for one patient to another and the administration of
incomplete course of medication to a patient. (MMD, 2008)
In a review of reported medication errors incidents
between 2005 and 2010 carried by Medicines and
Healthcare Products Regulatory Agency (MHRA) and NHS
England, 525, 1860 medication error incidents were
reported. Of this number, 86,821 (16%) reported actual
3
patient harm and 822 (0.9%) resulted in death or severe
harm (MHRA, 2013). It must be emphasised that there are
many unreported cases of medication errors in our
hospitals because cases are mostly reported when harm is
involved or when there is a courageous whistle blower at
the point of incident.
Many strategies and ideas have been developed and put
forward to reduce the possibility of prescribing,
dispensing and administering medication in error. The
American Society of Hospital Pharmacists (ASHP, 1993) has
suggested that to reduce medication errors:
..effective systems for ordering, dispensing,
and administering medications should be
established with safeguards to prevent the
occurrence of errors. These systems should
involve adequately trained and supervised
personnel, adequate communications, reasonable
workloads, effective drug handling systems,
multiple procedural and final product checks by
separate individuals, quality management, and
adequate facilities, equipment, and supplies
(ASHP, 1993).
Even with these checks in place, current medication
procedure in our mental health hospitals which involves
the use ledgers and charts to manually checks and
document medication administration is prone to errors.
4

This paper will discuss how electronic medication such as
bar coded medication, automated dispensing machine and
electronic medication recording can significantly reduce
medication errors. The paper will show how Kurt Lewin’s
change management theory can be used to guide the process
of implementing this change in a mental health setting.
We will discuss how Kurt Lewin’s change management theory
can be use to support staff especially nurses many of
whom are sceptical, or lack confidence in the face of new
technologies and transitions. Through a careful planned
change, the theory will be used to identify areas of
strength, weakness and resistance prior to implementation
of the change to ensure that mistakes that could have
adverse effects on the patients are not made.
The Importance of Electronic MedicationThe National Patient safety Agency (NPSA) define
medication errors as “incidents in which there has
been an error in the process of prescribing,
dispensing, preparing, administering, monitoring, or
providing medicine advice, regardless of whether any
harm occurred” (NPSA_NHS, 2007. p. 9). Medication
error occurs in healthcare establishments all over
the world and can result in serious harm or death,
longer stay of patients in hospital, increase in
5
cost of treatment and the lost of public confidence
on healthcare practitioners. The department of
health estimates that 4.7 percent of the total
admissions in NHS hospitals, England are due to
avoidable (definitely preventable) harm from
medicines and medication errors. It estimates the
financial cost of these admissions to be in the
ranged of £200- £400 million annually (NPSA_NHS,
2007). The department of health also estimates that
around 7% of inpatients experience adverse drug
reactions (ADRs), in NHS England (NPSA_NHS, 2007).
Assuming that a similar percentage of inpatient
medication incidents were preventable, it will add
up to an annual cost of £410 million to NHS England
(NPSA_NHS, 2007). If what is known about litigation
cost was added to the costs mentioned above, we
could say that the cost of preventable harm from
medicines to NHS England exceeds £750 million a year
(NPSA_NHS, 2007). We must also add that very little
is know about preventable harm from medicines at
community level in NHS England where most drugs are
prescribed and administered by the GPs and the
community health care system (NHS_NPSA 2007, p. 12).
The less recognised and discussed aspect of
medication error is the harm to morale, lost of work
time or very often lost of job suffered by nurses
who are the last line of defence against error
medication error. The nurse is expected to combine
6
the knowledge and work of the doctor and pharmacist,
recognise any potential harm from a medication and
stop the administration otherwise she faces the
consequences of administering the medication in
error because according to the NMC ‘Standards for
medicines management’, medication “is not solely amechanistic task to be performed in strict compliance
with the written prescription of a medical
practitioner…... It requires thought and the exercise
of professional judgement...” (NMC, 2007 p. 3)
The technology involved in medication that have been
tested and are being used in different countries of the
world and in some NHS hospitals are: bar coding scanning
medication administration (BCMA), electronic medication
recording (EMR), computerised physician order entry
(CPOE) and automated pharmacy dispensing machines (APDM)
(Appari, et al, 2011). Bar coding (BCMA) technology
involves the scanning of bar codes on medicine packets,
patients’ wrist bands and codes on the medication charts
(Appari, et al, 2011). Mental health patients may not
like to wear a hand band as inpatients in general
hospital but the bar code on the medicine packets and the
patient’s chart will fill that vacuum. The computerised
physician order entry (CPOE) will save the amount of
papers needed for medication documentation, reduce
transcription errors from bad or ineligible handwriting
and remove the problem of missed signature. Electronic
7

medication recording (EMR) will save documentation
resources, ensure that the time, date and signature of
the person who administered the medication are visible
and accurate and that the record is available to all
departments of the hospital who might need them in real
time. The automated pharmacy dispensing machines (APDM)
will reduce the error of dispensing underdose or overdose
and will also reduce the chances of wastage through
medication slipping from the fingers to the floor. In
all, electronic medication system verifies several
elements of the patient to make sure that the right
medicine is being administered to the right patient at
the right time, dose, route and frequency and it does so
in speed and accuracy thereby saving time and error that
could occur through manually flipping through piles of
paper work.
Change Management: Lewin’s Change ManagementTheory
In any healthcare system, nurses are major players in the
implementation of health policies and are therefore
expected to be up to date and embrace developments that
will lead to improvement in health care delivery.
Unfortunately however, once it is agreed that change is
necessary by the policy makers, nurses are expected to
buy into it without given enough chance to say how they
are affected by the new change. Managing change is
challenging and it is even more challenging in a hospital
environment where such a change involves lives. According
8
to (Bozak, 2003) nurses ‘buy in’ is vital to a successful
transition of technological project in hospitals because
many of them can be unsure or just simply resistive to
new technological devices. Other barriers that have been
identified when implementing technological changes in an
hospital environment are lack of cooperation from staff
and even patients, lack of confidence and fear of using
the new technique, slow implementation of the change and
the technique with the believe and hope that the new
technological will not last (Spetz, et al. 2012). In a
mental health hospital, there may be cases of some
patients refusing to wear the bar coded hand band; this
problem can simply be solved by sticking the bar code
onto the patient’s chart. Other challenges that could
face the implementation of electronic medication are
‘short cuts’ like pre-pouring of medication and
‘workarounds’ which bypasses technological failures. Any
technology that involves computer networking will at some
point experience a break down as we do often experience
in clients’ software applications like Rio and Jade.
Fortunately, networking technology has evolved to a level
that stability is becoming very reliable. “Backbone”
which backups networking application software now exists
to take care of breakdowns and networking computers have
been upgraded to operate as “stand alone” in the event of
a network outage.
Lewin’s Field Analysis of the Electronic Medication System in Mental Hospitals
9

The process of using Kurt Lewin’s theory frame work to
understanding human behaviour as it would react to change
is known as ‘Kurt Luwin’s Field analysis’(Bozak, 2003).
The model involves three phases: unfreezing, moving stage
and refreezing phase. The aim of the model is to
identify: factors that can prevent change from taking
place; factors that oppose change from occurring often
referred to as ‘static force’; and factors that promote
change also referred to as ‘driving forces’. In other to
implement a change, the work force must recognise theses
forces. When the positive driving forces are promoted and
strengthened against the restraining forces, a change can
be implemented successfully (Bozak, 2003).
10
The unfreezing stage involves a thorough understanding of
the identified problems and formulation of strategies to
overcome them. A meeting is held with the individuals
that will be affected by the change and lists of the
driving and static forces that will affect the change are
created. Individuals during this stage recognise that
change is coming and are prepared for it (Bozak, 2003).
There may be a feeling of apprehension and stress during
this period among staff involve in the change process.
The second stage is the moving stage where the actual
change takes place. The opposing forces, that is the
restraining forces and the driving forces meet. The
moving force is strengthened to propel the change until
it occurs successfully. The last stage is the unfreezing
stage. This is the stage in which change that occurred is
incorporated in the routines practices of the
organization. To prevent retrogression and falling back
to previous ways of doing things, staffs are supported
with training, rewards and policy updates to make the a
part of the culture of the organization (Kaminski, 2011).
Application of the Change Management Theory
Unfreezing Stage
The first step in Kurt Lewin’s change process is
unfreezing the change which involves identifying the
change focus. In our case, it means implementation
electronic medication in NHS mental health hospitals.
This stage step involves communicating and holding
11
meetings with stakeholders such as the doctors, nurses,
pharmacists, managers and administrators. According to
(Bozak, 2003), it is important that lines of
communication are kept open to build trust and a sense of
security during this stage. Frontline staffs have to be
involved in the planning and decision making process and
they should be taking place. Round table discussions are
held during this stage and the driving and restraining
forces are identified and listed. Some of the restraining
forces likely to be face by this change will be: poor
computer experience across members of staffs, reluctance
to learning new technology, workarounds and shortcuts to
bypass procedures, and lack of trust in the change. The
driving forces are those that will make the change takes
place such as: availability of finance, support from the
upper management level, a good a training to support
staff and make the system easy to use. Briefly, this
stage involves engaging staff that will be using the
system to work together using the driving forces to
overcome the restraining forces.
Moving Stage
This is the stage in which the actual change takes place.
It involves perusing the plans that were put in place in
step one and implemented them (Sassen, 2009). The various
hospital teams particularly those involved clinical
service will be part of this implementation stage.
Nursing staff play a vital role in the medication chain
12
hence and in the view of Bozak (2003) they must be give
prominent role and should be made to realise that the
success or failure of the scheme depends on them. There
should be a timeline that must be adhere to and executed
during this phase, equipment should be tested for
reliability, continuing education program should be
planned to support staff and a project leader should be
appointed to oversee the implementation of the change.
Refreezing StageThis is the stage in which the mental health hospitals
are now using electronic medication system to prescribe
order and administer medication to patients. This is a
time of stability and re-evaluation of the change that
has taken place. Continue education is provided for
support, functional equipment with necessary literatures
guides and other resources are made available to support
end users, staff training program for old and newly
recruited staff should be put in place and policy
guideline regarding and regulating electronic medication
should be drawn up by the hospital management.
Medication error will always occur but it is the view of
this essay that electronic medication system will reduce
it.
Criticism of Lewin Change Management Theory
The third stage of Lewin’s model has provoked much
criticism. Many people argue that changes in modern
13
business is too fast to allow room and time for
refreezing after a change process have taken place. But
Lewin himself according to Longo (2011) anticipated this
criticism and wrote in 1757 that : “The refreezing stage
is not intended as a final, conclusive and stable point,
but as the point necessary to determine from which point
and/or state the following process of change starts”.
Clinical Governance Framework and Change Management
Clinical governance was introduced into the NHS in 1997
in the aftermath of many failures in NHS in the 1990s
(Braine, 2006). According to the Department of Health,
the elements and framework of Clinical governance is
important to improve the quality of services in NHS (DOH,
1997). Where and when a change is necessary in the way a
service is delivered, adopting the framework of clinical
governance helps to maximise the quality of care. The
basic themes of clinical governance are: patient
involvement and experience, clinical audit, education and
training, use of information, staff and staff management
(Leadership), clinical effectiveness and research
(Nicholls et al 2000, Starey 2001).
Clinical governance emphasises clinical audit; which in
the context of our change to electronic medication system
mean a system is put in place to evaluate progress. Is
the electronic medication being implement accurately? Are
there any shortcomings against what we ought to be doing?
14
What has worked and what has not worked? Nurses must not
see auditing as a job for the quality control commission
(CQC) alone. When it is well carried out, clinical audit
according to Wilson (1998) “provides reassurance to
patients, practitioners and managers that an agreed
quality of service is being provided within the resources
available”.
Leadership
Change is a process and at every level of that process
leadership is important to harness the efforts of the
workers and achieve a desired goal (Ajmal, et al, 2014).
And in order to survive according to Ajmal, et al. (2014)
every establishment must respond to local, national and
international need for change in technology or other
fields of life. Leaders are the “Champions of Change”.
They keep the process of any change in an establishment
going and maintain operational reliability (Ajmal, et al
2014). Leadership means having the vision, enthusiasm and
the desire to meet challenges (Bishop 2009). It is about
having the ability to get the best out of other people
and not simple contended with the tag of being the boss
(Frampton 2009). A leader must have the ability and
patience to listen to others’ opinions and he must be
able to reflect on these opinions and turn them into
durable policy for the progress of the organization
(Manley et al, 2011).
15

The Prime Minister’s commission on the future Nurses and
Midwifes in England have challenged senior nurse managers
to accept full managerial and professional accountability
for high quality care (DOH, 2010). This means statements
like “many nurses can be unsure and resistive to new
computer aided devices in practice” and that “new
technologies often incite resistance from nurses” by
Bozak, (2003) are no longer acceptable because nurses are
not only suppose to be agents of change but must take
charge and lead that change. According to McKenzie
and Manley (2011) ‘Nurses and nursing staff lead by
example develop themselves and other staff, and influence
the way care is given in a manner that is open and
responds to individual needs.’
Leadership Framework
In a change to electronic method of medication for
example, it is the responsibility of the ward manager to
provide the nursing staff the policy guideline and
supervision for the change taking place. The Royal
College of Nursing (RCN) (2009) identifies clinical
16
leadership as “vital for assuring and sustaining quality
care through the supervisory role of the ward sister or
team leader and the creation of an effective workplace
culture”.
Change Management Method
The National Institute for Health and Clinical Excellence
(NICE) offers a three levels structural approach on how
to manage and implement change in a healthcare setting
titled “How to change practice”. The three layers are:
Understand the barriers to change, identify the barriers
to change and overcome the barriers to change. The guide
aims to improve the quality of patients’ care by
encouraging healthcare professionals to use latest
guidance in their practice. (NICE, 2007). The method is
similar to Lewin’s management theory except that, it is
designed for health care setting although it can be
applied to other fields.
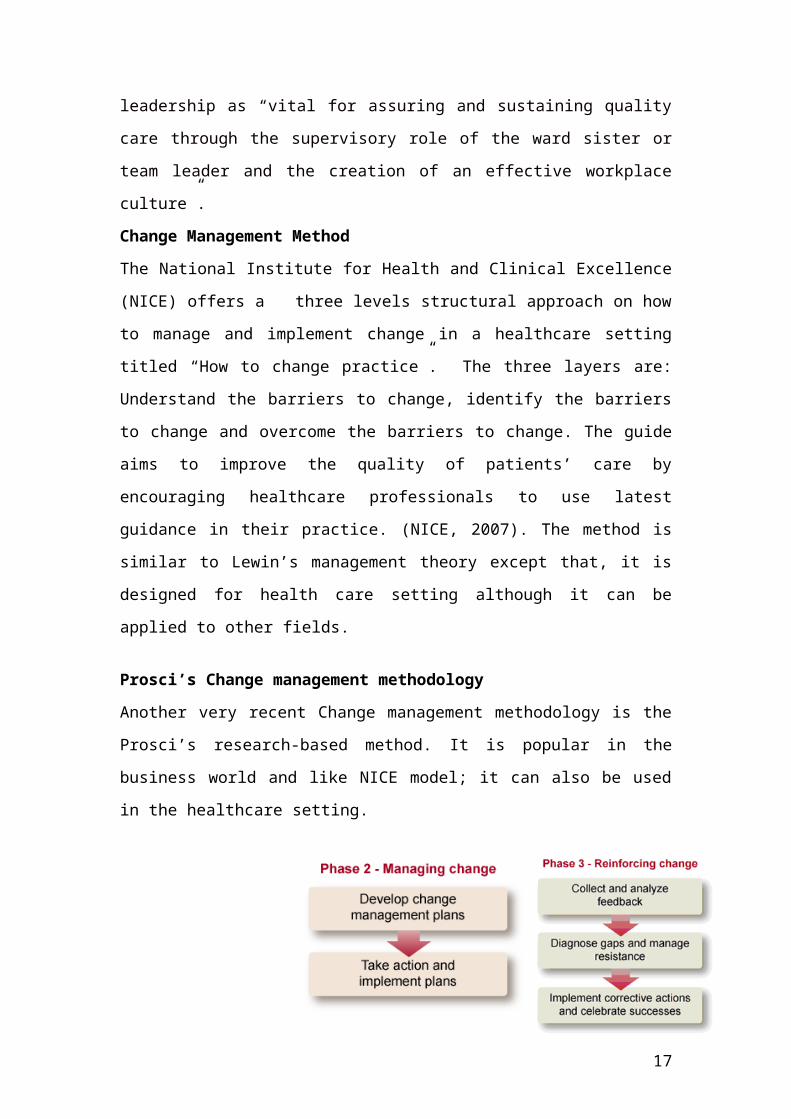
Prosci’s Change management methodology
Another very recent Change management methodology is the
Prosci’s research-based method. It is popular in the
business world and like NICE model; it can also be used
in the healthcare setting.
17
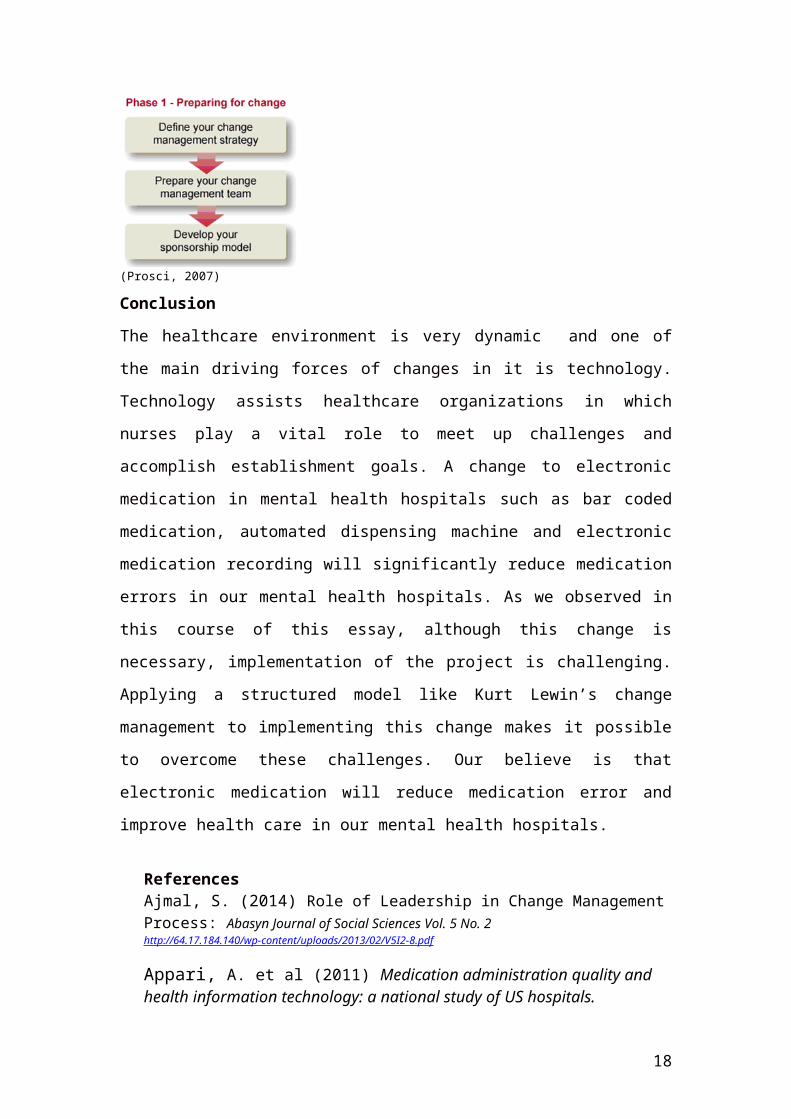
(Prosci, 2007)
Conclusion
The healthcare environment is very dynamic and one of
the main driving forces of changes in it is technology.
Technology assists healthcare organizations in which
nurses play a vital role to meet up challenges and
accomplish establishment goals. A change to electronic
medication in mental health hospitals such as bar coded
medication, automated dispensing machine and electronic
medication recording will significantly reduce medication
errors in our mental health hospitals. As we observed in
this course of this essay, although this change is
necessary, implementation of the project is challenging.
Applying a structured model like Kurt Lewin’s change
management to implementing this change makes it possible
to overcome these challenges. Our believe is that
electronic medication will reduce medication error and
improve health care in our mental health hospitals.
ReferencesAjmal, S. (2014) Role of Leadership in Change ManagementProcess: Abasyn Journal of Social Sciences Vol. 5 No. 2 http://64.17.184.140/wp-content/uploads/2013/02/V5I2-8.pdf
Appari, A. et al (2011) Medication administration quality and health information technology: a national study of US hospitals.
18
[Online]. Available at: http://jamia.bmj.com/content/early/2011/10/28/amiajnl-2011-000289.full.html. (Accessed: 02 June, 2014) American Society of Hospital Pharmacists. [ASHP] (1993)guidelines on preventing medication errors in hospitals. Am J Hosp Pharm. 1993; 50:305–14.
Bishop, V. (2009) Leaders of the future. Nursing Standard.24, 10, 62-63.
Bozak, M., (2003) Using Lewin’s force field analysis inimplementing a nursing information system. Computers, Informatics, Nursing, 21(2), pp.80-85.
Braine, M. (2006) Clinical governance: applying theory to practice. Nursing Standard. 20, 20, 56-65. Date of acceptance: November 15 2005.
Curtis, C. (2007). Nursing evaluation of electronic documentation systems. Retrieved from http://healthfieldmedicare.suite101.com/article.cfm/electronic_health_records
Department of Health (2010) Front Line Care: the future of nursing and midwifery in England. Report of the Prime Minister’s Commission on the Future of Nursing and Midwifery in England. London: Department of Health
Frampton, L. (2009) Changing Culture on the Front Line. [Online] Available at: www.clinicalservicesjournal.com/Story.aspx?Story=5857 (Accessed: June 10, 2014)
Getz, L. (2010). The Benefits of Bar Coding: For the Record [Online]. Vol. 22 No. 23 P. 20. Available at: http://www.fortherecordmag.com/archives/122010p20.shtml (Accessed June 02, 2014)
Kaminski, J. (2011) Theory applied to informatics – Lewin’s Change Theory Canadian Journal of Nursing Informatics Volume 6 No 1. 23 Mar 2011
19
Longo, R. (2011), Is Lewin’s change management model still valid?, HR Professionals, [online]. Available at: http://rosariolongo.blogspot.co.uk/2011/05/is-lewins-change-management-model-still.html (Accessed June 18, 2014)
McKenzie, C, Manley, K (2011) Leadership and responsivecare: Principle of Nursing Practice H. Nursing Standard25(35) 4 May pp.35-37 (PDF 94KB)
Manley, K. et al. (2011) Person-centred care: Principleof Nursing Practice D. Nursing Standard. 25, 31, 35-37.
MHRA (2013) Improving Medication Error Incident Reporting and Learning: [Online]. Available at: http://www.mhra.gov.uk/home/groups/comms-po/documents/news/con341187.pdf
(Accessed 28 May 2014)
Mosby's Medical Dictionary, (MMD) (2008) 8th Edition, Elsevier
NHS Leadership Council (2011) NHS Leadership Framework.NHS Leadership Website (http://www.leadershipacademy.nhs.uk/discover/leadership-framework/
NHS England (2013) Information Governance Policy Issue Document Number: POL_1008
NHS Executive (1999) Clinical governance: quality in the new NHS. Health Service Circular. HSC 1999/065. The Stationery Office, London.
Nicholls et al (2000) Clinical governance: its origins and its foundations. Clinical Performance and Quality Health Care. 8, 3,172-178,
NPSA_NHS (2007) Safety in doses: medication safety incidents in the NHS [Online]. Available at: http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=61392
(Accessed 27 May 2014)
Nursing and Midwifery Council (NMC), (2007): Standards formedicines management Pg. 3. [Online] Available at: www.nmc-uk.org/.../NMC- Standards-for-medicines - management .pdf (Assessed 15 June 2014)
20
Prosci (2007).Change management methodology overview. http://www.change-management.com/prosci-methodology-overview.pdf
PricewaterhouseCoopers. (2001). Patients or paperwork: The regulatory burden facing America’s hospitals. [Online]. Available at: www.aha.org/content/00-10/Final Paperwork Report.pdf (Accessed: June 08, 14)
Poissant, L. et al. (2005). The impact of electronic health records on time efficiency of physicians and nurses: A systematic review. JAMIA: Journal of the American Medical Informatics Association, 12(5), 505-516. doi: 10.1197/jamia.M1700
Sassen, E. (2009). Love, hate, or indifference: How nurses really feel about the electronic health record system. Computers, Informatics, Nursing, 27(5), 281-287
Spetz, et al. (2012) What determines successful implementation of inpatient information technology systems? The American Journal of Managed Care, 18 (3), 157-162.
Saranto, K. & Kinnunen, U. (2008) Evaluating nursing documentation – research designs and methods: Systematic review. Journal of Advanced Nursing, 65 (3), 464-476. doi:10.1111/j.1365-2648.2008.04914.x
The Royal College of Nursing (RCN) (2009) Breaking Down Barriers, Driving Up Standards: The role of the ward sister and charge nurse [Online]. Available at: http://www.rcn.org.uk/__data/assets/pdf_file/0010/230995/003312.pdf
Wilson, J (1998) Incident reporting, British Journal of Nursing. 7 11. 670-671
21