1226837470-img04609.pdf - kiu institutional
TRANSCRIPT
EMPLOYEE PERFORMANCE AND HEALTH SERVICE DELIVERY IN
NAKASONGOLA DISTRICT
ACASE STUDY OF NAKASONGOLA HEALTH CENTRE IV
BY
NAKAFEERO DOREEN
1153-05194-00760
:~ RESEARCH REPORT SUBMITTED TO THE COLLEGE OF ECONOMICS
AND MANAGEMENT IN PARTIAL FULLFILMENT OF THE
REQUIREMENTS FOR AWARD OF BACHELORS
DEGREE OF SCIENCE IN STATISTICS OF
KAMPALA INTERNATIONAL
UNiVERSITY
AUGUST, 2018
DECLARATION
I, declare that the research report entitled “Employee performance and health service delivery in
Nakasongola District is my own work and that all the sources that I have used or quoted have
been indicated and acknowledged by means of complete references.
Signature Date
APPROVAL
This research report has been done under my supervision and is now ready for submission to
Kampala international University examinations board with my approval as the University
supervisor.
Signed....~ Date ~.~&(Super~ isor)
oI~Ii~ ~
DEDICATION
I dedicate this work to my parents father Lukwago Tom Mande and mother Namanda Efridah
and family members for their moral support and the encouragement that they gave me during the
study.
iu
ACKNOWLEDGEMENTS
I wish to acknowledge and be grateful to God for enabling me to reach this point in my academic
life and I am so thankful for His unconditional protection.
Many thanks to my supervisor Mr. Okello Moses for the advice and making numerous revisions
and helped me make some sense of the project.
Fourth acknowledgement goes to my research assistants who devoted their time and energy
towards the accomplishment of this research project.
The moral support that they gave me too was overwhelming and came in handy at times when I
was being challenged by various issues in the field. And finally, thanks to my family, tutors and
numerous friends who provided me with consolidated support vital for the success of this
pr~i eeL
As well as acknowledgement goes to my beloved brothers and sisters all these brothers and
sisters showing me support and encouraging me all the time to educate and improve my learning.
Finally. I thank for my all classmate students.
iv
ACRONYMS
DuO Director of Health Organization
D1IS Demography and Health Survey
GOC Government of Uganda
1lCs I lealth Centers
I IC’l I lealth Communication Technology
IIIV human Immune Virus
1MM Integrated Management of Malaria
KDI IS Kenya Demographic I health Survey
\1CI I Ministfy of Health
~. I Nadonal I Icaith Planning
NI ISSP National health sustainable Scale Program
PFP Private for Profit
PNFP ProPt not for Profit
Tuberculosis
~N I Igaucia Bureau of Standards
UN United Nations
USF Uganda Sanitation Fund
WI 10 World I Iealth Organization
V
TABLE 01? CONTENTS
DECLARATION.).)~t ~I ~
~ S •~ibDV 11
DEDICATION iii
.
ACRONYMS v
ABSTRACT ix
‘‘II \Pl’ERONF 1
.S fEODI ‘CT!ON 1
1.! Background of the study I
1 .1 .1 1 listorical Perspective I
1.1.2 Theoretical Perspective 6
.! .3 Conceptual Perspective 7
.: .4 Contextual perspective 8
1.2 Problem Statement 9
1.3 Purpose of the study 10
1.3.IObjectives of the Research 10
1.3.2 Research Questions 10
1.~.3 Ilypothesk 10
1.4 Scope of the Study 10
1.4.1 CottcntScope 10
l.4.2meoretical Scope 10
1.4.3 Geographical Scope 10
1.4.4 Time Scope 11
1.5 Significance of the Study ii
1.6 Definitions of Key Concepts 11
C1IAPTERTWO 13
LITERATURE REVIEW 13
2.0 Introduction 13
2.1 Performance of Ilealth Worker 13
2.2 health Service Delivery 15
2.3 Relationship between employee Performance and Health Service Deliver) 17
vi
2.4 Related studies . 19
2.5 Conceptual Frame Work. 21
Ci-IAPTER THREE 23
METHODOLOGY 23
3.0 Introduction 23
S Research Design 23
3.2 Target Population 23
3.3 Sample Size 23
3.3.2 Sampling Procedure 24
3.4 Data Collection Instrument 25
3.5 Data Collection Method 25
3,6: Validity of the Instrument 25
3.7 Reliability of Instruments 25
3.8 Data Processing and Analysis 25
3.9 Ethical Considerations 26
CHARTER FOUR 27
PRESENTATION, INTERPRETATION AND ANALYSIS OF FINDINGS 27
4.0 introduction 27
4.1 Demographic Profile of respondents 27
4.1 .1 Findings on Gender of respondents 27
4. 1 .2 Findinps on Age categories of respondents 28
4.1 .3 Findings on educational qualifications of respondents 28
4.1 .4 Findings on Marital status of respondents 29
4.1.5 Findings on duration respondent’s in the health centers 29
4.2 State of employee performance in E-Iealth Centre IV Nakasongola District 30
4.3 State of health service deliver)’ in health centers in Nakasongola District 33
4.4kelationship between employee performance and health service delivery in Nakasongoladistrict 34
4.4.2 Chi-Square tests for the variables 35
CHAPTER FIVE 37
DISCUSSION OF FINDINGS. SUMMARY, CONCLUSION, RECOMMENDATIONS 37
5.() Introduction 37
5.1 Discussion of findings 37
vii
5.2 Summary of Findings. 38
5.3 Conclusions 39
5.4 RecommendaHons 40
5.5 Areas of further research 40
REFERENCES 41
Appendix i: Questionnaire for health workers 46
Appendix ii: Questionnaire for Clients/ Community 49
viii
ABSTRACTThe purpose of study was to establish how health workers performance affects health service
delivery in Nakasongola District. The study objectives included establishing the state of
employee performance and to find out the state of health service delivery and the third objective
was to find out the relationship between employee performance and health service delivery, The
study was conducted in Nakasongola health centre iv, where data was collected from clients and
the employees of the health centre who were 80 in number who provided information through
the research questionnaires, the study employed correlation research designs where the data was
analyzed using descriptive statistics of mean and standard deviation and then after using Pearson
correlation coefficient to determine relationship between employee performance and health
service del iverv. The study findings on the first objective revealed that employee performance
was low. The study findings are justified by the poor rate according to the mean of 2.276,
SD=.$92 interpreted as poor. The study results revealed that the health services delivery was
poor at 2.504, SD= 0.802. The study findings on the third objective revealed a significant
negative relationship between employee performance and health service delivery in Nakasongola
district (r~ -275). further more chi—square test suggest that retention had significant influence on
efficienes, motivation had a significant effect with quality and accessibility. The study concludes
ihat improved working conditions, accountability and retentions could have a high bearing on
employee performance in the health centers, the state of health service delivery in health centers
was considerably low and that low performance levels of workers negatively affect health
service delivery. The study recommends for improvement in the motivation in terms of
payments, therefore improvement of the state of workforce efficiency by establishing a strong
working environment for the workers. The study also recommends that the health service
delivery need to be improved through improving accessibility, the quality of health care through
purchase of tools and equipment required in the health centers and finally government strengthen
social service accessibility for improving the functionality employees for improved health
services.
ix
CHAPTER ONE
INTRODUCTION
.1 i.iackground of tue study
.1. ,.i . .i.H.istorical .Perspective
Service delivery has significance relationship with customer satisfaction (Swanson and Davis,
2004) in any health system, good health services are those that deliver effective safe good quality
personal and non-personal care to those that need it, when needed with minimum waste. The
service deliver building block is concerned with how inputs and services are organized and
managed to ensure access, quality and continuity of care across health conditions, across
different locations and over times.
In East Africa for instance in Kenya , health services are provided through a network of over
4700 health facilities country wide with public sector system accounting for about 51 %of the
lhcilities. The public health sector consists of the following levels of health facilities: national
referrals, provincial general hospitals, district hospital, health centers and dispensaries.
According to the 201 5 Kenya Demographic and Health survey (KDHS, 2015) more married
women are using modern contraceptive methods.
ivlalaria is the leading cause of outpatient morbidity in Kenya, accounting for one—third of all
new cases reported. After malaria, the most common illnesses seen in outpatient clinics are
diseases of the respiratory system, skin diseases. diarrhea, and intestinal parasites In 2003. full
immunization coverage declined to under 60 percent (from 65 percent in 1 998 and 78 in 1 998 to
6 percent in 2003. The major causes of this decrease in coverage are the declining availability,
access to. and quality of public health services; the increasing level of poverty is a main
underlying factor. in addition, because fewer people are dying from immunisable diseases, the
focus on immunization services has reduced, and funding has decreased (Hill and Kazembe,
2(106)
The challenge facing the government is to reverse this decline. The National Development Plan
of 2008- 20 14 states that the health care system in its current form (at the time of the National
Plan’s preparation) does not operate efficiently. Some of the areas targeted in the plan include
drugs. personnel, and facility utilization. Drugs, which account for 14 percent of the health
budget. were deemed to he the most promising area for improvement, particularly in drugs~
selection and quantiOcation. Staffing norms for key cadres would he developed for deployment
purposes. The plan also calls for formulating a health manpower policy, to develop and retain
human resources in the sector.
in a renewed effort to improve health service delivery, the Ministry of Health and stakeholders
have reviewed the NIEISSP service delivery system in order to devise a new strategy for making it
more effective and accessible to as many people as possible (KMOH, 2015a). Services are atthe
provincial and district level, as a result of health sector reforms that have decentralized health
services, services are integrated as one goes down the hierarchy of health structure from the
national level to the provincial and district levels. Under decentralization, the district handles
supervisory responsibilities. Unfortunately, supervision has not been very effective, as one
technical person may supervise several technical areas of service delivery at lower levels.
Since independence in 1961, the Government of Tanzania has consistently focused its
development strategies on combating ignorance, diseases, and pmierty. The investment in
primary health services is recognized as a potential tool in fighting diseases at the same time
improving the quality of~-~ lives of the majority of people. Progress has been made in Tanzania’s
health sector; however, more can be done to improve service delivery. Perception of quality at
facilities is often a deciding factor in service utilization. Like many countries, Tanzania faces an
inequitable geographic distribution of service quality. Quality and provider availability is often
best in urban areas, particularly in Dares Salaam. While Dares Salaam is home to about 10
percent of the population, about 45 percent of the country’s doctors are concentrated in Dar es
Salaam (World Bank. 2015). The availability of medical equipment and diagnostic accuracy are
also higher in urban areas than rural areas.
laazania periorms relatively well in the availability of medical equipment in facilities.
Infrastructure and drug availability, however, are major challenges. Only half the facilities in
Tanzania have the required components for infrastructure. Drug availability, particularly for
mothers and children were also pool’ (Makuru, 2012).
A major challenge for Tanzania’s health sector is the shortage of skilled human resources for
health (HRI—l). The provider knowledge and abilities are not adequate to deliver quality services.
Caseload per provider and absenteeism are relatively low. so the issue is not overburdened
providers, There seems to be ample room for a significant increase in the caseload of Tanzanian
providers, i.e. the level of productivity in health service delivery, without jeopardizing quality. In
addition to increasing the volume of skilled HRI—I to address the shortage of providers,
improvements in management, supervision and training is important to improving service
delivery. llealth for all in Tanzania means the simultaneous availability of widely accessible
inputs and skilled providers.
Over the past 5—1 0 years. Rwanda has seen great improvements in several key health indicators,
including most health outcomes in the domain of maternal health. Maternal mortality decreased
signidcantly: the 2010 Demographic and Health Survey (DHS) estimated Rwancla’s maternal
mortality ratio (MMR) at 476 deaths per 100,000 live births, down from 1071 deaths per 100,000
in the year 2000. The 201 2 report of the Countdown to 2015 Collaboration ranked Rwanda as the
country with the highest average annual rate of maternal death reduction, at 9 %. Recent
estimates by several ON agencies and the World Bank categorised Rwanda among 11 countries
that are ~on track~ to achieve target 5A of the Millennium Development Goals, which involves a
decline 01 me MMR by at least 75 % between 1990 and 2013 (World Bank, 2014).
Fhese achievements are often attributed to a combination of improved population coverage and
improved health service quality. In terms of coverage of maternal health services, the proportion
of institutional deliveries increased from 69 % in 2010 (DI-IS 2010) to 90% in 2013 according to
the national health management information system. Despite all these achievements, there is also
evidence of deficiencies in Rwanda’s health system; for instance in the delivery of emergency
and essential surgical services, particularly at district hospitals, which underlines the scope to
Firther improve maternal and neonatal health.
From 1960’s to mid-l 970. Uganda had one of the most effective public service systems in sub
Saharan Africa. The country’s health system in particular was one of the finest with an effective
refdrral system from the village dispensaries and district hospitals to the national referral
hospital. During the 1970’s and early 1980’s. many of these institutional systems collapsed.
i’esulting into substantial deterioration of the health outcome indicators ( UBOS, 2009).By 1996,
‘3
~ne Lj.th sector was in a state of near collapse, with dilapidated and very poorly equipped public
neatu~ facilities, and in addition, public funding for the sector was unreliable ( National Health
rolicv. 1 999).While several policies have been undertaken in the health sector with a view to
improve health sector indicators, progress has stagnated since the late 1 990’s, The immediate
reform emphasis was on the rehabilitation of the existing facilities to restore functional capacity
and shill of emphasis to primary health care in order to improve service delivery.
i lcalth care services in Uganda are delivered by both public sector (government) and private
entities that include private—not—for—profit (PNFP) and private—for—profit (PFP) organisations as
nail as complementary health service providers such as the traditional medicine providers. The
~uhiic health facilities make up 55% of the total health care facilities in Uganda. while PNFP and
i’l”P make up 1 6% and 29%. respectively. Nearly all (90%) of the private-for-profit facilities are
located in one district Kampala district which also hosts Uganda’s capital city (Martens and I lall.
2002).
eanda’s health service delivers’ structure, the national level stewardship functions are
pcrfurmed by the Ministry of I lealth (Mol I). In the public sector, health services are delivered
through the national referral hospitals. regional referral hospitals and district health services. The
ii~~o~~al referral hospitals are autonomous and have a target population of 1 0 million people.
fhe~ provide referral services for the regional and general hospitals across the country. National
referral hospitals arc expected to offer highly specialized medical and surgical services.
ncR aneed diagnostic services, advanced research and training for medical doctors, nurses and
paramedical oflicers such as orthopedic officers and laboratory technologists (Morel, Lauer and
Rvnns, 2005).
h~ lisirict-lceel health service includes the district health management team. general hospitals
ann ni nrrn~ ci prin~1ry care facilities (also known as health centres (HCs)). The district health
ser\ ice is under a District health Officer who is appointed by and accountable to the district
local government. Because the decentralized system of governance adopted in 1995 devolved
must ilinctions and powers to districts, the district health services are administratR ely
4
independent of regional hospitals and report directly to the MoH (Utzinger. Tozan and Singer.
2001).
Uganda has three levels of primary care facilities: level II (lower-level primary care facility), III
(mid—level primary care facility) and IV (higher—level primary care facility) all focusing mainly
on prevention and treatment of infectious illnesses. A level II primary care facility is the lowest
level of formal health care delivery. It is mostly staffed by nurse aides and qualified nurses. A
level III primary care facility has provisions for basic laboratory services, maternity care, and
inpatient care (often for onward referral). It is usually staffed by nurse aides, qualified nurses and
clinical officers (physician assistants). A level IV primary care facility is the level immediately
below a district hospital and has a target population of 100,000 people. It has provisions for an
operating theatre, in—patient and laboratory services, and is a referral facility for 20-30 level II
and Ill primary care ihcilities under its jurisdiction. A level IV primary care facility is staffed by
nurse aides. qualified nurses, clinical officers and doctors, although the majority does not have
doctors (Morel. Lauer and Evans, 2005).
Along with increased literacy rate and vibrant economic growth, health outcomes are improving
which translates to better health indicators. Over the past two decades has increased the
government of republic of Uganda has increased access to health services two fold. By 1997.
onlv 47% of the population who needed health care could access outpatient services (NHP
1 998). During that time, health facilities were few and far from communities, and the health
system that was degraded by years of civil strife and mismanagement was just beginning to
recover. This figure has since improved to about 110 pe1’ce~t underscoring the ease of access to
health facilities by the population (D1dIS. 2015/2016). These improvements are attributed to
I nccstn ~en~ in health infrastructure and decentralization of the health system, abolition of the user
fee (2001). and increase in health resources in nominal terms; number of workers increased for
52%in 2010 to 70% in 2016 and availability of medicines from about 35% in 2007/2008 to 75%
in 2015/16. Health indicators as pci’ UN estimates have significantly improved over the last 15
veai’s (2000-205)MMR 506/100000 live births to 360/100000 live births. IMR 56/1000 live
birDs to 38/1000 live births, NMR 27 /1000 live births to 19/1000 live births and life expectancy
43 years at birth up for 35 years in 1986. (MOH, 2017)
Sakasongola district has got 30 health facilities with 263 beds in the health facilities: Most of the
population in the district does not have access to the health services with only 38% of the
population within the radius of 5km of health center. Deliveries in the health facilities ~ere at 32
percent the top illnesses being malaria at 48 percent followed by pneumonia at 30 percent in
health centers. ‘I’he district’s top ten causes ofmorbidity include malaria 25.7%, acute respiratory
infection 20.8%. trauma/accidents 5.7%. intestinal worms 5.5%. diarrheal diseases 6.3%. dental
diseases 5.4%. anemia 3.2%. protein energy malnutrition 1.9%. and maternal complications
3.4% among others human resource is the greatest resource an organization can have. if~ the
district had all the approved staff then it would improve its health services. The general
.mvirc nment of the employee performance as of 2017 is low according to the health service
r:port jI)isLrict i Icalth report. 2017).
a.12 Theoretical Perspective
According to llerzberg’s two f~etor theory of motivation (2002). employee motivators
ichallenging work . recognition. responsibility) give positive satisfaction and hygiene factors
status. job security. salary. fringe benefits work conditions) that do not give positive satisfaction
.~a.ugn bring cissatisfaction due to their absenteeism (Fincham& Rhodes . 2005)
Self-motivated employees tend to exhibit good performance even if they are never provided with
much external motivation and their performance increases if they are provided with motivation
thus high quality health care delivery. Great stress is placed on the importance of qualit> in the
~~ork place. with an emphasis on the perceptions of work improvement and satisfaction in the
industry ((‘lake 2000) and also on the ways that management can create a motivational
~~orkplace in which retention and employee satisfbction lead to improved health care delivery.
.Jood performance by staff is enabled via a supportive working environment. This encompasses
.noic than lust having sufficient equipment and supplies it also includes systems issues such as
it inn ia&kiiig ant. capacity issues as worked, support services and infrastructure (Potter
&Lsrough. 2004)
Understanding performance begins with understanding that the workers are not necessarily to be
blamed if their performance is not what is expected. instead of assuming what the workers in
6
question are unskilled or unwilling to perform the task at hand, the wise manager seeks to
understand why the worker are not performing to their expectations. While it may be that the
workers do not possess the required skills, there may be other factors involved which are more
compi icateci and which reach to the heart of effective management. Assuming that the workers
are being willfully disobedient or unproductive is to put responsibility where it does not belong.
1.1.3 Conceptual Perspective
Employee performance can be defined as the job activities expected of a worker and how well
those activities were executed many employees are assessed on an annual or quarterly basis in
order te help identii~’ gaps in their performance.
Poor performance of service providers leads to inaccessibility of care and inappropriate care
which thus contributes to reduce health outcome as people are not using services or are
mistreated due to harmful practices.
The health workers number. quality and type of professionalism determine output and
productivity that greatly influence progress. A number of articles and documents have reported
problems relating to service provision due to poor performance of health workers.
Foor performance results from too few staffs or from staff not providing care according to
standards and not being responsive to the needs of the community and patients. As Hughes et al
state ~most peri~ormance problems can be attributed to unclear expectations skill deficit resource
or equipment shortage or a look of motivation (Hughes et al, 2002). These causes are rooted in a
failing health system, low salaries, difficult working and living conditions and inappropriate
training.
Health worker performance barriers such as unclear roles and expectations, unclear guidelines,
Poor rocesses of work, inappropriate skills mix in the work setting, competency gaps. lack of
feedback . difficult work environment and unsuitable incentives mean that even where are no
critical workforce shortages health workers may still fail to provide quality care/ delivery while
substantive evidence of the effectiveness of different types of interventions to improve worker
IDelormance and service delivery is still limited salient feature are emerging from existing
7
studies and country experiences that can help inform a strategy for optimizing the performance
a~d producu vitv health workers (Green and Kreuter. 2005).
1.1.4 Contextual perspective
The health of the Uganda population is central to the socio economic transformation of the
country. The poor health status of our people undermines the economic by 2020, if health service
delivery is not improved. The inadequacy of interventions against common health conditions and
the inefficient use of available health resources is a challenge that must overcome as we move
towards middle income status. Improving health service delivery continues to be recognized as
the district health priority.
Throuh environmental health, which component aims at contributing to the attainment of a
signi ticant reduction of morbidity and mortality clue to poor sanitation and hygiene, indoor
pollution, poor food hygiene and supply unsafe water accessibility and other environmental
health related conditions, Nakasongola di strict through implementation of activities supported by
the GOU and the Uganda Sanitation Fund (USF) program whose emphasis was put on improved
hygiene and sanitation. for instance training and capacity building of health workers,
commemoration of district sanitation weeks. This has led to improvement in latrine coverage
and safe drinking water with 59% and 46.8% respectively (WHO, 2003).
Nakasongola local government in partnership with the community based organization throughout
reaches have caused a positive change in health seeking behavior by disseminating health
messages and conducting household monitoring. The out reaches involves provision of dental
services. UCT services. Distribution of Albendazole and imnwmization of all immunisable
diseases
Sensitizing communities on the 7 tips for a healthy life style for instance Eating healthy and
exercising regularly immunizing children and others at risk, observing personal hygiene and
sanitation. fighting malaria , TB. HIV and other common infections . Avoiding drugs and
alcohol abuse. practicing responsible sexual behavior and safe parenthood. Attending regular
medical checkups and seeking medical care early.
AMREF in partnership with the District local government initiated a project of enhancing the
capacity for prevention and treatment of malaria. This was a response to strengthen community
8
support structures scale up malaria prevention and treatment interventions in Nakasongola
district. Through behavioral communication change (BCC) which is the deliberate use of
communication to promote positive health outcome based on proven theories and models of
behavior changes. This improved the prevention of malaria among school children from 76.6%
to 90%. among pregnant women 24% to 78% and the overall mosquito net coverage of 91.6%
(IJBOS. 2014). In the bid to continuously ensure that staff at service delivery points has the
requisite skills for diagnosis and management that they are up dated on the malaria control
policies, integrated management of malaria (1MM) training has been conducted in Nakasongola.
Rapid diagnostic kits for testing malaria and anthmalaria medicines have been procured.
1.2 Problem Statement.
The health status of Nakasongola has improved over the last five years, approximately 45% of
the population has adequate access to health service and latrine coverage has increased from 15%
to 60 % (IJBOS. 2016). As a result. child and maternal mortality rates have fallen significantly.
and i Os expectancy at birth increased to 61 years of age. With respect to health indicators, 60.4
of he population has access to safe drinking water. Additionally 86.5% of children reaching
the first birth clay are fully immunised, (UBOS, 2016). Despite these achievements, the district
has some of the worst health status indices in the country, with fertility rate of 6.8%, malaria
accounts for 46% of the disease burden in Nakasongola district compared to 26% of the total
burden on the national rate (Uganda). The mortality rate stands at 505/10000 and under 5
:nnstaiit\ rate a 129/1000 live births (UDhIS, 2016).
The district faces a number of issues concerning health performance which is relevant to
successful service delivery for instance the doctor to population ratio and midwives to population
ration is 1:142800 and 1:347 respectively (D1-IO’s office, 2014). This is evidenced by the district
deal [P performance evaluation of 6t).9% for FY 201 5/16 by the district league table (DLT.
20 1 5~20 1 6) and the failure to meet the minimum national health standards of 75% as by the
Auditor General report 2016 of Nakasongola District. A full understanding of the concept of
employee’s performance variable influencing health service delivery is needed to improve the
health service delivery.
9
.3 H rpose of the study
the purpose of study was to establish how health workers performance affects health service
aulk cry in Nakusongula District
.3.lObjectlves of the Research
I) To establish the state of employee performance in Health Centre IV Nakasongola
District.
-) lb find out the state of health service delivery in health centres in Nakasongola District
3) 1o find out the relationship between employee performance and health service delivery in
Nakasongola district.
a .a.2 aesearca Questions
I) ~Vhat is the state ofemployee performance in health centres in Nakasongola District?
) ~‘hat s the state of health service delivery in Health Centre IV in Nakasongola District?
3) What is the relationship between employee performance and health service delivery in
Nakasongola district?
~.3.3 Hypothesis
lucre is a significant relationship between the performance of health workers and health service
‘.: ~
- .1
.4.1 Con:cnt Scope
health worker performance was independent variable and service delivery will be the dependent
~ariablc. The study looked at the performance attributes and how these attributes influences the
c3uzility of health service delivery.
a.-., :a~uret;ca1 ScGpe
The study was based on the Two-Factor Theory propounded by Herzberg 1959 which states that
there are certain factors in the workplace that cause job satisfaction, while a separate set of
factors cause dissatisfaction. According to Herzberg. individuals are not content with the
• atis.èction of sower-order needs at ~ork. for example. those associated with minimum salary
.a ~ls ts safe and pleasant working conditions.
1.4.3 ~Jeographical Scope
This study was conducted at Nakasongola health centre IV in Nakasongola district
10
1.4.4 Time Scope
The study was carried out in the period of 5 months in 2018.
1,5 Significance of the Study
The proposed research will help the researcher in understanding how poor performance of the
health worker affects the health service delivery.
The study will help the researcher to gain confidence as it will enable me to apply the theory
work and interact with the practicing member who will enable me gain the insight of the actual
fhe study will he of vital use to me as it is a partial fulfillment for the Bachelor of statistics at
Kampala international university
The study will he of vital use to the Nakasongola health centre IV as it will help them to
understand the impact of their performance on the service delivery.
•L6 .Definitions of Key Concepts
aLl Oua~~tv 01 care
This is the function of the health care delivery system to deliver safe, effective and patient
centered care in an efficient, timely and equitable manner. The institute of medicine (loM)
defInes quality of care as the degree to which health services for individuals and populations
increase the likelihood of desired health outcomes and are consistent with current professional
knowledge.
.1. .6.2 Perforn~az~ce
Performance of health worker includes the quality of their work, the technical skills they use, the
care they deliver and the impact of their work on health outcomes
1. .6.3 Productivity
i~rocluctivitv of health worker is determined by the setting in which they work. their levels of
motivation, work organization, work organization, management capacity, the division of labour
and other resources.
11
.6.4 llealthcare workers
icaith ~~orker are known as Human Resource for health (IIRH) or healthcare providers
‘omprise of all people whose main activity is to enhance health by providing health services in a
s ci&lly desired and technologically/professionally standard quality. Such workers include
doctors, nurses, pharmacists. laboratory technicians, the management team, supporting staff such
as financial officers and cleaners (WHO Factsheet 2006).
.~.6.5 ~VorK morale
~‘or& morale is the job satisfaction or outlook that comes with wellbeing of someone in a
s,ecific i~ork place. It has a direct effect on performance and one on the key detenninants of
productivity.
.6.6 Work Environment
Work environment is the designated location where a task is to be done or completed such as a
,l~n. t)f Lpl ~> merit. The physical conditions that surround the place in which work is done
.6.7 ~Ies.thca.e ser’ice delivery
It defines the quality and availability of its healthcare and describes how and when it is delivered
to the intended persons in need of healthcare both at the hospitals and at home.
12
CHAPTER TWO
LITEI~TURE REVIEW2.0 Introduction
This chapter shows what other scholars have written about the employee performance and health
service delivery. The focus was on the objectives of the study, it also presents the conceptual
framework and linallv the related studies based on the topic of the study. This section shows all
the literature that was used in the study.
2.1 Performance of Health Worker
Performing service providers are defined according to the definition in WHO report of 2006 as a
workiorce that works in ways that are responsive, fair and efficient to achieve the best health
oui,comes possible given the available resources and circumstance: Performance can be defined
as a combination of equipment and staff being available, competence, productive and responsive.
Staff performance is often perceived as a function of skills and knowledge. In recent years it has
been recognized that performance has been influenced by additional factors (WI-JO 2006) if staff
members are to perform to their full capacity, it is not only staffing issues that must be
midresserk but also systems and facility issues.
The perlormance of health workers depends not only on their availability, productivity,
responsiveness and competence as well as the availability of infrastructure, equipment and
support systems such as the management information system, resources and accountability
systems that are in place (Zurn et al 2005). The elements of staff performance are influenced by
retention, absence. motivation and job satisfaction, obtaining knowledge, skills and attitudes.
accoumahility and working conditions and are interrelated.
2.i~1 Absenteeism
Absenteeism by health providers is a frequently occurring phenomenon in many health facilities,
especially in resource poor areas. Reasons for absenteeism may include income generating
opportunities etsewhere or personal problems. An important factor contributing to absence is the
elects of HI’v’! AIDS on the health workforce (Aitken & Kemp. 2003).
2.1,2 Obtaining skills, knowledge and attitudes
inadequate knowledge, skills and inappropriate attitudes can all form obstacles to good health
care delivery. Advances in insights into treatment and diagnosis as well as changes in roles and
1—,I 3
responsibilities require continuous professional development among health workers. The method
most frequently used to upgrade skills and knowledge in the health care sector in resource poor
settings is oil site training courses and seminars. As an intervention to improve practices of
health providers these have not proven to be very effective (Rowe et a] 2005) , this can be due to
lack of problem analysis and training needs assessment (Potter&Brough 2004) lack of
competences occurs because of limited access to training and inadequate training methods.
2.1.3 Motivation and job satisfaction
I )cmotivaiion and dissatisfaction with work lead to poor attitudes on the part of providers
to\vardls worlds and their patients, not using standards protocols for treatment or behaving
rudely towards patients and stigmatizing patients.
Motivation is defined as an inclividuaks degree of willingness to exert and maintain an effort
towards organizational goals (France et al, 2002). Various studies show that financial incentives.
thougn inilDorlani. are not the sole reason. and often not the main reason, for motivation. Other
important motivating factors include recognition, appreciation and opportunities for career
advancement. Factors relating to clemotivation include high load, lack of equipment and supplies
and the lack of supervision and training opportunities,
Motivation and job satisfaction are two different things in that when someone is satisfied with
his or her job. he/she ~s not necessarily motivated to perform well, however job satisfaction does
influence motivation and is related to turnover and absenteeism.
2.1.4 Accountability
l-lealth service providers might not adhere to standard guidelines for diagnosis, treatment and
communication with patients. and may engage in harmful practices in consequence of lack of
accountability mechanisms. Health worker / patient relationships can be severely disrupted as a
result of health \vorkers’ attitudes. (IVlodibaet al 2002, wood &Jewkes 2006), Occurrence of
inadequate behavior towards patients is possible when staff members are not held personally
responsible for their performance towards clients, managers or peers. Various reasons form a
bundation for these practices, such as a lack of supervision and follow up. patient perspectives
and characteristics.
14
2.1.5 Working conditions
Good performance by staff is enabled via a supportive working environment. This encompasses
more than just having sufficient equipment and supplies. It also includes systems issues such as
decision making and information exchange processes and capacity issues such as workload,
supoort services and infrastructure (potter &Brough, 2004).
Protection from HIV/A1DS at work has become a very important issue in countries with a high
IJIV prevalence. A lack of protective measures increases fear of infection and limits quality of
services due to stress and delegation of tasks to non-qualified staff (KAT/CHAZ, 2005, Doulo
2005)
This is evident to poor health systems with lack of equipment, supplies and poor productivity,
limited competences and poor responsiveness. The root cause that result in suboptimal
~eriormance in these areas consists of a complex set of factors which are interrelated. For
instance, low salaries can lead to increased absence to earn extra income and also to decreased
motivation to he willing to provide quality of care. At the same time, motivation is influenced by
lee 2 at equipment supplies, management support and supervision.
2.2 Health Service Delivery
There is a vast literature conceptualizing and measuring various aspects of health service
delivery which is the dependent variable of interest, ideally, the chosen outcome variables should
be sensitive to the impact of performance. The study considers proximate process indicators of
the perlGrmance of health service delivery; process indicators include quality, efficiency and
access. It is important to bear in mind that even these intermediate indicators may be influenced
by factors beyond the performance of health workers.
2,2,1 Quality
i-lisa ricaliv, much of the research on health care delivery has focused on clinical quality.
investigating whether the care provided to a patiei~t was safe and medically appropriate
(Donoabedian 1980, lOM 2001). Clinical quality refers to whether the provider’s care conformed
to best clinical practice for those who use the services of the organization. It does not refer to
outcome measure of population health Such as vaccination or antenatal care coverage, in which
15
the denomination is the population. Although clinical quality remains a major objective of heath
service delivery, managerial quality and patient experience with in the quality intermediate
outcome domain, managerial quality refers to the degree to which administrative system such
..s atiman resources and data management support the delivery of high quality Clinical care
~Itgg1zc et al 2005). Administrative systems also influence other organisational intermediate
outcomes like efficiency and access. Patient experience is included with in quality because of the
importance of patient centred service delivery, for which patient experience is often used as a
measure and a counter point to the technical standards of clinical and managerial quality. (Safran~, ii. :006)
‘.2.t ~.teiency
Efficiency is relative measure that compares inputs used (human. teclmological, financial) to
outputs attained (number and level of services) (Hollingsworth. 2008). Efficiency has been
received in high income countries due to shills in technology, market structure and demographic
rroii iCS.
“.2.3 Access
Acecss relbrs to the potential ability of an organization’s potential clients to obtain its services.
~Vhcn this potential ability is realized, it results in observable utilization which is why studies
oftet ‘iso utilization as a proxy variable for access; conversely, lack of utilization can signal the
existeace ol’ barriers to access (0 mahony. 2008). However access and utilization are
conceptually distinct intermediate out come as an individual may have access to an organization
but choose not to utilize service there.
Access can also be used to refer to the availability. accessibility, accommodation, affordability
3nd aeccpLabi!ity of health services (Peters et al. 2008). Access is sometimes discussed in terms
of ~x1uity or geographical or financial coverage of health services but these latter terms tend to
a,ply more to health system perspective on service delivery rather than organization level
models. Although enabling ph>sical and financial access for geographically dispersed population
or providing discretionary health care services are typically beyond organization’s jurisdiction.
tb:. aspects of access are nonetheless influenced by organizational action and are therefore
;nciuded as organization level intermediate outcomes.
16
~c ~io s ~‘n act~een employee Performance and Health Service Delivery
ontz and Weihrich (2009) argued that considering the role of employees in service
organizations, they need to be equipped to carry out their functions successfully. Technically and
otherwise. they need to be reinforced and motivated to be able to span boundaries. The link
between employee’s behavior, their motivation, competencies, satisfaction. and commitment.
fimpio~ cc satisfaction levels were caused by latitude given to employees by their management to
custonie: needs authority given to tnem serve customers and possession of knowledge and
~ki1ls needed to serve customers.
Maicihi (2007) argued that employee performance has a positive relationship with service
cleli\ cry. As a result the human resource practices play a crucial role in the management of
~arvice operations. Suggests that a complex combination of strategies is needed to ensure that
~er~ ice employees are willing and able to deliver quality services and that they stay motivated to
perii~rm in customer-oriented, service-minded ways. Paying attention to competencies and their
continuous development, establishing collaborative relationships, and empowering service
employees should he reflected in I luman Resource practices for services.
Nisgrove & ~Neighten (2003) argued that there is relationship between employee performance
and service delivery associated with deficiencies in the incentive structure of’ health systems.
nrtceu most services delivery systems in developing countries present front line providers with
set of incentives that negate the impact of pure based polices . therefore while resource alone
ap~ea: to nave a limited impact on the quality of health in developing countries . it is possible
npu~s are complementary to changes in incentives and so coupling improvements in both may
lia~ e large and significant impact.
Nielsen (2013) contends that employee performance and a significant relationship with service
ielhcrv in the public sector. First. recent research shows that the ps~ chological role of applicants
a nt,1 lie ohs is largely determined by adjustable features of the position. most importantly the
~agc. Second. research shows that personality traits are malleable, providing a potential avenue
ibr policy. Thirdly. psychometric measures might be useful as diagnostics in hiring or promotion
decisions. The degree of correlation between personality measures. doctor attendance. and the
-cs~onsivencss of senior oflicials to acifonahle data on absence we suggest that substantial
17
improvements can be made by changing the role of hired workers, either through changes in
hiring and/or promoting practices through offering more attractive jobs or through working to
chance individuals traits over time. Our findings additionally imply that improvements in
performance max he achievable even in a system where incentives to attend work are extremely
weak.
Redman and Wilkinson (2015) set to study the impact of employee performance on health
service delivery, using and focusing on the local governments in Kenya. the study right as
measured by bottom-line results seem to follow all if not most of the following ten best practices
in implementation of succession planning. These include: commitment and involvement of the
CEO and Board, regular talent reviews, identifying viable successors for key positions, taking a
“pipeline” approach to development, holding the executive team accountable, aligning the
succession plan with business strategy, managing the irrational, political, and emotional
dynamics of succession, assessing performance of potential successors, integrating succession
sPanning with performance management. recruitment, selection, development and rewards and
making a serious commitment to development in terms of time and resources. Molina (2013)
cites three succession planning best practices geared towards growth and business continuity
namely: Benchmarking, looking into the future and keeping it dynamic.
Berthal (201 6) did a comparative study on achieving health service delivery through employee
performance at Malaysian Institutions and found that while focus on competitive pay packages to
attract and retain talented cadres is clearly effective in manifesting job motivation.
complimentary strategic HR practices are profoundly important in reducing staff turnover.
Walker (2016) did an exploratory study on the relationship between employee performance and
service delivery employee retention in public organizations at the United Arab Emirates and
established that lack of empowerment and management style are factors that influenced the
retention of employees in UAE public organizations. This was attributed to the fact that the
organization appropriately redirects its retention intervention strategy in consonance with the
valence of employees such that pay rise always factors in the inflation rates. Talent management
and staff retention at the bank of Zambia and concluded that employees felt motivated by
realist:c objective setting, continuous learning opportunities, valued ideas and encouraging
creativity which largely contributed to their retention.
1 C)I0
• weording to Wright & Gem> (2014) argued that employee performance positively affect service
,.eii~ e.y. “fle results improves the overall performance of the employees to efThctively perform
the current job but also enhance the knowledge. slcills and attitude of the workers necessary for
the future job. thus contributing to superior organizational performance. Through training the
employee competencies are developed and enable them to implement the job related work
‘ilieentl>. mid &chicve firm objectives in a competitive manner. Further still, dissatisfaction
‘o1n1)laints. absenteeism and turno~ er can be greatly reduced when emplo> ees are so ~vell trained
that can experience the direct satisfaction associated with the sense of achici ement and
knowledge that they are developing their inherent capabilities.
4 belated studies
‘za’ o> a (2015) conducted a study on employee performance and health service delivery in
Uganda. The study ‘~as conducted based on employees of Kampala capital city authority head
office and data collection was done through the use of the questionnaire. The study findings
reveal that employee compensation had a positive effect on health service delivery. The study
concluded that employees expressed the desire to execute duties under the corporate settings
a.. a.: .iun the existing leadership styles. Similarly. following the second objective, the
:sctacher i’urher eoreluded that employee performance created dislike to work and reducing the
iaherent motivation to work freely for health service delivery. Further still. in respect of the third
ub~~etive. the researcher concluded that employee performance was mostly applied to lower
depa.iments that had no formal work procedures of performance and these transfonned to
;rnpro~’ed health service delivery.
A study on the retention of health workers in Ndetei & Kbasakhala & Omolo (2016). the study
was conducted employee performance and health service delivery in Busia district ‘l’he study did
.iol find out that heaith service delivery practices among the major determinants of employee
::ti.t.on :aaoig tne a.urses in public health facilities in Uganda. The study instead found out that
urs~s retainitag depended on salaries, access to house and car loans, availability of training
opportunities. good living conditions. communications, health care and educational opportunities
for themselves and their families. This study sampled a variety of health stakeholders across the
country and combined a cross-sectional field survey with key informant int~rviewi (primary
L.a) tad a,n anal~ sk ii secondary data from internet websites.
19
Mukasa (2016) conducted a study on employee perfonnance and health service delivery in USA,
flexible job descriptions are vital options that promote developmental opportunities and
succession management plans especially in the library industry. This study used supportive
literature from both within and outside librarianship to examine the impact of flexible job
descriptions on succession management process. The focus of the paper was to address expected
library management and leadership gap expected in the years ahead as current library managers
from the baby boomer generation retire in record numbers. The study findings suggest that
written job descriptions may limit the ability of current library managers to provide opportunities
for learning and growth for those employees who will fill leadership roles in the coming years.
However, more flexible job descriptions was found to provide richer, more creative learping
professional and developmental opportunities for identifying high potential employees within
organizations for succession planning.
Omar (2016) conducted a study on the effect ofperformance contracting on service delivery. The
study was conducted in Gulu district, the study was conducted from the employees of the district
The study concluded of the study findings are advanced based on the relationships that were
established for each of the different research objectives. From the foregoing summary, it can be
concluded that the process of performance contracting implementation at the municipal council
of Gulu district has transformed the once inefficient council into a vibrant entity that is able to
provide efficient and quality service to its customers. It has moved from being a tool that the
employees loathed to one which they look forward to in order to help them achieve their share of
service, several challenges notwithstanding. From the findings further research are suggested as
follows; to begin with, a study on the perceptions of the residents of Gulu district on the quality
of service delivery.
Naomi, Lusala & Kabasingwa (2015) conducted a study on the local government councils’
perfonnance and public service delivery in Uganda, Jinja District Council. The performance of
the Local Government Council, the District Chairperson, the Speaker and individual Councilors
who are vested with powers and responsibilities to ensure effective governance of the respective
Local Governments as stipulated in the Local Governments Act (CAP 234). The score-card is
intended to build the capacity of leaders to deliver on their mandates and empower citizens to
20
Jemai1d ibr accountability fiom elected leaders. The objective of this report therefore is to
prot jde inlbrmation and analysis based on an assessment conducted during the FY 2011/12. The
report is based on a comprehensive review of existing documents which include: planning and
budgeting. service delivery monitoring, and Jinja District Local Government performance
reports. Qualitative analyses of minutes of standing committees and council sittings was also
jnde:take~i to inlbrm the report particularly about the performance of the council, chairperson
~nd individual councilors, The major challenges to the performance of the council and political
.eadcrs mainly arose from internal weaknesses characterized by internal conflicts, poor contact
vi .h the electorate, poor monitoring of government projects. poor record keeping. low civic
wareie~s especially ~nong the new councilors, and poor budget performance.
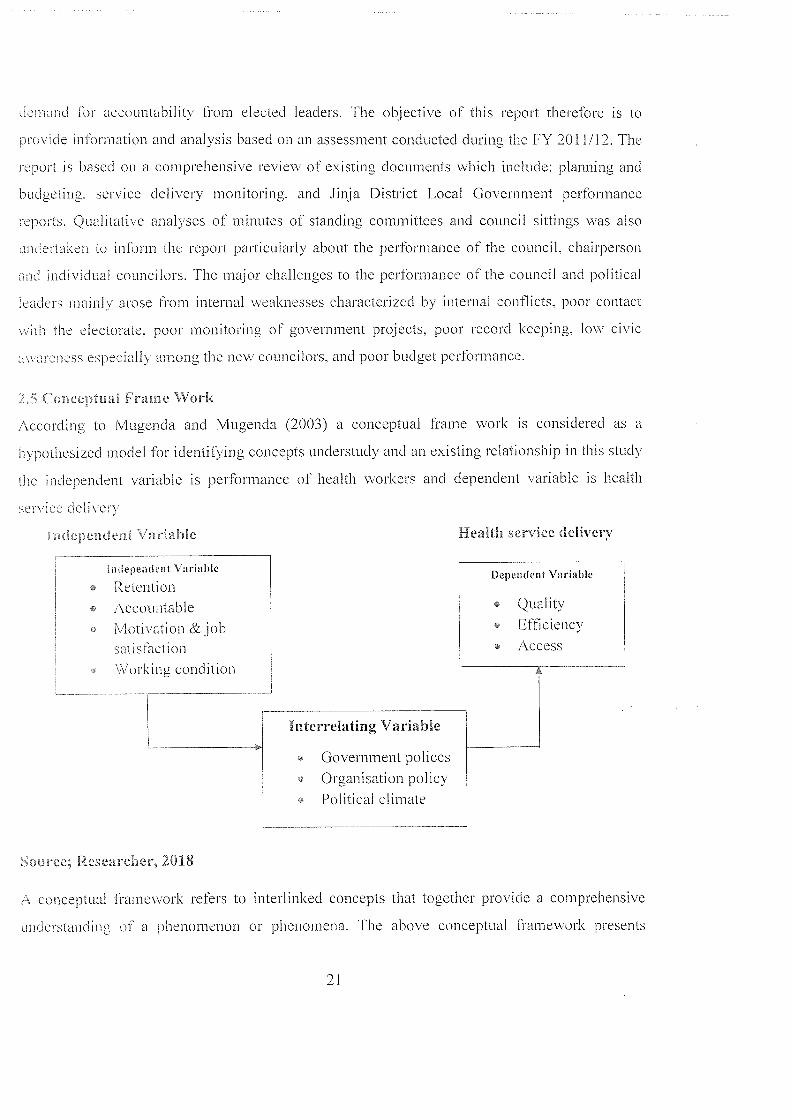
‘~ (~ineep~uai Frame Work
According to Mugenda and Mugenda (2003) a conceptual frame work is considered as a
hypothesized model for identifying concepts understudy and an existing relationship in this study
the independent variable is performance of health workers and dependent variable is health
sereice dcl i\ ~f\
i uel,dnoem v~-:~ible Health service delivery
Independent Variable I.Dependent VariableRetentionAccountable ~ Qualityi~4otivation & job • EfficiencySat:slaction Access\~~orking condition- Interrelating Variable
Government policesOrganisation policyPolitical climate
source; Researcher, 2018
A conceptual framework refers to interlinked concepts that together provide a comprehensive
un3erstandinf of a phenomenon or phenomena. The above conceptual 1i’amework presents
21
factors aifecting performance of health workers as the independent variable with four
dimensions: retention. accountable, motivation, and working condition. Service delivery on the
othar hand is presented as the dependent variable which is measured in terms of efficiency.
quality. effectiveness, and access. In healthcare services, there are different viewpoints to quality
service delivery. hrom the provider’s standpoint, the WI—lO (2004:15) asserts that quality means
providing the best possible care available to the patient. From healthcare administrator
persiective. quality is seen as providing ‘~effective care in a cost—conscious environment that may
include rationing of health care especially when resources are limited
‘2’2
CHAPTER THREE
METHODOLOGYZJ~ I’OOJCLGfl
l’his chapter covered the method that is used in the study. It included the research design, the
study population, target population and sampling size population. sampling techniques, data
~oJecion ins~run~ent. reliability, and validity of the instruments, data collection procedure, data
r rocessing and analysis, ethical consideration.
3. kescarch Design
rtvsearch design is the conceptual structure within which research is conducted. In this study.
correlation research designs were used to determine the relationship between employee
er hrmancc and health service delivery (Amin. 2006). The design is deemed appropriate
aecaasc ~t provides an assessment on the assessment of the relationship between variables. The
correlation design on the other hand involved inferential statistics to determine the relationship
bet\\ecn the ~ ariables. The research designs were guided by both quantitative research
approache.~. ~lic quantitative data collection approach was undertaken using closed ended
~u ~s.i 3.15 in eakccting quantitative daLa or numerical data or data which was presented
~. or iaatheniatically into mean and standard deviation.
.i.2 ~‘arget Pop alation
.\ population may be a group of people~ organizations. houses, i’ecords. legislators. and so on
(~\acamias and Nachmias. 2012). The target population for this study included two categories of
respoi ~dents. [he study involved this category included the patients and employees of health
workers, ‘[he population in this category included because is the ones who receive the services.
‘[he stud included the health workers 35 and the people 65 who constituted 100 people as
lopulation.
~p~e Siz
SIZL c I ~() respondents u as selected. This got by the use ol’ Slovene Formular
~he sample Size was calculated mathematically using the formula below:
I’I=I .Vu~
~cv: a ~he sample size
N = total target population, that is 100.
a = the level of significance, that is 0.05
N‘7=
l+Nr
n= 100
I + 100 (0.05). (0.05)
100
1+100* 0.0025
n= 100
1.25
n =80
A sample size of 80 respondents were selected to participate in the study
Table 3.1: The Sample size
Categories Population Sample Size
l-leahh workers 35 28
Patients 65 52
Total 100 80
3.3.2 Sampling Procedure
The researcher used simple random and purposive sampling technique in order to get target
respondents. The random sampling technique was used in order to give each targeted
respondents’ equal chance to participate in the study by being part of the sample. Simple random
sampling was used through rotary to select the respondents on the basis of pick and play. The
simple random technique was solved biasness for selection of health staffs were given equal
chance to be selected and provide data for this study. The health staff was purposively selected
from the employees through purposive sampling.
24
3.. Ln.ta CoHesion instrument
:~ semi structured questionnaire for this study used for ease and expression by the respondents.
The questionnaires were designed to ask questions in the four areas of the study; retention.
presence. motivation and job satisfbction of the employees and health service delivery delivered
to the community.
.,.3 l,ata .olaction Metaod
)ata lbr the stud) collected from both primary and secondary sources. Semi structured
questionnaires were administrated to the randomly selected respondents and focus group
discussions with purposive clients to collect the primary data. The secondary data consisted of
!sublisI~ed literature about previous studies and contemporary practices
q1( Cy o ttae I istrument
~alidit> refer~ to the extent to which a method of data collection presents what it is supposed to
do. or the extent to which methods of data collection measure what it is supposed to measure
(Bell. 1997). Content validity ensured by subjecting the researcher devised methods of data
.c.llection on employee performance on health service delivery by the judgments from the
.~ e.~s ~c!,o e’ainiate the validity on the basis of their experience.
.~s.i f~eliability of Insbruments
aeliability according to Amin (2005) refers to the degree to which the instrument consistently
measures vhatever it is measuring. A test is reliable only if it consistently measure s what it is
supposed to measure. The researcher requested her supervisor to review the instrument. The
~ )fllfl.ICCS .n~pro’ ed and adjusted according to the recommendations were provided by the
54’C?¼ isor.
3.8 Data P1ocessing and Analysis
After completion of the field work in Nakasongola health centre IV. questionnaire were given
s:ral ,umbers before data entry. data was entered and analyzed by using SPSS version 21.0 was
ii. . in.t lrcquei:cy ‘tnd percentages was used for demographic characteristics of respondents.
unu a1can and standard deviation for computation of the state of employee performance and
health service delivery. Also the researcher used correlation analysis to measure the association
25
~tv~ am no ~ariab1es (independent and dependent variables) and the strength of their
:~lationship.
ieaa Ra~ige Response Interpretation
3.26 - 4.00 Strongly Agree Very Good
‘.5. ‘.25 Agree Good
i.73 -...50 Disagree Poor
1.00-1.14 Strongly Disagree Very Poor
3.9 Ethical Consderations
i~thica1 issues arose during the study include authorization to conduct the study. permission from
who •jy~~, and acquisition informed consent of the participants. The power differences between
he rcscarcher and the participants. privacy and confidentiality of the participants and
information (~~ine. 2010) addressed.
Introductory letter was granted from the university and permission to conduct research requested
≥om i~Ievant authori y. The participants was informed about the objectives of the stud) and they
..a i.11,z~ie~ 1hat tacir participation was voluntary and there is no any kind of force that
employed to have them participated.
26
CHAPTER FOUR
d~i~SZNTATION, INTERPRETATION AND ANALYSIS OF FINDINGS
~ larroocehen
This cha~rer comprises of the findings that were gathered by the researcher from the employees
and clients of Nakasongola health centre iv. The purpose of study was to establish how health
workers pcrihrmance affects health service delivery, The study objectives were to establish the
:iate ( f enlpl( ~ cc performance. to find out the state of health service delivery and finally to find
oL.I in relationship between employee perlbrmance and health service delivery in Nakasongola
uisirict. The presentation and interpretation of data in this chapter has been done with the aid of
quantitative and qualitative methods for example the use of tables, figures and personal analysis
and interpretation are all presented.
b~n ~o~:a~wi vrofile of respondents
~his was easer. on the gender of respondents. age. education, marital status. departments in an
organization, position of i’csponclents and period of work in the organization.
.1.1 i~indings on Gender of respondents
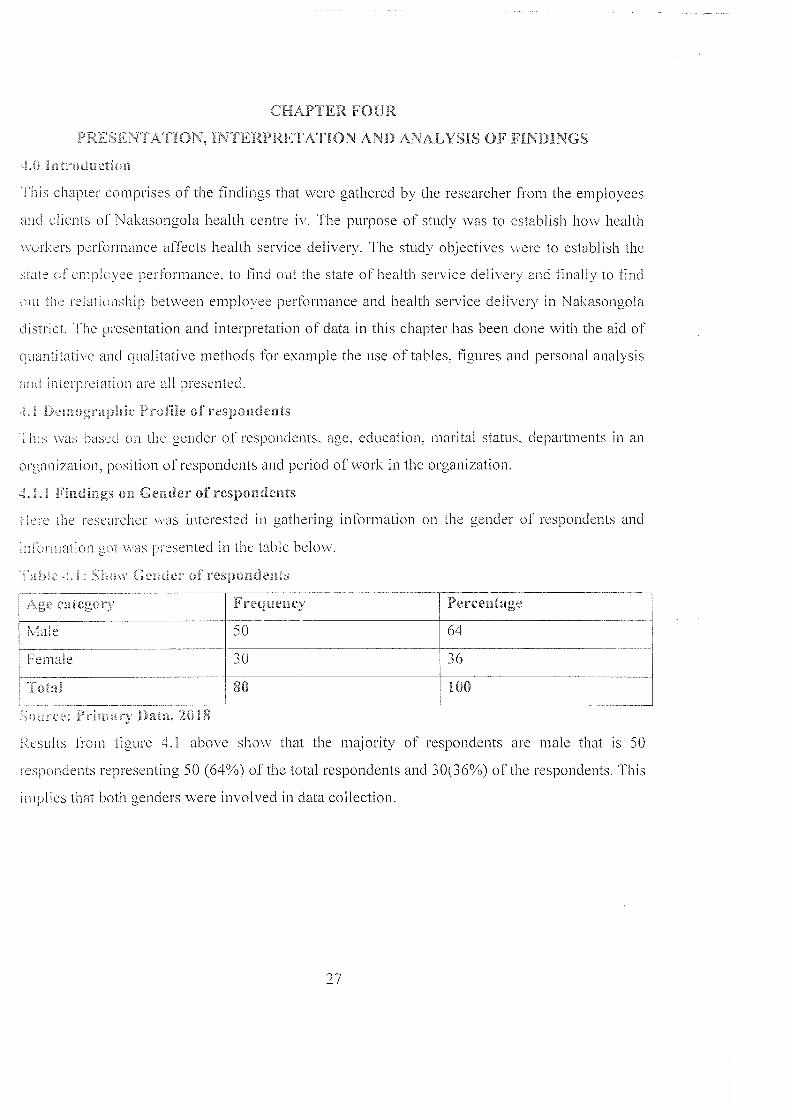
[etc the researcher was interested in gathering information on the gender of respondents and
n tation cii v as I resented in the table below.
~ 0 N C~ uer of res1)oIideIhs
Age carcgsirc Frequency Percentage
Male 50 64
~Female 30 36
~otaI 80 100
~ cc ~knacy Cant, 2018
~<Nsults from figure 4.1 above show that the majority of respondents are male that is 50
respondents representing 50 (64%) of the total respondents and 30(36%) of the respondents. This
imphes that both genders were involved in data collection.
27
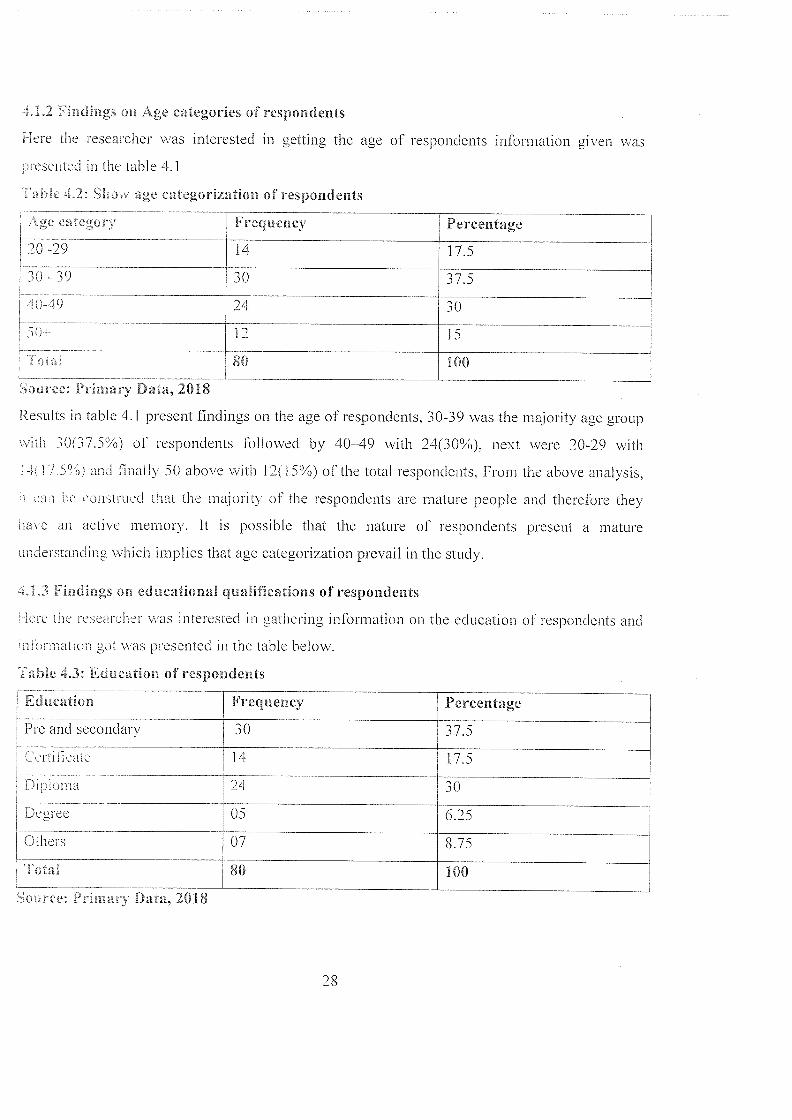
~.L2 vindings on Age categories of respondents
I lere the researcher was interested in getting the age of respondents information given was
presented in the table 4.1
0 mc -~.2: SLnv age categorization of respondents
4ge ~ategor~
20-29 14 17.5
30 - 39
40-49
~80 ______________
Soarce: Primary Data, 2018
Results in table 4.1 present findings on the age of respondents. 30-39 was the majority age group
with 30(37.5%) of respondents followed by 40—49 with 24(30%). next were 20-29 with
4 1 7 5° o) and Iinall\ 50 above with 12(15%) of the total respondents. From the above analysis.
be ansi uccl that the majority om the respondents are mature people and therefore they
have an active memory. It is possible that the nature of respondents present a mature
understanding which implies that age categorization prevail in the study.
~.i.3 Findings or. educational qualifications of respondents
Ie:e the r ‘sear her ~ as interested in gathering inlbrmation on the education ol’ respondents and
elar ~iatioi~ gal ~ as presented in the table below.
lame ~.3: Education of respondents
Education
L~’~_secondary 30 37.5CenilicaL 14 1 7,5
~ L i~( 1~i 24 30
~ Dearee 05 6.25
Others 07 8.75
l~~I 80 100
Frequency
3
Percentage
24
-
~
3
15
100
Frequency Percentage
ieee: P:imarv Da a, 2018
28
vrun. i.e ~ahlc above it shows that the majority of the respondems were pre and secondary level
ceerec holders representing 30(37.5%) followed by diploma holders at 24(30%) followed b~
certiticate holders representing 14(17.5%). then others at 7(8.75%) and finally degree
respondents who were 5(6.25%). This implies that the respondents from the xvell educated and
lherctore the information obtained from them can be relied upon for the purpose of this study.
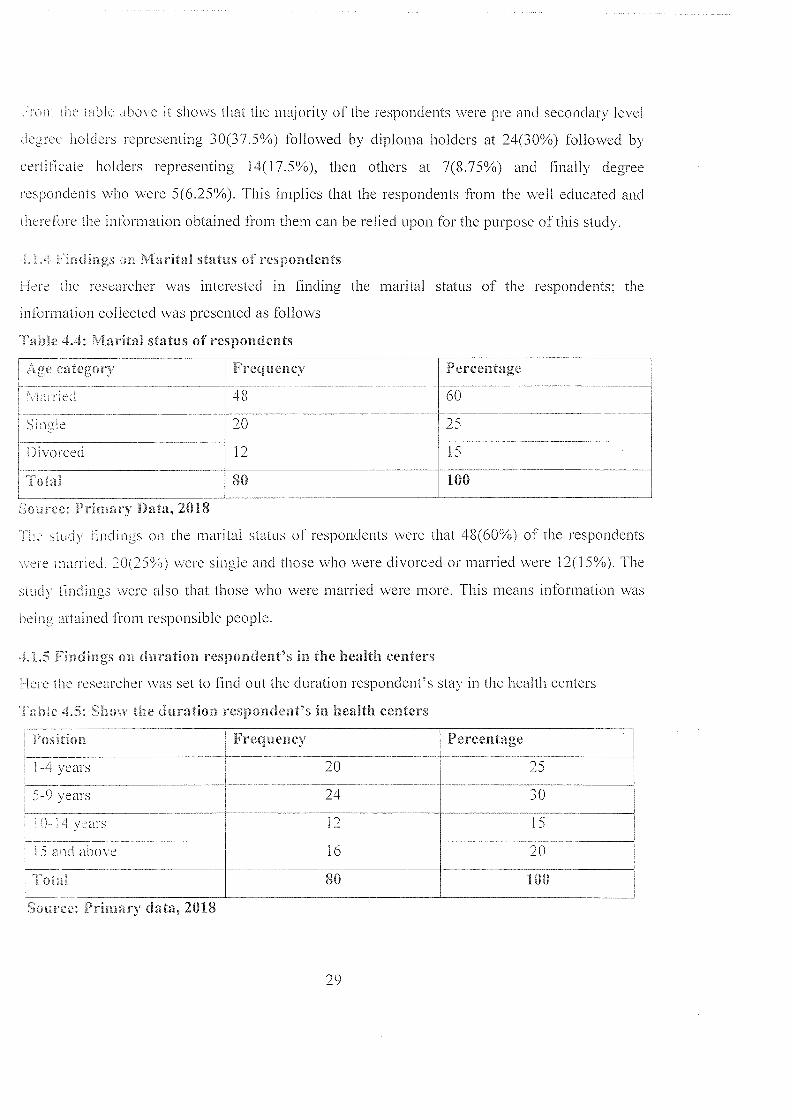
.dacings ot Marital status o~’ respondents
lere tne researcher was interested in finding the marital status of the respondents; the
information collected was presented as follows
~able 4,4: Marital status of respondents
category Frequency ~Percentage
a~rDi 48 60
Sin~&tc 20 25
Divorced 12 15
4ota~ 80 100
fiource: Prin~ary Data, 2018
.u’ s~ud~ linJngs on the marital status of respondents were that 48(60%) of the respondents
.t etc ~aarried. 20(25° ~ were single and those who were divorced or married were 12(15%). The
sLud~ findings were also that those who were married were more. This means information was
being attained Dom responsible people.
.1.5 ‘indmgs on duration respondent’s in the health centers
I lere the researcher ~a as set to find out the duration respondent’s stay in the health centers
~Th~ne ~.5: Sl~o,v the duration respondent’s in health centers
Postion Frequency Percentage
1-ivears 20 25
5-bvears 24 30
12 15
15 and above 16 20
80 100
Source: drimary data, 2018
29
i’he results in table 4.5 on the duration respondents time of association with the organization had
heeti there for 5-9years 12(30%). 1-4 years had 1O(25%) of the respondents. 15 and above had
~ 1 ~) of the re~ pondents while 10-14 years had 6(1 5%) of the respondents. 1 his implies that
marn :esponcients have information about the health centre.
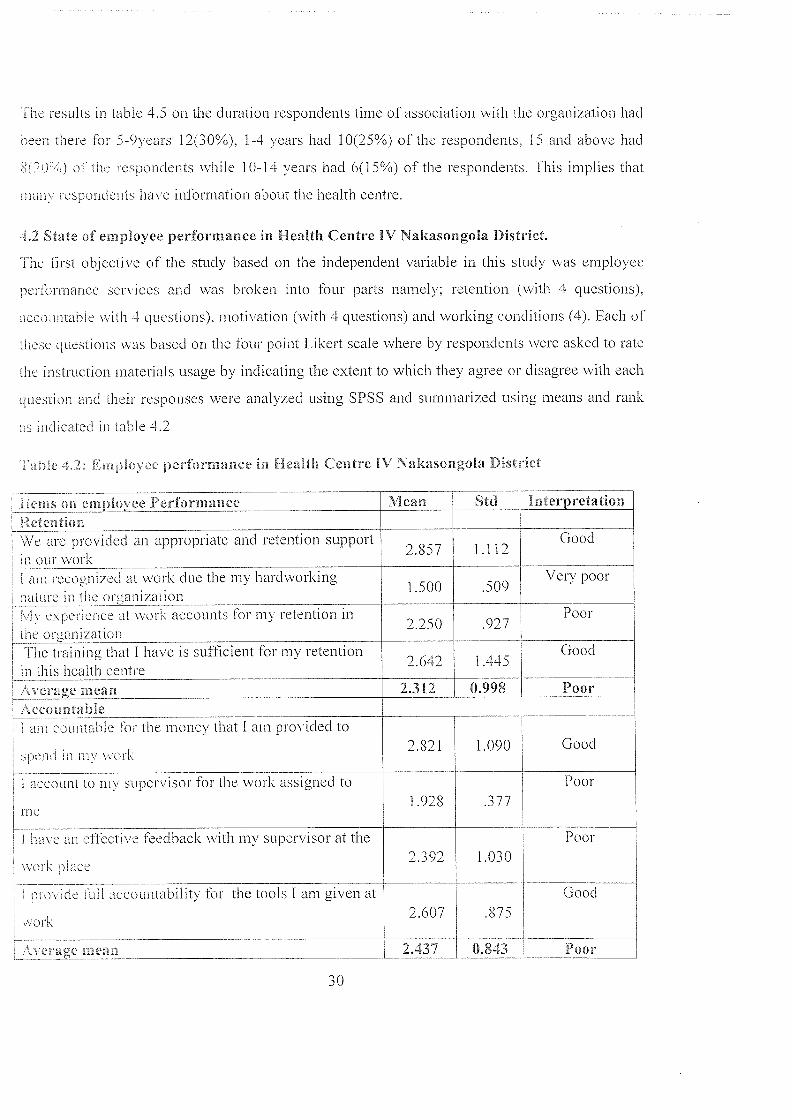
4.2 State of employee performance in Health Centre IV Nakasongola District.
The Orsi objecti\ e of the study based on the independent variable in this study was employee
perlormance services and was broken into four parts namely: retention (with 4 questions).
~cc unahle with 4 questions). motivation (with 4 questions) and working conditions (4). Each of
th~sc cjuestions was based on the four point Likert scale where by respondents were asked to rate
the instruction materials usage by indicating the extent to which they agree or disagree v~ith each
question and their responses were analyzed usmg SPSS and summarized using means and rank
as indicated in table 4.2
4 ne ~.2. iG ~lnvee performance in health Centre
H erage mean~cccou nta b Ic _______________________ ________________________
am conmable Ib: the money that I am provided to
~ in a a worf
account to my supervisor for the work assigned to
roe
I have anel’lèctive feedback with my supervisor at the
v~ ark ulace
ptov:c.eiull accountability for the tools 1 am given at
aork
:erage InearL
IV Nakasongola District
Lerns on eniployce Performanceketen tion
IVlean Std Interpretation
We are provided an appropriate and retention support ~ 857 1 1 1’? Goodin our work ~. . —
tam recognized at work due the my hardworking -~ Very poornat ire in the organizanon.‘ IV experience at work accounts lhr my retention ~ 2.250 .927 Poorthe organizationThe training that I have is sufOcient for my retention
. . 2.642 1.44tn this health eent:e
2.312 0.998 Poor
2.821 1.090 Good
1.928 .3
Poor
2.392 1.030
Poor
2.607
Good
.875
2.337 0,833 2oor
3
I h~ ~ ~F ‘isIrs p:oviJe an appropriale supervisory
an vi ionment in the organization
There is authority on the employees in decision
making
~ ciage ~iea ; ________ ________
a~4~ mean _______ _________ _______
a~ nay tla~, 2018
a1ea~i Range Response
3.26 4.00 Strongly Agree
2.5l~ 3.25 Agree Good
.75 -2.50 Disagree Poor
.00-1.74 Strongly Disagree Very Poor
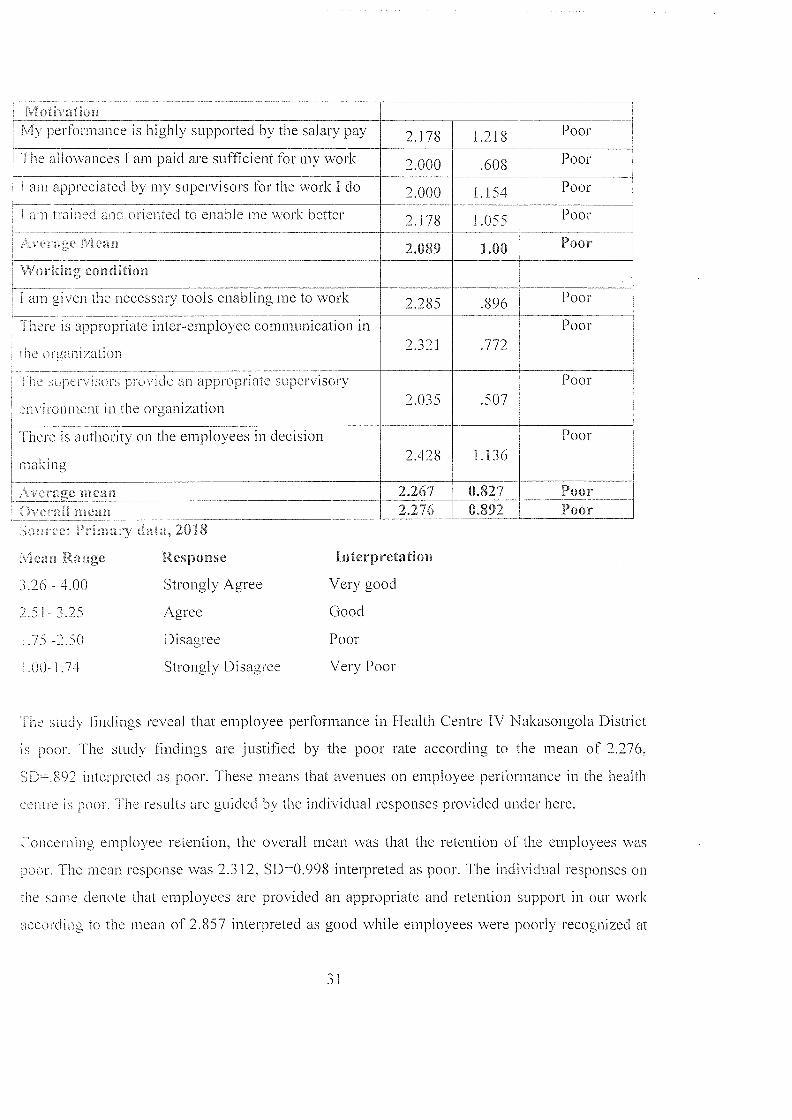
‘1’he siudy lindings reveal that employee performance in Health Centre IV Nakasongola District
is poor. The study lindings are justified by the poor rate according to the mean of 2.276.
SD—.892 interpreted as poor. These means that avenues on employee performance in the health
a is poor. <<<he results are guided by the individual responses provided under here.
~<oneerning employee retention. the overall mean was that the retention of the employees was
poor. fhe mean response was 2.3 12. SD=0.998 interpreted as poor. The individual responses on
the same denote that employees are provided an appropriate and retention support in our work
according to the mean of 2.857 interpreted as good while employees were poorly recognized at
.1 th I ~<it EloilMy perlormance is highly supported by the salary pay 2.178 1.218 Poor<I he allowances I am paid are sufficient for my work 2.000 .608 Poor
~ am appreciated by my supervisors for the work I do 2.000 1.154 Poor
am trained aad oriented to enable me n ork better 2. 178 1 .055 Poor
~ C.5 yC .~CI4d 2.089 1.00 Poor
4ic4rklng conthtion
I am given the necessary tools enabling me to work 2.285 .896 Poor
~ I here is appropriate inter-employee communication in Poor. . 2,321 .772
he organi/atlon
Poor2.035 .507
2.428 1.13
Poor
2.2672.276
0.827 Poor0.892 _____
Interpretation
Very good
-43
work due the my hardworking nature in the organization. the mean was 1 .500. The experience at
nih iceounts lhr my retention in the organization was poor 2.25() and finally the training that
flO~ iS sLilliCient lbr my retention in this health centre. the mean was 2.642
interpreted as good.
Concerning accountability of the employees, the result reveals that there was low and poor
seen jntabil i i~ ~upported by a 2.437 mean interpreted as poor. The poor responses are attributed
res; ‘osses m employees are countable for the mone that I am provided to spend in my
\\ork. tis was good. mean was 2.821 interpreted as good while I account to my supervisor for
the work assigned to me . the mean was 1 .928 interpreted as poor while I have an effective
feedback with my supervisor at the work place, the mean was 2.392 interpreted as poor and
dual ~ employees are not provided full accountability for the tools I am given at work according
sieni. a 2.~07 tnterpreted as good.
Concerning motivation, the state of employee motivation was poor. The sludy results reveal that
the average mean was 2.089. The responses were that the performance is highly supported by the
salary pay had the mean of 2.1 78. the allowances I am paid are sufficient for my work. had the
mean 2.00. The stuth revealed that i am appreciated by my supervisors for the work I do have
~an J.Oi and Ilitally the results on being trained and oriented to enable me work better had
the mean of 2. 1 78 interpreted as poor. responses on the respect to the study.
The study lindings concerning the working conditions reveal that the working conditions of the
stud~ was. The study results were guided by the responses on I am given the necessary tools
enabling me to work. the mean 2.285. the responses were poor while there is appropriate inter
cnyoyee communication in the organization. the mean was 2.321 while the supervisors provide
m appropriate supervisory environment in the organization had the mean of 2.035 and iinallv
regarding there is authority on the employees in decision making had the mean of 2.428.
accorc. i ug to thL~ response.
32
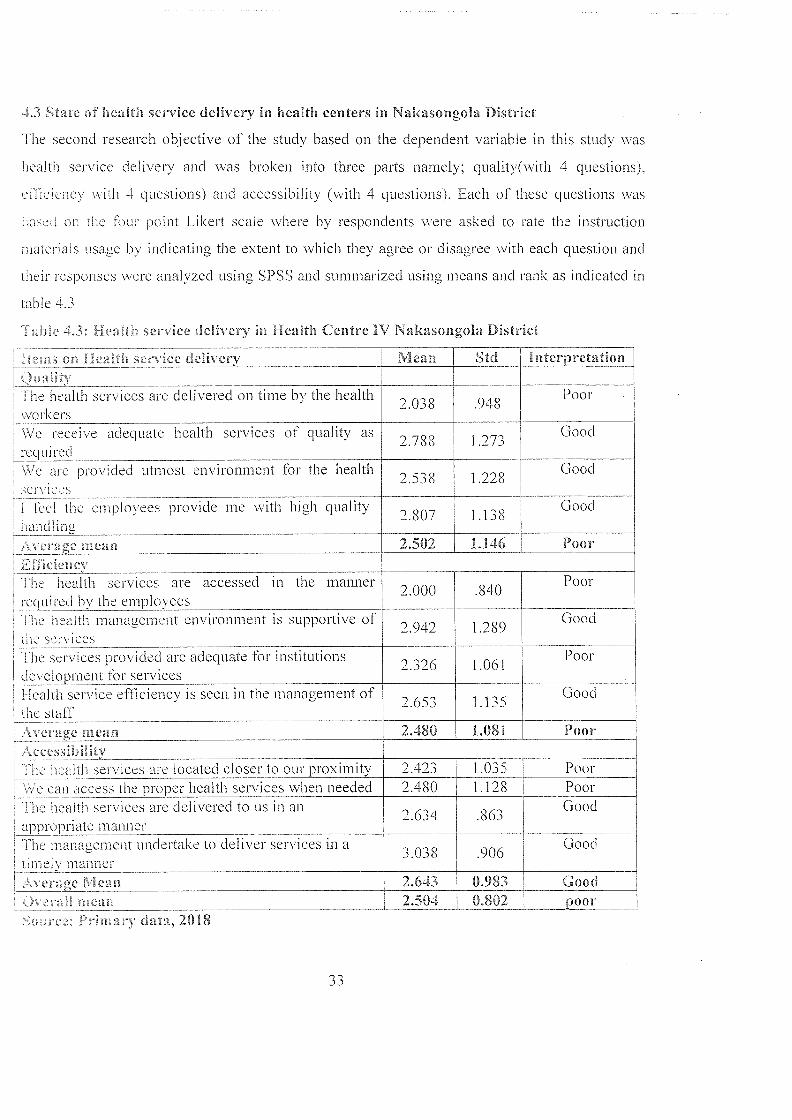
4.3 State of health service delivery in health centers in Nakasongola District
The second research objective of the study based on the dependent variable in this study was
health service delivery and was broken into three parts namely; quality(with 4 questions).
ebb cieney with 4 questions) and accessibility (with 4 questions). Each of these questions was
based on the four point Likert scale where by respondents were asked to rate the instruction
materials usage by indicating the extent to which they agree or disagree with each question and
their responses were analyzed using SPSS and summarized using means and rank as indicated in
table 4.3
Table 4.3: Health service delivery in Health Centre IV Nakasongola District
rums on Health service delivery Mean Std interpretationQualityThe health services are delivered on time by the health Poor~ 2.0~8 .94SworkersWe receive adequate health services of quality as 2.78$ 1 .273 Goodrequired
We are provided utmost environment for the health Good. 2.~8 1.22$
lurlthuumplo\ccs piovide mc nith high quality 2 807 1 138 Goodliandling
Average mean 2.502 1.146 Poor.l.smciencyThe health services are accessed in the manner ~ 000 840 Poorrequired by the employees —.
The health management environment is supportive of 2.942 1 .289 Goodthe servicesThe services provided are adequate for institutions ‘~ 3~6 1 061 Poordevelopment for servicesHealth service efficiency is seen in the management of Good
.,. 2.6e 1.liathe s~afrAverage mean 2.480 1.081 PoorAccessibilit~u health services are located closer to our proximity 2.423 1.035 Poor
We can access the proper health services when needed 2.480 1.128 PoorThe health services are delivered to us in an Good
. 2,6j4 .86aappropriate mannerThe mana~ement undertake to deliver services in a Good~ 3.038 .906timely manner
Average Mean 2.643 0.983 GoodOverall mean_______ 2.504 0.802 poor5o~”t’c~’ Primary data, 2018
fl,,3-,
~he s~uth rc.ults iii table 4.3 concernina the health service delivery in I lealth Centre l\’
\a~asangoia District. The study results revealed that the health services delivery was poor at
2.504. SDz~~ 0.802. this was supported by the results presented below.
The quality of health service delivery was that the quality, the health services are delivered on
~in~e [a Dc health wurkers. the mean was 2.308. SD=.948 interpreted as poor. The we receive
~d ~ cc heal .h ser~iees oi quality as required according the mean of 2.788 interpreted as good.
\Vc are pro~vided utmost environment Ibr the health services, the mean was 2.538 interpreted as
good. I feel the employees provide me with high quality handling had the mean of 2.807
interpreted as poor in the service delivery.
i~ a~alt1i se. jc~s are accessed in the manner required by the employees had the mean of 2.000
~vhilc the healta management environment is supportive of the services had the mean of 2.942.
SD D .289. The study findings the services provided are adequate for institutions development
br services, the mean was 2.326 and finally the health service efficiency is seen in the
management of the staff. the mean of 2.653 interpreted as good based on the assessment of the
1 he study findings the health services are located closer to our proximity had the mean was
2.423. interpreted as aoor. We can access the proper health services when needed had the mean
of 2.430. SD—i .128. The health services are delivered to us in an appropriate manner, the mean
a as 2.634 and finally the management undertake to deliver services in a timely manner had the
mcai~ of 3.03$ interpreted as good.
~Re~ationship between employee performance and health service delivery in Nakasongola
~isrricl
The third objective in this study was to examine the relationship between employee performance
mi ieaith service delivery in Nakasoi~gola district. To achieve this objective the researcher
corralated the mean on employee performance usage and that on health service delivery using the
Pearson’s Linear Correlation Coefficient. as indicated in table 4.4.
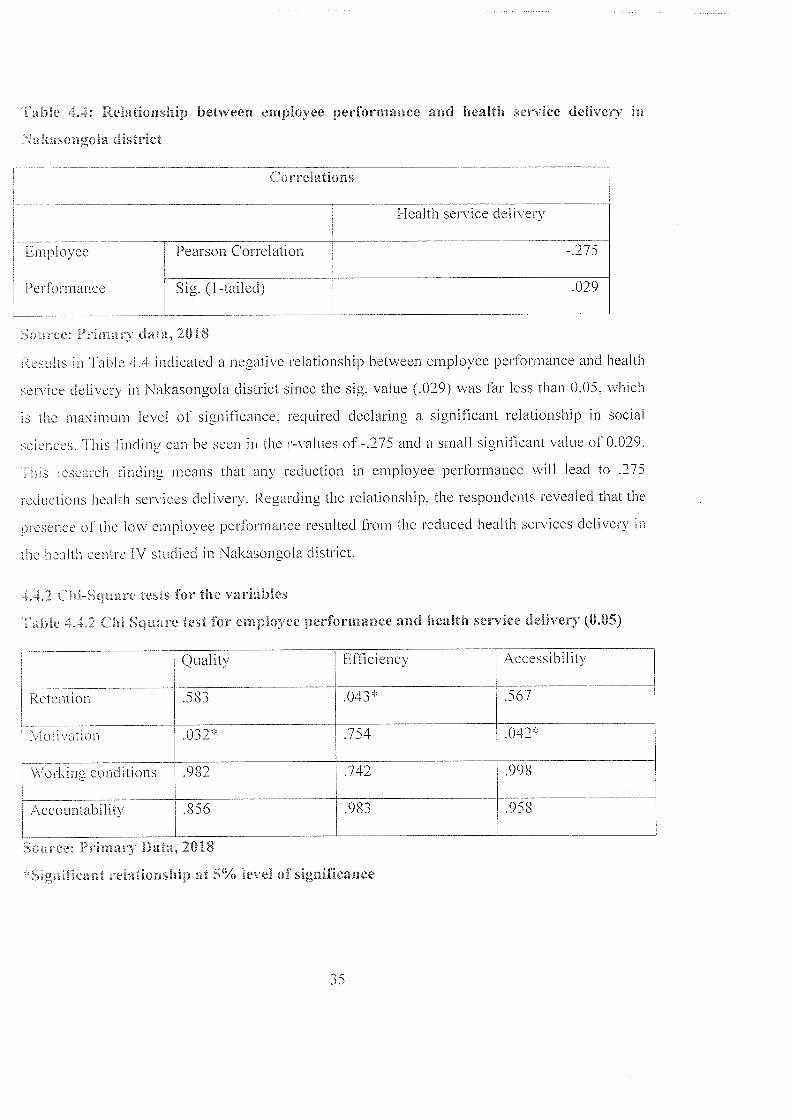
Table 4.4: Relationship between employee performance and health service delivery in
Nakasongola district
Correlations
Health service delivery
Employee Pearson Correlation - .275
Performance S ig. ( I -tai led) 029
Source: Primary data, 2018
Results in Table 4.4 indicated a negative relationship between employee performance and health
service delivery in Nakasongola district since the sig. value (.029) was far less than 0.05, which
is the maximum level of significance, required declaring a significant relationship in social
sciences. This finding can he seen in the r-values of -.275 and a small significant value of 0.029.
This research iinding means that any reduction in employee performance will lead to .275
reductions health services delivery. Regarding the relationship, the respondents revealed that the
presence of the low employee performance resulted from the reduced health services delivery in
the health centre IV studied in Nakasongola district.
4,4,2 Chi—Square tests for the variables
Table 4,42 Clii Square test for employee performance and health service delivery (0.05)
Quality Efficiency Accessibility
Retention .583 .043* .567
Motication .032* .754 .042*
Working conditions .982 .742 .998
Accountability .856 .983 .958
Source: Primary Data, 2018
‘~Significant relationship at 5% level of significance
iD
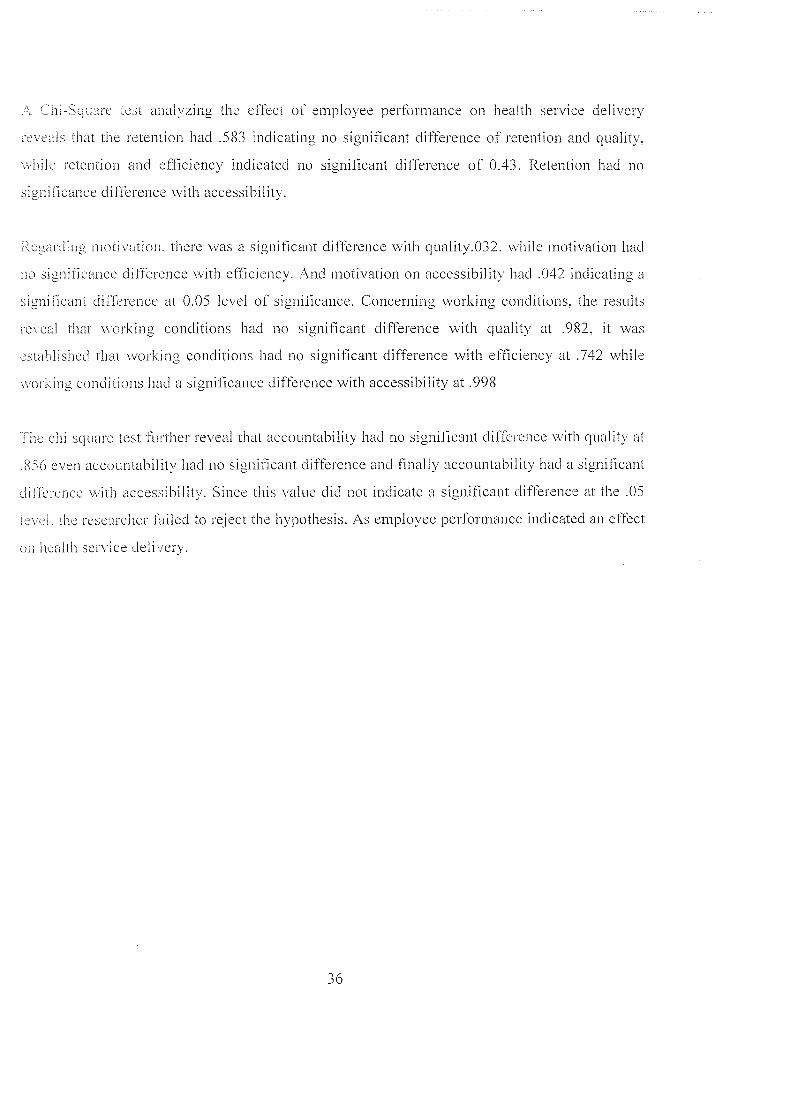
.‘.. “a.-Sc1aare test analyzing the effect of employee performance on health service delivery
1n eals that the retention had .583 indicating no significant difference of retention and quality.
~~hi1e retention and efficiency indicated no significant difference of 0.43. Retention had no
significance difference with accessibility.
ceg~ rding motivation, there was a significant difference with quality.032. while motivation had
no significance difference with efficiency. And motivation on accessibility had .042 indicating a
significant dilThrence at 0.05 level of significance. Concerning working conditions. the results
reveal that working conditions had no significant difference with quality at .982. it was
~stabll shed that working conditions had no significant difference with efficiency at .742 while
~soi king conditons had a significance difference with accessibility at .998
The eN square test further reveal that accountability had no significant difference with quality at
£56 even accountability had no significant difference and finally accountability had a significant
Jifference with accessibility. Since this value did not indicate a significant difference at the .05
nfl’i the researcher failed to reject die hypothesis. As employee performance indicated an effect
on health sen ice delivery.
36
CHAPTER FIVE
DISCUSSION OF FINDINGS, SUMMARY, CONCLUSION, RECOMMENDATIONS
5.0 Introduction
This chapter presents the discussions, summary, conclusions and recommendations made based
on the study fmdings. They were made basing on the research questions. It also gives areas of
further study.
5.1 Discussion of findings
The study findings reveal that employee performance in Health Centre IV Nakasongola District
is poor. The study findings are justified by the poor rate according to the mean of 2.276,
SD’.892 interpreted as poor. The study findings are in agreement with previous authors such as
Modibaet at 2002, wood & Jewkes (2006) argued that health service providers might not adhere
to standard guidelines for diagnosis, treatment and communication with patients, and may
engage in harmful practices in consequence of lack ofaccountability mechanisms. Health worker
/ patient relationships can be severely disrupted as a result of health workers’ attitudes. Even
Potter & Brough (2004) argued Good performance by staff is enabled via a supportive working
environment This encompasses more than just having sufficient equipment and supplies. It also
includes systems issues such as decision making and information exchange processes and
capacity issues such as workload, support services and infrastructure.
KAT/CHAZ (2005) and Doulo 2005) argued that A lack of protective measures increases fear of
infection and limits quality of services due to stress and delegation of tasks to non-qualified staff
Protection from HIV/AIDS at work has become a very important issue in countries with a high
HIV prevalence.
On the second objective, the study results revealed that the health services delivery was poor at
2.504, SD= 0.802. The study in terms of efficiency, quality and accessibility in tenns of the
health services provided in the context, the study findings were in agreement with the previous
authors such as Omahony, (2008) who argued when this potential ability is realized, it results in
observable utilization which is why studies often use utilization as a proxy variable for access,
conversely, and lack of utilization can signal the existence of barriers to access.
37
Safrat (2006) argued that patient experience is included with in quality because of the
importance of patient centered service delivery, for which patient experience is often used is a
measure and a counter point to the technical standards of clinical and managerial quality.
.1 he lard objective was that a negative relationship between employee performance and health
sen’ix deliver> i1i Nakasongola district since the sig. value (.029) was far less than 0.05. which
is the maximum level of significance. required declaring a significant relationship in social
sciences. The study reveal that Ndetei & Khasakhala & Omolo (2016). the study was conducted
employee performance and health service delivery in Busia district. The study did not find out
gnat hcalth service delivery practices among the major determinants of employee retention
~mni~. the nutses in public health facilities in Uganda. The results were in agreement with Omar
(2016) conducted a study on the effect of performance contracting on service delivery. The study
‘~as conducted in Gulu district, the study ~as conducted from the employees of the district. The
stud> concluded of the study findings are advanced based on the relationships that were
‘stat lished for each of the different research objectives. From the foregoing summary. it can be
o11clwed that the process of performance contracting implementation at the municipal council
of Gulu district has transformed the once inefficient council into a vibrant entity that is able to
procide efliciei.t and 4uality service to its customer. The study findings are contrary to those of
.(a~~3oya (2015) conducted a study on employee performance and health service delivery in
~j,w.c a. The stud> ~as conducted based on employees of Kampala capital city authority head
,facc and ua~a collection was done through the use of the questionnaire. The study findings
reveal that employee compensation had a positive effect on health service delivery
~.2 St mmary of Findings
lliis sxtion presents the summary of findings which were based on the research questions and a
~ nl.ariscsn a ‘other authors’ views on the findings.
I’he sLud> findings reveal that employee performance in Health Centre IV Nakasongola District
is poor. The study findings are justified by the poor rate according to the mean of 2.276.
SD.892 interpreted as poor. These means that avenues on employee performance in the health
Centre is poor. The results are guided by the individual responses provided under here.
38
The study results in table 4.3 concerning the health service delivery in Health Centre IV
• tkaso1~goIa Disaict. The study results revealed that the health services delivery was poor at
- .:u. SD— 0.802. The study in terms of efficiency. quality and accessibility in terms of the
health sen ices provided in the context.
The stud) findings on the third objective reveal a negative relationship between employee
erR ri~ance and health service delivery in Nakasongola district since the sig. value (.029) was
fir less than 0.05. which is the maximum level of significance. required declaring a significant
relationship in social sciences. This finding can be seen in the r-values of -.275 and a small
significant value of 0.029. This research finding means that any reduction in employee
perltrmance will lead to .275 reductions health services delivery. Regarding the relationship, the
r’spoitdents r:cealed that the presence of the low employee perfonnance resulted from the
:.xiu~.ed acaith sen ices delivery in the health centre IV studied in Nakasongola district.
~‘.3 Conclusions
The purpose of study was to establish how health workers performance affects health service
.ieli~e1y in Nakasongola District. On the first objective, the study concludes that the state of
nployee performance in Ilealth Centre IV Nakasongola District was poor. these was due to
poor motivation, working conditions. accountability and employee retention. The study
concludes that improved working conditions, accountability and retentions could have a high
bearing on employee performance in the health centers. On second objective conclude that the
sate of health service delivery in health centers in Nakasongola District was poor. the
~ ~.ibiF y to Ll’e nealth services. ~juality and efficiency in the services was poor. these imply
.aac tvisions of the health services was considerably low. On the third objective, the study
Ibund that a negative relationship between employee performance and health service delivery in
Nakasongola district. The study concludes that the state of health service delivery was reduced
by the employee performance constraints hence improving the working conditions, retention and
~t ILabiliL) a n . r,~tention.
‘S3
kccoIhmcnth~tions
~cegar. hog the first objective, the study recommends that there is need for improvement the
\vorkinC conditions of the health workers in Nakasongola. The study also recommends for
imprJ ~‘ement in the motivation stances such as payments. the study also recommend for
:uprocement of the state of workforce efficiency by establishing a strong working environment
1hr the workers.
The saidy also recommends that the health service delivery need to be improved through
nor ring accessibility, the quality of health care through purchase of tools and equipment
:ccuired in the health centers. The study hence provides and recommends that the mechanisms
for the management of the efficiency of the health workers need to be buttressed.
I he government should strengthen service delivery and improve social service accessibility even
hh Uircct provisions from central government or create a mechanism that will effectively
health ser~ ices to citizens so as to improve on people’s standards of living that is
i~eeessary for the service delivery. The central government, the district officials should give all
me necessary help to enable its operation in health centers with less inconveniences.
~ reas of furtaer cesearch
hecause of time and resource constraints, the researcher suggests the following as possible areas
tdr flu nier rcsrarch on employee performance and health service delivery.
An assessment of the impact of employee motivation on health service delivery
The impact of employee retention on health service delivery
The i’ole of employee performance in policy implementation for health service
ie~ :er\,
40
REFERENCES
African Medical and Research Foundation AMREF (2004). Tracking Human Resource and
Wage Bill Management in the Health Sector. Kampala: AMREF and Ministry of Health.
Aitken .JM, Kemp J (2003). H1V/AIDS. equity and health sector personnel in southern Africa.
Regional Network for Equity in Health in Southern Africa and Oxfam
(http://www.eq uinetatrica,org/bibl/docs/hivpersonnel.pdf/, accessed 1 7 March 2018)
Aitkcn JM. Kemp .1 (2003). HI V/AIDS. equity and health sector personnel in southern Africa.
Regional Network for Equity in Health in Southern Africa and Oxfam
(http://www.equinetafrica.org/bibl/docs/hivpersonnel.pdf/, accessed 12 March 201 8).
Amin, ME. (2005). Social sciences research Concepts, Methodology and Analysis. Kampala:
Makerere University Printery
13db, 1. S. (2004). Knowledge and utilization of Information Technology among Healthcare
professionals and students in Ile-Ife, Nigeria: a case study of a University Teaching
Hospital. Journal of Medical Internet Research, 6(4), 45-57.
Bcrthai. 2. (201 2). Succession Management Practices: Survey report issuel vol.2.
Chalker J, Chuc NT, Falkenberg T, Do NT, Tomson 0 (2000). STD management by private
pharmacies in Hanoi: practice and knowledge of drug sellers. Sexually Transmitted
Infections. 76(4):299—302.
Dm1 ii o et ml.. (2(1 3) The external pressures on the internal governance of universities’. Higher
Education Quarterly, Vol. 3 (3): 245-256.
Decker, Strader& Wise, (1997); Russomagno,(2000.) The use and usefulness of performance
measures in the public sector’. Oxford Review of Economic Policy. Vol. 1 9(2): 250-267.
Donabedian, A. 1980. The Definition of Quality and Approaches to Its Assessment. Ann Arbor.
Mi: I-lea ltd Administration Press.
Egger. D.. P. Travis, D. Dovlo, and L. Hawken. 2005. Strengthening Management in Low
Income Countries. Working Paper No. I, Making Health Systems Work. Geneva: World
Health Organization.
41
Fiedler. J. 1 981. “A Review of the Literature on Access and Utilization of Medical Care with
Special Emphasis on Rural Primary Care.” Social Science and Medicine. 15C: 129-42.
Fishinan. P.. fyI. Hornbrook. R. Meenan. and M. Goodman. 2004. ~Opportunities and
Challenges for Measuring Cost. Quality, and Clinical Effectiveness in Health Care.”
Medical Care Research and Review. 61(3 Supplement):124S-43S.
Gish. 0. (1990), Some Links between Successful Implementation of PHC Interventions and
Overall Utilization of Health Services. Social Science Medical Journal, 30.
Green. LW.. Kreuter, M.W. (2005). Health program planning: an educational and ecological
approach. New York, USA: McGraw-Hill, pp. 672.
Heckman et al. (2006) Performance measurement and institutional processes: a study of
managerial responses to public sector reform’, Management Accounting Research, Vol.
12:43764.
Hill. .1., Kazembe. P. (2006). Reaching the Abuja target for intermittent preventive treatment of
malaria in pregnancy in African women: a review of progress and operational challenges.
Tropical Medicine & International Health, Vol. 11, No.4, pp. 409—418.
Hughes RL. Ginnett RC, Curphy 0.1 (2002). Leadership, enhancing the lessons of experience.
New York. McGraw-Hill/Irwin
Ikamari. ODE. (2004). Maternal F-Iealth Care Utilization in Teso District. African Journal of
Health Sciences, 11, 1-2.
Joint Learning Initiative (2004). Human resources for health: overcoming the crisis. Cambridge,
Global Equity lnitiative/ Harvard University Press.
Katende C. (1 994). The Impact of Access to Health Services on Infant and Child Mortality in
Rural Uganda. Africa Journal of’ Medicine, Vol. 1. Cairo.
Kawooya N (201 5) employee performance and health service delivery in Kampala capital city
Authority Uganda
KIT/CI-IAZ (2005). Coping with the impact of HIV/AIDS on health workers in Zambia: a pilot
studvin two districts. Amsterdam, Royal Tropical Institute.
42
L~~oiaz 11 and \Veihrich, 11. (2009). Management 7th Edition, Tokyo: McGraw-Hill Book
Company.
Kothari. C.R (2008). Research Methodology. Methods and Techniques. New Age Inter National
Publication. New Delhi
I:uci i .\, .\. (2007). 1 luman Resource Management Success: The tips for HRM theorist’s and
Pracutioners. Kampala: Makerere University Printer.
Martens, P.. hall. L. (2002). Malaria on the Move: Human Population Movement and Malaria
lransmission. Perspectives. Vol. 6, No. 2, Pp. 103-109.
\linistry of health (MOH) [Ugandaj. 2010. Health Sector Strategic Plan. 2010/1 1—2014/15.
Lamp Ja. ~ ‘gaada: \401 I
l:nis~r\ al 11 ~a1th (Mol I: Annuai I lealth Sector Performance Report. (Al ISPR) Kampala:
government of Uganda; 2014/5.
Ministry of health. health sector strategic investment plan 2010/11-2014/15: promoting people’s
health to enhance socio-economic development. Kampala: Ministry of Health, 2010.
LH C ~l. ~auer .1. A.. and Evans. I). B.. (2005). Cost efFective analysis of strategies to
combat malaria in developing counties. achieving the millennium development goals for
health. I3ritish Medical Journal. Vol. 331. PP. 1133-1136.
Niugenda M and AhelG (2003). Mugenda. Research Methods. Quantitative and Qualitative
Approaches.
J ~kasa .J (2016 . Rewards and I luman Resource Retention. A case study of selected private
Secondary schools in Wakiso and Masindi Districts. A research dissertation submitted to
the higher degrees department in the partial fulfillment of the requirements for the award
of Masters of Management Studies of UMI.
\ lusgrove& Creighton (2003) Employee training & development at Wells Fargo . Retrieved on
March I.ongman. Birmingham.
uuia A Lusala .1 2. Kabasingwa L. (2(115) Local Government councils’ perlhrmance and
public service deli\ cry in Uganda. Jinja District Council Score-Card Report 2014/20 15
Nielsen. A. (2013). Performance Management, Managerial Authority, and Public Service
Performance. Journal of Public Administration Research and Theory. 3(1) 19— 135.
‘f J
‘Y~iahony S.. J. Mcllenry. D. Snow. C. Cassin. D. Schumacher. and P. Selwyn. 2008. “A
Revinv of Bacriers to Utilization of the Medicare Hospice Benefits in Urban Populations
11111 Staaegies for Enhanced Access.” Journal ofUrban health. 85(2): 28 1-90
Ornar A A (2016)effect of performance contracting on service delivery in (Mu district,
Kampala Publishers.
Pelizer. K. (2005). Factors Influencing the Utilization of PMTC Services by Pregnant Women in
the Eastern Cape. South Africa. health SA Gesonhcid. 10(1).
~ters D.. A. Garg. 0. Bloom, D. Walker. W. Brieger, M. Ilafizur Rahman. (2008). toverty
and access to Health Care in Developing Countries.” Annals of the New York Academy
ofSciences. 1136: 16171.
?ottcr C. Brough R (2004). Systemic capacity building: a hierarchy of needs. I lealth Policy and
ritual w. I 9(5):336—345
Redman. and Wilkinson. (2015).Contemporary Human Resource Management: Pearson
Education Limited, England
Roberts et al.. (2006) Performance Management: a Framework for Management Control
systems R~seaech’. Management Accounting Research. Vol. 10(4): 363-382.
.%OW%~ AR. DC ~aviw~, D. Lanata CF. Victora C (2005). flow can we achieve and maintain high
quaht) perfonnance of health workers in low-resource settings? The Lancet. 366:1026—
1035. Royal
.wanson. S.R. and Davis. J.C. (2003). The relationship of differential loci with perceived
quality and behavioral intentions. Journal of Services Marketing, 17.202-19
L Iganda Bureau of Statistics (UBOS) and ORC Macro. 2006. Uganda Demographic and Health
Survey 2006. Kampala: UBOS and Calverton. MD: ORC Macro. Uganda
Uganda Bureau of Statistics (UBOS). 2014. Uganda National Household Survey 2014.Kampala.
Uganda: UBOS.
Ctzingcr. J.. i’ozan. Y.. Singer. 8.11. (2001). Efficacy and cost-effectiveness of enviromnental
management for malaria control. Tropical Medicine & International health. Vol. 6, No.
9. pp.677487.
44
c~’alkcr. .1. (2002). 1 Juman Resource Planning: Mcgraw Hill Incorporation. USA.
WI It) (2003a1. Framework for developing. implementing and updating national antimalarial
drug policy: A guide for countr malaria control programmes. WHO Regional Office for
Africa llrazzaville.
~‘~J IA Je~v~es R (2006). Blood blockages and scolding nurses: barriers to adolescent
contraceptive use in South Africa. Reproductive health Matters. 14(27): 109—118.
World llealth Organization (2010).World health report. Health system financing: a path to
universal coverage. Geneva: World Health Organization Press. 2010
uAr~c I ic~ltl Diganization (WI 10). 2009. Report of Assessment Review of the Medicines
Rcgulat3rv Authority of Uganda. Geneva.
\Vorld I Icalth Organization (WHO).(201 5). Trends in maternal mortality: 1990 to 2015:
estimates by WhO, UNICEF. UNFPA. World Bank Group and the United Nations
Population Division. Geneva: WIlD.
A4~hL. 0. \\riglt. C.. & Parker. M. (2014). Social studies: Classroom activities l~r New
Zealand schools. Greenwood. W.A: Ready-Ed Publications
Zurn P. Dolca C. Stilwell B (2005). Nurse retention and recruitment: developing a motivated
workforcc. Geneva, World I-lealth Organization
45
Appendix i: Questionnaire for health workers
KAMPALA INTERNATIONAL UNIVERSITY
SCHOOL OP ECONOMICS AND MANAGEMENT
RE: Questionnaire on Assessment of Impact of employee performance on health service
delivery at Nakasongola health centre iv in Nakasongola district
Dear respondent, I am Nakafeero, student of Bachelor of statistics at Kampala international
university. You are kindly requested to fill/tick questionnaire as honesty as you possibly can.
This information obtained will be used for academic purposes only.
NB TICK WHERE ISAPPLICABLE
Back ground information
SECTION A - Characteristics of respondents
1. Gender
a)Male I Ib) Female I I
2. Age
a) 20—29 I Ib) 30—39 I Ic) 40-49 I Id)50+ I I
3. Qualification academically
a) Certificate
b) Diploma
c) Degree
d) Masters
4. Marital status ______
a) Single I Ib)Married I Ic) Separated/divorced I I
46
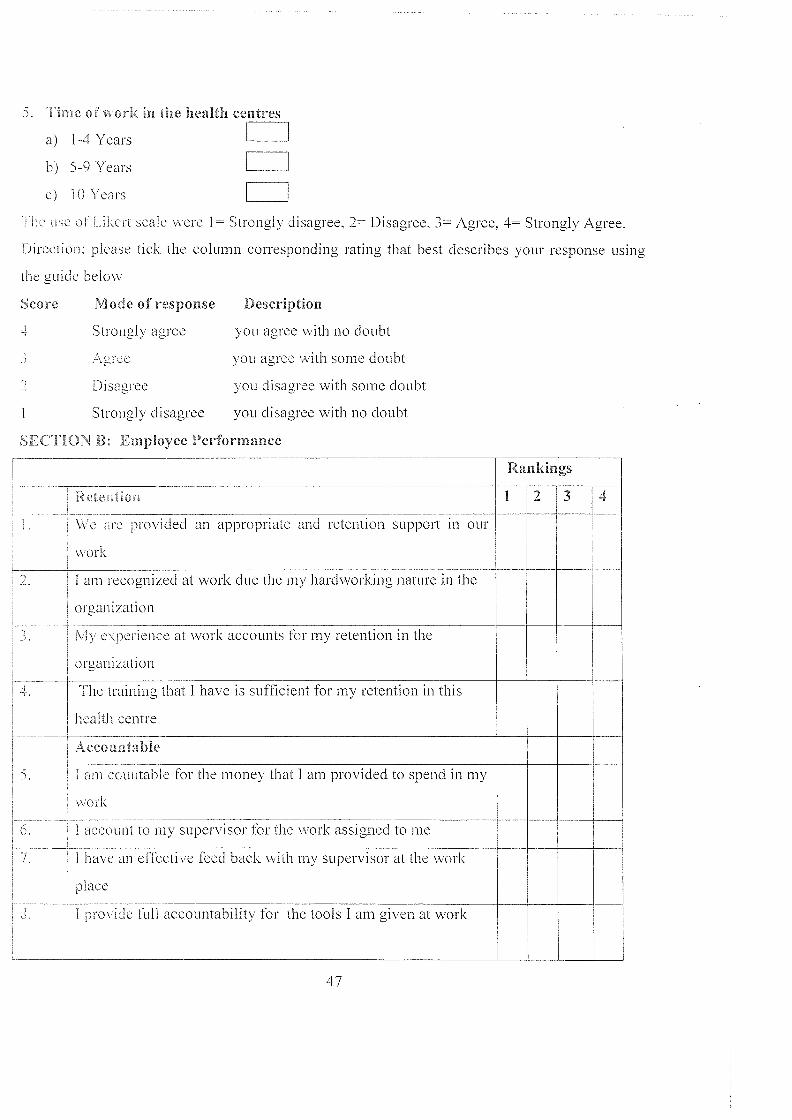
5. Time of work in the health centres
a) 1-4 Years
h) 5-9 Years _____
c) 10 Years _____
1 ha use of Lihert scale were 1= Strongly disagree, 2= Disagree, 3= Agree, 4= Strongly Agree.
Direction: please tick the column corresponding rating that best describes your response using
the guide below
Score Description
you agree with no doubt
you agree with some doubt
you disagree with some doubt
you disagree with no doubt
Rankings
Re~ntion 1234
I \Veare pro\’idecl an appropriate and retention support in our
work
2. 1 am recognized at work clue the my hardworking nature in the
organ jzation
7. Mv experience at work accounts for my retention in the
organ izat ion
Li. — The training that I have is sufiScient for my retention in this
health centre
Acco a ntable
5. I am countable for the money that I am provided to spend in my
work
6. 1 account to my supervisor for the work assigned to me
7. 1 have an effective feed back with my supervisor at the work
p1 ace
7. I provide full accountability for the tools I am given at work
Mode of response
Strongly agree
3 Agree
2 Disagree
Strongly disagree
SECTION B: Employee Performance
47
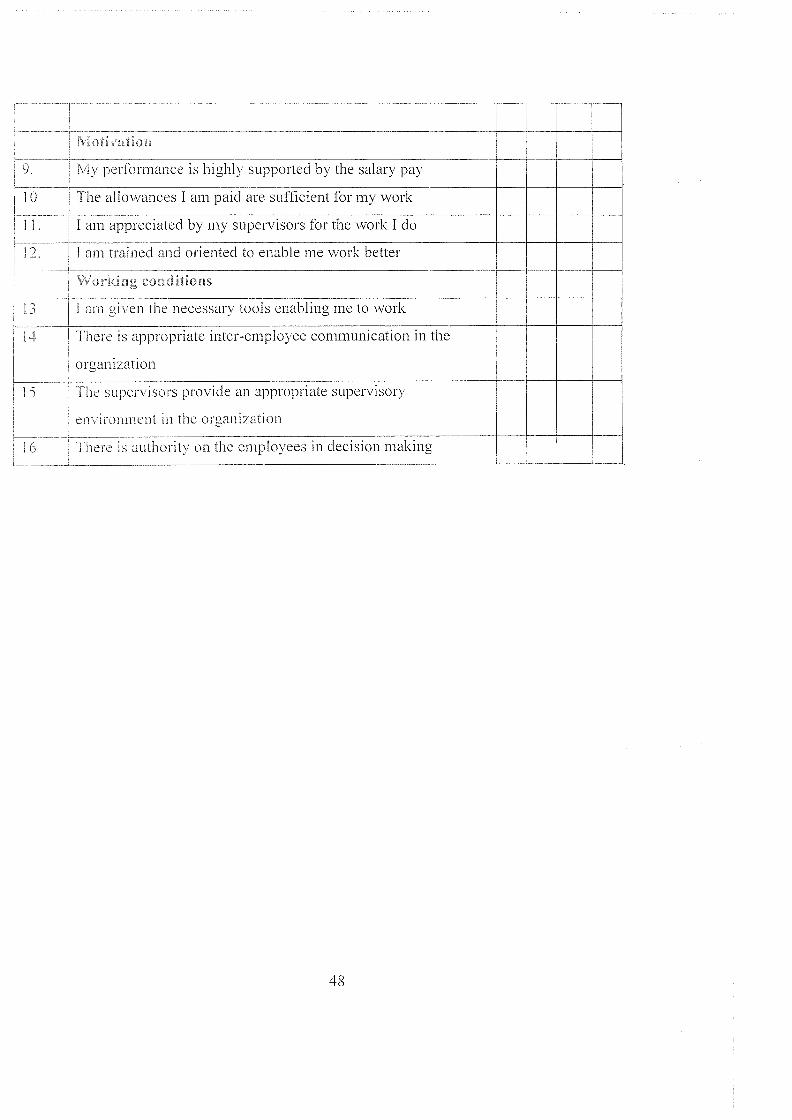
1Li~.t~Ofl
Nlv performance is highly supported by the salary pay
The allowances I am paid are sufficient for my work
1 1 1 am appreciated by my supervisors for the work I do
1 2. I am trained and oriented to enable me work better
~ co~ditioas
13 1am given the necessary tools enabling me to work
I 4 There is appropriate inter-employee communication in the
organization
I ‘ I he supervisors provide an appropriate supervisory
en irai tn ~eiit in the organization
1 6 [here is authority on the employees in decision making
48
Appendix ii: Questionnafre for Clients! Community
RE: Questionnaire on assessment of impact of employee performance on health service
delivery at Nakasongola health centre IV in Nakasongola district
Dear respondent, I am Nakafeero, student of Bachelor of statistics at Kampala international
university. You are kindly requested to filUtick questionnaire as honesty as you possibly can.
This information obtained will be used for academic purposes only.
NB TICK WHERE ISAI’PLICABLE
Back ground information
SECTION A - Characteristics of respondents
1. Gender
a)Male I Ib) Female I I
2. Age
a) 20—29 I Ib) 30—39 I Ic) 40-49 I Id)50+ I I
3. Qualification academically
a) Primary
b) Secondary
c) Certificate
d) Diploma
e) Degree
4 Time for stay in the area? _____
a)1-4Years I Ib) 5-9Years I Ic) loYears I I
49
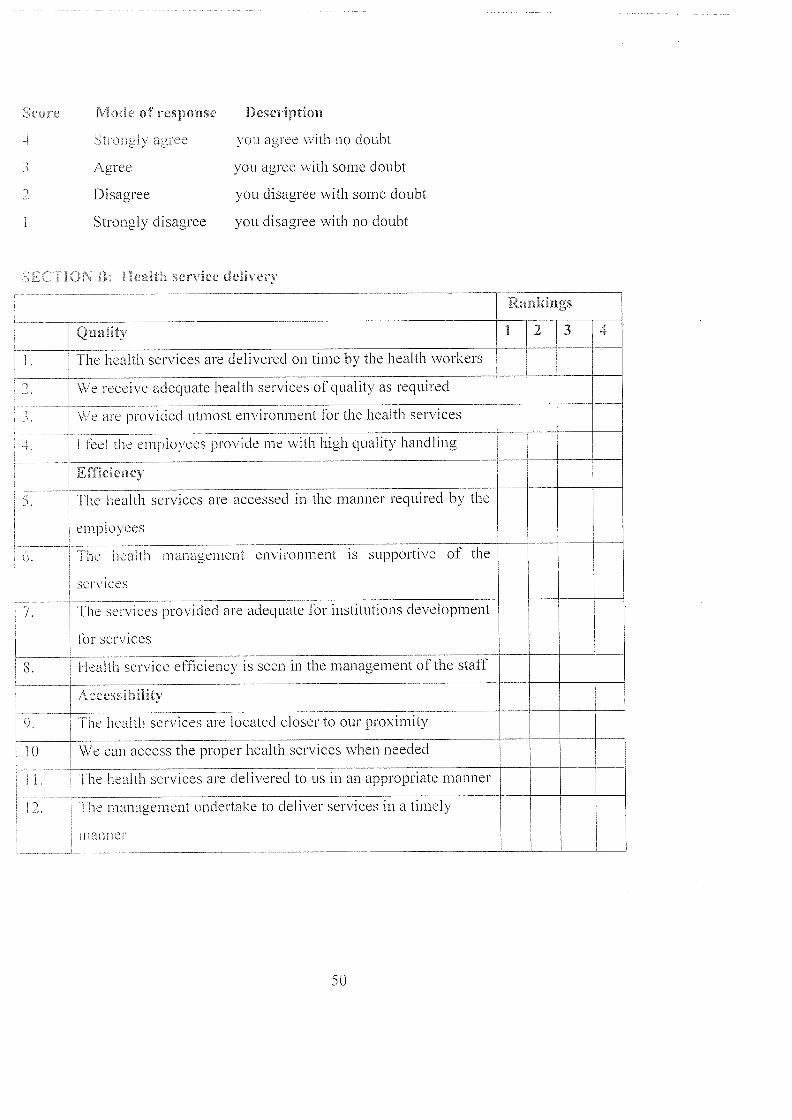
Quality 1 2 3
The health services are delivered on time by the health workers
4
We receive adequate health services of quality as required
\\‘eare provided utmost environment for the health services
I feel the employees provide me with high quality handling
Efficiency
The health services are accessed in the manner required by the
employees
‘[he ucaith management environment is supportive of the
services
services provided are adequate for institutions development
for services
8. health service efficiency is seen in the management of the staff
Accessibility
9. [ne health services are located closer to our proximity
We can access the proper health services when needed
‘[he health services are delivered to us in an appropriate manner
[he management undertake to deliver services in a timely
aimer
Mode of response I)escription
‘ti ongly agree ~ ou agree with no doubt
3 Agree you agree with some doubt
2 Disagree you disagree with some doubt
Strongly disagree you disagree with no doubt
~ ~ ~t ~1ea~t service delivery
Rankings
50
II KAMPALA Ggaba Road, Kansanga
IiiNTERNATIO NAL P.O. Box 20000, Kampala, UgandaEmail: [email protected]
_____ I *Website:http://www.kiu.ac.ug
COLLEGE OF ECONOMICS AND MANAGEMENT
OFFICE OF THE HEAD OF DEPARTMENTECONOMiCS AND STATISTICS
15t March, 2018TO WHOM IT MAY CONCERN
Dear Sir/Madam,
SUBJECT: PERMISSION TO CONDUCT A RESEARCH STUDY IN YOUR ORGANIZATION
With reference to the above subject, this is to certify that NAKAFEERO DOREEN REG.NO. 1153-05194-00760 is a bonafide student of Kampala International Universitypursing a Bachelors Degree of Science in Statistics.She is currently conducting a field research entitled “Employee Performance andHealth Service Delivery in NakasongoLa District. A case study of NakasongolaHeaLth Centre IV”.
This area has been identified as a valuabLe source of information pertaining to herresearch project. The purpose of this letter therefore is to request you to avail herwith the pertinent information as regards to her study.
Any data shared with her will be used for academic purposes only and shall be keptwith utmost confidentiality.
‘ ~t•J ~ .Any ~. endered to her will be highly appreciated.I
~ truty, )fHI
II U1MAR2Q ~‘:‘‘I I
~ l.~ I I. ‘~COV~)~1/(~. / 1
Mi~fi’E’ 9~1~ANKLINHea~~fi ~ - partmeritTel: 0777094955Email: [email protected]
~pthth~g tfie %eigfits