disruption, danger, and droperidol: emergency management of the agitated patient
TRANSCRIPT
disruption, danger, and droperidol: emergency management of the agitated patient
reuben j. strayer emupdates.com
what patient defines emergency medicine?
what patient defines emergency medicine?
what patient defines emergency medicine?
sickwell
what patient defines emergency medicine?
undifferentiated chest pain undifferentiated abdominal pain undifferentiated headache undifferentiated dizzy undifferentiated back pain undifferentiated fever
undifferentiated agitation
what patient defines emergency medicine?
an immediate threatrequires use of dangerous maneuversdrunk or dying
simultaneous control, resuscitation, and risk stratification
undifferentiated agitation

3 types of emergency department agitation
agitated but cooperativedisruptive without dangerexcited delirium
agitated but cooperative
responds to suggestionno concern for dangerous condition
have someone sit with themor small dose oral benzo
assessable - low concern for dangerous condition
conversant but disruptive
sleep it off
disruptive without danger
safety prioritized over speed and efficacy
often “observed” in unmonitored bed
very common in many ED’s
disruptive without danger
disruptive without danger
haldol 5, lorazepam 2is fine. better than fine:
droperidoldroperidol is the most effective agent for undifferentiated agitation
disruptive without danger
Chan 2013 Isbister 2010 Martel 2005 Resnick 1984 Richards 1998 Thomas 1992
droperidol is the safest agent for undifferentiated agitation
droperidol
disruptive without danger
Isbister 2010 Knott 2006 Martel 2009 Spain 2008
is nonsense
droperidol
disruptive without danger
Calver 2013 Calver 2015 Chase 2002 Chambers 1999 Nuttall 2007 Perkins 2015 Richards 2002 Shale 2003 Szuba 1992
the QT black box
and suspicious
droperidol
disruptive without danger
is nonsense Bailey 2002 Horowitz 2002 Jackson 2007 Kao 2003 Lenzer 2002 Mullins 2004 Newman 2015 van Zwieten 2004
the QT black box

disruptive without danger
Clindamycin Clopidogrel Factor VIIa Dihydroergotamine Flumazenil Haloperidol NSAIDs Metformin Methotrexate Metronidazole Midazolam Nitroprusside Procainamide Succinylcholine Warfarin
the QT black boxis nonsense
droperidol
Clindamycin Clopidogrel Factor VIIa Dihydroergotamine Flumazenil Haloperidol NSAIDs Metformin Methotrexate Metronidazole Midazolam Nitroprusside Procainamide Succinylcholine Warfarin
is nonsense
droperidol
disruptive without danger
the QT black box
is no longer available in the US
long live droperidol
droperidol
disruptive without danger
5-10droperidol
disruptive without danger
midazolam
disruptive without danger
midazolam
disruptive without dangeri
Hung 1996 Nobay 2004 McMullan 2010 Rey 1999
midazolam
disruptive without danger
hypoventilationparadoxical response benzo resistancevs. droperidolvs. haloperidol
5-10
Spain 2008 Mancuso 2004
monitor
no monitor
haldol 10 versed 2
*
faster than haloperidol*but narrow therapeutic window

disruptive without danger
re-dosing is okvs. excited delirium
droperidol 5-10 IMmidazolam 5-10 IMhaldol 10 midaz 2 IM

excited delirium
uncommon outside citiesdelirium and danger
to himself to others from dangerous conditions
*except in australia
disruptive vs. delirious
cannot engage / incoherentfluctuating sensoriumabnormal vitals - don’t fight for vitals
screaming and thrashing
err on treating as excited deliriumdrunks exist to embarrass emergency doctors
disregard for futility, pain, fatigue
Vilke 2012
1. adequate forcemake sure it’s safe to approach the patient
code white - partner with hospital security
how to manage excited delirium
2. put face mask oxygen on the patientcontrols spitprovides oxygen
whatever the patient position

[pic of choke hold / neck compression]

[pic of knee on back of face down patient preventing chest excursion]

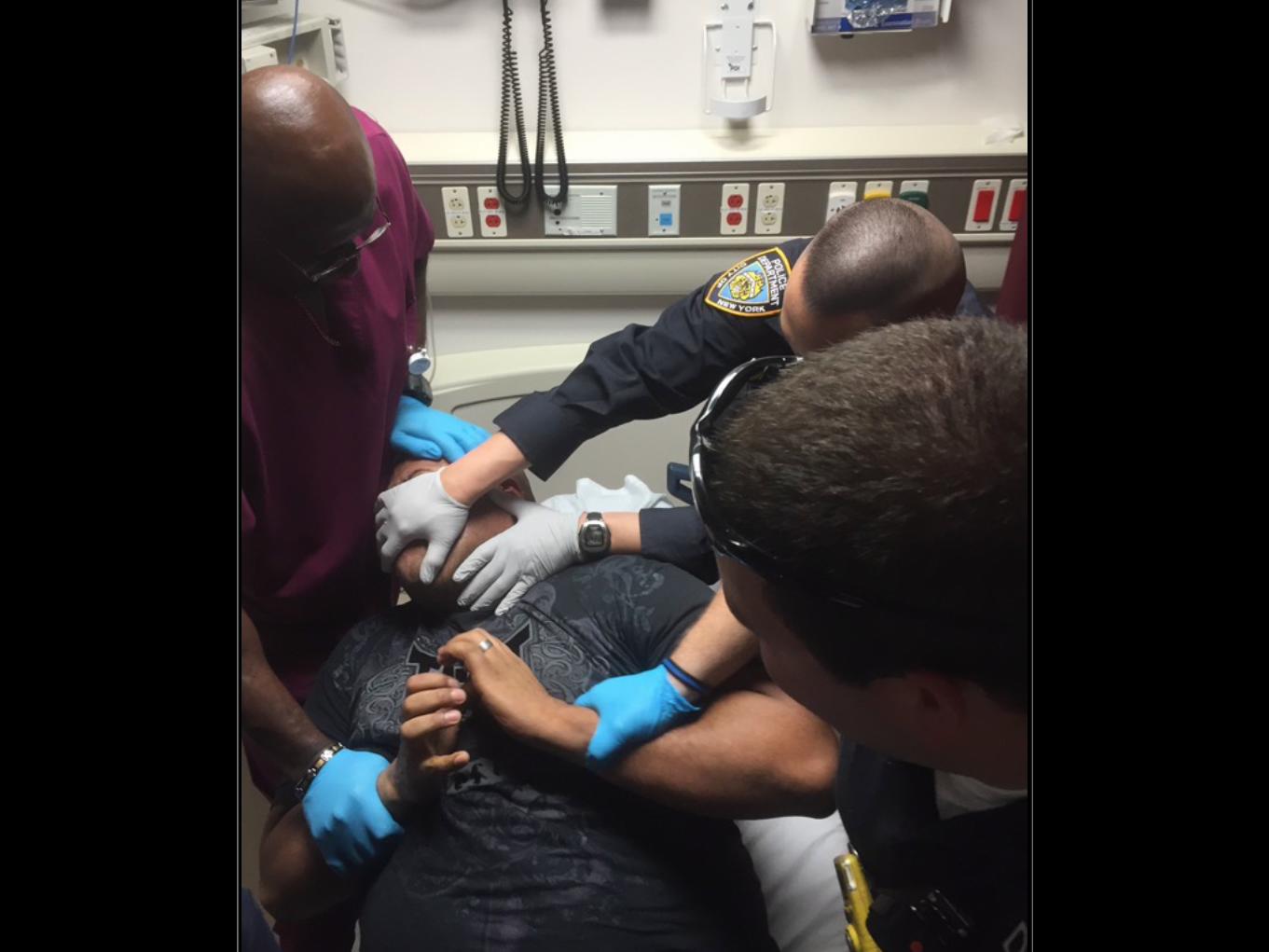
[pic of pulling the officer’s hand off the face of the patient by holding a face mask]
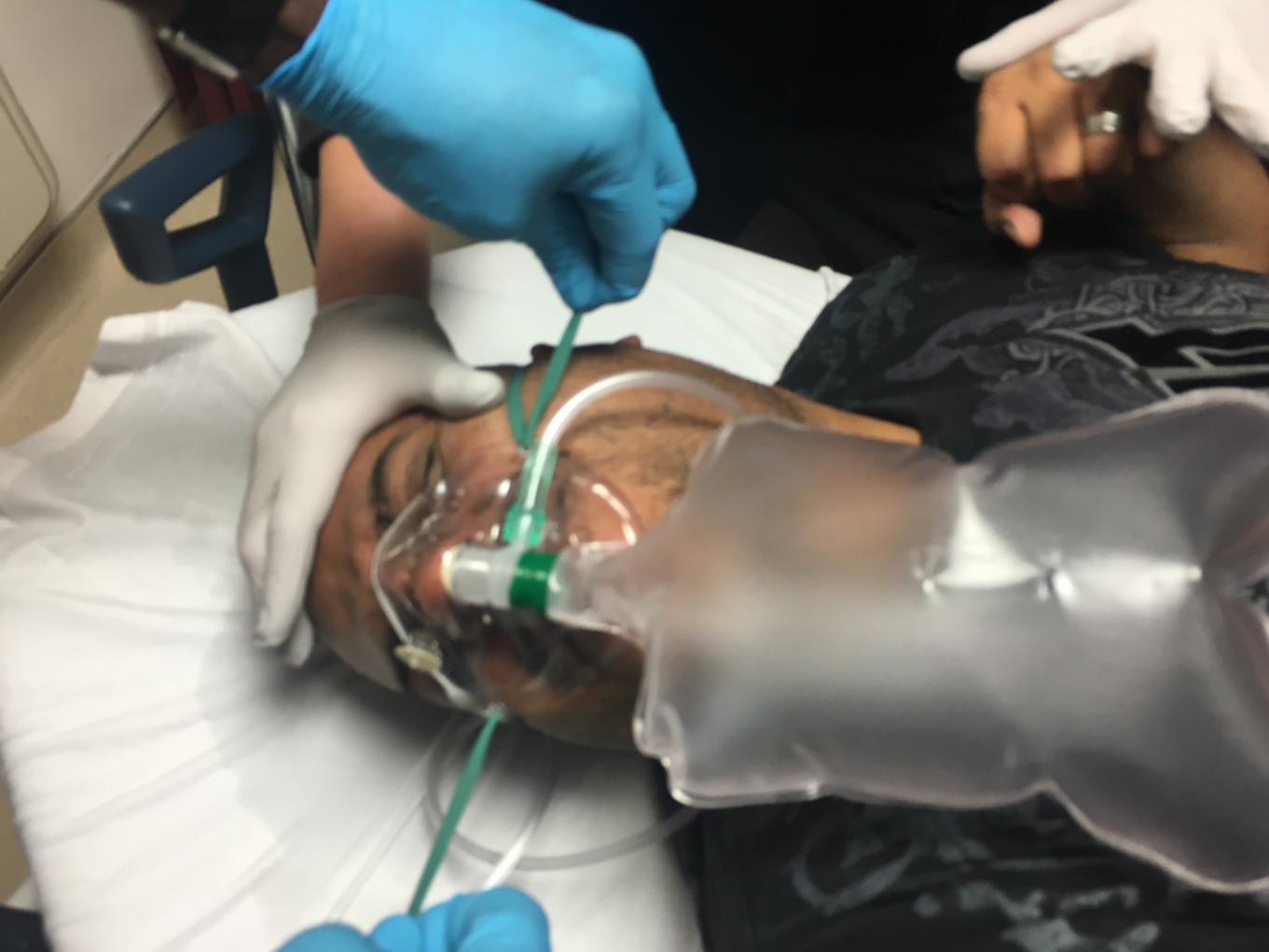
[pic of pulling the straps tight to the face of the patient, strongly securing the face mask to the face]
3. relieve dangerous restraint holdsneck or chest compression

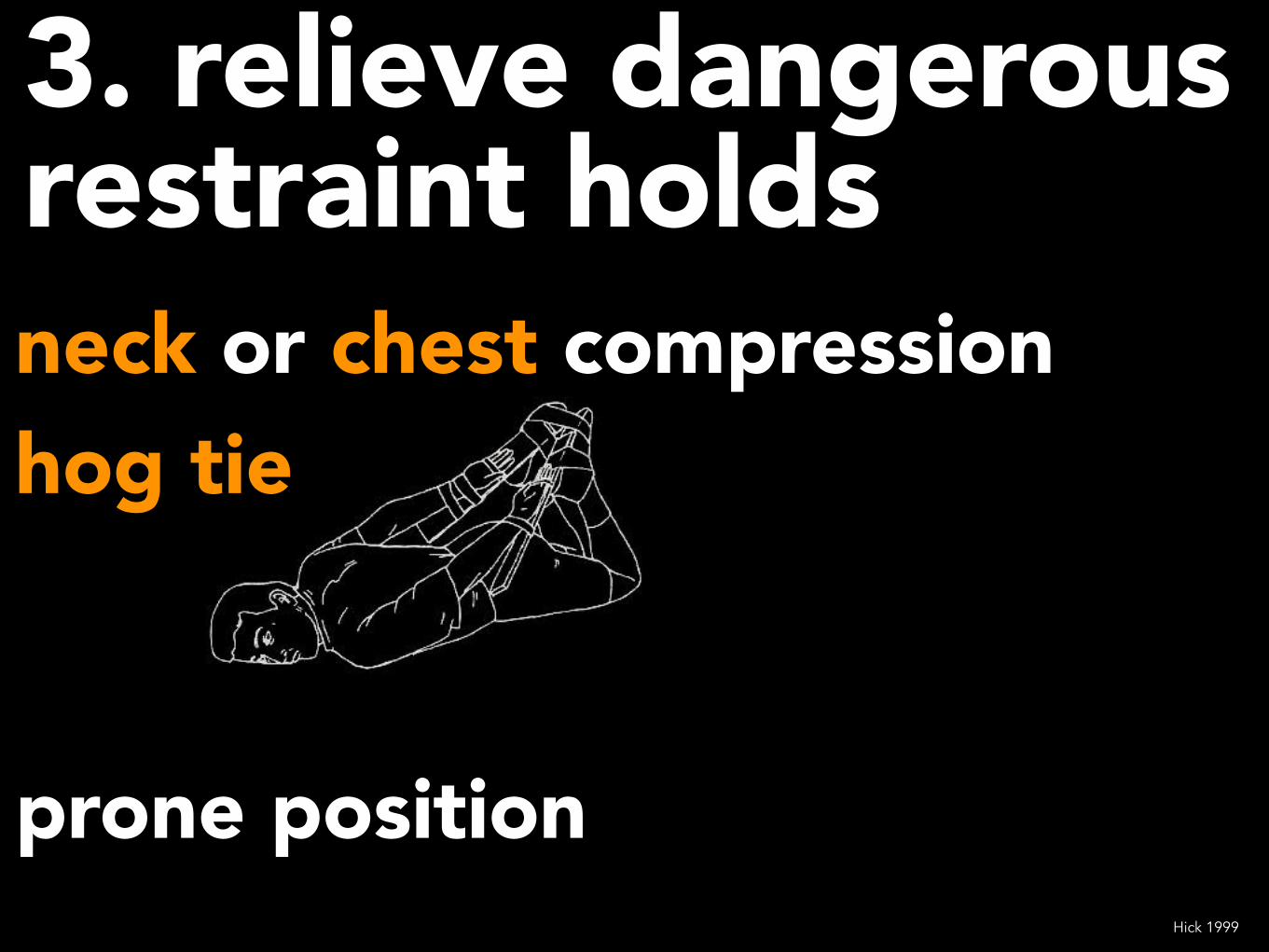
3. relieve dangerous restraint holdsneck or chest compressionhog tie
prone positionHick 1999
4. chemical restraintNOT physical restraintsclock is ticking danger is unaddressedovercome this unfortunate tradition
focus on sedation

IM not IV
through clothing
SPEEDSAFETY
4. chemical restraint
Calver 2010
speed and efficacy trump concern for over-sedation
(respiratory depression)
intubating the excited delirium patient is good care
4. chemical restraint
rapid single shot success4. chemical restraint
ketamine“but this patient has elevated HR and BP!” NO PROBLEM - ketamine will normalize hyperdynamic vitals in most cases
Isbister 2016 Burnett 2012 Hopper 2015 Iwanicki 2014 Keseg 2015 Melamed 2007 Roberts 2001 Scheppke 2014
this is procedural sedation requires PSA monitoring
500 mg4-6 mg/kg IM
ketaminerapid single shot success4. chemical restraint
do not apply tight restraints, continue to hold the patient
loose restraints are ok but should be unnecessary and should not delay resuscitation
loosen existing tight restraints
head of bed up
as the patient calms

5. vitalstemp fingerstickroom air saturation
or capnography
6. vascular access and crystalloid bolus
7. identify and treat dangerous causes and effects of severe agitation
hypoxia hyperthermia hypoglycemia hypoperfusion
first
hyperkalemia acidemia ICH CNS infection
second

sedative withdrawal serotonin syndrome NMS thyrotoxicosis sepsis seizure/postictal Na, Ca, Cr, NH3
third
CK, trauma
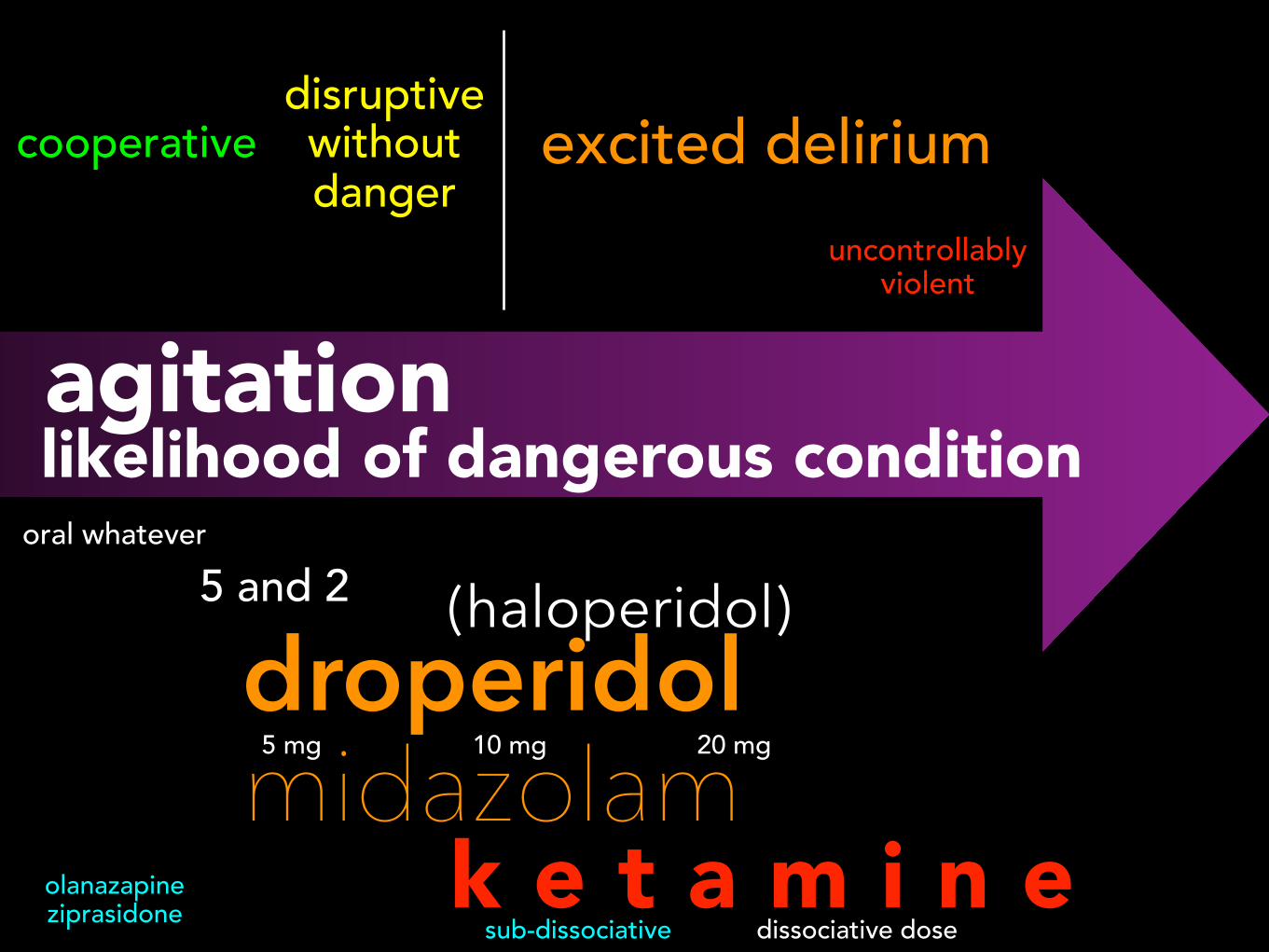
oral whatever5 and 2
droperidol midazolam
k e t a m i n e5 mg 20 mg10 mg
dissociative dose
(haloperidol)
agitationlikelihood of dangerous condition
cooperativedisruptive without danger
excited deliriumuncontrollably
violent
sub-dissociativeolanazapine ziprasidone
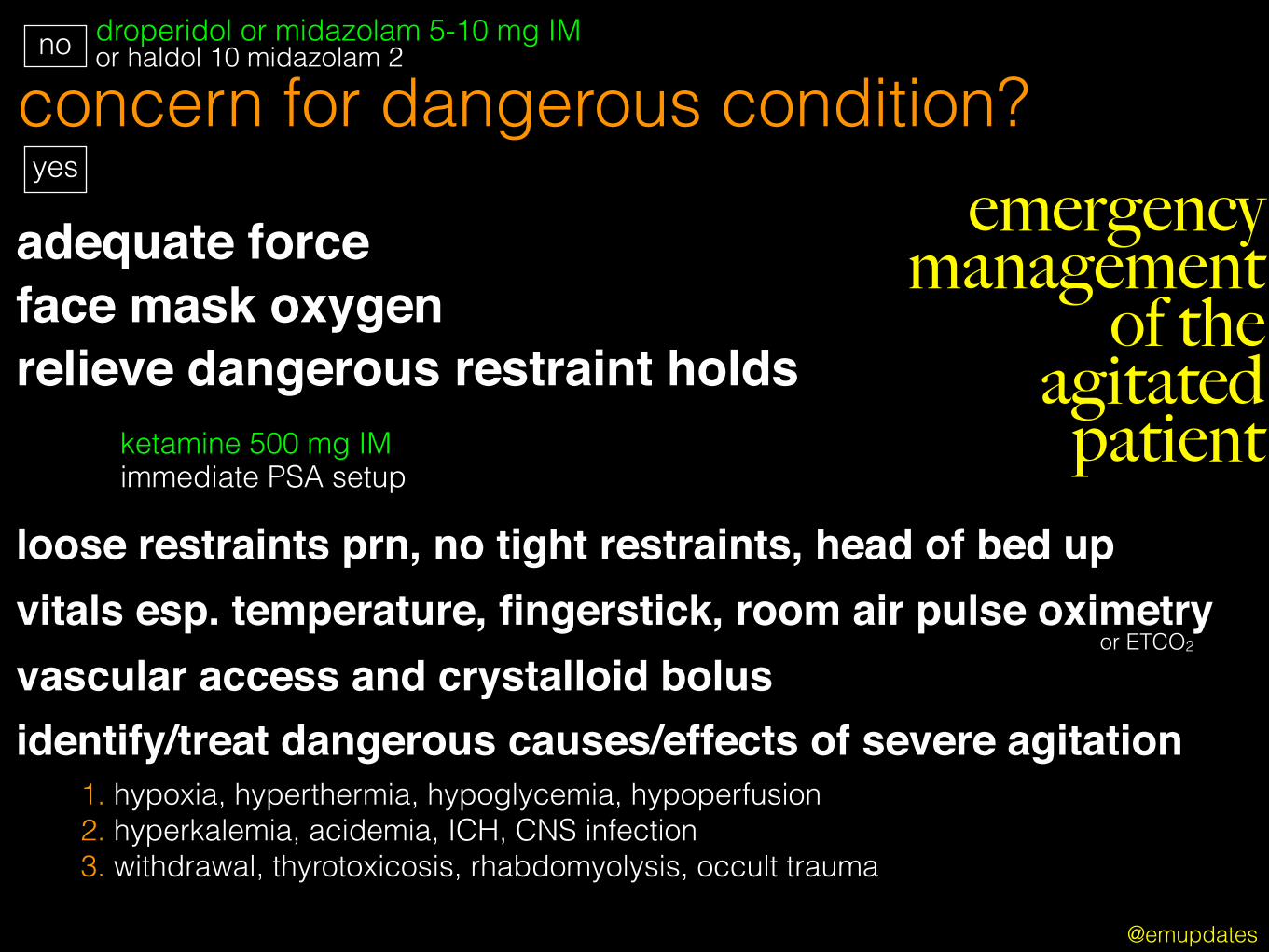
concern for dangerous condition?droperidol or midazolam 5-10 mg IM or haldol 10 midazolam 2
ketamine 500 mg IM immediate PSA setup
adequate forceface mask oxygenrelieve dangerous restraint holds
identify/treat dangerous causes/effects of severe agitation
loose restraints prn, no tight restraints, head of bed up
vascular access and crystalloid bolus
yes
no
1. hypoxia, hyperthermia, hypoglycemia, hypoperfusion 2. hyperkalemia, acidemia, ICH, CNS infection 3. withdrawal, thyrotoxicosis, rhabdomyolysis, occult trauma
@emupdates
emergency management
of the agitated patient
vitals esp. temperature, fingerstick, room air pulse oximetryor ETCO2

www.kickstarter.com/bringbackdroperidol

@emupdates
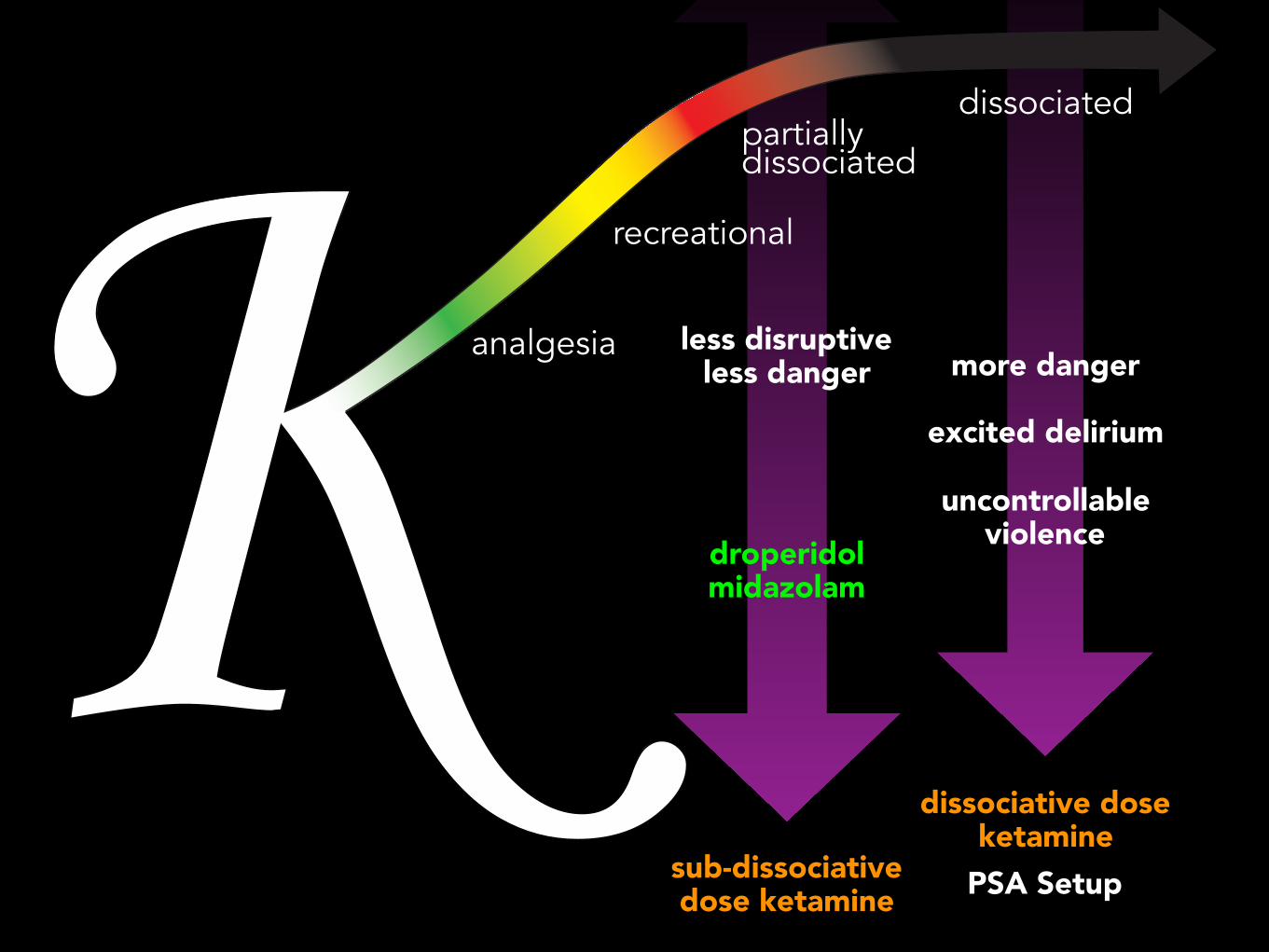
droperidol midazolam
sub-dissociative dose ketamine
dissociative dose ketamine
more danger
excited delirium
uncontrollable violence
analgesia
recreational
partially dissociated
dissociated
less disruptive less danger
PSA Setup
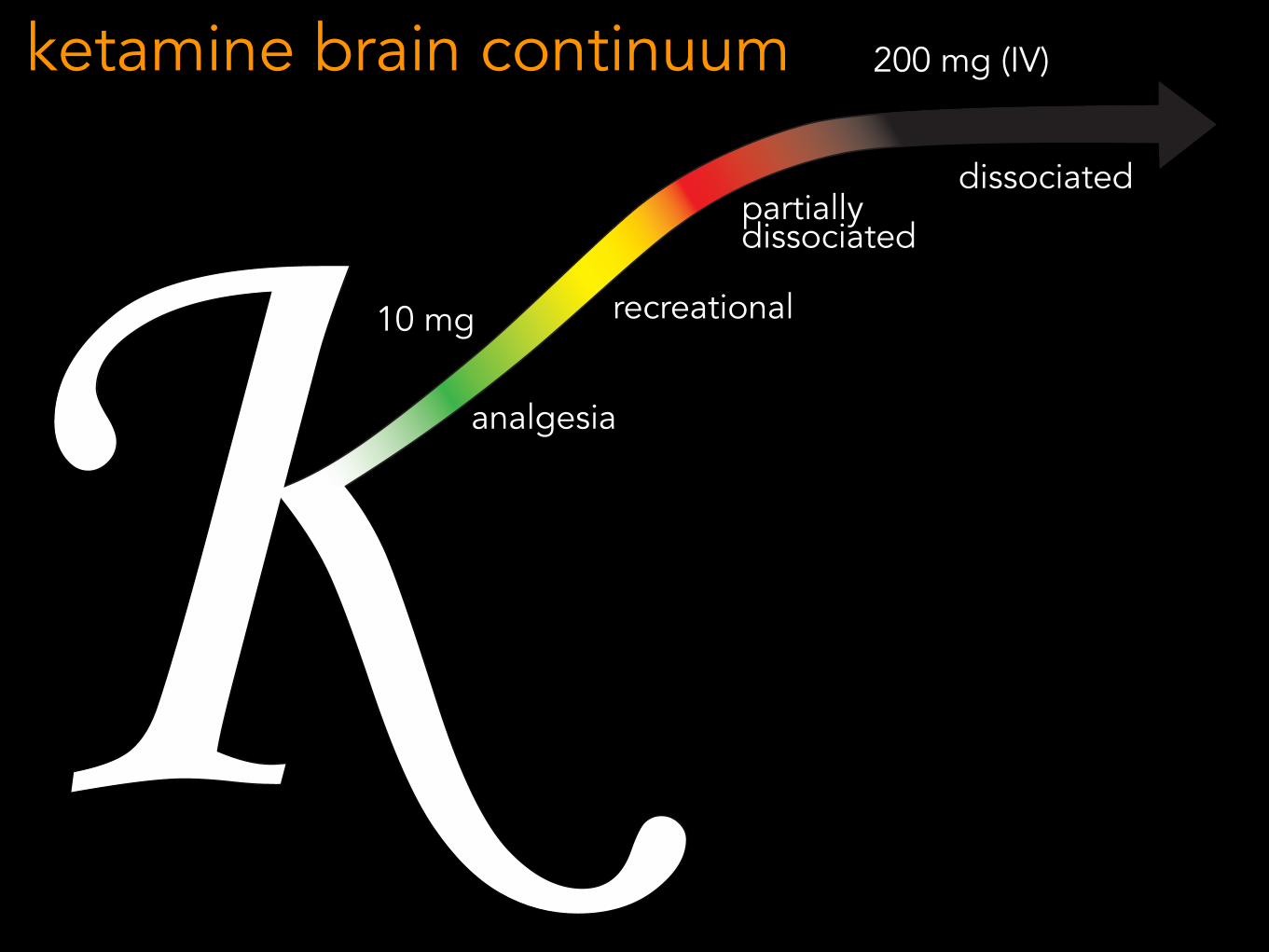
analgesia
recreational
partially dissociated
dissociated
10 mg
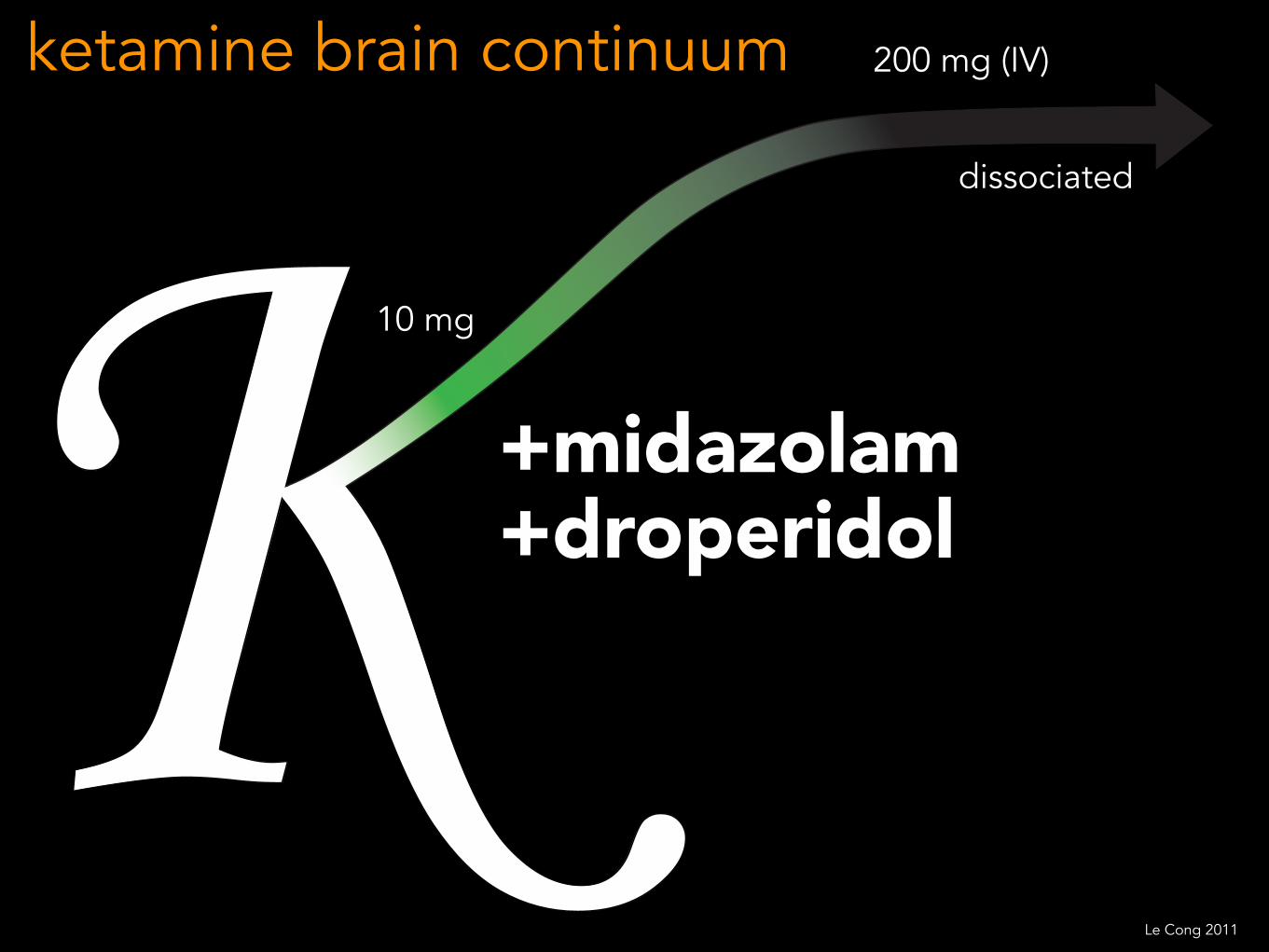
200 mg (IV)ketamine brain continuum
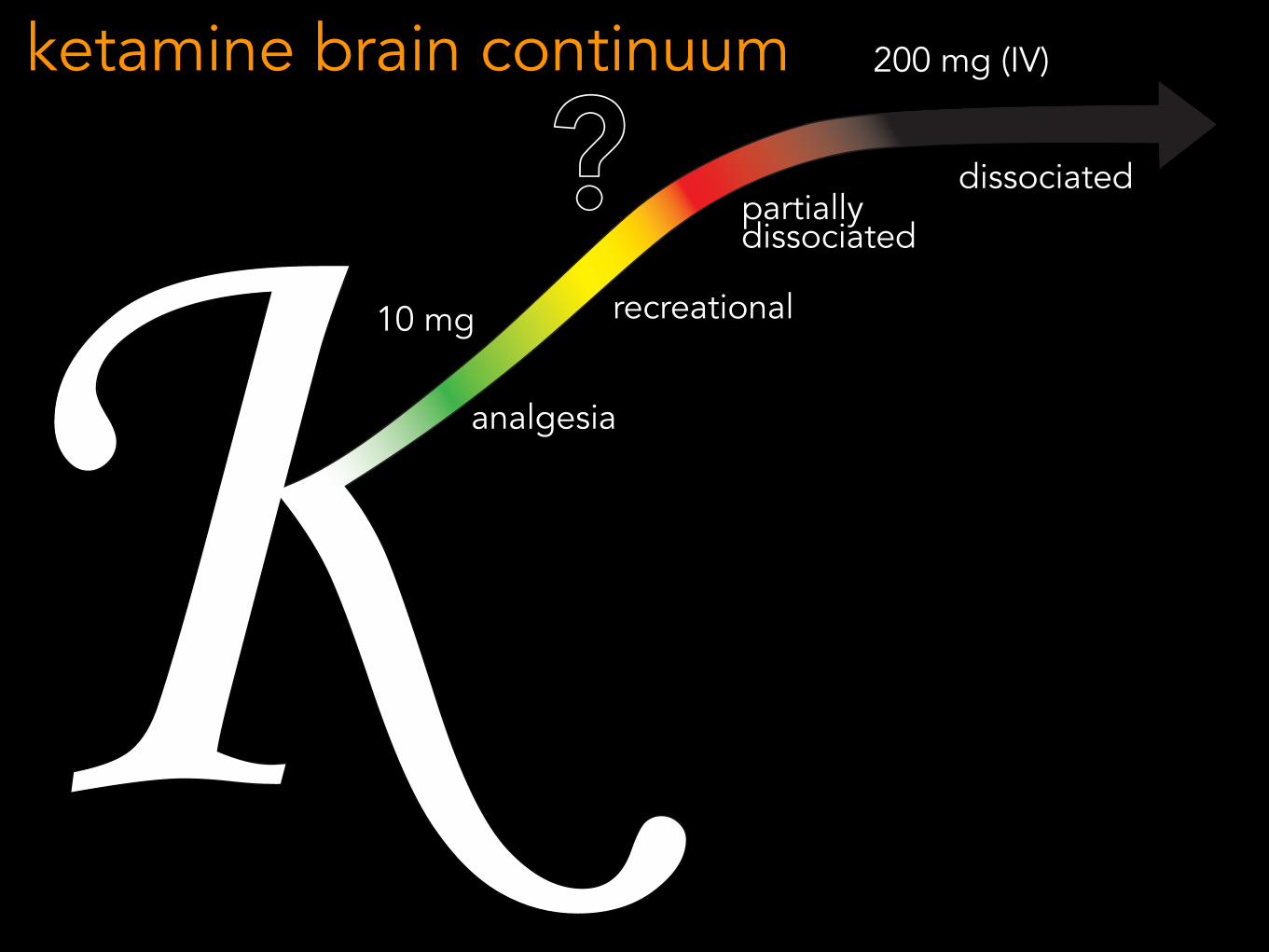
analgesia
recreational
partially dissociated
dissociated
10 mg
200 mg (IV)ketamine brain continuum
?
dissociated
200 mg (IV)ketamine brain continuum
+midazolam+droperidol
10 mg
Le Cong 2011
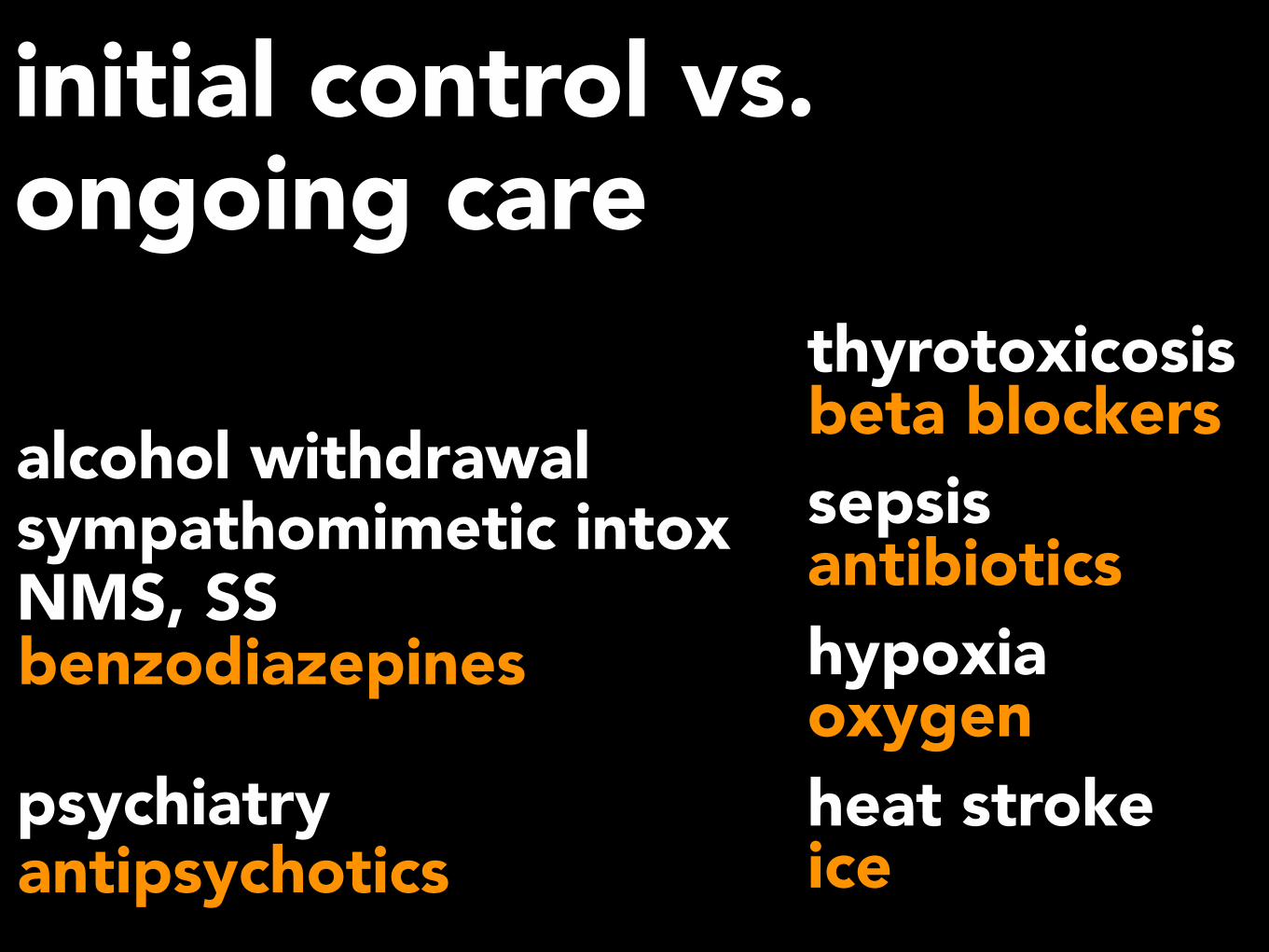
initial control vs. ongoing care
alcohol withdrawal sympathomimetic intox NMS, SS
psychiatry
benzodiazepines
antipsychotics
thyrotoxicosis beta blockerssepsis antibioticshypoxia oxygenheat stroke ice