division of education annual report fy2014
DESCRIPTION
Division of Education Annual Report FY2014TRANSCRIPT

Innovative Education for Exceptional Care
D i v i s i o n o f E D u c a t i o n
A n n u A l R e p o R t F Y 2 0 1 4

What’s Inside?Highlights from FY2014
Opening message from our administrator..........................................................................................p.3Framework for how the Division of Education is helping LVHN meets its Triple Aim.......................p.4Industry trends shaping how we education, train, and prepare healthcare
Training the next generation of physicians............................................................................................p.14
A data-driven, performance learning organization through metrics and analystics............p.8
Educational services for LVHN’s clinical staff......................................................................................p.16Nurse Residency Program......................................................................................................................p.18Interdisciplinary faculty development...................................................................................................p.20Providing opportunities for students..................................................................................................p.21Simulation center and standardized patients.................................................................................p.22Innovative uses of eLearning, social media, and virtual reality..................................................p.24Improving patient care and patient engagement..........................................................................p.26
SELECT medical students engage in a simulation learning activity at the Division of Education’s Interdisciplinary Simulation Center.
Budget and Administration.....................................................................................................................p.10The Dorothy Rider Pool Health Care Trust grant utilization........................................................p.12
SELECT medical school program..........................................................................................................p.15
professionals at LVHN and elsewhere....................................................................................................p.6
2 | D i v i s i o n o f E d u c a t i o n

Who our education touches:
Staffphysicans, nurses, advanced practice clinicians, nurse practitioners, physician assistants, pharmacists
Studentsresidents, fellows, medical students, nursing students, graduate nurses
Professional Stafftechnical and support partners, home healthcare personnel
$10.26Million dollars of actual operating
expenses
Optimizing Health Systems Performance
and Transforming Patient CareHelping Lehigh Valley Health Network toward the strategic goals of the Triple Aim
The Division of Education (DOE) remains committed to improving the health of our community through enhancing the effectiveness of Lehigh Valley Health Network (LVHN) as a network.
Our operational success is built upon the talents of an excep-tional team of clinical and non-clinical educators, physician and nurse faculty, instructional designers, curriculum specialists, technologists, analysts, and others. The educational services of the DOE reaches nearly every employee of LVHN.
Our Mission
Create a learning organization that delivers and supports innovative education for exceptional care!
Our Vision
We champion an environment of life-long and self-directed learning. We promote a culture of ongoing growth and development by creating innovative systems that produce transformational change in the vital processes of teaching, learning, and the application of knowledge and skills.
What’s In This Annual Report?
The following sections in this Annual Report are just a snapshot highlighting some of what DOE does for LVHN and the Lehigh Valley community. The multitude of educational activities, teaching, mentoring, projects, consultations, collaborations, materials, support, research, presentations, and publications within DOE, and with other departments in LVHN, the University of South Florida, business and academic partners in the Lehigh Valley would be too overwhelming. A more comprehensive summary of the individual teams (e.g., eLearning, clinical staff services, medical education, etc), the services they provided, and the metrics describing their work during FY2014 and previous years can be found on our intranet webpage.
A Special Thank You
We are grateful for the continued support of The Dorothy Rider Pool Health Care Trust in supporting the mission of LVHN to heal, comfort, and care for our community, and in particular their commitment to support education. We have previously presented evidence of our stewardship in various forums and welcome the opportunity to provide feedback to the Trustees, LVHN senior management, and our greater LVHN community on our progress at any point. Our sincere appreciation to the Pool Trust for helping make possible so much of what you will read about in this report.
84,984To t a l l e a r n e r
contacts
1:1,368Staff Ratio
253Residents and
fellows
421Medical and physician assistants students
1,038Nursing students
A n n u a l R e p o r t F Y 2 0 1 4 | 3

Opening message from our administrator
The Division of Education’s (DOE) mission is to innovate education for exceptional care. Our goal is to provide the culture, environ-ment, and tools to support ongoing solutions that meet the educational needs of the people at LVHN and the communities we serve. In 2007 we created a framework built on the use of emerging education theory, methodology, and state-of-the-art instructional technologies. This became the foundation for our work in teaching & learning, instruction & curriculum, and assess-ment & evaluation, and our vision for LVHN as a high performing learning organization.
Informed from an extensive site visit sponsored by The Dorothy Rider Pool Health Care Trust (Pool Trust) in 2009 we authored our first multiyear grant Essential Infrastructure and Project Support, Interdisciplinary Simulation Center, Standardized Patient Program, Social Media Research and Development, Online Case Based Continuing Education, and Art of Observation also known as grant number 20120118 or simply grant 118. Grant 118 was approved and initiated in July 2010 providing support and resources contributing to our core services, developing new metrics and outcomes measures, growing our faculty development programs, attracting youth from our community into healthcare careers, establishing our simulation center, expanding our use of distance learning technologies and social media, and experi-menting with several mixed method interdisciplinary courses. The original grant was for $4,317,074 for a 3-year period July 2010 – June 2013. During the life cycle of this grant, especially at its inception, we experienced several slow starts on many of the grant projects, with some projects experiencing delays of up to 15 months. These along with the early completion of two sub-projects left us with considerable financial resources and unfinished work within the scope of the grant allowing for the 4th year grant extension. In June 2013 a one year extension was approved
with a final expenditure as of June 2014 of $3,972,479 or 92% utilization across the cumulative 4 years.
A portion of the Pool Trust Grant supplemented hospital funds sustaining certain positions within the DOE associated with program innovation in the areas of patient safety, quality of care, compliance, resident and physician education, nurse education, unlicensed healthcare professional development, youth programs, eLearning, and patient and consumer education. When reading this report, please keep in mind that this places Pool Trust grant funded innovations in just about every aspect of DOE operations and delivery of our services.
The Pool Trust has always played a key role helping the DOE conceptualize, initiate and sustain innovative high-impact projects that have value in evolving a flexible workforce that meets the changing healthcare needs of our region. By design the DOE has always supported an interprofessional and multi-disciplinary approach, training professionals to practice at the top of their licensed capability, while remaining focused on increased quality and decreased cost of care. The tremendous resources the Pool Trust provides, creates for the DOE a protected space for talented people to explore, innovate and implement value laden programs that benefit our community and our network.
In this report you will read about how the DOE leverages all its available resources to fulfill our mission, including: -Average program growth from year to year (see supplemental document)- New programs that emerged- Adoption of new instructional technologies- Adoption of new instructional methods- Highlights of innovative, collaborative, or exemplary projects and activities- Integration of metrics- Implementation of the SELECT medical school- Growth of online digital library- How the DOE contributes to LVHN’s Triple Aim
Alexander J. Lemheney, Ed.D. Administrator, Division of Education
Conceptual model of what informs DOE’s services
4 | D i v i s i o n o f E d u c a t i o n

Workforce Development
Patient Engagement
Value Added Care
Data Driven Performance
Building a strategically flexible, interprofessionally competent, emotionally intelligent health-care workforce that meets the
needs of the individual and population health needs of our
community.
Enable value-added care at LVHN by providing training and simulation environments that facilitate broad
adoption of LEAN principles, network integration, and improved processes, including the electronic health record
to optimize health system perfor-mance.
Engage Patients, families, and focused populations more directly in their care by educating health-care practitioners on methods of engagement and providing effec-tive education tools and content.
Position LVHN as a premier, data-driven performance-focused learning
organization through optimization of knowledge management and skill
transfer, application of enhanced learning metrics, and dissemination of best practices at local, regional,
and national levels.
We provide education and training for physicians, nurses, advanced
practice clinicians, technical partners, and others so that they
can provide the best care possible for our patients.
Better CareKeeping people healthy in the
Lehigh Valley and beyond is impor-tant to us. We produce and offer patient and community educa-
tional programs and materials to help people better take care of themselves and their families.
Better HealthImproving patient satisfaction on HCAHPS and Press Ganey through topics like emotional intelligence, crucial conversations, and effec-tive teamwork is one of the ways
we help improve quality and reduce costs in LVHN. We are also
integral in the roll-out of Epic, our integrated electronic medical
records system.
Better Cost
A framework for how the Division of Education is helping LVHN meetits Triple Aim
A n n u a l R e p o r t F Y 2 0 1 4 | 5

Industry trends shaping how we educate, train, and preparehealthcare professionals at LVHN and elsewhere
Care of Patients
Network Culture
Optimization of System
Network Human Environment
Health Care
Professional
Attitudes Skills
Adapted from the Mandala Health Model (Hancock, 1985)
Local Community
Large-Scale Health Sphere (Regional, National, Global)
6 | D i v i s i o n o f E d u c a t i o n

Social Determinants of HealthEncouraging healthcare providers to focus on environmental, social, behavioral, and ethnomedical determinants of health can increase patient care and quality according to the Institute of Medicine (IOM). Furthermore, outpatient, population-based, and individual non-clinical preventative inter-ventions are needed to help prevent or delay cases of costly chronic diseases.
Emotional IntelligenceImproving the patient experience positively transforms and improves health care and community health. Training physicians, nurses, and other clinical and non-clinical healhcare professions in emotional intelligence, a hallmark of the SELECT medical school, represents a significant shift in the attitudes and culture of how we care for patients, but for businesses, education, and leadership development.
ReferencesIOM (Institute of Health). (2014). The role and potential of communities in improving population health.IOM (Institute of Health). (2014). Graduate medical education that meets the nation’s health needs.
Innovations in Technology Help to Enhance Collaborative LearningThe demands of a “knowledge society” require new models of collaborative and inquiry-oriented learning and teaching that engage learners in sustained motivation, agency, and autonomy. New, exploratory technologies such as intelligent conversational agents, crowd-based innovations, technology augmented human facilitation, digital badges, and social networking can help promote innovate ideas.
Building Better Processes to Handle Value-Based CareAccountable cost organizations (ACOs) need to be nimble and responsive to be able to negotiate changing value-based payments that increase the risk of reduced payments for poor quality of care and patient experience. Healthcare systems that are built upon LEAN processes, higher efficiencies, and more effective sharing and transfer of knowledge and information will be better adapted to changing healthcare requirements than previouis models of patient care.
Potential Changes in the Financing of Graduate Medical EducationThe IOM recently conducted an independent review of the governance and financing of the GME system, concluding that there is an “unquestion-able imperative to assess and optimze the effectiveness of the public’s investment in GME” (IOM, 2014, p.1). In their report, the IOM suggests that there is “great potential to leverage Medicare’s investment in GME by redesigning the system to reward desired outcome and program performance” (IOM, 2014, p. 2)
New Forms of Health Care Providers That Promote Patient EngagementWith the shift to more preventative measures to ensure the health of patients and the community, new forms of health care professionals may lead to substantial improvements in the overall health of individuals in our communities. For example, greater use of health coaches in the outpatient setting or in the home through physical face-to-face appointments, telemedicine, or other mobile technologies can potentially increase patient engagement, awareness of risk factors, compliance with treatment plans, and the likelihood that challenges and barriers to improved health outcomes can be met in a timely manner.
Big Data That is Integrated and MobileElectronic medical records that link disparate records and data systems and allow them to “talk” to each other has recently become a priority among health care systems to improve patient safety, quality, and satisfaction while reducing costs and inefficiencies. The success of mobile communica-tions technologies (e.g., smart phones, tablets) offers the potential transfer of ideas, such as open-source application programming tools that allow innovators and developers to create custom apps for mobile devices that brings the right information quickly to healthcare providers, learners, patients, and the community.
Partnerships That Utilize Community PartnershipsRecognizing that improving health, especially from a preventative perspective in the outpatient or community health environment, has led to some non-traditional partnerships throughout the United States, including those involving hospitals, drug chains, and grocery stores. Expanding formal partnerships could potentially include social service agencies, gyms, transportation systems, nature centers, and religious organizations.
Workforce Development
Patient Engagement
Data-Driven Performance
Value-Added Care
A n n u a l R e p o r t F Y 2 0 1 4 | 7

LVHN staff participate in a continuing education activity coordinated by the DOE.
Data-driven program evaluations, metrics, and analytics
The DOE continually looks for ways to improve the services we provide LVHN to better serve our patients and community. We do this by systematically, establishing relevant, meaningful metrics, collecting data, and applying analytics to improve how our educators train our clinical staff, increase engagement in our learning activities, and establish well designed programs.
DOE’s metrics and analytics are funda-mental to every part of DOE, including clinical staff development, graduate medical education, eLearning, simula-tion, the SELECT medical program, and youth programs.
Level 1 Evaluation MetricsWe use a standard evaluation for most of our learning activities and programs to determine, from the participants’ perspective, satisfaction with the activity, increases in productivity, gains in knowl-edge, applicability to job functions, and how engaging the speakers were.
Qualitative Data AnalysesThe comments that our participants write in our standard level 1 evaluations are important to us as we continually seek to improve our educational training and activities. Through a rigorous thematic coding and categorization of the partici-pant’s comments, we are able to gain insight into their training experiences.
Level 2 Evaluation MetricsAssessments and exams provide objec-tive measurements of knowledge and skill gains and allows us to know if our learning activities are effective. Many of activities utilize level 2 evaluations.
Online Evaluation SystemOver the last three years, we have transi-tioned from paper evaluations to an online evaluation system. By doing this, we have dramatically increased our efficiency in collecting data on our learning activities, and decreased turn-around time for data analyses and providing feedback to our educators.
Centralized Data WarehousingAs part of our metrics and analytics process, we have consolidated data warehousing of our level 1 evaluation data to a centralized databased. This allows us a one-stop source for important learning and program metrics that are easily comparable across the entire DOE. Additionally, we continually utilize our learning management system, the Learning Curve (TLC) to provide a central location for eLearning modules, registration for live events and activies, and transcript of learners’ training at LVHN.
Metrics and Analytics in the Upcoming YearAlthough we have made great strides in transforming DOE into a lean, data-driven perforance focused organization through improvements in how we identify, collect, analyze, and utilize quantitative and qualitative data, we have ambitious plans for the upcoming year. Among our goals is the refinement our metrics and analytics capabilities through the application of an overarching develop-mental evaluation framework to guide
how we use metrics to promote rapid improvements in the service we provide.
Our Metrics and Analytics Capabilities Are Essential to:- Internal residency reviews- CME and CNE accreditations- Epic implementation- LVHN research projects- Magnet designation- Department of Health reviews- Joint commission accreditation- Network wide needs assessments- Improving the teaching in all of our learning activities and events.- LEAN process iimprovements
Our Metrics Trends- Consistently exceeds internal (3.50) and expternal benchmarks for all standard level 1 evaluation questions.
Note: If interested in more detailed metrics, please refer to the separate Learner Evalu-ation Report.
8 | D i v i s i o n o f E d u c a t i o n

Overall Level 1 Evaluation Metrics
Overall Satisfaction (4.36)
Objectives Met (4.43)
Pacing Appropriate (4.38)
Speaker(s) Engaging (4.37)
New Knowledge Learned (4.36)
Applies to Job (4.35)
Improves Job Performance and Productivity (4.25)
Credentials of Level 1 Evaluation Respondents
No. of Course Occurrences By Teaching Methodology
How learners responded to: “I will be able to apply learning to improve job performance.”
Level 2 Evaluation ImprovementsStrongly Agree (41%)
Agree (50%)
Undecided (7%)Disagree (2%), Strongly Disagree (0%)
Always (17%)
Most of the time (42%)
Sometimes (35%)
How continuing education (CE) outcomes evaluation respond-ents answered: “How often did you use the knowledge and skills learning in this activity in your job?”
Rarely (4%), Never (2%)
Average Pre-Test Score
Average Post-Test Score
68%
88%
How contiuing education (CE) outcomes evaluation respond-ents answereed: “How continuing education (CE) improved...”
Students (2%)
Registered Nurses (57%)Other Unlicensed,
Non-Clinical (17%)
Physicians (13%)
Other Licensed, Clinical (11%)
Instructor-Led (82%)
eLearning (6%)Simulation (6%) Instructor-Led
Simulation (6%)
My Knowledge (32%) Quality, Patient Safety, or Patient Health (18%)
Little or No Improvement (4%)
My Job Performance and Productivity (14%)
My Attitude(s) Towards the Topic(s) (17%)My Competence (17%)
By the Numbers...
303
Number of distinct activities
evaluated
1,247
Number of activities evaluated
18,984
Number of level 1 evaluation
responses
48%
Total response rate for level 1
evaluations
134
Number of instructor-led activities in the
highest volme month
Qualitative Evaluation Data - Major Themes
1. Learning activity were effective, practical, timely, and relevant.
2. The content of the learning activity was engaging and effective.
3. The teaching techniques used in the learning activity helped in explaining concepts, including collaborations, and were effective in making me think.
4. The speaker(s) in the learning activity were clear, effective, knowledgeable, and engaging.
A n n u a l R e p o r t F Y 2 0 1 4 | 9

Budget and administration
Division of Education Expenses- $2.67 million DOE variance under expenses- DOE’s expenses represent 0.005% of 2014 total hospital expenses Note: several labor and non-wage expense budge reductions were made during the year.
$4.41 operating (non-wage)
expenses
$3.78 actual operating
(non-wage) expenses
$4.99 actual labor wages
$6.66 labor wages
$1.16 actual labor benefits
$1.53 labor benefits
Actual operating budget$9.93 million
Division of Education Revenues- $1.10 million DOE variance over revenues
Operating budget $12.6 million
$1.20 operations (including SELECT)
$1.20 operations (including SELECT)
$3.03 grants and funds
$1.93 grants and funds
Actual Revenues$4.23 million
Budget$3.13 million
Patient Care Services (PCS) Expenses PCS pass-through accounts accumulate the wages and expenses for participants in Patient Care Services nurse internships and mandatory training. These expenses are not part of DOE operations.
- $9.96 million PCS operating budget- $6.00 million PCS actual operating expenses- 3.96 million PCS variance under expenses
Nursing Education (18%)
SELECT Staff (10%)
1 0 | D i v i s i o n o f E d u c a t i o n

Continuing Education (1%)
Distance Learning (1%)
eLearning (3%)
Patient Education (2%)
DOE Administration (9%)
Ethics Program (<1%)
Nursing Education (7%)
SELECT (16%)
Simulation (1%)
Medical Library (6%)
Library (M) (1%)Combined Pass-Through Accounts (32%)
Grants and Funds (15%)
Medical Education (3%)
DOE Administration (M) (3%)
Total Expenditures = $18.7 million (including pass through accounts, grants and funds)
Continuing Education (3%)
Distance Learning (2%)
eLearning (5%)
Patient Education (3%)
DOE Administration (16%)
Ethics Program (1%)
Nursing Education (13%)
SELECT (30%)
Simulation (3%)
DOE Admin (M) (5%)
Medical Education (5%)
Library (M) (2%)
Medical Library(12%)
Total Expenditures = $9.9 million (excluding pass through accounts, grants and funds)
Distribution of Approved 62.1 FTEs Distribution of Actual 55.7 FTEs
Revenue, Grants, and Fund Sources
Library (M) (2%) Medical Education (7%)
Continuing Education (6%)
DOE Admin (M) (9%)
eLearning (4%)
Patient Education (6%)
DOE Admin (10%)
Nursing Education (19%)
SELECT Staff (13%)
Library (8%)
Simulation (2%)
SELECT Faculty (12%) Distance Learning (2%)
Library (M) (2%) Medical Education (7%)
Continuing Education (5%)
DOE Admin (M) (9%)
eLearning (4%)
Patient Education (6%)
DOE Admin (9%)Nursing Education (18%)
SELECT Staff (10%)
Library (8%)
Simulation (1%)
SELECT Faculty (19%)
Distance Learning (2%)
USF SELECT (30%)
SELECT (28%)
Other* (2%)
Pool Trust Grant (34%)
Unrestricted Fund (6%)
Continuing Education
Clifford Cholarship Fund
Wagner Scholarship Fund
Butz Nursing Education Fund
Library Education Fund
Temp Restricted Fund
Workforce Investment Board Grant
USF General Scholarship Fund
*Note: Each account for <1%
A n n u a l R e p o r t F Y 2 0 1 4 | 1 1

ActualBudget
Budget Actual
The Dorothy Rider Pool Health Care Trust grant utilization
Pool Trust Grant Utilization by Projects, FY2011 to FY2014
Pool Trust Grant Monetary Utilization by Fiscal Year, FY2011 to FY2014
Pool Trust Grant Percentage Utilization by Fiscal Year, FY2011 to FY2014
$4,313,074$3,917,903
Total
$1,528,606$1,247,310
FY14
$1,507,752$1,074,131
FY13
$1,475,709$936,388
FY12
$1,333,613$660,074
FY11
82%
91%Total
Year 4 (FY14)
71%Year 3 (FY13)
Year 2 (FY12)
Year 1 (FY11)
63%
49%
Essential Infrastructure Support
Interprofessional Faculty Development
Metrics and Analytics
Youth Education and Student Enrichment
Simulation Center
Standardized Patient Program
Social Media Research and Development
Online Case-Based Continuing Education
Art of Observation
Evaluation and Realignment Education
$403,450$199,390
$285,000$247,939
$424,800$325,035
$586,512$633,106
$1,298,585$1,739,262
$466,859$407,176
$343,968$318,825
$447,900$19,718
$60,000$7,447
$0$20,005
1 2 | D i v i s i o n o f E d u c a t i o n
Pool Trust Grant Utilization by Projects, FY2011 to FY2014
The Dorothy Rider Pool Health Care Trust Grant Utilization Explanation
It is important to keep in mind the original scope of the grant was spread over three years however as previously mentioned we experienced several slow starts on many of the grant projects with some projects experiencing delays of up to 15 months during the first year. The most common causes of these delays included difficulty in recruiting needed talent, obstacles related to experimental instructional technology and associated security restrictions and limited support, and delayed capital renova-tion projects expanding our simulation and learning facilities. These along with the early completion of two sub-projects left us with unfinished work within the scope of the grant and considerable unused financial resources allowing us to create a 4th year extension of the grant.
Essential Infrastructure (134%): Resources were reallocated to extend this into a 4th year, thus what appears as 34% over the original budget is the extension of this project. The essential infrastructure support represents a portion (6.1FTE) of the core human resources that are at the foundation of our leading-edge research and implementation of our educational innovations and services. The Pool Trust funds were matched with LVHN labor budget realizing a total of 13.6 FTE. This has been one of the primary ways Pool Trust funds were diffused throughout the work DOE accomplished.
Interprofessional Faculty Development (49%): One key program was evaluated early on and stopped; that was for an externally accredited faculty certification. There was not sufficient interest or commitment for such a program. Other less significant changes involved fewer honorariums paid to outside guest lecturers. Greatest challenge of delivering faculty development is the aggressive schedules and conflicting priorities our clinician and physician faculty face.
Metrics and Analytics (87%): Majority of these resources funded an (1) FTE whose primary responsibility was implementing standardized metrics, strategies for analytics, and lead (co-chair) our departmental metrics and research committees. Unused resource is associated with a small portion of funding to contract services.
Youth Education & Student Enrichment (77%): Underuse of these funds is associated with an early decision not to implement the Medical Leader Pipeline Program and a strategic decision by LVHN to eliminate our Youth Program Coordinator. This constrained our current youth programs and placing attention on our core nursing and medical student programs.
Interdisciplinary Simulation Center (108%): As with other projects, resources were reallocated to extend this into a 4th year, thus what appears as 8% over the original budget reflects the extension of this project. This funding represents a staff (4.0 FTE) of simulation specialists and technicians matched with LVHN funding realizing a full staff of 6.0 FTE. Pool Trust funding acceler-ated the momentum behind establishing simulation as a core instructional methodology. During this time LVHN invested over $2mm capital in the laboratory infrastructure.
Standardized Patient Program (82%): This line item represents labor costs of developing and maintaining a pool of trained patient actors and 1 FTE who acted as a full time coordinator. A slower than projected startup of the standardized patient program is associated with the startup of our SELECT medical education and the needed training of faculty to incorporate SPs into teaching scenarios.
Social Media Research and Development (93%): While there was a slow start to this project we were later able to accelerate its progress. After failed attempt to attract technical talent associated with non-competitive wages, we changed strategy and recruited brilliant entry level talent from our Research Scholars program. Funding covered an (1) FTE and additional ad-hoc support by engaging talented Research Scholars in part-time work. We then needed to narrow the scope of this research to specific emerging technologies including; social learning, virtual reality, gesture based interface, gaming, and augmented reality. We encountered several technical challenges working with emerging technology in a highly secured corporate computing environ-ment. Evaluating certain technologies for data security risks precluded them from further development. We also encountered limitations from our Information Services department to support corporate wide implementation of non-standard technologies. Most significant progress was made with virtual reality and gaming.
Online Case Based Continuing Education (4%): In the first year we experimented with wonderful technology that provided highly engaging interactive case based multimedia learning scenarios. The target audience was physicians and residents. We also found several vendors who were willing to contract with us eliminating the budgeted need for staffed programmer. However we encountered resistance in adoption by the intended audience. An early decision was made to terminate the project.
Art of Observation (12%): This project was completed ahead of schedule and significantly under budget! This project also met with some adoption issues.
A n n u a l R e p o r t F Y 2 0 1 4 | 1 3

Resident Central Venous Catheter Line Insertion Training
The training utilized a blended, interprofessional design that included a mixture of pre-training with required videos on the technical aspects of the procedure, sterile procedure, and expectations for interprofessional communication. The communication module incorporated video clips and reflective cues that demonstrate the expected communication around the procedure, including consent, pre-procedure time-out verifica-tion, and two needle stick challenges.
Hands on practice included a station utilizing ultrasound for target vessel identification, post-test station for knowledge assessment, simulation skills demonstration, and opportunities for additional technical practice. Nurses reinforced collegial teamwork behaviors including participation in “time out”, requesting sedation/analgesia, and coaching residents in calling for back up when necessary. Resident physicians are directly observed by physician faculty using a technical checklist to determine competency.
New Innovation Duty Hour Tracking Improvements
DOE and the residency program coordinators collaborated to revise the current duty hour module in New Innovations. As part of this improvement there was a significant reduction in the number of duty types available in the system from 88 to 13 standard duty types. This standardization helped to align rotations and resident assignments with the proper duty type. The ACGME and AOA duty hour rules were also reviewed and aligned to provide for more uniform reporting of duty hour violations as an institution.
Residents partipate in a surgery simulation utilizing a manikin.
The importance of investing in knowl-edgeable, skills, and competent future physicians continues to be an essential role of DOE. The DOE has an established history of providing high quality support of LVHN’s medical education programs. through oversight of graduate medical education (GME) and the University of South Florida’s Morsani College of Medicine/LVHN SELECT medical school program.
Residents and fellows are an integral part of the high quality care that LVHN provides to the region. Here in the Division of Education, we provide support and oversight of the residency programs through eLearning training modules for residents, faculty, and residency program
coordinators. Furthermore, the Division of Education coordinates site visits, internal program reviews, and onboarding orientation. Residents receive valuable training and education that help them provide better care for our patients, better health for the Lehigh Valley community, and better costs through improved patient safety and quality.
Training the next generation of physicians
85Visiting residents
253Medical residents and
fellow
102 Residency graduates
in FY2014
2,718Applicants to LVHN
residency programs
1New residency program
14Allopathic (ACGME) accredited programs
4osteopathic (AOA) accredited programs
41% of applicants from allopathic accredited
medical schools
22% of applicants from osteopathic medical
schools
16% of applicants from international medical
schools
37% of applicants from Pennsylvania medical
schools
1 4 | D i v i s i o n o f E d u c a t i o n

Dr. Ronald Swinford, former LVHN CEO and one of the founders of the SELECT program, speaks to a 4th year SELECT medical student.
This July the SELECT program increased to its full complement of four classes (Classes of 2015, 2016, 2017, and 2018) across all four years. The DOE focused on preparing for the Class of 2015 to enter their fourth year, updating the 3rd year curriculum based on feedback and lessons learned with our inaugural class, and continuing to build the infrastructure to support the program. This year we also focused heavily on preparing documentation for an accreditation site visit by the Liaison Committee on Medical Education (LCME) scheduled for February 2015.
- Created a scheduling process for SELECT students that meshed with the scheduling of visiting students from other institutions;
- Updated the orientation course for the Class of 2016 based on feedback from our launch of the course in 2013.
- Expanded our National Board of Medical Examiners (NBME) exam and logistics to accommodate 42 students.
-Initiated a career planning workshop in September, a career fair in November, and a residency planning workshop in March.
- Created a process for SELECT student induction into the Alpha Omega Alpha Honor Medical Society.
- Uploaded over 100 clinical simulation scenarios into the DOE simulation center learning management system.
- Conducted comprehensive clinical practice exams which consisted of 12 live standardized patient encounters providing
Highlights1:1 feedback on communication and interpersonal skills, professionalism, medical decision making, data gathering and interpretation skills to assist the student in preparing for the National Step 2 Clinical Skills exam.
- Offered 11 procedural courses for our SELECT students and other visiting medical students to introduce commonly performed procedures including central line insertion, airway management, thorocostomy, foley catheter insertion, airway management, nasogastric tube insertion, paracentesis, lumbar puncture and intravenous catheter insertion.
SELECT medical school program
82Syllabi developed for fourth year electives
433rd year SELECT
students
164th year SELECT
students
3New SELECT-
specific courses
A n n u a l R e p o r t F Y 2 0 1 4 | 1 5

Better Care Through Learning Activities and Events That Covered:- Increased knowledge, skill and competency of clinicians attending conferences.- Documented outcome surveys support knowledge gained, changing practice.- Discussion of ethically challenging clinical situations and available LVHN resources available for resolution.- Role of the Advanced Practice RN in a community-based (nurse-led) practice (Palliative Medicine).- Discussion of treatment plan options that match the Patient’s Goals of Treatment.
Better Costs Through:- Funds in many departments help defray costs. Employees attend free or with little tuition.- Effective care reduces cost.
Core
Ser
vice
s
Educational services for LVHN’s clinical staff
The Division of Education facilitates educa-tion and training for clinical staff, including physicians, nurses, and other health care providers that support the LVHN’s commit-ment to patient safety, quality, and clinical excellence. A variety of activities are offered, including orientation for new staff, continuing education, and other activities. Educational activities for clinical staff are organized into clinical staff development (i.e. nurses, technical partners, etc.) and continuing education (i.e. physician and nurse continuing education, grand rounds, etc.).
Continuing Education (CE) partners with network members to provide effective and efficient learning solutions that integrate quality educational experiences for our colleagues and the clinical professional
community. This encompasses Continuing Medical Education (CME) and Continuing Nursing Education (CNE), while supporting other forms of accredited continuing education for clinical personnel. Education is delivered in traditional classrooms, through conferences and symposia, and multi-media based digital productions for employees and our professional clinical community.
- Interdisciplinary orientation classes - Registered Nurse orientation and development- Graduate Nurse internships- Orientation and training of unlicensed assistive personnel- Competency Based Education consultation- Consultation in the role of nurse planner on continuing education planning committees- Clinical product consultation
14,146Clinical Staff Develop-ment learner contacts
79,240Clinical Staff Develop-ment instructional hours
and coordination of related education- Instruction and curriculum consultation for other profes-sionals engaged in learning- Accredited by the Pennsylvania Medical Society to provide AMA PRA Category 1 Credit™ - Approved provider of CNE by the Pennsylvania State Nurses Association- Guide planning teams in meeting accreditation standards for
92%Of learners satisfied with their CSD learning activity.
542Newly hired staff completed a DOE orien-
tation programs.
28,792Continuing education
participants
8,672Physicans that attended Continuing Medical
Education activities
5,912Nurses that attended Continuing Nursing
Education activities
94%CE participants that indicated they used the information from
the event.
continuing education credit - Provide tools for analysis, design, development, imple-mentation and evaluation of continuing education activities - Facilitate teams in obtaining other continuing education credits such as Respiratory, Pharmacy, Social Work and others
Edith Gray, an education specialist provides hands-on learning to newly graduated nurses.
1 6 | D i v i s i o n o f E d u c a t i o n

Critical Care Course Redesign
The revised course was launched in March 2014 with a focus on adult critical care and progressive care clinical environments. Redundant topic covered elsewhere in the DOE and LVHN were eliminated and the length of the course was reduced from 11 to 5 days of instructor-led workshops. The result was over 40 clinical hours available to participants to spend at the bedside learning patient care during orientation. The course is reviewed quarterly while maintaining congruency between American Associal of Critical Care Nurses: Essentials of Critical Care Orientation 2.0 eLearning modules and DOE-led workships.
Teaching methodologies for the course were also improved to promote a more learner-centered, technology-enhanced, and interactive approach. Among the changes are group presentations, gaming, formative evaluations, and an iPad app to complete case studies while viewing a patient monitor.
Additionally, the course redesign included collaboration with the Respiratory Services Department to include hands-on demon-stration and practice with advanced therapy equipment and use of the simulation center.
Highlights
A Great Catch That Improved Patient Care and Safety
In December of 2013 during an educational session Amy Droskinis, MSN RN CCRN, Education Specialist, was questioned by a learner regarding the use of the pediatric hands-free defibrillation pads. In order to properly answer the question Amy reviewed the Heartstart XL Defibrillator manufacturer manual and recommendations. This uncovered the actual recommenda-tion was not to use the hands-free pads for pediatric patients under 8 years old in AED mode. This recommendation was not congruent with the LVHN current practice and education being delivered.
Amy notified the pediatric and neonatal Patient Care Specialists which sparked the involvement of the Pediatric Code Blue Committee, Risk Management, and led to a hospital wide notification and change in practice related to the hands-free pads and AED mode. Amy’s attention to detail and follow-up with the issue contributed to avoiding serious potential patient safety events. Amy was nominated for and received an LVHN “Great Catch Award” which recognizes the outstanding performance of employees for catching these issues before serious events occur.
Changes in FY2014
Audience for the Navigations orientation program expanded to include Medevac, Population Health, Rehabilitation Services, and Pastoral Care.
The number of new products in-serviced in FY 2014 was 17 with several of them focusing on supporting the opening of the new facility at Tilghman.
The volume of new hires for the network decreased significantly this year which allowed the CSD team to focus efforts on several redesign projects.
A full electronic registration and payment system was incorporated into all single CE events, conferences, and symposiums. CE event attendees can now register 24 hours a day, 7 days a week from a computer or mobile device.
Amy Droskinis is presented an award for LVHN’s Great Catch award.
A n n u a l R e p o r t F Y 2 0 1 4 | 1 7

Picture on the left: Partners in the develop-ment of the Nurse Residency Program at the formal kickoff of the program in April.
Picture on the right: Nurse residents present their evidence-based practice posters during the Nurse Residency Program graduation in June.
What is the UHC/AACN Nurse Residency Program?Since the pre-published release of the Future of Nursing: Leading Change, Advancing Health report from the Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing LVHN has been developing action plans for implementing the Institute of Medicine’s (IOM) recommendations.
LVHN is a member of the University Health Systems Consortium (UHC) and the American Association of Colleges of Nursing (AACN). LVHN has partnered with DeSales University and Cedar Crest College to develop a dynamic, rigorous curriculum within the UHC/AACN Nurse Residency ProgramTM framework while incorporating the priorities and goals of LVHN. Financial support for LVHN’s Nurse Residency Program is provided by The Dorothy Rider Pool Health Care Trust. On April 22, 2013, the UHC/AACN Nurse Residency Program was formally introduced to LVHN.
Under the leadership of the Division of Education, the Nurse Residency Program is a network-wide, interdisciplinary, collabora-tive effort. Throughout their 12 months in the program, the Nurse Residents gain valuable training from experienced nurses, medical educators, evidenced-based researchers, medical ethicists, and organizational leadership consultants.
Who are the Nurse Residents?Newly licensed registered nurses are admitted to the Nurse Residency Program upon hire. All Nurse Residents are graduates of baccalaureate nursing programs. The Nurse Residents are provided 7 eight-hour seminar days over their first 12 months of employment as newly licensed registered nurses.
Why is the Nurse Residency Program important to LVHN?Research has shown that nurses new to the profession experience significant challenges and stress and many leave the profession within the first 12 months. The Nurse Residency Program aims to provide support to our newly hired nurse by engaging them in their practice, building self-satisfaction of their roles as nurses, developing them as bedside clinical leaders, training them to become critical thinkers utlizing evidenced-based practices, and empowering them to positively transform their units and LVHN.
Nurse Residency Program
Outcomes of the Nurse Residency ProgramNurse Residents take part in outcomes measurement through UHC/AACN, completing surveys upon hire, at 6 months and 12 months using the Casey Fink Graduate Nurse Assessment tool and the UHC/AACN Progression Survey. Demographic and retention data are also maintain. Data is then benchmarked within all UHC/AACN Nurse Resident Programs, and can be sub-divided and individually reported for LVHN and compared against other Magnet™ hospitals. Nurse Resident graduates will also be measured at 2 and 3 year intervals as additional survey periods have been added to the UHC/AACN Nurse Residency Program™.
The data shows that, for the first 66 Nurse Resident graduates, their results mirror that of other Magnet facilities as well as all NRP partici-pants. The one area of variance is in the degree of stress experienced by the Nurse Residents at 12 months. We attribute this additional stress to the current staffing levels and vacancy rates in the clinical units.
As a complete year of data has just been received, it is now incum-bent on the NRP and DOE to interpret the data and make necessary improvements in the program seminars and/or support systems to ensure that LVHN has a Nurse Residency experience that meets or exceeds the UHC/AANC benchmarks and other Magnet™ hospitals.
Performance Improvements for LVHNTwenty-five evidenced-based practice projects were completed to address patient safety and improved quality.
“The residency program is a great tool to have to integrate new graduate
nurses from academics into the ‘real world.’”
- Nurse Resident, July 2014
“I believe the nurse residency program helped
significantly with the transition from student
nurse to RN.”
-Nurse Resident, June 2014
1 8 | D i v i s i o n o f E d u c a t i o n

A n n u a l R e p o r t F Y 2 0 1 4 | 1 9

Interdisciplinary faculty development
Developing the quality of LVHN’s faculty is critically important to the learning and educational experiences of our learners, including clinical staff, residents, fellows, nursing students, SELECT medical students, and others. Among the goals of our faculty development efforts include facilitating greater interprofessional collaboration among clinical educators across traditionally siloed boundaries and developing the teaching and research skills of medical faculty members.
As part of DOE’s interdisciplinary faculty development, education grand rounds provides great topics and speakers, information and skills to take network teaching to a new level, and opportunities to collaborate with other educators throughout the Network. Following each workshop participants are asked to complete an evaluation of the session.
Online Faculty Development- Teaching in the Outpatient Setting
The LCME requires that residents and faculty have training in how to teach medical students. This online module was developed as part of an online set of faculty development eLearning courses focused on topics aligned with the responsibilities of teaching and learning inside of our clinical areas.
This module provides additional support to our facility and residents who interact with our medical students in the outpatient setting. The modules discussed feedback, teaching tips, teaching strategies and reflection. This is part of our other series of courses on effective feedback as a tool for improving a student’s clinical skills, the micro skills that should be mastered in order to be an effective preceptor, and teaching at the bedside as a tool for improving a student’s clinical skills.
The benefit of this online series is that they are available to suit the various scheduling needs of residents and they can serve as predecessors to live training or as enrichment for those that desire it.
4.52Rating of participants when asked if they learned new knowledge
4.39Rating of participants when asked if activity will improve job performance
Quotes from Faculty Development Participants
“Great suggestions and mentoring took place!.”
“Love the conversational style and in the room coaching.”
“It was an excellent basic overview of writing curricula, which I can directly apply to a project I’ve been tasked to complete.”
“Increase my comfort level when presenting a subject or topic.”
“Learned many new skills to which I can apply to my job working as a clinical educator.”
“Sharing of current practices and identification of barriers.”
287Responses to a network wide faculty develop-ment needs assessment
635Grand rounds sessions
46Grand rounds series
Workshops Offered in FY2014
Curriculum designPresentation skillsLearner engagementDesigning education with the learner in mindThe “RIME” method of assessmentDesigning effective assessment itemsEmotional intelligenceVideo-assisted debriefing and assessment: can I see that again?Written presentations, poster presentations, abstracts: a guideYou did what? Observing emotional intelligence competenciesGiving effective feedback
2 0 | D i v i s i o n o f E d u c a t i o n

Research Scholars learn on the laparoscopic task trainers in the Surgical Education Center.
EHP alumni Jessica Hartner (2nd from right) and McKenna Bast (far right) participate in the 2014 Research Scholars Program
Providing opportunities for students
Bridging the Gaps (Graduate Students) This program offers health care professions students the opportunity to work in interdisciplinary teams providing community health services to the Lehigh Valley.This year’s students worked with community partners such as the AIDS Activity Office, Sixth Street Shelter, and Neighborhood Health Centers of the Lehigh Valley.
Clinical Rotations (Undergraduate Students) We continued to offer clinical rotations at LVHN for students, particularly nursing, medical, and physician assistant students, from a variety of colleges and universities, including Cedar Crest College, Northamp-tion Community College, DeSales University, Lehigh Carbon Community College, Wilkes University, East Stroudsburg University, and Penn State University. This is our largest student program. Research Scholar Program (Undergraduate Students) A summer only program now, the Research Scholar Program again drew a large number of applicants for 61 positions in 33 LVHN departments. This year’s program included a seminar component in addition to the students’ research projects.
Research Scholars’ Work Demonstrates Standardization and Cost-Efficiencies As Research Scholars in the Perioperative Services Department, Lauren Boulay (College of William and Mary) and Sally Trout (LaFayette College) worked on a project to eliminate practice variation of two laparoscopic procedures. Using quantitative data analysis and LEAN theory, the research scholars created two possible solutions: one simply replaced certain items with more cost effective equivalents, and the other created a standard pick list that allowed variation within certain classifications of materials, ensuring quality and safety standards were maintained. Their analyses estimated cost savings between $28,000 and $142,000 depending on the two proposed implementation options.
Emerging Health Professionals (High School Students) The dual-enrollment program for Lehigh County high school students interested in a healthcare career had its largest class in its nine years, with 56 students total. Select EHP students participated in the Health Occupations Students of America (HOSA) competition, which ten state winners advancing to the national HOSA competition in Orlando, Florida. This year, two alumni from the EHP program also selected for this year’s Research Scholar Program.
437Students enrolled
12Bridging the Gaps
students
56Emerging Health Profes-
sionals Graduates
1,707Nursing student rotations
193Physician assistant
rotatations
Our programs give high school and college students valuable real-world training and understanding of a complex healthcare system that help them become engaged, innovative, emphathetic, and competent healthcare professionals. The programs that we offer include:
Research Scholar Program: By the Numbers
The Program The Applicants Accepted Scholars
8 weeks33 departments
6 seminar sessions
Seminar Topics:- Systems-based practice - Practice-based learning - Social determinants of health - Professionalism - Research design - Manuscript writing
403 applicantsAverage applicant GPA: 3.48
Number of colleges represented: 87
Senior applying: 162 (40.1%)Juniors applying: 170 (42.1 %)
Sophomores applying: 71 (17.9%)
61 scholarsAverage scholar GPA: 3.61
Number of collegesrepresented: 29
Live in the Lehigh Valley: 27
Live outsidethe Lehigh Valley: 36
A n n u a l R e p o r t F Y 2 0 1 4 | 2 1

3,342Learner contacts
65Courses
13SELECT Simulation
Exams
62%Response rate on level 1 evaluations
4.43Overall average satisfaction on level
1 evaluations
26Number of New Courses in Simulation
Audience members at the Innovations in Education Symposium participate in SIMWARS®.
RNs practice their skills on a manikin in the simulation center.
Simulation and learning center and standardized patients
The simulation and learning center supports the network by creating an educational, innovative learning environment in which learning occurs through the uses of live standardized patient encounters, high and low fidelity manikins, and virtual reality to increase quality of care delivered to patients while reducing safety concerns.
Over the last year, the simulation center has experienced tremendous growth by expanding our services to include family medicine, pastoral care, hospice and palliative medicine, periop services, pharmacy and Lehigh Valley Physicians Group (LVPG) practices while continuing to support and grow our already extensive programs. We continue to focus on the Triple Aim to improve healthcare in our community by improving quality and safety, optimizing health for individuals, while reducing costs.
Improving Quality of Standardized Patient Program
The standardized patient program was redesigned through an A3 process to improve scheduling, provide education, and standardize the interview and orientation process resulting in higher quality education for learners and reduced costs. The mission of the standardized patient program is to deliver high-quality standardized patient programming to train and assess healthcare learners at various stages of their education and training. Standardized patients are used extensively in medical education allowing learners to practice and improve their clinical and conversational skills and develop professional conduct in challenging situations.
The program expanded the number of standardized patients, including ones to represent different cultures, races, ethnicities, and disabilities in order to meet the growing demands of our community. Training was provided to the standardize patient on physical assessment, providing meaningful feedback, and debriefing to enhance the quality of educa-tion offered in simulation.
What’s new in the Upcoming Year- Equipping 20 simulation rooms with Epic equipment to prepare for go-live implementation.- Continue to expand the standardized patient program.- Improve SELECT clinical practice exam testing through revised scenarios.- Offer ACLS, PALS, and BLS course to SELECT students.- Continue to expand variety and frequency of learning activities.
2 2 | D i v i s i o n o f E d u c a t i o n

Better Care Through Learning Activities and Events That Covered:
Interprofessionalism- advanced practice clini-cians, nurse practitioners, physician assistants, pharmacistsTeam Performance - promoted TeamSTEPPS skillsCommunications - objective structured clinical exams (OSCEs) focusing on interpersonal and communications skills, professionalism, and patient careCritical Emergent Situations - OBGYN code pink, interdisciplinary code blueFocus on safety - standardized patient encoun-ters developed in partnership with Risk Management
Better Costs Through:
Epic Preparation - developing scenarios for Epic credentialed trainers for Wave 1 and Wave 2 implementationBetter Patient Satisfaction - cultural sensitivityClinical Efficiency - development of supply carts for CVC, foley, lumbar punctiure, and paracentesis. Standardization - cart standardization for Broselow pediatric codes, adult codes, and neonatal resus-citation post-partium hemorrhages
Better Health Through:
Promoting Health at Home - technical and support partners, home healthcare personnel
Obstetrics Interdisciplinary Cases
The simulation center works in collaboration with the Division of Obstetrics and Gynecology to train nurses, physicians and residents taking part in high fidelity and standardized patient simulations of real-life in-hospital and outpatient scenarios.
Most OB staff can attend at least one or more of these sessions throughout the year. These sessions promote teamwork and enhance practical skills, clinical competence and interdisciplinary collaboration.
One of the sessions this year focused on a high risk pregnant patient who had a genetic complex medical problem called catecholaminergic polymorphic ventricular tachy-cardia (CPVT). Given this condition carries a high risk of sudden cardiac death, the OB and simulation staff worked to develop a scenario surrounding this condition in a pregnant patient and conducted simulated adverse outcomes in order to educate and prepare the staff should these issues develop during this patient’s delivery.
Sample Programs
“This helps the OB department to work more efficiently as a team”
“Participation in this event helped to increase communication with
providers and nurses”
-Obstetrics Interdisciplinary participants
MICU Interdisciplinary Code Blue Insitu’s
On a monthly basis, the simulation team members in collaboration with the Internal Medicine Department and the Medical Intensive Care Unit team, conducts code blue simulations integrated in the intensive care environment for the medical residents, medical students, respiratory, and pharmacy staff.
These insitu events create realistic experiences for the learners allowing them to practice skills. Afterwards the learners are given the opportunity to debrief and reflect on the experience with faculty to discuss concepts that can be improved upon and new ideas to improve the quality and safety of practice. A pretest and posttest is captured to measure the effect of learning.
A learner is assessed during an obstetrics interdisciplinary simulation.
A n n u a l R e p o r t F Y 2 0 1 4 | 2 3

Better Care Through Instructional Materials That...Help LVH Improve Patient Experience such as:-Moisture Associated Skin Breakdown eLearning, Implanted Port Care Video, Fall prevention eLearning, restraints eLearning, disability etiquette video, Children’s Hospital Awareness eLearning, patient lift video
Improve quality and safety measures including:-Surgical care improvement program eLearning, Cardiac Rhythm Interpretation eLearning courses, CLABSI eLearning, minimally invasive gyneco-logic surgery video, cardiac virtual simulation scenarios, Patient Safety Week vidoes, media site recordings for topic presented at Grand Rounds, CORE annual education
Better Costs Through:Supporting the implementation of Epic electronic records through:-Epic TLC registration process, Epic eLearning courses, Super User Program, Epic Certifica-tion Proctors
Helping LVHN employees reduce waste and improve performance by providing:-Management of training resources and electronic content- TLC learning management system, online registration system, online training transcript, video remote conferencing to USF campus, ICD-10- Basic Education introduction to ICD-10 eLearning, Advanced Education ICD-10 eLearning
- Resource Management- Waste Stream eLearning and online game, Hazardous communication OSHA updates eLearning, Human Resources- Labor Relations training, Score Card eLearning, LVPG Compensation Education, API
Better Health Through...Supporting LVHN Wellness through:-the Wellness University conference with registra-tion, attendance, and videos of key presenters caring for our caregivers videos
New technologies offer ways to meet diverse learning styles to reduce costs and improve outcomes. These technologies include social media, virtual worlds, eLearning, and other innovative technologies that can be harnessed for improved instructional effectiveness and learning outcomes.
Many of the learning activities offered by DOE are supported or enhanced through the use of technology. The Learning Curve (TLC) learning management system provides eLearning modules to LVHN staff and registration for other educational events throughout the network. To address the need for technology to support educational offerings, DOE will shift towards more consultation, rapid design processes, and a train-the-trainer model.
What’s new in the upcoming year
Epic project support- Build infrastructure for Epic instructional designers to create LVHN-specific Epic workflow eLearnings activities- Support operationalization of Epic training (eLearning, registration, New Hire Orientation)- Roll out Epic serious games to network to assist in change management- Design a platform in our virtual reality platforms to allow for access to Epic- Support curriculum innovation of Epic new hire orientation
Innovations- Develop an augmented reality applications- Fully integrate virtual simulation- Expand our use of interactive multimedia in decision-based education
ICD-10- Work with the network planning team to support the integration of both eLearning and instructor education to prepare the network for ICD-10 implementation
16,181Enabled eLearning
System Users
911Support tickets resolved by TLC administrators
68Different educators building content
Innovative uses of eLearning, Social Media, and Virtual Reality
553,019TLC User Enrollments
100,457Hours of on-line training consumed
by learners
1,220Course, including
Epic
$23.42License Cost per TLC
user
4.21Average response to “this activity will improve my job performance and
productivity”
2 4 | D i v i s i o n o f E d u c a t i o n

Tapping into the potential of virtual reality and educational games
DOE has continued collaborations with LVPG to research and use 3D virtual environments in the training of office-based clinical teams.
Specifically, the virtual reality environment project seeks to: - identify and evaluate key design elements for realism, pacing, flow of events, group interactions, and transfer ability of knowledge and skills. - provide LVPG clinical trainers with virtual reality cases and the necessary training and support to implement the platform as a training solution for geographically dispersed practice sites.
Three virtual simulation scenarios were developed focusing on teaching high-risk, low-volume problem-prone office-based medical emergencies. The three scenarios included cardiovas-cular, neurological, and behavioral health emergencies.
Additionally, DOE utilized the Unity3D game development platform to create two educational training games. The games were designed to increase knowledge acquisition and retention regarding LVHN waste management policies and Epic system termi-nologies and functions.
Art of Observation
An innovative, interdisciplinary series of three sessions (fine arts, music, and performance art) was developed to enhance healthcare providers’ ability to get at the “heart” of patient encoun-ters by opening pathways to intuition and perception, thinking more broadly about patients’ social and cultural contexts, and moving beyond mechanistic thinking often reinforced by traditional medical education. Ultimately, the goal was to improve diagnostic and communica-tion skills of physicians, nurses, and other medical staff.
The Art of Observation received very positive feedback from participants. However, overall participation numbers were limited because of clinicians’ schedule constraints.
Art of Observation Sessions
Fine Arts (Muhlenberg College)Sharpen observation skills by obsrving the fine details in art and making the clinical connection to improved-history taking.
Music (Sartori Chamber Music Group)Enhance active listening skills through this dynamic and interactive session of focused listening to selected music pieces. The pieces connect to improved detection of heart and lung sounds.
Performance Art (Touchstone Theatre Group)Enhance visual skills through the obser-vation of selected performance art pieces specific to the biomechanical movements of the human body.
Virtual reality simulation involving LVPG participants.
A member of the Touchstone Theatre Group demonstrates biomechanical movements for the participants.
“As a PT, this activity was
useful because it applies to our
job of analyzing movements-so
it is a nice tool to perhaps
sharpen our observational
skills.”
From a partipant in the
performance art session
A n n u a l R e p o r t F Y 2 0 1 4 | 2 5
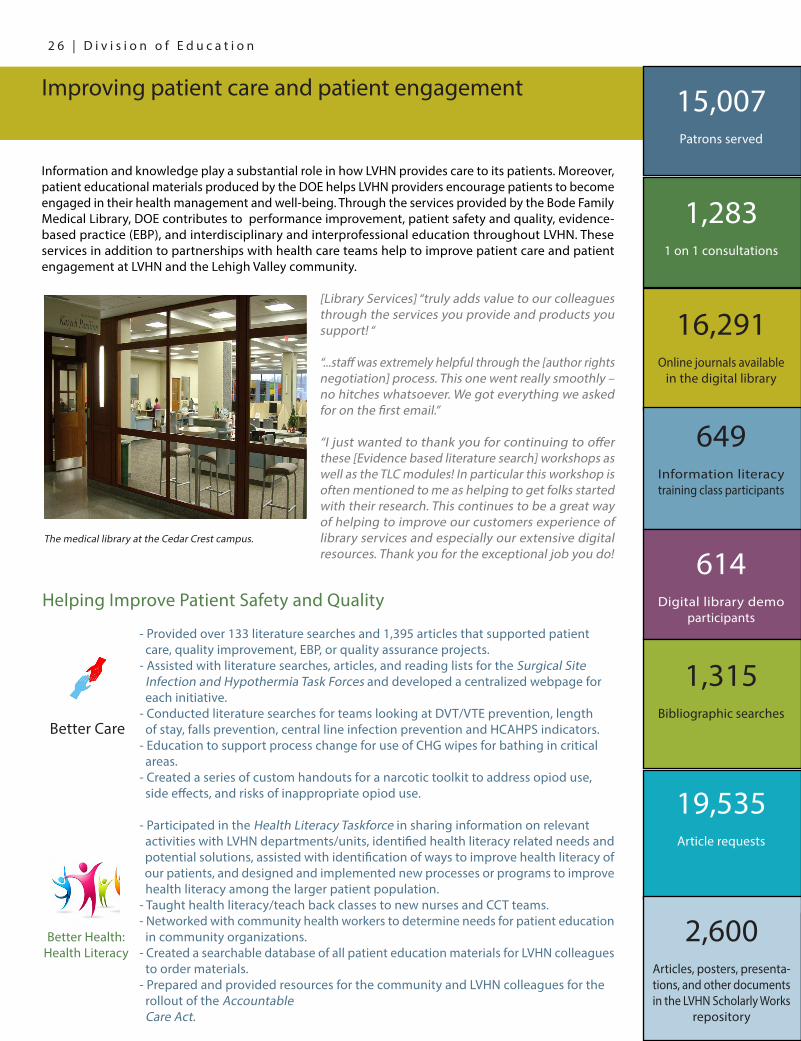
Information and knowledge play a substantial role in how LVHN provides care to its patients. Moreover, patient educational materials produced by the DOE helps LVHN providers encourage patients to become engaged in their health management and well-being. Through the services provided by the Bode Family Medical Library, DOE contributes to performance improvement, patient safety and quality, evidence-based practice (EBP), and interdisciplinary and interprofessional education throughout LVHN. These services in addition to partnerships with health care teams help to improve patient care and patient engagement at LVHN and the Lehigh Valley community.
[Library Services] “truly adds value to our colleagues through the services you provide and products you support! “
“...staff was extremely helpful through the [author rights negotiation] process. This one went really smoothly – no hitches whatsoever. We got everything we asked for on the first email.”
“I just wanted to thank you for continuing to offer these [Evidence based literature search] workshops as well as the TLC modules! In particular this workshop is often mentioned to me as helping to get folks started with their research. This continues to be a great way of helping to improve our customers experience of library services and especially our extensive digital resources. Thank you for the exceptional job you do!
The medical library at the Cedar Crest campus.
Helping Improve Patient Safety and Quality
Improving patient care and patient engagement 15,007Patrons served
1,2831 on 1 consultations
16,291Online journals available
in the digital library
649Information literacy training class participants
614Digital library demo
participants
1,315Bibliographic searches
19,535Article requests
2,600Articles, posters, presenta-tions, and other documents in the LVHN Scholarly Works
repository
Better Care
- Provided over 133 literature searches and 1,395 articles that supported patient care, quality improvement, EBP, or quality assurance projects. - Assisted with literature searches, articles, and reading lists for the Surgical Site Infection and Hypothermia Task Forces and developed a centralized webpage for each initiative.- Conducted literature searches for teams looking at DVT/VTE prevention, length of stay, falls prevention, central line infection prevention and HCAHPS indicators. - Education to support process change for use of CHG wipes for bathing in critical areas. - Created a series of custom handouts for a narcotic toolkit to address opiod use, side effects, and risks of inappropriate opiod use.
Better Health: Health Literacy
- Participated in the Health Literacy Taskforce in sharing information on relevant activities with LVHN departments/units, identified health literacy related needs and potential solutions, assisted with identification of ways to improve health literacy of our patients, and designed and implemented new processes or programs to improve health literacy among the larger patient population.- Taught health literacy/teach back classes to new nurses and CCT teams.- Networked with community health workers to determine needs for patient education in community organizations.- Created a searchable database of all patient education materials for LVHN colleagues to order materials. - Prepared and provided resources for the community and LVHN colleagues for the rollout of the Accountable Care Act.
2 6 | D i v i s i o n o f E d u c a t i o n

Helping expecting mothers maintain and improve physical health
The Healthy Expectations team and the department of obstetrics and gynecology developed the Healthy Expectations booklet to educate mothers at risk for developing gestational diabetes. The booklet focused on meal planning, exercise, and goal setting to improve health and pregnancy outcomes.
Sample Patient Education Material
HealthyExpectations
L E H I G H V A L L E Y H E A L T H N E T W O R K
Wall Squats • Placestabilityballbetweenyourlowerbackandawall.Leanagainstthestabilityballwith yourfeetfirmlyplantedabout2feet(0.5meters)infrontofyou. • Slowlyloweryourbody,bendingatthehipandknees.Comedownalittlebitatfirsttoget familiarwiththemotion.Onceyoufeelready,slowlyloweryourselftoacomfortable position.Don’tletyourbuttsinkbelowyourknees.
•Straightenlegsandreturnbacktothestartingpositiontocompleteonerep. • Repeat8to12times. Works quads, butt and hamstrings.
AB
90 degrees
0 degrees
90 degrees
45 degrees
28
Cover and sample page from the Healthy Expectations booklet.
Better Cost
- Collaborated with quality blue core measures reimbursement team to reorganized Krames health sheets that affect network reimbursements.- Provided articles, books, and other resources to Legal Services to support LVHN legal cases.
Better Health: Patient Engagement
- Created a custom patient education booklet for the Mechanical Heart Assist Device Program.- With LVPG, created descriptive materials on the roles of mid-level and ancillary HCP’s such as chiropractors. - Participated in PCE Project 22– Pain Management by updating LVHN custom patient education materials relating to pain and assisting in securing licensing to Wong-Baker FACES pain scale. - Participated in PCE Project 26– Children’s Hospital by providing input into content and introduction of network- wide employee needs survey and providing reference documents on aspects of patient education to be included.
108New text items written in FY2014
105,480Items printed and
distributed
75%Order fulfillment
time reduction from process improve-
62Items uploaded to Scholarly Works with a resident or fellow author
226Illustrations (hand-drawn, computer-generated, and
photos)
1,653,650Health sheets
printed from Krames onDemand
A n n u a l R e p o r t F Y 2 0 1 4 | 2 7

Division of EducationLehigh Valley Health Network1247 S. Cedar Crest Blvd. 2nd Floor