distal radius fractures- volar plating for all distal radius fractures-volar plating for all...
TRANSCRIPT

1
Distal Radius Fractures-Volar Plating for All
Francisco Rubio, M.D. Miami Hand and Upper Extremity Institute
Miami, FL
Frontiers in Upper Extremity Surgery 2017
Disclosure
Skeletal Dynamics- Consultant
• 85% Dorsal
• 15% Volar

2
• Anatomical Reduction
• Early Function
• Stable Fixation
1970 - AO
Dorsal Plate Fixation
Extensor Tendon Disturbance
• Limited Motion
• Plate Removal

3
Fragment Specific Fixation
1994
- Distal fragment does not toggle
- Provides stable distal fixation in comminuted or osteoporotic bone
1995 - Distal Radius Locking Plate Fixation
“π - Plate”
Extensor Tendon Ruptures

4
- Plate redesign
The Dogma
Dorsal Fracture – Dorsal Plate
Palmar Fracture – Palmar Plate

5
PQ
PQ
The volar approach seldom presents flexor tendon problems
Operative Treatment of Volar Intra-Articular Fractures of the Distal End of the Radius. - Jupiter JB, Fernandez DL, Toh CL, Fellmann T, Ring D. J Bone and Joint Surg. 78A: 1817-1828 1996

6
A new method of treatment
Volar management of
the dorsal fracture
1997
Ineffective for Dorsal Fractures
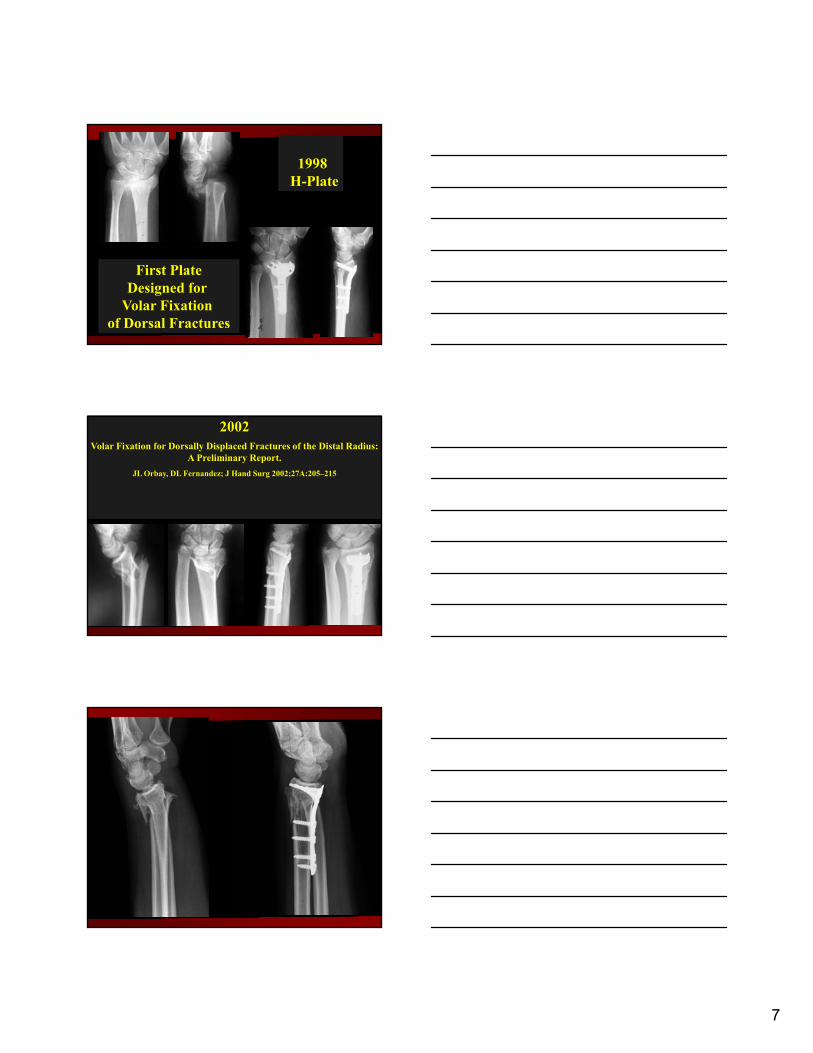
7
First PlateDesigned for
Volar Fixation of Dorsal Fractures
1998H-Plate
2002Volar Fixation for Dorsally Displaced Fractures of the Distal Radius:
A Preliminary Report.
JL Orbay, DL Fernandez; J Hand Surg 2002;27A:205–215

8
4-6 weeks post-op
1998 - 2013Volar Plate Evolution
Fixed Angle FixationStrongest Possible Interface

9
Plate acts as template and drill guide
Subchondral Support Scaffold
Ligament Contribution to Patterns of ArticularFractures of the Distal Radius
Daniel G. Mandziak, MBBS, Adam C. Watts, MBBS, Gregory I. Bain, PhD, MBBS
Journal of Hand Surgery. 2011.07.014

10
LRL
RSCVRU
DRU
DRC
AMF
LFPMF
SRL
Load Transmission Through the Wrist in the Extended Position
Masataka Majima, MD, Emiko Horii, MD, Hiroshi Matsuki, MD, Hitoshi Hirata, MD, Eiichi Genda, MD
( J Hand Surg 2008;33A:182 – 188.)
Fracture fixation methods
• Pins/wires

11
Hand (NY). 2014 Jun; 9(2) 230-236
Fracture fixation methods
• Pins/plates
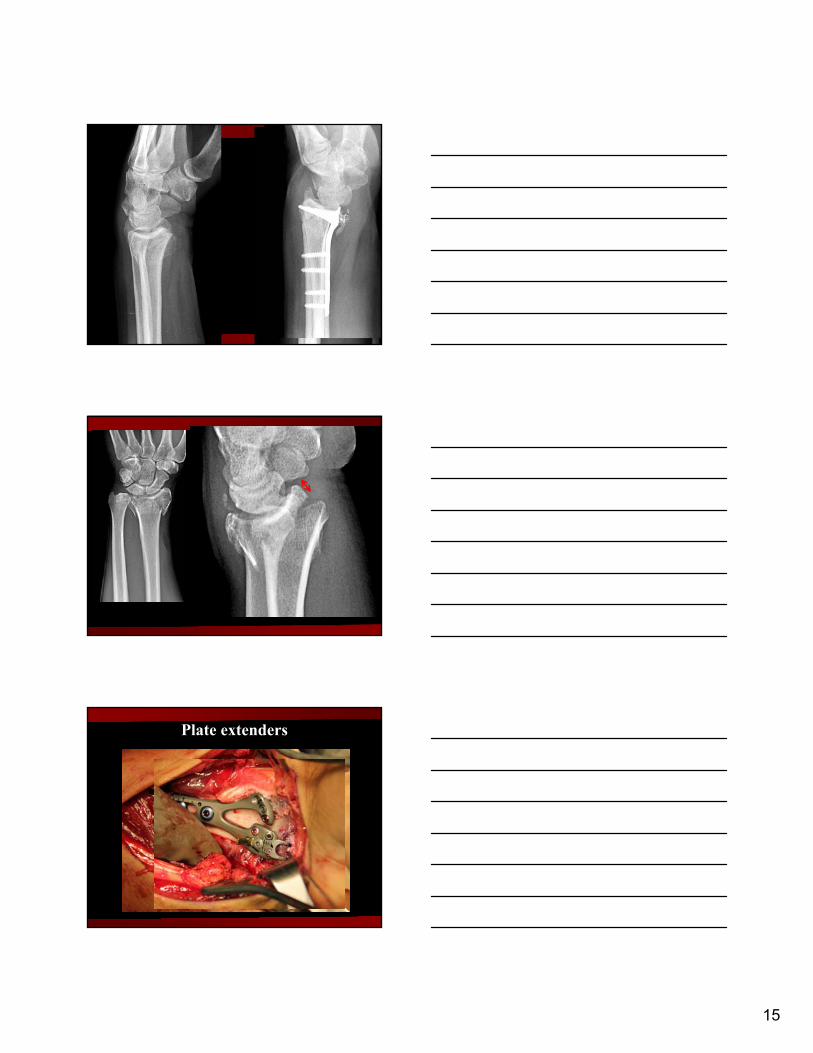
Fracture fixation methods
• Plates and extenders

12
Scaphoid Fossa Fixation
Lunate Fossa Fixation

13
Lunate Fossa
Watershed Line
Watershed Line

14
3 mm
Watershed Line
2 mm
Watershed Line
Watershed Line to Plate Distance
5 mmVolar Marginal Fragment
Volar Lunate Fragment
15
Plate extenders

16
Plate extenders
Radiographic Evaluation of Dorsal Screw Penetration After Volar Fixed-Angle Plating of the Distal
Radius: A Cadaveric Study
Steven D. Maschke & Peter J. Evans & David Schub &
Richard Drake & Jeffrey N. Lawton
Hand. 2007 Sep; 2(3): 144–150

17
18
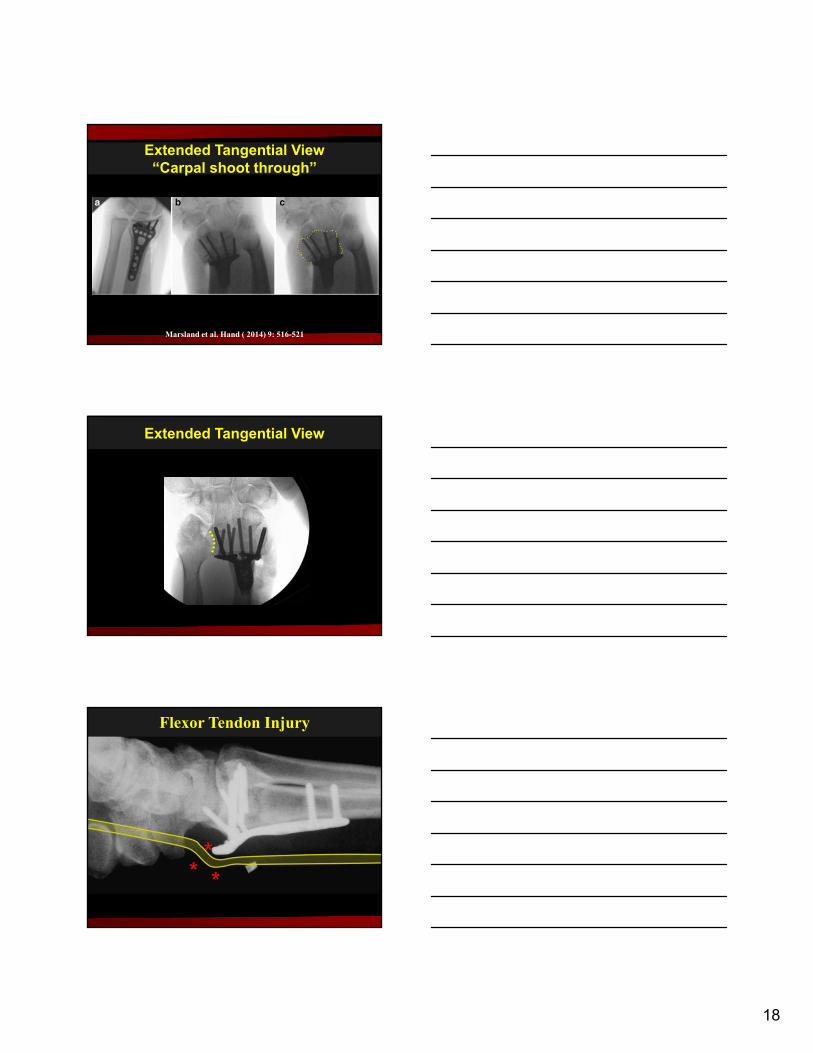
Extended Tangential View“Carpal shoot through”
Marsland et al. Hand ( 2014) 9: 516-521
Extended Tangential View
MWFlexor Tendon Injury

19
FDP IIFPL
Most Frequently Ruptured Tendons
#1 #2

20
--------Volar Rim Lunate Fossa
Volar Radial -------Tubercle
Inter Fossa Sulcus
Tendon Center to Bone 4.5mmPlate to Tendon Surface ≈ 0mm
FPL

21
0 1 2
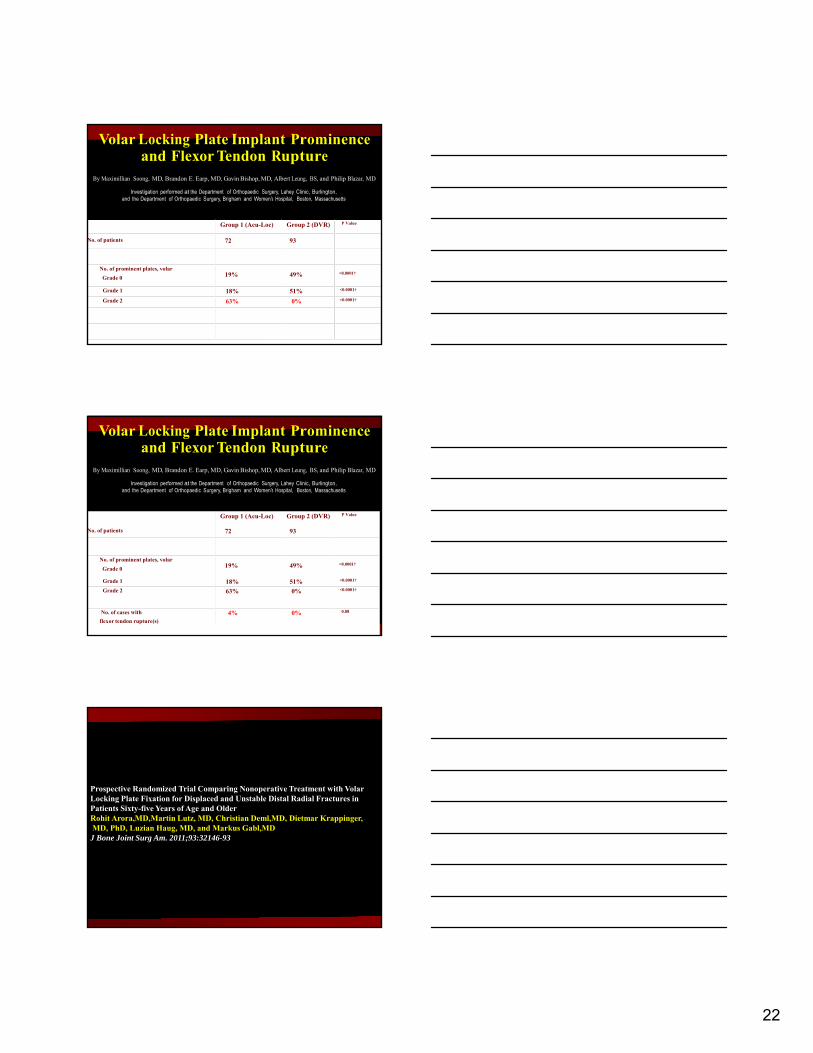
Volar Locking Plate Implant Prominence and Flexor Tendon Rupture
By Maximillian Soong, MD, Brandon E. Earp, MD, Gavin Bishop, MD, Albert Leung, BS, and Philip Blazar, MD
Investigation performed at the Department of Orthopaedic Surgery, Lahey Clinic, Burlington, and the Department of Orthopaedic Surgery, Brigham and Women’s Hospital, Boston, Massachusetts
“The Critical Line”
168 DRFs treated with volar plating
• Grade 0 0 Ruptures
• Grade 1 1 Rupture
• Grade 2 2 Ruptures
Volar Locking Plate Implant Prominence and Flexor Tendon Rupture
By Maximillian Soong, MD, Brandon E. Earp, MD, Gavin Bishop, MD, Albert Leung, BS, and Philip Blazar, MD
Investigation performed at the Department of Orthopaedic Surgery, Lahey Clinic, Burlington, and the Department of Orthopaedic Surgery, Brigham and Women’s Hospital, Boston, Massachusetts
Group 1 (Acu-Loc) Group 2 (DVR) P Value
No. of patients 72 93
Volar Locking Plate Implant Prominence and Flexor Tendon Rupture
By Maximillian Soong, MD, Brandon E. Earp, MD, Gavin Bishop, MD, Albert Leung, BS, and Philip Blazar, MD
Investigation performed at the Department of Orthopaedic Surgery, Lahey Clinic, Burlington, and the Department of Orthopaedic Surgery, Brigham and Women’s Hospital, Boston, Massachusetts
22
Group 1 (Acu-Loc) Group 2 (DVR) P Value
No. of patients 72 93
No. of prominent plates, volar
Grade 0 19% 49% <0.0001†
Grade 1 18% 51% <0.0001†
Grade 2 63% 0% <0.0001†
Volar Locking Plate Implant Prominence and Flexor Tendon Rupture
By Maximillian Soong, MD, Brandon E. Earp, MD, Gavin Bishop, MD, Albert Leung, BS, and Philip Blazar, MD
Investigation performed at the Department of Orthopaedic Surgery, Lahey Clinic, Burlington, and the Department of Orthopaedic Surgery, Brigham and Women’s Hospital, Boston, Massachusetts
Group 1 (Acu-Loc) Group 2 (DVR) P Value
No. of patients 72 93
No. of prominent plates, volar
Grade 0 19% 49% <0.0001†
Grade 1 18% 51% <0.0001†
Grade 2 63% 0% <0.0001†
No. of cases with
flexor tendon rupture(s)4% 4 4 4 4 0% 0.08
Volar Locking Plate Implant Prominence and Flexor Tendon Rupture
By Maximillian Soong, MD, Brandon E. Earp, MD, Gavin Bishop, MD, Albert Leung, BS, and Philip Blazar, MD
Investigation performed at the Department of Orthopaedic Surgery, Lahey Clinic, Burlington, and the Department of Orthopaedic Surgery, Brigham and Women’s Hospital, Boston, Massachusetts
Prospective Randomized Trial Comparing Nonoperative Treatment with Volar Locking Plate Fixation for Displaced and Unstable Distal Radial Fractures in Patients Sixty-five Years of Age and OlderRohit Arora,MD,Martin Lutz, MD, Christian Deml,MD, Dietmar Krappinger,MD, PhD, Luzian Haug, MD, and Markus Gabl,MD
J Bone Joint Surg Am. 2011;93:32146-93

23
• Randomized: VLP vs Casting.
• “Simple volar approach” @ 1-2 weeks
• Operative group did better first 6 months.
• At one year both groups were almost equal.
• 36% vs 14% complication rate
• Total: 13 5
• Flexor 4 (plate prom) 0
• Extensor 6 (long screws) 0
• CTS 1 0
• CRPS 2 5
Operative Non Operative
• Total: 3 5
• CTS 1 0
• CRPS 2 5
Operative Non Operative

24
Standard Fixation Technique
Complication rate and patient satisfaction after volar plating of distal radius fractures
J. L. Orbay, F. Rubio, E. J. Balaguer, L. Vernon
Unpublished data
- 808 consecutive patients
- 443 evaluated thus far (54.8%)
- 9.2% overall complication rate
- 4.3% required a second operation
- <0.5% infection rate
Complication rate and patient satisfaction after volar plating of distal radius fractures
J. L. Orbay, F. Rubio, E. J. Balaguer, L. Vernon
Unpublished data
- Overall satisfaction 91.4%
- 90.1% would have the same procedure again
- 92.6% would recommend their surgeon

25
Volar Approach for Dorsal Fracture Not Trivial
Anatomical Plates
RequireAnatomical Reduction

26
Using the Extended FCR Approach
• Release the radial septum
• Intrafocal Exposure
• Pronate the proximal fragment
• Release FCR tendon sheath
Standard Fixation Technique
Standard Fixation Technique
Removing dorsal hematoma allows reduction

27
Dorsal rim fracture

28

29

30
Bone Graft Support
2 mm Rule
2 mm
2 mm

31
1- Reduce and Pin Lunate Fossa
2- Reduce and Pin the Scaphoid Fossa

32
Volar rim fracture

33

34
Prevent Collapse and Salvage Failures of theVolar Rim of the Distal Radius
J. L. Orbay, F. Rubio, L. Vernon
Journal of Wrist Surgery 2016;00:1–5.
21 patients
- 17 had volar marginal fixation at primary surgery
- 4 had volar marginal fixation as a revision
- No failures in primary VMF fixation group
- 2/4 had failure after revision
- 91% successful overall VMF fixation
- failure associated with revision fixation
Prevent Collapse and Salvage Failures of theVolar Rim of the Distal Radius
J. L. Orbay, F. Rubio, L. Vernon
Journal of Wrist Surgery 2016;00:1–5.
- For failed VMF fixation, opening wedge osteotomy
- Correct volar tilt to 5 degrees dorsal
- Restores supination loss seen after failed VMF fixation

35

36

37
A combination

38

39

40
Is there any role for a dorsal approach?

41
42

43
Thank You!