diseases, ao ospedale niguarda ca’ granda, milano el 1 · • responsabile dr. issa el hamad...
TRANSCRIPT
Epidemiological profiles of viral hepatitis in Italy:
effect of migration
HIV
Chiara PezzoliDept of Infectious DiseasesUniversity of BresciaBrescia
Issa El Hamad1st Dept of Infectious Diseases,AO Spedali Civili Brescia
Massimo PuotiDept of Infectious Diseases,AO Ospedale Niguarda Ca’ Granda, Milano

ASL di BresciaD.G. Dr. Carmelo Scarcella
D.S. A. Dr. Francesco Vassallo
• Centro di Salute Internazionale –Ambulatorio di Medicina del Disagio
• Responsabile Dr. Issa El Hamad 1° Divisione Malattie Infettive AO Spedali Civili Brescia
• Dirigenti Medici– Dr.ssa S. Rossi – ASL di Brescia
– Dr.ssa C. Scolari – ASL di Brescia
• Dirigenti e consulenti 1991‐2011– Dr. Salvatore Casari – Clinica Malattie Infettive Università di Brescia
– Dr. Silvio Caligaris ‐ Clinica Malattie Infettive Università di Brescia
– Dr. Massimo Puoti ‐ Clinica Malattie Infettive Università di Brescia
Epidemiological profiles of hepatitis in Italy efect of migration: HIV & Hepatitis coinfections
• Impact of immigration on HIV epidemiology in Italy
• Hepatitis B and HIV coinfection • Special issues in HIV management in immigrants and relationship with concurrent liver diseases
• HBV genotypes in HIV‐HBV coinfection• Impact of late presentation of HIV infection in HBV coinfected immigrants
Epidemiological profiles of hepatitis in Italy efect of migration: HIV & Hepatitis coinfections
• Impact of immigration on HIV epidemiology in Italy
• Hepatitis B and HIV coinfection • Special issues in HIV management in immigrants and relationship with concurrent liver diseases
• HBV genotypes in HIV‐HBV coinfection• Impact of late presentation of HIV infection in HBV coinfected immigrants

Proportion of immigrant in all cases of AIDS in Italy by year of diagnosis
7.9 % of all cases in Italy

Proportion of new diagnosis of HIV infection immigrants vs italians (immigrants : 9% in 1992 vs. 29% in 2010)
(Valle d’Aosta, Piemonte, Liguria, Lombardia, Friuli Venezia-Giulia, Veneto, Bolzano, Trento, Emilia-Romagna, Lazio, Puglia, Marche, Calabria, Pescara, Sassari e Catania)
COA, Notiziario ISS 2010

88Source: Not Ist Super Sanità, 2010; 23(4 suppl. 1)
Proportion of AIDS cases whose HIV infection was previously unknown at the moment of diagnosis (1996-2009)
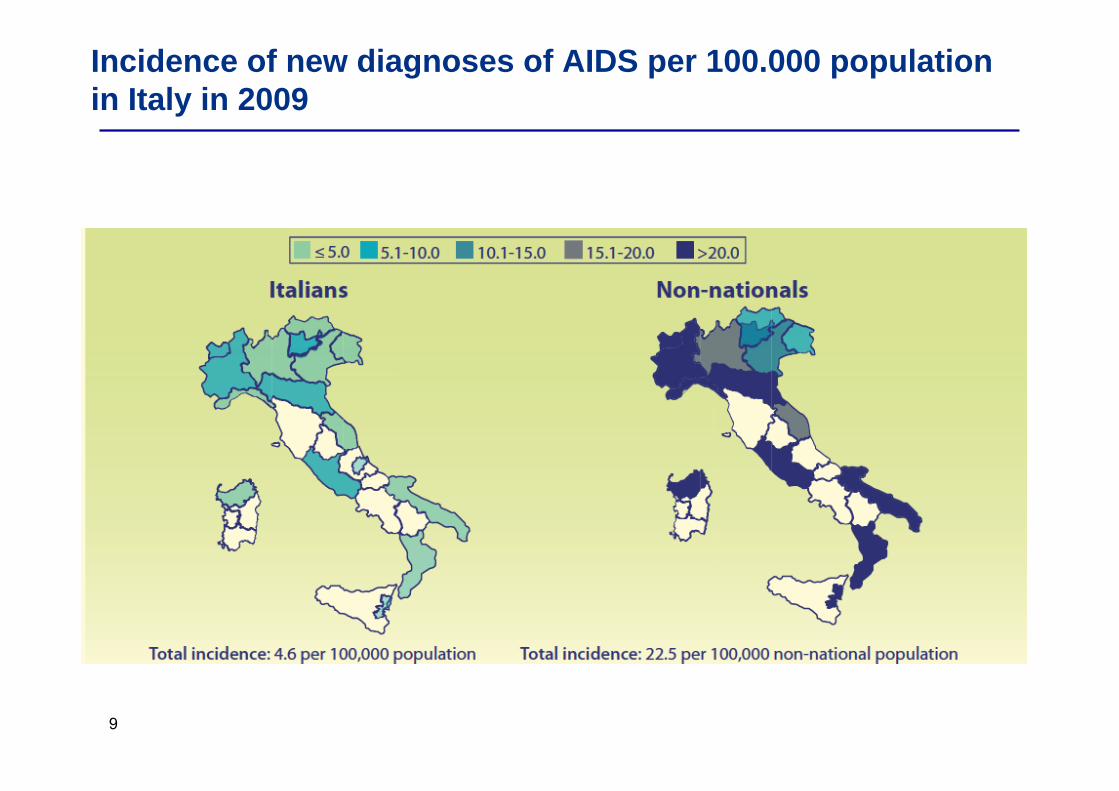
Diagnosis of HIV is later in immigrants
Potential causes of late diagnosis:
• Infection acquired in the native
country(Akinsete OO et al, AIDS Patient Care STDs, 2007)
• Culture and language(Sobrino-vegas P et al. Current
HIV Research, 2009)
• No targeted information campaign
• Low perception of risk and of the
importance of diagnosis
• Other priorities (job, home, permesso di
soggiorno...)
• Stigmatization
• Institutional barriers
• Political and legal issues
9
Incidence of new diagnoses of AIDS per 100.000 population in Italy in 2009
10
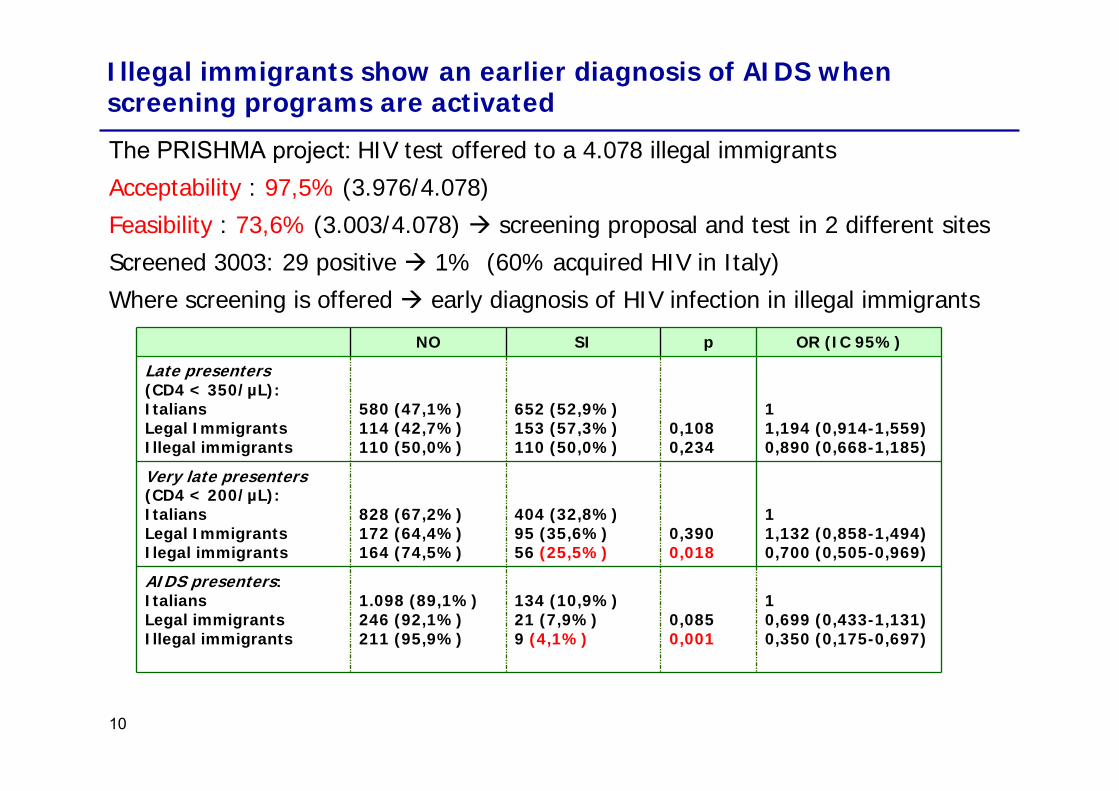
NO SI p OR (IC 95%)
Late presenters(CD4 < 350/µL):ItaliansLegal Immigrants Illegal immigrants
580 (47,1%)114 (42,7%)110 (50,0%)
652 (52,9%)153 (57,3%)110 (50,0%)
0,1080,234
11,194 (0,914-1,559)0,890 (0,668-1,185)
Very late presenters(CD4 < 200/µL):ItaliansLegal ImmigrantsIlegal immigrants
828 (67,2%)172 (64,4%)164 (74,5%)
404 (32,8%)95 (35,6%)56 (25,5%)
0,3900,018
11,132 (0,858-1,494)0,700 (0,505-0,969)
AIDS presenters:ItaliansLegal immigrantsIllegal immigrants
1.098 (89,1%)246 (92,1%)211 (95,9%)
134 (10,9%)21 (7,9%)9 (4,1%)
0,0850,001
10,699 (0,433-1,131)0,350 (0,175-0,697)
Illegal immigrants show an earlier diagnosis of AIDS when screening programs are activated
The PRISHMA project: HIV test offered to a 4.078 illegal immigrants
Acceptability : 97,5% (3.976/4.078)
Feasibility : 73,6% (3.003/4.078) screening proposal and test in 2 different sites
Screened 3003: 29 positive 1% (60% acquired HIV in Italy)
Where screening is offered early diagnosis of HIV infection in illegal immigrants

11
Immigrants are one third of HIV patients on follow up in Bresciafrom 2000
Year of HIV Dx ≥ 2000First visit no more than 1 year after HIV positive testART naive at first visit
N (%)
All HIV+ 1.719 (100)
Italians 1.232 (71,7)
Immigrants487 (28,3)
N (%)
Status :- Legal immigrants-Illegal immigrants
267 (54,8) 220 (45,2)
Country of birth - Africa-South America- Eastern Europe- Asia- ND
268 (55)110 (22,6)50 (11,9)30 (6,2)21 (4,3)

Patients ethnicity and nationality of antiretroviral naives HIV+in Icona foundation Study

Epidemiological profiles of hepatitis in Italy efect of migration: HIV & Hepatitis coinfections
• Immigrants are a growing subgroup of HIV infected patients: HIV screening in high risk behaviour and in those coming from high endemicity areas is mandatory
Epidemiological profiles of hepatitis in Italy efect of migration: HIV & Hepatitis coinfections
• Impact of immigration on HIV epidemiology in Italy
• Hepatitis B and HIV coinfection • Special issues in HIV management in immigrants and relationship with concurrent liver diseases
• HBV genotypes in HIV‐HBV coinfection• Impact of late presentation of HIV infection in HBV coinfected immigrants
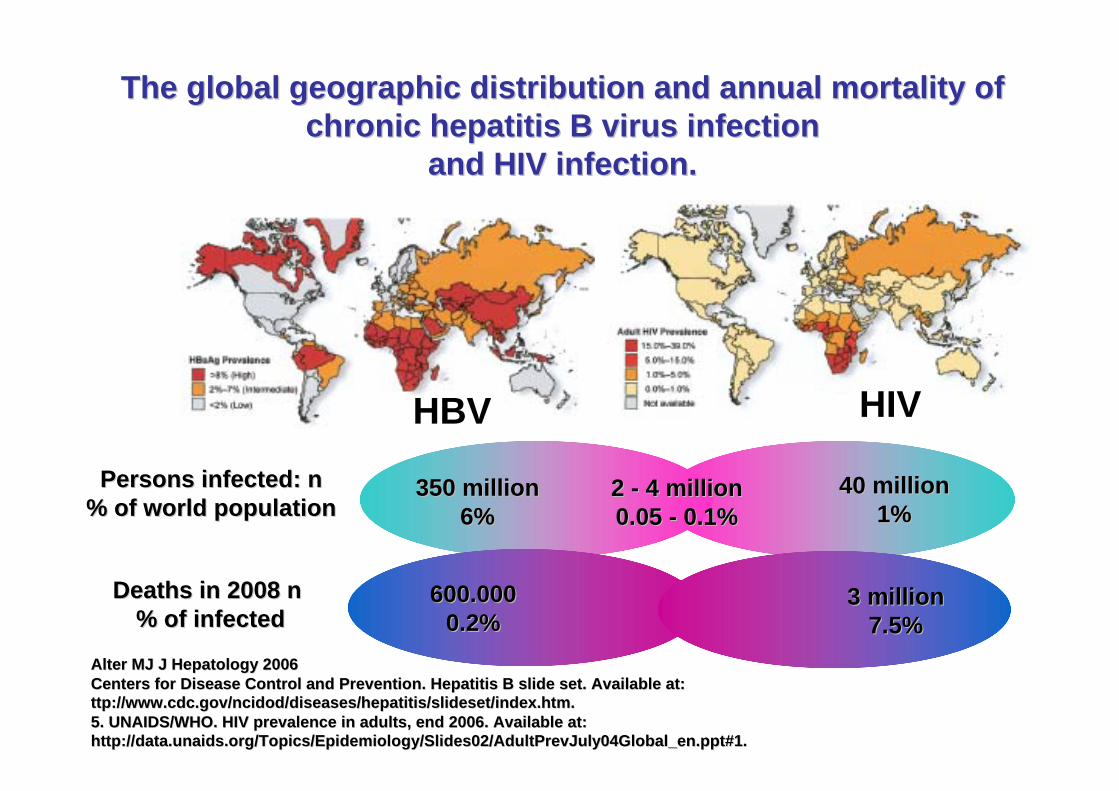
The global geographic distribution and annual mortality of The global geographic distribution and annual mortality of chronic hepatitis B virus infection chronic hepatitis B virus infection
and HIV infection.and HIV infection.
Alter MJ J Hepatology 2006Alter MJ J Hepatology 2006Centers for Disease Control and Prevention. Hepatitis B slide seCenters for Disease Control and Prevention. Hepatitis B slide set. Available at: t. Available at: ttp://www.cdc.gov/ncidod/diseases/hepatitis/slideset/index.htm. ttp://www.cdc.gov/ncidod/diseases/hepatitis/slideset/index.htm. 5. UNAIDS/WHO. HIV prevalence in adults, end 2006. Available at:5. UNAIDS/WHO. HIV prevalence in adults, end 2006. Available at:http://data.unaids.org/Topics/Epidemiology/Slides02/AdultPrevJulhttp://data.unaids.org/Topics/Epidemiology/Slides02/AdultPrevJuly04Global_en.ppt#1. y04Global_en.ppt#1.
350 million350 million6%6%
40 million40 million1%1%
2 2 -- 4 million4 million0.05 0.05 -- 0.1%0.1%
Persons infected: n Persons infected: n % of world population % of world population
Deaths in 2008 n Deaths in 2008 n % of infected% of infected
600.000600.0000.2%0.2%
3 million3 million7.5%7.5%
HBV HIV
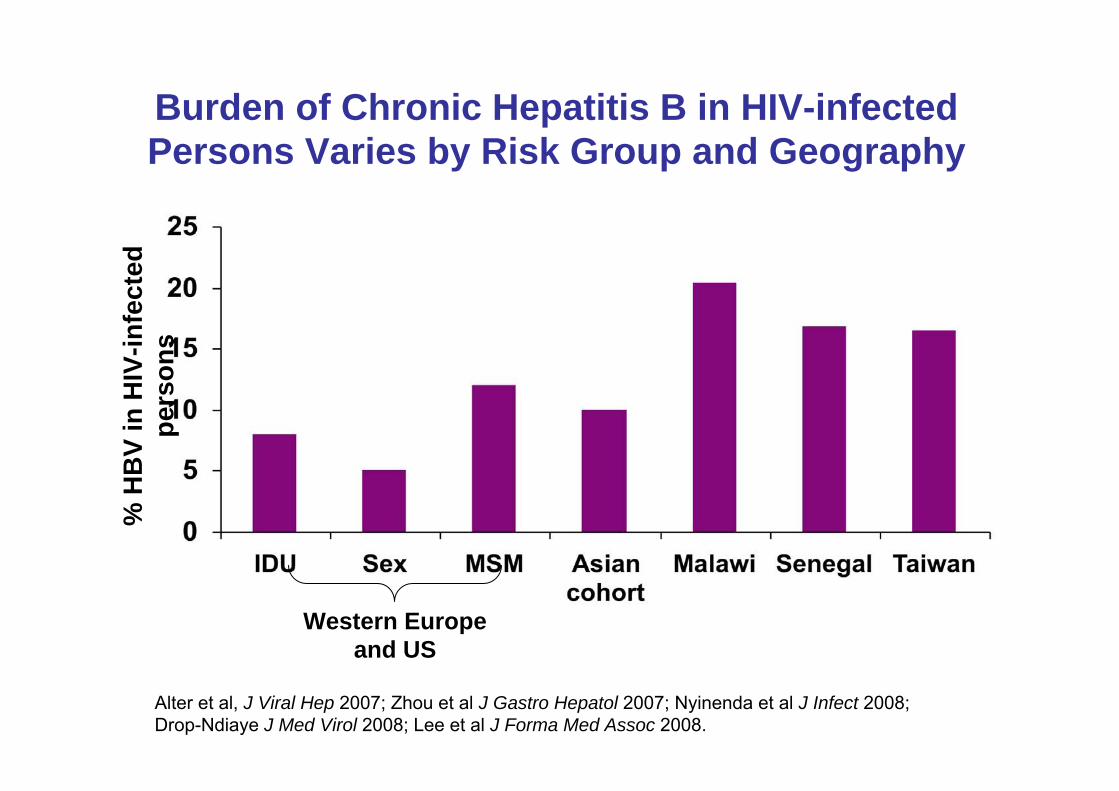
Burden of Chronic Hepatitis B in HIV-infected Persons Varies by Risk Group and Geography
Western Europe and US
% H
BV
in H
IV-in
fect
ed
pers
ons
Alter et al, J Viral Hep 2007; Zhou et al J Gastro Hepatol 2007; Nyinenda et al J Infect 2008; Drop-Ndiaye J Med Virol 2008; Lee et al J Forma Med Assoc 2008.
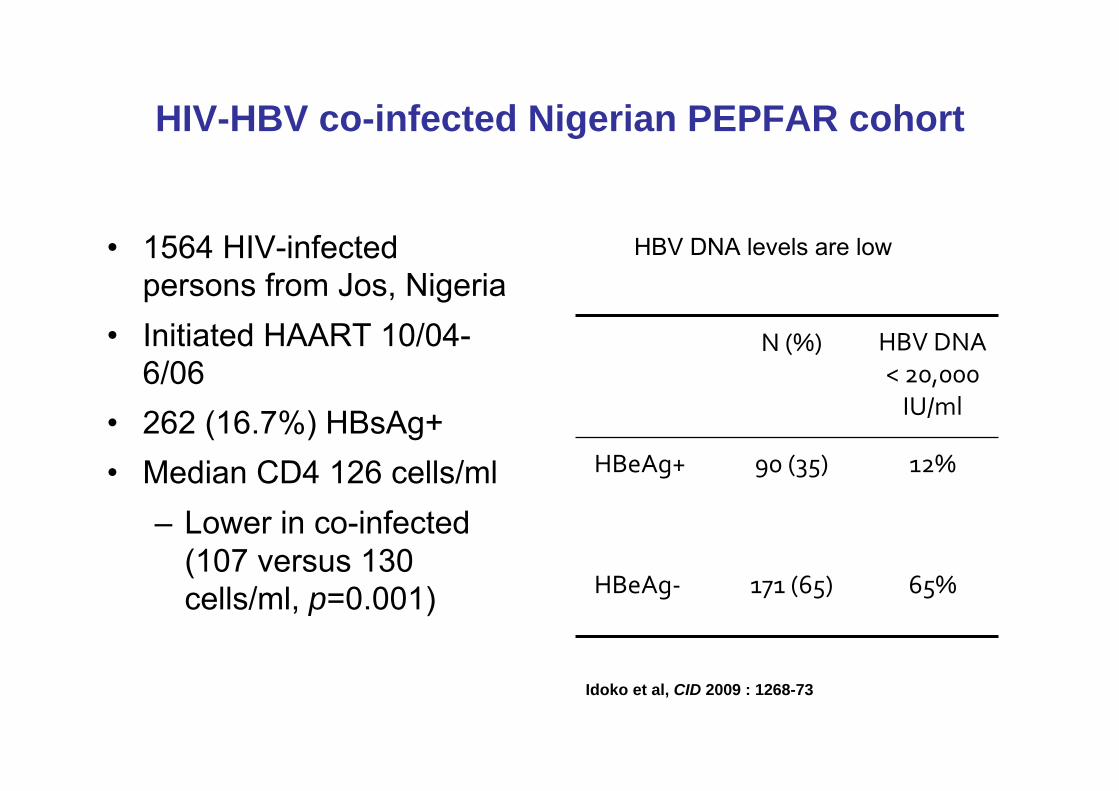
HIV-HBV co-infected Nigerian PEPFAR cohort
• 1564 HIV-infected persons from Jos, Nigeria
• Initiated HAART 10/04-6/06
• 262 (16.7%) HBsAg+• Median CD4 126 cells/ml
– Lower in co-infected (107 versus 130 cells/ml, p=0.001)
N (%) HBV DNA < 20,000 IU/ml
HBeAg+ 90 (35) 12%
HBeAg‐ 171 (65) 65%
HBV DNA levels are low
Idoko et al, CID 2009 : 1268-73

HBV DNA levels low in majority of HIV-HBV co-infected individuals in ACTG A5175 and A5208
HBsAg negativeN=1914
HBeAg negativeN=57
HBeAg positive
N=55Age, years* 34 34.5 35.1CD4, cells/mL* 161 137 117HIV RNA, log cp/ml* 5.05 5.15 5.07ALT (U/L) 23 23 28.4AST (U/L) 28.6 34.2 45.4HBV DNA (IU/mL)* -- 2.7 7.7HBV DNA <2000 IU/mL 68% 6%
HBV DNA <20,000 IU/mL
77% 10%
*median values Thio et al, CROI 2010
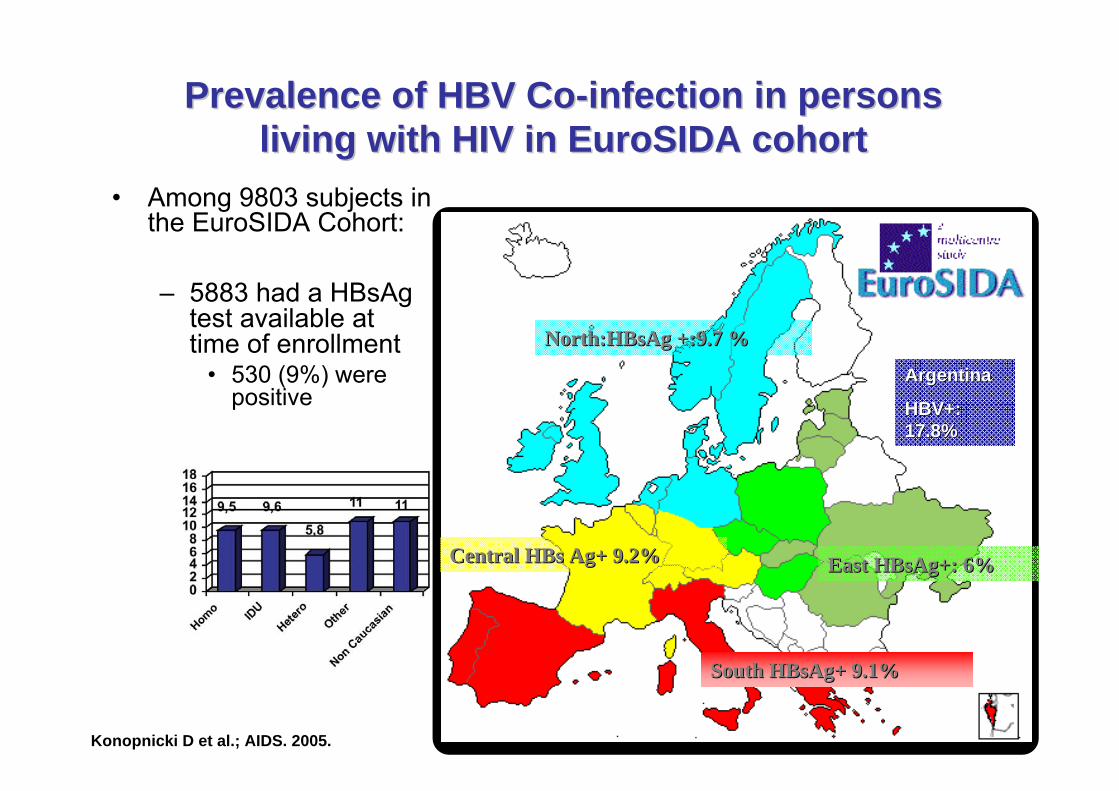
Prevalence of HBV CoPrevalence of HBV Co--infection in persons infection in persons living with HIV in EuroSIDA cohortliving with HIV in EuroSIDA cohort
• Among 9803 subjects in the EuroSIDA Cohort:
– 5883 had a HBsAgtest available attime of enrollment
• 530 (9%) were positive
North:HBsAg +:9.7 %North:HBsAg +:9.7 %
Central HBs Ag+ 9.2%Central HBs Ag+ 9.2%
South HBsAg+ 9.1%South HBsAg+ 9.1%
East HBsAg+: 6%East HBsAg+: 6%
ArgentinaArgentina
HBV+: HBV+: 17.8%17.8%
Konopnicki D et al.; AIDS. 2005.
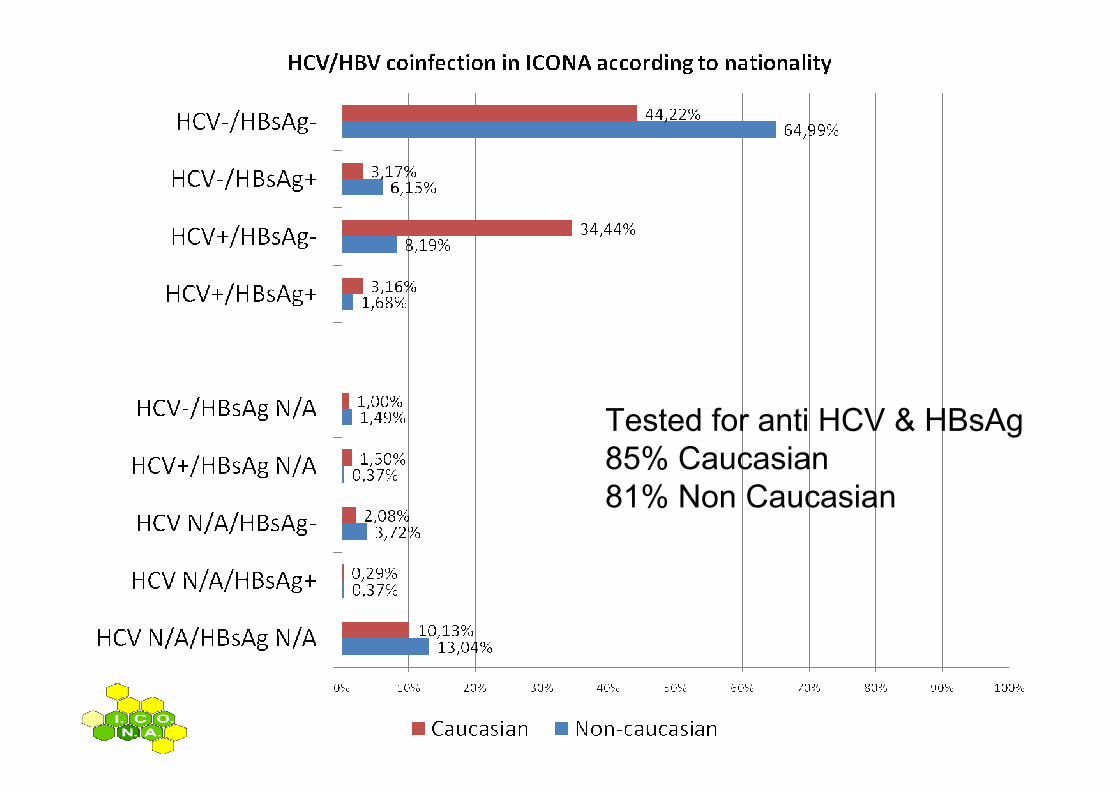
Tested for anti HCV & HBsAg85% Caucasian81% Non Caucasian
Epidemiological profiles of hepatitis in Italy effect of migration: HIV & Hepatitis coinfections
• Immigrants are a growing subgroup of HIV infected patients: HIV screening in high risk behaviour and in those coming from high endemicity areas is mandatory
• Hepatitis B coinfection is common in HIV+ immigrants (7.83%) as in italian natives (6.33%); HCV is less common in immigrants (9.87% vs. 37.6%)

Epidemiological prophiles of hepatitis in Italy effect of migration: HIV & Hepatitis coinfections
• Impact of immigration on HIV epidemiology in Italy
• Hepatitis B and HIV coinfection • Special issues in HIV management in
immigrants and relationship with concurrent liver diseases
• HBV genotypes in HIV-HBV coinfection• Impact of late presentation of HIV infection in
HBV coinfected immigrants
23
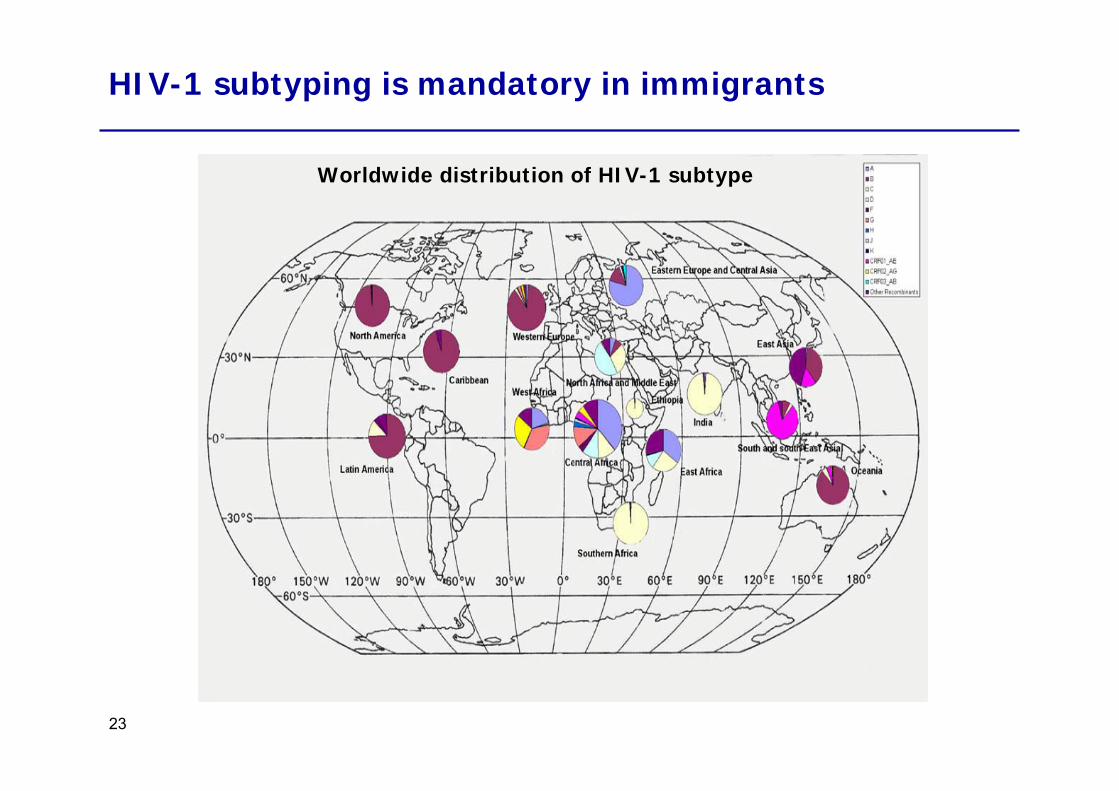
HIV-1 subtyping is mandatory in immigrants
Worldwide distribution of HIV-1 subtype
24
0102030405060708090100
1983‐1985 1986‐1988 1989‐1991 1992‐1994 1995‐1997 1998‐2000 2001‐2003 2004‐2006
Anno
% patients
A1 C CRF02_AG F1 G Altri
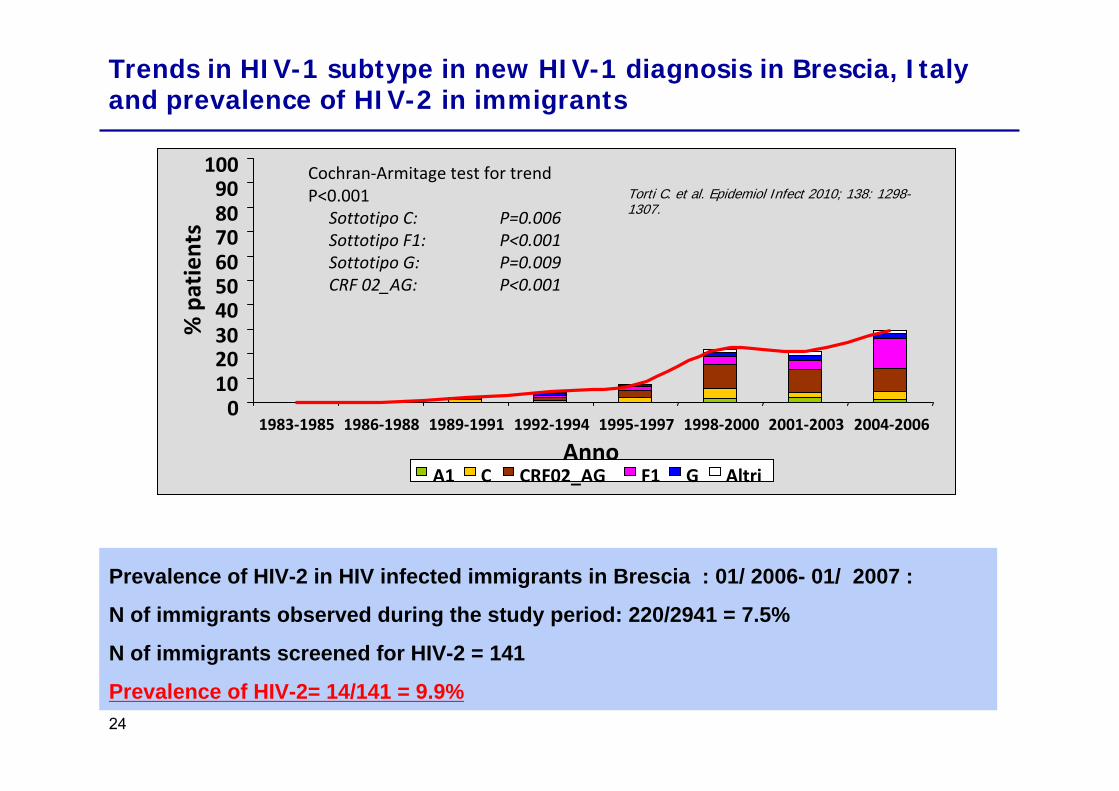
Cochran‐Armitage test for trend P<0.001
Sottotipo C: P=0.006Sottotipo F1: P<0.001Sottotipo G: P=0.009CRF 02_AG: P<0.001
Torti C. et al. Epidemiol Infect 2010; 138: 1298-1307.
Trends in HIV-1 subtype in new HIV-1 diagnosis in Brescia, Italy and prevalence of HIV-2 in immigrants
Prevalence of HIV-2 in HIV infected immigrants in Brescia : 01/ 2006- 01/ 2007 :
N of immigrants observed during the study period: 220/2941 = 7.5%
N of immigrants screened for HIV-2 = 141
Prevalence of HIV-2= 14/141 = 9.9%

Implication of high prevalence of non B HIV-1 subtype and HIV-2 in immigrants
•Need for HIV subtyping:●Correct meausurement of HIV RNA [1,2];● Identification of more aggressive subtypes ( ie subtype D)
need for closer monitoring off and on therapy] [3-4];●HIV-2: NNRTI uneffective fosamprenavir, enfuvirtide null or
partial efficacy [2, 5-7];●Correct interpretation of resistance testing [8-9].
25
1. Rodes B et al. J Clin Microbiol, 2007; 45(1): 88-92.2. Easterbrook PJ et al J Int AIDS Soc, 2010; 13(1): 4.3. Bousheri et al. JAIDS, 2009; 52(5): 548-552.4. Rodes B. et al. Clin Infect Dis, 2005; 41: e19-e21.5. Van der Ende ME AIDS, 2003; 17(suppl 3): S55-S61.6. Poveda E et al. AIDS Res Hum Retroviruses, 2004; 20(3): 347-348.7. Geretti AM. Curr Opin Infect Dis, 2006; 19(1): 1-7.8. Kantor R. et al. PLOS Medicine, 2005.9. Holguin A et al. AIDS Rev. 2006 Apr-Jun;8(2):98-107.
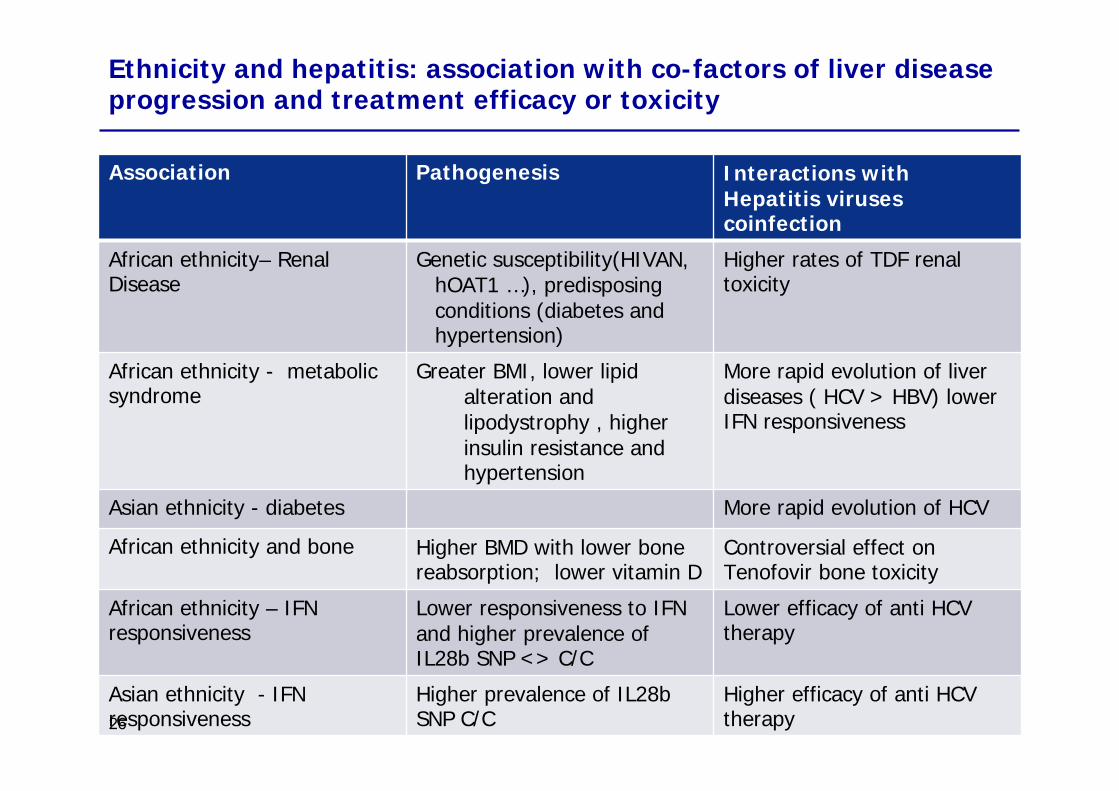
Ethnicity and hepatitis: association with co-factors of liver disease progression and treatment efficacy or toxicity
Association Pathogenesis Interactions with Hepatitis viruses coinfection
African ethnicity– Renal Disease
Genetic susceptibility(HIVAN, hOAT1 …), predisposing conditions (diabetes and hypertension)
Higher rates of TDF renal toxicity
African ethnicity - metabolic syndrome
Greater BMI, lower lipid alteration and lipodystrophy , higher insulin resistance and hypertension
More rapid evolution of liver diseases ( HCV > HBV) lower IFN responsiveness
Asian ethnicity - diabetes More rapid evolution of HCV
African ethnicity and bone Higher BMD with lower bone reabsorption; lower vitamin D
Controversial effect on Tenofovir bone toxicity
African ethnicity – IFN responsiveness
Lower responsiveness to IFN and higher prevalence of IL28b SNP <> C/C
Lower efficacy of anti HCV therapy
Asian ethnicity - IFN responsiveness
Higher prevalence of IL28b SNP C/C
Higher efficacy of anti HCV therapy26
27
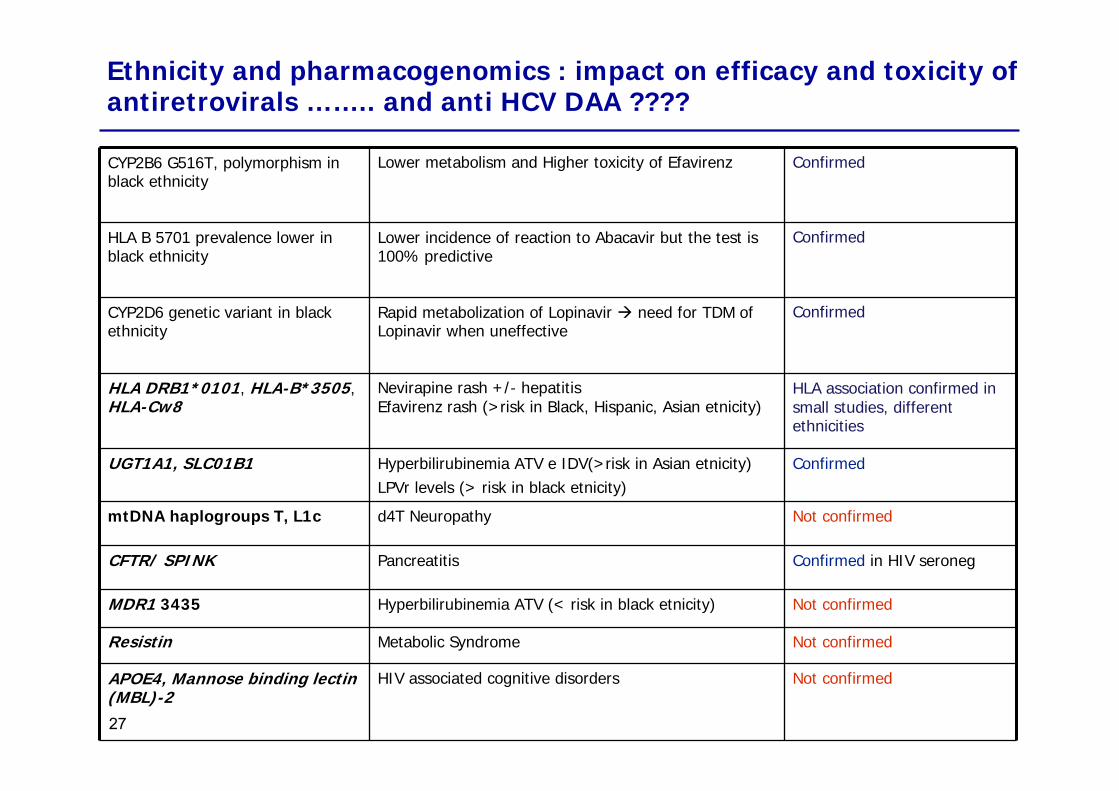
CYP2B6 G516T, polymorphism in black ethnicity
Lower metabolism and Higher toxicity of Efavirenz Confirmed
HLA B 5701 prevalence lower in black ethnicity
Lower incidence of reaction to Abacavir but the test is 100% predictive
Confirmed
CYP2D6 genetic variant in black ethnicity
Rapid metabolization of Lopinavir need for TDM of Lopinavir when uneffective
Confirmed
HLA DRB1*0101, HLA-B*3505,HLA-Cw8
Nevirapine rash +/- hepatitisEfavirenz rash (>risk in Black, Hispanic, Asian etnicity)
HLA association confirmed in small studies, different ethnicities
UGT1A1, SLC01B1 Hyperbilirubinemia ATV e IDV(>risk in Asian etnicity)LPVr levels (> risk in black etnicity)
Confirmed
mtDNA haplogroups T, L1c d4T Neuropathy Not confirmed
CFTR/ SPINK Pancreatitis Confirmed in HIV seroneg
MDR1 3435 Hyperbilirubinemia ATV (< risk in black etnicity) Not confirmed
Resistin Metabolic Syndrome Not confirmed
APOE4, Mannose binding lectin (MBL)-2
HIV associated cognitive disorders Not confirmed
Ethnicity and pharmacogenomics : impact on efficacy and toxicity of antiretrovirals …….. and anti HCV DAA ????
Epidemiological profiles of hepatitis in Italy effect of migration: HIV & Hepatitis coinfections
• Immigrants are a growing subgroup of HIV infected patients: HIV screening in high risk behaviour and in those coming from high endemicity areas is mandatory
• Hepatitis B coinfection is common in HIV+ immigrants (7.83%) as in italian natives (6.33%); HCV is less common in immigrants (9.87% vs. 37.6%)
• HIV is different in immigrants:– Need for subtyping– Different toxicities & interaction with liver disease
pathogenesis– Different pharmacogenomics
Epidemiological profiles of hepatitis in Italy effect of migration: HIV & Hepatitis coinfections
• Impact of immigration on HIV epidemiology in Italy
• Hepatitis B and HIV coinfection • Special issues in HIV management in
immigrants and relationship with concurrent liver diseases
• HBV genotypes in HIV-HBV coinfection• Impact of late presentation of HIV infection in
HBV coinfected immigrants
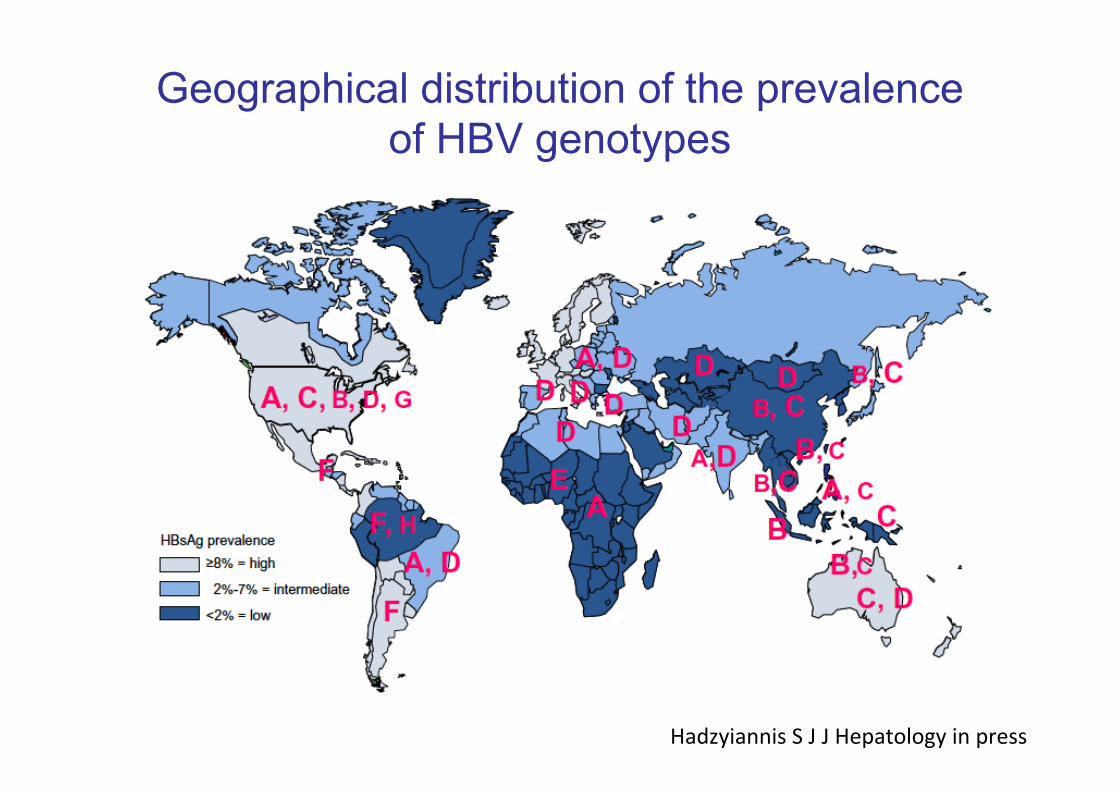
Geographical distribution of the prevalence of HBV genotypes
Hadzyiannis S J J Hepatology in press
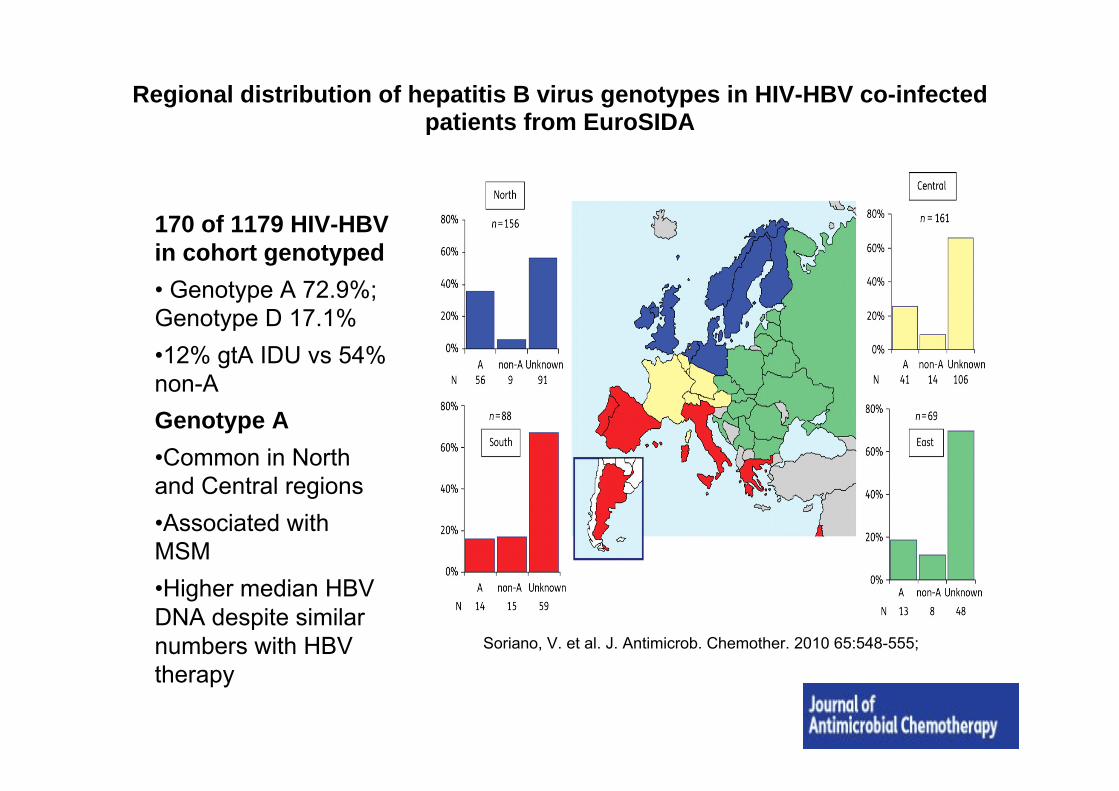
Soriano, V. et al. J. Antimicrob. Chemother. 2010 65:548-555;
Regional distribution of hepatitis B virus genotypes in HIV-HBV co-infected patients from EuroSIDA
170 of 1179 HIV-HBV in cohort genotyped• Genotype A 72.9%; Genotype D 17.1%•12% gtA IDU vs 54% non-AGenotype A •Common in North and Central regions•Associated with MSM•Higher median HBV DNA despite similar numbers with HBV therapy
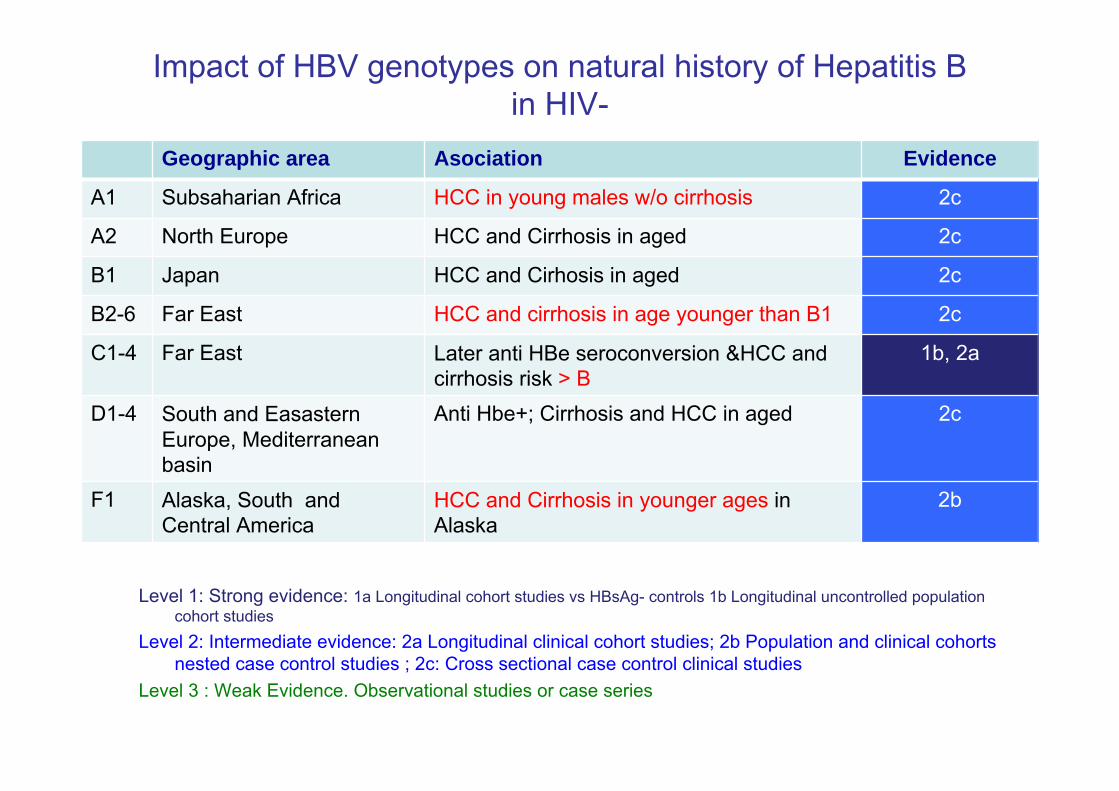
Impact of HBV genotypes on natural history of Hepatitis B in HIV-
Geographic area Asociation Evidence
A1 Subsaharian Africa HCC in young males w/o cirrhosis 2c
A2 North Europe HCC and Cirrhosis in aged 2c
B1 Japan HCC and Cirhosis in aged 2c
B2-6 Far East HCC and cirrhosis in age younger than B1 2c
C1-4 Far East Later anti HBe seroconversion &HCC and cirrhosis risk > B
1b, 2a
D1-4 South and Easastern Europe, Mediterranean basin
Anti Hbe+; Cirrhosis and HCC in aged 2c
F1 Alaska, South and Central America
HCC and Cirrhosis in younger ages in Alaska
2b
Level 1: Strong evidence: 1a Longitudinal cohort studies vs HBsAg- controls 1b Longitudinal uncontrolled population cohort studies
Level 2: Intermediate evidence: 2a Longitudinal clinical cohort studies; 2b Population and clinical cohorts nested case control studies ; 2c: Cross sectional case control clinical studies
Level 3 : Weak Evidence. Observational studies or case series
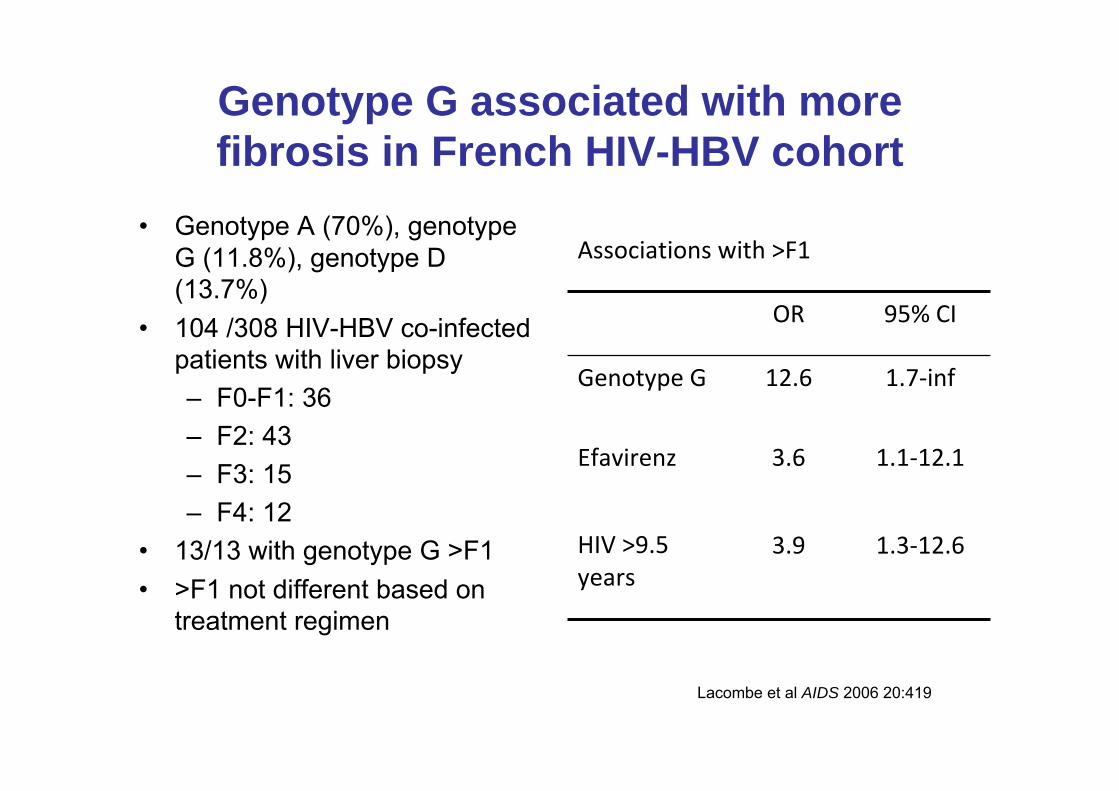
Genotype G associated with more fibrosis in French HIV-HBV cohort
• Genotype A (70%), genotype G (11.8%), genotype D (13.7%)
• 104 /308 HIV-HBV co-infected patients with liver biopsy– F0-F1: 36 – F2: 43 – F3: 15 – F4: 12
• 13/13 with genotype G >F1• >F1 not different based on
treatment regimen
Lacombe et al AIDS 2006 20:419
Associations with >F1
OR 95% CI
Genotype G 12.6 1.7‐inf
Efavirenz 3.6 1.1‐12.1
HIV >9.5 years
3.9 1.3‐12.6

Additional HBV genotype studies
• In 40 Taiwanese HIV-HBV patients, HBV genotype B had higher HBV DNA and more rapid development of LMV-R (Hsieh TH et al AVT 2009 14(8):1157-63.
• Two other studies demonstrate genotype A associated with HIV-HBV MSM
– In Japanese cohort, 20/32 (62.5%) of MSM or bisexuals were genotype A compared to 1/9 (11%) of heterosexuals and 1.9% of HBV monoinfected (Shibayama et al J Med Virol 2005 76:24)
– Spanish study of 23 HIV-HBV subjects (Perez-Olmeda. AIDS Res Hum Retro 19:657)
Genotype A Genotype DMSM, % 67 33IDU, % 33 67

Epidemiological profiles of hepatitis in Italy effect of migration: HIV & Hepatitis coinfections
• Immigrants are a growing subgroup of HIV infected patients: HIV screening in high risk behaviour and in those coming from high endemicity areas is mandatory
• Hepatitis B coinfection is common in HIV+ immigrants (7.83%) as in italian natives (6.33%); HCV is less common in immigrants (9.87% vs. 37.6%)
• HIV is different in immigrants:– Need for subtyping– Different toxicities & interaction with liver disease pathogenesis– Different phatrmacogenomics
• HBV is different in immigrants: peculiarities of HBV subtypes

Epidemiological profiles of hepatitis in Italy effect of migration: HIV & Hepatitis coinfections
• Impact of immigration on HIV epidemiology in Italy
• Hepatitis B and HIV coinfection • Special issues in HIV management in
immigrants and relationship with concurrent liver diseases
• HBV genotypes in HIV-HBV coinfection• Impact of late presentation of HIV infection in
HBV coinfected immigrants

3737Source: Not Ist Super Sanità, 2010; 23(4 suppl. 1)
Proportion of AIDS cases whose HIV infection was previously unknown at the moment of diagnosis (1996-2009)
Diagnosis of HIV is later in immigrants
Potential causes of late diagnosis:
• Infection acquired in the native
country(Akinsete OO et al, AIDS Patient Care STDs, 2007)
• Culture and language(Sobrino-vegas P et al. Current
HIV Research, 2009)
• No targeted information campaign
• Low perception of risk and of the
importance of diagnosis
• Other priorities (job, home, permesso di
soggiorno...)
• Stigmatization
• Institutional barriers
• Political and legal issues

Hepatitis Flares in HIV-HBV coinfected patients starting anti HBV active HAART(TICO trial substudy)
•TICO Trial substudy: •36 antiretroviral naïve HIV/HBV in Thailand
randomized to receive:● TDF vs LAM vs TDF + LAM as part of an Efavirenz based
HAART● 8 (22%) cases with Hepatic Flares ( ALT > 5 x VN or > 200
within 12 weeks) 1 died for LF (3%)● Predictors of flares:
● High HBVDNA● High ALT● Low CD4
● Pathogenesis of flares: Immune Restoration Diseases by cytokines substudy: ● T cell and NK activation markers ↑↑↑ in cases IP-10 and sCD30 & ● markers of IFNγ induction (IL-18) and activity (MCP-1) ↑↑↑
Crane et al Hepatology 2009 JID 2009
Epidemiological profiles of hepatitis in Italy effect of migration: HIV & Hepatitis
coinfections• Immigrants are a growing subgroup of HIV infected patients:
HIV screening in high risk behaviour and in those coming from high endemicity areas is mandatory
• Hepatitis B coinfection is common in HIV+ immigrants (7.83%) as in italian natives (6.33%); HCV is less common in immigrants (9.87% vs. 37.6%)
• HIV is different in immigrants:– Need for subtyping– Different toxicities & interaction with liver disease pathogenesis– Different phatrmacogenomics
• HBV is different in immigrants: peculiarities of HBV subtypes• Late presentation in HIV HBV coinfected higher risk of
decompensation in cirrhotics after immune restoration
Epidemiological profiles of hepatitis in Italy effect of migration: HIV & Hepatitis coinfections
• Immigrants are a growing subgroup of HIV infected patients: HIV screening in high risk behaviour and in those coming from high endemicity areas is mandatory
• Hepatitis B coinfection is common in HIV+ immigrants (7.83%) as in italian natives (6.33%); HCV is less common in immigrants (9.87% vs. 37.6%)
• HIV is different in immigrants:– Need for subtyping– Different toxicities & interaction with liver disease
pathogenesis– Different phatrmacogenomics
• HBV is different in immigrants: peculiarities of HBV subtypes• Late presentation in HIV HBV coinfected higher risk of
decompensation in cirrhotics after immune restoration

ASL di BresciaD.G. Dr. Carmelo Scarcella
D.S. A. Dr. Francesco Vassallo
• Centro di Salute Internazionale –Ambulatorio di Medicina del Disagio
• Responsabile Dr. Issa El Hamad 1° Divisione Malattie Infettive AO Spedali Civili Brescia
• Dirigenti Medici– Dr.ssa S. Rossi – ASL di Brescia– Dr.ssa C. Scolari – ASL di Brescia
• Dirigenti e consulenti 1991-2011– Dr. Salvatore Casari – Clinica Malattie Infettive Università di
Brescia– Dr. Silvio Caligaris - Clinica Malattie Infettive Università di
Brescia– Dr. Massimo Puoti - Clinica Malattie Infettive Università di
Brescia

Dipartimento Malattie Infettive AO Spedali Civili di Brescia
Malattie Infettive 1 Divisione
direttore Dr. Alfreedo Scalzini
Clinica di Malattie Infettive e Tropicali
direttore Prof. Giampiero Carosi

Icona Foundation StudyGOVERNING BODY- M. Moroni (Chair), G. Angarano, A. Antinori, G. Carosi, R. Cauda, A. d’Arminio Monforte, G. Di Perri, M. Galli, R. Iardino, G. Ippolito, A. Lazzarin, C.F. Perno, P.L. Viale, F Von Schlosser.SCIENTIFIC SECRETARY- A d’Arminio MonforteSTEERING COMMITTEE A. Ammassari, M Andreoni, A. Antinori, C. Balotta, P. Bonfanti, S Bonora, M Borderi, M.R. Capobianchi, A. Castagna, F . Ceccherini-Silberstein, A. Cozzi-Lepri, A. d’Arminio Monforte, A. De Luca, M Gargiulo, C. Gervasoni, E. Girardi, M Lichtner, S. Lo Caputo, G Madeddu, F Maggiolo, S Marcotullio, L Monno, R. Murri, C. Mussini, M. Puoti, C. TortiSTATISTICAL AND MONITORING TEAM A Cozzi-Lepri, I Fanti, T FormentiPARTICIPATING PHYSICIANS AND CENTERS Italy M. Montroni, A. Giacometti, A Costantini, A. Riva (Ancona); U. Tirelli, F. Martellotta (Aviano-PN); G. Angarano, L Monno, N. Ladisa, (Bari); F. Suter, F. Maggiolo (Bergamo); PL: Viale, G. Verucchi, B Piergentili, (Bologna); G. Carosi, G. Cristini, C. Torti, C. Minardi, D. Bertelli (Brescia); T. Quirino, C Abeli (Busto Arsizio); P.E. Manconi, P. Piano (Cagliari); J Vecchiet, K Falasca (Chieti); G Carnevale, S Lorenzotti (Cremona); L. Sighinolfi,D. Segala (Ferrara); F. Leoncini, F. Mazzotta, M. Pozzi, S. Lo Caputo (Firenze); G. Cassola, G Viscoli, A. Alessandrini, R. Piscopo, G Mazzarello (Genova); C. Mastroianni, V. Belvisi (Latina); P. Bonfanti, C Molteni (Lecco); A. Chiodera, P. Castelli (Macerata); M Galli, A. Lazzarin, G. Rizzardini, M. Puoti, A. d’Arminio Monforte, AL Ridolfo, A Foschi, A Castagna, S Salpietro, S. Merli, L Carenzi, M.C. Moioli, P Cicconi, T Formenti (Milano); R. Esposito, C. Mussini (Modena); A Gori, V Pastore (Monza), N. Abrescia, A. Chirianni, M. De Marco, (Napoli); C. Ferrari, R Borghi (Parma); F Baldelli, B Belfiori (Perugia); G. Parruti, F Sozio (Pescara); G. Magnani, M.A. Ursitti (Reggio Emilia); M. Arlotti, P. Ortolani (Rimini); R. Cauda,M Andreoni, A. Antinori, G. Antonucci, P. Narciso, V Tozzi, V. Vullo, A. De Luca, M. Zaccarelli, L Gallo, R. Acinapura, P. De Longis, L Ceccarelli, R Libertone, M.P. Trotta, A Miccoli, (Roma); AM Cattelan (Rovigo); M.S. Mura, G Madeddu (Sassari); P. Caramello, G. Di Perri, G.C. Orofino, M Sciandra (Torino); E. Raise, F. Ebo (Venezia); G. Pellizzer, D. Buonfrate (Vicenza).The Icona Foundation Study is supported by unrestricted educational grants of Abbott , Bristol-Myers Squibb Gilead