2-pre-operative assessment and pre-operative optimazation
TRANSCRIPT
PreoperativePreoperative Evaluation and Evaluation and
MedicationMedication
Learning AimsLearning AimsGoals of preoperative evaluation
What we do during preoperative evaluation
Airway evaluationASA classificationFasting protocols
Learn From A CaseLearn From A Case A 24-year-old healthy male was scheduled for an laparoscopic cholecystectomy. The induction of anesthesia was uneventful, the anesthesia was maintained with sevoflurane and fentanyl. 30 minutes after surgery, the EtCO2 rose to 70, and the temperature rose to above 40oC
Q: what happened? What’s the problem with the anesthesia?
After asking his family history, it showed that his sister was died during a minor surgery ten years ago, because of unknown reason, manifested with “high fever”, “shock”, and “muscle spasm” etc.!
What’s the problem of our practice of anesthesia?
Goals of Preoperative Goals of Preoperative evaluationevaluationThe preoperative evaluation consists of gathering information about the patient and formulating an anesthetic plan.
The overall objective is reduction of perioperative morbidity and mortality.
Inadequate preoperative planning and errors in patient preparation are the most common causes of anesthetic complications
Anesthesia and elective surgery should not proceed until the patient is in optimal medical conditions
If any procedure is performed without the patient’s consent, the physician may be liable for assault and battery
ROUTINE PREOPERATIVE ROUTINE PREOPERATIVE ANESTHETIC EVALUATIONANESTHETIC EVALUATIONHistory◦Current problem◦Other known problems◦Medication History
Allergies Drug intolerances Present therapy Non therapeutic
◦Previous anesthetics, operation◦Family history◦Review organ systems◦Last oral intake
ROUTINE PREOPERATIVE ROUTINE PREOPERATIVE ANESTHETIC EVALUATIONANESTHETIC EVALUATIONPhysical examination◦Vital signs◦Airway◦Heart◦Lungs◦Extremities◦Neurological examination
ANESTHETIC PLANANESTHETIC PLANPremedicationsType of Anesthesia: General Anesthesia
• Airway management• Induction• Maintenance
ANESTHETIC PLANANESTHETIC PLANRegional Anesthesia◦Technique◦Agent
Monitored Anesthesia Care (MAC)◦Supplemental oxygen◦Sedation
ANESTHETIC PLANANESTHETIC PLANIntra-operative management◦Monitoring◦Positioning◦Fluid management◦Special techniques
ANESTEHTIC PLANANESTEHTIC PLANPost-operative management◦Pain control◦Intensive care
Postoperative ventilation Hemodynamic monitoring
SYSTEMS APPROACHASYSTEMS APPROACHAAirway Basic concern of the anesthesiologist is always the patient’s airway
InductionMaintenanceMuscle Relaxation
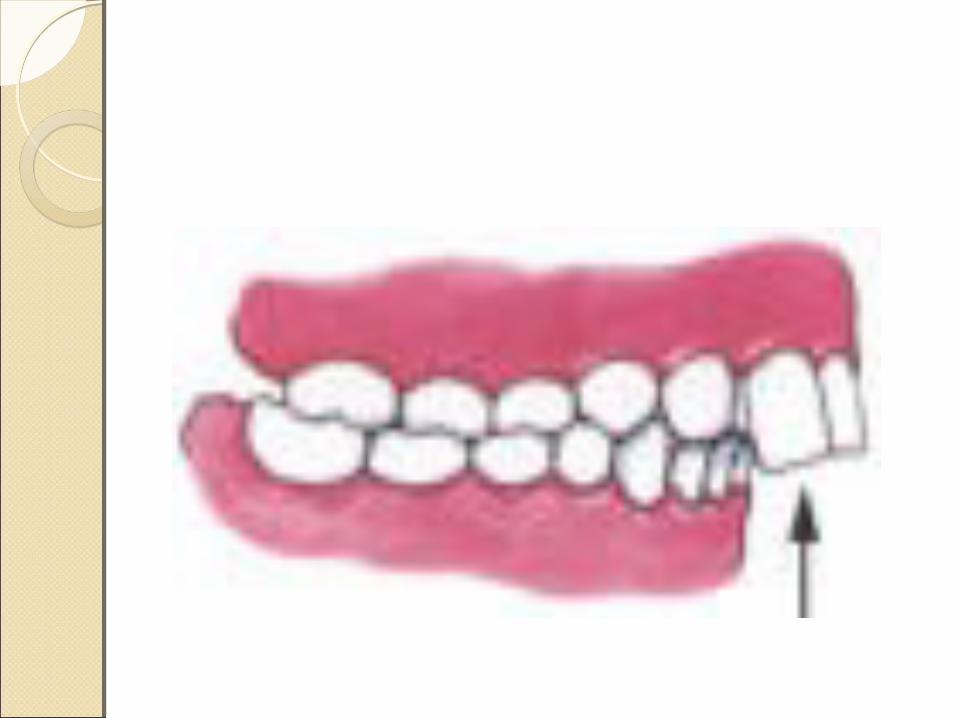
COMPNENTS OF THE AIRWAY COMPNENTS OF THE AIRWAY PHYSICAL EXAMINATIONPHYSICAL EXAMINATION Length of upper incisors Condition of the teeth Relation of maxillary and mandibular incisors
during normal jaw closure Ability to protrude or advance lower incisors in
front of upper incisors Interincisor distance 3FB Tongue size Visibility of uvula Shape of palate Compliance of mandibular space Thyromental distance with head in maximum
extension 6cm Length of neck: mentosternal distance 15cm Thickness of neck Range of motion of head and neck Facial hair
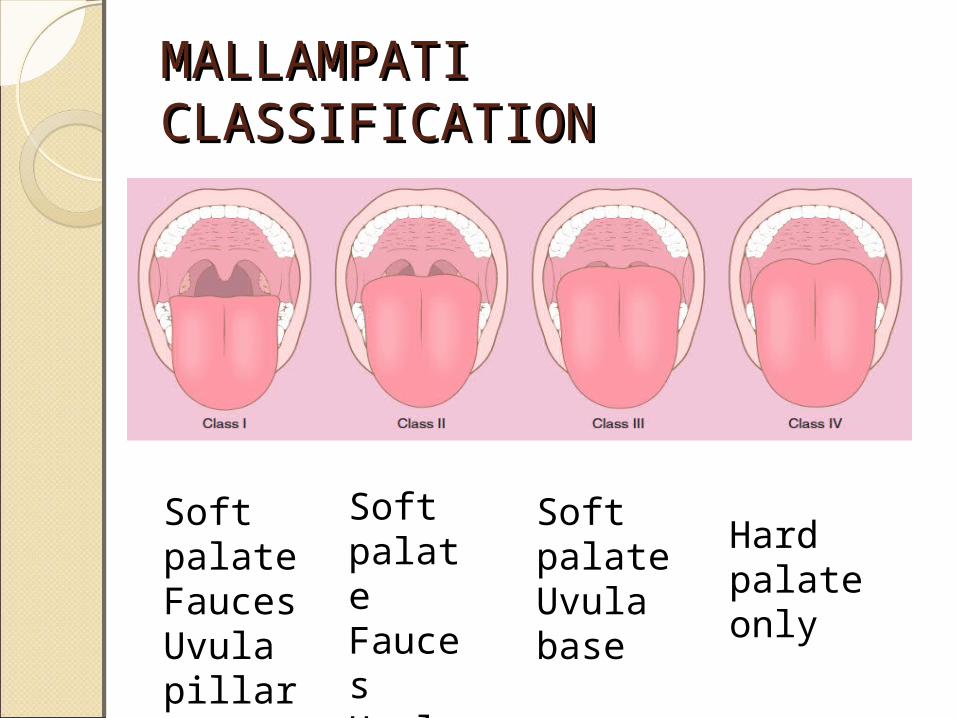
MALLAMPATI MALLAMPATI CLASSIFICATIONCLASSIFICATION
Soft palateFaucesUvulapillars
Soft palateFaucesUvula
Soft palateUvula base
Hard palate only
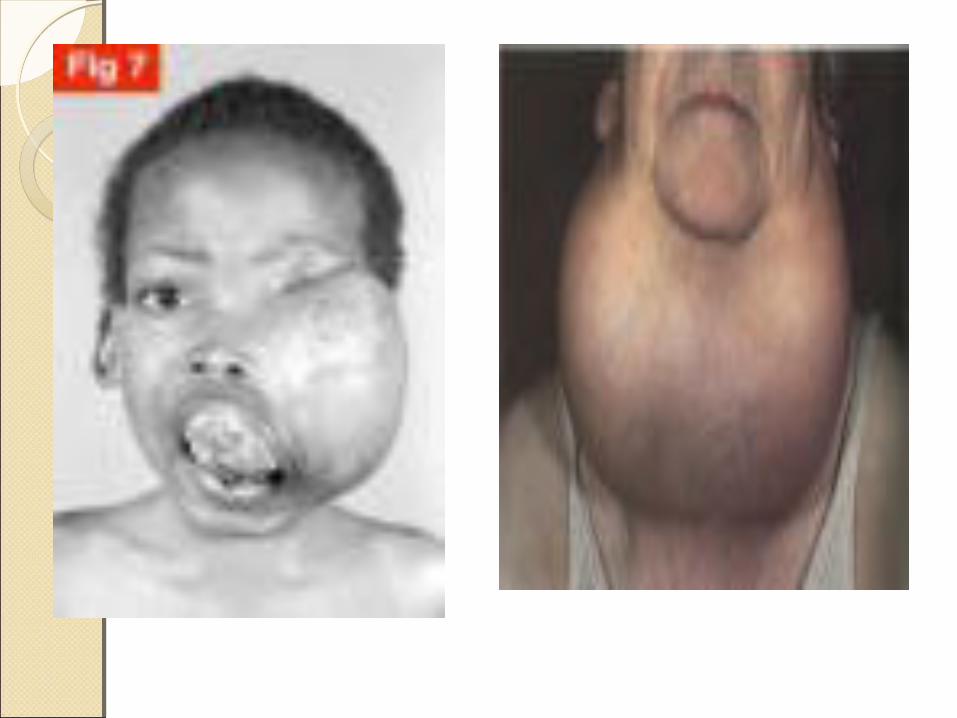
Difficult intubationDifficult intubationMouth opening less than 3 cmLimitation of neck movementMicrognathiaMacroglossiaProtrusion of teethShort neckMorbid obesityTumor in the face and neck


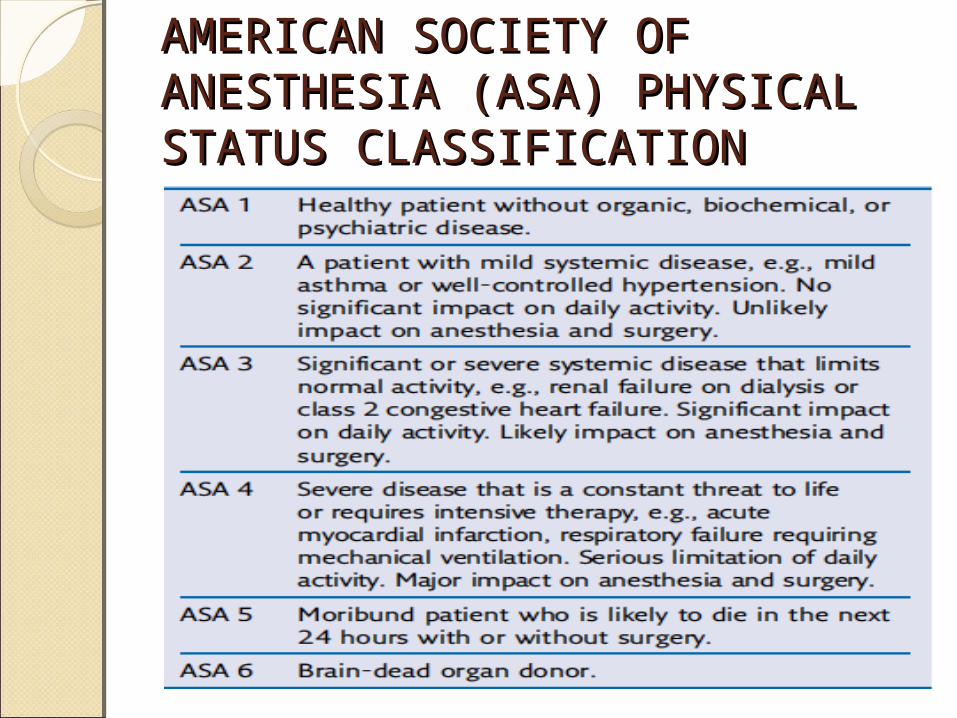
AMERICAN SOCIETY OF AMERICAN SOCIETY OF ANESTHESIA (ASA) PHYSICAL ANESTHESIA (ASA) PHYSICAL STATUS CLASSIFICATIONSTATUS CLASSIFICATION
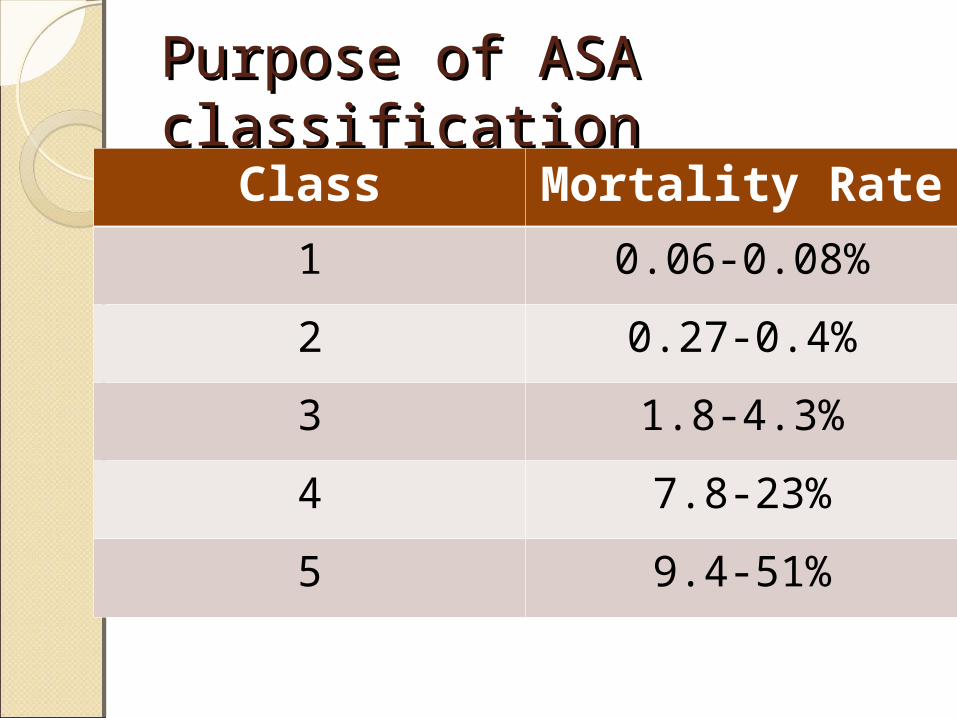
Purpose of ASA Purpose of ASA classificationclassification
Class Mortality Rate1 0.06-0.08%2 0.27-0.4%3 1.8-4.3%4 7.8-23%5 9.4-51%
SYSTEM APPROACHSYSTEM APPROACHPulmonary Pulmonary complication remain a major cause of morbidity and mortality for patients undergoing surgery and anesthesia
Preoperative risk factors Preoperative risk factors for pulmonary complicationsfor pulmonary complicationsThoracic and upper abdominal surgeryPreoperative history of chronic obstructive pulmonary disease
Preoperative purulent productive coughAnesthesia time greater than 3 hoursHistory of cigarette smokingAge older than 60 yearsObesityPoor preoperative state of nutritionSymptoms of respiratory diseaseAbnormal findings upon physical examination
Abnormal findings on chest radiographs
PULMONARYPULMONARYPerioperative pulmonary complications include: atelectasis, pneumonia, bronchitis, bronchospasm, hypoxemia, exacerbation of CPOD, and respiratory failure requiring mechanical ventilation
The site and type of surgery are the strongest predictors of complications
PULMONARYPULMONARYPatient related factors Patient with pre-existing pulmonary disease should include assessment of the type and severity of the disease, as well as the reversibility
PULMONARYPULMONARYTobacco◦Smoking increase carboxyhemoglobin levels, decrease ciliary function and increase sputum production and stimulation of CV system 2nd to nicotine
◦Cessation of smoking for 2 days◦Cessation for 4-8 weeks to reduce rate of postoperative pulmonary complications
◦Administer a bronchodilator such as albuterol preoperatively
PULMONARYPULMONARYAsthma◦During interview important to elicit information regarding inciting factor, severity, reversibility, and current status.
◦Frequency of using bronchodilators, hospitalization for asthma and requirement for systemic steroids
◦Perioperative steroids as prophylaxis for severe asthmatic
PULMONARYPULMONARYObstructive Sleep Apnea◦Obstruction of upper airway during sleep leading to episodic oxygen desaturation and hypercarbia
◦Propensity for airway collapse and sleep deprivation, patients are susceptible to respiratory depressant and airway effects of sedatives, narcotics and inhaled anesthetics
PULMONARYPULMONARYContinue medicationAerosol medication before surgeryRisk reduction of pulmonary complication◦Smoking cessation◦Education of lung expansion maneuver and deep breath exercise
◦Treatment of obstruction◦Antibitotic ◦hydration
SYSTEM APPROACHSYSTEM APPROACHCardiovascular preoperative evaluation◦Clinical risk indices◦Surgical procedure◦Exercise tolerance
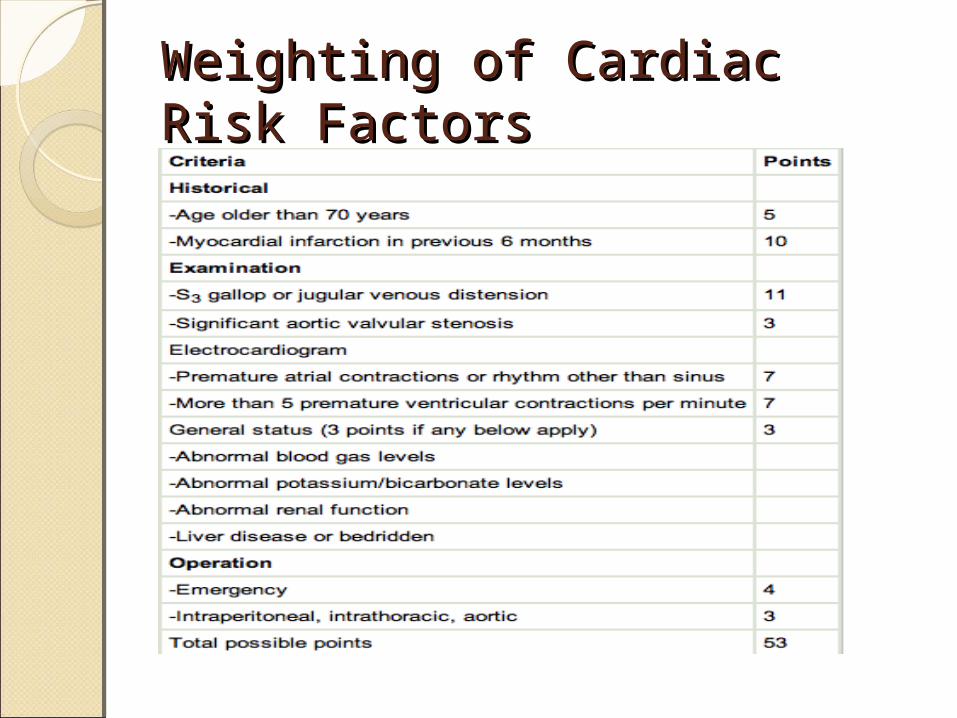
Weighting of Cardiac Weighting of Cardiac Risk FactorsRisk Factors
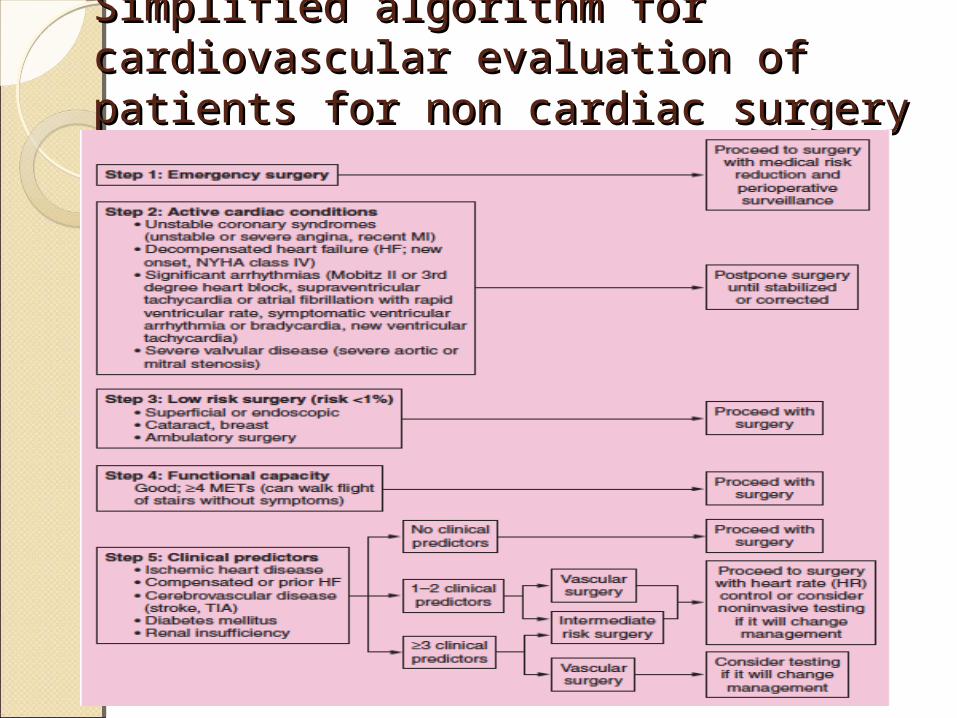
Simplified algorithm for Simplified algorithm for cardiovascular evaluation of cardiovascular evaluation of patients for non cardiac surgerypatients for non cardiac surgery
CARDIAC RISK STRATIFICATION FOR CARDIAC RISK STRATIFICATION FOR NONCARDIAC SURGICAL PROCEDURES IN NONCARDIAC SURGICAL PROCEDURES IN PATIENTS WITH KNOWN CADPATIENTS WITH KNOWN CAD
High (reported cardiac risk >5%)◦Emergent major operation, particularly in elderly, aortic and other major vascular peripheral vascular
◦Anticipated prolonged surgical procedures associated with large fluid shifts and blood loss
Intermediate (reported cardiac risk<5%)◦Carotid enarterectomy◦Head and neck◦Intraperitoneal and intrathoracic◦Orthopedic◦Prostate
Low (reported cardiac risk <1%)◦Endoscopic procedures◦Cataract and breast
Exercise tolerance◦4METs: walk at 6km/hr, run short distance, heavy work around house, golf, bowling, dancing
CARDIOVASCULARCARDIOVASCULARCardiovascular test◦Electorcardiogram information of patient’s myocardium and coronary circulation
◦Abnomal Q waves in high risk paitent are highly suggesitve of past MI
◦The risk of reinfarction during an elective procedure performed within 3 months after a myocardial infarction exceeds 30%, while the reinfarction rate decreases to 4.5% after 6 months
SYSTEM APPROACHSYSTEM APPROACHEndocrine system◦Diabetes mellitus
Most common endocrinenopathy Hyperglycemia, blood glucose>200mg/dl
DM increase risk of CAD, hypertension, congestive heart failure and perioperative MI
At intermediate risk
Diabetes MellitusDiabetes MellitusPerioperative stress may increase serum glucose concentration secondary to the release of cortisol and catecholamine
Control of glucose within a range of 100-150mg/dl
Administer insulin in the form of infusion or regular infusion
Thyroid and Thyroid and Parathyroid DiseaseParathyroid DiseaseHistory and clinical manifestationThyoid function test more sensitive◦Thyroid-stimulating hormone (TSH)◦Thyrotropin◦Thyroxine (T4)◦Triiodothyronine (T3)
Hyperparathyroidism usually have hypercalcemia, indicating the need of serum calcium level monitoring
PREOPERATIVE LABORATORY PREOPERATIVE LABORATORY TESTINGTESTING
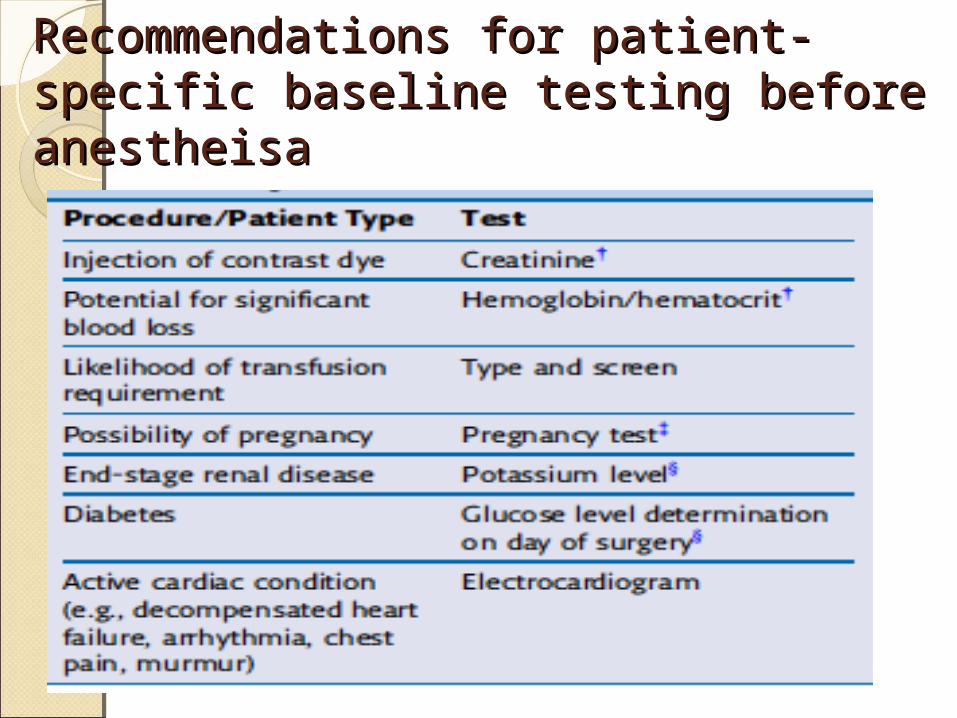
Recommendations for patient-Recommendations for patient-specific baseline testing before specific baseline testing before anestheisaanestheisa
Complete Blood Count and Complete Blood Count and Hemoglobin concentrationHemoglobin concentrationBaseline hematocrit is indicated in any procedure with a risk of blood loss
Hemoglobin level of 7g/dl is acceptable in patient without systemic disease
In patient with systemic disease signs of inadequate systemic oxygen delivery (tachypnea and tachydia) are indication for transfusion
ElectrolytesElectrolytesCreatinine and glucose has been recommended in older patient
Blood urea nitrogen and creatinine are indicated in patient with systemic disease or on medication that affect kidney
Patient has kidney disease may has hyperkalemia
Coagulation studiesCoagulation studiesHave significant impact on the surgical procedure and perioperative management
PT and aPTT analysis are indicated in patient with history of bleeding problems
Bleeding time advocated to determining the presence of qualitative platelet defect
Avoid regional anesthesia in patient with clinical bleeding diathesis
Pregnancy testingPregnancy testingPregnancy testing should be limited to female patient who believe they are pregnant or cannot tell if they are pregnant
To avoid specific agent that may harmful to the fetus
Chest X-RayChest X-RayCan identify abnormalities that may lead to delay or cancellation of planned surgical procedure or modification of perioperative care
Pneumonia, pulmonary edema, pulmonary nodules or mediastinal mass
Preoperative MedicationPreoperative Medication
GoalsGoalsRelief of anxietySedationAmnesiaAnalgesiaDrying of airway secretionsPrevention of autonomic reflex responses
Reduction of gastric fluid volume and increase pH
Antiemetic drugReduction of anesthetic requirementFacilitation of smooth induction of anesthesia
Prophylaxis against allergic reaction
Anesthetic managementAnesthetic managementPreoperative Psychological preparation
Preoperative medicine
Psychological Psychological preparationpreparationPreoperative visit and interview with patient and family members
Explain anticipated events and the proposed anesthetic management in an effort to reduce anxiety and allay apprehension
An informative and comforting preoperative visit may replace many milligram of depressant medication
Preoperation Preoperation medicationmedicationPatient condition, patient physical status and age must be considered
Surgical procedure and its duration are important factors
Must know patient weightTime and route of administration is important
Sedatives-Hypnotics and Sedatives-Hypnotics and TranquilizersTranquilizersBenzodiazepines anxiolysis, amnesia, and sedation
site of actions in CNS, little depression of ventilation and CV
wide therapeutic index with low toxicities
OpioidsOpioidsThe analgesic properties and respiratory depressant effects of opioids usually go hand in hand. The decrease in the carbon dioxide drive at the medullary respiratory center may be prolonged. Consider supplement oxygen for patient receiving opioids premedications
Nausea and vomitingCholedochoduodental sphicter spasm. Not with fentanyl and meperidine
Preanesthesia Medication Preanesthesia Medication InstructionInstruction
Antidepressant, antianxiety, and psychiatric medications should be continued on the day of surgery
Antihypertensives◦Generally to be continued◦Consider discontinuing ACEI or ARB 12-24 hr before surgery
Aspirin◦Continue on the day of surgery
Patients with known vascular disease Patients with drug-eluting stents for <12 months
Patients with bare metal stents for < 1 month Before cataract surgery Before vascular surgery Taken for secondary prophylaxis
◦Discontinue 5-7 days before surgery If risk of bleeding > risk of thrombosis For surgeries with serious consequences from bleeding
Taken only for primary prophylaxis
Clopidogrel◦Continue on the day of surgery
Patients with drug-eluting stents for < 12 months
Patients with bare metal stents for < 1 month
Before cataract surgery◦Patients not included in the group recommended for continuation
Warfarin◦Continue on the day of surgery
Cataract surgery with no bullbar block
◦Discontinue 5 days before surgery
Insulin◦Continue on the day of surgery
Type 1 diabetes: take 1/3 intermediate to long acting
Type 2 diabetes: take up to ½ of long acting
◦Discontinue Regular insulin Discontinue if blood glucose level < 100
Gastric Fluid pH and Gastric Fluid pH and VolumeVolumeSummary of fasting recommendations to reduce the risk of pulmonary aspiration
For healthy adult with no risk of aspiration, the following time of fasting is recommended:◦For solids 8 hours◦For light meal 6 hours ◦For fluids that are not clear 4hours (breast milk)
◦For clear fluids 2 hours
A CASEA CASEA healthy 24 man had a car accident at about 10 am after he his breakfast at 8am. His suffered from femur fracture and need for surgery. About 18 pm, after finished routine preoperative examinations, the patient was delivered to the OR.
Q: whether the fasting time of the patient is adequate? Why? What should we do?
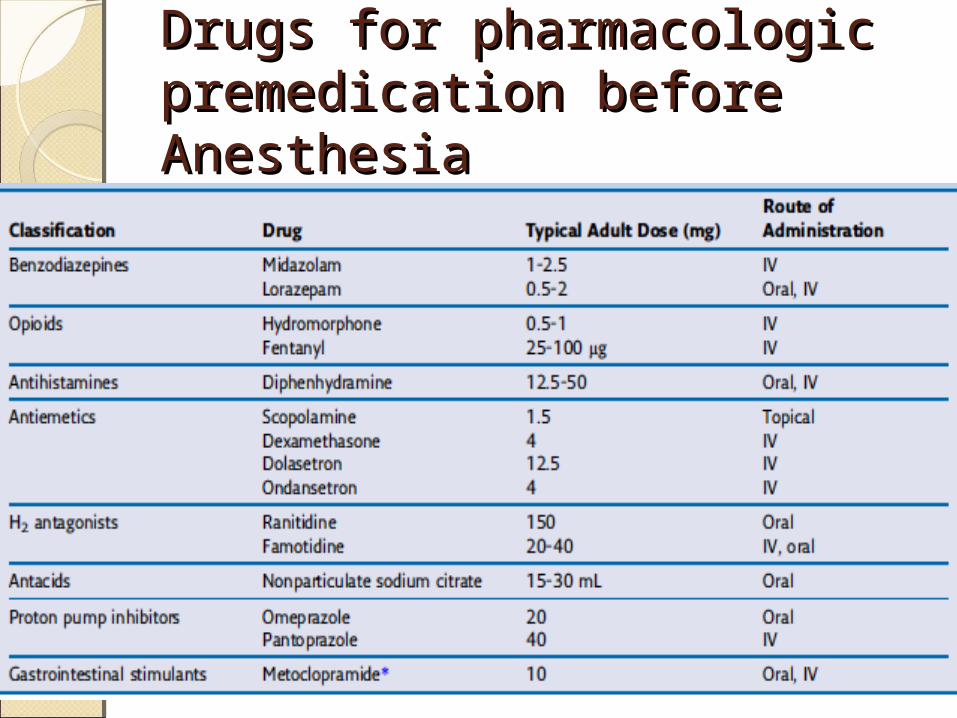
Drugs for pharmacologic Drugs for pharmacologic premedication before premedication before AnesthesiaAnesthesia
THE ENDTHE END