disorders of the superior labrum: review and...
TRANSCRIPT

CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 400, pp. 77–87© 2002 Lippincott Williams & Wilkins, Inc.
77
Advancements in shoulder arthroscopy have ledto a better understanding of the anatomy anddisorders of the superior labrum biceps tendonanchor complex and the role that lesions of thesuperior labrum anterior and posterior lesionsplay in pain and instability of the shoulder. Var-ious injury mechanisms have been suggestedand studied and it is likely that different mech-anisms produce different types and areas ofdamage to the superior labrum. Classificationsystems have been proposed to describe the spe-cific pathoanatomy of lesions of the superiorlabrum anterior and posterior lesions and toguide treatment. Presenting symptoms often arenonspecific and physical examination maneu-vers have varying degrees of sensitivity andspecificity making diagnosis challenging. Diag-nostic ability is enhanced by the ultimate diag-nostic test, arthroscopy. A clear appreciationfor the various lesions and the potential result-ing joint dysfunction is necessary to determinethe appropriate treatment of this complex re-gion of the shoulder. The current authors reviewthe anatomy, classification, presentation, evalu-ation and treatment results of superior labrumanterior and posterior lesions, and includes novelevaluation methods and treatment guidelinesuseful in treating these lesions.
The use of shoulder arthroscopy in the diagno-sis and treatment of shoulder disorders has leadto increased understanding of superior labrumanterior and posterior (SLAP) lesions. The cur-rent authors reviewed current knowledge par-ticularly in the areas of classification, presenta-tion, evaluation, treatment, and results. Alsoincluded are novel evaluation and treatmentguidelines.
Andrews and coworkers2 described a su-perior labral lesion in a group of 73 throwingathletes, in which the anterosuperior labrumwas pulled off the glenoid by traction fromthe biceps tendon. They thought that the trac-tion occurred as the elbow was deceleratedduring the follow-through phase of throwing.In 1990, Snyder et al45 coined the term SLAPlesion in a retrospective review of 700 shoul-der arthroscopies in which 27 SLAP lesionswere identified and classified into a four-partscheme.
The awareness of SLAP lesions and their po-tential role in shoulder pain and disorders has in-creased rapidly during the past 10 years. Con-comitant advancements in shoulder arthroscopyalso have resulted in significant improvement indiagnosis and treatment of SLAP lesions. Yet,the pathoanatomy sometimes is more complexthan previously described and treatment re-mains uncertain. The current authors will re-view classification, presentation, evaluation,treatment, and results, and will include novel
Disorders of the Superior Labrum:Review and Treatment Guidelines
Michael A. Parentis, MD*; Karen J. Mohr, PT, SCS**; and Neal S. ElAttrache, MD**
From *The Knee Center of Western New York, Buffalo,NY; and **The Kerlan-Jobe Orthopaedic Clinic, Los An-geles, CA.Reprint requests to Neal S. ElAttrache, MD, The Kerlan-Jobe Orthopaedic Clinic, 6801 Park Terrace, Los Ange-les, CA 90045.

evaluation methods for SLAP lesions andguidelines that have aided in treatment.
ClassificationMany authors use the four-part classificationof Snyder and coworkers45 to describe SLAPlesions. Type I lesions have degeneration orfraying of the labrum without instability. TypeII lesions are most common, accounting formore than 50% of SLAP lesions, and involvedetachment of the superior labrum from theglenoid. A Type III lesion is characterized bya bucket-handle tear of the superior labrumwith firm attachment of the remainder of thelabrum. Type IV lesions also remain attachedto the labrum but have an associated bucket-handle tear of the labrum that extends into thebiceps tendon. Snyder et al45 developed thisscheme from a retrospective evaluation of 700shoulder arthroscopies in which only 27 pa-tients had SLAP lesions. Therefore, it is notsurprising that all SLAP lesions do not fallinto the initial classification of Snyder et al.
Morgan and coworkers32 developed a sec-ondary classification of Type II lesions froma retrospective review of 102 SLAP lesions.Three Type II lesions were described basedon the anatomic location (anterior, posterior,or combined anterior and posterior.) Posteriorand combined lesions occurred three timesmore frequently in throwing athletes and an-terior lesions usually were seen in patientswith trauma. Morgan et al think that patientswith SLAP lesions with posterior componentsdevelop posterosuperior instability that leadsto chronic superior instability and rotator cufftears.
Maffet and coworkers28 retrospectively re-viewed 84 superior labral lesions and foundthat 38% could not be classified according toa four-part scheme. Types V to VII wereadded to the four-part classification. A Type Vlesion is an anteroinferior Bankart lesion thatcontinues superiorly to include separation ofthe biceps tendon. A Type VI lesion includeda biceps separation with an unstable flap tearof the labrum. Finally, a Type VII lesion is asuperior labrum-biceps tendon separation that
extended anteriorly beneath the middle gleno-humeral ligament.
The current authors think that the classifica-tion of SLAP lesions can be simplified by not-ing whether the lesion would contribute to in-stability of either the biceps tendon anchor orthe glenohumeral ligaments. Lesions producingsignificant labral defects at the site of attach-ment of critical capsuloligamentous structuresgenerally require repair of these structures backto the bony glenoid rim. Lesions producing sig-nificant defects extending into the biceps ten-don may require biceps tenotomy with or with-out tenodesis.
PresentationMechanism of Injury
Most patients with SLAP lesions present withnonspecific shoulder pain associated with ac-tivity. The complicating factor in the presen-tation is that the majority of SLAP lesions re-ported in the literature are associated withother shoulder disorders such as rotator cufftears, acromioclavicular joint disorders, andinstability.1,4,10,14,17,18,32,36,39,41,44,48 In a reviewof 140 lesions, which is the largest review inthe literature, only 28% of the SLAP lesionswere isolated.44
Traction and compression injuries arethought to be the source of the majority ofSLAP lesions.7,9,10,18,25,28,29,32,39,44,45 Most com-pression injuries are traumatic in nature,whereas traction injuries occur most often inoverhead athletes. Bey and coworkers6 showed,in a biomechanical model, that traction on thebiceps tendon can create Type II SLAP lesionsand that inferior subluxation of the shouldermay lead to the creation of more unstable le-sions. Seven of the eight shoulders with infe-rior subluxation led to lesions but only two ofthe shoulders that were reduced had unstablelesions develop. Several authors9,10,32 de-scribed the peel-back mechanism for the cre-ation and extension of Type II lesions. Theystated that when the shoulder is in the ab-ducted and external rotated position, the bi-ceps assumes a more vertical and posterior an-gle, which produces a twist at the base of the
Clinical Orthopaedics78 Parentis et al and Related Research

biceps. This transmits a force to the postero-superior labrum, which causes it to rotate me-dially and peel off the glenoid.
Pathoanatomy
The superior labrum-biceps-glenohumeral lig-ament complex is attached to the superior andperipheral portions of the glenoid rim. Thelabrum is a fibrocartilaginous tissue that isanatomically and histiologically distinct fromthe shoulder capsule.12,37 The superior and an-terosuperior portions of the labrum are at-tached more loosely to the glenoid than the in-ferior portion of the labrum. Although theinferior labrum is a rounded, elevated structureclosely adherent to the glenoid, the superiorlabrum is attached less firmly, more mobile,and meniscoid in appearance.12 The labrumadds to the depth of the glenoid and increasesthe diameters of the glenoid surface to 75% ofthe humeral head vertically and 57% in thetransverse direction.38
The overall anatomy of the shoulder hasbeen described by Cooper and coworkers13 inan exhaustive anatomic study of 17 cadavers.Steinbeck and coworkers46 additionally delin-eated the intraarticular anatomy of the shoul-der. The current authors think that there is astrong relationship and interplay between thesuperior labrum, biceps tendon, and superiorand middle glenohumeral ligaments. In astudy of 24 shoulders from cadavers,35 the bi-ceps tendon was found to blend with the supe-rior labrum 75% of the time, with only a smallportion inserting on the supraglenoid tubercle.In a study of 100 shoulders from cadavers,Vangsness et al47 found that approximately50% of the biceps arose from the supraglenoidtubercle and the remainder arose directly fromthe superior labrum. In more than 1⁄2 of thespecimens, the main labral origin was poste-rior but a small percentage (8%) had attach-ment mainly anterior to the biceps tendon.
The anatomic association between the su-perior labrum and glenohumeral ligaments hasbeen well documented. In an anatomic studyof 104 cadavers by Steinbeck and cowork-ers,46 all of the superior glenohumeral liga-
ments originated from the superior labrum,whereas approximately 30% of the middleglenohumeral ligaments also arose from theanterosuperior labrum. In 17% of the cases,the superior and middle glenohumeral liga-ments originated together from the 1 o’clockposition of the labrum. Some authors have ob-served that the anteroinferior glenohumeralligaments can insert directly onto the superiorlabrum.17
Prior studies indicated there was a relation-ship between the superior labrum-biceps-glenohumeral ligament complex and shoulderinstability. Rodosky and coworkers40 deter-mined that the superior labrum and biceps ten-don contributed to anterior shoulder stabilityby increasing resistance to torsional forces inthe abducted and externally rotated position.They also found that SLAP lesions created asignificant increase in the strain in the inferiorglenohumeral ligament. Kumar and cowork-ers24 showed that the long head of the bicepsacted to prevent humeral head migration whenthe arm was at the side. Itoi and coworkers20
concluded that the long head and the shorthead of the biceps contribute to the anteriorstability of the shoulder in the abducted andexternally rotated positions and showed thattheir role as anterior stabilizers only increasedas shoulder instability worsened. In a biome-chanical model creating tension through thebiceps tendon, Bey and coworkers6 showedthat the incidence of SLAP lesions was in-creased if the shoulder was unstable. Finally,Pagnani and coworkers34 found that completelesions of the superior labrum resulted in sig-nificant increases in anteroposterior and su-peroinferior glenohumeral translation.
The current authors think and the literaturesupports the concept that the superior labrum,long head of the biceps, and the superior andmiddle glenohumeral ligaments work togetherto provide shoulder stability. Currently, the ex-act contribution of each structure is not com-pletely clear but the relationship between supe-rior labral lesions and instability has been welldocumented.1,10,14–18,28,29,32,40,41,44,45,48 Burkhartet al,10 Burkhart and Morgan,9 and Morgan et
Number 400July, 2002 Disorders of the Superior Labrum 79

a132 reported that patients with SLAP lesionswith a posterior component have posterosupe-rior instability develop, which results in under-surface rotator cuff tears. The incidence of rota-tor cuff disorders, which includes incompleteundersurface tears and complete tears, has beenreported between 10% and 48% of the time tooccur with a SLAP lesion.1,10,18,28,32,39,44,45 Thequestion remains, however, whether the SLAPlesion leads to shoulder instability or whethersubtle shoulder instability leads to the SLAP le-sion and then increased shoulder instability.
EvaluationPhysical Examination
The studies regarding SLAP lesions generallyindicate that the diagnosis of SLAP lesions isdifficult.29 The current authors have found thatthe diagnosis of SLAP lesions in isolated casesis more straightforward but, as the current au-thors have described, it is much more commonto have associated disorders that complicateand cloud clinical findings. Numerous authorsdescribe the use of Hawkins’ test, Neer’s test,Speed’s test, Jobe’s relocation test, and Yer-gason’s tests and generally report that they arenonspecific.10,15,18,28,29,32,44,45 As a result, nu-merous authors have developed specific teststhat they reported to be sensitive and specificin the diagnosis of SLAP lesions.5,22,23,26,31,33
Mimori and coworkers30 developed the painprovocation test and reported a 100% sensitiv-ity and 90% specificity regarding Type II SLAPlesions. However, 1⁄2 of the 22 patients in thestudy who were thought to have a Type IISLAP lesion had their definitive diagnosismade by magnetic resonance imaging (MRI)only. Liu and coworkers27 described the cranktest in a group of 62 patients in which 30 hadSLAP lesions; however, the type of tear wasunclear. The crank test was reported to have asensitivity of 91%, a specificity of 93%, a pos-itive predictive value of 94%, and a negativepredictive value of 90%. Kibler22 developed theanterior slide test and described its use in astudy with 88 arthroscopically-confirmed SLAPlesions, although the lesions were not classi-fied. He found that the anterior slide test had a
sensitivity of 78.4% and a specificity of 91.5%.Kim and coworkers23 described the biceps loadtest in patients with instability and SLAP le-sions. Although only 10 patients had Type II le-sions they determined that the test had 90.9%sensitivity and a specificity of 96.9% with apositive predictive value of 83% and a negativepredictive value of 98%. Finally, O’Brien andcoworkers33 described the active compressiontest that they thought could be used to diagnoseSLAP lesions and acromioclavicular joint dis-orders. In their study, which included 53 SLAPlesions that were repaired but not classified, theactive compression test had a sensitivity of100%, a specificity of 98.5%, a positive predic-tive value of 94.6%, and a negative predictivevalue of 100%.
Morgan and coworkers32 thought that theSpeed and O’Brien tests were helpful in the di-agnosis of anterior lesions with sensitivities of100% and 88% and specificities of 70% and42%, respectively. The Jobe relocation testwas particularly useful for posterior lesionswith 85% sensitivity and 68% specificity.
The current authors recently completed aprospective clinical study to determine themost effective provocative maneuver withwhich to diagnose SLAP lesions. The follow-ing tests were included: active compression,anterior slide, pain provocation, crank, reloca-tion, Hawkins’, Neer, Speed’s, and Yergason’stests. A series of 132 consecutive patientsscheduled to have diagnostic arthroscopy wereexamined preoperatively with each of theaforementioned tests. The final diagnosis ineach case was made arthroscopically. Fortypatients had either a Type I (17 patients) or aType II (23 patients) SLAP lesion. The re-mainder of the diagnoses included completerotator cuff tears, partial rotator cuff tears, im-pingement, and instability. The two most sen-sitive tests for Type II SLAP lesions were theactive compression (65.2%) and Hawkins’tests (65.2%) followed by Speed’s (47.8%),Neer (47.8%), and the relocation test (43.5%)(Table 1). None of the remaining tests had asensitivity greater than 17.4% for Type II le-sions. When Type I and Type II lesions were
Clinical Orthopaedics80 Parentis et al and Related Research

combined the sensitivities were similar for allof the provocative tests (Table 2). However,none of the sensitive tests were specific for ei-ther Type II lesions alone or when Type I andII lesions were combined. There were no sig-nificant differences between the tests whenpositive and negative predictive values wereassessed.
The current authors’ results may have dif-fered from those previously reported becauseunbiased investigators evaluated numeroustests in a random population and arthroscopywas used as the final diagnostic tool in all pa-tients. These results indicated that no test is
sensitive and specific for diagnosis of SLAPlesions and diagnostic arthroscopy remainsthe best means to definitively diagnose SLAPlesions. Yet the active compression test al-though not as sensitive or specific as describedby O’Brien and coworkers,33 may be the mostuseful test. The mechanism of this test was re-ported to be that when the shoulder was in theinternally rotated position, the superior labrumwas tensioned from medial and inferior dis-placement of the biceps tendon. Tension thencould lead to mechanical symptoms by dis-placing an unstable superior labrum into thejoint. O’Brien and coworkers33 also reportedthat the active compression test was an excel-lent test for evaluation of the incongruous ordegenerative acromioclavicular joint. The ac-tive compression test was 100% sensitive and96.6% specific for detecting acromioclavicu-lar joint disorders. They thought the greatertuberosity “locked and loaded”33 an unstableor degenerative acromioclavicular joint by el-evating the lateral aspect of the acromion inthe internally rotated position.
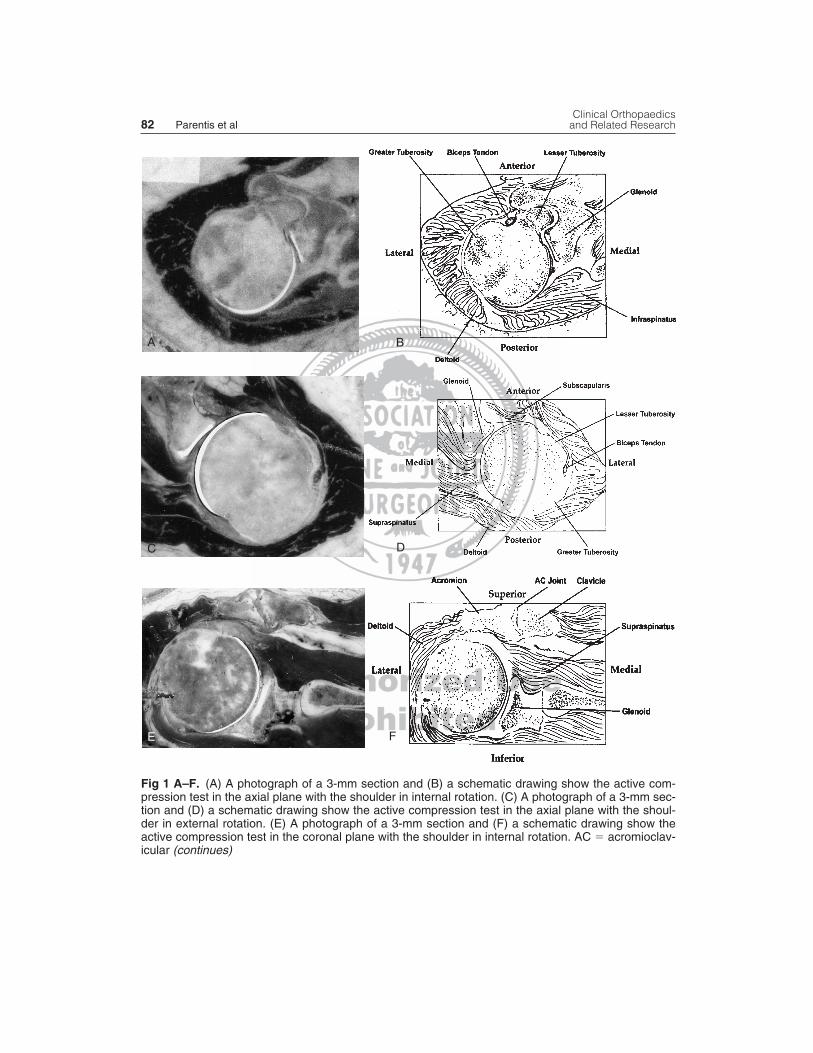
To better understand the mechanism, thecurrent authors did a study to describe the in-traarticular and extraarticular anatomic rela-tionships during the active compression test.Four matched pairs of fresh-frozen shouldersfrom cadavers were positioned statically in theinternally or externally rotated positions of theactive compression test. The shoulders thenwere embedded in polyurethane and sequen-tially sectioned at 3-mm intervals in the axialand coronal planes using an industrial planer.Each section was reviewed independently todetermine anatomic contact areas.
In the axial plane, shoulders in the inter-nally rotated position had consistent contactbetween the lesser tuberosity and subscapu-laris tendon and the superior aspect of the gle-noid and the labrum (Fig 1A–B). In the exter-nally rotated position, there was no contactbetween the superior structures of the shoulder(Fig 1C–D). The lesser tuberosity and sub-scapularis tendon likely displace an unstableor torn superior labrum, leading to a positiveclinical result in the internally rotated posi-
Number 400July, 2002 Disorders of the Superior Labrum 81
TABLE 1. The Sensitivity andSpecificity of Nine Provocative Tests forType II SLAP Lesions
Specificity Sensitivity Test (%) (%)
Yergason’s test 92.7* 13.0Pain provocation test 89.9* 17.4Anterior slide test 83.5 13.0Crank test 82.6 8.7Speed’s test 67.9 47.8*Relocation test 51.4 43.5*Neer test 51.4 47.8*Active compression test 48.6 65.2*Hawkins’s test 30.3 65.2*
* � p �.05
TABLE 2. The Sensitivity andSpecificity of Nine Provocative Tests forType I and Type II SLAP Lesions
Specificity Sensitivity Test (%) (%)
Yergason’s test 93.5* 12.5Pain provocation test 90.2* 15Crank test 82.6 12.5Anterior slide test 81.5 10Speed’s test 67.4 40Relocation test 53.3 50*Neer test 52.2 50*Active compression test 50 62.5*Hawkin’s test 30.4 67.5*
* � p �.05
Clinical Orthopaedics82 Parentis et al and Related Research
Fig 1 A–F. (A) A photograph of a 3-mm section and (B) a schematic drawing show the active com-pression test in the axial plane with the shoulder in internal rotation. (C) A photograph of a 3-mm sec-tion and (D) a schematic drawing show the active compression test in the axial plane with the shoul-der in external rotation. (E) A photograph of a 3-mm section and (F) a schematic drawing show theactive compression test in the coronal plane with the shoulder in internal rotation. AC � acromioclav-icular (continues)
A B
C D
E F

tion. However, when the shoulder is rotatedexternally, contact from the lesser tuberosityand subscapularis tendon is relieved and theclinical result is a negative test.
In the coronal plane, the internally rotatedspecimens revealed contact between the supra-spinatus tendon and the lateral aspect of theacromion (Fig 1E–F). There was no contactbetween the supraspinatus tendon and theacromion when the shoulders were rotated ex-ternally in the coronal plane (Fig 1G–H). Inthe case of a Type II or Type III acromion, onewould expect periacromial pain in the inter-nally rotated position. The pain should im-prove in the externally rotated position be-cause no contact was seen between the tendonand the acromion in the externally rotated po-sition. This provides an anatomic explanationfor the clinical results of the active compres-sion test. It can be used to assist in diagnosisof SLAP lesions and impingement includingrotator cuff disorders.
Radiographic Analysis
Short of arthroscopic evaluation, the clinicalhistory and physical examination are the bestindicators of the presence of a SLAP lesion butcontrast magnetic resonance imaging (MRI)can improve the diagnostic acumen of the clin-
ician. Numerous studies have been done inwhich the use of noncontrast and contrast MRIwas used to diagnose superior labral lesionsof the shoulder.3,11,21,27,31,42,43 Retrospectivestudy was used to ascertain the effectivenessof noncontrast MRI in the diagnosis of SLAPlesions. Smith and coworkers43 reviewed sixMRI scans from shoulders with SLAP lesionsconfirmed at arthroscopy and found only oneto have been read positive. Even with retro-spective review, only four of six could be la-beled positively torn. All six had increasedsignal intensity in the superior labrum. Monuand coworkers31 similarly reviewed eight pa-tients with proven SLAP lesions and foundthat noncontrast MRI of the superior labrumwas abnormal on all coronal images, 88% ofaxial images, and 50% of sagittal images.These studies are problematic in that they arepurely retrospective and therefore give littleinformation to the true accuracy of noncon-trast MRI in the diagnosis of SLAP lesions.
Karzel and Snyder21 compared noncontrastMRI with contrast MRI in seven lesions andfound that four were diagnosed correctly withcontrast MRI whereas all seven were missedwith the noncontrast MRI. They also reportedfalse positive results in three patients who hadcontrast MRI scans. They thought that the ad-
Number 400July, 2002 Disorders of the Superior Labrum 83
Fig 1 G–H. (continued) (G) A photograph of a 3-mm section and (H) a schematic drawing show the ac-tive compression test in the coronal plane with the shoulder in external rotation. AC � acromioclavicular
G H

dition of contrast material to standard MRIcould aid in diagnosis of SLAP lesions. Re-cently, Bencardino and coworkers3 found MRIarthrography to have a sensitivity of 89%,specificity of 91%, and accuracy of 90% in thediagnosis of 19 SLAP lesions in 52 patients.Furthermore, the MRI classification was cor-rect in 13 of 17 cases. Chan and coworkers11
added arm traction in a cadaver model andfound that this improved the diagnostic accu-racy of contrast MRI, most likely by displac-ing the unstable superior labrum.
The current authors use MRI arthrography asan adjunctive tool to clinical history and physi-cal examination. Some studies support that theaddition of contrast improves the accuracy ofMRI in the diagnosis of unstable superior labrallesions.3,21 One must be aware, however, thatfalse positive results occur. In a study on cadav-ers by Smith and coworkers,42 73% of the 26shoulders had a sublabral recess that can be thesource of false positive MRI arthrography re-sults. Furthermore, anatomic variants, such asthe cordlike middle glenohumeral ligament, orBuford complex,49 can complicate results.
TreatmentThe treatment of SLAP lesions has evolvedsignificantly since first described. At the timeSLAP lesions first became recognized, mostwere treated by either debridement alone or re-moval if the SLAP lesion was unstable. Cor-dasco and coworkers14 reviewed 52 cases oflabral debridement in which there were 27SLAP lesions. They found that with debride-ment alone, 78% of patients had good resultsat 1 year but this decreased to 63% at the sec-ond year. Seventy percent of the patientswith SLAP lesions had shoulder instability onphysical examination and only 44% returnedto prior athletic levels. Similarly, Altchek andcoworkers1 debrided 40 anterosuperior labrallesions and found that only 7% of patients hadsymptomatic relief at 2 years. Segmuller andcoworkers41 repaired 17 unstable SLAP le-sions with the Suretac device and 83.3% of pa-tients had good results at 17 months but only53% returned to preinjury levels of activity.
Field and Savoie16 prospectively reviewed 20unstable SLAP lesions that were repaired andfound good results in all patients at 21months. All of the patients in that study re-turned to their preinjury activity level butonly six were athletes. Yoneda and cowork-ers50 arthroscopically stapled 10 unstableSLAP lesions and had 80% good results at 2years. Second look arthroscopy at an averageof 4 months revealed that all of the lesions hadhealed solidly to bone. Finally, Resch andcoworkers39 reviewed 18 cases of unstableSLAP lesions in which 14 were repaired andfour were debrided only. Five lesions were re-paired with an arthroscopic screw and ninewere repaired with a Suretac. The mean fol-lowup was only 18 months and revealed thatof the patients who had lesions repaired, eightpatients had excellent results, four had im-proved results, and two patients had failed re-sults. Only one patient with debrided lesionshad improvement in symptoms. Morgan andcoworkers32 described preliminary 1-year re-sults on 102 repaired Type II lesions in pitch-ers with 83% excellent, 14% good, and 3%fair results. All of the 37 pitchers returned topitching and 83% thought they returned to thesame level.
Although the current authors do not thinkthat Snyder’s four-part classification is com-pletely inclusive, treatment recommendationsare described according to this scheme becausemost orthopaedists are familiar with it. Type Ilesions by definition are stable and only shouldrequire gentle debridement of frayed labral tis-sue. Type II lesions, or any lesion determined tobe unstable, should be repaired using eitherarthroscopic sutures or tacks (Fig 2). The suc-tion test can greatly assist with the determina-tion of whether the superior labrum is unstable.In this test, the distended joint is suctioned andan unstable superior labrum is pulled awayfrom the superior glenoid rim. Various methodsto repair the superior labrum have been de-scribed in the literature.10,17,29,32,39,41
Type III lesions only may require debride-ment of the damaged portion of the labrum in-volved in the bucket handle tear. Type IV le-
Clinical Orthopaedics84 Parentis et al and Related Research

sions are characterized by a bucket-handletear of the superior labrum that extends intothe biceps tendon. The treatment algorithmfor these lesions is determined by the extentof injury to the biceps tendon because the re-mainder of the superior labrum is attached bydefinition, to the glenoid. The biceps can bededrided if less than 40% is involved and ei-ther should be repaired or tenodesed if greaterthan 40% to 50% is involved.8,29 In the cur-rent authors’ experience, however, bucket-handle tears of the superior labrum (Type IIIand Type IV) often are superimposed on a
Type II avulsion of the remaining labral tis-sue. If this is observed, and the labral remnantis adequate, repair as described for a Type IIlesion should be done.
Gartsman and Hammerman17 stated thatone must be aware that a normal superiorlabrum is not always well attached to the su-perior glenoid. They reported that if the gle-noid underlying the superior labrum is cov-ered with smooth cartilage and the labrum andglenoid show no outward signs of trauma, thesuperior labrum should be considered a nor-mal variant.
Number 400July, 2002 Disorders of the Superior Labrum 85
Fig 2 A–D. Sequential repair of the superior labrum with suture anchor is shown. (A) Posterior to an-terior arthroscopic view shows superior labral avulsion from the glenoid rim. (B) The suture anchor isshown in place in the anterosuperior quadrant. The anterior limb of the suture is shown through rota-tor cuff interval cannula and the posterior limb of the suture is shown through superolateral periacro-mial portal. (C) The suture passer with prolene loop penetrating the anterosuperior labrum is shown.The prolene loop is used to pull the posterior suture limb through the labrum. (D) The completed repairwith simple arthroscopic knots is shown.
A B
C D

The current authors have observed a strongassociation between the presence of paralabralor spinoglenoid notch cysts and tears of the su-perior labrum. Therefore, when such cysts arefound on diagnostic imaging studies, the supe-rior labrum should be evaluated carefully forthe presence of a tear. Successful arthroscopiccyst decompression has been reported19 and inthe current authors’ experience, repair of thetorn labrum results in resolution of the cyst.
Shoulder surgeons need to be aware of theexistence of superior labral lesions and thenormal anatomy of the superior labrum-biceps-glenohumeral complex when treating patientswith shoulder pain. Hopefully, the next decadewill provide as much growth in the under-standing of these lesions as has the past. Theauthors think that the superior labrum works asa complex with the long head of the biceps andthe glenohumeral ligaments to provide stabil-ity to the anterosuperior shoulder. The contin-uum of superior labral disorders and instabilityis a result of the interplay between the superiorlabrum, biceps tendon, and superior and mid-dle glenohumeral ligaments.
References1. Altchek DW, Warren RF, Wickiewicz TL, Ortiz G:
Arthroscopic labral debridement: A three-year fol-low-up study. Am J Sports Med 20:702–706, 1992.
2. Andrews JR, Carson WG, Mcleod WD: Glenoidlabrum tears related to the long head of the biceps.Am J Sports Med 13:337–341, 1985.
3. Bencardino JT, Beltran J, Rosenberg ZS: Superiorlabrum anterior-posterior lesions: Diagnosis with MRarthrography of the shoulder. Radiology 214:267–271,2000.
4. Berg EE, Ciullo JV: The SLAP lesion: A cause offailure after distal clavicle resection. Arthroscopy13:85–89, 1997.
5. Berg EE, Ciullo JV: A clinical test for superior gle-noid labral or “SLAP” lesions. Clin J Sport Med8:121–123, 1998.
6. Bey MJ, Elders GJ, Huston LJ, et al: The mechanismof creation of superior labrum, anterior, and poste-rior lesions in a dynamic biomechanical model of theshoulder: The role of inferior subluxation. J Shoul-der Elbow Surg 7:397–401, 1998.
7. Burkhart SS, Fox DL: SLAP lesions in association withcomplete tears of the long head of the biceps tendon: Areport of two cases. Arthroscopy 8:31–35, 1992.
8. Burkhart SS, Fox DL: Case report: Arthroscopic re-pair of a Type IV SLAP lesion-the red-on-white le-sion as a component of anterior instability. Arthroscopy9:488–492, 1993.
9. Burkhart SS, Morgan CD: The peel-back mecha-nism: Its role in producing and extending posteriorType II SLAP lesions and its effect on SLAP repairrehabilitation. Arthroscopy 14:637–640, 1998.
10. Burkhart SS, Morgan CD, Kibler WB: Shoulder in-juries in overhead athletes: The “dead arm” revisited.Clin Sports Med 19:125–158, 2000.
11. Chan KK, Muldoon KA, Yeh L, et al: Superior labralanteroposterior lesions: MR arthrography with armtraction. Am J Radiol 173:1117–1122, 1999.
12. Cooper DE, Arnoczky SP, O’Brien SJ, et al:Anatomy, histology, and vascularity of the glenoidlabrum. J Bone Joint Surg 74A:46–52, 1992.
13. Cooper DE, O’Brien SJ, Warren RF: Supporting lay-ers of the glenohumeral joint: An anatomical study.Clin Orthop 289:144–155, 1993.
14. Cordasco FA, Steinmann, Flatow EL, Bigliani LU:Arthroscopic treatment of glenoid labral tears. Am JSports Med 21:425–431, 1993.
15. Craig EV: Shoulder arthroscopy in the throwing ath-lete. Clin Sports Med 15:673–700, 1996.
16. Field LD, Savoie FH: Arthroscopic suture repair ofsuperior labral detachment lesions of the shoulder.Am J Sports Med 21:783–790, 1993.
17. Gartsman GM, Hammerman SM: Superior labrum,anterior and posterior lesions: When and how to treatthem. Clin Sports Med 19:115–124, 2000.
18. Handelberg F, Willems S, Shahabpour M, HuskinJP, Kuta J: SLAP lesions: A retrospective multicen-ter study. Arthroscopy 14:856–862, 1998.
19. Iannotti JP, Ramsey ML: Arthroscopic decompres-sion of a ganglion cyst causing suprascapular nervecompression. Arthroscopy 12:739–745, 1996.
20. Itoi E, Kuechle DK, Newman SR, Morrey BF, AnKN: Stabilizing function of the biceps in stable andunstable shoulders. J Bone Joint Surg 75B:546–550,1993.
21. Karzel RP, Snyder SJ: Magnetic resonance arthrog-raphy of the shoulder. Clin Sports Med 12:123–136.
22. Kibler WB: Specificity and sensitivity of the anteriorslide test in throwing athletes with superior glenoidlabral tears. Arthroscopy 11:296–300, 1995.
23. Kim SH, Ha KI, Han KY: Biceps load test: A clini-cal test for superior labrum anterior and posterior le-sions in shoulders with recurrent anterior disloca-tions. Am J Sports Med 27:300–303, 1999.
24. Kumar VP, Satku K, Balasuramaniam P: The role ofthe long head of the biceps brachii in the stabilizationof the head of the humerus. Clin Orthop 244:172–175,1989.
25. Levine WN, Flatow EL: The pathophysiology ofshoulder instability. Am J Sports Med 28:910–917,2000.
26. Liu SH, Henry MH, Nuccion SL: A prospective eval-uation of a new physical examination in predictingglenoid labral tears. Am J Sports Med 24:721–725,1996.
27. Liu SH, Henry MH, Nuccion S, Shapiro MS, DoreyF: Diagnosis of glenoid labral tears: A comparisonbetween magnetic resonance imaging and clinicalexaminations. Am J Sports Med 24:149–154, 1996.
28. Maffet MW, Gartsman GM, Moseley B: Superiorlabrum-biceps tendon complex lesions of the shoul-der. Am J Sports Med 23:93–98, 1995.
Clinical Orthopaedics86 Parentis et al and Related Research

29. Mileski RA, Snyder SJ: Superior labral lesions in theshoulder: Pathoanatomy and surgical management. JAm Acad Orthop Surg 6:121–131, 1998.
30. Mimori K, Muneta T, Nakagawa T, Shinomiya K: Anew pain provocative test for superior labral tears ofthe shoulder. Am J Sports Med 27:137–142, 1999.
31. Monu JUV, Pope TL Jr., Chabon WJ: MR Diagno-sis of superior labral anterior posterior (SLAP) in-juries of the glenoid labrum: Value of routine imag-ing without intraarticular injection of contrast material.Am J Radiol 163:1425–1429, 1994.
32. Morgan CD, Burkhart SS, Palmeri M, Gillespie M:Type II SLAP lesions: Three subtypes and their re-lationships to superior instability and rotator cufftears. Arthroscopy 14:553–565, 1998.
33. O’Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wil-son JB: The active compression test: A new and ef-fective test for diagnosing labral tears and acromio-clavicular joint abnormality. Am J Sports Med26:610–613, 1998.
34. Pagnani MJ, Deng XH, Warren RF, Torzilli PA,Altchek DW: Effect of lesions of the superior portionof the glenoid labrum on glenohumeral translation. JBone Joint Surg 77A:1003–1010, 1995.
35. Pal GP, Bhatt RH, Patel VS: Relationship betweenthe tendon of the long head of biceps brachii and theglenoidal labrum in humans. Anat Rec 229:278–280,1991.
36. Pearce CE, Burkhart SS: Case report: The pitcher’smound: A late sequela of posterior Type II SLAP le-sions. Arthroscopy 16:214–216, 2000.
37. Prodromos CC, Ferry JA, Schiller AL, Zarins B: His-tological studies of the glenoid labrum from fetal lifeto old age. J Bone Joint Surg 72A:1344–1348, 1990.
38. Rames RD, Karzel RP: Injuries to the glenoidlabrum, including SLAP lesions. Orthop Clin NorthAm 24:45–53, 1993.
39. Resch H, Gosler K, Thoeni H, Sperner G: Arthro-scopic repair of superior glenoid labral detachment(the SLAP lesion). J Shoulder Elbow Surg 2:147–155,1993.
40. Rodosky MW, Harner CD, Fu FH: The role of the
long head of the biceps muscle and superior glenoidlabrum in anterior stability of the shoulder. Am JSports Med 22:121–130, 1994.
41. Segmuller HE, Hayes MG, Saies AD: Arthroscopicrepair of glenolabral injuries with an absorbable fixa-tion device. J Shoulder Elbow Surg 6:383–392, 1997.
42. Smith DK, Chopp TM, Aufdemorte TB, WitkowskiEG, Jones RC: Sublabral recess of the superior glenoidlabrum: Study of cadavers with conventional nonen-hanced MR imaging, MR arthrography, anatomic dis-section, and limited histologic examination. Radiology201:251–256, 1996.
43. Smith AN, McCauley TR, Jokl P: SLAP lesions ofthe glenoid labrum diagnosed with MR imaging.Skeletal Radiol 22:507–510, 1993.
44. Snyder SJ, Banas MP, Karzel RP: An analysis of 140injuries to the superior glenoid labrum. J ShoulderElbow Surg 4:243–248, 1995.
45. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD,Friedman MJ: SLAP lesions of the shoulder.Arthroscopy 6:274–279, 1990.
46. Steinbeck J, Liljenqvist U, Jerosch J: The anatomy ofthe glenohumeral ligamentous complex and its con-tribution to anterior shoulder stability. J Shoulder El-bow Surg 7:122–126, 1998.
47. Vangsness CT, Jorgenson SS, Watson T, JohnsonDL: The origin of the long head of the biceps fromthe scapula and glenoid labrum-an anatomical studyof 100 shoulders. J Bone Joint Surg 76B:951–954,1994.
48. Warner JJP, Kann S, Marks P: Arthroscopic repair ofcombined Bankart and superior labral detachmentanterior and posterior lesions: Technique and pre-liminary results. Arthroscopy 10:383–391, 1994.
49. Williams MW, Snyder SJ, Buford D: The Bufordcomplex: The “cord-like” middle glenohumeral lig-ament and absent anterosuperior labrum complex: Anormal anatomic capsulolabral variant. Arthroscopy10:241–247, 1994.
50. Yoneda M, Hirooka A, Saito S, Yamamoto T, OchiT: Arthroscopic stapling for detached superior gle-noid labrum. J Bone Joint Surg 73B:746–750, 1991.
Number 400July, 2002 Disorders of the Superior Labrum 87